Danny Bonvissuto, Paul Govern, Nancy Humphrey, Sid Sadler, Tom Wilemon
Photography/Illustration
Amanda Bailey, Donn Jones, Erin O. Smith, Susan Urmy
Design & Art Direction
Diana Duren
Director of Publications
Christina Echegaray
Executive Director of Digital Publications
Wayne Wood
Cover Photograph
Erin O. Smith
Editorial Office
Vanderbilt University Medical Center Office of News and Communications
T-5200 Medical Center North Nashville, TN 37232-2390 615-322-4747
Editorial Board
Deb Friedman, MD, Laura Goff, MD, Theresa Sberna, MPH, Scott Hiebert, PhD, Orrin Ingram, Beth Jones, MA, Teresa Knoop, MSN, RN, Ben Ho Park, MD, PhD, Sydnie Hochstein, Julie Bulger
Olivia Leow is part of a group of people who have joined together to invest more resources into glioma research
Raising funds for childhood and adult cancer initiatives at Vanderbilt-Ingram Cancer Center
Chemo Allergy
Researchers seek biomarkers to identify patients with chemotherapy allergies
Glioma Warriors
People affected by brain cancer have joined forces and invested in research to develop more
Sound Power
New
Grateful Goal
A clinical trial saved Lily Hensiek’s life when she relapsed with childhood leukemia, and now she’s helping other patients
We have made great progress in recent decades with cures and better treatments for many cancers, but that has not been the case with gliomas — tumors that originate in the brain — and particularly glioblastoma, the most aggressive form. With the assistance and support of families who have been affected by gliomas, we are establishing a Brain Tumor Center at VanderbiltIngram Cancer Center that will develop new therapies, expand the availability of clinical trials and train more glioma specialists. The cover story of this Momentum describes the people behind this initiative and explains the goals for the Brain Tumor Center.
Also in this issue, we celebrate our clinical trial successes. Children who relapse from the most common subtype of acute lymphoblastic leukemia (ALL) now have better survival because of blinatumomab, a therapy our pediatric oncologists offered through a clinical trial that has become the standard of care. A young woman — who was diagnosed with ALL at age 7, fought the cancer into remission and then relapsed at age 15 — shares her journey and career path to help others with cancer.
We continue to achieve breakthroughs with clinical trials. One of our oncologists is the principal investigator of a national trial that has shown that through a dual immunotherapy regimen, plus short-course radiation, patients with rectal cancer that is termed “microsatellite instability-high” can avoid chemotherapy and colostomy-requiring surgery. We have teams of researchers that continue to keep us at the vanguard of another immunotherapy, CAR-T (chimeric antigen receptor T cell). Interim results from a new “off-the-shelf” CAR-T therapy — one that bypasses the time-consuming process of reengineering a patient’s own immune cells to target cancer by instead using donor cells — demonstrated a 91% overall response rate for
From the Director
BEN HO PARK, MD, PHD
patients with multiple myeloma who had not responded to existing treatments or who had relapsed. Developing an off-the-shelf CAR-T is important because it will speed time to treatment for patients and offer an option for patients who are not healthy enough for their own T cells to be harvested and reengineered. Collectively, our experts are investigating several potential new CAR-T therapies, including one that involves an emerging medical treatment called CRISPR, a gene-editing technology.
Vanderbilt-Ingram’s surgical oncologists are also at the forefront of innovative technologies. A recent addition is histotripsy, which directs focused ultrasound waves to destroy metastatic tumors in the liver that would otherwise be inoperable. This is a groundbreaking technology recently approved by the Food and Drug Administration. While we develop new therapies, we simultaneously refine existing treatments to make them more tolerable and effective. A case in point is ongoing research to identify biomarkers that can help physicians predict who is at risk for allergies to chemotherapies, using ovarian cancer treatments as a model, so therapy protocols can be put into place to desensitize those patients and prevent anaphylactic reactions.
You can read about these treatment achievements and our initiatives to lessen the cancer burden for patients and their families in this Momentum. We could not do this without people who participate in clinical trials, advocate for cancer research funding, share about their journeys to increase awareness and provide financial support.
“We continue to achieve breakthroughs with clinical trials.”
News and Notes
FROM AROUND THE CANCER CENTER
Fever Mysteries
Researchers seek to understand and harness the power of fever at the cellular level
FEVER IS A common symptom that occurs with many illnesses, but the effect that high body temperatures have at the cellular level is not fully understood. Vanderbilt researchers recently discovered that prolonged fever causes mitochondrial stress, DNA damage and cell death in a particular subset of T cells and published their findings in the journal Science Immunology. On another front, Vanderbilt researchers are also seeking to develop a new cancer immunotherapy utilizing nanobody delivery and temporary targeted heating of tumors, an initiative that has received funding from the Waddell Walker Hancock Cancer Discovery Fund. n
CLINICAL TRIAL SUCCESS
Data from a clinical trial shows that a dual immunotherapy regimen plus short-course radiation for the treatment of rectal cancer that is microsatellite instability-high (MSI-H) or mismatch repair deficient (dMMR) can be effective enough to avoid chemotherapy and colostomy-requiring surgery.
