50, 60 and 70 year acknowledgements
Drs Graham Wheeler, Peter McKerracher OAM and Gerard (Bruce) Barblett CPD spotlight
Meet Lalima Tiwari

WA REGIONAL COMMITTEE
50, 60 and 70 year acknowledgements
Drs Graham Wheeler, Peter McKerracher OAM and Gerard (Bruce) Barblett CPD spotlight
Meet Lalima Tiwari
WA REGIONAL COMMITTEE



FRI, 5 SEP
8:00AM - 5:00PM
ALOFT
Join leading voices in the profession for a full day of evidence-based insights, clinical case presentations, and innovation in dental care.
Keynote Speakers

Dr Adam Hamilton Specialist Prosthodontist
Open to all General Dentists, Specialist Dentists and Oral Health Professionals
Emeritus Professor Laurence Walsh Specialist in Special Needs Dentistry
Also featuring presentations from:
Dr Lisa Bowdin - Paediatric Dentist

Dr Tom Huang - Dento-Maxillofacial Radiologist
Dr Sonny Lee - General Dentist
Dr Melanie McAlpine - Periodontist
Dr Justina Teo - General Dentist
Mr Tom Truong - Lab Technician
Dr Nathan Vujcich - Oral and Maxillofacial Surgeon
Dr Chris Wholley - Orthodontist
Dr Mostafa Elkholy - Endodontist
NOW TO SECURE YOUR PLACE



Dr Gwen Chin ADAWA President
As we reach the midpoint of 2025, I want to take a moment to reflect on the strength and continuity of our profession — a theme that resonates strongly in the latest edition of The Western Articulator. This issue features a special tribute to some of our most enduring members, whose careers have been a testament to the values and commitment of the dental profession in Western Australia.
We proudly acknowledge Dr Graham Wheeler for reaching the extraordinary milestone of 50 years in dentistry. His reflections, shared in the feature article, highlight not only the evolution of the profession but also the enduring spirit of service and mentorship that characterise our members.
We also celebrate Dr Peter McKerracher OAM, recognised for 60 years of contribution to the profession, and Dr Bruce Barblett, who marks an incredible 70 years in dentistry. Their legacies are interwoven with the growth and strength of the ADAWA community,
CEO Trevor Lovelle President Dr Gwen Chin
and we are grateful for their ongoing presence and wisdom.
This edition of the Western Articulator also includes a timely finance feature, offering practical financial tips for members as we begin the new financial year. Whether you're just starting out or planning for retirement, it’s worth a read for all members.
A gentle reminder to those who haven’t yet done so — subscription renewals are now due. Maintaining your ADAWA membership ensures continued access to our highquality CPD program, member benefits, advocacy support, and collegial community. We thank all our members who have already renewed for another year of professional support and connection.
As always, ADAWA remains committed to supporting every stage of your professional journey. Whether you are a recent graduate or a member celebrating seven decades of practice, your role in our profession is valued and vital.
Editorial Brooke Evans-Butler Designer Michelle Walker Advertising Business Development Manager Shaden Kanaan

Trevor Lovelle
In a previous CEO Comment, I wrote about sensible regulation and the need to balance benefits against economic and social costs. This was specifically in relation to Government’s proposed regulatory change for private dental clinics that provide IV sedation.
I am pleased to report that ADAWA successfully advocated against the proposed changes to regulations of the Health Services Act that would have significantly impacted private dental practices across the state.
The Minister for Health has confirmed that the previous plan of revising only specific sections of the Act (i.e. related to IV sedation) would not be commenced but there is now a commitment to undertake a comprehensive review of the Act – which is a significant revision that ensures greater transparency and an evidentiary approach to potential change.
In November 2022, the Department of Health’s Licensing and Accreditation Regulatory Unit (LARU) initiated a review of the Health Services (Day Hospital Facility) Determination. The “Determination” is subsidiary legislation made under the Act and defines what constitutes a "day hospital facility" for the purposes of the Act.
One key recommendation to arise from the review was the introduction of a licensing framework for all private dental
clinics performing procedures under intravenous (IV) sedation.
The practical effect of this proposed regulatory expansion would have been considerable. Clinics administering IV sedation — regardless of the sedation level — would be required to retrofit facilities to meet Day Hospital specifications. This could include physical upgrades to clinic infrastructure and hiring additional clinical staff, placing a heavy compliance burden on practices and potentially reducing patient access.
ADAWA responded decisively, arguing that not all IV sedation techniques necessitate Day Hospital-level oversight. While we support licensing for clinics offering ‘deep’ IV sedation, we consistently opposed regulatory measures that would include ‘light’ or conscious sedation, which is commonly and safely used in routine dental procedures. ADAWA’s position was reinforced by the absence of unambiguous clinical evidence supporting the proposed change. Consequently, Government has chosen not to pursue changes to the Health Services (Day Hospital Facility) Determination at this time. This outcome affirms ADAWA’s commitment to protecting practical and evidence-informed standards in oral health care delivery.
ADAWA continues to support our members in advancing balanced, sensible policy. We sincerely thank our members for your continued support—your engagement remains vital in driving meaningful change.

After a remarkable career, Oral and Maxillofacial Surgeon, Professor Raymond Williamson, will be retiring soon.
Professor Raymond Williamson has a long reputation as a respected Oral and Maxillofacial Surgeon, with qualifications including BDS (Sydney), MDSc (UWA), PhD (UWA), FRACDS (Aus), FFDRCS (Ireland), FDSRCS (England), FRACDS (OMS), FICD and is Life Member of the International Association of OMS. He has also worked In Sports Medicine, Anthropology and Archaeology with his main interest in Egyptology. He was the first person in Australia to carry out CT scans in Egyptian Mummies in the early 1990s, and was a founding member of the Ancient Egypt Society of Western Australia. He has worked as an archaeologist in Egypt as part of the Macquarie University Egyptian Excavation Team on a site called Qift, north of Luxor, Egypt and on the restoration of mummies in the Cario Museum.
He began his career in the Royal Australian Navy as a Dental Officer, Diving Officer and he trained in Underwater Medicine. He was in charge of the only Recompression Chamber here in WA and oversaw treatment of all diving accidents,
including the Bends from all over Western Australia. He rose to the rank of Surgeon Commander before transferring to the RAN Reserve to begin his training in OMS here in Perth. On completion of his training, he was offered a position at Queen Victoria Hospital, East Grinstead, UK. On return from the UK to Perth, Prof Williamson took up a joint appointment with the UWA Dental School and Royal Perth Hospital. During his 33 years at UWA and Royal Perth Hospital, as Head of OMS, he oversaw the OMS undergraduate and postgraduate teaching programs was the Western Australian Coordinator of OMS Training. In addition, he was on the RACDS College Board of Surgeons as the WA representative.
He was also a member of the Specialist Medical Team for the Wallabies Rugby Union team, Western Force Rugby Union team and the WA Reds Rugby League team. He also toured the UK as a Medical Officer for his son's Rugby Team.
In 2013 Prof Williamson was head hunted for the position of the Head of Oral Surgery, Oral Medicine, Oral

Pathology and Radiology at Queens University and Queen Victoria Hospital in Belfast, UK. While in Belfast Prof Williamson gained a five Accreditation for the University.
Prof Williamson returned to the Gold Coast in 2016 and took up a position at Bond University. Following retirement from Bond University in 2020, he returned to Perth where he was offered a position in Private Practice and participated in teaching courses at CTEC and UWA.
When asked what initially drew him to study dentistry, Raymond reveals his grandfather was a dentist. The decision to later specialise in Oral and Maxillofacial Surgery was made because he saw OMS gave a greater opportunity to deal with patients’ facial problems.
"(Highlights of my career is) a difficult question, but I would answer it by saying my career in OMS has allowed me to carry my knowledge and expertise into many other fields, ensuring I have been able to have a broad and full experience of the tapestry of life as well as leaving a legacy of having the pleasure of teaching all the people under my guidance the over the years,” he says.
To someone considering specialising in oral and maxillofacial surgery, Raymond says: “OMS is the longest training program of any dental or medical specialty, so it will take dedication and commitment but will give a rewarding and fulfilling career.”
Retirement will not mean slowing down for Raymond – he plans to
continue swimming three kilometres a day and plans to get back to his archaeology digs and lots of travel. He will also continue to be part of training courses at CTEC and UWA.
“I first met Ray Williamson when I returned from London in the early 80s. Ray had moved to Perth with the Navy, and we had a common goal of Specialising in Dentistry. We have kept in touch professionally over our entire careers. Ray’s clinical and academic career has been so varied and exceptional.
Most recently, he and his wife Jan, having returned to Perth after considerable family challenges, and as we both move towards the end of our careers, we have re-engaged and worked clinically again together with Dieter Gebauer in Mount Lawley.
Above all things, Ray’s inquisitive nature, his life long quest for answers, has led him to explore deeply into so many fields including receiving his PhD in Head and Neck Radiation Biology, and external to dentistry, his love of Archaeology, Underwater and Sports Medicine, rugby and other passions, but to name a few.
On a lighter note, in 1997, I remember having a very deep discussion about the recently released, Mercedes SLK 230 convertible roadster.
I’d had the first one to come into Western Australia and Ray was getting impatient, still being on the 18-month waitlist.

