
FEATURING
• Rectus femoris injuries: what currently informs our practice?
• Women’s rehabilitation following anterior cruciate ligament reconstruction – what factors should be considered?
• 2025 Member Survey: Your feedback, our focus

• Rectus femoris injuries: what currently informs our practice?
• Women’s rehabilitation following anterior cruciate ligament reconstruction – what factors should be considered?
• 2025 Member Survey: Your feedback, our focus
02
From the Chair
Dr Kay Copeland reflects on recent progress, governance reform and new partnerships, as SMA evolves with its members and the sporting community.

From the CEO
Posters, partnerships, and packed-out events – Jamie Crain recaps a high-impact half-year as SMA sharpens its focus on safety, growth, and national reach.

Opinions expressed throughout the magazine are the contributors’ own and do not necessarily reflect the views or policy of Sports Medicine Australia (SMA). Members and readers are advised that SMA cannot be held responsible for the accuracy of statements made in advertisements nor the quality of goods or services advertised. All materials copyright. On acceptance of an article for publication, copyright passes to the publisher.
04
The future is here: using non-invasive electrical brain stimulation to improve outcomes following Anterior Cruciate Ligament Reconstruction
Dr Myles Murphy leads a proof-ofconcept study exploring whether anodal-tDCS alters quadriceps function during ACL rehab.


11
The prevention of ankle injuries in elite adolescent male Australian footballers
Jessica McDonald presents a targeted program to prevent ankle injuries in junior Australian Football, based on SANFL U18 data.
Publisher Sports Medicine Australia State Netball and Hockey Centre – Parkville 10 Brens Drive, Parkville VIC 3052 sma.org.au ISSN No. 2205-1244 PP No. 226480/00028
Copy Editors
08
The comfort of ASICS now in a Work Boot
Our major partner, ASICS, has partnered with Dr Chris Bishop to test a new work boot combining comfort and safety for physically demanding jobs.

Archie Veera and Rosie Davis
General Manager,
Membership Development
Sarah Hope
Design/Typesetting
Perry Watson Design
Cover photograph
Getty Images / Ilona Shorokhova
Content photographs
Author supplied; www.gettyimages.com.au
14
2025 Member Survey: Your feedback, our focus
SMA’s 2025 Member survey results reflect insights from professionals, students, and sports trainers.

22
2025 ASICS SMA Conference –Meet your keynote speakers
We’re excited to welcome our Conference keynote speakers, sharing cutting-edge research, insights, and fresh perspectives.


16
Rectus femoris injuries: what currently informs our practice?
Sam Pietsch examines the prevalence, biomechanics, and limited clinical guidance surrounding rectus femoris injuries in sport.

24
Women’s rehabilitation following anterior cruciate ligament reconstruction – what factors should be considered?
Melissa Haberfield highlights the lasting impact of ACL ruptures, with women facing poorer outcomes and lower return-to-sport rates.
29
Improving neck strength to reduce the risk of concussion in contact sports
Dr Felix Leung evaluates the high concussion risk in school rugby and investigates whether neck strength can help identify players at greater risk.

Physician Focus: Dr Trevor Law

People who Shaped SMA: Professor Dara Twomey

Sports Medicine in Finland

Sports Trainer Spotlight: Liesl Turley


At Sports Medicine Australia, we continue to evolve and grow with the needs of our members and the wider sporting community.
This year, the SMA Board has commenced a full review of our Constitution to ensure it remains fit for purpose, reflects contemporary governance expectations, and supports the long-term sustainability of our organisation. Member forums began at the end of May, providing an opportunity to walk through the review and invite feedback on the proposed changes. Your input will help shape the final recommendations to be presented for member approval at the AGM later this year.
Our annual Member Survey once again offered valuable insights into the priorities and perspectives of our community. A clear theme this year was the professional credibility that membership of SMA provides. It’s evident that being part of our multidisciplinary, national organisation is seen as a marker of quality and a commitment to best practice, and that trust in SMA continues to guide our work.
We’re pleased to announce a new strategic partnership with AUSactive, opening the door to fresh opportunities for collaboration across the health and active living sectors.
Our 2025 ASICS SMA Conference is also taking great shape, with early registrations indicating high interest. We have an exciting line-up of keynote speakers confirmed and are delighted to welcome Professor Nick Brown as this year’s Refshauge Lecturer. The calibre of abstract submissions has been exceptional, and our Conference Co-Chairs, A/Prof Kat Mills and A/ Prof Ryan Timmins, have curated a dynamic program that integrates keynote presentations with the breadth of research received. We’re pleased to see such enthusiasm and
thank our long-standing partner ASICS for their continued support. We look forward to seeing many of you in Hobart this October.
Each year in June, applications for ASMF Fellowship open, inviting eligible members to be considered for this important recognition. The new Fellows will be formally announced at the Fellows Dinner during the Conference – always a highlight as we celebrate the outstanding contributions of our Fellowship community, both new and longstanding.
We’re also pleased to announce a new strategic partnership with AUSactive, opening the door to fresh opportunities for collaboration across the health and active living sectors. By working together, we can promote safer, more inclusive participation in physical activity.
SMA remains committed to advancing sports medicine and supporting the broader sporting community. As we move through the second half of the year, we look forward to continued collaboration, innovation, and meaningful progress across our shared goals.

Dr Kay Copeland Chair, Sports
Medicine Australia

FROM THE CEO
As we approach the end of the financial year, it’s a great time to reflect on our achievements for the year and some of the strategic investments made to strengthen SMA’s profile and member value.
Our joint conference with ACSEP at the MCG in October was a real highlight and we are pleased to say we are currently working with the College on the next version of this important collaboration for 2026. Our major campaign for this year included a national Concussion Awareness Poster, developed by SMA off the back of the Australian Concussion Guidelines for Youth and Community Sport. Mailed to 38,000 schools and sporting clubs across the country and downloaded by another 5,000 users, this poster has helped continue raising awareness of the importance of the guidelines and adhering to the Graded Return to Sport Framework amongst grassroots sport. In our Education business, we’ve made significant upgrades to our core systems paving the way for new growth and opening up new opportunities.
Our first-ever Super Early Bird offer for the 2025 Conference in Hobart has
Our first-ever Super Early Bird offer for the 2025 Conference in Hobart has been a resounding success, with an exceptional response from members keen to secure their place early.
and quality of our speakers to our field. Visit our Events page to register.
We recently launched a significant three-year partnership with AUSactive, which will see SMA deliver First Aid and CPR courses to fitness professionals across the country. This reflects our continued commitment to supporting safe participation in sport and physical activity. A reminder to SMA members – you receive 15% off all SMA courses. Simply log in to the Member Portal to access your discount code and keep up to date.
been a resounding success, with an exceptional response from members keen to secure their place early. It’s encouraging to see such strong engagement in what promises to be another outstanding event. The Conference is our flagship, however throughout the year we run up to 50 events covering an ever-expanding array of topics, curated and facilitated by subject matter experts from within our membership and around the world. Attendee feedback typically averages more than 4.5 out of 5, a great testament to the contribution
In this edition of Sport Health, we feature emerging research on injury prevention and rehabilitation. Highlights include novel use of electrical stimulation in ACL rehab, targeted ankle injury prevention in junior football, insights into rectus femoris injuries, sex-specific challenges in women’s ACL recovery, and the role of neck strength in concussion risk.
We hope you find this edition of Sport Health insightful and engaging.

Jamie Crain CEO, Sports Medicine Australia
DR MYLES MURPHY, Nutrition and Health Innovation Research Institute, School of Medical and Health Sciences, Edith Cowan University WA; Institute for Health Research, The University of Notre Dame Australia, Fremantle WA (2024 SMA & ACSEP Conference – ASICS Medal for Best Paper Overall)

Following anterior cruciate ligament reconstruction, exercise-based rehabilitation is known to be the gold-standard intervention to optimise function and facilitate return to sport. Despite this people with anterior cruciate ligament reconstruction struggle to regain full quadriceps muscle activation and strength. As poor strength is associated with the ongoing dysfunction following anterior cruciate ligament reconstruction and has been linked to the progression of knee osteoarthritis progression, it is something that must be addressed. People with anterior cruciate ligament reconstruction have large deficits in voluntary muscle activation of both their reconstruction, leg, and their non-injured leg. These deficits are almost identical to what is seen in people with knee osteoarthritis.
It has been proposed that these deficits in muscle activation are the result of arthrogenic muscle inhibition, or AMI, which is associated with poor outcomes following anterior cruciate ligament reconstruction. This means that if an athlete cannot sufficiently contract and activate a muscle, it is harder to provide that muscle with sufficient loading and cause physiological adaptation. Essentially, you may be trying to work a muscle to its physiological limits, but neurophysiological changes are preventing that. One of the major drivers of AMI is dysfunction of the primary motor cortex of the brain and available evidence suggests that changes in cortical excitability persist and drive continued weakness following anterior cruciate ligament reconstruction.
One neurophysiological intervention that has been shown to alter primary motor cortex excitability is noninvasive brain stimulation. Transcranial direct current stimulation (tDCS) is one type of non-invasive brain stimulation whereby a direct current is sent through the cortex of the brain. Depending on stimulation parameters, tDCS can alter primary motor cortex excitability (e.g., it can increase excitability with anodal stimulation and decrease excitability with cathodal stimulation). Anodal-tDCS has been shown to increase primary motor cortex excitability, improving strength and motor control in both healthy and pathological populations. TDCS has also improved patient-reported outcomes in clinical populations, such as knee osteoarthritis.

Transcranial direct current stimulation (tDCS) is one type of non-invasive brain stimulation whereby a direct current is sent through the cortex of the brain.
Therefore, the primary objective of this proof-of-concept study was to determine if anodal-tDCS can alter quadriceps intracortical inhibition and facilitation in an anterior cruciate ligament reconstruction population after 6-weeks of application during exercise (from week 2 post- anterior cruciate ligament reconstruction). Our secondary objective included the evaluation of whether anodaltDCS can alter quadriceps maximal voluntary contraction.
I led a randomised, triple-blind, controlled trial for proof-of-concept comparing anodal-tDCS to sham-tDCS following anterior cruciate ligament reconstruction. Both the anodaltDCS or sham-tDCS was delivered
to the primary motor cortex for 20 minutes, three times per week, for 6-weeks from week 2 following anterior cruciate ligament reconstruction.
The tDCS devices were preprogrammed by a research team member to ensure the trial physiotherapists and participants were unaware of group allocation. Participants simply had to turn the device on and press the ‘go’ button until they felt the stimulation. We covered the bottom half of the tDCS device screen, so only the amount of stimulation ramping was displayed. However, in the sham group the stimulation ramping was incorrect.
The anode was positioned over the primary motor cortex and held in place using standardising sporting caps. The cathode was then secured on the upper arm (contralateral to the injured knee) via a fabric sweatband. The anode and cathode were connected to the underlying skin via 35mm x 35mm sponges. Saline solution was used to wet sponges, allowing enhanced conduction. All participants (both anodal-tDCS and sham-tDCS) were shown how to check sufficient sponge contact and confirmed that they received a sensation of tingling under the anode when the device was used and were advised this would fade. Therefore, the procedures for both anodal-tDCS and sham-tDCS were identical, except for the amplitude of the stimulation.
Using non-invasive electrical brain stimulation to improve outcomes following Anterior Cruciate Ligament Reconstruction
Both tDCS groups received the stimulation during routine exercise rehabilitation sessions. The exercise rehabilitation was delivered over 6-weeks and physiotherapistprescribed. Exercise rehabilitation was based on the standard post-operative protocol of the Orthopaedic Surgeon and informed by the research team. Exercise rehabilitation templates were stored within Physitrack®. Participants had access to the complete program on their smartphones using the PhysiApp®. The duration of the exercise intervention varied and became longer over the 6-weeks intervention window, but it was always within 20 to 60 minutes. Whilst templates were used as a guide, the program was adapted to the individual participant as able based on the judgement of the physiotherapist, however at a minimum, all programs comprised of:
1. A single joint exercise for each of the following muscle groups: abdominals; hip extensors; hip flexors, hip abductors; hip adductors; knee flexors; knee extensors; and ankle plantar flexors.
2. A multi-joint squat pattern (e.g., squat) and bend pattern (e.g., deadlift) movement.
3. One balance-based exercise (e.g., star excursion balance).
Participants completed the exercise intervention daily. However, only three sessions per week were required to be completed on-site at the rehabilitation gymnasium. During that time, the tDCS intervention would be delivered for the first 20 minutes of the exercise session, and then participants typically removed the device to complete the remainder of the exercises.

The excitability of the brain was assessed using transcranial magnetic stimulation, and we quantified inhibition [short-interval intracortical inhibition (SICI); long-interval intracortical inhibition (LICI)] and facilitation [short-interval intracortical facilitation (SICF)] of the quadriceps representation of the brains motor cortex. Quadriceps maximal voluntary contraction was measured using the VALD Force Frame.
We included 21 participants who were randomised to anodal (n=11) or sham (n=10) tDCS. Participants were predominantly male (n=13) and had a mean (standard deviation, SD) age of 24.4 (4.7) years.
Inhibition of the quadriceps representation in the primary motor cortex
For quadriceps SICI there was a significant group-by-time effect for anodal-tDCS (ß=0.519, p=0.028) and a significant effect for time
(ß=-1.421, p<0.001). For quadriceps LICI there was no significant group by time effect (ß=-0.217, p=0.543) or effect for time (ß=0.039, p=0.928).
Facilitation of the quadriceps representation in the primary motor cortex
For quadriceps SICF there was a significant group by time effect for anodal-tDCS (ß=-0.764, p=0.020) but not time (ß=0.504, p=0.383).
Quadriceps maximal voluntary contraction
For quadriceps maximal voluntary contraction there was no significant group by time effect for anodaltDCS (ß=-10.667, 95%CI=-59.166 to 37.953, p=0.667) or group effect (ß=-9.911, 95%CI=-78.145 to 58.323, p=0.776). However, there was a significant effect for time (ß=60.667, 95%CI=19.166 to 102.167, p=0.004).

