Center for Oral & Maxillofacial Surgery Newsletter: Summer 2024
COMMITTED TO EXCELLENCE
Welcome to the new issue of our clinical update newsletter! We hope you find it helpful and invite you to suggest any topics you’d like to see covered (just give us a call to request).
We welcome referrals from colleagues and invite you to speak to any of our surgeons to discuss the needs of your patients. We look forward to hearing from you!
Warm regards,
Emily J. Van Heukelom, DDS
Roseanna P. Noordhoek, DDS, FACS
Chris Bulcher, DMD, MD
Dillon Feigenbaum, DDS, MD
Contact one of our surgeons at 616-361-7327
4349 Sawkaw Drive NE Grand Rapids, MI 49525
158 Marcell Drive, Suite B Rockford, MI 49341
Welcoming New COSDI Doctors: CHRIS BULCHER, DILLON FEIGENBAUM
WHAT DO south-central Idaho and New York’s Long Island have in common? Each was the original home of an oral surgeon who will bring his talents to the Center for Oral Surgery and Dental Implants (COSDI) in the summer of 2024. That’s when Long Islander Dillon Feigenbaum, DDS, MD, and Idahoan
Christopher Bulcher, DMD, MD, will join the practice.
Actually, they have more
in common than that. They share a zeal not just for the technical art of surgery, but also for their profession’s human aspect: being sensitive to individual patients, making them comfortable and relieving their pain. Meeting the standard of care isn’t the end for Drs. Bulcher and Feigenbaum; it’s the beginning.
“Algorithms exist, but there’s a reason we don’t just have
robots following a flow chart,” says Dr. Feigenbaum, noting that patients are often fearful when they arrive at the oral surgeon’s chair—or even the dentist’s. “You need to have the emotional component, to be able to interpret and use your experience to know the best thing to do.” From the patient’s point of view, he says, “you want a person who can talk to you, make you feel better and put you at ease. Because any kind of surgery is scary.”
“It’s unique in oral surgery that a lot of our work can be done with the patient awake,” says Dr. Bulcher. “But we also have the ability to sedate patients, and that’s great for people who are anxious about their treatment. So regardless of the treatment, whether it’s wisdom teeth, implants or major surgery, my goal is to create as safe and pleasant an experience as possible.”
Third year’s the charm
For both of COSDI’s new oral surgeons, the third year of dental school was a critical decision point on the path to becoming oral and maxillofacial surgeons. During Dr. Bulcher’s third-year rotation in oral
CONTINUED
Welcoming New COSDI Doctors
CHRIS BULCHER, DILLON FEIGENBAUM
surgery, he watched corrective jaw surgery. “After that,” he says, “I couldn’t really imagine myself doing anything else. I loved the impact, the surgery and all the planning that goes into this kind of work.”
Dr. Feigenbaum’s third dental-school year saw him shadowing oral surgeons in the hospital, and, though he had long known he wanted to specialize, that was when the decision crystallized.
“For the more consequential reconstructions—auto-accident injuries, wounds to the face, bad animal bites—I decided that the best way to help those people was to go into oral surgery and learn about oral-maxillofacial reconstruction.”
Dr. Feigenbaum practiced for six years in Detroit as a resident with Ascension Michigan. “In Detroit, I did a lot of orthognathic surgery, repositioning the jawbones when they didn’t align properly,” he says. Such procedures are often the answer when braces alone can’t do the job, he explains. At COSDI, he anticipates doing more of that work—and whatever else is called for. “I’m trying to help expand their reach and continue to help patients however I can,” he says.
Dr. Bulcher completed his residency at Cleveland’s Case Western Reserve University in 2022 and recently practiced in the San Francisco Bay area. He, too, is interested in orthognathic surgery. One clinical passion of his? He would
like medical clinicians to be more alert to the risks to oral health that come with the use of antiresorptive medications, such as bisphosphonates to treat osteoporosis. “They can have a devastating effect on patients who need oral surgical care,” he explains.
That doesn’t mean antiresorptives are invariably a bad idea—medications often come with trade-offs. But it does mean, says Dr. Bulcher, that many patients who will require treatment for osteoporosis should be evaluated for oral health care needs first so that any necessary oral surgery can be performed before treatment with antiresorptives begins.