The data from the EA2201 study was so promising that the clinical trial is being redesigned to investigate whether radiation treatment can also be avoided. Most patients in the study — 57% — had a complete clinical response according to scan results, or a complete surgical response. Of those who had rectal surgery, which was the standard of care when the clinical trial began, 100% had no cancer cells left, according to pathology reports. The study participants, who had Stage 2 or Stage 3 MSI-H/dMMR rectal cancer, were treated with nivolumab plus ipilimumab before and after receiving short-course radiation therapy.
Kristen Ciombor, MD, MSCI, Ingram Associate Professor of Cancer Research and co-leader of the Translational Research and Interventional Oncology Research Program at Vanderbilt-Ingram Cancer Center, presented the data in Munich during the European Society for Medical Oncology Gastrointestinal Cancers Congress 2024.
She is the principal investigator of the EA2201 study, which is sponsored by the National Cancer Institute and being administered through the ECOG-ACRIN Cancer Research Group. Around 5% of rectal cancer patients have MSI-H tumors, characterized by a higher number of repeated DNA base sequences. n
News and Notes
Colorectal Cancer
Endeavor seeks to expand immunotherapy efficacy
The Robert J. Kleberg, Jr. and Helen C. Kleberg Foundation has awarded a $1 million grant to support research at Vanderbilt aimed at dramatically expanding the efficacy of immunotherapy for colorectal cancer.
Currently, only people with microsatellite instability-high colorectal cancer, which accounts for about 10% of patients, respond to immune checkpoint inhibitors, but Vanderbilt researchers have discovered proteins that could be targeted to potentially benefit the other 90%. The work is the latest collaboration between Robert Coffey, MD, Ingram Professor of Cancer Research, and Ken Lau, PhD, professor of Cell and Developmental Biology, to understand the mechanisms of colorectal cancer. It builds on recent discoveries by their research teams.
Notably, the researchers identified three immune exclusion biomarkers associated with the 90% of colorectal cancer cases that are microsatellite stable and have a paucity of CD8 T cells. These three genes, DDR1, TGFBi and DPEP1, take part in cancer cell packaging of proteins into nanoparticles, including small extracellular vesicles and newly discovered “supermeres,” which are secreted to regulate the extracellular microenvironment.
Coffey’s research team discovered supermeres and reported their study in the journal Nature Cell Biology on Dec. 9, 2021. Two years later, in another study published Dec. 7, 2023, in the journal Cell, Coffey and Lau reported the
role of the immune exclusion genes in human colorectal cancer.
The Kleberg Foundation will support the next step in their research. Coffey and Lau plan to uncover the mechanistic underpinnings of supermeres in the tumor microenvironment, look for other immune exclusion biomarkers, and evaluate the efficacy of immunotherapy when immune exclusion proteins are targeted.
DDR1 will be targeted with the antibody PRTH-101, which binds to and blocks DDR1. Vanderbilt University Medical Center is a Phase 1 and Phase 2 clinical trial site testing PRTH-101. The researchers also have access to a TGFBi-neutralizing antibody being developed for clinical trials. DPEP1 will be targeted by an inhibitor that is already approved by the Food and Drug Administration to block the protein’s enzymatic activity, while clinical trials are underway to study the drug’s effect on the protein’s receptor function.
The work will involve multiomics analysis, machine learning,
patient-derived organoids and other research technologies. The overarching goal is to find a way to transform “immune cold” tumor molecules into “immune hot” ones, so that immunotherapy can unleash CD8 T cells to kill cancer cells.
“We are proud to continue investing in novel cancer research at Vanderbilt-Ingram Cancer Center,” said Helen Alexander, president of the Robert J. Kleberg, Jr. and Helen C. Kleberg Foundation. “Our longtime partnership has yielded many advancements in therapies for cancers of all types; this latest grant will support crucial next steps in Vanderbilt-Ingram’s quest to find more effective treatments for historically untreatable colorectal cancers.” n
SMITH
Ken Lau, PhD, left, and Robert Coffey, MD, both lead research labs.
Preventive Treatment
Therapies to prevent stomach cancer receive funding
YEARS OF RESEARCH by Vanderbilt University Medical Center investigators to determine how precancerous cells in the stomach transition to gastric cancer and to develop strategies to prevent this transition have received federal funding to test two potential treatments.
