ILUMETRI ® is indicated for the treatment of adults with moderate to severe plaque psoriasis who are candidates for systemic therapy. 2
Efficacy
ILUMETRI® offers early and long-term control and proven effectiveness in skin treatment including sensitive areas*2-4
Wellbeing
ILUMETRI® restores patients’ wellbeing from week 16 up to week 52 in line with general population averages7,9
Flexibility and safety
ILUMETRI® is the only anti-IL-23 giving the flexibility to individualise therapy whilst maintaining an acceptable safety profile1,5,6
Could any of your patients benefit from ILUMETRI® and our enhanced value support services?
*Sensitive areas such as scalp, nails, genitals and palmo-plantar2-4
1. ILUMETRI® SmPC. Almirall. 2. Thaçi D, Piaserico S, Warren RB, et al. Br J Dermatol. 2021;185(2):323–334. 3. Thaçi D, Gerdes S, Jardin K, et al. Dermatol Ther.2022;12(10):2325-2341. 4. Magnolo N, et al. Presented at DDG Congress, Mar 1-3 Wiesbaden, Germany, 2024. P030. 5. Tremfya® Summary of Product Characteristics. Janssen. 6. Skyrizi® Summary of Product Characteristics. AbbVie. 7. Mrowietz U, Augustin M, Sommer R. Abstract presented at 25th World Congress of Dermatology, Singapore, 3–8 July, 2023. 8. Dauden E, Mrowietz U, Sommer R, et al. Presented at 51st National Congress AEDV, 22-25 May; Madrid, Spain. 2024. Current SPA version: 166/2374/199. 9. EuroFound “European Quality of Life Survey - Data visualisation. Eurofound https://www.eurofound.europa.eu/data/european-quality-of-life-survey. Last accessed August 2024.
ILUMETRI® (tildrakizumab) PRESCRIBING INFORMATION
Please consult the Summary of Product Characteristics (SmPC) before prescribing ILUMETRI® is available as 100 mg and 200 mg solution for injection in pre-filled syringes. Active Ingredient: Each pre-filled syringe contains 100 mg or 200 mg of tildrakizumab in 1 mL or 2 mL. Tildrakizumab is a humanised IgG1/k monoclonal antibody produced in Chinese Hamster Ovary (CHO) cells by recombinant DNA technology. Also contains 0.5 mg/mL polysorbate 80 (E 433). Indication: ILUMETRI is indicated for the treatment of adults with moderate to severe plaque psoriasis who are candidates for systemic therapy.Dosage and Administration: The recommended dose of ILUMETRI is 100 mg by subcutaneous injection at weeks 0, 4 and every 12 weeks thereafter. In patients with certain characteristics (e.g. high disease burden, body weight ≥ 90 kg) 200 mg may provide greater efficacy. Consideration should be given to discontinuing treatment in patients who have shown no response after 28 weeks of treatment. Some patients with initial partial response may subsequently improve with continued treatment beyond 28 weeks. Injection sites should be alternated. Elderly: No dose adjustment is required. Renal or hepatic impairment: No dosage recommendations can be made. Paediatric population: No data available. Contraindications, Precautions and Warnings: Contraindications: Hypersensitivity to the active substance or to any of the excipients listed in SmPC section 6.1. Clinically important active infection, e.g. active tuberculosis. Precautions: To improve traceability always record the batch number of the administered product. ILUMETRI has the potential to increase the risk of infections. If a patient develops a serious infection, the patient should be closely monitored and treatment with ILUMETRI should not be administered until the infection resolves. Exercise caution in patients with a chronic infection or a history of recurrent or recent serious infection. Instruct patients to seek medical advice if signs or symptoms of an infection occur. Patients should be evaluated for tuberculosis (TB) prior to initiation of treatment and monitored for signs and symptoms of active TB during and after treatment. In patients with a history of latent or active TB, consideration for anti-TB therapy should be given. Discontinue
use if a serious hypersensitivity occurs. All appropriate immunisations should be completed prior to start of treatment with ILUMETRI. If a patient has received live viral or bacterial vaccination it is recommended to wait at least 4 weeks prior to starting treatment with ILUMETRI. Patients treated with ILUMETRI should not receive live vaccine during treatment and for at least 17 weeks after treatment. This medicine contains polysorbate. Polysorbates may cause allergic reactions. Fertility, pregnancy and lactation: Women of childbearing potential should use effective methods of contraception during treatment and for 17 weeks after treatment. As a precautionary measure, it is preferable to avoid the use of ILUMETRI during pregnancy. A decision must be made whether to discontinue breast-feeding or to discontinue/abstain from ILUMETRI therapy taking into account the benefit of breast-feeding for the child and the benefit of therapy for the woman. The effect of ILUMETRI on human fertility has not been evaluated. Adverse Reactions: Very common (≥1/10): Upper respiratory tract infections. Common (≥1/100 to <1/10): Headache, gastroenteritis, nausea, diarrhoea, injection site pain, back pain. Immunogenicity: In pooled Phase 2b and Phase 3 analyses, 7.3% of tildrakizumab-treated patients developed antibodies to tildrakizumab up to week 64. Of the subjects who developed antibodies to tildrakizumab, 38% (22/57 patients) had neutralizing antibodies. This represents 2.8% of all subjects receiving tildrakizumab.
Please consult Summary of Product Characteristics for further information.
Legal Category: Ireland: Subject to prescription which may not be renewed (A).
United Kingdom & UK/NI: POM Price & Pack: United Kingdom 100 mg pre-filled syringe - £3,241; 200 mg pre-filled syringe - £3,241 Ireland 100 mg pre-filled syringe Price to wholesaler 200 mg pre-filled syringe Price to wholesaler
Further information available from: Almirall Limited, Harman House, 1 George Street, Uxbridge, Middlesex, UB8 1QQ, UK.
Date of Revision: 08/2024 Item code: UK&IE-ILU-2400045
UK-Adverse events should be reported. Reporting forms and information can be found at MHRA https://yellowcard.mhra.gov.uk or search for MHRA Yellow Card in the Google Play or Apple App Store. Adverse events should be also reported to Almirall Ltd. Tel. 0800 0087 399
IE-Adverse events should be reported. Reporting forms and information can be found at HPRA Pharmacovigilance, Website: www.hpra.ie. Adverse events should be also reported to Almirall Ltd. Tel: +353 1800849322
Dr Hannah Saunders
ichthyosis vulgaris and introducing the emollient circle of choice
Julie Van Onselen
Could teledermatology in the community aid and reshape the future of NHS care?
Rebecca Ramdeen-Thomas, Kurt Ayerst Professional development
Entering dermatology as a newly qualified nurse
Dawn Holt
On becoming a research nurse in dermatology: Challenges and achievements
Rebekah Higgins
Is it a dermatological panacea?
Reflections on dermatological emergency preparedness: Implementing a dedicated emergency trolley
Eimear Duff, Sheila Ryan
Skin of colour and dermatology nursing: A specialised focus – part one
Modupe O Soji-Adeyemo
the Pharmacist
making dietary changes improve disease severity in psoriasis?
Ensuring acne patients avoid a spot of bother
Rod Tucker, Simone Calvert
new in the world of research?
Rod Tucker Wellbeing for the workforce
Fighting for change in India Christina Raj
Setting sail to improve wellbeing Sandra Lawton
trek up Kilimanjaro and journey of self-discovery Lucy Moorhead
news
DN
British Dermatological Nursing Group
Editorial
Jackie Tomlinson
Chair of the Editorial Board
Dermatology Clinical Nurse Specialist, Addenbrooke’s Hospital, Cambridge University Hospitals Foundation Trust
Polly Buchanan
Clinical Editor
Community Dermatology Nurse Specialist, NHS Fife pauline.buchanan2@nhs.scot
Consultant Dermatologist, University Hospitals of Derby and Burton NHS Foundation Trust
Julie Brackenbury
Aesthetic Nurse Practitioner, JB Cosmetic, Bath
Ivan Bristow
Podiatrist and Associate Professor, Southampton
Sara Burr
Senior Lecturer, Centre of Postgraduate Medicine and Public Health, University of Hertfordshire and Community Dermatology Specialist Nurse/Clinical Lead Community Skin Integrity Team, Norfolk Community Health and Care NHS Trust
Elfie Deprez
PhD student and Psoriasis Nurse Specialist, University of Ghent, Belgium
Steven Ersser
Professor of Nursing and Dermatology Care and Head of Department of Nursing Science, Bournemouth University
Senior Lecturer, Postgraduate Medicine, University of Hertfordshire and Dermatology Specialist Nurse, Dermatology Clinic Community Services, Cambridgeshire
Kathy Radley
Senior Lecturer, School of Life and Medical Sciences, University of Hertfordshire and Dermatology Nurse Specialist, Dermatology Community Clinic Services, Cambridgeshire
Sue Rice
Clinical Development Manager, CD Medical
Alison Schofield
Head of Education, Tissue Viability Nurse Consultant at NHS Pioneer Wound Healing and Lymphoedema centres.
Karen Stephen
Dermatology Specialist Nurse, NHS Tayside
Delia Sworm
Trainee Advanced Clinical Practitioner – Skin Cancers (Oncology), St Luke’s Cancer Centre, Royal Surrey NHS Foundation Trust
Rod Tucker
Community Pharmacist/Researcher with a Special Interest in Dermatology, East Yorkshire
Dermatological Nursing (ISSN 1477-3368) is published by the BDNG, 82 Antrim Street, Lisburn BT28 1AU Tel: 02892 793 981. www.bdng.org.uk
All rights reserved. No part of this publication may be reproduced, stored or transmitted in any form or by any means without the prior written permission of the BDNG. Opinions expressed in articles are those of the authors and do not necessarily reflect those of the BDNG or the editorial/advisory board. Advertisements have no influence on editorial content or presentation.
The advertisements in this journal are for a UK audience only.
Adex Gel has been shown to improve atopic eczema from moderate to mild in 2 weeks without corticosteroids1
Summary of trial results
In a recent trial of children with moderate atopic eczema, conducted in NHS GP practices (to reflect real-life settings), the mean disease severity score (SCORAD) improved significantly:
• from 37.14 (moderate atopic eczema) at baseline
• to 22.56 (mild atopic eczema) after 2 weeks
• and to 18.48 (mild atopic eczema) after 4 weeks, per protocol analysis of 41 children.
Adex Gel
Bridges the gap between plain emollients and topical corticosteroids.
Adex Gel is an emollient with an ancillary anti-inflammatory, nicotinamide 4%, to help reduce inflammation.
Adex Gel can be used continuously, for as long as necessary, all over the body including on the face, hands and flexures. Available on NHS prescription and suitable for patients aged 1 year+.
In addition, the mean children’s dermatology life quality index score (CDLQI) improved significantly from 9.3 (moderate effect on child) at baseline, to 3.7 (small effect on child) after 4 weeks.
Application of Adex Gel in the trial
Three times daily, for 4 weeks, instead of usual emollient or as the first-line treatment for moderate atopic eczema, in both scenarios, without supplementary use of any oral or topical steroids or immunomodulators.
Adex Gel has been shown to be an effective treatment for moderate atopic eczema in children in a real-world setting.
SCORAD is a tool used in clinical trials to assess atopic dermatitis severity based on disease area, intensity and subjective symptoms (itch and sleeplessness). The CDLQI is designed to measure the impact of any skin disease on the lives of children.
Product name: Adex™ Gel. Key ingredients: Isopropyl myristate 15%, liquid paraffin 15%, nicotinamide 4%. Uses: Highly moisturising and protective emollient with an ancillary anti-inflammatory medicinal substance for the treatment and routine management of dry and inflamed skin conditions such as mild to moderate atopic dermatitis, various forms of eczema, contact dermatitis and psoriasis. Package sizes: 100g tube and 500g pump pack. Further information is available from: Dermal Laboratories Ltd, Tatmore Place, Gosmore, Hitchin, Herts, SG4 7QR, UK. ‘Adex’ is a trademark.
Adverse Events/Incidents should be reported. Reporting forms and information for the UK can be found at yellowcard.mhra.gov.uk, and for the Republic of Ireland at www.hpra.ie. Adverse Events/Incidents should also be reported to Dermal.
SCORAD, SCORing Atopic Dermatitis. CDLQI, Children’s Dermatology Life Quality Index.
Reference: 1. Gallagher J. et al. Evaluation of a nicotinamidecontaining emollient for moderate atopic eczema in paediatric patients:
A prospective, multi-centre GP study reflecting real-life settings. Data presented at the Annual Meeting of the Austrian Society of Dermatology and Venereology (ÖGDV), November 2024, Graz, Austria.
Reflecting on reflective practice
Polly Buchanan
Ihave been thinking quite a bit about ‘reflective practice’ recently 1 Not only was I asked to provide five reflective accounts for my NMC revalidation, but I also experienced a difficult consultation with a patient where the outcome was not what either of us had anticipated. My subsequent reflective learning on that occasion was profound as I considered the event, my feelings, and the social situation.
We hear a lot about ‘reflection’ in the caring professions and all the supposed benefits, but do we actually reflect enough? How can we make time to reflect? Or is it just a paper exercise for the NMC?1
Certainly, reflective practice is encouraged in every health and social care environment, as it fundamentality aims to keep us (and patients/clients) safe. It is not just about reflecting on negative aspects but also considering positive events and achievements. The most significant thing within any reflective exercise is to be analytical about experiences, actions, emotional impact and feelings.
This is important in healthcare, as we work with colleagues caring for other individuals. Our work can be fast paced at times, stressful and emotional, whether you are a lone worker or a team member. Therefore, taking time to reflect regularly as an individual, or within a group, fosters support, care and compassion for us and others.
The benefits of reflective practice are many, such as refinement of knowledge, new knowledge, better understanding of oneself, increased motivation, understanding specific goals and rationale
in decision making, enhancing compassion and empathy for self and others, as well as improving the quality of care provided. Reflection can be anticipatory (undertaken before an event) or carried out during and/or after an event. What is important is the understanding that different situations may warrant different types and levels of reflection.
So, how can we incorporate reflection into our daily practice? Reflection can be formal or informal. It can be at a surface level (superficial) or more thorough (deeper) and it always follows six key steps. The ‘Reflective Cycle’ as described by Gibbs2 includes:
1. Description
2. Feelings
3. Evaluation
4. A nalysis
5. Conclusion, and 6. Action Plan.
How these steps are undertaken is very individual. Some people like to thoughtfully consider a narrative in their head, others may wish to write a journal or complete a specific reflective template. Some may use reviews and articles to shape their reflection, e.g. a ’Patient’s Voice’ article in the Dermatological Nursing journal. Some may wish to share with a confidant, a colleague or within a group.
Group reflections can be beneficial for teams working together. Schwartz Rounds3 have come into vogue in healthcare environments to provide mutual support for team members. These rounds are regular gatherings of clinical and non-clinical team members meeting to understand the rewards and
challenges of working within healthcare settings. Staff can feel the benefit of being supported in their roles having time and space to reflect.
Evidence3 suggests staff have greater insight and appreciation of other team members’ roles, feel less anxious or stressed and less lonely or isolated. They focus on the relational aspects of providing care and help reduce the hierarchies between staff. If you think implementing a Schwartz Round into your working environment would support the team, you can find out more at www.transformationpartners.nhs.uk and searching for ‘What is a Schwartz Round’.
In conclusion, reflective practice is here to stay in healthcare environments. It is not just a paper exercise for the NMC. How we undertake reflection is up to each individual, but it is vitality important that we do reflect for our ongoing professional development and quality improvement. Reflection can greatly enhance our emotional intelligence, empathy and compassion which will directly influence our approach to care.
References:
1. NMC Reflective Practice Guidance Sheet. Available at: www.nmc.org.uk [last accessed February 2025]
2. University of Edinburgh. Gibb’s Reflective Cycle: Reflection Toolkit. Available at www. reflection.ed.ac.uk [last accessed February 2025]
3. Health & Care Professions Council. Reflective Practice: Schwartz Rounds. Available at www. hcpc-uk.org [last accessed 27 Feb 2025].
Polly Buchanan is the Clinical Editor of Dermatological Nursing.
From young atopic eczema to elderly varicose eczema
Dermol Cream knocks out Staph. and soothes very dry and itchy skin conditions
• Rich hydrating emollient cream with antimicrobials and soap substitute
• Preferred by the majority of patients to their previously used emollients for relief of itching, relief of dryness and cosmetic acceptability1
*Image used with permission of DermNet NZ www.dermnetnz.org.
Uses: An antimicrobial emollient cream for the management of dry and pruritic skin conditions, especially eczema and dermatitis, and for use as a soap substitute.
Directions: Adults, children and the elderly: Apply direct to the dry skin or use as a soap substitute.
Contra-indications, warnings, side effects etc: Please refer to SPC for full details before prescribing. Do not use if sensitive (especially generalised allergic reaction) to any of the ingredients or if there is a possible history of allergic reaction to a chlorhexidine compound. In the unlikely event of a reaction, stop treatment. Local skin reactions are very rare (<1/10,000 based on spontaneous reporting). Reactions have been observed occasionally when used excessively as a leave-on application in the anogenital area. When breast-feeding, if use on the nipples is necessary, apply sparingly and after feeds. Take care to avoid
Proven activity against Staph. aureus including MRSA, 2 FRSA, 2
Mupirocin-resistant Staph. aureus, 3 as well as, Pseudomonas aeruginosa, 4
Streptococcus pyogenes5 and Malassezia furfur 6 when tested in vitro.
slipping in the shower or bath, when using as a soap substitute. Keep away from the eyes.
Instruct patients not to smoke or go near naked fl ames. Fabric (clothing, bedding, dressings etc) that has been in contact with this product burns more easily and is a potential fi re hazard. Washing clothing and bedding may reduce product build-up but not totally remove it.
Package quantities, NHS prices and MA number: 100g tube £3.08, 500g pump dispenser £7.19, PL00173/0171.
Adverse events should be reported. Reporting forms and information can be found at yellowcard.mhra.gov. uk. Adverse events should also be reported to Dermal.
References: 1. Data on File. Dermal Laboratories. January 2005; 2. Gallagher J. et al. Routine infection control using a proprietary range of combined antiseptic emollients and soap substitutes –their effectiveness against MRSA and FRSA. Poster presented at 18 th EADV Congress, October 2009, Berlin, Germany;
3. Gallagher J. and Rosher P. Topical antiseptic products –Antimicrobial activity against mupirocin resistant Staphylococcus aureus. Data presented at the 16 th Annual Maui Derm for Dermatologists, January 2020, Maui, USA; 4. Gallagher J. and Rosher P. Infected wounds – in vitro activity of topical antiseptic products against P. aeruginosa. Poster presented at the 23 rd EADV Congress, October 2014, Amsterdam, The Netherlands; 5. Gallagher J. and Rosher P. Evaluation of the bactericidal activity of two antiseptic emollient formulations against Streptococcus pyogenes. Poster presented at the 73 rd Annual Meeting of the American Academy of Dermatology, March 2015, San Francisco, USA; 6. Gallagher J. & Rosher P. In vitro antimicrobial activity of two topical antiseptic products against Malassezia furfur. Poster presented at the 10 th EADV Spring Symposium, May 2013, Cracow, Poland.
Just cosmetic? Accessing healthcare for disfigurements
Dr Hannah Saunders
As an alliance of charities supporting people with disfigurements and facial differences, we hear a lot about healthcare from our community. Many people with facial differences rely on, and are tremendously grateful for, the medical care they receive. But we often hear of frustrations too, about a feeling that people with conditions and injuries affecting appearance (rather than bodily function) are deprioritised and misunderstood on several levels within the health service.
In a 2017 survey by the charity Changing Faces1 about the experiences of people with disfigurements, 19.8% of respondents felt that their healthcare professionals had no understanding of the psychosocial impact of living with their condition, and a further 38.9% reported very little understanding from their healthcare teams. Moreover, 77% of respondents had experienced an NHS worker making an assumption about them because of their appearance.
So, why do some patients with visible differences feel misunderstood and ‘low priority’ in the medical world? One reason relates to perceived unfairness in treatment decisions. Earlier this year, NICE refused to recommend the drug ruxolitinib to treat vitiligo on NHS prescription. The reasons cited for its rejection included cost-effectiveness and uncertain quality of life benefits,2 but many in the community were devastated by the decision, and an appeal is believed to be pending.
Another reason for disillusionment with healthcare interactions is the terminology used. In the words of one
survey respondent “My GP is useless and classes my condition as cosmetic. It’s all cosmetic and we don’t do cosmetic.”3 This terminology may be felt as trivialising the reality of living with a visible difference, because many people associate the word ‘cosmetic’ with elective beauty treatments, rather than restorative medical treatment for an illness or injury.
The word ‘disfigurement’ is difficult for many too, but not everyone agrees on the best terminology to use instead. Best practice, where possible, is to reflect the wording which that individual chooses to describe their difference, but there are clearly challenges doing this in a medical context.
We believe that opportunities do exist to improve the healthcare experience for people with facial differences, and consultation with the community is urgently needed as a first step. We need greater recognition within the health sector about what it’s like to live with a facial difference. This is dependent on working together as an alliance to put the lived experiences of the patient groups we represent at the centre, and to ensure our advocacy efforts are recognised by the health sector.
Many years of research and community accounts confirm that people with disfigurements often face extreme social barriers – including being stared at and abused in the street, bullied at school, discriminated against at work and during recruitment, and trolled online. Just last month, there were media reports of a man with a facial difference being asked to leave a London restaurant because of his face, and sadly this is not an isolated
incident.4 Many people – although not all – also suffer psychologically. An understanding of common day-to-day realities – and a willingness to listen to individual experiences – is needed to ensure that people feel understood by their healthcare teams.
Training frontline healthcare workers about terminology may be helpful too, to put an end to the use of phrases such as ‘it’s just cosmetic’. Greater availability of psychosocial support for people with facial differences may also be needed, to help the many people in this community who experience high levels of anxiety, depression or social phobia or who struggle to adjust to a change in appearance.
As a charity, we offer a training programme to inform organisations about the lived experience of visible difference and how they can become more reflective and inclusive of this community.
Our training is evidence-led and run by community members. Do reach out to us at info@faceequalityinternational.org to find out more.
References:
1. Changing Faces, Disfigurement in the UK, 2017, p32
2. Hurrell A. Appeal update: First licenced vitiligo drug won’t be available on NHS. Vitiligo Society 2024. Available at: https:// vitiligosociety.org/vitlife/first-licencedvitiligo-drug-wont-be-available-on-nhs/ [last accessed March 2025]
Dr Hannah Saunders is Head of Policy and Education at the charity Face Equality International
Fight infected dermatoses with the POWER OF 3
FOR SKIN IRRITATED BY INFECTED DERMATOSES
Recommend Nystaform HC Cream – now available and ready to prescribe
Reference: 1. Perspectus Global; omnibus survey of 1,000 adults; July 2023. Job code: 1/NYS/12/2404/970. Date of preparation: April 2024. Abridged Prescribing Information Nystaform HC Cream. See Nystaform HC Cream Summary of Product Characteristics (SmPC) prior to prescribing. Presentation: Cream containing nystatin (100,000 I.U./g), chlorhexidine hydrochloride (1.0% w/w) and hydrocortisone (0.5% w/w) for topical administration. Indications: Treatment of infected dermatoses where fungal (particularly monilial) and/or bacterial infections are present. Posology and Method of Administration: Adults and children: For topical application only. Apply to the infected area 2-3 times daily. Treatment should be for a maximum of 7 days. If the condition does not improve within seven days, return to doctor. Contraindications: Known sensitivity to the active substances, especially those with a history of chlorhexidine-related allergic reactions. Tuberculous lesions of the skin. Special Warnings and Precautions for Use: For external use only. Avoid contact with the eyes. If sensitivity occurs or if new infection appears, discontinue use and institute alternative therapy. Cetostearyl alcohol may cause local skin reactions (e.g. contact dermatitis). Chlorhexidine is known to induce hypersensitivity, including generalised allergic reactions and anaphylactic shock. Should not be administered to anyone with a potential history of an allergic reaction to a chlorhexidine-containing compound. In infants, long-term continuous topical steroid therapy should be avoided. Adrenal suppression can occur when extensive areas are treated, particularly under occlusion. Long term continuous or inappropriate use of topical steroids can result in the development of rebound flares after stopping treatment (topical steroid withdrawal syndrome). A severe form of rebound flare can develop which takes the form of a dermatitis with intense redness, stinging and burning that can spread beyond the initial treatment area. It is more likely to occur when delicate skin sites such as the face and flexures are treated. Should there be a reoccurrence of the condition within days to weeks after successful treatment a withdrawal reaction should be suspected. Reapplication should be with caution and specialist advise is recommended in these cases or other treatment options should be considered. Pregnancy and Lactation: Nystatin and corticosteroids should be administered with caution during the early months of pregnancy and its use requires that the anticipated benefits outweigh the possible risks. Undesirable E ects: Skin disorders: Allergic skin reactions such as dermatitis,
Managing ichthyosis vulgaris and introducing the emollient circle of choice
Julie Van Onselen
Declarations of Interest: The author has worked in consultancy and educational capacities for L’Oreal, Alliance, Menarini and Viatris.
What is ichthyosis?
Ichthyosis was first described 200 years ago. It is a genetic disease of cornification which affects the whole integumentary system (skin, hair, and nails), characterised by dryness and scaling. Ichthyosis consists of many different presentations and is classified into common, congenital (including keratoderma), and acquired ichthyosis. This article will focus on common forms of ichthyosis and management.
All HCPs ned to be aware of ichthyosis and know the difference between ichthyosis and eczema – it is very important to understand that ichthyosis is not just dry skin. Ichthyosis is a lifelong genodermatosis, affecting children and adults. It is a chronic condition, which does not resolve throughout life. The management of ichthyosis is specific to the condition. This article will a focus on skin care and complete emollient therapy and how to support patients with IV and their families or carers.
Summary:
This ar ticle discusses the evidence-based management of ichthyosis vulgaris (IV), the most common form of ichthyosis affecting 1:250 people in the UK. Complete emollient therapy (CET) with bland medical emollients is the first-line treatment for all patients with IV. Humectant emollients are preferable due to loss-of-function mutations in the filaggrin gene (FLG mutation), and patient preference is the single most important factor. Adhering to the emollient ladder or having limited formularies can be restrictive for patients with ichthyosis and other chronic inflammatory skin conditions. This article introduces the emollient circle of choice (ECC), a visual aid as an alternative to the emollient ladder, which incorporates different emollient formulations that can be used at any time, to help equip patients with an individual emollient toolkit.
Classification and symptoms of ichthyosis
Ichthyosis is either congenital (develops at birth) or vulgar (develops in the first year of life), or it can be acquired (develops anytime throughout life). Ichthyosis vulgaris (IV) is the most common form, and is often not diagnosed, or misdiagnosed, as eczema, in childhood. IV has a prevalence of 1:250 of the European population. Signs and symptoms of ichthyosis vulgaris include a progression of fine scaling from three months of age, which progresses to light grey scales covering extensor surfaces of limbs, and the trunk; the groins are larger flexures and are generally spared.1 Despite dry skin, patients with IV do not present with skin inflammation.2 Acquired ichthyosis is commonly misdiagnosed. It is a non-hereditary condition and associated with malignancy, infections, drugs, endocrine, metabolic and autoimmune conditions.3
Rarer types of ichthyoses include congenital non-syndromic and syndromic forms, which are caused by mutations in the STS gene encoding recessive X-linked (caused by mutations in the STS gene encoding) affects males exclusively. Recessive x-linked ichthyosis is a mild form, with a prevalence of 1:1,500 in Caucasian and Asian populations.1 Rare congenital forms of ichthyosis are grouped into autosomal recessive congenital ichthyosis
Citation: Van Onselen J. Managing ichthyosis vulgaris and introducing the emollient circle of choice. Dermatological Nursing 2025. 24(1):10-14.
Julie Van Onselen is a Dermatology Lecturer Practitioner with a portfolio role working at Dermatology Education Partnership Ltd, Oxford, Check4Cancer Ltd, Cambridge, National Eczema Society, London and an Executive Committee Member and Primary Care Practitioner Sub-Group Lead at The Primary Care Dermatology Society (PCDS).
(ARCI), with a prevalence of 1:35,000. These is a mild-to-severe spectrum of lamellar and congenital ichthyosiform (including Netherton’s, collodion baby, harlequin, epidermolytic ichthyosis).
Clinical features vary in the ARCI group. In harlequin ichthyosis, gross thickening of the stratum corneum occurs, causing armour-like plates of scale and fissuring; in lamellar ichthyosis, there is a spectrum of generalised brown hyperkeratosis to generalised erythroderma with fine white scaling. ARCI is diagnosed at birth/infancy and managed by dermatologists in a multidisciplinary team at specialist centres. Other congenital forms include epidermolytic palmoplantar keratoderma, which is a rare localised autosomal form of ichthyosis, characterised by diffuse yellow thickening of palms and soles.1
Ichthyosis vulgaris and atopic eczema – relationship with FLG mutation
Clinical assessment needs to differentiate between atopic eczema (AE) and ichthyosis vulgaris (IV). Loss-of-function mutations in the filaggrin gene (FLG mutation) can be found in both AE and IV. Filaggrin is a key protein, essential for differentiating the epidermis and forming the stratum corneum (skin barrier). Around 40 loss-of-function filaggrin mutations have been identified in both IV and AE.4 FLG mutation is the cause of IV and a predisposing factor for AE.5 In IV, FLG mutation is an autosomal dominant trait; two FLG gene mutations are seen in two-thirds of people with IV, and in one-third, one FLG mutation causes palmer and plantar creases and dry skin.6
In AE, FLG mutation in gene encoding is a subset of 20-30% of people with AE, and a genetic predisposition for AE. It is known that 2.5-37% pf people with AE have clinical evidence of IV, so there is an overlap between the two conditions.7 FLG mutations physiologically cause altered loading and disorganisation in the lamellar bodies, resulting in lipid disruption in the stratum corneum. Clinically, FLG mutations causes skin barrier defect and reduces levels of natural moisturising factors (NMFs)
while also elevating skin surface pH, which increase trans-epidermal water loss (TEWL).6
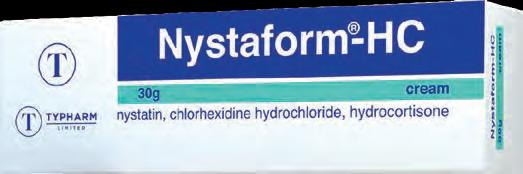
The normal chemical composition of NMFs in the skin is illustrated in Figure 1. The inherent reduction of FLG metabolites seen in patients with IV reduces the levels of NMFs. NMFs hydrate the skin, maintain acidic pH balance, improve skin elasticity and limit overgrowth of microbiomes.2
Loss-of-function FLG mutations cause a genetic reduction in skin hydration, which results in elevated skin surface pH, and increased TEWL. The reduction of
chemical composition of NMF is present in all patients with IV; as loss-of function FLG prevents the breakdown of normal FLG into NMFs, such as trans-urocanic acid (UCA) and pyrrolidone carboxylic acid (PCA).8 The significance of FLG mutations on the ichthyotic skin barrier was first discovered 40 years ago. Knowledge of NMF deficit in ichthyotic skin should dictate first-line emollient treatment choice.