Why COSDI?
With their geographically varied backgrounds and their professional credentials, Drs. Bulcher and Feigenbaum had numerous options. It speaks volumes that they chose COSDI. The organization attracted Dr. Feigenbaum, he says, because its practice philosophy emphasizes both education— offering continuing education courses for dentists and other professionals—and involvement with the community. Dr. Bulcher appreciated COSDI’s full range of oral surgery and dental implant services and its autonomy as a practice.
“I was pleased to see that Dr. Rosie [Noordhoek, DDS, FACS] and Dr. Emily [Van Heukelom, DDS] still provide services at a Level 1 Trauma Center, treating
GET TO KNOW COSDI’S TWO NEWCOMERS
Learn more about our practice’s new oral surgeons, Christopher Bulcher, DMD, MD, and Dillon Feigenbaum, DDS, MD, in this quick “lightning-round” summary.
DILLON FEIGENBAUM, DDS, MD
CHRIS BULCHER, DMD, MD
College Drew University, 2013 University of Idaho, 2012
Dental school State University of New York, Buffalo, 2018
Favorite movie Inglourious Basterds, 2009 Heat, 1995
Favorite food Indian cuisine Ramen
What would you be if you weren’t an oral surgeon?
Formula One race-car driver Drummer for a rock band
Bucket-list goal To own a coffeeroasting shop To scuba-dive with a whale shark
“Outside-the-box” accomplishment “I’ve fenced against Olympic fencers.” “I did eight years of jazz and tap dancing.”
facial traumas, in addition to their private practice, where they do the bread-and-butter outpatient dentoalveolar work,” says Dr. Bulcher. His own goals, he says, include maintaining a similar breadth of practice and minimizing “the number of outside influences that dictate one’s quality and level of care.”
Dr. Noordhoek believes that both of these new doctors will fit superbly into COSDI’s professional culture. “It’s very important in our office to have people who not only are clinically very competent,
but also have a good bedside manner,” she says. “And we know Dr. Feigenbaum and Dr. Bulcher will pass that test. We know that they will care for our referring doctors’ patients just as we would.”
Dr. Noordhoek is particularly encouraged by the two new doctors’ enthusiasm for being part of the West Michigan community. Confident as both Dr. Bulcher and Dr. Feigenbaum are in their skills, they’re downto-earth individuals who can relate to the needs and goals of COSDI’s patient population.
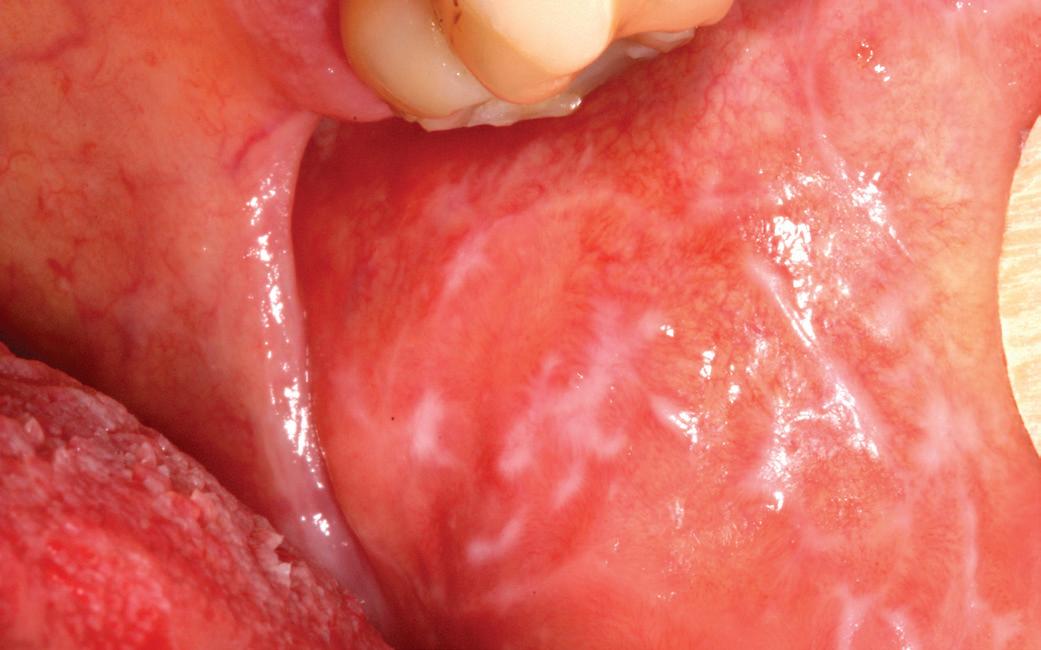
SEEING MORE ORAL LICHEN PLANUS?
