For Filing purposes DC ID DC NHI DC Phone #
DC Name DC Address
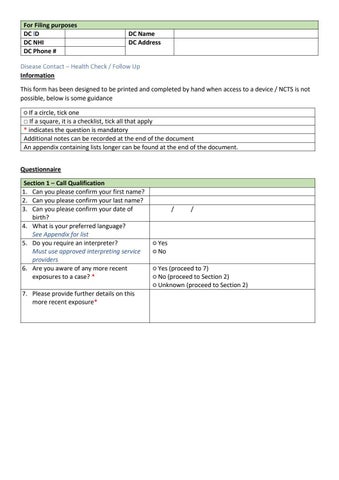
Disease Contact – Health Check / Follow Up Information This form has been designed to be printed and completed by hand when access to a device / NCTS is not possible, below is some guidance ○ If a circle, tick one □ If a square, it is a checklist, tick all that apply * indicates the question is mandatory Additional notes can be recorded at the end of the document An appendix containing lists longer can be found at the end of the document. Questionnaire Section 1 – Call Qualification 1. Can you please confirm your first name? 2. Can you please confirm your last name? 3. Can you please confirm your date of birth? 4. What is your preferred language? See Appendix for list 5. Do you require an interpreter? Must use approved interpreting service providers 6. Are you aware of any more recent exposures to a case? * 7. Please provide further details on this more recent exposure*
/
/
○ Yes ○ No ○ Yes (proceed to 7) ○ No (proceed to Section 2) ○ Unknown (proceed to Section 2)