This study provided proof of the efficacy of anodal-tDCS following anterior cruciate ligament reconstruction in reducing maladaptive quadriceps inhibition and facilitation. Further, we demonstrated that quadriceps strength was maintained even with a reduction in both primary motor cortex inhibition and facilitation. Thus, following anodaltDCS the brain is working less ‘hard’ to achieve the same motor output. If these results are maintained at longterm follow up this may mean that some complications of overactivity of the motor cortex will be less likely (e.g., activation of visual pathways of the brain for simple motor actions).
The entire study has been published in BMJ Open Sport and Exercise Medicine (BOSEM) and is available open access: https://bmjopensem. bmj.com/content/10/4/e002080


Dr Myles Murphy is an early-career clinician researcher at Edith Cowan University and a Sport and Exercise Physiotherapist consulting at SportsMed Subiaco. In 2022, Myles was awarded his PhD by the University of Notre Dame Australia (which was selected for an academy award by the British Journal of Sports Medicine) and he was inducted as a fellow of the Australian Sports Medicine Federation. Myles has > 75 peer-reviewed research publications on a variety of topics. He is an associate editor at leading sports medicine journals, such at the British Journal of Sports Medicine, BMJ Open Sport and Exercise Medicine, and the Journal of Orthopaedic and Sports Physical Therapy. Dr Murphy also has an established clinical career. Myles has worked for sporting organisations such as the Western Australia Cricket Association and consults for a number of national and international organisations, predominantly for tendon injuries. Myles is currently engaged in injury prevention partnerships with organisations such as the Perth Wildcats, West Coast Eagles Football Club and Western Australia Police Force.

The complete citation for this research is: Murphy MC, Sylvester C, Whife C, D’Alessandro P, Rio EK, Vallence AM. Anodal transcranial direct current stimulation (tDCS) modulates quadriceps motor cortex inhibition and facilitation during rehabilitation
following anterior cruciate ligament (ACL) reconstruction: a triple-blind, randomised controlled proof of concept trial. BMJ Open Sport Exerc Med. 2024 Dec 9;10(4):e002080. doi: 10.1136/bmjsem-2024-002080.
Many Australian workers in physically demanding jobs struggle to find comfortable footwear that meets the strict safety standards required to protect against workplace hazards. Conventional work boots have typically prioritised safety features like reinforced toe protection and elevated ankle support over comfort. ASICS has identified a market gap for work boots that blend superior comfort with crucial safety elements.

ASICS has long been committed to providing comfort and quality in footwear. We are now extending this dedication to the worksite with our new work boot range. In 2025, ASICS has released the CP6 S3 GTX BOA® MID-CUT work boot. Our boots are engineered to keep workers feeling agile while offering the necessary protection throughout their workday. ASICS work boots merge the renowned comfort of ASICS athletic footwear with robust safety features necessary for demanding work environments.
Upper Design: Our work boot features a lightweight upper with a breathable GORE-TEX™ membrane, effectively keeping water out. The innovative BOA® Fit System offers precise, micro-adjustable fitting that performs reliably in harsh conditions, ensuring easy customization for the perfect fit.
Safety Features: The composite toe cap, made of glass fiber-reinforced resin, provides robust protection capable of withstanding 200-joule impacts, meeting worksite safety requirements. As an added benefit, these boots are airport security-friendly, allowing wearers to pass through checkpoints without removal.
Comfort and Support: The midsole incorporates ASICS’ proprietary FLYTEFOAM™ technology and rearfoot fuzeGEL™, enhancing underfoot comfort. A 10mm heel gradient helps reduce stress on the lower limbs during long workdays.
Traction and Durability: The outsole features an advanced tread pattern for superior grip, making the boot slip resistant. Additionally, these boots are puncture-resistant, anti-static, and oil-resistant, ensuring durability and safety in various work environments.
To test and compare the new ASICS innovative work boot design in reference to industry-standard safety boots, ASICS Oceania partnered with Dr Chris Bishop PhD and his team at The Biomechanics Lab to complete testing of ASICS products.
When speaking to Dr Bishop, he said: “Clinically, we know footwear comfort is a significant barrier for millions of Australians who engage in active jobs that pose specific safety considerations / needs in footwear because of occupational hazards encountered as part of employment. These tradespeople experience some of the highest loads on their feet during a workday. When we sat down with groups of builders, plumbers and electricians, they told us they can clock up north of 20,000 steps per day on a mix of muddy sites, concrete slabs and uneven dirt terrain, not to mention being up and down ladders and on roofs. Their overwhelming feedback relating to footwear requirements was the need for comfort, lightweight and stability”.
Based on the feedback of talking to over 100 industry representatives, the team at The Biomechanics Lab went


about designing an analysis protocol that assess footwear’s ability to provide the needs outlined by the industry. Dr Bishop said “The range of footwear available to these workers has largely focussed on protective capacity associated with steel cap forefoot protection, high cut heels for ankle stability, and zip sided lacing systems to facilitate ease of putting on. What we tried to do in our study is design a methodology that investigated the actual comfort of the footwear, whilst still providing an assessment of the relevant safety features and protection
on job.” To assess the footwear, The Biomechanics Lab used advanced force platform and 3D motion capture data to assess the actual function of the boot, as well as the comfort of the boot out on the building site, compared to other industry comparators.
In compiling the results, when compared to industry comparators, the ASICS Work boot was the most comfortable boot tested in this study, as assessed by the tradespeople included. Not only was it the most comfortable boot tested, but it was the boot most likely to be purchased for purposes of work. In explaining the results, Dr Bishop said “what the participants loved was the lightweight nature of the boot, as well as the comfort of the midsole. It felt like they had a sneaker on, yet still felt they were secure and protected on site. What was most pleasing however was the lab data was consistent with the subjective feedback we got. The biomechanical data showed the ASICS boot was most stable side-to-side, without compromising the efficiency of walking.”
ASICS work boots merge the renowned comfort of ASICS athletic footwear with robust safety features necessary for demanding work environments.


Official journals of Sports Medicine Australia
Submission deadline:
30 September 2025

Learn more:
Sport-related traumatic brain injuries, especially concussions, are receiving increased attention from researchers and clinicians, yet many uncertainties remain, particularly in football (soccer), which is underrepresented in research despite its global popularity. Given the large number of players at all levels, football-specific research is needed to drive football-specific health-related protocol adaptations and potential rule changes.

Submit your research:

Read the special issue:

This special issue will consider articles on all aspects of concussion and head impacts in football including, but not restricted to:
Sport-related traumatic brain injuries, especially concussions, are receiving increased attention from researchers and clinicians, yet many uncertainties remain, particularly in football (soccer), which is underrepresented in research despite its global popularity. Given the large number of players at all levels, football-specific research is needed to drive football-specific health-related protocol adaptations and potential rule changes.
1) Prevention
2) Diagnosis
3) Treatment / Management
This special issue will consider articles on all aspects of concussion and head impacts in football including, but not restricted to:
4) Return-to play, /-competition, /-performance
1) Prevention
5) Long term health of veteran players
2) Diagnosis
3) Treatment / Management
4) Return-to play, /-competition, /-performance

5) Long term health of veteran players
This special edition of ‘Exercise-Oncology’ examines the emerging discipline of exercise-oncology, which explores the role of exercise in cancer control. Despite improvements in survival rate for most cancers, there is a growing population of cancer survivors living with side-effects and an increased risk of developing health complications from their treatment. Cancer survivors also experience increased risk of recurrence and mortality, and subsequently often have a reduced quality of life.
This special edition of ‘Exercise-Oncology’ examines the emerging discipline of exercise-oncology, which explores the role of exercise in cancer control. Despite improvements in survival rate for most cancers, there is a growing population of cancer survivors living with side-effects and an increased risk of developing health complications from their treatment. Cancer survivors also experience increased risk of recurrence and mortality, and subsequently often have a reduced quality of life.
The field of exercise-oncology has rapidly grown over the past 10 years, with benefits in physical, psychological and clinical outcomes for patients. This evidence is growing across different cancer types, and across the cancer continuum including before treatment (prehabilitation), during treatment, and after treatment.
The field of exercise-oncology has rapidly grown over the past 10 years, with benefits in physical, psychological and clinical outcomes for patients. This evidence is growing across different cancer types, and across the cancer continuum including before treatment (prehabilitation), during treatment, and after treatment.
JESSICA MCDONALD, University of South Australia (2024 SMA & ACSEP Conference – ASICS Best Poster in Sports Injury Prevention)
Background
Australian Football (AF) has the highest incidence of injuries when compared to other football codes like soccer and rugby. At the junior AF level, ankle injuries are consistently one of the most common injuries reported by injury surveillance studies. Indeed, a multi-season injury surveillance undertaken by our research team in the South Australian National Football League (SANFL) under-18 (U18) competition across the 2015 to 2021 season highlighted that ankle injuries were the most common injury type. This finding is not surprising due to the frequent changing direction, jumping, landing, and physical contact, that occur during AF- all of which are all considered risk factors for ankle injuries.
To counter this problem, our research team developed and tested a targeted ankle injury prevention program. The intervention program was designed based on previously successful ankle injury exercises and programs in sports with similar physical capabilities such as the FIFA 11+ program in soccer. Prevention of ankle injuries in junior AF was considered important not only due to the high incidence, but also because junior AF injuries increase the risk of future AF injuries throughout a senior playing career. As a result, each junior AF ankle injury prevented has long term flow on benefits to reducing injury risk.

Prevention of ankle injuries in junior AF was considered important not only due to the high incidence, but also because junior AF injuries increase the risk of future AF injuries throughout a senior playing career.
in elite adolescent male Australian footballers
The specific research aims were to:
1. Develop an injury prevention program specifically targeted at ankle injury prevention.
2. Determine the effectiveness of the specific program on ankle injury incidence compared to usual practice.
3. Determine changes in ankle stability and function before and after the program.
4. Explore the acceptability of the program by participating players and coaches.
The ankle injury prevention program was designed based on previously successful interventions, the collective expertise of the research team, and collaboration with relevant organisation staff at the SANFL. Previous interventions were identified using a search of academic research databases.
This experimental study was a nonrandomised control trial. A total of
214 male players (age ranging from 15-18) in the SANFL U18 competition consented to participating in the intervention in the 2022 season. The control data were historical ankle injury observations from 1,728 players participating in the same competition between 2015-2021. Ankle stability and function were measured for the intervention cohort at the start of preseason and the end of the competitive regular season. Player surveys and coach interviews were performed at the end of the competitive season.
Injury surveillance was conducted throughout the regular competitive season (18 games) using injury report forms provided to medical staff at each club. An ankle injury was recorded if a player was to miss at least one competitive season game. Ankle injury incidence (absolute number of ankle injuries), severity (number of games a player misses due to ankle injury), and burden (the product of ankle injury incidence and ankle injury severity per player) were the specific injury
outcomes. The same injury surveillance processes were in place for both the intervention and historical control seasons due to the long history of injury surveillance research collaboration between the research team and the participating competition.
The multiple hop test was used to a test ankle stability and function. Players were required to hop along a diagonal course as fast as possible with their hands on their hips without losing their balance. Players had three attempts on each leg. The outcome measures were: (1) average time to complete the course and (2) total number of balance errors. All attempts were video recorded and reviewed to determine error counts.
The ankle intervention program was developed as a gradual, progressive 3-stage program. The intervention program increased in intensity and difficulty across three stages. Stage one


was activation and strength exercises focussed on balance, stage two focussed on change of direction and sport specific movements, and stage three involved jumping and landing exercises. The author can be contacted if access to the full program is desired. Each session from each stage was designed so that it could be completed in 10 minutes prior to trainings or games, and was implemented before two sessions per week. The total program duration was 36 weeks and was designed so that stage one, two and three were completed during preseason with stage three continuing throughout the competitive season.
There was no significant or clinically relevant difference in ankle injury incidence, severity, or burden between the intervention season and control seasons. Ankle stability and function significantly improved following the ankle intervention program (i.e., faster time to complete and reduced number of stability errors). Over 90% of players rated the program positively (i.e., considered it worthwhile and valuable use of training time) and coaches reported that the program was easily implemented. However, a common challenge reported by coaches was maintaining player engagement throughout the season, suggesting that an increase in competitive elements would make the program more engaging.
Although the program did not reduce ankle injury incidence, severity, or burden, it did facilitate improvements in ankle stability and function and was accepted by participating players and coaches. It is unclear on why the intervention didn’t change injury rates considering it was based on other successful programs. It is theorised that more information is required about injury mechanisms in the U18 cohort to help make the current injury prevention program more specific to those mechanisms.
Therefore, more research into specific ankle injury mechanisms and how they can be prevented is required.
As suggested by the coaches, increasing engagement and adherence to the program would be beneficial to the players. Ways to do this would be to include footballs into the warmup or introduce some competitive aspects as this is what the cohort requires to be engaged. By increasing engagement, adherence, and effort towards a program, it is likely that the preventative effect will increase.
Due to the nature of junior AF training which typically has 1-2 coaches to manage a full squad of players, individualised player supervision/ coaching is difficult to achieve in injury prevention programs. If possible, it would be recommended to have the strength and conditioning coach and an assistant or another coach present for the warm-up to ensure players are performing the exercises correctly.
For article references, please email info@sma.org.au

Jessica McDonald completed her Masters by Research degree at the University of South Australia. Her research was focussed on injury prevention at the elite junior Australian Football level, in partnership with the South Australian National Football League. Her poster presentation titled “Does a targeted exercise program reduce ankle injuries in elite male adolescent Australian Footballers?” won the ASICS best poster – Sports Injury Prevention at the 2024 SMA ACSEP Conference in 2024.
Jessica was supervised and supported by Dr Samuel Chalmers (UniSA), Dr Hunter Bennett (UniSA), Dr Steve Milanese (UniSA), and Dr Joel Fuller (Macquarie University) – who attended the SMA conference on Jessica’s behalf.
EACH YEAR, SMA SURVEYS ITS MEMBERS TO LEARN MORE ABOUT WHAT MATTERS TO THEM – WHAT’S WORKING WELL, WHERE WE CAN IMPROVE, AND HOW WE CAN BETTER SUPPORT THEIR GROWTH AND CONNECTION. THE 2025 MEMBER SURVEY CAPTURED THOUGHTFUL AND CONSTRUCTIVE INSIGHTS ACROSS OUR DIVERSE COMMUNITY OF PROFESSIONAL MEMBERS, STUDENTS AND SPORTS TRAINERS.
97% of member responses said SMA’s overall performance is the same or better than last year.
Satisfaction and performance
Overall sentiment remains positive. Members cited professional development, credibility, and being part of a multidisciplinary community as the top reasons for maintaining their SMA membership. This is supported by a strong belief in the reputational value of belonging, with more than 82% of respondents agreeing that SMA membership adds credibility
to their professional status, with 38% saying it “definitely” enhances how they are perceived in the field.
Many members also reinforced the importance of SMA’s national profile and advocacy presence, calling for continued leadership in public education, safe sport, and injury prevention.

