A self-fulfilling prophecy: A fourth-year medical student’s misinformed decision
4 Interview
New SVS president seeks to enhance communication with members, tighten focus on outcomes
11 Corner Stitch
A vascular resident explores how to say, ‘I messed up’
13 Vascular practice
‘Parenthood in vascular surgery a personal choice, not a professional deadline’
www.vascularspecialistonline.com
Vascular unity: ‘Let’s stop standing on the sidelines while others define what vascular care looks like’
Outgoing SVS president casts vision for the future of vascular surgery as he delivers the 2025 presidential address during the Vascular Annual Meeting.
By Bryan Kay
VASCULAR SURGERY HISTORY: PUTTING SPECIALTY ON THE MAP IN A BROADER SENSE
By Bryan Kay
THE PEOPLE, DISCOVERIES, innovations and events that brought the vascular surgery profession to where it is today formed the bedrock of the subject matter for this year’s John Homans Lecture—“Who put the vascular in vascular surgery?”—at VAM 2025.
Jerry Goldstone, MD, an adjunct professor at Stanford University College of Medicine, pored over some of the most important developments in the field since the founding of the SVS in 1946, an occurrence which set the stage for the modern vascular surgical specialty.
“When the 31 founding members were gathered for their first meeting in 1947, how could they possibly have imagined what vascular surgery is like today,” Goldstone told Vascular Specialist. “They formed this organization because there was no organization devoted to vascular surgery. Most were general surgeons with a special interest in vascular, some were cardiac people with a special interest in vascular.”
What they helped shape
See page 9
Matthew Eagleton, MD, did not go looking for vascular surgery—it found him. His vascular journey started when his grandfather was a patient of a cardiac and vascular surgeon. That surgeon’s calm, focused demeanor sparked something in the chief of the Division of Vascular and Endovascular Surgery at Mass General Brigham and Harvard Medical School in Boston, he told attendees during the 2025 Society for Vascular Surgery (SVS) Vascular Annual Meeting (VAM) presidential address in New Orleans (June 4–7). That encounter led Eagleton down the vascular path, from a position as a college sophomore where he was “uncertain and unfocused.” Invoking that personal journey, he used the address to make a call for the SVS to choose unity, excellence and each other to make vascular surgery’s next chapter a proud one.
See page 4
By Marlén Gomez
THE SVS HAS ANNOUNCED a new partnership with group purchasing organization (GPO) Provista in an effort to help provide a cost-slashing benefit to private practice physicians amid ongoing financial pressures in outpatient care. The initiative,
4
Medical Editor Malachi Sheahan III, MD
Associate Medical Editors
Bernadette Aulivola, MD | O. William Brown, MD | Elliot L. Chaikof, MD, PhD
| Carlo Dall’Olmo, MD | Alan M. Dietzek MD, RPVI, FACS | John F. Eidt, MD | Robert Fitridge, MD | Dennis R. Gable, MD | Linda Harris, MD | Krishna Jain, MD | Larry Kraiss, MD | Joann Lohr, MD | James McKinsey, MD | Joseph Mills, MD | Erica L. Mitchell, MD, MEd, FACS | Leila Mureebe, MD | Frank Pomposelli, MD | David Rigberg, MD | Clifford Sales, MD | Bhagwan Satiani, MD | Larry Scher, MD | Marc Schermerhorn, MD | Murray L. Shames, MD | Niten Singh, MD | Frank J. Veith, MD | Robert Eugene Zierler, MD
Resident/Fellow Editor
Saranya Sundaram, MD
Executive Director SVS
Kenneth M. Slaw, PhD
Senior Director for Public Affairs and Advocacy
Megan Marcinko, MPS
Communications Specialist
Marlén Gomez
GUEST EDITORIAL
A self-fulfilling prophecy based on a fourth-year medical student’s misinformed decision
By Sarah Lauve, MD
“How many programs conducted in-person interviews this year?”
“Which programs conducted in-person interviews?”
“Oh wow, I didn’t realize that many programs were conducting in-person interviews.”
All of these are questions gleaned from last year’s Match process.
Published by BIBA News, which is a subsidiary of BIBA Medical Ltd.
Publisher Stephen Greenhalgh
Managing Editor Bryan Kay bryan@bibamedical.com
Editorial contribution Jocelyn Hudson, Will Date, Jamie Bell and Éva Malpass Design Josh Lyon and Terry Hawes
Advertising Nicole Schmitz nicole@bibamedical.com
Letters to the editor vascularspecialist@vascularsociety.org
BIBA Medical, Europe 526 Fulham Road, London SW6 5NR, United Kingdom
BIBA Medical, North America 155 North Wacker Drive – Suite 4250, Chicago, IL 60606, USA
Vascular Specialist is the official newspaper of the Society for Vascular Surgery and provides the vascular specialist with timely and relevant news and commentary about clinical developments and about the impact of healthcare policy. Content for Vascular Specialist is provided by BIBA News. Content for the news from SVS is provided by the Society for Vascular Surgery. | The ideas and opinions expressed in Vascular Specialist do not necessarily reflect those of the Society or the Publisher. The Society for Vascular Surgery and BIBA News will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services, or the quality or endorsement of advertised products or services, mentioned herein. | The Society for Vascular Surgery headquarters is located at 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. | POSTMASTER: Send changes of address (with old mailing label) to Vascular Specialist, Subscription Services, 9400 W. Higgins Road, Suite 315, Rosemont, IL 60018. |
RECIPIENT: To change your address, e-mail subscriptions@bibamedical.com | For missing issue claims, e-mail subscriptions@bibamedical. com. Vascular Specialist (ISSN 1558-0148) is published monthly for the Society for Vascular Surgery by BIBA News. Printed by Ironmark |
To be sure, the Association of Program Directors in Vascular Surgery (APDVS) has demonstrated a tireless commitment to finding best interview practices, developing new residency programs, and increasing training resources and recruitment. Looking at the 2024 Electronic Residency Application Service (ERAS) preliminary data, the APDVS efforts have clearly been successful. Diagnostic radiology and integrated vascular surgery were the two specialties experiencing the largest growth, characterized by increases in applicant numbers, average applications submitted per applicant, and average applications received per program. Despite this demonstrated growth and the efforts of the APDVS, these sentiments from the interviewers during the 2024 interview cycle identified a large discrepancy between the success the APDVS has had in these measures and the current interview process for a residency position in this field.
The Match process was a frequently discussed topic at the Houston Methodist intern boot camp. Out of curiosity, I began intentionally interviewing my fellow incoming interns about their experiences. I fully expected the first interview to fail, assuming people either wouldn’t participate or the conversations would be vague and superficial. Wrong. I was met with a shocking level of engagement that catapulted more interviews, shared experiences and inquisitive questions. I was excited to share what these conversations uncovered and knew if anyone would be interested in my findings, it would be my program director, Dr. Malachi Sheahan. In his 2021 article, “It is time to end the interview,” Dr. Sheahan thoroughly describes the faults of our current surgical trainee and faculty selection processes, impressions vs. assessment tools, the interviewer’s bias, and the overly confident assumption that we make as humans that we conduct interviews well. The guidelines made by the APDVS during the 2024 interview cycle for best interview practices were followed by only 64 programs. Eleven programs conducted in-person interviews, and one program conducted a combination of in-person and virtual interviews. Thus, my first question was born: how are integrated vascular surgery residency applicants affected by their own bias in the current in-person/virtual/hybrid interview era?
