SCCMA is a professional association representing over 4,500 physicians in all specialties, practice types, and stages of their careers. We support physicians like you through a variety of practice management resources, coding and reimbursement help, training, and up to the minute news that could affect your practice. The Bulletin is our quarterly publication.
SCCMA OFFICERS
President | Fahd Rahman Khan, MD
President-elect | Santosh Pandipati, MD
Secretary | Veena Vanchinathan, MD
Treasurer | Shahram Gholami, MD
Immediate Past President | Gloria Wu, MD
VP-Community Health | Paul Wang, MD
VP-External Affairs | Christine Doyle, MD
VP-Member Services | Sam Wald, MD
VP-Professional Conduct | Lewis Osofsky, MD
SCCMA STAFF
CEO/Executive Director | Marc E. Chow, MS
Director of Operations | Angelica Cereno
Director of Governance & Advocacy | Emily Coren
Facilities Manager | Andie Campanilla
Executive Assistant/Member & Program Manager | Rashida Mirza
SCCMA COUNCILORS
El Camino Hospital of Los Gatos | Jaideep Iyengar, MD
El Camino Hospital – Mountain View | Carol A. Somersille, MD
Good Samaritan Hospital |Judong Pan, MD
Kaiser Foundation Hospital - San Jose | Haritha Reddy Rachamallu, MD
Kaiser Permanente Hospital - Santa Clara | John Truong, MD
O’Connor Hospital | David Cahn, MD
Regional Medical Center | Raj Gupta, MD
Saint Louise Regional Hospital | Kevin Stuart, MD
Santa Clara Valley Medical Center | Open Stanford Health Care/Children’s Health | Karen Kim, MD
Managing Editor | Emily Coren
Production Editor | prime42 – Design | Market | Host
Opinions expressed by authors are their own, and not necessarily those of The Bulletin or SCCMA. The Bulletin reserves the right to edit all contributions for clarity and length, as well as to reject any material submitted in whole or in part. Acceptance of advertising in The Bulletin in no way constitutes approval or endorsement by SCCMA of products or services advertised. The Bulletin and SCCMA reserve the right to reject any advertising.
Address all editorial communication, reprint requests, and advertising to:
Emily Coren, Managing Editor
700 Empey Way
San Jose, CA 95128
408/998-8850
Fax: 408/289-1064
emily@sccma.org



Fahd R. Khan, MD SCCMA President
Dear Colleagues,
Medicine is more than a science—it is a moral practice. Every clinical decision we make carries ethical weight, whether we’re navigating a complex prognosis, obtaining informed consent, or weighing risks and benefits of a novel therapy. Bioethics is not a peripheral concern—it is a core part of our daily work.
This issue of the Santa Clara County Medical Association Bulletin focuses on the essential role of bioethics in modern medical practice. The foundational principles of autonomy, beneficence, nonmaleficence, and justice guide our interactions with patients and their families. These values shape decisions around end-of-life care, reproductive health, vaccination, experimental therapies, and the equitable distribution of limited resources.
In the hospital setting, bioethics provides a structured forum to address difficult questions. Ethics committees—often composed of physicians, nurses, chaplains, legal counsel, and community members—support clinicians when facing challenging cases involving capacity, surrogate decision-making, goals of care, and conflicts between medical recommendations and patient or family wishes. These committees uphold the rights of patients to be informed, to consent (or refuse), to privacy, and to receive care that aligns with their values and dignity.
With the emergence of artificial intelligence in diagnostics, gene editing technologies, and expanding data collection in medicine, we must also consider the ethical implications of innovation. Are these tools safe, equitable, and aligned with the patient’s best interests? How do we safeguard privacy while promoting progress? Ethical literacy among physicians has never been more critical.
Physicians must also be aware of the legal dimensions that directly impact their practice—not only at the bedside, but also behind the scenes. Employment contracts, compensation structures, non-compete clauses, and termination provisions all carry significant legal and ethical implications. Understanding the fine print of these agreements is not just a matter of financial prudence—it’s about protecting our professional integrity and ensuring we can advocate for patients without compromise. As the landscape of healthcare employment continues to shift, physicians must stay informed, ask questions, and seek guidance when
necessary.
Physicians can get involved in bioethics in several meaningful ways:
• Join your hospital’s ethics committee to participate in real-time consultations and policy development.
• Advocate for patients’ rights by ensuring transparency, informed consent, and shared decision-making.
• Stay informed about developments in medical law, research ethics, and health policy.
• Engage in public discourse —our experience as frontline clinicians offers insights that the broader community and policymakers need to hear.
If these issues resonate with you, I strongly encourage you to connect with our Bioethics Committee. This is an opportunity to help shape the ethical culture of our institutions, guide colleagues through difficult moments, and keep the patient’s voice and dignity at the heart of everything we do.
Thank you for your commitment to ethical, compassionate, and just care.
Sincerely,

Fahd R. Khan, MD President Santa Clara
County Medical Association

Delegates represent their counties in the California Medical Association (CMA) house of delegates by attending and actively participating in delegation caucus meetings and in all sessions of the house.
Delegates monitor business put before the house to consider, including business at the annual session, and items presented during the year-round resolution process. Delegates are represent their overall constituency and not just their own personal views on issues.
Delegate candidates are team-oriented, knowledgeable on policy issues, willing to play an active role in the delegation and support the goals of the delegation.
Positions are for a two-year term. If you are interested in becoming an alternate delegate to participate in future meetings of the House of Delegates please contact Governance & Advocacy Associate at emily@sccma.org.
ADD YOUR VOICE TO ORGANIZED MEDICINE!


