


VOLUME 6/ISSUE 12 - NOVEMBER 2019 Uniform Policies Staffing specialist Victoria Vilas advises on how to implement a fair dress code policy Dermal Filler Blindness Miss Elizabeth Hawkes explores approaches for immediate dermal filler-related blindness Special Feature: Static Lateral Canthal Rhytids Practitioners discuss considerations around treating crow’s feet Forehead Anatomy CPD RANGE OF THE WORLD’S MOST EXPLORE COUNTLESS POSSIBILITIES WITH COMPLEMENTARY TECHNOLOGIES NASHA & OBT TO CREATE YOUR OWN SIGNATURE TREATMENT #INSPIREDBYYOU FOLLOW US ON FACEBOOK & INSTAGRAM @RESTYLANEUK RES19-10-0716c DOP October 2019 References 1.Data on file (MA-33939) 2. Öhrlund A. Poster presented at AMWC 2019 Mr Dalvi Humzah and nurse Anna Baker provide an update on forehead anatomy TOCHANCELAST BOOK! AESTHETICSAWARDS.COM

Mr Dalvi Humzah and nurse prescriber Anna Baker provide an update on forehead anatomy
Dr Xavier Goodarzian provides an overview of performing deep peels
Advertorial: Merz Innovation Partner Programme
Presenting a Belotero Lips masterclass with Lee Garrett 42 Understanding Brow Shapes
Permanent makeup artist Karen Betts discusses the importance of eye brow shapes in facial aesthetics 45 Considering Dermal Filler Blindness
Miss Elizabeth Hawkes identifies the approaches for immediate dermal filler-related blindness 49 Using Growth Factors: Part 2
In the second of her two-part article Dr Anna Hemming uncovers the use of growth factors within aesthetic medicine 53 Understanding Ocular Rosacea

Miss Jennifer Doyle discusses presentation and treatment of ocular rosacea 57 Treating Strabismus with Toxin
Miss Joanne Hancox details the use of toxin for eye squints 61 Abstracts
A round-up and summary of useful clinical papers IN PRACTICE 62
Starting Pro Bono in Aesthetics
Nurse Frances Turner Traill shares advice for successful pro bono work 65
Introducing Uniform Policies
Victoria Vilas explains how to create a dress code for aesthetic clinics 68 Tips for CQC Success



Dr Julia Sevi provides her top tips for CQC registration 73 In Profile: Dr Tahera Bhojani-Lynch
Dr Tahera Bhojani-Lynch reflects on her career in aesthetics and shares her passion for treating the upper face 74 The Last Word: Treatment Duration

Dr MJ Rowland-Warmann argues why practitioners should stop the length of advertising treatment times for filler procedures

Rhytids
Clinical Contributors
Mr Dalvi Humzah is a consultant plastic surgeon and delivers his clinical practice through PD Surgery in the West Midlands, Gloucester, and The London Welbeck Hospital. He is also director Dalvi Humzah Aesthetic Training and clinical director of Derma-Seal Ltd.

Anna Baker is an aesthetic nurse prescriber, and qualified educator. She works as a trainer and KOL for a number of aesthetic companies, and is a board member for the BACN. Baker is a course coordinator and tutor at Dalvi Humzah Aesthetic Training.

Miss Jennifer Doyle has a Bachelor in Medicine and a Bachelor of Surgery, as well as a Master’s in Medical Sciences from the University of Oxford. Miss Doyle currently works as an NHS registrar in ophthalmology, as well as leading her clinic, Oxford Aesthetics.
Dr Anna Hemming is the owner and medical director of Thames Skin Clinic in Twickenham and associate doctor at Cranley Clinic on London’s Harley Street.
Dr Hemming is a GP who has worked at Buckingham Palace and spent five years as an army doctor.
Miss Elizabeth Hawkes is a consultant ophthalmologist and oculoplastic surgeon at the Cadogan Clinic in Chelsea, London. Miss Hawkes leads the emergency eye care service for the Royal Berkshire NHS Foundation Trust.
Karen Betts has clinic locations in Cheshire, Yorkshire and on Harley Street and has been performing permanent makeup and medical tattooing for more than 20 years. Betts offers a variety of permanent makeup training courses under the K.B Pro brand.
Dr Xavier Goodarzian is the medical director and co-owner of Xavier G. Clinic in Southampton. He is a lecturer and trainer at major conferences throughout the UK and abroad, and the past lead trainer for Innomed Training.
Miss Joanne Hancox is a consultant ophthalmologist specialising in complex adult and paediatric strabismus, with extensive experience in botulinum toxin injections. She is strabismus service director and North Thames training programme director.

Last chance to book tickets! Aesthetics Awards 2019 www.aestheticsawards.com Contents • November 2019 Subscribe Free to Aesthetics Subscribe to Aesthetics, the UK’s leading free-of-charge journal for medical aesthetic professionals. Visit aestheticsjournal.com or call 0203 196 4367
Special Feature: Treating Static Lateral Canthal
Page 27
News
14
20
23
NEXT MONTH • IN FOCUS: Evolution • 30 Years in Aesthetics • Neck Rejuvenation 06
The latest product and industry news
On the Scene Out and about in the specialty
News Special: Medical Device Regulations The latest on the new medical device regulations set by the MHRA
CCR: A Huge Success Highlights from the recent CCR conference 24 ACE 2020: Another Exciting Event Ahead After this year’s success, Aesthetics showcases what you can expect CLINICAL PRACTICE 27 Special Feature: Treating Static Lateral Canthal Rhytids Aesthetics explores the causes, assessment and treatment approaches for static lateral canthal lines 32 CPD: Forehead Anatomy for Injectables
36 Performing Deep Chemical Peels
40


Intensive Pigment Corrector Meeting the needs of your business, delivering high satisfaction to your patients Call us on 01234 313130 info@aestheticsource.com www.aestheticsource.com Help your patients. Reduce their pigmented marks. Reclaim their natural beauty. 1.Mansouri et al (2015)British Journal of Dermatology 173 (1) 209 –217 2.Farshi et al (2018) Journal of Dermatological Treatment, 29 (2) 182–189 67% 90% noticed moderate to significant improvements after 16 weeks.2 melanin pigment reduction in pigmented lesions.1
Chloé Gronow Editor & Content Manager
What a fantastic time we had at CCR! After joining forces earlier this year, the Aesthetics Media and CCR team worked hard to deliver a stellar conference and exhibition that united both the surgical and non-surgical communities, with the BAAPS annual meeting also taking place at the event. Hundreds of new treatments and products were showcased across the exhibition floor, while renowned speakers presented their most innovative techniques and valuable advice for best practice. If you were there then you would have seen the fantastic display of more than 2,000 journals in our Sales Lounge, where the editorial team were positioned to interview delegates and catch up with all our contributors. As always, it was great to see everyone and CCR has got us even more excited for ACE 2020 on March 13 and 14! Before that, though, it’s the Aesthetics Awards on December 7! Tickets are selling fast, so I do really encourage you to book soon so you don’t miss out. We have hilarious comedian Tom Allen confirmed as our host and a new band booked for after the ceremony, which I am
Clinical Advisory Board
particularly excited about! Of course, the entertainment is a huge part of the Awards, but our main focus is rewarding those who do so much to uphold high standards in aesthetic practice and ensure patients are treated safely. Join us in coming together to recognise and celebrate all the companies and individuals who work so hard to do so. Our issue this month focuses on the Upper Face. To honour this, our Advisory Board Clinical Lead Mr Dalvi Humzah and nurse prescriber Anna Baker share an update on forehead anatomy on p.32 – essential CPD reading for all practitioners. We also explore the treatment of static lateral canthal rhytids on p.27, ocular rosacea on p.53 and the causes and treatment approaches for dermal filler-related blindness on p.45. Consultant ophthalmic surgeon Miss Joanne Hancox gives an interesting overview of how squints can be treated with toxin, while permanent makeup artist Karen Betts outlines how brow shapes should influence aesthetic treatments on p.42 Finally, for our In Profile this month, ophthalmologist and aesthetic practitioner Dr Tahera Bhojani-Lynch tells us what she loves about treating the upper face and the lessons she’s learnt throughout her fascinating career. Catch her advice on p.73.
Leading figures from the medical aesthetic community have joined the Aesthetics Advisory Board to help steer the direction of our educational, clinical and business content

Sharon Bennett is chair of the British Association of Cosmetic Nurses (BACN) and the UK lead on the BSI committee for aesthetic nonsurgical medical standards. She is a registered university mentor in cosmetic medicine and has completed the Northumbria University Master’s course in non-surgical cosmetic interventions.

Mr Adrian Richards is a plastic and cosmetic surgeon with 18 years’ experience. He is the clinical director of the aesthetic training provider Cosmetic Courses and surgeon at The Private Clinic. He is also member of the British Association of Plastic and Reconstructive and Aesthetic Surgeons and the British Association of Aesthetic Plastic Surgeons.
Jackie Partridge is an aesthetic nurse prescriber with a BSc in Professional Practice (Dermatology). She has recently completed her Master’s in Aesthetic Medicine, for which she is also a course mentor. Partridge is a founding board member of the British Association of Cosmetic Nurses and has represented the association for Health Improvement Scotland.
Dr Christopher Rowland Payne is a consultant dermatologist and internationally recognised expert in cosmetic dermatology. As well as being a co-founder of the European Society for Cosmetic and Aesthetic Dermatology (ESCAD), he was also the founding editor of the Journal of Cosmetic Dermatology and has authored numerous scientific papers and studies.
Dr Raj Acquilla is a cosmetic dermatologist with more than 12 years’ experience in facial aesthetic medicine. In 2015 he won the Aesthetics Award for Aesthetic Medical Practitioner of the Year and in 2012 he was named Speaker of the Year. Dr Acquilla is a UK ambassador, global KOL and masterclass trainer for botulinum toxin and dermal fillers.
Dr Tapan Patel is the founder and medical director of PHI Clinic. He has more than 16 years’ clinical experience and has been performing aesthetic treatments for more than 14 years. Recently, he was listed in Tatler’s Top 30 AntiAgeing Experts. Dr Patel is passionate about standards in aesthetic medicine.

Mr Dalvi Humzah is a consultant plastic, reconstructive and aesthetic surgeon with more than 20 years’ experience and is director of P&D Surgery. He is an international presenter, as well as the medical director and lead tutor of the multi-award-winning Dalvi Humzah Aesthetic Training courses. Mr Humzah is founding member of the Academy of Clinical Educators at the Royal College of Physicians and Surgeons of Glasgow. ARTICLE


Do you have any techniques to share, case studies to showcase or knowledge to impart?
Email editorial@aestheticsjournal.com
Dr Stefanie Williams is a dermatologist with special interest in aesthetic medicine. She is the founder and medical director of the multi-award winning EUDELO Dermatology & Skin Wellbeing in London. She lectures in the Division of Cosmetic Science and has published more than 100 scientific articles, book chapters and abstracts.
Dr Souphiyeh Samizadeh is a dental surgeon with a Master’s degree in Aesthetic Medicine and a PGCert in Clinical Education. She is the clinical director of Revivify London, an honorary clinical teacher at King’s College London and a visiting associate professor at Shanghai Jiao Tong University.

PDFs AND REPRO
Courtney Baldwin
Event Manager T: 0203 196 4300 | M: 07818 118 741 courtney.baldwin@easyfairs.com Judith Nowell • Business Development Manager T: 0203 196 4352 | M: 07494 179535 judith@aestheticsjournal.com
MARKETING
Aleiya Lonsdale • Head of Marketing T: 0203 196 4375 | aleiya.lonsdale@easyfairs.com

Annabelle Arch • Marketing Manager
T: 020 3196 4427 | annabelle.arch@easyfairs.com
CUSTOMER LIAISON
Chloe Carville • Customer Liaison Executive
T: 0203 196 4367 | contact@aestheticsjournal.com
Lian Graham • Customer Liaison Executive T: 0203 196 4368 contact@aestheticsjournal.com


Material may not be reproduced in any form without the publisher’s written permission. For PDF file support please contact Chloe Carville, contact@aestheticsjournal.com © Copyright 2019 Aesthetics. All rights reserved. Aesthetics is published by Aesthetics Media Ltd, which is registered as a limited company in England; No 9887184
ABC accredited publication
Editor’s letter
DISCLAIMER:
PUBLISHED
MANAGEMENT
The editor and the publishers do not necessarily agree with the views expressed by contributors and advertisers nor do they accept responsibility for any errors in the transmission of the subject matter in this publication. In all matters the editor’s decision is final.
BY PORTFOLIO
•
Director
Gronow • Editor & Content Manager
Kilgariff • Deputy Editor
196 4351 M: 07557 359 257 shannon@aestheticsjournal.com Megan Close • Journalist
196 4363 M: 07557 359 257
Johnson • Senior Designer
196 4359 |
& SPONSORSHIP
Jenny Claridge
Commercial
T: 0203 196 4364 | jenny@aestheticsjournal.com EDITORIAL Chloé
T: 0203 196 4350 | M: 07788 712 615 chloe@aestheticsjournal.com Shannon
T: 0203
T: 0203
megan@aestheticsjournal.com DESIGN Peter
T: 0203
peter@aestheticsjournal.com ADVERTISING
•
Aesthetics Journal @aestheticsgroup Aesthetics @aestheticsjournaluk
Mr Dalvi Humzah, Clinical Lead
WE WANT TO HEAR FROM YOU!
Aesthetics Media Part of
Talk #Aesthetics
#Celebration
Aesthetics Media
@aestheticsjournaluk TODAY WE HIT 10K INSTAGRAM FOLLOWERS!

Since starting this channel a few years ago, so much has changed as the team has grown and adapted to what content YOU like to see. We want to thank you for your continued support, day after day. We couldn’t have done it without you!
#AestheticsTeam #Milestone
#Networking
Dr Marcus Mehta @dr_marcus_mehta
A great day at CCR Expo today catching up with everyone including my London colleague Dr Martin Kinsella #CCRexpo2019

#Surgeons
Mr Marc Pacifico @marcpacifico Wow! An amazing past few days of electric debate and thought provoking ideas all led by the world’s leading #plasticsurgery thinkers and innovators. #baaps2019

Dermal fillers
Croma Pharma rebrands filler range
Pharmaceutical company Croma Pharma has rebranded its hyaluronic acid filler brand Princess to saypha. The company explains that the rebranding, starting in Europe, became necessary due to its ongoing globalisation process and the advancing approval procedures of bio-pharmaceutical company Hugel, Inc.’s botulinum toxin product Botulax requiring a more medical HA filler brand, exclusively for medical professionals. Croma has licensed the product Botulax for Europe and recently established a joint venture with the company in order to develop and commercialise Croma’s HA filler and PDO thread products together with the toxin in the US, Canada, Australia and New Zealand. Managing director, Andreas Prinz, said, “By replacing Princess with saypha we pursue several different purposes. Primarily, Princess is not a suitable and approvable brand for all our current and future markets.” He continued, “In the course of our progressing internationalisation process, this standardised appearance of the company towards our primary target audience, the medical professionals, becomes absolutely essential. Apart from that, all saypha products are easy to distinguish which was a customers’ request that we are happy to follow. The saypha brand also reflects medical science and evidence-based medicine. By introducing saypha we are creating a strong global HA filler brand that stands for comprehensive quality, reliability and medical effectiveness.”
Partnership
SkinCeuticals launches clinical centre with Cavendish Clinic

After a successful five-year partnership, skincare company
#Learning
Dr Raul Cetto @drcetto
Fantastic weekend with the North East Aesthetics Group on stage with my #teobro @leewalker_academy @drtijionesho and @sueyoungaesthetics Great group of engaging delegates attended can’t wait to see you all again. #Teoxane

#Education
Alice Hart-Davis @alicehartdavis
Brilliant weekend at the @tamcongress in Dubrovnik. Huge congrats to @drnickmilojevic who in just two years has established this conference in the hearts and minds of the international medical aesthetics community.

#Conference
SkinCeuticals and Cavendish Clinic in London have launched SkinCeuticals’ first advanced clinical centre. Named SkinCeuticals by Cavendish Clinic, the centre was officially launched in September and aims to provide patients with advanced knowledge and experience alongside the SkinCeuticals product offering. In the centre, patients can take advantage of the Custom D.O.S.E machine, a professional service that combines high-potency ingredients with professional expertise to create a personalised corrective serum. There is also an express peel bar and SkinScope skin analysis. Consultant plastic surgeon at The Cavendish Clinic Mr Matt James, said, “We are thrilled to partner with SkinCeuticals in Kensington to become a flagship clinic. As a skincare centre of excellence, we look forward to creating an engaging, bespoke experience for both our loyal and new patients.”
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Follow us on Twitter @aestheticsgroup and Instagram @aestheticsjournaluk
Toxins
Evolus receives EU marketing approval for Nuceiva
Medical aesthetic company Evolus Inc has announced that the European Commission (EC) has approved the marketing of Nuceiva prabotulinumtoxinA (branded Jeuveau in the US and known in other markets as Nabota). The marketing has been approved for the temporary improvement in the appearance of moderate to severe glabellar lines. The EC’s decision is applicable to all 28 European Union member states plus Iceland, Norway and Liechtenstein. “With the approval in Europe, we have now achieved all key research and development milestones around the world,” said Rui Avelar, chief medical officer and head of research and development at Evolus Inc. He added, “This approval further validates our transparency clinical development programme, which included the largest aesthetics head-to-head pivotal study conducted in Europe and Canada versus Botox out to 150 days.” Aesthetics Clinical Advisory Board lead, and consultant plastic, reconstructive and aesthetic surgeon Mr Dalvi Humzah, said the approval is a very positive step for the UK market. He commented, “I welcome a new toxin in the aesthetic arena. This marketing approval means that both patients and practitioners will have more choice and it opens further competition between the toxin companies. From a practitioner’s perspective, they need to consider that it’s only approved for the glabella; we know that this product has been used successfully in other markets so it will be very interesting to see what the future holds.”
Education Allergan hosting education at ACE 2020
For the first time, global pharmaceutical company Allergan will host unmissable free clinical education on complication management, as well as exhibit at the annual Aesthetics Conference and Exhibition (ACE) next year. Nancy Ghattas, associate vice president, country manager UK and Ireland at global pharmaceutical company Allergan said, “We are very excited to be at ACE 2020. It is a milestone event for us where education and training is key for all of our stakeholders and customers in aesthetics. We are going to showcase Juvéderm and CoolSculpting at the Allergan stand and we are going to bring some really exciting developments so please watch this space!” There will be four identical ‘Allergan Experience’ sessions taking place in the Masterclass agenda on Saturday March 14. Spaces are limited, so delegates must register their interest for these sessions and complete DocCheck to confirm their medical registration in advance. She added, “For Allergan, education and training is key – we firmly believe that the higher we raise the standards for education and training the higher the standards are for the entire aesthetics market. Every year we look at how we can rise, elevate and empower our customers through training and education and how we can bring innovative products and techniques into the space as well so we are delighted to be sponsoring education at ACE 2020.” ACE 2020 will be held at the Business Design Centre on March 13-14. To register free, go to aestheticsconference.com.
Vital Statistics
Last year, 3,153 blepharoplasty surgeries were performed in the UK, 89% of these procedures were on female patients (BAAPS, 2019)
61% of mobile users are more likely to contact a local business if the business has a mobile-friendly site (Junto, 2019)

Out of the 616 dermal filler-related complaints reported to Save Face last year, 13% related to the tear trough (Save Face, 2019)
According to a survey conducted amongst 738 HR managers, employees are nearly two times as likely to enjoy working for a company when they are satisfied with how life events are celebrated in the workplace (GloboForce, 2018)
In a survey of more than 2,000 women, 96% admitted that they use a filter to improve the appearance of their skin (FOREO, 2019)
There was a 12% rise in PRP treatments in the US last year with 127,394 patients undergoing treatments, compared to 113,356 the previous year (ASPS, 2018)
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Events Diary
2nd November
WACS Annual Conference www.welshaesthetics.com
7th-8th November
British Association of Cosmetic Nurses Conference www.bacn.org.uk
4th-6th December
British Association of Plastic Reconstructve and Aesthetic Surgeons Winter Scientific Meeting www.bapras.org.uk
30th January - 1st February 2020
IMCAS World Congress www.imcas.com/en
Exhibition CCR 2020 moves to ExCeL London
After the success of CCR 2019, Easyfairs, the company behind CCR, has confirmed that the exhibition will be moving to London’s ExCeL centre next year, taking place on October 1 and 2. This is to secure the best conference facilities and transport links in London for both the exhibitors and delegates. “CCR is delighted to host the next event at ExCeL London in 2020, a truly powerful forum for members of the aesthetic medical community,” said Alison Willis, divisional director of CCR. She added, “The move is in response to customer demand for continual growth and development of the scientific meeting and ExCeL London is the best place to support our ambitious educational plans. We are committed to providing the greatest possible customer and delegate experience. ExCeL London’s location and facilities enable us to better cater for attendees coming from outside London and all over the UK and to organically grow our international audience with the proximity to London City Airport.”

7th December
The Aesthetics Awards 2019 www.aestheticsawards.com
13th-14th March
The Aesthetics Conference and Exhibition www.aestheticsconference.com
Skincare
iS Clinical applauds UK distributor
UK aesthetic distributor Harpar Grace has been named as skincare company iS Clinical’s second most successful distributor in the world at its global conference in Warsaw, Poland.
Alana Chalmers, director of Harpar Grace International said, “We are delighted to secure recognition as the second largest iS Clinical distributor in the world. We have achieved this success with not only being one of its youngest distributors but also with the most refined number of accounts.”
She added, “This achievement demonstrates our commitment and success of taking a selective distribution strategy here in the UK, which involves growing our partners’ business by taking a much more collaborative and supported approach, tailored to the needs of each clinic.”
Appointment
Celluma announces new recruit

Light emitting diode (LED) device manufacturer Celluma has appointed Jim McKenney as its new vice president of global sales. McKenney joined the team in August to manage the company’s international growth and develop new global markets for the series of devices. McKenney brings more than 20 years of leadership experience in business development and sales management. In addition to his experience in contract manufacturing and healthcare, he has successfully started and exited two real estate investment firms. Celluma CEO Patrick Johnson said, “We are excited to add Jim to our growing senior leadership team. He brings a wealth of experience and refined skillset to the company. I have no doubt Jim will make an immediate contribution to the company’s continued success, growing our top-line sales and expanding our global footprint beyond the 74 countries we already sell into.”
Botulinum toxin
Positive results for liquid toxin
Global pharmaceutical company Galderma’s liquid formulation of botulinum toxin type A has achieved positive results for the treatment of glabellar lines in a phase 2 clinical trial. The results of the phase 2 multicenter, randomised, double-blind, placebo-controlled clinical trial using QM1114 ready-to-use investigational botulinum toxin demonstrated initial safety and efficacy at all doses in the treatment of glabellar lines in more than 350 patients, with high patient satisfaction. QM1114 is derived from Galderma’s proprietary strain of Clostridium botulinum bacteria and manufactured using an animal-origin free process. It is designed and developed specifically for use in aesthetics as a liquid formulation, aiming to reduce preparation time needed in clinic as it is ready-to-use rather than requiring reconstitution before administration. Following the trial results, Galderma has received a manufacturing license from the Swedish Medical Products Agency (MPA) for a new state-of-the-art manufacturing facility at the Center of Excellence, located in Uppsala, Sweden. Phase 3 trials for Galderma’s liquid formulation of botulinum toxin type A for the treatment of glabellar lines are expected to begin soon and will involve approximately 1,500 subjects.
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
13 & 14 MARCH 2020 / LONDON
Digital
Clever Clinic now available
Patient management app Clever Clinic launched at the industry-leading event for non-surgical and surgical aesthetic professionals, CCR. Developed by aesthetic supplier Healthxchange Group, the app aims to help practitioners comply with regulatory requirements and ensure that patient safety and good record keeping becomes a part of every patient consultation. According to Healthxchange Group, the key features of the app include a patient consultation platform, which allows practitioners to quickly and easily complete patient records, fully documenting clinical plans using bespoke visuals specific to the aesthetics industry. The app also features smart consenting that captures patient and practitioner signatures, date and time stamps, and specific highlighted areas in each patient record. Practitioners can also utilise smart treatment planning and automatic Healthxchange e-pharmacy orders, which aims to significantly cut down admin work for aesthetics practitioners. Finally, the app includes a flexible calendar booking system with advanced booking and scheduling, live notifications and customisable calendars. Clever Clinic is available on the Apple iOS iPad app store. Users must have a valid Healthxchange ePharmacy account to log in.
Tickets selling fast for the Aesthetics Awards

With just over one month until the most prestigious event in the aesthetics specialty takes place, those wishing to attend are encouraged to secure their seat by booking tickets soon. The ceremony will be taking place on December 7 at the Park Plaza Westminster Bridge Hotel and guests will receive entry to the dazzling ceremony, prosecco on arrival, a three-course meal with drinks, and entertainment from top comedian Tom Allen throughout the night. Commercial director, Jenny Claridge said, “The Aesthetics Awards 2019, is set to be a fantastic night. We are expecting more than 850 guests from all areas of the specialty and the very best clinics, products, training providers, distributors and other aesthetic companies will be recognised for their continued hard work and achievements over the past year. To make sure that you do not miss out, get in contact with our team today.” Also announced this month is SkinCeuticals sponsorship of the Energy Device of the Year category. To find out more, visit aestheticsawards.com
Event
Aesthetic Exchange to take place this month
Laser manufacture CynoSure UK will host its third symposium as part of its Aesthetic Exchange educational platform in London on November 22-23 in collaboration with cosmeceutical brand iS Clinical. The event is titled Topicals and Lasers; Maximising Outcome and Income, and will provide practitioners with the opportunity to attend seminars, discussions and live demonstrations. The sessions will discuss pigmentation, scarring, vascular issues, laser hair and tattoo removal and body contouring. It will be led by cosmetic laser surgeon Dr Dianne Quibell and clinical director of iS Clinical, Dr Charlene DeHaven who will be joining from the US to share their experience in light-based technology and epigenetics, and how best to combine the power of lasers and cosmeceuticals for superior patient outcomes.
Jackie Partridge, aesthetic nurse prescriber

What attracts young adults to the service you provide?
In the industry, I am well known for giving an honest opinion to my patients and guiding them appropriately. With the prevalence of social media, the younger generation are more aware of their overall image and try to be the best versions of themselves. They have a much better appreciation of treatments that can be used to beautify themselves including nonsurgical options, where perhaps 10-15 years ago it was only possible with surgery, for example, chin enhancement and jawline sharpening.
What does a ‘complete approach’ mean to you and how do you offer this?
It’s all down to a full assessment of the face. I’ll explain the anatomy to the patient and why we should or shouldn’t do certain treatments. I have had patients talk about how they are unhappy with their mouth or jawline area, but it might well be a small addition of dermal filler to the chin area that can put the proportions back in sync. Once I’ve done a full assessment, I can guide them to what’s in their best interest. They might be focused on that one line, but it might be something completely different we’re looking at, and I can see with my aesthetic eye and years of experience what outcome that patient is going to get from such a service.
Do you think there are any misconceptions relating to dermal filler treatment?
Quite often, patients are unaware of specific treatments that can make a profound change to their entire appearance. For example, when treating the cheeks, we are putting in the scaffolding to support the whole face which gives a subtle enhancement, and this is where product choice is key. I always use the Restylane range; it’s my toolbox. It has an amazing broadspectrum portfolio of dermal fillers and I can absolutely deliver what my patients require.
This column is written and supported by
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
60
RES19-10-0696 DOP October 2019
Lasers & skincare
BACN UPDATES
A roundup of the latest news and events from the British Association of Cosmetic Nurses

CCR
The BACN had a fantastic time at CCR this year – the BACN Nursing Lounge was busy over the two days, and it was great to catch up with existing members and to encourage other nurses to join the association. The opportunity to meet with BACN partners in aesthetics and attend presentations by a number of BACN nurses, including Anna Baker, Mel Recchia, and BACN Chair, Sharon Bennett was brilliant. As the leading professional association for aesthetic nurses in the UK, it was warming to see that CCR invested so much for nurses who were front and centre throughout the two days – roll on 2020!
MONTHLY PAYMENTS AND ANNUAL CHANGES
Historically, the BACN has run a strict April-March Membership year, along with asking members for upfront annual payments. At CCR, the BACN launched the new flexible membership year, whereby no matter when you join, you get a full year of benefits, opportunities to attend events, and the BACN Autumn Aesthetic Conference. In addition to this, there is now availability to either choose an annual membership payment, or select a monthly payment option which will renew each month. More information concerning this can be found on the membership page of the BACN website or alternatively you can contact Gareth Lewis, BACN Membership and Marketing Manager at glewis@bacn.org.uk
BACN AUTUMN AESTHETIC CONFERENCE
This month, the BACN will be holding its Autumn Aesthetic Conference, with a Professional Sessions Symposium held on the first day, and the more traditional exhibition area and networking on the second day, which is included as part of the BACN membership. At the conference, the BACN will also be launching its new ‘I am a BACN nurse’ campaign, which will showcase the dedication to professionalism and commitment to patient safety that all BACN nurses adhere to through the BACN Code of Conduct. Alongside this, BACN nurses will be encouraged to promote their membership throughout the year via BACN social media channels and at BACN events.
This column is written and supported by the BACN
Buttock lifts
BAAPS announces formal review for BBL
The British Association of Aesthetic Plastic Surgeons (BAAPS) will launch a formal review of emerging new evidence into the safety and techniques used for the fat grafting procedure, the Brazilian Butt Lift (BBL).
Last year, the association advised its members to stop performing this procedure until more data could be collated. At the BAAPS Annual Scientific Meeting, which took place at CCR on October 10 and 11, leading plastic surgeons presented emerging evidence with respect to safety and techniques of buttock fat grafting. This has resulted in BAAPS undertaking a formal review that will include a survey of each of its members and examine emerging, peer-reviewed published evidence. Aesthetic practitioner and British College of Aesthetic Medicine (BCAM) spokesperson Dr Uliana Gout supported this, “BCAM advises practitioners and patients to note the BAAPS cautionary statement regarding the BBL treatments which have had a lot of recent international publicity and interest. Patient safety is paramount to BCAM and we are aligned with BAAPS that all treatments should be backed by evidence-base to ensure safety and efficacy are optimised.”
Topical New PDT formulation released
Private label cosmeceutical supplier 5 Squirrels has partnered with Alamed Technologies UK Limited to launch a new photodynamic therapy (PDT) treatment to the UK and Irish aesthetic market, GlycoAla. The companies claim that the glycosphere nanoparticle encapsulation of GlycoAla’s photodynamic ingredient enables enhanced penetration into the skin to provide safe improvement of skin tone, sun damage, ageing, hydration and moisture retention. Gary Conroy, co-founding director at 5 Squirrels Ltd, said, “This really is a game changing product. I have been working in PDT for the past decade and have often been frustrated that the benefits of this technology have never been widely adopted due to the complicated legacy protocols. GlycoAla changes all of that, it is a great fit with the range to finally deliver truly remarkable outcomes.” According to Conroy, the partnership with Alamed Technologies UK Limited will also allow healthcare professionals working in medical aesthetics to gain competence in PDT through training provided by aesthetic practitioner Dr Robin Stones and nurses prescriber Jan Birch, along with the commercial and business support of 5 Squirrels.

