SCCMA is a professional association representing over 4,500 physicians in all specialties, practice types, and stages of their careers. We support physicians like you through a variety of practice management resources, coding and reimbursement help, training, and up to the minute news that could affect your practice. The Bulletin is our quarterly publication.
Santa Clara County Medical Association
SCCMA OFFICERS
President | Fahd Rahman Khan, MD
President-elect | Santosh Pandipati, MD
Secretary | Veena Vanchinathan, MD
Treasurer | Shahram Gholami, MD
Immediate Past President | Gloria Wu, MD
VP-Community Health | Paul Wang, MD
VP-External Affairs | Christine Doyle, MD
VP-Member Services | Sam Wald, MD
VP-Professional Conduct | Lewis Osofsky, MD
SCCMA STAFF
CEO/Executive Director | Marc E. Chow, MS
Director of Operations | Angelica Cereno
Director of Governance & Advocacy | Emily Coren
Facilities Manager | Andie Campanilla
Executive Assistant/Member & Program Manager | Rashida Mirza
SCCMA COUNCILORS
El Camino Hospital of Los Gatos | Jaideep Iyengar, MD
El Camino Hospital – Mountain View | Carol A. Somersille, MD
Good Samaritan Hospital |Judong Pan, MD
Kaiser Foundation Hospital - San Jose | Haritha Reddy Rachamallu, MD
Kaiser Permanente Hospital - Santa Clara | John Truong, MD
O’Connor Hospital | David Cahn, MD
Regional Medical Center | Raj Gupta, MD
Saint Louise Regional Hospital | Kevin Stuart, MD
Santa Clara Valley Medical Center | Open Stanford Health Care/Children’s Health | Karen Kim, MD
Managing Editor | Emily Coren
Production Editor | prime42 – Design | Market | Host
Opinions expressed by authors are their own, and not necessarily those of The Bulletin or SCCMA. The Bulletin reserves the right to edit all contributions for clarity and length, as well as to reject any material submitted in whole or in part. Acceptance of advertising in The Bulletin in no way constitutes approval or endorsement by SCCMA of products or services advertised. The Bulletin and SCCMA reserve the right to reject any advertising.
Address all editorial communication, reprint requests, and advertising to:
Emily Coren, Managing Editor
700 Empey Way
San Jose, CA 95128
408/998-8850
Fax: 408/289-1064
emily@sccma.org
New and Noteworthy
A Message from the President
Fahd R. Khan, MD SCCMA President
Dear Colleagues,
I hope you were able to enjoy some moments of rest and relaxation this summer. Taking time away from the demands of practice is essential to sustaining our well-being and keeping us motivated as physicians so that we may continue to serve our patients and communities at our very best. It has also been a busy and productive summer at SCCMA. I am grateful to all who joined us for our recent gatherings, including the Young Physicians Mixer at Tipsy Putt, the Family Picnic at Shoreline Park in Mountain View, the Summer Social at Meso in Santana Row, the Wellness Retreat, and the Healthy Cooking Class. Looking ahead, we have an exciting slate of programs this fall, including our Artificial Intelligence and Innovation Forum, the House of Delegates in Los Angeles, a half-day wellness event, and more. These events are opportunities not only to learn but also to reconnect with colleagues, strengthen professional relationships, and reinforce our sense of community.
This issue of the Bulletin focuses on environmental health—a subject of growing urgency. The environment has always shaped human health through factors such as infections, toxins, water and air pollution, and now, more visibly than ever, climate change. Each day we are reminded that rising temperatures, extreme weather, and degraded ecosystems are no longer distant threats but pressing realities affecting our patients. As our understanding of these connections deepens, so too does our responsibility as physicians to address them.
From a health equity perspective, climate justice is especially relevant for the diverse populations of Santa Clara County. Climate justice recognizes that those who contribute least to climate change, often low-income, immigrant, and other vulnerable communities, are among the most severely affected, while wealthier groups and major emitters bear greater responsibility. At its core, climate justice demands fairness in how the burdens and benefits of climate action are shared, accountability for historical emissions, and a just transition that protects workers and communities while advancing public health and sustainability.
Physicians have a unique and trusted voice in this conversation. Beyond caring for individual patients, we are well positioned to:
Influence policy by engaging with local, state, and federal officials to advocate for evidence-based climate and health solutions.
Educate the public, including our patients, about steps they can take to reduce disease risk— such as reducing exposure to environmental toxins, staying safe during heat waves, or making sustainable lifestyle choices.
Inform and empower our colleagues in health care by sharing knowledge about the health impacts of climate change and promoting environmentally responsible practices within our workplaces.
Promote healthy, sustainable diets, such as plant-forward eating patterns, which benefit both patient health and the environment.
Partner with nonprofits and community groups that champion environmental health, climate justice, and health equity, adding our medical expertise to broader coalitions for change.
Our Environmental Health Committee is deeply engaged in these issues. If you are passionate about climate change, climate justice, environmental toxins, or public health, I encourage you to consider joining this active group. Together, we can amplify our impact—advancing not only the health of our patients but also the resilience and well-being of our communities.
Warm regards,
Fahd R. Khan, MD
President,
Santa Clara County Medical Association
Santa Clara County Physician’s
testify against the repeal of the EPA Endangerment Finding
On July 29, 2025, EPA proposed to rescind the 2009 Greenhouse Gas Endangerment Finding. The Endangerment Finding is a prerequisite for regulating emissions from new motor vehicles and new motor vehicle engines. Absent this finding, EPA lacks statutory authority under Section 202 of the Clean Air Act to prescribe standards for GHG emissions. Therefore, EPA also proposed to remove GHG regulations for light-, medium-, and heavy-duty on-highway vehicles. As a result of these proposed changes, engine and vehicle manufacturers would no longer have any future obligations for the measurement, control, and reporting of GHG emissions for any highway engine and vehicle, including model years manufactured prior to this proposal.1
SCCMA signed onto a group letter organized by the American Lung Association in opposition to the proposed rescinding of the Endangerment Finding as well as a group letter authored by the Alliance of Nurses for a Healthy Environment, American Thoracic Society, and the Medical Society Consortium on Climate and Health.
“As health professionals, we urge the Trump Administration to recognize and respond to the urgent health and economic crisis that global climate change poses for our nation and the world. The science is clear: Climate change is real, driven primarily by human-caused emissions, and harming both our health and the economy today. Contrary to the EPA’s claim that “the projections relied upon in the Endangerment Finding appear unduly pessimistic in light of empirical observations made after it was finalized in 2009 through 2024,” the potential climate impacts of increased greenhouse gas emissions were well understood as early as the 1950s and 1960s, based on research conducted by the fossil fuel industry. Since that time, predictive models have only improved, and recent research notes that climate models published over the past five decades have generally been quite accurate in predicting global warming trends.1 Without rapid action, health threats will escalate—condemning future generations to a crisis that will jeopardize their well-being and eco-
nomic stability.
The health harms of climate change caused by greenhouse gas (GHG) emissions are well understood and acknowledged by the American medical and scientific communities. At least 32 medical societies and 18 national nursing organizations from across the United States, plus the International Council of Nurses, have adopted or published position papers, statements, or policies recognizing the health threat of climate change. In 2023, 42 national, state, and academic nursing organizations and institutions signed on to a joint commitment on climate change and health. That same year, over 200 health journals coordinated the release of an editorial declaring climate change a global health emergency, warning that vulnerable communities will bear the greatest burdens.”” 2
In addition to the organizational sign-ons to the two group letters, as representatives on behalf of SCCMA both Dr. Cindy Russell and Dr. Robert Gould testified at the EPA hearings in opposition to the repeal of the Greenhouse Gas Endangerment Finding. These actions are in-line with the Environmental Health Policy developed by the Santa Clara County Medical Association’s Environmental Health Committee. If you are interested in joining County these efforts, please reach out to staff member emily@sccma.org.
“I’ve never seen anything like it, and no one is sure what this patient has.”
— Neurology resident to Dr. William Langston, Santa Clara Valley Medical Center, 1982
EMILY VALENCIA AND RAY DORSEY, MD
Center
for
the
Brain
& Environment, Atria Research and Global Health Institute
On July 16, 1982, at Santa Clara Valley Medical Center, a neurology resident interrupted Dr. William Langston’s morning cup of coffee. “Dr. Langston, you have to come down here,” he said. “I’ve never seen anything like it, and no one is sure what this patient has.”
Down in the psychiatric unit, 42-year-old George Carillo, who had a history of substance use, presented with symptoms mimicking advanced Parkinson’s disease: profound rigidity, tremor, slowed movement, a fixed gaze, and near-total loss of speech. Most alarming, however, was that these symptoms had emerged virtually overnight.
Within days, five more patients showed up across Northern California with nearly identical symptoms. Each had developed nearly all of the motor symptoms typically seen in Parkinson’s disease, including tremors, stiffness, and slowed movement. As Langston and his team investigated further, they discovered a common thread: all six patients had recently used a new synthetic heroin that had recently hit the streets in several Northern California cities.
After obtaining samples of this synthetic heroin from the local police department, Langston and his colleagues found that the drug contained a chemical called MPTP.
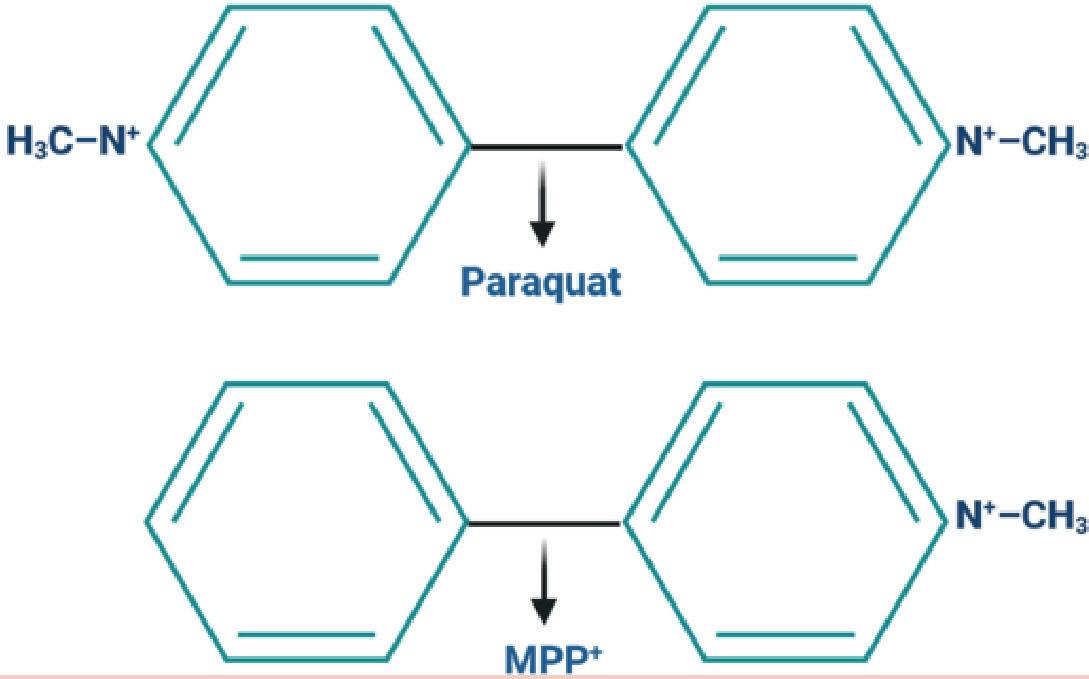
Once inside the body, MPTP crosses the blood–brain barrier and is converted into MPP+ , a neurotoxic metabolite that selectively destroys dopaminergic neurons in the substantia nigrathe very same population of neurons that is lost in Parkinson’s disease. For the first time, scientists had clear, causal evidence that an environmental toxin could directly induce parkinsonism in humans.
The discovery marked a turning point in the field, and established MPTP as a powerful tool for studying the disease. And it also raised an unsettling question: if one man-made substance could trigger parkinsonism overnight, what else in our environment might be doing the same?
