Researchers continue to wrestle with TAVI-related stroke riddle
Continued from page 3
Cardiology (ACC) scientific sessions (29–31 March, Chicago, USA) have dashed hopes of a significant reduction in stroke rates associated with the technique. The trial’s results suggest that there is “no evidence to support a recommendation for the routine use of cerebral embolic protection in TAVI,” according to investigator Rajesh Kharbanda (John Radcliffe Hospital, Oxford, UK) .
BHF PROTECT-TAVI enrolled 7,635 patients undergoing TAVI for aortic stenosis at 33 centres in the UK from 2020–2024. Participants were randomised 1:1 to undergo TAVI with the Sentinel device or TAVI without cerebral embolic protection.
In a third planned interim analysis, the trial’s primary endpoint—the incidence of stroke at 72 hours post-TAVI or at the time of hospital discharge, if sooner—occurred in 2.1% of patients assigned to the Sentinel device and in 2.2% of patients assigned to the control group, showing no evidence of a difference between the two study arms. Results for secondary endpoints including all-cause mortality, stroke severity, disabling stroke and cognitive outcomes were also similar between groups. Recruitment for the trial was stopped after the interim analysis based on these findings. No differences in outcomes were seen in any subgroups that were analysed.
Although BHF PROTECT-TAVI showed current cerebral embolic protection devices do not improve outcomes, Kharbanda did not close the door on the technique entirely, stating that it is possible that nextgeneration devices could reduce stroke risk for certain groups, although further trials would be needed to demonstrate this. “We need to understand which patients are at higher risk of stroke during TAVI and whether a more stratified approach to delivering therapy to those people is beneficial,” he said.
Flushing TAVI valves and stent grafts for thoracic endovascular aortic repair (TEVAR) with CO2 prior to their implantation is another technique that has been touted as offering promise in stroke reduction, with findings from two studies investigating CO2 flushing in TEVAR and TAVI shared at the recent Charing Cross (CX) Symposium (23–25 April, London, UK).
“In recent years, many centres have started using carbon dioxide flushing as a more effective way to de-air the stent grafts in order to reduce cerebral air embolisation,” said Lydia Hanna (Royal Holloway University of London, London, UK), an investigator in the INTERCEPTevar and INTERCEPTavi trials, who presented insights from the trials at CX 2025.
The research was designed to test the hypothesis that
CO2 flushing of aortic valves could reduce cerebral air embolisation and cerebral infarcts in diffusion-weighted magnetic resonance imaging (DW-MRI), and whether this could potentially result in improved clinical outcomes when compared with standard saline flushing.
Hanna revealed that though the results of both trials showed a trend towards a reduction in neurological injury amongst the patients who received CO2 flushing, crucially there was no overall difference in rates of stroke.
“Because you don’t see a difference in clinical strokes here, and with the recent publication of the findings of the Sentinel device in TAVI—which showed no difference in clinical stroke—is this field still alive in the TAVI world?”
session moderator Nimesh Desai (Perelman School of Medicine at the University of Pennsylvania, Philadelphia, USA) asked Hanna in response to the findings.
Hanna responded that adequately identifying and defining stroke makes it difficult to study as a hard outcome in trials and that understanding the impact of cerebral injury in the long term will be important in
We need to understand which patients are at higher risk of stroke during TAVI.”
assessing the efficacy of this intervention in improving outcomes for patients.
“Most of these trials have not had a neurologist to examine the patients, and that is the problem with how we define stroke and how we look for it, or how hard we look for it. It is definitely still relevant,” she said. “I think stroke is obviously clinically important and we have much to learn about that, but in terms of the impact of the cerebral injury that is visible in MRI scans it is a concern that with all that happens to the brain, we don’t follow the patients for long enough to understand the impact of this for the long term.”
Further analysis is being done by the INTERCEPTevar and INTERCEPTavi team to assess quality of life data, six-month MRI findings, and to correlate the effect of brain injury with neurocognitive data, Hanna revealed.
Editor-in-chief: Simon Redwood | Publisher: Stephen Greenhalgh
Senior editor: Will Date will@bibamedical.com | Editorial contribution: Jamie Bell, Jocelyn Hudson
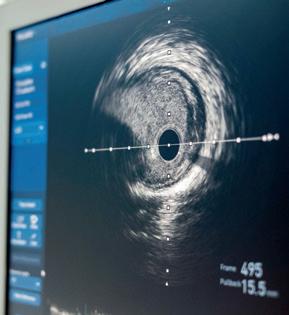
Findings of a new study support the routine use of intravascular imaging to guide percutaneous coronary intervention (PCI) for the treatment of calcified coronary artery lesions, researchers state, but in certain regions, uptake of the technology remains low. With recent guideline recommendations advocating its use, could intracoronary imaging become mainstream in the near future?
For more on this story go to page 8.
n TRILUMINATE TRIAL:
Two-year findings from the largest randomised trial to date to investigate the use of Abbott's Triclip system for the treatment of tricuspid regurgitation, the TRILUMINATE trial, have shown that patients treated with the device were less likely to be hospitalised for heart failure compared to those receiving medical therapy alone, in what has been described as a significant development for the transcatheter therapy.
For more on this story go to page 19.
n CARDIOVASCULAR AWARDS:
The second ever Global Cardiovascular Awards, hosted by Cardiovascular News brought together leading lights from the field of cardiovascular medicine to celebrate innovation and excellence. Winners were chosen in 13 categories recognising the contributions of academia, clinicians and industry to advancing the cause of cardiovascular healthcare worldwide.
For more on this story go to page 22.
Scan the QR code to subscribe
If you have comments on this issue or suggestions for upcoming editions write to will@bibamedical.com
Lydia Hanna at CX 2025
“Urgent
need” to move
away
from lead in mitigating cath lab radiation exposure
With an increasing focus on the harmful impact of radiation exposure, as well as the risk of orthopaedic injury related to prolonged usage of lead amongst cath lab staff, new study results have brought into focus the stark need for alternative protective technologies to shield cath lab teams, interventional cardiologists say.
Presented at the 2025 Society for Cardiovascular Angiography and Interventions (SCAI) annual meeting (1–3 May, Washington, DC, USA), results of the ERGO-CATH study—a single-centre analysis of ergonomic strain on interventional cardiology teams—have shown that the use of the traditional lead apron may cause as many as 43% of operatives to experience discomfort.
The ERGO-CATH study, conducted by researchers at Brigham and Women’s Hospital (Boston, USA), saw electromyography electrodes and inertial monitoring units (IMUs) placed on the cervical, thoracic, torso-pelvic, and lumbar regions of the spine on participating cath lab team members.
The primary endpoint was the percentage of time spent in high-risk positions (+/-20°) such as cervical axial rotation (moving the head and neck to the right or left), cervical flexion (the bending of the head towards the chest), and thoracic flexion (bending forward and rounding of the upper back).
Radiation was measured by using a real-time dose monitoring system and divided by the use of a leadless apron (Rampart device) versus a traditional lead apron approach.
There were 20 operators (38% female, mean age of 40.7 years) including attendings, fellows, and physician assistants/associates (PAs). The comprehensive cohort time spent in a high-risk position was: 35.8% (cervical axial rotation), 15.6% (cervical flexion), and 5.7% (thoracic flexion).
When comparing traditional lead and the lead-less approaches, researchers noted a similar percentage of time spent in high-risk positions: cervical axial rotation (lead: 35.9% versus lead-less 35.6%), and thoracic flexion (lead: 6.4% versus lead-less: 4.4%). Overall, 32% of study participants experienced discomfort (34% in the lead arm and 27% in the Rampart arm), while the average measured radiation for the traditional lead was 55.8 mrem versus 0.5 mrem for the lead-less approach.
“Working in the setting of high radiation exposure, interventional cardiologists and cath lab staff need radiation-related protection traditionally in part through the use of lead vests and skirts. These traditional lead vests/skirts provide reasonable protection from radiation but dramatically increase the axial load on these clinicians. ERGO-CATH shows several important insights (i) it quantifies that interventional cardiologists are in high-risk cervical position for one-third of total case duration and (ii) the reduction in radiation is dramatic with the Rampart device as compared with the traditional approach,” said Ajar Kochar (Brigham and Women’s Hospital, Boston, USA), lead author of the research.
An additional sub-analysis of the study sought to examine cath lab operator ergonomic strain by stratifying for sex-based differences and laboratory
roles, with the findings suggesting cath lab operators in fellow and PA positions are exposed to high-risk ergonomics more often and at longer durations than those in attending positions, leading to a strong likelihood of occupationally caused pain.
Female operators were more likely to be fellows or PAs (47%). When separated by sex, average times in high-risk positions were determined as cervical flexion: 17.6% (female) versus 14.1% (male), cervical axial rotation: 33.4% (female) versus 37.6% (male), and thoracic flexion: 6.5% (female) versus 5.1% (male). When graded by operator role, mean times in high-risk positions were cervical flexion: attending (11.9%) versus non-attending (16.6%), cervical axial rotation: attending (32.2%) versus non-attending (36.7%), and thoracic flexion: attending 4.4% versus non-attending 6.1%.
Our study underscores the urgent need to adopt novel solutions to radiation protection.”
“Our study underscores the urgent need to adopt novel solutions to radiation protection; many of these novel innovations allow cath lab operators to work without any lead or with ultra-light lead which will help reduce the axial load and presumptively decrease musculoskeletal discomfort,” said Greta Campbell, a clinical research coordinator at Brigham and Women’s Hospital. Future clinical studies will be necessary to determine if differences exist between the ergonomic injuries of male and female operators.
As a society, SCAI has been working to raise awareness of the dangers associated with radiation exposure and prolonged lead use through recent activities. Survey results published recently by the organisation suggest that as many as 60% of respondents had reported facing orthopaedic injuries, with 6% having reported a cancer diagnosis. Other types of radiation injury, such as cataracts, were shown to be threefold higher than what is observed in the general population, highlighting the stark need for technologies to protect cath lab teams, the organisation has said.
Technological developments are seeking to meet the needs of cath lab teams to reduce their radiation exposure, but as one operator and researcher told Cardiovascular News, even simple solutions can be difficult to gain traction.
A think tank session addressing radiation at
Washington, DC, USA), Giorgio Medranda (NYU Langone Health, New York, USA) presented results of the ATTENUATE trial, a large single-centre randomised trial of a protective scatter radiation absorbing shield—Radpad Orange (Worldwide Innovations & Technologies).
The trial demonstrated that the use of the antimony and bismuth drape peripheral shield significantly reduced proximal operator radiation exposure by 50.7% when compared to procedures that did not use the shield system.
Looking at 500 procedures in each arm, including a mixture of structural, coronary and diagnostic procedures, investigators assessed dose-area product (DAP)-normalised operator dose as the trial’s primary endpoint, as well as looking at operate dose, fluoroscopy time and DAP as secondary endpoints.
The study showed that the primary endpoint, DAPnormalised operator dose stood at 3.1uSv/mGycm for procedures that used Radpad, compared to 6.3uSv/ mGycm2 among procedures that did not use Radpad. Operator exposure stood at 9uSv for procedures using Radpad, and 14uSV without.
Speaking to Cardiovascular News, Medranda said that the study’s results highlight that relatively simple and inexpensive solutions can make a difference to radiation exposure amongst cath lab operators.
“It is strange, and I can’t put myself in everyone’s perspective—but it seems like a no-brainer,” he responded, when asked why he felt there was not a greater uptake of technological solutions like Radpad to address harmful radiation in the cath lab.
“People have done things the way they have done things for 30 years and it is hard to argue with success. Radiation is tricky for some people because you don’t see it or feel it up front. It is like high blood pressure or diabetes. For many years you may be doing tonnes of damage and feel fine, so why are you going to take an antihypertensive or insulin? It is not until the back end of the whole thing that you realise that maybe there is room for improvement.”
Additional research presented at the CRT meeting compared the EggNest (Egg Medical) and Rampart Defender scatter radiation protection systems in reducing radiation exposure around the X-ray table. Both systems are designed to eliminate the need for teams to wear lead.
