David Heath details how to enhance the patient experience via ‘smart clinics’


VOLUME 7/ISSUE 12 - NOVEMBER 2020
Creating a Smart Clinic
Treating Migraines with Toxin
Using Radiofrequency Microneedling
2020 Allergan. All rights reserved. Model treated with Juvéderm. Individual patient results may vary. Produced and Funded by Allergan Aesthetics. UK-JUV-2050344 October 2020 Adverse events should be reported. Reporting forms and information can be found at https://yellowcard.mhra.gov.uk/. Adverse events should also be reported to Allergan Ltd. UK_Medinfo@allergan.com or 01628 494026. THEIR LOOK Juvederm_AnyLevel_MagazineCover_Aesthetics Key Visual_V2.0.indd 1 14/10/2020 14:29 EXCLUSIVEBEAUTYBEYOND P.36-37! Muscle Stimulation CPD Dr Nestor Demosthenous introduces muscle-stimulating technologies
Practitioners discuss using botulinum toxin to treat chronic migraine
Practitioners highlight the benefits of RF microneedling We believe the most natural looking, long lasting results are achieved by enhancing your client’s features, not changing them. That’s why this year we’ll be launching a striking new campaign to educate your clients about our Juvéderm® Vycross range. In fact, our versatile range of fillers includes five tailored products, each designed to benefit a specific area of the face at the optimum dermal level. Which means you can offer your clients a more bespoke and tailored treatment to suit their needs. So, for good results for your clients and your business, choose Juvéderm®. *Juvéderm® offers a range of facial fillers to answer a variety of needs, each of which is administered at a different dermal layer. To find out why Juvéderm® could work for your clinic on every level, visit juvederm.co.uk
Light Therapy







































































THE DIGITRX AWARD FOR PRODUCT INNOVATION OF THE YEAR
Treating Migraines with Toxin
Dr Paul Charlson and Dr Vikram Swaminathan explain how botulinum toxin type A can be used to treat migraines 51 Supporting Patients with PCOS
Dr Aileen McPhillips looks at polycystic ovarian syndrome and skin 55 Abstracts

A round-up and summary of useful clinical papers IN PRACTICE 57 Incorporating LED into Your Practice
Dr Simon Ravichandran provides his tips on purchasing LED devices 58 Creating a Smart Clinic
Medical device researcher Dr David Heath explores the patient experience via ‘smart clinics’ 61 After Foundation Training: What Next?
Dr Manav Bawa shares advice for new practitioners 64 Improving Clinic Processes
Dr Askari Townsend discusses standard operating procedures 66 Optimising Website for Mobile
Digital consultant Rick O’Neill looks at the user mobile experience 69 In Profile: Dr Tapan Patel
The man behind PHI Clinic shares an insight into his clinical life 70 The Last Word: Video Calls and Aesthetic Treatments
Dr Yiannis Valilas and psychologist Jacqui Finnigan explore the ‘Zoom phenomenon’
Clinical Contributors
Dr Nestor Demosthenous obtained his medical degree and BSc Hons Neuro from the University of Edinburgh in 2006. He has 10 years’ experience in aesthetic medicine and is a KOL for Allergan and Cutera Medical Ltd.

Miss Jennifer Doyle has a Bachelor of Medicine and a Bachelor of Surgery and a Master’s in Medical Sciences from the University of Oxford. She has completed the Level 7 in Injectables and is a lead trainer at Harley Academy.
Dr Emmaline J Ashley received a first class honour’s degree in biology from Carleton College in the US. She works in the NHS and in her private aesthetic practice, Ashley Aesthetics. Dr Ashley is currently the aesthetics KOL for ZoomClinic.
Dr Paul Charlson has a background in general practice and 19 years’ experience in aesthetic medicine. He is the past president of the British College of Aesthetic Medicine. Dr Charlson has clinics in London and Yorkshire.

Dr Vikram Swaminathan has aesthetic clinics in the North West and London. He is a faculty member of the British Society of Aesthetic Examiners and Assessors (BSAEA), and an educational supervisor.

Dr Aileen McPhillips currently works as a GP as well as at her aesthetic clinic Aesthetics by Dr Aileen. She is a member of the RCGP and has completed a Level 7 certificate in Injectables for Aesthetic Medicine.




Contents • November 2020 Special Feature Using Radiofrequency Microneedling Page 21 News Special MPs Support Child Regulation Page 16
NEXT MONTH
06 News The latest
16 News
18
19
20
21
27
34
36
39
In Focus: Evolution in Aesthetics • Ultrasound in Aesthetics • Aesthetics Across the Globe • Treating Lipoedema
product and industry news
Special: Children & Injectables Aesthetics reports on the developments to make dermal fillers and botulinum toxin illegal for under 18s
Advertorial: Galderma Reasons to choose Restylane
Advertorial: Help Fund 40,000 Operations Change the lives of children living with facial differences
Advertorial: Holistic Facial Rejuvenation Dr Kate Goldie shares her approach to creating structure with BELOTERO Volume CLINICAL PRACTICE
Special Feature: Using Radiofrequency Microneedling Practitioners highlight the benefits of RF microneedling
CPD: Exploring Muscle Stimulation Dr Nestor Demosthenous introduces muscle-stimulating technologies
Understanding Alternative Uses of Hyaluronidase Miss Jennifer Doyle discusses the different uses of hyaluronidase
Introducing Beyond Beauty Educating and inspiring the public to make safe and ethical choices in aesthetic medicine
Analysing Photobiomodulation
47
Dr Emmaline Ashley outlines benefits of photobiomodulation


































Meeting the needs of your business, delivering high satisfaction to your patients Call us on 01234 313130 info@aestheticsource.com www.aestheticsource.com THE CLINICSOFTWARE.COM AWARD FOR AESTHETIC PRODUCT DISTRIBUTOR OF THE YEAR This weekly at-home treatment peel delivers advanced antiaging benefits to visually improve skin imperfections for more radiant, healthy-looking skin. Clinically shown to improve skin clarity, brightness, texture and radiance. KEY INGREDIENTS BENEFITS 20% blend of Glycolic Acid and antioxidant Citric Acid Visually improves fine lines, wrinkles and uneven skin tone and smoothes blemish-prone skin Pigmentation/clarity3+ WEEK 0 WEEK 8 *% of subjects reporting improvement + After 2 months of weekly use, along with a daily PHA regimen 94% REPAIR CITRIATE SOLUTION Single Use Pad, 1.5 mL / 0.05 fl oz; NEOSTRATA® SKIN ACTIVE REPAIR COLLECTION IMPROVED SKIN TEXTURE*+ + 1x per week SUNBURN ALERT: This product contains an Alpha Hydroxy Acid (AHA) that may increase your skin’s sensitivity to the sun and particularly the possibility of sunburn. Use a sunscreen, wear protective clothing, and limit sun exposure while using this product and for a week afterwards. This weekly at-home treatment peel delivers advanced antiaging benefits to visually improve skin imperfections for more radiant, healthy-looking skin. Clinically shown to improve skin clarity, brightness, texture and radiance. KEY INGREDIENTS BENEFITS 20% blend of Glycolic Acid and antioxidant Citric Acid Visually improves fine lines, wrinkles and uneven skin tone and smoothes blemish-prone skin Pigmentation/clarity3+ WEEK 0 WEEK 8 *% of subjects reporting improvement + After 2 months of weekly use, along with a daily PHA regimen 82% 94% 88% REPAIR CITRIATE SOLUTION Single Use Pad, 1.5 mL / 0.05 fl oz; NEOSTRATA SKIN ACTIVE REPAIR COLLECTION IMPROVED SKIN TEXTURE IMPROVED SKIN RADIANCE*+ HEALTHIER LOOKING SKIN*+ 1x per week CITRIATE SOLUTION This weekly at-home treatment peel delivers advanced anti-ageing benefits to visually improve skin imperfections for more radiant, healthy-looking skin. Clinically shown to improve skin clarity, brightness, texture and radiance. Key Ingredients 20% blend of Glycolic Acid and antioxidant Citric Acid Single Use Pad, 1.5 mL / 0.05 fl oz; AT-HOME PEEL NEW Complete your daily skin care regimen to correct visible signs of ageing 88% IMPROVED SKIN RADIANCE*+ HEALTHIER LOOKING SKIN*+ PIGMENTATION/CLARITY3+ WEEK 0 * % of subjects reporting improvement + After 2 months of weekly use, along with a daily PHA Regimen This weekly at-home treatment peel delivers advanced antiaging benefits to visually improve skin imperfections for more radiant, healthy-looking skin. Clinically shown to improve skin clarity, brightness, texture and radiance. KEY INGREDIENTS BENEFITS 20% blend of Glycolic Acid and antioxidant Citric Acid Visually improves fine lines, wrinkles and uneven skin tone and smoothes blemish-prone skin Pigmentation/clarity3+ WEEK 0 WEEK 8 *% of subjects reporting improvement + After 2 months of weekly use, along with a daily PHA regimen 82% 94% 88% REPAIR CITRIATE SOLUTION Single Use Pad, 1.5 mL / 0.05 fl oz; NEOSTRATA® SKIN ACTIVE REPAIR COLLECTION IMPROVED SKIN TEXTURE*+ IMPROVED SKIN RADIANCE*+ HEALTHIER LOOKING SKIN*+ 1x per week WEEK 8 94% IMPROVED SKIN TEXTURE*+
Chloé Gronow Editor & Content Manager @chloe_aestheticseditor
Hands up if you leave your copy of the journal out for patients to read?!
With such a lack of quality education on aesthetic procedures available in mainstream media, we can see why. But the journal isn’t for them – it’s your resource, written with your medical experience in mind.
So, you may ask, what can you recommend for patients to read instead? Is there a trusted magazine out there that will separate the facts from fiction, share honest reviews of what to expect from treatment and, importantly, give valuable advice on how to choose an appropriately-qualified aesthetic practitioner? No – there isn’t. Until now.
Beyond Beauty – the ultimate aesthetic resource for patients and consumers – will launch in January. Created by us here at the journal, you can be confident that we’ll educate and inform readers, without using scare tactics, and have a bit of fun thrown in! Our ethos
Clinical Advisory Board
is to enhance knowledge, build trust and promote positivity in the specialty, which we will do in our four issues released throughout the year, as well as across our website and social media platforms.
The team and I are so excited to bring this to you, with a free copy gifted to every subscriber in January. We know you’ll love it, so you’ll also have the opportunity to pre-order additional copies for your patients, which you can then give out or sell for a recommended retail price. Our website will be up and running soon, but until then follow our new Instagram account –@beyondbeauty_mag – for all the latest updates!
Now, time for our November issue for you! This month, we’ve packed the journal with articles all about devices! Covering radiofrequency microneedling, muscle stimulation and LED, we aim to help you make decisions on devices to invest in to enhance your treatment offering and build a profitable practice. Let us know what you found useful by tagging us on Instagram @aestheticsjournaluk.
Leading figures from the medical aesthetic community have joined the Aesthetics Advisory Board to help steer the direction of our educational, clinical and business content
Mr Dalvi Humzah is a consultant plastic, reconstructive and aesthetic surgeon with more than 20 years’ experience and is director of P&D Surgery. He is an international presenter, as well as the medical director and lead tutor of the multi-award-winning Dalvi Humzah Aesthetic Training courses. Mr Humzah is founding member of the Academy of Clinical Educators at the Royal College of Physicians and Surgeons of Glasgow.


Dr Raj Acquilla is a cosmetic dermatologist with more than 12 years’ experience in facial aesthetic medicine. In 2015 he won the Aesthetics Award for Aesthetic Medical Practitioner of the Year and in 2012 he was named Speaker of the Year. Dr Acquilla is a UK ambassador, global KOL and masterclass trainer for botulinum toxin and dermal fillers.
Miss Elizabeth Hawkes is a consultant ophthalmologist and oculoplastic surgeon at the Cadogan Clinic in Chelsea. She specialises in blepharoplasty surgery and facial aesthetics. Miss Hawkes was clinical lead for the emergency eye care service for the Royal Berkshire NHS Foundation Trust. She is an examiner for the Royal College of Ophthalmologists.
Mr Adrian Richards is a plastic and cosmetic surgeon with 18 years’ experience. He is the clinical director of the aesthetic training provider Cosmetic Courses and surgeon at The Private Clinic. He is also member of the British Association of Plastic and Reconstructive and Aesthetic Surgeons and the British Association of Aesthetic Plastic Surgeons.

PORTFOLIO
WE WANT TO HEAR FROM YOU!
Sharon Bennett is chair of the British Association of Cosmetic Nurses (BACN) and the UK lead on the BSI committee for aesthetic nonsurgical medical standards. She is a registered university mentor in cosmetic medicine and has completed the Northumbria University Master’s course in non-surgical cosmetic interventions.
Jackie Partridge is an aesthetic nurse prescriber with a BSc in Professional Practice (Dermatology). She has recently completed her Master’s in Aesthetic Medicine, for which she is also a course mentor. Partridge is a founding board member of the British Association of Cosmetic Nurses and has represented the association for Health Improvement Scotland.
Dr Souphiyeh Samizadeh is a dental surgeon with a Master’s degree in Aesthetic Medicine and a PGCert in Clinical Education. She is the clinical director of Revivify London, an honorary clinical teacher at King’s College London and a visiting associate professor at Shanghai Jiao Tong University.

ADVERTISING & SPONSORSHIP
Courtney Baldwin • Event Manager T: 0203 196 4300 | M: 07818 118 741 courtney.baldwin@easyfairs.com

Judith Nowell • Business Development Manager T: 0203 196 4352 | M: 07494 179535 judith@aestheticsjournal.com


Chloe Carville • Sales Executive T: 0203 196 4367 | chloe.carville@aestheticsjournal.com

MARKETING
Aleiya Lonsdale
Head of Marketing
T: 0203 196 4375 | aleiya.lonsdale@easyfairs.com
Katie Gray • Marketing Manager
T: 0203 1964 366 | katie.gray@easyfairs.com
DESIGN
Peter Johnson • Senior Designer T: 0203 196 4359 | peter@aestheticsjournal.com
Do you have any techniques to share, case studies to showcase or knowledge to impart?
Email editorial@aestheticsjournal.com
Dr Tapan Patel is the founder and medical director of PHI Clinic. He has more than 16 years’ clinical experience and has been performing aesthetic treatments for more than 14 years. Recently, he was listed in Tatler’s Top 30 AntiAgeing Experts. Dr Patel is passionate about standards in aesthetic medicine.

Dr Stefanie Williams is a dermatologist with special interest in aesthetic medicine. She is the founder and medical director of the multi-award winning EUDELO Dermatology & Skin Wellbeing in London. She lectures in the Division of Cosmetic Science and has published more than 100 scientific articles, book chapters and abstracts.

ARTICLE PDFs AND REPRO
Material may not be reproduced in any form without the publisher’s written permission. For PDF file support please contact Chloe Carville, contact@aestheticsjournal.com
Aesthetics Media
© Copyright 2020 Aesthetics. All rights reserved. Aesthetics is published by Aesthetics Media Ltd, which is registered as a limited company in England; No 9887184
DISCLAIMER: The editor and the publishers do not necessarily agree with the views expressed by contributors and advertisers nor do they accept responsibility for any errors in the transmission of the subject matter in this publication. In all matters the editor’s decision is final.
Editor’s letter
PUBLISHED BY Aesthetics Journal @aestheticsgroup Aesthetics @aestheticsjournaluk
Mr Dalvi Humzah, Clinical Lead
MANAGEMENT
Alison Willis Director T: 07747 761198 | alison.willis@easyfairs.com EDITORIAL Chloé Gronow Editor & Content Manager T: 0203 196 4350 | M: 07788 712 615 chloe@aestheticsjournal.com
Shannon Kilgariff Deputy Editor T: 0203 196 4351 | M: 07557 359 257 shannon@aestheticsjournal.com
Holly Carver Journalist | T: 0203 196 4427 holly.carver@easyfairs.com
Talk #Aesthetics
Follow
#Conference
Dr Firas Al Niaimi @drfirasalniaimi
Finally! After 7 months of lockdown and no travels and virtual meetings the time has come for my first international trip and face-to-face conference. A great honour and privilege to be invited to the German Laser Dermatology Association Conference and be given the keynote lecture.

#Clinic
Dr Tristan Mehta @dr.tristan.m So here begins the next chapter! The team behind Harley Academy are proud to announce STORY. Despite so many hurdles to navigate this year, we have just launched in Marylebone and Southwell! I can’t take the credit – Shout out to Emily, Alex, Marcus, Tim, Gina and Aneta for getting this over the line!
#Training
Dr Vincent Wong @drvincentwong
My first teaching session for Definisse Threads by ReLife as the lead trainer. A pleasure to have the opportunity to work with these experts to standardise the training for the UK. #ReLife #definisse #training
#Podcast
Dr Ali Garnham @dr_ali_ghanem Podcast with @sinclair_uk on minimally invasive #aesthetic interventions! Love #scarlessaesthetics @raeclinic

#Skincare @8westcosmetic Happy #NationalAestheticianDay! We’d like to take a special moment of appreciation for all the skin care professionals out there. Thank you to our dear medical aestheticians, we’re only half a team without you!


Advertising ASA rules against advertising of weight loss injections
Three weight loss injection clinics have had their adverts banned by the ASA after promoting the prescription-only weight loss medicine liraglutide.
The adverts also claimed that people could lose a precise amount of weight within a stated time frame, as well as using images of already slim women promoting the use of the product. The complaints challenged whether the ads breached the code because the rates of weight loss were unlikely to be compatible with good medical and nutritional practice. They also implied that the product could be used by people who were not overweight when the product is indicated for those with a BMI of 30+ or ≥27kg/m2 to <30kg/m2 in the presence of at least one weight-related comorbidity, and because they promoted a prescription-only medicine.
The claims for all three clinics were upheld, and the posts were found to go against the Committee of Advertising Practice (CAP) code. The CAP code states that marketing communications must not contain claims that people can lose precise amounts of weight within a stated period, that marketers should ensure advertising was prepared with a sense of responsibility to consumers and to society, and that the advertising of prescription-only medicines to the general public was prohibited by the Human Medicines Regulations 2012.
The ASA concluded that the ads must not appear again in their current form, and all clinics have removed the posts from their social media accounts.
Fillers
Allergan acquires Luminera filler ranges
Global pharmaceutical company Allergan, an AbbVie company, has entered an agreement with privately-owned aesthetics company Luminera. The agreement means that Allergan will acquire its full dermal filler portfolio including HArmonyCa, a dermal filler intended for facial soft tissue augmentation, which comprises a combination of cross-linked hyaluronic acid (HA) with embedded calcium hydroxyapatite (CaHA) microspheres. The Luminera dermal filler portfolio also includes a line of HA dermal fillers, as well CaHAbased fillers commercialised across several markets. Brands include Crystalys, Hydryalix and Hydryal. Luminera chairman Dadi Segal commented, “We believe bringing together key, innovative Luminera assets with the support of Allergan Aesthetics will provide an even brighter future for our people, products and a more expanded offering for our customers. This is a tremendous opportunity to further build, develop and collaborate with a leading global aesthetics company.” Carrie Strom, senior vice president AbbVie, and president, Global Allergan Aesthetics, said, “The addition of the Luminera assets adds innovative technology, complementing our leading Juvederm filler franchise. We welcome the Luminera team as we continue to build our global aesthetics company and a world-class product offering for healthcare professionals and patients around the world.”

us on Twitter @aestheticsgroup and Instagram @aestheticsjournaluk
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Patient education
Aesthetic magazine for patients launching January
Beyond Beauty – a revolutionary new magazine that will educate patients and consumers on non-surgical and surgical cosmetic treatment – will launch in January 2021.
Created by the Aesthetics team, safety and education will be at the heart of the publication, providing content that is factual, informative and engaging.
Beyond Beauty will feature impressive case studies and expert commentary alongside articles on injectables, skincare, energy devices, surgery and all the services aesthetic practitioners provide.
Editor and content manager Chloé Gronow said, “There is a real need for quality information for patients and consumers that does not scare or misinform them about aesthetic treatment. At the Aesthetics journal we work extremely hard to fact check everything we publish, while working with the best names in the industry, to ensure everything we cover is safe and efficacious for patients. The same approach will be used for Beyond Beauty, offering a unique and valuable tool for clinics and brands to engage with consumers!”
Deputy editor Shannon Kilgariff added, “Every day the public hears about the shocking horror stories of complications and treatments gone wrong in the mainstream media, but rarely is the light shone upon positive experiences and life-changing journeys in a way that is factual, educational, and fun! I am thrilled to debunk the biggest misconceptions and champion positivity in our growing industry through Beyond Beauty.”
An accompanying event for the magazine – Beyond Beauty Live – will then take place in early 2022, leading on patient safety by uniting thousands of consumers with key associations, practitioners and brands. Four issues of Beyond Beauty will be published throughout the year, with exclusive subscription offers for Aesthetics readers. You will be able to purchase multiple copies for your clinic at a discounted rate, which you can then retail from your clinic at a recommended retail price. Stay updated by following our Instagram @beyondbeauty_mag which will go live soon!
VIVACY launches profiloplasty competition
Aesthetic product manufacturer VIVACY has launched an international competition for practitioners to showcase their profiloplasty enhancements using the STYLAGE range of dermal fillers.

Before and after photos should be submitted on social media and the competition will run between November 9 and January 6. It is open to practitioners in the UK (England, Wales and Scotland), Russia, Poland, Canada, Benelux, Italy, Israel, Belarus, Ukraine and Mexico. Two local winners will be chosen from each country, and they will then all be compared by the VIVACY scientific medical board, which will choose the two final international winners. The final winners will be announced during the VIVACY Symposium at IMCAS Paris 2021, on January 28-30.
Vital Statistics
53% of respondents cited self care as a motivating factor in purchasing grooming products (HYPEBEAST, 2020)
30% of facial skincare users said they had moisturised more since the outbreak of COVID-19, while one in five spent longer on their routine (Mintel, 2020)
40% of 400 people surveyed said they engaged with stories the most on social media platforms (Visual Objects, 2020)
89% of 700 perioperative practice staff in the UK stated they had been a victim of bullying (Association for Perioperative Practice, 2020)
Out of the 1,000 adults surveyed, one in 10 said a romantic relationship had ended because of their eczema (National Eczema Society, 2020)
In a survey of 2,000 11-21-year-old girls, eight out of 10 revealed they had considered changing how they look (Girlguiding, 2020)
Dermal fillers
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
BRINGING THE WORLD OF AESTHETIC MEDICINE TO YOU
Plastic surgery
BAAPS elects first female president
DHAT introduces business training
Dalvi Humzah Aesthetics Training (DHAT) will host a one-day business training agenda on January 21 to help newly qualified or soon to qualify aesthetic plastic surgeons get set up in private practice. Speakers at the event will be consultant plastic surgeons Mr Dalvi Humzah and Mr Jeyaram Srinivasan. The agenda’s opening session will focus on the core elements of setting up a clinical practice, such as how to work with the Medical Advisory Committee of private hospitals, how to deal with insurance companies and the best ways to manage hospital politics. Other sessions at the training event will include web marketing, social media, tax planning, brand creation, content writing, working with the media, investment and customer service. These sessions will be led by experts in each area. The event will be held at Resort World in Birmingham, and will be sponsored by InMode, Étre Vous and SkinGenuity.
Launch
ReLife launches in the UK
Italian pharmaceutical company Menarini Group has launched Definisse threads, fillers and peels by ReLife in the UK.
The British Association of Aesthetic Plastic Surgeons (BAAPS) has appointed consultant plastic surgeon Miss Mary O’Brien as its first ever female president. Miss O’Brien was previously vice-president of the association and replaces former president Mr Paul Harris.

Commenting on her new role, Miss O’Brien said, “I am very grateful to many mentors both male and female who helped me to pursue a career that I love. Plastic surgeons are not defined by their gender, but rather their training and skillset. I hope to be able to continue to contribute to training future generations of plastic surgeons in this fulfilling career. With regard to the BAAPS, it is an association that primarily treats female patients. I hope that a professional female perspective will provide a healthy balance and contribution to its leadership.”
According to the company, the Definisse peel range offers a choice of oily and dry skin pre-peels, classic or lightening peels and a neutralising buffer to use following the peel. Menarini explains that Definisse Threads use a combination poly lactic acid/caprolactone and have bidirectional and convergent barbs that aim to stimulate the body’s fibroblasts to synthesise the extracellular matrix and collagen in the skin. The Free Floating Threads are designed for use in the cheek, the Double Needle Threads for the eyebrow and lower jaw, and the Ancourage Threads are to be inserted into the mid-face. The Definisse Filler range comes in four different variations: the Definisse Core Filler for shaping and building facial contours; Definisse Restore Filler for medium lines and wrinkles; Definisse Touch Filler for fine lines; and Definisse Hydrating Filler for treating the superficial dermal tissue. Zoe Phillips, UK senior brand manager at ReLife, said, “ReLife UK is happy to announce the launch of its new range of aesthetic products. The range includes a skin specific peel programme, Definisse fillers and Definisse threads, for lifting and repositioning of the skin. With our full range of products and KOL led training programmes, we believe ReLife can provide a one-stop shop for aesthetic practitioners.” ReLife is available in the UK exclusively through Church Pharmacy.
Conference
Rising Star initiative launches
The Aesthetics United Charity Conference (AUCC) has launched a Rising Star initiative for registered doctors, dentists or nurses who have been practising in the aesthetics industry for 12 months or less. Successful applicants will get the opportunity to present alongside a headline speaker on the main stage at the AUCC, and will gain mentorship from the same headline speaker. Practitioners can apply on the AUCC website. Dr Lara Watson, co-founder of the AUCC alongside Dr Priyanka Chadha, said, ‘Through our surgical training and the running of training group Acquisition Aesthetics, Dr Chadha and I really understand the importance of strong mentorship and a supportive working environment. The objectives of the Rising Star initiative are simply to identify and nurture talent, to provide opportunities for mentorship and collaboration, and to support the progression of our industry through facilitating the next generation of leaders.” The conference will take place on June 19, at the Sofitel, St James in London.
Education
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020 Events Diary MARCH 12 & 13, 2021 | LONDON AESTHETICSCONFERENCE.COM 12 & 13 MARCH 2021 / LONDON
Cynosure to host webinar on new RF device
On November 10 laser manufacturer Cynosure will present a webinar, hosted by Aesthetics, discussing its new radiofrequency microneedling device. According to Cynosure, the webinar will cover how the Potenza device can help you provide customised treatments and address more tissue per treatment, as well as how to combine it with your existing treatment offerings. The session will be hosted by Dr Dianne Quibell, vice president of the American Board of Laser Surgery and a fellow of The American Society for Laser Medicine and Surgery. The talk will begin at 2pm and delegates can register via the Aesthetics journal website.
Industry
Intraline announces new medical director
Medical aesthetic company Intraline has appointed Dr Huw Jones as its new medical director. Dr Jones has been working in aesthetics for more than 25 years and owns clinics on Harley Street and Henleyon-Thames. Terry Fraser, Intraline president, said, “We are thrilled to appoint Dr Jones as medical director of Intraline. His lifetime approach as both student and teacher, satisfaction in developing new techniques and the care he puts into every treatment he gives make him a perfect fit with Intraline’s values.” Dr Jones commented, “I am delighted and honoured to be joining Intraline as medical director. It is exciting to work with such an ambitious company who are driving to increase education and confidence.”

Mental health
New report indicates lack of support for skin disease patients
A report published by the All Party Parliamentary Group on Skin (APPGS) suggests that there is a lack of mental health support available for patients with skin conditions. Evidence was collected by the APPGS in March and April from more than 500 UK patients with a range of skin conditions, as well as 100 clinicians and 16 organisations operating in the field of dermatology. It found that 93% of people with skin disease reported a negative impact on their self-esteem and 69% reported a negative impact on their work or education. In addition, 100% of the 27 under 18-year-olds who responded to the survey indicated that their skin condition affected their psychological wellbeing. Dr Tony Bewley, consultant dermatologist and chair of the APPGS’s expert committee, said, “As this vital report illustrates, children and young people who can be particularly vulnerable to mental health issues and bullying related to their skin health and appearance have been particularly let down in this area. We are keen to urge commissioners to recognise the evidence highlighted in this report which shows that investment in specialised mental health services for people with skin conditions is cost effective compared to the alternatives.”
ACE IS BACK
The highly anticipated Aesthetics Conference and Exhibition (ACE) 2021 will take place on March 12-13 in London, featuring expert-led education covering both clinical and business advice. The educational sessions will cover all aspects of the aesthetic speciality from technique and training to the support of developing a successful aesthetics business. As well as world-class education from more than 60 speakers in the conference agenda, the exhibition will boast dozens of highly anticipated product launches. With so many launches having been delayed this year, ACE will be the perfect place to discover the latest aesthetic services and technologies for your clinic. You will be able to discover first-hand dozens of products launched exclusively at ACE – to widen your clinic offering, helping you stand out from your peers.
EXPERT-LED EDUCATION FROM TEOXANE
The headline sponsor of next year’s ACE is aesthetic manufacturer TEOXANE Laboratories, a major player in aesthetic medicine and skincare, and one of the top manufacturers in the world of hyaluronic acid-based dermal fillers. As the headline sponsor, they will host unmissable education in the main auditorium exclusive to healthcare professionals. The free-to-attend sessions will be CPD-certified offering high-quality education and best practice from expert trainers and injectors.

