
VOLUME 10/ISSUE 3 - FEBRUARY 2023 Managing No-Shows Max Hayward advises on reducing your no-show clinic appointments Addressing Acne Scarring Hannah Depledge treats a patient’s active acne and scarring holistically Treating SOC with Devices Practitioners discuss skin rejuvenation using energy-based devices in SOC patients CPD: Facial Rejuvenation Emma Coleman provides an overview of four treatments for facial rejuvenation by Adverse events should be reported. For the UK, Reporting forms and information can be found at www.mhra.gov.uk/yellowcard or search for Yellow Card in the Google Play or Apple App Store. For Ireland, Suspected adverse events can be reported via HPRA Pharmacovigilance, Website: www.hpra.ie; Adverse events should also be reported to Galderma (UK) Ltd, Email: medinfo.uk@galderma.com Tel: +44 (0) 300 3035674 UKI-RES-2200360 DOP December 2022 FOR ANY & EVERY LOOK ACE2023 REGISTRATION OPEN!
One device. Endless possibilities for your business.
Get the best skin of your life.











































A single device for head-to-toe glow: deliver face, body, lips and scalp treatments. Limitless personalisation options. @hydrafacialuk www.hydrafacial.co.uk 01788 572 007
Inject more beauty into your life
The Teoxane drop is where innovation meets beauty. In every drop of Teoxane’s designer fillers and dermocosmetics, you will find a concentrate of Swiss science that enriches lives from within.

THE LEADING SWISS EXPERT IN THE SCIENCE OF HYALURONIC ACID VISIT TEOXANE.COM
News
The latest product and industry news
16 News Special: Exploring Filler Longevity
Aesthetics gets industry perspectives on discussions about filler longevity
18 Advance Your Skills with TEOXANE at ACE
Headline Sponsor TEOXANE reveals unmissable ACE 2023 clinical content
CLINICAL PRACTICE
21 Special Feature: Treating Skin of Colour with Devices

Three practitioners discuss skin rejuvenation using devices in SOC patients
29 CPD: Analysing Facial Rejuvenation Treatments
Emma Coleman outlines four treatments for facial rejuvenation
35 Providing Bespoke Lip Service to Your Patients
Galderma puts a smile on patients’ lips with innovative HIT Kiss & Smile
39 Understanding Ablative vs Non-Ablative Lasers
Miss Jennifer Doyle discusses ablative and non-ablative laser resurfacing
42 Exploring Hand and Feet Perspiration
Dr Ros Jabar outlines the causes and treatments of excessive perspiration
45 Case Study: Treating Acne Scarring
Hannah Depledge combines RF microneedling with skincare to treat active acne and scarring
49 Achieving Clinical Efficacy when Performing Microneedling Treatments
Dermalogica focuses on upskilling practitioners to meet industry standards

50 Case Study: Utilising Laser for Fat Loss
Dr Abs Settipalli shares a case study using green laser for reducing fat
53 A History of Radiofrequency
Dr Uliana Gout and Dr Samantha Hills outline the development of radiofrequency in aesthetics
58 Our Antioxidant Answer for What Your Skin Needs
SkinCeuticals provides insight into 30 years of research in every drop
59 Abstracts
A round-up and summary of useful clinical papers
IN PRACTICE
60 Addressing Unconscious Bias
Kimberley Cairns explores how unconscious bias can potentially impair aesthetic practice
63 Managing No-Show Appointments
Max Hayward advises how to manage and reduce no-show clinic appointments
66 Understanding Data Analytics
Carla Jones discusses the importance of using data analytics for your business
69 In Profile: Dr Saleena Zimri
Dr Saleena Zimri shares how her passion for skin led her to run her own clinic franchise

70 The Last Word: Purchasing New Devices
Dr Nestor Demosthenous and Amanda Demosthenous debate the pros and cons of investing in the latest devices
News Special: Exploring Filler Longevity
Page 16
Special Feature: Treating Skin of Colour

Page 21
Clinical Contributors
Emma Coleman is an aesthetic nurse who opened her first aesthetics clinic in Orpington in 2015 and completed a dermatology diploma with distinction in 2019. She has recently opened a second clinic in Bromley, and her passion lies in providing holistic treatments.

Miss Jennifer Doyle is a consultant ophthalmic and oculoplastic surgeon based at The Clinic at Holland Park and at Milton Keynes University Hospital. She has completed the Level 7 diploma in Injectables and served as a lead trainer for Harley Academy.

Dr Ros Jabar is an aesthetic practitioner and divides her time between the polytrauma unit in the University Hospital of Wales and Ros Medics, an aesthetic, cosmetic and skincare clinic. Dr Jabar has a background in accident and emergency, acute and general medicine.
Hannah Depledge is an aesthetic nurse prescriber with more than seven years’ experience in the aesthetics specialty with a special interest in treating skin. She was an NHS palliative care nurse for 11 years before opening Eterno Aesthetics Medical Skin Clinic in Sheffield in 2019.
Dr Abs Settipali has practised and studied aesthetics under some of the world’s most renowned cosmetic doctors. He brings his wealth of experience to doctors, dentists and nurses across the world through lecturing cosmetic medicine internationally.
Dr Uliana Gout is an aesthetic practitioner and founder of London Aesthetic Medicine Clinic in Harley Street, London. She is also general secretary of the International Peeling Society and is heavily involved in international research and medical textbooks.

Dr Samantha Hills is the clinical director at Lynton Lasers and oversees the company’s Clinical and Training Programme. In 2017, Dr Hills was appointed an honorary lecturer in the Department of Musculoskeletal and Dermatological Sciences at the University of Manchester.


Become a Member of Aesthetics! Join the Aesthetics Community as a Full Member to receive the monthly Aesthetics journal, among many other exclusive benefits. Visit aestheticsjournal.com to sign up!
Contents • February 2023
MONTH IN FOCUS: GROWING YOUR PRACTICE • A History of Dermal
in
NEXT
Fillers • Networking
Aesthetics 08
go go go


Letybo® brings practitioners a new option to the current aesthetic market and provides aesthetic professionals and their patients with a notable efficacy and confirmed tolerability.















1. Mueller DS, Prinz V, Adelglass J, Cox SE, Gold M, Kaufman-Janette J et al. Efficacy and Safety of Letibotulinum Toxin A in the Treatment of Glabellar Lines: A Randomized, Double-blind, Multicenter, Placebo-controlled Phase 3 Study. Aesthet Surg J. 2022; 42(6): 677- 88. ; 2. Letybo® smPC, https://www.medicines.org.uk/emc/product/13707 2022


Undesirable
effects:






new ways ADLET0822UKf (QR: VID2LET0822UK) Date of preparation: August 2022
1,2,*
*Letybo® is indicated for the temporary improvement in the appearance of moderate to severe vertical lines between the eyebrows in adults <75 years old seen at maximum frown (glabellar lines), when the severity of the facial lines has an important psychological impact. **Response rate was defined as a ≥ 1-point reduction in FWS at maximum frown based on the investigators assessment. References:
Most
SmPC. Legal Category: POM; Pack size: Packs containing 1 5ml vial. Multipack containing 2 (2 packs of 1) vials; Price list: UK - 1x5ml: 65GBP, 2x5ml: 120GBP; MA Number: PL 29863/0002; PA Number: PA0846/001/001; MA Holder: Croma-Pharma GmbH, Industriezeile 6, 2100 Leobendorf, Austria; Date of preparation: 11/04/2022; Unique ID no CRP001/001; Adverse events should be reported. Reporting forms and information can be found at: UK - http://yellowcard.mhra.gov.uk/ or search for MHRA Yellow Card in the Google Play or Apple App Store. IE - HPRA Pharmacovigilance Website: www.hpra.ie. Adverse events should also be reported to Croma Pharma GmbH on 0118 206 6513 94% response rate 4 weeks post injection 1,** Demonstrated high patient satisfaction2 Proven consistent effi cacy and tolerability with repeated injections for up to 12 months 1,2 Scan for Reconstitution Instructions Finalist
Letybo 50 units powder for solution for injection; Abbreviated Prescribing Information: Please refer to the Summary of Product Characteristics (SmPC) before prescribing. Presentation: One vial contains 50 units botulinum toxin type A produced by Clostridium botulinum. After reconstitution each 0.1 mL of the solution contains 4 units. Indication: For the temporary improvement in the appearance of moderate to severe vertical lines between the eyebrows in adults <75 years old seen at maximum frown (glabellar lines), when the severity of the facial lines has an important psychological impact. Dosage and administration: Should only be administered by physicians with expertise in this treatment. Posology: The recommended dose is a total of 20 units divided into five injections of 4 units (0.1 mL) each: 2 injections in each corrugator supercilii muscle and 1 injection in the procerus muscle. Botulinum toxin units are not interchangeable from one product to another. Doses recommended are different from other botulinum toxin preparations. Treatment interval should not be more frequent than every three months. In the absence of any undesirable effects secondary to the previous treatment session, a further treatment session with at least a three-month interval between the treatment sessions is possible. The efficacy and safety of repeat injections beyond 12 months has not been evaluated. Special populations: No specific dose adjustment is required for use in the elderly older than 65 years of age. Letybo is contraindicated in patients 75 years or older. There is no relevant use in the paediatric population. Method of administration: Intramuscular use. Care should be taken to ensure that Letybo is not injected into a blood vessel. Contraindications: Hypersensitivity to the active substance or to any of the excipients. Generalised disorders of muscle activity (e.g. myasthenia gravis, Lambert-Eaton syndrome, amyotrophic lateral sclerosis). Presence of acute infection or inflammation at the proposed injection sites. Patients with bleeding disorders. Warnings and Precautions: Injection into vulnerable anatomic structures must be avoided. Avoid use when the muscle shows excessive weakness or atrophy. Risk of eyelid ptosis following treatment. Procedurerelated events: Needle-related pain and/or anxiety have resulted in vasovagal responses, including transient symptomatic hypotension and syncope after treatment with other botulinum toxins. Pre-existing neuromuscular disorders: Patients with unrecognised neuromuscular disorders may be at increased risk of clinically significant systemic effects including severe dysphagia and respiratory compromise from typical doses of botulinum toxin type A. Hypersensitivity reactions: An anaphylactic reaction may occur after injection of botulinum toxin. Epinephrine (adrenaline) or any other anti-anaphylactic measures should therefore be available. Local or distant spread of toxin effects: Adverse reactions possibly related to the spread of toxin distant from the site of administration have been reported. Patients may experience exaggerated muscle weakness. Swallowing and breathing difficulties are serious and can result in death. Use not recommended in patients with a history of dysphagia and aspiration. Patients should be advised to seek immediate medical care if swallowing, speech or respiratory disorders arise. Pregnancy & Lactation: Not recommended during pregnancy or lactation and in women of childbearing potential not using contraception.
common effects are headache and injection site reaction. Very rarely aspirational pneumonia. For full list of side effects, consult
2023
Shannon Kilgariff Editor & Content Manager @shannonkilgariff

You must have noticed the hype surrounding dermal filler longevity this past month. If you haven’t, then I suspect you are either still in holiday mode or working so hard following the festive period that you haven’t had a chance to check the news. As a recap, well-known beauty journalist Alice Hart-Davis published a report in the Daily Mail sharing an MRI scan showing her face is still full of fillers, even though she hadn’t had an injection in four years!
The imagery is undoubtedly impactful, and I see why it comes as a shock to so many people in the public that fillers are lasting longer than they say on the label. Like many of you, I know this concept isn’t new and I have heard of many anecdotal reports as well as ongoing research in this area. However, it’s sparked some fascinating discussions, which we have reported on in our News Special this month (p.16). I think it’s exciting that awareness and research in this area is growing – the journal will be sure to share anything new that comes to light on this fascinating topic.
Clinical Advisory Board
Also in the journal this month, we have a lot of content focusing on energy-based devices and how you can utilise different technologies in your practice. On p.21 we delve into how to safely rejuvenate skin of colour with devices, alongside lots more insightful content including the differences between ablative and non-ablative lasers (p.39), laser for fat reduction (p.50) and a history of radiofrequency (p.53), among many other useful articles.
For those who are keen to learn more about how aesthetic devices can benefit your patients’ results as well as your revenues, then the upcoming ACE 2023 conference is the best place for you! There will be more than 20 companies showcasing the latest lasers, HIFU and radiofrequency machines, plus many more products and treatments you can add to your treatment offering. Go to p.18 to register free.
Of course, next month on March 11, we are also hosting The Aesthetics Awards! I’m so excited to find out who this year’s Winners are and to see everyone glammed up! I hope you can join us – tickets are selling out fast so get yours now by scanning the QR code on p.68 – see you there!
Leading figures from the medical aesthetic community have joined the Aesthetics Advisory Board to help steer the direction of our educational, clinical and business content
Sharon Bennett is chair of the British Association of Cosmetic Nurses (BACN), previous UK lead of the BSI committee for aesthetic non-surgical standards, and member of the Clinical Advisory Group for the JCCP. She is a trainer and registered university mentor in cosmetic medical practice, and is finishing her MSc at Northumbria University. Bennett has won the Aesthetics Award for Nurse Practitioner of the Year and the Award for Outstanding Achievement.
Sharon Bennett, Clinical Lead
Mr Naveen Cavale has been a consultant plastic, reconstructive and aesthetic surgeon since 2009. He has his own private clinic and hospital, REAL, in London’s Battersea. Mr Cavale is the national secretary for the ISAPS, president of the Royal Society of Medicine, and vice-chair for the British Foundation for International Reconstructive Surgery.

Jackie Partridge is an aesthetic nurse prescriber with a BSc in Professional Practice (Dermatology). She has recently completed her Master’s in Aesthetic Medicine, for which she is also a course mentor. Partridge is a founding board member of the British Association of Cosmetic Nurses and has represented the association for Health Improvement Scotland.
Mr Adrian Richards is a plastic and cosmetic surgeon with 18 years’ experience. He is the clinical director of the aesthetic training provider Cosmetic Courses and surgeon at The Private Clinic. He is also a member of the British Association of Plastic and Reconstructive and Aesthetic Surgeons and the British Association of Aesthetic Plastic Surgeons.

PORTFOLIO MANAGEMENT
PUBLISHED BY
Alison Willis • Director T: 07747 761198 | alison.willis@easyfairs.com
EDITORIAL
Shannon Kilgariff • Editor & Content Manager
T: 0203 196 4351 | M: 07557 359 257 shannon@aestheticsjournal.com
Holly Carver • Senior Journalist | T: 0203 196 4427 holly.carver@easyfairs.com

Ellie Holden • Journalist | T: 0203 196 4265 ellie.holden@easyfairs.com
Kate Byng-Hall • Journalist | T: 0203 196 4265 kate.byng-hall@easyfairs.com
DESIGN
Peter Johnson • Senior Designer
T: 0203 196 4359 | peter@aestheticsjournal.com
Miss Elizabeth Hawkes is a consultant ophthalmologist and oculoplastic surgeon. She is the lead oculoplastic surgeon at the Cadogan Clinic, specialising in blepharoplasty and advanced facial aesthetics. Miss Hawkes is a full member of the BOPSS and the ESOPRS and is an examiner and fellow of the Royal College of Ophthalmologists.
Dr Tapan Patel is the founder and medical director of PHI Clinic. He has more than 16 years’ clinical experience and has been performing aesthetic treatments for more than 14 years. Recently, he was listed in Tatler’s Top 30 Anti-Ageing Experts. Dr Patel is passionate about standards in aesthetic medicine.

Dr Souphiyeh Samizadeh is a dental surgeon with a Master’s degree in Aesthetic Medicine and a PGCert in Clinical Education. She is the founder of the Great British Academy of Medicine and Revivify London Clinic. Dr Samizadeh is a Visiting Teaching Fellow at University College London and King’s College London.


ADVERTISING & SPONSORSHIP
Courtney LeBorgne • Event Director
T: 0203 196 4300 | M: 07818 118 741 courtney.leborgne@easyfairs.com
Judith Nowell • Business Development Manager

T: 0203 196 4352 | M: 07494 179535 judith@aestheticsjournal.com
Chloe Carville
• Sales Executive
T: 0203 196 4367 | chloe.carville@aestheticsjournal.com
Emma Coyne • Sales Executive
T: 020 3196 4372 | emma.coyne@easyfairs.com
MARKETING
Aimee Moore • Marketing Manager

T: 020 3196 4370 | aimee.moore@easyfairs.com
Emma Kurzyca • Marketing Assistant
T: 020 3196 4306 | emma.kurzyca@easyfairs.com
WE WANT TO HEAR FROM YOU!
Do you have any techniques to share, case studies to showcase or knowledge to impart?
Email: editorial@aestheticsjournal.com
Dr Stefanie Williams is a dermatologist with a special interest in adult acne, rosacea and aesthetic medicine. She is the founder and medical director of multi-award winning EUDELO Dermatology & Skin Wellbeing in London, and creator of Delo Rx skincare. She is the author of three books and has published more than 100 scientific articles, book chapters and abstracts.
ARTICLE PDFs AND REPRO
Material may not be reproduced in any form without the publisher’s written permission. For PDF file support please contact Chloe Carville, contact@aestheticsjournal.com
Aesthetics Media
Editor’s letter
DISCLAIMER: The editor and the publishers do not necessarily agree with the views expressed by contributors and advertisers nor do they accept responsibility for any errors in the transmission of the subject matter in this publication. In all matters the editor’s decision is final.
© Copyright 2023 Aesthetics. All rights reserved. Aesthetics is published by Aesthetics Media Ltd, which is registered as a limited company in England; No 9887184
Aesthetics Aesthetics @aestheticsjournaluk
Talk #Aesthetics
#Aestheticsjournal
Dr Salma Haque

@saya.aesthetics
Essential Sunday reading – the new Aesthetics journal! Great way to start the year.

Prescribing HIS releases Scottish regulation update
Healthcare Improvement Scotland (HIS) has released an exclusive statement to the Aesthetics journal clarifying its plans to regulate non-prescribing medical aesthetic practitioners. This comes following reported confusion and shock among non-prescribing medical aesthetic practitioners in Scotland, who were told in December they may no longer be able to perform dermal filler injections without a prescriber present on-site following updated guidance surrounding Regulation 12.
#Demonstrations
Dr Vincent Wong
@drvincentwong
At ReLife’s Anatomical Cadaveric Aesthetic Demonstration meeting. There’s so much to learn and discuss!
In the statement, head of service review at HIS Kevin Freeman-Ferguson explained that the reason for implementing regulation changes was an increase in individual practitioners establishing private aesthetic clinics. This has triggered concerns that not all clinics have enough qualified professionals on-site to deal with emergencies when they arise, such as when hyaluronidase is required to treat adverse events related to dermal filler. He emphasised that the number of qualified staff at each premises should be proportionate to how many patients it treats.
Freeman-Ferguson reiterated that safety is at the core of HIS’ aims when introducing new regulation, so it will be prioritising addressing adequate training for all practitioners, meaning any new and existing clinics must be able to demonstrate that they are planning to introduce a prescriber to the practice within an agreed time frame. Other training requirements HIS is considering include basic or advanced life support, anaphylaxis and managing aesthetic complications.
#TheAestheticsAwards
Dr Arreni Somasegaran
@dr.arreni
I’m so excited and honoured that I’m officially a Finalist for The AlumierMD Award for Rising Star of the Year 2023!
#Wellness
Dr Ashwin Soni
@thesoniclinic
A lovely event with wellbeing consultant Anni Hood chatting all things wellness.

Freeman-Ferguson commented, “Private clinics that provide cosmetic interventions in Scotland and HIS share a common goal: ensuring that people who receive cosmetic interventions do so in an environment that is as safe as possible. Most private clinics in Scotland are well run and have safety as a clear priority, as can be seen in our inspection reports. However, it has become increasingly clear to us that we need to do more to keep people safe.”
To read the full statement, go to www.aestheticsjournal.com and read ‘Special Report: HIS Update to Scottish Regulation’ online now.
Toxin
JCCP announces national toxin complications survey

#Education
Anna Kremerov
@anna_medical_aesthetics
We had such a great day filming with the lovely Sinclair UK team. So much exciting and educational content coming soon!
The Joint Council for Cosmetic Practitioners (JCCP) has announced a national survey into patients’ experiences of botulinum toxin complications in the UK. The survey, conducted in collaboration with researchers at University College London (UCL) and the British Association of Aesthetic Plastic Surgeons (BAAPS), will aim to document patients’ experiences of toxin complications. The organisations hope this collation of evidence can be used to improve practitioners’ knowledge of potential adverse events connected to the treatment. Professor David Sines, chair of the JCCP, said, “The JCCP is delighted to be a partner in this collaborative research project. The JCCP is committed to encouraging the collection of objective empirical data to assist in the construction of a robust and reliable evidence base upon which responsive systems of clinical governance and national oversight can be based for the UK aesthetic sector.” The survey can be accessed via UCL online now.

Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Follow us on Instagram @aestheticsjournaluk
First details of ACE 2023 agenda revealed
The first details of the unmissable talks at this year’s ACE have been revealed, with 16 CPD points on offer across five conferences.

ACE 2023 will return to the Business Design Centre in London on March 10-11, providing a range of clinical and business content for practitioners across the Innovation Stage, In Practice Theatre, Masterclasses, Symposiums and Teoxane Conference. The industry’s top companies and organisations will be presenting educational content, including Allergan, Croma and Galderma, as well as some of the industry’s biggest names performing live demonstrations. On the Friday evening at 5pm, Hydrafacial will be hosting networking drinks on its stand for visitors to make new connections. As well as this, HA-Derma is ACE’s VIP sponsor, providing refreshments throughout the conference, and a VIP hair and makeup lounge and drinks reception for Finalists and guests to get glam and celebrate before The Aesthetics Awards on the Saturday. Alongside this, there will be an exhibition of more than 80 aesthetic companies, from dermal filler and toxin brands to aesthetic devices and skincare, ready to chat about new innovations. Also discover business and clinic management solutions to help boost your business at the In Practice Zone.
Courtney LeBorgne, event director of Aesthetics, commented, “I am so excited for all our delegates to see the wonderful agenda we have prepared for ACE 2023. Medical innovation and excellence is our top priority, so I also look forward to welcoming our wonderful exhibitors who are keen to share their knowledge and insights. I can’t wait to see you all there!”
Advertising
Vital Statistics
Scan the QR code to view the agenda and register for free today.
ASA issues ruling against weight loss injection ads
The Advertising Standards Authority (ASA) has issued a ruling against an aesthetic clinic following Whatsapp and Instagram advertisements of prescription-only weight loss injections.
The ASA found that the clinic, situated in Hertfordshire, England, had used two Whatsapp messages and one Instagram story post to promote the use of Ozempic injections – a form of semaglutide injection – as a weight management solution for its patients.
The advertisements, disseminated in November 2022, stated, “We only have enough dosage for 10 clients so please message ASAP to be added to waiting list,” alongside patient testimonials and before and after images. The ASA ruled that semaglutide injections are prescription-only medications (POMs), so should not be advertised to patients. The clinic in question was willing to remove and retract the advertisements, and the ASA emphasised that no ads promoting POMs can be distributed going forward.
Between
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Of 3,500 respondents, 78% of those considering aesthetic treatments feel the cost of living crisis will impact them
(RARE: Group, 2022)
Out of 47,000 13- to 24-year-olds, 68% said that members of their social group have undergone a cosmetic procedure
(VICE UK, 2022)
Bell’s palsy accounts for around 80% of all facial palsy cases, affecting 20-30 people per 100,000 each year
(Facial Palsy UK, 2022)
Of 5,000 UK students, 37% refuse to buy products with ingredients harmful to the environment
(UNiDAYS, 2022)
Of 2,000 menopausal women, 43% said they avoid looking in mirrors due to body and skin issues
(Dr Yusra Clinics, 2022)
5% and 15% of aesthetic patients meet the diagnostic criteria for BDD
(Nuffield Council Bioethics, 2022)
Conference
Events diary
10th February
Menopause in Aesthetics (MIA) www.menopauseaia.co.uk
10th-11th March
ACE 2023 www.aestheticsconference.com
11th March
The Aesthetics Awards 2023 www.aestheticsawards.com
21st April
BACN Spring Symposium www.bacn.org.uk/events
23rd May
British Association of Sclerotherapists Conference www.bassclerotherapy.com/events
Galderma to hold launch event for Alluzience

Pharmaceutical company Galderma is hosting a launch event for its new liquid neuromodulator Alluzience. Following a soft launch in 2022, Alluzience has been trialled in selected practices across the UK and Ireland and is now available to purchase at Medfx in the UK and BFM in Ireland. The launch event will be invite only for in-person guests, but will be live-streamed for registered healthcare professionals to watch. The full agenda is still to be confirmed but will be taking place on March 9 at 8 Northumberland Avenue, London, with doors opening at 4:30pm and the event being held between 5pm-7pm GMT. Galderma will be revealing more details about Alluzience at ACE, with a spot on the Symposium Agenda at 12:30pm on March 11. Turn to p.18 to register now.
Croma-Pharma releases new detox mask
IN THE MEDIA
BBC podcast puts spotlight on BDD
An episode of the BBC podcast ‘Room 5’ with host Helena Merriman has shone a light on the struggle of coping with a diagnosis of body dysmorphic disorder (BDD). The episode features BDD sufferer Tilly sharing her experience of coping with symptoms of BDD since the age of 13. With a 2017 NHS study finding that more than one in 20 (5.6%) 17- to 19-year-old girls in the UK experience BDD, aesthetic practitioners must be aware of the pertinence of the disorder.
Skin flooding skincare hack trends on TikTok
Another skincare trend is taking over social media platform TikTok – this time, it’s ‘skin flooding’. This refers to the method of moisturising the skin as much as possible through layering serums, face mists and lightweight moisturisers to address dryness and dehydration. The theory is that keeping skin damp will optimise absorption of serums such as hyaluronic acid. Aesthetic nurse prescriber Alice Henshaw said, “Skin flooding can be very beneficial if you do suffer from dry skin as it helps product absorption, which in turn can help to keep your skin hydrated for longer.”
Aesthetic pharmaceutical company Croma-Pharma has unveiled its new detox face mask.
According to the company, the mask aims to purify the skin and provide a smooth-looking and radiant skin appearance. The sheet material is made of 40% charcoal powder to provide the benefits of charcoal without creating a mess.
Key ingredients include bakuchiol, white willow bark and magnolia leaf for gentle exfoliation; charcoal powder to remove impurities from the skin; hyaluronic acid and poly-y-glutamic acid to hydrate, plump and reduce dryness as well as nutgrass to help smooth skin texture, explains the company.
Aesthetic practitioner Dr Amiee Vyas, said, “The detox mask is a great addition for congested and blemish prone skin. It is particularly useful for those patients who experience dehydration with their breakouts and for those that may be using prescription preparations as it leaves the skin calm, supple and moisturised post-use.”
Recruitment
Teoxane introduces new team member
Aesthetic manufacturer Teoxane has welcomed Grace Hoskins as its new digital marketing manager. Hoskins has 10 years of digital marketing experience, knowledge and skills and will be focusing on continuing to create a space for aesthetics within the wellness environment.
According to the company, Hoskins and the digital team will be supporting Teoxane customers with their own digital infrastructures, offering advice and insights to further support clinics in all areas of their business. She commented, “I am so excited to have joined the team at Teoxane UK. With a plethora of exciting campaigns and events planned for 2023, it’s a fantastic time to have come on board and I’m looking forward to aligning Teoxane’s digital marketing activities with the hard work that has been completed already, further cementing the brand as a leading hyaluronic acid dermal filler and dermocosmetics provider.”

Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
What’s trending in the consumer press Toxin
Skincare
BFIRST unveiled as Aesthetics Awards charity partner
The British Foundation for International Reconstructive Surgery and Training (BFIRST) will be returning as the charity partner for The Aesthetics Awards 2023. BFIRST, the official charity of the British Association of Plastic, Reconstructive and Aesthetic Surgeons (BAPRAS), prioritises high global standards in surgery through training and local organisation. This includes face-to-face trips such as a visit in September 2022 to Tumbi Regional Referral Hospital in Tanzania, during which plastic surgeons Mr Naveen Cavale, Mr Foiz Ahmed and Mr Asmat Din offered hands-on learning about treating congenital hand abnormalities and burn deformities. At the Awards ceremony at Grosvenor House, London on March 11, BFIRST representatives will be taking donations for this worthy cause.
Mr Cavale, chair of BFIRST, commented, “I’m really grateful and happy that BFIRST has been chosen as the charity partner of The Aesthetics Awards once more. The Awards guests were amazingly generous last year, raising just short of £15,000 in one evening! We are hopeful that we can all out-do ourselves this year as BFIRST’s work has restarted in earnest, following the end of COVID-19 restrictions. We are so looking forward to a fantastic night!”

Head to p.12 to get your tickets to the glamourous Aesthetics Awards today!
Research
Link between perceived age and health issues unveiled
New research has shown a link between how old a person looks and their risk of age-related health issues, suggesting that our physical and mental age is reflected on our faces.
The research, published in the British Journal of Dermatology, involved 2,679 men and women (median age 65.8 years). High-resolution facial photographs from the front and side were taken with any cosmetics, creams or jewellery removed. An independent panel was asked to estimate the age of each participant using the photographs.
The perceived age of the participants was scored by taking the difference between the actual age and the age guessed by the panel. Researchers from Erasmus University Medical Centre Rotterdam and Unilever Research and Development grouped participants based on perceived age scores and reviewed lifestyle and health data. Lifestyle factors included body mass index (BMI), UV exposure and smoking status, while the health data included renal, cardiovascular and lung conditions as these were strongly associated with age. Researchers also looked at muscle and bone health issues, eye health issues, age-related hearing loss and a measure of cognitive impairment.
The youngest-looking group was guessed to be on average five years younger than their chronological age, and was predominantly male (61%), less often a smoker and had the highest BMI (probably due to the filler effect of facial fat, according to the authors). Looking younger was linked with higher cognitive function and a lower risk of chronic obstructive pulmonary disease, age-related hearing loss, cataracts and osteoporosis. To conclude, researchers believe the concept of perceived age could be used as a diagnostic clue in clinical settings, and used to create easy-to-use models that map shared causes of ageing across different organ systems.
BACN UPDATES

A round-up of the latest news and events from the British Association of Cosmetic Nurses

BACN SPRING SYMPOSIUM
We’re thrilled to announce our second annual Spring Symposium, set to take place at the prestigious Royal Society of Medicine in London on Friday April 21, 2023!
The day-long event will have a robust agenda filled with a wide range of fascinating subjects, exhibiting an extremely high calibre of content for those who are interested in deepening their knowledge and experience.
In addition to the educational programme, the Symposium offers a chance for members and guests to network with their peers and establish valuable connections within the industry.
“We are thrilled to be hosting the Spring Symposium at the Royal Society of Medicine,” said BACN chair Sharon Bennett, “This is a fantastic opportunity for our members to learn from the best in the industry and to stay up-to-date with the latest developments in aesthetic medicine. We hope to see as many of our members as possible at the event.”
This is a real highlight of the BACN 2023 calendar, and not one to be missed! We’ve already had a fantastic response from members, with tickets flying off the shelves. Tickets are available at the fixed rate of just £99 via the BACN events website, and spaces are limited. You can purchase your Spring Symposium tickets on the BACN event page now – just scan the QR code below!
BACN MAP-IQ ASSESSOR PROGRAMME
On November 18 2022, the BACN officially opened applications to BACN MAP-IQ Assessor Programme. Since then, we’ve had more than 50 applications from members wanting to take part in the course. The BACN, working alongside MAP-IQ, has agreed to sponsor a new L3 Certificate in Assessing Vocational Qualifications in Aesthetics. This is part of the BACN strategy to develop its own in-house assessment capabilities alongside the introduction of its ‘Career Structure for Aesthetic Nurses’. The qualification is recognised and enables those who have successfully completed the programme to assess across any vocational area, focusing specifically on aesthetics. With the overwhelming response to the scheme, the sponsorship programme is set to run again in March 2023 following the first intake of members this winter.
This column is written and supported by the BACN
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Awards
Development
AWARDS
Join Your Colleagues at The Aesthetics Awards

With voting and judging having come to a close, finalising the results for each Aesthetics Awards category is well underway, and there is now just over one month left until this year’s Winners are revealed! With only five weeks to go, tickets to the ceremony are selling out fast so make sure you get yours now to avoid missing out on the biggest event in the aesthetics calendar.
Merz Aesthetics offers new features on Events platform
Pharmaceutical company Merz Aesthetics has relaunched its Events platform with new features and content. The company explains that some of the new content includes dermal fillers, patient journey, consultation, ultrasound technology, business, marketing and insurance. The content is not CPD certified.
Gillian Kennedy, country manager, said, “We have an opportunity to elevate standards and bring more inclusion and equity in our industry through the Events platform. Available to clinic teams as well as the healthcare professional, the Events educational offering aims to empower everyone in the clinic to be clear about the positive role they can have on patients’ lives.”
Finance
PLIM officially launches payment solution
Experience a brand new venue
The ceremony will take place on March 11 after the second day of ACE and will be held for the first time at the dazzling Grosvenor House, London. With greater capacity than ever, The Aesthetics Awards will play host to all the biggest names, companies and brands in the medical aesthetic specialty. Make the most of your evening by building connections with both established and upcoming practitioners and the minds behind breakthrough products, all while celebrating the wonderful achievements of the industry throughout the last year.
Get your tickets now!
You can take part in the evening of glitz and glamour by purchasing either a single ticket or a table of 10. Prices are as follows:
Single ticket: £340
Table of 10: £3,400
By purchasing a ticket, you will receive a delicious three-course meal; champagne on arrival and half a bottle of wine per person at dinner; a live band and DJ so you can dance into the night; professional photographs; entertainment and the chance to be the first to know who and what are the stars of the aesthetics industry for 2023.
To purchase your ticket, scan the QR Code below. The Aesthetics team can’t wait to see you all there!
Scan the QR code to book your tickets now!
Aesthetic service provider PLIM has officially launched its payment solution platform after a successful beta launch in August 2022. PLIM Finance aims to make UK beauty and aesthetics services available to all with a buy now, pay later scheme. The platform offers the ability to spread upscale treatment payments over four or 12 months. The company explains that it provides full payment with a 25% deposit, with every customer awarded a credit limit tailored to them. CEO of PLIM, Nada Ali Redha said, “We are very excited to go live and curious to see how the market reacts to our product. We strive to make wellbeing accessible to everyone.”
PLIM is sponsoring the In Practice Theatre at ACE 2023 on March 10-11, with talks across both days. Turn to p.18 to register today.
Device
Sofwave cellulite technology receives FDA clearance
Medical device company Sofwave has received US Food and Drug Administration (FDA) clearance for a cellulite treatment to add to its SUPERB (synchronous ultrasound parallel beam) technology.

According to the company, SUPERB can already be used to treat wrinkles and fine lines on the face and neck, and this new clearance means cellulite treatment is now recommended to UK users, expanding the device’s potential.
Aesthetic practitioner and Sofwave user Dr Mahsa Saleki said, “We are thrilled that we can now treat cellulite with our Sofwave device. Non-invasive treatment of cellulite is one of the hardest concerns to treat, but also the most desired body treatments in medical aesthetics. Sofwave fills a gap in the market with incredible results.”
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Counterfeit Profhilo surfaces in the UK
There have been reports of counterfeit Profhilo circulating in Europe and Asia and affecting UK and Ireland markets, according to the product’s manufacturer IBSA Derma.
The company emphasised in a statement that packaging of the counterfeit product is so similar to the genuine one that the counterfeit is undetectable if not examined by the manufacturer. Even the unique product codes on each box have been replicated on the counterfeits. It is unknown how many counterfeit units of Profhilo have been produced or sold, and it is also unknown what the counterfeit products contain from box to box, so it is possible that it could be harmful when used.

IBSA states that the only way to guarantee the product is genuine is to purchase Profhilo directly from HA-Derma or HA-Derma’s exclusive partner pharmacies. Due to the patented technology used by IBSA to produce Profhilo, it is impossible to recreate it, according to the company. In addition, IBSA highlights that purchasing from outside of the official supply chain may affect your insurance cover. Other suppliers not on HA-Derma’s list could be sourcing the products from the European suppliers where the counterfeits are circulating. According to IBSA, as the officially appointed distributor for this region, HA-Derma is the only company procuring Profhilo directly from IBSA Derma and securely delivering to the UK and Ireland while compliant with the requirements IBSA imposes on the transport of its medical devices.
According to Iveta Vinkler, director of HA-Derma, “This is a serious issue. IBSA Derma has issued the statement to warn those who purchase Profhilo from unauthorised sources that IBSA cannot guarantee the authenticity, stability nor safety of the product unless it is sold directly by IBSA Derma or its authorised distributors.”
Appointment
Harpar Grace welcomes new chief operating officer

Aesthetic distributor Harpar Grace International (HGI) has welcomed Peter Atkin as its new chief operating officer after his promotion from operations director.
HGI says that with a specialism in data, Atkin will focus on supporting founder Alana Marie Chalmers across operations, business delivery and project success during the company’s phase of international expansion, including its new Caribbean territory. Atkin said, “I am truly excited to accept the role of chief operating officer at this point of HGI’s journey. Our strong and continued delivery of success, which is my goal, will provide the foundation for our future plans. I am determined that through my insightful leadership, our wonderful portfolio of brands and of course the HGI team, we will deliver benefit to our clients. I look forward to meeting as many of our partners as possible this year.”
Expert Insights Dr Rita Rakus

Aesthetic practitioner Dr Rita Rakus has decades of experience in aesthetic medicine. Dubbed ‘The London Lip Queen’ by the consumer media, she is a co-founder of BCAM and represents a number of global brands alongside running her clinic in Knightsbridge.
Here, Aesthetics shares her recommendations and top tips for success in the specialty…
What treatments work best for body contouring?
EMSCULPT NEO from BTL Aesthetics is wonderful for muscle stimulation which patients love, and I’ve been enjoying using the new Deleo Cristal Body-Layering programme for efficient fat dissolving. Cellulite treatment using Sofwave’s SUPERB technology has also been a miracle procedure for me.
What devices work well for the lips?
People don’t tend to put devices and lips together, but it’s great for younger patients or those nervous about injectables. We use the ADVATx laser on the lips, as well as Hydrafacials.
What are some tips for providing a successful consultation?
You must be a good listener and explain patients’ options in straightforward language. Reviewing a thorough medical history is key for safe and effective treatment, and sensitivity around budget is essential to avoid embarrassment. I also tell patients I’m happy to discuss any concerns post-consultation as well.
What are the best ways to seek education and support in aesthetics?
Attending events like ACE and CCR provide the latest industry updates and allow you to learn more about the products and devices on offer. I recommend becoming a member of associations like ACE Group World, BACN, BAD, BCAM or CMAC to learn from colleagues and establish a support network.
What top three treatments would you recommend a new practitioner to offer?
You have to start with the bread and butter – dermal fillers and toxin – and then I would recommend a device that can treat the face and body, such as Exilis ULTRA 360, Hydrafacial or Sofwave SUPERB.
What is a new treatment you’re excited about?
BTL has recently released EMFACE – a muscle tightening device for the face – and my clinic is one of only three in the UK to have it so far. The Thermage FLX radiofrequency device has also been a great new addition to my offering.
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Distribution
Cosmetic Courses unveils new consultation training
Aesthetic training provider Cosmetic Courses has launched a new online learning course for practitioners to advance their consultation skills. Led by clinical lead of Cosmetic Courses Dr Fiona Durban, the training will take delegates through the stages of consultations: medical history, facial and photographic assessment, treatment planning and more, according to the company.

Dr Durban said, “We are delighted to be offering a brand-new online course covering the consultation process. This course has been developed using our wealth of experience and will be taking delegates through the various stages of a consultation. We believe that conducting a thorough consultation is one of the most important parts of your patients’ journey, and we hope this online course helps practitioners in creating a successful consultation which not only your patients will benefit from, but also yourself.”
Recruitment
VIVACY welcomes two new sales reps
Aesthetic product manufacturer VIVACY has appointed two new sales representatives to its UK team. Keelan Butler will be representing London whilst Sharen McBride will represent the North of England, covering maternity leave. Butler has a background in health economics where he worked as a consultant. McBride is a registered general nurse and has 23 years of experience in medical aesthetics, helping to launch premium brands into the market.
Butler said, “Meeting the needs of our clients is imperative and is the pinnacle of my everyday focus. I look forward to making new connections in the aesthetic world and helping VIVACY grow.”
Technology
The Aesthetic Entrepreneurs partners with Erchonia
Business growth company The Aesthetic Entrepreneurs has announced an upcoming partnership with aesthetic device company Erchonia UK. According to the companies, the partnership will lead to the creation of bespoke resources to support Erchonia UK customers when using its technologies.
Founder of The Aesthetic Entrepreneurs Richard Crawford-Small said, “We are thrilled to be partnering with Erchonia UK. Its innovative technologies have the potential to revolutionise the aesthetic industry, and we are excited to help its clients successfully launch and grow their businesses with these products.”

Simon Ramshaw, Erchonia’s managing director, also stated, “The Aesthetic Entrepreneurs is the perfect partner to help our clients achieve success with our technology. Their expertise in the industry and dedication to their clients makes them a valuable asset to our team.”
Education
PCA Skin launches new training platform
Skincare company PCA Skin has launched a new online learning platform for aesthetic practitioners.
According to PCA Skin, the platform provides interactive learning resources covering its Professional Peel Certification, which incorporates skin anatomy, treatment planning for various skin concerns, product knowledge and application techniques.
Lizzie Shaw, brand manager of PCA Skin UK, said, “We are delighted to launch the PCA Skin UK Academy platform and to provide aesthetic practitioners with a new way to learn and improve their skills. Our platform is intended to be user-friendly and convenient, allowing practitioners to learn on their schedule and at their own pace. We believe that this new platform will be a valuable resource for professionals looking to advance their careers while also providing the best service to their patients.”
Expansion
Candela opens new Irish office


Aesthetic device company Candela has opened a new office in Naas, Ireland. According to Candela, the Irish office is the next step in the company’s expansion, offering Irish practitioners the opportunity to learn more about Candela’s devices. Senior sales manager Grace McCormack commented, “It’s great to have a new office space which allows existing and new customers to visit and see demonstrations of our devices, undertake training and attend workshops. We have an exciting schedule of workshops planned to support our customers in 2023.”

Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com Training
Prollenium unveils new consumer website
Aesthetic manufacturer Prollenium Medical Technologies has launched its consumer-focused brand website. According to the company, the website uses real case studies rather than photographic models and stock photography to headline its design and showcase the dermal fillers’ capabilities. The website aims to promote real-life, attainable results while educating consumers about the products, including the safety profile, efficacy, clinical claims and data, Prollenium explains. Melissa Kang, chief marketing officer at Prollenium, commented, “With an ever-expanding family of Revanesse users all over the UK, we feel it is the right time to communicate our message to patients directly, giving them a suitable level of information and real-life case studies to help them make an informed decision about treatment.”
Expansion
Crown Aesthetics appoints new sales director
Aesthetic manufacturer Crown Aesthetics has announced the appointment of Simon Ofei as director of sales for the UK and Ireland (UKI).
Ofei has 25 years’ experience in the aesthetics industry, and in his new role, he will oversee the expansion of aesthetic device SkinPen Precision, as well as new launches for 2023.

He said, “I am super excited to be joining Crown Aesthetics as it is already gaining great traction in the UKI market, with a strong reputation for SkinPen Precision along with superb customer service by the sales, marketing and training team. My aim is to accelerate the sales growth in the UKI and to help develop our people. I am thrilled to be taking up this new role in 2023.”
Organisation
Facial Palsy Association established
New organisation the Facial Palsy Association (FPA) has been established to raise awareness of best practice when treating facial palsy.
The association, set up by aesthetic nurse prescriber Michelle McLean, is designed to offer support to those suffering with facial palsy, as well as assist practitioners worldwide through sharing information on safe and efficient treatment of the disorder with surgery, aesthetics and other therapies. According to FPA, the association will address a knowledge gap regarding facial palsy in the specialty.
McLean commented, “After conversations with multiple facial palsy patients, it was clear there was a lack of knowledge within the industry. I am so excited for the FPA to grow, support and spread awareness. My biggest enthusiasm comes from the prospect of linking up professionals within the industry to share vital knowledge in best practices and successful treatment, and explore new innovative treatment options. The FPA is a positive and exciting thing to be a part of.”
News in Brief
Lumenis appoints new country manager
Aesthetic device company Lumenis has announced the appointment of Andrew Greenwell as its new UK country manager. Greenwell commented, “I’m joining Lumenis at an exciting time of growth. As a firm believer that the customer experience is at the heart of everything we do, I’m very much looking forward to meeting as many of our existing customers as possible this year to understand how we can improve our existing offering, as well as working towards expanding our community of professional providers in the UK both this coming year and beyond.”
Neauvia unveils new Dubai training centre
Medical aesthetics company Neauvia has opened a new international training centre in Dubai. According to the company, the centre’s one auditorium and two treatment and consultation rooms will offer face, body and gynaecological treatments. Jean-Sébastien Ricard, Neauvia’s chief operating officer, commented, “We’re delighted to officially open our new international training centre located in the heart of the vibrant and trendy Dubai. For us, Dubai is a perfect location and is very much aligned with our multicultural values and lifestyle brand positioning.”
InDesk launches clinic support app Clinic management system InDesk has revealed the launch of new app InDesk Go. According to the company, InDesk Go allows practitioners to view new and upcoming appointments on a mobile device, monitoring correspondence and which treatments are receiving the most bookings. Dave Roe, CEO of WhatClinic.com, InDesk’s parent company, said, “We are delighted to further enhance the functionality of InDesk, giving our customers the transparency and peace of mind that they need to place their patient communication with the InDesk team.”
Glow Skin Health becomes WiQo’s UK distributor
Aesthetic distributor Glow Skin Health has been named as the sole UK and Ireland distributor of skin resurfacing product company WiQo. Morag Hague, director of Glow Skin Health, said, “We have already been working with WiQo for three years now. The quality of the entire portfolio of products is excellent and produces high-quality results. We are excited to be the sole distributors and have developed multiple training levels to ensure that PRX-T33 and all the other products are properly taught in foundation and advanced courses.”

Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Digital
Exploring Filler Longevity
Aesthetics gains industry perspectives on recent discussions about filler longevity
Last month, a story exploded in the consumer media looking into the reality of dermal filler longevity.1 This has been a topic of discussion in the medical aesthetic community for some time, but a recent Daily Mail article written by beauty journalist and author of The Tweakments Guide Alice Hart-Davis has put a spotlight on this concept for members of the public.
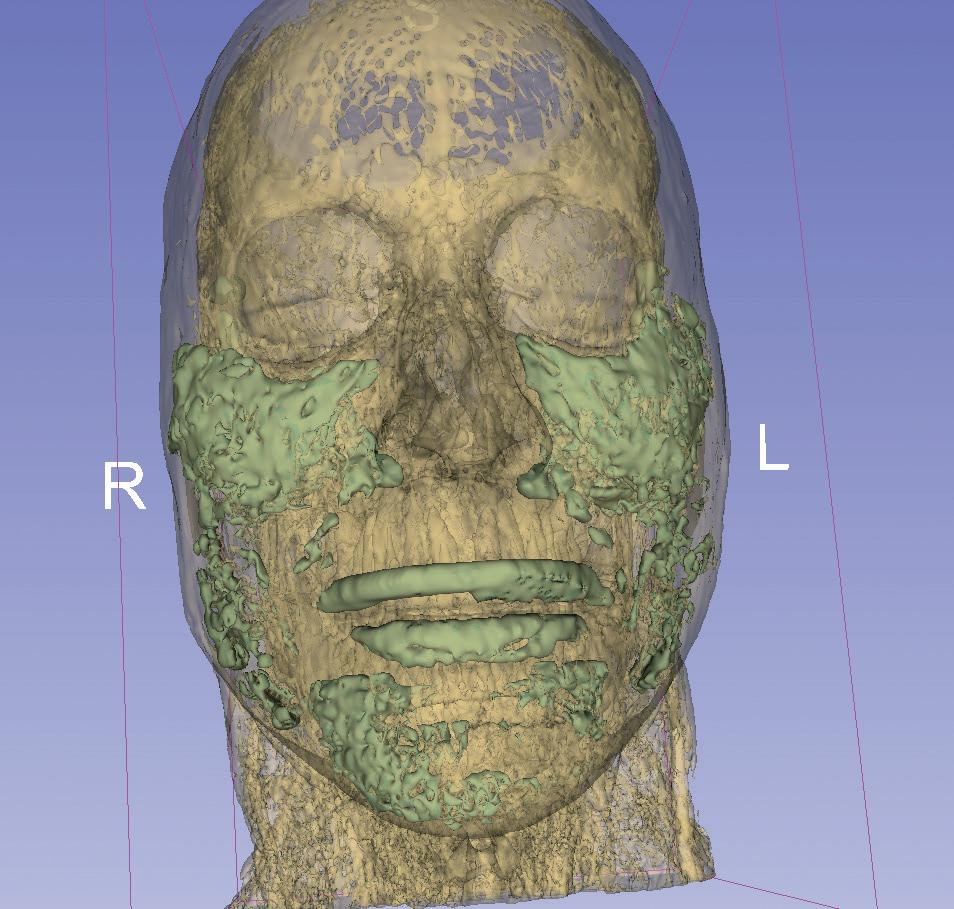
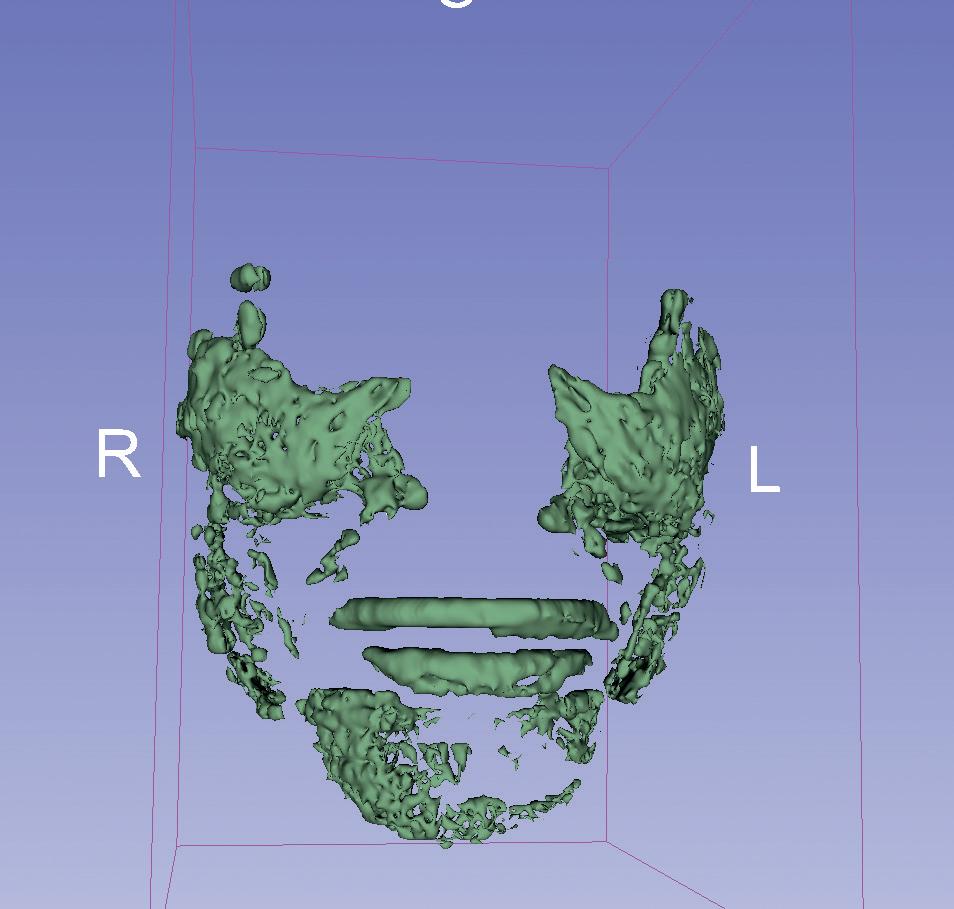
In the article, Hart-Davis wrote about the results of a 2021 MRI scan showing that despite not having had injectables for four years, there was still a total of 35ml of filler in her face (Figure 1&2). This contrasts the notion that dermal fillers are a short-term solution lasting between six and 18 months.2
On the general reaction to the story, Hart-Davis says there has been a massive response to the article, with doctors, nurses, surgeons, dentists and dermatologists sharing it around the world. She explains, “Many aesthetic professionals have commented that this is not news to them – they have for years seen evidence in their own clinics of filler that is hanging around for much longer than expected. But everyone else – patients, consumers – were astonished, because it doesn’t fit with the general perception of hyaluronic acid (HA) fillers as something that will dissolve in time, certainly within a couple of years. They were concerned even though the filler in my face is all in the right place and is not causing any problems.”

