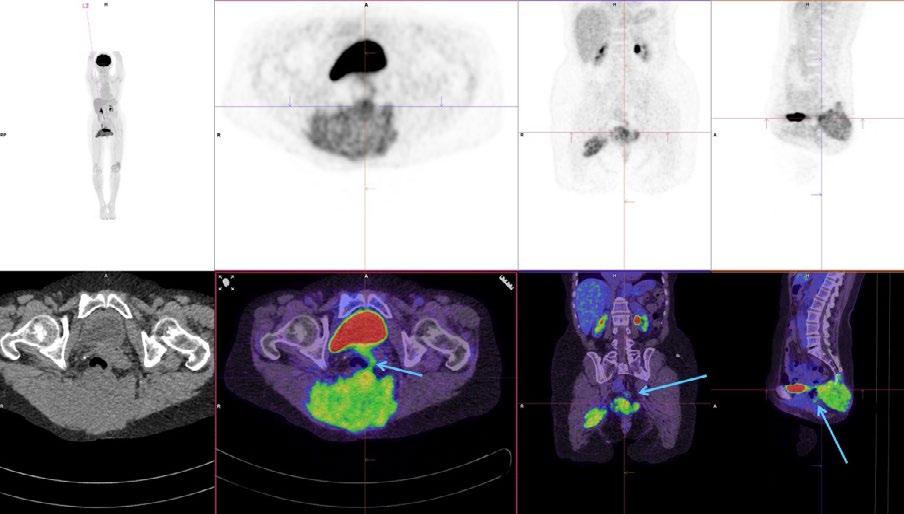
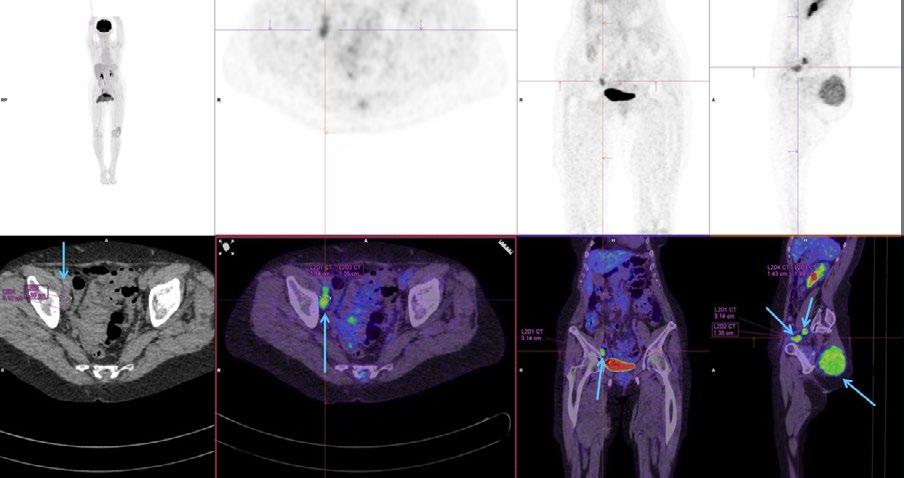
The Role of 18F-FDG PET/CT In Diagnosing Metastatic Chordoma
Rural realities: a case study on health inequities and the role of nuclear medicine in regional areas
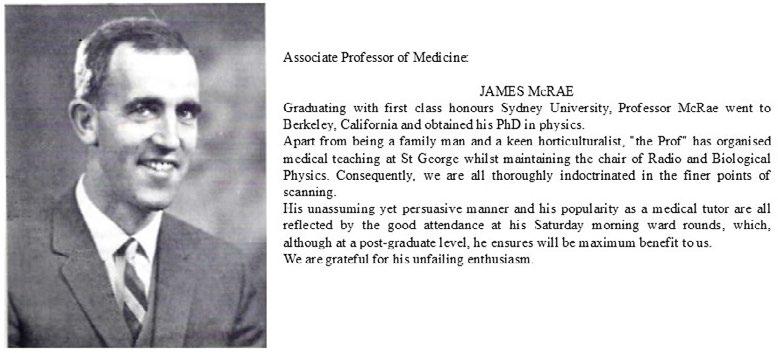
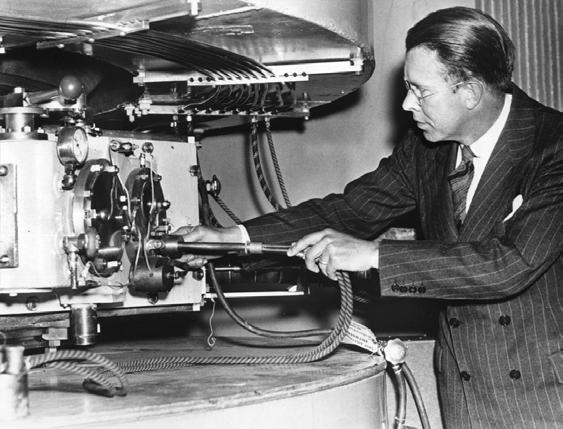
Reminiscences and Thoughts on Nuclear Medicine by Jim McRae
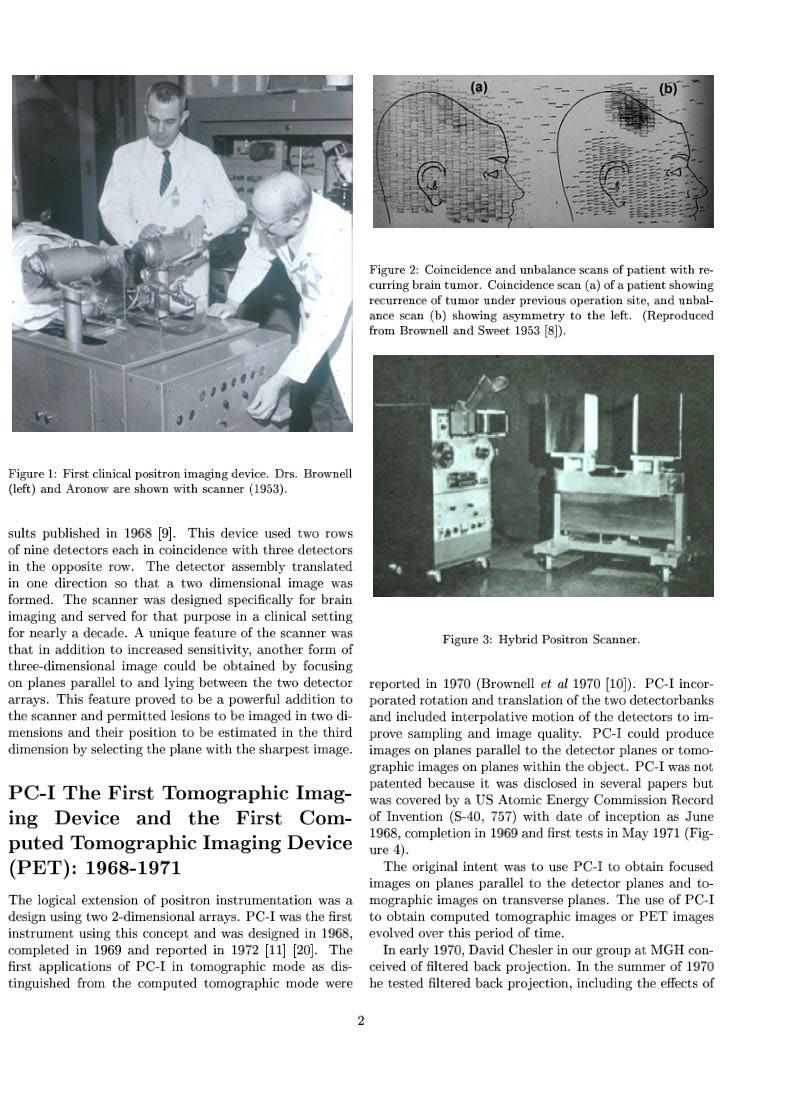
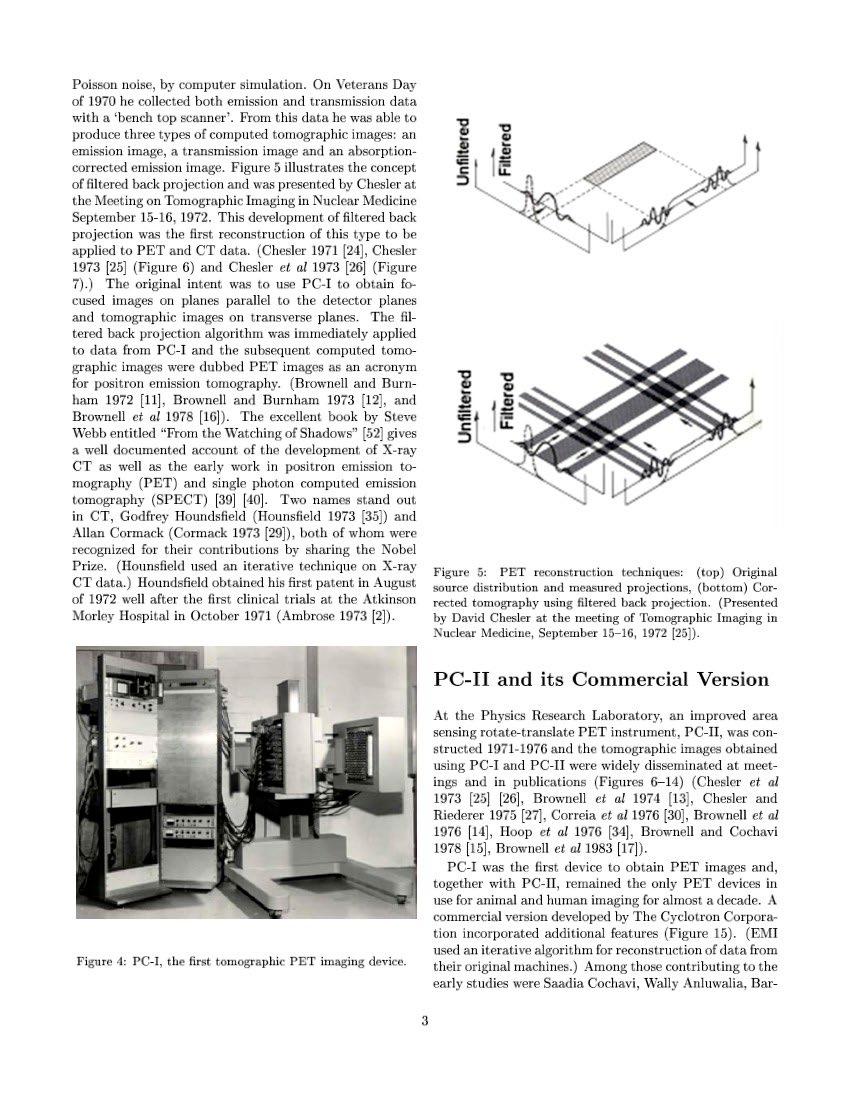
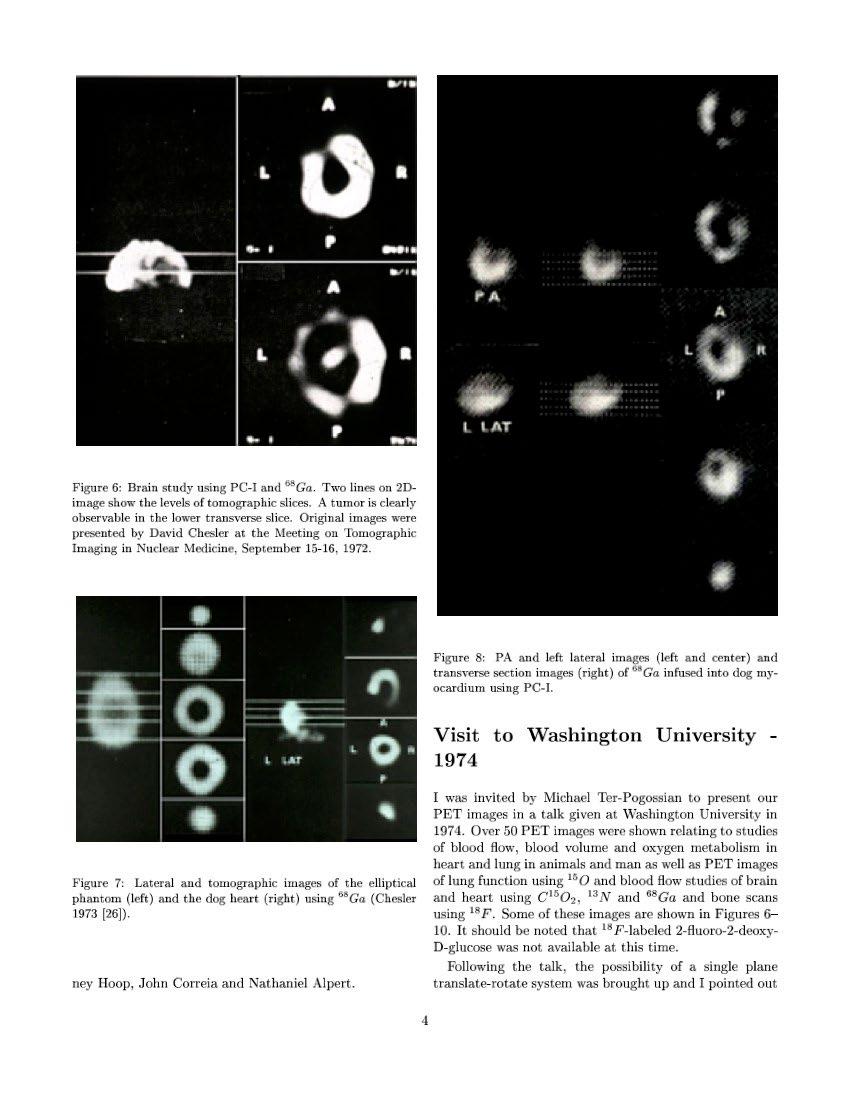
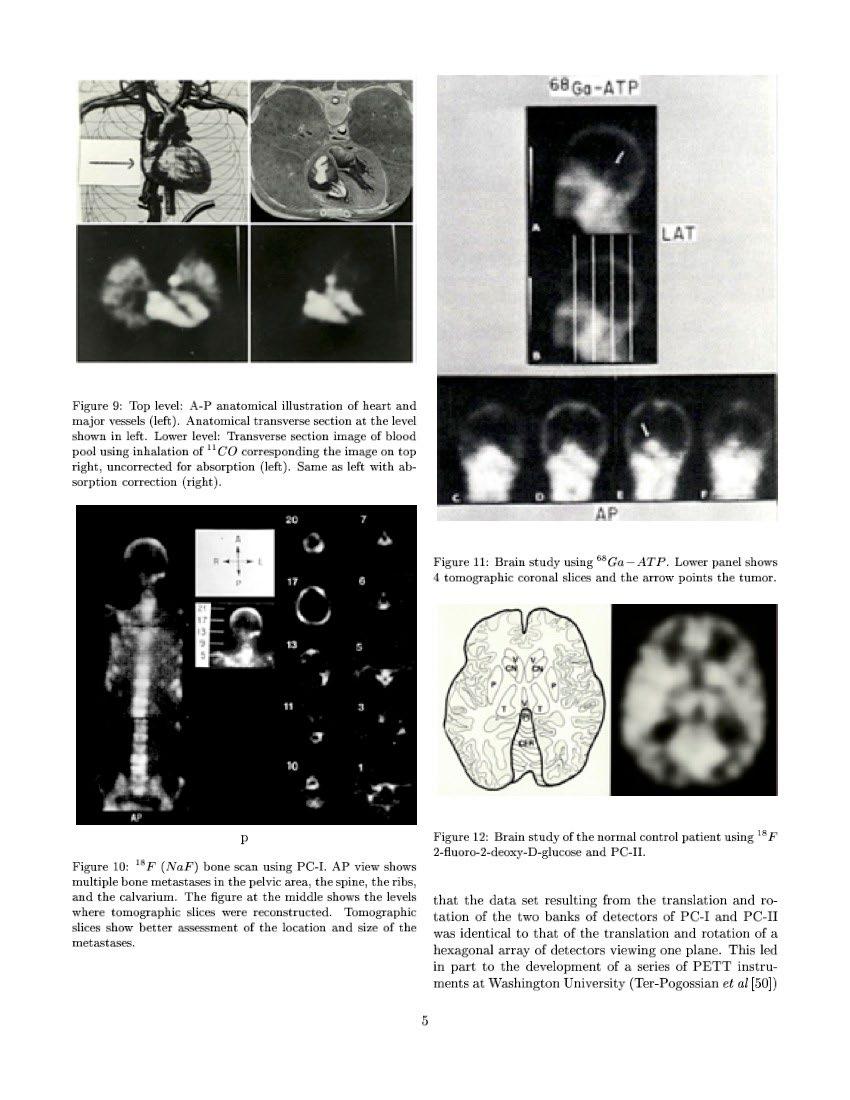
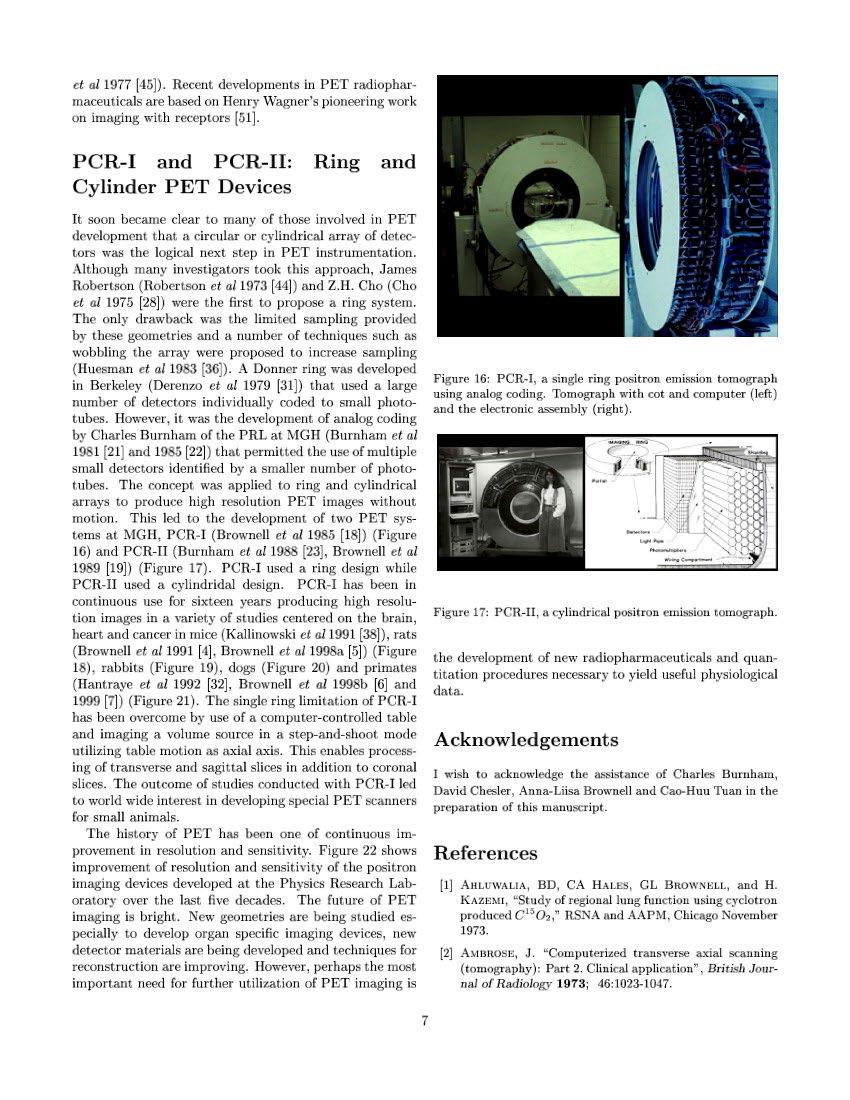
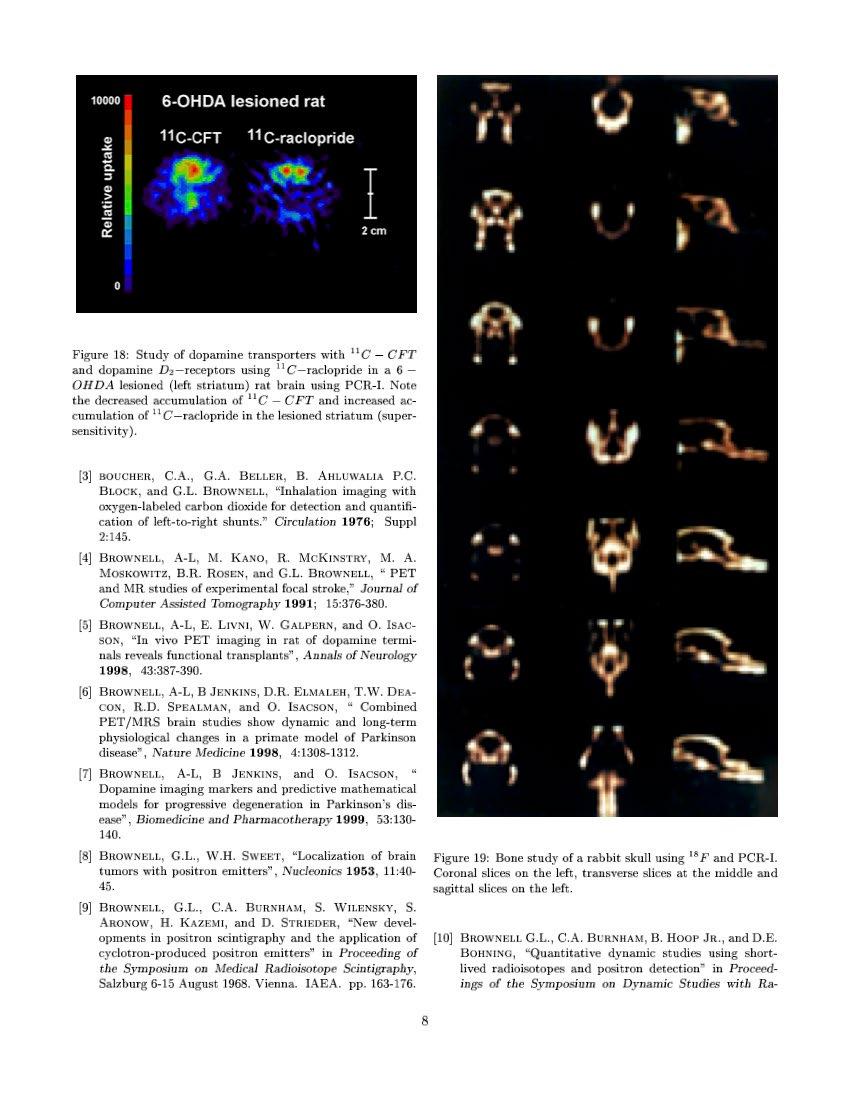
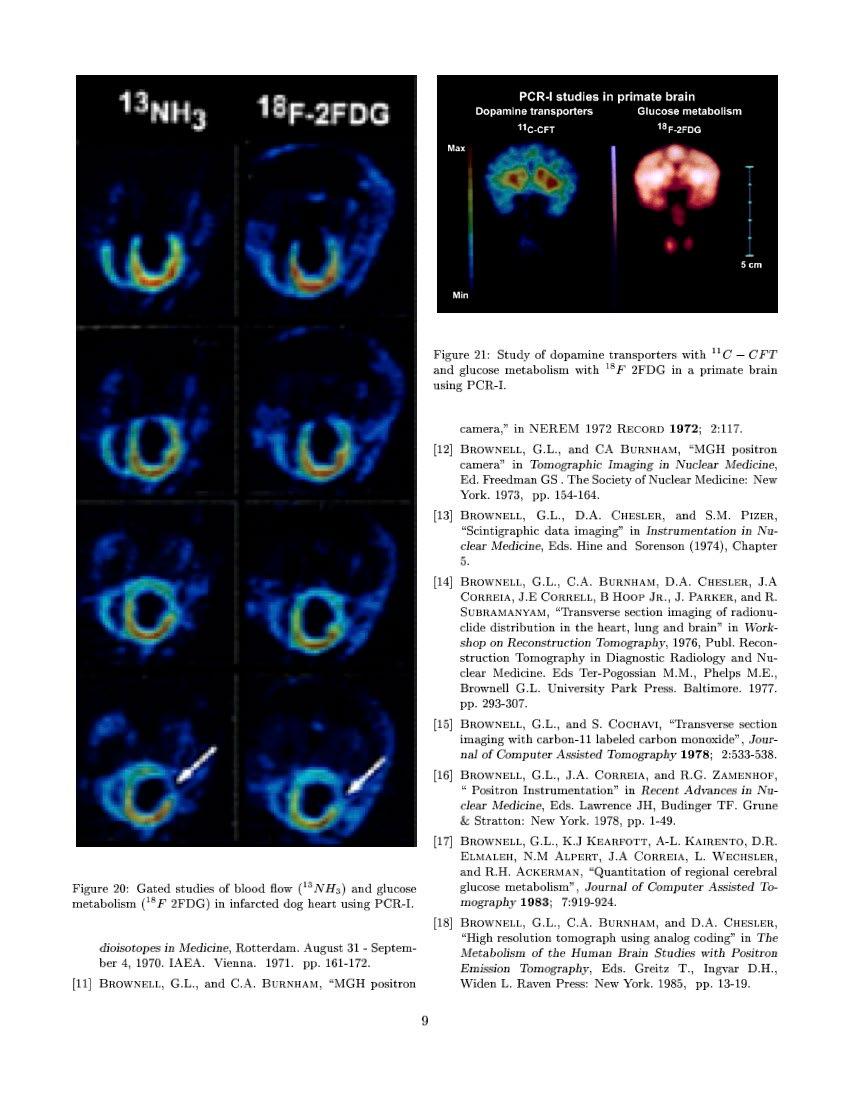
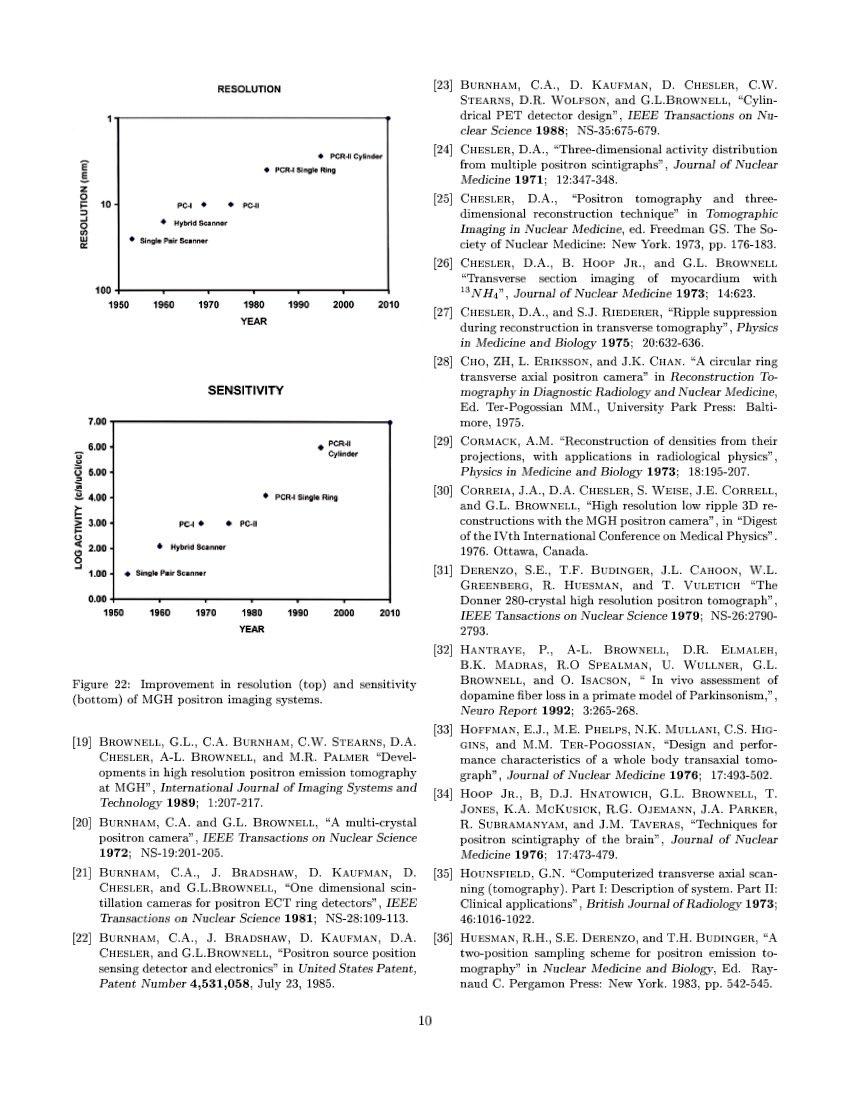
A History of Positron Imaging
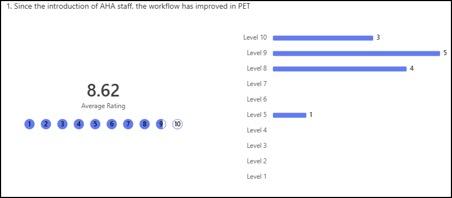
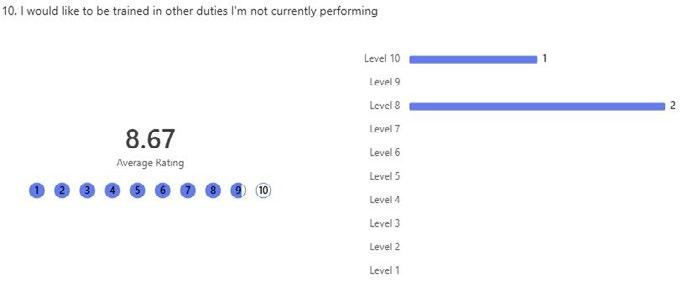
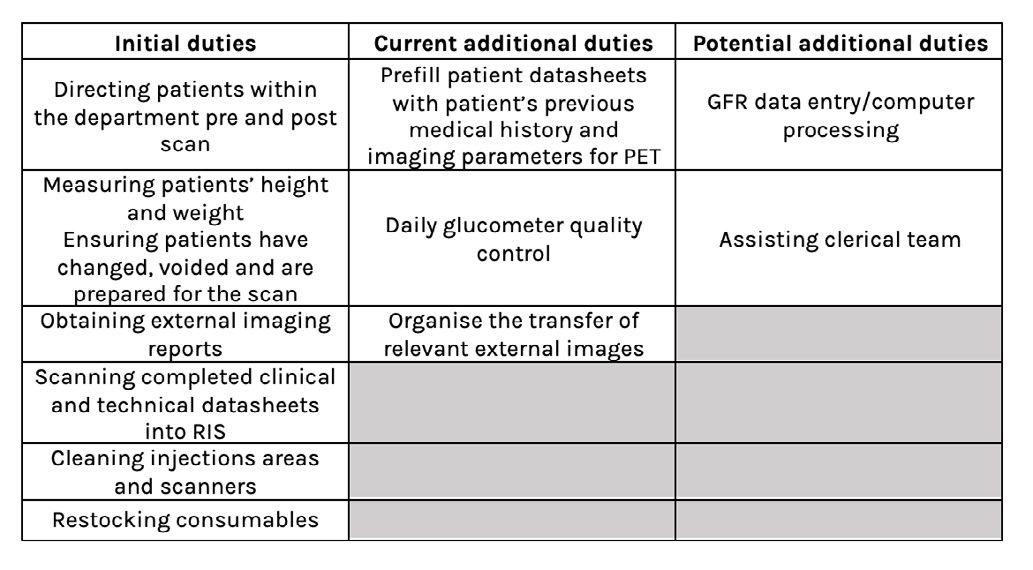
An Allied Health Assistant Model in Nuclear Medicine
Vale Maria Triantafillou
FROM THE PRESIDENT
Welcome to the 2025/26 SUMMER EDITION of the Gamma Gazette
“We must have perseverance and, above all, confidence in ourselves.”
Marie Curie (1867-1934)
Hello Fellow ANZSNM members,
Karen Jones President
As we move into a new year, I am gratified to reflect on how much we have achieved together during the past 12 months. Guided by the principles of perseverance and confidence that Marie Curie exemplified, the ANZSNM has continued to grow and thrive. This year saw the formation of the Medical SIG, strengthening representation for medical colleagues within our Society, and an exceptional Annual Scientific Meeting (ASM) held in Melbourne that attracted a record number of delegates, including many leaders from around the world. Important milestones at the ASM were the launch of the Human Molecular Imaging Translational Network, funded by the National Imaging Facility (NIF) and the signing of a new MOU between NIF and ARTnet, representing a shared commitment to the support of research and clinical access related to imaging.
Momentum has been equally strong across our Special Interest Groups (SIGs). The Physics SIG held its first post-COVID Joint Symposium with the ACPSEM. The TSIG organised a highly successful Technologist Day Symposium on the Gold Coast, in collaboration with the Queensland Branch, highlighting rural and regional nuclear medicine. The Radiopharmaceutical Sciences SIG also launched their webinar series. We continued to support the next generation of nuclear medicine technologists through the ANZSNM/AANMS Student Placement Grants, an initiative that addresses placement poverty and champions equity and opportunity.
It has been a landmark year internationally. The resolution on Strengthening Medical Imaging Capacity, co-led by Professor Andrew Scott, was adopted by the World Health Organisation in February and endorsed by the World Health Assembly in May. This represents a major step forward to address the global burden of non-communicable diseases by improving access to advanced medical imaging and nuclear medicine, particularly in low- and middle-income countries.
Australia and New Zealand were honoured as the Highlight Countries at the SNMMI Annual Meeting in New Orleans in June, featured in this edition of the Gamma Gazette. Both the breadth and significance of our global collaborations continue to increase. An important initiative is the establishment of the Nuclear Medicine Technologist in Theranostics International Consortium, NMT-TIC, a partnership between the ANZSNM TSIG, EANM-TG, SNMMI-TS and the IAEA directed at the worldwide standardisation of technologist practice in theranostics. The recent MOU between the SNMMI Clinical Trials Network (SNMMI-CTN), EANM EARL and ARTnet represents an important step towards global standardisation and harmonisation of quantitative PET imaging, with far reaching implications for both clinical trials and patient care.
There are now less than six months remaining in my presidency. It is a role that I continue to enjoy and find immensely rewarding, particularly because of the numerous talented people that I interact with. I am proud of what has been achieved and confident that the Society is in very sound hands with the future leadership, including Vice President A/Professor Grace Kong and Vice President-elect Suzi McGavin. Our membership continues to grow, now exceeding 1000 - I thank all who have renewed for 2026. Our momentum is strong, our partnerships are thriving, and our community is more connected than ever.
In this issue of the Gamma Gazette, you will find Branch and Committee reports, an introduction to our new ANSTO representative, Annah Skillen, a feature on the SNMMI Highlight Countries, insights from the EANM meeting and several interesting case studies and articles. I extend my sincere thanks to all the contributors.
