
Bronchiectasis is an old disorder that had been described in 1819 by Laennec after postmortem examination of the lung of an infant who died following whooping cough (1). The word bronchiectasis derived from Greek words bronchon and ektasis that mean wide pipe stretching out. Despite it is an old disease still there are various opinion about bronchiectasis; is it a separate disease, complication of other disorder or it is a consequence of disorders, but in any way it represent an end stage of variety of pathology (1). Because of these variation there is different definitions of bronchiectasis, but the most comprehensive one is that bronchiectasis is an irreversible abnormal dilatation of one or more bronchi with chronic airway inflammation associated with chronic sputum production, recurrent chest infection and airflow obstruction (2). This definition contain pathology, pathogenesis, symptoms, common eatiology and common complications. The prevalence of bronchiectasis exactly not known because of many factors such as wide range of eatiology, the fact that it is end result of different pathology and that its symptoms and presentation similar to many respiratory disorders and this is the situation in study area, Port Sudan, eastern Sudan. In general There are three theories for developing of bronchiectasis; these are traction theory(infection), atelectatic theory ( collapse) and pressure of secretion theory ( infection) (1), all these theories result from infection or obstructive insult. Despite different eatiology such as infection, primary impaired of mucus clearance, immune deficiency, developmental defect and alpha antitrypsin deficiency (3) bronchiectasis shows few symptoms such as cough, sputum production, small or massive haemoptysis from insult of mucus membrane or from pulmonary artery insult respectively and general feature of inflammation (4). Diagnosis of bronchiectasis depend on CT chest which may be normal in significant percentage of cases and lead to delay in diagnosis. The outcome of bronchiectasis depend on several factors such as underline cause, duration of disease, comorbidity, age,
Conclusion: Mortality of bronchiectasis in Port Sudan is low comparing to other areas. Respiratory failure due to pulmonary fibrosis and subsequent inflammation and lung destruction or due to due to recurrent bronchiectasis exacerbation and pulmosepsis is the commonest direct cause of death in those patients.
1 Respiratory medicine Associate professor, Red sea university2 Assistant professor, Umm Al Qura university
I. Background
Result:152 patients with bronchiectasis enrolled in this study, male to female is 3: 1, tuberculosis represent the most common cause of bronchiectasis in this area occur in (76.3 %) of patients , mortality is ( 5.3%), and 5 years survival rate is( 94.7%). the risk factor for mortality are; infectious exacerbation (87%), pleuroparenchymalfibroelastosis (37.5%), cystic fibrosis (25%), bronchopleuralfistula (25%),and pneumothorax (12.5%)
1 Dr. Murwan Mohamed Saeed 2 Dr. LailaSulmanAbdElrmanFaki MD.
Introduction: Bronchiectasis is an old disease return to 1819, despite this still there are many different ideas about it, and different definitions but the most comprehensive definition is that bronchiectasis is an irreversible, abnormal dilatation of one or more bronchi with chronic airway inflammation, associated with chronic sputum production, recurrent chest infection and air flow obstruction. Bronchiectasis is an end stage of various respiratory disorders and it may occur as complication of non respiratory disorders and its symptomatic presentation overlapping symptoms of its eatiology therefore it is difficult tobe studied an there are very few studies regarding its outcome. In Port Sudan, eastern Sudan the prevalence and outcome of Bronchiectasis are not known so this study done to assess bronchiectasis mortality and its risk factors.
Keywords: Bronchiectasis, Risk factor, Mortality, Exacerbation, Respiratory failure.
Bronchiectasis outcome and risk factors of mortality In Port Sudan
Abstract:
American Journal Of Multidisciplinary Research & Review (AJMRR) 2022 AJMRR Journal Page | 29 American Journal of Multidisciplinary Research & Review (AJMRR) E ISSN: 2378 228X Volume 01, Issue 02, pp 29 33 www.ajmrr.comResearchPaper Open Access
Method: this is a prospective analytical hospital base study done in Port Sudan, eastern Sudan from April 2014 to April 2019 to study outcome, morbidity and mortality of bronchiectasis and to assess risk factor for both.

FEV1 at the beginning of study were> 80% in 142 patients ( 93.4%) , 80 50 % in 10 patients (6.6%). In second year > 80 % in 102 patients (67.1%), 80 50 % in 102 patients ( 32.9 %), in third year > 80 % in 89 patients (58.6), 80 50 % in 63 patients (41.4% ) and in the fourth year < 80% in 52 patients (34.2% ), 80 50 % in 96 patients ( 63.2%) and 50 30 % in 4 patient (2.6%). 42 patients (27.63 %) developed exacerbation in the first year, in second year 132 patients (86.84% ) have recurrent exacerbation and from third year all patients . Throughout the study 23 patient (15%) developed pulmonary hypertension, 6 patients (4%) developed respiratory failure, 4 patients (2.6%) developed pneumothorax and other 4 patients ( 2.6%) developed bronchopleural fistula. 8 patients died ( 5.3%) 6 ( 3.95%) of them in the fourth year and 2 (1.32% ) in the fifth year, 3 (37.5%) of those who died have pleuroparenchymalfibroelastosis; developed recurrent exacerbation and end with respiratory failure
3 5: Inclusion criteria: Patients more than 17 years old who have bronchiectasis, attend to chest hospital referred clinical and accept to be enrolled in this study.
