March - April 2023


March - April 2023
Editorial Summary
The prevalence of chronic venous disease (CVD) can vary depending on the population studied and the diagnostic criteria used, but is estimated to affect up to 30% of adults worldwide. There is an increasing prevalence with age, with rates as high as 50% in people over the age of 50. Females are more likely than men to develop CVD, as are patients who are smokers, overweight or obese. In severe cases, CVD can lead to complications such as venous leg ulcers (VLU), deep vein thrombosis (DVT), and pulmonary embolism (PE). Wound bed preparation and irrigation are important steps in wound care that help to remove debris and promote healing. The options for wound bed preparation and irrigation include normal saline irrigation, antiseptic solutions containing agents that can kill bacteria and other microorganisms in the wound bed. Examples include povidone-iodine, chlorhexidine, and hydrogen peroxide. These should be used with caution. Enzymatic debridement agents break down and remove necrotic tissue and debris from the wound bed. Examples include collagenase and papain-urea. Mechanical debridement involves physically removing debris from the wound bed using methods such as wet-to-dry dressings or irrigation with a syringe. Negative pressure wound therapy (NPWT) is a specialized wound dressing to promote wound healing. It can help to remove excess fluid from the wound bed and promote the growth of healthy tissue. The choice of wound bed preparation depends on the type and severity of the wound, as well as individual patient factors. This article examines the potential for synergistic use of pure hypochlorous acid (pHA) with ovine forestomach matrix for patients with venous leg ulceration.

Chronic venous disease is a huge spectrum of medical conditions, and is one of the most prevalent medical conditions in the world affecting 25 - 40 million Americans; however, there are 2 - 4 million, or even more, that have advanced chronic venous insufficiency; 500,000 - 1 million patients have venous ulceration.



Chronic wounds progress from hemostasis to inflammatory, proliferative, and remodelling phases, but wounds become a chronic wound if they are stalled in the inflammation phase and have not entered the proliferation phase after 4 weeks of standard of care (SOC) therapy.
Venous ulceration is associated with older age groups, however many of these individuals are still actively working, resulting in significant economic cost due to time taken off work due to the condition, or as happens frequently, the condition leading to a decision to take early retirement, which will often involve a reduced quality of life.1
 Dr Peter Gloviczki
Dr Peter Gloviczki
“Micronutrient components can maximize nitric oxide production which improves lymphatic function, micro arterial vasodilation, venous tone, and immune function which are all incredibly beneficial to these patients who may be micronutrient deficient.”
Of the 2.5 million leg ulcer cases per year, 80% are venous leg ulcers (VLUs), and with an everincreasing elderly population, there is increasing incidence. The costs involved are substantial, on an individual basis and also considering the wider economic impact, including:
early, managing the venous hypertension as a basis for wound healing.
In the 4 weeks of SOC, there should be a 50% reduction in the wound size; if not, it may be necessary to signal for a change, or additional therapies, or advanced extracellular matrices (ECM). This is important, because generally wound area reduction after 4 weeks is predictive of complete wound healing by 24 weeks.
It is important to run a typical VLU checklist, like an airplane pilot’s pre-flight checks, to maximize outcomes. Local and national guidelines should be followed, with incorporation of evidence-based modalities that lead to the highest quality outcomes with the most appropriate resource utilization. The goals are to alleviate pain, rapidly heal the ulcer, and to prevent long term sequelae.
Investigation with venous competency ultrasound is critical, identifying both saphenous and non-saphenous reflux, as well as perforator status. Studies suggest that axial and non-axial venous reflux should be treated
A nutrition evaluation typically, in practical terms, ranks low on the checklist. Micronutrient components can maximize nitric oxide production which improves lymphatic function, micro arterial vasodilation, venous tone, and immune function which are all incredibly beneficial to these patients who may be micronutrient deficient. Focusing on the B vitamins (B12, B6 folate), and high dose vitamin C can help with decreasing reactive oxygen species and antioxidants. A caveat on vitamin C is that if the patient has a history of renal stones, it may be necessary to be careful and discuss with the primary care physician. Vitamin D can also have an impact, not just on bone health, but on microvascular perfusion. Arginine certainly contributes to nitric oxide production and Micronized Purified Flavonoid Fraction (MPFF).
Certainly, looking at the medication list is important, because medications like amlodipine or other calcium channel blockers, can contribute directly to lower extremity edema; typically amlodipine needs to be stopped to maximize edema control. Oncology patients undertaking chemotherapy or who are on hydroxyurea are certainly at a high risk of inhibited long term healing.
It is prudent to consider biopsy; with atypical vs typical ulcerations, if an atypical is missed such as a malignancy, or pyoderma gangrenosum, and it is treated as a typical venous leg ulcer, then there will not be a good outcome.
There is of course a focus on reducing wound pH; peer reviewed validated data confirms that decreasing the wound pH can help with decreasing bacteria population, improve angiogenesis, and improve accelerated epithelialization, combined with other types of adjunctive modalities.
Another important consideration is compression, and it is pivotal to get certified lymphedema therapists involved and begin utilizing inelastic Velcro; this is applied and removed over the top of dressings, and it is vital not to forget about both the foot component and the calf component.
Cost effective wound bed modulation, as shown with ovine forestomach later in this article, should also be opted for. Also, smoking has to be ceased, including vaping.
To conclude, the steps should include the checklist for VLUs with special attention to avoiding missing the identification of Peripheral Arterial Disease (PAD); it has been observed in a growing demographic with diabetes and metabolic syndrome in the population. Another focus point is avoiding undertreating lymphedema; recognizing malnutrition and treating it appropriately, focusing not just on the protein component but on the micronutrient component. In terms of investigations, venous ultrasounds must be done early. It is necessary to be vigilant with medications contributing to lower extremity edema and to modify them. Of course, tobacco cessation is another vital component.
Pure hypochlorous acid can be utilized to manage microbial adherent aggregates, decreasing the pH to 5.5. Ovine forestomach matrix can be incorporated for extracellular matrix modulation; for both there is supporting evidence, both micro to macro, for wound modification and healing.