As we approach the holiday season, I wish everyone a restful break. My thanks go to the Secretariat, our Branches, Committee members, and the Federal Council for their ongoing dedication and support. Most importantly, thank you to our members. Your expertise, energy, and commitment continue to strengthen our Society and advance our field in meaningful ways.
The quote from Marie Curie captures the spirit of our members and the achievements we have celebrated this year - with dedication, collaboration, and self-belief, positive progress will occur. Best Wishes.
OUR CONTRIBUTORS
EDITORIAL COORDINATOR
Rajeev Chandra General Manager PO Box 6178, Vermont South, VIC 3133 T 1300 330 402 F (03) 8677 2970 gm@anzsnm.org.au
EVENTS & ADVERTISING ENQUIRIES
secretariat@anzsnm.org.au
SUBMISSIONS
secretariat@anzsnm.org.au
PUBLISHED IN
Winter & Summer
CONTENT SUBMISSIONS
Scientific submissions on all aspects of nuclear medicine are encouraged and should be forwarded to the Secretariat (instructions for authors published at https://www. anzsnm.org.au/activities/gamma-gazettecontent-submission-and-guidelines/).
Letters to the Editor or points of view for discussion are also welcome.
If original or public domain articles are found and considered to be of general interest to the membership, then they should be recommended to the Editor who may seek permission to reprint.
The ANZSNM Gamma Gazette is published two times per year. Deadlines for each issue of the journal can be found on our website anzsnm.org.au
DISCLAIMER
The views expressed in any signed article in the journal do not necessarily represent those of the Society. The individual rights of all authors are acknowledged.
Rochelle Bird Prince of Wales & Sydney Children's Hospitals
Karen Jones
The University of Adelaide
Annah Skillen Gold Coast University
Prue Lamerton Canopy Imaging
Caitlin Burt Royal Darwin Hospital
Samantha Hawkins ARTNet
Zhipeng Cao Olivia Newton-John Cancer Research Institute
BRANCHES NEWS
As 2025 draws to a close, our ANZSNM Branches reflect on another productive and engaging year across the regions. From hosting educational meetings and workshops to supporting members’ professional growth, strengthening collaboration, and engaging with local communities, each Branch has contributed to advancing nuclear medicine practice and strengthening the Society’s national network. We extend our sincere thanks to all Branch Committee volunteers for their dedication, time, and commitment throughout the year. Your efforts are vital to the continued success of ANZSNM and the vibrancy of our professional community.
Queensland News
Queensland has had a strong year with significant progress across education, events, and regulatory developments. We successfully partnered with TSIG to deliver a full-day symposium at HOTA on the Gold Coast, featuring outstanding speakers and excellent engagement. Our final in-person event for 2025, RadPharm, was held on 11 November. The Joint ESM Program with RMIT has completed its first year with great success, attracting over 80 statewide applicants for the 2026 intake, reflecting strong interest in workforce development. On 1 October, changes to the Radiation Safety Regulation 2021 (Qld) introduced prescribed licensee arrangements for AHPRA-registered NMTs/NMS, removing the need for a Radiation Use Licence for CT imaging, nuclear medicine imaging, and bone mineral densitometry. The Queensland Branch Committee has also seen changes, with Heather Biggs stepping down, and we will be looking to refresh the team at the end of 2026. Thank you to all members for your continued support, we look forward to an even stronger year ahead.
Anisa Kumari
QLD Chairperson
South Australian & Northern Territory News
The SA/NT Branch has experienced a successful few months and would like to express our gratitude to our members for their continued engagement and support.
Recent meetings have all been held online, including the first collaborative meeting between the SA/NT Branch and the Rural/Regional Branch. In partnership with the Rural/Regional Branch committee, we hosted an event focused on rural patient care, the Australian workforce, and the establishment of the Rural/Regional Branch. The event was both enriching and motivating, fostering a
sense of unity across the two branches.
Our final-year nuclear medicine technologist students from the University of South Australia are currently completing their 6-week placement. We wish them the best of luck as they embark on their careers in nuclear medicine.
Additionally, we are proud to congratulate Dr. Ashleigh Hull, a member of the SA/NT Branch, who has been named a finalist for the PhD Research Excellence Award at the 2025 SA Science Excellence and Innovation Awards.
We hosted our SA/NT Branch Radpharm Night on Thursday, 6th November, followed by our AGM and Quiz Night on Friday, 21st November. We were excited to welcome all members to these in-person events.