At the recent Cardiovascular Research Technologies (CRT) meeting (8–11 March,
The study, presented by Thom Dahle (CentraCare Heart & Vascular Center, St Cloud, USA) looked at radiation exposure at five positions around the X-ray table, including the primary operator, assistant, nurse, anaesthesiologist and electrophysiologist or echocardiographer positions. The study showed that scatter radiation was not evenly distributed around the X-ray table, with dose rates at the head of the table greater than at other positions.
SCAI 2025
TUESDAY
11–12 NOVEMBER
IN PERSON
COURSE DIRECTORS
ECLIPSE study results support routine use of intravascular imaging during PCI of calcified lesions, investigators say
Using intravascular imaging (IVI) to guide drug-eluting stent implantation during complex percutaneous coronary intervention (PCI) is safer and more effective for patients with severely calcified coronary artery disease than conventional angiography, results of the ECLIPSE trial have shown.
PRESENTED DURING A
featured clinical research session at the 2025 American College of Cardiology (ACC) scientific sessions (29–31 March, Chicago, USA) by Gregg W Stone (Icahn School of Medicine at Mount Sinai, New York, USA), results of the study “could shift treatment options for high-risk patients”, according to investigators.
“The ECLIPSE trial shows that use of IVI to guide coronary stenting in severely calcified lesions prevents death, stent thrombosis, and unplanned repeat procedures in this high-risk patient population,” said Stone, the first author of the study. “These results extend the strong recommendations from recent US and European societal guidelines that intravascular imaging with either optical coherence tomography (OCT) or intravascular ultrasound (IVUS) should be routinely used during complex
coronary stent procedures.
“Currently, IVI is performed in only 20 to 25% of these cases in the USA. I suspect its use will rapidly accelerate given study after study now showing reductions in death, stent thrombosis, and nearly every other adverse outcome after PCI when intravascular imaging is used.”
of these cases in the USA—hundreds of thousands a year—have moderate or severely calcified lesions, where calcium builds up in the arteries. Ten percent of those cases are severe, meaning the blood vessels in the arteries essentially turn to bone, making the stenting procedure more challenging and higher-risk. Interventional cardiologists most commonly guide the PCI catheter by using angiography, which involves a special dye (contrast material) and X-rays to see how blood flows through the heart arteries to highlight any blockages.
In the ECLIPSE study, researchers analysed the outcomes of PCI in severely calcified lesions of 2,005 patients to see if IVI guidance improves survival without adverse cardiac events compared with angiography guidance.
Patients with coronary artery disease—plaque buildup inside the arteries that leads to chest pain, shortness of breath, and heart attack— often undergo PCI, a non-surgical procedure in which interventional cardiologists use a catheter to place stents in the blocked coronary arteries to restore blood flow. About one-third
AGENT IDE trial results “consistent” out to two years using DCB
in ISR
Consistent results have been seen out to two years in the AGENT investigational device exemption (IDE) trial, the first US randomised trial investigating the safety and efficacy of the use of a drug-coated balloon (DCB) for the treatment of coronary in-stent restenosis (ISR).
JEFFREY MOSES (COLUMBIA UNIVERSITY Medical Center, New York and St Francis Heart Center, Roslyn, USA) presented the trial’s two-year findings at the 2025 Cardiovascular Research Technologies (CRT) meeting (8–11 March, Washington DC, USA), where he commented that the data support the use of the Agent DCB (Boston Scientific) for the treatment of coronary ISR.
Agent, a paclitaxel-coated balloon, is the first DCB to gain approval from the US Food and Drug Administration (FDA) for the treatment of coronary ISR, which is estimated to make up around 10% of percutaneous coronary intervention (PCI) procedures.
The AGENT IDE trial, a prospective, randomised, multicentre, superiority trial enrolled a total of 600 patients across 40 US sites, who were randomised 2:1 to undergo either DCB-PCI with the Agent device or plain balloon angioplasty. Moses described the trial population as being a “varied group”, with an average age of 68 years, 26% women and 25% non-white.
Patients with severely calcified coronary lesions were randomised at 104 sites across the USA. One group, 1,246 patients or 62%, had PCI with either OCT or IVUS guidance, and the other 759 patients, or 38%, had PCI with angiography guidance. The primary endpoint was the one-year rate of target vessel failure, the composite occurrence of either cardiac death, target-vessel myocardial infarction, or ischaemia-driven target-vessel
Importantly, he said, over 40% of patients had multi-layer stents.
At one year, the trial demonstrated that Agent outperformed conventional balloon angioplasty against a primary endpoint of target lesion failure (TLF)—defined as a composite of target lesion revascularisation, target vessel myocardial infarction (MI) or cardiac death—at 12 months, with the investigatory device demonstrating statistical superiority to uncoated balloon angioplasty (17.9% vs. 28.7%).
Detailing the two-year results at CRT 2025, Moses reported that TLF stood at 27% for the Agent DCB compared to 34% for balloon angioplasty, with a hazard ratio (HR) of 0.73. Analysis of recurrent events showed that patients had nearly twice as high a likelihood of a subsequent target lesion revascularisation (TLR) event in the plain balloon angioplasty group compared to DCB.
“To look at it another way, if you look at the first event, it is 28% vs. 19%, but there is also a two-thirds reduction in subsequent events in patients with multiple TLRs,” said Moses.
In terms of other endpoints, mortality was similar, myocardial infarction (MI) trended lower, and target vessel revascularisation (TVR) was 22% for the Agent DCB vs. 31.4% for the plain balloon group, whilst target vessel failure (TVF) was 28% for Agent, compared to 36% in the comparator group.
revascularisation.
Overall rates of target vessel failure were 26% lower among patients who had IVI guidance than among those with angiography guidance. Researchers also observed a significant reduction in all-cause death, stent thrombosis, and target lesion and vessel revascularisation among patients in whom intravascular imaging was used compared with angiography.
Researchers further analysed the two imaging modalities—IVUS and OCT—to determine whether one was more effective. In the unadjusted analysis, patients had better outcomes with OCT compared to IVUS; however,
Currently, IVI is performed in only 20 to 25% of these cases in the USA.”
the differences between the two were no longer significant when adjusting for factors including age, diabetes, and the number and severity of lesions.
“Overall, both OCT and IVUS were effective; additional studies are required to determine whether OCT is more beneficial in severely calcified lesions,” Stone adds. “Regardless, IVI with either OCT or IVUS should be used rather than angiography guidance to guide PCI in patients with severely calcified lesions.”
angioplasty).
“AGENT IDE is the first randomised trial conducted in the USA examining the efficacy and safety of DCBs, it was superior to conventional balloon angioplasty for the target lesion endpoint at one year, and consistent results were observed on the two-year follow-up with a significantly reduced instance of target lesion failure, with 37% reduction,” said Moses in his concluding remarks.
“The recurrent TLR analysis shows significantly more repeat events with placebo balloon angioplasty. There were no definite or probable thromboses that occurred with the Agent balloon, so these data support the use of the Agent DCB for treatment of coronary ISR.”
27%
Agent DCB 24%
Moses was asked by session moderator Gregg W Stone (Icahn School of Medicine at Mount Sinai, New York, USA) how to view these data when deciding whether to use a DCB or a drug-eluting stent (DES), the current standard of care, and whether there are certain scenarios that may favour the DCB.
“The easy one is multi-layer stenting. Most of us are quite hesitant to add a third layer. Smaller vessels also, [it is] a matter of real estate, and I also see complex bifurcation restenoses which are pretty common. Those are the sweet spots,” commented Moses.
Subgroup analysis showed that TLF occurred more often in patients with multiple layers of existing stents (35.4% in the Agent arm and 44% in the balloon angioplasty arm) compared to those with a single layer of stent (20.7% for Agent and 26.6% for balloon
“As far as the first restenosis in a large vessel, we will have randomised data to help guide us in the future. It is a fielder’s choice at this point and you can make arguments on both sides, recent meta-analyses are literally all over the map so I can’t give you guidance on that, we will wait for the real randomised data.”
DCB
Target lesion failure at two years
Balloon angioplasty
New TAV-in-SAV data underline importance of aortic valve sizing at index procedure
New data on the outcomes of transcatheter aortic valve-in-surgical aortic valve (TAV-in-SAV) following bioprosthetic surgical valve failure have demonstrated low rates of mortality and stroke at up to five years among low and intermediate surgical risk patients undergoing the procedure.
THIS IS ACCORDING TO FINDINGS FROM THE PARTNER 3 aortic-valve-in-valve study, presented at the 2025 Cardiovascular Research Technologies (CRT) meeting (8–11 March, Washington DC, USA) by S Christopher Malaisrie (Northwestern Medicine Bluhm Cardiovascular Institute, Chicago, USA). Malaisrie, a cardiothoracic surgeon, tells Cardiovascular News that the data provide an important contribution to decision-making when plotting lifetime management strategies for patients with aortic stenosis— particularly as increasing numbers of patients receive bioprosthetic surgical valves in the first instance.
“The trend now, certainly in the USA, is increased usage of bioprosthetic valves, especially in younger patients. Guidelines in Europe go down to 60 years, guidelines in the USA go down to 50 years old, so as more younger patients get aortic valve replacement with bioprosthetic valves, that means they are going to be at risk for structural valve deterioration later and will need a procedure later in life,” comments Malaisrie.
rate of 3.2% for disabling stroke. A fifth of patients (21%) faced rehospitalisation, with aortic valve reintervention required in 14% of patients. Investigators were keen to understand risk factors for aortic valve reintervention, examining reintervention rates by valve size. What they noted was that valve reinterventions were more common in patients with valves sized between 17–21mm, occurring in seven out of the 40 patients with these valves, whilst four of the 27 patients with valves between 22–23mm required reintervention, compared to none of the 23 patients with valves between 24–27mm.
“The published data already well establish that we should avoid 19–21mm valves because they are most at risk for gradients after valve in valve,” reported Malaisrie. “I think what this study sheds some light on is that medium-sized valves also are at risk of reintervention after valve-in-valve. You are really not free and clear unless at the index aortic valve replacement the patient had a large sized valve. In our cohort, none of those patients had an aortic valve intervention and that translated nicely to stratification in mortality from low, medium to big sized valves.”
Mean gradients remained stable at five years, with a mean of 19.6mmHg at one year, which stood at 17.6mmHg after five years. Ninety per cent of patients were free from any aortic regurgitation, with the figure standing at 94.2% after five years. Malaisrie also reported that quality of life measures appeared favourable after five years, with 70% of patients remaining in NYHA class I, and KKCQ scores stable out to five years, having improved by an average of over 20 points following the index procedure. He noted some limitations of the study, including the lack of a comparator group, that most patients were male, and a lack of consistency in the availability of post-surgical mean gradients.
Malaisrie and colleagues previously published oneyear data from the PARTNER 3 registry, showing that aortic valve-in-valve procedures using the Sapien 3 (Edwards Lifesciences) transcatheter aortic valve implantation (TAVI) valve improved haemodynamic and functional status at one year, with 0% mortality. The five-year follow-up, reported at CRT 2025, also includes data on rates of rehospitalisation, aortic valve reintervention, echo parameters, valve durability, New York Heart Association (NYHA) class and Kansas City Cardiomyopathy Questionnaire (KCCQ) scores.
The study included 100 low or intermediate surgical risk patients—defined as having a Society of Thoracic Surgeons (STS) score >8—treated at 29 US sites between 2016–2019 for a failed bioprosthetic aortic valve due to either aortic stenosis or regurgitation with surgical valves sized from 18.5mm out to 28.5mm. Patients had to have suitable anatomy to accommodate transfemoral access, and those with patient prosthesis mismatch (PPM) after the index procedure were excluded, as well as those with a mean gradient >20mmHg. Patients had an average age of 67 years, and most were male, with an average STS score of 2.9 and mean gradients of 39mmHg at baseline.
Malaisrie revealed that the event rate for death and stroke at five years stood at 14.7%, describing this as a “good outcome” and “remarkably low, considering these patients would otherwise have gotten a reoperative aortic valve replacement”. Breaking down the composite outcome, Malaisrie noted that following no deaths at one year, the five-year mortality rate stood at 11.5%.
