A Hole in One: Uncovering A Diaphragmatic Leak with Nuclear Medicine
ARTnet Delivering Impact to Enhance Clinical Trial Site Accreditation and Dosimetry
Silly
Technologists
Radiopharmaceutical Sciences Special Interest Group
ARTNet
Quality and Technical Standards Committee
International Relations Committee
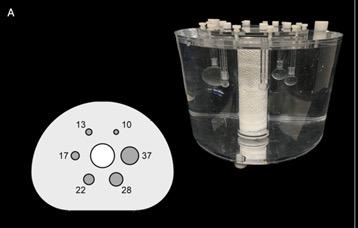
Silly Splenunculus - A Case Study
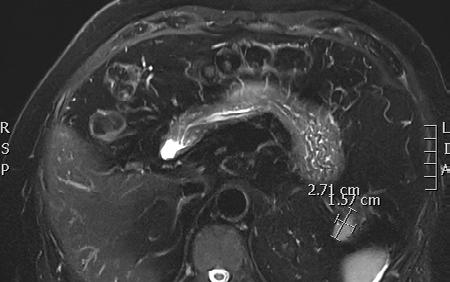
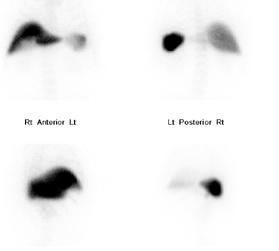
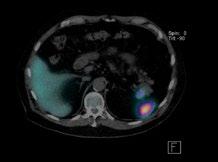
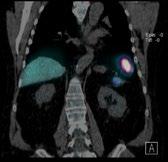
A Hole in One: Uncovering A Diaphragmatic Leak with Nuclear Medicine.
ARTnet Delivering Impact to Enhance Clinical Trial Site
Accreditation and Dosimetry
Piloting a paediatric nuclear medicine colouring-in book in Australia and New Zealand
Prue Lamerton, ONZM
Prof Andrew Scott
Prof Michael Hofmann
FROM THE PRESIDENT
W
elcome to the 2025 WINTER EDITION of the Gamma Gazette
Karen Jones President
The achievements of an organisation are the results of the combined effort of each individual.” Vince Lombardi (1913-1970)
Hello Fellow ANZSNM members,
The first half of 2025 has been filled with energy, growth, and a strong sense of connection, both within our Society and across the global nuclear medicine community.
Locally, our 55th Annual Scientific Meeting (ASM) in Melbourne was a landmark event, drawing a record number of 845 delegates. The diverse program featured leading national and international speakers, research presentations, case studies and invaluable networking opportunities. The event’s success was made possible through the outstanding efforts of Kunthi Pathmaraj and the Local Organising Committee, along with members of the Conference Convening Committee, whose commitment created a vibrant and memorable experience for all attendees.
In a key development for the ANZSNM, the newly formed Medical Special Interest Group (MSIG) held its inaugural meetings and began shaping its Terms of Reference. Led by Chair, A/Professor Grace Kong, who now sits on Federal Council, this group provides a distinct medical specialist voice within the ANZSNM, addressing issues unique to nuclear medicine specialists and a formal pathway onto Federal Council.
Supporting the future nuclear medicine workforce remains a priority, with the student placement grant program, in collaboration with the AANMS, continuing to alleviate the burden of placement poverty for nuclear medicine technologist students. The success of these grants reinforces our commitment to nurturing the next generation of nuclear medicine professionals and enhancing workforce sustainability.
Internationally, the World Health Organisation (WHO) Resolution on Strengthening Medical Imaging Capacity, adopted by the World Health Assembly (WHA) in Geneva in May, marks a pivotal moment for equitable access to advanced imaging, particularly in low- and middle-income countries. This resolution will foster improved healthcare outcomes through enhanced diagnostic and therapeutic capabilities. We congratulate Professor Andrew Scott for his tireless advocacy and leadership, which played a vital role in this international success.
The Nuclear Medicine Technologist International Consortium (NMT-TIC) continues to advance under the guidance of TSIG Chair, Suzi McGavin. This initiative unites technologist leaders from multiple international organisations, including the EANM, SNMMI-TS, ANZSNM, and IAEA, to develop best-practice technologist guidelines in theranostics. Suzi’s leadership exemplifies our commitment to both local excellence and global collaboration for nuclear medicine technologists. It was a profound honour to represent ANZSNM at the SNMMI Annual Meeting in New Orleans (21–24 June), where Australia and New Zealand were proudly featured as the 2025 Highlight Countries. This prestigious recognition provided a unique platform to showcase the innovation, research, and clinical excellence of our community on the international stage. The ANZSNM booth was a hub of activity throughout the meeting, delighting visitors with traditional Australian and New Zealand foods and wines, generously sponsored by Telix Pharmaceuticals, and lots of Tim Tams!
A standout was the recognition of Professor Andrew Scott, who was awarded both the prestigious Henry Wagner Jr. Lectureship and the Minoshima-Pappas Transformative Leadership Award at the SNMMI Annual Meeting. These honours acknowledge his exceptional contributions to the global advancement of theranostics and molecular imaging, as well as his visionary leadership in the field. His achievements are a source of immense pride for the ANZSNM and underscore the international influence of our region’s leaders.
Photos from the meeting can be found on our website, and a full recap will feature in the Summer Edition of the Gamma Gazette. Thank you to all who contributed to this outstanding representation of our region on the international stage at the SNMMI Annual Meeting. As legendary American football coach Vince Lombardi once said, “The achievements of an organisation are the results of the combined effort of each individual.”
We look forward to continuing this momentum and all the exciting initiatives planned for the rest of the year.
Best wishes
OUR CONTRIBUTORS
EDITORIAL COORDINATOR
Rajeev Chandra General Manager PO Box 6178, Vermont South, VIC 3133 T 1300 330 402 F (03) 8677 2970 gm@anzsnm.org.au
EVENTS & ADVERTISING ENQUIRIES
secretariat@anzsnm.org.au
SUBMISSIONS
secretariat@anzsnm.org.au
PUBLISHED IN
Winter & Summer
CONTENT SUBMISSIONS
Scientific submissions on all aspects of nuclear medicine are encouraged and should be forwarded to the Secretariat (instructions for authors published at https://www. anzsnm.org.au/activities/gamma-gazettecontent-submission-and-guidelines/).
Letters to the Editor or points of view for discussion are also welcome.
If original or public domain articles are found and considered to be of general interest to the membership, then they should be recommended to the Editor who may seek permission to reprint.
The ANZSNM Gamma Gazette is published two times per year. Deadlines for each issue of the journal can be found on our website anzsnm.org.au
DISCLAIMER
The views expressed in any signed article in the journal do not necessarily represent those of the Society. The individual rights of all authors are acknowledged.
Selina Warrington Sunshine Coast University Hospital
BRANCHES UPDATE
All the branches have had a fruitful start to 2025, with several committees welcoming new office bearers who have energetically carried on the work of their predecessors in putting together engaging events for their members. I had the pleasure of meeting many of the incoming branch chairs and committee representatives in person at the recent ASM.
This will be my final report as I exit the Chair of Branches role, handing over the reins to New Zealand branch chair Jessica Fagan. I wish Jessica all the best in carrying on what has been a truly rewarding endeavour for me within the society. It has been an absolute privilege to work with all the current and former branch chairs during my time in this role. Their energy and enthusiasm for their branches is truly inspiring, and I express my gratitude to them for their tireless efforts. I wish them every success for their future endeavours.
Queensland News
Queensland nuclear medicine departments have eagerly embraced the pilot Embedded Student Model (ESM) program in conjunction with RMIT University. There has been overwhelmingly positive feedback from the technologist workforce and students alike, and we are hopeful that the success of the model will lead to its rolling out in other parts of the country.
Our first branch meeting was held in March via Zoom, which was focussed on theranostics and was kindly sponsored by Siemens. We had 3 speakers and 60 online attendees. Our next branch meeting, sponsored by Telix Pharmaceuticals, will be held in June and will focus on regulation concerning the use of pharmaceuticals by nuclear medicine technologists.
The branch also looks forward to hosting members at the upcoming TSIG Annual Day Symposium at Home of the Arts on the Gold Coast on 2nd August.
Victoria & Tasmania News
The VIC/TAS branch opened the year as per tradition with our annual visit from Dr. Kim Williams on the 21st January. The hybrid event was well-attended and Dr. Williams delivered an engaging presentation.
It was a great pleasure to welcome the wider nuclear medicine community to the recent ASM in Melbourne, and we express our sincere thanks to committee members Kunthi Pathmaraj and My Linh Diep for leading the Local Organising Committee, whose indefatigable
efforts ensured the ASM was a resounding success.
The committee is busy at work planning for our remaining events for 2025, details to come soon!
South Australian & Northern Territory News
The SA/NT branch has been delighted to host our first two meetings for the year to excellent attendance. We look forward to welcoming members to our two upcoming events in June:
• Our first Technologist Group meeting, taking place on Wednesday 11th June, and
• The next SA/NT branch meeting hosted by Flinders Medical Centre on Thursday 26th June
We also congratulate Jess Watson on being awarded the 2024 Academic Student Prize by the University of South Australia. Well done Jess!
We encourage members to start looking out for case studies to enter for this year’s Radpharm Awards, taking place on Thursday 6th November, with further details to come.
Western Australia News
Our last Meeting of 2024 and AGM was hosted by PCH and sponsored by Siemens. Presentations were paediatric themed covering Theragnostics and PET they were given by Dr Shoba Ratnagobal, Dr Elizabeth Thomas, Dr Russell Troedson and Dr Sam Wellman.
Christian Testa, MANZSNM Outgoing Chair of Branches
We welcomed Cassandra Koudela as our new Chair taking over from Tiffany Briggs. WA Branch also has two new committee members Isabella Michael and Taylor Hope.
In 2025 we have held 2 inperson meetings hosted by SKG, GenesisCare and PRC. Sponsored by Siemens and GE Health Care. The first meeting was focused on pharmaceuticals and new therapy trials. A big thank you to our presenters, Kim Tao, Cindy Ha, Kylie Denis, Prof Joe Cardaci.
The second meeting had talks on thyroid, neurology and pregnant PET. These were done by Dr Shoba Ratnagobal, Stefanie Greyson, Dr Heidi Espedal and Richard Hampson.
Many WA Nuclear Medicine community members attended the ANZSNM conference in Melbourne. We are very proud Shiphrah Tagore of PRC and TelemedVET won the Radpharm award!
New South Wales & Australian Capital Territory News
It was a glowing start to the year for the NSW/ACT branch with a networking event held on 21 February. A wonderful crowd of nuclear medicine techs, biochemists and medicos from across the public, private and industry sectors ascended the heights of Babylon Rooftop and Garden Bar in Sydney CBD. We gathered not just to discuss cyclotrons or SUVmax, but to toast, mingle and make connections. A highlight of the evening were the hilarious and rowdy team games. Thank you to the efforts of the organising committee, and the ANZSNM for subsidising the event and facilitating the delicious spread.
Our CPD event ‘Molecular Imaging in Breast Cancer’ 9 April was very popular with 86 members registering. Special note of thanks to Dr Edward Hsiao, Lara Tomlin and Dr Zahra Sabahi for their insights on FDG PET/CT and the less well known role of FES and NeoB PET/CT. Congratulations to Zahra who was the lead author of a study on the diagnostic potential of NeoB PET/CT in ER/ PR positive breast cancer which was published in the Journal of Nuclear Medicine in March this year.
We look forward to welcoming you at the following upcoming events:
24/07/2025 Paediatrics in Focus
19/08/2025 Student Placement Information Night 30/10/2025 Radpharm & Student Award and AGM
Rural / Regional News
The rural and regional branch are currently seeking expressions of interest for new committee members. If you are a society member working in nuclear medicine in a regional or remote area and want to make an impact in this domain, we would love to hear from you! The committee is currently working on events for the remainder of the year, and welcomes ideas from regional, rural and remote members on event themes and other initiatives which would benefit your experience in nuclear medicine.
New Zealand News
Business as usual across Aotearoa NZ so far for 2025. We are looking forward to the upcoming NZ Symposium, September 13 & 14th in Palmerston North. Registrations are open and we encourage members to submit abstracts. We are also accepting entries for The Radpharm Award and Aotearoa NZ Remembrance Award to be presented at the Symposium.
MEET THE NEW MEDICAL SPECIAL INTEREST GROUP (MSIG)
Formation of the ANZSNM Medical Special Interest Group (MSIG)
Within the ANZSNM, Special Interest Groups (SIGs) provide a voice for specific professional cohorts, including the Technologist SIG (TSIG), Radiopharmaceutical Scientists SIG (RPS SIG), Physics SIG, and the Student Representative Council (SRC). However, a longstanding gap in this structure has been the absence of a medicalfocussed group to represent nuclear medicine specialists within the Society. This has been increasingly apparent as the ANZSNM is frequently invited to provide input on matters specifically impacting nuclear medicine specialists, often independently of other organisations. A further impetus came from a 2023 constitutional amendment, ratified at the 2023 AGM, requiring two nuclear medicine specialists to sit on the Federal Council. Unlike other professions within our society, however, there was no formal mechanism for medical specialists to be nominated or elected to Council.
The concept of a Medical SIG (MSIG) was discussed with AANMS President, Dr Paul Beech, during one of our regular Presidents’ meetings. I was pleased to receive his support, recognising the value of a medical group within the ANZSNM that could complement the role of the AANMS.
Following this, a survey was distributed in March to 148 ANZSNM members who are nuclear medicine specialists. The survey included four statements rated on a fivepoint Likert scale to assess interest in establishing a Medical SIG. We received 29 responses (~20% response
rate) from across Australia and New Zealand. Feedback was overwhelmingly positive, and the Federal Council formally endorsed the formation of the MSIG. Expressions of Interest were subsequently invited to form the inaugural MSIG Executive Committee, tasked with establishing the group and drafting its Terms of Reference.
The following members were appointed and elected their Chair at the first meeting:
• Associate Professor Grace Kong (Chair)
• Dr Kevin London
• Dr Jeremy Hoang
• Dr Tehereh Erfani
• Dr Edward Hsiao
At the recdnt AGM, Grace Kong was formally appointed as a Director on Federal Council. Since its formation, the MSIG has been highly active. Its Terms of Reference were endorsed by Council in May, and both Grace and Ed represented by ANZSNM at the AMA meeting in Canberra in June. Grace now joins me at the monthly Presidents’ meetings, providing an open line of communication between the ANZSNM MSIG and the AANMS.
I am confident the MSIG significantly strengthens ANZSNM’s capacity to advocate for our medical members and I look forward to working closely with Grace and the MSIG Committee in the months ahead.
Professor Karen Jones
ANZSNM President
A/Prof Grace Kong, MSIG Chair Nuclear Medicine Physician at the Peter MacCallum Cancer Centre (PMCC), Clinical Associate Professor at the University of Melbourne.
Being a member of the MSIG within the ANZSNM provides an important opportunity for nuclear medicine specialists to liaise and work with the other established ANZSNM special interest groups and collaborate with key medical organisations such as the AANMS to further advance the Nuclear Medicine specialty through the ANZSNM nationally and internationally. I respect and enjoy collaborating with people from different craft groups, representing the ANZSNM.
MEET THE NEW MEDICAL SPECIAL INTEREST GROUP (MSIG)
Dr Kevin London - MSIG Committee Member
Nuclear Medicine Physician at The Children’s Hospital at Westmead and, Alfred Nuclear Medicine and Ultrasound.
Over the years, I have had the privilege of contributing to various ANZSNM committees and serving on the Federal Council, including as President from 2022 to 2024. Through these roles, I have come to appreciate that the strength of ANZSNM’s relationships with other organisations in the nuclear medicine space is critical to advancing the field both nationally and internationally.
By joining the MSIG, I hope to help strengthen ANZSNM’s collaboration with key medical organisations such as the AANMS and to enhance our collective advocacy for nuclear medicine. I believe that through strategic partnerships and unified efforts, we can amplify the visibility, capacity, and impact of nuclear medicine in Australia and beyond.
Dr Jeremy Hoang, MSIG Committee Member
Nuclear Medicine Physician at Royal North Shore Hospital & Endocrinologist at Hornsby Hospital.
I am honoured to be part of the inaugural ANZSNM MSIG. I believe this will help strengthen the engagement and collaboration of the ANZSNM with key medical organisations such as the AANMS and I will endeavour to advocate for the interests of our medical members.
Dr Tahereh Erfani, MSIG Committee Member
Staff specialist in Nuclear Medicine and PET at John Hunter & Calvary Mater Hospitals and Conjoint Senior Lecturer at University of Newcastle.
As a passionate advocate for nuclear medicine specialists, I am committed to contributing to the advancement of our field through my involvement with the ANZSNM MSIG committee. The ANZSNM is a leading scientific organisation dedicated to development and promotion of nuclear medicine, and I am honoured to support its mission.
Through my role with MSIG, I aim to contribute to the strategic direction and growth of molecular imaging, while fostering collaboration with medical and nuclear medicine communities both nationally and internationally.
Dr Edward Hsiao, MSIG Committee Member
Senior Staff Specialist in Nuclear Medicine and PET at Royal North Shore Hospital
As a dual-qualified radiologist and nuclear medicine specialist, I am passionate about advancing patient care through the use of innovative imaging techniques. My work is concentrated on the clinical applications and research of PET/CT, molecular imaging, and theranostics, particularly within oncology. I am eager to contribute my expertise to the MSIG of ANZSNM, collaborating with peers to drive progress and to promote the latest advancements in our field.
TECHNOLOGIST SPECIAL INTEREST GROUP (TSIG)
Suzanne McGavin, MANZSNM TSIG Chair
As I reflect on the last Gamma Gazette report from Summer 2025, it’s remarkable to see just how much the TSIG has accomplished in only six months. This period has been one of growth, transformation, and impact. One thing that remains clear and unwavering is TSIG’s role as a strong, consistent advocate for Nuclear Medicine Technologists and Scientists (NMT/S) across our profession
We’ve continued to evolve and adapt, undertaking critical initiatives, engaging in consultations, awarding student grants, and forming new subcommittees—all with the aim of shaping TSIG into a forward-thinking Special Interest Group that responds to the changing needs of our workforce and industry.
Leadership Transitions and Acknowledgements
In May, we held our Annual General Meeting (AGM), where I reviewed our achievements over the past 12 months, outlined our strategic direction for the year ahead, and farewelled some of our valued committee chairs.
