Dr Tara Francis introduces the skin barrier in aesthetic medical practice
Hyaluronidase Dosage

Dr Jordan Faulkner discusses the correct hyaluronidase dosage for vascular occlusions
Practising Self-Reflection
Dr Brian Franks offers his tips for reflective practice for medical aesthetic practitioners
VOLUME 9/ISSUE 12 - NOVEMBER 2022
Understanding the Skin Barrier
outlines managing thread complications CPD: Thread Lift Complications M-MA-UKI-2448 Date of Preparation October 2022 WE BRING THE EXPERTS TO YOU merz-aesthetics.co.uk/events EDUCATION ON DEMAND Face-to-face events | Live webinars | On demand education ACE REGISTRATION OPEN!
Dr Uzma Qureshi
One Treatment. Endless Options.
HydraFacial is for everyone. It’s suitable for all skin types and addresses all skincare needs. The HydraFacial delivers immediate, noticeable results, with no downtime, that keep your customers returning regularly.
HydraFacial is your connection to millions of believers that know that beauty is more than a physical attribute – it’s a feeling. Our customers’ want to give their clients the best experience possible.


The HydraFacial Company helps them deliver it.
Consumers want to be pro-actively offered personalised solutions for skin health and provide them with education on their ideal, easy-to-follow skin health regimen1.
And your clients needs are as individual as they are, which is why HydraFacial has partnered with the best brands in aesthetics to bring you advanced booster options that meet the emerging consumer trends that are influencing our industry more than ever before.
HydraFacial is scored as a ‘99% Worth It’ rating by www.realself.com and on average, somewhere in the world, a HydraFacial treatment is now carried out every 10 seconds!
1 EddieWouldGrow Facial Research 2018, n=2000; 2 Mintel Trends 2017

Simplification Multi-benefit solutions that save time1 Personalisation Treatments tailored to specific skin concerns2 Recommendation Skin health technology and regimen education1 give your customers what they want!
Boosters to Target Skin Concerns
Tips Tailored FOR Skin Type


Only HydraFacial uses a unique, patented Vortex-Fusion delivery system to exfoliate, extract and hydrate skin. The spiral design of HydroPeel® Tips, used in conjunction with the HydraFacial proprietary vacuum technology and serums, creates a vortex effect to easily dislodge and remove impurities while simultaneously delivering hydrating skin solutions.
• Convenient, single use, saves time; eliminates the need for sterilisation equipment • Range of exfoliation levels allows for custom treatment results • Spiral design delivers painless extractions
INTRODUCING KERAVIVE SCALP HEALTH


Expand into a new category with HydraFacial Keravive scalp heath treatment that leads to fuller looking hair. HydraFacial Keravive is a first of its kind 3-step treatment that includes an in-clinic component, as well as a 30-day take-home spray.

we deliver Personalisation...
How
HydraFacial delivers personalised skin health through boosters that are designed to: • Smooth and Refine • Restore and Firm • Brighten • Hydrate • Calm • Revitalise Lips & Eyes
W: hydrafacial.co.uk E: infoUK@hydrafacial.com T: 01788 572 007 To see the HydraFacial in action follow us @hydrafacialuk















































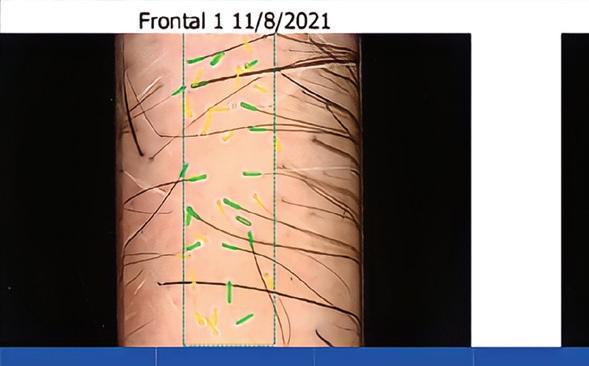
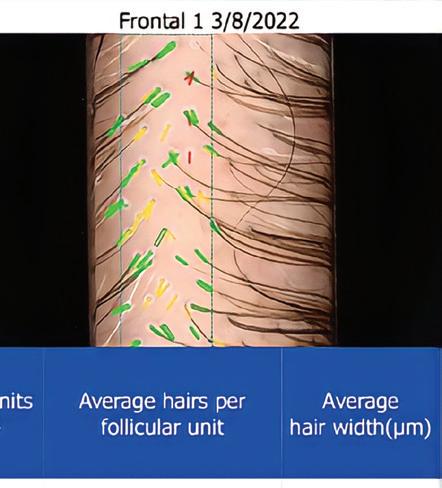

BEFORE CELLUMA 16 WEEKS Images courtesy of S-Thetics Clinic in Beaconsfi eld, Buckinghamshire, UK 2022 Aesthetics Awards Winner for Best Clinic South England No products, supplements, or other modalities were used. Hair Restoration FDA-CLEARED MEDICAL CE MARK 01462 481500 www.celluma.co.uk infoUK@celluma.com COUNTER Male and Female Pattern Balding PREVENT Further Hair Loss REJUVENATE Aging Skin IMPROVE Circulation REVERSE Hair Loss REQUEST MORE INFO
The latest product and industry news
News Special: Prioritising Diversity in Aesthetics

Aesthetics explores a new report on diversity and inclusivity in the aesthetics industry 20 CCR 2022: The UK’s Biggest Aesthetics Event
Marking the UK’s most highly-anticipated aesthetic conference of the year, Aesthetics reflects on the best CCR yet!
CLINICAL
PRACTICE
25 Special Feature: Utilising the Full-face Approach
Practitioners discuss methods for treating the full-face with dermal fillers
Dr Kiran Kandola shares his approach to treating the perioral area with BELOTERO Soft
Dr Uzma Qureshi outlines the potential complications of thread lifting

Mr Dean Rhobaye presents a case study showing a full-face transformation on a female patient
An Unmissable Two Days of Networking and Content
ACE and The Aesthetics Awards are back with a BANG in 2023!
Treating Temple Hollowness
Dr Harry Singh details his approach to rejuvenating the temples 48 Understanding the Skin Barrier
Dr Tara Francis provides an introduction to the skin barrier and its relevance to aesthetics
News Special: Prioritising Diversity in Aesthetics Page 18
The Power of Integrating Skincare In-Clinic
SkinCeuticals explores integrating skincare with aesthetic treatments 53 Case Study: Correcting Lip Filler Migration
Dr Sana Sadiq shares how she corrected a poor dermal filler result in the perioral area 59 Exploring Hyaluronidase Dosage
Mr Jordan Faulkner discusses hyaluronidase dosage for vascular occlusions
Case Study: Treating the Lower Face
Dr Chris Rennie rejuvenates the lower and mid-face in a female patient
Clinical Contributors
Dr Uzma Qureshi is an NHS GP partner who runs a CQC-registered medical aesthetics clinic. She taught anatomy at Cambridge University, has a background in surgical training, including a few years in plastic surgery and is a member of the Royal College of Surgeons.



Mr Dean Rhobaye is a specialist in minimallyinvasive and non-surgical facial aesthetic procedures. He is now the clinical director of Sloane Clinic on Harley Street and is a key opinion leader in advanced aesthetics and evidence-based professional skincare.
Dr Harry Singh is a mentor, business coach, keynote speaker, key opinion leader and founder of training academy the Botulinum Toxin Club. Dr Singh has worked in the aesthetics industry for more than 20 years, helping to build aesthetic clinics in combination with dentistry.

Dr Tara Francis is co-creator and director of The London Academy of Aesthetic Medicine, aesthetic director at Twoth, an Obagi Medical ambassador and Teoxane UK regional associate. Dr Francis has a special interest in skin and a holistic aesthetic approach.
Dr Brian Franks provides his tips for self-reflection in medical practice
Miss Sherina Balaratnam outlines a typical working day at her clinic
The Last Word: Pros and Cons of Instagram
Rick O’Neill argues why Instagram may provide challenges for your clinic
Special Feature: Utilising the Full-face Approach Page 25 NEXT MONTH
IN FOCUS: THE FUTURE OF AESTHETICS • Toxin Evolution • Biostimulating Fillers
Dr Sana Sadiq is an aesthetic practitioner and cosmetic dentist. She acquired her Master’s in chemical research followed by her Bachelor of Dental Surgery from King’s College London. She is now the co-founder and medical lead for By Design Aesthetic Academy.
Mr Jordan Faulkner is the founder of Allo Aesthetics and runs clinics in South West London and South Yorkshire. He is an aesthetics instructor at Interface Aesthetics and maintains a role as a surgical SHO at Chelsea and Westminster Hospital.


Contents • November 2022
08
News
18
30 Rejuvenating the Perioral Area with BELOTERO Soft
33 CPD: Understanding Thread Lift Complications
37 Case Study: Achieving Facial Harmonisation
40
43
51
64
66
71
65 Abstracts A round-up and summary of useful clinical papers IN PRACTICE
Selling in a Financial Downturn Vanessa Bird highlights selling skills and strategies to help drive sales
Utilising Social Media Effectively
Cait McLaughlin shares advice for maximising online video content 74 Practising Clinical Reflection
77 In The Life Of Miss Sherina Balaratnam
78
go go go


Letybo® brings practitioners a new option to the current aesthetic market and provides aesthetic professionals and their patients with a notable efficacy and confirmed tolerability.1,2,* *Letybo® is indicated for the temporary improvement in the appearance of moderate to severe vertical lines between the eyebrows in adults <75 years old seen at maximum frown (glabellar lines), when the severity of the facial lines has an important psychological impact. **Response rate was defined as a ≥ 1-point reduction in FWS at maximum frown based on the investigators assessment. References: 1. Mueller DS, Prinz V, Adelglass J, Cox SE, Gold M, Kaufman-Janette J et al. Efficacy and Safety of Letibotulinum Toxin A in the Treatment of Glabellar Lines: A Randomized, Double-blind, Multicenter, Placebo-controlled Phase 3 Study. Aesthet Surg J. 2022; 42(6): 677- 88. ; 2. Letybo® smPC, https://www.medicines.org.uk/emc/product/13707 2022













Letybo 50 units powder for solution for injection; Abbreviated Prescribing Information: Please refer to the Summary of Product Characteristics (SmPC) before prescribing. Presentation: One vial contains 50 units botulinum toxin type A produced by Clostridium botulinum. After reconstitution each 0.1 mL of the solution contains 4 units. Indication: For the temporary improvement in the appearance of moderate to severe vertical lines between the eyebrows in adults <75 years old seen at maximum frown (glabellar lines), when the severity of the facial lines has an important psychological impact. Dosage and administration: Should only be administered by physicians with expertise in this treatment. Posology: The recommended dose is a total of 20 units divided into five injections of 4 units (0.1 mL) each: 2 injections in each corrugator supercilii muscle and 1 injection in the procerus muscle. Botulinum toxin units are not interchangeable from one product to another. Doses recommended are different from other botulinum toxin preparations. Treatment interval should not be more frequent than every three months. In the absence of any undesirable effects secondary to the previous treatment session, a further treatment session with at least a three-month interval between the treatment sessions is possible. The efficacy and safety of repeat injections beyond 12 months has not been evaluated. Special populations: No specific dose adjustment is required for use in the elderly older than 65 years of age. Letybo is contraindicated in patients 75 years or older. There is no relevant use in the paediatric population. Method of administration: Intramuscular use. Care should be taken to ensure that Letybo is not injected into a blood vessel. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Generalised disorders of muscle activity (e.g. myasthenia gravis, Lambert-Eaton syndrome, amyotrophic lateral sclerosis). Presence of acute infection or inflammation at the proposed injection sites. Patients with bleeding disorders. Warnings and Precautions: Injection into vulnerable anatomic structures must be avoided. Avoid use when the muscle shows excessive weakness or atrophy. Risk of eyelid ptosis following treatment. Procedurerelated events: Needle-related pain and/or anxiety have resulted in vasovagal responses, including transient symptomatic hypotension and syncope after treatment with other botulinum toxins. Pre-existing neuromuscular disorders: Patients with unrecognised neuromuscular disorders may be at increased risk of clinically significant systemic effects including severe dysphagia and respiratory compromise from typical doses of botulinum toxin type A. Hypersensitivity reactions: An anaphylactic reaction may occur after injection of botulinum toxin. Epinephrine (adrenaline) or any other anti-anaphylactic measures should therefore be available. Local or distant spread of toxin effects: Adverse reactions possibly related to the spread of toxin distant from the site of administration have been reported. Patients may experience exaggerated muscle weakness. Swallowing and breathing difficulties are serious and can result in death. Use not recommended in patients with a history of dysphagia and aspiration. Patients should be advised to seek immediate medical care if swallowing, speech or respiratory disorders arise. Pregnancy & Lactation: Not recommended during pregnancy or lactation and in women of childbearing potential not using contraception. Undesirable effects: Most common effects are headache and injection site reaction. Very rarely aspirational pneumonia. For full list of side effects, consult SmPC. Legal Category: POM; Pack size: Packs containing 1 5ml vial. Multipack containing 2 (2 packs of 1) vials; Price list: UK - 1x5ml: 65GBP, 2x5ml: 120GBP; MA Number: PL 29863/0002; PA Number: PA0846/001/001; MA Holder: Croma-Pharma GmbH, Industriezeile 6, 2100 Leobendorf, Austria; Date of preparation: 11/04/2022; Unique ID no CRP001/001; Adverse events should be reported.

ADLET0822UKg (QR: VID2LET0822UK) Date
preparation: August
of
2022
Reporting
94% response rate 4 weeks post injection 1,** Demonstrated high patient satisfaction2 Proven consistent effi cacy and tolerability with repeated injections for up to 12 months 1,2 Scan for Reconstitution Instructions
forms and information can be found at: UK - http://yellowcard.mhra.gov.uk/ or search for MHRA Yellow Card in the Google Play or Apple App Store. IE - HPRA Pharmacovigilance Website: www.hpra.ie. Adverse events should also be reported to Croma Pharma GmbH on 0118 206 6513
As you know, the areas of the face are most often the first places aesthetic patients want to target. As such, we have some great content this month focusing on treating the face. Don’t miss the Special Feature with top tips from three practitioners on the full-face approach with dermal fillers (p.25), thread lifting complications (you can get 1 CPD point by reading this on p.33!), as well as articles on temple treatment approaches (p.43), and rejuvenating the perioral area (p.30). We also have three fantastic case studies; one on a full-face treatment (p.37), a lower face treatment (p.64) and one on correcting a lip adverse event (p.53). Our News Special this month is also worth a read. It covers the important topic of diversity in aesthetics, following a report released by the DREAM initiative. With stats like ‘only 17% of women think racial beauty is accepted by society’, it’s important we as an industry strive to make improvements in this area. Have a read on p.18 As an event organiser and media provider, Aesthetics is trying hard
Shannon Kilgariff Editor & Content Manager @shannonkilgariff

to help drive change in the sector. Recently we featured a fantastic panel discussion on skin of colour at CCR, which was extremely well attended and popular with delegates – there will be more to come. If you attended CCR on October 13-14, you will know that it was a fantastic event uniting the aesthetic specialty! Have a read of the highlights on p.20 and note that our next event is ACE 2023 on March 10-11 and The Aesthetics Awards on March 11. Find out how to register and buy tickets on p.40 Speaking of events, the November calendar is jam packed! I think it’s great to see so many opportunities for education and learning, which is so important in aesthetic medicine. I’m really looking forward to attending the MINT Academic Symposium on the 12th and IAAFA conference and charity ball on the 19th. The Aesthetics team will also be at CMAC on November 19-20, and on the 27th they will be at both FACExpo and the annual Cutera University Clinical Forum. Be sure to say hello to myself and the team and let us know if you’d like to write for the journal or become a Member of the Aesthetics community. We look forward to seeing you soon!
Clinical Advisory Board
Leading figures from the medical aesthetic community have joined the Aesthetics Advisory Board to help steer the direction of our educational, clinical and business content
Sharon Bennett is chair of the British Association of Cosmetic Nurses (BACN), previous UK lead of the BSI committee for aesthetic non-surgical standards, and member of the Clinical Advisory Group for the JCCP. She is a trainer and registered university mentor in cosmetic medical practice, and is finishing her MSc at Northumbria University. Bennett has won the Aesthetics Award for Nurse Practitioner of the Year and the Award for Outstanding Achievement.
Mr Naveen Cavale has been a consultant plastic, reconstructive and aesthetic surgeon since 2009. He has his own private clinic and hospital, REAL, in London’s Battersea. Mr Cavale is the national secretary for the ISAPS, president of the Royal Society of Medicine, and vice-chair for the British Foundation for International Reconstructive Surgery.

Jackie Partridge is an aesthetic nurse prescriber with a BSc in Professional Practice (Dermatology). She has recently completed her Master’s in Aesthetic Medicine, for which she is also a course mentor. Partridge is a founding board member of the British Association of Cosmetic Nurses and has represented the association for Health Improvement Scotland.
Mr Adrian Richards is a plastic and cosmetic surgeon with 18 years’ experience. He is the clinical director of the aesthetic training provider Cosmetic Courses and surgeon at The Private Clinic. He is also a member of the British Association of Plastic and Reconstructive and Aesthetic Surgeons and the British Association of Aesthetic Plastic Surgeons.

PORTFOLIO
Alison Willis • Director
T: 07747 761198 | alison.willis@easyfairs.com
EDITORIAL
Shannon Kilgariff
T: 0203 196 4351 | M: 07557 359 257
shannon@aestheticsjournal.com
Holly Carver • Senior Journalist | T: 0203 196 4427 holly.carver@easyfairs.com

Ellie Holden • Journalist | T: 0203 196 4265 ellie.holden@easyfairs.com
Kate Byng-Hall • Journalist | T: 0203 196 4265 kate.byng-hall@easyfairs.com
DESIGN
Peter Johnson • Senior Designer
T: 0203 196 4359 | peter@aestheticsjournal.com
Miss Elizabeth Hawkes is a consultant ophthalmologist and oculoplastic surgeon. She is the lead oculoplastic surgeon at the Cadogan Clinic, specialising in blepharoplasty and advanced facial aesthetics. Miss Hawkes is a full member of the BOPSS and the ESOPRS and is an examiner and fellow of the Royal College of Ophthalmologists.
Dr Tapan Patel is the founder and medical director of PHI Clinic. He has more than 16 years’ clinical experience and has been performing aesthetic treatments for more than 14 years. Recently, he was listed in Tatler’s Top 30 Anti-Ageing Experts. Dr Patel is passionate about standards in aesthetic medicine.

Dr Souphiyeh Samizadeh is a dental surgeon with a Master’s degree in Aesthetic Medicine and a PGCert in Clinical Education. She is the founder of the Great British Academy of Medicine and Revivify London Clinic. Dr Samizadeh is a Visiting Teaching Fellow at University College London and King’s College London.


ADVERTISING & SPONSORSHIP
Courtney LeBorgne • Event Director
T: 0203 196 4300 | M: 07818 118 741
courtney.leborgne@easyfairs.com
Judith Nowell • Business Development Manager T: 0203 196 4352 | M: 07494 179535

judith@aestheticsjournal.com
Chloe Carville • Sales Executive T: 0203 196 4367 | chloe.carville@aestheticsjournal.com
Emma Coyne • Sales Executive T: 020 3196 4372 | emma.coyne@easyfairs.com
MARKETING
Aimee Moore • Marketing Manager
T: 020 3196 4370 | aimee.moore@easyfairs.com
Abigail Larkin • Marketing Executive T: 020 3196 4306 | abigail.larkin@easyfairs.com

WE WANT TO HEAR FROM YOU!
Do you have any techniques to share, case studies to showcase or knowledge to impart?
Email: editorial@aestheticsjournal.com
Dr Stefanie Williams is a dermatologist with a special interest in adult acne, rosacea and aesthetic medicine. She is the founder and medical director of multi-award winning EUDELO Dermatology & Skin Wellbeing in London, and creator of Delo Rx skincare. She is the author of three books and has published more than 100 scientific articles, book chapters and abstracts.
Carville, contact@aestheticsjournal.com
© Copyright 2022 Aesthetics. All rights reserved. Aesthetics
published by Aesthetics Media Ltd, which is registered as a limited company in England; No 9887184
Editor’s letter
Aesthetics Journal @aestheticsgroup Aesthetics @aestheticsjournaluk
Sharon Bennett, Clinical Lead
ARTICLE PDFs AND REPRO Material may not be reproduced in any form without the publisher’s written permission. For PDF file support please contact Chloe
is
DISCLAIMER: The editor and the publishers do not necessarily agree with the views expressed by contributors and advertisers nor do they accept responsibility for any errors in the transmission of the subject matter in this publication. In all matters the editor’s decision is final. PUBLISHED BY
Aesthetics Media
MANAGEMENT
• Editor & Content Manager
Botulinum toxin
Talk #Aesthetics
Follow us on Instagram
@aestheticsjournaluk
#CCR
Shannon Kilgariff
@shannonkilgariff
Wow CCR London - what an event! CCR is such a special event bringing the whole aesthetic community together and I had an absolute blast catching up with friends and colleagues!

#Appointment
British Association of Aesthetic Plastic Surgeons @thebaaps
Congratulations Mr Marc Pacifico, the new President of the BAAPS!

#Networking
Dr Ahmed El Houssieny
@bankmedispa
It’s been a busy week of events, conferences and seminars, but it was great to catch up with some of the amazing team from the Aesthetics journal at CCR!


Evolus launches new neurotoxin in the UK
Medical aesthetic company Evolus has launched its first botulinum toxin A product in Great Britain. According to the company, Nuceiva (prabotulinumtoxin A) has been approved for temporary improvement in the appearance of moderate to severe vertical lines between the eyebrows.
The safety and efficacy of the product was evaluated through the company’s Transparency programme. A multicentre, randomised, double blind, placebo-controlled, single dose, phase III, non-inferiority study took place in adult patients comparing prabotulinumtoxin A and onabotulinumtoxin A for the treatment of moderate to severe glabellar lines. In the 150-day study, 540 patients were randomised to receive a single treatment (0.1ml injected into each of five glabellar sites) of 20U prabotulinumtoxin A, 20U onabotulinumtoxin A or placebo. Responder rates for the primary efficacy endpoint were 87.2% (prabotulinumtoxin A), 82.8% (onabotulinumtoxin A) and 4.2% (placebo). Patients’ level of satisfaction 30 days following injection showed that 91.5% (Nuceiva patients) were either satisfied or very satisfied, compared to 86.5% (onabotulinumtoxin A patients) and 6.3% (placebo patients). No serious adverse events were assessed but the most frequently reported were headache and nasopharyngitis. The study therefore suggested that a single treatment of 20U prabotulinumtoxin A was safe, effective and non-inferior to 20U onabotulinumtoxin A. David Moatazedi, president and CEO of Evolus, said, “We are excited to introduce Nuceiva to Great Britain, the largest market for aesthetic neurotoxins in the European region, and Europe is the second largest market for aesthetic neurotoxins globally. Our expansion there will form the foundation for a potential future of aesthetic products.”
Best practice
BAAPS releases new gluteal fat grafting guidance
#Conference
Dr Tapan Patel
@drtapanp
Welcome to TAMC from the scientific board! Powerful and inspiring opening, followed by a truly excellent plenary keynote session.

#Education
Dr Dev Patel
@drdevpatel1
Enjoyable evening sitting on the ‘Expert Panel’ at Erchonia’s Emerald event hosted at the beautiful Hurlingham Club.
The British Association of Aesthetic Plastic Surgeons (BAAPS) has released new guidance on how to safely perform gluteal fat grafting procedures after dissuading its members from performing Brazilian buttock lift (BBL) surgery in 2018.
After four years of clinical research, BAAPS has released its gluteal fat grafting (GFG) guidelines to promote responsible buttock-enhancing surgery, following concerns about the high mortality rate associated with BBLs.
The guidelines state that GFG is safe to perform under two key conditions: the injection is into the subcutaneous plane only, and intraoperative ultrasound is used during the placement of fat in the gluteal area.
GFG is currently the fastest-growing plastic surgery procedure worldwide, with an increase of around 20% every year.
BAAPS president Mr Marc Pacifico explained, “The new BAAPS guidelines are very robust and comprehensive, and the evidence has been critically analysed. The deaths recorded with BBLs have all had breeches of the fascia with fat injected into the muscle. So, it’s no to BBL but yes to superficial gluteal lipofilling where the fascia is not compromised.”
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Regulation Details for new industry licensing scheme unveiled
The Joint Council for Cosmetic Practitioners (JCCP) has released more details of the proposed licensing scheme for cosmetic procedures in England, which is laid out in the Health and Care Act 2022. Clause 180 of the Act states that the licensing scheme may be introduced ‘for the purposes of reducing the risk of harm to the health or safety of members of the public’. This includes the concept of ‘personal licences’ which would authorise an individual to carry out cosmetic procedures, and ‘premise licences’ which would authorise a premises to be used for carrying out cosmetic procedures.
The Clause defines cosmetic procedures as the injection of a substance, the application of a substance that penetrates into or through the epidermis, the insertion of needles into the skin, the placing of threads under the skin, and the application of light, electricity, cold or heat therapy.
More details of this scheme will be finalised following a period of engagement and public consultation, which is likely to begin in early 2023, with a further consultation to follow later in the year.
Chair of the JCCP Board of Trustees, Professor David Sines said, “The JCCP has been working alongside national organisations, such as the British Beauty Council and the Chartered Institute of Environmental Health, to support the design of a new scheme of licensing for non-surgical cosmetic practice. The JCCP remains committed to ensuring the implementation of a robust system of licensing to enable public protection and patient safety that are embedded across the aesthetic sector by 2025.”
The details of the Clause are available to view via the JCCP website.
Ceremony
Cherry Healey announced as Aesthetics Awards host
Television presenter Cherry Healey will return as the host of The Aesthetics Awards 2023.

Healey is a television personality who has presented programmes such as 10 Years Younger in 10 Days and Women’s Health: Breaking the Taboos. Healey will host the prestigious Awards ceremony at Grosvenor House, London on March 11, where guests will be treated to a delicious three-course meal, live entertainment and dancing, plus a professional photographer.
Healey said, “I’m absolutely thrilled to be hosting The Aesthetics Awards again this year! Not only is it such an honour to be part of celebrating the achievements of such dedicated experts, but it also happens to be the most fun night of the year! Can’t wait to see you there.”
Editor of Aesthetics, Shannon Kilgariff, added, “I am delighted to welcome back Cherry, who was a fantastic host last year. With her experience helping people feel the best version of themselves, she is well suited to present the Aesthetics Awards trophies.”
A new sponsor has also been announced for 2023 – HydraFacial is supporting the Best New Clinic, UK & Ireland Award. Early Bird tickets are available until December 31. Turn to p.40 to purchase your tickets.
Vital Statistics
Of 51,000 13 to 24-year-olds in the UK, only 34% said they didn’t want to change any of their facial features through non-surgical procedures (VICE UK, 2022)
Across 730 pages from 41 beauty brands’ websites, the term antiageing appeared almost 3,000 times (Lifestyle Packaging, 2022)
Only 35% of practitioners in the UK would still train as healthcare professionals if joining the industry now (YouGov & World Innovation Summit for Health, 2022)
In a survey of 320 US surgeons, 76% reported seeing increased demand for procedures compared to pre-pandemic levels
(The American Society of Plastic Surgeons, 2022)
Among the UK population, 60% of people currently have a skin condition or have had one in the past (British Skin Foundation, 2022)
In a survey of 1,000 UK adults, 24% said dental implants or veneers would be their dental treatment of choice to improve their smile (Sunstar, 2022)
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Events diary
10th-12th November
BACD Conference bacd.com/annual-conference
19th November
IAAFA Conference & Ball www.iaafa.net/iaafa-events
19th-20th November
CMAC Conference www.cmac.world/conference
27th November
FACExpo www.facexpo.com
10th-11th March ACE www.aestheticsconference.com
11th March
The Aesthetics Awards www.aestheticsawards.com
Injectables
Allergan celebrates 100 million syringes milestone
Aesthetic pharmaceutical company Allergan has announced a company milestone as it has manufactured 100 million syringes of its Juvéderm dermal filler.
The brand began producing Juvéderm in 2004, and reached the 100 million milestone in April 2022 as the filler is now distributed worldwide.
Djamshid Ghavami, general manager at Allergan Aesthetics UK&I, said, “We are hugely proud of this achievement of reaching such a significant milestone. For us it represents so many patient experiences, and empowering confidence. We couldn’t have reached this milestone without the collaboration between the Allergan Aesthetics team and the expert skill of our practitioners. We recognise that despite reaching a significant milestone, our journey continues and there is still so much more to come as we go beyond 100 million syringes!”
Women’s health
New survey reveals embarrassment over menopausal experience
A new British Skin Foundation (BSF) survey has found that nearly a quarter of those who have gone through the menopause felt ashamed to talk about it.
In the survey, 85% of 100 respondents experienced some skin changes during the menopause, with 24% feeling embarrassed to discuss them.
The most common symptom was excessive sweating, followed by skin laxity, excessive signs of ageing, alterations in pigment, rosacea or broken blood vessels and late onset acne. Only 15% reported no changes to their skin.
IN THE MEDIA What’s trending in the consumer press
Shannon Kilgariff features on Aesthetics Unlocked podcast
Aesthetics journal editor and content manager Shannon Kilgariff has starred as a guest on the new series of Hamilton Fraser’s Aesthetics Unlocked podcast. In the episode, Kilgariff shares her vision for the journal, CCR and ACE as live events return post-COVID, as well as discussing how she ensures Aesthetics stays relevant under her stewardship among discussions about regulation, diversity and mental health.
Skin A&E returns to Channel 5
Skin A&E has returned for its fourth series on Channel 5, with members of the public receiving advice on their skin conditions from dermatological practitioners after failing to secure treatment from the NHS. On the programme, consultant dermatologists including Dr Emma McMullen and Dr Natalia Spierings treat cysts, lipomas, skin tags, rashes and more.
Despite how common menopausal skin changes are, 22% of respondents felt uninformed before going through it.
Eleanor Lloyd, communications officer at BSF, said, “It is evident from our survey results that the menopause causes a whole host of skin symptoms, with varying degrees of severity, for a lot of people. Unfortunately, some stigma is still associated with the menopause which may cause a barrier for people to talk about it and ultimately seek help and guidance.”
Microneedling
SkinPen Precision approved for new indications

Aesthetic manufacturer Crown Aesthetics has announced three new approved indications for microneedling device SkinPen Precision.
The device has a certification confirming its use to help improve the appearance of surgical scars, stretch marks and enlarged pores on all areas of the body. The device has also been approved for medical purposes to treat facial acne scars in adults aged 22 years or older and for aesthetic purposes to help improve the cosmetic appearance of fine lines, wrinkles and pigmentation conditions (dyschromia), explains the company.
Vice president of sales international for Crown Aesthetics, Andy Moulton, said, “This new certification not only solidifies our status as the leading, most advanced skin remodelling treatment system, but it also enables us to further our global consumer reach. We are committed to supporting our customers’ skin health journey by helping them visibly transform and improve the appearance of their skin without surgical intervention.”
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Aesthetics community invited to register for ACE 2023
Registration is now open for ACE 2023 at the Business Design Centre, London on March 10 and 11.
ACE 2023 is set to welcome more than 2,500+ attendees, 95 exhibitors and 60 speakers for two days of discovery, learning, business advice and networking for the non-surgical aesthetic community. Aesthetic manufacturer Teoxane is Headline Sponsor of this year’s conference and will be running two days of excellent educational content in the Main Auditorium. Event director Courtney LeBorgne said, “ACE 2023 is set to be our biggest yet! Being reunited with the aesthetics specialty and seeing the amazing exhibitors, sponsors, speakers, and delegates unite is incredible. Running ACE alongside The Aesthetics Awards went so well last year that we’re excited to do it again even bigger and better this year, with 950+ guests at the dazzling Grosvenor House.”

