


A publication of the Florida Podiatric Medical Association Vol. 77, #1, SPRING 2024 SAM 2024 RECAP PAGE 26 A Young Physician’s Insight on Employment PAGE 14 Florida’s Future Legislative Leaders PAGE 18 FPMA 2024 Summer Conference Registration Forms PAGE 36




Florida Podiatric Medical Association | 3 28 From the Editor: Provider Attendance at SAM 2024 Highest Ever 5 Cary M. Zinkin, DPM President’s Perspective: Let the Good Times Roll 8 Larissa Schmidt, DPM Membership: Milestone Members 10 New and Returning Members 10 FPMA Component Presidents 2024 11 In Memoriam 12 Check Out the FPMA Career Center! 13 A Young Physician’s Insight on Employment 14 Insurance Affairs: Insurance Report Update: Navigating Challenges and Advocacy Efforts 16 Legislative Update: Florida’s Future Legislative Leaders ........................... 18 Legal: Employing a Nurse Practitioner in Florida – an Update 20 FPMA Corporate Affinity Partner Article: Complications Resulting in Amputation –Reducing the Risk for You and Your Patients 22 www.fpma.com CONNECT WITH FPMA CONTENTS Conference News: SAM 2024 Recap 26 Keeping the Passion in Practice 34 Attending SAM 2024: A Student’s Perspective 35 FPMA 2024 Summer Conference Registration Forms 36 20 VOL. 77, #1, SPRING 2024 26
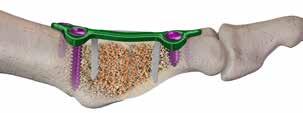
Managing Partial Foot
Amputations
• Limb Preservation
• Gait Restoration
• Propulsion with Proximal Stability



Studies have shown destructive forces are distal to the residuum using BlueROCKER®, thereby preserving the residual foot.


 Carbon footplate
SAFO
BlueROCKER
Carbon footplate
SAFO
BlueROCKER

Larissa M. Schmidt, DPM President
David M. Schweibish, DPM President-Elect
Adriana P. Strimbu, DPM Vice President
Liana G. Seldin, DPM Treasurer
Diana E. Rogers, DPM Secretary
Alissa B. Zdancewicz, DPM Immediate Past President STAFF
Karen N. Lambert CEO/Executive Director
Becky Reese Public Affairs/Website Coordinator
Gin Grand Membership Coordinator
Dee Muller Administrative Manager EDITOR
Cary M. Zinkin, DPM
The recommendation of any benefits, products, or services to our membership does not constitute a warrantee by the Florida Podiatric Medical Association, Inc., or the Florida Podiatric Medical Society, Inc. Each member must decide for himself or herself as to the value and benefit of any product purchased. The Florida Podiatric Medical Association, Inc., or the Florida Podiatric Medical Society, Inc., is not liable for any defects or failure of any benefit, product, or service purchased by any member.
Provider Attendance at SAM 2024 Highest Ever
 By Cary M. Zinkin, DPM
By Cary M. Zinkin, DPM
I hope everyone enjoyed the SAM 2024 conference at the Hyatt Regency Orlando this past January! This year we celebrated the highest attendance of providers in FPMA history, proving that the FPMA Science & Management Symposium is the No. 1 podiatric conference in the country! We also inducted our new president, Dr. Larissa Schmidt, as well as our new secretary, Dr. Diana Rogers.
Did you know that FPMA is the largest podiatric state component in the United States? As a result, we send more delegates to the APMA House of Delegates in Washington, D.C., than any other state! The APMA House of Delegates, which took place March 16 and 17, was a huge success.
Some FPMA delegates also participated in Legislative Day on Capitol Hill, visiting our U.S. representatives and senators. Our team discussed subjects that affect our members, our patients and our ability to offer top-quality professional medical and surgical treatments.
The FPMA Summer Conference will once again take place at the Hyatt
Regency Coconut Point Resort in Bonita Springs on June 7-9, offering CECH and required courses in a casual family atmosphere. This has been a favorite of our members, and we hope to see you there!
On a personal note, a short time ago, we lost a good friend and past FPMA president, Bradley Haves. Dr. Haves was active in FPMA for more than 20 years and served as a delegate to the APMA House of Delegates. He was well known and well loved. We will keep his fun spirit and love of great restaurants with us forever. Rest in peace, my friend, and may your memory always be a blessing.
Florida Podiatric Medical Association | 5 FROM THE EDITOR Published April 2024 • Volume 77 Issue 1 • 2024 FPMA Footprints is published by Innovative Publishing. Direct all inquiries to Aran Jackson at (844) 423-7272. 10629 Henning Way, Suite 8 Louisville, KY 40241 (844) 423-7272 www.innovativepublishing.com FPMA Footprints is published by The Florida Podiatric Medical Association 3375-F Capital Cir. NE, Ste. 201 Tallahassee, FL 32308 Phone: (800) 277-3338 Fax: (850)
Website: www.fpma.com Permission to reprint FPMA Footprints articles may be obtained by contacting the editor.
681-0899
OFFICERS
The New ICD-10-CM Coding Summary is Here! Brought to you exclusively by BakoDx!
Aspiration Biopsy (Soft Tissue Mass)
CPT® 20612 Aspiration and/or injection of ganglion cyst(s) any location
ICD-10-CM codes to consider for aspiration biopsy:
M67.4- Ganglion
D49.2 Neoplasm of unspecified behavior of bone, soft tissue, and skin
D21.2- Benign neoplasm of connective and other soft tissue of lower limb, including hip
D48- Neoplasm of uncertain behavior of other and unspecified sites
Aspiration / Arthrocentesis (Joint or Bursa)
CPT® 20600 Arthrocentesis, aspiration and/or injection; small joint or bursa (eg, toes)
CPT® 20605 Arthrocentesis, aspiration and/or injection; intermediate joint or bursa (eg, ankle)
ICD-10-CM codes to consider for : M19.07- Primary osteoarthritis, ankle and foot
M19.17- Post-traumatic osteoarthritis, ankle and foot M19.27- Secondary osteoarthritis, ankle and foot M65.87- Other synovitis and tenosynovitis, ankle and foot
Bone Biopsy
CPT®
CPT®

ICD-10-CM Coding Summary
Biopsy, bone, trocar, or needle; superficial Biopsy, bone, open; superficial
CPT® 11102
ICD-10-CM codes to consider for bone biopsy: Osteomyelitis
M86D49.2
D16D48.0
CPT® 1110
Neoplasm of unspecified behavior of bone, soft tissue, and skin
CPT® 11106
CPT® 1130X
Tangential Biopsy, Punch Biopsy, Incisional Biopsy, Shave Excision
Benign neoplasm of bone and articular cartilage
Neoplasm of uncertain behavior of bone and articular cartilage
M87Osteonecrosis
© Copyright 2023
Tangential biopsy of skin (e.g. shave, scoop, saucerize, curette, single lesion)
Shaving of epidermal or dermal lesion, single lesion
ICD-10-CM codes to consider for :
D49.2 Neoplasm of unspecified behavior of bone, soft tissue, and skin
Punch biopsy of skin (including simple closure when performed), single lesion
Incisional biopsy of skin (e.g. wedge), (including simple closure when performed), single lesion
D23.7Other benign neoplasm of skin of lower limb, including hip (need laterality)
L98.0 Pyogenic granuloma
D22.7Melanocytic nevi of lower limb, including hip (need laterality)
ENFD
D04.7Carcinoma in situ of skin of lower limb, including hip (need laterality)
D48Neoplasm of uncertain behavior of other and unspecified sites
L98.8 Other specified disorders of the skin and subcutaneous tissue
Punch Biopsy
CPT® 11104
L92Granulomatous disorders of skin and subcutaneous tissue
G64
Punch biopsy of skin (including simple closure when performed), single lesion
ICD-10-CM codes to consider : G60Hereditary and idiopathic neuropathy
G62Other and unspecified polyneuropathies
G63 Polyneuropathy in diseases classified elsewhere
Other disorders of peripheral nervous system
Nail Unit Biopsy
E10.4Type 1 diabetes mellitus with neurological complications
CPT® 11755
E11.4Type 2 diabetes mellitus with neurological complications
E13.4Other specified diabetes mellitus with neurological complications
ICD-10-CM codes to consider for nail unit biopsy:
Biopsy of nail unit (e.g. plate, bed, matrix, hyponychium, proximal and lateral nail folds)
D49.2 Neoplasm of unspecified behavior of bone, soft tissue, and skin
L60.3 Onychodystrophy
D48Neoplasm of uncertain behavior of other and unspecified sites
D23.7Other benign neoplasm of skin of lower limb, including hip
D22.7Melanocytic nevi of lower limb, including hip (need laterality)
855-422-5628
L98.8 Other specified disorders of the skin and subcutaneous tissue
6 | FPMA Footprints Download your copy today!
Bako Diagnostics
770-475-0528 info@bakodx.com
bakodx.com
PRACTICE ESSENTIALS™
InnovaMatrix® AC
Placental ECM
The first FDA-cleared placental-derived extracellular matrix medical device for wound management
Suitable for a range of wounds, including:*
• Diabetic ulcers
• Venous ulcers
• Partial and full-thickness wounds
• Tunneled/undermined wounds
*See package insert for full list of indications

