

VOLUME 9/ISSUE 6 - MAY 2022 Adverse events should be reported. Reporting forms and information for United Kingdom can be found at www.mhra.gov.uk/yellowcard. Reporting forms and information for Republic of Ireland can be found at https://www. hpra.ie/homepage/about-us/report-an-issue/mdiur. Adverse events should alsobe reported to Merz Pharma UK Ltd at the address above or by email to UKdrugsafety@merz.com or on +44 (0) 333 200 4143. REVIVE YOUR PATIENT‘S DREAMS OF YOUTHFUL SKIN BELOTERO® Revive is the newest product in the BELOTERO® portfolio of fillers indicated to revitalise the signs of early onset photodamaged facial skin. 1. Belotero Revive IFU 2. BELOVE 2019 Facial skin revitalization with CPM-HA20G an effective and safe early intervention • Improves skin hydration1 • Increases skin elasticity and firmness1 • Smooths skin texture1 • Reduces pigmentation2 M-BEL-UKI-1355 Date of Preparation April 2022 @merzaesthetics.uki merz-aesthetics.co.uk merzaesthetics.uki Summer Marketing Julia Kendrick shares tips to upgrade your marketing for the summer months Understanding Sunscreens Kirsty Whitworth explores the basics of sun care and safeguarding patients Managing Pigmentation Concerns An overview of complaints and treatment approaches Extrinsic Factors of Ageing CPD Practitioners present the factors that accelerate ageing of the skin






To see how one powerful device provides everything you need to power your business, contact us today:
Treatment. Endless Options. give your customers what they want! Simplification Multi-benefit solutions that save time1 Personalisation Treatments tailored to specific skin concerns2 RecommendatioN Skin health technology and regimen education1 HydraFacial is for everyone. It’s suitable for all skin types and addresses all skincare needs. HydraFacial delivers immediate, noticeable results, with no downtime, that keep your customers returning regularly. HydraFacial is your connection to millions of believers that know that beauty is more than a physical attribute – it’s a feeling. Consumers want to be pro-actively offered personalised solutions for skin health and provide them with education on their ideal, easy-to-follow skin health regimen1 And your clients needs are as individual as they are, which is why HydraFacial has partnered with the best brands in aesthetics to bring you advanced booster options that meet the emerging consumer trends, which are influencing our industry more than ever before. HydraFacial is scored as a ‘99% Worth It’ rating by www.realself.com and on average, somewhere in the world, a HydraFacial treatment is now carried out every 10 seconds! 1 EddieWouldGrow Facial Research 2018, n=2000; 2 Mintel Trends 2017 hydrafacial.co.uk infouk@hydrafacial.com @hydrafacialuk 01788 572 007
One
DESTINATION GLOW
HydraFacial opens immersive new Flagship in London.




The doors are now open and aestheticians are assured a radiant reception at HydraFacial’s latest venture in the capital – HydraFacial LDN Flagship. Located on Portman Square in the bustling West End, the hybrid space has been designed to help drive consumer demand and connect the European-wide HydraFacial community with innovative training, education and marketing opportunities. Following a two-year renovation, the state-of-the-art LDN Flagship is HydraFacial’s largest investment to-date and underpins the company’s ‘skin health’ ambitions for the UK and EMEA markets.
“Our UK HydraFacial community is valued and everything about our new LDN Flagship has been designed to support their commercial success”, says UK & Ireland Country Manager, Lauren Gibson.

Every month, the LDN Flagship will deliver up to 750 deluxe treatments for registered members of the public, allowing the treatment-curious to - just once - ‘try before they buy’. This novel ecosystem is designed to socially-inspire and source new patient prospects, before converting them to a skin health programme with a recommended local provider.

In 2022, the new LDN Flagship will play a part in delivering more than 2.5 million treatments globally.
Alongside media masterclasses on trending wellbeing topics, the venue will play host to collaborative brand events and expert-led forums with doctors, facialists and makeup artists alike. A new VIP suite means celebrities and journalists can be treated in comfort and with West End stars and sporting legends already lined up to experience a radiance-reset.

To visit the new LDN Flagship, register for accredited CONNECT training or book a demo & learn how to enhance patient loyalty in your clinic or medispa, visit: www.hydrafacial.co.uk/london-flagship/

Congratulates



Miss Sherina Balaratnam









UK Medical Aesthetic Practitioner of the Year 2022 Aesthetics Award Winner












S-Thetics Clinic













Beaconsfield, Buckinghamshire (UK)
Best Clinic South England 2022 Aesthetics Award Winner
| PAIN DERMAL
ACNE | ANTI-AGEING
WOUND HEALING FDA-CLEARED AND MEDICAL CE MARK
Miss Sherina Balaratnam
MBBS MRCS (Edin). MSc (UCL), Medical Director, S-Thetics Clinic
“My Celluma devices have taken our patients’ results and satisfaction to the next level.”
of ultrasound in aesthetic medicine 45 Diagnosing Skin Lesions
Dr Keli Thorsteinsson explains how to diagnose different skin lesions 49 Treating Hip Dips Using Dermal Fillers

Dr Lucy Glancey discusses using PLLA fillers for hips dips 53 Case Study: Full-face Rejuvenation


Dr Jeremy Isaac explores his tips for facial restoration using TEOXANE fillers 56 Joining the Spherical Revolution
Dr Johanna Ward outlines why she decided to join the Spherical Revolution
A round-up and summary of useful clinical papers
Julia Kendrick shares her tips to upgrade your seasonal marketing
Optimising Landing Pages
Rick O’Neill discusses the best Website tools that will help yield more enquires
Max Hayward outlines why practitioners should use online appointments 68 In Profile: Dr Euan Mackinnon
Dr Euan Mackinnon details his enjoyment at using the Merz portfolio 69 In The Life Of: Mr Paul Banwell
The plastic surgeon discusses the different commitments he fits into his busy schedule 70 The Last Word: Australian Perspective
Dr Jake Sloane outlines the challenges facing the Australian injectables industry
Special Feature: Managing Hyperpigmentation Page 19

Clinical Contributors
Dr Nihull Jakharia-Shah is an internal medicine trainee with an interest in dermatology. Dr JakhariaShah held a position at Acquisition Aesthetics training academy for four years, gaining exposure to clinical aesthetic practice.

Miss Lara Watson is a maxillofacial surgery doctor and a UK key opinion leader for various pharmaceutical companies. She is a director at Acquisition Aesthetics training academy, which recently won the Clinisept+Skin Award for the Independent Training Provider of the Year.
Miss Priyanka Chadha is a plastic surgery doctor and a global key opinion leader and speaks regularly on the national and international stage. Her academic CV comprises of national and international prizes. She is a director at Acquisition Aesthetics training academy.
Dr Saleena Zimri is a former GP with a special interest in cosmetic dermatology. She has been practising aesthetics for 13 years and is the co-founder of the Skin Doctor Clinics and set up her first aesthetic skin and laser clinic 12 years ago in Yorkshire.


Dr Lauren Hamilton began her medical career in the field of surgery. She went on to achieve a Master’s Degree in Medical Education from University College London. Dr Hamilton is co-founder of Victor & Garth, a clinic in Shoreditch.
Dr Miriam Adebibe is a UK-trained surgical doctor with more than 15 years of experience. She is actively involved in medical education, training, and has published many research reports in scientific literature. She is co-founder of Victor & Garth clinic in Shoreditch.

Kirsty Whitworth is a highly qualified registered adult nurse, independent nurse prescriber, advanced aesthetics nurse. She is registered with the Nursing and Midwifery Council and an active member of the British Association of Cosmetic Nurses.
Dr Keli Thorsteinsson is a specialty doctor in secondary care NHS dermatology and a cosmetic practitioner. He has more than a decade of experience in skin cancer diagnosis and medical aesthetics. He is the co-owner and director of Freyja Medical.

Dr Lucy Glancey is an aesthetic practitioner who owns the Dr Glancey clinics in London and Essex. She is a member of the Royal College of Surgeons of England and the British College of Aesthetic Medicine. She is currently joint president of the British Association of Body Sculpting.

Contents • May 2022
NEXT MONTH IN FOCUS: COMPLICATIONS • Using Ultrasound for the Nose • Complications and Radiofrequency 08 News The latest product and industry news 16 News Special: Training in Menopause
explores the limitations on current menopause training CLINICAL PRACTICE 19 Special Feature: Managing Hyperpigmentation An overview of common complaints and treatment approaches 27 CPD: Assessing the Extrinsic Factors of Skin Ageing Three practitioners present factors which accelerates skin ageing 31 Exploring Skin of Colour in Summer
discuss conditions that may affect SOC in the summer 34 Treating Gynoid Lipodystrophy
Zimri discusses radiofrequency as a treatment for cellulite 36 Supporting the Future of Aesthetics at Beauty Uncovered LIVE The event is great for patients, but what about practitioners? 39 Understanding Sunscreens
explains the basics of sun care 42 Ultrasound Technology in Aesthetics
at the use
Aesthetics
Practitioners
Dr Saleena
Nurse prescriber Kirsty Whitworth
Dr Simon Ravichandran looks
57 Abstracts
IN PRACTICE 59 Leveraging Summer Marketing Strategies
62
65 Managing Online Appointments


100+ ADVANCED LEARNING & CLINICAL TRAINING MATERIALS Search for Merz Aesthetics Ecademy today EXPLORE TODAY SCAN ME M-MA-UKI-1913 Date of Preparation February 2022. Developed and funded by Merz Aesthetics UK & Ireland. CLINICAL TRAINING POWERED BY ECADEMY FOR HEALTHC ARE PROFESSIONALS ONLY
As the days start to become warmer, the excitement of summer begins! With the change in seasons, you will likely be noticing a shift in the types of treatments patients are asking for and you’ll need to strengthen your efforts towards summer skincare. In this month’s summer issue, we have a look at the causes and treatments of hyperpigmentation, which becomes more prevalent in the warmer months (p.19). We also have a great article on the extrinsic factors that impact ageing, from the sun to diet, pollution and stress – it’s CPD-verified so you can use it for your medical revalidation and appraisals (p.27). As well as this, we cover how you can take care of your patients with skin of colour in the summer on p.31, diagnosing skin lesions, which is vital for patient safety (p.45), and we go back to the basics of sun protection on p.39 Don’t forget, many people fail to apply their sunscreen properly and much more education is needed in this area. According to a YouGov survey commissioned by Cancer Research UK, almost a quarter do
Shannon Kilgariff Editor & Content Manager @shannonkilgariff

not apply sunscreen during the summer or when on holiday, with men twice as likely as women to forego protection. Another YouGov survey commissioned by Cancer Research UK and NIVEA SUN found that 24% thought it was false or didn’t know that if skin goes pink but then a tan develops, it still counts as being burnt. So, it’s important you educate your patients about the importance of sun protection not only to prevent skin cancers but to strengthen your treatment results and reduce the risk of photoageing. Speaking about patient education… this month sees the first ever Beauty Uncovered LIVE event! With so much negativity and misunderstanding around the aesthetic industry, I personally can’t wait to open up the world of medical aesthetics to the public to enhance their knowledge, build trust and promote positivity. It’s a first-of-its-kind event to really support the whole industry. We hope to welcome aesthetic professionals as well as the public to the Business Design Centre in London on May 7 & 8 – turn to p.36 for more information and to get your free tickets. I look forward to seeing you there! Remember to tell us what you’ve enjoyed reading in the journal this month by tagging us on Instagram @aestheticsjournaluk
Clinical Advisory Board
Leading figures from the medical aesthetic community have joined the Aesthetics Advisory Board to help steer the direction of our educational, clinical and business content
Sharon Bennett is chair of the British Association of Cosmetic Nurses (BACN), previous UK lead of the BSI committee for aesthetic non-surgical standards, and member of the Clinical Advisory Group for the JCCP. She is a trainer and registered university mentor in cosmetic medical practice, and is finishing her MSc at Northumbria University. Bennett has won the Aesthetics Award for nurse practitioner of the year and the Award for Outstanding Achievement.
Mr Naveen Cavale has been a consultant plastic, reconstructive and aesthetic surgeon since 2009. He has his own private clinic and hospital, REAL, in London’s Battersea. Mr Cavale is the national secretary for the ISAPS, president of the Royal Society of Medicine, and vice-chair for the British Foundation for International Reconstructive Surgery.
Jackie Partridge is an aesthetic nurse prescriber with a BSc in Professional Practice (Dermatology). She has recently completed her Master’s in Aesthetic Medicine, for which she is also a course mentor. Partridge is a founding board member of the British Association of Cosmetic Nurses and has represented the association for Health Improvement Scotland.
Mr Adrian Richards is a plastic and cosmetic surgeon with 18 years’ experience. He is the clinical director of the aesthetic training provider Cosmetic Courses and surgeon at The Private Clinic. He is also a member of the British Association of Plastic and Reconstructive and Aesthetic Surgeons and the British Association of Aesthetic Plastic Surgeons.

Miss Elizabeth Hawkes is a consultant ophthalmologist and oculoplastic surgeon. She is the lead oculoplastic surgeon at the Cadogan Clinic, specialising in blepharoplasty and advanced facial aesthetics. Miss Hawkes is a full member of the BOPSS and the ESOPRS and is an examiner and fellow of the Royal College of Ophthalmologists.
Dr Tapan Patel is the founder and medical director of PHI Clinic. He has more than 16 years’ clinical experience and has been performing aesthetic treatments for more than 14 years. Recently, he was listed in Tatler’s Top 30 Anti-Ageing Experts. Dr Patel is passionate about standards in aesthetic medicine.

Dr Souphiyeh Samizadeh is a dental surgeon with a Master’s degree in Aesthetic Medicine and a PGCert in Clinical Education. She is the founder of the Great British Academy of Medicine and Revivify London Clinic. Dr Samizadeh is a Visiting Teaching Fellow at University College London and King’s College London.



ADVERTISING
Courtney Baldwin • Event Manager T: 0203 196 4300 | M: 07818 118 741
courtney.baldwin@easyfairs.com
Judith Nowell • Business Development Manager T: 0203 196 4352 | M: 07494 179535

judith@aestheticsjournal.com
Chloe Carville • Sales Executive
T: 0203 196 4367 | chloe.carville@aestheticsjournal.com
Emma Coyne • Sales Executive T: 020 3196 4372 | emma.coyne@easyfairs.com
MARKETING
Aleiya Lonsdale • Head of Marketing
T: 0203 196 4375 | aleiya.lonsdale@easyfairs.com
Aimee Moore • Marketing Manager T: 020 3196 4370 | aimee.moore@easyfairs.com

Abigail Larkin • Marketing Executive T: 020 3196 4306 | abigail.larkin@easyfairs.com
WE WANT TO HEAR FROM YOU!
Do you have any techniques to share, case studies to showcase or knowledge to impart?
Email: editorial@aestheticsjournal.com
Dr Raj Acquilla has more than 12 years’ experience in facial aesthetic medicine. In 2015 he won the Aesthetics Award for Aesthetic Medical Practitioner of the Year and in 2012 he was named Speaker of the Year. Dr Acquilla is a UK ambassador, global KOL and masterclass trainer for botulinum toxin and dermal fillers.


Dr Stefanie Williams is a dermatologist with a special interest in adult acne, rosacea and aesthetic medicine. She is the founder and medical director of multi-award winning EUDELO Dermatology & Skin Wellbeing in London, and creator of Delo Rx skincare. She is the author of three books and has published more than 100 scientific articles, book chapters and abstracts.
ARTICLE PDFs AND REPRO
Material may not be reproduced in any form without the publisher’s written permission. For PDF file support please contact Chloe Carville, contact@aestheticsjournal.com
Editor’s letter
Aesthetics Journal @aestheticsgroup Aesthetics @aestheticsjournaluk
Sharon Bennett, Clinical Lead
All rights reserved. Aesthetics is published by Aesthetics
which is registered as a limited company in
DISCLAIMER: The editor and the publishers do not necessarily agree with the views expressed by contributors and advertisers nor do they accept responsibility for any errors in the transmission of the subject matter in this publication. In all matters the editor’s decision is final. PUBLISHED BY
Media PORTFOLIO MANAGEMENT Alison Willis Director T: 07747 761198 | alison.willis@easyfairs.com
Kilgariff Editor & Content Manager
196 4351 | M:
359 257 shannon@aestheticsjournal.com
Carver Journalist | T:
196 4427
Holden Content Writer |
Johnson • Senior Designer
196 4359 |
© Copyright 2022 Aesthetics.
Media Ltd,
England; No 9887184
Aesthetics
EDITORIAL Shannon
T: 0203
07557
Holly
0203
holly.carver@easyfairs.com Ellie
T: 0203 196 4265 ellie.holden@easyfairs.com DESIGN Peter
T: 0203
peter@aestheticsjournal.com
&
SPONSORSHIP
Talk #Aesthetics
Follow us on Twitter @aestheticsgroup
#Aestheticsjournal
Claire Newman
@soft_touch_aesthetics
Thank you
@aestheticsjournaluk for publishing my article on managing the needle phobic patient

JCCP launches new consumer website
The Joint Council for Cosmetic Practitioners (JCCP) is introducing a new consumer website for aesthetics and launching it at Beauty Uncovered LIVE on May 7-8. Over the past two years, the JCCP and CDM Communications, a PR agency which focuses on health issues, has researched concerns associated with patient safety and awareness. They decided that a new user friendly website, named JCCP & Me, should be designed which provides basic information for patients who are looking to undergo non-surgical treatments, guidelines on the key questions to ask when considering a treatment and who and what to look for when considering a practitioner.
#Education
Jackie Partridge
@mrsjackiepartridge
I love presenting to colleagues in aesthetics! We had an amazing group of aesthetic nurses in Manchester for the BACN regional meeting #anatomy
#Training
Dr Lee Walker
@leewalker_academy
Train the trainer for our amazing Brazilian colleagues… big thanks to @drcetto for incredible lectures and support

Professor David Sines, executive chair of the JCCP, said, “The launch of JCCP & Me represents a milestone in raising public awareness about issues surrounding patient safety in the world of non-surgical aesthetics. We are very grateful for all the work undertaken by CDM in this area and the support from Beauty Uncovered.”
Editor and content manager of the Aesthetics journal and Beauty Uncovered magazine, Shannon Kilgariff, said, “We are so excited to launch the new JCCP + Me consumer website at our first patientfocused event Beauty Uncovered LIVE. Our event aims to build trust, promote positivity and enhance education for patients in the aesthetics specialty. The new website launched by the JCCP embodies this, so it is the perfect opportunity and event for it to be showcased at.” The new consumer website will be live on May 5 and will be officially launched at Beauty Uncovered LIVE on May 7-8. Turn to p.36 to find out more about the event.
Education
Dr Jean Carruthers to present at BCAM Conference

#Conference
Dr Manav Bawa
@drmanavbawa
What an amazing time at the AMWC Medical Aesthetics conference in Monaco! It was great to spend time with and get to know my colleagues

#Malehealth
Dr Shirin Lakhani
@drshirinlakhani
I had a great day yesterday sharing ideas and knowledge on the management of male intimate health with @harbornept and @function2fitness
Canadian aesthetic practitioner and pioneer of the use of botulinum toxin for wrinkles, Dr Jean Carruthers, will present at the British College of Aesthetic Medicine (BCAM) Conference in September.


The following day, Dr Carruthers will stage exclusive masterclasses for College members only which are due to be announced soon. BCAM vice president Dr Catherine Fairris said, “We are honoured to have such an inspirational speaker at this year’s event. It’s a fitting way to celebrate our return to a physical conference after two successive virtual events. Dr Carruthers is a global leader in the field of aesthetic medicine and we look forward to sharing her expertise and experience. It’s a rare opportunity for delegates to have close contact with the pioneer of botulinum toxin treatments and benefit from her incredible knowledge.”
The BCAM conference will take place on September 10 at Church House, Westminster.
Patient Safety
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Botulinum Toxin
New toxin receives national approval in the UK
Aesthetic manufacturer Croma-Pharma has announced the national approval of its new botulinum toxin Letybo in the UK. The launch is the first toxin to be approved in the UK since 2008. According to the company, Letybo has been approved for the treatment of glabellar lines. The neurotoxin, letibotulinum toxin A, aims to provide practitioners and patients with efficacy and tolerability. According to a study of 355 subjects, it received a 94% response rate four weeks after injection. Managing director at Croma-Pharma, Andreas Prinz, commented, “We are proud to be the first Austrian family-owned pharmaceutical company launching its own neurotoxin to the aesthetic market. In the upcoming weeks and months, we expect national approvals for Letybo in additional European countries. With this completed portfolio, we will now be able to meet our customers’ needs even better.”
Galderma expands sales team




Pharmaceutical company Galderma has expanded its UK sales team with five new positions.
According to the company, the new positions aim to provide strategic support and servicing across the country because of an increased demand for its products. The new team includes Lucy Dean, who will be focusing on Manchester and Liverpool; Jayne John to oversee Wales and the Southwest; Kirsty Pesticcio will cover the South coast region; Karen Houlihan will be based across Central London; and Hannah Miller will cover Birmingham and the West Midlands.
Galderma will be exhibiting at Beauty Uncovered LIVE on May 7-8. Turn to p.36 to find out more!
MINT masterclass to take place
HansBiomed Corp, creator and distributor of MINT, will be holding a masterclass in May. The MINT PDO World masterclass will be presented by 20 global speakers discussing the MINT PDO threads and the opportunities that using MINT PDO offers. The name MINT stands for ‘minimally invasive non-surgical thread’. Speakers include medical director, Dr Irfan Mian, aesthetic practitioners Dr Zunaid Alli and Dr Kam Lally, aesthetic nurse Lisa Waring, consultant physician Professor Syed Haq and nurse prescriber Sandy Green, as well as other practitioners from the US, Europe, Middle East, Africa and Asia, explains the company. The masterclass will cover topics on essential assessment and anatomy for PDO threads, the latest techniques, outcome analysis, and how to get registered by the Care Quality Commission. Attendees will be able to gain access to the lectures to rewatch after the masterclass. The masterclass will be taking place on May 14 at 9am-5pm GMT at the Royal College of General Practitioners, London.
Vital Statistics
More than 210,000 cases of non-melanoma skin cancers are diagnosed annually in the UK with a prediction to reach almost 400,000 per year by 2025 (skcin.org, 2022)
80% of 1,000 respondents said that they’ll watch a live stream from a brand rather than read a blog from the same company (Findstack, 2022)
In a survey of 2,000 women, 73% do not feel able to talk openly about their menopausal symptoms with their colleagues (Koru Kids, 2022)
According to 54 dermatologists from 23 countries, 90% said applying a moisturiser to the body daily is important for overall skin health (CeraVe, 2022)
In a survey of 18,100 marketers, 62% consider Facebook as the most effective platform for reaching business goals (Hootsuite, 2022)
91% of 991 people would not consider receiving a non-surgical treatment from somebody who was not a medical professional (Cosmetic Surgery Solicitors, 2022)
Recruitment
Threads
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Events Diary
7th-8th May
Beauty Uncovered LIVE beautyuncovered.com 15th-16th September
The BACN Autumn Aesthetic Conference bacn.org.uk 13th-14th October CCR ccrlondon.com 9th September
IAPCAM iapcam.co.uk 10th September
BCAM conference bcam.ac.uk
Training Cutera introduces learning series
Complications conference to be held in Ireland
Aesthetic practitioner Dr Patrick Treacy will host a new complications conference in July. The International Medical Aesthetics and Complications Conference (IMACC) will be held in-person and will feature live sessions split across multiple stages. The conference will also be available via a virtual platform and anchor studio.
The first day will see talks on botulinum toxin and dermal fillers, energy-based devices, DNA, growth factors and stem cells, cosmeceuticals, chemical peels and what is new in dermal fillers. The second day will discuss genital rejuvenation, hair transplants, cosmetic surgery, threads, dermal filler techniques, the role of the media in aesthetics and the future of aesthetic medicine. Speakers include aesthetic practitioners Professor Bob Khanna, Dr Raj Acquilla, Dr Tapan Patel, Dr Martyn King, Dr Beatriz Molina, Dr Uliana Gout and consultant plastic and reconstructive surgeon Mr Dalvi Humzah.
The conference will take place on July 15-16 at O’Reilly Hall, University College Dublin.
Skin mesoestetic unveils bodyshock range
Aesthetic manufacturer Cutera has launched a new on-demand virtual learning series. The series is in partnership with the company’s Secret RF Advisory Board, a group of practitioners who currently use the brand’s range of radiofrequency microneedling technologies. The company explains that the goal of the initiative is to provide a clear understanding of the mechanism of action used in radiofrequency microneedling technologies, using the board’s insights and feedback, backed by clinical demonstrations. The first part of the series is hosted by Dr Tapan Patel, who discusses a multi-layered approach to skin rejuvenation. He explores the Cutera Secret Pro device and provides his thoughts and insights about the current clinical possibilities of Cutera technology and explains how he uses it to achieve optimal results. Dr Patel said, “Both microneedling RF and fractional CO2 lasers have seen considerable success in treating a variety of indications. Combining two gold standard energy sources takes skin rejuvenation to new heights, offering a safe and effective way of treating a wide range of concerns whilst minimising downtime.”
Pharmaceutical company mesoestetic has introduced the new bodyshock range to its portfolio. According to the company, the range aims to treat areas such as cellulite, localised fat, flaccidity and stretch marks. The range comprises four products, including the intensive mist which aims to reduce the fat located in stubborn areas, such as the stomach and hips. The bodyshock celluxpert is a cream-gel designed to prevent cellulite, while moisturising and helping firm the skin. The firm’ up cream aims to treat areas with flaccidity and loss of turgor. The massage roller increases the absorption of ingredients and aims to provide firmer and toned skin, whilst the essential cream helps to mitigate and prevent the appearance of stretch marks, explains mesoestetic.
The range also has products specifically for in-clinic use with three phases. The preparation phase includes an exfoliator gel to prepare the skin for the application of active ingredients. The personalisation phase contains a lipactive booster which aims to decrease the number of fat cells; the firmactive booster to restore skin elasticity; drainactive booster to stimulate microcirculation; stretchactive booster to reduce stretch marks and the intensive drops to reduce fat accumulation. The completion phase includes a sculpting mask to reduce volume; the tightening mask to tighten the skin; and the intensifying cream to prolong the effect of the treatment.

Takeover
Galderma to host webinar with Aesthetics
Pharmaceutical company Galderma will be hosting a webinar in partnership with the Aesthetics journal. The webinar will focus on the Restylane Skinboosters range. Aesthetic practitioners Dr Yusra Al-Mukhtar and Dr Kishan Raichura will discuss the benefits and features of Restylane Skinboosters whilst demonstrating how to inject the product on patient cases. The webinar will take place in May, with the date to be confirmed on the Aesthetics website soon. To keep up to date, sign up for the Aesthetics newsletter.

