• Diet, disordered eating and risk of running injuries
• Effects of acute cycling exercise bout on resistance training-induced changes in arterial stiffness
• Understanding concussion disclosure in elite female Rugby League players: Insights from the NRLW Premiership
Contents
REGULARS
02
From the Chair
Dr Kay Copeland discusses the Constitution review, welcomes new Council and Student Network members, highlights SMA’s involvement in the Play Well initiative, and looks ahead to the 2025 ASICS SMA Conference.
03
From the CEO
From concussion awareness to extreme heat response, CEO Jamie Crain shares how SMA is driving change to protect athletes at every level, with members’ support keeping health and wellbeing at the centre of sport.
Opinions expressed throughout the magazine are the contributors’ own and do not necessarily reflect the views or policy of Sports Medicine Australia (SMA). Members and readers are advised that SMA cannot be held responsible for the accuracy of statements made in advertisements nor the quality of goods or services advertised. All materials copyright. On acceptance of an article for publication, copyright passes to the publisher.
FEATURES
04
Understanding Impact Perception and Concussion Experience in Female Rugby League Players
Catherine de Hollander examines female players’ perceptions of impacts, risk, and recovery, along with key insights to inform prevention, education, and safer return-to-play as participation grows.
14
2025 ASICS SMA Conference: Preview & highlights
From global experts to emerging voices, this year’s Conference delivers inspiring keynotes, practical education, and the chance to connect with peers in the heart of Hobart.
Publisher Sports Medicine Australia State Netball and Hockey Centre – Parkville 10 Brens Drive, Parkville VIC 3052 sma.org.au ISSN No. 2205-1244 PP No. 226480/00028
09
Effects of acute cycling exercise bout on resistance training-induced changes in arterial stiffness
Prof Anthony Leicht explores how adding aerobic exercise after resistance training can reduce arterial stiffness and cardiovascular stress, supporting safer and more effective strategies for heart health.
Copy Editors
Archie Veera and Caitlin Ficken
General Manager,
Membership Development
Sarah Hope
Design/Typesetting
Perry Watson Design
Cover photograph
Getty Images / Michele Ursi
Content photographs
Author supplied; www.gettyimages.com.au
16
Breaking Barriers: Supporting Young People with Limb Difference in Sport. What Sports Medicine Practitioners Need to Know
Dr Free Coulston and Dr Rachel Toovey share powerful insights into supporting young people with limb difference in sport, highlighting practical strategies for coaches, clinicians and organisations.
28
Understanding Concussion Disclosure in Elite Female Rugby League Players: Insights from the NRLW Premiership
Shreya McLeod explores concussion disclosure among professional women’s rugby league players, revealing barriers to reporting and highlighting strategies to improve athlete safety and symptom recognition.
22
Diet, disordered eating and risk of running injuries
Erin Colebatch and Dr Alison Hill examine how diet, energy availability, and nutrient intake influence running-related injury risk in distance runners, highlighting strategies to support injury prevention and long-term participation.
5
People who Shaped SMA: Mark Brown
Sports Trainer Spotlight: Jeremy Lubrano
Sports Medicine in Malta
Minutes With: A/Prof Melanie Hayman
FROM
THE CHAIR
Strengthening Governance and Growing Together
SMA
IS STRENGTHENING ITS FOUNDATIONS THROUGH GOOD GOVERNANCE, MEMBER ENGAGEMENT AND NATIONAL INITIATIVES. FROM THE CONSTITUTION REVIEW TO THE PLAY WELL PARTNERSHIP AND THE 2025 ASICS SMA CONFERENCE, THE ORGANISATION REMAINS FOCUSED
ON BEING RESPONSIVE, SUSTAINABLE AND IMPACTFUL.
Good governance is foundational to any successful organisation. As we enter the second half of 2025, I want to acknowledge the strategic work underway to ensure that SMA remains responsive, sustainable, and future-focused – and to thank our members for continuing to place their trust in us.
One of our major focus areas this year has been the review of our Constitution. It has been more than a decade since our last comprehensive review, and as SMA continues to evolve, it is vital that our governing document reflects contemporary governance expectations and supports long-term growth. A Constitution Review Committee has invested significant time and care in preparing a revised version of the Constitution.
In May and June, two national member forums were held to walk through the proposed changes and get feedback directly from members. The final version of the revised Constitution will be put to a member vote, ahead of our Annual General Meeting at the ASICS SMA Conference on 30 October in Hobart.
As SMA continues to evolve, it is vital that our governing document reflects contemporary governance expectations and supports long-term growth.
I also want to take this opportunity to welcome the newly appointed members of our State Councils and the SMA Student Network, and to thank all those across our Councils and Committees who generously give their time and expertise to help drive our initiatives forward. Your leadership and contribution play a vital role in shaping the direction and impact of the organisation.
I am also pleased to share that SMA has become an Affiliate of the Australian Sports Commission’s Play Well initiative. Play Well is a national strategy aimed at creating safe, welcoming and inclusive environments for sport and physical activity. We are proud to stand alongside 16 other organisations in supporting this important work. Our contribution will include promoting injury prevention and safer sport, which is central to ensuring that participants of all ages, backgrounds, genders and abilities can take part with confidence.
As always, the highlight of our calendar year is the scientific Conference, and the 2025 ASICS SMA Conference is shaping up beautifully. With a strong scientific program, excellent keynote speakers and a host of networking opportunities, it promises to be an inspiring few days in Hobart. I look forward to connecting with many of you there.
Thank you for your continued support of SMA.
Dr Kay Copeland Chair, Sports Medicine Australia
FROM THE CEO
Safeguarding Health Across the Sporting Landscape
SMA CONTINUES
TO PRIORITISE PLAYER SAFETY, FROM CONCUSSION AWARENESS TO PRACTICAL EXTREME HEAT GUIDELINES, SUPPORTING SAFE SPORT AT
EVERY LEVEL.
As we move through the second half of the year and towards the warmer months, it’s a natural time to reflect on the issues that have defined the winter sporting season and to look ahead to the challenges and opportunities on the horizon. At Sports Medicine Australia, our focus remains firmly on safeguarding the health and wellbeing of all participants, from elite athletes to grassroots players.
One issue that continues to demand attention is concussion. While our National Awareness Campaign has been well received and is making strong inroads, there is still significant work ahead to shift culture, improve recognition, and ensure consistent management across all levels of sport. SMA will continue to work closely with partners and stakeholders to keep concussion on the agenda and to ensure that player welfare remains a priority in every sporting decision.
As we prepare for warmer weather, our attention also turns to extreme heat: a growing challenge in a climate of increasing variability and unpredictability. SMA has recently endorsed the Extreme Heat Risk and Response Guidelines, developed by Professor Ollie Jay, Dr Federico
SMA will continue to work closely with partners and stakeholders to keep concussion on the agenda and to ensure that player welfare remains a priority in every sporting decision.
Formenti, Dr James Smallcombe, Dr Carolyn Broderick from the Heat and Health Research Centre at the University of Sydney.
These evidence-based guidelines are complemented by a live web tool that delivers real-time heat risk assessments down to postcode level. This provides community sport organisers with practical guidance on whether to proceed with the schedule, delay the game until a cooler part of the day, or postpone the activity to another day. This serves as a critical decision-making resource for leagues and clubs to protect participants, particularly in grassroots settings where expert advice can be limited.
Finally, I want to thank our dedicated members. Your ongoing support drives SMA’s mission forward, and membership remains one of the most effective ways for medical and allied health practitioners to demonstrate leadership and commitment to sports and exercise medicine.
In this edition of Sport Health, we feature research and insights to support safer, more inclusive participation. Articles include female rugby league players’ perceptions and disclosure of concussion; the effects of acute cycling on resistance training-induced arterial stiffness; supporting young people with limb difference in sport; the influence of diet and energy availability on running injury risk; and strategies to improve concussion disclosure in elite female rugby league players.
With our annual scientific conference in Hobart fast approaching, I look forward to seeing many of you there for what promises to be another outstanding event of learning, networking and collaboration.
Jamie Crain CEO, Sports Medicine Australia
Understanding Impact Perception and Concussion Experience
in Female Rugby League Players
IN RESPONSE TO GLOBAL CONCERNS ABOUT THE SHORT- AND LONG-TERM CONSEQUENCES OF CONCUSSIONS AND REPEATED HEAD TRAUMAS IN CONTACT SPORTS, THE AUSTRALIAN SENATE LAUNCHED AN INQUIRY IN 2022.
CATHERINE DE HOLLANDER, James Cook University
Photo:
The findings of the inquiry reported a lack of comprehensive data (such as the incidence, severity, recurrence, and long-term outcomes) on concussion and repeated head traumas) within Australian contact sports, particularly across different levels of play and among female athletes. As a result, the inquiry recommended that identifying, managing and reducing the risk of concussion and repeated head traumas be made a priority for all Australian contact sports.
One of the most popular contact sports in Australia is rugby league, which exposes athletes to impacts or collisions that have a high risk of injury, including concussion. Female athletes may face sex specific differences in impacts and impact-induced injuries compared to males. Research indicates females tend to experience less tackle events (the main cause of impacts) per match (females = 512 per match), and males = 1068 per match), however, female athletes have higher rates of concussion, experience more severe symptoms, and have longer recovery periods than their male counterparts. This is concerning as the number of females playing rugby league is growing worldwide. From 2015 to 2021, participation in Australia grew 141%. While the increased media focus and participatory rates for female rugby league players has been tremendous, research about impacts/collisions and their outcomes (i.e. concussion) has been limited.
There is a clear need to address this growing evidence gap, in order to develop effective and equitable
Females tend to experience less tackle events per match (females = 512 per match), and males = 1068 per match), however, female athletes have higher rates of concussion, experience more severe symptoms, and have longer recovery periods than their male counterparts.
strategies that respond to the specific risks faced by female athletes. It is essential to explore not only the physical aspects of concussion, but also how female players perceive, understand, and respond to these injuries within the context of their sport. Understanding female rugby league players’ perceptions of impacts and concussion is critical for designing effective prevention strategies, educational programs, and return to play protocols.
Previous research across various contact sports has shown that athletes’ knowledge and attitudes toward impacts and concussion can significantly influence reporting behaviours and recovery outcomes. Both male and female athletes may downplay or normalise concussion symptoms due to external pressures, such as team expectations or fear of losing their place in the squad. However, female athletes may experience additional or unique challenges. For example, cultural and social dynamics within traditionally
Photo: gorodenkoff/Getty Images
Understanding Impact Perception and Concussion Experience
in Female Rugby League Players
male-dominated sports, such as rugby league, can shape how female athletes perceive injury severity, toughness, and the legitimacy of symptoms. These dynamics may include expectations to conform to masculine ideals of resilience, limited representation in leadership roles, and the need to prove their legitimacy in a male-dominated environment. Prior concussion history can also influence attitudes, as athletes with previous concussions have shown more negative attitudes and lower likelihood of reporting symptoms. This is especially important in rugby league, where tackles and collisions are not only frequent but often associated with performance and perceived toughness. Without a genderspecific understanding of these perceptions, concussion management strategies may not be as effective.
While studies on impacts and concussion in female athletes are increasing, they have predominantly focused on sports such as soccer, ice hockey, and rugby union, with limited attention paid to rugby league. This is problematic, as rugby league differs significantly in its match structure (e.g. 13-a-side format and 10-metre defensive line), tackle frequency, and contact intensity compared to these sports. For example, players in rugby league engage in more frequent tackles per match than in rugby union or soccer, with shorter rest periods between collisions, potentially increasing cumulative impact exposure. Additionally, many female rugby league players participate at a semi-professional or amateur level, which may limit access to educational programs, medical support, and tailored return-to-play protocols. Addressing these gaps requires sport- and gender-specific research that captures players’ perspectives and recognises the broader systemic and environmental factors that shape their experiences.
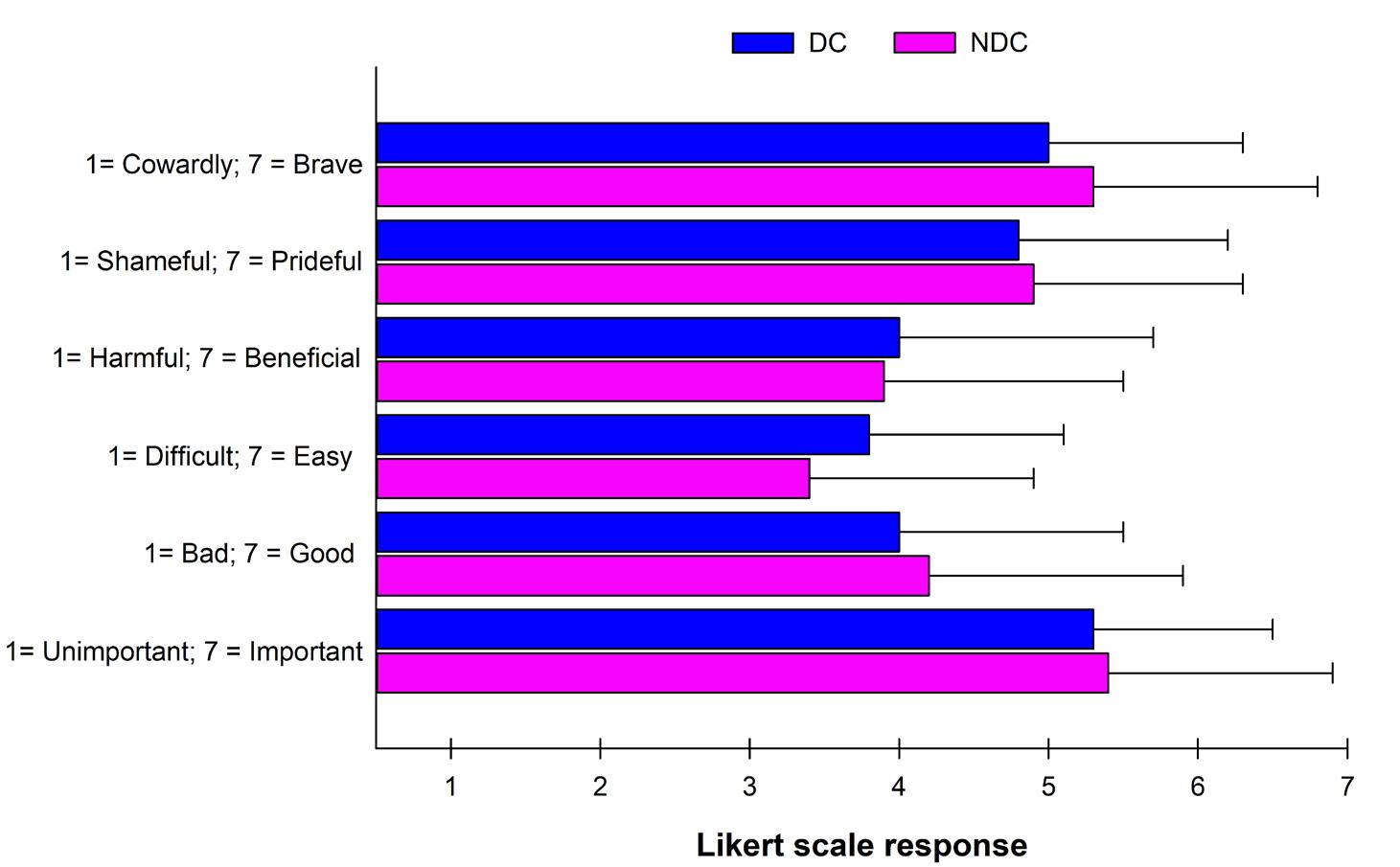
Subsequently, our study explored perceptions of risk, attitudes, values, beliefs, and behaviours related to impacts and concussion among female, semi-professional, rugby league players. We also wanted to examine how this differed between female athletes with a history of a prior Diagnosed Concussion (DC) and those with No Diagnosed Concussion (NDC). Understanding female rugby league players’ perceptions of concussion is essential to improving injury prevention, promoting symptom reporting, enhancing return-to-play safety, and ensuring the sport evolves in an equitable, evidence-based way.