With patients concerned about what the news might mean for them and their future treatment plans, we spoke to aesthetic practitioner
Dr Sophie Shotter and aesthetic radiologist Dr Mobin Master to get their advice on how to speak about filler longevity with your patients, and whether it should impact your treatment planning/consultation.
An emerging concept
Dr Master has been a pioneer in bringing filler longevity to greater attention, first noticing it back in 2019. He comments, “I started getting referrals for facial MRIs of patients who had eyebags of unknown cause, who denied having filler for more than two years. Many of the MRIs showed filler still present in the tear trough area. As more of these referrals started coming in, many had residual or large volumes of HA filler despite denying any treatments, ranging from two to 15 years.”
Following this, Dr Master then started his own retrospective trial, looking at patients who have had persistent or misplaced filler in the face.3 He comments, “This trial showed the value of MRI as a great ‘snapshot’ of the face and a roadmap to dissolving unwanted areas.”
Dr Shotter has also been aware of longer-lasting dermal filler for some time, commenting, “I personally am not surprised by this news. I’ve seen patients who clinically still have filler present many years after treatment, and anecdotally we know from patients who have had positron emission tomography (PET) scans that filler can appear on those even 10 years later.”
Changing treatment approaches
As a result of the growing evidence that HA dermal filler is lasting for longer than expected, Dr Master advises that practitioners need to ensure they are taking good clinical photos before any filler treatment, as well as progress photos to assess how the face has been filled or potentially ‘over-filled’. He explains, “It means when we use HA filler, we need to position it correctly from the start. Any errors or poor outcomes will remain for a very long time and may still be seen.”
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
“The refill process should have a visual, clinical basis and looking back at baseline photos is very important”
Dr Mobin Master
He adds that this will be a positive for aesthetic medicine, as it will stop practitioners using guesswork and therefore minimise the risk of error. He explains, “As more become aware, they are more likely to review their face and work off the clinical photography, rather than assumption. Practitioners are stopping refilling purely on a ‘time’ or ‘recommended’ basis. This has made the use of filler far more scientific and evidence based, which is refreshing! The refill process should have a visual, clinical basis and looking back at baseline photos is very important.”
continue to assess my patients at regular intervals and treat only if they have a clinical indication. It doesn’t change our clinical assessment of their needs, but we shouldn’t dismiss a treatment done five years ago as irrelevant.”
What to communicate to patients
Dr Master advises that if patients present to you with concerns, you should reassure them that all treatments will be tailored to individual patient requirements. He says, “At this stage, as clinicians, I believe it’s a good approach to address those concerns and make it clear that the use of the filler will be related to the photography and progress photos. Filling according to the six-to-24-month recommendations is no longer relevant if the face still seems full. Clinicians can reassure that the face will not be ‘overfilled’, and this is best prevented by filling carefully and gradually.”
Progressing the concept of filler longevity
Dr Shotter believes this increased awareness is a huge positive for patients and practitioners. She notes, “I very much hope it makes patients think more carefully about what they have injected, and to consider that fillers involve having something injected into the face that could be there for as long as a surgical implant. This means it should be treated with the same degree of respect. They should ensure they have treatment with a qualified and respected medical practitioner, and they should ask what products they use. I see it as a chance for ethical medical injectors to credit themselves appropriately.”
However, Dr Shotter adds that more research needs to be done in this area to fully understand what this means for the specialty, noting, “We need to do significantly more research to determine how common a case like Hart-Davis’ really is. Currently we don’t have this data available to us.” She adds that it’s important for medical practitioners to stay abreast of the latest developments so they are in a better position to educate patients.
Dr Master also acknowledges that there needs to be further research into this area for practitioners to further assess what this might mean for aesthetic medicine. He concludes, “Indeed there needs to be larger trials, as per my first paper in Plastic Surgery USA 3 In fact, I have just completed the largest cohort study on longevity, which I am working on submitting this month.”
Aesthetics will be following developments in this area as they emerge.
REFERENCES
1. Daily Mail, I’ve got 20 years of filler stuck in my face, 2023, <https://www.dailymail.co.uk/femail/ article-11620871/Ive-got-20-years-filler-stuck-face-meant-dissolve-MRI-scan-revealed-truth.html>
2. Alice Hart Davis, How Much Filler Did Alice’s MRI Scan Show, 2022, <https://thetweakmentsguide. com/blog/how-much-filler-did-alices-mri-reveal/?fbclid=IwAR3fZML9I0-u-BcXoIWD394rtOpsLehKs5N 2ktc8G7cdtHjm7T4Ye9cynfQ>
Dr Shotter doesn’t believe practitioners need to change their current approach to consultations, noting, “The outcomes of this news coverage shouldn’t impact our patients or how we interact with them. However, I do think that we have a responsibility as the consulting practitioner to discuss these things frankly when asked. I have always been honest with my patients that the results of fillers usually last between one and two years, but that doesn’t mean all the filler disappears then.”
She adds that she won’t change the frequency of treatments for patients either, commenting, “The ageing process still continues to progress and the visible results of fillers do ‘wear off’. So, I will
3. Mobin Master, Hyaluronic Acid Filler Longevity and Localization: Magnetic Resonance Imaging Evidence, 2021, <https://pubmed.ncbi.nlm.nih.gov/33002985/>
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
“It doesn’t change our clinical assessment but we shouldn’t dismiss a treatment done five years ago as irrelevant”
Dr Sophie Shotter
Figure 1&2: MRI Scan imagery showing 35ml of filler. Images courtesy of Alice Hart-Davis
Advance Your Clinical Skills With TEOXANE
Headline Sponsor TEOXANE reveals its unmissable clinical agenda for ACE 2023

ACE 2023 is fast approaching. As the UK’s leading event in non-surgical aesthetics, you can expect a world-class educational programme, unmissable networking opportunities and the chance to gain up to 16 CPD points.
Returning for the second year in a row, we can finally reveal the official agenda for this year’s Headline Sponsor TEOXANE! The TEOXANE symposium brings a stand-out line-up of expert KOLs providing injectable demonstrations for delegates to watch and
discover new techniques. Taking place on March 10&11, these free-to-attend sessions are the perfect place to learn about the newest treatment styles, anatomy and products, keeping you up-to-date with all the latest in medical aesthetics.

20 Years of Changing Lives with TEOXANE
SESSION 1 – Beauty is Personal
Live demonstration by Dr Saleena Zimri
Speakers to include:
• Dr Sabrina Shah-Desai
• Dr Tahera Bhojani-Lynch
• Rachel Goddard

• Dr Saleena Zimri
DAY 1
SESSION 2 – Every Lip is Unique
Including three live lip demonstrations on how to approach different patient profiles
Speakers to include:
• Dr Lee Walker
• Dr Raul Cetto
• Dr Saleena Zimri
• Dr Sabrina Shah-Desai
Rachel Goddard, independent nurse prescriber, commented, “I am truly delighted to be part of TEOXANE’s female-only symposium panel during their first session at ACE, and having the opportunity to not only showcase the physical results of using TEOXANE dermal fillers for natural outcomes, but also investigating the positive emotional impacts that these treatments can have on our patients. I cannot wait to be able to share my knowledge and experience of using the TEOXANE approach to achieve optimal results when performing a full-face treatment, alongside my colleagues on the TEOXANE Medical Faculty!’
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
SESSION 1 – Beauty is Personal
Live demonstration by Dr Benji Dhillon

Speakers to include:
• Dr Wassim Taktouk
• Dr Kam Lally
• Dr Lee Walker
• Dr Benji Dhillon
SESSION 2 – Every Lip is Unique
Including three live lip demonstrations on how to approach different patient profiles
Speakers to include:
• Dr Benji Dhillon
• Dr Lee Walker
• Dr Kam Lally
• Dr Jeremy Isaac
Dr Jeremy Isaac, aesthetic practitioner, commented, “When it comes to treating the perioral area, there really is no ‘one size fits all’ approach. The key to creating a natural outcome, tailored to the patient, comes down to three fundamental factors: versatility of technique, a deep understanding of the products rheology and knowledge of the appropriate anatomical boundaries. During these symposiums, the delegates will have a fantastic opportunity to observe the TEOXANE Faculty showcasing three different techniques, demonstrating a variety and flexibility in approach and product when treating the perioral area, in order to maintain a natural outcome.”

WHAT ELSE CAN YOU EXPECT?
As well as world-class clinical education from TEXOANE, ACE 2023 has lots of other incredible content available. The In Practice Zone, a dedicated space for clinic service providers, will provide you with all the latest business insights and developments, covering topics ranging from social media and marketing to patient relations and finance. At the
CROMA – Symposium Stage
Beauty needs No Filter – Introducing a New Injectable Polynucleotide (with Live Demo)
Speakers to include:
• Professor Syed Haq
• Dr Mayoni Gooneratne
• Dr Uche Aniagwu
GALDERMA – Symposium Stage
Turn your AART into a HIT: SHAPE UP (with Live Demo)
Speakers to include:
• Dr Munir Somji
• Miss Priya Chadha
• Dr Rikin Parekh
• Jackie Partridge
GALDERMA – Symposium Stage
The New Era in Neuromodulation
Speakers to include:
• Miss Lara Watson
• Dr Kuldeep Minocha
• Dr Munir Somji
Innovation stage, you can discover the products set to take the industry by storm through demonstrations and workshops, and at our Masterclass agenda, KOLs will take a deep dive into the latest clinical education for your favourite procedures. Finally, at our Symposium stage, the industry’s top pharmaceutical brands will showcase their innovative techniques through live demonstrations.
Here’s a sneak peak of what you can expect:
HA-DERMA – Innovation Stage
The Key Factors of Successful Integration of Profhilo® Into Your Clinic
Speaker:
• Julie Scott
SKINCEUTICALS – Masterclasses
Integrated Skincare: How to combine evidence-based skincare within clinic procedures to optimise treated outcomes and protect your results
Speakers to include:
• Dr Ana Mansouri
• Mr Dean Rhobaye
REGISTER NOW FOR ACE 2023
Further details of the ACE agenda will be released soon. Keep an eye out for our Agenda at a Glance in the next issue, which will help you to plan your visit and ensure you’re attending the sessions which suit your learning needs the most.

Make sure you register now to further your clinical and business knowledge!
All sessions are free-to-attend and seats will be filled on a first-come, first-served basis. Please arrive 10 minutes before sessions start as spaces will fill quickly.
Please check the individual sessions listed on the website for full details of session accessibility.
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
DAY 2
REGISTER FREE NOW
Headline Sponsor
THE SECRET IS OUT





The #1 RF microneedling technology chosen by aesthetic professionals who prioritise patient comfort and efficacy ahead of anything else.
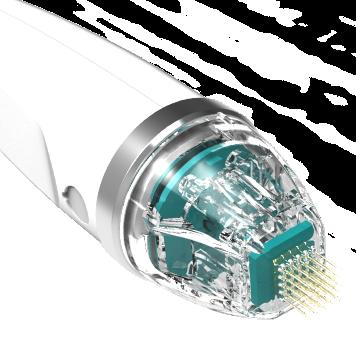












aesthetic
The technology trusted by the UK & Ireland’s leading
professionals
Mr Kambiz Golchin
Dr Tapan Patel
Dr Tatiana Lapa
Dr Manav Bawa
Dr Yusra Al-Mukhtar
Dr David Eccleston
Dr Anna Hemming
Dr Ana Mansouri
Learn more about our award-winning technology at cutera.co.uk CHOICE AESTHE T I C I NDUSTR Y + R F MICRONEED L I N G TECHNOL O G Y + RF A C T I ONAL CO 2 L ASER
Treating Skin of Colour with Devices
Exploring Skin of Colour in Summer
Dr Lauren Hamilton and Dr Miriam Adebibe discuss conditions that may affect skin of colour in the summer months
Three practitioners discuss their methods for skin rejuvenation using energy-based devices in skin of colour patients
People seeking clinical skin treatments vary widely in ethnicity. Though people with skin of colour (SOC) constitute the majority of the world’s population, they are under-represented in scientific studies, medical textbooks, and practical training where light skin tones have historically featured most frequently.1 This bias causes delays in diagnosis and treatment, resulting in greater morbidity and mortality, with the need for more oppressive treatment.2
certain skin concerns among their patients are heightened in the summer months.
Hyperpigmentation
where possible, I ask my patients about their ethnic background, as it isn’t just the colour of the skin which determines how the skin will react, but also its response to UV radiation, according to Fitzpatrick skin types.” She continues, “In my clinic, scarring is one of the main concerns SOC patients face due to being more prone to PIH, melasma, age and sunspots, leading to a darkening of the skin and marks. Therefore, I make sure to always conduct a thorough examination of the patient’s skin before advising treatments.”
In the aesthetics specialty, injectables are commonly considered the bread and butter of the industry, however, devices are also becoming increasingly popular among patients. According to business consulting and market research company DelveInsight, the global energy-based aesthetic device market is estimated to be valued at US $4.96 billion by 2026.1 This highlights that patients could be investing their money into treatments which are considered less painful and less invasive, while still delivering those all-important results.
We have found that the warmer months are a key time for enquiries and advice sought by patients with SOC at our clinic, because sun exposure worsens certain conditions and draws greater attention to them. In this article, we provide aesthetic practitioners with an overview of considerations for treating individuals with SOC in the summertime.
Understanding the differences in the structure and function of SOC is important to facilitate timely diagnosis and prevent adverse outcomes. Thankfully, this call is starting to be addressed. Several large-scale studies have been conducted examining the genetic and phenotypic differences among racial groups3 dedicated training for SOC has been included in the UK dermatology training syllabus since 2021.
Pigmentation is the most obvious difference between skin types. Melanin is a natural skin pigment that protects the nucleus and DNA from damage by UV radiation.8 Melanocytes in the basal layer of the epidermis make melanin in melanosomes for the purpose of transfer to neighbouring keratinocytes. One melanocyte distributes melanin to approximately 40 keratinocytes.8 We all have roughly the same number of melanocytes, though in darker skin these are located throughout epidermal layers, containing larger melanosomes and producing more melanin.9
Dr Ejikeme reiterates the importance of understanding that pigment production is ultimately a protective mechanism. She notes, “The goal for practitioners when treating is to try and calm the pigment producing cells, so there isn’t an exaggerated response. It is also important to note that if there is a mild response such as some PIH, this is normal, and it should settle itself down. Therefore, when I’m thinking about treating skin, I always start preparing it by using specific products or altering my process to avoid overstressing the skin.”
Classification of skin types
Another key difference is the melanocyte activity between the skin types, with eumelanin being more present than pro-melanin in melanin rich skin, Dr Ejikeme states. “Melanin is a protective mechanism,” she says, “Therefore it is produced, distributed and increased in the skin in response to skin stress. This stress can be caused by prolonged pressure, scrubbing the skin, heat and sunlight, which encourages the body to trigger this protective mechanism and increase pigment. As a result, this presents itself as uneven skin tone, darkening of the skin, discolouration, PIH, or in extreme cases, hypopigmentation.”5,7
Dr Beckhurst notes that PIH is the main concern to be aware of when treating SOC patients, as well as the risk of keloid and hypertrophic scarring. “In my consultations,
Skin is famously known as the largest organ of the body and functions as a protective barrier, a temperature regulator, a toxin eliminator, the best source of vitamin D production, and our environmental sensor through tactile touch.4 Under the microscope, the structure of skin is similar across all skin types, however there are morphological differences apart from the inherent SOC that are most often seen in the outermost layer of the epidermis, the stratum corneum.4
Despite energy-based treatments being available for all patients regardless of skin type, practitioners may need to take some precautions for skin of colour (SOC) patients.2 Due to having higher melanin production, SOC patients may be provided with specific pre-treatment and post-procedure care to avoid complications such as post-inflammatory hyperpigmentation (PIH).3 Using the Fitzpatrick classification, we are referring to SOC as those patients with skin types IV-VI, whilst lighter skinned patients fall into I-III (Figure 1).4
Aesthetics spoke to aesthetic practitioners Dr Rehanna Beckhurst, Dr Ifeoma Ejikeme and Dr Yusra Al-Mukhtar to discover their advice for treating SOC patients with devices and what practitioners should be aware of before treatment.
So, what do we mean by SOC? Ethnologically all humans are of African ancestry. The colour of our skin, determined by melanin pigment, is on a continuum ranging from pale white to darkest brown. Ethnicity and race fall short of the scientific description needed. While ethnicity relates to broad populations with a common culture or language, race defines a specific population with genetic similarities, such as Caucasian, African or Australasian.5
Type 1
• Skin colour (before sun exposure): ivory
• Eye colour: light blue, light grey or light green
• Natural hair colour: red or light blonde
• Sun reaction: skin always freckles, always burns and peels, and never tans
Type 2
Potential complications
All the practitioners agree that PIH is the main complication to avoid when treating SOC with devices such as radiofrequency microneedling, laser and high-intensity
Pheomelanin (yellow-red pigment) predominates in light skin (Fitzpatrick I-II) and eumelanin (brown-black pigment) in darker skin tones (Fitzpatrick V-VI), with a mix of both in Fitzpatrick III-IV.10 Melanogenesis commences with the conversion of L-Tyrosine to dopaquinone, by the key enzyme tyrosinase, which then serves as a substrate for eumelanin and pheomelanin production.11 Regulation of melanin synthesis by inhibiting tyrosinase is an important target in the prevention of hyperpigmentation. Although all skin types undergo photoageing due to sun exposure, darker phototypes
• Skin colour (before sun exposure): fair or pale
• Eye colour: blue, grey or green
• Natural hair colour: blonde
• Sun reaction: skin usually freckles, burns and peels often, and rarely tans
Type 3
• Skin colour (before sun exposure): fair to beige
• Eye colour: hazel or light brown
• Natural hair colour: black, dark blonde or light brown
• Sun reaction: skin might freckle, burns on occasion, and sometimes tans
Differences between SOC and white skin
The Fitzpatrick classification (phototypes I-VI) categorises skin of all colours according to its response to UV radiation (Figure 1).6
Generally, SOC refers to Fitzpatrick skin types IV-VI, ranging from olive to dark brown skin tones that tan easily and rarely burn. This includes people of Latino, African diaspora, East and South Asian, Australasian, and indigenous descent.7
Skin conditions in skin of colour
Most skin conditions occur in people of all skin types. However, some conditions may affect darker skin tones more frequently or more severely. Practitioners may find that
The physiology and anatomy of SOC and white skin differs, causing patients to present to practitioners with contrasting concerns. Dr Al-Mukhtar explains, “The collagen density tends to be higher in SOC people compared to white skin, meaning they are less likely to suffer with issues like fine lines and wrinkles.5,6 Instead, their main concerns are usually scarring, acne, pigmentation or textural issues such as enlarged pores. For lighter skinned patients, the concerns are likely to be thin, crepey skin, lines and wrinkles and wanting to improve skin texture.”
Type 4
• Skin colour (before sun exposure): olive or light brown
• Eye colour: dark brown
• Natural hair colour: black, dark brown

• Sun reaction: doesn’t really freckle, burns rarely, and tans often
Type 5
• Skin colour (before sun exposure): dark brown
• Eye colour: dark brown to black
• Natural hair colour: dark brown to black
• Sun reaction: rarely freckles, almost never burns, and always tans
Type 6
• Skin colour (before sun exposure): deeply pigmented dark brown or darkest brown
• Eye colour: brownish black
• Natural hair colour: black
• Sun reaction: never freckles, never burns, and always tans darkly
Figure 1: Classification of skin type using the Fitzpatrick scale4
Figure 1: Classification of skin type using the Fitzpatrick scale6
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 9/Issue 6 - May 2022 Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
For more information, please contact Lutronic









D i s c o v e r t h e B a b y F a c e p r o t o c o l , o n e o f t h e w o r l d ’ s m o s t i n - d e m a n d L a s e r F a c i a l s . Pigmented lesions | Melasma | Radiance | Texture Skin rejuvenation | Active acne | Wrinkles | Large pores Book your Demo to see why LaseMD Ultra™ is revolutionising skin rejuvenation! 48 George Street London W1U 7DY www.lutronicpbsuk.com General enquiry: info uk@seriderm com Phone: 0207 486 5429
2 0 M I N U T E S , 3 S T E P S t o m e e t a l l n e e d s Before After 2 treatments W i t h t h e c o u r t e s y o f M e g a n S o t i r o p o u o s , ( R N , B S N ) Finalist 2023
PBS UK & Ireland.
focused ultrasound. Dr Al-Mukhtar reiterates that PIH can be a long-term complication if not treated appropriately. “In essence, PIH is the skin’s response to a wound. It causes the skin to be angry and inflamed, so the skin deposits more melanin in response to the heat trauma it is experiencing. PIH can most commonly occur after treatments like microneedling or CO2 laser,” she notes.8 Dr Beckhurst agrees, highlighting that dark spots can also occur as a reaction to the injury on the skin. She says that hypertrophic scarring is also riskier in SOC patients and should be managed accordingly.
Furthermore, Dr Ejikeme believes that although complications can occur in melanin rich patients, they are rare and can usually be rectified. She notes, “Hypopigmentation and PIH are our main concerns, but if you pick the right treatment option, these are rare. If they do happen, it’s relatively straightforward to address them. Despite this, it’s important to advise your patient to use SPF regularly, avoid direct sunlight and continue using the skincare products recommended by their practitioner to maintain results.”
Before treatment
All three practitioners conduct a thorough medical history and skin assessment during their consultations, as well as advising a skincare regime before treatment, including the use of SPF 50.
Dr Beckhurst recommends vitamin C pre-treatment, and rarely prescribes hydroquinone cream to her SOC patients unless they are suffering from PIH. She explains, “I try to avoid prescribing hydroquinone creams if the patient has no clear history of PIH, because if used long-term or not used strictly, it can cause dyschromias. I will only advise hydroquinone if I want to hasten the rate of PIH on the skin. Therefore, I advise using a vitamin C serum from PCA Skin (C&E advanced), as well as PCA Skin Pigment Bar and Pigment Gel Pro to inhibit tyrosinase and melanogenesis. I also recommend the PCA Skin Vitamin B3 to even
out skin tone and hydrate the skin.”
Dr Al-Mukhtar chooses to put her patients on a skincare regime using either prescription tyrosinase inhibitors alongside a retinoid to reduce the activity of the melanocytes, improve collagen density and mitigate the risk of PIH prior to an energy-based treatment.

On the other hand, Dr Ejikeme notes that it is important to consider whether you are going to cause an exaggerated stress response to the skin, further causing inflammation. If so, she recommends regulating the pigment producing process beforehand. “In my clinic, I use a number of different options including Obagi products to regulate pigment. There are lots of different ones on the market, but the one you choose will determine the amount of inflammation you’re intending to cause post-treatment,” she notes.
Dr Ejikeme reiterates that if you are intending to carry out a mild treatment after which you don’t think there will be any pigment production or inflammation, she recommends the patient use a consistent broadband sunscreen. If the treatment is mild/moderate such as microneedling, she uses products to optimise the skin such as vitamin C, arbutin and SPF. Lastly, for resurfacing treatments, she would use tretinoin and SPF, as well as hydroquinone for two to four weeks prior to treatment.

Choosing your device
When choosing a new device for your clinic, Dr Al-Mukhtar advises checking that it has been tried and tested on SOC and to ensure they provide clinical data to back this up. “In the past, devices were trialled on Fitzpatrick skin types I-III, including skincare,” she says. “With the conversation surrounding diversity becoming more topical, practitioners and patients are advising company manufacturers to test their products on SOC.”
Dr Al-Mukhtar uses the Secret Pro radiofrequency microneedling and CO2 combination device by Cutera, for epidermal and dermal focused skin rejuvenation applications. This particular device allows her to tailor her treatment specifically for SOC patients. She comments, “The device has the option of using semi-insulated needles rather than just the non-insulated option, which allows me to prevent unnecessary heat and trauma to the epidermis and deliver energy to the deeper dermal tissues, which is the aim with SOC patients. This mechanism of action helps reduce incidence of melanogenesis (new pigmentation), which is a priority. To further reduce risk, the Secret Pro also allows me to tailor my target depth within 0.1mm increments, depending on skin type and treatment indication.” Furthermore, Dr Beckhurst uses a similar technique when treating SOC with radiofrequency, choosing to use insulated needles and a lower energy output with the Gentlo device from Beamwave Technologies. She explains, “Gentlo gives me a choice of needles (insulated or non-insulated). For darker skin types, I use insulated needles as they deliver radiofrequency from the tip at a deeper depth. In lighter skin types, we aren’t as concerned about upsetting melanocytes
Before After
Figure 2: 44-year old patient before and four months after melasma treatment using chemical peels and skincare. Image courtesy of Dr Ifeoma Ejikeme.
“Hypopigmentation and PIH are our main concerns, but if you pick the right treatment option, these are rare”
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Dr Ifeoma Ejikeme




hello@beamwave.co.uk 0208 191 7117 Beamwavetech Beamwavetechnologies wwww.beamwave.co.uk Before two treatments Cutting-edge technology built on a revolutionary combination of RF Microneedling and Plasma. ǐ Stimulate collagen production ǐ Target a variety of skin concerns ǐ Non-invasive procedure ǐ Minimal downtime and recovery ǐ Long lasting results ǐ Safely treat all Fitzpatrick skin types Book your FREE demo today by emailing hello@beamwave.co.uk
and increasing melanin production, but in darker skin, we want to bypass those layers and deliver radiofrequency at a deeper level, targeting collagen production safely.”
Dr Al-Mukhtar notes that she adapts her protocol based on the patient’s concern, goals and skin type, by changing the energy, depth, and needle size. She states that she might add additional CO2 into her treatment if necessary. “In the past, CO2 laser was completely avoided in SOC patients with Fitzpatrick skin types III-V,” she says, “However, with advancements in the efficiency of the technology available to practitioners, we can tailor the treatment to suit SOC. This means we can alter the depth of the CO2, and the amount of skin coverage meaning we can deliver a fraction
She reflects, “I like to use the Secret Pro device for any radiofrequency microneedling procedures too. For laser hair removal, I use the Nd:Yag laser by Fotona because I believe it is the safest modality for SOC.”
After treatment
Dr Beckhurst reiterates that post-treatment skincare (the same products used in pre-treatment) is advised, as well as regular follow-up appointments to catch any complications early. She says, “I try to make it clear to patients that our main concern is PIH occurring, so I advise vitamin C and SPF, alongside topical skinboosting enzyme products to slow down melanin production by inhibiting tyrosinase. We also give my patients a courtesy call two days post-treatment to see how they are, and then a follow-up one or two weeks later depending on how the call goes. We then have an additional radiofrequency microneedling treatment booked in for six weeks’ time after the original to maintain results.”
Similarly, Dr Ejikeme offers post-procedure care to all patients regardless of skin colour to maintain results. “When patients come
sun protection is pivotal in preventing further hyperpigmentation and dark spots. Once the healing has completed after an energy-based treatment, I will follow up with tyrosinase inhibitors and a retinoid again to improve the results and reduce the risk of PIH.” In the past, SOC patients may have been reluctant to seek out energy-based treatments due to a higher risk of PIH and other skin complications. Dr Al-Mukhtar adds that with appropriate pre- and post-care, practitioners can offer patients treatments that they might have been reluctant to have previously. If melanin production is managed, SOC patients can be treated without the additional fear of complications.
Treat SOC with caution
Dr Ejikeme concludes that practitioners should be confident in treating all ethnicities and make expectations clear to patients before treatment. She says, “Patients with melanated skin are not a uniform group. From African and Middle Eastern to Indian and Southeast Asian, every group has a different skin tone and concern. Therefore, make clear to patients the results they can expect from your treatment. There must be a match between what you think you can achieve and what the patient wants. If you achieve this, you can get great results and happy patients!”
Dr Beckhurst advises practitioners to refer patients to other colleagues if they are unsure of how to treat. “Always treat SOC patients with caution! If you are unsure, refer to a practitioner who specialises in SOC, especially if there is something in a patient’s medical history which raises concerns such as if they had complications from treatment before. If in doubt, always refer.”
REFERENCES
1. DelveInsight, ‘The energy based aesthetic market’, 2021 <https://www.delveinsight.com/report-store/energy-basedaesthetic-devices-market>
2. Anderson A, ‘Special Feature: Dermatologic Concerns in Skin of Colour’, Aesthetics journal, 2019, <https://aestheticsjournal.com/ feature/dermatologic-concerns-in-skin-of-colour>
of the laser so that it is fractionally ablative rather than fully ablative. By ensuring we spend time preparing the skin pre-treatment by prescribing melanin inhibitors such as hydroquinone, we can then deliver a more controlled, lower energy output of the CO2 10,600 nm, avoiding unnecessary trauma to the skin. The advancements in technology have enabled us to offer our SOC patients gold-standard CO2 resurfacing treatments, which they might previously have been told wasn’t suitable for them.9”