Accepting a new physician employment offer is a major milestone in any medical career. But before signing on the dotted line, it is critical to take the time to carefully review the proposed contract. These agreements are more than just paperwork—they are legally binding documents that define your rights, responsibilities, compensation, and long-term career trajectory. As a healthcare attorney, I have seen firsthand the legal and professional consequences of overlooked contract terms. Here are five key elements that every physician should scrutinize before entering into any employment agreement.
One of the first—and most important—questions to ask is whether you are being hired as an employee or as an independent contractor. This distinction significantly affects your eligibility for benefits, tax treatment, malpractice coverage, and legal protections.
Employees typically receive W-2 income, health and retirement benefits, paid time off, and employer-covered malpractice insurance. They also benefit from workplace protections under state and federal employment laws.
Independent contractors receive 1099 income and are responsible for their own taxes, insurance, and benefits. These arrangements may offer more scheduling flexibility, but they come with added legal and financial risks.
If you are offered an independent contractor agreement, make sure it is explicit about your obligations regarding professional liability insurance, tax reporting, and operational expenses. Confirm whether you are required to purchase “tail” coverage for malpractice claims and whether you will be reimbursed for licensing, continuing education, or administrative support.
In California, employment classification also implicates the Corporate Practice of Medicine (CPOM) doctrine, which prohibits lay corporations from employing physicians to practice medicine. The legal foundation for this doctrine is grounded in Business and Professions Code §§ 2052 and 2400, which together prohibit unlicensed persons—including corporations—from practicing medicine or employing licensed physicians to do so. The purpose of this doctrine is to preserve physician autonomy and protect patient care by preventing corporate interference in clinical decision-making. Courts and the California Attorney General have consistently interpreted these provisions to restrict non-physician control over medical services.
Only entities with specific statutory or regulatory authority are exempt from the CPOM restrictions on physician employment. Permitted entities include:
• Professional medical corporations, which must be majority-owned and controlled by physicians as authorized by the Moscone-Knox Professional Corporation Act (Corp. Code §§ 13400–13410);
• Nonprofit community clinics licensed under Health & Safety Code § 1204(a), provided they meet certain conditions and do not interfere with medical judgment;
• Academic institutions and teaching hospitals under Bus. & Prof. Code § 2401;
• Narcotic treatment programs and certain nonprofit research clinics;
• Health maintenance organizations (HMOs), which are permitted under federal and state law, including the Knox-Keene Health Care Service Plan Act of 1975.
Even within these narrow exceptions, however, state law strictly prohibits lay control over essential medical decisions, including determining treatment protocols, supervising medical staff, or selecting billing practices. See Bus. & Prof. Code § 2400; People ex rel. State Bd. of Med. Examiners v. Pac. Health Corp., 12 Cal. 2d 156, 158, 82 P.2d 429, 430 (1938). Physicians should be wary of arrangements that place medical practice in a non-physician entity’s hands—whether through employment or de facto control. Even where an entity claims exemption, it is imperative to confirm that the structure complies with the CPOM doctrine.
Equally important is ensuring that your job description is clearly defined in the contract. It should outline your scope of clinical duties, expected hours and on-call responsibilities, administrative tasks, and any teaching, supervisory, or research expectations. Ambiguity in job responsibilities can lead to conflict or exploitation, such as being assigned non-clinical duties without additional compensation. Additionally, the agreement should state what the employer is obligated to provide, such as clinical support staff, office space, electronic medical record systems, malpractice coverage, and billing services. A well-drafted job description helps preserve physician autonomy and ensures clarity about each party’s obligations.
Understand exactly how you will be paid. Physician compensation models can vary widely and may include:
• Fixed salary (common in employee arrangements)
• Productivity-based pay (e.g., RVUs or percentage of collections)
• Hybrid models
If you are paid based on collections, ask:
• How are collections calculated?
• How often will you be paid?
• What happens if patients don’t pay or if there are insurance clawbacks?
Make sure the agreement defines all key terms and clearly outlines the reconciliation process for disputes over pay. Watch for “withhold” provisions—where your compensation may be held back pending completion of documentation or audits. Additionally, consider whether you will be expected to take call—and if so, whether you will be compensated for it. Call duties can significantly impact your time, stress level, and worklife balance, especially in high-acuity or understaffed settings. It is entirely appropriate to request call pay, and many institutions provide it either as a daily stipend, per-shift rate, or as part of a pooled bonus structure. Do not assume that taking call is simply part of your salary unless the contract says so clearly. Confirm how call is scheduled, whether there are protections against excessive call burdens, and whether additional compensation is provided. Asking for and receiving call pay is not only appropriate—it is a standard and justified practice in many clinical environments.
Your contract should outline how the employment relation-
ship can be ended by either party. Look for:
• Notice requirements for termination without cause (e.g., 90 days’ written notice)
• Termination for cause provisions and what constitutes a breach
• Obligations after termination, such as completing medical records or returning equipment
Importantly, determine whether termination affects your eligibility for bonus pay, collections, or reimbursement. Clarify what survives the agreement’s expiration—some obligations (e.g., confidentiality, non-solicitation) may remain enforceable. Also, carefully review any non-disparagement clause, which typically prohibits you from making negative statements about your employer or colleagues—even after termination. While these clauses may seem benign, they can potentially restrict your ability to speak out about problematic conditions or defend your professional reputation. Ensure the language is not overly broad, vague, or indefinite in duration.
Non-compete clauses may be enforceable in other states but are generally void in California under Business and Professions Code §16600. However, physicians may still be subject to non-solicitation clauses, which can limit your ability to recruit former patients or staff if you leave.
Review:
• The geographic scope and duration of any restrictions
• Whether restrictions apply to referrals, partnerships, or consulting
• Whether the contract allows you to work elsewhere concurrently or post-termination
Always consult with an attorney to determine whether a restrictive covenant is enforceable under your state’s laws.
Pay close attention to how disputes will be resolved:
• Is arbitration mandatory? If so, who pays the costs?
• Where will arbitration or litigation take place?
• Are attorney’s fees awarded to the prevailing party?
Many contracts waive the right to jury trial and limit the types of remedies available. These clauses may seem procedural, but they can drastically affect your rights in the event of a legal conflict.
Employment contracts are legally binding documents. Even provisions that seem minor—such as reimbursement for CME, call coverage pay, or patient assignment policies—can have lasting consequences for your finances and job satisfaction. Don’t hesitate to ask for clarification or request changes before you sign.
And most importantly, have your contract reviewed by a knowledgeable healthcare attorney. Resources like the California Physician’s Legal Handbook (CPLH) and CMA’s Center for Legal Affairs provide physicians with state-specific guidance on employment law, corporate practice prohibitions, and contract negotiations.
Your employment agreement is the foundation of your professional future. Treat it with the care and attention it deserves.

An invaluable resource unlike any other, the California Physician’s Legal Handbook (CPLH) is designed to equip health care professionals with comprehensive legal insights tailored to the evolving landscape of California’s health care industry.
CPLH not only provides legal information to help physicians, medical groups, practice managers, risk management groups and legal practitioners understand and comply with the law, but it also helps shape the law by approaching issues from a physician’s perspective.
CPLH is updated by California Medical Association (CMA) attorneys on a rolling basis throughout the year to ensure CPLH remains a go-to resource for legal guidance and insights. Chapters include eMedicine, FQHC, Medical Staffs, Professional Liability, and many more.
CMA members have free access to CPLH content via CMA’s online Health Law Library at cmadocs.org/health-law-library. Non-members can purchase individual documents for $3 per page. The entire CPLH library is also available as an annual subscription for $575.00 at cplh.org.
Far from being just a bridge between the 2 professions of law and medicine, MLPs have been proposed as a crucial hinge by which shared concerns may be addressed constructively.
By Jin K. Park
Medical legal partnerships (MLPs) are interprofessional collaborations between medical and legal professionals designed with the goal of identifying patients’ health-harming legal and social needs. The pressing need for such collaborative endeavors is highlighted by the broader pattern of health status in the United States. According to some estimates, access to health care services accounts for 10% to 20% of modifiable health outcomes.1 As is now wellknown, health status is influenced by broader social and economic factors—the so-called structural determinants of health (SDoH)—apart from individual behavioral or genetic risk factors. Indeed, physicians now increasingly insist upon the social nature of disease, such that those seeking to systematically understand the drivers of poor health are expected to account for the fact that “disease is always generated, experienced, defined, and ameliorated within a social world.”2 Of course, SDoH matter because they adversely impact not only our health, but also genuine human flourishing in a variety of ways.3 As Michael Marmot has written: “so intimate is the connection between our set of social arrangements and health that we can use the degree of health inequalities to tell us about social progress in meeting basic human needs.”4 While this close connection between health and human flourishing is now widely understood, an important tension remains: how to balance health care provision with prevention and with broader goals of social justice.5
Similar questions have long-occupied legal academics and practitioners. As a general proposition, the law has often shaped our understanding of what fundamental forms of social support we may expect from one another—particularly with regard to our health.6,7,8 As legal scholars have argued, the law has been a crucial determinant of health in a variety of circumstances and has often been the setting in which

Read the entire AMA Journal of Ethics Issue: Standards in Medical-Legal Partnerships It is available free, online at the QR Code above.
health promoting social reforms have been made.9 And, as Lawrence Gostin and Lindsay Wiley demonstrate in their landmark contribution, Public Health Law: Power, Duty, Restraint, many of the significant public health interventions in the 20th century—vaccinations, workplace protections, food and safety regulations, and child welfare—relied fundamentally on obligations generated by the law.10 It is in these cases that the law has been called upon to help resolve fundamental tensions between population health and well-being, on one hand, and personal liberty and other pro-social goals, on the other. As novel methodologies are brought to bear to systematically study the impact of the law on population health over time11—in particular, the role of law itself in determining health outcomes—the potential of the law to promote health will continue to be central.
Far from being just a bridge between the 2 professions of law and medicine, MLPs have been proposed as a crucial hinge by which shared concerns may be addressed constructively.12,13,14 Since at least 1993, when pediatricians and lawyers worked together at the Boston Medical Center to construct one of the first MLPs, the MLP model has been replicated across the country,15 generating significant interest and attention for its potential to address SDoH. However, the unique ability of MLPs to identify and address many health-harming social and legal needs means that the MLP model has— often for good reason—come to encompass an increasingly diverse set of interventions.16
Contributions to this issue seek to answer several fundamental questions that must be addressed if MLPs are to gain