Conference
The BACD announces upcoming annual conference
The British Association of Cosmetic Dentistry (BACD) is to hold its 18th annual conference on November 10-12 at the ICC Wales, Newport.
The three-day agenda will feature headline speaker and aesthetic dentist Dr Frank Spear, alongside multiple courses, workshops and talks.
The BACD has also been announced as a new partner of Aesthetics and CCR, increasing support for dentists and ensuring they have access to the right educational information when entering the aesthetics specialty. Dr Sam Jethwa, director of communications at the BACD, said, “We are very pleased to have collaborated with CCR on their event, and on our BACD annual conference. The event is bringing the world-class Dr Spear to the UK after many years and provides a chance to see our loyal and talented members from all over the world.”
Parliament
MPs launch inquiry on complementary therapies
MPs on the All-Party Parliamentary Group on Beauty and Wellbeing (APPG BAW) have launched an inquiry into the utilisation of complementary therapies in promoting patients’ physical health, mental health and wellbeing.
The APPG BAW will look into the possibility that complementary therapies including massages, acupuncture, chiropractic, osteopathy, homeopathy and others, could optimise overall health, support those with existing health conditions and prevent deterioration in health, as well as bring potential business benefits to the sector.
Carolyn Harris and Judith Cummins, MPs and co-chairs of the APPG BAW, said, “Great steps have been made to secure the beauty industry recognition in Parliament and Government, however the value of complementary therapies in supporting everyone’s health is not being adequately recognised.”
The deadline for Call for Evidence submissions is midnight on November 11.
BACN UPDATES

A round-up of the latest news and events from the British Association of Cosmetic Nurses


BACN REGIONAL MEETINGS
After a busy year, the BACN is back with our final round of Regional Meetings for 2022! Events will be running throughout November and December, with educational content and networking opportunities for both BACN members and guests. These meetings provide a platform for attendees to hear industry updates, attend educational presentations, engage in peer-to-peer reviews and take part in our all-important networking opportunities before, between and after sessions.
Speakers and topics will range from leading brands such as Galderma and Church Pharmacy, to local leaders discussing their personal aesthetics journeys and sharing business and complication guidance. This round, many of our Regional Meetings will run as half-day sessions taking place in the morning, followed by an optional lunch at a restaurant nearby for members to get together and network in a more informal setting. The day is a fantastic opportunity to network with nurses in your local area, learn something new, and feel just that little bit more connected. Spaces are available to reserve online on the BACN website now. Visit www.bacn.org.uk/ events or scan the QR code below!
CCR
As always, CCR was a fantastic couple of days for the BACN, and we want to thank everyone who popped by the stand – a big welcome to all our new members who signed up at the conference! We hope to see many of you at our upcoming events this winter. Also, a big thank you and well done to the CCR team for organising such a successful event!
AGM
The BACN recently held its Annual General Meeting on October 31. Members can view all the details and minutes in the Member’s Area of the BACN website.
This column is written and supported by the BACN
Education
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Enjoy a night of glitz and glamour at the most prestigious awards ceremony in aesthetics!
With entry to The Aesthetics Awards now officially closed, it’s time to look forward to the most glamorous event of the year – the Awards ceremony! This time it will be taking place on March 11 in a BRAND NEW location, the dazzling Grosvenor House, so it’s one you won’t want to miss.
Industry NHS nurses urged to go on strike over pay
The Royal College of Nursing (RCN) has urged all UK members to engage in strike action in November. The strike is expected to be predominantly regarding pay, and will not affect emergency care services.
The RCN has commissioned research showing average nurses’ pay had fallen by 6% between 2011 and 2021 once inflation had been taken into account, according to the union. The British Association of Cosmetic Nurses (BACN) has seen a growth in membership in recent years, with 1,200 additional nurses from just over 700 in 2018 – a 71% increase in four years.
Aesthetic nurse prescriber and chair of the Aesthetics Clinical Advisory Board Sharon Bennett said, “It saddens me to see so many nurses unhappy within their roles in the NHS. Although the mainstream news tends to focus mostly on pay, I know it’s not just about this but also about nurse workload and working conditions.”
Get your early bird tickets now!
Join your colleagues at the ‘Oscars of Aesthetics’!
The Aesthetics Awards is the perfect opportunity to celebrate the hard work and achievements of the industry over the past year, while also getting dolled up to the nines!
Like last year, the event will be taking place after the second day of ACE, so whether you’re a Finalist or not, the ceremony is still a great way to round off and celebrate two days of incredible education.
Early Bird tickets are only available until December 31. Tickets will sell out, so make sure you grab yours now and avoid disappointment!
Why should you attend the The Aesthetics Awards?

By purchasing an Awards ticket, you’ll receive:
• A celebratory glass of bubbles on arrival at the networking reception
• Professional photographs at The Aesthetics Awards pressboard
• A delicious three-course meal
• Live music and dancing into the night
• An opportunity to celebrate with your peers
Do you have to be invited?
The Aesthetics Awards isn’t an invite-only event, and is open to everyone in the medical aesthetic specialty. If you’re a colleague of someone up for an Award and want to come along to show them support, or just want to enjoy the celebrations and networking opportunities, you can purchase tickets! We can’t wait to see you all there!
Scan the QR code to book your early-bird tickets or if you have any questions, please call our team on 0203 096 1228.
Bennett went on to say that many nurses are choosing to work in areas such as medical aesthetics, dermatology or even private midwifery either part-time or full-time in the hope of a better work-life balance, improved working environments, and greater financial gains in comparison to the NHS. The BACN, of which Bennett is the chair, has seen a large increase in membership in the past year. “This has been partly due to NHS nurses venturing into the aesthetics industry,” Bennett said, “but we are also seeing people choosing to go into nursing purely to become medical aesthetic practitioners.”
She concluded, “For the aesthetics specialty, this highlights the importance of a distinct medical career path for individuals hoping to get into this field which will help them in their new career pathway.”
Education
New conference launches for aesthetic beginners

A one-day scientific meeting for entrylevel healthcare professionals (HCPs) starting out in aesthetics will take place next month. FACExpo, created by oral and maxillofacial surgery registrar Mr James Olding, will consist of an educational programme, workshops, breakout sessions, networking and research presentations. Speakers at the event include Mr Olding, alongside aesthetic practitioners Dr Zainab Al-Mukhtar, Dr Jordan Faulkner, Dr Jane Leonard and Dr Eithne Brenner and Dr Arthur Gasperazzo; oral and maxillofacial surgeons Miss Caroline Mills and Miss Sieuming Ng; independent nurse prescriber Julie Scott; and chair of the Joint Council for Cosmetic Practitioners, Professor David Sines. The event will take place on November 27 at the Royal Society of Medicine, London, with Allergan Spark as the headline sponsor.
Mr Olding said, “Our vision is to empower HCPs to make the best first steps into the industry, and this links up closely with our creation of pioneer schemes in mentorship. We have been able to put together a comprehensive educational programme spanning education, clinical practice, business and regulation that will leave delegates inspired and empowered.”
Celebrate the achievements in medical aesthetics
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
HEADQUARTERED IN CALIFORNIA
global corporate headquarters in Newport have been growing since 2012. We have more associates with some amazing skills – from R&D digital engineers and sales and marketing thing unites us - we love being disruptive!
SOME OF OUR NEWEST RECRUITS ARE IN THE UK
skinbetter science debuts brand new regimens

We are super excited to introduce our shiny new team. Headed up by industry pioneer, Dan Stewart, we have assembled a stellar cast of Evolusionaries.
Medical-grade skincare company skinbetter science has launched three new skincare regimens following its latest clinical research. The Where to Start Regimen combines the Alto Advanced Defense, Repair Serum and AlphaRet Overnight Cream for those starting out on their skincare journey. The company reported that of 22 patients aged between 40 and 63, 64% saw an improvement in skin dullness, and 54% in skin texture. 100% reported that their skin’s overall appearance had improved.
Introducing the Evolus UK team (drum roll, please)

Suse Alexander, Evolus UK general manager
Who are you and what’s your superpower?
Suse Alexander, our UK General Manager, and all-round superstar
The Clarity Regimen is designed to combat ageing and blemishes using the AlphaRet Clearing Serum, Hydration Boosting Cream and AlphaRet Exfoliating Peel Pads. Of 11 patients aged 30-52, skinbetter science says that 80% reported their skin to be healthier looking with less visible pores, and 100% agreed that their skin was hydrated and not flaky.
Finally, the Even Glow Regimen is geared towards addressing sub-related discolouration through a combination of the Even Tone Correcting Serum, AlphaRet Overnight Cream and AlphaRet Exfoliating Peel Pads. According to the company, 96% of 10 patients aged 30-65 reported their discolouration had lessened and their skin tone had become more even.
Lorna Bowes, CEO of skinbetter science’s UK distributor AestheticSource, said, “These new regimens are a real step forward in treatment protocols, and with the supporting clinical data helping our understanding of the results that are possible, we now can see clearly how to put the products together for best results – and share the information with patients to increase compliance and therefore even further improve results.”
BAAPS elects new president
EXPANDING AROUND THE WORLD
company, we are flourishing. In 2021, over 1,400 new joined Evolus, bringing the total number of we support to more than 7,500 in the US alone. are excited to expand our operations outside of America, starting with Great Britain, Germany and us, this is another significant step in our strategy a leading, global, multi-product performance company.

I’m really pleased to have recently been appointed as the general manager for Evolus in the UK. I’m returning to aesthetics and beauty after a few years of working within another health and wellness sector. It’s good to be back! Being part of a company that’s starting up in the UK, I’m really enjoying a new set of challenges and opportunities. It’s great fun reinvigorating connections and meeting new customers, mixing fresh ideas with deep expertise. I’m all about listening and learning so that we are orientating our operations around our customer experience.
What makes Evolus UK different?
EVOLVE WITH US.
In the last three years, we’ve had a lot of conversations and learned a lot from our North American customers about what works, and what doesn’t work. We’re taking these lessons, and evolving what we do in Europe and beyond to meet your needs.
Consultant plastic surgeon Mr Marc Pacifico has been elected to take over from Miss Mary O’Brien as the new president of the British Association of Aesthetic Plastic Surgeons (BAAPS).
Consultant plastic surgeon Ms Nora Nugent will become vice president.

Yet there is one thing that comes across clearly. Our North American customers are delighted to have choices.
Mr Pacifico has been the vice president of BAAPS for the past two years, during which he set up and became actively involved in the BAAPS mentorship programme, training junior plastic surgeons. Mr Pacifico said, “I feel honoured and privileged to be leading BAAPS at a very exciting time for UK plastic surgery. BAAPS is leading the way in training the aesthetic plastic surgeons of the future through our mentorship scheme. We are continuing to campaign for patient safety with our petition to prevent non-surgeons from performing aesthetic surgery; we are supporting our members with the latest evidence-based guidelines for different plastic surgery procedures and we are building links with international sister organisations around the world.”
We take fun seriously! One of the reasons I said yes to this new role is the culture at Evolus UK. The mantra is Fun, Transparency, Grit and Impact. I’ve worked at several companies with long descriptions of their cultural ideal. None of them had FUN featured at all! It’s empowering as a manager of a hard-working team to inject some spirit and zest into how we work together. I’m convinced this will influence how we show up for our customers. Performance beauty really does represent a shift in the industry, and it’s being driven by people with a millennial mindset. They are informed, they want choices, they see beauty as part of their everyday routines. These consumers are walking through clinic doors now and fueling the boom. These consumers certainly aren’t standing still, and neither should we. While we are starting up Evolus in the UK, we’ve been growing and thriving from our California home base since 2012. More than 8,000 customers across the US are now supported by Evolus, with more growth anticipated.
What are you most proud of?
Now, we want to hear from the aesthetics community in the UK about the trends you are seeing and how your business is evolving.
Visit www.hello-evolus.com to find out more.
Ah! Having an impact by contributing to patients feeling better about themselves. Sharing the buzz after establishing a growth business. Watching my team fly and doing a great job every day for our customers. Oh, and perhaps being a little bit disruptive along the way. Visit hello-evolus.com to learn more and find out how you can evolve the future of beauty with us.
We look forward to partnering with you as we launch a different type of company. and join us at our CCR symposium Thursday October 13 at 1230 – 1330, Dr Steve Fagien and guests.
Ms Nugent has been a member of council of BAAPS since 2018 and chair of BAAPS support from 2020-2022.
Ms Nugent said, “My vision for BAAPS is to maintain its core aims while adapting to future needs and circumstances to be a modern and innovative aesthetic plastic surgery organisation that is true to its values and responsive to its membership.”
Don’t stand still , evolve with
60
DOP October
This advertorial was written and supplied by Evolus UK UK-UNB-2200059
2022
the future of beauty with us.
Jean Johnston, Scotland and the North, Wearer of Killer Heels
Hilary Gates, Southern and West England, Equestrian Queen
Nichola Smith, Central and Eastern-ish England, outdoor enthusiast
Holly McDonald, London and the South East, also known as Hollywood
Amy Wood, Manchester and the North West, our Peloton junkie
Samuel Oladiran, Medical Science Liaison, and community champion
us
Skincare
Appointment
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Merz Aesthetics reveals new brand identity

Conference IAAFA conference returns in November
Pharmaceutical company Merz Aesthetics has unveiled a new corporate visual identity. The company explains that the new branding aims to put the definition of beauty back into the hands of the individual through a vibrant colour palette along with strong photography. The new identity includes shades of orange, yellow, green, red and blue contrasted by black and white typography. The typography is enhanced by photography representing diverse ages and cultural backgrounds which highlight personal authenticity, explains Merz Aesthetics. Bob Rhatigan, CEO of Merz Aesthetics, said, “It was important to create a cohesive and clear visual identity for Merz Aesthetics that reflects who we are and our purpose to fuel confidence. It drives everything we do to support our customers and patients. Launching this new visual identity reaffirms to our customers, employees and patients that we stand behind the shared vision of a more confident world.”
BTL launches EMSCULPT

NEO EDGE applicators
Device manufacturer BTL Aesthetics has launched the new EMSCULPT NEO EDGE applicators. According to the company, the device aims to target and treat the entire lateral abdomen. The design allows for a closer fit on the curvier areas of the body offering a solution which addresses all fat deposits and muscle groups in the abdominal area, explains BTL Aesthetics. The new EDGE applicators feature a specifically engineered double coil system allowing the energy to penetrate through all three layers of the oblique muscles resulting in consistent muscle contouring and fat reduction. Ron Borsheim, vice president of product development, said, “With the exciting new addition of the EDGE applicators, BTL is continuing to raise the bar in the aesthetics industry and innovate for versatility by extending the sculpting power of the award-winning EMSCULPT NEO therapy. The unrivalled device treats more key muscle groups than any other non-invasive treatment.”
The International Academy of Advanced Facial Aesthetics (IAAFA) annual conference and awards ceremony will be taking place on November 19 at the De Vere Beaumont Estate, Windsor. Speakers at the conference will include aesthetic practitioners

Miss Sherina Balaratnam and Dr Manav Bawa, dentists Dr Rita Poddar, Dr MJ Rowland-Warmann and Professor Bob Khanna, as well as business coaches Ron Myers, Pam Underdown and Adam Houghton. Topics include enhancing your patient journey, developing and maintaining a five-star clinic, sustainability in aesthetics and revolutionary innovations in energy-based devices.
Professor Khanna, president and founder of IAAFA, said, “I’m so excited for this year’s IAAFA conference. After a day of education, we will be continuing the event with our annual charity ball which grows in success each year. Delegates can enjoy a Moët champagne and canapé reception, three-course meal, with a free bar all night plus all entertainment including a raffle and auction, with all proceeds going to the Make a Wish Foundation.”
Thread lifting
MINT to hold threads symposium
HansBiomed Corp, creator and distributor of MINT PDO threads, will be holding a symposium in November. The MINT Academic symposium is intended for beginners who are seeking to perform PDO threads, with lifting techniques that can be applied to their patients. The symposium includes lectures as well as hands-on experience on the fundamentals of MINT PDO threads, presented by the MINT Education Board.
Speakers include aesthetic practitioners Dr Kam Lally, Dr Zunaid Alli, Dr Jeremy Isaac and Dr Chike Emeagi with topics including the scientific approach to MINT PDO threads, anatomy and assessment, complications and contradictions, as well as a case study highlighting what can be achieved with MINT, and a Q&A session.
Afterwards, attendees will enjoy a drinks reception and be awarded a digital certificate of attendance. The symposium will take place on November 12 at 12:30pm at JW Marriott Grosvenor House, London.
Design
Body contouring
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Skin Medical Aesthetic Group debuts new treatment protocol at CCR
At this year’s CCR, medical aesthetic distributor Medical Aesthetic Group released a new skincare treatment protocol designed to target acne and photodamaged skin. According to the company, GlycoAla is a stable form of photosensitising drug 5-aminolevulinic acid. The product uses glycosphere nanotechnology to deliver both 5-ALA and hyaluronic acid into the skin before red LED light energy is used to produce a photodynamic response, according to Medical Aesthetic Group.

Patrick King, commercial director at Medical Aesthetic Group, said, “We are pleased to introduce this unique and highly effective innovative treatment. Following a long trial period, we believe it will enable unprecedented treatment of these distressing problems with life-changing outcomes.” Education

Dermapen to hold microneedling masterclasses in London
Microneedling device company Dermapen has announced two CPD-accredited masterclasses in November to educate practitioners on usage of Dermapen to treat pigmentation and acne.
The Dermapenworld Masterclasses will be hosted at the Walford Hotel, London, where practitioners will be led by mesotherapist Dr Andrew Christie in learning about skin indications, treatment parameters, combination therapies and homecare protocols. Dr Christie will also perform live demonstrations on both days. Ahead of the event, Dr Christie said, “These masterclasses deliver the most innovative, evidence-based material to revolutionise skin-needling practice and protocols. A true synergy of mechanical and chemical regenerative medicine can be achieved.” The Dermapenworld Masterclasses will take place at the Walford Hotel, London on November 21 and 22.
Recruitment
Croma Pharma welcomes new brand manager
Aesthetic pharmaceutical company Croma has appointed Nikki Jones as the company’s new brand manager.

Jones is bringing more than 30 years’ sales and training experience to the role, helping the brand coordinate the global launch of its new prescription medicine.
Jones said, “I am so thrilled to have the opportunity to join not only a global industry leader with a peerless portfolio of minimally-invasive aesthetic medicine, but also such an experienced team of experts within the aesthetics industry and their own fields.”
She continued, “Naturally, I can’t wait to fully envelop myself in all aspects of my new role, from working with the Croma team, key opinion leaders and customers’ existing and new, to getting to know the brands, products and technologies.”
News in Brief
Charity ball to raise funds for veterans’ cosmetic procedures
Charitable organisation Back on Track is holding its annual ball on November 26 to raise money to offer cosmetic treatments to veterans affected by service injuries. Back on Track was founded by aesthetic practitioner Dr Aamer Khan and Lesley Reynolds, founders of Harley Street Skin Clinic, to provide service people with aesthetic treatments for scar tissue damage or burn injuries. The ball will be a night of music, dance and comedy and is open to everyone.
Prollenium appoints new commercial manager
Aesthetic manufacturer Prollenium Medical Technologies has appointed Sinead Golden as its new commercial manager in London. Golden will be managing existing accounts, maintaining brand relationships and acquiring new accounts in the London area, as well as supporting training and general enquiries. Golden commented, “This is a dream role, having come from an aesthetics and beauty background I can lean on my 14 years of experience working closely with practitioners in this space.”
IBSA Derma expands into Australia and New Zealand Pharmaceutical company IBSA Derma has launched its Profhilo line in Australia and New Zealand. During a tour in Sydney, Melbourne and Adelaide, IBSA presented its products and technologies to industry professionals and scientific and business partners, supported by key opinion leaders including Mr Dalvi Humzah, Dr Gabriel Siquier, Dr Cara McDonald, Dr Steven Liew and Dr Robin Chok. Leo Magnani, international sales manager at IBSA, said, “Australia and New Zealand are key markets for IBSA’s expansion journey on the international scene that confirms the successful strategic choice of enhancing authentic beauty.”
Promoitalia launches iWave body contouring device
Cosmetic product company Promoitalia has released its new body microwave contouring device, iWave. The device combines two technologies – MicroWave RD offering focused radial microwaves, and Cold HP Oxygen offering molecular propulsion therapy – with the company saying these combat localised adiposity, cellulite and skin relaxation. CEO and founder Valerio Matano said, “Our clinical studies have shown that the device uses safe and effective technology, as well as being comfortable and non-invasive, with instant visible results and no downtime.”
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
On The Scene
Out and about in the specialty this month
SkinPen Global London Symposium

Aesthetic manufacturer Crown Aesthetics held the SkinPen Global London Symposium on October 1. More than 450 delegates tuned into the event, and 100 attended in-person. The event hosted a full day of clinical advice on using SkinPen to drive patient results, live treatment demonstrations and business talks. Speakers included aesthetic practitioner Miss Sherina Balaratnam, education manager Kat Coleman, plastic surgeon and burns specialist Mr Andy Williams and digital marketing consultant Rick O’Neill. Reena Sandhu, head of marketing and operations UKI, said the event was another overwhelming success with excellent customer feedback. “Our SkinPen symposiums aim to provide clinical education to our customers and provide them with detailed treatment protocols to enhance patient results further,” she explained. She added that SkinPen is already working on the next Symposium, which will be in mid-2023.
The Sciton Rockstar Experience
Aesthetic laser company Sciton kicked off its Rockstar Experience at the Hyatt Regency Churchill Hotel in London on September 30 and October 1.

The Experience provided healthcare professionals with clinical demos, advanced treatment techniques and talks on emerging industry trends from aesthetic practitioners, plastic surgeons and dermatologists.
Over the two days, more than 70 attendees were treated to nine talks by oculoplastic surgeon Dr Maryam Zamani, cosmetic surgeon Mr Benji Dhillon, ophthalmologist Miss Jennifer Doyle and aesthetic practitioner Mr Cormac Convery. Richard Crawford-Small from The Aesthetic Entrepreneurs also presented on business strategy for aesthetic clinics. Attendees were also treated to networking drinks and a prize draw during the event. Sciton’s Rockstar Experience is a live tour with monthly dates across the US, and the next UK event is expected to take place in September, 2023.
EvoCyte Regenerative Aesthetic Exosome Summit, London
On October 15, aesthetic distributor EvoCyte held its second Regenerative Aesthetic Exosome Summit (RAES) at The Intercontinental Hotel Park Lane, Mayfair. After officially launching its exosome technology at CCR, RAES offered further information and education on exosomes’ clinical applications for skin and scalp rejuvenation. The event hosted an array of speakers, including CEO of ExoCoBio Byong Cho, aesthetic practitioner Dr Shameema Damree and Dr Inigo De Felipe, who all spoke on how the science of exosomes can be applied to aesthetics.

Consultant plastic surgeon Mr David Gateley said, “The emerging peer-reviewed science behind exosome isolation, purification and its role in managing inflammatory skin conditions is absolutely astonishing. A real game changer!” EvoCyte will be holding a masterclass at ACE in March, 2023.
Aesthetics Business Conference
On October 4, aesthetic insurance company
Hamilton Fraser held the fifth Aesthetics Business Conference (ABC) at the Royal College of Physicians in London. ABC 2022 brought together business professionals and aesthetic practitioners to share their expertise on running an aesthetic business, starting out in the field and maintaining success. Mark Copsey, head of healthcare at Hamilton Fraser, said, “We are delighted to bring practitioners our fifth conference, together with the support of so many of our valued expert partners from across the industry, to help practitioners establish themselves in the sector Hamilton Fraser is proud to be a part of.”
Speakers in the morning included aesthetic practitioner Dr Tristan Mehta, tax and VAT advisor Veronica Donnelly, British Association of Cosmetic Nurses CEO Paul Burgess, plastic surgeon Miss Priya Chadha and aesthetic business development consultant Lucy Peacock. The talks in the afternoon began with an inspiring guest session from businesswoman and winner of The Apprentice Michelle Dewberry. She was followed by co-founder of Aesthetic Nurse Software Max Hayward, CEO of AestheticSource Lorna Bowes, psychologist Kimberley Cairns and Hamilton Fraser’s healthcare account executive Nicola Bowtell. The conference was rounded off with a champagne reception in the building’s library. At the end of the day, Hamilton Fraser events executive Viki Hooker said, “At Hamilton Fraser, we pride ourselves on the educational aspect of the aesthetics industry. We’ve noticed that the industry events touch on the business side, but there was nothing dedicated to practitioners starting up, so that’s why we started ABC. People come back each year because the education around business and marketing is so important to the success of the clinics.”
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
























Aesthetic Technology Ltd. T: 0845 689 1789 E: info@aesthetictec.com W: dermaluxled.com
POWERFUL PROVEN PERFORMANCE
Ayodele believes that SOC people are underrepresented in the aesthetics industry in both marketing and education. “There is a definite lack of diversity in the industry,” she says, “However, it has improved in the last two to three years as awareness has grown. Platforms such as the BSD have forced the industry to do more deep thinking, but the overall lack of diversity is down to many things. This ranges from the lack of appropriate education and biased marketing, to SOC practitioners not feeling as if they have a voice that would be listened to by the industry,” Ayodele notes.
Prioritising Diversity in Aesthetics
Aesthetics
explores a new report on diversity and inclusivity in the beauty and aesthetic industry
As medical professionals, you are taught to treat each patient equally and fairly, regardless of their gender, body type or skin colour. In the last decade, there has been an increased awareness surrounding diversity in adverts, publications, events and marketing materials, and this has been accelerated by the Black Lives Matter movement in 2020.1 Despite this, a recent report has highlighted that diversity and inclusion in the beauty and aesthetic industry is still not where it needs to be.
The Forces of Beauty report was recently published by Driving Racial Equity in Aesthetic Medicine (DREAM).2 The DREAM initiative was developed by Allergan Aesthetics and skinbetter science to advance racial and ethnic diversity, inclusion, equity and sensitivity in the fields of dermatology and plastic surgery.
The report involved 4,000 women aged 21-65 years old across numerous ethnicities and geographical locations. In the survey, only 11% agree society makes them feel beautiful, while 30% believe society pressures them to look a certain way.2 A further 38% believe that the biggest change they want to see in the beauty industry is ‘real women in beauty and advertising’.2
Diversity in mainstream media advertising was explored in a recent Parliamentary report in which MPs outline their desire to work with advertisers to feature a wider variety of body aesthetics, as well as introducing a logo to state when any part of the body, including its proportions and skin tone, is altered in advertisements.3,4
To find out how this new report affects the aesthetics industry and steps that practitioners can take to be more diverse, we spoke to founder of the Black Skin Directory (BSD) Dija Ayodele, and aesthetic practitioner and member of the Black Aesthetics Advisory Board, Dr Amiee Vyas.
Lack of diversity
Within the DREAM report, the ideals of beauty were scrutinised, with many skin of colour (SOC) women feeling they need to conform to society’s beauty standards. Only 17% of all women surveyed, regardless of race and ethnicity, feel like their racial beauty is accepted by society.2 The benchmarks of female beauty have been typically understood as light skin, straight hair, thin physique, able-bodied, large eyes and a small nose.5

