EDITOR
Dr Jay Hsing
EDITORIAL TEAM
Dr Matthew Nangle
Dr Gary Smith
Ms Lisa Rusten
Ms Melissa Kruger
PRODUCTION
Published by the
Dental Association (Queensland Branch)
CONTACT
24 Hamilton Place
Bowen Hills Qld 4006
PO Box 611, Albion Qld 4010
Phone: 07 3252 9866
Email: adaq@adaq.com.au
Website: adaq.com.au
ADVERTISING KIT
Information on advertising, deadlines and artwork specifications are available in the ADAQ Advertising Kit: adaq.com.au/advertising
GRAPHIC DESIGN
Kristen Willis, Tondo Creative
COVER ART DESIGN
Kristen Willis, Tondo Creative
ADAQ DENTAL MIRROR 2 CONTENTS 04 FROM THE PRESIDENT Dr Matthew Nangle's Final Address as ADAQ President 06 IT TAKES TWO Interview with the Dental Team 08 ADAQ TRAINING STUDENT PROFILE Ms Megan Moody 10 Understanding Run-off Cover 22 MEMBER SPOTLIGHT Dr Michael Foley AM 24 MUSEUM OF DENTISTRY The Grave History of Dentistry 27 CPD Cycle is Ending Soon–Are you Compliant? 34 IN MEMORY OF Dr Andrew Cole & Dr Robert Mabin
ADAQ Dental Mirror is published for the information of Members only and is not for general distribution. Copyright is reserved throughout. No part of this publication may be reproduced in part or whole without the written consent of the publisher. This publication is for the purpose of promoting matters of general interest to Members of the Association. The views expressed in this magazine do not necessarily reflect the views and policies of ADAQ or ADA. Publication of advertisements for products or services does not indicate endorsement by ADAQ. All material is positioned and published at the discretion of ADAQ.
DISCLAIMER
Australian
ADAQ COUNCILLORS
PRESIDENT
Dr Matthew Nangle
SENIOR VICE PRESIDENT
Dr Jay Hsing
JUNIOR VICE PRESIDENT
Dr Kelly Hennessy
COUNCILLORS
Dr Kevin Ang (Peninsula)
Dr Jiten Rao (Northern)
Dr Kaye Kendall (Moreton)
Dr Norah Ayad (Gold Coast)
FEDERAL COUNCILLORS
Dr Martin Webb
Dr Oleg Pushkarev (Western)
Dr Keith Willis (Moreton)
Mr Andrew Waltho (Skills-based)
IMMEDIATE PAST PRESIDENT
Associate Professor Alex Forrest AO
ADAQ SUB-BRANCHES
Bundaberg
Dr Paul Dever
Ipswich
Dr Andrew Wong
Kingaroy
Dr Man Chun (Simon) Lee
Cairns
Dr Brian James
ADAQ COMMITTEES
Conduct and Honours Committee
Chair: Dr Matthew Nangle
Volunteering in Dentistry Committee
Chair: Dr Jay Hsing
Mackay Dr Peter Monckton
Sunshine Coast Dr Peter Jorgensen
Gladstone Dr Patrick Dohring
Recent Graduates and Students Committee Chair: Dr Phillip Nguyen
Asset Management Committee Chair: Dr Jay Hsing
Toowoomba Dr Rob Sivertsen
Gold Coast Dr Roslyn Grant
Rockhampton Dr Kelly Hennessy

Dental History Preservation Committee Chair: Dr Gary Smith
Finance, Audit & Risk Management Committee Chair: Dr Martin Webb
Remuneration Committee
Chair: Dr Matthew Nangle
3 SPRING 2022
Dear Members,
FROM THE PRESIDENT: DR MATTHEW NANGLE
Thank you for having me as your President for the year of 2021 to 2022. It is my honour to give one final address to our Members.
This is my last address to you as President of our wonderful Association. I have thoroughly enjoyed working with colleagues on ADAQ Council, with our CEO Lisa Rusten, and all ADAQ’s staff over this last year. I have served on Council since 2017 and have seen board members come and go, but it has been a privilege to work with some of our profession’s brightest minds during this time. ADAQ Council is unified in its commitment to see growth not only in its membership base, but also in its provision of member services, and engagement with stakeholders and the community at large.
The overarching principles of what we do and the decisions we make are to meet our core objectives: the improvement of public health

and the practice and development of dentistry in Queensland through the design, support, and delivery of educational and professional services to member dentists and dental students. This includes the promotion of oral health in the community at large via interaction with government, regulators, and relevant professional, industry, and dental education bodies.

Telling the ship in which direction it should sail is all very easily said. However, keeping it functioning and at full speed is another matter. I believe our CEO, Lisa Rusten, deserves all the support our members can muster to help her in this demanding task. I have thoroughly enjoyed working with Lisa, she is a consummate professional, though I leave it to her to determine if this has been a mutually beneficial relationship – I am not renowned for meeting deadlines! I have also enjoyed working with ADAQ’s senior management and all other staff, be it help with editing and filming updates and reports to working on the ground at events and other business dealings. This year’s Dental Health Week in August garnered a lot of member and public interest, and I and others gave media interviews as part of spreading the positive message of the benefits of a healthy mouth and dentition on behalf of ADAQ. Advocacy will always be a key element of our existence. I have written before and will reiterate that member apathy is our greatest threat, so I thank all active and engaged members for the work they do that often goes unsung.
As I look back over the last year it would be inappropriate for me not to make mention of two major events that impacted our profession. First, the ongoing COVID-19 pandemic. In my first month at the helm, the Omicron wave began in Australia, and I was receiving many member emails confused as to government mandates and practice restrictions. I recall one E-blast in December 2021 that was written with due diligence and care and sent with good intention but became largely outdated within a matter of hours as government updates followed. With almost daily health updates from government during this period dentistry-specific messaging was unfortunately a difficult process, however I was mindful of the nature of disease and the
ADAQ DENTAL MIRROR 4
Image Dr Nangle at ADAQ General Meeting 2021
inevitable transition to an endemic status even then.
As we began 2022, I wrote in ADAQ’s Dental Mirror that: “I am no clairvoyant but am hopeful that we will continue to be able to work and meet the oral health needs of our patients with minimal disruption as we adapt to living with COVID-19”. Whilst this has proven to be largely true, it has coincided with a grim statistic, as more than two thousand Queenslanders will likely have succumbed to COVID-19 by the end of this calendar year alone, with many thousands more incapacitated to some degree impacting working environments across the entire healthcare sector. Nonetheless, our members have played a pivotal role during the pandemic, by helping to reduce the number of potentially preventable hospitalisations related to dental care.
The dental profession’s ongoing commitment to the highest standards of infection prevention and control is to be commended, and I thank members for continuing to carry out their role in healthcare provision be they private, public, or any other forms of activity. This has served the community well, and with time will hopefully have engendered greater public trust and understanding of the important interplay between oral and general health.
A second major event this year was the catastrophic flooding that affected many homes and practices across Southeast Queensland, from the Gold Coast up to the Wide Bay-Burnett regions. I heard many stories of support that helped practices get back on their feet, but this was nonetheless a very stressful and upsetting period for many members. Again, I offer praise and thanks to ADAQ staff, who have shown great capacity to adapt and work productively through these challenging times to provide support where it was badly needed.

ADAQ has achieved a lot in the last year, but this is not due solely to strong personal convictions of my own. I have always tried to encourage Council to reach consensus on any important decisions, and this can only be done by encouraging alternate and dissenting opinions to be heard so that all the pieces of the puzzle can be considered. We can be proud of continued increasing membership over the last few years (bucking trends in many other health professions), a discount in ADAQ fees this year, increased support for new and recent graduates including tailored CPD offerings and mentorship programs, and better engagement within and beyond the profession too. We have successfully expanded our reach across all dental sectors in Queensland, and this includes celebrating the first year of our ‘Dental Team Access’ program, offering appropriate (free and fee-based) resources and support to non-dentist members of the dental team.
During the year I have attended regular meetings with ADA federal bodies including the National Advisory Council and Inter-Organisation Working Forum and held important networking and advocacy meetings at ADAQ headquarters and online. For example, I have held productive meetings with Queensland Health’s Chief Dental Officer and Chief Allied Health Officer, representatives from the national health regulator (Ahpra), professional bodies including various representatives of the dental team, e.g., the Australian Dental Prosthetists Association, charities including the Australian Dental Health Foundation, and met with dental students and journalists across the state. It has been a particular pleasure to have visited many of ADAQ’s sub-branches as well. This has been of bidirectional benefit, as I have not only been able to update members directly on the activities of ADAQ this year but have received useful feedback on what we are doing well, and of course what we could do better.
Finally, I want to thank all ADAQ staff and members including fellow Councillors for supporting the Association in all its varied activities over the last year.
I look forward to continuing to work with a new President of the Association next year, with your professional and personal interests at the heart of all advice that may be requested of me.
Best wishes,
Dr Matthew Nangle, ADAQ President