Dr Ejikeme prefers to use different devices depending on the patient’s condition.
for their treatment and the skin seems hyperactive, I may give 1% hydrocortisone after treatment to reduce hyperpigmentation. For all treatments we do, everybody would get an emollient and SPF 50,” she adds. Dr Al-Mukhtar reinforces the point that protecting the skin post-treatment is vital. She notes, “Aftercare is not one size fits all approach – it depends on the patient’s previous history of treatments, what skincare they’ve been on and reactions to previous devices. The number one thing I would say is that patients need to protect their skin after treatments and keep it hydrated. Applying
3. Czerkasij V, ‘Skin of Colour: A Basic Outline of Unique Differences’, The Nurse Practitioner, 2013, p.34-40.
4. Pathak, M.A. Acute and chronic effects of the sun. In: Fitzpatricks dermatology in general medicine, 1999.
5. Rawlings AV, ‘Ethnic skin types: are there differences in skin structure and function?’, Int J Cosmet Sci, 2006.
6. Twijiri S, Jamali Y, ‘Exploring the Physiology of Black Skin’, Aesthetics journal, 2021, <https://aestheticsjournal.com/feature/ exploring-the-physiology-of-black-skin>
7. Rajput M, ‘Exploring Hyperpigmentation in Skin of Colour’, Aesthetics journal, 2021, <https://aestheticsjournal.com/feature/ exploring-hyperpigmentation-in-skin-of-colour>
8. Close M, ‘Special Feature: Treating Skin of Colour with Lasers’, Aesthetics journal, 2019, <https://aestheticsjournal.com/feature/treating-skin-of-colourwith-lasers>
9. Kronemeyer R, ‘Aesthetic Device Considerations for Skin of Colour’, Dermatology Times, 2021, <https://www. dermatologytimes.com/view/aesthetic-device-considerationsfor-skin-of-color>
Before After
Figure 3: 46-year-old female patient before and 12 weeks after three sessions of Gentlo fractional radiofrequency microneedling. Image courtesy of Dr Rehanna Beckhurst.
“With the conversation surrounding diversity becoming more topical, practitioners and patients are advising company manufacturers to test their products on SOC”
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Dr Yusra Al-Mukhtar

This information is intended for Healthcare Professionals only. This advertisement has been created and funded by Galderma. Prescribing information can be found on the adjacent page.
by
Botulinum toxin type A
Over 100 million treatments delivered worldwide for aesthetics indications to date 1
Fast-acting and long-lasting, patients saw results as early as 24 hours 2-5 and for up to 5 months. 2-4,6-9
Please refer to the Prescribing Information for important safety information and to the Summary of Product Characteristics before use.
Azzalure
Prescribing Information (UK)
Presentation: Botulinum toxin type A (Clostridium botulinum toxin A haemagglutinin complex) 125 Speywood units (powder for solution for injection)
Indications: Temporary improvement in appearance of moderate to severe:
• Glabellar lines seen at maximum frown, and/or
• lateral canthal lines (crow’s feet lines) seen at maximum smile in adult patients under 65 years, when severity of these lines has an important psychological impact on the patient.
Dosage & Administration: Azzalure should only be administered by a healthcare practitioner with appropriate qualifications and expertise in this treatment and having the required equipment, in accordance with national guidelines. Botulinum toxin units are different depending on the medicinal products. Speywood units are specific to this preparation and are not interchangeable with other botulinum toxins. Reconstitute prior to injection. Intramuscular injections should be performed using a sterile suitable gauge needle. Glabellar lines: recommended dose is 50 Speywood units divided equally into 5 injection sites, 10 Speywood units to be administered intramuscularly, at right angles to the skin; 2 injections into each corrugator muscle and one into the procerus muscle near the nasofrontal angle. Lateral canthal lines: recommended dose per side is 30 Speywood units divided into 3 injection sites; 10 Speywood units to be administered intramuscularly into each injection point, injected lateral (20 - 30° angle) to the skin and very superficial. All injection points should be at the external part of the orbicularis oculi muscle and sufficiently far from the orbital rim (approximately 1 - 2 cm); (See summary of product characteristics for full technique). Treatment interval should not be more frequent than every three months. The efficacy and safety of repeat injections of Azzalure has been evaluated in Glabellar lines up to 24 months and up to 8 repeat treatment cycles and for Lateral Canthal lines up to 12 months and up to 5 repeat treatment cycles. Not recommended for use in individuals under 18 years of age. Contraindications: Hypersensitivity to botulinum toxin A or to any of the excipients. In the presence of infection at the proposed injection sites, myasthenia gravis, Eaton Lambert Syndrome or amyotrophic lateral sclerosis. Special warnings and precautions for use: Care should be taken to ensure that Azzalure is not injected into a blood vessel. Use with caution in patients with a risk of, or clinical evidence of, marked defective neuro-muscular transmission, in the presence of inflammation at the proposed injection site(s) or when the targeted muscle shows excessive weakness or atrophy. Patients treated with therapeutic doses may experience exaggerated muscle weakness. Not recommended in patients with history of dysphagia, aspiration or with prolonged bleeding time. Seek immediate medical care if swallowing, speech or respiratory difficulties arise. Facial asymmetry, ptosis, excessive dermatochalasis, scarring and any alterations to facial anatomy, as a result of previous surgical interventions should be taken into consideration prior to injection. Dry eye has been reported with the use of Azzalure in the treatment of glabellar lines and lateral canthal lines. Reduced tear production, reduced blinking, and corneal disorders, may occur with the use of botulinum toxins, including Azzalure. Injections at more frequent intervals/higher doses can increase the risk of antibody formation to botulinum toxin. Clinically, the formation of neutralising antibodies may reduce the effectiveness of subsequent treatment. Botulinum toxin units are not interchangeable from one product to another. Doses recommended in Speywood units are different from other botulinum toxin preparations. To be used for one single patient treatment only during a single session. In order to improve the traceability of biological medicinal products, the name and the batch number of the administered product should be clearly recorded. There is a potential risk of localised muscle weakness, visual disturbances or asthenia linked with the use of this medicinal product which may temporarily impair the ability to drive or operate machinery. Interactions: Concomitant treatment with aminoglycosides or other agents interfering with neuromuscular transmission (e.g. curare-like agents) may potentiate effect of botulinum toxin. Pregnancy, Breast-feeding and Fertility: Pregnancy: Azzalure should not be used during pregnancy. There are no adequate data from the use of botulinum toxin type A in pregnant women. Studies in animals have shown reproductive toxicity at high doses. The potential risk for humans is unknown. Breast-feeding: There is no information on whether Azzalure is excreted in human milk. The use of Azzalure during lactation cannot be recommended. Fertility: There are no clinical data from the use of Azzalure on fertility. There is no evidence of direct effect of Azzalure on fertility in animal studies.
Side Effects: Most frequently occurring related reactions are headache and injection site reactions for glabellar lines and; headache, injection site reactions and eyelid oedema for lateral canthal lines. Generally, treatment/ injection technique related reactions occur within first week following injection and are transient. Undesirable effects may be related to the active substance, the injection procedure, or a combination of both. For glabellar lines: Very Common (≥ 1/10): Headache, Injection site reactions (e.g. erythema, oedema, irritation, rash, pruritus, paraesthesia, pain, discomfort, stinging and haematoma). Common (≥ 1/100 to < 1/10): Temporary facial paresis (due to temporary paresis of facial muscles proximal to injection sites, predominantly describes brow paresis), Asthenopia, Eyelid ptosis, Eyelid oedema, Lacrimation increase, Dry eye, Muscle twitching (twitching of muscles around the eyes). Uncommon (≥ 1/1,000 to <1/100): Dizziness, Visual impairment, Vision blurred, Diplopia, Pruritus, Rash, Hypersensitivity, Rare (≥ 1/10,000 to < 1/1,000): Urticaria, Eye movement disorder. For lateral canthal lines: Common (≥ 1/100 to < 1/10): Headache, Temporary facial paresis (due to temporary paresis of facial muscles proximal to injection sites), Eyelid ptosis, Eyelid oedema and Injection site reactions (e.g. haematoma, pruritus and oedema). Uncommon (≥ 1/1,000 to <1/100): Dry eye. Post-marketing experience: frequency not known (cannot be estimated from the available data): asthenia, fatigue, influenza-like illness, hypersensitivity, hypoaesthesia and muscle atrophy.
Adverse reactions resulting from distribution of the effects of the toxin to sites remote from the site of injection have been very rarely reported with botulinum toxin (excessive muscle weakness, dysphagia, aspiration pneumonia with fatal outcome in some cases).
Prescribers should consult the summary of product characteristics in relation to other side effects.
Packaging Quantities & Cost: 2 Vial Pack (2 x 125u) £126.00 (RRP)
Marketing Authorisation Number: PL 06958/0031
Legal Category: POM
Further information is available from: Galderma (UK) Limited, Evergreen House North, Grafton Place, London, NW1 2DX, UK.
Tel: +44 (0) 300 3035674
Date of Revision: August 2022
Adverse events should be reported.
Reporting forms and information can be found at www.mhra.gov.uk/yellowcard or search for Yellow Card in the Google Play or Apple App Store. Adverse events should also be reported to Galderma (UK) Ltd, E-mail: medinfo.uk@galderma.com Tel: +44 (0) 300 3035674
References: 1. Galderma Data on File MA-52573; 2. Kassir R et al. Dermatol Ther (Heidelb) 2013;3(2):179–189; 3. Maas C et al. Aesthet Surg J 2012;32(1 Suppl):S8–S29; 4. Monheit GD et al. Dermatol Surg 2020;46(1):61–69; 5. Moy R et al. Arch Facial Plast Surg 2009;11(2):77–83; 6. Warren H et al. Plast Surg Nurs 2020;40(1):37–44; 7. Brandt F et al. Dermatol Surg 2009;35(12):1893–1901; 8. Rzany B et al. Dermatol Surg 2007;33(1 Spec No):S18–S25; 9. Gubanova E et al. Aesthet Plast Surg 2018;42(6):1672–1680. GB-ALD-2200014 DOP December 2022 United
Order now at www.medfx.co.uk
This information is intended for Healthcare Professionals only. This advertisement has been created and funded by Galderma.
Dr David Eccleston Sebastian Cotofana M.D., Ph.D*
Dr Victoria Dobbie Dr Raj Thethi Dr Sabika Karim
Dr Kam Lally Dr Fab Equizi Dr Steven Land and your Evolus team present
Hello FUTURE tourUK
Edinburgh | Norton House Hotel
Bristol | Aztec Hotel
London | Hallam Conference Centre
Birmingham | National Conference Centre
Manchester | Marriott Hotel Airport
Durham | Hotel Indigo
| 20 February ‘23
| 6 March ‘23
| 7 March ‘23
| 13 March ‘23
| 14 March ‘23
| 27 March ‘23
12:00 - 16:00 (Lunch included)
Join the discussion on anatomy science products industry trends evolving the future of beauty

Register today on:
https://www.hello-evolus.com/uk-tour




Promotional meetings, that will discuss Evolus and its products, initiated, developed and funded by Evolus. For UK doctors, dentists and nurses only.
Speakers will vary based on location.
*
Pre-recorded bespoke content from Sebastian Cotofana.
January 2023 | UK-NUC-2200186
Adverse events should be reported. Reporting forms and information can be found at www.mhra.gov.uk/yellowcard or search MHRA Yellow Card in the Google Play or Apple App store. Adverse events should also be reported to Evolus International Ltd. Please contact Evolus Europe medical information by emailing Evoluseurope@druginfo.com or calling 08000541302.
Analysing Facial Rejuvenation Treatments
Aesthetic nurse Emma Coleman provides an overview of four treatments for facial rejuvenation
Facial ageing is believed to be caused by intrinsic (genetic) and extrinsic (environmental) factors, including sun exposure, pollution, smoking, diet and general lifestyle elements.1 Ageing may also be defined as a complex process brought about by cultural and societal factors reflecting biological, environmental and genetic influences.2 Cutaneous changes include wrinkles, pigmentation and loss of elasticity, which often vary according to ethnic origin.2 Pollution may also play a role.3
Rejuvenation treatments include any injectables or skin intervention that makes the face appear younger 4 When considering a patient for facial rejuvenation, it is important to focus on facial harmony and realistic aims and outcomes.5 There is significant evidence to support implementing different methods to effectively rejuvenate the face in a variety of ways, and that combining two therapies together often yields more profound and longer-lasting results 6-13
In this article, I discuss four popular treatment options and present recent, relevant clinical data for each therapy with the aim of highlighting efficacy in treating specific issues.
Botulinum toxin
Botulinum toxin A (or BoNT-A) has its roots in ophthalmology, where it was first utilised in strabismus (squint) treatment.14 Allergan acquired the rights to distribute the drug in 1988, and the drug has been used cosmetically to reduce and prevent wrinkles in the upper face, periorbital and perioral regions since 1989.14 Its uses have expanded to treatment of the neck platysma bands, gummy smile and masseter muscles.15 It exerts its ‘muscle-relaxing’ action by gradually blocking release of the neurotransmitter Acetylcholine from presynaptic terminals of neuromuscular junctions at injection sites.16
From my readings, the highest proportion of trials provide evidence for the efficacy of BoNT-A in glabellar treatment. One open-label, phase 4 study (n=42) provided evidence that 85.4% of subjects displayed significant reduction in frown lines two days after treatment with 20U of the toxin Nabota.17 A larger scale American trial (n=156) treated and assessed healthy subjects in the glabellar, (GFL – 20U), frontalis (HFL – 10-20U) and periorbital line (LPL – 24U) regions, using a percentage scoring system.18 At 30 days post-treatment, a mean improvement of 71.3% across all treated areas was recorded in the study group, versus mean of 0.06% improvement in the control group 18 Another multicentre randomised, controlled trial conducted over five months and employing the four-grade facial wrinkle scale (FWS) focused on aesthetic results of treatment of the crow’s feet with 24 units of BoNT-A in 445 subjects. Findings provided evidence that the BoNT-A-treated group experienced a 66.7% wrinkle reduction at day 30, versus 6.7% in the placebo group.19
The effects of toxin may also go beyond wrinkle smoothing, with one study (n=40) providing evidence that female subjects who received a solitary treatment displayed significant improvements in
cutaneous hydration, elasticity and a reduction in trans epidermal water loss (TEWL) at week 12 post-treatment, compared to the control group.12 The same study also provided evidence that toxin therapy had positive effects on quality of life and psychological benefits on study group subjects, scoring significantly higher on the physician‘s global assessment and subject satisfaction score, compared to the control group 12
BoNT-A results vary according to a number of factors:16,20
1) Antibody resistance – the lowest possible dose to attain the optimal outcome should always be used, and treatment intervals of more than three months should be instated
2) Sex – outcomes of BoNT-A treatment may vary between males and females due to differing muscle anatomy
3) Age – there is evidence to suggest that patients over 51 may require significantly higher doses
4) Length of toxin storage after reconstitution
There is some data to support the theory that the type of toxin used affects the dosage required to reach optimum results; for example, one trial used 50U of Dysport (Azzalure) in the glabellar to achieve an average 86% improvement,21 whilst one Japanese trial provided evidence that lower doses of Botox – 10 to 20U – are required to achieve effective subject and physician-rated results up to a period of 16 weeks 22 This variation could be attributed to the presence or absence of complexing proteins across different brands, with protein-free toxins requiring lower dosage to achieve results.23 On the other hand, a single-blind, split-face trial compared two toxin brands with 10 female subjects and reported no significant difference in clinical results.24 Therefore, further large-scale, specific trials are required to substantiate this.
A 2022 study (n=40), provided evidence that combining toxin with hyaluronic acid dermal filler yielded a lower FWS in glabellar treatment, compared to toxin alone.25 Another provided significant evidence that combining application of cosmeceutical hyaluronic acid (HA) serum with toxin injections lengthened the duration of action of the BoNT-A.26 Study reviews have shown toxin to be a well-tolerated and safe treatment option for facial rejuvenation.23 Uncommon adverse side effects include ectropion, ptosis, heavy upper eyelids, bruising and transient headaches.16
Hyaluronic acid dermal filler
Injectable dermal fillers are commonly used to treat signs of facial ageing and provide enhancement in specific areas. There is much evidence to suggest that injection of HA filler improves skin volume, texture, elasticity, smoothness and hydration, as well as greater type I collagen expression, and can be used to attain natural, youthful results.27-29,30-35
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
HA is a linear glycosaminoglycan containing a disaccharide unit36 and is hygroscopic, meaning it has the capacity to absorb water extensively, creating lift and volume in the face.27 Dermal filler products can be classified as biphasic or monophasic, based on the type of cross-linking technology they possess; cross-linking is essential in maintaining product longevity and stability.27,37 Products will also vary based on HA concentration, particle size, gel consistency, viscosity and hardness, plus water solubility.37 There is evidence to suggest that monophasic HA fillers are more cohesive, cause less localised erythema and display less risk of migration compared to biphasic fillers following injection.38,39
Understanding the rheological properties of dermal filler –viscoelasticity and cohesivity – assists practitioners in selecting the correct product for treatment of a particular part of the face.40 A thorough knowledge of facial anatomy, ideal proportions, bone degradation, and the facial fat pads and vasculature, is essential to attain optimal results and safety when injecting.29,41
Tear trough rejuvenation is a popular choice of treatment with HA filler.30 Under-eye hollows are believed to occur due to anatomical changes including descent of the cheek and underdevelopment of the infraorbital malar complex.27,42 Natural, effective results can be achieved in this area through depot, periosteal HA placement.29
An American study (n=100), assessed tear trough treatment outcomes based on patient satisfaction, downtime and side effects following injection of Perlane 0.59ml beneath each eye. The mean downtime was one day, 85% reported marked or moderate satisfaction, and 10% were dissatisfied.31 A recent prospective study assessed 24 subjects treated with Teosyal PureSense Redensity 2 in the medial tear trough. At two and four weeks post-procedure 75% were satisfied with the outcome, whilst 25% required further filler to be satisfied, and side effects such as bruising and swelling were mild and minimal.32 A systemic review has highlighted that complications of tear trough treatment can occur up to a mean of 52 months following initial treatment, including lumps, migration, discolouration and swelling.43 Thorough consultation, patient selection incorporating skin analysis in the lower eyelid and rigorous consent help to reduce risks.29
Mid-face rejuvenation and volume replacement with HA filler is essential in establishing rejuvenation in other areas, particularly in the nasolabial and lower face regions, and requires a thorough understanding of facial anatomy, particularly of the vasculator.34,44 Successful treatment in this area should combine deep fat injections with periosteum placement, considering the sex and natural bone structure.44
Zygomatic region rejuvenation using biphasic HA filler has shown improvements in elasticity, zygomatic curvature, volume and skin smoothness, as well as a high level of subject satisfaction at three months following treatment.33 One split-face study highlighted that placing HA filler lateral to the line of ligaments versus medially in 12 subjects created a sculpted cheek, successfully volumised the infraorbital and upper cheek areas, whilst also achieving optimal patient satisfaction.45
In terms of the efficacy of hyaluronic acid in combination with other treatments, a recent small-scale trial (n=12) provided evidence of 25-50% improvement in acne scarring following HA filler and ablative laser therapy,46 whilst an earlier trial in 2013 highlighted greater improvement in static perioral rhytids when treated with a combination
of HA filler, lipolysis injection and ablative laser, compared to HA and lipolysis alone.47
The most common reactions to HA filler include erythema, swelling and bruising, and less frequently, Tyndall effect, migration and vascular occlusion.48 Appropriate patient selection, skin preparation and a sterile technique are essential in preventing infections.27
Microneedling
Microneedling is a minimally-invasive procedure implementing fine needles to repeatedly puncture the epidermis, with limited risk of adverse effects.49 Dating back to 1905, the micro-wounds created during the needling process stimulate the release of growth factors and induce collagen production 49 Improvements in scars, discolouration and skin texture brought about by microneedling were accidentally discovered during camouflage tattoo treatments to hypopigmented facial scars 50
There are two types of microneedling devices. Roller devices have a cylindrical head which is rolled back and forth to induce tiny incisions over the skin; electronic pen devices have adjustable settings to control speed and depth of needle penetration 51 One review paper has provided evidence that roller devices are more likely to cause adverse effects, particularly erythema and pain, however, a 2015 pilot trial (n=22) used a roller device to improve facial melasma and reported no adverse side effects 52,53
Few studies are available that focus purely on the effects of microneedling on overall facial rejuvenation, with most implementing combination therapies, making it difficult to analyse the benefits of microneedling alone 53-57 This could be because a performance
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Understanding the rheological properties of dermal filler assists practitioners in selecting the correct product for treatment of a particular part of the face
bias is inevitable because blinding subjects and practitioners for the procedure is impossible.51 The most widely researched area is acne scarring, and most trials analyse results using computerised images, optical profilometry, biopsy, visiometer and exometers 51,53,55,56 From my readings, biopsy and resulting histological staining provides the clearest view of the impact microneedling has on epidermal changes at a cellular level 57-59
Skin darkening and pigmentation have shown significant improvement for up to 24 months following a combination of two sessions of microneedling treatment, using 1.5mm depth and topical skin lightening agents 34 However, it is difficult to substantiate the exact effect of the needling in this case.53 One Korean trial (n=25) provided evidence that a combination of stem cell and microneedling therapies at a depth of 0.25mm had a significant impact on wrinkles and hyperpigmentation following five treatments.54 There is evidence to suggest that hypertrophic and atrophic acne scarring is significantly improved with three to six treatments of microneedling alone, reporting the most significant results three to 12 months following treatment 51,55,58
A small 2015 study (n=10) administered six roller needling sessions spaced two weeks apart, at 1.5mm depth to subjects with atrophic scars.58 The biopsy results highlighted a favourable effect on enhancing collagen formation, particularly collagen III, which increased significantly between one and three months following treatment.58
A 2014 German murine study used biopsy to compare changes in epidermal thickness and collagen synthesis in 30 rats divided into five equal groups.57 Increases in epidermal thickness and growth factor occurred across groups C to E with a clear, significant trend. Group C experienced epidermal growth of 115% after one session of microneedling at 1mm depth, versus group D with an increase of 205% following four needling sessions at 1mm depth. Group E received four sessions at 1mm depth plus skincare and exhibited growth of 658% compared to control. The same trial also observed that skin tightening occurred in all microneedling groups 57
Furthermore, a small-scale human study (n=10) treated subjects with six microneedling sessions at 14-day intervals, and provided evidence that various types of collagen – specifically I, III and VII – plus tropoelastin significantly increased (P<0.05) in response to treatment. This led to a reduction in wrinkles in all subjects.60
When combined with chemical peels and platelet-rich plasma therapy, microneedling may yield faster and more profound results in treating acne scarring, due to increased upregulation of growth factors.61,62 Microneedling is usually well tolerated with minimal risk of side effects.53,57,63 Deeper treatment depth leads to longer recovery periods due to erythema and swelling 64 Post-inflammatory hyperpigmentation should be considered as a realistic potential side effect, particularly in patients with darker skin, and therefore, microneedling should be avoided in patients with obvious signs of sun exposure.65
Intense pulsed light
The basic principle of intense pulsed light (IPL) devices is selective thermal damage of tissue and chromophores – water, melanin and haemoglobin – to boost cellular rejuvenation.66 IPL devices use light and filters to emit incoherent high-intensity pulsed light at a specific wavelength range, fluence, pulse duration and intervals, making it suitable for treatment of a wide range of skin issues associated with ageing.66,67 The patient’s skin type must be recorded according to the Fitzpatrick scale pre-treatment68 as well as its specific condition, as
this determines the choice of suitable cut-off filters and therefore the spectrum of wavelengths to be emitted.66 Photo documentation is highly recommended at each IPL session.66
For this review, I have focused on data specifically linked to the effects of IPL on pigmentation, wrinkles and epidermal thickness. From my readings, IPL shows significant efficacy in skin rejuvenation, although differences in devices, wavelengths, numbers and intervals of treatments present limitations in comparing and drawing conclusions about the efficacy of IPL.66-72 Additionally, trials with greater subject numbers, different skin types and longer-term follow ups are required to assess the prevalence of skin changes 66 Trials have used a range of techniques to assess IPL efficacy, including patient and physician assessment photography and biopsy,68-73 blinded evaluation of pre- and post-treatment photographs,68 Fitzpatrick Wrinkle Severity Score67 and Melasma Area Severity Index (MASI).69
Before treatment of pigmentation, lesions must be identified as non-malignant and precisely diagnosed. Darkening and sloughing of treated spots can be expected in the days following IPL.66 Q-Switched ruby laser (QSRL) therapy is often recognised as the gold standard in pigmentation treatments;74 one trial (n=25) combined IPL with QSRL in Korean females with >2 pigmented lesions, at three to four-week intervals. A good to excellent improvement in lesions was reported by 76% of the subjects, whilst physician analysis reported 60% of subjects displayed 76-100% improvement in lesions.69 Yet a larger Chinese trial (n=89) yielded similar results in hyperpigmented subjects treated with IPL alone at wavelengths ranging from 560-640 nm; from patient analysis, 70.8% reported improvement of 50% or higher, whilst the physician’s report provided evidence that 77.5% of subjects experienced improvements of 51-100%.70
Another trial (n=58) used biopsy and photography to analyse skin changes following three sessions of IPL therapy.71 Marked improvements in wrinkles and pigmentation were displayed in 62.1% and 84.6% of patients respectively, whilst pathological examination provided evidence of an increase in fibroblast activity, a rise in types I and III collagen, but a decrease in elastin fibres.66 Conversely, a quantitative murine study highlighted significant increases in both collagen and elastin fibres directly proportionate to the number of
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Combination treatment involving three sessions of IPL and continuous fractional radiofrequency showed significant improvements in wrinkles, pigmentation and vascular lesions
IPL treatments administered. This could explain the physical changes behind the improvement in skin texture we see following IPL, but further trials are required to clarify exact cellular changes.66
The effects of IPL on wrinkles are unclear. One open-label study (n=38), treated periorbital rhytids with three IPL sessions using 572 nm at four weekly intervals, and provided data to show that 30.3% of subjects reported considerable to excellent improvement in the wrinkling in this area, whilst 27.2% were dissatisfied or noticed little or no improvement.73 Similarly, another small-scale, split-face trial (n=32) provided evidence that application of three sessions of monthly IPL therapy at 530-750 nm had no significant effect on rhytids, although pigmentation and skin texture improved with optimum results recorded one-month post-treatment.8 However, the effects of IPL on epidermal thickness appear promising; a 2018 trial provided evidence that five sessions of IPL significantly improved thickness of the stratum corneum, epidermis, basal layer and dermal papillae in 10 Asian subjects.73 Combination treatment involving three sessions of IPL and continuous fractional radiofrequency showed significant improvements in wrinkles, pigmentation and vascular lesions at six and 12 weeks in 11 subjects.75 The trials I have reviewed provide evidence that IPL is generally well tolerated and safe, with the most common side effects recorded being transient erythema and discomfort. Transient post-inflammatory hyperpigmentation, linear hypopigmentation, swelling and blistering also occur in rare cases.8,66-75
Consider your treatment options
This article has presented data available on the efficacy, safety and limitations of four different clinical approaches to facial rejuvenation. BoNT-A is highly effective in reducing wrinkles in the glabellar area,18 improving skin tone and texture.12,24 Dosing and brands vary between studies making evaluation difficult and extensive research into the effects of BoNT-A on other facial muscles and longer-term skin improvements is limited 16 Microneedling possesses the strongest evidence for long-term increase in both collagen production leading to greater epidermal thickness and wrinkle reduction54,57-59 although patients should be made aware of potential downtime following each treatment.64

HA dermal fillers can restore fat and skeletal depletion in the mid and lower face, improve skin hydration and promote collagen production.27- 35 Care should be taken in patient selection, and treating conservatively and appropriately according to age and sex to maintain facial harmony.34,44
In trials, IPL has comparable results to laser in facial rejuvenation, particularly in treatment of pigmentation and collagen stimulation,69-73 whilst its effect on wrinkle reduction is controversial.8,73 Most of the trials reviewed used IPL wavelength 530-650 nm, and as there is much variation between devices, this presents a challenge in assessing optimum wavelengths for different skin issues, and larger scale studies with long-term follow-up are required.66 This review also suggests that if implemented appropriately, combinations of these modalities used together in patient treatment programmes could help to rejuvenate the facial skin and structure longer term, although more large-scale trials are required to substantiate this.
Aesthetics Reviewing Panel member and nurse prescriber
Julie Scott commented...
This article provides a really nice overview of key aesthetic treatments, underpinned with relevant clinical data. In this article, the author has taken four of the staple treatments and explained them very well. It’s a holistic overview from ingredients and drug actions, to rheology, treatment considerations and possible reactions. I want to thank the author for bringing it back to grassroots in this article and reminding us of the basics of treatment. I find this to be a must-read for newer injectors and a wonderful recap for others.
Emma Coleman is an aesthetic nurse who opened her first aesthetics clinic in Orpington in 2015 and completed a dermatology diploma with distinction in 2019. She has opened a second clinic in Bromley, and her passion lies in providing holistic treatments to create aesthetically pleasing and natural results.