• HCPCS code = A2001 Learn

• No product preparation required
• No tissue tracking or special storage requirements
• Effectively decellularized ECM can encourage the body toward the wound healing phase1,2
1. Keane, T. J., Londono, R., Turner, N. J., & Badylak, S. F. (2012). Consequences of ineffective decellularization of biologic scaffolds on the host response. Biomaterials, 33(6), 1771- 1781. doi:10.1016/j.biomaterials.2011.10.054
2. Sicari, B. M., Dziki, J. L., Siu, B. F., Medberry, C. J., Dearth, C. L., & Badylak, S. F. (2014). The promotion of a constructive macrophage phenotype by solubilized extracellular matrix. Biomaterials, 35(30), 8605-8612. doi:10.1016/j. biomaterials.2014.06.060
MKT-2023-0287 V01 Convatec Triad Life Sciences,
1770 Moriah Woods Blvd., Suite 18 Memphis, TN 38117
LLC
how InnovaMatrix®
can benefit
and
AC
your patients
practice by visiting InnovaMatrix.com. 901.333.6000
Let the Good Times Roll
 By Larissa Schmidt, DPM FPMA President
By Larissa Schmidt, DPM FPMA President
In following the Mardi Gras theme of this year’s FPMA Science & Management Symposium … “laissez les bons temps rouler!” SAM 2024 was a great springboard to the 2024-25 season ahead! It’s a theme as well as a perspective of energy to “let the good times roll.”
We are a great collective group of practitioners with vast talents spanning from our offices to the larger scale of association involvement. FPMA stands true in promoting podiatrists as the leading professionals of foot, ankle and lower extremity care throughout the state of Florida. We should be proud of our accomplishments and continue to strive for our members’ best interests in promoting our profession.
I have a unique perspective on podiatry dating back to the golden days of the 1950s. My grandmother, Dr. Lubow Pronchick, was affected by polio as a young adult and required reconstructive foot surgery for her deformities. Soon thereafter, she attended Temple University School of Chiropody, started her family and practiced not too far away in King of Prussia, Pennsylvania. As a young girl, I remember hearing about the support from her prestigious colleagues when her health was not the best. Some of our history’s greats were there humbly supporting her clinic when she and her patients needed them the most. In that sense, I believe we are at our best when working to promote each other.
It is an honor to carry on my family’s trade, and after 10-plus years of seeing the inner workings of this association, it’s a familiar, collegial feel. Beyond
the vast array of personal, practice and group benefits to which I hope you are familiar, FPMA has a lot of excitement to roll out in the coming year. Our goal is to support our fraternal variety pack of ages, ideas, interests and needs. I urge you to stay up to date via text, email and the FPMA website for information we are working hard to provide for you.
As our digital world has become more nuanced, FPMA has launched our complimentary Career Center, where members can connect as employers and future employees. This site also has portals to career-building insights and tips. So far, it has been a fruitful opportunity to connect physicians beyond interview opportunities at our SAM and Summer conferences. A large focus of FPMA is supporting our students, residents and fellows within our state. We are continuing to evolve in education and programming, but when it comes down to it, a valued need is a link to a future employer!
We also look forward to the upcoming FPMA Summer Conference this June in Bonita Springs, Florida. If you’re looking for a conference with esteemed educational content, a half-day lecture series, a variety of vendors, extracurriculars on-site and ample family entertainment, look no further.
It truly is a great time to connect, learn and unwind.
Another collective energy boost this year is happening with our legislative efforts. This year we sent the largest delegation to APMA’s House of Delegates in Washington, D.C. Within this event, we not only represented the Sunshine State with APMA endeavors, but on a larger scale, we secured one-on-one time with congressional appointments on Capitol Hill. Although this is a valued, thoughtfilled and productive opportunity, we’re not done there! This fall, we anticipate our formal Meet the Candidates Forum, where statewide politicians visit with our Executive Committee, Executive Board and Committee Members at Large to share thoughts and converse openly about our impact leading into the next legislative session.
As we continue to roll, I assure you there is much more happening that is not covered in this article. I’d like to encourage each of you to engage. With every perfect post-op X-ray, there is effort, experience and sweat behind it. You have a dedicated FPMA staff and leadership crew with good intentions on moving our profession forward. We want you to connect and take advantage of the opportunities your membership provides you, so “laissez les bons temps rouler!”
8 | FPMA Footprints PRESIDENT’S PERSPECTIVE

















































































Florida Podiatric Medical Association | 9 ELEVATE COMFORT, MINIMIZE EXPENSES, NO HIDDEN FEES, NO ANNUAL COSTS. EMPOWERING PODIATRY PROFESSIONALS DIGITAL CUSTOM ORTHOTICS W ITH EASYSNAP 3D THE SMART WAY! IN-HOUSE SOLUTION $10 AT JUST IN RAW MATERIALS sensormedica.us info@sensormedica.us Product distribuited by Sensor Medica: CALL US +1 (772) 530-3411 Our dedicated team offers 24-48 hour turnaround time for routine pathology cases. We offer mycology services and web-based reporting. When you call our lab, one of our customer service representatives will answer the phone. Contact us at 954-977-7959 or visit our website and read testimonials at lauderdalepathology.com G i v i n g Y o u A n E d g e i n t h e F i g h t A g a i n s t D i s e a s e These are just some of the ways we work to provide our clients with the highest level of care for their patients without compromise!
Milestone Members
Congratulations to our Milestone Members. We heartily thank you for your commitment to the profession of podiatric medicine — past, present and future.
25-YEAR MEMBERS
Constantine Barbounis
Craig Breslauer
Jaime Carbonell
Jose Concha
Michelle Detweiler
Jorge Dopico
Lisa Farrar
Robert Herbold
James Koon
Bradley Makimaa
David Morris
Marc Nathanson
Nicholas Przystawski
Robert Snyder
Paul Sommer
50-YEAR MEMBERS
Philip Adler
Meyer Buchbinder
Jerald Carmel
Howard Imanuel
Ellis Jacobs
Peter Mason
William McLay
Marc Novell
Ralph Reed
Lee Winthrop