Event
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Patient Education
Beauty Uncovered LIVE launches on May 7-8

The inaugural consumer-facing event Beauty Uncovered LIVE will be taking place on May 7-8 at the Business Design Centre, London.
The event will be jam-packed with educational content for your patients to learn more about the aesthetics specialty, as well as watch live demonstrations, discover new products and leave with a goody bag worth £150+.
Editor and content manager of the Aesthetics journal and Beauty Uncovered magazine, Shannon Kilgariff, said, “We are so excited to launch our first patient-focused event in May! Our aim is to enhance your patients’ education on the world of aesthetics, promote positivity around the treatments they can get and build trust by only recommending qualified and reputable practitioners. Don’t forget to tell your patients about this wonderful event and grab your FREE ticket to attend by using the code VIPHCPJOURNAL at the checkout!”
Read more about the event on p.36
HydraFacial opens new flagship premises

Aesthetic manufacturer HydraFacial has opened a new flagship in London. According to the company, the flagship has been designed to help consumer demand and connect the European-wide HydraFacial community with training, education and marketing opportunities. Every month, the flagship will deliver up to 750 treatments for members of the public. This is designed to inspire and source new patient prospects, before converting them to a skin health programme with a recommended local provider, explains HydraFacial.
The venue will also play host to collaborative brand events and expert-led forums with medical professionals, facialists and makeup artists, adds HydraFacial. UK and Ireland country manager, Lauren Gibson, said, “Our UK HydraFacial community is valued and everything about our new London flagship has been designed to support their commercial success.”
HydraFacial is the Headline Sponsor at Beauty Uncovered LIVE on May 7-8. Turn to p.36 to find out more.
BACN UPDATES
A round-up of the latest news and events from the British Association of Cosmetic Nurses

SPRING SYMPOSIUM
On April 29 the first ever BACN Spring Symposium was held at the prestigious Royal College of Physicians in London. This was our first national event since 2019, and second only to our annual conference, was the biggest event we’ve put on.
We welcomed more than 100 members, guests, and speakers along for a jam-packed day of educational talks, exclusive exhibitors, BACN updates, and networking opportunities.
A special thank you to Galderma UK for sponsoring this event, and to all the fantastic speakers who took to the stage – Anna Baker, Julie Scott, Rachel Goddard, Jude Dunican, Sharon King, Dr Elizabeth Hawkes, Jackie Partridge, Dr Tapan Patel and Dr Tristan Mehta. The evening ended with a drinks reception and canapés held in the beautiful Royal College grounds. Thank you so much to everyone who came along and made the day a success!
REGIONAL MEETINGS
Our regional meetings came to an end in early April after hosting 13 meetings over three months across the UK! We had more attendees than ever before, and 95% of those who came along gave the events a 5* review.
Our Liverpool meeting (which was postponed due to storm Eunice) is now rearranged for May. If you would like to attend this meeting, you can find all information on the BACN events page, along with a link to book.
Our next full round of meetings will take place in autumn 2022.
AUTUMN AESTHETIC CONFERENCE
The BACN’s annual Autumn Aesthetics Conference returns this year, with a brand-new venue – The Eastside Rooms. Taking place over two days on September 15-16, this is the biggest event dedicated to aesthetic nurses in the UK.
We are offering a limited number of hotel package options for members who are attending the first day of the event. Tickets to the event as well as hotel packages are available to buy on the BACN website now.
This column is written and supported by the BACN
Expansion
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Revision Skincare introduces new lip treatment
Clinical distributor AestheticSource has launched the Revision Skincare YouthFull Lip Replenisher. According to the company, the product aims to replenish lip volume, plump lips and smooth fine lines and wrinkles, defend against environmental stressors and sooth dry, dehydrated lips.
Ingredients include hyaluronic acid to hydrate the lips, shea butter to retain moisture and restore a natural, healthy lip colour, green tea and vitamin E to support long-term skin health and palmitoyl tripeptide-1 to strengthen lip structure. Lorna Bowes, CEO of AestheticSource, said, “Skin on the lips is more sensitive and prone to ageing than facial skin, so we are delighted to announce the launch of Revision Skincare YouthFull Lip Replenisher. Created to be used as a three-times daily topical treatment, it gives both immediate and long term results, leaving lips hydrated and plumper-looking, while defending against damaging environmental stressors.”

Partnership
The BACN collaborates with Aesthetic Nurse Software
The British Association of Cosmetic Nurses (BACN) has partnered with software company Aesthetic Nurse Software (ANS). According to ANS, the collaboration has been designed to drive standards and promote professionalism within aesthetics. The partnership aims to offer members a range of benefits, including a 10% discount on annual payments for BACN membership for existing ANS members. BACN members will also benefit from a one-month subscription for free when joining ANS, explains the BACN. Throughout June, ANS will be taking over the BACN digital channels for an episode of ‘In Conversation…’ with nurse prescriber and founder of ANS Jo Hayward, as well as an extended ‘In Focus’ webinar. Hayward commented, “We are delighted to be partnering with the BACN after building a great relationship with the team over many years. It is clear that we share the same goals, to support aesthetic nurses to maintain high standards of professionalism and run compliant, successful aesthetic practices. We’re looking forward to working together to support our respective members through educational content and sharing best practice in all areas of their business including practice management and record keeping.”
ANS will be exhibiting at the BACN Spring Symposium on April 29 and will be attending the BACN annual Autumn Conference on September 15-16.
Training Mr Daniel Ezra launches tear trough masterclass
Consultant oculoplastic surgeon Mr Daniel Ezra is hosting a tear trough masterclass at his Harley Street clinic in May. The masterclass includes an in-depth understanding of the anatomy of the tear trough, patient and filler selection, recognising and treating complications, as well as the use of hyaluronidase therapy in this area, explains Mr Ezra.

Mr Ezra will be joined by ophthalmic and oculoplastic surgeon Miss Caroline Wilde and 10 delegates are able to join per course. The surgeons will demonstrate the three-point tangent injection technique with each delegate receiving one-to-one injection training on patients. The course will take place on May 29 and a second one will take place on November 6.
Eco-friendly
BCAM unveils new sustainability initiative
The British College of Aesthetic Medicine (BCAM) has launched a new sustainability initiative. The College is encouraging its members to make their clinics more sustainable by sharing tips in newsletters and collaborating with others who are driving change in the industry.
BCAM explains it has introduced the initiative to help its members make small changes which have a big impact such as recycling waste, employing non-paper-based clinic systems and choosing suppliers who use ethical packaging.
The College is collaborating with business development consultant Ron Myers who launched the ‘Sustainability in Aesthetics’ Facebook group to share best practice and engage with those who are committed to making a change. BCAM is also publishing regular sustainability tips in its fortnightly newsletter and has asked members to share their own ideas so they can be passed on to others.
BCAM trustee Dr Bhavjit Kaur said, “As the UK’s leading organisation for doctors and dentists practising aesthetic medicine, BCAM is taking the initiative and providing members with practical solutions to make their clinics more sustainable. We also plan to encourage suppliers to offer greener options with their packaging, and it’s encouraging that there are already a handful of pharma companies that are taking sustainability seriously.”

Skincare
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Cynosure acquires MyEllevate System
Aesthetic device manufacturer Cynosure has acquired the MyEllevate Surgical Suture System.

According to the company, the patented light-guided suture system allows practitioners to easily place a suture support system without incisions, helping to define and enhance the jawlines, elevate the sub-dermis and underlying muscle with a quick recovery.
Cynosure launched the system in the UK at an exclusive training event, hosted by plastic surgeon and inventor of the MyEllevate System Dr Gregory Mueller. The company explains that it will be making the MyEllevate procedure available to plastic surgeons in the UK.
Todd Tillemans, chief executive officer at Cynosure, said, “MyEllevate broadens Cynosure’s already extensive surgical product portfolio, enabling us to offer this ground-breaking procedure in combination with other energy-based skin tightening technologies for optimal, long-lasting results. It’s a cutting-edge treatment, and we’re thrilled to be able to offer this highly sought-after procedure to selected UK customers so that they can bring out the beautiful energy in everyone.”
Education
Wigmore Medical conference returns

Aesthetic supplier Wigmore Medical will be hosting Wigmore Medical Presents in May. The event will offer two CPD-accredited agendas across two days with seven points available for each day. Highlights include aesthetic practitioner Dr Rita Rakus and plastic surgeon Mr Stephen Mullholland discussing the future of the aesthetics industry, as well as business consultant Wendy Lewis leading a morning with experts on business development.
Consultant dermatologist Dr Mukta Sachdev will be discussing treating skin of colour whilst giving a glimpse into the new training course that Wigmore is developing. The weekend will also have talks on toxins, fillers, threads and hair restoration with, consultant dermatologist Professor Nick Lowe, nurse prescriber Anna Baker consultant plastic and reconstructive surgeon Mr Dalvi Humzah and nurse practitioner Julie Scott. Alongside the talks, exhibitors at the event include Merz, Teoxane, Rosmetics and Aesthetic Technology. Croma-Pharma will be conducting workshops and InMode and HA-Derma will offer insights into their products. Wigmore Presents will take place on May 7-8 at the Royal College of Physicians, London.
Invite Your Patients to Beauty Uncovered LIVE
With so many new procedures and devices being launched each year, it can be difficult for your patients to know where to start. This is where Beauty Uncovered LIVE comes in. This two-day event will empower your patients and patients-to-be to make safe and ethical choices when choosing the right treatment for them. All while understanding why going to a qualified medical practitioner is so vital!
On May 7-8 2022, your patients will get the unique opportunity to enhance their knowledge and speak to more than 40 aesthetic and skincare brands, many of which will already be featured in your clinic. Headline sponsor HydraFacial is giving away free treatments and Skinade will have a collagen bar with a free drink for every ticket holder. Plus, we have top injectable companies Galderma, Teoxane and Neauvia hosting live demos and sponsored sessions specifically aimed at patients who want to expand their knowledge. The show floor will be packed with samples and demos showing patients the incredible products, devices and aesthetic treatments available in your clinic.

As healthcare professionals, we want to help you build trust and loyalty with your patients by educating them on new and existing treatments, and the long-term benefits both mentally and physically. We have gathered leading UK practitioners, beauty journalists, aesthetic-loving celebs, and real-life patients to uncover the treatments and products that will help them to achieve their beauty goals. Taking to the stage will be Dr Tapan Patel, Dr Munir Somji, Miss Jonquille Chantrey, Mr Naveen Cavale, Dr Nina Bal from E4’s ‘Body Fixers’, beauty guru and journalist Nadine Baggott, Love Island star Sharon Gaffka, model and entrepreneur Caprice, and many more.
Beauty Uncovered LIVE will allow you to get to the heart of what patients really want, to learn how leading practitioners speak to them, to explore current trends and to attend Q&A sessions alongside them. Let’s work together to open up the world of aesthetic medicine by promoting safe practice, a comfortable environment and overall, a healthy patient experience.
We are giving away free VIP tickets to the next 500 medical professionals to register. The offer code is HCPVIPJOURNAL and the discount will be automatically applied when you select your ticket.
Device
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
TO GET TICKETS FOR YOUR
SCAN HERE
PATIENTS
News in Brief
AlumierMD partners with GetHarley
Skincare platform GetHarley has partnered with skincare brand AlumierMD. The company explains that any medical practitioner using the GetHarley service can add AlumierMD products to their digital shelves, following full training with the brand. Charmaine Chow, founder and CEO of GetHarley, said, “AlumierMD is a forward-thinking brand that the medical community loves to recommend in-clinic and for patients at home. We are delighted to officially welcome this brand and look forward to partnering with AlumierMD.” AlumierMD will be exhibiting at Beauty Uncovered LIVE on May 7-8. Turn to p.36 to find out more.
Cosmetic Courses releases new training course
Aesthetic training provider Cosmetic Courses has launched a new online course on treating Asian patients. According to the company, the ‘East Asian Full-face Rejuvenation’ course will explore the use of aesthetic procedures for East Asian patients and how they differ from Caucasian skin types. The course allows practitioners to understand and appreciate different clientele and also learn a holistic approach to aesthetic treatments, with two full-face rejuvenation demonstrations performed by aesthetic trainer Dr Tracy Xu.
Hannah McClune unveils new online image library
Photographer Hannah McClune has launched the Visible Image Library. The library has been designed to sit alongside existing brand photos or to use alone, to support your aesthetic brand, explains McClune. The library has a mixture of work and lifestyle images in different colour palettes and is suitable for aesthetic business owners who have had a photoshoot before and need a ‘top up’; haven’t invested in a shoot but need professional images; or don’t have time to take their own pictures.
BMLA conference to take place
The British Medical Laser Association (BMLA) is hosting its annual conference in May. The conference will be held in-person to provide delegates with an opportunity to learn about the field of lasers and light-based devices. The event will begin with core of knowledge and specialised skin courses with speakers including medical physicist Mr Graham Hart, independent laser and radiation protection advisor Mr Stan Batchelor and consultant scientist Professor Harry Moseley. The conference will take place on May 25-27 at the Surgeons Quarter in Edinburgh.
Skin skinbetter science releases new peel system
Distributor AestheticSource has launched the new skinbetter science AlphaRet Professional Peel System 50. The peel system is for professional-use only and contains the pre-peel solution to prepare the skin for application of the peel, a triple-acid peel gel 50 which is a high strength 50% blend of lactic, glyolic and salicylic acid and the AlphaRet Peel Solution, a patented retinoid, alpha-hydroxy acid conjugate formulation, explains AestheticSource.

In a clinical study where one peel treatment was administered once every four weeks, 100% of patients agreed the overall condition of their skin improved from baseline after one peel. Lorna Bowes, CEO at AestheticSource, said, “We are delighted to announce the launch of the new skinbetter science AlphaRet Professional Peel System 50. The system is an exciting addition to the skinbetter science range, which is just one more reason I am excited that we are able to bring it to aesthetic professionals in the UK and Ireland.”
On the Scene
The MaiLi Experience, London
On April 4 pharmaceutical company
Sinclair Pharma hosted the MaiLi Experience, an educational event for its new hyaluronic acid filler.

Delegates were welcomed with tea, coffee and pastries as they arrived at the Royal College of General Practitioners, London, and the day began with a presentation about MaiLi, hosted by head of marketing Chloé Antunes.
Attendees had the opportunity to enhance their knowledge of treating different areas of the face – the upper face, mid-face, and lower face – by being split into small groups and watching demonstrations by the company’s key opinion leaders and trainers Dr Sabika Karim, Dr Charlotte Woodward and Dr Sheila Nguyen. With a five to one training ratio, delegates were able to closely observe treatments and share peer-to-peer engagement, trading best practice and tips.
During the day, the trainers also shared recommendations about patient selection and the consultation process, in addition to tips about identifying vessels and landmarks on the face to ensure a safe and effective treatment.
Dr Karim commented, “The MaiLi Experience was a brilliant chance to raise industry standards by having intimate groups of people training on the whole face. Whether people are experienced injectors or have only been injecting for a few years, we were able to share ideas and best practice techniques together. One of the best parts of the day was not only discussing injection techniques, but tips and tricks on how to get the best possible results for our patients.”
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Skinade manufacturing site, St Margarets
On April 5, Aesthetics was invited to the Skinade global headquarters in St Margarets, London, to see first-hand how the award-winning Skinade skincare drinks are manufactured.
Despite nearly two years of forced closures and disruption due to the pandemic, Skinade have built and launched two state-of-theart manufacturing facilities in London and Washington, with the capability of producing 46 million units of Skinade bottles per year.
The family-run company has certainly come a long way from the tiny start-up in 2013. Upon arrival at the site, Skinade enforce strict biological protocols to ensure the highest
food safety standards. Skinade report that according to their onsite tests, even a clean pair of hands carries a bacterial count of over 1,500 – the target is less than five! Inside the factory clean rooms, there are HEPA filter positive pressure environments and no jewellery can be worn. Hands must be thoroughly washed, and a protective coat, shoes, and hair net coverings must be worn. Manufacturing professional grade nutraceuticals demands the highest quality ingredients. Skinade create their own water using industrial level reverse osmosis membrane units – tap water contains too many impurities. In the first clean room, the
patented formulation is made using a high velocity entrainment process, combining peptides with added ingredients such as vitamin C, methylsulfonylmethane, l-lysine, vitamin B complex and omegas 3 and 6; accuracy is crucial.
This solution is then piped into the second clean room where the bottle production line begins. In-house trained production staff operate the line checking quality control and full track and trace.
Piers Raper, CEO and founder of Skinade, explains, “Our product is designed to trigger a physiological response in the body to stimulate natural production of collagen, elastin, and hyaluronic acid with an overall aim of normalising skin function. One of the reasons our product works so well is that all ingredients in the drink are in solution, achieving a bioavailability of more than 95%. This is only made possible through the liquid engineering process we have designed.”
Skinade will also be exhibiting at Beauty Uncovered LIVE from May 7-8 at the Business Design Centre. Raper continues, “We have provided limited-edition branded Skinade bottles for Beauty Uncovered LIVE. You can find us at the Skinade bar, where all show attendees are entitled to a bottle. We’re very excited to see everyone there!”

IMCAS World Congress
After a year’s hiatus, the International Master Course on Aging Science (IMCAS) returns to the Palais des Congrès, Paris on June 3-5
The 23rd edition of IMCAS will take place in-person with the new addition of offering all participants the possibility to live stream the event online. The congress provides innovative and in-depth learning opportunities for all aesthetic practitioners. The key themes will cover a range of updates which took place in minimally invasive treatments such as injectables, lasers, threads, cosmeceuticals, peels, microneedling, and more.
This year, the scientific programme includes new elements designed to help delegates refine their medical knowledge and treatment techniques in 2022.
Some of the major focuses will include ultrasonography as an essential ally for aesthetic procedures, the latest trends and innovations for artificial intelligence (AI) and robotics, updates on how to manage complications, and understanding the female and male patients in 2022. On Friday, the anatomy on cadaver workshops will combine live cadaver dissections and patient demonstrations so delegates can see the anatomy on one hand and the procedure on the other. The first day also puts the spotlight on threads, from combined techniques to complications management for different types of threads.
On Saturday, delegates will have the opportunity to interact with leaders of the aesthetics market during the IMCAS Global Market Summit. The summit involves meeting international start-ups and their solutions, receive knowledge to achieve higher returns from the market and learn about the latest market segment figures, mergers and acquisitions. The day will focus on cosmeceuticals and nutraceuticals where delegates can learn about skin ageing treatments. The final day will focus on AI and robotics and discover the future of aesthetics during sessions on new technology and research and development. Dedicated sessions on botulinum toxins and new toxins to be released in 2022 will take place.

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Factory Visit
Training in Menopause
By 2025, the number of postmenopausal women is expected to rise to 1.1 billion worldwide 1 Despite this, it has been recently highlighted by the Government that many women feel isolated and unable to seek guidance from their doctor or nurse. In the Women’s Health Strategy report published in April, it was outlined that healthcare professionals (HCPs) in England need better and more standardised training on the menopause.2
The report involved a public survey of 100,000 women aged 16 and over who discussed areas such as menstrual health, fertility, mental health and the menopause. According to the survey, 64% of respondents felt uncomfortable talking to HCPs about the menopause as women often had their symptoms dismissed. The reasons behind this were that they were classed as ‘too young’ or they were not displaying the ‘obvious’ symptoms such as hot flushes, night sweats and mood changes.2 Respondents also felt they were provided with limited treatment options and often had their preferences ignored, particularly when requesting hormone replacement therapy (HRT).2
The report detailed that gaps were found in clinician education, including a reluctance to prescribe HRT due to existing guidelines issued by the National Institute for Health and Care Excellence (NICE) which highlighted the risks rather than the benefits.2,3 In addition, menopause training is often not mandatory so some GP placements may not be trained by someone with sufficient knowledge. Another issue was that the symptoms associated with the menopause, such as mood swings, can overlap with other conditions, leading to HCPs prescribing antidepressants to treat symptoms, which might not help.2
Upon reading the report, aesthetic practitioner and former GP, Dr Shirin Lakhani, who has a special interest in women’s health and holds a diploma of the Royal College of Obstetricians and Gynaecologists, said, “Women regularly present to me saying they have given up work or turned down a promotion because of their menopausal symptoms. It astounds me that the menopause isn’t given the same consideration as other hormone deficiencies, such as diabetes or hypothyroidism, despite the lack of these hormones leading to considerable morbidity and mortality in women.”
Training in the menopause
Currently in the UK, menopause is included in the Royal College of General Practitioners curriculum, however, training programmes are short. Practitioners therefore have to invest in additional training courses to gain further knowledge. Dr Lakhani believes it’s causing a lack of understanding amongst medical professionals when it comes to patient care. “Gaps in training for professionals hinders effective menopause care. Further training around the menopause should be mandatory for HCPs as it has a myriad of symptoms and signs, not just the well-known flushes and sweats,” she says. The gap in practitioner training, Dr Lakhani notes, presents an opportunity for those working within aesthetics to help patients by providing a holistic approach to their consultations. Dr Lakhani says practitioners should complete a full examination of their patient and factor in the menopause as a possible cause. “Aesthetic professionals should seek additional training and be equipped to recognise the symptoms of the menopause and signpost women to the correct services, or be able to successfully treat and guide patients in your own clinic,” she says. For aesthetic practitioners interested in furthering their knowledge, Dr Lakhani recommends joining the British Menopause Society, and seeking out training with The Marion Gluck Clinic, American Academy of Anti-Ageing Medicine and the European College of Aesthetic Medicine and Surgery.
Understanding the treatment options
The NHS states that HRT is advised as the main option to help relieve symptoms such as hot flushes, mood swings and vaginal dryness. Other treatment approaches include cognitive behavioural therapy or clonidine.4 Dr Lakhani notes, “In my experience, HRT is still regularly
feared by HCPs who can actively discourage their patients from taking it, rather than having a discussion, considering up-to-date evidence instead of older flawed studies.”
Dr Lakhani refers to the results of two large studies which raised concerns in the early 2000s about the safety of HRT, particularly with regards to breast cancer and heart disease.5,6 However, she highlights that newer research has found that bioidentical HRT does not carry the same risks as traditional HRT, so this is something she actively recommends to her patients and believes should be more widely available.7
According to Dr Lakhani, the NHS does not promote the use of other well-known interventions commonly found in clinics which may also help patients. These include skin treatments to tackle pigmentation, sagging and dryness, hair treatments to improve hair loss, radiofrequency tightening treatments for vaginal dryness and laxity, or supplements to help calcium and vitamin D levels.
“A large proportion of our aesthetic patients fall into this demographic, and there has been an increase in clinics broadening their offering to meet the medical needs of post-reproductive women. In my clinic, we offer radiofrequency technology to help with vaginal laxity, platelet-rich plasma for menopausal atrophy, intimate fillers and hydrating skinboosters as well as the usual aesthetic treatments to tackle the face and body,” Dr Lakhani comments.
Taking the menopause seriously
To ensure that patients receive the correct diagnosis and optimal treatment options available, Dr Lakhani believes that extended education on the menopause should be implemented. Dr Lakhani concludes, “I hope the report will help to highlight the need for practitioners to understand the menopause and its symptoms. I believe that with thorough training, menopausal management is a holistic service that many clinics can add. Holistic care is what differentiates us from the number of non-medical clinics, so let’s start to take the menopause more seriously!”
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
VIEW THE REFERENCES ONLINE! WWW.AESTHETICSJOURNAL.COM
Following the release of a new report on women’s health, Aesthetics explores the limitations on current menopause training and how the aesthetics industry can help patients


















Aesthetic Technology Ltd. T: 0845 689 1789 E: info@aesthetictec.com W: aesthetictec.com
Letybo�
Botulinum toxin type A
*Letybo® is indicated for the temporary improvement in the appearance of moderate to severe vertical lines between the eyebrows in adults
years old seen at maximum frown (glabellar lines),
the severity of the facial lines has an important psychological impact. **Response rate was defined as a ≥ 1-point reduction in FWS at maximum frown based on the investigators assessment. References: 1. Mueller DS, Prinz V, Adelglass J, Cox SE, Gold M, Kaufman-Janette J et al. Effi cacy and Safety of Letibotulinum Toxin A in the Treatment of Glabellar Lines: A Randomized, Double-blind, Multicenter, Placebo-controlled Phase 3 Study. Aesthet Surg J. 2022; Jan 29: sjac019. doi: 10.1093/asj/sjac019. Epub ahead of print. PMID: 35092418.; 2. Letybo SmPC, revision date: 08.04.2022 Letybo 50 units powder for solution for injection; Abbreviated Prescribing Information: Please refer to the Summary of Product Characteristics (SmPC) before prescribing. Presentation: One vial contains 50 units botulinum toxin type A produced by Clostridium botulinum. After reconstitution each 0.1 mL of the solution contains 4 units. Indication: For the temporary improvement in the appearance of moderate to severe vertical lines between the eyebrows in adults <75 years old seen at maximum frown (glabellar lines), when the severity of the facial lines has an important psychological impact. Dosage and administration: Should only be administered by physicians with expertise in this treatment. Posology: The recommended dose is a total of 20 units divided into five injections of 4 units (0.1 mL) each: 2 injections in each corrugator supercilii muscle and 1 injection in the procerus muscle. Botulinum toxin units are not interchangeable from one product to another. Doses recommended are different from other botulinum toxin preparations. Treatment interval should not be more frequent than every three months. In the absence of any undesirable effects secondary to the previous treatment session, a further treatment session with at least a three-month interval between the treatment sessions is possible. The efficacy and safety of repeat injections beyond 12 months has not been evaluated. Special populations: No specific dose adjustment is required for use in the elderly older than 65 years of age. Letybo is contraindicated in patients 75 years or older. There is no relevant use in the paediatric population. Method of administration: Intramuscular use. Care should be taken to ensure that Letybo is not injected into a blood vessel. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Generalised disorders of muscle activity (e.g. myasthenia gravis, Lambert-Eaton syndrome, amyotrophic lateral sclerosis). Presence of acute infection or inflammation at the proposed injection sites. Patients with bleeding disorders. Warnings and Precautions: Injection into vulnerable anatomic structures must be avoided. Avoid use when the muscle shows excessive weakness or atrophy. Risk of eyelid ptosis following treatment. Procedure-related events: Needle-related pain and/or anxiety have resulted in vasovagal responses, including transient symptomatic hypotension and syncope after treatment with other botulinum toxins. Pre-existing neuromuscular disorders: Patients with unrecognised neuromuscular disorders may be at increased risk of clinically significant systemic effects including severe dysphagia and respiratory compromise from typical doses of botulinum toxin type A. Hypersensitivity reactions: An anaphylactic reaction may occur after injection of botulinum toxin. Epinephrine (adrenaline) or any other anti-anaphylactic measures should therefore be available. Local or distant spread of toxin effects: Adverse reactions possibly related to the spread of toxin distant from the site of administration have been reported. Patients may experience exaggerated muscle weakness. Swallowing and breathing difficulties are serious and can result in death. Use not recommended in patients with a history of dysphagia and aspiration. Patients should be advised to seek immediate medical care if swallowing, speech or respiratory disorders arise. Pregnancy & Lactation: Not recommended during pregnancy or lactation and in women of childbearing potential not using contraception. Undesirable effects: Most common effects are headache and injection site reaction. Very rarely aspirational pneumonia. For full list of side effects, consult SmPC. Legal Category: POM; Pack size: Packs containing 1 5ml vial. Multipack containing 2 (2 packs of 1) vials; Price list: UK - 1x5ml: 65GBP, 2x5ml: 120GBP; MA Number: PL 29863/0002; PA Number: PA0846/001/001; MA Holder: Croma-Pharma GmbH, Industriezeile 6, 2100 Leobendorf, Austria; Date of preparation: 11/04/2022; Unique ID no CRP001/001; Adverse events should be reported. Reporting forms and information can be found at: UK - http://yellowcard.mhra.gov. uk/ or search for MHRA Yellow Card in the Google Play or Apple App Store. IE - HPRA Pharmacovigilance Website: www.hpra.ie. Adverse events should also be reported to Croma Pharma GmbH on 0118 206 6513; ADLET0322UKa