Dr Vyas has also noticed a lack of diversity in the industry, and thus conducted a diversity survey in 2020 alongside the Aesthetics journal.6-8 She explains, “For many years, I’ve been seeing patients of colour in my clinic who have been treated incorrectly or were unable to receive treatment because of a lack of practitioner knowledge. Many of the comments on the diversity survey reflected that practitioners were not competent in confidently treating darker skin types and lacked both knowledge and experience in this. Since this survey, I have seen aspects of the industry improving, but I believe that more still needs to be done.” Dr Vyas notes that this is primarily due to Western medicine having a larger focus on Caucasian anatomy and clinical presentations without accounting for other ethnicities.
In the last census, 15.2% of people in the UK identified as having skin of colour, highlighting that any practitioner across the country is likely to have SOC patients at some points, and they should therefore be actively making them feel welcome in their clinic.9
Increasing education
Ayodele and Dr Vyas agree that to obtain a better understanding of SOC needs, practitioners should be proactive in seeking out education.
In the report, many of the DREAM ambassadors explain that medical professionals must understand the unique needs of deeply melanated skin and how to adapt their treatment plans to cater for different skin colours. As a result, healthcare professionals must be able to decipher whether patients of colour feel a heightened sense of pressure to undertake treatments due to stereotypes or are doing so freely, and therefore should adjust their approach as needed to better understand their patients’ motivations.2
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Ayodele believes that increased education in the industry will help SOC patients when seeking treatments. She notes, “If practitioners are better educated, not just in psychological aspects of skin and aesthetics, but also in cultural expectations, marketing and branding, it will enable us to connect with a diverse clientele. As a result, the BSD launched the Practical Guide to Treating Skin of Colour platform this year, which enables practitioners at all levels to deepen their understanding of key concerns of women of colour and how to approach with cultural understanding and empathy.”
Dr Vyas reiterates that education and sharing knowledge is key to treating SOC patients. “Practitioners need to be accessible and share experiences they have with SOC. I share information on the training courses I offer and the updates I personally do for my own learning. I also have a clinic policy to only include treatments that are safe for all skin tones. Diversity is reflected in my marketing, social media and clinic team, and this is what helps my patients feel confident in my ability to look after their needs appropriately,” she reflects. There are numerous ways for
practitioners to increase their knowledge, including reading the latest studies in SOC, attending SOC talks at events like CCR, encouraging your suppliers to give you SOC training on their products and joining associations which focus on SOC.
Essential progression in aesthetics
The release of this new report is pivotal to keep the topic of diversity at the forefront of the industry, explains Ayodele. “It is another tool that enables us to deepen our understanding of how women of colour navigate the beauty and aesthetics world and the unseen barriers that they can be up against. For practitioners, it allows us to examine our work and seek ways in which we can ensure we improve and serve a diverse market.”
Dr Vyas concludes the report is a huge step for the industry to understand the beauty standards of a diverse population. She adds, “With two well-respected global brands –Allergan and skinbetter science – leading the way for the entire industry, now is the time to take a more inclusive and in-depth approach to treating SOC patients.”
REFERENCES
1. Gronow C, ‘Special Feature: Celebrating 10 Years of Aesthetics’, Aesthetics journal, 2022, <https://aestheticsjournal.com/feature/special-featurecelebrating-10-years-of-aesthetics>
2. Driving Racial Equity in Aesthetic Medicine, ‘Forces of Beauty’, 2022, <https://media.allergan.com/allerganaesthetics/ dreamforequity/reports/UNB157406-DREAM%20Forces%20 of%20Beauty%20Report.pdf>

3. House of Commons, ‘The impact of body image on mental and physical health’, Health and Social Care Committee, 2022, <https://committees.parliament.uk/ publications/23284/ documents/170077/default/>
4. Holden E, ‘News Special: Tackling Body Image Advertising’, Aesthetics journal, 2022, <https://aestheticsjournal.com/feature/tackling-body-imageadvertising>
5. Chen T, Lian K, et al., ‘Occidentalisation of Beauty Standards: Eurocentrism in Asia. Across the Spectrum of Socioeconomics’, 2020, p.218-22.
6. Aesthetics journal, ‘Practitioners encouraged to take part in diversity survey’, 2020, <https://aestheticsjournal.com/news/ practitioners-encouraged-to-take-part-in-diversity-survey>
7. Gronow C, ‘Voicing the Specialty’s Diversity Concerns’, Aesthetics journal, 2020, <https://aestheticsjournal.com/ feature/voicing-the-specialty-s-diversity-concerns>
8. Kilgariff S, ‘Improving Diversity in Aesthetics’, Aesthetics journal, 2020, <https://aestheticsjournal.com/feature/ improving-diversity-in-aesthetics>
9. Census 2021, ‘Population estimates by ethnic group and religion, England and Wales: 2019’, 2021, <https:// www.ons.gov.uk/peoplepopulationandcommunity/ populationandmigration/populationestimates/articles/popul ationestimatesbyethnicgroupandreligionenglandandwales/ 2019#ethnicity-in-england-and-wales>
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Discover the most advanced PDO Threads – exclusively available from Eden Aesthetics 3 CE Marked 3 Manufactured in ISO approved facility 3 Made in Korea 3 KFDA Approved Beginner and advanced training available. Contact Eden Aesthetics to book. Tel: +44 (0)1245 227752 E-mail: info@edenaesthetics.com www.edenaesthetics.com
CCR 2022:
The UK’s Biggest Aesthetics Event
The eagerly-awaited CCR conference returned to ExCeL London on October 13 and 14.




Over the two days, 120+ speakers, 140+ exhibitors and 3,400+ attendees gathered to learn, share innovations and discuss advancements in the surgical and non-surgical world of medical aesthetics. With live demonstrations, masterclasses, symposiums, product launches and a plethora of chances to learn and network, this year’s CCR was one of our most educational and engaging events to date.
Courtney LeBorgne, event director at Aesthetics and CCR, commented, “CCR 2022 was a huge hit! It was an honour to bring the industry together in the post-COVID boom that we are lucky to witness in our community. Exhibitors showcased new products, innovations and portfolios at the show and reached almost 3,500 healthcare professionals. We were supported by the most expert speakers, sponsors and associations who delivered unrivalled CPD-certified content. Thank you to everyone who came along and supported CCR, and we hope you loved the show as much as we did. We can’t wait to share more quality content and opportunities at ACE in March, 2023!”
Highlights from CCR
For the second year in a row, pharmaceutical company Galderma was CCR’s Headline Sponsor. The company ran the wonderful Networking Lounge across the two days, providing delegates with refreshments in between talks. Galderma also staged two symposiums about the company’s new Holistic Individualised Treatments (HITs) protocol, featuring head of medical education and training at Galderma Michele Di Giacomo, plastic surgeon Miss Priya Chadha, aesthetic practitioner Dr Rikin Parekh and aesthetic nurse prescriber Jackie Partridge. Joanna Neal, brand manager at Galderma, said, “It has been a real privilege for Galderma to be Headline Sponsor at CCR for the second year in a row. We had a really great meeting showcasing our new HITs protocol, and our training team were on the stand with our new mannequins so people could come and play with our products which I think works super well. We’re already looking forward to being back next year!”
Skincare company SkinCeuticals was the sponsor of our networking drinks at the Galderma Networking Lounge on the first evening, giving delegates a chance to network further, complete with a saxophonist to start the party. Throughout the conference, CCR VIPs were treated to cocktails, canapés and complementary treatments in the HydraFacial VIP Lounge. A new feature for this year was the Innovation Trail, which showcased 10 companies that have introduced innovations to the industry in the past year: Aesthetic Technology Ltd, Allergan, Cutera, Dr Mayoni Human Health, Evenswiss UK, EvoCyte, Galderma, Nuchido, Prollenium and Sofwave.
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Marking one of the UK’s most highly-anticipated aesthetic conferences of the year, Aesthetics reflects on the best CCR yet!
Latest developments at the Innovation Stage

Across the two days, some of the industry’s top brands hosted talks on the latest developments in aesthetic medicine. Some of these fascinating sessions included aesthetic practitioner Miss Sherina Balaratnam discussing her utilisation of BTL’s EMSCULPT NEO devices and the new EDGE applicators; aesthetic practitioner Dr Marcus Mehta and aesthetic nurse prescriber Sharon Bennett speaking on using the Prollenium portfolio to create anatomical architecture; aesthetic practitioner Dr Magdalena Bejma sharing how she uses VIVACY’s STYLAGE dermal fillers for medical profiloplasty; and aesthetic practitioners Dr Ian Strawford and Dr Selena Langford introducing Sinclair’s MaiLi fillers. On both days, oral and maxillofacial surgery registrar Mr James Olding and aesthetic practitioner Dr Tapan Patel hosted pharmaceutical company Allergan’s lunchtime takeovers, during which they discussed oral architecture while treating the lower face, before introducing HArmonyCa hybrid injectables in a live demonstration.
Live injectables at the Aesthetics Arena

The Aesthetics Arena was the place to be for independent educational content across the two days and brought the Aesthetics journal to life. Talks on the first day included aesthetic practitioner Dr Souphiyeh Samizadeh speaking on innovations in botulinum toxin; a live demonstration on jaw sculpting from aesthetic practitioner Dr Joshua Van Der Aa; an explanation of lip anatomy from aesthetic practitioner Dr Steven Harris; and a tear trough transformation live demonstration from consultant oculoplastic surgeons Miss Rachna Murthy and Professor Jonathan Roos.
The second day welcomed aesthetic practitioner Dr Manav Bawa demonstrating lower face augmentation; guidance on treating younger patients from Professor Bob Khanna; a live demonstration of mid-face rejuvenation with aesthetic practitioners Dr Raul Cetto and Dr Jeremy Isaac; Dr Vincent Wong treating a transgender patient in another live demo; and a panel discussion on the future of ultrasound innovations with consultant surgeon Mr Ansar Mahmood, consultant plastic surgeon Mr Dalvi Humzah and consultant ophthalmologist and oculoplastic surgeon Mrs Sabrina Shah-Desai. Many other brilliant practitioners took to the stage across the two days, informing delegates with their years of expertise.
Top business tips at the In Practice theatre



Throughout the conference, delegates were provided with practical advice on progressing in the industry and maintaining their own clinics at the In Practice Theatre, sponsored by SkinCeuticals. A brand-new agenda this year was A Dentist’s Guide to Aesthetics, curated by aesthetic practitioner and dentist Professor Bob Khanna. Talks from Professor Khanna, Dr Nina Bal, Dr Ian Hallam and Dr Anjuli Patel offered dentists an insight into how to get started and excel in the aesthetics industry. Professor Khanna reflected on the agenda, saying, “It was a pleasure to share almost three decades of my knowledge with dentists and other emerging aesthetic practitioners at this year’s CCR. I’m seeing more and more interest from dentists wanting to enter the aesthetics specialty, and it is wonderful to see an event as big as CCR supporting their journey.”
The second day was geared towards providing business advice, covering topics such as social media from communications manager Cait McLaughlin; aesthetic trends from founder of marketing and insights consultants Rare: Group Ben Pask; effective consultations from aesthetic nurse Mel Recchia; and red flag patients from British College of Aesthetic Medicine president Dr Catherine Fairris. The day was rounded off with a panel discussion on the developments of the aesthetics specialty to celebrate the Aesthetics journal going into its tenth year, featuring Aesthetics Clinical Advisory Board members Dr Souphiyeh Samizadeh, Mr Adrian Richards and Sharon Bennett, chaired by editor and content manager Shannon Kilgariff.
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
New concepts at the Skin and Wellness Agendas
Two new agendas were introduced at this year’s CCR, in the form of Skin and Wellness. The Skin agenda featured aesthetic nurse prescriber Anna Baker sharing knowledge on managing photodamage; aesthetic nurse prescriber Julie Scott advising on skincare for pregnant patients; and aesthetic practitioners Dr Amiee Vyas, Dr Ayah Siddiqi and Dr Sharon Belmo collaborating to discuss treating skin of colour. Wellness is a hot topic in the industry right now, as shown in the Wellness Agenda, led by aesthetic practitioner Dr Mayoni Gooneratne. Topics covered included the connection between inflammation and disease from Dr Gooneratne; the science of ageing from molecular biologist Dr Nichola Conlon; prioritising mental health in clinics with psychologist Kimberley Cairns; and responsible weight loss services from aesthetic nurse prescriber Tracey Jones. Dr Gooneratne reflected, “The event was a fantastic opportunity for us to get the concept of aesthetic wellness out to the profession. We know that when our patients feel good on the inside they can really shine on the outside, and we believe that the aesthetics clinic environment is the perfect place for a more in-depth consult. This was also our reason for launching the Human Health Affiliates programme to deliver training in this approach to consulting.”

Complications advice at the ACE Group World Conference
CCR played host to the annual Aesthetic Complications Expert (ACE) Group World Conference for a second time, sharing the most recent developments in managing and preventing aesthetic complications. Professor David Sines, chair of the Joint Council for Cosmetic Practitioners (JCCP), spoke on the government’s proposed new aesthetic licensing scheme; aesthetic nurse prescriber Lou Sommereux provided expert advice on the prevalence and

identification of mental health issues and body dysmorphia in aesthetic patients; independent nurse prescriber Sharon King presented on complications relating to fat dissolving injections; and consultant resuscitation practitioner Paul McVittie shared knowledge on resuscitating patients. Finally, chair of the ACE Group World, Dr Martyn King presented evidence and guidance on managing delayed onset nodules and reactions which have increased significantly since the pandemic. Dr King said, “The ACE Group World Conference, held at CCR, was again a huge success with leading practitioners providing evidence-based lectures on a range of complications and important updates and industry news. Feedback we have received following the conference has been extremely positive and the need for a whole agenda on the management of complications was recognised!”
Surgical insights at the ISAPS Symposium UK
CCR was the host of the fifth International Society of Plastic Surgery (ISAPS) Symposium UK, inviting top UK plastic surgeons to discuss the latest advancements and best practice in the specialty. Topics addressed included facelifts from Mr Dan Saleh; patient satisfaction with Mr Francisco Bravo; non-surgical scar management with Mr Ernest Azzopardi; and building a hospital with UK national secretary of ISAPS Mr Naveen Cavale. After the symposium, Mr Cavale said, “Once again, it was really good to be working alongside CCR for the fifth time. The interface between the surgical and non-surgical specialties was so good to see, with experts from all over the world contributing to the ISAPS Symposium UK this year. The speakers were inspirational to our delegates, and it was great to hear about innovations in the industry.”
Expert injection techniques at Dr Tapan Patel’s Masterclass
Aesthetic practitioner Dr Tapan Patel provided a packed roster of facial injectable live demonstrations in his highly-anticipated masterclass. Within the session, Dr Patel demonstrated treatment techniques for the temple, cheeks, nose, lips, chin and jaw, as well as offering advice on danger zones and safety tips. He was joined by a team of practitioners including Dr Manav Bawa and Dr Amanda Penny. Following six hours of live demos, Dr Patel said, “It’s always a
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Networking at the PHI Lanthropy Diwali Party
CCR threw its first ever after party this year, recruiting Dr Tapan Patel to be the face of the PHI Lanthropy Diwali Party! The party at Trinity Buoy Wharf next to the Thames raised funds for charitable causes: The Childhood Trust, the Children’s Burns Trust, the Society of Friends of the Sassoon Hospital and Mahatma Gandhi School.
Party guests were greeted with champagne and delicious Indian food, before dancing the night away to DJ tunes and Indian drummers in the festively decorated venue, with a photobooth and photo wall for guests to mark the occasion with colleagues and friends.


We would like to thank our wonderful sponsors Church Pharmacy, Cutera, Hamilton Fraser, HYAcorp, Pabau, Prollenium and SpringPharm for making this amazing evening possible!
pleasure to perform live demos at conferences, especially CCR because it attracts such an array of aesthetic practitioners, both established and new to the specialty. I enjoyed sharing my expertise with so many delegates, and already look forward to more learning next year.”
Newest trends at the CCR Press Conference
In the Harley Academy Press Lounge, the CCR Trends Report was presented to both trade and consumer press. Compiled by former Aesthetics editor Chloé Gronow and co-edited by the editor of Tatler’s annual Beauty & Cosmetic Surgery Guide Francesca Ogiermann-White and Aesthetics journal editor and content manager Shannon Kilgariff, the Trends Report highlights the year’s most innovative advancements and launches.
Exclusive data obtained by Rare: Group revealed that 32% of 25-32-year-olds and 29% of 33-40-year-olds in the UK have had treatment or are considering doing so in the next 12 months. Shockingly, 13% of 16-17-year-olds in the UK have had or are considering treatment in the next year.
The report also announced the launch of several new products and technologies at CCR, including Evolus’ first UK aesthetics conference, showcasing its newly-approved toxin Nuceiva (prabotulinumtoxin A) for use between the eyebrows. New polynucleotide company Plenhyage XL also made its debut, providing injectable treatments to stimulate fibroblasts, encourage cell turnover, improve elasticity, boost collagen production and hydrate skin.
Prollenium’s brand new topical hyaluronidase Topilase, Cutera’s innovative acne treatment device AviClear, AestheticSource’s pigment correcting Cyspera Intensive System, skincare company Evenswiss’ new patented Dermatopoietin technology and Eden Aesthetics’ updated DermaFrac device were all also on show at CCR 2022, among many others.
After presenting the report to members of the press from publications including The Sunday Times, Forbes and HELLO, Kilgariff said, “We created the annual CCR Trends Report to educate both the consumer
press and wider aesthetics community about the latest statistics, exciting product launches and developments we are seeing in our speciality. CCR is the perfect stage to showcase this, and we are proud to be a part of the movement to make the aesthetic specialty more accessible to everyone.”
See you next year!
And with that, CCR 2022 has come to a close! To attend next year’s event, reserve October 19-20 in your diary and keep an eye out for registration to open for CCR 2023.
Our next event will be ACE on March 10-11, 2023 at the Business Design Centre, London for two more days of exceptional education. This will be followed by the prestigious Aesthetics Awards on the evening of March 11, marking all the year’s most impressive achievements in the world of aesthetics.
Find out more about how to register for ACE and get your tickets for the Awards on p.40.

“The speakers were inspirational, and it was great to hear about innovations in the industry”
Mr Naveen Cavale
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com

Providing a reputable and trusted service in medical aesthetic and clinic supplies since 2005. Shop our special offers: *Real Church Pharmacy Team Member! ChurchPharmacyUK @ChurchPharmacy ChurchPharmacy.co.uk 01509 357300 info@churchpharmacy.co.uk Committed to delivering excellence for your medical aesthetic and clinic needs.
Utilising the Fullface Approach
complement the face as a whole and it means we, as aesthetic practitioners can achieve better, more natural results.”
Aesthetic practitioner Dr Mohsin Ghor adds that the continuous development of aesthetic products has also aided practitioners’ ability to treat the full-face effectively, noting, “Around 10-15 years ago, there were only a handful of dermal fillers. However, now there are so many different ranges, which each consist of a variety of fillers designed for specific areas and even different indications in that area. This has meant that we as practitioners are able to choose products based on individual concerns, so we can be a lot more dynamic with how we treat faces.”

Assessing the full-face
Dr Ghor notes that regardless of the indication his patient has come in for, he always conducts a full-face assessment. He explains, “This is because most of the time patients aren’t sure themselves what they really need. They just feel they want to address X, Y and Z but they’re unsure what treatments are needed to correct that, and what needs to be treated to achieve that. They simply see on social media that there’s treatments such as lips or nose available, and they feel maybe those can help correct their problem areas. When practitioners assess the full-face, we can tell them what it is that would actually be needed.” Dr Ghor adds that he always takes full-face photos of each patient from different angles to help explain his thought process to the patient, as well as helping to show the impact each treatment could have on those specific areas.
When understanding an individual patient’s objectives and motivations for treatment, Henshaw advises managing their expectations of treatment outcomes and taking these factors into account when devising an individualised treatment plan. She notes, “This is critical to achieving high patient satisfaction. In order to do that, the whole treatment starts with a thorough consultation. The facial assessment can vary from person to person. I personally like to use the Galderma facial assessment, which consists of looking at skin quality, facial shape, proportions and contour, symmetry, animation and emotional suitability (excluding the possibility of BDD).”
Gone are the days when aesthetic treatments were synonymous with having boundless amounts of filler injected into your lips. Nowadays, patients are seeking a more holistic approach, looking for tweaks across the full-face that can subtly address their concerns. According to aesthetic practitioner Dr Kam Lally, this is due to a mixture of both patient and practitioner education. He notes, “Our patients are now more informed about aesthetic treatments and have also seen the negative results of isolated treatments in the media. As such, they’re looking for a more holistic approach to their treatments and one that helps to keep their tweakments under the radar – full-face treatments help to mask this more as you aren’t drawn to one area of the face that looks out of place.”
He adds that at the same time, more education means practitioners are moving away from an era of treating static parts of the face, allowing them to respect dynamism by learning that you need to look at neighbouring areas to get a good result.
Aesthetic nurse prescriber Alice Henshaw agrees, noting, “As practitioners become increasingly advanced and experienced with injectables, we understand more about how treating one area can produce subtle, indirect improvements for other areas. There are a number of key benefits that full-face filler treatments offer, including providing more harmonious, beautifully balanced results which
When assessing his patients, Dr Lally uses a top to bottom approach, focusing on the areas that the patient has identified as bothersome and then looking at the areas surrounding it. He notes, “Of course, we have to be aware that not everyone needs a full-face approach. Younger patients, for example, will not experience as many facial changes due to ageing, so it might be fine for them to just have one area done in isolation. However, older patients have more signs of ageing across the whole face that subsequently contribute to aesthetic concerns, such as ptosis, wrinkles and volume loss. If this is addressed in one area but not another, the result can look obvious and so we need to be wary of this and explain it to the patient when creating our treatment plans.”
Selecting products and choosing techniques
In terms of product choice, Henshaw uses the Restylane range of dermal fillers when treating her patients. She notes, “The Restylane portfolio offers a diverse range of fillers by using two complementary gel technologies, Non-Animal Stabilized Hyaluronic Acid (NASHA) and Optimal Balance Technology (OBT). These technologies provide personalised, natural-looking results which, in my experience, deliver long-term satisfaction.”
In terms of technique, Henshaw adds that she usually uses a combination of needle and cannula techniques depending on the
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Three practitioners discuss their methods for addressing the full-face with dermal fillers and provide tips for consultation, assessment and treatment
Beauty flows through us
Blunt-tip reduces friction and glides through dermal tissue

Ultra-thin cannula wall increases lumen diameter and reduces injection forces
Premium quality single-use cannula used by clinical and industry leaders
Made in Britain for over 30 years

OVER 100 MILLION SOLD
AESTHETIC +44 1527 501480 ● www.sterimedix.com AESTHETIC CANNULA
individual’s needs. However, when doing a full-face approach, she tends to use cannulas for most of the treatments. She explains, “This is because of its suitability to fill a large area of the face in the subdermal or supra-periosteal plane. Regions such as the tear troughs, mid-face, temples, forehead, cheeks and marionettes require an even ‘filling’, rather than the more focused ‘projection’ approach, where a needle may be more appropriate. Another advantage of using a cannula is that it reduces the risk of bruising and vascular occlusions because it moves a blood vessel out of the way rather than hitting it (if used correctly).1 However, in some areas, such as the lips, it is my opinion that the use of needles achieves the optimal cosmetic outcome.”

Dr Lally agrees, noting that he also prefers a cannula when treating the full-face. He comments, “As well as for safety reasons,1 it’s also ideal because you only need one entry point to treat multiple areas. This is particularly important for the full-face approach as it means that there is minimal trauma to the patient’s face. For example, an entry point in the jowl can be used to treat the jawline, chin, marionette lines and nasolabial fold and so this reduces the amount of bruising and swelling in more than one area.” Dr Lally notes that he does, however, use a needle for areas in which he needs more precision, such as the cheekbone or the nose.
When treating his patients, he uses injectables from the Teosyal portfolio. He explains, “Their range of fillers are a toolbox, consisting of a good variety of products that are for all ages of patients. This means I can create a bespoke plan for each individual based on their unique needs. For example, when treating the jawline of an older patient I would use Teosyal Ultra Deep because this helps restore structure to the bone foundation that the soft tissue envelope is draped over. However, when treating the jawline of a younger patient I would use RHA 4 because this dynamic volumiser will give great definition and blend seamlessly with their tissues when used, so can be used more superficially.”


Like the other two practitioners, Dr Ghor also uses a combination of both needle and cannula when treating. He explains, “Different areas require different instruments – for example, I almost always use a cannula when injecting the jawline to get the right angles and be able to create good shape and structure. However, if I’m injecting an area such as the cheeks, lips or nose, where I want to restore volume, I will use a needle to superficially inject and create shape. For jawline, I typically use a combination of the two. Every patient is different, so it really depends on what their individual needs are.”
In terms of product choice, Dr Ghor uses the STYLAGE range, as well as Teosyal Ultra Deep. He explains, “I tend to use STYLAGE XXL and RHA 4 for volume loss and restoration, and for the lips I use STYLAGE Lips Plus. For me, the beauty of STYLAGE fillers is that less is more, and I always see good results as it hydrates and integrates well.”
Considerations for success
Henshaw notes that budget is often one of the main considerations for a patient when a full-face approach is suggested, as well as how often they will be required to touch up the treatments. She advises that practitioners need to manage expectations of results, explaining, “Patient education is needed to clarify how much filler may be
Figure 1: Patient before and after full-face treatment using the Restylane portfolio. Images courtesy of Alice Henshaw
Figure 2: Patient before and after treatment using the Teosyal portfolio. Images courtesy of Dr Kam Lally
education is needed to clarify how much filler may be required at each treatment session”
Before After After After “Patient
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Alice Henshaw

HIGH LEVEL TRAININGS KEY OPINION LEADERS NEW VIDEOS EACH MONTH REGULAR LIVE WEBINARS FACIAL & INTIMATE AESTHETICS
required at each treatment session and how much improvement could be expected, ensuring that patients understand the expected result and duration of the effects. This helps them to make an informed decision about treatment. The interval between sessions may vary according to the issue being addressed, the type of products being used, the timeframe required to achieve the patient’s desired look and how many follow-up appointments will be needed to maintain the results.”
She recommends a two-week follow-up consultation in order to provide the patient with feedback on the effectiveness of the chosen treatment plan, helping to maintain consistency and structure during consultations and plan and plot out dates for future treatments.
Dr Lally notes that it is important to consider ethnicity when treating the full face. He comments, “We are sometimes subconsciously biased towards the western ideal of aesthetics. However, this is not necessarily the desirable aesthetic elsewhere – for example, in the Middle East and parts of Africa a fuller, rounder mid-face is preferred to a contoured, sculpted appearance.”
Dr Lally adds that another important consideration is price. He says, “After I go through my treatment plan with my patients, I discuss their budget with them. Then according to this, we can space treatments out over a time period that the patient feels comfortable with. There are finance options available, but I strongly advise my patients to not overstretch themselves, but rather work with us to create a flexible timeline that accommodates their budget.”
Dr Ghor notes that practitioners need to ensure they are also giving
their patients in-depth aftercare advice, with more injection points meaning a greater risk of more minor side effects such as bruising. He advises, “I always tell my patients to rest appropriately for 48 hours, so this means avoiding things such as the gym or heavy lifting. It’s also important for patients to lie on their back when sleeping for three to four days post-treatments, because if they sleep on their side it may mould the filler out of place. Things like arnica gel can also really help the bruising.”
Top practitioner tips
Henshaw summarises that using an assessment tool or guide helps her to ensure consistency for full-face rejuvenation, particularly for those newer to this concept. She notes, “For all of my patients, I perform a full-face approach during the consultation and gently suggest treatments that would help balance their profile and create more harmonious results. Using this method also offers consistency if you have multiple practitioners working at your clinic. It gives patients a better chance to achieve results aligned with their needs resulting in a higher level of satisfaction with aesthetic treatments. The agreed treatment plan should define the treatment objectives, the rationale and the order in which each objective will be addressed.”
When treating the full-face, Dr Lally advises that one of his top tips is to keep reassessing the patient as you go. He notes, “One area impacts all other areas, so it’s important not to be shy to reassess after each injection. Look at your patient in static and dynamic repose – get them to smile and pout! See how your injections in the lips, for example, have affected the neighbouring areas, and then adapt your treatment plan if necessary. Don’t be scared to change what you originally thought was needed.”