Resources
Sinclair Pharma releases Instagram media packs
Pharmaceutical company Sinclair Pharma has released a monthly-subscription service to ensure that its customers have the latest content to promote the Sinclair product range on Instagram. The company explains that the media pack provides practitioners with social media ready content which can be used to support their activity on social networking sites, with a main focus on Instagram. Each media pack is specifically designed for each of Sinclair Pharma products; Ellansé, Perfectha, Silhouette Soft and InstaLift in their retrospective markets and languages.
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Skincare
iS Clinical introduces the GeneXC Serum

Skincare company iS Clinical has launched a new serum, the GeneXC. It is suitable for all skin types and aims to activate genes to enhance skin cells’ ability to respond to stress, renew cells, brighten the skin and improve the overall skin function, the company explains. iS Clinical has also stated that the serum provides antioxidant protection, improvement in skin tone and elasticity, support in cellular regeneration and metabolism, and improve signs of ageing. The key ingredients include, l-ascorbic acid (20% stabilised), trehalose, hydrolysed eruca sativa leaf, plankton extract, lecithin, terminalia ferdinandiana fruit extract, plankton extract, arginine ferulate, mixed fruit acid extracts and superoxide dismutase. In a clinical study the skin was exposed to GeneXC Serum and gene expression was measured. Gene expression panels including 107 target genes and five endogenous control genes were analysed. Skin that was exposed to GeneXC showed increased antioxidant protection, improved hydration, enhanced skin barrier function, improved extracellular matrix integrity, enhanced cell renewal and repair and enhanced immune response.
Derma-Seal secures EU trademark
UK-based company Derma-Seal has successfully obtained trademark registration of its post-treatment product in the UK and member states of the EU. Mr Dalvi Humzah, consultant plastic, reconstructive and aesthetic surgeon and clinical director at DermaSeal, said that following the company’s Commendation in The Barry Knapp Award for Product Innovation of the Year in last year’s Aesthetics Awards, the product has seen increased interest nationally and internationally. Alan Hillier, finance director at DermaSeal added, “We have seen increased sales in the UK and Europe with interest in the Far East and the US. We are in discussion with key players in these new markets. We hope Derma-Seal will be of clinical use to practitioners there.” Derma-Seal is available in the UK through distributors Church Pharmacy, John Bannon, You Can Pharmacy and Wigmore Medical.
Association
BCAM confirms plans for student membership
The British College of Aesthetics Medicine (BCAM) is planning to introduce a special membership option for medical and dental students. BCAM president Dr Paul Charlson told Aesthetics that the organisation has seen an increase in students going straight into aesthetic medicine following their medical training, rather than into their normal clinical practice. “There is a lot of interest in the aesthetic field from new doctors and dentists and many are going straight into aesthetics following their qualifications,” Dr Charlson said. He explained, “One of our concerns is that these practitioners don’t have as much experience and grounding in medical practice, so as an association we need to support them. The aim is to introduce a student membership that will be applicable to dental and medical students. We want to make sure that these practitioners are confident in areas such as recognising mental illness, consultation skills and other practice that doctors and dentist gain through experience working in the field.” Dr Charlson further emphasised that it’s important for the aesthetic specialty to recognise that many are training to become doctors and dentists, but do not actually aspire to work in the traditional way and instead desire to a career in aesthetics. Further plans for student membership are expected to be released by the end of the year.
FLOOR
By attending ACE, delegates can learn the latest technologies and best practise from industry leading practitioners over two days. Plus, there is so much more on offer at the event than just the incredible content.
Set over 2,500m2, 80+ aesthetic exhibitors will be showcasing over 4,000 of the newest and most innovative products and treatments, exclusive to this event. There are multiple opportunities to try out the latest equipment, so delegates can be confident in their understanding and requirements. By attending ACE, delegates have a true insight into this specialty and what’s in store for the year ahead.

AESTHETIC PRACTITIONER, LONDON
AESTHETIC CLINIC MANAGER, LONDON
VISIT aestheticsconference.com
Use registration key 10001
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com 13 & 14 MARCH 2020 / LONDON
HEADLINE SPONSOR
EXPLORE THE EXHIBITION
“There is no better place to learn than in one big room, where you can compare different machines and equipment!”
“Excellent display from the whole spectrum of the aesthetics industry”
Post-procedure
Training
Cutera announces new training programme
Laser and light-based medical provider Cutera Medical Ltd has launched a new laser and IPL training programme with free of charge spaces on its first Core of Knowledge course, running on December 2. The new programme will be based at the company’s facility in London but will also see Cutera participate in a laser training roadshow around the UK. Tim Taylor, UK country manager stated, “I am delighted to be bringing the worldrenowned training programme direct to the UK. We will now be offering UK delegates a range of specialist laser training courses, including the Core of Knowledge and Level 4 and 5 qualifications in both hair reduction and skin rejuvenation.” Cutera has also stated that its new training team will include established industry specialists, which will ensure delegates receive the highest quality laser training available.
Support
Limited support for dermatology issues
The British Skin Foundation, a charity dedicated to raising funds for skin disease research, has conducted a survey amongst 245 dermatologists indicating that 87% believe that there is a lack of access to psychological support for those suffering with skin conditions in the UK. Dr Andrew Thompson, practitioner clinical psychologist at the University of Sheffield and Sheffield Health and Social Care NHS Foundation Trust commented, “This survey demonstrates that dermatologists recognise some patients experience psychological distress associated with their skin condition. It also indicates that whilst dermatology is making great advances in treating the medical aspects of skin disease, perhaps not enough is being done to address the accompanying psychological effects. Clearly, we need more research that looks to develop effective psychological treatments or support for both children and adults living with skin conditions.”
IMCAS World Congress Preview

On January 30 to February 1, the International Master Course on Aging Science (IMCAS) will host its 22nd Annual World Congress in Paris. More than 12,000 international attendees and 300 exhibitors are expected to attend, with 345 educational sessions planned for the event. According to IMCAS, one of the highlights for 2020 will be artificial intelligence (AI) robotics. A spokesperson said, “Advances in diagnostic algorithms, sophistications in surgical robotics, imaging technologies for accurate and affordable scans and other technological developments all serve as examples of the emerging revolution that will change the practice itself. The sessions of this series aim to provide insight into how AI and robotics can specifically apply to aesthetics, what technologies are currently available, and what it entails for physicians and patients in their everyday interaction.” Two live events will also take place, showcasing a simultaneous transmission and screening of live cadaver dissections alongside live procedures on patients. IMCAS notes that the Anatomy on Cadaver Workshop focuses on the anatomy and techniques pertaining to injectables and threads, as well as echographic scanning to avoid danger zones, while the Live Aesthetic Surgery Course will enable attendees to follow a range of different surgical procedures performed live, juxtaposing with the anatomy of the relevant areas. Those interested in attending can book tickets via the IMCAS website.
News in Brief
HydraFacial expands UK footprint
Skincare treatment brand HydraFacial has increased its presence in the UK by purchasing assets of the Consulting Room, an aesthetic information website and distributor. The new acquisition, called HydraFacial UK, will see 19 Consulting Room employees transition to the HydraFacial UK team to ensure continuity of service with existing customers. As well as this, it will increase the company’s international profile by adding northern Europe into a portfolio already including China, Japan, Spain and Canada, the company states.
Mediderma releases lip peel
Clinical skincare and aesthetic company Mediderma has launched the FERULAC DUBAI LIPS, a two-step system that the company explains is formulated to target lip photoageing. Step one prepares the skin with the FERULAC DUBAI LIPS TRX MIST, which is formulated with tranexamic acid that aims to reduce pigmentation. Step two is to apply the FERULAC DUBAI LIPS PEEL, lactic and ferulic acid. This should be applied with one to two coats and allowed to work for six to eight minutes, Mediderma states. To further prolong the effects, the company recommends following this with its lip balm.
Image Skincare launches exfoliant Skincare company Image Skincare has introduced a new product, the ORMEDIC balancing gel polisher. According to the company, its combined physical, enzymatic and alpha hydroxy acid (AHA) exfoliates dead skin without harsh scrubbing, leaving skin smooth, clean and refreshed. It includes caviar lime extract, a natural AHA, pomegranate fruit enzyme, which aims to increase cellular renewal, and olive seed powder, bamboo spheres and eco-friendly beads to provide physical exfoliation.
New clinic to open in Belgravia
A collaboration of worldwide doctors and surgeons have joined forces to open Tempus | A Nu Yu Concept clinic in Belgravia London. Amongst the founders are aesthetics practitioner Dr Kuldeep Minocha, dermatologist and founder of the Nu Yu brand Dr Nada Soueidan and surgeon Ms Veerle Rotsaert. “Tempus incorporates the experience of a team of global experts in aesthetic education and treatments for face, body and mind. We have come together to create something really special for our London clinic in the heart of prestigious Belgravia. We treat to achieve the best results, with integrity in luxurious surroundings, keeping safety as our priority,” said Ms Rotsaert.
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
International conference


Hair Removal, Reinvented. abclasers.co.uk A NEW ERA OF SPEED ™ 0845 170 7788 TECHNOLOGY for unrivalled results FINALIST
On the Scene
Out and about in the specialty
Belotero Lips Masterclass
SkinPen press launch
Aesthetics invited eight aesthetic practitioners to attend the first Belotero Lips London Masterclass

On October 12, aesthetic
Lee Garrett. The day saw Garrett present the anatomy of the lips, the science and clinical trials behind the Belotero Shape and Contour products and his technique to achieve a more outlined, full and natural lip using both a needle and cannula. He them demonstrated this technique on his model before each practitioner was able to perform this on their own models, under Garrett’s close supervision. The intimate setting of the day enabled practitioners to freely ask questions and learn about the products and techniques, which was well received by all delegates.
Garrett said of the event, “The training session has gone so well and there is a good collection of delegates. I’m delighted to be part of the Merz innovation partner event and hosting the first one in London!”

Maria Rodrigues, marketing assistant at Merz Aesthetics added, “Lee has done a very professional job – he was very interactive with the group addressing all of their questions and guiding on best practice technique. The delegates have thoroughly enjoyed the Masterclass and have learnt something new to take home to their own practice.” The Merz Innovation Partner Masterclass series continues into 2020.
French Kiss Conference
Journalists were invited to learn about SkinPen Precision microneedling at its official UK press launch at the AllBright Club in London on October 3. The event had a good presence from consumer press, with representatives from VOGUE, TATLER, Harper’s Bazaar, the Daily Mail You Magazine and the Daily Telegraph in attendance. The talks started with Thomas Hitchcock, the chief science officer for medical affairs at Crown Laboratories, the owners of SkinPen manufacturer Bellus Medical. Then, oculoplastic surgeon and aesthetic practitioner Dr Maryam Zamani, burns and plastic surgeon at Chelsea and Westminster hospital Mr Andrew Williams, and aesthetic surgeon Mr Benji Dhillon all spoke about their experiences with SkinPen. The presentations had a large focus on helping the press to understand the science of microneedling and safety regulations to protect the consumer market, as well as the impact the SkinPen can have on a variety of skin concerns. Kathy Taylor-Brewin, managing director of BioActive Aesthetics, distributor of SkinPen in the UK, said following the event, “We are delighted with the high level of interest into the SkinPen Precision. It’s great that the press are interested in not only the device itself, but also the safety elements of the potential cross-contamination within microneedling treatments and how SkinPen protects against that issue.”
The new Art Filler Lips Soft was launched by aesthetic company FILLMED Laboratories at the London Cabaret Club on October 9 at its Aesthetics French Kiss Conference. More than 80 guests enjoyed a drinks and networking reception, before being invited to take a seat for a mix of live entertainment and lectures. Andrew Hansford, education ambassador at FILLMED welcomed guests, which was followed by a vocal performance by Rebecca Denham, head of FILLMED UK and Ireland. Throughout the evening, guests learnt about anatomy, filler techniques and the FILLMED range by dermatologist Dr Ferial Fanian, and aesthetic practitioners Dr Phillipe Hamida Pisal, Dr Fabien Giausseran and Dr Riekie Smit. They also gained business and profile advice from communications consultant Jason Gale. In between each lecture guests enjoyed live cabaret performances. The highlight of the event was the launch of the Art Filler Lips Soft by Dr Smit. She said, “FILLMED now uniquely offers two distinctly different lip products, Art Filler Lips and Art Filler Lips Soft. Art Filler LIPS SOFT is can be used to improve contour and shape for people with already full lips and is good for fixing imperfections and lines.” FILLMED is distributed in the UK by Medical Aesthetic Group and Med-fx.
Aesthetics Business Conference
The Aesthetics Business Conference (ABC) returned for its third year at the Royal College of Physicians on September 28. Organised by Hamilton Fraser

Cosmetic Insurance, around 100 delegates met to learn about how to build or expand their business. The day covered business insights from well-known speakers in the industry, including aesthetic entrepreneur Richard Crawford-Small, dentist and aesthetic practitioner
Professor Bob Khanna, cosmetic account handler at Hamilton Fraser, Shelly Hemmings, amongst others. CEO of Hamilton Fraser Cosmetic Insurance, Eddie Hooker, said of the day, “ABC is about teaching people to run and operate a successful business. We sold out this year, which was great, and in 2020 we want it to be bigger and better. Hamilton Fraser is about giving back, education, support and ultimately running a successful business.” Hamilton Fraser is planning its next ABC event to take place on September 24, 2020.
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
manufacturer Merz
hosted by nurse prescriber and Merz innovation partner




Harmony XL PRO TM TM TM AWARD WINNING LASER PLATFORM 70+ FDA APPROVED TREATMENT INDICATIONS Skin Remodelling Vascular Lesions Pigmented Lesions Tone & Texture Hair Removal Acne & ‘Hollywood Facelift’ the world’s most advanced antiageing laser with no pain & no downtime. Perfecting problematic complexions with a cooling, vacuum-assisted laser. HOME TO: abclasers.co.uk 0845 170 7788 info@abclasers.co.uk 4D











0208 748 2221 info.uk@venusconcept.com www.venusconcept.com THE MOST VERSATILE MULTI-TREATMENT SYSTEM • Intense Pulsed Light (IPL) with SmartPulse™ technology and advanced real-time cooling • NanoFractional RF™ with SmartScan™ • Proprietary (MP)2 technology, which combines Multi-Polar Radio Frequency (RF) and Pulsed Electro Magnetic Fields (PEMF). Venus Versa™ is the most adaptable device for the needs and growth of your business, enabling you to maximize treatments and yield the highest possible ROI. DIAMONDPOLAR™ & OCTIPOLAR™ NANOFRACTIONAL™ RADIO FREQUENCY IPL APPLICATORS 1 SR IPL, 1 DiamondPolar™ & 1 NanoFractional RF™ treatment Courtesy of venus Concept 8 DiamondPolar™ & 1 NanoFractional RF™ treatment Courtesy of Glow Permanent Cosmetics BEFORE AFTER BEFORE AFTER APPLICATOR for skin resurfacing APPLICATORS for photorejuvenation, acne reduction and hair removal APPLICATORS for anti-ageing, body contouring, skin tightening
Croma Pharma Visit, Vienna
“Do you know where Croma got its name from?”, asked founder and pharmacist Gerhard Prinz. “I have three children; Corinna, Martin and Andreas,” he explained, “I wanted all of their names to be reflected in the company name so took their initials and Croma was formed.” Now, more than 40 years after its creation, the business still has a large focus on family, with both sons working across the management board. With the recent relaunch of the Princess hyaluronic acid dermal fillers, which are now known as saypha, a portfolio comprising PDO threads, a platelet-rich-plasma (PRP) system, two skincare lines and more developments on the horizon, Croma opened its doors to the UK press to share its history and plans for the future. The Croma headquarters is based in Leobendorf, Austria, and is housed across three floors. There are more than 500 employees worldwide and the site manufactures between 5,000-7,000 of saypha dermal filler syringes per hour.
The company uses a fully automated manufacturing process, has strict sterilisation requirements and has developed a proprietary hyaluronic acid crosslinking technology. Stefanie Höhn, director of corporate communications, explained, “We try to limit the potential negative influence of the environment during the process and therefore the requirement of people by having a high automation level throughout. To reduce the potential for human-error, individuals who check the fillers through the microscope during the final stages are only allowed to work for 20 minutes before they are swapped. To further support this, one of the floors within the building is dedicated to delivering a sufficient and clean air flow. The air that feeds into the 1,000m2 clean room is changed 30 times per hour. Prinz told Aesthetics, “We produce 50 to 200L batch sizes, which, from my knowledge, is significantly more than other manufacturers out there. This means that we can provide competitive cost of goods and
ensure consistently high-quality products.” He continued, “But a company is only as good as its employees – it’s of upmost importance to me that my people are happy. Every fortnight, I take a walk around our office and talk to everyone to make sure they are happy and catch up on the work they are doing. We also have a resident doctor onsite, a state-of the art gym and fitness classes, and we also work closely with Light for the World charity, which aim to restore sight to blind people in low-income countries.”
The second half of the trip saw a visit to Yuvell Clinic, one of Croma’s official partner clinics. Here, Croma conducts a large number of clinical trials for its products and use it as a training centre too. So, what can be expected from Croma in the future? Prinz said, “Next year we will be releasing a new toxin and that will be a huge step as we will have a very complete and broad portfolio. One thing is for sure, we will never compromise on quality for any of our future products.”
IAPCAM Symposium, London
Aesthetics reports on the third International Association for Prevention of Complications in Aesthetic Medicine (IAPCAM)

Symposium
On September 20, 140 delegates attended the Church House Conference Centre in Westminster for the third IAPCAM Symposium to learn the latest information and advice on complication recognition, management and prevention. Conference director and aesthetic practitioner Dr Beatriz Molina welcomed guests to the event, along with consultant dermatologist Dr Sandeep Cliff, who chaired the meeting for the rest of the day. The morning’s talks focused on the most common complications in the upper and mid-face, utilising detailed anatomy videos, presentations and live demonstrations which were delivered by maxilloplastic surgeon Mr Jeff Downie, oculoplastic surgeon Mr Phillipe Berros and Dr Molina. Ophthalmologist Dr Tahera Bhojani-Lynch and aesthetic practitioners Dr Sophie Shotter, Dr Anna Hemming and Dr Shirin Lakhani then shared a number of case studies to support this.
Throughout the event, delegates were encouraged to interact with the speakers by casting their vote via a mobile app. During the afternoon, the attention shifted to common complications in the lower face which was presented by Mr Downie, Dr Molina, Dr Hemming and Dr Lakhani. Following this, the panel presented their complication case studies and encouraged the audience participation once again. Aesthetic practitioner Dr Mayoni Gooneratne also shared her concerns around the lack of clinical evidence for energy-based devices used for vaginal rejuvenation, while referencing informative case studies of the
complications that can and have occurred. Medical device specialist Feza Haque from the MHRA then gave an important update on the new medical device regulations taking place in 2020 and reiterated the importance of Yellow Card Reporting. There was also a small exhibition which featured well-known companies including Enhance Insurance, AestheticSource, Galderma, HA-Derma, SkinCeuticals and Medical Aesthetic Group. Dr Molina said of the event, “We were delighted at the success of IAPCAM 2019. This year we hosted the highest number of delegates from all specialities who came together to deliver, discuss and debate the management of complications, presented in 20 case studies. We welcome everyone to join us at our event next year on September 18.”
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Aesthetics tours Croma Pharma’s headquarters and explores the company’s history and plans for the future
Teoxane Academy UK Conference, London
Aesthetics reports on the second Teoxane Academy Conference in the UK


Swiss aesthetic manufacturer Teoxane held its annual Teoxane Academy UK Conference at the Leonardo Royal Hotel St Paul’s in London on Monday September 23. A total of 270 aesthetic practitioners attended the event to learn about the latest product innovations from Teoxane and to see new techniques from its key opinion leaders. The day kicked off with a welcome from Sandra Fishlock, director of Teoxane UK, who emphasised the company’s commitment to medical education and scientific excellence. Speakers included aesthetic practitioner Dr Lee Walker, ENT surgeon Mr Raul Cetto, plastic, reconstructive and aesthetic surgeon based in Paris Mr Patrick Trevidic, ophthalmologist Dr Tahera BhojaniLynch, aesthetic surgeon Mr Ayad Harb, aesthetic practitioner Dr Wassim Taktouk and aesthetic surgeon Mr Benji Dhillon. Speakers throughout the day explored many aspects of facial ageing. In his talk, Dr Walker said,
“Dynamic movement is real-life, so we need a hyaluronic acid product that can mimic the movement of the face for natural results. It’s important to match the personality of the product to the personality of the tissue.” In his presentations, Mr Trevidic discussed in-depth anatomy through video cadaver dissections. The highlight was a demonstration of the ‘smiling cadaver’, which illustrated the importance of injecting the right product in the right layer of the mid-face. Jordan Sheals, head of marketing and medical education at Teoxane UK, said of the event, “We are so pleased with the feedback we have received from delegates. Teoxane UK strives to deliver the best-inclass, comprehensive and clinically relevant training and it was fantastic to see our faculty of expert speakers deliver this so well.” She continued, “During the Teoxane Academy Conference, we discussed, demonstrated and launched our brand-new
BCAM Conference 2019, London
Aesthetics reports on the British College of Aesthetic Medicine’s annual conference
The British College of Aesthetics Medicine’s (BCAM) 24th annual conference welcomed 326 aesthetic doctors and dentists at the Church House Conference Centre in Westminster, London on Saturday September 21. BCAM conference director Dr Ruth Harker welcome guests and opened the event. Live demonstrations and clinical and business talks took place throughout the
day. Consultant plastic, reconstructive and aesthetic surgeon Mr Dalvi Humzah gave an update on the international guidelines for blindness and urged practitioners to become familiar with the free-to-access AIIVL Consensus. Aesthetic practitioner Dr Beatriz Molina gave an interactive presentation on treating younger patients with accompanying video demonstrations, and aesthetic practitioner Dr Kate Goldie demonstrated how to optimise filler placement to support the lower face structures. Another useful session detailed VAT and medical exemptions with partner at accounting company BDO, Glyn Woodhouse. He said, “Make sure you demonstrate in
product Teosyal RHA KISS and are looking forward to seeing healthcare professionals in attendance trying this new product and applying the techniques they learnt during the conference in their own practices.’’
Teoxane is planning to extend its annual conference to two Teoxane Academy UK Conferences in 2020, with the dates yet to be released.
Teoxane UK will also be hosting two days of free clinical education at the Aesthetics Conference and Exhibition (ACE) 2020 on March 13 and 14 in London.
ACE registration is free: www.aestheticsconference.com
every treatment case whether it is therapeutic or cosmetic and clearly record this so you can use this as evidence.” The event also featured an exhibition with around 25 exhibitors.
Vikki Baker, marketing manager at exhibitor AestheticSource, said, “AestheticSource was delighted to have supported BCAM again this year, as well as the IAPCAM conference the day previously. It was a buzzing two days, with lots of new enquiries and interest in our Cyspera pigmentation product.” The day ended with a drinks and canapés networking reception sponsored by Healthxchange, which showcased its patient management app Clever Clinic to delegates. BCAM president Dr Paul Charlson said of the day, “The event has been fabulous this year. It was great to introduce our new CEO Greg White, and tell delegates about our membership qualification exam, which is being launched very soon. BCAM is also continuing to work closely with the Joint Council for Cosmetic Practitioners (JCCP) and the regulatory bodies to affirm aesthetic medicine as a recognised credentialed medical specialty.”
The 2020 BCAM Conference will take place at the Church House Conference Centre in Westminster on Saturday September 19.
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Medical Device Regulations

As the end of 2019 approaches, we edge closer to the enforcement of the new EU Medical Devices Regulations (MDR). But, after speaking with those in the specialty, it is apparent that many do not feel ready for the changes or feel adequately informed about how it is going to affect the industry going forward.
Aesthetic practitioner Dr Beatriz Molina reiterates, “We know that the industry is in need of regulation and anything that is going to support this is a good thing. In my opinion, the changes haven’t been communicated as effectively as they could be and there is still some confusion within the specialty.”
The changes
The EU MDR 2017/745 was implemented on May 25 2017 and marked the beginning of a three-year transition period. Therefore, the MDR will fully apply from May 26 2020.1 The MHRA states that the changes aim to modernise the current system to ensure better protection of public health and patient safety. These changes will primarily affect manufacturers, importers, distributors, authorised representatives and health institutions.1 Health institutions are defined as ‘an organisation with the primary purpose of care or treatment of patients or the promotion of public health’.1
The key changes relevant to the aesthetics sector include: raising the threshold for clinical evidence required for the regulation of devices, increasing the requirements placed on notified bodies to ensure they are applying the changes consistently and supporting traceability of devices through Unique Device Identification (UDI), and issuing implant cards to patients.1,2
As well as this, the MDR expands the scope of what is considered to be a medical device. This means that certain groups of products without an intended medical purpose, listed under Annex XVI, will be regulated as medical devices for the first time.1 This includes dermal fillers without any medical purpose, as well as body
contouring equipment and light-based devices.1 Additionally, all current medical devices will need to be reassessed for compliance and recertification, which means that companies have had to review the data used to support their products and ensure it meets new requirements.
One of the most significant changes is that dermal filler manufacturers will be required to provide device information and a physical implant card containing: device name, serial number, lot number, the UDI, device model, as well as the name, address and website of the manufacturer, amongst other requirements including life expectancy and warnings.2 Health institutions must also give their patients this physical implant card with their name on it.2 The implant cards should provide information during an emergency, information or safety requirements regarding reciprocal interference, improve patient awareness of warnings/precautions and limitations of normal activity and improve data to implant registries, to identify failed components.2 The aim of this, the MHRA confirms, is to place emphasis on traceability throughout the whole supply chain and provide the patient with information about implanted medical devices, such as dermal fillers and threads, that will make information easily accessible and available.2
How have the changes been received?
Nancy Ghattas, associate vice president, country manager UK and Ireland at global pharmaceutical company Allergan, welcomes the MDR and the changes that it brings, which will affect the company’s dermal filler and body contouring products. She says, “As a responsible company we appreciate any changes that increase the regulatory oversight and transparency of our industry. The purpose of the new MDR is principally to increase the safety of consumers; something which Allergan is very passionate about. We see the changes as a way for the whole industry to become better, to benefit patients.”
Dr Molina shares her view as a practitioner, stating, “Although it’s important that practitioners understand what’s going on in regulatory changes, I don’t think it’s going to have too much of an impact on us as the main focus seems to be on the companies, but within time, this will filter down to clinics and could affect which products and devices we can use.”
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
The latest on the new medical device regulations and what they will mean for the industry going forward
Certain groups of products without an intended medical purpose, listed under Annex XVI, will be regulated as medical devices for the first time
Will the implant cards mean a safer specialty?












Dr Molina believes one of the most notable differences within the MDR are the implant cards. Because of this, she says there is the potential to track and stop any faulty products in the market. Regarding dermal fillers, she also notes that having the ability to know what filler a patient has had could aid in treating and preventing complications.
Dr Molina explains, “I’m very much looking forward to seeing how the implant cards are implemented. I think if we make patients aware of this process then it will also help them to decipher between the good and the not so good practitioners.”

However, she says that for this to work, there needs to be patient awareness of the requirement to receive an implant card following a procedure. “Patients should know that receiving this implant card is a standard, involuntary procedure and anyone that doesn’t issue this may not be as reputable as they say they are,” she explains.
Ghattas echoes this point and believes the implant cards will have a positive impact across the board. She says, “Implant cards will enable customers to have easy access to information on the products they have been treated with. We think it is very important for consumers to be further educated on the products that are being used on them and empowered to ask for more information.”
Future considerations
Whilst Dr Molina recognises that the changes are overall positive, she says it could affect newer companies and products coming to the market. She says, “I think it may be harder for smaller companies and may stop the development of newer products due to the costs associated with additional research and time implications. It’s fantastic that it gives us a guarantee of safety, but I question whether it will limit the progression of the specialty.”
Dr Molina concludes, “My dream is to see all of the top associations collaborate and receive ongoing data from the MHRA regarding reported products. The only way a change is going to come is if we all join forces. I’m hoping that the changes are going to be a step in the right direction and I look forward to seeing a more regulated specialty in time to come.”
REFERENCES
1. MHRA, Guidance for products without an intended medical purpose (Annex XVI) under the new medical device regulation (EU 2017/745) <https://assets.publishing.service.gov.uk/government/ uploads/system/uploads/attachment_data/file/748131/Guidance_leaflet_on_Annex_XVI_ products_.pdf>





2. Madden K, MDR Article 18, BSI, January 2019 <https://www.bsigroup.com/globalassets/localfiles/ fr-fr/dispositifs-medicaux/ressources/bsi-md-article-18-implant-card-webinar-presentation-24jan-2019.pdf>
3. Gov.uk, Regulating medical devices in the event of a no-deal Brexit, October 2019 <https://www. gov.uk/guidance/regulating-medical-devices-in-the-event-of-a-no-deal-scenario#registrations>
FURTHER READING
• Boumans R, New European MDR guidance on medical device implant cards, Emergo by UL, July 2019 <https://www.emergobyul.com/blog/2019/07/new-european-mdr-guidance-medicaldevice-implant-cards>
• European Commission, Medical Devices: Guidance document Implant Card relating to the application of Article 18 Regulation, July 2019 < https://ec.europa.eu/docsroom/ documents/36167>

BUILD MUSCLE & BURN FAT ARE YOU IN? NO SURGERY – NO DOWNTIME 799-79EMCADAJENGB100; Emsculpt_AD_Aesthetic-journal_85x225_ENGB100 Results and patient experience may vary. Patients shown in the B&A pictures are within +/- 5 lbs of their original weight unless specified. As with any medical procedure, ask your doctor if the Emsculpt procedure is right for you. The Emsculpt procedure is U.S. FDA cleared for improvement of abdominal tone, strengthening of the abdominal muscles, development of firmer abdomen, strengthening, toning and firming of buttocks. ©2019 BTL Group of Companies. All rights reserved. BTL® and EMSCULPT® and HIFEM® are registered trademarks in the United States of America, the European Union and/or other countries. The products, the methods of manufacture or the use may be subject to one or more U.S. or foreign patents or pending applications. Trademarks EMSCULPT®, EMSELLA®, EMBODY® and HIFEM® are parts of EM™ Family of products. EMSCULPT.COM SALES@BTLNET.COM I NSTALLEDUNITS WORLDWIDE 1000 + #clubemsculpt OVER250000TX IN12 MONTHS Emsculpt_AD_Aesthetic-Journal_85x255_EN100.01.indd 2 15/07/2019 16:27:21

yo uth & age in plastic surgery, dermatology and aesthetic science in 2020 jan 30 - feb 1 paris .france
“One of the best medical congress of the world. I participate every year for 15 years now."
Dr Paleologos, Dermatologist, Greece
“Excellent congress. I am super impressed about the content, the speakers, the live surgeries, everything this year.It keeps getting better”
12,00 ATTENDEES – 800 SPEAKERS – 265 SESSIONS
Dr Conde Green, Plastic Surgeon, USA Browse imcas.com and view hundreds of attendees’ feedback
CCR: A HUGE SUCCESS
Aesthetics reports on the highlights of ACE’s sister conference, CCR
On October 10 and 11, thousands of practitioners from across the UK attended CCR at Olympia London for two days of live demonstrations, exclusive brand takeovers, independent education and unmissable networking opportunities.