“If you remember the low-risk trials—both with Edwards and Medtronic valves—with the Edwards valve at five years, the main group for native aortic stenosis was roughly 10% mortality, and the mortality for the Medtronic trial which was reported at four years was roughly 11%. So, this is good, it is comparable to TAVI for patients who have native aortic stenosis,” he said. The rate of stroke was also low, 5.4% at five years, with a
“In low and intermediate risk patients with a failing surgical bioprosthetic valve, aortic valve-in-valve with Sapien 3 demonstrated low mortality and stroke rates at five years,
Surgeons are doing more aortic root enlargements— a procedure that is designed to increase the size of the aortic annulus.”
sustained haemodynamic improvement, and this is despite aortic valve reintervention rates that are higher than in native valves,” Malaisrie said in his concluding remarks. “We think that aortic valve reintervention is associated with the index valve replacement in accordance to the size of the initial valve prosthesis the surgeon puts in, but despite that aortic valve reintervention mortality, and stroke, are comparable with the low-risk trials with native aortic stenosis. So, reinterventions did not affect mortality and stroke in this study.”
Speaking to Cardiovascular News, Malaisrie stressed that the sizing of the initial surgical valve plays an important role in the outcome of any subsequent valve-in-valve procedure, and urged heart teams to consider root enlargement in cases where patients, who may require a later procedure, have small aortic annuli.
“As this strategy of aortic valve-in-valve has been proven, it has gotten surgeons to think about how to optimise the first aortic valve replacement. One way we can do that is to put in as large a valve as possible. That means that surgeons are doing more aortic root enlargements, a procedure that is designed to increase the size of the aortic annulus, in order to place a larger aortic valve, and this will make the second procedure—a valvein-valve—more successful.”
First EACTS innovation grants announced at summit
INNOVATIONS IN ROBOTIC surgery, novel valve technologies and the advent of artificial intelligence (AI) for the cardiothoracic surgery community were in focus for the third European Association for CardioThoracic Surgery (EACTS) Innovation Summit (11–12 April, Paris, France).
The-event saw surgeons, cardiologists, health professionals, engineers, industry, biochemists, scientists, health economists and academics convene to explore the future of cardiothoracic surgery.
Speaking at the Innovation Summit, past EACTS president Friedhelm Beyersdorf (Heart Center Freiburg University, Freiburg, Germany), said: “We are here to change the world. Innovation is important for the EACTS community because we are always looking to collaborate and find better ways to treat our patients. I look forward to learning new approaches to medicine and taking practical next steps.”
At this year’s event, EACTS announced the first recipients of its Innovation Grants scheme, intended to support earlystage, exploratory research and innovation initiatives. Recipients include projects involving AIenhanced virtual reality training for extracorporeal membrane oxygenation (ECMO) in cardiothoracic surgery and a novel total artificial heart.
“It’s a huge honour for the team and it honours the dedication that the team put into the development of this device over the last four years,” said Daniel Zimpfer (University of Vienna, Vienna, Austria), of the receipt of grant funding for the ShuttlePump valveless pulsatile total artificial heart. “The funding will create a lot of momentum and we will be able to validate everything we simulated. It’s a huge catalyst for the entire project.”
Elsewhere the event saw clinically relevant examples presented and discussed, such as robotic-assisted aortic valve replacement and heart transplantation.
S Christopher Malaisrie
Bioresorbable scaffold technology has “potential to be a new paradigm for femoropopliteal endovascular intervention”
In the 2025 Charing Cross (CX) Symposium (23–25 April, London, UK) peripheral arterial programme, which hosted several podium-first presentations, lower limb drug-eluting technologies took centre stage—signalling a potential shift in the treatment paradigm for chronic limb-threatening ischaemia (CLTI). Investigators shared compelling new data from studies ranging from first-in-human trials to large-scale registries, which vie to redefine durability and safety, as well as cost-effectiveness, in the peripheral arterial treatment landscape.
Opening the session, Sahil Parikh (Columbia University Medical Center, New York, USA) delivered an economic analysis of the Espirit below-the-knee (BTK) drug-eluting resorbable scaffold (Abbott) in the treatment of patients with CLTI. The two-year results demonstrated superior long-term outcomes for Esprit BTK compared to percutaneous transluminal angioplasty (PTA), particularly in terms of vessel patency and limb salvage.
Parikh stated that the incremental cost-effectiveness ratio at two years was determined by the difference in total cost divided by the difference in clinically driven target lesion revascularisation (CD-TLR) endpoint failure.
“Esprit BTK showed a lower adjusted event rate compared to PTA [27.5% vs. 49.4% for primary efficacy endpoint; 10.5% vs. 21.6% for CD-TLR] showing a sustained benefit,” Parikh stated. He concluded that use of the Esprit BTK device resulted in US$3,206 per primary efficacy endpoint avoided, and US$6,068 per CD-TLR avoided.
Michel Bosiers (University Hospital Bern, Bern, Switzerland) shared an update on the three-year results of the MOTIV-BTK trial. The trial sought to evaluate the Motiv (Reva Medical) bioresorbable scaffold in 58 patients, the majority with Rutherford 4 or 5 lesions, Bosiers added.
At three years, the speaker reported 99% technical success and 80% primary patency for the Motiv device, with 93% freedom from CD-TLR at three years. Limb salvage at follow-up was 95%, with a recorded 16 deaths, although Bosiers notes that these were not device- or procedure-related.
Presenting one-year EFEMORAL I data, Andrew Holden (Auckland City Hospital, Auckland, New Zealand) shared that the trial has the “lowest [percentage of] residual stenosis in any reported study of femoropopliteal intervention”.
EFEMORAL I is a first-in-human trial evaluating the Efemoral scaffold (Efemoral Medical) for the treatment of symptomatic peripheral arterial occlusive disease from atherosclerosis of the femoropopliteal artery across four sites in Australia and New Zealand. Concerning maintenance of arterial patency, even after scaffold dissolution, Holden reported 100%
This, the largest study of sirolimus drug-eluting balloons in complex peripheral arterial disease patients, is proof that this technology works.”
primary patency and freedom from TLR at three years. He also highlighted sustained improvement in clinical outcome and walking tolerance at follow-up. Among other outcomes, the speaker shared a 0–15% post-procedure residual stenosis and no acute or subacute thrombosis—the lowest ever reported for a femoropopliteal trial. Meanwhile, Holden reported that the mean minimal lumen diameter of 4.74mm recorded at six months was the “highest ever reported”.
“This has potential to be a new paradigm for femoropopliteal endovascular intervention,” he added.
The peripheral arterial programme also featured a series of podium-first presentations that sought to demonstrate the graduation of devices past ‘proof of patency’, to evidence of their “major clinical benefit” in lower limb arterial intervention for CLTI.
Michael Lichtenberg (Arnsberg Clinic, Arnsberg, Germany) began with the first report of the 12-month SUCCESS-PTA trial data, which evaluated the Selution SLR (Cordis) drug-eluting balloon in patients with CLTI. The trial investigators enrolled 723 patients from 27 sites across Europe, Asia, and South America
Lichtenberg reported positive 12-month outcomes, including consistent haemodynamic, functional and clinical improvements, with 91.1% freedom from CD-TLR overall, and 90.3% for the CLTI subgroup. Among other outcomes, the speaker reported sustained improvements in ankle-brachial index (ABI), Rutherford classification, and EQ-5D from six- to 12-month follow-up.
“These data continue to demonstrate the consistency of positive results across this new technology, even
for patients with severe CLTI,” said Lichtenberg, addressing CX delegates. “This, the largest study of sirolimus drug-eluting balloons in complex peripheral arterial disease patients, is proof that this technology works,” he stated.
Elsewhere in the session, Edward Choke (Northern Heart Hospital Penang, Georgetown, Malaysia) delivered three-year real-world outcomes from the HOPE registry, evaluating MagicTouch (Concept Medical) sirolimus-coated balloon versus plain balloon angioplasty in the below-the- knee (BTK) subgroup.
“At three years, sirolimus-coated balloons were associated with lower BTK interventions,” Choke reported, showing a 76.5% versus 64.9% freedom from TLR for MagicTouch and plain balloon angioplasty, respectively. He added that sirolimus was superior to plain balloon angioplasty regarding amputation-free survival (AFS), showing 60.9% and 47.4% rates, respectively, in the two groups.
“Survival was somewhat surprising,” said Choke, who detailed that, at three years, sirolimus was associated with better survival, hypothesising that this was due to higher rates of reintervention in the plain balloon angioplasty group, and therefore, “in this high-risk and highly frail group of CLTI patients, any procedures done will confer a risk to life”.
Choke ended pragmatically: “This is real-world data, and there are confounders both known and unknown,” he said. “Although sirolimus was associated with better outcomes, we should wait for the final data to emerge in the next one to two years before making definitive conclusions.”
Next, Brian DeRubertis (New York Presbyterian–Weill Cornell Medical Center, New York, USA) shared 12-month amputation and readmission rates between the Eluvia (Boston Scientific) drug-eluting stent versus bare device therapies in a large contemporary realworld peripheral arterial disease (PAD) cohort.
He outlined that their evaluation was based on de-identified electronic health records (EHR) which granted his team access to data for approximately 10,000 patients. Of these, the investigators identified 881 patients treated with the Eluvia device and 5,156 treated with the non-drug-eluting device. They found that race and ethnicity distributions differed between groups, with Eluvia being more frequently used in Black and Hispanic patients.
“This is important because these two groups of patients are known to have worse outcomes in the United States in terms of amputation rates,” DeRubertis told the CX audience. Following propensity score matching to “reduce bias associated [with] device selection”, DeRubertis outlined that above-ankle amputation and any readmission within 12 months occurred “significantly more frequently” with non-drug-eluting therapy versus the Eluvia drugeluting stent.
Considering these results, DeRubertis restated the significance of reducing amputations to “not only save cost to the patient, but to the healthcare system”. Showing a decline in amputation and readmission rates, the speaker confirmed the dual benefit of the drug-eluting stent in saving limbs and reducing the economic burden that major amputation places on global healthcare.
Subsequent audience questions and panel discussion focused on differentiating characteristics of these technologies, including lesion coverage protocols and drug aggressiveness. However, when asked how interventionists decide on what device to use during daily practice, presenter Thomas Zeller (University Heart Centre Freiburg–Bad Krozingen, Bad Krozingen, Germany) brought the discussion back to “reality”, stating that what drives device selection in daily practice comes down to cost. “You have to take what’s on your shelf and use it,” he said. “With free choice, you can tailor these technologies to lesion characteristics.”
FAVOR III identifies major risk factors of cardiovascular events after PCI
New findings from the FAVOR III China trial demonstrate that kidney function, followed by body mass index (BMI), is the strongest predictor of serious cardiovascular events two years after quantitative flow ratio-guided (QFR) percutaneous coronary intervention (PCI) treatment.
RESEARCHERS ALSO FOUND
that QFR can reduce the risk of major cardiovascular events by nearly 15% compared to angiography-guided procedures. The data were presented as late-breaking science at the Society for Cardiovascular Angiography & Interventions (SCAI) 2025 scientific sessions (1–3 May, Washington, DC, USA).
The FAVOR III China trial, a multicentre, randomised, shamcontrolled trial conducted at Fuwai Hospital in Beijing, China, explores the long-term outcomes of PCI procedures guided by QFR. Two post-hoc analyses focused on identifying the likelihood of major adverse cardiovascular events (MACE) two years after treatment and highlighting the potential benefits of using physiological assessments to guide PCI treatment decisions.
In the first subset of the FAVOR III trial, researchers explored the impact of using physiological assessments, such as QFR, to guide treatment decisions aimed at restoring blood flow. Before treatment, physicians identified which blood vessels would receive PCI as part
of a pre-randomisation treatment plan.