5
Image
Dr Nangle’s President’s Investiture at Annual Clinic Day 2021
Image Dr Nangle at 'Dental Topics in the Tropics' 2021
Image Dr Nangle at ADAQ Council Meeting 2021
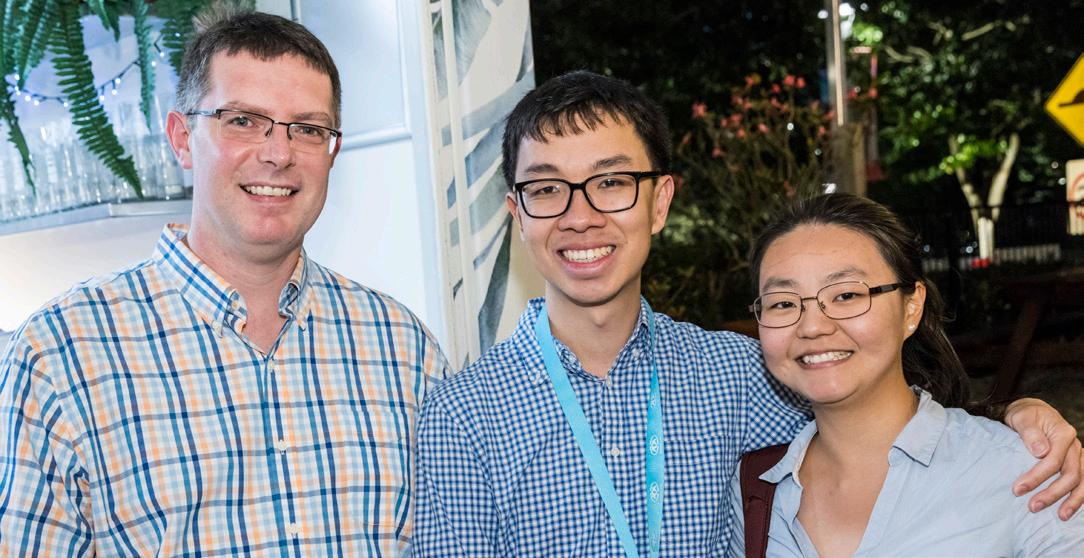
IT TAKES TWO
To celebrate the one year anniversary of ADAQ Dental Team Access, Dr Andrew Zischke, and Practice Manager Ms Kylie Horsburgh, share their perspectives on the profession and the ADAQ resources that benefit the whole Dental Team.
MS
KYLIE HORSBURGH — DENTAL TEAM ACCESS
Practice Manager and Dental Assistant, Grange Road Dental Group
WHAT ADVICE WOULD YOU GIVE TO SOMEONE WHO WANTS TO WORK IN THE DENTAL TEAM?
Dental assisting is such a rewarding career. Dentistry is both a science and an art. Getting to be a part of that is like nothing else. Seeing the changing smiles and confidence of your patients is a great feeling to take with you.
In many cases you will be treating a patient, or even family, throughout many stages of life. Spend the time to get to know your patients. A friendly face goes a long way to making patients feel relaxed and happy to attend their appointments.
Emulate more experienced staff. Practise, practise, practise. Repetition is the key to proficiency.
AS A PRACTICE MANAGER AND DENTAL ASSISTANT, WHAT ADVICE WOULD YOU GIVE TO A NEW DENTIST STARTING OUT IN A PRACTICE?
We’ve all heard it before. Communication.
Communication is the ultimate key in forging strong relationships with your team and patients. Dental Assistants may be known to ‘read minds’, but sharing the procedural information certainly makes the process much easier.
Going to run 10 mins late? Quickly communicating this can allow the team to prepare the patients as they arrive, rally other staff to aid in turnover and reduce the downtime.
Really lean on your staff, they know the procedures and the patients. They will be key in quickly forming the rapport and quiet confidence your patients are looking for.
That, and never passing up an opportunity to have a laugh and enjoy the process of building relationships with your patients and team.
WHAT SUPPORT DOES ADAQ GIVE TO YOU IN YOUR ROLE AS A PRACTICE MANAGER AND DENTAL ASSISTANT?
As a Dental Assistant, ADAQ gives me access to resources and courses to progress my career.
As a Practice Manager, I have access to materials that ensure the staff are supported and fully trained, so the practice is running smoothly and efficiently.
I am included in networking with other dental professionals and aid in the sharing of information to support my clinic and team members.
WHY DO YOU THINK DENTAL TEAM MEMBERS SHOULD ENGAGE WITH ADAQ?
We are all in this together. The information being given to providers is relevant to the Dental Team as well and aids in the training of new procedures.
Our industry is ever changing. Being able to access upto-date information, changes, and supportive material directly from ADAQ means I can seamlessly update the SOPs and staff.
The resources I have had access to over the past year

Members of a dental team can gain access to relevant ADAQ services & resources, through the ADAQ website.

ADAQ DENTAL MIRROR 6
Ms Kylie Horsburgh
DR ANDREW ZISCHKE
Dentist and Practice Owner, Grange Road Dental Group
AS A DENTIST AND PRACTICE OWNER, WHY IS IT IMPORTANT THAT YOUR TEAM HAS ACCESS TO ADAQ UPDATES AND RESOURCES?
To have good quality professional support is invaluable. Reassurance from our professional body helps us keep abreast of updates and advancements in the dental field. We can access practice tools and templates, that we use in our practice.
Being part of a larger group of like-minded people inspires us to continually improve.
AS A DENTIST AND PRACTICE OWNER, WHAT ADVICE WOULD YOU GIVE TO A NEW DENTIST STARTING OUT IN A PRACTICE? ESPECIALLY IN TERMS OF BUILDING RELATIONSHIPS AND WORKING EFFECTIVELY WITH THE DENTAL TEAM?
Seek out mentorship from experienced Dental Team members. Those who have been in the industry for a while have the benefit of already seeing what works and what doesn’t. Use them as a valuable resource. Also treat all Dental Team members with the respect they deserve and enjoy working with each other as a cohesive unit.
Be willing to learn ‘tricks of the trade’ that can often only be developed with experience.
Dr. Andrew Zischke
Continue growing with further education to build a pool of knowledge and skills that can benefit your patients.
AS A DENTIST AND PRACTICE OWNER, WHAT DO YOU LOOK FOR IN A DENTAL TEAM MEMBER?
Being a positive team member, with patient care and looking out for other staff members is the number one priority.
Conscientiousness and the willingness to take initiative within the practice environment. We have a term in our practice called, ‘situational awareness’, which means being aware of the flow of the day and what needs to happen to keep on top of things and to care for our patients.
Resilience and the ability stay in control under the pressures that day-to-day life and work can throw at us.
WHY DO YOU THINK DENTAL TEAM MEMBERS SHOULD ENGAGE WITH ADAQ?
Feeling connected to a larger professional body will enhance the journey one takes in the dental profession and help provide additional support with the day-to day workplace environment.
It is valuable to feel part of a large group that will help with your individual growth and benefit the entire profession.
Every member of the Dental Team should have access and utilise the benefits of ADAQ to its full potential.

Dr Andrew Zischke and Ms Kylie Horsburgh work together at Grange Road Dental Group located in Ipswich. Learn more about their work here:

GRANGE ROAD DENTAL GROUP

7 SPRING 2022
ADAQ STUDENT PROFILE
MS MEGAN MOODY | ADAQ TRAINING STUDENT
ADAQ Training offers qualifications in Dental Assisting with learning materials written and designed by dental professionals. Hear from one ADAQ Training student who recently completed a Certificate III in Dental Assisting.

ADAQ DENTAL MIRROR 8
WHAT DREW YOU TO DENTAL ASSISTING?
I have always been really interested in all things medical, right from when I was young. I thought I would try a dental assisting traineeship straight out of school and see if it was right for meand it was! I found being part of the dental team and being able to help patients very rewarding.
WHICH COURSES DID YOU COMPLETE/ARE IN THE PROCESS OF COMPLETING WITH ADAQ TRAINING?
I completed my Certificate III in Dental Assisting last year (my previous qualification was over 10 years old and out of date!) This year I embarked on Certificate IV in Dental Assisting specialising in Dental Radiography.
HOW DID YOU LEARN ABOUT ADAQ TRAINING?
I first learned that ADAQ provided training when I spoke to the wonderful Davina Barker, who came to visit my practice in the Northern Territory to provide updated infection control training. We have no dental training available in Darwin, so I was really excited to hear that I could complete my studies through the ADAQ in a flexible way as an interstate student.
WHY DID YOU PURSUE A QUALIFICATION IN DENTAL ASSISTING?
For my current role as a Treatment Coordinator in an orthodontic practice I need to be able to take radiographs. As my original Cert III no longer met the requirements for direct entry into Cert IV, I needed to gain new qualifications.
WHY WOULD YOU RECOMMEND
ADAQ TRAINING?
The ADAQ teaching staff are all very approachable and knowledgeable. Studying through ADAQ, you know that you are being given the most up to date information that meets healthcare guidelines.
The staff are active in not only teaching, but workplace visits and support. They can provide you with the practical know-how to implement what you have learnt in theory to your workplace –because let’s face it, not all dental surgeries are laid out the same!
WHAT DID YOU ENJOY ABOUT ADAQ TRAINING?
I enjoyed having a supportive network of teachers. ADAQ Trainers are always quick to reply to any questions and are very approachable. The practical unit for radiography was also amazing. We were learning in a nice small group, which allowed for a good student to teacher ratio. I could always get the help I needed, and ongoing support was easily accessible during the entire course. I feel like this course equips you for real life patients.
WHAT DO YOU ENJOY MOST ABOUT DENTAL ASSISTING?
In my current role in orthodontics, I enjoy seeing the positive transformations that patients go through during treatment.
Patients first attend the practice very nervous and self-conscious. I enjoy supporting them through their treatment and watching their confidence grow as not only their teeth start to align but they
become comfortable with the friendly faces of the dental team through seeing them every 6 weeks.
Looking after people provides a great deal of job satisfaction.
WHAT IS THE MOST CHALLENGING PART OF DENTAL ASSISTING?
The most challenging part for me is trying to fit everything into the day! Unlike the clinicians who just work in the mouth, a dental assistant usually juggles being chairside, sterilisation and reception all throughout the day.
WHAT DO YOU THINK MAKES A GOOD DENTAL ASSISTANT?
You need to care about people first and foremost. The dental surgery is a very scary place for many patients and having the level of empathy to put your patients at ease is first and foremost.
Attention to detail and procedures is also paramount – you must always strive to maintain your standards no matter how late the day is running, your clinician and your patients are relying on you to provide an excellent level of service and teamwork regardless of running late or not!
LEARN MORE ABOUT ADAQ DENTAL ASSISTANT TRAINING HERE"