a broader foothold in health care delivery. First, there are questions about value—what fundamental normative goals and priorities are MLPs best suited to fulfill? Next, there are questions about scope—can we expand the scope of services and activities MLPs are engaged in apart from the well-known I-HELPTM (income and insurance, housing and utilities, education and employment, legal status, personal and family stability) model?16 Relatedly, are there particular domains in which MLPs have been uniquely demonstrated to be effective? Lastly, there are questions about evidence—what kinds of evidence are necessary to evaluate the efficacy of various MLP programs? While these questions are by no means exhaustive of the many issues in which the current theme issue intervenes, the issue helps to put forward a diverse set of perspectives on these questions and seeks to set the agenda for MLP research and practice going forward.
References
1. Magnan S. Social determinants of health 101 for health care: five plus five. National Academy of Medicine. October 9, 2017. Accessed October 5, 2023. https://nam.edu/socialdeterminants-of-health-101-for-health-care-five-plusfive/
2. Jones DS, Podolsky SH, Greene JA. The burden of disease and the changing task of medicine. N Engl J Med. 2012;366(25):2333-2338.
3. Wilson J. Not so special after all? Daniels and the social determinants of health. J Med Ethics. 2009;35(1):3-6.
4. Marmot M. Foreword. In: Venkatapuram S. Health Justice: An Argument from the Capabilities Approach. Wiley; 2011:ix-x.
5. Glied S, D’Aunno T. Health systems and social services—a bridge too far? JAMA Health Forum. 2023;4(8):e233445.
Jin K. Park is a MD/JD candidate at Harvard Medical School in Boston, Massachusetts, and Yale Law School in New Haven, Connecticut. His research interests focus on legal and political determinants of health.
6. National Federation of Independent Business v Sebelius, 567 US 519 (2012).
7. Graham v Richardson, 403 US 365 (1971).
8. Fuse Brown EC, Lawrence MB, McCuskey EY, Wiley LF. Social solidarity in health care, American-style. J Law Med Ethics. 2020;48(3):411-428.
9. Benfer EA. Health justice: a framework (and call to action) for the elimination of health inequity and social injustice. Am Univ Law Rev. 2015;65(2):275-351.
10. Gostin LO, Wiley LF. Public Health Law: Power, Duty, Restraint. 3rd ed. University of California Press; 2016.
11. Wagenaar AC, Pacula RL, Burris S, eds. Legal Epidemiology: Theory and Methods. 2nd ed. Wiley; 2023.
12. Healton EB, Treanor WM, DeGioia JJ, Girard VW. Training future health justice leaders—a role for medical-legal partnerships. N Engl J Med. 2021;384(20):1879-1881.
13. Zuckerman B, Sandel M, Lawton E, Morton S. Medical-legal partnerships: transforming health care. Lancet. 2008;372(9650):1615-1617.
14. Teitelbaum J, Lawton E. The roots and branches of the medical-legal partnership approach to health: from collegiality to civil rights to health equity. Yale J Health Policy Law Ethics. 2017;17(2):343-377.
15. Lawton E. A history of the medical-legal partnership movement. Community Health Forum. 2014;(Fall/Winter):12-13. Accessed March 6, 2024. https://medical-legalpartnership. org/wp-content/uploads/2015/01/NACHCMagazine-A-History-of-the-Medical-Legal-Partnership-Movement.pdf
16. Regenstein M, Trott J, Williamson A, Theiss J. Addressing social determinants of health through medical-legal partnerships. Health Aff (Millwood). 2018;37(3):378-385.
AMA Journal of Ethics, Copyright 2024 American Medical Association. All rights reserved. The AMA Journal of Ethics® is a registered trademark of the American Medical Association. journalofethics.org. Reprinted with permission. AMA Journal of Ethics® August 2024, Volume 26, Number 8: E593-595
BY DR. SONYA MISRA AND ANN MONGOVEN Co-chairs of the SCCMA Bioethics Committee
The SCCMA Bioethics Committee is a true county-level committee of the chairs and co-chairs of the ethics committees of all hospitals in Santa Clara County, along with ethicists and some community members, including clergy. The committee both is informed by and supports hospital ethics committees within the county, especially through the development of model ethics policies that can serve as advisory guidelines. (See https://www.sccma.org/programs/bioethics.aspx).
This article introduces the service of the committee and describes its interrelationship with hospital ethics committees.
Both hospitals ethics committees and the SCCMABC address three core functions, at different and mutually reinforcing levels:
• Ethics case consultation
• Clinical ethics education
• Ethics policy development
Hospital ethics committees began developing in the 1960s and 1970s and became a standard element of hospital/ health-system structure during the 1980s
and 1990s. Their development reflected several factors: increasing awareness that social and ethical issues are intertwined with scientific issues in medical care; resistance to overly paternalistic and overly physician-driven models of medical decision-making; the increasingly teambased organization of medicine itself.
For a brief history of the development of hospital ethics committees, see https://journalofethics.ama-assn.org/article/why-did-hospital-ethics-committeesemerge-us/2016-05
Hospital/health-systems ethics committees typically are comprised of clinicians (physicians and nurses), social workers and chaplains, and community representatives who together address bioethical challenges in the clinical setting. Some ethics committee members may have formal education/degrees in conceptual ethics, but most are professionals with other primary roles who have a track record of reflectiveness and leadership helping the institution respond to ethical challenges, and who are provided training and mentoring in ethics to support their ethics committee service. Any hospital staff, patients, or patient-families may request assistance
from their hospital ethics committee.
The SCCMABC developed to provide a forum for cross-hospital deliberation of ethics challenges, sharing of resources, and policy deliberation. While the committee primarily serves hospital ethics committees within the county, it welcomes enquiries from other health professionals or policy-makers in the county.
One of the primary roles of hospital ethics committees is to provide case consultation in real time to difficult bioethical cases. Cases that can generate request for consult include:
• Cases in which ethical principles conflict
• Cases in which there are conflicts among people involved in the case
• Cases in which both those kinds of conflicts are at stake.
Cases in which ethical principles or ideals are in tension or conflict. Conflicts may be true dilemmas, requiring a choice of which principle to be undermined for the sake of the other. Or they may be tensions shy of a direct conflict that can be resolved by restructuring some aspects of care/communication so that a true dilemma is avoided and all
Case Consultation Clinical ethics case consultation in real time.
Ethics Education In-house education, including rounding participation, etc.
Policy Development Development or review of official hospital policies on ethics matters.
Review of de-identified challenging cases that have come before county hospital committees; discernment of patterns and identification of related policy/process issues.
Education is geared to hospital ethics committee chairs to share and take back to their hospital committees. Includes briefings by guest experts and policy updates.
Development of model policies that serve as advisory guidelines which can be adopted or adapted by hospitals within the county. Focuses on common challenges identified across institutions. The influence of SCCMABC model policies has resulted in highly deliberative policies and consistency across healthcare institutions in the county, establishing ethical practice as standard of care.

ethical principles one normally wishes to uphold can be upheld.
Some examples of dilemmatic or tension-ridden cases of ethical principles include: patients declining overwhelmingly beneficial care; or conversely, patients/ families insisting the patient should receive care the medical team does not consider beneficial. Conflicts between medical duty and other administrative or legal duties; e.g., should a physician lie or stretch the truth to get insurance coverage for a treatment considered essential for a patient?
Cases in which there are conflicts or tensions among people involved in the case. These cases may revolve around different conceptions of who should be the treatment decision-maker, or about who should lead the medical team. They may revolve around different conceptions of beneficence and nonmaleficence in the case among family members or among medical staff. They may revolve around aspirations to or resentment of power among various parties. They may be impacted by alternately clear, unclear, sensitive, or insensitive communication.
Examples include: different family members of an incompetent patient – or different members of a medical team--disagree on the desirable care plan. Or, family members and/or consulting medical staff disagree or have distrust.
Of course, sometimes tensions between ethical principles and between people involved in a case are intertwined. Whatever the nature of the tension, by listening to patient/family/staff, case consultants from the hospital ethics committee can help to articulate the eth-
ical tensions at play. They also can make recommendation aimed at helping those involved with the case either to negotiate the dilemma, or to restructure care or improve communication to lessen ethical conflicts or reduce tensions among people involved with the case. Ethics committee recommendations are non-binding. They generally (a) describe ethical principles and tensions at play; (b) describe a range of defensible options; and (c) recommend options.
While hospital ethics committees provide time-sensitive ethics consultation to the actual parties in a challenging case within the hospital, the SCCMABC considers challenging cases in retrospect. Members discuss de-identified recent challenging cases from all the hospitals. Crucially, in the process they identify and address troubling patterns among cases across hospitals. This pattern-identification feeds SCCMABC policy-development processes. For example, when many ethics committees in the county reported an increasing number of challenging cases involving noncompetent unrepresented patients with no surrogate, the committee developed a model policy for unrepresented patients.
In addition to case consultation, hospital ethics committees may sponsor a variety of clinical ethics educational initiatives within the hospital. Education ranges from informal to more formal— from a quick 1-on-1 with a requesting physician or nurse, to formal educational forums offering CME credit.
The SCCMABC directs its educational activities to hospital ethics committees, sharing conversations from national bioethics discourse and flagging changes in law or policy that affect bioethical de-
cision-making. Occasionally the committee may sponsor educational forums for the broader community.
Policy development is the third role of ethics committees. Hospital ethics committees often participate in writing or reviewing official ethical policy guidelines for the institution. In contrast, the SCCMA Bioethics Committee provides a meeting ground where all county hospitals can support each other and discuss ethical challenges that affect all the hospitals. The SCCMABC develops advisory model policies on pervasive ethical challenges in health systems that county hospitals can adapt or adopt in their development of hospital-specific official policies. Model policies are drafted by subcommittees of the SCCMBC, then deliberated, revised, and adopted. These are then deliberated and approved at the committee. Advisory model policies are then utilized by individual hospital committees who revise them to suit unique institutional exigencies and incorporate them into function. Recently developed or updated model policies/Guidelines include: Crisis standards of care guidelines for allocation of scarce resources in a pandemic; model policy for medically ineffective interventions; model policy on health care decision-making for incapacitated patients without surrogates.
The SCCMMABC welcome issues for discussion and looks to support SCCMA members! Feel free to contact the committee though the SCCMA office. For more information on the SCCMA Bioethics Committee and links to its model policies, go to: https://www.sccma.org/ programs/bioethics.aspx