87% of Parkinson’s Cases Have No Known Genetic Link
Parkinson’s is now one of the world’s fastest growing brain diseases and among the least heritable. A 2024 study in Brain found that among thousands of Americans with the disease, only 13% have a genetic cause or risk factor for the disease1. 87% do not. The principal causes of Parkinson’s lie not within us but outside, in our environment. Among the toxicants linked to Parkinson’s are certain pesticides and dry-cleaning chemicals, both of which plague Santa Clara and surrounding communities.
Certain Pesticides Increase the Risk of Parkinson’s by 150%
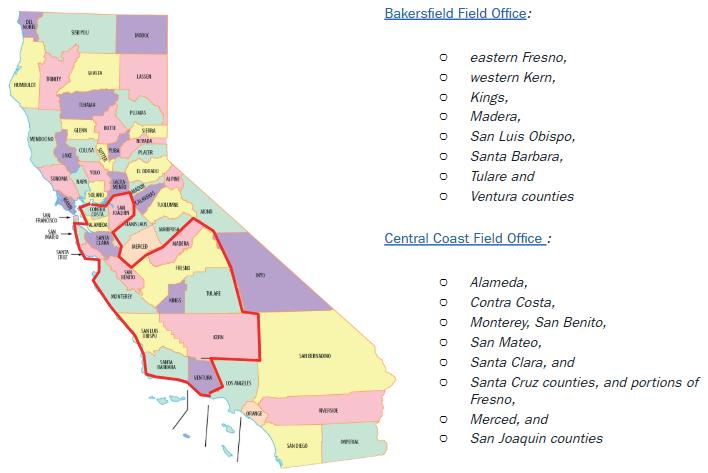
son’s. Structurally, paraquat bears a striking resemblance to MPP+ , the neurotoxin that caused the Santa Clara cases2.
In the Central Valley of California, a region with some of the highest agricultural pesticide use, paraquat is widely sprayed. In 2011, Dr. Langston, Dr. Caroline Tanner (now at UCSF), and colleagues found that farmers who worked with the chemical had a 150% increased risk of developing Parkinson’s disease. A decade later, researchers at UCLA found that simply living or working near where paraquat is sprayed is associated with a doubling of the risk of Parkinson’s.
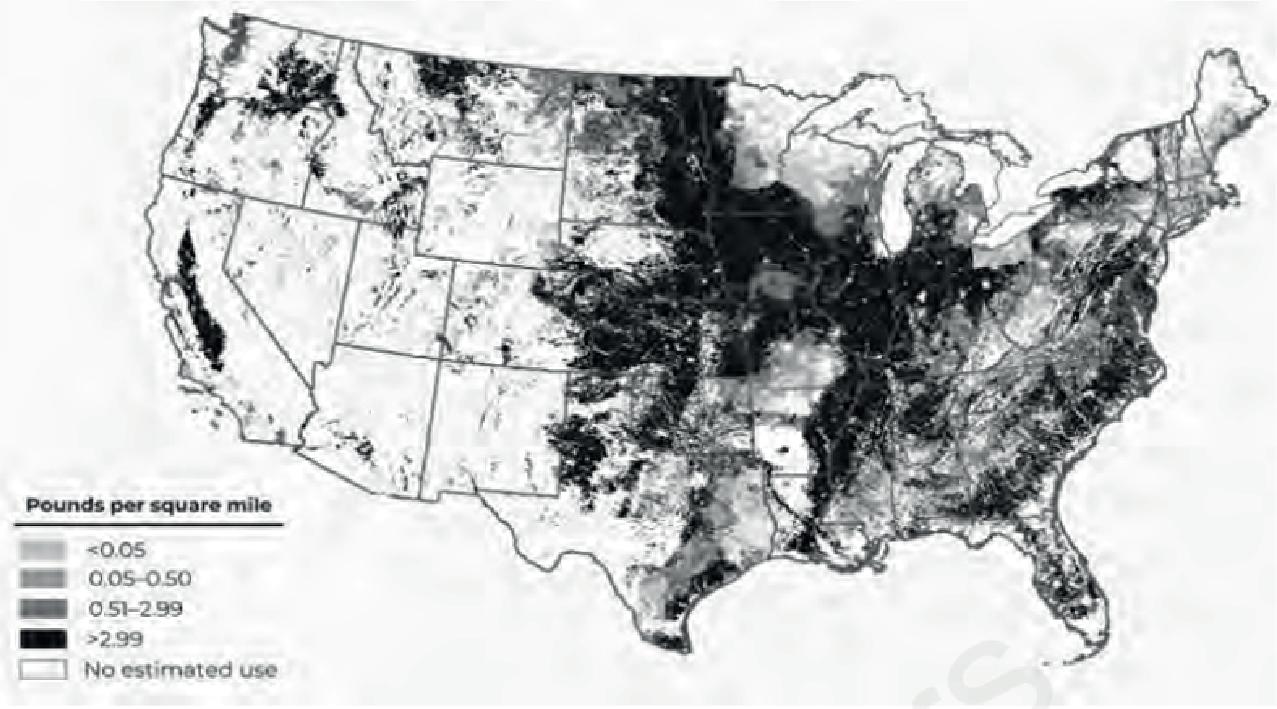
Despite being banned in over 70 countries, paraquat remains in widespread use across the U.S., and is sprayed on crops including soybeans, cotton, corn, and grapes. The EPA’s own website says, “One Sip Can Kill,” yet continues to re-authorize its use3. More than 50 countries, including China, have banned paraquat, but over the last five years, for which data are available, use of paraquat in the U.S. has doubled.
Preliminary estimated agricultural use of paraquat in the United States, 2018, which includes “more extensive estimates of pesticide use not reported in surveys.” Map created by the US Geological Survey.
Paraquat dichloride, a widely used herbicide, is among the most consistently linked environmental risk factors for Parkin-
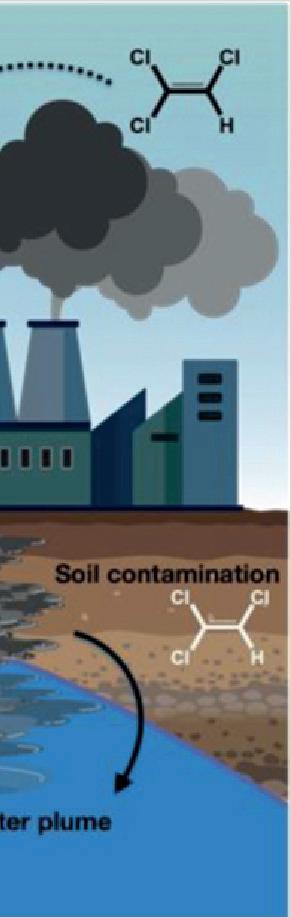
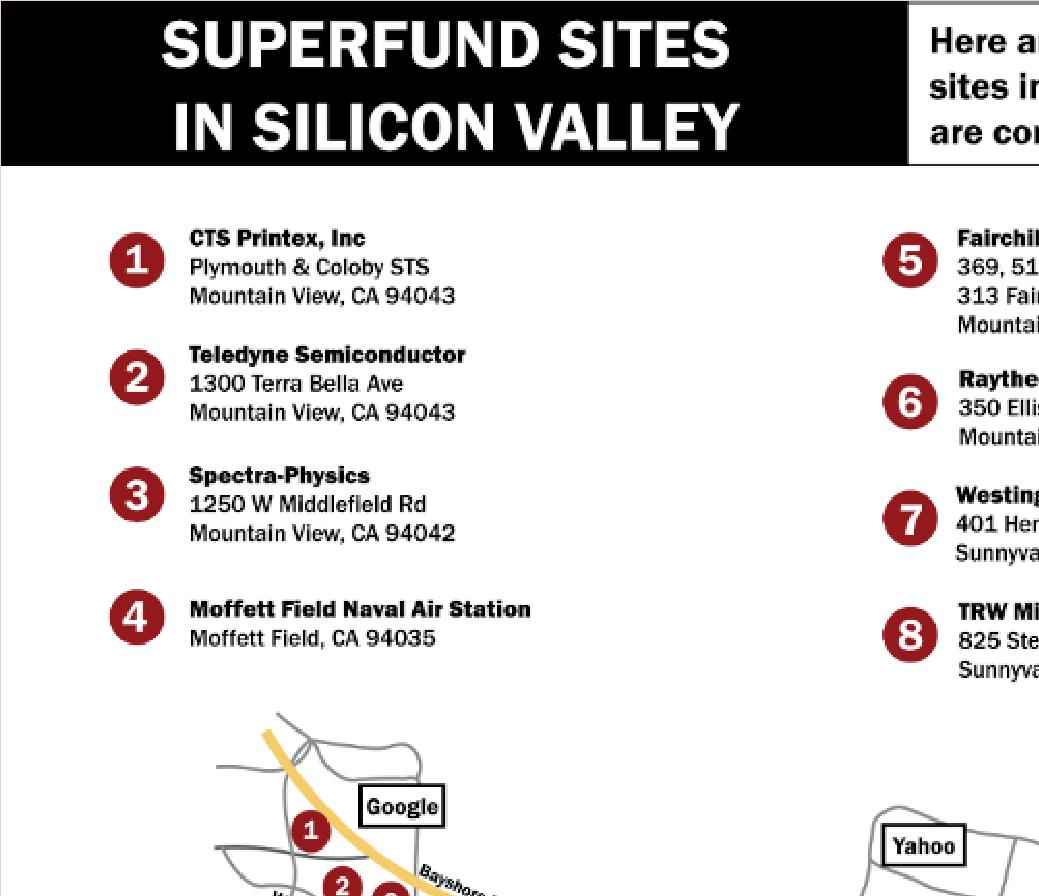
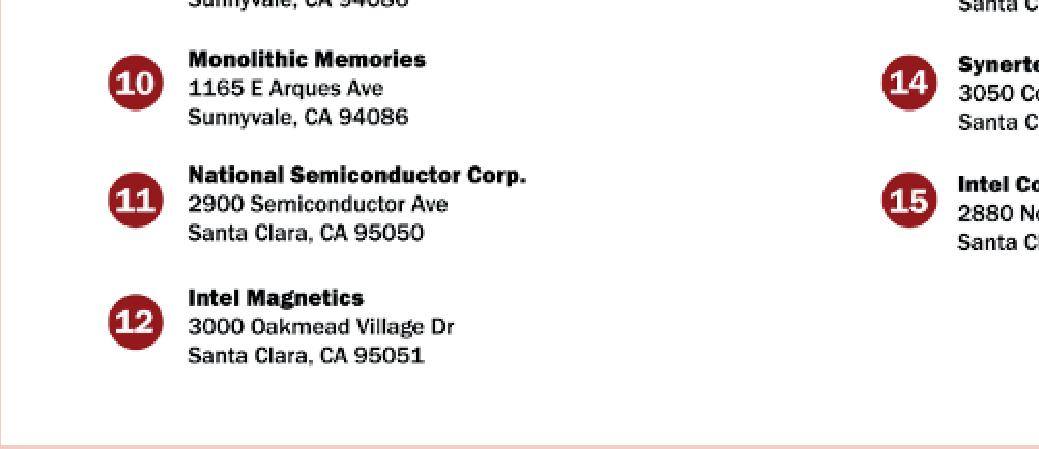
The Toxic Solvent Lurking Beneath Silicon Valley
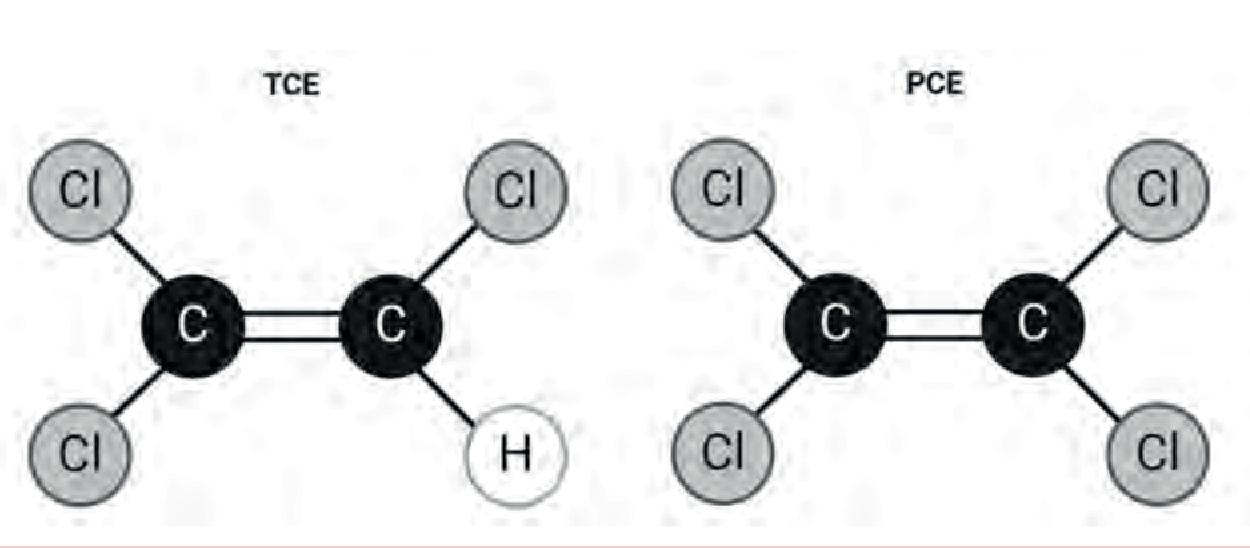
Another chemical with a troubling track record is trichloroethylene or TCE. A small molecule composed of two carbon atoms, one hydrogen, and three chlorines, TCE is a known carcinogen that was once used in everything from degreasing met-
al and dry cleaning clothes to decaffeinating coffee. Its close structural cousin, perchloroethylene (PCE), contains an additional chlorine atom, is classified as a likely carcinogen, and is widely used in dry cleaning (California has banned this use as of 2023). Both chemicals have been linked to neurotoxicity, and TCE in particular has been associated with a 500% increased risk of Parkinson’s disease4
tionally.