What did we do?
During the pre-season periods of 2023 and 2024, 103 female players (mean age 17.9±3.6 years; range: 15-39) within two semi-professional, rugby league clubs completed a self-report survey. Players invited were competing within the U17 representative (n=45), U19 representative (n=35) and/or open age semi-professional (n=23), state-wide competitions. The survey included the following topics/questions:
ٚ Diagnosed and suspected (undiagnosed) concussion history
– Example: Have you ever had a DIAGNOSED concussion (i.e. by a medical professional such as a doctor)? If so, how many, and in what year/s did they occur?
ٚ Risk perception and attitudes toward impacts and concussion
– Example: Rate your level of concern of personally experiencing the following in your current sport/s: (rated on a 1–7 scale with 1 being not concerned and 7 being very concerned)
ڇ Muscle injury
ڇ Ligament/joint injury
ڇ Broken bones and fractures
ڇ Concussion
ڇ Cuts/lacerations/abrasions
ڇ Repetitive impacts (that don’t result in the injuries listed above)
ٚ Beliefs about concussion recovery
– Example: How many days on average does it take to recover from a concussion?
Photo: Chinnapong/Getty Images
Likert Scale with 1 = No Concern/Risk and 7 = Extreme Concern/Risk
My concern for personally experiencing a muscle injury whilst participating in rugby league
My concern for personally experiencing a ligament/ joint injury whilst participating in rugby league
My concern for personally experiencing a broken bone whilst participating in rugby league
My concern for personally experiencing a cut whilst participating in rugby league
My concern for personally experiencing a concussion whilst participating in rugby league
My concern for personally experiencing a repetitive impact injury (e.g. Parkinson’s disease, Alzheimer’s disease or Chronic Traumatic Encephalopathy) whilst participating in rugby league
*p<0.05 vs. DC
Approximately 40% of players (n=38) reported a history of at least 1 diagnosed concussion in their lifetime.
ٚ Use of protective equipment – Example: Do you currently wear any of the following protective gear? If yes, please explain why you wear it?
ڇ Mouthguard
ڇ Headgear
ڇ Chest plate
ڇ Shoulder pads
ڇ Shin guard
ڇ Knee guard
ڇ Other
Independent samples t-tests and chi-squared tests were used to compare responses between the DC and NDC groups.
What did we find?
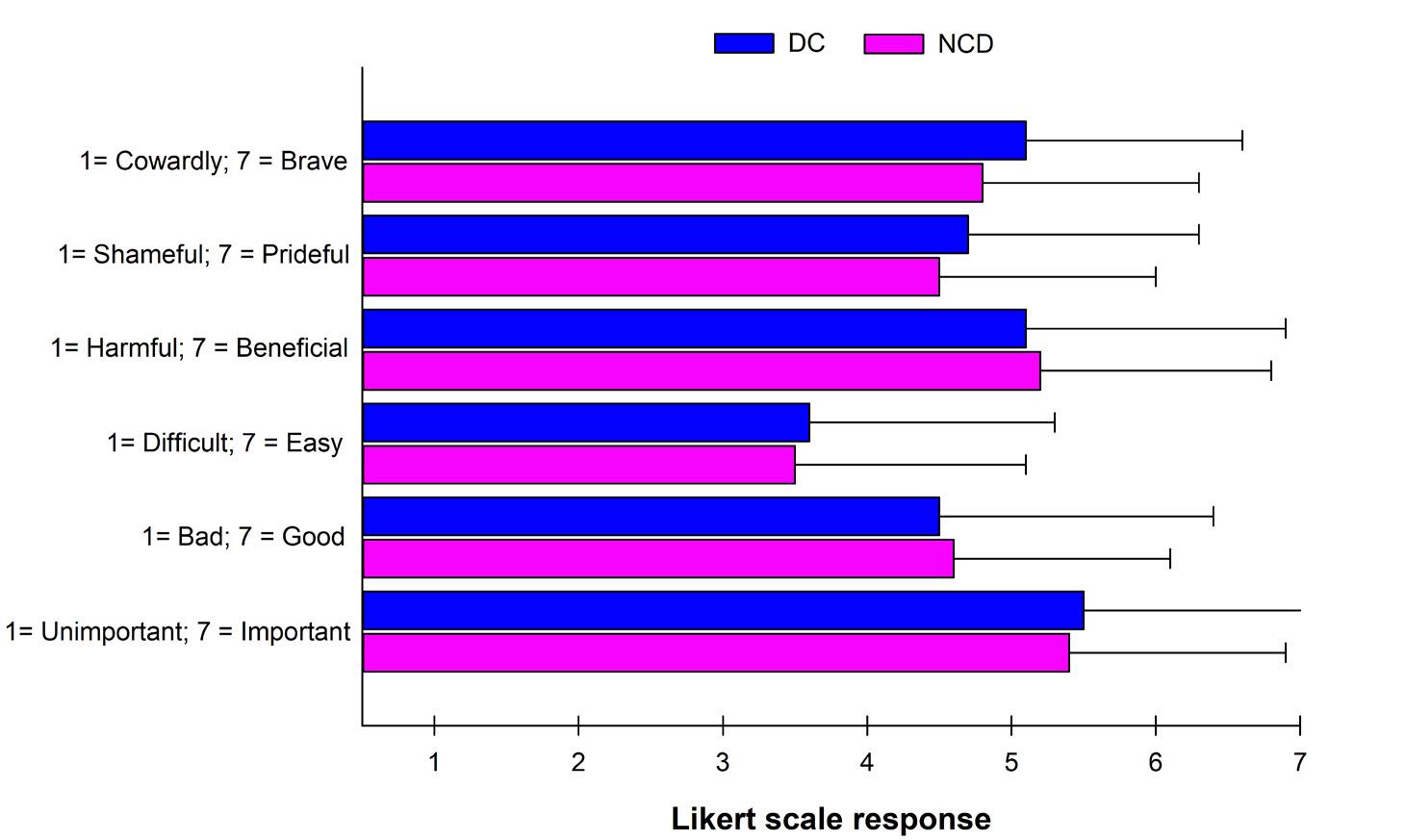
Approximately 40% of players (n=38) reported a history of at least 1 diagnosed concussion in their lifetime. The DC group reported a significantly higher incidence of suspected concussions in their lifetime compared to the NDC group (1.2±2.0 vs. 0.4± 0.8 concussions, p=0.016). The DC group was more concerned about experiencing a concussion during rugby league participation (Table 1), and both groups reported similar attitudes (Figures 1 and 2) and values (Table 2). The DC group reported significantly greater personal knowledge about the effects of impacts (including concussion) compared to the NDC group, and both groups (p>0.05) believed that a concussion resolved within an average ~12-14 days (Table 3). Both groups reported similar use of protective equipment against concussion, with 74% of all players (n=76) wearing a mouthguard during matches.
Figure 1. Attitudes Towards a Teammate Who is Exposed to a High Frequency of Impacts During the Rugby League Season
Figure 2. Attitudes Towards A Teammate Who is Exposed to a High Frequency of Impacts During the First Half of a Rugby League Season & Requests to Be Benched for the Remainder of the Season
Table 1. Perception of Risk to Injury
Understanding Impact Perception and Concussion Experience
in Female Rugby League Players
Table 2. Player Values
Likert Scale with 1 = No Value and 7 = Extremely Valuable
My
Table 3. Beliefs on Impacts and Concussions
Likert Scale with 1 = No Knowledge and 7 = Very Knowledgeable
My knowledge on the effects of impacts (including concussion)
How long does a concussion take to fully recover from (days)
*p<0.05 vs. DC
What do the findings mean?
Female rugby league players with a history of DC were found to be at a heightened risk of experiencing further suspected concussions. These players also reported greater concern about sustaining future concussions while participating in their sport. One possible explanation for this increased risk is a premature return to play following a previous concussion, before neurological recovery has occurred. Additionally, the tendency for some players to not seek medical attention and continue playing despite experiencing symptoms may be influenced by negative personal or observed experiences related to concussion management and outcomes.
Interestingly, having a history of concussion did not appear to influence female players’ perceived risk of sustaining other types of injuries, nor did it affect their attitudes towards teammates or personal values related to sport participation. However, players with prior concussion experience demonstrated greater knowledge of the concussion recovery process. Their understanding was generally consistent with the National Rugby League’s (NRL) mandatory stand-down period of 11 days for adult players (≥19 years). In contrast, this duration was shorter than the 19-day stand-down period required for players aged ≤18 years under NRL policy, and also shorter than the 21day stand-down period recommended by the Australian Concussion Guidelines for Youth and Community Sport.
Although the use of personal protective equipment, such as headgear or mouthguards, is not mandatory in rugby league, the majority of players reported wearing a mouthguard. This choice appeared to be motivated by a desire to protect against
orofacial injuries and may also reflect a growing awareness of the role mouthguards can play in reducing concussion risk. However, around 26% of female athletes reported not wearing a mouthguard during play, highlighting a potential gap in protective behaviours. This may be due to discomfort, cost, lack of awareness, or scepticism about their effectiveness, factors which should be explored further to inform targeted education and injury prevention strategies.
These findings highlight the urgent need for further sportand gender-specific research to better understand the factors influencing concussion risk, reporting behaviours, and recovery in female rugby league players. Such research is critical to developing effective education programs, refining return-to-play protocols, and guiding policy decisions that prioritise player safety and long-term health.
Take home message
Athletes’ understanding of concussion recovery generally aligns with the NRL’s 11-day stand-down policy for adults. However, under-reporting of suspected concussions remains an issue, particularly among those with a history of diagnosed concussion. Practitioners are encouraged to educate players on the importance of reporting all suspected concussions. Additionally, players’ indifferent attitudes toward the long-term effects of repeated head impacts highlight the need for ongoing education and awareness from support staff and sporting organisations.
For article references, please email info@sma.org.au
About the Author
Catherine de Hollander is a Bachelor of Exercise Physiology (Honours) graduate who is currently undertaking her PhD at James Cook University. Her PhD is examining the impacts/collisions experienced by semi-professional female rugby league players and their effects on health. Her PhD is an exciting collaboration between government, community and industry partners.
Effects of acute exercisecycling bout on resistance traininginduced changes in arterial stiffness
CARDIOVASCULAR DISEASE (CVD) REMAINS THE LEADING CAUSE OF DEATH GLOBALLY WITH MORE THAN 525 MILLION PEOPLE WORLDWIDE AFFECTED. WHILE FACTORS SUCH AS POOR DIET, SEDENTARY LIFESTYLE, AND SMOKING ARE WELL KNOWN, ONE LESSER-KNOWN BUT POWERFUL PREDICTOR OF CARDIOVASCULAR HEALTH IS ARTERIAL STIFFNESS.
Arterial stiffness refers to the rigidity and reduced ability of an artery to expand and contract in response to pressure changes. Healthy arteries are elastic, allowing them to buffer the pulsatile output of the heart and maintain steady blood flow. As we age, or due to conditions like hypertension, diabetes, and chronic inflammation, arteries can become rigid. This stiffness can contribute
to increased vascular resistance and cause the heart to work harder, increasing CVD risk. In fact, arterial stiffness can be a key monitoring tool for cardiovascular health and risk for CVD. Regular exercise can provide a potent, non-pharmacological means to address arterial stiffening however, not all exercise is created equal.
Aerobic exercise, activities that increase heart rate and breathing over sustained
periods, has long been championed for improving cardiovascular health and function. Acutely, aerobic exercise such as running and cycling were reported to reduce arterial stiffness for 30-240 minutes following an exercise bout. However, not all acute exercise bouts have produced beneficial changes in arterial stiffness. Pierce et al. reported that arterial stiffness was significantly elevated for up to 50 minutes in 21 recreationally active males following a 30-minute bout of resistance exercise. While resistance exercise may be beneficial for musculoskeletal health, its acute elevation of arterial stiffness and associated increased vascular resistance and cardiac load, may pose a substantial cardiovascular risk to those regularly undertaking resistance exercise. The addition of aerobic exercise to the end of a resistance exercise session may provide a simple way to reduce
PROFESSOR ANTHONY LEICHT, James Cook University
Photo: Ryan McVay/Getty Images
Effects of acute cycling exercise bout on resistance traininginduced changes in arterial stiffness
arterial stiffness responses following resistance exercise bouts and manage future development of CV risks. Therefore, the current study aimed to determine the effects of a bout of aerobic exercise performed after a resistance bout on cardiovascular function including arterial stiffness.