Managing ichthyosis – what do HCPs need to know Ichthyosis (except for acquired ichthyosis) is a chronic and life-long
“Complete emollient therapy (CET) with bland medical emollients is first-line treatment for all patients with IV”
Chemical composition and percentages of NMF in normal skin
(Adapted from Fowler, 2012)9 Copyright Alliance Pharmaceuticals Ltd, 2024
Figure 1.
condition. It is not a predominant childhood condition – differing from AE – meaning incidence and prevalence do not reduce in adulthood. The whole skin is likely to be affected, with eye and ear involvement. There is a range of treatments for different types of ichthyoses; IV is treated with complete emollient therapy and keratolytics, which is first line therapy for all forms of ichthyosis. Rarer forms of ichthyosis are managed in secondary care, and advanced therapies will vary depending on the type of ichthyosis, for example, oral retinoids (acitretin). Some rarer types of ichthyoses do not have specific treatments. Some are in development, (such as treatments for Netherton’s) and these include molecular treatments such as immunoglobulin, biologic and genetic therapies.10
A key point in the management of all ichthyoses is to ensure individualised emollient treatment. Prescribing must be tailored to patient choice, and not necessarily guided by formulary, as emollients are first-line treatment in IV and for other types of ichthyoses.
Complete emollient therapy and emollient choice
CET with medical emollients is firstline treatment for all patients with IV. CET is defined as using emollients for moisturising and replacing all soaps and washing products with emollientbased products.11 Emollients can be creams, lotions, gels, ointments and washes. All emollients act by leaving an occlusive layer of lipids or oil on the skin surface to prevent TEWL. Emollients with additional humectant qualities enhance skin barrier repair and are longer lasting than basic water-oil creams, lotions and gels.12 The role of humectants in IV is important, as due to FLG mutation, the ichthyotic skin lacks humectants and is very dry. Therefore, humectant emollients which add NMFs to the ichthyotic skin should be first choice for IV. Humectant emollients are therapeutic in IV, include urea, propylene glycol and ceramide-based creams to help with dryness and scaling. There is no known curative treatment for IV, and lifelong emollient treatment will help alleviate the symptoms.2
Individual patient choice, in terms of formulation and product, is a crucial factor, as an emollient that suits one patient may not necessarily suit another. Therefore, the best emollient for a patient with IV is the one that suits them and the one they will use. Emollient formularies should have a wide range of formulations available on prescription, and the appropriate amount of emollient for monthly use should be on repeat prescription. Generally, adults should aim for 500g per week and younger children, 250g week. It is good practice to add a monthly amount to a repeat, i.e., 2kg. Patient education and demonstration in emollient use and application is very important, (e.g., downwards stroking rather than ‘rubbing in’).13
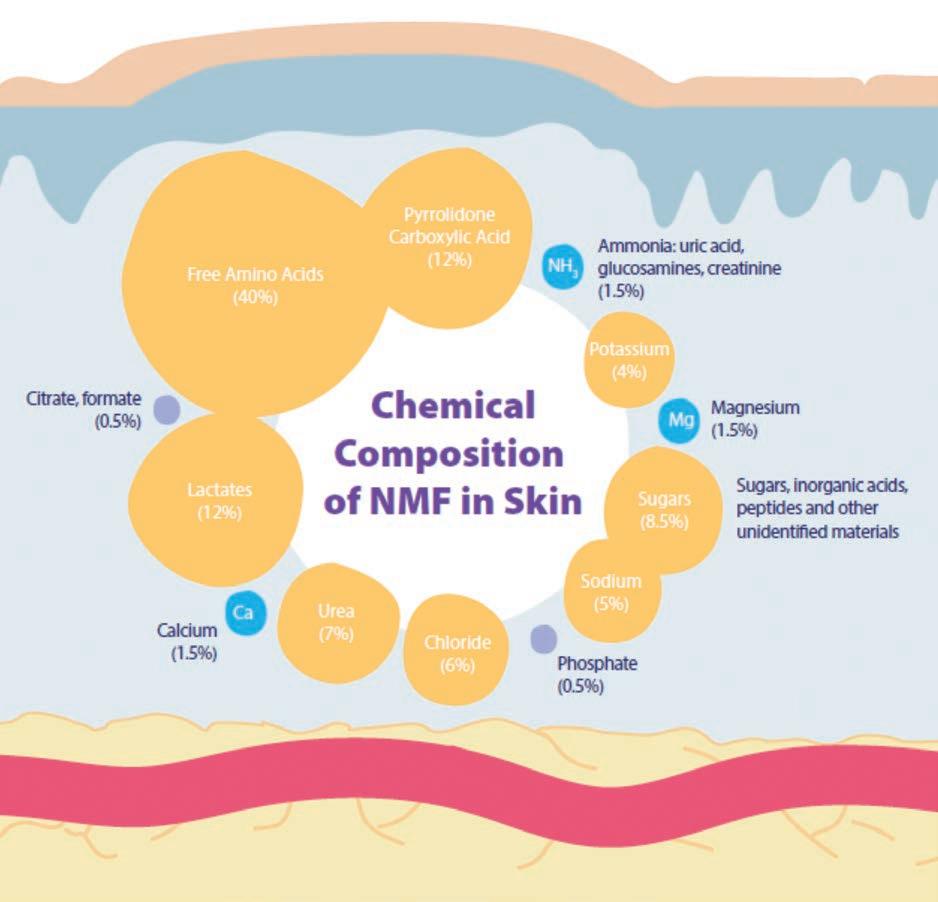
Emollient prescribing is often informed by the formulary, and the emollient ladder (Figure 2) is a tool used widely
by the NHS. It can be debated that it is not a treatment ladder, but a list of formulations from the least (lotions) to most greasy (ointments). Emollients with humectant ingredients are not specifically listed, only those which contain urea. Emollient action is not addressed in the emollient ladder. This is key in emollient choice, as emollients with added humectants, for example hyaluronic acid and glycerin, can give hydrating effects for 24 hours,14 which is an important consideration for patients with ichythosis. Furthermore, this may lead to a perception (especially by nondermatology specialists) that emollients are prescribed from the bottom of the ladder upwards. It could be argued that the emollient ladder is not beneficial for patient choice and does not account for matching emollient action with clinical parameters of skin dryness, which are very important factors in ichthyosis care.
“The best emollient for a patient with IV is the one that suits them and the one they will use”
l Lists formulation and products only
l Does not explain emollient actions
l Guides HCPs to start with light and ‘climb the ladder’
l Emollients are not stepped up and down (like topical steroids)
l The emollient ladder often guides local formularies
Figure 2. The emollient ladder and limitations for IV
Details about the Ichthyosis Support Group Aims
l To preserve and protect the health of and to relieve persons affected by ichthyosis and any associated condition
l To advance the education of the medical profession and the public on ichthyosis and its implications for the family
l To promote research into the management of ichthyosis and to publish the useful results thereof, and to support organisations promoting research into ichthyosis.
Membership Benefits
l Information packs
l Newsletters and ebulletins
l National Family Conference
l Children’s residential camps
l Family days
The Ichthyosis Support Group raises awareness of ichthyoses by attending and speaking at various dermatology related conferences and events around the UK and Ireland. They also attend the British Association of Dermatologists (BAD) Conference, one of the largest gatherings of consultant dermatologists in the UK, and the British Dermatological Nursing Group (BDNG)’s annual conference to help raise the profile of the condition and the support group.
More information about the work of the Ichthyosis Support Group can be found at: https://www.ichthyosis.org.uk/
CET includes emollients for washing and bating, and patients with IV often find bath additives a helpful component of their CET regimen. A current challenge is that many formularies have removed bath additives, following the BATHE study, which showed no clinical benefit from emollient bath additives in the standard management of eczema in children under 12 years of age.15 The NHS website recommends ichthyoses treatment may include moisturising treatments and bath oils; therefore these should be prescribed for the patient with IV, if required and not restricted, as the BATHE study was conducted in children with atopic eczema and cannot be generalised to patients with ichthoyses.16
The Emollient Circle of Choice
The Emollient Circle of Choice (ECC) is a new concept, and an alternative to the emollient ladder, for patients with IV. The ECC centres on the patient and their skin hydration needs. For CET to achieve a reduction in skin dryness and scaling for one patient, it may just require one emollient for washing and
moisturising; alternatively, for another patient, a bath oil and two different emollients may be required. The ECC is≈a concept that works on patient choice, rather than following a rigid ladder or formulary where one emollient is tried and then ‘stepped up’ in formulation or brand. Patients with IV should not be restricted in the emollient ladder of
choice and there is not ‘one size fits all’ or a progression from lighter to heavier formulations.
The adoption of the ECC would help ensure individual patient choice and improve adherence for patients with IV. The value of the ECC is to help patients with IV chose the emollients that suit them and their need for effective daily complete emollient therapy. Patients can use the ECC to help build a personalised emollient toolkit, choosing the formulations which suit their skin, and which they will use. The emollients in the toolkit may change depending on skin flares, changes in skin dryness and seasonal changes.
The suggestion is that local formularies adopt and list emollients as the ECC, and this will give patients greater choice while removing the rigidity of following a ladder approach, which often restricts choice and the need for more than one emollient, depending on patient need. The patients can then visually see emollient choice, and the HCP can prescribe the emollients chosen by the patients, rather than following a stepped ladder approach, which is not individualised.
Complications and psychological issues
HCPs need to be aware of complications of IV and psychological issues. Dry skin itself can cause skin fissures, which can mean the patient is more susceptible to infection. Due to loss of skin function,
“The adoption of the ECC would help ensure individual patient choice and improve adherence for patients with IV”
IV can cause vitamin D deficiency.2 Tight skin may impair fine and gross motor function; for example it may impair the use of hands, while on the soles of the feet it can cause problems with mobility. Certain materials in school or the workplace may irritate the skin, including sand, clay, and paint. People with IV may be more susceptible to over-heating due to the body’s inability to sweat through pores blocked by thickened skin, which may also cause dehydration.17 Body odour can be a problem, due to the normal accumulation of bacteria between dry skin and scales.
Eyes and ears are often affected. Ectropion of the eyelids results in eyes not fully closing, which causes dry eye and can lead to keratitis; cataracts are also more common in patients with IV.2 Hearing loss and ear pain is caused by scales binding with ear wax. The ear canal can become blocked; one study showed that 74% of patients with IV over 74 years of age had hearing loss, and 50% of children under 18 had abnormal hearing tests.18
The psychological impact of IV should never be underestimated. Coping with physical symptoms on a daily ongoing basis and ongoing treatment can be difficult to cope with, while body image, daily activities and social life can be affected.19 A study showed quality of life was severely affected for people with all types of ichthyosis, including IV; adults suffered more effect on quality of life than children.19 The Ichthyosis Support Group (ISG) provides information and support for anyone with ichthyosis and their families. See Box 1 for more details.1,7
Conclusion
Most people with IV will be cared for in primary care. Dermatology nurses need to have good knowledge of IV and
understand how to support patients and families, as well as provide guidance, support and management help to primary care colleagues.
IV can be wrongly diagnosed as AE, as the two conditions can co-exist. IV is a long-term chronic condition that does not resolve or remit. Management of IV is done via an emollient toolkit, which includes emollients that are the patient’s choice and the one(s) they want to use. Patients and their families need support in manging this distressing and chronic long-term condition, and key to this is effective complete daily emollient therapy and choice of emollients for washing and moisturising.
The ECC can help facilitate individual choice for complete daily emollient therapy for patients with IV. The ECC has been introduced for patients with IV, future work will be on developing a theoretical framework for this concept and incorporation into clinical practice and guidelines.
References
1. Oji V, Dieter M, Traupe H (2016) Urticaria. In Griffiths C, Barker J, Bleiker T, Chalmers R, Creamer D (eds). Rook’s Textbook of Dermatology – 9th Edition. Oxford: WileyBlackwell, Part 2, Chapter 65: 1-41
2. Jaffar H, Shakir Z, Kumar G, Ali IF. Ichthyosis vulgaris: An updated review. Skin Health Dis 2022. 3(1)
3. Haber R, Feghali J, Nadir U et al. Acquired ichthyosis: a clinical review. Arch Dermatol Res 2023. 315(9):2529-2543
4. Osawa R, Akiyama M, Shimizu H. Filaggrin gene defects and risk of developing allergic disordres. Allergol Int 2011. 60(1):1-9
5. Hoyer A, Rehbinder EM, Färdig M et al. Filaggrin mutations in relation to skin barrier and atopic dermatitis in early infancy. British Journal of Dermatology 2022. 186: 544-552
6. Thyssen JP, Godoy-Gijon E, Elias PM. Ichthyosis vulgaris: the filaggrin mutation disease. British Journal of Dermatology 2013. 168(8):1155-1166
7. Singh M, Pawar M. Eyelash length for the diagnosis of atopic dermatitis and ichthyosis vulgaris in children—a case control study. Eur J Pediatr 2018. 177(6):955-60
8. Leman G, Moosbrugger-Martinz V, Blunder S, Pavel P, Dubrac S. 3D-organotypic cultures to unravel molecular and cellular abnormalities in atopic dermatitis and ichthyosis vulgaris. Cells 2019. 8(5):489
9. Clar et al. (1980), L’acide Pyrrolidone Carboxylique et la peau, International Journal of Cosmetic Science, 3, 110-113; cited by Fowler J (2012) Understanding the role of natural moisturising factor in skin hydration. Practical Dermatology. Available at: https://assets. bmctoday.net/practicaldermatology/pdfs/ pd0712_ftr_nmfreview.pdf [last accessed January 2025]
10. Joosten MDW, Clabbers JMK, Jonca N. et al. New developments in the molecular treatment of ichthyosis: review of the literature. Orphanet J Rare Dis 2022. 17:269
11. Cork MJ. The importance of the skin barrier function. Journal of Dermatological Treatment 1997. 8 (supplt 1): S7-13
12. Cork MJ, Danby S. Skin barrier breakdown: a renaissance in emollient therapy. British Journal of Nursing 2009. 181(14): 872-877
13. PCDS 2024. Emollients Treatment Pathway. Available at: https://www.pcds.org. uk/files/general/Emollient-Treatment-web.pdf [last accessed January 2025]
14. Milani M, Sparavigna A. The 24-hour skin hydration and barrier function effects of a hyaluronic 1%, glycerin 5%, and Centella asiatica stem cells extract moisturizing fluid: an intra-subject, randomized, assessor-blinded study. Clin Cosmet Investig Dermatol 2017. 11(10):311-315.
15. Santer M. Emollient bath additives for the treatment of childhood eczema (BATHE): multicentre pragmatic parallel group randomised controlled trial of clinical and cost effectiveness. BMJ 2018. 361
16. NHS. Ichthyosis. 2024. Available at: https:// www.nhs.uk/conditions/ichthyosis/ [last accessed January 2025]
17. Ichthyosis Support Group 2025. Available at: https://www.ichthyosis.org.uk [last accessed January 2025]
18. Huang JT, Mallon K, Hamill S, Ohlms LA, Liang MG. Frequency of ear symptoms and hearing loss in ichthyosis: a pilot survey study. Pediatr Dermatol 2014. 31(3):276-80
19. Diaz LZ, Browning JC, Smidt AC, Rizzo WB, Levy ML. Complications of ichthyosis beyond the skin: non-cutaneous complications of ichthyosis. Dermatol Ther 2013. 26(1):39-45.
Fludroxycortide 4 micrograms per square centimetre Tape: A steroid tape to treat inflammatory skin conditions.
Flexible. Versatile. Waterproof.
Knowing that their dermatosis is covered by a clear tape providing a constant steroid treatment, goes a long way in helping your patients feel more confident in everyday life.
Reference: 1. Scars & Keloids. BAAPS. Available at https://baaps.org.uk/patients/procedures/16/ scars_and_keloids. 2. Ogawa R et al. J Nippon Med Sch 2016; 83(2): 46-53.
FLUDROXYCORTIDE TAPE PRESCRIBING INFORMATION: Fludroxycortide 4 micrograms per square centimetre Tape See full Summary of Product Characteristics (SmPC) before prescribing. Presentation: Transparent, plastic surgical tape impregnated with 4 micrograms fludroxycortide per square centimetre. Indications: Adjunctive therapy for chronic, localised, recalcitrant dermatoses that may respond to topical corticosteroids and particularly dry, scaling lesions. Posology and Method of Administration: Adults and the Elderly: For application to the skin, which should be clean, dry, and shorn of hair. In most instances the tape need only remain in place for 12 out of 24 hours. The tape is cut so as to cover the lesion and a quarter inch margin of normal skin. Corners should be rounded off. After removing the lining paper, the tape is applied to the centre of the lesion with gentle pressure and worked to the edges, avoiding excessive tension of the skin. If longer strips of tape are to be applied, the lining paper should be removed progressively. Paediatric population: Courses should be limited to five days and tight coverings should not be used. If irritation or infection develops, remove tape, and consult a physician. Fludroxycortide Tape is waterproof. Cosmetics may be applied over the tape. Contraindications: Chicken pox; vaccinia; tuberculosis of the skin; hypersensitivity to any of the components; facial rosacea, acne vulgaris, perioral dermatitis, perianal and genital pruritus; dermatoses in infancy including eczema, dermatitic napkin eruption, bacterial (impetigo), viral (herpes simplex) and fungal (candida or dermatophyte) infections. Warnings and Precautions: Not advocated for acute and weeping dermatoses. Local and systemic toxicity of medium and high potency topical corticosteroids is common, especially following long-term continuous use, continued use on large areas of damaged skin, flexures and with polythene occlusion. Systemic absorption of topical corticosteroids has produced reversible hypothalamic-pituitary-adrenal (HPA) axis suppression. Long-term continuous therapy should be avoided in all patients irrespective of age. Application under occlusion should be restricted to dermatoses in very limited areas. If used on the face, courses should be limited to five days and occlusion should not be used. In the presence of skin infections, the use of an appropriate antifungal or antibacterial agent should be instituted. Long term continuous or inappropriate use of topical steroids can result in the development of rebound flares after stopping treatment (topical steroid withdrawal syndrome). A severe form of rebound flare can develop which takes the form of a dermatitis with intense redness, stinging and burning that can spread beyond the
Including hand eczema and finger tip fissures1
Waterproof protection once in place
Can be cut to size for awkward areas
For both children and adults
Scan the QR code to view the application video.
initial treatment area. It is more likely to occur when delicate skin sites such as the face and flexures are treated. Should there be a reoccurrence of the condition within days to weeks after successful treatment a withdrawal reaction should be suspected. Reapplication should be with caution and specialist advise is recommended in these cases or other treatment options should be considered. For children, administration of topical corticosteroids should be limited to the least amount compatible with an effective therapeutic regimen. Children may absorb proportionally larger amounts of topical corticosteroids and thus may be more susceptible to systemic toxicity. Pregnancy and Lactation: Use in pregnancy only when there is no safer alternative and when the disease itself carries risks for mother and child. Caution should be exercised when topical corticosteroids are administered to nursing mothers. Undesirable Effects: The following local adverse reactions may occur with the use of occlusive dressings: burning, itching, irritation, dryness, folliculitis, hypertrichosis, acne form eruptions, hypopigmentation, perioral dermatitis, allergic contact dermatitis, maceration of the skin, secondary infection, skin atrophy, miliaria, striae and thinning and dilatations of superficial blood vessels producing telangiectasia. Transient HPA axis suppression. Cushing’s syndrome. Hyperglycaemia. Glycosuria. Adrenal suppression in children may occur. Infected skin lesions, viral, bacterial, or fungal may be substantially exacerbated by topical steroid therapy. Wound healing is significantly retarded. Local hypersensitivity reactions. Stop treatment immediately if hypersensitivity occurs. Withdrawal reactions - redness of the skin which may extend to areas beyond the initial affected area, burning or stinging sensation, itch, skin peeling, oozing pustules. Precautions for Storage: Store in a dry place, below 25oC. Pack Size and Price: Polypropylene dispenser and silica gel desiccant sachet in a polypropylene container, with a polyethylene lid, packed in a cardboard box, containing 20 cm or 50 cm of translucent, polythene adhesive film, 7.5 cm wide, protected by a removable paper liner. 7.5 cm x 20 cm £21.44. 7.5 cm x 50 cm £37.49 Legal Category: POM Marketing Authorisation Number: PL 00551/0014 Marketing Authorisation Holder: Typharm Ltd., Unit 1, 39 Mahoney Green, Rackheath, Norwich, NR13 6JY. Tel: 01603 722480, Fax: 01603 263804. Date of Revision of Text: January 2025
Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events should also be reported to Typharm Limited on 02037 694160.
Could teledermatology in the community aid and reshape the future of NHS care?
Rebecca Ramdeen-Thomas, Kurt Ayerst
Declarations
Conflicts of Interest
The authors are both contracted by ScreenCancer UK.
Financial Support and Sponsorship
Nil
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Abstract:
In England and Wales, 13.2 million people see their general practitioner (GP) annually regarding dermatology concerns. Skin cancer accounts for half of all cancers in England and Wales and is increasing by 8% annually.1,2 In England and Wales, the NHS dermatology units surgically remove 200,000 skin lesions yearly.1 Our patient population is substantial, with 54% of individuals affected by skin disease each year, with between 23-33% of the population experiencing a skin condition at any given time that would benefit from medical attention.3 Melanoma is responsible for 90% of skin cancer-related mortality, and is often first detected in primary care, where differentiating it from benign lesions
Aim: The aim of this research was to assess the effectiveness of DermoSight Teledermoscopy in primary care for both patients and healthcare professionals, as well as to evaluate its impact on reducing inappropriate referrals to secondary care.
Method: A non-selective retrospective study was conducted over a 12-month period. Patients who presented to their GPs with skin condition(s) or skin lesion(s) were referred to the DermoSight Service.
Results: The service received a total of 4,633 submissions from 3,920 patients. Of these, 74% were managed with advice and guidance by their GP, while 12% were handled in community clinics. This means 86% of cases did not require referral into secondary care. A total of 12% were referred to secondary care, with just over 8% directed to the rapid access clinic. Only 0.4% were incomplete, requiring additional information.
Conclusion: DermoSight Teledermoscopy Service has proven valuable in supporting Healthcare Professionals with management advice by quickly diagnosing skin lesions and conditions, thereby reducing the need for in-person appointments with dermatologists. It allows patients to receive accurate results promptly while safely reducing unnecessary referrals into secondary care or redirecting to alternative teams.
Key sentences:
l T he DermoSight USB connected camera is a United Kingdom Conformity Assessed (UKCA) registered device that can be used for macroscopic and dermatoscopic imaging.
l I t was used in the Primary Care setting to upload information and images to a secure platform for an analysis report for patients presenting with skin lesions and conditions.
l I t provides a method to expand healthcare within the primary care setting, helping to streamline the patient journey and improve referral pathways into secondary care.
Author info: Rebecca RamdeenThomas is a Dermatology Specialist Nurse at ScreenCancer UK, Medway, Kent, and Kurt Ayerst is a Dermatology Consultant in the independent sector, based in Kent.
Citation: Ramdeen-Thomas R, Ayerst K. Could teledermatology in the community aid and reshape the future of NHS care?
Dermatological Nursing 2025 24(1):17-21.
can be challenging.4 Skin conditions are commonly encountered in general practice, however, dermatology training is inadequately addressed in undergraduate medical education.5 This disparity can place considerable strain on dermatology departments, as there is an ongoing rise in referrals.3 Additionally, it may be inconvenient for patients who require multiple appointments in the treatment pathway, such as visits to the GP, followed by hospital consultations and subsequent follow-up or minor surgery appointments.
Dermoscopy is a skin visualisation tool which is commonly used for diagnosing skin lesions in secondary care. However, its role in primary care remains uncertain,4 and GPs will usually have to undergo further specialised training in dermoscopy to become confident in diagnosing and differentiating different skin lesions and skin conditions. An area of dermatology which is on the rise is the use of teledermatology.
Teledermatology operates primarily through two pathways.
l L ive Interaction: This involves dermatologists using a phone or computer to conduct consultations in real-time with their patients. 6
l S tore-and-forward: This involves information and images uploading on a system for a dermatologist to review at a later stage .7
Teledermatology was first reported in Norway in 1993, and the uses were first published in 1995.3 In 2019, during the COVID-19 pandemic, there was an increase in demand for teleconsultations, including teledermatology services, and one can argue that it has now become accepted as an integral part of dermatology practice.4
DermoSight
DermoSight is a software and camera device which uses the store-andforward system of teledermatology, hence teledermoscopy. It holds a Class 1 registration under the Medical Device Regulation (MDR), with both European Conformity (CE) and United
Kingdom Conformity Assessed (UKCA) certifications, including the UKCE mark. This ensures compliance with the standards outlined in the National Health Service Data Security and Protection Toolkit (NHS DSP), the General Data Protection Regulation (GDPR), and applicable cybersecurity protocols.
Regulatory and information security
FDA 510K Clearance
CE MDR Class 1 Approved
UKCE Approved
NHS DSP Toolkit
GDPR
Cybersecurity Certification
DermoSight helps deliver specialised care to patients promptly without always having to visit secondary care. The information gathered for the dermatologist includes macroscopic images, dermoscopy images and specific information in the form of questions in relation to the skin lesion or skin condition.
The dermatologist can assess and review all the information collected to formulate a management plan for the patient.
Figure 1 illustrates the use of DermoSight in a clinical setting, showing the camera device with images uploaded to secure cloudbased software. The device can capture
Figure 1.
DermoSight in a clinical setting
Figure 2. Application of stabiliser stick for macroscopic images
multiple dermoscopy images. The nose cone can be detached, and a stabiliser stick can be attached to capture the macroscopic images. This setup ensures images are standardised and also provides stability, as seen in Figure 2.
Objectives
In April 2020, a medium sized Clinical Commissioning Group (CCG) with 10 GP practices was keen to improve their existing teledermatology eReferral System (eRS) service. They were interested in the store-and-forward system of Teledermatology. DeepX Health (DXH) offered a solution to treat patients with the DermoSight Teledermoscopy (DST) service. All patients presenting with a skin complaint that needed specialised advice from a dermatologist were booked into the DST clinic. These patients clinically presented with either a skin condition(s) or a skin lesion(s). All skin phototypes, as per the Fitzpatrick Skin Type Scale, were included, ensuring representation of all ethnicities and skin types.
The primary objective of this study was to determine the effectiveness of using DST in primary care for patients, healthcare professionals and
CCGs. Secondary outcomes included prevention of unnecessary referrals to secondary care, thus burdens of over referrals, using integrated services to enhance patients’ journey and reducing costs for the NHS and achieving financial savings.
Method
A non-selective retrospective study was conducted over a 12-month period from August 2021 to July 2022. Patients who visited their GP with a skin condition or skin lesion(s) were referred to the DST service. The skin lesion(s) included both pigmented and non-pigmented lesions. Some patients had multiple skin concerns and were also seen in this clinic. All the information was uploaded to a secure cloud-based server. A dermatologist was able to access and review all the submissions remotely and provide a management plan in the form of a personalised report.
In the DST clinic, the process involved a trained healthcare professional filling out a pre-set online questionnaire to document the patient’s history and capturing both macroscopic and dermoscopy images.
Before using DermoSight, healthcare professionals were required to undergo specialised training. This included one online training session and three practical case submissions. Healthcare professionals could submit as many practice cases as they chose, but at least three of them needed to be approved as competent before gaining access to the live system. Additional training, such as face-to-face sessions or further online courses, were available if required by individuals.
Out of the 10 GP practices, there was a combination of healthcare professionals using DST, including GPs, nurses and healthcare assistants (HCAs). In clinics, where nurses and HCAs were designated to manage the DST, GPs were not involved in gathering information for the dermatologists. However, the GPs played an active role once the dermatologists generated the management plans. These management plans, in the form of a report, were completed within 72 hours for every patient.
The outcome of each patient’s assessment was designated to one of seven categories, with additional advice provided in the free text area. This has been outlined in Table 1.
1. Advice and Guidance Patients who were provided with a diagnosis and management plan for skin conditions or lesions appropriate for management in Primary Care were designated as having received Advice and Guidance and the pathway was completed. Examples include benign skin lesions, acne and eczema.
2. Rapid Access Pathway Patients were upgraded to the Rapid Access Pathway to be seen in secondary care cancer clinics. Examples included any high-risk or suspected melanoma or squamous cell carcinoma lesions.
3. Secondary Care Patients referred to Secondary Care routine clinics for management in that sector included higher risk basal cell carcinomas (BCCs) or inflammatory conditions requiring systemic therapy.
4. Primary Care Surgical Clinic
5. Primary Care Community Dermatology Clinic
The Primary Care Surgical Clinics saw patients who were not suitable to be treated in secondary care but still needed intervention. Examples were low risk BCCs and benign symptomatic lesions for management in the community.
The Local Community Dermatology clinics saw patients requiring intermediate level dermatologic care for management in the community. Examples include problematic inflammatory conditions.
6. Other Outcome Other Outcome was used for patients who fell outside of dermatology management pathways with the recommendation to refer to other teams, or when advice or an interim management plan was provided with review required for final diagnosis.
7. Incomplete If further information or images were required to formally assess the patient, they would be designated as Incomplete and request kept pending awaiting resubmission
Table 1: Summary of the assessment outcome following DST consultation
“Dermatology teams face an additional burden with over-referrals received from primary care”
Results
The DST service accepted a total of 3,920 referrals. This included 3,470 and 450 participants with lesions and skin conditions respectively. Some patients had multiple skin lesions submitted. There were 4,633 submissions in total.
Figure 3 illustrates the total number of patients who visited the DST clinic. It reveals that for approximately every eight patients with a skin lesion, one had a skin condition.
All the outcomes were recorded and analysed for the DST clinics. The findings were:
l 74.1% (n=3,435) were managed with advice and guidance alone
l 8 .8% (n=406) were referred via the cancer pathway for rapid access assessment
l 8 .6% (n=397) were recommended for management in the primary care surgical clinic
l 1.8% (n=82) were listed as Other Outcome. These patients were outside the referral pathway
l 3 .1% (n=143) were sent to the local community dermatology clinic
l 3 .2% (n=150) were referred to secondary care
l Only 0.4% (n=20) submissions were incomplete. These included images that breached inclusion criteria. Additionally, it included patients that had to return as the original information submitted was incomplete. The patients were re-assessed and the information updated for resubmission.