Lastly, we extend our sincere thanks to our sponsors for their ongoing support throughout 2025:
Platinum Sponsor: Global Medical Solutions
Gold Sponsors: Bayer, Siemens Healthineers, South Australia Medical Imaging
New South Wales & Australian Capital Territory News
It has been a busy 6 months for the NSW/ACT branch since the last Gamma Gazette.
In July, we held our Paediatrics in Focus event. A highlight was to see Dr Kevin London at the Children’s Hospital brilliantly act out the role of a nuclear medicine staff as well as an anxious mother, simultaneously, to drive home the joy and challenges of working with children in nuclear medicine.
August was all about the future, with our Student
Jessica Fagan, MANZSNM Chair of Branches
Placement Night. We shared tips, tricks, and stories to help students navigate their placements with confidence.
We wrapped up our CPD year with our Radpharm Award Presentations
held on 30 October, at the Kolling Institute of Medical Research, Royal North Shore Hospital. While the format of the meeting was hybrid, there was a strong turn-out in person. Congratulations to our winner, Sasha Aurisch from Royal Prince Alfred Hospital. Well done Sasha! As we are coming to the end of the year, we reflect on our efforts and look ahead. 286 people registered for the
Branch’s events over the past year, and our membership grew by 11%. A big thank you to all our guest speakers. We extend our appreciation to the ANZSNM Federal Council and our sponsors for their support. And of course, a huge shout-out to my tireless committee members: Holly Spooner, Karan Singh and Yolanda Chan. Your energy, ideas, and ability to answer WhatsApp messages before 7am are what keep the NSW/ACT branch running!
Jeremy Hoang
NSW/ACT Chairperson
New Zealand News
The New Zealand Branch hosted its annual NZ Symposium in Palmerston North on 13 & 14 September 2025. It was an outstanding event. At our AGM we elected Branch Secretary Rebecca Manglesen and Branch Treasurer Anna Whitten, as well as welcomed some new members to the branch committee. I look forward to working with you all as we continue to support the nuclear medicine
community in New Zealand. I would like to take this opportunity to thank Salome Lingenfelder and Trish Mead for their dedication and commitment as previous Treasurer and Secretary. Both Salome and Trish served in their roles for multiple back-to-back terms and the NZ Branch is extremely grateful for your service.
As the year closes, I wish all members a relaxing and joyful holiday period and summer! I am looking forward to what 2026 has in store!
Jessica Fagan
NZ Chairperson
NZ Symposium 13 &14 September 2025
The symposium in Te Papaioea/Palmerston North was another great meeting of the nuclear medicine community from around Aotearoa New Zealand. It was an excellent opportunity to network between the private and public service providers and to find out what everyone around the motu was doing. It was a good opportunity to provide both the charge technologists forum and the student event on Friday to enable these two groups to be able to get together and network before the commencement of the official programme on Saturday morning.
The highlights of the first day were the dynamic and informative team who delivered the workshop on ‘Gender Diversity’ and the energy from the Niuvaka Trust team who delivered the workshop on ‘Engaging with Pasifika in Health’. It was great to be able to learn such valuable lessons about how to make the health service a more inclusive place for both the Rainbow Community and Pasifika peoples. It also embraced the symposium’s theme of ‘Moving to the Future’ by providing valuable tips to take into our future practice.
The scientific programme provided a variety of talks that were both amusing and informative and our congratulations go out to Prue Lamerton for being awarded the Paul Orr Award for her talk ‘Breaking From Cold to Very Hot, is Not so Bad’ and to Je’nine HornLodewyk for her audience nominated winning Case Race entitled ‘MIBI Impossible’.
Holly Spooner, Karan Singh, Mei Yee Chan, Jeremy Hoang
Prue Lamerton and Je’nine Horn-Lodewyk
BRANCHES UPDATE (CONTINUED)
The ‘Moooooving and Groooooooving’ farm themed social event on Saturday evening was an exceptional display of flannel shirts, gumboots, cowboy outfits, cow onesies and of course, the prize-winning ‘Cherno-bulls’ from Allevia. Everyone enjoyed a delicious meal, had a lot of laughs and showed off their moves on the dance floor. It was a great opportunity to socialise with the sponsors who attended the symposium and to meet other technologists from around the country.
All in all it was a fun, informative and educational event and we thank our sponsors for their contributions that enabled us to provide yet another well-run event for the local nuclear medicine community.
Clare McKenzie
NZ Symposium Convenor, Palmerston North
Victoria & Tasmania News VIC/TAS Branch Annual Symposium
Jessica Welch, Dr Bonnia Liu, Dr Lewis Crawford
A/Prof James McMahon
Dr Bonnia Liu
Western Australia News
For the second half of 2025 we have held 2 in-person meetings hosted by Perth Children’s Hospital. Sponsored by Qscan, Envision and Siemens.
The first meeting in June focused on Theranostics and a summary of the 2025 Melbourne ASM. Thank you to Dr Zeyad Al-Ogaili, Joe Cardaci and Rosemary Dallen.
The second meeting in September contained several PET presentations and some interesting Paediatric cases. Shout out to Rikki Nezich, Andrew Hohnon and Rosemary Dallen. This was also our state Radpharm night, congratulations to Taylor Hope.
We finished off the year with our final meeting on November 12th followed by our AGM.
Looking forward to 2026, we are planning 5 in-person meetings and a half day in-person workshop.
Cassandra Koudela
WA Chairperson
Jessica Welch
Dr Lewis Crawford
MEET THE NEW ANZSNM ANSTO REPRESENTATIVE ANNAH SKILLEN
We are delighted to introduce Annah Skillen, the newly appointed ANZSNM ANSTO Representative. With a strong background in nuclear medicine, Annah brings a wealth of expertise and enthusiasm to the role. As the connection point between ANSTO and the Society, Annah will play an important part in strengthening collaboration, sharing insights, and supporting initiatives that advance nuclear medicine across Australia and New Zealand. To help members get to know Annah a little better, we’ve put together a short Q&A covering their background, priorities, and personal reflections.
Can you tell us a little about your professional background and what led you to this role?
I’ve worked in nuclear medicine for over 20 years, across both public and private sectors, in Australia and internationally. During that time, I’ve had the opportunity to work in diverse settings in leadership positions. That experience gave me a strong understanding of the unique challenges that we face during supply shortages. While I’ve always enjoyed the clinical side of the profession, I felt inspired to take on a new challenge. I also felt that, with the depth and variety of my experience, I was wellpositioned to take on a representative role.
What excites you most about becoming the ANZSNM ANSTO Representative?
To be honest, I didn’t think my application would be successful, so when I found out I’d been selected, I was genuinely surprised.
What excites me most is the opportunity to represent our Nuclear Medicine community in discussions that directly impact our field. It’s a chance to help strengthen the connection with ANSTO and ensure that the practical, day-to-day challenges we face in clinical settings are heard and considered. I’m also passionate about promoting equality in access to healthcare services, and I see this role as a platform to advocate for that.
I’m very thankful to the ANZSNM committee for trusting me with this responsibility. Vicky Sigalas made a meaningful contribution as the liaison and is now working in a role that I didn't even know was possible for a Nuclear Medicine Technologist. With her stepping down, I know I have big shoes to fill. Their support means a lot, and I’m genuinely looking forward to contributing in a way that makes a difference.
Annah Skillen Advanced Nuclear Medicine Technologist, Gold Coast University
What does your role at ANSTO involve on a day-to-day basis?
Day-to-day, I work clinically as an Advanced Nuclear Medicine Technologist at Gold Coast University Hospital. As the ANZSNM ANSTO representative I can be called upon at any time if there is an emergent issue, for example, a supply chain breakdown or unexpected disruption. Balancing this responsibility with clinical duties will be challenging, but I’m fortunate to work within a supportive team that understands the importance of this liaison role.
Occasionally, ANSTO will also reach out about planned shutdowns or changes in isotope supply. When that happens, I’m responsible for relaying any concerns or feedback from a clinical Nuclear Medicine perspective to ensure our operational needs are considered and patient care remains uninterrupted. This means I may engage with state representatives or individual departments from time to time, to gain a better understanding of our industry's needs.
MEET THE NEW ANZSNM ANSTO
REPRESENTATIVE ANNAH SKILLEN (CONTINUED)
How do you see ANSTO’s collaboration with ANZSNM benefiting the nuclear medicine community?
I think it’s incredibly important that we work together. Collaboration between ANSTO and the ANZSNM helps ensure that the clinical voice is heard when decisions are being made about isotope supply, production planning, and broader strategic directions. It creates a direct line of communication between those producing the products and those using them in patient care, which is essential for maintaining quality, consistency, and responsiveness to clinical needs. By working together, we can also better advocate for the profession, support workforce sustainability, and promote equitable access to nuclear medicine services.
What are your key priorities as the ANSTO Representative over the next year?
My key priorities as the ANSTO Representative over the next year are to maintain and strengthen the positive relationships we’ve already established with ANSTO, and to build from that. I can see my priorities evolving over time, and I’m committed to remaining responsive and transparent as situations develop. As a representative
for all members of the society, I do welcome input. If there’s a priority you’d like to see addressed, please don’t hesitate to reach out.
What inspired you to pursue a career in nuclear medicine?
After I finished high school, my parents told me that if I didn’t go to university, they wouldn’t buy me a car. So, I grabbed the course guide, flipped through it, and picked something that sounded interesting. I’d enjoyed learning about radiation and nuclear reactors in school, so Nuclear Medicine caught my eye. So off I went to university, in my new car, and I had no idea what I was getting into. Fast forward 23 years, and here I am. So maybe I was a little bit inspired but mostly bribed!
What do you find most rewarding about your work?
For me, the most rewarding aspect is being part of an industry that’s constantly advancing and transforming. With the rapid development in theranostics and the push to establish radionuclide therapy as a first-line treatment option, we’re in a unique position in our industry.
TECHNOLOGIST SPECIAL INTEREST GROUP (TSIG)
Suzanne McGavin, MANZSNM
TSIG Chair
I always find writing the Gamma Gazette article both a daunting and rewarding task. Capturing the tireless work of our committees over the past six months can feel like a monumental challenge, but once it’s written, it’s immensely satisfying to reflect on the dedication and achievements of our society in supporting Nuclear Medicine Technologists.
For those following along with our monthly newsletters, much of this will be familiar. The newsletter may seem to come around quickly, but it has provided a valuable and consistent channel to keep members informed about the detailed work of the TSIG and our various committees.
So, let’s recap what has been happening within the Technologist Section of the ANZSNM over the past six months!
Changes and Committee Updates
As mentioned in the last Gamma Gazette, Emma Brook stepped down as University Liaison. Emma was the inaugural holder of this position and set the foundation for meaningful communication, consultation, and engagement with our university partners and student groups. I would like to personally thank Emma for her leadership and for establishing the framework that allows the TSIG to strengthen our ties with the tertiary education sector.
After a brief vacancy, we were delighted to welcome Erin Hemingway back to the team as our new University Liaison. Erin recently stepped down as CPD&E Chair, and we’re fortunate to once again benefit from her expertise and enthusiasm.
Both our CPD&E and Workforce Advocacy Committees have undergone some membership changes, which you’ll read about in the reports from Melissa Shields (CPD&E Chair) and Kunthi Pathmaraj (WFA Chair) below. I extend my sincere gratitude to the outgoing members for their invaluable contributions, and a warm welcome to our new members, we look forward to your fresh perspectives and energy as we move forward.
Tertiary Education Space
In the absence of a University Liaison, I had the privilege of chairing both the Student Representative Committee (SRC) meeting and the inaugural Academic Reference Group meeting.
I’ll admit, there’s always a moment of anxiety before a first meeting, wondering if people will attend, but I was thrilled by the turnout and inspired by the SRC’s energy and ideas. We now have representation from all universities, and it’s exciting to see the passion and creativity of this group, particularly their insights on engaging younger students and using social media in new ways. The ANZSNM has also proudly sponsored events at UniSA and the University of Newcastle, reinforcing our visibility and commitment to supporting students — our future professionals. The SRC has decided not to limit participation, so any interested students are warmly invited to join.
The Academic Reference Group meeting was also a significant milestone. As a former academic, I felt privileged to be among colleagues from universities across Australia and New Zealand, all dedicated to advancing Nuclear Medicine education. Despite the diversity of program delivery models, the group’s collaboration promises great opportunities for sharing ideas, resources, and innovation. Many common themes emerged, and I foresee exciting joint projects and presentations ahead. Thank you to Kathy Guerrero (University of South Australia) for taking on the role of Chairperson.
We have also recently announced another $10,000 in ANZSNM/AANMS Student Placement Grants. This round saw almost double the number of applications, highlighting the significant financial pressures faced by students during placements.
Suzanne McGavin, MANZSNM, TSIG Chair
While we wish we could support everyone, congratulations to the successful recipients and to those who missed out this time, please apply again in future rounds. I will be reaching out to universities to clarify eligibility requirements to ensure all students can put forward strong applications.
And as I’ve said before, if you have a student on placement, never underestimate the simple gesture of offering lunch, a drink, or a coffee. Here in Darwin, we have a rotating “gift bag” of non-perishables passed along to locums and students, a small but meaningful act that can make a difference.
International Engagement
Karen Jones and I continue to represent the ANZSNM on the Nuclear Medicine Technologists in Theranostics International Consortium (NMT-TIC). You may have seen the launch of our international survey on the roles of Nuclear Medicine Technologists in Theranostics — an exciting first public project for the group. The survey required approval from the executive boards of the EANM, SNMMI, IAEA, and ANZSNM, a significant achievement in itself. The data collected will help shape future universal standards and educational pathways for Nuclear Medicine Technologists globally, with plans to publish findings and support ongoing professional development.
Our meetings connect colleagues from across the USA, Poland, the UK, Portugal, and Australia, a truly global collaboration. I encourage all departments with NMTs involved in Theranostics to complete the survey. It was also a privilege to attend the SNMMI Conference in New Orleans this year. I met with leadership from across the organization, presented, and supported our Australian colleagues as we proudly served as the Host Country. You can find my full conference review in this edition.
Additionally, I was invited to join the SNMMI NuMe Mentor App working group, which has successfully launched a digital mentorship platform for members. We hope to partner with SNMMI in the future to adapt this technology for our own mentorship program. While our 2025 program didn’t progress as planned, we are committed to relaunching and reinvigorating it in 2026.
Collaborations and Advocacy
As the TSIG representative on the ARPANSA Working Group, I’ve been involved in reviewing and rewriting the Radiation Safety guidelines for Nuclear Medicine. It’s been a challenging but essential process, ensuring the updated documents reflect current practices and standards across the profession.
I’ve also met with representatives from Indigenous Allied Health Australia (IAHA) to discuss recognising Nuclear Medicine as an Allied Health profession. These discussions have been insightful, and we’re exploring opportunities for collaboration, including possible site visits for Allied Health students to experience Nuclear Medicine firsthand. If you identify as Indigenous and would like to connect or assist with this project, please reach out, your involvement would be greatly valued. Finally, we’ve met with MRPBA regarding the new Professional Capabilities, which will launch in November 2025 and become mandatory by March 2026. Key updates include mandatory training in anaphylaxis management and recognition of leadership within practice. The TSIG is already engaging with facilitators to deliver educational sessions to help members meet these new standards. And a quick reminder: don’t forget to renew your registration!
Closing Thoughts
I hope you feel that the TSIG has been working effectively to represent and support you as professionals. I always welcome feedback or ideas for new initiatives that could benefit our members.
My heartfelt thanks go to all committee members and ANZSNM members for your contributions — creating events, completing consultations, and helping our profession continue to grow.
As I finish writing this, the tropical storm outside my window has rolled in, heavy rain hammering the roof like a thousand drums. Here in the Top End, we’re always grateful for the rain: it breaks the humidity, refreshes the air, and soon enough, the sun will glisten again on the grass.
Wishing you all a wonderful festive season, may you find time to rest, recharge, and enjoy the company of friends and family.
SNMMI 2025 TSIG REPORT
Suzanne McGavin, MANZSNM TSIG Chair
Attending the Society of Nuclear Medicine and Molecular Imaging (SNMMI) Annual Conference in 2025 was an absolute honour. Reflecting on the experience, three key themes stood out to me:
1. Representing Australia and New Zealand as the Highlight Countries — both through our booth and speaker sessions.
2. Collaborating with international colleagues and professional groups to enhance ANZSNM’s visibility and share knowledge.
3. Gaining new insights into the evolving field of nuclear medicine and identifying ideas to bring back to the TSIG.
As a full conference recap will no doubt be covered elsewhere, I’ll focus my reflections on aspects most relevant to my role as TSIG Chairperson.
Representing ANZSNM as Highlight Countries
They say a picture tells a thousand words — and if you’ve seen the photos, you’ll know the ANZSNM booth was a showstopper. The vibrant artwork, friendly atmosphere, and constant stream of visitors made it one of the busiest spaces at the conference. Many delegates came by to learn about working in Australia and New Zealand (and to ask about our famous wildlife — yes, the spiders came up! I may have told a story about a massive Huntsman my sister had on her back when we were kids, and I locked myself in the bathroom and screamed. I thought it was a funny story, the look on the poor young girls’ face made me reconsider what I had just said. The next 5mins was spent explaining they are harmless…). Our opening night event, complete with plush koalas, kiwis, and local wines, was a huge success. I’ll quietly skip over the Fosters beer, though it did seem to be a crowd favourite!
Our representatives were constantly engaging with visitors, taking meetings, and proudly showcasing the expertise, professionalism, and warmth of our members. Personally, I relished every moment, speaking about Nuclear Medicine all day felt like a dream come true. Our booth chocolates became an unofficial conference staple, and the overall atmosphere reflected the pride we all feel in our profession.
Many attendees were curious about Technegas, which is only now being introduced in the United States. It was rewarding to see their astonishment at how advanced Nuclear Medicine practice is in Australia and New Zealand — something reinforced by the exceptional plenary presentation from Prof Karen Jones, the Henry Wagner
Award to Prof Andrew Scott, and numerous outstanding talks by our Australian contingent.
For the Technologist stream, Karen, Nerida Newman, and I presented an ANZSNM-sponsored session early on the final day, and despite a late-night concert the evening before, the turnout was fantastic! Nerida presented on Technegas application, Karen on gastric emptying research, and I discussed Australian cultural safety initiatives. The positive feedback was overwhelming, and it was a privilege to highlight the hard work of our Darwin department. I may have even convinced a few attendees that the Top End (crocodiles and all) is worth a visit.
We were also proud to see Kunthi Pathmaraj present on a patient audit tool improving nuclear medicine patient experiences at the Austin, and Dr Melissa Shields, our Curium Award winner, speak on workplace burnout.
It was clear throughout the conference that our ANZSNM nuclear medicine professionals are recognised as world leaders — respected for our skill, innovation, and professionalism across both physician and technologist domains.
Collaborating Internationally to Expand ANZSNM’s Reach
One of the greatest benefits of attending international conferences is the opportunity to connect with professionals from around the globe who share our passion for nuclear medicine.
Suzanne McGavin, MANZSNM, TSIG Chair
During the SNMMI, I met with the SNMMI Technologist Section (TS) Leadership Team, where we discussed initiatives supporting early-career professionals, such as the Leadership Academy and Mentor Program. These align closely with the TSIG’s priorities, and it was valuable to exchange insights and learnings from both sides. The global workforce shortage was another key topic. The USA and Canada are facing similar recruitment and retention challenges. At an Educators Forum, we explored creative solutions, such as a “base year” in Medical Radiations with later specialisations (for example, PET-only practitioners), as a means to expand workforce entry pathways. I also shared details of our Embedded Student Model, which drew interest as a potential solution for “education deserts” in the U.S.