A heartfelt thank you goes to Erin Hemingway, who chaired the CPD&E Committee for the past two years. Under Erin’s leadership, the committee not only organised a series of impactful CPD events and launched the CPDValet app, but also hosted our largest TSIG Symposium to date—an incredible achievement. Thank you, Erin, for your energy, innovation, and commitment. We also said goodbye to Sarah Daniel, Chair of the WFA Committee. Sarah’s depth of experience and insight into workforce issues has been invaluable, and her leadership has helped drive important conversations around the workforce challenges our profession continues to face. Thank you, Sarah, for your thoughtful contributions and dedication.
As we bid farewell to our outgoing chairs, we warmly welcome our new leaders:
• Dr. Melissa Shields will lead the CPD&E Committee
• Kunthi Pathmaraj will chair the WFA Committee
I’m looking forward to collaborating with Melissa and Kunthi as we move into an exciting new chapter for the TSIG.
Broadening Our Scope
Beyond the CPD&E and WFA Committees, the TSIG now includes the Student Representative Council and our newly established Academic Reference Group, both under the University Liaison portfolio. These subcommittees, while distinct in their focus, share a common purpose: to support emerging technologists by understanding and addressing the evolving educational and training needs within the NMT/S community. I look forward to their renewed activity in the coming months and to seeing their positive impact grow.
Highlights from the Past Six Months
TSIG’s key accomplishments since the Summer 2025 report include:
Awarding an additional $10,000 in ANZSNM/AANMS Student Clinical Placement Grants, supporting 16 students (total now $20,000) and easing financial burdens during clinical placements.
• Engaging with the MRPBA and MRTB to strengthen relationships with our regulatory bodies and remain aligned with current and forthcoming changes.
• Nominating a TSIG member to represent ANZSNM on the Professional Capabilities Working Group, contributing to the development of future standards.
• Collaborating with the Indigenous Allied Health Association (IAHA) to develop a formal Acknowledgement of Country, soon to be endorsed by Federal Council.
Suzanne McGavin, MANZSNM, TSIG Chair
• Awarding academic excellence prizes to the topperforming NMT/S students of 2024.
• Partnering with ASMIRT to co-produce a career video promoting Nuclear Medicine as a dynamic and rewarding profession.
A Global Vision: NMTs in Theranostics
Among our most exciting undertakings is the formation of the Nuclear Medicine Technologists in Theranostics International Consortium (NMT-TIC). This global initiative brings together major professional bodies—including SNMMI, EANM, IAEA, and ANZSNM—to collaboratively assess, standardise, and improve education and competency frameworks for NMT/S in the growing field of Theranostics.
As Theranostics continues to evolve rapidly, the consortium’s work aims to provide clarity and support for NMT/S professionals striving to upskill and prepare their departments. This international partnership has been made possible through TSIG’s ongoing advocacy efforts and the strong global relationships we have cultivated through representation at key events.
Looking Ahead: What's Next for TSIG?
The remainder of 2025 promises to be both vibrant and productive. Planned activities include: Allocation of a further $10,000 in Student Clinical Placement Grants
• Revitalisation of our Mentorship Program— supporting early-career professionals and fostering guidance from experienced colleagues
• Attendance at SNMMI 2025, where ANZSNM is the
host society—showcasing the talents of Australian and New Zealand NMT/S through presentations, panels, and leadership roles
• Participation in the ARPANSA Medical Radiation Safety Guides Working Group
• Representation on the SNMMI-TS NuMe Advisory Group, contributing to the development of their mentoring application
• Hosting the Annual TSIG Symposium on August 2 in the beautiful Gold Coast
• Presentation of the prestigious Nuclear Medicine Technologist Award, honouring an outstanding leader in our field
Continued exploration of national or reciprocal licensing frameworks across Australia
Inaugural meeting of the Academic Reference Group
In Closing
Being part of the TSIG and its committees is both professionally rewarding and personally fulfilling. Our members work tirelessly—often outside of their clinical roles and personal commitments—to strengthen and uplift the profession. I am truly grateful for their passion, dedication, and service.
As we head into the colder months, I hope everyone finds time to rest, recharge, and reflect. Here in Darwin, the Dry Season brings cool evenings, golden sunsets, and a full calendar of festivals—an invigorating contrast to the winter blues experienced further south.
Stay well, Suzi
ANZSNM/AANMS Semester
1 2025 Student Clinical Placement Grant Recipients
Emily Fraser RMIT
Mikaela Burrows University of Newcastle
Landon Tesoriero University of Newcastle
Lachlan Thomas University of Newcastle
James Stevens University of Newcastle
Meghan Andren University of Newcastle
Jason Good University of Newcastle
Hanna John University of Newcastle
Kate Gilmour University of Newcastle
Alicia Langley Charles Sturt University
Ebony Rayner University of Newcastle
Bianca McCann University of Newcastle
Erin Brown Charles Sturt University
Jacob Cobner University of Newcastle
Joey Da Zhao Tan RMIT
Ashleigh Innes University of Newcastle
CPD&E UPDATE
Dr Melissa Shields, MANZSNM Chair TSIG CPD&E Committee (cpdechair@anzsnm.org.au)
The TSIG CPD & E committee has recently changed chairs, with Melissa Shields taking over from Erin Hemingway. Erin has done a wonderful job over the past two years, growing the committee from strength to strength. Over the past 12 months, highlights from the CPD & E committee include:
The committee had six meetings and a further eight symposium planning meetings.
Delivered four engaging webinars:
• Winner’s Circle – celebrating the ASM Technologist winners (June 2024)
• Nuclear Medicine & Molecular Imaging Week (October 2024)
• CPDValet Information Webinar (November 2024)
• International Women’s Day Webinar (March 2025) –in collaboration with Women in Nuclear (WiN) and European Association of Nuclear Medicine Women’s Empowerment (EANM WE)
Held the Annual TSIG Day Symposium in the Hunter Valley, NSW (August 2024). Our successful collaboration with the Hunter Technologists Group led to a record attendance of 105 delegates from six states and territories.
Trialled and endorsed CPDValet as the new CPD logging platform for ANZSNM members, providing feedback and support during its rollout.
Contributed feedback via consultations on key sector documents, including:
MRPBA Low-value care and informed consent
ANZSNM Quality and Technical Standards
• AHPRA Good Clinical Practice Document
• MRPBA Professional Capabilities
Additional initiatives include:
• Supported the ANZSNM Student Representative Council (SRC) committee
• Investigated Diagnostic CT credentialling for NMTs
• Contributed to a Nuclear Medicine Fact Sheet for the ANZSNM website
The current CPD & E committee comprises of eight women from three different states and New Zealand.
• Melissa Shields (Chair) – University of Newcastle, NSW
• Erin Hemingway (Immed Past Chair) – Gosford Hospital, NSW
• Kym Barry – Charles Sturt University, NSW
• Ellie Kelliher – Royal North Shore Hospital, NSW
• Clare McKenzie – Palmerston North, New Zealand
• Stephanie Schultz – Gold Coast, Qld
• Shikha Sharma – St Vincent’s Hospital, NSW
• Elaine Tija – Perth, WA
These women volunteer their time to deliver a diverse range of CPD opportunities for technologists while actively representing members interests.
We have an exciting year ahead, filled with further initiatives to foster learning and collaboration. These include:
The 2025 Annual TSIG Day symposium at HOTA on the Gold Coast QLD on Saturday 2nd August. In collaboration with the ANZSNM QLD Branch, this event promises a day of high quality, technologist focused presentations.
• Launching a journal club for ANZSNM members.
• Continuing to support the ANZSNM SRC committee and provide new support to the ANZSNM Mentor/ Mentee program.
• Undertake the biannual review of the ANZSNM awards.
Melissa Shields Bio
Melissa was a nuclear medicine technologist for 24 years, working in various departments throughout Wollongong and Sydney. She has been an academic at the University of Newcastle for 6 ½ years. Melissa was recently awarded her PhD titled “Burnout in Australian Nuclear Medicine Technologists”. She is passionate about providing education for nuclear medicine technologists, from students through to qualified NMTs, and is a firm believer that we are all life-long learners.
Erin Hemingway and Melissa Shields, CPD&E Committee
The ANZSNM TSIG WFA committee is currently focusing on critical aspects that impact the nuclear medicine community, such as the national workforce shortage of nuclear medicine technologists, understand and interpret issues relevant for ANZSNM technologist members from the Medical Radiation Practitioners Board of Australia (MRPBA), the New Zealand Medical Radiation Technologists Board (NZMRTB) and other health authorities such as the Department of Health, work with educators, universities and high schools to promote nuclear medicine as a profession, and review applications via the Overseas Qualification Assessment program.
The TSIG WFA is currently represented by the following membership:
• Elizabeth Brettschneider
• Pru Burns
• Louise Campbell
• Sarah Daniel
Katherine Guerrero
Lauren Marks
Suzanne McGavin (Chair, TSIG OC)
Kunthi Pathmaraj (Chair, TSIG WFA)
We are currently seeking expressions of interests from our colleagues in NSW/ACT, WA and NZ to join the WFA team. Please write to the ANZSNM secretariat if you would like to join the WFA team, we look forward to interested members contributing to our committee.
As the incoming chair, I would like to thank Sarah Daniel for the leadership she has provided thus far. I look forwards to working with the TSIG WFA committee, the TSIG CPD & Education Committee, TSIG Oversight Committee and the wider nuclear medicine community towards achieving meaningful outcomes for our workforce and profession.
Kunthi Pathmaraj, Chair, TSIG WFA
As I sit down to write this report, my final “official” duty as the outgoing TSIG WFA Chairperson - I want to begin by acknowledging the incredible time and effort contributed by members of the WFA and other TSIG committees. We’ve worked diligently to ensure ANZSNM has responded to and provided consultation on key issues, regulatory changes, and policies impacting Nuclear Medicine Scientists/Technologists across Australia and New Zealand. The dedication shown by each member, outside of their regular duties, is a true testament to their commitment to our profession.
Some highlights since my last report in the Gamma Gazette include (but are not limited to):
• The Occupation Standard Classification for NMT/S has been updated to be more descriptive, offering greater clarity on roles and responsibilities.
NMT/S remains on the Occupation Shortage List for 2025.
In Queensland, amendments to legislation have allowed students enrolled in accredited tertiary programs to bypass the previously lengthy application process for student radiation licences through prescribed licences. This has significantly reduced the workload for education providers, students, and clinical facilitators.
NMT/S has been added to the Core Skills Occupation List (CSOL).
Although I’m stepping down as Chairperson, I will remain an active member of the TSIG WFA. I’m confident that our newly appointed Chairperson, Kunthi, will bring her extensive experience, passion, and expertise to the role—fostering growth and aligning with the strategic direction of the organisation.
Sarah Daniel, Immediate Past Chair, TSIG WFA
Kunthi Pathmaraj, MANZSNM, WFA Committee
UNIVERSITY LIAISON UPDATE
Emma Brook, MANZSNM University Liaison
Farewell from the TSIG University Liaison
As I come to the end of my term as University Liaison for the TSIG, I want to take a moment to reflect on what has been an incredibly rewarding and impactful journey.
Over the past three years, it has been amazing to help shape and influence this new role - working alongside an inspiring group of passionate and dedicated nuclear medicine technologists across Australia and New Zealand. Collaborating with such a committed community has been both energising and humbling, and I’m deeply grateful for the trust, support, and encouragement I’ve received along the way.
During my time in this role, I’ve had the privilege of:
Being involved in the early development of the Academic Advisory Committee — an evolving initiative that aims to strengthen collaboration between academia and the profession. I look forward to watching this exciting initiative continue to grow and make a lasting impact. Supporting dialogue between the ANZSNM TSIG and educators to bridge academic and clinical practice, with a focus on enhancing the student experience.
• Mentoring and advocating for the Student Representative Council — an energetic and engaged group who continue to bring fresh ideas and strong representation to the profession.
• Overseeing the introduction of the Student Grant Program — a collaborative initiative between the AANMS and ANZSNM — which provides financial support for students during clinical placements and enables greater access to professional development opportunities, particularly for rural, interstate, or other high need regions.
One of the greatest honours has been the opportunity to support and influence the next generation of nuclear medicine professionals. To have played a part in mentoring emerging talent and helping shape future leaders is something I will always hold close.
As I hand over this role, I encourage anyone with a
passion for education, mentorship, and connection to consider stepping in. It’s a role that offers deep professional fulfilment, meaningful relationships, and the chance to leave a lasting impact.
Thank you again to everyone who has collaborated, challenged, and inspired me during this time. It’s been a true privilege.
Emma Brook UniSA - Kathy Guerrero
In April academic staff attended the graduation ceremony of the 2024 graduates. This is a wonderful celebration for graduands as they celebrate their achievements over the course of the program. Congratulations to Jess Watson, recipient of the ANZSNM prize for academic achievement. We also congratulate Jess on being the awarded the UniSA University Medal. This is an outstanding achievement awarded to the top 0.5% of graduands across the university. Wishing all the graduates all the very best for your future in nuclear medicine. It has been a pleasure to teach you all over the last 4 years and we look forward to continuing to see you in the nuclear medicine community as professional colleagues.
We have increased the enrolment of students to the program in response to workforce need and recognized the important of early program and industry engagement of new students. The first years have completed a series of professional workshops to introduce them to the profession. They recently attended a “meet and greet” that allowed them to meet with many industry professionals. They also attended a tour of the Women and Children’s Nuclear medicine department and met staff as well as fourth year students. It was fantastic to see the first years engaged and excited about embarking on their nuclear medicine journey.
Emma Brook, MANZSNM, University Liaison
The UniSA Nuclear Medicine team recently attended the ANSZNM ASM. Here we celebrated UniSA Honours student Jess Watson being awarded the Sumitomo Student award for her honours thesis “Evaluating the expression pattern of MUC1-CE in head and neck cancers for potential application in radioimmunotherapy.”
2026 will bring the merger of UniSA and University of Adelaide as the new Adelaide University is launched. The Nuclear Medicine program will initially remain largely unchanged in structure. Longer term we envision the merger expanding opportunities and resources in both teaching and research. Adelaide University launched into the 2026 QS World rankings at 82nd confirming its place in the global top 1%.
Charles Sturt University update – Kym Barry
This year has been off to a great start with welcoming a new first year cohort to both our Wagga Wagga and Port Macquarie campuses in March and then celebrating graduation ceremonies for our graduates occurring in May. It was great to catch up with the graduates and hear about their first few months working since graduation. We congratulate our recent graduates and wish them well in their future as nuclear medicine technologists!
We have participated in several outreach and information events already this year, taking these opportunities to spread the word and tell prospectives students about careers in nuclear medicine. Here are a couple of events from this year so far:
Explore Day
Explore Day is an on campus event at both campuses where students can visit our campuses and get a chance to experience university life. As part of this, we held some hands-on workshops in our nuclear medicine spaces. These workshop sessions saw excellent numbers of students attending and feedback from students was really positive.
Careers Expo
Nuclear medicine was showcased at a local careers market in Port Macquarie in May. Over 1000 school students from mid north coast schools attended this expo event. Nuclear medicine was represented at our Medical Radiation Sciences booth where students were shown some nuclear medicine images and asked to guess what was being imaged. This provided a great opportunity to talk to students about nuclear medicine and the role nuclear medicine plays in patient management. There was a lot of engagement at this event, with many students who we talked to who had some understanding of nuclear medicine, which was very encouraging.
University of Auckland - Pippa Bresser PGDipHSc (Nuclear Medicine)
We currently have ten students who hold clinical training positions that are enrolled in various courses across the Nuclear Medicine programme at different stages in their programme. We are anticipating at least another three students to be onboarded in clinical training positions shortly in preparation for semester two. A new student mentoring programme was established in the Postgraduate Diploma in Health Sciences in Nuclear Medicine. The purpose of this mentor programme is to connect our current students (as mentees) to recent graduates (mentors). We have matched the mentees and mentors for this year and we are looking forward to hear about their progress and engagements later in the year.
Autumn graduation
Students who completed their programmes in 2024 were invited to graduate at a ceremony on Tuesday 14th May at Spark Arena. It was wonderful to see our undergraduate and postgraduate students including four Nuclear Medicine graduates walk proudly across the stage to receive their diplomas and degrees. Congratulations to Kate Harvey, Shelly Lyford, Holly Stirling and Olivia Wallace who ALL received their postgraduate diplomas with Distinction.
PGCertHSc (PET-CT) Certificate
We are pleased to announce that Te Poari Ringa Hangarau Iraruke | the Medical Radiation Technologists Board confirmed accreditation of the Postgraduate Certificate in Health Sciences in PET-CT (PGCertHSc PET-CT) on 11 April 2025. The programme has officially launched this year with the first cohort of students undertaking their academic courses online while gaining clinical experience. The programme consists of a combination of academic and clinical components, both of which students must successfully complete to demonstrate competency.
Students may choose to complete one or two courses each semester with the maximum time allowed for completion being two years. The students received access to their electronic clinical portfolio (e-Portfolio) on our new e-Portfolio platform, PebblePad. We look forward to seeing some of the students in this first cohort over the finish line in November.
Theranostics course
The new 15-point course (MEDIMAGE 729: Theranostics) is currently being developed. We are excited to roll out this course for the first time as part of the PGDipHSc Nuclear Medicine suite of courses from next month (Semester 2, 2025). The course is also suitable to be undertaken as a one-off course (Certificate of Proficiency) for registered Nuclear Medicine Technologists for their Continuing Professional Development (CPD). For more information please see the course outline here: https://courseoutline. auckland.ac.nz/dco/course/MEDIMAGE/729/1255.
RADIOPHARMACEUTICAL SCIENCES SPECIAL INTEREST GROUP (RPS)
Nigel Lengkeek, MANZSNM Chair, RPS SIG
The RPS SIG of the ANZSNM is in the best shape I have seen since joining the ANZSNM. We have a committee of six RPS members committed to improving member engagement and community content. In April we launched the RPS seminar series with three speakers, Nikita Safonov, Adam Kennedy and Saikat Ghosh, with over 30 members attending. Details for the second seminar will be announced soon. If you are interested in presenting in a safe and supportive environment of community members, please reach out to the RPS committee. If you missed the presentations, head over to EduTrace to watch them on demand.