Dr Ghor agrees, also warning against the danger of overfilling. He explains, “Do each treatment area slowly, bit by bit, and then assess and reflect on what you’ve done. I think that sometimes treating over several sessions is preferable, as it gives the filler you have injected time to settle before you inject more and you can assess the patient without swelling. In a situation where you would need significant filler to get a good result, such as a class II malocclusion, I would recommend doing this as the filler can integrate in different ways for different people.”
He adds that it’s also important so as not to overwhelm the patient, noting, “Having too much in their face at once can be scary, particularly if they’ve never really had treatments before, and if it seems like a big difference, they may be worried. So, it also gives them time to adjust to their treatment before anything else is added.” Dr Ghor also advises taking before and pictures after each treatment, and at each appointment, so that you can track and monitor the progression. Dr Lally also uses the ‘less is more’ approach with his patients, concluding, “You can always add more filler, but you can’t take it away easily! So, I think it is best to undertreat and then add more if and when you think it is necessary. Again, this is why it is important to keep reassessing – take your time with it, and don’t rush!”
REFERENCES
1. Marcus Mehta, Using Cannulas, 2022, <https://aestheticsjournal.com/feature/using-cannulas>
After Before
Figure 3: Patient before and after treatment using the STYLAGE and RHA ranges. Images courtesy of Dr Ghor
“Look at your patient both static and dynamic – get them to smile!”
Dr Kam Lally
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Rejuvenating the Perioral Area with BELOTERO® Soft
TO REGISTER SCAN THE
I have always been inspired by the natural sciences. Additionally, I am an extremely detail orientated and precise person. This makes my practice as a consultant anaesthetist a very natural fit for me. My clinical experience in the NHS informs my patient-focused approach to aesthetic medicine. I have also found that my skill using ultrasound and precise injectables in anaesthesia continues to be of great help and relevance in medical aesthetics.
At a recent anaesthetic and critical care meeting with a senior medical leader in my NHS trust, I suddenly realised why it was that I have always needed more – professionally speaking. He said something which may well resonate with you too, so I shall share it. Addressing a few of us in a group at a coffee break (as is so often the way at professional meetings), he was sharing luminescent pearls of wisdom and as junior consultants we were listening intently. “Chaps, you know what you really have to guard against?” he sipped thoughtfully at his coffee and ruminated with a furrowed brow, “Intellectual redundancy.” How can that be I wondered? As are you all, we are medical professionals working
in a challenging environment, often making life or death decisions – what about that is intellectually redundant? He expanded; over time in any profession, we wedge our minds into narrower and narrower gaps, squeezing the essence of who we are out, contorting around the challenges of our day-to-day existence. His point was that we need to pause, reflect and refract. Refraction into the composite parts of who we are – in my case I have a huge interest in anaesthesia, but equally in more creative and communicative vocations. This is how I found a natural and enjoyable match in the field of medical aesthetics.
This advertorial is sponsored by
M-BEL-UKI-1406 Date of Preparation September
For me, this counterweight provides energy and interest to my professional life. In working with Merz Aesthetics and using their products I have found a company which is on my wavelength. Rigorous and ethical science in conjunction with a thoughtful and supportive group of colleagues, underpinned by an excellent range of products. Which neatly brings me to the exquisite BELOTERO® Soft. BELOTERO® Soft is used to treat perioral lines with a blanching technique.1 I have also utilised superficial subcision in a comparable
30 Aesthetics | November 2022 @aestheticsjournaluk Aesthetics @aestheticsgroup aestheticsjournal.com Advertorial Merz Aesthetics
Dr Kiran Kandola shares his approach to the treatment of the perioral area with BELOTERO® Soft in a 37-year-old female patient
FOR HEALTHCARE PROFESSIONALS ONLY
“In working with Merz Aesthetics and using their products I have found a company which is on my wavelength”
plane with a 29 gauge cannula to augment the rejuvenation of the superficial dermis. My patient is a 37-year-old and a perfect candidate for this treatment given that her perioral lines are not established at rest, they are dynamic.
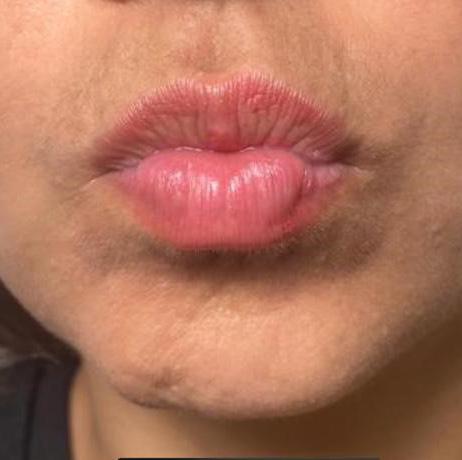

As such, BELOTERO® Soft ensures an extremely natural looking finish and is a linchpin in my arsenal of treatments. The prevention rather than restorative treatment modality (preventing worsening of dynamic wrinkles or delaying them from becoming static) is clearly a hugely expanding field given the wider appreciation of aesthetic medicine in general and specifically an understanding that treatments grow and evolve with you over time; with the initial preventative ones, such as this, forming the backbone of future treatments.
When patients understand the rationale behind a preventative, rather than restorative approach, their mindset changes for the better; it is a healthier way
maintenance of natural facial movement and appearance by virtue of its 3D tissue expansion and rheological tailoring.2,3 It is also distributed evenly in the superficial dermis, with consistent results – especially important when practising the blanching technique.2,4


BELOTERO® Soft also has extremely high
to approach treatments psychologically and I take great pleasure in assisting them to maintain their freshness and confidence over time.
BELOTERO® Soft, along with Revive, forms the basis of my preventative strategy at my clinic (Just Skin Time, 108 Caerphilly Road, Cardiff, CF14 4AG) and I have excellent feedback to give you regarding them.
BELOTERO® Soft helps ensure

cohesivity, low viscosity and CPM (Cohesive Polydensified Matrix) technology.2 This makes it ideal for use in the blanching technique and also in the superficial reticular dermis, with studies suggesting it has optimal properties for this.2,5 Also, because BELOTERO® products generate a low immune response and integrate uniformly with the dermal tissue, I know I am practising in the interests of my patients and providing
them with optimal advice and care.4,6 My mode of treatment using BELOTERO® Soft in the perioral area consists of the blanching technique (0.01-0.5ml), aiming to evenly distribute boluses in a focused vertical plane along the dynamic rhytids. I aim to take a very shallow angle and pass the tip of the needle just into the skin – with the 30 gauge needle tip still visible through a translucent sliver of skin and dermal tissue; I then proceed to inject and raise a tiny bleb. This vertical aspect of treatment is literally underpinned by subcision and injection of tiny droplets (0.01-0.5ml) via 29 gauge cannula at 90 degrees to the vertical rhytids. Results are to an extent immediate, with a gradual improvement over a few weeks and lasting 6-12 months,2 in my experience. When explaining the treatment to patients I ensure to mention swelling and bruising as there are multiple (albeit very small) injection points; I also make play of the fact that the perioral area is a dynamic area and the focus of communication, so to err on the side of slight under-treatment in the first instance is prudent.
31 Aesthetics | November 2022 @aestheticsjournaluk Aesthetics @aestheticsgroup aestheticsjournal.com Advertorial Merz Aesthetics
M-BEL-UKI-1406 Date of Preparation September 2022 This advertorial is sponsored by Merz Aesthetics UK & Ireland TO REGISTER SCAN THE QR CODE OR VISIT 24/7 ACCESS TO EDUCATION AT YOUR FINGERTIPS M-BEL-UKI-1406 Date of Preparation September 2022 This advertorial is sponsored by Merz Aesthetics UK & Ireland TO REGISTER SCAN THE QR CODE OR VISIT 24/7 ACCESS TO EDUCATION AT YOUR FINGERTIPS REFERENCES 1. BELOTERO® Soft IFU 2. Van Loghem J, et al. Clin Cosmet Investig Dermatol. 2021;14:1175-1199. 3. Sundaram H, et al. Plast Reconstr Surg. 2015;136(5 Suppl):149S-163S. 4. Micheels P, et al. Dermatol Surg. 2012 ;38(7 Pt 2):1162-9. 5. Micheels P, et al. J Clin Aesthet Dermatol. 2017;10(1):29-36. 6. Edwards PC, et al. Clin Interv Aging. 2007;2(4):509-19. This advertorial is sponsored by Merz Aesthetics UK & Ireland M-BEL-UKI-1431 Date of Preparation October 2022
Date of Preparation September 2022 This advertorial is sponsored by Merz Aesthetics UK & Ireland TO REGISTER SCAN THE QR CODE OR VISIT 24/7 ACCESS TO EDUCATION AT YOUR FINGERTIPS “BELOTERO® Soft ensures an extremely natural looking finish and is a linchpin in my arsenal of treatments” Dr
anaesthetist, medical aesthetic doctor and Merz Innovation Associate. Qual: MBBCH, FRCA, MRCP (UK)
M-BEL-UKI-1406
Kiran Kandola is a consultant
Before After














THE AESTHETIC DEVICE EVENT OF THE YEAR 27 NOVEMBER 2022 DE VERE BEAUMONT ESTATE SCAN HERE REGISTRATION IS NOW OPEN! REGISTER TODAY AT CUCF.CO.UK 8CPD ACCREDITED The essential event for all aesthetic professionals seeking to remain at the forefront of device-led treatments! Gain valuable insights into the latest industry trends, experience live product demonstrations, and socialise with your peers. Dr Tapan Patel Dr Tatiana Lapa Dr Rishi Mandavia Dr Nestor Demosthenous Dr Nima Mahmoodi Dr Yusra Al-Mukhtar Mr Kambiz Golchin FEATURED PRESENTERS MORE SPEAKERS WILL BE ANNOUNCED SOON Device Demonstrations Treatment Techniques Trends & Development Q&A Panel discussion Network at
Ball FUNDRAISING INITIATIVE
Gala
Understanding Thread Lift Complications
Thread lifts are minimally-invasive procedures where sutures are placed in the subdermal region to help lift sagging tissues. They are growing in popularity as patients seek treatments to tackle facial sagging with less downtime, risk and costs compared with the standard incisional surgery for facial rejuvenation.1
There are a variety of sutures on the market, but broadly the main types used are absorbable and contain synthetic polymers such as polydioxanone (PDO), poly-L-lactic acid (PLLA) or polycaprolactone (PCA).2 Many threads have collagen stimulating properties; newer ones may also contain hyaluronic acid.3 The sutures can be smooth, barbed, with cones, cogs or springs to hook and lift the skin. Complications are, however, generic across the board and not specific to one type of thread. Recently, many horror stories have occurred in the press and usually involve unregulated non-medics performing this treatment, with Save Face reporting complaints about thread treatments having tripled in the last year.4,5 Risk of adverse effects include infection, acute inflammatory reaction, pain, swelling/oedema, bruising, haematoma, dimpling and rippling, nerve injury, thread migration, protrusion, palpable threads and sensitivity/ allergic reactions.6
With a growing number of procedures being performed, it’s important to be aware of the risks and potential complications that can arise from thread lift suture insertions. Even if you don’t perform thread lifts, being aware of the complications can help manage patients who may present at your clinic for other treatments.
Infection and related complications
The incidence of post-operative infection following thread lifts varies significantly in the literature, with reported rates in threads fluctuating between 0.01% to 31%. However, it is one of the most common complications of thread lifts.6,7
Active infection can present in the early post-operative period or later when associated with inflammation or foreign body reaction.6 It can present with pain, persistent swelling, redness or warmth/heat. If there is no abscess, then antibiotic treatment consisting of co-amoxiclav 625mg (amoxicillin and clavulonic acid) acid three times a day would be recommended.6 One study that retrospectively reviewed the records of 61 patients, found that two thirds of infections resolved with pharmacological intervention.6
Many practitioners in the UK use prophylactic antibiotics as part of their protocol and National Institute for Health and Care Excellence (NICE) guidance states that ‘clean surgery involving placement of a prosthesis or implant’ requires antibiotic prophylaxis.8 However, there is no clear evidence in the literature of a consensus or if the use of prophylactic antibiotics accounts for the low infection rate.9
Azithromycin, a macrolide, may be a suitable prophylactic antibiotic due to its broad-spectrum nature, ability to target skin and soft tissue infections and tolerability. Dosing regimens that would be appropriate would be 500mg BD for two to three days starting either
one day pre-procedure or on the day of procedure.10 Prevention is also paramount here, in that the thread lifting should be viewed as a surgical procedure performed in a clinical setting, using chlorhexidine or betadine prep, use of drapes and aseptic techniques.
Abscess
In line with widely accepted good surgical practice, an abscess would require incision and drainage (I&D).11 Any infection that is not responding to antibiotics would need extraction of the thread material to remove the nidus of infection, followed by irrigation of the wound site.6,12 Adjuvant antibiotics alongside I&D are usually reserved for where there appears to be signs of cellulitis.13,11 Granulomas are nodules representing chronic inflammation and are a rare complication of thread lifts. They would present as hard nodules that may be red and can be tender. Diagnosis requires histological analysis. Management includes excision of the thread and nodule with subsequent scar management.14,15 As there is an inflammatory process involving the initial foreign body, consideration should be given to prescribing a tapering course of oral steroids (prednisolone).15
Pain
Pain can be expected in the immediate post-operative period due to swelling and bruising or the threads being pulled too taut.7 It is not unusual for these symptoms to last one to two weeks and in most cases settle within that time frame. Pain that is due to initial swelling should settle with management of the swelling using simple measures such as cool packs, simple analgesia (paracetamol and/or NSAIDS, depending on patient allergies) and antihistamines as well as sleeping propped up and on the back.7,12
Where the pain is due to threads being too taut, in most cases this can be alleviated by gently massaging the threads to release the tension. Clinicians should be wary of unremitting pain as it can be an indicator of infection or nerve injury.16,29
Bruising, haematoma and swelling
Swelling is a common post-procedure occurrence. One study, which conducted a meta-analysis of 26 studies (8,190 patients and 642 cases of complications), had a pooled incidence rate of 35%, which settled spontaneously.17 Although a minimally-invasive procedure, ecchymosis and bleeding due to damage of structures such as superficial temporal artery and sentinel vein can occur. Both these vessels are sited at entry points and along paths of thread insertions for both eyebrow lifts and mid-face lifting. If noticed at the time of procedure, management with compression is usually sufficient. Use of blunt cannulas, adrenaline in the local anaesthetic and appropriate anatomical knowledge can help minimise the risk of significant bleeding.29
Haematoma management includes compression in the form of bandages and observation for secondary complications such as
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dr Uzma Qureshi outlines the potential complications of thread lifting identified in the literature and how to manage them
infection. Patient factors should also be addressed, and steps taken, for example patients on antiplatelets should be forewarned of the risk of bruising and bleeding and a full risk assessment carried out at the consultation stage to ensure the thread lift benefits outweigh potential risks. Anticoagulants are listed as relative contraindications for thread lifts for most of the major thread lift suppliers.18
Dimpling and contour irregularities
Dimpling and skin irregularities are also common complications with incidence cited between 10-20% according to the literature.7,17,19 They occur where the sutures have been placed superficially and are caught on the dermis or catch during animation. These tend to occur due to incorrect positioning of the thread, typically too superficial. Many cases will simply resolve spontaneously, but persistent dimpling can be improved with gentle massage at the site of dimpling, which can result in release of the suture that was caught. Use of heat, for example radiofrequency, has also been shown to help to improve contour irregularities due to tethering.7 It has been identified that persistent cases can be released with subcision techniques. Using a large bore needle, such as an 18 gauge needle, it is recommended to make an entry point close to the area of dimpling and proceed to release any tethering and scar tissue by sliding the needle under the tethered area. This procedure can be repeated at intervals if some success is seen with the initial process.19 If this fails to correct the dimpling or skin irregularity, then the thread can either be removed or allowed to absorb naturally. If left to absorb naturally, the addition of dermal fillers to smooth out contours whilst waiting is also an option.19
Visible threads, protrusion and thread migration
Complications directly related to threads include those that are visible or palpable under the skin or protrude through the skin. Causative factors including using the wrong type of thread for the indication, too long a thread, incorrect placement, migration due to thread breakage or potential infection. Reported incidence rates in the literature range from around 4% for palpability to 2% for protrusion.6,17,20 It is important to correct these, as prolonged protrusion or irritation of the skin from a thread poking or rubbing increases the risk of infection and granuloma formation.19,29,30 In cases where the thread is protruding through the entry point, gently pulling and trimming the end so that the remainder of the thread is in the subdermal region may be all that is needed.16
Migration can occur due to breakage or loss of anchoring, followed by the muscles pushing the thread on animation. Where there has been migration and the thread is palpable superficially or poking the skin, then a small incision needs to be made and the area gently probed to locate the thread to then extract it.6,16
Nerve injury
Branches of the facial nerve can be subject to injury during a thread lift procedure. Incidence of injury is reported as 3% for facial nerve injury and 19% for paresthesia.6,17,12 Nerves most at risk of injury are the temporal branch of the facial nerve, which has been reported to be damaged during eyebrow lifts, zygomatic and buccal branches during mid-face lifts, and marginal mandibular branches of the facial nerve during lower face and neck lifts.16
Use of tumescent local anaesthesia is a method of administering dilute local anaesthetic into the subcutaneous tissue to allow for a comfortable procedure. It is commonly used pre-thread insertion and allows the use of lidocaine with adrenaline to provide prolonged analgesia in a larger area as opposed to regional blocks. Initial temporary paralysis can occur due to tumescent local anaesthetic effects, but generally these wear off by the following day.16
Having a good understanding of facial anatomy can help reduce the chances of inadvertent injury, for example, one cadaveric study looked at each side of 10 cadaveric heads and has shown a consistent relationship between the temporal branch of the facial nerve and the sentinel vein.21 Knowledge of this can help a clinician proceed cautiously in the zone where the sentinel vein is located.
The use of blunt-ended cannulas can help avoid more permanent damage to the nerves and avoid damage to blood vessels that can lead to haematomas and compression of nerves.31
Nerve injury can present as paralysis, paraesthesia, numbness or pain.22 Investigations such as nerve conduction tests and MRI scans may be utilised in the assessment of the injury.23
Management of persistent pain is to prescribe neuropathic medications such as gabapentin or amitriptyline.6,7 Where there is paraesthesia or paralysis, close observation with watchful waiting is first line management. An improvement would be expected at four weekly intervals, but early involvement from specialist plastic surgeons is advisable if no evidence of recovery or incomplete recovery is seen at three months. Possible interventions include physical therapy, pharmacological therapy, chemodenervation, facial nerve exploration, decompression or repair.6,7
Asymmetry and patient dissatisfaction
Most studies report high patient
rates post-procedure
selection and pre-treatment counselling is essential to ensure realistic expectations and avoid patient dissatisfaction.
Patient
satisfaction
use of blunt-ended cannulas
Complications No of Patients Treatment Infections 19 (31.2%) Dressings, oral/topical antibiotics Dissatisfaction with facial contour 14 (23%) Physiotherapy Parathesia 12 (19.7%) Physiotherapy, oral analgesics, oral neurotrophic drugs Dimpling and irregularity 10 (16.4%) Local massage and application of heat Subcutaneous induration 8 (13.1%) Intralesional steroid injections Chronic swelling 8 (13.1%) Oral detumescent drugs Thread extrusion 3 (4.9%) Subcision Allergic reaction 3 (4.9%) Topical glucocorticoid ointment Scarring 3 (4.9%) Silicone scar gel and laser therapy Facial nerve disturbance 2 (3.3%) Oral neurotrophic drugs
Complications and treatments6 Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com CPD Thread Lifting
The
can
help avoid more permanent damage to the nerves and avoid damage to blood vessels
Table 1:
Clinical Advisory Board Member Dr Souphi Samizadeh says...
A whole range of procedures carried out with various threads are known as ‘thread lifting’ in the market by both practitioners and consumers. This term is not correct and can be misleading;
however, accepted. Patient education is paramount, in particular, informing patients not to expect miracles or surgical results from this procedure and that in almost all cases, multi-modality and multi-step treatments are needed to get optimal results. Both practitioners and patients need to understand that these treatments are not always minimally
invasive, are to be carried out in a clinical environment under an aseptic technique, and the post-care instructions should be adhered to. This article effectively covers many main complications and treatment options post-thread lifting procedure.
ranging from 98% to 76%.7,24 One study reviewed the records of 311 patients and reported that patient satisfaction in thread lifting is independent of the patient’s age, treatment area, type of thread used, and the number of threads used.25 Dissatisfaction rates are reported at 23% in another study that looked at 61 patients and are related to unhappiness with facial contour and asymmetry.11 One of the indications for thread insertion is correction of asymmetry, but asymmetrical correction can occur post-procedure. It is important to conduct a full pre-treatment assessment to note and point out to patients any pre-existing asymmetry so that it isn’t attributed to the procedure. Asymmetry post-procedure can occur due to overcorrection or under-correction of a side and is reported to occur in approximately 3% of reported cases, as reported in one study that retrospectively looked at the records of 6,098 patients who had undergone approximately 12,000 procedures.26 Swelling can occur post-tumescent and post-procedure which can affect the judgement of how much lift is required when assessing patients during the procedure. Asymmetry may also occur due to weakening of the thread lift capability on one side. Mild asymmetry may be corrected with gentle manipulation of the threads, but more noticeable asymmetry will require further procedure on the side that needs more correction or removal of the threads.26
Allergy/sensitivity reactions
There are very few reported sensitivity reactions to thread sutures in the literature. One study described a sensitivity reaction where a patient experienced a skin rash which was managed with topical steroids.11 Anaphylaxis reactions have not been reported in the literature but should be managed in line with local resus council guidelines.27
Rarer complications
Damage to the parotid gland is a rare complication of thread lift procedures, however, often the entry points for mid-face lifts are over the parotid region and the parotid duct generally runs above the line connecting the tragus and angle of the mouth, a trajectory for thread insertions. Problems could present as pain on chewing, swelling or infection. Management involves removal of the thread and involvement of ENT surgeons if ongoing symptoms occur.16 Alopecia has also been reported with the mechanism cited as traction ischaemia from the taut threads. Full recovery was made after thread removal.14
Conclusion
Thread lifting using absorbable sutures carries low risk of long-term sequelae, provided that the procedures are conducted by appropriately trained medical professionals, in appropriate clinical settings with correct infection control measures in place.7,9,26 Most complications associated with thread lifts are transient and
self-resolve. Those that persist mostly required simple measures of pharmacological intervention. The exception is injuries to nerves/ surrounding structures or infection/inflammation.28 However, the literature does not cover the complications caused by non-medical professionals conducting thread lifts, which inevitably increases the risks of serious adverse events presenting in our aesthetic practices.
Dr Uzma Qureshi is an NHS GP partner who runs a CQC-registered medical aesthetics clinic. She taught anatomy at Cambridge University, has a background in surgical training, including a few years in plastic surgery and is a member of the Royal College of Surgeons. Qual: MBChB, MRCGP, MRCS


THE REFERENCES ONLINE! AESTHETICSJOURNAL.COM Questions Possible answers 1. Commonly available threads in the UK market can be made of which synthetic polymers?
2. In prevention of infection, a suitable antibiotic to use as prophylaxis would be... a.
3. In order to minimise bruising what measures can a clinician take? a. Use a blunt cannula b. Use adrenaline in anaesthetic c. Address patient factors such as antiplatelets d. All of the above 4. Tethering, dimpling and skin irregularities usually occur due to... a. Placing the thread in the deep tissues b. Superficial
of the thread c. Placing the
the
d. Patient
the
too vigorously 5. Nerves at risk of damage during an eyebrow lift include... a. Buccal branch of facial nerve b. Auriculotemporal branch of
nerve c.
of
d. Zygomaticofacial
of the
nerve
and go
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com CPD Thread Lifting
VIEW
a. Polydiaxonone b. Polyethelene c. Polyprolene d. Polystyrene
Trimethoprim b. Azithromycin c. Amoxicillin d. Flucloxacillin
placement
thread in
wrong direction
massaging
thread
mandibular
Temporal branch
facial nerve
branch
maxillary
Test your knowledge! Complete the multiple-choice questions
online to receive your CPD certificate! Answers: A,B,D,B,C



AESTHETICSJOURNAL.COM Keep up-to-date with the latest aesthetic developments and best practice guidance on your desktop, tablet or phone AESTHETICSJOURNAL.COM @aestheticsjournaluk Aesthetics @aestheticsgroup
Case Study: Achieving Facial Harmonisation
Mr Dean Rhobaye presents a case study showing a full-face transformation on a young female patient
A 24-year-old woman presented to my clinic seeking an overall aesthetic facial enhancement, with the motivation being a desire to feel more confident about her appearance. She also had a specific request to enhance her chin projection and improve the shape and volume of her lips. Apart from mild acne, the patient was fit and well, was not on regular medication, and had no known allergies.
Primary assessment
Using clinical assessment aided by 3D imaging device Canfield Vectra H2 and high-quality photography (Figure 1&2), the following issues were identified:
Upper third
Forehead and glabellar rhytids (principally dynamic with a mild static component) and relatively low brow positioning.
Middle third
Under-projected cheek bone structure with an inadequate definition and periorbital issues such as tear trough/nasojugal sulci, maxillary hypoplasia and negative orbit-rim vector. In the nasal area, she had suboptimal nasolabial angle, under-defined nasal tip and supra-tip break as well as septal and columellar deviation (minimal functional symptoms).
Lower third
In the chin and jawline area, the patient had mandibular retrognathia and secondary retrogenia, suboptimal chin height, mentalis strain with dermal puckering, slightly obtuse cervicomental angle and an under-defined jawline. She also had dental malocclusion with a moderate overjet and overbite, as well as suboptimal lip volume, an ‘M-shaped’ upper lip, excessive eversion of lower lip secondary to mentalis strain, lip incompetence, dynamic muscle discord and excess gingival show.
Skin
When assessing her skin, I found she had combination-type skin with T-zone oiliness, acne, dull complexion lacking radiance, and an uneven skin tone with ephelides and lentigines.
Discussion of treatment options
The degree of mandibular retrognathia/ retrogenia presented in this case would typically be treated by alloplastic implantation or orthognathic surgery. However, the range of aesthetic concerns that the patient presented with would have potentially necessitated additional surgical procedures to optimise her aesthetic outcome (for instance, malar implants, fat transfer, temporal brow lift and rhinoplasty). We discussed the principal advantages of the surgical options, as well as the limitations and risks. However, the patient was reluctant to undergo surgical intervention, particularly when multiple procedures might be required to achieve the aesthetic outcome she sought. Consideration was therefore given to the non-surgical, minimally-invasive option of non-autologous soft tissue augmentation with hyaluronic acid (HA) fillers in combination with neurotoxin. The concept of facial harmonisation was explained to the patient as a staged process of creating aesthetic enhancement and balance within and between facial regions and improving the overall facial shape and structural framework. I have devised the following fundamental principles that underlie facial harmonisation, which were highlighted and discussed with the patient:
1. Optimising the facial proportions
2. Enhancing the soft tissue structural support
3. Improving the definition of the facial contours
4. Smoothening of any surface contour irregularities and the transitions between and within facial zones and aesthetic units
5. Reshaping or optimising the position of individual facial features
6. Reducing the appearance of rhytids
Discussion of aesthetic challenges
This patient presented with an interesting array of aesthetic challenges due to various soft tissue issues complicated by the inadequacy of the underlying structural skeletal support. These challenges were particularly evident in the perioral region and surrounding structures.
Lower face structural deficiencies
A significant retrognathia/retrogenia resulted in inadequate skeletal support for the overlying soft tissue, manifesting as reduced lower face definition and a slightly obtuse cervicomental angle. Furthermore, the retrognathia and associated dental malocclusion (overjet and overbite) resulted in an intrinsic discrepancy in the position of the patient’s lips in repose. Consequently, she displayed a degree of lip incompetence with an inability to comfortably approximate her lips to form an adequate seal without straining her perioral muscles. The commonly associated pattern of retrognathia, malocclusion and lip incompetence is typically accompanied by hypertonicity of the mentalis muscle, as seen in this case. The mentalis muscle normally provides vertical support and stability for lower lip elevation and everts the lower lip on maximal contraction. A possible explanation for the mentalis strain in this context is that it occurs to increase the lower lip elevation to improve the approximation of lower and upper lips, hence reducing the intrinsic lip incompetence. However, the mentalis strain also results in excessive eversion of the lower lip and visible dermal puckering, which in this case were both more evident on the patient’s right side.
Lips and perioral dynamic muscle discord
Significant mentalis strain is often observed with a similar but weaker ‘resting-state’ hypertonicity of the depressor anguli oris (DAO) muscles. This hypertonicity possibly occurs as a mechanism to provide an additional mechanical force that potentiates the mentalis contraction and central lower lip elevation. However, the DAO hypertonicity also resulted in a subtle downward pull (negative-axis tilt) of the oral commissures. Anatomically, muscle fibres of the extrinsic lower lip depressors and upper lip elevators intermingle with fibres of the orbicularis oris muscle (OOM). Consequently, a mechanical dominance at rest resulting from the hypertonicity of the lower lip depressors can slightly attenuate the sphincteric action of the OOM by conferring an opposing vector force. Consequently, the reduced OOM sphincteric action leads to a slight relaxation of both the lower and, paradoxically, upper lip. This relaxation results in a minor but perceptible elongation of both lips in the coronal plane at rest in association with a loss in vertical height. The imbalance between opposing facial muscle groups, resulting in a shift of mechanical vectors favouring the dominant muscle action, has
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
previously been termed dynamic muscle discord or DMD.1 DMD occurs in the highly mobile areas of the face, specifically the perioral, periorbital and forehead regions, which are affected by intrinsic and extrinsic muscles acting within those areas. Where evident, it is an important consideration when planning a treatment strategy as it necessitates a holistic approach that may involve the correction of a deficiency in a different, often neighbouring, facial region that is not the direct target for treatment. The patient’s lips also had an intrinsic deficiency in volume and shape in proportion to her other facial features, and her upper lip displayed excessive gingival show in animation.
Mid-face structural deficiencies
Assessment of the patient’s mid-face revealed maxillary hypoplasia, evident as a suboptimal anterior soft tissue projection in the patient’s medial malar region. The resulting negative orbit-rim vector was associated with bilateral tear trough sulci. In addition, the patient’s lateral zygoma and zygomatic arch were also under-projected, further contributing to a lack of soft tissue definition in the malar region.
Procedure and results
Mid-face
A mid-face augmentation of the soft tissue overlying the maxilla, zygoma and zygomatic arch was performed bilaterally. Juvéderm Voluma and Juvéderm Volux were injected at the deep pre-periosteal layer and deep fat compartments to improve the malar shape and projection. Pre-periosteal HA filler implantation on the zygomatic process of the maxilla and lateral surface of the zygoma (facies lateralis) resulted in a projective displacement force and increased soft tissue projection. The improved structural framework compensated for the negative orbit-rim axis and indirectly attenuated the inferolateral portion of the tear trough sulci. Additional direct treatment of the tear trough sulci was then performed to optimise the results further. The submalar/pre-auricular concavity was also augmented in the pre-parotid fat layer using a cannula with a standard fanning technique.
Mentum
The structural foundation in the lower face was improved through chin augmentation, addressing the patient’s significant chin recession. Two sessions were necessary to optimise the results, using a combination of



high and mid-cohesivity HA fillers (Juvéderm Volux, Voluma and Volift) injected at different tissue depths and regions of the chin. The soft tissue pogonion, gnathion and mentum were augmented to provide anterior and inferior projection and chin definition. The labiomental sulcus was treated to reduce the concavity. The displacement force produced by filling the sulcus resulted in an infero-anterior rotation of the mentum in the coronal plane, increasing the mental height and anterior projection.
Perioral region
The improved chin projection and mechanical block secondary to the chin augmentation attenuated the patient’s mentalis strain and dermal puckering, while enhancing the lower lip support. Her lip incompetence and excessive lower lip eversion were corrected through this myodmodulatory action. In the third session, a residual excessive downward pull on the right side of the lower lip resulting from persistent DAO hypertonicity was treated with neurotoxin.
A lip augmentation was performed to optimise the upper and lower lips’ volume, shape, and definition. In addition, care was taken to preserve the topographical features
of the lips (such as the mucosal tubercles) and natural wrinkle patterns (sulci labiorum) as seen in Figure 3 in the online version of this article. M-shaped lips are challenging because of a lack of dry mucosal surface area that restricts volumisation. M-shaped lips also typically present with perioral muscle hypertonicity. The increased muscle activity at rest and on animation pulls on and compresses the vermillion lips, resulting in a loss of shape and apparent thinning. Therefore, a relatively viscoelastic and cohesive gel product (Restylane Defyne) was used to counter the deformation forces and reduce the likelihood of filler migration resulting from the perioral muscle hypertonicity. The downside of using a more cohesive product is the resistance of the treated lips to fully compress when in animation resulting in a residual slightly excessive projection of the white roll of the upper lip.
The patient’s upper lip excess gingival show was treated by soft tissue augmentation of the piriform fossae and nasolabial folds, which increased the mechanical resistance to the levator muscles during animation (see online Figure 4).
Figure 1&2: Patient before and eight months after treatment using 14.45ml of HA dermal filler
Before Before Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022
After After @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Anatomical area Approximate volume (ml) HA filler per side Total (ml) full-face
Main session (Day 0) Review session (Day 28) Refinement session (Day 49)
Mid-face
Zygomatic arch 0.3 0.5 1.6
Submalar concavity 0.7 1.4 Malar eminence/zygoma 0.3 0.5 1.6
Maxillary body and zygomatic process 0.2 0.4
Tear trough sulcus 0.5 1 Nose 0.25 0.5
Lower face
Angle of ramus 0.5 0.5 2
Labiomental sulcus 1 2
Pogonion / Gnathion 0.25 0.225 0.95 Menton 0.5 1

