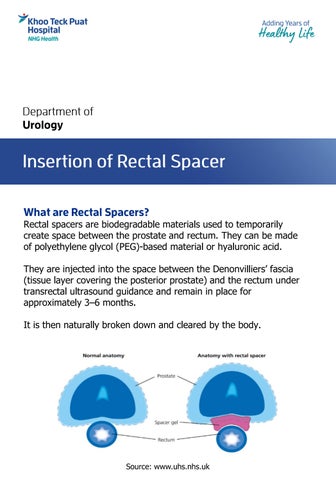
Rectal spacers are biodegradable materials used to temporarily create space between the prostate and rectum. They can be made of polyethylene glycol (PEG)-based material or hyaluronic acid.
They are injected into the space between the Denonvilliers’ fascia (tissue layer covering the posterior prostate) and the rectum under transrectal ultrasound guidance and remain in place for approximately 3–6 months. It is then naturally broken down and cleared by the body.
Source: www.uhs.nhs.uk