Qual: RGN
Test your knowledge!
Complete the multiple-choice questions and go online to receive your CPD certificate!
Possible answers
Questions
1. According to this review, what is the most likely number of microneedling sessions required to achieve an increase in collagen production?
2. According to studies, which type of filler is most suitable for tear trough rejuvenation in reducing risk of adverse events?
3. Which statement is most accurate:
a. Five
b. Three
c. Six
a. Monophasic HA filler
b. Profhilo
c. Biphasic HA filler
a. Toxin injections are designed to freeze muscles
b. Significant improvements in cutaneous hydration and elasticity, as well as a reduction in trans-epidermal water loss (TEWL) is seen in subjects at week 12 after toxin treatment
c. There is significant loss of skin hydration and elasticity in subjects at week 12 following toxin injections
4. According to clinical evidence, IPL is most likely to exert positive effects on:
5. Which statement is true?
a. Pigmentation and collagen production
b. Forehead lines and crow’s feet
c. Fibroblast activity
a. Skin ageing is influenced by genetic and cultural factors, pollution and sun exposure
b. Combining two therapies together into one patient programme often yields more profound and long lasting effects on skin ageing
c. When considering a patient for facial rejuvenation, it is important to focus on facial harmony and realistic aims and outcomes
d. All of the above
Answers: C,A,B,A,D
VIEW THE REFERENCES ONLINE! AESTHETICSJOURNAL.COM
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com














SHAPED BY SCIENCE

Patented technologies, the most sought-after ingredients in dermatology and significant clinical data. ALLSKIN | MED will bring something different to your clinic with results your clients will love.



Exclusively available from professional skin clinics. Expect more from your skincare.














UK & Ireland distributor: aestheticare.co.uk/allskin-med






















Providing Bespoke Lip Service to Your Patients
Galderma puts a smile on patients’ lips with innovative holistic individualised treatment (HIT) Kiss & Smile

As part of Galderma’s new, increasingly holistic approach towards aesthetics, the HITs methodology helps patients discover more individualised and natural results, and how they work in conjunction with one another. Their method teaches the use of AART™ – Assessment, Anatomy, Range and Treatment – in order to deliver ‘Holistic Individualised Treatments’ (HITs), a simplified approach to facial aesthetic needs, based on cross-usage of products for different areas of concern.
Galderma has designed five HITs for different areas of the face. Focusing on the lips and perioral area is Kiss & Smile, providing dynamic and natural results for the lips while treating concerns regarding static lines around the perioral area.
The Kiss & Smile HIT™ is a patient-centric, science-based, individualised treatment approach which enables injectors to leverage their expertise with the renowned Galderma portfolio to optimise aesthetic outcomes, while prioritising patient satisfaction. Every patient has a unique lips story and a different definition of the perfect lips. Regardless of age or gender, everyone is looking for their perfect smile, which calls for a truly individualised approach. The Kiss & Smile HIT™ begins with Galderma’s Lip Assessment Scale, which has been specifically developed to help practitioners systematically assess the lips and surrounding facial structures. It focuses on five individual facets, including Lip Shape, Proportions, Symmetry, Perioral tissue and Dynamic evaluation. These five facets are then graded according to their level of severity, before treatment priorities are identified and visualised with the patient.
The Galderma Lip Assessment Scale can then be complemented with the Galderma Facial Assessment Scale. A thorough facial assessment is important for recognising individual needs and creating a personalised treatment plan for patients. Galderma’s AART™ methodology uses Assessment with a facial assessment scale to identify patients’ needs and priorities, Anatomy analysis to fully assess the patient, a Range of solutions from the Galderma aesthetics portfolio and tailored Treatment plans for holistic individualised treatment. The recommended products in Galderma’s Kiss and Smile HIT™ approach are from the
Restylane range and can be used to target the various areas of concern within the lips and perioral region. These include:
• Restylane® KYSSE™ for smooth, plump and natural-looking lips1-3
• Restylane® DEFYNE™ for providing flexible support where definition is still needed in areas such as the chin4-7
• Restylane® REFYNE™ to treat static or fine lines in the dynamic perioral region, but still providing mobility for true expression4,8,9
Miss Priyanka Chadha, Acquisition Aesthetics director and Galderma KOL, said, “Now that Galderma has introduced HITs, the methodology enables practitioners to adopt a logical approach to their practice. It enables clinicians to ensure that no area of the patient treatment journey is overlooked by actively addressing anatomy, assessment, the Restylane range and treatment delivery. This in turn enhances the holistic approach, overall patient satisfaction and treatment outcomes. Addressing practice in this way ensures that it is not random or ad hoc, and that there is science and thought behind the treatment planning and delivery.”
This advertorial has been produced and sponsored by Galderma.
UKI-RES-2200363 DOP December 2022
REFERENCES
1. Hilton, Said et al. “Randomized, Evaluator-Blinded Study Comparing Safety and Effect of Two Hyaluronic Acid Gels for Lips Enhancement.” Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.] vol. 44,2 (2018): 261-269.
2. Bertucci, Vince et al. “Subject and partner satisfaction with lip and perioral enhancement using flexible hyaluronic acid fillers.” Journal of cosmetic dermatology vol. 20,5 (2021): 1499-1504
3. Restylane Kysse IFU, May 2022.
4. Philipp Dormston, W. G, et al. Perceived naturalness of facial expression after hyaluronic acid filler injection in nasolabial folds and lower face. J Cosmet Dermatol 2020;19:1600–1606.
5. Nikolis, A et al. “An Objective, Quantitative Assessment of Flexible Hyaluronic Acid Fillers in Lip and Perioral Enhancement.” Dermatologic Surgery: official publication for American Society for Dermatologic Surgery. 2021;47(5):e168-e173.
6. Solish, N. et al. Dynamics of hyaluronic acid fillers formulated to maintain natural facial expression. J Cosmet Dermatol 2019;18:738–746.
ADVERSE EVENTS SHOULD BE REPORTED
For the UK, report forms and information can be found at www.mhra.gov.uk/yellowcard or search for Yellow Card in the Google Play or Apple App Store. For Ireland, suspected adverse events can be reported via HPRA Pharmacovigilance, www.hpra.ie; Adverse events should also be reported to Galderma (UK) Ltd. Email: Medinfo.uk@galderma.com Tel: +44 (0) 300 303 5674.
7. Restylane Defyne IFU, 2020.
8. Williams, S, et al. Changes in skin physiology and clinical appearance after microdroplet placement of hyaluronic acid in aging hands. J Cosmet Dermatol 2009;8:216–225.
9. Restylane Refyne IFU, 2020.
Galderma’s AART™ methodology uses Assessment with a facial assessment scale to identify patients’ needs and priorities
35 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com Aesthetics | February 2023 Advertorial Galderma


AWARDS 11 March, Grosvenor House, London aestheticsconference.com Attend ACE 2023 for CPD accredited content including live injectable demos, the latest aesthetic trends, business insights and more. Headline Sponsor Co-located with AWARDS 11 March, Grosvenor House, London
5 conferences dedicated to injectables, innovation, leading brands, techniques and business, provide an unmissable 360 learning opportunity for practitioners.





16 CPD points for your appraisal



Conference Speakers


Teoxane Main Auditorium Innovation Stage Symposiums Masterclasses In Practice Theatre
Aesthetic
Cosmetic Doctor
Dr Raul Cetto
Doctor Dr Wassim Taktouk
Cosmetic Dermatology Doctor
Aesthetic Oculoplastic
Bhojani-Lynch Laser Eye
Aesthetic Doctor
Dr Lee Walker Dental Surgeon Dr Saleena Zimri
Dr Sabrina Shah-Desai
Surgeon Dr Tahera
Surgeon &
Rachel
Nurse
Prescriber
Dr Benji Dhillon
Cosmetic Surgeon
Goddard
Independent
Cosmetic
REGISTER FREE NOW @aestheticsjournaluk @aesthetics
Dr Kam Lally
Doctor Dr Jeremy Isaac
Cosmetic Doctor
Understanding Ablative vs Non-Ablative Lasers
Miss Jennifer Doyle discusses the differences between ablative and non-ablative laser resurfacing in aesthetics
In aesthetic medicine, lasers and light are commonly used to treat pigmentation, vascularity and textural issues in the skin. Treatments such as intense pulsed light (IPL) and broadband light (BBL) use a broad spectrum of wavelengths to absorb melanin and hemoglobin within the skin. Treatment of photodamaged skin with IPL or BBL has been proven to be an effective non-invasive method for skin rejuvenation, resulting in the clearance of redness and pigmentary blemishes.1
Conversely, lasers use individual wavelengths targeting specific chromophores and depths. Different laser devices have also been commonly used for skin resurfacing, and this article will discuss the important concepts for these applications.
Skin anatomy
In order to understand the specific treatment area, a basic understanding of the skin anatomy is important when looking at the role of different ablative and non-ablative resurfacing devices. The skin: the body’s largest organ: can be divided into three distinct layers.2
1. Epidermis: the outermost layer of the skin is comprised of several layers, with the stratum corneum being the most superficial.
2. Dermis: lies below the epidermis and is comprised of a vascular connective tissue. It is divided into the more superficial and thinner papillary dermis, and the deeper and thicker reticular dermis.
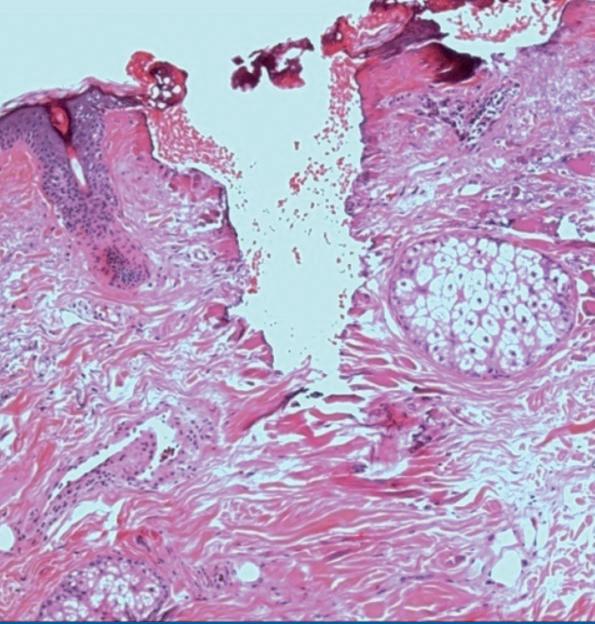
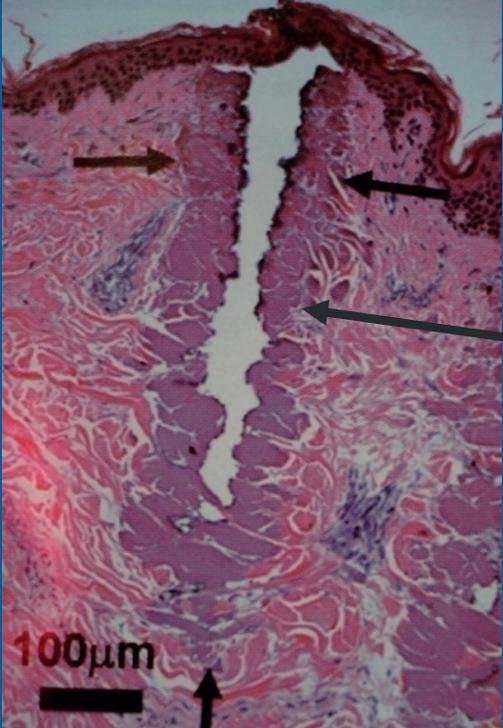
3. Hypodermis: the subcutaneous layer containing the major blood supply and adipose tissue.
Different laser wavelengths translate to varying peak absorption depths which coincide with these layers of skin.3 Common skin conditions such as scarring, wrinkles, pigmentation and vascularity exist at different levels in the skin and require different penetration depths for effective treatments.3
Ablative laser resurfacing
Ablative laser resurfacing is the process of removing tissue in the epidermal and dermal layers of the skin.2 When you look at the history of laser resurfacing, carbon dioxide (CO2) lasers have been an effective tool since the early 1990s.2 The CO2 wavelength is 10,600 nm and it targets water within the tissue to create a controlled wound.2 Later, Erbium (Er:YAG) lasers were introduced which have around 10 times the absorption efficiency in water than CO2. As a result, CO2 ablates some tissue but has leftover energy which is absorbed and causes a ‘zone of thermal necrosis’.2 Conversely, Er:YAG lasers cause almost pure ablation with the higher affinity for water.4 The role of CO2 vs Er:YAG is often debated as they are both considered similar treatments in terms of efficacy.5 In general, both ablative wavelengths offer similar quantifiable results, however Er:YAG has been shown to have quicker healing with less incidence of hypopigmentation due to the lack of thermal necrosis in the wound.4 Caution is advised when treating skin of colour with ablative lasers. Darker skin types tend to absorb more energy, resulting in a greater risk of side effects such as scarring, hypo or hyperpigmentation.6 There is little evidence suggesting that use of a short-term topical corticosteroid post-procedure can help minimise the risk of post-inflammatory hyperpigmentation for patients with Fitzpatrick skin type IV or above.7
The first ablative lasers were used for full-field application, meaning 100% of the skin surface was treated with the laser.8 Later, fractional lasers were developed to decrease downtime and minimise the risk of side effects like scarring, hypo and hyperpigmentation. Fractional lasers produce tiny wound arrays at different densities while leaving the surrounding tissue untouched by the laser. While downtime is less, fractional treatments generally require multiple sessions for optimal results.8
In the UK, there are many ablative lasers available commercially, some of which include: the CO2RE laser, JouleX Dual-Mode Erbium-YAG laser and SmartSkin CO2 laser.

Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Figure 1: Zone of tissue coagulation seen adjacent to CO2 laser defect. Image courtesy of Sciton.
Figure 2: Erbium ablation leaving no detectable coagulation zone adjacent to laser defect. Image courtesy of Sciton.
Figure 1
Figure 2
IT’S THE ONE
SWT ®: The only way to IPL
Selective Waveband Technology (SWT®) delivers precise narrowband IPL.¹︐² With 50% less fluence required than broadband IPL, this improves comfort, keeps downtime low, and enables use of multiple technologies in a single session – all without compromising patients' safety and comfort, as well as results.¹︐²︐³︐⁴
The Nordlys system is a multi-application platform with in-demand treatments across 24 indications, including pigmentation, vascularity, skin resurfacing, and hair removal.¹︐⁵︐⁶



Four timeless technologies: SWT® IPL, high-ROI Frax 1550™ and Frax 1940™ , and Nd:YAG 1064 nm¹
Grows with your practice – add handpieces to extend treatment options¹
Compact and quiet, with software modes ranging from guided to expert¹
Treats a wide range of skin tones¹
For more information, contact your local Candela sales professional or visit candelamedical.com

National Databank
2019. Available
https://www.surgery.org/sites/default/files/Aesthetic-Society_Stats2019Book_FINAL.pdf. Accessed Jan 25, 2022. ©
and unregistered trademarks,
service
brand names of
Corporation and its
other
owners. All rights reserved. PU02255EN, Rev. A
1. Nordlys User Manual, 2021. 2. Candela, data on file, 2022. 3. Bjerring P, et al. Lasers Surg Med. 2004;34(2):120-126. 4. Schallen KP, Murphy M. Treatment of photodamaged skin with a combined dual-filter intense pulsed light and fractional 1550-nm laser system. Lasers Surg Med Suppl. 2020;52(S32). 5. Nordlys and Frax Pro with Frax 1940 , CE mark. 6. The Aesthetic Society.
Aesthetic Plastic Surgery
Statistics
from
2022 Candela Corporation. This material contains registered
trade names,
marks and
Candela
affiliates. All
trademarks are the property of their respective
candelamedical.com
Non-ablative laser resurfacing
Non-ablative lasers first came to the market in the late 1990s.9 They achieve skin resurfacing outcomes by inducing controlled injury in the dermis to stimulate remodelling and collagen production. Compared to Er:YAG and CO2 ablative lasers, non-ablative lasers offer a reduction in recovery for patients.9 This is achieved by heating the tissue to the point of necrosis but not actually removing tissue, therefore leaving the skin intact after treatment. Patients experience less downtime but may have an increased number of treatments and more subtle improvements.9 Additionally, darker skin types can safely be treated with non-ablative lasers as risk of post-inflammatory hyperpigmentation is reduced.9
There are numerous lasers available, but the most common nonablative wavelengths include 1550 nm Erbium:glass for textural issues (1400u treatment depth) and 1927 nm Thulium for pigmentation (200u treatment depth).10 Treatments with non-ablative laser create microscopic treatment zones where the laser produces small columns of thermal injury to the skin.10 These thermal zones are rapidly repaired by the body, sending the injured dermal tissue to the epidermis to create microscopic epidermal necrotic debris (MENDs).10 These MENDs will naturally flake off after several days, leaving fresh new skin behind.10 In the UK, some of the popular non-ablative lasers include: Fraxel, Icon, Moxi and ResurFX.
Hybrid laser resurfacing
As resurfacing has continued to evolve, the latest advance in laser resurfacing uses a hybrid approach to simultaneously deliver two wavelengths. A 1470 nm non-ablative laser for tissue coagulation is combined with ablative 2940 nm Er:YAG for tissue vaporisation. As discussed, both ablative and non-ablative skin resurfacing are well-established aesthetic treatments. Both treatments have limitations tied to downtime as ablative procedures offer the best results with the most downtime, while non-ablative procedures offer quicker recoveries but with more limited results after multiple sessions.11
The hybrid approach allows providers to treat several skin conditions with high efficacy and reduced patient downtime compared to ablative lasers. This method of ‘combination laser therapy’ is an option to bridge the gap between ablative and non-ablative lasers.12 Practitioners should continue to be careful when treating skin of colour patients, however, hybrid technology enables the patient to
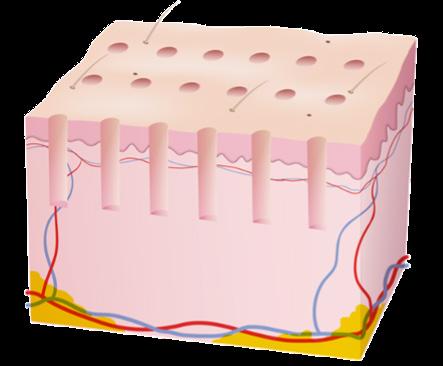
receive a high efficacy result compared to non-ablative and with a reduction in downtime. Hybrid laser technology is available in the UK commercially as Halo and Alma Hybrid.
Side effects and considerations
Though some variance exists between devices, in general there are common considerations with all laser resurfacing. Manufacturer protocols should be followed in accordance with patient skin type, and desired downtime may impact the treatment settings. Providers should conduct a thorough consultation and understand the patient’s medical history, recent sun exposure and fillers or injectables conducted in the past six to 12 months as possible contraindications. Patients should be made aware of possible side effects, including redness, swelling and dry/flaking skin. These usually resolve with time and will be dependent on the depth and strength of the treatment. Pre-treatment might be needed for patients with a history of herpes simplex (anti-viral) or melasma (hydroquinone).13 Possible complications include severe oedema, hyperpigmentation, hypopigmentation, burns and scarring. Practitioners can minimise the risk of these complications by ensuring the patient has no contraindications before treatment, patient selection, considering skin type and adjusting the treatment accordingly.8
Suiting your patient’s needs
Over the years, laser resurfacing technology has evolved significantly and there are many favourable treatment options available to providers in the UK. Ablative technology offers good results but with longer recovery and potential side effects. Nonablative technology offers an easier recovery with more moderate results. Hybrid technology combines both types of lasers and potentially shows some of the best aspects from both types. This wide selection of options allows providers to choose the technology and experience that is most appropriate for their patients.
Miss Jennifer Doyle is a consultant ophthalmic and oculoplastic surgeon based at The Clinic at Holland Park and at Milton Keynes University Hospital. She has a Bachelor’s in Medicine and a Bachelor of Surgery with distinction, as well as a Master’s in Medical Sciences from the University of Oxford. She is the non-surgical lead clinician at The Clinic at Holland Park. She has completed the Level 7 diploma in Injectables and served as a lead trainer for Harley Academy.
Qual: BMBCh, MA(OXON), L7Cert, FRCOphth
 Figure 3: Diagram showing isolated wound arrays created by a fractional laser. Image courtesy of Sciton.
To find out more about the latest devices in aesthetics, attend ACE on March 10-11. Scan the QR code to register for free.
Figure 3: Diagram showing isolated wound arrays created by a fractional laser. Image courtesy of Sciton.
To find out more about the latest devices in aesthetics, attend ACE on March 10-11. Scan the QR code to register for free.
VIEW THE REFERENCES ONLINE! AESTHETICSJOURNAL.COM Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Exploring Hand and Feet Perspiration
Dr Ros Jabar outlines the causes of excessive perspiration along with suitable treatment options
Most people have had sweaty palms at some point, usually when they’re nervous, but the vast majority of those do not have a medical condition. However, there are some who do. Hyperhidrosis is a relatively common condition that can cause a person’s palms, as well as their feet, armpits and other parts of their body, to sweat excessively, and it’s not always related to exercise.1 Patients with hyperhidrosis can experience heavy sweating to the point that it soaks through clothes and drips off their hands. This can understandably become a cause of social anxiety and embarrassment, as well as disrupting a patient’s day-to-day life to the extent that they feel they need to seek treatment.1
Background
For all mammals, sweating is a response that fulfils a number of functions. It helps with thermal regulation and offers an equilibrium for our pre-historic instinct to self-protect and survive. Sweating can also be an indicator of a patient’s psychological state. As humans, we possess three different types of sweat glands (eccrine, apocrine and apoeccrine), which all contribute to these regulations and functions.2
Eccrine glands are found throughout the body and are in abundance on the hands and feet. While physiological sweating of the face, neck, armpits and back is an important part of thermoregulation, the eccrine glands on the hands and feet are stimulated by the nervous system, which is why it’s common to get sweaty palms when nervous.3
Humans have between two and four million eccrine sweat glands across their bodies, which can be found on hairy (non-glabrous) skin such as the face and limbs, and smooth (glabrous) skin as found on the palms and soles of the feet. Eccrine gland density differs across the surface area of the body, with the highest gland densities found on the palms and soles.3 The density of the eccrine glands on non-glabrous skin is between two and five times greater than it is on glabrous skin.3
Eccrine sweat glands primarily produce sweat in response to an increase in body temperature, but skin temperature and increased blood flow can also stimulate the glands.3 The rate at which people sweat is down to the density of their active sweat glands, as well as the rate of secretion per gland.3
Hyperhidrosis
As medical professionals, we look to investigate when these typical sweat responses are not a reaction to heat, and are instead a response to a patient’s tolerance being full and their usual coping mechanisms for stress and self-soothing are ineffective. When diagnosing hyperhidrosis, I look for ‘emotional sweating’ which is not caused by heat but by mental stress, deep respiration and local tactile stimulation including the warming, drying and rubbing of the soles of the feet. This emotional sweating can create challenges for patients and make slips more likely, even when doing gentle, everyday holding and stepping. In my consultations, I will ask the patient questions such as when they notice the sweating is worse and if they are prone to any other sweaty areas.
There are two types of hyperhidrosis:1,3,4
1. Primary hyperhidrosis: This is caused by an overactivity of the sympathetic nervous system which leads to the narrowing of arteries and the excessive stimulation of eccrine sweat glands, causing excessive sweat production. It commonly occurs in the hands (palmar hyperhidrosis), feet (plantar hyperhidrosis) and armpits (axillary hyperhidrosis). There isn’t a known medical cause, but it’s thought to have a genetic link, with 40% of patients having a family member with the condition.5
2. Secondary hyperhidrosis: This condition is caused by an underlying medical condition such as diabetes, thyroid issues, some cancers (leukaemia, Hodgkin’s lymphomas, liver cancers for example), menopause, infections or nervous system disorders. It can also be a side effect of certain medications, including antidepressants, pain relievers and some hormonal and diabetes medication. Secondary hyperhidrosis can cause sweating all over the body, although it’s typically worse in the palms, feet and underarms due to the relatively high concentration of sweat glands in these areas.
The psychological and emotional impact of excessive sweating can damage a patient’s confidence and have a significant impact on their day-to-day life. The condition can cause social, psychological and occupational problems, with many hyperhidrosis sufferers reporting negative impacts on their social life, sense of wellbeing and emotional and mental health.5,6 A total of 5% of sufferers take antidepressants or anti-anxiety medications due to their sweating.5,6 Although hyperhidrosis can have a detrimental impact on sufferers’ lives, excessive sweating from eccrine glands is not a source of odour. Eccrine glands secrete a clear, odourless fluid. The ‘body odour’ we associate with sweating is produced by another type of sweat gland called the apocrine gland.6 These glands are found in the armpits and genital region, and produce a thick fluid which produces a potent odour when it comes into contact with bacteria on the skin’s surface.6
Treatment options
There are a number of non-surgical treatment options for hyperhidrosis, including:7
• Toxin – injections can be applied to the hands and armpit area, with multiple injections given in a single session
• Iontophoresis – a low-voltage direct electrical current is applied to the patient’s hands and feet when they are submerged in water
• Laser for underarms – laser light can be used to permanently destroy axillary sweat glands without damaging the surrounding tissue
• Thermal energy for underarms –technology which emits microwave energy into the skin, heating and destroying the sweat glands
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
• Oral medications such as anticholinergics – anticholinergic medications can be effective but also decrease sweating over the entire body, not just the problem areas, increasing the risk of overheating
• Natural remedies – some natural remedies are still used, including witch hazel, which acts as an astringent and antiperspirant There are also several methods of surgically treating hyperhidrosis by cutting, clipping or removing the affected nerves. Although this can be effective for the treatment of palmar hyperhidrosis, improvement in plantar and axillary sweating is less consistent.
Case study
A 14-year-old boy was referred to me by his mother and school teacher. The patient had to change his cotton gloves six times a day just to be able to hold his pen at school. He also didn’t want to hold hands with anyone or play any ball games or sports, and sadly became a withdrawn teenager. As the patient was under 18, we could only provide treatment with a legal guardian present, and as the procedure was deemed medical, it could only be performed in a registered establishment. His treatment therefore occurred at the University Hospital of Wales Medicentre which is registered with Healthcare Inspectorate Wales. If treating hyperhidrosis in other regions of the UK, the establishment should be registered with the Care Quality Commission, Health Improvement Scotland or The Regulation and Quality Improvement Authority in Ireland. The first stage of the treatment was a full and thorough consultation with both the patient and a parent present due to his age. During the consultation, I learnt that a toxin had previously been administered by another medical practice, but the patient had found this traumatic due to too many healthcare professionals being in the room, as well as the use of diabetic needles causing pain. He was reluctant to try this treatment again, so we decided to explore other options.
patient’s choosing and his parent waited in the waiting room at the patient’s request. I explained the process to the patient in full before the treatment began, and made it clear to him that he could leave and change his mind at any point. I chose not to perform the starch test so as not to put the patient through any more unnecessary stress. However, I would usually perform this to identify moisture released from the sweat glands/skin. A thin layer of iodine tincture is applied to the area until it dries. After, a thin layer of starch powder is applied, showing a pale brown colour. When moisture/sweat is produced, the starch and iodine mix to form a polyiodide that has a blue/purple appearance, indicating the prescence of moisture/sweat.8
I applied topical anaesthesia and then drew a grid on the palm of the patient’s hand to help deliver the toxin in equally spaced 1-2cm aliquots of 2-3 units.8 We also did the same on the medial and lateral aspects of his fingers and thumbs (Figure 1). I used high gauge 32 needles to apply the treatment and used multiple syringes to deliver the toxin to keep the needles sharp and reduce any discomfort. The toxin was delivered just below the skin’s surface, leaving small blebs. I delivered 50 units of toxin to each hand, and the treatment was completed in no more than 10 minutes. The speed and precision of the treatment were central to the patient’s comfort and confidence. There are potential side effects to any treatment including pain, bleeding, bruising and infection, all related to the needles and breaking of the skin, but this patient did not experience any side effects. The aftercare provided to the patient included avoiding activities involving the hands for the next four to six hours, avoiding hot baths/showers, avoiding other hand treatments and refraining from moisturising or massaging the hands.