ESTABLISHING A PRACTICE AND STANDING OUT FROM THE CROWD
With regulations and advertising standards constantly changing, new safety measures to adhere to, technology developing rapidly, and the recovery of a global pandemic thrown into the mix, managing a successful clinic or practice is becoming increasingly challenging. The free Business Track agenda at ACE is designed to successfully establish a private practice to stand out from the crowd. Topics will cover advice on PR, marketing, software, social media and more, making it a must-attend event for practitioners.
FIND OUT MORE
12 & 13 MARCH 2021 / LONDON
aestheticsconference.com Education
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
HEADLINE SPONSOR
BACN UPDATES
A roundup of the latest news and events from the British Association of Cosmetic Nurses

BACN CONFERENCE
November has been the month for the BACN Autumn Aesthetic Conference for a number of years. Unfortunately, like many other events in aesthetics, the conference has been postponed until mid-2021 at the earliest. After the success of the regional digital conferences held in September and October, the BACN is looking at offering more content online and making this content varied and useful for its membership base. More information regarding 2021 events will be announced in the coming months alongside the strategic approach the BACN will be taking in 2021. During the regional conferences the BACN ran polls to gather the opinions of members to decide on the best approach for the BACN Conference going forward. Tara Glover, BACN Events Manager has been analysing this feedback – please get in touch with Tara at tglover@bacn.org.uk if you have any thoughts.
BACN MEMBER SURVEY
Members of the BACN were contacted in September to complete a short member survey; we had a brilliant 337 responses – 40% from new members and 60% from renewed members. Some of the results can be seen below. Members will be updated with a full set of results along with comments from Paul Burgess MBE, BACN CEO and Sharon Bennett, BACN Chair.
• The reasons for joining were focused on the need to be part of a professional association and wanting support from fellow practitioners
• 55% of respondents had been qualified in aesthetics for over five years
• 62% work part time in aesthetics
• 71% are prescribers
• 25% are prescribing for others
The BACN Management Committee had a long discussion about the implications of these results for the BACN and provision of services. It was clear that the membership was split between inexperienced new entrants and highly experienced, longstanding aesthetic practitioners. The need to reflect these trends in membership services will be a critical task going forward to 2021.
This column is written and supported by the BACN
Collagen
Totally Derma releases sugarfree drink supplement
Nutraceutical collagen drink company
Totally Derma has created a sugar-free version of its bovine collagen drink supplement.
According to the company, the new Totally Derma sweetener contains the polyalcohol xylitol and vanilla flavour only and the drink is formulated using arthred amino acid peptide powder, synovoderma hyaluronic acid, vitamin C, grape seed extract, green tea extract, alpha lipoic acid, zinc citrate, manganese citrate, and copper sebacate. Following a 10-week clinical study conducted by Totally Derma, 100% of group participants said that their skin felt more hydrated with a smoother texture, was firmer, and had more volume, and 80% said they had experienced less redness. Anita Eyles, owner and director of Totally Derma, commented, “It’s very tricky trying to establish the best taste when formulating a collagen drink supplement. Previously, Totally Derma contained stevia and erythritol and a small amount of cane juice. But, even that was a red flag for some aesthetic practitioners, dermatologists and of course dentists, for whom sugar is an absolute no-no, despite the product containing even the tiniest amount of sweetener. So, the holy grail is to contain no sugar at all on the ingredient list. Apart from adding sweetness for better palatability, from a science point of view, xylitol is a prebiotic and has been shown in animal studies to increase collagen production in the skin when used as a supplement. Totally Derma is also safe for diabetics.” The company explains that once all stock of the current nutraceutical collagen formulation (with stevia, erythritol, cane juice) are depleted, it will be offering the sugar-free version only to customers.
 Skincare
Skincare
iS Clinical introduces new serum for the body
After seeing a rise in patients requesting more active skincare for the body, iS Clinical has launched the Youth Body Serum. According to the company, the serum is designed to provide the skin with hydration and antioxidant protection against environmental aggressors. The serum is formulated using hyaluronic acid, potent extracts of watermelon, blue microalgae, liquorice root and holy herb, vitamin B5 and proprietary extremozymes.
Alana Marie Chalmers, director of UK distributor Harpar Grace International, said, “There has been a growing number of body device launches recently and this new product offers practitioners a topical cosmeceutical product to offer patients for home-use with benefits. iS Clinical Youth Body Serum is formulated with active ingredients more commonly found in facial skincare to create a epigenetics-led, antioxidant serum for use on the body. Containing natural micro-organisms that endure extreme environments and conditions, it not only protects skin cells and macromolecules from external factors but also repairs skin, and provides antioxidant protection against environmental aggressors.”

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
NeoStrata launches new products in company rebrand
Skincare company NeoStrata is introducing new products to its portfolio as part of its company rebrand. The new NeoStrata Restore Deluxe Mini Kit will contain the Neostrata PHA Facial Cleanser, Ultra Moisturising Face Cream and Bionic Face Cream, which NeoStrata states is designed to help with aggravated or unsettled skin as a result of face coverings, masks and PPE.
The brand is also releasing the Comprehensive Retinol Eye Cream, containing a dual peptide which aims to target dark circles and reduce the appearance of wrinkles; and the Comprehensive Retinol 0.3% Night Serum, which is formulated with 0.3% pure retinol, neoglucosamine and hyaluronic acid.
The company states that it will also be upgrading its packaging, in-clinic toolbox and training. Vikki Baker, marketing manager at AestheticSource, commented, “We are particularly excited about this rebrand as it represents who NeoStrata are today, their focus on skin inclusivity, and how they respect and represent the dermatological needs of a diverse patient demographic. The introduction of the new packaging design, together with the category name updates, will support the practitioners to be able to explain how the products work in the range.”
Industry New distribution company opens
DermaFocus, a new distribution company, has launched in the UK.

The company states that it offers the the Pistor Eliance mesotherapy injector, Venusian Carboxytherapy and the Quantificare 3D LifeViz system which takes 3D images.

The company explains that it also offers peels, serums and injectable preparations, as well as products patients can use at home. It will also provide product training and support with all clients.
Milad Bemana, executive director, commented, “We are excited to bring innovative and niche aesthetic products in the market and look forward to offering our solutions to aesthetic practitioners around the UK with ongoing support and training.”
Charity
AlumierMD releases holiday kit to support children’s education in Africa
Skincare brand AlumierMD has launched a new holiday kit to help support the education of 500 primary school students in South Africa through the Alumier Foundation. The Power Peptide Duo holiday set brings together the Ultimate Boost Serum and Everactive C&E + Peptide for the first time and for every purchase the company will donate £5 to the Alumier Foundation to support its Nhlengelo Primary School project in Mpumalanga, South Africa. AlumierMD’s UK medical communications manager Victoria Hiscock said, “We are delighted to be launching the Power Peptide Duo. Not only will these potent serums work symbiotically to deliver great patient outcomes, a portion of the sales will support the children of Nhlengelo Primary School through the Alumier Foundation.” The Everactive C&E+ Peptide is designed to improve skin tone and texture, neutralise free radicals and reduce the appearance of fine lines and wrinkles. The product is formulated with vitamin C, Matrixyl Synthe’6 peptide and vitamin E. The Ultimate Boost Serum contains niacinamide, sodium hyaluronate and Matrixyl Synthe’6, which aims to deliver hydration and enhance elasticity. Aesthetic practitioner Dr Nina Bal said of the new holiday kit, “AlumierMD is one of my absolute favourite medical grade skincare brands. They couldn’t have chosen two better products. This duo not only restores skin health and defends against free radicals, it also delivers potent antiageing benefits and comfort to the skin in colder months.”

International
Cynosure introduces new device in the US
Laser manufacturer Cynosure has launched FlexSure, a wrapabble radiofrequency (RF) applicator, to US and Canadian markets.
The company explains that FlexSure’s ‘peel-andstick’ disposable applicators allow practitioners to deliver hands-free, deep tissue heating to multiple areas, including the abdomen, back, arms, buttocks, thighs and above the knees. The applicators, available in multiple sizes, are equipped with six customizable zones and temperature-sensing capabilities.
Todd Tillemans, chief executive officer of Cynosure, commented, “We at Cynosure are committed to driving innovation forward and delivering technology like FlexSure that not only meets our growing base of consumer needs, but practitioner needs as well, helping them to maximise both time with each patient and resources to remain productive and profitable. Created with these considerations, the FlexSure device is the ideal product for practices to integrate as its single-use, disposable applicators help meet the needs expressed by consumers for more hygienic treatment options.” The FlexSure will launch in the UK in 2021.
Skincare
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Breast surgery
GC Aesthetics introduces new implant range
Silicone breast implant manufacturer GC Aesthetics Ltd (GCA) has launched a new round breast implant called PERLE. PERLE uses BioQ-Surface, which is developed with reverse surface technology. According to GC Aesthetics, this allows for reduced inflammation, easier implant placement and incision, as well as a lower risk of capsular contracture. The implant also has Emunomic Breast Tissue Dynamic Gel, a protective GCA 360 barrier that aims to inhibit gel diffusion and an enhanced GCA ultra-link shell to prevent fractures. Carlos Reis Pinto, CEO of GC Aesthetics said, “With PERLE, we complete our range of breast implants to best suit each patient’s and plastic surgeon’s individual needs. We back our commitment of being a global medical device company focused on aesthetic surgery, women’s health and patient security through a broad portfolio of secure and innovative solutions.” GC Aesthetics states that PERLE breast implants are covered by the GCA Comfort Plus Warranty; a lifetime warranty on all GC Aesthetics’ breast implants.
Muscle stimulation
Aesthetic Technology Ltd releases body contouring device
The manufacturer of the Dermalux LED systems, Aesthetic Technology Ltd, has introduced the CM Slim Contour Master to its portfolio and will be the exclusive UK distributor for the electromagnetic body contouring device. According to the company, the device uses High Intensity Electromagnetic Muscle Training (HIEMT) to target the stomach, buttocks, arms or legs by simultaneously increasing muscle and decreasing fat. Aesthetic Technology Ltd states that the technology causes 30,000 contractions every 30 minutes and recommends four to six sessions to achieve optimum results, with The Contour Master package also including a chair targeted to help strengthen pelvic floor muscles. Louise Taylor, founder and director of Aesthetic Technology Ltd said, “The medical device industry is a fast-moving market and we recognise that partnering with stand-out products enables us to bring solutions to market faster, which helps our clients stay ahead. As an IS013485 Medical Device manufacturer, we offer assurance that any products distributed under the ATL name have been through strict due diligence to ensure, compliance, safety and efficacy.”


Allergan establishes new brand identity
Global pharmaceutical company Allergan Aesthetics has launched a new brand identity to empower confidence and promote diversity. According to the company, the new identity is designed to recognise people from different genders, ethnicities and skin tones to help the company express its dedication to developing aesthetic medicine for everyone. Fernando Alvarez, general manager at Allergan Aesthetics UK and Ireland, commented, “I am delighted to share the fresh new look of Allergan Aesthetics, an AbbVie company. Our new brand is full of passion, energy and a continued focus on customers. More than ever before, Allergan Aesthetics aims to empower confidence and create products and technologies that drive the advancement of aesthetic medicine. The new brand is a clear articulation of what
Alice HartDavis launches new book
Aesthetic and beauty journalist Alice Hart-Davis has released a second book titled The Tweakments Guide: Start with Skincare The book follows on from The Tweakments Guide: Fresher Face and discusses what products are best for different skin concerns such as acne, rosacea and wrinkles, as well as what ingredients work best and her top product recommendations. On her decision to write the book, Hart-Davis said, “For 20 years I’ve had a ringside seat as skincare has moved from being ‘hope in a jar’ into the realms of high science. I have interviewed scores of brand founders, formulators and dermatologists. I’ve reported on all the new ‘miracle creams’ and ‘beauty-science breakthroughs’ and this book tells consumers everything I’ve learnt along the way. I’ve sifted through the details to give people an in-depth insight into the truth about modern skincare, what’s fact, what’s hype and what’s opinion, so they can work out what’s best for their skin.”
we stand for at Allergan Aesthetics and reflects the principles that we have long held: putting science at the core of all that we do, connecting to patients, and being inclusive to all people.”
Carrie Strom, senior vice president of AbbVie, and president of Global Allergan Aesthetics, said, “At Allergan Aesthetics, we believe in the impact confidence can have on the businesses, careers and lives of those we serve. The new brand better reflects who we are today and where we are going in the future. It represents our company – full of passion, energy, and solely focused on aesthetics. Empowering confidence is important to our work and our industry. We believe this new brand brings that purpose to life – for colleagues, customers and consumers around the world.”
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Consumer education
Diversity
world’s first and only ‘Pain-Free’ hair removal platform to deliver the two gold-standard lasers for treating ALL skin typesTRUE Alexandrite & Nd:YAG.

For the practitioner that values efficacy...
And the client who chooses ‘Pain-Free’ Call Lynton on 01477 536 977 Visit lynton.co.uk/motus Now Supported in the UK by Lynton
The
Market growth
Botulinum toxin market set to experience large growth
According to a report published by Fortune Business Insights, the botulinum toxin market will reach US $8,309 million by 2026, exhibiting a compound annual growth rate of 8%. Companies analysed in the Botulinum Toxin Market: Global Market Analysis report included Allergan, Ipsen Pharma, Merz Pharma, Medytox, US WorldMeds, LLC (Solstice Neurosciences, LLC), Galderma Laboratories, Lanzhou Institute of Biological Products Co Ltd, and Revance Therapeutics.
According to the report, the rising demand for improved aesthetic appearance following COVID-19 has created a demand for botulinum toxin procedures around the world. Resulting from the high demand, there has been a subsequent rise in the number of product launches worldwide. Fortune Business Insights predicts that increasing product launches will constitute an increase in the overall botulinum toxins market value. Key industry developments outlined in the report included the South Korean company launch of Liztox, a botulinum toxin in Korea for the treatment of moderate to severe glabellar wrinkles, and the US FDA approval of Evolus Inc’s cheaper botulinum toxin for the treatment of frown lines.
Radiofrequency
New hair restoration device available for UK clinics
UK distributor Belle is now supplying the HairWave device to aesthetic practices in the UK. HairWave is a radiofrequency hair restoration device manufactured by INDIBA. According to Belle, the radiofrequency device offers both thermal and subthermal effects, aiming to boost metabolic activity in the hair capillary network leading to a reduction in hair loss and an increase in hair strength and density. According to Belle, the HairWave device can also be used in combination with stem cell therapies, PRP, botulinum toxin, LED devices and mesotherapy. Ben Sharples, director of Belle, commented, “We are excited to add INDIBA’s HairWave device to our already strong portfolio of devices and products for hair restoration. HairWave is a relaxing, non-invasive therapy that can be used as a stand-alone option or in conjunction with existing therapies such as Kerastem Stem Cell Hair therapy, PRP or hair transplantation. It’s a must have for anyone who deals with hair and hair loss.”

Education
Dr Harry Singh to release new book
Aesthetic practitioner and dentist Dr Harry Singh is publishing a new book called The BTC Injectable Guide. He explains that the book contains information on the best techniques for administering prescription-only medicines and fillers, including his own tailor-made method. Dr Singh commented, “During my Botulinum Toxin Club workshops, it dawned on me that delegates wanted to take pictures of our markings, injection sites and techniques whilst undertaking the practical hands-on element of the workshop. I then had an ‘a-ha’ moment and started the journey to creating a pictorial atlas, with high-quality images and descriptive text explaining the treatment parameters for commonly requested procedures. It will be a ‘manual’ that you can refer to, time after time, giving you the confidence to deliver outstanding results for your patients.” The book will be available for purchase on November 15.
News in Brief
BAHRS to host virtual meeting
The British Association of Hair Restoration Surgery (BAHRS) is hosting a hair restoration product showcase on November 14 via Zoom. According to the BAHRS, the event will allow providers of hair restoration and scalp treatments to give educational talks about the products they use to benefit patients. The day will also include a session on business support tools. Danny Large, president of BAHRS, commented, “As our partners have supported us during 2020 we hope that we can provide a showcase of some of the best hair restoration products on the market. We look forward to welcoming non/members alike to a fantastic day.”
IBSA Derma receives packaging award
Pharmaceutical company IBSA Derma has won a gold award for its Profhilo packaging at the 2020 Carton E-vent and Awards in the ‘European Carton Excellence’ category. The award was announced at the online event on October 7, hosted by the European Association of Carton and Cartonboard manufacturers, Pro Carton. Maria Bisogni, marketing and communication manager at IBSA, said, “For Profhilo, a product based on innovative technology that has created a new concept of hyaluronic acid, the packaging that has been created is a real work of art, expressing the IBSA Derma philosophy that each of us is a masterpiece.”
WOW Facial appoints new head of sales Skincare brand WOW Facial Ltd has recruited Caroline Gwilliam to be its new head of global sales. The company explains that Gwilliam will be launching the existing WOW Facial brand and commercialising its upcoming product launches. Gwilliam previously worked as sales and business development manager for AestheticSource, UK regional sales manager for Thermi and head of the surgical division at ABC Lasers. Gwilliam commented, “This role is truly a huge challenge but also massively exciting and incredibly rewarding. Every day I am inspired by the team at WOW and what we are achieving.”
Initial Medical launches infection containment kit Waste management service Initial Medical has launched the Infection Containment Kit designed to help medical professionals with the cleaning and disinfection of potentially contaminated surfaces. The company explains that the kit contains personal protective equipment, specialist cleaning supplier Steri-7 infection control products such as hand sanitiser, workplace barrier tape and a rigid container for waste disposal. The kit also comes with complete step-by-step guidelines on how to use each of the items inside, and once used the waste will be collected and disposed of by the Initial Medical team.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Christmas Gift Sets!
SkinCeuticals


Cosmeceutical company SkinCeuticals is launching two limited edition holiday kits called Radiance and Illumination. The Radiance kit is recommended for normal and dry skin types and is made up of the Gentle Cleanser to clean and hydrate skin and the C E Ferulic, an antioxidant vitamin C serum designed to target fine lines. The Illumination kit is for combination and oily skin types and consists of the Simply Clean gel cleanser to exfoliate the skin and Phloretin C F, an antioxidant vitamin C serum which aims to target discolouration and visible signs of ageing. Jackie Tuzee, head of branding at SkinCeuticals, commented, “Expertly crafted, each kit contains a skin-type specific duo to provide recipients with the perfect foundation to their morning skincare regime. Drier more mature skin types should use the Radiance kit (Gentle Cleanser + C E Ferulic) and combination, oily or pigment-prone skin types should use the ‘Illumination’ kit (Simply Clean + Phloretin C F). These duos are both efficacious, educational and highly shoppable during this holiday season.”
Nimue Skin Technology
Skincare company
Nimue Skin Technology has launched six new giftsets to celebrate the approaching festive season.

The gift sets include the Healthy Skin Essentials set, the Healthy Skin Essentials set Lite, the Radiance Reveal set, the Ultimate Collagen Boost set, the Ultimate Anti-Ageing Boost set, and the Ultimate Hydration Boost set. The Healthy Skin Essentials set contains the company’s Cleansing Gel, Conditioner, Exfoliating Enzyme, and Sun-C SPF40. The Healthy Skin Essentials set is also available in ‘Lite’ for those with sensitive skin. The Radiance Reveal set is made up of the Exfoliating Enzyme and the Sun-C SPF40.
The Ultimate Collagen Boost set contains the Multi Rejuvenating Booster Serum 60ml, the Ultimate Anti-Ageing Boost contains the Stemplex Booster Serum 60ml and the Ultimate Hydration Boost set contains the Hyaluronic Ultrafiller Serum 60ml. Each of the boost sets has a Glyco Mask At-Home treatment, a Nimue Mask Brush and three disposable compresses.
mesoestetic
Pharmaceutical company mesoestetic is launching The Element, a new limited edition antiageing cream, for Christmas 2020. mesoestetic explains that the cream is designed to protect the skin from external aggressions and prevent premature signs of ageing. According to the company, the cream is formulated using the company’s Agebiome Complex, which aims to help increase bacterial diversity; the Defence Shield which protects the skin from oxidative stress; and the Powercell System, a peptide complex which works to redensify and restructure the skin. Adam Birtwistle, managing director of mesoestetic UK, said, “The Element represents a very special and limited edition luxury everyday moisturiser developed by mesoestetic especially to give patients a little indulgence this Christmas. I think we all could do with a bit of a treat this festive season!”

AestheticSource
Aesthetic distributor AestheticSource has launched eight Cosmeceutical Crackers and two Deluxe Trial gift sets featuring NeoStrata, Exuviance, Peel2Glow by Skin Tech and SkinBetter Science products that are exclusively available over the Christmas period. The NeoStrata Skin Active Repair and Firm cracker contains the brand’s Intensive Eye Therapy, Triple Firming Neck Cream and Tri-Therapy Lifting Serum, and the Neostrata Clarify cracker contains the Mandelic Clarifying Cleanser, Oily Skin Solution, Exfoliating Mask and Sheer Hydration SPF40. The NeoStrata RESTORE Deluxe Mini Kit features the PHA Facial Cleanser, Ultra Moisturising Face Cream and Bionic Face Cream, and the NeoStrata SKIN ACTIVE Deluxe Mini Kit contains four Citriate Solutions, Peel Pads, Matrix Support with SPF 30, Dermal Replenishment and Intensive Eye Therapy. The Exuviance normal/oily skin cracker features the Gentle Cleansing Crème, Glycolic Polish and Deep Hydration products and each Peel2Glow cracker will contain two kits. The SkinBetter Power Trio cracker contains the Alto Defense Serum, the Even Tone Correcting Serum and the AlphaRet Overnight Cream, while the SkinBetter Interfuse Collection cracker features the Treatment Creams for the Eyes and Face and Neck.

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Last month, MPs voted in favour of the Botulinum Toxin and Cosmetic Fillers (Children) Bill 2019-21 following its second reading at the House of Commons. Brought to Parliament by MP for Sevenoaks Laura Trott after numerous consultations with industry professionals, the Bill aims to:1
• Make it an offence to administer botulinum toxin or a ‘subcutaneous, submucous or intradermal injection of a filler for a cosmetic purpose’ to those under 18

• Make business owners liable if a ‘person other than an approved person’ administers botulinum toxin or a ‘subcutaneous, submucous or intradermal injection of a filler for a cosmetic purpose’ to those under 18
• Make corporate bodies liable if the offence is proved to have been committed with consent of ‘any director, manager or secretary of the body corporate or any person who was purporting to act in any such capacity’
It will now move to the committee stage of Parliament where clauses may be added and points will be considered by MPs in the House of Commons line-by-line (Figure 1). MP Edward Argar, Minister of State for the Department of Health and Social Care (DHSC), also gave his support and noted that the DHSC is exploring a range of options for increased oversight of practitioners, including a system of registration or licensing.
Specialty support
The developments have been hugely celebrated by members of the aesthetic community, with Dr Uliana Gout, president of the British College of Aesthetic Medicine saying, “This is a welcomed step toward long-overdue tightening of regulation surrounding the accessibility of aesthetic interventions, particularly from non-medically qualified practitioners. BCAM fully endorses the Private Member’s Bill and increased regulation in our specialty.”
The Joint Council for Cosmetic Practitioners also welcomed this update, with executive chair Professor David Sines commenting, “We are at a pivotal point in the debate about regulation in the aesthetics sector and we are really encouraged by the interest shown by Parliament.” The JCCP also stated that it is of the opinion nothing less than statutory registration for all practising cosmetic practitioners should become a legislative requirement in the UK to afford public protection and patient safety and set out a 15-point plan for Government to utilise, detailed on our website.2
What will the regulation mean?
If the Children’s Bill comes into force, treatment with toxin or filler in under 18s will be allowed if a medical professional can demonstrate a medical need for the procedure, for example for migraines. As nonmedics cannot make a medical diagnosis, it will ultimately mean that they will be acting illegally if they treat anyone under the age of 18 with toxin or filler, for any purpose.
According to the Bill, medical professionals will not be liable if they can demonstrate that they took reasonable steps to establish the patient’s age and reasonably believed they were aged 18 or over. Should the Bill become law, regulation will be enforced by local authorities that will be able to issue unlimited fines.
MPs’ response
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
highlighting
the physical risk,
with House of Commons House of Lords
Bill started in the House of Commons Progress of the bill Firstreading Firstreading Secondreading Secondreading Committeestage Committeestage Reportstage Reportstage Thirdreading ThirdreadingConsiderationsofamendments 1 1 2 2 C C R R 3 3 A Figure 1: Diagram demonstrating stages of the Bill – latest completed stage marked in black1
After
not only
but also the psychological concerns
Royal Assent
Children & Aesthetic Procedures Regulation Aesthetics reports on the developments to make injection of toxin and fillers for cosmetic purposes in children illegal
MPs Support



AESTHETICSJOURNAL.COM Keep up-to-date with the latest aesthetic developments and best practice guidance on your desktop, tablet or phone AESTHETICSJOURNAL.COM @aestheticsjournaluk Aesthetics @aestheticsgroup
REASONS TO CHOOSE
Restylane
WORLD’S FIRST NON-ANIMAL HA FILLER WITH 40 MILLION TREATMENTS OVER 24 YEARS1
Restylane is the world’s first non-animal stabilised hyaluronic acid (HA) dermal filler.1 Restylane has been delivering results for 24 years with 40 million treatments completed across the world.1 Restylane sets the standard for dermal fillers, delivering results time after time.
RESTYLANE NASHATM: CLOSER TO NATURAL HA THAN ANY OTHER FILLER3
The hyaluronic acid (HA) in NASHATM gels (Restylane and Restylane Lyft) is closer in composition to the HA that occurs naturally in the body than any other fillers on the market today.3 Rather than adding more BDDE or other chemicals, Restylane’s NASHATM gels largely use the natural entanglement of HA. This means that the body is more likely to accept the HA and Restylane is considered to be generally well-tolerated.4,6 Restylane Lyft has the highest G’ on the market and has been shown to last 24 months with one retreatment.2,7 It’s used on the nose, chin, jawline and cheekbone - where projection is needed, without volume.

STRONG CLINICAL EVIDENCE: 60 TRIALS CITED IN 320 PAPERS5
The effectiveness and safety of Restylane has been evaluated in 60 clinical trials cited in 320 peer-reviewed clinical papers.5 That’s a lot of data and means every claim can be substantiated with incredibly strict and high standards. The world’s leading practitioners trust Restylane. You can too.
References
1. Data on file (MA-39680).
2. Data on file (MA-39364).
3. Kablik J et al. Dermatol Surg 2009;35(Suppl1):302–312.
4. Weiss RA et al. Dermatol Surg 2016;42:699–709.
5. Pubmed search for ‘Restylane’ Available at: www.ncbi.nlm.nih.gov/ pubmed/?term=restylane Accessed October 2020.
6. Narins RS et al. Dermatol Surg 2011;37:644–650.
7. Data on file (MA-43049)
RES20-10-0932a
Date of preparation October 2020
Aesthetics | November 2020 18 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial Galderma
Help fund 40,000 Life-changing Operations

Change the lives of children with facial differences

It’s coming to the end of the year and there’s still funds to raise. As a result of COVID-19, many training opportunities and operations have been put on hold, meaning children in Vietnam are still living with the physical and psychological difficulties of their facial difference. Your donations will go towards training Vietnamese doctors in the skills needed to carry out such challenging operations.
Dr Bui Tuan Anh is an ENT surgeon from Hong Ngoc Hospital in Hanoi. He came to the UK with Facing the World in 2017 and was so grateful for the experience.1
Dr Bui Tuan Anh said, “In Vietnam, sever malocclusion and skeletal discrepancies are met quite a lot, especially in poor patients because they have less chance to be examined and don’t always take care of their oral health. It is really hard for me to treat them

because I do not have knowledge and experience in treating such severe cases.”
He continued, “I was so grateful for the opportunity to come to London. While there, I met so many experts, all who are so excellent and kind in sharing their knowledge. What I have learned will help me so much in diagnosing and treating my patients in Vietnam. The experience I had in London was so amazing and unforgettable. Your support for me is so precious and I really appreciate it.”
We’re all hoping for a better 2021, so why not help these children achieve it?
Donate today to fund scholarships for medics in Vietnam.
 Dr Bui Tuan Anh
Dr Bui Tuan Anh
To donate to this special charity scan the QR Code using the camera on your phone or visit www.justgiving.com/fundraising/aestheticsmedia

REFERENCES
Katrin
Training Program
<https://facingtheworld.net>
1.
Kandel, Vietnam
, Facing the World
“Your support is so precious to these children”
Aesthetics | November 2020 19 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Charity Facing the World
Case Study: Holistic Facial Rejuvenation


with BELOTERO® Volume

Assessment and consultation
My 58-year-old patient presented with general ageing concerns and sought a rejuvenated and refreshed appearance. I assessed the patient both statically and dynamically as, while we know that shadows and lines can indicate a person’s age, it’s really when we’re speaking to them and seeing their face in animation that gives their age away. I noted that my patient’s age was most notable upon smiling. While she had volume loss to both sides of her face, previous overtreatment had left her with ‘apple-like’ cheeks upon animation. With such a distinct difference between her medial and lateral face, we needed to create a treatment plan that would address everything holistically. It’s extremely important that facial movement is coordinated and, unfortunately for a number of people, it can become disjointed if treatment has previously only been focused in one area.
Merz Pharma UK Ltd.
260 Centennial Park, Elstree Hill South, Elstree, Hertfordshire, WD6 3SR Tel: +44 (0) 333 200 4140
BELOTERO ® is a registered trademark of Merz Pharma GmbH & Co. KGaA.








Treatment plan and technique
My aim was to create harmonious structure and shape through injecting different layers. My product of choice was BELOTERO® Volume, which is a HA dermal filler with patented CPM technology for seamless integration into the skin.1 Its optimal elasticity and plasticity allows injectors to create natural contours, harmonious shapes and introduce lift where it is needed most. BELOTERO® Volume is ideal for treating volume loss in the mid to upper face, creating natural-looking results.2 A multi-cannula technique was used, with three injection sites on each side of the face. BELOTERO® Volume can be injected into multiple layers; deep, on the supraperiosteal plane and more superficially at the subcutaneous level.3 I utilised each of these to slim the patient’s face, redistribute volume laterally from the cheeks and create an overall rejuvenated and youthful appearance.
As with all treatments, I advised the patient not to put pressure on their face or wear make-up for 24 hours. Given the current situation with COVID-19, she was also given a fresh mask to wear upon leaving.
Adverse events should be reported. Reporting forms and information for United Kingdom can be found at www.mhra.gov.uk/yellowcard. Reporting forms and information for Republic of Ireland can be found at https://www.hpra.ie/homepage/about-us/report-an-issue/mdiur.
Adverse events should also be reported to Merz Pharma UK Ltd by email to UKdrugsafety@merz.com or on +44 (0) 333 200 4143.
1 MERZ Data on File: Merz Aesthetics Global Patient Survey, >7.000 patients, 2015 & 2017

2 Prager W, Kravtsov M, Kerscher M. J Drugs Dermatol. 2017; 16(4): 351-357
3 Micheels P et al. Thérapeutiques en Dermato-Vénérologie, Sep.2014 (Mensuel 235, Cahier 3)


4 Micheels P et al. J Clin Aesth Derm. 2015; 8(3): 28-34
5 Kerscher M et al, Clin Cosm Inv Dermatol. 2017:10 239-247
6 BELOTERO® Volume Instructions for Use 12/2018
7 Garvard MS et al. J Med Behav Biomed Mater. 2016; 61: 290-298
Results
For me, the best reaction to treatment is when the patient says they look like ‘themselves’ again, which was exactly the case for this lady. She was delighted with the result and, being conscious of her ‘apple cheeks’, couldn’t believe how adding more volume could make her look slimmer. The treatment with BELOTERO® Volume delivers optimal modelling capacity that ensures the filler maintains projection and blends contours in each individual patient’s face for up to 18 months.4
To learn more about Dr Kate Goldie’s techniques for treating the mid-face with BELOTERO® Volume, get in touch with Merz Aesthetics.
Dr Kate Goldie is an internationallyrenowned aesthetic practitioner and the medical director of Medics Direct training. She is a trainer, key opinion leader and global faculty member for Merz Aesthetics, travelling the world to educate practitioners on how to successfully use the Merz portfolio. Dr Goldie has private practices in Harley Street and Henley on Thames, as well as being a member of the British College of Aesthetic Medicine.