Patients were randomly assigned to either the QFR-guided or angiographyguided procedure group. Following treatment, researchers retrospectively evaluated both the original plans and final procedures using QFR to determine whether they aligned with physiological measurements.
compared to 17% in the angiographyguided group. Furthermore, across all patients, those whose final treatment strategies matched physiological assessments had a lower two-year MACE rate than those whose treatments did not (8.8% vs. 17.2%).
In another subset of the FAVOR III trial, researchers developed a machine learning prognostic model for identifying the clinical, angiographic, and procedural features of patients likely to have two-year MACE despite online QFRguided PCI.
Hao-Yu Wang
Results showed that patients whose treatment strategies were aligned with physiology, particularly those guided by QFR, experienced fewer MACE. Specifically, the QFR-guided group with physiology-concordant plans had a primary MACE rate of 8.9%, compared to 10.4% in the angiographyguided group with physiologyconcordant plans.
Among patients whose original treatment plans were not physiologically concordant, only 7.6% in the QFRguided group experienced MACE,
Low-dose colchicine seen to reduce coronary plaque progression in EKSTROM trial
Low-dose colchicine (0.5mg per day) significantly reduced the total plaque volume progression by 1.1% among patients with stable coronary artery disease compared to placebo, but failed to significantly reduce low attenuation plaque.
THESE ARE FINDINGS OF THE EKSTROM trial, presented during a late-breaking trial session at the 2025 American College of Cardiology (ACC) scientific sessions (29–31 March, Chicago, USA).
The randomised, double-blind, placebo-controlled trial evaluated the effects of low-dose colchicine (Lodoco, Agepha Pharma) on atherosclerotic plaque. A total of 84 participants were enrolled, of which 72 completed the trial, with participants randomised to receive either colchicine 0.5mg/day or placebo (n=36 per treatment group) as add-on to their standard of care.
All participants underwent coronary computed tomography angiography (CCTA) to assess coronary
Using data from 1,913 patients, researchers tested eight different machine learning algorithms, each trained on 47 clinical features, to predict the likelihood of two-year MACE. Key variables included estimated glomerular filtration rate (eGFR, a measure of kidney function), BMI, LVEF (or how much blood the left ventricle pumps out with each heartbeat), stent length, age, lesion location, anatomic SYNTAX score (a tool used to assess the complexity of coronary artery disease), and history of PCI.
Findings revealed that 161 patients (8.4%) experienced MACE within two years of QFR-guided PCI. Among all variables examined, eGFR emerged as the strongest predictor, followed by BMI. Notably, in a subset of 375 patients whose planned PCI was
artery anatomy and stenosis, at baseline and at 12 months. The primary endpoint was change in lowattenuation plaque volume, a quantification of noncalcified, lipid-rich plaque, compared to placebo as measured by CCTA.
Secondary endpoints included change in total plaque volume, and change in total non-calcified plaque, fibro-fatty, fibrous and dense calcified plaques.
The results demonstrate that low-dose colchicine significantly reduced the total plaque volume compared to placebo at 12 months (change in percent atheroma volume [PAV] was 1.1% between treatment groups; p=0.015), though the trial did not meet its primary endpoint, as low-attenuation plaque volume was not significantly reduced with low-dose colchicine treatment (p=0.344).
Low-dose colchicine treatment significantly
Together with statins, antihypertensives, and other standard of care treatments, this antiinflammatory therapy may become a vital pillar in cardiovascular disease management.”
deferred, researchers identified the lesion location involving the left circumflex artery (LCX), or the location of the coronary blockage, as the most significant risk factor for future events.
“The FAVOR III trial continues to provide valuable information that encourages prioritisation of personalised treatments for patients and the use of artificial intelligence,” said Hao-Yu Wang (Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China), lead author of the study. “By identifying key risk factors like kidney function, BMI, LVEF, and lesion location involving LCX, we’re moving towards better predicting and preventing heart complications after PCI.”
By identifying key risk factors like kidney function, BMI, LVEF, and lesion location involving LCX, we’re moving towards better predicting and preventing heart complications after PCI.”
reduced dense calcified plaque volume (-0.9% PAV between treatment groups; p=0.009). Similarly, lowdose colchicine treatment demonstrated trends toward regression of non-calcified plaque, fibrous and fibrofatty plaque.
Future analyses are needed in a larger population of patients to confirm these findings.
“The results from the EKSTROM trial offer powerful evidence that low-dose colchicine has potential to directly reduce inflammation, which plays a substantial role in the formation and progression of atherosclerotic plaque leading to heart disease,” said Matthew J Budoff (David Geffen School of Medicine at the University of California Los Angeles, Los Angeles, USA). “Together with statins, antihypertensives, and other standard of care treatments, this anti-inflammatory therapy may become a vital pillar in cardiovascular disease management, and could help reduce hospitalisations and cut long-term healthcare costs.”
In his presentation at the ACC meeting, Budoff pointed out a number of limitations of the study, including that due to its funding, investigators were limited in enrolment to only 84 patients. Additionally, the stable coronary artery disease population enrolled in the trial had lower levels of both low attenuation plaque and C-reactive protein (CRP) than prior acute coronary syndrome imaging trials using this therapy.
“The EKSTROM trial findings demonstrate that anti-inflammatory treatment with low-dose colchicine, 0.5mg improved several measures of plaque volume changes over a period of 12 months in patients with stable coronary artery disease,” Budoff adds.
How important is it for aspiring interventional cardiologists to see people in senior positions who reflect their background?
When I was training, I was trying to become something that perhaps did not exist. There was no such thing as a female, Mexican interventional cardiologist working in the USA at that time that I know of. I think it is very important that we have role models.
Many things have changed in the 20 years since I started, and I am happy to be able to look back and see all the things that we have been able to achieve. The progress in technology has been great, but the progress in the representation of women at many levels—whether it is as physicians in the field of interventional cardiology, in academic positions, or in leadership positions—has been very slow. This has an impact in patient care and the inclusion of women in clinical trials. Most trials only recruit around 20–30% women, and that is a big disparity that has not changed at the pace we would want.
We have to participate at all levels. Societies need to provide support and funding, agencies need to put up guard rails and ensure that trials meet requirements to include women. A 20% enrolment rate is not good enough, and that goes into the design of the trial.
We also need to ensure that there is diversity in the leadership of trials too. When teams are diverse everybody wins, and diversity in leadership positions is essential to improve enrolment of women and minorities in trials. Unfortunately, this is all going to take time. We are making progress, and we need to keep trying harder and not give up.
For those who were able to achieve what they wanted it is also our responsibility to help the next generation. It wasn’t until I got to Mayo Clinic that I started to analyse the 20 years of my career, and I couldn't believe how far I had made it. That is when I realised how difficult it was, and it helped me understand that it should not be that way.
We need to make it easier for the next generation. At the same time, I have a
“There should not be borders in science.”
profound feeling of gratitude that I was given this without looking for it. That is what makes me want to give back.
What does your life outside of medicine look like?
I love riding my bike, especially around the Lake Shore Drive in Chicago. Now that I am based in Rochester, I cycle the trails in nature. But, I also spend time in Chicago, almost every weekend that I am not on call or traveling for meetings. I love seeing sun rises and particularly running whilst the sun comes up. Wherever I go I wake up early, go for a run, and watch the sun rise at least once during that trip. I have so many pictures of sun rises. Spending time with family and friends is the most important thing to me. As physicians, we spend a lot of time at the hospital. When you work hard at the hospital, taking care of really sick people, it helps you to appreciate a regular day with your family and friends on a deeper level and to be grateful for all the blessings you have.
Structural Heart Interventions
Acurate neo2 shows “reassuring” performance in observational study after stuttering IDE trial
Observational data from Sweden’s national SWEDEHEART registry have shown no difference in rates of mortality, heart failure hospitalisation and stroke among patients receiving the Acurate neo2 (Boston Scientific) when compared to Sapien 3 (Edwards Lifesciences) and Evolut (Medtronic) transcatheter aortic valve implantation (TAVI) systems.
The results of the analysis, presented during a late-breaking trial session at the 2025 Cardiovascular Research Technologies (CRT) meeting (8–11 March, Washington, DC, USA), offer some reassurance over the performance of the Acurate neo2 platform, after the device failed to meet non-inferiority for the same endpoints in the ACURATE IDE trial, a randomised study, intended to support US regulatory approval for the Acurate platform in the USA, which is already widely used outside of the country.
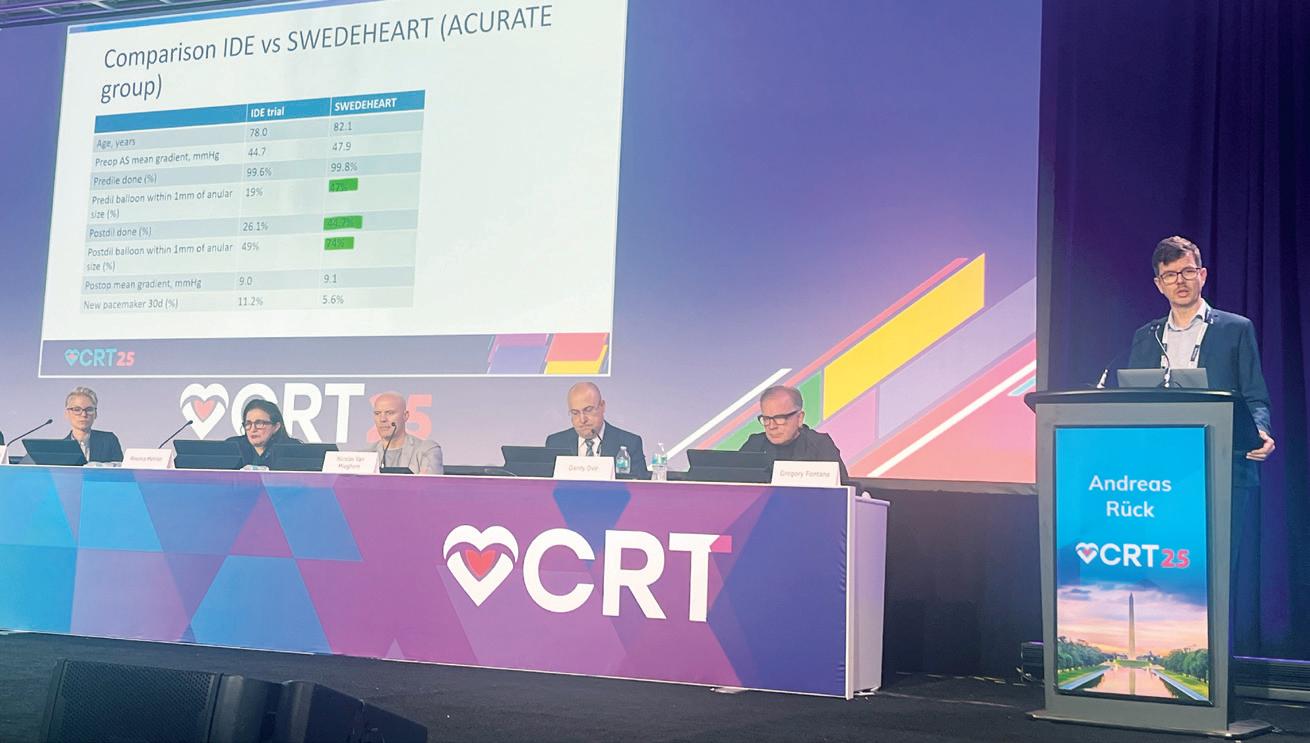
Andreas Rück (Karolinska University Hospital Stockholm, Stockholm, Sweden) presented the analysis of SWEDEHEART data, explaining that the study—a “target trial emulation study”—sought to address some of the concerns thrown up by the results of the ACURATE IDE trial.
Results of ACURATE IDE, reported at the 2024 TCT meeting (27–30 October, Washington, DC, USA), showed that one-year composite rates of all-cause mortality, stroke or rehospitalisation stood at 16.16% among patients receiving Acurate neo2 compared to 9.53% in the control arm with the comparator device, meaning that Acurate neo2 did not meet the prespecified 8% margin for non-inferiority.