For nine months of the year, the patient’s palms were completely dry. We would see him for a follow-up after this time. He has since gone on to complete his GCSEs and A-Levels and is now studying engineering at university. His confidence has increased exponentially – he is excelling at his studies, socialising assuredly and is in a healthy relationship.
Combatting hyperhidrosis
Excessive hand and feet perspiration is usually the result of a condition known as hyperhidrosis. Although it’s not clear why hyperhidrosis develops, it’s thought to have a genetic element (primary hyperhidrosis), but could also be caused by a medical condition or by taking certain medications (secondary hyperhidrosis). Patients with palmar (hand) or plantar (feet) hyperhidrosis should see a healthcare provider if the sweating disrupts their daily routine or causes emotional distress or social withdrawal. Treatments, both surgical and non-surgical, can be very effective.
Throughout the consultation, it was evident that the patient suffered from palmar hyperhidrosis, which was most likely to be primary hyperhidrosis. His mental health had been affected and his confidence was low. His academic progress had also been negatively impacted. Despite the patient’s previous experience with a toxin, I decided this was the most appropriate treatment in this case. Although the patient found the treatment painful, he had noticed a reduction in sweat and his mother agreed. However, I wanted to deliver the treatment in a much calmer and more comfortable environment to reduce the patient’s anxiety and discomfort. I reduced the number of staff present in the room, played music of the
Dr Ros Jabar is an aesthetic practitioner and divides her time between the polytrauma unit in the University Hospital of Wales and Ros Medics, an aesthetic, cosmetic and skincare clinic. Dr Jabar has a background in accident and emergency, acute medicine and general medicine. Previous to undertaking her medical degree, Dr Jabar was a consultant pharmacist. Qual: MBBCh, BSc Pharm

TO VIEW THE REFERENCES GO ONLINE AT WWW.AESTHETICSJOURNAL.COM Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Figure 1: Markings on patient’s hand to show the points to inject

Case Study: Treating
Acne Scarring


Nurse prescriber Hannah Depledge presents a case study combining radiofrequency microneedling with skincare to treat active acne and scarring
Over the last couple of years, we have seen a shift in the way patients want to look. The days of looking ‘overdone’ have been replaced with a want for good skin health and a more natural appearance. Many people suffer with acne and often come into a medical skin clinic as a last resort after they have tried a range of over-the-counter topical skin products and been prescribed oral antibiotics by their doctor with little improvement. Acne and acne scarring can have a huge impact on a patient’s self-esteem and confidence, and the scarring can often be permanent.1 When managing acne, treatment starts with topical home care to treat the acne, followed by a range of in-clinic treatments such as microneedling, skin peels, fractional radiofrequency and laser. In this article, I have included the case of a patient I treated to address her acne and scarring, detailing the treatment plan and the results achieved.
Case study
A 27-year-old female patient contacted us at the start of the first lockdown in April 2020. The pandemic caused our clinics to shut, and the only way we could help patients was by providing topical skincare advice and posting products out. The patient had been suffering from moderate hormonal acne for more than 10 years since she
was a teenager because of her polycystic ovarian syndrome, and the acne had a massive impact on her self-esteem.
Consultation
As the clinic was shut, I was unable to consult and review the patient’s skin in-person, so I performed a consultation via a video call. I asked her to send photographs of her skin prior to the consultation so that I could have a closer look. Video consultations have their limitations when assessing the skin as we are unable to see it clearly and up close. This meant that the before treatment images were not of the best quality. From the photographs, I could see that the patient was suffering with severe acne that was concentrated on her lower face, jawline and chin (Figure 1). The skin was red and inflamed, with congested pores and comedones over her face, and she had active acne as well as pigmented acne scarring mainly to the lower face and jawline. She was using a drug store skincare brand without little advice or recommendation from anyone and had been taking oral doxycycline prescribed by her doctor for three weeks. She had been prescribed this before and noted that it had little effect with the acne coming back when she stopped taking the tablets. I suggested that she continued to take the course of doxycycline prescribed and would reassess the use of these once the topical skincare treatment had started.
The consultation consisted of discussing the patient’s past medical history and asking her to list what products and treatments she had tried. She had been prescribed topical benzoyl peroxide 5% cream by her GP, but she didn’t tolerate this well and described it as ‘burning her skin’. The cream was prescribed without further advice about what other products to use alongside it to build the skin’s barrier and soothe the irritation. We discussed the importance of clearing the acne first before starting any scar reduction treatments. It was important that there wasn’t any active acne present before performing needling treatments as if the needles encountered the bacteria under the surface of the skin, it could spread and possibly worsen the flare ups. She had both hypertrophic scarring, some atrophic scarring and post-inflammatory hyperpigmentation.
I discussed the options we had for treating her acne scarring in-clinic as soon as we were able to reopen and gave her suggestions to suit her budget as this can be a deciding factor about how far a patient can proceed. Our usual plan for acne scarring is a course of microneedling and regular skin peels. However, just before lockdown we purchased our first device from InMode, the Optimus platform which included the Morpheus8 fractional radiofrequency handpiece. The patient was keen to try the Morpheus8 due to the good reviews from other acne sufferers. Therefore, we planned to get her in for a course of this once the clinic reopened.
Skincare
I decided to start the patient on a ZO Skin Health acne programme as we have had positive results from using these products to treat acne in the past. This programme included a twice daily skin routine using the Exfoliating Cleanser, Exfoliating Polish, Complexion Renewal Pads, Daily Power Defence, Daily Sheer SPF 50 and Complexion Clearing Masque. This is a mild treatment plan for acne,
Figure 1: 27-year-old patient’s initial consultation picture of her active acne and scarring
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Sofwave™ SUPERB™ ultrasound technology is the new non-invasive FDA-cleared way to lift the eyebrow, lift lax submental and neck tissues, improve facial lines and wrinkles, and short-term improvement in the appearance of cellulite











Groundbreaking and proprietary technology with integrated cooling that enables treatment at the optimal depth in the mid-dermis for collagen production, making sure you look more lifted every time you look in the mirror.
What Sets Sofwave™ Apart?

Simple and delegate-able protocol
Patented integrated cooling system
Safe for all skin types

Quick procedure (30-45min)
Non-invasive with no delays to daily routine
WINNER OF
 BASELINE 4-MONTH FOLLOW UP
BASELINE 1-MONTH FOLLOW UP
Photos Courtesy of Skye Dermatology & Dr Oliver Spencer
BASELINE 4-MONTH FOLLOW UP
BASELINE 1-MONTH FOLLOW UP
Photos Courtesy of Skye Dermatology & Dr Oliver Spencer
MK00076_V2
which allows the patient’s skin to become tolerant before moving on to stronger products.
I suggested the patient did this for six weeks because a typical skin cycle, i.e. the time it takes for an old skin cell to be replaced by a new skin cell in a younger person, is usually between 21-45 days.2 After six weeks, we knew that the old skin cells would have been replaced by new ones and therefore would be stronger and more compliant to harsher products. In our experience, if we are too aggressive at the start and introduce retinols too early, patients often give up as they believe the products do not suit them.
After six weeks, I had a phone call with the patient to discuss how she was getting on with the at-home skincare regime. She had been sending me regular photos as an update and her acne had started to clear well. She did still have some redness and dryness but found this tolerable. Her skin had begun to clear, was smoother, looked less dull and had a glow to it. She was thrilled with how her skin had improved and was keen to carry on and increase the treatment plan. As she was tolerating the regime well and her skin barrier was improving, I moved her from the mild acne protocol to the severe protocol in the ZO Skin Health regime, adding Oil Control Pads to replace the Complexion Renewal Pads containing 2% salicylic acid. These pads are beneficial in helping to reduce sebum in the pores and encourage exfoliation of the dead skin cells. I swapped the Exfoliating Polish to a Dual Action Scrub as this was stronger, medicated and better at treating acne. I also added in an Exfoliation Accelerator which contained glycolic and lactic acid and tretinoin 0.5% to begin treating the scarring. She used the ZO products at home for three months, which cleared up most of her active acne. When the clinic reopened, the patient was able to come in to have some treatment to improve her scars.
Treatment
Before we purchased our Morpheus8 device, we treated acne scarring with peels and standard microneedling using a SkinMed Derma FNS pen. Whilst I achieved some good results, I felt we needed something that would treat severe acne scarring better and therefore I chose the Morpheus8 device. Fractional radiofrequency is indicated for the face, neck, chest and back of the hands.3 The treatment induces ablation, thus improving the appearance of rough texture, fine lines, wrinkles and depressed scars, along with superficial pigmentation. The treatment also induces skin rejuvenation by heating the dermis, which stimulates collagen generation and replenishment.3
I usually recommend a course of three treatments, four to six weeks apart, as this gives the skin a chance to heal and the skin cells to shed, but this patient only had two before we went into lockdown again. I performed the first full-face Morpheus8 treatment in July 2020. This treatment can be quite uncomfortable, so I always numb the skin for one hour using a topical numbing cream, to ensure the patient is comfortable. Morpheus8 has little side effects, the main ones being redness and dry skin for a few days after the treatment. It can also be performed on all skin types, even darker skin following a period of skin preparation using hydroquinone and tretinoin and a reduction in the energies used.4
I used the 24-pin tip and performed two passes over the skin. The first pass at 3mm depth fixed used a double stacking approach which delivers two shots of radiofrequency when the needles remain in the skin, while using an energy of 50. On the second pass, I performed a single pass at a depth of 2mm and used an energy of 35. A total of 420 shots of radiofrequency was given in this treatment. The patient did notice improvements following the first treatment. Her atrophic acne
scarring looked better and her skin generally was tighter and smoother. I usually recommend a gap of six weeks in between treatments, so the patient’s second Morpheus8 procedure was performed in September with the same treatment specifics carried out. She did struggle this time with some discomfort. Patients can struggle more on their second and third treatments without any real explanation. We were unable to perform as many shots but concentrated on the scarring rather than performing on the full-face. A total of 246 shots of radiofrequency were performed. Unfortunately, another lockdown meant she couldn’t have her third treatment but we recommended that she came back for a review when she could to make a plan for the future. She did eventually have her third treatment.
Results
When we reviewed the patient six months after her two Morpheus8 treatments, I was able to see how it had transformed her skin. It was clear of acne, she had virtually no scarring and the pigmented red lesions had almost gone. The patient was thrilled with her results and described them as ‘life changing’. Her confidence has vastly improved as a result. We plan to maintain the results with regular Hydrafacials, ongoing skincare maintenance with ZO products and a yearly Morpheus8 treatment. The only product we changed in the ZO regime was stopping the tretinoin and adding a maintenance retinol named Wrinkle + Texture Repair as it could be used daily without continuous irritation.

A combination treatment
This case study highlights how a combination of treatments can bring about life changing results for our patients. Results take time and patients must be willing to commit to the treatment plan and follow the recommended advice. When they do commit, the results can be transformative as we can see from the images above.
Hannah Depledge is an aesthetic nurse prescriber with more than seven years’ experience in the aesthetics specialty with a special interest in treating skin. She opened Eterno Aesthetics Medical Skin Clinic in Sheffield in 2019. Prior to this, Depledge was a palliative care nurse in the NHS for 11 years.

Qual: RGN, BSc, MSc, NMP
 Figure 2: Patient before and 12 months after Morpheus8 device treatment. Results show an improvement in acne scarring, facial lifting and tightening.
Figure 2: Patient before and 12 months after Morpheus8 device treatment. Results show an improvement in acne scarring, facial lifting and tightening.
Before After VIEW THE REFERENCES ONLINE! WWW.AESTHETICSJOURNAL.COM Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com

by Adverse events should be reported. For the UK, Reporting forms and information can be found at www.mhra.gov.uk/yellowcard or search for Yellow Card in the Google Play or Apple App Store. For Ireland, Suspected adverse events can be reported via HPRA Pharmacovigilance, Website: www.hpra.ie; adverse events should also be reported to Galderma (UK) Ltd, Email: Medinfo.uk@galderma.com Tel: +44 (0) 300 3035674 FOR ANY & EVERY LOOK Your expertise, meets ours. The world’s most diverse range of individually designed dermal fillers and skinboosters.1-3 Matching your mastery, with their vision. References: 1. Data on file. MA-43049. 2. Data on file. MA-34483 3. Nikolis A et al. Aesthet Surg J Open Forum. 2020; 2(1):1-12 UKI-RES-2200358 DOP December 2022
Achieving Clinical Efficacy When Performing Microneedling
Upskilling the aesthetic practitioner to meet industry standards

Microneedling has rapidly gained popularity in the past decade. As one of the most requested aesthetic treatments, this minimally-invasive service targets a variety of concerns including hyperpigmentation, lines, wrinkles and even visible pores. However, the device and products used in the service can influence the extent of results and minimise downtime further. Microneedling stimulates collagen and elastin production by inflicting micro-injuries in the
are not a qualification, however, regulated qualifications are developed in line with these standards.
Endorsed programmes and regulated qualifications

skin, leading to skin rejuvenation. The manner in which these perforations are made is vastly different between a manual roller versus a pen. Roller devices will leave a pyramid shape wound on the skin by nature of the action of the drum rolling over the surface. This is in contrast to a pen which will puncture straight down into the skin. This means using a pen device will result in more controlled trauma to the skin, while also influencing the efficacy of the treatment. Finer needles provide cleaner and more effective perforation. Cartridges that have fewer needles and larger spacing between each pin can also drastically reduce the Fakir Effect. This phenomenon results in the skin being pushed downwards as the needle plate makes contact with the skin, therefore reducing penetration of needles to the desired depth. This effect can also be influenced by devices with extremely high stitch speeds. The result is more scratching or tearing of the tissues instead of a clean puncture.
The products used to facilitate the movement of the pen over the skin can accelerate results and reduce downtime. One of the most recent advances is an innovative approach called pro-resolution using omega-3, delivered through the new Pro Pen device. This not only accelerates wound healing, but also resolves overexpression of inflammation, limiting potential downtime and amplifying tissue regeneration. The use of these ingredients at home by the patient can further improve skin recovery.

Meeting industry standards
Patient safety and clinical results are central to all aesthetic procedures. Quality training elevates skills and enables aesthetic practitioners to deliver high-standard services that deliver the desired outcomes. With increased patient demand for aesthetic treatments such as microneedling, finding the right training that builds confidence and expertise is essential. When training focuses on protocol and procedure but is missing the underpinning and supporting knowledge, it can prevent effective treatment decision-making. Professionals can find it difficult to benchmark their practice and ascertain whether they meet the National Occupational Standards (NOS) for these services.
The NOS specify the knowledge, skills and behaviours an individual needs to be competent in an occupation. With no real industry regulation for non-surgical cosmetic procedures, the NOS provide a clear industry standard to which they should be performed. The NOS
Since 2019 Dermalogica has been investing in upskilling their own skin therapist staff, and to date 52 of the professional team have achieved their CIBTAC Level 4 Diploma in microneedling and chemical peels. Dermalogica has also been carefully aligning training in advanced services including Pro Microneedling and Pro Power Peel, along with Pro Pen Manufacturer training to meet with these standards and training recommendations. Dermalogica has developed the Pro Pen Endorsed programme, which is directly mapped to NOS and the Level 4 Microneedling qualification specification. Dermalogica is proud to have the programme CIBTAC endorsed. With a renowned legacy in high-quality training, Dermalogica has been planning the introduction of a regulated qualification offering through the International Dermal Institute. In 2023, this programme will offer professional skin therapists the opportunity to complete CIBTAC Level 4 awards in microneedling and chemical peels, with the current Pro Pen Endorsed programme eligible for credits towards the award.
Aurelian Lis, CEO of Dermalogica, commented, “As the leaders in professional skincare education with nearly 40 years of expertise, we’re always innovating to help skin practitioners achieve new levels of success in their business. With changing consumer requirements and growing excitement around aesthetic services, we see this launch as a way to get a whole new generation into this industry, which is both good for the livelihoods of those who work in the industry, but also for skin health in general. There are other needling pens on the market, but what’s exciting to me is that because Dermalogica knows peels as well as needling, we can actually create procedures and treatments which combine the two and show fabulous results.”
49 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com Aesthetics | February 2023 Advertorial Dermalogica
This advertorial was written and supplied by To find out more scan the QR code
Case Study: Utilising Laser for Fat Loss
Dr Abs Settipalli treats a female patient using green laser to reduce body fat
The body contouring market is one of the fastest evolving and in-demand markets to date, with new devices appearing regularly 1 Low-level laser therapy (LLLT) – also known as photobiomodulation, cold laser therapy, low-intensity light therapy or soft laser therapy – is a non-invasive, painless, no-trauma light source treatment that has started to be used for aiding fat loss in more recent years. Here, we will present a case study showing a successful treatment for fat reduction using green laser.
What is LLLT?
Hungarian physician and surgeon Mr Endre Mester is credited with the discovery of the biological effects of low-power lasers, which occurred a few years after the 1960 invention of the ruby laser and the 1961 invention of the helium-neon (HeNe) laser. Mester accidentally discovered that low-level ruby laser light could regrow hair during an attempt to replicate an experiment that showed that such lasers could reduce tumours in mice.2 Since then, studies have shown that LLLT has excellent pain-relieving properties, as well as the ability to improve the functioning of various cells.2,3
For a long time, non-thermal LLLT has been confused with light emitting diode (LED).
The main difference is that non-thermal lasers are collimated, unidirectional and monochromatic so this optimises photonic energy into the mitochondria of the fat cell, not losing any photonic energy en route as with a non-coherent light like LED.4 Research has shown the benefits of this modality through mitochondrial actions, cellular proliferation, intra and extra cellular communication, not to mention a restoration of mitochondrial DNA and other essential processes. As such, the benefits of low-level lasers are known to reduce pain, inflammation and oedema, prevent cell death and tissue damage and promote wound healing.3
Laser for fat reduction
In the last few decades, we’ve learnt a lot more about how light treatment, and more recently how green light treatment, works on fat reduction. For example, one study showed that low-powered green lasers in particular can help people lose body weight and achieve a smaller waist size.5 The study recruited 60 participants with a body mass index (BMI) between 25 and 30. All the participants took part in 12 identical LLLT treatments. The green lasers were targeted at the abdomen and central back for 30 minutes during each session. The participants were
split into three groups of 20. They examined the participants before the study began and again at weeks four, six and 12. During the study, the participants did not make any drastic diet changes, simply drinking two litres of water and reducing sugar intake. All 60 of the participants lost 1-2kg of body weight. The waist measurements suggested that much of this weight loss came from the abdominal area.5 Other studies have also shown the effectiveness of green light on fat reduction.6,7 There are no reported side effects for this treatment.5-7
In our experience, green light therapy appears to achieve a significant improvement in fat loss treatment. Here, we will present a case study to evidence the positive effect of green LLLT therapy on a female patient and explain how we achieved this result in our practice.
Case study
A 54-year-old female patient presented to our clinic citing her main aesthetic concern as being her stomach and legs, as well as generally feeling tired and old. Her primary goal was to look slimmer and feel more confident. The patient was unsure what treatment would be best for her, but she was undergoing a weight loss programme at the time and wanted something that would speed up her progress. The patient had realistic expectations and understood that anything non-surgical was not a miracle, but she opted not to go down the surgical route as she wanted little downtime and found surgery to be less cost-effective. The patient was a non-smoker, had no medical conditions and had also never received any non-surgical aesthetic treatments in the past. The patient walked twice a day as a form of exercise and had a generally healthy diet.
The consultation
During the consultation, we ran an analysis to record the patient’s weight, skeletal muscle mass and percentage body fat to ensure that this could be monitored throughout the treatment journey. We used the InBody device at our practice, and there are other such analysis machines on the market. Various treatment modalities were discussed with the patient. The options presented to her included LLLT for fat loss, high-intensity focused electromagnetic (HIFEM) therapy for muscle stimulation and strengthening and radiofrequency for skin tightening.
It was discussed during the consultation that LLLT would be the best treatment option over the other modalities available in our clinic
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
The patient noted that she felt more confident in her appearance, her jeans fit better and her energy levels had increased tremendously
because it was found that the patient had a body fat percentage of 44%, a BMI of 30 and a visceral fat score of 19/20. The patient had an overall wellness score of 57/100. The total score reflects the evaluation of composition, based on the weight of total body water (intracellular water and extracellular water), protein, minerals and body fat mass. This patient therefore had to debulk the body first and reduce body fat percentage before we could focus on body contouring, as she would not see optimal results with the other options until this had been done. At our clinic we use Emerald, which has a 532 nm wavelength, and an eight-session treatment programme with once-a-week treatments being advised. The patient’s lifestyle, water intake and diet were also discussed in the consultation, and she was advised to drink a minimum of two litres of water per day before treatment began for a total of seven days. The patient was also advised to reduce sugar intake and saturated fat intake, but to continue with a balanced diet. We asked her to keep track of daily changes and she was handed an Emerald Journey Diary whereby change in energy levels, sleep levels and lifestyle changes could be monitored daily. This would then be reviewed every week.
The procedure
The patient did not require any disinfectant prior to treatment, as this specific laser does not disrupt the skin barrier, nor ever touch the patient’s skin. The patient laid comfortably
on the treatment couch, while her abdomen was exposed and 10 low-intensity 532 nm lasers were applied for 15 minutes. The laser diodes target the subcutaneous fat creating a transitory pore in the adipose fat cells. Once this pore opens, the triglycerides and fatty material inside seep out into the interstitial space between the cells, causing the adipocytes to collapse and shrink in size. From there, the lymphatic system safely excretes fatty material through its normal process of detoxification.
The patient then had to lie on her front, where this process was repeated.5,6,7 The same was done for each of the following six sessions. Emerald laser has no pain or downtime, so the patient was able to return to her usual routine straight away following treatment.


Results
Although the patient was advised a programme of eight treatments, she stopped after treatment seven as she was pleased with the results she had already achieved. After seven treatments over a period of seven weeks, the patient’s wellness score increased to 62/100, and her visceral fat decreased with a new score of 17/20. Her body fat percentage decreased to 40% and her BMI also dropped to 27. Our analysis showed her abdomen held 18.8kg of fat prior to treatment, but at the end the results showed 16.6kg –a decrease of 2.2kg in seven treatments. Following treatment, she felt more confident


in her appearance, her jeans fit better and her energy levels had increased tremendously. The patient was advised to live a healthy, balanced, active lifestyle and to continue with ongoing maintenance treatments once every six weeks for as long as the patient deemed necessary, as in our clinical experience, this can prolong and enhance the results. The patient was also advised a series of four HIFEM device treatments using the EMSCULPT NEO device to contour the body and strengthen the core, however, due to personal reasons, she has been unable to undergo the procedure as of yet. We do typically recommend using HIFEM for patients after treatment using laser, because after the fat has been emulsified with the Emerald, HIFEM can help release this emulsified fat from the body.
Utilising LLLT

In recent years, LLLT has been used for many reasons such as to reduce pain, inflammation, and oedema, promote the healing of wounds, deeper tissues and nerves, as well as preventing cell death and tissue damage. More recently, green lasers have been used to tackle fat and fat reduction, with little to no downtime or side effects.
Dr Abs Settipalli graduated from the University of Leeds in Dentistry and then went on to complete his Master’s Programme in Italy. He practises mainly in the UK splitting his time between treating his own patients, teaching university students and professionals, research in clinical trials and authoring publications. Qual: MChD, BChD, BSc
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
After Before After Before VIEW THE REFERENCES ONLINE! AESTHETICSJOURNAL.COM
Figure 1: 54-year-old patient before and after seven treatments using Emerald LLLT
Erchonia are exhibiting at ACE 2023 on March 10&11. Scan the QR code to register for free.