The outcome for each patient who visited the DST clinic can be categorised into one of seven groups, as shown in Figure 4. For further details, please refer to Table 1.
Discussion
This study highlights that DST is an effective and efficient method for managing patients with both pigmented and non-pigmented skin lesions, as well as other skin conditions, in the primary care setting. DST has demonstrated its value by facilitating timely patient consultations without requiring physical visits to secondary care, while still providing access to expert advice and treatment.
Additionally, it has proven effective in delegating appropriate tasks to nurses and healthcare assistants, allowing GPs to prioritise their workloads and patient care while maintaining best practices. The GPs that did use DST found it was quick and easy to use.
The effectiveness of DTS in the community was assessed by evaluating the potential number of inappropriate referrals that were prevented. Overall,
86% of cases did not require referral into secondary care. Additionally, when comparing patients treated solely in the community to those treated in secondary care, the figures are 82.7% and 17.3%, respectively.
Figure 5 illustrates the number of patients treated in the community and referred into secondary care. These community patients potentially avoided referrals to secondary care and were appropriately triaged and treated within the community locally.
Dermatology teams face an additional burden with over-referrals received from primary care.8 However, by utilising the DST in the community GP setting, patients were able to receive specialist advice promptly and enhance the diagnostic accuracy and condition(s) management. Moreover, patients were seen and treated in the appropriate clinical settings, ensuring that those needing urgent referrals were accurately identified and directed to the correct pathway.
All DTS outcomes
Figure 3.
The
Figure 4.
Category outcomes for every patient that used the DTS
Patients treated within the community received the appropriate treatment plans, and where surgical intervention was needed, they were treated in the correct clinical setting without the need for an initial secondary care in-person visit. This integrated approach reduced the need for multiple visits to other clinics for the patient, and managed the workload received in secondary care.
Teledermatology services remain effective, eliminating the need for face-to-face appointments with a dermatologist.9 DST has successfully reduced the need for travel and in-person appointments with dermatologists. Teledermatology facilitated collaboration between dermatologists and GPs, enabling patients to obtain accurate results promptly while minimising unnecessary referrals to secondary care.10
Despite the restrictions imposed by the COVID-19 pandemic, GP practices considered the DST solution to be a valuable asset for both the surgeries and their patients. As a result of this success, additional sites requested access to the DST service.
Patients classified in the incomplete category were reviewed. It was found that for skin lesions, the issue was primarily blurry images, while for skin conditions, key missing information was identified. These limitations were addressed by reviewing and adapting the software to improve image clarity for blurry skin lesion images. Additionally, extra time is now dedicated during training for healthcare professionals to emphasise the importance of completing all questions in the questionnaire.
Conclusion
This study has shown that DST has been useful in assisting GPs with management advice by rapidly diagnosing skin lesions and skin conditions. Assigning the DST clinic to nurses and healthcare assistants was considered successful in optimising and integrating workloads.
Most cases that would have typically been referred to secondary care were successfully managed within the community, eliminating the necessity for hospital visits. By strengthening
“Most cases that would have typically been referred to secondary care were successfully managed within the community”
community services and improving integration, management pathways can be enhanced, supporting care in the community and reducing the demand for secondary care.
This contributes to meeting cancer and elective care waiting times, enhancing patients care as well as saving the NHS time and money, amongst other benefits.
References
1. NHS England. Getting it right first time. Dermatology overview. [online]. NHS: England 2022. Available at: https://gettingitrightfirsttime. co.uk/medical_specialties/dermatology/ [last accessed February 2025]
2. Ulrike L, Ulrike K, Garbe C. Epidemiology of skin cancer: Update 2019 [online]. Advances in Experimental Medicine and Biology 2020. Available at: https://link.springer.com/ chapter/10.1007/978-3-030-46227-7_6 [last accessed February 2025]
3. Jones OT, Jurascheck LC, Utukuri M, Pannebakker MM, Emery J, Walter FM.
Dermoscopy use in UK primary care: a survey of GPs with a special interest in dermatology. Journal of the European Academy of Dermatology and Venereology 2019: 20: 111-115
4. M Cnudde, C Thomas, C Aldridge. Inpatient dermatology referrals: what is the burden? A retrospective review of 14 years of dermatology inpatient referrals. Clinical and Experimental Dermatology 2024: 498
5. Andrees V, Klein TM, Augustin M, Otten M. Live interactive teledermatology compared to in-person care- a systematic review. JEADV. Journal of the European Academy of Dermatology and Venereology 2019. 34(4)733-745. Available at: https://doi.org/10.1111/jdv.16070 [last accessed February 2025]
6. Jiang WS, Flynn SM, Kwock TJ, Nicholas MW. Store-and-forward images in Teledermatology: Narrative Literature Review. JMIR Dermatology 2022. 5(3):e37517. Available at: https://derma.jmir.org/2022/3/e37517 [last accessed February 2025]
7. Tommasino N, Cacciapuoti M, Villani S, Martora A, Ruggiero F, Potestio L. The Past, the Present and the Future of Teledermatology: A Narrative Review. Clinical, Cosmetic and Investigational Dermatology 2024. 17: 717–723
8. Nickles AM, Rustad MA, Lio AP. Teledermatology: The future is Now. Journal of the Dermatology Nurses’ Association 202. 14: 82-88
9. Mehr tens S, Shall L, Halpern S. A 14year review of a teledermatology service: experience of over 40 000 teleconsultations. Clinical and Experimental Dermatology 2019. 44: 874-881
10. Barbieri JS, Nelson CA, James WD. The reliability of teledermatology to triage inpatient dermatology consultations. JAMA Dermatology 2014. 4: 419-424.
Dermatology nursing with 18 Week Support
18 Week Support
Dermatology nursing offers a uniquely rewarding career, blending clinical expertise with the opportunity to transform lives through patient-centred care. At 18 Week Support, we’re proud to partner with the NHS, delivering innovative solutions through insourcing to address the challenges of long waiting lists and ensure timely care.
By joining our highly professional team, you’ll become part of a company dedicated to making a tangible difference in patients’ lives while advancing your own career in a supportive and dynamic environment.
A day in the life of a dermatology nurse in charge
Every day as a dermatology nurse with 18 Week Support brings new challenges, opportunities, and the satisfaction of knowing you’re making a real difference.
Dermatology nurses play a pivotal role in delivering care across various settings, from outpatient clinics to surgical procedures. Working collaboratively with consultants and healthcare assistants, you’ll be at the forefront of patient care.
My day begins
The day starts with a briefing with the local NHS team, reviewing the schedule and patient needs. From there, I prepare for a day of skin assessments, wound care, or assisting in minor dermatological surgeries. Each patient brings a unique case, keeping the day engaging and educational.
Leading the team
As a nurse in charge, I oversee the clinic’s workflow, ensuring all team members have the resources they need to provide high-quality care. Communication is key, as I liaise with both 18 Week Support’s central team and local NHS staff to maintain seamless operations.
Balancing responsibilities
Throughout the day, I balance clinical duties with mentoring newer team members and addressing patient concerns. This
Summary:
This ar ticle provides an outline of the work carried out by 18 Week Support, including details of a day in the life of an 18 Week Support dermatology nurse.
“18 Week Support’s proposition was originally developed from our founder Dr Conal Perrett’s vision to support Trusts and reduce patient waiting lists in dermatology services. Whilst we now cover multiple specialties nationwide, dermatology remains front and centre of the quality care we deliver through insourcing solutions to the NHS.”
– Josh Collins, CEO, 18 Week Support.
variety keeps my role dynamic and fulfilling, with every interaction offering the chance to learn and grow.
Wrapping up
At the end of the day, I review patient outcomes and clinic feedback, ensuring everything is in place for the next session. Knowing I’ve contributed to reducing waiting times and improving patient experiences is deeply gratifying.
Keywords:
18 Week Support, Patient-centred care, Dermatology
Citation:
Dermatology Nursing with 18 Week Support. Dermatological Nursing 2025. 24(1):22-23.
The role of insourcing in dermatology
Insourcing is a patient-focused initiative where clinical teams work within NHS trusts utilising available estate, ensuring patients are seen in familiar settings. Unlike outsourcing, it keeps care local and leverages the expertise of trusted NHS-trained professionals.
Insourcing plays a crucial role in reducing waiting times for dermatology patients, enabling faster diagnosis and treatment. By joining 18 Week Support, you’ll help deliver seamless, high-quality care that aligns with NHS standards while advancing your professional skills.
18 Week Support is a leading partner to the NHS, founded by eminent
“At 18 Week Support, we’re proud to partner with the NHS through insourcing, delivering fast access to care for patients while reducing waiting lists, improving productivity, and enhancing outcomes. By working collaboratively, we support the NHS in ensuring patients receive the care they need, when they need it most.”
– Jack Player, Director of Workforce, 18 Week Support
“Working with a team of dedicated professionals has moulded me into a better and more effective leader. Starting as an HCA while awaiting my NMC registration, I progressed to Nurse in Charge with support from 18 Week Support. The organisation’s commitment to excellence and innovation has been a constant source of pride and professional growth.”
– Lucy, dermatology nurse and nurse in charge
“Joining 18 Week Support has been incredibly rewarding. I’ve had the privilege of working in diverse units, handling unique cases, and collaborating with inspiring consultants. This variety has sharpened my clinical skills and deepened my passion for dermatology nursing. The supportive team culture makes it a truly inspiring place to work.”
– Phoebe, dermatology nurse
“I find clinics very educational, being a HCA we don’t normally get the opportunity to sit in clinics in our daily jobs but with 18 Week Support we’re able to sit in clinic and learn the different type of dermatological procedures and conditions while also being able to learn the different treatments used to treat these conditions. I also enjoy being able to work with clinicians and nurses from all different hospitals sharing experiences. Working with 18 Week Support have fun working together as one great team members.”
– Chevelle, dermatology HCA
dermatologist Dr Conal Perrett. For over 10 years, we have been at the forefront of insourcing, delivering clinical excellence through our dermatology services.
Why join us?
Professional Growth: Gain exposure to various cases, advanced treatments, and opportunities for continuous learning whilst working with industryleading consultants and nurses.
Flexibility: Experience flexible scheduling and different workplace settings to match your lifestyle.
Competitive Benefits: Receive attractive pay rates and a team-oriented environment.
Rewarding Work: Contribute to an organisation focused on clinical outcomes where your work impacts patient care.
Want to find out more?
Join 18 Week Support and become part of a dedicated team delivering exceptional care and shaping the future of dermatology.
Enstilar® is indicated for the topical treatment of psoriasis vulgaris in adults.1 Produced and
once-daily treatment for 4 weeks during the active flare… 1-3
twice-weekly maintenance treatment for up to 52 weeks in responders1,4*
1,4 Enstilar® should be applied twice-weekly on two nonconsecutive days to previously affected areas.1 Between applications there should be 2-3 days without Enstilar® treatment.1 The most frequently reported adverse reactions during treatment are application site reactions.1 Local reactions can occur after topical use, especially during prolonged application, including skin atrophy, telangiectasia, striae, folliculitis, hypertrichosis, perioral dermatitis, allergic contact dermatitis, depigmentation, and colloid milia.1 Long-term use of corticosteroids may increase the risk of local and systemic adverse reactions.1 Treatment should be discontinued in case of adverse reactions related to long-term use of corticosteroid.1 For a full list of adverse reactions please refer to the Enstilar® SPC.1 The total dose of all calcipotriol containing products should not exceed 15 g per day.1 The total body surface area treated should not exceed 30%.1
Prescribing Information for Ens tilar ® (calcipotriol/betamethasone)
50 micrograms/g + 0.5 mg/g cutaneous foam
Please refer to the full Summary of Product Characteristics (SmPC) (www.medicines.org.uk/emc) before prescribing.
Indication: Topical treatment of psoriasis vulgaris in adults. Active ingredients: 50 µg/g calcipotriol (as monohydrate) and 0.5 mg/g betamethasone (as dipropionate). Dosage and adminis tration: Flare treatment: Apply by spraying onto affected area once daily. Recommended treatment period is 4 weeks. If it is necessary to continue or restart treatment after this period, treatment should be continued after medical review and under regular supervision. Long-term maintenance treatment: Patients who have responded at 4 weeks’ treatment using Enstilar once daily are suitable for long-term maintenance treatment. Enstilar should be applied twice weekly on two non-consecutive days to areas previously affected by psoriasis vulgaris. Between applications there should be 2-3 days without Enstilar should be re-initiated Maximum dose: The daily maximum dose of Enstilar should not exceed 15 g, i.e. one 60 g can should last for at least 4 days of treatment. 15 g corresponds to the amount administered from the can if the actuator is fully depressed for approximately one minute. A two-second application delivers approximately 0.5 g. As a guide, 0.5 g of foam should cover an area of skin roughly corresponding to the surface area of an adult hand. If using other calcipotriol-containing medical products in addition to Enstilar, the total dose of all calcipotriol-containing products should not exceed 15 g per day. Total body surface area treated should not exceed 30%.
below 18 years have not been established. Shake the can for a few seconds before use. Apply by spraying, holding the can at least 3 cm from the skin, in any orientation except horizontally. Spray directly onto each affected skin area and rub in gently. If used on the scalp, spray into the palm of the hand
used to treat the hands) to avoid accidentally spreading to other parts of the body as well as unintended drug absorption on the hands. Avoid application under occlusive dressings since systemic absorption of corticosteroids increases. It is recommended not to take a shower or bath immediately after application. Let the foam remain on the scalp and/or skin during the night or during the day. Contraindications: Hypersensitivity to the active substances or any of the excipients. Erythrodermic and pustular psoriasis. Patients with known disorders of calcium metabolism. Viral (e.g. herpes or varicella) skin lesions, fungal or bacterial skin infections, parasitic infections, skin
manifestations in relation to tuberculosis, perioral dermatitis, atrophic skin, striae atrophicae, fragility of skin veins, ichthyosis, acne vulgaris , acne rosacea, rosacea, ulcers and wounds. Precautions and warnings: Adverse reactions found in connection with systemic corticosteroid treatment, e.g. adrenocortical suppression or impaired glycaemic control of diabetes mellitus, may occur also during topical corticosteroid treatment due to systemic absorption. Application under occlusive dressings should be avoided since it increases the systemic absorption of corticosteroids. Application on large areas of damaged skin, or on mucous membranes or in skin folds should be avoided since it increases the systemic absorption of corticosteroids. Visual disturbance may be reported with systemic and topical corticosteroid use. If a patient presents with symptoms such as blurred vision or other visual disturbances, the patient should be considered for a referral to an ophthalmologist for evaluation of possible causes which may include cataract, glaucoma or rare diseases such as central serous chorioretinopathy (CSCR) which have been reported after use of systemic and topical corticosteroids. Due to the content of calcipotriol, hypercalcaemia may occur. Serum calcium is normalised when treatment is discontinued. The risk of hypercalcaemia is minimal when the maximum daily dose of Enstilar (15 g) is not exceeded. Enstilar contains a potent group III-steroid and concurrent treatment with other steroids on the same treatment area must be avoided. The skin on the face and genitals is very sensitive to corticosteroids. Enstilar should not be used in these areas. Instruct the patient in the correct use of the product to avoid application and accidental transfer to the face, mouth and eyes. Wash hands after each application to avoid accidental transfer to these areas as well as unintended drug absorption on the hands. If lesions become secondarily infected, they should be treated with antimicrobiological therapy. However, if infection worsens, treatment with corticosteroids should be discontinued. When treating psoriasis with topical corticosteroids, there may be a risk of rebound effects when discontinuing treatment. Medical supervision should therefore continue in the posttreatment period. Long-term use of corticosteroids may increase the risk of local and systemic adverse reactions. Treatment should be discontinued in case of adverse reactions related to long-term use of corticosteroid. There is no experience with the use of Enstilar in guttate psoriasis. Enstilar contains butylhydroxytoluene (E321), which may cause local skin reactions (e.g. contact dermatitis), or irritation to the eyes and mucous membranes. Pregnancy and lactation: There are no adequate data from the use of Enstilar in pregnant women. Enstilar should only be used during pregnancy when the prescribing Enstilar to women who breast-feed. The patient should be instructed not to use Enstilar on the breast when breast-feeding. Side effects:
There are no common adverse reactions based on the clinical studies. The most frequently reported adverse reactions are application site reactions. Uncommon (≥1/1,00 0 to <1/100): Folliculitis, hypersensitivity, hypercalcaemia, skin hypopigmentation, rebound effect, application site pruritus, application site irritation, application site pain (including application site burning). Not known (cannot be estimated from available data): Blurred vision, application site erythema, hair colour changes. Calcipotriol: Adverse reactions include application site reactions, pruritus, skin irritation, burning and stinging sensation, dry skin, erythema, rash, dermatitis, psoriasis aggravated, photosensitivity and hypersensitivity reactions, including very rare cases of angioedema and facial oedema. Systemic effects after topical use may appear very rarely causing hypercalcaemia or hypercalciuria. Betamethasone: Local reactions can occur after topical use, especially during prolonged application, including skin atrophy, telangiectasia, striae, folliculitis, hypertrichosis, perioral dermatitis, allergic contact dermatitis, depigmentation and colloid milia. When treating psoriasis with topical corticosteroids, there may be a risk of generalised pustular psoriasis. Systemic reactions due to topical use of corticosteroids are rare in adults; however, they can be severe. Adrenocortical suppression, cataract, infections, impaired glycaemic control of diabetes mellitus, and increase of intra-ocular pressu re can occur, especially after long-term treatment. Systemic reactions occur more frequently when applied under occlusion (plastic, skin folds), when applied onto large skin areas, and during long-term treatment. Precautions for storage: container. May burst if heated. Protect from sunlight. Do not expose to temperatures exceeding 50°C. Do not pierce or burn, even after use. Do not Legal category: POM. Marketing authorisation number and holder: PL 05293/00 08. LEO Pharma A/S, Ballerup, Denmark. Basic NHS price: £39.68/60 g, £79.36/2 x 60 g. Last revised: April 2023.
Reference number: REF-23176.
Reporting of Suspected Adverse Reactions
Adverse events should be reported
Reporting forms and information can be found at: www.mhra.gov.uk/yellowcard or search for MHRA Yellow Card in the Google Play or Apple App Store. Adverse events should also be reported to Drug Safety at LEO Pharma by calling +44 (0)1844 347333 or e-mail: medical-info.uk@leo-pharma.com
References: 1. Enstilar® (calcipotriol/betamethasone) SPC 2022. 2. Leonardi C et al. J Drugs Dermatol 2015;14(12):1468–1477. 3. King C and Lowson D. Poster 237 presented at the 5th Psoriasis International Network Annual Meeting, Paris, France, 5–7 July 2016. 4. Lebwohl M et al. J Am Acad Dermatol 2021;84:1269-77.
Entering dermatology as a newly qualified nurse
Dawn Holt
The misconception which many healthcare professionals may have about dermatology could be one of the leading reasons as to why it has been historically challenging to attract newly qualified nurses to choose this specialty.1 It is widely assumed, incorrectly, that there is no established career pathway for staff nurses in an outpatient setting, let alone in dermatology outpatients, which is often regarded as a less attractive clinical area among healthcare professionals and students.
Why dermatology?
Throughout my undergraduate degree, I did not have the opportunity to have a placement within any dermatology unit, and exposure to any dermatology theory was extremely minimal. Practice placement experiences have a major impact on newly qualified nurses, and this impact typically determines the speciality which they may pursue as they begin their nursing career. 2 The level of exposure to a speciality is another element which may influence newly qualified nurses’ interest in their chosen speciality.3 This has been reflected in research studies that have looked at preferred speciality choices among healthcare students, with one systematic review between 2010 to 2022 highlighting a greater preferences for emergency, intensive care and surgical paediatrics, with no nursing students expressing a preference for dermatology.4
Regardless of the minimal exposure to any dermatology centres, I would often
Summary:
encounter patients with skin conditions in acute settings. During my final placement, which was a primary care pilot trial in Lancashire, I had the opportunity to manage the care of my own patients with the support of registered nurses and other clinicians at the practice. The hands-on approach to this placement exposed me to a variety of commonly presenting skin conditions in primary care, including eczema, psoriasis and acne, in addition to suspicious lesions. It became clear to me during lesion checking appointments – which would be referred to dermatology – that there is a large theory gap for dermatology within the undergraduate nursing degree.
It is noted that a large portion of newly trained nursing practitioners do not feel confident in assessing patients with skin disease or potential skin cancers.5 As the rate of skin cancer diagnoses in the UK continue to rise, with an expectancy for melanoma incidence rates to rise by 9% between 2023-2025, 6 it is imperative that undergraduate nursing degree courses take this into consideration when planning the curriculum for nursing students.
“A large portion of newly trained nursing practitioners do not feel confident in assessing patients with skin disease or potential skin cancers”
In this ar ticle, the author, a recently qualified staff nurse, describes the factors which influenced her decision to pursue a career in dermatology. The author started her nursing career in a large dermatology department at a prominent teaching hospital in the North West of England.
Keywords:
Newly qualified nurse, Skin cancer, Competency framework, Role descriptors
The result of early stage detection and diagnosis of skin cancers has proven to be beneficial, for both survival rates and the overall treatment costs to hospitals, compared to skin cancers diagnosed at a much later stage, or those which have progressed to metastatic disease. 7,8 This realisation also led me to reflect on the NMC code,9 particularly
Author info:
Dawn Holt is a Dermatology Clinical Nurse Specialist and Staff Nurse at Dermatology Outpatient Department at Salford Royal Hospital, part of Northern Care Alliance.
Citation: Holt D. Entering dermatology as a newly qualified nurse. Dermatological Nursing 2025. 24(1):25-28.
Professional development
around safe and effective practice. Regardless of the specialty area of nursing, it is important for registered nurses to be able to recognise basic skin concerns and have some understanding of how to effectively manage the care of these patients.
The consultations at this placement allowed me to provide patient-centred care which demonstrates some of the key values held by the Nursing and Midwifery Council (NMC), 9 prioritising people and treating patients with dignity. However, it became clear to me during my placements that there is an active stigma towards many skin conditions. The stigma and disapproving attitudes which dermatology patients face has a significant impact on their mental health and several studies would appear to support my view.
Conceptual models which were created to measure stigmatisation among patients with visible skin conditions, identified that the key themes which were prevalent were rejection, discrimination, and alienation. 10 In some countries, people with visible conditions, such as vitiligo, are rejected from public facing professions, including the armed forces, 11 which indicates the need for awareness of these conditions to be spread globally. One observational cross-section study analysed results from 17 centres across European countries in 2023, 12 which had consistent findings of increased perception of stigmatisation felt by people with visible skin conditions, in comparison to those with a healthy appearance of skin. The importance of demonstrating the NMC9 code of treating people with respect and dignity should be emphasised to nurses by such studies, especially when dealing with patients who have dermatological conditions that make them targets of discrimination in society. My natural interest and passion for dermatology grew over the period I was at this placement. I had realised that for each dermatology referral I had recommended for patients, my desire to be a part of their treatment journey only grew larger.
An additional advantage of choosing this speciality at a teaching hospital, was the opportunity to work alongside multiple clinicians within each sub-speciality, as teaching hospitals usually consist of larger groups of clinicians.
Continuous learning and professional development are recommended within the NMC Code,9 and this is easier to do in an environment that encourages teaching and training regularly. Within the department, many of the consultant dermatologists also have a background in teaching, commonly as an additional career. This has proven to be helpful to me as a newly qualified nurse, as I have been able to learn valuable skills from working with a range of clinicians.
It is widely known that retention of newly qualified nurses within the NHS is difficult, with many leaving the profession shortly after qualifying due to common themes of burnout and the lack of a supportive environment.14 Contrasting factors may encourage newly qualified nurses to continue with their career, such as trusts which value a culture built on support, empowerment and team working.15
“My knowledge of dermatological conditions has significantly developed due to the rotational nature of my role”
The environment created within this department allows for a novice to become equipped with the needed skillset to progress further within dermatology. The local clinical competencies required for band five staff nurses to achieve within their role reflect the British Dermatology Nursing Group’s (BDNG) clinical competencies16 and role descriptors,17 which aids staff nurses within this speciality. The role descriptors and clinical competencies offer a supportive guide to nurses by preparing them in advance for what the requirements are for roles which they aspire to work towards.
Dermatology and continuous development
Upon my decision to enter dermatology, I became excited to learn that there was a vacancy available for a staff nurse in one of the largest dermatology centres in Europe which places itself at the forefront of pioneering research in skin disease. 13 One of the main benefits of choosing this dermatology centre in Salford was the opportunity to explore multiple sub-specialities which exist within dermatology, from both medical and surgical perspectives.
The appeal to progress in dermatology, specifically at Salford, is rooted within the multidisciplinary approaches towards patient care which I have witnessed at this centre across all sub-specialties. Clinicians at this dermatology centre actively demonstrate collaborative working with patient care treated as a true priority. Within the dermatology centre there is an active research presence taking place within most sub-specialties of dermatology, which further validates the use of evidence-based practice in nursing and gives the dermatology speciality a ‘modern’ appeal to recently qualified nurses.
In-house training during the preceptorship period
The preceptorship period for any newly qualified nurse may seem daunting initially, particularly if there has
been limited prior experience in the specific speciality. However, going into dermatology with a positive attitude to learn, paired with some basic knowledge from my own research, allowed me to have an idea of what I may be expecting within my role. During the initial months, my eyes had been opened to discover just how large of a specialty area dermatology is, to the extent that dermatology almost feels like a well-kept secret which many student nurses are yet to discover. The exposure to a wide range of dermatology subspecialties offered an excessive amount of reassurance to me as a newly qualified nurse, contradicting stigmatised opinions of outpatient departments within the nursing profession.
Having now completed one year post qualifying, I am delighted to share that I have been feeling an immense amount of joy to be part of the team at Salford. I have been through various phases of in-house training, including venepuncture, clinics, emergency admissions, surgical scrub nurse assisting in addition to scrub nurse assisting in Mohs micrographic surgery. Exposure to a variety of sub-specialties has allowed me to acquire new skills and develop my knowledge, whilst working towards completing the competencies required for a dermatology nurse. The in-house training which is provided for dermatology nurses blends seamlessly with the preceptorship programme period for newly qualified nurses. Having a structured training programme in dermatology allows nurses to continuously develop their skills and gain confidence in practising safely as per the NMC code,9 while also allowing them to explore which area may be of interest to them in terms of future career progression.
Professional development
in a position where I have been able to learn an extensive amount about different types of presenting conditions, both inflammatory and cancerous (as well as potentially cancerous) in dermatology theatres. The competency frameworks which are in place in the dermatology centre are structured in a way that allows myself and other staff nurses completing their training to thoroughly understand every single component of dermatology theatre. It should also be mentioned that being able to work closely with a range of professionals, including registrars, consultants, advanced nurse practitioners and nurse consultants, within surgical dermatology has been rewarding and educational. From the perspective of a newly qualified nurse, being able to work closely with highly experienced healthcare professionals in this field is important as it has helped me to learn different approaches over time.
“The feeling of supporting patients and their families through part of a cancer diagnosis and treatment is quite like no other”
My knowledge of dermatological conditions has significantly developed due to the rotational nature of my role. I have also been provided with a new skill set particularly within surgical dermatology. Whilst most general nursing roles may focus solely on either medical or surgical, the role of a dermatology nurse combines both surgical and medical care to treat patients. Entering any speciality without prior experience in the area may be perceived as challenging. In contrast to this, the local competencies, which have been set for band five staff nurses to complete, have allowed me to feel supported as it is structured in a way that encourages continuous learning in multiple areas of interest.
The in-house dermatology scrub nurse training has proven to be an exciting challenge, as it has put me
One area of in-house training that has had a significant impact on me has been training to assist in Mohs micrographic surgery. This has particularly sparked my interest in patient skin cancer support, as this aspect of nursing has always been of interest to me. Providing emotional support to patients and their relatives throughout surgical procedures is an element which I have found rewarding, as it has required me to explore more deeply into communication techniques and strategies that are helpful in relation to how patients are affected by cancer. It has been highlighted, across several studies, that patient centred communication can significantly influence outcomes for patients receiving cancer care.18 Studies have found that therapeutic communication techniques heavily influence elements of the patient’s quality of life, such as levels of anxiety and symptom control, both of which may be improved due to the style of communication being used by the practitioner.19
An additional suggestion for the in-house competencies that would appeal to newly qualified staff members may be to have additional training material provided, such as the use of digital learning through the trust’s e-learning portal; having theoretical training alongside practical in-house training may be beneficial, as the foundation of knowledge learned through theory learning may improve alongside the practical skills, and vice versa. Although practical learning has proven to be valuable to learners, theory-based learning provides cognitive engagement, whereby nurses are able to understand, evaluate and apply their scientific knowledge into practical scenarios which they encounter. 20
Future goals and progression
My current intentions for career progression would be to develop my knowledge and skills in relation to skin cancers, working towards the goal of becoming a skin cancer clinical nurse specialist. One key driver behind my decision to work towards a skin cancer role is due to my positive experience working within the department, most specifically in Mohs micrographic surgery. The feeling of supporting patients and their families through part of a cancer diagnosis and treatment is quite like no other. The NMC strategy21 emphasises the value of acting with kindness to others, which can be demonstrated in situations such as surgical procedures and clinic appointments in dermatology. Expanding my knowledge through practical exposure and theoretical learning would allow me to provide a high level of care for this specific patient group. Additionally, in the future, I wish to contribute towards the support services available for patients with a melanoma diagnosis, as it is important to recognise how health outcomes are influenced by cancer support.
The experiences which I have gained from a combination of medical and surgical dermatology have led me to the conclusion that the aspect of my career which I enjoy most is providing support to patients, during moments where they need it most. Furthermore, I believe that if more student nurses were exposed to this speciality throughout their undergraduate training, it would attract more newly qualified nurses to join the dermatology speciality as they would be able to view dermatology in a positive light and see the support that is in place to allow them to progress through their nursing career.