New and Returning Members
Congratulations to our new and returning members for 2024.
Brevard Component
Sienna Day, DPM
Broward Component
Sharon Cuffy, DPM
Brian Finke, DPM
Bert Henkel, DPM
Aric Swancutt, DPM
Christopher Tveter, DPM
Central Florida Component
Phillip Calaj, DPM
Kale Meeks, DPM
Channa Williams, DPM
Charlotte Component
Julio Gutierrez, DPM
Collier Component
Karan Malani, DPM
Dade Component
Abir Zafar, DPM
East Central Florida Component
Maikhoi Pham, DPM
Lake-Sumter Component
Andrew Franklin, DPM
Samuel Mason, DPM
Lee Component
Michael Black, DPM
Ola El-Sheikh, DPM
Austin Hansen, DPM
North Central Florida Component
Nisha Krishnan, DPM
Michael Reed, DPM
Bruce Wolosky, DPM
Northeast Florida Component
Michael Monter, DPM
Palm Beach Component
Robert Clements, DPM
Brian Frenchman, DPM
Tommy McCain, DPM
Julio Ortiz, DPM
Martha Solomon, DPM
Pinellas Component
Todd Behrmann, DPM
Sharmila Das Wattley, DPM
Katie Ferraro, DPM
Jacqueline Lucke, DPM
Danielle Mustico, DPM
Bonnie Sanchez, DPM
Polk Component
Lya Basha, DPM
Nichole Didley, DPM
Shayne Erman, DPM
Trey Iakovidis, DPM
Louis Polizzi, DPM
St. Johns Component
Nicole Gortaire, DPM
Students and Residents
Broward Component
Claudia Barnett, DPM
Valentina Bocanegra
Leiah Burgess
Anthony Masih
Dade Component
Sarah Bergmann
Rafael Betancourt
Samuel Birman
Luke Drouillard
Richard Hannig
Rachael Juszczak
Yasemin Kahveci
Zaib Latif-Jangda, DPM
Chloe Leverson
Lisa Mesa
Heather Negru
Chukwudumebi Nwachokor
Mansi Patel
Paxtan Perry
Alejandro Pujol Quintana
Faraazullah Quadri
Seth Riker
Andrew Shkolnik
Tasmia Unnoor
Ethan Warnock
Hernando Component
Malisha Pahari, DPM
Joel Santana, DPM
Manasota Component
Carol Paez
Palm Beach Component
Andrew Immler, DPM
10 | FPMA Footprints MEMBERSHIP
25 YEARS 50YEARS
FPMA Component Presidents 2024
BREVARD
Dr. David M. Schweibish
2020 N. Hwy. A1A, Ste. 101 Indian Harbour Beach, FL 32937
(321) 777-4774, 777-4788 (FAX) david311@me.com
BROWARD
Dr. Adam J. Oxios 17013 Pines Blvd. Pembroke Pines, FL 33028 (954) 450-4200 aoxios@gmail.com www.thebcpma.com
CENTRAL FLORIDA
Dr. Timothy J. Miller
3701 Avalon Park W. Blvd., Ste. 225 Orlando, FL 32828 (631) 312-7581 timothymiller63@gmail.com
CHARLOTTE
Dr. Andre M. Williams
352 Milus St. Punta Gorda, FL 33950 (941) 626-1804, 347-7271 (FAX) awilliam33dpm@yahoo.com
COLLIER
Dr. Jenny W. Adams 3435 Pineridge Rd., Ste. 102 Naples, FL 34109 (239) 260-7476, 260-7608 (FAX) dradams239@gmail.com
DADE
Dr. Lucita M. Clersaint 58 NE 167th St. Miami, FL 33162 (305) 944-1610, 944-1670 (FAX) lmclersaint@aol.com www.miamidadepod.com
EAST CENTRAL FLORIDA
Dr. Macalee Harlis Jr. 1680 SE Lyngate Dr., Ste. 201 Port St. Lucie, FL 34952 (772) 210-3339, 404-7819 (FAX) macaleeharlisjrdpm@gmail.com
EMERALD COAST
Pending
GULF CENTRAL FLORIDA
Dr. Bryan A. Spooner 1866 Buford Blvd. Tallahassee, FL 32308 (850) 894-1820, 656-9293 (FAX) bas@tlhpodiatry.com
HERNANDO
Dr. John E. Baker 6317 Sealawn Dr. Spring Hill, FL 34607 (352) 597-2223, 597-2061 (FAX) jebaker@tampabay.rr.com
HILLSBOROUGH
Dr. Zenobia A. Bowen 6632 Glencoe Dr. Temple Terrace, FL 33617 (813) 261-0382 zeebowen@aol.com
INDIAN RIVER
Dr. Amberly C. Paradoa 3735 11th Cir., #201 Vero Beach, FL 32960 (772) 299-7009, 562-7138 (FAX) ircpma2018@gmail.com
LAKE-SUMTER
Dr. Chad C. Watkins 914 E. Dixie Ave. Leesburg, FL 34748 (352) 805-4317, 805-4298 (FAX) watkins207@comcast.net
LEE
Dr. Michael J. Wilkins 5238 Mason Corbin Ct., #102 Fort Myers, FL 33907 (239) 936-5400, 936-9572 (FAX) mikewilkinsdpm@gmail.com
MANASOTA
Dr. Louis S. Giannone 411 Commercial Ct., Ste. G Venice, FL 34292 (941) 412-3000, 412-3005 (FAX) l.s.giannone@gmail.com
NORTH CENTRAL FLORIDA
Dr. Diana E. Rogers 7915 SW 85th Ter. Gainesville, FL 32608 (954) 401-2610 drogers@fpma.com
NORTHEAST FLORIDA
Dr. Jorg A. Bober 1409 Kingsley Ave., Ste. 9G Orange Park, FL 32073 (904) 637-0037, 639-6017 (FAX) julbober@gmail.com
NORTHWEST FLORIDA
Dr. Mark S. Isenberg
4311 Bayou Blvd., #A8 Pensacola, FL 32503 (727) 639-1973, (866) 258-9993 (FAX) msidpm@thefootdoctors.org
PALM BEACH
Dr. Xavier A. Sanchez
8645 N. Military Trl., Ste. 501 Palm Beach Gardens, FL 33410 (561) 838-7250, 619-2928 (FAX) xaviersanchezdpm@gmail.com
PINELLAS
Dr. Robin M. Katz
6600 34th Ave. N.
St. Petersburg, FL 33710 (727) 343-2244, 347-0777 (FAX) rkatz4@gmail.com
POLK
Dr. James E. Koon
635 First St. N. Winter Haven, FL 33881 (863) 294-0670 cypresspodiatry@aol.com
ST. JOHNS
Dr. Craig S. Schein
508 Sebastian Sq.
St. Augustine, FL 32095 (904) 824-0869 podno2@msn.com
VOLUSIA
Dr. Andrew B. Green
21 Hospital Dr., Ste. 170 Palm Coast, FL 32164 (386) 586-7373, 586-7346 (FAX) gatorpod1@gmail.com
Florida Podiatric Medical Association | 11 MEMBERSHIP
GULF CENTRAL NORTH CENTRAL EMERALD COAST NORTHWEST HERNANDO LAKE-SUMTER HILLSBOROUGH MANASOTA DADE BROWARD PALM BEACH EAST CENTRAL INDIAN RIVER POLK CENTRAL VOLUSIA ST. JOHNS NORTH EAST COLLIER LEE CHARLOTTE PINELLAS BREVARD
In Memoriam
Dr. Christopher N. Chiodo passed away on November 13, 2023, at the age of 80. Dr. Chiodo was a member of FPMA for 54 years. He practiced in Palm Beach County for 50 years. He started his surgical career in Broward County with Dr. Henry Merritt prior to Palm Beach County allowing podiatrists on staff. He was instrumental in gaining hospital privileges in Palm Beach County and
was on the staff of Bethesda Memorial Hospital and JFK. He loved podiatry, his employees and his patients. Dr. Chiodo is survived by his wife, Linda, three children, five grandchildren and two great-grandchildren.
Dr. Bradley C. Haves passed away on November 13, 2023, at the age of 62. Dr. Haves received his podiatric degree from the Barry University School of
Podiatric Medicine in 1990. He was later recognized by his alma mater when he received the Alumni of the Year award. Dr. Haves was a member of FPMA for 25 years. He served as FPMA president in 2009 and was the former president of the FPMA Dade and Broward components. Dr. Haves had his own practice in Miami, Florida. He is survived by his wife, Milly, his mother, and a son and daughter.

12 | FPMA Footprints MEMBERSHIP
Lapiplasty® Just Got Even Better. Introducing To learn more, visit Lapiplasty.com Pat. treace.com/patents ©2024 Treace Medical Concepts, Inc. All rights reserved. M2486B Designed to deliver the stability of a titanium locking plate* with the speed and compression of a staple.

Check Out the FPMA Career Center!
In November, 2023 FPMA launched its new Career Center, which is available to FPMA members seeking career opportunities as well as FPMA members seeking new employees.
FPMA members can easily access the FPMA Career Center via a link on the FPMA website at FPMA.com. Simply click on the Careers tab at the top of the page and select the FPMA Career Center link.
<Career Center Name>
Check out FPMA's newest member benefit today!
Job Seekers: Employers:
l EMAIL your job directly to job seeking professionals
l PLACE your job in front of our highly qualified members
l SEARCH our resume database of qualified candidates
l MANAGE jobs and applicant activity right on our site
l LIMIT applicants only to those who are qualified
l FILL your jobs more quickly with great talent
l POST multiple resumes and cover letters or choose an anonymous career profile that leads employers to you
l SEARCH and apply to hundreds of fresh jobs on the spot with robust filters
l SET UP efficient job alerts to deliver the latest jobs right to your inbox
l ASK the experts advice, get resume writing tips, utilize career assesment test services, and more
https://fpma.careerwebsite.com
Florida Podiatric Medical Association | 13 MEMBERSHIP