What did this study do??
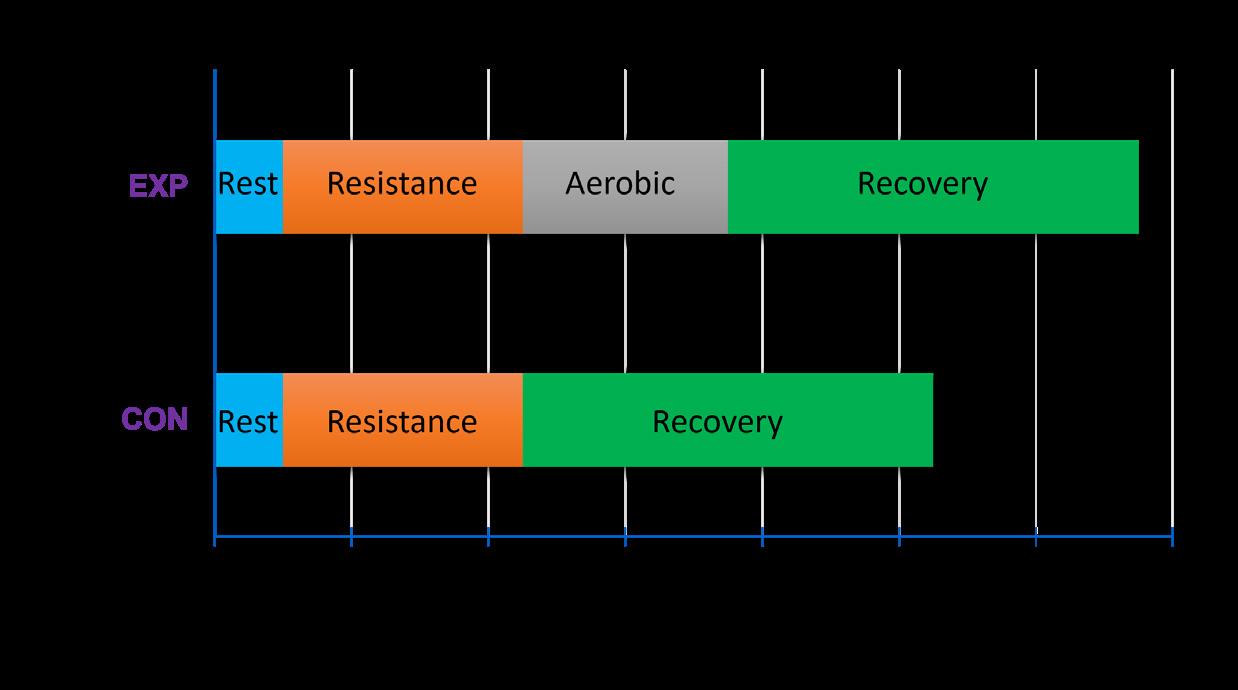
Moderately-active, male (n=12) and female (n=8) individuals (mean age of 35.0 ± 10.5 years) volunteered for this study. Following a familiarisation session, participants completed two individual sessions with each separated by at least three days. The sessions included the recording of seated cardiovascular function (e.g. heart rate, blood pressure, etc) during a 10-minute seated rest period, 35-minute resistance bout (i.e. paired superset of six exercises at 80% of 10-repetition maximum) and a 90-minute recovery period. The sessions were identical, except for the recovery periods, which consisted of either 90-minutes of seated rest (Control) or 30-minutes of aerobic cycling (70-75% maximum heart rate) followed by 60-minutes of
Figure 1: Study design and assessment protocol during Control (CON) and Experimental (EXP) sessions. *Assessment of heart rate, brachial blood pressure and augmentation index corrected for a heart rate of 75.
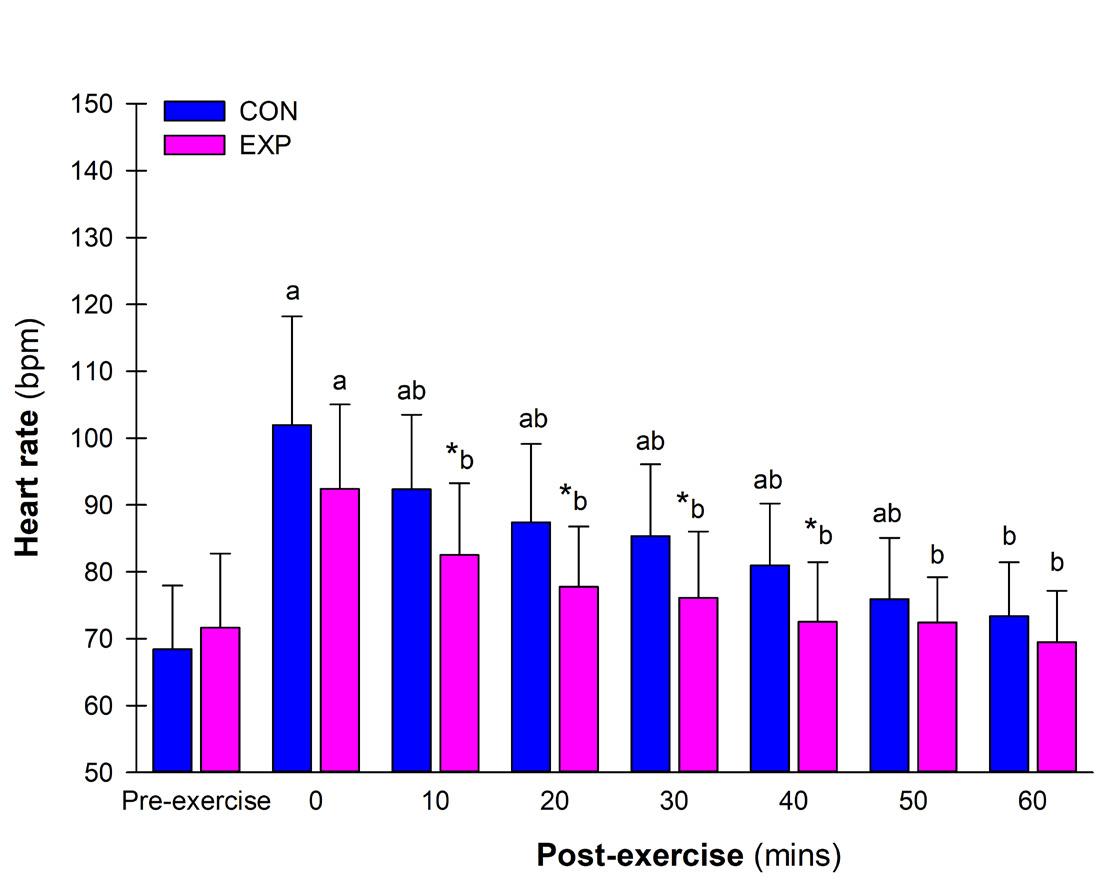
Figure 2: Heart rate prior to and during recovery for the Control (CON) and Experimental (EXP) sessions. ap<0.05 vs. Pre-exercise within session; bp<0.05 vs. 0 minutes within session; *p<0.05 vs. CON at timepoint
Photo: Bojan89/Getty Images
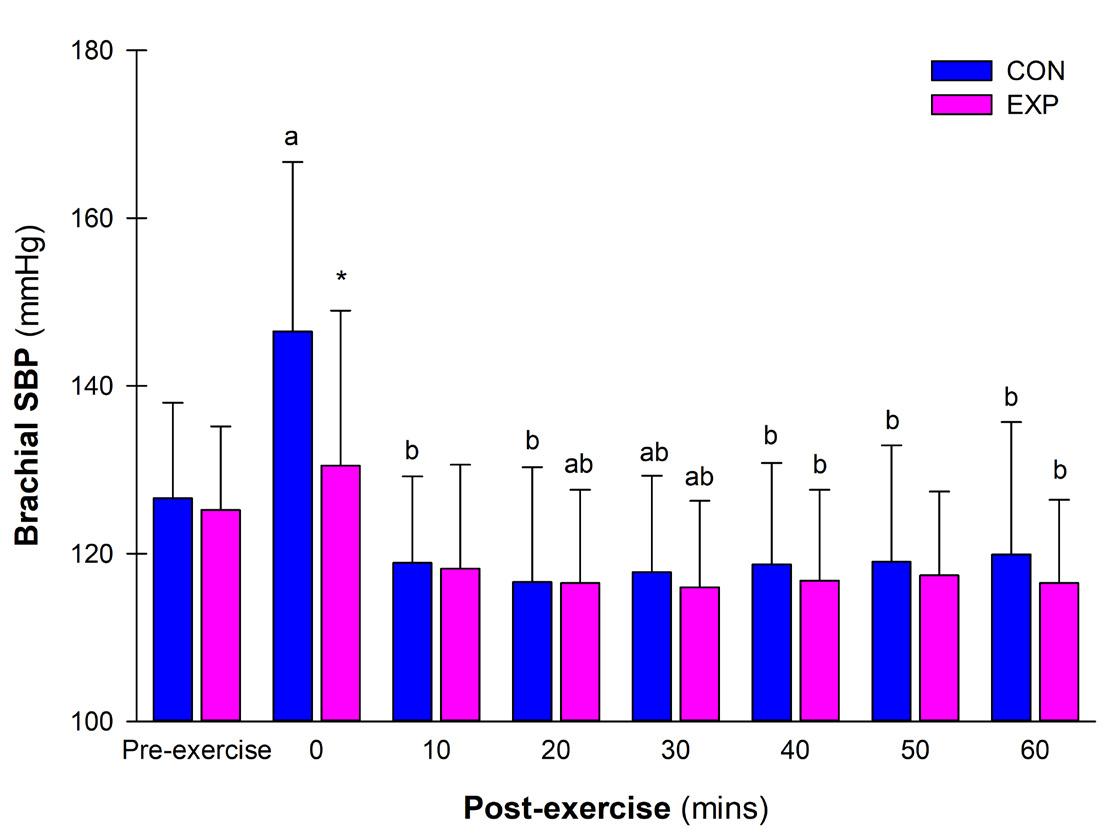
Figure 3: Brachial systolic blood pressure prior to and during recovery for the Control (CON) and Experimental (EXP) sessions. ap<0.05 vs. Pre-exercise within session; bp<0.05 vs. 0 minutes within session; *p<0.05 vs. CON at timepoint
During recovery, heart rate was significantly greater compared to preexercise values and had returned to resting values by minute 10 for the Experimental compared to minute 60 for the Control session
seated rest (Experimental). The order of session completed by participants was randomly allocated. Heart rate (HR), brachial blood pressure and arterial stiffness via augmentation index (corrected for heart rate of 75, AIx 75) were recorded at the end of seated rest, after resistance or resistance/aerobic exercise, and then every 10 minutes of seated recovery (Figure 1). Comparisons between conditions (Control vs. Experimental) over time (pre-exercise vs. recovery) for variables were examined using two-way repeated measures analysis
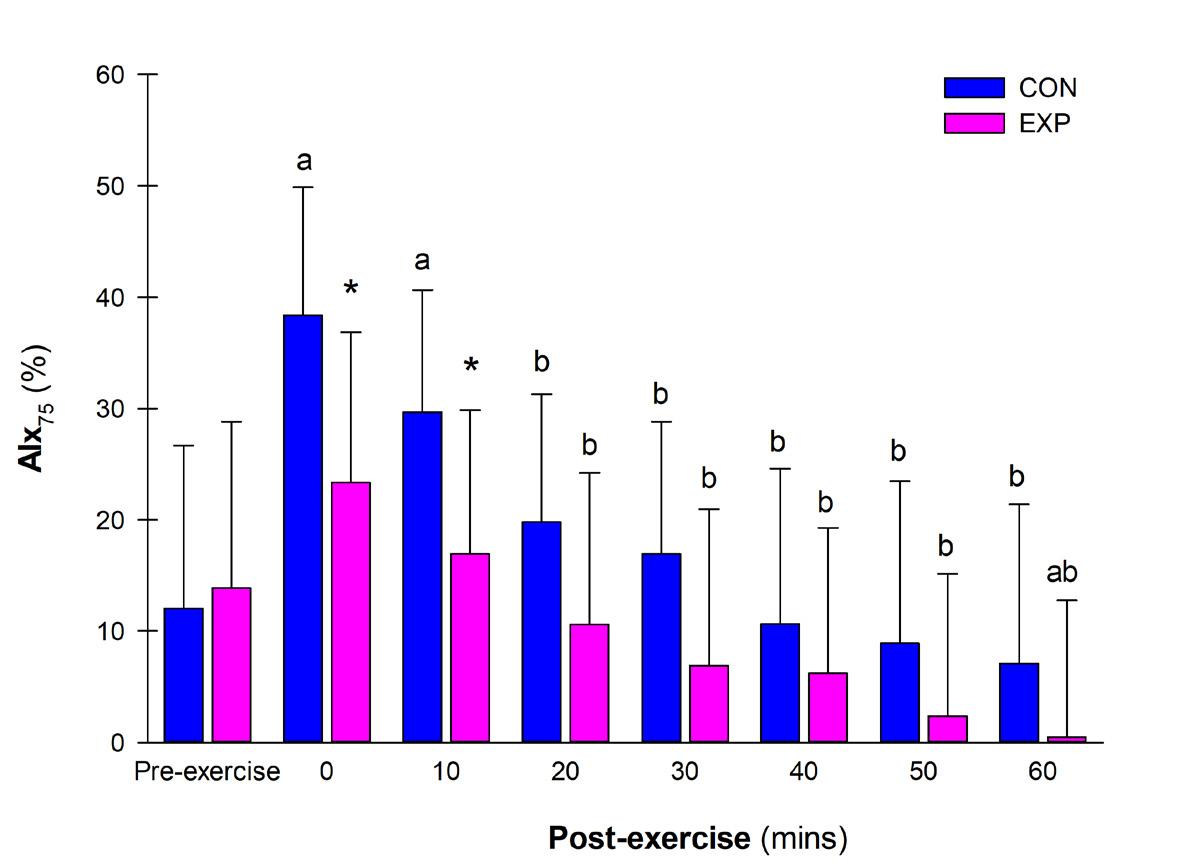
Figure 4: Augmentation index corrected to a heart rate of 75 (AIx 75) prior to and during recovery for the Control (CON) and Experimental (EXP) sessions. ap<0.05 vs. Pre-exercise within session; bp<0.05 vs. 0 minutes within session; *p<0.05 vs. CON at timepoint
Photo: jacoblund/Getty Images
Effects of acute cycling exercise bout on resistance traininginduced changes in arterial stiffness
of variance and post-hoc pairwise contrasts with a Bonferroni correction.