Investigators looked at possible factors contributing to the finding, discovering that as many as 21% of Acurate neo2 valves implanted were under-expanded.
“This result was shocking, but at least led to the fact that we, as big users of Acurate, needed to reassure ourselves that this valve is safe to use,” explained Rück of the rationale for the analysis.
Using the observational data from SWEDEHEART, Rück and colleagues emulated all aspects of the ACURATE IDE trial protocol including eligibility criteria, follow-up time and outcomes. They found 1,943 TAVI patients who fit the criteria for the study, 644 receiving Acurate neo2 and 1,299 receiving either Evolut or Sapien 3 valves.
The population was described as typical for those seen in European TAVI practice, with a mean age of 81.2 years and 49.8% female. Most patients
(99.8%) receiving Acurate neo2 underwent predilatation, whilst post-dilatation was also frequent, occurring in 44.7% of cases compared to 26.1% of cases in the IDE trial.
Rück reported that the primary endpoint of allcause mortality, heart failure hospitalisation and stroke occurred in 11.9% of patients receiving Acurate neo2 compared to 12.3% in the control group. Event rates for each of the components of the composite endpoint were virtually identical, with all-cause mortality trending lower the Acurate neo 2 valve.
Outlining key differences in the procedures within the Swedish study and the ACURATE IDE trial among patients receiving the Acurate neo2 valve, Rück noted that predliatation was done in almost all cases in both trials, though there was a big difference in balloon sizing between the two datasets, with very few balloons within a 1mm annular diameter range in the IDE trial.
Additionally, Rück reported a substantial difference in the post-dilatation balloon sizing, with 74% within 1mm of the annular range in the Swedish data compared to 49% in the IDE trial.
“If we try to compare our data from Sweden with the IDE trial, we see that our patients were a little bit older, and the severity of the aortic stenosis was actually a little bit higher, both of those would lead to more events potentially,” Rück summarised. “Predilatation was done almost in 100% in both, but the balloon sizing was a big difference in the IDE trial, with very few balloons within 1mm. Post-dilatation was less frequent in the IDE and there was also a big difference in the sizing.
“At the end of the day, the postoperative mean gradient was very
similar between these two, and interestingly the rate of new pacemakers at 30 days was actually lower in the Swedish data.”
The presenter noted that the findings were limited by the observational nature of the data, and it was not possible to ascertain how many of the valves were fluoroscopically under-expanded—which is thought to have been a major contributor to the negative result seen in the IDE trial.
“Under-expanded valves had higher flows, turbulent flow and reduced washout. That is a very plausible reason for platelet activation and clumping possible micro-emboli which could affect later strokes and later myocardial ischaemia. When we look at time to event, what we saw with under-expanded valves was that you had double the risk of all-cause mortality and triple the risk of stroke,” ACURATE IDE trial investigator Michael Reardon (Houston Methodist DeBakey Heart & Vascular Center, Houston, USA) commented of the results.
Reflecting on the SWEDEHEART data at CRT 2025, Nicolas van Mieghem (Thoraxcenter, Erasmus University Medical Center, Rotterdam, The Netherlands) noted differences in handling of the valves in each study.
“There are a lot of learnings and takeaways from this study. The main one is how we handle the Acurate valve in Europe is definitely different to how the valve was handled in the IDE trial.
“You demonstrated the importance of balloon dilatation pre and post, and the rule of thumb these days is that when you do a balloon dilatation for the Acurate valve it is a 1:1 sizing, for preand post-dilatation. That means that you just rely on one balloon for both.”
Speakers at CRT were asked if these
latest data could support a regulatory submission for Acurate neo2 to the US Food and Drug Administration (FDA), in lieu of positive data from the IDE trial.
“There’s no question that it is encouraging to see that the hypothesis that under-dilatation was the issue and you show us that with diligent work that could be fixed,” said Roxana Mehran (Mount Sinai Hospital, New York, USA) on this point. “Am I convinced in a nonrandomised study 100% that I feel like this is just as good? It is a difficult one to sell, because it is observational, but I think it is great to see that and hopefully in a smaller sized [trial] in a randomised fashion, I am certain there are ways that we could do this so that they could continue to be looked at.”
Commenting on the data presented by Rück at CRT, Reardon described the findings as “reassuring”.
“In the IDE study we failed to meet our non-inferiority endpoint. This led us to do a post hoc analysis where we found almost a quarter of the Accurate valves were under-expanded. Fully expanded valves had no difference in mortality or stroke at one year compared to the control valves. Under-expanded valves had an increased risk of both death and stroke at one year compared to control.
“The IDE trial was enrolled during the Covid-19 pandemic waves and took 47 months to enrol. The average time between Accurate neo2 implantation at sites was 3.9 months.
“In the SWEDEHEART study, operators were implanting the Acurate neo2 valve as part of their normal TAVI program. The SWEDEHEART implanters also followed the guidance for pre-implantation balloon dilatation sizing much more commonly than what was done in the IDE study.
“We have now clearly defined for US operators how to recognise and treat under-expansion. The hope, of course, is that this will lead to results seen in the expanded group of the IDE which matched control valves. With the excellent results seen in Europe, we are hopeful to find a path forward in the USA.”
Andreas Rück at CRT 2025
Novel leaflet modification technique shows promise in reducing LVOT obstruction in mitral valve replacement
A novel technique to reduce left ventricular outflow tract (LVOT) obstruction during transcatheter mitral valve replacement (TMVR) has been shown to be safe and effective, and to result in shorter procedure times. This is according to new data from an international registry presented by Gennaro Giustino (Morristown Medical Center, Morristown, USA) at the 2025 Society for Cardiovascular Angiography & Interventions (SCAI) scientific sessions (1–3 May, Washington, DC, USA).
BALLOON-ASSISTED
anterior mitral leaflet modification, known as the BATMAN technique, involves deploying the transcatheter mitral valve within the anterior mitral valve leaflet. It is intended to prevent LVOT obstruction— which is associated with mortality and screen failure for TMVR—by causing posterior translocation of the anterior leaflet tip and chords, mimicking surgical posterior translocation during mitral valve replacement.
Current strategies to prevent LVOT obstruction include percutaneous laceration of the anterior mitral leaflet, or LAMPOON, which operators say has a steep learning curve, is technically challenging and time consuming.
To date there have been no studies to demonstrate the safety and efficacy of the BATMAN procedure, prompting the current analysis. The study included 41 patients at high risk of LVOT obstruction undergoing transseptal
TMVR with balloonassisted anterior mitral leaflet modification across 12 structural heart centres in the USA, Canada, and Europe.
The primary efficacy endpoint was the rate of successful TMVR with freedom from LVOT obstruction (LVOT mean gradient >50 mmHg) and no procedural death.
The primary safety endpoint was the in-hospital composite of death, stroke, or major cardiac structural complications according to the mitral valvular academic consortium (MVARC) criteria.
Giustino reported that the primary efficacy endpoint was met in 92.7% of patients. Leaflet traversal and balloon laceration were successful in all cases, and there were no cases of residual LVOT obstruction.
The median time between leaflet traversal and valve implantation was only 28 minutes. The primary safety endpoint occurred in 9.8% of patients due to two deaths in the valve in mitral annular calcification group and one death in the valve-invalve group. There were no primary safety events in the valvein-ring group.
BATMAN may be considered as an alternative to LAMPOON associated with excellent efficacy and safety.”
There were no cardiac structural complications attributed to the technique, and no cases of stroke.
“Traditionally, the LAMPOON technique and its various iterations has been used to enable TMVR in patients at high risk of LVOT obstruction; however, this technique has a steep learning curve and is technically more challenging and time-consuming,” said Giustino, the lead author of the study.
“The findings from this study highlight that BATMAN may be considered as an alternative to LAMPOON associated with excellent efficacy and safety, particularly for valve-in-ring and valve-in-valve procedures, providing another option for physicians.”
First-in-human cases using robotic-assisted TMVR system performed in Chile
Details of the successful first-in-human cases of robotic-assisted transcatheter mitral valve replacement (TMVR) using the Capstan system (Capstan Medical), which is remotely controlled using a controller modelled on the type used for the Xbox gaming console, were shared at the 2025 Cardiovascular Research Technologies (CRT) meeting (8–11 March, Washington, DC, USA).
SANTIAGO GARCIA (CHRIST HOSPITAL, Cincinnati, USA) presented details of the two cases, which were performed by Gonzalo Martinez, the director of the Endovascular Therapy Center at Pontifical Catholic University of Chile (Santiago, Chile) and his team, in February.
“Capstan is a fully integrated, robotically controlled TMVR system, designed to maximise physician control of the implant and also expand the pool of patients that can benefit from TMVR,” Garcia said in his presentation.
The system consists of three main components, he
detailed, including the mitral valve implant, which consists of a “dual-stent” system with a valve housing unit of 27mm intended to provide an effective orifice area (EOA) of 3.3cm2; a delivery catheter (33Fr); and, the catheter control system. The implant is manipulated using the controller which can be used to navigate the mitral valve anatomy. Deployment is staged and controlled, and the operator retains the ability to modify the catheter trajectory, depth and position until close to the end of the procedure.
Detailing the first-in-human case performed in Chile, Garcia noted that the patient was not a suitable
Drug therapy may slow progression of aortic valve stenosis
RESEARCHERS HAVE DEMONSTRATED the potential of a new drug—ataciguat—to significantly slow the progress of aortic stenosis. Results of the drug’s effectiveness have been shown in preclinical and clinical studies, published in Circulation, and the team behind the research are seeking to launch a pivotal trial to demonstrate the long-term safety and effectiveness of the treatment.
“This research represents a significant advancement in the treatment of aortic valve stenosis,” comments Jordan Miller, director of the Cardiovascular Disease and Aging Laboratory at Mayo Clinic (Rochester, USA), a co-author on the research paper. “Ataciguat has the potential to substantially delay or even prevent the need for valve replacement surgery, significantly improving the lives of millions.”
The research is part of a collaboration between Mayo Clinic, the National Institutes of Health (NIH), the University of Minnesota (Minneapolis, USA), and Sanofi Pharmaceuticals, conducted under an academic-industry partnership grant administered by the National Center for Accelerating Translational Sciences and a Minnesota Biotechnology and Genomics Partnership grant.
In their Circulation paper, the researchers write that they tested the hypothesis that reactivation of oxidised soluble guanylate cyclase (sGC), the primary receptor for nitric oxide, with ataciguat is a safe and effective strategy to slow the progression of fibrocalcific aortic valve stenosis.
The study team used quantitative real-time reverse transcription polymerase chain reaction, Western blotting, and immunohistochemistry to characterise sGC signalling and the biological effects of the drug on signalling cascades related to nitric oxide, calcification, and fibrosis in excised human aortic valve tissue, aortic valve interstitial cells, and mouse aortic valves. They then conducted randomised placebo controlled phase I and II trials, showing 14-day safety and tolerance and six-month efficacy, respectively, in patients with moderate aortic valve stenosis. The phase II trial in 23 patients showed a 69.8% reduction in aortic valve calcification progression at six months compared to placebo, and patients receiving ataciguat tended to maintain better heart muscle function.
candidate for surgery due to the presence of multiple comorbidities. The case took around 120 minutes to complete, and final results were “excellent”, he said, with no evidence of paravalvular leakage (PVL) and complete elimination of mitral regurgitation (MR). A second case, performed the following day, was also successful, and took a total of 90 minutes to complete.
Both cases had an excellent result, there was no residual MR, no issues with the left ventricular outflow tract (LVOT), no PVL, no wire in the left ventricle and no rapid pacing was required, he described.
“This is a technology that provides unparalleled control and simplicity in navigating the very complex mitral valve anatomy,” Garcia commented. “It is a dual stent system that conforms to the native anatomy, [has a] very low profile in the ventricle to minimise interaction with the LVOT and it is a staged deployment that is very controlled and allows for hemodynamic stability throughout the procedure.”
More cases using the Capstan system are expected to be carried out in Canada and Australia in the near future, Garcia outlined, and a US early feasibility study (EFS) using the system is slated for 2026.