A Young Physician’s Insight on Employment
 By Jemaar Graham, DPM, FACPM, CWSP
By Jemaar Graham, DPM, FACPM, CWSP
I was told podiatrists eat their young. This was largely the motivation for me to practice with an orthopedic group for the past five years.
My first associate position after residency was with a small podiatry group. Responsibilities included independently managing a busy clinic, hospital rounding, taking the lead in a wound care clinic, and training podiatry residents and students. After nine months, I was approached with discussions of contract nonrenewal. There was a lack of transparency concerning the revenue I had generated while suggesting that I had not worked hard enough. It was then that the echoes of wisdom from my upperclassmen came to mind. I took a leap of faith and applied for a position that was initially listed as temporary and required a minimum of one year of post-residency experience.
Five years later, my time working as a podiatrist within an orthopedic practice has, for the most part, been rewarding, autonomous and insightful to an alternative approach. Occasionally I have been asked by students and residents about my experience working as a podiatrist within an orthopedic practice.
Here are three initial responses that come to mind:
1. Read the Fine Print
The orthopedic group I joined had a history of well-trained podiatrists predating my arrival. Nevertheless, I found multiple instances where there were third-party contracts that would exclude equal pay and rights to DPMs. For example, a contract with a local hospital to treat uninsured/ underinsured patients made a stipulation that I, as a podiatrist, was not authorized to dispense CAM walking boots, while my MD and DO colleagues could. Clearly, this was impractical and a detriment to patient care. Surprisingly it was not known among the management and other physicians in the group. With the support of my group bringing awareness to this outdated policy, it was put to rest and equal terms were agreed upon. In another instance, changes to fee schedules that would seemingly benefit the group were found to bring a reduction in allowable fees for DPMs. Once again, it was necessary to establish alternative parameters to ensure that I was provided with my maximum earning potential. Even in 2024, there remains much work to be done so the parity of podiatry exists in every space we occupy.
This experience has reminded me of the necessity of assuming nothing. Trust, but verify, and be keenly aware of how podiatrists may be uniquely impacted.
2. Code Switch
I delight in the spectrum of perspectives patients present regarding what it
means to be a podiatrist. In southwest Florida, many seasonal residents seek out podiatrists specifically because they understand fully our focus of training and expertise. At other times, patients have stated directly to me that they “will never see another podiatrist again” because of poor prior experiences. Seemingly they assume that I am an orthopedic surgeon due to my practice affiliation. In those instances, my association with an orthopedic group provides reassurance of my subspecialization and ability to treat their pathology in a more effective way than what was previously offered. Though “DPM” is appropriately noted in all advertisements, my title as “Foot & Ankle Surgeon” appears to be more palatable to laypeople.
Another situation in which I code-switch is when a new patient has been dissuaded from surgery due to a “matter-of-fact” type of orthopedic surgeon. They delight in seeing a podiatrist as an alternative option. They will likely appreciate that as podiatrists, we are equally skilled in nonsurgical and surgical options. In these cases, I find it helpful to provide alternative conservative treatment options to earn a patient’s trust. My willingness to be creative and take the additional time to explain foot and ankle pathology in practical terms is frequently rewarded with positive feedback. Taking this approach results in patients eventually returning to my office requesting to proceed with surgery because they’ve noted a distinction in the approach.
14 | FPMA Footprints
MEMBERSHIP
I encourage students and residents to be confident in their skillset while having situational awareness. The literature and trends in orthopedic medicine and podiatry offer valuable insight on a hybrid approach to patient care.
3. Ride the Wave
Inevitably there will be those who are stuck in the past, with a limited view of our role in the podiatry profession. But take heart — as podiatrists continue to receive better surgical training and more podiatry schools become affiliated with larger multidisciplinary institutions, the medical community at large will be forced to acknowledge how far we have progressed. I expect to see more shared workspaces between podiatric surgeons and orthopedic surgeons in the coming years. We have more in common than in difference.
In the same way that nurse practitioners and physician assistants continue to push for more autonomy and better pay, podiatry must do the same. I have overwhelmingly received respect from
my orthopedic colleagues for my unique skillset. After training, our medical colleagues are more concerned about what problems we can solve and the revenue we can generate, than our degree. If approached with the right perspective, podiatry offers a dynamic approach to patient care and revenue offerings within the tide of orthopedic surgery. I am often reminded, “Where there are scalpels, there will be wounds.” As a profession, no one is better trained in wound care than podiatrists. I encourage new graduates to initiate discussions with orthopedic groups in the area where they desire to work, regardless of previous podiatrist employment. The ability to provide insight into wound care techniques, ancillary revenue streams and expanding an established referral base is an obvious asset.
I encourage new podiatry graduates to strategically develop their toolbox of treatment options to the utmost of their skillset and scope of practice. Maintaining an autonomous entrepreneurial mindset within the
I encourage new podiatry graduates to strategically develop their toolbox of treatment options to the utmost of their skillset and scope of practice. Maintaining an autonomous entrepreneurial mindset within the context of a larger group can reap great benefits.
context of a larger group can reap great benefits.
My hope is that in the future, greater fellowship between orthopedic surgeons and podiatrists will advance both disciplines, provide better patient care/ access and elevate public opinion of podiatry.



Florida Podiatric Medical Association | 15
© 2024 PediFix, INC. FPM524 To order or get more information… Call: 800-424-5561 Email: info@pedifix.com Contact: your favorite supplier Fight Fungus, Reinfection & Recurrence Don’t Ignore Their Shoes The Most Advanced Shoe Sanitizer, Ever Kills Fungus & Bacteria That Cause Onychomycosis, Athlete’s Foot, Odor, More Buy 3, Get 1 FREE! Mention Code: FPM524 Offer Expires 7/1/24 Use Dispense Recommend

Insurance Report Update: Navigating Challenges and Advocacy Efforts
 By Mark S. Block, DPM
By Mark S. Block, DPM
Since my previous article, and as expected, new provider challenges have emerged. As in the past, my latest insurance report will contain a detailed update of issues and material that should be of interest to FPMA members. The following are some specific and timely items I felt would be appropriate for this publication.
CMS/OIG SNF Recoupment Initiative
In November, I corresponded with First Coast Service Options (FCSO) regarding the Centers for Medicare & Medicaid Services/Office of Inspector General Skilled Nursing Facility (CMS/OIG SNF) initiative targeting payment recoupment based on the place of service (POS). The burden on providers is extreme, and economic challenges persist.
Coordinated efforts with APMA are underway to address this issue. Following FCSO’s directives in a timely manner cannot be overemphasized to avoid additional penalties. As previously advised, providers receiving recoupment letters should contact their malpractice carriers if they have a policy rider that addresses these issues.
For more information and guidance, visit the APMA members’ site:
www.apma.org/practicingdpms/ content.cfm?itemnumber=57366.
Key Issues I Communicated to FCSO
CMS/FCSO Recoupment
Request
Based on POS:
• POS 32 – “Nursing Facility”
• POS 31 – “Skilled Nursing Facility”
Providers, especially those serving nursing homes, received overpayment letters triggered by a misclassification of POS. This led to refund requests, creating economic challenges. Some key concerns raised include:
1. The difficulty of segregating a patient classified as SNF when a provider had been treating the patient for several encounters under a different classification. Often the patient was in the “same bed,” but the designation/SNF had changed. For the provider, their service had not. Additionally, the physical location of
the treatment in several cases was the same as during previous encounters.
2. In some cases, the facility did not clearly delineate the change of classification and/or since the designation was recently changed, some of the documentation or records were not updated or did not clearly indicate the status.
3. Technically, a provider would have to research the status of a patient to determine if the designation (POS) had changed since the last encounter.
4. A substantial economic burden was placed on providers to comply with the requested refund.
Many providers were frustrated that reimbursement was at a lower level merely due to a POS change in classification. The services they were providing did not differ based on the change in designation. Additionally, the patient often was in the same
16 | FPMA Footprints INSURANCE AFFAIRS
bed at the same facility regardless of POS designation.
In summary, the following challenges were encountered:
1. Difficulty segregating patients classified as SNF.
2. Lack of clear documentation on classification changes.
3. The economic burden on providers for compliance.
FCSO Response
“Upon review of the provider’s letter and claim/invoice examples an OIG audit was conducted and determined the provider should have been paid under POS 31 (SNF) in place of POS 32 (nursing home). Therefore, the OIG audit concluded an overpayment was made to the provider based on the place of service (POS) review. Please refer the provider to the appeal rights located on page 4 of the letter if they disagree with the recoupment decision. Of note, the provider has 30 days from




the date of the recoupment letter to submit an appeal….”
Positive Change to ‘Surgical Treatment of Nails’ Policy
In a recent “FPMA Insurance Alert,” I shared a “win.”
The following was stated:
The updated current “Surgical Treatment of Nails” policy has presented challenges to providers and, ultimately, our patients. The word “ recently ” has been changed to “ previously .”
After presenting concerns and substantiating the rationale for a change in the policy requirements, FCSO subsequently agreed to my requested recommended edit. This positive editorial change to the policy will eliminate another problematic area that could have resulted in denials or recoupment.