What did this study find??
During recovery, heart rate was significantly greater compared to pre-exercise values and had returned to resting values by minute 10 for the Experimental compared to minute 60 for the Control session (Figure 2). During the Control session, postexercise brachial systolic blood pressure was elevated immediately and then returned to pre-exercise values by minute 10 whereas during the Experimental session, it was similar to pre-exercise values throughout and then significantly lower at 2030 minutes post-exercise (Figure 3). Likewise, post-exercise AIx 75 was significantly increased immediately and at minute 10 during the Control condition before returning to preexercise levels. In contrast, postexercise AIx 75 during the Experimental session was similar to pre-exercise values throughout and decreased significantly below pre-exercise values at minute 60 of recovery (Figure 4).
What are the conclusions of this study??
A typical resistance exercise bout caused notable and immediate increases in heart rate, brachial systolic blood pressure and arterial stiffness (AIx 75) measures that returned to preexercise levels within 10-60 minutes. These results were similar to prior studies and demonstrated that a resistance bout induces significant cardiovascular stress that subsides with time. Importantly, the addition of an aerobic cycling bout after the resistance bout (Experimental) resulted in an accelerated return of, and favourable, cardiovascular and arterial stiffness measures compared to resistance exercise only (Control). This favourable response may represent a faster cardiac autonomic transition (i.e. parasympathetic reactivation, reduced sympathetic contributions) that remains to be confirmed in
future studies. The inclusion of aerobic exercise following resistance exercise, typical of a concurrent training session, may provide beneficial short-term changes in cardiovascular function and arterial stiffness with long-term cardiovascular benefits remaining to be determined.
Arterial stiffness may be a silent threat, but it’s one we can fight with every run, pedal and lift. Aerobic exercise remains
the gold standard for improving arterial elasticity (and reducing stiffness), but resistance training, when done wisely, can complement and enhance overall health. Together, aerobic and resistance exercise form a powerful prescription for lifelong cardiovascular health.
For article references, please email info@sma.org.au
About the Author
Professor Anthony Leicht is an experienced exercise scientist and active educator/ researcher with an international reputation in the assessment of health, human performance and physiological responses to exercise/sport/occupational tasks across a range of populations. He is a Fellow of Exercise and Sports Science Australia, European College of Sport Science and Sports Medicine Australia. This study was a collaborative effort by Honours student Mani Gregson, Dr Kenji Doma and Professor Anthony Leicht at James Cook University, Townsville.
Photo:
INTRODUCTION
The 2025 ASICS SMA Conference is the premier event for sports medicine and science, uniting leading experts, researchers, and practitioners from around the world. It is the place to connect, collaborate, and shape the future of the field – continuing SMA’s proud tradition of hosting Australia’s leading multidisciplinary sports medicine conference.
HIGHLIGHTS
ٚ Hear from seven global leaders – Prof Nick Brown, Prof Michael Rathleff, A/Prof Michelle Smith, Dr Enda King, Dr Carly McKay, Prof Ollie Jay, and Prof Silvia Blemker – sharing insights from research and real-world practice.
ٚ Start each day with practical workshops covering topics like movement variability, concussion rehab, ankle injuries, and Athletic Disordered Eating (ADE).
ٚ Join symposia featuring experts and emerging voices on REDs, hamstring injuries, brain health, trail running, concussion prevention, and the IOC FAIR Consensus.
ٚ Explore research across ACL rehab, knee OA, adolescent injury, women’s health, tendons, and more, with $23,000 awarded to standout free papers presentations
ٚ Reconnect with peers and expand your professional network through a vibrant and inclusive social program
ٚ Discover the latest tools and technologies to support your practice at a dynamic trade exhibition featuring leading industry partners.
ٚ Enjoy Hobart’s culture and dining with the centrally located Hotel Grand Chancellor just steps from Salamanca Place, Battery Point, and the MONA Ferry.
Over 20 hours of high-quality podium paper presentations across the following topics:
ٚ Hip and knee OA
ٚ Upper limb
ٚ ACL
ٚ Workforce
ٚ Feet and shoes
ٚ Performance testing and evaluation
ٚ Injury surveillance and trauma
ٚ Women’s health
ٚ PFP and knee
ٚ Neurophysiology and exercise
ٚ Concussion and mental health
ٚ Lower limb bone and soft tissue
ٚ FAIR follow-up
ٚ Post ACL reconstruction
ٚ Hip and FAIS
ٚ Adolescent injury and evaluation
ٚ Tendons
ٚ Women’s sport evaluation and performance
OUR SPONSORS, PARTNERS AND EXHIBITORS *
Industry Partners & Supporters
Session Sponsors
Trade Exhibitors
Breaking Barriers
Supporting Young People with Limb Difference in Sport
What Sports Medicine Practitioners Need to Know
DR FREE COULSTON and DR RACHEL TOOVEY,
The University of Melbourne
“Just treat me like everyone else” – these words from a 16-year-old triathlete with a lower limb difference capture the essence of what young people with limb difference want from their sports experiences. But as sports doctors, allied health professionals and sports trainers, how do we balance this desire for equality with the reality that individualized support is often essential?
A groundbreaking Australian study involving nine young athletes with limb difference and their parents has
revealed powerful insights that can transform how we approach sports participation for this population. The research, led by researchers from The University of Melbourne in collaboration with the START Foundation, investigators with lived experience of limb difference, prosthetists and orthotists from the Royal Children’s Hospital, and researchers from La Trobe University, offers a roadmap for creating inclusive sporting environments where young people with limb difference can thrive.
The Reality Check: More Than Just Participation
When 14-year-old Alex (name changed) started soccer training, their coach spent individual time assessing their capabilities before introducing them to the squad “The soccer coach, before he threw ‘Alex’ in the deep end, he did spend a bit of one-onone time just getting to know their capability, like “Show me if you can do this,” or “how do you do this for me, can you copy what I do?” Alex’s mother recalls. “I think ‘Alex’ just had that solid time to build up a bit of
confidence and go “Yeah, I’m good at this” and then [be guided] into the group.” This approach exemplifies what the research identifies an essential approach: equitable participation. It’s not about lowering expectations or providing special treatment. Instead, it’s about recognizing differences to enable equal opportunities for success.
The study revealed three critical themes that sports professionals should understand:
1. “Just Treat Me Like Everyone Else” – The Equity Paradox
Young people with limb difference face a fundamental tension. They want
to be seen as “no different” from their teammates, yet they often require individualized support to achieve this equality. The key lies in how professionals navigate this paradox.
What This Looks Like in Practice:
ٚ High Expectations: Assume competence and set performance standards equal to peers. One study participant described feeling frustrated when coaches underestimated their abilities, saying they were often “discarded” in competitive situations.
ٚ Subtle Support: Provide necessary modifications without drawing unnecessary attention. A soccer coach in the study exemplified this by conducting one-on-one assessment sessions before group integration, allowing them to provide seamless support during team activities.
ٚ Genuine Competition: Treat the young person as a legitimate opponent or teammate. As one participant noted, “They will genuinely play against me without caring about my disability – that’s what I want.”
Practice Alert: Coaches who assume limitations without assessment or are “overly cautious” in ways that exclude the young person from full participation should be supported to shift their practice. You are the perfect person to help with this mindset change!
2. “Provide Them Opportunities and Let Them Take the Lead” – The Choice Revolution
Genuine choice emerged as a fundamental need, but it’s more complex than simply offering options. The research identified two crucial components:
ٚ Availability and Accessibility of Opportunities: The study found that organizational attitudes significantly impact access. One parent reported calling eight different recreation centres to find swimming lessons, with most responding, “I don’t think I can help you.” Contrast this with organizations that proactively state, “What do you need? How can we help?”
ٚ Young People’s Agency in Decision-Making: Participants chose sports where they felt “powerful” and could demonstrate competence. Functional elements played a major role – some preferred sports with natural rest breaks to manage fatigue, others chose activities where prostheses weren’t required to reduce preparation time.
What This Looks Like in Practice:
ٚ Ask open-ended questions: “What draws you to this sport and how can we support you best?” rather than “Try an easier sport”
ٚ Provide clear information about pathways, including para-sport classification opportunities
ٚ Respect the young person’s preferences – there’s sound reasoning behind their choices
Practice Alert: Organizations that restrict young people to certain sports or make participation contingent on extensive negotiations are a core barrier to sports participation. Encouraging organisations and coaches to be sensitive to families when they call seeking information is essential, as they may have faced rejection or dismissal from other organisations.
3. “I Wish They Were Easier to Get” – The Equipment Game-Changer
Photo: Cristina Villar Martin/Getty Images
Breaking Barriers
Supporting Young People with Limb Difference in Sport What Sports Medicine Practitioners Need to Know
Participants who used sports-specific prostheses often described them as transformational. One young person explained: “ I can use a shoddy prosthetic for walking, but I cannot use it for running, I can’t use it for playing any sports. So, like when my mobility aids and things are affected, that’s when I’m affected in what I have, like the choices that I have.” However, it was often a rocky road to the right prosthetic.
ٚ The Multi-Prosthetic Reality: The research revealed that young athletes often need multiple prostheses:
– Different prostheses for different sports (running blade vs. swimming fin)
– Regular replacements due to rapid growth (one participant had three prostheses in 11 months)
– Backup equipment for training vs. competition
ٚ The Funding Challenge: While Australia’s National Disability Insurance Scheme (NDIS) provides support, the application process can
It’s not about lowering expectations or providing special treatment. Instead, it’s about recognizing differences to enable equal opportunities for success.
their current equipment.
ٚ Multiple Equipment Justification: Help families understand they may need to advocate for multiple prostheses – particularly to enable equitable choice in trying multiple sports.
be time-consuming, complex and emotionally challenging. Parents described having to focus on their child’s limitations rather than aspirations, with one noting: “you have to sort of say all the things that they can’t do that you want them to be able to do which you know, that can be a bit upsetting.”
What This Looks Like in Practice:
ٚ Early Equipment Planning:
Start conversations about sportsspecific prostheses early, before the young person outgrows
ٚ Strengths-Based Reporting: When writing professional reports for funding applications, frame needs in terms of participation goals and potential rather than deficits. Focus on “to enable participation in chosen sport” rather than “due to inability to...”
ٚ Timing Advocacy: Recognize that equipment delays directly impact participation. A young athlete missing a season due to funding delays or equipment fitting issues loses valuable development opportunities.
ٚ Family Expertise: Acknowledge that families often become equipment modification experts out of necessity. Support their innovations and advocate for funding of proven adaptations.
Practice Alert: Support parents to re-engage with funding processes using a strengths-based approach, as some have relegated it to the “too hard basket”.
The Four-Level Action Plan
The research mapped barriers and facilitators across four levels of influence, providing a clear framework for intervention:
Level 1: Individual Factors
Your Role: Ensure optimal equipment function and build confidence and competence
ٚ Advocate for proper prosthetic fit and functionality
ٚ Support skill development that builds confidence
ٚ Recognize signs of equipment issues affecting performance
Photo: Rawpixel/Getty Images
Success story: One parent described their child’s running prosthetic as “an enhancement. It’s like any athlete. It’s like Thorpey with his swimsuit. They’re doing the hard work, and […] this will allow them to reach their full potential.”
Level 2: Interpersonal Relationships
Your Role: Be the professional who makes the difference
ٚ Assessment Before Integration: Spend time understanding capabilities before group activities
ٚ Learn and Adapt: You don’t need para-sport expertise, but you need willingness to problem-solve collaboratively
ٚ Family Partnership: Work with families who often become expert advocates and equipment modifiers
Success Story: One family’s father modified his child’s bike by hack-sawing the prosthetic attachment and creating a custom handlebar connection using plumbing pipes – simple innovation that enabled safe cycling.
Level 3: Community/ Organizational Systems
Your Role: Champion sporting organizational change
ٚ Advocate for inclusive policies in workplaces you are linked with
ٚ Provide education to coaches about capabilities vs. limitations
ٚ Support clear information provision about available programs and pathways
Success story: A national sporting organization immediately embraced a young triathlete, asking “What do you need? How can we help you?” and offering pathway support to Paralympic competition. The family described it as “like a big warm hug […] you’re in the loop so you can actually see what the future looks like.”
Level 4: Societal/Policy Level
Your Role: Systems advocacy
ٚ Support families navigating funding applications
ٚ Provide professional reports that emphasize function and potential rather than deficits
ٚ Advocate for timely equipment provision that keeps pace with growth and activity changes
The “Moving Through Childhood” Framework
The research culminated in a practical model called “Moving Through Childhood: Participation supports for young people with limb difference.” This framework recognizes that effective sports participation support must account for:
ٚ Age-Related Changes:
– Early childhood: Focus on unstructured recreation and family activities
– Later childhood: Support exploration of multiple sports and competitive pathways
– Adolescence: Enable highlevel performance and specialization choices
ٚ Key Success Elements:
– Appropriate Adaptive Equipment: Right tool, right time, right fit
– Supportive Coaches: Willing to learn and adapt
The study found that organizational attitudes significantly impact access. One parent reported calling eight different recreation centres to find swimming lessons, with most responding, “I don’t think I can help you.” Contrast this with organizations that proactively state, “What do you need? How can we help?