If Parkinson’s Is Man-Made, It Can Be HumanEnded
Experimental studies have repeatedly shown that exposure to paraquat, TCE, and airborne pollutants can reproduce hallmark features of Parkinson’s in animal models, including tremor and motor dysfunction7,8 Since Dr. Langston’s insight in Santa Clara Valley Medical Center over forty years ago, the evidence from the lab, the clinic, and populations are all directing us to the environmental roots of Parkinson’s disease.
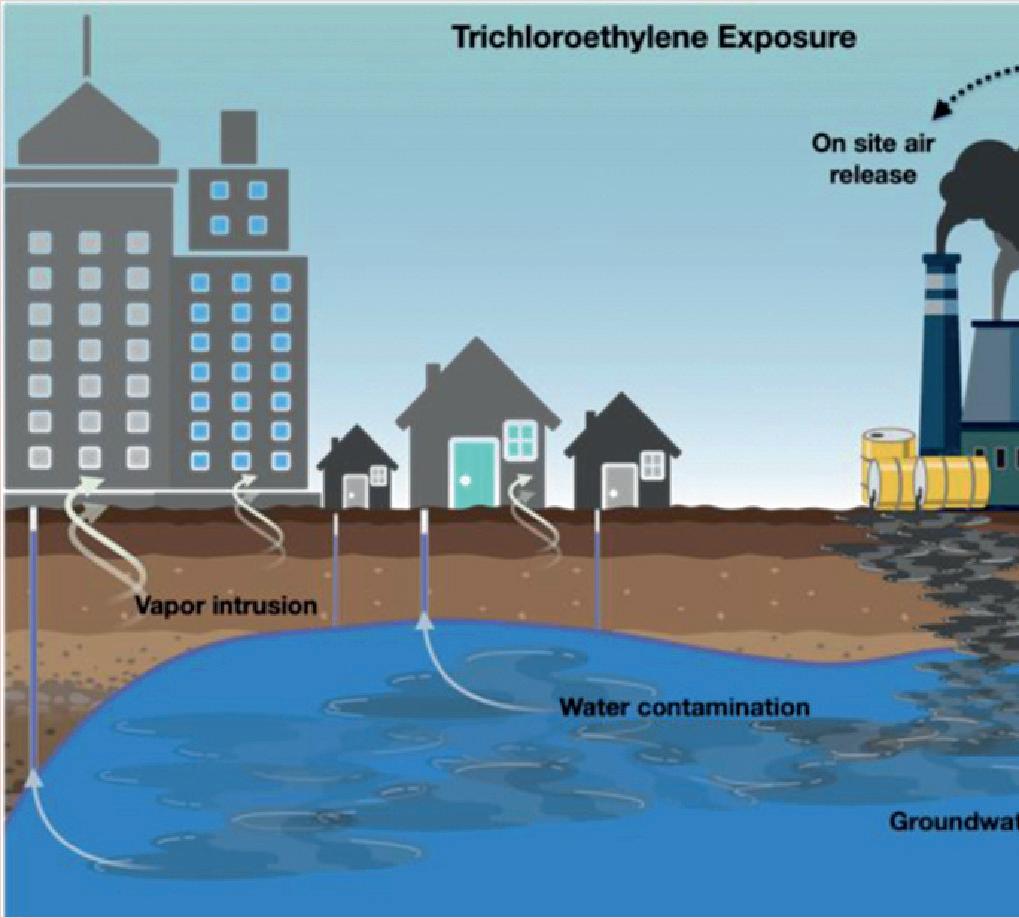
In Silicon Valley, TCE was heavily used during the rise of the semiconductor industry in the 1960s and 70s to clean silicon chips. Over time, the chemical seeped into the ground, forming vast underground plumes that continue to release toxic vapors into homes, schools, and offices. A 7-mile stretch of Highway 101 in Mountain View is now home to 15 EPA Superfund sites, representing one of the highest concentrations of toxic cleanup sites in the country.
Much like radon, TCE can evaporate from contaminated soil or groundwater, migrating into buildings through cracks and utility lines in a process known as vapor intrusion. As a result, TCE has been detected not only in indoor air, but also in butter stored in refrigerators and even in the breast milk of nursing mothers4.
One of the most tragic examples of TCE exposure occurred at Camp Lejeune, a Marine Corps base in North Carolina. For more than 35 years, over a million Marines, civilians, and their families were exposed to drinking water contaminated with TCE and PCE at levels up to 280 times the federal safety limit. Veterans stationed at the base, even for just a few years, were later found to have a 70% higher risk of Parkinson’s disease compared to those stationed at another Marine base in California5 Nationwide, annual EPA testing shows that between 4.5% and 18% of U.S. drinking water sources contain some level of TCE contamination6. And because groundwater plumes can stretch for 1.5 miles or more, toxic chemicals can travel far beyond their original source, often silently and without detection. In 2024, the EPA banned the use of TCE and PCE. However, the ban does little to address the thousands of contaminated sites in California and na-
To the extent that Parkinson’s is a man-made disease, it can be ended by humans. By reducing harmful exposures and driving change in our homes, communities, and societies, we can tackle the disease at its source, and with enough momentum, make Parkinson’s a disease of the past.
About the Authors
Ray Dorsey, MD, is a neurologist and directs the Center for the Brain & Environment at Atria Research and Global Health Institute. He is the author of The Parkinson’s Plan and a leading advocate for preventing neurological diseases by addressing their environmental causes.
Emily Valencia is the Clinical Research Program Manager at Atria Research and Global Health Institute, where she leads studies in preventive and longevity medicine in collaboration with Dr. Ray Dorsey.
References
1. Cook, L., Verbrugge, J., Schwantes-An, T. H., Schulze, J., Foroud, T., Hall, A., & Alcalay, R. N. (2024). Parkinson’s disease variant detection and disclosure: PD GENEration, a North American study. Brain, 147(8), 2668-2679.
2. Miller, G. W. (2007). Paraquat: the red herring of Parkinson’s disease research. Toxicological Sciences, 100(1), 1-2.
3. U.S. Environmental Protection Agency. (n.d.). Paraquat dichloride: One sip can kill. https://www.epa.gov/ pesticide-worker-safety/paraquat-dichloride-one-sip-can-kil
4. Dorsey, E. R., Zafar, M., Lettenberger, S. E., Pawlik, M. E., Kinel, D., Frissen, M., Schneider, R. B., Kieburtz, K., Tanner, C. M., De Miranda, B. R., Goldman, S. M., & Bloem, B. R. (2023). Trichloroethylene: An Invisible Cause of Parkinson’s Disease?. Journal of Parkinson’s disease, 13(2), 203–218. https://doi.org/10.3233/JPD225047
5. Goldman, S. M., Weaver, F. M., Stroupe, K. T., Cao, L., Gonzalez, B., Colletta, K., ... & Tanner, C. M. (2023). Risk of Parkinson disease among service members at marine corps base camp Lejeune. JAMA neurology, 80(7), 673-681.
6. Agency for Toxic Substances and Disease Registry. (2023, September 25). Toxicological profile for trichloroethylene (Chapter 6). Center for Disease Control and Prevention (CDC).
7. De Miranda, B. R., Castro, S. L., Rocha, E. M., Bodle, C. R., Johnson, K. E., & Greenamyre, J. T. (2021). The industrial solvent trichloroethylene induces LRRK2 kinase activity and dopaminergic neurodegeneration in a rat model of Parkinson’s disease. Neurobiology of disease, 153, 105312.
8. Shan, L., Heusinkveld, H. J., Paul, K. C., Hughes, S., Darweesh, S. K., Bloem, B. R., & Homberg, J. R. (2023). Towards improved screening of toxins for Parkinson’s risk. npj Parkinson’s Disease, 9(1), 169.
Neurological Conditions and Environmental Exposures: The Role of Pesticides
Laya Khan, Student, University of Southern California and
Fahd Khan, MD Neurological Surgery
Introduction
Neurological disorders are often perceived as being driven primarily by genetics or aging. While these factors are important, mounting evidence underscores the significant influence of environmental exposures, particularly pesticides, on neurological health. For physicians, understanding these connections is essential not only for patient care but also for broader advocacy on behalf of public health.
Parkinson’s Disease
Among the most well-documented links between environmental exposures and neurological disease is the association between pesticide exposure and Parkinson’s disease (PD). Epidemiological studies consistently show that agricultural workers and individuals living near areas of high pesticide use are at increased risk of PD. Specific chemicals, such as paraquat and rotenone, have been implicated in damaging dopaminergic neurons, the very cells that degenerate in Parkinson’s. Animal models provide biologic plausibility, demonstrating that these agents induce oxidative stress and mitochondrial dysfunction, which are pathways central to PD pathology.
Cognitive Decline and Dementia
The relationship between pesticide exposure and cognitive impairment is also an area of growing concern. Long-term, low-level exposure to organophosphate and organochlorine pesticides has been associated with memory loss, decreased attention, and an increased risk of dementia. A 2016 meta-analysis found a statistically significant link between occupational pesticide exposure and higher rates of Alzheimer’s disease. Mechanistically, pesticides can disrupt cholinergic transmission, increase oxidative damage, and promote neuroinflammation, all of which contribute to neurodegenerative processes.
Neurodevelopmental Disorders
Children are particularly vulnerable to environmental toxins due to their developing nervous systems and higher exposure relative to body weight. Prenatal or early-life exposure to pesticides has been linked to increased risk of neurodevelopmental disorders, including autism spectrum disorder (ASD) and attention-deficit/hyperactivity disorder (ADHD). Studies from agricultural regions of California demonstrate that maternal exposure to organophosphates during pregnancy correlates with impaired cognitive development and higher rates of ASD in offspring. These findings highlight the intergenerational consequences of environmental exposures.