References
1. Penzer-Hick R. Career pathways for dermatology nurses. Dermatological Nursing 2022. 21(3):3-5 Available at: https://bdng. org.uk/wp-content/uploads/2022/09/25BDNGDN.pdf [last accessed December 2024]
2. Wareing M, Taylor R, Wilson A, Sharples A. Impact of clinical placements on graduates’ choice of first staff-nurse post. British Journal of Nursing 2018. 27(20):1180-5
3. Anyango E, Adama E, Brown J, Ngune I. The impact of finalyear clinical placements on nursing students’ career planning for the graduate year and beyond. Nurse Education in Practice 2024. 76:103944
4. Stanley N, Binti Bakar RS, Cheng KY, Nwedu AB, Binti Hassan II. Career intentions and the determining factors among health science students: A systematic review. Creative Nursing 2023. 29(1):65-97
5. Woodmansee R, Turnage D, Loerzel V. Nurse practitioner student knowledge and attitudes toward skin cancer assessments. Journal of the Dermatology Nurses’ Association 2018. 10(2):115-9
6. Cancer Intelligence Team at Cancer Research UK, Melanoma skin cancer incidence statistics 2023. Available at: https://www. cancerresearchuk.org/health-professional/cancer-statistics/statisticsby-cancer-type/melanoma-skin-cancer/incidence#ref-10 [last accessed December 2024]
7. Ahmed B, Qadir MI, Ghafoor S. Malignant melanoma: skin cancer− diagnosis, prevention, and treatment. Critical Reviews™ in Eukaryotic Gene Expression 2020. 30(4)
8. Serra-Arbeloa P, Rabines-Juárez ÁO, Álvarez-Ruiz MS, GuillénGrima F. Cost of cutaneous melanoma by tumor stage: a descriptive analysis. Actas Dermo-Sifiliográficas (English Edition) 2017. 108(3):229-36
9. Nursing and Midwifery Council. The Code. NMC 2023. Available at: https://www.nmc.org.uk/standards/code/read-the-code-online/ [last accessed December 2024]
10. Germain N, Augustin M, François C, Legau K, Bogoeva N, Desroches M et al. Stigma in visible skin diseases–a literature review and development of a conceptual model. Journal of the European Academy of Dermatology and Venereology 2021. 35(7):1493-504
11. Silveira LP, Grijsen ML, Follador I, Dellatorre G. How persistent stigma and discrimination keep people with visible skin diseases out of jobs: vitiligo in Brazil today. The Lancet Regional Health–Americas 2023. 23
12. Van Beugen S, Schut C, Kupfer J, Bewley AP, Finlay AY, Gieler U et al. Perceived stigmatization among dermatological outpatients compared with controls: an observational multicentre study in 17 European countries. Acta Dermato-Venereologica 2023. 103
13. Northern Care Alliance. Dermatology – Salford Royal. NHS Foundation Trust 2024. Available at: https://www. northerncarealliance.nhs.uk/our-services/dermatology [last accessed December 2024]
14. Ho SS, Stenhouse R, Snowden A. ‘It was quite a shock’: A qualitative study of the impact of organisational and personal factors on newly qualified nurses’ experiences. Journal of Clinical Nursing 2021. 30(15-16):2373-85
15. Northern Care Alliance. Our Values – Salford Royal [Internet]. NHS Foundation Trust 2024. Available at: https://www. northerncarealliance.nhs.uk/about-us/our-values [last accessed December 2024]
16. British Dermatology Nursing Group, Dermatology Nursing Competencies. BDNG 2012. Available at: https://bdng.org.uk/ wp-content/uploads/2017/02/nursing_competencies_2.pdf [last accessed December 2024]
17. British Dermatology Nursing Group, British Association of Dermatologists. Clinical Dermatology Nursing Role Descriptors: Guidance on scope of practice. BDNG 2023. Available at: https:// bdng.org.uk/wp-content/uploads/2017/02/Clinical-DermatologyNursing-Role-Scope-of-practice-guide-bands-5-8-FINAL2.pdf [last accessed December 2024]
18. Ong LM, Visser MR, Lammes FB, De Haes JC. Doctor–patient communication and cancer patients’ quality of life and satisfaction. Patient Education and Counseling 2000. 41(2):145-56
19. Supportive PD, Board PC. Communication in Cancer Care (PDQ®). National Cancer Institute (US). In PDQ Cancer Information Summaries 2008
20. Norris Waller M, Newsome Wicks M. Is There Still Value in Teaching Nursing Theory? Journal of Nursing Education 2021. 60(11):603-4
21. Nursing and Midwifery Council. NMC Regulate Support Influence Strategy 2020-2025. NMC 2020. Available at: https:// www.nmc.org.uk/globalassets/sitedocuments/strategy/nmcstrategy-2020-2025.pdf [last accessed December 2024].
KLISYRI® (tirbanibulin) is indicated for the field treatment of non-hyperkeratotic, non-hypertrophic actinic keratosis (AK, Olsen grade 1) of the face or scalp in adults.1
A PREFERED AK TREATMENT EXPERIENCE FOR YOUR PATIENTS3
KLISYRI® (TIRBANIBULIN) PRESCRIBING INFORMATION
Please consult the Summary of Product Characteristics (SmPC) before prescribing. Klisyri 10 mg/g ointment Active Ingredient: Each gram of ointment contains 10 mg of tirbanibulin. Each sachet contains 2.5 mg of tirbanibulin in 250 mg ointment. Excipients with known effects: Propylene glycol 890 mg/g ointment Indication: Klisyri is indicated for the field treatment of non-hyperkeratotic, non hypertrophic actinic keratosis (Olsen grade 1) of the face or scalp in adults. Dosage and Administration: Tirbanibulin ointment should be applied to the affected field on the face or scalp once daily for one treatment cycle of 5 consecutive days. A thin layer of ointment should be applied to cover the treatment field of up to 25cm2 Consult SmPC and package leaflet for full method of administration. Contraindications, Precautions and Warnings: Contraindications: Hypersensitivity to the active substance or to any of the excipients listed in section 6.1 of SmPC. Precautions: Contact with the eyes should be avoided. Tirbanibulin ointment may cause eye irritation. In the event of accidental contact with the eyes, the eyes should be rinsed immediately with large amounts of water, and the patient should seek medical care as soon as possible. Tirbanibulin ointment must not be ingested. If accidental ingestion occurs, the patient should drink plenty of water and seek medical care. Tirbanibulin ointment should not be used on the inside of the nostrils, on the inside of the ears, or on the lips. Application of tirbanibulin ointment is not recommended until the skin is healed from treatment with any previous medicinal product, procedure or surgical treatment and should not be applied to open wounds or broken skin where the skin barrier is compromised. Local skin reactions in the treated area, may occur after topical application. Treatment effect may not be adequately assessed until resolution of local skin reactions. Due to the nature of the disease, excessive exposure to sunlight (including sunlamps and tanning beds) should be avoided or minimised. Tirbanibulin ointment should be used with caution in immunocompromised patients. Changes in the appearance of actinic keratosis could suggest progression to invasive squamous cell carcinoma. Propylene glycol may cause skin irritation. Consult SmPC and package leaflet for more information. Fertility, pregnancy and lactation: No human data on the effect of tirbanibulin ointment on fertility are available. Tirbanibulin
Reference: 1. KLISYRI® SmPC. Almirall. 2. Blauvelt A, et al. N Engl J Med. 2021;384(6):512-520. 3. Schlesinger T et al. Skin, 2023: 7(3); 771-787. PROVEN EFFICACY2
ointment is not recommended during pregnancy and in women of childbearing potential not using contraception. It is unknown whether tirbanibulin/metabolites are excreted in human milk. A risk to the newborns/infants cannot be excluded. Consult SmPC and package leaflet for more information. Adverse Reactions: Very common (≥1/10): Application site - erythema; exfoliation; scab; swelling; erosion. Common (≥1/100 to <1/10): Application site - pain, pruritus and vesicles. Consult SmPC and package leaflet for further information. Legal Category: Ireland: POM Subject to prescription which may not be renewed (A). United Kingdom & Northern Ireland: POM Price: Ireland: Price to wholesaler United Kingdom & Northern Ireland: UK NHS Cost: £59.00 (excluding VAT). Marketing Authorisation Numbers: Ireland and Northern Ireland: EU/1/21/1558/001 Great Britain: PLGB 16973/0043 Marketing Authorisation Holder: Almirall, S.A., Ronda General Mitre, 151 08022 Barcelona, Spain Further information available from: Almirall Limited, Harman House, 1 George Street, Uxbridge, Middlesex, UB8 1QQ, UK. Date of First Issue: August 2021 Item code: IETIRBA-2100011 Complete information on where to find reportingforms and information for adverse events search MHRA Yellow Card in the Google Play or Apple App Store.
UK and UK(NI)-Adverse events should be reported. Reporting forms and information can be found at MHRA https:// yellowcard.mhra.gov.uk Adverse events should be also reported to Almirall Ltd. Tel. 0800 0087 399
IE-Adverse events should be reported. Reporting forms and information can be found at HPRA Website: www.hpra.ie. Adverse events should be also reported to Almirall Ltd. Tel. +353 (0) 1431 9836
Aklief is a topical retinoid indicated for the cutaneous treatment of moderate acne vulgaris of the face and/or trunk in patients from 12 years of age and older when many comedones, papules and pustules are present
Aklief is contraindicated during pregnancy or for women planning a pregnancy.
On becoming a research nurse in dermatology: Challenges and achievements
Rebekah Higgins
Throughout this piece I will be sharing my experiences on becoming a research nurse. To provide a bit of background on myself, I qualified as a Registered Nurse in 2018 and started my role as a Dermatology Staff Nurse in 2021. It’s safe to say that I fell in love with dermatology.
An exciting opportunity became available in the department, and after expressing my interest, I was fortunate enough to have been selected for a three-month secondment as a Dermatology Research Nurse for two days a week. Before this experience, I was completely new to the research role. After the secondment finished, the opportunity arose again for me to apply for a two days per week post as a Dermatology Research Nurse, this time over 12 months, and I was fortunately successful.
Working as a Dermatology Research Nurse, given my background in dermatology, is very useful. I have an understanding of the main types of skin conditions that are commonly seen in the department, and this means I have knowledge of medical terminology of the skin, and I am familiar with skin assessments that may be required for a study.
The main types of skin conditions that are seen in the department are psoriasis, eczema and acne, and these cohorts of patients are mainly who I see as a research nurse.
Becoming a research nurse
The first significant hurdle in my transition to research nursing was completing Good Clinical Practice (GCP)
Summary:
training.1 My organisation generously allowed me the time to focus entirely on this course, which proved invaluable. GCP training has equipped me with foundational knowledge about clinical research processes, ethical standards, and patient safety – a starting point for anyone entering this field.
“The first significant hurdle in my transition to research nursing was completing Good Clinical Practice (GCP) training”
Joining the research team, I felt nervous for the change. I was completely new to research nursing, and I am currently the only Dermatology Research Nurse. However, I am surrounded by so much support from all who I have met in the research department in my organisation, especially the management team who have given me the support and guidance to feel confident in my role.
When I first started my secondment and completed my Good Clinical Practice training, I was able to start working on two studies that were currently running in my department. I was able to shadow other research
In this ar ticle, the author describes how they managed to build on their passion for dermatology by embracing research. The article considers the author’s achievements and challenges, as well as discussing what they would like to achieve as they become more confident in the research world.
Author info:
Rebekah Higgins is a Staff Nur se and Research Nurse in Dermatology at Hull University Teaching Hospitals NHS Trust
Citation:
Higgins R. On becoming a research nurse in dermatology: Challenges and achievements Dermatological Nursing 2025 24(1): 31-34.
Keywords: Research, Dermatology, BADBIR, Clinical study
Professional development
teams in the hospital where I work and get a general feel for the research nursing role. I got to spend time with experienced members of staff who were very knowledgeable. I was also able to shadow the research nurses’ approach to patients taking part in a research study and how to obtain informed consent.
I was then shown the online databases that are used for inputting data for the studies running in my department and completed the appropriate training to use them. I was also introduced to the wider study teams.
“One of my primary responsibilities during the secondment was working on BADBIR”
Achievements
One of my primary responsibilities during the secondment was working on BADBIR (British Association of Dermatologists Biologic and Immunomodulators Register),2 an observational study that tracks the long-term safety of biologic treatments for psoriasis. When I joined the team in January 2024, there had been a gap in research nurse coverage for several months, resulting in a backlog of 65 outstanding follow-up entries.
My main responsibilities as a research nurse when working on BADBIR have
been to gather information from the notes from follow-up clinics. A patient will have a follow-up with a doctor or a nurse specialist, and I will collect the data and input into the electronic database. Another responsibility is ensuring that adverse events are inputted into the system. If I am not certain about any adverse event, I will seek help from the study Principal Investigator (PI). I also am responsible for answering data queries. I need to show data analysis skills to answer data queries, as finding the correct data in the notes is not always easy. I have reached out to the study team many times to talk through queries and advice on how to respond to certain questions that could be difficult to answer. This has helped me with answering queries, as I have been able to work as a team with the study provider and PI to make joint decisions on inputting data.
Over the course of the secondment, I worked diligently to complete these follow-ups. By the end of three months, I had successfully cleared the backlog of 65 entries and had catalogued, analysed and reported on them answering any queries that were raised.
Detailed results of the analysis are in Table 1.
Summary of key achievements in BADBIR
Our efforts were recognised when BADBIR awarded our centre ‘Centre of the Month’, which was a proud moment for our team.
I also had the honour of presenting at the British Dermatology Nursing Group (BDNG) Conference. Sharing my experience working on BADBIR and offering tips for handling data queries was a nerve-wracking but rewarding
Task Completed Entries Queries Answered Adverse Events Documented Follow-Up Data
experience. My presentation included a step-by-step guide to data collection, entry, and organisation – all skills that had helped me excel in my role.
My intention when presenting was to share with other healthcare professionals, who may be in the same situation as myself, the benefits of reaching out for help from the study provider. I received such good guidance and help from the team at BADBIR to help build my confidence working on their study, and this has helped me when working on future studies.
“As the sole research nurse in the department, I have developed strategies to manage my workload, including setting weekly targets and creating structured plans”
I also received a lot of support and guidance from the PI, speciality doctor and clinical nurse specialist working on BADBIR in my department. The feedback from attendees was overwhelmingly positive, and I felt gratified to know my insights might assist others managing BADBIR at their organisations. This experience also opened another exciting opportunity: I was invited to write an article for the BDNG’s journal –which you are now reading!
When I completed the queries for BADBIR, I had to do a lot of problem solving. Some queries were backdated to before I was part of the team, so it took a lot of time to capture the correct data to respond to the
Table 1: Summary of key achievements in BADBIR (January-March 2024)
Professional development
queries. I really enjoyed taking the time to respond to the queries, as this gave me my first taste into research nursing, learning how to be analytical and provide attention to detail to find correct data.
I have been able to give the department updates on the current research studies in our monthly newsletter, and this has been a benefit to the team as they can see what they are a part of. Some members of the team in the department are new, and these updates can help to inspire newer staff members to be part of the upcoming research studies if it gains their interest.
Challenges
Even with these achievements, I have faced some challenges.
Learning a new role
As someone with six years of nursing experience, but no prior research background, I found it challenging to familiarise myself with research terminology, protocols, and processes. To address this, I dedicated time to self-study and relied on the expertise of consultants, doctors, specialist nurses, and senior research staff within my department. Their guidance was invaluable.
Time management
I balance two distinct roles within the dermatology department: working two days a week as a research nurse and three days a week as a staff nurse. This dual role requires careful prioritisation and time management.
In my staff nurse role, patient care and workload are shared responsibilities among the team, ensuring collaborative care delivery. In contrast, my research nurse role is more individualised, involving the identification and recruitment of patients for clinical studies. Patients are typically referred to me by healthcare professionals within the department, based on potential eligibility for a study. If I miss seeing a patient in the clinic, I follow up to provide additional information about the study. For those expressing
interest, I coordinate their return to the department at a time when the PI is available.
Teamwork is crucial in managing my responsibilities effectively. Ensuring the department team is familiar with the studies and their eligibility criteria streamlines the process of identifying participants. Additionally, having the PI present during patient visits enhances efficiency, as the PI can assess suitability, engage in joint decision-making with me, and address any patient questions that extend beyond my expertise.
As the sole research nurse in the department, I have developed strategies to manage my workload, including setting weekly targets and creating structured plans. While this role comes with challenges, I find it deeply rewarding. The autonomy and responsibility of this position has allowed me to grow professionally and contribute meaningfully to both patient care and clinical research.
“I am excited to grow in my role as a Dermatology Research Nurse, gaining new skills, deepening my experience and exploring where this path may lead”
Limited experience
When I started in my role, I started working on a study that was already ongoing and established within the department. It has taken me some time to complete the relevant training needed for the study and to go through the protocol and site file to become familiar with the study. I am
currently setting up new studies in the department, and being involved from the beginning offers a clearer understanding of a study’s requirements and processes.
Being completely new to the role, I do have a lack of knowledge regarding research compared to others. I am trying my best to work on this, while being aware that I respect my limitations and always seek help and guidance from someone senior before doing something I am unsure of.
Communication and collaboration
Research nursing has required me to step out of my comfort zone, liaising with a wide range of individuals, including consultants, study teams, and non-clinical staff. Building these relationships and honing my communication skills have been integral to my growth in this role.
Skills development
Due to these new challenges, the role has enabled me to develop a range of new skills:
l A nalytical thinking: Due to addressing data queries, this has taught me to be thorough and specific, especially when working with historical data
l B eing organised: Working part time in this role has developed a new range of time management skills and the ability to prioritise tasks effectively
l Co mmunication: Engaging with new colleagues, patients, and external study teams has allowed me to develop my communication skills, which is needed to ensure clear and professional communication
l P roblem-solving: I have been able to navigate unexpected challenges, such as long-standing data queries, which has strengthened my adaptability.
Working as a research nurse
Whilst working on other studies in the department, I have been able to recruit new patients.
Professional development
I place great emphasis on providing quality time and compassionate care when working with patients who are being considered for clinical studies. When a healthcare professional identifies a patient as potentially eligible for a study, I allocate myself sufficient time during our first session to ensure a detailed and supportive conversation. This dedicated time allows me to provide detailed information about the study, address patient concerns through active listening, and ensure the patient is reviewed by the PI. This collaborative process, with input from the PI and the referring healthcare professional, ensures that decisions regarding the patient’s suitability are made as a team, carefully considering the study’s inclusion and exclusion criteria and adhering to the protocol requirements.
The initial meeting with the patient is pivotal. Through active listening, I aim to create a space where patients feel heard, valued, and comfortable voicing their concerns. Having the PI present ensures that all questions, including those outside my scope of knowledge, are answered promptly and accurately. This approach not only enhances the patient’s understanding of the study but also facilitates informed consent, ensuring that they feel confident and supported in their decision to participate.
Building trust and fostering relationships with patients is a significant aspect of my role. Many studies span long periods, requiring me to engage with patients at regular intervals, either face-to-face or over the phone. As the primary point of contact for study-related concerns, I strive to be approachable and provide reassurance. I encourage patients to reach out whenever needed, reinforcing their trust in me and in the process.
By prioritising quality time, compassionate communication, and teamwork, I bring significant value to patients navigating the complexities of clinical research. This approach not only ensures their comfort and understanding but also enhances the overall quality of care and their experience as study participants.
Looking ahead
Since COVID-19, the research in my department has been limited. I hope to expand and develop dermatology research to help contribute to the advancements in dermatology care.
I am excited to grow in my role as a Dermatology Research Nurse, gaining new skills, deepening my experience and exploring where this path may lead. My aim is to continue a long career in dermatology research and take on new trials that are offered
to the department. I will try to build up the portfolio for the department as my experience and knowledge increases. I have also booked onto some further training regarding informed consent to consolidate my knowledge and display that into practice in the near future.
I am surrounded by so many knowledgeable and supportive colleagues in my department and I feel like this has led to the achievements I have made so far, such as presenting at a national conference and contributing to a professional journal. I am very grateful. For anyone considering a similar role, my advice is to embrace the opportunities and challenges, seek out support, and take pride in the work you do and the contributions you make to patient care.
Conflict of interest
The author declares no conflict of interest.
References
1. Good Clinical Pr actice (GCP) Training Manual. Medicines and Healthcare Products Regulatory Agency (MHRA). Stationary Office, 2012
2. Br itish Association of Dermatologists Biologic and Immunomodulators Register (BADBIR). Available at: http://www.badbir. org/ [last accessed February 2025].
Call for papers
Each year, the Dermatological Nursing Editorial Board actively seeks and encourages colleagues to write up their work and publish. As Clinical Editor, I support this and would like to highlight this call for papers.
l A re you interested in having your work published?
l Have you completed some work or project which enhances knowledge, skills or dermatology nursing?
l Do you have a patient case study that would be of interest to our readership?
l Have you recently completed an audit that has informed practice development or service delivery?
l Have you recently completed a dissertation or a literature review?
l Is there a particular clinical area that interests you and you wish to share?
l Do you have a medical or nursing colleague who would like to write for publication?
If so, please consider submitting a paper to Dermatological Nursing
Support and advice is available to guide you through the writing process, so please, do not hesitate to contact myself, Jackie, Rob or any member of the Editorial Board for advice. (Email addresses are listed in the journal).
For the treatment of moderate to severe atopic dermatitis in adult and adolescent patients 12 years and older who are candidates for systemic therapy1,2
Prescribing Information for Adtralza® (tralokinumab) 150 mg solution for injection in pre-filled syringe and Adtralza® (tralokinumab) 300 mg solution for injection in pre-filled pen Please refer to the full Summary of Product Characteristics (SmPC) (www.medicines.org.uk/emc) before prescribing.
This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions. Indications: Treatment of moderate-to-severe atopic dermatitis in adult and adolescent patients 12 years and older who are candidates for systemic therapy. Active ingredients: Each pre-filled syringe contains 150 mg of tralokinumab in 1 mL solution (150 mg/mL). Each pre-filled pen contains 300 mg of tralokinumab in 2 mL solution (150 mg/mL). Dosage and administration: Posology: The recommended dose of tralokinumab for adult and adolescent patients 12 years and older is an initial dose of 600 mg (four 150 mg injections by prefilled syringe or two 300 mg injections by pre-filled pen) followed by 300 mg (two 150 mg injections by pre-filled syringe or one 300 mg injection by pre-filled pen) administered every other week as subcutaneous injection. Every fourth week dosing may be considered for patients who achieve clear or almost clear skin after 16 weeks of treatment. The probability of maintaining clear or almost clear skin may be lower with every fourth week dosing. Consideration should be given to discontinuing treatment in patients who have shown no response after 16 weeks of treatment. Some patients with initial partial response may subsequently improve further with continued treatment every other week beyond 16 weeks. Tralokinumab can be used with or without topical corticosteroids. The use of topical corticosteroids, when appropriate, may provide an additional effect to the overall efficacy of tralokinumab. Topical calcineurin inhibitors may be used, but should be reserved for problem areas only, such as the face, neck, intertriginous and genital areas. Missed dose: If a dose is missed, the dose should be administered as soon as possible and then dosing should be resumed at the regular scheduled time. Special populations: No dose adjustment is recommended for elderly patients, patients with renal impairment or patients with hepatic impairment. For patients with high body weight (>100 kg), who achieve clear or almost clear skin after 16 weeks of treatment, reducing the dosage to every fourth week might not be appropriate. The safety and efficacy of tralokinumab in children below the age of 12 years have not yet been established. Method of administration: Subcutaneous use. The pre-filled syringe and pen should not be shaken. After removing the pre-filled syringes or pre-filled pens from the refrigerator, they should be allowed to reach room temperature by waiting for 30 minutes before injecting a pre-filled syringe or 45 minutes before injecting a pre-filled pen. Tralokinumab is administered by subcutaneous injection into the thigh or abdomen, except the 5 cm around the navel. If somebody else administers the injection, the upper arm can also be used. For the initial 600 mg dose, four 150 mg tralokinumab injections or two 300 mg tralokinumab injections, should be administered consecutively in different injection
Adtralza® has demonstrated up to 3 years of skin clearance: 73% of patients achieved a 75% improvement in Eczema Area and Severity Index (EASI-75) at 3 years (n=29/40).1-3 Based on a 3-year subgroup interim analysis of ECZTEND.3
The most common adverse reactions with Adtralza® are upper respiratory tract infections (23.4%; mainly reported as common cold), injection site reactions (7.2%), conjunctivitis (5.4%) and conjunctivitis allergic (2.0%).1,2
Not an actual patient. For illustrative purposes only. Individual results may vary.
There is limited amount of data from the use of Adtralza® in pregnant women.1,2 As a precautionary measure, it is preferable to avoid the use of Adtralza® during pregnancy.1,2
sites within the same body area. It is recommended to rotate the injection site with each dose. Tralokinumab should not be injected into skin that is tender, damaged or has bruises or scars. A patient may self-inject tralokinumab or the patient’s caregiver may administer tralokinumab if their healthcare professional determines that this is appropriate. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Precautions and warnings: If a systemic hypersensitivity reaction (immediate or delayed) occurs, administration of tralokinumab should be discontinued and appropriate therapy initiated. Patients treated with tralokinumab who develop conjunctivitis that does not resolve following standard treatment should undergo ophthalmological examination. Patients with pre-existing helminth infections should be treated before initiating treatment with tralokinumab. If patients become infected while receiving tralokinumab and do not respond to antihelminth treatment, treatment with tralokinumab should be discontinued until infection resolves. Live and live attenuated vaccines should not be given concurrently with tralokinumab. Interactions:
See SmPC for full details on interactions. Fertility, pregnancy and lactation: There is limited data from the use of tralokinumab in pregnant women. Animal studies do not indicate direct or indirect harmful effects with respect to reproductive toxicity. As a precautionary measure, it is preferable to avoid the use of tralokinumab during pregnancy. It is unknown whether tralokinumab is excreted in human milk or absorbed systemically after ingestion. Animal studies did not show any effects on male and female reproductive organs and on sperm count, motility and morphology. Side effects: Very common (≥1/10): Upper respiratory tract infections. Common (≥1/100 to <1/10): conjunctivitis, conjunctivitis allergic, eosinophilia, injection site reaction. Please see SmPC for full list of side effects. Precautions for storage: Store in a refrigerator (2°C-8°C). Do not freeze. Store in the original package in order to protect from light. Legal category: POM. Marketing authorisation number and holder: Pre-filled syringe: PLGB 05293/0182, EU/1/21/1554/002. Pre-filled pen: PLGB 05293/0189, EU/1/21/1554/004. LEO Pharma A/S, Ballerup, Denmark. Basic NHS price: 4 pre-filled syringes: £1,070 (each syringe contains 150 mg of tralokinumab in 1 mL solution (150 mg/mL)). 2 pre-filled pens: £1,070 (each pen contains 300 mg of tralokinumab in 2 mL solution (150 mg/mL)). Last revised: January 2024. Reference number: MAT-70774.
Reporting of Suspected Adverse Reactions
Adverse events should be reported.
Reporting forms and information can be found at: www.mhra.gov.uk/yellowcard or search for MHRA Yellow card in the Google Play or Apple App Store.
Adverse events should also be reported to Drug Safety at LEO Pharma by calling +44 (0)1844 347333 or e-mail: medical-info.uk@leo-pharma.com
® Registered trademark
Roflumilast: Is it a dermatological panacea?
Rod Tucker
Background
The ability of cells to process and respond to extracellular signals from hormones and cytokines is crucial to life. This processing of external signals is accomplished via intracellular secondary messenger molecules, and one that has been extensively studied is cyclic adenosine monophosphate (cAMP). First discovered in 1958, it has become clear that cAMP has an important role in several biological processes. In relation to inflammatory diseases, for example, elevated levels of cAMP reduce the production of pro-inflammatory mediators and increase expression of anti-inflammatory agents within immune cells.1 cAMP is hydrolysed by a series of phosphodiesterase (PDE)-4 enzymes. What’s more, the activity of PDE-4 enzymes is elevated in immune-mediated inflammatory conditions such as psoriasis.2 Consequently, targeting the PDE4 enzyme has become an important approach in the management of inflammatory diseases, because this action upregulates cAMP and increases expression of anti-inflammatory mediators.3
This method has been utilised in the management of airway inflammatory conditions such as COPD and asthma, but more recently PDE-4 inhibitors have been explored in the management of psoriasis. The first PDE-4 inhibitor used was apremilast, which received European approval for treating moderate to severe psoriasis in 2015. As a PDE-4 inhibitor, roflumilast has also been investigated as a possible treatment for psoriasis. But since PDE-4 activity is elevated in a number of inflammatory conditions, roflumilast has the potential to treat other inflammatory-mediated conditions.
Summary:
Roflumilast is a selective phosphodiesterase-4 inhibitor initially approved for maintenance treatment of chronic obstructive pulmonary disease (COPD). Yet in recent years, the drug has been approved for the management of psoriasis, atopic eczema and seborrhoeic eczema in the US. Moreover, on-going studies are exploring the value of roflumilast for other skin conditions. But where might roflumilast sit in the dermatology treatment landscape and is it a valuable addition to the dermatologist’s armamentarium? Rod Tucker takes a closer look at the evidence.
This article reviews the available evidence for roflumilast in psoriasis, atopic eczema and seborrhoeic eczema, but also considers how the drug may be of benefit in other dermatological conditions.
Efficacy in psoriasis
The first study to examine a topical formulation of roflumilast in psoriasis was undertaken in 2020. In a phase 2a, double-blinded study in 89 patients with mild to moderate plaque psoriasis, roflumilast was studied at concentrations of 0.5% and 0.15%.4 Applied once daily, both concentrations of drug were used for 28 days and the efficacy compared to the vehicle cream. The results showed significant improvements for roflumilast 0.5% (p = 0.007) and roflumilast 0.15% (p = 0.011) compared to vehicle. Furthermore, statistically significant improvements were seen after only two weeks. In addition, treatment emergent adverse effects were mild or moderate and included application site erythema and pain.
Following this early success, a randomised, double-blind phase 2b trial was undertaken in patients with psoriasis affecting roughly six percent of their body surface area. Participants were equally assigned to roflumilast 0.15%,
“As a PDE-4 inhibitor, roflumilast has also been investigated as a possible treatment for psoriasis”
Rod Tucker is a pharmacist with a special interest in dermatology and a member of the Dermatological Nursing Editorial Board.
Citation: Tucker R. Roflumilast: Is it a dermatological panacea? Dermatological Nursing 2025. 24(1):37-41.
0.3% cream or vehicle for a period of 12 weeks.5 Assessment was made using a 5-point investigator’s global assessment (IGA) scale, ranging from 0 (clear), 1 (almost clear) through to 4 (severe). The IGA assessment considered plaque thickening, scaling and erythema. For the study, a treatment success (the primary outcome) was defined by an IGA score of 0 or 1 at week six. The trial also considered a number of secondary outcomes. For instance, the change in the Worst Itch Numeric Rating Scale (WI-NRS). This ranged from 0 (no itch) to 10 (worst itch imaginable) during the preceding 24 hours. A treatment response was defined as a 4-point improvement in WI-NRS score. Roflumilast also appeared to improve intertriginous psoriasis. Consequently, the trial also included an intertriginous area IGA score as a secondary outcome. For this measure, treatment success was defined as an IGA score of 0 or 1(clear/almost clear) plus a 2-point grade improvement from baseline, when assessed at week 12 for patients with an IGA score greater than 2. These results are summarised in Table 1.