Lateral mental protuberance 0.5 1
Upper + lower lips 0.5 1
Session totals
Total volume (ml) full-face 11 0.45 3 14.45
Table 1: Soft tissue augmentation volume summary
Jawline
Fillers do not fundamentally ‘lift’ the soft tissues. However, depending on the patient’s anatomy, the localised projection created by the soft tissue augmentation can lead to a pull on the neighbouring regions. This ‘pull vector’ can, in turn, lead to an apparent ‘pseudo-tightening’ of the adjacent area along the axis of the projective force. However, the observable magnitude of this effect depends on the degree of pre-existing soft tissue laxity versus underlying structural support. Indeed, the apparent soft tissue pull is predominantly observable in patients who do not have significant laxity. In this patient, the increased chin projection following treatment indirectly resulted in an improved definition of the lateral jawline and a slightly more acute cervicomental angle. Soft tissue augmentation of the ramus angle was also done to improve the definition and projection of the postero-lateral jawline.
Brows and rhytids
A non-surgical brow lift was performed using Botox, which was also used to reduce the appearance of the rhytids in the upper face. The injection points and doses were based on a dynamic mapping assessment of the patient’s facial expression patterns, muscle movement, specific muscle mass and shape.
Nose
A mild non-surgical augmentation rhinoplasty was also performed for a slight enhancement of the nasal tip definition and supra-tip break using Teosyal Ultra Deep.
Skin
An evidence-based skincare plan was formulated for home use consisting of the Gentle Cleanser (alternating with Blemish and Age Cleanser at night twice a week), Equalising Toner, Phloretin CF, Blemish and Age Serum, H.A. Intensifier and Brightening UV Defence – all from SkinCeuticals. The patient also had a six-session course of hydradermabrasion, light glycolic acid peels and LED phototherapy using the DermaLux FlexMD, with the sessions one month apart.
Treatment summary
During the facial harmonisation process, 14.45ml of HA filler was injected over a main session, an intermediary review session, and a refinement session (Table 1). These filler sessions were combined with two sessions of neurotoxin. Figure 1 shows the treatment results taken eight months post-procedure, demonstrating a significant aesthetic enhancement. The patient’s overall facial shape and profile conveyed more optimised proportions, with improved contour definition in the middle and lower thirds. There was a notable reduction in her perioral dynamic muscle discord with the restoration of her
lip competency and attenuation of the chin dimpling. The aesthetic profile was also improved, resulting from the increased chin projection, malar and nasal tip definition, enhanced lip projection and shape, and elevated brow positioning. The periorbital region was also rejuvenated through amelioration of the tear trough sulci and pericanthal rhytids, and the brow lift. Notably, the patient’s aesthetic enhancement was apparent both at rest and in animation (see Figure 5 online). Her smile pattern was improved due to the correction of the upper lip excess gingival show, reduced lower lip depressor muscle dominance and a secondary increase in the zygomaticus and risorius muscle pull. Furthermore, her brow was maintained at a relatively elevated position during smiling, and the pericanthal rhytids were less evident, further enhancing her appearance during expression. Finally, her skin tone and radiance were markedly improved with a reduction in her acne blemishes and a smoother skin texture. The patient reported high satisfaction levels and psychosocial wellbeing with an elevated sense of confidence and outlook.
Conclusion
Conceptually, facial harmonisation represents a paradigm shift in the role of fillers in facial aesthetics. This case presentation demonstrates the versatility of soft tissue augmentation and myomodulation in a patient that would otherwise have traditionally been regarded as needing surgical intervention. This case also highlights the importance of careful assessment, including identifying facial intricacies that are often overlooked such as dynamic muscle discord, as well as proper procedural planning and staging.
GO ONLINE TO VIEW MORE IMAGES OF THE TREATMENT JOURNEY AND THE REFERENCES
Mr Dean Rhobaye is a specialist in minimallyinvasive/minimal access and non-surgical facial aesthetic procedures with 13 years’ experience in plastic and reconstructive surgery. He is now the clinical director of Sloane Clinic located on Harley Street. Qual: MBBS, BSc (Hon), MRCS, PhD
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
An Unmissable Two Days of Networking and Content
ACE and The Aesthetics Awards are back with a BANG in 2023!
After the monumental return of ACE this year, this incredible event will return once more in 2023 to deliver even more first-class learning, innovations and clinical sessions from leading aesthetic brands.


Taking place on March 10 & 11 at the Business Design Centre in London, ACE 2023 is the must-attend event for all medical aesthetic professionals. The conference provides clinical sessions, business updates and masterclasses for aesthetic practitioners, delivered by leading brands, trainers and experts. All content is free and gives attendees CPD points towards their annual accreditation.

Teoxane takeover
Teoxane once again returns as the Headline Sponsor of ACE, and will be hosting two full days of free talks, reinforcing the company’s dedication and commitment to co-creating the future of medical aesthetics. Jordan Sheals, deputy country manager, commented, “Following the successful return of ACE in March 2022, Teoxane is thrilled to exhibit once again as the Headline Sponsor in 2023!

Conferences such as ACE represent an excellent opportunity to shape and co-create the future of aesthetics, which is why in 2023, Teoxane will offer even more opportunities for healthcare professionals to engage with each other, with our expert faculty and with our science. In 2023, we will host four masterclass symposiums, each seating hundreds of practitioners, to cover a wide range of topics, all emphasising the fundamentals of assessment, anatomy, techniques and rheology.”
Explore brand new innovations from world-leading brands
The industry’s most respected manufacturers, suppliers and brands will be back again once more at ACE 2023. As host to 80+ exhibitors, the show will provide you with the opportunity to keep your practice
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
All education is free to attend, CPD certified and hosted by leading medical aesthetic providers
up-to-date by showcasing exclusive new products and techniques. Key exhibitors include Teoxane, Galderma, Prollenium, HA-Derma, Merz Aesthetics, Allergan and VIVACY.
Free unmissable education
Throughout the course of the two days, ACE will provide masterclasses and symposiums with leading aesthetic practitioners taking a deep dive into innovative techniques and delivering excellent standards.

Teoxane as the Headline Sponsor will run two days of back-to-back symposiums in the Main Auditorium for a first-hand look at how experts utilise the Teoxane filler range. ACE also delivers more high-level education in the Symposiums, Masterclasses and Expert Clinics, with LIVE demos and in-depth guidance on developing your clinical offering.
The In Practice agenda will also return, providing attendees with essential commercial support to drive the success of your clinic business. Led by entrepreneurs and established practitioners, discover everything you need to improve your business acumen and run a profitable practice.
Register NOW!
Attending ACE will provide you with valuable opportunities to learn, network and keep up-to-date with the latest technologies and clinical advancements in medical aesthetics.
All educational content is free to attend, CPD-certified and hosted by leading medical aesthetic providers. Register FREE now to keep your skills up-to-date and stay ahead of the competition!
Attend the most prestigious ceremony in aesthetics
The Aesthetics Awards brings together the very best in medical aesthetics to celebrate the achievements of the industry over the past year. Dubbed ‘The Oscars of Aesthetics’ we can’t wait to yet again bring the industry

The glamourous event will be taking place after the second day of ACE on March 11, making it the perfect way to round off two days of unmissable educational content. Attended by a record number of practitioners in 2022, we are delighted to have moved this year’s ceremony to a brand new location, the dazzling Grosvenor House. The largest and most glamorous awards venue in London, The Aesthetics Awards 2023 will truly be a night like no other. With all the entries in, shortlisting is taking place right now and early bird tickets are available to purchase until December 31, so make sure you get yours as soon as possible to avoid missing out. By purchasing your ticket you will receive:
• A celebratory glass of bubbly on arrival at the networking drinks reception
• Professional photographs at The Aesthetics Awards pressboard
• A delicious three-course meal including a ½ bottle of wine per person
• Live music and dancing into the night
• An opportunity to celebrate with your peers
Single tickets or tables of 10 are available. Make sure to head to our website to get them now and keep an eye out for the Finalists to be revealed in the January Aesthetics journal.
SCAN TO REGISTER FREE
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
together for a dazzling evening of recognition and positivity.
10 & 11 MARCH 2023 BUSINESS DESIGN CENTRE, LONDON
HEADLINE SPONSOR
(Botulinum Toxin Type A)
Observational Masterclass.
Bocouture® (botulinum toxin type A (150 kD), free from complexing proteins) 50/100 unit vials*. Prescribing information: M-BOC-UK-0432. Please refer to the Summary of Product Characteristics (SmPC) before prescribing. Presentation: 50/100 units of Clostridium Botulinum Neurotoxin type A, free from complexing proteins as a powder for solution for injection. Indications: Temporary improvement in the appearance of moderate to severe upper facial lines (glabellar frown lines, crow’s feet lines, horizontal forehead lines) in adults ≥18 and <65 years when the severity of these lines has an important psychological impact for the patient. Dosage and administration: For intramuscular use only. Unit doses recommended for Bocouture are not interchangeable with those for other preparations of botulinum toxin. BOCOUTURE should only be administered by an appropriately qualified healthcare practitioner with expertise in the treatment of the relevant indication and the use of the required equipment, in accordance with national guidelines . The intervals between treatments should not be shorter than 3 months. Reconstitute with 0.9% sodium chloride. Glabellar Frown Lines: Total recommended standard dose is 20 units. 4 units into 5 injection sites (2 injections in each corrugator muscle and 1 injection in the procerus muscle). May be increased to up to 30 units. Injections near the levator palpebrae superioris and into the cranial portion of the orbicularis oculi should be avoided. Crow’s Feet lines: Total recommended standard dosing is 12 units per side (overall total dose: 24 units); 4 units injected bilaterally into each of the 3 injection sites. Injections too close to the Zygomaticus major muscle should be avoided to prevent lip ptosis. Horizontal Forehead Lines: The recommended total dose range is 10 to 20 units; a total injection volume of 10 units to 20 units is injected into the frontalis muscle in five horizontally aligned injection sites at least 2 cm above the orbital rim. An injection volume of 2 units, 3 units or 4 units is applied per injection point, respectively. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Generalised disorders of muscle activity (e.g. myasthenia gravis, LambertEaton syndrome). Infection or inflammation at the proposed injection site. Special warnings and precautions: It should be taken into consideration that horizontal forehead lines may not only be dynamic, but may also result from the loss of dermal elasticity (e.g. associated with ageing or photo damage). In this case, patients may not respond to botulinum toxin products. Should not be injected into a blood vessel. Not recommended for patients with a history of dysphagia and aspiration. Caution in patients with botulinum toxin hypersensitivity, amyotrophic lateral sclerosis, peripheral neuromuscular dysfunction, or in targeted muscles displaying pronounced weakness or atrophy. Bocouture should be used with caution in patients receiving therapy that could have an anticoagulant effect, or if bleeding disorders of any type occur. Too frequent or too high dosing of botulinum toxin type A may increase the risk of antibodies forming. Should not be used during pregnancy unless clearly necessary. Should not be used during breastfeeding. Interactions: Concomitant use with aminoglycosides or spectinomycin requires special care. Peripheral muscle relaxants should be used with caution. 4-aminoquinolines may reduce the effect. Undesirable effects: Usually, undesirable effects are observed within the first week after treatment and are temporary in nature. Undesirable effects independent of indication include; application related undesirable effects (localised pain, inflammation, swelling), class related undesirable effects (localised muscle weakness, blepharoptosis), and toxin spread (very rare - exaggerated muscle weakness, dysphagia, aspiration pneumonia). Hypersensitivity reactions have been reported with botulinum toxin products. Glabellar Frown Lines: Common: headache, muscle disorders (elevation of eyebrow). Crow’s Feet Lines: Common: eyelid oedema, dry eye, injection site haematoma. Upper Facial Lines: Very common: headache. Common: hypoaesthesia, injection site haematoma, application site pain, application site erythema, discomfort (heavy feeling of frontal area), eyelid ptosis, dry eye, facial asymmetry, nausea. For a full list of adverse reactions, please consult the SmPC. Overdose: May result in pronounced neuromuscular paralysis distant from the injection site. Symptoms are not immediately apparent post-injection. Legal Category: POM. List Price: 50 U/vial £72.00, 50 U twin pack £144.00, 100 U/vial £229.90, 100 U twin pack £459.80. Product Licence Number: PL 29978/0002, PL 29978/0005 Marketing Authorisation Holder: Merz Pharmaceuticals GmbH, Eckenheimer Landstraße 100,60318 Frankfurt/Main, Germany. Date of Preparation:August 2021. Further information available from:. Ground Floor Suite B, Breakspear Park, Breakspear Way, Hemel Hempstead, Hertfordshire, HP2 4TZ Tel: +44 (0) 333 200 4143

Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard for the UK. Adverse events should also be reported to Merz Pharma UK Ltd at the address above or by email to UKdrugsafety@merz.com or on +44 (0) 333 200 4143.
*Botulinumtoxin type A, purified from cultures of Clostridium Botulinum (Hall strain)2 M-BOC-UK-0468 Date of Preparation: June 2022

BOCOUTURE®
(Botulinum toxin type A) Free from complexing proteins
FEEL GOOD LOOK GOOD
information
and
to
For
about dates
locations and
reserve your place, scan the QR code. Join us at a half-day course, designed to kickstart your journey with BOCOUTURE® Our experienced aesthetic practitioners will guide you through the scientific and clinical aspects BOCOUTURE®, and demonstrate a treatment in all three upper facial line indications.
Treating Temple Hollowness
In a youthful face, the temples are full, convex, round or oval. As we age, this turns into a skeletal shape due to loss of temporal fascia, reduction in volume and the temporal fossa becoming more apparent and concave. One of the secondary effects is a loss of support for the eyebrows.1 This loss of volume is a result of the temporalis atrophies and the temporal fat pads decreasing, resulting in an undesirable, hollow appearance.1
Achieving a balanced and youthful appearance whilst counteracting volume loss can be achieved through dermal filler augmentation.2 Some facial manifestations of ageing reflect the combined effects of gravity, progressive bone resorption, decreased tissue elasticity and redistribution of subcutaneous fullness.3 Fat may reposition or shift within facial compartments due to gravity, causing an inferomedial displacement of the overlying skin envelope. This movement increases hollows in the cheeks and flattens the angles of the face.4




There are several changes in facial structures as we age. Bones remodel in specific areas, ligaments increase in laxity, the fat deflates, muscles decrease in mass and there is also tonus change, with the skin experiencing gradual laxity increase.5 As a result, faces present with an increased visible vasculature, lateral orbital rim, and upper zygomatic arch as well as a descent of the eyebrow tail.6
In this article, I will be discussing the different protocols I like to implement in my clinic for treating temple hollowness.
Patient selection
Most patients will be unaware of a loss of volume in the temple area and the effect this has on the attractiveness of the face. The ageing process can alter the symmetrical and balanced facial features found in youth. This impacts a patient’s physical attractiveness but also their self-esteem.7
In addition to the generic consultation questions, I will also ask specific questions and make personalised assessments based on the patient. I will compare the patient’s pre-treatment photos of the temporal area with a set of photos from a patient I’ve treated with temple filler and ask the patient to ‘spot the difference’. It is imperative that the patient can see in themselves the temple deformity. Then, during the assessment, I’ll get the patient to clench their teeth and feel for any hypersensitivity in the temporal muscle and warn of any potential chewing issues post-treatment.
Medical history
As well as general contraindications for treatment such as active infection near the site of injection, a known allergy/ hypersensitivity to the material or lidocaine, pregnancy and anticoagulant therapy, it
is important for a full medical history to be taken before treatment.8 As noted in the guidelines by the Aesthetic Complications Expert (ACE) Group World, a history of allergic reaction to wasp or bee stings represents an increased risk of allergic reaction to hyaluronidase and should be considered as a relative contraindication, so it’s my personal preference to avoid treating patients with dermal fillers.9
Practitioners should also be aware of medications that predispose to bruising which include painkillers, non-steroidal anti-inflammatories, anticoagulants or vitamin E.10
Practitioners should also be aware of patients who are using isotretinoin. There are divided opinions as to whether this drug for acne treatment affects dermal fillers. It has been advised in the literature not to inject dermal fillers for at least six months following cessation of isotretinoin.11 This recommendation is challenged, and some clinicians believe that the drug has no effect on outcomes and are happy to use dermal fillers while the patient is undergoing this medication, as there is no conclusive evidence.12 Personally, I will be cautious and wait six months before treating the patient.
Tissues and structures of the temple
It is important for practitioners to have a strong anatomical knowledge and understand the properties of the product being used to maximise the efficacy of the treatment as well as minimising complications.13 The temporal region is based on a bony platform consisting of the parietal, frontal, sphenoid and temporal bones. The overlying soft tissues are arranged in layers, which contain the temporal neurovascular structures.5 The temples form the lateral boundary of the periorbital region of the upper third of the face.14
Figure 1: Technique for addressing volume loss in the temporal area Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dr Harry Singh details his approach to rejuvenating the temples and provides his considerations for those newer to injecting this area



HINNAO® Longevity Range The perfect trio for daily internal skincare • PRACTITIONERS RANGE • Join our training to become an Advanced Qualified Wellness Practitioner
The temporalis muscle is a large, flat muscle that lies within the temporal fossa of the skull. This fan-shaped muscle arises from the entirety of the temporal fossa below the temporal line, as well as the deep surface of the temporal fascia.15 Its muscle fibres converge anteriorly to form a tendon, which runs deep to the zygomatic arch. The tendon inserts on the apex and medial surface of the coronoid process, and the anterior border of the ramus of the mandible.15
In the temporal region, the blood supply is acquired from the superficial temporal, middle temporal, deep temporal, posterior auricular, transverse facial, zygomatico-orbital, zygomaticotemporal, zygomaticofacial and middle meningeal arteries.16 Branching off the maxillary artery in the infratemporal fossa, it travels through the foramen spinosum to supply the dura mater and the calvaria, which is deep.16
The superficial temporal artery supplies the temporal and parietal area, which originates in the parotid gland. This runs superficially upward along the vein and the auriculotemporal nerve, between the ear tragus and the posterior root of the zygomatic arch. It then divides into two branches: the frontal branch and the parietal branch.17 As a result, these vessels and nerves are not, theoretically, at risk if the practitioner refrains from injecting past the lateral safety line.17
The sub-temporalis space is the safe area for dermal filler injection, located in the upper area of the temporal region adjacent to the frontal border. Whilst inferior to the middle temporal vein and near to the zygoma, the superficial temporal fat pad is the targeted area for safe injection.18
Product selection
I use hyaluronic acid-based dermal filler products because of the hydration effect that we encounter and the ability to reverse these fillers. These products are temporary, but practitioners can expect results to last between six to 12 months.

Practitioners should consider the different viscoelastic, elastic modulus, cohesivity, hyaluronic acid concentration and viscosity properties.19-21 For treating the temples, I prefer to use plastic surgeon Dr Arthur Swift’s technique to address volume loss by using a product with a large particle size, to restore volume, and a high G prime, to help with lifting.22
Techniques
I prefer the multi-layer approach to gain the maximum result and optimise product usage.22 My approach is to insert a deep vertical depot high up in the thinner fibres of the temporalis muscle.23
It is important to ensure that you are on the bone with a needle, and secondly a deep horizontal depot with a cannula. I use the TSK Laboratory 25 gauge, 50mm cannula.
Volume loss
Personally, I use Dr Swift’s technique to address volume loss, however, I’m aware of there being up to eight different techniques which practitioners can use to treat the temples.22 The injection technique for the temples is injecting 1cm up from the lateral orbital rim and 1cm lateral to the temporal fusion line, high up in the thinner fibres of the temporalis muscle. The depth here is 4mm before you hit bone.23 Again, ensure that you are on bone, as you may puncture an artery or vein that you couldn’t palpate. As with all filler treatments, there are risks of complications, such as bruising, swelling or vascular occlusion which can, in extreme cases, result in blindness.24,25 On the temporal bone in this region there are no vessels of concern, as the terminations of the deep temporal arteries are small and posterior. I advise keeping a finger medial to the injection point while injecting so the product doesn’t diffuse medially.
It’s rare that I use more than 0.5ml of product here. I chose a higher G prime product, as it will try to lift and hit the undersurface of the deep temporal fascia, spreading between it and the muscle. You can see the product
flowing towards the zygoma.22 I prefer to leave the temple area flat after injecting and not convex, as I’m trying to recreate a triangle of youth and a V-shaped outline would require flat temples.
Temporal lifting
The result with this technique is to soften the transition from the upper face to the mid-face. I use a 23 gauge needle for the insertion point, 1cm anterior to the tragus. I’ll then use a 22 gauge cannula with a high G prime HA filler. I inject subcutaneously into the subdermal plane. There are no major arteries located here so I inject into the temporal hairline, close to the lateral border of the eye and place 0.2-0.5ml of filler per side (Figure 1).26 Adjunct treatment may include toxin around the orbicularis oculi as well as fillers laterally to lift eyebrows or for mid-facial volumisation. This creates a result where the volume loss is restored and temporal lifting has taken place. As an example, see the treatment in Figure 2, which was carried out with 1.2ml of Teosyal RHA 4 on each side to restore volume deficit. Then 0.6ml of RHA 4 on each side with a 22 gauge cannula for temporal lifting.
Consider temple rejuvenation
Treating the temple can have impactful results for patients experiencing the signs of ageing. There are several techniques that practitioners can choose from. It’s important to identify the suitable patient and the underlying cause of the deformity. This allows you to choose not only the appropriate product, but the suitable technique too. Despite this, the temples are a highly skilled and advanced procedure to treat and should be undertook by trained practitioners with many years of experience.

Dr Harry Singh is a mentor, business coach, keynote speaker, key opinion leader and founder of training academy the Botulinum Toxin Club. He has worked in the industry for more than 20 years helping to build aesthetic clinics in combination with dentistry and has written four books.
Qual: BChD, MFGDP

Before After
Figure 2: Patient before and after temple treatment using 1.2ml of Teosyal RHA 4
VIEW THE REFERENCES ONLINE! AESTHETICSJOURNAL.COM Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com

WE PROVIDE THE COLLECTION YOU PROVIDE THE LOOK UKI-RES-2200306 DOP October 2022 5 5



References: 1. Restylane KYSSE EU IFU; 2. Restylane DEFYNE EU IFU; 3. Restylane VOLYME EU IFU; 4. Restylane LYFT EU IFU; 5. Data on file (MA-39680). Adverse events should be reported. For the UK. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard or search for Yellow Card in the Google Play or Apple App Store. For Ireland. Suspected adverse events can be reported via HPRA Pharmacovigilance, Website: www.hpra.ie; Adverse events should also be reported to Galderma (UK) Ltd, Email: medinfo.uk@galderma.com Tel: +44 (0) 300 3035674 For exclusive offers on the full Restylane range, visit Medfx.co.uk today Restylane® KYSSE™ Adds volume, enhancing the shape of the lip to give a natural and balanced look.1 Restylane® VOLYME™ Creates natural volume and shape in the face. For the correction of facial volume in areas such as the cheeks.3 Restylane® DEFYNE™ Shapes facial contours where definition and flexibility is required, such as augmenting the chin.2 Restylane® LYFT™ Provides lift and structure for a pronounced effect. Recommended for areas of contour and structure where precision is required.4
Understanding the Skin Barrier
As such, we should recommend that our patients use a broad-spectrum sunscreen, minimum SPF 30, and reapply throughout the day or after swimming and sweating. In my experience, mineral sunscreens are better than chemical sunscreens for some patients, such as those who suffer with rosacea. This is because mineral sunscreens sit on the skin and block UV rays, whereas chemical sunscreens will absorb active ingredients that deactivate UV rays, which can cause heat and therefore irritation.4

Have a healthy diet
The human skin comprises of three main layers: the epidermis (outermost layer), the dermis (middle layer) and the subcutaneous layer. The most upper layer of the epidermis is the stratum corneum, and is typically given a likeness to a ‘brick and mortar’ arrangement microscopically; the bricks being corneocyte cells, and the mortar being fats such as ceramides, cholesterol and fatty acids.1 The stratum corneum (SC) acts as a skin barrier and is the body’s first line of defence to the percutaneous penetration of exogenous substances, both accidentally encountered as well as deliberately (outside-inside barrier), whilst also allowing your body to retain water and other components of the body (inside-outside barrier).1,2
The barrier to water permeation is not absolute and the normal movement of water through the SC into the atmosphere is known as transepidermal water loss (TEWL). Any changes in the cellular composition and arrangement results in altered barrier function, leading to conditions such as eczema and psoriasis, as well as symptoms such as dry skin, sensitive or inflamed skin, pigmentation, wrinkles and infection.1,2 It’s important as medical practitioners we are educated and knowledgeable on the
skin barrier function, as some patients are compromising theirs. Some of the treatments we carry out in-clinic could also be contributing to damage.
How to protect the skin barrier
As we know, prevention is better than cure, and so protecting the skin barrier should be the practitioner’s aim. Below is some advice we can pass onto our patients.
Avoid excessive sun exposure
Patients should avoid too much sun exposure because UV rays can cause cellular damage.
Causes of skin barrier damage
Practitioners should encourage their patients to include nutritious foods in their diet. For example, recommend foods that contain omega-3 fatty acids (like oily fish and flaxseed) as these can improve TEWL and skin hydration. Avocados also have the potential to protect skin from sun damage through some of the compounds they contain.5 Another example is broccoli, as this contains a compound called sulforaphane, which can protect against sun damage by neutralising harmful free radicals. Practitioners should become aware of how eating habits impact the skin’s barrier and there are many good resources available to build knowledge in this area.5,6,7
Consider other relevant lifestyle factors
Patients should try not to irritate their skin with long hot baths, pat dry their skin with a towel instead of aggressively rubbing, and to pick spots or scabs. This is because the break in skin causes a defective barrier and also allows bacteria into the skin, which can cause irritation.8 Patients should also try to manage stress levels where possible – a study carried out on 25 healthy women suggests that one mechanism contributing to stress-
Potential causes of skin barrier damage include:1-2
• Environmental factors – dry or humid environment, hot or cold weather, allergens, pollutants, cuts or wounds
• Lifestyle factors – smoking, too much sun exposure, hot baths or showers, an unhealthy diet, lack of sleep, stress, poor skincare
• Patient factors – family history of skin conditions, ageing, ethnicity
• Iatrogenic factors – certain prescribed medications such as steroids, treatments in-clinic such as chemical peels, laser, microneedling, inappropriately prescribed active ingredients for topical use
• pH – normal human range of the stratum corneum pH is 4.5-5.5, and higher pHs have been associated with acute dermatitis
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dr Tara Francis provides an introduction to the skin barrier and its relevance to aesthetic practitioners
Figure 1: Structure of the skin barrier
induced exacerbation of some chronic hyperplastic and inflammatory skin disorders is stress-induced impairment of skin permeability barrier homeostasis.9
The same study showed that there was a significant reduction in skin barrier function recovery after sleep deprivation, so practitioners should advise patients to try and get enough sleep consistently. The generalised and known recommended amount is seven to nine hours of actual sleep, rather than simply resting in bed.9
Look into skincare Moisturisers
The term ‘moisturiser’ implies that the substance applied adds water and/or retains water in the SC. This is true for many of the products in use today, although the mechanism by which this is accomplished may vary. Urea, propylene glycol, glycerin and hydroxy acids (especially lactic acid) are humectants (water holding) and are used in many moisturising formulations; however, they all also function as exfoliants (they promote desquamation).10
Another mechanism for moisturising skin is to provide an exogenous barrier to TEWL so that more water is retained in the SC – a ‘barrier cream’. This is the mechanism by which petrolatum works.10
Ceramides
Formulations that include ceramides are extremely beneficial to protecting the skin barrier function. Research shows that products containing pseudo-ceramides may help improve the dryness, itchiness and scaling caused by a poorly functioning barrier.11 Ceramide-rich moisturisers may also strengthen the structural integrity of the skin barrier.10
Lipids
When applied topically, constituents of lipids (plant oils such as triglycerides, phospholipids, free fatty acids, phenolic compounds and antioxidants) may act synergistically by several mechanisms:13
1. Promoting skin barrier homeostasis
2. Antioxidative activities
3. Anti-inflammatory properties
4. Direct and indirect anti-microbial properties
5. Promoting wound healing
6. Anticarcinogenic properties. Some of the most effective plant oils include coconut oil, jojoba oil and almond oil
Niacinamide
Niacinamide, a form of vitamin B, can help to decrease inflammatory activity, decrease TEWL and increase SC thickness. In one study of 20 healthy patients, areas treated with formulations containing niacinamide were significantly different to pre-treatment baseline and untreated/vehicle-control treated sites, with larger and more mature corneocytes.14
pH
Enzymes in the SC function optimally in an acidic environment and are responsible for the production of ceramides and free fatty acids which affect diffusion through the epidermis. The acidic skin surface, together with an intact SC, prevents colonisation with pathogens and supports the normal skin microbiome.2
As the clinical benefits of acidification are becoming increasingly evident, wherever possible or appropriate, reduced pH emollients and cleansers should be deployed to prevent and treat acute dermatitis.15
Creating a plan for your patient
In my opinion, when consulting patients, you should always gain a thorough understanding of the patient’s skin history, lifestyle, medical history, diet, habits and current skincare regimes.
My advice is to repair the barrier function as best as possible before carrying out any in-clinic treatments such as skin peels, microneedling or heat-based treatments, and before prescribing any active ingredients. This is done by applying knowledge from the guidance above and stripping back to only necessary high quality skincare products – a cleanser, a moisturiser and an SPF is important in my view. I have found that once the skin barrier is functioning better, healing will be quicker after treatments and results will be more effective. When introducing active skincare ingredients, I advise to go slowly and create a gradual approach so as not to over challenge the skin barrier.
Focus on skin health
The skin is a complex organ and the skin barrier has many intricacies in its makeup, cellular activity and influencing factors. What has been mentioned in this article is just a brief snippet of the science behind the skin barrier. There is yet more to be discovered, and more to be investigated, however, from research to date it is clear of some of the things that disrupt the barrier and things we can do to protect it. Our role as medical aesthetic practitioners is to treat the patient as a whole. Most patients come to us with the desire to minimise the signs of ageing or to help with their appearance, including skin quality. However, keeping the skin barrier healthy is an absolute responsibility on our end, as it is not just an aesthetic concern, it is also an overall health concern.
Dr Tara Francis is co-creator and director of The London Academy of Aesthetic Medicine, aesthetic director at Twoth, an Obagi Medical ambassador and Teoxane UK regional associate. Dr Francis has a special interest in skin and includes a holistic approach when consulting with patients who seek her aesthetic services.
Qual: BDS

Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Stratum corneum
VIEW THE REFERENCES ONLINE! AESTHETICSJOURNAL.COM
Sebum barrier Corneocyte Ceramides

The Power of Integrating Skincare In-Clinic
Since 1997, SkinCeuticals has led the way, integrating skincare into the aesthetic treatment space with its vast, potent range of active-rich skincare treatment products, making it the gold standard for aesthetic clinics globally. Long-lasting comprehensive results are achieved through the combination of state-ofthe-art clinical procedures, professional treatments and advanced homecare. Integrated Skincare is a programme built around clinical procedures. Before and after in-office procedures, SkinCeuticals offers homecare for pre-conditioning, post-treatment, and daily use. To maintain and complement results, SkinCeuticals also offer in-office professional treatments such as chemical peels and antiageing protocols. The benefits of Integrated Skincare are clear: a comprehensive regimen that combines homecare, clinical procedures and professional treatments which yields long-lasting results as well as healthier, younger-looking skin.
SkinCeuticals integrated treatment procedures
SkinCeuticals has curated a perfect regime of home-use products to suit all skin types and skin needs to be used daily, or as treatments in conjunction with all the in-clinic treatments listed. For more information about the regimes and the product portfolio, speak to your SkinCeuticals representative.
Professional treatments
SkinCeuticals professional treatments are chemical peels and facial protocols performed by a licensed aesthetician or expert. Designed to work in conjunction with clinical procedures and a SkinCeuticals homecare regimen, these treatments utilise potent technologies available exclusively through professionals. SkinCeuticals skincare professionals are extensively trained to customise these treatment protocols for specific skin types, conditions and skin improvement goals.
Laser
Non-ablative laser patients benefit from skincare that helps reduce downtime, healing and the immediate inflammation post-laser treatment:
o C E FERULIC – is clinically suitable to use immediately post-ablative and non-ablative laser and is clinically proven to reduce downtime post-procedure.* It improves radiance, skin firmness and overall appearance after laser treatment.
o PHYTO CORRECTIVE MASQUE – 83.3% of subjects felt post-laser discomfort was soothed immediately upon product application* plus it reduces skin temperature by up to 2.8 degrees.**
Ablative laser patients benefit from products that are well tolerated after treatment and help reduce downtime post-procedure:
o C E FERULIC – is clinically proven to reduce downtime post-ablative laser treatment.*** It helps against free radicals and improves the skin’s overall appearance
Microneedling
o HYDRATING B5 – is clinically proven to be used at slip agent in treatments as well as post-procedure and is clinically proven to be well tolerated after microneedling treatment helping to replenish moisture with its hyaluronic acid and panthenol.****
Professional chemical peels
In-clinic chemical peels are essential for
Injectables and skincare
Dr Ana Mansouri

commented, “I recommend SkinCeuticals H.A. Intensifier to patients who want to slow down the ageing process and maintain the plumpness of the tissues, a preventative measure alongside injectables. I always say that the things that you do every day (medical-grade skincare) are so much more important than the treatments you do once in a while (such as injectables). I think it is so important to target the ageing process in the skin on a daily basis with medical-grade skincare alongside any treatments you have done in the clinic.”
o H.A. INTENSIFIER – clinically proven to be used pre- and post-neurotoxins/ injectables which helps to improve firmness and plumpness of the skin to complement in-clinic injectable treatments
o MINERAL EYE UV DEFENSE SPF 30 – ideal for use post-treatment in the orbital area
o AOX LIP REPAIR – ideal for use posttreatment in the lip area
maintaining and restoring skin’s health and appearance. SkinCeuticals peels are available exclusively through an authorised SkinCeuticals skincare professional and work synergistically with SkinCeuticals homecare to yield optimal results. Patients are able to prolong their results by incorporating glycolic acid-rich skincare into their regime. Two specific products are clinically proven to help maintain the results of a chemical peel:****
o Glycolic Renewal Cleanser
o Glycolic 10 Renew Overnight
REFERENCES
*Self-assessment, 30 subjects
**Clinical study, 30 subjects
***Three-month clinical study, 40 subjects
****10-week clinical trial, 30 subjects. Candidates used the Glycolic
Renewal Cleanser twice a day and one application of the Glycolic 10
Renew Overnight each evening
*****Instrumental evaluation of 27 subjects
This advertorial was written and supplied by SkinCeuticals
Contact@SkinCeuticals.co.uk https://www.skinceuticals.co.uk/

SkinCeuticals explores how to integrate skincare with aesthetic treatments in your clinic
51 Aesthetics | November 2022 @aestheticsjournaluk Aesthetics @aestheticsgroup aestheticsjournal.com Advertorial SkinCeuticals




Case Study: Correcting Lip Filler Migration

Dr Sana Sadiq shares how she corrected a poor aesthetic result from dermal filler in the perioral area
Dermal filler procedures can cause migration and unnatural results if not performed appropriately. Lip fillers are a common procedure for these complications to occur in. Over recent years, I have observed an increasing visibility in the media and general populous of over-filled, migrated and unnatural lip proportions owing to lip filler. For many aesthetic practitioners, there is a reluctance to try to rectify these cases.1,2,3
There are many reasons for this. Often, these cases have unidentifiable fillers with an unknown safety or composition profile, there is a reluctance to touch other practitioners’ work, practitioners may be uncertain how to dissolve appropriately or may not be confident that they can adequately refill these cases while managing patient expectations. This article follows a case study from presentation through to assessment, planning and retreatment, and offers an algorithm which I prepared based on the Aesthetic Complications Expert (ACE) Group World guidance for managing such cases.2,4
Treating another practitioner’s complication
Unfortunately, due to a poorly regulated market, we see different levels of quality
aesthetic treatments from questionable sources, such as beauticians and lay injectors. As a result, many practitioners are reluctant to deal with cosmetic complications from unknown origins as there is a lot of undisclosed information surrounding the treatment performed, including filler choice, injection technique, aseptic preparation and pre-treatment lip appearance, to name a few. One of the reasons practitioners might avoid involving themselves in another practitioner’s complication is to not be connected in an indemnity investigation against themselves or a previous treating practitioner. When you start treating a patient, the duty of care becomes yours, and although you may be acting in your patient’s best interest, the nature of aesthetic work is subjective and emotional for patients. Starting a treatment on a difficult baseline, which you have little prior knowledge about, sets up both practitioners and patients for a potentially stressful treatment experience. Practitioners should be cautious when considering

whether to treat a complication from another injector. Efforts should be made to collect accurate information regarding the filler used, the date of the treatment, and where appropriate, contacting the previous practitioner, as this may aid retreatment. It is likely that all practitioners will face a complication in their career, however this should not be a point of anxiety and stress if we are trained and confident in managing them prior to treatment. It should also be emphasised that practitioners must only work within their scope and competency. Therefore, if a practitioner feels unable to adequately resolve a complication, they should convey this to the patient and be aware of experienced practitioners to whom they may refer these more complex cases.
Consultation
A 41-year-old female patient presented to my clinic having had lip filler successfully in the past, however, her most recent lip treatment two years ago had resulted in an undesirable aesthetic result. The patient had exclusively seen facial surgeons and dermatologists for her treatments as she was fearful of experiencing complications or poor outcomes and therefore wanted to see someone who could achieve safe and natural results. The patient noticed she had lumps from the beginning of her most recent filler treatment but felt they had become more obvious over time. She also felt the shape was unnatural and her upper lip was bulging in the wet-dry border and was becoming more prominent with time. The patient felt that her lips had always been ‘wonky’, but they had become more unsymmetrical and lacking in definition. She hoped to achieve fuller looking lips with more definition in the cupid’s bow, better symmetry and a more natural shape without lumps. The patient had a breakdown of
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Figure 1: Patient’s pre-treatment lips showing migration of dermal filler
Visible lumps
Visible lumps Distorted smile line contributing to unnatural appearance
Migration into the upper cutaneous lip and upper wet-dry border
A MULTI-LAYERED TECHNIQUE
Using a combination of two volumizing HA fillers: RHA® 4, a dynamic gel that offers soft volume enhancement, alongside Ultra Deep, a static, projecting HA filler that is specifically designed to provide deep structural support, Teoxane can provide the multi-layered approach to treating the mid and lower face.


These complementary products are perfectly positioned to offer your patient optimal lifting and volume, whilst maintaining facial dynamism and natural expressions.
RHA® 4 DYNAMIC & SOFT VOLUMIZING

Manufactured to boast resilience and strength when placed within dynamic anatomical zones, this volumizer will provide soft volume within the superficial fat to naturally enhance and contour the mid cheek.
• High strength & stretch
• Low BDDE + High Molecular Weight
ULTRA DEEP DEEP SUPPORT FOR LIFT & PROJECTION
Designed to provide support that has depleted from the deep fat layers during the ageing process. This static, projecting volumizer with high cohesivity offers structural support with optimal lift capacity to the mid-face.
• High cohesivity
• High resistance to compression
TEOSYAL® PureSense ULTRA DEEP and TEOSYAL RHA® 4 are trademarks of the firm TEOXANE SA. These products are gels that contain hyaluronic acid, and 0.3% by weight of lidocaine hydrochloride (local anesthetic can induce a positive reaction to anti-doping tests). In the case of known hypersensitivity to lidocaine and/or amide local anaesthetic agents, we recommend not use lidocaine-containing products and please refer to products without lidocaine. TEOSYAL® PureSense Ultra Deep exists also without lidocaine: TEOSYAL® ULTRA DEEP. TEOSYAL® PureSense ULTRA DEEP and TEOSYAL RHA® 4 are class III medical devices and are regulated health product bearing the CE marking (CE2797) under this regulation. For professional use only. Please refer to instructions for use. The product availability depends on registration, please contact your local distributor. Please inform the manufacturer TEOXANE of any side effects or any claim as soon as possible to the following address: medical@teoxane.com.
RHA® 4 = TEOSYAL RHA® 4 ULTRA DEEP = TEOSYAL® PURESENSE ULTRA DEEP
communication with the original practitioner as she felt pressured into aesthetic treatments by them. As a result, the patient didn’t want to return to the practitioner to rectify her complication. In the consultation, the patient appeared fit and healthy with no medical conditions or social history to note. She was unsure what dermal filler product had been injected into her lips by her previous practitioner.

Assessment
On visual assessment, the frontal view showed bulging contours at the wet-dry border. This created an exaggerated ‘key-hole’ aperture between the upper and lower lips in the midline when at rest. There was also an unnatural fullness coincident with her upper second incisors and canines bilaterally. Despite having 10 aesthetically optimised upper porcelain veneers placed, the patient’s lip line was distorted when smiling. The lip covered a significant portion of the labial surfaces of all her upper anterior teeth, except her central incisors. The bulging areas had a non-homogenous and firm texture on palpation, with discrete lumps present near the wet-dry border. Her lower lip covered her upper left incisors when smiling due to a large, firm, palpable lump. This created a clear asymmetry upon smiling despite her oral commissure positions being
roughly equal bilaterally. Sagittally, her lips were over projected on Rickett’s E-line (Figure 1).5
Re-treatment and complications
I agreed with the patient that the outcome of the most recent lip filler treatment was not satisfactory and explained in detail the clinical findings. I advised that poor aesthetic outcomes are possible even in the hands of a qualified medical professional and there is always a risk of lumps occurring following a lip filler treatment.

I advised that certain lip anatomy features, such as pocketed lips in this case, can increase the risk of migration and lumps. The
reason for this is there is a natural tendency for filler to collect in the areas of the lip with the least tension, so if too much filler is administered, it will preferentially cluster in a pocketed area. I recommended dissolving the filler and allowing the lips to recover from the current distortion for a period of at least four weeks before attempting to refill them in a careful manner.4 I advised that although the filler will be dissolved within two weeks after hyaluronidase administration, allowing longer for the lips to recover from distortion may decrease the risk of getting an unsatisfactory aesthetic result again.4 I also advised a slow and steady approach, with gradual additional volume to lower the risk of filler migration.
The patient did have some anxiety about dissolving the filler as she was concerned about having small lips while waiting to recover. I reassured her that her lips would not appear significantly smaller than they were prior to her first lip filler treatment and that to achieve natural results, I could not continue to add product to the existing lip filler. I referred to the ACE Group World guidance and converted its advice into an easy flow chart, which helped me come up with the correct plan (Figure 2).4
I informed the patient of the risks of dissolving the filler with hyaluronidase.6 These included local irritation or a severe allergic reaction. I did not perform a patch test on the patient as literature highlighted the poor sensitivity of intradermal patch testing as there’s no validated test concentration.7 If the patient had a history of bee/wasp allergies, then I’d refer to a specialist allergy testing clinic.
I reassured the patient that in the event of the latter, I was able to appropriately manage the complication with adrenaline administration. I also advised her that there is a possibility that the filler used is
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Figure 2: Algorithm for managing poor aesthetic outcomes of lip filler treatment4
annotated
correction Are the lips larger than desired? Dissolve with hyalase +/- refill Dissolve with hyalase +/- refill Dissolve with hyalase +/- refill Dissolve with hyalase +/- refill Monitor Monitor Is there migration to the cutaneous lip? Do they have lumps? Has vigorous massage and heat resolved them? Are they visible? Are they affecting function? Monitor or dissolve with hyalase +/-refill No No No Yes Yes Yes No No No Yes Yes Yes Before After
Figure 3:
Patient
six weeks after dissolving with hyaluronidase and three months post-filler treatment. New smile lines
in black and asymmetry









D i s c o v e r t h e B a b y F a c e p r o t o c o l , o n e o f t h e w o r l d ’ s m o s t i n - d e m a n d L a s e r F a c i a l s . Pigmented lesions | Melasma | Radiance | Texture Skin rejuvenation | Active acne | Wrinkles | Large pores Book your Demo to see why LaseMD Ultra™ is revolutionising skin rejuvenation! 48 George Street London W1U 7DY www.lutronicpbsuk.com General enquiry: info uk@seriderm com Phone: 0207 486 5429 For more information, please contact Lutronic PBS UK & Ireland. 2 0 M I N U T E S , 3 S T E P S t o m e e t a l l n e e d s Before After 2 treatments W i t h t h e c o u r t e s y o f M e g a n S o t i r o p o u o s , ( R N , B S N )
not dissolvable, in which case, aspiration or referral would be required for surgical excision. The patient felt that the general lip size had become larger so I was concerned that it could be a poly-methyl methacrylatebased filler. I also discussed the risks of lip filler treatment, including vascular occlusion, which could lead to skin necrosis, migration, infection and lumps.8 The patient understood and agreed to proceed.
Dissolving the filler
The patient admittedly had a low pain threshold, and therefore was numbed with 2ml of plain 2% lidocaine which was added by labial infiltrations intraorally across the upper and lower lip. The lips were disinfected with hypochlorous acid solution. I prepared 1500IU of hyaluronidase in 5ml of 0.9% bacteriostatic saline. A total of 2ml (600IU) was injected across the upper and lower lips using a 30 gauge 8mm needle. A serial puncture and fanning technique was used with a focus on the palpable lumps and bulging areas. The lips were vigorously massaged until the lumps were softened. Post-procedure instructions were provided, which included no makeup, exercise, alcohol, sunbathing or saunas for 24 hours. I also recommended the patient to avoid omega three supplements to reduce post-procedure swelling. I advised the patient that swelling and bruising were normal and would be strongest in the first 48 hours. A review and retreatment visit were arranged for six weeks later.
Review and retreatment
After six weeks, I reassessed the patient’s lips (Figure 3). They no longer had unnatural contours, bulging or palpable lumps. Her smile line was restored to a natural aesthetic arc, revealing an optimal amount of the labial surfaces of her maxillary teeth. There was still some asymmetry in her lower lip, however no palpable lumps were evident, and her lower lip covered her upper incisors when smiling. The lips had a pocketed appearance and there was some skin laxity in the upper lip in the region of the wet-dry border. I recommended retreating with a soft hyaluronic acid filler. The patient was numbed with 2ml of plain 2% lidocaine which was added by labial infiltrations intraorally across the upper and lower lip and cleansed with hypochlorous acid solution. I used 0.5ml of Teosyal RHA 2 using a 30 gauge needle. This product
was selected due to its low G prime, high flexibility and dynamic stretch. Care was taken to keep all injections within the body of the lips, whilst avoiding injection near the wet-dry border. No vertical threads or tenting technique was used as this carried a larger risk of allowing migration into the lax and previously bulging wet-dry border. In my experience, a vertical thread involves deposition close to the wet-dry border. Horizontal linear threads and fans were administered in a superficial plane. The lips were massaged throughout to ensure no residual lumps, and post-procedural instructions were provided.
Results
The patient was pleased with the outcome and has not required further filler administration since treatment three months ago. Upon smiling, no migration has occurred, and the natural contours achieved at the treatment appointment have been maintained. The patient experienced no side effects or bruising.
Respect the anatomy
This case highlights the importance of anatomy, technique and product selection, respecting the unique natural anatomy of each patient’s lips, and not continuing to build on an already compromised result. It is key that medical practitioners assess facial anatomy and risks for potential complications prior to treatment. Practitioners should also consider the drawbacks of taking on another injector’s complication and whether they are experienced enough to help the patient. If not, practitioners should inform the patient
and refer them to a competent injector. If a practitioner feels they can appropriately manage the case, referencing the simple algorithm in Figure 2 may provide a guide for which cases may require dissolving and which alternative options may be employed to achieve the best possible aesthetic outcomes for our patients.
Dr Sana Sadiq is an aesthetic practitioner and cosmetic dentist. She acquired her Master’s in chemical research followed by her Bachelor of Dental Surgery from King’s College London. She graduated with distinction, winning the highly prestigious University of London Gold Medal Award. She is now the co-founder and medical lead for By Design Aesthetic Academy.

Qual: BDS (Hons), AKC, MSc, BSc (Hons)
REFERENCES
1. Land S, ‘The Last Word: Complication Management’, Aesthetics journal, 2021, <https://aestheticsjournal.com/feature/ the-last-word-complication-management>
2. Ranjbar H, ‘Addressing Filler Complications’, Aesthetics journal, 2021, <https://aestheticsjournal.com/feature/addressing-filler-complications>
3. Bennett S, ‘The Last Word: Other Practitioner’s Complications’, Aesthetics journal, 2017, <https://aestheticsjournal.com/feature/ the-last-word-other-practitioner-s-complications>
4. King M, Convery C, Davies E, ‘This month's guideline: The Use of Hyaluronidase in Aesthetic Practice (V2.4)’, J Clin Aesthet Dermatol, (2018).
5. Ricketts R, ‘A foundation of cephalometric communication’, American Journal of Orthodontics, (1960), p.330-357.
6. Jung H, ‘Hyaluronidase: An overview of its properties, applications, and side effects’, Arch Plast Surg, (2020).
7. Murray G, Convery C, et al., ‘Guideline for the Safe Use of Hyaluronidase in Aesthetic Medicine, Including Modified HighDose Protocol’, Journal of Clinical and Aesthetic Dermatology, 2021, <https://jcadonline.com/guideline-hyaluronidase-aesthetic/>
8. Snozzi P, van Loghem JAJ, ‘Complication Management following Rejuvenation Procedures with Hyaluronic Acid Fillers-an Algorithm-based Approach’, Plast Reconstr Surg Glob Open, (2018).
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Practitioners should also consider the drawbacks of taking on another injector’s complication and whether they are experienced enough to help the patient
Important Safety Information
During the procedure patients may experience sensations of pulling, tugging, mild pinching, intense cold, tingling, stinging, aching and cramping at the treatment site.2 These sensations subside as the area becomes numb.2 Following the procedure, typical side effects include redness, swelling, blanching, bruising, firmness, tingling, stinging, tenderness, cramping, aching, itching, skin sensitivity and numbness. Numbness can persist for up to several weeks. A sensation of fullness in the back of the throat may occur after submental treatment.2 These rare and very rare adverse events have the following incidence rates (approximate occurrences per number of treatments): paradoxical hyperplasia (1/3000 [0.033%]), visibly enlarged tissue volume within the treatment area, which may develop two to five months after treatment, surgical intervention may be required; late-onset pain (1/6000 [0.017%]); severe pain (1/6000 [0.017%]); hyperpigmentation (1/11000 [0.009%]); freeze burn (1/15000 [0.006%]); treatment area demarcation (1/20000 [0.005%]); vasovagal symptoms (1/30000 [0 .003%]); subcutaneous induration (1/30000 [0.003%]); cold panniculitis (1/60000 [0.002%]) and hernia (1/185000 [0.001%]).2,6 The CoolSculpting® procedure is not for everyone. Patients should not have the CoolSculpting® procedure if they suffer from cryoglobulinaemia, cold agglutinin disease or paroxysmal cold haemoglobinuria.2 The CoolSculpting® procedure is not a treatment for obesity.7 CoolSculpting® is not a weight loss procedure and should not replace a healthy diet and active lifestyle.
1. Sasaki GH, et al. Aesthet Surg J 2014;34:420–31. 2. Allergan Inc. CoolSculpting® Elite User Manual. CS-UM-CM3-04-EN-D. February 2021. 3. American Society for Dermatologic Surgery. Survey on Dermatological Procedures: Report of 2019 Procedures. Available from: https://www.asds.net/portals/0/PDF/procedures-survey-results-presentation-2019.pdf [Accessed October 2022]. 4. American Society for Dermatologic Surgery. Survey on Dermatological Procedures 2019: Results infographic. Available from: https://www.asds.net/portals/0/PDF/procedures-survey-results-infographic-2019.pdf [Accessed October 2022]. 5. Allergan Inc. Unpublished Data. Number of CoolSculpting® treatment cycles to date. INT-CSC-2150323. June 2021. 6. Zeltiq Aesthetics, Inc., An AbbVie Company. Full safety information: https://www.coolsculpting.com/pdfs/CSC146039-v2-CoolSculpting_Elite_Full_Important_Safety_Information.pdf [Accessed October 2022]. 7. FDA. K193566. ZELTIQ® CoolSculpting® System. January 2020. CoolSculpting®, the CoolSculpting® logo, the CoolSculpting® ELITE logo, and the Snowflake design are registered trademarks of Allergan Aesthetics. CoolSculpting® systems, applicators and cards are medical devices Class I or Class IIa CE0197. ZELTIQ® is part of Allergan Aesthetics, an AbbVie company. © 2022 AbbVie. All rights reserved. The suitability of CoolSculpting® treatment on an individual patient basis should always be considered as part of the assessment and consultation process. CoolSculpting® is not suitable for all patients. Please consult the Directions for Use prior to the procedure. Patient results may vary.