Members who engage with SMA’s PD event program and annual Conference reported strong value. For others – particularly those not regularly attending events – there is an opportunity to better connect them with practical benefits and offerings.
For Sports Trainers, insurance continues to be a key reason for joining. Some are also calling for more structured support, ongoing education, and clearer progression pathways following their initial training.
Members appreciate the core inclusions, such as insurance, discounted CPD, free access to JSAMS and JSAMS Plus, Sport Health, member updates, and professional credibility, however they would like these benefits to be easier to find, understand and use.
More than 82% of respondents agree that SMA membership adds credibility to their professional status, with 38% saying it “definitely” enhances how they are perceived in the field.
Notably, 97% of member responses said SMA’s overall performance is the same or better than last year, reflecting steady confidence in the organisation’s direction.
Sports Trainers are particularly seeking quicker, more direct access to support and information, while others noted the need for a more intuitive digital experience.
SMA has already taken steps to address these areas, with recent updates to the renewal process, enhancements to the member portal, and improvements to our course registrations. Further upgrades are underway to strengthen navigation, personalisation, and the clarity of member value.
Professional development continues to be the most valued aspect of membership. Respondents consistently highlighted CPD opportunities, the quality of education, Conference access, and practical learning as key benefits.
This year’s feedback reinforces a consistent message: SMA is a credible, respected organisation with strong goodwill among members, but there is more we can do to fully deliver on our value promise.
Members described a deep trust in SMA’s heritage, national leadership role, and evidence-based focus. Many also called for a stronger public profile, encouraging SMA to take a more visible position on key
Members described a deep trust in SMA’s heritage, national leadership role, and evidence-based focus.
sector issues and continue to act as a national voice for sports medicine, public health, and safer sport. This broader advocacy was seen as a key way to reinforce the credibility and influence of membership.
Core offerings like CPD, insurance, networking, and publication access were frequently noted as valuable. At the same time, members are looking for greater visibility of what’s included, and better tools to engage with their benefits.
Importantly, this feedback doesn’t signal disengagement, instead it reflects a desire for deeper connection. Members want to be heard, supported, and part of a growing national community that recognises and represents them at every stage of their journey.
Thank you to every member who contributed their voice to this year’s survey. Your insights continue to shape the way SMA evolves. We remain committed to listening, responding, and delivering a stronger, more connected membership experience.
SAM PIETSCH, Sports and Exercise Physiotherapist
(2024 SMA & ACSEP Conference – Early Career Researcher –ASICS Best Paper in Sports Injury Prevention)

QUADRICEPS MUSCLE INJURIES, PARTICULARLY THOSE INVOLVING THE RECTUS FEMORIS, ARE PREVALENT ACROSS A RANGE OF SPORTS THAT DEMAND HIGHSPEED RUNNING AND REPETITIVE KICKING. THESE INJURIES CAN POSE A SIGNIFICANT CHALLENGE TO BOTH ATHLETES AND THEIR SUPPORT TEAMS, CONTRIBUTING TO PROLONGED TIME AWAY FROM COMPETITION.
In elite male professional football (soccer), quadriceps strains are the third most common muscle injury, accounting for approximately 5% of all time-loss injuries and 19% of all muscle injuries. Recovery times of 19 days following an index injury have been described, with longer time required for recovery following reinjuries. Recurrence rates between 16% and 21% have been reported. Similar outcomes are observed in Australian Football, where quadriceps strains also rank as the third most common muscle strain injury, taking on average 25 days to return to play with a 18% rate of recurrence. Quadriceps injuries are not limited to the football codes with an average return-to-training time of
In elite male professional football (soccer), quadriceps strains are the third most common muscle injury, accounting for approximately 5% of all time-loss injuries and 19% of all muscle injuries.

20 days reported in elite track athletes.
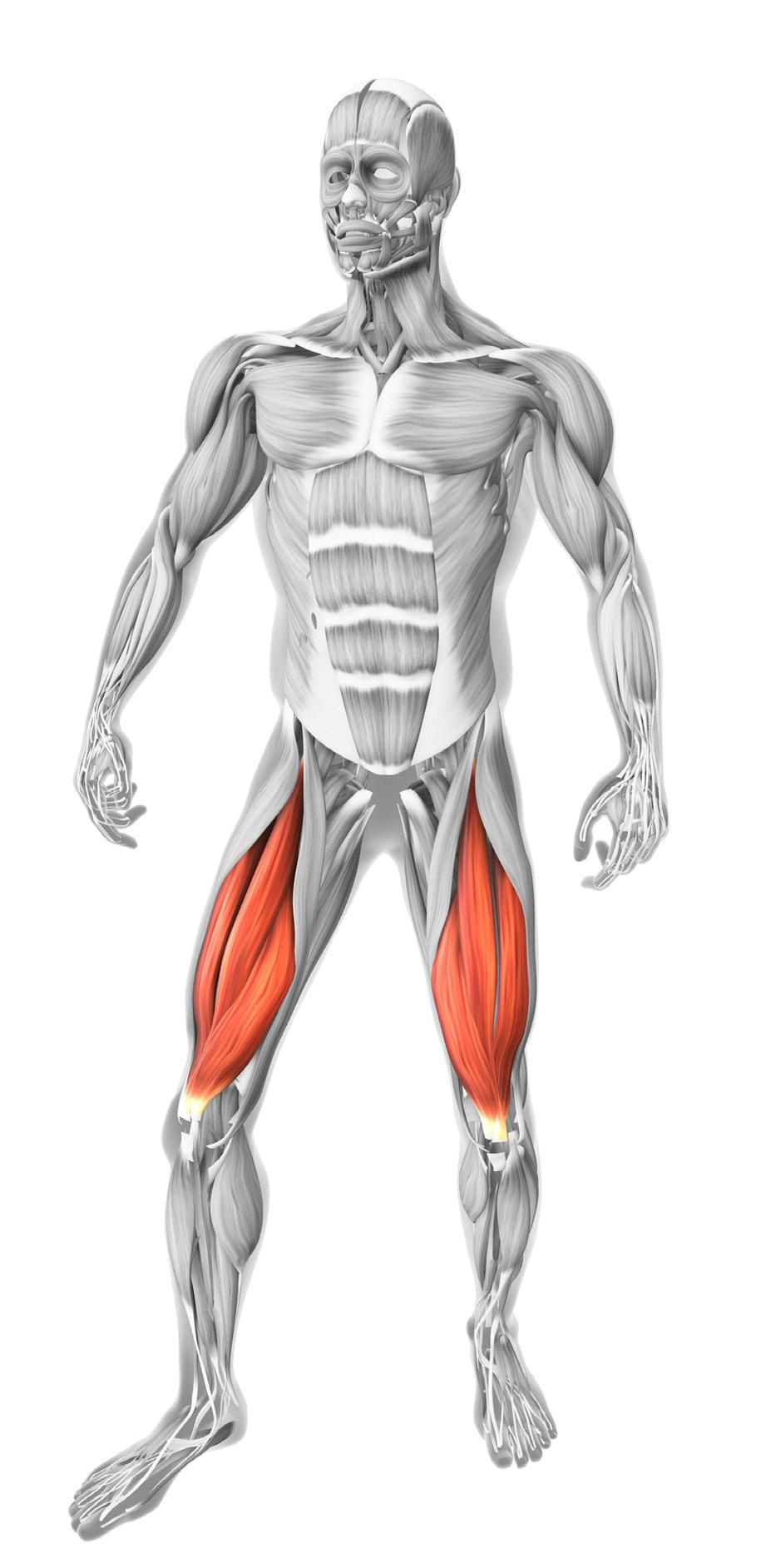
The quadriceps muscle groups’ primary function is to concentrically extend the knee and eccentrically control knee flexion to absorb ground reaction forces during landing and deceleration activities. The rectus femoris is the only quadriceps muscle that is bi-articular crossing both the hip and knee, and therefore also plays a key role in hip flexion. Due to this biarticular function, the rectus femoris plays a critical role in both high-speed sprinting and kicking.
During sprinting, the rectus femoris contributes substantially to hip flexion during the early swing phase, where it must rapidly transition
from eccentric (to decelerate hip extension) to concentric contraction (to initiate hip flexion). During kicking the rectus femoris also experiences high eccentric loading during the backswing as the hip extends while the knee flexes, with peak muscle activation occurring during the windup phase when the rectus femoris reaches its maximum length. The muscle must then work concentrically to generate rapid hip flexion and knee extension, to accelerate the leg forwards and generate foot speed for ball strike. These movements require the rectus femoris to produce rapid high force contractions in a lengthened position, making it especially vulnerable to strain.
Despite the prevalence of rectus femoris injuries, clinical guidance for rehabilitation and prevention of quadriceps muscle strain injuries remains limited. Compared to hamstring and calf injuries, there is a relative lack of high-quality evidence to inform practitioners. Key clinical questions remain around risk factors for injury, mechanisms of injury, the prognostic value of imaging, and whether specific rehabilitation strategies may improve outcomes.
Prior to our recent work, no systematic review or meta-analysis had focused exclusively on identifying risk factors for quadriceps muscle strain injuries in sport. Our systematic review revealed strong evidence that athletes are more likely to sustain a quadriceps strain in their dominant (kicking) leg and are at increased risk if they have any history of quadriceps injury or a recent hamstring strain. In contrast to well-established risk profiles for hamstring and calf injuries, there was strong evidence that increasing age is not associated with an elevated risk of quadriceps strain injury. Additionally, moderate evidence indicated that muscle flexibility is not a contributing risk factor. Evidence regarding the influence of sex and height was conflicting, highlighting the need for further research in these areas.
For extrinsic factors, the review found strong evidence that quadriceps muscles strain injuries are more likely to occur during competitive match play compared to training. There was also moderate evidence suggesting an increased injury risk
what currently informs our practice?
during the preseason period, while findings related to playing surface and climatic region were inconclusive.
Identifying modifiable risk factors is essential for guiding targeted preventive strategies. Clinicians can use these insights to monitor at-risk athletes (e.g. those with a history of quadriceps injury on their dominant kicking leg) more closely during highrisk periods such as when returning to preseason training, when reintegrating into high-load activities involving the dominant leg (e.g. returning to kicking post injury), or when returning to competitive match play.
Our recent epidemiological study analysing data taken from the Soft Tissue Registry of the Australian Football League (STRAFL) investigated quadriceps muscle strain injuries in elite AFL players. We found nearly 50% of all quadriceps strains occurred during kicking, with a high prevalence in the athlete’s preferred kicking leg. Running-based mechanisms accounted for approximately 31% of injuries, predominantly associated with acceleration and high-speed efforts. Importantly, when isolating rectus femoris injuries, 74% occurred during kicking activities, and 80% of re-injuries were in the dominant kicking leg. This highlights the high occurrence rectus femoris pathology from kicking mechanism.
On average, return to play following a rectus femoris injury took approximately 28 days, significantly longer than injuries affecting the vasti muscles (14 days). The longer recovery time for rectus femoris injuries likely reflects the unique anatomical and biomechanical role of the biarticular rectus femoris, which must manage high tensile loads during both hip flexion and knee extension in sprinting and kicking activities.
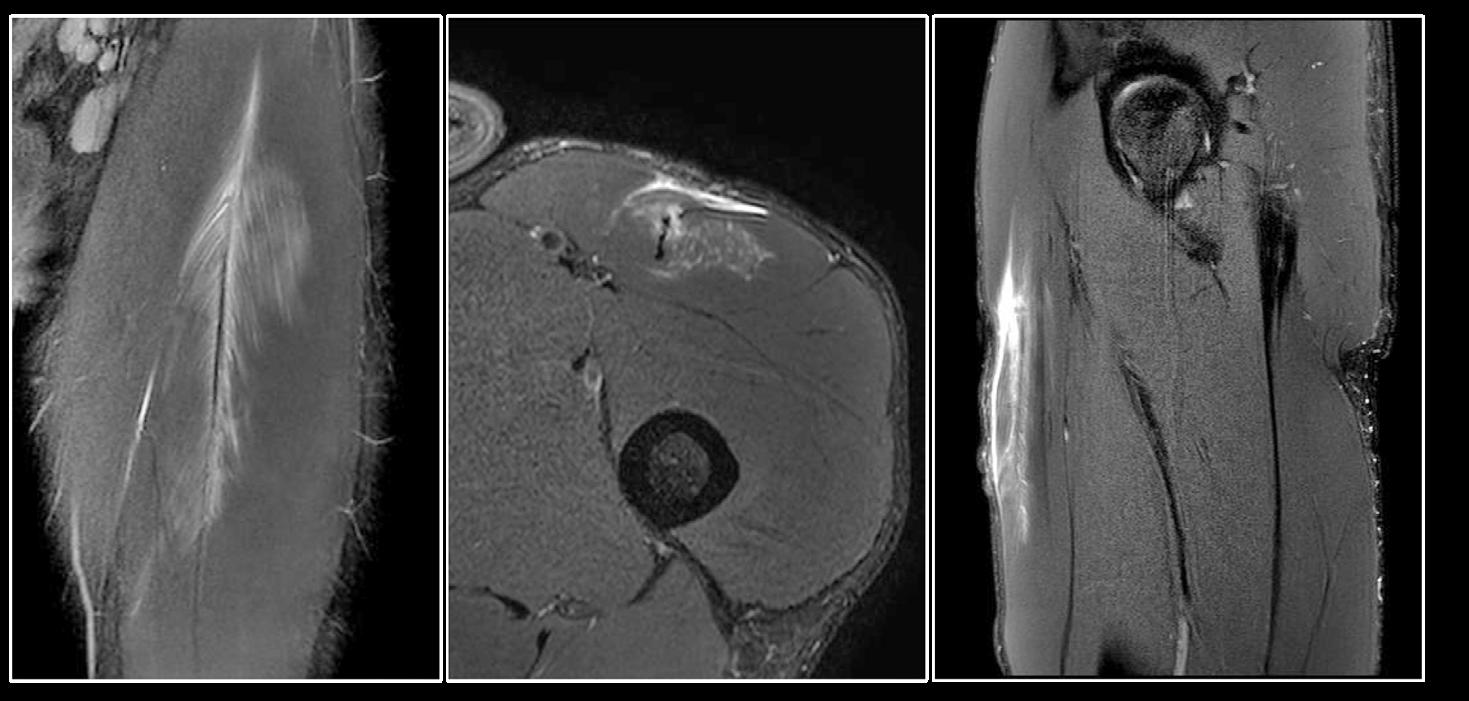
Understanding the factors that influence prognosis following injury is crucial for effective management. Evidence indicates that both the anatomical location and the severity of tissue disruption significantly affect rehabilitation timeframes. Injuries involving the connective tissue structures of the rectus femoris, particularly those with retraction of the central tendon, have been associated with longer rehabilitation periods. Our preliminary data from elite AFL athletes, presented at the 2024 SMA conference, revealed that over 75% of rectus femoris injuries were located at or within myo-aponeurotic regions (e.g., the anterior aponeurosis, central aponeurosis/tendon, or posterior aponeurosis), with 60% showing some degree of connective tissue disruption. Return-to-play timelines varied significantly by anatomical location, with proximal free tendon injuries requiring the longest recovery time (average of 53 days). Greater severity of aponeurotic disruption was correlated with prolonged return to play, particularly in injuries involving the central intramuscular aponeurosis/ tendon. Reinjuries, nearly all of which involved the rectus femoris, were also associated with a significantly longer rehabilitation period, taking on average an extra two weeks to return to play.
Importantly, kicking was identified as the predominant injury mechanism in cases of proximal free tendon injuries and aponeurotic disruption. As such, clinicians should consider the likelihood of more severe pathology when athletes present with proximal rectus femoris pain following an acute kicking-related injury. Accurate differential diagnosis is essential, and imaging may be necessary to identify free tendon injuries that could warrant surgical evaluation, or possible avulsion injuries, which are especially common in adolescent athletes. While imaging
A phased approach to recovery that addresses muscle inhibition and atrophy, strength development, and the restoration of function through targeted training strategies can be utilised.
can assist in diagnosis and help guide prognosis in elite sport settings, it should not be used in isolation. Instead, comprehensive clinical assessment, athlete-reported feedback, and symptom response to loading should drive the rehabilitation process.
Rehabilitation following rectus femoris injuries requires an individualized approach that considers anatomical location, injury severity, and the specific demands of the athlete’s sport. Although standardised rehabilitation protocols for rectus femoris injuries are still evolving, several evidence-informed frameworks and strategies have emerged from both research and clinical practice.
A phased approach to recovery that addresses muscle inhibition and atrophy, strength development, and the restoration of function through targeted training strategies can be utilised. Key components of rectus femoris rehabilitation should include initial restoration of muscle capacity and cross-sectional area through use of isometric and low intensity, high repetition loading, progressing to maximal strength training exercises aimed at enhancing knee extensor capacity and loading the muscle eccentrically at long lengths.
Research has demonstrated that eccentric exercises, such as the reverse Nordic, can significantly increase fascicle length and thickness in the vasti muscles. Additionally, training the rectus femoris at longer muscle length using a reclined leg extension (in 40 degrees of hip flexion), has resulted in greater hypertrophy across both proximal and distal regions of the muscle compared to training in a shortened position (in 90 degrees of hip flexion). These findings suggest
that eccentric loading at greater muscle lengths may be particularly effective in promoting positive strength and structural adaptations in the quadriceps during rehabilitation.
Strengthening of the hip flexors through full range while developing trunk and pelvic co-ordination in positions relevant to running and kicking may also help reduce the load on the rectus femoris. Additionally,
progressive exposure to ballistic, sport-specific movements, including plyometrics, high velocity running, kicking and deceleration at the knee, is essential for successful return to play.
Running can be reintroduced as soon as the athlete is able to comfortably control knee deceleration (e.g., demonstrated through a hop or lunge test) and has regained sufficient range of motion to accommodate the swing phase of the running cycle. Running should commence at a slow pace, with speed gradually increased as tolerated and guided by symptom response.
Returning athletes to kicking sports following rectus femoris injury presents unique challenges. Rehabilitation models for reintroducing kicking