3 4: Study duration: This study done from April 2014 to April 2019.
3 1: Study design: This is a prospective, analytical, hospital base study.
3 3: Study population: Patients who are diagnosed as bronchiectasis on base of HRCT and accept to be enrolled in the study.
American Journal Of Multidisciplinary Research & Review (AJMRR) 2022 AJMRR Journal Page | 30 BMI, stage of pulmonary function, type of organism that cause exacerbation and radiological severity; because of these different factors and wide range of eatiology the outcome of bronchiectasis being difficult to studied and very few studies done to assess the prognosis and outcome of bronchiectasis. In Sudan no study done to assess the outcome of bronchiectasis so this study done to know the mortality of bronchiectasis and its risk factors. II. Objective
This study aim to know the outcome of bronchiectasis, morbidity and mortality and to assess risk factors of mortality.
3 6: Exclusion criteria: Smoker patients, patient who have bronchial asthma, COPD or Cardiac disease.
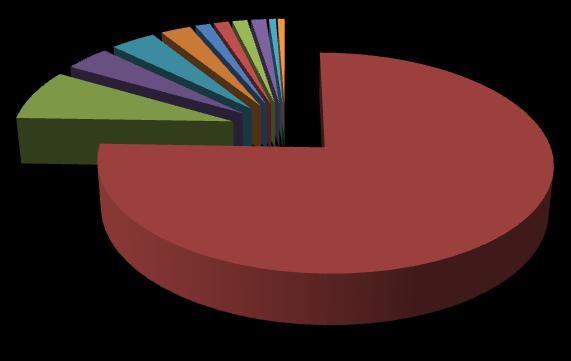
3 8: Data collection and method: Data was collected through modified St George's questionnaire ( SGRQ) That contain sex, age, time of diagnosis, diagnostic evidence, comorbidities and history of exacerbation and hospital admission. Patients followed regularly and on daily base during exacerbation. HRCT chest done for all patients as base and then annually, CBC, renal profile, liver function test, and inflammatory markers done at every visit. ANA profile, Z N smear, total IgE, IgE for aspergillosis,and retroviral screening done at first visit. BMI calculated annually and Pulmonary function test with simple spirometry done annually. Then data analyzed using SPSS program. Result: 152 patients of bronchiectasis enrolled in this study. Male to female 3:1, the causes of bronchiectasis in those patients were tuberculosis in 116 ( 76.3% ),12 patients HIV (7.9% ),rheumatoid arthritis in 6 patients (4%), kyphoscoliosis in 4 patients (2.6%), pleuroparenchymalfibroelastosis in 4 patients (2.6%), measles 2 patients (1.3%), cystic fibrosis 2 patients (1.3%), aspergillososis 2 patients (1.3%), 2 patients yellow nail syndrome (1.3%), 1 patient (0.7%) IgA deficiency and 1 patient (0.7%) monierKhon syndrome.
3 2: Study area: This study done in Port Sudan chest hospital, Port Sudan, eastern Sudan.
3 7: Ethical consideration: Ethical approval from ministry of health and verbal accepting from patients after explanation of study objective and methods.
Using bronchiectasis severity index (BSI) at beginning of study 105 patients (69.1% ) were mild bronchiectasis, 29 patients (19.1% ) moderate bronchiectasis and 18 patients (11.8%) were sever bronchiectasis. BMI at the beginning of study was < 18 in 21 patients (13.8%), 18 25 in 122 patients (80.3%) and 25 30 in 9 patients ( 5.9%). In second year < 18 in 39 patients (25.7%|), 18 25 in 109 patients (71.7%) and 25 30 in 4 patients (2.6%). In third year < 18 in 92 patients (60.53%), 18 25 in 42 patients (27.63%) and 25 30 in 18 patients (11.84%) which not changes in 4th year and in fifth year 6 patients were died and BMI became < 18 116 ( 76.32%), 18 25 in 28 patients (18.42%) and 25 30 in 2 patients (1.32%).