Beyond Pesticides: A Broader Environmental Lens
While pesticides represent one of the most studied groups of environmental neurotoxicants, they are not the only concern. Air pollution, heavy metals (such as lead and mercury), and industrial solvents also play important roles in neurological disease burden. However, pesticides remain unique in their widespread use, persistence in the environment, and potential for both acute and chronic neurotoxicity.
The Role of Physicians
Physicians have several avenues to make a difference in this area. At the clinical level, taking an environmental exposure history can be invaluable when evaluating patients with neurological symptoms. Counseling patients about reducing exposure—such as using protective equipment, washing produce, or avoiding areas during pesticide application can be practical preventive steps. At the community level, physicians can advocate for policies that limit the use of the most harmful pesticides and promote safer alternatives. Finally, as trusted voices, physicians can educate patients, colleagues, and policymakers about the connections between environmental health and neurological disease.
Conclusion
Neurological conditions linked to pesticides remind us that health is inseparable from the environment. The evidence connecting these exposures to Parkinson’s disease, dementia, and neurodevelopmental disorders is growing stronger. Physicians are uniquely positioned to translate this knowledge into action through patient care, education, and advocacy, helping to reduce disease burden and protect the health of future generations.
References
• Hertz-Picciotto, I., & Delwiche, L. (2009). The rise in autism and the role of age at diagnosis. Epidemiology, 20(1), 84–90
• Sagiv, S. K., et al. (2021). “Gestational Exposure to Organophosphate Pesticides and Attention-Deficit/Hyperactivity Disorder–Related Behaviors in Childhood and Early Adolescence.” American Journal of Epidemiology, 190(11),
• Yan D., Zhang Y., Liu L., et al. (2016). “Pesticide exposure and risk of Alzheimer’s disease: a systematic review and meta-analysis.” Scientific Reports, volume 6, article 32222
How the American Lung Association Is Working to Clean Up California’s Air and What Health Professionals Can Do to Protect Our Hard-Earned Progress
As longtime California residents can attest, the state’s air quality has substantially improved in recent decades. Much of that progress stems from innovative clean air policies and regulations, many of which the American Lung Association and other health organizations have strongly supported. Unfortunately, the gains made in recent years to clean up California’s air are at risk due to efforts at the federal level to roll back strong protections. Keep on reading to learn about what’s at stake and how health professionals can use their trusted voices to defend critical safeguards that help keep our air clean.
tor vehicles, like cars and trucks, release harmful pollutants into the air, such as particle pollution and diesel particulate matter, a known carcinogen. Tailpipe emissions are also comprised of nitrogen oxides (NOx) and volatile organic compounds (VOCs), which react with sunlight to form ground-level ozone.
Breathing smog, soot, and other types of air pollution is associated with numerous short- and long-term health risks. These range from coughing, wheezing, and shortness of breath to asthma attacks, heart attacks, stroke, and preterm birth. Exposure to particle pollution is also linked to increased risk of dementia, lung cancer, and even early death. Unfortunately, these pollutants do not affect Californians equally: communities of color are more likely to live near high pollution sources, such as warehouses, ports, highways, and railyards.
California’s Air Pollution Challenges
Even after decades of progress, California remains home to the nation’s most polluted air. According to the American Lung Association’s 2025 “State of the Air ” report, 156 million people, nearly half of people in the U.S., live in communities with unhealthy levels of air pollution. In California, that number is much higher: over 34 million people, or 88% of residents, live in counties with unhealthy levels of poor air quality. The report also found that California cities are among the most polluted in the nation. Notably, California is home to five of the ten most polluted cities for ozone (smog) and particle pollution (soot).
So where is all this pollution coming from, exactly? The transportation sector in California is the largest contributor to air and climate pollution in the state. Gasoline and diesel-powered mo-
Recent Clean Air Wins in California
To address its worst-in-the-nation air quality, California has led the charge to implement some of the country’s most cutting-edge clean air policies and regulations to address different types of transportation pollution. Given the serious health risks air pollution poses to Californians, the American Lung Association and a broad coalition of health and medical organizations around the state have spent years advocating for rules that support a widespread transition to zero-emission technologies as well as stronger pollution controls for cars, trucks, ships, leaf blowers, lawnmowers and more. A few major regulatory achievements over the last several years include:
ELISE WALLIS, MPH
• Advanced Clean Cars II – Stronger emission standards and increasing zero-emission sales standards for passenger vehicles beginning on model year 2026 and beyond.
• Heavy-Duty Inspection and Maintenance (Clean Truck Check) – Ensure heavy-duty vehicles meet emissions control standards as a condition of registration, similar to “Smog Check” programs for passenger vehicles.
• Advanced Clean Trucks – Ensuring increasing sales of zero-emission trucks over time in California.
According to a report released by the American Lung Association in California last year, the suite of California clean air policies that were adopted in recent years would generate a total of $200 billion in public health benefits and save over 20,000 lives in California if fully implemented over the coming decades.
In addition to state-level progress, there were numerous clean air rules that were strengthened at the federal level under the Biden administration that the Lung Association had spent years advocating for. These clean air wins included stronger nationwide standards for particle pollution, cleaner cars and trucks rules, limits on methane from the oil and gas industry and updated rules to reduce mercury and carbon emissions from power plants.
What’s At Stake
Today, the significant clean air progress that has been made in California and nationwide is now being threatened. Through the Clean Air Act, California has been able to adopt stronger air pollution standards than those set by the federal government due to the state’s unique air pollution issues for decades. Unfortunately, over the course of this past year, the federal government revoked the “waivers” California had received that enabled the state to set stronger standards on cars and trucks. Further, the administration has proposed eliminating provisions of the Clean Truck Check program.
Additionally, at the federal level, the U.S. Environmental Protection Agency has proposed to weaken virtually all of the clean air rules that were strengthened under the Biden administration. Most recently, the current administration took one of its most aggressive steps yet to undermine clean air and climate protections. In July, the U.S. EPA issued a proposal to overturn the Endangerment Finding and rollback all greenhouse gas standards for vehicles. This finding serves as the legal underpinning for the federal government’s ability to regulate climate pollutants like carbon and methane. Furthermore, greenhouse gas standards for vehicles have served as a critical tool over the last several decades to reduce harmful emissions from cars and trucks. At the same time important clean air rules are attempted to be rolled back, climate change is leading to worsening wildfires and hotter temperatures which generate more air pollution.
Where Health Professionals Come In
Now more than ever, health and medical professionals play a critical role when it comes to advocating for clean air and a safe climate. Physicians, along with nurses, respiratory therapists and other health professionals, are on the front lines of the climate crisis. This firsthand experience, as well as the fact that health professionals are highly trusted by the public, allows them to be a powerful voice to stand up for the health of their patients and communities.
The American Lung Association offers a variety of ways for health professionals to get involved and leverage their unique perspective to advocate for change. One of the easiest ways to stay up to date on the Lung Association’s clean air and climate advocacy efforts is by signing up for their “Health Professionals for Clean Air and Climate Action” community and monthly newsletter. In addition to updates on the Lung Association’s advocacy work, the monthly newsletter includes news, resources and ways for health professionals to take action. You can learn more and sign up for the newsletter at Lung.org/ClimateChangesHealth.
Another great way to get involved with the American Lung Association’s advocacy work is by joining the Lung Action Network. By signing up at Lung.org/TakeAction, you will receive regular email updates with opportunities to contact your elected officials and other key decision makers about important lung health issues. Finally, here are three positions you can join today to help defend critical clean air protections and programs:
• Don’t Let EPA Dismantle Clean Air Rules: Please urge Congress to ensure protections are funded, implemented and enforced. Oppose EPA efforts to roll them back.
• Defend the Experts and Mission of the Environment Protection Agency: Huge swaths of EPA staff are being fired. Congress must act to stop these actions that put people’s health at risk. Contact your members of Congress today and urge them to save EPA’s expert staff and lifesaving programs.
• Protect Energy Efficiency Programs That Save Americans Money, Cut Pollution and Improve Health: Call on Congress to defend ENERGY STAR and federal energy efficiency standards. Tell your representatives these programs are a win for our wallets, health and environment.
The Lung Association is always looking for health voices to get involved in their advocacy work in other ways, such as testifying at public hearings, authoring letters to the editor or opeds, and speaking with elected officials about clean air and climate issues. If you’re looking for opportunities to get involved, please complete this advocacy interest form or email Elise. Wallis@Lung.org.
Join us on October 9th to help stop new oil drilling on our California public lands – in order to protect health
The evidence is clear, climate change and dirty fossil fuel energy cause myriad health harms. Fossil fuel related air pollution costs over 8 million lives a year worldwide, clean, renewable energy is now cheaper than fossil fuel energy– and yet this administration’s Bureau of Land Management (BLM) is paving the way to open over one million acres of our public lands in California to new oil and gas drilling– from the San Joaquin Valley all the way up to the Central Coast and the San Francisco Bay Area– including Santa Clara county The project’s draft Environmental Impact Report is expected October 24th. We can work together to stop this. The most important action we can take is to mobilize health professionals to submit comments on the report documenting the health harms of expanded drilling during the comment window.
Climate Health Now is hosting a meeting on Thursday October 9th @12:30-1:30p to review the evidence showing the health impacts of oil and gas drilling, the resources you can use to provide impactful comments on the health harms of this proposal, and to show how we can get involved in stopping this proposal (there will be an upcoming public comment period). The BLM must respond to every substantive comment, making each health professional’s voice important to stopping the massive expansion that threatens air quality and everyone’s health in California.
We hope you will join us to learn more and take meaningful action together. Please Register HERE to join health colleagues on Thursday October 9th at 12:30pm!
Written by Alexandra Johnson, PhD, and edited by Ashley McClure, MD ashley@climatehealthnow.org
When Does Disease Begin?
Lanphear, MD, MPH
Let me take you back to medical school, where I learned to see disease in binary terms: you either had it or you didn’t. Over time, I came to see how wrong that was. Most diseases exist on a continuum.
When does cancer begin? When a person starts smoking? When a rogue cell mutates? When the immune system fails to keep it in check? Or only when a doctor makes the diagnosis? I was also taught that chemicals had “safe” exposure levels—and if exposures stayed below those thresholds, we had nothing to worry about.
Cause and effect were simple: one agent, one disease, one
safe level. An agent could be a microbe, a toxic chemical, or a missing nutrient. Case closed.
But life, like medicine, is messier than that.
Most chronic diseases and conditions—premature birth, heart disease, autism, lung cancer—don’t arise from a single event. They accumulate, quietly and gradually, like junk in a garage. And the most studied toxic chemicals show a disturbing pattern: even tiny exposures can do measurable harm, especially when they’re widespread.