Gennaro Giustino
ALIGN-AR reports positive outcomes with dedicated TAVI device for aortic regurgitation
Data from 500 patients treated for aortic regurgitation with the Trilogy (JenaValve) transcatheter aortic valve implantation (TAVI) system point towards positive safety and efficacy outcomes with the device, alongside favourable valve performance at up to two years.
THE FINDINGS, PRESENTED during a late-breaking trial session at the 2025 American College of Cardiology (ACC) scientific sessions (29–31 March, Chicago, USA), build upon previous results from the trial’s first 180 patients, in which the device was shown to meet its safety and efficacy endpoints.
Design features of the Trilogy valve are intended to make it suitable for the dedicated treatment of aortic regurgitation and include locators that clip onto native leaflets and enable secure anchoring in the absence of calcium. These features may also help to facilitate commissural alignment which can be important when treating aortic stenosis, and the device also features large open cells that are designed to support future coronary access.
The trial—ALIGN-AR—enrolled 500 patients between 2018–2024, with 180 patients enrolled in a premarket approval cohort and 320 patients in a continued access cohort. All patients had moderate to severe symptomatic aortic regurgitation and underwent TAVI with the Trilogy valve. To date, about 360 patients have at least one year of followup after their procedure and 200 have about two years of follow-up. Data from the investigational device exemption
(IDE) study are intended to support US Food and Drug Administration (FDA) approval for the device.
Reporting the latest data at ACC 2025, Raj Makkar (Cedars-Sinai, Los Angeles, USA), commented: “Once approved [Trilogy] will actually provide a new and a much-needed therapeutic option for those who have aortic regurgitation and are high risk for surgery.”
The trial’s primary endpoint was mortality at one year, with a prespecified threshold of 75% survival or better indicating that the valve is not inferior to outcomes that would be expected in the absence of a valve replacement. With a survival rate of 91.9% at one year, the trial met and exceeded this endpoint.
The study reported a device success rate of 96.4% and low rates of residual regurgitation, with only 1.5% of patients experiencing more than mild regurgitation at 30 days and valve embolisation noted in only 1.6%. The 30-day mortality rates were also lower in the continued access cohort (0.9%) compared to the initial premarket approval cohort (2.2%), likely due to a combination of improved patient selection and procedural improvements.
Furthermore, Makkar reported that there was evidence of the device having
Post-TAVI pacemaker implantation linked to long-term increase in mortality rates
Pacemaker implantation within 30 days after a transcatheter aortic valve implantation (TAVI) procedure has been found to correlate with significantly higher rates of all-cause and cardiovascularrelated mortality at up to 10 years of follow-up, as per data from the nationwide SwissTAVI registry.
LATE-BREAKING RESULTS FROM THIS registry were presented by Patrick Badertscher (University Hospital Basel, Basel, Switzerland) at the recent European Heart Rhythm Association (EHRA) congress (30 March–1 April 2025, Vienna, Austria). Within the SwissTAVI registry, researchers assessed a total number of more than 30,000 patients undergoing TAVI procedures in Switzerland between 2011 and 2022. They stratified these patients into three groups: those who already had a pacemaker implant prior to TAVI (n=1,366); those who received a pacemaker <30 days post-TAVI (n=2,028); and those who did not undergo any pacemaker therapy (n=9,966). The median age of this patient population
Trilogy will provide a new and a much-needed therapeutic option for those who have aortic regurgitation.”
a favourable impact on left ventricular (LV) valve remodelling, demonstrated by reduced LV end systolic volumes,
was 82 years, 47% were female, and roughly one-third had a history of atrial fibrillation (AF).
The researchers’ primary endpoint was all-cause death evaluated at the one-year follow-up timepoint, as well as at five and 10 years of follow-up, while notable secondary endpoints included cardiovascular death, decreases in left ventricular ejection fraction (LVEF) ≥10%, and occurrences of heart failure (HF) symptoms.
As per the registry’s primary endpoint, all-cause mortality rates at one year revealed a significantly worse prognosis in patients who received a pacemaker <30 days post-TAVI compared to those who received no pacemaker therapy (hazard ratio [HR], 1.28). And, similarly, patients who had a pacemaker implant prior to TAVI also had a significantly worse prognosis as compared to those in the registry’s non-pacemaker group (HR, 1.39).
Analyses relating more specifically to one-year cardiovascular-related mortality ultimately revealed similar trends—patients who received a pacemaker post-TAVI experienced a significantly worse prognosis, on average, versus those who did not receive pacemaker therapy (HR, 1.39). However, those with a prior pacemaker implant did not experience statistically significantly worse prognoses compared to those without a pacemaker in terms of cardiovascular death (HR, 1.28).
“When comparing patients receiving pacemaker therapy within 30 days after TAVI to patients with no pacemaker therapy, these patients had a significantly
from 38.4ml/m2 at baseline to 30.5ml/ m2 at two years, and decreased LV mass, from 152.3g/m2 to 114.3g/m2
Around 23% of patients required a new pacemaker, with further analysis ongoing to understand the underlying causes and potential mitigating factors, Makkar said.
Further study of the Trilogy valve is set to commence with the initiation of the ARTIST trial, which is due to begin enrolment shortly. The ARTIST trial is a randomised study comparing TAVI with Trilogy to surgical aortic valve replacement (SAVR) in non-high-risk patients with severe and moderate-tosevere aortic regurgitation.
worse outcome regarding all-cause death and cardiovascular death at one year,” Badertscher told the EHRA audience, referencing conclusions from a model adjusted for multiple cardiac risk factors, before going on to outline results from extended follow-up data. “These findings were mirrored when using fiveyear follow-up data, and when using 10-year follow-up data, with significantly worse prognoses for patients receiving a pacemaker within 30 days after TAVI.”
This trend indicating inferior outcomes in patients implanted with a pacemaker post-TAVI—as compared to those without a pacemaker—was maintained across a number of additional study endpoints, including rates of decreased LVEF ≥10% and HF symptom occurrence, as well as a composite measure combining cardiovascular death, LVEF decline and HF symptoms.
Prior to concluding, Badertscher outlined a handful of the SwissTAVI registry’s limitations, such as its observational nature and resulting susceptibility to residual confounding, a lack of information on ventricular pacing during follow-up, and the fact that the potential clinical impact of different pacemaker types and indications was not assessed.
“Novel pacemaker implantation techniques, such as conduction system pacing [CSP], may result in different outcomes,” he added. “However, this is yet to be demonstrated in the TAVI population.”
Long-term outcome data from the SwissTAVI registry were also published in JACC: Cardiovascular Interventions shortly after Badertscher’s presentation.
Innovation and excellence celebrated at second Global Cardiovascular Awards
One of interventional cardiology’s master operators, known globally for his landmark work in the field of coronary stenting, intravascular ultrasound (IVUS) and stent thrombosis, was recognised for his stellar career at the second annual Global Cardiovascular Awards (13 March, London, UK).
Antonio Colombo (San Raffaele Scientific Institute, Milan, Italy) was given the Lifetime Achievement Award for his groundbreaking work across nearly 50 years in practice.
The awards, hosted by Cardiovascular News with support from the European Cardiovascular Research Institute (ECRI), Cardialysis and Boston Scientific, seeks to recognise the innovators and pioneers at the forefront of efforts to improve the treatment of cardiovascular disease worldwide.
Across 14 categories, awards were presented to some of the individuals, industry leaders and nonprofit organisations who are helping to shape the future of cardiovascular care. Each award category was adjudicated by a panel assembled by Cardiovascular News, and the winners were announced at a ceremony at London’s Grand Sheraton Hotel on the evening of 13 March hosted by the comedian and entertainer Patrick Monahan.
“I’m proud of optimising stent implantation with use of intravascular ultrasound, high-pressure balloon inflation, and dropping coumadin switching initially to ticlopidine and then clopidogrel. If I had to stop my career I would stop after I did that,” Colombo said in an address to the Global Cardiovascular Awards audience, reflecting humbly on his career. “It is acceptable for one life of a person to solve one problem, at least one problem has been solved!”
Simone Fezzi (University of Verona, Verona, Italy) was named as the recipient of the Future Leader award, recognised for his contributions to several notable studies in interventional cardiology, particularly focusing on coronary physiology and advanced imaging techniques in percutaneous coronary intervention (PCI), as well as drug-coated balloon (DCB) PCI, and his work on the DCB-Academic
Research Consortium (ARC) working group.
The team behind the BHF SENIOR-RITA trial, led by Vijay Kunadian (Translational and Clinical Research Institute, Newcastle University and Freeman Hospital, Newcastle upon Tyne, UK), were handed the Clinical Research Excellence Award for their work comparing an invasive and a conservative strategy to treat patients over the age of 75 years with a non-STelevation myocardial infarction (NSTEMI).
Among the industry awards, Medtronic was named the winner in the Best Cardiovascular Product Launch category, for the launch of its Aurora Extravascular Implantable Cardioverter Defibrillator (ICD) system. Siemens Healthineers’ Hero Campaign was named as the best educational campaign, for its work to raise awareness for cardiovascular care by bringing the ‘heroes of daily work’ to the forefront.
Ahmed Elmouelhi, CEO of the tricuspid valve innovator TriCares, was named as the CEO of the year. The Medtronic and Atricure veteran paid tribute to his team, in collecting the award.
In the Best Startup category, Egg Medical, whose pioneering products seek to limit radiation exposure for cath lab teams, was named as the winner, recognised for key milestones including the global launch of its EggNest XR radiation protection system, as well as the EggNest Protect and EggNest Complete Radiation Protection systems in 2024. The company has already obtained US Food and Drug Administration (FDA) and CE-mark approvals, and has systems in 50 US and 10 global hospitals.
Global Heart Hub was named as the winner of the Best Prevention Campaign award for its Manifesto for Change, which seeks to drive early detection and diagnosis of cardiovascular disease.
Boston Scientific’s health equity initiative, Close
the Gap, was named as the winner in the category recognising the Contribution to Equity and Diversity in Cardiovascular Care. The award was presented by ECRI’s Ernest Spitzer, who commented: “Innovation continues to deliver better therapies for patients in need. But, clinical investigations supporting these therapies sometimes lack adequate representation of all patients who suffer from the specific condition.
“Clinical trials have traditionally underrepresented women, the elderly, demographic minority groups, and lower-income families. Becoming conscious of these information gaps has motivated numerous initiatives to increase high-quality data in underrepresented patient populations.
“The Close the Gap initiative from Boston Scientific has pioneered on this mission and continues to create better pathways to address disparities. Almost 20 years since its beginnings in cardiovascular disparities, it has evolved into other areas such as asthma and colon cancer. On behalf of the organisers, it is an honour to dedicate this award to Boston Scientific, which continues to lead in many different areas within cardiovascular care.”
Innovation was a central theme running through the awards, and several categories sought to recognise the ingenuity and novel use of technology to improve outcomes for patients with cardiovascular disease.
In the Digital Innovation category, the Acarix CADScor system, an AI-powered acoustic diagnostic aid to rule out coronary artery disease, was crowned as the winning entry, whilst the HeartFlow ONE system picked up the Innovation in Cardiac Imaging award.
In a highly competitive Innovation in Interventional Cardiology category, Medtronic’s Symplicity Spyral renal denervation system won out. Presenting the award, Adrian Banning (Oxford Heart Centre, John Radcliffe Hospital, Oxford, UK) underlined the important collaboration between industry and clinicians need to drive advances in the field.
Highlighting the important recent developments in improving the safety of interventional procedures, Rampart IC was selected as the winner in the Innovation in Patient and Operator Safety category for its fully adjustable, portable radiation shielding system that provides proven, full-bodied radiation protection for interventionalists.
In the Collaboration of the Year category, the Redo TAV App, which provides guidelines for assessing the suitability of a transcatheter aortic valve for Redo-TAV procedures, was recognised by judges for its cross-industry participation. The initiative was led by Vinayak Bapat (Minneapolis Heart Institute Foundation, Minneapolis, USA).