The 2025 ANZSNM ASM was a resounding success driven by the outstanding efforts of the local organising committee and the record number of attendees at the meeting. If you attended the ASM I hope you picked up your membership badge during the conference, and if not, reach out to you local state branch representatives to collect one. Despite potential competition from the iSRS 2025 meeting held the week prior the RPS community had an excellent showing at the ASM with some of our best presentations to date. Well done to everyone who made it out for the Saturday morning ‘Fun Run’, it was thankfully a litter warmer than the previous mornings in Melbourne and it made the run along the Yarra enjoyable.
At the ASM, Talia Enright (Austin Health), announced the 2025 Survey of the Radiochemist Workforce in Australia, Survey 1 - Current State of Radiochemistry. This is a crucial first step in building an understanding of the RPS workforce across Australia, and from it developing training and development initiatives for the current and future RPS workforce. The initiatives will only be as good as the data the survey collects so I encourage you to complete the survey (thank you if you already have) and share amongst your colleagues in the community across hospitals, universities, research institutes and private industry. Thank you to Talia for spearheading this
initiative.
As we shift gears to planning for the 2026 ANZSNM ASM in Canberra it presents a unique opportunity for the Nuclear Medicine community to engage with federal government ministers and departments, as well as our regulators. Promoting the importance and impact of our work to government while highlighting the challenges and barriers we face will allow us to work with government on solutions to deliver better patient care through the advancement of Nuclear medicine. As per previous years the Australasian Cyclotron users group meeting will be held just prior to the ASM, so look out for details if you are part of that community as well.
To turn a bad pun, the hottest emerging radioisotope at the iSRS 2025 was At-211, an alpha emitter with a simplified decay chain compared to other Target-AlphaTherapy radioisotopes such as Ac-225 and Pb-212, a favourable half-life of 7.2 hours and radiochemistry similar to iodine radioisotopes. Check out this open access review, Astatine-211 radiolabelling chemistry: from basics to advanced biological applications | EJNMMI Radiopharmacy and Chemistry | Full Text, if you want to learn more. Production of At-211 requires a ~28-29 MeV alpha beam (via 209Bi(α,2n)211At) that is currently inaccessible in Australia. The ANZSNM maintains a position paper on the need for a medium-to-high energy cyclotron in Australia through the Scientific Advisory Panel, but there is much more work we need to do as a community to justify and fund such a facility to benefit the clinical and research communities. Stay safe and well over Winter,
Nigel Lengkeek, RPS SIG Chair
Nigel Lengkeek, MANZSNM, RPS SIG Chair
ARTNET UPDATE: ARTNET WELCOMES EXCITING NEW PARTNERSHIP!
Samantha Hawkins Project Manager, ARTnet
ARTnet is excited to announce a new strategic collaboration with the National Imaging Facility (NIF), through their Human Molecular Imaging Translational Network, a national-scale initiative aimed at transforming cancer imaging, dementia diagnosis, and radiopharmaceutical development. Launched at the recent ANZSNM annual meeting in Melbourne, this $10 million, 3-year project brings together 10 imaging research facilities across Australia to streamline molecular imaging research and create new opportunities for clinical trials.
Through a newly signed Memorandum of Understanding (MOU), ARTnet and NIF will work together to enhance the capacity and capabilities of molecular imaging across Australasia. This partnership will help harmonize imaging protocols, expand the ability to conduct multicentre clinical trials, and drive innovations in the treatment of cancer, dementia, and more.
ARTnet’s Executive Chair, Dr Kevin London, expressed enthusiasm for the partnership, stating, “This collaboration marks a significant milestone in advancing
molecular imaging
research in Australia.”
Professor Roslyn Francis, ARTnet's
Scientific Committee Chair, also highlighted the potential impact: “We are eager to combine ARTnet’s goals with the NIF’s mission to deliver high-quality imaging capabilities and better patient outcomes across critical health areas.”
This partnership supports ARTnet’s ongoing commitment to accelerating research and improving patient care through radiopharmaceutical trials and innovative nuclear medicine. We look forward to working closely with NIF to achieve our shared objectives and bring cutting-edge therapies to the clinical stage.
Stay tuned for more updates on this exciting collaboration!
What the committee is working on ... what should we be working on?
The committee is still working on updates to the PET quality standard, the in-house production of radiopharmaceuticals, looking at some aspects of GFR measurements/results reporting, collecting information on dosimetry practices in radionuclide therapy, and the routine quality control of radiopharmaceuticals. Work on the minimum QC schedule for dose calibrators and the routine quality control of gamma cameras have both been paused awaiting reports from other organisations. We are also waiting on the ACPSEM to release the results from the ACPSEM-ANZSNM survey on radiation safety in radioiodine therapies. Thanks again to all those who contributed to that survey.
What should we be working on? If you have a technical or quality standard concern, or an idea you would like to propose, please discuss it with your Branch or SIG representative, or email the QATSC chairperson, Darin O’Keeffe, at QATSC@anzsnm.org.au
Recent changes to technical standards and practice guidelines
Some recent changes to technical standards and guidelines that may be of interest to members and of relevance to future ANZSNM guidelines.
NEMA NU-2 2024 - PET
In October 2024 the National Electrical Manufacturers Association (NEMA) published an update to the NU-2 standard for “Performance Measurements of Positron Emission Tomographs”. The listed changes are rather minor (they are documented in the Forward of the free preview – click on “Buy” using the above link) but do include a move from regions of interest (ROIs) to volumes of interest (VOIs) for image quality checks – changing the number and location of background variability measurements, for example. It will likely be a while before manufacturers specify equipment performance against the new 2024 standard, but we wanted members to be aware of the change.
ACR Nuclear Medicine QC Manual
Late last year the American College of Radiology (ACR) released a document called the “Nuclear Medicine Quality Control Manual”. The document is structured similar to the other free ACR quality control manuals: a Physician’s Section, a Technologist’s Section, and a Medical Physicist’s Section. The technologist and medical physicist checks are similar to the ANZSNM minimum quality control schedule for gamma cameras, except the ACR manual includes dose calibrator, thyroid uptake probe, and well counter QC checks as well. It’s worth a read if these checks are your responsibility.
The ACR have also just closed submissions on a draft PET Quality Control Manual. Hopefully it won’t be long before that is available as well.
QATSC session at the Annual Scientific Meeting in Melbourne
We held another very successful QATSC session at the Annual Scientific Meeting in Melbourne in May 2025. The session was titled “Theranostics Confidently: The Beta Emitters” and featured a line-up of three speakers and chairperson, Alicia Corlett, from the Peter MacCallum Cancer Centre. Lachlan McIntosh spoke on “Dose calibration of non-standard radioisotopes”, Michael Gilhen on “The role of radiation safety in the growth of nuclear medicine”, and Lisa MacFarlane on “Post radionuclide therapy imaging - practical considerations”. Thanks to all those who contributed to the session.
The feedback we received was great and we plan to negotiate with future conference convenors to run further QATSC sessions.
Resources Update
The ANZSNM does not necessarily endorse these free resources. They are provided here simply to notify members of their existence. If you come across a useful quality or technical standard, or other resource, please email the details to QATSC@anzsnm.org.au so it can be considered for inclusion in future QATSC updates.
This publication fits under the category of “Other resources”: Springer have a series of texts on diagnostic imaging, referred to as the IDKD Springer Series. The most recent update is on the chest, heart, and vascular system. The claim of the IDKD series is that “The world-renowned International Diagnostic Course in Davos (IDKD) represents a unique learning experience for imaging specialists in training as well as for experienced radiologists and clinicians".
The open access texts are all dated to reflect the need for regular updates and they certainly look interesting. Perhaps someone would like to share their thoughts on the quality and accuracy of the contents?
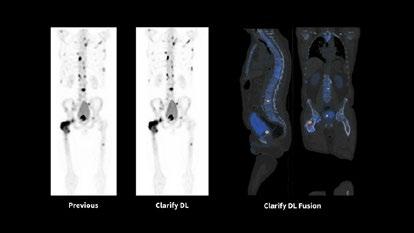
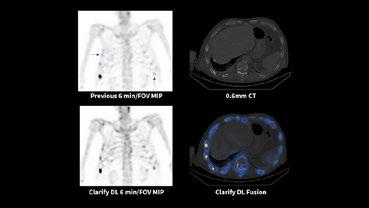
One Powerful Platform. Future-Proofing Clinical Possibilities.
Introducing the NEW Siemens Healthineers Biograph Trinion – a fully integrated digital PET/CT system that combines bestin-class PET, CT, and syngo.via software into one highperformance platform1.
Designed with both patient comfort and user efficiency in mind, Biograph Trinion redefines the imaging experience through intelligent AI-supported workflows, seamless automation, and a compact, modern footprint that supports energy-saving features and on-site scalability.
Delivering outstanding small lesion detectability, excellent quantification, and ultra-fast time-of-flight performance2, the Biograph Trinion enables personalised scan times and the use of any radiotracer without compromising image quality. Intelligent Applications power motion-free images without external gating devices—helping you advance clinical confidence across oncology, cardiology, neurology, theranostics, and more3
Biograph Trinion - your next-generation PET/CT.
Make confident diagnostic decisions backed by improved small lesion detectability and effective sensitivity.
Have intelligent imaging tools and advanced reading solutions for molecular imaging and CT at your fingertips.
Offer patients the latest in diagnostic image quality, speed, and dose reduction with nextlevel CT.
PET
PET/CT CT
INTERNATIONAL RELATIONS COMMITTEE
Andrew Scott, MANZSNM Chair, IRC
Following the announcement of Australia and New Zealand as the Highlight Countries of the SNMMI annual scientific meeting in June, the IRC has been involved in the co-ordination of the activities and the planning for the Continuing Education sessions which ANZSNM will be presenting at the conference. This will be an opportunity to highlight the accomplishments and forward plans of our nuclear medicine community in policy, workforce training, clinical practice and evidence-based clinical trials.
The IRC has continued to engage with SNMMI and EANM regarding harmonisation of PET and SPECT camera credentialling, with Dale Bailey playing a key role in the validation and acceptance of final protocols. It is proposed to have a memorandum of understanding signed by ANZSNM, SNMMI and EANM (EARL) regarding mutual acceptance of credentialling by each group in the next few months.
In conjunction with all major International nuclear
medicine organisations, a Resolution on “Strengthening Medical Imaging Capacity” is to be voted on at the World Health Organisation (WHO) World Health Assembly in May this year. ANZSNM through the IRC has had a key role in this Resolution being developed, and which builds on the impactful Lancet Oncology Commission on Medical Imaging and Nuclear Medicine, and Lancet Oncology Commission on Radiotherapy and Theranostics, for which ANZSNM has been a formal supporter. This WHO Resolution will have major impact on policy at a Government level throughout the world, and we look forward to the outcome of this vote.
The ANZSNM ASM will have representation from the SNMMI and EANM leadership during the meeting, and the IRC has been involved in planning and facilitation of the attendance of these leaders at the meeting.
Members of the IRC have also had input into policy and guideline meetings at the IAEA over the last 6 months, in the areas of Theranostics training and global access.
ANZSNM ASM 2025 Highlights
Kunthi Pathmaraj Chair of the Local Organising Committee (LOC), on behalf of the LOC (Jessica Welch,
MyLinh
Diep,
Mohammad
Haskali, Sze Ting Lee and Bonnia Liu)
The 55th Annual Scientific Meeting of the ANZSNM was held at the Melbourne Exhibition and Convention Centre between May 23-25, 2025, based on the theme, “Fusion of Foundation and Frontiers”.
Our ASM brought together the different multidisciplines in our profession, including nuclear medicine physicians, radiologists, nuclear medicine technologists, radiopharmaceutical scientists, medical physicists, nurses, researchers, industry partners, students, educators and volunteers from Australia and around the world.
The total number of registrations was a staggering 845, a testament to the dedication of our nuclear medicine community to their efforts in growing and developing our profession to international best standards of practices, both in the clinical space and research space. There were 96 oral presentations and 83 poster presentations via the formal abstracts submission pathway. Australian and New Zealand states and territories made their presence felt, 48 from New Zealand, 4 from Australian Capital Territory, 206 from New South Wales, 5 from Northern Territory, 92 from Queensland, 50 from South Australia, 6 from Tasmania, 332 from Victoria and 19 from Western Australia. Overseas attendees totalled 75 and they came from far and wide including Canada, Austria, China, France, Germany, Hong Kong (SAR China), India, Indonesia, Israel, Italy, Japan, Kenya, Malaysia, Netherlands, Pakistan, Republic of Korea, Singapore, Switzerland, Taiwan (Province of China), United Kingdom, United States Minor Outlying Islands, and United States of America.
Industry partners, sponsors and exhibitors were strongly represented at the ASM. We had 36 sponsors, in the trade hall, promoting strong networking amongst stake holders. Our sponsors and exhibitors are vital to the growth and strength of nuclear medicine, and we are grateful for their contributions to the nuclear medicine community.
Two noteworthy local speakers delivered the highly esteemed Pioneer Lecture and Lowenthal lecture this year.
Professor Vijay Kumar, Head of Radiopharmaceutical Research, at the Department of Nuclear Medicine & PET at Westmead Hospital & The Children's Hospital at Westmead, NSW, and Clinical Professor, at the Sydney Medical School, Sydney University, could not attend the meeting in person to deliver the Pioneer Lecture, but he provided an excellent recorded presentation. Vijay eloquently described his perspectives on the pioneer lecture reflecting that if we are enjoying advanced technology in nuclear medicine today, it is due to the fact that we stand on the giant shoulders of our pioneers in this field. He spoke about Charles de Hevesy as a pioneer who was the first to demonstrate the tracer uptake in plants and the circulation of tracer drug in rabbits. He spoke of Theranostics being the state of the art for certain types of cancer management and that the pioneers in the field have contributed enormously by way of advancements in PET, cyclotrons, PET scanners, Ga-68 generators, bifunctional chelators,
and generated a huge volume of clinical data in a short period, enabling the success in Theranostics that we witness today.
This year’s Lowenthal Lecture was delivered by ANZSNM President Karen Jones and was entitled ‘From gut feelings to facts - solving the mysteries of the stomach’. Karen shared a deeply personal and inspiring journey, tracing her path from childhood curiosity to qualifying as a nuclear medicine technologist, and ultimately pioneering a research pathway by completing a PhD, at a time when no formal program existed for medical radiation graduates in Adelaide. She went on to establish an independent research program, highlighting the power of perseverance, innovation, and serendipity in shaping a purposeful career. Karen’s lecture reflected on her 33 year contribution to clinical research, focusing on the pivotal role of gastric emptying in regulating blood glucose and blood pressure in both health and diabetes. She also emphasised the importance of collaboration and complementary expertise, reinforcing the value and strength of diversity, not only in clinical research but within the ANZSNM community.
We were very fortunate to have amidst us renowned
international and local speakers, who accepted our invitation to speak and share the latest developments in their areas of expertise. We were witness to high calibre presentations by international speakers, Prof Cathy Cutler, Prof Prem Soman, Prof Bital Savir-Baruch, Julie Bolin and Dmitry Beyder from USA, Prof Felix Mottaghy from Germany, Dr Savvas Frangos from Cyprus, Prof John Buscombe from UK. Dr Ngai, Prof Bailey, Dr Owen, Dr Liu, Prof Emmett, Prof Better, Dr Danon, A/Prof Sivaratnam, A/Prof Taubman, A/Prof Shembri, Dr Hogg, Prof Rowe, and Prof Scott presented outstanding lectures and updates, showcasing the talent and expertise in the local landscape. Invited speakers made excellent contributions to the pre-conference symposium which was themed on neuroscience, the three plenary sessions (Oncology, Cardiology and Musculoskeletal), scientific sessions, panel discussions, special interest group sessions, breakfast and lunch sessions, read with expert sessions and panel discussions which generated healthy debates. The sessions ran smoothly thanks to the speakers and chairpersons.
There was fierce competition for the scientific awards and research grants, making it quite challenging for the judges to single out winners. The ANZSNM extends warm congratulations to the award winners of the 55th ASM: Dr Bonnia Liu (ANSTO / ANZSNM Research Grant), Ya Ruth Huo (AANMS Registrar Research Grant), Lisa Nguyen (Landauer Award), Nicole Ayars (GMS Poster Award), Catherine Dickmann (The RAPHAEL Student
Research Award), Jess Watson (The Sumitomo NMT Research Award), Giang Ngo (2025 ANZSNM Victoria/ Tasmania Student Oral Presentation Award), Shiphrah Tagore (RadPharm Award), Zhipeng Cao (Shimadzu Award) and Jessica Van Zuylekom (Telix, ‘Best of the Best’ Award). A Special Recognition Award was presented to Russell Booth, a highly respected Victorian Nuclear Medicine Technologist. Russell recently retired after an extraordinary 50 years of service at St Vincent’s Hospital, Melbourne. A true pioneer of nuclear medicine, his quiet leadership, unwavering dedication, and tireless advocacy have profoundly shaped the profession, leaving a legacy for generations of technologists across Australia and New Zealand.
The social events were a huge success, starting with the Welcome Reception on the opening night. It would be a great injustice not to mention the awe created by the oyster shucking theatrics at the welcome reception!
The Award Dinner was an evening of celebration and elegance; inspired by our beloved imaging techniques, our dress theme was “Black & White with a Twist” with the intent to embrace the timeless greyscale aesthetic, accentuated by the dynamic hues of our favourite colour spectrum. To quote Bonnia Liu, the intent of the theme was “Feel free to adjust your personal style as boldly or subtly as you wish. After all, you control the windowing!” The band was hugely popular, and it was hard to find space on the dance floor.
The fun run was a resounding success too; we had close to 40 runners and walkers, the much feared Melbourne rain didn’t eventuate and people still made it on time to the plenary session.
The trade hall, plenary theatre, breakout rooms and the foyer were constantly abuzz with a positive vibe and sense of comradery, thanks to the record attendance, the high level of engagement from sponsors and exhibitors, the superb scientific presentations and fun at the social events.
Finally, a special acknowledgement and thanks are warmly extended to our RMIT student volunteers, their help was valuable and appreciated by many. They patiently worked through many issues, their enthusiasm was palpable, and it was fantastic to have them participate at the ASM.
The 55th ANZSNM ASM concluded with the ceremonial passing of the hoe to the Co-Convenors of the 56th ASM, Kevin London and Justine Trpezanovski, who will lead our 2026 meeting in Canberra. In Māori culture, the hoe (paddle) is a powerful symbol of unity, collaboration, and shared journeys. Just as paddlers in a waka (canoe) must move together to reach their destination, so too does our ANZSNM community, across professions and across our two nations, Australia and New Zealand, working in harmony towards our common goal: advancing nuclear medicine. We wish Kevin and Justine every success in their preparations for ASM 2026.