THE CORONAVIRUS PANDEMIC changed everyone’s lives, and oral health care providers didn’t escape. Yes, they returned very quickly to their offices to treat patients in person while other professionals embraced remote work. But some things had changed, and research now suggests that one of them may be a clinical residue from the pandemic: a sharply increased incidence of oral lichen planus and oral lichenoid mucositis
The causation of these chronic inflammatory dermatologic disorders isn’t fully known. But scientists believe that antigens on the surface of epithelial basal cells can trigger what Patricia Burgos-Blasco, MD, and her co-authors have called “an abnormal T-cell cytotoxic reaction” that produces these skin lesions. And while such antigens may have varied sources, they write, “infection by SARS-CoV-2 may represent an exogenous antigen that triggers this inflammatory cascade.” The authors add that dermatologists should be “vigilant” for such skin lesions when they evaluate patients who have had COVID-19.¹
That finding coincides with what oral surgeons Roseanna Noordhoek, DDS, and Emily Van Heukelom, DDS, have encountered anecdotally at the Center for Oral Surgery and Dental Implants (COSDI). “Since COVID-19 hit I have seen probably 5 to 10 times more evaluations for lichen planus or lichenoid-like reactions than I did before,” says Dr. Noordhoek.
But COVID isn’t the only newly revealed culprit. Additional research has
Photograph by Ian Furst, CC BY-SA 4.0 https://creativecommons.org/licenses/by-sa/4.0, via Wikimedia Commons
suggested that, although no hard-andfast causation can yet be established, booster vaccinations for COVID may also be triggers for oral lichen planus or oral lichenoid mucositis.²
In doing further research on the subject, Dr. Noordhoek found that in recent years multiple studies have been published on an increase in lichenoid reactions with all vaccinations. “This has brought a learning experience for our practice,” she says, “because previously when one or two patients connected their lesions to vaccines we tended to be skeptical.”
Now she has a different view. But she emphasizes that the threat of oral lichen planus is no reason for patients to avoid COVID booster shots or other vaccinations and risk their health. She now tells them, “If you get COVID, it’s just as likely to cause these sores in your mouth. So let’s get them treated—and keep getting your booster.” (Lichen planus reactions have also been associated with vaccinations for hepatitis B, influenza and herpes zoster.)³
Avoiding unnecessary biopsies
While COSDI receives many requests to biopsy patients for lichen planus, says Dr. Noordhoek, a formal biopsy with immunofluorescence isn’t always strictly necessary.
“I send the sample in a regular formaldehyde solution, and the diagnosis I get back is ‘lichenoid mucositis—if present on bilateral buccal mucosa, could represent oral lichen planus.’ Those are the exact words.”
While lichen planus can be persistent in some patients—symptomatic or not—the cases of newly occurring lesions that are attributable to COVID-19 or COVID-19 vaccination appear to be fully resolved by one or two months’ treatment with topical steroids. “So if you have patients with new-onset oral lichen planus or oral lichenoid mucositis— especially if it’s ulcerated or painful find out if they’ve recently had COVID or a vaccination,” Dr. Noordhoek tells referring dentists. “Then provide topical steroid treatment if you’re comfortable doing so and send the patient for pathology referral to our office.”
One telltale sign of the new postpandemic world? That would be a slight change in the routine of COSDI’s oral surgeons. Dr. Noordhoek says she and Dr. Van Heukelom used to write up oral lichen planus cases afresh each time. But they see the phenomenon so often that in order to save time, Dr. Noordhoek says, “I now have a template about it that I didn’t used to have, and a printout for patients for home care. I can just add specific information for the patient and the history of present illness.”