The $2.5 million Department of Defense Translational Team Science Award provides funding over four years to launch a clinical trial in the U.S. with one of the therapies and compare it with another therapy from an ongoing clinical trial in Japan.
James Goldenring, MD, PhD, the Paul W. Sanger Professor of Experimental Surgery, and professor of Surgery and Cell and Developmental Biology, is the lead principal investigator. Eunyoung Choi, PhD, associate professor of Surgery and Cell and Developmental Biology, is a co-principal investigator along with Katherine Garman, MD,
associate professor of Medicine at Duke University.
The U.S. clinical trial will be conducted under Garman at Duke to evaluate the effectiveness of pyrvinium, an existing medicine that has been used for the past 70 years to treat pinworms in children, for a new purpose — reversing metaplasia of stomach cells and killing dysplastic precancerous cells.
While metaplasia is a reparative process in the stomach lining and is less likely to lead to cancer, dysplasia develops from metaplasia and is considered the critical step toward carcinogenesis. Choi and colleagues have validated that pyrvinium can be repurposed as a preventive treatment for stomach cancer, having previously demonstrated in human organoids and mouse models that the drug induces cell death in precancerous dysplastic lesions.
The ongoing clinical trial in Japan, which is led by Sachiyo Nomura, MD, PhD, in collaboration with Goldenring, is testing a targeted therapy using low-dose trametinib, which is an inhibitor of the MEK signaling pathway. MEK, an abbreviation for the mitogen-activated extracellular sig-
nal-regulated kinase pathway, plays an integral role in the development of stomach cancer. Pyrvinium also blocks the MEK pathway, the researchers have shown.
Using patient samples from the clinical trial in Japan, they will seek to determine how trametinib is changing cells that line the stomach as well as immune cells and other cell types found in the stomach.
They will compare cell changes from both treatments in the individual patients with the goal of developing personalized or precision preventive strategies.
“These trials are the first ever attempted to utilize directed therapeutic interventions to arrest and reverse precancer as a general strategy for decreasing patient risk for developing gastric cancer,” said Goldenring.
While stomach cancer is one of the three highest causes of cancer-related deaths worldwide, its incidence is lower in the U.S. In the U.S. most stomach cancers are diagnosed at late stages when they are more difficult to treat.
Infection of the stomach with the bacterium Helicobacter pylori leads to a loss of acid-secreting cells within the lining of the stomach, and their absence leads to metaplasia, the development of a new set of lining cells.
The overall goal of the study is to develop and implement prevention strategies for stomach cancer for high-risk pop-ulations and improve mortality rates from the disease. n
HOSPITAL EXPANSION HONORS JIM AYERS
Vanderbilt University Medical Center will name the new expansion tower for Vanderbilt University Hospital the Jim Ayers Tower in recognition of Janet and Jim Ayers’ philanthropic legacy and abiding interest in improving the health care and quality of life for Tennesseans.
The naming of the 15-level, 470,000-square-foot tower, currently under construction between 21st Avenue South and Medical Center Drive on VUMC’s main campus in Nashville, honors the couple’s steadfast community leadership and longtime connection to VUMC. The tower is scheduled to open its first floor — Level 7 — in October.
A Parsons, Tennessee, native, Ayers has achieved business successes in financial services, real estate and health care ventures, and he is widely recognized for increasing educational opportunities for young people. In 1999, he established The Ayers Foundation, now known as the Ayers Foundation Trust, which supports a wide range of programs and institutions.
At VUMC, the Jim Ayers Institute for Precancer Detection and Diagnosis at Vanderbilt-Ingram Cancer Center was established in 2005 to help researchers find early markers for colorectal cancer that could improve diagnosis and potentially save lives.
“To have my name connected with empowering access to health care is the honor of a lifetime,” Ayers said. “This isn’t just a building but rather a space for families to receive care that can improve their lives. n
News and Notes
DRAKE ROBIDEAU, 7, puts his handprint on a car with the help of Nashville SC mascot Tempo during the Hyundai Hope on Wheels check presentation and handprint ceremony in September 2024. Since 2007, Hyundai Hope on Wheels, which includes funding from Hyundai Motor America and local dealerships, has awarded more than $2 million in funding to pediatric cancer researchers at Monroe Carell Jr. Children’s Hospital at Vanderbilt. n
BY THE NUMBERS
BREAST CANCER
The American Cancer Society’s Breast Cancer Facts & Figures 2024-2025 provides incidence and mortality data for the disease.
1 IN 8
Approximately 1 in 8 women in the U.S. (13.1%) will be diagnosed with invasive breast cancer.
1 IN 43
One in 43 women (2.3%) will die from the disease.