typically begin with isolated, uniarticular loading of hip flexion and knee extension in a gym-based setting. This progresses to combined hip and knee movements that replicate the biomechanics of the kicking action with graduated resistance (e.g. starting with standing kicking in the pool or against resistance bands).
As the athlete improves, the speed and resistance of these exercises are gradually increased, leading into field-based kicking. If necessary, initial kicking drills can be performed using a lighter or smaller ball. Once the athlete can kick over short distances without pain, both the distance and velocity of kicks should be progressively increased until they can execute all types of kicks at high intensity without symptoms.
Kicking prescription should be individualized based on the specific demands of the athlete’s sport and playing position, as the intensity and type of kicks required will vary significantly (e.g., a goalkeeper versus a midfielder in soccer). In cases involving connective tissue disruption, a more cautious rehabilitation approach may be warranted, with slower progression to high-load eccentric and stretchbased loading that occurs in highvelocity sprinting and kicking.

ٚ Quadriceps muscle injuries are common in kicking sports.
ٚ Injuries involving the proximal and central connective tissue elements of the rectus femoris appear to require longer time to return to play.
ٚ Rehabilitation strategies focussed on increasing the capacity of the rectus femoris at longer lengths and strengthening of the surrounding muscle synergists are important in the rehabilitation and prevention of rectus femoris injures.
ٚ Graduated progression of kicking frequency, distance and intensity specific to the demands of the sport is required for rehabilitation of kicking athletes.
ٚ Further research into specific rehabilitation protocols and strategies following rectus femoris injury are required.
For article references, please email info@sma.org.au
On average, return to play following a rectus femoris injury took approximately 28 days, significantly longer than injuries affecting the vasti muscles (14 days)

Sam Pietsch is an APA Sports and Exercise Physiotherapist with over 15 years experience working in elite sport in both Australian football (AFL) and soccer (A-league). He is currently the Senior Physiotherapist at Melbourne City FC, and also consults in private practice at Alphington Sports Medicine. As a current PhD candidate at La Trobe University, Sam is researching factors that effect prognosis and best practice rehabilitation for quadriceps muscle strain injuries in sport.



CONNECT. LEARN. INSPIRE.



THIS YEAR, SMA IS HEADING TO VIBRANT HOBART FOR THE 2025 ASICS SMA CONFERENCE, BRINGING TOGETHER SOME OF THE WORLD’S LEADING SPORTS MEDICINE RESEARCHERS AND PRACTITIONERS TO CONNECT, COLLABORATE, AND EXCHANGE IDEAS. AS ALWAYS, WE HAVE ORGANISED A RICH PROGRAM OF THOUGHT-PROVOKING PRESENTATIONS AND ARE EXCITED TO ANNOUNCE OUR KEYNOTE SPEAKERS WHO WILL BE SHARING CUTTINGEDGE RESEARCH, INDUSTRY INSIGHTS, AND FRESH PERSPECTIVES.

2025 REFSHAUGE LECTURE
Professor Nick Brown
Nick will deliver SMA’s prestigious Sir William Refshauge Lecture at the 2025 ASICS SMA Conference, recognising his significant contribution to sports and exercise medicine and science.
Nick is Head of the School of Clinical Sciences at Queensland University of Technology (QUT), leading multidisciplinary education and research across allied health and biomedical science.
He previously served as Director of the University of Canberra Clinical School and Deputy Director of Performance Science and Innovation at the Australian Institute of Sport, overseeing sport science, applied research, and innovation for elite athletes.
A qualified Podiatrist, Nick began his career in Brisbane before completing a PhD in Biomechanics and a postdoctoral fellowship in Bioengineering at the University of Texas at Austin. He also held research roles in Orthopaedics and Biomedical Engineering at the University of Utah and is widely published in lower extremity biomechanics.

Professor Michael Rathleff
Michael is a physiotherapist and Professor at Aalborg University, where he directs PRIMA, a new centre for primary care research, and leads the MSK-Health group. His research focuses on improving lifelong musculoskeletal health through effective, real-world care models. He collaborates with clinicians, patients and stakeholders, and has published over 250 peerreviewed papers in sports medicine, physiotherapy and primary care.

Dr Carly McKay
Carly is Director of Research at Podium Analytics and Reader in Injury Prevention at the University of Bath, where she co-leads the Centre for Health, Injury and Illness Prevention in Sport (Chi2PS). Her research focuses on psychosocial and behavioural factors in sport injury. She is an executive member of UKCCIIS and Associate Editor for JSAMS, with experience in policy, advocacy, and prevention initiatives.

Associate Professor Michelle Smith
Michelle is a Sports & Exercise Physiotherapist and Director of the Masters of Sports Physiotherapy program at The University of Queensland. She co-directs a research unit focused on preventing and managing lower limb injuries, especially ankle conditions, to enhance lifelong participation in sport. She is also Co-director of the International Ankle Consortium and Associate Editor for Physical Therapy in Sport.

Professor Ollie Jay
Ollie is Professor of Heat and Health and Director of the Heat and Health Research Centre at The University of Sydney. He has led internationally influential research on heat policy, partnered with Google on global alerts, advised major sports bodies, and chairs a Lancet Countdown group. Ollie has authored over 220 peer-reviewed publications and held senior editorial roles at JSAMS.
Dr Enda King, PhD, MSc
Enda is a sports physiotherapist, strength and conditioning coach, researcher, and educator. He is Head of Elite Performance and Development at Aspetar, Qatar, where he integrates 3D biomechanics with high-level rehabilitation. Specialising in hip, groin, and ACL injuries, he has over 40 publications and global experience across elite and professional sports. Enda holds a PhD, MSc, and BSc in physiotherapy.

Professor Silvia Blemker, PhD
Silvia is co-founder and Chief Scientific Officer of Springbok Analytics and Professor of Biomedical Engineering at the University of Virginia. She leads R&D on AI-driven muscle analytics for applications from sport to disease. Her lab develops advanced methods to study skeletal muscle biomechanics and physiology. Silvia is a fellow of ASB, AIMBE, and the National Academy of Inventors.
MELISSA HABERFIELD, La Trobe Sport and Exercise Medicine Research Centre (2024 SMA & ACSEP Conference – Wendy Ey Award for Best Paper for Women in Sport)

Anterior cruciate ligament (ACL) ruptures are devastating knee injuries often experienced by otherwise active and healthy young people. Beyond the immediate disruption to sport and daily life, ACL ruptures can have lasting health consequences. In young people, osteoarthritis rates are low, but following an ACL rupture, rates are much higher, affecting up to 50% of people before the age of 40 years. Many also experience ongoing symptoms such as knee pain, reduced
knee function, lower physical activity levels and poorer quality of life (QoL).
In women, the post-ACL rupture burden is magnified compared to men. In the first five years following ACL rupture and reconstruction, women have 25% lower odds of returning to sport than men. Women also report worse knee pain, poorer function, and reduced QoL than men. Psychological distress, including anxiety, is more common in women who have concerns about how an ACL injury
may impact their lives. Confidence in managing their recovery – selfefficacy – is also lower in women than men. Such discrepancies in outcomes highlight the importance of comprehensive and effective rehabilitation strategies to address the needs of women following ACL rupture.
Sex and gender are distinct but interconnected concepts. Sex refers to biological attributes (e.g. female or male), while gender relates to a person’s identity, social roles and characteristics (e.g. woman or man).

an ACL rupture. Factors such as social roles, expectations, and access to healthcare may affect how well rehabilitation works, and whether it’s accessible or accepted. If such factors aren’t considered, it may add to the burden women face following an ACL rupture. Current clinical rehabilitation guidelines emphasise individualised, criterion-based exercise therapy and education as key components of ACL rehabilitation programs. However, they offer little direction on addressing the broader range of factors affecting women’s recovery, such as managing interrelated individual, sociocultural, and environmental factors. Barriers for women may include access to rehabilitation services, dislike of gyms or lack of confidence in gym environments, and a lack of social support. Sex-specific factors may include the impact of female health factors including menstrual/ pelvic health and pregnancy.
In the first five years following ACL rupture and reconstruction, women have 25% lower odds of returning to sport than men.
Importantly, neither sex nor gender is strictly binary – people may identify outside of traditional female/male and/or woman/man categories. In our study (outlined below), we used the term woman to reflect our focus on the gendered context of ACL rehabilitation. We use the term female when referring to biological (sex-based) factors.
Current ACL rehabilitation approaches
There is a growing recognition that sex and gender-based factors can shape how people experience healthcare and rehabilitation after
Co-creation could be the key to enhancing outcomes for women
One way to help close the sex/gender gap is by co-creating solutions with those people affected most, including patients, practitioners and consumer groups. Involving end-users in developing tailored solutions for women ensures that ACL rehabilitation is both relevant and practical. Understanding both the biological and social influences on and considerations for ACL rehabilitation is critical to improving outcomes for women and creating gender-responsive approaches that reflect women’s lived experience of ACL rehabilitation.
what factors should be considered?
The aim of our study
We sought to identify considerations for women’s ACL rehabilitation from the perspective of women with lived experience of an ACL reconstruction (ACLR) and rehabilitation, and health and exercise practitioners who work with them. This study is the first step to inform co-creation and development of a tailored ACL rehabilitation program for women.
was involved
We invited women patients with recent lived experience of an ACLR and rehabilitation, and a range of health and exercise practitioners (including physiotherapists, sports medicine physicians, exercise physiologists, strength and conditioning professionals, dietitians) with self-reported experience rehabilitating women post ACLR.

We used a mixed-methods research approach called concept mapping Briefly, this approach combines qualitative and quantitative techniques to gather, sort, and rate ideas from the participants. Using specialised online software, participants brainstormed ideas in response to a focus prompt (described below). Participants then sorted these ideas into themes and rated each idea (relative to all other ideas) for both importance and feasibility in clinical practice on a 5-point scale (1=least to 5=most). The result, following analysis and statistical modelling, was a visual ‘concept-map’ showing key themes, or ‘clusters’ of key considerations that may assist practitioners and researchers in designing targeted and nuanced ACL rehabilitation solutions for women.
The focus prompt “What factors should be considered in ACL rehabilitation for women (18-45 years)? Think about what might be needed or could be done to support activity (e.g., walking, jogging, sport, activities of daily living), improve quality of life (e.g., physical, mental wellbeing, social), enhance participation (e.g., work, sport, family), reduce symptoms (pain, instability, range of motion), regain knee confidence and prevent reinjury”.
Forty-seven participants (19 women patients and 28 practitioners) brainstormed, sorted and rated 90 unique ideas in response to the prompt. Seven key themes were identified as important considerations for women’s ACL rehabilitation. There was a high level

of overlap between patients and practitioners in sorting and rating ideas, indicating both groups may have similar priorities on enhancing ACL rehabilitation for women.
The 7 key themes
From highest to lowest importance, the 7 themes were:
(1) Foster goal-driven rehabilitation;
(2) Promote mental and emotional wellbeing;
(3) Create adaptable and supportive environments;
(4) Provide education and resources;
(5) Engage the whole team for the whole woman;
(6) Address accessibility and competing demands; and
(7) Build peer, group and social support.