REFERENCES
1. Patricia Burgos-Blasco, MD, et al., “COVID-19: A Possible Trigger for Oral Lichen Planus?” International Journal of Dermatology, July 2021; 60(7); pp. 882-883.
2. Lama Alabdulaaly, DMSc, et al., “New Onset and Exacerbation of Oral Lichenoid Mucositis Following SARS-CoV-2 Infection or Vaccination,” Oral Diseases, May 31, 2022: 10.1111/odi. 14257 (E-publication ahead of print).
3. Ibid.
HOW TO HELP PATIENTS FIND INFORMATION THEY CAN TRUST
“IT AIN’T what you don’t know that gets you into trouble,” Mark Twain supposedly said. “It’s what you know for sure that just ain’t so.”
Medical and dental professionals today face a patient population better armed with health care information than ever before— and that’s a good thing. The more people know, the more they can make healthy decisions about their lives and be effective partners when it’s time for treatment.
But, as with many good things, there’s a downside: Some patients come in with health information they’ve confidently culled from the Internet, TV, radio, magazines or newspapers—or even from social media or neighbors—that has misled them. The information could be from a report that they’ve misinterpreted, that is perfectly valid but doesn’t apply to them or, in some instances, that is flat wrong.
The Internet may be the biggest offender because, online, the boundaries are less clear than in older media between people trying to tell you something and people trying to sell you something.
“Much of what’s on the Internet boils
down to advertising,” warns Emily Van Heukelom, D.D.S., of the Center for Oral Surgery and Dental Implants (COSDI).
Dr. Van Heukelom says the Internet and other media can be great as sources for questions patients can ask their clinicians. But a patient seizing upon them for answers can be a problem.
When patients get it wrong
“I’ve had patients after wisdom-tooth surgery who have diagnosed themselves,” says the oral surgeon. “They’re sure they have an infection or a dry socket. And I’ll say, ‘Actually, I think this is more straightforward. There’s a suture there, and some food is trapped underneath it. Let’s just flush that out and let you sit for ten or fifteen minutes. I think it’s going to feel much better.’”
When Dr. Van Heukelom turns out to be right on such occasions, she says, little harm has usually been done beyond the patient’s “excessive worry.” “But in occasional cases,” she says, “the incorrect information has undermined the patient’s relationship of trust with the clinician.”
Sensitivity to the patient’s point of view is a bedrock principle for COSDI, and that doesn’t stop when it’s time to gently correct misinformation. But Dr. Van Heukelom has three points she stresses with patients to help them make sure the health information they find online isn’t biased or problematic:
• Don’t trust social media Today’s proliferation of instant digital get-togethers and comparisons can be fun and useful for sharing many things. But patients shouldn’t use social media—ever—for diagnosing and treating medical or dental conditions, says Dr. Van Heukelom, just as they shouldn’t take pills handed to them by a neighbor over the back fence.
• Find out a website’s purpose. Many sites offer information about dental or medical conditions as a prelude to a pitch for a product or service that may or may not be right for your patient.
Often, the information is couched to make the product or service seem like the perfect answer to the patient’s problem— perhaps a new breakthrough just being announced. “But if it sounds too good to be
true,” says Dr. Van Heukelom, “it probably is.”
• Check a site’s domain name. As a government website explains, four suffixes that are part of web addresses can tell you something about the evenhandedness of a site’s approach.¹
-.gov: a U.S. government agency, usually reliable and kept up-to-date with the latest research.
-.edu: an educational institution. Such a site may extol the virtues of its university or research center and be in that sense biased—it may boast, for example, of that institution’s own research accomplishments—but its health care content can usually be trusted because intellectual credibility is its stock in trade.
-.org: a nonprofit organization, such as a medical society, an advocacy group or a treatment facility—the Michigan Dental Association, the American Heart Association and the Mayo Clinic are examples. These sites may advocate for a professional community or a disease constituency (a specialty society’s site, for instance, may not provide equal coverage of another specialty that offers similar services), but their content about medical or dental issues is usually unbiased and drawn from peer-reviewed science.
-.com: a commercial enterprise, which may sometimes have splendid information, but which is driven by a business mission, not an informational one. Read with a cautious eye.