This advertorial was written and supplied by Merz Aesthetics
www.merzaesthetics.com M-BEL-UKI-0868 Date of Preparation October 2020


REFERENCES
@merzaesthetics.uki
1. Micheels P et al. 2017;5: e1222
2. Micheels P et al. J Clin Aesth Derm. 2015; 8(3): 28-34


3. BELOTERO® Volume Instructions for Use 12/2018

4. Kerscher M et al, Clin Cosm Inv Dermatol. 2017:10 239-247
Aesthetics | November 2020 20 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial Merz Aesthetics





9 Sundaram H. et al. Poster presented at American Academy of Dermatology Meeting (AAD), 4 - 7Mar. 2016, Washington, DC (Merz data on file) 10 Prasetyo AD et al. 2016:9 257-280 11 Micheels P et al. 2017;5: e1222 12 Micheels P et al. Clin Cosm Inv Dermatol. 2019:12: 1-10 13 Tran C et al. Dermatol. 2014; 228(1): 47-54 14 Patent family publication number WO2005 / 085329

Dr Kate Goldie shares her approach to creating harmonious structure and shape
95% of BELOTERO® Volume patients were satisfied with their results for up to 18 months and would repeat the treatment and recommend it to their friends2
8 Sundaram H et al. Plast Reconstr Surg. 2015;136(4): 678-86 BELOTERO® Cross-linked sodium hyaluronate 26.0 mg/ml Lidocaine hydrochloride 3.0 mg/ml Phosphate buffer pH 7 q.s. 1.0 ml Focus indication restore facial volume Product pack contains 2 syringes of 1.0 ml of gel / 2 x Silkann 27G Cannulas
Before After
Using Radiofrequency Microneedling
Practitioners
Microneedling devices and radiofrequency technology are both extremely common treatments in an aesthetic clinic setting. Studies suggest that puncturing the skin’s surface through microneedling can help to improve a variety of different indications such as scars and wrinkles, as well as rejuvenate skin and improve its overall cosmetic appearance.1 Radiofrequency meanwhile, aims to induce thermal damage to stimulate neocollagenesis in deep layers of the skin and subcutaneous tissue to help with concerns like wrinkles and skin laxity.2 Put these two treatments together and you get a two-pronged approach to skin rejuvenation. A recent 2020 review paper by two board-certified dermatologists concluded that they believe practitioners should consider adding radiofrequency microneedling (RFM) devices to their treatment offering for a variety of indications such as acne scars, hyperhidrosis, cellulite, rosacea, skin laxity, striae and skin rejuvenation.3 Here, Aesthetics speaks to three practitioners about their experiences using RFM devices in their clinics, specifically for facial skin rejuvenation, and explores their tips for treatment success.
How radiofrequency microneedling works

ENT, head and neck surgical doctor Mr Rishi Mandavia, managing director of the Dr Tatiana Aesthetic Dermatology Clinic, explains that RFM involves the penetration of small needles that enter the skin at different depths – usually between 1-4mm for the face depending on the treatment area and severity. He says, “Once the needles have penetrated the skin, they release radiofrequency energy that heats the dermis in a controlled manner, stimulating the production of collagen and elastin via a wound-healing response.” According to Mr Mandavia, RFM devices can be used for various different patient concerns. “RFM can be a beautiful treatment for retexturing the skin and improving its quality, as it remodels the skin’s surface as well as improves sagging skin via the generation of collagen and elastin,”
he explains. Aesthetic nurse prescriber Eve Bird, owner of Botastic Medispa, adds, “I have found that the combination of radiofrequency with microneedling means you achieve a much quicker result compared to just one of the treatments on its own. For example, if you use regular microneedling for severe acne you will probably need about six treatments over the course of a year; whereas, with RFM you can half that treatment to about three or four procedures and over a shorter period of time, depending on the device used.”
According to consultant obstetrician and gynaecologist Dr Hina Sra, who works as an aesthetic practitioner at Cosmebeauté clinic, patients are particularly drawn to the ‘natural’ element of this treatment. “RFM doesn’t give quick results like an injectable,” she says, explaining, “As the treatment stimulates the body’s own collagen and elastin production, the results get better over time. I think this is appealing to patients because people tend to look a lot more natural and it doesn’t involve adding anything artificial.” From a practitioner’s point of view, she notes, RFM can have high patient satisfaction and can really help gain the patient’s trust in you as a clinician.
Patient selection
All practitioners highlight the importance of patient selection and conducting a thorough medical history to exclude any contraindications,4,5,6 as well as manage expectations, suggesting that the treatment is not a ‘quick fix’. “You can get fantastic results using this technology if you choose the right patients,” says Dr Sra, adding, “When you are treating the face, you can address fine lines, wrinkles, crepeyness and give the face a nice uplift and tightening effect. I usually treat women and men in their middle age, right up to those in their 60s or 70s. If they have a large amount of loose skin and clearly need a surgical facelift, ensure you refer because no non-surgical machine will help them.”
Dr Sra doesn’t treat younger patients with her RFM device; she says, “This is an aggressive treatment, and I find that younger patients can benefit greatly from other treatments such as regular microneedling and active skincare – they don’t usually need that lift that the older patients require.”
Bird has a similar approach, explaining that she usually treats patients with skin texture issues and fine lines in patients around the ages of 45-65. “I will consider it for those under 45 who have acne scarring – we find our Asian ladies have particularly bad scarring from acne in their youth and have really quite pitted skin as well as hyperpigmentation – the results we are getting for these concerns are excellent (Figure 1).” As Mr Mandavia uses two different RFM devices in his clinic, he is able to treat younger patients in their 30s by using lighter settings to target fine lines and wrinkles while improving skin texture.
Radiofrequency microneedling devices
There are many RFM devices available in the UK, such as Fractora, Infini, Intensif, INTRAcel, Morpheus8, Profound and the newest
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
highlight the benefits of radiofrequency microneedling devices for facial
rejuvenation
skin

02 M i l l i o n HAinjections In 40 countries ove r 2 5 sraey . 20 MILLION INJECTIONS 02 M i l l i o HAinjections countries ove r 2 5 sraey . 20 MILLION INJECTIONS “I have found YVOIRE® Volume to be a great addition to my practice. It’s a very versatile product with great lifting potential which helps me to successfully treat various areas of the face.” - Dr Vikram Swaminathan, Director of Clinic @. Safety Lower cross-linkers ensuring high biocompatibility Longevity High concentration and enzymatic stability Elasticity High molecular weight and lifting capacity Exclusively available at ChurchPharmacy.co.uk/Yvoire 01509 357300 info@churchpharmacy.co.uk A partner for confidence by
It has fractionated pulse mode technology and gold plated noninsulated needles that can penetrate to a controlled depth of up to 5mm. You can adjust the needle length to suit the treatment indication and area.” The Intensif involves a course of three to six treatments about three weeks apart, Bird says, depending on how severe the concern is. She adds, “In most people, you start to see an improvement three weeks after the first treatment with the final result visible 12 weeks after the final treatment.”
Dr Mandavia has two RFM devices, which he will choose according to the extremity of the patient’s concern. “I have the Morpheus8 in my clinic which is excellent for patients with less severe skin sagging, fine lines, pores or acne scarring.” The Morpheus8 delivers fractional treatments with programmable energy and features 24 coated needles with a penetration depth of up to 4mm.5 Dr Mandavia adds, “I will treat the whole face and neck if needed, even around the eyes, and although you can see noticeable results after one treatment I almost always do a course of three treatments, four to six weeks apart, for optimum results, which are natural but significant (Figure 2).”
He also has the Profound device, which he will consider for older patients with moderate ageing concerns. “I do sometimes use the Morpheus8 using a higher setting, but for patients who have more significant skin sagging, particularly around the jawline and neck, I usually choose the Profound since it represents a more aggressive treatment, heating the tissue for longer and at a specific temperature of 67 degrees, providing a non-surgical lift,” he explains. The Profound includes two separate handpieces for both dermal and subcutaneous penetration. To target the dermis, the Dermal Handpiece features five pairs of bipolar microneedles at a depth range of 1-2mm and the SubQ Handpiece has a set of seven needles at a range of 2.9-5.8mm to treat the subcutaneous layer.7 One consideration Mr Mandavia will make when choosing between the two different devices for those with moderate concerns is the lifestyle of the patient. “The Profound only requires one treatment session, which usually takes about an hour and a half for the face, so is better suited to patients who don’t want to come back three times. Of course, the downtime is much greater – from seven days up to two weeks – because there’s more facial bruising and oedema, whereas the Morpheus8 is about two to three days.” He continues, “I can use the Morpheus8 to treat the whole face since I am able to vary the depth of needle penetration; however, I only
use the Profound below the cheekbones due to the depth of needle penetration. I tend to combine the Profound and the Morpheus8 for patients with skin sagging around the jawline and neck, also looking to improve their skin texture and fines lines higher up on the face, including for patients with periorbital laxity.”



Dr Sra uses the Profound device as the sole RFM technology in her practice and will use it to treat across the whole face, if the patient requires. “I feel that it gives the best results as it works deep in the tissue. The device has two heads and they go at various depths for the face and body – the dermal head is what I use on the face and it has a depth of 1.5mm that goes into the dermal layer. I love that you only need one treatment and the results continuously get better over time. You start seeing results from a month onward; I see the patient for their review at three months because we know this is how long we need for collagen to form. At six and nine months their results are even better (Figure 3).”
A big consideration to make before purchasing a RFM device is who will be performing the treatments, practitioners note. Some RFM devices such as the Morpheus8 and Endymed Intensif can be used by an aesthetic therapist under medical supervision, while others such as the Profound are doctor-led. “From a practical standpoint, for my business it’s important for me that my therapist can be trained to do the treatment after I have consulted the patient and created the treatment plan,” adds Bird.
aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
“RFM can be a beautiful treatment for retexturing the skin and improving its quality”
Mr Rishi Mandavia
Figure 1: 25-year-old Asian patient presenting before and after six Endymed Intensif treatments spaced three weeks apart. After picture taken 12 weeks following final treatment. Images supplied by Eve Bird of Botastic Medispa.
Figure 2: A 61-year-old patient before and after two treatments using the Morpheus8 device. After picture was taken at two weeks following final treatment. Images supplied by Mr Rishi Mandavia of the Dr Tatiana Aesthetic Dermatology Clinic.
Before Before After After






Before After
Tips for treatment success
The practitioners all agree that the main challenge with RFM treatments is pain management, so a good protocol must be put in place for comfort.
Bird says for the Intensif device, 30-40 minutes of topical anaesthetic is sufficient, and numbing cream can also be appropriate for the Morpheus8 if it is used in a low setting, Mr Mandavia states. “The Morpheus8 and the Profound are painful treatments so you must be open and honest with your patients and manage their expectations about pain. I tend to use a topical anaesthetic cream then 2% lidocaine with adrenaline in very specific areas because unfortunately the lidocaine injections are themselves quite painful.”
Mr Mandavia advises to always check the patient’s pain levels throughout the procedure. “Constantly look at your patient’s face while you’re performing the treatment and if you notice any discomfort consider increasing the local anaesthetic dose. I tend to initially apply topical anaesthetic cream, followed by injecting small amounts of local anaesthetic in areas which are more tender.”
Dr Sra’s approach is to inject anaesthetic across the treatment area on the face before the procedure. “This is because the pain can be significant with the Profound so it’s really important the patient can tolerate it. The anaesthetic does increase the swelling and bruising, but after this they don’t usually feel anything at all. I will ice the area in the clinic before they leave to help with the after effects of the anaesthetic.” All practitioners also highlight the importance of before and after images for this treatment. “If anyone takes anything away from this article it is to get really good before and after pictures with good consistent lighting, angles and positions with the same backdrop,” Bird states, reiterating, “This is because comparing pictures is the only way that your patient can truly see how the treatment has helped improve their skin.” Dr Sra adds, “Also ensure to show before and after images in the consultation prior to treatment so that they know what the results look like; they are subtle and get better month after month.” Practitioners all note that patients of all skin types can benefit from RFM, however Mr Mandavia highlights the need for practitioners to have really good procedures and protocols in place that specifically cater for different skin types. Mr Mandavia says, “You don’t want to over-treat areas with RFM as this can denature the collagen, limiting results. Patients with darker skin will have a higher risk of post-inflammatory hyperpigmentation (PIH) so you will need to tailor the energy levels and depth of needle penetration to prevent this. If using a device that requires more than one treatment I recommend starting modestly, monitor the patient’s response and adjust the settings as needed for the second and third treatment.” You should share
your results regularly with your team as well as with other experts, Mr Mandavia advises, so to continue to develop your protocols. “We have developed over 20 versions of our Morpheus8 protocol because we are constantly learning and improving and you certainly get better results if you embrace this approach,” he says.
For patients more prone to PIH, practitioners advise to put them on preventative skincare before treatment. “For skin types III-VI I put patients on a vitamin C lotion and 4% hydroquinone – I use Obagi as this is what I trust,” says Dr Sra. Dr Mandavia will recommend a hydroquinone as well as retinol for patients with darker skin types to prepare for the procedure.
Following Profound treatment, Dr Sra says that good aftercare advice to avoid infection is vital. “In the first three days I advise patients to sleep upright to reduce swelling, and I will advise arnica to help with bruising. There is risk of infection, so I will tell patients not to wear makeup during this time, and also have a clean towel and pillow every night. They shouldn’t let pets come near them, avoid touching their face and only with clean hands if necessary. The last thing you want is an infection that will increase their recovery time,” she says, adding that patients should always have a number they can call or message if they have any concerns or questions that will get through to you at all hours. Other side effects can include prolonged swelling, PIH and burns, amongst others.3,6,7,8 Practitioners also note that it’s important to tell the patient to stop using any active skincare when their skin barrier is compromised to avoid irritation. “We tell patients to stop using their active skincare for about three to six days, depending on how long it takes for their skin to settle and give them an aftercare kit to use instead. This contains products with the barest ingredients, such as a light moisturiser and an SPF, to reduce the risk of reactions,” Bird explains.
Consider implementing into your practice
RFM can be a useful tool to add to your portfolio if you are looking for a treatment that can utilise your patient’s own response to produce collagen and elastin. As well as its use on the face, it can be used for a variety of other indications on the body. It can also be used in combination with other modalities, such C02 lasers and dermal fillers. Appropriate parameters must be used, including energy level and needle depth, according to individual patients and treatment areas.8 Practitioners are advised to ask their current patients if this kind of treatment would be of interest to them before introducing into practice, and of course implementing abundant training of all staff members who will be involved with the use of the device is paramount.

REFERENCES
1. T Alster & P Graham, Microneedling: A Review and Practical Guide, August 2017 Dermatologic Surgery 44(3):1 <https://www.researchgate.net/publication/318997589_Microneedling_A_Review_ and_Practical_Guide>
2. A Rodrigues de Araujo, et al. Radiofrequency for the treatment of skin laxity: mith or truth*, An Bras Dermatol. 2015 Sep-Oct; 90(5): 707–721. <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4631236/>
3. K Kesty & DJ Goldbery, Radiofrequency microneedling for acne, acne scars, and more, March 2020, Dermatological Reviews, Volume 1, Issue 1. <https://onlinelibrary.wiley.com/doi/10.1002/der2.9>
4. E Dayan, et al., Adjustable Depth Fractional Radiofrequency Combined With Bipolar Radiofrequency: A Minimally Invasive Combination Treatment for Skin Laxity, 2019, Vol 39(S3) S112–S119.

5. Safety and Efficacy of the EndyMed Pro System Using RF Micro-needles Fractional Skin Remodeling <https://clinicaltrials.gov/ct2/show/NCT02368626>
6. HJ Park, et al., Clinical Study of Facial Wrinkle Treatment with Fractional Microneedle Radio Frequency System, Medical Lasers; Engineering, Basic Research, and Clinical Application 2014; 3(2): 59-64. http://www.jkslms.or.kr/journal/view.html?doi=10.25289/ML.2014.3.2.59
7. T Puiu, et al. A Comparative Analysis of Electric and Radiofrequency Microneedling Devices on the Market, Journal of Drugs in Dermatology, September 2018, Volume 17, Issue 9. <https://jddonline.com/ articles/dermatology/S1545961618P1010>
8. SJ Lee et al., Consensus Recommendations on the Use of a Fractional Radiofrequency Microneedle and Its Applications in Dermatologic Laser Surgery, Med Laser 2014;3(1):5-10.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Figure 3: 40-year-old patient before and six months after one Profound treatment to the face and neck. Images supplied by Dr Hina Sra of Cosmebeauté.


1,2 The Process of Muscle Hypertrophy, Robin Nye, RN, BSN; Alysa Hoffmeister, BS ©2020 Cutera, Inc. All rights reserved. Model; Not actual patient. AP002774 rA Well, now you can. The next-generation muscle-sculpting technology is here; offering more targeted treatments, across more areas (8x) than any other device –simultaneously. What makes truSculpt flex® truly unique is its proprietary MDS
Stimulation) technology. This allows users to target specific muscles using three
treatment modes, all designed to continually confuse and challenge the muscle,
30% increase in muscle mass2 Personalised and Selective 3 treatment modes Treat 8 areas simultaneously IMAGINE REPLICATING 54,000 CRUNCHES1? REDEFINING MUSCLE SCULPTIN G Learn how truSculpt flex® can strengthen your practice at cutera.co.uk/truSculptflex Cutera UK. Head Office 42 Kingston Space Ltd, Molly Millars Lane, Wokingham RG412PQ 0118 3272640 | info.uk@cutera.com | cutera.co.uk #WHYCUTERAUK Designed and manufactured in the San Francisco Bay Area, USA, our world-leading portfolio of laser & energy-based aesthetic devices provide professionals with the innovation, quality, and performance required to provide unrivalled clinical results for their patients.
(Multi-Directional
different
resulting in an average
Exploring Muscle Stimulation Technology
with a focus on EMS and the evidence behind its efficacy
Non-surgical body contouring/sculpting is one of the fastest growing treatments in the world.1 The ‘little-to-no’ downtime with few associated risks is appealing to many. Muscle stimulation devices promise to build muscle, increase strength and improve tone, therefore appealing to those who strive for aesthetic perfection, as well as those who are serious about reaching peak fitness levels. The earliest known use of electric muscle stimulation dates back to around 500 BC. The Egyptians discovered that certain fish emit electrical impulses; these fish were used to treat pain.2 There is plenty of emerging science into the benefits of muscle stimulation, whether this be through direct electric stimulation or indirect electromagnetic stimulation. In this article, I look at the science of both of these modalities and discuss their potential uses in aesthetic medicine, the fitness industry and rehabilitation, as well as providing a brief overview of the in-clinic devices available in the UK.
Types of muscle-stimulating technologies
There are currently three types of technologies which stimulate muscle contraction. These include transcutaneous electrical nerve stimulation (TENS), electrical muscle stimulation (EMS) and electromagnetic field devices, of which high intensity focused electromagnetic field (HIFEM) devices and functional magnetic stimulation technologies are included.1 There are several manufacturers of each type of device and Figure 1 lists some of the devices available in the UK.3 As TENS is the use of an electric current produced by a device to stimulate the nerves for therapeutic purposes, rather than muscles, this article will not be looking at this modality in detail.4,5
Electrical muscle stimulation
EMS, also known as neuromuscular electrical stimulation (NMES), is the evocation of muscle contraction using electric impulses. EMS provides an electrical current at a specifically designed frequency to target motor nerves causing them to depolarise, as shown in Figure 2.6 This stimulation creates muscle contractions that can be quick and frequent, fast with long pauses, or contractions that are held for several seconds or minutes at a time. Normally, electrical impulses from the brain travel through the central nervous system (CNS) and reach the neuromuscular junction where a neurotransmitter crosses the junction and stimulates muscle contraction. Muscle recognises a stimulus, regardless of the source, and reacts to it.7 EMS allows for deep, intense, and complete muscular contractions without activating the CNS. It is the contraction type that determines whether the session will result in a warm up, increase in strength, muscle hypertrophy or even recovery. EMS works directly on the muscles and bypasses the body’s own energy conservation system, which means that there’s no limit to the percentage of muscle fibre that can be activated.8
During an EMS treatment, similar to strength training, muscle fibres undergo microscopic tears, and then cells attempt to repair the damage which results in increasing muscle size and strength. This repair process, known as hypertrophy, begins after each treatment and involves releasing hormones, such as testosterone, to activate cell recovery, form new blood capillaries, repair muscle fibres, and manage the gain in muscle mass. The body needs to repair, build and increase muscle size over several weeks.
This simulation continually confuses and challenges the muscle at an intensity and duration that is beyond the level that can be achieved
Figure 1: Physician led, in-clinic muscle-stimulating devices in the UK3,26
technologies,
Device Manufacturer Technology Sessions needed Exercise equivalent Applicators/hand pieces CMSlim Contour Master Daeyang Medical & distributed in the UK by Aesthetic Technology Ltd High-intensity electromagnetic muscle training 4-6 30,000 contractions per 30-minute session 2 EMsculpt BTL Aesthetics High intensity focused electromagnetic technology 4-8 20,000 crunches per 30-min session 2 StimSure Cynosure Electromagnetic field technology 6-8 24,000 muscle contractions per 20-30 min session 1 or 2 TESLAFormer Iska Medical Functional magnetic stimulation technology 4-8 50,000 contractions per 30min session 2 TruSculpt Flex Cutera Medical Ltd Multi-directional direct muscle stimulation (form of electrical muscle stimulation) 4-6 54,000 crunches per 45-min session 8 3D-PowerSculpt 3D-Lipo High intensity focused electromagnetic technology 6-8 20,000 crunches per 30-min session 2 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Dr Nestor Demosthenous introduces muscle-stimulating

EMS in the literature
documented since the late 1980s In 1988 Lai et al randomly assigned 24 participants to a control group, a low intensity EMS group and a high intensity EMS group They showed that low and high intensity EMS training resulted in statistically significant strength improvement in quadricep muscles 8 More recently, Liu et al conducted a systematic review and found that neuromuscular electrical stimulation improved muscle strength in a cohort of 576 patients who had developed ICU-acquired weakness 10 There is also evidence that EMS can improve functional performance in a variety of strength tasks 11 Two mechanisms have been
during regular exercise. A typical abdominal workout, for example, may include up to 10 minutes of various movements to contract, hold and relax the abdominal muscles. Accessory muscles can also be recruited to facilitate sit ups/crunches such as latissimus dorsi and splenius capitis. Varying the frequencies can change which types of muscle fibres are stimulated. Three ranges of frequencies stimulate three kinds of motor-neuron muscle fibre types (the slow, medium, and fast twitch fibres).9 As we will see, the literature supports higher frequencies to achieve results.
proposes that augmentation of muscle strength with EMS occurs in the same way as augmentation of muscle strength with voluntary exercise, where a low number of repetitions with high external loads and a high intensity of muscle contraction leads to increase strength 11 The second mechanism proposes that the muscle strengthening seen following EMS training results from a reversal of voluntary recruitment order (where type II muscle fibres are selectively augmented) Type II fibres have a higher specific force than type I fibres, while selective augmentation of type II muscle fibres will increase the overall strength of the muscle 11
EMS in the literature
The positive effects of EMS on improved strength has been documented since the late 1980s. In 1988 Lai et al. randomly assigned 24 participants to a control group, a low intensity EMS group and a high intensity EMS group. They showed that low and high intensity EMS training resulted in statistically significant strength improvement in quadricep muscles.8 More recently, Liu et al. conducted a systematic review and found that neuromuscular electrical stimulation improved muscle strength in a cohort of 576 patients who had developed ICUacquired weakness.10
The use of EMS to prevent muscle atrophy associated with prolonged knee immobilisation following ligament reconstruction surgery or injury has been extensively studied According to a 1992 literature review,
strength, muscle mass and the oxidative capacity of thigh muscles following knee immobilisation 11
Filipovic et al 2012 conducted a systematic review of more
There is also evidence that EMS can improve functional performance in a variety of strength tasks.11 Two mechanisms have been suggested to explain the training effects seen with EMS. The first proposes that augmentation of muscle strength with EMS occurs in the same way as augmentation of muscle strength with voluntary exercise, where a low number of repetitions with high external loads and a high intensity of muscle contraction leads to increase strength.11 The second mechanism proposes that the muscle strengthening seen following EMS training results from a reversal of voluntary recruitment order (where type II muscle fibres are selectively augmented). Type II fibres have a higher specific force than type I fibres, while selective augmentation of type II muscle fibres will increase the overall strength of the muscle.11
The use of EMS to prevent muscle atrophy associated with prolonged knee immobilisation following ligament reconstruction surgery or injury has been extensively studied. According to a 1992 literature review, EMS was shown to be effective in preventing the decreases in muscle strength, muscle mass and the oxidative capacity of thigh muscles following knee immobilisation.11
strength, speed strength, power, jumping and sprinting ability amongst untrained subjects, trained subjects, and elite athletes 12 The analysis showed that trained and elite athletes, despite their already high level of fitness, are able to significantly enhance their level of strength to the same extent as is possible with untrained subjects After a stimulation period of three to six weeks, significant gains (p<0 05) were shown in maximal strength, speed strength and power Developing these parameters increased vertical jump height by up to +25% and improved sprint times by as much as 4 8% in trained and elite athletes 12
In 2015, Kim et al
Filipovic et al. 2012 conducted a systematic review of more than
therapy on the abdominal obesity levels of young women and whether it could be used to lose body fat 13 22 obese women were enrolled into either a control (12) or treatment group (10) The treatment group received treatment (30 minutes) three times a week for six weeks After those six weeks, the researchers measured the subjects’ waist circumference, body mass index, subcutaneous fat mass, and total body fat percentage Without modifying their exercise or diet,
abdominal obesity, subcutaneous fat mass, and body fat percentage 13
200 published studies looking at EMS effects on maximal strength, speed strength, power, jumping and sprinting ability amongst untrained subjects, trained subjects, and elite athletes.12 The analysis showed that trained and elite athletes, despite their already high level of fitness, are able to significantly enhance their level of strength to the same extent as is possible with untrained subjects. After a stimulation period of three to six weeks, significant gains (p<0.05) were shown in maximal strength, speed strength and power. Developing these parameters increased vertical jump height by up to +25% and improved sprint times by as much as 4.8% in trained and elite athletes.12
five-week EMS training programme on muscular strength (quadriceps), kicking velocity, sprint, and vertical jump performance in football players 14 20 male football players were randomly divided into two training groups The EMS group received treatment on quadricep muscles (three sessions of 12 minutes per week for five weeks) and regular football training The control group only had regular football training The athletes were tested after three weeks and five weeks of training and, at both assessments, the EMS group showed significant improvements in quadricep muscle strength parameters as well as in ball speed performance These improvements were not seen in the control group 14
In 2015, Kim et al. looked at the effects of high frequency EMS therapy on the abdominal obesity levels of young women and whether it could be used to lose body fat.13 22 obese women were enrolled into either a control (12) or treatment group (10). The treatment group received treatment (30 minutes) three times a week for six weeks. After those six weeks, the researchers measured the subjects’ waist circumference, body mass index, subcutaneous fat mass, and total body fat percentage. Without modifying their exercise or diet, EMS led to significant effects on decreasing waist circumference, abdominal obesity, subcutaneous fat mass, and body fat percentage.13 A French study used an EMS device to investigate the effect of a five-week EMS training programme on muscular strength (quadriceps), kicking velocity, sprint, and vertical jump performance in football players.14 20 male football players were randomly divided into two training groups. The EMS group received treatment on quadricep muscles (three sessions of 12 minutes per week for five weeks) and regular football training. The control group only had regular football training. The athletes were tested after three weeks and five weeks of training and, at both assessments, the EMS group showed significant improvements in quadricep muscle strength parameters as well as in ball speed performance. These improvements were not seen in the control group.14
In 2018 Mettler et al found that after just 30 minutes of a high frequency EMS treatment, there was an up-regulation of anabolic signalling as shown on staining of muscle biopsies in eleven healthy volunteers (six men, five women) This suggests that high frequency stimulation may provide a stronger stimulus for processes that initiate muscle hypertrophy 9 Exercise has numerous benefits for patients with cancer, but implementation is challenging because of practical and logistical hurdles Therefore, in a recent 2020 study, Toth et al examined whether EMS can serve as a surrogate for classical exercise by eliciting an exercise training response in skeletal muscle of women diagnosed with breast cancer undergoing chemotherapy Of the 22 patients enlisted, 17 completed the trial and showed a statistically significant increase in muscle fibre hypertrophy15
In 2018 Mettler et al. found that after just 30 minutes of a high frequency EMS treatment, there was an up-regulation of anabolic signalling as shown on staining of muscle biopsies in eleven healthy volunteers (six men, five women). This suggests that high frequency stimulation may provide a stronger stimulus for processes that initiate muscle hypertrophy.9
Aesthetics | January 2019 3 g p j aestheticsjournal
During an EMS treatment, similar to strength training, muscle fibres undergo microscopic tears, and then cells attempt to repair the damage which results in increasing muscle size and strength
Figure 2: Action potential of electrical muscle stimulation6 Action potential V o l tag e ( m V ) Time (ms) 0 -70 -55 0 +40 1 2 3 4 5 Stimulus Failed initiations Refractory period Threshold Resting state Depolarisation Repolarisation Figure 2: Action potential of electrical muscle stimulation6 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
During an EMS treatment, similar to strength training, muscle fibres undergo microscopic tears, and then cells attempt to repair the damage which results in increasing muscle size and strength
EMSCULPT is the only procedure to help both women and men burn fat, while toning the underlying muscle, backed up by 20 peer-reviewed publications.
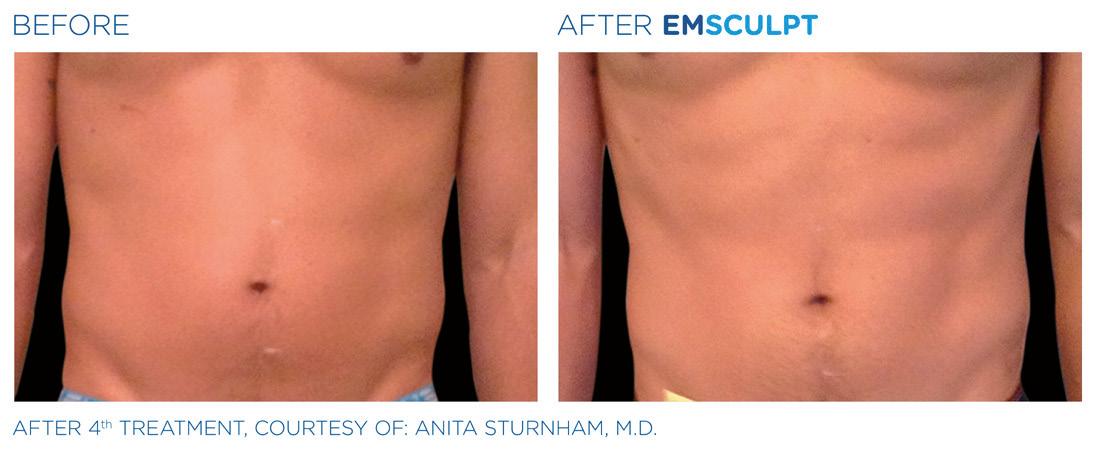