Our findings reinforce what many clinicians already know: ACL rehabilitation is about more than physical recovery, and there is no one-size-fits-all approach. While individualised and holistic rehabilitation is vital for all patients, adopting a gender-responsive approach may help address rarely considered barriers and enablers unique to women (e.g. competing demands, gender-specific strength training needs, and menstrual/obstetric health during knee injury recovery).
The goal-setting environment and process may be just as important as the goals themselves. Key clusters such as foster goal-driven rehabilitation and promote mental and emotional wellbeing highlight the importance of clinicians creating a therapeutic environment where women feel supported, encouraged
Understanding both the biological and social influences on, and considerations for ACL rehabilitation is critical to improving outcomes for women and creating gender-responsive approaches that reflect women’s lived experience of ACL rehabilitation.
and empowered. Goals should reflect their needs, motivations and life circumstances (beyond simply returning to sport) and promote resilience and adherence throughout the rehabilitation journey.
Other clusters including, create adaptable and supportive environments and provide education and resources, highlight the pressing need to reflect on how we deliver strength training during women’s rehabilitation. Lack of confidence or supervision, gendered stigmas, or competing life demands may make this core component of ACL rehabilitation difficult for women to access and/or sustain. To fully engage in rehabilitation, women may need tailored strength training education and support, and flexible options like home-based programs/ equipment or safe gym environments.
what factors should be considered?
While often overlooked in traditional ACL rehabilitation approaches, female health factors (including menstrual health, pelvic health, energy availability and pregnancy) were highlighted in clusters – engage the whole team for the whole woman and address accessibility and competing demands Rehabilitation may intersect with female health factors, life stages, or broader sociocultural roles and responsibilities, and therefore could influence rehabilitation planning and participation for women. Clinicians should be willing to have open discussions with their patients and refer to relevant professionals when required (e.g. dietitians, pelvic health physios, sports doctors).
Although build peer, group and social support was rated as the least important and feasible cluster overall, its emergence as a distinct theme suggests that consideration of social connection still has value in women’s ACL rehabilitation. Clinicians can use strategies such as group-based rehab, connection with teammates and peer support from online communities to maintain motivation and adherence, particularly during more challenging phases of rehabilitation.
Key take-home messages
While awaiting future research, clinicians can refer to our 7-cluster framework as a practical guide to enhance ACL rehabilitation and outcomes for women. Clinicians should tailor strategies to the woman in front of them; recognise what motivates her, what gets in the way, and what kind of support she really needs. From there, more nuanced factors—like menstrual

health, caregiving responsibilities, or the value of peer support—can be layered into the rehabilitation plan to further personalise care.
Key tips
ٚ Check their own biases and ensure ACL rehabilitation is a gender-responsive and flexible approach, accounting for unique barriers and enablers for women (including social, psychological, and female-health factors).
ٚ Create a supportive and empowering therapeutic environment with open
communication and clear milestones throughout the rehabilitation journey.
ٚ Individualise goals so they are tailored to women’s lives, values and broader participation aspirations beyond sport.
ٚ Deliver strength training and education in safe, accessible, supervised environments.
ٚ Collaborate across disciplines, particularly to address femalespecific health factors that may impact rehab.

Melissa Haberfield is a physiotherapist with over 16 years of clinical experience and a current PhD candidate at La Trobe University’s Sport and Exercise Medicine Research Centre. Melissa’s PhD is exploring sex/gender differences following ACL injury, and how to optimise outcomes for women. In 2024, she won the Wendy E Award for best paper- Women in Sport at the SMA Conference. As a clinical physiotherapist, she has worked across all facets of the profession, most notably in the elite female sporting space. She has been team physio at a National and state level in Basketball and gymnastics, as well as an AFLW physiotherapist for North Melbourne Football Club – winning the 2024 AFLW premiership. Her particular interests are knee injury, women’s health in sport, and women working in sport.
DR FELIX LEUNG, Lecturer in Physiotherapy, Griffith University QLD

CONCUSSION IS ONE OF THE BIGGEST CONCERNS FOR ATHLETES PARTICIPATING IN CONTACT SPORTS. IN AUSTRALIA, OVER 1 MILLION ADULTS AND 685 000 KIDS PLAY POPULAR TEAM SPORTS SUCH AS RUGBY UNION, RUGBY LEAGUE OR AUSTRALIAN FOOTBALL [AUSTRALIAN SPORTS COMMISSION].
The physical and unpredictable nature of these sports where athletes collide with each other while tackling and contesting for the ball leads to a high risk of athletes sustaining a concussion. A study conducted in Australia found that one concussion occurs in every eight games of school rugby union, with tackling or being tackled the most common mechanism associated with a concussion (Leung et al., 2017). A concussion is a traumatic brain injury that results from an impact to the head, neck or body that transmits an impulsive force to the brain (Patricios et al., 2023). This sets off a neurotransmitter and metabolic cascade with possible axonal injury, blood flow change and inflammation in the brain. Following a concussion, athletes present with a range of clinical signs and symptoms that may occur immediately and can evolve
over hours to days. In most athletes, symptoms resolve within 14 days and they return to sport by 20 days (Putukian et al., 2023), however, 30% of athletes remain symptomatic greater than 30 days (Schneider et al., 2023).
A lot of attention has been placed on the negative consequences of concussion, including prolonged symptom burden, impact on mental and physical health of athletes, and long-term neurodegenerative diseases (Patricios et al., 2023).
At the 6th Consensus Conference for Concussion in Sport, held in Amsterdam 2022, there was a concerted effort among the scientific community to identify strategies for prevention of sports-related concussion (Patricios et al., 2023). Primary prevention is a key priority for
reduce the risk of concussion in contact sports
sport governing bodies and health care practitioners. There is added concern about the safety of contact sports at the youth levels, with children and adolescents having a greater risk of concussion. Prevention strategies such as rule changes, use of protective equipment and implementation of neuromuscular training programmes have been effective in reducing concussion injuries (Eliason et al., 2023), however, the rate of concussions remain high.
There is growing interest in the role of modifiable factors such as an athlete’s physical attributes and sports-specific skills that could mitigate the risk of concussion in athletes participating on contact sports. The cervical spine is an important region when considering its functional role in stability and control of the head. Muscles around the neck provide a protective role in preventing impact forces during collisions from being transferred to the head and brain. Stronger neck muscles are proposed to stiffen the neck region and prevent the whiplash like movements that often occur resulting in concussions (Elliott et

al., 2021). Recent systematic reviews have highlighted conflicting evidence regarding the relationship between neck strength and concussions, however, due to the heterogeneity of sports included in the reviews and methods of assessing neck strength, it is difficult to rule out neck strength as a potentially modifiable risk factor for mitigating concussion injury risk (Garrett et al., 2023, Cooney et al., 2022).
The aim of our study was to determine whether strength of the neck muscles was associated with in-season concussions in a cohort of adolescent rugby union and rugby league players. If a significant relationship was found, we aimed to establish clinical cutoff values which could be used to identify athletes that were at a greater risk of sustaining a concussion.
A prospective cohort study was conducted to investigate the relationship between neck strength and in-season concussion injury risk. Assessment of neck strength took place during the 2023 preseason period between January and February. Concussion injuries were monitored during the school rugby union (March to June) and rugby league (June to September) playing season. A concussion was recorded if a player was taken off the field for a suspected concussion and met the criteria as published in the 6th Consensus Statement for Concussion in Sports. Concussions sustained during training and games were recorded.
A total of 43 adolescent (aged 15 to 18 years) male rugby union and rugby league players were recruited from one school in Queensland, Australia. Players were recruited from the preseason training squad of the school’s Firsts and Seconds rugby union and rugby league teams. Players were excluded from the study if they had sustained a recent concussion (within 30 days),
reported neck pain greater than 2/10 on a numerical pain rating scale during screening of neck range of motion and manual examination, or were currently not cleared to train or play due to any injury to the neck region.
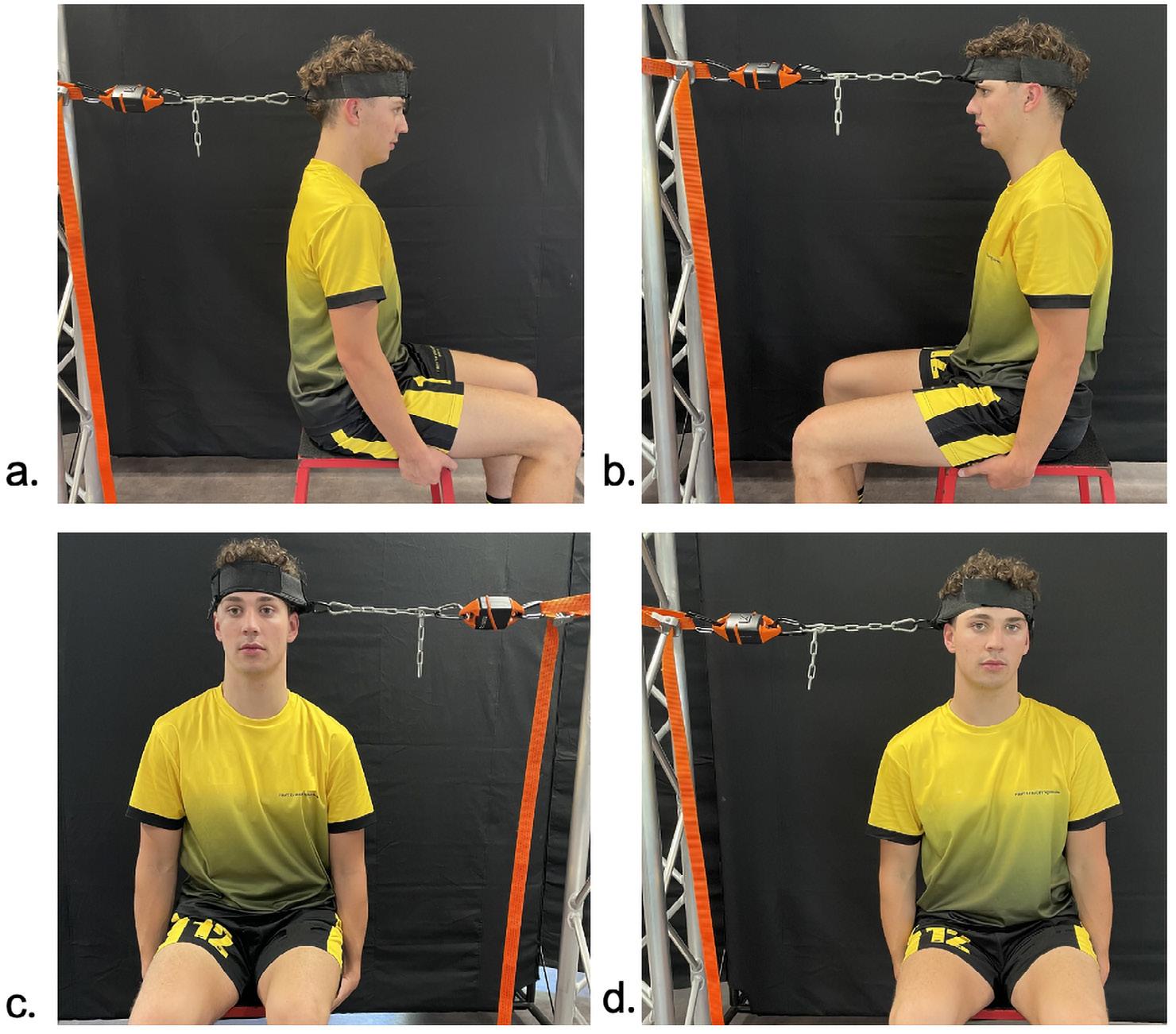
For this study we utilised a protocol with demonstrated reliability to assess the strength of the neck muscles (Fuller et al., 2022). The protocol has previously been used in high school
rugby union athletes and uses portable equipment that can be easily set up in a clinic or gym environment (Figure 1). A pull dynamometer (K-Pull KINVENT, Montpellier, France) was used to assess maximal isometric neck strength for the directions of flexion, extension and lateral flexion (left and right) (Figure 2). The dynamometer is synced to an App which displays the strength outputs on a tablet. Participants were seated on a 45 cm high bench, in an upright position with their feet positioned hip width apart and flat on the floor, and arms placed by their side holding onto the seat. The head was positioned in neutral during the testing for all directions. A warm-up was conducted prior to the testing, with participants completing self-resisted isometric contractions for 10 s at 70 % maximal voluntary contraction in all four directions. A head harness was placed around the head above the ear line and across the frontal and parietal bones. For the maximal strength testing, participants were instructed to produce “a maximal effort as quickly as possible” whilst maintaining their