The Strange Curve of Toxicity
Regulatory science rests on two key assumptions:
Bruce
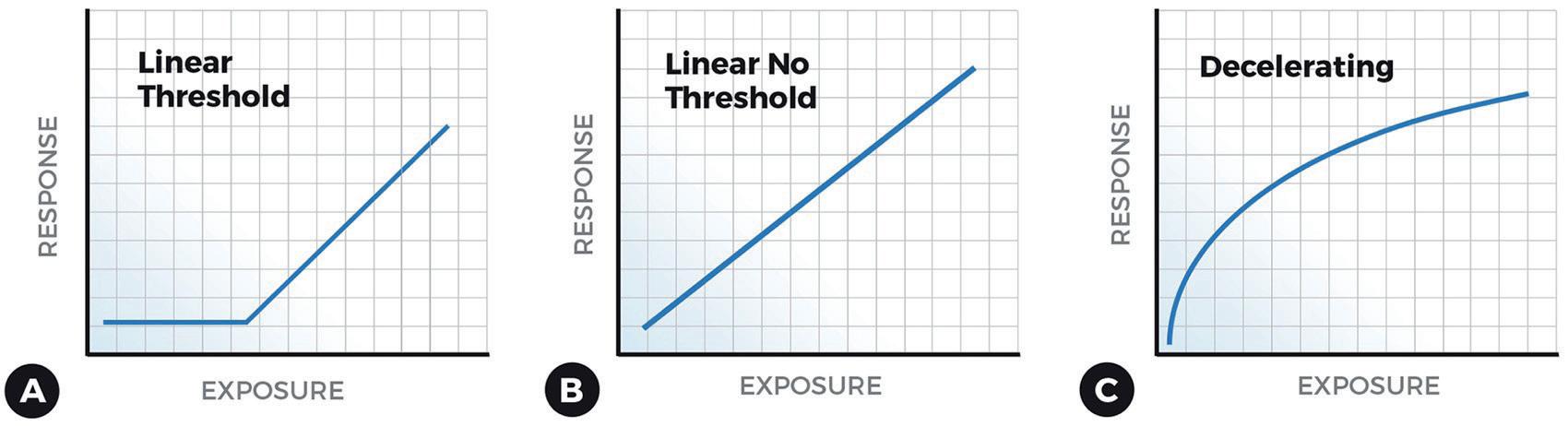
• Non-carcinogens are safe below a threshold. The is the so-called threshold model (Figure 2A)
• Carcinogens follow a linear model—double the dose, double the risk. This is the linear, no threshold model (Figure 2B)
Turns out, both assumptions are wrong. For some of the most well-studied and widely disseminated toxic chemicals and pollutants.
For decades, researchers have studied toxic chemicals and chronic disease. Again and again, the same pattern has emerged: the greatest harm occurs at the lowest levels of exposure. Imagine a graph that rises or drops steeply, then flattens. That’s a decelerating dose-response curve (Figure 2C).
At first, I thought it was a blip in my own data. But the same pattern kept showing up—in study after study, chemical after chemical.
Lead and the Myth of “Safe”
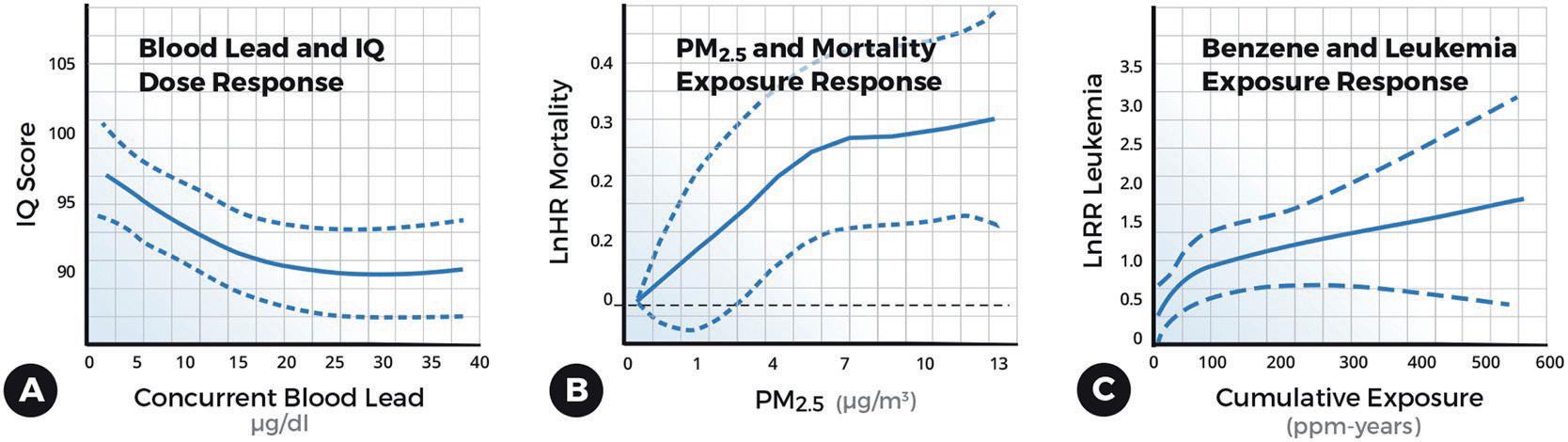
Lead is the poster child of industrial-era pollution. Early studies found that blood lead levels below 10 micrograms per liter (µg/dl)—once considered safe or “acceptable”—were linked to a large IQ drop; the biggest drop was at the lowest exposures (Figure 3A).
A rise in blood lead from under 1 µg/dl to 30 µg/dl was linked to a 9-point drop in IQ. But two-thirds of that loss occurred before the level even reached 10 µg/dl.
Translation: most of the damage occurred at levels still considered low by today’s standards. This finding has been rep-
licated more than a dozen times. No safe level of lead has been identified
The Air We Breathe
Another culprit is particulate air pollution—PM2.5, or particles smaller than 2.5 microns, about the size of bacteria. They are small enough to penetrate deep in the lungs. Arden Pope at Brigham Young University found a similar steep curve linking PM2.5 to heart disease, with the steepest rise in risk at the lowest levels of exposure (Figure 3B).
Going from “clean” air to moderately polluted air is more dangerous than going from moderately polluted to filthy air. Yet regulatory agencies set air quality standards at “moderate.”
A Canadian study found increased mortality at PM2.5 levels as low as 1 µg/m³. That’s almost nothing—at least by contempo-
action level—we prevent just 18% of the damage.
In other words, most harm happens below what was the “threshold” for low-level lead poisoning.
This is Geoffrey Rose’s “prevention paradox”: the greatest number of cases comes from people at low and moderate risk— not the high-risk few.
We think of lead as a threat to children’s brains, but the damage extends further. Even in adults, low-level lead exposure increases risk of cardiovascular disease. In a national study of 14,000 U.S. adults, we estimated that nearly 400,000 deaths annually—more than one in six—could be attributed to lead, including 250,000 from heart disease.
And again, most of those deaths occurred at blood lead levels below 5 µg/dl—levels still widely considered acceptable.
Why the Silence?
rary standards—and still harmful.
When cities ban indoor smoking or reduce air pollution, health improves almost immediately: fewer heart attacks, fewer preterm births, even among non-smokers. Low-level exposures aren’t subtle after all.
Benzene, Asbestos, Radon—Same Story
We’ve seen the same pattern with other toxic chemicals:
• Benzene: causes leukemia; risk is steepest at low exposures.
• Asbestos: causes mesothelioma; low exposures still kills.
• Radon: raises lung cancer risk; steepest rise at low levels.
These aren’t outliers. They’re part of a pattern.
But Why?
The biology isn’t fully understood. With benzene, toxic metabolite production slows at higher doses—like the body saying “enough” (Figure 3C). For other chemicals, we don’t know why the exposure-response curve bends.
Is it a fluke? Unlikely. This curve appears across chemicals, studies, populations, and continents. Some critics blame confounding or poor measurement. But those critiques don’t hold up—not when the evidence is this consistent.
The Prevention Paradox
Why haven’t regulators responded?
Because accepting that low-level exposures cause widespread harm would open the floodgates. It would mean admitting that millions more people are at risk. That we need near-zero exposure standards for lead, PM2.5, benzene, asbestos, and radon.
That’s politically and logistically daunting.
Regulators walk a fine line: protect public health, but also reassure the public. Those aren’t always the same thing. Saying “no level of lead is safe” makes headlines—and headaches.
Then there’s cost. Reducing exposures is expensive. The benefits—fewer heart attacks, smarter kids, less cancer, and economic savings—are real, but spread out over time and across populations. In a market-driven health system, that’s a hard sell.
What We Need to Do
If low-level exposures to the most widely disseminated cause the most harm, our current system of risk assessment needs a major overhaul.
Take lead again. David Bellinger at Harvard estimated that U.S. children born over six years lost 23 million IQ points due to lead. Lead levels have dropped a bit since then. Still, if we only protect kids whose blood lead exceeds 5 µg/dl—the WHO’s
We need to abandon the myth that low exposures are harmless.
That means:
• Rethinking chemical regulations for air, water, and consumer products.
• Protecting people with even low-to-moderate exposures.
• Recognizing that for some toxic chemicals, zero may be the only safe number.
“It won’t be easy. But the alternative is to keep pretending a little poison is no big deal—until someone you care about gets sick, and then it is.”
SCCMA’s 2025 Environmental Health Webinar Series: Advancing
Physician Education and Advocacy
This spring, the Santa Clara County Medical Association (SCCMA) hosted a powerful three-part Environmental Health webinar series, bringing physicians, researchers, and public health experts together to explore how environmental issues— from climate change to toxins—directly impact patient health.
Each session focused on an urgent, actionable topic:
Plant-Based for the Planet (March 25): Drs. Ulka Agarwal and Tamiko Katsumoto discussed how plant-based diets support both personal health and climate sustainability by reducing chronic disease and lowering carbon emissions.
Climate Change & Public Health (April 22 – Earth Day): Drs. Nathaniel DeNicola, Bruce Bekkar, and Dr. Rupa Basu highlighted the health effects of rising greenhouse gases, urging physicians to become advocates for climate action in their communities.
The Legacy of Lead Poisoning (May 20): Dr. Bruce Lanphear exposed the lasting public health threat of lead exposure, particularly in vulnerable populations, emphasizing that no level of lead is safe.
This series is part of SCCMA’s strong Environmental Health initiative, which equips healthcare providers with the knowledge and tools to be leaders in sustainability and health equity.
All webinars are recorded and available to everyone on the SCCMA website—offering accessible, on-demand education to support physician advocacy and informed care.
Watch the full series today and join us in making environmental health a medical priority.
Scan the QR code to watch all the webinars
Creating Our Own Diseases
Plasticene, n. & adj. an era in Earth’s history, within the Anthropocene, commencing in the 1950s, marked stratigraphically in the depositional record by a new and increasing layer of plastic1
“It is seldom recognized that each type of society has diseases peculiar to itself—indeed, that each civilization creates its own diseases.”
(René Dubos: The Dreams of Reason: Science and Utopias, 1961)
Ted Schettler MD, MPH
The origin of the term plasticene as an era in earth’s history is uncertain, although there is general agreement that it began in the 1950s when plastic production dramatically accelerated. Since then the term has become more firmly established with exponential increases in production—and pollution.
City streets, streams, rivers, ocean gyres, and beaches strewn with plastic debris became common throughout the world. Less visibly, tiny fragments of plastic containing biologically active chemicals also began contaminating all of earth’s ecosystems. Now ubiquitous in soil, sediments, air, food, and water, micro- and nano-plastics (MNPs) are embedded in plants, wildlife and people everywhere.
encountered in the real-world, many effects are likely to be missed.
3. Nanoplastics are particularly challenging to study because of their small size. Yet they probably have more marked effects than larger particles since they can be more readily absorbed and penetrate tissue barriers.
4. Since exposures are difficult to quantify, little is known about dose-response relationships—how much, or little, of this complex mixture is sufficient to elicit an adverse response.
Health effects of MNPs
These tiny time-release granules leach chemicals that can cause obesity, diabetes, cardiovascular disease, reproductive and development disorders, cancer, and more2. Microplastic exposures and associated health effects are certain to grow rapidly as plastic production is expected to double or triple from current levels by 2050.
The complexity of micro- and nanoplastics
Microplastics are tiny particles less than five millimeters in size, while nanoplastics are a smaller subset, at less than one-thousandth of a millimeter. They largely come from the chemical and mechanical breakdown of food packaging, synthetic fabrics, paint, tires, and other plastic products.
Plastic products are made from various polymers with combinations of additional chemicals that impart certain features and functions. The list of potential additives is estimated at over 15,000 individual chemicals, most of which have not been studied for their toxic properties3. Those that have been studied can have strikingly diverse health effects, often after even low-level exposures. In addition to chemicals intentionally added to a plastic polymer, MNPs pick up additional chemicals from the ambient environment. Biofilms that form on MNPs in the environment introduce a microbial component to the diverse exposures, adding to the complexity.