Feeling uninformed when applying to and selecting away rotations is a sentiment commonly expressed by many fourth-year medical students
on a mentor’s, resident’s or another applicant’s opinion/experience was reported by nearly all the matched applicants with whom I spoke. This was reported regardless of presence/absence of a home program, and if their most positive and impactful experience was inperson or virtual. This was one of, if not the most, influential factors for both females and males when making their rank lists, yet the characteristics of their rank lists were drastically different. Roughly 30 interns were at the Houston Methodist boot camp, representing roughly a third of current vascular interns in the country. There was not a single female intern who ranked a program number one at which she hadn’t completed an away rotation, interviewed at in person, and/or visited in person. There were several males who ranked a program number one at which they had only interviewed virtually. Although it is uncertain if these trends are significant, the VISIT trial cohort consisted of a similar number of residents that responded and completed the survey—similar in size to the number who participated in my discussion. The VISIT trial was used by the APDVS to make recommendations for best interview practices this past interview cycle, but should other factors—such as the effects of gender—be included? Are females affected differently than their male colleagues by the increasing number of programs conducting in-person interviews? If so, can the APDVS utilize this information to reduce bias and create a more consistent interview experience? This led me to reflect on my own experience with away rotations and how this influenced my rank list. I decided to then ask how recently matched interns selected away rotations to apply to and subsequently attend. Again we saw the influence of word of mouth. Every single person I asked said they chose to apply to and accept at least one away rotation solely based on program reputation and/or their mentor’s opinion. Additionally, the entire cohort of interviewees said they would significantly change where they applied and attended away rotations after having completed interview season. All interns I spoke with wished there was more information about programs provided by the programs themselves, either on their websites or by the SVS/APDVS.
In their 2023–2024 guidance statement, the APDVS references the data from the VISIT (Vascular in-person for students in the Match) trial to showcase the impact that in-person visits have on an applicant’s rank list. The VISIT trial reported that the most impactful factors to applicants when visiting a program were esprit de corps of the program, the people and physical setting. Within minutes of conducting the first conversation it was evident that a program’s reputation, as it pertains to the experiences of fellow applicants during away rotations and the opinions of an applicant’s mentor, far outweighed anything gained from an interview, regardless of format or an in-person visit. It is well known that many applicants also vet their impression of a program with a mentor or trusted colleague. This is especially influential in vascular surgery, which is a smaller, well-connected field. Placing highest value
Sarah
Lauve
The SVS currently provides a full listing of Accreditation Council for Graduate Medical Education (ACGME)accredited vascular surgery training programs. Program descriptions are listed if available but vary drastically in the information provided. In my experience, this is not specific to integrated vascular surgery residency applicants. Feeling uninformed when applying to and selecting away rotations is a sentiment commonly expressed by many fourth-year medical students. However, if integrated vascular surgery—one of the fastest growing residency programs—is a specialty so heavily impacted by networking and away rotations, should opportunities such as these be a topic addressed by the APDVS? Other specialties have begun to implement changes to address away rotation and interview practices. Integrated plastic surgery has created a specific task force dedicated to away rotations. This task force has been responsible for developing numerous resources for prospective applicants, including well-organized, updated and consolidated information on away rotations, application cycle webinars, and application process advice.
Integrated vascular surgery residency is one of—
continued on page 11
SAME SHOCK, BIGGER WAVES
Shockwave Medical is Now Part of J&J MedTech
As part of J&J MedTech, we’ll continue to deliver our same unmatched commitment to innovation, customer service and improving patient outcomes — with the added energy of the global leader in healthcare.
NEW SVS PRESIDENT SEEKS TO ENHANCE COMMUNICATION WITH MEMBERS, TIGHTEN FOCUS ON OUTCOMES
By Marlén Gomez
WITH ANOTHER VASCULAR Annual Meeting (VAM) in the books, that means the flag unfurls on a new presidential year. And that means Philadelphia-based vascular surgeon Keith Calligaro, MD, now leads the SVS as president. And Calligaro, who brings decades of experience to the role, has outlined a clear vision for his year at the helm, and he has his sights fixed on helping address some of the key areas of priority for vascular surgery and the SVS.
“At the end of the year, I want our members to reflect on the projects we have completed or at least made significant progress on. To me, this will be the measure of our success in achieving our priorities,” he tells Vascular Specialist after the conclusion of VAM 2025 in New Orleans (June 4–7).
Calligaro’s presidency comes at a pivotal time for the SVS, as the organization continues to evolve in response to changes in healthcare delivery, technology and growing membership. He says three key initiatives will define his term: a resolution on the current deliberations regarding the optimal model for the Vascular Surgery Board (VSB),
promoting the uptake of the Vascular Verification Program (VVP), and engaging in strategic realignment and rebalancing of the SVS’ primary efforts.
“One of the biggest lessons I’ve learned is the value of getting input from others,” he explains.
“I always like to hear different perspectives, especially on controversial issues. It helps shape my thinking.”
He highlights the importance of having a clear structure and a sense of accountability in leadership roles. His approach to leadership and oversight emphasizes discipline and the establishment of deadlines—without these elements, tasks often remain unfinished, he says. Transparency and accountability are principles he consistently aims to instill in the teams with which he collaborates, and this will continue in the SVS.
The SVS has recently completed an assessment of the pros and cons of supporting the current VSB within the American Board of Surgery (ABS) or moving toward the establishment of a free-standing—or
independent—board for vascular surgery. After a year of deliberation, the task force presented survey results at VAM 2025, indicating a near-even split among members’ opinions. Calligaro aims to provide further clarity on this issue, recognizing the members’ desire for a resolution on what the SVS Executive Board (EB) recommendation will be. He plans to finalize a governance decision during the EB retreat at the end of July. The EB will communicate the decision to members shortly thereafter. Calligaro emphasizes that the rapidly evolving healthcare environment requires flexibility and adaptability. Therefore, any decisions made at this moment will likely require ongoing monitoring, he says.
The VVP, developed in collaboration with the American College of Surgeons (ACS), aims to recognize hospitals and outpatient centers as vascular centers of excellence. Calligaro notes that participation has lagged since the program’s establishment.
To address this issue, Calligaro plans to schedule meetings and set deadlines with the Strategic Board of Directors (SBOD), comprising approximately 30 members, as well as with centers that have a high volume of participation in the Vascular Quality Initiative (VQI) registry. These discussions will focus on providing strategies for applying for the program.