I attended the SNMMI Leadership Meeting, where we discussed the Theranostics International Consortium for Nuclear Medicine Technologists (NMT-TIC) — a collaboration between ANZSNM, EANM, SNMMI, and the IAEA. It was inspiring to have all professional bodies represented in one room, united in advancing global standards for NMTs in Theranostics. I only wish we’d taken a group photo to capture the moment! The consortium’s first survey (at time of writing) is nearing completion, and we look forward to publishing soon.
Conversations with the EANM Technologist Section were equally enlightening. Their varied training models, similar to the U.S. system — provide flexibility but also create challenges around skill consistency. It made me appreciate the rigor and high standards of Australian education, and the global recognition our NMTs enjoy. We also connected with the Canadian Association, who plan to hold a workforce summit inspired by the ANZSNM’s 2023 event. Additionally, discussions with American educators highlighted opportunities for collaboration, particularly in education around Technegas, which is new to many of their programs. I may have surprised them by explaining that, in Australia, Technegas is our go-to lung imaging modality (unless the machine is down and we’re back to aerosol DTPA!).
These discussions, formal and impromptu alike, are exactly why international conferences matter. They strengthen global relationships, inspire innovation, and create new opportunities that ultimately benefit our local NMT community.
Learning and Bringing Ideas Home
Between meetings, presentations, and supporting our ANZSNM colleagues, I made time to attend sessions aimed at professional growth. Topics such as leadership, paediatric nuclear medicine, career pathways, and the expanding role of the NMT offered valuable insights we can adapt for the TSIG.
Many of these ideas, from mentorship and career development to professional advancement, will inform future symposiums, webinars, and sessions at the ANZSNM ASM. Building career pathways and leadership capacity is key to improving workplace satisfaction and retention, and I left feeling inspired to further develop initiatives that support NMTs at all stages of their careers. The leadership workshops, in particular, resonated with me, exploring the differences between mentors, coaches, and supervisors, and the unique value each brings at different career stages.
Overall, attending the SNMMI was an incredibly positive and productive experience. There’s something uniquely powerful about connecting face-to-face: the conversations, the shared ideas, and the energy are simply unmatched. Whether it’s the ANZSNM ASM, the TSIG Symposium, or an international meeting, these experiences remind us that our profession is vibrant, collaborative, and world-class.
Representing the ANZSNM as TSIG Chair, speaker, and part of the Highlight Country delegation, was an honour and a celebration of “us”: the talented, passionate nuclear medicine professionals of Australia and New Zealand. I look forward to bringing these insights back to our TSIG committees and continuing to build opportunities for our members at home.
ANZSNM/AANMS Semester 2 2025 Student Clinical Placement Grant Recipients
The ANZSNM and AANMS are delighted to announce the recipients of the Semester 2, 2025 Student Clinical Placement Grants. These grants support students undertaking clinical placements away from their home location, helping to reduce financial barriers and ensure equal access to high-quality training opportunities across the profession. The Placement Grants are an initiative of the ANZSNM and supported by the AANMS and commenced in 2024. We bring to you some of the recipients and future members of the profession.
Ashlee Brown University of Newcastle
Sam Anderson Charles Sturt University
Erin Brown Charles Sturt University
Jacob Cobner University of Newcastle
Celeste Peh RMIT
Isabella Reitano University of South Australia
Alexanda Le University of South Australia
Sarah McIldowie University of South Australia
Andrew Lay RMIT
Kate Gilmour University of Newcastle
Clare Davine RMIT
Juliette Palce University of South Australia
Jesse Filkin University of South Australia
Meri Lioulios University of South Australia
Leah Mitsis RMIT
Join Queensland’s largest private radiology practice group
Led by an experienced team of radiologists and imaging specialists, Queensland X-Ray is one of the largest private imaging groups in Queensland, with over 50 practices state-wide.
Queensland X-Ray is part of the Sonic Healthcare group, an ASX top-40 listed company focused on delivering medical excellence in radiology, nuclear medicine, pathology, general practice and occupational medicine.
Why join Queensland X-Ray?
▷ Opportunity to work across major hospitals, community practices, and specialised sites.
▷ Gain exposure to a broad range of procedures, including complex hospital-based cases, cardiac imaging, emergency, and on-call work.
▷ Access structured training across all Nuclear Medicine modalities. Learn from Queensland’s leading providers of PET/CT and benefit from CPD opportunities.
▷ Take advantage of pathways for advancement, with career progression opportunities across our Nuclear Medicine network.
▷ Enjoy competitive remuneration, paid parental leave, and ongoing support for continued professional growth.
For more information please contact Queensland X-Ray Human Resources on 07 3422 8800 or email humanresources@qldxray.com.au
CAIRNS
TOWNSVILLE
MACKAY
BRISBANE GOLD COAST
TOOWOOMBA
CPD&E UPDATE
Dr Melissa Shields, MANZSNM Chair TSIG CPD&E Committee (cpdechair@anzsnm.org.au)
The second half of the year has been busy for the TSIG CPD&E committee.
TSIG Annual Day Symposium
It started with the TSIG Annual Day Symposium, held on the 3rd August on the sunny Gold Coast at the Home of The Arts (HOTA). The symposium sub-committee, comprising of members of the TSIG CPD&E committee as well as members of the Queensland branch of the ANZSNM, worked hard to ensure the program and venue met the needs of our delegates. The presentations had a distinctly Queensland feel on topics such as the enduring value of nuclear medicine, contemporary CTPA and Lung V/Q radiation exposure, CZT camera experience, RMIT embedded module, Rural practice in Queensland and the hurdles faced, career pathways, workforce expansion and one of the most popular presentations of the day, wellness in healthcare. Thank you to all of the presenters who helped make another successful TSIG Annual Day Symposium.
Another highlight of the day was the awarding of the ANZSNM Nuclear Medicine Technologist Award to Vicky Sigalas. Her honest and thought-provoking presentation made a lot of us reflect on our journey through life (and wish we had some tissues handy).
I would like to extend a heartfelt thank you to the committee who organised the symposium, the presenters who took time to prepare and deliver great presentations, the delegates who turned up and the generous sponsors, without whom this event would not be able to be as successful as it is.
TSIG Webinars
The TSIG CPD&E committee have also celebrated two significant dates in the calendar with themed webinars. Firstly, NAIDOC Week was celebrated with presentations from Randy Williams & Freddie Liuvale, discussing Pasifika Cultural Centeredness Training and Liz Jarvis, discussing Cultural Safety in Regional and Rural Settings. We also delayed our 2025 Winners Circle webinar until October to coincide with Nuclear Medicine Week. This is such a great webinar as it celebrates the talented technologists who won the Radpharm and Landauer (previously Curium) Awards and Sumitomo NMT Student
Award at the ANZSNM ASM. For the second year in a row, a nuclear medicine technologist also won the Telix “Best of the Best” Award. Thank you and congratulations to Shiphrah Becker (Tagore), Lisa Nguyen and Jessica van Zulekom. Unfortunately, Jess Watson was unable to make the webinar, but congratulations to Jess as well for winning the Sumitomo NMT Research Award in 2025.
TSIG CPD&E Committee
The committee has met twice in the second half of 2025 and is busy planning webinars for 2026 and the 2026 TSIG Annual Day Symposium, to be held in South Australia on 1st August. Committee members have also provided feedback on various consultation papers, mainly from AHPRA.
The membership of the committee is also changing. Unfortunately, Ellie Kelliher and Alicia Corlett have stepped down from the committee, we thank Ellie and Alicia for all of the hard work they have done in the past few years. We would like to welcome Kirralee Davies and Megan Stirrat on to the committee, we can’t wait to work with you both.
Moving forward, the CPD&E eagerly await the new MRPBA Professional Capabilities, due to be released in November. We then hope to produce learning activities to help our members meet any new capabilities. The CPD&E committee will also be introducing a journal club for technologist members in 2026. More information can be found on the following page.
Thank you to all of the committee members, who tirelessly give up their spare time to be on the CPD&E committee. If you have any ideas on how the CPD&E committee can help you with your continuing education, please reach out to me at cpdechair@anzsnm.org.au
I wish all of our members a Merry Christmas and a Happy and Prosperous New Year.
Melissa Shields, MANZSNM, CPD&E Committee
TSIG CPD&E JOURNAL CLUB
TSIG CPD&D Journal Club
The TSIG CPD&E committee will be introducing a journal club for nuclear medicine technologist members of the ANZSNM in 2026. The journal club will help foster an interest in current literature relevant to our diverse roles, as well as help meet the MRPBA professional capabilities (at the time of writing this is Domain 4: Evidence-informed Practitioner, however this is likely to change with the rollout of the new MRPBA professional capabilities). The journal club will also provide participants with CPD hours.
The journal club has been put together by Clare McKenzie, a member of the TSIG CPD&E committee and a nuclear medicine technologist at Palmerston North Hospital in New Zealand and Melissa Shields, the chair of the CPD&E committee and academic at the University of Newcastle.
Why a Journal Club?
Journal clubs are a long-established and valuable method of educational strategy in healthcare and are a platform where health professionals can engage with current literature, while also developing participants’ skills in foundational concepts of research design and critical evaluation.
By using their clinical experience, participants are able to support and/or challenge the article’s content and comment on the relevance and usefulness of the research findings to clinical practice. Not only do journal clubs inform a participant’s professional knowledge, they can also educate the participants in research design and manuscript preparation. In turn, this will increase participants’ confidence in reading current literature and facilitate the development of lifelong learning attributes in nuclear medicine technologists (NMTs), something that can only benefit the profession.
The journal club will bring together a group of enthusiastic NMTs, providing a supportive environment for learning and encouraging NMTs to share their opinions about current literature and facilitate reflection through discussion on their own clinical practice. Whether you are a recent graduate or have many years of experience, the journal club will provide some sort of learning experience for everyone.
Adult learners are motivated to learn those things they see the need to learn, so by carefully choosing locally relevant articles, the TSIG CPD&E Journal Club will help to bridge the gap between research and clinical practice.
How will it
work?
The TSIG CPD&E journal club will run online (via Zoom)
for one hour, quarterly. This will be of an evening, outside of work hours, trying to accommodate the different time zones of participants. There will be one person who is the coordinator of the journal club, and they will delegate roles to other participants. These roles may include picking an article for the following journal club meeting and leading the discussion.
The journal article will be circulated well in advance, giving participants ample time to review the article. Participants are encouraged actively contribute to the journal club meetings, being prepared to discuss the research. There will be a guideline distributed to help participants with their critical appraisal skills. However, there are known barriers to a successful journal club. These include a lack of time (for both volunteer organisers and participants), a lack of access to the journal articles, and a lack of research methodology knowledge. Therefore, we are aiming for quarterly journal club meetings, so participants don’t feel like they are constantly having to read and evaluate articles. The chosen articles will open access, meaning that everyone will be able to freely access the chosen journal article. Lastly, an educational resource will be available for participants to refresh their skills on how to critically appraise a journal article.
Goals of the CPD&E Journal Club
1. Enhance critical appraisal and research literacy
2. Bridge the gap between research and clinical practice
3. Foster lifelong learning and professional development
4. Cultivate a collaborative learning environment
5. Develop research and scholarly communication skills
What Next?
The 2026 journal club meetings will be held in February, May, August and November, at the end of the month. The journal article will be sent out in the month prior to the meeting. Therefore, for the inaugural February meeting, the journal article will be sent out in early January.
To register your interest in the TSIG CPD&E Journal Club, please email Melissa Shields, the TSIG CPD&E Chair, at cpdechair@anzsnm.org.au. Please include your name, best contact email address, and what areas of interest or topics you would like to see covered in the journal club.
We look forward to working with our technologist members to grow the TSIG CPD&E Journal Club into a fantastic learning opportunity for all involved.
TSIG Workforce Advocacy (WFA) committee currently has a full complement of membership representing New Zealand and the states and territories of Australia. I am pleased to extend a warm welcome to our new members Olivia Amsterdam, Emily Jeffriess, Ellen Mason and Lauren Marks and I am grateful to the ongoing support from existing members, Elizabeth Brettschneider, Louise Campbell, Sarah Daniel, Katherine Guerrero, Lauren Marks and Suzanne McGavin.
The WFA committee has been actively providing feedback on consultations that are relevant to our profession, initiated by the Australian Government, MRPBA, MRTB and other relevant organisations. We have had the opportunity to work with the TSIG CPD&E committee on some consultations, and this has been a rewarding exercise.
Our committee is also refocussing on the priority areas identified by the ANZSNM Nuclear Medicine Technologist Work Force Summit held in Melbourne in 2023. We have successfully addressed some priorities that were identified by the summit report, such as creating a nuclear medicine power point to target high school students, collaborating with ASMIRT to produce a video targeting high school students describing the role of an NMT in the workforce and promoting new
methods of program deliver to prospective students.
Some priority areas that are currently in progress include continuing to advocate for the profession via consultation processes and approaching stakeholders of nuclear medicine for placement support. We have identified a number of future priority areas such as working with SNMMI-TS and EANM-TC to understand how they address workforce challenges and facilitating education with overseas tertiary institutions.
Allied Health Assistants are being increasingly utilised in nuclear medicine departments to support the nuclear medicine technologist workforce and is one of the discussion points of our committee.
The WFA committee is committed to building and nurturing the NMT workforce and we welcome suggestions and feedback from our NM colleagues. Please reach out to us via email: wfachair@anzsnm.org.au
Kunthi Pathmaraj Chair, TSIG WFA
Kunthi Pathmaraj, MANZSNM, WFA Committee
RESEARCH STUDY INVITATION
A team from Monash University, University of Sydney, and University of Newcastle are seeking Medical Radiation Practitioners in Australia who are either currently practicing clinically or who have left clinical practice within the last 6 months to participate in a research study. The aim of the research study is to understand the factors that influence Australian medical radiation practitioners’ decisions to remain or leave the profession. The research study involves a short demographic survey and a 45-minute online interview.
If you think you might be interested in participating, please read the explanatory statement linked here for more information.
If you wish to proceed as a participant in this research study, please review and complete the consent form via this link
If you have any questions about this study, you can contact principal investigator Dr Kristie Matthews kristie.matthews@monash.edu
UNIVERSITY LIAISON UPDATE
Erin Hemingway, MANZSNM University Liaison
Hello everyone,
My name is Erin Hemingway, and I am delighted to be stepping into the role of ANZSNM University Liaison. It is a privilege to support our student and academic communities, and I’m looking forward to working closely with members across Australia and New Zealand as we continue strengthening the educational landscape of nuclear medicine.
I would like to extend a sincere thank you to our outgoing University Liaison, Emma Brook. Emma has provided outstanding leadership and advocacy in her time establishing this relatively new role within the ANZSNM, and I’m grateful for the strong foundation she leaves behind.
Following Emma’s departure, the University Liaison role was briefly vacant, during which time Suzi as TSIG Chair held meetings with both the Student Representative Committee (SRC) and the newly formed Academic Reference Group (see TSIG Chair report for more details). These meetings have already set a positive trajectory for
UniSA Amazing Race
2026, and it’s great to step into this role with momentum already underway.
Erin
MANZSNM, University Liaison
Looking ahead to 2026, I’m excited to contribute to the newly established Academic Reference Group as the TSIG representative, helping to strengthen the connection between academic programs and the ANZSNM. I also look forward to supporting the passionate Student Representative Council (SRC) as they continue expanding student participation in the society. On that note, any students wishing to join the SRC please get in contact! I welcome anyone to reach out with enquiries, ideas, or suggestions. Collaboration is at the heart of what we do, and I look forward to hearing from you.
Erin Hemingway uniliaison@anzsnm.org.au
The ANZSNM is committed to supporting the development of undergraduate Nuclear Medicine Technologist students. We were pleased to sponsor the University of South Australia’s (UniSA) 2025 Amazing Race, an event designed to promote collaboration and interdisciplinary teamwork as fourth-year Nuclear Medicine, Medical Imaging, and Radiation Therapy students worked together through a series of clinical and theoretical challenges.
The UniSA academic team delivered an exceptionally well-organised event, showcasing a range of industry professionals and catering by second-year Nuclear Medicine student Aneiki, through her matcha business.
Hemingway,
MEDICAL SPECIAL INTEREST GROUP (MSIG)
Associate Professor Grace Kong, MANZSNM
Chair, Medical SIG
This is the first Gamma Gazette report from MSIG! This group is newly formed within the ANZSNM, established in April 2025. The MSIG provides an important opportunity for nuclear medicine specialists to work closely with the other established ANZSNM multidisciplinary special interest groups to enhance our collective advocacy for nuclear medicine. MSIG can provide advice on matters affecting Nuclear Medicine specialists across Australia and New Zealand, strengthen ANZSNM collaborations with key medical organisations such as the AANMS, and further advance the Nuclear Medicine specialty through the ANZSNM nationally and internationally.
MSIG is represented by 5 medical specialists within the Society:
• Grace Kong. Peter MacCallum Cancer Centre, Vic (Chair).
Kevin London. Children’s Hospital at Westmead and Alfred Nuclear Medicine, NSW.
Jeremy Hoang. Royal North Shore & Hornsby Hospitals, NSW.
• Tahereh Erfani. John Hunter and Calvary Mater Hospitals, NSW.
• Edward Hsiao. Royal North Shore Hospital, NSW,
Since its formation, MSIG has been highly active. Its Terms of Reference were established and endorsed by the Federal Council. Nine Government documents were reviewed with formal feedback provided. Two MSIG members represented ANZSNM and attended the AMA meeting in Canberra. The chair of MSIG attended the
EANM/ANZSNM leadership meeting at the annual EANM Congress 2025 in Barcelona and the Nuclear Medicines
Australia National Rountable in Canberra. The MSIG chair also attends the monthly Presidents’ meetings providing regular direct communication between the ANZSNM MSIG and the AANMS.
We look forward to further strengthening the ANZSNM’s capacity to advocate for our medical members, and through collaborations to advance the impact of Nuclear Medicine in Australia and internationally.
Grace Kong, MANZSNM, Medical SIG Chair
A/Prof Grace Kong, A/Prof Gabrielle Cehic AM & Professor Karen Jones at the Nuclear Medicines Australia National Roundtable
ARTNET UPDATE: CELEBRATING ACHIEVEMENTS
Samantha Hawkins Project Manager, ARTnet
ARTnet is proud to celebrate some recent milestones and ongoing progress across several ARTnetaffiliated clinical trials. These achievements reflect the dedication and collaboration of our investigator teams and their shared commitment to advancing clinical research in nuclear medicine and theranostics.
Primary 2 Trial – Recruitment Completed!
We’re delighted to announce the successful completion of recruitment for the Primary 2 trial, with a total of 660 patients enrolled.
Congratulations to Prof Michael Hofman and his team at Peter maccallum Cancer Centre, and Prof Louise Emmett and her team at St Vincent’s Hospital, Sydney, on reaching this significant milestone. Follow-up is now underway, and primary endpoint results are anticipated in 2026.
Ongoing Recruitment Progress
We also recognise the continued recruitment progress across the following ARTnet studies:
• FIG
• I-FIRST
• SNAP
Led by Prof Andrew Scott and his teams, each of these trials continues to advance steadily. We extend our gratitude to all investigators and site teams for their ongoing commitment and collaboration.
Spotlight on the TheraP Trial
A special mention goes to the TheraP trial, which has now produced another high impact publication — a testament to its ongoing influence and importance in the field of theranostics.
Read the full article: [177Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): a randomised, open-label, phase 2 trial
Recent Publications
We’re pleased to share that the World Journal of Nuclear
Medicine has published an article titled “ARTnet Perspectives and Contributions to Theranostics”, highlighting ARTnet’s collaborative impact and leadership in advancing theranostics across Australia and New Zealand.
This publication underscores the strength of the ARTnet network and the dedication of its members to innovation in nuclear medicine.
Read the full article: ARTnet Perspectives and Contributions to Theranostics.