The event featured seven conference streams, comprising the Non-surgical Arena, Aesthetics Masterclasses, Live Demo Stage, Practice Management Theatre, Dermatology and Injectables Symposia, Dr Tapan Patel Masterclass and the BAAPS Annual International Conference. Each agenda offered valuable CPD points and covered the latest in aesthetic education.
Renowned speakers from across the globe delivered talks on injectables, body contouring, and skincare, alongside business advice on developing your practice and standing out from the crowd.
Delegate and aesthetic practitioner Dr Bhavjit Kaur commented, “I have been attending CCR for many years now because it’s a great place to network and meet new people, as well as a fantastic place to learn from excellent speakers.” CCR speaker and consultant ophthalmic and oculoplastic surgeon Mrs Sabrina Shah-Desai added, “It’s been a fantastic amalgamation of reconstructive and medical aesthetics, which is exactly what I enjoy.”
First-time CCR delegate Dr Martin Kinsella also exhibited his new business at the event.
He said, “This is my first time at CCR and I have been really impressed. As a practitioner I am always on my own, I don’t work with a big group of people, so to come to events like this to see what everyone else is doing,
at Large, said, “The industry is evolving at an impressive rate and I think I can speak for all the visiting media when I say how amazing it has been to see so much innovation under one roof. I am wowed by the number of expert all-stars in attendance from both the surgical and non-surgical disciplines, delivering hours of educational content to packed audiences. It’s been a real coup to be able to spend time talking to so many of them.” Delegate Dr Marwa Ali, commented, “It’s so encouraging to see so much press interest at the show this year, not only their interest in aesthetic innovations but also in the general elevation and betterment of the industry as a whole in terms of safety and ethics too.” Feedback from exhibitors was also positive, with many expressing the benefits of CCR to showcase their new products and treatments. Hayley Jones, sales and marketing director at Lynton Lasers said, “There is new technology everywhere. The industry is incredibly strong at the moment and it’s offering people life-changing treatments and it’s really good to be a part
Dr Bhavjit Kaur
the latest procedures and the high standard of work that’s going on is excellent – it offers very good education. The networking is also brilliant – I’ve had a great opportunity to catch up with people I haven’t seen for a while. On the other side of the coin, I’m an exhibitor, and the stand has been busy so it’s been great.” This year, after working closely with aesthetic PR company, Mantlepiece PR, press turnout exceeded CCR’s seven-year history, with journalists and camera crews from BBC Radio, ITV, SKY TV, Talk Radio, The Guardian, Grazia and The Telegraph all in attendance. CCR’s press ambassador, Francesca White, editor of the Tatler Beauty and Cosmetic Surgery Guide and Health & Beauty Editor
Next on the educational agenda is ACE 2020. Taking place at the Business Design Centre in Islington, London, the event will be brought to delegates by the leading medical aesthetic providers in the specialty, including Galderma, Teoxane UK, Allergan and many more. Turn to the next page to find out more!

Following ACE, CCR 2020 will take place on October 1 and 2. Next year the event will be held at a new location, ExCeL London, which will offer delegates and exhibitors ease of access, along with an enhanced conference offering.

Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
of that.” Raffi Eghiayan, marketing director of Wigmore, added, “CCR is a fantastic platform for us to launch and that’s exactly what we are doing today.”
“A fantastic place to learn from excellent speakers”
ACE 2020 ANOTHER EXCITING EVENT AHEAD
After the success of last year’s conference and exhibition, and last month’s CCR, Aesthetics showcases what you can expect to see at ACE 2020
The next edition of the award-winning Aesthetics Conference and Exhibition (ACE), will be taking place on March 13 and 14 at the Business Design Centre in London. Across the two days of ACE 2020, leading aesthetic providers will reveal their latest products and treatments, with demonstrations and education delivered by





renowned key opinion leaders. The education will be free-of-charge for all delegates, with an upsurge of attendees expected. The event will offer unmissable networking opportunities, as well as the chance to visit more than 80 exhibition stands showcasing the latest innovations in medical aesthetics.

Main Auditorium
Galderma
(250 delegates per session)
Main Auditorium
For the first time ever, the Headline Sponsor of ACE will be delivering an unmissable education agenda, led by international speakers. Global pharmaceutical company Galderma will take over the Main Auditorium to present its latest innovations in four two-hour sessions across Friday and Saturday. With content to be revealed soon, this is a fantastic opportunity for 250 delegates per session. There will be two two-hourlong sessions each day – 11:00-13:00 and 15:00-17:00.
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Symposium
Teoxane Training Academy (200 delegates per session) Symposium, Room A
After the hugely popular Symposium agenda last year, aesthetic manufacturer and training academy Teoxane UK will host four two-hour informative learning experiences, led by its Country Experts. All sessions will feature a range of topics with a focus on anatomy, techniques and product rheology for safe and effective practice. This involves the Teoxane approach to 4D volumisation, perioral treatment and a full facial treatment algorithm. Teoxane will also be running two two-hour-long sessions each day – 10:0012:00 and 14:00-16:00.


Masterclasses
Allergan Medical Institute, Church Pharmacy, HA-Derma, SkinCeuticals (120 delegates per session) Masterclass, Rooms E & F
On Friday, three renowned aesthetic providers will present one-hour Masterclasses on the latest products and treatments, with best-practice advice on their use, alongside live demonstrations. On Friday see the latest from Church Pharmacy, SkinCeuticals, and HA-Derma, while on Saturday you can find out how to prevent and overcome complications, with advice led by Allergan Medical Institute in four sessions throughout the day.
Expert Clinic & Business Track
17 leading aesthetic providers will deliver half-hour Expert Clinic session on their latest innovations, while 19 industry professionals will share their expertise and experiences of running an aesthetic practice at the Business Track. These sessions are aimed at aesthetic practitioners, those in administrative roles, and individuals working in management. One delegate last year said, “Being able to receive the latest information in the specialty in all areas of the profession, from regulations to patient retention, was fantastic!” Delegates attending ACE can learn from five different agendas, totaling over 45 CPD points across both days.
Note that some sessions are restricted to doctors, dentists and nurses. Delegates wanting to attend these sessions will need to provide evidence of their qualifications via DocCheck before the event. More information is available upon registration.
HEADLINE SPONSOR Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com 2020 50+ EDUCATIONAL SESSIONS 80+ EXHIBITORS 60+ SPEAKERS 45+ CPD POINTS 1 UNMISSABLE EVENT 13 & 14 MARCH 2020 / LONDON SAVE THE DATE AND SECURE YOUR TICKET NOW FOR ACE 2020 Head to our website and enter code 10001 aestheticsconference.com Key stats for ACE 2020










NUTRACEUTICAL SUPPLEMENT PREMIUM once-a-day Collagen DRINK Supplement Skin • Hair • Nails • Joints • Bones • Gut Health • Peri/Post Menopause FOR AGE MANAGEMENT Once a day supplement mixed with water, smoothie or fruit juice Expect results in 3-12 weeks CLINICALLY PROVEN SCIENCE www.totallyderma.com Tel: 020 3126 6795 | Email: info@totallyderma.com Tel: 020 3868 6242 | Email: enquiries@harpargrace.com • Added revenue stream • Full marketing support Also available from our distributing partner hair skin joints arteries gut bladder urethra vagina nails ligaments tendons bone Enhances the effect of topical medical aesthetic treatments Stimulates collagen and hyaluronic acid sites ALL OVER the body • evidence based and results-driven • pharmaceutical-grade ingredients • 95% bioavailable (pre-digested collagen amino acid peptides) • visible difference in skin firmness, skin elasticity, skin hydration, improved hair and nails • helps to improve cartilage thickness and pain in joints • anecdotal evidence shows a connection between Totally Derma® and improved gynaecological menopausal dryness • promotes recovery post-procedure up to 200% more Collagen than current market players at least 300% more Hyaluronic acid up to 300% more L-Ascorbic Vitamin C Key antioxidants and anti-inflammatory ingredients: Grape Seed Extract, Green Tea Extract, Alpha Lipoic Acid, Zinc, Copper, Manganese
Treating Static Lateral Canthal Rhytids
Aesthetics explores the causes, assessment and treatment approaches for static lateral canthal lines
Static lateral canthal rhytids, commonly known to patients as crow’s feet, are one of the most common concerns patients will present with. In one study of 603 women between 30-65 years of age, 82% chose lateral canthal rhytids as the facial feature they were most likely to seek treatment for first. The same group identified the lines as the number one facial feature that bothered them the most.1
According to aesthetic practitioner Dr David Jack, around 95% of his patients aged 45-50 will have concerns regarding lines in this area. Surgeon and aesthetic practitioner Miss Sherina Balaratnam adds, “Lateral canthal lines are a very common concern amongst patients and we see this presentation daily with our patients. The eyes are a key facial feature – they are ‘the window to the soul’. The eyes are what we look into, what we communicate and express ourselves with, and hence patients naturally want their eyes to look as aesthetically pleasing as possible.” While male patients may also present to clinic with concerns in this area, this article will focus on the assessment and treatment approaches of lateral canthal rhytids in females, while also addressing how to maintain successful results.

Causes
Before constructing a treatment plan, it is important practitioners understand the underlining causes of static lines in the periorbital area and what the patient’s individual needs are. Ageing in the periorbita is associated with a combination of muscle movement, loss of volume within the fat pads, skeletal changes and a reduction in skin quality.2
Consultant aesthetic oculoplastic surgeon Mrs Sabrina Shah-Desai explains, “The orbicularis oculi muscle is a large free-floating muscle that is situated around the eye and attached to its inner corner. When we are young, the activity of this muscle, as well as the zygomaticus muscle, through movements such as smiling, is hidden by a fat layer
below and above the muscle, which is protecting and translating its movement to the skin above. In youth, when you have that fat pad between the muscle and the skin, every time you smile or crinkle your eyes, the movement is happening, but you don’t see it as lines and wrinkles because of the fat pad. With age, the fat pad gradually shrinks and movements are eventually relayed to the skin.” These factors cause dynamic lines, or those that are only apparent with movement, explains Mrs Shah-Desai.
The deeper lateral canthal lines that appear without movement (known as static lines) usually come with additional decrease in skin quality and thickness in the area, Mrs ShahDesai says. Aesthetic nurse prescriber Jackie Partridge explains that there is a decrease in bone density associated with ageing that has an effect. “Changes in volume of the temple and orbit, for example, can have an impact on the appearance of the periocular area as you don’t have the same skeletal support for the tissue and muscle above,” she says.
Partridge adds that individuals who have not had the best lifestyle will get particularly bad lines in this area, and may be likely to get them earlier. For example, she says, “Those who have had a lot of sun exposure, are smokers, have a poor diet, live in polluted areas, or have been overly exposed to the elements, for example, through a lot of outdoor activity, are more likely to present with severe lines.”
Partridge also mentions that expressive people, such as those who smile a lot, or who do activities that might cause them to squint or express their face in anticipation such as mountain bike riding or skiing, might be more likely to have worsening lines. “Many patients who present with deep lateral canthal lines have also generally not been on an active skincare regime or used SPF as a preventative ageing measure,” she adds.
Miss Balaratnam agrees that lifestyle factors play a huge part in the ageing of the periorbital area. She says, “In this digital era, I am especially noticing a connection between the increasing use of gadgets, smartphones and technologies which in turn causes an
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
“Many patients who present with deep lateral canthal lines have also generally not been on an active skincare regime or used SPF as a preventative ageing measure”
Jackie Partridge
the pursuit of skin perfection
PLEXR ® Plus Plasma System

The Medical Choice for Soft Surgery

• Effective alternative to non-invasive blepharoplasty, face lift & neck lift procedures
• Three separate handpieces with micro plasma in different power frequencies dependent on tissue to be treated
• Wireless hand pieces allowing use between clinics
• Touch screen display to control settings and treatment videos
• Upgradable software via USB



• Bloodless treatment with no need for anaesthesia
Ideal to treat:
• Non surgical blepharoplasty
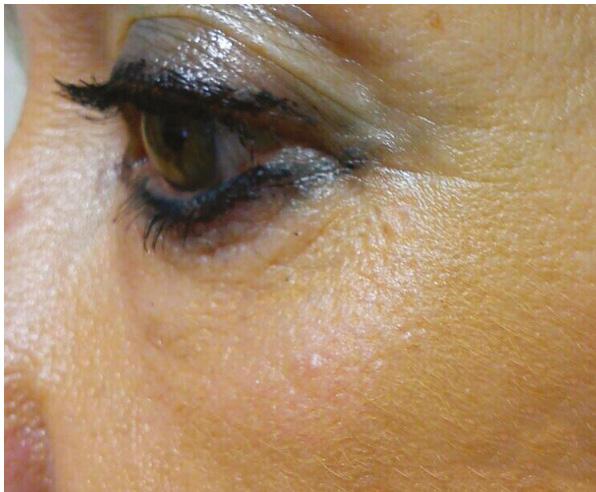

• Face, neck and body lifting
• Scars
• Stretch marks
• Cysts and spots
• Hyperpigmentaion
• Keloids
“I am truly passionate about PLEXR ® and the plethora of conditions it can treat never ceases to amaze me. With so many copycat devices out there, I want to help ensure that appropriately qualified practitioners obtain this device and that they receive the highest standard of training to ensure safe yet effective use of the PLEXR ®.” Dr Dev Patel, PLEXR® Ambassador
COMMENDED 2017 TREATMENT OF THE YEAR HIGHLY COMMENDED 2017 DISTRIBUTOR OF THE YEAR TREATMENT OF THE YEAR EQUIPMENT SUPPLIER OF THE YEAR DERMAPEN 0333 358 3904
Interested in Learning More? Join us at an
DATES: Wednesday
November or
Book your workshop space today by calling 0333 358 3904 or email us on
info@naturastudios.co.uk naturastudios.co.uk
Introductory Workshop with Dr Dev Patel at Natura Academy, Elstree London for an overview on the system, learn about plasma itself, what treatment PLEXR® can offer as well as LIVE demonstrations.
6th
*February date TBC*
info@naturastudios.co.uk
EXCLUSIVE TO
BEFORE AFTER
sure you’re taking photos of people at rest and animation. Then, when the patient returns for their review, you can show them the static lines that were there before and how your treatment approach has helped. It’s not only for a reassurance and a best practice point of view, but also many insurance policies are invalid if you haven’t got before and after photographs,” she advises. As with all other aesthetic procedures, ensuring the patient has realistic expectations and understands the risks associated with treatment is paramount, practitioners state. Partridge also advises to effectively communicate to the patient about prices and budget, as this can really impact treatment strategy.
increased frequency of repetitive eye movement and blinking. This then impacts the lines in the periorbital region, causing many patients to have a faster degree of accelerated ageing, due to increased dynamic movement with the periorbital muscles.” Mrs Shah-Desai agrees that this constant muscle action is having an effect on her patients’ periorbital ageing too.
Consultation and assessment
As lifestyle factors can play such a large part in the causation of these lines, Miss Balaratnam explains that they should always be identified and discussed in the consultation. “I will always tell patients that doing nothing is an option and highlight the importance of addressing lifestyle factors such as smoking, sun exposure, sugar intake, alcohol and pollution; however, patients don’t present to clinic to do nothing,” she says, adding, “They present for solutions.”
In the consultation, practitioners will commonly grade the severity of the lines before planning their treatment approach and determine whether they are static or dynamic. In 2008, a 5-point photonumeric rating scale to objectively quantify the severity and type of lateral canthal lines at rest (static) and at maximum contracture of the orbicularis oculi (dynamic) was developed.3 The lines are graded on the Crow’s Feet Grading Scale from 0 (none) to 4 (severe).3
• 0 – no wrinkles
• 1 – minimal wrinkles
• 2 – mild wrinkles
• 3 – moderate wrinkles
• 4 – severe wrinkles
Mrs Shah-Desai will also perform what’s called ‘the snap test’ to assess the patient’s skin quality and laxity. “I do this by pinching the skin in the area to assess the active recall. If it snaps back well, then I know that my patient will likely respond well to an injectable approach, whereas if it is lax and stays put, I know their skin quality and laxity also needs addressing,” she explains.
As well as the physical assessment, Miss Balaratnam and Mrs Shah-Desai also do a digital assessment using a VISIA digital skin imaging. “With this, we are able to review the skin closely to assess the severity of these lines, and whether there may be contributing factors like hydration and photodamage. This will determine where patients will start on their treatment ladder,” explains Miss Balaratnam. Partridge also emphasises the importance of clinical photography in every consultation. “For static lines in particular, make
Treatment
The practitioners interviewed have slightly different approaches to management but recognise that treatment will depend on what is most needed to be addressed: volume replacement, skin quality, muscle movement or a combination. All acknowledge the important role skincare plays in both pre-treatment and maintenance of results, and advise patients are on a good quality skincare regime, with daily use of SPF.
The mainstay of lateral canthal line treatment remains to be botulinum toxin. Partridge reiterates, “Toxin is going to be my first choice 99% of the time when treating somebody with all types of lateral canthal lines.” Although, for patients displaying deep, static lateral canthal lines with skin quality concerns, a multifactorial treatment approach is appropriate, according to practitioners.
Mrs Shah-Desai explains, “It’s important to understand that static wrinkles need combination therapy and, in this area, the combination is either fillers and botulinum toxin, or if there is a lot of skin laxity associated with those wrinkles then you will need additional methods such as radiofrequency.”

Dr Jack adds, “My approach for treatment would be multifactorial and really depends on the individual patient and how far they want to go, how much time they have, how much they can tolerate and what sort of the expectations they have.”
Dr Jack usually treats with injectable first, then moves on to skin quality treatments if needed. “I would consider the use of botulinum toxin to relax the downward pull of the muscle and lightweight dermal fillers such as Teosyal Redensity I or Juvéderm Volite. I would offer injectables first because I find you can get to a stage where the lines are so improved that you don’t necessarily need to perform resurfacing treatments through methods such as radiofrequency or soft surgery. I think these approaches can have more variability in the eventual outcome and they are different for each patient.” Dr Jack likes using a controlled micro-droplet technique in the area and says that using injection pens such as Teosyal Pen or Juvapen work well for him to monitor injection depth and product quantities.
Partridge has a similar approach to Dr Jack. Two weeks following toxin injection, she will assess the impact it has made, before planning further intervention. “For less severe static lines, Skinboosters can be really good for both skin quality and hydration. For older patients with deep, severe lines I would need to consider radiofrequency – I use the Exilis Elite, which I find great for stimulating collagen and elastin. For those requiring extra skin rejuvenation I use the RevLite laser, which I find is effective for
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
6 months after Before
Figure 1: Static lateral canthal line treatment of 51-year-old patient. Treatment involved VISIA and consultation, new skincare regime using iS Clinical Youth Eye Complex, Firming Complex, Cleansing Complex, Super Serum, Extreme Protect SPF 30 and monthly HydraFacials. Images courtesy of Miss Sherina Balaratnam.
New skinade | MD ®
As a plastic surgeon, I am excited by the Skinade | MD® launch, which will enhance my patients’ experience for better results and reduced downtime.
“
Mr Dalvi Humzah
Consultant Plastic Surgeon
A 4 - step programme specifically designed to be integrated into aesthetic surgical procedures.
“
stimulating the fibroblasts for collagen production.”
To improve skin quality, Dr Jack advises practitioners choose treatments that will stimulate the dermis. “I would consider using a resurfacing radiofrequency device such as the Morpheus8. This is great for people who are 40-50 with crepey, lax skin,” he says. Dr Jack adds that soft surgery can also be used in this area, “I sometimes use Plexr, but the downtime is usually seven to 10 days and there is a risk of redness that remains for a period after, which can deter patients. I always advise practitioners against treating the line directly with soft surgery – treat the skin either side of the line, which should create tension and draw the line out outwards.”
Conversely, Mrs Shah-Desai would always address skin laxity before using injectables. “This is when I go down the energy-based devices route, and will be looking at Tixel, or the Morpheus8 radiofrequency microneedling device. I always tighten before I volumise because as you tighten the skin it thickens itself and I find that it retains the filler better. In my experience, if you try to revolumise something that’s loose, it’s not as effective. Once I start seeing improvement in the skin quality, I will start looking at dermal fillers,” she says, adding, “There are so many lovely hyaluronic acid products that will improve the structure and hydrobalance in the skin such as Skinboosters, Viscoderm, Redensity I, RHA I, or mesotherapy products.”
Miss Balaratnam also likes to address skin quality prior to the injectable route. Following a good skincare routine and lifestyle advice, Miss Balaratnam says, “My treatment ladder will often involve high-tech facials. Facials such as the HydraFacial encourages increased oxygenation to the skin which in turn produces new cell formation. We have a very specific eye treatment called the HydraFacial Perk, which gives a greater degree of controlled exfoliation and skin conditioning to the skin around the eye area and pushes active topicals onto the epidermal layer of the skin to hydrate this area.”
After skin conditioning treatments, Miss Balaratnam will take patients to the next stage, which she says involves energy-based devices. She explains, “My top treatment for addressing the skin causing lateral canthal lines would be the EndyMed 3DEEP Fractionated Skin Resurfacing, which creates superficial microchannels for skin resurfacing and collagen stimulation. Something new in my clinic that is getting excellent and fast results for treating pigmentation and skin texture is the PicoSure laser. This works in a trillionth of a second, targets the epidermal tissue causing a focused and photomechanical injury to the skin without breaking the tissue. This elegant injury to the skin causes cell signaling which brings about skin revitalisation.”
Miss Balaratnam continues, “To address skeletal issues, I will use dermal fillers in the temple, lateral cheeks and periorbital area to provide volume from within which in turn supports the skin – I use the MD Codes techniques and use the Juvéderm Vycross range of facial fillers to address this. Following this, if there is remaining muscle
activity, I will also address this with botulinum toxin. I administer toxin after the fillers as, in my experience, muscles will behave differently once you use dermal fillers underneath and around them. We call this concept myomodulation.” Toxin is also usually last on Mrs ShahDesai’s treatment plan. “I would look to do toxin if the patient has a lot of dynamic movement. I also find that when we restore the volume and take the underlining anatomy back to where it used to be, we tighten the skin, so we don’t necessarily need to inject very much toxin,” she explains.
Aftercare and maintenance
“You can’t underestimate the importance of maintenance,” highlights Partridge, noting, “If a patient thinks they can come in, have a treatment and then go home and not do anything to support their welfare then they won’t achieve their best results. I always stress the importance of hydration, diet, SPF, and general lifestyle factors,” she says. Dr Jack likes to keep his maintenance advice simple. “Skincare is really important; I always recommend vitamin C, SPF and a light retinol. I also recommend supplementation with vitamins such as C, E, and biotin, which I think can really benefit patients,” he says.
Mrs Shah-Desai also values supplements for skin maintenance, she says, “There is not a lot of literature on this, but just from my own use I have noticed that it helps my own skin, particularly my periocular lines and wrinkles. I stock both bovine collagen – Totally Derma – and marine collagen – Skinade – to give my patients a choice.” Mrs ShahDesai also recommends microchanneling patches such as Radara, which she says can help encourage new collagen and deeper penetration of hyaluronic acid into the skin.
The practitioners also acknowledge that it’s important to tell patients that their results will need to be preserved through regular maintenance of in-clinic treatments, as per the treatment protocols.
Summary
As with many other aesthetic concerns, practitioners have various different approaches for rejuvenation of the static lateral canthal rhytids. Dr Jack’s top advice is, “Treatment of these lines requires a multifactorial approach, as with anything these days, for the best outcome.” Miss Balaratnam adds, “My approach very often is a blend of skin conditioning and energy based-treatments, with topical skincare driving the results forwards. As practitioners we need to do more than provide a quick fix and really understand how we can help in the long-term. Our profession is a minefield and each of us will have different treatment options, hence patient education is key, so that patients will have a better understanding as to the science behind the treatments they are receiving.”
Finally, Miss Balaratnam says, “When treating static lateral canthal lines in an older patient, I always ‘leave a little bit behind’ so that patients just look more real, with a natural result. This keeps their friends and family second-guessing, which I believe is a nice place to be, instead of saying, ‘Where did you have your work done?’ If they pass this test and go unnoticed, then I have done my job well.”
REFERENCES
1. Narurkar V , Shamban
3. Carruthers A, et al., A validated grading scale for crow’s feet.Dermatol Surg. 2008 Nov;34 Suppl 2:S173-8. <https://www.researchgate.net/publication/46179758_A_validated_facial_grading_scale_ The_future_of_facial_ageing_measurement_tools>
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
A , Sissins P , Stonehouse A , Gallagher C . Facial treatment preferences in aesthetically aware women . Dermatol Surg . 2015 ; 41 ( suppl 1 ): S153 - S160 . 2. Tung, R, et al., Treatment of lateral canthal rhytides with a medium depth chemical peel with or without pretreatment with onabotulinum toxin type A: a randomized control trial. International Journal of Women’s Dermatology, Volume 2, Issue 1, 1 March 2016, Pages 31-34. <https://www.sciencedirect. com/science/article/pii/S2352647515000751>
“As practitioners, we need to do more than provide a quick fix and really understand how we can help in the long-term”
Miss Sherina Balaratnam
Forehead Anatomy for Injectables
To develop treatment strategies, it is imperative that practitioners understand the current anatomy of the area being treated. Anatomical knowledge and the aesthetic considerations around forehead treatment is an evolving area in aesthetics. In this article, the topographic and skeletal anatomy of the forehead and agerelated changes will be explored and its importance in clinical aesthetic practice discussed. The forehead anatomy will be reviewed and applied to current and possible future clinical practice for injectable treatments.

Forehead definition
It is generally accepted that the forehead represents the part of the face above the eyebrows.1 For the basis of this discussion, the forehead will be defined as the area demarcated inferiorly by the superior part of the orbital rim, laterally by the temporal crests and superiorly by the hair-bearing area of the scalp. This may immediately pose a problem as with a receding hairline in androgenetic alopecia, the area of the forehead will change with time.2 To overcome this, a fixed superior border such as the coronal suture of the frontal bone may be used as a definition for the superior border. This superior border would only be seen on imaging views and so is not a practical border to be used in clinical practice. Therefore, the practitioner must formally use one of these two possible superior borders in demarcating the area of the forehead. This has implications which will be discussed further with regards to facial profiles and proportions.
Importance of the forehead
The forehead is of major significance to the aesthetic appearance of patients when it is considered in terms of anthropometrics and
cephalometrics and the ideals of beauty. Anthropometrics looks at dimensions and relationship of facial soft tissues. It is the study of the human body to define size and weight measurements and proportional relationships.3 Cephalometrics is the measurement of parts in relation to bony and soft tissue points using a radiograph known as a cephalogram.3 Dividing the face into proportions are based on ‘neoclassical canons’ developed by Renaissance artists such as da Vinci and Durer who defined the ideal facial proportions in art.4 Horizontally, the whole face may be divided into thirds – the forehead comprising the upper third.5 Farkas et al. reviewed the neoclassical canons and confirmed the upper third ratio as 1:1 with variability of the mid-face and lower face in actual subjects. Any change in the horizontal height of the forehead will, therefore, change the proportions of the face.5 A change in the position of the brow due to brow ptosis will elongate the horizontal length of the forehead; a low or high hairline will also change the forehead length.3 When analysing the forehead, these possible configurations should be considered. This is of primary importance when considered in the concept of ‘profiloplasty’ when the relative length of the forehead and the angle of inclination of the upper forehead is considered with respect to the nose and chin relationship.6 The angle of inclination of the upper forehead has both a gender difference as well as agerelated changes, explored in more detail below.7 Male and female foreheads may require different outcomes, with females preferring a shapely brow compared to a more horizontal male brow.8 There is also an ethnic aspect of beauty; in Asian cultures for example, the shape of the forehead has social implications and there is an aesthetic requirement for forehead contouring.9 In one study comparing Japanese women with Korean women, the majority of the former preferred the forehead height to be roughly one-third of the overall facial height. Korean women had a wider range of desirability, with 50% preferring the forehead height to be one third of the total facial height, while more than 33% of respondents preferred a large forehead. Both groups, however, preferred a negative slope over straight inclination of the forehead.9 A firm knowledge of the layers of the forehead will enable the practitioner to ensure that a safe layer is approached in relation to product placement.
Anatomical considerations
Anatomically, the forehead may be considered as a layered structure of five components. This is often referred to in the mnemonic ‘SCALP’ to represent the following layers: skin, subcutaneous tissue, aponeurotic layer, loose areolar tissue and periosteum.10 This simplified concept does not, however, represent the interaction between the layers.
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dalvi
and nurse
Figure 1: Bones in the head Frontal bone Lacrimal bone Nasal bone Zygomatic bone Maxilla bone Mandible Zygomatic arch Styloid process of temporal bone External acoustic meatus Mastoid part of temporal bone Squamous part of temporal bone External occipital crest External occipital protuberance Superior nuchal line Occipital bone Parietal bone Superior temporal linea Inferior temporal linea Orbital lamina of ethmoid bone Greater wing of sphenoid bone
Mr
Humzah
prescriber Anna Baker provide an update on forehead anatomy and review the current literature to assist with clinical practice
The recent work on the deep layers of the forehead reveal the presence of distinct septae between the periosteum and the frontalis muscle; the superior and inferior frontal septum.11 These structures act as anchor points for the overlying frontalis muscle. The result of this arrangement is that the frontalis muscle can act as an elevator in its inferior attachment between the brow and inferior frontal septum. The muscle attachment between the inferior forehead septum and the upper fibres of frontalis acts as a depressor of the frontal hairline.11
The clinical relevance of this is that botulinum toxin injections below the inferior frontal septum are more likely to result in brow ptosis.12 Often the position of this frontal septum is about 2-3cm above the superior orbital rim – hence the rationale for botulinum toxin being placed above this level in the forehead.12
The separate linear lines on the forehead represent the unique muscle arrangements that have recently been described. The arrangement of the underlying frontalis muscle is different in individuals with four different variations described to date (Figure 2).13 Clinically, this is important when considering placement of botulinum toxin as the traditional five-point horizontal points do not correspond to the underlying frontalis muscle arrangement; which can result in either wastage of toxin or under-treatment in some areas.14
The lateral extent of the frontalis is also not clearly defined. It has been stated that the frontalis does not extend beyond the temporal crest; this being the border between the temple and forehead compartments.15 However, recent directed dissections in 49 cases have shown that the lateral border of the frontalis shows variability in its position to the temporal crest.16 The frontalis was also observed to overlap the orbicularis occuli up to 2cm from the frontotemporal (FT) region and the musculoaponeurotic junction extended superiorly to up to 9cm from the FT region. The lateral margin of the frontalis extended further laterally in 9/49 cases (18.4%).16
Considering this research, the implication on the placement of lateral injection of botulinum toxin would be to place the lateral injection points at least 2cm from the FT region (to avoid the orbicularis oris). Placement medial to the temporal crest in the majority of cases would treat the lateral margin of frontalis with a limit of the superior extent to 9cm from the FT region as the muscle is aponeurotic beyond this point.16