With the SVS’ rapid growth over the past decade and projections to reach close to 8,000 members by 2030, Calligaro believes the time is ripe to reassess the organization’s top-most priorities, as well as its volunteer
FROM THE COVER VASCULAR UNITY: ‘LET’S STOP STANDING ON THE SIDELINES WHILE OTHERS DEFINE WHAT VASCULAR CARE LOOKS LIKE’
Early on, Eagleton recognized that people in the vascular community exerted incredible influence on others aspiring in the field. Take the late Roy Greenberg, MD, an intern then, and Karl Illig, MD, a senior resident, who were both major influences when he started out. They would go on to grapple with the future of aortic repair, as well as introduce Eagleton to invaluable future mentors such as Dick Green, MD, and Ken Ouriel, MD—“people who didn’t just do vascular surgery, but lived it. The intensity, the pace, the sense of urgency at times—it was a world I couldn’t turn away from,” he said.
Eagleton was convinced, even as a fourth-year medical student, that one of the great strengths of vascular surgery was in its ability to deliver longitudinal care. And the early experience of presenting his research at a regional conference opened the door to interaction with the giants in the field, like former SVS President Frank Veith, MD. “Be prepared. Vascular surgery doesn’t hand you anything. But if you’re willing to show up, stay humble and learn fast—it gives back in ways few other fields can,” Eagleton said.
He highlighted the successes that the SVS has achieved—advocacy, reform and often “quiet” progress— but he also listed the numerous challenges, notably a
continued from page 1
heterogeneous and growing group of members that confronts the organization. The faultlines of the struggle lie in fragmentation and disconnection.
“Our biggest internal challenge right now is fragmentation and disunity. And it’s been a problem growing over the past several years,” he noted. “We’re not just disagreeing—we’re disengaging. And that weakens us. It weakens our credibility. It weakens our voice.”
Yet, patients and purpose are always at the heart of vascular surgery, Eagleton argued. And beyond this dual bedrock, he called for a different kind of leadership, one that is layered, brave and collaborative.
“We need bridge-builders. People who can bring together our fragmented membership—who can sit in a room of differing opinions and find common ground without compromising our core values,” he said.
Vascular surgery’s relationship with other specialties has too often been defined by tension, Eagleton told attendees. And yet, the volume of vascular disease is rising fast, and “we are not enough. We can’t serve this population alone. That doesn’t mean we dilute our identity. It means we must instead lead with clarity, not defensiveness.” He added: “Let’s stop standing on the sidelines while others define what vascular care looks like. […] Because this is our house.”
and staff support structure. “We’ve expanded significantly, but our members have likely hit their limit regarding increases to dues going forward, and we can’t expect ever-increasing support from the same group of loyal sponsors,” he says. “We need to prioritize and streamline our efforts to ensure sustainability while we also explore expanding the pool of potential sponsors and seek new sources of revenue.”
Calligaro plans to address the growing demand for vascular surgeons, particularly in underserved areas. He points to the SVS Foundation’s Vascular Care for the Underserved (VC4U) program, which supports research and workforce development in less populated regions. “About 50% of trainees stay where they train, so we need to be strategic,” he explains. “We’re also exploring telemedicine as a way to extend care and expertise to remote areas.”
As vascular surgery continues to evolve, Calligaro underscores the need to support mid-career surgeons. “We must be open-minded and adaptable,” he says. “Through the Clinical Practice Council and simulation-based learning, the SVS is working to optimize education and help surgeons stay current.”
So, what is his vision for his presidency? “Transparency,” he responds. “I want members to know what we’re doing and why. Even if there’s disagreement, we must speak with one voice and always act in the best interest of the Society,” he adds. “I hope people will say that I—and the Executive Board—did our best to serve the vascular community with honesty, openness and a commitment to excellence.”
FROM THE COVER SVS LAUNCHES PARTNERSHIP TO HELP PRIVATE PRACTICE VASCULAR SURGEONS CUTS COSTS
continued from page 1
unveiled during a Section on Ambulatory Vascular Care (SAVC) session at the Vascular Annual Meeting (VAM) on June 6 in New Orleans, aims to help smaller practices reduce expenses by leveraging collective buying power.
“The GPO is something that the SVS has been working on for a while, and it’s finally come to fruition,” said Anil Hingorani, MD, chair of the SAVC. “This is a potential lifeline for smaller outpatient practices.”
Hingorani noted that rising costs and inflation have led to the closure of many office-based labs (OBLs) in his area. He emphasized that the GPO model allows smaller practices to access the same discounted pricing typically reserved for large hospital systems.“For example, a small group like ours with three practitioners might pay half a cent per piece of gauze,” Hingorani said. “But when a larger group buys in bulk, they might pay a quarter of a cent. The GPO brings those smaller practices together to achieve similar savings.”
He continued: “We did some beta testing with practices of various sizes, asking them to identify their top 10 or 20 high-cost items. The results were promising, especially for smaller practices that don’t already benefit from economies of scale.”
Email sections@vascularsociety.org or visit vascular. org/GPO.—Marlén Gomez
Keith Calligaro
How likely are your surgical patients to have disruptive bleeding?
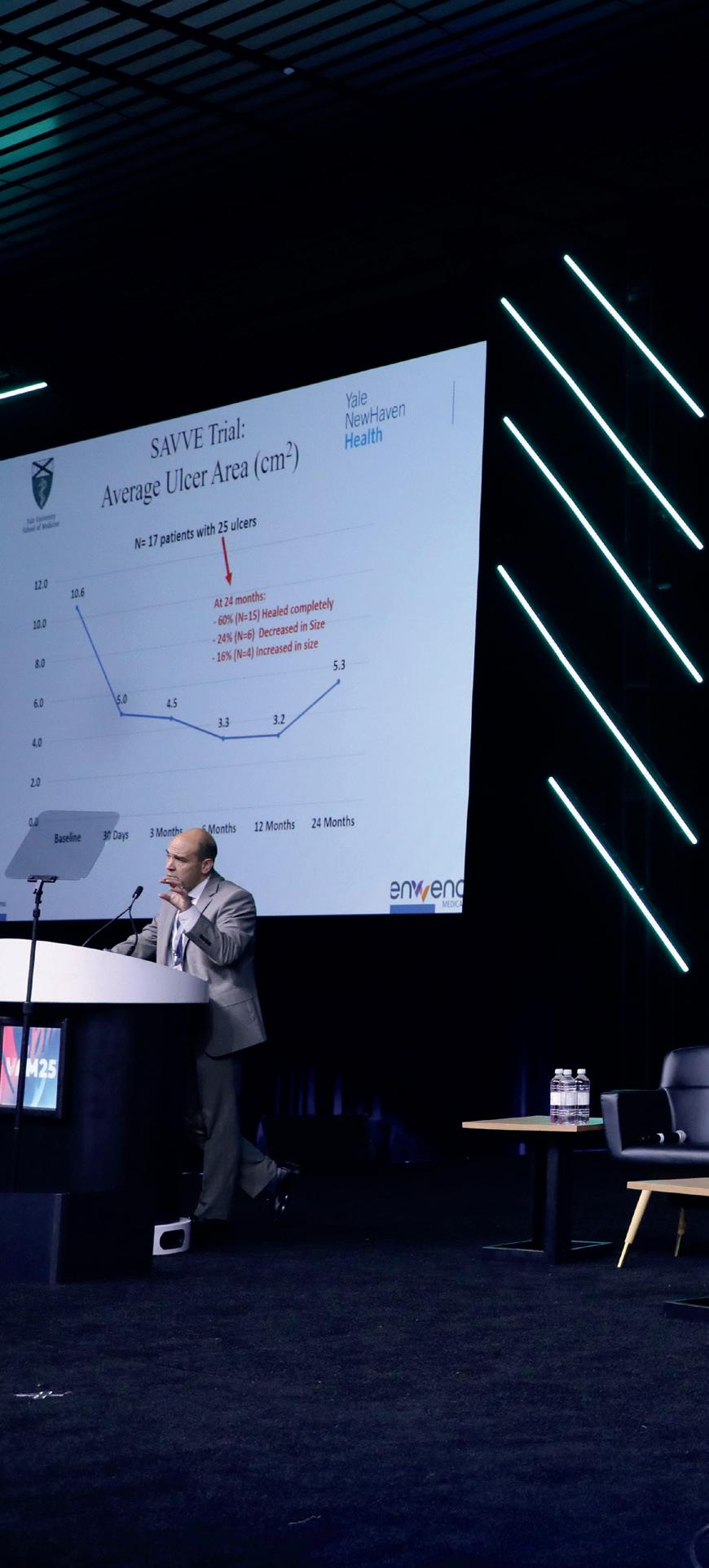
VAM THROUGH THE LENS » 25
The 2025 Vascular Annual Meeting in New Orleans (June 4–7) brought together the vascular meeting for four days of scientific and educational sessions amid sweltering heat on the outside but robust content on the inside of the host venue.