Global Harmonization Milestone: Unified PET Accreditation Framework
On October 6, 2025, ARTnet joined with EARL and SNMMI-CTN to endorse a unified PET/CT, PET/ MR scanner accreditation framework designed to harmonize quantitative PET imaging worldwide. This landmark agreement introduces a contrast recovery coefficient (CRC)-based accreditation system replacing older SUV RC metrics, streamlining protocols, reducing duplication, and improving data consistency. The new framework will be fully implemented from January 2026, driving global standardization and efficiency in clinical trials and patient care.
“By adopting CRC-based accreditation, we are creating a scalable and adaptable framework that meets the evolving needs of quantitative PET/CT imaging, ensuring robust, reproducible data while streamlining efforts across the global research community.”
Together, these achievements highlight the collective strength, collaboration, and impact of the ARTnet community.
Thank you to all investigators, collaborators, and site teams for your continued contributions to the success of ARTnet trials.
Samantha Hawkins, ARTnet Project Manager
INTERNATIONAL RELATIONS COMMITTEE
A YEAR OF ACHIEVEMENTS
Professor Andrew Scott, MANZSNM Chair, IRC
The IRC continues to be involved in a number of major international policy initiatives for nuclear medicine. In May this year, at the WHO World Health Assembly in Geneva, a Resolution was adopted on "Strengthening Medical Imaging Capacity" (https://apps.who.int/ gb/ebwha/pdf_files/WHA78/A78_R13-en.pdf), which will have major impact on global government policy on improving access to imaging (including nuclear medicine) in all UN countries. This was based on data in two recent Lancet Oncology Commissions on Medical Imaging and Nuclear Medicine (https://www.thelancet. com/journals/lanonc/article/PIIS1470-2045(20)30751-8/ abstract), and Radiotherapy and Theranostics (https:// www.anzsnm.org.au/public/28/files/24TLO0655%20(1). pdf?_zs=JG6Km&_zl=01jA3), both of which were formally supported by ANZSNM. A steering Committee, co-led by Prof Andrew Scott (https://imagingcommission.org/) and supported by many global professional organisations, worked tirelessly to navigate the requirements for this Resolution, the outcomes of which are summarised in a recent Nature Medicine Commentary (https://www. nature.com/articles/s41591-025-04007-9). ANZSNM will have an important role in the Asia-Pacific region for workforce training and implementation of improved access to nuclear medicine in our region.
The SNMMI conference in June this year was a tremendous success for ANZSNM, with Australia and New Zealand being the designated Highlight Countries, and was represented by President Karen Jones in the Plenary Opening Session. The IRC was involved in discussions with the SNMMI Executive on a range of issues including workforce and training, global harmonisation of nuclear medicine studies for clinical trials (see below), clinical practice guidelines, and theranostics initiatives.
At the EANM conference in Barcelona in October a Memorandum of Understanding was signed between ARTnet, EANM and SNMMI for the mutual recognition of PET camera credentialling protocols between the
organisations. This means that for multi-centre clinical trials the PET camera credentialling of sites will be accepted if any organisation has approved the site PET cameras. This work was led by an expert physicist group, with Prof Dale Bailey representing ARTnet and ANZSNM in this endeavour, and a paper published in the Journal of Nuclear Medicine earlier this year outlined the process for harmonisation of PET camera credentialling (https:// jnm.snmjournals.org/content/jnumed/66/10/1506.full. pdf). Further work is being performed to standardise SPECT camera credentialling by this expert group, which will further assist clinical trials that are multi-national and involve therapeutic studies.
Professor Andrew Scott and Professor Dale Bailey
Signing of the Memorandum of Understanding between ARTnet, EANM and
(left to right)
Ivalina Hristova – Chief Scientific Officer, EARL
Ronald Boellaard – Scientific Chair of PET Accreditation Program, EARL
Bonnie Clarke – Senior Director, Research and Discovery, SNMMI
Virginia Pappas – Chief Executive Officer, SNMMI
John Sunderland – Co Chair, SNMMI Clinical Trials Network
Henrik Silber – Executive Director, EANM
Andrew Scott – Chair, International Relations Committee, ANZSNM
Giuseppe Esposito – Chair, Scientific Program Committee, SNMMI
SNMMI
SNMMI 2025 - ACCELERATING THE CURE Highlight Countries: Australia & New Zealand
Professor Karen Jones
ANZSNM President
Selection as the 2025 Highlight Countries for the Society of Nuclear Medicine and Molecular Imaging (SNMMI) Annual Meeting represented an extraordinary honour for Australia and New Zealand, and one that reflects the outcome of decades of productive scientific, educational, and cultural contributions from the members of both nations. Accordingly, this recognition was the culmination of the sustained and effective leadership, innovation, collaboration, and advocacy across our region.
My initial reaction when informed of our selection was excitement, followed quickly by recognition of both the enormity of the responsibility and challenges ahead. What some of you may be unaware of is the enormous amount of planning that takes place ‘behind the scenes’. Our preparation necessitated countless meetings, brainstorming sessions, and creative decisions over many months e.g. selecting images, designing the Highlight Countries booth, producing the Highlights video, writing the President’s letter (featured in the 2025 SNMMI Annual Meeting Magazine – and reproduced in this edition of the Gamma Gazette), preparing my Opening Ceremony address for which a precise timing was required, coordinating the ‘Australian and New Zealand’ food and wine for the Opening Reception, and selecting both topics and speakers for our Continuing Education (CE)
sessions. We also grappled (successfully) with the logistics of transporting ‘essential’ infrastructure/ consumables i.e. ANZSNM flyers, as well as large boxes of Tim Tams, Caramello koalas, Whittaker’s chocolates, NZ chocolate fish, clip-on koalas and plush kiwis. - My suitcase weighed 10kg less on the journey home!
Following our arrival in New Orleans for the meeting (June 21-24), all our planning proved effective and what we had hoped came together in the most rewarding way.
A Strong Opening and Vibrant Presence
From the beginning of the conference, ANZSNM’s presence was highly visible and impactful. I was privileged to present during the Opening Ceremony, an anxiety provoking, but also exhilarating, experience. I sought to convey the bond shared by Australians and New Zealanders, a sibling-like relationship, marked by good-natured teasing, and jokes at each other’s expense, but underpinned by trust and mutual respect. As an example of humour, I referred to former New Zealand Prime Minster, Robert ‘Piggy’ Muldoon, who remarked, during a period of high migration from New Zealand to Australia in the 1980s, that ‘New Zealanders who leave for Australia raise the IQ of both countries’. With the pivotal support of Telix, we showcased a professionally produced video highlighting the remarkable history of nuclear medicine in Australia and New Zealand, as well as the strengths of our contemporary practice,
SNMMI 2025
research, and innovation. I was also delighted to meet the Opening Ceremony MC, Dr Margie Warrell, an internationally recognised leadership strategist, keynote speaker, author, coach and fellow Australian, who gave an inspiring address. The Opening Ceremony concluded with a vibrant Big Band that led us out to the Exhibition Hall for the Welcome Reception.
Our Highlight Countries booth rapidly became a lively, welcoming hub. Attendees predictably enjoyed Australian and New Zealand favourites, including sausage rolls, fairy bread, lamingtons, our wines – and, of course, the Tim Tams, in addition to clip-on koalas and plush kiwis. Attendees left with a deeper appreciation of the substantial and broad-based strengths of our region. ANZSNM members helped serve food. - I have a photo of Prof Andrew Scott adjusting the lid on a bain-marie while welcoming visitors to the booth. My sincere thanks go to Telix, particularly Simone Leyden, Sam Rebbechi and Stewart Holmstrom, for producing the booth artwork, the Highlights video, and their sponsorship of the food and wine for the Welcome Reception. Without their generous support, this success would not have been achieved.
Throughout the meeting, our booth continued to draw considerable international interest so that by Day 3, supplies of Tim Tams, chocolate frogs, Caramello Koalas, and plush kiwis, were nearly exhausted - perhaps the most reliable metrics of our popularity!
A very big thank you to all of those who helped ‘man’ the booth during the meeting. This represented a mammoth task of organisation and scheduling to ensure that someone was always available to greet guests and promote our region.
Scientific Excellence on the Global Stage
The scientific program reflected the depth of talent and broad expertise across Australia and New Zealand. Highlights included:
• Professor Andrew Scott delivered the prestigious Dr Henry Wagner Jr. Lectureship and received the Minoshima-Pappas Transformative Leadership Award . These awards represent appropriate recognition of his major global impact.
Three Highlight Countries CE Sessions, each very well-attended:
1. Contemporary SPECT/CT V/Q Scanning Protocols – Pearls & Pitfalls (Prof Dale Bailey, Dr Raef Boktor, Dr Ghee Chew)
2. The Art of Clinical Trials – Generating Evidence for Changing Practice (Profs Ros Francis, Dale Bailey, David Pattison, Andrew Scott, and Bonnie Clarke)
3. Quality Management in Nuclear Medicine (A/ Prof Soma Somanesan, Kunthi Pathmaraj, Dr Diana Paez)
• ANZSNM Technologist CE Session (in partnership with the SNMMI-Technologist Section (TS)), featuring presentations from Nerida Neumann, Suzi McGavin, and I, related to Technegas, cultural safety and gastric emptying, respectively.
It was also wonderful to see Melissa Shields recognised by the SNMMI-TS for her work on technologist burnout, following her ANZSNM Landauer Award in 2024.
Collegiality, Culture, and Connection
The SNMMI Meeting provided opportunities to interact with SNMMI and SNMMI-TS leadership. There were valuable discussions about current issues of mutual importance, and areas for potential future collaboration.
Beyond the scientific program, the meeting offered several social events to connect with colleagues. A memorable moment was during the 2025 SNMMI Hot Trot (and it was extremely hot and humid!), where A/Prof David Pattison surged ahead while Suzi, Melissa and I ‘walked with purpose’ along the Mississippi River. David’s
SNMMI 2025
cheerful ‘Go ANZSNM!’ as he passed us on the return leg captured the spirit of camaraderie that characterised the entire meeting. The social events were also exceptionally well planned. The International Dinner was a highlight for me, providing the opportunity to meet Presidents of Nuclear Medicine Societies from around the globe. The Technologist International Dinner was held the same evening, and from all accounts it was also a wonderful night. The Presidents’ Reception took place at The Cabildo. Located in Jackson Square, it is one of New Orleans’ most historically important buildings, completed in 1799 as the seat of the Spanish colonial government. It is perhaps best known as the site of the 1803 Louisiana Purchase ceremonies, when the United States doubled its territory in a single momentous transaction. Over the years, it has served various roles,from government headquarters to the home of the Louisiana Supreme Court, before becoming part of the Louisiana State Museum. Entertainment was provided by the band ‘Of Sea and Stone’, featuring the daughter of the outgoing SNMMI President, Dr Cathy Cutler. A charming touch was the selection of two iconic New Orleans cocktails to represent each of the outgoing Presidents: the Vieux Carré, French for ‘old square’ (a nod to the French Quarter), a cocktail containing rye whiskey, cognac, sweet vermouth and Benedictine liqueur, for Cathy Cutler (outgoing SNMMI President) and the Sazerac, signature cocktail of New Orleans with French cognac as the base for Julie Bolin (outgoing SNMMI-TS President). Both drinks are not recommended for the faint of heart.
A Fitting Finale
The meeting concluded with Professor Sze Ting Lee’s Henry Wagner Jr. Meeting Highlights presentation for General Nuclear Medicine, an excellent, comprehensive overview of standout work presented during the conference. As the final visitors left our booth, many with
koalas pinned to their lanyards or kiwis tucked under their arms (or both), leaving a very large bowl devoid of Tim Tams, I felt an immense sense of pride. Being chosen as the SNMMI Highlight Countries for 2025 allowed Australia and New Zealand to showcase not only our substantial and longstanding scientific achievements, but also our culture, marked by generosity, warmth, humour and effective collaboration.
Gratitude and Final Reflections
I am most grateful to Professor Dale Bailey, Professor Sze Ting Lee, Professor Ros Francis, Professor Andrew Scott, and Suzi McGavin for their unwavering support, guidance, and contributions throughout the many months of preparation, to those who assisted on the booth, presented in the Highlight CE, and Technologist, sessions and to Telix for their generous sponsorship.
This story of success reflects the efforts of all of us - researchers, nuclear medicine specialists, radiopharmaceutical scientists, nuclear medicine technologists, physicists, industry partners, and the wider nuclear medicine community across Australia and New Zealand. Together, we demonstrated the excellence, innovation, collaboration and good will that define our region.
SNMMI 2025
A MESSAGE FROM THE PRESIDENT Highlight Countries: Australia & New Zealand
Professor Karen Jones
ANZSNM
President
Reproduced from the 2025 SNMMI Annual Meeting Magazine
On behalf of the Australian and New Zealand Society of Nuclear Medicine (ANZSNM), I would like to express our profound gratitude and heartfelt thanks for the great honour of selecting Australia and New Zealand as the Highlight Countries at the 2025 SNMMI Annual Meeting to be held in New Orleans, Louisiana, June 21-24, 2025. It is a privilege for our region to be recognised on this prominent global stage, and we are very excited to have the opportunity to share the history, innovations, and future directions of nuclear medicine in both Australia and New Zealand with our international colleagues.
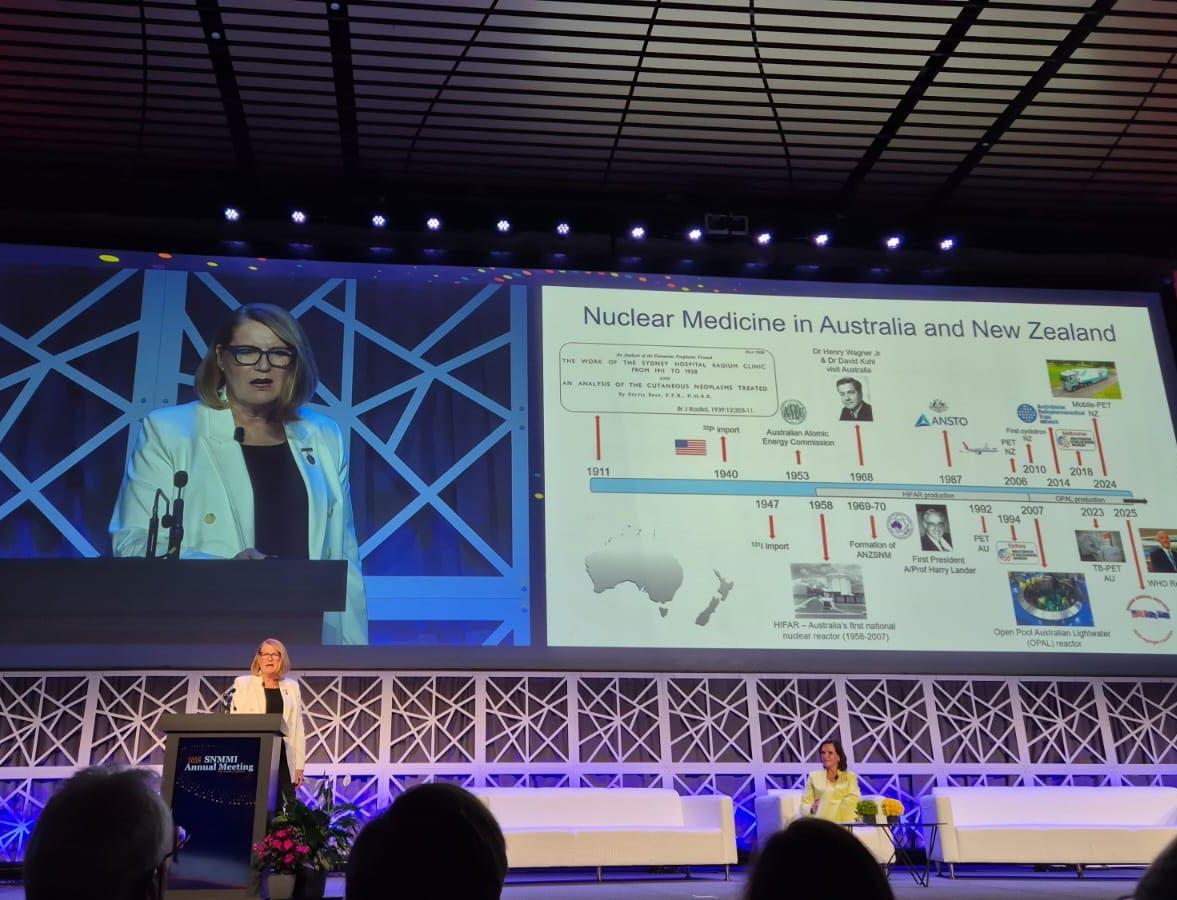
The history of nuclear medicine in Australia and New Zealand is long. The earliest recorded use of radionuclides in medicine in Australia was in 1911, with radium needles employed at Sydney Hospital for treating skin and gynaecologic lesions. During World War II, partnerships with American forces stationed in Queensland facilitated the import of 32P and other unsealed sources, establishing nuclear medicine as a clinical discipline in the region. Australia began importing 131I in 1947, with New Zealand following closely in 1948. These early efforts, not surprisingly, had to address a number of logistical challenges, one of which was the vast distances involved in the transport of radionuclides, an issue that still, on occasion, affects us today.
Australia took a major stride toward selfsufficiency in ~1958 with the commissioning of the
HIgh-Flux Australian nuclear Reactor (HIFAR), which began to produce and distribute medical radionuclides in the late 1960s. This allowed daily deliveries across Australia and also supported the requirements of our New Zealand colleagues. The evolution of technology was predictably associated with the development of our capabilities, of which a seminal milestone was the installation of Australia’s first medical cyclotron in 1989. HIFAR was decommissioned in 2007 and replaced with the multi-purpose Open Pool Australian Lightwater (OPAL) reactor, which is located at the Lucas Heights site of the Australian Nuclear Science and Technology Organisation (ANSTO), which celebrated their 70th anniversary in 2023. Today, Australia and New Zealand are both well-equipped with hybrid medical imaging systems (including SPECT/CT, PET/CT, PET/MRI) and medical cyclotrons, to support a robust, and expanding, clinical and research infrastructure. The formation of the ANZSNM represented a pivotal moment in our shared history. Inaugurated in May 1969 as the Australian Society of Nuclear Medicine, it became the Australian and New Zealand Society of Nuclear Medicine
SNMMI 2025 - A MESSAGE FROM
THE PRESIDENT
in 1970 attesting to the importance of a growing trans-Tasman collaboration. From the outset, the ANZSNM embraced a multidisciplinary, complementary membership of nuclear medicine specialists, technologists, radiopharmaceutical scientists, physicists, nurses and industry partners; current membership approximates 1000 across both countries and our diversity continues to represent a major strength. Since its inception, our Society has maintained a commitment to excellence in education, training, and innovation – we have had had the honour of hosting the World Congress of the World Federation of Nuclear Medicine and Biology (WFNMB) twice, first in Sydney in 1994 and, more recently, in Melbourne in 2018. In addition to these major events, we continue to play a key role in education and training of nuclear medicine professionals across the world through the International Atomic Energy Agency (IAEA) and Regional Cooperative Agreement (RCA), with our multidisciplinary experts contributing to their ongoing programs.
It is particularly gratifying that, at this year’s SNMMI Annual Meeting, Professor Andrew Scott, one of our most distinguished researchers, is the recipient of the prestigious Henry N. Wagner, Jr. Lectureship, as this honour is of particular relevance to our Society. Dr Wagner, along with Dr David Kuhl, played a foundational role in shaping nuclear medicine in Australia – during their visit enroute to the IAEA meeting in Vienna in 1968, together they delivered 48 lectures across the country, promoting nuclear medicine – and in only 16 days! Dr. Wagner’s sustained relationship with our nuclear medicine community further strengthened the significance of this recognition. Nuclear medicine in Australia and New Zealand continues to flourish today. We lead innovative clinical trials through the Australasian Radiopharmaceutical Trials Network (ARTnet) and maintain a strong international profile, particularly in the rapidly expanding
field of theranostics. Several innovative radiopharmaceutical companies have emerged in Australia including ANSTO Health, Telix Pharmaceuticals, Clarity Pharmaceuticals, Radpharm Theranostics and AdvanCell, to name a few.