The vertical lines observed in individuals also have an anatomical significance; the medial glabellar lines (often referred to by patients as number 11s) may serve as a marker for the underlying supratrochlear arteries in 50% of cases.17 The artery is, however, variable in its arrangement. The superficial branch is always present, but the deep branch is not present in over 80% of cases. This has been used as a
basis of dividing the arterial patterns of the forehead into two types: type I – with superficial branches of the supratrochlear and supraorbital artery, with the deep branch of the supraorbital artery – and type II – with both superficial and deep branches of the supratrochlear and supraorbital artery.17 The types are further divided depending on whether a central dorsal artery is present medial to the superficial branch of the supratrochlear artery.18 This variability should be considered when dermal filler injections are being performed in the forehead and deep placement with a cannula is recommended by these authors.17,18 In some individuals, an oblique ‘crease’ is observed in the forehead (Figure 3) and this is related to the deep branch of the supraorbital artery and the boundary between the medial superficial forehead fat compartment and lateral temporal fat compartment.19
The supraorbital artery runs superolaterally and becomes superficial in three different areas between the superficial branches of the supratrochlear, temporal superficial artery and itself. The deep branches continue the path of the supraorbital artery superolaterally or are divided into medial and deep branches.18
There are distinct differences in the skeletal shape of a male and female forehead. For example, with males, there is more frontal bossing and central concavity and this is accentuated with ageing.20 Notable structural differences between the male and female upper faces can manifest with females showing a straighter forehead with the glabellar curved and less pronounced and the supraorbital rim less noticeable than in men.20 The sexual dimorphism among human skulls is well established in the anthropological literature, however not all bones in the skull undergo resorption. Although the mid-face recedes, the forehead suffers continuous expansion, due to bone deposition in the external wall of the frontal bone, especially in the supraorbital rim.20 This is an important structural consideration, which in part can influence the activity of the frontalis, through increased hypertonicity.21 The muscles of facial expression on the upper third of the face are separated into two antagonistic groups.13 The eyebrow elevator muscle is composed of the medial, intermediate and lateral fibres of the frontalis, and the eyebrow depressor muscles made up of the procerus, the corrugator supercilii, and the orbicularis oculi.22 Careful assessment and appropriate patient selection can usually negate an unwanted brow ptosis, which may arise from misplacement
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Figure 3: Oblique ‘crease’ sometimes observed in the forehead19
Figure 2: The four different arrangements that have been reported of the underlining frontalis muscle13
Frontalis 1 Frontalis 2 Frontalis 3 Frontalis 4
with toxin as the frontalis has been recently described to potentiate a depressor effect within its superior portion, and elevates inferiorly.23 Many individuals may present with evidence of frontal bone ageing (flattening anteriorly) and may benefit initially from structural (volume) replacement initially, which alleviates the hypercontraction of the frontalis muscle.24
Rohrich and Pessa delineated the presence of three superficial frontal fat compartments through the injection of dye into 15 unembalmed specimens. These findings demonstrated that the subcutaneous fat of the forehead is compartmentalised, bounded by fibrous septa.19 Additionally, Gierloff et al. described findings from their study which incorporated computed tomographic scans and three-dimensional reconstruction of nine unembalmed specimens.25 The advantage of this method was that the authors did not disturb the septa through dissection, but the sample size is a poignant limitation. These findings did confirm the presence of the central superficial frontal compartment, but not the lateral superficial forehead compartments. Cotofana et al. have updated these significant findings with a study that included both contrast-enhanced computed tomographic scans and anatomical dissections on 20 subjects, mixed cohort of embalmed and unembalmed, Caucasian, male and female.26
One of the most significant findings from this study was the presence of longitudinal fibrous adhesions extending from the fascia covering the posterior side of the frontalis muscle to the periosteum. In addition, the septum appeared to connect both temporal ligamentous adhesions from each side, noted as the inferior frontal septum and the middle frontal septum, and were noted to limit the migration of volumeenhancing material to the forehead.26 These are significant findings for the practitioner undertaking volume correction of the forehead as it gives unique clarity on important anatomical boundaries.
The motor supply to the frontalis has been studied with a combination of anatomical dissection (30 cases) and electro stimulation in parotidectomy patients (14 cases). In one particular study, the frontalis muscle was always innerved by the temporofacial trunk of the facial nerve with no accessory innervation.27
The trigeminal nerve (cranial nerve V) branches supply the sensory innervation to the forehead and has three branches: ophthalmic, maxillary and mandibular.28
The ophthalmic nerve is the superior point of division for the trigeminal nerve and divides into three branches: the lacrimal, frontal and nasociliary branches, with the frontal nerve subdividing again into two branches – the supratrochlear and supraorbital, with the supratrochlear supplying the medial angle of the eye, the upper eyelid and part of the glabellar.29
The frontal nerve subdivides again into two branches –supratrochlear and supraorbital, with the supratrochlear nerve supplying the medial angle of the eye, the upper eyelid and part of the glabellar.29 The supraorbital nerve emerges from the supraorbital foramen to supply the lateral canthus, the upper eyelid and the temporal and frontoparietal regions of the head.30
The supraorbital and supratrochlear arteries travel with corresponding nerves and the supraorbital branch exits the medial aspect of the orbital rim along its superior course to the frontalis.21 An accessory foramen may be located just superior to the supraorbital foramen, which is a possible and significant anatomical variation to note when assessing an individual’s glabellar complex. This potential variance may increase the risk of an eyelid ptosis as this additional
foramen facilitates a path where botulinum toxin may pass to inadvertently weaken the levator palpebrae superioris. The clinician may proceed cautiously at this region and ensure intradermal placement of botulinum toxin.31 Whilst it is acknowledged that the glabellar is considered a higher risk area owing to the medial and variable anastomosis of the supratrochlear vessels, the practitioner is advised to remain mindful of the extensive and varied anastomosis of the entire facial vasculature.31
Botulinum toxin can provide an effective and subtle elevation of the lateral brow. Careful assessment of the periorbital area is advised to elicit suitability and degree of response, such as degree of skin laxity and extent of bone resorption.22 Ahn et al. report findings from their small cohort study of 22 patients, which demonstrated an average brow elevation from the mid pupil with botulinum toxin A was 1.02mm, with an average brow elevation from the lateral canthus of 2.83mm.32 Subjects were treated with 5U of onabotulinum toxin A at the inferior tail of the lateral eyebrow as an intradermal injection and evaluated two weeks after treatment. Outcomes were measured by the primary change in brow elevation along vertical axis extending from both mid-pupil and lateral canthus to the caudal row of brow hairs with eyes at neutral gaze and the head at Frankfort plane.32 Additional weakening of the corrugator, procerus, and depressor supercilii muscles can also accentuate the brow position.16
Treatment considerations
An individualised and integrated approach is advised in the assessment and treatment planning of the upper facial areas prior to injection with botulinum toxin.33 Additionally, it is recommended that treatment with toxin is performed as the primary or combination treatment, only if the target muscle is the primary aetiology of the facial disharmony to be addressed.33
There are many techniques within the literature concerning toxin placement and dosing for improving horizontal forehead lines through treating the frontalis muscle. When assessing the upper face, the clinician is advised to closely note the extent of lateral versus medial muscle activity, asymmetry, compensation for brow ptosis, muscle mass as well as brow width and height of forehead.23 Variants in the frontalis muscle have been well described by the recent work of Abramo et al.13 and treatment of the frontalis muscle can directly affect brow position, as the shape and height are influenced by the interplay between the frontalis and the medial glabellar complex.34 The number of injection sites can be determined by the extent and location of muscle contraction, and techniques have been described comprising five to seven injection points, as well as multiple injection sites.34
Individuals who manifest structural changes and loss of contour of the forehead can benefit from volume replacement as first-line treatment as this additional support to the frontal eminence, deep to the frontalis muscle, can smooth the forehead as well as reposition a ptotic brow.35
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Careful assessment of the periorbital area is advised to elicit suitability and degree of response
A number of approaches have been described in the literature. For male patients, retrograde threads of high G prime dermal filler can be placed deep to the muscle on the supraperiosteal plane, from an entry point medial to the temporal crest using a 25 gauge 38mm or 50mm cannula. This cannula size is recommended to allow the cannula to be placed deeply and to minimise risk of vessel compromise.35 Augmenting the left and right frontal eminences can be very effective for restoring strength to the male upper face. The volume of product required may vary and will depend upon the choice of product as well as the degree of correction required. For female foreheads, a smoother and more convex eminence across the full-frontal region is aesthetically pleasing. An alternative correction can be utilised at the superior midline aspect of the forehead, placing retrograde threads on the supraperiosteal plane to smooth and strengthen the anterior aspect of the forehead; however, the lateral correction described for male foreheads can be combined if the clinical need is evident.30 An additional approach which may further enhance the result of forehead contouring, specifically to target static lines, is a type of hyaluronic acid dermal filler technology which is designed to be placed intradermally in the skin to create a blanching appearance, which is a clinical indication of the product’s close proximity the surface of the skin. This technique was first described by Micheels et al. in 2013 whereby a 30 gauge needle was used with the bevel of the needle placed down, depositing small quantities of product until the visible appearance of the line had reduced, or fully corrected, depending on the depth of the line. The treated area is gently massaged following placement to ensure integration.36
Summary
Our anatomical understanding of the forehead structures continues to change as more detailed anatomical and clinical studies are performed. Previous concepts of anatomy and treatment plans must be challenged in light of new studies. These new findings will allow clinicians to fine tune their treatment strategies to apply safer techniques and approach this area to obtain improved outcomes. The underlying anatomy is fundamental in order to approach this; many dissection studies remain comparatively small and continual updates of these studies will allow more details to emerge. Using these studies, clinically targeted strategies can be applied to our medical patients.
REFERENCES
1. Oxford English Dictionary (2019) Oxford University Press UP.
2. Trueb R.M. (2002) Molecular mechanisms of androgenetic alopecia. Exp Gerontol, 37 981-990
3. Lehocky, B (2006 Ch 41 Anthropometry and Cephalometric Facial Analysis in Plastic Surgery 2nd Ed Mathes Vol 2 Elsevier Inc
4. Guyuron B., Cohen S.R. (1997) Facial Evaluation for Orthognathic Surgery. In: Ferraro J.W. (eds) Fundamentals of Maxillofacial Surgery. Springer, New York, NY
5. Farkas L.G, Hreczko T.A,Kolar J.C, Munro I.R. (1985) Vertical and Horizontal proportions of the face in young adult North American Caucasians:revisionof neoclassicalcannons. Plast. Recon. Surg. 75: 328-33
6. Gonzalez-Ulloa M. (1962) Quantitative principles in cosmetic surgery of the face (profileplasty). Plast Reconstr Surg Transplant Bull. Feb;29:186-98.
7. Shaw R.B., Katzel E.B., Koltz P.F., Yaremchuk M.J., Girotto J.A., Kahn D.M., Langstein H.N. (2011) Plast Reconstr Surg 127(1): 374- 383
8. Capitán, L., Simon, D.; Kaye, K; Tenorio, T.(2014) Facial Feminization Surgery: The Forehead. Surgical Techniques and Analysis of Results. Plastic and Reconstructive Surgery: 134 (4) 609–619
9. Dobke, M., Chung, C. & Takabe, K. Facial Aesthetic Preferences Among Asian Women: Are All Oriental Asians the Same?Aesth Plast Surg (2006) 30: 342
10. Mendelson B.C. Jacobson S.R. (2008) Surgical Anatomy of the Midcheek: Facial Layers, Spaces, and the Midcheek Segments. Clinics in plastic surgery 35(3):395-404; discussion 393
11. Cotofana S., Mian A., Sykes J.M., Redka-Swoboda W., Ladinger A., Pavicic T., Schenck T.L., Benslimane F., Ingallina F., Schlattau A. (2017) An Update on the Anatomy of the Forehead Compartments Plast.. Reconstr. Surg. 139:864e-872e
12. Kane M. A. C., (2013 Commentary: Asian Consensus Recommendations on the Aesthetic Usage of Botulinum Toxin Type A, Dermatologic Surgery, 39, 12, (1861-1867).
13. Abramo A.C., Amaral T.P.A.D., Lessio B.P., De Lima G.A. (2016) Anatomy of Forehead, Glabellar, Nasal and Orbital Muscles and Their Correlation with Distinctive Patterns of Skin Lines on the Upper Third of the Face: Reviewing Concepts Aesth Plast Surg 40:962-971
14. Blitzer A, Binder WJ, Aviv JE, Keen MS, Brin MF. (1997)The Management of Hyperfunctional Facial Lines With Botulinum Toxin: A Collaborative Study of 210 Injection Sites in 162 Patients. Arch Otolaryngol Head Neck Surg.;123(4):389–392.
15. Costin B.R., Plesec T. P. Sakolsatayadorn N., Rubinstein T. J., McBride, J. M., Perry J. D (2015) Anatomy and Histology of the Frontalis Muscle Ophthalmic Plastic & Reconstructive Surgery: 31(1):66–72
16. Choi Y-J, Won S-Y, Lee J-G, Hu K-S, Kim S-T, Tansatit T, Kim H-J (2016) Characterizing the Lateral Border of the Frontalis for Safe and Effective Injection of Botulinum Toxin Aesthetic Surgery Journal, 36(3): 344–348
17. Vural E., Batay F., Key J. M. (2000) Glabellar frown lines as a reliable landmark for the supratrochlear artery. Otolaryngol Head Neck Surg. 123(5):543-6.
18. Kapur E. Salihagic S. Gracic E. Dracic A. Hadžović-Džuvo A. (2017). Vascular structures relevant in facial dermal filler injections and their complications. Medical Journal 23(2):
19. Rohrich R.J., Pessa J.E. (2007) The fat compartments of the face: Anatomy and clinical implications for cosmetic surgery Plast. Reconstr. Surg.
20. Avelar L.E.T., Cardaso M.A., Bordini L.S., Avelar L .D.M., Avelar J.V.D.M. (2017) Aging and Sexual Differences of the Human Skull Plast. Reconstr. Surg. Glob. Open. e:1297
21. Sykes J.M., Cotofana S., Trevedic P., Solish N., Carruthers J., Carruthers A., Moradi A., Swift A., Massry G.G., Remington B.K. (2015) Plast Reconstr. Surg. 136: 240s-218s.
22. De Maio M., Swift A., Signorini M., Fagien S. (2017) Facial Assessment and Injection Guide for Botulinum Toxin and Injectable Hyaluronic Acid Fillers: Focus on the Upper Face Plast. Reconstr. Surg. 140: 265e-276e
23. Gart M.S., Gutowski K.A. (2015) Aesthetic Uses of Neuromodulators: Current Uses and Future Directions Plast Reconstr Surg 136:62s-71s
24. Hwang K (2017) Topographic Analysis of the Supratrochelar Artery and the Supraorbital Artery: Implication for Improving the Safety of Forehead Augmentation Plast. Recons. Surg
25. Gierloff M, Stöhring C, Buder T, Wiltfang J. (2012) The subcutaneous fat compartments in relation to aesthetically important facial folds and rhytides. J Plast Reconstr Aesthet Surg.65:1292–1297.
26. Cotofana S., Mian A., Sykes J.M., Redka-Swoboda W., Ladinger A., Pavicic T., Schenck T.L., Benslimane F., Ingallina F., Schlattau A. (2017) An Update on the Anatomy of the Forehead Compartments Plast.. Reconstr. Surg. 139:864e-872e
27. De Bonnecaze G., Vergez S., Chaput B., Vairel B., Serrano E., Chantalat E., Chaynes P. (2019) Variability in Facial -Muscle Innervation: A Comparative Study Based on Electrostimulation and Anatomical Dissection. Clinical Anatomy 32: 169-175
Visit our website to test your knowledge and complete our Multiple Choice Questions based on this article.
You will then receive a certificate confirmation of your CPD point.
Mr Dalvi Humzah is a consultant plastic surgeon and delivers his clinical practice through PD Surgery in the West Midlands, Gloucester, and The London Welbeck Hospital. He is also director of the award-winning Dalvi Humzah Aesthetic Training and clinical director of DermaSeal Ltd. He has wide experience in teaching and training nationally and internationally.

Anna Baker is an aesthetic nurse prescriber, trainer qualified educator. She is a works as a trainer for a number of aesthetic companies as a KOL and is a board member for the BACN. Baker has worked as a course coordinator and tutor at Dalvi Humzah Aesthetic Training since 2012 and presents at a national and international level, practising from Marylebone, London and Sussex.

28. Moss J.C., Mendelson B.C., Taylor G.I. (200) Surgical Anatomy of the Ligamentous Attachments in the Temple and Periorbital Regions, Plast. Reconstr Surg, 105 (4):1475-1489.
29. Sundaram Sinnatamby CS (2006) Lasts Anatomy Regional & Applied. 11th Edition. Churchill Livingstone Elsevier, London
30. Humzah D, Baker A. (2015) Forehead rejuvenation and contouring strategies Aesthetics Journal: 27-30 31. Kim B.W., Park G.H., Yun W.J., Rho N.K., Jang K.A., Won C.H., Chang S.E.,Chung S.J., Lee ~M.W. (2013) Adverse events associated with botulinum toxin injection: A multidepartment, retrospective study of 5310 treatmentsadministered to 1819 patients Journal of Dermatological Treatment 32. Ahn M.S., Catten M., Maas C. (2000) Temporal Brow Lift Using Botulinum Toxin A Plast Reconstr Surg 105:1129-1135 33. Sundaram H., Signorini M., Liew S., Trinidade de Almeida A.R., Wu Y., Braz A.V., Fagien S., Goodman G.J., Monheit G., Raspaldo H. (2016) Global Aesthetics Consensus: Botulinum Toxin Type A-Evidencebased Review, Emerging Concepts, and Consensus Recommendations for Aesthetic Use, Including Updates on Complications Plast. Reconstr. Surg.137:518e-529e 34. Anido J., Arenas D., Arrubarrena C., Dominguez-Gil A., Fajardo C., Mira M., Murillo J., Ribe N., Rivera H., del Cueto S.R., Silvestre H., Tirado M. (2017) Tailored botulinum toxin type A injections in aesthetic medicine: consensus panel recommendations for treating the forehead based on individual facial anatomy and muscle tone Clin Csomet Investig Dermatol 10:413-421
35. Muhn C., Rosen N., Solish N., Bertucci V., Lupin M., Dan sereau A., Weksberg F., Remington B.K., Swift A. (2012) The evolving role of hyaluronic acid fillers for facial volume restoration and contouring: a Canadian overview Clin Cosmet Investig Dermatol 5:147-158
36. Micheels P.,Sarazin D.,BesseS .,Sundaram H.,FlynnT.C.‘A Blanching Technique for Intradermal Injection of the Hylauronic Acid Belotero’, Plastic And Reconstructive Surgery, 132(4S-2) (2013), pp. 59S-68S.
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
patient can have severe sun damage or laxity, for example lines around the eyes or the mouth such as smoker’s lines. The rest of the face may not be bad enough to require a phenol peel, hence why sometimes it is appropriate to divide the face as you can see in Figure 2 and 3
Why perform a deep chemical peel?
Deep peel treatment enables complete removal of most wrinkles on the face and, as such, can create a ‘facelift effect’ due to the post-procedure collagen and elastin repair of the skin.2
Compared to many other resurfacing procedures on the market, both ablative and non-ablative, the results are, in my opinion, superior. However, the downtime of the procedure may put many practitioners and patients off, which I discuss in more detail later on.
Performing Deep Chemical Peels
It’s fair to say that deep chemical peels have received their fair share of bad press. Both patients and doctors are familiar with the devastating complications that can happen in the hands of an inexperienced practitioner.1 However, when performed by an experienced doctor, I believe that the results of this treatment can be far superior to any other including fractional and ablative lasers. In this article, I will explore when a deep chemical peel is suitable for your patient and discuss considerations around this. It is important to note here that these treatments should only be performed by highly qualified and experienced doctors who have undergone specialised training in performing phenol peels.
What is a deep chemical peel?
A deep chemical peel is performed using a substance called phenol. This procedure has been around since the 1930s and has been adapted and altered by many practitioners throughout the decades.2,3 The most common adaptation is the variation of the components that make a phenol peel, including the phenolic acid itself and croton oil, discussed in more detail below.


Various formulations are currently available on the market with different percentages of phenol mixed with other substances and varying percentages of croton oil, which is another substance that enhances phenol penetration.2 In short, the higher the croton oil percentage, the deeper the peel will go. Due to these variations, many of the phenol-containing peels on the market do not give the results of a deep peel but instead enhance the tolerance of other peels such as trichloroacetic acid (TCA). Deep peels can only be performed on the face and not on any body parts. This is because the skin outside of the facial area is too thin and contains far less pilosebaceous units, therefore it cannot recover itself and will scar.2 They can be performed on the entire face or in separate cosmetic units. My preference is to treat the full face (shown in Figure 1 and 4), however sometimes a
Who is the ideal candidate?
The most ideal candidate would be Caucasian with a Fitzpatrick skin type between I-III who has moderate to severe sun damage and/or skin laxity. This is because, as we know, darker skin types run the risk of hypo and hyperpigmentation after such treatment. With this in mind, I would strongly recommend that phenol is avoided on skin types IV, V and VI, purely because of a severe risk of permanent hypopigmentation and possibly scarring.
I would suggest that a deep peel is not great for acne-scarred skin and, in my experience, TCA medium-depth peels or TCA pixel peels (combined with microneedling) are far more effective to treat acne scarring.4,5 In my experience, deep peels are also not suitable to treat pigmentation disorders as there are far safer options available. I would also not recommend deep peels for patients with minor imperfections or very few fine lines. Again, they would get much better results with TCA peels. It’s all about understanding your patient, their concerns and ensuring that you are able to recommend the most suitable, safe option to achieve fantastic results.
Pre-peel preparation
First of all, spotting the ideal candidate during your consultation is key, as many patients do not come in asking for this procedure or may have not even heard of it. Secondly, explaining the procedure in detail is extremely important.
If I believe a patient would benefit from a deep phenol peel, I would present this solution during their consultation, briefly explaining the procedure and showing them before, during and after pictures. If the treatment interests the patient and they are not put off by the pictures, I would generally organise a second consultation to go through the procedure in full detail. My consent form for this procedure is more than 20 pages long so that should give you an idea of how much detail I go into.

Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Figure 1: Patient before and three months after a full-face phenol peel. Images courtesy of Dr Xavier Goodarzian.
Before After
Dr Xavier Goodarzian provides an overview of performing full face deep chemical peels
It explains the procedure in minute detail and explains what they need to do to get the best results such as skincare preparation, medication, prepeel tests, medical history and so forth. I feel this is very important as patient cooperation is crucial to the success of the procedure. Once the consultation is done, I give the patient the full consent form and the extended medial history questionnaire to take home to read and sign in their own time. It’s important procedures such as these are not rushed or forced. I also ask their spouse, next of kin or whoever will be looking after them for the first couple of days post procedure to read and sign the consent form. I also recommend that they come along to the second consultation. The process begins with skin preparation. This is an important step
recovering. I also recommend a full blood count, liver function tests and urea and electrolytes (U&Es) to be done before the peel. An electrocardiogram may be necessary if there is a history of cardiac illness, all of which I perform in my clinic.1 This is because phenol is detoxified by the liver and kidneys and is also toxic to the heart, potentially causing cardiac arrhythmia.2
Several medications are then prescribed for the patient including strong analgesia, benzodiazepines, sedating antihistamines, antivirals and antibiotics. A chart is given to the patient explaining exactly when and how frequently to take these drugs on a daily basis for a period of two weeks.
Performing the peel
in any peeling procedure and unfortunately can often be omitted by practitioners to cut down cost. In my experience, well-prepared skin with effective topicals has a much higher chance of good recovery after any peel and enhances the results dramatically.6 I would recommend a three-week skin preparation cycle as the absolute minimum. This would consist of a good twice daily routine, containing antioxidants, SPF (lots of it) possibly skin-lightening agents and sometimes retinoids, although a long gap is required between the use of strong retinoids and a phenol peel. All of which would be discussed in the consultation.
It is also my preference to always include a full-face botulinum toxin treatment about one to two weeks before the peel as this will prevent the expression lines from deteriorating post peel on fresh skin that is



The patient arrives at least an hour before the procedure and is offered analgesia and benzodiazepines to relax. An intravenous (IV) cannula is inserted and a half litre of saline is administered slowly, sometimes with additional IV non-steroidal antiinflammatory drugs (NSAIDs). This is primarily for pain relief and hydration to cleanse the kidneys. Blood pressure, pulse and oxygen saturation levels are monitored during the procedure and a small cardiac monitor can be used to assess the heart rhythm if there are any palpitations or for random checks. In my experience, it is always beneficial to have an assistant present to help with anything from setting up the room or prepping various steps of the peel. The assistant can be a medical professional or a therapist who has been specifically trained to assist the doctor in this procedure. The face is cleansed, disinfected and degreased thoroughly with alcohol and acetone and then a full-face local anaesthetic block is performed to anaesthetise the majority of the face. This allows a full phenol peel to be performed without sedation or general anaesthetic which can significantly increase the risk of arrhythmia during the procedure.2 The face is then divided into several cosmetic units using a white eyeliner/marker pen and the peeling process can begin. The phenol is applied in specific quantities and in a specific number of coats to each cosmetic unit with a gap of at least 10 minutes between to ensure phenol detoxification and avoid cardiac side effects. For the eyelid, I would use two coats, however for the top lip, I would use three of four. Once the full face has been treated, an occlusive tape can be applied over the entire face which will remain in place for about 12-24 hours. This process of occlusion allows epidermal maceration and further penetration of the phenol.2 Once the procedure has finished, the patient is generally unable to open their eyes due to oedema and their ‘carer’ should get them home with accurate instructions. Hygienic environments are absolutely crucial at this stage, so I always recommend no contact with pets, young children, no touching and no scratching. You can also advise patients to change their pillowcases and towels daily. The following day the ‘carer’ brings the patient back to the practice

Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
It is important to note, that these treatments should only be performed by highly qualified and experienced doctors who have undergone specialised training in performing phenol peels
Figure 2: Patient before and three months after a phenol peel around the eyes. Images courtesy of Dr Xavier Goodarzian.
Before After
Figure 3: Patient before and three months after a phenol peel around the eyes. Images courtesy of Dr Xavier Goodarzian.
Before After
where the occlusive mask is removed and bismuth subgallate is applied to the face. This allows the skin under the powder to heal while protecting it from the outside world. This mask, which becomes semi solid, has to remain in place for seven days and should under no circumstances be removed. At this point the practitioner is able to help open the eyes for the patient, which gives them back a bit of their independence after not being able to see for almost 24 hours. During this week there is really not much the patient can do except to stay at home and rest. The medication allows prolonged and deep sleep for the patient at home which makes this week much more tolerable. Any form of exercise is strictly forbidden. Solid foods and excessive chewing have to be avoided so most people stay on a liquid or semi-liquid diet for the week.
At the end of this healing and isolation period, the patient applies a thick layer of occlusive ointment to their face at night which allows the mask to come off the following day. Of course, there are variations to this description as sometimes the occlusive mask may not be applied, or only a part of the face will be treated with phenol, such as the periorbital region.
Aftercare
The skin is very red and very sensitive for at least six weeks, but it’s sometimes longer. The patient should accurately follow the post-peel protocols with their topicals, instructed by their practitioner to avoid any complications such as infection or scarring.2 Usually, there is minor skin shedding in the following 10 days as the new skin starts settling and adapting. I also advise that makeup can be applied almost as soon as the yellow crust comes off to cover
redness and provide further SPF. It is crucial for the patient to be seen at the practice several times during the following weeks to ensure potential complications don’t go unnoticed. As a minimum, I like to see my patients at day 10 and one, two, three and six months’ following treatment.
Full sun protection (no lower than SPF 30) and sun avoidance are compulsory for the first few months. This is because new skin will be very sensitive and can burn or pigment very easily.
I would say that even though the immediate results are great, the full effect can only be appreciated around three to six months’ post procedure, as this waiting period is necessary for the collagen and elastin fibres to rebuild and restructure.2 I would recommend that the final ‘after’ pictures are taken around that time. The results from this type of peel are very long lasting without promising permanent results. Histologically, the skin changes can be seen decades later.7 As we very well know, the face continues to age, and sun exposure is inevitable even when all sun protection measures have been complied with. Generally, the more sun damaged and wrinkled the face, the more dramatic and long lasting the effects.
Considerations
As mentioned, cardiotoxicity is one of the most dangerous side effects of performing this treatment.2,8 If a patient has any form of cardiac medical history, the treatment should not go ahead.
Once all medical contraindications such as diabetes, infections, autoimmune illness, genetic collagen abnormalities have been excluded, it still comes down to the practitioner’s discretion to decide if the patient is a good candidate or not.
As mentioned, there is a high risk of infection immediately after the peel.2 The yellow mask acts as an antimicrobial shield and prophylactic antibiotics are also prescribed. The most important thing is to communicate all of the risks associated with this procedure clearly and document that you have done so. Reiterating the importance of hygienic environments will also aid in making treatment outcomes successful.
Dr Xavier Goodarzian is the medical director and coowner of the national award-winning Xavier G. Clinic in Southampton. He is a lecturer and trainer at major conferences throughout the UK and abroad and the past lead trainer for Innomed Training. Dr Goodarzian is a member of the Royal College of General Practitioners and has postgraduate degrees is clinical dermatology and cosmetic medicine. He is a member of BCAM and also a past committee board director.
REFERENCES
1. Nikalji N, Complications of medium depth and deep chemical peels, Journal of Cutaneous and Aesthetic Surgery, October 2012 <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3560165/>


2. Deprez P, Textbook of chemical peels second edition, July 2016
3. Shuster M, The Baker Phenol Peel, Plastic and Reconstructive Surgery, July 1998 <https://journals. lww.com/plasreconsurg/Citation/1998/07000/The_Baker_Phenol_Peel_Formula.60.aspx>
4. Castillo D, Keri J, Chemical peels in the treatment of acne: patient selection and perspectives, Clinical, Cosmetic and Investigational Dermatology, July 2018 <https://www.ncbi.nlm.nih.gov/pmc/articles/ PMC6053170/>

5. Hay A et al., Interventions for acne scars (review), Cochrane Library, 2016 <https://www. cochranelibrary.com/cdsr/doi/10.1002/14651858.CD011946.pub2/pdf/full>
6. Rendon M, Berson D et al.,Evidence and considerations in the application of chemical peels in skin disorders and aesthetic resurfacing, Journal of Clinical and Aesthetic Dermatology, July 2010 <https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2921757/>
7. Bensimon R, Croton Oil Peels, Aesthetic Surgery Journal, ,January 2008 <https://academic.oup.com/ asj/article/28/1/33/218367>
8. Landau M, Cardiac complications in deep chemical peels, Dermatologic Surgery, February 2007 <https://www.ncbi.nlm.nih.gov/pubmed/17300604>
@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019
The results from this type of peel are very long lasting without promising permanent results. Histologically, the skin changes can be seen decades later
Figure 4: Patient before and three months after a full-face phenol peel. Images courtesy of Dr Xavier Goodarzian.
Dr Goodarzian would like to thank Dr Phillippe Deprez for his extensive work involving chemical peels







13 & 14 MARCH 2020 / LONDON HEADLINE SPONSOR 2020 FIND OUT MORE AND REGISTER FOR FREE www.aestheticsconference.com use code 10001 @aestheticsgroup @aestheticsjournaluk Aesthetics REGISTER TODAY FOR ACE 2020 BY ATTENDING ACE, YOU CAN DEVELOP YOUR OWN PERSONAL LEARNING, INCREASE YOUR CPD POINTS AND LEARN EXCLUSIVELY FROM: Note that some sessions are restricted to doctors, dentists and nurses. Delegates wanting to attendthese sessions will need to provide evidence of their qualifications via DocCheck before the event. More information is available upon registration. 19 BUSINESS TRACK WORKSHOPS 80+ RENOWNED EXHIBITORS CUTTING EDGE TECHNOLOGY AND TREATMENT ADVANCES KEY INSIGHT FROM INDUSTRY LEADERS BROUGHT TO YOU BY THE LEADING MEDICAL AESTHETIC PROVIDERS
Merz Innovation Partner Programme
To further support our educational and training programme, MIAA has a dedicated online educational platform; the Merz Institute of Advanced Aesthetics Online via www.merz-institute.co.uk. This website hosts a variety of educational courses and videos with CPD accreditation. The Merz Institute Online is open to healthcare professionals registered and based in the UK.

of Advanced Aesthetics (MIAA) is the training and education umbrella brand for Merz Aesthetics. As part of our training and education strategy, in early June this year MIAA partnered with 10 expert healthcare professionals from the UK and Ireland to create the Merz Innovation Board and Merz Innovation Partners. We hosted a four-day intensive Merz Innovation Partner Conference in London, which covered scientific product knowledge as well as injection techniques for the Merz Aesthetics injectable portfolio. This conference was led by four members of the Merz Innovation Board: Dr Kate Goldie, Mr Dalvi Humzah, Dr Simon and Dr Emma Ravichandran. The goal of this conference was to enhance the skills and knowledge of the future Merz Innovation Partners. They are now leading Merz customer training and education via the Merz Innovation Partner programme, an exclusive series of masterclasses for the Merz Aesthetics injectable portfolio.