9
UNDERSTANDING RUN-OFF COVER
BY CHRIS MCGILL | ADAQ COMPLIANCE & ADVISORY SERVICES
It is a statutory requirement to ensure that you are appropriately covered by professional indemnity insurance and Ahpra enforce this statutory requirement through their auditing of practitioners to ensure compliance with the Professional Indemnity Insurance Registration Standard.
When you cancel your practising registration as a dentist, maintaining your PI insurance is no longer a statutory requirement.
However, this does not mean that you can simply let your insurance lapse when you cease practice.
In healthcare and dental specifically, it is common for patient complaints, formal claims, and allegations of negligence to arise a long time after the treatment was performed or concluded.
CLAIMS MADE INSURANCE POLICIES
Professional Indemnity Insurance policies in Australia typically operate on a “claims made” basis, as opposed to “occurrence based”. This means the claim will be made to the insurance provider you hold a current policy with at the time the claim is made or notified, rather than against the policy you had at the time the treatment was provided or incident occurred.
WHAT IS “RUN-OFF COVER”
When a dentist had occurrence-based coverage and continues to pay their insurance premiums until they cease practice, they will be covered if an incident occurs which then results in a future claim, and the dentist would be covered for any incidents which occurred in their period of coverage in perpetuity. For example, if you practised negligently and then retired the next day and ceased your insurance coverage, even if the complaint is made two years later, you will still be covered as the incident that gave rise to the claim occurred during your period of coverage.
However, claims made coverage does not afford the same protection. In the event of retirement or cessation of practice under a “claims made” policy arrangement, you must maintain your professional indemnity coverage in case a claim arises in the future.
However, most of the time, you are not required to continue
paying for a new professional indemnity insurance policy each year after you retire. That is where run-off cover comes in. Runoff cover extends the period of coverage for a policy beyond the end of the policy period and allows coverage to extend to future claims without the need for payment of continued policy premiums.
SUMMARY
As dental complaints and claims are often made long after the treatment was actually completed, run-off coverage is a necessary part of any claims made professional indemnity insurance policy.
You need to investigate your insurer’s run-off policy and terms and conditions well in advance of when you cease practice so that you can ensure their requirements meet your needs and you are not surprised when it comes time to retire.
If you have already retired and are unsure if you have run-off indemnity arrangements in place from your insurer, I recommend you contact your last professional indemnity insurance provider to confirm that you have coverage.
If you are retired and you do not have adequate run-off indemnity in place, there is a risk that you will be personally liable for defending yourself if a claim is brought against you regarding treatment you completed while you were in practice.
ADAQ RUN-OFF COVER
Under the ADAQ/QBE professional indemnity insurance policy, members are offered unlimited run-off coverage as part of the policy terms and conditions provided you have been insured with ADAQ for at least three years, have had no claims, and notify ADAQ of your cessation of practice within 90 days.
If you do not meet these terms and conditions, alternative run-off arrangements can be made upon application.
If you want to call and discuss the ADAQ run-off arrangements, please contact the ADAQ Compliance and Advisory team on (07) 3252 9866, or assist@adaq.com.au
ADAQ DENTAL MIRROR
TYPES OF INDEMITY COVER OCCURANCE-BASED COVER POLICY PREMIUMS STOP Policy in force Policy no longer in force Cinical incident occurs Dentist covered by the policy Claim is made by patient* Dentist covered by the policy Claim is made by patient * this is subject to the policy being in force when the patient received treatment CLAIMS-MADE COVER POLICY PREMIUMS STOP Policy in force Policy no longer in force Cinical incident occurs Dentist covered by the policy Claim is made by patient Claim is made by patient 10 X Dentist not covered by the policy *Unless the claim is made within an agreed extended reporting period (known as "run-off")
Member Assistance Program (MAP)
As part of our commitment to Members, we have partnered with Workplace Wellness Australia, an independent support service, to provide you with a range of wellness services.
24/7 access to the Member Assistance Portal
• Informative and practical well-being resources
• Topical fact sheets and podcasts
• Confidential self check-ins
• Links to well-being services in the community.
Access to three confidential counselling sessions from Workplace Wellness via the 1300 326 350 support line number.
Counselling by highly qualified professionals. Confidentiality standards are maintained on behalf of all members and no identifiable information is provided to ADAQ.
membership@adaq.com.au



A monthly wellness newsletter covering various well-being topics


adaq.org.au/map
11 SPRING 2022
Celebrating one year of Dental Team Access
It takes a team. ADAQ is the first and only ADA state branch to offer Dental Team Access to better support the whole team.
We recognise that the whole dental team is responsible for Queensland’s oral health – so we want to make sure everyone can access important resources and services.
If you are a dental prosthetist, oral health therapist, dental therapist, dental hygienist, dental technician, practice manager or dental assistant, we welcome you to ADAQ.
Regulatory advice
Discounted CPD courses
ADAQ news and updates
Wellness resources

Practice support
Learn more at adaq.org.au/dentalteam


Study Dental Assisting with us
Cert III and Cert IV Dental Assistant training courses available.
Developed by experienced dental experts
Self-paced learning, start anytime
Qualified trainers, one-to-one support
State-of-the-art hands-on training facilities
SPRING 2022
training.adaq.org.au RTO 30621
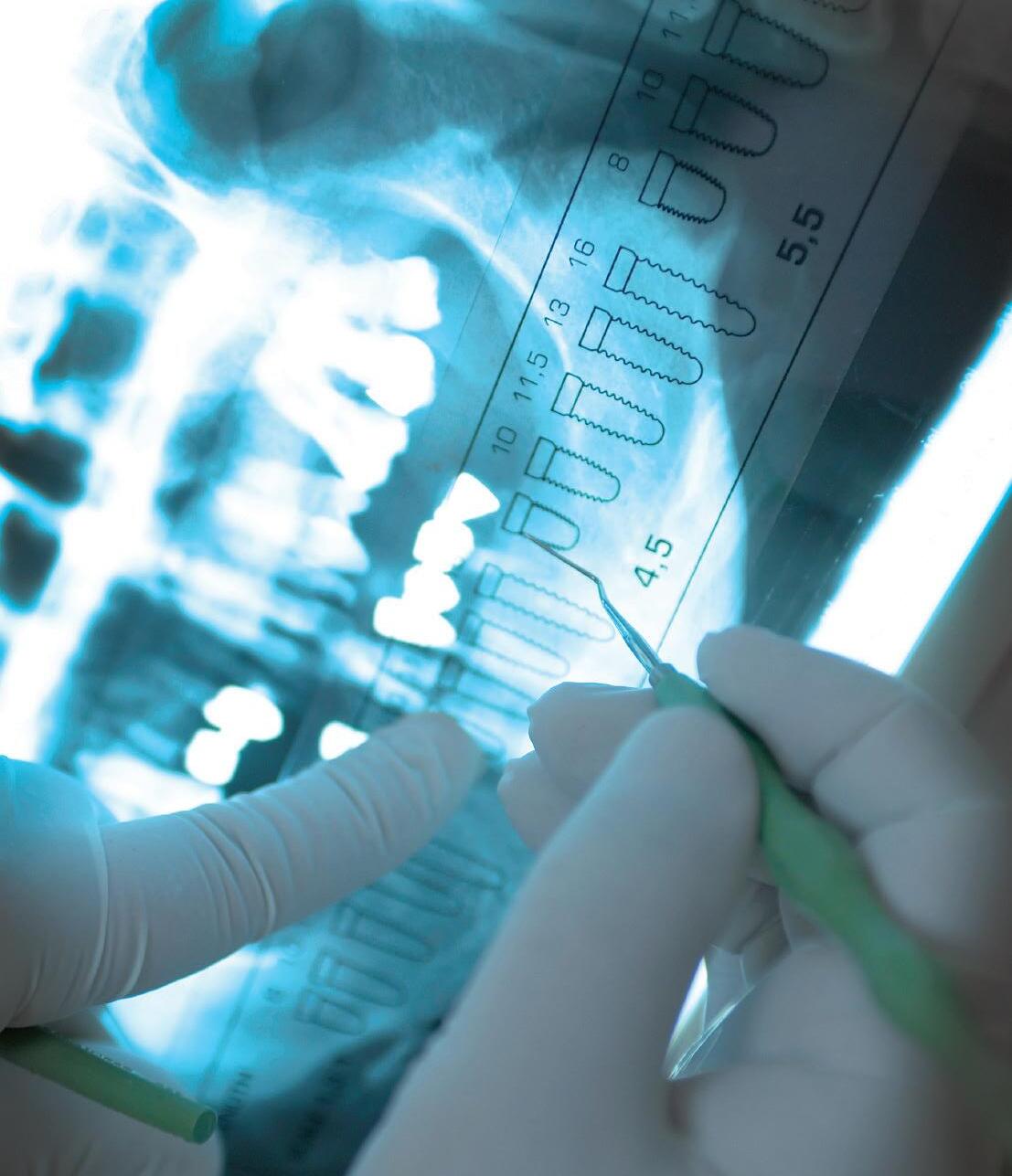
RADIATION SAFETY UPDATES
DAVINA BARKER | ADAQ TRAINING AND PRACTICE CONSULTANT
Would your practice pass an audit from Radiation Health? Here are some useful resources and regulatory advice to help your practice.
RECORD KEEPING CHECKLIST
9 Approval to Acquire and Removal/Destruction notice
9 Compliance Requirements and Quality Assurance
9 Inventory List, Servicing and Maintenance documents
9 Possession Licence and Use Licence
9 Radiation Safety Protection Plan (RSPP) and RSO certificate
9 Shielding Report of the room
9 Dose Monitoring Reports
All documents and certificates should be kept onsite in your practice, in the event a Radiation Safety Audit takes place from Radiation Health.
COMPLIANCE TESTING
Radiation apparatus must be compliance tested, following the Queensland Health Radiation Safety standard: Standard for ionising radiation apparatus–medical imaging (2021).
Compliance certification is renewed every 3 years.
All new radiation apparatus must be compliance tested once installed and before being used.
READ MORE