BY: JENNIFER S. SINGH, MD, DIPABLM Chief Mission Officer, Performance Kitchen

California is leading a revolution in chronic disease care - by covering food as part of medical treatment. For busy clinicians who often feel helpless to deeply support their patients’ knowledge and skills around nutrition, being able to literally prescribe nutritious food is groundbreaking. Through the expansion of Food-is-Medicine (FIM) benefits under Medi-Cal
and Medicare Advantage plans, patients with chronic conditions are now eligible for medically tailored meals (MTMs), produce prescriptions, grocery support, and more. The implications for clinical outcomes, healthcare spending, patient satisfaction, and even provider satisfaction are profound.
Mr. Thomas is a 76-yearold man with congestive heart failure (CHF), type 2 diabetes, and limited mobility. He lives with his adult daughter, who works fulltime and struggles to manage his appointments and special dietary needs, as he usually handles his meals alone at home, often resorting to processed foods that are easy to consume. Mr. Thomas has been hospitalized twice in the last nine months for CHF exacerbation, been to the emergency department twice for shortness of breath, and he makes frequent calls to the nursing line for elevated daily weights and diuretic adjustments. Despite having visited the diabetic teaching nurse and a registered dietitian, he states he feels discouraged about his health and just cannot seem to master his diet.
needs of patients managing chronic conditions like diabetes, congestive heart failure, chronic kidney disease, cancer, HIV, and more. Patients prescribed a DASH or ADA diet, for example, can receive meals designed to support those guidelines - without needing to learn new cooking or shopping skills overnight.
The clinic’s social worker helped initiate a medically tailored meal benefit through his Medi-Cal Managed Care Plan. Within two weeks, Mr. Thomas was receiving two RD-designed meals per day, along with telephone nutrition support. At his next visit, his blood pressure was improved, and his daughter shared that his daily weights were more stable than ever. He was so encouraged that he has begun checking his blood glucose on a schedule. Mr. Thomas said the meals had relieved their stress and drastically reduced the number of urgent calls they had made to the nurse advice line. But he was most excited about feeling well enough to begin taking short walks.
His story isn’t rare. It’s becoming common to those of us in the MTM world.
Medically tailored meals are more than “healthy” food delivery. These are condition-specific, home-delivered meals developed by registered dietitians to meet the precise nutritional
MTMs are proven to boost dietary adherence, ease the transition from hospital to home, and give patients practical support in applying their treatment plan. And although they do relieve food insecurity, they also relieve “nutrition insecurity,” a newer term that describes the problem of receiving adequate supplementary calories, but not necessarily in the form of nutrient-dense foods that are known to support health (i.e., vegetables, fruits, lean protein, whole grains, legumes, nuts, healthy fats).
California’s CalAIM initiative, launched in 2022, introduced “Community Supports”—optional services available through Medi-Cal Managed Care Plans (MCPs) to address health-related social needs (HRSNs). Among the most widely adopted of these supports is the Medically Tailored Meals benefit. CalAIM was specifically designed to move Medi-Cal beyond clinical care and into whole-person care, with food and nutrition recognized as central to long-term health and cost control.
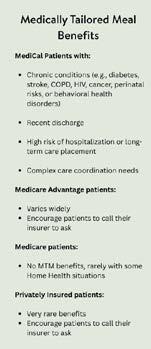
Eligibility varies slightly by plan, but Medi-Cal patients typically qualify if they:
• Have one or more chronic conditions (e.g., diabetes, stroke, COPD, HIV, cancer, perinatal risks, or behavioral health disorders)

• Were recently discharged from a hospital or skilled nursing facility
• Are at high risk of hospitalization or long-term care placement
• Require ongoing care coordination In Santa Clara County, all three MCPs—Santa Clara Family Health Plan, Anthem Blue Cross, and Kaiser Permanente—offer this benefit. In most cases, a physician referral is not required. A clinic staff member or a patient can contact the insurer to begin benefit activation.
While traditional Medicare does not yet cover medically tailored meals, over 70% of Medicare Advantage (MA) plans
nationwide now offer some form of meal benefit, often post-discharge or as part of chronic disease management. In California, however, only 10% of MA enrollees are currently in plans that offer food or produce support.
Original (Traditional) Medicare provides extremely limited meal coverage—typically only when combined with certain home health services. This leaves many older adults without access to MTMs, even if they have qualifying conditions. While advocacy is growing to expand coverage, these benefits are not yet part of standard Medicare.
Private plans may offer limited MTM coverage, particularly in employer-sponsored or high-risk population plans. Encourage all patients to check with their insurers, because coverage is evolving rapidly.

The clinical and financial benefits of MTMs continue to emerge. A 2019 JAMA Internal Medicine study found that MTM recipients had 37–52% fewer hospital readmissions and significantly better adherence to diet and medication.¹ A 2022 publication from Tufts University used data modeling to predict that implementing MTMs nationally could save $13.6 billion annually and prevent 1.6 million hospitalizations.²
More recently, a Cleveland Clinic study (2025) found that patients receiving MTMs for three months experienced an average cost reduction of $12,046 per patient over six months, with decreases in both emergency department visits and inpatient days. Patient satisfaction was high, and most participants reported improved energy and confidence in managing their conditions.³
As of 2024, MTMs and medically supportive food services served more than 156,000 Medi-Cal members statewide. According to the California Department of Health Care Services (DHCS), MTMs are associated with a 21.4% reduction in inpatient use and a 22% reduction in emergency department use over six months.⁴ These outcomes reflect not only improved chronic disease management but also reduced avoidable healthcare utilization.
Medi-Cal Members in Santa Clara County:
• Does the patient have a qualifying condition? (chronic medical condition, recent discharge, at risk for hospitalization, complex care)
• Clinic staff, case managers, or patients can call the health plan to begin a referral
Medicare Advantage Members:
• Many MA plans only offer a Discharge Benefit, available only after a hospitalization, but some offer more chronic benefits
• Coverage and benefits vary widely in length and
number of meals; some include groceries or produce prescriptions
• Patients should call their plan and ask about “meal” or “food” benefits
Traditional Medicare Members:
• Original Medicare does not include MTM coverage, except in rare instances involving home health services.
• These members should be advised that this benefit is not currently included in their plan.
Private Insurance:
• Less common, but worth asking (especially in employer-based plans)
California has created a replicable model for integrating nutrition into clinical care. Most physicians and patients don’t realize this benefit exists—and that’s the gap we must close.
The story of Mr. Thomas highlights that the elusive “Quadruple Aim” of healthcare may have found a surprising ally in the medically tailored meal. Improving patient experience, population health, cost-effectiveness, and provider well-being are all being seen where
MTMs are implemented. For providers, when patients return to clinic not only feeling better, but showing measurable improvements in blood pressure, blood glucose, and energy levels, their care team sees firsthand the impact of food as an intervention. These moments can reignite a provider’s sense of purpose, reminding them why they entered medicine in the first place: to help people heal in ways that truly matter.
References:
1. Berkowitz SA, Terranova J, Randall L, Cranston K, Waters DB, Hsu J. Meal Delivery Programs Reduce the Use of Costly Health Care. JAMA Intern Med 2019;179(6):786–793. doi:10.1001/ jamainternmed.2019.0198
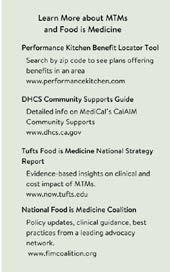
2. Rimm EB, Mozaffarian D, Flatt J, et al. The Case for Food is Medicine: National Strategy Report. Tufts University Friedman School of Nutrition Science and Policy. October 2022.
Accessed June 6, 2025. https://now. tufts.edu/2022/10/17/food-medicine-could-save-13-billion-annually
3. Haddad EH, Miles R, Alejandro-Rodriguez M, et al. Feasibility of self-investment in a medically tailored meals program by a large health enterprise: Cleveland Clinic experience. Nutr Health. 2025. doi:10.1177/02601060241307980
4. California Department of Health Care Services. Community Supports, or In Lieu of Services (ILOS), Annual Report: Department of Health Care Services (DHCS) 1915(b) Waiver Report to the Centers for Medicare & Medicaid Services (CMS) for Calendar Year (CY) 2024. Published April 2025. Accessed June 6, 2025. Available at: https://www. dhcs.ca.gov/Documents/MCQMD/ DHCS-1915b-Annual-Report-on-ILOS-STC-B20-2025.pdf