ANSTO/ANZSNM Research Grant
Dr
Bonnia Liu, Austin Health
The utility of 18F-FDG-PET/CT for the diagnosis of giant cell arteritis: A cost of illness analysis at an Australian tertiary centre
…CLICK
TO READ
2025 Lowenthal Lecture Award
Professor Karen Jones, The University of Adelaide
From gut feelings to facts - solving the mysteries of the stomach
…CLICK TO WATCH
2025 Pioneer Lecture Award
Professor Vijay Kumar, The University of Sydney
Pioneer Lecture
…CLICK TO WATCH
AANMS Registrar Research Award
Dr Ruth Huo, Nepean Hospital
Ketogenic FDG-PET/CT: Clinical Audit at an Australian Hospital to assess use of blood ketone levels and other risk factors for inadequate myocardial glucose suppression
Ketogenic FDG-PET/CT: Clinical Audit at an Australian Hospital to assess use of blood ketone levels and other risk factors for inadequate myocardial glucose suppression
Ya Ruth Huo1, Sandeep Gupta 2, Natalie Rutherfor2, Megan Saul2
1Nepean Hospital, 2Department of Nuclear Medicine / John Hunter Hospital
AIM: 18F-FDG PET/CT is used to diagnose myocardial inflammation such as sarcoidosis, requiring preparation with a ketogenic diet to achieve myocardial glucose suppression (MGS). Despite this, incomplete MGS remains a common problem. This study aims to assess the benefit of blood ketone levels and identify other risk factors for inadequate MGS.
METHODS: In April 2024, our department introduced improved dietary guidelines, dietary logbook, patient questionnaire and blood ketone level testing. Retrospective study from Aug 2022 to April 2024 and prospective study from April 2024 to January 2025 of all patients who underwent a ketogenic 18F-FDG PET/CT at two Australian Hospitals was performed. All patients were instructed to follow a 24hr high-fat, low-carbohydrate diet. Images were classified as either adequate or inadequate myocardial suppression.
RESULTS: The overall rate of inadequate MGS was 22% (95 patients from Aug2022-April2024 and 92 patients from April2024-January2025). Following the introduction of improved dietary guidelines and a dietary logbook in April 2024, the rate of inadequate MGS reduced from 26% down to 17% (pvalue 0.14). Mean blood ketone levels were significantly lower in patients with incomplete MGS (0.34mmol/L vs 0.76mmol/L, p-value 0.04). On univariate analysis, significant risk factors for inadequate MGS included prednisolone use (75% vs 14.9% for no prednisolone use, OR: 17.1 [95%CI 1.65-177.04], p=0.009), a low blood ketone level (0.3mmol/L or lower) (OR: 5.77 [95%CI 1.6919.68], p=0.003) and female sex (27.5% vs 9.6% in males, OR: 3.57 [95%CI 1.12-11.3], p=0.025). On multivariate analysis, prednisolone use, low blood ketone levels and <24hr ketogenic diet remained significant risk factors for inadequate MGS. The rates of inadequate MGS were 50%, 26% and 7% for patients with blood ketone levels of 0.1, 0.2-0.3 and ≥0.4mmol/L, respectively. If patients were on prednisolone, 100% had inadequate MGS if the blood ketone level was 0.3mmol/L or lower despite 24hrs on a ketogenic diet.
CONCLUSION: Providing clear dietary guidelines and dietary logbook may improve patient compliance with the ketogenic diet. Risk factors of inadequate MGS include low blood ketone levels (0.3mmol/L and lower), prednisolone use and inadequate ketogenic diet adherence (<24hrs).
Landauer Award
Lisa Nguyen, Austin Health
The impact of the external iliac artery on Hilson’s Perfusion Index 99mTc MAG3 Renal Transplant Scans
The impact of the external iliac artery on Hilson’s Perfusion Index 99mTc MAG3 Renal Transplant Scans
Lisa Nguyen1, Wesley Ng1, Kunthi Pathmaraj1, Sze Ting Lee1, Andrew Scott1,2 1Austin Health, 2ONJCRI
AIM: Renal scintigraphy using 99m Tc mercaptoacetyltriglycine [MAG3] plays a crucial role in the accurate assessment of graft function after renal transplantation. The Hilson’s Perfusion Index [Hilson’s Index] is a useful parameter to evaluate graft function (including acute tubular necrosis) and rejection. Early detection of complications is vital to allow for early intervention to ensure success of transplantation. The external iliac artery often overlaps the transplanted kidney and there is little consensus in the current literature as to whether the inclusion or exclusion of the artery whilst processing makes a difference to the Hilson’s Index.
The aim is to evaluate the impact of inclusion or exclusion of the external iliac artery during processing on the calculated Hilson’s Index in renal transplants during the perfusion phase.
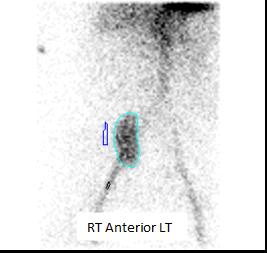
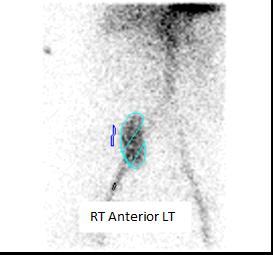
METHOD: 100 consecutive day one MAG3 renal transplant scans were retrospectively processed and analysed. Each scan was processed twice by a technologist, once with the entire kidney and any overlying iliac artery included and then again with minimal iliac artery inclusion [Figures 1A & 1B]. The Hilson’s Index was calculated using the ratio of the area under of the arterial curve to peak divided by the area under the renal curve to peak multiplied by 100, with normal being <150.
RESULTS: The 100 patients consisted of 70 males and 30 females ranging in age from 18 to 75 years. The mean Hilson’s Index when the external iliac artery was included was 213.55 [range 28.99 - 3083.27] versus 273.55 [range 28.9 - 4546.97] when the external iliac artery was excluded. The paired ttest showed a significant difference [p-value = 0.0015] in the Hilson's Index of scans processed including and excluding the external iliac artery.
CONCLUSION: The external iliac artery should be excluded during post-transplant MAG3 renal scan processing (where possible), to ensure more accurate estimation of the Hilson’s Index. 1A. Entire kidney with any overlying iliac artery included
Kidney with minimal iliac artery included in region of interest
GMS Poster Award
Nicole Ayars, SAMI Royal Adelaide Hospital
Amyloid Imaging in AL Amyloidosis – A Case Study
Amyloid Imaging in AL Amyloidosis – A Case Study
Nicole Ayars1,2, Kari Hughes2, Sophie Thoo1,2, Dylan Bartholomeusz1,2 1South Australia Medical Imaging, 2Royal Adelaide Hospital,
A 49 year old male had been experiencing severe autonomic dysfunction including gastroparesis and postural drops for two years, as well as a 60kg weight loss. Small bowel biopsies showed minute deposition of amyloid within the stroma and blood vessels and with immunostaining for Amyloid A, TTR Prealb and Kappa/lambda IHC all negative. An Echocardiogram demonstrated moderate concentric LV wall thickening with an ejection fraction of 45%, noting there was apical sparing. The differential diagnosis was primary amyloidosis or POEMS syndrome.
For investigation of cardiac amyloid, the patient was referred for a 99mTc-HDP Cardiac Amyloid scan. He was injected with 800MBq of 99mTc-HDP and whole body and cardiac scans were performed three hours post injection. Images showed no abnormal activity in the myocardium on both planar and SPECT/CT images, Perugini grade (0).
Noting that the patient had previously had a lytic lesion identified in the clavicle, the differential diagnosis was expanded to include multiple myeloma or plasmacytoma. A skeletal survey performed didn’t demonstrate any areas of concerns and CT of the chest, abdomen and pelvis performed due to worsening gastrointestinal symptoms was unable to provide additional information.
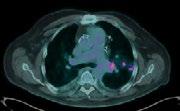
Amyloidosis continued to be a differential, resulting in the patient being referred for an 18FFlorbetaben (FBB) PET scan. FBB PET scanning is an established method of assessing amyloid deposits in the brain and recently usage has increased to assess for systemic amyloid disease. FBB uptake variations have also been noted to differentiate between Transthyretin (ATTR) amyloidosis vs light chain (AL) amyloidosis.
The patient was injected with 244MBq 18F-FBB and images of the whole body toes to vertex obtained at 1-hour post injection. The scan demonstrated diffuse increased tracer uptake in the heart, spleen, mesorectum and tongue, suggesting amyloid infiltration. There was also soft tissue uptake in the right lower leg.
The negative HDP scan along with the positive FBB scan suggest the presence of AL Amyloidosis in this patient. This study highlights the complementary use of two Nuclear Medicine studies in seeking a diagnosis of amyloidosis.
RAPHAEL Student Research Award
Catherine Dickmann, University of Cambridge
Development of a halofluorocarbon, chromatography-free radiosynthesis of fluorine-18 difluorocarbene on the GE TracerLab FXFN module
Development of a halofluorocarbon, chromatography-free radiosynthesis of fluorine-18 difluorocarbene on the GE TracerLab FXFN module
Catherine Dickmann1, Selena M Sephton1, Franklin I Aigbirhio1 University of Cambridge,
BACKGROUND: In recent years, the development of [18F]difluoromethyl radical ([18F]2),1 and [18F]difluorocarbene prosthetic groups ([18F]4),2 has paved the way towards direct [18F]difluoromethylation in routine PET tracer synthesis with high molar activity (Figure 1). However, some limitations in their syntheses are perhaps hindering their widespread adoption. These include the requirement of ozone-depleting dibromofluoromethane for the synthesis of precursors 1 and 3 and the lengthy syntheses of both [18F]2 and [18F]4 requiring semi-prep purification on cartridge-based radiosynthesis modules.
AIMS: The aim of this work was to develop a haloflurocarbon-free, chromatography-free, fullyautomated synthesis of [18F]difluorocarbene reagent [18F]4 on the GE Tracerlab FXFN module.
RESULTS: Precursor 3 was synthesised in 54% yield from decarboxylative bromination of 5 which circumvented the need for dibromofluoromethane. Difluorocarbene reagent [18F]4 was first radiosynthesised on the GE TracerLab FXFN module with semi-prep purification in 2% RCY The semi-prep purification step was then eliminated in favour of a cartridge-based trapping and elution approach (on an aluminium cartridge loaded in series with a C18 SepPak plus cartridge) to give [18F]4 in 7.3% ±1.8% (n=6) RCY (97% ± 3% RCP, 1.5 to 34 GBq/μmol) Finally, a fully automated [18F]difluoromethylation radiosynthesis with [18F]4 was developed on two Tracerlab FXFN modules linked together to yield the model [18F]difluoromethylated compound in adequate amounts for biological studies, including in vivo PET, in under two hours (99.0 MBq, 0.8% RCY, 1.5 GBq/μmol, 103 min total synthesis time). Therefore we have established a path forward for routine automated synthesis of radiotracers via [18F]difluorocarbene insertion with [18F]4
Conclusions: A halofluorocarbon, chromatography-free synthesis on the GE FXFN Tracerlab module afforded difluorocarbene reagent [18F]4 in 7.3% ± 1.8% yield. Additionally, a fully-automated three-step [18F]difluorocarbene insertion radiosynthesis is described for the first time.
Figure 1 Previous and current radiosyntheses of [18F]difluoromethyl prosthetic groups.
REFERENCES:
1. Trump, L. et al. Late-Stage 18F-Difluoromethyl Labeling of N-Heteroaromatics with High Molar Activity for PET Imaging. Angew. Chem. Int. Ed. 58, 13149–13154 (2019).
2. Sap, J. B. I. et al. [18F]Difluorocarbene for positron emission tomography. Nature 606, 102–108 (2022).
SUMITOMO NMT Student Award
Jess Watson, Royal Darwin Hospital
Evaluating the expression pattern of MUC1-CE in head and neck cancers for potential application in radioimmunotherapy
Evaluating the expression pattern of MUC1-CE in head and neck cancers for potential application in radioimmunotherapy
Jess Watson1, Ashleigh Hull2, Eva Bezak2, Katherine Guerrero1, 1Royal Darwin Hospital, 1University of South Australia
AIM: Head and Neck Squamous Cell Carcinomas (HNSCCs) are aggressive and invasive cancers with high recurrence rates following conventional therapies. Unsatisfactory patient outcomes warrant the development of novel treatment options, such as radioimmunotherapy. Mucin-1 (MUC1) is an antigen present on HNSCCs that is prone to tumour-associated mutations, exposing cancer-specific MUC1 epitopes (MUC1-CE). C595 antibody specifically targets MUC1-CE. This study aimed to assess the feasibility of radioimmunotherapy directed at MUC1-CE, by evaluating its expression in HNSCC cells, HNSCC tissue, and healthy tissue samples using C595 antibody.
METHODS: MUC1-CE expression was quantified in three HNSCC cell lines (UM-SCC-1, UM-SCC17A, UM-SCC-22A) using indirect immunofluorescence flow cytometry. Fluorescence intensity from cells incubated with the C595 antibody was compared to an isotype control to determine the percentage of MUC1-CE-expressing cells Immunohistochemistry with C595 antibody was performed to identify MUC1-CE expression in HNSCC and healthy head and neck tissue samples. MUC1-CE expression in tissues was measured via immunoreactive score, pixel analysis and textural analysis (Haralick Features)
RESULTS: Flow cytometry revealed MUC1-CE expression in HNSCC cell lines was 27% (UM-SCC1), 32% (UM-SCC-22A), and 38% (UM-SCC-17A). Immunohistochemistry showed significantly higher MUC1-CE expression in HNSCC tissues compared to healthy tissues, with mean immunoreactive scores of 4.6 and 2.6, respectively (p = 0.0072). Pixel analysis revealed higher mean pixel values in HNSCC tissues (175.6) versus healthy tissues (171.6), though this difference was not statistically significant (p = 0.0649). Texture analysis via Haralick Features identified significantly greater heterogeneity of MUC1-CE expression in HNSCC tissues compared to healthy tissues (p = 0.0022).
CONCLUSION: MUC1-CE was moderately expressed in HNSCC cell and tissue samples, and mildly expressed in healthy tissue. These preliminary results indicate radioimmunotherapy directed at MUC1-CE may be feasible. Further in-vitro studies are warranted to assess the binding efficiency, internalisation and cytotoxicity of C595-radioimmunoconjugates to further explore the potential of MUC1-CE as a radioimmunotherapy target.
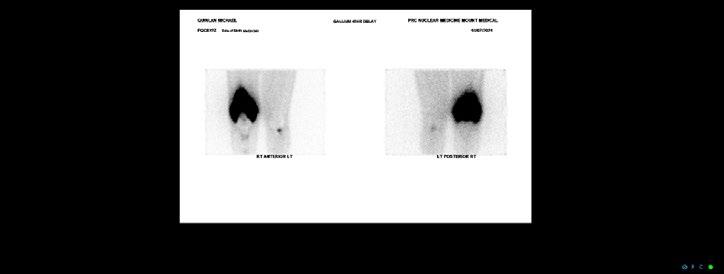
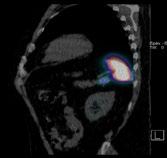
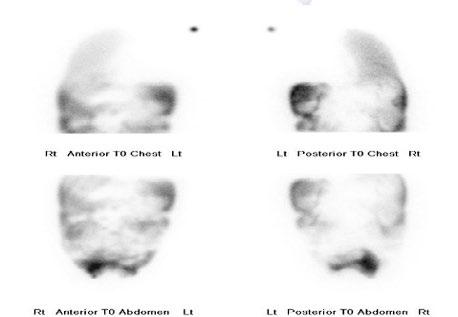
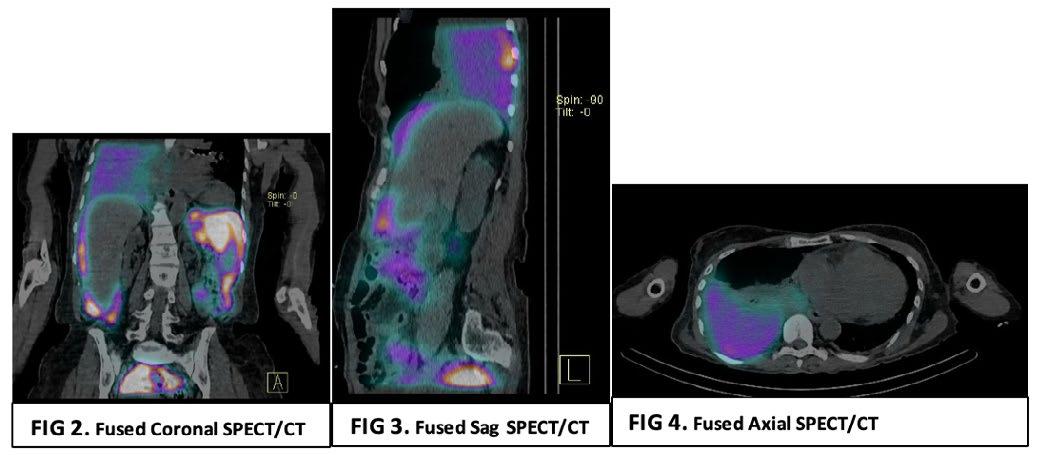
RADPHARM Award
Shiphrah Tagore, Perth Radiological Clinic
Glow and Behold, Nuclear Medicine's Bright Role
Glow and Behold: Nuclear medicine’s bright role
Shiphrah Tagore
INTRODUCTION: Nuclear medicine imaging plays a pivotal role in evaluating complex prosthetic joint cases, particularly when conventional modalities are compromised by metal artifacts and nonspecific findings. This case study illustrates how the combined use of Gallium-67 scintigraphy and FDG PET imaging guided surgical intervention and evaluated disease progression with superior diagnostic sensitivity
CLINICAL PRESENTATION: A 61-year-old military veteran with a right total knee replacement presented with several months of knee swelling and severe pain. Initial evaluations including CT, bone scan, XR, ultrasound with fluid aspiration and MRI were inconclusive due to metallic artifacts and complex prosthetic fractures with adjacent oedema. The patient subsequently underwent Gallium-67 scintigraphy following an intravenous injection of 150 MBq Gallium-67 citrate, with imaging performed 48 hours later using a GE Discovery 670 system. The Gallium-67 scan demonstrated a significantly abnormal periprosthetic uptake, consistent with clinical concerns for infection. This result expediated surgical intervention and tissue biopsy of the affected area. The biopsy results revealed an extremely rare form of Diffuse Large B-cell Lymphoma involving the joint prosthesis. An FDG PET scan was then performed on a GE Omni PET system which revealed intense metabolic activity within the right knee and left knee, subcutaneous upper back activity and an FDG-avid right iliac fossa lymph node, suggesting systemic involvement. The patient underwent 6 cycles of R-CHOP and is awaiting further surgical intervention for the affected knee.