“For me, the key criteria in choosing equipment are the reputation of the system and manufacturer, supporting clinical data and public brand awareness. BTL have set these benchmarks and this gives me confidence to offer EMsculpt to my patients”
Dr.
Rita Rakus MBBS FBCAM Global Ambassador

BUILD
SCULPT YOUR
CLINICALLY PROVEN – GLOBALLY RECOGNISED Emsculpt_AD_Aesthetic-Journal_A4_ENGB100 799-79EMCFMA2JENGB100 Results and patient experience may vary. Patients shown in the B&A pictures are within +/- 2,25 kg of their original weight unless specified. As with any medical procedure, ask your doctor if the Emsculpt procedure is right for you. In the EU EMSCULPT® is intended for the treatment of obesity by fat reduction through neuromuscular stimulation and increase of the blood flow. ©2020 BTL Group of Companies. All rights reserved. BTL® and EMSCULPT® are registered trademarks in the United States of America, the European Union, and other countries. The products, the methods of manufacture or the use may be subject to one or more U.S. or foreign patents or pending applications. Trademarks EMSCULPT®, EMSELLA®, EMTONE®, EMBODY®, and HIFEM® are parts of EM™ Family of products. *Data on file. EMSCULPT.COM | SALES@BTLNET.COM | 01782 579060
MUSCLE &
BODY
Exercise has numerous benefits for patients with cancer, but implementation is challenging because of practical and logistical hurdles. Therefore, in a recent 2020 study, Toth et al. examined whether EMS can serve as a surrogate for classical exercise by eliciting an exercise training response in skeletal muscle of women diagnosed with breast cancer undergoing chemotherapy. 22 patients with stage I,II or III breast cancer scheduled to receive neoadjuvant or adjuvant chemotherapy were randomised to eight weeks of bilateral electrical muscle stimulation to their quadricep muscles or control. Biopsy of the vastus lateralis was performed at baseline and after eight weeks of intervention to assess muscle fibre size, contractility, and mitochondrial content. EMS promoted muscle fiber hypertrophy (P < 0.001), particularly in fast-twitch, myosin heavy chain (MHC) IIA fibres (P < 0.05) and tended to induce fibre type shifts in MHC II fibers.15 A Cochrane systematic review (Jones et al. 2016) looked at 18 studies with 933 participants who had EMS treatments. It considered EMS a valid therapeutic intervention to improve muscle weakness in adults with conditions such as chronic obstructive pulmonary disease, chronic respiratory disease, chronic heart failure, or thoracic cancer.16 A recent study (submitted for publication) by Yezak et al. from the Houston Spine and Rehabilitation Centre looked at EMS therapy on 20 patients with chronic lower back pain who were unresponsive to physical therapy and pain management injections. They received six 45-minute EMS treatments to the abdominal region (rectus abdominis, abdominal obliques, and transverse abdominis). At baseline and eight to 10 days post final treatment, the patients completed disability questionnaires and were functionally evaluated
for lumbar flexion, as well as muscular endurance and strength. Pain levels were recorded pre- and post-testing by questionnaire. Six treatment sessions with the muscle stimulator, twice weekly for three weeks, demonstrated clinically and statistically significant improvement in chronic lower back pain that was unresponsive to physical therapy and pain management injections, in addition to clinically and statistically significant improvements in lumbar flexion and core muscular endurance and strength.17
A preliminary study by Dr Stephen Ronan treated 28 patients with EMS technology (up to six treatments spaced two to four days apart) and found it to be a safe and efficacious treatment to firm and tone the abdominal muscles.18 Digital photos and ultrasound measurements were obtained at baseline and at four, eight, and 12 weeks post treatment. The electrodes were placed on the abdomen and flanks. These areas were treated for 45 minutes with varying intensities of energy. The author found an average of 30% increase in muscle mass and a modest reduction in fat thickness. All patients tolerated the procedure well with minimal pain. Minor erythema was reported by two patients following the treatments.18
Despite positive reports in the literature, in 2002, Porcari found no significant improvement in measures such as strength, muscle mass and body weight.19 It is important to note that there are many EMS devices on the market that are inexpensive, over-the-counter homeuse devices; however, there is only one physician led, in-clinic device currently available on the UK market (TruSculpt). For this reason there is a plethora of conflicting data.
High intensity focused electromagnetic therapy
There are not many electromagnetic field devices available for in-clinic use in the UK. A few HIFEM devices have been listed in Figure 1. It is a relatively new technology for body contouring. Electromagnetic fields are composed of both electric and magnetic fields. Electric fields are a result of electric charges (measured in volts per metre), while magnetic fields arise from movement of electric charges and are measured in Tesla (T).20 There are four basic principles for understanding electromagnetic theory:20
1. Electric charges attract or repel each other with a force that is inversely proportional to the distance between them.
2. Magnetic poles attract or repel each other like electric charges and exist in pairs.
3. Electric current in a wire generates a circumferential magnetic field surrounding the wire. The direction of the magnetic field is perpendicular to the wire.
4. An electric current is induced in a loop of wire when moved towards or away from a magnetic field or a magnet is moved towards or away from it.
measurements were obtained at baseline and at four, eight, and 12 weeks post treatment The electrodes were placed on the abdomen and flanks These areas were treated for 45 minutes w varying intensities of energy The author found an average of 30 increase in muscle mass and a modest reduction in fat thickness
In HIFEM technology, a rapidly varying magnetic field induces an electric current in the target tissue, as demonstrated in Figure 3 20 The first difference we see between EMS and HIFEM is that the latter relies on a magnetic field to produce an electric current in the tissue, which depolarises motor nerves resulting in muscular contractions. The magnetic field intensities delivered are up to 2.5T.20 An important safety issue that needs to be addressed is the dosage of electromagnetic field being generated per treatment. The World Health Organization has established potential longterm effects of childhood leukaemia from average magnetic field exposures in the 0.3T range.21 Kinney et al. (2019) treated 22 patients with HIFEM technology. Patients received four
A Cochrane systematic review (Jones et al 2016) looked at 18 studies with 933 participants who had EMS treatments It considered EMS a valid therapeutic intervention to improve muscle weakness in adults with conditions such as chronic obstructive pulmonary disease, chronic respiratory disease, chronic heart failure
All patients tolerated the procedure well with minimal pain Minor erythema was reported by two patients following the treatments Despite positive reports in the literature, in 2002, Porcari found no significant improvement in measures such as strength, muscle mass and body weight 19 It is important to note that there are man EMS devices on the market that are inexpensive, over-the-count home-use devices; however, there is only one physician led, inclinic device currently available on the UK market (TruSculpt) For this reason there is a plethora of conflicting data
High intensity focused electromagnetic therapy There are not many electromagnetic field devices available for in-cli use in the UK A few HIFEM devices have been listed in Figure 1 It is
News @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Clinical Practice
or thoracic cancer 16
Wire loop Magnetic field Electric current induced Figure 3: A rapidly moving magnet induces an electric current in HIFEM technology20
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
There is also evidence that EMS can improve functional performance in a variety of strength tasks




AESTHETICSJOURNAL.COM Get the best experience... VISIT WWW.AESTHETICSJOURNAL.COM TO JOIN FREE TODAY Keep up-to-date on the latest aesthetics developments and best practice guidance on your desktop, tablet or phone
our Library for a huge range of categorised content and tools
to your specialism and interests
training to your personal Training Record for easy reference
accredited CPD articles and receive digital certification
our comprehensive supplier Directory for useful business partners
and advertise products and devices you may wish to buy and sell
the Classified section
Search
relating
Add
Complete
Browse
Review
in
30-minute abdominal treatment sessions spaced two to five days apart. They found a 15.4% increase in rectus abdominis muscle thickness. They also found an associated 18.6% reduction of adipose tissue thickness, which was attributed to adipocyte apoptosis.22 In 2020 Zachary et al. treated six patients (who were to undergo abdominoplasty) with the same device.23 Superficial and deep subcutaneous adipose tissue was harvested at set timepoints post treatment. The presence or absence of an inflammatory response was evaluated using standard haematoxylin and eosin (H&E) staining. Perilipin immunofluorescence was used to assess irreversible fat cell injury. Following H&E histological analysis at three, 10, 11, and 17 days post treatment, no HIFEM-treated samples showed an inflammatory response in either the superficial or deep subcutaneous adipose tissue. The persistence of perilipin staining of adipose tissue indicated that all fat cells were viable.23 Patient satisfaction appears to be high with HIFEM technology. Jacob et al. (2018) looked at patient satisfaction using a HIFEM device and found patients initially dissatisfied with the appearance of their buttocks reported a significant 85% improvement after the fourth treatment based on two seven-point Likert scale questionnaires.24 Unpublished data by Kent and Jacob who treated 16 patients found a 15.8% increase in abdominal muscle thickness on CT scan evaluation before and after four treatments.25
EMS vs. HIFEM
There are currently no studies comparing these technologies. Most studies for HIFEM devices have looked at muscle hypertrophy of abdominal muscles, or patient satisfaction of the gluteal region. As we can see from Figure 1, treatment protocols range from four to eight half-hour treatment sessions. Result times will therefore vary depending on the device. Additional studies are needed to evaluate these devices in a standardised manner.
Muscle stimulation devices are relatively new and still require more robust clinical studies to definitively show their efficacy. While large double blind randomised controlled trials are lacking, increasing numbers of level three and four studies are showing promising results in favour of these devices.
Conclusion
Non-surgical body treatments have developed past just contouring and are now looking to sculpt and define our patients, with the use of muscle-stimulating devices developing rapidly. There is a great interest in the ability to push patients passed their physical limits of training and improve their strength as well as muscle mass. Clinicians are extending its use past the aesthetics of muscle hypertrophy, but applying it to strength and core training, as well as rehabilitation such as for lower back pain.
HIFEM shows a high patient satisfaction as well as good evidence of muscle hypertrophy of abdominal muscles and, potentially, abdominal adipocyte reduction. The future of EMS devices is interesting for the management of lower back pain, muscle hypertrophy in chemotherapy patients, and rehabilitation following lower limb surgery. Whatever device a clinic decides to use, they should market treatments responsibly. It must be made clear to our patients that these devices will help them on their journey to achieving a healthier, more aesthetic physique. These devices do not replace a healthy diet and exercise. Instead, they complement a healthy lifestyle. As with all treatments, a lengthy consultation is needed to understand patient expectations and advise if these can be met.
Dr Nestor Demosthenous obtained his medical degree and BSc Hons Neuro from the University of Edinburgh in 2006. He has completed core surgical training followed by four years as a clinical fellow in trauma and orthopaedic Surgery. Dr Demosthenous obtained his MSc in Aesthetic Medicine from QMUL in 2019. He has 10 years’ experience in aesthetic medicine and is a KOL for Allergan and Cutera Medical Ltd.

Qual: MBChB, BSc Hons Neuro, MSc (Aesthetic Medicine)
aestheticsjournal.com/cpd
REFERENCES
1. Alexandra K. Rzepecki, et al., Update on Noninvasive Body Contouring Techniques. Cutis 2018 Apr;101(4):285-288.
2. Heidland et al., Neuromuscular electrostimulation techniques: historical aspects and current possibilities in treatment of pain and muscle wasting, Clin Nephrol, 2013 Jan;79 Suppl 1:S12-23.
3. Carver, H, Introducing Muscle Stimulating Technology, Aesthetics journal, April 2020. <https:// aestheticsjournal.com/feature/introducing-muscle-stimulating-technology>
4. Dubinsky RM, Miyasaki J, ‘Assessment: Efficacy of transcutaneous electric nerve stimulation in the treatment of pain in neurologic disorders (an evidence-based review): Report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology”. Neurology 74 (2): (2009) 173–176.
5. Khadilkar A, Odebiyi DO, Brosseau L, Wells GA , Brosseau, Lucie (ed.), ‘Transcutaneous electrical nerve stimulation (TENS) versus placebo for chronic low-back pain,’ The Cochrane Library (4): 2008.
6. Aarushi Khanna, ‘Action Potential’, TeachMe Physiology, 2020. <https://teachmephysiology.com/ nervous-system/synapses/action-potential/>
7. The Editors of Encyclopaedia Britannica, Neuromuscular junction, Encyclopaedia Britannica, <https:// www.britannica.com/science/neuromuscular-junction>
8. Hon Sun Lai, et al., The effect of Different Electro-Motor Stimulation Training Intensities on Strength Improvement. The Australian Journal of Physiotherapy. Vol. 34, No.3, 1988
9. Joni A Mettler, Dillon M Magee, Barbara M Doucet. High-Frequency Neuromuscular Electrical Stimulation Increases Anabolic Signaling.Med Sci Sports Exerc 2018 Aug;50(8):1540-1548.
10. Miao Liu, Jian Luo, Jun Zhou, Xiaomin Zhu, Intervention effect of neuromuscular electrical stimulation on ICU acquired weakness: A meta-analysis, Int J Nurs Sci 2020 Mar 10;7(2):228-237.
11. D A Lake, Neuromuscular Electrical Stimulation. An Overview and Its Application in the Treatment of Sports Injuries. Sports Med1992 May;13(5):320-36.
12. Andre Filipovic et al., Electromyostimulation – a Systematic Review of the Effects of Different Electromyostimulation Methods on Selected Strength Parameters in Trained and Elite Athletes. J Strength Cond Res 2012 Sep;26(9):2600-14.
13. Jin-Seop Kim, Duck-Won Oh, Effects of High-Frequency Current Therapy on Abdominal Obesity in Young Women: A Randomized Controlled Trial. J Phys Ther Sci 2015 Jan;27(1):31-3. doi: 10.1589/ jpts.27.31. Epub 2015 Jan 9.
14. Maxime Billot, et al., Effects of an Electrostimulation Training Program on Strength, Jumping, and Kicking Capacities in Soccer Players. J Strength Cond Res 2010 May;24(5):1407-13
15. Michael J Toth et al. Effect of Neuromuscular Electrical Stimulation on Skeletal Muscle Size and Function in Patients With Breast Cancer Receiving Chemotherapy. J Appl Physiol (1985) 2020 May 7.
16. Jones, S., et al., Neuromuscular electrical stimulation for muscle weakness in adults with advanced disease. Cochrane Database Syst. Rev. (2016) 10:CD009419.
17. Mark C. Yezak, et al., Effect Of Bio-Electrical Muscle Stimulation On Chronic Low Back Pain And Abdominal Muscular Endurance And Strength. Paper provided by Cutera Medical.
18. Stephen J. Ronan M.D. Facs A Novel Bio-Electric Current Stimulation Device For Improvement Of Muscle Tone: The TruSculpt et al
19. JOhn P. Porcari, et al., Effects of Electrical Muscle Stimulation on Body Composition, Muscle Strength, and Physical Appearance. Journal of Strength and Conditioning Research, 2002, 16(2), 165–172.
20. Macrene Alexiades. High Intensity Focused Electromagnetic Field (HIFEM) Devices in Dermatology. Journal of Drugs in Dermatology. 2019, 18(11), pg 1088.
21. WHO, Electromagnetic fields (EMF): Electromagnetic fields and public health, 2007. <https://www.who. int/peh-emf/publications/facts/fs322/en/>
22. Kinney B, Lozanova P, High Intensity Focused Electromagnetic Therapy Evaluated by Magnetic Resonance Imaging: Safety and Efficacy Study of a Dual Tissue Effect Based Non-Invasive Abdominal Body Shaping Lasers in Surgery and Medicine 51:40–46 (2019)
23. Zachary C, Burns AJ, Pham LD, Lozano JNJ, Clinical Study Demonstrates that Electromagnetic Muscle Stimulation Does Not Cause Injury to Fat Cells, Lasers Surg Med 2020 May 8.
24. Jacob C, Kinney B, Busso M, Chilukuri S, McCoy JD, Bailey C, Denkova R. High Intensity Focused Electro-Magnetic Technology (HIFEM) for Non-Invasive Buttock Lifting and Toning of Gluteal Muscles: A Multi-Center Efficacy and Safety Study. J Drugs Dermatol 2018 Nov 1;17(11):1229-1232.
25. Kent DE, Jacob CI, Computed Tomography (Ct) Based Evidence Of Simultaneous Changes In Human Adipose And Muscle Tissues Following A High Intensity Focused Elelctro-Magnetic Field (Hifem) Application: A New Method For Non-Invasive Body Sculpting. Study provided by BTL Technologies.
26. CM Slim Contour Master, Aesthetic Technology Ltd, <https://www.aesthetictec.com/cmslim.html>
Test your knowledge with our multiple-choice questions to receive your CPD certificate online!
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Understanding Alternative Uses of Hyaluronidase
Hyaluronidases are a family of enzymes which are able to degrade hyaluronic acid (HA);1 a glycosaminoglycan molecule of the extracellular matrix (ECM) and the main constituent of many dermal fillers.2 Long before HA fillers became popular, hyaluronidase had been used for many other applications within medicine.3,4,5 Its use for correcting problems secondary to dermal filler is off-label, and much of the safety data we have is based on its uses from other areas of medicine. In this article, we aim to summarise the other uses of hyaluronidase within medicine in order to improve aesthetic practitioners’ understanding of how the drug works.
What is hyaluronidase?
Hyaluronidase is an enzyme which is considered a ‘spreading factor’5 as it degrades HA, which is an essential constituent of the ECM. It was initially discovered in 1929 by Dr Francisco Duran-Reynals, a doctor from Barcelona who became well known in the field of experimental pathology.6 It had been found in certain strains of streptococcal bacteria7 and as HA was found to be its primary substrate, it was named hyaluronidase. Hyaluronidase leads to the degradation of HA by hydrolysing the disaccharides at hexosaminidic β-1 through β-4 linkages.8 There are several sources of hyaluronidase, and they are generally divided into three subgroups: mammalian (obtained from the testis), hookworm/leech and microbes.9,10 Recombinant human hyaluronidase is now available (Hylenex), and has a purity of 100 times higher than some of the bovine preparations.11 The long-term data for this product is awaited, however it is speculated to have a lower incidence of allergic reactions.9 The current hyaluronidase available in the UK (Hyalase) is available in a 1500 international unit ampoule of powder for reconstitution and is of ovine (sheep) origin.12
Use in aesthetics
Within aesthetics, hyaluronidase is widely used off-label for dealing with a variety of HA fillerrelated complications, including vascular occlusion, nodules, lumps and poor cosmetic result such as overtreatment, asymmetry or Tyndall effect.12,13
Vascular occlusion secondary to HA filler can be relieved by injecting hyaluronidase. This recommendation forms part of the Aesthetic Complications Expert (ACE) Group guidelines for the management of vascular occlusion.14 Whilst this is an off-label indication, there is a wealth of
evidence in the literature supporting its use in this situation to prevent tissue necrosis.15-19 ACE guidelines also support the use of hyaluronidase in other non-emergency situations related to HA filler, where it is in the patient’s best interest, and the patient has agreed to the treatment as part of the informed consent process.12 Hyaluronidase is often considered the quick solution to many filler complications, however we ought to remain mindful that the use of hyaluronidase is not without risk, with bruising, swelling and allergic reaction all being reported possible complications.20
As well as in relation to filler, in the past there has been interest in whether hyaluronidase can be used to treat cellulite. It has been suggested that intradermal mesotherapy use of hyaluronidase can aid in reducing its appearance. It was initially thought that fibrosclerosis of the tissues contributed towards the development of cellulite,21 and interest in the use of hyaluronidase as a ‘spreading factor’ grew. The pathophysiology of cellulite however, remains largely unknown, and there is a lack of studies demonstrating a beneficial effect through treatment with hyaluronidase.22
Applied to medicine
Before the popularity of HA-based fillers and its use in management of HA-related complications, hyaluronidase was, and still is, used for many other applications within medicine. It is licenced for use to enhance permeation of subcutaneous or intramuscular injections, to enhance permeation of local anaesthetics, to enhance permeation of
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Hyaluronidase leads to the degradation of HA by hydrolysing the disaccharides at hexosaminidic ẞ-1 through ẞ-4 linkages
Ophthalmologist Miss Jennifer Doyle discusses the different uses of hyaluronidase in the medical field
ophthalmic local anaesthetics, for hypodermoclysis and to treat extravasation injuries and haematomas.23
As a ‘spreading factor’, hyaluronidase’s action to degrade HA in the ECM has long been utilised as an adjuvant treatment. By rendering tissues more permeable to injected fluids, it can aid the spread and effectiveness of local anaesthesia. In particular, it has been used for decades in ophthalmic surgery to aid anaesthesia and akinesia.24,25 This use is becoming less popular, with a recent Cochrane review concluding that the beneficial effect of adding hyaluronidase to ophthalmic local anaesthetic is uncertain due to the low quality of evidence available.25 The authors did, however, also conclude that there was no harm attributed to the use of hyaluronidase in any of the studies, which is also an important finding in terms of considering the safety of its use.26
Hypodermoclysis or subcutaneous infusion of fluids is a method of providing hydration, and is often used as an alternative to intravenous (IV) infusion in patients where IV access is difficult, such as in elderly care or palliative medicine.26,27 It is thought that the addition of hyaluronidase to subcutaneous hydration may aid in enhanced dispersion and absorption of the fluid.28 The benefits of its use are also still widely debated, with no conclusion that its use is justified.29 Extravasation injury can occur if an infused drug leaks out of a blood vessel into the surrounding tissue during IV infusion.30 Hyaluronidase is currently recommended for extravasation of certain cytotoxic drugs such as vinca alkaloids.31 It is suggested to help treatment of such injuries by facilitating drug diffusion and dilution.27 This ability as a ‘spreading factor’ is why it is also used in the treatment of haematomas, by facilitating the absorption of the haematoma through lymphatic vessels and capillaries as a result of the increase of local intercellular permeability.32
Due to its action on the ECM it is thought that there is high potential in medicine, surgery and aesthetic medicine for future uses of hyaluronidase.8 Further research is still required to elucidate the exact mechanisms of HA catabolism within the ECM.8 An example of a new potential use within medicine is its role in cancer metastasis and therapy. Novel non-invasive tumour imaging using hyaluronidase activity as a marker of tumour aggressiveness is being investigated.33-34
Over the past few years it has been shown that the combined overexpression of HA synthesising enzymes with hyaluronidases confers tumorigenic potential.34 The degradation of high molecular weight HA-generated proangiogenic breakdown products.33 Thus, by expression of hyaluronidase, tumour cells can influence the angiogenic balance of their microenvironment.33 As hyaluronidase activity correlates with progression and metastatic spread, detecting hyaluronidase activity by magnetic resonance imaging (MRI) can be useful in investigating tumour aggressiveness.33
There is future potential for hyaluronidaise
The rising popularity of HA fillers within the aesthetic industry has led to the increase of use and interest in hyaluronidase. As an off-label indication it can successfully be used in emergencies such as vascular occlusion, as well as correction of HA filler-related complications, such as delayed onset nodules or poor cosmetic result correction. It acts as a ‘spreading factor’, degrading HA in the ECM allowing increased permeability of the ECM for other medications. Before its popular use in aesthetics, it was used in other fields of medicine such as anaesthetics, ophthalmology and oncology. Further studies to elucidate its exact mechanism of action within the ECM are needed, and it is anticipated that hyaluronidase will have many future potential uses across a variety of medical specialities.
Miss Jennifer Doyle has a Bachelor of Medicine and a Bachelor of Surgery with distinction, as well as a Master’s in Medical Sciences from the University of Oxford. She is a Fellow of the Royal College of Ophthalmologists. She has completed the Level 7 in Injectables and is a lead trainer at Harley Academy. Miss Doyle currently works as an NHS registrar in ophthalmology, as well as leading her clinic, Oxford Aesthetics.
QUAL: BMBCh, MA(OXON), L7Cert, FRCOphth
REFERENCES
1. Maurizio Cavallini, Riccardo Gazzola, Marco Metalla, Luca Vaienti, The Role of Hyaluronidase in the Treatment of Complications From Hyaluronic Acid Dermal Fillers, Aesthetic Surgery Journal, Volume 33, Issue 8, November 2013, Pages 1167–1174. <https://doi.org/10.1177/1090820X13511970>
2. Gold MH. Use of hyaluronic acid fillers for the treatment of the aging face. Clin Interv Aging 2007;2(3):369-376.

3. Atkinson WS. Use of hyaluronidase with local anaesthesia in ophthalmology: preliminary report. Arch Ophthalmol. 1949;42(5):628–633.
4. Zenk KE, Dungy CI, Greene GR. Nafcillin Extravasation Injury: Use of Hyaluronidase as an Antidote. Am J Dis Child. 1981;135(12):1113–1114.
5. Watson D. Hyaluronidase. British Journal of Anaesthesia, 1993; 71: 422-425
6. Obituaries. Nature; No 4649 December 1958. <https://www.nature.com/articles/1821549b0.pdf>
7. Duran-Reynals F. The effects of extracts of certain organs from normal and immunised animals on the infecting power of vaccine virus. Journal of Experimental Medicine 1929; 50: 327-340.
8. Buhren BA, Schrumpf H, Hoff NP, et al. Hyaluronidase: from clinical applications to molecular and cellular mechanisms. Eur J Med Res. 2016;21:5.
9. King M, Convery C, Davies E. This month’s guideline: The Use of Hyaluronidase in Aesthetic Practice (v2.4). J Clin Aesthet Dermatol. 2018;11(6):E61-E68.
10. Meyer K. Hyaluronidases. In: Boyer PD, editor. The Enzymes. New York, NY: Academic Press; 1971. pp.307–320.
11. Andre P, Levy PM. Hyaluronidase offers an efficacious treatment for inaesthetic HA overcorrection. J Cosmet Dermatol. 2007;6(4):159–162.
12. ACE group. The Use of Hyaluronidase in Aesthetic Practice. <https://s3-eu-west-2.amazonaws.com/ ace-group-wp/app/uploads/2019/02/19170806/ACE-Group-Hyaluronidase-v2.6.pdf>
13. Claudio DeLorenzi, Complications of Injectable Fillers, Part I, Aesthetic Surgery Journal 2013 33: 561
14. ACE Group. Management of a vascular occlusion associated with cosmetic injections. <https:// s3-eu-west-2.amazonaws.com/ace-group-wp/app/uploads/2019/02/05184455/Vascular-Occlusionv2.5.pdf>
15. Souza Felix Bravo, B., Klotz De Almeida Balassiano, L., Roos Mariano Da Rocha, C., Barbosa De Sousa Padilha, C., Martinezt Torrado, C., Teixeira Da Silva, R. and Carlos Regazzi Avelleira, J. (2015) ‘Delayed-type Necrosis after Soft-tissue Augmentation with Hyaluronic Acid’, J Clin Aesthet Dermatol, Dec;8(12), pp 42-47.
16. Ozturk, C.N., Li, Y., Tung, R., Parker, L., Peck Piliang, M. and Zins, J.E. ‘Complications following injection of soft-tissue fillers’, Aesthetic Surgery Journal, 33(6), pp 862-877.
17. Grunebaum, L., Allemann, I., Dayan, S., Mandy, S. and Baumann, L. (2009) ‘The risk of alar necrosis associated with dermal filler injection’, Dermatol Surgery, 35, pp 1635-1640.
18. Urdiales-Gálvez, F., Delgado, N.E., Figueiredo, V. et al. (2018) ‘Treatment of Soft Tissue Filler Complications: Expert Consensus Recommendations’, Aesthetic Plast Surg, 42(2), pp 498–510.
19. Deok-Woo, K., Eul-Sik, Y., Yi-Hwa, J., Seuna-Ha, P., Byung-Il, L. and Eun-Sang, D. (2011) ‘Vascular complications of hyaluronic acid fillers and the role of hyaluronidase in management’, Journal of Plastic, Reconstructive & Aesthetic Surgery, 64, pp 1590-1595.
20. King M, Convery C, Davies E. This month’s guideline: The Use of Hyaluronidase in Aesthetic Practice (v2.4). J Clin Aesthet Dermatol. 2018;11(6):E61-E68.
21. Bassas Grau, E. and Bassas Grau, M. Consideraciones clinicas etiopatogenicas y terapeuticas sobre la mal nomada ‘cellulitis’. Ann. Med., sect especial 16, 2–17 (1964).
22. Malinowska Sylwia & Mlosek Robert Krzysztof (2017) Efficacy of intradermal mesotherapy in cellulite reduction – Conventional and high-frequency ultrasound monitoring results, Journal of Cosmetic and Laser Therapy, 19:6, 320-324.
23. British National Formulary, 10.3 Drugs for the treatment of soft-tissue disorders and topical pain relief, 10.3.1 Enzymes, Hyaluronidase.
24. Sarvela PJ, Paloheimo MP, Nikki PH. Comparison of pH-adjusted bupivacaine 0.75 % and a mixture of bupivacaine 0.75% and lidocaine 2 %, both with hyaluronidase, in day-case cataract surgery under regional anesthesia. Anesth Analg. 1994;79(1):35–39.
25. Nicoll JM, Treuren B, Acharya PA, Ahlen K, James M. Retrobulbar anesthesia: the role of hyaluronidase. Anesth Analg. 1986;65(12):1324–1328.
26. Rüschen H, Aravinth K, Bunce C, Bokre D. Use of hyaluronidase as an adjunct to local anaesthetic eye blocks to reduce intraoperative pain in adults. Cochrane Database of Systematic Reviews 2018, Issue 3. Art. No: CD010368.
27. Humphrey P. Hypodermoclysis: An alternative to I.V. infusion therapy. Nursing 2011: November 2011Volume 41- Issue 11- p.16-17.
28. Thomas JR, Yocum RC, Haller MF, von Gunten CF. Assessing the role of human recombinant hyaluronidase in gravity-driven subcutaneous hydration: the INFUSE-LR study. J Palliat Med. 2007;10:1312-1320.
29. Constans T, Dutertre JP, Frogé E. Hypodermoclysis in dehydrated elderly patients: local effects with and without hyaluronidase. J Palliat Care. 1991;7(2):10-12.
30. Al-Benna S, O’Boyle C, Holley J. Extravasation injuries in adults. ISRN Dermatol. 2013;2013:856541. Published 2013 May 8.
31. Bertelli G. Prevention and management of extravasation of cytotoxic drugs. Drug Safety 1995;12(4):245–255.
32. Nelson RE, Carter JM, Moulthrop TH. Hyaluronidase injection for the treatment of facial and neck hematomas. Laryngoscope. 2015;125:1090–2.
33. Shiftan L. Magnetic resonance Imaging Visualisation of Hyaluronidase in Ovarian Carcinoma. Cancer Res .November 15 2005 (65)(22) 10316-10323
34. McAtee CO, Barycki JJ, Simpson MA. Emerging roles for hyaluronidase in cancer metastasis and therapy. Adv Cancer Res. 2014;123:1-34.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Introducing…

EDUCATING AND INSPIRING THE PUBLIC TO MAKE SAFE AND ETHICAL CHOICES IN AESTHETIC MEDICINE
With the medical aesthetic market set to be worth $15.9 billion by 2025, we know it is a fast-evolving specialty, booming with new products and treatments, life-changing procedures and revolutionary science.
Yet, unfortunately, there is a lack of quality education on what’s available and media coverage can be largely negative; leaving patients and consumers misinformed, afraid of complications and hesitant to talk openly about aesthetic treatments and procedures. This is where Beyond Beauty comes in.
The ground-breaking new magazine, with four issues a year, will be filled with educational content that is factual, informative and engaging. We’ll also be hosting an experiential event for consumers – Beyond Beauty Live – in early 2022, so stay tuned!