The Santa Clara County Medical Association (SCCMA) is proud to introduce our revitalized educational series: “Elevating Your Medical Practice”—formerly known as Saving Private Practice. This rebranded initiative continues our commitment to empowering solo, small, and medium-sized medical practices with the tools, insights, and strategies needed to thrive in today’s ever-changing healthcare landscape.
Whether you’re a physician or office manager, this program is designed to provide you with practical guidance, expert-led education, and real-world strategies that can be applied across all specialties. Our focus is clear: supporting your success in practice management while navigating regulatory changes, operational challenges, and opportunities in innovation.
Our first three webinars in the series have been a resounding success, each delivering targeted content tailored to help physicians and their teams elevate their practices.
Speaker: Russell K. Ryan
Healthcare law is evolving rapidly, and staying current is essential for compliance and operational success. In this session, attendees learned:
• The latest updates in California’s employment rules and regulations
• How to manage the changing landscape of paid and unpaid leave policies
• Critical updates to personnel policies for healthcare providers
• Key legal developments impacting physician practices
Webinar
Speaker: Debra Phairas
As 2025 ushers in a new administration, major shifts in health-
care policy are anticipated. This webinar focused on proactive strategies to maintain profitability and patient care quality in a challenging environment. Highlights included:
• Financial and operational strategies to manage decreased reimbursements and rising overhead
• Creating effective patient education materials to optimize visit time
• Exploring the risks and benefits of incorporating AI and new technologies into practice
Webinar 3: Personal Branding for Physicians – Elevate Your Online and Social Media Presence
Speaker: Vanessa Errevarte
In the digital age, your online presence is as critical as your in-person reputation. This engaging session equipped physicians with:
• Tools to create impactful online content that highlights expertise and leadership
• Strategies to transform LinkedIn presence from passive to powerful
• Frameworks for building a personal brand across multiple platforms
• Practical tips for translating online branding into real-world recognition
Missed one of the webinars? Recordings of all sessions are available on the SCCMA website. We encourage all members to take advantage of these valuable resources and continue learning at their own pace.
This is just the beginning. SCCMA is committed to bringing more relevant, expert-led programming through Elevating Your Medical Practice—covering topics from finance and staffing to patient engagement and digital transformation.
Stay connected, stay informed, and let’s elevate your medical practice—together.
On April 9th, 2025, the Santa Clara County Medical Association participated in the California Medical Association (CMA) Annual Legislative Advocacy Day. Our SCCMA team sent fifteen physician and resident participants to Sacramento to meet with our legislative offices. We had nine legislative meetings in one day, including meetings with the offices for Assemblymembers Berman, Kalra, Lee, Ahrens, Pellerin, and Rivas, as well as Senators Becker, Cortese, and Wahab. Many of our meetings were held jointly with colleagues from neighboring county medical societies where our legislative districts overlapped.
Our group gathered in the Capitol at the Sheraton Grand Sacramento Hotel with hundreds of other physicians, residents, and medicals students from throughout California in the morning before heading to our meetings with our local representatives. Physicians were lobbying their legislators in support of CMA’s priority issues, including Prior Authorization, Physician Health and Wellness Program, Pandemic Exceptions for Medical Liability and Stop the Devastating Medicaid Cuts.
The key messages that were shared with legislators were:
Stop the Devastating Medicaid Cuts
Medi-Cal, California’s Medicaid program, provides essential health coverage to one in three Californians and is foundational to the state’s health care delivery system and economy. 15 million Californians depend on Medicaid – children, pregnant women, seniors, the disabled, veterans and low-income families. If Medicaid is cut, patients will lose their coverage, get sicker, crowd emergency rooms and end up in debt. Californians are already waiting weeks or months to see a specialist, particularly in rural parts of the state and Contact Your Members of Congress: It is extremely urgent that members of Congress hear directly from their constituents about how devastating a potential $880 billion cut to Medicaid would be. CMA has made

it easy and quick, with sample letters written from both the physician and patient perspectives.
Prior Authorization Reform
Health plans’ overuse of prior authorization as a blunt cost-control tactic has placed profits over patient safety and intruded on physicians’ ability to make health care decisions that best serve their patients’ interests. Patients and their physicians are forced to wade through red tape, delays and denials, all while their medical conditions worsen. More than one in four (29%) of physicians say that prior authorization burdens have led to a serious adverse event – such as hospitalization, permanent bodily damage, and even death – for a patient in their care. Physicians and medical professionals are also spending numerous hours a week on unnecessary paperwork – time they could otherwise be spending with patients. On average, a physician practice completes 43 prior authorizations per week, and physicians and their staff spend nearly two working days out of the week completing prior authorizations.
AB 408 – authored by Assemblymember Marc Berman (D-Menlo Park) – would establish a physician health and wellness program (PHP) that aligns with national best practices. PHPs that incorporate these best practices provide a proactive approach to address mental health and burnout issues. This bill would enable the Medical Board of California to prevent patient harm by connecting impaired or at-risk physicians with treatment. CMA supports AB 408 because it creates an effective, confidential program – similar to those in other states – that supports physicians’ health and wellness and protects patients by allowing physicians to be at their best. CMA is working with the medical board and the author to ensure the bill will be most effective in meeting its goals of ensuring that physicians have access to support when they need it.
SB 29 seeks to permanently extend pandemic-era exceptions in medical malpractice cases, despite the fact such exemptions


Fahd Khan, Veena Vanchinathan, Seema Sidhu, Assemblymember Pellerin, Jack Watson, Madison Meeks, and John Christensen.




were intended to be temporary to address the issue of backlogged courts during the pandemic. These exceptions were passed through SB 447 in 2021, in the midst of the pandemic. CMA is seeking amendments to carve out medical malpractice claims from SB 29 because of the historic reforms to California’s Medical Injury Compensation Reform Act, made through AB 35 in 2022, which were implemented with the understanding that the exceptions in SB 447 would sunset. Under AB 35, pain and suffering awards in cases involving a patient death increased to $500,000 on the effective date of January 1, 2023, with incremental increases over the next 10 years to $1 million.
What stood out this year where the skill with which the physician members conducted the legislative meetings. SCCMA has had a core group of physician members regularly attend this event for the last three years. The experience that they have gained is reflected in the nuanced ability of the physicians to work as a team to highlight textural examples of the CMA issue priorities in their own medical practices. These transferable skills apply broadly to the advocacy work that SCCMA does with other legislative engagements throughout the year. There were four newer or resident participants this year. Experienced SCCMA physicians supported newer participants in learning how to do advocacy engagement. If you are a SCCMA member who is interested in learning how to do advocacy, please join us next year. This is a wonderful opportunity to connect in person with experienced advocacy leadership and to practice team advocacy. Legislative Advocacy Day is open to the membership at large. We encourage interested physician members to register early as this free event, which is a membership benefit, and fillsup quickly. We hope that you will join our team for next year! Thank you to our physician leaders for their participation and advocacy!

Meeting with Speaker of the Assembly Robert Rivas staff member, Roz Pulmano. From left to
Jack Watson, John Christensen, Roz Pulmano, Michael Jadali, John Christensen, Madison Meeks, Sofia Rojasova, Donna Odryna and Don Hernandez.
Meeting with Assemblymember Ash Kalra’s Chief of Staff, Ryan Guillen. From left to right: Veena Vanchinathan, Lewis Osofsky, Randal Pham, Ryan Guillen and Fadh Khan.
Dr. Christine Doyle receives a warm welcome from newly elected Assemblymember Ahrens.

Meeting with Senator Aisha Wahab, Legislative Aide on Human Services & Health, Karen Bernal. Attended by Christine Doyle, David Li and Carol Shi with AlamedaContra Costa Medical Association members.