2,790
Breast cancer also affects men with an estimated 2,790 diagnoses occurring in 2024.
38%
Although Black women have a 5% lower incidence of breast cancer than white women, they have a 38% higher mortality rate.
44%
The breast cancer death rate has dropped by 44% since 1989 because of advances in treatment and earlier detection, resulting in approximately 517,900 averted deaths.
The Food and Drug Administration approved in July 2024 the first blood test as a primary screening for people at average risk for colon cancer. The test checks blood for circulating tumor DNA shed by tumors.
The test detected colorectal cancers in more than 83% of participants in a study who were also found to have colorectal cancer on colonoscopy, but its sensitivity for detecting precancerous growths was much lower –only 13%.
Another FDA-approved screening, the fecal immunochemical test (FIT), works by checking stool for evidence of colorectal cancer. It’s an at-home kit that you ship via UPS.
A colonoscopy remains the gold standard for colorectal screening because it is more accurate than either the blood test or the FIT test. People at average risk for colorectal cancer should start screening at age 45, according to the U.S. Preventive Services Task Force and the American Cancer Society, but earlier screening is recommended for those at higher risk or who experience symptoms.
News and Notes
Q A
Scalp Cooling at Vanderbilt-Ingram
Treatment helps mitigate chemotherapy hair loss
Q How does scalp cooling mitigate hair loss during chemotherapy?
A Scalp cooling prevents chemotherapy-induced alopecia in two ways. First, it reduces blood flow to the scalp. Cooling causes the blood vessels in the scalp to constrict, which reduces the amount of medication reaching the follicles. Secondly, when our scalp’s temperature is lowered, our metabolism is reduced. This causes the follicles to absorb
Appointments can be made in several ways: Patients’ oncologists can inform them of the benefits of scalp cooling, then send me a message through Epic, our electronic health record system. Oncology staff nurses can call me or send a message through Epic if they have patients who are interested. If patients are familiar with our Belle Meade clinic, they can directly reach out to me. I like to schedule the patient’s entire treatment plan at one time, so when new scalp cooling patients inquire, I can quickly look at my calendar to see if we have availability.
Q Which cancer patients undergoing chemotherapy are suitable for scalp cooling?
A DigniCap is FDA-approved for solid tumors. Many of our scalp cooling users are breast cancer patients. However, we have had a couple of men successfully use the system.
Q How long does the procedure take, and is it painful or uncomfortable?
Q How many patients have undergone scalp cooling, and are they pleased with the results?
A About 75 patients have used scalp cooling since we implemented the program in March 2023. Our patients have been extremely happy with their results.
Q Is there a certain group of patients who respond better to scalp cooling than others?
A We have not found any significant correlation between age, ethnicity, hair length and the effectiveness of scalp cooling. However, we have observed that the condition of the hair at the beginning of treatment plays a crucial role. For instance, individuals who have regularly colored or bleached their hair may not respond as effectively to the treatment compared to those who have not. It’s important to note that this information is not meant to discourage anyone from trying scalp cooling, but rather to set realistic expectations.
Q Are there any plans to expand scalp cooling to other locations?
less chemotherapy. The key to keeping as much hair as possible is to keep the scalp cold for an extended period. Each chemotherapy has a set post-cool time in which chemotherapy is finished but the scalp cooling continues.
Q Where is scalp cooling offered, and how do patients make appointments to receive it?
A Currently scalp cooling is offered at Vanderbilt-Ingram Cancer Center Belle Meade.
A The duration of treatment varies based on each patient’s chemotherapy plan. DigniCap includes a specific cooling period after chemotherapy, typically ranging from 90 to 120 minutes. For breast cancer patients, the total time spent on treatment day is approximately five to six hours. While scalp cooling may be uncomfortable, it is not typically painful. The initial 15 minutes during which the scalp is cooling and reaching peak temperature can be the most challenging. However, once the scalp is numb, patients can relax in our heated recliners with warm blankets and often find themselves drifting off to sleep.
A Yes, Vanderbilt-Ingram Cancer Center Hendersonville has just received their DigniCap machine. Their staff has completed training and will begin accepting patients soon. There are talks of a few more clinics starting scalp cooling in the future. n
“Patients have been extremely happy with their results.”
— AMY ADLICH, RN
Amy Adlich, RN, is the Belle Meade charge nurse for VanderbiltIngram Cancer Center.