VAM 2025 got off to a belated start after the lights went out in the main meeting hall just before the day one kick off (right). But, once started, the event ran the full gamut of VAM staples and 2025 special sessions, including the Greenberg Lecture from Sherene Shalhub (top left) and the latest in the SVS Keynote Speaker Series: U.S. Olympic hockey team legend Jim Craig (pictured second from top right with Matthew Eagleton)
“Welcome to VAM 2025, our new motto: No power, no problem”
MATTHEW EAGLETON
FROM THE COVER VASCULAR SURGERY HISTORY: PUTTING SPECIALTY ON THE MAP
yielded some tremendously important advances over the years, minting vascular surgery as a bona fide, standalone specialty in its own right, Goldstone told VAM 2025. After canvassing colleagues in the field, he landed on “about 10 of the most important things that got us from 0 to a place, now, where there is one big society, 6,000 members, our own journals, recognition internationally, good science,” he explained.
Among the topics he charted were the formation of the SVS and its merger with the American Association for Vascular Surgery (AAVS), previously the North American Chapter, International Society for Cardiovascular Surgery (NA-ISCVS); the development of grafts; the coming of the vascular lab and duplex ultrasound; carotid endarterectomy (CEA); two innovations in venous disease in the shape of the Greenfield filter for pulmonary embolism (PE) and laser ablation of the great saphenous vein; the founding of the Journal of Vascular Surgery (JVS); and the birth of the vascular surgery fellowship.
continued from page 1
related. But much earlier, the development of grafts brought vascular surgery from a place of few repair options to one in which, from the early 1950s, a vein graft became available for the lower extremity, continuing on with further developments for larger vessels. The coming of the first textile graft emerged and “changed everything,”
Goldstone continued. “So now, by the mid-50s, we’ve got grafts that can basically repair any artery anywhere—that’s a huge jump forward for the profession.”
The vascular lab and duplex ultrasound machine, meanwhile, “literally changed the nature of the diagnosis,” he said. They brought diagnosis directly into the hands of vascular surgeons, now with the tools in their offices. “You get real anatomic information, and at the time all of this was going on, angiography existed, but it’s risky, painful, expensive and it’s a little complicated. So, now [with the lab and ultrasound], we have non-invasive things that allow for better diagnosis, follow-up and management of patients.”
own little cocoon, as maybe a little different from general surgery. It put vascular surgery as a profession on the map in a broader sense.”
Goldstone also focused on important developments in venous disease treatment, referencing how the surgeon for whom the lecture is named, John Homans, MD, had a special interest in veins. “One was the Greenfield filter, because PE is still a common problem and still can be deadly,” he noted. “In the old days, they were tying off veins to prevent clots from going to the lung, and there had been a bunch of efforts to do things to the vena cava that didn’t work very well, and then Greenfield came up with this filter that really changed the management of that condition.”
For one, the merger that created the modern SVS in 2003 brought together a society that was exclusive with one that bore a larger, more unlimited membership base “into one big organization that has 6,000 members.”
That’s one of the major developments, Goldstone
CRAWFORD FORUM
The rise of CEA helped push the vascular specialty further forward, Goldstone said. “After all, we are a surgical specialty, and known by the operations we do, and one of the most common and distinctive is CEA,” he explained. “It put vascular surgeons into contact with other people, in other specialties, and elevated the profession beyond its
PRESENTING A UNITED FRONT TO ADDRESS VASCULAR SURGERY’S STRUCTURAL AND FINANCIAL CHALLENGES
By Will Date and Bryan Kay
VASCULAR SURGEONS MUST present a unified front in order to address structural and financial challenges facing the specialty, SVS President-Elect Keith Calligaro, MD, said in summing up this year’s E. Stanley Crawford Critical Issues Forum at the 2025 Vascular Annual Meeting (VAM) in New Orleans. This year, the annual forum explored ways to “empower” the vascular community to confront these head on and covered topics ranging from vascular surgery’s position within heart and vascular centers, to unionization and fair financial reimbursement.
First up, Malachi Sheahan III, MD, chair of surgery at the Louisiana State University Health Sciences Center in VAM host city New Orleans, addressed one of the thorniest topics: the issue of heart and vascular centers and vascular surgery’s position within them. Fundamentally, he asked whether the specialty’s role is being a peripheral part of the heart and vascular center?
“If we cohabitate heart and vascular, I just see no way we are going to come out on top,” he told those gathered. “For most of us here, we are at too much of a disadvan-
tage for this to be a successful paradigm for our care.”
Next, Faisal Aziz, MD, the chief of vascular surgery at Penn State University in Hershey, Pennsylvania, contemplated the position of departments of vascular surgery in both academic and community hospital settings, ultimately asking, “Are they worth fighting for?” “The best interests of vascular surgery are not served by being a part of heart and vascular institutes, or by departments of surgery—I think it is about time that we declare our independence,” he said.
Sunita Srivastava, MD, assistant professor of surgery at Massachusetts General Hospital in Boston, addressed how vascular surgeons can attain fair financial reimbursement from a marketing and fair compensation perspective. Her talk, based on a report of the SVS Population Health Task Force, looked at outside pressures impacting fair compensation. “The financial advantage of a vascular surgeon to healthcare is severely underestimated and very difficult to measure,” she told VAM 2025 attendees. “We contribute the technical revenue to a service, we are not given credit for it. When
“It put vascular surgeons into contact with other people, in other specialties, and elevated the profession beyond its own little cocoon”
JERRY GOLDSTONE
our operative assistance is needed, we drive the complexity, we drive the financial value, and the contribution margin to the hospital.”
Last up, Enrico Ascher, MD, professor of surgery at New York University in New York City and CEO of the Vascular Institute of New York, tackled the question of potential unionization, asking, “How can vascular surgeons unionize when 95% of payments come from Medicare?” he said. “As issues with full time employees and patients increase, the topic of unionization is not going to go away, it is just going to become deeper and [more] robust.”