94% response rate 4 weeks post injection1,** Consistent efficacy and safety also with repeated injections for 12 months1,2 Demonstrated high patient satisfaction2
new
Letybo® is the new neurotoxin. Here to change the aesthetic market with notable performance and confirmed tolerability.1,2,*
go go go
ways
<75
when
the different layers of the skin will determine its colouration.2
In the epidermis, it will appear tan, brown, or dark brown and may take months to years to resolve without treatment. In the dermis, PIH has a blue-grey appearance and may either be permanent or resolve over a significant amount of time if left untreated. PIH can worsen with sun exposure and persistent or recurrent inflammation.2
Melasma
More common in women, melasma generally occurs as a result of hormonal changes. Birth control and hormone replacement medication can have an effect, while research suggests that up to 50% of pregnant women experience melasma.3
Managing Hyperpigmentation Concerns
Practitioners would agree that an even skin tone is fundamental to fresh and healthy-looking skin. You could provide a patient with the very best injectable treatment; reducing lines and wrinkles, volumising cheeks and enhancing facial features, yet this cannot guarantee ultimate satisfaction – for you and them.
Addressing skin tone concerns and, in particular, managing hyperpigmentation, could make all the difference. First, it’s vital to understand what hyperpigmentation is and why it occurs. Here we will explore the three most common types and consider how it is best treated.
Understanding hyperpigmentation
Hyperpigmentation occurs when there is excess production of melanin; the pigment produced by melanocytes which are the cells that give skin its colour.1
“The darker your skin, the more melanocytes you have,” says consultant dermatologist Dr Hiba Injibar, explaining that this subsequently means that those with darker skin types have a higher risk of hyperpigmentation. That said, she notes, lighter-skinned individuals are also affected –particularly those who’ve had excessive sun exposure.
However, sun isn’t the only cause. Aesthetic practitioner Dr Lori Nigro explains that hormonal, systemic, inflammatory and structural triggers can all lead to various forms of hyperpigmentation. And as consultant dermatologist Dr Jinah Yoo highlights, hyperpigmentation is simply a description. She emphasises that to appropriately treat the concern, it’s vital to identify exactly which pigment disorder your patient is suffering from. The three most common are: post-inflammatory hyperpigmentation, melasma and solar lentigines.
Post-inflammatory hyperpigmentation

When skin is irritated or injured, for example through acne, eczema, or burns, it triggers an inflammatory response whereby more melanin is produced leading to post-inflammatory hyperpigmentation (PIH). Research has indicated that the location of the excess pigment within
It usually appears on the cheeks, forehead, upper lip, nose, and chin, but can also occur on the other areas of the body exposed to the sun. Melasma becomes more noticeable in the summer and can improve with hormonal adjustments.3
Solar lentigines
Often referred to as sun, age, or liver spots, solar lentigines usually appear on sun-exposed areas of the skin such as the face, hands, neck and chest. They can be various shapes and sizes, and most don’t go away unless treated.4
There are other types of lentigines, which can be present from birth or form following radiation treatment, however they are outside the scope of this article.4
Prevention
“The sun is a major culprit in all forms of hyperpigmentation,” says Dr Injibar; whether it’s causing or exacerbating the condition. She emphasises that sun protection is key to prevention. “Wearing SPF50, a broad, widebrimmed hat, seeking shade and staying out of the sun in peak hours – between 11am and 3pm – is prime advice we should be giving all of our patients,” says Dr Injibar, with both Dr Nigro and Dr Yoo agreeing. “I tell my patients that if they are leading an active lifestyle, they are really using up their full quota of sun exposure. Sun tanning and sunbeds do not and should not be part of their beauty routine,” says Dr Nigro. She adds, “I remind them that there are really great and fully adequate bronzers available and try not to make them feel bad for wanting to do it. We must instead give patients better options.”
Particularly in cases of melasma, the practitioners recommend reviewing patients’
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
An overview of common complaints and best treatment approaches for hyperpigmentation



™
hormonal balance in order to target the cause, prior to tackling the effect. They suggest looking at different medication; for example, switching the combined oral contraceptive to an intrauterine device instead. Likewise, for those suffering from PIH, the practitioners believe it’s beneficial to review the condition that may be causing it if it’s something treatable such as acne.
“It’s a discussion to have on a case-by-case basis,” says Dr Nigro. She emphasises, “We must have a prevention strategy for every patient who walks through the door. We as aesthetic practitioners need to be able to treat our patients differently and accept that they have different requirements. And if we cannot, then we should refer to colleagues who can.”
Treatment
There are a number of different ways in which hyperpigmentation can be treated, with the deciding factor being led by the type and severity.


Skincare
For low-severity hyperpigmentation, the practitioners recommend that prescriptionstrength skincare is a good place to start. Hydroquinone is a well-known ingredient, however if this isn’t suitable for your patients there are other effective ingredients. Some of these are:5
• Vitamin C: blocks tyrosinase, an enzyme the body uses to produce melanin and, as an antioxidant, protects cells from further damage from the sun or pollutants.
• Kojic acid: similarly to vitamin C, also works by inhibiting tyrosinase enzymes and protects skin thanks to antioxidants.
• Retinol: encourages cell turnover, bringing healthier skin cells to the surface while exfoliating older, darker ones.
• Niacinamide: a form of vitamin B3 which can interrupt the process of cell pigmentation and brighten skin, while also being used to treat acne and prevent future hyperpigmentation.
• Azelaic acid: anti-inflammatory properties and can suppress melanin production –considered suitable to use in pregnancy so especially beneficial for melasma treatment.
• Mandelic acid: an alpha-hydroxy acid that helps exfoliate the skin.
• Arbutin: considered to be a natural form of hydroquinone – a chemical that bleaches the skin – so can be a preferred method.
Dr Yoo has seen success with Cyspera; the product uses a formula that contains cysteamine, which aims to regulate melanin synthesis in the skin. While it can be used as an intensive treatment when used daily for 16 weeks, Dr Yoo says that she finds it a valuable tool to maintain results if used twice weekly.6
For Dr Injibar, Eucerin Sun Pigment Control sunscreen or a mineral sunblock such as Bioderma Photoderm Mineral are her go-to skincare recommendations, while Dr Nigro advocates the use of the mesoestetic range.
Chemical peels
Of course, these ingredients can also be used in chemical peels – one of the most popular methods for treating hyperpigmentation. “In terms of peels, you need to have the preparation phase, the treatment phase and the maintenance phase,” explains Dr Nigro, adding that the preparation phase is arguably the most important in order to limit localised skin reactions to the peel itself. She says, “Localised skin reactions can include redness, swelling, tenderness and tightness. By adequately preparing the skin, we can avoid this and amplify results.”
To prepare the skin, Dr Nigro advises you could either provide patients with fortnightly superficial peels or recommend a homecare regime, with less intensive products, which they would use every day for a period of two to six weeks, depending on their concern. When it comes to the peel itself, Dr Nigro is quick to remind practitioners that a medium peel can always become deep, whereas a deep peel cannot become superficial, so always take caution, and select a weaker ingredient to start. Dr Nigro’s go-to products are cosmelan for the preparation phase and dermamelan for the main peel; both from mesoestetic. She explains that they can be used on all skin types and use respected ingredients such as vitamin C, ferulic acid, niacinamide and vitamin E, that address more than the pigmentation. She notes, “If
you use a treatment which has the intensive treatment phase and the maintenance phase, you can modulate the melanocyte response for years after a treatment, so patients’ results can be prolonged and they can get the best possible long-term outcome.”
For Dr Yoo, the Exuviance 20-30% glycolic acid peel is her product of choice. She says, “It’s a gentle superficial peel which allows me to combine with other treatments such as laser or radiofrequency microneedling.”
Energy-based devices
For solar lentigines, Dr Injibar prefers the use of the Synchro QS4 Q-switched laser from DEKA and also recommends a pico laser. She explains that short bursts of laser cause the pigment to shatter into tiny, microscopic fragments under the skin, which are absorbed by the body or peel off externally. “In my experience, Q-switched laser is very effective. I can often peel off the hyperpigmentation completely,” she says. Topical anaesthetic should be used, but Dr Injibar says pain and downtime are minimal. “Side effects can include scabbing in the area and, as practitioners will know, any time you break the skin barrier, there’s always a very slight risk of infection. This is of course low if you keep the skin clean,” she says. Dr Injibar adds that there is also always a risk of scarring and further hyperpigmentation but, in her experience, this is low if the device is used correctly so appropriate training is essential for all users. CO2 lasers are also an option, however, she notes that this risk is higher as they break the skin.
Generally, Dr Injibar says effective treatment will require between three and 10 sessions with the device she uses but
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Figure 1: 43-year-old patient before and 120 days after one dermamelan peel. Images courtesy of mesoestetic.
Before After

acknowledges that more densely pigmented areas will need more treatments, so managing patient expectations is key. To help with this and incentivise booking, she offers patients a discounted package of treatments based on predicted sessions. This, she says, helps them acknowledge that it won’t be an overnight fix.
Dr Nigro also offers laser treatment, with her device of choice being the C02RE – a C02 laser – from Candela. She says it can be particularly beneficial for patients with lighter skin suffering from acne scarring. “As well as being able to treat the PIH, you’ll also be able to refine the skin and see further improvement,” she explains.
For darker-skinned patients with a strong family history of hyperpigmentation and who’ve tried all the prevention strategies, Dr Nigro says there’s no justification for using a laser. “In my view, you must stick with combination peels as they’re much safer,” she advises.
Dr Yoo also uses laser, choosing to utilise the Hollywood Spectra from Lutronic. She says the Q-switched device has different modes to target different sizes of pigment. “I use a laser toning technique every two weeks for five to 10 sessions when treating PIH and melasma, which breaks down pigments into smaller fragments to be removed through the lymphatic system,” she explains. Dr Yoo also uses the Clarity II long pulse device, again from Lutronic, which she claims has a unique temperature monitoring feature, which allows it to be safely used to treat darker skin types.
Dr Yoo, on the other hand, uses a radiofrequency microneedling device called Sylfirm X. She explains, “This device reaches a 300micron depth where it is targeting fibroblasts in the papillary dermis to modify the crosstalk between fibroblasts and melanocytes in melanogenesis.” With minimal downtime and discomfort, she has found it to be a reliable addition to her practice. Dr Yoo notes, “As radiofrequency microneedling works by delivering radiofrequency energy through the microneedle in a controlled way and it is not affected by chromophores – such as pigments like in laser – it is safe to use as long as not too much heat is delivered.” To treat melasma, Dr Yoo says the device is suitable for all skin types and uses 0.3mm needles and offers five sessions every two to four weeks.
Hyperpigmentation in the intimate area
Dr Nigro says there is often an assumption that only facial hyperpigmentation is a concern. Yet, she has found that many patients are bothered by the condition occurring in intimate locations. Hormones and factors such as friction can contribute to skin darkening,7 and it’s vital that practitioners are able to offer safe treatments before patients turn to unregulated products found online. She highlights, “Culture has suggested that only porn stars should want to treat their intimate area but, the reality is, when your body starts to change you may not like it and that’s nothing to be ashamed of.” Dr Nigro uses the mesoestetic dermamelan intimate product, which contains a combination of active ingredients with depigmenting efficacy, as well as formula that aims to control the inflammation. Useable in the genital-perineal area, perianal area, mons pubis, inner thighs and groins, Dr Nigro says she’s seen excellent results with the product. She emphasises, however, that if you don’t feel confident or comfortable treating intimate areas, then always refer your patient to a practitioner who does.
Considerations
The practitioners recommend always performing a patch test on a patient prior to laser or peels which, as well as checking the treatment is appropriate for them, allows the patient to see the effect after one treatment and get an idea of expected downtime and help manage expectations.
When investing in a laser device, Dr Injibar says it’s important to understand the technology before making a selection. She advises, “Try different machines before you invest, research its track record and get to know the company itself. The laser company is very important as you will need the postpurchase support.” Dr Injibar recommends finding out what training is available, what their upgrade policy is and the maintenance service they offer. “I would recommend investing in a company that is here in the UK, so if something does go wrong, they will have local engineers who can fix any error as soon as possible. They’re very fancy machines but something can go wrong on the spot and, if you have patients booked, what do you do?” she highlights.
Dr Injibar also advises being cautious of new technology – sometimes the latest doesn’t mean it’s the best, she says, adding, “It has to stand the test of time, so do your research by checking clinical studies and sourcing first-hand experiences of the devices you plan to purchase!”
Of most importance, is recognising when and when not to treat, agree the practitioners. “Skin cancer is pigmented,” says Dr Injibar, emphasising what you assume is simply hyperpigmentation, could be more sinister. “If it’s suspicious or you’re unsure, always refer to a dermatologist,” she warns.
And, as always, sun protection is key to avoid and reduce the chance of severe hyperpigmentation. The practitioners conclude that SPF50 and above should be recommended for maximum protection, while educating patients on the sun’s impact on skin overall is imperative to achieving healthy, aesthetically-pleasing skin.
REFERENCES
1. MaryAnn De Pietro, What You Should Know About Hyperpigmentation (Healthline, 2022) <https://www. healthline.com/health/hyperpigmentation#outlook>
2. Erica C Davis, Valerie D Callender, ‘Postinflammatory Hyperpigmentation’, The Journal of Clinical and Aesthetic Deramtology, 2010. <https://www.ncbi.nlm.nih.gov/pmc/ articles/PMC2921758/>
3. What Is Melasma? (British Skin Foundation, 2022) <https:// knowyourskin.britishskinfoundation.org.uk/condition/ melasma/>
4. S. Behring, Lentigo (Liver Spots) (Healthline, 2022) <https:// www.healthline.com/health/lentigo#types-of-lentigo>
5. Kate Watson, The best ingredients to treat hyperpigmentation and brighten your complexion, according to dermatologists (Insider, 2022) <https://www.insider.com/ best-ingredients-for-hyperpigmentation>
6. Cyspera Intensive Pigment Corrector (Face the Future, 2022) <https://www.facethefuture.co.uk/products/cyspera-intensivepigment-corrector>
7. Intimate Area Hyperpigmentation: A Common But Personal Concern (Cyspera, 2022) <https://www.cyspera.com/intimateareas-hyperpigmentation/#:~:text=Darkening%20of%20 the%20skin%20of,can%20contribute%20to%20skin%20 darkening.>
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022



YVOIRE ® Training Modules


Develop strong theortical knowledge with our pre-learning webinar and establish new techniques with confidence from our 1:1 practical session.

Modules
Mid Face Lower Face Temples HEXA Ligment Lift
Upcoming Training Dates 2022
London
Thursday 23rd June
Tuesday 12th July
Tuesday 9th August
Tuesday 6th September
Monday 24th October
Tuesday 15th November
Manchester
Tuesd ay 7th June Friday 12th August Tuesday 4th October
Bristol
Wednesday 13th July
Wednesday 23rd November
Loughborough
Wednesday 15th June
Wednesday 13th July
Wednesday 10th August
Wednesday 14th September
Wednesday 12th October
Wednesday 16th November
Training will be carried out by renowned experts and dermal filler specialists: Dr Andrew Greenwood BDS Dr Vikram Swaminathan MB ChB Yvette Newman RGN
High Lifting Capacity | High Enzymatic Stability | High Biocompatibility ChurchPharmacyUK training@churchpharmacy.co.uk
Exclusive to Healthcare
HICE Cross-Linking Technology
ChurchPharmacy
professionals only.
Assessing the Extrinsic Factors of Skin Ageing
Dr Nihull Jakharia-Shah, Miss Priyanka Chadha and Miss Lara Watson present
the extrinsic factors that accelerate skin ageing
Ageing is universal. However, the physical manifestations of ageing vary greatly between individuals. Skin ageing is typically defined morphologically as the development of wrinkles, uneven texture, pigmentation and telangiectasia.1 The drivers of skin ageing can be classified into intrinsic and extrinsic factors. Intrinsic factors are those that we cannot control, namely our genes, whereas extrinsic factors are modifiable and often environmental, such as those caused by smoking, sun exposure and nutrition.2 Intrinsic ageing is unavoidable but its impact is superimposed by extrinsic factors, thus better understanding and control of extrinsic factors is key to limiting the impact of time on the skin.
Intrinsic factors of skin ageing
The intrinsic factors of skin ageing (i.e. one’s genes) are predetermined. Those of genetically male sex have an increased predisposition to demonstrate the physical signs of skin ageing over their female counterparts.3 A recent meta-analysis has suggested that there is no clear association between skin colour and skin ageing, but variability between different ethnicities has been seen.3 It has been suggested that intrinsic factors contribute more to the development of the signs of ageing than extrinsic factors.4 However, as we cannot yet alter our intrinsic risk, attempts to minimise skin ageing will focus on reducing extrinsic factors.
As intrinsic ageing cannot be altered, it is important to note that a degree of skin ageing is inevitable and should be embraced as part of the natural, healthy ageing process.
Extrinsic factors of skin ageing
A number of factors contribute to extrinsic skin ageing, including: sun exposure, smoking, diet, pollution, stress, skincare, weight and sleep.
Sun exposure
Sun exposure refers to ultraviolet (UV) radiation-induced damage to the skin. Both UVA and UVB have been implicated in this process, though UVB is thought to play a greater role.5 UV radiation causes direct damage to the DNA of skin cells (keratinocytes, fibroblasts for example) leading to reduced function of the cells and even cell death.6 UV exposure also generates oxygen free-radicals which damage local structures and cells within the skin.7 Free radicals lead to the breakdown of, and a reduction in the production of collagen and elastin in the skin.8 Exposure to UV radiation is the greatest extrinsic contributor to skin ageing.9 Photoageing has been shown to
have a greater impact in people of lighter skin types, due to the protective properties of melanin against UV radiation.10 It should also be noted that UV radiation is a carcinogen and exposure is directly linked to increased risk of all types of skin cancer, including malignant melanoma.11
Adequate UV exposure is, however, vital for the production of endogenous vitamin D.12 Vitamin D is directly linked to a number of positive health outcomes.13 Thus, global public health campaigns strongly advise maintenance of adequate vitamin D levels, with supplementation if required. Many foods in the UK are fortified with vitamin D, such as cereal. However, these doses are generally not sufficient to achieve healthy levels without adequate sun exposure and possibly external supplementation.14
The UK NHS advice on sun safety includes the following suggestions: spend time in the shade between 11am and 3pm, make sure you never burn by covering up with suitable clothing and sunglasses and using at least factor 30 sunscreen.15 This advice has inconsistent compliance due to practical difficulties and social behaviours, for example wearing covered clothing during summer months. However, the use of sunscreen is paramount for minimising the ageing effect of UV radiation whilst being socially unrestricted. In order to be effective, a sunscreen of at least SPF 15 is required to adequately protect against UVB (93% protection).16 This should be applied as a thin layer over all sun-exposed areas of skin and reapplied every two to four hours. As the impact of UV radiation on skin ageing has become clearer, the pharmaceutical industry has endeavoured to create sunscreens to cater for all skin types and preferences.
Figure 1: The effects of sun damage

Smoking
Not only is smoking the most preventable cause of morbidity and mortality worldwide, it produces a significant damaging effect on the skin.17 Smoking is associated with premature skin ageing, melanoma, oral cancer, acne and psoriasis.18 Smoking leads to the breakdown of collagen and elastin as well as generating harmful free radicals. It alters the intra-cellular matrix, changing the consistency of the skin.19
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
The act of smoking also directly causes wrinkles around the mouth, known colloquially as smoker’s lines.20
Smoking has established links to poor wound healing outcomes. This is likely due to damage of microvasculature around wound sites and the deposition of toxins.21 Therefore, in the event of seeking any cosmetic procedure to counteract the effects of ageing, smokers will be prone to poor wound healing and risk worse aesthetic outcomes from the resulting scar. Cognitive behavioural therapy and nicotine replacement therapy are amongst a number of recognised methods to facilitate smoking cessation.22 Help can be sought via the general practitioner and local specialist smoking cessation services.

Diet
A number of dietary compounds have been associated with improved skin appearance, however a well-rounded diet is vital for maintaining good physical health across all body systems. Fruits, fatty acids and vegetables have all been associated with reduced appearance of skin ageing.23,24,25 Fatty acids in particular play an important role in the skin barrier and hydration of skin.26
Vitamin A, vitamin C, vitamin D and other compounds believed to have antioxidant properties, such as curcumin, polyphenols and flavonoids are all documented to promote younger looking skin.27,28 Retinoids are vitamin A derivatives and are the most commonly used antiageing drugs. They are proven to regulate genes and the extracellular matrix proteins and they also prevent photodamage.29
Consumption of water is important for cellular function and keeping the skin hydrated. Hydrated skin appears fuller, reducing wrinkles and evening contour.30 Trace elements such as zinc, iron and copper are involved in healthy cell biology and formation of the extracellular matrix. They should be consumed in safe amounts (less than 25mg, 17mg and 10mg per day, respectively).31,32
Alcohol consumption has generally shown to have non-significant associations with skin ageing, however at excessive levels (>40 units per day) the association becomes significant.33 Excessive sugar in the diet has shown to promote inflammation within the skin resulting in long-term damage to cellular structures.34 Advice on diet and alcohol consumption as per the UK government guidelines should be recommended to all patients.35,36
Pollution
Skin ageing, in particular dyspigmentation and skin wrinkling, is associated with air pollution. Compounds such as nitrogen dioxide, fossil fuels, second hand smoke, traffic-associated particulate and carbon monoxide have been associated with progressive skin ageing.38
It is documented that molecular interactions between pollutants and UV radiation produce exaggerated damaging effects to the skin, accelerating the ageing process. Ozone, O3, at ground level is a harmful pollutant gas.39
Alongside other molecular (e.g. poly-aromatic hydrocarbons) and particulate matter, a cascade of reactions occur within the skin resulting in the release of reactive oxygen species (free radicals) which damage cellular structures, DNA and matrix proteins, resulting in signs of skin ageing.40 Pollutant matter is also responsible for destruction of the atmospheric ozone layer, exposing us to higher levels of UV radiation, which in turn contributes to skin ageing.41 A rising number of cosmeceutical products contain antioxidants. These active ingredients are aimed at reducing the effect of pollution on the skin. Though few objective trials have been conducted to quantify their effect, anecdotal and theoretical studies all suggest a beneficial effect on skin ageing from the use of topical antioxidant.42,42,44 Finally, engaging with activities to reduce/reverse climate change is important as yet another long-term health measure is detrimentally affected by these changes.
Stress
Psychological stress is one of the less researched contributors to skin ageing, though anecdotally the association is well defined. Chronic stress has shown to alter gene regulation, increasing an individual’s vulnerability to ageing.45 This genetic dysregulation causes decreased proliferative capacity and altered biosynthetic activity of cells resulting in a disorganisation of the dermal matrix. Epigenetic studies evaluating DNA methylation patterns seek to identify targets for gene alteration in response to stressful stimuli. Finding these biomarkers will enable quantification of the impact of stress on ageing but also possibly identify targets for future therapies.45 Glucocorticoids, such as cortisol, are known to be released in excess in response to stress. These are likely to be responsible for also triggering adverse physiological responses which contribute to extrinsic and intrinsic (gene-related) ageing.46 Chronic stress is also known to activate and alter other physiological systems, such as the hormonal hypothalamic-pituitary axis, the autonomic nervous system and the immune system. Each of the above lead directly or indirectly to increased susceptibility to the ageing processes.47 Complete avoidance of stress is unattainable; instead, identifying effective coping mechanisms is crucial for maintaining good physical and mental health.
Skincare
Skincare routines are highly variable and can utilise a range of products, including medicated preparations. At its simplest level, regular moisturising of skin is an essential activity for maintaining good skin function as well as aesthetic skin. Dry skin leads to disorganised keratin structures and reduced extracellular matrix volume, which creates uneven surfaces and makes skin appear sunken.48 Wrinkle appearances are exaggerated in individuals with
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Figure 2: The presentation of smoker’s lines
dry skin.49 The list of active compounds that are utilised in skincare products is vast and beyond the scope of this article. However, literature suggests that the hydrating component of moisturisers, such as glycerine or petrolatum, leads to a greater impact on improved skin appearance than the advertised active ingredients.50 The choice between ointment, cream or gel-based moisturisers is individual. Compliance is key, thus, the best choice of product is the one a patient is happy to use consistently. It is important to note that sunscreen also falls into this category of topical skincare and, for reasons covered in the previous section on photodamage, should be a component of every basic skincare regime alongside moisturising.
Body mass index
Studies suggest that genes encoding proteins involved in skin structure, blood supply and healing are altered in obese (BMI 35-50) individuals compared to those within the defined healthy range (BMI 18-26).51,52 At both ends of the scale, individuals with underweight BMI (<18) and obesity were shown to be more susceptible to skin infections.53 Infections and the resulting inflammation can cause scarring and permanent damage to the skin structure. This can manifest as signs of aged skin and leave the skin more susceptible to other extrinsic factors. UK government’s advice on weight management, as well as dietary advice referenced above, should be relayed to all patients.54
Sleep
Sleep plays an important role in the regulation of a number of physiological systems.55 The biological and physiological mechanisms of its effect on skin ageing are not well documented, however, observational studies suggest that sleep deprivation and poor-quality sleep results in the appearance of less healthy, more aged skin.56,57 Both referenced studies focused on female participants. In the former, a cohort of 20 female participants were subjected to sleep deprivation and photo comparisons were made, with each volunteer acting as their own control, to identify skin changes. Increasing wrinkles, drooping corners of the mouth and hanging eyelids were identified in the sleep deprived group and are also signs consistent with skin ageing.58 The precise quantity of sleep needed for optimal health is likely to vary between individuals but in one study, and anecdotally, a good night’s sleep is defined as eight hours.
Consider the extrinsic factors of ageing
Significantly aged skin is associated with perceived negative aesthetic and health characteristics. Though ageing is a natural phenomenon, there exists a multi-billion pound industry dedicated to preventing and reversing the effects of age on skin. The effects of extrinsic factors can be mitigated, if understood. UV-radiation-induced damage is by far the greatest contributor to extrinsic ageing. Simple steps, such as application of moisturisers containing SPF 15+, can be highly effective in preventing UV damage and maintaining healthy skin. Other significant, modifiable factors include diet, stress and sleep. Pollution is becoming more of a concern but is difficult to alter on an individual basis. Whilst steps to minimise extrinsic factors of skin ageing can reduce the rate of skin ageing, it is important to stress that a degree of ageing (intrinsic) is inevitable and should be embraced. Also, activities to minimise skin ageing should take into context the wider health of an individual such that other body systems are not adversely affected by any interventions.
Dr Nihull Jakharia-Shah is an internal medicine trainee with an interest in dermatology. Dr Jakharia-Shah held a position at Acquisition Aesthetics training academy for four years, gaining exposure to clinical aesthetic practice. Qual: MBBS, BSc(Hons)


Miss Lara Watson is a maxillofacial surgery doctor and a UK key opinion leader for various pharmaceutical companies. She is a director at Acquisition Aesthetics training academy.