We also played a pivotal role in the recent Lancet Oncology Commission in Medical Imaging, co-led by Professor Andrew Scott, working collaboratively with our international colleagues on the World Health Assembly resolution on Strengthening Medical Imaging Capacity, that is critical to our collective efforts to combat the growing burden of non-communicable diseases (NCDs), particularly in low- and middle-income countries (LMICs), by improving access to advanced medical imaging and nuclear medicine. We are passionate about supporting our workforce and training the next generation of nuclear medicine professionals to ensure that our field continues to go from strength to strength. Our commitment to clinical excellence, training and academic innovation has positioned us as a major contributor and global leader in the nuclear medicine community.
We look forward to celebrating our history, world-class innovations and achievements at the Opening Ceremony at the SNMMI meeting and encourage you to attend our three CE sessions during the meeting:
• The Art of Clinical Trials – Generating Evidence for Changing Practice
• Quality Management in Nuclear Medicine
We also warmly invite you to visit our booth in the Exhibition Hall (Booth #1229). During the Opening Reception, you will have the opportunity to experience a ‘taste’ of what Australia and New Zealand have to offer (proudly supported by Telix Pharmaceuticals) – and, of course, say G’day! Thank you again for this incredible opportunity.
EANM ANNUAL CONGRESS 2025 Inside EANM 2025
Miriam Prieto
ANZSNM Societies Village Hostess
The ANZSNM Societies Village Hostess, Miriam Prieto, caught up with Dr Zhipeng Cao, recipient of the 2025 Shimadzu Award, to discuss his experience attending the European Association of Nuclear Medicine (EANM) 2025 Congress. Zhipeng reflected on the highlights of the event, sharing key insights, emerging trends in nuclear medicine, and how this opportunity has contributed to his professional development.
What were the standout themes or innovations that caught your attention at EANM 2025?
The EANM 2025 included a wide range of themes covering different aspects and applications of nuclear medicine, from oncology to neurology . Theranostics remain a central focus, with many sessions highlighting its expansion into new targets and the growing interest in alpha-emitters for therapeutic use. It was encouraging to see several novel targets and corresponding theranostic agents developed, some of which have progressed into clinical trials, demonstrating the rapid growth and transformative potential of nuclear medicine in improving patient outcomes. In addition, a series of sessions on dosimetry and AI workflows highlighted how emerging technologies are improving sensitivity, workflow efficiency, and clinical decision-making.
Was there a particular session, presentation, or technology that you believe will have the greatest impact on the future of nuclear medicine in Australia and New Zealand?
One session that particularly impressed me and could have a significant impact on the future of nuclear medicine in Australia and New Zealand was the Plenary Session – “World’s Best Theranostics Comes to EANM’25”. In this session, our very own Australian nuclear medicine physician, Dr Grace Kong from the Peter MacCallum Cancer Centre, joined several world-leading experts to present the latest advances in theranostics for oncology. Beyond the well-established 177Lu-based PSMA radioligand therapy, the plenary also highlighted the emergence of alphaemitters and novel molecular targets showing powerful
therapeutic potential and encouraging clinical outcomes. These developments represent the next frontier for nuclear medicine and could guide the future direction of theranostic practice in our region.
How did the discussions at EANM compare with what we’re seeing in our region. Are there any gaps or opportunities that Australia and New Zealand should focus on?
The discussions at EANM benefited from the its large and diverse membership, representing many countries and covering a wide range of nuclear medicine topics. In Australia and New Zealand, we have several unique strengths, including robust clinical practice standards, active theranostic centres, and the ability to rapidly initiate clinical trials. However, there are also some gaps and opportunities that we could address to stay aligned with international progress:
Alpha-emitter (e.g., 225Ac) readiness: The implementation of alpha therapies (e.g., 225Ac-based agents) in Australia and New Zealand still depends heavily on isotope supply. Expanding local production and supply-chain capacity would be essential for clinical translation.
Cohesive translational pathways: The EANM has a dedicated M2M/TROP track which specifically focuses on preclinical and translational outputs. While our ANZ research activity is strong, developing a more cohesive and coordinated national program could enhance collaboration and accelerate first-in-human studies.
• Infrastructure and regulatory harmonisation: Establishing a well-integrated theranostics ecosystem would facilitate national coordination and interdisciplinary collaboration. This includes harmonising regulatory frameworks and building stronger links between academic, clinical, and industrial partners. This is an approach that aligns closely with current initiatives under development by the National Imaging Facility.
EANM ANNUAL CONGRESS 2025 (CONTINUED)
From your perspective, what global collaborations or trends emerging from Europe could benefit practitioners or researchers here?
Europe has been co-leading the development of large, coordinated theranostic trial networks, enabling multicountry clinical studies at advanced phases. These initiatives rely on strong harmonisation and wellstructured collaboration models. Aligning our studies, led by cooperative groups such as ANZSNM and the National Imaging Facility, with these European frameworks would allow Australia and New Zealand to participate more actively in global theranostic trials and generate more impactful, internationally comparable outcomes. In addition, establishing a standardisation program for training, quality control, quality assurance, and regulatory practices in radiotheranostics would provide a consistent framework for all centres across Australia and New Zealand. This would not only strengthen our local expertise and confidence in theranostic practice but also facilitate TGA approvals and streamline clinical translation. Creating national data registries that capture dosimetry, clinical outcomes, and toxicity profiles would be a valuable step forward to enable Australia and New Zealand as active contributors to the international theranostics community.
What was your personal highlight from attending EANM, either professionally or culturally in Barcelona? Professionally, my highlight was attending the M2M/TROP
session – “Combination Therapy - Shaping the Future of TRT”, where, I along with researchers from around the world, presented and discussed how combination therapies could represent the next major direction for improving efficacy, overcoming resistance, and reducing toxicity in targeted radiopharmaceutical treatments. I had several insightful discussions with both academic and industry partners on the feasibility and design of future theranostic combinations in oncology, which was particularly inspiring and relevant to our ongoing work in Australia.
Culturally, I found Barcelona to be a remarkable host city. Walking past Gaudi’s masterpieces after the conference sessions was a wonderful reminder of how creativity and perseverance can transform both architecture and science. The blend of modern innovation and timeless artistry truly reflected what the conference stood for — combining technical excellence with visionary thinking.
Dr Ingrid Burvenich, Dr Christian Wichmann, Dr Zhipeng Cao
EANM ANNUAL CONGRESS 2025 (CONTINUED)
THE ROLE OF 18 F-FDG PET/CT IN DIAGNOSING METASTATIC CHORDOMA CASE STUDY
Rochelle Bird, MANZSNM and Associate Professor Ivan Ho Shon, MANZSNM
Department of Nuclear Medicine & PET, The Prince of Wales & Sydney Children’s Hospitals, Randwick, NSW 2031
This case report describes the presentation of a large chordoma arising in the pelvis, with rare metastatic involvement of disease spread to adjacent iliac pelvic lymph nodes.
Abstract
Chordomas are slow growing rare malignant bone tumours that present many significant diagnostic and therapeutic challenges (2). The mean survival rate for patients with sacral chordoma is about 6 years, with approximately 67% surviving 5 years after a wide tumour resection (3).
This case report demonstrates the role of Fluorine-18 Fluoro-Deoxy-Glucose ( 18 F-FDG) positron emission tomography/computed tomography (PET/CT) in evaluating metastatic sacral chordoma, with a particular focus on local pelvic nodal involvement, a feature rarely described in literature. PET/CT imaging provides critical information for chordoma disease assessment and treatment planning, complementing conventional imaging modalities such as CT and MRI (1).
The report shows the fundamental role of a multidisciplinary team (MDT) in collaboratively developing appropriate treatment strategies for advanced sacral chordoma, ensuring that providing personalised care remains the primary focus.
Introduction
Chordomas are rare malignant tumours that originate from remnants of the notochord along its embryological pathway (2)(3). They most commonly arise in the skull base, mobile spine, or sacrum (2). Although typically slow growing, chordomas are locally aggressive and account for 1–4% of primary bone tumours, with the sacrum and pelvis being the most frequent sites of reported primary disease occurrence (3). Chordomas represent the most common primary tumour of the sacrum with a distribution and growth rate of 29.2%.
The reported incidence of chordoma metastasis in literature ranges from 3-48%, with the lungs, liver, bone, and lymph nodes being the most affected sites (4).
Barber et al. (2021) provide an overview of the current understanding and treatment approaches for
chordoma. Their review reports an incidence of 0.08 cases per 100,000 people, with variation between sexes. Specifically, males have a higher incidence rate of 0.10, with chordoma cases more frequently reported in men than in women. The incident rate for females is 0.06, with a known peak age of between 50-60 years old. It’s worth noting that less than 5% of cases were reported in children and adolescents (2).
A chordoma is considered life threatening due to local invasion of multiple surrounding tissues as it develops (2). These tumours are unfortunately diagnosed at a stage where prognosis is considered poor. They are difficult to treat and are often associated with a poor patient prognosis and interventional outcomes. Aggressive wide tumour resection is the most important predictive indicator for chordoma (2).
Chordomas frequently present as large tumours, sometimes detectable as an external palpable mass. Clinical symptoms vary depending on tumour location. In sacral chordomas, patients may present with localised pain, discomfort, radiculopathies, myelopathy as well as bowel or bladder dysfunction (3).
Key characteristics of chordomas –Location/Origin: Typically occurs along the spinal column at two main sites - the base of skull (upper spine) or the sacrum (lower spine) (2).
Growth : They have a slow devious onset and most patients are asymptomatic, often going unnoticed for years. As it grows it becomes a locally aggressive tumour attaching to surrounding tissues such as muscle and nerves (2).
Symptoms : Symptoms can vary depending on the location of the tumour within the body. Some skin decolourisation can occur near the tumour growth site. Patients can experience either discomfort or pain. As the tumour grows it can all cause some nerve pain or discomfort (3).
Diagnosis: Chordomas are commonly diagnosed in the later advanced stages of growth and development. Patients are eventually diagnosed when the tumour is well advanced and extensive in size (3).
Treatment options: The first-line treatment typically involves wide surgical resection when appropriate,
Case Study: THE ROLE OF 18 F-FDG PET/CT IN DIAGNOSING
METASTATIC CHORDOMA (Continued)
though suitability varies depending on the individual patient’s case (3).
Case Report: A Rare Presentation of Disease Spread
A 76-year-old female underwent an 18F-FDG PET/CT staging scan to further assess a large posterior pelvic mass that was palpable on examination. She reported no specific pain but described increasing pelvic discomfort, developing gradually over two years and worsening in the last six months, particularly when lying supine or sitting for extended periods. Skin discolouration was observed over the palpable area. Otherwise, she had no significant medical history.
Before the PET/CT scan, the patient underwent a pelvic CT and an ultrasound-guided fine needle aspiration biopsy. The clinical question was tumour staging to guide management.
Pelvis CT comment: There is a soft tissue mass with mild heterogeneous enhancement, destroying the distal sacrum and coccyx, infiltrating the gluteal muscles bilaterally, and touching the rectal wall. Ultrasound guided biopsy comment: Findings are consistent with chordoma, a rare malignancy. Correlation with imaging and surgical consultation is recommended.
18F-FDG PET/CT to assess a large pelvic chordoma
On the day of the scan, the patient’s weight was 52 kg, height 155cm, and fasting blood glucose 5.8 mmol/L.
Scan Technique
The scan was performed from a on a Philips Ingenuity, skull vertex to feet, 63 minutes after intravenous administration of 235 MBq of 18F-FDG, using standard imaging parameters and low-dose 128-slice CT.
Scan Findings
Tumour: There is intense abnormal FDG uptake (SUVmax 6.9) within the large soft tissue mass involving the distal sacrum and coccyx, with extension into the gluteal muscles bilaterally, more pronounced on the right. Uptake along the posterior and left lateral rectal walls is highly suspicious for direct invasion. The mass extends predominantly into the right buttock region.
Node: A small focus of mild–moderate FDG uptake is seen between the proximal right quadratus femoris and gluteal muscles, highly suspicious for a small nodal metastasis. Intense uptake is present in two right external iliac lymph nodes, with additional moderate uptake in a right common iliac node at the L5 level. Several right axillary nodes demonstrate mild uptake, likely inflammatory. Metastases: There is no focal abnormal FDG accumulation to suggest distant visceral or skeletal metastatic disease. Comment: The pelvic chordoma demonstrates intense metabolic activity with extensive local involvement. Moderately to intensely active nodal metastases are present between the proximal right quadratus femoris and gluteal muscles, as well as in the right external and common iliac regions. No metabolically active distant metastatic disease is identified.
Figure 1: The PET images show extensive posterior pelvic involvement, extending into the distal sacrum, coccyx, and bilaterally into the gluteal muscles, with greater involvement on the right. In addition, several FDG-avid lymph nodes are visible inferior to the primary mass (arrowed).
Case Study: THE ROLE OF 18 F-FDG PET/CT IN DIAGNOSING METASTATIC CHORDOMA (Continued)
Figure 2: The PET/CT fusion images demonstrate the chordoma mass involving the distal sacrum and coccyx, with extension into the adjacent gluteal muscles (arrowed).
Figure 3: The PET/CT fusion images demonstrate direct tumour extension into the posterior and left lateral rectal wall (arrowed).
Case Study: THE ROLE OF 18 F-FDG PET/CT IN DIAGNOSING METASTATIC CHORDOMA (Continued)
Figure 4: The PECT/CT fusion images demonstrate intense FDG uptake in two right external iliac lymph nodes (arrowed).
Discussion
Systemic therapy options for chordoma are limited (2). Following completion of the staging 18F-FDG PET/CT scan, the patient’s case was reviewed twice at the sarcoma multidisciplinary team (MDT) meetings to assess surgical suitability and explore alternative local treatment options. Both reviews determined that the mass was too large for a wide resection, with minimal chance of achieving clear margins. Consequently, the disease was considered incurable in this patient.
Although surgical resection is the preferred first-line treatment, it carries substantial risks, including injury to the proximal sacral nerve roots and infection, which may lead to urinary and bowel incontinence, sexual dysfunction, and lower limb weakness. Resection of sacral chordomas is particularly challenging due to the complex neurovascular anatomy of the pelvis, and surgery is often associated with considerable morbidity that can significantly affect quality of life (2). Additionally, the patient’s age of 76 years old was an important factor in decision making to obtain the most appropriate treatment options. Surgical removal of the large mass was considered highly morbid, requiring procedures such as tumour debulking, pelvic
floor reconstruction, and extensive skin flap repair, all associated with a prolonged and difficult recovery and significant risk of postoperative complications (2).
Curative radiotherapy was not appropriate due to the extensive tumour size however, high-dose palliative radiotherapy was considered a suitable option to alleviate pain and discomfort, slow tumour growth, and improve quality of life (2).
The staging PET/CT also revealed FDG-avid pelvic lymph nodes, which could be biopsied to confirm metastatic involvement and guide treatment planning. If confirmed, targeted radiation therapy could be considered to help slow disease progression through the lymphatic system (1).
This case is of particular interest as, while chordomas are rare, FDG-avid iliac nodal involvement is even less frequently reported. The nodal disease sites in this patient were atypical and rarely described in the literature. The FDG-avid iliac nodes (Figures 1 and 4) demonstrated uptake and SUVmax values comparable to the confirmed sacral tumour. Importantly, there was no clinical history of inflammatory disease that could explain the nodal uptake as a false positive.
Case Study: THE ROLE OF 18 F-FDG PET/CT IN DIAGNOSING METASTATIC CHORDOMA (Continued)
Conclusion
18F-FDG PET/CT is an effective, non-invasive imaging modality that provides valuable functional information for diagnosis, staging, and treatment planning in sacral chordoma. In this patient, PET/CT clarified the extent of disease and surrounding structures at risk, supporting clinical decision making and guiding care.
References
1. Ahmad Almuhhaideb, N. P. (2011, January-February). 18F-FDG PET/CT Imaging in Oncology. Ann Saudi Med, 31(1), 3-13. doi:10.4103/0256-4947.75771
2. Barber, S. M., Sadrameli, S. S., Lee, J. J., Fridley, J. S., Teh, B. S., Oyelese, A. A., Telfeian, A. E., & Gokaslan, Z. L. (2021). Chordoma — Current understanding and modern treatment paradigms. Journal of Clinical Medicine, 10(5), 1054. https://doi.org/10.3390/jcm10051054
3. S. Pillai, S. G. (2018, April 29). Sacral Chordoma: A review of literature. Journal of Orthopaedics, 15(2), 679-684. doi:10.1016
4. Saurabh Rohatgi, N. H. (2014, September 7). Metastatic Chordoma: Report of the Two Cases and Review of the Literature. The Eurasian Journal of Medicine, 47(2), 151-154. doi:10.5152/eurasianjmed.2015.52
RURAL REALITIES: A CASE STUDY ON HEALTH INEQUITIES AND THE ROLE OF NUCLEAR MEDICINE IN REGIONAL AREAS CASE STUDY
Caitlin Burt, MANZSNM
Royal Darwin Hospital
Introduction
Approximately 7 million Australians (28% of the population) live in rural and remote Australia and because of their geographical location face unique health challenges (AIHW, 2025). Data shows that Australians living in rural and remote areas have a lower life expectancy, higher rates of preventable disease and poorer access to primary health care services compared to people in metropolitan areas (AIHW, 2024).
Additionally, living in the Northern Territory (NT), presents its own challenges. Many patients living in rural and regional communities across the NT need to travel by plane, boat or many hours by car just to receive basic health care services. As Darwin is an isolated capital city, patients who require specialised health care may even need to travel interstate. This isolation makes patients hesitant to address health concerns, and thus are likely to present with disease that is far progressed due to a delayed diagnosis. A study by Grimson et al. 2013, highlights the impact of geographical location on health outcomes, showing that patients with cancer who live in rural and regional areas have poorer survival rates in comparison to patients in metropolitan areas.
Case Study
A referral was received for a Lymphoscintigraphy of the lower legs. Upon review of the patient, the patient had already waited 3 months for a vascular specialist to fly up to investigate their situation, to receive this referral for the nuclear medicine study. This study was re-prioritised as urgent and performed at the patient’s earliest convenience.
An 80-year-old female presented to the Darwin nuclear medicine department for a lymphoscintigraphy study with very swollen legs, the right worse than the left which spontaneously occurred overnight 3 months prior (figure 1).
In the preceding 3 months, the patient underwent an ultrasound to rule out blockages, attempted compression
bandaging, physiotherapy and massaging. The patient noted the treatment had provided some relief, yet the swelling remained the same.
Figure 1: Patients lower legs upon presentation to the department
Additional patient history included diagnosis of uterine cancer 10 years prior, treated with radiation therapy. The patient recalled some swelling occurring on the left due to lymphedema during treatment, however, was adamant the new swelling was unrelated. The patient also had a coronary angiogram performed where the catheter was inserted into the right femoral region.
Method
4 x 10 MBq of 99mTc NanoScan was injected intradermally into the webs between the 1st and 2nd phalange and the 3rd and 4th phalange. A physician and nuclear medicine technologist injected simultaneously to allow for direct comparison.
Case Study: RURAL REALITIES: A CASE STUDY ON HEALTH INEQUITIES AND THE ROLE OF NUCLEAR MEDICINE IN REGIONAL AREAS (Continued)
120 second dynamic images were acquired over the injection site, the popliteal and pelvic region at t=0 to track the tracer movement.
At t=20, 45, 60 and 90 minutes, images were acquired from pelvis to toes.