News and Notes
Cathy Eng, MD
Cathy Eng, MD, FACP, FASCO, the David H. Johnson Professor of Surgical and Medical Oncology, has been named associate director of Strategic Relations and Research Partnerships for Vanderbilt-Ingram Cancer Center. In this new position, she will elevate Vanderbilt-Ingram’s profile locally, regionally, nationally and internationally through stakeholder engagement, programmatic development and targeted marketing. It is an expanded role for Eng, who has served as director for Strategic Relations and is an internationally known expert on colorectal cancer and earlyonset cancers. Her new responsibilities will include promoting clinical research by developing new strategic relationships with pharmaceutical and biotech companies. She will review their pipeline portfolios and engage with them about the clinical, basic and translational research capabilities at Vanderbilt-Ingram.
Katrin Karbstein, PhD
Katrin Karbstein, PhD, Ingram Professor of Cancer Research and professor of Biochemistry, has been appointed co-leader of the Cancer Cell Biology Research Program at Vanderbilt-Ingram Cancer Center. She will develop and implement program aims, participate in strategic decisionmaking, direct pilot project funding, facilitate interactions among members, and assist in the recruiting activities for the 42-member program with over $11.7 million in annual peer-reviewed funding. Karbstein is a highly accomplished and recognized leader in understanding how ribosomes are assembled, a process critical for the translation of the genetic code into protein molecules — a fundamental process for all organisms. She was recruited to Vanderbilt University from The Herbert Wertheim UF Scripps Institute for Biomedical Innovation & Technology (formerly The Scripps Research Institute) where she was professor of Integrative Structural and Computational Biology. She was a Damon Runyon postdoctoral fellow at the University of California, Berkeley, earned her PhD in biochemistry from Stanford University, and earned degrees in chemistry and biochemistry from Ruhr University Bochum and Witten/Herdecke University, respectively.
VA recognizes physicians for improving lung screening for veterans
Two physician-scientists at Vanderbilt University Medical Center have been recognized by the Department of Veterans Affairs Quality Scholars (VAQS) Fellowship program for implementing and evaluating innovative lung cancer screening programs for veterans.
Lucy Spalluto, MD, MPH, professor of Radiology and Radiological Sciences, and Jennifer Lewis, MD, MS, MPH, assistant professor of Medicine, are the recipients of the 2024 VAQS Team Award for work they began in 2017 as VAQS fellows enrolled in the Vanderbilt
Master of Public Health program.
In 2019, upon completing their joint project, developing a lung cancer screening program for the VA Tennessee Valley Healthcare System, Lewis and Spalluto were selected to co-lead an evaluation of the national Veterans AffairsPartnership to Increase Access to Lung Screening (VA-PALS).
Funded through the VA Office of Rural Health and the Bristol Myers Squibb Foundation, an independent charitable organization, VA-PALS evaluated the implementation of 10 lung cancer screening
Carla Strom, MLA
Carla Strom, MLA, has been appointed administrative director for Community Outreach and Engagement at Vanderbilt-Ingram Cancer Center She is responsible for working with colleagues to develop initiatives for supporting community engagement and addressing health care education as well as translational research across all programs at Vanderbilt-Ingram. Strom was recruited from Atrium Health Wake Forest Baptist Comprehensive Cancer Center in North Carolina, where she served as director of the Office of Cancer Health Education and assistant direc-tor for Community Outreach and Engagement. Strom has 25 years of experience in oncology education, research, and health policy. Her interest in cancer research began as a teen volunteer at The University of Texas MD Anderson Cancer Center. She has an undergrad-uate degree in sociology with a minor in Spanish from Texas A&M University and a Master of Lib-eral Arts with an emphasis on international stud-ies from the University of St. Thomas. Strom has a personal connection with underserved com-munities and is a two-time, young adult cancer survivor.
programs across the Veterans Health Administration.
The project was conducted in collaboration with VA physician-scientists and the Vanderbilt Center for Clinical Quality and Implementation Research.
As of 2023, more than 20,000 veterans had been screened for lung cancer at VA-PALS sites. To date, the evaluation project has generated 10 scientific articles on
lung cancer screening co-authored by Lewis and Spalluto.
Their work influenced the VA to establish a National Center for Lung Cancer Screening, and together they leveraged their shared skill sets to obtain more than $6 million in grant funding since completing their fellowship.
Lewis, whose faculty appointment is in the Division of Hematology and Oncology, has focused her efforts on understanding providers’ perspectives in implementing lung cancer screening, while Spalluto has focused on the patient’s experience in imaging-based cancer screening through community-engaged research.
LEWIS SPALLUTO
Only half of young cancer patients report discussing fertility preservation
Only half of people with early-onset cancers reported discussing fertility preservation options prior to their oncology treatments, according to results of a cross-sectional study published Nov. 12, 2024, in JAMA Network Open. Young patients with thyroid, lung, ovarian and colorectal cancers reported the lowest prevalence of a fertility preservation discussion with a health care professional involved in their cancer care. Only 21.4% of patients with ovarian cancer reported a discussion about fertility preservation. The percentages reporting a discussion were 44.2% for patients with colorectal cancer, 21% for lung cancer, and 3.6% for thyroid cancer. The patient population represented 30 types of early-onset cancers.