DISCUSSION: Prosthetic joint-associated lymphoma is an exceedingly rare phenomenon, with fewer than 20 cases documented in the global literature. The utility of 67Ga in lymphoma diagnosis is historically well demonstrated and this case underscores the complementary value of Gallium-67 scintigraphy and FDG PET imaging in complex prosthetic joint scenarios. While traditional imaging modalities were hampered by metal-induced artifacts and non-specific findings, nuclear medicine techniques facilitated the critical differentiation between infection and malignancy. This case also highlighted the importance of evaluating 67Ga-citrate imaging in complex clinical presentations with a comprehensive understanding of the mechanism of uptake in relevant pathologies The integrated imaging approach not only prompted surgical management but also informed systemic treatment planning, highlighting the evolving role of nuclear medicine in addressing challenging diagnostic dilemmas
Figure 1. 67Ga-citrate scan
Shimadzu Award
Zhipeng Cao, Olivia Newton-John Cancer Research Institute
Preclinical Evaluation of DNA Damage Response Inhibitors and 225Ac-DOTA-girentuximab Combination Therapy
Preclinical Evaluation of DNA Damage Response Inhibitors and 225Ac-DOTA-girentuximab Combination Therapy
Zhipeng Cao12, Christian Wichmann1, Alesia Ivaskevich3, Astrid Zimmermann4, Fiona E Scott1, Michael Wheatcroft3, Andrew Scott1,5, 1Olivia Newton-John Cancer Research Institute, 2La Trobe University, 3Telix Pharmaceuticals Limited, 4The healthcare business of Merck KGaA, 5Austin Health
AIM: DNA Damage Response inhibitors (DDRi) have been developed to enhance the biologic effect of anti-cancer treatments such as chemotherapy and radiation therapy, which can induce DNA damage in cancer cells This study aims to investigate anti-tumour effect of combining DDRi with 225Ac-DOTA-girentuximab targeting CAIX-positive cancer
METHODS: Girentuximab was conjugated with DOTA (1,4,7,10-Tetraazacyclododecane-1,4,7,10tetraacetic acid) chelator for 225Ac radiolabelling. The half-maximal inhibitory concentration (IC50) values for lartesertib targeting ataxia telangiectasia mutated protein (ATM) and peposertib targeting DNA-dependent protein kinase (DNA-PK) were evaluated by clonogenic assay Levels of molecular markers related to DDR were quantified by Meso Scale Discovery (MSD) and Luminex assays The in vitro anti-tumour efficacy of combined treatment comprising 225Ac-DOTA-girentuximab and DDRi was studied
RESULTS: Lartesertib and peposertib exhibited IC50 values of 3.543 µM and 0.7712 µM, respectively, for SK-RC-52 cells The IC50 value for 225Ac-DOTA-girentuximab in SK-RC-52 cells was 0.1505 kBq/mL. Synergy mapping analysis revealed an additive effect between 225Ac-DOTAgirentuximab and lartesertib (Figure 1A) The combination of 225Ac-DOTA-girentuximab with peposertib, in contrast, exhibited a synergistic effect (Figure 1B). Combination Index (CI) analysis showed a CI value of 0.760 for the 225Ac-DOTA-girentuximab + peposertib combination therapy, corroborating the observed synergistic effect. The CI value for 225Ac-DOTA-girentuximab + lartesertib was 0.985, indicating an additive effect (defined by 0.8 < CI < 1.2) (Figure 1C) The MSD assay demonstrated a positive correlation between DNA-PK phosphorylation and the doses/treatment duration of 225Ac-DOTA-girentuximab While increased phosphorylation of ATM and KRAB-associated protein (KAP) was also observed with higher doses and longer treatment durations of 225Ac-DOTAgirentuximab, the trend was less pronounced compared to phosphorylated DNA-PK.
CONCLUSION: The combination of 225Ac-DOTA-girentuximab and DDRi proved to be more effective than either monotherapy alone The synergistic effect was evident with 225Ac-DOTA-girentuximab + peposertib, whereas 225Ac-DOTA-girentuximab + lartesertib exhibited an additive effect. Analysis of DDR biomarkers indicated elevated levels of DNA-PK phosphorylation, with phosphorylated ATM showing a comparatively lesser increase Future studies will be extended to in vivo models to determine the anti-tumour efficacy of these combinations.
Telix ' Best of the Best ' Award
Jessica Van Zuylekom, Peter MacCallum Cancer Centre
Modelling
resistance to PRRT in NET in vivo
Modelling resistance to PRRT in NET in vivo
Jessica Van Zuylekom1, Kelly Waldeck1, Jeannette Schreuders1, Benjamin Blyth1, Carleen Cullinane1, Rodney Hicks2
1Peter MacCallum Cancer Centre, 2Melbourne Theranostics Innovation Centre
AIM: The development of resistance to peptide receptor radionuclide therapy (PRRT) in neuroendocrine tumour (NET) patients, without loss of the target, is a poorly understood resistance mechanism. This reduces effectiveness and durability of treatment, thus worsening patient outcomes. Whilst multiple NET models display inherent resistance to PRRT, none mimic developed resistance without target loss. To allow investigation of this phenomenon, we describe a method of generating in vivo models of ‘developed resistance’ to 177Lu-DOTA-octreotate (177LuTATE) with retention of somatostatin receptor type 2 (SSTR2) expression
METHODS: Immunocompromised mice bearing one of three different subcutaneous xenografts (AR42J, H1299-7 or H69) were serially treated with 30 MBq of 177LuTATE until tumours showed no response (Fig.1a) These tumours were resected and ‘177LuTATE resistant’ cells isolated. A new cohort of mice were inoculated with these cells, alongside mice inoculated with parental cells naïve to 177LuTATE. These cohorts were either utilized in efficacy studies, with tumours treated with a single dose of 17 MBq of 177LuTATE or vehicle (n=5-8), or underwent 68GaTATE PET imaging and/or immunohistology (IHC).
RESULTS: Resistance was confirmed in AR42J and H1299-7 models, with treated resistant tumours showing tumour growth corresponding to untreated tumours (Fig.1b). The H69 model however did not show a difference in response between parental and ‘resistant’ tumours or treated and untreated mice. SSTR2 expression was confirmed in resistant tumours via PET imaging and IHC, which displayed similar 68GaTATE uptake (Fig.1c) and staining (Fig.1d) to parental tumours
CONCLUSION: Two SSTR2 expressing models of developed resistance were established which mimic the resistance phenotype seen in a subset of NET patients These will be utilised to investigate mechanisms of resistance in vivo and in turn assess treatment options for overcoming this resistance This translational approach can lead to clinical development and improved patient outcomes
Figure 1. a) NETs were serially treated with 30 MBq of 177LuTATE until tumours became unresponsive. These tumours were resected, cells isolated, and reimplanted into naïve mice These mice were used to b) confirm resistance with an efficacy study, and SSTR2 expression with c) 68GaTate PET imaging and d) IHC
ANZSNM Special Recognition Award
Mr Russell Booth
Recognising 50 Years of Service as a Nuclear Medicine Technologist in Victoria
It was a true honour to present an ANZSNM Special Recognition Award to Russell Booth at the Gala Dinner during our recent Annual Scientific Meeting, celebrating his extraordinary achievements during his 50 years of service as a Nuclear Medicine Technologist in Victoria.
Throughout his remarkable career, Russell has been a tireless advocate for technologists, a passionate educator, a trusted mentor, and a shining example of professionalism and dedication. It was deeply heartwarming to see so many former colleagues and friends come forward to congratulate him, and to witness him share this special moment with his wife, Julia.
I would also like to acknowledge and thank the many people who shared their reflections and memories of working alongside Russell over the years. In particular, sincere thanks to Liz Parkinson and Jo Pinson for nominating Russell for this well-deserved honour, and for thoughtfully collating the stories and insights and drafting the speech I delivered on the evening.
Please find the full speech below.
There are many great reasons to be ANZSNM President, and tonight is absolutely one of them.
It’s a real pleasure to be here to acknowledge and celebrate a remarkable Nuclear Medicine Technologist from Victoria, Mr Russell Booth
In 2023, Russell marked 50 years of service at St Vincent’s Hospital in Melbourne, an extraordinary milestone, and retired shortly thereafter. - Hopefully to enjoy a wellearned break!
But in all seriousness, back in 1973, Russell was a true pioneer in what was then a new and rapidly evolving specialty: Nuclear Medicine.
His journey began alongside the late Dr Rudolph
Chmiel, as they established the Nuclear Medicine Department at St Vincent’s. I’m told they started with a rectilinear scanner, then moved to a gamma camera, then multiple gamma cameras, followed by ultrasound, the creation of a new private practice, and eventually to SPECT/CT and PET, technologies now central to our practice.
Now, there are many in our Nuclear Medicine community with rich, clinically focused careers, but what I want to shine a light on tonight is Russell’s exceptional influence beyond the clinic
Russell has been a quiet force, a visionary whose dedication, commitment, foresight, and humility have helped shape the profession for Nuclear Medicine Technologists in Victoria and, subsequently across Australia.
He never sought the spotlight, but his impact has been deeply felt. As one of his long-time colleagues, David Bell, noted: “Russell was about making connections that endured, moving the chess pieces, and providing encouragement, wisdom and support.”
Professor Andrew Scott reflected “Russell would frequently reach out to colleagues to provide guidance and support for professional and personal matters and would not hesitate to give advice. His support and friendship have always been very much appreciated by colleagues and friends.”
Julia Booth, Liz Parkinson, Russell Booth
ANZSNM Special Recognition Award - Mr Russell Booth
(Continued)
So what does that behind-the-scenes influence look like?
Let me share just a few highlights: Russell was a long-standing member of the RMIT Course Advisory Committee — first for the Diploma of Medical Nucleography (yes, that’s what it was called!), and later for the Bachelor of Medical Radiations (Nuclear Medicine) — helping to ensure the course aligned with evolving clinical needs.
• In the 1980s, he championed Australia’s first Nuclear Medicine degree at RMIT and played a key role in the long, ultimately successful push for professional recognition and wage reclassification based on this new academic status. This laid the foundation across Australia.
• In the early 1990s, Russell was instrumental in reviving the ANZSNMT, uniting and empowering technologists across Australia and New Zealand. And just look at where we are today!
• He helped create the Professional Internship Program in Victoria, supporting new graduates in their first year of practice, with funded supervisor roles hosted at St Vincent’s.
• In 2009, as President of the Victorian Society of Nuclear Medicine Technologists, Russell conceived the idea of the first CT course for Nuclear Medicine Technologists, well ahead of its time. Developed in collaboration with Monash University, the Australian Institute of Radiography, and approved by the Medical Radiation Practitioners Board of Victoria and the Radiation Safety Committee, this course redefined the way Nuclear Medicine Technologists performed SPECT/CT and PET/CT, and paved the way for CT training to be embedded in all tertiary Nuclear Medicine programs.
These are just some of the reasons we are celebrating Russell tonight.
Russell - thank you. On behalf of myself, and on behalf of the entire ANZSNM community - thank you for everything you've done, often quietly and without fanfare, to advance our profession.
And to close, I want to share a few words from Adam Reinhard, Executive Officer of Medical Radiation Practice at Ahpra: “Russell is a man of energy and action—something you can
see reflected in the flair and style of his glasses. But more importantly, he’s a man of compassion, humility, and great humour.
People like Russell don’t just change how we see the world, they change how we engage with it. He leads with integrity, inspires with passion, and engenders confidence through his openness and adaptability.
Russell’s dedication and vision are the foundation upon which meaningful and lasting progress is made.
Congratulations on your well-deserved award, Russell. It recognises not only your lasting professional contributions, but in you, it reflects the very best of who we are.”
Please join me in warmly welcoming our Special Recognition Award recipient: Mr Russell Booth.
Karen Jones
ANZSNM President
Professor Karen Jones, Russell Booth
Celebrations
WE ARE SEEKING EXPERIENCED NUCLEAR MEDICINE TECHNOLOGISTS
Join Queensland’s largest private radiology practice group
Led by an experienced team of radiologists and imaging specialists, Queensland X-Ray is one of the largest private imaging groups in Queensland, with over 50 practices state-wide.
Queensland X-Ray is part of the Sonic Healthcare group, an ASX top-40 listed company focused on delivering medical excellence in radiology, nuclear medicine, pathology, general practice and occupational medicine.
Why join Queensland X-Ray?
▷ Opportunity to work across major hospitals, community practices, and specialised sites.
▷ Gain exposure to a broad range of procedures, including complex hospital-based cases, cardiac imaging, emergency, and on-call work.
▷ Access structured training across all Nuclear Medicine modalities. Learn from Queensland’s leading providers of PET/CT and benefit from CPD opportunities.
▷ Take advantage of pathways for advancement, with career progression opportunities across our Nuclear Medicine network.
▷ Enjoy competitive remuneration, paid parental leave, and ongoing support for continued professional growth.
For more information please contact Queensland X-Ray Human Resources on 07 3422 8800 or email humanresources@qldxray.com.au
CAIRNS
TOWNSVILLE
MACKAY
BRISBANE GOLD COAST
TOOWOOMBA
Conference Sessions
Official Welcome and Opening
Oncology - Paul Roach, Louise Emmett, Bital Savir-Baruch, John Buscombe, Dale Bailey, Grace Kong
ANZSNM President, Karen Jones with EANM representatives, Michel
Raelee McNab Nuclear Medicine Technologist - QLD Health - Townsville University Hospital, QLD
Introduction
Heat Denatured Tc-99m labelled Red Blood Cell Labelling. 99mTc- labelled heat-denatured red blood cells allow a non-invasive diagnosis of splenosis or a splenunculus. Splenosis is a condition that occurs from seeding of splenic cells after trauma, ruptured spleen, or splenectomy. Essentially it is remaining spleen cells that have been deposited elsewhere. Splenunculus is defined as an accessory spleen. A congenital condition in which there is an additional benign functional part of the spleen located separate from the spleen. Both these conditions are commonly found within the abdomen near the spleen/pancreas bed.
The spleen consists of white and the red pulp. This procedure utilises the function of the red pulp, that contain macrophages which filter and remove the damaged or aging red blood cells out of the body. By radiolabelling and subsequently damaging the red blood cells, then re-administering the blood to be able to visualise the splenic tissue located within the abdomen. As the red pulp in the spleen will filter out the heat-denatured red blood cells, accumulating the tracer and be visualised on the images.
CT scans have also been useful in assisting in the characterisation of lesions in which a splenunculus or splenosis is a differential diagnosis. The density and enhancing characteristics of the lesion will be compared with that of the spleen.
MRI can also be utilised and has similar detection of diagnosing the lesion as CT. However, the gold standard for identifying splenic tissue has been shown to be 99mTc- Heat Denatured RBC scintigraphy, as it can differentiate between splenic tissue and non-splenic tissue, allowing for more conclusive results.
Patient Background and Previous Imaging
The patient had a CT previously for an unrelated condition that found an incidental solid lesion on the pancreatic tail. Additional MRI imaging was performed. The CT report stated the incidental finding as a ‘hypoattenuating focus’ at the tail of the pancreas could not be ruled out as a pancreatic malignancy. Dedicated
pancreatic MRI imaging was performed to assist in the characterisation the lesion.
The MRI report stated three possible differentials: an adenocarcinoma, pancreatic NET or splenic tissue. A full clinical work up was suggested to identify the lesion.
After the MRI imaging, a 99mTc- Heat Damaged Red Blood Cell scan was performed to exclude or define the lesion as splenic tissue.
The patient had not experienced any symptoms associated with pancreatic malignancy, no unintentional weight loss or fevers, no difficulty with exocrine insufficiency or jaundice. Patient had not experienced any pain or discomfort, no nausea or diarrhoea.
Figure 1: CT Key Images of Incidental finding of lesion on pancreatic tail
Figure 2: MRI of Pancreas Key Image of uncharacterised lesion on pancreas
Case Study: SILLY SPLENUNCULUS
(Continued)
Imaging Technique
99mTc-Ultratag kit was utilised for labelling as shown in Figure 3.
Patient was cannulated – a 20 Gauge cannula was used to reduce the risk of damaging any red blood cells when withdrawing or re-administering the blood. Three millilitres of blood were withdrawn into a syringe prepared with 45 Units of Heparin (10-15 Units of heparin per ml of blood). The blood was transferred into the reaction vial included in the Ultratag Kit, allowed five minutes for incubation/ reaction. Firstly, the contents from Syringe I were injected into the reaction vial, inverted five times. Secondly the contents from Syringe II were injected into the reaction vial and inverted five times.
1.5GBq of 99mTc-Pertechnetate in 3mls of Saline were added into the reaction vial. Incubation period of 20 minutes followed.
The reaction vial was placed into a dry heat block (pre heated up to 49.5 °C) and allowed to denature for 30 minutes whilst swirling intermittently.
Reaction vial was removed from the dry heat block after 30 minutes and allowed to cool prior to administering a dose of 200MBq to the patient.
Images were acquired one hour post reinjection. Images acquired over the abdomen included 4-minute Planar images (Anterior, Posterior, and Laterals).
Additional SPECT/CT imaging was performed (20 seconds per frame for 32 frames).
Discussion
Focal tracer uptake is seen in the known lesion in the tail of the pancreas. This is in keeping with a diagnosis of intrapancreatic accessory splenule.
These findings rule out the possibility of a pancreatic malignancy and supports the differential diagnosis of an accessory spleen. This non-invasive diagnostic imaging technique allows the treating team to characterise the lesion and manage accordingly.
As the patient is non-symptomatic and the lesion is not located within a region of the abdomen that could cause possible bowel obstruction, the proposed management was to monitor the patient for symptoms.
If the accessory spleen was located within the region of the bowels or be at immediate risk of rupturing, surgical management is recommended.