Finally, two phase 3 randomised, placebocontrolled double-blind trials (DERMIS-1 and Dermis-2), published in a single paper, examined roflumilast 0.3% in 881 patients with mild to moderate plaque psoriasis.6 Again, the primary efficacy outcome was an IGA score of 0 or 1. At week 8, 42.4% and 39.6% of roflumilast assigned patients achieved a treatment success which was significantly higher than those using the vehicle cream.
As with the earlier trials, there was a significant improvement for intertriginous IGA scores among those assigned to roflumilast. Finally, a foam formulation containing roflumilast 0.3% has also been shown to significantly improve scalp psoriasis compared to placebo foam.7
In total, four randomised trials including 1,403 patients with plaque psoriasis have been undertaken, and these were summarised in a recent systematic
review and meta-analysis, focusing on the efficacy of roflumilast 0.3%.8 As before, the primary outcome was an IGA score of 0 or 1 and a secondary outcome, an intertriginous IGA treatment success. The findings for the primary outcome are shown in Figure 1. Similarly at week eight, a significantly higher proportion of participants assigned to roflumilast 0.3% achieved an intertriginous IGA treatment success (71.9% vs 20.5%, p < 0.01).
Proportion (%) of participating patients achieving an IGA score of 0 (clear) or almost clear (1) at week 8. (Adapted from reference 8).
From figure 1 it is clear that after eight weeks of treatment, 39.6% of patients on roflumilast achieved IGA 0/1, significantly higher than vehicle. This suggests that roflumilast is an effective option for mild to moderate plaque psoriasis.
Secondary outcomes (week 12)
4-point change in WI-NRS score (where baseline value > 6)
Table 1. Summary of primary and two secondary outcomes from the phase 2b trial (adapted from reference 5)
Figure 1.
Finally, the longer-term efficacy and safety of roflumilast in plaque psoriasis was examined in a 52-week openlabel trial, phase 2 trial in 332 patients who had either completed the earlier phase 2b study or were newly enrolled and treatment naïve.9 The same two previous outcome measures were used. At week 52, 244 patients had completed the trial with 44.8% achieving an IGA treatment success and 36.4% achieving an intertriginousIGA success. Only 12 patients reported treatment-related adverse events, none of which were serious.
A topical cream containing roflumilast 0.3% received FDA approval for the treatment of plaque psoriasis in 2022. Despite this, there is also data from a trial supporting the use of oral roflumilast 500 micrograms, for patients with moderate to severe psoriasis.10 The study included 46 patients with a median PASI score of 10, equally randomised to roflumilast 500mcgm or placebo. The primary outcome was a PASI75 at 12 weeks which was achieved by 35% of participants receiving roflumilast but none of those in the placebo arm.
Efficacy in atopic eczema
The first study of roflumilast in patients with atopic eczema gave rise to a nonsignificant effect on EASI scores (the primary outcome).11 This randomised, double-blind, phase 2, proof of concept study enrolled 136 patients with atopic eczema who received a cream containing two strengths of roflumilast (0.05% or 0.15%) compared against matching vehicle. However, the findings of two phase 3 randomised, controlled trials (INTEGUMENT-1 and 2) did provide robust evidence for the efficacy of roflumilast 0.15% cream in patients aged six years of age and older with mild to moderate atopic eczema.
In the two trials, 1,337 patients were randomised 2:1 to roflumilast 0.15% or vehicle applied once daily for four weeks. The primary outcome was based on a validated Investigator Global Assessment-AD (vIGA-AD) score. This ranged from 0 (clear) to 4 (severe) and a treatment success was defined as a vIGA-AD score of 0 or 1 plus a greater
than 2-point improvement from baseline at week four. Changes in EASI (50, 75, 90 and 100) were used as secondary outcomes. The results for the primary outcome are shown in Figure 2.
In addition, significantly more patients treated with roflumilast achieved an EASI50 (69.2% vs 44.4%, p < 0.0001) and an EASI75 (41.5% vs 21.2%, p < 0.0001). To date, these findings are only available as a conference abstract,12 yet the FDA did approve roflumilast 0.15% cream for atopic eczema in July 2024. Although currently unapproved, a 0.05% roflumilast cream has been trialled in children aged two to five years of age. According to a recently published abstract of a phase 3 randomised, controlled trial, a higher proportion of children using roflumilast achieved the primary outcome (a vIGA-AD score of clear or almost clear) than those applying the vehicle (25.4% vs 10.7%, p < 0.0001).13
Seborrhoeic eczema
In a study of 30 patients with seborrhoeic dermatitis, crisaborole (another PDE-4 inhibitor) was found to be effective and well tolerated.14 As a result, Zirwas et al15 undertook
a phase 2a randomised, double-blind, placebo-controlled trial, with a 0.3% roflumilast foam, applied once daily, in 226 patients with seborrhoeic dermatitis. Using an IGA score of 0 or 1 to denote a treatment success, after eight weeks, a significantly higher proportion of patients were successfully treated (73.8% vs 40.0%, p < 0.001). Furthermore, a second randomised phase 3 trial in 457 adolescents and adults with seborrhoeic dermatitis and treated with the same strength foam, found that 79.5% of those assigned to roflumilast achieved a treatment success.16 As a result, topical
“Although currently unapproved, a 0.05% roflumilast cream has been trialled in children aged two to five years of age”
From Figure 2 above it can be seen that 4 weeks of treatment with roflumilast, 31.1% of patients achieved a vIGA-AD score of 0 or 1. This suggests that roflumilast is an effective option for mild to moderate atopic eczema.
Figure 2. Proportion of patients with atopic eczema achieving a treatment success (adapted from reference 12).
Table
approvals for roflumilast and other currently available treatments for the different conditions
Drug treatments Mild to moderate psoriasisAtopic eczema Seborrheoic eczema
Roflumilast
FDA approved/not approved by EMA/UK
CrisaboroleNot approved
RuxolitinibNot approved
Topical corticosterioids
FDA approved
roflumilast has also received FDA approval for use in seborrhoeic eczema in April 2023.
Other potential roles in dermatology
Vitiligo
It has been suggested that in vitiligo, melanocytes have a greater susceptibility of oxidative stress,17 especially from hydrogen peroxide.18 In addition, there is some, albeit limited, data showing how apremilast can control the progression of vitiligo.19 Furthermore, roflumilast has been found to enhance melanin synthesis and attenuate hydrogen peroxide-induced oxidative stress, but only in combination with forskolin, a cAMP stimulator.20 This suggests that the drug may have a role in the management of vitiligo, particularly as lesional skin in active vitiligo was shown to have increased PDE activity. To date, however, no studies have examined whether roflumilast is of value in the management of vitiligo.
FDA approved/not approved by EMA/UK
FDA approved in adults and children from 3 months
EMA withdrew license in 2020
FDA approved in adults and children from 12 years
FDA approved
Behcet’s disease-associated aphthosis
Oral roflumilast has also been explored as a treatment for Behcet’s diseaseassociated aphthosis and there is some limited supportive data.21 Moreover, given how there are a number of case studies using apremilast22 for conditions such as hidradenitis suppurative, erosive oral lichen planus and nummular eczema, it is reasonable to assume that roflumilast may also be of value in these conditions.
Papulopustular rosacea
Topical roflumilast has also recently been examined in a trial for patients with papulopustular rosacea. However, at the time of writing, the results have not been published.
Comparison with other currently approved treatments
A summary of the current indications for which roflumilast has been approved are shown in Table 2, together
“Where exactly PDE-4 inhibitors like roflumilast will sit in the treatment of common conditions like psoriasis and atopic eczema and for the management of other dermatological diseases conditions is presently unknown”
FDA approved/not approved by EMA/UK
Not approved
Not approved
FDA approved
with other topical therapies used in the management of these conditions. As shown in Table 2, there are several other currently available treatments for the management of psoriasis, atopic and seborrhoeic dermatitis.
Adverse effects
The type of adverse effects identified from clinical trials for roflumilast foam, with a reported frequency exceeding 1% are listed below.
l N asopharyngitis 1.5%
l N ausea 1.3%
l H eadaches 1.1%.
Other, less common adverse effects include diarrhoea and insomnia (0.3%). For the topical cream formulation when used in either psoriasis or atopic eczema, the most common adverse effects were:
l D iarrhoea, headache, nausea, application site pain, upper respiratory tract infections and urinary tract infections (all greater than 1%).
Using topical roflumilast
There is currently limited information on how to use topical roflumilast. Patient resources available from the manufacturer’s website, Zoryve, simply state that the cream formulation should be applied once daily and rubbed into the skin until no longer visible. The patient product information
2. Comparison of
also adds how the cream can be applied to all affected areas of the body, including the face, eyelids, torso, hands and feet. The patient information for the foam product is equally vague when used for seborrhoeic eczema. The product literature simply suggests that a small amount of foam is dispensed into a hand and then a thin layer applied and rubbed in completely, to affected areas of the skin and scalp. However, both the cream and foam are recognised as being flammable, with advice to avoid flames and smoking when applying both formulations.
Final thoughts
While approved for use in the US, topical formulations of roflumilast are yet to receive approvals within Europe or the UK. Despite this, no clinical guidelines for psoriasis include a recommendation for the use of PDE-4 inhibitors. But as roflumilast is effective and well tolerated in the management of intertriginous psoriasis (see Table 1) this might represent an important use for the drug. PDE-4 inhibitors are also currently not recommended in the management of atopic eczema, especially following the withdrawal of the marketing authorisation for crisaborole in Europe. However, in the US, roflumilast is now included in the management options for seborrhoeic eczema,23 and hence subsequent European recommendations may include the drug.
Where exactly PDE-4 inhibitors like roflumilast will sit in the treatment of common conditions like psoriasis and atopic eczema, and for the management of other dermatological conditions, is presently unknown. But an important first step would be head-to-head studies with existing psoriasis and eczema treatments. Such a move would provide the much-needed clarity on how and where roflumilast might sit in the dermatological treatment landscape.
References
1. Raker VK, Becker C, Steinbrink K. The cAMP Pathway as Therapeutic Target in Autoimmune and Inflammatory Diseases. Front Immunol 2016. 7:123
2. Schafer PH, Truzzi F, Parton A, Wu L, Kosek
J, Zhang LH, et al. Phosphodiesterase 4 in inflammatory diseases: Effects of apremilast in psoriatic blood and in dermal myofibroblasts through the PDE4/CD271 complex. Cell Signal 2016. 28(7):753-63
3. Sakkas L, Mavropoulos A, Bogdanos, DP. Phosphodiesterase 4 inhibitors in immunemediated diseases: mode of action, clinical applications, current and future perspectives. Curr Med Chem 2017. 24(28):3054-67
4. Papp KA, Gooderham M, Droege M, Merritt C, Osborne DW, Berk DR, et al. 15309 ARQ-151, roflumilast cream, improved psoriasis in phase 2a study. J Am Acad Dermatol 2020. 83(6)
5. Lebwohl MG, Papp KA, Stein Gold L, Gooderham MJ, Kircik LH, Draelos ZD, et al. Trial of Roflumilast Cream for Chronic Plaque Psoriasis. N Engl J Med 2020. 383(3):229-39
6. Lebwohl MG, Kircik LH, Moore AY, Stein Gold L, Draelos ZD, Gooderham MJ, et al. Effect of Roflumilast Cream vs Vehicle Cream on Chronic Plaque Psoriasis: The DERMIS-1 and DERMIS-2 Randomized Clinical Trials. JAMA 2022. 328(11):1073-84
7. Kircik LH, Alonso-Llamazares J, Bhatia N, Bukhalo M, Devani AR, Draelos ZD, et al. Once-daily roflumilast foam 0.3% for scalp and body psoriasis: a randomized, doubleblind, vehicle-controlled phase IIb study. Br J Dermatol 2023. 189(4):392-9
8. de Moraes-Souza R, Chahine Chater R, Pera Calvi I, Mesquita Y, Sarto R, Lapenda I, et al. Efficacy and Safety of Topical Roflumilast for the Treatment of Psoriasis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin Drug Investig 2024. 10
9. Stein Gold L, Adam DN, Albrecht L, Alonso-Llamazares J, Ferris LK, Gooderham MJ, et al. Long-term safety and effectiveness of roflumilast cream 0.3% in adults with chronic plaque psoriasis: A 52-week, phase 2, open-label trial. J Am Acad Dermatol 2024. 91(2):273-80
10. Gyldenlove M, Meteran H, Sorensen JA, Fage S, Yao Y, Lindhardsen J, et al. Efficacy and safety of oral roflumilast for moderate-tosevere psoriasis-a randomized controlled trial (PSORRO). Lancet Reg Health Eur 2023. 30
11. Gooderham MK, L, Zirwas, M et al. The Safety and Efficacy of Roflumilast Cream 0.15% and 0.05% in Patients With Atopic Dermatitis: Randomized, Double-Blind, Phase 2 Proof of Concept Study. J Drug Dermatol 2023. 22:139-47
12. Eichenfield L, Boguniewicz M, Simpson E, et al. Once-daily roflumilast cream 0.15% for atopic dermatitis: pooled results: From INTEGUMENT-1/2 phase 3 trials. Ann Allergy Asthma Immunol 2023. 131(5):s91
13. Eichenfield L, Browning J, Funk, T, et al. 639 - Efficacy and safety of once-daily roflumilast cream 0.05% in pediatric patients 2 to 5 years of age with mild to moderate atopic dermatitis (INTEGUMENT-PED): a phase 3 randomized controlled trial. Br J Dermatol 2024. 191
14. Pena SM O, ASW, Smith AM, et al. Topical crisaborole is an efficacious steroidsparing agent for treating mild-to-moderate seborrhoeic dermatitis. J Eur Acad Dermatol Venereol 2020. 34(12):e809-10
15. Zirwas MJ, Draelos ZD, DuBois J, Kircik LH, Moore AY, Stein Gold L, et al. Efficacy of Roflumilast Foam, 0.3%, in Patients With Seborrheic Dermatitis: A Double-blind, Vehicle-Controlled Phase 2a Randomized Clinical Trial. JAMA Dermatol 2023. 159(6):613-20
16. Blauvelt A, Draelos ZD, Stein Gold L, Alonso-Llamazares J, Bhatia N, DuBois J, et al. Roflumilast foam 0.3% for adolescent and adult patients with seborrheic dermatitis: A randomized, double-blinded, vehiclecontrolled, phase 3 trial. J Am Acad Dermatol 2024. 90(5):986-93
17. Jian ZL, K, Song P, et al. Impaired activation of the Nrf2-ARE signaling pathway undermines H2O2-induced oxidative stress response: a possible mechanism for melanocyte degeneration in vitiligo. J Invest Dermatol 2014. 134(8):2221-30
18. Shalbaf MG, N. C., Wood JM, et al. Presence of epidermal allantoin further supports oxidative stress in vitiligo. Exp Dermatol 2008. 17(9):761-70
19. Majid I, Imran S, Batool S. Apremilast is effective in controlling the progression of adult vitiligo: A case series. Dermatol Ther 2019. 32(4):e12923
20. Chen Z, Li Y, Xie Y, Nie S, Chen B, Wu Z. Roflumilast enhances the melanogenesis and attenuates oxidative stress-triggered damage in melanocytes. J Dermatol Sci 2023. 110(2):44-52
21. Leal R, Hoyos, CL, Ruiz, JAP, et al. Treatment of Behçet disease with oral roflumilast, an observational study. Clin Exp Dermatol 2024. 10.1093/ced/llae284. Online ahead of print
22. Mansilla-Polo M, Gimeno E, MorgadoCarrasco D. [Translated aticle] Topical and Oral Roflumilast in Dermatology: A Narrative Review. Actas Dermo-Sifiliográficas 2024. 115(3):T265-T79
23. American Academy of Dermatology Association. Seborrheic dermatitis: Diagnosis and treatment 2024. Available at: https://www.aad.org/public/diseases/a-z/ seborrheic-dermatitis-treatment [last accessed January 2024].
ADDITIONAL DOSING OPTION
Adolescents with moderate to severe atopic dermatitis who do not adequately respond to 15 mg can now be escalated to 30 mg once daily
The recommended dose of RINVOQ for the treatment of moderate to severe AD in adults and adolescents 12 years and older who are candidates for systemic therapy is 15 or 30 mg once daily depending on individual patient presentation:
x A dose of 15 mg is recommended for patients at higher risk of VTE, MACE and malignancy.
x A dose of 30 mg once daily may be appropriate for patients with high disease burden who are not at higher risk of VTE, MACE and malignancy or patients with an inadequate response to 15 mg once daily.
x In adolescents (12 to 17 years and ≥30 kg), a dose of 15 mg is recommended. If the patient does not respond adequately to 15 mg once daily, the dose can be increased to 30 mg once daily.
x The lowest effective dose to maintain response should be used.
x For patients 65 years of age and older, the recommended dose is 15 mg once daily.
RINVOQ® (upadacitinib) is indicated for the treatment of moderate to severe atopic dermatitis (AD) in adults and adolescents 12 years and older who are candidates for systemic therapy.
Some patients may not be suitable for RINVOQ® (upadacitinib). You are strongly advised to read the prescribing information available by scanning the QR code.
RINVOQ should be initiated and supervised by healthcare
professionals experienced in the diagnosis and treatment of AD. RINVOQ is contraindicated in patients with: hypersensitivity to active substance or excipients; active tuberculosis (TB) or active serious infections; severe hepatic impairment; pregnancy. Women of childbearing potential have to use effective contraception during treatment and for 4 weeks following the final dose of RINVOQ. RINVOQ should not be used during breast
feeding. Female adolescent patients and/or their parents/caregivers should be informed about the need to contact the treating healthcare professional once the patient experiences menarche while taking RINVOQ.
JAK inhibitors, including RINVOQ, should only be used if no suitable treatment alternatives are available in patients ≥65 yrs and other specific patient groups.
Adverse events should be reported. Reporting forms and information can be found at https://yellowcard.mhra.gov.uk or via the MHRA Yellow Card app, available in the Google Play or Apple App Stores. Adverse events should also be reported to AbbVie on GBPV@abbvie.com
Reference: RINVOQ Summary of Product Characteristics.
WReflections on dermatological emergency preparedness: Implementing a dedicated emergency trolley
Eimear Duff, Sheila Ryan
hile most dermatology centres are now outpatient based, the need for emergency inpatient care remains. Patients with severe, and sometimes potentially life-threatening1 cutaneous events – such as Stevens–Johnson syndrome (SJS), toxic epidermal necrolysis (TEN) staphylococcal scalded skin syndrome, bullous pemphigoid and generalised pustular psoriasis – are cared for on general medical wards, intensive care settings, or in burn centres.2
Stopping offending medications where relevant, supportive management, and specialist skin evaluation and care are key pillars of treatment in dermatologic emergencies.3 The required specialised dermatology dressings and sufficient quantities of emollients are generally unavailable in such contexts to support patient care. In some hospital pharmacies, the storage of large volumes of emollients may prove difficult. Furthermore, limited availability of nonadherent wound dressings such as Exu-Dry® has been a significant concern for dermatology departments due to supply chain issues.
Funding information: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement: None to declare.
Summary:
This article will explore the use of a dermatological emergency trolley (Figure 1) in our department to ensure preparedness for the management of severe and acute dermatoses in our centre, an acute tertiary referral hospital in Ireland.
Emergency trolleys for the management of high-risk conditions, where timely access to emergency supplies should be fast and easy, are used by many specialties to improve outcomes for patients. In life-threatening cardiac resuscitations, crash trolleys are essential tools.4 It has also been useful for postpartum haemorrhage,5 and critical procedures such as central lines, arterial lines,6 airway emergencies7 and sepsis management.
What’s on the trolley?
The dermatological emergency trolley is kept in an easily accessible location in the dermatology department main corridor, where it is readily available on weekends and
“In some hospital pharmacies, the storage of large volumes of emollients may prove difficult”
This shor t article explains the rational behind the implementation of a dedicated emergency trolley in a dermatology department.
Author info:
Eimear Duff is a Specialist Registr ar in Dermatology. Sheila Ryan is an Advanced Nurse Practitioner in Dermatology. Both work at the Charles Centre for Dermatology, University Hospital Limerick, Dooradoyle, Limerick, Ireland
Keywords: Drug reactions, Immunobullous disease, Nursing
Citation: Duff E, Ryan S. Reflections on dermatological emergency preparedness: Implementing a dedicated emergency trolley. Dermatological Nursing 2024. 24(1):43-45.
Clinical practice
out-of-hours. It is mobile and can be easily moved to locations around the hospital. Contents, enumerated in Table 1, can be transferred to an emergency kit bag for use in satellite centres such as the maternity hospital when required. This minimises inefficiencies in gathering supplies from various locations, and avoids delays caused by missing equipment. We keep laminated copies of useful guidelines (e.g., management of SJS/TEN2) mounted on the inside doors. A separate biopsy equipment bag is also used.
The trolley contents align with recommendations from UK guidelines for the management of SJS/TEN, which are the most widely followed guidelines in Ireland for this condition.
Our trolley contents place a focus on equipment that is not routinely available in general storerooms across the hospital. For example, although the conservative approach to SJS/TEN requires sterile water, saline, or an antimicrobial
Equipment
Topical corticosteroids +/- pots for decanting these
Bland, greasy emollient 10 x 500g pots
Example (tradename)
such as chlorhexidine (1/5000) for cleansing or irrigation of wounds and skin, these are widely available outside the dermatology context and are therefore not maintained in our trolley.
“Our trolley contents place a focus on equipment that is not routinely available in general storerooms across the hospital”
Indication
From mild to very potent classes
50% white Soft Paraffin with 50% Liquid Paraffin (50/50)
Sterile 10ml syringes and 21 gauge hypodermic safety needles n/a
Tongue depressors n/a
Wound swabs n/a
Exu-Dry® sheets, vests, arm and leg dressings
Non-adherent dressings
Silicone film dressings
Paraffin-based dressings
Silicone foam dressings
Securing silicone dressings
Soft silicone tape and low adherence film dressing
Low-adherent, absorbent dressing bulk roll 50cm x 7m (MELOLIN)
Mepitel®
Adaptic™ (requires changing daily in acute cases)
Mepilex® XT (standard thickness)
Mepilex® transfer (thinner and more malleable – useful on difficult-to-dress areas such as ears, under breasts)
Mepitel® film
Mepitac®
Mepitac® Mepitel® film
Gauze swabs n/a
Disposable surgical mob capn/a
Management of acute inflammatory conditions where indicated
Supportive skin care
Decompression of bullae
Oral examinations
Decanting of emollients from containers
Microbiology and virology swabs as needed
Suitable for total body coverage
Can be adapted to paediatric population if needed
Alternative to Exu-Dry®, needs to be cut to appropriate size
For application to localised areas
Can also be used to indirectly apply topical corticosteroids to skin rather than applying topical creams to eroded sites
For skin protection of localised areas
Useful for securing lines
Useful for securing intravenous lines and nasogastric tubes
Cleaning skin, application of gentle pressure when decompressing blisters
Hairnet for protection and containment of hair when full body dressings being applied
Other equipment recommended for acute skin failure is more challenging to obtain urgently outside dermatology departments, such as greasy emollients; non-adherent dressings for denuded dermis (e.g., Mepitel™); and secondary foam or burn dressings for collecting exudate (e.g., Exu-Dry®). These are therefore prioritised for storage in our emergency trolley. While our centre has an intensive care unit (ICU) for critical care management and specialist nursing, it is not a burn centre, and the preferred equipment and topical preparations may vary according to location, hospital trust, and availability of surgical management for SJS/ TEN. Furthermore, departments without space for a trolley may wish to maintain a checklist of supplies required, an emergency bag, or an emergency cupboard.
Here, we suggest a convenient solution to the problem of dressing and emollient accessibility for emergencies in clinical practice. We hope this solution can enhance the preparedness of other dermatology departments, who could replicate this, customising solutions according to their needs.
References:
1. Hsu DY, Brieva J, Silverberg NB, Silverberg JI. Morbidity and mortality of Stevens-Johnson syndrome and toxic epidermal necrolysis in United States adults. Journal of Investigative Dermatology 2016. 136(7):1387-97
2. Creamer D, Walsh SA, Dziewulski P, Exton LS, Lee HY, Dart JKG, et al. U.K. guidelines for the management of Stevens–Johnson Syndrome/toxic epidermal necrolysis in adults 2016. British Journal of Dermatology 2016. 174(6):1194-227
3. Freiman A. Dermatologic emergencies. Canadian Medical Association Journal 2005. 173(11):1317–9 doi:10.1503/cmaj.050783
4. Jacquet GA, Hamade B, Diab KA, Sawaya R, Dagher GA, Hitti E, et al. The Emergency Department crash cart: A systematic review and suggested contents. World Journal of Emergency Medicine 2018. 9:93
5. Phillips M. A ‘crash cart’ for postpartum hemorrhage. American Journal of Nursing 2022. 122:14–14
6. Johnson K, Smith C, Barker LG, et al. Implementation of a resident-designed procedure cart in a busy emergency department. Cureus 2023. 15(7):e42211
7. Heller M, Worobetz N, Grischkan J, Lind M, Jatana KR, Hamersley ERS. Improving emergency airway cart efficiency in compliance with Joint Commission standards. International Journal of Pediatric Otorhinolaryngology 2022. 158:111161.
Corresponding author: Eimear Duff, Charles Centre for Dermatology, University Hospital Limerick, Dooradoyle, Limerick, Ireland, +353 061 301 111, eimear.duff2@hse.ie
Metvix (Methyl aminolevulinate) is indicated for treatment of thin or nonhyperkeratotic and non-pigmented actinic keratoses on the face and scalp in adults above 18 years of age.
SUSTAINED AK CONTROL
METVIX® offers your AK patients a high AK lesion response rate2 and a low recurrence rate.3†
High response rate at 3 months (87% with DL-PDT and 91% with c-PDT) and low recurrence rate at 12 months† (13% with DL-PDT and 10% with c-PDT)3,4
Please refer to the full Prescribing Information available via the QR code.
GB-MVR-2500001 | Feb 2025
Treatment with METVIX is tailored to your patients affected by this chronic disease with three flexible illumination options:1,5 YEARS
ADVERSE EVENTS SHOULD BE REPORTED. Adverse Event Reporting For the UK: Reporting forms and information can be found at www.mhra.gov.uk/yellowcard or search for MHRA Yellow Card in the Google Play or Apple App Store. For Ireland: HPRA Pharmacovigilance, Website: www.hpra.ie Adverse events should also be reported to Galderma (UK) Ltd E-mail: medinfo.uk@galderma.com; Tel: +44 (0)300 3035674
Indication: METVIX (methyl aminolevulinate) photodynamic therapy (PDT) is indicated in adults (≥18 years) for the treatment of: thin or non-hyperkeratotic and non-pigmented actinic keratoses on the face and scalp, treatment of superficial and/or nodular basal cell carcinoma unsuitable for other available therapies due to possible treatment related morbidity and poor cosmetic outcome (such as lesions on the mid-face or ears, lesions on severely sun damaged skin, large lesions, or recurrent lesions) and squamous cell carcinoma in situ (Bowen´s disease) when surgical excision is considered less appropriate.1 Abbreviations: AK, actinic keratosis; PDT, photodynamic therapy. † Lesion recurrence rate defined as number of lesions cleared at three months, and recurring at 12 months /number of lesions cleared at three months. References: 1. Galderma. Metvix 160 mg/g cream SmPC, March 2021. Available at:https://www.medicines.org.uk/emc/product/6777/smpc. Accessed February 2025. 2. METVIX® Product Monograph. May 17, 2019 3. Fargnoli MC, et al. Eur J Dermatol 2017;27 (1 ):89– 91. 4. Sotiriou E, et al. J Eur Acad Dermatol Venereol 2018;32 (4 ):595-600 5. Cramer P and Stockfleth E. Expert Opin Emerg Drugs. 2020;25(1):49–58.
Skin of colour and dermatology nursing: A specialised focus –part one
Skin of colour (SOC) encompasses a variety of skin tones, particularly in those of African, Latin, Asian, Middle Eastern, and Native American descent.1 This is due to the increased melanin in the skin.
The emphasis in dermatology care for SOC patients requires educational competence, specialised knowledge, and a deep and broad understanding of how skin conditions manifest differently in darker skin tones in relation to the Fitzpatrick skin type scale.2
The role of dermatology nurses is very important in providing comprehensive and personalised care to this group of patients.3 According to the British Association of Dermatologists (BAD), understanding and addressing the unique characteristics of SOC is essential for effective dermatologic care.4
Some common changes to the skin (pallor, cyanosis, jaundice, flushing) are not easily detectable when assessing people who have dark skin tones. Skin tone and pigmentation are regulated by melanogenesis, a complex process directly linked to genetics. Melanocyte cells in the skin produce melanin pigment which help protect skin against sun damaging UV rays. Although the colour of the
Funding information: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflict of interest statement: None to declare.
skin may change due to UV exposure, a person’s Fitzpatrick skin phototypes (FSP) classification does not change. Skin tone is best assessed in areas of the body that are not frequently exposed to UV radiation.5
“Skin tone and pigmentation are regulated by melanogenesis, a complex process directly linked to genetics”
Understanding dermatological differences in skin of colour
Post inflammatory hyperpigmentation (PIH) is a major concern in patients with SOC and it is important that this is addressed. The variations in PIH in SOC often shows differences in pigmentation, such as hyperpigmentation or hypopigmentation in response to skin conditions.6
The common conditions in SOC are:
l Eczema: Also known as atopic dermatitis, eczema can be more difficult to diagnose and manage in patients with SOC. Symptoms, including dry, itchy patches, may appear less obvious due to the skin’s pigmentation, which can delay diagnosis and treatment.7 The BAD has previously highlighted the challenges
Summary:
The Chair of the BDNG’s new Skin of Colour Subgroup explains why the group is needed and sets out some of the challenges practitioners face when working with patients with darker skin tones.
Citation:
Soji-Adeyemo MO. Skin of colour and dermatology nursing: A specialised focus – part one. Dermatological Nursing 2024. 24(1):47-49.
Author info:
Keywords:
Skin of colour, Fitzpatrick skin type, Subgroup, Nursing
Modupe O Soji-Adeyemo is an Advanced Nurse Practitioner in Adult Medical Dermatology at Guy’s and St Thomas’s NHS Foundation Trust.