Ray arranged to come around and have a drive and see if he was going to wait. We roared around the eastern suburbs with the top down and were like a couple of kids.
I’m uncertain if Ray still has his, unlikely due to his International career, but I still have mine. Maybe it’s time to go for another ride.
A loyal colleague and teacher to so many, we all congratulate Ray and wish him, the very best in his upcoming retirement.”
Dr John Owen AM, Orthodontist
“The most important memory that I have of Ray was that he was instrumental in organising and applying the new regulations at that time for training for the RACDS Maxillofacial exam and qualification. This required the coordination of consultants and trainees passing through Royal Perth Hospital, Charles Gairdner Hospital and Princess Margaret Hospital (now Perth Children’s Hospital). This took some doing, to be sure that the trainees fulfilled requirements for training and examination. He also needed to make sure that the Consultants were aware of the requirements. Ray was always approachable, sympathetic and easy to deal with as the Head of Department. He is definitely worthy of special recognition.”
Dr Ian Rosenberg, Oral and Maxillo-Facial Surgeon
“I found Ray a very diligent, dedicated and eager trainee who was both inquisitive and able to grasp his subject enthusiastically with great
determination to get things right and perform his duties with professional and skilled ability.
Ray went on after finishing his training to a position in the University where he acquitted himself admirably as both a clinician and teacher, being involved in the training of many of current Maxillofacial surgeons in WA and some from the Eastern states.
Due to our very various commitments at different hospitals, I rarely had the opportunity to have any ongoing clinical or professional involvement with Ray apart from catching up at many OMFS Association meetings and conferences at which I always saw Ray in a very involved and committed role.”
Mr Dennis Gregory, Oral and Maxillo-Facial Surgeon
“Prof Williamson has had oversight of the training a significant number of Oral and Maxillofacial surgeons who are providing a service to the West Australian community and has educated many general dentists over a long and distinguished academic career. He is the only OMS in west Australia who has completed a PhD and has had an immeasurable impact on the West Australian dental community. I am grateful for the influence you have had over my training and career, and I wish you the best in your retirement.”
A/Prof Dieter Gebauer, Oral and Maxillofacial Surgeon

Dr Gerard (Bruce) Barblett was recently acknowledged with an incredible 70 years of continuous ADAWA membership. We look at his contribution to the dental profession.
Bruce graduated from the University of Western Australia in 1955 – and he has given much to the dental profession over seven decades.
After a short time working at the Perth Dental Hospital, Bruce moved to the United Kingdom, before returning to Perth in 1959 on invitation to teach at the UWA Dental School for one year. Teaching is a passion and Bruce continued sharing his wisdom with dental students as a tutor for many years (he was also the Australian Dental Association’s representative for the education and training of dental technicians/prosthetists). In 2003, UWA’s Dental Alumni Group
recognised Bruce by appointing him to the Campbell-Wilson Roll of Honour.
“Bruce was a stalwart tutor in the mid to late 80's and beyond at the original UWA Dental School in Wellington St,” says former student, Dr David McInerney. “His expertise in denture construction was second to none and his professionalism and good humour made him a favourite amongst our cohort. One of our professions' outstanding contributors, an amazing gentleman and good friend. Congratulations on your 70-year membership of the ADA."
In 1960, Bruce joined Cottesloe Dental as a partner – staying at the
practice and treating generations of patients until his retirement in 1999.
He celebrated the practice’s 100th anniversary with current and previous partners and staff at a celebration in 2023, which happened to fall on Bruce’s 90th birthday.
“Bruce’s long-term membership with ADA typifies his loyalty and dedication to all aspects of his life – his family, his profession, his church and his sporting clubs,” says Dr Max Trott, former colleague and fellow partner at Cottesloe Dental. “Anything he does, he does with passion.”
“Bruce is such an enthusiast with everything in dentistry,” adds Dr Colin O’Brien, one of the current partners at Cottesloe Dental, who worked with Bruce for over a decade.
“He maintained his memberships with various dental groups – and attended meetings until recent years.”
Outside of Bruce’s commitment to his patients, Bruce served on the Dental Board of Western Australia for six

years. In 1994, The Australian Dental Association (WA Branch) recognised Bruce with a Distinguished Service Award. Bruce has always been an active member of the dental community – serving on various dental groups. Bruce is a long-standing member of the Western Australian graduate chapter of Delta Sigma Delta –with his contribution recognised internationally. He has been a valued member of the Dental Study Group of WA, Australian Society of Prosthodontists, and the Australian Endodontic Society. He held committee positions with the UWA Dental Alumni Council and the National Dental Foundation. He is also a Fellow of the Academy of Dentistry International and a Member of the International College of Dentists.
Congratulations and thank you, Dr Barblett – for your remarkable contribution to dentistry.


Dr Peter McKerracher OAM has been an ADAWA member for an incredible 60 years.
Dr Peter McKerracher OAM was the CEO of ADAWA when the branch was planning to recognise its first 60-year member – the late Dr Ray Owen OAM. He now joins Dr Ray Owen OAM (dec), Dr Ronald Townsend (dec), Dr David Booth (dec), Dr Gary Davis, Dr Donald Lloyd and Dr Brian Atkinson – as well as Dr Ted Adler and Dr Gerard ‘Bruce’ Barblett (both now 70-year members) as ADAWA members for over six decades.
Dr Peter McKerracher cannot recall why he initially decided to study dentistry but says it appealed to him from about Year 10 in high school. Certainly, his career has been varied –giving much to the profession.
“After three years on the Perth Dental Hospital staff (Road Dental Clinic, Aero-dental service included), I spent three years in UK obtaining my Fellowship in Dental Surgery at the Royal College of Surgeons and returned to a group practice in Perth city,” he says.
“After five years I spent a year as Visting Professor in the Crown and Bridge Department of the University of Michigan Dental School.”
Back in Perth, Peter set up his own practice in West Perth, where he remained for 25 years.
He then took the reins as CEO of ADAWA in the early 2000s. “It was the first time a dentist had done so,” he says. “It was a great pleasure to take on the role. I retired in 2007

but returned on a half time basis as a Consultant to the Dental Cases Committee and then the Dental Cases Panel. I finally retired in 2017.”
In addition to these roles, Peter tutored at the Dental School for over 20 years and was active in many dental groups – including on the Council of RACDS for 14 years. He was recognised in the 2015 Queen’s Birthday Honours with a Medal of the Order of Australia (OAM) for services to dentistry, to professional associations, and to dental education.
When asked about some of the biggest changes he has seen in dentistry, he says it is difficult to know where to start, listing changes including:
• Composite resins in materials
• Implants in treatment planning
• Infection control in practice
• And advertising, corporate ownership and health fund intervention in practice management. However, after six decades in the profession, what he has most enjoyed about dentistry comes down to the patients. “(I have most enjoyed) developing long-term relationships with patients and helping restore their smile, comfort and self-confidence,” he says.
“I think one single highlight that I recall with considerable pride during my tenure as CEO was the conception and the gestation of the delivery of the History of Dentistry of Western Australia, which was launched by the then Governor, Dr Ken Michael AC, on the 100th anniversary to the day of the first meeting of organised dentistry in Western Australia,” Peter recalls. “If you haven’t read the book or at least looked at it, I know there are some in the ADAWA office and would recommend that you have a look and discover what dentistry was like in the past. A lot of work went into the book and a lot of people contributed.”
As a former CEO, and as an Honorary Life Member of the branch, ADAWA has clearly had a positive place in Peter’s career. Aside from the CEO role, Peter says ADAWA was always very good to him and supported him in many ways. “(ADAWA is) always supportive to practitioners and a source of valuable information in all aspects of dentistry,” he explains. To other dentists, Peter advises: “The more that one puts into the profession, the more one gets from it – in every respect.”