Qual: BM, BSc (Hons), BMedSci, MRCS(Eng), BDS(Hons)
Miss Priyanka Chadha is a plastic surgery doctor and global key opinion leader. She is a director at Acquisition Aesthetics training academy.
Qual: MBBS(Lond), BSc (Hons), DPMSA(Lond), MRCS(Eng), MSc(Lond)
Complete
Questions Possible answers
1. Which of these is not an extrinsic factor of skin ageing? a. UV-radiation exposure b. Genes c. Pollution d. Diet
2. Which extrinsic factor is the greatest contributor to skin ageing? a. UV-radiation exposure b. Smoking c. Sleep d. BMI
3. Which of the following is not in line with NHS advice on skin protection from sun exposure?
a. Apply regular sunscreen b. Avoid sunlight between 11am and 3pm c. Cover up with suitable clothing and sunglasses d. Encourage gentle burning of skin
4. Which dietary component is not associated with improved skin health? a. Excessive alcohol b. Copper c. Vitamin A d. Flavonoids
5. Excessive stress can accelerate skin ageing through which of the following mechanisms:
a. Vitamin D deficiency b. Photodamage c. Excess secretion of glucocorticoids d. Free radical generation
Answers: B,A,D,A,C
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
your knowledge!
the
questions
VIEW THE REFERENCES ONLINE! WWW.AESTHETICSJOURNAL.COM
Test
multiple-choice
and go online to receive your CPD certificate!







AESTHETICSJOURNAL.COM Keep up-to-date with the latest aesthetic developments and best practice guidance on your desktop, tablet or phone AESTHETICSJOURNAL.COM @aestheticsjournaluk Aesthetics @aestheticsgroup
Exploring Skin of Colour in Summer
Dr
Lauren
Hamilton and
Dr Miriam Adebibe
discuss conditions that may affect skin of colour in the summer months
People seeking clinical skin treatments vary widely in ethnicity. Though people with skin of colour (SOC) constitute the majority of the world’s population, they are under-represented in scientific studies, medical textbooks, and practical training where light skin tones have historically featured most frequently.1 This bias causes delays in diagnosis and treatment, resulting in greater morbidity and mortality, with the need for more oppressive treatment.2
Understanding the differences in the structure and function of SOC is important to facilitate timely diagnosis and prevent adverse outcomes. Thankfully, this call is starting to be addressed. Several large-scale studies have been conducted examining the genetic and phenotypic differences among racial groups3 dedicated training for SOC has been included in the UK dermatology training syllabus since 2021.
We have found that the warmer months are a key time for enquiries and advice sought by patients with SOC at our clinic, because sun exposure worsens certain conditions and draws greater attention to them. In this article, we provide aesthetic practitioners with an overview of considerations for treating individuals with SOC in the summertime.
Classification of skin types
Skin is famously known as the largest organ of the body and functions as a protective barrier, a temperature regulator, a toxin eliminator, the best source of vitamin D production, and our environmental sensor through tactile touch.4 Under the microscope, the structure of skin is similar across all skin types, however there are morphological differences apart from the inherent SOC that are most often seen in the outermost layer of the epidermis, the stratum corneum.4
So, what do we mean by SOC? Ethnologically all humans are of African ancestry. The colour of our skin, determined by melanin pigment, is on a continuum ranging from pale white to darkest brown. Ethnicity and race fall short of the scientific description needed. While ethnicity relates to broad populations with a common culture or language, race defines a specific population with genetic similarities, such as Caucasian, African or Australasian.5
The Fitzpatrick classification (phototypes I-VI) categorises skin of all colours according to its response to UV radiation (Figure 1).6
Generally, SOC refers to Fitzpatrick skin types IV-VI, ranging from olive to dark brown skin tones that tan easily and rarely burn. This includes people of Latino, African diaspora, East and South Asian, Australasian, and indigenous descent.7
Skin conditions in skin of colour
Most skin conditions occur in people of all skin types. However, some conditions may affect darker skin tones more frequently or more severely. Practitioners may find that
Type 1
• Skin colour (before sun exposure): ivory
• Eye colour: light blue, light grey or light green
• Natural hair colour: red or light blonde
• Sun reaction: skin always freckles, always burns and peels, and never tans
Type 2
certain skin concerns among their patients are heightened in the summer months.
Hyperpigmentation
Pigmentation is the most obvious difference between skin types. Melanin is a natural skin pigment that protects the nucleus and DNA from damage by UV radiation.8 Melanocytes in the basal layer of the epidermis make melanin in melanosomes for the purpose of transfer to neighbouring keratinocytes. One melanocyte distributes melanin to approximately 40 keratinocytes.8 We all have roughly the same number of melanocytes, though in darker skin these are located throughout epidermal layers, containing larger melanosomes and producing more melanin.9
Pheomelanin (yellow-red pigment) predominates in light skin (Fitzpatrick I-II) and eumelanin (brown-black pigment) in darker skin tones (Fitzpatrick V-VI), with a mix of both in Fitzpatrick III-IV.10 Melanogenesis commences with the conversion of L-Tyrosine to dopaquinone, by the key enzyme tyrosinase, which then serves as a substrate for eumelanin and pheomelanin production.11 Regulation of melanin synthesis by inhibiting tyrosinase is an important target in the prevention of hyperpigmentation. Although all skin types undergo photoageing due to sun exposure, darker phototypes
• Skin colour (before sun exposure): fair or pale
• Eye colour: blue, grey or green
• Natural hair colour: blonde
• Sun reaction: skin usually freckles, burns and peels often, and rarely tans
Type 3
• Skin colour (before sun exposure): fair to beige
• Eye colour: hazel or light brown
• Natural hair colour: black, dark blonde or light brown
• Sun reaction: skin might freckle, burns on occasion, and sometimes tans
Type 4
• Skin colour (before sun exposure): olive or light brown
• Eye colour: dark brown
• Natural hair colour: black, dark brown

• Sun reaction: doesn’t really freckle, burns rarely, and tans often
Type 5
• Skin colour (before sun exposure): dark brown
• Eye colour: dark brown to black
• Natural hair colour: dark brown to black
• Sun reaction: rarely freckles, almost never burns, and always tans
Figure 1: Classification of skin type using the Fitzpatrick scale6
Type 6
• Skin colour (before sun exposure): deeply pigmented dark brown or darkest brown
• Eye colour: brownish black
• Natural hair colour: black
• Sun reaction: never freckles, never burns, and always tans darkly
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
“It’s no mere figure of speech or empty marketing device to say that there is literally nothing else the same as Profhilo®” Dr Tracy Mountford

DETAILS OF BEAUTY. Unveiled on body.

EVERYONE IS A MASTERPIECE. ha-derma.co.uk 0208 455 4896 hadermauk @ha_dermauk Exclusive UK & Ireland distributor/ training provider of IBSA’s aesthetic products
exhibit less signs of ageing, such as wrinkles and skin laxity, compared to lighter skin tones due to the protective effect of melanin. However, they endure a higher risk of hyperpigmentation, which only increases in the summer, as UV light triggers further melanin production in the epidermis and deposition deeper in the skin.5 Melasma is a condition characterised by irregular hyperpigmented patches typically located on the forehead, cheeks, nose, chin, and upper lip. It is more common in darker skin types living in areas of intense radiation.12 Post-inflammatory pigmentation affects darker skinned patients with more frequency and severity than lighter skin tones.13 It may occur after minor injuries, such as mosquito bite scratches, or as a result of common skin conditions, such as eczema or acne. Treatment for hyperpigmentation must address three key items: prevention of further pigmentation using sunscreen, regulation of melanin production using tyrosinase-inhibitors, and exfoliation of existing hyperpigmentation using alpha hydroxy acids.13
Hydration
Hydration of skin is vital for optimal function as a protective barrier to the external environment. Dry skin, or xerosis, results in considerable compromise to this barrier function, where skin cells in the stratum corneum shrink, develop small cracks, and allow harmful particles to enter the body.14 The skin appears dull, flaky, and rough with increased levels of histamine and inflammatory cytokines under microscopic examination.14 Though dry skin occurs in all skin types, incidence increases with maturity and darker phenotypes due to differences in water loss, water content, lipid content, and skin reactivity. SOC has the lowest ceramide levels compared to Caucasian and Asian skin.15 Ceramides are long-chain fatty acids that help to reduce permeability of the skin and lock in moisture. Low ceramide
lipid levels are associated with greater transepidermal water loss (2.7 times higher than Caucasians) and a lower water content of the stratum corneum.15 Xerosis is often exacerbated in the summer due to heat, air conditioning, UV exposure, air travel, chlorine chemicals in pools, and salt in seawater.15 Treatment for xerosis comprises elimination of aggravating factors and moisturising skin to minimise relapses.16 Patients are advised to avoid excessive bathing and use of alkaline soaps, regular use of humectants which draw moisture into the skin (such as hyaluronic acid, alpha hydroxy acids and glycerin), emollient replace moisturising oils to smooth and soften the skin surface (such as ceramides, jojoba oil, rosehip oil), and occlusives which seal in moisture (such as shea butter, beeswax, and lanolin).16
Vitamin D deficiency
Darker skin is less efficient at synthesising vitamin D from sunlight, so ethnic minorities are at higher risk of deficiency, especially in cold climate countries such as the UK. A study of 4,046 British Afro-Caribbean subjects under 40 years of age, showed insufficiency in 41% and deficiency in a further 37%.17 Crucial for biological function, vitamin D calms skin inflammation, increases cell turnover, and has antiageing effects. Even in the summer, when levels of light are at their highest, people with SOC are advised to continue daily vitamin D supplementation to ensure optimal skin health.17 However, many patients are unaware of this as they believe the sun will improve their levels enough, leading to neglect. More health promotion around this is needed by both healthcare and aesthetic professionals.

Hypertrophic or keloid scarring
People with SOC are more susceptible to hypertrophic and keloid scar formation, characterised by dysregulated growth with excessive collagen formation in the wound healing process, causing a raised growth beyond the boundary of the original injury.18
This can occur with minor injuries such as cuts, piercings, tattoos, or acne more frequently in the warmer months where skin is more exposed, typically on the upper chest, shoulders, and ears. The pathophysiology is unclear but it is thought that increased papillary fibroblast activity seen in darker skin leads to increased wound response.19 Treatment of keloid scarring includes steroid injections, surgical removal, pressure dressings on wounds, silicone gels, laser or radiation treatment. Despite various treatment modalities, recurrence rates range from 20-100%.18
Educate your patients
Improving knowledge around common skin conditions affecting different skin types is essential to properly serve diverse populations. Patients with SOC are at a higher risk of inflammatory skin conditions, hyperpigmentation, xerosis, and vitamin D deficiency, and these are particularly prevalent during the summer months. Patients should be advised on how to manage their symptoms through lifestyle changes, avoidance of triggers, use of effective skincare, and when to seek help from a dermatology specialist.
Dr Lauren Hamilton began her medical career in the field of surgery. It was her experience within head and neck surgery that piqued her interest in aesthetic medicine. She went on to achieve a Master’s Degree in Medical Education from University College London and works as an advanced non-surgical trainer. Dr Hamilton is co-founder of Victor & Garth, a clinic in Shoreditch.
Qual: MBBS, MSc
Dr Miriam Adebibe is a UK-trained surgical doctor with more than 15 years of experience, specialising in weight loss surgery and the nutritional needs of obese patients at a university teaching hospital in London. She is actively involved in medical education, training, and has published many research reports in scientific literature. She is cofounder of Victor & Garth clinic in Shoreditch.
Qual: MBBS, MRCS

VIEW THE REFERENCES ONLINE!
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
People with SOC endure a higher risk of hyperpigmentation, which only increases in the summer, as UV light triggers further melanin production
WWW.AESTHETICSJOURNAL.COM
Treating Gynoid Lipodystrophy
Gynoid lipodystrophy (GLD) is a prevalent skin concern, and although data isn’t completely conclusive, the condition reportedly affects between 80-98% of post-pubertal women.1 Men can also experience GLD, although they are far less likely. GLD is more commonly known as cellulite, so for the purposes of this article we will refer to it as such. Cellulite is a multifactorial disorder of the subcutaneous tissue resulting in alterations to skin topography and creating a distinctive wavy or dimpled appearance.1,2 Cellulite occurs due to the herniation of subcutaneous papillae adipose through the dermo-hypodermal junction and is commonly identified on the gluteal, femoral, abdominal and brachial areas of the skin.2 Despite its prevalence, and although it is not considered to be a dangerous condition, cellulite has the propensity to affect self-confidence and selfesteem, with one consumer survey of 2,006 women revealing that 64% felt self-conscious about their cellulite, with 49% bothered ‘a great deal’ or ‘a lot’ by their cellulite.3 Another small study of 46 volunteers showed 50% of the study population reporting dissatisfaction regarding their appearance and 78% reporting the need to seek treatment.4



Causes
Several factors are known to contribute to the development of cellulite and the most common include, but are not limited to: age, weight, genetics and hormones.
Age
Skin loses elasticity as we age, making cellulite more likely to occur as we get older. There is limited literature to support this, but a few studies have demonstrated a connection between the two, with skin laxity noted as one of the major aggravators of this condition.5,6,7
Weight
Weight gain or a higher body fat percentage can increase visible cellulite due to the
way in which adipose tissue is distributed. However, it’s also been widely reported that weight loss may actually worsen cellulite for some individuals.8 Research has shown that 31% of the 29 women, who were enrolled in medically supervised weight loss programmes, saw their cellulite worsen.9
Genetics
Cellulite may run in families, since the distribution of adipose, metabolism, ethnicity and circulatory levels are influenced by genetics. Certain genes are required for cellulite development with one Italian study of 200 women identifying genetic variants in the ACE and the H1F1A gene are associated with cellulite in healthy women.11
Hormones
Research has suggested that hormones including oestrogen, insulin and catecholamines also play a role in determining predisposition to developing cellulite.12,13 All of these hormones are connected to fat breakdown and storage and oestrogen deficiency in life events such as menopause, which impacts production of type I and III collagen and elastin fibres, which also contributes to cellulite formation.13
Assessment of cellulite
Accurate assessment, classification and scoring of cases of cellulite is imperative to allow the practitioner to establish the best course of treatment to suit an individual’s need. There are several scales available to assist clinical assessment and grading of cellulite. However, Hexel’s photonumeric scale is recognised as the first standardised and objective method of grading cellulite severity and is widely used by practitioners.14 The scale identifies five key features of cellulite structure: the number of depressions, depth of depressions, clinical appearance of raised lesions, presence of flaccidity and the grade of cellulite. Each of these gets graded from 0 to three, helping to identify the final classification of cellulite as either mild,

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Figure 1: Patient before, after four treatments, and one month after six treatments using the Lumenis NuEra Tight RF device. Images courtesy of Lumenis.
radiofrequency as a suitable treatment for cellulite Before One month after six treatments After four treatments
Dr Saleena Zimri discusses
moderate, and severe.14 Although recognised as an effective method of assessing cellulite severity, Hexel’s model did not take into account patient assessment and so subsequent scales were developed such as the Clinician Reported Photonumeric Cellulite Severity Scale (CR-PCSS) and Patient Reported PCSS (PR-PCSS).15 So, although Hexel’s scale is the most used and still encouraged to use, it’s worth knowing that it has a limitation and practitioners should consider adding patient assessment in addition.
Treatment using radiofrequency
There are numerous cellulite creams, clinic treatments, and supplements on the market which promise to eradicate an individual’s cellulite. However, it’s important to note that currently nothing has been scientifically proven to completely ‘cure’ cellulite, so caution should be taken against making unrealistic efficacy claims when consulting with patients to ensure that realistic outcome expectations and the highest standards of clinical ethics are maintained.
I have personally found that an effective and popular intervention when treating patients presenting with cellulite is device-led using radiofrequency (RF) technology. RF is a type of non-invasive energy-based treatment that targets cellulite and delivers deep thermal heating via electrodes through the dermis to the subcutaneous adipose tissues.16
The depth and degree of thermal effects are directly related to the power, the wave frequency (the higher the frequency the greater the surface activity), the energy/tissue coupling mode (resistive or capacitive) and the conductivity characteristics of the treated tissue: in tissues with higher impedance, such as osseus, muscle and adipose tissue for instance, more heat is generated. The thermal action causes vasodilation, increased microcirculation and metabolism of adipose tissue improving topography.16
RF technology has a good safety and efficacy record that is supported by clinical data.17,18 It is effective and safe for use on all Fitzpatrick skin types, adverse events are rare and the treatment has the added benefit of zero downtime, making it a good option for treating cellulite for both patient and practitioner alike.17,18 As the treatment modality delivers thermal heating deep through the dermis to the subcutaneous tissues, it is suitable for treating all grades of cellulite.9 In my experience, I would expect on average to see the grade of cellulite decrease by one.
One study of 10 women demonstrated the following mean grading scores for the treated leg versus the control leg: dimple density of 2.73 vs 3.18 and dimple distribution 2.89 vs 3.32, following three to six treatments.19 It should be noted that treatment success is also dictated by the level of commitment by the patient in terms of lifestyle factors that include water intake and regular exercise.
Procedure
As with any procedure, it’s essential to perform an in-depth consultation and clinical examination of the area, along with careful skin analysis prior to treatment to ensure that the treatment modality is tolerable and suited to the needs of the individual. Performing a small spot test on a small, shaved area before carrying out the full treatment and waiting until the next day to assess the results is recommended by the manufacturers of my device of choice to assess for any possible unforeseen adverse event that is unique to the individual. This also allows the practitioner to select suitable fluence for the patient, ensuring not to exceed the maximum tolerable level for the individual.
The treatment area should be clean and free of lotions or fragrant products. Conductive cream or gel suitable for use with RF devices should be spread over the area to be treated as well as partially over the electrode surface, as recommended by the device manufacturer. In my experience it is beneficial to work in a circular motion directed towards lymph nodes located in the popliteal fossa until the patient experiences an intense, but not uncomfortable, heat. The electrode should always be kept in motion in order to avoid causing erythema or burning.20
Practitioners should also take electrode size into consideration. When having to treat large areas (such as femoral or abdominal areas) choose an electrode with a larger diameter. For my chosen device, the desired temperature can be achieved by setting the electrode size to the area you are treating and also by placement of the grounding pads. Remember, practitioners should refer to specific instructions from their device manufacturer for the most effective settings for that device.
The duration of each treatment can run from a minimum of 30-60 minutes according to the number and extent of areas to be treated. Treatment duration and length differs between individuals and will depend on factors that include age, lifestyle, location and severity of their cellulite. However, on average, patients could expect one
treatment every one to three weeks, for four to six treatments in total. In my experience, it is possible that some improvement could be visible up to six months after the last treatment in the course. My patients typically book a maintenance course of three treatments after 12-18 months.
Safety considerations
Although RF treatments are considered to have a good safety record, and adverse events are rare, they can be further minimised by ensuring that manufacturer instructions for your chosen device are followed and proper techniques are used. The patient’s medical history should also be taken into consideration at the consultation stage, especially if they are taking any medicines that increase sensitivity to heat or change the skin’s metabolism (antidepressant medication is one such example).
When it comes to aftercare, some patients require a cooling gel to calm localised swelling, but as RF is so well tolerated I have found that this is rare. A follow-up consultation should always form part of any treatment plan and should be discussed on an individual basis with the patient.
Consider RF for cellulite treatments
Cellulite is a prevalent skin concern that has several potential causes. In my experience, RF technology is a good treatment approach to improve its appearance. It is well-tolerated, is safe and effective for use on all Fitzpatrick skin types, requires little to no downtime and carries minimal risk of adverse events making it a beneficial treatment modality for patients and practitioners alike.
Dr Saleena Zimri is a former GP with a special interest in cosmetic dermatology. She has been practising aesthetics for the last 13 years and is the co-founder of the Skin Doctor Clinics and set up her first aesthetic skin and laser clinic 12 years ago in Yorkshire. The company has four branches located in Manchester, London, Leeds and York.
Qual: MBChB, MRCGP, PGDip

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
VIEW THE REFERENCES ONLINE! WWW.AESTHETICSJOURNAL.COM
Supporting the Future of Aesthetics at

The expert team behind CCR, ACE, The Aesthetics Awards and the Aesthetics journal are delighted that we are now in the month of Beauty Uncovered LIVE. A first for us and for our industry: an event that highlights the importance of regulated medical practice to our patients, live, at the UK’s first patient-facing aesthetics show of this size!

Taking place on May 7-8 2022 at the Business Design Centre, London, Beauty Uncovered LIVE is a two-day event combining the biggest names, practitioners and brands in the industry, with exciting live demonstrations and insights into products and treatments. All with the backing and expertise of our clinical advisory board members, incredible KOLs, leading brands and industry associations such as the JCCP, BCAM and BACN to ensure we promote safe practice and a healthy patient experience. After speaking to many clinic owners and medical practitioners, we understand there are reservations about inviting your patients to an aesthetics event, with the worry that it may be competitive for your clinic. To prove how we, and this event, continue to support the individuals in our industry, we have put together some FAQs on Beauty Uncovered LIVE, and why it is vital that you and your patients attend.
How will the event benefit my patients?
Beauty Uncovered LIVE is an aesthetics wonderland for all interested in aesthetic treatments, beauty and health. With three stages dedicated to live demos, myth busters, and the latest trends, there are tonnes of chances for patients to find out all they need to know. They will leave feeling informed, educated and empowered to take the next step in their aesthetic treatment journey.
How will the event benefit me and my clinic?
Rest assured we are not directly encouraging attendees to get treatments, nor are we telling them which clinics or practitioners to choose. Just how to make the right, safe and informed decisions. The event will uncover the various treatments available, introducing them to the full range of aesthetic solutions you can offer and the benefits of taking a holistic approach.

36 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Aesthetics | May 2022 Event Spotlight Beauty Uncovered
This event is great for patients, but what about practitioners?
In a study recently carried out by Beauty Uncovered, 20% of those surveyed said they were worried about side effects and complications, and 26% were worried about looking ‘fake’ and being unhappy with the results
Happy, well-informed patients will see the benefits of continuing their treatments (and maybe adding on some more) with their trusted clinic and practitioner, building their loyalty to you and the chances of referring you to their friends.
A continued undertone highlights the danger of unregulated and unqualified aesthetic practice. Though we are steering clear of botched jobs and scaremongering to promote positive aesthetic results, advice against ‘cowboy beauticians’ is offered, reinforcing the relationships your patients have with you, and deterring them from straying elsewhere for cheaper and unregulated treatments.

How will Beauty Uncovered Live support the
industry?
By enhancing knowledge, building trust, and promoting positivity. In a study recently carried out by Beauty Uncovered, 20% of those surveyed said they were worried about side effects and complications and 26% were worried about looking ‘fake’ and being unhappy with the results.
We know as well as anyone that aesthetics gets a bad rep. We are changing that. By working with respected practitioners, sharing honest and realistic before and afters, and covering a range of treatments and aesthetic solutions, we want to give patients the whole story. As our recent cover star Hanna Kinsella said, ‘I think we owe it to each other to actually say, yes, I’ve had treatments, and this will help break the taboo’.
Who will be there?
Sessions will uncover all things aesthetics with beauty editors, influencers and celebs as well as advice offered from the UK’s most respected practitioners. Attendees will get both honest and opposing opinions from patient case studies and live Q&As with top doctors, nurses, dentists and surgeons.

Taking to the stage will be Dr Tapan Patel, Dr Munir Somji, Miss Jonquille Chantrey, Mr Naveen Cavale, Dr Dev Patel and many more.
Beauty guru and journalist, Nadine Baggott will be sorting aesthetics fact from fiction, and Love Island’s Sharon Gaffka will share some home truths about her personal journey. Dr Nina Bal from E4’s ‘Body Fixers’, influencer and award-winning celebrity injector also joins our star-studded panel.
As well as amazing speakers, we also have more than 40 incredible aesthetics brands that we know and love. Headline Sponsor HydraFacial are giving away free treatments and Skinade have a collagen bar with a free drink for every ticket holder. Top injectable companies Galderma, Teoxane and Neauvia will be doing live demos and the show floor will be packed with more brands showing patients the incredible products, devices and treatments available in your clinic.
Be part of the bigger picture
It is a no brainer for patients. For clinic owners and medical practitioners, it is being part of the bigger picture, raising the public profile of the aesthetics industry as we take an altruistic approach to bettering it for both ourselves, our clinics and our patients. Patients will leave empowered, energised and full of knowledge. Knowing exactly how to choose the right treatment, confidently make safe choices and more importantly, how to choose the right practitioner.
If you would like to offer discounted tickets to your patients, please scan the QR code to receive your own discount code as well as a limited number of FREE VIP tickets for you and your team.
SCAN HERE TO GET TICKETS FOR YOUR PATIENTS
Tickets are on sale now and include a goody bag, plus a free Skinade collagen supplement. Group bundle tickets are also available to save even more by getting the whole gang involved! Tickets can be booked at beautyuncovered.com
Business Design Centre, Islington
Show opening times:
Saturday 7 May: 10:00 – 19:00

Sunday 8 May: 10:00 – 17:00

37 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Aesthetics | May 2022 Event Spotlight Beauty Uncovered
EXCLUSIVE POWER OF THREE MASTERCLASS
In association with Prima Ultima - the UK’s only purveyor of biorevitalising and bioregenerating HA dermal fillers


FRIDAY 20TH MAY 2022
Unit 13 Mercian Business Park, Felspar Road, Tamworth, B77 4DP
Gain an in-depth knowledge of the application of the full range of Zhoabex products, including training on the 4-point Bio Lift Technique and a practical demonstration by a clinical lead.
Value of £1500, exclusively for a limited number of delegates at £300 redeemable against product purchases following training.
Contact info@apothecaryaesthetics.co.uk or call 0345 319 1000 to register your interest and book.
Supplying a comprehensive catalogue of high quality, fully regulated aesthetics products to HCPs nationwide. Our trusted supply chain allows us to deliver whatever is required, whenever it’s needed and wherever it’s going.
Working in partnership with Apothecary Aesthetics Springpharm is an approved supplier of Zhoabex products
 The ONLY HA dermal filler on the UK market that combines 3 molecular weights, acts on all 3 levels of the skin, and triggers biorevitalisation, biostimulation and bioregeneration
The ONLY HA dermal filler on the UK market that combines 3 molecular weights, acts on all 3 levels of the skin, and triggers biorevitalisation, biostimulation and bioregeneration
Understanding Sunscreens
It’s no secret that SPF is a vital product in many antiageing regimes. With so many ingredients, factors and types on the market it can be difficult to get to grips with exactly which SPF would be most beneficial for yourself and patients. Products with varying star ratings, SPF values, and references to the words mineral, zinc oxide, organic and natural are often attached to SPF advertisements with little guidance on what they actually mean, the protection they offer, or any helpful information on their safety for use.
Misinformation about sunscreen is common, and so it is important to ensure myths or lack of understanding do not deter you from guaranteeing patients protect their skin.