Conclusion
99mTc- Heat-denatured red blood cell scintigraphy remains the gold standard in identifying a lesion as functional splenic tissue in lieu of a malignant neoplasm. This imaging technique provides a definitive diagnosis of functioning splenic tissue with regards to a lesion, whilst other modalities may have inconclusive results.
99mTc-Denatured RBC provide high specificity, being able to identify smaller lesions not always detected with other modalities. It provides a definitive diagnosis without the need to biopsy the site, as other modalities cannot conclusively characterise the lesion without pathology results.
As accessory spleens can often mimic tumours in appearance, other modalities might find it difficult to identify splenic tissue. Nuclear medicine as a functioning imaging modality provides an alternative that allows the definitive diagnostic characterisation of a lesion consisting of splenic tissue. Providing the grave possible diagnosis of pancreatic NET or adenocarcinoma it was a great outcome to be able to diagnose the lesion as an accessory spleen and actively contribute to the patient treatment pathway.
Figure 3: Contents of 99mTc-Ultratag RBC Labelling Kit. Including syringes I and II and one reaction vial.
Figure 4: Anterior, Posterior, Left and Right Lateral Planar Acquired Images
Figure 5: Axial Key Image of Accessory Spleen next to the Spleen. Figure 6: Coronal Key Image of the Accessory Spleen. Figure 7: Sagittal Key Image of Accessory Spleen.
Case Study: SILLY SPLENUNCULUS (Continued)
References
Belkhir, SM, Archambaud, F, Prigent, A & Chaumet-Riffaud, P 2009, ‘Intrapancreatic Accessory Spleen Diagnosed on Radionuclide Imaging’, Clinical Nuclear Medicine, vol. 34, no. 9, pp. 642–644.
Graziani, T, Baldari, G, Sammartano, A, Scarlattei, M, Migliari, S, Pescarenico, MG, Cidda, C, Bola, S & Ruffini, L 2020, ‘SPECT/CT with 99mTc labelled heat-denatured erythrocyte to detect thoracic and abdominal splenosis’, Acta Bio-Medica: Atenei Parmensis, vol. 91, no. 4, p. e2020098.
Holzgreve, A, Völter, F, Delker, A, Kunz, WG, Fabritius, MP, Brendel, M, Albert, NL, Bartenstein, P, Unterrainer, M & Unterrainer, LM 2022, ‘Detection of Splenic Tissue Using 99mTc-Labelled Denatured Red Blood Cells Scintigraphy—A Quantitative Single Center Analysis’, Diagnostics, vol. 12, no. 2, p. 486.
Kapila, V & Tuma, F 2023, Physiology, Spleen, PubMed, StatPearls Publishing, Treasure Island (FL).
Landauer 2023, Landauer Radiopharmaceuticals Pty. Ltd. - Curium - Mallinckrodt, Landauer Radiopharmaceuticals Pty. Ltd. - Curium - Mallinckrodt. Matthieu Pelletier-Galarneau, Ozimok, C, Sadri Bazarjani & Zuckier, L 2014, ‘Selective spleen scintigraphy using 99mTc-heat denatured red blood cells in the era of fusion SPECT-CT imaging’, Journal of Nuclear Medicine, vol. 55, Society of Nuclear Medicine, no. supplement 1, pp. 1994–1994, viewed 13 March 2025, <https://jnm.snmjournals. org/content/55/supplement_1/1994>.
Sammartano, A, Scarlattei, M, Migliari, S, Giorgio Baldari & Ruffini, L 2019, ‘Validation of in vitro labeling method for human use of heat-damage red blood cells to detect splenic tissue and hemocateretic function.’, PubMed, vol. 90, National Institutes of Health, no. 3, pp. 275–280.
A HOLE IN ONE: UNCOVERING A DIAPHRAGMATIC LEAK WITH NUCLEAR MEDICINE CASE STUDY
Selina Warrington & Remi Hillery Nuclear Medicine Technologists – Nuclear Medicine and PET Department, Sunshine Coast University Hospital
Introduction 62-year-old female presented to the Department of Emergency (DEM) with central chest pain, mainly on expiration, shortness of breath, difficulty lying flat and swollen legs. She had a known history of autonomic and peripheral neuropathy. This patient was receiving peritoneal dialysis for chronic kidney disease (secondary to ischaemic glomerulosclerosis), in which her latest treatment was performed the night before presenting to DEM.
A chest X-ray was performed which confirmed new rightsided pleural effusion, so a Computed Tomography (CT) of the chest, abdomen and pelvis was performed to further define the thorax and assess for underlying aetiology to explain the pleural effusion. The team also wanted to exclude any potential malignant changes to a right upper pole lesion that was under surveillance. No contrast was utilised in the CT study due to the patients end stage renal failure (ESRF) and current eGFR of 7. The scan demonstrated bilateral effusions with associated atelectasis, including partial collapse of the right lower and middle lobes. The effusions appeared non-specific, and the CT could not determine if they were infective or reactive in nature. The CT scan displayed no diaphragmatic defect, therefore unlikely to be a peritoneal leak, though without contrast, the scan accuracy was limited.
A repeat chest X-ray was performed 2 days later to assess the progress of the pleural effusion. The peritoneal dialysis was withheld during this time. No free subdiaphragmatic gas was evident, though the small effusions may have been due to positive fluid balance. A differential diagnosis of a peritoneal leak was still valid, so the treating team decided to push forward and perform a Nuclear Medicine Peritoneal Leak Study to assess any evidence of a diaphragmatic leak.
Method
206MBq of 99mTc-MAA was administered via infusion through the dialysate. Planar imaging of the abdomen and thorax were acquired immediately following this, followed by Single Photon Emission Computed Tomography (SPECT/CT) of the lower thorax/abdomen. Dialysate was drained at the conclusion of the study.
Findings
The imaging demonstrated abnormal radiotracer activity at the right hemithorax localising to the moderate/large volume right pleural fluid. There was no radiotracer activity at the left hemithorax and expected tracer accumulation throughout the peritoneal compartment. The low-dose CT demonstrated a subtotal collapse of the right lower lobe due to compression from the pleural effusion. The scan demonstrated a positive study with scintigraphic confirmation of a right pleuro-peritoneal communication.
Peritoneal leaks, or pleuro-peritoneal communication, are the result of egress of peritoneal dialysis (PD) fluid from the peritoneal cavity, occurring in 1-2% of dialysis patients (Faucon et al., 2022). This often occurs through defects created either during the catheter insertion process itself or through congenital or acquired defects in the peritoneal dialysis space (Kennedy et al., 2011).
The most common occurrence of peritoneal leaks is believed to be caused by an increase in intra-abdominal pressure induced by dialysis volume, hence the need for a conservative approach to increasing dialysis volume as tolerated by the patient (Kennedy et al., 2011).
Peritoneal leaks account for 6.9% of all PD failures and categorically 35% of mechanical failures in the first year of treatment according to a study by See et al., (2018). Patients with early technique (mechanical) failure were more likely to be male (58.7%), older than 70 years (34.7%); be Caucasian (72.4%); have a BMI between 18.5-30 kg/m2 (72.0%); have a history of ischemic heart disease (44.3%), cerebrovascular disease (18.1%), or peripheral vascular disease (29.6%); or be referred late to a nephrology service (25.1%) (See et al., 2018).
Typically, a peritoneal leak may be diagnosed through the study of dialysate, serum and pleural fluid for glucose and protein, where a ratio of pleural fluid to serum glucose with a positive gradient is highly suggestive of a peritoneal leak. Further corroboration is usually achieved with dynamic imaging methods such as CT and nuclear medicine scintigraphy (Kennedy et al., 2011).
Discussion
This patient is a 63-year-old, Caucasian, female with a BMI of 20.5 kg/m2, and did not meet any other increased risk factors listed above. They do, however, have a complex medical history including diagnosis of Stage V chronic kidney disease (secondary to biopsy proven ischaemic glomerulosclerosis), renal calculi, hereditary sensory and autonomic neuropathy, significant autonomic dysfunction manifesting as postural hypotension and post-prandial diarrhoea, anaemia and thrombocytopenia.
Initially, the patient was not thought to be a good candidate for haemodialysis due to know postural hypotension and was put on peritoneal dialysis to avoid blood pressure issues.
After presentation to DEM, multiple chest radiographs and a chest CT scan were completed without a conclusive diagnosis which led to the Nuclear Medicine Peritoneal Leak Study being performed. This study was able to provide a definitive diagnosis and allow the treating team to begin management planning. The patient was advised they would need to cease peritoneal dialysis for a minimum of 3 months to allow the site time to heal.
A permacath was inserted and the patient commenced haemodialysis instead. Despite not being a suitable candidate for haemodialysis, the peritoneal leak diagnosis left no other option. The patient has now successfully been undertaking haemodialysis for 6 months and will not be returning to peritoneal dialysis due to the increased risk of another leak occurring.
Case Study: A HOLE IN ONE:
(Continued)
The Nuclear Medicine Peritoneal Leak Study was able to identify and localise the pleuro-peritoneal communication in this patient, where other methods had been indeterminate or normal. Without Nuclear Medicine, it is unlikely the peritoneal leak would have been found, and whilst the treatment may have been similar, the patient would be far more likely to resist the change in dialysis, in turn, leading to poor health outcomes and further presentations with respiratory issues.
Conclusion
Nuclear Medicine Peritoneal Leak studies utilise functional imaging to demonstrate the transfer of radioactive tracer from the peritoneal to the pleural cavity and facilitates localisation of the leak site, providing a safe and reliable procedure in these cases (Faucon et al., 2022). It is a useful diagnostic tool in the management of this PD complication, as it can rapidly and effectively identify pleuro-peritoneal communication (Martins et al., 2015). This case study helps solidify the justification that pleuroperitoneal leaks being considered in the differential diagnosis of a pleural effusion, particularly a right-sided effusion, in patients undergoing peritoneal dialysis (Kenney et al., 2011).
References
Faucon, A., Messai, N., & Pardon, A. (2022). A sweet unilateral pleural effusion: pleuro-peritoneal communication in a patient on dialysis. The LancetClinical Picture, 400(10356), p920. A sweet unilateral pleural effusion: pleuroperitoneal communication in a patient on dialysis - The Lancet.
Kennedy, C., McCarthy, C., Alken, S., McWilliams, J., Morgan, R. K., Denton, M., Conlon, P. J., & Magee, C. (2011). Pleuroperitoneal leak complicating peritoneal dialysis: a case series. International journal of nephrology, 2011, 526753. https://doi.org/10.4061/2011/526753
See, E. J., Johnson, D. W., Hawley, C. M., Pascoe, E. M., Badve, S. V., Boudville, N., Clayton, P. A., Sud, K., Polkinghorne, K. R., Borlace, M., & Cho, Y. (2018). Risk Predictors and Causes of Technique Failure Within the First Year of Peritoneal Dialysis: An Australia and New Zealand Dialysis and Transplant Registry (ANZDATA) Study. American journal of kidney diseases : the official journal of the National Kidney Foundation, 72(2), 188–197. https://doi. org/10.1053/j.ajkd.2017.10.019
Martins, A.R., Branco, P., Gonçalves, M., Marques, M., Afonso, S.P., Gaspar, A., & Barata, J.D. (2015). Pleuroperitoneal communication on peritoneal dialysis patients – presentation of four cases. Portuguese Journal of Nephrology and Hypertension, 29(2), 165-172. https://cdn02.spnefro.pt/pjnh/54/n2_2015_ pjnh_10.pdf
ARTnet Delivering Impact to Enhance Clinical Trial Site Accreditation and Dosimetry
Dale Bailey PhD
Royal North Shore Hospital and The University of Sydney
There are two projects underway now trying to improve the site validation process for clinical trials and improving the standardisation of dosimetry from SPECT imaging in theranostics. The two projects are separate, but related. The ANZSNM and ARTnet have been able to have input directly into these projects as well as through ARTnet.
Project A - International Standardisation of Validation for Clinical Imaging Trials
Accurate The first project is an unfunded one that is aiming to develop a single, standardised site validation process for SPECT and PET imaging for enrolment in clinical trials. The motivation for this project arose out of the work that Hedi Hricak (MSKCC, NY), Andrew Scott (Austin Health, MEL) and others were doing putting together the first Lancet Oncology Commission report into Medical Imaging and Nuclear Medicine which, in part, examined issues related to global access to nuclear medicine (1). Andrew suggested to some physicists he knew that they give some thought to an improved way to initiate and standardise site validation for nuclear medicine imaging trials. This resulted in a small ad hoc group of physicists from the US, Europe and Australia got together to discuss whether this might be achieved by devising a site validation procedure that all three nuclear medicine societies could agree to standardise on. It was envisaged that the methodology would be used by the larger nuclear medicine clinical trials organisations: the Clinical Trials Network (CTN) of SNMMI, EANM Research Ltd (EARL) of EANM and the Australasian Radiopharmaceutical Trials Network (ARTnet) of ANZSNM/AANMS. It would have mutual international recognition for rapid and efficient site/scanner/radionuclide enrolment in clinical trials. Thus, if a radiopharmaceutical company based in Europe or North America wanted to run a trial in Australia then the sponsor would be able to accept the site accreditation for any site for the radionuclide that was assessed by ARTnet, as well as any other accreditation by EARL or the CTN, rather than having to repeat it. As it turns out, neither the CTN or EARL have considered site validation for SPECT systems and have been focussed until now on PET. ARTnet, however, has been using a technique for site validation that was common for both PET and SPECT. After some very
helpful interactions, the physicists from North America and Europe have decided to use the methodology that we have developed within ARTnet as the single testing procedure (2). This involves using a “standard” NEMA/IEC Image Quality (IQ) NU2 asymmetric phantom containing a series of spheres measuring from 10 mm to 37 mm internal diameter with a radio-concentration ratio of 8:1 between the spheres and the background compartment (Fig. 1). Those members who have participated in an ARTnet accreditation exercise would recall this procedure. Fortunately, ARTnet has been refining the testing process over the last 10 years of operation and now has a single syringe method for filling the phantom (both spheres and background) which is easy to perform and robust, even at sites without scientific support staff. The decision to use the ARTnet methodology involved the CTN accepting a different phantom to their anthropomorphic torso phantom containing a series of spheres and has seen EARL change the sphere to background concentration in the IQ phantom in their test procedure from 10:1 to 8:1. There is a strong suggestion in the future that the sphere sizes for PET will change, with the 37 mm diameter sphere replaced with a 6 or 7 mm diameter sphere, due to the constantly improving spatial resolution of Time-of-Flight PET systems, but for the moment the PET and SPECT testing remains identical.
The analysis will also be standardised by each of the trials organisations looking after their own region or any other country that wishes to engage their services. The phantom measurements provide a variety of measures including quantitative accuracy (e.g., Bq/cc or SUV), noise characteristics (“background variability”), plus spatial resolution estimation and recovery coefficient measures from the spheres.
ARTICLE: ARTnet Delivering Impact to Enhance Clinical Trial Site
Accreditation and Dosimetry (Continued)
The accreditation will be recognised by each of the three organisations as well. The benefits of this mutual co-operation include:
A single global site validation process
• Standardised analysis methodology
• Multicentre international standardisation for imaging trials
• Can reuse site accreditation for different trials
Less testing required
• Lower cost – no need for repeated measures of same radionuclide
Faster site validation & enrolment into a trial.
Importantly, trial sponsors will not need to devise their own testing procedures but can always request extra testing if needed (e.g., special reconstructions for organspecific studies such as brain imaging). The procedures developed will also recommend the frequency of testing that is required to maintain accreditation for the site.
A Memorandum-of-Understanding between the three nuclear medicine societies to adopt the standardised
Project B - The Precision Dosimetry Imaging Biomarker Project
The second international standardisation project that ARTnet is involved in is the Precision Dosimetry Imaging Biomarker (PDIB) Project, a fully funded initiative of the Foundation of the National Institutes of Health (FNIH), USA. This is operating under the umbrella of the Biomarkers Consortium of the FNIH which was established in 2006 and has activities in many areas of medicine such as cancer, inflammation and immunity, metabolic disorders and neuroscience. These projects bring together representatives from the US NIH, US FDA, Industry, non-profit organisations and academia to collaboratively address shortcomings in biomarker measurements related to monitoring disease. The FNIH seeks funding from industry representatives to address a larger picture than any one partner alone could achieve. A list of the partners at the time of writing is included at the end of this article.
PDIB seeks to standardise and improve the accuracy of radionuclide dosimetry measurements. The work
approach is currently being drafted and we hope to sign-off at the SNMMI Annual Meeting in New Orleans in June this year. It is likely that other nuclear medicine organisations in Asia, Africa and Latin America will follow this initiative and use the same methodology with industry expected to welcome this development as well. A manuscript describing the procedures has been written and is currently under review by the editor of the J Nucl Med.
has four distinct projects in two phases (Fig. 2): (i) establishment of secondary standards laboratories for all radionuclides used for therapy, (ii) harmonisation of SPECT/CT sensitivity calibration, and (iii) standardising dosimetry calculation workflows are all part of phase 1; (iv) empirical data collection in dose-escalation studies in radiopharmaceutical clinical trials is phase 2. The initiative has raised $US5m to fund this programme of work over the next five years and was officially launched on March 31, 2025 at the NIH, Bethesda, MD. From the Australian and
Figure 1: (A) The NEMA IQ (NU2) phantom shown has been selected for both SPECT and PET testing for site validation. The sphere diameters shown are in mm (B) The ARTnet NEMA test phantom kit in the transport case with the associated ancillary equipment to fill the phantom for the measurements.
ARTICLE: ARTnet Delivering Impact to Enhance Clinical Trial Site
Accreditation and Dosimetry (Continued)
New Zealand perspective there will be a number of ways that we will be involved. The ANSTO Nuclear Metrology Group, represented by Freda van Wyngaardt, will be involved in developing the calibration standards for all radionuclides involved (in order: 177Lu, 131I, 225Ac, 111In, 203Pb, 212Pb and 89Zr) of the first project. I will be leading the SPECT calibration of project 2 locally thru ARTnet, along with John Sunderland in the US and John Dickson in the UK and will involve asking sites to perform the validation testing so that all makes and models of SPECT imaging systems are covered. This project will also provide a multi=centre evaluation of the ARTnet Insert that we have developed to deal with the problem of storing large volume (10 L) long-lived radioactive phantoms (3). Price Jackson (PMCC) will be involved in the 3rd project, testing the dosimetry software workflows for kidneys and bone marrow. The 4th project, the collection of human data to test dose-response relationships, is the most ambitious phase and is contingent on success in the first three phases of the development. Every aspect of the project is fully costed so that the sites involved in the projects will be paid for their time, phantoms and standards will be provided, and all services being supplied will be appropriately funded.