YOU AND YOUR
To meet your potential with
get
with your
† ASDS Survey on Dermatologic Procedures. Data were collected for the 2019 experience and generalised to represent all ASDS members – 257,868 CoolSculpting® procedures out of
total
EXPERIENCE THE ELITE OFFERING RESULTS
PATIENTS CAN TRUST.1 Treat multiple areas at once with CoolSculpting ® ELITE. 2 Trust the leading non-invasive fat reduction treatment, 3,4† with over 11 million treatment cycles delivered to date.5¶ Model has received treatment with CoolSculpting ®. Individual treatments and patient results may vary.
CoolSculpting ® ELITE,
in touch
local Allergan Aesthetics representative by scanning the QR code or visit int.coolsculptinghcp.com Material produced and funded by Allergan Aesthetics an AbbVie Company. UK-CSC-220145 Date of preparation: October 2022 Adverse events should be reported. Reporting forms and information can be found at: UK adverse events reporting https://yellowcard.mhra.gov.uk Adverse events should also be reported to Allergan Ltd. UK_medinfo@allergan.com or 01628 494026 Irish adverse events reporting https://www.hpra.ie Adverse events should also be reported to Allergan Ltd. UK_medinfo@allergan.com or 01628 494026
1,007,532
body-sculpting procedures. The survey invitation was sent to 3,853 practising members, with 514 physicians reporting. ¶ Patients may require more than one treatment to reach their desired outcome. As of May 2021.
be repeated multiple times with intervals of 15 minutes to one hour.3,4 The reversal agent should be used to flood the affected area and does not need to be directed into the vessel lumen as hyaluronidase readily diffuses across the vessel wall into the intravascular space.4 The protocols clarify that these repeated doses should continue until evidence of re-established skin tissue perfusion.4 The primary indicator of this is the capillary refill time, which should be below two seconds.4
One key feature that I have found to be persistently absent from treatment guidelines is the potential maximum dose of hyaluronidase required. It would be prudent to extend treatment guidelines to include a minimum amount of available hyaluronidase to safely be equipped to manage a VO, should one occur. This would improve patient safety and reduce the risk of patients being part-managed, in the event of an acute HA-induced VO. In light of this, I performed a literature review to evaluate the total hyaluronidase dose required to successfully manage acute HA-related VO, not related to vision loss or blindness.
Exploring Hyaluronidase Dosage
Hyaluronic acid (HA) dermal fillers are the second most common form of minimallyinvasive aesthetic procedure across the globe.1,2 Of all HA dermal filler-related complications, vascular occlusion (VO) is one of the least frequent, yet generally the most feared by aesthetic practitioners and patients alike. The incidence is estimated to be as low as 0.001% of procedures performed.2

Typically, the symptoms of VO onset within minutes to hours, however there are reports of delayed onset VO up to a few days post-injection.1-4 The symptomatology can be quite variable.2,4 The most common symptoms include sudden, progressive pain (at the injection site, or elsewhere) and skin discolouration.2-5 Discolouration can also be variable, particularly depending upon time of onset to presentation. Acutely, it can present with pallor or cyanosis. Either of these, especially if combined with a reticular pattern, should prompt emergency management.4
The Complications in Medical Aesthetics Collaborative (CMAC) advises practitioners to attempt to dissolve HA fillers, no matter the point of presentation – even in the case of delayed presentation with established necrosis in the form of an eschar.4
Hyaluronidase treatment
There are many proposed treatment protocols for acute HA-related VOs, and the mainstay of treatment is enzymatic breakdown of the product with subdermal hyaluronidase injection.4 Although this suggested protocol is now ten years old, there are still relevant points which can be applied to managing a vascular occlusion in current practice. Emergency management protocols for HA dermal filler-induced VO advise doses of up to 1500 units of hyaluronidase per 1ml, dissolved in bacteriostatic 0.9% saline or 1% lidocaine (without adrenaline).2-4 It is clarified that this is not a one-off dose, and treatment should
Methodology and results
To review the literature, a PubMed search was performed. The search criteria were ‘hyaluronic acid AND vascular occlusion’, followed by ‘hyaluronidase AND vascular occlusion’. The search was limited to papers with free access to the full text. These searches yielded 36 and nine articles respectively. Of these articles, the inclusion criteria were any articles including:
1) A protocol for emergency management of dermal filler induced VO
2) A case report describing successful management with hyaluronidase
3) A case series or cohort study describing successful management of the above with hyaluronidase
Discussion
In 2012, Beer et al. devised a treatment protocol for emergency management of VO in the context of particulate soft tissue augmentation.4 The author commented on the obvious: the inability to perform high level evidence such as a randomised control trial (RCT) to compare rescue treatments for VO, for simple ethical reasons.4 Therefore, we rely on past experience (case reports or case series, as well as expert opinions). Beer et al presented two cases as such. Unfortunately,
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Mr Jordan Faulkner discusses the total dose of hyaluronidase required to successfully treat dermal filler-induced vascular occlusions
Case study
In my experience, the largest total dose of hyaluronidase required to successfully treat VO occurred in 2021, presented to me by Joanna Sillince, aesthetic nurse practitioner at S18 Face clinic. A female patient in her 30s was successfully managed for a VO to the chin following 15 initial pulsed doses of hyaluronidase. She had a total of 6x0.1ml boluses of a well known HA filler across the chin area, injected at the periosteal level. The clinician performed aspiration before every injection, all of those being negative. Shortly after the procedure, the injector noted an area of marked pallor, about 2x3cm on the left side of the chin, with a larger area of mild pallor and reticular changes spreading down the neck area between the midline and the anterior border of the sternocleidomastoid muscle. The capillary refill time (CRT) was about five seconds. The area was flooded immediately with 1500u of hyaluronidase in 2ml bacteriostatic saline and massaged firmly with a hot compress. 300mg oral aspirin was given. Following discussion with the ACE Group World, the hyaluronidase infiltration was repeated a total of 15 times, with 10-15-minute intervals. The clinic exhausted their emergency supply of hyaluronidase and had to contact other local practitioners to get hold of further doses before CRT was under two seconds, indicating re-established perfusion. The patient was reviewed the following day and further hyaluronidase was administered across the neck area, and the local emergency department was contacted to enquire about the possibility of ultrasound investigation. A further dose of hyaluronidase was administered the day after that. The patient was reviewed three days later, and the area was perfused throughout but tender bruised. The patient had no long-term scarring.
both cases describe patients treated with injectable calcium hydroxylapatite (CaHA) and are therefore not directly relevant to this discussion. Nevertheless, it is worth noting that the treatment for case two did include the employment of hyaluronidase – 600 units diluted in 5ml normal saline. Here, the aim was to dissolve the native HA to reduce external compression of the affected vessel, hence this treatment protocol can effectively be discounted from our discussion. However, looking at the bigger picture, this paper remains relevant, particularly given the introduction of Allergan’s HA and CA combination filler, HArmonyCa, to the market.
Cohen et al. wrote a more relevant consensus report on the treatment of HA-induced impending necrosis with hyaluronidase in 2015.2 Their suggested treatment algorithm advises starting with 200 units of hyaluronidase, and suggests mixing with lidocaine over normal saline, in view of its vasodilatory properties.2 They suggested one injection for every 3-4cm of skin showing signs of impending necrosis. Their suggested interval period was 60 minutes, at which point the dose should be repeated if resolution was not achieved repeating up to three to four cycles, thus suggesting 800 units of hyaluronidase should be adequate.2 They did include a disclaimer in their discussion, that different formulations of hyaluronidase may vary in
efficacy, and therefore this consensus is only applicable to the most widely used formulation in the US at the time, Vitrase.2 The transferability of this information to use of the UK’s current most widely used formulation, Hyalase, is questionable.
More recently, in 2018, an expert panel of aesthetic practitioners combined to develop consensus recommendations for the treatment of soft tissue filler complications.3 Again, this only provides low level (level V) evidence. Previous evidence referenced in this paper had recommended doses of 200-300 units of hyaluronidase.3 They go on to suggest repeating hourly until clinical resolution is achieved, permitting doses up to 1500 units.3 No specific brand names were given in this paper.
The most recently published guideline available from this PubMed search was produced by Murray et al. (CMAC), in May 2021.5 This guidance is UK-based and relates to the prescription-only medicine (POM) formulation of hyaluronidase produced by Wockhardt in Wrexham. Their guideline, referenced in the introduction to this article, suggests using 1500 units of hyaluronidase in 1ml of 0.9% bacteriostatic saline or 1-2% lidocaine.5 Murray et al. further developed their protocol in August 2021, when they updated their advice on the interval between repeated
doses of hyaluronidase. Based upon the half-life of hyaluronidase when injected subcutaneously or intramuscularly (5.1 and 7.5 minutes, respectively), they suggest repeating doses every 15 minutes until clinical resolution is achieved.6 This was the first time an author had taken the half-life into consideration when suggesting the appropriate interval, across papers in this review. In another single case report of delayed HA-induced VO, a patient presented with pain and discoloration at the injection site and beyond, with onset more than 48 hours post-injection.1 He was treated with three doses of 500 units of hyaluronidase in 10ml of solution hourly, more than three hours. At three hours, a remarkable change in skin colour was noted and after a further hour, the patient was sent home.1 He was followed up 14 hours later and received a further single injection of 500 units in 10ml.2 The diluent was not given in the article. He was reviewed at 15 days and had no residual scarring.1 In their discussion, they commented on the lack of unanimity of the correct dose or interval between doses between suggested protocols.1
Outcomes
Each of these papers have their own limitations, many of them shared. All evidence discussed in this article is of low level: case reports and expert opinions only. It is unlikely that we will ever overcome the impossibility of performing a large RCT, as it would be immoral to trial variable doses or concentrations of hyaluronidase in cases of VO, given the risk of undertreating an individual leading to long term facial disfigurement. Not to mention, the logistical nightmare that would be involved in enrolling enough clinicians to gather data prospectively for such an infrequent complication.
A key limitation of this article itself is the relatively small yield of articles that include information relevant to the question in hand. This is undoubtedly, in part, down to the inclusion of articles with free access to the full text only. However, this approach was taken with good reason. Many aesthetic practitioners in the UK work independently or in a private aesthetic clinic. Many of them no longer engage in clinical work in the NHS. Therefore, they are unlikely to remain affiliated with their university or a large NHS institution. This creates a financial barrier between those needing access to this information, and
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
a large percentage of the information itself. For reference, when the search was repeated without limiting it to those with free access only, the total number of articles yielded was 183, compared to only 45 with free full access. In practice, aesthetic clinicians are more likely to rely upon dedicated resources such as the Aesthetic Complications Expert (ACE) Group World or the CMAC than a PubMed search, especially in the event of an emergency. For reference, the ACE Group World guideline for emergency management of a VO does not include a potential total dose required.7
Next steps
In summary, we require a large scale, nationwide survey of medical injectors at all levels. This should be anonymous to reduce under-reporting. This survey should evaluate the understanding of injectors on the signs and symptoms of HA-induced VO. It should evaluate their opinion on the appropriate emergency management. Finally, it should collate information on the number of experiences of VO of each clinician, what dosing regimen of hyaluronidase was used in those cases, and whether the treatment was successful or not. This would provide higher-level evidence, in the form of a retrospective cross-sectional study. The information produced would allow us to describe the highest total dose of hyaluronidase required to resolve a VO to date, and from that suggest a minimum storage amount of hyaluronidase for injectors to work comfortably, knowing they will be able to adequately manage a VO, should one occur, with the stock they have immediate access to. Last of all, this protocol should be free and readily available to all medical injectors using hyaluronic acid dermal fillers.
Mr Jordan Faulkner is the founder of Allo Aesthetics and runs clinics in South West London and South Yorkshire. He is an instructor at Interface Aesthetics, and maintains a role as a surgical SHO at Chelsea and Westminster Hospital.

Qual: BMedSci, BMBS, MRCS
REFERENCES
1. Singh, S. and Chauhan, A., 2019. Management of delayed skin necrosis following hyaluronic acid filler injection using pulsed hyaluronidase. Journal of Cutaneous and Aesthetic Surgery, 12(3), p.183.

2. Cohen, J., Biesman, B., Dayan, S., DeLorenzi, C., Lambros, V., Nestor, M., Sadick, N. and Sykes, J., 2015. Treatment of Hyaluronic Acid Filler–Induced Impending Necrosis With Hyaluronidase: Consensus Recommendations. Aesthetic Surgery Journal, 35(7), pp.844849.
3. Urdiales-Gálvez, F., Delgado, N., Figueiredo, V., Lajo-Plaza, J., Mira, M., Moreno, A., Ortíz-Martí, F., del Rio-Reyes, R., Romero-Álvarez, N., del Cueto, S., Segurado, M. and Rebenaque, C., 2018. Treatment of Soft Tissue Filler Complications: Expert Consensus Recommendations. Aesthetic Plastic Surgery, 42(2), pp.498-510.
4. Beer, K., Downie, J., Beer, J., 2012. A Treatment Protocol for Vascular Occlusion from Particulate Soft Tissue Augmentation. The Journal of Clinical and Aesthetic Dermatology [online] 5(5), pp.44-47. Available at: < https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC3366448/>
5. Murray, G., Convery, C., Walker, L. and Davies, E., 2021. Guideline for the Safe Use of Hyaluronidase in Aesthetic Medicine, Including Modified High-Dose Protocol. The Journal of Clinical and Aesthetic Dermatology, [online] 14(8), pp.E69-E75. Available at: < https:// www.ncbi.nlm.nih.gov/pmc/articles/PMC8570661/>
6. Murray, G., Convery, C., Walker, L. and Davies, E., 2021. Guideline for the Management of Hyaluronic Acid Filler-induced Vascular Occlusion. The Journal of Clinical and Aesthetic Dermatology, [online] 14(5), pp.E61-E69. Available at: <https://www.ncbi.nlm.nih.gov/pmc/ articles/PMC8211329/>
7. King, M., Convery, C. and Davies, E., 2018. This month’s guideline: The Use of Hyaluronidase in Aesthetic Practice (v2.4). The Journal of Clinical and Aesthetic Dermatology, 11(6), pp.E61-E68.
Silicone gels such as KELO-COTE used for first-line preventation and treatments of hypertrophic and keloids have been shown to have better patient acceptability than silicone sheets, leading to better patient compliance.1,2



Helps soften and flatten scars
Helps relieve itching and discomfort
Available as a UV SPF30 gel, to protect from the harmful effects of the sun

Available as a spray for larger, sensitive scars
1. Monstrey S, et al. Updated Scar Management Practical Guidelines: Non-invasive and invasive measures. Journal of Plastic, Reconstructive & Aesthetic Surgery 2014;67:1017–25.
2. Chernoff WG, et al. Aesthetic Plastic Surgery 2007;31(5):495-500. JB-0001381. Date of Prep: April 2022
C-SECTION SCARS BURN SCARS SURGICAL SCARS COSMETIC SURGERY SCARS
Helps reduce redness
clinically proven preventative scar treatment that links your expert craft to patient satisfaction. 167156 KELO-COTE Half page print ads 95x265_FINAL.indd 2 06/05/2022 09:36
THE VITAL LINK A
100 MILLION
We have reached a significant milestone, the manufacturing of 100 million JUVÉDERM® syringes.1,*
While we are proud of this achievement, reaching this milestone means so much more than a number.
For us, it represents so many patient experiences, because we craft every JUVÉDERM® treatment to highlight our patients’ individuality. Since our launch in 2006, the JUVÉDERM® brand has experienced a remarkable evolution that is still ongoing today.
We couldn’t have reached this landmark without the collaboration between Allergan Aesthetics, the expert skill of practitioners… and of course the JUVÉDERM® experience that you continue to share. It is because of these partnerships that so many patients have been able to achieve their unique aesthetic goals.
Although 100 million syringes is a significant milestone for us, we recognise that our journey continues and there is so much more to come.
Adverse events should be reported. Reporting forms and information can be found at: UK adverse events reporting https://yellowcard.mhra.gov.uk/ Adverse events should also be reported to Allergan Ltd.
UK_medinfo@allergan.com or 01628 494026
Irish adverse events reporting https://www.hpra.ie Adverse events should also be reported to Allergan Ltd.
UK_medinfo@allergan.com or 01628 494026
At JUVÉDERM®, we believe that with our holistic treatment approach to individual beauty, combined with strong partnerships between Allergan Aesthetics and physicians, we can go beyond 100 million syringes.
* 100 million JUVÉDERM® syringes manufactured worldwide from 2004 to April 2022.1
1. Allergan Aesthetics. Data on File. REF-96563. FILLERS GLOBAL NUMBER OF SYRINGES. May 2022.
This content is intended for UK adult (>18 years) audiences only. ©2022 Allergan Aesthetics, an AbbVie company. All rights reserved. Produced and Funded by Allergan Aesthetics, an AbbVie company.
UK-JUV-220326 October 2022
Case Study: Treating the Lower Face
Dr Chris Rennie rejuvenates the lower and mid-face in a female patient
A 51-year-old female patient presented to my clinic with concerns about the appearance of her lower face and volume loss in the mid-face, feeling that she looked quite skeletal. When performing a consultation, I never sit in front of a patient and say ‘you need XYZ’, because I do not want them to leave feeling more self-conscious than they were when they arrived. So, I always ask the patient what their problem area is, and then after assessing them properly I suggest treatment options. I also look at them in three dimensions – from the front, the oblique and the side – taking into consideration how they look both when static and in animation. It’s important to note what the patient looks like when they’re smiling and moving to see how different areas of their face interact with each other. I then consider the face in thirds – upper, middle and lower – to see if there are any jarring or big contrasts between them. Next, I observe whether there’s any asymmetry between the left and right sides of the face. Throughout the assessment, I always explain to the patient what I’m seeing when I’m seeing it, and educate them on what treatment options might be the most beneficial as a result. From this, I determined that the patient had had poor lower face skeletal contour, with a small and retrognathic chin, gravitational descent of the superficial jowl fat pad, poor anterior projection of her


mid-face with focal volume loss in the deeper fat compartments. These regions were going to be my primary targets for treatment with a view to progressively improve other areas accordingly afterwards.
Product selection and technique
In terms of technique, I first wanted to create a structure and outline before I focused on volume loss, so as to make her face look more balanced and the proportions harmonised. To do so, I injected 2.4ml of Teosyal® PureSense Ultra Deep in the chin and posterior jawline, and then multi-layered that with 2.4ml of RHA® 4. I chose this product due to its unique rheological profile dedicated to respecting facial expression. Therefore, it can be used in the areas that traditional fillers can’t as these run the risk of becoming visible when the patient animates. When injecting, I was aware that her jowl fat pad had hypertrophied over time, meaning I needed to blend the other aspects of her face into the jowl fat pad to avoid any harsh contours and shadowing.
I also injected 1.2ml of PS Ultra Deep into the deep static fat pads in the mid-face to create some extra anterior projection and lateralisation, getting a taper and turning her longer, more oval face shape into a heart shape. For any of the deep periosteal work, I used a needle but for multi-layering, I used a microcannula to help create that
soft contouring. After the initial treatment, the patient had a follow-up session four weeks later so I could perform some small maintenance tweaks. Here I injected 1ml of RHA® 2 to address the perioral lines and deeper folds, and 3ml of the Redensity® 1. treatment to improve her overall skin quality.
Results
Both the patient and I were delighted with her results. When the patient first presented to my clinic, I found her demeanour could be considered quite harsh or somewhat abrupt, however when she came back for the review appointment she was softer and more personable. She explained that as her appearance had changed, this had translated into other areas of her life and had impacted how people responded to her/how she approached people. She also noted that she was a lot more confident in herself as a result.
Top tips for success
Remember that you are a medical professional and not a vending machine –what the patient is asking for does not mean that is what you have to give them. Assess them properly and decipher what the best treatment options really are depending on their individual anatomy. You should also always explain to your patient why you’re choosing the treatments you are, so that they can fully reflect on everything and make an informed decision. This will help build trust too, so it’s good for patient retention. Finally, I recommend following the principles of anatomy, technique and product. This is so that you can stand there and explain to your patient why you have chosen to treat the areas you have treated, why your techniques are beneficial for them and why you have chosen the products you have. I believe it is important to use a product portfolio where each product is designed for different indications of the face, to elevate the results.
Dr Chris Rennie obtained a degree from the University of Wales College of Medicine in 2005. He now works as the clinical director of Romsey Medical Practice in Hampshire, is a medical injectable doctor, and a country expert for the Teoxane UK Educational Faculty.

Qual: MBBCh, MRCS (Eng)
This advertorial was supplied by
Teoxane.com/uk
Figure 1: Patient before and after treatment of the mid and lower face 64 Aesthetics | November 2022 @aestheticsjournaluk Aesthetics @aestheticsgroup aestheticsjournal.com Advertorial Teoxane
Before After
A summary of the latest clinical studies
Title: Patient Comfort, Safety and Effectiveness of Resilient Hyaluronic Acid Fillers Formulated With Different Local Anaesthetics
Authors: Kaufman-Janette J, et al.
Published: Dermatological Surgery, October 2022
Keywords: Dermal Filler, Hyaluronic Acid, Local Anaesthetic
Abstract: Maximising patient comfort during hyaluronic acid gel injection is a common concern that is usually addressed by selecting fillers with lidocaine. Two randomised, double-blinded, split-face trials aimed to demonstrate non-inferiority of specific hyaluronic acid fillers incorporating mepivacaine (RHA-M), versus their lidocaine controls, at providing pain relief. Thirty subjects per trial received injections of RHA R-M versus RHA R, and RHA4-M versus RHA4, respectively, in the perioral rhytids (PR) and nasolabial folds (NLF). Pain was assessed on a visual analogue scale; aesthetic effectiveness was evaluated with validated scales, and safety was monitored based on common treatment responses (CTRs) and adverse events (AEs). RHA-M fillers proved as effective as their lidocaine counterparts at reducing pain (noninferior, p < .0002 and p < .0001). Bilateral wrinkle improvement was measured both in the PR (-1.5 ± 0.6 points on each side) and in the NLF (-1.8 ± 0.6 and -1.9 ± 0.5 points) trials at one month, with virtually identical responder rates (≥96.7%). Common treatment responses and AEs were similar between treated sides, and none was clinically significant. Resilient hyaluronic acid fillers with either mepivacaine or lidocaine are equally effective at reducing pain during treatment, and equally performant and safe for correction of dynamic facial wrinkles and folds.
Title: Use of Retinoids in Topical Antiageing Treatments: A Focused Review of Clinical Evidence for Conventional and Nanoformulations
Authors: Milosheska D, Roŝkar R
Published: Advances in Therapy, October 2022
Keywords: Antiageing, Retinoids, Skincare
Abstract: Retinoids are one of the most popular ingredients used in antiageing treatments. The most commonly used retinoids such as retinol, retinaldehyde and retinyl palmitate are contained in cosmeceuticals regulated as cosmetics. Since clinical efficacy studies are not required for marketing cosmetic formulations, there are concerns about the efficacy of these retinoids. From a formulation perspective, retinoids pose a challenge to researchers because of their proven instability, low penetration and potential for skin irritation. Therefore, novel delivery systems based on nanotechnology are being developed to overcome the limitations of conventional formulations and improve user compliance. In this review, the clinical evidence for retinoids in conventional and nanoformulations for topical antiageing treatments was evaluated. In addition, an overview of the comparison clinical trials between tretinoin and other retinoids is presented. In general, there is a lack of evidence from properly designed clinical trials to support the claimed efficacy of the most commonly used retinoids as antiageing agents in cosmeceuticals. Of the other retinoids, tazarotene and adapalene have clinically evaluated antiageing effects compared to tretinoin and may be potential alternatives for antiaging treatments. The promising potential of retinoid nanoformulations requires a more comprehensive evaluation with additional studies to support the preliminary findings.
Title: Comparative Study Between Topical Application Of Triamcinolone Acetonide After Fractional Carbon Dioxide Laser Versus Microneedling In Treatment Of Resistant Alopecia Areata
Authors: Omar M M, et al.
Published: Dermatologic Therapy, October 2022
Keywords: Alopecia Areata, CO2 Laser, Microneedling Abstract: The aim of this study was to compare the efficacy of topical application of triamcinolone acetonide after fractional carbon dioxide laser versus microneedling in the treatment of resistant alopecia areata from a clinical and dermoscopic perspective. Thirty patients were randomly divided into two groups of 15: the laser group received fractional CO2 laser treatment followed by topical application of triamcinolone acetonide, and the microneedling group received Dermapen treatment followed by topical application of triamcinolone acetonide. We found no statistically significant difference between the studied groups before and after treatment, except for black dot, which is higher in the microneedling group than in the laser group (46.7% versus 13.3%). There was a statistically significant difference between the studied groups in terms of treatment response at the first follow-up, with 13.3% of the laser group seeing terminal hair regrowth compared to 0 in the microneedling group after 12 weeks. Regarding the degree of improvement, there was no statistically significant difference between the laser group and the microneedling group. There was no significant difference between the two treatment methods in terms of their high effectiveness in the treatment of resistant alopecia areata.
Title: Evolving Concepts in Psoriasis: Special Considerations for Patients With Skin of Colour, Skin Barrier Dysfunction, and the Role of Adjunctive Skincare
Authors: Alexis A, et al.
Published: Journal of Drugs in Dermatology, October 2022
Keywords: Care Disparities, Psoriasis, Skin of Colour Abstract: Knowledge gaps in the clinical presentation, quality-of-life impact and approach to treating psoriasis in skin of colour (SOC) patients contribute to disparities in care. In addition, small studies suggest that using skincare products can reduce psoriasis symptoms, improve barrier function and result in higher patient satisfaction, yet patients with psoriasis may underuse skincare products. A structured literature search followed by a panel discussion and online review process explored best clinical practices in treating SOC psoriasis patients, including guidance on gentle cleansers and moisturisers. Racial/ethnic differences in genetic factors, clinical presentation and disease burden in psoriasis have been reported. Under-recognition of these differences contributes to racial/ethnic health disparities for psoriasis patients in the US. Several studies have shown a greater quality-of-life impact with psoriasis among SOC patients. Although the published data is limited, some studies have identified differences in skin barrier properties and suggest a role for adjunctive skincare in the management of psoriasis. Further studies are needed to understand racial/ethnic population variations in psoriasis and develop strategies to reduce disparities in care.
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Selling in a Financial Downturn
Business consultant Vanessa Bird outlines
With each passing day, we are bombarded with news about the financial status of the UK. Energy prices are hitting record levels with no signs of slowing down, impacting businesses and households who are sent record bills for energy use.1
The cost-of-living crisis is in full swing and people are naturally more cautious about spending, preferring to make cut backs on non-essentials to ensure they can pay their bills, fuel the car and feed their family. How can we stay positive in these economically challenging time when the word ‘recession’ is mentioned in the news on a daily basis? What can we do to bring in more sales, increase spend and keep our aesthetic businesses healthy when our patient base starts to cut back and spend less?
First and foremost, keep a clear head. Panicking is counterproductive. If you’re worried about how your clinic will survive or anxious about generating enough revenue, then this article will provide practical advice and actionable steps you can use to help sell more treatments and survive the financial downturn.
Why do people buy?
People have many motivations behind what they choose to buy, but the driver behind making the decision to proceed
with a purchase is emotion. Sales expert and author of Heart and Sell: 10 Universal Truths Every Salesperson Needs to Know, Shari Levitin, talks about the need to ‘connect with a customer’s deep emotional motivators’ in order to sell.1 Logic alone is not enough to trigger a sale. There needs to be an emotional connection too, and it’s that connection that results in the decision to invest in your services. Forging this emotional connection should be at the forefront of your mind when you are promoting and selling treatments. Something has to make sense (logic) and feel right (emotion) in order for the sale to proceed.
A financial squeeze may mean that someone’s budget is reduced, but they still have the same wants and needs they had before. Wanting to look more youthful or craving healthy skin is still important to patients. They want to feel confident in how they look and that may involve having non-surgical treatments that enhance their face and body and boost their self-esteem. People will always find money for things that make them look and feel fantastic.
Revisit existing demographics
When was the last time you looked at your patient demographics? You are attracting a particular type of patient because of the
treatments you provide and the results you deliver. Look again at each demographic and identify who they are and what they want. Are they younger patients in lower paid jobs who want regular injectable treatments? Perhaps you treat mid-lifers with more disposable income who want to tackle the signs of ageing by having courses of treatments? Or are they older patients who need a more intensive treatment regime and don’t mind spending to achieve this? How will the financial downturn affect them all?
Analyse each group. Are there better ways you can accommodate their needs, so they still have the results they want without having to drastically cut back on spending? Perhaps there are new treatments you can offer to meet other needs they have? It is easier and more cost effective to sell to and retain an existing customer than prospect for a new one. Existing patients have that emotional connection with you and the trust is there. So, it’s all about retention in the first instance. Not only will they spend more readily with you, but they are more likely to refer you to friends and family, growing your patient base further. After this, you should look at promoting packages and treatments on social media to draw in enquiries from new patients too.
Consider asking for referrals and rewarding patients who bring in a paying customer with a credit on their account or a treatment that doesn’t cost you much in terms of time or consumables such as a chemical peel or LED therapy. Always include skincare as part of the treatment package. Remember if they aren’t buying skincare from you, they are buying it elsewhere, so make it easy for them to purchase from you.
Repackage your treatments
Once you have reassessed each demographic and identified their common wants and needs, it’s time to refresh and repackage your existing treatments to provide more value for money. People will be looking for value right now, so if you can provide this in-clinic, you are more likely to retain patients.
Write down all the injectables, skincare and energy-based treatments you currently offer, then get creative. How can you combine some of these treatments to boost results?
What packages can you create that meet the most pressing needs of your patients? Don’t offer skincare as an optional extra. When times are hard, the customer may cut back. Instead, bundle in skincare so the average
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
how to improve your selling skills and provides strategies to help drive sales
sales value increases. Above all, don’t be tempted to discount. You’ll end up in a price war with your competitors and it will be a race to the bottom. Plus, when recovery happens, and it will, you will find it harder to increase your prices again.
Introduce the ‘Goldilocks’ approach and create three versions of each package so a patient can upgrade or downgrade to suit their budget. Options mean a patient is less likely to say no. The middle package will be the one you promote and recommend most frequently as it will meet the needs of the patient and also generate revenue. For an upgrade amount of a few hundred pounds, patients can opt for the premium package and receive greater value with perhaps more top-up treatments, added skincare or even a bonus peel or home care kit. It’s also important to offer a simpler solution, perhaps with less skincare or fewer treatments and this will be in a more affordable price range.
Why offer a cheaper solution? Your patient has something either side of the recommended package to measure value against and, if they wish, can upgrade (or downgrade if needing to save some money) accordingly. It’s better to downgrade if needed and provide some value than to lose a patient completely as they cannot afford the recommended package.
Stay visible and promote your new treatment packages. Social media is a great place to showcase new packages using reels, posts and stories. Update your website blog to announce the latest package options available, and don’t forget to reach out via newsletters or e-shots to your database so they are aware there is something new that provides exceptional results and value for money. Nobody wants to buy something from a clinic that looks like it’s struggling, so by promoting something new, you catch the eye of the patient and stay one step ahead of the competition.
Change tactics
There’s an age-old saying in sales – ‘features tell, benefits sell’. You may have a more expensive laser than your competitors and worry your patients will seek out a cheaper option. So, address the features and benefits from a financial point of view. Firstly, talk about the features of the laser. This could be the technology used, the superior results and the speed it takes to treat. Next talk about the benefits of the laser The technology used means you get better
results which last longer, saving the patient money in the long term. As the laser is more advanced, fewer treatments are needed which means the patient doesn’t have to make as many visits to the clinic, saving money on travel and parking. Help them see how investing more now will save money in the long term.
Brush up on selling skills
If you or your team don’t feel confident selling, invest in sales training or a coaching call with a sales trainer to teach you the basics. Although there will be an initial outlay, this should pay for itself within the first month or two post-training, as your team will have new skills to ethically sell to patients, increasing your average spend. Don’t forget there are plenty of helpful articles on sales in publications such as the Aesthetics journal, and some suppliers now include sales training as part of the support package they offer. Business webinars focusing on selling in clinics can also be a useful tool and you can usually find those linked with pharmacies, training academies or companies who sell to aesthetic clinics. Industry conferences like CCR and ACE have business agendas designed to help you grow, so try and soak up as much business advice as possible and act on it.
Invest in your team
The best people deliver the best results for your patients, so try not to lay staff off as you’ll need a good team to help you during this economic climate. Schedule weekly team meetings to keep staff motivation high, reminding them of the importance of customer care and recommending additional treatments and products to existing patients. Motivated staff who sell more treatments will help you generate more revenue to pay their wages. Make sure they know you value and appreciate them, so they are more willing to work together as a team to get through this challenging time. Incentivise the right behaviour such as converting enquiries to consultations, cross-selling, up-selling treatments and getting referrals. You can incentivise individually or as a group by setting targets and rewarding them with bonuses, commission or even a team lunch. These all positively impact your business. Good people are hard to find, so it’s better to train your team rather than start from scratch so you can avoid costly recruitment bills.
Stay in contact with your patients
Now is not the time to lose touch with your patients as everyone is vying for their hard-earned cash. Send out newsletters advertising new packages. Sending text messages or e-shots advertising last-minute cancellations will keep your diary (and bank account) full. Create a short survey, either through Instagram stories or an email questionnaire to ask patients for their opinions. Would they like you to open at weekends or introduce payment plans? What else can you help them with? Ask the question, listen, then deliver. It’s also important to improve response times. Whether a patient reaches out via your online form, telephone or social media, always respond within a few hours. If you don’t answer, they may enquire at another clinic which responds to them faster. Don’t lose business because you waited a day or didn’t have anyone checking the inbox over the weekend.
Stay positive
The aesthetics market is resilient even in times of recession, so concentrate on what you can control rather than on things that are out of your control. Start by implementing one or more of the methods in this article focus on what you’re good at and do more of it. Be flexible and ready to change, amending treatments or extending opening hours. Reach out to local businesses who will be facing similar challenges and discuss how you can support each other by referring customers. Remember you’re not alone –the aesthetics industry is fast-moving and responsive, with the ability to weather any financial storm. So, stay positive, remain calm and take action now.
Vanessa Bird is the founder of The Aesthetic Consultant. She has more than two decades of sales experience and 14 years in the aesthetics industry. She now works with companies, clinics and practitioners to help them increase sales and grow their businesses.