– Access and Inclusion: Organizational openness with practical support
– Moving Through Childhood: Recognition that needs change with growth and development
Photo: Jesus Rodriguez/Getty Images
Breaking Barriers
Supporting Young People with Limb Difference in Sport
What Sports Medicine Practitioners Need to Know
Practical Strategies You Can Implement Tomorrow
For Sports Medicine Professionals:
ٚ Assessment Approach: Focus on what the young person CAN do and wants to do, not their limitations
ٚ Equipment Advocacy: Understand the sports-specific needs and advocate accordingly
ٚ Family Education: Help families navigate funding systems and understand their advocacy rights
ٚ Professional Networks: Connect families with appropriate sporting organizations, pathways, and coaches
For
Sports Trainers and Coaches:
ٚ The One-on-One Rule: Always assess individually before making assumptions
ٚ Modification Mindset: Think adaptations, not restrictions
ٚ Team Integration: Focus on making the young person feel part of the group, not special or separate
ٚ Growth Planning: Anticipate equipment needs changing with growth and sport development
For Sports Organizations:
ٚ Inclusive Messaging: Make it clear that you welcome athletes with disability
ٚ Information Provision: Offer clear pathways including para-sport classification information
ٚ Staff Training: Educate personnel on capability-focused approaches
ٚ Policy Review: Ensure policies enable rather than restrict participation
The Bottom Line
The research delivers a clear message: young people with limb difference want genuine opportunities to excel in sports they choose. They want coaches who see their potential. They want teammates who view them as peers.
As one participant’s parent powerfully stated about their child: “For them essentially it was kind of saying, ‘my decision and the way I do life is I want to live my life without limitations’ […] sport has been
that beautiful vehicle that’s kind of enabled them to get there.”
Your role as a medical or health professional is to be the facilitator who removes barriers and creates opportunities. It’s to support the coach to take time to understand rather than assume. It’s to be the advocate who ensures equipment needs are met promptly and appropriately.
The young people are ready. They have the determination, the resilience, and the desire to participate. The question isn’t whether they can succeed in sport – it’s whether we’re prepared to create the conditions where they can thrive.
The research shows us the way forward. Now, let’s put these insights into action, one young person at a time. Because when we get it right, we don’t just
change their sporting experience – we change their entire relationship with what’s possible in their lives.
This article is based on research published in Disability and Rehabilitation by Toovey & Coulston et al. (2024), involving interviews with nine Australian young people with limb difference aged between 9-16 years, and their parents. The research was conducted in partnership with researchers, clinicians and people with lived experience on the lands of the Wurundjeri Woi Wurrung peoples of the Kulin Nation and won the 2024 Sports Medicine Australia Best Paper in Physical Activity & Health Promotion. A generative AI tool (claude.ai) was used by the authors to create an outline of this article based on the original research.
About the Authors
Dr Free Coulston (PhD, DPT, BSci, DipCircArts) started her career as an international circus performer, transitioning to become a physiotherapist a decade later. Another 10 years on has found Free combining these passions in a PhD, looking at how circus activities may influence participation and developmental outcomes for children born preterm. As a post-doc researcher Free continues to work alongside people with lived experience in research, including expanding her work in co-design and collaborative research practices. She also holds a lecturing position at The University of Melbourne where she teaches the next generation of physiotherapists and strives to make the student experience more inclusive.
Dr Rachel Toovey (PhD, MPHTM, BPhysio (Hons)) is a Senior Lecturer and Physiotherapist with the Department of Physiotherapy at The University of Melbourne. Dr Toovey’s research centres around working with individuals, families, communities and organisations to create change and improve health through inclusive participatory research and evaluation, with a particular focus on physical activity.
Dr Peter Harcourt AM inducted into Sport Australia Hall of Fame
Congratulations to SMA Member, Dr Peter Harcourt AM, inducted into the Sport Australia Hall of Fame for his outstanding contribution to sports medicine. Over more than four decades, Dr Harcourt has been a global leader in sports medicine and anti-doping, working with the AFL, International Cricket Council, Basketball Australia, and the Commonwealth Games Federation. His work has shaped policies and practices that protect athlete health, safety, and integrity at both national and international levels, leaving a lasting impact on Australian and global sport.
Dr Sharon Stay appointed CMO of the A-Leagues
Sport and Exercise Physician Dr Sharon Stay has been appointed Chief Medical Officer of the A-Leagues, where she will lead medical policy and player welfare across both the men’s and women’s competitions. Her responsibilities include concussion management, infectious disease protocols, antidoping, and injury surveillance. Dr Stay is also Chair of SMA’s Sports Doctors Committee and is spearheading the FIMS Team Physician Development Course being delivered by SMA
Dr Donald Kuah appointed CMO of the Australian Winter Olympic Team
Congratulations to SMA Member, Dr Donald Kuah, appointed Chief Medical Officer of the Australian Winter Olympic Team for the 2026 Milan-Cortina Games. Dr Kuah will lead the provision of medical services across six sites in Northern Italy, supporting athlete health, safety, and performance throughout the Games. He succeeds Dr Peter Braun and is supported by OWIA Medical Services Manager Peter Caine. The appointment reflects Dr Kuah’s extensive expertise and leadership in elite sport medicine, and he looks forward to the challenges of guiding the medical team on the world stage.
Diet, disordered eating and risk of running injuries
DISTANCE RUNNING CONTINUES TO GROW IN POPULARITY WORLDWIDE, DUE TO ITS AFFORDABILITY, INCLUSIVITY, AND WIDE-RANGING HEALTH BENEFITS.
Regular running improves cardiovascular fitness, and is associated with better mental health, mood and sleep quality. It is also linked to a reduced risk of death, including death from cardiovascular disease and some cancers. However, many runners report getting injured. Some studies suggest that running-related injuries (RRIs) are experienced by 4345% of runners, of all abilities. Novice runners (those not running regularly in the past year) have nearly double
the injury rate of recreational runners. Most injuries involve chronic soft tissue damage in the lower limbs, with symptoms typically lasting two to eight weeks. This can carry significant economic costs from health care use and time off work, not to mention discouraging long-term participation.
While many risk factors have been proposed, evidence remains limited. For short-distance runners (≤20 km/ week), higher injury risk is linked to male sex, older age, higher body mass
index (BMI), no running experience, and prior non-running injuries. Among long-distance runners (>20 km/week), previous RRIs are the strongest predictor of future injury. Other potential contributors include female sex and menstrual dysfunction, poor sleep, and sudden increases in training load.
Diet may also influence the risk of RRIs, with low energy availability (LEA) being a major concern. LEA occurs when energy intake doesn’t meet the demands of both exercise and essential physiological functions. While this energy mismatch can be intentional or unintentional, certain behaviours such as disordered eating, can exacerbate LEA risk. Chronic
ERIN A. COLEBATCH
DR ALISON M. HILL, University of South Australia
Photo:
lzf/Getty Images
LEA, where energy mismatch occurs over an extended period, can lead to nutrient deficiencies, which subsequently contribute to fatigue, low bone mineral density, and stress fractures. Hormonal changes, such as reduced estrogen in females and testosterone in males, may further increase injury risk. Research linking other dietary factors and RRIs is limited.
Two systematic reviews have included dietary components in their exploration of risk factors for RRIs. Both reviews are nearly a decade old and did not specifically target dietary factors. Only two prospective cohort studies with dietary data from young female athletes in the USA were included. The evidence was low-quality and inconsistent, making it difficult to draw clear conclusions. We determined that an updated analysis was necessary and sought to collate evidence from studies evaluating associations between diet, risk of disordered eating, and RRIs in adult distance runners. These findings may inform better nutrition strategies to support injury prevention, long-term participation, and population health outcomes.
Study selection and data extraction
We searched different databases (including Ovid MEDLINE, PubMed, Embase, Ovid Emcare, CINAHL, SPORTDiscus, PyscINFO, Scopus, and Web of Science) for articles that mentioned terms related to running and athletic injury. Dietary terms were intentionally excluded in our search to avoid missing studies where diet was a secondary outcome. This is because secondary outcomes may appear in the body of an article but are typically not mentioned in the title, abstract and key words, which is how articles are identified in the search. Once we identified studies looking at RRI, we download the full-text article and checked that it was written in English and published in a peer-reviewed journal. We then screened the article for the following:
ٚ Study design: prospective cohort (i.e. follow participants over time)
ٚ Participants: adult (≥18 years) distance runners whose primary sport was running
ٚ Outcome: running-related injury
ٚ Diet-related exposure: assessment of energy intake, energy availability (EA), nutrients, dietary patterns, or eating behaviours
Studies that met these criteria were included in our review, and we extracted data related to study characteristics (e.g. design, duration), population (e.g., age, gender, BMI, weekly running volume, athlete classification), injury definitions (general RRI or bone stress injury (BSI)), dietary assessment methods, dietary risk factors (e.g. energy, macroand micronutrient intake, alcohol, eating behaviour) and injury risk outcomes (e.g. injury counts, odds ratio). If data were unclear or missing, we attempted to contact authors. Studies were excluded if we couldn’t obtain the data. We also checked the methodological quality of each study using the JBI Checklist for Cohort Studies, with studies rated as low, moderate, or high quality.
Analyses
Meta-analyses were performed when 2 or more studies reported comparable outcomes. We used a random effects model to calculate standardised mean differences (SMD) or odds ratios (OR) with 95% confidence intervals. Heterogeneity was assessed using the I² statistic, and subgroup analyses were conducted by injury type and sex. Findings were deemed significant when p <0.05. Certainty of evidence was assessed using the GRADE framework. Studies were downgraded based on study quality, consistency, precision, and directness.
These processes are consistent with guidelines for conducting a systematic review and meta-analysis (i.e. PRISMA). The protocol was registered with PROSPERO (CRD42022323627).
Populations and injury types
Some studies suggest that running-related injuries (RRIs) are experienced by 43-45% of runners, of all abilities. Novice runners (those not running regularly in the past year) have nearly double the injury rate of recreational runners.
Fifteen studies with 5,942 runners were included in the review (details presented in Table 1). Participants were recruited from the USA, Australia, Japan, New Zealand, and the Netherlands. Six studies included only female runners, three only males, and six both sexes. General RRI was assessed in six studies (n=5,192, recreationally active to trained/ developmental runners), while BSI was the focus in nine studies (n=750, trained/developmental to elite/ international level runners). Compared to studies of general RRI (18-53 years, 22–23.6 kg/m²), studies investigating BSI involved younger runners (18–26 years) with lower average BMIs (19.3–22.9 kg/m²). Injury definitions for general RRI varied but mostly involved self-reported reductions in training, while BSI definitions were consistent across studies and confirmed with medical imaging. The follow-up period ranged from 9 days to 12 months for general RRIs and 1 to 2 years for BSIs.
Associations between diet and injury
Commonly investigated dietary factors included total energy intake (5 studies),
Diet, disordered eating and risk of running injuries
macronutrients (carbohydrates, protein, fat; 5 studies), micronutrients (calcium, iron, vitamin D; 6 studies), dietary fibre (3 studies), alcohol (6 studies), dairy (2 studies), and disordered eating risk (3 studies). Four studies used the Triad Cumulative Risk Score, including LEA with or without disordered eating. Single studies explored additional micronutrients and dietary patterns. No studies examined fat types or dietary preferences such as vegetarian or vegan diets. The findings from the meta-analyses are summarised in Table 2.
Energy intake and RRI
Contrary to previous inconclusive findings, our analysis found female
Table 1. Study characteristics
Author, date, country Runner
General RRI
Fokkema et al. 2023
runners with general RRI or BSI consumed significantly less total energy (-303 kcal/day) compared to uninjured runners (Figure 1). This association was independent of body weight or BMI, suggesting energy intake itself influences injury risk. The impact of energy intake on injury in males remains unclear due to limited and inconsistent data.
Nutrients and RRI
Carbohydrate intake, often reduced during energy restriction, has been implicated in impaired bone formation and immunity; however, our results found no association between carbohydrate intake and injury risk in either sex. Protein intake generally met
Netherlands Tier 1-2 runners
Male n= 551; Female n= 443
Data available for combined sex only
42 ± 12 years
BMI 23.5 ± 2.7kg/m2
Gerlach et al. 2008
USA
Lagas et al. 2019
Netherlands
Satterthwaite et al. 1999
New Zealand
van Middelkoop et al. 2008
Netherlands
van Poppel et al. 2016
Netherlands
Mostly tier 2 runners, few tier 3 runners
Female, n= 86
18-53 years (37 ± 9 years)
BMI 22 ± 2.4kg/m2, BF% 19 ± 5.2
Tier 1-2 runners
Male n= 1020; Female n= 909
Data available for combined sex only
42 ± 12 years
BMI 23.6 ± 2.9kg/m2
Tier 1-2 runners
Male n= 707; Female n= 168
Data available for combined sex only
<25 - >40 years (no mean, SD or range)
Tier 1-2 runners
Male n= 694
44 ± 10 years
BMI 23.5 ± 2.1kg/m2
Tier 1-2 runners
Male n= 412; Female n= 202
Data available for combined sex only
44 ± 11 years
BMI 23.1 ± 2.5kg/m2
6 weeks
12 months
Energy, protein, total fat, dietary fibre, vitamins A, B6, B12, C, D, E & K, calcium, copper, iron, magnesium, zinc, risk of disordered eating (Eating Attitudes Test-40)
Tier 2-3 track & field athletes in a variety of running events
Male n= 49; Female n= 46
Data available for sex combined and separated
20 ± 2 years
BMI female 21.1 ± 1.8kg/m2, male 21.8 ± 1.7kg/m2
Tier 2-3 runners
Female n= 71
22 ± 3 years (range18-26 years)
BMI 21.3 ± 2.0kg/m2, BF% 23.3 ± 5.4
Tier 2 & 3 cross country runners
Female n= 127
22 ± 3 years (range 18-26 years)
BMI 21.2 ± 1.9kg/m2, BF% 23.0 ± 5.3
Tier 3 middle & long distance runners
Male n= 80
20 ± 1 years
BMI 20.9 ± 1.6 kg/m2
Tier 2 & 3 runners
Female n= 125
22 ± 3 years (range 18-26 years)
BF% 18.4 ± 6.1
Tier 4 middle & long distance runners
Female n=114
19.0 ± 1.1 years
BMI 19.9 ± 1.5 kg/m2
Tier 4 cross country runners
Female n= 58
20 ± 1 years
BMI 22.9 ± 2.7 kg/m2 (for all athletes, no data for cross-country only)
Tier 3 long distance runners
Male n= 41
19 ± 1.0 year
BMI 19.3 ± 1.2kg/m2, BF% 7.5 ± 1.9
Tier 4 middle distance & distance runners
Male n= 24; Female n= 15
Data available for sex combined and separated
18-23 years
BMI: Male 21.2 ± 1.5kg/m2, Female 19.8 ± 1.0kg/m2
Study duration
12 months
Risk factors evaluated
Energy, carbohydrate, protein, total fat, dietary fibre, calcium, phosphorous, sodium, caffeine, alcohol, risk of disordered eating (Eating Attitudes Test-40)
2 years
Mean 1.85 years per person
Mean followup 1.96 years
2 years
Mean followup 2.2 ± 1.2 years
109 ± 80 days
Energy, calcium, risk of disordered eating (three subscales of the Eating Disorder Inventory – drive for thinness, bulimic tendencies and body dissatisfaction subscales)
Calcium, dairy products, risk of disordered eating (three subscales of the Eating Disorder Inventory – drive for thinness, bulimic tendencies and body dissatisfaction)
Risk of Male Athlete Triad (Modified Female Athlete Triad Cumulative Risk Assessment; includes a criterion of “Low EA with or without disordered eating/eating disorder*”)
Energy, total fat, dietary fibre, vitamins C & D, calcium, iron, phosphorous, potassium, dairy products, diet patterns, fruit and vegetables
Triad Cumulative Risk Assessment (includes low EA criterion determined from modified EDE-Q 6.0, physician notes and clinical evaluation)
or exceeded athlete recommendations (1.4-2.0 g/kg/day), and did not differ between injured and uninjured runners. In contrast, a lower total fat intake (-20g/day) was significantly associated with injury in females (Figure 2). Fat plays essential roles in nutrient absorption, hormone production, and inflammation regulation, all relevant
to musculoskeletal health. Injured females consumed fat at the lower threshold of recommendations (20% of total energy), while intake was similar between injured and uninjured males (~30%). Future research should explore the influence of specific fat types, such as omega-3 fatty acids, known for anti-inflammatory effects.