Another hint is to beware of online search algorithms that send users to paid content, which can be slanted. The label “sponsored,” often at the top of a list of search results, indicates such paid entries. The information they contain may be perfectly fine, but you should know—and consider—that someone has paid to have you directed to it.
What studies show—and don’t Digging a little deeper, some patients will come into the office having read about new clinical research and drawn conclusions
from it. Giving these individuals a bit of guidance about how to assess what they’ve read can be helpful. Take sampling error, for instance. “If you flip a penny a hundred times, then repeat that over and over,” says Dr. Van Heukelom, “once in a while, out of your first twenty flips, fifteen will be tails. That doesn’t change the fact that it’s a 50–50 probability. You’ve just had a sample error.”
Similarly, says the doctor, with some rare or newly discovered conditions the literature may only include case reports, which a patient may overinterpret. But case reports can differ widely just as those pennies can. “A retrospective study is stronger than case reports,” she explains, “and a prospective study is better still, because it’s designed to eliminate bias. Best of all is a randomized clinical trial, which has gone through an institutional review board.”
Even the soundest studies can be complex, and sometimes the portion of a study’s findings that is genuine new knowledge isn’t fully clear. That’s especially true if one is learning about those findings from headline writers or the writers of TV news or Internet lead-ins, who have simplified them with an emphasis on novelty to attract readers, viewers or clicks.
The consumer mindset
“Medicine is growing and changing, and so is dentistry,” says Dr. Van Heukelom. “But hopefully we are growing and changing for the benefit of our patients, by and large, and not just the shareholders of our companies.”
Today’s consumer has a new mentality that demands answers—and again, that can be very constructive. A patient with informed questions is one who is ready to be knowledgeably adherent in treatment and any necessary lifestyle adjustments. But patients should direct their skepticism wisely—they should, for example, be wary of professionals who make exact, lowball promises about cost or duration in matters that inherently resist such precise
WHERE PATIENTS CAN LEARN MORE
Valuable advice about how to assess medical and dental content on the Internet is available at https://medlinelus.gov/ evaluatinghealthinformation. html, a government site from the National Library of Medicine. And useful information on oral surgery topics is also to be found at the Center for Oral Surgery and Dental Implants (COSDI) site, www.grandrapidsoralsurgery.com.
prediction. “If you’re going to nickel-anddime things, you may not get the best result,” says Dr. Van Heukelom.
Even in the age of the Internet, she argues, what counts most is the relationship of trust a patient builds with his or her providers. They, after all, have gone to dental or medical school, while the patient usually has not—it’s simple prudence to tap their expertise. Dr. Van Heukelom tells patients: “You need to find a place where the practitioners meet your level of needs, offer you a path forward that makes sense, and don’t overtly try to push you towards one decision or another. There are many ways to replace a missing tooth, for example. Let’s talk about two or three of those and why I think one is the best choice for you. If you feel good about that, awesome—I’ll give you a plan. If you prefer to think more about it, fine—I’m not going to twist your arm. I’m just here to give you the information. And then, when you’re ready, if you’re ready, we’ll take good care of you.”
REFERENCES
1. https://medlineplus.gov/ evaluatinghealthinformation.html , accessed online May 7, 2024.
AN INGREDIENT IN TOOTHPASTE CAN CAUSE UNWANTED EFFECTS
PATIENTS MAY OR MAY NOT be familiar with sodium lauryl sulfate (SLS), but dentists know it as a surfactant—the sodium salt of lauryl alcohol—used in toothpastes and mouthwashes as well as some foods and household cleaning products. SLS aids solubility and thus appears to help facilitate plaque control and the cleaning of teeth. It also “maximizes the foaming action,” in the words of a September 2023 literature review by Hamoun Sabri, MScD, and co-authors. And it “reduces the surface tension of water, which allows a better application of toothpastes.”¹
So what’s not to like?
“Personally, I use an SLS-free toothpaste,” says Rosie Noordhoek, DDS, of the Center for Oral Surgery and Dental Implants (COSDI). “And I probably do get more tartar buildup. But at the end of the day, I believe my gingiva feels better.” (Her chosen toothpaste is without SLS, she emphasizes, but not without fluoride.)