A total of 43 male adolescent rugby players (aged 15-18) were recruited from the preseason training squads of one Queensland school’s Firsts and Seconds rugby union and league teams.
neck in a neutral position. For each direction, three repetitions of three second contractions were recorded with 30 second rest between each repetition. Participants were given a three second countdown before the verbal cue of “pull, pull, pull, pull, pull and relax”. The maximal contraction in kilograms were recorded.
A total of 43 adolescents participated in the study. All played in the rugby union season, and 24 also played in the subsequent rugby league season. The mean and standard deviation (SD) for age, height, weight and years playing rugby union or rugby league were 16.4 (0.8) years, 182.4 (5.6) cm, 86.6 (13.9) kg and 9.2 (3.2) years. There were 11 recorded concussions, with six concussions occurring in rugby union and five in rugby league. The demographic information and neck strength characteristics are presented in table 1.
The current study found that players with weaker neck strength were more likely to sustain a concussion during the playing season. Players who sustained a concussion injury had weaker neck extension strength in kilograms (p = 0.043, ES = 0.74) and when normalised to body weight (p = 0.041, ES = 0.74). The process of normalisation allowed the effect of bigger players possibly having stronger muscles to be accounted for. The flexor to extensor strength ratio was also different between the players who did and did not sustain a concussion (p = 0.039, ES = 0.81). Receiver operating characteristic (ROC) curves were used to determine an optimal cutpoint for each of these significant
Demographics
Strength (kg)
Means (SE)
Strength (N/kg)
* Significance at p < 0.05.
Table 1. Demographic information and neck strength characteristics for players who did and did not sustain a concussion injury during the playing season.
variables in predicting the concussion injury outcome variable (Table 2). This process determines the cut-off point for strength measurements that best predict whether a condition is present, in this case, whether the adolescent has experienced a concussion. The clinical cut-points for extension strength in kilograms (<32.05 kg), extension strength when normalised to body weight (<3.71 N/kg) and the flexor to extensor muscle strength ratio (>0.74) were able to correctly identify nine of the 11 concussion injuries. Each of these individual measures were able to identify seven of the 11 concussion injuries (Figure 3). The cut-points were then used to convert the continuous variables to
a binary form. The unadjusted odds ratios (ORs) for predicting injuries and concussions in the playing season were estimated from cross-tabulations.
Weaker neck extension strength is a risk factor
This is the first study investigating neck strength and concussion injury risk in adolescent rugby union and rugby league players. Players with less than 32 kg or less than 3.7 N/kg of neck extension strength had five-and three-times greater odds of sustaining a concussion during the season. Considering that the most common mechanism of sustaining a concussion injury occurs during collision events such as tackling or being tackled,
Table 2. Significant measures with area under the curve (AUC)
* Because this was an exploratory study aimed at identifying the priority for subsequent research, liberal p values < 0.1 were considered to help identify clinically meaningful effects and to avoid type II error.
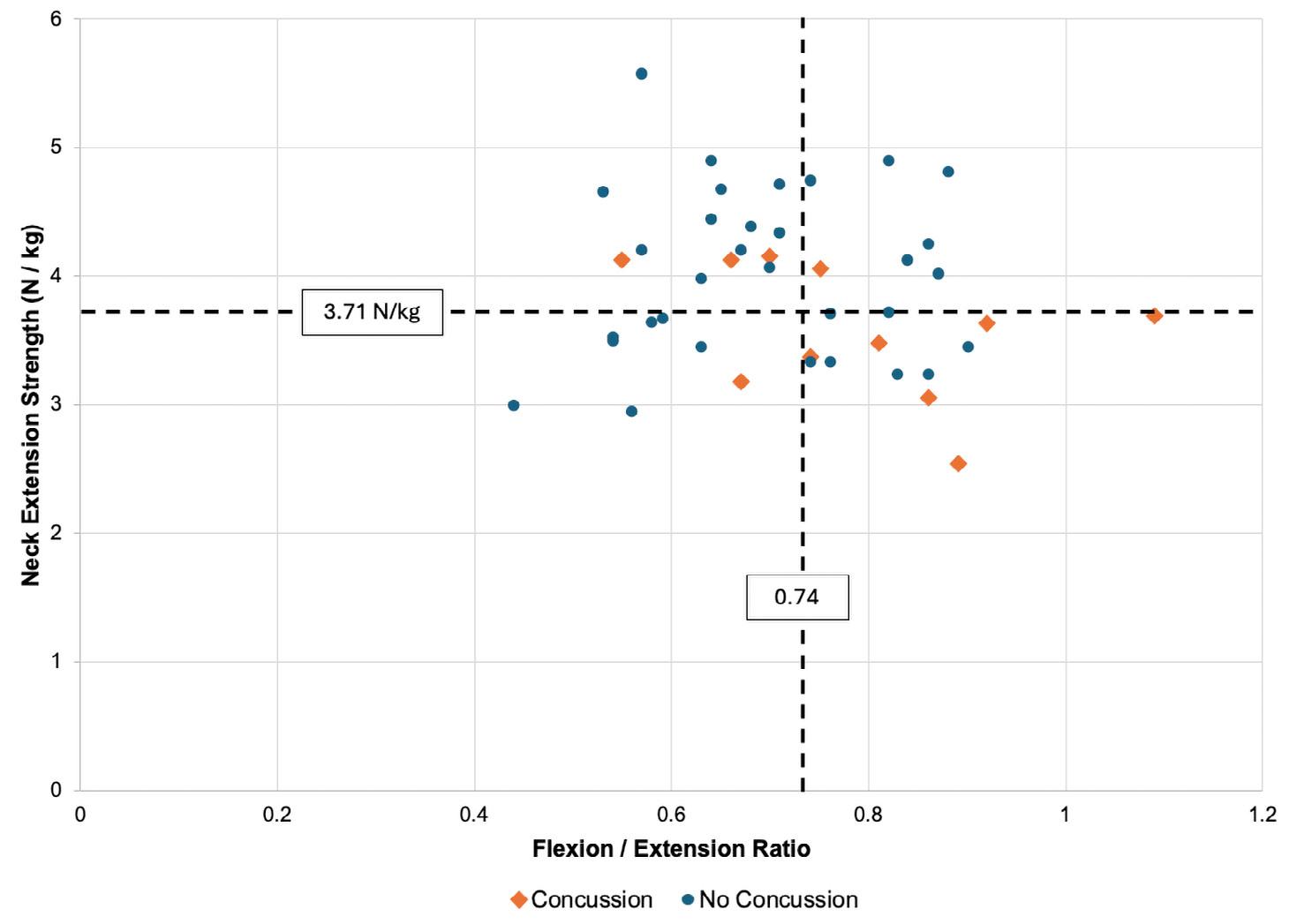
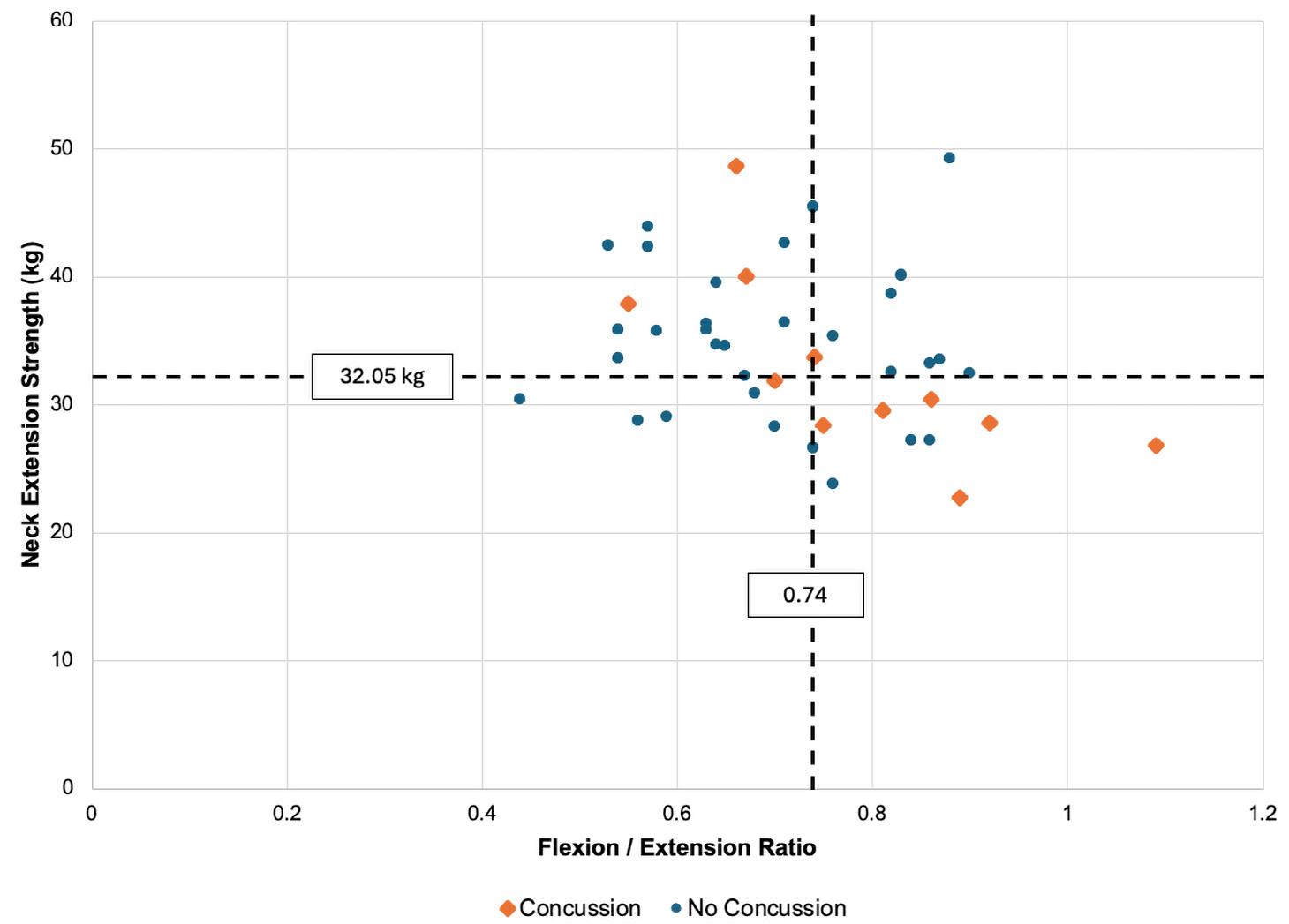
stronger neck muscles are thought to increase the ability to absorb impact forces and stiffen the neck to mitigate the whiplash-like movements that can occur and result in concussions. There are currently limited studies in adolescent athletes. A study by Collins et al. 2014, in adolescent basketball, lacrosse and soccer players found that decreased neck strength was a predictor of concussion injury. Emerging studies have published normative values for adolescent rugby union players (Fuller et al., 2022; Nutt et al., 2022), using similar neck strength testing protocols. Our results build on these studies and provide useful clinical values for healthcare practitioners which could be used to select players beneath the cut-off value and direct targeted interventions to these players.
Our study found that a greater neck flexor to extensor strength ratio increased the odds of sustaining a concussion, with players who had a ratio of 0.74 or greater, three-times more likely to sustain a concussion during the season. Co-contraction of the neck flexor and extensor muscles to stabilise the neck has been considered a mitigating factor in reducing head impacts and accelerations (Dezman et al., 2013; Peek et al., 2020). It has been proposed that a ratio close to one may be beneficial in mitigating head impacts and reducing head acceleration, however, this has been extrapolated from studies in soccer players during purposeful heading. Due to the demands of rugby union and rugby league, it is reasonable to
to reduce the risk of concussion in contact sports


expect that players will have stronger neck extensor muscles than soccer players, and therefore smaller neck flexor to extensor strength ratios. The neck extensors are the stronger muscle group and contribute the most to reducing sagittal plane impact forces common during rugby collisions (Farley et al., 2022). Our results suggest that a greater neck flexor to extensor strength ratio may indicate weaker neck extension strength relative to flexion strength and hence, increase the risk of concussion.
The results of our study are similar to those conducted in adult male rugby union and rugby league players that also found reduced neck extension strength was a risk factor for concussion incidence. The studies reported clinical cut-off for neck extension strength of 41 kg and 37kg in professional rugby union and rugby league players respectively (Farley et al., 2022; Hides et al., 2024). These values are higher than the value reported in our study, which is not surprising considering the likely differences between professional adult athletes and adolescent athletes. The results of our study need to be interpreted with caution and may not be generalisable to other sports and to female players. The clinical values determined in this study may not be transferable to other collision team sports such as Australian Rules Football or American Football as demands of those games are different from rugby union and rugby league.
As neck strength is modifiable, strength training of these muscles should be incorporated into athlete training schedules to contribute to concussion prevention. This study provides coaches and healthcare practitioners with strength values that could be used to identify at-risk athletes for targeted neck strengthening interventions to reduce their risk of sustaining a concussion.
Targeted neck strengthening exercises have been shown to increase isometric neck strength in athletes (Gillies et al., 2022). Neck strengthening interventions should target all directions of neck movement and may include the use of resistance bands, cable weights, or body weight resistance. Exercises should be performed in neutral and sports specific positions (Figure 4). While more research is needed to determine the optimal strength increases required to reduce concussion risk, this study provides a positive direction towards improving safety for athletes participating in contact sports.
For article references, please email info@sma.org.au

Dr Felix Leung is a Lecturer in Physiotherapy at Griffith University. He is a clinical and research physiotherapist with an area of expertise in sports and musculoskeletal injuries. Felix’s research focuses on sportsrelated concussions and how physiotherapy can be integrated into the management of athletes following a concussion. Felix was the recipient of an NHMRC postgraduate scholarship, and his PhD thesis investigated the sensorimotor system in adolescent rugby players, focusing on identifying the changes to the musculoskeletal and vestibular systems post-concussion. He is currently involved in research projects with elite athletes across several sporting organisations in Queensland with the aim of reducing concussion risk and optimising safe return to sport following concussion. Felix is an experienced clinician and currently works with high school athletes and representative-level rugby union teams in Queensland.