Aesthetics | November 2019 40 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial Merz Aesthetics
The Merz Institute of Advanced Aesthetics is an expert-led educational brand devoted to advancing knowledge and providing UK healthcare professionals with academic and practical skills to successfully compete in the area of aesthetics. The Merz Institute
The Merz Institute of Advanced Aesthetics presents a BELOTERO® Lips masterclass with Merz Innovation Partner Lee Garrett
The Merz Institute Online
Merz Innovation Partner Conference in June 2019. From left to right: Dr Kim Booysen, Lee Garrett, Dr Paula Mann, Dr John Tanqueray, Annie Cartwright, Mr Dalvi Humzah, Dr Kate Goldie, Dr Simon Ravichandran, Emma Chan, Aine Larkin, Anna Gunning, Dr Emma Ravichandran, Julie Redmond and Patricia Molloy.
“As an experienced injector I don’t always expect to learn anything new at meetings and conferences. However, I am really pleased to say that under Lee’s expert guidance I now have a new approach to using BELOTERO® Lip filler”
Dr Peter Forrester
BELOTERO® Lips Masterclass with Lee Garrett

Our vision at Merz is to become the world’s most Admired, Trusted and Innovative Company in aesthetics. Education continues to be a key part of how we aim to deliver against our Vision; this is why we have partnered with our Merz Innovation Partners to deliver The Merz Innovation Partner Programme. A Masterclass for BELOTERO® Lips is one of the many educational meetings that we will be running this autumn and in 2020. The objective of these Masterclasses is to help healthcare professionals expand their scientific and practical knowledge on the use of Merz products to deliver optimum clinical outcomes for patients. The BELOTERO® Lips Masterclass consists of a combination of lectures, live demonstration and hands-on injection experience. Delegates will bring their own model for the allocated guidance time, where they will receive guidance and supervision on the specific injection technique for BELOTERO® from the Merz Innovation Partner. BELOTERO® Lips (Shape and Contour) is the only combination hyaluronic acid therapy specifically for lip enhancement.1 BELOTERO® Lips Contour is indicated for lip enhancement (e.g. lip contour, perioral fine lines, moderate oral commissures).2 BELOTERO® Lips Shape is indicated to enhance soft tissue volume (e.g. lip volume).3 The patented Cohesive Polydensified Matrix (CPM®) Technology and rheologic tailoring reduces the risk of palpability and visibility, which means that patients are also less likely to feel BELOTERO® Lips Shape and Contour in the skin, with no reported Tyndall effect.4 For further information about BELOTERO® Lips (Shape and Contour) please contact your Merz Aesthetics account manager or our customer service team.

Meet Lee Garrett

Lee Garrett has a degree in adult nursing and is fully qualified as a staff nurse and an aesthetic nurse practitioner. Lee has sat on the steering committee for the aesthetic nurses forum, which was part of the Royal College of Nursing. With a highly regarded reputation as nurse practitioner, Lee plays a high profile and active role within the aesthetic industry, particularly in the London area. His values and ethical stance for high standards mean he is recognised as a credible expert, hence he is often the point of contact for fellow professionals for advice and is frequently called upon by national media to give his expert opinion. Lee has dedicated a large proportion of his time to training to a wide array of both new and experienced practitioners in both medical devices and injectables. Lee is truly passionate about teaching and focuses his time only training in what he truly believes in and advocates.
Highlights from the first London BELOTERO® Lips masterclass
On Saturday October 12, Merz Innovation Partner Lee Garrett hosted the first Londonbased Masterclass where eight aesthetic practitioners were invited to learn more about the specific anatomy of the perioral and oral area, as well as the BELOTERO® Lips technique using both the Shape and Contour products.


Lee then performed a live demonstration showcasing the technique, before delegates were encouraged to recreate this on their own models. The technique primarily focused on restoring the outline of the vermilion border for a more youthful appearance and enhancing the upper and lower lip, using both needle and cannula. Throughout the event, Lee offered his advice and recommendations to the practitioners, all of whom were able to speak with him, and showcase their injection techniques, on an intimate one-to-one basis. The day came to a close with a group discussion, where practitioners were able to converse over what they had learnt and what practical tips and advice they were able to take away with them and implement into their practice.
Merz Pharma UK Ltd. 260 Centennial Park, Elstree Hill South, Elstree, Hertfordshire, WD6 3SR Phone: 0208 236 0000 Email: customerservices@merz.com
M-MA-UKI-0638 date of preparation October 2019. Adverse events should be reported. Reporting forms and information for the United Kingdom can be found at www.mhra.gov.uk/yellowcard. Reporting forms and information for the Republic of Ireland can be found at https://www.hpra.ie/homepage/about-us/report-an-issue/ mdiur. Adverse events should also be reported to Merz Pharma UK Ltd by email to UKdrugsafety@merz.com or on +44 (0) 333 200 4143.

Aesthetics | November 2019 41 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com Advertorial
Aesthetics
Merz
Lee Garrett, NIP, Merz Innovation Partner
REFERENCES: 1. Ref BELOTERO® Data on File - REF-0946. 2. Ref IFU Lips Contour 3. Ref IFU Lips Shape. 4. Ref Micheels P et al. Two Crosslinking Technologies for Superficial Reticular Dermis Injection. A Comparative Ultrasound and Histologic study; J Clin Aestheti Dermatol 2017; 10(1) 29-36
Understanding Brow Shapes



Permanent
There is no denying that eyebrows are a big business in both the beauty and aesthetics specialty. Eyebrows have the power to define important features,1 express one’s emotions and play a role in facial recognition.1 I also believe they can have the power to provide a more youthful aesthetic to the face. Understanding how to properly design and shape a brow to suit a patient is the cornerstone of permanent makeup and equally important for aesthetic practitioners carrying out facial filler and botulinum toxin treatments.
Thanks to the likes of actress Brooke Shields and model Cara Delevingne – both of whom wear a fuller, bushier eyebrow – the beauty and cosmetic industry has swiftly turned its back on the minimal brow, popular in the 90s and early 2000s. This is clearly reflected in the growth of the UK brow market in relation to buying products to make brows appear fuller as well as














treatments that meet this requirement too, such as a HD Brows treatment (consisting of tinting, trimming, waxing and threading).
A number of years ago, it was estimated that the market was worth an estimated £6.5m and in 2016 it was worth £20m.2,3 More recent UK figures are not available, however in the US last year, brow products alone accounted for £60m,4 so it is likely that the UK follows suit.
The impact of the brow
The eyebrows frame the eyes, and we communicate a lot through our eyes. In my experience, a well-placed brow can lift and widen the eyes, whereas the wrong brow can make eyes look smaller and appear older. I find that a naturally full, well-groomed and correctly-positioned brow can open up the upper face and give a more youthful appearance. There have been numerous studies on the role of the eyebrow and what is generally considered the ideal.5-7
For example, in July this year Zhao et al., conducted a study that explored the attractiveness of an individual by combining the geometric and shape features of the eyebrows and the eyes, taking into consideration the shape of the face.
The study, which was conducted on 300 Asian female face images, found that high-bending eyebrows

with small eyes and a round face, and lowbending eyebrows with large eyes and a longer face, made the facial image have a higher attractiveness score.5 This has been illustrated by Aesthetics in Figure 1. In 2007, a study conducted by Feser et al., compared three different variations of eyebrows; the arched eyebrow with the maximum height in the middle, and two variations that had their maximum height in the lateral third, but differed in their position. It found that among a total of 357 subjects, 12 to 85 years of age, the preference for a specific eyebrow shape depended on the person’s age. The younger subjects (up to 30) preferred eyebrows in a lower position, and ruled out arched eyebrows. Those older than 50 years stated the opposite preference.6






Whilst both of these studies demonstrate that brows are considered a key component of what is deemed ‘attractive’ they also highlight the need for a personalised approach. Your brows are as unique as your fingerprints, they should complement your

Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
makeup artist Karen Betts discusses the importance of eyebrow shapes in facial aesthetics
While permanent makeup technicians can add width, shape and density to brows, it is very difficult to correct overly uneven brows in terms of height and where they sit on the face, so this is where aesthetic practitioners come in
Figure 1: Example of the aesthetic ideal according to Zhoo et al. study. Images interpreted by Aesthetics Media.
Brow and face shapes
Different face shapes are suited to different brow styles; it’s all about balance. If a person has a square jaw, I find that the brow should be gently arched, as a flat brow will make the face look heavy and overly angular. Long face shapes should opt for a soft, rounded brow arch, as a high arch will add more length to the face – something longer face shapes generally will want to avoid, in my experience. Round face shapes, in comparison, should be complemented by a brow with a slightly more angular arch. I recommend that practitioners always look at the face as a whole and consider how you can balance out any overly-prominent features with your non-surgical aesthetic treatments.9
Round: A round face is almost as wide as it is long. Gently curved brows, with no harsh angles, really complement this face shape.








Oval: This face shape suits most styles of brow.




















Oblong: A long and slender face is best complemented by flatter brows with a soft wide arch.





















Square: This shape is similar to the round face shape, proportion wise. However, people with a square face often have a strong, square jawline and a square hairline, as well as more angular features. Creating some height in the arch will give the illusion of length to the face.
Heart: The forehead and cheeks are usually the widest part of the face, and they will taper to a delicate chin. Soft angles in your brows or a softly curved brow that is shorter in length will help to balance out and complement features.
Diamond: The forehead and jawline are likely to be a similar width. As such, you want your brow shape to create balance between wide cheekbones and a narrow jawline and forehead. I recommend a soft angular shape with lift and width in the arch with a shorter tail.
features and as you age they may need to be adjusted to continue to do so. As mentioned, a higher arch gives the illusion of a more open eye – hence older women tend to prefer this style of brow.
Eyebrows in medical aesthetics
While permanent makeup technicians can add width, shape and density to brows, it is very difficult to correct overly uneven brows in terms of height and where they sit on the face, so this is where aesthetic practitioners come in. Regardless of the treatment type, any practitioner working on a patient’s upper face should have a full understanding of brow shapes and how they can impact the whole face. For example, if the patient has a prominent brow bone, it is important not to lift the tails of the brow too high when using injectables in the forehead and eye area as this can result in the brows ‘disappearing’ when looking at the face from certain angles. It’s important to be aware of the effects on the muscles surrounding the brow, especially the corrugator supercilii muscle. This is because any adjustments in this area can potentially affect the shape and movement of the brow.
I would also recommend all practitioners check their patients’ brow proportions, particularly where the bulb (front of the brow closest to the nose) of their brow
sits prior to a botulinum toxin treatment to ensure the procedure won’t negatively impact their brow shape or cause drooping. As we know, botulinum toxin can help patients with brows that naturally sit at different levels because of differences in muscle strength. It can also be used to adjust the arch of the eyebrow to give a more angular look.8
Summary
It is undeniable that the brows are a key component of the facial structure and have a huge impact on the overall facial aesthetic. Whilst a permanent makeup treatment focuses on the actual physical eyebrow (and the hairs/lack of), aesthetic treatments can impact how the brow sits on the face. Therefore, I think it is important for aesthetic practitioners to have a strong working knowledge of brow design when working with the upper part of the face. The brows sit on major facial muscles so any intervention in or around the eye area should most definitely take the brows into consideration.
As with a lot of treatments in the beauty and aesthetics field, fashions and trends come and go. So, it’s important that, first and foremost, patients’ eyebrow shape, positioning and design suits their face and complements their features.
Karen Betts has clinics in Cheshire, Yorkshire and on Harley Street. She has been performing permanent makeup and medical tattooing for more than 20 years and has recently developed her own range of pigments. She offers a variety of permanent makeup training courses under the K.B Pro brand.
REFERENCES
1. Sadr J, The role of eyebrows in face recgnition, Perception 2003 <https://web.mit.edu/sinhalab/Papers/sinha_ eyebrows.pdf>
2. BABTAC, The Brow Boom, December 2016 <https://www. babtac.com/blog/2016/12/95-the-brow-boom>
3. The Guardian, How brows became the beauty obsession of the decade, eptember 2016 <https://www.theguardian.com/ fashion/2016/sep/27/brows-beauty-obsession-eyebrowgrooming-cara-delevingne>
4. Nielsen.com, From lashes to brows: eye-opening trends in cosmetics, September 2018 <https://www.nielsen.com/us/ en/insights/article/2018/from-lashes-to-brows-eye-openingtrends-in-cosmetics/>
5. Zhao J et al., Data-driven research on the matching degree of eyes, eyebrows and face shapes, Psychology July 2019 <https://www.frontiersin.org/articles/10.3389/ fpsyg.2019.01466/full>
6. Feser D et al., Attractiveness of eyebrow postion and shape in females depends on the age of the beholder, Aesthetic Plastic Surgery, April 2007 <https://www.researchgate. net/publication/6568246_Attractiveness_of_Eyebrow_ Position_and_Shape_in_Females_Depends_on_the_Age_ of_the_Beholder>
7. Schroeder B, Eyes, eyebrows and their effect on the facial perception of hostility, Modern psychological studies, 2011 <https://scholar.utc.edu/cgi/viewcontent. cgi?article=1185&context=mps>
8. Woodward C, Manning V, Treating the brow, Aesthetics journal, August 2017 <https://aestheticsjournal.com/feature/ treating-the-brow-1>
9. Yalcinkaya E, Aesthetic analysis of the ideal eyebrow shape and position, European Acrives of Oto-RhinoLaryngology, October 2014 <https://www.researchgate.net/ publication/267742996_Aesthetic_analysis_of_the_ideal_ eyebrow_shape_and_position>
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Round Oval Oblong Square Heart Diamond

Considering Dermal Filler Blindness
of this artery results in sudden loss of vision and is classified as an ophthalmic emergency.5 Rapid treatment may prevent visual loss,6 although often this can be futile, and there is no clear consensus on its management. Hayreh et al. used a primate model of central retinal artery occlusion to show that the retina may recover within 97 minutes of retinal artery occlusion.7 Although human studies are lacking, this evidence has demonstrated the urgency of management in this scenario.
How the central retinal artery becomes occluded

With the high demand for non-surgical rejuvenation treatments, including dermal filler, it is expected that complications will occur. Whilst rare, the most devastating is dermal filler-associated visual loss. This article describes the anatomical principles and mechanisms of this serious complication, highlighting the need for all aesthetic practitioners to understand them clearly, as well as the necessary immediate management steps should visual loss present.
Classification
Dermal filler complications can be classified into ischaemic and non-ischaemic categories.1 Non-ischaemic complications include infection/biofilm, nodules and granuloma formation, Tyndall effect and prolonged oedema. Ischaemic complications are more concerning, and these include skin ischaemia, skin necrosis and visual loss.1 Hyaluronic acid (HA) has overtaken autologous fat as the leading cause of visual complications following filler procedures.2 A recent comprehensive global literature review identified 53 cases of HA filler-related visual loss between 2000-2018.3 This is likely to be underestimated due to the lack of rigorous complication reporting.
Anatomy of filler-related visual loss
Visual loss can occur from a facial dermal filler injection in almost every anatomical region, but the theme of visual loss, despite the location of the injection, is occlusion of the central retinal artery.4

The central retinal artery is the first branch of the ophthalmic artery (Figure 1), a branch of the internal carotid artery (the main blood supply to the brain). It is of crucial importance in providing oxygen and nutrients to the eye, allowing functional vision. Occlusion, therefore,
It is not possible to directly inject the central retinal artery with dermal fillers due to its deep location relative to the skin. However, there is a linked arterial network that includes branches from the ophthalmic artery to many areas of the face such as the supraorbital, supratrochlear, angular, and dorsal nasal arteries.5 Therefore, filler injected on the face distant to the eye can cause visual loss. In addition, the facial artery (a branch of the external carotid artery), supplies blood to the face. This artery has several vascular anastomoses providing connections between it and the blood supply to the eye.5 The mechanism of filler-associated visual loss is multifaceted due to the complexity of the facial anatomy. The main hypothesis is that direct arterial embolisation can occur and subsequent retrograde flow to the ophthalmic arterial circulation results in visual loss.8 Beleznay et al. postulated that when filler is injected into a vessel, it can travel in a retrograde manner against the arterial flow.2,8 The authors measured the vessel volume of the supratrochlear artery on cadaver heads from the glabellar region to the orbital apex to be 0.085ml, highlighting that injectors should be aware that a bolus of this critical volume may lead to a significant adverse outcome.2
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Anterior
Cornea Posterior
Central
Central
Vein Optic disc Retina Optic Nerve
Consultant ophthalmologist Miss Elizabeth Hawkes explores the causes and treatment
approaches for
immediate dermal filler-related blindness Figure 1: The anatomy of the eye. Occlusion of the central retinal artery results in sudden loss of vision and is classified as an ophthalmic emergency.4
segment
segment
Retinal Artery
Retinal
Central retina artery branches at the optic disc to supply the retina
• Inject slowly
• Use low volume boluses (<0.1ml per injection site)
• Aspirate prior to injection to ensure location
• Sound knowledge of facial vascular anatomy
• Be aware of the correct depth of filler placement
• Cautious use in high risk areas: nose, glabella, forehead and nasolabial regions
• Have a robust management strategy in place in case of complication
• Establish a link with a local ophthalmologist or eye casualty service9
Clinical features
Although it can occur at any facial injection point, the high-risk areas for dermal filler-associated visual loss are the nasal, glabella, nasolabial and forehead/temple regions.9 Most recent publications have confirmed that the nasal region is the most common area for filler-associated visual loss.3,9,10 This is due to the location of the dorsal nasal artery, which is a branch of the ophthalmic artery.5

The immediate clinical sign of central retinal artery occlusion is sudden reduced vision.11,12 In addition, patients may also describe eye pain, headache, ophthalmoplegia and ptosis, depending on which other vessels are involved.11,12 Due to this myriad of symptoms, clinicians must be vigilant and aware of any symptoms reported by the patient in the immediate period post-procedure and all aesthetic practitioners should consent for the risk of blindness and discuss with patients prior to treatment.
Management
There have been recommendations from US surgeons for a ‘blindness toolkit’ to be readily available in clinics administering fillers.13 This blindness toolkit would include the protocol and treatment for immediate management before referral to a specialist eye centre.
There are a series of protocol and treatment guidelines published by the Aesthetic Interventional Induced Visual Loss (AIIVL) consensus group, which is essential information for all aesthetic practitioners.14
The first step for management is a correct and rapid diagnosis following a quick examination, but treatment must be instituted with minimal delay. The examination should include an estimate of the visual acuity in each eye, eye movements, and pupillary responses. Once the diagnosis is suspected, it is essential to liaise with an ophthalmologist and local emergency eye care service immediately. It is advised that the injector provides a vial of hyaluronidase to the patient to pass on to the ophthalmologist.8 This avoids unnecessary delays and gives the patient the greatest chance for visual recovery. The practitioner should provide a detailed handover to the hospital specialist as part of good medical practice.8 AIIVL mentions that some patients who present at emergency facilities are not met by specialists who are up-to-date with recent specific guidelines, so it is also recommended that practitioners give the patient a printed set of guidelines to take to A&E with them so that they can choose to consider these in their treatment approach.14
The fundamental principle of management is to dissolve or dislodge the clot to the peripheral retina by delivering hyaluronidase to the arterial circulation. There is a lack of robust evidence for the definitive management and unfortunately many patients will not regain vision.8 Following immediate visual loss, AIIVL recommends the following path:14
Action
by injecting practitioner:
1. Stop injecting immediately and call ophthalmologist/local emergency eye care service.
2. Ask the patient to breathe in and out of a paper bag. This procedure increases carbon dioxide concentration and thus results in vasodilation, which can potentially encourage clot migration to the peripheral retina.14
3. High dose oral aspirin with appropriate gastric protection. This is usually recommended for one week.
4. Administer sublingual GTN to encourage vasodilation and product movement toward the periphery of the retinal system.
5. Ocular massage to theoretically encourage movement of the clot. This should be instituted immediately in conjunction with the above maneuvers. I recommend practitioners understand how this should work in practice through training.
6. Transfer patient to emergency eye care service.
Action by ophthalmologist:
1. Further ocular massage will be performed to further encourage movement of the clot. This is performed by an ophthalmologist using a special three-mirror lens on the eye.
2. Anterior chamber paracentesis with a 30G needle to remove 0.1ml of aqueous fluid. This aims to lower the intraocular pressure in the eye.
3. Further reduce the intraocular pressure using topical timolol 0.5% and intravenous acetazolamide 500mg
4. Inferotemporal peribulbar injection of hyaluronidase, 1500 IU (high dose).
5. Infiltration of hyaluronidase (1500 IU) around supratrochlear notch.
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Tips to help reduce the likelihood of dermal filler-related visual loss9
Figure 2: The most common injection points on the face that have been shown to result in blindness according to the most recent world literature.3
The role of hyaluronidase
A high dose of hyaluronidase (1500 IU) should be injected at the dermal filler entry point and along the arterial path as per any fillerrelated ischaemic complication.8 This can either be performed by the treating practitioner, as long as it does not delay referral to a specialist, or the ophthalmologist in A&E. Various methods of hyaluronidase administration direct to the central retinal artery have been studied and are beyond the scope of this article, but unfortunately the visual outcomes remain poor and the mode of delivery is controversial and carries further potential complications.8 Potential delivery options for hyaluronidase include retrobulbar, direct arterial and sub-tenon injection.8 There have also been reported cases of visual recovery with injection of hyaluronidase to the supratrochlear notch.15 The AVIIL consensus group advises inferotemporal peribulbar injection of hyaluronidase to target the central retinal artery.14
Although hyaluronidase is permeable to vessel walls it appears unable to diffuse across the optic nerve sheath where the central retinal artery lies.16 One paper by Adulkar et al. has therefore questioned the value of retrobulbar treatment of HA filler embolism.17
REFERENCES
Miss Elizabeth Hawkes is a consultant ophthalmologist and oculoplastic surgeon at the Cadogan Clinic

1. Hwang, Catherine J. et al. Filler Complications. Advances in Cosmetic Surgery, Volume 1, Issue 1, 143 – 150

2. Khan TT, Colon-Acevedo B, Mettu P, DeLorenzi C, Woodward JA. An anatomical analysis of the supratrochlear artery: considerations in facial filler injections and preventing vision loss. Aesthet Surg J. 2017;37(2):203-208.
3. Chatrath V, Bannerjee PS, Goodman G, Rahman E. Soft-tissue filler-associated blindness: a systematic review of case reports and case series. Plast Reconstr Surg Glob Open 2019; 7:e2173.
4. Ferneini E, Hapelas S et al. Surgeon’s Guide to Facial Soft Tissue Filler Injections: Relevant Anatomy and Safety Considerations, Journal of Oral and Maxillofacial Surgery, Volume 75, Issue 12, 2017, Pages 2667.e1-2667.e5, ISSN 0278-2391.
5. Snell RS & Lemp MA, Clinical Anatomy of the eye, second edition.
6. Hayreh SS. Central retinal artery occlusion. Indian J Ophthalmol. 2018 Dec;66(12):1684-1694.
7. Hayreh SS, Zimmerman MB, Kimura A, Sanon A. Central retinal artery occlusion: retinal survival time. Exp Eye Res. 2004;78:723-736.
8. Beleznay K, Carruthers JA, Humphrey S, et al. Update on avoiding and treating blindness from fillers: a recent review of the world literature. Aesthet Surg J 2019; 9:662 – 674.
9. Rzany B, DeLorenzi C. Understanding, avoiding, and managing severe filler complications. Plast Reconstr Surg 2015; 136(5 S):196S - 203S.
10. Carruthers JDA, Fagien S, Rohrich RJ, et al. Blindness caused by cosmetic filler injection: a review of cause and therapy. Plast Reconstr Surg. 2014;134:1197–1201
11. Hu XZ, Chen SQ, Zhang Q, Wu PS, Lu W. Clinical analysis of visual loss caused by facial cosmetic llers injection. Zhonghua Yan Ke Za Zhi. 2017;53(8):594-598.
12. Schelke LW, Fick M, van Rijn LJ, Decates T, Velthuis PJ, Niessen F. [Unilateral blindness following a non- surgical rhinoplasty with filler]. Ned Tijdschr Geneeskd. 2017;161:D1246.
13. Prado G, Rodriquez-Feliz J. Ocular pain and impending blindness during facial cosmetic injections: is your office prepared? AesthPlastSurg. 2017;41:199-203
14. Humzah MD, Ataullah S, Chiang C, Malhotra R, Goldberg R. The treatment of hyaluronic acid aesthetic interventional induced visual loss (AIIVL): A consensus on practical guidance. J Cosmet Dermatol. 2019 Feb;18(1):71-76.
15. Murthy R, Roos JCP, Goldberg RA. Periocular hyaluronic acid fillers: applications, implications, complications. Curr Opin Ophthalmol. 2019. Sep;30(5):395-400.
16. Adulkar N, Cheng C, Lee L, et al. In vitro evaluation of hyaluronidase && penetrating of the optic nerve sheath. Ophthalmic Plast Reconstr Surg 2019.
17. Murthy R, Roos JCP, Goldberg RA. Periocular hyaluronic acid fillers: applications, implications, complications. Curr Opin Ophthalmol. 2019. Sep;30(5):395-400.
18. Feza Haque & Mitul Jadeja, Understanding the Yellow Card Schee, 2019. <https:// aestheticsjournal.com/feature/understanding-the-yellow-card-scheme>
Following the complication
The AIIVL group advises that the follow-up of the patient should be combined between the injecting practitioner and ophthalmologist. In line with Good Medical Practice guidelines, the injector has a duty of candour to the patient to be honest about the event. The incident must be reported to the Medicines and Healthcare products Regulatory Agency (MHRA) via the Yellow Card reporting scheme18 and the appropriate medical indemnity provider should be informed. Documentation with photographs is essential and should include all correspondence between the patient, injecting practitioner and specialist, although note that photos in the emergency setting should not be a priority.
Conclusion
The prompt diagnosis and recognition of dermal filler-related central retinal artery occlusion is critical for all aesthetic practitioners. Patients should be consented for this complication prior to any facial filler injection. Due to the poor visual prognosis, injectors should have a good understanding of facial anatomy and practice safe aesthetic medicine to reduce the likelihood of this life changing complication.
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
in Chelsea, London. She specialises in cosmetic eyelid surgery and facial aesthetics. Miss Hawkes also leads the emergency eye care service for the Royal Berkshire NHS Foundation Trust.
SHARE YOUR EXPERTISE AND WRITE FOR THE AESTHETICS JOURNAL Do you have any techniques to share, case studies to showcase or knowledge to impart? CONTACT Email editorial@aestheticsjournal.com Tel 0203 196 4359
Although it can occur at any facial injection point, the high-risk areas for dermal filler-associated visual loss are the nasal, glabella, nasolabial and forehead/temple regions





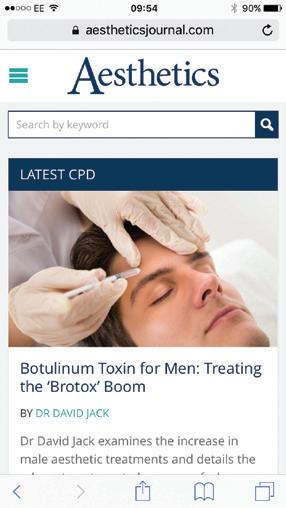
AESTHETICSJOURNAL.COM Keep up-to-date with the latest aesthetic developments and best practice guidance on your desktop, tablet or phone AESTHETICSJOURNAL.COM @aestheticsjournaluk Aesthetics @aestheticsgroup
Using Growth Factors
As detailed in my previous article published in the October issue of the Aesthetics journal,1 the depth of history and award-winning research behind the humble growth factor indicates how important these small molecules are.2-5 It is generally accepted that aesthetic medicine is becoming more and more focused on regenerative medicine and within this article I will explore the different types of growth factors, detail how to assess products for the best treatments and maximise the benefit to your patients. We know that as we age, we lose more cells than we can generate, the body slowly tires and cells become sluggish. We don’t have the stem cell reserves to maintain the demands of our skin and connective tissue to regenerate.
As a result, our collagen, elastin and fibrin depletes, our bone changes shape, our fat pads decrease and our skin increases in laxity. Sagging and wrinkles continue as we age, unless, of course, we do something about it.
The introduction of growth factors into aesthetic medical treatments and skincare can increase the stimulation of growth factors supplied to our tissues and trigger further signalling, in order to regenerate our connective tissue production at an improved rate.6 By replacing or helping to regenerate the cells that the body loses in the natural ageing process, we can help treat ageing skin.
Growth factors in aesthetic medicine
The science behind the creation of stem cells through therapeutic cloning has many potential uses in the field of regenerative and aesthetic medicine.7 Stem cells are important as they allow our body to regenerate and repair damaged tissue, replacing cells, which turn over with age. Growth factors play a fundamental role in this process as they provide the biochemical cues for stem cells to differentiate and are used to develop the right factors in tissue regeneration.8 The modulation of growth factors at the site of injury or within cells stimulates the most beneficial stem cell differentiation and tissue regeneration.8 Growth factors used in aesthetic treatments can be derived from different stem cell sources and not all stem cell-derived products are equal. It is important to select the correct stem cells to create growth factors, providing positive effects for regenerative medicine. There are various types of growth factors but less are suitable for aesthetic treatment:
• Plant-derived growth factors are taken from the stem of a plant. They are then homogenised under high pressure resulting in dead plant cells, similar to plant extract, which contain antioxidants. There is no data comparing plant-derived products to conventional creams to regenerate skin or stimulate collagen. In my opinion, basic logical understanding of science should conclude that plant stem cells produce plant growth factors that regenerate plants.
• Adipose-derived growth factors are strongly inflammatory fat growth factors that regenerate fat cells, not skin cells. They are obtained by liposuction waste and also used in fat grafting.
• Snail-derived growth factors are highly inflammatory as they are produced when the snail is stressed.9
• Human umbilical cord-derived growth factors produced from cord bank stores are a non-specific growth factor mix and their direct use is not allowed under EU law. In addition, extraction can be ethically challenging.10
• Mesenchymal growth factors are very non-specific but generally anti-inflammatory, however not allowed under EU law.11
The ideal growth factor is anti-inflammatory and stimulates cell growth and repair.12 They target areas in need for regeneration and healing. Growth factors work alongside antioxidants, retinols, hydroxyl acids, plant extracts and protective SPF to help form and complete skin health treatments, hence why there are a number of home treatments including post-
treatment serums and skincare. The mix of growth factors in the product should be anti-inflammatory, selective and targeted for wound healing and skin cell proliferation. There are many growth factors found in the body, with different functions that act on different cell types. Growth factors work best and most effectively when paired up with other growth factors and are used synergistically.13,14 Solutions of single growth factor products do not supply the variety of signalling to induce the correct combined effects of growth, proliferation, differentiation, healing and inhibition of inflammatory cytokines.15 In my experience, the most common growth factors used in popular brands Calecim and Skin Genuity and the ones I’d recommend to look out for include, IGF-1, TGF-beta3, aFGF, bFGF, IL-10, EFG, PDGF KGF for skin rejuvenation and IGF-2, VEGF for hair due to their positive effects on stimulating hair growth.
Growth factor selection
Generating and using specific targeted antiinflammatory growth factors to act on and in the skin stimulates new collagen, fibrin and elastin, along with cell proliferation, speeding healing and enhancing rejuvenation of the skin. By selecting specific growth factors, the use of unwanted inflammatory growth factors and killer cells can be avoided, which can cause apoptosis and cell death.6
Preparations should specifically omit these inflammatory growth factors as they inhibit the healing process and are irritant, especially if included in a daily skincare routine. The next challenge, once you have selected the growth factor solution, is which method you wish to use to get the chosen growth factors to their target inside the skin. Growth factors are large molecules, and as a result are unable to pass into the skin unaided. I have found that for best penetration into the skin, products can be injected, applied using trans-epidermal drug delivery systems such as Plasma Shower or through nano encapsulation via nanotechnology such as liposomes. They can also be delivered through microneedling.16 Liposomes are a spherical vesicle with at least one lipid bilayer which can be used to administer nutrients or pharmaceutical drugs.16 They are hydrophobic and pass easily through the skin’s protective barriers. It is generally accepted that the correct growth factors minimise downtime by reducing negative elements in inflammation and help stimulate the cells needed to improve skin quality without inducing trauma. Areas where
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
In the second of her two-part article Dr Anna Hemming discusses the use of growth factors within aesthetic medicine
It’s no Miracle, it’s Science
The World’s Only Anti-Aging System Powered by Umbilical Cord Lining Stem Cells*
Exclusively available at www.churchpharmacy.co.uk
*CALECIM ® cell-free conditioned media is derived from non-human mammalian umbilical cord.