‘Upgrade As You Grow’ LUMINA® the multi-treatment Laser and IPL Platform LUMINA® Call Lynton today on 01477 536 977 or visit lynton.co.uk THE TECHNOLOGY TO TRANSFORM #weuseLynton #illumiFacial Award-winning ResurFACE® fractional laser handpiece upgrade, available for ablative treatments with minimal downtime 4 Multiple IPL handpieces for hair removal & various skin rejuvenation treatments 1 Long-pulsed Nd: YAG upgrade available for those looking to treat all skin types including darker skins 2 Ergonomic, active Q-switched laser upgrade for removal of multi-coloured tattoos 3
A History of Radiofrequency
Aesthetic medicine is developing at a rapid rate, with energy-based technologies in particular gaining momentum. Radiofrequency (RF) – a technology first used in the medical sphere in the 1920s for electrocautery1 – is one of primary modalities used to address patient requests for rejuvenation, skin tightening and body contouring. Since its inception, RF has developed with several forms of energy delivery, as well as being used in combination with other aesthetic treatments.
Here, we will outline how the treatment has evolved and how it might be used in the aesthetic specialty going forward.
How radiofrequency works
Radiofrequency is a type of electromagnetic radiation with a frequency range from 30-300 GHz. It produces heat by generating electromagnetic energy, which passes through the tissue, creating vibrations at a molecular level. For skin treatments, the heat damages the body’s collagen, stimulating a wound-healing response which in turn causes neocollagenesis.2 For body shaping treatments, some manufacturers claim patients can experience apoptosis of the fat cells, while others say that they help to melt the fat by making the cell membrane more permeable so that fatty acids and lipids can be excreted via the lymphatic system.3 Subdermal temperatures from 65°C to 68°C and skin surface temperatures ranging from 38°C to 42°C are required to obtain optimal contraction.4
Developments over time
After its initial use for electrocautery, RF was further developed in medicine to treat a variety of indications, including tissue electrodesiccation electrocoagulation, joint capsular tightening, corneal curvature alteration, incompetent saphenous venous closure, aberrant cardiac electroconductive ablation and prostate and liver neoplasm eradication.5
When it comes to aesthetic medicine, the first method of delivering RF into the skin was brought into the limelight in the early 2000s for concerns such as laxity, wrinkle reduction, acne and skin tightening, and several methods of delivery have now been developed, including monopolar, bipolar, multipolar and fractional. RF technology can be used on all skin types.5
Monopolar
The first kind of RF device used in aesthetic medicine was delivered through a monopolar technology and was approved in 2002 by the Food and Drug Administration (FDA) for facial wrinkle reduction and periorbital rhytids.6 Monopolar devices deliver a current through one
singular active electrode, flowing from the device to a grounding pad placed on the treatment area.
Monopolar technology has been shown to be effective for treating skin laxity, with one study of 86 patients showing wrinkle score improvements of at least one point in 83.2% of treated periorbital areas. In addition, 50% of subjects were either satisfied or very satisfied regarding the degree of reduction in periorbital wrinkles.7
However, another study of 290 patients evidenced that 11.49% of patients experienced high levels of pain when undergoing the treatment. The appearance of second-degree burns occurred in 2.7% of the treatment sessions. Other side effects identified in the study were persistent erythema, headache, scarring, oedema, fat atrophy, burn in the return pad site, neuralgia and facial palsy.8
In 2004, monopolar RF was approved for use on the full-face.4 RF body contouring devices can be monopolar, but a limitation has been identified due to having small applicators treating large areas, for example the abdomen. While this may work for smaller areas such as the eyelids, it can be considered impractical from a time standpoint to use for these large areas.1
Bipolar
Bipolar RF devices were first used for aesthetic applications in 2004, designed to deliver the energy while focusing on optimising comfort and minimising downtime, as mentioned above.1 Although it treats the same indications, bipolar differs from monopolar because the current is transferred between two different positioned electrodes in the handpiece as opposed to just one, meaning practitioners can distance the poles to control the area that they are targeting. Less current is required with a bipolar device than with a monopolar device to achieve the same effect, because the current passes through a smaller volume of tissue.9
One study of 30 patients showed that bipolar RF gives an improvement in treated imperfections from the second session onward (six to eight sessions were performed), and they expressed their satisfaction at the end of the treatment cycle. Two patients did however report the formation of blisters on the treated area caused by excessively high RF settings.10 RF treatments do create a thermal effect in the skin, but with bipolar RF, are rare and generally
Dr Uliana Gout and Dr Samantha Hills provide an overview of the development of radiofrequency over the years
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
In the last five years, the main trend that we’ve observed with RF technology is its use in combination with other aesthetic treatments, sometimes in one device
Radiance revealed
A multi-tasking corrective serum powered by a unique blend of AHAs, PHAs and botanical extracts.

✓ Provides gentle exfoliation while hydrating and calming the skin
✓ Reduced the build-up of dead surface cells

✓ Leaves skin radiant, smooth and clear
EXCLUSIVELY AVAILABLE AT
@pcaskin_uk www.ChurchPharmacy.co.uk/PCASkin @pcaskin_UK
transient. Burns, scarring and post-inflammatory hyperpigmentation are all possible but rarely encountered. Side effects are usually limited to erythema and oedema, and usually resolve within a few hours. A challenge that has been identified with bipolar RF is that the practitioner can only treat one depth of skin or subcutaneous fat at a time.1 So, different handpieces are generally required for face and body treatments.
Multipolar
Building on bipolar technology, multipolar RF technology was created in 2005, again for skin laxity and tightening. This refers to a device with three or more electrodes, where the negative and positive poles rotate around the different electrodes. In this way, very uniform bulk heating can be achieved, while maintaining low epidermal temperatures.1 One study of 12 patients showed a significant reduction in upper arm circumference, following treatment with a tripolar RF device.11
Fractional RF / RF microneedling
In 2008, the first fractional RF technology was approved by the FDA.12 This type of technology delivers the energy through needles, with each needle acting as a probe. The needle tips carry a positive charge while the faceplate of the disposable handpiece carries a negative charge. As this allows practitioners to get deeper into the tissue, there is no need to have the energy as high, which results in lower epidermal temperatures and consequently safer and more comfortable treatments for patients.13 Fractional RF can be bipolar or monopolar.
Different types of needles can be used in this treatment, either insulated or non-insulated. Insulated needles deliver energy only at the tip of the needle, whereas non-insulated ones deliver it throughout the entire length of the needle. An advantage of using insulated needles is that they can deliver energy deep into the skin, and may offer safer treatments for skin of colour by reducing the risk of post-inflammatory hyperpigmentation, but can cause the patient to experience more bleeding than is generally seen in (the more cost-effective) non-insulated needles. As the skin is undergoing micro-wounds or punctures, it increases the downtime for the patient, however, the mechanical damage caused to the skin does work in synergy with the RF delivery for optimal collagenesis.14
Where RF is today
In the last five years, the main trend that we’ve observed with RF technology is its use in combination with other aesthetic treatments, sometimes in one device. The first dual device combined RF and electro-optical energy.4 This has now evolved to RF being paired with many other energy-based treatments. Many device companies are now choosing to create dual machines and pair RF with other modalities such as intense-pulsed light, fractional laser, ultrasound, fractional radiofrequency, high-intensity focused ultrasound and CO2 laser.
As aesthetic medicine is now becoming more holistic and we are beginning to treat the full-face and body rather than just one individual area, there is a growing interest in combining RF with other treatments to be delivered individually, such as with botulinum toxin and dermal filler.5 While there have many developments in terms of RF devices, there currently still isn’t an agreed consensus about whether you should perform these on the same day or not. Following an RF treatment the skin can be slightly swollen and if you inject botulinum toxin within the same area right after there may be an associated risk of botulinum toxin diffused in a wider area. Some practitioners choose to cool the treatment area post-RF and leave 20-30 minutes before injecting.
The future of RF in aesthetic medicine
Currently, there is no consensus protocol of how many RF treatments patients should receive, nor the best time-period to leave in between each treatment for optimal results, and is usually dependent on manufacturer guidelines. Personally, we recommend that patients have six treatments spread three to six weeks apart as we find this produces the best results. For the future, further research into consensus treatment protocols would be interesting to explore, alongside furthering the concept of combination treatments as further consensus would be ideal to explore optimising treatment outcomes.
The evolution of RF
Having been around for more than 20 years in the medical aesthetic sphere, RF technology has evolved into several forms of devices looking to provide patients with optimal results while also balancing downtime and safety. More recently, there has been a growth in the use of RF for the body and RF in combination with other energy-based technologies or injectable treatments. In the future, we recommend more research is done to determine best practice for all practitioners to follow, as well as a protocol for performing combination treatments.
Dr Uliana Gout is an aesthetic practitioner and founder of London Aesthetic Medicine Clinic in Harley Street, London. Dr Gout was the previous president of the British College of Aesthetic Medicine. She is also general secretary of the International Peeling Society and is heavily involved in international research. Dr Gout has co-authored numerous medical textbooks in the arena of non-surgical aesthetic medicine.
Qual: MBBS, BSc
Dr Samantha Hills is the clinical director at Lynton Lasers and oversees the company’s Clinical and Training Programme. In 2017, Dr Hills was also appointed an honorary lecturer in the Department of Musculoskeletal and Dermatological Sciences at the University of Manchester, in recognition for her ongoing contribution to the University of Manchester’s ‘Anti-Ageing and Aesthetic Medicine’ MSc course.

Qual: PhD

You can discover different radiofrequency devices at ACE 2023 on March 10-11 by visiting the following companies: Scan the QR code to register for free! • 3D Aesthetics • ABC Lasers • Beamwave Technologies • Cutera • Cosmeditech • Eden Aesthetics • InMode • Lumenis • Lynton • Neauvia • Solta Medical Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
the NEW depigmenting solution by mesoestetic®

NEW from the world leader in depigmentation treatments
now you can correct pigmentation imperfections and improve the quality, turgor and appearance of the intimate area in a single clinical session.
This is the latest innovation in pigmentation treatment brought to you by mesoestetic® through over 35 years of research and development.
Developed in collaboration with specialised gynaecologists.

versatility and effectiveness with clinically proven results mesopeel® advanced dermapeels by mesoestetic®
maximum
Our Antioxidant Answer for What Your Skin Needs
30+
of research in every drop
Prevent, Protect & Correct. A leader in advanced skincare, SkinCeuticals is on a mission to help improve everyday skin health with scientifically backed products. Its dedication to science has established the brand as a leader within the industry, and continues to pioneer nextgeneration products and innovations.
This collection of revolutionary serums is powered by scientifically backed ingredients and antioxidants, clinically proven to support the appearance of fine lines, wrinkles, discolouration, blemishes and uneven skin tone, while protecting the skin from everyday environmental stressors. SkinCeuticals vitamin C serums are backed by 30+ years of antioxidant research and demonstrated efficacy in independent, in-vivo (live skin) clinical studies, to deliver advanced environmental protection and targeted visible results.
Created to fight the modern day invisible stressors, SkinCeuticals hero product C E Ferulic reduces free radicals caused by the interaction of sunlight, pollution and metal for up to 48% less oxidative damage in skin* – delivering brighter and healthier looking skin. Metals such as iron and/or copper are known to contribute to the formation of reactive oxygen species, which eventually lead to skin damage – all the impactful stressors we forget are there!
Dr Emma Craythorne says, “For maximal protection of the skin, the addition of a topical antioxidant is essential alongside the use of a broad spectrum SPF. SPF helps to protect skin against UV radiation, which can be enhanced by the antioxidant, as well as adding protection against free radical damage. The SkinCeuticals range of antioxidant serums covers all bases to ensure each skin type can benefit.”

The range includes…
Oily skin - SkinCeuticals Silymarin CF
When the skin’s oils oxidise, free radicals are generated that can damage skin and create favourable conditions for blemishes. This powerful antioxidant helps reinforce the skin’s natural protection from free radical damage. This oil-free antioxidant serum is also formulated with L-ascorbic acid, ferulic acid, and salicylic acid. Together, the ingredients in this antioxidant serum are clinically proven to reduce oil oxidation by up to 76%**, reduce excess sebum/oil by up to 15%*** and refine skin texture, improve skin clarity and reduce oiliness.
Hyperpigmentation - SkinCeuticals Phloretin CF
A powerful triple antioxidant vitamin C serum enriched with 2% Phloretin, 10% pure vitamin C (L-ascorbic Acid) and 0.5% ferulic acid, specifically formulated for combination and discolouration-prone skin. This product is a synergistic vitamin C combination antioxidant that provides advanced environmental protection against damaging free radicals caused by UVA/UVB rays and pollution. Formulated to meet the Duke Parameters necessary for optimal vitamin C absorption and effectiveness, this potent serum also helps diminish the look of discolouration and fine lines while improving the skin’s overall tone and texture.
Dry/combination skinSkinCeuticals C E Ferulic

Ideal for dry/combination skin. This daily topical antioxidant delivers up to 8x environmental protection and helps to reinforce the skin’s natural protection against free radicals. Featuring a blend of 15% pure vitamin C (L-ascorbic acid), 1% vitamin E (alpha tocopherol) and 0.5% ferulic acid, this award-winning antioxidant serum has been proven to improve the appearance of fine lines and wrinkles, loss of firmness, and brighten the overall complexion.
Pioneering the stabilisation of vitamin C
Since 1997 SkinCeuticals has led the way, integrating skincare into the aesthetic treatment space with its vast, potent range of active-rich skincare treatment products, making it the natural choice for aesthetic clinics globally. The brand was founded by Dr Sheldon Pinnell, chief of dermatology at Duke University, North Carolina. As part of his research, Dr Pinnell was able to patent the Duke Antioxidant “The Duke Formulation Parameters”, stabilising vitamin C as far back as 1992 which has become a key ingredient in some of the best-selling SkinCeuticals products today and a real anchor ingredient in the antioxidant range.
The Duke Antioxidant patent outlines the formulation parameters required for the most effective delivery of the ingredient to skin.
1. Pure L-Sascorbic acid (vitamin C)
2. An acidic pH within the 2.0-3.5 pH range
3. A concentration between 10%-20%.
Award-winning skincare
Speak to your SkinCeuticals representative for more information about the range. If you do not have a dedicated contact, please email Contact@SkinCeuticals.co.uk
https://www.skinceuticals.co.uk/
58 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com Aesthetics | February 2023 Advertorial SkinCeuticals
This advertorial was written and supplied by *Measure of 4
lipid peroxidation marker indicative of oxidative stress. 4-day in vivo clinical study, 13 subjects. C E Ferulic applied daily vs untreated. Skin samples collected for 4HNE protein analysis at the end of study. Note: Sunlight interacts with oxygen or molecules in skin to form free radicals. C E Ferulic does not contain sunscreen. **Clinical study 35 subjects (China, 2020) ***12-week clinical study, 60 women (Brazil, 2020)
years
hydroxynonenal (4HNE)
A summary of the latest clinical studies
Title: Botulinum Toxin in Oily Skin: Advantage of a Multi-Needle Device for a Controlled Release
Authors: Guarino E.
Published: Journal of Drugs in Dermatology, January 2023
Keywords: Botulinum Toxin, Oily Skin, Microinjections
Abstract: Oily skin is one of the most common dermatological complaints. One of the treatments proposed to combat this is the use of onabotulinumtoxin-A injected sub-dermally. For an optimal result, the injections must be done on the whole area with numerous micro-injections located only in the sub-dermis. The procedure is often poorly tolerated by patients and sometimes accompanied by hematomas and bruises. This research aimed to test a disposable device to inject botulinum toxin at 1.5mm under the skin with a painless procedure and homogeneous distribution of the toxin. We treated patients with oily skin with the injection of 100 IU of onabotulinumtoxin-A (diluted in 5ml of a saline solution). All the patients were evaluated after two weeks, one month and three months. In 10 patients, after 15 days, we observed an improvement in skin quality. In all cases, the treatment appeared homogeneous in the entire face. All the patients considered the procedure virtually painless. In accordance with other authors, we confirm the real advantages of micro-botulinum toxin for oily skin. Moreover, the use of this simple and innovative device allows a homogeneous distribution of the drug in the correct plane, without pain, and reduces the risks of common complications.
Title: One-step Generation of Core-shell Biomimetic Microspheres Encapsulating Double-layer Cells Using Microfluidics for Hair Regeneration
Authors: Huang J, et al.
Published: Biofabrication, January 2023
Keywords: Follicles, Hair Loss, Hair Regeneration
Abstract: Tissue engineering of hair follicles (HFs) has enormous potential in the treatment of hair loss. HF morphogenesis is triggered by reciprocal interactions between HF germ epithelial and mesenchymal layers. Here, a microfluidic-assisted technology is developed for the preparation of double aqueous microdroplets that entrap double-layer cells and growth factors to ultimately be used for hair regeneration. Mouse mesenchymal cells (MSCs) and epidermal cells (EPCs) are encapsulated in gelatin methacrylate (GelMA) cores and photo-curable catechol-grafted hyaluronic acid (HAD) shells to fabricate GelMA-MSC/HAD-EPC (G/HAD) microspheres. The findings show that the G/HAD microspheres exhibit ultrafast gelation, aqueous phase separation, superior biocompatibility and favourable wet adhesion properties. G/ HAD microspheres can also support cell proliferation and sustain growth factor release. These composite cell microspheres are capable of efficient HF generation upon transplantation into the dorsal dermis of nude mice. This finding facilitates the large-scale preparation of approximately 80 double-layer cell spheres per minute. This simple double-layer cell sphere preparation approach is a promising strategy for improving current hair-regenerative medicine techniques and can potentially be applied along with other organoid techniques for extended applications.
Title: Non-invasive Hands-free Bipolar Radiofrequency Facial Remodelling Device for the Improvement of Skin Appearance
Authors: Labadie J, et al.
Published: Dermatologic Surgery, January 2023
Keywords: Ageing, Energy-Based Device, Radiofrequency
Abstract: Ageing is a multifactorial response to genetic preprogramming nuances, sun exposure and ultraviolet radiation. Recently, there has been a paradigm shift toward minimally invasive rejuvenation. This prospective multi-centre study aims to evaluate the efficacy and safety of a novel hands-free bipolar bulk radiofrequency (RF) device in terms of improvement in skin appearance. This study enrolled subjects aged 35 to 75 years old with visible signs of ageing. The primary objective was to evaluate skin appearance pre-treatment and at one, three and six months after the final treatment. Each patient received three total treatments to the chin and cheeks using the hands-free RF device spaced two weeks apart. In total, data from 87 patients were assessed from six treatment sites. The average age was 54 years. Most patients were female (97%), and Fitzpatrick skin types I to V were represented. Overall, patients found the procedures to be relatively pain-free, and both patients and investigators felt they noted some improvement in their skin appearance. Histological sections demonstrated an increase in collagen or elastic fibres within the papillary dermis. This study supports the use of this novel non-invasive hands-free bipolar facial remodelling device for the improvement of skin appearance.
Title: Surgical Management of Polymethylmethacrylate-Collagen Gel Complications in the Lower Eyelid: A Case Series
Authors: Durkin A, et al.
Published: Annals of Plastic Surgery, January 2023
Keywords: Complications, Granulomas, PMMA Collagen Filler
Abstract: Polymethylmethacrylate (PMMA)-collagen gel is unique among fillers in that the PMMA microspheres are not completely absorbed and phagocytosed by the body. This durability, coupled with the biophysical properties of PMMA, makes it a poor choice for periorbital rejuvenation. Between 2011 and 2018, 14 patients with PMMA granulomas in various facial areas self-referred to the senior author’s practice. Of these patients, 11 were managed non-surgically; however, all three patients who presented with granulomas in the infraorbital area required surgery to remove the filler and restore a natural aesthetic. The three patients with significant swelling and PMMA filler nodules in the infraorbital area with unacceptable cosmetic appearance were females between the ages of 50 and 55 years old. Non-surgical protocols were unsuccessful, and surgical removal was required. All subjects have been followed for a minimum of two years with no immediate- or long-term post-operative complications secondary to PMMA removal. Patients remain satisfied with the outcome of the surgery. Despite the evidence that the periorbital area is prone to adverse events when injected with particular fillers, misguided enthusiasm for PMMA-collagen gel as a durable treatment continues to lead to unnecessary and severe complications in patients. This product should not be introduced into the periorbital area.
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Addressing Unconscious Bias
On November 15, 2022, the world population reached eight billion people.1 The majority of these people tend to believe that they are fairer and less prejudiced than the average person.2 Yet, discrimination is an endemic social stressor that can lead to detrimental mental and physical health issues, which can have profound effects upon self-esteem, opportunity and agency in life.3,4 Unfortunately, this can subconsciously seep into the world of aesthetics.
What is bias?
Bias is a tendency to believe that some people, their ideas and beliefs are better than others, which can often result in treating people unfairly.5 How a person thinks can depend on their life experiences, and sometimes, people may hold beliefs and views about others that might not be fair, right or reasonable.6 Practitioner anxieties, business experiences, fear of complications, habits and even patient archetypes can stack up to form categories of bias within aesthetic practice.
In 1960, psychologist Peter Wason demonstrated how humans selectively collect and evaluate evidence based on preconceived ideas known as ‘confirmation bias’, which we are influenced by without realising.7 This is an invisible and unconscious filter that seeks and interprets information and evidence from sources that affirm existing beliefs, ideas and expectations of the world around us.8 Furthermore, experience and expectation simultaneously create a self-fulfilling prophecy that feeds into unconscious bias, which can lead to a set of entrenched associations through ‘grouping’.9 If an individual belongs to, or wishes to belong to, an ‘ingroup’ as determined by biases, they are more likely to respond positively to them, be more helpful and hold space for common ground. Conversely, an ‘outgroup’ member would not be so favourable, confirming pre-existing biases. Confirmation bias has been explained as a consequence of the limitations in our brain’s information processing systems, with prejudice and discrimination seen as inevitable consequences of flawed human cognition.10 Simply put in evolutionary terms, it takes too
long to assess each situation or person based on individual merits when survival is the priority. Unfortunately, this has a propensity to influence clinical practice, and it is something we must combat to treat our patients justly and compassionately.


Identifying your own unconscious bias



Explicit bias refers to visible, accessible attitudes and beliefs that are conscious, deliberately held and expressed about a person or a collective group. Implicit bias, on the other hand, includes attitudes and beliefs about other people that operate outside of conscious awareness.11 Unconscious biases are developed over time from lived experience, and are consequently learnt and consolidated over a lifetime through confirmation bias.7,12 Ogugbe et al. explored six types of implicit bias – race, weight, social class, sexual orientation, mental illness and ageing – when measuring physicians’ clinical decision-making skills.13 It was revealed that nearly 70% reported an adverse effect of bias on health outcomes. Two major biases identified were race and weight.13 These two biases could be considered major mediators of potential health disparities, and although unconscious (implicit) biases are difficult to access or be aware of, they still have an influence on behaviour and affect everyday opinions and decisions.
It may not always be clear which ‘ingroup’ you belong to, and it is not always easy to predict this for others either. Generally, our ‘ingroup’ is the group we would like to belong to. Thus, it is not surprising that women can be biased against other women, and people from black, Asian, minority, ethnic and refugee (BAMER) communities can be biased against other people from the same groups. Implicit or unconscious bias are fundamentally held by everyone, even those who are tasked with remaining ‘impartial’ or ‘objective’, regardless of job role and social status. We are all affected by unconscious bias.1-15
As humans, we notice differences. Physical characteristics such as skin colour, age, gender and disabilities are among the most frequently noticed differences.16 In 2018, Paganini et al. noted that gender bias was at play in the medical treatment of patients with cleft lip and palate (CLP), with women being overtreated and men being undertreated for second surgeries to address nasolabial aesthetic concerns.17
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Psychologist Kimberley Cairns explores how unconscious bias can potentially impair your aesthetic practice and how practitioners can combat it
Managing your unconscious biases
Accountability is key for unlearning, interrogating and shifting biases. To become more aware of your biases, reflect on the below with curiosity and a view to challenge your habits.21
1. What ‘ingroup’ do you belong to? Consider how many groups you are part of on a daily basis. This may involve your family, lifestyle, work, leisure or religion. Do you ever find yourself favouring members of common or desired ingroups?
2. When has an unconscious bias been useful in your medical aesthetic practice?
3. Question cultural stereotypes that seem truthful and examine your own unconscious biases and implicit thought processes. Are these inappropriately affecting the objectivity of your decision-making?
4. Identify patient-centred strategies to minimise the influence of unconscious bias when interacting with patients. Consider how your patients’ ingroups may affect their choices, rather than just looking at their basic characteristics.
5. Have you ever witnessed an act of unconscious bias from a patient, or between colleagues? E.g. ‘Because of your skin tone…’, ‘If you had started this 10 years ago…’, ‘How long have you worked here?’, ‘I’ve had a patient just like them before...’, ‘Let me get the door for you?’ Was it a positive or negative inference? What did you do when it arose?
6. Slow down the speed of decision-making to prevent subconsciously giving in to biases. This is especially significant at patient consultations and within HR operations.
7. Be open to seeing what is new and unfamiliar, and increase your knowledge of other groups.
8. Be prepared to call out bias when you see them; it is easier to detect unconscious bias in others than in yourself. Remember, we all fall into bias traps. Some biases are sensitive and even painful. Give people the benefit of the doubt – we are all here to learn and grow, and open exchanges are an essential part of that process.
9. Keep a written record of why business decisions were made where bias may be concerned; this is a requirement for Care Quality Commission inspections with regards to recruitment processes.22
10. Ask continuously, ‘Am I being fair in the way my staff and I practise?’ Do you need to enhance areas of your practice, or expand your multidisciplinary team?
11. Unconscious bias training may provide and improve awareness in your own self-discovery. The Harvard Implicit association test measures the strength of associations between concepts or stereotypes to reveal an individual’s hidden or subconscious biases, which you can then work on addressing.23
It is of note that those with CLP and other visual differences such as acne, rosacea and eczema are considered a vulnerable group as identified in the extensive research at the Centre of Appearance Research (CAR) in Bristol, featured in the recent Health and Social Care Committee report on the impact of body image on mental and physical health. It concluded that the aforementioned ‘vulnerable groups’ would benefit from specific and targeted psychological assessment when considering elective aesthetic treatments.18
Correlational evidence has revealed that healthcare professionals’ biases are likely to influence diagnosis, treatment decisions and levels of care in some circumstances, with further investigation required.15 Therefore, given the identified biases and healthcare
disparities, along with identified vulnerable groups, we are given an opportunity to increase understanding about racial, ethnic and cultural disparities to minimise damaging consequences of bias, especially concerning mental health, age, ethnicity, weight management, body shape and colour.18
Unchecked bias can be detrimental to all aspects of business and clinical function rooted in patient selection, recruitment and appraisal opportunities, complaint handling and care plan approaches, which can all negatively influence patient satisfaction, treatment and service expectations, as well as overall results and patient retention.19 In rare cases, this could even cost you a legal discrimination case from patients or staff if they feel they have been discriminated against based on age, race, sex, sexuality,
gender, disability, religion, marriage, pregnancy or maternity, in accordance with The Equality Act 2010.20 The good news is the influence of unconscious bias can be overcome or neutralised.
Exploring unconscious bias can uncover blind spots to overcome cognitive bias and build better relationships by allowing you to elicit and respond to individual perspectives and build trusting partnerships for superior outcomes.7 Tackling this head-on can better inform your business operation, enhancing personal and professional goals.
Combatting bias across the specialty
Accepting that everyone has unconscious bias, as well as knowing the difference between conscious and unconscious biases, can offer insight that could prevent a small mistake leading to huge problems if left unchecked. Improve your understanding of the most common forms of bias in the aesthetic workplace, hold yourself and others accountable to biases and learn how to challenge these biases if you see them unfolding. Use multiple frames of reference to encourage yourself and your patients to limit discrimination and challenge distortion, thus helping to progress the developments in diversity and cultural acceptance within our dynamic, inclusive and fast-paced sector. This will be instrumental to understanding and delivering aesthetic equity in elected interventions and treatment options.
Kimberley Cairns is an integrative psychologist who prioritises education, training and clinical opportunities to address the complex mental health challenges facing the aesthetic and non-surgical cosmetic sector. She is a psychology consultant, and holds numerous privileged positions in the sector including membership of the Aesthetics journal Aesthetics Reviewing Panel.
Qual: BSc, MSc, MBPsS

Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
VIEW THE REFERENCES ONLINE! AESTHETICSJOURNAL.COM

Become a HINNAO® Practitioner BENEFIT FROM Scan the QR Code TO LEARN MORE OR VISIT WWW.HINNAO.COM Hinnao HINNAO ® Starter Pack Your Business Featured Full Access Online Portal A starter pack containing discounted HINNAO ® products. Free product training is also included. Your business will be featured on our website as an approved HINNAO® stockist. Full access to our online portal where you can access HINNAO® training courses, webinars and much more.
Managing No-Show Appointments
Business director Max Hayward advises how to manage and reduce your no-show clinic appointments
When working within aesthetics, practitioners are probably familiar with the odd no-show appointment. However, if you do not address no-shows, your business quickly suffers from lost revenue and time. When patients fail to show up at all, you lose money – it’s as simple as that. There are many reasons why patients may not show up for their appointments, from forgetting their appointment completely, to not being able to attend due to work or family commitments. Whatever the reason, it’s important to understand why patients are not attending their appointments and begin to review your business against these missed appointments.
This article highlights the impact no-show appointments can have on your business and what practitioners can do to tackle them.
How much do no-show appointments cost your business?
Since running your aesthetics business, have you ever considered how much no-shows are costing your business?
Let’s say you have one no-show appointment each week for an anti-wrinkle
treatment in two areas. If a conservative charge for this appointment is £150, that’s £600 a month and £7,200 a year!
When patients miss their appointment, you’re not only losing revenue from their treatment, you should also consider the cost of any products you have already purchased. Especially when your business is growing, you do not want to be left out of pocket on a regular basis.
It’s probably time to address the number of no-shows and late cancellations your business has on average every month.
What can practitioners do about no-show appointments?
The first step is to monitor the number of no-shows you are experiencing. If you currently use a clinical software, you’ll be able to run a missed appointment report which will highlight your no-show appointments and cancellation levels in your clinic. Otherwise, this process will be done through your manual diary, noting how many appointments were cancelled or when patients did not attend. You should also consider if there are any
trends in your no-show appointments.
• Do you get more no-shows on a certain day or time?
• Is there a certain treatment receiving more no-shows?
• If so, is this treatment the cheapest or most expensive?
Whilst these patterns can help you to understand your patients and highlight areas of your business, they will not eliminate the no-shows you are experiencing.
Below are some suggestions of how you can start to take action to reduce your no-show rate.
Remind your patients
Everyone’s been there – you book an appointment months in advance and completely forget until a few hours before when a notification pops up in your calendar. By sending your patients a reminder 48 hours before, you give them an opportunity to rearrange within your clinic’s cancellation window (discussed below), preventing a potential no-show.
Automated reminders are designed to stop those late-night messages and give patients the little nudge they didn’t know they needed. Aimed to make a patient’s experience with your clinic as seamless as possible, these reminders provide any relevant information the patient may require before they arrive for their appointment.
When it comes to sending your reminders, consider using multiple channels. Whilst emails are great for booking confirmations, consider introducing text message reminders for your patients. With the open rate sitting at 98% for text reminders compared to only 20% for emails, this could be the trick needed to reduce your no-show rates.1
By also asking your patients to confirm their attendance at the end of your reminder messages, this prompts them to respond, and could prevent a missed appointment. You then have the opportunity to ring any patients who have not confirmed to double check their attendance. If you have still not got a response after these attempts, you may want to consider cancelling the appointment so that you can re-advertise the slot to other customers (of course, make sure to send confirmation of this cancellation to the patient).
Make it easy for patients to manage their appointments
Online booking systems are a great way to streamline your business and allow your patients to manage their own appointments.
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com








in Aesthetics Conference A FIRST-OF-ITS-KIND EVENT DEDICATED TO THE SYNERGY BETWEEN AESTHETICS AND MENOPAUSE Menopause in Aesthetics will unite professionals from a broad spectrum of specialties to discuss everything from hormones, weight reduction and referral pathways to nutrition, well-being, intimate health and facial aesthetics. A boutique-style hybrid conference offering both face-to-face and online delegate experiences. BOOK NOW to avoid disappointment Online and in person delegate passes £199.00 + VAT or visit www.menopauseia.co.uk Call 01702 870 190 In person includes lunch & champagne reception FRIDAY 10 FEBRUARY 2023 THE WALDORF HILTON, LONDON The Menopause in Aesthetics Conference 2023 is sponsored by Roseway Labs www.rosewaylabs.com To better serve women on their journey through menopause Menopause in Aesthetics is proud to be a member of the CPD Certi cation Service
Menopause
By introducing an online booking system to your business, your patients can quickly reschedule their appointment without needing to contact you, making their life easier and saving you time rearranging.
With service-based companies finding 40% of their appointments are being booked outside of their business hours, your business could be opened to a whole new reach of people by introducing an online booking system.2 When looking at why patients don’t turn up, people can sometimes feel uncomfortable ringing to reschedule or cancel their appointment as they feel they are a burden or are letting you down. With 81% of millennials experiencing apprehension anxiety ‘before summoning the courage to make a call’, you could significantly decrease your no-shows by offering an easy, self-service way for patients to reschedule or cancel their own appointments.3
Charging for deposits
After a no-show appointment, do you often wish you’d taken a deposit? As a service-based business, your time is your business, and this should not be wasted by a patient with no intention of attending.
Charging a deposit can sometimes be a difficult decision for practitioners out of fear that patients will stop booking appointments. However, under Chapter Four of the Consumer Law Act 2015, if a contract (appointment) is cancelled, the business is entitled to keep or receive an amount sufficient to cover their actual losses that directly resulted from the cancellation.4 This is usually in the form of a non-refundable deposit or a cancellation charge which must be a genuine estimate of the direct loss of the business. By charging a small percentage of your treatment price, you can cover the cost of that wasted appointment time. Plus, this gives more of an incentive for patients to turn up to their appointments.
Consider introducing deposits to your business dependant on trends you notice with your no-show appointments. Start to take a deposit to secure bookings for treatments that have the highest no-show rates or take up a larger amount of time. This is an excellent way to prevent loss of your income and time.
Document a clear cancellation policy
Do you have a clear and concise cancellation policy displayed on your website and online booking page? Some practitioners avoid or don’t consider displaying or enforcing a cancellation policy as they feel it could put patients off booking the appointment,
particularly if they are new to aesthetics and starting to build their patient base. However, this is not something to shy away from when running a business. By making your patients aware of what to expect and being clear about your boundaries, this indicates that your time is valuable and can help to reduce your no-show appointments. When creating your cancellation policy, consider the following:
• How much notice do you need for cancellations to allow you to refill that time slot?
• Make it clear whether any deposits paid will be refundable or not if the appointment is cancelled. For example, if cancelled with less than 24 hours’ notice.
• If you do not charge deposits, you could make it clear that repeated late cancellations or no-shows (e.g. more than once or twice) could result in you no longer accepting any further booking requests from them without a payment.
By creating a policy with a 24-hour window for patients to call or reschedule and sending a reminder message, you are giving them the opportunity to reach out if they cannot make an appointment. Of course, you can always exercise your discretion and waive a cancellation fee if the patient has a genuine reason for missing their appointment.
What should practitioners do when a patient fails to show up?
It’s unlikely that you’ll eliminate no-shows altogether. So, when the odd no-show appointment does occur, what steps should you take?
Always message your patients
Practitioners should always follow up with a patient who has missed an appointment. Reach out to them by either calling or texting. This usually helps to understand why the patient has not turned up, and gives them the opportunity to rebook. This helps to acknowledge the fact they did not attend without souring your patient-practitioner relationship. Patients can sometimes feel embarrassed about missing an appointment or may have completely forgotten. Sending the patient a polite message gives them the reassurance that you are happy to rebook their appointment without losing their custom. For example, you could say “Hi Jane, you missed your appointment today, I hope everything is well. If you’d like to reschedule,
please reply to this message or call us…” Your patients, just like you, are only human and sometimes life gets in the way. Therefore, following up after a no-show is important because it allows you to reconnect with your patient and avoid potentially losing them as a customer altogether.
Monitor regular no-show patients
Regularly review patients who cancel last minute or don’t show up despite your reminder messages. However, with repeat offenders, practitioners may consider if they want this type of patient within their business. Remember to think about the cost that these no-show appointments have on your clinic. Can you really afford to be out of pocket for a patient who frequently does not turn up? Consider booking these patients in at a time which is not going out of your way to accommodate them or insist on a deposit to secure their booking. As a last resort, you are well within your rights to turn this patient away next time.
Manage your no-shows!
No-show appointments within a service-based business like aesthetics can never be fully prevented. However, by adding a few simple processes into your business, they can be reduced. Reminder messages give patients the nudge they didn’t know they needed, a cancellation policy helps secure your appointment deposits and an online booking system enables patients to reschedule appointments with sufficient notice.
Max Hayward is the director of Aesthetic Nurse Software, a clinic management system designed specifically for aesthetic practitioners. Hayward has more than six years of experience working in the aesthetics industry, supporting practitioners nationwide to go paperless.

Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
VIEW THE REFERENCES BY HEADING TO AESTHETICSJOURNAL.COM
Aesthetic Nurse Software will be exhibiting at ACE 2023 at the In Practice Zone on March 10-11. Scan the QR code to register for free.
Understanding Data Analytics
It is estimated that 20% of small businesses fail in their first year, 30% by year two, 50% by year five and 70% close before their tenth year of business. This is reported to be largely due to a lack of vision, purpose or mission for where the business will go, no business strategy, no marketing plan, no clear agenda for how they intend to sell their business to generate income and no commitment to learning.1
In contrast, successful business owners are constantly looking for new and better ways to get clients, as well as to serve the ones they already have. They are aware of the latest trends and how these can benefit their clients. Taking one action that will increase your visibility or credibility can improve a business, and there are multiple options to do this.1
One main way you can further your business as a clinic owner is by utilising data analytics. These can highlight the good, the bad and the ugly, answering questions such as: How well are things actually going? Do you need to implement changes? What’s going well? How do you stay ahead of the game and maintain that competitive edge?
Just look at the example of Don Marler, a street food vendor. He used the data
available to him. Using his customer personal data, he was able to create a marketing strategy via SMS messaging. Subsequently, the Don Marler business was able to increase its financial profit by 35% in the first three months.2
Indeed, Ernst & Young stated ‘companies don’t have analytics problems; they have business problems that analytics can address’.3 It could be argued that all the factors leading to the failure of a small to medium sized enterprise (SME) such as an aesthetic clinic can be defined as a form of data analysis.
So, why are we not using it more? Speaking with colleagues and with smaller sized aesthetic clinics, it appears data analysis seems too overwhelming, or they just haven’t ever realised the hidden gem that is quantifiable data.
Collecting data
Social media
For smaller or newer businesses collecting data from their target markets, the simplest way is likely through social media. One such example is Facebook, where Facebook Business Manager makes data collection easy, even for those with very
little experience in data analysis. Facebook Business Manager is a free tool that enables businesses to view analytics for each post, increasing understanding of who their demographics are, and expanding their potential conversion to customers.4
Instagram also offers an insights function, which shows who your audience are. It gives you a window into their gender, age and what region they’re from, down to the time of day your audience is viewing your content. All this information can help you formulate a social media marketing plan. Letting your audience know about all the fabulous treatments you offer can then translate to an increase in bookings and revenue.5
Software systems
Outside of social media, you can look at utilising the software systems to collect data more efficiently. These systems use the data you input each day within your clinic – patient age, treatments booked, how much of the staff shifts are being used to carry out treatments, what are your monthly takings – and allow you to calibrate this data to specific reports, assessing staff revenue, time utilisation, the most popular and least popular treatments, month to month. You’re then able to have a pulse on your business, therefore reacting effectively. We can even break it down to each staff member and check what their most popular treatments are or if they’re meeting their targets each month – the list goes on. In our clinic we use the Pabau software system, however there are others available such as Aesthetic Nurse Software, Collums Clinic Software, e-clinic, iCLINICIAN, iMedDoc, Phorest, Rushcliff, Sellsio and Zenoti.
Patient feedback
Feedback forms could be paper based and provided in-clinic after treatment, or reviewed through the easy-to-read software reporting systems mentioned above. At our clinic, we have chosen to text feedback forms to patients after every treatment. Online reviews are also extremely helpful, and the autonomy of online reviews allows you to understand your patients at a deeper level.
The benefits of utilising analytics
Marketing
Looking at your data can highlight where your highest number of treatments come from and whether there are any treatments that aren’t as popular. This, alongside data evidencing your target demographic, can
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Nurse prescriber Carla Jones discusses the importance of using data analytics for your business
help you create a marketing strategy to promote your treatments more effectively to your patients. Your staff are already trained in those treatments, so it’s a good way to utilise what your business already has to offer.
Professional development
Similarly, data can be a great source of evidence which businesses can use towards staff professional development reviews. When I talk to other practitioners, I find that clinics very rarely take the time to evaluate patient feedback. This is something to change – they are the voice of your business and, most importantly, they are your revenue stream. You can uncover so much: what are your patients telling you? What is your staff doing well? What could they be doing better? All this data can be used to take your clinic forward and get it to that next level, and listening to their feedback can provide you with the tools to increase your patient satisfaction.
Clinic development
As well as professional development, the above data could be applied to potential clinic improvements, as it can help you to identify the most important areas to spend money. Is it to increase patient comfort in-clinic, health and safety improvements, or creating more space to increase your revenue per square foot of your aesthetic clinic? Identifying your most popular treatments can again help here, as it may signify that you should invest in space to add more aesthetic devices – or if these treatments are poorly performing, utilise that space for something else.
Considerations for success
Cost
One of the main concerns for data analysis is budget – is it expensive? To put it simply, the answer depends entirely on the extent of the analysis you wish to undertake. A small-tomedium-sized business can still utilise data analysis without breaking the bank. Although most of us have now moved into using various software systems, even clinics who are paper-based will still have data to be analysed. This could be something as simple as going through the diary and looking at your most frequently booked treatments, from which you can learn what you’re doing well, as well as highlighting the treatments you need to market more. As mentioned above, there are also many social
media tools which can be used at no cost. All this is free, so it just needs your time or the time of another staff member, such as your clinic manager or a member of your administration staff.
When it comes to clinic software systems, it gets slightly more expensive. In my clinic we pay a subscription fee each month. While this is more for your budget, I personally think having a patient software is a game changer. Not only does it provide an easily accessible patient information storage system, but it also allows you to calibrate your clinic data more easily, also making the data much more interpretable, especially for someone who is not a qualified data analyst.
Of course, you could also consider hiring a data analyst to help you make sense of the above, but the average salary is around £35,334 per year 6 In terms of finance, it may make more sense for your business to do it independently, especially with so many accessible tools.
Time
Some practitioners may be concerned that collating and analysing data can be too time consuming, especially when they already have a hectic schedule and many of us are balancing aesthetics and work in the NHS. However, it doesn’t need to be.
I allocate on average four hours at the end of each month where my clinic manager and I sit down and look at all the data for that month. We then compare the data against our targets, allowing us to make a business plan for the next three months.
Once this becomes part of your plan it just becomes routine, and allows you to keep a finger on the pulse of the business. We also block out time each quarter for a governance
meeting during which we review patient feedback and look for any patterns. This allows our clinic to increase our residual income in the business quicker.
Optimising your data
Data analytics don’t just apply to large corporations. SMEs can benefit from making time to carry out regular data analysis, too. As clinic owners, responsibility for covering the daily outgoings of our businesses, we should make time to analyse our business data on a regular basis. Not only will this support the sustainability and longevity of our businesses, it will also aid the future growth plans for the business.
Carla Jones is an independent nurse prescriber and aesthetic nurse with 10 years’ experience. She is the founder of C.J Aesthetics Clinic in North Wales. Jones has a passion for business and received a first-class degree in Business and Management in 2021. She also has a particular interest in promoting safety in aesthetics and is one of the BACN leaders for the North Wales/ North-West region.

Qual: RGN, INP, Bsc
REFERENCES
1. Forbes, and Laura Cowen. “Eight Common Reasons Small Businesses Fail.” Forbes, 2019, <https://www.forbes.com/sites/ ellevate/2019/10/24/eight-common-reasons-small-businessesfail/?sh=2f3348da4fbb>
2. Fitzpatrick, Luke. How Data Analytics Impacts Small Businesses in 2019, 2019, <https://www.business.com/articles/the-state-ofdata-analytics-in-2019/.>
3. Ernst & Young. “Big data and analytics.” Ernst & Young, 2020, <https://www.ey.com/en_uk/big-data-analytics>
4. Meta, Free Facebook Marketing Tools to Grow Your Small Business | Meta for Business. Facebook. Retrieved November 27, 2022, <https://business.facebook.com/business/smallbusiness/free-tools>
5. Instagram, View Account Insights on Instagram. Instagram Help Center, 2022, <https://help.instagram.com/1533933820244654>
6. Glassdoor Salary: Data Analyst | glassdoor, Data Analyst Salaries in United Kingdom. Glasdoor, 2023, <https://www. glassdoor.co.uk/Salaries/data-analyst-salary-SRCH_KO0,12.htm>
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
Data could be applied to potential clinic improvements, as it can help you to identify the most important areas to spend money

Celebrate the medical aesthetics specialty at the most glamorous night in the aesthetics calendar Each ticket includes: A three-course meal | Complimentary wine | Live entertainment aestheticsawards.com AWARDS GET YOUR TICKETS Co-located with @aestheticsjournaluk @aesthetics @aestheticsgroup 11 March, Grosvenor House, London
Since opening her first clinic straight out of medical school, aesthetic practitioner Dr Saleena Zimri has been championing dermatological skin health.

Dr Zimri grew up in Leeds and was inspired to study medicine at the University of Manchester by her father, who was also a doctor. She became a GP after qualifying in 2009, but her greatest interest always lay in dermatology. “When I was a teenager, I had really problematic skin with bad acne,” she says, “I would try everything and anything to combat it. That’s how I became passionate about skin.” NHS rotations in plastic, ear, nose and throat surgery also piqued her interest in facial aesthetics. Dr Zimri opened an aesthetic clinic – Skin Doctor Leeds – with her father in 2009 alongside full-time NHS work, further undertaking a dermatology diploma at Cardiff University in 2016 to become a GP with a specialist interest in dermatology.
When her first daughter was born eight years ago, Dr Zimri decided to prioritise her passion and left the NHS just as the Skin Doctor Clinics franchise opened its second location in York, followed by Manchester and London. She attributes her rapid expansion partly to effective and consistent use of social media, hopping on trends to increase reach. She explains, “Soon after our clinics began, I remember opening our Facebook page and we had reached 10,000 likes in one year. It just spiralled from there, and Instagram blew up too. It’s a great way to grow your patient base.”
Offering a range of device-led treatments has always been a priority in Dr Zimri’s clinics after she learnt about the many uses of lasers while studying dermatology in hospitals. She explains, “Even as a start-up, we went straight into providing a 360, holistic approach to treatments. It was
important that we were able to help patients improve their skin with devices and skincare as well as the more standard fillers and toxin.” Some of her favourite devices include the Lumenis multi-platform Alma Harmony and SPLENDOR X lasers.
As well as expanding her business, Dr Zimri prioritises clinical education. She is an international key opinion leader for aesthetic manufacturer Teoxane – the HA filler brand she uses most in-clinic. On top of this, she does some educational work with Lumenis, and is a faculty member for skincare companies SkinCeuticals and ZO Skin Health. She values welcoming practitioners for one-on-one shadowing days with her, saying, “It’s a natural progression over the years of wanting to pass on what you’ve learnt. I’ve found that it helps me think critically about my own practice.”
To stay abreast of the industry’s latest developments, she attends the largest educational events such as ACE, AMWC, CCR and IMCAS, where she can hear about everything new in the specialty. On top of that, she recommends attending a cadaver dissection session once a year. She explains, “We’re learning new things about the body all the time. Dissecting is a great way to refresh knowledge about
Top tip for success when treating the skin…
Have
Favourite
Currently
Advice
Have
the layers of the face and reemphasise the best placement for fillers and threads. For safety, I think it’s one of the best things you can do.”
Since entering the aesthetics specialty in 2009, Dr Zimri has seen huge growth, both in terms of demand from patients and the number of practitioners in aesthetics. However, as stigma around aesthetics reduces, she says, “I definitely think the growing demand for aesthetic treatments has outweighed the number of clinics opening, so there’s room for everyone to practise.” She has also seen an increase in the holistic treatment approach which she has always championed. “Skin has become a huge thing, and I think devices are going to come more into focus now.”
Dr Zimri remembers how hard it was to gain expertise at the beginning of her career, but believes today’s new practitioners have a wealth of resources to help them. “There are so many courses you can go on nowadays,” she says, “These can be skin-related, injectable-related, finance-related. Hone in on what you need to improve, and shadow more experienced colleagues as well.”
One of the highlights of her career has been owning her own clinics from the very beginning, but she stresses that it doesn’t have to be an isolating process. She highlights, “Investing in your staff is really important. I think when you’re a lone practitioner, it can be hard to let go of the desire to do everything by yourself, but when you do, it’s incredible.”
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com
“Skin has become a huge priority and devices are going to come even more into focus”
Dr Saleena Zimri shares how her passion for skin led her to run her own clinic franchise and teach on the global stage
skin health plan
the beginning.
a good diagnosis and
from
device treatment…
(IPL)
it’s intense pulsed light
therapy to help skin texture and quality.
for running a clinic…
of
patients
work ethic.
a good team, good knowledge
your
and good
Dr Saleena Zimri will be speaking on behalf of Teoxane at ACE 2023. Scan the QR code to register for free!
The Last Word
Dr Nestor Demosthenous and nurse prescriber
Amanda Demosthenous debate the pros and cons of investing in the latest devices
Purchasing a device is a huge investment for aesthetic clinic owners and is therefore something which requires a great deal of planning and thought. Whilst devices have the potential to add huge value to your clinic, they also require a large financial investment, so you need to be sure to do your homework properly before committing to anything.
In this article, we will be arguing the pros of onboarding the newest and latest devices and exploring why some practitioners may be reluctant to do so.
Positives of onboarding a new device
One of the pros of investing in the latest technologies is the possibility of having new and more effective solutions to better our patients’ results. They can also attract a whole new patient demographic, or allow existing patients to try something different that might be better suited to them (for example, with less downtime). This, of course, all helps increase your clinic’s revenue. We also feel it’s important to stay ahead of trends, otherwise your patients could go to a competitor who is offering solutions and technology you don’t.
In addition, we have found that newer devices carry the benefit that manufacturers often invest more heavily in assisting practitioners with marketing the device. When companies invest in marketing of new products, patients may already be aware of the technology, meaning you already have a potential patient base ready for when you do make the purchase. Companies may also invest much more in supporting you with the device, assisting in launching events, newsletters and so on, which in turn will generate more patients.
Choosing to wait
Some practitioners may decide it is best to hold off and not go for the newest bit of kit on the market. This might be because of the investment (both time and money) required or they may want to see how the device performs at other clinics before purchasing – we have all seen devices come and go across our career! Waiting can help reassure some practitioners that the technology is effective, safe and sells, which is particularly important for smaller businesses.
Of course, the main downside to this may be that you lose out to competitors who attract patients before you invest in the technology. Also, from an industry perspective, practitioners who are early adopters of new technology often become ‘experts’ in that area sooner than others, meaning they are likely to become leaders in their fields, and be asked to participate in clinical studies, represent companies for training and present at national and international events.
Key considerations
So, should you invest in the latest devices and technologies on the market? Research suggests early adopters of new tech can end up with 50% of the market share, and we personally feel that with the right
technology, it’s a good investment. However, it is pivotal to ensure you are conducting your own research first, allowing you to be more likely to invest in the best device for you.1 Before onboarding a new device, we consider the following points. Firstly, we research the company, technology and indications devices treat, and ask our patients if this would benefit them before investing.
It’s a good idea to do this via a questionnaire that includes how much patients would be willing to pay, as you want to ensure the device pays for itself quickly. It is also worth running a return on investment (ROI) calculator to see how many treatments would be required before you gain a profit. Price point must be considered, and what works in one region may not work in another. If the device company gives you a price point for a London patient, this may not be the price you can charge in your local area.
Secondly, we ensure the new device does what it says and the results are reproducible and consistent. We do thorough research and critique the clinical evidence of the technology in general, as well as the specific device, to accomplish this. Some manufacturers allow for trials or demos in-clinic prior to making a payment. This is worth doing so you can make sure you believe in it before purchasing. Being passionate about what a device is treating is an important factor to choosing the right technology and attracting patients. If you’re not a fan of treating skin, for example, buying a CO2 laser may be pointless. Furthermore, it’s vital that you have the staff and resources available to take on the new device. Lasers, for example, require extensive training before they can be used – do you have Level 4 trained staff, or do you need to recruit someone new? You also should consider levels of training for appropriate revenue. Be clear in your mind as to why you are bringing in the technology and why you want it.
Embrace new technology
There are many pros and cons when purchasing the latest technologies, as well as some considerations before purchasing. Overall, we feel new technology should be embraced, and devices in particular can bring enhanced results, patient satisfaction and retention, as well as a healthy revenue. Thorough research should be carried out prior to making an investment, and a great place to start is events like ACE and CCR, where you can meet companies and see the latest devices on the market. Understand what you are aiming to achieve, speak to friends and colleagues about their experiences and, importantly, ensure any new device will provide your patients with great results.
Dr Nestor Demosthenous obtained his medical degree and BSc Hons Neuro from the University of Edinburgh in 2006 and obtained his MSc in Aesthetic Medicine from QMUL in 2019. He is a KOL for Cutera and an Allergan Medical Institute Faculty member.

Qual: MBChB, BSc Hons Neuro, MSc (Aesthetic Medicine)
Amanda Demosthenous is a registered general nurse and nurse prescriber with a BSc (Hons) in Adult Nursing as well as a PGDip in Aesthetic Medicine. Amanda is the founder of ICAN aiming to help nurses with mentorship, training and development in aesthetics.

Qual: RGN, INP, PG Dip
REFERENCES
1. Timesheet Mobile, ‘5 Factors to Consider Before Investing in Technology for Your Business’, 2017, <https://blog.timesheetmobile.com/5-factors-to-consider-before-investing-in-technology-for-yourbusiness>
Reproduced from Aesthetics | Volume 10/Issue 3 - November 2023 @aestheticsjournaluk Aesthetics Aesthetics aestheticsjournal.com


Beauty flows through us OVER 100 MILLION SOLD Blunt-tip reduces friction and glides through dermal tissue Ultra-thin cannula wall increases lumen diameter and reduces injection forces Premium quality single-use cannula used by clinical and industry leaders Made in Britain for over 30 years AESTHETIC +44 1527 501480 ● www.sterimedix.com AESTHETIC CANNULA