How did you get started in sports medicine, and what inspired you to pursue this path?
My journey into sports medicine began with a lifelong love of sport. I grew up in Hong Kong where football, or soccer, is the number one sport, and I played it from a young age. After completing my residency in emergency medicine in 1990, I became aware of the only formal university course in sports medicine at the time, which was a full-time program at

the Royal London Hospital. I applied and was fortunate to be accepted as one of 20 international candidates.
That experience in London was pivotal, it gave me a solid foundation and confirmed how much I enjoyed this field. When I returned home, the AIS and the University of Canberra launched the first Master of Sports Medicine program. I was one of only four students in that inaugural cohort. From there, I have stayed in the field ever since. Sports medicine has really become my passion; it blends clinical expertise with something I’ve always loved, which is sport.
You’ve worked with athletes from the Olympics to grassroots, what’s one lesson that remains constant across all levels of sport? One of the key lessons I’ve learned throughout my career is that the principles of sports medicine stay consistent, regardless of the level of sport. Whether I’m working with elite athletes on national teams or supporting grassroots players in the community, the foundational concepts don’t change. What differs is the scale – elite and professional setups naturally have more funding, better facilities, and more staff. But that doesn’t mean those without such resources can’t deliver quality care.
A lot of people assume that if they’re not part of a major club or don’t have access to professional infrastructure, they can’t apply the same standard of care. But that’s not true. Money affects the scale of services, yes, but not the principles. If you understand those principles and are willing to apply them properly, you can still
achieve excellent outcomes, even on a limited budget. I always encourage grassroots practitioners not to be discouraged, what matters most is how you apply what you know.
What are some of the most common injury challenges you’ve seen in elite football, and how has your approach to managing them evolved?
In elite football, the most common injuries I see are ankle sprains, followed closely by knee injuries like ACL tears. At the elite level, groin injuries are also a significant concern, and many of these issues stem from overuse rather than just acute trauma.
One area I’ve come to focus on heavily is biomechanics. My master’s research explored biomechanics as a factor in injury, and while it may not always predict acute injuries, it’s highly relevant to chronic and overuse injuries. Poor biomechanics can place additional
stress on the body, increasing the risk of strain, especially in professional athletes with high-intensity schedules and limited recovery time.
Over time, my approach has shifted more towards prevention, rather than just treatment. Elite players can’t afford long breaks; they might be playing two to three games a week. So, by identifying and correcting biomechanical or underlying inefficiencies early, we can reduce their injury risk. It all comes back to that core medical principle: prevention is better than cure.
How has the field of sports medicine evolved since you first began, and what changes are you most excited about today?
Sports medicine has come a long way, especially in Australia, where it’s now a fully recognised specialty. When I first started, there was no formal training

or established field as we see today. In many countries, even now, sports medicine often falls under orthopaedic surgery. But orthopaedic surgeons typically focus on injuries they can operate on such as ACL tears, shoulder dislocations and fractures, whereas soft

tissue or non-surgical injuries often get overlooked. Rheumatology was the only field that somewhat addressed soft tissue issues, but it mainly focuses on autoimmune conditions, not sports injuries. Sports medicine has since filled that gap, tackling soft tissue and exercise-related problems that fall outside traditional specialties.
Now, I receive referrals not just from GPs but also from orthopaedic surgeons, which really highlights how the field has evolved. GPs are also becoming more aware of what we do, though there’s still work to be done in medical education, musculoskeletal medicine is often underemphasised in medical school curricula, and it’s usually taught from a surgical perspective.
You’re known for mentoring earlycareer doctors, what advice do you find yourself giving most often? The first thing I always say is that you really need to have a genuine interest in sport, because in the early stages, it’s not particularly financially rewarding. When I returned from London, I began by volunteering with local community sports clubs and looking after the ACT representative teams. Volunteering

So, my advice is: don’t be discouraged by where you start. Volunteering opens doors. If you’re passionate, build your skills, show people what you can do, and the opportunities will follow.
There’s a phrase I love that FIFA promotes: “Football is medicine.” It’s true, regular sport can help with cardiovascular health, obesity, diabetes, and even some cancers.
What do you enjoy most about working in the Sports Medicine Industry?
helped me gain experience, develop my skills, and build networks. That ultimately led me into the national team setup, and in 1995, I started working with Soccer Australia (now Football Australia) as a national team doctor. I stayed in that role for 20 years, retiring in 2015. One of the highlights was the 2015 Asian Cup, which Australia hosted and won. After that, I was invited to join the Asian Football Confederation’s medical panel and have since also done work with FIFA.
For me, sports medicine is such a rewarding and uplifting area of healthcare. Unlike general practice, where you often see patients with chronic diseases who may not be particularly motivated to get better, in sports medicine, people come to you because they want to recover and return to activity. It’s incredibly satisfying to help someone through that journey, making the right diagnosis, guiding their rehab, and seeing them return to the sport they love. And it’s not just elite athletes; I treat everyone from teenagers to older adults. We sometimes forget how important sport is for people’s physical and mental health, especially in middle age and beyond.
There’s a phrase I love that FIFA promotes: “Football is medicine.” It’s true, regular sport can help
with cardiovascular health, obesity, diabetes, and even some cancers. I currently work with a Masters-level footballer managing prostate cancer who is still playing and doing well. Sport improves mental wellbeing too, especially in older adults. So, while it may not be the most financially lucrative field, the personal reward and impact on people’s lives make it incredibly worthwhile
Seeing as you love soccer so much, who’s your favourite team?
The Tottenham Hotspurs! (Trevor was proudly wearing a Spurs jersey during the chat.)
Can you describe your experience being part of the SMA Sports Doctors group, or how your time has been with Sports Medicine Australia?
My experience with SMA has been positive, especially in recent years as things are really picking up. Initially,

we were part of SMA’s Sports Doctors of Australia (SDrA) group, which was recently rebranded. After our founder passed away, the group lost momentum, and membership declined. But I’m grateful to SMA for its persistence in keeping the group going, especially with the support of the current Chair, Dr Sharon Stay.
We’ve been able to rejuvenate the Sports Doctors group, and it’s been
great to see the growth of activities and the establishment of more structured courses to educate doctors. Thanks to SMA’s continued support, we’re starting to see more attention being given to the group, and it’s becoming more appealing for doctors to consider sports medicine as a special interest field. Australia is a big sporting nation, so the more sports doctors we can bring in, the better the care and safety for athletes.


Take us back to the beginning – what first sparked your interest in sports science?
I began my working life as a physical education and mathematics teacher in Ireland. After approximately three years, I had the opportunity to take part in a professional development course focused on posture. That course was a significant turning point as it ignited my interest in biomechanics. Since then, I haven’t been able to watch any kind of human movement without considering the biomechanical aspects. I took that knowledge back into the school setting and applied it to the PE classes and sports I was coordinating,
and realised it was something I was deeply passionate and curious about.
That curiosity led me to pursue a PhD in biomechanics, specifically focusing on the role of foot mechanics in fundamental motor skills in adolescents. While my research wasn’t sport-specific, it had considerable implications for sports participation.
During my doctoral studies, I also had the chance to work on sports injury prevention projects with my supervisor, Professor Andrew McIntosh, which helped solidify my interest in sports science and
particularly the role it plays in sports injury prevention. I am incredibly grateful for those opportunities, as it led to a post-doctoral position in sports injury prevention and my introduction to SMA.
Is there a piece of research or project from your career that you’re especially proud of?
The PAFIX project, Preventing Australian Football Injuries Through eXercise, was one project I’m especially proud to have contributed to. I had the privilege of securing a postdoctoral position with Professor Caroline Finch, a global leader in sports injury
prevention, to work on the PAFIX project. The project was focused on reducing lower limb injuries in community-level Australian football. We assessed the impact of a targeted warm-up routine against a standard warm-up across various teams in Victoria and Western Australia.
The experience gave me a deeper appreciation for the passion and commitment in community sport, especially the reliance on so many volunteers. Numerous stakeholders in the clubs involved expressed that they were incredibly grateful that research was being directed their way, not just toward elite athletes. It highlighted for me just how vital sport is to the social fabric of these communities, and it was a privilege to work with them.
During the project, a drought in Ballarat necessitated football teams to train on unconventional surfaces like basketball courts and hockey fields. This situation presented an opportunity to study the role of playing surfaces in injury risk. From there, the AFL and Cricket Australia approached us about developing national standards for playing on artificial turf, something I’d never done before. We successfully developed standards tailored to community-level Australian football and cricket, and that work opened so many doors for me broadening my professional opportunities.
How do you bridge the gap between academic research and real-world practice for coaches and clinicians? What an excellent question and an

important consideration in most research. For me, bridging that gap begins with co-designing research in collaboration with the end users, whether that’s coaches, clinicians, or others working directly in the field.
Involving them from the beginning ensures the research is grounded in real-world needs and challenges. Such collaboration not only improves the relevance and usability of the research but also builds mutual respect and trust between me as the researcher and the practitioners, which is key for achieving meaningful impact.
It is really about adopting a humancentric approach to thoroughly understand the environment where the findings will be implemented.


How did you first get involved with SMA and what has been your highlight so far
When I commenced my postdoc with Professor Caroline Finch, it was just a couple of months before the SMA Conference in Fiji. She very kindly supported me to attend, even though I wasn’t presenting. My responsibility was to network and get to know

Bridging
the gap between research and practice starts with co-designing studies alongside end users, whether that’s coaches, clinicians, or others working directly in the field.

people in the field, which was a relatively new area to me at the time. I only knew two attendees initially, and it was quite daunting attending without presenting as you don’t have that natural exposure as a delegate.
However, it was one of the best experiences of my career. Everyone was incredibly welcoming and since the conference took place in a single resort in Fiji, networking opportunities were abundant during breakfast, coffee breaks, and leisure activities. Many of the people I met there for the first time are now close colleagues and friends.
That was in 2006, and since then I’ve only missed one SMA conference due to unexpected circumstances. It remains as one of the highlights of my year.
After five years chairing the SMA Conference judging panel, how have submissions evolved, and what themes continue to impress you?
I was fortunate to assume the role of Judging Chair after some amazing predecessors who had done wonderful work in establishing robust processes. The awards are very prestigious and have remained highly competitive, so having a transparent fair process is paramount. Every year we have tried to refine the submission process and make it as fair, equitable and easy as possible.
Over the five years, we have adapted processes following feedback and reflections. I say “we” as there was a team of people involved, including SMA staff, my fellow conference committee members, SMA Board members, and all the judges and delegates who provide valuable feedback and suggestions. Some adaptations over the past five years include the development of a more detailed guide for reviewers, the removal of the additional 2-page submission required to be eligible for an award, sharing the judging process and grading criteria in a preconference webinar for the past two years, and capturing interest in judging at the abstract submission stage.


What’s been particularly impressive and exciting is seeing the calibre of early career researchers. The quality of their work is exceptional, and they are now competing right alongside senior researchers in the “Best of the Best” sessions, which wasn’t always the case. That increase in confidence and competitiveness has been one of the most interesting shifts in my time as Judging Chair.
What has been a standout moment or favourite aspect of your time on SMA’s Scientific Advisory Committee?
Firstly, I was honoured to be invited to join SMA’s inaugural Scientific Advisory Committee in 2019. It has been a wonderful opportunity to collaborate and learn from fellow committee members. It is a multidisciplinary group, so people from different discipline areas and levels of experience bring perspectives that often differ from mine.
One of the most appealing aspects is the variety of matters we get to provide advice on. To date, it has included reviewing applications for SMA endorsement, evaluating various SMA resources, and recommending the development of consensus statements on current issues.
For me, it presents an excellent opportunity to give back to SMA. SMA has played such an important role in my career, so to be able to contribute to the organisation in a meaningful way is truly gratifying.
Would you recommend SMA to those starting their career in sports medicine and what advice would you give them?
I highly recommend Sports Medicine Australia to anyone, especially those starting out in their careers. In fact, I actively encourage people, at all stages, to get involved. One of SMA’s notable strengths is its multidisciplinary nature, which unites professionals from numerous fields within sports medicine and science. In most workplaces, you might be surrounded by some related disciplines, but rarely do you get the full breadth of perspectives all in one place like you do with SMA.
My advice is to take advantage of opportunities to get involved, even if it seems challenging initially. Sometimes that may involve going to a conference where you don’t know anyone, volunteering for a committee position, or sharing your expertise with the community. Embracing those moments can lead to unexpected, valuable and rewarding connections.




The success of Finnish long-distance runners in the 1920s and 1930s sparked medical interest in studying the physical capabilities and health of both retired and actively competing athletes. Ahead of the Olympic Games originally scheduled for 1940 in Helsinki, there emerged a clear need and growing interest in establishing a medical society with a special focus on sports as a distinct discipline.
As a result, the Finnish Society of Sports Medicine (Suomen Urheilulääkäriyhdistys) was founded in 1938. However, the outbreak of World War II altered the course of the specialty’s development, and due to obvious reasons, the Helsinki Olympic Games were postponed until 1952. Nevertheless, immediately after the war, in 1946, the first sports medicine clinic was established at
the Helsinki Olympic Stadium. This clinic remained active until the 1980s and was restructured into Helsinki Sports Medicine Clinic (Helsingin Urheilulääkäriasema – HULA) in 1964.
The hosting of the Olympic Games in Helsinki served as a catalyst for the development of sports and exercise medicine as a specialized field. As the need to study training methods and physical performance grew, it became increasingly clear that fundamental scientific research was necessary to understand the physiological effects of physical activity on human performance and health.
In 1956, a sports medicine centre was founded in Turku with the assistance of the Department of Physiology at the University of Turku. This centre later became known as the Paavo Nurmi
Centre (PNK), named after the iconic Finnish runner Paavo Nurmi. Nurmi won nine Olympic gold medals and three silver medals between 1920 and 1928, and set 22 world records, becoming a symbol of excellence in endurance sports and a lasting influence on sports science. Paavo Nurmi Centre regarded as the first and, in many ways, a model for the six modern sports medicine centres currently operating in Finland.
The growth and development of research in sports and exercise medicine during the 1950s to 1970s laid the groundwork for the formal establishment of sports and exercise medicine as an independent academic and clinical specialty. During this formative period, sports medicine centres were founded in various forms, gradually contributing to the structural
and institutional development of the field. In 1964, the Helsinki Sports Medicine Centre was officially founded, followed by centres in Oulu, Oulu Diaconess Sports Medicine Clinic (1969), Jyväskylä, LIKES – The Foundation for the Promotion of Physical Activity and Public Health (1975), Kuopio, Kuopio Research Institute of Exercise Medicine (1976), and Tampere Research Centre of Sports Medicine (1980). These centres were primarily established in the geographical regions of Finland where major universities were located—particularly those with medical faculties, such as in Helsinki, Oulu, Tampere, Turku, and Kuopio, as well as the Faculty of Sport and Health Sciences in Jyväskylä. The foundation of the first professorship in sports medicine at the University of Jyväskylä in 1970 marked a significant step toward academic recognition of the discipline.
In the course of their development, each centre evolved based on regional needs and developed its own thematic focus. For instance, the Paavo Nurmi Centre (Paavo Nurmi Keskus) historically placed a particular emphasis on research in sports traumatology, ranging from the physiology of muscle injuries to epidemiological studies. In later years, its research trajectory shifted toward understanding the broader impact of physical activity on health, with an emphasis on the adverse effects of sedentary behavior.
While the first sports medicine clinic in close proximity to the Helsinki Olympic Stadium was established in 1946, the official founding year of the Helsinki Sports Medicine Clinic is considered to be 1964. Known as HULA, the clinic concentrated on investigating correlations between physical activity and health