American Journal Of Multidisciplinary Research & Review (AJMRR) 2022 AJMRR Journal Page | 31 and death, 2 patients (25%) with cystic fibrosis again developed several exacerbation attacks and pulmosepsis then died, 2 patients (25%) died bronchopleural fistula that cause respiratory failure and 1 patient ( 12.5%) developed tension pneumothorax, So mortality rate in this study is 5.3% and five year survival rate is 94.7% Figure(1):Causes Figure (2): Relation between FEV1 and duration 0 %76.30 %7.90 %3.90 %3.90 %2.60 %1.30 %1.30 %1.30 %1.30 %0.60 %0.60 HIVTBRAKyphoscoliosispleuroprenchymalfibroelastosis %93.40 %67.10 %58.60 %34.20 %6.60 %32.90 %41.40 %63.20 %2.60 %0.00 %10.00 %20.00 %30.00 %40.00 %50.00 %60.00 %70.00 %80.00 %90.00 %100.00 first yearsecond yearthrid yearforth year more80% %50%80 %5030
The outcome, prognosis, morbidity and mortality of bronchiectasis not fully studied worldwide because of many factors such as wide range of underline causes and overlapping of complications and similarity of symptoms of both bronchiectasis and its eatiology. In this area (Port Sudan) there is no previous study done to assess the outcome of bronchiectasis and also the prevalence of disease not known exactly. TB is the commonest endemic infectious disease in this area and it represent the common cause of bronchiectasis this return to weakness of TB program which follow patient through unqualified medical staff so many patients developed pulmonary fibrosis that lead to traction bronchiectasis in addition to drug interruption, this is similar to C. Hayoung, et al study in Korean patients which conclude that the incidence of bronchiectasis follow the prevalence of TB (5). The mortality rate of bronchiectasis in this areais 5.3% which is very low comparing to other areas as in M. R. Loebinger study's that done in Royal Brompton hospital (London, UK) in 91 patients mortality rate was 29.7% (6), this may be due to variation of both duration and sample size of two studies.
American Journal Of Multidisciplinary Research & Review (AJMRR) 2022 AJMRR Journal Page | 32
Figure (3): morbidity III. Discussion
Bronchiectasis is common respiratory problem in Port Sudan, eastern Sudan and tuberculosis represent the commonest cause of bronchiectasis in this area and its complications especially fibrosis are main cause of morbidity and mortality of Mortalitybronchiectasis.rateinthisstudy which is 5.3% is low comparing to other study and 5 years survival rate is high 94.7%. Respiratory failure which occur due to fibrosis, pulmosepsis or pulmonary hypertension is the commonest direct cause of death, this followed by sepsis while risk factors of both morbidity and mortality are pulmonary fibrosis, infectious exacerbation, and pulmonary hypertension. %2.60%2.60%5.30%2.60%3.90
Pulmonary fibrosis which lead destruction of lung parenchyma that progress to respiratory failure and result in death (3); fibrosis may occur secondary to tuberculosis or as part of both cystic fibrosis and pleuroparenchymalfibroelastosis and it may cause disability, hypoxic pulmonary hypertension, respiratory failure and death. Infectious exacerbation represent the second risk factor of morbidity and mortality as many factors in bronchiectasis predispose to recurrent infection and lung destruction such as accumulation of secretion that increase virulence of infecting organism, anatomical abnormality of both bronchi and lung parenchyma and immune compromise (7).
IV. Conclusion:
Pulmonary hypertension which occur in significant percentage in this study may result from destructive inflammation, scar or due to loss of alveolar bed that result in systemic to pulmonary shunt (3,8,9) and it may cause disability and respiratory failure that lead to death. Patients with cystic fibrosis are at risk of recurrent exacerbations and respiratory failure so it represent major risk for death in bronchiectatic patients through pulmosepsis or respiratory failure. Bronchopleural fistula occur in tuberculousbronchietatic patients due to fibrothorax in old tuberculosis or rupture of cavity during active tuberculosis (10) and it may lead to death through life threatening tension pneumothorax or due to sepsis.
%0 %20 %40 %60 %80 %100 %15 %100

References: [1]. Crofton and Douglas respiratory disease, S. Anthony, A. Gordon, fifth edition (2002), 394,795,804,805. [2]. Oxford hand book of respiratory medicine, C. Stephen, et al, third edition (2014), 154. [3]. Kumar & Clark clinical medicine, P. Kuma, Clark M. forth edition (2002), 822, 806. [4]. Harrison pulmonary and critical care medicine, L. Loscalzo, et al, 17th edition (2010), 168. [5]. 5 C. Hayoung, et al, ERJ open research 2020,6:00097 2020; DOI: 10 1183/ 23120541. 00097 2020. [6]. M.R. Loebinger, et al, Mortality in bronchiectasis: long term study assessing the factors infleuencing survival, European respiratory journal 2009 34:843 849; DOI: 10. 1183/ 09031936. 00003709. [7]. Fishman, manual of pulmonary diseases and disorders, Alfered P. Fishman, Jack a. Elias, third edition (2002), 671. [8]. Wieber BM, Laursen H. Lung morphometry by unbiased method in emphysema: bronchial and blood vessels volume, alveolar surface area and capillary length APMIS; 106 : 501 656. [9]. Setta M. Baraldo S, Carbino L, et al. CD8 +ve cell in the lungs of smoker with chronic obstructive lung disease. AMJ Respi Crit Care Med; 160:711 717. [10]. Tuberculous and post tuberculousbronchopleural fistula ten years clinical experience, J. Donath, et al, chest 1984. Nov pubMed. gov.
Strengthening of TB program and close monitoring of TB patient will decrease the incidence of bronchiectasis and decrease its morbidity and mortality.
American Journal Of Multidisciplinary Research & Review (AJMRR) 2022 AJMRR Journal Page | 33