In-clinic reconstruction of skin cancer defects costs less
Reconstruction of facial defects after skin cancer removal can occur in a traditional hospital-based operating room (OR) or an office clinic-based setting. Vanderbilt University Medical Center researchers compared cost-effectiveness for the reconstruction of facial skin cancer defects in the OR and clinic setting. The study, which was published Oct. 8, 2024, in OtolaryngologyHead and Neck Surgery, summarized the cost differences of head and neck reconstructive surgery for facial defects after skin cancer removal based on the procedural setting. Analyzing 1,206 patient cases from an insurance claim database, the researchers found that OR reconstruction cases had a higher median baseline cost of $2,308 compared to $987 for clinic procedures.
Study
shows cancer vaccine blocks tumor progression at early
lesion stage
A cancer vaccine that had little success in clinical trials for patients with advanced tumors could potentially have efficacy if administered earlier in the treatment cycle, according to a study from Vanderbilt researchers. The investigators demonstrated in a mouse model that the cancer vaccine can block tumor progression if administered when the lesions are at an early stage. Results of the study, which were published Oct. 3, 2024, in the Journal for ImmunoTherapy of Cancer, revealed that tumor-specific T cell populations are present in mice with early-stage lesions and can be therapeutically exploited by vaccination, but mice with advanced tumors do not retain these cells. The inquiry by the Vanderbilt researchers differed from most cancer vaccine studies, which have focused on patients with advanced tumors. The findings
support further vaccine investigation to make long-term, progression-free survival a reality for more cancer patients, said the study’s senior author Mary Philip, MD, PhD, associate director of the Vanderbilt Institute for Infection, Immunology and Inflammation.
Protocol improves follow-up for women at high risk for breast cancer
A nurse-led initiative at the Vanderbilt Breast Center offers women at high risk for breast cancer greater opportunities for recommended follow-up screenings and genetic counseling. Before the new protocol was implemented, every patient underwent a Breast Cancer Risk Assessment Tool (BCRAT) evaluation, yet there was no established protocol for sharing the results. A team of six advanced practice providers devised a system using Epic software. Each week, they searched electronic health records to identify patients who had BCRAT scores with a lifetime risk of breast cancer greater than 20%. The scores were sent through a secure electronic message to the patients’ referring physicians notifying them of the option for an additional referral to the Vanderbilt Breast Center high-risk clinic. Nurses also contacted patients directly to offer high-risk consultations. Results of the intervention, which were published in the August 2024 issue of the Clinical Journal of Oncology Nursing, showed that the protocol resulted in increases in breast MRIs, genetic counseling and genetic testing. The study’s lead author is Ashley Johnson, DNP, APRN.
Epigenetic change to DNA associated with cancer risk
A research team co-led by investigators at Vanderbilt University Medical Center and the University of Virginia has identified associations between DNA methylation and cancer risk. DNA methylation is an epigenetic change — the addition of “methyl groups” to DNA — that can affect gene expression without changing the DNA sequence. Most DNA methylation occurs on CpG sites in the genome. The new study, published in the journal Nature Communications, identifies 4,248 CpG sites associated with the risk of seven different types of cancer: breast, colorectal, renal cell, lung, ovarian, prostate and testicular germ cell cancers.
Innovations
Immunotherapy Revolution
Vanderbilt-Ingram pioneers new CAR-T discoveries and treatments
Remarkable. That’s how Bhagirathbhai Dholaria, MD, described responses to an ongoing clinical trial for patients with relapsed or refractory multiple myeloma who had run out of treatment options.
Dholaria, associate professor of Medicine, presented interim results from the Phase 1 trial for a new “off-the-shelf” chimeric antigen receptor-T cell (CAR-T) therapy at the 21st International Myeloma Society Annual Meeting in Rio de Janeiro on Sept. 27, 2024. CAR-T is an immunotherapy that the Food and Drug Administration first approved for a type of leukemia in 2017, but Vanderbilt-Ingram Cancer Center hematologists were already providing it to patients. They pioneered the treatment through clinical trials and remain at the vanguard of this revolutionary immunotherapy.
CAR-T is a treatment in which a patient’s T cells are harvested, reengineered in a laboratory to attack cancer cells, and then infused back into the patient’s body. It was revolutionary at the time it was developed because CART is a once-and-done, single-treatment therapy, but CAR-T discoveries have just begun. An “off-the-shelf” treatment option — engineered from healthy donors’ T cells instead of a patient’s own T cells — would expedite the manufacture of this immunotherapy and make it readily available, allowing patients to start treatment sooner. The FDA has not yet approved an “off-the-shelf” or allogeneic CAR-T therapy, but Vanderbilt-Ingram researchers are once again leading the way.