Pure Hypochlorous Acid (pHA) preserved cleanser (Vashe®, Urgo Medical North America, Fort Worth, TX), is manufactured at 300 ppm (parts per million), it has a pH range of 3.5 - 5.5, which is conducive to healing.2
It is not cytotoxic, unlike standard sodium hypochlorite solutions.3 This product is consumed by organic matter in the wound and dissipates in seconds, so it is safe to use with ECM in the same setting.4 For wounds that have microbial adherent aggregates, 5 - 8 minutes of wound contact with the solution should be considered, in combination with sharp debridement.5 This mechanical disruption of germs and associated necrotic debris is a rapid process, and does not require long exposure as some other modalities may.
Some very recent consensus documents and guidelines suggest discontinuation of use of cytotoxic cleansing agents such as Dakin’s, or solutions that contain cytotoxic agents, such as chlorhexidine gluconate.6
A paper published in 2022 also considers the use of hypochlorous acid versus sodium hypochlorite.7 The issue of margin of safety is discussed at length.
Another paper looks at the cytotoxicity of cleansers via the lens of the therapeutic indices of the cleansing agent preservative
“Another important consideration is compression, and it is pivotal to get certified lymphedema therapists involved.”
molecule.8 Hypochlorous acid has a higher therapeutic index compared to the hypochlorite present in Dakin’s, offering a higher effectiveness with a lower toxicity to the tissue.
The hypochlorous acid molecule, a naturally evolving substance inside the human tissue, forms part of the cellular barrier immunity; humans are designed to live with hypochlorous acid in their tissue, which explains the lack of cytotoxicity of the pHA based cleanser.
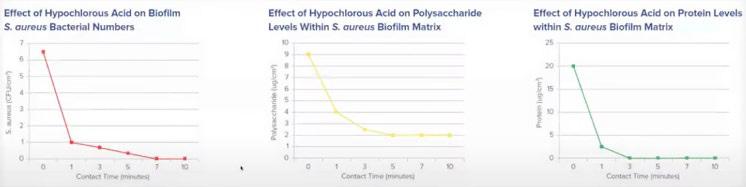
The pHA based cleanser has been studied extensively in its ability to disrupt microbial adherent aggregates. Laboratory studies have shown that hypochlorous acid has the ability to mechanically disrupt 90% of microbial adherent aggregates after a short exposure.
Microbial adherent aggregates, the exopolymeric substances secreted by and surrounding bacteria, has presented many problems in the healing of wounds. Estimates suggest they are present and potentially delaying healing in 60% of chronic wounds; disrupting them is a crucial element of any wound care clinician’s armamentarium in treating chronic wounds.
Hypochlorous acid has a stable shelf life of approximately 18 months, a pH of 5.5, and it is non-cytotoxic in wound and peri-wound environments; it decreases inhibitory wound bed pathogens. In many institutions, it is SOC with Negative Pressure Wound Therapy (NPWT) after surgical debridement, in order to maximize lowering of the wound pH, and not having a recurrence of microbial adherent aggregates. It is applicable to all wounds, including pyoderma, diabetic foot ulcerations and traumatic wounds.
On sulfamylon or mafenide and bacterial adherent aggregates, Murphy et al. report that the mafenide solution had a flat curve; very little effects occurred on the bacterial adherent aggregates, as compared