EXCLUSIVE DISCOUNTS FOR SUBSCRIBERS • All Aesthetics journal subscribers sent a complimentary copy in January • Option to purchase multiple copies for your patients at a discounted rate Follow us on Instagram for all the latest updates @beyondbeauty mag ENHANCING KNOWLEDGE | BUILDING
2021 BUILDING TRUST | PROMOTING POSITIVITY
LAUNCHING JANUARY
The newly developed Level 7 Diploma in Clinical Aesthetic Injectable Treatments brought to you by VTCT
The VTCT Level 7 Diploma in Clinical Aesthetic Injectable Treatments, is designed for regulated professionals who are registered with a healthcare statutory regulatory body.
The development of the qualification has been undertaken with support from Harley Academy, who have been instrumental in helping shape aspects of both content and delivery in order to ensure the highest standards are maintained across the sector of non-surgical aesthetics.

Exploring Photobiomodulation
Dr Emmaline Ashley discusses the current literature surrounding the use of photobiomodulation

Photobiomodulation (PBM) was discovered by accident in the 1960s.1 A Hungarian scientist, studying the effect of ruby lasers on tumours in mice, found that his lasers were producing very unusual results: the mice’s wounds were healing more quickly and new hair was growing on their shaved skin. From there, a novel field of investigation was born – and it has recently been gaining increasing momentum in multiple medical modalities. The underlying principle of photobiomodulation is that light has the ability to activate photoreceptors and chromophores naturally contained within the skin, with potential therapeutic effects. The vocabulary surrounding this process has been confused in the past, with various terminologies used interchangeably or inaccurately.2 It is therefore important to clarify the definition of PBM as a form of low-level light therapy utilising non-ionising, non-thermal light in the visible to infrared spectrum. These light sources include lasers and light-emitting diodes (LEDs), and they act on endogenous receptors to activate either stimulatory or inhibitory biological pathways.3 This phenomenon is distinct from the common use of light (often in the near infrared range) to heat tissues, relying on thermal light energy as the mechanism of action.3
Mechanisms of action
So how is light in non-photosensitive and extra-ocular tissue actually being received? At the most basic level, the process begins with the absorption of a photon of a specific wavelength by a receptor in the skin. Usually this causes excitation of an electron, and a signalling cascade is initiated. However, beyond these first steps, our explanations get murkier. Despite this ambiguity and initial skepticism, it is not in dispute that PBM is a very real phenomenon. It has been used in several areas of aesthetic medicine: in the treatment of acne, cellulite, body contouring, alopecia, and antiageing (Table 1).4-8
Cytochrome C oxidase
The majority of the research into PBM has examined light in the red (600-700 nm) and near-infrared (770-1200 nm) range.10 This is because the first proposed mechanism of action for PBM was mitochondrial cytochrome C oxidase, a copper-containing enzyme with a biphasic response to these two ranges of light. It is now one of the most well-known pathways described in the literature.13,14 After photon absorption by cytochrome C oxidase, there is an increase of mitochondrial activity leading to a proliferation of adenosine triphosphate (ATP), nicotinamide adenine dinucleotides (NADH), and ribonucleic acid
(RNA).15 There is also the release of nitric oxide (NO), a vasodilator, and reactive oxygen species (ROS), which act as transcription factors.15 It is proposed that the vasodilatory effects of NO and upregulation of growth factors may explain PBM’s ability to cause hair growth, although it is not completely understood yet.12 In addition, fibroblast stimulation and collagen synthesis may lead to improvement in scar appearances.11 This proliferation of gene transcription factors may also be involved in cells’ defence mechanisms against stress and hypoxia, which aid in wound healing.10
The cytochrome C oxidase pathway has also been described as the mechanism behind body contouring, where ATP synthesis leads to the up-regulation of cyclic adenosine monophosphate (cAMP), activating a lipase that breaks down intracellular triglycerides.9 Part of this pathway has been shown, via electron scanning microscopy, to create pores in the adipose cell membranes, allowing the release of broken-down fatty acids and glycerol into the extracellular space, and collapse (but not death) of the adipose cell.9
Blue and green wavelength opsins
Opsins are a group of G protein-coupled receptors that have been well-characterised and described in the skin of animals. They are responsible for all sorts of biological marvels from the camouflaging colour change of octopi to the thermoregulation seen in lizards.16 In humans, opsins primarily exist in retinal photoreceptors, but have also been described in the skin in melanocytes, keratinocytes, fibroblasts and hair follicle cells, responding primarily to blue light wavelengths.16 Initially it was unclear if these were just a vestigial evolutionary throwback, or still performed important physiological roles. However, early in vivo studies have suggested the possibility of opsins playing an important part in potential future therapies for hair loss and skin pigmentation disorders.17,18
The proposed mechanism is primarily via calcium channels.10 There is still much to discover, and opsins represent one of the most exciting and promising areas of exploration in photobiomodulation.
Nanostructured water
There is some speculation that longer wavelengths of light (>1000 nm) may be affecting nanostructured water in heat- and light-sensitive ion channels, opening them and leading to changes in intracellular calcium concentrations.19 Water
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
RHA
topical skin


INSTANTLY SMOOTHED, VISIBLY REJUVENATED
RHA ® topical skin booster is a cosmetic product according to European Regulation 1223/2009. Cosmetic products are not designed to b e injected.
®
booster THE FIRST RHA TOPICAL SKIN SOLUTION Hyaluronic Acid Sterile Gel
THE POST TREATMENT SKIN QUALITY BOOSTER With newly improved applicator
Colour Wavelengths (approximate)
Indication
Proposed mechanism of action
Blue 400-430 nm Acne vulgaris P. acnes inactivation via free radical formation5
Green 532 nm Cellulite
Red ~630 nm Antiageing
Red 630-670 nm Acne vulgaris
Unknown – potentially skin tightening secondary to collagen neogenesis9
Unknown – potentially via the p53 pathway’s anti-apoptotic effects and/or collagen and elastin reorganisation10
Unknown – likely via anti-inflammatory effects10
Red 620-750 nm Scarring Cytochrome C oxidase11
Red ~660 nm Body contouring Cytochrome C oxidase9
Red-Infrared 660 nm + 800 nm Alopecia Cytochrome C oxidase12
Infrared 820-830 nm Antiageing Unknown – most effective in combination with red wavelengths8
Infrared 940 nm Hyperpigmentation Melanocytes downregulate melanin synthesis and tyrosinase expression10
Table 1: Possible applications of PBM in aesthetic medicine
is omnipresent in biological tissues, and has been shown in some studies to act as an active molecule with the ability to affect physiological change.10,20 Water is not just a passive solvent, but capable of forming a multitude of complex structures with their own properties. Molecular biologists are just beginning to understand and appreciate the dynamic role it plays in the cell, donating and accepting protons, changing the environment of proteins, and influencing biomolecules around it.20 In PBM, it is proposed that absorption of a photon increases the vibrational energy of water, leading to a disruption of the protein structure at the ion channel, allowing it to open.10
Other mechanisms
There is also some evidence that infrared wavelengths activate melanocyte cells directly, decreasing melanin synthesis via the tyrosinase pathway and the p53 signalling pathway.21 Cryptochromes, which have an important role to play in the circadian rhythm, have also been implicated in photobiomodulation. They have a significant function as gene transcription regulators, with vital roles in metabolism and the immune system.15
PBM has been used in acne treatments and there is evidence that blue light acts on endogenous porphyrins produced by P. acnes bacteria, creating free radicals and destroying their cell membranes.5
Red light has also been used due to its anti-inflammatory effects, and combination therapy with both red and blue light has been beneficial for acne. However, the optimal wavelengths for this are not yet defined.9
Gaps in the literature
The multitude of currently proposed mechanisms of action for PBM (some better supported than others) points to the fact that there are many different receptors and pathways activated in this phenomenon.15 This is already a very complex tangle of biological cascades, and it is further complicated by the fact that there is still no consensus on parameters or protocols for the therapeutic uses of PBM. Despite the fact that there are thousands of published research articles on the subject, most utilise different variables with an unfathomable array of possible permutations.22 To make things even more convoluted, in many historical studies experimental parameters were just not adequately described. This represents the first big hurdle in gaining a true understanding of this process from the current research. There is probably an ideal range of wavelengths, dose, and intensity for PBM where it will be the most effective for any given condition – below this range there may be little benefit, and above this range there may even be inhibition or harm.10 Additionally, as part of the biphasic dose response, PBM can either stimulate or inhibit processes at the same wavelength, depending on the energy used.23 In addition to this, tissue optics further complicate things – our skin will absorb and scatter light differently, depending on where PBM is used on the body, our individual skin type and colour, the quality of the skin, and the existence of any skin conditions.10
The task now is defining what parameters PBM will be the most therapeutically effective at. In order to do this, the general
consensus moving forward is that the parameters in experiments must always be defined: laser or LED, wavelength, power, power density, fluence, energy, and the number of sessions.2,9,13,15
Are there risks to our patients?
As discussed, there is clearly a lack of understanding of how PBM works. And within the current body of literature, there are several other shortcomings in addition to the varied treatment modalities and unreported parameters. Many studies are in vitro, and the extent to which their results can be extrapolated to a patient population is not clear. The existing in vivo studies are also limited by small patient sample sizes.4,6-8,24,25 A few studies have been pointed out as having potential bias, when authors disclose existing financial conflicts of interest.10,13,26 In addition, not all studies have appropriate controls in place.10,21 A systematic review carefully analysed the discrepancy of some studies showing positive effects, and others have shown negative effects using the similar parameters.22 It is worth repeating that untangling this interplay is complicated. So, does the current lack of understanding of PBM pose a potential risk for our patients, especially as many assumptions are being made about efficacy and mechanism of action, which have not yet been clearly proven? Data on longterm effects of photobiomodulation is still lacking. However, despite this, there does seem to be a high benefit to low risk ratio for this treatment modality. In the past 50 years of its use, there has been a very low incidence of adverse effects associated with photobiomodulation. Adverse events that
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020






ZERO USAGE FEE PER TREATMENT CLINICALLY VALIDATED EFFECTIVENESS TWO TECHNOLOGIES, ONE DEVICE HIGH PATIENT COMFORT FINALIST 2019
have been reported include mild dryness, erythema, desquamation, and pain.27 However, these were mild and infrequent and, in the majority of studies no adverse events are reported at all, with no severe adverse events reported overall.9,27 Because of the rarity of these mild adverse effects, and as most studies either report none or mention very mild, self-limited events with little detail, it is difficult to comment on whether there are specific triggers or risk factors that would make a patient more likely to experience one. A recent review, compiling the results of 31 clinical studies and approximately 1,384 patients, recommended that clinical use of PBM in skin clinics should be ongoing due to the clear benefits, while research continues to explore the nuances of this fascinating phenomenom.27 Understanding the biology behind this phenomenon will hopefully take the guesswork out of it in the future.
Further directions
In considering how photobiomodulation can be incorporated into our aesthetic practice at present and in the future, PBM would be an excellent candidate for combination therapies. It can easily be used in conjunction with systemic and topical treatments. The devices are sometimes portable and generally easy to use, at home or in the clinic. There are fascinating applications for wound healing, which could be used to accelerate recovery after aggressive aesthetic treatments. The potential anti-inflammatory effects could also have implications for a variety of skin pathologies, with work currently being done in psoriasis and eczema.10 In conclusion, there are several key areas that need to be clarified in order to fully utilise this exciting mechanism for the benefit of skin
health. There needs to be consistency and a clear rationale behind the choices of optical parameters for different treatment modalities – all of which requires more research. There are multiple photoreceptors that could be involved in receiving the infrared to visible spectrum of light. While there has been some fascinating work done in trying to describe the underlying biology of these reactions, the proposed mechanisms do not yet explain the full extent of the physiological activity that is observed.
However, while our knowledge expands and refines the use of PBM in the future to be even more effective for our patients, the evidence currently suggests that we should continue using this powerful tool in clinic.
Dr Emmaline J Ashley received a first class honour’s degree in biology from Carleton College in the US. She completed her honour’s medical degree at University College Dublin and is finishing her Master’s in Surgery with the Royal College of Surgeons Ireland. Dr Ashley divides her time between working for the NHS and developing her own private aesthetics practice, Ashley Aesthetics. She is currently acting as the aesthetics KOL for ZoomClinic. Qual: BA, MCh, MBBChBAO
REFERENCES
1. P. E. McGuff, R. A. Deterling, Jr., and L. S. Gottlieb, ‘Tumoricidal Effect of Laser Energy on Experimental and Human Malignant Tumors’, N Engl J Med, 273 (1965).
2. M. R. Hamblin, ‘How to Write a Good Photobiomodulation Article’, Photobiomodulation, Photomedicine, and Laser Surgery, 37 (2019).
3. Juanita J. Anders, Raymond J. Lanzafame, and Praveen R. Arany, ‘Low-Level Light/Laser Therapy Versus Photobiomodulation Therapy’, Photomedicine and laser surgery, 33 (2015).
4. M. S. Nestor, N. Swenson, A. Macri, M. Manway, and P. Paparone, ‘Efficacy and Tolerability of a Combined 445nm and 630nm over-the-Counter Light Therapy Mask with and without Topical Salicylic Acid Versus Topical Benzoyl Peroxide for the Treatment of Mild-to-Moderate Acne Vulgaris’, J Clin Aesthet Dermatol, 9 (2016).
5. H. Ashkenazi, Z. Malik, Y. Harth, and Y. Nitzan, ‘Eradication of Propionibacterium Acnes by Its Endogenic Porphyrins after Illumination with High Intensity Blue Light’, FEMS Immunol Med Microbiol, 35 (2003).
6. R. F. Jackson, G. C. Roche, and S. C. Shanks, ‘A Double-Blind, Placebo-Controlled Randomized Trial Evaluating the Ability of Low-Level Laser Therapy to Improve the Appearance of Cellulite’, Lasers Surg Med, 45 (2013).
7. M. S. Nestor, J. Newburger, and M. B. Zarraga, ‘Body Contouring Using 635-Nm Low Level Laser Therapy’, Semin Cutan Med Surg, 32 (2013).
8. R. J. Lanzafame, R. R. Blanche, R. P. Chiacchierini, E. R. Kazmirek, and J. A. Sklar, ‘The Growth of Human Scalp Hair in Females Using Visible Red Light Laser and Led Sources’, Lasers Surg Med, 46 (2014).
9. M. Nestor, A. Andriessen, B. Berman, B. E. Katz, D. Gilbert, D. J. Goldberg, M. H. Gold, R. S. Kirsner, and P. Z. Lorenc, ‘Photobiomodulation with Non-Thermal Lasers: Mechanisms of Action and Therapeutic Uses in Dermatology and Aesthetic Medicine’, Journal of Cosmetic and Laser Therapy, 19 (2017).
10. D. Barolet, ‘Photobiomodulation in Dermatology: Harnessing Light from Visible to near Infrared for Medical and Aesthetic Purposes’, Medical Research Archives, 6 (2018).
11. A. Mamalis, D. Siegel, and J. Jagdeo, ‘Visible Red Light Emitting Diode Photobiomodulation for Skin Fibrosis: Key Molecular Pathways’, Curr Dermatol Rep, 5 (2016).
12. P. Avci, G. K. Gupta, J. Clark, N. Wikonkal, and M. R. Hamblin, ‘Low-Level Laser (Light) Therapy (Lllt) for Treatment of Hair Loss’, Lasers Surg Med, 46 (2014).
13. M. R. Hamblin, ‘Photobiomodulation for the Management of Alopecia: Mechanisms of Action, Patient Selection and Perspectives’, Clinical, Cosmetic and Investigational Dermatology, 12 (2019).
14. T. Karu, ‘Mitochondrial Mechanisms of Photobiomodulation in Context of New Data About Multiple Roles of Atp’, Photomed Laser Surg, 28 (2010).
15. C. Mignon, N. V. Botchkareva, N. E. Uzunbajakava, and D. J. Tobin, ‘Photobiomodulation Devices for Hair Regrowth and Wound Healing: A Therapy Full of Promise but a Literature Full of Confusion’, Exp Dermatol, 25 (2016).
16. S. Suh, E. H. Choi, and N. Atanaskova Mesinkovska, ‘The Expression of Opsins in the Human Skin and Its Implications for Photobiomodulation: A Systematic Review’, Photodermatol Photoimmunol Photomed (2020).
17. S. Buscone, A. N. Mardaryev, B. Raafs, J. W. Bikker, C. Sticht, N. Gretz, N. Farjo, N. E. Uzunbajakava, and N. V. Botchkareva, ‘A New Path in Defining Light Parameters for Hair Growth: Discovery and Modulation of Photoreceptors in Human Hair Follicle’, Lasers Surg Med, 49 (2017).
18. C. Oplander, S. Hidding, F. B. Werners, M. Born, N. Pallua, and C. V. Suschek, ‘Effects of Blue Light Irradiation on Human Dermal Fibroblasts’, J Photochem Photobiol B, 103 (2011).
19. F. Vatansever, and M. R. Hamblin, ‘Far Infrared Radiation (Fir): Its Biological Effects and Medical Applications’, Photonics Lasers Med, 4 (2012).
20. Philip Ball, ‘Water Is an Active Matrix of Life for Cell and Molecular Biology’, Proceedings of the National Academy of Sciences, 114 (2017) .
21. D. Barolet, ‘Dual Effect of Photobiomodulation on Melasma: Downregulation of Hyperpigmentation and Enhanced Solar Resistance-a Pilot Study’, J Clin Aesthet Dermatol, 11 (2018).

22. R. Zein, W. Selting, and M. R. Hamblin, ‘Review of Light Parameters and Photobiomodulation Efficacy: Dive into Complexity’, J Biomed Opt, 23 (2018).
23. M. R. Hamblin, ‘Mechanisms and Mitochondrial Redox Signaling in Photobiomodulation’, Photochem Photobiol, 94 (2018).
24. R. F. Jackson, D. D. Dedo, G. C. Roche, D. I. Turok, and R. J. Maloney, ‘Low-Level Laser Therapy as a Non-Invasive Approach for Body Contouring: A Randomized, Controlled Study’, Lasers Surg Med, 41 (2009)
25. S. Friedman, and P. Schnoor, ‘Novel Approach to Treating Androgenetic Alopecia in Females with Photobiomodulation (Low-Level Laser Therapy)’, Dermatologic Surgery, 43 (2017).
26. G. Ablon, ‘Phototherapy with Light Emitting Diodes: Treating a Broad Range of Medical and Aesthetic Conditions in Dermatology’, J Clin Aesthet Dermatol, 11 (2018).
27. J. Jagdeo, E. Austin, A. Mamalis, C. Wong, D. Ho, and D. M. Siegel, ‘Light-Emitting Diodes in Dermatology: A Systematic Review of Randomized Controlled Trials’, Lasers Surg Med (2018).
Data on long-term effects of photobiomodulation is still lacking, however despite this, there does seem to be a high benefit to low risk ratio for this treatment modality
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020


LEARN | NETWORK 12 & 13 MARCH 2021 / LONDON 12 & 13 MARCH BUSINESS DESIGN CENTRE, LONDON @aestheticsgroup @aestheticsjournaluk Aesthetics UNMISSABLE TWO DAYS AND RECOGNITION FIND OUT WWW.AESTHETICSJOURNAL.COM

NETWORK | CELEBRATE 13 MARCH ROYAL LANCASTER, LONDON DAYS OF LEARNING RECOGNITION OUT MORE WWW.AESTHETICSJOURNAL.COM

REJUVENATION AND WELL BEING FROM WITHIN CLINICALLY PROVEN SCIENCE www.totallyderma.com T: 020 3126 6795 | E: info@totallyderma.com T: 020 3868 6242 | E: enquiries@harpargrace.com • Evidence-based collagen supplement for medical aesthetic practitioners and their dermatology, dental and plastic surgery patients • Supports prescriptive strength skincare regimes, invasive and non-invasive medical aesthetic treatments • Once a day supplement, expect results in 3-12 weeks TOTALLY DERMA ® THE ULTIMATE NUTRACEUTICAL SUPPLEMENT NOW SUGAR FREE
Treating Migraines with Toxin
gaps in knowledge. There are complex neurochemical changes that create migraine headaches, and it has a strong genetic element.4 Botulinum toxin is not effective in other forms of headache such as tension headaches due to its mechanism of action. Botulinum toxin works in chronic migraine not by muscle relaxation, but the reduction of pain pathway expression in certain parts of the trigeminal system.5
Botulinum toxin in the form of Botox has a licence for use in chronic migraine, is recommended by NICE and can be used in the NHS within criteria that is locally determined and is invariably accessed via secondary-care contracts. NICE suggests that it may be an appropriate treatment in chronic migraine where patients have not responded to at least three prior pharmacological prophylaxis therapies and whose condition is appropriately managed for medication overuse.6
NICE guidance is generally used as a benchmark for local criteria.
NHS treatment of migraine with botulinum toxin is usually restricted to the NICE guidance, which states that three prophylactic drugs need to have been tried before botulinum toxin is used on a patient.7
Migraines are primarily a headache disorder, with acute attacks lasting between four and 72 hours. However, a migraine is not ‘just a headache’. It has a myriad of associated symptoms and is a debilitating condition for many, with an estimated 190,000 attacks per day in the UK and an estimated 25 million lost work days in the UK per year.1
When a patient is experiencing an acute migraine, there is usually a prodromal period prior to the headache which might consist of symptoms such as irritability, tiredness, dizziness, hunger, nausea, or yawning, followed by an often unilateral headache and sometimes aura such as tingling, visual and speech disturbance. A recovery period lasting up to a few days will then take place, followed by a clear period with no symptoms.2 A chronic migraine can be considered separately, and this is the category in which patients may seek the help of aesthetic practitioners to conduct botulinum toxin treatments.
Defining chronic migraines
The National Institute for Health and Care Excellence (NICE) guidance defines chronic migraine in accordance with the International Headache Society, stating it as the occurrence of headaches on 15 days or more per month, for at least three months, where the attacks

fulfil criteria for pain and associated symptoms of migraine. This must be without aura on at least eight days per month for at least three months, where there is no medication overuse, and where the headaches are not attributable to another causative disorder. To fulfil the criteria for chronic migraine, a person must previously have had at least five attacks fulfilling the International Headache Society’s criteria for migraine without aura. Despite these criteria, in clinical practice, there is a lack of consensus regarding the definition of chronic migraine.3
Using toxin for migraine
The pathophysiology of a migraine is complex and there remains many
NHS wait times and increased difficulties recently have resulted in patients not being commenced on botulinum toxin, or having their treatment programmes interrupted. In private practice, the decision to treat a patient is between the clinician and the patient based on clinical evaluation. Provided that the diagnosis is correct and red flags have been excluded, it is reasonable to start treatment. Although, it should be noted, that good communication with a patient’s GP is important and considered good practice. We would suggest writing to the patient’s GP to inform them that the patient has undergone migraine treatment with botulinum toxin, providing the number of units used.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Botulinum toxin works in chronic migraine not by muscle relaxation, but the reduction of pain pathway expression in certain parts of the trigeminal system
Dr Paul Charlson and Dr Vikram Swaminathan explain how botulinum toxin type A can be used to treat chronic migraines
Your patients with obesity have the will
You can offer them the way
If you would like to request a visit from a representative please contact us on SaxendaUK@novonordisk.com
For all product related enquires please contact us via our online information request form at www.novonordisk.co.uk
Indication: Saxenda® is indicated as an adjunct to a reduced-calorie diet and increased physical activity for weight management in adult patients with an initial Body Mass Index (BMI) of ≥ 30 kg/m² (obesity) or ≥ 27 kg/m² to < 30 kg/ m² (overweight) in the presence of at least one weight-related comorbidity such as dysglycaemia (pre-diabetes or type 2 diabetes mellitus), hypertension, dyslipidaemia or obstructive sleep apnoea. Treatment with Saxenda® should be discontinued after 12 weeks on the 3.0 mg/day dose if patients have not lost at least 5% of their initial body weight.
Prescribing Information
Please
Saxenda® Liraglutide injection 3 mg.
Saxenda® 6 mg/mL solution for injection in a pre-filled pen. One pre-filled pen contains 18mg liraglutide in 3mL.

Indication: Saxenda® is indicated as an adjunct to a reduced-calorie diet and increased physical activity for weight management in adult patients with an initial Body Mass Index (BMI) of ≥ 30 kg/m² (obesity) or ≥ 27 kg/m² to < 30 kg/m² (overweight) in the presence of at least one weight-related comorbidity such as dysglycaemia (pre-diabetes or type 2 diabetes mellitus), hypertension, dyslipidaemia or obstructive sleep apnoea. Posology and administration: Saxenda® is for once daily subcutaneous use only. Is administered once daily at any time, independent of meals. It is preferable that Saxenda® is injected around the same time of the day. Recommended starting dose is 0.6 mg once daily. Dose should be increased to 3.0 mg once daily in increments of 0.6 mg with at least one week intervals to improve gastro-intestinal (GI) tolerability. If escalation to the next dose step is not tolerated for two consecutive weeks, consider discontinuing treatment. Treatment with Saxenda® should be discontinued after 12 weeks on the 3.0 mg/day dose if patients have not lost at least 5% of their initial body weight. Daily doses higher than 3.0 mg are not recommended. No dose adjustment is required based on age but therapeutic experience in patients ≥75 years is limited and not recommended. No dose adjustment required for patients with mild or moderate renal impairment or mild or moderate hepatic impairment but it should be used with caution. Saxenda® is not recommended for use in patients with severe renal impairment including end-stage renal disease, or severe hepatic impairment or children and adolescents below 18 years.

Contraindications: Hypersensitivity to the active substance or to any of the excipients.