Calligaro, at the time SVS president-elect, now SVS president following the conclusion of VAM 2025, identified the need for vascular surgery unity. “The overriding theme from this whole session is that we need to be unified. There are disagreements on certain issues, but we really need to speak as one voice, get together and try to figure out what we can by working together.”
Calligaro, who as the incoming SVS president was responsible for organizing the forum, assembled the panel of four leading vascular surgeons to tackle some of the hottest topics of the day that speak to how vascular surgery is structured in hospitals and medical centers, as well as how vascular surgeons are reimbursed and organized.
“Fundamentally, we want to inform our SVS members what they can do to become better positioned with their hospital administrations and compared to other specialties, so that we are in a better position to take care of our patients for ourselves,” the chief of vascular surgery at Pennsylvania Hospital in Philadelphia told Vascular Specialist ahead of the event.
NEW OFFICERS
SVS reveals 2025 election results
THE SVS HAS ELECTED ANDRES Schanzer, MD, as the incoming vice president and Malachi G. Sheahan III, MD, as the new secretary.
The results from this year’s SVS elections were revealed during the Society’s Annual Business Meeting, which took place during VAM 2025.
As vice president, Schanzer will help coordinate the activities of SVS councils and committees. His term as vice president will be followed by terms as president-elect and president, ensuring continuity of leadership.
Schanzer, professor and chief of the vascular and endovascular division at UMass Medical School in Worcester, Massachusetts, is noted for his commitment to vascular surgery education and has taken on numerous leadership roles within regional and national surgical societies, including the presidency of the New England Society for Vascular Surgery (NESVS).
As secretary, Sheahan will serve a threeyear term, overseeing strategic alignment and coordination of SVS communications.
Sheahan is a professor of surgery at Louisiana State University Health Sciences Center (LSUHSC) in New Orleans. He serves as chair of the institution’s Department of Surgery and chief of the Division of Vascular and Endovascular Surgery. He serves as the medical editor of Vascular Specialist.—Marlén Gomez
Jerry Goldstone
CORNER STITCH COMMENT& ANALYSIS
How to say ‘I messed up’
By Anonymous
LITTLE, IF ANYTHING, IN LIFE PREPARES YOU FOR when you eventually cause harm to another human. Intentional or not, medical errors cause significant morbidity and mortality to those we care for. But how do we manage our errors and mitigate moral injury?
As a PGY2 in the surgical intensive care unit (ICU) I found myself in front of an elderly man who underwent emergent surgery overnight for cecal volvulus. He was extubated, stable, and his daughter was at bedside. When I introduced myself, the daughter recognized my last name on my white coat and asked if I was related to a local cardiologist who had performed her father’s transarterial aortic valve replacement. I said yes and immediately she trusted me. I found out later she was an RN who knew my father personally. His postoperative course was wholly unremarkable. We determined on rounds that, given his elevated CHADSVASC score, to restart anticoagulation on postoperative day two. The surgeon of record was even present to endorse hemostasis gained with low risk of bleeding and concluded the benefits of anticoagulation outweighed those risks. I ordered the heparin drip.
On postoperative day 3 the patient faltered in his otherwise unremarkable post-operative course. He now refused to ambulate and was in atrial fibrillation with rates of 150. He subsequently began to complain of worsening abdominal pain, decreased urinary output, and now had a fever to 102. The team decided on a complete blood count (CBC) in the afternoon to check on his white count. His partial thromboplastin time (PTT) was therapeutic, and his white blood cell (WBC) was 10. Focused on those details, when I checked the WBC, I neglected the hemoglobin drop from 10 to 8.5. In hindsight, he was bleeding. But in the moment, I was concerned with postoperative infection or possible leak/missed enterotomy. I continued to monitor him until end of shift and updated the daughter, who was reassured by my presence said she would see me again tomorrow. I left the hospital. Overnight the covering resident physician found the patient decompensating and repeat CBC showed a hemoglobin of 4 after fluid resuscitation for hypotension. I arrived at the hospital the following morning to find the patient being rolled back to the operative suite in extremis, blood hanging on the IV pole connected to the hospital bed. I was filled with dread. I missed something. After rounds
I made my way into the operative room to check in with the attending and chief resident scrubbed in the case. They found two liters of blood in the abdomen, which they controlled, and the patient was in the lethal triad (hypothermic, acidotic and coagulopathic). He was closed and brought back to the ICU for me to continue resuscitative efforts. I spent the entire shift in his room attempting to correct the error I knew I had played a part in. I warmed him back to normothermia, corrected his coagulopathy and acidosis back on the first night. The following day I battled atrial fibrillation with rapid ventricular response and hypotension. I tried everything. Eventually I was able to correct his hypotension, but I was using multiple vasoactive peptides. Near the end of my shift, I placed an ultrasound probe on his chest, and I couldn’t see his left ventricle contracting as well as I’d like, so I obtained a formal transthoracic echocardiogram and placed a Swan-Ganz catheter in the interim, which confirmed the diagnosis I had been dreading. The reading cardiologist called at one point wondering if the patient was even still alive. He told me over the phone the ejection fraction was maybe 5%, but he was unsure given how little the heart was contracting. My management changed to cardiogenic shock, and I reached out to the inpatient cardiology team to assist in efforts.
ble experience can fully prepare you for making a medical mistake that leads to a patient’s death. I regret that during the patient’s last hours I could not care for them. I was too emotional and was unable to think clearly. Thankfully my covering attending for the weekend was present and took over for me. She conducted the CMO discussions and managed the patient until he passed while I hid in the call room alone. I regret this decision daily. I think the toughest concept to reconcile was that the patient and his daughter trusted my medical decision making based on their experience from working with my father. I felt like I not only let them down, but my family as well. I missed a diagnosis that is sacrosanct in surgery and not a day goes by where I don’t think about this case. I lost countless hours of sleep, liters of tears, and a lot of my confidence. I know people say this kind of experience helps you avoid making the same mistake again, but it makes me sick to my stomach that in this situation, someone lost their loved one. Someone and their family put their trust in my management only to end up losing their loved one.
I don’t think any possible experience can fully prepare you for making a medical mistake that leads to a patient’s death
The following day was status quo. We started to see some improvement with de-escalation of the multiple drips the patient was receiving. I even started to feel better with newfound hope that he might recover, but I knew the only reason the patient is in the situation he’s in is because of my error. That night during sign-out I wrote out as many potential paths the patient may take, and detailed “if this, then that” scenarios and communicated with the overnight resident to follow the Swan numbers to keep track of the systemic resistance. I was losing control of the patient’s status but doing everything I thought possible to keep him from spiraling down. Overnight, the patient decompensated with what appeared to be distributive shock. I immediately sent blood cultures and started antibiotics, but it was too late. His family ultimately went for comfort measures only, and he passed shortly after. The following day his blood grew pseudomonas.