Defining SPF
SPF stands for ‘sun protection factor’ and refers to the amount of defence the sun protection sunscreen offers compared to unprotected skin. SPF 50+ is formulated to allow less damaging rays to reach the skin’s surface and therefore provide optimum protection.1
The lower down the numerical rating SPF products appear, as you would expect, the less protection they provide. Interestingly, from factor 15 to 50 there is only a 5% difference in the amount of UVB rays that are blocked, with SPF 15 blocking 93% of UVB rays, SPF 30 blocking 97%, and SPF 50 blocking 98%.1
Rising cancer rates and why selection matters
With the Food and Drug Administration (FDA) having removed 14 of the 16 chemicals found in sunscreens from its ‘generally accepted as safe and effective category’2 in 2019, there has never been a better time to raise awareness on the types of SPF products which are safe to use. The FDA reported that of the 16 chemicals utilised, only zinc oxide and titanium dioxide are generally regarded as safe and effective.2 In the UK and the EU,
sun protection products are defined as cosmetic products and are governed by the Cosmetics Regulation. In the US, the FDA governs the safety of these products.3
According to data from The Royal Marsden NHS, over 15,000 people each year in the UK are diagnosed with melanoma, with rates of malignant melanoma rising faster than any other cancer.4 Data from The British Skin Foundation indicated there were 14,000 new cases of melanoma and 147,000 cases of non-melanoma skin cancers reported in 2017. These types of skin cancer can be contracted through exposure to the sun’s rays, which comprise ultraviolet radiation in both UVA and UVB sunbeams.5
According to research from Cancer Research UK, within the last decade melanoma skin cancer rates have increased by 32%, with incidences in females doubling, and in males almost tripling.5 In light of shocking statistics such as these, it’s increasingly important for patients to be fully informed about the different rays which cause harm, and the products which can give them what they need in terms of protection and skin health.
Shielding the sun’s rays
The three types of rays emitted by the sun include ultraviolet A (UVA) ultraviolet B (UVB) and ultraviolet C (UVC) as shown in Figure 1. UVC is the shortest wavelength and most damaging ray, however it does not reach the earth’s surface and is filtered by the atmosphere, so therefore is not something we need to concern ourselves with here.6 UVA is the ray which penetrates the skin most deeply due to its longer wavelength. Exposure to UVA rays result in premature skin ageing and pigmentation. UVB causes burning and reddening of the skin. UVB is the ray most commonly linked to causing cancer, however information from the Skin Cancer Foundation states that unprotected exposure to both UVA and UVB damages the DNA in skin cells and can lead to skin cancer.6
Patients need to understand that SPF values only relate to their capacity to protect skin from the sun’s UVB rays and not UVA. From this perspective, any product, whether medically graded or not, cannot entirely protect skin from the damaging impact of the sun’s rays and it is important to limit time spent in direct sunlight and wear other protective items such as sunglasses, clothing and sun hats and to seek shade.
Practitioner recommendations therefore need to encompass not just product and application suggestions, but also common-sense guidance that can debunk misconceptions around ensuring
coverage and protection. Star ratings relate to the amount of UVA rays that sun protection products can block and range from 0 to 5. It is commonly understood that any product below 4 stars is not suitable in its capacity to protect the skin, as per advice from The British Skin Foundation.7
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
prescriber
explores the basics of sun care and how to safeguard patients
1: The different types of rays and their wavelength
Nurse
Kirsty Whitworth
Figure

Chemicals vs mineral sunscreens
When recommending different SPF products to patients, practitioners can explore the differences between chemical and physical sunscreens.
Chemical sunscreens known as organic or synthetic sunscreens are the most commonly used and recommended by The British Skin Foundation.7 They work through absorption of UV light and the release of it in heat form. Oxybenxone, avobenzone, octisalate, octocrylene, homosalate and octinoxate are the chemicals, amongst others, that will be found in this category of sunscreen.8
According to the Skin Cancer Foundation sunscreen needs to be applied to skin 30 minutes before sun exposure9 and is usually more popular with patients due to their typically thinner texture and easier-to-spread consistency. However, it may be less widely understood that due to the chemical composition of these types of sunscreens they can be ‘used’ up more quickly when in direct sun,7 and can require more regular application. They may also be more likely to cause skin irritation, due to the combination of ingredients and UV light. This irritation is referred to as ‘irritant contact dermatitis’ by The Cancer Council and is more common in those with sensitive skin10 or with a history of eczema. Patients should be aware of all the ingredients before application, so as to check for any contained fragrance or preservatives that they may be allergic to.
As many people under-apply their sun protection, it is important to offer guidance as to the amount required to ensure proper shielding from UV rays. A minimum of 2mg to every cm2 of skin should be applied, instead of the usual quarter or half of this amount that most people tend to apply.11
Mineral sunscreen, also referred to as physical sunscreens, work by absorbing and then scattering or deflecting the UV radiation, whilst also absorbing the UV light and releasing it as heat. Titanium dioxide and zinc oxide are the two main chemicals used in these products.12
Mineral sunscreens are quicker acting than chemical sunscreens, as they provide protection from the sun immediately after they have been applied. They also tend to last longer in the sun, but are washed off when they come into contact with sweat and water which is an important detail for patients to understand, as this factor alone will impact the amount of application required. With this in mind, larger amounts are often required to achieve adequate protection.13
Mineral products are less irritant on the skin than chemical sunscreens because they reduce the likelihood of long-term exposure to chemical ingredients. It is worth noting that mineral products often leave a whitish cast on the skin, and therefore are less cosmetically acceptable for people with darker skin tones.14
Although there are sunscreen products available which combine both mineral and chemical ingredients, research shows that mixing the two can lead to degradation of the sunscreen or sun block and hinder the product’s effectiveness. As a result, I only recommend usage of the mineral-based products.15
Product selection and daily habits
When recommending best practice to patients, medical practitioners should be advising, in line with the FDA and British Skin Foundation guidance that sunscreens or skincare products of at least SPF 15 and upwards need to be applied to ensure skin protection.6
Like many aspects of the aesthetic industry, consistency is key. A broad spectrum SPF should be applied as part of the daily morning skin routine. Broad spectrum SPF refers to sunscreen which offers protection against both UVA and UVB rays, safeguarding both the skin’s surface and deeper skin tissue when applied.6 This ensures
the skin is protected from the get go, and also offers a way for patients to incorporate skin health and protection into their daily routine. As not all sunscreens are broad spectrum, this can be another area of patient confusion. In terms of transparency, medical practitioners should be informing their patients that sunscreens which are broad spectrum, or are below SPF 15, are meant to contain warning labels on the products denoting the dangers of skin cancer and skin ageing via a clear ‘alert’ label.16 Checking products for these warning labels, however small, is a good way to assess their suitability before purchasing for your clinic and recommending to patients.
There are many different brands of sunscreens available and many are produced by high-quality cosmeceutical brands and pharmaceutical companies. In my clinic, I choose to recommend Heliocare 360° broad spectrum SPF and ZO Skin Health Smart Tone SPF 50.
Heliocare 360° is extensively studied, with more than 50 studies published in leading international medical journals. Evidence demonstrates that it is not only effective in photoprotection, but also for the prevention of skin ageing, actinic damage, sun allergies and dark spots. The Gel Oil-Free SPF is suitable for all skin types, including sensitive skin, and a great option for skin of colour due to its clear, barely there, matte finish, which my patients appreciate.17
I recommend the ZO Skin Health Smart Tone SPF 50 to patients who like a tinted SPF that blends into their natural skin tone and combats against the appearance of redness. I have found this is a particular favourite amongst patients who have rosacea skin concerns. This is due to its capacity to minimise redness, guard against the appearance of photodamage, and its 12-hour antioxidant time release which keeps the skin hydrated.18
Awareness is key
As responsible aesthetic practitioners we need to firstly understand the science of sun protection, and inform our patients about the best ways to research, purchase and apply sunscreen products. Raising awareness and being transparent is the best way to help patients protect themselves from the harm caused by sun exposure. Providing valuable, honest information ensures practitioners are the voices which our patients can trust, and establishes us as individuals who can help our community maintain youthful and healthy skin in the long term.
Kirsty Whitworth is a registered adult nurse, independent nurse prescriber, advanced aesthetics nurse, with a BMedSci (Hons) RGN, and Masters in Oncology. She is also registered with the Nursing and Midwifery Council and an active member of the British Association of Cosmetic Nurses (BACN). She has 10 years’ experience within NHS management and has also honed her impressive skillset as a specialist cancer nurse. Qual: INP, RGN
TO VIEW THE REFERENCES GO ONLINE AT WWW.AESTHETICSJOURNAL.COM

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Ultrasound Technology in Aesthetics
Dr Simon Ravichandran looks at the use of ultrasound technology in aesthetic medicine practice and training
With a technology-driven approach to teaching, Merz Aesthetics have incorporated a programme of education based around visualisation with ultrasound that brings to life the textbook concepts we typically learn about.
My journey with ultrasound
We started using ultrasound in our clinic – Clinetix, Glasgow – in about 2010. This was about the time that we started to inject deeper into the tissue planes and use cannulas alongside needles. We had a clinical device for vascular mapping, and we thought we could use that to see if we were right about the placement of our products. Was it in the right place? In the correct tissue plane? What I found was I wasn’t always where I thought I was. In fact, I was practically never where I thought I was. Initially, we found the ultrasound helpful in speeding up the learning curve with the new techniques that were evolving at the time. We also found it a useful tool from time to time when dealing with complications. For me, the learning process was initially slow, but this was a long time ago. I’m not a radiologist, and there wasn’t much available in terms of cranial/facial scanning courses at that time, so I gradually became familiar with the appearance of the different tissues and the different fillers over a long period of time. My first device actually cost me a lot of money and weighed as much as that same suitcase filled with bricks. It had really poor resolution with grainy green images that honestly were really difficult to interpret.
Now with the latest handheld, high-resolution, high-frequency devices, we can see so much more. These wireless devices can be carried around in a pocket, like a mobile phone, and produce much better images. It’s made it so much faster to learn and faster to scan with greater clarity and confidence. The skill of recognising and interpreting the images just comes with repetition. With each patient I now scan, I can see a little more, which enables me to identify the smaller muscles in the face and visualise the distribution of the arterial networks with relative ease.
I’ve realised that there are so many variations in the blood supply to the face, and we can never truly predict where we might cause a significant bruise or a vascular occlusion.
I’ve modified my treatment plan based on what I see on the scan enough times to now feel that I’m essentially flying blind without it. Ultrasound has now become a routine part of my treatment plan, just like putting on a seatbelt in a car, and I won’t run an aesthetic clinic without it. We use it for facial mapping, patient education and our own development. It allows us to tailor our treatment plans individually for every patient to get what we feel is a more effective, optimal result. Just from the routine scanning of patients presenting to our clinic, we can demonstrate that filler intended for the deep plane of the mid-face can actually be within the Superficial Musculoaponeurotic System (SMAS). And filler intended for the interfacial, or the plane of the temple can sometimes be subcutaneous, intramuscular or intrafascial, rather than interfacial. Ultrasound guidance means that we can see the tip of the cannula in the right place whilst we inject, rather than finding out afterwards that we have a suboptimal result.
This applies to the area, but what I’ve really found useful is using this guided injection method for the cheeks and for the temples. For the cheeks, when I thought I was in the deep plane, occasionally I actually found I was within this mass, Superficial Musculoaponeurotic System (SMAS). So I can reposition, get in the right place, use less product and get a much better aesthetic result. For the temples, ultrasound guidance means that I really can be sure that I’m in that interfacial plane when I want to be. And when I’m injecting on the bone, I can make sure I’m in a place that’s effective and has no visible vasculature. Visualisation means greater accuracy, greater effectiveness and greater safety of dermal filler implantation.
every patient undergoing a dermal filler procedure has an ultrasound
Now
42 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Aesthetics | May 2022 Advertorial Merz Aesthetics
“Ultrasound has now become a routine part of my treatment plan, just like putting on a seatbelt in a car, and I won’t run an aesthetic clinic without it”
Ready to Glow ?








TH
Diagnosing Skin Lesions

Is it a mole or melanoma? Is it harmless or not? Do I agree to treat it and how should I treat it? Should I refer? Examining our patients’ skin lesions can feel like tiptoeing through a minefield. Perhaps not unreasonably, our patients assume that as we work in medical aesthetics, we have expertise in ‘everything skin’, including moles. The problem is that most of us are not experts in skin lesion diagnosis. This raises the question: how should we approach our patient’s concerns and stay safe as medical practitioners?
We know that it takes years of specialist training in dermatology to gain the expertise required to diagnose and treat all the possible blemishes of the human skin. Luckily, many skin lesions are easy to diagnose, and you are probably already pretty good at recognising most of the ones we come across in daily practice. However, there are pitfalls, but you can improve your chances of avoiding them by sticking to a few simple rules.
In this article we will cover the presentation of common skin blemishes, with a focus on pigmented skin lesions and how to stay safe using a handful of simple safety rules for you to use in your day-to-day consultations.
What are skin lesions?
Skin lesions can arise from any organ of the skin. In medical terminology, we describe skin lesions as ‘naevus’ or ‘naevi’ in the plural form. If the naevus arises from the pigment cells (melanocytes) its correct name is a melanocytic naevus.
The medical shorthand for a melanocytic naevus is a ‘mole’. Patients tend to call everything a ‘mole’ and this colloquial meaning of the word can lead to confusion. To counter this, practitioners
should refer instead to ‘skin blemishes’ or ‘skin lesions’ in your consultation before a diagnosis is made. As you examine your patient, start making diagnoses and give skin lesions their medical names as you go. Begin with the non-pigmented skin lesions you feel confident in diagnosing, such as skin tags, cherry spots, sebaceous hyperplasia, cysts, and lipomata as you are likely to be good at diagnosing all of these. DermNet NZ has a fun diagnostic tool to hone your skills and even use in the clinical setting.1 Sebaceous hyperplasia can be a little tricker to the naked eye. These are overgrowths in the sebaceous glands and tend to affect the T-zone of the face. They are small yellow-white papules with a central dip.1 When there are multiple, the diagnosis is usually clear, but isolated ones can be hard to differentiate from a basal cell carcinoma.2,3
Pigmented skin lesions
Keeping pigmented and non-pigmented skin lesions separate for yourself in this way will help reduce the likelihood of missing or inappropriately treating a melanoma. In an ideal world, all pigmented skin lesions should be assessed with the aid of a dermatoscope and the National Institute for Health and Care Excellence (NICE) recommends this for any pigmented skin lesion referred to secondary care.4 This is not practical for most non-experts or for patients themselves and naked eye examination with good lighting is adequate for the vast majority of the blemishes you will see. Keep in mind that patients with darker skin types will invariably have darker skin lesions. This can make the clinical diagnosis more difficult and, sadly, most of the literature and the references in use are still too biased towards paler skin types. This situation is partly to blame for the later diagnosis of melanoma and other skin cancers in people with darker skin types.5 There is a host of other skin lesions which can have brown pigment in them but being familiar with the listed ones will cover most scenarios. Table 1 provides tips on how to differentiate common pigmented skin lesions from each other and what they will appear like.
Freckles
Freckles are common in paler, Celtic skin types. They are usually found on the sun exposed skin of the face, upper back, chest, arms, and legs in all age groups. Simple freckles are unlikely to catch you out.7
Solar lentigo
A solar lentigo is the medical term for a ‘liver spot’ or a ‘sunspot’. It is the most common type of lentigo, which refers to a well-defined, flat, uniformly coloured macule or patch of skin. They are larger than freckles and are common on the face and the back of hands as we get older. Diagnosis is usually straightforward, but practitioners should be wary of isolated lentigines or ones that don’t look 100% typical. Premalignant sun damage (pigmented actinic keratosis) or melanoma in-situ (lentigo maligna) can be subtle and mimic solar lentigines.8
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Dr Keli Thorsteinsson discusses how to diagnose different skin lesions in your patients and considerations before treating them
Diagnosis
Typical features
Common distribution
Freckle (ephelide)
Multiple pale brown macules
Face, chest, arms
Sun/liver spot (solar lentigo) Well-defined uniformly coloured macules and patches Face, dorsum of hands
Age spot (seborrhoeic keratosis)


Dermatofibroma
Raised warty lesions with well-defined ‘stuck on’ appearance
Face, neck, trunk
Firm papules, can be pinched Arms, legs
Pigmented basal cell carcinoma (BCC)
Moles (melanocytic naevi)
Shiny papules or nodules, can have crust or ulcer Head, neck, trunk

Pigmented macules or papules, soft to touch Any body site
Melanoma
Pigmented skin lesions with irregular features, see text Any body site
Table 1: Common and important pigmented skin lesions6
Seborrhoeic keratoses
Seborrhoeic keratoses arise out of lentigines as we start to feel (palpate) a raised surface or margin. We often refer to them as ‘Seb Ks’ for short. They are very common (even ubiquitous), so it’s easy to become complacent about them.9 I recommend that you consider them for what they are, a pigmented skin lesion. Proceed with care when examining likely Seb Ks and apply the safety rules outlined below. There are pitfalls here. Consider this for example: how do you pick out a melanoma in a patient with innumerable seborrhoeic keratoses?
Dermatofibromas
Dermatofibromas are small, firm pink or brown skin lesions on an extremity. They can be ‘pinched’ on examination, and you can find another similar lesion on patients who are prone to them. They are often pigmented, especially in darker skin types.9

Figure 1: Different types of moles
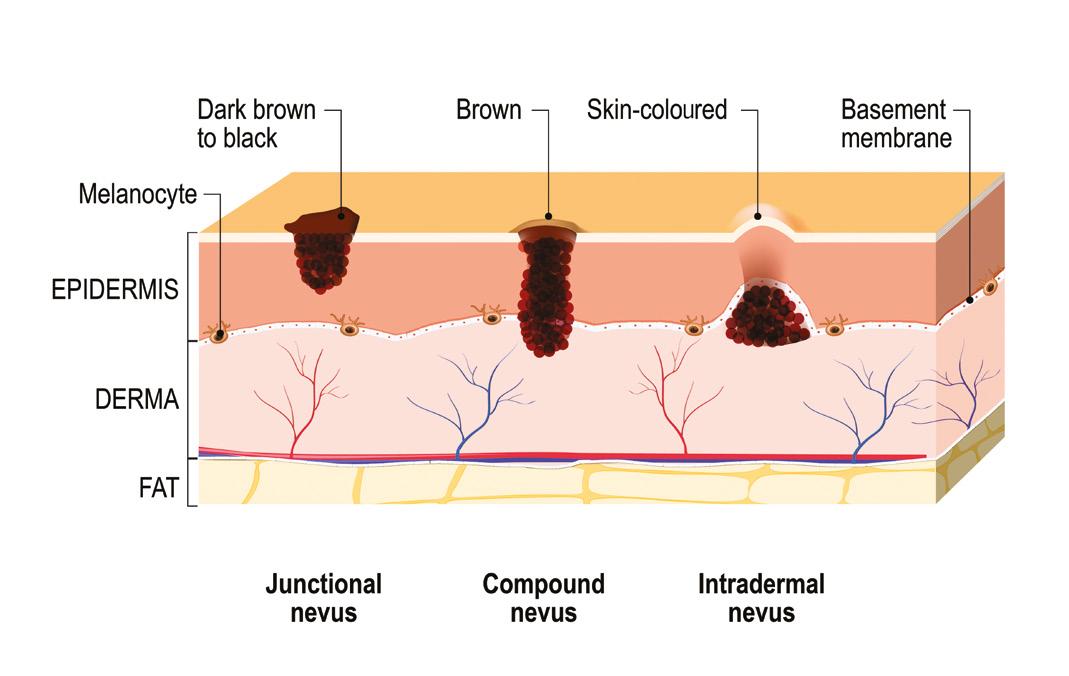
Basal cell carcinoma
Basal cell carcinoma (BCCs) are usually raised shiny nodules, often with a crust or small ulcer (nodular BCC) or flat eczema like patches of skin (superficial BCC). They often have brown pigment within them, or they can even be heavily pigmented in people with darker skin.10 Differentiating them from an atypical seborrhoeic keratosis or melanoma with naked-eye examination can be impossible.
Moles
Moles (melanocytic naevi) come in different shapes and sizes. To keep things simple, let us think of moles in three groups (Figure 1):
1. Flat, where the melanocyte accumulation sits at the junction between the dermis and epidermis (junctional naevi)
2. A combination of flat and raised elements (compound naevi)
3. Raised, where the melanocytes have started to clump together in the dermis, causing the overlying epidermis to rise and become palpable (intradermal nevus)11
Only 1% of us are born with moles.12 These are referred to as congenital naevi, and a discussion of these is outside the remit of this article. Instead, we are concerned with acquired melanocytic naevi. They accumulate throughout life but less so as we get older. Melanocytes have a general tendency to descend in the skin as we age. As they do so, they can bunch up in the dermis as shown in the cross sections (Figure 1). During this ‘maturation’, the surface of the mole tends to get paler, and the mole turns more ‘soft and wobbly’. This is a good sign and the risk of melanoma in these paler, soft, and wobbly moles is low. On the other hand, flat moles are considered of unknown potential and patients should observe them for any changes.11 Differentiating a slightly atypical mole from a superficial spreading melanoma can be tricky, even for experts using dermoscopy.

Safety rules for identifying melanoma


All of this may sound complicated or even scary. Fortunately, there are rules of thumb you can set yourself to minimise your risk of missing or treating a skin cancer inappropriately.
ABCDE rule
The first of these safety rules is the well-known ABCDE rule.13 Remember, when in doubt, consult an expert.
• ‘A’ stands for ‘asymmetry’ – can you in your mind’s eye draw a line through the mole and reflect it like a mirror image onto the other half?
• ‘B’ stands for ‘border’ – is the border of the skin lesion smooth or ragged? In other words, does the mole look like a small map of Mallorca?
• ‘C’ stands for ‘colour’ – are the colours within the mole even and symmetrical?
• ‘D’ stands for ‘diameter’ – is the lesion larger than the head of a pencil (> 6mm)?
• ‘E’ stands for ‘evolving’ – is the mole changing?
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
‘Ugly duckling’ rule
If you find a skin lesion you are not sure about, look for a skin lesion which looks near identical. If you find one this is clearly reassuring, since the chances of having TWO skin cancers on a single patient are clearly lower. That is not to say that you can’t have more than one skin cancer or precancerous lesion at the same time. This would normally apply more to people who have led an outdoor life, such as sportspeople or farmers, those who have lived in tropical countries, have pale skin (Fitzpatrick skin types I-II) and patients who are immunosuppressed. Fortunately, the chances of having two melanomas presenting at the same time (synchronous melanomas) are very low, even in these groups.14 The ‘ugly duckling’ rule is therefore a valid rule of thumb for many of our patients.
Beware of the isolated lesion
Any single skin lesion, however harmless looking, should get your attention. One classical pitfall is to treat an isolated verruca which later turns out to be a squamous cell carcinoma.15 Another pitfall is to be over-confident in your diagnosis of a seborrhoic keratosis. As we discussed before, seborrhoeic keratoses are best regarded as a pigmented skin lesion and, as such, the differential diagnosis is always melanoma.
Beware of the ‘new’ lesion
It is a common fallacy that most melanomas arise out of existing moles. They are more likely to come from normal skin but in the initial months or years they can mimic harmless moles.16 To catch melanomas and other skin cancers before the later stages, advise patients to be aware of any NEW skin lesions or moles.
Give it a name
This is a great rule for clinicians. If you can’t give a skin lesion a name, give yourself two options:
1. Send the whole lesion or a biopsy for histology analysis (or refer to an expert)
2. Bring the patient back for a follow-up in three to six months Reassurance or treating a skin lesion without histology analysis should NOT be an option when you cannot give it a name.
Seek professional help
Diagnosing skin lesions, moles and skin cancer is clearly a skill which takes specialists years to develop. It is, however, possible to be a safe practitioner through self-directed learning, attending courses and learning from those around you who have more experience. You can contact your local NHS dermatology department and ask if shadowing sessions are available. Increasingly, dermoscopy is considered an essential skill for those who treat skin lesions.
The Primary Care Dermatology Society runs fantastic courses, if you want to gain more expertise.17 Most importantly, know your limitations and be honest with yourself and your patients if you are not sure about a skin lesion. Ask them to see their GP for an assessment and NHS referral to a dermatologist where appropriate or refer them to a dermatologist privately if they prefer. If you already treat skin lesions you must follow guidance from NICE and the British Association of Dermatologists.4,18
Take skin lesions seriously
Consider your learning needs in the context of your practice and use the resources out there to address them. Use the simple safety rules we have outlined, know your own limitations, and refer to experts when in doubt. This way you are unlikely to contribute to harm for your patient by false reassurance or, worse, treating a skin lesion which later turns out to be cancerous.
Dr Keli Thorsteinsson is a specialty doctor in secondary care NHS dermatology and a cosmetic practitioner. He has more than a decade of experience in skin cancer diagnosis, reconstructive skin cancer surgery and medical aesthetics. He is the co-owner and director of Freyja Medical, a dermatology and aesthetic clinic in Wrexham and Nanwich. He and his business partner, Dr James Dean, also run Clinic Courses, a new academy teaching advanced aesthetic techniques to medical practitioners. Qual: MD, DPD