Inhaled, ingested, and potentially absorbed through the skin, MNPs contaminate human blood, urine, feces, breast milk, and semen4 5 Human brains, hearts, blood vessels, livers, kidneys, intestines, bones, testicles, lungs, and placentas are flecked with MNPs. These tiny geometrically, chemically, and biologically diverse fragments present difficult research challenges.
The National Academy of Sciences recently concluded a webinar series addressing what we know and would like to know about MNPs and their impacts. Among the research challenges identified:
The clearance of MNPs from tissues is exceedingly slow, if it occurs at all. They can cause oxidative stress, inflammation, immune system and metabolic disruption, decreased cell viability, and fibrosis6. Laboratory animal and human studies show a high likelihood that MNP exposures increase risks of lung inflammation and fibrosis, impaired sperm quality, gastrointestinal disorders including colon cancer, other malignancies, heart attacks and strokes7 8 9 10 Many of the animal studies do not account for the various chemical additives in MNPs that can also be harmful.
See the box for a partial list of known health effects from chemical additives present in plastics. For more see Minderoo Plastics Health Map11.
Managing MNP risks
In some places decision-makers have taken early policy steps intended to reduce MNP exposures. For example:
1. Collecting, identifying, and quantifying MNPs in environmental samples or in biologic tissues and fluids are extremely challenging. With no standardized protocols, different methods give different results, making it difficult to compare findings among studies.
2. Many experimental studies use manufactured MNPs that can yield valuable insights into their impacts. But since these MNPs are unlike the complex mixture of geometrically, chemically, and biologically diverse fragments
• Some countries, states, and cities have banned frequently littered single-use plastic items like shopping bags, clamshells, and plastic drink accessories.
• Several countries have restricted the sale of personal care products containing microplastics.
• Australia and France have introduced measures to phase in microfiber filters on new washing machines. (Microfibers from synthetic textiles are discharged from washing machines without filters into the waste water. MNPs migrate into sewage sludge, which is often spread on farm land.)
• Efforts are underway in the European Union to set tire
Partial list of health effects known to result from exposures to chemicals of concern in plastics
• Impaired fertility (e.g. bisphenol A (BPA), some phthalates)
wear abrasion limits intended to reduce a major source of MNPs
• California has adopted a comprehensive two-track strategy. One track outlines immediate, ‘no regrets’ actions and multi-benefit solutions to reduce MP pollution. The second track outlines a research strategy to enhance the scientific foundation for MP monitoring, source identification, risk assessment, and development of management solutions.
• The CA State Water Resources Control Board is establishing guidelines for acceptable levels of microplastics in drinking water.
The US EPA has the authority under the Toxic Substances Control Act (TSCA) to assess the risk of MNP exposures. Given the marked heterogeneity of MNPs, arguably a risk evaluation should consider MNPs as a single class during the assessment, as provided for in TSCA.
The Food and Drug Administration (FDA) says the agency “continues to monitor the research on MNPs. If the FDA determines, based on scientific evidence, that MNPs in food, including packaged food and beverages, adversely affect human health, the FDA can take regulatory action to protect public health.” 12
The United Nations convened international treaty negotiations in 2022 to address the growing global crisis of plastic pollution. Petro-states and chemical industry lobbyists vigorously opposed any curbs on plastic production, wanting to focus solely on waste management and recycling. Higher ambition countries recognized that constraints on production are necessary. The negotiations ended without any consensus resolution.
Upstream interventions are available to product manufacturers. Some plastic polymers and products are inherently less toxic throughout their life cycles than others and require fewer hazardous chemical additives. Extended producer responsibility (EPR) policies requiring manufacturers to be responsible for products at their end of useful life can help13 They are proven to reduce plastic waste, improve recycling rates, and stimulate product re-design. Common products subject to EPR are packaging, electronics, batteries, paint, pharmaceuticals, and textiles. Five states in the U.S. have adopted EPR policies addressing packaging14.
• Vacuum and dust more frequently to reduce MNPs in indoor air.
“Each civilization creates its own diseases” (René Dubos)
Undeniably, the material economy has radically changed with rapidly accelerating introduction of plastic products into all aspects of daily life. Now tiny fragments of plastics and their chemical additives are everywhere. Research into their health effects strongly support the plausibility that MNPs are contributing to documented disease trends. As Rene Dubos observed, “each civilization creates its own diseases.” This civilization has added plastics and MNPs to the mix of factors shaping the diseases and disorders of our time.
References
5. A Plasticene Lexicon - ScienceDirect
6. Plastic Health Map
7. https://doi.org/10.1038/s41586-025-09184-8.
8. Detection of microplastics in human tissues and organs: A scoping review - PMC .
9. Microplastics in the Olfactory Bulb of the Human Brain | Environmental Health | JAMA Network Open | JAMA Network
10. Microplastics: A Real Global Threat for Environment and Food Safety: A State of the Art Review .
11. Effects of Microplastic Exposure on Human Digestive, Reproductive, and Respiratory Health: A Rapid Systematic Review - PubMed
12. Immunotoxicity and intestinal effects of nano- and microplastics: a review of the literature - PubMed.
13. The alarming link between environmental microplastics and health hazards with special emphasis on cancerPubMed.
14. Microplastics and Nanoplastics in Atheromas and Cardiovascular Events - PubMed .
15. Plastic Health Map
Interventions are also available to institutional consumers. For example, hospitals rely more than necessary on single use plastic items for different purposes like surgical gowns15 Reusable gowns are shown to be as safe and effective as single use disposables. Hospital offices and cafeterias also can also move away from single-use disposable plastics. Some actions that can be undertaken by individuals to reduce their exposures include:
• Avoid using plastic cutting boards, a source of MNPs during use.
• Avoid plastic water bottles.
• Avoid microwaving food in plastic containers.
• A number of water filters will remove MPs from drinking water (check specifications).
• Reduce plastic food packaging as much as possible while maintaining food safety. For example, recent studies report billions of MP particles released from plastic polymer tea bags when heated in hot water.
16. Microplastics and Nanoplastics in Foods | FDA
17. Extended Producer Responsibility: Revolutionizing Plastic Waste Management | Plastics for Change | Plastics For Change
18. EPR Laws for Packaging in the United States: Where Are We Now? - Reverse Logistics Group
19. A prescription for change: Rethinking plastics use in healthcare to reduce waste, greenhouse gas emissions and costs - Eunomia
SCCMA sponsors the Silicon Valley Youth Climate Action Impact Summit
On August 9th at the Campbell Heritage Theater, high school and college students, young professionals, community stakeholders, educators, elected officials and industry leaders gathered for a day of learning, networking and discussion around innovative climate solutions and strategies. This year’s summit included action-oriented breakout sessions, panel presentations, and keynote speakers that empowered all attendees to make a difference and fight climate change.
The Santa Clara County Medical Association was a proud sponsor this year of the Silicon Valley Youth Climate Action Impact Summit1. Dr. Robert Gould, a longtime member of the
SCCMA Environmental Health Committee presented on the Health Impacts of Climate Change Panel. Dr. Ulka Agarwal will be joining the Silicon Valley Youth Climate Action as a guest speaker in an upcoming event. The summit brought together both youth organizers as well as a large number of the region’s legislators from different levels of governance as a testament to the strength of collective action supporting applied climate solutions.
Dr. Robert Gould presents on the Health Impacts of Climate Change Panel
Co-Chair, SCCMA Environmental Health Committee
STEPHEN M. JACKSON MD
SCCMA physicians are not alone among medical professionals advocating for healthy, sustainable and affordable water supplies. When our SCCMA Environmental Health Committee (EHC) endorsed local plans to produce advanced purified recycled water for potable reuse, we joined a growing movement of physicians serving as trusted sources of information about the process. I recently had the opportunity to join colleagues from Texas and Southern California who also endorse their local water utilities’ efforts to reuse water in a discussion about how physicians can help ensure their communities have adequate water supplies in the face of a changing climate.
Background
In late 2021, our EHC studied the science of water reuse and water pollution with professionals from Valley Water, the agency responsible for most of Santa Clara County’s water supply. Fortified with this scientific knowledge, the SCCMA accepted our recommendation to formally endorse Valley Water’s advanced water purification project. The EHC then authored a Resolution to the CMA’s House of Delegates in support of the safety and public health value of this advanced purification process for producing potable (drinking) water. The SCCMA also published a special issue of The Bulletin (2022) titled “Water and Health” in which we shared our understanding of the public health value and relevant technical and regulatory information. Since then, Valley Water has issued a request for proposals for the design of the Pure Water Silicon Valley demonstration facility direct potable reuse project, which is proposed to add 24 million gallons per day (mgd) to our local water supply by 2035. The project will reduce dependence on imported water, enhance drought resilience, and reduce land subsidence and saltwater intrusion.
In 2023, at the invitation of the national WateReuse Association, SCCMA physicians, Dr. Ken Yew and Dr. Santosh Pandipati, spoke about the benefits of creating a dialogue between physicians and water professionals. Their message inspired the Environmental Protection Agency (EPA) to sponsor a national initiative, led by SCCMA and Valley Water, to further develop this collaborative engagement by bringing together physicians and utility managers from around the country.
Panel on Physicians and Water Reuse
unfo to serve Los Angeles and Ventura Counties, one element of a larger strategy to recycle most of the wastewater produced in Southern California. Our conversation centered on the essential role that physicians play in educating the public about the need for clean purified water for potable reuse in our communities and the safety of advanced water reuse technology.
As El Paso’s public health officer, Dr. Ocaranza became aware of water reuse in response to questions about water from parents seeking the opinion of a knowledgeable and trusted physician. “We as practicing physicians get questions from our patients about the safety of the water, and they look to us as a trustworthy source of information,” Dr. Ocaranza said. “Even though a lot of people get their research through social media, when we see these patients in the office they ask us, which is an incentive to us to become more knowledgeable about water.”
On July 31, 2025, I joined two other physicians in a conversation facilitated by Valley Water about the nexus between water and health and how we communicate with patients and others about the need for water reuse in our communities. El Paso, Texas pediatrician Hector Ocaranza MD now serves as the county health officer and sits on the board of El Paso Water, which is currently building a Pure Water Center to supply 10 mgd of potable water by 2028. Cardiologist Sion “Shy” Roy MD, past president of the Los Angeles County Medical Association, supports the efforts of the Las Virgenes-Triunfo Joint Powers Authority (JPA) to build the Pure Water Project Las Virgenes-Tri-
After two decades of adding treated recycled water to their groundwater supplies, El Paso Water broke ground this year on a project to send further purified water directly to their water treatment facility. In view of the stringent regulations for direct potable reuse, Dr. Ocaranza emphasized that physicians need to know enough about the way water is purified to effectively communicate scientifically based information to the public. To that end, he recommended that doctors schedule a visit to the local water recycling plant. “Although we know a fair amount about microbiological contaminants in drinking water and the toxicology of chemical pollutants found in water supplies, until I saw the facility for myself, I had no idea that all this was going on right here in our community,” he recalled. “Now I can attest to the quality of the water and tell them for sure that this project is going to be good for those of us who live in a desert area.”
Dr. Roy offered a personal example of how important it is for physicians to become well-informed about the safety of purified water. “We’re in this age of incredible information dissemination,” he observed, “and I think everybody is having a hard time finding truth in all the information out there. I lost my home in the Palisades fire, and a lot of chemicals from ash and debris wound up in our underground aquifers. Even when the authorities told us that the water was safe to drink, I texted
Reverse Osmosis
people I knew who knew about water to ask, ‘Is this really true?’ So, if it’s hard for me as a physician to trust authority, then it’s really important for us to share with patients not only what we know but also where we get our information and to help them digest that information.”
Dr. Roy also recommended an in-person visit to a water purification plant or a demonstration facility like the JPA’s Pure Water Demonstration Facility that he toured in Calabasas, California. “When it comes to water reuse, we do not need to reinvent the wheel,” he added. “There are dozens of other communities that have used this water in a very safe way.”
I want to echo this sentiment because prior to SCCMA’s endorsement of the “Pure Water Silicon Valley” project, I personally visited the Silicon Valley Advanced Water Purification Center, located here in San José. I can attest that touring this water purification demonstration project is a powerful and engaging learning experience.