This case hurts, and it continues to hurt. I will never forget looking at the patient and his daughter knowing they trusted me. I let them down. I don’t think any possi-
I learned many lessons from my failure. Failure is necessary for growth. It allows us to learn and be better for it. But in a profession where failure might mean morbidity or mortality for someone, making those mistakes comes with a heavy burden to bear. Our training as surgical residents is extensive and demanding. Not just physically, but mentally. It is easy to say to yourself or an attending that you will improve, but that feeling of failure is always present. It can easily consume you until you find yourself in a dark place, alone. Having people around you for support is crucial. You are expected to compartmentalize emotions to allow yourself to care for the next patient, even when you’re hurting, but no one really teaches you this firsthand. Being a surgeon is not just about being technically excellent, else we would be robots. It is an all-encompassing, lifelong endeavor.
I hope by sharing my experience I can empower those with similar stories, or those who will one day find themselves caring for critically ill people, to take care of yourself as well. That way, that next patient and family you find yourself in front of will get 100% of you caring for them.
This commentary was submitted anonymously by a PGY-2 integrated vascular resident.
GUEST EDITORAL A SELF-FULFILLING PROPHECY BASED ON A FOURTH-YEAR MEDICAL STUDENT’S MISINFORMED DECISION
if not the only—residency specialty to not utilize signaling. Surprisingly, this was a topic of large debate amongst the recently matched integrated vascular surgery interns. Some advocated for the implementation of signaling within our specialty, others argued against this, and still others were neither for nor against but instead focused on risk/benefit analysis. Those who advocated for the implementation of signaling are simply of the mindset
continued from page 2
that if other specialties are utilizing it, then vascular should as well. Some argue that away rotations are the equivalent of signals in vascular surgery and the use of signals would compensate for the issues regarding away rotations. Those who are adamantly against the use of signals appreciate that uniqueness and lack of conformity of our specialty, and vote against signaling as they do not wish to go with the status quo. Others value that many vascular programs individually
review applications and the use of signaling may negate this.
I think the process of interviewing for residency will forever be a complex task that is met with constructive—and sometimes not so constructive—criticism.
I do not think any one specialty has or will ever figure out the “perfect” system. However, with the completion of the 2024–25 interview season, my curiosity regarding the interview practices within vascular surgery persists.
Are our current practices affecting genders differently? Are we lagging behind other specialties that are experiencing less growth? Most importantly, were the opinions expressed by interns in Houston specific to that class of interns, or do these trends persist amongst newly matched students?
SARAH LAUVE is a second-year integrated vascular surgery resident at Louisiana State University (LSU) in New Orleans.
THE OUTPATIENT COMMENT& ANALYSIS
BENEFITS OF A MULTISPECIALTY PRACTICE
By Jennifer Thomas, MD
WHEN I WAS ASKED TO BE PART OF the Section on Ambulatory Vascular Care (SAVC) committee, I was frankly surprised. My practice is a privately owned group of a single cardiologist and two vascular surgeons in the relatively small community setting of Anderson, South Carolina. After working as a hospital-employed surgeon for six years in this community, I made the risky but very rewarding choice to enter into a private practice and start an office-based lab (OBL). It’s been an interesting journey, from learning about business management to navigating the challenges of treating our patients safely in an outpatient setting. The obstacles continue daily, especially with reimbursement cuts as Dr. Anil Hingorani outlined in last month’s issue.
Besides being in a smaller community setting, I was surprised about being included in SAVC because some in the SVS could see me as “partnering with the enemy.” I never imagined when I started my career that I would end up sharing a practice with
a cardiologist. Like many of you, I was taught to guard against them at all costs, that they were trying to encroach on our territory in unsafe and unscrupulous ways. However, now that we have been in this marriage of sorts for eight years, I can say that it’s a natural fit. We all understand that our patients are largely the same, with overlapping risk factors and comorbidities. When cardiology and vascular surgery operate within the same practice, patients benefit from a cohesive evaluation that spans the entire arterial tree.
Pairing these specialties reduces delay in testing and treatment for patients and prevents fragmented care. From a practice growth perspective, co-locating vascular and cardiology services increases patient retention. However, there are guidelines that we’ve established over our time together as we collaborate to provide our patients’ care. You need to be very honest with your partners about how you’re going to share
patients to avoid turf wars, and our roles in patient care have evolved over the years. For example, my cardiology partner has now transitioned to outpatient medical cardiology, doing cardiac testing in the office and using the OBL for loop recorder insertions and cardioversions primarily. He refers patients who need cardiac catheterizations to our hospital-employed colleagues, again something I never expected to see but came about due to a dispute over call requirements when our former cardiology partner retired. While this seemed crazy in the beginning as we figured we would lose these folks in follow-up, patients love the ease and cost-effectiveness of our office so much that this system is actually working very well.
My vascular surgery partner focuses primarily on peripheral arterial disease (PAD), using the OBL for mainly chronic limb-threatening ischemia (CLTI) interventions, and we both provide office-based wound care. I have transitioned to mostly venous interventions. I also have an interest in wellness, so we are adding some newer cash-based services to the practice, another necessary move in my opinion to maintain financial independence.
Being willing to think outside the box when it comes to partnering with other specialties may allow you to enter or stay in a private setting if that’s your desire. For my vascular partner and I, we needed this well-established private cardiology group to help us negotiate insurance contracts, share overheads, and have the business acumen to start and run a successful OBL. Whether it’s cardiology, intervention radiology, nephrology or podiatry, partnering with other specialists who treat our patients can be a great option for all involved. My best advice is to have clear expectations, especially when discussing how to split overhead and profits. There are Stark Law issues to consider as well, so involve a healthcare attorney with experience in that arena. Bottom line, all of us need to fight for our worth, and for those in private practice, we need to be creative if we want to keep offering our patients an outpatient option. Speaking on behalf of myself and my patients, what we need is private choices in order to drive quality in healthcare, so let’s all continue sharing ways to maximize these options.
JENNIFER THOMAS is a vascular surgeon and part owner of Anderson Heart & Vascular, PC, in Anderson, South Carolina.
Jennifer Thomas
‘PARENTHOOD IN VASCULAR SURGERY A PERSONAL CHOICE, NOT A PROFESSIONAL DEADLINE’
By Marlén Gomez
WHEN IS THE RIGHT TIME TO START A FAMILY in vascular surgery? That was a core question posed during the 2025 Vascular Annual Meeting (VAM) in a dedicated session aimed at tackling issues around parenthood for those practicing in the specialty. A panel of vascular surgeons and trainees sought to address the crucial conundrum.
One answer: There is no definitive timeline for pregnancy in the operating room, said Christina Cui, MD, a vascular resident at Duke University in Durham, North Carolina, and a moderator and panelist representing the trainee perspective. She emphasized that pregnancy is a personal decision that individuals must navigate with their families, not with hospitals or program directors.
“There is so much self-imposed stigma around this topic,” she explained. “As women, we go through a lot of these issues on our own; the mental load you have to deal with on your own and [with] your partner—understand you can share that bargain.”
The session, titled “Carrying the Weight: Parenthood in Vascular Surgery,” featured perspectives from
trainees, faculty from private practice, and others sharing personal experiences.