Details on this issue can be found in the above referenced FPMA Insurance Alert from November 28, 2023. I, along with APMA, have been addressing this problematic policy and advocating for change that needs to align with “clinical realities.”
I continue to address problematic areas on behalf of the membership and profession. Every effort is made toward a positive outcome. I strive to provide timely updates and guidance, and to address emerging issues before they become a burden to the profession.
To access a detailed archive of past and present issues, log in to the FPMA website at www.fpma.com, click on the “DPM Resources” tab at the top of the website, click on the “Insurance News/Medicare Updates” link, and select the FPMA Insurance Report links.





Florida Podiatric Medical Association | 17
 By Chris Hansen, FPMA Lobbyist
By Chris Hansen, FPMA Lobbyist
Florida’s Future Legislative Leaders
Every two years, Florida has a change in its legislative leadership. In an election by their peers, a new speaker of the House of Representatives and president of the Senate are selected. What most people don’t know is that these leadership positions are decided years ahead of time. As an example, the speaker of the House for 2029 has already been decided. However, this is not a sure thing. A lot depends on future political developments: the same majority party being in control, future leaders winning their ensuing elections and no internal power struggle within the party.
All of the above scenarios have come to pass over the last 30 years. This is our system, and even with occasional disorder, it has worked pretty well for the last half-century. As we prepare for another election this November, I thought it would be helpful to introduce the future leaders in Florida government.
Speaker of the House – Florida House of Representatives

Committee Assignments Rules Committee, Chair Appropriations Committee
Biographical Information
City of Residence: Miami
Occupation: Attorney
Spouse: Stephanie Perez
Children: Camila Lucia Perez, Matias Daniel Perez
Education: Florida State University, BA, 2009; Loyola University New Orleans College of Law, JD, 2012
Born: June 22, New York City, New York
Religious Affiliation: Catholic
Legislative Service
Elected to the Florida House of Representatives on September 26, 2017; subsequently reelected

Committee Assignments Health Care Appropriations Subcommittee, Chair Appropriations Committee Joint Legislative Budget Commission Rules Committee
Biographical Information
City of Residence: Fleming Island
Occupation: Attorney
Spouse: Gayle Simpson Garrison
Children: Mary Beth, Jane
Education: Samford University, BA, International Relations, 1998; University of Illinois College of Law, JD, 2001
Born: November 13, 1976, Peoria, Illinois
Moved to Florida: 2001
Religious Affiliation: Anglican Recreational Interests: American history, music, reading, running
Legislative Service
Elected to the Florida House of Representatives in 2020; subsequently reelected
18 | FPMA Footprints LEGISLATIVE UPDATE
Rep. Daniel Perez R-Miami 2025-26
Rep. Sam Garrison R-Fleming Island 2027-28

Committee Assignments
Infrastructure Strategies Committee, Vice Chair
Education & Employment Committee
Education Quality Subcommittee
Energy, Communications & Cybersecurity Subcommittee
Health Care Appropriations Subcommittee
Insurance & Banking Subcommittee
PreK-12 Appropriations Subcommittee
Biographical Information
City of Residence: Lakeland Occupation: Teacher
Senate President – The Florida Senate

Committee Assignments
Select Committee on Resiliency, Chair
Fiscal Policy
Governmental Oversight and Accountability
Health Policy
Joint Legislative Budget Commission
Judiciary
Biographical Information
City of Residence: Wauchula
Occupation: Agribusiness owner
Spouse: Missy Albritton

Committee Assignments
Banking and Insurance, Chair
Agriculture, Vice Chair
Appropriations Committee on Agriculture, Environment, and General Government
Finance and Tax
Fiscal Policy Judiciary Rules
Biographical Information Occupation: Insurance and investments

Committee Assignments
Commerce and Tourism, Chair
Appropriations Committee on Transportation, Tourism and Economic Development, Vice Chair
Appropriations Committee on Agriculture, Environment and General Government
Banking and Insurance
Fiscal Policy
Select Committee on Resiliency
Transportation
Spouse: Charles T. Canady
Children: Julia Canady, Anna Canady
Education: Florida State University, BS, Elementary Education, 1995; University of South Florida, MA, Special Education, 2014
Born: July 22, 1973, Lakeland, Florida
Religious Affiliation: Presbyterian Recreational Interests: Gardening, hiking, reading, traveling
Legislative Service
Elected to the Florida House of Representatives in 2022
Children: Rebecca, Joshua, Ryan
Education: Florida Southern College, BS, Business/Citrus, 1990
Born in: Lakeland, Florida
Religious Affiliation: Christian Recreational Interests: Spending time with family, reading
Legislative Service
Elected to the Senate in 2018; subsequently reelected Senate Majority Leader, 2023-24
House of Representatives, 2010-18
Spouse: Sandra Woodard
Children: Ansley, Austin
Grandchild: Houston
Education: Florida State University, BS, 1978
Born in: Bradenton, Florida
Religious Affiliation: Baptist Recreational Interests: Golf, quail hunting
Legislative Service
Elected to the Senate in 2020; subsequently reelected House of Representatives, 2010-2018
Biographical Information
City of Residence: Panama City
Occupation: Business owner
Spouse: Brittany Fishel
Children: Merritt, Tripp, Emery
Education: Auburn University, 2011
Born in: Panama City, Florida
Religious Affiliation: Christian
Recreational Interests: Fishing, hunting
Legislative Service
Elected to the Senate in 2022
House of Representatives, 2014-2022
Florida Podiatric Medical Association | 19
Rep. Jennifer Canady R-Lakeland 2029-30
Sen. Ben Albritton R-Wauchula 2025-26
Sen. Jim Boyd R-Bradenton 2027-28
Sen. Jay Trumbull R-Panama City 2029-30

Employing a Nurse Practitioner in Florida – an Update

 By Diana Rogers, DPM, and Jason D. Winn, Esq., FPMA General Counsel
By Diana Rogers, DPM, and Jason D. Winn, Esq., FPMA General Counsel
As with our allopathic and osteopathic colleagues, there are divided opinions regarding the incorporation of NPs into our practice models. Many feel it is direct competition and a threat, while others see the potential for practice growth with lower overhead. Having practiced in a state that allows a podiatrist to supervise and collaborate with NPs, I can attest to the qualitative and quantitative benefits for both the practice and patient care.
Several years ago, the Medical Group Management Association (MGMA) reported that orthopedic surgeons that utilized a non-physician provider (NPP) increased their yearly salaries by approximately $100,000. Furthermore,
Nurse practitioners (NP) are rapidly changing the face of the health care model. With a shortage of primary care physicians, lack of access to care, rising health care costs, and the need to see more patients, states are transitioning to full practice authority for NPs. To date, 30 states allow NPs to have full practice authority, which means they can perform the full scope of practice without a supervising or collaborating physician.
the overhead associated with an NP can be significantly lower than adding another physician, and approximately 70 percent of the highest-performing groups employed NPPs. From a podiatric perspective, having an NP can certainly increase patient numbers, improve quality of care, reduce wait times and, when utilized, improve efficiency in the perioperative period.
The Florida Podiatric Medical Association (FPMA) regularly receives inquiries regarding a podiatric physician’s ability to hire an NP. Every state has written within their laws which physicians can supervise or collaborate with an NP. As Florida is now one of the states that has passed
legislation allowing for NPs to practice autonomously, what does that mean for us as podiatric physicians? I recently asked FPMA’s General Counsel, Jason Winn, Esq., to answer some of FPMA’s most frequently asked questions and provide a review of the current laws.
As a Florida DPM, can I supervise or hire a nurse practitioner?
In Florida, nurse practitioners, who meet the requirements of autonomous nurse practitioner, may engage in autonomous practice only in primary care practice, including family medicine, general pediatrics and general internal medicine, as defined by Board of Nursing Rule (F.S. 464.0123(3) (a)(1)(2023)). As the term implies, an
20 | FPMA Footprints LEGAL
autonomous nurse practitioner does not require a supervising physician and is not required to work in collaboration with a physician.
Also, the scope of practice is for primary care only . For example, an autonomous practitioner cannot perform brain surgery. They can, however, treat the common cold, occasional gout, and many other primary care conditions that can be treated without referral to a specialist.
Can I supervise a nonautonomous nurse practitioner/one who isn’t an autonomous nurse practitioner? No.
Florida law only allows for DPMs to supervise or direct a medical assistant as defined in §461.0155, F.S. A podiatric physician who supervises a medical assistant is governed by §458.3485, F.S. There is a list of duties a medical assistant can perform under the direct supervision of a licensed podiatric physician. It is the responsibility of the supervising podiatric physician to ensure competence in the field, ensure adherence to the ethical and legal standards of professional practice, recognize and respond to emergencies, and demonstrate professional characteristics.
Well, if I can’t supervise an autonomous nurse practitioner, nor a nurse practitioner, can I employ one at my practice?
Yes and No.
First, a medical office may employ an autonomous nurse practitioner to perform primary care services (they would be an employee of the practice). They would not be under the supervision of any physician in the practice, nor outside of the practice. They would work autonomously but work as employees. The employer would not be able to direct the autonomous nurse practitioner in any health care decisions and/or actions with patients. An autonomous nurse
practitioner could also be employed as an independent contractor for the practice. The practice could then provide primary care services through this autonomous nurse practitioner.
Secondly, you may not employ a nonautonomous practice nurse in your practice unless your practice also has an MD or DO. The MD/DO would act as the supervising physician, and as a podiatric physician you would have no authority to direct/supervise or interact with the practical nurse for patient care.
In conclusion, if you are considering adding an NP to your practice model, you must seek the advice of a specialized health care attorney who is knowledgeable on this subject.
The FPMA is dedicated to assisting our members in all aspects of practice. We
are listening to you and continue to follow trends in health care that can potentially impact our membership.
LEGAL DISCLAIMER
The information contained herein is provided to you “AS IS,” does not constitute legal advice, and is governed by our Terms and Conditions of Use. We make no claims, promises, or guarantees about the accuracy, completeness, or adequacy of the information.
The FPMA, its employees, agents, or others that provide information on or through this will not be liable or responsible to you for any claim, loss, injury, liability, or damages related to your use of this information. Seeking the advice of competent legal counsel is recommended.
If you are considering adding an NP to your practice model, you must seek the advice of a specialized health care attorney who is knowledgeable on this subject.