At t=120 minutes, static images were acquired over the popliteal and pelvic region.
In between imaging the patient walked around the department to promote lymphatic flow.
Findings
The study found rapid lymphatic clearance on the right with a back-flow phenomena occurring, demonstrating failure of lymphatic passage from the right inguinal region. This pattern is a diagnostic finding for lymphedema. The flow on the left limb was slower in comparison, however passage was noted into the inguinal nodes and passing more proximately (figure 2).
Discussion
This study was able to finally find the cause of the patients swelling, creating a clear graphical picture of where the issue is and what is happening in the leg. Due to the simple nature of the study, the scan was
conducted quickly once the referral was received, the patient was able to easily access their appointment, not delaying treatment any longer.
With the numerous options of imaging modality and scans available, lymphoscintigraphy is considered the gold standard for imaging the lymphatic system. It is also the only imaging modality that can assess lymphatic flow in a non-invasive method, with a 96% sensitivity and 100% specificity (Pappalardo & Ming-Huei, 2019).
Lymphoscintigraphy images the patient’s real-time bodily function to give an accurate representation of the flow of lymphatic fluid.
Lymphoscintigraphy is a tried and tested imaging technique and as technology continually advances, SPECT/CT can also be utilised for better anatomical localisation (Villa , et al., 2019). Other advances also include quantitative analysis to compare tracer movement between limbs and assess kinetics of proximal lymph node uptake (Nganga & Makhdomi, 2019).
This case endeavours to highlight nuclear medicine’s role in providing these studies in a timely manner, understanding that patients who are from rural and regional settings may already have a delayed treatment plan.
Figure 2. - Lymphoscintigraphy results
Case Study: RURAL REALITIES: A CASE STUDY ON HEALTH
INEQUITIES AND THE ROLE OF NUCLEAR MEDICINE IN REGIONAL AREAS (Continued)
Often, when working in rural and regional settings, nuclear medicine practitioners are challenged to adjust their mindsets and workflow. What may see as a nonurgent study in a metropolitan area, is rather urgent for the rural patient’s treatment plan. It is a common theme to feel pressure to get studies done more because “the patient will only be in town for that week” or “their specialist is flying in” rather than triaging by their clinical urgency. When these ‘non-urgent’ studies are completed, the results are often elevated to an urgent nature as the disease is often in more advanced stages.
Conclusion
A nuclear medicine practitioner may sometimes forget the role they play in a patient’s pathway. Our work becomes routine and predictable, and often we do not see the larger picture of the patient’s journey. This case demonstrates that a simple study, allowed a diagnosis for a debilitating condition for a patient, who has already endured challenges that many in metropolitan areas would have had addressed months earlier. It highlights our role as practitioners working in rural and regional settings in providing these studies in a timely manner, adjusting our understanding of urgent and non-urgent studies, particularly for patients that have already suffered health inequities, simply due to their geographical location in Australia.
References
AIHW. (2024). Rural & remote Australians. Retrieved from Australian Institute of Health and Welfare : https:// www.aihw.gov.au/reports-data/population-groups/ rural-remote-australians/overview
AIHW. (2025). Rural and remote health. Retrieved from Australian Institute of Health and Welfare : https://www. aihw.gov.au/reports/rural-remote-australians/rural-andremote-health
Grimson P, P. F. (2013). Are visiting oncologists enough? A qualitative study of the needs of Australian rural and regional cancer patients, carers and health professionals. Asia Pacific Journal of Clinical Oncology, 226-38.
Nganga, E. C., & Makhdomi, K. (2019). Comparison of quantitative analysis to qualitative analysis for interpretation of lower-limb lymphoscintigraphy. World Journal of Nuclear Medicine , 36-41.
Pappalardo , M., & Ming-Huei, C. (2019). Lymphoscintigraphy for the diagnosis of extremity lymphedema: Current controversies regarding protocol, interpretation, and clinical application. Journal of Surgical Oncology , 1-11.
Villa , G., Campisi, C. C., Ryan , M., Boccardo, F., Di Summa, P., Frascio, M., . . . Campsisi, C. (2019). Procedural Recommendations for Lymphoscintigraphy in the Diagnosis of Peripheral Lymphedema: the Genoa Protocol. Nuclear Medicine and Molecular Imaging, 4756.
Reminiscences and Thoughts on Nuclear Medicine by Jim McRae as related to Paul A.C. Richards as part of the ANZSNM Pioneer Witness Project (c.2007)
Readers should be aware that these comments are being written 56 years after their commencement and 18 years after I retired from Nuclear Medicine – Jim McRae
Edited by Dale L Bailey PhD
Sep 2025
Royal North Shore Hospital and The University of Sydney
In The Beginning
My first contact with radioactive tracers was in 1951 when I did a BSc(Med) with Professor de Burgh. We explored the replication of ectromelia virus in the mouse liver using 32P to measure the turnover of phosphorus in mitochondria, microsomes. Don Metcalf preceded me and Gus Nossal followed the next year with Professor de Burgh. Barry Firkin2 worked with Professor Thorpe in 1951. At the time I did not realize how early in tracer technology this work was. I was one of the Professorial Residents at RPAH in 1954 and was Medical Registrar in the Clinical Research Ward in 1956 and 1957 with Professor Blackburn3. Again, I had the opportunity to use radioactive tracers measuring hepatic blood flow.
At the end of 1957 I passed the Membership4 and at this time Professor Blackburn asked whether I would be interested in training at Donner Laboratory, which he had visited in 1956 and had arranged for a training position in the future. A fellowship was arranged (Lederle International Fellowship).
In January 1958 we (my wife, Elizabeth and a 3 month-old child, Amanda) left Sydney on a Qantas Super Constellation - 4 regular propeller engines and a top speed of 180 mph. On the 2nd day I awoke to see one propeller idling and fuel leaking out. Next came the captain’s voice to alert us to a stop on Canton Island, a minute spot 2 degrees south of the equator, and a refuelling airfield for fighters flown to Australia during WW2. We spent 24 hours waiting for a replacement engine and the onward flight to San Francisco.
We had left Sydney, not knowing the exact location of Berkeley to San Francisco, something not imaginable in this day of global positioning and maps on the internet. A bus ride (segregated) to downtown San Francisco and cab to the Shattuck Hotel in Berkeley answered the location of UC Berkeley and Donner Laboratory - a distance of 45 miles5. The room rate was $9. Accommodation was found in a small apartment about one mile from Donner Lab through the service to foreign students run by International House. The person was Mrs McGlaughlin and of interest is the fact that Mrs McGlaughlin is still active in community affairs and now at over 90 has participated in a protest to stop the University cutting down some oak trees to make way for an addition to the football stadium. This involvement is typical Berkeley. We lived in that apartment for three years paying first $80 per month and later $90.
Jim McRae’s entry in the University of Sydney Medical School 1963 Yearbook
ARTICLE: Reminiscences and Thoughts on Nuclear Medicine by
Jim McRae (Continued)
I met with John Lawrence the program director and the brother of Ernest Lawrence6, the inventor of the cyclotron and the reason Donner Lab had the earliest access to new radioactive isotopes. I learned that the program he offered was a PhD in Medical Physics involving courses in Math, Physics, Nuclear Physics, Nuclear Chemistry, & Radiation Biology with a usual time of 4 years. Not only was this the only option but I had already missed the first week of classes. The Medical Physics program centred at Donner was started in 1944 and drew physicians from the US and all over the world. It provided training in the use of radioactive tracers in medical research and in radiobiology. Candidates were assigned an advisor from the active research staff. Although Hal Anger7 was busy upstairs I did not meet him and was unaware of the major contributions he was about to make. There was no recognition of Nuclear Medicine as a field of medicine at Donner and it was not affiliated with a hospital.
I was assigned to work with Lola Kelly whose field was radiation biology. There was intense interest in radiation damage and in transplantation problems, specifically graft-versus-host reactions. This became the subject of my thesis and I treated the mouse with graft-versus-host syndrome as I would a sick patient. The anaemia was fully evaluated with iron kinetic studies, red cell and plasma volumes blood loss and plasma loss using the appropriate radioactive tracers. The basic course work was a constant background. In late 1959 we made a 56-day trip of over 12,000 miles visiting centres active in radiobiology and tracer methodology including Los Alamos, Brookhaven National Laboratory, Oak Ridge, and Bar Harbor in Maine. We made this trip in a 1952 de Soto lacking a heater, window defroster and air conditioner. This was typical for a cheap Californian car with its mild climate but not ideal in the snow and subfreezing conditions we experienced. We had two children in the back, our daughter now close to two and son of six months. My wife has uncovered a diary she kept on this adventure and it makes the experience live again and reinforces the joys and rashness of younger years.
E.O.Lawrence inspecting a cyclotron at Berkeley
On our travels we visited Tony Edwards at the Mayo Clinic, Barry Firkin in St Louis and Kaye Ellem at the Wistar Institute in Philadelphia to mention some Australians in the US in 1959. There was a Nuclear Medicine Department at the Massachusetts General Hospital and the diary mentions lots of equipment (it must have included the positron scanner) We also visited many National Parks on our route including Bryce Canyon which we saw on a brilliant morning but cold enough to freeze the dribble on the baby’s bib. I completed the course work and thesis for my PhD at the end of 1960 and was appointed Senior Lecturer in Medicine (Radiobiology) in 1961. My father commented that I had been a student for 14 years.
The laboratory design I requested was planned for bench work and tracer investigations as I did not foresee the major role that organ imaging was about to play. Following my appointment there was a news release about this:
ARTICLE: Reminiscences and Thoughts on Nuclear Medicine
by Jim McRae (Continued)
Radiation Medicine as New University Course
The Dwepartment of Medicine in the University of Sydney will soon provide general training in Radiation Medicine amongst its regular courses. A considerable amount of isotope detection equipment has been provided by the Postgraduate Medical Foundation. These steps have been taken because we have entered the nuclear age in which there is an increasing need for doctors, biologists, physicists and other groups to
The major emphasis of the news release was radiobiology with the disclaimer that Radiation Medicine was chosen in preference to Nuclear Medicine because the significance to man of radiations of all types will be a central theme. It was a time of great concern about nuclear weapons.
It was noted that particular medical uses of isotopes will be presented and late in the article it stated that "other scanning devices capable of precise localization will be required". In conclusion it was said that the courses were aimed to "achieve the safe and optimal peaceful use of atomic energy”.
Apart from my Nuclear Medicine activities I was assigned to St George Hospital to oversee the students and run the classes on history taking. My students did well in their exams and I took pleasure and pride in their success. Frank Broderick and I conducted Saturday morning rounds for interested physicians and these were also well received. A number of these students went on to enter Nuclear Medicine e.g., Andrew McLaughan, Fred Lomas, Peter Valk and others.
The clinical activities in the Radiation Medicine section quickly expanded to include a full range of radioisotope tracer techniques to investigate haematological problems. Other specialists were encouraged to participate and an early project was an evaluation of the anaemia of ulcerative colitis (Beal, Skyring et al Nov 63). Renograms were performed and I can especially remember performing studies with the patient erect (standing) to evaluate the effect of posture on renal blood flow noting that some kidneys drop some distance and the renal artery could kink. The department was not involved in radio-assays which commonly were major activities in early Nuclear Medicine Departments. With the delivery of the positron scanner in mid-1961 (chosen and finance found by Dr Rex Money, the senior neurosurgeon at RPAH)8 imaging was started. To provide patient oversight and technical support Sister Meredith McDade joined the group. Nurses were often the first to be Nuclear Medicine "technicians".
Throughout my career in nuclear medicine I performed many scans and camera studies. The doctors working with me followed this routine and became proficient in performing all studies. The tracer doses were prepared and administered by the medical staff. Millicent Marion communicated to me that she fell through a balcony at RPAH en route to a ward with a little lead pot of isotope. None spilt!! The fact that the MDs did many of the early studies adjusting the settings and positioning the patient greatly speeded the learning process. We (the medical staff) perused the history and examined the patient and as a result, the accuracy of the final report was enhanced as we became familiar with interpreting the images.
This policy led to John Morris' mantra9 "reports must be in the proper clinical context". I wonder if the reason we took this approach was our clinical medicine background unlike radiology where so may reports are read from film alone.
I returned to Donner Laboratory on sabbatical leave in 1968 and worked closely with Hal Anger. The nuclear medicine group was not closely integrated. Hal Anger always worked alone on instrument design apart from excellent technical support. Notable were Pete Dowling in the machine shop who fabricated much of the imaging equipment including
ARTICLE: Reminiscences and Thoughts on Nuclear Medicine by
Jim McRae (Continued)
housing, shielding and many collimators. Hal also had an engineering assistant, John Gurule, who worked on maintenance and continuous upgrades to the electronics. Both Pete Dowling and John Gurule have provided input to these musings. Hal actively participated in the evaluation of new isotopes and tracers to assess the need for instrument modifications. He worked with a series of physicians (Bill Myers and Alex Gottschalk) in the evaluation of his positron camera, whole body scanner, multiplane tomographic scanner (I was the first to report on this) transmission scintigraphy and rotational sciniscintigraphy. He designed numerous collimators for different sensitivities and energies. His primary camera had 3 collimators on a clover leaf support such that a low energy, medium energy or pinhole collimator could be rotated into position over the supine or prone patient. The patient was positioned by moving the bed as needed. The pinhole collimator had inserts of different apertures made of platinum. Most images were recorded on Polaroid film using a camera with a shutter opened at 6 different apertures to provide different levels of exposure.
With computer storage and manipulation available today this seems very simplistic. For dynamic studies the Polaroid film was manually pulled in a suitable time sequence. It was the first time that I worked with Hal Anger and realized the level of his achievements and his appreciation of what was needed to further imaging.
A brief review of Hal’s huge contributions to Nuclear Medicine seems appropriate: 1950: designed the well counter
• 1952: Pinhole camera 1
• 1953: Early whole-body scanner with 16 detectors
1956: Anger camera prototype
• 1959: Positron camera
1965: Whole body scanner with 64 detectors-a real work horse
• 1966-68: Multiplane Tomographic scanner
• 1968: Transmission imaging10
1970-72: Major upgrades of the positron camera and whole-body scanner
• 1973: Cardiac gated dynamic mobile probe for cardiac ejection
Professor Blackburn has found a letter I wrote to him in May 1968 which enthusiastically reported on the work at hand. The multiplane tomographic scanner was almost finished as was a new camera with 16” crystal. There was a new model of the Nuclear Chicago commercial camera on loan for his evaluation. We had just completed a series of transmission images to test their place in imaging. I wrote that continued experience has convinced me that "proper camera studies" take a long time - by the time you have done a dynamic study, early and late scintiphotos even a brain study takes an hour or more. Bearing in mind the clinical load at RPAH I recommended funding at least two cameras. I was not as enthusiastic about the immediate need for a positron camera. So happy was I with the rate of change in imaging that I asked "what would your reaction be to some extension of my stay in Berkeley if developments were booming at Donner and stationary in Sydney?" I do not have an answer to that request but as events unfolded it was not until the spring of 1969 that I returned to Sydney. I was most fortunate to have worked with Hal at the acme of his career.
1971 A Turning Point
In 1971 I was appointed research fellow at Donner Laboratory with the responsibility of conducting the imaging studies using Hal Anger's instruments and new isotopes and compounds prepared by Yukio Yano (Radiochemist working with Hal Anger) and myself. Examples included Kr81m and Rb81 generators and 99mTc-diphosphonate. I was particularly interested in determining the optimal amount of stannous chloride to formulate the Tc99m bone scan agent. Rats were injected immediately after preparation but there may well have been reasons to explore the effects of different amounts of tin on the stability of the bone scan agent over time. I never found that bone scanning
ARTICLE: Reminiscences and Thoughts on Nuclear Medicine by
Jim McRae (Continued)
agents obtained from radiopharmacies gave the same quality of images as did freshly prepared kits. Since stannous tin was being used so widely to produce Tc99m tracers I investigated the toxicity of tin in rats. The lethal dose was determined and the kidneys were the critical organ. As part of this study I explored the distribution of Tc99m pertechnetate at times following the injection of tin11. With smaller challenge doses of tin red cell uptake was pronounced. At this time there were reports of abnormal distribution of Tc99m pertechnetate in patients who had had a bone scan a few days previously. (Tony Walker contacted me because he had noted the altered distribution of pertechnetate in such patients.) From these observations came the method of in vivo labelling of red cells for blood pool and cardiac studies. Note that some tracer compounds "give up their tin to red cells better than others with pyrophosphate being a good primer". Handmaker, Hal and I explored rotational sciniscintigraphy. Multiple images of the liver and spleen were taken with the patient on a rotating turntable and recorded as a 16-frame film loop. When played, this loop gave a remarkable three-dimensional feel12. There seems to be an advantage in interpreting serial images focused around an area as multiple CT images are better interpretated in a moving sequence versus single frame viewing. In 1975, when Joe Kriss was on sabbatical leave, I substituted for him at the Stanford Nuclear Medicine Department two days a week for six months supervising the Nuclear Medicine trainees. There I saw a technetium “glove” resulting from the injection of the bone scan agent into the radial artery. The bones in the wrist and hand "light up " in a glove pattern.
In 1976 the funding at Donner was redirected and clinical-type programs reduced. I joined a private group in San Francisco with its own radiopharmacy (Radpharm) which supplied other hospitals. In 1978 I applied to Children's Hospital in Oakland to commence a Nuclear Medicine Service in house. Prior to this time a few studies had been done at nearby hospitals. From October 1978 until April 1989 I was the only person in the Department. I picked the children up from the ward, prepared, calibrated and injected all tracer doses, conducted every study and typed the reports. All the imaging was all done on a portable camera and numerous studies were performed in the intensive care nursery and ward. By studying the critically ill children and infants this way nursing assistance was available. In the Department the mother frequently provided helpful oversight. For infants a plywood extension was attached to the camera head which faced upwards. Excellent prone and supine images could be obtained.
For several years I also was the Quality Assurance Director and learnt much about tracking and addressing problems in clinical care. A quality control check was made on the accuracy of the Nuclear Medicine reports for random blocks of days against the discharge diagnosis. I provided emergency scans at night and weekends with call about every two weeks. With only a few odd holidays it was time to retire in 1969 and have an extended holiday in Scotland.
One of the last areas that I was exploring at Donner in 1973 was the use of a cardiac gate to image the heart in diastole and systole. In multiple studies over the chest. I had noted the variation in cardiac size and a gating circuit was built to trigger off the R wave and accumulate a series of images. This system was shown to visitors. At the same time, I had also had the electronic support group build a respiratory gate to see if image quality could be improved by freezing respiratory movement. Hal Anger was not involved with these gates.
While I was experimenting with the ECG gate to measure ejection fraction Donald van Dyke and Hal Anger were evaluating a detector (cardiac gated dynamic mobile probe) which was centred over the left ventricle as best as could be assessed by X-ray and an external lead marker. The probe had a central area which recorded activity in the left ventricle and a concentric ring of equal area recording the surrounding activity which was the subtracted background activity. The ejection fraction could be calculated and the results were judged of value. The parallel development of the probe and the fact that Hal was not directly involved with the gating approach was critical to advancing the technique and perfecting the ECG gate. Research proceeds better with a coordinated effort and a narrow focus. The ECG and respiratory gates remained after my departure and were not further developed at Donner. The alternate probe approach was superseded as gated cardiac studies proved so successful.
It is now 18 years since I retired and the contacts and memories involved in this project13 have been special.
ARTICLE: Reminiscences and Thoughts on Nuclear Medicine by
Jim McRae (Continued)
References
1 Paul AC Richards AO OBE has just turned eighty and published his 45th book. He still lives in Tasmania.
2 Editor’s note: In 1958 Jim McRae, Barry Firkin and Alan Skyring were the driving force behind the establishment of the Australian Society for Medical Research, (ASMR) of which Barry Firkin became the first president.