50-year acknowledgment
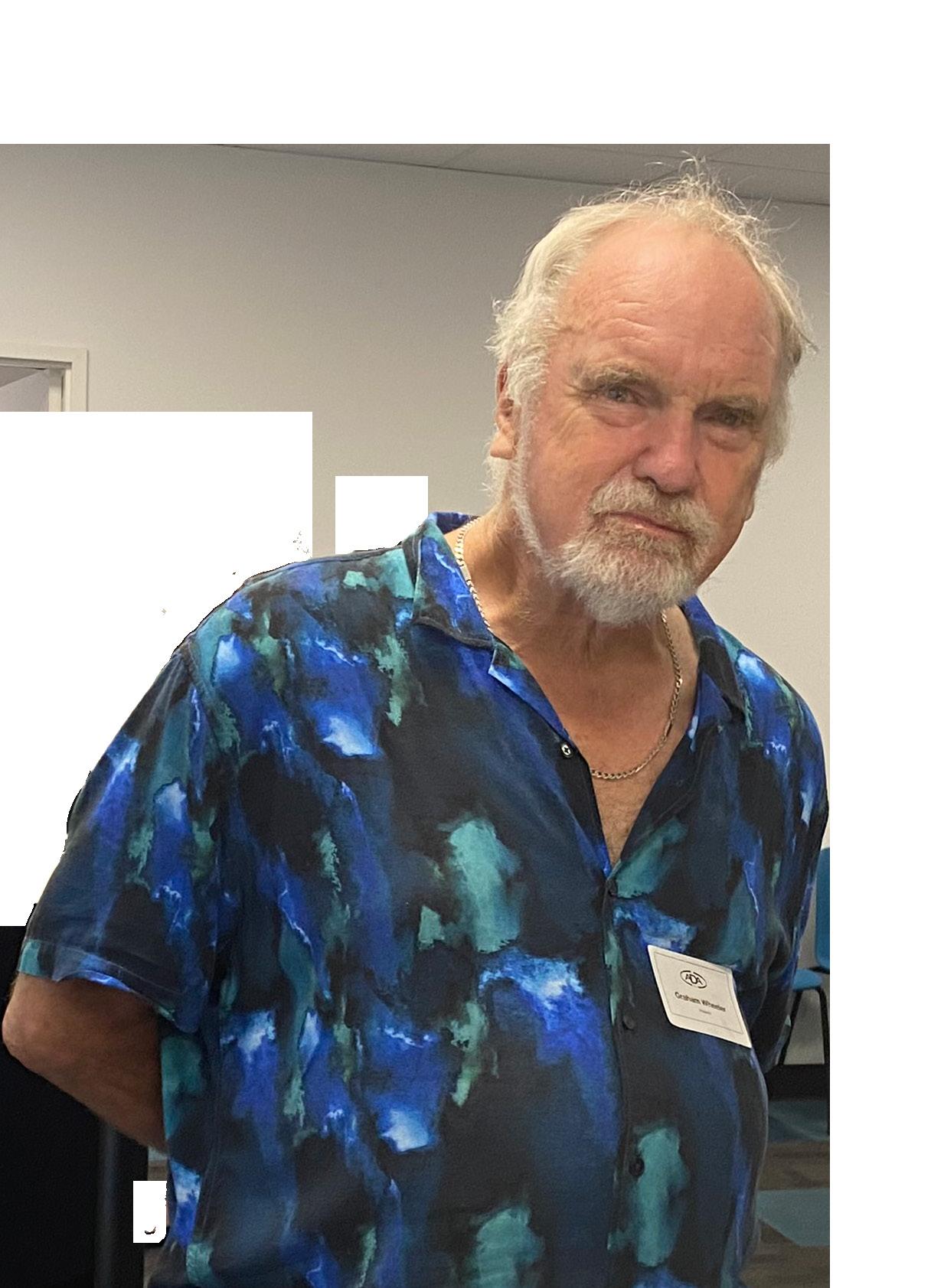
Dr Graham Wheeler was recently acknowledged with 50 years of continuous ADAWA membership. We spoke to him about his career.
As a dentist for over 50 years, Dr Graham Wheeler’s career has been as varied as it has been long – practicing in many locations both locally and internationally. After graduating, Graham started working for the government at the Fremantle Clinic – and was soon moved to the country. “I did short stint in New Norcia working on the mission kids,” he recalls. “It was freezing but good. I then went to Mt Newman and was then posted to Gnowangerup in the southeast. We then went to the UK.”
When Graham returned to Perth, he worked in various places including Fremantle Prison – before working full-time in a Mount Lawley practice for over 10 years. He then moved to a practice in Booragoon. He later relocated to a practice in South Perth and has since worked in practices around Roleystone, Craigie and is now in South Lakes.
Outside of dentistry he has given back in different ways – on the P&F (Parents and Friends) committee at his children’s primary school and later when they went to high school at MLC, Graham served as the president of the P&F and was on the college board. He also helped set up the Neighbourhood Watch in the Attadale area.
Graham has a long association with Rotary, and was the youngest
president his Rotary club had ever had back in 1988/89. He then went onto be President at another Rotary Club in 2017/18. He has even appeared on national television on ‘Insight’ on SBS in May 2008, on the topic ‘Pulling Teeth’. He also has a very loved family with two daughters, two granddaughters and a grandson. Things haven’t always been smooth sailing, but when asked about what he has enjoyed most in his career, he says it has been talking to people and giving them practical solutions to problems. He advises new practitioners to always think of the patient. “Always think of the practical solutions rather than what you can make money out of,” he says. “Get the best outcome for your patients.”
Congratulations Dr Wheeler!