Florida Podiatric Medical Association | 21
www.fpma.com CONNECT WITH US
Complications Resulting in Amputation –Reducing the Risk for You and Your Patients

As you could probably surmise, amputations are a leading factor in malpractice suits against podiatrists. So, how do you reduce the risk that a complication will result in amputation? And if amputation is necessary, how can you reduce the risk of a lawsuit being filed?
 Article courtesy of FPMA Corporate Affinity Partner PICA
Article courtesy of FPMA Corporate Affinity Partner PICA
In many instances, patients who end up with an amputation have multiple comorbidities such as diabetes and vascular disease, which lead to nonhealing or infected wounds. There could be a post-operative surgical complication, injury or other factor that leads to amputation. Regardless of the cause, amputation significantly impacts the patient’s quality of life.
It is important to effectively manage complications by addressing the patient’s condition and the potential for complications before they occur. And recognizing complications when they do occur so you can appropriately respond to complications is also critical.
Reduce Risk by Taking a Complete Patient History
One of the first steps in risk reduction is to obtain and document an appropriate history and physical exam prior to the initiation of treatment. Does the patient have other conditions that need to be co-managed with other specialists? Does the patient have risk factors for a potential complication? Is a patient’s hypertension or diabetes under control? Do not just take the patient’s word that all is well. Consider obtaining copies of the patient’s lab work and other physicians’ patient records.
Obtain and document the patient’s social history. The patient’s social history is also extremely important in ascertaining potential risks and determining the best course of treatment for that patient. Does the patient smoke? Is the patient able to comply with instructions? For example, does the patient have adequate support
at home? Can the patient afford to be off work for an extended period? Is the patient responsible for caring for small children or aging parents?
It is important to document both normal and abnormal physical exam findings. If abnormal findings are present, document your rationale for your decision to refer or not refer for further evaluation. Collaborating with vascular, cardiology, infectious disease, endocrinology and other specialists can help reduce the risk of complications and achieve better outcomes for your patients.
Education and ExpectationSetting with the Patient (and Their Family!)
Patient (and family) education is key in reducing the risk of complications leading to amputations. Explain the patient’s condition, treatment options and risk factors. Explain why you are referring the patient for further
22 | FPMA Footprints

testing. Explain the importance of following instructions and what may happen if instructions are not followed. Make sure the patient has realistic expectations regarding treatment and the outcome of treatment.
Documentation of all patient education and instructions in the patient’s record is a valuable risk reduction tool in the event a lawsuit is filed. You may have properly informed and instructed your patient, but if it is not documented,
It is important to effectively manage complications by addressing the patient’s condition and the potential for complications before they occur.
it is your word against the patient’s word that they were not informed. If you are performing surgery, document your medical justification for surgery, procedure options and your rationale for selection and obtain the patient’s written informed consent.
Pay Attention When Complications Arise and Act Fast
Recognize a complication when it first arises. Is a wound not healing as expected? Does the patient have a loss of vascularity? Is an infection not responding to antibiotics? Promptly document the abnormal findings and inform the patient.
Document your rationale for addressing the complication. Assess and document the patient’s compliance with instructions. Documentation of the patient’s noncompliance is another valuable risk reduction tool in the event of litigation. If the patient
is noncompliant, try to work with the patient (and family) to address the reasons for noncompliance. Inform the patient of the risks of noncompliance, including the risk of amputation. Promptly refer the patient to an appropriate specialist for further workup if appropriate.
Should a patient eventually undergo an amputation, documentation of your assessments, rationale for treatment decisions, patient education and prompt response to complications are key in reducing the likelihood a lawsuit will be filed or will greatly aid in your defense should a lawsuit be filed.
PICA is proud to have FPMA’s endorsement as the preferred provider of medical malpractice insurance for podiatrists. Please visit www.picagroup.com to learn more about the benefits of being a PICA policyholder or to request a free, no-obligation quote!
Florida Podiatric Medical Association | 23





24 | FPMA Footprints Visit PCCSoleMarketing.com or Call Randy Rosler (917) 572-5088 Take Your Orthotics Profit To The NEXT LEVEL ★ Email Campaigns To Promote Orthotics ★ Educate With In-Office Marketing Materials ★ Social Media Digital Orthotics Library ★ lncrease Your Orthotics Revenue Dispense More Orthotics TM Connection Podiatry Content Make This Revision Last with Compression That Doesn’t Quit. Gap Recovery¹ Continuous staple compression overcomes space between the fusing bones (i.e. gapping) caused by natural osteoclast resorption. Note: For recognized manufacturer, refer to the product label. Please refer to the instructions for use for a complete list of indications, contraindications, warnings and precautions. To order (USA): 800-523-0322 www.depuysynthes.com 1. CrossRoads Extremity Systems Report: CrossRoads Extremity Claims Substantiation Memo. CRE QMS 2022 Ref:ER22-0021. Apposition¹ The average contact surface area of the MTP joint is 38mm. Typical ag screws reduce this contact area by approximately 25%. Speed¹ Compared to lag screw preparation, inserting a staple is more efficient and can drastically reduce operating time. MTP Staple Compression Plates Quarter-Page Ad.indd 1 3/26/24 10:01 AM PEACE OF MIND STARTS WITH: Estate Planning Lawsuit Prevention License Protection Tax Reduction Did you miss Gary 's presentation or want to learn more? You can schedule a time to meet with Gary and learn all about how we can protect your assests and save you money on taxes (800) 375-2453 | legallymine com | 1337 E 750 N Orem UT 84097 -Estate Planning: What are the best tools to protect my family if something happens to me? -Asset Protection: Essential tools to ensure that your practice and family's assets are protected from the threat of lawsuits -Tax Strategies: Learn tax strategies that will work for you and put money back in your practice and family's pocket Free risk assessment available: visit this link to schedule a follow up call with Gary ht tps://legallyminewebinar as me/FollowUp




Clinically proven results www.swiftusa.com

hello@swiftusa.com



By combining the power of the American Podiatric Medical Association data registry, an award winning EHR with podiatric blueprints built in, and practice management, NextGen® Office is built for podiatry practices of the future. Learn more at nextgen.com/podiatry
Florida Podiatric Medical Association | 25
isn’t
85%+ Efficacy <1% “Swift
just a treatment, it’s a cure.”
Finally, an answer Dr. Robert Conenello, DPM Orangetown Podiatry No wounding, downtime, or at-home care
STAY A STEP AHEAD WITH AN APMA-supported EHR solution © 2024 NXGN Management, LLC. All Rights Reserved. NextGen is a registered trademark of NXGN Management, LLC. All other names and marks are the property of their respective owners. ©2024 Modernizing Medicine, Inc. All rights reserved. *2023 Black Book™ I have gained hours of time back in my day. GREGG NEIBAUER, DPM ALPINE FOOT & ANKLE CLINIC MISSOULA, MT YOUR PEERS ARE GAINING AN EDGE. EHR + PM + PATIENT COLLABORATION + ANALYTICS + RCM WHAT’S THEIR SECRET? Experience the podiatry solutions your peers voted #1* modmed.com/footprints | 561.710.FEET
Choose Function Over Fusion

