


Urethroplasty is a surgical procedure to repair a narrowing (stricture) of the urethra, the tube that carries urine from the bladder out of the body.
Sometimes, a graft may be required for the repair and this is commonly taken from the inside of the cheek (buccal mucosa) to reconstruct the urethra.
Depending on your medical condition, this may be performed as a staged procedure, requiring more than one surgery.
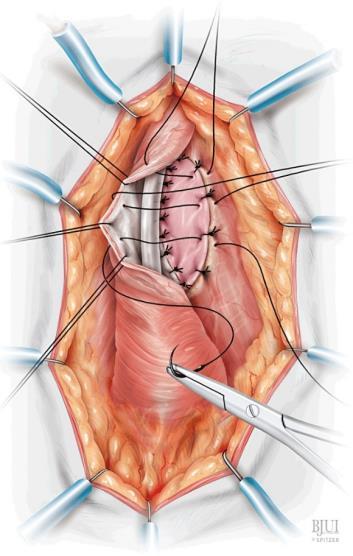
Source: Barbagli G et al. Dorsal Onlay Oral Mucosal Graft Bulbar Urethroplasty. BJUI (2012).
• This procedure is performed under General Anaesthesia
• Cystoscopy and intraoperative X-rays (urethrogram) are usually performed to assess the location and length of the stricture
• A small incision is made in the perineum or penis (for men) / vagina (for women)
• The site of the urethra stricture is identified
• The stricture will be excised or a graft placed at the site, depending on the intraoperative findings. A staged procedure may be required, depending on your clinical condition
• There will be a urinary catheter and if needed, a suprapubic urinary catheter may be inserted as well
Urethroplasty is performed to treat urethral strictures, especially those which are recurrent.
Urethral strictures can result in:
• Weak urine flow
• Straining to urinate
• Urinary retention (inability to urinate) requiring a urinary catheter
• Frequent urinary tract infections
• Painful urination
• Bladder stones
Depending on the severity and length of the stricture, alternatives include
• Conservative management: Observation, however this may result in difficulty in urine passing and urinary retention
• Urethral dilation: Stretching the urethra with progressively larger instruments
• Optical urethrotomy: Cutting the stricture via a cystoscope
• Intermittent self-catheterisation: regular selfcatheterisation to reduce the risk of stricture recurrence
• Permanent urinary diversion: Includes options such as suprapubic catheters. This is generally considered for poor surgical candidates, and is associated with lower quality of life
• High Success Rate: Urethroplasty is the definitive treatment for urethral strictures and has a long-term success rate of approximately 80-90%, depending on location, length, and previous treatments
• Improved Urinary Flow: Most patients experience a significant increase in urine flow rate and bladder emptying
• Reduced Recurrence Risk: Compared to other treatment options, the stricture recurrence rate after urethroplasty is lower
• Swelling and/or bruising at the wound site
• Wound infection
• Urinary tract infection
• Spraying of urine during micturition
• Erectile dysfunction which may require further treatment after the procedure
• Failure of the urethra to join completely, resulting in urine leakage (fistula)
• Painful sexual intercourse with reduced force of ejaculation (men)
• Recurrence of urethral stricture
• Urinary incontinence
• Hospital Stay: Usually 1–2 days.
• Catheter Duration: Typically, 2–3 weeks or longer.
• Pain Management: Pain medications will be provided upon discharge
• Activity Restrictions: Avoid heavy lifting and strenuous activities for at least 4–6 weeks.
• Follow-Up: Follow up Xray (urethrogram /cystourethrogram) and uroflowmetry to assess voiding function and to look for recurrence; a repeat cystoscopy may be performed if required as well.