Now that we are in a new financial year, we spoke to the experts in finance about their tips for dentists.
Marcus Parkinson and Christopher Ninyett from Smith Coffey say whether you’re a newly qualified dentist or a practice owner, effective tax and financial planning is essential. Here are some key tips tailored to different stages of your career.
Buying property is a common goal, but many dentists delay because they think they need a larger deposit. The key is starting early. Create a separate savings plan dedicated to your deposit and automate contributions from each pay. A 5% deposit (plus costs) is typically needed through Smith Coffey’s recommended lender, and the earlier you act, the more you benefit from long-term capital growth.
Income Protection - Protecting Your Earning
Your ability to earn is your most valuable asset. Income protection insurance is a must, especially policies tailored to dental professionals with “own occupation” definitions, ensuring benefits if illness or injury stops you from practising dentistry specifically.
New Practitioners – Understand the Tax Landscape
When new Dentists come into the industry most of them are contracting or earning ABN untaxed income. Its imperative to set aside funds for tax, register for GST correctly, and understand the difference between employee and contractor arrangements.
Owning a practice? Ensure to utilise tax-effective structures (e.g. trusts, companies, or service entities) to legally reduce tax, limit liability, and plan for succession. Don’t leave profits in your personal name unnecessarily exposed to top marginal tax rates. The right advice at the right stage of your career can make a significant difference. smithcoffey.com.au
Briony Gouldthorp, David Hartley and Kasey Cuff from AMA Financial Services share some valuable tips for dentists from various stages of their career.
Seek help when you need it: Seeking expert financial assistance helps you make informed decisions, avoid costly mistakes, and create a tailored plan to reach your goals. Professionals offer strategies you might not consider, help manage risk, and provide guidance through complex financial situations.
Address your contingency plans: establishing or managing a dental practice, particularly with others, offers significant advantages for dentists seeking to expand their practice and enhance patient care. However, will partnerships provide shared opportunities for growth and success, they also bring shared risks.
It is essential to consider the potential consequences if a partner were to pass away or become incapacitated.
Contribute to your retirement. Contributing to superannuation helps grow your retirement savings through compounding, offers potential tax benefits, and ensures you have enough funds to maintain your lifestyle when you stop working. The earlier you start, the more your money can grow over time.
Set goals early. Setting financial goals early gives you a clear direction, helps build discipline by living within your means, and maximizes the power of compound growth. It also prepares you for big life events, reduces financial stress, and increases your chances of long-term success. amafinancialservices.com.au
BOQ Specialist offers practical advice to help you stay financially fit and future-ready. Finance Specialist Josh van Bruchem shares his top tips.
Investing in modern dental equipment is essential to stay competitive. Upgrades can enhance patient outcomes and improve practice efficiency. Take advantage of any available government incentives and supplier promotions to make upgrades more affordable.
Healthy cash flow is the backbone of any practice. Set aside funds for unexpected expenses and seasonal revenue fluctuations. Being prepared ensures smoother operations year-round.
Whether you're purchasing a new practice, expanding your current one, or buying equipment, BOQ Specialist offers various financing solutions tailored to various needs. Knowing your options empowers you to make confident, informed decisions. boqspecialist.com.au
Credabl’s finance consultant, Ali Joyce, shares top strategies for building wealth from a finance perspective.
Whether you’re a contractor or practice owner, building a team of specialists who understand the dental profession can make a real difference. This might include a finance specialist, accountant, financial planner, and home loan broker. Their collective expertise helps ensure your financial decisions align with your growth goals and circumstances.
Not all debt is created equal. Understanding the difference between personal bad-debt (non-deductible) and investment or business-related good-debt (potentially deductible) is key. As a general rule, focus on repaying personal debt (like a home loan) before tackling business or investment debt, as the latter may deliver long-term financial advantages. A finance specialist can help you structure your loans in a way that supports your broader wealth-building goals. credabl.com.au/team#wa






Emily Chae
As well as dentists, oral health therapists play a pivotal role in treating patients in the TIMA Perth team.
After finishing high school without a clear career path, Emily was inspired to explore dental technology when she saw my grandmother struggle with ill-fitting dentures. “I trained as a dental technician and worked as a ceramist, fabricating crowns and veneers,” Emily recalls. “Over time, I became curious about how my work translated into patient outcomes, which led me to become a dental assistant. I found deep meaning in patient care and wanted to be more directly involved in treatment. After eight years as a dental assistant, I enrolled in an Oral Health Therapy course and am now a registered oral health therapist working in Armadale.”
Having worked as a dental assistant in private clinics for over a decade, Emily says she often witnessed patients referred to the public system endure long waiting periods. “While I was still a student, I felt a strong desire to contribute meaningfully to the community, especially for individuals from low socioeconomic backgrounds with limited access to dental care,” she recalls. “That motivation led me to begin volunteering with TIMA as a dental assistant before I graduated.”
Emily began volunteering regularly at TIMA’s monthly dental clinics and also participated at their first rural outreach program in Kalgoorlie, supporting disadvantaged patients, including those experiencing homelessness, people living in rural areas, and Indigenous Australians.
“With over ten years of experience as a dental assistant, I often support new volunteers, particularly those who have little or no dental experience or have just started studying in a dentistry-related course,” Emily explains. “I guide them through essential skills such as instrument names and infection control procedures. Since graduating, I have been volunteering as an oral health therapist, treating patients within my scope of practice and working closely with dentists.
I also assist by administering local anaesthetic or preparing patients so that dentists can begin treatment immediately.”
Emily adds she primarily focuses on managing periodontal disease for TIMA patients, which she believes is fundamental to achieving long-term oral health.
“I also provide restorative treatments within my professional scope as an oral health therapist,” she says. Volunteering with TIMA has been very rewarding – and she says the rural outreach program in Kalgoorlie was especially meaningful. “For several days, we gathered before sunrise and continued treating patients until 10pm, driven by a shared commitment to helping others,” she says. “Even when we were physically exhausted and some team members were unwell, what stayed with me most was seeing Indigenous patients who left home at three or four in the morning just to receive care. The dedication of both volunteers and patients was truly inspiring.”
To someone thinking about volunteering with TIMA, Emily says they welcome support in all forms.
“In addition to dental assistants and clinicians, there are important roles for interpreters, patient escorts, and other volunteers who help with many tasks that are often overlooked in regular clinics,” she explains. “Volunteering with TIMA is incredibly rewarding both personally and professionally. You will meet compassionate people, grow as a clinician, and make a real difference in communities that need it most.”
To enquire about volunteering with TIMA Perth, please email tima.perth@tzuchi.org.au
Our specialist lending team has deep experience in the dental sector so we understand what you need. We’re here to support you at every step of your professional and personal journey.


Ali Joyce 0411 602 084 ali.joyce@credabl.com.au


Deb Kiely 0413 427 601 debbie.kiely@credabl.com.au

Karyn Bailey 0490 851 159 karyn.bailey@credabl.com.au
Kym Bowker 0482 163 249 kym.bowker@credabl.com.au
Alison Gardner 0428 563 325 alison.gardner@credabl.com.au
Discover the difference that Credabl can deliver for you. Reach out to your local team today!

The Australian Dental Association (WA) Prize
Ms Elyssa Chan and Ms Yi Jia Yap
The Australian Dental Association (WA) Award for Leadership Excellence in Dentistry
Dr Josephine Santoso
The Australian Dental Association (WA) Prize for Academic Excellence in Dentistry
Dr Kaylee Wong
ADAWA were pleased to present awards at the 2025 UWA Dental School Prize-Giving Ceremony. We asked Dr Kaylee Wong about the honour.
Q: What does being awarded the ADAWA Award for Academic Excellence in Dentistry mean to you?
A: Receiving the ADAWA Award for Academic Excellence was an immense honour, one that I never expected. Throughout Dental School, my focus has always been on giving my best, absorbing as much information as possible, and providing the highest standard of care to my patients. To have my hard work recognised in this way is both humbling and deeply rewarding.
Q: Do you have a message for ADAWA and the Dental School regarding receiving this award?
A: I would like to express my heartfelt gratitude to ADAWA and the UWA Dental School for their unwavering support throughout our journey as dental students. I am very appreciative of the guidance, support and opportunities provided by both parties, which have been instrumental in helping me reach where I am today.
Q: What are you currently doing, since graduating from Dental School?
A: I am currently working in metro Perth, where I continue to grow and develop my skills as a new graduate. Transitioning from school to private practice has been a steep learning curve, but it is also a welcomed and exciting change! Additionally, I am also undertaking CPD courses to further enhance my learning.
Q: What would your advice be to current Dental School students to ensure they make the most of their degree?
A: My advice to current students would be to always be willing to ask questions and seek clarification. The tutors and lecturers have a wealth of knowledge, so make sure you tap into it while you have the opportunity. It is also important to find time for activities outside of studying—maintaining balance is key to both motivation and well-being!