Modupe O Soji-Adeyemo
Clinical practice
clinicians face in diagnosing eczema in darker skin tones. 8
l Psoriasis: Psoriasis can be harder to diagnose in darker skin tones as the typical red or silvery scales may appear darker and less pronounced. It is also more likely to present with post-inflammatory hyperpigmentation, complicating the management of the condition.9
l Keloids: Overactive scarring that is more prominent in African American and Hispanic populations.10
l Pseudo-folliculitis barbae: More common in people of African descent due to the curliness of hair and shaving habits.11
l Post-inflammatory hyperpigmentation: Darker spots that appear after an injury or inflammation, particularly in people with darker skin. 6
l Lupus and sickle cell anaemia: Both conditions have different dermatologic presentations in people with darker skin.9
Challenges for dermatology nurses
There are several challenges for dermatology nurses when working with patients with SOC. These include:
l Underrepresentation in research: SOC populations have historically been underrepresented in dermatology research, leading to a knowledge gap in how conditions manifest and are treated in diverse skin types.7
l D iagnostic challenges: Conditions like eczema, psoriasis, or skin cancer may look different in darker skin, making early detection more difficult.12 The BAD notes that diagnostic challenges arise when typical symptoms of conditions like eczema or psoriasis appear differently in darker skin tones, which can lead to delayed diagnoses.4
l Patient education: There may be unique challenges in educating SOC patients on skin care, sunscreen use, and treatments that are effective for their skin type.1
l Cultural sensitivity: Understanding and respecting cultural differences when discussing skin care practices, potential treatments, and the impact of certain conditions on daily life.9 The BAD emphasises the importance of cultural competence in dermatology care to improve patient outcomes and satisfaction.4
The role of dermatology nurses in addressing these challenges
l Patient-centred care: Nurses must build trust by acknowledging the unique needs of SOC patients and offering personalised care that considers cultural and individual preferences. 3
l E ducation and advocacy: Nurses can educate patients about the importance of sun protection, the risk of hyperpigmentation, and the need for early intervention in chronic skin conditions. 2 The BAD stresses that although darker skin provides some protection against
Eczema
Psoriasis
UV damage, it is still important for SOC patients to use sunscreen regularly to prevent skin damage and conditions like skin cancer.13
l Collaboration with dermatologists: Dermatology nurses often act as the bridge between the patient and the dermatologist. They can assist in diagnosis, follow-up care, and ensure appropriate treatment plans for patients with SOC.10 l Training and continuing education: Ongoing education for dermatology nurses is essential to stay up to date with the latest research and treatment options for SOC populations.7 The BAD offer resources and training for dermatology professionals to improve care for patients with SOC.4
Consideration of these points are what led to the creation of the BDNG’s SOC Subgroup, after an initial survey of BDNG members in 2023 found the need to raise awareness and educate nurses about patients in this category, as well as successfully delivering a good
Conclusion
The need for inclusion and the time to act is now. It can no longer be delayed as we now provide clinical care for a wider population of patients with SOC. Our awareness, education and good clinical practice will improve early diagnosis and result in the right treatment regimens for these cohorts.
The importance of specialised care for SOC patients and the critical role dermatology nurses play in this process cannot be underestimated.12 This is the time to engage in ongoing research, education, and advocacy, to ensure dermatology nurses are best placed to support diverse patient populations.9 The BAD emphasises the need for dermatology nurses to be proactive in addressing the unique dermatologic concerns of SOC patients, including providing culturally competent care and personalised treatment plans.4
Part two of this article will consider cultural beliefs, habits and traditional medical practices.
BAD 2021. Available at: https://www.bad. org.uk/education-training/skin-of-colourin-dermatology-education/ [last accessed February 2025]
5. Dar ker Skin Tones. American Academy of Dermatology Association. AAD 2010. Available at: https://www.aad.org/public/darkerskin [last accessed February 2025]
6. Naylor C, Hunter L. Post-inflammatory hyperpigmentation: A review of treatments and challenges in skin of colour. Dermatologic Surgery 2019. 45(7):937-945
7. Soltani AM, Landeck D. Darker skin tones and the risk of misdiagnosis in dermatology. The Journal of Clinical Investigation 2020. 130(4):2272-2281
8. Post-inflammatory Hyperpigmentation in Skin of Colour. British Association of Dermatologists. BAD 2020. Available at: https://www.skinhealthinfo.org.uk/supportresources/skin-of-colour/ [last accessed February 2025]
9. Elbuluk N, Roberts W. Cultural competence in dermatology: Addressing disparities in the care of patients with skin of colour. Journal of the American Academy of Dermatology 2020. 83(3):751-757
10. Kari RM, Dunn M. Keloid scarring: Pathophysiology, treatment, and challenges in skin of colour populations. American Journal of Clinical Dermatology 2020. 21(2):123-132
Can making dietary changes improve disease severity in psoriasis?
Rod Tucker
Rod Tucker, a pharmacist with a special interest in dermatology, answers more questions submitted by DN readers. If you have a burning question that you’d like answered in a future issue, please email it to susan. maguire@bdng.org.uk entitling your email: Ask the Pharmacist.
There’s no doubt that all of us should seek to eat a healthy diet. But could changing what we eat have a positive effect on the severity of skin diseases such as psoriasis?
Psoriasis is a common, chronic inflammatory skin disease which is estimated to affect up to 2.8% of the UK population.1 Although the presence of psoriasis negatively impacts a patient’s quality of life, sufferers are also recognised as having a higher incidence of other health conditions such as obesity, diabetes, heart disease and stroke.2 In fact, one study of 753 patients with psoriasis revealed how 73% had co-morbidities including hypertension, diabetes and heart disease.3 Even among those without psoriasis, the development of these adverse health sequalae can, to some extent, be attributed to a poor diet. So, what if anything, is the connection between a poor diet and the development of psoriasis or even a worsening of disease severity?
In trying to answer this question, it’s first necessary to look at the physiological changes associated with overweight or obesity and to see whether these are present in patients with psoriasis. Take for example, the adipocytokine, visfatin, secreted from visceral fat. It is recognised that levels of visfatin are elevated in patients with overweight and obesity.4 Moreover, according to the findings of a recent meta-analysis, serum levels of visfatin are also significantly higher in patients with psoriasis and correlated with disease severity.5 Given this connection, could dietary changes improve disease severity in psoriasis?
Dietary changes in psoriasis
Patients with psoriasis who change their diet with a view to losing weight experience improvements in disease severity, and this was shown in a review of 10 clinical trials published in 2019.6 However, the review did not provide a quantitative estimate of the amount of weight loss or even the best type of dietary change required to facilitate an improvement in disease severity. Perhaps, not surprisingly, patients themselves have also explored dietary changes in an effort to reduce the
extent of their psoriasis. In 2017, the US National Psoriasis Foundation surveyed members about any dietary modifications they had undertaken and the impact of these changes on their skin. A total of 1,206 responses were obtained7 and, overall, 86% of respondents said that they had employed some form of dietary intervention. Among those who reported improvements in their psoriasis, the biggest impact came from reducing the intake of either alcohol (53.8%) or gluten (53.4%). What’s more, addition of omega fish oils to the diet, led to improvements in 44.6% of respondents, as did inclusion of oral vitamin D (41%). Psoriasis severity also improved following the adoption of a particular type of diet. For instance, a high proportion of patients saw improvements after switching to a vegan (70%) or palaeolithic (68.9%) diet. However, the biggest change came from the Pagano diet (72.2%). This latter diet was introduced in 2008 by chiropractor John Pagano.
The central tenet of the diet, which doesn’t appear to have much supportive evidence, is that psoriasis is a manifestation of leaky gut syndrome,
“Patients with psoriasis who change their diet with a view to losing weight, experience improvements in disease severity and this was shown in a review of 10 clinical trials published in 2019”
causing toxins to leak out of the gastrointestinal tract via holes in the intestinal lining.
On the face of it, some of these dietary changes would appear to be rational. For example, vitamin D is effective when used topically, hence it is not unreasonable to expect to see improvements following oral supplementation of the vitamin.
Nevertheless, a recent meta-analysis of trials of oral vitamin D use in patients with psoriasis concluded that ‘no significant differences were found in PASI after 3, 6, and 12 months of supplementation’ and that ‘vitamin D supplementation did not seem to improve clinical manifestations.’8
The role of omega 3 fish oils also has some theoretical merit in that these long-chain fatty acids have an anti-inflammatory action. However, as noted by Wolters,9 while the evidence from uncontrolled studies is somewhat convincing, randomised trial data is less robust, with only one of four trials demonstrating any benefit from supplementing with omega 3 fish oils.
Finally, in recent years there has been a surge of interest in the role of the gut microbiome in a whole host of chronic conditions including psoriasis. To date, there is some evidence showing how the gut microbiome in patients with psoriasis is markedly altered compared to those without
the disease. In particular, there was a reduced abundance of Lachnospiraceae, which is observed in the autoimmune inflammatory disease, Sjogren’s syndrome.10 However, the authors made clear that further work is needed to confirm whether the gut microbiota and the subsequent overproduction of inflammatory cytokines is involved in the development of psoriasis.
“Dietary changes alone are unlikely to cure psoriasis”
There’s no doubt that dietary changes in psoriasis can affect disease severity. Unfortunately, there remains much uncertainty as to which specific changes provide the greatest benefit. Nevertheless, it is worthwhile for nurses to incorporate the importance of a healthy diet – whatever that might be – into their discussions with those who have psoriasis. Dietary changes alone are unlikely to cure psoriasis, but if such changes can ameliorate the inflammatory milieu that is characteristic of the disease, then this could serve as an important adjunct alongside conventional treatment.
References
1. Spr ingate DA, Parisi R, Kontopantelis E et al. Incidence, prevalence and mortality of
patients with psoriasis: a U.K. populationbased cohort study. Br J Dermatol 2017. 176(3):650-658
2. Far ley E, Menter A. Psoriasis: comorbidities and associations. G Ital Dermatol Venereol 2011. 146(1):9-15
3. Pearce DJ, Morrison AE, Higgins KB et al. The comorbid state of psoriasis patients in a university dermatology practice. J Dermatolog Treat 2005. 16(5-6):319-23
4. Chang YH, Chang DM, Lin KC, Shin SJ, Lee YJ. Visfatin in overweight/obesity, type 2 diabetes mellitus, insulin resistance, metabolic syndrome and cardiovascular diseases: a meta-analysis and systemic review. Diabetes Metab Res Rev 2011. 27(6):515-27
5. Zou Q, Si J, Guo Y et al. Association between serum visfatin levels and psoriasis and their correlation with disease severity: a meta-analysis. J Int Med Res 2021. 49(3):3000605211002381
6. Alotaibi HA. Effects of Weight Loss on Psoriasis: A Review of Clinical Trials. Cureus 2018. 10(10):e3491
7. Afifi L, Danesh MJ, Lee KM et al. Dietary Behaviors in Psoriasis: Patient-Reported Outcomes from a U.S. National Survey. Dermatol Ther (Heidelb) 2017. 7(2):227-242
8. For misano E, Proietti E., Borgarelli C et al. Psoriasis and Vitamin D: A Systematic Review and Meta-Analysis. Nutrients 2023. 15(15)
9. Wolters M. Diet and psoriasis: experimental data and clinical evidence. Br J Dermatol 2005. 153(4):706-14
10. Zhang X, Shi L., Sun T et al. Dysbiosis of gut microbiota and its correlation with dysregulation of cytokines in psoriasis patients. BMC Microbiol 2021. 21(1):78.
Scan for more information and to book your place
Kizoulis
Ensuring acne patients avoid a spot of bother
Rod Tucker, Simone Calvert
Simone Calvert originally worked as a beauty therapist before training as an aesthetics practitioner at a private skin clinic. This role provided her with a wide range of experience in cosmetic dermatology, including laser and chemical peel therapies. She subsequently trained as a general nurse but continued to work at the skin clinic for several more years. In 2020, Simone landed a job as a trainee dermatology nurse. Since 2022, she has been in her current post at Kingston hospital as a clinical nurse specialist.
Acne management clinics
In her current role, Simone focuses on inflammatory dermatoses including acne, eczema and psoriasis. For the latter two conditions, she runs clinics specifically for patients prescribed systemic agents, though in the near future, this will probably be expanded to include patients treated with biologics. Simone has two acne clinics per week in which she is involved with the monitoring of patients prescribed isotretinoin. Nevertheless, she adds how ‘I do see the odd patient on topicals who wants to continue to be seen because they are worried that their acne might come back’. In such cases, which she says are rare, the patients are seen six months post-isotretinoin and even possibly six months after that. Simone always suggests that these patients take photos during this sixmonth window to use during their review appointment.
“Pomade acne arises as a consequence of cultural practices and the use of heavily oil-laden gels”
Summary:
If their skin remains clear, she simply advises that patients continue with adapalene, alongside an appropriate skincare regimen. Simone does find that some patients become anxious at the prospect of being discharged from her care. In such cases, she seeks to reassure them by addressing their immediate concerns and ensuring that they have a plan in place on how to manage their skin.
Post-isotretinoin acne management
Once a course of isotretinoin is completed, most of her patients are commenced on adapalene gel which, she says, ‘helps to maintain the results they’ve achieved with isotretinoin’. With topical retinoids known to irritate the skin, Simone advises patients that ‘slow and steady is always the way’. She adds how ‘our general advice with adapalene is to apply the treatment once a week for the first week, twice a week on the second week and then three times a week on the third week or as tolerated’. But even after this slow build-up, some patients struggle with irritancy and end up using their topical retinoid only once a week. The clinics have also taught her the importance of being able to manage patients’ expectations. As she explains, ‘I like to gently remind patients that while isotretinoin can be highly effective, it’s still possible to get an occasional spot in the future, and that this is completely normal and these should be easy to manage with topical treatments and effective skincare.’
As with all specialist dermatology nurses, an important aspect of her role is patient education. However, this can be challenging, especially in the current era of social media, which is hugely influential and, in some cases, serves only to undermine her educational efforts. For example, Simone mentions how ‘ sometimes patients are firmly set on what they might have seen on social media ,’ even if the approach advocated by an influencer has not given rise to the same effects in her patient. Fortunately, most of her patients take note of what she has to say, but there is a small number who remain sceptical.
Simone Calvert is an NHS clinical nurse specialist in dermatology at Kingston Hospital. She spoke to Rod Tucker about her role in managing patients with acne.
Tucker R, Calvert S. Ensuring acne patients avoid a spot of bother. Dermatological Nursing 2024. 24(1):53-55.
Simone remains pragmatic and doesn’t just dismiss any products or approaches that her patients might have seen on social media. As she explains ‘ I’m a great believer in trying things out, swapping treatment around after about three to six months to see what does and doesn’t work .’ For example, some patients don’t wish to continue with topical therapy, in which case, provided it has been six months post-isotretinoin, she can refer them to a private clinic for photo-pneumatic or intense pulsed light therapy, together with gentle vacuum treatment to remove excess oil and dead skin cells, and/or chemical peel treatments.
Acne in patients with skin of colour
Dealing with acne patients with skin of colour (SOC) presents further challenges with large numbers developing pomade acne, which predominately occurs on the forehead and along the hairline. As a woman of colour herself, she fully understands how cultural practices lead to pomade acne and can address this with her patients.
Pomade acne arises as a consequence of cultural practices and the use of heavily oil-laden gels used by women who have a hairstyle where the characteristic baby hairs are tucked down the side of the face. This effect is achieved through the use of lots of oils and all sorts of other oil-based cosmetic products.
A further challenge to managing acne in patients with SOC is the need to emphasise the use of sunscreen to help minimise the extent of post-inflammatory hyperpigmentation (PIH), which can take 6 -12 months to completely fade. Simone also advises on the use of sunscreens and in particular, mineral gel-based, broadspectrum agents or even tinted gels to help match with a patient’s skin tone. ‘ There are many sunscreens available for SOC patients. I specifically recommend a mineral gel-based broad-spectrum SPF, such as Heliocare gel oil free SPF 50.’
Skincare routines
Six months post-treatment with isotretinoin, Simone provides her patients with advice on an appropriate skincare routine alongside their topical retinoid. As she says, ‘I suggest that patients use a wash three times a week that contains either glycolic or salicylic acid as an exfoliant ’ which are much more effective than a physical exfoliant, as these can be abrasive and damage the skin.
She also suggests a non-foaming gel cleanser, given that foaming agents like sodium lauryl sulphate can aggravate acne-prone skin. She is a big fan of hyaluronic acid as a humectant which she feels works well to increase skin hydration as well as products containing niacinamide which helps with ceramide and collagen production in addition to having an anti-inflammatory action.
Simone is also not averse to patients experimenting with other treatments alongside adapalene. As she says ‘they can explore chemical skin peels once a month to help remove dead skin cells; this also has an antibacterial and anti-inflammatory effect and reduces oil production in the skin.’ She finds that exfoliating chemical peels combining salicylic acid, lactic acid, and resorcinol or mandelic acid can be particularly helpful for those with hyperpigmentation. What’s more, Simone advises that rather than purchase such products, patients seek ‘a private dermatology clinic that offers these services so that patients get to consult with an aesthetic practitioner or a nurse or even a consultant dermatologist’.
Treatment delays
One of Simone’s biggest concerns is the length of time patients must wait to be seen at the hospital. The waiting time can often be in excess of 52 weeks following an initial referral from the GP and she is aware that in some trusts, the wait time can exceed 60 weeks. As she says, for many ‘acne is a debilitating condition that has a huge effect on patients at any age, especially during their teenage years when image is everything’.
Given this, Simone argues that the whole care pathway must be better engineered and utilised to support patients living with acne. She highlights the use of the NICE 2023 guidelines and PCDS 2019 for acne management,1,2 as evidence of the role primary care can play in this – even though she remains sympathetic to the demands placed on them.
Regarding more severe cases, she urges the need for referrals to be made in a timely manner, and especially so for those patients in psychological distress or with an unclear diagnosis.
One of Simone’s biggest concerns for patients is that, often, lengthy delays in reaching secondary care means their skin worsens by the time they finally see someone.
‘Sometimes, by the time they’ve been assessed, their acne scarring is so severe, it can be a challenging conversation to have with a patient when you have tell them that Isotretinoin does not treat scarring,’ she says.
Managing acne scars
Although early interventions for acne can help reduce the risk of scarring, many patients still develop some degree of scarring. Unfortunately, as Simone notes, the NHS does not currently offer any treatments for acne scars, which is frustrating, although she is aware that some trusts will offer their patients the option of having their scars managed privately. As she says, while isotretinoin is an effective drug, it can only go so far and a common concern among patients is whether they will also be treated for their scars, which have a huge negative impact on their self-esteem. The only real option is for patients to be treated privately but, as she says, ‘where is a 17-yearold boy going to get £3,500 from so he can get his scarring sorted out?’ Simone thinks that one possible solution could be for NHS trusts to offer subsidised scar treatments. In fact, with a limitless budget, Simone’s first task would be to establish clinics to treat acne scars with both lasers
and chemical skin peels. While acne scar treatment is generally not available on the NHS, some trusts do offer triamcinolone injections for patients who develop keloids and hypertrophic scarring. Simone is also eager to point out the value of resources such as Acnesupport.org, which provides well-rounded information on acne types, acne treatments and management and is both useful for patients and health professionals alike.
There’s no doubt that Simone is passionate about managing her acne patients. While she feels dissatisfied about the lack of access to scar treatments, she remains hopeful that in the future, her current service could evolve to provide an overall and complete acne management programme.
References:
1. National Institute for Health and Care Excellence. Acne vulgaris: Management (NICE Guideline No. 198). NICE 2021 (updated 2023). Available at: https://www.nice.org.uk/guidance/ ng198 [last accessed February 2025]
2. Primary Care Dermatology Society. Acne treatment guidelines. PCDS 2019. Available at: https://www.pcds.org.uk/files/general/ Acne_Treatment_2019-final-web.pdf [last accessed February 2025]
Focus on Alopecia
DN
Articles include:
l A natomy and physiology of hair growth: Understanding the intricacies
l A n overview of causes and presentations of different hair disorders: ‘Because it is not just hair!’
l Alopecia areata: The journey from the big black hole, via the roller-coaster, to acceptance of living with a visible difference
l Alopecia treatments
l The role of Janus kinase (JAK) inhibitors in the treatment of alopecia areata
Scan to download a FREE copy of the Focus on Alopecia
THIAMIDOL
Ellie Rashid Consultant Dermatologist, UK
HIDDEN SPOTS [UV CAMERA]
What’s new in the world of research?
Rod Tucker
Perhaps we need to get more sunlight
Encouraging patients to get more exposure to UV radiation is something of a no-no in dermatology. After all, UV radiation is a carcinogen and strongly implicated in the development of skin cancers, and in particular, malignant melanoma. So, spending more time in the sun is a potentially risky business. Or is it?
According to a new analysis by dermatologist Richard Weller’s group in Edinburgh, it seems that more exposure to sunlight has health benefits that potentially outweigh the risks. In his latest work,1 the team examined the association between UV exposure and mortality among older adults in the UK. They used data from the UK Biobank, a treasure trove of health information that is regularly collected from over half a million UK residents. The team focused on two measures of UV exposure: solarium use and the annual average residential shortwave radiation (SWR). The study included data on nearly 500,000 individuals who were followed for over 12 years. It turned out that those who used a solarium and lived in areas of higher annual average SWR, had a lower risk of all-cause, cardiovascular disease (CVD) and cancer mortality. Solarium users also had a lower risk of non-CVD/non-cancer mortality. However, while solarium users did have a higher incidence of melanoma, this was non-significant and not linked with greater melanoma mortality.
These observations are not new and have been previously reported by others. But before we all dash out into the sun, it’s important to recognise that this was an observation study demonstrating a correlation, i.e., that the reduction in mortality was only related to and not caused by, increased exposure to sunlight. Nevertheless, it is an intriguing finding that certainly provides plenty of food for thought and warrants further study.
Could metformin reduce the risk for nonmelanoma skin cancer?
Although recognised as an effective treatment for patients with type 2 diabetes, it seems that metformin
Summary:
In this column, Rod Tucker takes a look at some interesting pieces of current research in dermatology.
Author info:
could also be used to reduce the risk of non-melanoma skin cancers according to a retrospective analysis by US researchers.2 With some preliminary evidence that metformin might protect against squamous cell carcinoma (SCC) but not basal cell carcinoma (BCC), the research team retrospectively examined cases of both SCC and BCC in relation to metformin use. They matched all non-melanoma skin cancer cases with noncancer patient controls.
Overall, there were 4,111 cases of SCC and 8,047 BCCs. The adjusted odds of having an SCC among those with taking metformin was 0.45. In other words, the odds of developing an SCC were slightly more than 50% lower in patients taking metformin. In sub-group analysis, exposure to metformin decreased the risk of a BCC in both males and females as well as across different ethnicities. Similarly, the adjusted odds of developing a BCC for those prescribed metformin was 0.33. Interestingly, the risk of developing an SCC was not significantly lower among African Americans.
“It has been recognised since 1990 that the topical retinoid tretinoin is an effective treatment for patients with photo-ageing”
Quite how metformin provides this anti-cancer action is not entirely clear. It might be related to the ability of the drug to stimulate AMP-activated protein kinase, which serves as a cellular energy sensor and ultimately restricts both energy and nutrients to cancer cells. Although it seems that metformin does something to impede the development of cancer, the retrospective nature of the study is an important limitation, because clearly there
Rod Tucker is a pharmacist with a special interest in dermatology, and a member of the Dermatological Nursing Editorial Board.
Citation: Tucker R. What’s new in the world of research. Dermatological Nursing 2025. 24(1):47-48.
might be other factors at play. However, it is certainly an interesting analysis and should prompt future work examining the use of metformin as a strategy to reduce the risk of non-melanoma skin cancer.
Is tretinoin still the best treatment for photo-ageing?
Following long-term exposure to UV radiation, the skin becomes damaged, leading to fine lines, laxity, pigment changes and dryness. These symptoms represent the hallmark of photo-ageing and the underlying cause is thought to be related to a reduction in the level of two structural proteins in the dermis, type I collagen and elastin. It has been recognised since 1990 that the topical retinoid tretinoin is an effective treatment for patients with photo-ageing. The drug reduces wrinkling as well as the number of age spots (lentigines) and increases epidermal thickness.
“While Keloids are not harmful to patients, the lesions can have a significant impact on an individuals’ physical and emotional wellbeing”
Tretinoin targets nuclear retinoic acid receptors, leading to increased keratinocyte proliferation, together with a greater production of both collagen and elastin. Although tretinoin is clearly effective, a downside to its use is adverse effects including burning, scaling and dermatitis. What’s more, these adverse effects have limited the usefulness of tretinoin in practice. This begs the question as to the effectiveness of the available alternatives and whether these agents are more tolerable?
This question was addressed in a recent systematic review by researchers from New York.2 The team examined all other topical agents studied in randomised controlled trials and which were compared with tretinoin in photodamaged skin. Overall, there were a total of 25 eligible trials. Comparators included other retinoids such as retinol, adapalene, tazarotene and retinaldehyde, as well as several non-retinoids including 4% hydroquinone, betalipohydroxy acids, glycolic acid and herbal extracts.
The results showed that retinol (0.2% or higher) was often as good, if not better, than tretinoin and was more tolerable. Despite this, the quality of trials was invariably poor and often sponsored by the manufacturer. Although the authors concluded that topical tretinoin, remained the gold standard therapy for photo-ageing, it would seem
that some of the non-retinoid treatments held promise. Nevertheless, the current lack of robust data meant that further work was required before these alternatives could be recommended to patients.
Vitamin D for keloid scars?
Keloids are fibroproliferative lesions that arise from an abnormal wound healing process. While keloids are not harmful to patients, the lesions can have a significant impact on an individuals’ physical and emotional wellbeing, particularly when located in visible areas, causing pruritus, tenderness and even pain. Intralesional triamcinolone seems to be the most commonly used treatment for keloids. However, interestingly, some evidence indicates how patients with lower levels of serum vitamin D have more severe keloids. In fact, a case report of two patients, found that intralesional injection of vitamin D improved the appearance of keloids. But how does vitamin D compare with triamcinolone?
This was examined in a randomised, double-blind trial undertaken by a team from Chandigarh, India.4 For the trial, researchers recruited 60 patients and randomised them to receive either four injections of vitamin D (2,00,000 IU) or triamcinolone 20mg/ml at a four-weekly interval. The primary outcome of interest was the proportion of patients achieving a 50% reduction in their Vancouver Scar Scale (VSS) score. The researchers also explored the incidence of adverse effects, and changes in tissue expression of vitamin D receptors before and after treatment. The study found that following treatment, the mean VSS decreased in both groups but the response to triamcinolone was significantly better (p = 0.03). In fact, a more than 50% reduction in VSS score was achieved by more patients receiving triamcinolone (76.7% vs. 50%, p = 0.032). Based on these findings, the authors concluded that while triamcinolone was clearly more effective, intralesional vitamin D did show promise as a safer alternative for the management of keloids.
References
1. Stevenson AC, Clemens T, Pairo-Castineira E, Webb DJ, Weller RB, Dibben C. Higher ultraviolet light exposure is associated with lower mortality: An analysis of data from the UK biobank cohort study. Health Place 2024. 89:103328
2. Siddiqui Z, Zufall A, Nash M, Rao D, Hirani R, Russo M. Comparing Tretinoin to Other Topical Therapies in the Treatment of Skin Photoaging: A Systematic Review. Am J Clin Dermatol 2024. 25(6):873-890
3. Haq Z, Mirza FN, Abdi P, Diaz MJ, Libby TJ. Metformin Use and Risk of Non-Melanoma Skin Cancer: A Propensity-Matched CaseControl Study. J Drugs Dermatol 2024. 23(12):1089-1095
4. Goyal A, Mehta H, Narang T, Vinay K, Chhabra S, Shilpa, Kaushik H, Kaur M, Sachdeva N, Dogra S. A double-blinded randomised control study to compare the effectiveness and safety of intralesional vitamin D3 with intralesional triamcinolone and its correlation with tissue expression of vitamin D receptors in patients with keloid. Wound Repair Regen 2024. 32(5):696-703.
SUITABLE FOR USE ON FACE & BODY
ZERO IN ON THE PERSON BEHIND THE CONDITION
Full range allows personalised approach
Cost efficient, quality products
UK’s #1 prescription emollient company1
Proven patient satisfaction2
The entire Zeroderma® range is approved by the British Skin Foundation
Prescribing Information
Zerobase Emollient Cream. Manufacturer: Thornton & Ross Ltd, Linthwaite, Huddersfield, HD7 5QH, UK. Code # of Notified Body: N/A. Legal classification: Class I. Product name: Zerobase Emollient Cream. Ingredients: Purified Water, Liquid Paraffin 11% w/w, White Soft Paraffin, Cetostearyl Alcohol, Macrogol Cetostearyl Ether, Sodium Dihydrogen Phosphate, Chlorocresol, Phosphoric Acid. Indications: Zerobase Emollient Cream softens, moisturises and protects the skin, providing symptomatic relief for red, inflamed or dry skin. If you have eczema, the cream can also be applied before a bath to stop the skin drying further. It can be used as an alternative to soap. Adverse reactions: Zerobase contains cetostearyl alcohol and chlorocresol which may cause local skin reactions (e.g. contact dermatitis) or allergic reactions. Rarely, mild allergic reactions such as a skin rash may occur. If you notice any side effects; or your skin condition worsens, stop use and tell your doctor or pharmacist, they will tell you what to do. Precautions: For external use only. Do not use if you or your child have an allergy to any of the ingredients listed. If the skin is badly cracked, infected or bleeding do not apply; seek medical advice before use. Avoid contact with the eyes. Use during pregnancy and breastfeeding is unlikely to have any ill effects when used as directed. If unsure, talk to your doctor or pharmacist. Do not use if tamper evident collar is broken or missing at first use (500g pack). Do not use if tube seal is broken or appears tampered with at first use (tubes). Fire hazard. Do not smoke or go near naked flames; clothing & bedding with this product dried on them can catch fire easily. Washing clothing and bedding may reduce product build-up but not totally remove it. If you accidentally swallow some see a doctor straight away. Take the pack with you to show which product you have swallowed. Use within three months of opening. Keep out of the sight and reach of children. Keep in the original carton (tube packs). Use by the date shown on the label (500g pack). Use by the date shown on the side of the carton (tube packs). Contra-indications: Hypersensitivity to any of the ingredients. Method of administration: Pumps: Prime the pump before first use by depressing fully until cream appears. If the pump stops working do not dismantle the pack. Re-start by covering the nozzle, then fully depress the pump several times to expel air. Adults, the elderly and children: Apply to the affected areas of skin as often as required. Smooth gently into the skin, following the direction of the hair growth. Date of preparation: 14/11/2023.