Dawn Coleman, MD, division chief of vascular and endovascular surgery at Duke University, raised a question from the audience about the challenges vascular surgeons face in balancing patient care and team dynamics when a team member takes leave. She noted the emotional implications for both the individual on leave and the rest of the team.
“If we can solve this, we can solve world peace,” answered Dejah R. Judelson, MD, a vascular surgeon at UMass Memorial Health in Worcester, Massachusetts, and a panelist from the academic perspective.
Judelson pointed out that past discussions have focused on the additional workload for the remaining team members. The panel agreed that it is not practical to merely front-load or back-load calls to compensate for someone on leave. Instead, she believes the solution involves cross-field conversations to find equitable ways to address these situations.
“In terms of training, it’s crucial for attending physicians to step in and take on primary calls when needed,” Judelson said. During her first pregnancy, she chose to front-load her calls to avoid being a burden to her partners. However, during her subsequent pregnancies, she realized that she didn’t have that bandwidth or functional ability.
“It’s essential to acknowledge that everyone has their limits while also being sensitive to others’ feelings and opinions. We all need to support one another, regardless of the circumstances,” Judelson added.
VC4U grants advance vascular equity for underserved women SVS
THE SVS FOUNDATION IS CURRENTLY accepting applications for its 2025 Vascular Care for the Underserved (VC4U) Project Grants until Aug. 1.
The VC4U Project Grants help to address disparities in vascular care across the United States, providing $20,000 in funding for innovative, one-year projects.
This application cycle specifically supports projects dedicated to advancing women’s vascular health, encouraging bold, creative approaches to advance equity and outcomes in the field.
The SVS Foundation is proud to offer this award in partnership with the SVS Women’s Section. This initiative aims to address disparities in vascular care with a focus this year on advancing women’s vascular health in underserved communities. The initiative supports efforts to improve early detection, expand research inclusion and develop gender-specific interventions for vascular disease.
“Too often, women—especially those in underserved communities—are left out of the vascular health conversation,” said Audra Duncan, MD, chair of the SVS Women’s Section. “The VC4U grants are a powerful step toward changing that narrative.”
Ideal proposals will define the target underserved population, identify disparities in care and propose actionable, scalable solutions. Applications are open to SVS Active Members, Early Active Members and Society for Vascular Nursing (SVN) Active Members.
Learn more at vascular.org/VC4U.—Marlén Gomez
Attendees take part in VAM 2025 parenthood session
SOCIETY BRIEFS
Compiled by Marlén Gomez and Bryan Kay
Join us: SVS goes to D.C.
THE SVS INVITES MEMBERS TO register for its inaugural Advocacy and Leadership Conference, taking place Sept. 14–16, in Washington, D.C. The conference will bring together vascular surgeons, trainees, fellows and other key contributors to engage in the policymaking process, and to advocate for the specialty and patients.
Attendees will learn about crucial legislative and regulatory issues impacting vascular care, sharpen their advocacy skills through interactive training sessions and engage in direct discussions with members of Congress and senior policy staff during scheduled Capitol Hill visits. SVS members at all career stages can register. Space is limited.
To register, visit vascular.org/Advocacy.
Coding workshop to cover 2025 updates
REGISTRATION FOR THE ANNUAL
Coding and Reimbursement Workshop—and optional evaluation and management (E/M) coding workshop—opened July 9 with earlybird registration available until Aug. 6.
This 1.5-day intensive program, scheduled for Nov. 3–4 in Rosemont, Illinois, will provide expert guidance and actionable strategies to ensure proper reimbursement and compliance.
The course will address significant coding changes made in 2025, with faculty breaking down new developments and their implications for practice. Major vascular surgery coding changes will go into effect in January 2026. Those will include a major restructuring of lower extremity revascularization coding, as well as coding changes for thoracic branch endografts and baroreflex activation therapy. The optional E/M coding workshop will have updates available focused on coding and documentation rules for choosing a correct E/M category and level of service.
Learn more at vascular.org/Coding25.
CPVI Skills Course
REGISTRATION IS NOW OPEN FOR THE Complex Peripheral Vascular Interventions (CPVI) Skills Course, taking place from Sept. 20–21 in Rosemont, Illinois. The twoday course will provide participants with hands-on training in the latest techniques and technologies for treating complex peripheral arterial disease (PAD) and chronic limbthreatening ischemia (CLTI). Attendees will benefit from expert-led presentations and case-based discussions. This year, registration offers more than $400 off while maintaining the same high-caliber education.
Learn more at vascular.org/CPVI25.
THREE HONORED IN POSTER COMPETITION
THE FINAL DAY OF THE 2025 VASCULAR ANNUAL MEETING (VAM) IN New Orleans honored three winners in the championship round of the SVS Poster Competition. The audience voted to select the winners from more than 100 entries highlighting innovative research.
Hassan Chanseddine, MD, took first place and a $1,500 prize for “Time is intestine: The impact of timely intervention on acute mesenteric ischemia outcomes.”
Ben Li, MD, earned second place with a $1,000 prize for “Predicting one-year successful clinical use of an arteriovenous access for hemodialysis using machine learning.”
And Samantha Fountain, MD, was awarded third place and a $500 prize for “Racial disparities in cardiac risk index calculators for vascular surgery complication rates.”
SVS VQI to host webinar on updated smoking cessation variables
THE SVS PATIENT SAFETY Organization (SVS PSO) will host a webinar on Tuesday, July 15, at 1 p.m. Eastern Time to present updates to the National Quality Initiative Smoking Cessation variables within the SVS Vascular Quality Initiative (VQI) Registry.
Caroline Morgan, PSO director of clinical operations, will lead the one-hour session and highlight recent revisions, as well as other registry changes.
Walk for wellness
GET READY TO JOIN THE SVS Foundation this September for the 2025 Vascular Health Step Challenge. Hosted during National Vascular Disease Awareness Month, the annual challenge promotes healthy vascular habits and raises critical funds for research, education and awareness initiatives.
This year’s challenge will feature new prizes, competitions and ways to fund the future of vascular health.
Registration for the challenge opens Aug. 1. Learn more at vascular.org/Step2025
Landmark paper presented at VAM 2025
THE SVS HAS HIGHLIGHTED findings from a comprehensive 20year clinical study that demonstrate treatment of functional popliteal artery entrapment syndrome— particularly in combination with fasciotomy for exertional compartment syndrome—has shown highly effective outcomes, with 82% of patients returning to prior level of athletics.
As the largest reported cohort to date, this research summarizes two decades of experience in standardized radiographic evaluations and surgical decompressive treatments.
The paper was presented at VAM 2025 in New Orleans and simultaneously published in the Journal of Vascular Surgery (JVS).
The senior author of the study was Jason Lee, MD, chief of vascular surgery at Stanford Health Care in Palo Alto, California.
From left: Jason Lee, Dawn Coleman, Hassan Chanseddine and Matthew Eagleton
CLINICAL&DEVICENEWS
Compiled by Jocelyn Hudson, Bryan Kay and Jamie Bell
Gore announces MDR expanded indication for the Viabahn VBX balloon-expandable endoprosthesis as a bridging stent
W.L. GORE ANNOUNCED CE-MARK approval of an expanded indication for the Gore Viabahn VBX balloon-expandable endoprosthesis (VBX stent graft) when used as a bridging stent with branched and fenestrated aortic endografts in the treatment of aortic aneurysms involving the renal and mesenteric arteries.