1. Best Cardiovascular Product Launch –Aurora Extravascular Implantable Cardioverter Defibrillator System – Medtronic
2. Best Education Campaign – Hero Campaign Cardiovascular Care – Siemens Healthineers
3. Best New Startup – Egg Medical
4. Best Prevention Campaign – Achieving early detection and diagnosis of cardiovascular disease: A Manifesto for Change –Global Heart Hub
• Highly Commended – ‘Til I Died – British Heart Foundation
5. CEO of the Year – Ahmed Elmouelhi – TriCares
6. Contribution to Equity and Diversity in Cardiovascular Care – Close the Gap: A Boston Scientific Health Equity Initiative
7. Collaboration of the Year: Redo TAV App –Vinayak Bapat
8. Digital Innovation Award – CADScor System
• Highly Commended – HeartFlow ONE
9. Innovation in Cardiac Imaging – HeartFlow ONE
• Highly Commended – CADScor System
• Highly Commended – CaRi-Heart Technology
10. Innovation in Interventional Cardiology –Sympliity Spyral Renal Denervation System
Edwards’ Sapien 3 lands US FDA approval for the treatment of asymptomatic severe AS Edwards Lifesciences has announced US Food and Drug Administration (FDA) approval for its Sapien 3 transcatheter aortic valve implantation (TAVI) platform for the treatment of severe aortic stenosis (AS) patients without symptoms, marking the first FDA approval for TAVI in asymptomatic patients.
Approval of the Sapien 3 platform— Sapien 3, Sapien 3 Ultra and Sapien 3 Ultra Resilia—is based on data from the EARLY TAVR trial, in which it was demonstrated that asymptomatic severe AS patients randomised to TAVI with Sapien 3 experienced superior outcomes compared to guidelinerecommended clinical surveillance.
“There is an urgent need to change practice and TAVI guidelines for the treatment of aortic stenosis patients, which currently recommend ‘watchful waiting’ until symptoms develop,” said Philippe Genereux (Morristown Medical Center, Morristown, USA), the principal investigator in the EARLY TAVR trial. “As we saw in the EARLY TAVR trial, patients originally designated as asymptomatic became symptomatic in sudden and unpredictable ways, underscoring the importance of early evaluation by a heart team to improve patient outcomes and benefit the healthcare system.”
“This approval is a powerful opportunity to streamline patient care and improve the efficiency of the healthcare system,” said Larry Wood, Edwards’ corporate vice president and group president, Transcatheter Aortic Valve Replacement and Surgical. “We are proud to partner with leading physicians to advance our knowledge of this deadly disease with high-quality science and optimise the treatment pathway for patients.”
Additionally, the company has announced that its Sapien M3 mitral valve replacement system has received CE mark for the transcatheter treatment of patients with symptomatic (moderate-to-severe or severe) mitral regurgitation (MR) who are deemed unsuitable for surgery or transcatheter edge-to-edge (TEER) therapy. Leveraging the company’s Sapien technology, the Sapien M3 system is the world’s first approved transcatheter valve replacement therapy using a transfemoral approach to treat MR, Edwards Lifesciences says in a press release.
Elixir Medical launches LithiX Hertz Contact IVL system in Europe Elixir Medical has announced EU medical device regulation (MDR) CE mark approval and commercial launch of its LithiX Hertz Contact (HC) intravascular lithotripsy (IVL) system in Europe.
The first cases were completed by Stefano Galli (Centro Cardiologico Monzino, Milan, Italy), Eric Van Belle (Lille University Hospital, Lille, France), and Nikos Werner (Hospital Barmherzigen Bruder Trier, Trier, Germany).
The LithiX lithotripsy mechanism of action to create calcium fractures is based on the Hertz Contact Stress principle and does not require an external energy source or capital equipment, delivering the expected performance of IVL with additional versatility to treat complex calcified lesions based on the unique design, Elixir Medical says in a press release.
The LithiX Hertz Contact IVL system is a transcatheter device comprised of multiple lowprofile metal hemispheres uniformly distributed and integrated across the surface of a semi-compliant balloon. Under low balloon inflation pressure, the hemispheres create highly localised points of contact with calcium and amplification of force to create deep and wide fractures based on Hertz Contact Stress mechanics, while minimising vessel injury when in contact with soft non-calcified vessel tissue.
require any pre-procedure step, further simplifying the procedure.
“Vascular closure remains a challenge for the growing cardiovascular procedures that require large-bore access. The introduction of PerQseal Elite is an exciting advancement for large-bore cardiovascular procedures,” said Mohamed Abdel-Wahab (Leipzig Heart Center, Leipzig, Germany). “Having a fully absorbable, sutureless closure option simplifies the procedure and has the potential to reduce complications associated with traditional closure methods. We look forward to utilising this technology to treat our patients.”
Anteris Technologies has announced that the biomimetic DurAVR transcatheter heart valve (THV) has been used to treat over 100 patients.
These include de novo aortic stenosis, valve-in-valve (ViV) patients and complex anatomies such as bicuspid aortic valve patients. Sixty-five patients have successfully completed the primary endpoint measures of safety and efficacy, including haemodynamic benefit at 30 days post implant.
Michael Reardon (Houston Methodist Hospital, Houston, USA), study chair of the DurAVR THV pivotal trial, said:
“We are building on a strong foundation of clinical evidence, and we remain committed to rigorous scientific evaluation as we progress toward the all-risk, head-tohead DurAV registration trial.”
at Scripps Clinic in San Diego, USA, by Paul Teirstein and Curtiss Stinis.
“SoloPace has modernised pacing during TAVI valve deployment,” said Teirstein. “The device takes variability out of the procedure by giving the operator full control while automating ramp-up and back-up algorithms. The TAVI procedure is simplified, reducing physician and staff workload. We preprogramme pacer settings to reliably deliver the same procedure every time. This allows us to focus on the patient and free up resources—especially at centres where nurses and technologists currently control the pacemaker generation.”
The SoloPace control system's operator-specific protocols and automated pace capture checks may improve procedural efficiency, while the intuitive interface and sterile remote -control operation are designed to reduce communication errors, the company further claims. In addition, the system is compatible with patient cables for all common procedural pacing methods, making it easy to integrate into current practice.
First US commercial cases performed with ShortCut leaflet modification device
Pi-Cardia has announced the first commercial procedures with its ShortCut dedicated leaflet modification device, enabling valve-in-valve (ViV) transcatheter aortic valve implantation (TAVI) procedures in patients at risk of coronary obstruction. This follows de novo market clearance granted by the US Food and Drug Administration (FDA) in September 2024.
“Optimal calcium modification is very important in achieving good percutaneous coronary intervention (PCI) outcomes, and LithiX Hertz Contact IVL fulfils that goal as a simple-to-use and versatile option with excellent clinical performance,” said Galli.
PerQseal Elite vascular closure system gains CE mark Vivasure Medical has announced European CE mark approval of the PerQseal Elite vascular closure system, a sutureless and fully bioresorbable large-bore vessel closure device. The company plans to launch the product in select European markets this summer.
Leveraging Vivasure’s PerQseal technology, the PerQseal Elite vascular closure system is designed for sutureless and fully absorbable largebore closure following percutaneous cardiovascular procedures such as transcatheter aortic valve implantation (TAVI) and endovascular aneurysm repair (EVAR). Currently, there are no fully bioresorbable devices available for closure following large-bore procedures. Moreover, unlike other current devices, PerQseal Elite does not
The company remains on track to commence the DurAVR THV pivotal trial in the third quarter of 2025, pending US Food and Drug Administration (FDA) approval, the press release adds.
One-year performance data for the DurAVR valve were recently presented at Sydney Valves (20–22 March, Syndey, Australia), where Rishi Puri (Cleveland Clinic, Cleveland USA) reported that the valve demonstrated a favourable haemodynamic profile sustained to one year, with an effective orifice area (EOA) of 2.1+0.2cm2 , a mean pressure gradient (MPG) of 8.6+2.6mmHg and Doppler velocity index (DVI) of 0.58.
SoloPace announces US FDA clearance and first-in-human use of TAVI temporary pacing system SoloPace has announced both US Food and Drug Administration (FDA) clearance and first-in-human use of its SoloPace control system for temporary pacing in transcatheter aortic valve implantation (TAVI) procedures. With standardised workflows, the control system is engineered to improve temporary pacing efficiency and reduce patient risks, according to a recent company press release.
Initial cases were completed in April
The initial procedures were successfully performed at institutions including the Gagnon Cardiovascular Institute (Morristown, USA) by Philippe Généreux and Gennaro Giustino, at Cedars-Sinai Medical Center (Los Angeles, USA) by Raj Makkar and Wen Cheng, and Piedmont Heart Institute (Atlanta, USA) by Vinod H Thourani and Pradeep Yadav.
“The ShortCut device is a true gamechanger, addressing one of the most significant challenges in structural heart,” says Makkar. “It will play a fundamental role in the lifetime management of aortic stenosis patients who may require multiple valve interventions. Given its quick and intuitive nature and seamless integration into the standard TAVI workflow, I am confident this tool will become highly adoptable across TAVI centres.”
Sapien 3
ShortCut
DurAVR transcatheter valve
Clinical News
Abbott to begin TECTONIC trial of IVL therapy prior to coronary stenting Abbott has announced that the US Food and Drug Administration (FDA) has approved an investigational device exemption (IDE) for its coronary intravascular lithotripsy (IVL) system to evaluate the treatment of severe calcification in coronary arteries prior to stenting. The TECTONIC CAD IVL clinical trial will enrol up to 335 people in 47 sites in the USA.
“For people living with coronary artery disease, severe calcification can make treatment more challenging, often limiting the effectiveness of standard interventions like angioplasty or stenting,” said Eric Secemsky (Beth Israel Deaconess Medical Center, Boston, USA) and co-principal investigator for the TECTONIC CAD IVL trial. “The TECTONIC CAD IVL trial will evaluate a possible new treatment option to prepare the vessel prior to stenting and optimise stent placement.”
Abbott’s investigational coronary IVL technology builds upon the company’s existing vascular portfolio and is designed to address challenges of currently available IVL systems, the company says in a press release. Abbott’s coronary IVL system is an investigational device and not commercially available.
Transverse Medical completes first patient series involving Point-Guard embolic protection device
Transverse Medical has announced the completion of the first series of patients under its feasibility clinical study at the Victorian Heart Hospital in Melbourne, Australia.
Patients undergoing transcatheter aortic valve implantation (TAVI) procedures were treated using the company’s next-generation PointGuard cerebral embolic protection device, marking what Transverse describes as a “major milestone” in the clinical evaluation of this innovative technology.
“Point-Guard was easy to use, simple to deploy and retrieve, and was free of adverse events in this first phase of the study,” said Robert Gooley (Victorian Heart Hospital, Melbourne, Australia), the study’s physician investigator. “Positioning the Point-Guard in the arch anatomy was predictable and the asymmetric design of the filter provided a unique approach for complete coverage of all the major arch vessels.”
Transverse’s Point-Guard device is designed to provide maximum protection against periprocedural stroke and brain ischaemia during transcatheter procedures by preventing embolic particles from reaching the brain. The “innovative and simple” design of the device, in addition to ease
of use for the operator, and the fact it represents a solution for “complete coverage” of all the major arch vessels, provides a positive outlook regarding enhanced patient safety and improved clinical outcomes. That is according to a Transverse press release.
“We are incredibly proud of the progress we’ve made with the PointGuard cerebral embolic protection (CEP) technology,” said Michael Reardon (Houston Methodist Hospital, Houston, USA), chief medical officer at Transverse. “Complete embolic coverage of the aortic arch and the great vessels supplying blood to the brain is clearly the next step for the CEP market. The Point-Guard solution and technology brings us one step closer to providing full brain protection for patients undergoing high-risk procedures like TAVI, which will be life-changing for so many.”
Shockwave commences trial of Javelin IVL catheter in complex coronary disease
Shockwave Medical, part of Johnson & Johnson MedTech, has initiated its pivotal FORWARD CAD investigational device exemption (IDE) study, assessing the safety and effectiveness of the Shockwave Javelin coronary intravascular lithotripsy (IVL) catheter for the treatment of calcified, difficult-to-cross stenotic de novo coronary artery lesions prior to stenting.