Zerocream Emollient. Manufacturer: Thornton & Ross Ltd, Linthwaite, Huddersfield, HD7 5QH, UK. Code # of Notified Body: N/A. Legal classification: Class I. Product name: Zerocream Emollient. Ingredients: Purified Water, White Soft Paraffin 14.5% w/w, Liquid Paraffin 12.6% w/w, Cetyl Alcohol, Glyceryl Monostearate, Sodium Cetostearyl Sulfate, Lanolin, Citric Acid Monohydrate, Carbomer, Sodium Hydroxide, Sodium Methyl Hydroxybenzoate, Sodium Propyl Hydroxybenzoate, BHT. Indications: Zerocream Emollient is used for the relief of symptoms of flaking, dry skin, ichthyosis, dermatitis, the dry stage of eczema and dry cases of psoriasis. It can be used as an alternative to soap. Adverse reactions: Zerocream contains methyl and propyl parahydroxybenzoates, cetyl alcohol and lanolin which may cause local skin reactions (e.g. contact dermatitis) or allergic reactions which may not appear immediately. Rarely, mild allergic reactions such as a skin rash may occur. If you notice any side effects; or your skin condition worsens, stop use and tell your doctor or pharmacist, they will tell you what to do. Precautions: For external use only. Do not use if you or your child have an allergy to any of the ingredients listed. Avoid contact with the eyes. If the skin is badly cracked, infected or bleeding do not apply; seek medical advice before use. Use during pregnancy is unlikely to have any ill effects when used as directed. If unsure, talk to your doctor or pharmacist. Wash and dry hands before use. Do not use if tamper evident collar is broken or missing at first use. Fire hazard. Do not smoke or go near naked flames; clothing & bedding with this product dried on them can catch fire easily. Washing clothing and bedding may reduce product build-up but not totally remove it. If you accidentally swallow some see a doctor straight away. Take the pack with you to show which product you have swallowed. Treated feet may be slippery. Take extra care when walking on smooth surfaces. Use within 12 months of opening. Keep out of the sight and reach of children. Keep in the original carton (tube packs). Do not use after expiry date shown on the side of the label (500g pack). Do not use after expiry date shown on the side of the carton (tube packs). Contra-indications: Hypersensitivity to any of the ingredients. Method of administration: Pumps: Prime the pump before first use by depressing fully until cream appears. If the pump stops working do not dismantle the pack. Re-start by covering the nozzle, then fully depress the pump several times to expel air. Adults, the elderly and children: Apply as required to the affected areas of skin, two or three times daily. Smooth gently into the skin, following the direction of hair growth. Date of preparation: 14/11/2023. Zeroveen Emollient. Manufacturer: Thornton & Ross Ltd, Linthwaite, Huddersfield,
HD7 5QH, UK. Code # of Notified Body: N/A. Legal classification: Class I. Product name: Zeroveen Emollient. Ingredients: Purified Water, Glycerol 12.6% w/w, Liquid Paraffin 5% w/w, Isopropyl Palmitate, Distearyldimonium Chloride, Avena Sativa Kernal Flour, Cetyl Alcohol, Dimeticone, White Soft Paraffin, Benzyl Alcohol, Allantoin, Stearyl Alcohol, Microcrystalline Wax, Myristyl Alcohol, Sodium Chloride. Indications: Fragrance-free 2-in-1 moisturising cream and wash with natural oatmeal (avena sativa kernal flour) for use in the management of dry skin conditions as may be found in eczema, psoriasis, dermatitis, ichthyosis, elderly pruritus and other dry skin conditions. Adverse reactions: Rarely, mild allergic reactions such as skin rash can occur. If you notice any side effects or the condition worsens while using the product, stop use and tell your doctor or pharmacist. They will tell you what to do. Zeroveen contains benzyl alcohol and cetyl, myristyl and stearyl alcohols which may cause local skin reactions (e.g. contact dermatitis) or allergic reactions which may not appear immediately. Precautions: Do not use if you or your child have an allergy to any of the ingredients listed. If the skin is badly cracked, infected or bleeding do not apply; seek medical advice before use. Avoid contact with the eyes. Use during pregnancy or breastfeeding is unlikely to have any ill effects when used as directed. If unsure, talk to your doctor or pharmacist. Wash and dry hands before use. Do not use if tube seal is broken or appears tampered with at first use (tubes). Fire hazard. Do not smoke or go near naked flames; clothing or bedding with this product dried on them can catch fire easily. Washing clothing and bedding may reduce product build-up but not totally remove it. Always replace the cap after use (tubes). If you accidentally swallow some see a doctor straight away. Take the pack with you to show which product you have swallowed. Treated feet may be slippery. Take extra care when walking on smooth surfaces. Keep out of sight and reach of children. Keep in the original carton (tubes). Do not use after expiry date shown on the side of the label (500g pack). Do not use after expiry date shown on the side of the carton (tubes). Contra-indications: Hypersensitivity to any of the ingredients. Method of administration: Pumps: Prime the pump before first use by depressing fully until cream appears. If the pump stops working do not dismantle the pack. Re-start by covering the nozzle, then fully depress the pump several times to expel air. All packs: Apply cream to the skin. Adults, the elderly and children: Apply as required to the affected areas of skin. Smooth gently into the skin, following the direction of hair growth. Date of preparation: 14/11/2023.
Zerodouble Gel. Manufacturer: Thornton & Ross Ltd., Linthwaite, Huddersfield, HD7 5QH, UK. Code # of Notified Body: N/A. Legal classification: Class I. Product name: Zerodouble Gel. Ingredients: Purified Water, Isopropyl Myristate 15% w/w, Liquid Paraffin 15% w/w, Glycerol, Triethanolamine, Phenoxyethanol, C10-C30 Alkyl Acrylate Cross Copolymer, Sorbitan Laurate. Indications: Highly moisturising emollient gel for dry skin conditions, as may be found in eczema, psoriasis, dermatitis, ichthyosis, elderly pruritus, and other dry skin conditions. It can also be used as an alternative to soap. Adverse reactions: Rarely, mild reactions such as skin rash may occur, or allergic skin reactions on extremely sensitive skin. These effects tend to occur during the first few uses. If you notice any side effects, stop use and tell your doctor or pharmacist, they will tell you what to do. Precautions: For external use only. Do not use if you or your child have an allergy to any of the ingredients listed. If the skin is badly cracked, infected or bleeding do not apply; seek medical advice before use. Avoid contact with the eyes. Use during pregnancy and breastfeeding is unlikely to have any ill effects when used as directed. The ingredients have been in widespread use for many years, without reports of problems. However, safety trials have not been conducted. If unsure, talk to your doctor or pharmacist. The ingredients in this product are not considered likely to affect or be affected by other medicines. Fire hazard. Do not smoke or go near naked flames; clothing & bedding with this product dried on them can catch fire easily. Washing clothing and bedding may reduce product build-up but not totally remove it. Check that the tube seal is not broken before first use (tubes). Do not use if tamper evident collar is broken or missing at first use (pump pack). If you accidentally swallow some, see a doctor straight away. Take this pack with you to show which product you have swallowed. Keep out of the sight and reach of children. Keep in the original carton (tubes). Use within 12 months of opening (100g tube & 500g pump pack). Use within 28 days of opening (20g tube). Use by the expiry date shown on the side of the carton (tubes). Use by the expiry date shown on the side of the label (pump pack). The expiry date refers to the last day of that month. Contraindications: Hypersensitivity to any of the ingredients. Method of administration: Tubes: Unscrew the cap, check and remove the foil seal, then replace the cap. Pump pack: Prime the pump before first use by depressing fully until gel appears. If the pump stops working do not dismantle the pack. Re-start by covering the nozzle, then fully depress the pump several times to expel air. All: Apply the gel only to the skin. Make sure your hands are clean and dry before applying the gel. Adults,
Pump format in line with NICE guidance3
Expert dermatology training & education
Request FREE Patient Evaluation Products!
Allow your patients to try our range of emollients and check their acceptability before a prescription is written. Simply scan the QR code or visit zeroderma.co.uk/pep
Experts in dry skin conditions
the elderly and children: Apply the gel to the affected area on a regular basis and as often as required. Smooth gently into the skin following the direction of the hair growth. Alternatively apply as directed by your doctor or pharmacist. Zerodouble Gel may also be applied before washing or bathing in order to prevent further drying of the skin. Date of preparation: 14/11/2023.
Zeroderm Ointment. Manufacturer: Thornton & Ross Ltd, Linthwaite, Huddersfield, HD7 5QH, UK. Code # of Notified Body: N/A. Legal classification: Class I. Product name: Zeroderm Ointment. Ingredients: Liquid Paraffin 40% w/w, White Soft Paraffin 30% w/w, Cetearyl Alcohol, Polysorbate 60. Indications: Zeroderm Ointment is a rich emollient used to moisture and soften dry skin in eczema, dry cases of psoriasis and other dry skin conditions. It is suitable for all ages and may also be used as a skin cleanser or bath additive. Adverse reactions: The product contains cetearyl alcohol which may cause local skin reactions (e.g. contact dermatitis). If you notice any side effects, stop use and tell your doctor or pharmacist. They will tell you what to do. Precautions: For external use only. Do not use the ointment if you or your child have an allergy to any of the ingredients listed. If the skin is badly cracked, infected or bleeding do not apply; seek medical advice before use. Avoid contact with the eyes. Using Zeroderm Ointment during pregnancy and breastfeeding is unlikely to have any ill effects. If unsure, talk to your doctor or pharmacist. Baths and showers may become slippery. Take care not to slip. Clean away any residues with household cleaner using warm water. Fire hazard. Do not smoke or go near naked flames; clothing & bedding with this product dried on them can catch fire easily. Washing clothing and bedding may reduce product build-up but not totally remove it. Do not use if tear-tab is broken or appears tampered with at first use. If you accidentally swallow some see a doctor straight away. Show this label or pack. Use within 12 months of opening. Keep out of the sight and reach of children. Do not use after the expiry date. Contra-indications: Hypersensitivity to any of the ingredients. Method of administration: Adults, the elderly and children: As an emollient: Apply to the affected area as often as required. Smooth gently into the skin, following the direction of the hair growth. As a bath additive: Melt about 4g (roughly a teaspoonful) of Zeroderm Ointment in hot water in a suitable container. Then add to the bath ensuring that the water has sufficiently cooled before getting in. As a soap substitute: Take a small amount of Zeroderm Ointment from the tub, lather it under warm water and use as required when washing or in the shower. Pat skin dry. Date of preparation: 14/11/2023.
Do not smoke or go near naked flames – risk of severe burns. Fabric (clothing, bedding, dressings etc) that has been in contact with this product burns more easily and is a serious fire hazard. Washing clothing and bedding may reduce product build-up but not totally remove it.
Medical advice should be sought before use of emollients if the skin is broken, badly cracked, infected or bleeding.
Adverse events should be reported. Reporting forms and information can be found at https://yellowcard.mhra.gov.uk or search for MHRA Yellow Card in the Google Play or Apple App Store. Adverse events should also be reported to Thornton and Ross Limited by emailing thorntonross@medinformation. co.uk or by calling 01484 848164.
Zeroderma, Zerobase, Zerocream, Zeroveen, Zerodouble and Zeroderm are registered trade marks of Thornton & Ross Ltd.
References: 1. IQVIA RXA Unit Sales ending March 2024. 2. Thornton & Ross, data on file. 3. NICE, Which emollient product should I prescribe? Available at: https://cks.nice. org.uk/topics/eczema-atopic/prescribing-information/emollients/#choice-of-product accessed August 2024.
STADA UK, Thornton & Ross Ltd., The Globe (3rd floor), Bridge Street, Slaithwaite, Huddersfield, HD7 5JN
Telephone: +44 (0)1484 500283 www.zeroderma.co.uk UK-ZERO-303(1) | August 2024.
Do your patients suffer never-ending itch? Discover how
Rapid itch relief within minutes 1 Hydrated skin starts with Hydromol
Fighting for change in India
Christina Raj
Iwas born as a premature collodion baby in 1967.
The medical fraternity in India hadn’t seen a collodion baby that survived. The nurses were too scared to touch or hold me. My mother, Dr Mary Victoria Ross, was a gynaecologist and had to quit her job for two years to take care of me as I was in a neonatal intensive care unit (NICU).
Her professor in medical college was also my paediatric dermatologist who diagnosed my condition as severe ichthyosis. He consulted dermatologists in the USA and UK and guided my mother on skin care and management. I was bathed often and doused in liquid paraffin as that was the only available and affordable emollient in India. I had severe growth and development challenges and didn’t speak until I was seven years old. My Mom thought I was deaf and dumb. I couldn’t stand and walk till the age of five. My skin used to be so dry that my limbs would contort, causing me pain.
Throughout my life, my mother and I faced many challenges. She was a single parent after my father left upon seeing my skin condition. We were never part of family gatherings and my mother’s siblings mistreated both of us. As my mother’s savings started to dwindle, she was forced to start work again. But after I was abused so badly by my aunt she felt it was safer to lock me in a room alone before leaving for work. She used to make me stand inside a wooden stool that was turned upside down, which was like a crib for me, leaving with a prayer that God would take care of me.
Strangers would stare, spit and make snide remarks, and this continued into adulthood where my neighbours ridiculed me, calling the police on me and trying to ban me from walking in the corridors due to misconceptions about my skin being contagious.
Summary:
A different perspective for this issue’s patient voice, with the author talking about her experience of growing up with harlequin, lamellar and epidermolysis ichthyosis in India.
Citation: Raj C. Fighting for change in India. Dermatological Nursing 2024. 24(1):61-62.
Finding work was a challenge due to many denying me and my appearance, but I did find work in the corporate world where I was valued and appreciated, making a few solid friends. That said, I was mistreated consistently throughout by managers, who would make fun of me and force me to work in conditions that would exacerbate my pain and the cracking of my skin.
Helping others
These challenges are why I set out to help others who perhaps didn’t have the support of a fierce mother with a medical background. We started out very small. I got to know a handful of patients across India, tracking their families and doing my best to reach out to show them that I too had the condition and could help. About 98% are poor and uneducated, and so feeding a family in itself is a challenge, let alone having money to pay for creams. As ichthyosis has not been classed as a rare disease or disability in India, this is a huge burden. I have tracked these families across India, teaching them skin care and management with products that are available at home or in the kitchen to ease pain.
Patients across Africa and India are neglected, forgotten about, and yet suffer the most. These challenges go beyond the daily health issues, to the way people are treated. From being denied admission to school, to students and teachers refusing to touch them or mark their work. The misconception around contagion plays a big part. One small boy and his family in India were shunned by their entire village and forced to pay 10,000 rupees, which is a huge amount for a daily wage labourer, all to feed the entire village a feast to appease the local deity as this would then supposedly heal the child.
Author info:
Chr istina is the Founder and Director of the Centre for Ichthyosis Related Members India (CRM). She has devoted herself to supporting others across the globe through support with wellbeing, advice on managing the condition, and helping people to access treatment such as creams and the necessary financial support. More recently, with the support of Face Equality International, Christina has taken on a mission in advocacy, successfully seeking legal recognition of ichthyosis as a disability in India.
by Sujata Setia
The World Health Organization (WHO) are aware there is no cure, but many families are desperate and so fall prey to extortion, being fed fake cures, which they’re often forced to crowd fund for.
Constantly addressed as a ‘demon’, ‘snake’, ‘alligator’, or ‘lizard’, this dehumanisation is also reinforced by the way in which such crowd funders and reputable newspapers report on the experiences of patients and families. But pushing back against mistreatment, or challenging discrimination, is too fearful for many.
Starting the mission
It was my mother who first started the mission, struggling for 30 years, approaching officials locally and nationally to have ichthyosis recognised as a disability in India as a means of helping patients to seek support in managing life with this disabling condition. I have carried on her fight for inclusion, writing to ministers, lawyers, appealing to celebrities for support, with nothing in return but pity. All my efforts were futile.
This all changed in 2023 when, after five decades of fighting, things started to change for us. After meeting with Phyllida Swift, CEO of Face Equality International, on her trip to interview people with disfigurements in India, I told her about our battle to have ichthyosis recognised as a disability. She spoke of how India had ratified the United Nations Convention on the Rights of Persons with Disabilities, and that any disfigurement should be
legally recognised. She invited me to join her in meeting the academic, Amita Dhanda, a lawyer who was instrumental in crafting this convention, and as fate would have it, was also based in Hyderabad.
After meeting Amita, she instilled in me a renewed faith in asserting the multidisabling nature of ichthyosis, and so I set out to pursue this legal battle again.
I then met Advocate Arvind, a Supreme Court lawyer from New Delhi. He has cerebral palsy and is a strong advocate for disability rights. I connected with the Advocate Arvind and sought his help to represent ichthyosis in the National Supreme Court. He was unsure about our condition and state. It took a few months for him to better understand our experiences. When Advocate Arvind was ready to represent the Centre for Ichthyosis Related Members India (CIRM) Foundation, he said he would want every detail of every patient explained well. Sushma Sirisha, a core member of our CIRM Foundation, and I worked and collected data, speaking to the patients for days, writing every detail of their condition, the challenges presented and the disabling nature of the condition. I had to call and track all 33 patients, whose data I had shared. I spoke to them every day, to be sure that we presented accurate and real time data to the court.
I remembered all the anxious faces of the ichthyosis community, especially from the marginalised members who do
not know anything about the process or the financial aspect of the case, but they knew that I was there for them. All address me as ‘Godmother’ of our ichthyosis community. I knew that everyone’s hopes were on me.
Achieving justice and recognition
In November, Amita Dhanda presented to the Supreme Court on the explicit inclusion of underrepresented disabilities such as ichthyosis, in directions to the union government to frame mandatory rules on accessibility of public spaces. A milestone moment for us all.
On December 1, I flew to Delhi. I got there at midnight and spent the night at a terrible hotel in cold, dust and dander. The next morning, I rushed to court at 8am. I was the first person at the Delhi High Court – I was so early the staff were surprised to see me! I did not have breakfast, nor could I shower in the hotel. I prayed the entire time, until 11am, when I entered the court hall. I waited for our turn. The entire court listened to our case that was read by the honourable Justice Manmohan. The entire hall was silent except for Justice Manmohan and Advocate Arvind who explained more details of our case.
I waited with bated breath to hear the outcome. Justice Manmohan said that this is a genuine case of many patients who suffer. He said that the Ministry of Social Justice and Empowerment should form a committee and list ichthyosis in the category of disability.
Justice Manmohan signed and put a seal on the order and said that the matter should be expedited as patients need urgent help.
A day of victory. After 55 years of fighting, a mission started by my mother and I carried on. December 2 2024; a day for the ichthyosis community to remember.
For more information on Face Equality International and the work of the CIRM Foundation please visit: https:// faceequalityinternational.org/
Images
BIMZELX was well tolerated, the most frequently reported adverse reactions were: upper respiratory tract infections and oral candidiasis . Other common reported adverse reactions include tinea infections, ear infections, herpes simplex infections, oropharyngeal candidiasis, gastroenteritis, folliculitis, headache, rash, dermatitis, eczema, acne, injection site reactions, fatigue, and vulvovaginal mycotic infection (including vulvovaginal candidiasis). Please refer to the SmPC for further information. 2 ¥co-primary endpoints PASI 90 and IGA 0/1 at Week 16 were met *secondary endpoints 1,3
Stay connected with UCB by scanning the QR code and set your digital preferences
§N= modified non-responder imputation (mNRI), missing data were imputed with mNRI (patients with missing data following treatment discontinuation due to lack of efficacy or a treatment-related adverse event were counted as non-responders; multiple imputation methodology was used for other missing data). BIMZELX® (Bimekizumab) is indicated for the treatment of moderate to severe plaque psoriasis in adults who are candidates for systemic therapy. Bimzelx, alone or in combination with methotrexate, is indicated for the treatment of active psoriatic arthritis in adults who have had an inadequate response or who have been intolerant to one or more disease-modifying antirheumatic drugs (DMARDs). Bimzelx is indicated for the treatment of active moderate to severe hidradenitis suppurativa (acne inversa) in adults with an inadequate response to conventional systemic HS therapy. Please refer to the SmPC for further information. 2
Setting sail to improve wellbeing
As I start to write this article, Storm Bert is hopefully calming down and the waters are less bouncy. Yes, I have been on board our yacht through many a storm and have been warm and cosy.
As a family we have sailed for 30 years mostly in Scotland, although we have explored the Cumbrian coast, Isle of Man and Ireland. As our family has grown, so have our boats to accommodate them. The plan had always been to spend more time on the boat, and when I took on the role with Eczema Outreach Support it helped us make the decision to live on board, in Scotland. My daughter had also moved to the area.
Summary:
In this ar ticle, Sandra Lawton explains how life on the sea is beneficial to her mental health and wellbeing.
“As a family we have sailed for 30 years mostly in Scotland, although we have explored the Cumbrian coast, Isle of Man and Ireland”
Author info:
Sandr a Lawton is a dermatology nurse and a volunteer ambassador at Eczema Outreach Support.
Citation: Lawton S. Sailing and living on board a boat. Dermatological Nursing 2025. 24(1):64-65.
Sandra Lawton
What is it like to live on board?
Well, you may wonder what sailing skills I have after many years. I must admit I have not achieved many competencies, as I have more of a supervisory role and keep the crew on their toes (aka husband and family/friends who often join us). The flexibility of where we go and where we anchor or moor is very relaxing, visiting places where the only neighbours are the wildlife or other anchored boats, or going into marinas to stock up on supplies.
We have made new friends in the sailing community, and I am able to work remotely from wherever we are. We are self-sufficient through solar power, and we make our own
“From a wellbeing point of view, at times it can be challenging, but overall, for most of the time, it is relaxing and enjoyable”
water, which makes you much more aware of these needs that we take for granted on land.
My life is not only about work but also the weather, as we are governed by the weather and elements.
From a wellbeing point of view, at times it can be challenging, but overall, for most of the time, it is relaxing and enjoyable. Life is less stressful with many benefits, both mentally and physically.
I have time for me, my family, friends and grand fur babies; I love knitting and can go ashore for walks. I know my dermatology colleagues Patricia Cowan and Nicola Housam go wild swimming and Lucy Moorhead paddle boards, and swimming is something I have considered doing, maybe later this year, as we settle into sea life and plan to venture further afield in the next few years. Paddle boarding though, probably not at this stage.
I acknowledge that sailing may not be for everyone and a few of my derm colleagues have been on board. Nicola, who loves the swimming, joined us and swam ashore for a park run, was not so keen on the heeling when we went up the Sound of Mull, but she survived.
Did you know that YOU can give scaly scalp sufferers faster access to treatment?
Treating scaly scalp conditions can sometimes feel like a dark art. However, a simple, well-established and quality treatment like Sebco TM, that is used by 1000s of dermatology professionals nationwide to soften and remove dry, scaly skin on the scalp, can be provided quickly and easily at every touch point in the patient’s journey.
Sebco TM scalp treatment can also be initiated via:
as dandruff use intermittently as necessary, e.g., once a week. If symptoms persist after 4 weeks consult your doctor. For children 6-12 years use under medical supervision only. Not recommended for use on children under six years. Contraindications: Skin infections of the scalp or known sensitivity to any of the ingredients. Use in Pregnancy and Lactation: To be used at the discretion of the prescribing doctor. Warnings and Precautions: Instruct patients not to smoke or go near naked flames - risk of severe burns. Fabric (clothing, bedding, dressings etc) that has been in contact with this product burns more easily and is a serious fire hazard. Washing clothing and bedding may reduce product build-up but not totally remove it. Avoid contact with eyes, and any areas of broken skin. Coal tar may stain clothes and jewellery. Remove or protect these items during treatment.
Effects: May cause skin irritation, folliculitis and rarely
A trek up Kilimanjaro and journey of self-discovery
Icompleted school at a time when gap years had not been conceived and have always been envious of those who have had the opportunity to travel and have an adventure. With a significant birthday looming and having spent a lot of 2023 caring for my mother as she quickly died from a brain tumour, I was forced to reassess my life a little and I realised I wanted to grab things whilst I still can. I have a very good friend, Fiona, with whom over the years, as a means to catch up, we would train and take part in ultra-challenges or climb UK mountains such as Ben Nevis. We had always talked of climbing Kilimanjaro ‘one day’. Fiona was preparing for an imminent empty nest, so 2023 made us both realise that we needed to nail ‘one day’ in the diary as soon as possible, so we booked a trip to climb Kilimanjaro this past October.
Kilimanjaro is a dormant volcano in Tanzania. It is the highest mountain in Africa and the highest free-standing mountain in the world above sea level. It stands 5,895 metres above sea level (altitude sickness can occur above 2,500 metres – more about that later). There are seven routes to reach the summit. Summit success has been averaged at around 60%, but the route chosen can improve or hinder your chances of success. You do not need oxygen or climbing equipment but, let me assure you, it is not a walk in the park.
After a lot of research, we chose to walk the Lemosho route. This takes eight days with seven days camping on the
Summary:
Lucy Moorhead documents her char ity trek up Kilimanjaro, in memory of her mother.
Lucy Moorhead
mountain. It is considered to be the best route for success as you have longer to acclimatise and it is also noted for its remoteness and beauty.
Once the trip was booked training commenced. I would walk up to the 32nd floor at Guy’s hospital every day I was on site, and started swimming to improve my lung capacity. I carry a heavy rucksack to work daily, so that box was ticked. Both Fiona and I had serious doubts at times as to whether the trip was one of our better ideas, but thankfully not at the same time. Personally, I found when I
started worrying, if I bought something to counteract my concerns it would assuage my worry. This did not help my rapidly depleting bank account!
Before long, departure day arrived. I felt a bit like I did before my A level exams when I hoped my appendix would burst, but appendix intact and, as dormant as Kilimanjaro, I was soon on a flight to Addis Ababa. Once there, we transferred to the flight to Kilimanjaro. En route, we met fellow walkers (easily spotted with hiking boots in situ) and shared stories about why we were
“Kilimanjaro is a dormant volcano in Tanzania. It is the highest mountain in Africa and the highest free-standing mountain in the world above sea level”
Author info:
Lucy Moorhead is a nurse consultant in inflammatory skin disease at Guy’s and St Thomas’ NHS Foundation Trust.
Citation: Moorhead L. A trek up Kilimanjaro and journey of self-discovery. Dermatological Nursing 2025. 24(1):67-70.
It takes a village to climb a mountain! Team Simba as we chose to call ourselves
Wellbeing for the workforce
doing this and how we had prepared. It was reassuring that all were daunted by the task ahead of us. One concern had been if we arrived and our luggage did not, so we had been advised to carry essentials in our hand luggage as the trek would not wait for our bags. Before long we were reunited with our bags and entertained by Masai dancers on the runway as we disembarked – Luton airport could learn a thing or two!
The first night was spent in a remote coffee plantation where we met our group of 13 fellow trekkers – lucky for us. As well as Fiona and I, there were two other nurses, making nursing the most prevalent profession. Eleven of the 13 were women with most of us being similar ages, which made for a fab group. Once we had been introduced and met our guides – also female, which is a relatively new concept that was welcomed by all – we had an early night sleeping for the last time in proper beds under a mosquito net.
Setting off
The next day we set off to our start point. We had still not seen Kilimanjaro
due to cloud cover. It was a four-hour drive to our starting point, but we enjoyed the scenery and getting to know each other. Highlights were seeing wild giraffe and a dirt track that was a free massage. Arriving at the start point we registered our presence on the mountain and met our crew. Altogether, it would take nearly 50 people to get us up and down Kilimanjaro.
The first day was an easy walk through the rain forest to our first camp. We had monkeys in the trees and porters dashing past us carrying the camp, so all was set up when we arrived. We all used poles but walking was easy and it was good to be on our way.
We arrived at camp mid-afternoon. Each campsite was shared by several groups and was literally just an area of land with a ranger’s hut, a helipad and long drop toilets. Some campsites did not have running water, so all had to be carried by our crew. The set up was normally one or two in a tent, a kitchen tent and a mess tent for each group. We had booked the ‘luxury option’ and had two chemical toilets between the 13 of us, which
“The second and third days were fun and easy, whereby we climbed higher and higher but nothing too taxing”
meant we did not have to venture near the dreaded long drop toilets, but this was at the camp only!
Each day, as we arrived at camp, we would be given a bowl with some water for ‘washy washy’ and then would meet for tea and popcorn. The late afternoons were spent relaxing; reading, chatting or playing cards. We would then meet for dinner and retire to our tents for an early night as we would be woken at six in the morning to start walking at 7.30. Meals were three courses – soup, rice and beans/vegetables/meat and pudding. No alcohol was allowed, and tasty, nutritious, unprocessed food was freshly prepared for us at each meal. We were encouraged to eat and amazingly we all lost weight despite eating way more than normal. Each morning, as we set off, our porters would be clearing the entire site and moving the camp to our next location to set up before we arrived.
The second day, we left the rainforest zone and entered the afro-alpine moorland zone. This also meant we were over 2,800 metres, so we needed to be vigilant for signs of altitude sickness. As
Above: Alpine desert zone – on our way to camp after lunch at Lava point
Left: A soon-to-be cloudy camp with the dreaded Barranco Wall in the background
we left the rainforest behind, we walked through changing vistas with spectacular views. We also started to be able to see the summit of Kilimanjaro looming in front of us covered in snow.
By now, all of us could identify we were feeling symptoms that we could attribute to altitude. Fiona and I found we spent a lot of time ‘faffing’ in our tents trying to find things we thought we had lost or coming up with new systems to prevent
us from losing things. There was a lot of laughter in our tent throughout the trip. We had shared a bedroom at university so already knew each other pretty well. We were only allowed to have 15kgs in one bag, which our porter would carry. In our bags everything was further divided into dry bags to keep it all safe. There was a lot of organising to do.
Acclimatising to the challenge
The second and third days were fun and easy, whereby we climbed higher and higher but nothing too taxing. We ate lots of food and snacks, drank four litres of water a day to minimise chances of altitude sickness and, whilst feeling short of breath, could still do all we needed.
Before long, day four was upon us. This was the day we had to climb the Barranco Wall. This was high up my worry list. It’s a scramble which requires four limbs to ascend 257 metres (but I am sure they have mis-measured). It takes approximately two hours and involves the famous ‘kissing rock’ whereby you must edge yourself around a precipice ‘kissing’ the rock. By now, we had all gelled as a group. Our guides were fantastic at
Wellbeing for the workforce
keeping our morale up with shouts of ‘non-stop, to the top’, ‘one team, one dream’. I don’t know whether it was the lack of oxygen or my fantastic group, but this turned out to be my favourite part. Climbing up the rock face, waiting on a ledge till several porters had passed me carrying tables, chairs and tents before attempting the next bit, all under the watchful eye of our guides, with a helping hand when needed, was an experience I will never forget. Each day we would climb higher than we needed and then descend to sleep at a lower elevation to help us acclimatise. By the end of this day, we were at 3,995 metres.