Dr. Noordhoek doesn’t recommend to all patients that they avoid SLS. But she does stress mounting evidence that SLS has a downside, especially for older patients who have, or are at risk for, underlying xerostomia (dry mouth) or certain other conditions. “Many of our patients, as they age and are on more medications, have salivary glands that are drying out and are therefore more apt to have a topical dermatitis reaction to additives in toothpaste such as SLS and whiteners,” she says. “These
ingredients put them at increased risk for desquamative gingivitis and a burning sensation, which then leads to more decay and pain and all the things that go along with them.”
A 1998 study by J. L. Jensen and P. Barkvoli noted that “salivary hypofunction” can lead to an increased frequency of “candidiasis, burning mouth syndrome, and white lesions of the oral mucosa.” Precautions recommended by the authors included “refraining from smoking and avoiding toothpastes containing sodium lauryl sulfate.”²
Sloughing and canker sores
In 1978, a pioneering study warned of such SLS side effects as “dosedependent irritative dermal reactions in high-dose usage” and “oral mucosal desquamation [sloughing] and reduction in the function of the protective barrier of oral epithelium” (though the authors attributed that to several factors, not just SLS).³
That 1978 study, by W. C. Rubright and co-authors, described a case in which desquamation in a 50-year-old woman “appeared as grayish-white gelatinous membranes on the floor of the mouth, lips, vestibules and gingiva.” Such sloughing, they wrote, was “caused by synthetic dentifrice detergents (foaming agents)…”⁴
Anecdotal experience bears out the research. Says Dr. Noordhoek: “Sometimes I’ll be evaluating someone for another purpose—an implant,
say—and I’ll rub my finger over his or her gums, and the outer layer, the desquamative gingiva, comes right off in my glove. That’s when I’ll say, ‘Tell me about the toothpaste you’re using,’ and usually it’s one with lots of additives in it, perhaps one that boasts of ‘total gum care.’”
At that point, Dr. Noordhoek asks if the patient has been experiencing symptoms. A typical reply, she says, is: “Well, yes, my gums are a lot more sore lately, but I just thought I needed to brush harder.”
Then there’s the matter of recurrent aphthous stomatitis—canker sores. There’s evidence that SLS can make these both more frequent and longerlasting. Looking at four crossover clinical trials in human subjects, the Sabri, et al. literature review found that patients using SLS toothpastes reported more pain than their SLS-free counterparts, and that “SLS-free dentifrice significantly reduced the ulcers’ number, ulcer duration, episodes’ number, and ulcer pain compared to SLS-containing.”⁵ One reason may be a retardant effect that SLS can have on wound healing. The authors call for more investigation of this topic, but suggest that an SLS-free toothpaste be recommended “to be on the safe side.”⁶
That foaming feeling
Besides its foaming and solubilizing action in toothpastes and mouthwashes, SLS clearly seems to be a factor in their
“Just over one in four people suffers from xerostomia, with higher rates observed among older people.” ⁸
consumer appeal. And a 2016 study by S. Sälzer and co-authors in the journal Clinical Oral Investigations hints that the latter may be its decisive advantage. In a randomized clinical trial, researchers compared toothpastes with and without SLS as to their effects on “plaque, gingivitis and gingival abrasion” in young adults. Their conclusion:
“The test dentifrice without SLS was as effective as a regular SLS dentifrice on gingival health and plaque index scores. In addition to the expected foaming effect, an SLS-containing dentifrice was also significantly more appreciated toward taste perception, freshness and duration of taste.”⁷ In other words, both toothpastes did the job equally well, but the SLS product felt more satisfying to use—more fun.
For many patients, this SLS tradeoff is fine. For older individuals with or at risk for xerostomia or certain other conditions, however, the fun may not be worth it.
“I tell all my patients, “Your mouthwash doesn’t have to have blue dye in it,’” says Dr. Noordhoek. “‘Your toothpaste doesn’t have to suds up and be sparkly. That’s not doing anything good. Those are marketing gimmicks.’”
Of course, if a sense of satisfying and effective foaming when they brush leads patients to brush more often or more thoroughly, that fact must be entered on the positive side of the SLS ledger. But that may be mostly a matter of habit, and habits can be changed in the face of better information. Whatever the benefits of SLS, either psychologically or as a cleaning agent, research has been making its drawbacks clearer.