REFERENCES
1. Levitin S, ‘Heart and sell: 10 Universal Truths Every Salesperson Needs To Know’, 1st edition, 2017.
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com



THE NEXT GENERATION OF PROFESSIONAL SKINCARE IS HERE
Allowing you to foster close, long-term relationships with your clients. Transforming your clinic business and earning you money even while your doors are closed. Create a completely unique skin health journey with the eventis business solution from iiaa.
For more information, please contact us on 02037458310 or email stockists@iiaa.eu

REGISTER INTEREST HERE NOW

Utilising Social Media Effectively
Communications manager Cait McLaughlin shares advice for staying abreast of the ever-changing social media landscape and using video to promote your clinic
We’re busy people. We have clinics to run, patients to see and business critical tasks to take care of. As the pandemic proved, social media is an integral tool in our marketing arsenal and one that demands our attention. It acts as the shop window to our businesses, and it’s often the first place prospective patients will find us. With Instagram desperately trying to compete with the likes of TikTok, and video content being more heavily prioritised in our customers’ feeds, what can we do as busy business people to make adapting to social media changes as manageable as possible?
Ultimately, our social media platforms give us an incredible opportunity to build trust with prospective patients, allowing them to get to know us before they even pick up the phone to book an appointment. The old marketing mantra of ‘The Seven Times Rule’, developed by marketing guru Dr Jeffrey Lant, states that a consumer has to see a particular advertisement, service or product seven times before the message will really
resonate.1 When a social media user sees an advert or a piece of content, it often takes creative repetition for the message to truly sink in and encourage the user to take action by seeking more information, booking an appointment or buying a product. That’s why it’s so important that as business owners, we utilise social platforms confidently, using them to their maximum potential to yield the best results.
How video is transforming social media
Following the rise in popularity of short-form video app TikTok, Instagram – which had previously been an image-focused platform –has been in a perpetual state of diversification in order to compete. In 2019, Instagram introduced Reels – full-screen, vertical videos that can be several minutes long. In 2021, head of Instagram Adam Mosseri declared that the platform is ‘no longer a photo-sharing app’, and that it will ‘embrace video’ going forward.2 Creators are therefore encouraged
to up their video game in order to stay at the top of followers’ feeds.
It comes as no surprise that video content resonates more effectively with audiences. On a basic human level, our brain enjoys video content because it’s easier to retain visual information, and users on social platforms fundamentally find videos more engaging than static imagery. According to a report by software company DataBox, 60% of marketers said that video content drives more clicks on Facebook, compared to just 30% who said that static imagery is the most engaging.3
So, with these changes in mind, it’s important to consider how we rely on social media to remain a valuable marketing tool for our businesses, while not allowing it to completely overwhelm our already hectic workload.
Outlining short-term goals
Firstly, when it comes to managing a successful social media account, it’s important to set out some goals for the month ahead. Do you want to increase brand awareness? Do you have a specific campaign you’d like to promote? Would you like to better understand your audience? Increase traffic to your website? Publicise your successes? Share news? Thinking about the ‘why’ in advance will allow you to shape the type of content you’ll be creating, and it’ll feel less like you’re posting for the sake of posting.
Bulk scheduling content ahead of time will prove an excellent way to make the most of the time you spend on social media. Using tools like Meta Business Manager, Hootsuite or Later, you can develop content well in advance and post to your social platforms at a date and time that suit you, and your followers. By dedicating a few hours to writing content, preparing video/imagery and loading them into the scheduling tool, you’ll free up valuable time in the month ahead.
Bulk filming is also an excellent time-saving technique. If you have time to film a video, why not try filming a few and bank them to use later? Many practitioners will block out time in their calendars each month –even for a couple of hours – to film several videos back-to-back for use on social media. Consider video content such as showcasing new products and treatments or introducing your audience to members of your team. If
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com





THE ONE
Selective
delivers
The
skin resurfacing, and hair removal.¹︐⁵︐⁶ 1. Nordlys User Manual, 2021. 2. Candela, data on file, 2022. 3. Bjerring P, et al. Lasers Surg Med. 2004;34(2):120-126. 4. Schallen KP, Murphy M. Treatment of photodamaged skin with a combined dual-filter intense pulsed light and fractional 1550-nm laser system. Lasers Surg Med Suppl. 2020;52(S32). 5. Nordlys and Frax Pro with Frax 1940 , CE mark. 6. The Aesthetic Society. Aesthetic Plastic Surgery National Databank Statistics 2019. Available from https://www.surgery.org/sites/default/files/Aesthetic-Society_Stats2019Book_FINAL.pdf. Accessed Jan 25, 2022. © 2022 Candela Corporation. This material contains registered and unregistered trademarks, trade names, service marks and brand names of Candela Corporation and its affiliates. All other trademarks are the property of their respective owners. All rights reserved. PU02255EN, Rev. A Four timeless technologies: SWT® IPL, high-ROI Frax 1550™ and Frax 1940™ , and Nd:YAG 1064 nm¹ Grows
Compact
software
Treats
For more information, contact your local Candela sales professional or visit candelamedical.com candelamedical.com
IT’S
SWT ®: The only way to IPL
Waveband Technology (SWT®)
precise narrowband IPL.¹︐² With 50% less fluence required than broadband IPL, this improves comfort, keeps downtime low, and enables use of multiple technologies in a single session – all without compromising patients' safety and comfort, as well as results.¹︐²︐³︐⁴
Nordlys system is a multi-application platform with in-demand treatments across 24 indications, including pigmentation, vascularity,
with your practice – add handpieces to extend treatment options¹
and quiet, with
modes ranging from guided to expert¹
a wide range of skin tones¹
editing a video for social media makes you feel a little out of your depth, not to fear – free tools such as Canva, Splice or Adobe Premier Rush provide easy-to-use templates where you can slot in your own video clips to create quick, easy and professional-looking Reels and Stories.
If standing in front of a camera sends shivers down your spine, just remember, we’re not aiming for perfection. Users like to see the real, authentic side of the individuals, clinics and companies they follow, not necessarily the polished version reading from a script. You might even have some talented videographers ready for the spotlight in your team! Mix things up and take turns to get in front of the camera, sharing stories and voices from across the business.
Instagram stories are another quick and easy way to bring both current and prospective patients on a journey with you each day, letting them see behind the curtain and, importantly, building trust and rapport. Filming short videos to give followers a window into your journey to clinic, chatting about your day, providing clinic updates or receiving your copy of the Aesthetics journal can prove really effective and engaging ways to keep your audience interested in what you’re up to.
Engaging with your audience
Networking and engaging with your community, whether they may be prospective patients, existing customers or colleagues within the industry, is critical to your success. It’s easy to maintain your profiles on social media and develop a good routine for updating them, but engaging with the community on the platform is also important for growth and engagement.
There are several easy ways to keep on top of community engagement. Firstly, it’s important to be seen as a participating member of the community, so make sure you’re prompt in responding to enquires and direct messages. Many social platforms facilitate the option to send automated messages when you might not have time to respond straight away, letting people know you’ve received their message and will reply as soon as you can. Use the tools within the Instagram stories feature to pose questions and create polls. Ask people what they’d like to see from you, why they’re following you and what kind of information they’re there to see. Like any business strategy, social media
marketing is most effective when goals and plans are underpinned by real data. Social media data analytics provide information that helps you understand what’s working and what isn’t. When using social media for your business accounts, you’ll automatically gain access to ‘Insights’ via your Professional Dashboard (on Instagram) and ‘Analytics’ via the Meta Business Suite (on Facebook). By analysing the data at the end of each month, you can make the right business decisions and refine your strategy as you move forward.
Important statistics to be aware of are your ‘reach’ – the number of people who see content from your page whether they follow you or not, and ‘impressions’ – the number of times any content from or about your page is visible on a person’s screen. By analysing these detailed insights, it allows you to find out what content resonates most effectively with your audience and what has the greatest reach to new users, as well as providing information about your follower demographics, meaning you can get to know your audience better.4
Embracing the platforms
Lastly, lean in. Changes to platforms and algorithms can be frustrating, especially when it feels as though it’s only been a week since you got your head around the last update. It’s very easy to put off learning how new features work or ignoring them altogether in the hope that they’ll eventually go away. More often than not, when a new update goes live, social networks will let you know when elements of their platform have changed and offer the opportunity to read more, learn the basics and get top tips on utilising new features effectively. The reality is that we must move with the times, embrace the updates and get into the swing of things to avoid being left behind.
Many of us now also face an interesting dilemma: is Instagram enough, or do I need to consider TikTok too? While many of us would assume that TikTok is a young person’s game, full of memes and viral dance routines, you may be surprised to learn that as of April 2022, over 30% of TikTok’s users were females aged 25 and up.5 It’s also the fastest growing social media platform, and has a 57% female user base.6 So, if the question remains, ‘are my patients likely to be on TikTok?’, the answer is, they very well could be!
The best way to find out if your patients
are using the platform is to simply ask them when they come into clinic so you can find out if engaging with TikTok is going to be worthwhile. If managing all platforms at once seems overwhelming, focus on your bread and butter platforms – usually Facebook and Instagram – but ensure you’ve got accounts set up with your bespoke username and profiles before they are snapped up on any additional platforms. This way, you can maintain a low-key, hands-off approach, maybe only updating the likes of TikTok once every fortnight initially until you build confidence and get into a good routine of publishing content on there.

Maximising success
To maximise your success on these ever-changing, ever more video-centric platforms, it really does come down to getting into a robust routine. Plan ahead by thinking about what your goals are for the month, schedule content and bulk record video content when you can, network and respond to any incoming enquires as promptly as you can, analyse the data at the end of each month and, critically, be brave. Throw yourself in to embracing new features, put your face out there and let current and prospective patients see the authentic you. Remember, social media should be one of several digital strategies to promote your business, and you should complement this with other factors such as a website and email marketing.
Cait McLaughlin is the communications manager at SJ Partnership and an industry specialist in communications, marketing and social media within the medical aesthetics field. Working across all industry sectors, and with a range of manufacturers, distributors, clinics and clinicians, McLaughlin uses her years of experience to guide clients through the complex digital landscape.
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
VIEW THE REFERENCES ONLINE! AESTHETICSJOURNAL.COM
Practising Critical Reflection
Reflective practice is the process of retrospectively examining a certain procedure or experience and analysing it to determine whether things could have been done better. This now forms part of the undergraduate education in most medical fields due to its continuing value throughout practitioners’ careers.1 It allows practitioners to evaluate their own level of skill and knowledge, and create ways to improve clinical outcomes. Reflective practice is also described as ‘critical and deliberate enquiry into professional practice in order to gain a deeper understanding of oneself, others, and the meaning that is shared among individuals. This can happen during practice or following a treatment, and can either be done alone or with others.’2
Donald Schön’s 1983 book, The Reflective Practitioner: How Professionals Think in Action, not only focuses on reflection-inaction (how professionals reflect during practice), but also on reflection-on-action, when reflection takes place after the event.3 This book, in my opinion, is a cornerstone of reflection as part of professional practice. Reflective practice is extremely important as it looks at all the factors that may have contributed to decision-making. According to Professor David Seedhouse, we are more inconsistent than we think on a daily basis
depending on our mood, how stressed we are, our level of knowledge and many other external factors.4 Looking at ourselves, our experiences and our values will help us understand how these relate to our treatment of patients and their clinical outcomes.5,6 Reflective practice can be especially key in aesthetics, when you’re not working in your core medical field anymore.
Reflective pathways
Reflective writing is a way of processing one’s practice-based experience to produce learning. It integrates theory and practice while identifying a learning outcome from an experience.7 As such, it is a powerful tool for self-development in any field, and has become a mainstay within the medical field to promote an ethos of continuous development and self-awareness.8 Reflection itself is a type of self-regulated learning which incorporates cognition, metacognition and motivation.9 Cognition is the mental process of knowing, understanding and learning, while metacognition is the conscious planning, monitoring and evaluation of one’s own learning. As such, motivation to undergo metacognition can lead to cognition. In order to wrestle these abstract concepts into workable action plans, several authors
have created reflection models in order to provide more defined processes and endpoints and I believe all of these can be applied to aesthetic practice.
Sociologist and psychologist Graham Gibbs’ created the Reflective Framework (Figure 1), which is commonly taught to clinicians, and prompts us to consider what happened and how we felt at the time of an event, what the good and bad points were during the experience and what alternative actions could have been taken.10 This then leads to the formulation of an action plan when encountering similar situations in the future.
An alternative framework is presented by American educational theorist David Kolb, in which he stipulates that learning ‘is the process whereby knowledge is created through the transformation of experience’.11 Kolb suggests that for this transformation to occur, an individual must progress through a four-stage cycle.
The key skills for reflective practice include the ability to:12
• Problem solve
• Build on existing knowledge
• Explore questions in depth
• Be critically aware
• Be open-minded
• Motivate themselves
• Be self-aware
• Recall
• Use theoretical perspectives appropriately
• Gather information and critically evaluate it
• Learn from experience
• Create personal knowledge
• Question professional assumption, values and beliefs
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Brian Franks
and how it can
your
Figure 1: Gibbs’ Reflective Framework10 Figure 2: Kolb’s Cycle of Experiential Learning11 Action plan (if the event arose again, what would you do?) Conclusion (what else could you have done?) Analysis (what sense can you make of the situation?) Evaluation (what was good and bad about the experience?) Feelings (what were you thinking and feeling at the time of the event?) Concrete experience (doing or having an experience) Reflective observation (reviewing or reflecting on the experience) Active experimentation (planning or trying out what you have learnt) Abstract conceptualisation (concluding/ learning from the experience) Description (what happened)
Dr
outlines his tips for self-reflection
help improve
practice
Putting it into practice
When reflecting on the many aesthetic non-surgical treatments I have provided over the years, many factors come into play and need to be assessed before any treatments are undertaken. These are summarised in the Interconnected Circle (Figure 3) which I created over time and share with my students. I would go so far as to say that any aesthetic treatment, including the use of botulinum toxin and dermal filler, should not be carried out until we have an understanding of all the aspects of the circle. This will enable us to question any professional assumptions and beliefs regarding the provision of treatments.
By reflecting in this way, we can continually learn from both the positive and negative outcomes of treatments.
The Interconnected Circle
The Interconnected Circle helps me not only with treatment planning, but also with reflection. For example, the Anatomy/ Ageing Anatomy subheading highlights the importance of the aesthetic practitioner having a sound understanding of anatomy. A practitioner trained in functional anatomy is better set to create, alter and/or reconstruct to achieve aesthetic success. Understanding the anatomy enables us to more accurately reflect on the treatments provided.
In my mind, the consultation is the most important aspect of a patient’s journey, as the practitioner may identify:13
• Poor rapport
• Unrealistic expectations
• Minor or non-existent defect (a potential sign of body dysmorphic disorder)
• Attitude of perfectionism
• Vagueness (unable to describe wishes)
• Impulsiveness
• Previous unsatisfactory surgery
• Litigation against other doctors
• Emotional crisis (such as death in the family, divorce, loss of job)
• Demanding personality
• Demeaning of others, especially your staff
• Disapproval by family for the surgery
Case study
In this case study, reflection played an important role in determining the reason for an undesired treatment outcome of one of my patients. A female patient in her late 40s was treated for upper and lower lip augmentation with non-permanent dermal fillers. Immediately after the treatment, the patient expressed her satisfaction with the results of the treatment and no adverse events were noted, i.e. no obvious bruising or abnormal swelling. The patient was given post-treatment instructions both verbal and written, and was discharged. Approximately five days later, the patient contacted me by email, with photographs which showed severe bruising on both upper and lower lips. On contacting the patient, it was elucidated that there was no pain or infection. The patient was reassured and advised to continue to follow the post-treatment instructions, which included application of cold packs. The patient was contacted regularly for follow-up, and after approximately 10 days the bruising, had greatly reduced and any residual bruising could be concealed with the use of makeup. On the next follow-up appointment with the patient two weeks later, the bruising had completely subsided. Why had severe bruising occurred? My first evaluation was to determine whether it was the patient, the practitioner (myself!) or both. Using the Interconnected Circle as my template, I determined that there were no factors associated with the patient which could have contributed to this severe bruising. The finger was then pointed at me!
On reflection, the following factors were deemed to be potential, singular or multiple,
causes of this bruising, in that I:
1. Injected too deeply
2. Injected in the proximity of a major vessel
3. Injected too quickly
4. Injected too ‘vigorously’
5. Injected too much product
6. Injected too viscous a product
My evaluation and reflection of these points enabled me to conclude that the bruising was probably caused by injecting too deeply, causing some degree of superficial laceration of a blood vessel(s). By utilising tools for reflection, I was able to refine my skills for injecting.
Start reflecting
I find that using the Interconnected Circle as a reference point focuses my mind during the consultation to ensure provision of the ultimate patient outcomes. Additionally, when things don’t go as well as expected, or the outcomes are not as one would hope, I find the Interconnected Circle to be a useful tool to revert back to. I believe there are two main criteria regarding patients and aesthetic non-surgical interventions. The first occurs at the consultation – as previously, stated, I believe this is the most important aspect of any treatment modality – where we determine whether or not the patient is treatable. If not, they are politely shown the door. If we feel that they are treatable, the second criterion is to ‘avoid the unhappy patient’ and all that entails.15
Experience and reflection give us more understanding of these critical issues and amplify the value of reflection and how it can improve practitioners’ practice.
Dr Brian Franks is visiting professor, City of London Dental School for the MSc Programmes, University of Bolton. He is the programme clinical director and co-producer, MSc Specialist Practice of Clinical Aesthetic Non-Surgical Interventions.
He is also the principal of Dr Brian Franks Facial/Medical Aesthetics Non-Surgical Interventions Training.
Qual: BDS, LDS, RCS, MSc, MFGDP, FPFA, FEWI, ACIArb

Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
VIEW THE REFERENCES ONLINE! AESTHETICSJOURNAL.COM
Toxin
Dermal Fillers Anatomy/ Ageing Anatomy Life Events Culture and Ethnicity Smoking Wellbeing Medical History Skincare Dentition Sleep Nutrition and Exercise Psychology Other Treatments Sun Stress
Figure 3: The interconnected circle created by Dr Brian Franks.
Botulinum
&

Book your tickets now! 11 March 2023 Grosvenor House, London aestheticsawards.com Tickets include: •Entry to the Aesthetics Awards ceremony •Networking drinks reception •A delicious three course meal •Live entertainment and dancing •A professional photographer & press board Scan to book your tickets @aestheticsgroup @aestheticsjournaluk @aesthetics
In The Life Of Miss Sherina Balaratnam
Aesthetic
A typical working day…
Every morning I wake up at 6am, and my first pleasure is to go downstairs and cuddle my dogs Spartacus and Thor. I then take them for a walk, which is a great way to set up the day. When I get home, I have a 20 minute Peloton session, followed by 20 minutes of weight-training. I’ve been into fitness since growing up in Malaysia and I have always loved being strong – my nickname in my 20s was ‘shoulders’ because of all the weight-lifting I did.
After my workout, I pour a mug of Japanese Genmaicha tea, hop in the shower and have eggs for breakfast which I love. I enjoy my car journey to work through Beaconsfield, during which I greet my social media followers with a short video and listen to TED Talks or podcasts to get my inspiration flowing. I arrive at my clinic S-Thetics by 8:30am, and prepare for the day ahead. Before the doors open at 9am, my team and I meet to get organised and fire each other up for the day. My days are extremely varied, which I love. One of my favourite parts of my job is consultation and treatment planning because I enjoy getting to know my patients. When doing this, I always remember my mentor Dr Mauricio de Maio – I actually have a picture of him on my clinic wall! In 2019, Dr de Maio selected me as one of 12 international doctors to join him for an elite masterclass as part of the Allergan Medical Institute faculty. What I have learned from him informs and inspires my practice to this very day. As well as facial treatments, my clinic offers a range of body-sculpting treatments. I use BTL’s EMSCULPT NEO applicators to assist in skeletal muscle regeneration, which is crucial post-COVID. We had a tremendous launch party of the latest EDGE applicators at S-Thetics last month with our most loyal patients. Patient education is at the core of my practice and I believe in giving back to patients every day, and our clinic events are a great way to do both.
I will have a quick lunch in between patients at around 1pm. On every last Friday of the month, my team and I have a reflective day
Sherina Balaratnam

and watch Netflix which is a great way to switch off – Schitt’s Creek is my current favourite. On the days I finish earlier, we will take the dogs for a walk together, have a joint personal training session and relax.
Other work commitments…
I am very selective with the treatments I offer, and the companies I work with represent that. I have been a faculty member of the Allergan Medical Institute since 2012, and enjoy the training and education side of my work with them. In 2018, we converted space in my clinic to be a National Allergan Training Centre, and we have also just been approved as one of Allergan’s 10 global research sites for a new treatment indication, which I am very excited about.
together, followed by a multidisciplinary team meeting where we will celebrate the month by having lunch together and my team orders whatever they wish.
I fill my afternoons with botulinum toxin and dermal filler treatments, consulting new patients and making sure all follow-up and treatment plans are completed. During late clinic days, I will have an early dinner at 6pm. I love sushi so that is normally what I will go for.
I love fruit and can eat it all day, so will always have watermelon and mango in the fridge.
I treat a large number of corporate patients who finish work late, hence we close at 9pm twice a week to give these patients access to have their treatments. On these days, I will go home after work, unwind with my husband
Career if I wasn’t a surgeon…
I’d
Favourite
I
Country I’d move to…
I work closely with BTL and had the pleasure of presenting on their behalf at CCR last month, including research results from my wonderful team which makes this all the more fulfilling. My patients’ skin health is important to me, and I enjoy working with iS Clinical to emphasise that healthy skin is a core foundation to successful aesthetic results. Juggling these responsibilities while running my clinic can be challenging, but it is equally rewarding and teaches me to become a better practitioner and leader. Whenever my team and I feel like we are stuck, we imagine being 100 feet up in the air looking down at the clinic, enabling us to think strategically and make the best decisions to progress confidently.
Proudest day…
My proudest day was opening my clinic S-Thetics in May, 2015 – it is my baby. A close second has to be receiving The GetHarley Award for Medical Aesthetic Practitioner of the Year at The Aesthetics Awards 2022.
Shortly after the Awards, iS Clinical invited me to present for them in my hometown Kuala Lumpur, Malaysia, and I brought my trophy back home for my family to bless in their prayer room. That was an incredibly humbling, proud and special moment for me.
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
practitioner and surgeon Miss
outlines a typical working day at her clinic and how she juggles her other commitments
be a chef – I love my scrubs, so I think I’d like chefs’ whites too.
treatment
perform…
to
love facial dermal filler treatments
they
me
because
give
the chance to be artistic.
I’d move back to Malaysia – it’s my home after all!
The Last Word
In medical aesthetics – and the wider beauty industry – there is something of an obsession with Instagram. This is no surprise: Instagram is above all a visual medium, and aesthetics literally means ‘visual appeal’. Therefore, it makes perfect sense to show what our aesthetic practices can achieve in a visual way. Modern Aesthetics magazine, for example, reported that 83% of consumers researching cosmetic surgery would not consider a practice which did not feature before and after photos.1
Instagram deserves its place in the aesthetic marketer’s toolkit – in a recent survey of 4,500 active Instagram users, almost two thirds of people said that the network helped them foster meaningful interactions with brands. However, it does have challenges, too.2 In an industry described as ‘fragmented’ with many small practices and self-employed health professionals, marketing budgets are not endless.3
Challenges of Instagram
Instagram has increasing competition and throughput. Even more practitioners are entering the aesthetics field, and they are all tuned in to the value of publishing content on social media as an essential, low-cost route to promoting their individual clinics. But the consumer’s feed hasn’t grown in size, and neither has their attention span. According to Meta (the owner of Instagram), the average user spends around 1.7 seconds on any one piece of content.4 Instagram’s business is simply predicated on maximising the value of the advertisements they squeeze into that feed and their ability to keep their audience scrolling. Practitioners therefore have two choices: pay for advertising, or hope that Instagram’s algorithm favours you against other aesthetic clinics, products and offerings clamouring for space. There are no points for guessing which of these Instagram would prefer. This has created a spiral where practitioners end up posting more content, and ultimately putting off followers that do see the content due to saturation. In addition, if the business has increasingly been prioritising advertising, it further reduces the opportunity for organic (i.e. unpaid) reach. Instagram’s organic reach currently hovers at below 1%- meaning that even among consumers who have interacted with your brand, fewer than one in 100 will see an unpaid post or story.5 There is a second challenge. As we saw above, Instagram deserves its place in the aesthetic marketer’s toolkit, but that doesn’t mean it should be 100% of that toolkit. There are plenty of experts and agencies who will sell you the dream that it’s possible to build a multi-million-pound clinic on Instagram alone. That’s a seductive thought, especially when you’re looking from the perspective of a start-up at the glamour of heavily retouched pictures of elegant white consulting rooms. It’s my moral duty to tell you that you can’t build an empire on one social channel. If you could, everyone would be doing it. You might have heard that you can build your social following relatively quickly. This is also not true. In the early days on any social platform, it is possible for early adopters to establish a reputation. But on mature social channels, it’s not the case. Those who succeed have done so through hard work over a long period of time as well as other factors.
A solution
If all this sounds negative, let me recommend a solution. Firstly, don’t ditch Instagram completely. Recognise that it is part of a rounded approach to marketing with many ingredients. Secondly, note that all social media operates the same way: highly tuned algorithms optimised for the profit of the platform, which decide what gets shown and to whom. To some extent, everything I said about Instagram also applies to Facebook, TikTok and others. Therefore, thirdly, you should balance your social media activity with other online marketing resources such as Google optimisation, content marketing and email marketing. In my experience – and this is advice I give every day to my aesthetic clients – an excellent balancing activity is to commit to Google Local.6 This is the map with results at the top of Google when anyone searches for physical businesses. Aesthetic practitioners
are just that – and they target a locality, too. Google Local is ideal in that it brings you potential patients who are in your local area and at their highest point of intent –rather than just scrolling on their Instagram feed, they are proactively looking for the sorts of services you provide. In order to capitalise on the new traffic you achieve from Google Local, you need to put focus and investment into a website that gives a great first impression, works well on a mobile and provides a seamless on-boarding experience for new patients.
While Instagram needs the constant fuel of new content, Google Local only requires you to invest regular effort into writing, editing and optimising your Google business profile. There are plenty of ways to do this, but most obviously you should include keywords such as particular treatments you offer or skin conditions which you can remediate. To get started, ensure you claim your Google Business Profile, have your location and profile ‘verified’ by Google, then optimise its content, keywords and posts on a weekly basis.
Broadening your approach

If you put effort into all your social media channels as well as Google Local – supported by a first-class website – you will gain an increasing share of localised, qualified, high-intent search traffic. In fact, some of those people will also check you out on Instagram, follow you on social media and therefore increase your social credibility, too. Instagram isn’t bad in itself, it’s just a highly competitive environment. You can choose to run harder in an ever-bigger pack, or you can conserve your energy by broadening your approach.
Rick O’Neill is a digital consultant to the medical aesthetics, cosmetic surgery and pharma sectors. With more than 20 years’ experience in digital marketing, O’Neill is the founder and owner of the award-winning digital agency ‘Look Touch & Feel’, a founding partner of The Aesthetic Entrepreneurs, digital consultant to Merz Aesthetics, and investor/advisor to several other digitally focused businesses.
Rick O’Neill argues why Instagram may prompt challenges for your clinic and how to broaden your approach to gain potential patients
Reproduced from Aesthetics | Volume 12/Issue 9 - February 2022 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
VIEW THE REFERENCES ONLINE!
AESTHETICSJOURNAL.COM




SIMPLY RADI ANT SKIN FROM HEAD TO TOE Phone: 020 2218 1108 Email: uksales@sciton.com ©2021 Sciton, Inc. All rights reserved. dable quality and • BBL® HERO™ with 4x the speed, 3x the peak power, and 2x the cooling will forever change how you treat skin from head to toe • MOXI™, a 1927nm fractionated thulium laser, opens the door to a younger prejuvenation patient • Versatile and synergistic treatments • Single targeted treatments to regular skin care regimens • Affordable and expandable; choose both or one, add second modality in the future ® MOXI | courtesy of Steven Swengel, MD MOXI + BBL | courtesy of Steven Swengel, MD LEARN MORE HERE! D E S IGN & BUIL D IN US A Transform your practice and your patients with the latest innovation by Sciton. Learn More www.sciton.co.uk
The delicate eye area, needs the strongest expertise

MaiLi Precise, is our safest and effective HA formula yet. Created to help you refresh and rejuvenate the most tired of eyes with care, precision and most importantly confidence*.

This deluxe treatment harnesses the power of the world’s first OxiFreeTM HA technology and uses lidocaine to make your clients comfortable, so you can focus on your work and help turn back the clock.
®
MaiLi.com
Actual patient, individual results may vary. * The application of MaiLi Precise in the periorbital area is reserved to specialists specifically trained in this technique and having sound knowledge of the anatomy and physiology for this area CE mark CE2797. MaiLi devices are intended for correction of facial wrinkles or folds, for the definition or enhancement of the lips, and for the restoration or enhancement of the facial volume.
Refresh with the power of MaiLi Precise.