By Enore Panetta Panetta McGrath Lawyers
In recent months, increased regulatory scrutiny has been directed toward the use of early access to superannuation via the Compassionate Release of Superannuation (CRS) scheme to fund dental procedures. While the scheme is administered by the Australian Taxation Office (ATO), it is the actions of some health practitioners in facilitating or encouraging these applications that have prompted concern.
On 30 May 2025, Ahpra and the Dental and Medical Boards of Australia issued a joint statement addressing reports of financial harm suffered by patients who accessed substantial amounts of superannuation to fund dental and medical treatments. The tone of the release was pointed. Practitioners were put “on notice” and warned that conduct prioritising financial gain over patient care would be met with regulatory action.
This article highlights the key regulatory risks and ethical concerns that arise in this context and what practices should be doing to avoid exposure.
It is not unlawful for patients to access their superannuation to pay for dental treatment under CRS, nor is it necessarily improper for a dental practitioner to provide clinical evidence to support an application. However, what is lawful is not always ethical, and what is ethical may still carry regulatory or reputational risks if poorly handled.
The real concern is the potential for misuse: where patients are encouraged to pursue early release of superannuation without full understanding of the risks, or where dental
practices become too closely involved in the application process. When that occurs, issues of consent, privacy, clinical justification and financial pressure all come into play.
The joint statement from Ahpra and the Boards makes it clear that they are actively investigating:
• Practitioners with high volumes of CRS support letters, potentially without adequate patient assessment;
• Reports of misleading or exaggerated documentation provided to facilitate applications;
• Practices engaging in predatory conduct, such as demanding upfront payments, pushing costly or unnecessary treatments, or requesting patient myGov login credentials.
Ahpra CEO Justin Untersteiner stated:
“We are deeply concerned by reports that some practitioners may be putting their own financial gain ahead of their patients’ best interests.”
This kind of commentary is significant. It suggests that CRS-related conduct is being viewed through the lens of public protection, not just technical compliance. Relevant Professional Standards
The obligations on dental practitioners are not new. The Dental Board of Australia’s

Code of Conduct and the ADA’s Code of Ethics both set out clear standards:
• Patient interests must be prioritised over personal or commercial gain;
• Treatment recommendations must be evidence-based and clinically appropriate;
• Financial consent must be fully informed and documented;
• Privacy obligations must be respected, particularly when it comes to patient identification and online portals such as myGov.
Where practices blur the lines between clinical care and financial facilitation, they expose themselves to complaints, investigations, and potential disciplinary proceedings.
From a legal and governance perspective, there are several practical steps that dental practitioners and clinic owners should take:
1. Avoid handling CRS applications
Patients should complete their own applications. Practitioners may provide factual clinical reports but must not log in to or submit applications on behalf of patients.
2. Never request myGov credentials
Doing so not only violates ATO guidelines but could give rise to serious privacy and security breaches.
3. Ensure financial consent is documented
Patients should receive written estimates, with all fees, payment options, and refund policies made clear before treatment commences.
4. Don’t link treatment to CRS availability
Refrain from implying that access to superannuation is required or encouraged. Discuss treatment on its own merits, and direct patients to seek independent financial advice.
5. Review marketing and sales practices
Audit your messaging and patient interactions to ensure no pressure tactics, upselling, or inducements to commit to large treatment plans.
While the overwhelming majority of dental practitioners act ethically and with integrity, the recent regulatory commentary makes it clear that a handful of cases have prompted real concern.
This is a good time for dental practices to pause and reflect:
• Are your current financial consent processes sufficient?
• Do your staff understand the boundaries around CRS involvement?
• Is your clinical documentation robust and defensible if later scrutinised?
Patients accessing superannuation to fund treatment are often vulnerable. The decision to sacrifice future financial security for present dental care is not one to be taken lightly, and not one for dental practitioners to steer.
Practices that operate transparently, separate financial and clinical processes, and adhere to ethical standards are unlikely to attract regulatory interest. But those that conflate care with commercial gain, or step too far into a patient’s financial affairs, are entering dangerous territory.
In an increasingly regulated environment, the best defence is a well-governed practice. If your systems, communications, and culture reflect a commitment to ethical care, you are on the right side of both the law and your patients.
The content of this article is intended to provide a general overview and guide to the subject matter. Specialist advice should be sought about your specific circumstances.

COURSE OUTLINE
This workshop will look at a range of traditional, and not so traditional approaches to restorative management of the ageing dentition. The workshop will also provide participants with hands-on exercises on minimally invasive conservative restorative techniques that provide cost effective and efficient options for managing the older patient.
Learning outcome
• Protecting exposed root surfaces – reducing sensitivity and improving aesthetics
• Root surface caries – is it manageable?
• The hopeless tooth – to restore or extract?
• Techniques for the deep interproximal posterior restoration
• Fibre reinforced restorations - for compromised and missing teeth
• And more
ABOUT THE PRESENTER
Professor Ian Meyers is a general dental practitioner in Brisbane Australia, and an honorary professor at The University of Queensland School of Dentistry. Professor Meyers has over thirty five years of combined experience in dental research, clinical dentistry, private practice, university clinics and hospital based dental clinics. He is a Fellow and Board Member of the Royal Australasian College of Dental Surgeons and of the International College of Dentists and is a Fellow of the Academy of Dentistry International and the Pierre Fauchard Academy. In 2017 he received the Order of Australia Medal for services to dentistry, to professional associations, and to tertiary education.
As a general dental practitioner, Ian Meyers has extensive experience in comprehensive patient care and has a special interest in diagnosis and management of worn and broken down dentition, geriatric and aged care dentistry, adhesive restorative dental materials, fibre-reinforced composites, and the management of patients through minimum intervention dentistry.


Dr Lalima Tiwari is one of the respected team of experts who will be presenting a course about oral medicine red flags.
Dr Lalima Tiwari says she always enjoyed Science and Human Biology so when it came to choosing a university course, she knew that something in healthcare would be a good match.
“During that time, my cousin had started Dentistry and so I was able to gain good insights into what Dentistry at UWA was like and a feel for how it could be as a career,” she recalls. “The combination of healthcare and a career that can provide work-life balance seemed very inviting.”
When asked what attracted her to the field of oral medicine, Lalima says she had the opportunity to observe Dr Arrabelle Clayden, Oral Medicine Specialist, whist working in Brisbane as a general dentist for Queensland Health. “Dr Clayden opened my eyes into how incredible
Oral Medicine can be and how much impact it can have on a patient,” she says. “Patients presenting for an Oral Medicine consult are often suffering with chronic, debilitating orofacial conditions, and are often very anxious about their condition. The combination of using problemsolving skills to diagnose their oral condition, care for them in a nurturing manner, and empower them to manage their condition was what attracted me to the field of Oral Medicine.”
Lalima says the aim of the oral medicine reg flags course is to provide attendees the latest knowledge on what “Red Flags” to watch out for in both oral mucosal and orofacial pain conditions. “We will cover ‘red flags’ for a variety of conditions including gingival
pathology, mucosal pathology, swellings, temporomandibular disorders and orofacial pain,” she says. “Attendees can expect lots of real-life case discussions to highlight these red flags.”
It will be the first time that oral medicine specialists Lalima, Janina, Ramesh, Bobby and Robert will be presenting a course together. “It is an incredible collaboration, as all of us have varying experiences, skills and knowledge that we hope to share with the attendees,” she says.
Lalima says the course is perfect for anyone who practices clinical dentistry. “At some point in time you will have a patient present with a “red flag” condition and will be required to provide appropriate management for them,” she says. “We hope attendees will leave the course with confidence in recognising and managing patients with urgent needs in relation to their oral pathology or orofacial pain,” she adds.
What three words best describe you? Empathic, Introspective and Adventurous.
What do you enjoy doing in your spare time? Spending time with my family, especially my little baby, and travelling and hiking.
What is your favourite book? Wild by Cheryl Strayed.
Is there anything someone might be surprised to learn about you? I love reading about space, the universe and enjoy stargazing – I’m keen to buy my own telescope one day! At the same time, I love trashy reality TV. Love is Blind, anyone?
You also hold a senior lecturer appointment at UWA Dental School.
“I think the course serves as an excellent opportunity to hear from a variety of speakers. We each have our own lecturing style which hopefully serves a larger audience.”
Lalima, along with Dr Janina Christoforou, A/Prof Ramesh Balasubramaniam OAM, A/Prof Bobby Joseph and Adjunct Professor Robert Delcando, will be presenting Oral Medicine Red Flags on Saturday 20 September at ADA House. To book, visit our website cpd.adawa.com.au
What do you enjoy most about teaching others? I find it extremely rewarding to teach Oral Medicine. I suppose that is how I fell in love with Oral Medicine – I had someone enthusiastically show me the impact it can have on a patient.
I love discussing cases with the DCD Oral Medicine Registrars, engaging in the latest literature, and most of all seeing them gain confidence as clinicians within the field.
What future plans are on the horizon for you? I have recently commenced my PhD in Oral Medicine. It’s a long road ahead as I am pursuing it parttime alongside private practice, my senior lecturer position as well as recently being a new Mum! In saying that, I am very excited about it, as it also focuses on improving how we teach Oral Medicine!