HI GH CONCENTRATIONS OF REJUVENATING CONDITIONED MEDIA SIGNIFICANT REDUCTION IN DOWNTIME CALMS, SOOTHES & RESTORES SKIN IMMEDIATE RESULTS LONG-TERM AESTHETIC BENEFITS
growth factors can be beneficial include facial rejuvenation, hair treatment, vaginal tightening and skin whitening,17-20 with more indications being researched. We know that stem cells release growth factors but platelets also release growth factors, and this is the basis of platelet-rich plasma (PRP) treatment. Platelets produce growth factors and their use has been well documented in aesthetic and orthopaedic medicine.6,8,21 Containing autologous non-selective growth factors when re-injected, the platelets trigger a cascade to promote healing and cell growth, however the growth factors produced are non-selective and the practitioner must be able to take a blood sample and have a centrifuge to spin the blood separating the plasma.21 Growth factors can also be applied following invasive treatments and within bespoke facials to aid skin healing or in daily treatment following skin trauma. For example, they can be used to decrease inflammation and swelling in the days after plasma blepharoplasty, fractional laser and other invasive skin treatments. Once modified to penetrate the skin, targeted and focused growth factors are at the top of the pyramid of skin ingredients according to Mayoral et al., shown in Figure 1 22 This diagram was published in the Journal of Drugs and Dermatology in 2013 and used extensive research of scientific literature and study reviews of ingredients, formulations and technologies affecting the skin. The result of this was an effective yet simple tool to help professionally guide patients towards. It highlights the optimal, transform and fundamental use of topical products to achieve the best outcomes for skin health.22
Considerations
Critical considerations include the method within which the product enters the skin in the appropriate concentration, as well as ensuring any equipment has the correct FDA or CE marking and doesn’t put the patient at risk, which is beyond the scope of this article. Growth
factor product selection should be from reputable safe and effective research-led companies. When selecting growth factor products, it is essential to understand the manufacturing process to ensure they comply with EU law.23 There should be product details and certification available from distributors.
Summary
I believe growth factors are part of the future in all aesthetic treatments and medical skin health programmes. Practitioners can consider using growth factors in a bespoke facial treatment or as part of a combined treatment plan. Serums with growth factors are available as add-on products for patients to take home and can be highlighted in clinic and unlikely to be sold on the high street. We can demonstrate their ability to enhance the effect of invasive therapies including microneedling and laser and help reduce the downtime associated with these procedures. For the successful use of growth factors in aesthetic medicine, the growth factors have to be able to enter the skin, have high enough concentrations to be effective, contain multiple focused and targeted growth factors, be easy to apply, available for all healthcare professionals to use, affordable and patiently friendly to allow for more at-home use.
Dr Anna Hemming has more than 11 years’ experience in medical aesthetics. She is the owner and medical director of Thames Skin Clinic in Twickenham and associate doctor at Cranley Clinic on London’s Harley Street. Dr Hemming is a GP who has worked at Buckingham Palace and spent five years as an army doctor. She speaks at aesthetic conferences worldwide about growth factors.

REFERENCES
1. Hemming A, Understanding growth factors, Aesthetics journal, October 2019
2. Goujon E, Recherches expérimentales sur les propriétés physiologiques de la moelle des os, J Anat Physiol, 1869
3. Gurdon J.B, The developmental capacity of nuclei taken from intestinal epithelium cells of feeding tadpoles, Journal of Embryology and Experimental Morphology, 1962
4. Gurdon JB, The egg and the nucleus: a battle for supremacy, Development, 2013
5. Takahashi, K., Yamanaka, S, Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors, Cell, 2006
6. Schuldiner M et al., Effects of eight growth factors on the differentiation of cells derived from human embryonic stem cells, PNAS, October 2000
7. Mason C, Dunnill P, A brief definition of regenerative medicine, Regenerative Medicine, 2008
8. Mao A S, Mooney D J, Regenerative medicine: Current therapies and future directions, Proc Natl Acad Sci USA, 2015
9. Vuitton D et al., Cross-reactivity between terrestrial snails (Helix species) and house-dust mite (Dermatophagoides pteronyssinus), Allergy, 1998
10. Dessels C, Factors influencing the umbilical cord blood stem cell industry: an evolving treatment landscape, Stem Cells Translational Medicine, May 2018 <https://stemcellsjournals.onlinelibrary.wiley. com/doi/full/10.1002/sctm.17-0244>
11. Ullah I et al., Human mesenchymal stem cells - current trends and future, Bioscience Reports, Department of Theriogenology and Biotechnology, College of Veterinary Medicine, 2015
12. Ueda M, A novel approach for skin rejuvenation by regenerative medicine: delivery of stem cellderived Growth Factors through an iontophoretic system, Int J Oral Maxillofac Implants, 2014
13. Lindeboom J A., Mathura K R et al., Influence of the application of platelet-enriched plasma in oral mucosal wound healing, Clin. Oral. Implants Res, 2007
14. Lacci K M, Dardik A, Platelet-rich plasma: Support for its use in wound healing, Yale J. Biol. Med, 2010
15. Barrientos S et al., Growth factors and cytokines in wound healing, Wound Repair Regen, Sept 2008 <https://www.ncbi.nlm.nih.gov/pubmed/19128254>
16. Kimball’s Biology Pages, Cell Membranes, January 2009 <https://web.archive.org/ web/20090125224255/http://users.rcn.com/jkimball.ma.ultranet/BiologyPages/C/CellMembranes. html> 17. Aldag C et al., Skin rejuvenation using cosmetic products contaiing growth factors, cytokines and matrikines: a review of literature, Clin Comset Investig Dermatol, November 2016 18. Lyons A et al., A randomised, double-blind, placebo-controlled, split-face study of the efficacy of topical epidermal growth factor for the treatment of melasma, Journal of Drugs in Dermatology, September 2018 19. Garza L et al., Bald scalp in men with androgenetic alopecia retains hair follicle stem cells but lacks CD200-rich and CD34-positive hair follicle progenitor cells, Journal of Clinical Investigation, November 2010 20. Isaza P et al., Use of growth Factors for Vulvo/Vagiinal Bio-Stimulation, Surgical Technology International, May 2019
21. Tallquist M, Kazlauskas A, PDGF signaling in cells and mice, Cytokine & growth factor reviews, 2004 22. Mayoral F, Kenner J, Draelos Z, The skin health and beauty pyramid: A clinically based guide to selecting topical skincare products, Journal of Drugs in Dermatology, April 2014
23. Hilling C, Human growth factors as natural healers: current literature application, April 2013 <https:// www.cosmeticsandtoiletries.com/formulating/function/active/premium-Human-Growth-Factors-asNatural-Healers-Current-Literature-and-Application-204553091.html#targetText=The%20FDA%20 allows%20the%20use,cosmetics%20in%20the%20European%20Union.>
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Figure 1: The pyramid of skin ingredients22 STEM CELL CYTOKINES & GROWTH FACTORS Stimulation RETINOIDS & AHAS Moisturisation, Exfoliation & Cell Turnover STEM CELL CYTOKINES & GROWTH FACTORS Protection & Repair FUNDAMENTAL TRANSFORM OPTIMISE
Growth factors can also be applied following invasive treatment and within bespoke facials to aid in skin healing











Get in touch to find out more about becoming a stockist and all about the new product launches! 0800
322
heliocare.co.uk Nothing protects
like Heliocare 360°
0195
info@aestheticare.co.uk
skin
Exclusive UK and Ireland distributor NEW @AesthetiCareUK
Heliocare 360° provides daily protection against UVA, UVB, visible light and infrared-A. The award-winning range protects skin at its surface and defends skin from within with clinically proven anti-oxidant, Fernblock® plus DNA repair enzymes. With a choice of beautiful formulations, every one of your clients will find a Heliocare 360° product they’ll love to use every day. The Water Gel is the latest addition to the family, providing intense hydration with a barely-there matte finish.
Rosacea is a treatable yet incurable common chronic inflammatory skin condition.1 Many aesthetic treatments including medical grade skincare,2 chemical peels3 and laser treatments4 can improve the skin redness and visible blood vessels that are associated with the concern. With this in mind, rosacea patients are often seen within aesthetic practice. Ocular involvement can occur in 58-72% of rosacea patients.5,6 With rosacea being a common disease particularly amongst Caucasians; with a prevalence of up to 22% in some populations,7,8 this amounts to a significant number of people being affected. This article aims to help practitioners understand the nature of ocular rosacea, the eye conditions that it can cause, and what treatments are available.
What is ocular rosacea?
Rosacea can be split into four subtypes: erythematotelangiectatic, papulopustular, phymatous and ocular (Table 1).9 Ocular rosacea is a subtype of rosacea that presents around the periorbital region and can lead to sight-threatening complications,10 which can usually be avoided with prompt recognition of the condition and referral to an ophthalmologist. Aesthetic practitioners may be the first point of contact for rosacea patients, so knowing the signs and symptoms
of ocular involvement is important as they may be able to help patients seek specialist advice in a timely manner. The exact pathological mechanisms of rosacea remain poorly understood, although several studies indicate that an inflammatory response is involved.11-16 Ocular rosacea results in inflammation of the eyelids and the ocular surface itself.17,18 Studies analysing the tears of patients with ocular rosacea have found increased levels of pro-inflammatory cytokines such as interleukin 1α & β and metalloproteinase-8 and 9.11-14 Patients with ocular rosacea may complain of symptoms including: eye irritation, foreign body sensation, stinging or burning sensation, sensitivity to light, watering of the eyes and blurriness of vision.18 Symptoms can range in severity and often patients with ocular rosacea will also present with other subtypes. However, no correlation has been found between the severity of the ocular disease and facial rosacea.19
Presentation of ocular rosacea
Ocular rosacea can affect the eyelids as well as the ocular surface, resulting in blepharitis, conjunctivitis or even corneal involvement in more severe cases.
Blepharitis
Blepharitis, or inflammation of the eyelid margin, can occur with ocular rosacea.20 You may notice that the eyelid margin and along the lash line looks red. The skin can become thickened and there may be telangiectatic blood vessels. Meibomitis is a type of blepharitis typically affected in rosacea and occurs when inflammation is located specifically to the meibomian glands on the posterior edge of the lid margin. This is different to anterior blepharitis which results in build-up of debris and bacteria along the base of the eyelashes. The meibomian glands (also known as tarsal glands) within the eyelid, secrete the oily part of our tear film. When they become inflamed or blocked this can result in a swelling known as a chalazion or ‘stye’.21 These glands are often involved in ocular rosacea.20,21 As the meibum (the oily part of the tear film) is not properly secreted in patients with meibomitis, the tears evaporate more easily, leading to dry eye disease. Patients experience ocular irritation as a result, and it can lead to the surface of the eye becoming inflamed or damaged. It can also lead to redness of the surface of the eye.
The mainstay of managing meibomitis is different to anterior blepharitis and involves conservative treatment such as lid hygiene, which involves applying hot compresses to the lids followed by massaging the eyelids.19 The aim of this treatment is to use heat to liquify the stagnant secretions in the glands, before massaging the lids to express these secretions to the tear film.
It has been found that this treatment improves the tear film stability and reduces the damage to the ocular surface.22,23
Conjunctivitis
Inflammation of the eyelids and poor tear film quality can lead to inflammation of the conjunctiva, the thin transparent layer that covers the inner surface of the eyelids and the sclera (white of the eye). When this layer of tissue becomes inflamed, this is called conjunctivitis.24,25 Practitioners may notice that the white of the eye looks red

Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
and Subtype Characteristics Subtype 1 Erythematotelangiectatic • Flushing • Telangiectasia • Facial Erythema Subtype 2 Papulopustular • Papules • Pustules • Facial erythema Subtype 3 Phymatous • Thickening of the skin • Irregular skin surface Subtype 4 Ocular Eye symptoms • Eye irritation • Photophobia • Blurred vision • Red eyes • Watering eyes Table 1: The four subtypes of rosacea9
Ocular Rosacea Ophthalmologist Miss Jennifer Doyle explores the diagnosis and treatment of ocular rosacea
Understanding
sore. In patients with rosacea, this can become chronic, resulting in longstanding sore and red eyes.25 Inflammation of the conjunctiva is thought to be due to dryness of the ocular surface, along with the underlying inflammatory response that is believed to relate to the disease process of rosacea, as mentioned above.24
Dry eye drops, also known as lubricating eye drops, are often the first treatment approach and can help to protect the ocular surface.23 For flare-ups of conjunctivitis related to rosacea, topical steroid eye drops can be used temporarily to settle the inflammation.24 These should
only be used under the supervision of an ophthalmologist and only for short-term therapy, as they can cause problems such as increased pressure within the eye and cataract.25
Corneal involvement
In more severe cases, ocular rosacea can affect the cornea. The cornea (shown in Figure 1) is the clear window at the front of the eye, which is in front of the iris or coloured part of the eye. When the cornea becomes inflamed, this is called keratitis. As the cornea is the clear window that we see out of, if this area becomes affected, it can result in a reduction of vision. It is thought that up to one third of patients with rosacea have corneal involvement at some stage of their disease.5,26 This normally starts in the top layer of the cornea, the epithelium, resulting in a superficial punctate keratitis. Once this barrier is breached, it can lead to deeper layers of the cornea becoming involved and corneal ulcers and vascularisation can occur.19 In these cases, as well as topical and conservative treatments, oral therapeutics may be recommended. Oral tetracyclines such as doxycycline not only have an antibacterial effect, but also have an immunomodulatory effect.27,28,29 They have been shown to reduce the expression of MMPs,28 which as mentioned, are thought to play a proinflammatory role within rosacea. A typical regimen that may be used would be 100mg doxycycline taken once a day orally for a threemonth period.30 It must be noted that advice or referral to a specialist in this field should be sought before offering treatment.

Other considerations
It is important to remember that suffering with a chronic disease like rosacea can take its toll psychologically, affecting the patient’s quality of life and having socioeconomic impacts.31 As the disease primarily affects the skin of the face and the eyes, it is easily visible to others and difficult to hide. Whilst the skin complaints affect a person cosmetically, it is important to remember that the ocular effects can, in severe cases, result in sight loss.10 It has been reported that up to a third of patients with ocular rosacea have potentially sight threatening corneal findings.10 I recommend that if any rosacea patient describes any symptoms or exhibit any signs of ocular involvement, practitioners advise them to seek specialist input from an ophthalmologist. For mild and non-acute cases, a local optometrist (optician) may be a good first point of call. They can examine the eyelids and ocular surface, and in mild cases of blepharitis they can advise patients on conservative treatments such as lid hygiene, and can recommend and supply lubricating eye drops. Optometrists can also check for signs of more severe disease and arrange referral to an ophthalmologist if necessary. If practitioners are worried about a patient presenting with severe acute eye symptoms, knowing the referral pathways to the local eye casualty service for advice and assessment is important. Catching the ocular disease early and arranging for the patient to have education and guidance on how to manage it can mean avoiding the more severe complications later down the line.
Summary
Rosacea can affect the eyes as well as the skin, and can result in complications affecting vision. It affects the eyelids and ocular surface including the conjunctiva and cornea. Symptoms and signs you may notice are irritation of the eyes, and redness of the eyes or eyelids. If you do identify a patient with ocular involvement, referring them to an optometrist or ophthalmologist as appropriate can help prevent more serious
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Cornea Optic disc (blind spot) Vitreous body (filled with vitreous humour) Pupil Lens Iris Sclera Posterior chamber Suspensory ligaments Ciliary body and muscle Medial rectus muscle Lateral rectus muscle Eye lid Lacrimal caruncle Tear duct Retina Choroid Sclera Optic nerve and retinal blood vessels Anterior chamber (filled with aqueos humor) Figure
eye32 Aqueous layer Mucous layer Lipid layer Tear film Studies analysing the tears of patients
ocular rosacea have found increased levels of pro-inflammatory cytokines such as interleukin 1α
and metalloproteinase-8 and 9
ocular disease.
2: The anatomy of the
with
& ß
Miss Jennifer Doyle has a Bachelor in Medicine and a Bachelor of Surgery with distinction, as well as a Master’s in Medical Sciences from the University of Oxford. She has completed the Level 7 in Injectables and is a lead trainer at Harley Academy. Miss Doyle currently works as an NHS registrar in ophthalmology, as well as leading her clinic, Oxford Aesthetics.

REFERENCES
1. Trebing D. (2014) Ocular Rosacea. In: Zouboulis C., Katsambas A., Kligman A. (eds) Pathogenesis and Treatment of Acne and Rosacea. Springer, Berlin, Heidelberg
2. Aaron F Cohen, Jeffrey D Tiemstra. Diagnosis and treatment of rosacea. The Journal of the American Board of Family Practice May 2002, 15 (3) 214-217
3. Michael S Kaminer MD, Kenneth A Arndt. et al. Atlas of Cosmetic surgery. (2008) Page 124
4. Michelle T Pelle MD, Glen H Crawford MD, William D James MD. Rosecea: II. Therapy. Journal of the American Academy of dermatology. Volume 51, Issue 4, October 2004, Pages 499-512
5. Starr PA, McDonald A. Oculocutaneous aspects of rosacea. Proc R Soc Med. 1969; 62(1):9-11. 2.
6. Bakar O, Demircay Z, Toker E, Cakir S. Ocular signs, symptoms and tear function tests of papulopustular rosacea patients receiving azithromycin. J Eur Acad Dermatol Venereol. 2009;23(5):544-9
7. van Zuuren EJ. (2017) Rosacea. New England Journal of Medicine. 377(18):1754–64.
8. Spoendlin J, Voegel JJ, Jick SS, Meier CR. (2012) A study on the epidemiology of rosacea in the U.K. British Journal of Dermatology. 167(3):598–605.
9. Wilkin J, Dahl M, Detmar M, Drake L, Liang MH, Odom R, Powell F (2004). “Standard grading system for rosacea: report of the National Rosacea Society Expert Committee on the classification and staging of rosacea” (PDF). J Am Acad Dermatol. 50 (6): 907–12. doi:10.1016/j.jaad.2004.01.048
10. Ghanem VC, Mehra N, Wong S, Mannis MJ. The prevalence of ocular signs in acne rosacea: comparing patients from ophthalmology and dermatology clinics. Cornea. 2003;22(3):230–233.
11. Afonso AA, Sobrin L, Monroy DC, Selzer M, Lokeshwar B, Pflugfelder SC. Tear fluid gelatinase B activity correlates with IL-1alfa concentration and fluorescein clearance in ocular rosacea. Invest Ophthalmol Vis Sci. 1999;40(11):2506-12. 20.
12. Barton K, Monroy CD, Nava A, Pflugfelder SC. Inflammatory cytokines in tears of patients with ocular rosacea. Ophthalmology. 1997;104(11):1868-74. 21.
13. Sobrin L, Liu Z, Monroy DC, Solomon A, Slezer MG, Lokeshwar BL, et al. Regulation of MMP-9 activity in human tear fuid and corneal epithelial culture supernatant. Invest Ophthalmol Vis Sci. 2000;41(7):1703-9.
14. Määttä M, Kari O, Tervahartiala T, Peltonen S, Kari M, Saari M, et al. Tear fluid levels of MMP-8 are elevated in ocular rosacea - treatment effect of oral doxycycline. Graefe’s Arch Clin Exp Ophthalmol. 2006;244(8):957-62. 23.
15. Yamasaki K, Kanada K, Macleod D, Borkowski AW, Morizane, S, Nakatsuji T, et al. TLR2 expression is increased in rosacea and stimulates enhanced serine protease production by keratinocytes. J Invest Dermatol. 2011;131(3):688-97. 24.
16. Pisella PJ, Brignole F, Debbasch C, Lozato A, Creuzot-Garcher C, Bara J, et al. Flow cytometric analysis of conjunctival epithelium in ocular rosacea and keratoconjunctivitis sicca. Ophthalmology. 2000;107(10):1841-9.
17. Bron AJ, Tiffany JM, The contribution of meibomian disease to dry eye, Ocul Surf, 2004;2:149–65.
18. R Amamurthi S, Rahman AQ, Dutton GN, et al., Pathogenesis, clinical features, and management of recurrent corneal erosions, Eye, 2006;20:635–44.
19. Mikkelsen CS, Holmgren HR, Kjellman P, et al. Rosacea: A Clinical Review. Dermatol Reports. 2016;8(1):6387. Published 2016 Jun 23. doi:10.4081/dr.2016.6387
20. Taliana Freitas Bernardes & Adriana Alvim Bonfioli (2010) Blepharitis, Seminars in Ophthalmology, 25:3, 79-83
21. Geerling G, Tauber J, Baudouin C, et al. The international workshop on meibomian gland dysfunction: report of the subcommittee on management and treatment of meibomian gland dysfunction. Invest Ophthalmol Vis Sci. 2011;52(4):2050-64. Published 2011 Mar 30. doi:10.1167/iovs.10-6997g
22. Matsumoto Y, Dogru M, Goto E, et al. Efficacy of a new warm moist air device on tear functions of patients with simple meibomian gland dysfunction. Cornea. 2006;25:644–650
23. TFOS International Dry Eye Workshop (DEWS II) The Ocular Surface Volume 15, Issue 3, Pages A1A10, 269-650 (July 2017)
24. Örnek N, Karabulut AA, Örnek K, Onaran Z, Usta G. Corneal and conjunctival sensitivity in rosacea patients. Saudi J Ophthalmol. 2015;30(1):29-32.
25. Butcher JM, Austin M, McGalliard J, Bourke RD. Bilateral cataracts and glaucoma induced by long term use of steroid eye drops. BMJ. 1994;309(6946):43.
26. Ghanem VC, Mehra N, Wong S, Mannis MJ. The prevalence of ocular signs in acne rosacea: comparing patients from ophthalmology and dermatology clinics. Cornea. 2003;22(3):230-3
27. Quarterman MJ, Johnson DW, Abele DC, Lesher JL Jr, Casco DS, Davis LS. Ocular rosacea. Signs, symptoms, and tear studies before and after treatment with doxycycline. Arch Dermatol. 1997;133(1):49-54. Comment in: Arch Dermatol. 1997; 133(1):89-90. 61.
28. Odom R, Dahi M, Dover J, Draelos Z, Drake L, Macsal M, Powell F, Thiboutot D, Webster GF, Wilkin J; National Rosacea Society Expert Committee on the Classification and Staging of Rosacea. Standard management options for rosacea, part 2: options according to rosacea subtype. Cutis. 2009;84(2):97104
29. Sapadin AN, Fleischmajer R. Tetracyclines: non-antibiotic properties and their clinical implications. J Am Acad Dermatol. 2006;54:258–265
30. Valentín S, Morales A, Sánchez JL, Rivera A. Safety and efficacy of doxycycline in the treatment of rosacea. Clin Cosmet Investig Dermatol. 2009;2:129–140. Published 2009 Aug 12.
31. Silva D, Tavares C, Santos L, Alves M, Franca A. Rosecea: Quality of life and ocular evaluation in a Latin population: 7494. Journal of the American Academy of Dermatology. 79(3):AB249, Sept 2018.

32. NHS, Moorfields, Anatomy of the eye, 2019. <https://www.moorfields.nhs.uk/content/anatomy-eye>

@aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
CONCERNED ABOUT TAKING CLINICAL PICTURES ON YOUR PHONE WITH THEIR LEGAL CONSEQUENCES? www.clinicalcam.com “Clinical Cam” allows you take pictures safely Get “Clinical Cam” on







Treating Strabismus with Toxin
Consultant ophthalmic
There is widespread awareness of the use of botulinum toxin as an antiageing treatment, but it is a lesser-known fact that it can also be an excellent treatment for misalignment of the eyes, known as strabismus. Adults with strabismus (commonly referred to as squint) suffer clinically significant levels of depression and anxiety; higher than those with other chronic illnesses such as diabetes and rheumatoid arthritis. Patients undergoing corrective restoration of eye alignment report significantly better quality of life on both functional and psychosocial scores after treatment.1-6
In some cases, surgery is not possible or patient preference is towards a less-invasive treatment. In the majority of cases, botulinum toxin to the extraocular muscles provides an alternative treatment.7-10 This article aims to highlight how effective treatment with botulinum toxin A (BoNT-A) can be in adult strabismus and increase awareness of its benefit for this condition, which can have debilitating functional and emotional consequences. It is important to note here that this treatment is highly specialised and should only be performed by strabismus surgeon specialists. I do believe that it is important, however, that aesthetic practitioners are aware of the condition as patients may present or discuss it amongst their aesthetic concerns in clinic. Knowing when to appropriately refer patients on for treatment of strabismus is imperative.
Presentation of
strabismus
Strabismus is a condition where the two eyes are not correctly aligned and one eye is deviated. Approximately 4% of the adult population are affected by strabismus and it is a common misconception that nothing can be done for this condition in adulthood.11
The eyes can be misaligned horizontally with an esotropia, where the eye turns in, and exotropia, where the eye turns out. They can also be vertically misaligned with one eye sitting higher (hypertropia) or lower (hypotropia) than the other. Rarely, the eyes experience rotational misalignment (torsional strabismus).11 The severity of the squint can vary on eye movement and in different directions of gaze.
Strabismus may be present from birth or arise at any time in life. Some adults will have had squints as children that were not corrected, and others may have had surgery, but the squint has recurred in later life. Some adults may even have no childhood history of a squint, but the control over eye movement has become more difficult over time and the squint becomes evident (decompensated phorias).11
Frequently, no actual cause is identified, although there are a number of different medical and neurological conditions that can give rise to squints in adulthood. These include orbital, cranial nerve palsies or muscular conditions. Direct ocular trauma and head injury can also cause squints.11
Psychosocial and economic impact of strabismus
If the squint is uncorrected, the effects on visual function can include double vision, visual confusion, loss of stereopsis (3D vision) and the inability to use the two eyes together.11 This can result in loss of independence, inability to drive, increased risk of falls and decline in workplace performance. Psychosocial difficulties that may also be encountered include low self-esteem, anxiety and depression, reduced quality of life, poor employment opportunities and discrimination.11 Studies have shown strabismus to have a debilitating effect on a person’s quality of life, mood, independence and livelihood. It has also been shown that employers are likely to discriminate against those with a squint compared to straight-eyed individuals. Studies in children have shown that as early as six years old, children show a significant preference for straight-eyed individuals in preference to those with a squint.11
Treatment of strabismus
The most frequent intervention in the long-term management of strabismus remains to be surgery. It is recognised, however, that in some patients, surgery may be technically difficult or impossible. Some patients prefer to undergo a less invasive procedure with little disruption to daily life. In these cases, botulinum toxin provides a safe and suitable alternative to surgery.11
The first use of botulinum toxin in the treatment of strabismus was in the mid 1970s by US-based ophthalmologist Mr Alan Scott, who was the first to pioneer work in the use of BoNT-A for strabismus. He published his initial work on the benefit in monkeys with induced strabismus in 1973 and the first success in human strabismus in 1979. Scott also led the way in its subsequent use in the aesthetic industry as it was noted that patients being treated for hemifacial and blepharospasm reported improvement in their wrinkles and migraines. The widespread use of BoNT-A in the aesthetic industry today, owes it legacy to the pioneering work of Scott in ophthalmology. Ophthalmologist Mr John Lee visited Scott in 1982 and introduced it in to the UK by setting up the first BoNT-A clinic for strabismus in 1984, at Moorfields Eye Hospital in London.12
From my observations, between 50-65 BoNT-A injections for strabismus are given in the two clinics that run at Moorfields on a weekly basis, likely more than anywhere else in the world. Much work has been done and published on the indications of BoNT-A in strabismus. Its effects are beneficial in a range of different squints. Those that have been shown to benefit include:
• Deviations as a consequence of previous childhood squint, consecutive or residual deviations13
• Deviations as a result of poor eyesight – sensory or secondary deviations14
• Intermittent deviations with poor ability to keep the eyes straight (reduced fusion)15-17
• Cranial nerve palsies (third, fourth, sixth)18-21
• Squints as a result of other ocular surgery22,23
• Congenital squints, such as Duane syndrome24
• Small angle squints25
• Complex pathologies such as chronic progressive external ophthalmoplegia, thyroid eye disease and myasthenia gravis12
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
surgeon Miss Joanne Hancox details the use of botulinum toxin in the treatment of eye squints
BoNT-A mechanism of action
The mechanism of action in treating squints with BoNT-A is the same that occurs when treating other muscles in the body, but the doses are much smaller. This ranges from 1-5 units depending on the centre. After the initial work done by Mr Lee at Moorfields the dose given is consistently 2.5 units in 0.1ml, compared to the typical single dose of 20 units that may be injected into a forehead. The BoNT-A causes a blockade at the neuromuscular junction of the chosen extraocular muscle that has been injected.12 It is not the intention to paralyse the muscle completely as this would affect the motility of the eye. The desired effect is a weakening of the injected muscle such that the eyes are able to take up normal alignment, with little or no effect on eye movement. The paralysis should not be excessive, such that the injected muscle is limited in its direction of action and the eye is unable to move normally. No effect is seen for two days and then weakening of the affected muscle is observed. The maximum effect occurs two weeks following the injection of the toxin. After reaching a peak at two weeks following the injection, the effect gradually wears off over the following three to four months. Some patients, however, find much longer-term benefit.
The injection of BoNT-A into the extraocular muscles is an extremely skilled procedure and, as mentioned above, can only be performed by a trained strabismus surgeon specialist. This is due to the fact that the muscles are not visible when viewing the eyeball and an injection given too deeply could penetrate into the eye, through the sclera and result in permanent sight loss.12
For a safe, low-risk procedure, all injections are performed under electromyography (EMG) guidance. During the preparation for the procedure, anaesthetic drops are applied to the surface of the eye and electrodes are attached to the forehead above the eye that is to be injected.
The BoNT-A needles are pre-loaded and attached to a further electrode. When these electrodes are plugged into the EMG machine, they complete a circuit. Once it has been confirmed that the patient is comfortable and cannot feel any discomfort, they are first asked to look away, then back into the direction of the muscle that requires the injection. This movement gives a signal when the appropriate muscle is firing. This signal confirms the correct presence of the needle in the muscle and the BoNT-A is only injected when a suitably strong signal is detected. This minimises the risk of complications.
Patients are reviewed again two weeks following the procedure, where a top-up injection can be given if the effect was only partial. A further appointment is made for three to four months where the patient can discuss if they found the treatment useful and wish to proceed with a further injection. There is no limit to the number of injections that can be performed over time. Studies have shown that with long-term BoNT-A use, the average angle of the strabismus decreases significantly over time and the frequency of required injections decreases.12,25 Patients who have had multiple injections over time have demonstrated much higher quality of life (QoL) scores than new adult patients with squints. Following the toxin injection, their QoL score compared favourably with straight-eyed controls.25
Considerations
Potential complications that can occur are ptosis, leakage of the toxin to the levator muscle of the lid, or unwanted ocular deviations due to leakage to the other extraocular muscles. The potential for this is reduced by leaving the injection in situ for 30 seconds before
removing the needle.12 Occasionally, bleeding on the surface of the eye (subconjunctival haemorrhage) or bruising around the eye can occur, but the effects are temporary. The serious risk of the needle penetrating the eye (globe perforation) is extremely rare and occurs in about 1 in 10,000 cases.12
Conclusion
It’s important for aesthetic practitioners to be aware of the treatments available for strabismus as, in the majority of cases, there is no need for adults to remain untreated and suffer the functional and emotional consequences. Long-term injections with BoNT-A is a good treatment approach for maintaining ocular alignment. It is a convenient and straightforward procedure that takes only minutes to perform, with excellent benefits in improved ocular alignment. Treatment provides the potential to correct strabismus in cases where surgery would not be possible and where the patient finds it preferable to surgery.
Miss Joanne Hancox is a consultant ophthalmologist specialising in complex adult and paediatric strabismus, with extensive experience in botulinum toxin injections. She is strabismus service director and North Thames training programme director. She also has a Psychology BSc allowing her better understanding of the functional, psychological and emotional consequences of her patients.
REFERENCES
1. McBain HB, MacKenzie KA, Au C, et al Factors associated with quality of life and mood in adults with strabismus British Journal of Ophthalmology 2014;98:550-555.
2. Marsh IB. We need to pay heed to the psychosocial aspects of strabismus. Eye (Lond) 2015;29(2):238–240. doi:10.1038/eye.2014.283
3. Hatt S.R., Leske D.A., Kirgis P.A., et al: The effects of strabismus on quality of life in adults. Am J Ophthalmol 2007; 144: pp. 643-647
4. Hatt S.R., Leske D.A., Bradley E.A., et al: Development of a quality-of-life questionnaire for adults with strabismus. Ophthalmology 2009; 116: pp. 139-144