By day five, whether it was the adrenalin come down from the day before or the altitude, we were all noting we were moving more slowly and becoming more out of breath. Getting my sleeping bag out now required major effort. Deflating and rolling up my little mattress required a two-minute rest. Our sats at times measured 86%. We were now high in the alpine desert zone, so the only creatures we ever saw were little mice-like critters with stripes down their back. We stopped for lunch at Lava Point – this is a notorious spot for climbers to deteriorate. The only way down, if not walking, is by helicopter or a wire contraption with a bicycle tyre fixed to
the bottom. The weather by now was hugely changeable – one-minute glorious sunshine and the next literally covered in cloud. Nights were cold, but with hot water bottles and our artic sleeping bags we were toasty.
The push for the summit
On day six we arrived at Barafu camp, which is at 4,673 metres. This is the last camp before summit night. You arrive midday, have lunch, rest, have dinner, rest, and then start your trek to the summit at 23:00. By now, shortness of breath is a thing. Many of us were struggling to eat (anyone who knows me knows this is never an issue) and sleeping was tricky.
Before long, we had put on almost every piece of clothing we had and set off walking ridiculously slowly (cos that is all we could do!) to the summit. The phrase is ‘poley poley’ which translates as ‘slowly slowly’. The summit required lots of climbing over and up rocks with only a headtorch for light which was disconcerting. Ahead and behind you could see all the other climbers with their lights which made for a spectacular sight. The plan was to reach the summit at seven in the morning for sun rise. By this point in our group there were those who were more adversely affected by altitude than others. Fiona was like a mountain goat, but I could not get enough air in me
Above: Camp under the summit of Kilimanjaro
Left: View of the Arusha and Moshi from one of our campsites
Wellbeing for the workforce
to move. With the help of Frank, one of our guides, I reached a summit point at nine having enjoyed the sunrise on my super slow walk to the top. As Kilimanjaro is a dormant volcano with a crater at the top if you reach the top of the crater it is considered a summit. Annoyingly, I was not allowed to walk a further two hours to climb just 100 metres higher to reach the highest point of Kilimanjaro due to signs of altitude sickness. At Stella Point, in the artic zone, 5,756 metres above the sea, I am not ashamed to say I shed a tear before I began my descent down. Frustratingly, as soon as I ducked under 5,000 metres I felt completely fine.
The next two days we made our way down over 3,000 metres (a good test for the knees) to the exit point where we signed out and made our way back to the coffee plantation for a shower, wine and first contact with loved ones – maybe not in that order!
I think I am still processing the whole experience. It taught me that I can leave my comfort zone. I was surprised at how well I coped with no mobile, showers, toilet or make-up. It also taught me to not worry – it turned out the bits I worried about the most where actually the most fun and the hardest part for me, the summit, I had thought I could do with mind over matter. I will never forget the stars in the sky over Kilimanjaro at night and looking down on the towns
below from up high! So, if anyone has an adventure in mind but is putting it off, I would say go and book it now – you will not regret it.
Although we arranged and paid for the trip ourselves we did take the opportunity to raise money for the Brain Trust Charity. I would like to thank
“I was surprised at how well I coped with no mobile, showers, toilet or make-up”
everyone who very kindly and generously donated. I raised over £1,600 in memory of my dear mum. If anyone else would like to the page can be found at:
Doing something for charity or a good cause and want to tell us about it?
Email rob.mair@pavpub.com
Above: Sunrise over Mount Mera on my plod to the top! Left: My summit point – its -8 degrees but I am feeling hot
Start prescribing QV for your patients with dry skin conditions.
Dermatologically tested emollients
Sources:
In-line with NICE Guideline recommendations first-line atopic eczema treatment1–4
Suitable for a range of dry and sensitive skin conditions, including eczema, dermatitis, and psoriasis
Available both on prescription and over the counter
1. National Institute for Health and Care Excellence (NICE). Eczema — atopic. Emollients. [Internet]. London: National Institute for Health and Care Excellence, April 2022 [cited August 2023]. Available from: https://cks.nice.org.uk/topics/ eczema-atopic/prescribing-information/emollients/emollients/.
2. National Institute for Health and Care Excellence (NICE). Eczema — atopic. Scenario: Mild eczema. [Internet]. London: National Institute for Health and Care Excellence, April 2022 [cited August 2023].Available from: https://cks.nice.org. uk/topics/eczema-atopic/management/mild-eczema/.
3. National Institute for Health and Care Excellence (NICE). Eczema — atopic. Scenario: Severe eczema. [Internet]. London: National Institute for Health and Care Excellence, April 2022 [cited August 2023]. *Fifth Quadrant, Sponsored by Ego Pharmaceuticals, OTC Skincare, n=374 (Australian Dermatologists, GPs and Pharmacists). October 2023
UK Dermatology Clinical Trials Network Update
Carron Layfield
Please note all studies mentioned below are funded by a range of National Institute for Health and Social Care (NIHR) funding programmes. These are just a selection of studies developed with UK DCTN support – for a full list please see http://www.ukdctn.org/ourclinicaltrials/index.aspx.
Ongoing studies
Acne-ID
Low dose isotretinoin study recruits first patients and needs more sites.
We are delighted to let you know that ACNE-ID (co-chief investigators Dr Ether Burden-Teh and Prof Kim Thomas, Nottingham) has recruited its first participants, with 18 recruited so far. The study is comparing a low-dose isotretinoin strategy (intervention 0.2-0.3 mg/kg/day) with standard care (comparator >0.5mg/kg/day) and aims to recruit 800 people aged 12-24 years with acne over a 12-month period. Each participant will be followed up for 12 months. The primary outcome for the study is acne clearance at the end of treatment course. Secondary outcomes include side effects and tolerability, change in mood, quality of life, treatment satisfaction and recurrence of acne, along with costs to patients and the NHS.
The study is now open at five sites across the UK and is looking for more sites. If your department has an acne service, please encourage them to complete the site selection questionnaire on the study website https://www.acne-id.ac.uk/.
SCC-AFTER
High-risk cutaneous squamous cell carcinoma study opens to recruitment.
SCC-AFTER is investigating whether adding in a course of radiotherapy following surgery in ‘high-risk’ squamous cell carcinoma patients will help prevent local recurrence. If effective, the use of adjuvant radiotherapy will be incorporated into NHS treatment pathways. Led by Dr Agata Rembielak (Manchester) and Prof Catherine Harwood (London), the study aims to recruit 840 patients over four years from 25 sites across the UK. We’re pleased to let you know that SCC-AFTER opened to recruitment in December and is now open at six sites. Additional sites are being opened over the next few months, with over 40 recruitment centres having expressed an interest in taking part.
Please see https://www.cardiff.ac.uk/centre-for-trials-research/ research/studies-and-trials/view/scc-after for further information.
PEARLS
LS study recruits over 140 patients and exciting new ‘LS Guide’ website launched.
The PEARLS study, investigating proactive versus reactive therapy for the prevention of vulval lichen sclerosus (LS) exacerbation and progression of disease, has now recruited 146 out of a target of 400 participants. A total of 16 sites are open to recruitment, with an additional three sites due to open shortly. Although recruiting well (with strong patient interest in taking part), the study team are applying to the funder for a six-month non-cost extension to enable them to extend the recruitment period to October 2025. Further information is available at https://www.nottingham.ac.uk/pearls/.
PEARLS is part of a wider package of vulval LS work led by Dr Rosalind Simpson (Nottingham), and we wanted to take this opportunity to highlight the new ‘Lichen Sclerous Guide’ website that was launched earlier this year. Developed by a team including healthcare professionals, researchers and patients, this site (funded by Wellbeing of Women, the British Association of Dermatologists and the British Society for the Study of Vulval Disease) is a wonderful resource for both those living with LS and those supporting them. Including sections on causes, symptoms and signs; treatment; everyday life with LS and information for healthcare professionals, it can be found at https:// www.lichensclerosusguide.org.uk/. Please do take a few minutes to look at this site and share with your colleagues and LS patients.
BEACON
Adult eczema study adds fourth arm (abrocitinib) and needs more sites.
BEACON is a multi-centre, assessor blinded RCT in adults with moderate-severe eczema requiring systemic therapy. Aiming to assess the effectiveness, tolerability, and cost-effectiveness of key systemic treatments, BEACON has been set up as a platform study to enable emerging systemic therapies to be added to the trial over time. To date, 115 participants have been recruited.
We are really pleased to let you know that in addition to the
original three therapies (ciclosporin, methotrexate and dupilumab), abrocitinib has been included as a fourth arm to the study. This means that the sample size of the study has increased from 402 to 536 participants and so the study team are seeking an additional five recruiting centres to get on board. Please get in touch with the study team on BEACON@kcl.ac.uk if you can help.
In addition to recruitment from hospital sites, patients can self-refer to BEACON, and over the next few months the study team will also be looking to identify GP practices to act as Patient Identification Centres (PICs) for the self-referral pathway. They are initially looking for GP practices in Central London, so again please follow up if you work in primary care or know GPs that may be able to help. Further information is available at https://www.beacontrial.org/.
TIGER
Recruitment end date extended to August 25 for paediatric study of IgE food allergy tests.
The TIGER study, investigating if dietary advice based on food allergy tests improves disease control in children with eczema, has now recruited 322/493 participants. Children under two years of age with eczema are randomised into two groups: “usual care” or “test guided dietary advice”. Those in the testing group will have skin prick tests to common allergycausing foods (milk, egg, wheat, and soya) with parents advised to exclude or include one or more foods for one month. To help meet the recruitment target, the study has now been given funder approval to extend its recruitment period to August 2025, with the study end date extended to October 2026 to allow participant followup and analysis of results.
TIGER is recruiting children through GP practices in South-West Central, South Central and North Coast (specifically Greater Manchester) NIHR Research Delivery Network areas. If you work in these areas and see children aged threemonths to under two years with eczema, please ask their parents/carers if they are aware of the study and encourage them to take part.
Parents can self-refer by emailing: tigerstudy@bristol.ac.uk but they must be registered at one of the participating GP surgeries which can be found at www.bristol.ac.uk/tiger-study along with eligibility criteria and further information about participation.
Saying goodbye to Prof Fiona Cowdell
After joining the UK DCTN Steering Committee in 2012 as the dermatology nursing representative and going on to become a member of our Executive Committee in 2016, we are saying a fond farewell to Prof Fiona Cowdell in March when she retires from her substantive post at Birmingham City University.
Fiona has been a staunch advocate of ensuring that the needs of the dermatology nursing community have been considered in all aspects of the UK DCTN. This has included encouraging study teams to bring nurses into their trial development groups, inspiring dermatology nurses to become actively involved in research activities such as Priority Setting Partnerships and supporting the development of research education initiatives including the UK DCTN Nurse Fellowship Award.
We would like to take this opportunity to formally thank Fiona for her much-valued contributions to the Network – she really will be missed.
Other UK DCTN news
The 2024 UK DCTN Annual report is now available - please see https://issuu. com/ukdctn/docs/final_version_uk_ dctn_annual_report_2024 for highlights of the past year. A PDF version is also available on our website https://www. ukdctn.org/about-us/reports-andpublications/index.aspx.
The theme for our 2025 Annual Evidence Based Update Meeting will be hidradenitis suppurativa (HS) and this one-day, online meeting is taking place on Thursday May 22. It will cover a mixture of recent RCT results, systematic reviews and expert opinions (with the ever-popular Q&A session of course!) from speakers including Dr John Ingram, Prof Falk Bachara and Prof Brian Kirby.
Further details, including how to book, are available at https://www.nottingham.ac.uk/ conference/fac-mhs/medicine/evidencebased-update-meeting/ (reduced delegate fee of £30 for nurses, standard rate £90).
The topic for our 2025 Themed Call Award is ‘Skin of Colour’. Up to £10,000 funding is available for work that will inform the development of an RCT in this area. The closing date is Monday 21 July 2025. Please see https://www.ukdctn. org/funding-awards/ukdctn-fundingawards.aspx and get in touch to discuss your ideas.
Please keep an eye out for dates for our new UK DCTN research clinics. These informal sessions are aimed at supporting study teams who have ideas for dermatology clinical trials and need some advice. Further information is available at https://www.ukdctn.org/idea-for-a-trial/ index.aspx. We can only provide input and feedback into research that has a trajectory to an RCT – if you are seeking support for other types of research then please consider contacting your local NIHR Research Support Service. You can find more details here https://www. nihr.ac.uk/support-and-services/researchsupport-service.
How to get involved
Membership of the UK DCTN is free and open to anyone with an interest in dermatology research and you can join via the website https://www.ukdctn.org/join-thenetwork/index.aspx#healthcare.
Correspondence
Carron Layfield (UK DCTN Network Manager)
UK DCTN Co-ordinating Centre, Centre of Evidence Based Dermatology, Applied Health Research Building, Main University Campus, University of Nottingham, Nottingham NG7 2RD e-mail carron.layfield@ nottingham.ac.uk
Podcast update
Teena Mackenzie
Welcome back to the BDNG podcast update where the Education Team are bringing you the latest insights and updates in dermatology. I’m Teena Mackenzie and I am excited to share what’s coming in our regular podcast series. Our episodes are designed to keep you informed and inspired, whether you’re a long-term listener or tunning in for the first time we have some incredible topics and there’s something for everyone.
Listen to expert insights, discussions and top tips from a variety of healthcare professionals. Fed up with that boring commute, instead tune into a BDNG podcast available on the website, Apple and Spotify. These podcasts can contribute to your appraisal or revalidation. Also, if you would be interested in recording a BDNG podcast with a member of the Education Team, please reach out to EDLead@bdng.org.uk. We are always happy to hear your ideas and support you with creating a BDNG podcast.
The Education Team continue to work closely with many dermatology charities, promoting the valuable work they do and allowing patients to have a voice. In the past few months, I have been working with Mandy AldwinEaston who many of you will know as the Medical and Communications Manger of the Ichthyosis Support Group. Mandy kindly reached out to members of the Ichthyosis Support Group, and we recorded two excellent podcasts. David represented the male voice of living with a rare form of ichthyosis and Georgia discussed being a parent of a child with ichthyosis and navigating the
healthcare system. Both contain valuable insights, and I would recommend a listen.
In addition, we record BDNG podcasts supported by pharmaceutical companies. In December, Derma UK supported two podcasts focusing on Sebco® and Methoderm®. I interviewed Val Anderson, who is known to many and Dr Angela Razzaque, who provide many top tips. Both podcasts are also available on the Derma UK website and are well worth a listen.
Education Nurse Molly Connolly has been busy recording podcasts focusing on sunshine research with Professor Weller, whilst Emma Button interviewed Paula Oliver and David Clements on home PDT initiatives. Kunsang Dolma provided valuable insights into skin cancer initiative and Claire Frazer discussed biologic treatments form a primary care perspective.
The Education Team are dedicated to sourcing new and interesting topics. We are pleased to say that, as a result of recording some of these podcasts, the guests have agreed to present at the main BDNG Conference 2025 in Harrogate. Save the dates now – September 30 to October 2.
We always love to hear from you. Please reach out to me at EDLead@bdng.org.uk if you know someone or you yourself are interested in recording a BDNG podcast.
An update for members
Lynne Skrine
Since my last update, things have slowed up a little as I was off for a period.
You may have noticed that in the BDNG’s regular Friday alert I asked for the dermatology leads for services around England, Scotland, Wales, Ireland and Northern Ireland. I am still in the process of building a database which contains these leads, as it will help us know where our dermatology nurses are.
If you haven’t already notified me, please let me know by dropping me a line at lynne@bdng.org.uk so I can add your service. I do realise everyone has been busy, manly due to the usual winter illnesses and pressures within their own services.
I hope you are all managing well and that you have been able to listen to or watch the brilliant webinars put on by the BDNG over the winter period. They have all been well received and attended.
Future plans
Recently, the BDNG President and trustees, alongside myself and the educational team, have been busy putting together the conference programme for 2025.
I have also been in conversation with Sara Burr, who is on the editorial board for the Community Skin Health journal, which is part of the International League of Dermatological Societies, and we are hoping to write an article for that journal, highlighting the work of the BDNG and my role in 2025.
Write for Dermatological Nursing
Why write for Dermatological Nursing?
Dermatological Nursing is a quarterly, peer-reviewed publication that aims to provide cutting-edge articles on the treatment and management of dermatological conditions and the care of patients with skin problems. While the focus is on dermatological nursing, the information included will be relevant to other healthcare professionals. Writing for Dermatological Nursing can be a useful way to help develop and crystallise ideas about a specific topic, and may encourage exploration of an area in greater depth and lead to further understanding. Once you have made the decision to write for Dermatological Nursing, please contact the Managing Editor to ensure that what you are planning to write has not already been commissioned, and that it is appropriate for the readership. The article should be unpublished and have not been submitted for publication elsewhere.
Dermatological Nursing is available online to BDNG members at bdng.org.uk,which also offers a searchable archive of previously published articles.
Dermatological Nursing welcomes submissions for publication broadly in the following categories:
l C linical Skills/Clinical Review
l S cience in Practice
l R esearch/Audit
l P ractice Development
l Policy Review
l C ase Reports
Once your idea has been given the all clear, you will be sent the guidelines that should be adhered to when preparing your paper for submission.
Find out more
For further information, please email Rob Mair, Managing Editor, at rob.mair@pavpub.com
Cosentyx is indicated for the treatment of: moderate to severe plaque psoriasis (PsO) in adults, children and adolescents from the age of 6 years who are candidates for systemic therapy; active psoriatic arthritis (PsA) in adults (alone or in combination with methotrexate [MTX] who have responded inadequately to disease-modifying anti- rheumatic drug therapy; active ankylosing spondylitis (AS) in adults who have responded inadequately to conventional therapy; active non-radiographic axial spondyloarthritis (nr-axSpA) with objective signs of inflammation as indicated by elevated C-reactive protein and/or magnetic resonance imaging evidence in adults who have responded inadequately to non-steroidal anti-inflammatory drugs; active moderate to severe hidradenitis suppurativa (HS; acne inversa) in adults with an inadequate response to conventional systemic HS therapy; active enthesitis-related arthritis in patients 6 years and older (alone or in combination with MTX) whose disease has responded inadequately to, or who cannot tolerate, conventional therapy; active juvenile psoriatic arthritis in patients 6 years and older (alone or in combination with MTX) whose disease has responded inadequately to, or who cannot tolerate, conventional therapy.2 1. Cosentyx®: European Public Assessment Report (EPAR) Product Information. https://www.ema.europa.eu/en/documents/product-information/cosentyx-eparproduct-information_en.pdf. Accessed 13 February 2025; 2. Cosentyx (secukinumab) Summary of Product Characteristics.
Adverse Event Reporting. Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard. Adverse events should also be reported to Novartis online through the pharmacovigilance intake (PVI) tool at www.novartis.com/report or alternatively email medinfo.uk@novartis.com or call 01276 698370.
This promotional material has been developed and funded by Novartis Pharmaceuticals Ltd. It is intended to UK Healthcare professionals.
Scan or click (if viewing digitally) the QR code to view Prescribing Information.
Clinical trial supports use of Adex Gel in moderate to mild atopic eczema
New data presented at the Annual Meeting of the Austrian Society of Dermatology and Venerelogy (OGDV) supports the use of Adex Gel for moderate to mild eczema, pharma Dermal has announced.
In the meeting, held in November 2024, in Graz, Austria, the study revealed that Adex Gel has been shown to improve atopic eczema from moderate to mild in two weeks without corticosteroids.1
The trial evaluated the performance of Adex Gel in the treatment of moderate atopic eczema in children and was a multi-centre study to reflect real-life settings.
In a trial of children with moderate atopic eczema conducted in NHS GP practices, the mean disease severity score (SCORAD) improved significantly from 37.14 (moderate atopic eczema) at baseline, to 22.56 (mild atopic eczema) after two weeks, and to 18.48 (mild atopic eczema) after four weeks, per protocol analysis of 41 children.
Additionally, the mean children’s dermatology life quality index score (CDLQI) improved significantly from 9.3 (moderate effect on the child) at baseline to 3.7 (small effect on child) after four weeks.
Further trial information can be found at: www.AdexGel.com/evidence
Adex Gel is a highly moisturising emollient gel with an ancillary anti-inflammatory, nicotinamide 4%, a form of vitamin B3, to help reduce inflammation and redness for dry skin conditions prone to inflammation.
Scan the QR code for Adex Gel essential information and adverse event reporting.
1. Gallagher J. et al. Evaluation of a nicotinamide-containing emollient for moderate atopic eczema in paediatric patients: A prospective, multi-centre GP study reflecting real-life settings. Data presented at the Annual Meeting of the Austrian Society of Dermatology and Venereology (ÖGDV), November 2024, Graz, Austria.
Think ROSACEA
Think SOOLANTRA®
SOOLANTRA® (ivermectin) is indicated for the topical treatment of inflammatory lesions of rosacea (papulopustular) in adult patients1
TOPICAL IVERMECTIN
IS RECOMMENDED BY NICE AND PCDS as a first-line treatment for mild to moderate papulopustular lesions of rosacea2-4
SOOLANTRA® Cream has anti-inflammatory and antiparasitic activity offering an alternative approach to help reduce inflammatory lesions of rosacea1
This convenient, once-daily treatment is more effective at reducing infl ammatory lesions at 16 weeks7 and gets more patients to clear (IGA 0)8 vs topical metronidazole 0.75%.
Most commonly reported adverse reactions are skin burning sensation, skin irritation, pruritus and dry skin, all occurring in 1% or less of patients treated with the medicinal product in clinical trial.
Soolantra is not recommended during pregnancy.
Please refer to the full Prescribing Information available via the QR code.
ADVERSE EVENTS SHOULD BE REPORTED.
Adverse Event Reporting For the UK: Reporting forms and information can be found at www.mhra.gov.uk/yellowcard or search for MHRA Yellow Card in the Google Play or Apple App Store. For Ireland: HPRA Pharmacovigilance, Website: www.hpra.ie
Adverse events should also be reported to Galderma (UK) Ltd E-mail: medinfo.uk@galderma.com; Tel: +44 (0)300 3035674
References: 1. Galderma. SOOLANTRA® (ivermectin) 10 mg/g Cream. Summary of Product Characteristics. June 2020.
2. NICE. Scenario: Rosacea. March 2024. Available at: https://cks.nice.org.uk/topics/rosacea/management/rosacea/. Accessed: Feb 2025.
3. Primary Care Dermatology Society Primary Care Treatment Pathway. October 2019. Available at:https://www.pcds.org.uk/files/general/Rosacea_ Treatment_2019-web.pdf. Accessed: Sept 2024. 4. Primary Care Dermatology Society. Rosacea. 2023. Available at: http://www.pcds.org.uk/clinical-guidance/ rosacea. Accessed: Feb 2025. 5. Taieb A, et al. Br J Dermatol 2015;172;1103–1110. 6. Webster G, et al. J Dermatolog Treat 2017;28:469-474.
7.Taieb A, et al. Br J Dermatol 2015;172;1103–1110. 8. Taieb A, et al. J Eur Acad Dermatol Venereol 2015;829–836.
Dates for the diary
The BDNG has a busy year ahead and we’d like to give you a sneak peek of what’s to come.
Spring Meeting 2025
This will be held in Manchester on the 12-13 May 2025 at the Mercure Manchester Hotel, Portland Street, M1 4PH.
12 May agenda
Rare Disease Day: This will have a unique focus involving support groups including DEBRA and the Ichthyosis Support Group. Professor Andrew Thompson and Olivia Hughes will be discussing the Toolkit for Parents of Children with Epidermolysis Bullosa.
Advances in Aesthetics for Dermatology Nurses Day: This would be a great opportunity for delegates practicing in both aesthetics and dermatology to gain more knowledge in the subject area. This stream is aimed at those already practicing in aesthetics but want to discuss hot topics and advancements further. The subgroup is led by incredibly experienced practitioners with dual skillsets. A full agenda is available on the BDNG website.
Psychodermatology Day: This will be hosted by Teena Mackenzie and Karen Stephen, who both hold a specialist interest and have experience in this area.
It’s Just Skin? Day: Molly Connolly will be taking you on a journey to think about this skin in a unique way with a practical workshop. Want to learn some
tips and tricks for managing patients with inflammatory conditions? Then this is the day for you.
13 May agenda
PDT Day: With a view to support delegates new to photodynamic therapy and for those requiring a refresher. A full agenda for the sessions is available on the BDNG website.
Patch Test Day: Are you in need of a refresher? Or are you new to patch testing? Either way, this day is for you. This session will be delivered by Liza Benfield, a Clinical Nurse Specialist in Inflammatory Dermatology, who has a wealth of experience and knowledge on this topic area.
Biologics Day: This day is great for those practicing in biologic therapies, with case studies and consideration for other interventions, such a psychdermatology, as well as red flags.
Wound Care Day: We will be discussing ‘red leg syndrome’, assessment of wounds, whether it is an infection and best techniques to treat. This day will include a practical element. Full details are available on the BDNG website.
12-13 May agenda
Advancing Knowledge and Skills in Phototherapy Days: This will run across both days, and will be led by Dermatology Clinical Nurse Specialist
Stephanie Greenleaf, who has significant experience in running a nurse led service.
The two-day event would be suitable for those practicing in phototherapy and looking to enhance, refresh and gain new knowledge and skills.
Future events
The BDNG will be hosting an introductory to phototherapy in Birmingham in the autumn. The date for this is 11 November 2025.
Stay up to date on future events
Please remember to check your weekly online newsletter informing you of upcoming supportive educational streams, including webinars, podcasts and e-learning.
Please check your BDNG email updates for future events and educational opportunities.
Follow us on twitter @BDNG / Instagram / Facebook
COMING SOON
The British Dermatological Nursing Group Clinical Handbook
A practical guide to managing common skin conditions.
The handbook features:
l Chapters on many of the common skin conditions seen in primary care
l A description, defining clinical features, differential diagnosis, general management measures, treatment and referral guide for each common condition
l A guide on emollient usage
l Details of a patient assessment
The information in the Handbook is suitable for use in primary care settings, but may be useful for those new to secondary care.
Keep an eye on the BDNG website for more information.
Starting the year with a bang
Teena Mackenzie
Christmas celebrations are now a distant memory, and the long month of January is now over. The BDNG Education Team has been looking forward to 2025 and has been focusing on events, podcasts, e-learning and working with many BDNG members on specific projects.
I do hope you have saved the date for many of our face-to-face events that are advertised via the e-newsletter and social media. Education Nurse Emma Button has written an events update for this copy of the journal, so please have a read. We look forward to seeing many of you at these events.
Our main BDNG conference will be held in Harrogate at a slightly later date this year, running from September 30 to October 2. We look forward to seeing you there. The Education Team and the Executive Team have been busy planning a packed agenda, with a focus on many aspects of dermatology. Of course, we don’t have to remind you that a trip to Betty’s Tearoom is always a must and remember your gym kit to wear off those calories as we are planning an early risers run session. Additionally, Molly Connolly will be running wellness sessions so you can relax at the end of a busy day.
We are always very grateful to those involved in the BDNG subgroups who are dedicated members providing education and support in their own time. Emmanuel Toni, as chair of the Research Group, organised the first BDNG journal club, which was welcomed by members that joined. This provides an insight into critiquing a research paper and allowing members to be actively involved in research, which can often be a difficult pillar to achieve.
We are advertising the journal club quarterly, with the next one being held in February. A research paper of interest will be shared via the BDNG, and a Teams link will be available, allowing members to join. Discussion will focus on the paper and aspects of research. We look forward to seeing you at the next one. Please reach out to a member of the Education Team if you need any further details.
“We have welcomed a new subgroup, chaired by Modupe (Bunmi) Soji-Adeyemo and Alice Mwale, focusing on skin of colour”
We have welcomed a new subgroup, chaired by Modupe (Bunmi) SojiAdeyemo and Alice Mwale, focusing on skin of colour. They have already welcomed fantastic members to this group, and I know they will contribute enormously to the BDNG. Both Bunmi and Alice are presenting at various BDNG face-to-face events and have contributed to the BDNG journal. The Education Team look forward to working alongside this dynamic subgroup.
Over the last few weeks, we have been focusing on a General Pustular Psoriasis (GPP) Project supported by Boehringer Ingelheim, who have had no influence in development. A fantastic group has
taken part, led by Lucy Moorhead, with national nursing representation. Scotland is represented by Dianne Ross, Ireland by Lorraine Gribben, Tracy Bale from Wales and Ben Sarapuddin for England. This productive group has been developing documentation, podcasts and education on the topic of GPP, which will greatly benefit patients that have this rare condition. This project is presently being developed, so watch out for future updates. The BDNG will also be providing resources.
Further topics of e-learning have been made available on the BDNG website. As a team, we always have e-learning in development along with podcasts, webinars and face-to-face meetings. At present, I have been working with Karen Stephen to develop a series of psychodermatology e-learning modules. A series of four modules will be available on the website soon, and these will support the two face-to-face meetings we have prepared. This is a vast subject area, and the modules will provide an insight into this topic which we hope you will find helpful.
The Education Team continue to enjoy meeting and working alongside BDNG members who provide continuing inspiration and education. We thank you all for your continued time and support. Please get in touch with any new ideas or education topics you would like covered by emailing me, Teena, at EDLead@bdng.org.uk.
This article has focused on only a small amount of work that has been completed over the last three months. For further details on our activity, please log into the BDNG website, listen to the latest podcasts or check out the e-newsletter for further updates.
The British Dermatological Nursing Group
Corporate Sponsors
The BDNG would like to thank all our corporate sponsors for their support and continued investment with the BDNG
Introducing EBGLYSS®
A NICE-recommended treatment for moderate-to-severe atopic dermatitis (AD) in eligible patients1,2
EBGLYSS is indicated for the treatment of moderate-to-severe AD in adults and adolescents 12 years of age and older with a body weight of at least 40 kg who are candidates for systemic therapy.1
NICE has recommended EBGLYSS for treating moderate-to-severe AD that is suitable for systemic treatment in people 12 years and over with a body weight of 40 kg or more, only if:2
• the AD has not responded to at least 1 systemic immunosuppressant or these treatments are not suitable, and
• dupilumab or tralokinumab would otherwise be offered, and
• the company provides it according to the commercial arrangement
Contact Almirall today for further information and evidence to support inclusion of EBGLYSS on your hospital formulary or local guideline
and
AD, atopic dermatitis; NICE, National Institute for Health and Care Excellence.
References: 1. EBGLYSS (lebrikizumab). Summary of Product Characteristics. 2. National Institute for Health and Care Excellence. Lebrikizumab for treating moderate to severe atopic dermatitis in people 12 years and over. Available at: https://www.nice.org.uk/guidance/ta986/ chapter/3-Committee-discussion [Last accessed: November 2024].