When Dr. Noordhoek believes that a patient would benefit from switching to an SLS-free toothpaste, she suggests
either the prescription Colgate PreviDent 5000 Dry Mouth (be sure to select the “Dry Mouth” version) or one of these over-the-counter products.
• Sensodyne Fresh Mint
• Hello “Naturally Whitening”
• Closys
Because these same brands also offer different varieties, the doctor cautions that patients should be sure to choose a formulation that does contain fluoride but does not contain SLS.
Personal preference will always play a role in the choice and use of toothpastes and mouthwashes. But for patients, especially elderly ones, who are at risk for xerostomia, desquamative gingivitis, recurrent aphthous stomatitis or similar conditions, getting rid of SLS may be a wise move—even if that foamy feeling when they brush or gargle with the new product isn’t quite the same.
REFERENCES:
1. Hamoun Sabri, MScD, et al., “The Yin and Yang of Sodium Lauryl Sulfate Use for Oral and Periodontal Health: A Literature Review,” Journal of Dentistry (Shiraz University of Medical Sciences), Sept. 2023; (24)3: pp. 262–276. Accessed online at https://www.ncbi.nlm.nih.gov/ pmc/articles/PMC10506142/, April 23, 2024.
2. J. L. Jensen and P. Barkvoli, “Clinical Implications of the Dry Mouth. Oral Mucosal Diseases,” Annals of the New York Academy of Sciences, April 1998; 15:842, pp. 156–162. Accessed online at https:// pubmed.ncbi.nlm.nih.gov/9599305/, April 23, 2024.
3. Sabri et al., op cit., (see under “Introduction.”)
4. William C. Rubright, DDS, et al., “Oral Slough Caused by Dentifrice Detergents and Aggravated by Drugs With Antisialic Activity,” Journal of the American Dental Association, August 1978, 97:2, pp. 215–220. Accessed online at https://pubmed. ncbi.nlm.nih.gov/277594/, April 23, 2024.
5. Sabri et al., op cit. (Table 1, pulldown sections 11 and 12.)
6. Ibid., (see under “Wound Healing.”)
KEY SYMPTOMS
Regardless of cause, patients with xerostomia usually report these symptoms:
• A sensation of oral dryness
• Oral burning or soreness
• Diminished or altered taste
• The need to sip water when swallowing—patients usually carry a water bottle at all times
• Difficulty swallowing dry foods, e.g., crackers
• A sensation of thickened saliva
• Sensitivity to acidic or spicy foods
• Loss of appetite and weight loss
SOURCE: National Institutes of Health
CLINICAL SIGNS
Examination findings might include:
• Fissured tongue and lips
• Filiform papillae atrophy
• Erythematous and parched oral mucosa
• The finger may adhere to the oral mucosa during palpation
• Evident lack of saliva on the floor of the mouth
SOURCE: National Institutes of Health
7. S. Sälzer et al., “The Effectiveness of Dentifrices Without and With Sodium Lauryl Sulfate on Plaque, Gingivitis, and Gingival Abrasion—a Randomized Clinical Trial,” Clinical Oral Investigations, 2016, 20: pp. 443–450. Accessed online at https://www.ncbi.nlm.nih.gov/pmc/ articles/PMC4799265/, April 23, 2024.
8. Agostini BA, Cericato GO, Silveira ERD et al. How Common is Dry Mouth? Systematic Review and Meta-Regression Analysis of Prevalence Estimates. Braz Dent J 2018;29(6):606-18. doi: 10.1590/01036440201802302.
JOIN US!
Center for Oral Surgery and Dental Implants is pleased to invite you to our fall open house. Come and enjoy complimentary food and beverages along with the company of your colleagues. Mark your calendars now!
Be on the lookout for a printed invitation and small gift, which will be delivered to your office at the end of August. You can RSVP early to events@grandrapidsoralsurgery.com.
WHEN: Thursday, October 3 from 4 to 7 p.m.
WHERE:
Center for Oral Surgery & Dental Implants 4349 Sawkaw Dr. NE, Grand Rapids