We are fortunate in Australia and New Zealand to have had over a decade of experience now in the trials space co-ordinated by ARTnet. This has provided us with valuable lessons in how to achieve site accreditation and
the logistics involved with the test objects and analyses that are required (4). This has allowed ARTnet/ANZSNM to have a place at the table in both of these international initiatives.
Figure 2: The first three sub-projects in Phase 1 of the PDIB trial are shown in the main boxes on the left. All phases are run in parallel.
ARTICLE: ARTnet Delivering Impact to Enhance Clinical Trial Site Accreditation and Dosimetry (Continued)
PDIB Partners
Radiopharmaceutical Innovator Partners
• Eli Lilly and Company
• Fusion Pharmaceuticals (a member of the AstraZeneca Group)
• Novartis US
• RayzeBio, a Bristol Myers Squib Company
Biotechnology Companies
• ITM
• Lantheus
• NorthStar
• Perspective Therapeutics
• Telix Pharmaceuticals
Start Ups & Software/Device Developers
• Capintec (a Mirion Medical Company)
• Hermes Medical Solutions
• MIM Software (a GE Healthcare Company)
• RAPID
• VOXIMETRY
Public Sector Partners
• ANSTO
• Belgian Nuclear Research Centre (SCK CEN)
• National Cancer Institute (NCI, US)
• National Physical Laboratory (NPL, UK)
• NIST (US)
• National Research Council of Canada (CNRC)
• US FDA
Medical Societies
• ANZSNM
• SNMMI
Academic Partners
• BC Cancer (CAN)
• Institute of Nuclear Medicine (GBR)
• Oslo University Hospital (NOR)
• Peter MacCallum Cancer Centre
• University College London (GBR)
• University of Alabama at Birmingham (USA)
• University of Iowa (USA)
• University of Sydney
References
1. Hricak H, Abdel-Wahab M, Atun R, et al. Medical imaging and nuclear medicine: a Lancet Oncology Commission. Lancet Oncol. 2021;22:e136-e172
2. Bailey DL, Willowson KP, O'Keefe GJ, et al. A Method for Validating PET and SPECT Cameras for Quantitative Clinical Imaging Trials using Novel Radionuclides. J Nucl Med. 2025;66:315-322
3. Bailey DL, Willowson KP, Muñoz-Ferrada C. A Practical Method for Assessing Quantitative Scanner Accuracy with Long-Lived Radionuclides: The ARTnet Insert. Asia Oceania J Nucl Med Biol. 2024;12
4. Francis RJ, Bailey DL, Hofman MS, Scott AM. The Australasian Radiopharmaceutical Trials Network (ARTnet) - Clinical Trials, Evidence and Opportunity. J Nucl Med. 2020;62:755-756.
Reproduced with permission from JMIRS
Journal of Medical Imaging and Radiation Sciences 56 (2025) 101919
www.elsevier.com/locate/jmir
Piloting a paediatric nuclear medicine colouring-in book in Australia and New Zealand
Rebecca J. Mangelsen a,∗,Ruby R. Holman a,Katherine Guerrero
a andKaren L. Jones a,b
a Allied Health and Human Performance Academic Unit, University of South Australia, Adelaide, SA, 5000, Australia
b Centre of Research Excellence in Translating Nutritional Science to Good Health, Adelaide Medical School, University of Adelaide, SA, Australia
ABSTRACT
Background: Well-informed paediatric patients experience reduced anxiety and improved outcomes during medical procedures. While age-appropriate education materials exist for alternate medical imaging modalities, only two resources exist globally for nuclear medicine. This student-led project aimed to develop a nuclear medicine colouring-in book for children aged 7-10 years, and to evaluate its impact from the nuclear medicine technologist (NMT) perspective.
Methods: A colouring-in book was developed following an extensive literature search and personal communication, with NMTs in the field. A total of 1000 colour A5 books were printed and distributed to nuclear medicine departments in Australia (n=8) and New Zealand (n=3), based on geographical location and paediatric workload. Twomonths after distribution, NMTs were surveyed via Microsoft Forms to assess the book’s application and utility with five Likert scale, and two short-answer, questions.
Results: Gender, race, rural accessibility, and age were identified as important factors for paediatric health education and incorporated in the colouring-in book. Survey responses were received from 8 of the 11 departments, yielding a response rate of 73%. Of respondents, 75% (n=6) found the book “quite valuable”for paediatric patients, and “quite beneficial”for parents/caregivers. Additionally, 75% (n=6) stated the book was most helpful for patients aged 4 to 6 years, with reported benefits including engagement, distraction, and serving as an icebreaker activity.
Conclusions: This pilot project was a worthwhile experience for patients, departments, and students, yielding positive feedback upon de-
partmental application. Further data is required to evaluate the patient and caregiver experience.
RÉSUMÉ
Contexte: Les patients pédiatriques bien informés ressentent moins d’anxiétéet obtiennent de meilleurs résultats lors des procédures médicales. Bien qu’il existe du matériel éducatif adaptéàl’âge pour d’autres modalités d’imagerie médicale, il n’existe que deux ressources au niveau mondial pour la médecine nucléaire. Ce projet menépar des étudiants visait àdévelopper un livre de coloriage sur la médecine nucléaire pour les enfants âgés de 7 à10 ans, et àévaluer son impact du point de vue des technologues en médecine nucléaire (TMN).
Méthodologie: Un livre àcolorier a étédéveloppéàla suite d’une recherche documentaire approfondie et de communications personnelles avec des technologues en médecine nucléaire (TMN) sur le terrain. Au total, 1 000 livres àcolorier en format A5 ont étéimprimés et distribués aux services de médecine nucléaire en Australie (n = 8) et en Nouvelle-Zélande (n = 3), en fonction de leur situation géographique et de leur charge de travail pédiatrique. Deux mois après la distribution, les technologues en médecine nucléaire ont étéinterrogés via Microsoft Forms pour évaluer l’application et l’utilitédu livre àl’aide de cinq questions sur une échelle de Likert et de deux questions àréponse courte.
Résultats: Le sexe, la race, l’accessibilitéen milieu rural et l’âge ont été identifiés comme des facteurs importants pour l’éducation àla santé pédiatrique et ont étéintégrés dans le livre àcolorier. Des réponses à
Funding: This project was supported by funding from the Australian and New Zealand Society of Nuclear Medicine (ANZSNM).
Competing interests: All authors declare no conflict of interest. Contributors: All authors contributed to the conception or design of the work, the acquisition, analysis, or interpretation of the data. All authors were involved in drafting and commenting on the paper and have approved the final version.
Ethical approval: The protocol was approved by the Human Research Ethics Committee of the University of South Australia, HREC approval number: 205065.
l’enquête ont étéreçues de 8 des 11 services, ce qui représente un taux de réponse de 73 %. Parmi les répondants, 75 % (n = 6) ont trouvé le livre «assez précieux »pour les patients pédiatriques et «assez bénéfique »pour les parents/tuteurs. De plus, 75 % (n = 6) ont déclaréque le livre était particulièrement utile pour les patients âgés de 4 à6 ans, les avantages signalés étant notamment l’engagement, la distraction et le fait qu’il s’agissait d’une activitébrise-glace.
Keywords: Paediatric; Nuclear Medicine; Colouring-in; Book
Introduction
Children, particularly younger children, who do not understand their medical procedure tend to be less cooperative and experience heightened anxiety, leading to a reduction in overall patient well-being [1,2] Children between the age of three and four years start to develop their own beliefs and desires, hence, it is important that they are informed before undergoing a medical procedure [3]. Moreover, from the age of five years, children demonstrate a reasonable understanding of language, with logic reasoning developing from six years of age [3] This does not imply competence for all children, rather an indication of average competence given substantial variation in developmental capacities and external factors [3].
Lack of understanding combined with an unfamiliar environment may culminate in reduced cooperation which, within nuclear medicine, may impede workflow, imaging methods, and image quality [1,2]. The use of sedation and general anaesthesia can be employed to obtain a diagnostic scan [4,5]; however, use should be minimised where possible due to the risk, cost, and associated stressors for patients and caregivers [6] To optimise patient wellbeing and imaging outcomes, thorough patient preparation and the implementation of distraction techniques are crucial [4].
Stutey & Wubbolding discuss that drawing as a therapeutic strategy is challenging for some children lacking fine motor skills [7] However, it is important to note that the application of play therapy is limited in a nuclear medicine department by healthcare hygiene standards, supervision, and space availability. In today’s society, children are readily exposed to digital devices and the tradition of paper-based children’s books is often replaced by an iPad. However, the question remains - what is the most effective medium to portray health literacy information? A meta-analysis conducted by Furenes et al. [8] compared children’s story comprehension and vocabulary development across the two mediums of digital versus paper and found that children aged 1-8 years with adult support had lower comprehension scores with digital books. This highlights the importance of a tangible book that allows children the opportunity to read at their own pace to ensure they comprehend the presented information.
Healthcare-specific colouring-in books have proven successful as educational resources [9-14]. One colouring-in book for general outpatient medical imaging modalities i.e. computed
Conclusions: Ce projet pilote a étéune expérience enrichissante pour les patients, les services et les étudiants, et a donnélieu àdes retours positifs lors de l’application au sein des services. Des données supplémentaires sont nécessaires pour évaluer l’expérience des patients et des soignants.
tomography (CT), fluoroscopy and nuclear medicine procedures has been evaluated [10] They evaluated anxiety levels of children aged 3-10 years by surveying parents. Parents reported that providing a child with an instructional colouringin book did not significantly reduce the child’s anxiety immediately prior to the imaging test [10]. However, surveys determined that access to the book was appreciated by nearly all parents and caregivers [10] One additional radiology book series has been created, however, no analysis of their application has been performed [15]
The integration of play aims to promote a positive experience by reducing anxiety and building confidence within the healthcare environment [16] Hence, colouring-in books can provide a mechanism to introduce play to the nuclear medicine setting, with the added benefit of providing information to the child and caregiver in an age-appropriate format.
The aims of this project were two-fold: (i) to develop a nuclear medicine specific paediatric colouring-in book and (ii) to distribute and evaluate the colouring-in book, from the perspective of the NMT, in a pilot study of nuclear medicine departments spanning Australia and New Zealand.
Methods
Development of the colouring-in book
A preliminary search of common public-facing search engines (Google and Yahoo), in addition to PubMed and MEDLINE, using the key words “nuclear medicine”, “colouring-in”, “book”, and “paediatric education”, demonstrated one nuclear medicine specific colouring-in book and one iteration specific to positron emission tomography (PET) with CT (PET/CT) [15] Both are authored by the same organisation in the United States of America and offer different versions based on gender [15]. However, no formal evaluation of their application was performed and a gap in Australian and New Zealand resources was identified [15]
"Raju’s colouring-in book" was created to complement existing resources and fill the gap in paediatric nuclear medicine resources, offering a fun, hands on approach that would integrate seamlessly into everyday clinical practice. The consultation process played a key role in shaping the development of the book. Through discussion with two experienced paediatric NMTs from the Women’s and Children’s Hospital in Adelaide,
South Australia, and direct observation of the paediatric nuclear medicine department, valuable insights were gained into the most commonly performed procedures, and the local workflow where the book would be used. This contact informed the design and content, ensuring it was practical and relevant. The book prototype was then developed and designed by the authors who were in their second-year of a four-year bachelor’s degree in nuclear medicine at the time of the project.
Design rationale
A general nuclear medicine study (rather than a specific radionuclide bone or renal scan) was selected due to versatility. The lengthy wait time between topical anaesthesia cream activation time, radiopharmaceutical injection and scan time provided an opportunity for the book to be utilised by children within nuclear medicine departments.
The book is comprised of 27 A5-pages with a flexible gloss cover and colour print to highlight key words. The pages include the storyline (63%), and child-appropriate activities e.g. a word-search, a maze, blank spaces to draw, “about the creators” sections tailored to both children and adults, a colourable logo, and a thank you page. All text and illustrations were designed by the authors.
The book’s content focused on inclusion, with gender, race, and access to healthcare as considered features. The protagonist was gender neutral, had a traditionally Hindi name, ‘Raju’, and was described as travelling 3 hours to receive the scan. The inclusion of children who travel far from home for their medical procedure was incorporated to cater for children from rural and regional areas, by asking the reader how long it took them to reach the department. Inclusion spanned to the multidisciplinary nature of nuclear medicine: key staffin the patient’s journey were introduced, such as the receptionist, nurse, NMT, radiopharmacist, physicist, and nuclear medicine physician.
The language, content, and design of the book were intentionally chosen to create a light-hearted and optimistic approach. Language focused on descriptive words with positive connotations such as ‘you are now super strong and brave’ and ‘star of the show’ to promote a sense of emotional validation for the audience. The language used in the book also reflected common phrases heard in paediatric nuclear medicine departments, as advised by NMTs. For example, immobilisation techniques were described using terms like “wrap you like a sausage roll”and “put your seat belts on to keep you extra safe.”Injection techniques were described as putting a ‘special medicine in your arm’; no mention of words with negative connotations, such as ‘pain’, ‘needles’, ‘injection’, etc. were included to reduce fear and medical anxiety.
Keywords were highlighted using bright colours to enhance the tone of the book. The inclusion of phonetic syllable breakdowns of difficult works, such as “nuclear”and “technologist”, provided the reader (be that the child or the parent reading aloud to the child) with an opportunity to learn and engage.
All illustrations were made to colour-in, introducing the child to the surrounding nuclear medicine environment and
further enhance their understanding of the procedure. Illustrations included Raju with common nuclear medicine elements, such as the gamma camera and their pictures. Play elements, such a “Parts of the Body”word search and a “Find the Gamma Camera”maze were included to promote engagement and distraction.
A physical copy book was chosen over an internet application due to versatility, cost, and accessibility, minimising reliance on technology and reducing socioeconomic barriers. A cost comparison of internet application development revealed it to be prohibitively expensive for this pilot project. In contrast, physical books are cost effective and the compact A5 sizing ensures portability, allowing the book to be easily taken home before or after appointments.
Taking all of the factors above into consideration, “Raju’s interactive colouring-in book”was produced (Fig. 1).
Upon completion, a graphic designer assisted with the book’s layout, design, and aesthetic considerations. A final print copy was created, and 1000 copies of the book were printed.
Distribution of the colouring-in books
For this pilot study, 1000 colouring-in books were distributed to nuclear medicine departments across Australia (n=8) and New Zealand (n=3). Crayons were not included due to logistical and financial limitations. Departments were selected on the basis of their geographical location, ensuring that all states and territories in Australia, and both islands in New Zealand were represented. Paediatric workload also influenced the quantity of books delivered to each site. New South Wales and Te Ika-a-Maui (North Island) of New Zealand each received 180 copies of the book. South Australia, Western Australia, Queensland, Victoria, and Te Waipounamu (South Island) of New Zealand each received 90 copies. Tasmania and Northern Territory each received 50 copies, and 90 copies were distributed at the Australia and New Zealand Society of Nuclear Medicine (ANZSNM) Annual Scientific Meeting held in Adelaide, May 2023. The suggested application for departments was to use the book while patients were waiting for topical anaesthetic activation or radiopharmaceutical uptake. However, it was at the discretion of the NMT to determine when patients received the book, as patient needs vary.
Questionnaire for evaluation of the colouring-in book
A questionnaire was developed using the Microsoft Forms platform. The survey included 7 questions to assess staffperceptions of the book using 5-point quantitative Likert scale questions (n=5), and qualitative open-ended questions (n=2). The following 5 questions were included in the survey: (1) “How valuable is the colouring-in book as a resource for paediatric patients?”, (2) “How beneficial do you think the colouring-in book is for the parents/caregivers?”, (3) “How engaging was the colouring-in book for your patients?”, (4) “How versatile was the colouring-in book in relation to different scans?”, (5) “Please indicate the age group you think benefits the most from
the colouring-in book.”. Questions 1-4 required participants to select from the following scale: “not at all”, “limited”, “somewhat”, “quite”, “extremely”. Question 5 required the participants to select the recommended age group from the following options: “0-3 years”, “4-6 years”, “7-10 years”, “10-12 years”, “12 years +”. The following open-ended questions (n=2) were included in the survey: (6) “What do you perceive as the main benefits of using the colouring-in book in your department?”, and (7) “Do you have any suggestions to improve the colouringin book?”. The survey did not assess children or parental anxiety due to ethics limitations.
The questionnaire was distributed via email, with a link to Microsoft Forms, two months after receipt of the books to assess their application and utility. Survey participation was not mandatory; however, departments were encouraged to respond to the survey and all responses were anonymous.
Data analysis
Data is presented in tables with both quantitative values based on the Likert scale questions and open-ended qualitative answers.
Results
Evaluation of the colouring-in book
A total of 8 of the 11 departments (73%) chose to take part in the survey and completed the questionnaire. The senior NMT who was responsible for book implementation was instructed to complete the survey on behalf of their department. One respondent (Respondent 6) completed the Likert scale questions but did not respond to the open-ended questions.
Responses to Likert scale questions are summarised in Figs. 2 and 3. A positive response to the colouring-in book was
seen for all questions. The suggested target age group was 4-6 years old (75%), with a minority (12%) supporting a target age group of 7-10 years old. Survey results on the perceived benefits of a colouring-in book in nuclear medicine departments, and suggested improvements are presented in Table 1
Surveyed departments demonstrated a similar perceived value of the colouring-in book as a resource for paediatric patients, and the benefit of the colouring-in book to parents/caregivers. One respondent (12.5%) ranked the value as “somewhat valuable”, six respondents (75%) found the application “quite valuable”, and one (12.5%) found the book “extremely valuable”. The one department that found the book “somewhat valuable”also perceived the book as “somewhat beneficial”. All departments that found the book “quite valuable”also ranked its application as “quite beneficial”, and the department that perceived the book as “extremely valuable”also ranked the application as “extremely beneficial”. The versatility of the book, which focused on the relevance of the book for different nuclear medicine scans, revealed an even division of responses between “somewhat versatile”(n = 4) and “quite versatile”(n = 4).