The FDA has approved six CAR-T autologous therapies, which are made from a patient’s own T cells, for lymphomas, leukemias and multiple myeloma. Other clinical trials are underway to potentially expand their approvals, and Vanderbilt-Ingram is offering them to patients who meet the medical protocols.
The FDA has given the therapy for which Dholaria presented interim data, P-BCMAALL01, designation as a regenerative medicine
advanced therapy through the 21st Century Cures Act to accelerate development.
P-BCMA-ALL01 demonstrated a 91% overall response rate for the 23 patients participating in the optimized dose cohort with multiple myeloma who had not responded to existing treatments or who had relapsed disease. Vanderbilt-Ingram accrued the most participants of the study’s 15 sites.
“The high overall response rate of 91% is remarkable because most study participants in my center had rapidly proliferative refractory disease in contrast with those treated in the pivotal clinical trials of FDA-approved autologous CAR-T therapies,” Dholaria said. “Such patients treated in the current trial of P-BCMAALL01 would not have qualified for standard of care autologous CAR-T therapy. All patients in the Phase 1 trial have been treated quickly once enrolled with no waiting for manufacturing and with no need for apheresis or bridging therapy, demonstrating key advantages of allogeneic CAR-T cell therapy.”
Dholaria is part of a team of physicians at Vanderbilt-Ingram who are CAR-T experts. Collectively, they are conducting several clinical trials for potential new CAR-T therapies. The trials include another potential “off-theshelf” therapy that also involves an emerging medical treatment called CRISPR. This is a gene-editing technology that allows scientists to precisely cut and insert DNA into the human genome.
Olalekan Oluwole, MD, MPH, associate professor of Medicine, is the investigator for this Phase 1 clinical trial involving CRISPR and CAR-T, which is called ANTLER. It is offered to patients with relapsed/refractory B cell non-Hodgkin lymphoma who meet the trial criteria. Oluwole also pioneered an outpatient treatment protocol for CAR-T at Vanderbilt-Ingram that other cancer centers are implementing. When the first cancer patients in Tennessee underwent CAR-T therapy at Vanderbilt-Ingram in 2015, they had to be
hospitalized for an extended period and closely monitored for serious reactions. He and colleagues demonstrated that patients could receive CAR-T liberated from a hospital room.
In 2017 Vanderbilt also pioneered CAR-T treatment for pediatric cancer patients in Tennessee. Carrie Kitko, MD, Ingram Professor of Pediatric Oncology and associate professor of Pediatrics, began offering it for a subset of pediatric acute lymphoblastic leukemia patients. At the time, Vanderbilt was one of only 32 health care institutions in the U.S. certified to offer the therapy.
Other physicians on the CAR-T team are Eden Biltibo, MD, MSCI, Andrew Jallouk, MD, PhD, Adetola Kassim, MD, Reena Jayani, MD, MSCI, James Jerkins, MD, Bipin Savani, MD, and Richard Ho, MD, MSCI. n
Find a clinical trial
Search Vanderbilt-Ingram Cancer Center clinical trials by disease, physician/investigator, treatment type and drug names at: vicc.org/clinical-trials or call 800-811-8480.