1.
On May 2nd, the Santa Clara County Medical Association (SCCMA) had the privilege of hosting a special lunch event with medical residents from Stanford’s Internal Medicine Health Equity, Advocacy, and Research (HEAR) Program and pediatric residents engaged in media and advocacy training. This collaborative gathering, held in partnership with the California Medical Association (CMA), was more than a shared meal—it was an intentional space for mentorship, reflection, and meaningful dialogue about the intersection of medicine and advocacy.
The HEAR program, founded and led by Dr. Lisa Chamberlain and coordinated by Dr. Christine Santiago and Dr. Vivien KonEa Sun, is designed to cultivate the next generation of physician advocates. It offers Internal Medicine residents dedicated training in health equity, public policy, and community engagement. Through structured curriculum and hands-on experiences, HEAR prepares residents to think beyond the clinic walls—to serve as leaders in addressing health disparities and influencing systemic change.
The pediatric residents in attendance, many of whom are completing specialized rotations in media and advocacy, bring a unique and complementary lens to this shared mission. Their work focuses on harnessing the power of communication, storytelling, and policy to elevate pediatric health concerns and advance child health equity.
During the lunch, SCCMA Immediate Past President Dr. Gloria Wu and current President Dr. Fahd Khan joined the conversation—offering their insights and encouragement to the group

of emerging leaders. Their presence underscored SCCMA’s ongoing commitment to supporting physicians at every stage of their career and reaffirmed the role that county medical societies can play in nurturing civic-minded, community-connected clinicians.
The event also gave residents an opportunity to learn more about organized medicine—how institutions like SCCMA and CMA advocate on behalf of physicians and patients alike at the local and state levels. It was a chance to bridge generations and roles within the medical profession, emphasizing that advocacy is not just a specialty—it’s a shared responsibility.
SCCMA continues to expand its programming around physician wellness, advocacy, and leadership development. This lunch is one of many efforts to highlight the non-clinical dimensions of medical training that are vital for shaping a responsive and compassionate healthcare system.
As SCCMA looks ahead, we remain committed to creating opportunities for connection, conversation, and change. We extend our deepest thanks to our colleagues at Stanford, the residents who participated, and our partners at CMA for making this event possible.
Stanford’s Health Equity, Advocacy, and Research (HEAR) pathway supports internal medicine residents with a structured curriculum on public policy, equity, and social justice in medicine. Learn more: https://medicine.stanford.edu/residency/mentorship/merit/stanford-health-equity--advocacy-and-research-hears.html


“Get involved, and get involved early,” said Dr. Khan, as he welcomed the group.

“CMA’s complimentary student membership enables me to actively participate in the progress of health care as a medical student. It’s a great way to stay informed and engaged in shaping the future of medicine.”
Cathy Tran Medical Student
CHSU’s College of Osteopathic Medicine
CMA provides many avenues for you to strengthen your CV, with federal, state and local leadership opportunities.
CMA Provides FREE Memberships to Medical Students and Residents: Shape the future of medicine with invaluable leadership and advocacy training, professional development, access to scholarships, grants, and more!
Student Loan Discounts: CMA members save an average of $22,000 when they refinance their student loans through our partner SoFi®.
Physician Workforce: CMA is committed to ensuring California is training enough physicians to meet current and future demand. Our CalMedForce GME grant program to date has allocated over $251 million to 180 GME programs across California to support and expand residency programs.
Loan Forgiveness: Our CalHealthCares program provides loan repayment grants of up to $300,000 to pay down educational debt for physicians and dentists who care for Medi-Cal patients. To date, 1,414 providers have received grants for a combined total of $323 million.
Career Center: CMA’s California PhysicianTM Career Center provides job opportunities, career advice and helpful resources at careers.cmadocs.org.
Be an advocate and have a direct impact on public health and the future of medicine in California.
Connect, network and learn with physician colleagues from across the state.
On the evening of Thursday, May 29, the Santa Clara County Medical Association (SCCMA) brought together a vibrant crowd of early-career physicians for an unforgettable night of connection, relaxation, and fun at the Young Physician Social, hosted at the lively Tipsy Putt in Sunnyvale.
From 6:00 to 9:00 PM, attendees were treated to an evening that hit all the right notes—mini golf with a creative twist, an array of engaging tabletop games, delicious food, and free craft cocktails or beer. The event offered a perfect opportunity for young physicians to unwind outside of the clinical setting and enjoy the camaraderie of peers navigating similar career stages.
The venue’s unique ambiance and playful atmosphere made for a relaxed and inviting backdrop as colleagues laughed, networked, and even got a little competitive over putters and shuffleboard. With a full dinner menu and an impressive drink selection, the event was both a social and culinary success.
More than just a fun night out, the social underscored SCCMA’s commitment to fostering community and connection among its members. Events like these offer essential space for physicians to build supportive networks, recharge, and remember that they’re not alone in the journey.
Here’s to many more evenings like this—where good food, great games, and even better company bring our medical community closer together.

“Our Young Physicians events are designed to foster meaningful connections early in our members’ careers. It’s rewarding to see the next generation of medical professionals building relationships and engaging with the SCCMA community in such a fun, relaxed setting.” - Fahd Khan, MD, SCCMA President

“Events like these are a reminder that professional growth doesn’t happen in isolation—it thrives in community. SCCMA is committed to creating spaces where young physicians can grow, connect, and feel supported.” - Fahd Khan, MD, SCCMA President




In addition to better malpractice protection and benefits, CAP offers practice resources and risk management tools to help you thrive during this transformational time in healthcare. Apply now or contact dleong@CAPphysicians.com


Meriwest Credit Union, one of Silicon Valley’s largest and most established financial institutions, provides innovative banking products and services to over 80,000 members throughout the Greater Bay Area.
Christina Thach cthach@meriwest.com

Transforming Healthcare with AI-powered workflow. Long Health uses AI to transform complex healthcare data into actionable insights, improving care coordination and outcomes.
Rohit Patil rohitrpatil@longhealth.io
Thriving Practice Community is a specialized collective where practice owners:
• Accelerate growth while maintaining quality care
• Share wisdom with peers facing similar challenges
• Access expert business solutions and strategies
• Build sustainable practices that honor work-life balance
• Resource Library: Immediate access to practice-building templates, guides, and tools
A special invitation to SCCMA for up to 20 Founding Members.
FOUNDING MEMBER BENEFITS:
• Complimentary June Access
• Founding Member Status
• Exclusive Pricing ($4000 savings)
• Expert Network Access
• Exclusive Platform: End the isolation of private practice
Contact Tracy Cherpeski to claim Founder Spot at tracy@tracycherpeski.com
On a bright sunny, Saturday afternoon, the Santa Clara County Medical Association (SCCMA) hosted Family Day at Shoreline Lake, offering members and their families a memorable day filled with fun, food, and fellowship—all complimentary for SCCMA members.
Set against the scenic backdrop of Shoreline Lake in Mountain View, the event provided a perfect opportunity for members to unwind and enjoy a variety of water-based activities. Attendees took to the lake for kayaking, pedal boating, and rowing, with all equipment and life jackets generously provided on-site. Whether paddling across the calm waters or relaxing along the shoreline, there was something for everyone to enjoy.
In addition to water activities, a delicious lunch was served, giving members a chance to gather, share a meal, and catch up with colleagues and new acquaintances. The event created an inviting space for socializing and building community bonds.
SCCMA President, Fahd R. Khan, MD, MSE, MPH, FAANS, FCNS, FACS, was also in attendance, mingling with members and their families throughout the day. The presence of lead-

ership added a personal touch to the event and reinforced SCCMA’s ongoing commitment to member engagement and wellness.
“Events like Family Day remind us that SCCMA is more than just a professional association—it’s a community. We’re proud to support opportunities that strengthen both personal and professional bonds.” – SCCMA President, Fahd R. Khan, MD
Shoreline Lake offered a wide range of additional activities for those looking to explore more. These included sailing, windsurfing, and stand-up paddleboarding. For land lovers, recreational options like hiking, biking, bird watching, and kite flying were extra activities to round out the day’s offerings.
Family Day at Shoreline Lake was not only a relaxing escape from daily routines but also a celebration of the vibrant SCCMA community. It was a day that showcased the strength of our professional network, the value of connection, and the joy of spending quality time with family and peers.
Thank you to all who attended and made the event such a success. We look forward to seeing you at future SCCMA gatherings!



Meriwest Credit Union, one of Silicon Valley’s largest and most established financial institutions, provides innovative banking products and services to over 80,000 members throughout the Greater Bay Area.
Christina Thach cthach@meriwest.com
Thriving Practice Community is a specialized collective where practice owners:
• Accelerate growth while maintaining quality care
• Share wisdom with peers facing similar challenges
• Access expert business solutions and strategies
• Build sustainable practices that honor work-life balance
• Resource Library: Immediate access to practice-building templates, guides, and tools
A special invitation to SCCMA for up to 20 Founding Members.
FOUNDING MEMBER BENEFITS:
• Complimentary June Access

• June Meetings: 06/13 6:00 PM - 7:00 PM and 06/17 5:30 PM - 7:00 PM
• Founding Member Status
• Exclusive Pricing ($4000 savings)
• Expert Network Access
• Exclusive Platform: End the isolation of private practice
Contact Tracy Cherpeski to claim Founder Spot at tracy@tracycherpeski.com

To register for any of these events, please visit www. sccma.org or scan the QR code