3 Charles Ruthven Bickerton Blackburn AC (1913 – 2016), Professor of Clinical Medicine at the University of Sydney
4 Royal Australian College of Physicians
5 Editor’s note: from downtown SFO
6 Nobel Prize in Physics in 1939 for inventing the cyclotron
7 Editor’s note: inventor of the gamma (“Anger”) camera
8 Planar positron scanning with 74As on a Baird Atomic positron rectilinear scanner
9 Professor John G Morris AO (1934 - 2022), Director of Nuclear Medicine at RPAH 1967 - 1994
10 Editor’s note: McRae’s work was unknown to me at the time, but dual radionuclide emission and transmission imaging was the topic of my Masters’ thesis in 1986: “Towards Quantification in SPECT: A Dual Radionuclide Approach”. It was initially commercialised by ADAC in the mid-1990s as a method to correct for photon attenuation in myocardial perfusion scans with other vendors implementing variations later, prior to the introduction of combined SPECT/CT.
11 J Nucl Med Vol 15, 151-155 1974
12 Editor’s note: unaware of this work, a very similar study was the subject of my undergraduate honours project thesis “Rotating & Planar Display in Nuclear Medicine” in 1983 using a GE400T camera, with similar findings to McRae’s remarks.
13 This is an annotated and re-edited version of the recollections by Jim McRae that appear in the ANZSNM history book Isotopes, Imaging & Identity which was collected by Paul AC Richards and published in 2013.
An Allied Health Assistant Model in Nuclear Medicine: Preliminary Findings
Claire Farrell, Jessica Welch, Wesley Ng, Kunthi Pathmaraj Department of Molecular Imaging and Therapy
Austin Health, Victoria, Australia
Background
Health Care Assistants have been employed in healthcare for more than a decade in the hope of relieving the increasing pressures on the healthcare system from a variety of reasons; one reason being the shortage of skilled healthcare professionals (1). Depending on the area of healthcare in which assistants are employed, the assigned tasks and duties may vary greatly.
A critical shortage of Nuclear Medicine Technologists (NMTs) across Australia has had a significant impact on maintaining optimal clinical service provision in Nuclear Medicine (NM) departments. Education institutions, medical industries and professional societies are working on initiatives and solutions to address this issue. The Allied Health Assistants (AHAs) model is being trialled in a few NM departments as one possible solution. Since this was the first time our department employed AHAs, we needed to ensure they fully understood their roles and responsibilities, felt comfortable and competent, maximising the value of this resource. To benefit the field of Nuclear Medicine, the AHA Position Description (PD) and recruitment process were targeted towards nuclear medicine students.
Aims
The primary aim of this study was to assess how AHAs may assist NMTs as a supplementary workforce and the impact of AHAs on the departmental clinical workflow; a secondary aim was to evaluate the effectiveness of this model in supporting AHAs in their learning and professional development.
Methods
The AHA Position Description (PD) and recruitment process was designed to best suit the needs of a NM service and the role targeted towards NM students. Duties set out in the PD included assisting with clinical procedures under the supervision of NMTs and performing administrative tasks that support our service provision. A clear scope of practice was established, with differentiation between allocated duties, and supplementary NM training.
At Austin Health, four AHAs were recruited from different university year levels to maintain adequate staffing during periods of university schedules and student clinical placements to ensure consistent availability of AHA staff.
Surveys were designed and distributed to technologists and AHAs to evaluate the model at three months post recruitment of AHAs. Surveys were designed to address the overall impact of the AHA model as well as department specific aspects such as shift allocation and AHA model satisfaction. Responses were collected using three formats: a 10-point Likert-type scale, where 1 indicated strong disagreement and 10 indicated strong agreement; multiple-choice items, for which results are reported as the percentage of respondents selecting each option; and free-text questions, which were analysed qualitatively. The technologists' survey was formulated to specifically assess the impact of the AHA model on workflow and pressures felt by staff within our NM and PET departments. It also considered the amount of training offered to AHAs by NMTs, specific to NM theory and clinical applications.
ARTICLE: An Allied Health Assistant Model in Nuclear Medicine: Preliminary Findings (Continued)
The AHA survey was developed to assess the impact of the AHA role on their NM studies. It also focussed on their current duties, and how these could be adjusted in future to further refine the model.
The initial AHA and NMT survey questions were revised and repeated 12 months after the initiation of the AHAs to determine the success or limitations of the AHA model.
For the technologists, the revised survey enquired about the performance level of AHAs, scope expansion and the consequences of AHA unavailability.
For the AHAs, the revised survey focussed on their confidence level in performing their tasks, their new learning experiences and their overall job satisfaction.
Results Technologists
The initial survey revealed that supplementing NMT rostering with the AHA model has provided support to maintain optimal clinical services and has been pivotal in achieving the following outcomes:
i. AHA assistance has streamlined processes which allows NMTs to focus on clinical and technical duties which are beyond the scope of AHA staff
ii. enabling a smoother workflow within both NM and PET departments. PET results shown in figures 3. and 4.
iii. NMTs were able to facilitate and create teaching opportunities for AHAs pertinent to their undergraduate program/course.
Figure 1. Initial survey questions: Nuclear medicine technologists
Figure 2. Initial survey questions: AHA
ARTICLE: An Allied Health Assistant Model in Nuclear Medicine: Preliminary findings (Continued)
AHAs being tasked with responsibilities such as cleaning, directing patients through the department, and assisting with administrative tasks, has allowed NMTs to focus on more technical duties. This has played a critical role in softening the impact of the workforce shortages on NMTs and has enhanced the service provision of our department.
It was noted that when AHAs were not available for a full shift, technologists found it more beneficial to have AHAs rostered in the morning and over lunch, to maintain an efficient workflow.
Sequential surveys at twelve months indicated that technologist believed:
i. AHAs are currently performing appropriate duties
ii. There were some areas for scope expansion identified
iii. Unavailability of AHA staff was most notable in the morning and over lunch, however; not to the extent of detrimentally affecting the critical workflow of the department.
AHAs
Feedback from AHAs indicated:
i. they had ample time to perform their allocated duties
ii. there was a strong interest from AHAs to be trained in additional duties
iii. the role has been beneficial to their NM undergraduate program
Figure 3. Initial technologists survey results on improved workflow in PET.
Figure 4. Revised technologists survey results on improved workflow in PET.
ARTICLE: An Allied Health Assistant Model in Nuclear Medicine: Preliminary Findings (Continued)
6. Revised AHA survey results on performing additional duties.
These results demonstrate an eagerness of AHAs to learn, taking opportunities to engage in additional training specific to the role of a NMT (figures 5 and 6). This has proven to be advantageous to their NM studies, providing a foundation for strong fundamental knowledge for the future NMT workforce.
It was noted in sequential surveys at twelve months, that all AHAs attributed their improved communication skills, and better understanding of departmental workflows to their current role as AHA. They indicated high levels of job satisfaction, with all AHAs stating they would recommend the role to future NM students.
Discussion
Initial evaluations of the AHA model have been positive. Once AHA staff are adequately trained, their presence can markedly improve departmental workflow, allowing for better utilisation of qualified Technologists and optimisation of service provision.
By employing undergraduate NM students, we found the training period to be relatively short, due to their familiarity with the unique and varied workflows in Nuclear Medicine. AHAs indicated they envisaged working in the role for 1-3 years, emphasising the fact that the model needs to be dynamic and flexible to work for both the AHA staff and the department.
We have found it advantageous to employ multiple AHAs from different university year levels, enacting a rolling workforce that is flexible and ensures adequate staffing during periods of student placements. It also allows us to maintain a degree of experience amongst AHAs within our department, while others
Figure 5. Initial AHA survey results on performing additional duties.
Figure
ARTICLE: An Allied Health Assistant Model in Nuclear Medicine:
Preliminary Findings (Continued)
progress to becoming qualified NMTs.
Certain areas for improvement were identified following the initial surveys, particularly in relation to additional duties AHAs could be trained to perform. While cognoscente of the fact that AHAs cannot perform all technical or clinical duties of NMTs, there is certainly scope to enhance their administrative assistance within the department. The willingness of AHAs to take on additional duties, and NMTs being able to facilitate the necessary training, raises the potential to further explore this aspect of the model.
Shift allocation and rostered locations is another aspect we have been able to refine and improve over the past twelve months. Noting that early shifts if PET appeared to facilitate the best use of AHA resources. Similarly, having AHA staff available during lunch breaks, supplemented the technologist workforce, allowing us to maintain a consistent workflow throughout the day.
Conclusion:
The AHA model has proven successful in supplementing the NMT workforce, allowing for NMTs to prioritise critical patient related tasks, and improving workflow within the department. It has also proven to be beneficial to the NM undergraduate studies of our AHAs. This invaluable experience will allow AHAs to enter the workforce as NMTs with sound theoretical knowledge, and a more in-depth understanding of the clinical application. As such, the AHA model is not only beneficial in supporting our current workforce but may play a crucial role in growing and protecting the future workforce of NMTs.
References:
1. Bosley S, Dale J. Healthcare assistants in general practice: practical and conceptual issues of skill-mix change. Br J Gen Pract. 2008 Feb;58(547):118-24. doi: 10.3399/bjgp08X277032. PMID: 18307856; PMCID: PMC2233962.
VALE - MARIA TRIANTAFILLOU, VICTORIAN NMT
35
YEARS YOUNG
A biography written by Maria Triantafillou back in 2021, prior to her retirement from Monash Health in 2023.
I just cannot believe 35 years have flown by and in a blink of an eye.
I was asked to contemplate and go over what those 35 years mean to me.
My goodness where to start
In 1986 in joined the Nuclear Medicine team at the Queen Victoria Hospital, as a newly graduate Nuc. Med Tech, back then I was only working part-time.
In 1987, Queen Victoria Hospital closed its doors and moved to Clayton. I had the privilege of literally moving in the furniture/equipment that came along from the Queen Victoria Hospital. A new hospital and many opportunities to advance my knowledge and advance my career.
In 1989 Prince Henry’s Hospital also closed its doors and amalgamated with us expanding the department even further.
Over the years I had many opportunities and learning experiences.
In 2002 I completed my Post graduate Masters in Health Service Management through Monash University and Clinical School of Medicine at the Alfred Hospital. Back then all our classes were held in the building which also housed the American embassy. Getting in through security in 2002 was quite the feat with security being escalated due to unrest outside the American embassy in Pakistan.
I have had the opportunity over the years to publish scientific papers to and do oral and poster presentations. I thank all the staff for the support and encouragement in helping me with my presentations.
I was also an active committee member in two associations VSNMT and the ANZSNM.
I helped with the organisation of many CPD programs/ lectures/seminars. Was fortunate to organise a very successful annual conference for the ANZSNM in Melbourne back in 2005 and over 500 delegates nationally and internationally attending the conference. A few years later was again given the privilege of sitting on the committee to organise another annual conference for the ANZSNM in Melbourne.
In 2004 when Casey hospital opened its doors as a senior technologist, I was asked to set up the Nuclear Medicine department. Creating protocols and workflow processes. Overall, I work across the four hospitals in the network. It’s
amazing as each site has a different demographic of patients and different workloads and demands and yet our imaging protocols are uniform throughout.
In 2012 I was given the opportunity to learn Bone densitometry and be a member of the department.
So now I can say I work at four sites and in 5 departments. Through the years I have gained a wealth of experience has worked with an amazing group of people and have made many connections and lifelong friendships. And today I continue to keep learning and keep evolving.
I love to share knowledge and love to participate in education continuously.
In my spare time, I am very family oriented, and I am a proud grand aunt to three amazing kids, Marri, Christian and Kingston.
I love to travel, dinning out any time of the day (even have breakfast early in the morning before work).
Love live theatre, musicals, plays, the ballet. Love cooking and sharing recipes and bring lots of cakes to work (though for now we cannot share as we use to in the past). I also like reading, knitting going for walks, And shopping.
The last two years COVID has not allowed us to do a lot of these things. 2022 is ahead of us now. New opportunities, new beginnings.
And another year to my tally.
I would like to thank everyone in Monash Imaging for the amazing people you all are the amazing friendships we all have that make coming to work a pleasure.
2025 ANZSNM PAUL ORR MEMORIAL AWARD
PRUE LAMERTON, ONZM
Abstract - Breaking from cold to very hot, is not so bad
In 2022 plans began to design and build a transformative approach to a Molecular Imaging and Therapy healthcare facility with a shift away from the typical clinical atmosphere. The design elements integrated cultural awareness and cutting-edge molecular and therapy technologies to prioritise patient comfort and wellbeing.
The Hot Lab was strategically designed to facilitate the synthesis of Gallium-68 and Lutetium177 alongside the production of Technetium-99m radiopharmaceutical (RP) cold kits. Key priorities included optimizing space efficiency and ensuring robust radiation safety. Dedicated zones were established for the cold bench, hot bench and quality control equipment to maintain clear functional separation. Working closely with Bayer Radiology, the final design incorporated all the clinical requirements including the integration of the Intego® dose injector as well as ensuring that Canopy Imaging remains adaptable to future advancements in RP synthesis and therapeutic applications.
In New Zealand, Nuclear Medicine Technologists have historically broadened their scope to encompass
aspects of radiopharmacy and medical physics. However, the transitioning to performing RP synthesis and quality assurance for both diagnostic and therapeutic applications has introduced a level of complexity and specialisation that surpasses prior training and expectations.
While the initial Hot Lab synthesis and QA proved challenging, they offered valuable learning opportunities. We can now say Breaking from cold kits to Hot Synthesis is not so Bad.
2025 RAMACIOTTI MEDAL FOR EXCELLENCE
PROF MICHAEL
HOFMANN
Prof Michael Hofmann is the recipient of the 2025 Ramaciotti Medal for Excellence. Prof Hofmann has led transformational research in prostate cancer including landmark clinical trials contributing to the development of the PSMA PET/CT, a new whole body cancer scan, and PSMA radioligand therapy, a new targeted treatment. This has contributed to global change in clinical practice guidelines and management for men with prostate cancer
2025 SOUTH AUSTRALIAN SCIENCE EXCELLENCE + INNOVATION AWARDS FINALIST
DR ASHLEIGH HULL
Dr Ashleigh Hull’s research is advancing the development of novel radiopharmaceuticals for the detection and treatment of challenging cancers, including pancreatic cancer. Her work focuses on designing targeted agents capable of localising to, imaging, and destroying malignant cells which has has shown promising results in identifying and killing pancreatic cancer cells in earlystage studies and has potential to improve outcomes for people with hard-to-treat cancers.
In addition to her scientific contributions, Dr Hull has played an important role in strengthening Australia’s nuclear medicine capability. She has supported the development of safety protocols for emerging radioactive materials in South Australia, contributed to public education on the value and safety of nuclear technologies, and mentored early-career researchers to help build a skilled nuclear medicine workforce.
Dr Hull has secured more than $470,000 in competitive funding, over $20,000 in awards and scholarships,
and contributed to initiatives attracting over $5 million in investment, including a national $5 million training centre aimed at advancing Australia’s leadership in nuclear science and technology. Her work continues to drive innovation, capability development, and improved patient outcomes across the nuclear medicine sector.
2025 ANZSNM NUCLEAR MEDICINE TECHNOLOGIST AWARD
VICKY SIGALAS
Vicky was awarded the 2025 Nuclear Medicine Technologist Award recognition for her leadership in the field of nuclear medicine. In her current role, she provides high-level strategic guidance to the Australian Government on matters relating to the nation’s current and emerging nuclear industries, with responsibilities spanning nuclear safety, nuclear security and nuclear safeguards.
She has recently represented Australia on the international stage, including as part of the national delegation to the International Conference on Nuclear Security in Vienna alongside the Deputy Minister of Foreign Affairs. She also contributed to the establishment of a long-term international collaboration with Sweden and the United States focused on advancing nuclear safety in radioactive waste management, a program of work that will influence global nuclear safety initiatives for the decade ahead.
Her career has been shaped by courageous decision-
making, beginning with the installation of the first hybrid camera in clinical use in Australia and extending to her decision to step beyond the clinical environment at the height of her NMT career. By embracing vulnerability and navigating unfamiliar roles, she has set a powerful example for nuclear medicine technologists seeking diverse and impactful career pathways.
PRESIDENT
Prof Karen Jones (SA/NT)
Vice President
A/Prof Grace Kong (VIC/TAS)
Immediate Past President
Dr Kevin London (NSW/ACT)
Treasurer
Dr Daniel Badger (SA/NT)
FEDERAL COUNCIL
Prof Karen Jones (President)
Dr Kevin London (Immediate Past President)
Dr Daniel Badger (Treasurer)
Ms Suzanne McGavin (Vice President-Elect, Chair TSIG)
A/Prof Grace Kong (Vice President, Chair MSIG)
Dr Nigel Lengkeek (Chair RPS SIG)
Dr George McGill (Chair Physics SIG)
Ms Jessica Fagan (Chair of Branches/NZ Rep)
Prof Andrew Scott (IRC/Medical Rep)
SPECIAL INTEREST GROUPS/ COMMITTEES
Technologists
Chair: Ms Suzanne McGavin
Medical
Chair: A/Prof Grace Kong
Radiopharmaceutical Science
Chair: Dr Nigel Lengkeek
Physics
Chair: Mr George McGill
Quality and Technical Standards Committee
Chair: Dr Darin O’Keeffe
Scientific Advisory Panel
Chair: Prof Dale Bailey
International Relations Committee
Chair: Prof Andrew Scott
Conference Convening Committee
Chair: Prof Paul Roach
Scientific Education Committee
Chair: Prof Andrew Scott
ANSTO Representative
Annah Skillen
BRANCH
SECRETARIES
New South Wales/Australian Capital Territory
Holly Spooner
Queensland
Ms Neena Sunny and Ms Stephanie Schulz
South Australia/Northern Territory
Mr Jagi Sandhu and Ms Emily James
Victoria/Tasmania
Ms My Linh Diep
Western Australia
Ms Rosemary Dallen
New Zealand
Ms Rebecca Mangelsen
Rural/Regional Branch
Mr Lachlan Patterson
GENERAL MANAGER & SECRETARIAT
All Correspondence
Mr Rajeev Chandra, General Manager ANZSNM Secretariat, PO Box 6178, Vermont South, Victoria 3133
Tel: 1300 330 402 | Fax: (03) 8677 2970
Email: secretariat@anzsnm.org.au
AIMS AND OBJECTIVES OF THE AUSTRALIAN AND NEW ZEALAND SOCIETY OF NUCLEAR MEDICINE
1. Promote:
• The advancement of clinical practice of nuclear medicine in Australia and New Zealand;
• Research in nuclear medicine;
• Public education regarding the principles and applications of nuclear medicine techniques in medicine and biology at national and regional levels;
• Co-operation between organisations and individuals interested in nuclear medicine; and
• The training of persons in all facets of nuclear medicine.
2. Provide opportunities for collective discussion on all or any aspect of nuclear medicine through standing committees and special groups:
• The Technical Standards Committee sets minimum standards and develops quality control procedures for nuclear medicine instrumentation in Australia and New Zealand.
• The TSIG Committee is the group overseeing the Technologist Special Interest Group (TSIG) and ensures that all projects, committees and activities of the TSIG align with the values and strategic plan of the ANZSNM. It reports directly to the ANZSNM Federal Council and oversees the two TSIG working groups: CPD & Education Working Group and Technologist Workforce Advocacy Working Group. The committee is able to form working groups to perform specific tasks as required to provide opportunities for the benefit of Technologist members of the ANZSNM after consultation with the ANZSNM Federal Council.
• The Radiopharmaceutical Science SIG and a Physics SIG that maintain standards of practice for their particular speciality and provide a forum for development in Australia and New Zealand.
Scan the QR code to stay informed about job offers in the field of Nuclear Medicine.