Queensland Compliance Testing:
XRAY MACHINE COMPLIANCE
XRAY PREMISES COMPLIANCE
3 years (1 year —CBCT) 5 years
Previously, cone beam computed tomography (CBCT) machines, had no compliance requirement or certificate of compliance issued other than a yearly quality assurance testing. From 1st September 2021, all CBCT machines must now be compliance tested annually and issued with a QLD Certificate of Compliance.
DENTAL X-RAY LEGAL REQUIREMENTS IN QUEENSLAND
9 Appoint a radiation safety officer as per s35 of the Radiation Safety Act 1999 (QLD)
9 Develop a radiation and protection plan (RSPP) for the radiation practice. This document covers the licence holder’s radiation obligations, radiation governance, accountability, and risk management.
9 Apply for possession licence for the radiation practice. Submit the RSPP together with the licence application.
9 Submit an approval to acquire form for all apparatus. This form details the type of radiation apparatus you are acquiring (to be completed between supplier and the purchaser of the Xray apparatus).
9 Apply for Use Licence for the individual operating the specific type of radiation source.
9 Certificate of compliance for the premises as per the standard for premises – ionising radiation source (2021) before use and every 5 years thereafter.
9 Annual Certificate of compliance for CBCT as per the Standard for ionising radiation apparatus – medical imaging 2021.
9 Shielding design for radiation premises.
RADIATION SAFETY AND PROTECTION PLAN (RSPP)
This document must be readily available to all staff members and in the dental practice.
• If you wish to add an x-ray machine not covered by your current possession licence, you need to update your current possession licence and submit a new RSPP to QLD Radiation Health for approval.
• All persons involved in radiation work must read and action all the required safety measures and practices in the RSPP.
Your current approved Radiation Safety and Protection Plan (RSPP) with the Queensland Radiation Health Authority must be updated to reflect the current radiation safety standards and the contact information for the RSO. READ MORE

ADAQ DENTAL MIRROR 14
RADIATION SAFETY OFFICER (RSO)
Under the updated standard for premises, the name and contact information of the RSO must be displayed at each entrance to the radiation source room or in the radiation source room. Without the display of RSO contact information, the accredited person cannot pass the compliance requirement and is therefore unable to issue the certificate of compliance.
Please note that under the Radiation Safety Act 1999 (Qld), a radiation practice can only be carried out if a RSO has been appointed for the radiation practice.
The RSO must have a current QLD RSO certificate that stipulates the exact radiation machine type. There may be exemption for RSO appointment under the Act. Please contact Radiation Health to discuss if these exemptions are applicable to you and your practice.
A RSO has a specific skillset that includes: being aware of legislative responsibilities, radiation knowledge and skills relevant to the radiation practice, radiation knowledge and its biological effects, applying radiation safety, monitor radiation measurements and interpreting guidelines and code of practice and standards.
Green sticker (premises) and Yellow Sticker (machines) are no longer in use. These stickers have been made obsolete with the new compliance standards regime from 1st September 2021. Current stickers remain compliant until the next cycle of compliance testings.
All subsequent compliance certificates issued against the new standards are to be displayed. READ MORE

USE LICENCE
The user must hold a Use licence under the Radiation Safety Act 1999 to use the nominated radiation apparatus. Only intra oral x-ray users who are registered dentists do not require a specific Use licence, however a copy of the Ahpra membership should be kept on site. Licences should be kept current regardless of any extended periods of leave or absences. It is the user’s responsibility to ensure that the use licence covers all modalities being used by the user.
READ MORE

POSSESSION LICENCE
A possession licence is not the same as a Use licence and a possession licence may cover multiple sites. Possession licences must cover all equipment you own. If you introduce new equipment to your clinic, you need to update your possession licence with a new application to update the possession licence and must be submitted together with a Radiation Safety Protection Plan (RSPP).
READ MORE

PERSONAL MONITORING DEVICES
This is mandatory for all extra-oral users and are not to be shared. It must be always worn at chest or waist height while in the practice. Personal monitoring devices must be kept at the practice. The control device must be stored away from the radiation source, for example in an admin area or reprocessing area. Testing records must be kept for at least 30 years or until users are 75 years old.
RADIATION WARNING SIGNS
Must be placed at every public entrance into the radiation room. Must be placed on/near each control of the radiation apparatus to warn users.
REFERENCES
1. Radiation Health Queensland 2. Sieverts Radiation



15
LOOK BEFORE YOU LEAP FROM OUR PARTNER - BOQ SPECIALIST
Securing your dream practice requires thorough consideration, plenty of research and advice from a trusted source.

Buying a commercial property can set up dental professionals for life—if they get it right. There are a multitude of factors to consider to ensure you get a property that is fit for purpose, not only today, but is also able to deliver long-term value. According to our finance specialists, here are some things to weigh up.
LOCATION, LOCATION, LOCATION
A commercial area that seems perfect today could lose its lustre in the future.
However, assessing the strengths of a suburb and checking out past business trends in the area can minimise any risks. Is the population on the rise? Does the site have access to public transport? Are there anchor tenants in the commercial zone or planned development within the area? “Practices located near shopping precincts with a strong anchor tenant will give the greatest exposure to foot traffic” says Nicole Rigo, Commercial Product Manager at BOQ Specialist.
She adds that buying on a site with good street frontage and the potential to erect eye-catching signage can make a real difference.
Nicole says it also often helps if practice owners have exposure to the area and its demographics prior to looking to purchase their own site. Another option for dental professionals could be to acquire property within close proximity to other healthcare providers. A thorough review of competition or potential synergies within the area should also be part of your extensive research.
THE STATE OF THE ECONOMY
Before signing on the dotted line for a commercial property, consider how the economy is performing.
Commercial property owners are more exposed to financial ups and downs than residential owners because people always need
Some practitioners might only have a one or two room practice, but their goal might be to expand in the future. One thing I always ask my clients is ‘Does the property you’re looking at accommodate where you would like to be in 10 years?’”
Nicole Rigo, BOQ Specialist
16
a place to live, whereas demand for high-end service providers can wax and wane. A sudden downturn could reduce an owner’s personal income, and limit their capacity to lease additional space to other businesses. Nicole recommends speaking to financial experts to gain an understanding of current economic and market trends.
SUPPORT SERVICES AND ACCESSIBILITY
A second-floor dental clinic without a satisfactory lift is a sure turn-off for potential patients, especially the elderly, disabled or parents with children. “A practice needs to be easily accessible and accommodating to the needs of your patient base,” Nicole says.
Other factors such as parking, security and access to IT infrastructure should also be part of the equation. Superior and well thought-out property facilities can aid your practice in the day-to-day, but also could ultimately contribute to a higher potential resale value of the site in the future as well.
EXISTING LEASES AND TENANTS
An investor in commercial property should understand their legal obligations when it comes to taking on an existing leasing arrangement when acquiring a property. If, for example, a tenant’s current leasing arrangement or terms are inconsistent with market norms, this may impact profitability on the property. Conversely, if the leases of high-paying tenants are about to expire, the new owner runs the risk of purchasing suites that could soon be vacant. “So it’s important to look at the tenancy demand and vacancies within an area, including the profiles of the existing tenants,” Nicole says.
GROWTH GOALS FOR YOUR PRACTICE
Nicole says prospective commercial property owners should understand the growth plans for their practice before agreeing to a purchase.
“Some practitioners may currently be operating out of a one or two room practice, but their goal might be to expand in the future,” she says. “Does the property you’re looking at accommodate those growth plans?”
Failing to account for the anticipated growth could result in significant costs should a bigger site be required within a few years, particularly if your practice requires purpose-built fixtures and fittings such as plumbing for dental chairs.
OTHER ELEMENTS TO THINK ABOUT INCLUDE:
Zoning and heritage-list guidelines – converting an existing house or property into a purpose-built dental practice could be subject to strict council planning laws.
Taxing times – the purchase of commercial premises can attract GST, especially when buying off the plan, and that can make a significant difference to cashflow or the financial viability of the site. Also factor in costs such as stamp duty, initial set-up costs and signage.
Contract of sale – such a contract will typically set out the terms and conditions for the sale of the property, including a description of the property, the purchase price, a list of any fixtures or fittings that are included in the sale, and the settlement date.
Doing your due diligence on a commercial property is a must, according to Nicole. That means paying attention to financial and legal considerations, having a building and pest inspection that discloses any underlying structural concerns with the property and infrastructure. It is also important to check that the property is correctly zoned for the intended use and relevant permits held if required.
This often exhaustive checklist underlines the importance of seeking advice from trusted banking, finance and legal advisers before finalising a commercial property deal.
“We have the industry knowledge and can help clients ask the right questions,” Nicole says. “This is what we do every day.”
We have the industry knowledge and can help clients ask the right questions. This is what we do every day, and we are focussed on helping dentists achieve their professional goals.
Nicole Rigo, BOQ Specialist