As physicians, we understand that our patients and others in our community (including elected officials and regulators) value our opinions about health-related issues, and certainly, water reuse is one of them. Moreover, we know that the process of obtaining informed consent is an ethical and effective way to obtain permission for medical treatments. In the same light, I have tried to incorporate this model to inform our physicians, who in turn can inform their patients, with the overall objective of gaining the public’s consent, acceptance and support for advanced water purification for potable reuse.
Over the years, we have had the opportunity to work closely with Valley Water professionals, and we plan to continue this collaboration to respond to public concerns about water quality. This applies not only to pathogens, but also chemical toxins such as medications patients flush down their drains, and perand polyfluoroalkyl substances (PFAS), the “forever chemicals” prevalent in our food supplies and linked to a wide range of health issues. Our nation needs to become more responsible and effectively responsive to all facets of water contamination and pollution. It is especially imperative that there be efforts to decrease upstream pollutants, such as commercial- and industrial-related chemical contaminants that negatively impact water. As medical professionals committed to public health, we have a
great opportunity to help accomplish this.
As physicians, there are several ways we can support direct potable reuse in Santa Clara County. We can tour the Silicon Valley Advanced Water Purification Center, either virtually or in-person. Once having educated ourselves, we can also offer educational materials about purified water in our offices and be willing to answer questions from patients and the public.
As affirmed by our colleagues in El Paso and Los Angeles, physicians play a critical role in advocating for direct potable reuse. This point was reiterated by Valley Water Board Chair Tony Estremera who acknowledged the contributions of SCCMA: “We depend upon the physicians in our community to help educate the public about the need for Pure Water Silicon Valley and the safety of potable reuse, and we are grateful to SCCMA for their endorsement. We will continue to work closely with them throughout the development of this program.”
SCCMA members can visit https://purewater4u.org/ or call 408-630-3533 to schedule a guided tour of the Silicon Valley Advanced Water Purification Center.
“I wish to thank Francesca Lomotan, MPH, Supervising Program Administrator in Valley Water’s Office of Civic Engagement, for her review and editing of this article.”
References
1. https://issuu.com/18621/docs/q2_2022
Ultraviolet Light Disinfection
Lee Anna Botkin MD,
Telina Martinez-Barrientos,
Yun Annie Wu MPH
Preventing firearm violence of all kinds involves both individual and community efforts. Recently the Santa Clara County Public Health Department launched the “We All Play A Role” campaign which promotes several ways to strengthen community protective factors and prevent violence.
In 2022, the New England Journal of Medicine published data showing that firearm violence was the leading cause of death of children and adolescents ages 1 to 19 years old in the United States. Every day, more than 120 Americans are killed by gun violence and more than 200 are shot and wounded. In Santa Clara County during the years 2017-2021, there were a total of over 140,000 newly purchased firearms. In addition, there are significant concerns about the numbers of ghost guns present in the community. Over the years 2016-2020 in Santa Clara County, there were 394 deaths from firearms and 610 non-fatal firearm injury-related emergency department visits. Of the types of gun violence fatalities in Santa Clara County, 60% are suicide, 33% are homicide, and 7% are categorized as other.
We invite you to look at the We All Play a Role website for ways physicians can be active in reducing firearm violence. Three options are raising awareness on firearm storage practices (including SB 53 which takes effect Jan 1, 2026), promoting healthy relationships and behaviors, and encouraging communities to address violence before it happens.
One specific way physicians can raise awareness is to participate in Wear Orange days at your worksite during each June to commemorate National Gun Violence Prevention Month. This event began in 2013 to honor Hadiya Pendleton, a 15-year-old who was mistakenly shot and killed at a playground in Chicago. Hadiya’s family and friends wore orange items in her memory. For the past several years health care staff at Santa Clara Valley Healthcare have participated in Wear Orange days during June to raise awareness of the magnitude of the issue and to learn more about violence prevention strategies. Staff have developed patient materials in several languages and a pilot program to distribute firearm locks in pediatric primary care clinics. How do you plan to get involved? Here are some ways to get started.
Learning for Health Care Providers
• Take a free CME course. Here are three options.
• Clinicians & Firearms, affiliated with Stanford.
• Preventing Firearm Injury: What Clinicians Can Do, affiliated with UC Davis.
• Counseling on Access to Lethal Means to Prevent Youth Suicide, from the American Academy of Pediatrics (AAP membership not needed).
• Learn about national resources like the Brady Campaign to End Gun Violence, the Giffords Law Center, and Everytown for Gun Safety
Patient Education
• Reinforce with patients that to reduce the risk of firearm harm for everyone in the household, firearms must be stored locked and unloaded. Store ammunition separately, also locked up.
• Become familiar with patient resources. Here are three.
• Lock to Live, an interactive tool for safety planning, available in English and Spanish.
Use this QR code for a live version of the document with working links.
• AAP’s gun safety campaign toolkit, which includes patient materials in English and Spanish.
• Be SMART | Secure Gun Storage (besmartforkids. org)
Mental Health Support
• Understand how to have conversations about firearm safety with people who may be at risk of suicide and what mental health resources are available.
• Learn about gun violence restraining orders (GVROs), or red flag laws.
• Read about safe storage, voluntary relinquishment, and GVROs at Suicide and gun safety | Behavioral Health Services | County of Santa Clara
Community Engagement
• Learn about local primary violence prevention efforts and ways to address domestic violence.
• Promote activities for children and youth that build resilience and connection.
• Organize a Wear Orange event at your workplace.
• Join a regional group focused on physicians and firearm violence prevention like SAFE (Scrubs Addressing the Firearm Epidemic)
Let’s come together and make a difference. We can each do something to help.
Resources
• Wear Orange | Brady United
• Everytown Research & Policy
• Cost of Gun Violence in Santa Clara County
• Goldstick, J. E., Cunningham, R. M., & Carter, P. M. (2022). Current Causes of Death in Children and Adolescents in the United States. New England Journal of Medicine, 386 (20). https://doi.org/10.1056/nejmc2201761
Celebrating Community and Connection:
SCCMA’s 2025 Annual Summer Social Lights Up Santana Row
The Santa Clara County Medical Association (SCCMA) kicked off the summer in style with its much-anticipated Annual Summer Social, held on Thursday, June 26, at the elegant Meso Restaurant in Santana Row, San Jose. From 6:00 PM to 9:00 PM, the outdoor patio buzzed with laughter, conversation, and camaraderie as members came together to celebrate the season—and each other.
Nestled in one of Silicon Valley’s most iconic and vibrant destinations, Meso proved to be the perfect backdrop for a warm and welcoming evening. The restaurant’s Mediterranean-inspired ambiance and beautifully appointed patio set the tone for an event that felt both festive and intimate.
More Than Just a Social—A Celebration of Community
The SCCMA Summer Social has long been a favorite among members, and this year was no exception. With complimentary registration for SCCMA members, the evening was a thankyou to the physicians, specialists, and healthcare professionals who give so much throughout the year. It was a moment to press pause, step away from the day-to-day demands of medical practice, and reconnect with colleagues in a relaxed and joyful atmosphere.
Attendees enjoyed gourmet small plates and signature summer cocktails, carefully curated to reflect the fresh flavors of
the season. The Meso team delivered exceptional hospitality, ensuring everyone felt both cared for and celebrated.
Connections Made, Stories Shared
From early arrivals to last guests lingering under the patio lights, the energy was vibrant throughout the night. Members new and seasoned had the chance to mingle, share experiences, and engage in meaningful conversations—many of which continued well past sunset. For new members and first-time attendees, the event offered an open door to the SCCMA community in a welcoming, no-pressure setting.
Raffles, Music, and a Few Fun Surprises
A lively raffle kept guests on their toes, with prizes that included gift cards to Meso Restaurant and one admission to SCCMA’s Annual Wellenss Retreat at 1440 Multiverstiy. Background music added to the ambiance without overpowering the conversation, and a few surprise treats made the evening even more memorable.
Looking Ahead
The Annual Summer Social was more than just an event—it was a celebration of the strong bonds and shared commitment that unite SCCMA’s diverse and dedicated membership. As the sun set over Santana Row and guests said their goodbyes, there was a clear sense of momentum and excitement for the rest of the year’s events.
Whether you’re a longtime member or just getting involved, gatherings like these remind us that while medicine is a calling, community is what sustains us.
We thank everyone who attended for making the night so special—and we look forward to seeing you at future SCCMA events.
Physicians Table: Cook, Connect, Celebrate SCCMA Hosts First-Ever Cooking Class: A Night of Food, Fun, and Community
On the evening of Thursday, August 28, the Santa Clara County Medical Association (SCCMA) traded scrubs for aprons at its first-ever Italian cooking class, held at Cucina Bambini in Willow Glen. The event brought together 18 physician members from small practices, Permanente Medical Group, and Santa Clara Valley Medical Center for a two-hour culinary experience that blended creativity, camaraderie, and cuisine.
The class marked a new kind of gathering for SCCMA, part of a broader initiative to introduce fresh, exciting events that go beyond traditional networking to offer members meaningful ways to unwind, connect, and explore new interests together outside the clinical setting.
Participants learned to craft a full Italian bistro menu from scratch, guided by a professional chef in the cozy, hands-on environment of Cucina Bambini. From rolling fresh pasta to mastering the perfect sauce, attendees got a true taste of Italian culinary artistry—complete with a vegetarian option for inclusive dining. With wine flowing and laughter echoing through the kitchen, the atmosphere was equal parts educational and entertaining.
This cooking class is just one example of how SCCMA is investing in its members—not only as professionals, but as people. These events are planned with our members in mind, as a benefit of membership and a way to say thank you. Whether it’s a social night out, a well-
ness activity, or a unique hands-on experience, we do this for YOU—to support your well-being, build stronger connections, and bring more enjoyment to your professional community.
“This event was about more than just food,” said SCCMA President Fahd Khan, MD. “It was about connection—sharing stories, stepping out of our daily routines, and getting to know fellow members in a whole new way.”
At just $50 per person, the event filled up quickly, highlighting the demand for creative, community-focused offerings among SCCMA’s diverse membership. With such a warm response, the success of the cooking class signals a promising future for more unique member events to come.
Stay tuned for upcoming activities—and if you missed out this time, don’t worry. More experiences like this are on the way!
For questions or to get involved in future events, please contact Membership and Programs Manager, Rashida Mirza, at Rashida@sccma.org
Fossil fuel polluters, not taxpayers, should pay for climate damage
ISABEL PENMAN,
Northern California Organizer, Food & Water Watch
There were 52,000+ premature deaths from wildfire smoke (2008-2018), with an associated economic impact of $432-$456 billion1. Seven extreme heat events (2013-2022) resulted in nearly 460 deaths, 5,000+ hospitalizations, and 10,600+ emergency visits, costing over $4.8 billion.2
The Polluters Pay Climate Superfund Act, authored by Sen. Menjivar and Asm. Addis, is a common-sense bill that will assess a fee to the largest fossil fuel polluters to pay their fair share of the climate damage caused by their products, relieving taxpayers who otherwise bear these costs.
This legislation could raise hundreds of billions of dollars to protect Californians and fund solutions that build affordable, resilient and sustainable communities at the municipal level. The current state budget crisis and the Trump Administration’s threatened cuts to disaster relief make it more important than ever to find new funding sources to address these urgent concerns.
The campaign to pass the Polluters Pay Climate Superfund Act in the California legislature is growing momentum. However, the fossil fuel industry has flooded the legislature with misleading ads and lobbyists so many legislators still haven’t committed to supporting the bill.
We need to counteract Big Oil’s misinformation and fearmongering by showing our legislators overwhelming demonstrations of support for the bill in their district to win their votes and move the bill forward.
We can pass resolutions through city councils and county boards of supervisors to demonstrate and lever-
age the growing support behind the bill. When we pass these resolutions in target legislators’ districts we create political cover for them to vote yes and intensify pressure on them to do the right thing. Legislators will vote on the bill in January 2026 so the time to get local elected support for the bill is now!