REFERENCES
1. DermNet NZ, ‘DermDiag’, <https://dermnetnz.org/dermdiag>
2. Skin Cancer Foundation, ‘Basal Cell Carcinoma Overview’, 2022, <https://www.skincancer.org/ skin-cancer-information/basal-cell-carcinoma/>
3. Zaballos P, et al., ‘Dermascopy of Sebaceous Hyperplasia’, Archives of Dermatological Research, 2005, <https://jamanetwork.com/journals/jamadermatology/article-abstract/395657>
4. National Institute for Health and Care Excellence, ‘Melanoma: assessment and management NICE guidelines (NG14), 2015, <https://www.nice.org.uk/guidance/ng14>
5. Ramji R, et al., ‘Melanoma in skin of colour’, DermaNet NZ, 2017, < https://dermnetnz.org/ topics/melanoma-in-skin-of-colour>
6. Mowlabaccus W, et al., ‘Common benign skin lesions’, DermaNet NZ, 2020, < https://dermnetnz.org/topics/benign-skin-lesions>
7. Griffiths C, et al., ‘Rook’s Textbook of Dermatology’, ninth edition, 2016.
8. Chan B, ‘Solar Lentigo’, DermNet NZ, 2014, < https://dermnetnz.org/topics/solar-lentigo>
9. Tanaka M, et al., ‘Key Points in dermatoscopic differentiation between lentigo maligna and solar lentigo’, Journal of Dermaology, 2011, p.53-8.
10. Nasr I, et al, ‘British Association of Dermatologists guidelines for the management of adults with basal cell carcinoma 2021’, Wiley Online Library, 2021, <https://onlinelibrary.wiley.com/ doi/10.1111/bjd.20524>
11. McCalmont T, ‘Melanocytic Nevi’, Medscape, 2019, <https://emedicine.medscape.com/ article/1058445-overview>
12. Jacobs A, Walton R, ‘The incidence of birthmarks in the neonate’, Pediatrics, 1976, p.218-22.
13. Cancer Research UK, ‘Symptoms’, 2020, https://www.cancerresearchuk.org/about-cancer/ melanoma/symptoms
14. Claeson M, et al., ‘Multiple Primary Melanomas: A Common Occurrence in Western Sweden’, Advances in Dermatology and Venereology, 2016, <https://www.medicaljournals.se/acta/ content/html/10.2340/00015555-2598>
15. Keohane SG, et al, ‘British Association of Dermatologists guidelines for the management of people with cutaneous squamous cell carcinoma 2020’, Wiley Online Library, 2020, <https:// onlinelibrary.wiley.com/doi/full/10.1111/bjd.19621>
16. Cymerman R, et al., ‘De Nova vs Nevus – Associated Melanomas: Differences in Associations with Prognostic Indicators and Survival’, Journal of the National Cancer Institute, 2016, <https:// pubmed.ncbi.nlm.nih.gov/27235387/>
17. Primary Care Dermatology Society, ‘General Dermaology Events’, <https://www.pcds.org.uk/ events/general-dermatology>
18. British Association of Dermatologists, ‘NICE Diagnostic Assessment Programme: Vivascope 1500 and 3000 for detecting and monitoring skin lesions’, 2015, https://www.bad.org.uk/ ResourceListing.aspx?sitesectionid=1139&itemid=7111
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Patients tend to call everything a ‘mole’ and this colloquial meaning of the word can lead to confusion
Arthur Swift’s Mastering of the Midface with Revanesse
A leading global voice in nonsurgical aesthetics, Dr Arthur Swift roused widespread anticipation when he took to the stage to reveal his worldrenowned injection techniques.
The aesthetics heavyweight spilled his secrets in a symposium on the OMGEE Curve: Mastering of the Midface with REVANESSE®. A play on the Ogee Curve, the name given to the double S-shaped curvature along the cheeks that gives the face contour and dimension, the symposium uncovered Swift’s secrets to creating mid-face masterpieces, unveiling the injection techniques he uses to counteract the downward protection that occurs with age.
Citing the amazing rheology of REVANESSE®, Swift explained how he uses SHAPE™ deep in the periosteal plane to project and lift, followed by CONTOUR™ deftly layered with a cannula to create the soft, S shape curves he’s famous for. He cast a spotlight on two of his most illustrious techniques, united in the idea that a systematic approach to cheek enhancement means using less product to achieve better results.
‘ The Doorstep’
Using the tacky texture of REVANESSE® CONTOUR™, Swift performs what he calls the ‘Doorstop Technique’. Pulling the skin of the jawline back towards the upper ear, he injects a small bolus of the product to act as a doorstop, preventing the retaining ligaments from folding forward. While he proceeds to inject the other side, the patient is tasked with holding the face in place with a cold compress.
‘The Double Scoop’
Likening the product to a scoop of ice cream, Swift layers two boluses on top of one another to project the cheek upwards. Using REVANESSE® SHAPE ™ , he injects a small bolus down onto the bone before lifting the skin up vertically and injecting a second bolus directly on top. The two balls of product sit on top of each other and push the midface up, as opposed to projecting it outwards.
‘
The Swift Seal of Approval’
One of only 5 companies to receive FDA approval, REVANESSE® has already become a big player in
®
the USA and Canada, where it has revolutionised the aesthetics market with its unique formula, commitment to high-quality ingredients, and innovative manufacturing technique.
The state-of-the-art dermal filler has spherical particles which give it it’s key selling points of safety and performance. The gels smooth integration can be linked to their particle shape and low levels of modification, which can reduce immune responses and inflammation 12 The spherical shape is designed to be accepted by the body and provide smooth, beautiful results that perform throughout the lifecycle of the skin.
Trial the collection of REVANESSE ® fillers for an introductory price of £504 for 8 x1 2ml syringes exclusively at Healthxchange pharmacy contact info@prollenium co uk for information
1.Edsman K, Nord LI, Ohrlund A, et al. Gel properties of hyaluronic acid dermal fillers. Dermatol Surg. 2012;38:1170–1179.
2.Laeschke K. Biocompatibility of microparticles into soft tissue fillers. Semin Cutan Med Surg. 2004 Dec;23(4):214-7. doi: 10.1016/j.sder.2004.09.005.
3.FDA Premarket Approval (PMA) Database (P040024/S072). Approval OrderStatement for Restylane® SilkTM, 2014. Restylane® is a registered trademark of Nestlé Skin Health SA. 4.Revanesse 1.2ml EU IFU.
Treating Hip Dips Using Dermal Fillers
Dr Lucy Glancey discusses the use of PLLA dermal fillers for contouring the hips
Aesthetic practitioners have augmented the body for more than 100 years. Before the development of dermal fillers that we recognise today, surgeons used the body’s own fat (known as autologous fat) and for the first 20 years of the 20th century, foreign substances such as paraffin to enhance both the face and body.1 Hyaluronic acid (HA) was the first ingredient used contemporaneously which we still harness in our practice today.2 They were first used for breast augmentation, as well as correcting small body irregularities, particularly post-liposuction.2 In my experience, these fillers required large quantities to achieve satisfactory results and the results were often short-lived, which was costly for the patient, meaning they could become disillusioned with the outlay required.
In more recent times, we have been using fillers to meet the demand for curvier figures, which I have found is often influenced by reality television stars. I find that it is younger patients driving this demand – image conscious consumers who want to improve their already slim bodies.
There are studies which have established the most attractive waist to hip ratios for women. The results show patients have an overall preference for a ratio of 0:7, with researchers noting that consumers deem this ratio healthier and more youthful.3,4

The rise of buttock augmentation
The popular Brazilian Butt Lift (BBL) procedure involves the transfer of fat to help create more fullness in your backside. In the UK, we have
HA vs PLLA fillers
been advised by the British Association of Aesthetic Plastic Surgeons (BAAPS) to not carry out the BBL surgery until more is known about safer techniques of fat injection into the bottom.5,6 Although recent studies have suggested that the procedure can be safe and effective when safety protocols are adhered, it is almost impossible to get an indemnity cover for carrying out the procedure in the UK.5 This has inspired aesthetic manufacturers to innovate their filler offerings to include a non-surgical alternative.
However, even if the fat transfer treatment was reinstated by BAAPS, in my view there are many prospective patients who aren’t suitable for the procedure. There is a large patient group seeking bigger hips or buttocks, but who are very slim. They simply don’t have the excess fat needed to transfer, as these areas require a substantial amount of fat to make a difference in their appearance. When you undertake a fat transfer treatment, 50% of the injected fat does not survive.5 As a result, some patients may request another treatment to reach their desired volume, and these patients are prime candidates for body fillers instead. I have also noted that there a large amount of my patients who do not wish to undergo an invasive procedure due to downtime and risk, and so body fillers provide a good alternative.
As mentioned, HA fillers have been used to treat the body for some time. HA is produced naturally by skin cells in a bid to maintain moisture levels. It is well known for its skin benefits, especially alleviating dry skin, reducing the appearance of fine lines and wrinkles and speeding up wound healing. HA filler is a biocompatible and biodegradable gel which is injected directly into the treated tissue to restore volume, shape and symmetry.7 More recently, poly-L-lactic acid (PLLA) fillers have been indicated for body treatment. Formulation of PLLA induces collagenasis and fibroblast proliferation by stimulating the body’s inflammatory
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Many patients do not wish to undergo an invasive procedure due to downtime and risk so body fillers provide a good alternative

HIGH LEVEL TRAININGS KEY OPINION LEADERS NEW VIDEOS EACH MONTH REGULAR LIVE WEBINARS FACIAL & INTIMATE AESTHETICS
Case study
Before Before After
A 50-year-old patient presented to the clinic wanting to improve the appearance of her hip dips. She had two treatment sessions spaced four weeks apart. The first session aimed to improve the shape of the area, while the second session improved the projection and shape of the area treated, using 0.5ml on each side


of the body. Across the two sessions, I used 2mls in total. Ahead of treatment, the defect is outlined, and the area is divided into evenly spaced squares. Each square equals an injection point. I inject into the subcutaneous tissue, filling the area. For larger areas I use a longer needle, ensuring that my patient has fewer injection sites.
response.8 The bio-stimulation helps to restore the skin’s inner structure and shape.8 For my patients, the added firmness from the collagen production is a significant benefit. The injected filler is absorbed by the body, and then over time the new reshaped appearance emerges, which has a longevity of more than two years, far longer than conventional HA filler results which are six to 12 months.9 PLLA lasts longer than HA fillers as it has regenerative properties restoring collagen in the skin. It also has a continuous improvement effect compared with the immediate effects of HA fillers.9 Therefore, while practitioners may opt for HA fillers when looking to treat the face, neck and hands, I find that PLLA is a better option for larger surface areas of the body. Recently, I have seen an increased demand for treatment of the buttock area, especially amongst patients who do their own research. In my experience, fat transfer and traditional HA fillers can actually give a puffy appearance to these areas where the skin is thinner, and doesn’t provide the desirable skin tightening. Therefore, I find that collagen stimulating filler is better suited for these delicate areas, as well as offering greater longevity, making it more cost effective for my patients. Depending on the size of the area to be remedied, I’ve found that the best results from PLLA fillers come after two to four treatments are performed four to six weeks apart depending on the results from the previous session. PLLA fillers can give results after just one session, as the skin is volumised and rehydrated.9
Considerations
In my experience, PLLA body filler patients need to be compliant as there is a need to massage the treated area post-procedure for five weeks to bring about the best results and distribute the filler evenly in any treated area, no matter the placement on the body. As with any injected treatment, patients may experience minimal bruising and minimal acute inflammatory tissue reaction.10 There are medical contraindications; for example patients with autoimmune diseases aren’t suitable for treatment, as there is a higher chance of having an adverse reaction.11

Figure 1: 50-year-old patient before and one year after hip dip treatments using PLLA dermal filler Lanluma.
The patient was delighted with her results following the treatment. The patient was advised to massage the area to distribute the filler, with no side effects experienced. Typically, the treatment is expected to last for 18-24 months, after which the patient will need to come back for a top-up.

The future of body augmentation
The latest body fillers have seen great improvements, meeting an increased demand for safe, effective buttock augmentation. Using careful application, we as practitioners can use PLLA fillers to enhance curves, add volume, or rejuvenate lax skin to encourage a firmer texture. Encouraging the body’s own collagen production gives better firmness and greater longevity than the equivalent HA fillers.7
Dr Lucy Glancey is an aesthetic practitioner with a background in cosmetic surgery, trauma and orthopaedics in the NHS. She owns the Dr Glancey clinics in London and Essex and is a member of the Royal College of Surgeons of England and the British College of Aesthetic Medicine. She is currently joint president of the British Association of Body Sculpting (BABS).
Qual: MRCS, MAACS
REFERENCES
1. J Glicenstein, ‘The first “fillers”, vaseline and paraffin. From miracle to disaster’, Annales de Chirurgie Plastique Esthétiqu, Volume 52 (2007) https://pubmed.ncbi.nlm.nih.gov/16860452/ [25.11.2021] (157-61)
2. Michael Gold, ‘Use of hyaluronic acid fillers for the treatment of the aging face’, Clinical Interventions in Aging, Volume 2007:2(3) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2685277/ [03.12.2021] (369—376)
3. Adrian Furnham, Joanna Moutafi, Peter Baguma, ‘A cross-cultural study on the role of weight and waist-to-hip ratio on female attractiveness’, Personality and Individual Differences, Volume 32 (2002) https://www.sciencedirect.com/science/article/abs/pii/S0191886901000733#:~:text=A%20ratio%20 of%200.7%20can,proposed%20by%20Henss%20. [25.11.2021] (725-745)
4. Sybil A Streeter, Donald H McBurney ‘Waist-hip ratio and attractiveness: New evidence and a critique of “a critical test”’, Evolution and Human Behavior, Volume 24, Issue 2 https://www.sciencedirect.com/ science/article/abs/pii/S1090513802001216 (2003) [03.12.2021] (88-98)
5. Surgical Fat Transfer (UK: NHS.UK, 2020) <https://www.nhs.uk/conditions/cosmetic-procedures/ surgical-fat-transfer/> [25.11.2021]
6. The Bottom Line (BAAPS, 2018) https://baaps.org.uk/about/news/1630/the_bottom_line/ [05.04.2022]
7. Brandt FS, Cazzaniga A., Hyaluronic acid gel fillers in the management of facial aging, Clin Interv Aging, 2008

8. David Goldberg, Adriana Guana, Andrea Volk, Elizabeth Daro-Kaftan, ‘Single-arm study for the characterization of human tissue response to injectable poly-L-lactic acid’, Dermatol Surg, Volume 39 (2013) https://pubmed.ncbi.nlm.nih.gov/23464798/ [08.12.2021] (915-922)
9. Rhoda S Narins et al ‘A randomized study of the efficacy and safety of injectable poly-L-lactic acid versus human-based collagen implant in the treatment of nasolabial fold wrinkles’, J Am Acad Dermatol, Volume 62 (2010) https://pubmed.ncbi.nlm.nih.gov/20159311/ [08.12.2021] (448-62)
10. De Boulle K, Heydenrych I. Patient factors influencing dermal filler complications: prevention, assessment, and treatment. Clin Cosmet Investig Dermatol. 2015;8:205-214. Published 2015 Apr 15. doi:10.2147/CCID.S80446
11. De Boulle K, Heydenrych I, Patient factors influencing dermal filler complications: prevention, assessment, and treatment, Clin Cosmet Investig Dermatol, 2015
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
After
Beauty flows through us
Blunt-tip reduces friction and glides through dermal tissue

Ultra-thin cannula wall increases lumen diameter and reduces injection forces
Premium quality single-use cannula used by clinical and industry leaders
Made in Britain for over 30 years

OVER 100 MILLION SOLD
AESTHETIC +44 1527 501480 ● www.sterimedix.com AESTHETIC CANNULA
Case Study: Full-face Rejuvenation
Dr Jeremy Isaac explores his tips for facial restoration using the TEOXANE range of dermal fillers


Assessment, ageing and anatomy
This 48-year-old peri-menopausal patient presented to my clinic because she felt reserved and self-conscious about her appearance, wanting to look fresher and younger. She had undergone no previous aesthetic treatments in the past and there were no contraindications found following a medical consultation.
The face was assessed using a global full-face approach. It was clear that the forehead, temples, mid-face and jawline were all showing the paradigm of ageing. The upper face appeared quite skeletal with temporal hollowing and there was the presence of decent, deflation and disproportion in the mid-face. Through dermal filler treatment, the aim was to achieve an overall softening of the face, developing feminine curves rather than sharp angles. The goal was a natural, subtle accentuation and avoiding abnormal exaggeration, our patient’s greater fear. I always begin treatment from the upper face, working through to the lower face. It is important to ensure the upper face is supported and elevated first as it has a direct impact on the anatomy and appearance of the mid-face. I then augment the mid-face before the lower face.


Technique and product selection
I choose the Teosyal RHA dermal filler range for their rheology. The genesis of the resilient hyaluronic range is to mimic natural hyaluronic acid. The TEOXANE range is the first resilient hyaluronic acid dedicated to facial dynamics2 and has an unparalleled viscoelastic region making the hydrogel very dynamic. The consequence is the gel is capable of stretch and compression with excellent biomechanical endurance, enabling it to mimic the natural movements of the face. They also have an excellent safety profile, and all the products in the range are approved by the US Food and Drug Administration.1 For this treatment, I used both needles and cannulas. I believe it is important for practitioners to be able to use both instruments to achieve a multi-layer approach. To access the superficial fat for example, you need a cannula to ensure you are in the correct tissue plane and when targeting the deep fat compartments of the face, then a needle or cannula could be used to access these anatomical landmarks.
I started with deep compartments and used the whole of the Teosyal RHA toolbox. By placing the right product in the right plane we were going to get the right outcome. A total of 7.8ml of product was used to get this outcome (Figure 1).
RHA 4 was used in the mid-face and multi-layered into the deep and superficial compartments. The target for the injection was the anterior mobile face and the lateral aspect of the periauricular area. The volume loss of ageing seen in the temple, jawline, pre-jowl sulcus and chin were addressed using RHA 4. RHA 3 was used in the marionettes and RHA 2 was
injected into the body of the lips. RHA 1 was used to augment the depleted upper cutaneous lip with a cannula and the perioral rhytids effaced using a flat blanching technique. In her review, the patient said she was very happy with the outcome. She’s got so much more confidence because of having this treatment, saying she feels she can face the world again. In my assessment, I deemed no further dermal filler treatment was necessary.
Top tips for success
It is important to understand the patient’s list of priorities when it comes to treatment and know what they want to achieve for their final outcome. Don’t rush your treatments because hyaluronic acid products react differently amongst individuals and consequentially, you may not need as much product as you may think. As hyaluronic acid takes on 1,000 times its weight in water, underestimate what you think you may need and then review. Remember, it is better to do a touch-up than overtreat and have to electively dissolve the product. Finally, for excellent aesthetic outcomes, it is essential to understand the anatomy and the stage of ageing of the patient to have a skillset of techniques to address the patient’s concerns and products with rheological properties you can trust within the targeted tissue. Each product has different characteristics and acts differently so choose dynamic products above the SMAS and more static products for the deep fat compartments for a natural outcome.
Dr Jeremy Isaac practises at Wish Skin Clinic in Port Talbot. He is a country expert for Teoxane and is a national trainer for Teoxane and Aesthetic Medicine Pathways. He is on the JCCP training and education committee and is a founder of MAP-IQ.
Qual: BDS, MSc (CosMed), PGCert (MedEd), LDS, RCS REFERENCES
1. US FDA, Premarket Approval (PMA), Teoxane, 2022. <https:// www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfPMA/pma.cfm> 2. Faivre J, et al. Advanced Concepts in Rheology for the Evaluation of Hyaluronic Acid-Based Soft Tissue Fillers. Dermatol Surg. 2021 Jan.
53 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Aesthetics | May 2022 Advertorial Teoxane
This advertorial was supplied by Teoxane.com/uk
Figure 1: 48-year-old patient before and after full-face rejuvenation treatment using the Teosyal RHA toolbox in one treatment session
Before After
FEEL GOOD

LOOK GOOD
Bocouture® (botulinum toxin type A (150 kD), free from complexing proteins) 50/100 unit vials*. Prescribing information: M-BOC-UK-0432. Please refer to the Summary of Product Characteristics (SmPC) before prescribing. Presentation: 50/100 units of Clostridium Botulinum Neurotoxin type A, free from complexing proteins as a powder for solution for injection. Indications: Temporary improvement in the appearance of moderate to severe upper facial lines (glabellar frown lines, crow’s feet lines, horizontal forehead lines) in adults ≥18 and <65 years when the severity of these lines has an important psychological impact for the patient. Dosage and administration: For intramuscular use only. Unit doses recommended for Bocouture are not interchangeable with those for other preparations of botulinum toxin. BOCOUTURE should only be administered by an appropriately qualified healthcare practitioner with expertise in the treatment of the relevant indication and the use of the required equipment, in accordance with national guidelines . The intervals between treatments should not be shorter than 3 months. Reconstitute with 0.9% sodium chloride. Glabellar Frown Lines: Total recommended standard dose is 20 units. 4 units into 5 injection sites (2 injections in each corrugator muscle and 1 injection in the procerus muscle). May be increased to up to 30 units. Injections near the levator palpebrae superioris and into the cranial portion of the orbicularis oculi should be avoided. Crow’s Feet lines: Total recommended standard dosing is 12 units per side (overall total dose: 24 units); 4 units injected bilaterally into each of the 3 injection sites. Injections too close to the Zygomaticus major muscle should be avoided to prevent lip ptosis. Horizontal Forehead Lines: The recommended total dose range is 10 to 20 units; a total injection volume of 10 units to 20 units is injected into the frontalis muscle in five horizontally aligned injection sites at least 2 cm above the orbital rim. An injection volume of 2 units, 3 units or 4 units is applied per injection point, respectively. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Generalised disorders of muscle activity (e.g. myasthenia gravis, Lambert-Eaton syndrome). Infection or inflammation at the proposed injection site. Special warnings and precautions: It should be taken into consideration that horizontal forehead lines may not only be dynamic, but may also result from the loss of dermal elasticity (e.g. associated with ageing or photo damage). In this case, patients may not respond to botulinum toxin products. Should not be injected into a blood vessel. Not recommended for patients with a history of dysphagia and aspiration. Caution in patients with botulinum toxin hypersensitivity, amyotrophic lateral sclerosis, peripheral neuromuscular dysfunction, or in targeted muscles displaying pronounced weakness or atrophy. Bocouture should be used with caution in patients receiving therapy that could have an anticoagulant effect, or if bleeding disorders of any type occur. Too frequent or too high dosing of botulinum toxin type A may increase the risk of antibodies forming. Should not be used during pregnancy unless clearly necessary. Should not be used

during breastfeeding. Interactions: Concomitant use with aminoglycosides or spectinomycin requires special care. Peripheral muscle relaxants should be used with caution. 4-aminoquinolines may reduce the effect. Undesirable effects: Usually, undesirable effects are observed within the first week after treatment and are temporary in nature. Undesirable effects independent of indication include; application related undesirable effects (localised pain, inflammation, swelling), class related undesirable effects (localised muscle weakness, blepharoptosis), and toxin spread (very rare - exaggerated muscle weakness, dysphagia, aspiration pneumonia). Hypersensitivity reactions have been reported with botulinum toxin products. Glabellar Frown Lines: Common: headache, muscle disorders (elevation of eyebrow). Crow’s Feet Lines: Common: eyelid oedema, dry eye, injection site haematoma. Upper Facial Lines: Very common: headache. Common: hypoaesthesia, injection site haematoma, application site pain, application site erythema, discomfort (heavy feeling of frontal area), eyelid ptosis, dry eye, facial asymmetry, nausea. For a full list of adverse reactions, please consult the SmPC. Overdose: May result in pronounced neuromuscular paralysis distant from the injection site. Symptoms are not immediately apparent post-injection. Legal Category: POM. List Price: 50 U/vial £72.00, 50 U twin pack £144.00, 100 U/vial £229.90, 100 U twin pack £459.80. Product Licence Number: PL 29978/0002, PL 29978/0005 Marketing Authorisation Holder: Merz Pharmaceuticals GmbH, Eckenheimer Landstraße 100,60318 Frankfurt/Main, Germany. Date of Preparation:August 2021. Further information available from:. Ground Floor Suite B, Breakspear Park, Breakspear Way, Hemel Hempstead, Hertfordshire, HP2 4TZ Tel: +44 (0) 333 200 4143
Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard for the UK. Adverse events should also be reported to Merz Pharma UK Ltd at the address above or by email to UKdrugsafety@merz.com or on +44 (0) 333 200 4143.
*Botulinumtoxin type A, purified from cultures of Clostridium Botulinum (Hall strain)1
References: 1. BOCOUTURE® (incobotulinumtoxinA) Summary of Product Characteristics. Merz Pharmaceuticals GmbH. 2. Vistabel® (onabotulinumtoxinA) Summary of Product Characteristics. Allergan Ltd. 3. Dysport® (abobotulinumtoxinA) Summary of Product Characteristics. Ipsen Ltd. M-BOC-UK-0443 Date of Preparation: December 2021
BOCOUTURE®
is the only toxin that can be transported and stored prior to reconstitution without the need for cold chain1–3
(Botulinum
type A)
toxin
Free from complexing proteins
Joining the Spherical Revolution
Having launched in October 2021, REVANESSE® from Prollenium is a relatively new name on the UK filler market, but it is now my go-to product. I have moved all my patients over to the brand and a key reason behind this was because of the product’s safety profile,1 I am now one of the most experienced doctors using the product in the UK.
New to the UK, but well established across the pond, Prollenium have two state-ofthe art facilities based in Toronto, Canada. They are one of only five filler brands to receive US FDA approval, which I think is very important when choosing new products for patients.2
The REVANESSE® collection has lovely clean products made from exclusively high molecular weight, HA which not only has anti-inflammatory properties but also knots with itself needing very low levels of BDDE to cross-link. The gels are shaped into spherical particles, which poses a number of benefits. I had already heard of the benefits of spheres in the body during my research and I was thrilled to see these benefits combined into a forward-thinking hyaluronic acid (HA) filler.
The body accepts spherical shapes well and spherical particles tend to have a reduced inflammatory profile compared to irregular shapes which can irritate the body.4 The particles also smoothly inject and integrate1into the tissue which has allowed me to achieve beautifully crisp results which look incredibly natural. In the UK, we now have an almost entire
adult population who have had COVID-19 or are vaccinated and there are more people than ever before who are on medication for auto-immune conditions, and this is having an impact on the way we treat patients.
One of the main problems I experienced with other filler brands was immune excitation. Filler was getting tickled up and excited in ways I had not experienced before the pandemic. None of us want complications, they can drag on for months and cause enormous amounts of stress for both the practitioner and the patient.
All fillers are foreign objects to the body, so the risk of adverse events is of course present for all brands. However, REVANESSE® piqued my interest for its dedication to minimising this risk to the lowest possible.
At Prollenium they’ve researched into all HA technology, reverse engineering iconic brands to take benefits and learnings alongside innovating and pushing the boundaries further on HA technologies. The state-of-the-art manufacturing process yields an advanced benefit at every step. Many of which are complicated intricate details which greatly contribute to the perfect combination. One step which resonated with me when looking into the products was the dialysis stage where the gels sit for seven days. This is to remove any excess BDDE and impurities, but cleverly hydrates the gels simultaneously,
portfolio
so when injecting REVANESSE® they’re close to their equilibrium and have a very low swell factor.1,5,6 My experience with the range so far has proven this point perfectly. I’m able to achieve precise results and my patients require less post-treatment management.
I think the glass syringe that REVANESSE® uses is very pioneering too and I hope this practice will be adopted by the whole industry in the future. We know that toxins seep and leech out of plastics so storing dermal fillers in plastic syringes that can be used in injections into live tissue is counter intuitive. I don’t need a clinical study to know the potential harm that comes from plastics. It’s common sense. I much prefer using a product that has been stored in a glass syringe for my patients because I want them all to receive as pure a product as possible. Everything that REVANESSE® has tried to do in terms of delivering a clean, pure filler resonates with me as a clinician. From the spherical particles to the clearance of any free BDDE, it all creates a better, superior and safer hyaluronic acid product that I as a clinician am happy to welcome into my practice.
REFERENCES
1. Gold MH, et al. J Drugs Dermatol. 2018 Jan 1;17(1):66-73. PMID: 29320589.
2. Testing from Prollenium Medical Technologies Inc. Data on file.
3. Rheologic and Physicochemical Properties Used to Differentiate Injectable Hyaluronic Acid Filler Products, Plast Reconstr Surg, 2019, 143(4): 707e-720e
4. Laeschke K. Semin Cutan Med Surg. 2004 Dec;23(4):214-7. doi: 10.1016/j.sder.2004.09.005. PMID: 15745227.
5. Edsman K, et al. Dermatol Surg. 2012;38:1170–1179
6. Julie Woodward, MD, et al American Society for Dermatologic Surgery, Inc. 1 (2021)