COURSE OUTLINE
The purpose of this course is to demystify endodontics over two days, so that attendees improve their confidence in root canal treatment. This course will involve hands on training first using plastic blocks to get used to simplified two preparation systems (ProTaper ULTIMATE and Wave One Gold) and then graduating to extracted teeth, with both systems. Warm gutta percha obturation techniques will also be explored. In addition to lectures on preparation and filling techniques, there will be lectures on treatment of endodontic pain and complications in endodontics..
Topics include
• Hands on training using plastic blocks and the latest endodontic equipment
• The opportunity to use microscopes
• Filling canals using the latest techniques
• And more
ABOUT
Dr Omar Ikram was born in Christchurch, New Zealand and attained his Bachelor of Dental Surgery qualification from Otago University, Dunedin. After graduation Omar worked in private practice in New Zealand and then moved to London in the UK where he attained significant experience in endodontics.
In 2005, he completed his Fellowship of the Royal Australasian College of Dental Surgeons and began specialist training in Endodontology at King's College, London. His groundbreaking research at King's, entitled 'Micro-computed tomography of tooth tissue changes following root canal treatment and post space preparation' was published in the International Endodontic Journal during his final year. This research has enabled him to lecture in the United States of America, the United Kingdom, Australia and Malaysia.

By David McMullen, Principal Lawyer – Practice Leader, Commercial and Sean Foy, Senior Associate Panetta McGrath
Recently, we were asked to advise on obligations arising under the Superannuation Guarantee (Administration) Act 1992 (Cth) (SGAA). More particularly, the extent to which the use of dental Facility and Services Agreements (FSAs) (which can go by a variety of names, but which are to be distinguished from contracts of employment and dental contractor agreements) can give rise to unintended obligations for dental practices under the SGAA.
It is opportune therefore to remind dentists and dental practices about some key principles; including those discussed by Full Court of the Federal Court of Australiain in Dental Corporation Pty Ltd v Moffet [2020] FCAFC 118 (Moffet).
The SGAA’s expanded definition of employee and employer
Under the SGAA, “employee” and “employer” have their ‘ordinary meaning’, but also an expanded meaning; such that ‘if a person works under a contract that is wholly or principally for the labour of the person, the person is an employee of the other party to the contract’. The SGAA therefore treats contractors as employees for superannuation purposes if they are engaged under a contract that is ‘wholly or principally’ for their labour. For the avoidance of doubt, a deemed employee for SGAA purposes is not an employee for all legal purposes. If they are a contractor having regard to the totality

of their relationship to the dental practice and the established legal tests, then they retain their character as a contractor. They are merely treated as an employee for the purposes of the SGAA.
The expanded meaning covers any natural person (ie individual) who works under a contract that is wholly or principally for the labour of the person. In our view, it follows that:
(a) A sole trader dentist who provides dentistry services to a dental practice under contract may be an employee for SGAA purposes.
(b) Sole traders who procure facilities and services from a dental practice under a genuine FSA are not likely to be employees for SGAA purposes.
(c) Corporations that supply dentistry services to a dental practice, or procure facilities and services from a dental practice under an FSA, are not employees for SGAA purposes. (However a corporation

in this situation may have superannuation obligations with respect to its own employees and subcontractors).
The Moffet decision
Dr Moffet’s company, Immediate Dental Pty Ltd (Immediate Dental), was trustee of the Moffet Family Trust and conducted a dental practice in Parramatta NSW. In 2007 Immediate Dental sold the dental practice to Dental Corporation Pty Ltd (Dental Corporation) and the parties agreed that Dr Moffet would continue to work in the practice.
Under the parties’ agreement
• Dr Moffet was required to treat patients, and he was incentivised to manage the practice profitably. His remuneration was comprised of multiple commission components calculated with reference to his own patient billings and the overall profits of the practice, as well as other components. Dr Moffet was able to set his working hours; he maintained his own insurances; and he had clinical autonomy.
• Dental Corporation was required to provide equipment and staff to enable the dental practice to operate efficiently.
• Dr Moffet was described as a contractor and not an employee of Dental Corporation.
• In 2014, Dr Moffet resigned. Some time afterwards, Dr Moffet commenced legal proceedings asserting he was an employee and entitled to payments with respect to superannuation as well as unused leave.
It was held
• Dr Moffett was a contractor – not an employee – of Dental Corporation, according to established legal principles. He was not entitled to employment leave.
• Although he was a contractor, Dental Corporation was still obliged to make superannuation contributions on Dr Moffet’s behalf because he met the ‘extended definition’ of employee at section 12(3) of the SGAA.
• It did not matter that Dr Moffet was paid substantially by commission.
The risk that every dental practice will want to avoid, is the risk of unwittingly incurring superannuation liability in respect of dentists who were never thought to be employees. The same will apply to dentists who subcontract with a third party (a locum, for example) to provide cover during periods of leave or other absence. The risk can materialise in several ways:
• A party that is required to make superannuation payments to another party under the SGAA, but does not do so, may be required to pay a superannuation guarantee charge (SGC) assessed by the Australian Taxation Office. SGC is typically assessed as a higher amount than the unpaid superannuation contribution.
• Alternatively, as in Moffet, the party to whom superannuation is owed may commence legal proceedings insofar as section 116B of the FW Act requires the superannuation to be paid.
• Although parties may think they have agreed that no superannuation is payable, it is in fact difficult and sometimes not possible to contract out of superannuation entitlements.
• Although a contract may on the face of things be an FSA under which superannuation is not applicable, the effect of wording in a written contract may be modified, supplemented or superseded by other factors. The ATO or a court may still consider that overall, the contract is better classified as being one for the provision of the dentist’s labour to the dental practice.
Careful decision making at the point of entering into a contract is critically important. In our view, parties should consider whether they want to contract as or with corporations or natural persons and whether an FSA, employment or contractor arrangements are better suited to their needs. Of course, superannuation is just one factor to
consider; and whatever the arrangements, they need to be satisfactory to all parties.
Additionally, parties should ensure that the basis of their contract is clear, particularly with respect to who is acquiring and who is supplying services. Parties should also maintain discipline about the correct and accurate implementation of their contract terms.
Every relationship between a dental practice and a dentist will be highly fact-specific, and dependent on the parties’ written (and sometimes unwritten) contract terms. To reduce the risk of unintended liabilities and duties, dentists and dental practices should always seek advice about the character and terms of their agreements; their respective rights and obligations; and their actual day to day performance of contracts when issues arise.
If you would like more information, or to discuss your circumstances, our firm would be pleased to hear from you. We offer free initial consultations and reduced fee arrangements to ADAWA members.

Dr Sheyda Khadembaschi generously donated her time and talent to create the first piece of art for our member gallery at ADA House.
“The intention for ‘Still Life Art versus Science’ was a nod to Dentistry in Western Australia,” Sheyda says.
“Skulls appear frequently in the European still-life tradition, serving as reminders of the fleetingness of life. To many of our colleagues, I hope it brings back fond memories of the days studying facial and dental anatomy. The colours in the ‘science experiment’ or ‘abstract bunch of flowers’ represent the colours of the native wildflowers of Western Australia.”
If you are a member who also happens to be an artist, who would like to donate or lend a piece of art for the gallery, please contact our office.