RECAP
By Becky Reese, FPMA Public Affairs/Website Coordinator

SAM 2024 returned to the Hyatt Regency Orlando and ran from Wednesday, January 24, through Sunday, January 28, 2024. In addition to podiatric physicians, separate conference programs were offered for podiatric medical assistants and initial/recert podiatric X-ray assistants.
The FPMA General Membership Meeting (GMM) and annual election of officers took place the afternoon of Wednesday, January 24, after a short day of scientific lectures. Members of the 2024 FPMA Executive Committee were sworn in during the GMM and include:
• Dr. David M. Schweibish, President-Elect
• Dr. Adriana P. Strimbu, Vice President
• Dr. Liana G. Seldin, Treasurer
• Dr. Diana E. Rogers, Secretary
• Dr. Alissa B. Zdancewicz, Immediate Past President
The 20th Annual SAM Residents Forum took place during SAM 2024 on Saturday, January 27. A total of seven resident case presentations were submitted by representatives from residencies throughout the state. The three winning case presentations included:
• First Place: Hector Santiago, DPM, of Bethesda for the entry titled “CAR Trauma to TAR Solutions”
• Second Place: Andrew Immler, DPM, of HCA Florida Westside for the entry titled “Extensor Tendons & Nerve Laceration with Surgical Repair”
• Third Place: Tiffany Cerda, DPM, of HCA Florida Mercy for the entry titled “Nailed It, Management Challenges in Charcot Neuroarthropathy”
The Seventh Annual SAM Poster Competition took place during the conference as well. A total of 34 posters were submitted by podiatric residents and fellows, and the posters were displayed outside the SAM 2024 exhibit hall for all SAM attendees to view. The five winning posters included:
• First Place: Josh Ekladios, DPM, for the entry titled “Iatrogenic Medial Malleolar Fracture and Stress Fracture Considerations in Total Ankle Joint Replacement: A Multicenter Retrospective Study”
• Second Place: Liset Perez, DPM, for the entry titled “Synovial Sarcoma of the Foot”
• Third Place: Jacob Ivey, DPM, for the entry titled “Exertional Compartment Syndrome”
• Fourth Place: Jimmie Watkins, DPM, for the entry titled “The Romash Test – Reliable Tool or Dusty Relic?”
• Fifth Place: Donovan Perry, DPM, for the entry titled “Word to the Weiss”
FPMA held the annual Student Quiz Bowl Competition in the SAM 2024 exhibit hall on Saturday, January 27. SAM 2024 Quiz Bowl winners included:
• First Place: London Elrod
• Second Place: Tailor Foreman
• Third Place: Hajar Ouassari
FPMA congratulates the winners of all these competitions and is proud to support young practitioners in striving for podiatric education and advancing the profession.
Additional events that took place during SAM 2024 included a Women
26 | FPMA Footprints
CONFERENCE NEWS
in Podiatry Breakfast, Ultrasound Workshop, Stop the Bleed training program, Non-CECH Breakfast & Learns, and a Non-CECH Lunch & Learn. The Florida Board of Podiatric Medicine held a meeting during SAM 2024 on Friday, January 26.
On Saturday, January 27, SAM attendees enjoyed the FPMA Annual Presidential Reception, which took place on-site at the Hyatt Regency Orlando. The theme of the reception, like the conference, was Mardi Gras and attendees enjoyed posing for pictures with Mardi Gras props, refreshments and dancing. Dr. Larissa Schmidt, FPMA’s new president, was sworn in during the event.
The FPMA annual awards ceremony was also held on Saturday, January 27, during the FPMA Annual Presidential Reception. The following recipients were honored for their outstanding contributions, continued leadership and dedicated service:
• Jason Winn, FPMA General Counsel/Lobbyist and Chris Hansen, FPMA Lobbyist – FPMA President’s Award
• Dr. Timothy Miller – Young Practitioner of the Year Award
• Dr. Andre Williams – Podiatric Physician of the Year Award
The SAM 2024 exhibit hall was open Thursday through Saturday during the conference, with 125 exhibitors participating. This year’s exhibit hall had a new, more spread-out layout to improve traffic flow. FPMA also provided food bars for the two-and-a-half-hour SAM attendee lunch break in the exhibit hall. Non-CECH Learning Labs were also provided by several exhibitors for SAM attendees. FPMA would like to thank all SAM 2024 sponsors and exhibitors for their support.
Thanks also go out to FPMA Convention Committee members, including General Co-Chairs Dr. Dennis Frisch and Dr. Robert Frimmel, Dr. Samir Vakil, Dr. Andrew Belis, Dr. Joseph Agostinelli, Dr. John Goggin, Dr. John Baker and Dr. Andre Williams.
The FPMA CEO/executive director and staff, who worked hard organizing SAM 2024 during the months leading up to the event as well as on-site during the conference, included Karen Lambert, Becky Reese, Gin Grand, Andy JeanBaptiste and Dee Muller. They were assisted by Doug Lambert, Sarah
Lambert, FPMA member volunteers and Barry student volunteers.
We look forward to seeing you at SAM 2025, which will once again take place at Disney’s Coronado Springs Resort in Lake Buena Vista, Florida, on January 29 -February 2, 2025.



Florida Podiatric Medical Association | 27






28 | FPMA Footprints CONFERENCE NEWS Conference Photos








Florida Podiatric Medical Association | 29
2024 Exhibit Hall
SAM








30 | FPMA Footprints Presidential Reception CONFERENCE NEWS


Florida Podiatric Medical Association | 31 Office: (786) 534-2555 Fax: (786) 703-7745 WWW.FLINTERVENTIONAL.COM