So far eight cities and counties have passed resolutions or sent in letters endorsing the bill including 3 of California’s 4 largest cities: LA, San Diego, and San Francisco.
The longer we wait, the worse the financial and health burden on Californians will be. The faster we act, the more we can save.
This document contains a stepby-step guide to get started on your own campaign to pass a local resolution and achieve these goals:
SCCMA Wellness Retreat Offers Healing, Reflection, and Reconnection for Physician Members
In the heart of the serene Santa Cruz Mountains, the Santa Clara County Medical Association (SCCMA) hosted its annual Wellness Retreat, a transformative getaway from Friday, August 15 to Sunday, August 17 at the renowned 1440 Multiversity campus in Scotts Valley. Surrounded by 75 acres of redwoods and quiet walking paths, physician members stepped away from the daily demands of medicine to focus on something essential yet often overlooked—their own well-being.
This three-day, two-night retreat offered more than just rest. It provided intentional, uninterrupted time for attendees to reflect, reconnect, and recharge. Designed in direct response to the stress, burnout, and emotional fatigue affecting healthcare professionals—especially in the wake of the pandemic and ongoing staffing shortages—the retreat delivered an immersive experience in mental health support, resilience-building, and personal growth.
• Grief and Healing
• Sustainable Emotional Well-Being: Flexible Strategies that Support Meaningful Work
These sessions were led by expert facilitators who tailored their content to address the unique emotional challenges faced by physicians today. In addition to the educational component, the retreat included a welcome session and ice breaker, encouraging connection and community-building among peers.
“This retreat has been such a godsend. I feel refreshed and fulfilled each time I have had the good fortune to be able to attend. I am grateful for the opportunity. Thank you! ”
— Lily Lee, MD, SCCMA Member
These types of events are part of SCCMA’s continued commitment to serving our members beyond the professional realm. We organize wellness retreats like this because we care—about your health, your happiness, and your ability to thrive both in and outside of your practice. This is a benefit of SCCMA membership, created specifically for you. Supporting physician well-being isn’t just a priority—it’s a core part of our mission.
Through a thoughtfully curated lineup of CME-accredited sessions (3 credits), attendees engaged in workshops such as:
• Cultivating Emotional Balance: Enhancing Emotional Awareness and Compassion for Healthcare Providers
True to 1440 Multiversity’s integrated wellness philosophy, participants enjoyed fresh, organic, plant-based meal sprepared with a “food as medicine” approach— nourishing the body while supporting a healthy, mindful lifestyle. Nestled in nature, attendees had the opportunity to unplug, take peaceful walks, or simply breathe deeply in an environment designed to foster inner calm.
Registration included single or double-occupancy accommodations, all meals, and full participation in programming—all designed to remove barriers to self-care and make the experience as accessible and restorative as possible.
The resounding success of the Wellness Retreat has reinforced SCCMA’s dedication to organizing future events that support physicians’ mental health, resilience, and overall quality of life.
MEMBERSHIP
CMA calls on physicians to speak out against Cigna’s unlawful downcoding policy
The California Medical Association (CMA) is urging physicians and medical groups to contact Cigna and demand the withdrawal of its new automatic downcoding policy. The policy appears to violate California law, undermines nationally recognized coding standards, and creates unnecessary administrative burdens.
CMA is urging physicians and medical groups to also make their concerns known directly to Cigna. Please contact Cigna Customer Service at (800) 88-Cigna (882-4462) or via the provider portal and request that the company rescind the R49 downcoding policy. CMA has also prepared talking points practices can use when communicating with Cigna on this issue. For full article, visit www. cmadocs.org/newsroom/news
CMA urges Congress to act on year-end health care priorities
CMA is calling on Congress to address urgent health care priorities before the end of the year to protect access to care for California patients. Without congressional action, millions could lose coverage, seniors will face growing barriers to care and physician shortages will grow more severe. CMA is also urging Congress to increase Medicare payments, noting that Medicare physician reimbursement has dropped 33% since 2001 with no annual inflation adjustment.
In a letter to the California congressional delegation, CMA stressed that Congress must not wait until the eleventh hour to act on these critical priorities. Each delay increases uncertainty for patients, drives more physicians out of practice and erodes California’s progress in expanding health coverage.
Understanding the MultiPlan antitrust
case – find out if your practice qualifies
A federal antitrust lawsuit against MultiPlan and several major insurers is moving forward, alleging a price-fixing scheme that systematically underpaid out-of-network physicians. The case could result in substantial financial recoveries for affected providers, and CMA is hosting a webinar to help practices determine eligibility and protect their rights. The free webinar is on Tuesday, Sept. 16, 2025 – Navigating the MultiPlan Litigation: What Physician Practices and Facilities Need to Know. Presented by AGG Healthcare Litigation partner Matt Lavin, a member of the Executive Committee for direct-action plaintiffs in the case. Lavin will walk through the origins of the litigation, key legal developments, strategies for joining the case, and why now is the time to act. For more information or to register, visit www.cmadocs.org/events. This webinar is free to all interested parties.
CMA supports bipartisan PBM reform legislation
Bipartisan legislation introduced in Congress aims to increase transparency and accountability in the pharmacy benefit manager (PBM) industry. The bill would ban spread pricing in Medicaid, require fair reimbursement for pharmacies, decouple PBM compensation from drug prices, and give patients and employers more insight into drug costs and access decisions.
The California Medical Association has long been concerned with the lack of information related to formulary placement, utilization requirements such as step therapy, and patient cost-sharing obligations, all of which are heavily influenced by PBMs and often hidden from both prescribing physicians and patients.
Need help reviewing a contract? CMA members get exclusive discounted services
CMA members have access to two valuable member benefits that provide legal analysis of physician contracts – such as employment agreements, managed care contracts, hospital recruitment contracts and more – at reduced rates.
Kessenick Gamma, LLP
Through CMA’s lonstanding partnership with Kessenick Gamma, LLP, members receive discounted rates (typically 20–25% off) on comprehensive legal analysis of physician contracts. Services include a paragraph-by-paragraph review for legal compliance and business risk, with personalized consultations before and after the written analysis. For more information, including rates, see CMA health law library document #7076. To request a contract review, contact Frank Gamma at fgamma@kessenick.com or (415) 362-6412.
Resolve – Physician Contract Review and Compensation Data
CMA members also receive discounted services through Resolve, a trusted provider of physician contract review and compensation benchmarking. Resolve offers physician-focused contract analysis backed by market data, to help physicians understand how their offers compare to the market—and negotiate with confidence. Call CMA’s legal help line at (800) 786-4262 to request your 10% discount code.
Whether you’re reviewing your first employment offer or renegotiating an existing agreement, these trusted partners can help you evaluate and negotiate your contract with confidence.
“Since its founding, the CDC has been central to protecting Americans from disease. But recent leadership changes, reduced transparency, and the sidelining of long-trusted advisory bodies have impaired the agency’s capacity to prepare the nation for respiratory virus season and other public health challenges. In a vacuum of clear, evidence-based vaccine guidance, manufacturers lack reliable information to plan production, health care providers struggle to provide consistent plans of care, and families face uncertainty about access and coverage.
In June, California, Oregon, and Washington condemned Secretary Robert F. Kennedy Jr.’s removal of all 17 members of the CDC’s Advisory Committee on Immunization Practices. Today, we reaffirm our commitment to science-driven decision-making. We will continue to provide clear, evidence-based guidance to people living in our states, look to scientific experts in trusted medical professional organizations for recommendations, and work with public health leaders across the country to ensure all Americans are protected. The absence of consistent, science-based federal leadership poses a direct threat to our nation’s health security. To protect the health of our com-
munities, the West Coast Health Alliance will continue to ensure that our public health strategies are based on best available science.” - Quote from California, Oregon, and Washington to launch new West Coast Health Alliance to uphold scientific integrity in public health as Trump destroys CDC’s credibility
For more information, please see:
• AAP releases evidence-based immunization schedule; calls on payers to cover recommendations
• Governor signs new law safeguarding vaccine access in California
• California, Oregon, and Washington to launch new West Coast Health Alliance to uphold scientific integrity in public health as Trump destroys CDC’s credibility
AAP releases evidence-based immunization schedule; calls on payers to cover recommendations
Governor signs new law safeguarding vaccine access in California
1 - California, Oregon, and Washington to launch new West Coast Health Alliance to uphold scientific integrity in public health as Trump destroys CDC’s credibility
EndtheIsolation.ScaleYourPractice.ReclaimYourLife. Areyousuccessfulclinically,butstrugglingwiththebusinessside? Workingharderisn'ttheanswer—workingstrategically is. Theharshreality? Anotheryearof"I'llfigurethisoutlater"meansmore time-for-moneycycles,risingoverhead,andsacrificingyourwellbeing.
THETHRIVINGPRACTICECOMMUNITY
YourGatewaytoExceptionalHealthcarePracticeSuccess
Your comprehensivegrowthecosystem wherepracticeowners buildtheirbusinessaroundtheirlife.
CMA Webinar: Navigating the MultiPlan Litigation - What Physician Practices and Facilities Need to Know
Date: Tuesday, September 16, 2025
Time: 12:15pm-1:15pm
A sweeping federal antitrust lawsuit is moving forward against MultiPlan, Inc. and several major insurers, including Aetna, Cigna, UnitedHealth and Blue Cross Blue Shield, alleging a price-fixing conspiracy that artificially suppressed out-ofnetwork payment rates and cost providers billions of dollars. Following a key court ruling in June, the case is headed into discovery, with potential damages tripled under federal law for successful claims. Join the California Medical Association for a timely webinar on what this case means for physician practices and facilities nationwide. The session will conclude with a Q&Aand open discussion is welcome and appreciated. All participant information will be kept private.
CMA Webinar: Managing Adverse Events in the Office Practice
Date: Thursday, September 18, 2025
Time: 12:15pm-1:15pm
Are you and your staff equipped to handle an adverse patient safety event or unexpected health care outcome in your practice? Managing adverse patient safety events and unexpected health care outcomes in a medical office setting can be challenging due to the uniqueness of the situation, or lack of standard processes, resources, or trained staff. Join this webinar to learn about the most frequent types of claims and risk issues arising in outpatient care. The session will provide a framework for responding to an adverse patient safety event or unexpected health care outcome in an office practice, including transparent communication and disclosure to the patient and their family, documentation of the event, and creating a culture of safety to learn from these unexpected events.
To register for any of these events, please visit www. sccma.org or scan the QR code
MEDFUTURE: SCCMA AI & Innovation Forum “Where Physicians and Technology Meet Tomorrow’s Healthcare”
Date: Saturday, September 20
Time: 8:00 AM to 2:00 PM
Location: SCCMA - 700 Empey Way, San Jose, CA 95128
Discover groundbreaking insights, connect with industry leaders, and be part of the conversation shaping tomorrow’s healthcare solutions. Keynote, panel discussions, exhibits and more. Register now, space is limited.
This AI & Healthcare event will be held in-person only and will not be recorded or streamed. Please contact rashida@sccma.org for questions and registration assistance.
SCCMA Webinar: Health Equity: An Analysis of Santa Clara County
Date: Friday, September 26
Time: 6:00 PM - 7:00 PM
Speakers: Dr. Tony Iton and Dr. Corneliu Delogramatic
Join our health equity analysis of the county, hosted by the Santa Clara County Medical Association’s Health Equity Intern, Theodore Bussell. This webinar discusses health equity priorities and themes within Santa Clara County as identified through a comprehensive literature review and several in-depth interviews with local providers and public health stakeholders. We will also go over actionable steps that providers can take within their own practices to initiate or continue making progress toward more equitable health outcomes for their diverse patient communities. In the second half of our presentation, a panel of speakers will share their experiences implementing health equity projects within their own work and larger organizations within Santa Clara County. A short, moderated Q&A will follow the panel.