No association was found between calcium intake and injury, possibly due to adequate calcium consumption (>1000 mg/day) across participants. Interestingly, while injured runners had lower dietary fibre intake (-3 g/ day, combined sexes) compared to uninjured runners, their average intake exceeded recommendations.
Diet, disordered eating and risk of running injuries
Table 2 . Effect of energy and nutrient intake on risk for injury based on sex
1: Forest plot of studies comparing differences in total energy intake (kcal/day) between injured and uninjured runners, by sex.
Bennell et al. 1996*
Cobb et al. 2007*
Gerlach et al. 2008**
Test for heterogeneity: Q(2) = 0.36, p = 0.83, I2 =
Test for overall effect: z = -2.59, p = 0.01
Bennell et al. 1996*
Toraishi et al. 2020*
Test for overall effect: z = 0.43, p = 0.67
Test for overall effect: z = -1.67, p = 0.10
Test of group differences: Qb(1) = 3.86, p = 0.05
Emerging evidence suggests dietary fibre may influence injury risk via gut microbiome modulation and antiinflammatory pathways. However, excessive fibre intake in female endurance athletes may contribute to energy deficits and menstrual dysfunction, highlighting a complex balance that requires further research.
Alcohol intake was not linked to increased RRI risk in combinedsex analyses. However, studies were limited by short durations, had varied definitions of “high intake,” and relied on self-reported injury, making conclusions tentative. Longer-term studies with standardised intake measures and sex-specific analyses are needed.
No increased injury risk was found in female runners with higher disordered eating risk. Several studies were not included in the meta-analysis due to inconsistent statistical reporting (i.e. they did not report an odds ratio). These studies also showed no significant differences in eating disorder risk between injured and uninjured runners. This was unexpected, given the relationship between disordered eating, lower energy intake, and LEA. More research is needed to explore the influence of risk of disordered eating on RRI risk in males.
Strengths and limitations
Strengths include a broad search capturing relevant dietary and eating behaviour data and inclusion of prospective cohort studies focused solely on runners. Limitations involve small sample sizes, heterogeneity in injury definitions (particularly general RRI), and methodological variability limiting some analyses. Most studies were of moderate quality with potential biases from self-report and confounders. Evidence certainty ranged from moderate for outcomes in females to low or very low for outcomes in males and combined sexes.
Figure
What next?
High-quality, long-term prospective studies using validated dietary and disordered eating risk assessments are needed. Adoption of the consensus definition of RRI developed by Yamato and colleagues will assist in standardising outcomes, and inclusion of diverse runner populations will improve applicability. Research gaps relevant to RRI include sexspecific effects of alcohol, and the role of dietary fibre intake and risk of disordered eating in males. Clinicians working with distance runners should assess LEA and fat intake, especially in female runners, and offer guidance to ensure adequacy of intake to reduce risk of RRI. Whilst the relationship between other dietary factors and RRI remains uncertain, it is advisable to support runners to meet national and sports nutrition guidelines. Education on LEA and the importance of screening should be extended to all support staff working with distance runners. Referral to professionals with expertise in LEA assessment and management is encouraged to better support athlete health.
For article references, please email info@sma.org.au
Figure 2: Forest plot of studies comparing differences in fat intake (g/day) between injured and uninjured runners, by sex.
Female
Bennell et al. 1996*
Gerlach et al. 2008**
Test for heterogeneity: Q(1) = 0.26, p = 0.61, I2 = 0%
Test for overall effect: z = -3.55, p = 0.00
Male
Bennell et al. 1996*
Toraishi et al. 2020*
Test for heterogeneity: Q(1) = 0.05, p = 0.82, I2 = 0%
Test for overall effect: z = 0.74, p = 0.46
Overall
Test for heterogeneity: Q(3) = 7.46, p = 0.06, I2 = 61%
Test for overall effect: z = -1.15, p = 0.25
Test of group differences: Qb(1) = 7.14, p = 0.01
Random-effects REML model
About the Authors
Erin Colebatch is an Accredited Sports Dietitian with 17 years’ experience across clinical dietetics and private practice. She holds a Bachelor of Science (2003) and a Bachelor of Nutrition and Dietetics (2008). In 2018, Erin completed the Sports Dietitians Australia Sports Nutrition Course, merging her professional skills with her personal passion for running. This led her to establish an online practice dedicated to supporting distance runners around the world with personalized nutrition strategies to enhance health and performance. Currently, Erin is in the final stages of a Master’s by Research, investigating the relationship between dietary and health-related risk factors for running-related injuries in masters (aged ≥35 years) distance runners. Her research aims to identify practical, evidence-based strategies to reduce injury risk and support masters distance runners to achieve lifelong participation in their sport.
Alison Hill is a Senior Lecturer at the University of South Australia and a member of the Alliance for Exercise, Nutrition and Activity (ARENA) research centre. An Accredited Practising Dietitian with training in sports nutrition and human movement, her research examines the effects of diet quality, nuts, polyphenols, and macronutrient composition on metabolic, cardiovascular, exercise, and musculoskeletal outcomes, including pain. With a strong focus on clinical trials, she has co-authored over 70 peer-reviewed publications, including randomised controlled trials, systematic reviews, and meta-analyses. Alison provides leadership within the nutrition research community through roles with the Nutrition Society of Australia and mentors allied health clinicians and early-career researchers, advancing evidence-based practice and innovation in clinical, sports, and pain-related nutrition research.
Photo: Jacob Wackerhausen/Getty Images
Understanding Concussion Disclosure in Elite Female Rugby League Players
Insights from the NRLW Premiership
SHREYA MCLEOD, Australian Catholic University
Despite these advancements, the on-field diagnosis of concussion remains challenging. In some instances, observable signs such as loss of consciousness, balance disturbances, or a blank or vacant look may be visible to trained spotters and the medical team. However, symptoms such as visual disturbances, headaches, sensitivity to light and noise and/ or cognitive difficulties are only perceived by the player and often not apparent to medical staff. Further, symptoms may be delayed or evolve over time, making it difficult for players to link them to a concussion. Therefore, the diagnosis of concussion relies heavily on athletes self-reporting their symptoms, along with sideline surveillance systems and clinical decision making by the medical team.
RESEARCH INTO SPORT RELATED CONCUSSION HAS GROWN RAPIDLY IN RECENT YEARS, ENHANCING OUR UNDERSTANDING OF THE IMMEDIATE AND LONGER-TERM EFFECTS OF THIS COMPLEX INJURY.
STUDIES HAVE EXAMINED PRE-INJURY RISK FACTORS, MECHANISMS OF INJURY, RECOVERY OUTCOMES AND RETURN TO PLAY PARADIGMS.
Studies have found that between 20 to 60% of potential sport related concussions are under-reported across all ages and sports. Increasing attention has been given to the behavioural factors influencing concussion disclosure, which are critical to ensuring athlete wellbeing and safety. Players’ decisions to disclose their symptoms may be influenced by their concussion knowledge, peer and coach attitudes towards reporting, and the broader sociocultural environment. Common barriers include fear of removal from play, concerns about letting their teammates or coaching staff down, not recognising symptoms as concussion related and perceiving symptoms as not serious enough to report. This may be a strong reason to downplay or not disclose symptoms, particularly when there is an important game. The fear of being perceived as weak or risk averse, combined with entrenched norms in sporting culture
that emphasise toughness or winning at all costs may discourage athletes from speaking up. These pressures may also be reinforced by social expectations to avoid disappointing teammates and/ or coaches.
When athletes who have sustained a concussion are not identified and removed from play, they are at increased risk of a prolonged recovery, which may include persistent physical, cognitive, emotional, and sleep-related symptoms. Continuing to participate in sport while concussed also raises the risk of second impact syndrome, a rare but potentially fatal condition that can occur when a second concussion is sustained before the first has fully healed. Moreover, repeat concussions, particularly those that are not managed appropriately, can increase the risk of secondary musculoskeletal injuries due to altered neuromotor control or impact overall brain health.
Improving concussion recognition and reporting is therefore critical to safeguarding athlete health and ensuring timely and effective management of head injuries.
Rugby league is a physically demanding, collision sport associated with a relatively high risk of head contact and concussion. In the National Rugby League (NRL), the incidence rate has been reported as 14.7 concussions per 1000 playing hours. Our research team identified an incidence rate of 11 concussions per 1000 match hours during the first three seasons of the NRLW Premiership. At that time, the competition consisted of four teams playing over seven rounds. Since then, the NRLW Premiership has undergone significant expansion. As of 2025, the Premiership features
12 teams, following the inclusion of the Canterbury-Bankstown Bulldogs and New Zealand Warriors, reflecting the growing scale and depth of the competition. During each preseason, NRLW players are provided with concussion education through mandatory club-based sessions. In addition to receiving concussion education, players undergo baseline assessments using validated tools such as the Sports Concussion Assessment Tool (SCAT) along with computerised cognitive testing through the Cognigram™ platform.
In professional men’s rugby league, 17% of 151 surveyed NRL players admitted to not reporting concussion symptoms during the 2018–2019 seasons, despite 85% receiving mandatory concussion education at their clubs. Similarly, in the U.K. super league, 20% of players surveyed did not report concussion symptoms to medical staff during the 2020 and 2021 seasons.
Our research team identified an incidence rate of 11 concussions per 1000 match hours during the first three seasons of the NRLW Premiership.
Research on concussion disclosure in professional women’s contact and collision sports remains limited. While some evidence suggests that female athletes may be more aware of their symptoms and more likely to report them, under-reporting still occurs.
Therefore, our study aimed to explore the extent of symptom disclosure and the reasons for non-disclosure among NRLW players in Australia, with the goal of informing future concussion education strategies.
Understanding Concussion Disclosure in Elite Female Rugby League Players
Insights from the NRLW Premiership
We conducted a cross-sectional survey, based on the survey administered by Longworth and colleagues (2021) to all NRLW players during the 2022 preseason. Of the 132 contracted NRLW players, 86 (65%) responded to the online survey. The survey was voluntary and anonymous in order to reduce bias.
The findings from this study offer valuable insights into concussion disclosure behaviours among NRLW Premiership players and serve as a preliminary reference point for future research in this area. Among the 86 respondents, 63% (n = 54) reported that they always disclosed a possible concussion during the past two seasons. However, 34% (n = 29) admitted to not reporting a suspected concussion on one or two occasions, and a small number (3%, n = 3) reported multiple instances of non-disclosure.
Additionally, 27% of players did not disclose symptoms during a medical assessment, which may have resulted in missed diagnoses, premature return-to-play decisions, or both.
These findings highlight a critical gap in symptom reporting, even in clinical settings where disclosure is essential for safe management.
The two most common reasons for not reporting symptoms were:
ٚ Concern about being ruled out of play or training (8/23; 35%)
ٚ Uncertainty about whether symptoms were related to concussion (8/23; 35%)
Despite these findings, the majority of players (86%; 74/86) reported attending mandatory concussion education sessions at their clubs.
When compared with available data from the NRL men’s competition, it appears that female players in the NRLW may be less likely to report concussion symptoms, potentially leading to a higher rate of undiagnosed concussions in women’s rugby league. This underscores the need for targeted strategies to improve symptom recognition, reduce barriers to disclosure, and foster a culture that prioritizes player health and safety.
This issue may be particularly relevant in the NRLW Premiership, which now spans approximately 14 weeks, compared to the 27-week season of the NRL men’s competition. Given this shorter timeframe, a concussion diagnosis in the NRLW could result in a player missing a slightly larger proportion of the season, increasing the pressure to remain available for selection. In high-stakes environments, this pressure may contribute to nondisclosure of symptoms, as players weigh the risk of missing games against their desire to compete.