Photo: Dmitry Naumov/Getty Images
Since 1986, a total of 92 individuals have completed training in sports medicine in a country with a population of 5.4 million.
parameters, the long-term impacts of high-performance sport on elite athletes, and conducted pioneering studies in areas such as exerciseinduced asthma, environmental adaptation to altitude, hypoxic training, and overtraining syndrome.
Kuopio Research Institute of Exercise Medicine is renowned for its extensive research on the effects of exercise in large population cohorts, including numerous randomized controlled trials investigating the impact of physical activity on cardiovascular health. Studies conducted in Kuopio have led to several original discoveries, such as the role of exercise in influencing blood coagulation through platelet activity, the beneficial effects of physical activity on HDL cholesterol levels, and its positive impact on blood pressure regulation in patients with hypertension. A consistent strength of research in Kuopio has been the use of large, well-characterized cohorts and high methodological quality. In
1982, Kuopio hosted the first Puijo Symposium, which later evolved into a flagship international congress in the field of exercise medicine.
The Tampere Sports Medical Centre, established in association with the Urho Kaleva Kekkonen Institute, originally focused its efforts on the analysis of physical activity safety and the prevention of musculoskeletal injuries. Notably, it became a pioneering site for tendon biology research and the investigation of tendinopathies.
At the Oulu Deaconess Sports Medicine Clinic, a longstanding tradition in sports traumatology has been maintained, with early contributions including documentation of operative interventions and the characterisation of medial tibial stress syndrome. This line of inquiry subsequently evolved into comprehensive research on the cardiovascular effects of physical exertion.
The Foundation for the Promotion of Physical Activity and Public Health in Jyvsäskylä has focused its clinical work on key areas such as musculoskeletal adaptation to exercise, weight management, sports injuries, and training effects. Research conducted in these domains has generated socially impactful insights, notably that increased physical activity correlates with a reduced risk of injury. These findings underscore the importance of exercise in promoting both individual and public health.
Thus, in the post-war decades of the 20th century, a body of scientific evidence was gradually established, providing what was then considered a sufficient foundation for the development of sports medicine as a medical specialty. By the end of the 1970s, it had become evident that the time was ripe for the institutionalisation of sports and exercise medicine as a formally recognized medical field. Consequently, in 1981, with support from the Finnish Olympic Committee, the Finnish Society of Sports Medicine (Suomen Urheilulääkäriyhdistys), and the Finnish Society of Physiology (Suomen Fysiologiayhdistys), an official proposal and application were submitted. A dedicated working group was subsequently formed, and in 1983, it presented its conclusions, recommending the formal recognition of sports and exercise medicine as a distinct medical specialty.
According to the working group, the key objectives for establishing sports and exercise medicine as a specialty were:
1. To promote healthy lifestyles among individuals and the general population through increased physical activity, and to direct the application of
Photo: Vladislav Zolotov/Getty Images

In 1981, with support from the Finnish Olympic Committee, the Finnish Society of Sports Medicine (Suomen Urheilulääkäriyhdistys), and the Finnish Society of Physiology (Suomen Fysiologiayhdistys), an official proposal and application were submitted.
exercise in ways that preserve, enhance, or restore health.
2. To prevent, minimise, and treat sports-related injuries and risk factors associated with physical activity.
3. To apply medically appropriate and ethically acceptable methods and strategies aimed at improving individual physical performance, supported by scientific research and accompanied by educational and public health initiatives.
Among the key target populations identified by the working group were recreational exercisers, competitive athletes, school-aged children, the elderly, and persons with disabilities. Already in the early 1980s, the development of sports and exercise
medicine was seen as part of a broader societal effort to promote health-enhancing activities.
Sports and exercise medicine was viewed as a means of contributing positively to public health outcomes. This perspective on the role of the specialty has not only endured but grown stronger over the decades.
This vision of the specialty’s societal role has not only persisted but has become increasingly central. The working group suggested that education and training would be best organized through Finland’s six national centers of sports and exercise medicine.
This process culminated in the official establishment and recognition of sports medicine as a medical specialty in 1986.

The six centres previously mentioned have played a central role in the development of sports and exercise medicine in Finland. Their primary focus has been on advancing scientific research related to physical activity and its effects – both beneficial and detrimental – on human health, including in the context of disease. From the outset, the core missions of these centres have included research, specialist training of physicians, public education, and dissemination of scientific knowledge.
To specialise in sports and exercise medicine, physicians must first complete a nine-month mandatory rotation in general practice. This is followed by optional 3–6-month rotations in a range of disciplines, including gynecology and
obstetrics, cardiology, internal medicine, pulmonology and allergology, clinical physiology and nuclear medicine, traumatology and orthopedics, rheumatology, physical and rehabilitation medicine, psychiatry, acute and emergency medicine, laboratory medicine, radiology, occupational medicine, pediatrics, and neurology.
After fulfilling these prerequisites, candidates may enter a dedicated two-year training program in sports and exercise medicine. Certification is achieved through a written examination. Since 2023, however, the training system has been transitioning to a model grounded in entrustable professional activities (EPAs).
Thus, the training of sports and exercise medicine specialists
provides a comprehensive and multidimensional skill set across a wide range of medical disciplines. Although the official duration of the specialisation is a minimum of five years, each rotation must be applied for through a competitive process. As a result, the actual time to completion typically averages around eight years, offering extensive clinical exposure and professional development.
The curriculum is built to develop expertise in evaluating physical activity eligibility – an individual’s capacity for physical activity – across diverse pathologies; administering exercise as a therapeutic intervention in coordination with multidisciplinary teams comprising physiotherapists, dietitians, and other specialists; and managing musculoskeletal disorders. Furthermore, trainees are prepared to function as sports physicians for athletic teams and competitions, contributing both preventive and acute care expertise in field-based settings.
Since 1986, a total of 92 individuals have completed training in sports medicine in a country with a population of 5.4 million. Approximately 38% (35 individuals) possess a secondary specialization, including fields such as clinical physiology, physiatry and rehabilitation, occupational medicine, internal medicine, orthopedics, and clinical chemistry. Furthermore, a significant portion of these specialists also hold academic degrees: 47 out of 92 have earned a doctoral degree (PhD), among whom 10 are associate professors (docents) and 14 are full professors across a range of disciplines.
Due to the limited number of positions in the public sector, the majority of specialist physicians are employed in
the private sector, primarily working with professional and competitive athletes. Some also work in sports medicine centres, often holding concurrent positions in related disciplines. In 2015, through joint efforts, the first public sector sports medicine clinic was established at the Central Hospital of Jyväskylä – NOVA. This clinic represents the first of its kind in exercise medicine within the public sector and operates within a major central hospital alongside other secondary-level specialties.
In the same year, the sports and exercise medicine responsibilities of Jyväskylä’s LIKES (The Foundation for the Promotion of Physical Activity and Public Health) were transferred to KIHU – the Finnish Institute of High Performance Sport, which continues to lead national efforts in elite athlete health and performance research.
It is also noteworthy that in 2015, the first professorship in sports medicine was established at the University of Eastern Finland (Itä-Suomen Yliopisto) in Kuopio. Significantly, this position was created within the university’s Faculty of Medicine, marking an important milestone in the academic development of the specialty. The position was awarded to Professor Heikki Tikkanen.
In the same year, as the field continued to grow, a decision was made to establish a dedicated professional society to represent and advocate for the interests of sports and exercise medicine specialists. As a result, the Finnish Society of Sports and Exercise Medicine was founded. This organization has gained national recognition and is officially endorsed by the Ministry of Health and Social Affairs, the Ministry of Education and Sports, the Finnish Olympic Committee, and the Finnish Medical Association.


Sergei Iljukov, MD, PhD, is a specialist in sports and exercise medicine. He earned his medical degree from the University of Tartu (Estonia) while also studying sports sciences. After specialty training in Finland at KIHU and the Kuopio Research Institute, he completed a fellowship at Aspetar Hospital in Qatar. Now based in Helsinki, he combines clinical work with research and defended his PhD titled “Athlete Performance Profiling – A New Approach in the Fight Against Doping.” Sergei has over 20 years of anti-doping expertise, has worked with elite teams and Olympians, and serves as Vice President of the Finnish Society of Sports and Exercise Medicine and UEMS delegate.

Heikki Tikkanen, MD, PhD, is a specialist in sports and exercise medicine and clinical physiology. He earned his medical degree and PhD from the University of Helsinki, focusing on cardiovascular physiology and exercise testing. He works with elite athletes and national teams and is Professor of Sports and Exercise Medicine at the University of Eastern Finland. His research explores exercise physiology, wearable technology, and physical activity’s role in managing chronic diseases. He also contributes to national health guidelines and lectures internationally. A founding member of the Finnish Society of Sports and Exercise Medicine, he currently serves as its acting president.


What motivated you to pursue certifications like the SMA Level 1 and Level 2 Sports Trainer Courses, and how have they influenced your career?
I started in my late teens as a volunteer ambulance officer with St John Ambulance in South Australia. I really enjoyed it, and it sparked an interest in health and first aid, so I began teaching first aid to local communities. I originally completed a Bachelor of Education, aiming to become a high school teacher, but I discovered quickly I much preferred working with adults.
When my kids started playing sport, their club needed first aid support, so I stepped in as I thought that sounded like fun and I could use my skills! That’s when I completed the SMA Level 1 Sports Trainer course and was lucky enough to be mentored by Peter Felton, who inspired me to go further and complete the Level 2 Sports Trainer course. I maintained my skills in first aid and sports training whilst I was living remotely and realised it sat well next to my passion for Work Health and Safety (WHS), as well as my work in First Aid and Advanced Resuscitation training, and team management. So, I guess I fell into it and saw an opportunity to progress in a paid role in a field that I loved.
Ultimately, becoming a Sports Trainer has helped me bring my two passions together. Now, as a facilitator with SMA, I not only deliver course content but also focus on preparing sports trainers for the practical realities of the role. It’s been a great blend of experience, and I feel lucky to work in a space that I genuinely enjoy.
What are the toughest challenges Sports Trainers face during live games or events?
One of the big challenges, especially for newer trainers, is dealing with pressure, particularly when games are filmed. Knowing that they are potentially open to a higher level of scrutiny, even if they’re doing
everything right, can make them second-guess themselves, which can affect their performance on the field.
Another major issue is communication. Sports trainers need to interact with a wide range of people, coaches, referees, parents, club officials, and that’s not always easy, especially in high-pressure moments. Assertive and respectful communication is vital, but it is not something that is covered much in training or that everyone has had a chance to develop.
There’s also pressure that can come from the sidelines, especially around injuries like concussion. I’ve seen situations where a parent has said

to their child to “be careful what you say” so they can stay in the game. That’s tough to manage, especially when the player is young and just wants to get back on the field.
I always remind young trainers: take control of your space, stand firm, and prioritise the athlete’s health, because their well-being is more important than the game.
You mentioned communication skills earlier, but what other qualities or skills do you believe the next generation of sports trainers should develop?
Communication is still a core skill, but moving forward, I think inclusivity and cultural awareness are going to be just as important. We’re seeing a broader range of people participating in sport, whether that’s across cultures, genders or neurodiversity and sports trainers need to be equipped with the skills to work respectfully and effectively.
They also need to be able to support athletes with different abilities and mental health needs. While we’re not mental health professionals, players can often open-up to trainers, especially when you are working with them over a season, so knowing how to respond appropriately matters.
Adaptability is key, too, whether you’re working at a single event or with a team long-term, the demands can be very different. And of course, the foundational skills still apply such as time management, triage and thinking under pressure.
Reflecting on your career, is there a moment that truly defined your journey as a Sports Trainer? It’s hard to pick just one moment but for me, it’s been the ability to

combine my first aid background with a sports injury-specific care, that’s been really fulfilling. One case that comes to mind is a young athlete who thought he’d pulled a stomach muscle, but something didn’t feel right as he was in a lot of pain. We encouraged him to get checked out, and it turned out to be appendicitis. You develop a kind of gut instinct after years in the field, and that moment reinforced how important that can be.
Another defining moment for me was helping a 12-year-old player who was really beating herself up after missing a goal. She was in tears, feeling like she’d let her team down. I sat with her and asked what she’d say to her best friend in the same situation. When she said, “It’s okay, it’s just a goal,” I told her to treat herself in the same way she would treat her best friend. That moment really stayed with me. It highlighted how important it is for sports trainers to support athletes not just physically, but emotionally and psychologically as well.
As a member of the SMA QLD State Council, what inspired your involvement? Are there any standout contributions or events you’re especially proud of?
I saw the Expression of Interest go out and at first, I hesitated, thinking, “I’m just a sports trainer,” in a space full of allied health and medical professionals. But then I realised Sports Trainers
I always remind young trainers: take control of your space, stand firm, and prioritise the athlete’s health, because their wellbeing is more important than the game.
students studying teaching with a PE major It’s all about growing the profession and making sure trainers feel supported and seen.
You’re currently assisting with the review of the Sports Trainer e-book. Are there any key elements that would benefit future sports trainers?
Yes, WHS is a big one. It’s often misunderstood by both trainers and clubs, and it’s so important. Trainers need to know things like whether they’re covered by the club’s insurance, how to assess risks, and what hazards to look out for, basic knowledge that can prevent serious incidents.
need a voice, and I wanted to advocate for better access to professional development opportunities. So, I decided to put my name in.
Since joining, I’ve really enjoyed being the voice that helps to promote the wide range of PD that’s now available to other Sports Trainers. I’ve also been able to identify gaps from the sports trainer’s perspective and make practical suggestions, like offering recorded sessions post-event for a fee, which I believe has since been adopted. There is also so much to learn from the other members of the council.
One of the things I’m most excited about is our upcoming student networking event in Brisbane. There’s such a need for more sports trainers, and this is a great step toward building that pipeline. I’d love to see more outreach, maybe even a roadshow to connect with more universities and students studying a broad range of disciplines, for example
It is a cultural issue as much as an educational one. It’s that old “She’ll be right, mate” attitude that still lingers in some areas of sport. We need to shift that mindset and perhaps offer a mandatory WHS module for sports trainers. It doesn’t have to be complex, but it should be clear, accessible, and taken seriously.
Another area I’d love to see added or built out more is post-training support. Once a trainer completes their course, that can’t be the end of the journey. A mentoring scheme or structured support system would help reinforce learning and build confidence, especially for younger or less assertive trainers just entering clubs.
Beyond that, I think the manual should continue to grow in areas like child safety, cultural awareness, and ethical practice especially as our teams become more diverse and expectations on trainers evolve. We need to equip them not just with technical skills, but with a broader understanding of the role they play in creating safe, inclusive sporting environments.