to the pHA based cleanser solution.17
Chronic wounds tend to be deficient in a good quality extracellular matrix (ECM), which is comprised of a complex process of cells, blood vessels, and macromolecules.10 The ECM is important for structural and biochemical support. Chronic wounds often have deficient ECM, senescent fibroblasts and increased Matrix Metalloproteinases (MMPs). Enhancing and optimizing the ECM with a replacement ECM to heal these ulcers more effectively should be considered.
It is an important consideration to try to focus on decreasing interstitial edema, and by maximizing lymphatic functionality resulting in immune function enhancement, as well as decreasing subcutaneous edema, microvascular arterial perfusion can be maximized, resulting in
“Hypochlorous acid has a higher therapeutic index compared to the hypochlorite present in Dakin’s, offering a higher effectiveness with a lower toxicity to the tissue.”Figure 3: Pure Hypochlorous acid versus Mafenide profile.
immune function enhancement, and when also decreasing subcutaneous edema, microvascular arterial perfusion can be maximized at the 5-micron level. Peri-wound lymphatic stasis occurs in almost every wound; the epiboly seen in wounds is actually built-up lymphatic stasis, and when lymphatics are static, the immune system doesn’t function well. By maximizing peri-wound lymphatic stasis resolution, we can improve overall wound healing.11,14,15
The matrisome is defined as the ensemble of more than 1000 genes encoding ECM and ECM-associated proteins vital for numerous processes in living tissue, including homeostasis, wound healing, growth, and development. The sheer number of proteins and the differences in their abundance in different tissue types demonstrates how complex a system is being orchestrated between cells and the many proteins of the ECM.

Overall, the ideal skin substitute graft would have the following criteria:
An effective advanced ECM for use in VLUs is Ovine Forestomach Matrix (OFM) (Endoform™ Antimicrobial; Endoform™ Natural; Myriad Matrix™, Aroa Biosurgery, Auckland, New Zealand). After years of research, the forestomach of sheep in New Zealand was identified as an ideal starting tissue to construct advanced ECM technologies for soft tissue repair. This source tissue from juvenile sheep (less than 12 months of age) is highly abundant in New Zealand, and the animals are disease free. The forestomach, even from these young animals, is very large, meaning large sheets of ECM can be easily manufactured. The forestomach is a highly vascular tissue, designed for digestion that is integral for rapid nutrient absorption. This also means that residual vascular channels in the graft help it to revascularize more quickly, and then this tissue undergoes more rapid remodelling, where soft tissues are continuously renewed in the body; it has a high concentration of secondary macromolecules, which are known to be important for healing.12
“By maximizing peri-wound lymphatic stasis resolution, we can improve overall wound healing.”
In terms of the ECM, OFM is recommended for use in the operating room, and Endoform™ Antimicrobial or Endoform™ Natural (Aroa Biosurgery, Auckland, New Zealand) in the clinic. Myriad Morcells™ (Aroa Biosurgery, Auckland, New Zealand) is another option that is available; it is a structured retention of architecture from the forestomach of young sheep, typically less than 12 months old. The stomach of sheep has to heal very quickly to maintain the health of the animal, so the OFM has a diverse array of collagens including 1, 2, 3, and 5, as well as an abundance of glycoproteins and proteoglycans. All these are preserved through a very specific process and retention of vascular channels, and it is cost effective.
A study of OFM usage in a military veteran hospital in 2017 shows that in 9 months, cellular or tissue-based graft unit usage decreased by 60%; expenditures on these grafts decreased by 66%, with a higher and faster rate of healing.13