Although some studies suggest that female athletes may be more attuned to their symptoms, the ‘win-at-all-costs’ mindset—observed in both male and
Among
the 86 respondents, 63% reported that they always disclosed a possible concussion during the past two seasons. However, 34% admitted to not reporting a suspected concussion on one or two occasions.
female contact sport athletes—can override health concerns, leading to decisions that prioritize performance over wellbeing. Compounding this challenge is the non-specific nature of concussion symptoms, which can overlap with common experiences such as dehydration, fatigue, or migraines. This ambiguity can make it difficult for athletes to recognize when symptoms warrant reporting.
These findings also align more broadly with previous research in other professional sports, including the U.K. based Super League, men’s and women’s rugby union and collegiate athletes where under-reporting of suspected concussions remain a concern. The tendency for athletes to not disclose their concussion related symptoms, particularly during or immediately after games, suggests the need for more objective assessment tools to support clinical decision-making, potentially with the addition of head acceleration exposure via instrumented mouthguards, fluid biomarkers and gait-based
assessments, to compliment the SCAT and cognitive testing measures.
Our study was not without its limitations. The retrospective design relied on self-reported data, which may have been affected by recall bias—particularly as the survey was conducted during the pre-season. The absence of open-ended questions limited deeper insights into reasons for non-disclosure. Additionally, anonymisation meant players could potentially complete the survey more than once and although responses were evenly distributed across clubs, they primarily reflected contracted NRLW players, rather than those in the reserve grade or under-20s.
Encouraging athletes to speak up about symptoms requires addressing the personal, social, and cultural factors that influence disclosure. Creating an athlete-centred environment— where wellbeing is prioritized and disclosure is normalized—can empower players to report symptoms, especially in the heat of competition.
Effective concussion education could also go beyond basic symptom recognition. It should:
ٚ Address common barriers to disclosure, such as fear of exclusion or uncertainty about symptoms
ٚ Be delivered in multiple formats and at various time points throughout the season
ٚ Include peer-led discussions and role model storytelling, especially from experienced players
ٚ Be designed with a developmental lens, embedding good practices from grassroots through to elite levels
Ultimately, all stakeholders—including coaches, medical staff, administrators, and teammates—play a role in fostering a supportive culture. This includes reframing injury disclosure as a positive and responsible action, discouraging the notion of playing through pain, and actively participating in education initiatives that promote athlete safety and long-term health.
For article references, please email info@sma.org.au
About the Authors
Shreya Mcleod is a Senior Lecturer and Course Coordinator of the Master of Sports and Exercise Physiotherapy program and an Early Career Researcher at the Sports Performance, Recovery, Injury and New Technologies Research Centre at Australian Catholic University. Her PhD focus was the identification of sport related concussion in women’s rugby league. She is also an APA Titled Sports and Musculoskeletal Physiotherapist and is a Queensland based contractor for Cricket Tasmania. She has previously been a Contract Physiotherapist for Cricket Australia, Cricket NSW, the Hobart Hurricanes WBBL, Singapore Sports Council and the WTA.
Photo: AleksandarNakic/Getty Images
For elite performance
People who Shaped SMA
Mark Brown
Q1: Can you briefly describe your journey from starting out in physiotherapy to your current role in research and sport?
A: I began my career in 1983 working in the NSW public hospital system, largely in intensive care and rehabilitation units including patients with amputations and spinal cord injuries. Some of the things I learned there turned out to be highly transferable to my later work in sports medicine including critical care skills and the ability to handle on-field emergencies, and also better informed me when working with athletes with a disability.
After a few years, I moved to private practice and became increasingly involved with sports medicine team roles including in rugby union, judo, and cricket. My personal background in cricket, particularly as a fast bowler with a history of stress fractures, motivated me to pursue postgraduate study in sports physiotherapy in 1995. After that I became involved in research as well, initially on spinal muscle control in fast bowlers. Around this time, I also had a career shift and moved into management roles in in health professional organisations, including the Australian Physiotherapy Association and Sports Medicine
A mentor once told me: “Think global, act local…” That principle stuck with me.
Presenting at the Fiji Association of Sports and National Olympic Committee in 2015
People who Shaped SMA
Mark Brown
Australia, and later completed an MBA to broaden my leadership capabilities.
One of the most formative experiences of my career came in 1997, when I was appointed Director of Physiotherapy Services for the Sydney 2000 Olympic and Paralympic Games. The 3 years in the lead up to the Sydney Games went like a blur. I was responsible for organising the host nation physiotherapy services at 63 venues, coordinating more than 530 physiotherapists. Sydney 2000 was a turning point for Olympic sports medicine programs as it was the first-time the IOC sanctioned physiotherapists to operate as primary contact practitioners at an Olympic Games, often acting autonomously at some venues due to limited medical staffing.
Following the Sydney Olympics, I was invited to contribute to physiotherapy and medical planning and training for subsequent events including the Athens and Vancouver Olympics. I also led the coordination of medical programs for the Pan Pacific Masters Games, the Australian University Games and Bridge to Brisbane for many years, and also the 2015 Pacific Games in Papua New Guinea, where I helped upskill local clinicians in sportspecific medical protocols. From 2014 to 2017 I was also an Australian Olympic Committee representative on the Oceania National Olympic Committees Medical Commission and as part of that developed a training program for sports medicine personnel that has since been run in many countries throughout the Pacific.
Since 2017, I’ve been based at Australian Catholic University, coordinating student delivered health clinics, and developing and teaching into units in the postgraduate Masters of Sports and Exercise Physiotherapy program. I’m also undertaking a PhD on musculoskeletal master’s athletes, with a focus on improving injury prevention and injury management strategies for older athletes, with the goal of improving lifelong participation in sport and physical activity.
Q2: What emerging trends in your research show the most promise for reducing injury risk or boosting performance in elite or community sport?
A: My research focus has been on improving safety and sustainability in sport including in community and Masters levels, where an injury can have significant long-term health implications. One area of interest is neuromuscular training for injury prevention. There is strong evidence that Interventions that improve muscle control may reduce knee, ankle, and hamstring injuries across a range of sports. But a challenge has been convincing injury some coaches and athletes that injury prevention is on the same continuum as athlete availability and performance. Another area of interest is sports taping, including the effects of injury prevention taping techniques on measures of sporting performance. There has been ongoing debate about whether taping hinders performance. Our research has found that appropriately applied taping doesn’t compromise athletic performance, although it might affect an athlete’s perception of performance. This is good news for athletes who use tape as a preventive measure.
Fiji CPR training in 2015
Q3: How do you juggle clinical work, research and sport involvement, and what keeps you motivated?
A: The balance works because there is an overlap between all three areas. Clinical work keeps me connected with the athletes who hopefully will be the beneficiaries of research and the subsequently improved approaches to preventing and managing sports related injuries.
What drives me is the ability to make a measurable difference. Whether it’s helping an individual athlete return from injury, shaping a national training framework like I did when I was working for SMA, or mentoring a student into a fulfilling career, there’s impact at every level. Whether working
The best opportunities often emerge at the intersections of clinical, academic, and sporting environments.
with elite athletes or community sport there is a sense of belonging that comes with being part of a team. Also, even after decades in the profession and within the sports medicine world, I still find everything to do with human movement and performance very interesting! On top of that, the landscape keeps changing with new technologies, new sporting codes and rules, new generations of clinicians. It’s exciting to be part of that evolution.
Q4: How has being part of Sports Medicine Australia shaped your career and opened up opportunities?
A: SMA has played a defining role throughout my career, offering opportunities, networks, and direction that have shaped both my clinical and academic work. Early on, SMA provided a gateway to professional development and multidisciplinary networking. It connected me to a national community of like-minded professionals and introduced me to mentors and collaborators not only from physiotherapy, but also medicine, psychology, podiatry and sports science. Straight away I recognised that we shared goals, not just our ability to provide effective recommendations and interventions, but also that SMA was a vehicle to educate and encourage the community to be involved in safe physical activity.
My involvement also led directly to opportunities that accelerated my career, including developing my teaching skills through involvement in the Safer Sport Program, contributing to the development of training modules, and participating in policy and position paper development. These roles helped build my skills, confidence, and credibility working in elite sport and academic settings.
With fellow sports physiotherapist Maria Constantinou at the Vancouver 2010 Winter Olympics, whom I met at Athens 2004 and have now been married to for 20 years.
People who Shaped SMA
Mark Brown
In 2004, I formally began working for SMA as the Queensland Executive Officer. At the time, I’d recently moved to Queensland and had just stepped away from a role with the Australian Physiotherapy Association. What was initially described to me as a short-term transitional appointment turned into a 13-year tenure. During that period, SMA Queensland underwent major structural and strategic changes. The organisation had been heavily reliant on state government funding, a model I recognised as unsustainable. Working closely with the Queensland Board, we restructured operations, shifted to a more self-reliant model, and later contributed to SMA’s transition to a unified national structure.
With my background in physiotherapy, I contributed to content development, including editing the 10th edition of Sports Medicine for Sports Trainers and updating several of SMA’s
SMA has played a defining role throughout my career, offering opportunities, networks, and direction that have shaped both my clinical and academic work.
educational fact sheets. I also led the implementation of SMA becoming a registered training organisation.
Internationally, along with Michael Kenihan and Nello Marino, I managed the expansion of SMA’s Safer Sport program through train-the-trainer
initiatives in Hong Kong and Papua New Guinea. The model involved educating local health professionals to adapt and deliver SMA’s safety content for their own communities, and it has since been adopted in other countries as a blueprint for grassroots sports safety education.
One of the more rewarding initiatives we developed in Queensland was the Emerging Researchers Award, part of our annual state conference. It gave Honours and Masters students the opportunity to present their work using the same criteria and format as SMA’s national conference. Many participants later progressed to national presentations and even further academic or professional achievements. Supporting the next generation of researchers and clinicians in this way was a meaningful part of the role.
During this time, we also responded to emerging issues in sport. Working with Dr Anita Green, we developed tailored resources for women in contact sports, an area previously underserved in sports medicine. In parallel, we were increasingly focused on the growing awareness of concussion and its long-term consequences, contributing to resource development and advocacy in that space as well.
Looking back, my time as Executive Officer was marked by significant change, both within SMA and in the broader sports health landscape.
A mentor once told me: “Think global, act local.” That principle stuck with me. Whether developing a local training program or contributing to national policy, I always approached the work with that mindset, aiming for quality and impact, regardless of scale.
Director of Physiotherapy for the 2000 Sydney Olympics and Paralympics.
One of SMA’s greatest strengths is its ability to bridge theory and practice. The emphasis on evidenceinformed care, supported through access to high-quality education, research, and thought leadership has been invaluable in keeping my work current and clinically relevant.
Equally important is the sense of community SMA fosters. Through conferences and events, as well as within sports medicine teams, I’ve collaborated with sports physicians, sports scientists, dietitians, and psychologists. These relationships have enhanced the quality of care we deliver to athletes and reinforced the importance of a truly interdisciplinary approach.
Q5: You’ve been actively involved in several SMA Member Committees, offering valuable insight. Could you briefly share your experience and the focus of your contributions?
A: Over the years, I’ve contributed to several SMA committees. My earliest involvement with SMA was with the NSW Branch teaching community education courses especially around injury prevention and acute injury management. Initially, I think I learned more than I contributed from the more experienced people who were already involved. In the late 1990’s I was on the NSW SMA Board of Directors and was involved with developing protocols for responding to serious incidents at sporting events, including spinal injuries and cardiac arrests, and an education package for clinicians attending the Paralympic Games, focusing on issues relevant to athletes with disabilities such as pressure injury prevention and differences in thermoregulation and other topics often missing in standard
training. After concluding my time as an employee of SMA in 2017 I’ve continued to be involved, including on the Executive Board of the SMA Fellows as Treasurer since 2020.
Q6: How do you support and mentor the next generation of physiotherapists entering clinical and research careers?
A: Mentoring is one of the most fulfilling parts of my current role. At ACU, I teach undergraduates and the postgraduate Master of Sports and Exercise Physiotherapy program, where I help students develop both technical competencies and broader professional skills. I also supervise research students, guiding them through the research process while encouraging a strong clinical foundation.
I try to model a well-rounded professional identity as someone who
can operate across academic, clinical, and sporting environments. Students often think they need to pick one lane early, but I encourage them to remain open. The best opportunities often emerge at the intersections.
Outside the classroom, I promote involvement in organisations like SMA. Getting engaged in the professional community early helps young physiotherapists build networks, stay current, and understand how policy and research shape practice.
I also share stories including what’s gone well, and what hasn’t. It’s important for early-career clinicians to know that success doesn’t follow a straight line. There are setbacks, shifts in direction, and unexpected opportunities. The key is staying curious, committed, and willing to grow.
Venue Medical Manager for Triathlon, Marathon, and the Aquatics Centre at Gold Coast Commonwealth Games 2018.
5 minutes with Associate Professor Melanie Hayman
Q1. Can you briefly share your career journey in health sciences and what first sparked your interest in the field?
From a young age, I had a deep love for sport, it was a constant in my life and naturally led me to pursue a Bachelor of Human Movement Science at CQUniversity, majoring in Sport Management. After graduating, I began my career at Bond University on the Gold Coast in a sport and recreation role. While I loved the job, I found it challenging to work behind the scenes while others were out on the field.
After three years, I shifted direction and completed a Masters of Educational Practice at Bond University. For 18 months, I balanced full-time work with full-time study, graduating with high distinction. I then returned to Rockhampton to take on a Director of
Sport role, which perfectly blended my interests, coordinating and managing sport while also teaching HPE.
When I became pregnant with my son, I faced a career crossroads. I couldn’t return to my Director role part-time, and I didn’t want to work full-time. Throughout my pregnancy, I remained highly active but was frustrated by the inconsistent and sometimes outdated advice I received from health professionals. This frustration sparked a desire to explore the area further.
A pivotal moment came over coffee with my mentor, Professor Peter Reaburn, who encouraged me to consider a PhD. I had little idea what I was getting into but embraced the challenge, completing my doctorate with the support of an APA scholarship while also running a personal training business and teaching casually.