17 SPRING 2022
Disclaimer – The issuer and credit provider of these products and services is BOQ Specialist – a division of Bank of Queensland Limited ABN 32 009 656 740 AFSL and Australian credit licence no. 244616 (“BOQ Specialist”). Terms, conditions, fees, charges, eligibility and lending criteria apply. Any information is of a general nature only. We have not taken into account your objectives, financial situation, or needs when preparing it. Before acting on this information, you should consider if it is appropriate for your situation. BOQ Specialist is not offering financial, tax or legal advice. You should obtain independent financial, tax and legal advice as appropriate. WANT TO KNOW MORE ABOUT A BOQ SPECIALIST COMMERCIAL PROPERTY LOAN? Visit boqspecialist.com.au/commercial, or call the Client Service Centre on 1300 160 160

ANNUAL CLINIC DAY 25.11.22
Achieving excellence with contemporary dentistry.
25 November 2022
Victoria Park Function Centre
MORELEARNAND REGISTER NOW!














19 SPRING 2022 ADAQ EVENTS CALENDAR 2022 OCTOBER 01-02 Botulinum Toxin and Intraoral Dermal Fillers Dr Mahmoud Bakr & Dr Mohammed Meer 07 Challenges in Endodontics Dr Bill Kahler & Dr Andrew Thomson 08 First Aid and CPR Upgrade BLS First Aid 08 Restoration of Root Filled TeethImproving the Success Dr Bilal El Masoud 12 Minimally Invasive Restorative Techniques Prof Ian Meyers OAM 13 In-Office Whitening Emeritus Professor Laurence Walsh AO 15 Geriatric DentistryManaging your Senior Patients Dr Matthew Nangle, Dr Lydia See & Dr David Fu 26 Evening Bites: Stress Management for the Busy Professional Susan Long NOVEMBER 05 Effective Record Keeping Dr Elizabeth Milford 12 Botulinum Toxin and Intraoral Dermal Fillers Dr Mahmoud Bakr & Dr Mohammed Meer 19 Extra-Oral Radiography and Cone Beam Pre-Licensing Course Emeritus Prof Paul Monsour 23 Head and Neck Anatomy - Applications in General Practice Dr Mahmoud Bakr SCAN TO LEARN MORE SCAN TO LEARN MORE
• Opening Breakfast
• Free childcare
• Free business growth seminars
• Latest technology & innovations
Brisbane Convention & Exhibition Centre

•
20
• Women in Dentistry Breakfast
REGISTER NOW AUSTRALIA’S PREMIER DENTAL EVENT @ausdental / ADXexpo @ ad x expo adxbrisbane.org.au FREEENTRY
CPD program presented by Highlights include: 27 - 29 October 2022
#ADXexpo #ADXBrisbane

WITH PRESENTATIONS FROM:
Prof. Laurence Walsh
Dr Raahib Dudhia
Dr Bharat Agrawal

Prof. Ian Meyers
William Buck
Dr Michael Mandikos
Dr Martin Webb
Dr Marina Kamel
Dr Michael Lewis
Dr Zeb McNamara AND MORE!
VIEW THE CPD PROGRAM
ADX Brisbane CPD proudly presented by ADAQ
DAY PASS ONLY $149.00 FOR ADA MEMBERS.
HOURS OF CPD ON OFFER!
EXPLORE THE LATEST IN DENTAL TECHNOLOGY AND INNOVATION AND GET YOUR CPD POINTS AT ADX BRISBANE! CPD
49
MEMBER SPOTLIGHT
DR MICHAEL FOLEY AM
In June this year, Michael Foley was appointed a Member of the Order of Australia (AM) for his “significant service to community health and to dental education”.

Dr Michael Foley AM, UQ Senior Lecturer and Dentist
22
Michael is a past ADAQ President and although now residing in NSW, he continues his valuable contribution to Queensland as one of our dental historians.
Those privileged to have worked closely with him, either on ADAQ business or at the Brisbane Dental Hospital, are not surprised by this recognition:
“Michael’s respect for scientific method and encyclopaedic knowledge of all things related to fluoridation are legendary but his willingness to share this knowledge for the benefit of all sets him apart. His good nature and generosity of spirit never falter” (Rick Olive, past ADAQ and ADA President).
His old BDH team described him as a ‘solid’ leader: approachable, reasonable, responsive and rational.
CONGRATULATIONS MICHAEL! HOW DID IT FEEL TO BE RECOGNISED THIS WAY FOR YOUR SERVICE AND ACHIEVEMENTS?
The Governor-General's office e-mailed out of the blue in March regarding the award nomination. I was really surprised when the award was confirmed in May. When I started out, I imagined I would have a quiet career in public sector dentistry, so this is wonderful to be honoured in this way.
I've loved being a public sector dentist, caring for Queenslanders from disadvantaged groups in society. We operate as a big team, and I'm lucky to have worked with so many good people. I've also enjoyed being on ADAQ Council and ADA committees - you never know where it might lead… Thank you, Don!
YOU WERE HEAVILY INVOLVED IN THE SUCCESSFUL ADAQ FLUORIDATION CAMPAIGN OF THE NOUGHTIES. HOW DID YOUR RESEARCH INTO FLUORIDATION BEGIN?
I was on ADAQ Council in 2003. At the time, despite decades of lobbying, <5% of Queenslanders had access to fluoridated drinking water, and we had the poorest dental health in the country. I prepared all responses to all the anti-fluoridation arguments floating around.
A bigger fluoridation campaign developed slowly, and this time the planets aligned: strong support from then Chief Health Officer Jeannette Young, the AMA and other health professions, the state government taking over control of water from councils in a time of drought, a level of cross-party support in parliament, and many others. It all led to Premier Anna Bligh's announcement of fluoridation legislation in December 2007.
It was an exciting time. Helping ADAQ and Queensland Health debunk the misinformation and deceit from anti-fluoridation fringe groups encouraged me to study for master's degrees in Public Health and Epidemiology, then lecturing and research and my current PhD studies.
WHAT DO YOU WANT PEOPLE TO KNOW ABOUT FLUORIDATION?
That it benefits people of all ages, not just children. The dental health of Australians has improved dramatically over the past few generations, and fluoride in drinking water and toothpaste has played a big part. Importantly, water fluoridation also reduces health inequities in society - the big differences in health status between people from advantaged and disadvantaged socioeconomic groups.
YOUR PHD RESEARCH FOCUSES EXACTLY ON THESE SOCIO-ECONOMIC VARIABLES IN (ORAL) HEALTH INEQUALITY. AN ESPECIALLY STRONG LINK EXISTS FOR YOUNG CHILDREN. IS GOVERNMENT-FUNDED DENTAL CARE
STILL THE BEST ANSWER TO ELIMINATE ORAL HEALTH DISPARITIES?
We've known for a long time that adults and children from what I call the WWW groups (wealthy, well-educated and white), tend to have better general and oral health than non-WWW people. Socio-economic variables such as education level, employment status and particularly household income have strong impacts on health behaviours and opportunities in life. Recent research supports them being considered 'causes' of health and disease, not just loosely 'associated with' health and disease. Society is remiss if we don't prioritise health promotion and address the upstream socio-economic and structural factors that drive poor health behaviours and disease outcomes. Prevention is always better than a cure.
But health inequalities will always exist, and a well-funded government dental service is essential for people who cannot easily access or afford private dental care. The measure of a society is how it treats its weakest citizens.
WHAT IS THE MOST REWARDING PART OF DENTISTRY?
At a clinical level, it's helping patients to better oral health, particularly if they have poor oral health or bad experiences in the past. It's sometimes said that healthcare and teaching are the noblest of the professions, and in dentistry we get to do both. I've also been very fortunate to manage public dental clinics, including six years at Brisbane Dental Hospital working with a superbly talented team. At a public health level, being one of the 'cast of thousands' over many decades who contributed to the (fairly) widespread introduction of water fluoridation in Queensland from 2008 was immensely rewarding.
WHAT IS THE MOST CHALLENGING PART OF DENTISTRY?
Providing quality dental care day in, day out is complex and difficult. I admire the GP and specialist dentists who are more skilful than I am!
WHAT WOULD YOU LIKE THE FUTURE OF ORAL HEALTH IN QUEENSLAND TO LOOK LIKE?
'Drill and fill' will always be part of dentistry, but if that's all we do, we're disease professionals, not health professionals.
We must constantly strive to improve the health and well-being of our patients and communities.
As one example, I would like to see water fluoridation introduced wherever practical in Queensland. More than 90% of residents in the rest of Australia enjoy the dental health benefits of water fluoridation, but only 72% of Queenslanders do so.
Most regional towns and cities and almost all our Aboriginal and Torres Strait Islander communities miss out. That's completely unacceptable, and has to change. Better dental health should not be a residential lottery.
23 SPRING 2022
THE ‘GRAVE’ HISTORY OF DENTISTRY: WATERLOO
AND WITCHES’ TEETH: ADAQ DENTAL HISTORY COMMITTEE & ALESSANDRA BOI
Friday, 28th. …Work’d two graves; one [body] bad, so drew the canines and sold them at St. Thomas…
From: The Diary of a Resurrectionist 1811-1812. To Which Are Added an Account of the Resurrection Men in London and a Short History of the Passing of the Anatomy Act. By James Blake Bailey.
In the 18th and early part of 19th centuries, sugar was England’s biggest import, and tooth decay was rampant. The replacement of lost teeth was a luxury treatment and could only be afforded by the very rich.
Bone and ivory were the most common materials, but animal teeth or wood were also used. However, these dentures rotted quickly and caused terribly foul odours. Even when porcelain techniques emerged, the results felt quite brittle and looked too artificial.
The best dentures were made of ivory and ‘natural teeth’: that is, human teeth which had been removed from cadavers or extorted from the desperately poor. Boiled and kept in bran, the teeth were skilfully embedded in hippopotamus or walrus ivory bases or held with gold braces to adjacent teeth.