“This is a landmark indication for a stent graft, equipping physicians with an on-label solution for more patients in complex pathologies,” said Luca Bertoglio, MD, from Spedali Civili Brescia in Brescia, Italy, co-ordinating investigator of the EMBRACE registry.
A total of 259 patients were enrolled in EMBRACE. Gore reports high rates of patency and freedom from endoleaks, target vessel instability and reinterventions were observed with the VBX stent graft in both branched and fenestrated endovascular aneurysm repair (BEVAR and FEVAR) cohorts at one year.
“We have studied performance in both
Cook Medical issues Class I recall for Beacon Tip angiographic catheters
COOK MEDICAL HAS initiated a Class I recall of its Beacon Tip 5F angiographic catheter. This follows reports of tip separation that could result in serious injury or death. The recall, identified as the most serious type by the Food and Drug Administration (FDA), involves the removal of affected devices from clinical and commercial use.
In its notification to customers, Cook advised immediate examination of inventory to identify and quarantine any unused affected devices. Distribution and use of the affected catheters must cease immediately. The manufacturer also stressed that the recall information should be communicated throughout relevant departments and to any third parties who may have received the devices.
Cook Medical initiated the recall after field complaints revealed that catheter tips were separating both before and during patient procedures. Tip separation poses significant clinical risks, including catheter fragmentation and embolization, which may lead to severe complications such as sepsis, vessel perforation, thrombosis, embolism, cardiac arrhythmia or death.
To date, three serious injuries linked to this issue have been reported, with no associated deaths. Healthcare providers and consumers in the U.S. are encouraged to report any adverse reactions to the FDA.
fenestrated and branched cohorts, and the results demonstrate that we can safely and effectively treat these patients with the VBX device,” Bertoglio added.
This multicenter, retrospective and prospective registry was conducted to evaluate the clinical performance and safety of the VBX stent graft as a bridging stent. A total of 14 centers in Europe enrolled 259 patients who have had treatment with the VBX stent graft. These patients will have prospective follow-up visits up to five years after the index procedure.
“Physicians have waited some time for an approved bridging stent indication for fenestrated and branched repair. Having a CE-marked indication is very important, as it is certainly of relevance to the endovascular community and the eligible patient population,” said Mauro Gargiulo, MD, from IRCCS S Orsola Hospital and University of Bologna in Bologna, Italy, principal investigator of the EXPAND registry. “I applaud Gore for recognizing the
Humacyte announces Symvess ECAT approval from US Defense Logistics Agency
HUMACYTE ANNOUNCED THAT Symvess has been awarded Electronic Catalog (ECAT) listing approval from the U.S. Defense Logistics Agency.
ECAT is an internet system that provides the Department of Defense (DOD) and other federal agencies with access to manufacturers’ and distributors’ products. The approval makes Symvess available to healthcare professionals treating military service members, veterans, and other patients receiving care at DOD and U.S. Department of Veterans Affairs facilities.
Symvess (acellular tissue engineered vessel-tyod) was approved in the extremity vascular trauma indication by the Food and Drug Administration (FDA) in December 2024.
Humacyte advises that, for uses other than the FDA approval in the extremity vascular trauma indication, the acellular tissue engineered vessel (ATEV) is an investigational product and has not been approved for use or sale by the FDA or any other regulatory agency.
need for a CE-mark indication and for being committed to conducting such thorough and expertly run clinical studies like EXPAND and EMBRACE.”
In the coming weeks, hospitals will start implanting the newly indicated VBX stent graft in BEVAR and FEVAR procedures. The official launch is planned after summer when many European and local congresses are taking place.
Gore shares that the VBX stent graft offers precise delivery and supports positive outcomes in a variety of complex applications. The device was developed utilizing the small diameter, expanded polytetrafluoroethylene (ePTFE) stent graft technology from the Viabahn endoprosthesis. The VBX stent graft is available in a range of diameters from 5 to 11mm and lengths of 15, 19, 29, 39, 59 and 79mm. It is currently the longest balloonexpandable stent graft available, according to Gore, covering a wide variety of treatment needs. The company adds that the VBX stent graft offers the largest range of diameter adjustability in a single device.
stent graft
GORE® VIABAHN® VBX
CGuard Prime carotid stent gains US and European approvals for stroke prevention
INSPIREMD HAS BEEN GRANTED premarket approval (PMA) from the Food and Drug Administration (FDA) for its CGuard Prime carotid stent system in the U.S.—news that follows the company’s recent announcement of CE-mark approval under the European Medical Device Regulation (MDR).
An InspireMD press release details that the FDA’s PMA is backed by “best-inclass evidence” from the C-GUARDIANS pivotal trial, first presented at the Leipzig Interventional Course (LINC) in May 2024. The study—which enrolled 316 patients across 24 sites in the U.S. and Europe— evaluated the safety and efficacy of CGuard Prime for treating carotid artery stenosis. CGuard Prime demonstrated the lowest 30-day (0.95%) and one-year (1.93%) primary endpoint major adverse event rates of any pivotal study of carotid intervention, the company claims.
In a separate press release announcing the CE-mark approval of CGuard Prime under the European MDR, InspireMD notes that development of the device incorporated extensive user feedback to optimize deliverability and deployment of the original CGuard stent.
Balloon Expandable Endoprosthesis
Consult Instructions for Use eifu.goremedical.com
INDICATIONS FOR USE IN THE U.S.: The GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis is indicated for the treatment of de novo or restenotic lesions found in iliac arteries with reference vessel diameters ranging from 5 mm–13 mm and lesion lengths up to 110 mm, including lesions at the aortic bifurcation. The GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis is also indicated for use with thoracoabdominal and pararenal branched devices indicated with the GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis as a branch component.* CONTRAINDICATIONS: Do not use the GORE® VIABAHN® VBX Balloon Expandable Endoprosthesis in patients with known hypersensitivity to heparin, including those patients who have had a previous incident of Heparin-Induced Thrombocytopenia (HIT) type II. Refer to Instructions for Use at eifu.goremedical.com for a complete description of all applicable indications, warnings, precautions and contraindications for the markets where this product is available.
With a 1 Fr profile reduction on most sizes, the VBX Stent Graft enables you to confidently address complex aortoiliac occlusive disease with greater versatility.
primary patency at 5 years per lesion1
89.5% of patients improved ≥ 1 Rutherford category from baseline at 5 years1 100%
freedom from target lesion revascularization (fTLR) at 5 years per subject1 89.1%
1. Holden A, Takele E, Hill A, et al. Long-term follow-up of subjects with iliac occlusive disease treated with the Viabahn VBX Balloon-Expandable Endoprosthesis. Journal of Endovascular Therapy. In press.
W. L. Gore & Associates, Inc. Flagstaff, Arizona 86004 goremedical.com
Please see accompanying prescribing information in this journal.
Products listed may not be available in all markets.
GORE, Together, improving life, VBX, VIABAHN and designs are trademarks of W. L. Gore & Associates.