By Dr Shahrzad Nazari, Endodontist
Dens Invaginatus (DI), a relatively uncommon developmental dental anomaly characterized by the invagination of enamel and dentin into the tooth structure, particularly the Type III variant which extends beyond the cementoenamel junction and possesses its own independent apical foramen, presents intricate endodontic challenges stemming from its often highly complex and unpredictable internal anatomy. Successful management requires a meticulous and tailored approach. This case report details the successful non-surgical root canal treatment of a Type III DI in a 15-year-old male's maxillary lateral incisor (tooth 12) with a pulpless, infected root canal system and a chronic apical abscess attributed to the DI defect. Preoperative evaluation involved clinical examination and periapical radiographs. While cone-beam computed tomography (CBCT) offers detailed visualization of such anomalies, its use was avoided to minimize radiation in this young patient. Clinical findings and conventional radiographs were deemed sufficient for treatment planning.
The endodontic therapy was conducted over four appointments. Access cavities were precisely prepared for both the main canal and the invagination, guided by a dental operating microscope. Working lengths were determined electronically and confirmed radiographically. The main canal was shaped using rotary files. The narrow, irregular invagination was meticulously instrumented with hand files, utilizing both EDTAC and copious sodium hypochlorite irrigation for thorough cleaning and disinfection. Calcium hydroxide mixed with Ledermix was used as the initial intracanal medicament to address infection and inflammation.
The fourth appointment involved re-access, final EDTA irrigation, and obturation. The main canal was obturated with a single gutta-percha cone and AH-26 Cement. Due to the invagination's complex morphology, a thermoplasticized injectable gutta-percha system ensured complete three-dimensional filling of this aberrant space. The access cavity was then permanently restored with composite resin to prevent microleakage.
A six-month clinical and radiographic follow-up demonstrated a successful outcome. The patient was asymptomatic with no tenderness, and the previously present sinus tract had resolved. Radiographic evaluation revealed a significant reduction in the periapical radiolucency, indicating healing of the chronic apical abscess.
In conclusion, this case underscores the critical role of meticulous chemomechanical preparation of both the main and invaginated canal systems, the strategic use of appropriate intracanal medicaments, and the application of tailored obturation techniques, such as thermoplasticized gutta-percha for complex anatomies, in achieving successful endodontic outcomes in challenging DI cases. While CBCT is a valuable diagnostic tool, this case highlights that thorough clinical assessment combined with carefully interpreted conventional radiographs can be sufficient for diagnosis and treatment planning in younger patients. Ultimately, a strong foundation in basic endodontic principles and the ability to adapt treatment strategies to the unique anatomical complexities of Dens Invaginatus remain paramount for successful management.




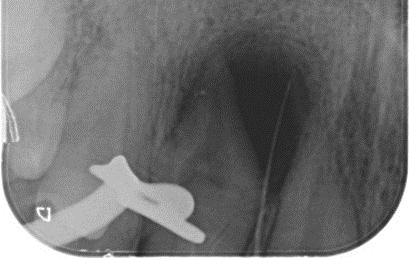
X-ray 1: A large periapical radiolucency in association with tooth #12, with a gutta-percha point tracing through the visible sinus tract originating from this area.




X-Ray 5: The six-month follow-up radiograph demonstrates a significant decrease in the dimensions of the radiolucent area, consistent with a favourable outcome of the endodontic treatment.


By Dr Colm Harney, Dentolegal Consultant at Dental Protection.
Orthodontics is that branch of dentistry concerned with growth of the face, development of the dentition, and the prevention and correction of occlusal anomalies.1
Abnormal alignment of the teeth and jaws is very common. The approximate worldwide prevalence of malocclusion was as high as 56% according to a recent meta-analysis.2
In COVID times, with people working from home and increasingly spending much more time looking back at themselves on screens in virtual meetings, there has been a significant uptick in demands for all forms of cosmetic dentistry, including orthodontics for cosmetic reasons –the so-called Zoom boom.
Any rise in demand unfortunately carries with it a rise in the number patients who are dis-satisfied with care. At Dental Protection, we see this especially when reviewing more elective or cosmetically driven cases where patients perceive that their expectations are not being met.
We know that most orthodontic cases involve a time span which can be viewed as a patient journey, from initial visit / referral to finish / review.
Along that road, Dental Protection regularly sees defined ‘pinch points’ in the treatment timeline that can lay the ground for a patient complaint.
So, by way of explaining, I will walk through a potential orthodontic case from start to finish highlighting some of the common themes and issues that arise. When referring to the patient, it is assumed that it includes parent / guardian / responsible person if the patient does not have capacity, such as a minor.
Taking a thorough history and having a good understanding of the patient’s presenting concerns and expectations as the starting point.
This should involve taking a history of previous treatments – for example an adult seeking clear aligner treatment due to relapse of previous orthodontic treatment may signal potential compliance discussions to be had, prior to any further course of care.
Communication
Effective and clear communication is paramount from the start, especially as orthodontic care often involves a significant time span and multiple visits.
Building a trusting relationship starts with something as simple as open disclosure about the practitioner’s qualifications –regrettably we sometimes see that general practitioners can be the subject of a complaint where the

patient reports they were under the impression the dentist was a specialist.
The quality and quantity of information gathered should be sufficient to evidence an assessment that is to standard, including consideration of the need for a lateral ceph and analysis of this. Pre-treatment ‘baseline’ records such as models / scans and good quality clinical photos are prudent practice. Are there any other dental considerations that may be impacted by treatment – for example periodontal considerations (including gingival biotype), existing recession, previous trauma? If so, this should be carefully assessed and documented and will serve as a baseline reference at the start of care. If there are sufficient concerns – for example periodontal issues - it may be in the patient’s best interest to undergo treatment or even see a specialist to ensure dental fitness prior to orthodontic treatment. With a history of trauma, baseline vitality testing of affected teeth might be indicated.
Putting all of the pieces (history, assessment, special tests) of the puzzle together. We often see cases where there is no diagnosis noted (even something as basic as an Angle’s classification), and it is difficult to justify relatively complex treatment without a diagnosis.
Following on from diagnosis, are all reasonable options presented (including benefits / risks / limitations / costs of each) appropriate to the case? Also, including the option of no treatment?
For example, are clear aligners going to achieve the outcome the patient expects? Is it an extraction vs non-extraction case?
Where mutual understanding is reached – a two-way conversation ensuring the patient has a good understanding of treatment options / limitations. The obligation is on the practitioner to ensure that the patient also understands their responsibilities (such as compliance, good oral hygiene, care of appliances, attendance as directed etc).
As orthodontic treatment is often elective, expensive and relatively complex, it is prudent to affirm any conversations with a written consent form which reiterates mutual understanding (signed before treatment commences) and / or a treatment letter setting out the practitioner’s findings and proposed care.
What is the cost, including any known additional costs such as retainers?
Who is responsible for payments?
Treating minors can create the additional level of consent required when a child lives with one parent, and another parent is paying for the treatment. To avoid dispute, there needs to be full clarity about who is paying for what and who is entitled to discuss the child’s care, give consent on their behalf (or withdraw it) and access the records, prior to the commencement of treatment.
Discussion of any concerns raised or unanticipated problems arising during treatment, for example a tooth that is not moving as anticipated or standards of oral hygiene that may put teeth at risk.
The practitioner should be working collaboratively with the patient / guardian to address these concerns wherever possible, in an open and transparent manner.
If a tooth is not moving or is going dark, it may be in the patient’s interest to have another opinion such as from
an endodontist. This may be a difficult conversation, especially if additional costs are going to be incurred. If there are difficulties finding a mutually agreeable resolution, there may be a need to reconsider merits of proceeding. For example, if a patient is not compliant with oral hygiene measures and is at risk of causing damage such as permanent marking around brackets, it may be in the patient’s best interests for the treatment to pause or cease.
At end of the planned course of care, was there a satisfactory outcomewithin the limitations discussed and agreed to at the start of treatment? This links back to options chosen and mutual understanding of limitations (consent) at the start.
Dispute about this is very common in surgical cases, where patients may have chosen a non-surgical compromised approach at the outset, only to be unhappy with the result at the end of treatment – everyone needs to be on the same page from the start.
We sometimes see patients / families who are tired and ‘burned out’ with treatment and want to finish / deband early – are they ceasing in full awareness of any compromises to the mutually agreed outcome at the start? For example, if there is still misalignment or bite discrepancies, is everyone aware and accepting of any compromises before a deband?
This should be a reiteration of conversations had at the start –such as need for retainers, ongoing compliance, any further potential costs (for example in case of continued lost or broken retainers) and spelling out what could happen in case of non-compliance (such as relapse and future need for partial / complete course of treatment again at the patient’s expense).
If we consider orthodontic care as a journey that a practitioner and patient travel on together, it is best practice to ensure that everyone is on the same page on what the journey looks like, including the end point or destination, before the journey starts. Once travelling, any unexpected roadblocks or diversions should be flagged and discussed. At the journey’s end, the practitioner needs to ensure that the patient is ‘dropped off safely’ at their destination and any ongoing mutual obligations are discussed and understood.
1. WJB Houston 1986; A Textbook of Orthodontics; Wright.
2. Lombardo G, Vena F, Negri P, Pagano S, Barilotti C, Paglia L, Colombo S, Orso M, Cianetti S (June 2020). "Worldwide prevalence of malocclusion in the different stages of dentition: A systematic review and meta-analysis". Eur J Paediatr Dent. 21 (2): 115–22.