Images

Dentures, Full lower denture. Ivory base and occlusal pads, human anteriors secured with metal pins. Note the spaces for attaching springs. Probably in use late 18th to early 19th century. ADAQ MoD collection.
The (in)famous Martin Van Butchell advertised a full set of ivory dentures with human teeth for £100 in 1782, the equivalent of £18,760 or $32,000 circa today.
‘Natural teeth’ appear in advertising as late as the 1870s, even though by then one could obtain Claudius Ash’s tube teeth quite easily instead.
‘RESURGAM HOMMO’ – THE LUCRATIVE TRADE OF THE RESURRECTIONISTS
Originally, human teeth were sourced only from executed prisoners; mostly murderers thanks to the Murder Act 1751. These bodies were delivered to medical schools for the additional indignity of dissection. In the process, healthy looking teeth were removed and sold, especially incisors and canines, the easiest to remove quickly. However, in the United Kingdom this supply did
not keep up with the demands of universities, and this is where grave robbers made their profit.
The Resurrection men, as they came to be known, were directly engaged by medical schools to exhume freshly buried corpses and deliver them secretly through back doors at night. Before handing the bodies over to medical students, the resurrectionists yanked out healthy looking teeth for sale to jewellers and ivory turners, and ‘dentists’ later on. Medical students themselves often also dabbled in the lucrative teeth trade. The first osteological preparations used for teaching in dental schools most likely also came from ‘resurrected’ corpses.


ADAQ DENTAL MIRROR 24
Images Osteological preparation. ADAQ MoD Collection. 19th Century.
The resurrection trade was so profitable that it became a temptation too great for some not to start ‘producing’ extra supply bodies, as the infamous Burke & Hare did in Edinburgh. Finally, the murder case of an Italian boy in London was the tipping point for the passing of the Anatomy Act 1832, which secured a minimum of ‘legal supply’ to anatomy schools.
WATERLOO TEETH
Body snatching from cemeteries did not provide enough good quality teeth. Dentists would often refuse to buy these teeth as they would have already started to turn yellow and brittle. The demand for human teeth was such that even the fresh cadavers secured through the Anatomy Act weren’t enough.
The largest supplies came from Anglo-French battlefields, and the Civil Wars across the Atlantic. Many resurrectionists left the trade to follow armies as sutlers: this enabled them easy access to the fresh bodies (and other valuables) of fallen young soldiers the night after a battle: over 50,000 died at Waterloo. The great influx of human teeth for dentures of those years secured the resulting dental products’ moniker of ‘Waterloo teeth’: many examples still survive in medical and dental museums worldwide.
WITCHES’ TEETH
Dentists weren’t the only ones in the market for zombie teeth. The Tooth Fairy was also involved! This is a shocking accusation, I know, but to understand why, we need to dig into the shady origins of the Tooth Fairy myth as we know it today.
In most cultures, teeth have acquired similar symbolic meanings revolving around the childhood shock of losing the first dentition, and perhaps acknowledging their importance for nutrition and wellbeing, and therefore survival.
This symbolism has translated into various magic beliefs that revolve around sacrificing or disposing of teeth to protect oneself and keep bad omens away (apotropaic magic).
In many Western cultures, the Middle Ages brought us the belief that witches could obtain complete power over a person just by holding their tooth. Teeth also routinely appear in witchcraft books as giving power to spells, especially to create links with the undead or summon the Devil. Witch bottles, for example, which are still randomly found hidden in old English houses, often contain human or animal teeth along with urine, hair and needles. Many spells involved taking away or bringing wealth, and that’s where the exchange of shed baby teeth for money comes into place in the form the superstition survives today for children: the Tooth Fairy, the Little Mouse, or even a Saint, depending on where you grew up.
‘The teeth of a hanged man are very efficacious for sorceries’, as spooky master painter Francisco Goya reminds us in his explanation for Plate 12 – Hunting for Teeth (1799), reproduced here courtesy of The Met Museum.
Incidentally, the tooth-death-magic link also works to protect someone’s teeth. In some European countries, like Italy, a piece of a hangman’s cord in the pocket had the power to keep toothaches away.
Our collective imagination still links teeth and supernatural pretty strongly, as proven by gothic tales and horror movies containing demonic teeth tropes.

Image
‘The teeth of a hanged man are very efficacious for sorceries…’ Goya, A caza de dientes. Hunting for Teeth. Plate 12 from Los Caprichos.1799. Etching. Source: The Metropolitan Museum of Art.
BRIS-BONES
It’s uncommon for the average home renovator to come across witches bottles here in Australia. However, interesting teeth are still being dug up from cemeteries, albeit mostly by chance when old burial sites are uncovered. For example, the excavation at Lang Park (Suncorp Stadium) on the site of the former North Brisbane Burial Grounds (Milton; 1843-1875) resulted in the discovery of several children’s teeth in one single coffin (Haslam et al., 2003).
The interest to today’s anthropologists, archaeologists and dental historians is not limited to real teeth, but also the artificial ones that lay with the buried remains. For example, the retrieval of ten Victorian-era dentures from the same North Brisbane excavation, showed us the sophisticated design and quality of dental appliances available at the time, for the few who could afford them (see for example: Morris & Akers, 2021; Morris, 2019).
REFERENCES
1. Michael Haslam, Jonathan Prangnell, Luke Kirkwood, Anthony McKeough, Adrian Murphy & Thomas H. Loy (2003) A Lang Park mystery: Analysis of remains from a 19th century burial in Brisbane, Queensland, Australian Archaeology, 56:1, 1-7, DOI: 10.1080/03122417.2003.11681743
2. Morris KE, Akers HF. Victorian-Era Dentures in Brisbane, Australia. J Hist Dent. 2021 Summer/Fall;69(2):74-93. PMID: 34734788.
3. The Diary of a Resurrectionist 1811-1812. To Which Are Added an Account of the Resurrection Men in London and a Short History of the Passing of the Anatomy Act. By James Blake Bailey.
25 SPRING 2022
DO NOT RECOMMEND ANY OF THESE TO YOUR PATIENTS...

BONUS: SCARY TEETH FOR THE SPO OKY SEASON
A CURATED LIST, NOT FOR THE FAINT HEARTED!
LITERATURE & FICTION
Berenice (1835). Gruesome short story by Edgar Allan Poe
Dracula (1897). Classic fangs by Bram Stoker
What-the-Dickens: the Story of a Rogue Tooth Fairy (2007). Fantasy fiction by Gregory Maguire
The Daughter of Smoke and Bone (2011). Young adult fiction by Laini Taylor.
MOVIES & TV
The Man Who Knew Too Much (1934) by Alfred Hitchcock.
Les Misérables (2019) the BBC production: just for Fantine’s tooth harvesting scene.
Marathon Man (1976) by John Schlesinger. The most famous dental torture scene: ‘Is it safe?’
Little Shop of Horrors (1986), by Frank Oz. The second most famous dental torture scene.
It (1986), for Pennywise’s smile of course.
The Dentist I and II (1996-98), by Brian Yuzna. Mad dentist.
Novocaine (2001) by David Atkins. Black comedy with violent self-extractions.
Darkness Falls (2003), by Jonathan Liebesman. Bad Tooth Fairy.
Tooth Fairy (2006), by Chuck Bowman. Bad Tooth Fairy again.
Teeth (2007), by Mitchell Lichtenstein – comedy horror revisiting psychological/horror trope of Freudian lore: vagina dentata.
Channel Zero – Candle Cove (2016). This Horror TV series may not be available in Australia, but just google the Teeth Child. I dare you.
A Cure for Wellness (2016) by Gore Verbinski. Psychological thriller and dental torture.
SPOOKY DENTISTRY