One department (12.5%) explained a reduction in patient anxiety as a perceived benefit. Education of patients regarding nuclear medicine scans was recognised by 37.5% (n = 3) of departments, and distraction was mentioned by 50% (n = 4) of departments as a benefit of the colouring-in book application.
Discussion
"Raju’s colouring-in book" serves as an engaging tour of a typical nuclear medicine department, which uses participatory methods to engage a child in their medical procedure, which is an important step in paediatric information exchange [17] Ultimately, the proposed book was created to improve clinical outcomes and patient well-being in paediatric nuclear medicine 4 R.J. Mangelsen, R.R. Holman, K. Guerrero et al. / Journal of Medical Imaging and Radiation Sciences 56 (2025) 101919
Fig. 1. The A5-sized paediatric nuclear medicine colouring-in book.
2. Department responses to Likert Scale questions (n =8).
Fig. 3. Department responses to statement “Please indicate the age group you think gains the most from the colouring-in book?”(n=8).
scans by educating children on the procedure whilst simultaneously providing distraction and entertainment.
Cultural and gender inclusivity greatly influenced the creation of the protagonist. In 2021, over 27.6% (7 million) of the Australian population were born overseas, not including second or third–generation Australians whose parents or grandparents were born overseas [18] In 2021, India was the second highest overseas country of birth, behind England, for the Australian
population [18] Thus, to reflect the multicultural society of modern Australia, a traditional Hindi name, Raju was selected for the protagonist. Raju was portrayed as a gender-neutral character, intentionally never referred to by any pronouns, providing an opportunity for both girls and boys to identify with the protagonist.
This pilot project, initiated and driven by two undergraduate nuclear medicine students at the University of South Aus-
Fig.
R.J. Mangelsen, R.R. Holman, K. Guerrero et al.
Table 1
Department responses to short-answer questions.
Respondent Question
What do you perceive as the main benefits of using the colouring-in book in your department?
1 An activity for the patients while they were waiting -
2 Patient engagement, occupies child whilst Elma cream is ‘working’
3 Distraction, desensitisation
4 Ice breaker for both parents and children
5 Takes away some of the mystery of Nuclear Medicine and reduces anxiety, making it seem a more “fun”place.
6 - -
7 Great way to educate the kids about the basics of a nuclear medicine scan, in a fun and engaging manner
8 Education, distraction and enjoyment
tralia, resulted in the creation of a valuable resource for departments who provide nuclear medicine services to paediatric patients. This is demonstrated by positive survey responses, with implementation perceived as beneficial for both children, caregivers and healthcare providers.
The book permitted further development of patients’ procedural understanding to complement the verbal explanations the children receive whilst in the department. Informed children, being those who are prepared and understand the procedure, are experience an improved clinical experience, and more often display cooperative behaviours [2,19] Thus, a colouring-in book was chosen as an age-appropriate tool to convey information to children.
In patient scenarios where health literacy is poor, such as in paediatrics, [20] healthcare providers should adapt their communication to match that of the developmental level of their patient to improve health outcomes [21] The book employed age-appropriate language to address the young target audience, deemed to be four to six years old by 75% of the departments surveyed. Phonetic syllable breakdowns of difficult words, such as technologist (tek-nol-o-jist) and nuclear (new-klee-ah) were employed to ensure the audience could understand the medical terminology. Additionally, positively connotated words including “special”, “smile”, “magic”, “cool”, “colourful”and “fun” were utilised throughout to promote a positive healthcare experience.
Current literature heavily focuses on the involvement of parental involvement in paediatric information exchange [20,22]. Parental anxiety is common in radiology procedures, often due to a lack of detailed information, which in turn may increase paediatric patient anxiety [10] Thus, the application of a colouring-in book serves as a valuable resource for not only children but also parents and caregivers to receive procedural information. This was reflected within the data as the majority (75%) of departments deemed the book “quite beneficial” for parents and caregivers, and “quite valuable”for paediatric patients (75%).
Do you have any suggestions to improve the colouring-in book?
Maybe change a few questions, to make it more relevant to be sent in advance with appointment letter.
Great idea and concept. Can be expanded to other areas of imaging, and life!
Not at the moment
Not really, great job!
Take the Elma away to standardise it (or have the pages removable for site specific)
Nil at this stage.
A study by Turturro and Drake, [23] assessed the psychological and psychophysiological effect of colouring-in and drawing in an adult population, and concluded that colouring-in and drawing successfully reduced anxiety in adults by employing distraction and expression. Hence, the book adopted an interactive colouring-in style, with games, rather than a traditional storybook style to promote distraction and engagement. Drawing prompts, such as “Draw yourself as a superhero”and “Draw what your pictures will look like”, promoted expression and individualism. Furthermore, asking the patient to “Draw what they see”encourages the patient to engage in their surroundings, fostering cooperation and a positive relationship with healthcare professionals and the environment. The book was written with fictional elements, such as superpowers resulting from topical anaesthesia (termed “magic cream”), and interactive components to encourage child engagement and participation in the procedure.
A general nuclear medicine study was selected due to versatility, allowing a larger audience to benefit from the book, which was reflected in the survey as 50% of departments found the application of the book quite versatile.
A study by Johnson et al., [10] assessed the effect of a radiology-specific colouring-in book on paediatric patient anxiety and reported no reduction in anxiety in the intervention group compared to the control group. However, most parents perceived the book as informative and were grateful to have received it [10] Although no parent/caregiver feedback was obtained in this study, Johnson et al.’s [10] equivalent results support NMTs’ perception of the book being “quite beneficial”for parents and caregivers. Assessment techniques vastly differed from Johnson et al., [10] as surveys were completed by NMTs, as opposed to patients and caregivers.
An additional benefit of the study was the ability to serve as a professional development exercise for two undergraduate nuclear medicine students. The exposure to industry partnerships, paediatric patient considerations, and project management highlight the importance of early industry involvement
to develop professional skills. Project implementation was facilitated through industry connections provided by the academic and industry mentors. Thus, the project also demonstrates the importance of academic and industry mentors in the success of extra-curricular projects for undergraduate students.
The pilot investigation of an educational colouring-in book for paediatric nuclear medicine applications in Australia and New Zealand has demonstrated the potential to improve clinical outcomes. In the results, NMTs highlight the importance of distraction in paediatric nuclear medicine procedures and demonstrate a colouring-in book can be an effective tool for the selective engagement and distraction of young patients. Results support current literature that health-based colouring-in books are valuable vectors in paediatric information exchange [9-14]
As a pilot project the study had some limitations. The colouring-in books were not distributed to all nuclear medicine departments in Australia and New Zealand, hence, the sample size of respondents was relatively modest. Furthermore, the evaluation was limited to the perceptions of the nuclear medicine staffrather than the children engaging with the colouring-in book or the caregiver(s). Further studies are therefore warranted to assess patient and caregivers’ perceived impact of the colouring-in book. Future directions may also include workflow efficiency evaluation, by assessing appointment duration with and without the application of the colouring-in book.
Conclusion
A paediatric nuclear medicine colouring-in book was successfully developed for use in Australia and New Zealand with survey results indicating that NMTs perceive the resource to be beneficial to patients, parents and caregivers. Colouringin books serve as an age-appropriate patient education material format, which may improve procedural understanding whilst providing a distraction from scan-associated unpleasantries. Further directions could include an assessment of the patient and parent or caregiver’s perceived value of the book.
Acknowledgements
The authors would like to thank all those who contributed to this research and the preparation of this manuscript. We are particularly grateful to Victoria Sigalas’ (Former Head Nuclear Medicine Paediatric Specialist Technologist, Women’s and Children’s Hospital) support with this project. Thanks, are also due to Ester Gomez (former ANZSNM graphic designer) for her assistance in the creation and distribution of the colouringin book and in its promotion on social media.
Data from this project was presented at the ANZSNM Annual Scientific Meeting, held in Adelaide in May 2023 and subsequently published in abstract form in the Internal Medicine Journal in the Special Issue: ANZSNM ASM, 26-28 May 2023, volume 53, issue S4 [24].
References
[1] Goodhue R, Dakin P, Noble K. Exploring Australia’sWellbeing Framework for Children and Young People What’s in the Nest?. Canberra, Australia: ARACY; 2021 https://www.aracy.org.au/documents/item/700#: :text=The%20Nest%20is%20Australia’ s%20wellbeing, young% 20person%20needs%20to%20thrive
[2] McQuattie S. Pediatric PET/CT imaging: tips and techniques. J Nucl Med Technol 2008;36(4):171–178. doi:10.2967/jnmt.108.051995
[3] Grootens-Weigers P, Hein I, Van Den Broek JM, De Vries MC. Medical decision-making in children and adolescents: developmental and neuroscientists aspects. BMC Pediatr 2017;17(1):120 -120. doi:10.1186/ s12887- 017- 0869- x
[4] Gernhold C, Kundtner N, Steinmair M, Henkel M, Oswald J, Haid B. Sedation rate reduction in paediatric renal nuclear medicine examinations: Consequences of a targeted audit. Children (Basel) 2021;8(5):424. doi:10.3390/children8050424
[5] Mandell GA, Cooper JA, Majd M, Shalaby-Rana EI, Gordon I, Smith WJM. Procedure guideline for pediatric sedation in nuclear medicine. J Nucl Med (1978) 1997;38(10):1640–1643
[6] Gelfand MJ, Clements C, MacLean JR. Nuclear medicine procedures in children: special considerations. Semin Nucl Med 2017;47(2):110–117. doi:10.1053/j.semnuclmed.2016.10.001
[7] Stutey DM, Wubbolding RE. Reality play therapy: a case example. Int J Play Ther 2018;27(1):1–13. doi:10.1037/pla0000061
[8] Furenes MI, Kucirkova N, Bus AG. A comparison of children’s reading on paper versus screen: a meta-analysis. Rev Educ Res 2021;91(4):483–517. doi:10.3102/0034654321998074
[9] McDonald R, Thomsen A, Belessis Y, Jaffe A. 292 CF and Me –a colouring book for children. J Cystic Fibrosis 2007;6:S71 –S71. doi:10.1016/ S1569- 1993(07)60267- 7
[10] Johnson AJ, Steele J, Russell GB, Moran R, Fredericks KP, Jennings SG. Decreasing pediatric patient anxiety about radiology imaging tests: prospective evaluation of an educational intervention. J Child Health Care 2009;13(4):370–382. doi:10.1177/1367493509344826
[11] Lerman J, CotéCJ, Steward DJ. Foundations of pediatric anesthesia. Manual of Pediatric Anesthesia Springer International Publishing AG; 2016:1–8. doi:10.1007/978- 3- 319- 30684- 1_1
[12] Morrison-Levy N, Knight-Madden J, Royal-Thomas T, King L, Asnani M. Improving disease knowledge in 6- to 10-year-olds with sickle cell disease: a quasi-experimental study. Child : Care Health Dev 2018;44(3):501–506. doi:10.1111/cch.12559
[13] Naumann PL, Huss K, Calabrese B, Smith T, Quartey R, Van de Castle B, Lewis C, Hill K, Walker J, Winkelstein M. A+ Asthma Rural Partnership coloring for health: an innovative rural asthma teaching strategy. Pediatric Nurs 2004;30(6):490–494
[14] Godshall M. Exploring learning of pediatric burn patients through storytelling ProQuest Dissertations Publishing; 2013
[15] Children’s Hospital of Pittsburgh (n.d). Adventure Series Color Book. UPMC Children’s Hospital of Pittsburgh. https://www.chp.edu/ our- services/radiology/coloring- book
[16] Russell B, Oh S, Dillman Taylor D. Integration of adlerian play therapy in pediatric hospitals. J Child Adolesc Couns 2019;5(1):61–72. doi:10. 1080/23727810.2018.1556987
[17] Lambert V, Long T, Kelleher D. Communication Skills for Children’s Nurses 1st ed. McGraw-Hill Education; 2012
[18] Australian Bureau of Statatics. (2022). Cultural Diversity of Australia. ABS. https://www.abs.gov.au/articles/cultural- diversity- australia#: : text=In%202021%2C%20just%20over%207,Australia%20who% 20were%20born%20overseas
[19] Bray L, Appleton V, Sharpe A. The information needs of children having clinical procedures in hospital: Will it hurt? Will I feel scared? What can I do to stay calm? Child: Care Health Dev. 2019;45(5):737–743. doi:10. 1111/cch.12692
[20] Bröder J, Okan O, Bauer U, Bruland D, Schlupp S, Bollweg TM, Saboga-Nunes L, Bond E, Sørensen K, Bitzer E-M, Jordan S, Domanska O, Firnges C, Carvalho GS, Bittlingmayer UH, Levin-Zamir D,
R.J. Mangelsen, R.R. Holman, K. Guerrero et al. / Journal of Medical Imaging and Radiation Sciences 56 (2025) 101919 7
Pelikan J, Sahrai D, Lenz A, Pinheiro P. Health literacy in childhood and youth: a systematic review of definitions and models. BMC Public Health 2017;17(1):361 –361. doi:10.1186/s12889-0174267-y
[21] Chau M. Cultural diversity and the importance of communication, cultural competence, and uncertainty in radiography. J Med Imaging Radiat Sci. 2020. doi:10.1016/j.jmir.2020.04.005.
[22] Jones E, Struik S. G199(P) Effective communication in paediatrics: what does this mean? Arch Dis Child 2016;101(Suppl 1):A106 –A106. doi:10. 1136/archdischild- 2016- 310863.190
[23] Turturro N, Drake JE. Does coloring reduce anxiety? Comparing the psychological and psychophysiological benefits of coloring versus drawing. Empir Stud Arts 2022;40(1):3–20. doi:10.1177/0276237420923290
[24] Abstracts. Intern Med J. 2023;53(S4):64–65. doi:10.1111/imj.16274.
PRUE LAMERTON, ONZM
Prue Lamerton, a longstanding member and great contributor to the profession and ANZSNM was recognised in the New Zealand New Year Honours List for "services to Nuclear Medicine" and as an Officer of the NZ Order of Merit.
PROF MICHAEL HOFMANN
Professor Michael Hofmann, received the Eric Susman Prize from the Royal Australasian College of Physicians. He was recognised for his pioneering work in theranostics – combining precision nuclear imaging with targeted radiotherapy – which is transforming the way prostate cancer is diagnosed and treated globally.
PROF ANDREW SCOTT
Professor Andrew Scott, was this year’s recipient of the the prestigious 2025 Henry N. Wagner, Jr., MD Lecture at the SNNMI Annual Meeting. Each year, a luminary in the field of nuclear medicine is invited by the SNMMI Scientific Program Committee to give this important lecture. Andrew was presented the award by SNNMI President Cathy Cutler and VP-Elect Heather Jacene at the meeting picturered above.
Andrew also received the Minoshima-Pappas Transformative Leadership Award as a testament to his dedication and international impact on Nuclear Medicine. Andrew is picturered with Sze Ting Lee above.
PRESIDENT
Prof Karen Jones (SA/NT)
Vice President
Vacant
Immediate Past President
Dr Kevin London (NSW/ACT)
Treasurer
Dr Daniel Badger (SA/NT)
FEDERAL COUNCIL
Prof Karen Jones (President)
Dr Kevin London (Immediate Past President)
Dr Daniel Badger (Treasurer)
Ms Suzanne McGavin (Chair TSIG)
A/Prof Grace Kong (Chair MSIG)
Dr Nigel Lengkeek (Chair RPS SIG)
Dr George McGill (Chair Physics SIG)
Ms Jessica Fagan (Chair of Branches)
Ms Jessica Fagan (NZ Rep)
Prof Andrew Scott (IRC/Medical Rep)
Vacant (ANSTO Rep)
Mrs Pru Burns (CCC Rep)
SPECIAL INTEREST GROUPS/ COMMITTEES
Technologists
Chair: Ms Suzanne McGavin
Medical
Chair: A/Prof Grace Kong
Radiopharmaceutical Science
Chair: Dr Nigel Lengkeek
Physics
Chair: Mr George McGill
Quality and Technical Standards Committee
Chair: Dr Darin O’Keeffe
Scientific Advisory Panel
Chair: Prof Dale Bailey
International Relations Committee
Chair: Prof Andrew Scott
Conference Convening Committee
Chair: Mrs Prudence Burns
Scientific Education Committee
Chair: Prof Andrew Scott
BRANCH SECRETARIES
New South Wales/Australian Capital Territory
Holly Spooner
Queensland
Ms Neena Sunny and Ms Stephanie Schulz
South Australia/Northern Territory
Mr Jagi Sandhu and Ms Emily James
Victoria/Tasmania
Ms My Linh Diep
Western Australia
Ms Rosemary Dallen
New Zealand
Ms Trish Mead
Rural/Regional Branch
Mr Lachlan Patterson
GENERAL MANAGER & SECRETARIAT
All Correspondence
Mr Rajeev Chandra, General Manager ANZSNM Secretariat, PO Box 6178, Vermont South, Victoria 3133
Tel: 1300 330 402 | Fax: (03) 8677 2970
Email: secretariat@anzsnm.org.au
AIMS AND OBJECTIVES OF THE AUSTRALIAN AND NEW ZEALAND SOCIETY OF NUCLEAR MEDICINE
1. Promote:
• The advancement of clinical practice of nuclear medicine in Australia and New Zealand;
• Research in nuclear medicine;
• Public education regarding the principles and applications of nuclear medicine techniques in medicine and biology at national and regional levels;
• Co-operation between organisations and individuals interested in nuclear medicine; and
• The training of persons in all facets of nuclear medicine.
2. Provide opportunities for collective discussion on all or any aspect of nuclear medicine through standing committees and special groups:
• The Technical Standards Committee sets minimum standards and develops quality control procedures for nuclear medicine instrumentation in Australia and New Zealand.
• The TSIG Committee is the group overseeing the Technologist Special Interest Group (TSIG) and ensures that all projects, committees and activities of the TSIG align with the values and strategic plan of the ANZSNM. It reports directly to the ANZSNM Federal Council and oversees the two TSIG working groups: CPD & Education Working Group and Technologist Workforce Advocacy Working Group. The committee is able to form working groups to perform specific tasks as required to provide opportunities for the benefit of Technologist members of the ANZSNM after consultation with the ANZSNM Federal Council.
• The Radiopharmaceutical Science SIG and a Physics SIG that maintain standards of practice for their particular speciality and provide a forum for development in Australia and New Zealand.
Scan the QR code to stay informed about job offers in the field of Nuclear Medicine.