Special warnings and precautions for use: There is no clinical experience in patients with congestive heart failure New York Heart Association (NYHA) class IV and Saxenda® is not recommended for use in these patients. It is also not recommended in patients with eating disorders or treatment with medicinal products that may cause weight gain, as Saxenda® for weight management was not investigated in subjects with mild or moderate hepatic impairment; it should be used with caution in these patients. Use of Saxenda® is not recommended in patients with inflammatory bowel disease and diabetic gastroparesis since it is associated with transient GI adverse reactions including nausea, diarrhoea and vomiting. Acute pancreatitis has been observed with the use of GLP-1 receptor agonists, patients
Adverse
Nordisk
Saxenda® is a trademark owned by Novo Nordisk A/S. 2020 © Novo Nordisk A/S, Novo Allé, DK-2880, Bagsvæd, Denmark
should be informed of the characteristic symptoms. If pancreatitis is suspected, Saxenda® should be discontinued. If acute pancreatitis is confirmed, Saxenda® should not be restarted. In weight management clinical trials, a higher rate of cholelithiasis and cholecystitis was observed in patients on Saxenda® than those on placebo, therefore patients should be informed of characteristic symptoms. Thyroid adverse events such as goitre have been reported in particular in patients with pre-existing thyroid disease. Saxenda® should be used with caution in patients with thyroid disease. An increased risk in heart rate was observed in clinical trials. For patients who experience a clinically relevant sustained increase in resting heart rate, treatment with Saxenda® should be discontinued. There is a risk of dehydration in relation to GI side effects associated with GLP-1 receptor agonists. Precautions should be taken to avoid fluid depletion. Patients with type 2 diabetes mellitus receiving Saxenda® in combination with insulin and/or sulfonylurea may have an increased risk of hypoglycaemia.
Fertility, pregnancy and lactation: Saxenda® should not be used during pregnancy. If a patient wishes to become pregnant, or pregnancy occurs, treatment with Saxenda® should be discontinued. It should not be used during breast-feeding.
Undesirable effects: Very common(≥1/10); nausea, vomiting, diarrhoea, constipation. Common (≥1/100 to <1/10); hypoglycaemia, insomnia, dizziness, dysgeusia, dry mouth, dyspepsia, gastritis, gastro-oesophageal reflux disease, abdominal pain upper, flatulence, eructation, abdominal distension, cholelithiasis, injection site reactions, asthenia, fatigue, increased lipase, increased amylase. Uncommon (≥1/1,000 to <1/100); dehydration, tachycardia, pancreatitis, cholecystitis, urticaria, malaise, delayed gastric emptying Rare (≥1/10,000 to <1/1,000); anaphylactic reaction, acute renal failure, renal impairment. The Summary of Product Characteristics should be consulted for a full list of side effects.
MA numbers and Basic NHS Price: 5 x 3 ml pre-filled pens EU/1/15/992/003, £196.20.
Legal category: POM.
Full prescribing information can be obtained from: Novo Nordisk Limited, 3 City Place, Beehive Ring Road, Gatwick, West Sussex, RH6 0PA.
Marketing Authorisation Holder: Novo Nordisk A/S, Novo Allé, DK-2880 Bagsværd, Denmark.
Date last revised: December 2019
Saxenda® is a trademark owned by Novo Nordisk A/S.
www.mhra.gov.uk/yellowcard
UK20SX00115 September 2020
.
.
events should be reported. Reporting forms and information can be found at
or search for MHRA Yellow Card in the Google Play or Apple App Store. Adverse events should also be reported to Novo
Limited (Telephone Novo Nordisk Customer Care Centre 0845 6005055). Calls may be monitored for training purposes.
of product
for
refer to the Saxenda® summary
characteristics
full information
Consultation
When consulting a patient, it is important to ensure you conduct a proper medical history. To do this thoroughly, there are a few important issues that need to be considered. Firstly, find out whether the patient in question has received a formal diagnosis of chronic migraine, by whom and when. Then, you should ask what previous treatments the patient has had – if any. We also often check which prophylactic medications they have had, their doses and duration of trial and side effects. It is important to look for drugs which might precipitate migraine such as oestrogen and nitrates as these might just need to be stopped to solve the problem.8 Liaison with the patient’s GP at this point is important to ascertain the patient’s main migraine triggers. For example, common migraine triggers include stress, dehydration, caffeine, alcohol, too much or too little sleep, or foods like chocolate, citrus fruits and cured meats, are all of which are implicated, as are hormonal changes.9 Because triggers are personal to each patient, it is essential for a diary to be kept as this provides vital clues which aid management. Even if you treat a patient with botulinum toxin, identifying triggers and reducing them will help to further reduce attacks.
Finally, ensure to check for ‘red flags’ which might indicate that the problem is something else, especially if your patient has not been to a specialist prior to seeing you.10 For example, headaches that occur in patients after the age of 50 and have not been present before. Most migraine suffers have had headaches since puberty or even before and follow a certain pattern which might change slowly over time. Worsening symptoms are also a sign that there may be something more sinister. In these cases migraines can be mistaken for thunderclap headaches, which are sudden onset severe headaches that raise suspicion of sub-arachnoid bleeds. Similarly, symptoms of temporal arteritis can appear alike to a migraine with sometimes an unilateral temporal tenderness, headache and visual disturbance. However, this generally occurs in over 50s and the headache pattern will be different to a patient’s migraine or they may have no pre-existing migraine. Glaucoma symptoms which are predominantly eye pain and redness of the eye may also mimic a migraine, and any additional neurological symptoms including meningism are concerning.11
Treatment approach
In 2009, pharmaceutical company Allergan conducted the seminal research into the use of botulinum toxin and migraines. The PREEMPT trials showed after 12 months of treatment of Botox (onabotulinum toxin A) at three monthly intervals, 70% of patients showed a greater than 50% reduction of headaches with minimal side effects.12
The PREEMPT protocol is 31 injections in the head and neck, with a total of 155 units of Botox used. There is the option of a further 40 units to be administered in the occipitalis, temporalis and trapezius areas if required. Treatment protocols are generally based upon the PREEMPT trials which were methodologically robust.13 There are criticisms of the PREEMPT trials mainly concerning the marked placebo effect in both PREEMPT trials and the fact that most patients enrolled were overusing acute migraine medications.11
A survey by Begasse de Dhaem et al. suggested that about 70% of clinicians varied the dose, sites and frequency of the toxin injections. Therefore, it would be interesting to explore the reasons behind this and develop new guidance as a result.14
There is a small sub-group of patients (around 10%) who fail to respond to treatment first time around, but research has shown that they do respond after two cycles of treatment at three months.15 Therefore, it is worth trying three cycles before considering ceasing treatment altogether. Dose should be at least 155 units of Botox, as earlier trials showed minimal difference from placebo below this dose.6 It is often worth treating trigger points and increasing the dose up to 195 units.11 Side effects of this treatment are fairly minimal. Brow ptosis can occur, but this is less likely in aesthetic practices as clinicians should be aware of this complication and may adjust the distribution of the injections as a result. Anecdotally, we have not found an issue with altering the distribution of injections in this site. There have been trials comparing prophylactic migraine medications to Botox and found them to be comparable, but the studies are small.16,17 Other toxins such as Bocouture and Azzalure can be used off label, but different units will need to be used and adjusted, for example where 1U Botox/ Bocouture is equal to 2.5U Azzalure.18
Summary
Botox is licenced for use in chronic migraine. The key elements of optimal treatment are ensuring appropriate patient selection, correct technique, identifying and minimising triggers, good liaison with
the patient’s GP and correct aftercare. It must be stressed that not all chronic migraineurs respond to Botox, so patient expectations need to be realistic and will need exploration at the initial consultation. Overall, treatment with Botox appears a safe method with long term tolerability.
Dr Paul Charlson has a background is in general practice. He has 19 years’ experience in aesthetic medicine and is past president of the British College of Aesthetic Medicine. Dr Charlson’s work is mainly confined to dermatology and aesthetics, with clinics in London and Yorkshire.

Qual: FRCGP,DRCOG, DPD, DOccMed, FBCAM
Dr Vikram Swaminathan has aesthetic clinics in the North West and in London. He is a faculty member of the British Society of Aesthetic Examiners and Assessors (BSAEA), Royal Society of Medicine (RSM) Aesthetics Sub-committee, and an educational supervisor.

Qual: MPhil, PGCertTLCP, MBCAM
REFERENCES
1. Steiner TJ et al., 2003, Cephalagia: The International Journal of Headaches, The prevalence and disability burden of adult migraine in England and their relationships to age, gender and ethnicity
2. John Hopkins Medicine, Migraine Headaches, <https://www. hopkinsmedicine.org/health/conditions-and-diseases/headache/ migraine-headaches>
3. National Institute for Health and Care Excellence, <https://www. nice.org.uk/guidance/ta260/documents/migraine-chronicbotulinum-toxin-type-a-final-scope>
4. Dodick DW, 2018, A phase-by-phase review of migraine pathophysiology. Headache 58(Suppl 1):4–16
5. Burstein R, Zhang X, Levy D, Aoki KR, Brin MF., 2014, Selective inhibition of meningeal nociceptors by botulinum neurotoxin type A: therapeutic implications for migraine and other pains
6. National Institute for Health and Care Excellence, <https://www. nice.org.uk/guidance/ta260/documents/migraine-chronicbotulinum-toxin-type-a-final-appraisal-determination3>
7. Ziegeler, C., Brauns, G., Jürgens, T. et al, 2019, The Journal of Headache and Pain, Shortcomings and missed potentials in the management of migraine patients - experiences from a specialized tertiary care centre
8. National Migraine Centre, Migraine and Headache Facts, <https:// www.nationalmigrainecentre.org.uk/migraine-and-headaches/ migraine-and-headache-facts>
9. NHS, Migraine, <https://www.nhs.uk/conditions/migraine/causes/>
10. Dr Suneeta Kochhar, 2018, <https://www.gponline.com/red-flagsymptoms-headaches/neurology/neurology/article/1332134>
11. Gooriah R, Ahmed F, 2015, OnabotulinumtoxinA for chronic migraine: a critical appraisal. Ther Clin Risk Manag. 2015;11:10031013
12. Dodick DW, Turkel CC, DeGryse RE, et al., 2010, Headache, OnabotulinumtoxinA for treatment of chronic migraine: pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program
13. Dodick DW, 2018, Headache, A phase-by-phase review of migraine pathophysiology.
14. Begasse de Dhaem O, et al. Headache, Modifications to the PREEMPT Protocol for OnabotulinumtoxinA Injections for Chronic Migraine in Clinical Practice
15. Aurora SK, Winner P, Freeman MC, et al. 2011, Headache, OnabotulinumtoxinA for treatment of chronic migraine: pooled analyses of the 56-week PREEMPT clinical program
16. Cady RK, Schreiber CP, Porter JA, Blumenfeld AM, Farmer KU, 2019, Headache, A multi-center double-blind pilot comparison of onabotulinumtoxinA and topiramate for the prophylactic treatment of chronic migraine
17. Magalhaes E, Menezes C, Cardeal M, Melo A., 2010, Clinical Neurology and Neurosurgery, Botulinum toxin type A versus amitriptyline for the treatment of chronic daily migraine.
18. C Blatchley, Treating Migraines, 2016, <https://aestheticsjournal. com/feature/treating-migraines?authed>
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
STERILE FACE SOLUTIONS
Remodel, tone, rebuild, firm, counter and correct facial skin imperfections


STERILE HAIR SOLUTIONS
Revitalize the scalp, support the hair growth and stimulate the development of the hair bulb



STERILE BODY SOLUTIONS
Combat fat deposits and cellulite, accelerate metabolism, and promote fluid drainage

“LITTLE, RARELY AND IN THE RIGHT PLACE”
Distributed exclusively by DermaFocus 02039941666 info@dermafocus.co.uk
Painless, Precise, Safe & Effective Mesotherapy Gun
www.dermafocus.co.uk
Supporting Patients with Polycystic Ovarian Syndrome
Dr Aileen McPhillips discusses polycystic ovarian syndrome, the common associated skin conditions, their management and relevance to aesthetic practice
Polycystic ovarian syndrome (PCOS) is one of the most common endocrine disorders in woman of reproductive age1 and is thought to affect one in five women in the UK.2 It impacts women of all races and ethnicities. PCOS tends to emerge at puberty and is characterised by hyperandrogenism, ovulation disorders and polycystic ovarian morphology.2 Clinically, PCOS may present with menstrual disturbance, anovulatory infertility and the manifestations of hyperandrogenism (possibly including hirsutism, acne, alopecia).3 Although not always present, an association between PCOS and obesity, impaired glucose tolerance, type II diabetes and sleep apnoea has been noted.1 Many woman with PCOS are obese and have a higher prevalence of impaired glucose tolerance, type II diabetes and sleep apnoea than is observed in the general population.1
In adults, PCOS can be diagnosed if two out of the three following criteria are present, provided other causes of menstrual disturbance and hyperandrogenism have been excluded:
• Clinical and/or biochemical signs of hyperandrogenism
• Oligo-anovulation or anovulation
• Polycystic ovaries (defined as the presence of 12 or more follicles in one or both ovaries and/or increased ovarian volume)2
Associated skin manifestations
Acne
PCOS should be considered for women with associated signs of hyperandrogenism, failure to respond to conventional therapy, menstrual irregularities, and insulin resistance.4 It is reported that 20-40% of those with PCOS suffer from acne.5 Androgens increase sebum production and cause abnormal desquamation of follicular epithelial cells, resulting in the formation of comedones, which in turn can lead to further inflammation and formation of pustules, cysts and scarring.4
Hirsutism

Hirsutism, defined as excessive growth of terminal hair in women in a male-like pattern, is the most commonly-used clinical diagnostic criterion of hyperandrogenism.6 It can be very distressing for the patient. In PCOS, there is increasing activity of 5-alpha reductase in hair follicles, which is also stimulated by hyperandrogenism, insulin-like growth factors, and insulin.7 Testosterone and dihydrotestosterone (DHT) alter the hair cycle resulting in the transformation of vellus hair into terminal hairs that are thicker and darker, especially in the face, neck, chest, and pubic region which are androgen-sensitive sites.6
Alopecia
Alopecia is characterised by progressive hair loss or thinning. Alopecia associated with PCOS usually displays a pattern of thinning at the vertex with maintenance of frontal hairline, however, in some, it is similar to androgenic alopecia in which there is loss of hairs in the central region of scalp.4 Hyperandrogenism causes increased levels of 5-alpha reductase, along with increased androgen receptors and decreased levels of cytochrome P450 enzyme, resulting in short anagen phase and miniaturisation of terminal hairs with eventual transformation to vellus hairs and therefore hair loss or thinning.8
Acanthosis nigricans
Acanthosis nigricans, which is associated with several endocrine and other conditions (obesity, insulin resistance, PCOS, diabetes, malignancy), is characterised by brown velvety moist, verrucous hyperpigmentation of skin, usually seen on the back of the neck and intertriginous areas like armpits and groins, underneath breasts and inside thighs. It is reported in approximately 5% of PCOS sufferers.9 The condition is due to excessive binding of serum insulin to IGF-1 receptors, which results in proliferation of keratinocytes and fibroblasts.4
Management
Along with addressing the menstrual disturbance and potential fertility issues, common dermatological manifestations need attention, which is of relevance to aesthetic practitioners. It is estimated that 72-82% of women with PCOS are seen with classical associated cutaneous signs, such as acne, hirsutism and androgenic alopecia.10 Hyperandrogenism may also manifest as acanthosis nigricans or seborrheic dermatitis.10 Patients with PCOS are frequently first seen by a dermatologist.11 Reports of
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
acne and hirsutism (the most common recognisable symptoms of androgen excess) should be taken seriously due to their potential association with medical disorders, their substantial effect of self-esteem and quality of life, and potential for psychosocial morbidity.12
Acne
Treatment choice for acne may be influenced by severity, affected area and patient choice. Topical options are usually used as first-line treatment, however hormonal therapy, such as the combined oral contraceptive pill (OCP), can also be considered an acceptable first-line treatment for patients who desire this method.12 The main ingredients that have been shown to be effective in topical treatments include salicylic acid, benzoyl peroxide, sulphur, alpha-hydroxyl acids and retinoids.14,15 There are many cosmeceutical ranges that provide treatments with the mentioned effective ingredients that would prove beneficial to those suffering from PCOS-associated acne.
Oral treatments (for example antibiotics, isotretinoin) are typically used for moderatesevere acne and more widespread acne affecting the back/chest.12 They are also appropriate when topical treatment has not been effective.
Hirsutism
Effective management of hirsutism includes lifestyle measures, physical hair removal and androgen suppression.13 Lifestyle measures include a healthier lifestyle and weight loss in overweight patients. Weight management and glycemic control can be helpful interventions to address symptoms of androgen excess.13 Androgen suppression examples include the combined contraceptive pill, spironolactone, finasteride and metformin.
Physical hair removal methods, such as bleaching, shaving, waxing, chemical depilatories, electrolysis and laser and IPL therapy can be used safely and effectively.13 However, only electrolysis and laser therapy offer a long-lasting treatment aimed at permanent hair reduction,13 therefore aesthetic clinics may offer effective and longterm treatments options to patients suffering for hirsutism.
Alopecia
Research has shown that mild-moderate androgenic alopecia in women can be treated with anti-androgens and/or topical minoxidil with good results in many cases.16
While many women using oral anti-androgens and topical minoxidil will regrow some hair, early diagnosis and initiation of treatment is desirable, as these treatments are more effective at arresting progression of hair loss than stimulating regrowth.17
Platelet-rich plasma (PRP) is a treatment modality which is gaining popularity for androgenic alopecia. Activated platelets are understood to release numerous growth factors and cytokines from their alpha granules as part of the woundhealing process.18 The process involves collecting blood from the patient to be treated, which is then centrifuged, therefore separating the specimen and providing concentrated platelets.20 PRP is injected sub- or intradermally into the affected area.18 Platelets in PRP become activated when injected into the scalp and release multiple growth factors, which promote hair growth. Several studies have shown PRP is beneficial. Alves and Grimalt performed a randomised, blinded, half-head study of 25 patients with androgenic alopecia.19 Each patient received three treatments of PRP one month apart and were evaluated using phototrichogram and global photography. At six months a statistical improvement in hair density was recorded. Gentile et al. conducted a randomised, evaluator-blinded, placebo-controlled, half-head group study of 20 patients with androgenic alopecia.20 Three treatments of PRP were performed, 30 days apart. Improvement in mean hair count and total hair density was noted after the treatments, compared to the placebo group. Microneedling has shown promising results as a treatment for androgenic alopecia. The minimally-invasive procedure uses fine needles on the skin to puncture the stratum
corneum.21 Microneedling induces a woundhealing cascade with minimal damage to the epidermis that induces collagen formation, neovascularisation, and growth factor production of the treated areas. Although there is limited research in this area it has been shown that microneedling combined with other hair-growth promoting therapies is beneficial. Dhurat et al. conducted a 12week randomised, comparative, evaluator blinded study, where 100 patients (with mildmoderate hair loss) were randomly allocated to treatment with microneedling plus minoxidil or minoxidil alone.22 Hair count was assessed at baseline and 12 weeks. The group treated with microneedling plus minoxidil showed statistically significant superior improvement in hair growth compared to minoxidil alone. Light therapy is a relatively new technique in the treatment of androgenic alopecia. It is thought that the cellular respiratory chain of mitochondria probably absorb the light energy, which results in increased electron transport and promotion of cellular signalling and, in turn, allows for hair regrowth.21 Leavitt et al. conducted a randomised doubleblind sham-device controlled, multi-centre trial to evaluate the effect of low level laser therapy to the scalp.23 A total of 110 patients completed the study over a 26-week period and were randomly allocated to treatment with a laser light energy device called HairMax Laser Comb or a sham device. Results showed that subjects in the HairMax LaserComb group exhibited a significantly greater increase in mean terminal hair density and significant improvements in overall hair growth over the 26-week period.
Hair transplantation may be an option for patients who do not have success with other therapies. It involves the relocation or
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Skin manifestations associated with PCOS are very common and are often the first presenting features
transfer of hairs from the occipital area to the bald area.21 To achieve a good result, the correct selection of the ideal candidate is important for this procedure. The adjunct use of PRP along with/prior to is becoming an increasingly popular trend.21 The growth factors and plasma components can be injected directly into the scalp before placement of the grafts.24
Although the studies mentioned above do not specifically look at a PCOS patient group, it can be concluded that treatment outcome should be similar in patients with PCOSassociated androgenic alopecia.
Acanthosis nigricans
Whilst treating the underlying cause is the ultimate goal, cosmetic treatment of acanthosis nigricans can be important for patients. For topical options, retinoids are considered first-line treatment. In a study of 30 patients, clinical improvement of treatment-resistant acanthosis nigricans was seen in all patients after 14 days of using topical 0.05% tretinoin. 80% showed total clearance at 16 weeks, however intermittent tretinoin was needed to maintain improvement as relapse was noted.25 Chemical peels are a relatively safe and effective treatment for acanthosis nigricans. Trichloroacetic acid (TCA) is a chemical exfoliating agent that causes destruction of the epidermis with subsequent repair and rejuvenation.21 This destruction is followed by inflammation and the activation of wound repair, causing re-epithelialisation with smoother skin.21 A pilot study was carried out to look at the safety and efficacy of TCA as a chemical peel in the treatment of acanthosis nigircans.26 Treatments were carried out weekly for one month. All patients showed improvement in hyperpigmentation, thickening and overall appearance. Patient numbers were small (six), however the results do suggest TCA peels are a useful and safe treatment for the skin condition.
Laser therapy has also been suggested as an effective treatment for acanthosis nigricans. A case report reviewed the effectiveness and safety of a long-pulsed alexandrite laser in the treatment of acanthosis nigricans of the axillae.27 Results showed 95% clearance after seven sessions with no recurrence after two years. The untreated axilla was unchanged. Further research is required, however this would suggest long-pulsed alexandrite laser can effectively and safely treat the condition. Although the studies mentioned above
do not specifically look at a PCOS patient group, it can be concluded that treatment outcome should be similar in patients with acanthosis nigicans associated with PCOS.
Summary
Management of PCOS often requires a multidisciplinary approach. Skin manifestations associated with PCOS are very common and are often the first presenting features. It is critical that the commonality of these conditions does not lead the clinician to dismiss them as trivial, as many can have severe and long-standing consequences, both physically and psychologically. Aesthetic practitioners can provide valuable input into the management of these common skin manifestations.
Dr Aileen McPhillips is a medical graduate of Queen’s University, Belfast and currently works as a GP and aesthetic practitioner, running her own clinic ‘Aesthetics by Dr Aileen – The Skin Health Clinic’ based in Aughnacloy, Co. Tyrone. She is a member of the Royal College of General Practitioners and has completed a Level 7 certificate in Injectables for Aesthetic Medicine. Qual: MB, BCh, BAO, MRCGP, DRCOG

REFERENCES
1. Royal College of Obstetricians and Gynaecologists, Consequences of Polycystic Ovary Syndrome (UK: RCOG, 2014) <https://www.rcog.org.uk/en/guidelines-research-services/ guidelines/gtg33/>
2. National Institute for Health and Care Excellence, Polycystic Ovarian Syndrome (UK: NICE, 2018) <http://cks.nice.org.uk/ polycystic-ovary-sndrome>
3. Guidelines, Diagnosis and management of polycystic ovarian syndrome (UK: Guidelines, 2020) <www.guildelines.co.uk/ womens-health/pcos-uk-guildeline>
4. Gainer S, Sharma B. ‘Update on Management of Polycystic Ovarian Syndrome for Dermatologists’. Indian Dermatology Online Journal 2019 March-April; 10(2):97-105.
5. Borgia F, Cannavo S, Guarneri F, Cannavo SP, Vaccaro M, Guarneri B. ‘Correlation between Endocrinological Parameters and Acne Severity in Adult Women’. Acta DermatoVenereologica 2004;84:201–4.
6. Yildiz BO. ‘Diagnosis of hyperandrogenism: Clinical criteria’. Best Practice & Research Clinical Endocrinology and Metabolism 2006;20:167–76.
7. Archer JS, Chang RJ. ‘Hirsutism and Acne in Polycystic Ovary Syndrome’. Best Practice & Research Clinical Obstetric & Gynaecology 2004;18:737–54.
8. Lee AT, Zane LT. ‘Dermatologic Manifestations of Polycystic Ovary Syndrome’. American Journal of Clinical Dermatology 2007;8:201–19.
9. Araujo LM, Porto MV, Netto EM, Ursich MJ. ‘Association of Acanthosis Nigricans with race and metabolic disturbances in obese women’. Brazil Journal Medicine and Biological Research 2002;35:59–64.
10. Schmidt TH, Khanijow K, Cedars M et al. ‘Cutaneous Findings and Systemic Associations in Women with Polycystic Ovary Syndrome’. JAMA Dermatology 2016; 152(4):391-398.
11. Sivayoganathan D, Maruthini D, Glanville JM, Balen AH. ‘Full Investigation of Patients with Polycystic Ovary Syndrome (PCOS) Presenting to Four Different Clinical Specialties Reveals Significant Differences and Undiagnosed Morbidity’. Human Fertility 2011; 14(4): 261-265.
12. Escobar-Morreale HF, Carmina E, Dewailly D, Gambineri A, Kelestimur F, Moghetti P et al. ‘Epidemiology, Diagnosis and Management of Hirsutism: a consensus statement by the Androgen Excess and Polycystic Ovary Syndrome Society’. Human Repro Update 2012; 18: 146-170.
13. Committee on Adolescent Healthcare, ‘Screening and Management of the Hyperandrogenic Adolescent’. Obstetrics &
Gynaecology 2019; 134(4): 106-114.
14. Mayo Clinic. ‘Acne Diagnosis and Treatment’, <http://www. mayoclinic.org/disease-conditions/acne/diagnosis-treatment/ drc-20368048>
15. Fox L, Csongradi C, Aucamp M, duPlessis J, Gerber M. ‘Treatment Modalities for Acne’. Molecules 2106; 21: 1063.
16. Bienova M, Kucerova R, Fiuraskova M, Hajduch M, Kolar Z. ‘Androgenic Alopecia and Current Methods of Treatment’. Acta Dermatovenerol Alp Pannonica Adria 2005 Mar; 14(1): 5-8.
17. Dinh Q, Sinclair R. ‘Female Pattern Hair Loss: Current Treatment Concepts’. Clinical Interventions in Ageing 1007; 2(2): 189-199.
18. Stevens J, Khetarpal S. ‘Platelet-Rich Plasma for Androgenic Alopecia: A Review of the Literature and Proposed Treatment Protocol’. International Journal of Women’s Dermatology, 2019 Feb; 5(1): 46-51.
19. Alves R, Grimalt R. ‘Randomised Placebo-Controlled, DoubleBlind, Half-head Study to Assess the Efficacy of PlateletRich Plasma on the Treatment of Androgenetic Alopecia’. Dermatologic Surgery 2016; 42(4): 491-497.
20. Gentile P, Garcovich S, Bielli A, School MG, Orlandi A, Carvelli V. ‘The Effect of Platelet-rich Plasma in Hair Regrowth: A Randomised Placebo-Controlled Trial’. Stem Cells Translational Medicine 2015; 4(11):1317-1323.
21. Fabbrocinic G, Cantelli M, Masara A, Annuziata MC, Marasca C, Cacciapuoti S. ‘Female Pattern Hair Loss: A Clinical, Pathophsiologic and Therapeutic Review’. International Journal of Women’s Dermatology 2018; 4(4): 203-211.
22. Dhurat R, Sukesh MS, Avhad G, Dandale A, Pal A, Pund P. ‘A Randomised Evaluator Blinded Study of Effect of Microneedling in Androgenetic Alopecia: A Pilot Study’. International Journal of Trichology 2013 Jan-Mar; 5(1): 6-11.
23. Leavitt M, Charles G, Heyman E, Michaels D. ‘HairMax LaserComb Laser Phototherapy Device in the Treatment of Male Androgenetic Alopecia’. Clinical Drug Investigation 2009; 29: 283-292.
24. Rose PT. ‘The Latest Innovations in Hair Transplantation’. Facial Plastic Surgery 2011; 27: 366-377.
25. Lahiri K, Malakar S. ‘Topical Tretinoin in Acanthosis Nigricans’. Indian Journal of Dermatology, Venereology and Leprology 1996; 62(3): 159-161.
26. Zayed A, Sobhi RM, Halim DMA. ‘Using Trichloroacetic Acid in the Treatment of Acanthosis Nigricans: a pilot study’. Journal of Dermatological Treatment 2014 Jun; 25(3): 223-225.
27. Rosenback A, Ram R. ‘Treatment of Acanthosis Nigricans of the Axillae Using a Long-Pulsed Alexandrite Laser’. Dermatological Surgery 2004 Aug; 30(8): 1158-1160.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020