5. Hatt S.R., Leske D.A., and Holmes J.M.: Responsiveness of health-related quality-of-life questionnaires in adults undergoing strabismus surgery. Ophthalmology 2010; 117: pp. 2322-2328
6. Durnian J.M., Owen M.E., Baddon A.C., et al: The psychosocial effects of strabismus: Effect of patient demographics on the AS-20 score. J AAPOS 2010; 14: pp. 469-471
7. Crouch ER. Use of botulinum toxin in strabismus. Current Opinion in Ophthalmology2006;17(5):435-40.
8. Marsh IB. Botulinum toxin and the eye. Hospital Medicine 2003;64(8):464-7.
9. Rayner SA, Hollick EJ, Lee JP. Botulinum toxin in childhood strabismus. Strabismus1999;7(2):103-11.
10. Scott AB. Botulinum toxin injection into extraocular muscles as an alternative to strabismus surgery. Ophthalmology 1980;87(10):1044-9.
11. Commissioning Guidance Strabismus surgery for adults in the United Kingdom: indications, evidence base and benefits RCOphth 2017 Adit Das, Joanne Hancox
12. Monheit g, Richett A, Abobotulinum toxinA: A 25 year history Aesthet Surg J 2017 May;37(suppl1): S4-S11
13. Gardener R, Dawson E, Adams G, Lee JLong-term management of strabismus with multiple repeated injections of Botulinum toxin J AAPOS 2008;12:569-575
14. Dawson EL, Sainani A, Lee JP. Does botulinum toxin have a role in the treatment of secondary strabismus?. Strabismus 2005;13(2):71-3.
15. Etezad Razavi M, Sharifi M, Armanfar F. Efficacy of botulinum toxin in the treatment of intermittent exotropia. Strabismus 2014;22(4):176-81.
16. Carruthers JD, Kennedy RA, Bagaric D. Botulinum versus adjustable suture surgery in the treatment of horizontal misalignment in adult patients lacking fusion. Archives of Ophthalmology 1990;108(10):1432-5.
17. Spencer RF, Tucker MG, Choi RY, McNeer KW. Botulinum toxin management of childhood intermittent exotropia. Ophthalmology 1997;104(11):1762-7.
18. Sanjari MS, Falavarjani KG, Kashkouli MB, Aghai GH, Nojomi M, Rostami H. Botulinum toxin injection with and without electromyographic assistance for treatment of abducens nerve palsy: a pilot study. Journal of AAPOS 2008;12(3):259-62.
19. Saad N, Lee J, the role of botulinum toxin in third nerve palsy Aust N Z J Ophthalmol 1992 20(2): 121-7
20. Garnham, Lawson, O’Neill, Lee Botulinum toxin in 4th nerve palsies Aust & NZ J Ophthalmol.25.31-5. 1997
21. Metz HS, Mazow M, Botulinum toxin treatment of acute sixth and third nerve palsies Graefes Arch Clin Exp Ophthamol 1988;226(2):141-4
22. Gardner R, Dawson EL, Adams GG, Lee JP. The use of botulinum toxin to treat strabismus following retinal detachment surgery. Strabismus 2013;21(1):8-12.
23. Bunting HJ, Dawson EL, Lee JP, Adams GG. Role of inferior rectus botulinum toxin injection in vertical strabismus resulting from orbital pathology. Strabismus 2013;21(3):165-8.
24. Dawson, Maino, Lee Diagnositic use of botulinum toxin in patients with Duanes’ syndrome Strabismus 2010:18(1) 21-2325. Dawson EL, Lee JP. Does botulinum toxin have a role in the treatment of small-angle esotropia?. Strabismus 2004;12(4):257-60.
25. Hancox J, Sharma S, MacKenzie K, Adams G. The effect on quality of life of long-term botulinum toxin A injections to maintain ocular alignment in adult patients with strabismus. Br J Ophthalmol. 2012 Jun;96(6):838-40
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com





introducing the neXT generation of HydraFacial™ MD Elite™ THE ELITE™ IS THE brand new HYDRFACIAL SYSTEM WITH unique ADVANCEMENTS TO ENSURE YOUR SUCCESS. With an enhanced user interface, LED light therapy, mechanical lymphatic drainage and a Perk delivery switch as standard... Personalised skin health has never been easier. for more information on the brand new elite: Tel: 01788 572 007 email: info@hydrateyourbusiness.co.uk HydraFacial UK is now a direct business and part of the global HydraFacial Companybringing you the same high level of customer service, combined with the benefits of greater brand visibility, more investment and the increased support that comes from being part of world wide business.
A summary of the latest clinical studies
Title: Analysis of U.S. Food and Drug Administration Data on Soft-Tissue Filler Complications
Authors: Ortiz AE et al
Published: Dermatologic Surgery, October 2019
Keywords: Complications, Dermal fillers, FDA
Abstract: The authors conducted a search of adverse events within the U.S. Food and Drug Administration database that involved injectable dermal fillers for soft-tissue augmentation from June 1993 to August 2014. Search terms included generic and trade names of commercially available soft-tissue fillers. Three thousand seven hundred eighty-two complications involving dermal fillers were identified in the MAUDE database. Forty-four percent of complications implicated hyaluronic acid fillers, 40% involved poly-L-lactic acid fillers, 15% complications included calcium hydroxylapatite fillers, and <1% complications arose from polymethylmethacrylate fillers. Common adverse events included lumps, infection, allergic reaction, ischemia, and swelling. Rare events included trigger of autoimmune reactions, visual disturbances, and stroke.
Title:
The Impact of Perceived Stress on Skin Ageing
Authors: CM Lee, REB Watson, CE Kleyn


Published: European Academy of Dermatology and Venereology, September 2019
Keywords: Stress, Ageing, Psychology
Abstract: Skin ageing can be divided according to phenotypical features into intrinsic (by the passage of time) and extrinsic (with the addition of the effects of environmental factors). Photoageing is by far the most researched factor of extrinsic ageing but the additional impact of other factors such as cigarette smoking and exposure to air pollution ought to be taken into account. One of the least researched topics in relation to extrinsic skin ageing is the impact of psychological stress. A contemporary review of response of human skin to stress describes the molecular mechanisms of extrinsic skin ageing, but has fallen short of explaining resilience to stress exhibited by people. Mechanisms to regulate gene expression, define cellular identity and promote functionality are responsible for the adaptive response to stressful events. Conversely, maladaptive response of human tissues to chronic stress appears to have an impact on gene regulation. Epigenetics is the study of heritable changes in organisms due to modifications in gene activity and expression, as opposed to the genetic code (DNA genome). Chronic stress appears to be an important factor in determining an individual’s vulnerability to ageing and age-related comorbidities via epigenetic modifications. Forerunners in epigenetic research recognized the necessity of a reliable biomarker in order to develop a better understanding of the role of epigenomics in ageing. Genomic DNA methylation patterns (DNAm) appear to be valuable in age prediction but variability in specificity exists across species of mammals, human races and tissues. Neuroscience research appears to be leading the way in epigenomics whilst the lack of a valid and reliable DNAm-associated age predictor compatible with human skin tissue hinders research endeavours for the epigenetics of skin ageing.
Title: Association of Lifetime Indoor Tanning and Subsequent Risk of Cutaneous Squamous Cell Carcinoma
Authors: Lergenmuller S et al.
Published: JAMA Dermatology, October 2019
Keywords: Skin cancer, Indoor tanning
Abstract: The objective of this study was to investigate the doseresponse association between lifetime indoor tanning and SCC risk, the association between duration of use and age at initiation with SCC risk, and the association between age at initiation and age at diagnosis. This cohort study included data from women born from 1927 to 1963 from the Norwegian Women and Cancer study, established in 1991 with follow-up through December 31, 2015. Baseline questionnaires were issued to participants from 1991 to 2007, with follow-up questionnaires given every 5 to 7 years. A total of 159 ,419 women (mean [SD] age at inclusion, 49.9 [8.3] years) were included in the study. During follow-up (mean [SD], 16.5 [6.4] years), 597 women were diagnosed with SCC. Risk of SCC increased with increasing cumulative number of indoor tanning sessions. The adjusted hazard ratio (HR) for highest use vs never use was 1.83 (95% CI, 1.38-2.42; P < .001 for trend). A significantly higher risk of SCC was found among women with 10 years or less of use (HR, 1.41; 95% CI, 1.08-1.85) and more than 10 years of use (HR, 1.43; 95% CI, 1.161.76) and among women with age at initiation of 30 years or older (HR, 1.36; 95% CI, 1.11-1.67) and younger than 30 years (HR, 1.51; 95% CI, 1.18-1.92) vs never users. The findings provide supporting evidence that there is a dose-response association between indoor tanning and SCC risk among women. The association between cumulative exposure to indoor tanning and SCC risk was the same regardless of duration of use and age at initiation.
Title: Development of Botulinum Toxin A-Coated Microneedle for Treating Palmar Hyperhidrosis
Authors: Shim DH et al.
Published: Molecular Pharmaceutics, October 2019
Keywords: Botulinum toxin, Microneedling, Hyperhidrosis
Abstract: Hyperhidrosis is a disorder that produces excess amount of sweat. The botulinum neurotoxin A (BoNT/A) has been used to treat hyperhidrosis through multiple intradermal injections at the site of condition. However, due to its toxicity, it is important to precisely deliver the proper dose of toxin to the target site. In addition, the use of conventional hyperdermic needle for multiple injections in the palm makes the approach undesirable and painful. Here, we designed a BoNT/A-coated microneedle (BoNT-MN) array and tested its efficacy as a substitute pain-free method to treat hyperhidrosis. BoNT-MNs were prepared by coating BoNT/A formulation on polylactic acid microneedles and were found to successfully penetrate in vitro thick skin. The coating formulations were then tested for its stability at 4°C, 25°C, and 37°C for 24 h. BoNT-MNs were found to be much more stable than its liquid state. Additionally, we carried out in vivo experiments by treating the right paw of mice with BoNTMNs and found that the treatment induced a significant reduction of sweating response in the mouse’s foot pads. Thus, BoNT/A treatment with microneedles is beneficial and may be used as a more efficient and less painful approach to treat hyperhidrosis.
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Starting Pro Bono in Aesthetics
The phrase ‘pro bono’ is derived from the Latin term ‘pro bono publico’, which means ‘for the public good’.1 The term often refers to legal work that is performed voluntarily and free of charge for the benefit of society, however it is also a common term known in medicine for the same reasons. This article will explain how I got into charitable pro-bono work in aesthetics for victims of violence and provide my tips and considerations before embarking on this journey.
My approach
There are various ways one can go about doing pro bono work in aesthetics. However, I find that working with a local charity, discussed later, is a great
approach. Some clinics treat disfiguring skin concerns such birthmarks, moles and pigmentation,2 but the mainstay of my pro bono work involves scar revision. From a psychological and sociological perspective, improving a disfiguring mark on someone’s face can significantly improve not only their aesthetic, but also their lives. Individuals within our society negatively judge and stereotype facial scars, which has a knock-on effect on aspects of people’s lives, such as employment and relationships.3 For successfully embarking on this journey, I think the main factor practitioners need to consider is implementing a strong process and strategy.
Explore your motivations
Firstly, ask yourself, why are you doing this? I believe you should be doing it because you have a genuine desire to use your unique skill-set help other people and to make a difference in society. My motivation to deliver pro bono work to patients who have been victims of violence comes from a nursing background in mental health, dermatology and working with vulnerable groups. I love that I can use my skills to give back to those most in need.
Contact local charities and associations
I would advise anyone looking to get into pro bono work to reach out to your local charities to see if you can offer your expertise or services in any way. I have worked with a Scottish charity called Medics Against Violence for a long time. Its aims are to not only treat injuries and deal with the medical consequences of violence, but to also help to reduce the likelihood of violence in the community.3 Through this charity, as well as Scottish Criminal Justice and Strathclyde Police, my clinic has a referral system in place. Someone who has been injured by violence will go through the NHS for treatment, and when they are discharged, they will likely have a support worker through the criminal justice system and will be connected with local charities.
However, sometimes they need a bit of extra assistance, such as scar revision, which isn’t available on the NHS, and that is when I will receive a referral from Medics Against Violence to see if I can help. I find this referral pathway extremely valuable and very important when doing pro bono work so that you are never the person to determine who gets access to treatment.
When working with your referral partners, ensure that you discuss and make what you can deliver, what you can’t, and that the pathway for referral is very clear to all parties.
I recommend that you write a standard operating procedure so that there is a clear set of step-by-step instructions that you and your referral partner will follow to ensure that the patient journey is mapped out. Having this in writing means that all parties know what their role is, their expectations and that everything is open and transparent.
Get clinic partners involved
It’s a great idea to get your clinic suppliers and distributors on board. I work with HADerma, Sinclair Pharma, Kelo-Cote, Church Pharmacy and Beamwave Technologies
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
would advise anyone looking to get into pro bono work to reach out to your local charities to see if you can offer your expertise or services in any way
I
tips for successful pro
work
Nurse prescriber Frances Turner Traill provides her
bono
in aesthetics
who will often donate their products for free, while I will give my time for free so there is no actual cost to me or my business, apart from my time. To achieve something similar with your own distributors, I would recommend contacting them to see if they will support you. I think that it’s perhaps best to at first become established with your pro bono work before approaching partners later to seek support in order to really demonstrate that you are serious about it. When I approached my suppliers, I provided them with evidence of the scar revision work I had done before and supplied mini case studies, which included before and after photographs, information on exactly how I got the results and the products used. When you are having the initial conversations with your suppliers, I recommend discussing and agreeing upon the logistics of how you will get your stock for these treatments. Sometimes I will get stock in advance, but often I will buy the stock and have it in clinic and then claim the expenses back through the company if I use it for any pro bono case. A lot of this is based on trust and I find that as long as you are communicating well with your suppliers they can be very generous and it can work well.
Know your limitations and work with others
Have a very clear definition of who you can help and who you can’t. As with any medical practice, you should work to your limits and not exceed this. The patients I treat have usually already gone through a great deal and do not deserve to be met with unrealistic expectations. There have been several times where a patient has come in and I have told them that the scar is outside my scope of practice or expertise. So, I will refer them to a surgeon, who I know also works with the
same charity, as they will be able to help them more than I can – we work together for the best outcome of the patient. Saying that, another great way to get into pro bono work is to approach local specialists like maxillofacial surgeons and ask them if you can help them in any way.
Practical advice
Treat your pro bono patients just like any other; however, always bear in mind that these patients have likely been through a traumatic experience. You therefore need to be extra sensitive to their situation and remember that they are not your usual ‘well’ aesthetic patient who is presenting for elective aesthetic intervention. I also avoid asking the patient about their past or the situations behind how they received their scar so not to cause any upset. Often we get this background from our referral partner, or sometimes the patient is comfortable talking about it, but we don’t want to instigate this conversation.
I always get my pro bono patients in on a quieter day in the clinic, particularly if they are violence victims as they may be feeling quite vulnerable, so you don’t want them waiting in a busy clinic. I opt for a Tuesday morning as it’s usually a bit quieter for us. I also ensure that the staff that are working at the clinic that day are well-aware that a pro bono patient is coming in, and that they are educated on how to sensitively communicate with these patients. Much like when adding a new treatment to your portfolio, always check with your insurance provider that pro bono work can be covered by your policy.
Marketing considerations
In Vietnam, one clinic markets their charitable activities on their website and even has an entire sub-clinic and dedicated page on their
website devoted to pro bono work.2 I also know of many UK practitioners who advertise their pro bono work on social media. Personally, I don’t do any marketing or social media around this because I don’t want to encourage patients to seek my help outside of referrals from my charity partners. The clinic in Vietnam seems to screen patients themselves,2 but I think it would be very difficult to have the time and resources to screen these people myself and help everyone who approaches me. I would personally find it very hard to decline a selfreferred patient who couldn’t self-fund, so I don’t put myself in that position. I think care should be taken if you do choose to do any marketing on your pro bono work and ensure you have a well-thought-out strategy in place. Remember your motivations for offering treatment; I wouldn’t advise practitioners get into pro bono work purely for marketing purposes or to increase your image or profile. Personally I haven’t gone public with my pro bono work until now so that I could share my experiences with other clinicians who may be interested in giving back.
Summary
My experience with pro bono work in aesthetics has been truly rewarding. It’s a great feeling to know that you are giving back, contributing to society and having a direct impact on someone’s life. If you are thinking of giving your time and expertise for pro bono charitable work, ensure you have a clear strategy, work with relevant partners and know your limitations. Remember, the end goal is to improve the patient’s aesthetic outcome so that they can move on with their lives confidently.
Frances Turner Traill is an independent nurse prescriber who is the clinical director of FTT Skin Clinics with clinics in Inverness and Hamilton, Scotland. She was previously the Scottish board member of the BACN and has represented BACN on new regulation changes with Scottish government and Healthcare Improvement Scotland.

REFERENCES
1. Pro Bono at LSE Law <http://www.lse.ac.uk/law/probono>
2. SW1 Clinic, 2019. <https://sw1vietnam.com/en/story/pro-bono/>
3. Changing Faces, Statistics. <https://www.changingfaces.org.uk/ education/health/patient-needs/statistics>
4. Medics Against Violence. <http://medicsagainstviolence.co.uk/>
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
When working with your referral partners, ensure that you discuss and make what you can deliver, what you can’t, and that the pathway for referral is very clear to all parties
EVOLUTION OF A PATIENT & PRACTICE JOURNEY; INTEGRATING TOPICALS & LASER TO MAXIMISE SUCCESS

AN EXCLUSIVE TWO

The Symposium will feature world experts Dr Qu i b e ll, Dr Charlene Dehaven and leading I ndustry expe r t Miss Sherina Balaratnam who will joi n forces to educate and explore an integrative a p proach of LASER & TOPICALS across a range o f F A C E & BODY condi tions to demonstrate how to achieve the best clinical results and co m mercial outcomes.






DAY EVENT
FACE & BODY SYMPOSIUM FRI 22 - SAT 23 NOVEMBER THE KING’S FUND 11-13 Cavendish Square, London ENGAGE Meet like minded peers and industry experts to grow your network EXPAND Experience hands on demonstrations to help develop programs for your practice EXCEL Learn new sales and marketing strategies A Partnership Education In itiative from & T O B OO K YO UR P LACE VISIT WW WCYNOSUREAEX.EVE NTBRITE.CO.UK o r Visit www.harpa r grace.com/training or CALL 01628 522 25 2
MISS BALARATNAM DR QUIBELLDR DEHAVEN
them a uniform, including requests that are easily achievable. It is not fair to include items that are too expensive for an average employee’s budget or too hard to find. For example, it may be easy to find suitably smart work clothing in black or grey, but to state that your employees must wear clothing only in a specific shade of green that matches your clinic logo may be asking the impossible.
Key things to consider for your
Though you may ensure that your clinic interior remains at a comfortable temperature year-round, people generally opt for clothing that is fitting with the season, so consider this when drafting your dress code. For example, if you do not want your employees to wear strappy tops in summer, include this in your policy.
Health and safety concerns: Those who perform treatments or are present in a treatment room to assist or chaperone will need to follow guidelines for cleanliness, hygiene and safety. For example, you could state that every person present during a treatment must remove rings before sanitising their hands, to avoid the risk of cross-infection from microorganisms trapped under jewellery. If you provide a uniform for your team, ensure you provide garments of the right size and condition. Employees may need to be responsible for their own laundry, but they may not have the skills to alter or fix clothing. If you do not provide a uniform for all team members, make clear what clothing is acceptable. For example, instead of saying that you would like your patient coordinators to wear ‘business attire’, specify that they should wear a black, grey or navy skirt or trousers with a neutral-coloured shirt or blouse. While it is legally acceptable for an employer to ask their employees to pay for their own work attire, you must ensure that any uniform cost deducted from a worker’s pay does not take their remuneration below the National Minimum Wage or National Living Wage.1
in terms of beauty looks and fashion trends, what is popular and acceptable on the high street may not be the look you want your clinic employees to have. For example, pastel-coloured hair and creative nail art may be seen as fashionable, but they are not always likely to be seen as professional. Though it would be unreasonable to expect staff members to have a specific haircut, it is reasonable to ask your team to avoid extreme fashion styles. These rules can apply to male staff members too, as it is reasonable to require men to keep their facial hair neat and tidy.
Cleanliness and smartness: When drafting what employees should wear, consider including rules on how they should wear those items. It may be common sense that work attire should be immaculately clean, crisp and neat, but it is worth reaffirming that if clothing is not presentable, employees may be asked to change.
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019







Light Therapy Medically CE Marked and FDA Cleared The most globally recognized and awarded LED Enhance outcomes & patient satisfaction Use to heal following surgery and LASER Increase post-surgery comfort levels Speed healing, reduce down time Forms to treatment area PROFESSIONAL ENQUIRY: www.celluma.co.uk +44 (0) 203 981 3993 “We are very excited to be using Celluma LED light therapy for treating capsular contracture. This is a difficult issue to treat and in the early stages of our trial we are seeing encouraging evidence to support its role as a nonsurgical option for treating this debilitating issue.” - Mr. Adrian Richards, Consultant Plastic Surgeon and Medical Director The Private Clinic, London Harley Street, Northampton and Princes Risborough, Buckinghamshire CELLUMA in the UK MEDICALLY CE MARKED AND FDA CLEARED Acne • Skin care • Dermal wound healing • Decreasing inflammation • Increasing micro circulation • General pain • Muscle & joint pain • Muscle tension, spasm & stiffness PROUD AESTHETICS AWARDS SPONSOR: Celluma Best Clinic-London Award HONORED AESTHETICS AWARDS FINALIST: Most Innovative Product
In practice...
Hannah Betts, clinic manager at Health & Aesthetics, Surrey

At Health & Aesthetics, we have branded grey tunics with our logo embroidered on them. Aestheticians must wear their hair tied back and black shoes with black smart trousers. These tunics are specifically made for the aesthetics industry so are comfortable, easy to move around in, hard wearing and don’t even need ironing. This means the team look exceptionally smart and professional at all times and are comfortable when doing their treatments. Our reception team have silk tops and black suits. These silk tops match our branding and logo colour. We provide the tops when a member of the team joins and ask for them to find a suit which is comfortable from a select store which we reimburse them for. This way the member of staff has time to find a suit which fits them comfortably and can try on various sizes and styles. To ensure our policy is communicated effectively, we go through it when someone joins the team and is also a part of our employee handbook. As well as this, it is discussed with members on each appraisal to ensure any questions can be answered.
Discrimination and dress codes
The Equality Act 20102 is legislation that protects certain groups of people from discrimination in the workplace and in society, with ‘protected characteristics’ including gender, disability, religion and more.2 Your workplace dress code must not be discriminatory in respect of the protected characteristics, so should only include rules that apply to both men and women and include reasonable concessions for those with religious beliefs and the disabled. For example, in 2017, corporate reception firm Portico changed their dress code policy after an employee brought to public attention how she was sent home from work on no pay for contravening a dress code policy that was clearly gender-biased. The company subsequently removed clauses from their policy that insisted on female employees wearing high heels and make-up at all times.3
In 2013 the European Court of Human Rights ruled that a British Airways employee suffered discrimination at work over her Christian beliefs after she was asked to remove a crucifix necklace, which was not seen to interfere with her work duties.4
In an aesthetic clinic, the majority of your employees may be female, but you should still create a dress code that is not overtly discriminatory to either gender. Sometimes there are differences that should be recognised, though. For example, it could be seen as discriminatory to insist that female employees wear a short, tight skirt while male employees can wear comfortable