General treatment algorithms for VLUs include commencing with standard compression, leg elevation, and then a thorough wound bed preparation with sharp excisional debridement; a high consideration for bacterial control with appropriate wound cleansers (a pure hypochlorous acid preserved wound cleanser is recommended); early use of advanced ECMs when appropriate for coverage of vital structures, dermal regeneration and accelerating primary healing of small VLUs (preferred option would be to use an OFM graft).
In patients that have failed healing of large venous ulcers with standard of care in conjunction with a granulated wound base, with no bone or tendon exposure, and where a high quality of skin coverage is desired, a Split Thickness Skin Graft (STSG) may be considered.
An ideal operative algorithm for STSGs could be considered as the following: a combination of performing a thorough intra-operative ultrasonic debridement with pure hypochlorous acid solutions; sharp debridement with a curette, and OFM coverage. The graft can then be stapled or sutured in place with a thrombin sealant. A standard dressing protocol can be used, which can include: a non-adherent silver silicone dressing with Negative Pressure Wound Therapy (NPWT); appropriate 4 or 5 layer compression wrap dressings, and then immobilization at the ankle or knee as indicated. The most complex patients are often admitted, put on bed rest, and some require a stay for optimal take of the graft, as well as compression and post-operative patient education.
“A study of OFM usage in a military veteran hospital in 2017 shows that in 9 months, cellular or tissue-based graft unit usage decreased by 60%; expenditures on these grafts decreased by 66%, with a higher and faster rate of healing.”
This patient was a 67-year-old male with chronic venous disease, 3 failed Cellular and Tissuebased Product (CTP) applications for VLU and a failed skin graft (failed STSG placement). He was referred to the center.








This second patient was a 66-year-old female with a 4 year history of VLU, compliant with compression and weekly debridement. She also had irrigation with Polyhydroxy Acid (PHA) solution.

7c:
7d: Week 24: the wound that had previously been so recalcitrant is now fully 100% epithelialized and healed.


The next patient was a 65-year-old male with a catfish spine through his leg. He had a history of VLU, hypertension and diabetes, and had developed a necrotizing soft tissue injury.




9a, 9b: Referred from the Long-term Acute Care Hospital (LTACH) with extensive injury, loss of soft tissue and crucial structures on the foot and leg, and necrotic fat on the dorsal foot.

9c: After debridement, application of OFM to obtain coverage over the exposed dorsal extensor tendons region.
9d, 9e: Application of OFM product over the remainder of the wound to help achieve this dermal regeneration coverage.
9f, 9g: 2 weeks postoperative: early granulation tissue showing through the graft.
9h, 9i: 13 weeks postoperative: fully granulated with an excellent contour restoration.

This patient had been immediately admitted to hospital with an inpatient wound team consultation, vascular surgery performed, and a venoplasty for improved outflow.

10b: An operative debridement of 1800mm2 wound had been performed twice with a pHA solution and sharp debridement.