A summary of the latest clinical studies
Title: Factors Influencing Pre‐injection Aspiration for Hyaluronic Acid Fillers: A Systematic Literature Review and Meta‐analysis
Authors: Kapoor KM, et al.
Published: Dermatologic Therapy, October 2020
Keywords: Hyaluronic acid, dermal filler, aspiration, injection
Abstract: Background: Pre‐injection aspiration of hyaluronic acid filler is a well‐recognized yet controversial safety technique. Many consider aspiration to be an important safety measure to prevent inadvertent intravascular filler injection. Objective: To assess factors influencing pre‐injection aspiration by understanding the relationship between aspiration time and a range of product, needle, and procedural characteristics. We conducted a systematic review and meta‐analysis of data, adopting the preferred reporting items for systematic reviews and meta analyses guidelines. Our literature search identified four articles presenting data on variables associated with aspiration time for different HA filler brands. Statistical models pooling data from the four articles suggest a robust association between aspiration time and a filler’s elastic modulus (G’), drop weight (cohesivity), and cross‐sectional area of the needle lumen. However there is insufficient evidence to confirm a robust association between aspiration time and HA concentration, viscous modulus (G’), needle length, and pullback volume. A deeper understanding of the relationship between product, needle, and procedural characteristics, and aspiration time can provide a sound base for discussing the role of pre‐injection negative aspiration as a safety measure. The understanding of the effect of various factors on pre-injection aspiration would further benefit from studies under clinical conditions.
Title: Adverse Events Associated With Cryolipolysis: A Systematic Review of the Literature
Authors: Hedayati B, et al.
Published: Dermatologic Surgery, October 2020
Keywords: Dermatology, body contouring, cryolipolysis
Abstract: Cryolipolysis is a popular procedure for people seeking non-invasive body contouring. As with any novel therapy, it is critical for providers to familiarize themselves with related adverse events (AEs), to provide appropriate information to patients before treatment. The objective was to describe reported complications and AEs associated with cryolipolysis. A systematic review was completed using the PubMed database and following search terms: “cryolipolysis” or “lipocryolysis” or “CoolSculpting.” Only randomized clinical trials, prospective cohort studies, retrospective studies, case series, and case reports describing AEs related to cryolipolysis as well as studies written in English were included for review. Fifty-three articles were included in this review. The most common AEs associated with cryolipolysis were treatment site erythema, numbness/paresthesia, bruising, and edema. More serious complications of cryolipolysis include severe/persistent pain, dysesthesia, skin hyperpigmentation, motor neuropathy, and paradoxical adipose hyperplasia. Cryolipolysis is a safe option for patients seeking noninvasive body contouring. Most reported AEs are minimal and resolve quickly. It is important to counsel patients appropriately before treatment.
Title: Brazilian Society of Dermatology Consensus on the Use of Oral Isotretinoin in Dermatology
Authors: Bagatin E, et al.
Published: Anais Brasileros de dermatologia, October 2020
Keywords: Acne vulgaris, dermatitis, seborrheic, isotretinoin
Abstract: Isotretinoin is a synthetic retinoid, derived from vitamin A, with multiple mechanisms of action and highly effective in the treatment of acne, despite common adverse events, manageable and dose-dependent. Dose-independent teratogenicity is the most serious. Therefore, off-label prescriptions require strict criteria. To communicate the experience and recommendation of Brazilian dermatologists on oral use of the drug in dermatology. Eight experts from five universities were appointed by the Brazilian Society of Dermatology to develop a consensus on indications for this drug. Through the adapted DELPHI methodology, relevant elements were listed and an extensive analysis of the literature was carried out. The consensus was defined with the approval of at least 70% of the experts. With 100% approval from the authors, there was no doubt about the efficacy of oral isotretinoin in the treatment of acne, including as an adjunct in the correction of scars. Common and manageable common adverse events are mucocutaneous in nature. Others, such as growth retardation, abnormal healing, depression, and inflammatory bowel disease have been thoroughly investigated, and there is no evidence of a causal association. Regarding unapproved indications, it may represent an option in cases of refractory rosacea, severe seborrheic dermatitis, stabilization of field cancerization with advanced photoaging and, although incipient, frontal fibrosing alopecia. In the opinion of the authors, indications for purely esthetic purposes or oil control are not recommended, particularly for women of childbearing age.
Title: Hyaluronidase in Dermatology: Uses Beyond Hyaluronic Acid
Fillers
Authors: Al-Niaimi F, et al.
Published: Journal of Drugs in Dermatology, September 2020
Keywords: Hyaluronidase, dermal filler, dermatology
Abstract: Hyaluronidase is mostly widely recognized for its offlabel use in correction of complications of hyaluronic acid fillers. However, its utility in other aspects of dermatology is less widely acknowledged. We describe the varied uses of hyaluronidase in dermatology and the underlying evidence base for its dermatological indications. This includes its uses in enhancing drug delivery (for local anesthesia, keloid and hypertrophic scars, and for Kaposi Rsquos sarcoma), in the treatment of disorders associated with mucin deposition (myxedema, scleroderma, scleroderma, and cutis verticis gyrata) and its potential uses in surgery (as a pre-operative adjuvant in dermatofibrosarcoma protuberans, for periorbital edema, and for hematomas). In select circumstances, hyaluronidase might be more efficacious than more established treatments with fewer adverse effects. We propose hyaluronidase as the latest addition to our global dermatological armamentarium and implore dermatologists to consider its use to enhance their practice.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Incorporating LED into your Treatment Offering
If your clinic is primarily focused on injectable procedures, you may have considered how you can grow your business by expanding your treatment offering with one of the various devices available on the market. From body contouring to laser hair removal, there really is a lot to choose from and knowing what to go for can be challenging. But have you ever thought about getting a light-emitting diode (LED) device? Studies suggest that LED can be effective in treating a variety of skin conditions, including acne and psoriasis, as well as helping general skin concerns on all skin types such as redness, uneven tone, and fine lines and wrinkles.1,2 With multiple benefits for a wide-range of patients, it can also be a good commercial entity to add to your treatment portfolio.
Benefits to your practice
Aesthetic practitioner and multiple clinic owner Dr Simon Ravichandran has a number of LED devices. He says they can be a lot cheaper than other types of devices and, if marketed and used correctly, can offer a good return-on-investment (ROI). “If you compare the price of LED devices to some laser technologies, it’s not that expensive. ROI can also be a lot easier to achieve as LED is such a versatile treatment modality – you can use it for every patient – as a standalone or in combination with other procedures.” In Dr Ravichandran’s experience, having the ability to add LED to a treatment package can not just improve the outcome or reduce the recovery time, but can also enhance each patient’s experience. “They’re getting more out of their visit and improving interaction with the clinic, which increases patient satisfaction and helps to grow your relationship and business overall,” he says. LED can particularly benefit clinics that employ therapists, as treatment can easily be delegated to them. “It can be generating revenue for you while you do other work,” says Dr Ravichandran, explaining that in his clinic, he will do the original consultation with a patient and any injectable treatment, before handing over to a therapist with instructions on the parameters to use to treat the patient’s concern with LED.
Choosing a device
Choosing an LED device is the first step, with a number of different brands available in the UK. Dr Simon Ravichandran uses the Dermalux Tri-Wave and Flex devices – but says there are a variety of others available that can benefit patients. As with any new treatment, he advises practitioners look at all the clinical studies available, ensuring they are efficacious, conform to safety standards and, for an added benefit, look to see if they’ve won any awards or are recommended by respected practitioners. He also notes that you should find one that invests in development; ensuring that the training on offer is concurrent with the latest research.
Tips for using LED
Basic training on how to operate an LED device can usually be completed in less than a day, according to Dr Ravichandran; however, he notes that some practitioners will always benefit from doing more research and developing a deeper understanding of its intricacies. He laughs, “If you’re like me, you can really get into the ‘nitty gritty’ of scientific papers and spend a lifetime learning and tweaking the controls!” Treatment outcome will depend on the condition being addressed. Generally, Dr Ravichandran says that significant results can be seen after 10 treatments and basic improvement in certain conditions can be seen after three. He says, “Take psoriasis as an example, I would recommend treatment two to three times a week – I have seen dramatic results after four weeks of LED alone. With concerns like general photorejuvenation to enhance collagen and improve skin texture, results won’t be as dramatic but you can definitely see visible results with 10 sessions or less.”
It is important to be aware that treatment with LED is contraindicated in those with lightsensitive conditions such as epilepsy or patients taking photo-sensitive medicine.1 Other than that, side effects are rare with no significant concerns reported.2
Marketing and pricing
Some may argue that one of the main challenges of introducing LED to your clinic is convincing patients to opt for treatment. Unlike injectable procedures, it does not offer instant results. For Dr Ravichandran, solving this problem is all about data segmentation, good communication and being fully educated on how to achieve results. He highlights that those who just come in for their lip filler top up every few months aren’t necessarily going to become phototherapy patients. Dr Ravichandran therefore advises, “Those who invest in skincare, though, and are really focused on improving their skin condition, are the patients you need to target.” Of course, the consultation is then equally as important. “Show good before and after images, showcase testimonials and, of course, talk potential patients through the scientific results in a way they can understand,” he says, adding, “Remember to explain that you cannot guarantee quick results, but LED will benefit their skin over time.”
Deciding a pricing strategy for your LED treatments can be tricky, but will usually depend on your location and patient demographic. Treatments across the UK are generally priced between £20 and £60 per 20-minute session, with most distributors able to advise what will be suitable for your clinic location. Dr Ravichandran says it’s important to consider your projected income at various price points before making a decision.

Dr Ravichandran concludes, “LED is solid technology that can offer high-quality results when the right device is used. In my opinion, any aesthetic practitioner that is serious about taking patients on a holistic journey through their clinic should be investing in device-led treatments and not solely relying on injectable treatment. Doing so will not only benefit your patients, but could reap commercial reward for your business too.”
For more information on all the devices available and to meet suppliers, attend ACE 2021 on March 13 and 14
Register FREE via aestheticsconference.com
REFERENCES
1. Opel, Daniel R et al., ‘Light-emitting Diodes: A Brief Review and Clinical Experience’, The Journal of clinical and aesthetic dermatology vol. 8,6 (2015): 36-44.
2. Cherney K, LED Light Therapy for Skin 9US: Healthline, 2019) <https://www.healthline.com/health/beauty-skin-care/led-lighttherapy>
Dr Simon Ravichandran shares his tips on purchasing an LED device and marketing it to patients
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Creating a Smart Aesthetic Clinic
Medical device researcher David Heath explores how to enhance the patient experience via ‘smart clinics’
COVID-19 has accelerated the need for businesses of all kinds to embrace digital technology. While the aesthetics profession was already equipped with many clever and high-tech devices, the events of recent months have magnified the opportunity for clinics to embrace all things ‘smart’ throughout the entire patient experience to help reduce physical contact.
As an industry which is so reliant on close physical proximity between the practitioner and the patient, aesthetic professionals have not had the easiest task of tackling COVID-19. In order to maintain strict adherence to social distancing measures and hygiene standards, clinics have been forced to operate at reduced capacity; either limiting length of appointments or number of sessions per day. As clinicians fight to remain commercially sustainable, implementing the right technology has become a necessity. Smart businesses are those that can effectively adopt emerging technologies to drive forward their business strategy and achieve operational excellence.1 This article will explore some of the types of devices and technologies you can adopt in your practice to help enhance the patient experience and reduce physical contact in this COVID-19 era and beyond.
Online from the onset
Many patient journeys begin with a Google search, which is where investing in a good website bodes well. Introducing ‘smart’ features such as live chats and contact forms can boost online rankings and search optimisation, while improving your patient’s initial impression of the brand. Adding internet ‘bots’ (software that runs automated tasks) to your website immediately streamlines the online experience, allowing potential patients to ask questions, engage with the brand and book automatically without leaving the page.2 Alongside this, with FAQs and popular enquiries actioned by this feature, clinicians can save valuable time which would have previously been spent compiling responses via email. Chatbots have been shown to produce three times the conversion rates of email marketing efforts,3 supporting brands to onboard new clients and recoup profits as they emerge from lockdown. What’s more, this technology is becoming more and more personalised, using customer search data behaviour to give accurate product recommendations, provide tailored advice, and ensure that the client gets the most out of their online experience.4 Once the patient has engaged with your business, technology can also be utilised to
reduce the amount of time they are in your clinic. While many practices are familiar with established online booking and customer registration management (CRM) systems –and if yours is not, now is the time to start – it is possible for clinicians to take this one step further and carry out consultations, medical questionnaires, therapist introductions and payment options from the comfort of the patient’s home.
Digital applications can help to automate many of these processes. Clinicians can directly connect apps with their onsite booking systems to ensure that the process from the first point of contact to the consultation and then to arrival at the clinic is highly streamlined. Transferring patient questionnaires and introductions online removes many of the physical touchpoints associated with the ‘check in’ process – such as clipboards, pens and personal records cards – helping the clinician to maintain their COVID-19 safety protocols and prevent contamination between patients.
Tailored apps are also a great way of opening up a line of communication with the patient, giving them a platform to ask questions, adjust appointment times and meet their consultant virtually. By introducing push notifications – small clickable messages that appear at the top of the user’s screen –practitioners can easily update their patients on appointment changes, revised COVID-19 guidelines and upcoming sessions, without asking the patient to log into their account or check their emails. By unburdening the patient in this way, push notifications can help increase repeat visits, user engagement and re-engagement, over and above what can be achieved via a traditional website.5
All of these efforts can save your clinic valuable time. Less time spent on manual administrative tasks potentially means that appointment times can be shortened, allowing clinics to accept more bookings each day without compromising the patient experience.
Augmented reality
While it can still sound like a futuristic concept, augmented reality (AR) is now very accessible within the health and beauty industry, with around 88% of medium-sized businesses implementing the tech in some capacity.6 AR is an interactive experience of a real-world environment. It layers digital elements onto the real world, typically through the camera on a smartphone, which is different from virtual reality, which offers a completely immersive experience separate from the
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
physical world.7
Within the beauty industry, this kind of tech is typically applied to virtually ‘try on’ products before purchase – a feature which is growing in popularity due to the pandemic with the absence of physical testers. AR adds a new dimension to the ‘try before you by’ prophecy, allowing consumers to experiment with lipstick shades, hairstyles and even clothes. One popular AR app found that consumers were 1.6 times more likely to buy beauty products, spending around 2.7 times more money than those not using the app.8 AR can be harnessed by clinicians during the virtual consultation: to assess skin needs, signpost possible problems, and allow consumers to get a ‘first look’ at treatment outcomes before completion of a procedure. This can be a great alternative for practitioners to collect individual patient data, compared to traditional methods. In turn, the patient will feel more empowered entering their appointment, while the clinician is equipped with initial diagnostic information to help them guide the session.9
Implement tech for treatments
Many aesthetic professionals focus on the injectable treatments – dermal fillers and botulinum toxin – however, investing in technology and devices like lasers and radiofrequency can be a huge advantage. Such devices can have short, more frequent treatments over longer timeframes, transforming the patient’s skincare journey into an all-round lifestyle change, guided by the clinician in the long term. Different treatments can also be carried out with many of these technologies in the same treatment session, such as a laser hair removal treatment and laser resurfacing treatment, shortening waiting times and eliminating the need to book and attend multiple appointments.
At home-devices such as LED devices can also be utilised by the patient, further enhancing their skincare journey without the need to come into your clinic. These types of
devices usually allow results and outcomes of treatments to appear immediately within a clinician’s databases and transfer directly to the patient’s app.
In addition to applying technology for the actual treatment, the rise in imaging devices for taking patient photographs and assessing their skin can also be utilised. This can be a great way to further enhance your patient’s journey and closely monitor their results.
Extending the patient experience

The patient experience does not end when your patient has walked out the door. In fact, this is the opportunity to really solidify the positive relationships created in the treatment room with the help of technology, by checking in with patients post-appointment, discussing their specific aftercare needs, and ensuring that progress continues to be made right up until the next appointment. Often, this is done by simply calling the patient. However, another way to do this is through using artificial intelligence (AI). AI, or machine learning, can offer an interactive and modern upgrade to the patient experience.
AI has the ability to continually learn and improve, and can build up a comprehensive bank of information about individual consumers. By building this software into apps, aesthetic practitioners can harness AI to continue monitoring the patient’s progress at home and learn more about their outcomes.
AI can also be used to create personalised regime trackers and monitor product use in real time. By gathering important data, clinicians can tailor their support to suit the needs of each individual, making for a more well-rounded and personalised experience.10
Fostering stronger relationships via technology allows practitioners to move towards educating their patients, empowering them with the knowledge to prevent issues reoccurring and reach their desired skin goals. This can be achieved by adding a ‘gamification’ element to apps using AI, whereby patients are ‘rewarded’ for taking positive steps in their skin journey,
such as adhering to their recommended regime or applying their treatment a set amount of times, subsequently gaining a deeper knowledge on how best to cater for their skin’s needs. In this way, the clinician becomes a ‘life coach’ for the patient’s skin, moving beyond the once transactional relationship associated with one-off treatments.11
It should be noted that AI is a relatively new concept, and there could be limitations to its use. For example, it is unknown if there is potential for patient complications to be missed by the AI, so a focus on mitigating this risk would be needed before implementing into practice.
Fostering a new ‘best practice’
Embracing a range of technologies within clinics can not only move towards a superior standard of treatment, but allow for a more holistic patient experience within the clinic. While some of these technologies can sit at the higher end of clinician budgets, there is scope for these to be rolled out gradually to save costs. Taking steps to optimise your website by including links to social media channels, adding blog content and transferring brochures online, can be a great and cost-effective way to make your clinic smarter, without breaking the bank. When implemented well, the benefits of tech extend far beyond COVID-19. Keep an open mind and consider how you can utilise new and upcoming technology to improve your practice. Try to embrace automation within clinics where you can to streamline the experience for patients, ensure increased consistency across practices, and help build and nurture long-term relationships.
Dr David Heath is an awardwinning entrepreneur with MSC degrees in both physics and engineering and a PhD in biomedical engineering. As a qualified medical device researcher, Dr Heath has a wealth of experience in multidisciplinary clinical, commercial and engineering teams. He is the CEO of Cutitronics, which is dedicated to revolutionising the way consumers take care of their skin with technology.
VIEW THE REFERENCES BY
ONLINE AT AESTHETICSJOURNAL.COM @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Aesthetic practitioners can harness artificial intelligence to monitor the patient’s progress at home
GOING







OUR EXPERT RANGE ALLOWS YOU TO RESHAPE , REGENERATE & REDEFINE WORKING WITH YOU TO DELIVER NATURAL LOOKING RESULTS Sinclair Pharma. 1st Floor Whitfield Court, 30-32 Whitfield Street, London W1T 2RQ. 0207 467 6920 Date of preparation: February 2020 For more product and training information visit www.sinclairpharma.com sinclair_uk @ellanse_global Collagen stimulating dermal filler 3D cone technology suspension sutures @silhouette_soft Full range of Hyaluronic Acid fillers @perfectha_global FINALIS T BE ST U K S U BSIDIA RY O F A G LO BA L M AN UFA CTURE R
After Foundation Training: What Next?
Consider a company name for your aesthetic clinic; this is certainly harder than many think! Your values, ethos, background and vision will all help you create your brand and company name. Remember this will represent you in the public domain, so consider your unique selling points, patient demographic and location.
Have you just finished your foundation course? Not sure what to do now? We have all been there! I remember walking out of training with a fantastic new skill set, and wondering what to do next? With many practitioners feeling like this, it is no wonder a high percentage of delegates do not move forward in medical aesthetics.1 Within this article I aim to guide those practitioners who have just finished their foundation training, or are about to begin, to get set up and start seeing patients, which is one of the first and hardest steps to being a successful aesthetic practitioner.
First steps
Prior to completing your foundation course, it is important to think about whether you would like a lifestyle business or an exit strategy2 as this will dictate what type of a business you will run, or how aesthetics will work within your lifestyle. A lifestyle business is one which can be set up around the practitioner’s current role, for example, to bring in a supplementary income for an NHS worker. There would be minimum expenses and it does not require a formal business structure. Many practitioners have started with this type of business including myself, renting clinical rooms on an ad-hoc basis and supplementing their income while they grow their patient database.
The typical entrepreneur would create a business with the sole aim of selling it, therefore have an ‘exit strategy’. They would invest in its value as much as possible and once a high enough profit can be obtained the business will be sold. For example, an entrepreneur could invest in the opening of a clinic and create a formal business structure with policies and processes in place, and employing staff to fill all levels. Once the business has grown and is worth a profit, the clinic could be sold to an established chain of clinics.
A business plan is essential,3 and many can be freely downloaded from the internet.4,5 It is certainly worth spending time completing this, as it will keep you on the right path in terms of financials and strategy. This will also help you to plan your future vision, which is a great concept to have, as it will give you something to work towards.
One of the most common questions I receive as a trainer is, “Where can I treat patients?” There are numerous ways, with one option being to rent a medical consulting room initially on an ad-hoc basis and progressing to a more regular sessional basis once you build your patient base. Many practitioners have built a successful practice by creating a clinic space within their home and mobile practice is an alternative method, however my concern has always been the difficulty in managing infection control when treating patients in their own home, which is even tougher in the current climate. It is also worth noting that the Joint Council for Cosmetic Practitioners (JCCP) emphasises that practitioners working from their home address should meet audit guidelines outlined in its Premises Standards,6 while the British Association of Cosmetic Nurses recently stated, ‘There is no risk assessment that can demonstrate fully all the stringent measures required to carry out a cosmetic medical aesthetic treatment in the home. The environment does not lend itself to all that is necessary to ensure adequate patient and practitioner safety of treating a patient in that setting, and therefore this practice is not recommended’.7 Instead, joining a larger and established clinic is a great way to be part of a larger team and to potentially learn from experienced practitioners. It can be daunting to approach a large clinic, however my advice would be to look at the transferable skills you have from your background, create a portfolio of your work and keep approaching clinics, as many look for inexperienced practitioners to train in their own philosophy and techniques. The most important part is to be yourself!
If you are looking for supervision, another option is to consider joining the JCCP which, along with the Cosmetic Practice Standards Authority (CPSA), recommend forming networks of practitioners and have devised a supervision matrix to enable everyone to have access to a practitioner as a supervisor or mentor.8 Supervision can be directly with the experienced practitioner or virtually, and junior practitioners can discuss complex cases, complications or anything they need help with.
Basics
The first thing to do after the foundation course is to organise indemnity. There are a number of insurance companies that specialise in the aesthetic medicine sector such as Cosmetic Insure, Enhance Insurance or Hamilton Fraser Cosmetic Insurance, so contact them to obtain a few details and quotes. Also speak to your current indemnity provider as they may be able to
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Dr Manav Bawa shares advice for new practitioners entering aesthetics
provide insurance for the aesthetic treatments you will be providing. Have you thought about which products you would use and where will you would purchase them from? There are numerous products on the market, and I would recommend researching and contacting product specialists of the reputable aesthetic medicine pharma companies. Discuss the range of products they have, how you would use each one to treat patients and what kind of support and additional training opportunities they offer. Remember to also do your own research to ensure you’re confident the products are reputable and safe.
The next step would be to register with an aesthetic pharmacy such as Church Pharmacy, Healthxchange Pharmacy, Med-fx or Wigmore Medical to purchase your products and consumables from a reputable establishment. Many pharmacies are now offering starter packs, which can be useful as they contain everything you would need for your first few patients.
To start with, I would recommend ordering a few products for stock or on a ‘per patient basis’ following a consultation, as the first few months can be unpredictable in term of treatments and revenue. This is exactly what I did when I started as I did not want to be left with stock getting near to its sell-by date. I also did not want to spend money on products I may not use. Regarding prescription-only medications, in England only doctors and dentists are allowed to keep stock, for all other practitioners, they must be prescribed and ordered for a specific patient. Remember that the General Medical Council says that you must undertake a physical examination of patients before prescribing non-surgical cosmetic medicinal products, so they should only be prescribed in the patient’s name following a face-to-face consultation. You should not prescribe these medicines by phone, video-link or online.9
One the biggest mistakes I made was to wait for almost a year for an ‘all singing all dancing’ website. When we went live, it was brilliant; however, for most of the time it was in the making, nobody knew that I was practising! So, I would certainly advise publishing a one-page website as fast as you can presenting who you are, your background and credentials, as well as the services and treatments you provide. When patients search online for a practitioner or service, for them to be able to find you, you must have an online presence. While a social media page is great for promoting your business, it doesn’t offer all the information a website can offer. Educating patients is a great way to engage with them, and ensure you cover the treatments you provide as well as details about each one including how it works, how long it takes and how much it costs. You therefore could create your own website or hire a digital marketing company to do this for you. It is also wise to create a Google business listing, known as Google My Business, so your clinic can be found on Google maps.
Marketing yourself can be extremely overwhelming with many platforms available. I recommend starting with simple social media such as Instagram and Facebook. They have their own algorithms which are constantly changing, so have an appreciation of them if you want to excel on these platforms. Post regular and engaging content to remain in your current and potential patients’ feed. Other ways to market yourself would be local advertising within lifestyle magazines or leaflet drops. Remember word of mouth can be a great way to grow organically, so treat your patients well, and they will tell their friends. Patient reviews are a great way to market and promote your work, so utilise a third-party service patients can leave reviews on, for example, TrustPilot or Google.
Getting started
Try to have a few patients lined up to treat as soon as you complete your course, as it is good to keep up the momentum and excitement, as well as to avoid deskilling. Patients could include family and friends, or through marketing prior to the course. A common question is how to market yourself when you haven’t got years of experience? I used my medical background to promote myself, the products I was using, and I focused on enhancing the patient journey as much as possible.
I started by approaching a local beauty salon prior to my foundation course, and I negotiated a collaboration where they would refer me patients, and in return they would receive a fee. This worked well as I built my experience through referrals from an established business. On the other hand, please do note that the General Medical Council has guidance for doctors that states they should not accept payment for referrals as it gives rise to a conflict of interest.10 Similar standards apply for nurses and dentists.11,12
Collaborating with local businesses can also bring in patients as they will have received a recommendation from a third party (your collaborator) and so will have a level of trust already formed. Local business networking can be very powerful in this way and can work well for all parties.
As you start to grow, you could use before and after photos to promote your work. Good quality photography is essential for this. Standardise your photos as much as possible, for example, always have the same plain screen behind patients, take pictures at the same angles before and after, as well as using a good quality camera. I started off using my iPad camera, then purchased a DSLR camera with a refurbished flash, a tripod and black screen, which didn’t cost too much.
It is essential to maintain detailed patient records for medicolegal reasons,13 as well as reviewing procedures, finances, diary management and tracking key performance indicators, which will help you grow. A digital patient management system can really help, as well as allowing before and after photography comparison. This can enhance the patient journey by showing your patients their progress at their review, as well as helping you learn from your results. There are numerous ones out there – from free to a significant fee – and choosing a robust and reliable system will really help to manage your time as well as aid business growth. Using an automated approach will also save time and money, thus boosting your profits; for example, in my experience, reminder emails or texts will reduce the number of patients who do not attend their appointments. Using a paperless system will also avoid storage issues and, currently, with heightened infection control, it is much easier as there is no paper, only a computer or tablet to clean. A good system could also integrate with your website or social media
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
You must undertake a physical examination of patients before prescribing non-surgical cosmetic medicinal products
allowing bookings to be made online, again saving time and costs. Some commonly used software systems include Aesthetic Nurse Software, Clever Clinic, Consentz, iClinician, iRejuvenation, Pabau, and Sellsio, to name a few.
Once you start building you patient database, it is important to spend time on retention, as it is more economical to retain current patients than obtain new ones.14 Ideas of how to do this could be to book patients in for their next treatment before they leave, newsletters to maintain a constant presence or even reaching out to patients with a quick phone call to see how they are and if you could help them in any way.
Work smart
Moving into a new industry can be daunting, as well as overwhelming initially when looking to become a successful practitioner – we have all been there! Get a head start by planning prior to your course, focusing on your own medical aesthetic journey, and working smart towards your own personal vision and goals by spending time on strategy and planning of your business.

Dr Manav Bawa is an aesthetic practitioner and GP with a surgical background. He is the medical director of Time Clinic in London, an injectables trainer, and has completed a Diploma in Aesthetic Injectable Therapies. Dr Bawa is an associate member of BCAM and is passionate about mentoring, education and patient safety. Qual: MD, PGDip(ESSQ), MRCS(Eng), M Ed(SE) & DIC, MRCGP, PGDip(CAIT)

REFERENCES
1. Harry Singh, Dr Harry Singh shares 10 traits found in successful entrepreneurs and explains how you can adopt them (Aesthetic Medicine, 2019) <https://aestheticmed.co.uk/site/ industrynewsdetails/building-the-machine>
2. Victoria Smith, The day to day running of an aesthetics clinic (PMFA NEWS VOLUME 4 ISSUE 2, 2017) <https://www.thepmfajournal.com/features/post/the-day-to-day-running-of-an-aestheticsclinic>

3. Hamilton Fraser, Creating an aesthetics business plan (Hamilton Fraser Knowledge Centre) <https://hamiltonfraser.co.uk/knowledge/creating-an-aesthetics-business-plan/>
4. Virgin Start Up Business Plan (Virgin Start Up) <https://www.virginstartup.org/business-plantemplate#download>
5. Barclays Business Plan PDF (Barclays Bank) <https://www.barclays.co.uk/content/dam/ documents/business/business-insight/guidetowritingbusinessplan.pdf>
6. BACN, Suggested Operational Plan Guidelines for COVID-19 (UK: BACN, 2020) < https://www. bacn.org.uk/content/large/documents/members_documents/reference_material/covid-19/ suggested_operational_plan_guidelines_for_covid-19_reintegration_of_medical_aesthetic_ services.pdf>
7. JCCP, JCCPWS 006 Work Standards for conferences, exhibitions and mobile working (UK: JCCP, 2017) <https://www.jccp.org.uk/ckfinder/userfiles/files/JCCPWS%20006%20 Conferences%20Exhibitions%20and%20Mobile%20Working.pdf>
8. CPSA, CPSA Supervision Matrix (CPSA) <http://www.cosmeticstandards.org.uk/ uploads/1/0/6/2/106271141/20180103_cpsa_supervision_matrix_final.pdf>
9. GMC, Remote Prescribing via telephone, video-link or online (GMC, Prescribing and managing medicines and devices, 20200<https://www.gmc-uk.org/ethical-guidance/ethical-guidance-fordoctors/prescribing-and-managing-medicines-and-devices/remote-prescribing-via-telephonevideo-link-or-online>
10. GMC, Competing interests and incentives, <https://www.gmc-uk.org/ethical-guidance/ethicalguidance-for-doctors/financial-and-commercial-arrangements-and-conflicts-of-interest>
11. NMC, Conflicts of interest joint statement, 2017. <https://www.nmc.org.uk/news/news-andupdates/conflicts-of-interest-joint-statement/>
12. GDC, Standards and guidance. <https://www.gdc-uk.org/information-standards-guidance/ standards-and-guidance>