Summer Social
Date: Thursday, June 26
Time: 6:00 PM - 9:00 PM
Location: Meso Restaurant, Santana Row, San Jose, CA
Registration: Free for all SCCMA Members! Advanced Registration Required
Let’s kick off summer in style! Join the Santa Clara County Medical Association (SCCMA) for an unforgettable evening of connection, conversation, and fun at the beautiful Meso Restaurant in Santana Row—one of Silicon Valley’s most vibrant destinations.
Virtual Grand Rounds: Tickborne Disease
Date: Tuesday, July 8
Time: 12:00 PM – 1:00 PM
Moving into summer, the ticks are out! As we and our patients explore the natural environments of California and travel to other states in the U.S., many will be exposed to ticks and the range of diseases that these insects can carry. Join us for an update on the epidemiology, research, diagnosis and management of tickborne illness. We will also review current epidemiology of COVID-19 and other summer infectious diseases. Register at www. CMAdocs.org
2025 Health Equity Summit
Date: July 10 – July 11
This event provides an opportunity for physicians, executives, advocates and allies to find community, engage in hands-on trainings and workshops, and hold in-depth conversations about how they are addressing the issue of health equity in California through their care of underserved communities throughout the state.
Attendees will leave feeling energized and inspired to continue their important work to improve the lives of all Californians. More info to come.
SCCMA Wellness Retreat
Date: Friday, August 15 to Sunday, August 17
Location: 1440 Multiversity – 800 Bethany Drive, Scotts Valley, CA 95066
Registration: $695 for single-occupancy room; $960 per pair in a double-occupancy room (all inclusive)
This Wellness Retreat is a three-day, two-night program at 1440 Multiversity, a 75-acre campus at Santa Cruz Mountains. Attendees will be immersed in a beautiful backdrop of nature as they unplug over the course of the weekend and participate in sessions aimed at delivering healing and supportive care. Register at www.sccma.org
Date: Thursday, September 18, 2025
Time: 12:15pm-1:15pm
This session will provide a framework for responding to an adverse patient safety event or unexpected health care outcome in an office practice, including transparent communication and disclosure to the patient and their family, documentation of the event, and creating a culture of safety to learn from these unexpected events.
The Centers for Medicare & Medicaid Services (CMS) recently opened the 2025 Merit-based Incentive Payment System (MIPS) Extreme and Uncontrollable Circumstances (EUC) Exception and Promoting Interoperability (PI) Hardship Exception applications. These updates offer critical flexibility to address unforeseen challenges that may impact MIPS reporting. Practices are encouraged to assess their eligibility and submit applications as needed to avoid potential payment penalties. If your application is approved, you will not be required to report data for the performance category or categories included in your approved application. Scan the QR code to read more or visit https://www.cmadocs.org/newsroom/news.
Medicaid is under threat. Physicians can help protect it – one text at a time.

The Senate is now considering HR 1, which threatens billions in Medicaid funding. If passed, states may be forced to cut coverage, eliminate benefits, or raise taxes. Your advocacy made a huge impact in the House—now we need that same energy in the Senate.
Thanks to support from Kaiser Permanente, the Protect Our Health Care Coalition has launched a voter-to-voter texting campaign. It’s fast, easy, and impactful.
David Ford, CEO of CMA Physician Services (CMA PSO), was recently featured on the Thriving Practice podcast to discuss MedWay – a new administrative solution supporting independent physician practices. The episode, “Independent Practice Isn’t Dead: How Physicians Can Thrive Outside Big Healthcare,” delved into how MedWay can help reshape the administrative landscape for independent practices across California.
In the episode, Ford discussed the mounting challenges faced by independent physicians—from staffing and compliance burdens to burnout—and how MedWay, CMA PSO’s newest initiative, aims to address them. To listen to the podcast, please visit https://www.podbean.com/media/share/pb-hub8j-18be533
The California Medical Association (CMA) is calling on state lawmakers to reject Governor Gavin Newsom’s proposal to divert billions in voter-approved health care funds from Propositions 35 and 56. The proposal will devastate access to care for Medi-Cal patients and betrays the trust of California voters. The Governor’s revised budget proposal diverts significant funding from Prop 35 to backfill the state’s budget shortfall instead of to increase provider rates, as the proposition requires. To read more, scan the QR code to enter CMA’s newsroom.
Thriving Practice Community is a specialized collective where practice owners:
• Accelerate growth while maintaining quality care
• Share wisdom with peers facing similar challenges
• Access expert business solutions and strategies
• Build sustainable practices that honor worklife balance
• Resource Library: Immediate access to practice-building templates, guides, and tools FOUNDING MEMBER BENEFITS:
• Founding Member Status
• Exclusive Pricing ($4000 savings)
• Expert Network Access

• Exclusive Platform: End the isolation of private practice
If you are interested in becoming a Founding Member with Thriving Practice Community, please email Angelica@sccma.org
The California Medical Association (CMA) has published a new fact sheet to help physician practices prepare for upcoming changes under SB 1061 (Limón, 2024)—a new law that reshapes how medical debt is handled in California. Beginning January 1, 2025, physicians and their billing partners will be prohibited from reporting medical debt to consumer credit reporting agencies. Additionally, starting July 1, 2025, any contract that creates a medical debt must include specific consumer protection language or it will be considered void and unenforceable.
To help practices understand and comply with these new requirements, CMA’s fact sheet outlines key provisions, offers compliance tips, and includes links to updated sample forms in the CMA Health Law Library. The fact sheet is available free to members on CMA website.
In a major step toward reducing delays in care and improving patient outcomes, three bills from the California Medical Association’s (CMA) Prioritizing Patients, Empowering Physicians legislative package have advanced out of their house of origin in the California State Legislature. Read more by scanning the QR code or visit https://www.cmadocs.org/newsroom/news




p u r p o s e .





Reprinted with permission from: https://publichealthproviders.santaclaracounty.gov/health-care-providers/diseases/measles. Please see the live website for linked information and forms.

A case of measles with rash onset on May 25, 2025 has been confirmed in Santa Clara County. The person tested positive after returning from international travel. The person was not hospitalized and is now isolating at home. Contact tracing to date has identified potential exposures at private locations including healthcare facilities where the individual sought care and testing, and several public locations. Read the health alert.
Healthcare providers are required to immediately report suspected or confirmed cases of measles to the Public Health Department. Call Public Health immediately, while the patient is still in your office, at (408) 885-4214 and select option 3. After hours, call (408) 998-3438 and ask for the Health Officer on call. Call, do not fax.
There has been an increase in measles cases in the United States in 2025, with outbreaks occurring in multiple states. While no outbreaks have occurred in California this year, several measles cases have been reported. Everyone who is not fully vaccinated against measles should get the vaccine, which is safe and highly effective.
Due to the recent cases, health care providers should be on alert for patients who have: (1) febrile rash illness and symptoms consistent with measles, and (2) travelled internationally, especially to countries with ongoing measles outbreaks or travelled domestically to areas experiencing measles outbreaks. Infected people are contagious from 4 days before the rash starts through 4 days afterwards.
For information on measles cases reported in California in 2025, refer to the California Department of Public Health’s Measles webpage.
Healthcare providers should consider measles in patients with:
• Clinical symptoms consistent with measles including fever, rash, and any of the “3 Cs” – cough, coryza (runny nose), or conjunctivitis.
• Epidemiological risk for measles including any of the following:
• International travel such as travel outside of North America, transit through U.S. international
airports, or interaction with international visitors (including at U.S. tourist attractions) in the last 21 days.
• Domestic travel to an area with known measles transmission in the last 21 days.
• Known exposure to measles
Ask about measles vaccination status, onset and duration of fever and rash, exposure to other persons with febrile rash illness, travel history, and contact with international visitors or visitors from areas with recent measles outbreaks in the three weeks prior to illness. When suspecting measles in your patient, immediately mask and isolate the patient per airborne precautions Infected people are contagious from 4 days before rash onset through 4 days after rash onset.
1. Mask and Isolate: Mask and isolate the patient immediately. Do not allow patients with suspected measles to remain in the waiting room or other common areas of the healthcare facility. Isolate patients in a single-patient airborne infection isolation room (AIIR) if available, or in a private room with a closed door until an AIIR is available.
a. Healthcare providers should be adequately vaccinated against measles and should adhere to standard and airborne precautions when evaluating suspect cases regardless of their vaccination status. All healthcare personnel entering the patient room, regardless of immune status, should use respiratory protection at least as effective as an N95 respirator per Cal/OSHA requirements.
2. Notify: Healthcare providers are required to immediately notify the Public Health Department of any suspected case of measles to ensure rapid testing and investigation. Call Public Health immediately, while the patient is still in your office, at (408) 885-4214 and select option 3. After hours, call (408) 998-3438 and ask for the Health Officer on call. Call, do not fax.
a. Be prepared to provide (1) a detailed description of fever and rash onset and evolution, (2) a photo of the rash, and (3) complete vaccination and travel history.
3. Test: If advised to test for measles by Public Health,