32 | FPMA Footprints CONFERENCE NEWS


Florida Podiatric Medical Association | 33
Keeping the Passion in Practice
 By Imani Graham, Student Doctor
By Imani Graham, Student Doctor
I am currently a second-year student at Barry University School of Podiatric Medicine (BUSPM). Having been born and raised in Indianapolis, Indiana, I grew up with a love of sports, basketball in particular. It wasn’t until I was playing a game of summer basketball in middle school that I found my true passion, shaping the rest of my future. During this particular game, I landed on an opposing player’s foot and immediately felt an excruciating pain in my right ankle. After being rushed to the emergency room and meeting with an orthopedic surgeon, I knew that I wanted to become a doctor and get my patients back on their feet as my doctor did for me.
Throughout college, I had to balance collegiate basketball and pre-med academics. However, I had the opportunity to secure internships at local hospitals each year of undergrad. During these, I realized I solely wanted to specialize in the lower extremity. Thankfully, during my junior year I had the opportunity to join a webinar that featured Dr. Ebonie Vincent from the show My Feet Are Killing Me , which I had grown to love. After this webinar, I did extensive research about what the field of podiatry had to offer and was quite impressed. From sports medicine to diabetic wound care to dermatology, the list of subspecialties in the field went on and on. I shared the news with my family, and they
were very supportive of my decision to change the avenue I wanted to pursue post-graduation.
I ultimately decided to attend BUSPM because of the opportunities available for me outside of the classroom, in addition to academia that could shape me into a better overall physician. Performing foot care at homeless shelters, coaching Special Olympics basketball and participating in local community initiatives made my passion for podiatry and giving back to my community grow more than I could ever imagine. I have come to realize that many of my classmates have become one-track minded with grades. School has become a competition to most rather than a steppingstone to reach a goal they once dreamed of.
As a former athlete, I love healthy competition. However, this competitive environment has made people believe they cannot have a life outside of school or participate in things they love outside of the numerous exams, additional assignments to complete, and labs we are required to attend. Being in the classroom for many years before embarking on clinical rotations and getting hands-on experience can be very tiresome, but there are many avenues to get involved in that help reinforce the passion we all started off with. Between volunteer initiatives through our schools, community programs readily seeking people to lend a helping hand, and all the possibilities offered in each subspecialty of podiatry, the opportunities are limitless. In addition to being great scholars, students need to be willing to give themselves a rest and adventure out to explore all that is available to them.
Attending conferences is a great way to spark interest in future endeavors. FPMA’s Science & Management Symposium is an amazing opportunity that many Barry students should experience. During my time at SAM, it was so fulfilling to talk to Barry alumni and discuss all the great achievements they have accomplished thus far in their practices. There were also great lecturers discussing many pertinent topics in the field, which inspired me to look more deeply into current research. Although SAM can be viewed as an event for physicians to obtain continuing education credits, it is quite informational for students. The “Dinner and Learn” event with Dr. Steve McClain was a student session where topics that we had questions about were discussed. There was even a Quiz Bowl Competition for students to participate in.
The opportunity to attend SAM helped me visualize what the end goal can look like for me, and I hope more students attend to gain the same experience. Regaining our passion for practicing can ultimately impact the relationships we have with our patients in the future. I have always been a firm believer that people gravitate to those who love the work they do and get involved in their communities. These attributes show in the work you perform and the care you provide to those around you. Patients want a physician who is not only committed to providing exceptional care to ensure they get back on their feet but who is also personable and sees them beyond their feet. We must be diligent about getting ourselves back on our own two feet and keeping the passion instilled within us to keep propelling us forward to the end goal.
34 | FPMA Footprints CONFERENCE NEWS
Attending SAM 2024: A Student’s Perspective
 By Malachi Brown, Student Doctor
By Malachi Brown, Student Doctor
I am currently in my second year at Barry University School of Podiatric Medicine (BUSPM). Originally from Miami, Florida, I’m a blend of Nicaraguan and Jamaican heritage and happen to be left-handed. For my undergraduate studies, I attended Florida International University (PawsUp!). Outside of the academic realm, I have the honor of holding the position of president-elect 2023-24 for the Florida Podiatric Medical School Association. My journey into podiatry began during my undergraduate years, when I worked part time in a clinic, participated in clinical service trips and shadowed various specialties. Podiatry emerged as the perfect convergence of disciplines I found intriguing, including orthopedics, dermatology, vascular, surgery and more. The field not only catered to my clinical interests but also opened doors to research, academia, leadership, community service, entrepreneurship and more.
Attending the FPMA Science & Management Symposium (SAM 2024)
proved to be a pivotal experience for me. SAM is designed to provide podiatric physicians with continuing education on the latest developments in foot and ankle health and surgery and practice management through seminars and workshops. Offering a glimpse into the broader spectrum of podiatry beyond the classroom, SAM exposes students to advanced topics that extend beyond our academic years, satisfying our curiosity about clinical practice. The symposium provides hands-on experiences in surgical skills, allowing us to familiarize ourselves with techniques we might not encounter until later in our education. Additionally, it serves as a platform for networking, enabling us to forge connections that offer both professional and personal benefits.
My recent attendance at SAM 2024 was nothing short of phenomenal. I had the privilege of presenting two research posters alongside my classmates, focusing on case studies provided by our clinical faculty. Volunteering at the event provided me with an insider’s view of the intricate planning that goes into such a significant gathering, allowing me to meet FPMA staff and Executive Board members. A highlight of the
weekend was the “Dinner and Learn” event hosted by McClain Laboratories. This included a captivating lecture by Dr. Steve McClain on podiatric pathological case reviews, emphasizing the collaborative approach between podiatric physicians and dermatopathologists in diagnosing dermatological conditions. The student session, facilitated by Dr. David Schweibish, featured lectures from various physicians and delved into topics of specific interest to students. Attending this session, which offered insights not covered in traditional coursework, proved to be one of my favorite days of the conference.
As we look toward the future of podiatric medicine and surgery, it is clear that young practitioners, residents and medical students play a crucial role. Conferences like FPMA’s SAM Symposium are integral to our medical education, contributing to knowledge expansion, networking, skill development and overall professional growth. These experiences enable us to immerse ourselves in the dynamic and evolving landscape of medicine, fostering a commitment to lifelong learning and excellence in our chosen field.
Florida Podiatric Medical Association | 35

Please use a separate form for each registrant. Some events may require separate fees. All communications regarding the FPMA 2024 Summer Conference coming from FPMA or exhibitors who purchase or capture registrant data on-site will be sent to the contact information provided below.
Attendee Information
PLEASE NOTE:
• Educational topics are subject to change as the program schedule develops.
• All registration fees must be paid in full, in advance.
• Payment must be received with your registration form.
• Registrations without complete payment will not be processed.
Cancellation Policy: Cancellation requests must be made in writing and received by May 24, 2024 Refunds will be processed after the event. No refunds available for no-shows or cancellations received after May 24, 2024
*Changes in registration, including changes in attendance preference after May 24, 2024, and no-shows are subject to a $125.00 fee.
36 | FPMA Footprints
June 7 - 9, 2024 Physician Registration Register by May 24, 2024 Visa MasterCard American Express Check Enclosed Card Number Cardholder Name Cardholder Signature Billing Address (if different from above) Hyatt Regency Coconut Point Resort and Spa 5001 Coconut Road Bonita Springs, FL 34134 Room rate (double, single occupancy): $219.00 For reservations, call 1-800-233-1234 To make reservations on-line, access the link at https://www.fpma.com/fpma_2024_summer_conference.php Reservation Deadline: May 14, 2024 admin@fpma.com 850-224-4085 FAX: 850-681-0899 City State Zip Phone (cell) License No. APMA No. Last Name Address Phone (daytime) Email (required to register) Additional Information Per the Americans With Disabilities Act of 1990, check here if you have a disability and may require accommodations to participate fully. Please provide details, and/or list any food allergies/dietary restrictions, on the line below: Guest Badge (Check to reserve) Guest badges are limited to one per attendee and are only for immediate family members aged 18+. Badges are required for access into the conference Exhibit Hall. All guests must be accompanied by a registered Summer Conference attendee. Receipt of Guest badge does not entitle holder to conference food and beverage. Registration Fees and Payment FPMA Member FPMA Life Member APMA Member Non-FPMA/ Non-APMA Member $200 $175 $299 $399
FPMA 2024 Summer Conference
$0 $125 $249 $349 By 4/26/24 After 4/26/24 First Name Degree Exp. Date Student $50 $25 Please make checks payable to Florida Podiatric Medical Society, Address: 3375-F Capital Circle NE, Ste. 201, Tallahassee, FL 32308 City State Zip Hotel Information CVV
* *

Florida Podiatric Medical Association | 37 FPMA 2024 Summer Conference June 7 - 9, 2024 X-Ray Assistant Registration Register by May 24, 2024 City State Zip Phone (cell) Attendee Information Last Name Physician/Employer Name Address Phone (daytime) Assistant Email (ALL information will be sent to this email address) PXA License # Per the Americans With Disabilities Act of 1990, check here if you have a disability and may require accommodations to participate fully. Please provide details, and/or list any food allergies/dietary restrictions, here: Registration Fees and Payment The X-Ray Assistant program consists of an 8-hour course on June 8, 2024 and an examination (for Initial Licensure ONLY) on June 9, 2024. X-Ray Assistant Registration Initial course for certification by the Florida Board of Podiatric Medicine Recertification: Florida Board of Podiatric Medicine PLEASE NOTE: • Educational topics are subject to change as the program schedule develops. • All registration fees must be paid in full, in advance. • Payment must be received with your registration form. • Registrations without complete payment will not be processed. • The X-Ray Assistant program is limited to 90 attendees. Visa MasterCard American Express Check Enclosed CVV Card Number Cardholder Name Cardholder Signature Billing Address (if different from above) Please make checks payable to: Florida Podiatric Medical Society Address: 3375-F Capital Circle NE Suite 201 Tallahassee, FL 32308 Cancellation Policy: Cancellation requests must be made in writing and received
May 24, 2024.
be
the event. No refunds
cancellations
after May 24,
Hotel Information Hyatt Regency Coconut Point Resort and Spa 5001 Coconut Road Bonita Springs, FL 34134 admin@fpma.com 850-224-4085 FAX: 850-681-0899 First Name Exp. Date 1st Assistant (By 4/26/24) $175 $175 2nd Assistant $160 $160 3rd Assistant $145 $145 Any Assistant (After 4/26/24) $190 $190
Room rate (double, single occupancy): $219.00 For reservations, call 1-800-233-1234
make
php Reservation Deadline: May
4 City State Zip
by
Refunds will
processed after
available for no-shows or
received
2024
Please use a separate form and separate email address for each registrant.
To
reservations on-line, access the link at https://www.fpma.com/fpma_2024_summer_conference.
14, 202

38 | FPMA Footprints CONFERENCE NEWS

IT’S TIME FOR A CONVERSATION WITH YOUR PATIENTS LEARN MORE AT JUBLIARX.COM JUBLIA is a trademark of Ortho Dermatologics’ affiliated entities. ©2020 Ortho Dermatologics’ affiliated entities. JUB.0051.USA.20

Florida Podiatric Medical Association 3375-F Capital Cir. NE, Ste. 201 Tallahassee, FL 32308