The first patient was treated recently by operators Evan Shlofmitz and Ziad Ali at St Francis Hospital & The Heart Center in Roslyn (USA).
“There is an opportunity to improve the treatment of cardiovascular patients with tight, calcific lesions in narrowed coronary vessels that are challenging to cross with balloon-based approaches as currently we have to rely on atherectomy technologies,” said Shlofmitz.
“We are delighted to enrol the first patient in the FORWARD CAD clinical trial to determine whether Shockwave’s novel forward IVL platform can help reduce the recognised risks of atherectomy in this patient population,” adds Ali.
A prospective, multicentre, singlearm study across approximately 35 sites in the USA and UK, FORWARD CAD aims to enrol up to 158 patients
with moderate-to-severely calcified, stenotic de novo coronary artery lesions presenting with stable angina or following stabilisation after acute coronary syndrome (ACS) and suitable for non-emergent percutaneous coronary intervention (PCI).
The global co-principal investigators of the study are Robert Yeh (Beth Israel Deaconess Medical Center, Boston, USA) and James Spratt (St George’s University NHS Trust, London, UK) and the US principal investigator is Robert Riley (Overlake Medical Center & Clinics, Seattle, USA).
The forward IVL platform is designed with a single distal emitter that creates ultrasonic shockwaves, with a spherical energy field that extends beyond the tip of the catheter. This novel design delivers lithotripsy closer to highly stenosed calcium lesions than balloon-based platforms.
Early feasibility study of Siegel 8Fr TAVI valve launches MiRus has announced the launch of the US multicentre early feasibility study (EFS) of the Siegel 8Fr aortic transcatheter heart valve.
The first two cases were successfully performed by Pradeep K Yadav and Vinod H Thourani, both of Piedmont Heart Institute (Atlanta, USA). Both patients were discharged without complications the next day.
The Siegel valve encompasses an 8Fr delivery sheath allowing less invasive procedures and broader patient access, a Nickel-free valve allowing treatment, lack of foreshortening and intrinsic commissural alignment and dry porcine pericardial leaflets with anticalcification treatment with the valve pre-mounted on the balloon.
“Our initial experience is very positive,” commented Yadav. “Siegel is much less invasive then current devices and can be placed very precisely due to the lack of foreshortening. This should lead to lower pacemaker rates. The haemodynamics are excellent due to the radial strength and porcine pericardial leaflets.”
“In these first two cases, the Siegel valve performance is impressive,” stated Thourani. “8Fr system with such precise placement and low gradients and no paravalvular leak (PVL) is not a combination I ever expected in a transcatheter heart valve. A transcatheter heart valve without nickel is also much needed.”
CONFORM IDE trial reaches enrolment milestone
Conformal Medical has announced the enrolment of its 500th patient in the CONFORM investigational device exemption (IDE) trial, the prospective multicentre, randomised controlled study evaluating the safety and efficacy of the Conformal CLAAS AcuFORM system compared to other commercially available left atrial appendage (LAA) devices.
This marks a significant milestone in the trial, reaching close to a third of the intended enrolment of 1,600
patients, and is a major step forward in validating the CLAAS system for patients with non-valvular atrial fibrillation (NVAF), Conformal Medical says in a press release.
Christopher Ellis (Vanderbilt Health Nashville, Nashville, USA), Vikrant Jagadeesan (West Virginia University, Morgantown, USA) and Devi Nair (St Bernards Medical Center and White River Medical Center, Jonesboro, USA) were among the first operators to implant the next-generation CLAAS AcuFORM left atrial appendage occlusion (LAAO) device.
The CLAAS system aims to provide an alternative option to seal the LAA with only two sizes.
Eight-year data “encouraging” for aortic valves using Resilia tissue technology Edwards Lifesciences has announced new eight-year data showing that patients receiving aortic surgical valves treated with its proprietary Resilia tissue technology have significantly improved long-term outcomes compared to those receiving nonResilia tissue bioprosthetic valves.
Presented at the Heart Valve Society annual meeting (16–19 April, Cairo, Egypt), the study of 947 patients marks the first long-term, propensity-matched comparison between Resilia tissue and non-Resilia tissue surgical aortic valves.
The Resilia tissue data from the trial reported encouraging results through eight years, with low rates of structural valve deterioration (SVD; 99.3% freedom from SVD in the Resilia tissue group versus 90.5% in the non-Resilia tissue group, p<0.0001) and freedom from reoperation due to SVD (99.2% in the Resilia tissue group versus 93.9% in the non-Resilia tissue group, p=0.0007).
Edwards developed the Resilia tissue technology more than two decades ago, and it is used in a wide range of Edwards’ surgical and transcatheter platforms, including the Inspiris Resilia aortic surgical valve, the Konect Resilia aortic surgical valve conduit, the Mitris Resilia mitral surgical valve and the Sapien 3 Ultra Resilia transcatheter aortic heart valve.
“These highly anticipated data provide strong clinical evidence of the excellent durability of Resilia tissue in surgical valves,” said Tsuyoshi Kaneko, John M Shoenberg chair of cardiovascular disease, chief of cardiac surgery at Washington University (St Louis, USA) and lead author of the study. “This level of performance is critical to reducing reinterventions and enabling more effective lifetime management for patients.”
Shockwave Javelin
CLAAS Implant
Industry News
Boston Scientific among investors in latest financing round for 4C Medical Technologies 4C Medical Technologies has closed a US$175 million series D financing round, led by existing shareholders and new investors, including Boston Scientific, which will be used to accelerate development and commercialisation of the company’s transcatheter mitral valve replacement (TMVR) technology AltaValve.
Funding will support the ongoing global pivotal trial, ATLAS, with enrolment of the trial having begun in October 2024.
“We are excited to welcome Boston Scientific and thank our shareholders for their support with our financing,” said Saravana Kumar, chief executive officer and president at 4C Medical. “The enthusiasm for participation in our ATLAS pivotal trial is palpable, and with this strong capital raise and the backing of Boston Scientific, we look forward to clinically demonstrating the safety and effectiveness of the AltaValve system in treating patients with mitral regurgitation (MR).”
New funding to support expansion of clinical programme for Supira Medical pVAD
Supira Medical has announced the successful completion of an oversubscribed series E financing round, raising US$120 million, with funds to be used to expand clinical programmes for the study of the company’s percutaneous ventricular assist device (pVAD) for both high-risk percutaneous coronary intervention (HRPCI) and cardiogenic shock (CS).
The funding round was led by new investors Novo Holdings and Qatar Investment Authority (QIA), along with participation from two undisclosed strategic investors.
Existing investors participated as well, including Cormorant Asset Management and The Capital Partnership (TCP), 415 Capital, AMED Ventures, PA MedTech VC fund, and Unorthodox Ventures.
The ATLAS pivotal trial is designed to assess the safety and effectiveness of AltaValve in treating moderate-tosevere or severe MR among patients who are unsuitable for surgery or transcatheter edge-to-edge repair (TEER). The trial is designed with two separate non-randomised cohorts: a moderate/severe mitral annular calcification (MAC) cohort, and patients with no or mild MAC.
Ron Waksman (MedStar Medical Center, Washington, DC, USA) is the chair of the ATLAS steering committee, with Paul Sorajja (Allina Health Minneapolis Heart Institute, Minneapolis, USA) and Yoshi Kaneko (Barnes-Jewish Hospital, St Louis, USA), sharing principal investigator responsibilities in the USA, while Vlasis Ninios (Interbalkan Medical Center, Thessaloniki, Greece) and Lenard Conradi (University Hospital Cologne, Cologne, Germany) sharing these responsibilities in Europe.
Conference calendar
19–23 May EuroPCR Paris, France pcronline.com
12–13 June
Actif 2025 Paris, France actif-cardio.com
In a statement, the company says that the clinical programme expansion includes the SUPPORT II US pivotal study for HRPCI, which will be used to seek US Food and Drug Administration (FDA) premarket approval (PMA).
Protembis names four-person advisory board
Protembis has announced establishment of a scientific advisory board (SAB) to provide objective advice and contribute to the strategic plans of the company.
The SAB will be comprised of Martin Leon (Columbia University, New York, USA), Anita Asgar (Northwestern Medicine, Evanston, USA), Samir Kapadia (Cleveland Clinic, Cleveland, USA), and Nicolas van Mieghem (Thoraxcenter, Erasmus University Medical Center, Rotterdam, The Netherlands).
Protembis is currently enrolling patients in the PROTEMBO pivotal investigational device exemption (IDE) trial, which aims to show that the ProtEmbo cerebral embolic protection system is superior to contemporary practice in reducing new cerebral lesion volume during transcatheter
aortic valve implantation (TAVI) when assessed by diffusion-weighted magnetic resonance imaging (MRI).
The novel trial randomises ProtEmbo against a hybrid control group: half receiving no cerebral embolic protection and half receiving the Sentinel (Boston Scientific) device.
The trial is led by Roxana Mehran (Mount Sinai, New York, USA) as the chair of the study executive committee, with Susheel Kodali (New York Presbyterian Hospital, New York, USA), Raj Makkar (Cedars Sinai, Los Angeles, USA) and Stephan Haussig (Herzzentrum, Dresden, Germany) as the global co-principal investigators.
Howard Herrmann appointed CMO for structural heart by Affluent Medical
Affluent Medical has appointed Howard Herrmann (Perelman School of Medicine at the University of Pennsylvania, Philadelphia, USA) as strategic chief medical officer (CMO) for its structural heart platform.
The appointment underscores the company’s commitment to enhancing clinical expertise and driving innovation as it advances its Kalios mitral ring and Epygon mitral valve, Affluent Medical says in a press release.
Herrmann is professor of medicine at the Perelman School of Medicine at the University of Pennsylvania and director of interventional cardiology at the Hospital of the University of Pennsylvania (Philadelphia, USA)..
Affluent’s urology platform.
“These appointments come at a crucial time as we enter our next phase of growth, transitioning into pivotal phases and continuing to progress towards commercialisation of our devices,” said Sébastien Ladet, chief executive officer (CEO) of Affluent Medical. “The addition of strong medical experts has been a deliberate move that demonstrates Affluent Medical’ commitment to execute and to offer the best available therapies worldwide.”
The company has also recently announced that it has coopted Liane Teplitsky as a new Board member. Recently appointed CEO of Artedrone, an autonomous robotic solution for mechanical thrombectomy, Teplitsky was most recently president, Global Robotics, Technology & Data Solutions at Zimmer Biomet where she led the global growth and development of the company’s portfolio of robotics and digital health technologies, having also held roles at Abbott and St Jude Medical.
He has over three decades of experience in transcatheter device therapies for valvular and structural heart diseases, and has authored over 500 publications and served as president of the Pennsylvania chapter of the American College of Cardiology (ACC).
Additionally, Affluent Medical has named Federica Azzimonti as director of clinical operations to lead the operational aspects of Affluent Medical clinical trials, ensuring streamlined execution as the company prepares for pivotal stages.
Nicolas Barry Delongchamps (Cochin Hospital, Paris Descartes University, Paris, France) has also been named as chief medical officer for
Evident Vascular raises Series B financing to advance AI-powered IVUS platform technology
Evident Vascular has announced the successful closing of its Series B financing, with the funding to be used to accelerate the development of the company’s advanced intravascular ultrasound (IVUS) technology to enhance vascular imaging and patient outcomes and support 510(k) US Food and Drug Administration (FDA) clearance ahead of US market launch.
“This significant investment underscores our investors’ confidence in Evident Vascular’s mission and technology while highlighting the vital role of intravascular imaging in optimising patient outcomes, clinical decision-making and procedural success,” stated Howard Rosen, chief executive officer and co-founder of Evident Vascular. “We will accelerate our progress toward FDA clearance and further the development of our AI [artificial intelligence]-powered IVUS solution which aims to set a new standard in vascular imageguided therapy.”
16–18 November PCR London Valves London, UK pcronline.com/courses