Image
David Solot. Le Dentiste a mal aux dents.
David Solot. Le Dentiste a mal aux dents. [The dentist’s toothache] Colour etching. 1940s. The nightmare of a dentist with an abscessed tooth: chased by the phantasm of animated dental instruments that have turned against him. Courtesy of National Library of Medicine Digital Collections, USA.
David Solot (1909-1985) was a French dentist and artist who used his dental tools as inspiration for his surrealist art. His disconcerting pictures make for a nightmarish collection where forceps are birds of prey, and molars stage uprisings.
ADAQ acquired artist-signed copies of three lithographs a few years back, which are sadly now somewhat faded: The Battle of the Forceps, Revolt of the Molars, and Medusa (1950 circa):

Image
The Battle of the Forceps
Image
Molar Medusa Image Molar Uprising
CPD CYCLE IS ENDING SOON – ARE YOU
COMPLIANT?
MADONNA MCMANUS | ADAQ CPD MANAGER
Dental practitioners are required to complete 60 hours of CPD activities over a 3-year period. The current CPD cycle closes 30 November 2022. Have you completed your required 60 Hours of CPD?
A minimum of 48 hours (80%) must be spent on clinical or scientific-based CPD activities and a maximum of 12 hours (20%) can be contributed to non-scientific CPD activities. To assist practitioners in complying with this requirement, the Dental Board of Australia has issued a Registration Standard and Guidelines. However, it does not detail mandatory CPD activities to be undertaken. Instead, it recommends dental practitioners undertake a varied range of CPD activities that they feel are in line with their learning needs.
The obligations of registered health practitioners in relation to CPD requirement is set out in the National Law (section 128):
“(1) A registered health practitioner must undertake the continuing professional development required by an approved registration standard for the health profession in which the practitioner is registered.
(2) A contravention of subsection (1) by a registered health practitioner…may constitute behaviour for which health, conduct or performance action may be taken”.
When renewing your registration with Ahpra, all dental practitioners must declare they have met the CPD Registration Standard. If audited, you must produce a logbook which includes details of the CPD activities undertaken, the number of hours spent, and whether the activity is clinically or scientifically based. The Board may also ask for evidence of your attendance (e.g. certificate of attendance).
Ahpra provides a portfolio template on their site CPD Portfolio Template to assist both identifying the requirements and maintaining a record of your continuing professional development.
READ MORE

Your CPD certificate of attendance can be added to your ADA CPD Logbook, to help you keep track of your CPD hours.
READ MORE

The standard requires you to keep a portfolio of your CPD activities for at least five years from the date you completed the CPD cycle. These records must be available for audit or if required by the Board as part of an investigation arising from a notification (complaint).
You must also keep evidence of CPD activities completed, such as:
• certificates of attainment or attendance, and
• your notes from the CPD activity such as conducting a literature review or reading case studies or journal articles. In this example, it is expected that these notes will provide a comprehensive summary of the key points of the review and reflect your learning from this activity.
What are my requirements and what happens if I don't comply?
READ MORE

DO YOU NEED MORE CPD HOURS? CHECK OUT THE ADAQ EVENT CALENDAR.

27 SPRING 2022

COST VS COST – CAN YOU AFFORD NOT TO HAVE A DEFIBRILLATOR IN YOUR PRACTICE?
FROM OUR PARTNER – DEFIBRILLATORS AUSTRALIA
A Sudden Cardiac Arrest (SCA) does not only stop the casualty, but it also stops the whole activity within the practice. Not to mention the trauma it causes to staff and patients having other treatments, possibly leading to long term effects such as stress leave and PTSD.
Sudden cardiac arrest (SCA) can happen to anyone—anywhere. SCA is usually caused by an electrical malfunction that makes the heart quiver ineffectively in an abnormal rhythm called ventricular fibrillation (VF). Sometimes triggered by a heart attack, SCA also can happen even without any blockage of blood flow to the heart. A lifesaving pulse of electricity must be delivered quickly to restore the heart’s normal rhythm and pump blood throughout the body. Defibrillation is the only effective treatment for sudden cardiac arrest caused by VF.
STA TIST ICS:
Consider if a patient or staff member has a SCA in your practice and you do not have access to a defibrillator.
• The chances of the person surviving are only 1 in ten
• CPR alone equates to a 16% chance of that person responding, a defibrillator increases these chances by up to 70% when administered immediately
• Cardiac arrest costs $35 Billion dollars each year in Australia
• Cardiac arrest affects more than 4 million Australians, killing 118 people every day or one person every 12 minutes
• It kills 40% more males than females
• Someone is hospitalised every minute, equating to a total of 1619 hospitalisations per day.
Over the last 10 years, deaths have been declining due to research into risk factors, medications, and interventions such as CPR and defibrillation.
RISK CONSIDERATION:
It is public perception that healthcare facilities within Australia are equipped with the appropriate medical and, OHS equipment in the event of an emergency. Such equipment includes First Aid Kits, Fire Extinguishers, Smoke Detectors, and a Defibrillator.
More and more businesses are recognising the importance of defibrillators in the workplace. If a patient has a cardiac arrest in the dental practice, they collapse and are not breathing starving their brain of oxygen and did not survive. The phone call to the next of kin is something none of us ever want to be faced with. Effective treatment is available, it just needs to be delivered fast—often before emergency responders arrive. Defibrillators work - SCA survival rates are more than four times higher when
bystanders use CPR and defibrillation than just CPR alone. When a SCA emergency happens, you want to be ready. As you can see, placing a defibrillator in your practice, and making sure people are trained to use them, can mean the difference between life and death.
FINACIAL IMPLICATIONS
The financial impact could be devastating impacting your business short and long term. According to seek.com.au, the average dental assistant's wage is $50 - $60K per year, about $152.00 per day plus super and tax. If you had 5 assistants in the practice on the day of the incident, that would be $835.00, not to mention other members of staff and the dentists wages.
Treatments being administered for the day will cease until the emergency is over, if the patient dies then the authorities will close the practice until the deceased has been examined and collected by either the coroner or the funeral directors. By installing a defibrillator in your practice, you will be giving peace of mind to your staff and your patients if the worst should happen.

11 93
29 SPRING 2022
TAKE ADVANTAGE OF THE EXCLUSIVE ADAQ MEMBER OFFER, SAVE OVER $1264.00. Call
or info@defibrillatorsaustralia.com.au
or email on 1300 33

Our experts in corporate finance, accounting, financial reporting and taxation have extensive knowledge, experience, and relationships within the Dentist industry sector.
We can assist with:
• General accounting, Bookkeeping, Structuring and Financial Reporting
• Starting and managing your practice
• Budgeting and Forecasting
• Taxation Advisory and Compliance
• Valuations
• Capital Raising
• Internal Audits, Controls Frameworks and Fraud Detection
• Strategic Planning, Benchmarking, Exit Planning and Retirement
For more information or to book a consultation, call or email us:
P: (07) 3229 5100
E: qld.marketing@williambuck.com
www.williambuck.com/industry/health/dentists/
STRATEGIC PLANNING - WHY IT SHOULD BE ON
YOUR 'TO DO' LIST
FROM OUR PARTNER WILLIAM BUCK
Imagine you are going on a long driving holiday in your prized prestige car. Compare in your mind the outcome of two different types of trips:
Trip One: You pack the car, make sure there are sufficient provisions for the trip, you might have the car serviced, you plan the stops and places to see and stay for the night.
Trip Two: No planning, no packing, no car service, no map, and you jump in the car and simply hope for the best.
I would take bets on which trip will go smoother, have less stress, and ultimately end up being a more pleasant and successful journey for all those involved. Your dental practice is your prestige car. Your ownership period is your journey. Running your practice without a clearly articulated business and strategic plan is like going on a long driving holiday without a plan.
DEVELOPING THE STRATEGIC PLAN – WHERE TO START?
Where to start, depends upon your practice’s operating and ownership structure. If you have multiple owners in a practice, alignment is essential. You should agree on the importance of developing a plan, what the actual plan is, and the implementation of said plan. If it is not supported by all key stakeholders, the plan will fail.
Ensuring support is key and maintaining it can be tricky, but alignment is critical for this process. Ensure that all owners are aligned from the start.
Strategic planning is about identifying where your practice wants to be - the Vision - then you take stock of where it is now and from there you formulate actions to bridge the gap.
DEVELOPING THE PLAN
Strategic planning is a process and not an event.
The process starts with a discovery and planning session. Indepth questioning uncovers what is important to determine the direction you wish your business to take. The practice is not purely clinical: all areas of the practice operations need to be considered, including staff, patients, processes, innovation, and the financial aspects of the business.
An effective planning session should provide a vision for your practice, and it will be clear, concise, achievable, and visible from all directions. Setting the vision is like placing a “flag on the hill”; it identifies and defines a common goal for the practice.
The session will also provide action points to implement the vision. These action points are a kick-start to change. Change comes from articulating a clear vision, providing resources and incentives to achieve it, and supporting the process, even when it becomes challenging. It is a roadmap.
Importantly, like any journey, the strategic plan is flexible and if you take a wrong turn, you can back up, reassess, and reposition. All the while continuing to move forward and build momentum.
WHAT HAPPENS IF A PRACTICE HAS A GOAL BUT NO STRATEGY?
Without a strategy, a practice runs the risk of inertia, a paralysis that causes it to stay where it is - not growing, not changing with it's environment and not being in touch with it's patients.
The ultimate example of a practice failing to move with the times is one that loses dentists, cannot recruit, has no succession plan for the owners and potentially will just close it's doors one day. A missed opportunity and a disservice to the community, it's staff, and owners.
The good news is that it is possible to work against a gradual decline using strategy. Having a goal is the first step and strategic planning sets the path and creates the actions to achieve this goal.
WHEN SHOULD A PRACTICE INVEST IN STRATEGIC PLANNING?
It is never too late nor too early to adopt a strategic approach irrespective of size or the business’s evolution. Without a plan, there can be no direction for the practice. Strategic planning provides that roadmap and action to drive the practice to be profitable, sustainable and to reach your flag on the hill.