Dr Johanna Ward is an award-winning GP with a special interest in clinical dermatology and nutrition. She studied English at Oxford University before studying Medicine at Guys, Kings and St Thomas’ in London. She is an advanced cosmetic injector and laser practitioner and trains other doctors nationally and internationally. Dr Ward has incredible attention to detail and artistic flair that has earnt her a fiercely loyal client following.
Qual: BA (Hons) MBBS, DRCOG, MRCGP, Dip Clin Derm (distinction)
This advertorial was written and supplied by Prollenium
To find out more, please contact info@prollenium.co.uk
IG: @prolleniumuk FB: Prollenium UK
56 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Aesthetics | May 2022 Advertorial Prollenium
Dr Johanna Ward outlines why she decided to join the Spherical Revolution with Prollenium and enjoys using the REVANESSE®
A summary of the latest clinical studies
Title: The Impacts of Sun Protection and Skincare Habits in the Biophysical and Morphological Properties of Men’s Skin
Authors: Infante V, et al.
Published: Journal of Cosmetic Dermatology, April 2022
Keywords: Radiation, Sun Protection, Sunscreen
Abstract: Studies have demonstrated that UVB radiation may cause changes in the epidermal permeability barrier and in the stratum corneum hydration. It is well known that sun exposure causes erythema, skin cancer and other physiologic alterations. The objective of this study was to evaluate the cosmetic use and sun protection habits of young men, correlating their lifestyle with the biophysical and morphological skin characteristics, as well as to study how skin unprotected can affect these features even in young people. 60 participants between 18 and 28 years old were divided into two groups: with photoprotection habits (PP habits) and without photoprotection habits (No PP habits). They were questioned about their sunscreen and cosmetic products use. The skin parameters were evaluated using biophysical and skin imaging techniques. 60% did not apply sunscreen often and 80% did not consume other skincare products. No PP habits group presented an increase in the transepidermal water loss – TEWL and sebum level, as well as a reduction in the stratum corneum water content and dermis echogenicity. The skin characteristics evaluated were correlated with the sun protection habits and skincare behaviour showing that men face some sociocultural barrier to start the use of cosmetic products.
Title: Presentation, Patterns and Surgical Management of the Complications of Thread Rhinoplasty
Authors:

 Jin H, Kim S
Jin H, Kim S
Published: Clinical and Experimental Otorhinolaryngology, April 2022
Keywords: Complications, Rhinoplasty, Threads
Abstract: Non-surgical rhinoplasty using threads has gained popularity in recent years. While the benefits of this procedure are being emphasised, possible complications and their management are not well-known. This study aimed to present the surgical management and results of the complications of a thread rhinoplasty. We retrospectively reviewed the medical records of seven patients who underwent revision rhinoplasty due to the complications of thread rhinoplasty from January 2018 to May 2021. The presentation of complications, detailed surgical procedure, and the outcomes of revision rhinoplasty were reviewed. Visible or extruded threads at the tip were the most common complication, followed by dorsum irregularity. All the threads were not absorbed and intact in shape, even several years after insertion. Thread removal required careful tissue dissection, resulting in the loss of tip support and dorsal irregularity. To restore the tip support and camouflage the dorsum shape, an autologous tissue graft was required. Removal of threads at the tip and dorsum accompanied structural weakening and partial tissue loss, which required tip support restoration and dorsum camouflage.
Title: Efficacy and Tolerability of a Microneedling Device for Treating Wrinkles on the Neck
Authors: Alqam M, et al
Published: Aesthetic Surgery Journal, April 2022
Keywords: Microneedling, Neck Ageing, Wrinkles
Abstract: A microneedling pen has been cleared by the US Food and Drug Administration and is indicated for improving the appearance of facial acne scars in adults. This study assessed the effectiveness of this pen for treating wrinkles. The paper focuses on the neck, an area of recent importance with video meetings placing stress on the neck area leading to wrinkles. Healthy adult men and women were enrolled. Subjects received four monthly microneedling procedures at depths up to 2.5 mm. Wrinkle assessments were performed by two trained blinded raters by comparing images of each subject at baseline and at 90 days post-procedure. The two raters were unblinded for the Clinician’s Global Aesthetic Improvement Scale (CGAIS) assessment. Subjects completed the Subject’s Global Aesthetic Improvement Scale (SGAIS) and a Satisfaction Questionnaire at 30- and 90-days post-treatment for the treatment areas of the face and neck. The study was completed by 32 subjects. Wrinkle assessments demonstrated significant improvement in the neck areas. The SGAIS and CGAIS showed significant improvements at 90 days posttreatment. Most subjects reported some level of improvement in their appearance at 30 days (73.3%) and 90 days (68.8%) post-treatment. The satisfaction questionnaire showed high levels of improvement in wrinkles (93.8%), satisfaction (87.5%), and would recommend microneedling to friends and family members (80.6%).
Title: Clinical Utility of Botulinum Toxin Type A Local Injection Therapy for Head and Forehead Hyperhidrosis
Authors: Ando Y, et al.
Published: Journal of Dermatology, April 2022
Keywords: Botulinum Toxin, Hyperhidrosis, Sweating Abstract: Head and forehead hyperhidrosis (HFH) is a disease that causes a large amount of sweating from the head region, and it significantly reduces patients’ quality of life. Only a few reports have shown the effectiveness of botulinum toxin type A (BTX-A) local injection therapy (BTX-A therapy) for HFH. To clarify the benefits of BTX-A for HFH, BTX-A therapy was performed in 15 patients, and its efficacy was evaluated. The amount of sweating was measured by the ventilation capsule method and Minor’s iodine-starch test. Evaluation was also performed using the Hyperhidrosis Disease Severity Scale (HDSS) and the Dermatology Life Quality Index (DLQI). In most cases, a remarkable antiperspirant effect was observed from 2 weeks after the injection, and the effect lasted for approximately 30 weeks. HDSS and DLQI improved along with the decrease in sweating. Two patients (13.3%) complained of transient mild ptosis. There were no serious side-effects. This study showed that BTX-A therapy is a safe and effective treatment for HFH.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022

Leveraging Summer Marketing Strategies
those consumer needs or desires as they shift through the year
• Do you want to position yourself as more of a leader, or tackle any key competitors? Are there opportunities to showcase your leadership and heritage – maybe a business award, or a clinic anniversary? Let people know if you’re launching a new brand, product, technique or service which nobody else in the area has!
Once clear on your short-term business objectives, you can layer in your planned marketing and promotional activities in advance. Don’t forget budget allocations – investment should maintain a consistent baseline all year (NEVER dropping off entirely!), with potentially additional budget required periodically to support big pushes like a new brand launch or social media ad campaign.
Marketing strategies must adapt seasonally
As business owners, we are aware that there are many factors driving customer spending habits. However there are certain times of the year when people may be more open and interested in buying your products and services. The finance industry has noted that the warmer months see a general increase in consumer spending; for example, a 2018 survey from a credit report provider showed 57% of Brits spend more money in the summer, which is typically £154 more a month.1 Whilst keeping on top of clinic marketing can often be a daunting prospect for many practitioners, you cannot afford to fall behind with efforts on marketing, promotion and positioning – and keeping your approach fresh to increase engagement throughout the year. Aesthetic customers are increasingly aware and discerning, so can easily be lured away to competitors if they don’t encounter regular touchpoints from your business across multiple channels (such as your website, newsletters, socials and traditional media) so planning ahead to tap into those increased spending habits as summer approaches is a smart business strategy. In this article, I will outline key strategies to help you keep your clinic marketing plan fresh for summer and targeted to maximise customer engagement.
Before you start
Bear in mind that any marketing effort done in isolation will never truly deliver the desired business results – PR and marketing work best when multiple activities are tied to the broader business strategy and objectives. To maximise your valuable time, energy and money, take some time to consider your overarching business objectives, such as:
• Are you aiming for growth, or maintenance? Set realistic targets and deadlines to measure your PR and marketing efforts against these goals
• Is there anything ‘new’ you can promote to existing and prospective customers? For example, new developments in-clinic, or bringing in new brands or treatments for the warmer weather. If there’s nothing new, don’t forget to re-educate your patients on existing hero treatments and explain how these work well for summer seasons – be that body shaping, hair removal, bridal season facials for example. You need to be tapping into
Consumers are more likely to ‘convert’ – to make a purchase or consultation appointment – if your service offerings are aligned with things they are already thinking about or planning for. This is a fundamental marketing technique known as the ‘next best offer’ (NBOs) – where analytical data about the customer (anything from demographics, past purchases, locations, browser history) allows businesses to create highly customised offers that steer consumers to the right merchandise or services at the right moment, at the right price, and in the right channel. One example is Microsoft’s tailored email ads based off Bing search engine users, which have lifted conversion rates by as much as 70% — dramatically more than similar but uncustomised marketing efforts.2 So, in the summer, you must ensure your messaging is reflecting their current thought processes – i.e getting rid of stubborn fat in time for their holiday to Majorca or clearing their acne so they can wear less makeup in the heat!
In addition, summer months can be challenging for clinics, as people are often away on holiday or spending less on discretionary items – so by planning your content marketing and PR in advance, you can help feed in educational and interesting topics to spark interest and enquiries to see you through the quieter period. Consumers are also more likely to engage with fresh messaging and information, rather than the same content pushed out all year-round.
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
PR consultant Julia Kendrick shares her top tips to upgrade your seasonal marketing efforts for business success




THE PROFESSIONAL ELECTRICAL MICRONEEDLING SYSTEM NEW
GET YOUR STARTERKIT INCL. CONSUMABLES FOR 30 TREATMENTS NOW! YOUR ADVANTAGES: Needle modules, XCELLARISPRO CIT Hyal & XCELLARISPRO Hydration Masks worth over 1300€ for 30 treatments included! Adjustable penetration depth from 0,25 - 2,5mm Active needle retrieval Class IIa medical device in Europe (93/42/EEC) Made in Germany XCellarisPRO by www.dermaroller.com MEET US @ BEAUTY Uncovered LIVE, London 7.-8. May 2022 BOOTH C23
Distribution by
Summertime is good for spending!
Interestingly, there is consumer retail data to suggest that the weather, particularly the change in seasons, has the biggest influence on consumer spending.3 Anecdotal data from retailers have also shown that exposure to sunlight will increase the number of impulse purchases3 – so the weather not only affects an individual’s emotional state, but also drives their purchase decisions!
Many aesthetic clinics will have a wealth of treatments which are ideal for ‘pitching’ to consumers ahead of and during the summer months – in particular, I’ve noticed that body shaping treatments ready for beachwear and laser hair removal for the summer wardrobe of shorts, dresses and skirts are key players to begin promoting. Travel skincare regimes, or products targeted towards pigmentation control and hydration could also be good to focus on.
Of course, many of these treatments require multiple sessions before the full results are seen, so it is critical to begin your summer marketing rollout ahead of the season, so you can secure bookings as people begin thinking about their summer preparations. For your summer campaign, think of it as a two or three month strategy with fresh topics, key profiling treatments and special offers tailored to attract your customers and split the approach into a ‘prep’ month with the more long-lead treatments (body shaping, laser hair removal), the activation month (skincare kits, quick turnaround treatments like facials, lymphatic drainage) and a post-holiday month (perhaps laser facials to tackle pigmentation, dry skin treatments). Summer also has some nice awareness days and milestones you can use for more short-term social media inspiration – for example National Bikini Day on July 5 – or you could create educational content about sun safety, SPF and even direct to mole checks or dermatology services if you offer these in-clinic.
Developing creative treatment packages for your clinic is also a clever way to leverage changing consumer purchase behaviour around the summer months – consider creating options with compelling pricing for more long-term prep (i.e. body shaping or hair removal treatments) alongside some short-term ‘impulse’ options (like skincare travel kits, or last-minute facials).
Content is king
Creating quality, engaging content is a critical success factor in any clinic PR and marketing
strategy. Now you know what treatments you’re focusing on for your summer marketing strategy, consider what this content should look like across your key channels: events, website, social media, blogs and newsletters. In addition, detailed planning at this stage will increase the chances of you eventually being able to delegate this work within your team or to an external supplier, if you haven’t done so already.
For each phase, brainstorm and plan out the content topics for at least:
• 1x patient newsletter – try to keep a consistent structure so it is easier to plan the content in advance and be sure to include links to your website in your newsletter. If you can send at around the same time each month, this can help with client expectations and time management
• At least x2 clinic blogs on the key seasonal topics – keep these primarily educational in tone, with perhaps some treatment information on your key offerings throughout. For optimum search engine optimisation (SEO), you should aim for 500 words minimum and post to your website
• 1x email campaign or social media advertising campaign – what do you want to promote that month and drive action for? Ensure you have a bank of good quality imagery – of you, the clinic, your brands, stock images – particularly with a bright, airy and summer-focused look and feel — the more you can stockpile in advance the less you will experience the daily ‘posting panic’
Teamwork and delegation
Now you should have a comprehensive overview of what your seasonal marketing campaign looks like, so if you have a team or clinic manager, consider delegating some of the responsibilities to them as part of their role – perhaps to compile the newsletter, or write one blog per month based on your plan. In addition, this plan could give you a strong brief and overview should you wish to engage an external PR or marketing supplier. Having clear actions and deadlines will help ensure that the marketing becomes an integral part of everyone’s function in the clinic – not an add-on or a burden which keeps getting forgotten.
Don’t forget to measure and evaluate
Successful marketing is contingent on accurate evaluation to determine if your
efforts are hitting the right note, and ultimately converting traffic into bookings, or sales. If your blogs aren’t driving website traffic, or customers aren’t opening your newsletter, or nobody is clicking on your social media posts – you need to know and adapt your strategy next time. Undertake regular reviews of your website analytics, also your customer relationship management (CRM) system and social channels to identify engagement, interaction and ultimately what is being delivered in terms of revenue. If something is not working effectively, it’s best to find out early on and adjust your strategy accordingly until you get it right!
Get ready for summer
Seasonal marketing campaigns are an effective and engaging way to connect with your customers and drive both new and repeat business into your clinic. With some advanced preparation, you can plan and create compelling content across your marketing channels (website, social, PR, events) to help boost awareness and profile, whilst driving treatment demand over the quieter months.
Julia Kendrick is an awardwinning PR with 18 years of experience across top London agencies and in-house at Allergan. In 2015, Kendrick founded her own consultancy and now leads a specialist team working with industry leaders, aesthetic brands, top-level practitioners and leading clinics to deliver a unique, full-service PR and marketing consultancy specialising in the medical aesthetics, wellbeing and beauty industries.

REFERENCES
1. Felicity Hannah, 2018, <https://www.independent.co.uk/money/ spend-save/summer-finances-sun-spending-holidays-moneydebt-a8355156.html>
2. Thomas H. Davenport, Leandro DalleMule, and John Lucker, Know What Your Customers Want Before They Do, 2011, <https://hbr.org/2011/12/know-what-your-customers-want-beforethey-do>
3. Joe Camberato, 2016, <https://www.nationalbusinesscapital. com/blog/change-seasons-spending-habits/>
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Marketing Summer Strategies
Optimising Website Landing Pages
Digital
Since the launch of the World Wide Web, businesses have sought to drive people to their landing pages in order to sell their wares, from books, to widgets, to vacuum cleaners. In medical aesthetics, we have an even tougher job to do with our landing pages. We need to communicate education, credibility, qualifications, social proof, and of course the treatments and services we offer, all with a view to giving the patient the confidence to book that first consultation. All of this in an increasingly competitive market, where patients have an almost overwhelming choice when it comes to choosing a clinician. In this article, I will lay out some of the fundamental principles of a strong landing page, as well as methods for testing and optimising them that have worked well for my clients.
What is a ‘landing page’?
Let’s start at the beginning. A landing page is a webpage specifically designed to convert visitors into leads or customers. Typically, a landing page is created for a specific audience or campaign. It might be the destination for a Facebook advert, email campaign or the search result for a high-traffic keyword, for example. Any page on your website can technically be a landing page if people tend to ‘land’ on it from certain searches on Google, but a
dedicated landing page typically converts at a higher percentage, has no navigation to the rest of the site, contains one focused offer or topic, and is ideal for paid ads on Google or Facebook, or targeted email campaigns. As an example, a popular blog article on your site could be considered a landing page when it ranks for certain terms and often people ‘land’ on that article from a search result, whereas a dedicated landing page would be created specifically for a particular campaign as described above.
Landing page best practice
As with all things in digital marketing, genuine success comes from continual trial and error, but as we enter the World Wide Web’s 25th year, there are thankfully some research-based best practices for landing page design that have been shown to increase the rate at which they convert a visitor into an enquiry. I’ll split out these best practices into three distinct types: design, content and layout; technical performance; and user experience.
Design, content and layout
Let’s start with the message. The message of your landing page needs to match the expectations of the visitor. Match the headlines and copy to that of the email campaign or social media advert. This
ensures the visitor immediately recognises that this is what they came here for, and will read on. If the message differs from the ad or email they came from, it can feel disjointed and less relevant and may lead to them leaving the page prematurely.
Next, consider your call to action (CTA). This needs to be clear, simple, and designed in a way that contrasts to all other elements to draw the visitor’s eye to it over all other page content. In fact, according to TechJury1 more than 90% of people who are directed to a landing page read the landing page’s headline as well as the CTA that took them there.2 In addition, think very carefully about the wording of your CTA. For example, research by HubSpot3 has shown that using the word ‘submit’ on a form can decrease conversion rates by 3%,4 this is typically because more ‘active’ language encourages users to take action more often. So get creative with your copy here and consider alternatives like ‘secure your consultation now’, or ‘get started’ and monitor the results by documenting the number of enquiries per month before you change the forms, then comparing the months after the form changes are published.
Use emotionally-driven ‘social proof’ that connects to the condition you’re treating or the service you are offering. Social proof can include patient testimonials, case studies, and data, and with 55% of online users considering customer reviews helpful in their buying decisions,5 it’s important to utilise this type of content at key points on your landing pages to reassure and educate your potential patients as they consider making an enquiry.
The position of your CTA also matters. But contrary to popular belief, this doesn’t mean that the CTA should necessarily be placed at the top of your page. In fact, a split test by Content Verve showed that moving the CTA to the bottom of their landing page contributed to a 304% uplift in conversions.6 This goes against a lot of the advice you will see online, but the test revealed that visitors that are motivated to take action are typically those that have read more copy and seen more social proof before doing so. Just as a great consultation will educate your patient to make an informed choice about their treatment, so must your landing page – and in my experience that in turn will lead to a greater percentage of your web visitors to convert into an enquiry. (I have observed this happening on many
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
consultant Rick O’Neill discusses the best practices and tools that will help yield more enquiries from your landing page visitors
client sites over the years).
Focus on the conditions you’re treating, the emotional attributes that these evoke, and the benefits of the treatment you’re offering, rather than the technical aspects or the clinical language around the medical device or capital equipment being used.
You are talking to a human, with emotions, frustrations, fears and desires on your landing page, just as you do when you consult, so it’s important to reflect this in the copy used to communicate your offer.
You should also consider the images you use carefully. Landing pages featuring images of real people are proven to convert at a higher rate (up to 33% higher according to a study by Taboola) than other types of graphics.7 Furthermore, images without text, and featuring a closer crop of the people are shown to increase conversion rates.8
Technical performance
For the ultimate landing page, you’ll need to consider more than just the content and layout. The technical performance of a landing page can also have a significant impact on its performance. Technical performance starts with speed – just a one second delay in load time on a landing page can decrease conversions by 7%, so ensure that your page has been tested and optimised accordingly to load in the shortest possible time (see later in regard to some of the tools that can help you here).6
It may sound obvious, but test, test, and test your forms again. According to WPForms,7 67% of users will abandon a form forever if they encounter any complications in submitting it.8 Sometimes your form may work perfectly in one web browser, but not at all in another. Other times it may work great on a laptop, but fall apart on a mobile. Testing is critical, and you will need to work with your web designer to ensure all forms function on all major browsers and devices.
User experience
With the content, layout and technical performance in check, turn your attention to the experience for your visitor. Make their life easier and try to reduce the information you ask for in forms. The average number of form fields (the different information you ask for in your forms, such as name, email) is 11, but according to Douglas Karr of SearchEnginePeople.com,9 reducing this to four can increase conversion rates by 120%.10 As tempting as it may be to try
and collect more data in the first contact, it’s more important to get the basics, and you can always follow up for more information at another stage in the onboarding process or when they visit for their consultation. Typically the four form fields I would recommend using would be name, email, mobile number and desired treatment.
Of course, user experience is more than just the forms on the page. Once the visitor has taken an action and completed an enquiry form, it’s still important to reassure and engage with them before they leave by including a separate ‘thank you’ page. Bringing them to a separate thank you page (or a pop-up) can create new opportunities. It not only lets them know the form has actually been submitted – a step some landing pages forget – it also gives you the opportunity to re-engage them. For instance, you can ask if they want to sign up for your newsletter or visit another part of your website to consume further educational content.
Lastly, if you can service it, live chat on a landing page is a great way to give potential patients fast answers to burning questions they may have. In fact, 60% of consumers will return to a website that offers live chat, according to a study by emarketer.com, and 38% of consumers are more likely to buy from a company that offers live chat support.11,12
Landing page tools
Over 55% of all web traffic is now via mobile device, and so your landing pages need to provide a seamless experience on a small screen.13 In fact, 86% of the world’s top performing landing pages are mobile optimised.14 To help with the design and optimisation of your landing pages, there are now a number of impressive tools to make the job easier and more effective. There are tools for building landing pages, and there are tools for testing and optimising them. I would recommend trialling a few to see which serve your needs best, but for page builders consider Unbounce, HubSpot, and InstaPage – all of which offer rapid tools for creating landing pages and deploying them as part of your campaigns.
For testing and optimisation, I would recommend Crazy Egg (which offers heat maps to show where visitors are engaging most on your pages), WordStream (which will grade your pages and offer suggested
improvements), and Optimizely (which offers a number of A/B testing tools and optimisation reports).
Get optimising!
Landing pages offer you a great opportunity to get results from your social media or email marketing campaigns. But in a competitive market such as medical aesthetics, success will take dedication to creating the very best content, layout, technical performance and user experience you possibly can, to ensure that the highest possible percentage of your visitors turn into enquiries for your practice. Make use of landing page builders and testing tools to make your job easier and create efficiencies in the building of your campaigns. I look forward to seeing your landing pages now that you’ve got the ultimate guide to creating them on your desk!
Rick O’Neill is a digital consultant to the medical aesthetics, cosmetic surgery and pharma sectors. With more than 20 years’ experience in digital marketing, O’Neill is the founder and owner of the award-winning digital agency ‘Look Touch & Feel’, a founding partner of The Aesthetic Entrepreneurs, digital consultant to Merz Aesthetics, and investor/advisor to several other digitally-focused businesses.
REFERENCES
1. TechJury, Landing Page Stats and BenchMarks, 2022, <https:// techjury.net/blog/landing-page-statistics/>
2. Daniel Burstein, Registration Forms, 3 steps to lead, 2012, <https://marketingexperiments.com/lead-generation/registration-form-optimization-steps>
3. HubSpot, Don’t Submit To Landing Page Button Text, 2022, <http://blog.hubspot.com/blog/tabid/6307/bid/6737/don-t-submit-to-landing-page-button-text.aspx>
4. Oli Gardner, How To Optimize Contact Forms, 2013, <https:// unbounce.com/conversion-rate-optimization/how-to-optimizecontact-forms/>
5. Nestor Gilbert, 60 Social Proof Statistics, <https://financesonline. com/social-proof-statistics/>

6. Neil Patel, Why the Fold is a Myth, <https://neilpatel.com/blog/ why-the-fold-is-a-myth/>
7. Taboola Trends, Image Trends, <https://trends.taboola.com/ images?_gl=1*1isgmrs*_ga*MTEyMDYwMzk3My4xNjQ0Njk4MDg1*_ga_ERHENNM7DM*MTY0NDY5ODA4NS4xLjAuMTY0NDY5ODA4NS42MA>
8. Neil Patel, How loading Time Affects Your Bottom Line, <https:// neilpatel.com/blog/loading-time/?wide=1>
9. SearchEnginePeople, How Many Questions Are On Your Landing Page Form, 2022, https://www.searchenginepeople. com/blog/150450955-how-many-form-fields.html
10. Lindsay Liedke, 2022, 101 Online Form Statistics, <https://wpforms.com/online-form-statistics-facts/#form-abandonment>
11. J Clement, Share of Global Mobile Traffic, 2022 <https://www. statista.com/statistics/277125/share-of-website-traffic-comingfrom-mobile-devices/>
12. Sharon Hurley Hall, 7 Examples of Mobile Landing Pages, <https://blog.taboola.com/how-to-create-high-converting-mobile-landing-pages/>
13. Insider Intelligence, How Helpful is Live Chat, 2009, <https:// www.emarketer.com/Article/How-Helpful-Live-Chat/1007235>
14. The Daily Egg. Best Live Chat Software, 2022, <https://www. crazyegg.com/blog/live-chat-software-solutions/>
15. WPForms, 101 Ubelievable Online Form Statistics & Facts for 2022, <https://wpforms.com/online-form-statistics-facts/#:~:text=length%20(27%25).-,3.,such%20as%20a%20free%20tool>
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022