10c: Inpatient installation of NPWT with the pHA preserved wound cleanser solution.
10d, 10e: The patient was transferred again to the long-term acute care hospital (LTACH) for a further 3 weeks after application of graft. The wound became resolved, and the patient transitioned to outpatient care, following a comprehensive team-based approach.
10g: 3 month follow up. Quality of life improved for this patient due to the success of treatment.
Pure Hypochlorous Acid is a non-cytotoxic, pH-balanced solution topical wound cleanser used to clean and irrigate acute and chronic wounds, formulated with hypochlorous acid (HOCl), a naturally occurring molecule that is produced by white blood cells to fight infection. Evidence shows that pHA is effective in reducing wound bioburden, promoting wound healing, and reducing the risk of infection. It is well-tolerated by patients and has a low risk of adverse reactions. It is effective against a broad range of microorganisms, including bacteria, viruses, and fungi. It can be used on a variety of wound types, including pressure ulcers, diabetic foot ulcers, venous stasis ulcers, surgical wounds, and burns.
Utilizing pHA in conjunction with ovine forestomach can lead to excellent results compared to STSG alone. For patients with these exposed structures such as tendons, or a significant volumetric defect, the ovine forestomach ECM helps achieve a robust granulation; this is likely due to the source of the tissue being highly vascular with the residual channels. It is a structure that is very used to a hostile environment of digestive enzymes, and so it seems to work well in these wounds that have significant microbial adherent aggregates and are difficult to heal; it may just be the ideal tissue for this difficult problem.
Considering the importance of maintaining volume and edema reduction of the leg following grafting, the compressive therapy and aftermath of the skin graft is vital. Immediately after surgery, after the negative pressure is applied, it is advisable to apply a 4 or 5 layer compression wrap; the Urgo K-Two wrap (Urgo K-Two, Urgo Medical North America, Fort Worth, TX) is an excellent option that is typically used in the clinical setting. A comproflex wrap can be applied on top, potentially as layer 5 for their long term compressive control, and also a venous edema leg pump can be used.
The biggest struggle must be considered recurrent ulcers due to recurrent edema, and so patient education is crucial, or they could be in the same condition again; an integrated approach to making sure that message is very clear is important.
Again, comparing using STSG alone to using
the ECM layer, the latter has clearly given a better contour on the overall end result of the leg. Considering case 3, this patient had significant 1cm contour deficit and although that tissue was viable, and could have tolerated an early skin graft, much more robust coverage and an excellent cosmetic result was achieved by utilizing a staged approach with the ECM with negative pressure.
Finally, it is worth noting that working with vascular surgeons and having evaluations conducted by the vascular team can be very beneficial.
This allows the patients to undergo evaluation by a vascular team and maybe some interventions, to treat the underlying venous problems. For the venous gangrene patient (case 4), the vascular team was consulted on admission, leading to an endovascular venoplasty; the expression ‘no flow no go’ is appropriate; improve the inflow and improve the outflow, and occasionally that is done outpatient or inpatient depending on the appropriateness of the setting, but this must be optimized before grafting, or there may be a failure of the graft.
The Society for Vascular Surgery and the American Venous Forum have published excellent guidelines, although it must be said that more recent venous ulcer guidelines are needed.
These guidelines need upgrades frequently, not only because there are a large number of new venous ulcer treatments that are not interventional, but because there have been tremendous changes in vascular reconstruction because of the endovascular revolution; during the last 2 decades, vein care has been changed forever.