In my final PhD year, I was offered a continuing academic position at CQUniversity, where I now work as an Associate Professor in Health Sciences. I teach research-related courses to students from a variety of health disciplines, and my research focuses on two key areas:
1. Improving exercise guidance for recreational and elite athletes during pregnancy and postpartum.
2. Shaping policy to better support female athletes from preconception to parenthood, so they are not forced to choose between athletic careers and motherhood.
Q2. Your research highlights physical activity during pregnancy. What key insights have emerged, and how have they shaped practice or policy?
Historically, pregnancy was viewed with caution, and many physical activity guidelines, though well-intentioned, were based on limited evidence. As a result, women were often advised to rest and avoid exercise. Despite strong contemporary evidence showing physical activity during pregnancy is both safe and highly beneficial, these outdated perceptions still linger.
Research now clearly demonstrates that regular physical activity during pregnancy reduces the risk of many pregnancy-related complications, including gestational diabetes, hypertensive disorders, excessive
(Left) At the IOC headquarters last year for a current research project (2024).
Best-practice recommendations launch, including Federal and State Ministers of Sport, Mattie Clements (Director of the AIS) Rach Harris (Female Performance Health Initiative (FPHI) – Lead) and my PhD students Boden and Jasmine.
weight gain, and the need for obstetric interventions. It also supports mental health and postpartum recovery. Yet, women still frequently receive inconsistent or conflicting advice such as being told they should not begin exercise once pregnant if they were not already active. Instead, inactive women should be encouraged to commence activity if not already active.
Healthcare providers play a critical role in changing this narrative, but inconsistent counselling and limited training in exercise prescription remain barriers. My research contributes to bridging this gap by informing national and international guidelines, creating educational resources, and promoting clear evidencebased recommendations, such as encouraging women to engage in 150–300 minutes of moderate to vigorous activity each week, including both aerobic and strength-based exercise.
For more guidance, see: https:// pubmed.ncbi.nlm.nih.gov/35418334/
Q3. What major challenges or gaps have you observed in public understanding or healthcare delivery around women’s health and exercise?
The biggest challenge is the persistence of outdated beliefs about safety and risk. Although the evidence base has grown substantially, these misconceptions continue to influence public opinion and, at times, clinical practice. Healthcare providers may lack confidence or the training to prescribe safe, appropriate exercise, which leads to women receiving vague, inconsistent, or overly cautious advice.
Addressing these gaps requires consistent, evidence-informed messaging across all health professions, as well as proactive encouragement for women to maintain or adopt healthy physical activity habits during pregnancy and postpartum.
Q4. You’re presenting in two symposia at 2025 ASICS SMA Conference. What key themes or takeaways can attendees expect, and why are they important?
The first symposium will discuss the newly released 2025 AIS Best Practice Policy and Practice Recommendations. Developed through a rigorous three-phase research process, these recommendations include over 100 individual support provisions grouped into 14 key themes, including communication, education, access to health professionals, childcare, travel, funding, facilities, and contract flexibility. Together, they form a practical blueprint for sporting organisations to better support athletes from preconception to postpartum, promoting athlete wellbeing, gender equity, and sustainable career pathways.
The second symposium will highlight the Women’s Tennis Association’s pioneering education initiative for female athletes. This intervention, integrated into the Annual Player Physicals, addresses femalespecific health considerations such as menstrual cycle, breast and pelvic health, pregnancy, and postpartum recovery. It offers practical recommendations for clinicians and sporting organisations, with the aim of promoting informed decision-making, peak performance, and long-term health.
(Left) Recent trip to Canada, working at the esteemed University of Alberta (2025).
At the WTA Miami Open (2024).
Sports and Exercise Medicine in Malta
DR
LUCIENNE ATTARD MD, University of Malta
MALTA, ONE OF EUROPE’S SMALLEST AND MOST DENSELY POPULATED NATIONS, HAS A VIBRANT AND GROWING SPORTS CULTURE.
Despite its modest size of just 316 square kilometres, the island supports a population of approximately 545,405, with an estimated 65,000 individuals actively involved in organized and recreational sports. This includes around 1,000 elitelevel athletes who compete on national and international stages. Within this dynamic environment, Sports and Exercise Medicine (SEM) has evolved from an informal, voluntary practice into a formalized and crucial medical specialty, gaining increasing recognition for its public health significance.
The Evolution of SEM in Malta
The journey of SEM in Malta began informally approximately four decades ago. It was pioneered by dedicated general practitioners and physiotherapists who, driven by a passion for sports, provided their services to local football teams and managed athletic injuries in other sports, many times on a voluntary basis. This foundational work was essential, providing early practitioners with invaluable field experience and establishing the groundwork for future development. Voluntary work still plays a big role in Maltese sport.
A pivotal moment occurred in 2011 with the passing of the Healthcare Professions Act, which formally recognized SEM as a primary medical specialty. This legislative milestone was a game-changer, paving the way for the creation of a Specialist Register.
In 2012, the first two SEM physicians were officially registered, marking the beginning of a new era. Today, the number has grown to eight registered SEM specialists, each bringing a diverse range of expertise from backgrounds such as military medicine, rheumatology, occupational medicine, orthopaedics, and family medicine. This multidisciplinary blend of knowledge enriches the specialty and allows for a holistic approach to patient care.
In 2015, SEM was fully integrated into Malta’s National Health Service (NHS) with the appointment of the
Photo: Krivinis/Getty Images
Sports and Exercise Medicine in Malta
first SEM Consultant. Currently, Mater Dei Hospital (which is Malta’s main and largest general hospital), offers SEM services, with two consultants providing dedicated outpatient care. The discipline is also established in the private sector, offering patients a wider range of options for specialized treatment.
A significant recent development is the approval of an in-house training program for SEM specialists. This comprehensive six-year program is designed to cultivate the next generation of experts. Eligible trainees are required to have a strong foundational experience in core medical fields, including medicine, surgery, accident and emergency (A&E), or general practice. The curriculum is meticulously structured, with rotations through SEM clinics, orthopaedics, and various medical and surgical departments. A strong emphasis is placed on key areas such as cardiology, rheumatology, respiratory medicine, and public health, ensuring trainees are well-rounded and equipped to handle the complex needs of athletes and the general population.
In 2012, the first two SEM physicians were officially registered, marking the beginning of a new era. Today, the number has grown to eight registered SEM specialists, each bringing a diverse range of expertise from backgrounds such as military medicine, rheumatology, occupational medicine, orthopaedics, and family medicine.
Medical Education and the Expansion of SEM Services
Malta’s long-standing and robust medical education system provides the essential support for specialized training like that required for SEM. The roots of medical education on the island date back to the 17th century,
influenced by Malta’s strategic role in Mediterranean healthcare and the legacy of the Knights Hospitalier of St John. The University of Malta was established in 1771, and it’s Medical School provides a five-year degree program that integrates academic teaching and clinical training at Mater Dei Hospital.
In recent years, Malta has expanded its medical education landscape through international partnerships, most notably with Queen Mary University of London, which established a medical campus in Gozo. This initiative marked the first foreign medical school on the island, further solidifying Malta’s position as a regional hub for medical training.
To obtain a license to practice medicine, newly graduated doctors are required to complete 24 months of Foundation training, rotating through different medical and surgical disciplines.
This strong educational foundation underpins the comprehensive services now offered by Maltese SEM professionals. They work collaboratively within multidisciplinary teams that include orthopedic surgeons, physiotherapists, and podiatrists to provide a wide array of services in both hospital and community settings, which include:
ٚ Injury prevention and rehabilitation: Offering specialized care for both acute and chronic conditions, from diagnosis to recovery.
ٚ Cardiac screening for athletes: A critical service that includes pre-participation screening and the thorough investigation of any abnormal results to ensure athlete safety.
ٚ Performance optimization: Working with both elite and recreational athletes to enhance their physical capabilities, improve technique, and prevent injuries.
Photo: Elvira Podolinska/Getty Images
Maltese SEM professionals have also adopted innovative and cuttingedge treatments to improve patient outcomes. This includes expertise in platelet-rich plasma (PRP) therapy and extracorporeal shockwave therapy (ESWT), which are used to treat a variety of musculoskeletal conditions. In a significant step forward, a dedicated Sports Cardiology unit has been established to conduct cardiac screenings and provide specialized rehabilitation services, ensuring the highest standard of care for athletes’ cardiovascular health.
Leadership and The Path Forward
The remarkable growth of SEM in Malta has been championed by key organizations. The Medical Commission of the Maltese Olympic Committee (MOC) has been instrumental in providing top-tier medical care for elite athletes and has actively promoted SEM education, particularly by offering scholarships for further sports-related education for doctors, physiotherapists and nutritionists. Similarly, the Maltese Association of Sports & Exercise Medicine (MASEM),
founded in 2008, has been a powerful advocate, successfully lobbying for the formal recognition of SEM as a primary specialty and fostering continuous education for healthcare practitioners.
Looking to the future, SEM is positioned as a core component of Malta’s National Strategy for HealthEnhancing Physical Activity (HEPA) 2025–2030. This ambitious strategy aims to increase physical activity levels across all age groups and recognizes SEM’s crucial role in combating sedentary lifestyles and the rising prevalence of chronic diseases.
As the field of Sports and Exercise Medicine continues to mature, ongoing investment in education, infrastructure, and policy will be vital. Fully realizing its potential means not only enhancing athletic performance and promoting safer sports participation but also leveraging SEM as a powerful tool for improving the overall health and well-being of the entire Maltese population. The transformation of SEM from its informal, voluntary roots to a structured, clinically and strategically important specialty is a testament to the dedication of its practitioners and a promising sign for the future of public health in Malta.
About the Author
Dr Lucienne Attard MD. MSc(SEM), FFSEM(UK), FFSEM(I)
Dr Attard is a Sports Physician currently serving as SEM Consultant at Mater Dei Hospital in Malta. She is also a Senior Lecturer at the University of Malta and the Chairperson of the Medical Commission of the Maltese Olympic Committee. President of the Medical and Scientific Commission of the International Committee for Mediterranean Games (ICMG). Recently-appointed member of the EOC (European Olympic Commission) Medical Commission. Founding member and General Secretary of MASEM. Former Chairperson of the Anti-Doping Commission (NADO Malta) and current TUE Committee member of several International Federations. She has served as Team Physician for Olympic Games, Commonwealth Games, Mediterranean Games and Games of the Small States of Europe.
JeremyLubrano Sports Trainer Spotlight
1. Can you walk us through your journey of becoming a sports trainer and what inspired this decision?
I’ve been involved in sport my whole life and played rugby league. Toward the end of my playing days at Eastern Suburbs in Brisbane, the club asked if I’d be interested in becoming a sports trainer. For a while, I was playing third grade, strapping first grade, and running water for the team, all at the same time. That hands-on experience made me realise how much I enjoyed helping athletes prepare, recover, and perform.
I did my Level 1 Sports Trainer course through SMA in 1996, followed closely by my Level 2 accreditation. I was living in Queensland then but later moved to New South Wales.
Two years ago, after a 35-year career in banking and financial services, I made the decision to shift into sports medicine and first response full time. Now I work as a subcontractor across a range of organisations, and currently I’m engaged with St George AFL and have just taken on a role with the GWS Giants AFLW team.
That includes on-field work as a sports trainer and massage therapy across training sessions and games.
2. What has been a standout moment in your experience as a sports trainer so far?
The most significant moment has been being offered the role with the GWS Giants AFLW team. I’ve worked in female professional sport before, including with the St George Dragons Tarsha Gale Cup side, but this is the first time I’ll be involved at the AFLW level. It’s a step up and a huge opportunity.
The role itself is diverse, I’m being employed in two different capacities, which keeps things interesting and allows me to use all my skills. Working at that level, and with such a professional team, is something I’m incredibly proud of.
3. How has your involvement with SMA impacted on your career as a sports trainer?
SMA has been central to my career from the very beginning. I completed my initial training through SMA and have always kept
my accreditations current, even while I was working within other systems like the NRL pathway.
What I appreciate most about SMA’s training is the strong guidance and evidence-informed content. It helped shape how I approach injury management, rehabilitation, and the overall role of a sports trainer. Wearing the SMA shirt also signals a level of professionalism, people notice it, enquire about it, and often associate it with quality training, which can open doors.
In fact, one client I initially worked with through an SMA contract later reached out and asked to work with me directly. That kind of trust and recognition really speaks to the credibility the organisation brings.
4. Can you share your experience with UniSport and how it has contributed to your knowledge and practice as a sports trainer?
My work with UniSport and the UniSport Indigenous Nationals has been incredibly valuable. In the early stages, I was often the least experienced trainer in the team, which gave me the chance to learn from those with broader backgrounds including paramedics and senior trainers. I picked up different ways to assess injuries, improve my taping technique, and improve my decision making under pressure.
Over time, I stepped into the role of senior trainer on site, taking on the responsibility of mentoring less experienced trainers. I made a point of not just showing them what to do but explaining the ‘why’ behind each clinical decision or technique. That process of guiding others deepened my own understanding, sharpened my communication skills, and ultimately strengthened my practice as a trainer. It reinforced that leadership in this space isn’t just about experience, it’s about elevating those around you.
UniSport has also exposed me to a wide variety of sports, including many I’d never worked in before, each one with its own demands and challenges. This exposure has pushed me to adapt quickly, broaden my clinical reasoning, and develop a deeper understanding of sport-specific needs, ultimately making me a more well-rounded and versatile trainer.
5. What is your advice to people wanting to get started as a sports trainer?
Take the jobs no one else wants! That’s honestly where the growth and connections happen. Be the person who says yes, who shows up early, stays late, and keeps learning.
Even if it’s a low-paying or three-hour gig at a trampoline centre, it still builds your experience and reputation. From there, people start to remember you, trust you, and offer you more work. That’s how I ended up in roles like the one I now have with the Giants.
I’d also strongly recommend continuing your education, the Level 1 Sports Trainer accreditation is a great start, but it’s not enough on its own. I went back to TAFE to undertake a massage course, trained under paramedics, and always looked for additional ways to upskill. Being calm and prepared in high-pressure situations comes from experience and good training. Finally, always be networking as in my experience your next opportunity is often one conversation away.