Managing Online Appointments
We’ve all been there, juggling multiple conversations, across several different apps… WhatsApp, Instagram, Facebook messenger, texts, and email. As your business grows this can quickly become chaotic, absorbing a lot of your personal time, and affecting your patient rapport.
In this article I will outline what you can do to manage appointments effectively and how technology can support you to create processes to benefit both your business requirements and the experience of your patients.
Updating your software
Firstly, think about how you currently manage your appointments. Is your beloved paper diary full of crossed out names and arrows showing the rescheduling of appointments from one time to another? If so, it might be time to jump into the 21st century (although this is easier said than done!). However, with the correct guidance and a supportive software company in place, this process can be a smooth transition.
Perhaps you are using a built-in calendar that comes with your phone, such as
Google or Apple calendar. This is probably your first go-to solution when removing your paper diary or just getting started in aesthetics due to it being free and it can quickly be amended when a patient makes an enquiry. However, this process can soon become just as time consuming as a paper diary because you will still need to schedule each appointment manually yourself. They also do not offer the opportunity to fully capture the patient’s details or create a link to a patient record, allowing you to access the history of each individual’s treatments.
If this sounds like you, then the first step for a cohesive aesthetic booking system would be to explore your options available with in-clinic management software. You should look for a software that is designed specifically for aesthetic practitioners with a dedicated diary. The system should be able to store all your patient records in one place and be quick to select returning patients. But how can practitioners work even more efficiently, saving themselves time and improving their patients’ experience? The answer is online booking.
What is online booking?
I believe an online booking system can be described as a software solution used for self-serve appointment management. This allows patients to book appointments themselves through your own unique booking page which can be linked to your website or social media. A range of different types of software offer online booking platforms which can manage your diary, display your treatment lists and practitioner availability. Some examples of these systems are Aesthetic Nurse Software, e-clinic and Pabau.
The benefits
Your business is always open
You will never miss a potential booking! Did you know that between 4pm and 8pm on a Sunday is the most popular time to book an appointment?1 This is likely when people usually have the most downtime, allowing them to plan for their weeks ahead. As a result, small independent businesses are typically losing out on a large amount of footfall. With an online booking system, whether you’re in-clinic, training or even having a week in the sun, patients can view the treatments you offer and your availability at a time that suits them. Essentially, it allows you to take bookings 24/7, removing the back-and-forth of messages or waiting until Monday for one of the team to pick-up. In an industry worth £3.6 billion, it’s time to make your business more accessible and hit the ground running in this competitive industry.2
Create a professional first impression Online booking systems can boost your first professional impression. In the UK, it is estimated that 45 million users are active on social media for an average of 110 minutes a day. Of these active users 28% research brands, products and services to buy.3 This equates to more than 12.6 million people looking for services online that, without an online booking system in place, practitioners could be missing out on. The first impression of a webpage is made within the first few seconds on the page meaning an efficient booking system with easy processes can boost the conversion rate from browsing activity to active bookings.
Appointment confirmations and reminders
In today’s busy society patients can sometimes lose track of their scheduled appointments. However, with an online booking system automatic confirmations and
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Business director Max Hayward outlines why practitioners should use online appointments to manage their clinic and his top tips for implementing this

JUNE 3 - 5, 2022 PARIS & ONLINE TOGETHER WITH THE BEST IN DERMATOLOGY, PLASTIC SURGERY & AGING SCIENCE «An amazing experience, very well organized and with a fantastic program. In my personal opinion, every physician who works in this field, should attend IMCAS» Leonardo Rossati, Plastic surgeon, Italy «An excellent reference and opportunity for practical and scientific exchange with colleagues from all over the world» Andreea Tunei, Dermatologist, Romania 12,000 ATTENDEES 700 SPEAKERS 280 LEARNING HOURS 23RD WORLD CONGRESS At Palais des Congrès de Paris or through www.imcas.live CHECK OUT THE PROGRAM & REGISTER ON IMCAS.COM
reminders will be sent to patients regarding their appointments. Therefore, this removes practitioners from the mind-numbing admin task of manually sending these reminders each day – eating into your own personal time. By creating set foundations and a rhythm for appointment confirmations and reminders this will reduce the number of no-show appointments and late cancellations. Allowing you to focus on what matters most, the patient experience and your clinical procedures.
Protect your time and business
There is nothing more annoying than a patient not turning up for their appointments or receiving a last-minute cancellation, effecting your business growth and causing loss of productivity.
Let’s say you have one no-show appointment each week for an anti-wrinkle treatment in two areas of the face. A conservative charge for this appointment is £150 – that’s £600 a month and £7,200 a year! However, deposits are a great way to prevent this loss of income and if a noshow or a late cancellation does happen, the deposit can be used as compensation for your wasted time. Now, you may already request deposits but if this method is through bank transfers, it can be a timeconsuming process to keep on top of, chasing payments before the appointment. Using an online booking system can allow you to charge patients a deposit at the time of booking to secure their appointment, stating your cancellation policy which patients must agree to before their booking is complete.
Also, this gives patients the ability to easily reschedule appointments. It can be easy to forget to get in touch to cancel or reschedule an appointment, especially when it’s out of hours. However, if you can make it possible for them to manage their own appointments by simply clicking a button then you are likely to reduce your last-minute cancellations and no-shows.
The paperless medical record rules which were introduced in 2018 is another reason for practitioners to move towards online booking services so the patients’ confidential information is logged into a centralised system. By doing this, your services are complying with General Data Protection Regulation (GDPR) and reduces the risk of having a potential data breach.4
The misconceptions
Although online booking systems have benefits, there are some misconceptions about using them within the industry.
I’m losing the personal touch with my patients
Some practitioners feel that taking away the communication between practitioners and patients can reduce the personal touch of your service – this is a fair point. However, now more than ever, people are used to booking appointments online and expect other services to offer the same speed and convenience when doing so. With 75% of millennials avoiding phone calls as they are deemed ‘too time consuming’ your business may be losing a valuable demographic.5
Patients will be able to book any time they want
Online bookings don’t give your patients 24/7 access to you; it simply gives them access to book an appointment. You will have control over the dates and times that you are available; with the ability to specify the clinics and dates you are working. You can also choose the specific treatments you wish to offer. Some practitioners will opt to just allow patients to book a consultation online. So, rest assured, you will not be receiving bookings for every waking hour of the day!
It’s a cost I can’t afford Yes, this software does come at a price. However, where software used to be expensive, you can find fantastic software that is affordable. Some have no long-term commitment and work out at just 50p a day!
You need to weigh up the small monthly cost compared to the time it will save you.
If you’re able to free up an hour each week that would have been spent on managing business admin, then that’s an hour you could use for an extra treatment – which covers the monthly cost.
Getting started
You will need to start by finding a software which suits you and your business’s needs.
You may want to consider the following:
• Does it link to patient records and medical/ consent forms?
• Is it specifically designed for aesthetics?
• Is it reasonably priced?
• Can it link to your website and social media?
• Are other medical practitioners
recommending it?
• Are there any hidden or additional fees?
Most software companies will offer a free trial, allowing you to manoeuvre through the software and access all elements including the online booking page. A good software system will have individuals on hand to help you set up and confidently use your online booking system as well as offer continued support going forward.
Introducing the new system
When launching your online booking platform there are several actions you can take to promote your transition.
• Social media – create a post to let patients know you have launched your new booking page or maybe create a short screen-recording or reel to show how easy it is to use and add to your highlights area
• Email marketing – send an email out to your patient list. Include the link to your booking page and a few simple steps for them to follow
• Website – add your online booking page to your website and include clear call to action buttons, such as ‘Book Now’
Try it yourself!
Online booking systems can split opinions about whether they should or shouldn’t be used within the industry. However, these systems are an easy way to convert extra traffic for your small business and are a real revenue generator when first trying to gain industry attention. With nearly half of all Google searches being for local services and having a conversion rate of 80%, it’s time to send your business into the world of online bookings.6
Disclosure: Max Hayward is the director of Aesthetic Nurse Software
Max Hayward is the director of Aesthetic Nurse Software, a clinic management system designed specifically for aesthetic practitioners. Hayward has more than six years of experience working in the aesthetics industry, supporting practitioners nationwide to go paperless.

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
VIEW THE REFERENCES ONLINE AESTHETICSJOURNAL.COM
ultrasound technology practice
Aesthetics
As a dual-qualified doctor and dentist, Dr Euan Mackinnon now has a mixed practice working as a maxillofacial surgery registrar and a cosmetic doctor in Knightsbridge He began working in aesthetics when he realised early on in his career that he was fascinated by the profound impact that surgical and non-surgical procedures had on patients’ wellbeing.
Now every patient undergoing a dermal filler procedure has an ultrasound scan, and it’s usually done immediately before the treatment, although we can sometimes do it at the consultation. The primary goal is to identify any vascular patterns that may make me consider my approach, particularly in the lip area where we’ve already found patients with very superficial superior labial arteries, where we would definitely be using a cannula over a needle and still be injecting with a degree of slow caution.
For particularly technically challenging areas, I often use the ultrasound for guided injection as well. For example, to ensure sure that I’m in the correct planes and away from blood vessels. Examples would be the forehead and the temples, and the nose.
the practitioner can use in their own practice with relative ease, suddenly makes that teaching more informative, more useful, more applicable, and more engaging.
a different area and find a similar stepwise process to identify those structures and keep going.
around made confidence.
facial mapping, patient education and our own development. It allows us to tailor our treatment plans individually for every patient to get what we feel is a more effective, optimal result.
In the right plane
which has for
Just from the routine scanning of patients presenting to our clinic, we can demonstrate that filler intended for the deep plane of the midface can actually be within the Superficial Musculoaponeurotic System (SMAS). And filler intended for the interfacial, or the plain of the temple can sometimes be subcutaneous, intramuscular or intrafascial, rather than interfacial. Ultrasound guidance means that we can see the tip of the cannula in the right place whilst we inject, rather than finding out afterwards that we have a suboptimal result.
Graduating from Newcastle University in 2012 after studying dentistry, Dr Mackinnon began his first training years in maxillofacial surgery. He knew from an early stage in his career that he was interested in the aesthetic branch of this specialty and was fascinated with facial reconstruction and re-animation. He explains, “After seeing dermal fillers and biostimulators being used in novel ways, such as in cleft lip reconstruction and gender re-assignment procedures, I quickly realised that there was a niche for surgeons who are proficient in both surgical and non-surgical aesthetics.”
The other area of interest for us is the management of complications. Being able to identify dermal filler and resolve with injection under ultrasound guidance means that I can be so much more confident in the outcomes of my treatments.
This applies to the area, but what I’ve really found useful is using this guided injection method for the cheeks and for the temples. For the cheeks, when I thought I was in the deep plane, occasionally I actually found I was within this mass, Superficial Musculoaponeurotic System (SMAS). So I can reposition, get in the right place, use less product and get a much better aesthetic result. For the temples, ultrasound guidance means that I really can be sure that I’m in that interfacial plane when I want to be. And when I’m injecting on the bone, I can make sure I’m in a place that’s effective and has no visible vasculature.
Visualisation means greater accuracy, greater effectiveness and greater safety of dermal filler implantation
Dr Mackinnon began practising in aesthetic medicine in 2014 after training with KT Training, who returned to teach for in 2018. He was taken on soon after as an associate at the Tracey Bell Clinic in Liverpool, which provided him with extensive training opportunities in injectable and energy-based treatments. He reflects, “Aesthetic medicine was a specialty that piqued my interest as I have always been fascinated with facial reconstruction. I quickly learned this during my early maxillofacial training when I saw the positive impact on wellbeing that can be achieved by restoring aesthetic harmony to the face. It made sense to me to branch into aesthetics at this early stage because I already knew that this was where I wanted my career to progress. I found that having a three-dimensional surgical perspective of head and neck anatomy gave me a comfortable platform to start injecting.”

to Liverpool Medical School in 2016 until 2019 to become a doctor, where he received Honours. He has also completed the Membership of the Royal College of Surgeons of England and the Membership of the Faculty of Dental Surgeons. Reflecting on his studies he adds, “Becoming a maxillofacial surgeon is hard work! You don’t stop studying and there’s always another exam to sit. Working as an aesthetic doctor has been a blessing to me during all my years of studying as it enabled me to finance my education whilst doing something I am truly passionate about. I’m very lucky to be able to say that!”
The use of ultrasound imaging in teaching with Merz Aesthetics and ATA really brings to life the concepts we talk about and gives the delegate an extra dimension of understanding.
How to get started
We used to give presentations and run training courses using ultrasound, and we used it mainly as a teaching aid because it was impractical to suggest that every clinic should have its own device. With modern ultrasound technology, this is no longer the case.
A vital training tool
A common theme in many of our teaching programs, both for Aesthetic Training Academy (ATA) and Merz, is a respect for and understanding of the anatomy of the patient. Now, that doesn’t just mean understanding the names and the branches and relations of a blood vessel or a nerve but also being aware of all the potential anatomical variations that may occur and could potentially be a problem.
That you need to know that is a truism, but given that you have no way of knowing what variations a given patient may have, the teaching can sometimes be more off-putting than useful. So bringing into play a simple, effective method for identifying your patient’s nasolabial artery, for example, and more so a method that
In 2019, Dr Mackinnon contacted aesthetic practitioner and owner of The Lovely Clinic in Knightsbridge, Dr Sarah Tonks. He adds, “Dr Tonks and associates Dr Kishan Raichura and myself are all dual-qualified and come from similar medical backgrounds. There aren’t a lot of dual-qualified practitioners around so when I discovered there were other doctors working in aesthetic medicine who were like me, I thought I would reach out. I didn’t go looking for a job, but it just so happened that Dr Tonks decided to take me on! I have now worked at the clinic for three years. We all

My advice is to buy an ultrasound device or borrow one, then pick an area that you are familiar with and get started. The basic principles of ultrasound imaging are that hyperechoic tissues bounce the signal back, and they’re white. Hypoechoic tissues allow the signal to pass through, and they’re dark. Fat is hypoechoic, water is hypoechoic, and muscles are mostly cells filled with water. Collagen fibres don’t have much water in them. They’re dense, and they bounce the signal back.
Then pick something simple and big, like the masseter muscle, hold the probe over it in different orientations and try to identify the structures, the skin, the fat, the muscle, and then the facial pedicle. Find those blood vessels and then look for the bone. And the bone is very dense. There’s no water, and it’s very hyperechoic, so it’s white. Do it a few times over the same areas and the same structures until you can always recognise them. And that’s the process of training your brain to interpret the light and dark images and build those into a representation of the tissues that are there. Then start moving into
Treatment you enjoy performing the most…
A difficult question but I guess cheek filler! The results you can get for a relatively low volume can be very impactful.
Industry
pet hate…
Dishonesty – usually demonstrated in deceptive or poor-quality clinical photography.
Plans for the future…
In 2015, Dr Mackinnon completed his Masters degree in Primary Dental Care and Oral Surgery with distinction. He returned
Of course, finish my surgical training. I would also love to advance to a key opinion lead role at Merz and take my skills internationally!
In conclusion
Ultrasound imaging brings us to the next evolutionary step in aesthetic medical practice. No longer having to inject blindly means that we have the ability to identify and avoid larger blood vessels, reducing the risk of bruising and potential vascular compromise.
Patients attending a practice where ultrasound imaging is used routinely can be confident that their practitioner is using every tool in the box to ensure that they have an effective treatment. Using ultrasound means that we can position our dermal filler exactly where we need it to be, meaning better aesthetic outcomes and potentially less product.
get on so well, it’s like working with your best friends. They are the most supportive and ambitious team and I’m thrilled to be there.” Dr Mackinnon’s recent venture has been working in partnership with Merz Aesthetics. He explains, “I have taken on the role of ‘Merz Innovation Associate’ for London. I approached Merz as I absolutely love their product portfolio, so I’m thrilled that this role has come to fruition. My primary role is to help develop the brand and to support other practitioners. I create educational content for Merz through editorials and showcase what the products can do – their range is so versatile! They are a truly forward-thinking company, and their product support is exceptional with patient safety always at the forefront. They’ve even provided me with an ultrasound scanning device and training in order to use their products with optimal precision. I couldn’t be happier with the partnership we have.”
We have already chosen the product with the best radiological profile for bio integration, and we use the products with a really good profile in terms of inflammatory reactions. We do this because we want the best for our patients, which means our patients trust us. Adding ultrasound is another obvious and visible step in the process. So, in addition to improving outcomes, reducing risk, improving the aesthetic outcome, we’re also improving trust alongside confidence, which itself leads to higher patient-reported satisfaction.
I think we’re approaching the point where guided injection and vascular mapping will become part a normal part dermal filler injections.
24/7 ACCESS TO EXPERT-LED CLINICAL
EDUCATION AT
Looking back at his career thus far, Dr Mackinnon urges practitioners who want to enter aesthetics to master the basics of aesthetics first. “I think if you want to be successful in aesthetic medicine, you’ve got to be resilient as it is a competitive and relatively saturated space with a woeful lack of regulation. You’ve got to commit to mastering the basics first. Don’t try and run before you can walk. Finally, remember to appreciate those in the business who have shown you kindness, opened doors for you and cheered on your successes. Try to emulate this one day when you’re in their shoes.” he reflects.
YOUR FINGERTIPS
REGISTER SCAN THE QR CODE OR VISIT
Date of Preparation February 2022 06/04/2022 13:29 68 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Aesthetics | May 2022 Advertorial Merz Aesthetics
TO
merz-aesthetics.co.uk/ecademy
M-MA-UKI-1892
“Build a portfolio of techniques which are truly competent to use and don’t push the boundaries too soon”
Dr Euan Mackinnon details his career into aesthetics and his enjoyment at using the Merz portfolio on his patients
M-MA-UKI-2150 Date
This article is sponsored by Merz Aesthetics
of Preparation: April 2022
In The Life Of Mr Paul Banwell
Consultant plastic surgeon Mr Paul Banwell details his typical working day and the different commitments he fits into his busy schedule

A typical working day…
As an early riser, my day usually begins at 5:30am, this allows time for some exercise before breakfast then I usually head off to work at 6:30-6:45am. One day a week, I do my NHS skin cancer work where I see urgent skin cancer cases. These include melanomas and squamous cell carcinomas, which have been sent urgently by a GP. I find that these are more prevalent in the summer months, so we are about to get busier! The rest of my week is dedicated to my private clinic, The Banwell Clinic. Our headquarters are based within the McIndoe Centre in East Grinstead, but we also have a beautiful clinic at The Harley Street Hospital in London.
My days vary between operating sessions, all day clinics or teaching and writing. In the mornings, I will do a ward round to check in on my patients who have stayed overnight or have arrived for surgeries and then do the crucial marking-up process. Whilst waiting for the team to get ready for the day ahead, I use my time wisely and complete my letters and any outstanding admin via our paperless computerised management system. Running a busy practice means replying to hundreds of emails throughout the day too in between of performing surgeries or seeing patients!
Career if I wasn’t a plastic surgeon…
I would be an art dealer! I love collecting modern art.
to review other colleagues submitted work for publication. I have lectured extensively around the world for many years, but I am trying to reduce these commitments now to focus on my novel writing, an art project and conservation work.
I am blessed to act as an ambassador and key opinion leader for several companies including RATIONALE skincare from Australia, Dermalux LED, and Motiva who manufacture the latest generation breast implants.
I also have my own health and wellbeing supplement company called ARTIS London, which was set up two years ago during the pandemic. Whilst the range was originally designed specifically for my own patients, it has gathered quite some momentum and we are now supplying to the aesthetics industry as a value-added offering to clinic treatment protocols and to enhance recovery following surgical procedures. We are now excited to be exporting to Southeast Asia and beyond!
I am currently writing two new books. One is an adventure novel with a medical connection, and another is a new edition of our book which has been published by Thieme in four languages already called Female Cosmetic Genital Surgery: Concepts, Classification and Techniques
Favourite thing about my job… Meeting lots of interesting people. Lords and ladies, film stars, authors, dustmen and cleaners – everyone has a story, and it is a privilege to be part of their journey.
Any hobbies…
I have many interests! I enjoy cycling, skiing, kayaking and martial arts.
My day will vary in terms of how many patients I see. Within an NHS clinic I will see 30-40 patients and more than 30 patients a day in my outpatient clinics (cosmetic surgery and skin cancer cases). This is a mix of new consults, follow-ups, local anaesthetic cases, injectables and threads. On an operating day I will perform between six to eight surgeries (many of which are combined cases). My surgical days will consist of breast augmentations, mummy makeovers, labiaplasties, liposuctions, abdominoplasties, eyelid surgery and breast reductions. I try and finish work earlier in the summer months as I think it’s important to enjoy the lighter and warmer evenings, so I try and finish at 6pm. However, in the winter months, I will usually finish at 9pm. In the evenings I like to get some fresh air, devote some time to mindfulness, recharge and take the dog for a walk.
Other work commitments…
As well as my clinical work, I have lots of other work commitments which I need to fit into my day and week! I write articles for medical journals and book chapters but also get asked
The book is a comprehensive review of contemporary practice in this rapidly emerging field and covers new concepts in anatomy, operative techniques and complications. It has received many plaudits and is a great learning tool for any young aspiring surgeons looking to excel in this field. Usually, my day finishes around midnight before catching up on some much needed shut eye!
Most memorable day…
My most memorable day professionally was when I was awarded the Visiting Harvard Professorship in Plastic Surgery. I had to travel to Harvard university and give a lecture in front of many esteemed professional colleagues which was very exciting! It was a standout moment for me and one I will not forget. I have been very blessed!
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
The Last Word
Australians per capita undergo more cosmetic procedures than the US, and the COVID-19 era has further exacerbated the insatiable demand for procedures.1 Yet, like in many other countries, Australia lacks any formal qualification or a consensus of standards that injectors must achieve to prove their competence, which I believe is the current downfall. This opinion piece aims to raise awareness about the issues in another country outside the UK so we can share information of what works, and what doesn’t.
Australian aesthetics
Australia permits doctors, registered nurses, nurse practitioners and dentists to inject. Unlike the UK, non-medics are prohibited from injecting. Each profession injecting is governed by its own college and each profession’s scope of practice is loosely defined by their respective college framework. But, in reality, there are continual inter-college issues that crop up and registered nurses currently cannot work independently; they must work under the supervision of doctors. The definition of ‘scope of practice’ is not explicit in any way when it comes to injecting, and this is where issues have cropped up.
The problem
Many injectors in Australia begin their aesthetic career within ‘chain clinics’ – large franchise models of clinics who typically employ multiple injectors per site.2 These injectors will usually be offered in-house training within their own clinic. The standard and length of this varies widely, from just some informal webinars up to eight full weeks. Injectors who work independently outside of the chain clinic will typically learn to inject via a variety of third-party foundational courses offered across Australia. According to some training provider websites, after doing their two day ‘combined’ course, ‘you will learn all 18 common procedures... after this course you will be able to get indemnity insurance and start treating paying patients straight away’. This model of training has clearly not evolved since the early days of cosmetic injectable training in the early 2000s and yet is still tolerated because there are currently no other credible alternatives. In 2017, a patient named Jean Huang died as a result of a botched breast filler procedure and this sparked a new round of introspection within the industry.3 Knee jerk reactions were made by the various state health departments,4 clinics were visited by undercover health inspectors and one notable prescribing doctor was sanctioned for unsatisfactory professional conduct.5 Some new definitions that mainly affected cosmetic surgeons were made and a clarification of the minimum expected standards,6 but no significant changes came and the status quo continued. In the aftermath of Jean Huang’s death, an enquiry was held in Parliament and representatives of some of the various colleges attended. Notably, the nurses had no cosmetic college of their own and were vulnerable to being sidelined, and so the ‘Cosmetic Nurses Association’ (CAN) was formed in 2020 to advocate for nurses providing non-surgical procedures.7
Suggested steps
Whilst the UK is often used as the worst example of the ‘Wild West’ of injecting, it does have an agreed standard known as the ‘Level 7 Qualification’ that was first adopted by Harley Academy.8 In February 2022, intentions for a newly-proposed license for non-surgical treatments in England were also announced in Parliament.9 So, steps are finally being taken to formalise facial aesthetics as a specialty in its own right.
What I believe is needed in Australia is an open and honest round table discussion to air views in a formal capacity but without government over-reach. We need to try and find a way forward for an agreed consensus in training standards, workplace regulations as well as continuing professional development. In my podcast Inside Aesthetics – Episode 126,10 we took the first step of doing this by bringing together the President of the Cosmetic Physicians College of Australia (CPCA), the President of the newly formed CNA in addition to globally-renowned key
opinion leaders from the plastic surgery and dermatology perspectives. Strong views were exchanged, controversies were brought up, but in the end more common ground was found than division. In the end, the President of the CPCA agreed to meet the President of the CNA for further discussions to resolve their long-standing concerns.
I think it has become increasingly obvious that if we want to recognise facial aesthetics as a true specialty, we’ll likely need to establish a facial aesthetic college that accepts all backgrounds of medical injectors under one united banner. Tribalism in medicine has always seemingly been tolerated but we need to end this immature mentality if we want to create a safer and better environment for both our patients but also the injectors. Without this, we are essentially accepting that poorly trained injectors can continue treating the public with impunity. This makes patients vulnerable to poor results and injuries whilst the territorial fights between the various groups of injectors over the control of the industry and their commercial interests will continue.
Final thoughts
Currently the ball is in the injectors’ hands. They can create change themselves if the will and motivation are there to evolve and elevate what we do. This would seem far more sensible than the prospect of sweeping and imposed changes led by the Government. If regulation is forced onto the industry from the top down, I think it will highly likely be done in way that is far less appealing to work in and will likely be detrimental to the current business model of many clinics. Going forward, we are watching what happens in the UK very closely to see what comes of the new legislation.
Dr Jake Sloane is an aesthetic doctor originally from London who now lives and works in Sydney. He’s an international key opinion leader for Allergan Aesthetics and is currently being mentored by Dr Mauricio De Maio. He co-hosts the aesthetic podcast, ‘Inside Aesthetics’. Qual: BSc, MBChB, MRCS

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022
Dr Jake Sloane outlines the prevalent challenges currently facing the Australian injectables industry as well as a proposed solution
VIEW THE REFERENCES ONLINE! AESTHETICSJOURNAL.COM


beautyuncovered.com/bul @beautyuncovereduk Headline sponsor 3 reasons your patients need to attend: 1. Highlights the importance of safe, regulated practice 2. Enhances their knowledge of the treatments you offer 3. Builds their trust in you & the aesthetics industry PLUS get your free VIP HCP tickets. Limited availability. Scan to get exclusive DISCOUNTS for YOUR patients


Did you know? 01 A reduced inflammatory profile 02 Uniform and even degradation in the skin 03 Smooth injection optimal tissue integration
INTERESTED IN THE LATEST HA TECHNOLOGY? PURCHASE REVANESSE ® FOR YOUR CLINIC EXCLUSIVELY THROUGH HEALTH XCHANGE 1. Gold MH et al. J Drugs Dermatol. 2018 Jan 1;17(1):66-73. PMID: 29320589. 2. Testing from Prollenium Medical Technologies Inc. Data on file. 3. Rheologic and Physicochemical Properties Used to Differentiate Injectable Hyaluronic Acid Filler Products. Plast Reconstr Surg. 2019; 143(4): 707e-720e. 4. Laeschke K. Semin Cutan Med Surg. 2004 Dec;23(4):214-7. doi: 10.1016/j.sder.2004.09.005. PMID: 15745227.
OTHER DERMAL FILLER