1. Gloviczki ML, Kalsi H, Gloviczki P, Gibson M, Cha S, Heit JA. Validity of International Classification of Diseases, Ninth Revision, Clinical Modification codes for estimating the prevalence of venous ulcer. J Vasc Surg Venous Lymphat Disord. 2014 Oct;2(4):362-7. doi: 10.1016/j.jvsv.2014.03.002. Epub 2014 May 10. PMID: 26993538.
2. Nagoba BS et al. Acidic environment and wound healing: a review, Wounds 2015;27(1):5-11
3. Hidalgo E et al. Cytotoxicity mechanisms of sodium hypochlorite in cultured human dermal fibroblasts and its bactericidal effectiveness. Chem Biol Interact. 2002 Mar 20;139(3):265-82.
4. C. Winterbourn et al. Modeling the Reactions of Superoxide and Myeloperoxidase in the Neutrophil Phagosome. Implications for Microbial Killing. J Biol Chem Volume 281. No. 52. Dec. 29, 2006. 39860 - 39869;
5. Robson MC. Treating chronic wounds with hypochlorous acid disrupts biofilm. Wound Prevention and Management 2020;66 (5):9-10
6. Swanson, T., Ousey, K., Haesler, E., Bjarnsholt, T., Carville, K., Idensohn, P., Kalan, L., Keast, D. H., Larsen, D., Percival, S., Schultz, G., Sussman, G., Waters, N., & Weir, D. (2022). IWII Wound Infection in Clinical Practice Consensus Document: 2022 Update. Journal of wound care, 31(S12), S10-S21. https://doi.org/10.12968/jowc.2022.31.Sup12.S10
7. Eriksson E, Liu PY, Schultz GS, Martins-Green MM, Tanaka R, Weir D, Gould LJ, Armstrong DG, Gibbons GW, Wolcott R, Olutoye OO, Kirsner RS, Gurtner GC. Chronic wounds: Treatment consensus. Wound Repair Regen. 2022 Mar;30(2):156-171. doi: 10.1111/ wrr.12994. Epub 2022 Feb 7. Erratum in: Wound Repair Regen. 2022 Jul;30(4):536. PMID:
35130362; PMCID: PMC9305950.
9. Wound Repair and Regeneration – the international journal of tissue repair and regeneration. Available from: https:// onlinelibrary.wiley.com/journal/1524475x
10. Melphine M. Harriott, Nayan Bhindi, Salam Kassis, Blair Summitt, Galen Perdikis, Blair A. Wormer, Timothy M. Rankin, Christodoulos Kaoutzanis, Mario Samaha, Charles Stratton, Jonathan E. Schmitz. Comparative Antimicrobial Activity of Commercial Wound-Care Solutions on Bacterial and Fungal Biofilms, Ann Plast Surg. 83(4): 404-410, 2019.
11. Optical Microscopy and the Extracellular Matrix Structure: A review, Cells 2021, 10(7),1760; https://doi.org/10.3390/ cells10071760
12. Sandi G. Dempsey, Christopher H. Miller, Ryan C. Hill, Kirk C. Hansen, and Barnaby C. H. May, Journal of Proteome Research 2019 18 (4), 1657-1668, DOI: 10.1021/acs.jproteome.8b00908
13. Topps J, Kay et al (1968). Digestion of concentrate and of hay diets in the stomach and intestines of ruminants. Br J Nutr
22, 261-280, 2. Engelhardt W and Hales J (1977). Partition of capillary blood flow in rumen, reticulum, and omasum of sheep.
American Journal of Physiology- Endocrinology and Metabolism 232(1 ): E53. 3. Baldwin, R. L; McLeod, K. R; Klotz, J. L.;
Heitmann, R. N.Rumen development, intestinal growth and hepatic metabolism in the pre- and post weaning ruminant. J. Dairy Sc. 2004, 87 (Suppl. E), E55-E65
14. Ferreras, D. T., S. Craig and R. Malcomb (2017). “Use of an Ovine Collagen Dressing with Intact Extracellular Matrix to Improve Wound Closure Times and Reduce Expenditure in a US Military Veteran Hospital Outpatient Wound Center”. Surg Technol Int 30:61-69
15. Dempsey SG, Miller CH, Schueler J, Veale RWF, Day DJ, May BCH. A novel chemotactic factor derived from the extracellular matrix protein decorin recruits mesenchymal stromal cells in vitro and in vivo. PLoS One. 2020 Jul 13;15(7):e0235784. doi: 10.1371/journal.pone.0235784. Erratum in: PLoS One. 2020 Sep 3;15(9):e0238964. PMID: 32658899; PMCID: PMC7357784.
16. Suami H, Scaglioni MF. Anatomy of the Lymphatic System and the Lymphosome Concept with Reference to Lymphedema. Semin Plast Surg. 2018 Feb;32(1):5-11. doi: 10.1055/s-0038-1635118. Epub 2018 Apr 9. PMID: 29636647;

PMCID: PMC5891651.
17. 1. Murphy RC, Kucan JO, Robson MC, Heggers JP. The effect of 5% mafenide acetate solution on bacterial control in infected rat burns. J Trauma. 1983 Oct;23(10):878-81. doi: 10.1097/00005373-198310000-00006. PMID: 6415293.