collect a throat swab and urine sample for reverse transcription polymerase chain reaction (RT-PCR). Collect specimens in-office rather than sending the patient to a laboratory.
a. Throat swab: Use a sterile synthetic swab. Place swab into viral or universal transport media.
b. Urine sample: Collect 10-50 mL urine in a sterile container.
c. Storage and transport: Store all specimens at 4°C. Transport all specimens on cold pack within 24 to 72 hours. Specimens should be dropped off at the Public Health Laboratory along with a submission form.
4. Manage: If discharged home: provide patient suspected to have measles with instructions to isolate at home until test results return. If transferred to a higher level of medical care: directly inform EMS and the accepting facility so that appropriate precautions can be put in place. In coordination with the Public Health Department, provide appropriate measles post-exposure prophylaxis (PEP) to close contacts without evidence of immunity, either MMR or immunoglobulin.
Measles can be prevented with measles-containing vaccine, which is primarily administered as the combination measles-mumps-rubella (MMR) vaccine. One dose of MMR vaccine is approximately 93 percent effective at preventing measles; two doses are approximately 97 percent effective.
The MMR vaccine is included in the routine childhood immunization schedule. CDC recommends children get two doses of MMR vaccine, starting with the first dose at 12 to 15 months of age, and the second dose at 4 to 6 years of age. Teens and adults should also be up to date on their MMR vaccination. There are also travel-related vaccine recommendations for people who are traveling internationally or to outbreak-affected areas in the United States.
For more information on the MMR vaccine, refer to the CDC’s Measles, Mumps, and Rubella (MMR) Vaccination: Information for Healthcare Providers webpage.
Measles and international travel
Measles cases often originate from unvaccinated or undervac-
cinated U.S. residents who travel internationally and then transmit the disease to people who are not vaccinated against measles. All international travelers over the age of 6 months should be vaccinated against measles before traveling.
Before traveling abroad:
• Infants 6 to 11 months old need 1 dose of MMR vaccine
• Children 12 months and older need 2 doses of MMR vaccine
• Adults born during or after 1957 without evidence of immunity against measles need documentation of two doses of MMR vaccine at least 28 days apart
After traveling abroad:
• Patients should monitor for fever and rash for 3 weeks after international travel
Measles and domestic travel
There have been multiple confirmed measles cases and outbreaks reported across the United States in 2025. Any person traveling to outbreak-affected areas should follow all vaccination recommendations issued by state, local, tribal, or territorial health departments. Healthcare providers can find updated outbreak-related recommendations issued by state or local health departments on the CDC’s Measles Cases and Outbreaks webpage.
Additional information:
• Measles case confirmed in Santa Clara County with public exposures (https://publichealthproviders.santaclaracounty.gov/measles-case-confirmed-santa-clara-county-public-exposures)
• Measles information for healthcare providers: (https://publichealthproviders.santaclaracounty.gov/ health-care-providers/diseases/measles)
• To share with your patients: sccphd.org/measles
• Press release: Public Health Departments of Santa Clara County and Alameda County announce locations of measles exposure and disease prevention recommendations (https://publichealth.santaclaracounty.gov/ news/media-advisory/public-health-departments-santa-clara-county-and-alameda-county-announce-locations-measles-exposure)
This spring, the Santa Clara County Medical Association (SCCMA) Environmental Health Committee hosted a timely and thought-provoking three-part webinar series addressing the crucial links between human health and environmental sustainability. The series brought together physicians, researchers, and public health experts to deepen our understanding of the health impacts of climate change, environmental toxins, and sustainable practices—and what we, as healthcare providers, can do about it.
From nutrition to climate science to toxicology, each session tackled urgent issues that directly affect the well-being of our patients and communities. Here’s a look back at the impactful sessions:
Session 1: Plant-Based for the Planet
Date: Tuesday, March 25
Presenters: Ulka Agarwal, M.D. and Tamiko Katsumoto, M.D.
Drs. Agarwal and Katsumoto kicked off the series by exploring how plant-based diets are not only essential for preventing and reversing chronic illnesses like diabetes, heart disease, and obesity—but also for preserving planetary health. The session emphasized that the agriculture sector, particularly livestock production, is a leading source of methane emissions and environmental degradation. The message was clear: shifting toward a plant-based diet is one of the most powerful actions individuals and communities can take to reduce carbon emissions and protect the environment.
2: Discussing
Date: Tuesday, April 22 (Earth Day)
Presenters: Nathaniel DeNicola, M.D., Bruce Bekkar, M.D., and Rupa Basu, Ph.D.
This Earth Day session brought a vital update on the trajectory of climate change, focusing on its rapidly accelerating impacts on public health. The panel outlined the science behind rising greenhouse gas levels and highlighted the mounting health risks, from heat-related illness to respiratory issues
and climate-related displacement. Physicians were urged to become not just informed, but active voices in climate advocacy, both in clinical settings and in broader public health policy.
Date: Tuesday, May 20
Presenter: Bruce Lanphear, M.D.

Scan the QR code to watch all the webinars
Dr. Lanphear delivered a compelling presentation on the history, health consequences, and ongoing public health threat of lead exposure. Despite significant reductions in exposure since the 1970s, the legacy of lead remains—particularly in marginalized communities and developing countries. The talk highlighted that no level of lead exposure is considered safe and discussed its links to developmental, cardiovascular, and neurological harm. Physicians were reminded of the importance of continued vigilance and advocacy in addressing this often overlooked but enduring threat.
All three webinars were recorded and are available on the SCCMA website for viewing at your convenience. Whether you missed the live events or want to revisit the insights, these recordings serve as valuable resources for healthcare providers interested in environmental health and advocacy.
This webinar series underscores SCCMA’s commitment to educating and empowering physicians to be leaders in environmental stewardship and health equity. As the impacts of climate change and pollution grow more evident, our role as trusted messengers and advocates for planetary health has never been more essential.
How do physicians manage the voice in their heads—the one that narrates their days, questions their decisions, and sometimes won’t stop even after the shift ends?
That was the central question of SCCMA’s recent physician book club gathering, which featured the bestselling book Chatter: The Voice in Our Head, Why It Matters, and How to Harness It by Dr. Ethan Kross. In a remarkable opportunity for attendees, Dr. Kross himself joined the event via Zoom for a live, interactive discussion.
The event was part of SCCMA’s ongoing efforts to explore wellness in its broadest and most meaningful sense—not just physical or clinical well-being, but mental and emotional resilience, especially for those working under the pressures of modern medicine.
Chatter: The Voice in Our Head, Why It Matters, and How to Harness It, offers an accessible yet scientifically grounded look into how our inner monologue affects everything from performance and decision-making to mental health. Drawing on decades of research in psychology and neuroscience, Dr. Kross explores why the voice in our head can either help or hinder us—and how to shift it toward being a force for clarity and calm.

During the conversation, book club members had the chance to ask questions directly. Topics ranged from the science of “distanced selftalk” to how physicians can apply these tools to reduce burnout and navigate high-stakes environments.
“WE ALL HAVE AN INNER VOICE. LEARNING TO HARNESS IT CAN BE THE DIFFERENCE BETWEEN ANXIETY AND FOCUS, BETWEEN BURNOUT AND RESILIENCE.” — DR. ETHAN KROSS


Dr. Kross also shared personal reflections from his research journey, including moments when chatter overwhelmed even him—and how the tools he teaches became ones he used himself.
Events like this align with a larger strategy to reimagine how wellness is supported in the medical community.
“Supporting physician wellness means looking at the whole picture,” Dr. Khan, SCCMA President, said. “It’s not just about clinical outcomes or physical health—it’s about managing stress, building self-awareness, and creating space for connection. A book club might seem like a small thing, but it creates a moment of reflection that can be very impactful.”
The event drew physicians from across specialties and stages of their careers, creating a rare forum for cross-disciplinary conversation grounded in shared human experience.
SCCMA plans to continue offering similar events—bringing together literature, lived experience, and expert voices—as part of its commitment to physician engagement and well-being.
For anyone who missed it, Chatter remains a recommended read for physicians seeking insight into their inner world—and tools to manage it with strength and grace.

By Ethan Kross
1. You Can Coach Your Inner Voice
When negative self-talk spirals, tools like distanced self-talk (e.g., using your own name) can help you step back and think more clearly under pressure.
2. Physical Space Can Bring Mental Space
Even small changes—like taking a walk in nature or organizing your desk—can reduce chatter and restore cognitive control.
3. We Need Reflective Time, Not Just Quiet Time
Suppressing our inner voice doesn’t work. Instead, reframing, journaling, and even talking to someone who helps us gain perspective can turn chatter into clarity.
SCCMA WOULD LIKE TO HEAR YOUR INPUT ON CONTENT AND THEMES YOU WOULD LIKE TO SEE FEATURED IN THE BULLETIN.

Scan the QR Code