ADA DHF Dental Rescue Day
“I didn’t have the ability to eat solid food properly. I have always been anxious about visiting a dentist. I have been given hope that I will have a complete smile in the future. Thank you from the bottom of my heart.”
Dental Rescue Day patient

This is the difference your dental practice can make by hosting a Dental Rescue Day!
The amazing team at Rockingham Dental Centre host Dental Rescue Days annually – with their latest one held on April 5. Five volunteer dentists: Drs Hari Menon, Vilas Menon, Jude Fernando, Zena Ibrahim, and Russell Gordon (Chair of WA ADA DHF), and their RDC volunteer team, including receptionist, Larrissa, and Dental Assistant’s: Michelle, Simone, Danielle, Taya, Jess, Ellen and Caitlyn, gave their time to provide urgent pro bono dental treatment to clients in desperate need of dental care.
If your practice is looking for a way to give back, please contact ADA DHF WA coordinator Andrea Paterson at WA@adahdf.org.au

Remember, Dental Health Week is from August 4-10! It is a great opportunity to remind your patients about the importance of taking care of their oral health. For Dental Health Week resources, visit teeth.org.au/dental-health-week
ADAWA recently acknowledged long-serving staff who have been employed for over 10 years. Congratulations to Andrea Paterson (who has been employed by ADAWA for 13 years), Jenny Catto (who has been employed by ADAWA for 11 years) and Andrea Andrys (who has been employed by ADAWA for 10 years).

Congratulations to the Healing Smiles team for winning the ‘Trailblazing Small Organisation’ at the Western Australian Council of Social Service (WACOSS) Community Service Excellence Awards. Healing Smiles’ Chair, Dr Lida Sayadelmi, was also a finalist in the ‘Outstanding Contribution’ category. Well done!

We would like to acknowledge the efforts of Volunteerism Coordinator, Sandra Wood, who, after five and a half years at ADA House, retired in June. Sandra was instrumental in coordinating the volunteerism efforts of Healing Smiles – liaising with volunteers, patients and referring organisations to help ensure the smooth journey of treatment of survivors of domestic violence. Her smile and bubbly personality will be very missed. The baton has been handed to Clinical Administration Coordinator, Rachel Mackie, the volunteers are in good hands! Any queries regarding volunteering with Healing Smiles should be directed to Rachel at admin@healingsmiles.org.au
It is good news for the teeth of residents of Donnybrook and Capel, with Fluoridation of drinking water commencing for the communities. About 94 per cent of WA’s population accesses fluoridated drinking water. For more details, see the media release: health. wa.gov.au/Media-releases/2025/June/ Fluoridation-of-drinking-water-forCapel-and-Donnybrook-communities
Join us at the next ADAWA General Meeting, with a lecture to follow by Dr Asheen Behari on: Composite Resin ‘Navigating common pressure points with posterior restorations’.
ADA House
54-58 Havelock St West Perth
6.15pm Eat and Meet
7.15pm Meeting Followed by Lecture
RSVP to adawa.com.au/adawa-general-meetings
ADA House was buzzing with enthusiastic attendees at June’s Practical Infection Control course with Dr Roslyn Franklin and Mr Steven Lines. Attendees heard lots of useful advice and took part in valuable hands-on components. Thank you to major sponsor/presenter STS Group Australia, as well as BOQ Specialist and Bunnings Trade, whose fantastic teams were here to talk and give merchandise to attendees. See what other courses we have coming up, cpd.adawa.com.au


At Dental Essentials, we’ll take care of all your insurance needs big and small.
As the leading insurance broker for dentists in Australia, our team will work closely with you to create a tailored insurance policy that offers ultimate peace of mind.
With our extensive services covering Practice Insurance, Management Liability, Practice Indemnity, Cyber Insurance and Personal Insurance, at Dental Essentials, we take care to do things right.


Dr Adam Hamilton – Increased Days
Dr Adam Hamilton, who is a prosthodontist with expertise in complex implant treatment, is now accessible an additional day each week. His private practice days are now Wednesdays and Fridays at The Centre for Prosthodontics South Perth. His team remains contactable throughout the week for any enquiries.
T (08) 9368 0888
E info@centreforpros.com.au
A 20 Lyall Street, South Perth W centreforpros.com.au

Dr Anchalee Jennings-Lowe new addition Taylor Road Periodontics & Dental Implants proudly welcomes Dr Anchalee Jennings-Lowe to the practice as a Specialist Periodontist. She is accepting referrals for all aspects of periodontics, implant surgery, and peri-implantitis prevention and management.
T (08) 6382 0699
E admin@taylorrdperiodontics.com.au
A 3/150 Stirling Highway, Nedlands WA 6009 W taylorrdperiodontics.com.au
New PerioPlus+ from Curaprox combines the treatment benefits of chlorhexidine (CHX) with CITROX® for great taste and reduced impact on your patient’s sense of taste.
Scientifically proven to be more effective than CHX alone, the PerioPlus+ range includes mouthwash, toothpaste and gel. For premium oral care choose PerioPlus+ from Curaprox.








Mortgage Broking, Financial Planning and General Insurance Broking. As financial planning, mortgage, and insurance broking specialists, we have a deep understanding of the unique complexities and challenges faced by businesses in your industry. Given our extensive experience working with health and medical professionals, we are pleased to offer exclusive discounts/benefits on our services to members of the ADA (WA). Phone 1800 262 346 or email info@amafinance.com.au

Medifit is an award-winning dental design and construction company, providing a comprehensive solution for dentists and dental specialists looking to build new premises or renovate their existing practices. Established in 2002, the company has designed and built hundreds of successful practices across Australia from their Head office in Perth. Contact Medifit and get the practice you deserve. medifit.com.au

We are excited to offer a member benefits program exclusive to ADAWA members. As a member of ADAWA, the member benefits program entitles you to an initial 30-minute consultation in person, by phone, or via video conference. ADAWA members are also eligible for a 15% discount on our standard hourly rates. ADAWA referral required pmlawyers.com.au

STS Group Australia is a family owned, WA business and industry leader in infection control and we have been serving the WA dental community for over 30 years. You’ll know us as Mocom Australia, offering a range of infection control and reprocessing equipment in Australia and New Zealand, STS Health, providing service and education throughout WA and STS Professional, manufacturer of infection control testing devices and related consumables. sts-group.com.au


For over 50 years, Smith Coffey has specialised in providing financial services for dentists. We offer expertise in taxation, superannuation, mortgages, and personal risk insurance. Trust us to help you achieve financial freedom while you focus on patient care. Contact us today! smithcoffey.com.au

Commonwealth Bank
At CommBank Health, we’re focused on delivering financial services for Dental Professionals at every stage of their careers. Services designed to increase productivity and enhance the patient experience. Tailored banking by experienced Health Bankers ensure your ambitions are fully supported. Flexible lending and insights enable business growth, Smarter payments can unlock efficiencies.
www.commbank.com.au/healthcare
At BOQ Specialist, we understand that a highly personalised service is what dental professionals need. We offer a full range of finance products and services, tailored to your needs no matter where you are in your career. With over 30 years of experience in dental finance, our focus is on building long-term relationships with our clients so that you can make financial decisions that are right for you. boqspecialist.com.au
Small Robot, a boutique technology company, provide business critical services covering IT, cyber security, and unified communications. Our highly experienced team leverage technology to protect, power and simplify your business. We provide consulting, engineering & managed services. We focus on the technology so you can focus on your business success. smallrobot.ai
SINCE 1997, SPADACCINI HOMES HAS DESIGNED AND BUILT SOME OF THE MOST DISTINGUISHED CONTEMPORARY HOMES IN PERTH. IF YOU HAVE THE VISION, WE HAVE THE EXPERTISE TO BRING IT TO LIFE. TOGETHER, LETS PUSH THE BOUNDARIES OF WHAT YOUR DREAM HOME CAN BE.