13. Mukta Sachdev and Gillian R Britto, ‘Essential Requirements to Setting up an Aesthetic Practice’, J Cutan Aesthet Surg. 7:3 (2014), 167–169.
14. Marcus Haycock, ‘Developing and retaining loyal aesthetic patients using a six-step process’, Journal of Aesthetic Nursing, 6:7(2017), 380–382.
“Our goal is for Beyond Beauty to take pride of place in every clinic waiting room and be the go-to information source for consumers. This special magazine is designed to inform patients of what to expect from treatments and encourage them to become loyal, returning visitors to aesthetic clinics. No frills, no fluff – the content will be purely educational, written in language that patients will understand and trust.”
BRINGING THE WORLD OF AESTHETIC MEDICINE TO YOU
| ENHANCING KNOWLEDGE | | BUILDING TRUST | | PROMOTING POSITIVITY | Follow us on Instagram for all the latest updates @beyondbeauty mag
JANUARY 2021
LAUNCHING
a missing or poor quality SOP (in which case we need to correct this) or whether the SOP was adequate but was not followed (in which case the solution is staff training).
problem was a missing or poor quality SOP (in which case we need to correct this) or whether the SOP was adequate but was not followed (in which case the solution is staff training).
2. Staff feedback – in every monthly team meeting, the agenda includes time for the staff to report any problems that they have encountered that have made their job more difficult or has affected the customer/patient experience. You don’t need to wait for a complaint – the goal is to improve things before they can become a problem.
2) Staff feedback – in every monthly team meeting, the agenda includes time for the staff to report any problems that they have encountered that have made their job more difficult or has affected the customer/patient experience. You don’t need to wait for a complaint – the goal is to improve things before they can become a problem.
Improving Clinic Processes
Improving Clinic Processes
Dr Askari Townsend discusses the use of standard operating procedures when running a clinic
Dr Askari Townsend discusses the use of standard operating procedures when running a clinic
Constant housekeeping is always essential to ensure an efficient and resilient business, but many people are unsure where to start. To begin, you should consider something most of us are already familiar with – the clinical audit cycle.1
Constant housekeeping is essential to ensure an efficient and resilient business, but many people are unsure where to start.
Although not the most exciting of tasks, or why we entered this field, applying this level of scrutiny and common sense to all aspects of your business can save you significant time and free up your staff to do other important tasks. The four stages of the clinical audit cycle refer to:
To begin, you should consider something most of us are already familiar with – the clinical audit cycle.1 Although not the most exciting of tasks, or why we entered this field, applying this level of scrutiny and common sense to all aspects of your business can save you significant time and free up your staff to do other important tasks. The four stages of the clinical audit cycle refer to:
This philosophy can be adopted for your business processes and can cover almost anything – ordering and stock management, cleaning, check-in/check-out, staff training/mentoring, complaint handling etc. An effective way of compiling these outcomes is by creating standard operating procedures (SOPs).
This philosophy can be adopted for your business processes and can cover almost anything – for example, ordering and stock management, cleaning, check-in/checkout, staff training/mentoring and complaint handling. An effective way of compiling these outcomes is by creating standard operating procedures (SOPs).
Standard operating procedures
1) Finding an area of your practice that could be improved
1) Finding an area of your practice that could be improved
2) Measuring the performance of that aspect
2) Measuring the performance of that aspect
3) Making the necessary improvements
3) Making the necessary improvements
4) Measuring again to see if the intervention gave the expected changes
4) Measuring again to see if the intervention gave the expected changes
SOPs are a set of step-by-step instructions created by an organisation or business that aim to help workers carry out complex routine operations.2 According to the UK Government, SOPs should also take account of regulatory requirements and security practices.2
Standard operating procedures
When creating or updating your business processes, ensure that you commit them to paper in the same way that you would with a treatment protocol. Have your staff read them and sign that they have understood and promise to follow them. The aim is to create a document detailing how your business works so that all staff understand what is required of them. These documents should be written after careful consideration of how you want each process in your business to be performed. As with all processes, it’s important to be clear what the benefits are and that they are real before implementing them permanently. Ensure that they are simple enough for all grades of staff to understand and remember when they are needed. The more unlikely an event, the more simple the SOP should be. If the event rarely happens, it’s highly unlikely that anyone will remember the SOP for it, let alone a complicated one.
It’s not just about efficiency but also quality control – ensuring that all employees are following the same process in order to deliver the same quality of service or product.
In the early days, new SOPs are often identified and created regularly as you become aware of the gaps. As your business matures, the focus often moves to improving existing SOPs. Practitioners shouldn’t see this as a chore but rather a valuable opportunity to make your business run more smoothly. In main events that result in reviewing our SOPs:
SOPs are a set of step-by-step instructions created by an organisation or business that aim to help workers carry out complex routine operations.2 According to the UK Government, SOPs should also take account of regulatory requirements and security practices.2 It’s not just about efficiency but also quality control – ensuring that all employees are following the same process in order to deliver the same quality of service or product. In the early days, new SOPs are often identified and created regularly as you become aware of the gaps. As your business matures, the focus often moves to improving existing SOPs. Practitioners shouldn’t see this as a chore but rather a valuable opportunity to make your business run more smoothly. In my business, there are two main events that result in reviewing our SOPs:
Many of my SOPs include asking for help from a senior which helps to cover all eventualities, including those that cannot be planned for. If the member of staff tries to manage a complicated situation that is outside of their capabilities, they can still be held to account for failing to involve a senior staff member. Ensure that your SOPs are reviewed as appropriate in the same way that you would with your clinical SOPs (e.g. consent procedure), especially as your business will change more often and quickly than clinical practice.
When creating or updating your business processes, ensure that you commit them to paper in the same way that you would with a treatment protocol. Have your staff read them and sign that they have understood and promise to follow them. The aim is to create a document detailing how your business works so that all staff understand what is required of them. These documents should be written after careful consideration of how you want each process in your business to be performed. As with all processes, it’s important to be clear what the benefits are and that they are real before implementing them permanently. Ensure that they are simple enough for all grades of staff to understand and remember when they are needed. The more unlikely an event, the more simple the SOP should be. If the event rarely happens, it’s highly unlikely that anyone will remember the SOP for it, let alone a complicated one. Many of my SOPs include asking for help from a senior which helps to cover all eventualities, including those that cannot be planned for. If the member of staff tries to manage a complicated situation that is outside of their capabilities, they can still be held to account for failing to involve a senior staff member. Ensure that your SOPs are reviewed as appropriate in the same way that you would with your clinical SOPs (e.g. consent procedure), especially as your business will change more often and quickly than clinical practice.
In my business, our SOPs are saved in a shared folder that all the staff can access and review at their leisure. As new SOPs are added, they are shared and discussed at the next team meeting.
In my business, our SOPs are saved in a shared folder that all the staff can access and review at their leisure. As new SOPs are added, they are shared and discussed at the next team meeting.
1. Complaints – every complaint is reviewed carefully to decide if the problem was
1) Complaints – every complaint is reviewed carefully to decide if the
Below I outline a few examples of how I identified areas of my business to be improved, implemented the changes and then added to my SOPs.
Below I outline a few examples of how I identified areas of my business to be improved, implemented the changes and then added to my SOPs.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Aesthetics | July 2019 2 Insider News @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
1 2 3 4
Bureaucracy
As medical professionals, we operate in a regulated sector and it can be easy to respond to this with bloated paperwork and processes. As a result, procedures need to be implemented that can increase productivity and reduce bureaucracy. For example, at my clinic, all my staff are required to have an hour long one-toone with their manager each month and I have an hour with each of my managers. Staff performance and expectations are discussed, in addition to training requirements and any problems that they may have. Each month we also have a three-hour team meeting that does much the same but for the business performance and team as a whole. Managers would write the notes for the one-to-ones they performed following the meeting, and a nominated staff member would write the minutes for the team meetings, which a manager will then review. When I first implemented this process, I hadn’t appreciated the amount of time staff spent writing these notes. As important as I thought this task was, realistically there is a limit on the amount of time that can be spent on them before the benefits begin to fall away. I made the decision to have the minutes typed up during the meetings. If necessary, these would be completed afterwards, but with a guide to what information is relevant and how much detail to include. The grand saving? Around four hours of employee time each month, enough time for a member of staff to perform several hundred pounds worth of treatments.
Payments
When I opened my clinic, we accepted both cash and card payments. However, I have realised that the time and effort of accepting and processing cash just wasn’t worth it. Whilst I believe it’s important we don’t move to a cashless society just yet as vulnerable groups may be excluded, these groups do not make up a significant part of our patient base. Additionally, with an average transactional value of well over £100 for aesthetic treatments, cash is not a significant method of payment so there was only a small number of cash payments. Alongside this, following COVID-19, few people want to handle cash that has passed through many hands. We therefore introduced a clinic management system with integrated payments which means that patients can enter their card
details and pay a deposit when booking online. When it comes to paying, they can choose to pay with that saved card. Staff click a button on the computer or device to take payment and the patient leaves without having to interact with anyone or anything. This will be done in the treatment room in future, leaving the patient to leave the premises without having to interact with the reception team again, leaving them clear to manage incoming patients. Changing well-established behaviour is always a challenge but in the case of payments, many people are used to having card details saved for quicker payment processes through e-retailers like Amazon. We’ve had a few people not wanting their details saved, so they simply use their card as normal. However, once they understand that our staff have no access to their card details other than the last four digits and expiry date, they often change their minds.
Efficiency
When faced with improving profitability, most consider the obvious areas – what supplies can I buy at a better price and which services can I charge more for? Buying low and selling high is business 101 and a strategy that most of us attempt to implement. However, improving efficiency and saving time will also improve your profit. If your team spends an extra five minutes on a process or wastes five minutes of your doctor’s time, there is a cost to that. Multiply this across the days and weeks that this problem occurs and it could be hours each month. The cost of this is easily calculated by how much they are paid per hour. Of course, this is the minimum cost as there may well be knockon costs such as lost sales or complaints. We had a problem with clinicians not always letting the staff know when consent forms were running low – on occasion, this would be overlooked until in the middle of a busy clinic, when there would be no consent forms. The knock-on effect on the clinic and business was extremely damaging for such a small issue with a simple solution. Until that time, there had been no formal SOP. I would simply let the staff know when I noticed that the forms were running low and I had asked other clinicians to do the same. The new SOP made my full-time staff responsible for checking forms and printing more if they were running low. There was a rota that ensured that management would know which member of staff had checked the
room on each day and so there was a record of who would be accountable if there was a problem.
Improving the team
Organisations are complex and whether they are documented or not, there are many processes to learn and remember. Aesthetic clinics are particularly difficult due to their specialist nature and level of regulation. SOPs are an important addition to an employee’s contract and job description. They ensure that a new member of staff is aware of what is expected of them and provide a source of information for when they forgot what to do or how to do it. It also enables employers to review staff performance and create training plans when SOPs have been forgotten. Ultimately, staff can be held to account when SOPs have been ignored. Ask your staff for their comments and include them in the process of drafting or signing off SOPs that affect them. If they feel included in the process, they will be more likely to remember and adhere to them.
Actioning and updating SOPs
Scrutinising business processes with the same vigour that we give to clinical processes is important to ensure a smooth running, productive and efficient business. This is an ongoing task where SOPs should be reviewed, improved and updated on a regular basis, especially as your business grows and faces new challenges. Ultimately, well written and adhered to SPOs will result in a better service for your patients, happier staff and more profit. All these are more important than ever at a time when business conditions are unpredictable.
Dr Askari Townshend has been practising aesthetics since 2006. He has founded two clinics, been a national trainer and was a senior doctor in the UK’s largest chain of aesthetic clinics. Dr Townshend’s multi-award winning clinic, ASKINOLOGY, recently celebrated five years in business. Qual: BMedSci, BMBS, MRCS

REFERENCES
1. NICE, Principles for best practice in clinical audit, 2002. <https:// www.nice.org.uk/media/default/About/what-we-do/Into-practice/ principles-for-best-practice-in-clinical-audit.pdf>
2. Gov.UK, Standard operating procedure guidelines, 2007. <https://www.gov.uk/government/publications/ standardoperating- procedure-guidelines>
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
Optimising Website for Mobile
Digital
I would be willing to bet my house that you own a smartphone. It’s probably either in your other hand, or placed in front of you while you read this issue of Aesthetics. It is our ‘go to’ device for initial queries, and of course it’s where we spend our social media lives (for more hours each day than any of us would like to admit). Statistics show that more than 70% of website visitors in the medical sector are using a mobile,1 and Google data shows that more than 63% of all Google searches are done on a mobile (2019).2 The laptop or desktop are no longer the primary device for searching or browsing online. Yet, despite evidence and data telling us how important and dominant mobile is, many aesthetic clinics and their web designers still focus the majority of their attention on how their website looks on a large screen, neglecting the mobile experience.
What is mobile experience?
Mobile experience refers to any and all interactions between a person on their smartphone, and your business in the digital world. This means your social media content, your website, your online store, your payment portal, your content, your clinic software, your email campaigns and
more. Mobile experience is important because it is often the first impression a potential customer has of your business, and it can be off-putting if it’s slow, confusing, or frustrating. Over time this kind of poor experience can affect your brand reputation and customer retention rates. Think about your own experiences interacting with other businesses online. How patient are you if you come across a website or booking system on your mobile that either doesn’t work at all, or is very slow and ‘clunky’? Do you stick with it? Or do you move on?
Making your website mobile friendly
The ‘mobile friendliness’ of your website is one of Google’s most important ‘ranking factors’ that it uses to determine your position in its search results. Mobileoptimised websites hold much higher positions on Google than those designed only for desktops. Not only that, but it is the mobile version of your website and its content that Google indexes by default, not the desktop version.3 So, which are the most important elements of the mobile experience that Google look at in order to determine your ‘rank’?
1. The content experience – don’t hide content from your main site on the mobile version
2. Speed – your site MUST load quickly on a mobile cellular connection (3G or 4G)
3. The visual – your mobile site needs to feel more like an App. Easy to use menu, intuitive navigation and functionality etc.
According to data from the website Think With Google, 76% of people who search on their smartphones for something nearby go on to visit a business within a day.4 For aesthetic clinics, this is absolutely vital. Therefore, it’s not only important that your website is optimised from a content, speed and interface perspective in order to rank well on Google, but it’s also critical that you ensure it is built to be easily and appropriately indexed by Google Local and Google Business listings (these are the listings that appear at the very top of Google search results, along with a map).
Where to start?
With so much riding on your mobile experience and mobile optimisation, where should you start and how exactly is this all achieved? First, it’s important to understand what state your website is in right now. There are some free tools you can use to check this within minutes, and will give you some pointers as to how to improve the technical performance (warning: it can get a bit geeky, so you may need a credible web designer/ developer to assist you).
• Test 1: Google’s Page Speed Insights Test (Found at developers.google.com/ speed/pagespeed/insights/)
• Test 2: Google’s Mobile Friendly Test (Found at search.google.com/test/ mobile-friendly)
These tests will let you know whether or not Google considers your site to be ‘mobile’ or not, and will also give you a score out of 100 for your website’s performance. The ultimate goal is to get the scores for both website and mobile to above 70. There are three score bands: 0-49 (red), 50-89 (orange), and 90-100 (green).5 However, it is unrealistic to aim for a score above 90. Not even multi-million pound sites like Apple.com have achieved above 80. Depending on how well your website is built, there could be up to 200 individual technical issues/optimisations to carry out to increase your score, which would usually need to be performed by an experienced web developer. However, the improvement in
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
consultant Rick O’Neill discusses why mobile user experience is important, explaining the common mistakes that aesthetic clinics make and provides ways to fix them
user experience and likely increase in Google rank as a result are often worth the effort and investment. This will take your website and certainly the mobile experience to another level in terms of user experience, speed, customer retention, and Google ranking.
Enhancing design and build
In terms of your website’s design and build, it must be ‘responsive’. This refers to the way a site changes its layout, content order, and navigational elements according to the screen it is being viewed on.
When you get beyond that basic premise, there are a number of elements for your design that you need to consider carefully to ensure a strong mobile experience:
• Make navigation easy and intuitive –consider a consolidated menu structure and look at how apps work for the ultimate user interface design principles. Everything should be designed for touch navigation (remember, mobile users are not pointing and clicking with a mouse, they are using their fingertips). This can also include making sure that phone numbers are ‘tap to call’ (meaning when tapped, a phone call is instantly initiated on the user’s smartphone).
• Keep a safe distance between functional elements – allow enough space for fingers and thumbs. Neither users nor smartphone screens like it when two functions are too close together. It can get very frustrating when you think you are tapping one thing, but something else happens instead!
• Design a ‘lean’ site – make sure that your web designer or agency are optimising the code, theme, templates, functionality, imagery and videos for speed.
• Use short forms – you can always ask for more information in a follow up. The key is to make the visit as convenient and efficient as possible for the user.
• Highlight your calls to action (links,
buttons, forms etc) – make it easy to identify them on a small screen, and for a fingertip to tap.
• Make sure text is a generous size and legible use just one or two text sizes on the mobile version of your website’s design – it’s better to keep it simple. You should also break the text down into bitesized chunks and use bullet lists and pullout quotes to make it easier for the eyes to ‘rest’ on each section. Large blocks of text are unpleasant to find your way through when staring at a smartphone screen.
• Avoid pop-ups – they are annoying on a mobile website, so don’t use them unless it’s legally necessary.
• Be careful of how you implement images and videos – your video player should be responsive and change shape on smaller screens. Make sure that you use current technology and be served by a fast video-hosting platform (such as EOOVI.com or Wistia.)
• Images should be optimised – in terms of their file size and format and avoid large JPG files. Instead look at SVG formats, or even CSS icons and sprites as alternatives to keep the site very ‘light’. SVG stands for scalable vector graphics and are files that end with ‘.svg’. They can be created with design tools such as the Adobe Creative Suite. Cascading Style Sheet (CSS) icons and sprites can be obtained from sites such as https://css.gg/

• Keep the elements and layout super clean and free from clutter – I always ask myself, ‘What would Google do?’ Just look at their homepage – it’s one of the most complex websites in the world, and yet it only has a single word and a search box. The beauty is in its simplicity. Apply this principle to your own mobile experiences wherever possible, whether it be your website, your next email newsletter, or your next Instagram story.
It doesn’t end with your website
Mobile experience isn’t just your website but also your booking software, eCommerce store, social content, email campaigns, and more. So, don’t stop once you’ve mobile optimised the website, make sure that optimised user experience designed for the small screen continues through every part of your customers’ journey with you. This might be from when they find you on Instagram, through to booking a consultation with you, to purchasing skincare products from your online store – the entire process should be an absolute joy and all from the convenience of a smartphone. Audit each of these areas carefully. Test them for yourself on your mobile and ask a select group of trusted partners and customers to do the same. Take the feedback to your digital consultant or web agency and carry out a mobile optimisation project to sort out the whole lot.
Think mobile first
For any aesthetic business, the importance of digital maturity is evident now more than ever. With more and more consumers using their smartphones to find clinics/ products and book appointments, the way that your website transfers over onto your mobile is crucial for gaining new patients and ensuring continued patient satisfaction. So, from now on remember to think ‘mobile first’ with everything you do for your aesthetic business!
Rick O’Neill, FRSA, is a digital consultant to the medical aesthetics, cosmetic surgery and pharma sectors. With more than 20 years’ experience in digital marketing, O’Neill is the founder and owner of the award-winning digital agency ‘Look Touch & Feel’, a founding partner of The Aesthetic Entrepreneurs, and is currently digital consultant for Allergan Aesthetics in the UK and Europe.
REFERENCES
1. Christel Lane et al., The Future of Professionalised Work: UK and Germany Compared (London: Anglo-German Foundation for the Study of Industrial Society, 2003) <http://www.agf.org.uk/pubs/ pdfs/1232web.pdf>
2. HitWise UK, Mobile OverTakes Desktop, October 2019, <https:// www.hitwise.com/en/2019/10/08/grow-mobile-web-conversionsuk/>
3. Oberio, 10 Google Search Statistics You Need To Know in 2020, April 2020, <https://www.oberlo.co.uk/blog/google-searchstatistics#5_Number_of_Mobile_Google_Searches>
4. Google Webmaster Central Blog, Announcing Mobile First Indexing For The Whole Web, March 2020, <https://webmasters. googleblog.com/2020/03/announcing-mobile-first-indexing-for. html>
5. Think With Google, Mobile Near Me Searches, May 2016, <https://www.thinkwithgoogle.com/data/mobile-near-mesearches/>
6. Page Speed Insights, Make Your Web Pages Fast On All Devices, <https://developers.google.com/speed/pagespeed/ insights/>
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
The key is to make the visit as convenient and efficient as possible for the user
Clever Consulting
A game-changing app, Clever Clinic transforms and simplifies every aspect of your clinical life, freeing you up to practice with the upmost excellence and safety. Every. Single. Time.


0.5 0.3
Wake up to Clever Clinic Innovative technology for the modern aesthetic practice
iPad only Group Free for Healthxchange customers. Visit cleverclinic.co.uk to find out more Preferential pricing available with an Allergan Commercial Policy. Commercial Policies now include VYCROSS® and ULTRA® packages, any five mix & match. Exclusive to Healthxchange Group. Healthxchange is proud to be Allergan’s Affiliated Pharmacy
0.7 0.3
NEW Injection Points feature for Clever Clinic.
In The Life Of Dr Tapan Patel
multi-award
I am a very early riser…
My day starts at 4:30am every morning, even on the weekends, and what gets me out of bed is my keen appreciation for fine coffee. In the mornings I catch up on my reading until about 6:30am. This can be medical, aesthetic or lifestyle related, or perhaps just a book I happen to be reading. I love the feel of paper and the printed word, and this time in the mornings is really anti-gadgets – no phone, no emails, or computer – just paper! Increasingly, I am also combining a bit of mindfulness into this time – yoga, meditation and breathing exercises.
At 6:30am I go to the gym for about an hour. I alternate resistance machines on one day with cardio the next – usually I run on the treadmill. Then I go home to get ready for work. Something I have been really getting into recently is cold immersion – there is an idea that cold water has multiple benefits for the body so I will have the coldest possible shower I can for a good five to 10 minutes, irrespective of the weather. There are studies that show that it improves mood, immunity, willpower and discipline and I can relate to this – it’s not something I look forward to, but really sets me up for the day.
After my morning vegan breakfast of oats, fruit, chia and flax seeds, and protein powder, I will prepare a plant-based lunch to take to work and will walk 7km from west London to PHI clinic on Harley Street – something I have started doing since COVID-19. As they say, ‘win the morning, win the day’ and this disciplined lifestyle is something I am really trying to embrace at the moment.
I drink endless cups of coffee in my working day…
I am at the clinic from around 10am until 6pm and my days are very varied; no two are the same! Before the pandemic I was doing an incredible amount of travelling – 20-30 trips abroad a year – to speak at international conferences or training for companies like Allergan. It wasn’t unusual for me to finish clinic and go to Heathrow airport straight after. This was fun and challenging, but also could be difficult and disruptive. Since COVID-19, putting a hold on this has been a welcome break and has been very grounding for me – I hope to find a good balance once travel returns.
Exciting me at the moment is… I’m working closely with Cutera and am really excited by their vascular Excel V and muscle sculpting truSculpt Flex devices, as we are seeing amazing results. I am also really eager for conferences and exhibitions to get started again, whenever that may be, so that we can begin to see even more product launches and just catch up with colleagues properly.
My tips for beginners… Invest in yourself and find a good mentor and team who can help you. Know that aesthetics is a marathon, not a sprint and you need to take the time to succeed.
When purchasing devices… I firstly look at whether it works and is safe. Then, I do market research amongst my patient base to see if there is demand for it and ask, is it easy to use for a range of practitioners at my practice?
During a typical clinic day I see three types of patients; those I need to consult, review and treat. The treatments I personally do are specific full-face advanced injectable procedures for patients who really want a total makeover. I am very well-known for having a wide variety of aesthetic devices

and have been heavily involved in bringing many to the UK. The devices I currently use the most day-to-day are for diagnostic purposes. I am very pedantic about recording everything and so I have not one, but several imaging devices that all do different things.
I have a VISIA for skin analysis, a VECTRA for 3D imaging, FotoFinder for consistency and I also use my own camera to take more creative or specific images.
Throughout my day it’s not uncommon to have a meeting or two as I work with a lot with companies and teach for them. Recently I have had a lot of meetings with TV producers because I have been taking part in 10 Years Younger in 10 Days, which I have loved. On the days we are filming I will just book a whole day out of clinic.
I also run my own aesthetic training academy. In 2017 I launched an online training platform called e-MASTR. We recently rebranded and relaunched as PHI College which involves both online and in-clinic training, so my day will usually involve some kind of work on this. What is very pivotal in my day is my team. I am not, by nature, a very organised person as I have so much going on, so my excellent team allows me to really focus on the tasks at hand. Without them, if I was doing all of this on my own, my day would be impossible!
My evenings are relaxed… I walk home and arrive at about 7:30pm. I try to spend this time doing something I enjoy – a small pleasurable thing. It could be that I cook something nice, or I like to draw, paint or sketch. During summer I was taking a lot of outdoor walks and just exploring London. I am also learning Italian on an app, so might do that while I walk. I go to bed relatively early at about 9:30 or 10pm. This contrasts a lot to how I used to live, which was completely the opposite; very late nights and blurry-eyed starts, usually travelling at 5,000 miles per hour! I am really focusing on looking after my health at the moment. In the past I probably did hours and days that were quite detrimental in the long run. I would probably tell my younger self not to rush things so much, but I think I have managed to pull back and slow down a bit, which has been a really positive thing for me.
The man behind the
winning PHI Clinic shares an insight into his daily clinical life
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
The Last Word
Video calling is now part of our everyday routine. It has enriched our lives during lockdown, ensuring we can still see our loved ones and has even allowed us to secretly wear pyjamas in business meetings! But despite video calling enabling good, solid communication between us during the lockdown period, it has also potentially had a negative impact on our wellbeing. “Oh No, I look old!”, “Is that a new spot on my face?”, “I’m getting a double chin!”, “Gosh, I look tired today.” Does this sound familiar? From speaking with our friends, family and patients, these are just some of the things people are saying to themselves internally whilst on a video call. While we should be focusing on the person who’s actually speaking, instead we can be too consumed by our own appearance on the video. And it is this affect that is leading to many people now seeking aesthetic treatments. Cosmetic surgeon and spokesperson for the British Association of Aesthetic Plastic Surgeons (BAAPS) Mr Gerard Lambe has voiced that he agrees that the use of video calling has led to more people seeking to change their appearance. Mr Lambe describes this as ‘the ‘Zoom factor’.1 People using cameras more than ever and their visual appearance being scrutinised on apps has certainly boosted enquiries for cosmetic tweaks and procedures. In addition, Mr Lambe argues that with many people working from home long-term, they will likely have more time to start planning their ‘dream procedures’.2 Although a demand in treatments is good news to practitioners, we highly believe the reasons behind the rise need to be considered, especially when consulting with new patients.
Mood and self esteem
Interestingly, there is psychology behind the trend, as using video conferencing is essentially the same as mirror gazing, which has been shown to have negative psychological impacts.3 When some people look at their reflection it can lead to a lot of self-criticism, leading them to compare themselves to other people. This is especially so if they are someone who has low selfesteem and focused on appearance or
grooming. Having to sit in front of a mirror, all day, would potentially lead to that person becoming more anxious and depressed about their appearance.4
Studies have demonstrated that prolonged periods of mirror gazing increases distress, causing more dissatisfaction with one’s appearance, while also increasing sadness.5 This is because the patient is spending more time checking, comparing, critiquing and criticising themselves. In one study in particular, participants mirror gazed for just two minutes and afterwards rated themselves as being more dissatisfied with their appearence.6
Mood can really influence how people think they look, especially if they already have low self-esteem. In one study, a standard moodinduction procedure was used to induce positive, negative, or neutral moods in low self-esteem and high self-esteem groups. They were asked to evaluate their specific qualities and characteristics, such as ‘How smart are you?’ and ‘How kind are you?’. Both self-esteem groups evaluated themselves favorably in a positive mood, but the low selfesteem group lowered their self-evaluations when in a negative mood.7
It is also important to find out where patients are sourcing their self-esteem from. How one looks is important, of course, but there are lots of other important things that should contribute to good self-esteem such as relationships and how well people are doing in their professional life, as well as in their social life and hobbies. Appearance is important and there is nothing wrong in taking pride in it and having aesthetic treatments, but it mustn’t be the only thing that boosts patients’ self-esteem. If video calling has made patients aware of new skin concerns, then conducting a thorough consultation, where self-esteem and video conferencing are discussed, could be hugely beneficial.
In consultations
If patients come to the clinic for treatment saying that video calls make them feel insecure about their appearance, and that’s why they want the procedure, then a thorough consultation needs to take place,
to see if aesthetic treatment is warranted or if, in fact, the patient would be better seeking treatment with a trained counsellor. Screening for body dysmorphic disorder, we believe, should always be part of the initital consultation process as standard.
Patients need to understand that cameras, angles, lighting, screens, different resolutions and colouring can accentuate certain facial features. This is not the way they appear in real life and video calling is only one way to interact with people. An injectable therapy or two will never solve complex psychological issues.
Overall, we have a responsibility to make our patients feel good about themselves and help them to appreciate their individuality, while encouraging them to develop a stronger sense of self-compassion. When consulting with patients, we should educate them that perfection does not exist; uniqueness is far more beautiful. We have the responsibility to steer them away from unnecessary procedures they may want but don’t need, refusing to treat when necessary. Patients should also be given enough time to process all information related to the treatment and encouraged to ask questions.
Patients need to be heard, feel appreciated and feel good about the way they look. They should only begin their facial aesthetics journey if they’re emotionally stable and realise how far this journey can take them.
Dr Yiannis Valilas is the director of the Anti Wrinkle Clinic in central London. He is a qualified general dentist with 13 years of experience in non-surgical facial aesthetics. Dr Valilas’s qualifications include an Msc in Restorative and Aesthetic Dentistry and a Diploma in Advanced Aesthetic Dentistry.

Qual: DDS, MSc
Jacqui Finnigan is a HCPC Registered Psychologist who holds Associate Fellowship and Chartership with the British Psychological Society. She has clinical experience providing psychological treatments for anxiety, body dysmorphic disorder and low self-esteem.
Qual: MSc, CPsychol, AFBPsS VIEW THE REFERENCES BY GOING ONLINE AT

Dr Yiannis Valilas and psychologist Jacqui Finnigan explain how the ‘Zoom phenomenon’ could be contributing to a rise in patients
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 7/Issue 12 - November 2020
AESTHETICSJOURNAL.COM
When you reveal beauty, we’re by your side.

Croma offers a wide range of state-of-the-art products in minimally invasive aesthetic medicine. This allows you to combine techniques for personally tailored treatment and ideal results. Learn more about Croma’s products and services at croma.at
HA Filler | Threads | PRP | ACA & SVF | Skincare
croma_inserat_210x297_NL_ada_1811_gch.indd 1 11.12.18 13:45
Scalp Health Matters

HydraFacial introduces a whole new market with...

Results of our recent study show just how effective HydraFacial Keravive can be for improving scalp health and helping consumers enjoy fuller, healthier-looking hair. Participants# undertook 3 consecutive monthly treatments combined with the topical take home spray in between and for 90 days afterward. Unretouched photographs of subjects at baseline and month 4 following 3 consecutive monthly in-clinic HydraFacial Keravive treatments plus 90-day continuous use of HydraFacial Keravive Take Home Spray.
After just 1 treatment, patients reported improvement in scalp itchiness, scalp dryness, scalp flakiness and hair fullness. After the full course of the treatments, patients reported:




Poor Scalp Health is a major contributor to damaged and thinning hair* which affects more than 30% of the population**. Thankfully, our exciting new treatment for optimising scalp and follicle health is here! HydraFacial™ Keravive™ is the first scalp treatment of its kind that uses a proprietary serum to target every aspect of scalp and follicle health to cleanse, nourish and hydrate the scalp for fuller and healthier-looking hair. contact us today: w: hydrafacial.co.uk | e: infouk@hydrafacial.com *Trüeb, R, Scalp Condition Impacts Hair Growth and Retention via Oxidative Stress, International Journal of Trichology, 2018. **American Hair Loss Association,2017. #Participants were 66% Caucasian, 18% African American, 11% Asian and 5% Other. Average age was 45 and the study was 55% females, 45% male.

improvement
72%
BEFORE AFTER BEFORE AFTER #GUNKIE improvement in hair fullness 75%
in overall hair appearance
improvement in overall confidence 64%