31
SPRING 2022
Angela Jeffery






ADAQ DENTAL MIRROR 32 UPCOMING SEMINARS with William Buck More information to come. Please email marketing@adaq.com.au for further details ADAQ and William Buck are proud to present a series of upcoming seminars from September through to December. Buying into a Practice Start & Finish time 6pm to 7:30pm Venue William Buck Office – Level 22, 307 Queen Street Brisbane 4000 Speakers Angela Jeffrey, Colin Taylor & Antony Harrison from William Buck Join Angela Jeffrey, Antony Harrison, and Colin Taylor as they unpack the various considerations when thinking about setting up or buying into a Dental Practice. Get key insights from our expert speakers as they delve into and discuss the legal, financial, business, and financing considerations to help you set up your Practice in the best way possible. 29 SEP Optimising a Practice 10 NOV Selling a Practice 8 DEC To Be Announced TBC DEC LEARN MORE
BRUCE TRUSLER, TONY SHIELDS, BRENDAN FITZPATRICK, JULIE CREAGH AND PREM PATEL ARE VERY PLEASED TO ANNOUNCE THAT DR CHRISTOPHER FRANCO HAS JOINED THE TEAM AT SHINE ORTHODONTICS.
Chris completed his Bachelor of Dental Surgery in 2014 and obtained a Doctorate in Orthodontics in 2018 from the University of Queensland. Chris holds certification with the Australasian Orthodontic Board (AOB) and is a member of the Australian Society of Orthodontists (ASO), American Association of Orthodontics (AAO) and World Federation of Orthodontists (WFO).
Chris will be available for appointments at our City practice as well as the branches at Kenmore, Caboolture, Strathpine and North Lakes.
MARKING 45 YEARS OF DENTISTRY UTILISING GENERAL ANAESTHESIA IN BRISBANE
Dr Anthony Speed, in association with anaesthetists from the Wesley Anaesthetic Group, wishes to advise that they can facilitate treatment for patients requiring general anaesthesia in our outpatient facility at Holland Park. This is particularly useful for patients who have no private hospital insurance. With an extensive range of experience, the team is willing to undertake wisdom tooth removal, implant placement and perform routine restorative dentistry on all age groups including children aged 3 and above. Anxiety sufferers, local anaesthetic problems, severe gag reflex sufferers, special needs patients, and dementia sufferers have all been successfully treated over the years.
Additionally, we are now able to offer Cerec single visit crowns so that the patient does not have to return for subsequent cementation. Patients who are medically compromised can be treated at St Andrew’s Private Hospital by arrangement.
CONTACT
If this service can be of assistance to some of your patients, please phone the reception staff on 3397 1339 for further information. Referral booklets available on request
The
should be “It’s
your dental
Responsive Efficient
Knowledgeable Trained
Experienced Professional






33 SPRING 2022
informed of opportunities and announcements exclusive to the ADAQ community Meet Brian Gardiner, Ian Colley and the QDS Team at ADX22 Brisbane, Stand 415.
CLASSIFIEDS Stay
people
installing and servicing
all
supplying,
equipment
about the People”
(Opposite the ADA booth). 1300 77 09 77 qlddentalservices.com.au Brian Gardiner Sales and Marketing Manager Our Technicians are all of the above, but first they are: Ian Derek M Derek P Corey Brett Daniel John Jake Jonathan Kym Kate Michele Rhonwyn +
OBITUARY ANDREW JOHN COLE
Andrew’s achievements were both simple and immense.
October 1st 1960 – July 9th 2022
The funeral service to celebrate the life of Andrew Cole was held at Marist Brothers Ashgrove on Wednesday 20th July. Andrew leaves behind his wife of almost 40 years, Anne-Maree; three children, Michael, David and Megan; two grandchildren, Hattie and Mia; and three more on the way. He also leaves innumerable friends from across the world and from across all walks of life. What Andrew does not leave behind are acquaintances – if you met Andrew even once, you recognised that you had met one of the truly remarkable men of this world and you would always consider him as a friend; and that consideration was returned.

Andrew’s achievements were both simple and immense. Andrew met the love of his life when he and AnneMaree were children. They became a couple early in their undergraduate years and lived, loved, laughed, and worked for each other for the rest of their life together. On graduation in 1982, Andrew and Anne-Maree went from dental school students to practice principals in one step when they opened a squat together in a vacant shop at Strathpine and built that up into the hugely successful Cole Dental.
Andrew’s other career was as an international rugby referee. He was one of the truly great referees of his time – players, coaches and spectators were pleased to see his name on the game sheet. He refereed 31 internationals, including All Blacks vs British and Irish Lions and retired from the international ranks on his own terms in 2005 to spend more time with his young family, of whom he was immensely proud. Andrew did not retire from rugby but accepted a post on the International Rugby Board as a referee coach. He mentored successive generations of rugby referees for the rest of his life.
Andrew’s son David once expressed some difficulty in understanding Andrew’s career choices. “Dad, you are a dentist and a referee; didn’t you want anyone to like you?” One of the remarkable aspects of Andrew’s funeral service was in the speeches commemorating his life. There was a speaker who had been a friend from primary school, another who represented international rugby referees, one of his sons, David and finally, his wife Anne-Maree. The stories from each speaker were different, but the sentiment that they had shared in the life of a great man was the common theme expressed repeatedly by each of them.
Vale Andrew Cole, a man who saw more potential in those around him than they recognised in themselves and then showed a way to allow that potential to flourish. He will be missed by all who knew him, but never forgotten.

34
OBITUARY
DR ROBERT MABIN
Born Maryborough Queensland 1941 – 2021
Dr Robert Mabin built small boats for the family, enjoyed gardening, hiking and their many British friends.
Born Maryborough Queensland 1941.
Attended primary school at Indooroopilly State School and completed his education at Brisbane Boys College.
Studied dentistry at University of Queensland and graduated in 1965.
Worked as a government dentist in Alice Springs 1966/7, after marrying Susan.
The couple travelled to the UK in 1967 and Rob worked in several practices in London.
Sons, Andrew and Rodney were both born during this period.
In 1970, Rob bought a dental practice in Dover, and the family moved to St Margaret’s Bay.
Eight happy years were spent here, Rob sailed in cross channel races at weekends, built small boats for the family, enjoyed gardening, hiking and their many British friends.
On returning to Australia in 1978, Rob went into partnership with the late Dr. Paul Kelly at Maroochydore. A second practice was set up at Coolum and eventually Rob took over this practice independently.
In retirement, Rob and Susan enjoyed active travelling holidays including motor cycling, bicycling and walking, world- wide, as well as ballroom dancing on cruise ships. He also now had more time for his beloved garden. Sadly missed by Sue, wife of nearly 59 years, sons, Andrew and Rodney, grandchildren and many friends.

35 SPRING 2022



Borrow up to 100% of the purchase price of your practice premises and pay no establishment fees^ ^Subject to credit approval. Credit provided by BOQ Specialist – a division of Bank of Queensland Limited ABN 32 009 656 740 AFSL and Australian credit licence no. 244616 (“BOQ Specialist”). Lending criteria, T&Cs and fees apply. Limited time offer only available for new commercial property finance applications received between 1 August 2022 and 31 October 2022 (inclusive) and that settle by 31 December 2022. Not available for the refinance, restructure or switches of commercial property loans within BOQ Group, which includes BOQ, ME Bank, Virgin Money (Australia) and BOQ Specialist. Client will be eligible for a waiver of the full upfront documentation fee and legal fees up to $1,705 upon settlement, provided the minimum total lending amount is at least $200,000 and the maximum lending amount is $3,000,000. Full valuation fee applies. For SMSF borrowers, the offer is only available to SMSF’s purchasing their practice premises. Other fees and charges may apply. This offer expires on 31 December 2022 and is subject to change without notice at the discretion of BOQ Specialist. Feel secure owning the space you operate from BOQ Specialist. The bank for dental professionals At BOQ Specialist, we want you to experience the security and freedom of running your practice from a space that you own. By giving your practice its own home, you can enjoy operating without the worry of potential rent increases, forced relocation or compromising on your fit-out. Our commercial property loans offer you the ability to borrow up to 100% of the purchase price of your own practice premises. What’s more, for a limited time we’re also waiving establishment fees when you finance your commercial property purchase with us.^ For over 30 years we’ve helped many dental professionals invest in their business, rather than their landlord’s. Now, let us help you. Visit boqspecialist.com.au/commercial or speak to your local finance specialist on 1300 160 160. 36