trousers, but your policy can include a clause on acceptable makeup, even if it does not apply to male employees. It is not considered discriminatory for an employer to ask an employee to cover tattoos or remove piercing jewellery when at work. Tattoos or body art are not included in the Equality Act 2010 as a ‘protected characteristic’.2
How to implement your dress code policy
When you recruit new team members, don’t assume they will know what you expect in terms of appearance. Make your dress code policy clear before their first day so they can start on the right note.
You may think it obvious that a certain standard is expected across the aesthetics industry, but a previous employer may have had slightly different rules in place. Define what you expect of your clinic team and communicate it to them clearly. Explain the reasons for setting the policy, why certain rules are non-negotiable, and what the consequences will be if the rules are broken. For example, you could state that if an employee arrives at work wearing unsuitable attire, they will be sent home to change.
If you notice an employee flouting the rules, remind them of your policies as soon as possible, so it doesn’t appear to others that you have relaxed the rules and allowed a change to your dress code. Speak to your employee in private, or send a confidential email, so as not to risk embarrassing your team member. If you wish to give an
employee an official warning, ensure you put it in writing, so it is formalised, and can be recorded and filed. The consequences of contravening a dress code policy can be the same as breaking any other rule set in an employee’s contract. So, an employee could be given an informal warning, followed by a formal warning, and ultimately, an employee could be dismissed if they continued to flout the rules stated in their contract.
Exceptions to the rules
If an employee is pregnant or perhaps has an injury, they may need to make changes to their working uniform to make it comfortable.5,6 If an employee needs to make a change to their workwear, they should seek approval first, so add a clause to your policy to advise staff that they should put their request to a manager before going ahead and making a change to their work attire.
Summary
If you make your rules reasonable and attainable for employees, and you communicate your desired dress code clearly, employees should have no major issue adhering to your policy. Having a clear policy in place should also help you appear consistent and objective if you do ever need to take disciplinary action against an employee who refuses to toe the line.
Victoria Vilas is the operations and marketing manager at ARC Aesthetic Professionals. A manager of teams and projects in the health and wellness content sectors for over a decade, Vilas has spent recent years focusing on the issues of staffing and practice management in the aesthetic medicine industry.
REFERENCES
1. Business Advice, Can I require my employees to pay for their own uniforms? , October 2018 <https://businessadvice.co.uk/hr/ employment-law/employees-pay-for-work-uniforms-minimumwage/>
2. Legislation.gov.uk, Equality ACT 2010 (UK: Legislation.gov.uk, 2010) <http://www.legislation.gov.uk/ukpga/2010/15/contents>
3. Ross A, High heels row: government response ‘a cop-out’, The Guardian, April 2017
4. BBC, British Airways Christian employee Nadia Eweida wins case, January 2013 <https://www.bbc.co.uk/news/uk-21025332>
5. Government Equalities Office, Dress codes and sex discrimination, May 2018 <https://assets.publishing.service.gov. uk/government/uploads/system/uploads/attachment_data/ file/709535/dress-code-guidance-may2018-2.pdf>
6. Equality and Human Rights Commission, During pregnancy <https://www.equalityhumanrights.com/en/managingpregnancy-and-maternity-workplace/help-and-supportemployees/faqs-employees/during-2>
FURTHER READING
ACAS, Dress Code (UK: ACAS, 2016) <https://www.acas.org.uk/ dresscode>
WorkSmart, Dress Regulations (UK: WorkSmart 2019) <https:// worksmart.org.uk/work-rights/discipline-and-policies/dressregulations>
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Tips for CQC Success
Engaging in the registration, inspection and rating process of the UK’s independent regulator of health and social care in England, the Care Quality Commission (CQC), is like scaling a mountain. It can be strenuous, painful, sometimes tedious, yet hopefully culminating in a triumphant summit. Wales, Scotland and Northern Ireland have their own individual regulatory systems, but like the CQC share the aim of providing people with safe, effective, high-quality care, with emphasis on continued improvement.1 Our clinic was graded ‘outstanding’ at our recent CQC inspection, the first doctor-led aesthetic clinic to achieve this grade,2 but the true reward has been the training and commitment required to succeed, and its positive impact on every aspect of our organisation. This article aims to dispel anxieties and reframe CQC registration as an opportunity for a positive and formative experience.
Why register?
Unlike general practice and dental clinics, aesthetic clinics are not automatically required to register with CQC, so why would some of us voluntarily take on this challenge? For many clinics, it is mandatory by virtue of the services they offer, while for others, registration is a voluntary choice to set aspirational standards that improve quality of care and promote patient confidence.
Essential registration
CQC registration and inspection is a requirement when a healthcare professional (doctor, nurse or dentist) working within a provider (individual, partnership or company) performs or supervises any ‘regulated activities’.3 The ‘regulated activities’ most relevant to aesthetic clinics are:
1. Treatment of disease, disorder or injury
2. Surgical procedures
3. Diagnostic and screening procedures
4. Services in slimming clinics
Indeed, in this situation, it is a prosecutable offence to carry out a regulated activity without CQC registration.4 In a non-surgical aesthetic clinic a ‘regulated activity’ might be ‘treatment of disease, disorder or injury’. The common diagnoses we as aesthetic practitioners may make while performing this regulated activity might include:
• Dermatological conditions such as acne, acne scarring, rosacea, seborrheic dermatitis, melasma, post-inflammatory hyperpigmentation, alopecia, photodamage and pre-cancerous lesions, hirsutism, hyperhidrosis
• Bruxism
• Migraine
• Psychological distress from appearance (face or body) such as scars and transgender concerns.
Elective registration
Essential registration is subject to some exceptions e.g. botulinum toxin for cosmetic purposes rather than medical concerns. Hence, there is a perception that many aesthetic clinics fall outside the jurisdiction of CQC, which indeed they could, if they choose to provide their services in a manner that does not include the regulated services above. For these clinics, registration is therefore voluntary. Simply put, if an aesthetic clinic chose NOT to make a medical diagnosis and NOT to treat disease i.e. only treat cosmetically not medically, then it would not need to CQC register, but would need to pay VAT over the threshold. Alternatively, the same clinic could register with the CQC, perform the same treatments with diagnoses, write treatment plans, record therapeutic purpose and then potentially not charge VAT on those treatments now deemed as medical.5
Benefits of elective registration
Although CQC registration is not an easy process, when embraced, I find that it facilitates and supports delivery of optimal patient care, through a clear framework to drive continuous improvement and quality. Aesthetic clinics wishing to pursue registration can design their services to fall within the CQC’s remit, but will only be inspected on their regulated services.6 I believe the requirements that need to be fulfilled in order to become registered with the CQC do make for better practice; consequently, many clinics opt to apply the same rigorous standards to all their services, not only the regulated ones. For example, a medical aesthetic clinic could choose to underpin its skin services by medical diagnosis, and therefore treat diseases such as acne and rosacea, in which case some treatments could be considered ‘regulated activities’ and be managed according to CQC standards. This is because if you make the diagnosis and are therefore treating the disease, then the use of the laser for example would be CQC regulated. If you are using the laser without having diagnosed a disease, it is not necessary to regulate its use. In addition to increasing quality, the regulatory improvements to process, policy and procedure that accompany CQC registration are certainly valuable. Also notable are the benefits to confidence and cohesion within the team, measurable improvements to services and the opportunity to focus on refining the culture and leadership of the organisation. For example, following the CQC process, feedback from staff in our clinic demonstrated that uniting around the CQC challenge improved team morale and unity. In addition, following this intense period, the team instinctively embraced the aims, visions and values of the clinic. Some clinics would willingly pay a business consultant who claimed to be able to deliver all of this, and yet colleagues often cite the cost of registration and maintenance of standards as a detractor for CQC. In our clinic, when we estimate the positive financial impact of being CQC registered, let alone the other benefits, we believe it to be a worthwhile investment.
Furthermore, the new grading system introduced in aesthetic clinics this year, which evaluates evidence for regulated activities as ‘outstanding, good, requires improvement or inadequate’, helps to establish quality benchmarking, which could promote greater patient confidence.7
The challenges of registration and inspection
Whilst initial CQC registration involves copious P-words (paperwork, processes, policies, procedures, pain and panic), the essence of it is more focused on creating a learning organisation that uses the CQC assessment framework to drive continuous improvement and quality. The inspection framework sets out five ‘domains’, assessing
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dr Julia Sevi provides her top tips for successfully registering your clinic with the Care Quality Commission
providers on whether they are: safe, effective, caring, responsive to patient needs, and well-led, outlined in more detail in ‘the five domains of CQC assessment’ section.8
Registering with CQC and preparing to be inspected on the five domains can be a lengthy, challenging and expensive process. Every clinic procedure, policy and process must be created or updated, and in addition to the extra staff costs incurred, there is the added expense of CQC fees, as well as external consultancy advice if you choose to use it. The registration and preparation phase can take between three to 12 months depending on the standards already in place and, once registered, a clinic is then subject to regular inspections, which can range from six months to five years.9 Clinics should have at least 48 hours’ notice of an inspection, but the CQC does have the right to make unannounced inspections (usually if they have concerns).9
Tips for inspection preparation
1.
Familiarise yourself with CQC hot topics
Inspectors must see evidence that a clinic fulfils ‘The Fundamental Standards’ which include the presence of person-centred care, treating patients with dignity and respect, informed consent, safety for patients and staff, safeguarding from abuse, a good standard of premises and equipment, good governance, duty of candour and an adequate number of fit and proper staff.10
In our experience, there are certain areas that you can expect CQC inspectors to concentrate on. These include health and safety for patients and staff, infection control, safeguarding and other mandatory training. We would also recommend that HR and staff qualifications, patient engagement, clinical records, confidentiality and GDPR, information provided for patients, participation in care, respect, dignity and chaperones, are also be considered.
Each year there are particular topics of current focus, so in addition to speaking with your inspector prior to the visit to ascertain the domains they will be inspecting, it can be helpful to gather local intelligence by speaking to other clinics who have recently been inspected. Reading the reports of other clinics on the CQC website can also be a further source of useful information, demonstrating what clinics are doing to achieve high ratings or what might require improvement.11
2. Prepare the evidence
The onus is on the clinic to use evidence to demonstrate that it is meeting each essential standard;12 if it is not evidenced then the CQC cannot report on it, for example showing documentation in patient notes of a patient’s involvement in decisions about care. The evidence does not all have to pertain to perfect situations. One key factor is to identify areas for potential improvement and develop an action plan for change to achieve the desired improvements. For example, if a mistake in care has occurred, demonstrate how you have used duty of candour to disclose this openly and honestly to the patient, as well as evidencing how the clinic has learnt from the mistake and put a process in place to prevent a recurrence.
3. Train your staff
All staff should understand the essence of CQC, as well as knowing about CQC essential standards and what the clinic is doing to meet them. Inspectors may speak with anyone in the clinic, so you need to prepare the staff to be confident and informative when interviewed.
We usually do this by holding a whole clinic meeting where we cover the following:
• CQC essential standards
• Location and content of policies and procedures
• Safeguarding situations
• How the clinic meets essential standards
• Areas to be inspected and what the inspectors are looking for
All the managers and directors are involved in delivering the training using powerpoint presentations, quizzes, role play and discussions. Our external CQC advisors also provide an invaluable ‘mock CQC visit’, which highlights areas requiring attention.
4. Organise paperwork and clinical records
Inspectors may request a sample of clinical records, so prepare for this by regularly screening to check they are up to date and correctly filed. Ensure your paperwork is current and reflects any new changes, including statement of purpose, visions values and culture, policies and procedures, emergency numbers e.g. local social services contact.
5. Inform patients
Inform the patients who will be in-clinic on the day of the inspection that the CQC might ask to interview them, although they are entitled to decline to speak to the inspectors. Involving regular patients in the CQC process usually supports a good outcome for the clinic as these patients are likely to be ‘clinic fans’ and happy to be advocates of your services.
6. Be authentic
Be confident to permit the inspectors to see a real day in the life of the clinic, remembering we have no need to hide. Recently, the CQC process has become more akin to peer review13 and, as such, we stand to gain from any issues raised as they signpost routes to improved care. Last year our inspectors highlighted the absence of a portable defibrillator, something that had been pricking our consciences for a while. We were grateful for this nudge and felt it was just what we needed to help us dive in, purchase one and train the whole team.
7. Consider your inspector
Imagine a day in the life of the inspector; look through their eyes at your clinic and try to make their day go more smoothly by being well prepared. They are not trying to find fault, are certainly willing to celebrate quality, and are simply trying to do their job. Plan carefully so that they have access to key people in order to gauge your organisation and ensure the evidence required for them to perform the assessment is readily accessible.
8. Go the extra mile
Our experience taught us that to achieve a ‘good’ clinic grading you should fulfill ALL mandatory CQC requirements and all five domains. However, to be considered ‘outstanding’ you need to provide evidence for regulated activities that you are really going the extra mile. Find innovative solutions to inequalities, problems, or unmet patient needs. While examples do not have to be original, many examples of ‘outstanding’ practice show innovative approaches to solving a problem or delivering a service.
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
www.inspiretooutstand.co.uk | info@inspiretooutstand.co.uk @inspiretooutstand Inspire to Outstand @Outstandto Contact: Tracey Jones - 07825 311 900 Inspire to Outstand supports organisations and businesses with CQC registration and preparation for inspection. We are an independent company based in Cheshire who have education and experience around the CQC inspection process.
9. Focus on regulated activates
Focus only on regulated activities during an inspection. As an aesthetic clinic, you may exceed in other areas, but these are not considered in inspection. It will not help your case if you evidence exceptional outcomes and patient satisfaction from purely cosmetic botulinum toxin treatments because the CQC cannot take these into consideration, they will only be looking for audit data from medical treatments such as bruxism or hyperhidrosis.
10. Seek external help with CQC registration
Unless somebody in your organisation has experience with CQC registration, I find it is helpful to consider the use of medical and healthcare regulatory compliance consultants There are several such organisations, ranging in price from £1,500-£3,500. In general, companies can help with:
• Pre-application: advice on eligibility, criteria and requirements for registration
• Support with application: preparation and completion of the online application forms
• Policies and procedures: development of the policies and procedures required to meet the fundamental standards
• Provision of supporting documentation: required to evidence compliance with audit and good clinical governance
• Facility development: advice regarding the suitability and development of premises to meet regulatory standards
• Training for registered persons: including the Nominated Individual and Registered Manager14
• Infection prevention and control: site audit with action plan
• Laser and IPL safety: including local rules, risk assessments and clinical protocols
• Ongoing advice and support: including pre and post inspection support on compliance issues
Conclusion
CQC registration can be a difficult and lengthy process. However, I have found that it builds confidence, morale and quality in your business. It also provides a continuous process of growth that nurtures an organisational culture focused on learning and the delivery of highquality compassionate care. When embraced and managed positively, the CQC process is formative for the clinic and the individuals within it, affording self-reflection and growth, with net consolidation of clinic culture, team cohesion and confidence, and measurable improvements to services.
Dr Julia Sevi is an aesthetic practitioner with more than 25 years’ medical experience.

Dr Sevi has completed a Bachelor of Medicine and Bachelor of Surgery, and studied acupuncture and Chinese medicine in China. She is director of Aesthetic Health and is a KOL, speaker and trainer specialising in the combination of aesthetic and antiageing medicine.
REFERENCES
The five domains of CQC assessment
CQC inspectors ask themselves whether a clinic fulfills the five domains during their assessment, and to be graded ‘outstanding’ a clinic would need to demonstrate the following. Remember, inspectors are able only to evaluate evidence for regulated activities at your clinic when considering what grade to award.12
1. Safe
People are protected by a strong comprehensive safety system, and a focus on openness, transparency, and learning when things go wrong.
2. Effective Outcomes for people who use services are consistently better than expected when compared with other similar services. Audits demonstrate tangible, improved outcomes for patients or improved access to services.
3. Caring
People are truly respected and valued as individuals and are empowered as partners in their care. The whole practice is involved, and often other practices in the area, in addition to demonstrating that they are playing an active role in ongoing initiatives in their local area.
4. Responsive to patient needs
Services are tailored to meet the needs of individual people and are delivered in a way to ensure flexibility, choice, and continuity of care. Services should be scalable, sustained, and robust. Examples are not just about delivering good care to one person, but are regularly done for a range of patients (often there is a process in place to demonstrate this). Services go above and beyond the minimum expected contractual obligations or are significantly more impressive than other similar providers.
5. Well-led Services find innovative solutions to inequalities, problems, or unmet patient needs. While examples do not have to be original, many examples of ‘outstanding’ practice show innovative approaches to solving a problem or delivering a service. The leadership, governance, and culture are used to drive and improve the delivery of high-quality personcentred care.
1. Regulatory Systems for Healthcare Quality across the United Kingdom, British Medical Association <https://www.bma.org.uk/collectivevoice/policy-and-research/nhs-structure-and-delivery/monitoring-quality-in-the-nhs/regulatory-systems-for-healthcare-quality>
2. Aesthetics journal, CQC rates first aesthetic clinic as ‘Outstanding’, 2019. <https://aestheticsjournal.com/news/cqc-rates-first-aesthetic-clinicas-outstanding>
3. CQC, Regulated Activities, July 2019. <https://www.cqc.org.uk/guidance-providers/registration/regulated-activities>
4. Enforcement Policy, Care Quality Commission <https://www.cqc.org.uk/sites/default/files/20150209_enforcement_policy_v1-1.pdf > p27
5. Should you be paying VAT, Aesthetic Medicine <https://aestheticmed.co.uk/site/industrynewsdetails/should-you-be-paying-vat>
6. CQC, Treatment of disease, disorder or injury, February 2019. <https://www.cqc.org.uk/guidance-providers/registration/treatment-diseasedisorder-or-injury>
7. CQC, Ratings, June 2018. <https://www.cqc.org.uk/what-we-do/how-we-do-our-job/ratings>
8. CQC, The five key questions we ask, July 2018. <https://www.cqc.org.uk/what-we-do/how-we-do-our-job/five-key-questions-we-ask>
9. CQC, When we will inspect independent doctors and clinics, March 2019. <https://www.cqc.org.uk/guidance-providers/independentprimary-medical/when-we-will-inspect-independent-doctors-clinics >
10. CQC, The fundamental standards, May 2017. <https://www.cqc.org.uk/what-we-do/how-we-do-our-job/fundamental-standards>
11. CQC, Inspection Reports, June 2017. <https://www.cqc.org.uk/what-we-do/how-we-do-our-job/inspection-reports>
12. CQC, Key lines of enquiry for healthcare services, June 2018. <https://www.cqc.org.uk/guidance-providers/healthcare/key-lines-enquiryhealthcare-services>
13. The King’s Fund Consultation Response. A New start – Consultation on changes to the way the CQC regulates, inspects and monitors care <https://www.kingsfund.org.uk/sites/default/files/field/field_publication_file/consultation-cqc-regulate-inspect-monitor-care-aug13.pdf>
14. CQC, Regulation 7: Requirements relating to registered managers, 2017. <https://www.cqc.org.uk/guidance-providers/regulationsenforcement/regulation-7-requirements-relating-registered-managers#guidance>
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com







PARK PLAZA WESTMINSTER BRIDGE HOTEL NETWORKING Catch up with friends and colleagues, and meet leading aesthetic professionals at the glamorous drinks reception CELEBRATION Recognise your achievements and celebrate the specialty’s successes for 2019 at the UK’s most prestigious ceremony for medical aesthetics DINNER Indulge in a delicious three-course meal with complementary drinks in the dazzling ballroom before the main ceremony gets underway INDIVIDUAL TICKET: £305 +VAT TABLE OF 10: £2,900 + VAT BOOK NOW LAST CHANCE TO BOOK AESTHETICSAWARDS.COM Join your colleagues from across the specialty for the Aesthetics Awards 2019 and be entertained by comedian Tom Allen, before a live band gets the party started following the ceremony HOSTED BY TOM ALLEN CATEGORY SPONSORS PHARMACY
“I love aesthetics because it’s happy medicine”
As an established ophthalmologist with more than 20 years’ experience in medical aesthetics, it’s fair to say that Dr Tahera Bhojani-Lynch is a well-recognised figure within the specialty. She is a key opinion leader for aesthetic manufacturer Teoxane, sits on the board for the International Association for Prevention of Complications in Aesthetic Medicine and has worked as a consultant for the likes of Galderma, Merz and Teoxane. As well as this, she was the first British woman to perform LASIK eye surgery in the UK in 2001. So, where did it all begin for Dr Bhojani-Lynch?

“I graduated from Aberdeen Medical School in 1989 and always had a passion for ophthalmology. I was short-sighted as a child and so, being the curious and idealistic child that I was, I had the idea that I was going to find a cure for it. I started my training at Worcester Eye Hospital, before moving to North Riding Infirmary in Middlesbrough, then to Derby Royal Infirmary and to one of the largest eye departments in the UK, the Queen’s Medical Centre in Nottingham, undertaking various positions,” she shares.
In 1997, her marriage saw her take a move further down south to Amersham where she was first introduced to the world of aesthetics. “I remember seeing a job opening at Allergan, which was primarily an ophthalmology business at the time, and reading the description thinking ‘this was written for me’ – it was for a medical advisor in the research and development department. I was actually pregnant with my first son at the time and started working for them when I was almost full-term, but I just couldn’t pass up the opportunity which went on to change my life. I was Allergan’s first resident ophthalmologist in Europe and this really was my first introduction to Botox as we know it,” says Dr Bhojani-Lynch.
Fast forward three years, with two young children, Dr BhojaniLynch wanted to have more flexibility in her work and moved to Loughborough to be closer to family where she opened her clinic, The Laser & Light Medical Skin Clinic. She explains, “I also owned an optometric business at the time and was performing regular laser eye surgery at Optimax Laser Eye Clinics. I was working three jobs at once and it was a lot of work and pressure. So, I set up the laser clinic as something that I could do part-time whilst my children were young and put my other roles on hold. I had always planned to go back into ophthalmology full-time but what I never expected was how much I would love doing aesthetics.”
She continues, “You develop a passion for making people happy in aesthetics; it’s a happy medicine. There are lots of areas that aren’t; for example, in my past experience in ophthalmology I would have to tell someone they have lost their sight, which would be very difficult. I’d also get rid of people’s glasses and treat a cataract which was fantastic, but I generally find that in aesthetics, you have the opportunity to empower patients about their appearance like no other specialty.” Speaking specifically about her love for treating the upper face, Dr Bhojani-Lynch states, “The periorbital really is my forte. My
signature treatment is performing an outer canthal lift using a needle to lift the corner of the eye and recreate an almond shape. The results are fantastic.”
Not only is Dr Bhojani-Lynch academically minded, she also has a keen interest in business and a strong eye for spotting opportunity. In 2005, Dr Bhojani-Lynch found herself frustrated when her orders from her pharmacy weren’t being fulfilled. This, she explains, became the reasoning behind her and her husband founding Church Pharmacy. She reflects, “I remember losing a chemical peel patient because the peel I ordered didn’t arrive. This patient had taken a week off work and the impact to her and my business was huge. I said to my husband, a businessman, ‘Can you set up a distribution company?’. My brother is a pharmacist and he was our resident pharmacist from the beginning, and so Church Pharmacy was born.” She continues, “I remember the first time we got an order; it took us half a day to pack the box because we were so excited! Church was born from a letdown customer and the one unique-selling point about this business was our communication; if we were unable to fulfil an order we would inform clients and try to give them a solution. In 2011, my husband retired and so we sold the business to my brother and his two sons; I’m very proud of what they are still achieving.” When considering her biggest achievement, Dr Bhojani-Lynch says that it is yet to come. She adds, “There’s so much to be learnt so I don’t think I’ve reached my biggest achievement yet. But the thing I’m most proud of is a clinical paper I wrote in 2017 about late onset inflammatory response. It got published in the Journal of Plastic and Reconstructive Surgery and in November last year I found out I had won the prize for the best paper in the whole of Europe. Flying out to Chicago with my two sons to receive my award was a very proud moment for sure.”
What are your hobbies?
I have always been a workaholic, but relaxation is found in a good book, good music, good company and good food.
What’s your favourite patient group to treat?
I love assessing and sculpting a man’s face to make him look younger, whilst keeping it angular and masculine – it is my passion. We generally find some signs of maturity on a man’s face attractive – just look at David Beckham – so injecting men in-keeping with their masculinity is really satisfying!
Do you have an ethos that you follow?
We are healthcare professionals first and businesspeople second. We have to always remember that this is somebody’s face and they have to live with what we do.
What’s your advice for those starting out?
Go on at least two training courses for the same treatment. It’s a really good way to compare techniques and find one that suits you.
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Ophthalmologist Dr Tahera Bhojani-Lynch reflects on her career in the aesthetics specialty and shares her passion for treating the upper face
The Last Word
Advertising how quickly a procedure can be carried out is the latest fad. A 10-minute lip filler here, a five-minute non-surgical rhinoplasty there, facial volume replacement promising recontouring in five minutes… Is this good practice or is promoting accelerated aesthetic treatments potentially harmful? Is ‘fast’ really what our patients want?
In this article, I explore whether promoting and promising speedy treatments is actually beneficial for both the patient and the practitioner, while discussing what I believe to be best practice.

Patient perception
Some practitioners want to minimise their patients’ time in the chair, one of their reasons being that faster treatments equate to a better patient experience. But is this really true? Patients are surprisingly unconcerned about many aspects of their treatments if they feel they are being adequately cared for.5 In a recent straw-poll of around two dozen of my patients, not one mentioned treatment time when asked what their priorities were during a procedure. It’s not news that what patients really worry about is the standard of care given to them and the effectiveness and quality of that treatment. The latter has been shown to influence patients’ intent to revisit a service.5 Supporting this concept is research into patient satisfaction.5,6 As a key quality
indicator in healthcare, satisfaction is directly linked to not only retention and outcomes, but also malpractice claims.5,6 Whilst time waited before receiving treatment is often cited as a contributing factor to satisfaction (especially in public healthcare systems such as the NHS), the speed of the treatment is not.6 Conversely, there is a strong link between increased time spent with the patient and increased satisfaction.6 This indicates that, in fact, your patients want to spend longer with you, not be ‘over and done with’ in just 10 minutes. As providers of luxury medical procedures, I believe we should strive to provide a compelling patient experience. In my opinion, perceived indifference, the act of making a patient feel unvalued and unimportant, can occur when the patient is not awarded with enough time. According to John Gattorna of Macquarie Graduate School of Management, perceived indifference is the reason 68% of all customers switch to competitors.2,8 I must presume that these five-minute non-
surgical rhinoplasties being offered by some clinics don’t include greeting the patient, photography, consent, and preparation of the patient or the room, as well as making sure the patient is comfortable and happy. At the very least this mismanages the patient’s expectations for treatment, as the actual time spent surrounding the procedure is not made clear. If it is the case, I have serious misgivings about significant aspects of the treatment procedure being omitted. Expectation setting is a key ingredient in the practitioner-patient relationship and should start at the advertising stage with clear and transparent statements.
Practitioner perception
There is an obvious difference between working efficiently and rushing procedures. Yet in my opinion, many practitioners seem to get the two confused. They fall into the trap of believing that if they can do it faster, they must be better. A tried and tested USP is usually the basic faster is better model. This is certainly what some customers want in some industries, however I would argue that patients simply aren’t interested in express aesthetic treatments. What I see is practitioners advertising internal KPIs in place of a competitive selling proposition in a ‘race to the bottom’ that is not good for patients, the aesthetic market as a whole and the perilous incidence of serious complications. Just because you see someone else promoting their services in this way, it doesn’t mean that you have to.
Clinical considerations
It cannot be disputed that there is a correlation between injection speed and the incidence of complications.1 Rapid injection and flow rate increase the amount of filler volume placed, increasing discomfort, swelling and bruising at best and possibly resulting in disastrous adverse events such as obstruction of vessels or even blindness at worst.1,3 On the contrary, slow injection of micro-volumes are less likely to result in complete blockage of vessels, or retrograde flow capable of blocking the ocular circulation.1,3 Injecting slowly and with caution allows practitioners to monitor the patient and change technique
Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
Dr MJ Rowland-Warmann explains why she believes practitioners should stop advertising the length of treatment times for dermal filler procedures
It cannot be disputed that there is a correlation between injection speed and the incidence of complications
intra-procedurally should the need arise.7 I would argue that boasting about taking five minutes to complete a potentially risky aesthetic procedure undermines the seriousness of its medical nature. It has also been suggested that it would likely be indefensible in a negligence action, should it come to light that a complication had arisen when the practitioner spent such little time on the procedure.7 I would strongly encourage practitioners to consider your position if a patient raises a grievance or negligence action for a complication. Imagine arguing at the tribunal that you took care of the patient and were doing a splendid job, yet opposing counsel produce your advert promoting your five-minute procedure.
So, with that information in mind, practitioners who continue to inject quickly and carry out treatment as quickly as possible, with a disregard for these obvious elements of safety, will soon be graduating from ‘negligence’, when your patient suffers harm as a result of a breach of a duty of care, to ‘recklessness’, where you are deliberately and unreasonably disregarding risks that could potentially result in injury to
the patient, vitiating consent and constituting a criminal assault.9
Moving forward
I believe the way to grow a patient base and have the practice and patients you want is to spend more time with patients. You must be caring, build relationships, do a good job and get repeat business. In my experience, patients respond well to values of basic decency in any service or retail business. Advertise your excellence in care, not speed. As complications are becoming more widely reported, in part due to the growth of the industry and its unregulated nature, we should consider it our responsibility to not to contribute to them, but to conduct safe and careful procedures.
REFERENCES
1. Ablon, G, Understanding How to Prevent and Treat Adverse Events of Fillers and Neuromodulators. Plast Reconstr Surg Glob Open, 2016
2. Aesthetic Business Transformations, How to maximise your medical aesthetic business profits, 2019 <https://www. aesthetic-bt.com/grow-your-practice-in-todays-economy/>


3. DeLorenzi, C, Complications of injectable fillers, part 2: vascular complications. Aesthet Surg J, 2014
4. Glogau, R G., Kane, M. A, Effect of injection techniques on the rate of local adverse events in patients implanted with nonanimal hyaluronic acid gel dermal fillers, Dermatol Surg, 2008
5. Kim, C E et al., Quality of medical service, patient satisfaction and loyalty with a focus on interpersonal-based medical service encounters and treatment effectiveness: a crosssectional multicenter study of complementary and alternative medicine (CAM) hospitals. BMC Complement Altern Med, 2017
6. Prakash B, Patient Satisfaction. J Cutan Aesthet Surg, 2010
7. Urdiales-Galvez, F et al., Preventing the Complications Associated with the Use of Dermal Fillers in Facial Aesthetic Procedures: An Expert Group Consensus Report. Aesthetic Plast Surg, 2017
8. CustomerThermometer.com, CSAT Stat of the Month: 68% <https://www.customerthermometer.com/customersatisfaction/csat-stat-68-percent/>
9. Loveless J, Intention, recklessness, negligence and gross negligence, Complete Criminal Law: text, cases and Materials, 2016 Dr MJ Rowland-Warmann is the founder and lead clinician at Smileworks in Liverpool. She is highly committed to continuing professional development, in 2016 completing her MSc in Aesthetic Medicine (with distinction) from Queen Mary University of London. She has a special interest in the management of complications, writing extensively on the subject.

Reproduced from Aesthetics | Volume 6/Issue 12 - November 2019 @aestheticsgroup @aestheticsjournaluk Aesthetics aestheticsjournal.com
BOOK YOUR TICKETS NOW! AESTHETICSAWARDS.COM
A PARTNERSHIP YOU CAN COUNT ON CELEBRATING OUR 10TH ANNIVERSARY IN AESTHETIC TREATMENTS

As your trusted partner in aesthetics, Azzalure is a truly global toxin approved in 72 countries with 40 million glabellar line treatments in Europe and the United States alone.1,2 Here’s to another decade of natural-looking results and high patient satisfaction.3
Botulinum
Speywood units
specific to this preparation and are not interchangeable with other botulinum toxins. Reconstitute prior to injection. Intramuscular injections should be performed using a sterile suitable gauge needle. Glabellar lines: recommended dose is 50 Speywood units divided equally into 5 injection sites, 10 Speywood units to be administered intramuscularly, at right angles to the skin; 2 injections into each corrugator muscle and one into the procerus muscle near the nasofrontal angle. Lateral canthal lines: recommended dose per side is 30 Speywood units divided into 3 injection sites; 10 Speywood units to be administered intramuscularly into each injection point, injected lateral (20 - 30° angle) to the skin and very superficial. All injection points should be at the external part of the orbicularis oculi muscle and sufficiently far from the orbital rim (approximately 1 - 2 cm); (See summary of product characteristics for full technique). Treatment interval should not be more frequent than every three months. The efficacy and safety of repeat injections of Azzalure has been evaluated in Glabellar lines up to 24 months and up to 8 repeat treatment cycles and for Lateral Canthal lines up to 12 months and up to 5 repeat treatment cycles. Not recommended for use in individuals under 18 years of age. Contraindications: In individuals with hypersensitivity to botulinum toxin A or to any of the excipients. In the presence of infection at the proposed injection sites, myasthenia gravis, Eaton Lambert Syndrome or amyotrophic lateral sclerosis. Special warnings and precautions for use: Care should be taken to ensure that Azzalure is not injected into a blood vessel. Use with caution in patients with a risk of, or clinical evidence of, marked defective neuro-muscular transmission, in the presence of inflammation at the proposed injection site(s) or when the targeted muscle shows excessive weakness or atrophy. Patients treated with therapeutic doses may experience exaggerated muscle weakness. Not recommended in patients with history of dysphagia, aspiration or with prolonged bleeding time. Seek immediate medical care if swallowing, speech or respiratory difficulties arise. Facial asymmetry, ptosis, excessive dermatochalasis, scarring and any alterations to facial anatomy, as a result of previous surgical interventions should be taken into consideration prior to injection. Injections at more frequent intervals/higher doses can increase the risk of antibody formation. Avoid administering different botulinum neurotoxins during the course of treatment with Azzalure. To be used for one single patient treatment only during a single session. There is a potential risk of localised muscle weakness or visual disturbances linked with the use of this medicinal product which may temporarily impair the ability to drive or operate machinery. Interactions: Concomitant treatment with aminoglycosides or
other agents interfering with neuromuscular transmission (e.g. curare-like agents) may potentiate effect of botulinum toxin. Pregnancy, Lactation & Fertility: Not to be used during pregnancy or lactation. There are no clinical data from the use of Azzalure on fertility. There is no evidence of direct effect of Azzalure on fertility in animal studies. Side Effects: Most frequently occurring related reactions are headache and injection site reactions for glabellar lines and; headache, injection site reactions and eyelid oedema for lateral canthal lines. Generally treatment/injection technique related reactions occur within first week following injection and are transient. Undesirable effects may be related to the active substance, the injection procedure, or a combination of both. For glabellar lines: Very Common (≥ 1/10): Headache, Injection site reactions (e.g. erythema, oedema, irritation, rash, pruritus, paraesthesia, pain, discomfort, stinging and haematoma). Common (≥ 1/100 to < 1/10): Temporary facial paresis (due to temporary paresis of facial muscles proximal to injection sites, predominantly describes brow paresis), Asthenopia, Eyelid ptosis, Eyelid oedema, Lacrimation increase, Dry eye, Muscle twitching (twitching of muscles around the eyes). Uncommon (≥ 1/1,000 to <1/100): Dizziness, Visual impairment, Vision blurred, Diplopia, Pruritus, Rash, Hypersensitivity, Eye movement disorder. Rare (≥ 1/10,000 to < 1/1,000): Urticaria. For lateral canthal lines: Common (≥ 1/100 to < 1/10): Headache, Temporary facial paresis (due to temporary paresis of facial muscles proximal to injection sites), Eyelid ptosis, Eyelid oedema and Injection site disorders (e.g. haematoma, pruritus and oedema). Uncommon (≥ 1/1,000 to <1/100): Dry eye. Adverse reactions resulting from distribution of the effects of the toxin to sites remote from the site of injection have been very rarely reported with botulinum toxin (excessive muscle weakness, dysphagia, aspiration pneumonia with fatal outcome in some cases). Prescribers should consult the summary of product characteristics in relation to other side effects. Packaging Quantities & Cost: UK 1 Vial Pack (1 x 125u) £64.00 (RRP), 2 Vial Pack (2 x 125u) £128.00 (RRP), IRE 1 Vial Pack (1 x 125u) €93.50, 2 Vial Pack (2 x 125u) €187.05 (RRP) Marketing Authorisation Number: PL 06958/0031 (UK), PA 1613/001/001 (IRE) Legal Category: POM Further Information is Available From: Galderma (UK) Limited, Meridien House, 69-71 Clarendon Road, Watford, Herts. WD17 1DS, UK. Tel: +44 (0) 1923 208950 Fax: +44 (0) 1923 208998 Date of Revision: September 2018
Adverse events should be reported.
For the UK, Reporting forms and information can be found at www.mhra.gov.uk/yellowcard
For Ireland, Suspected adverse events can be reported via HPRA Pharmacovigilance, Earlsfort Terrace, IRL - Dublin 2; Tel: +353 1 6764971; Fax: +353 1 6762517. Website: www.hpra.ie; E-mail: medsafety@hpra.ie. Adverse events should also be reported to Galderma (UK) Ltd.
References: 1. Azzalure SPC 2018. 2. Data on File MA-39613.
3. Molina B et al. J Eur Acad Dermatol Venereol 2015;29(7):1382–8.
Date of Preparation: April 2019 Job code: AZZ19-03-0018a
Azzalure Prescribing Information (UK & IRE) Presentation: Botulinum toxin type A (Clostridium botulinum toxin A haemagglutinin complex) 125 Speywood units of reconstituted solution (powder for solution for injection) Indications: Temporary improvement in appearance of moderate to severe: • Glabellar lines seen at maximum frown, and/or • lateral canthal lines (crow’s feet lines) seen at maximum smile in adult patients under 65 years, when severity of these lines has an important psychological impact on the patient. Dosage & Administration: Azzalure should only be administered by physicians with appropriate qualifications and expertise in this treatment and having the required equipment.
toxin units are different depending on the medicinal products.
are