KITKO
DHOLARIA
OLUWOLE
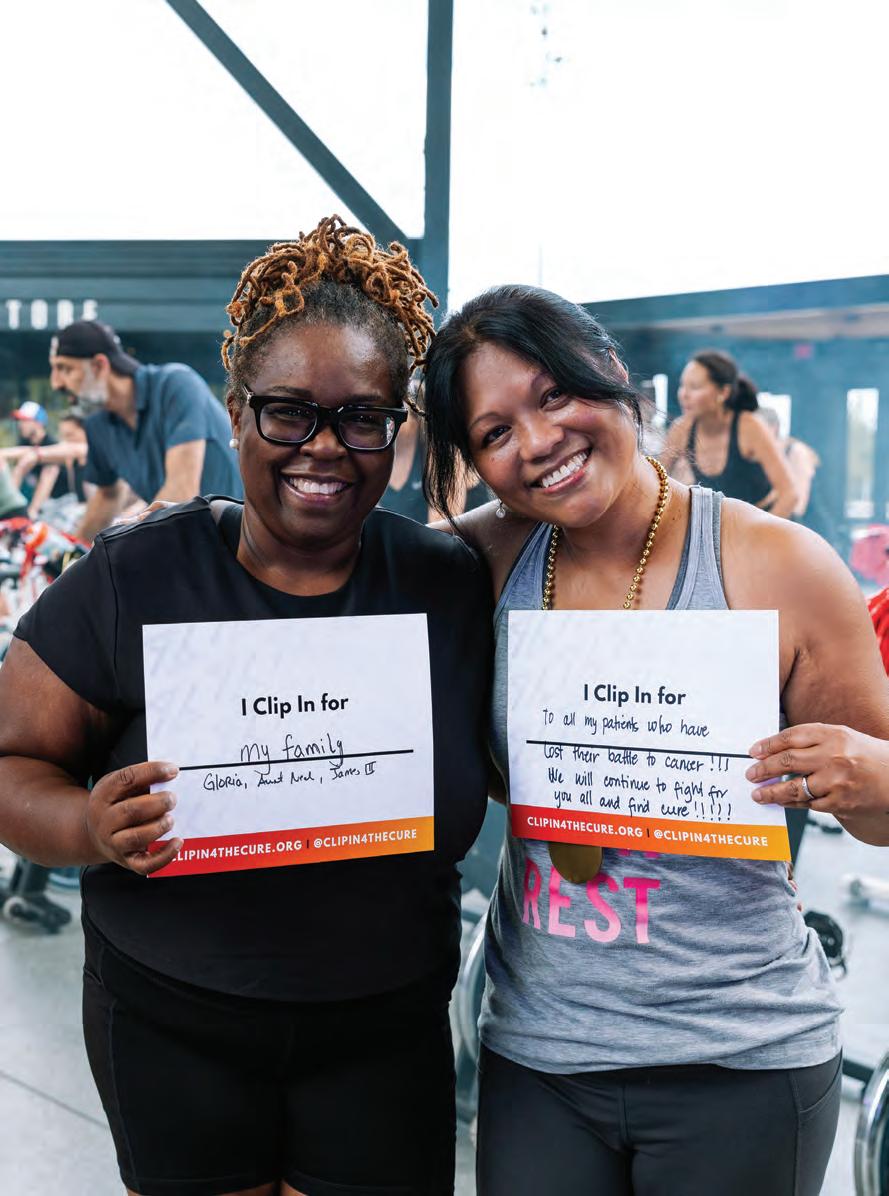
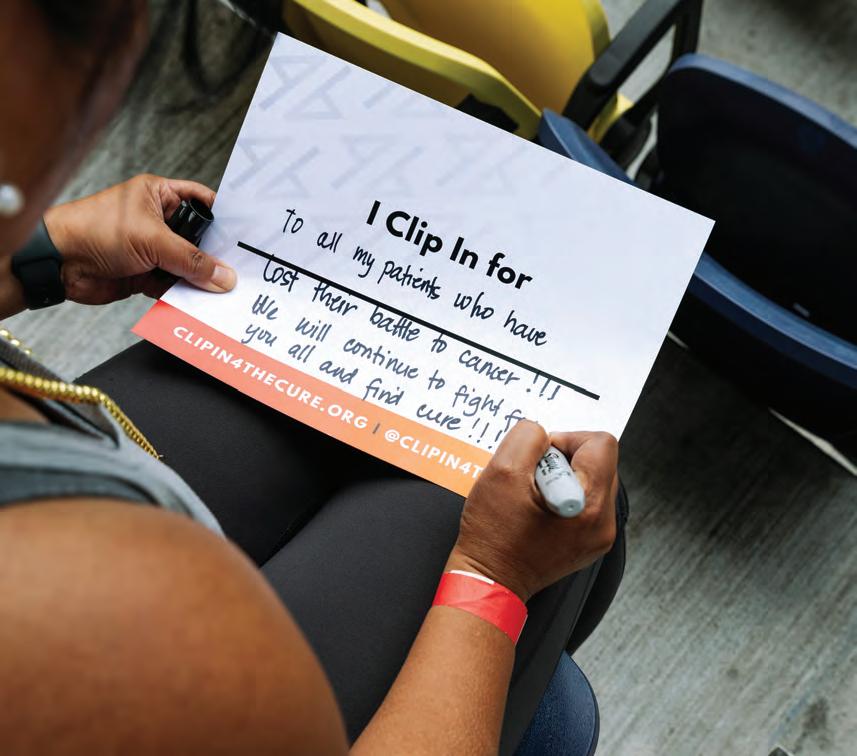
Clip In 4 the Cure
Benefiting childhood and adult cancer initiatives at Vanderbilt-Ingram Cancer Center
Clip In 4 the Cure 2024 brought people together on Sept. 14, 2024, for an inspiring day of cycling and raising money for cancer research. This year’s event was the most successful yet, with more than 400 attendees at GEODIS Park and over $277,000 raised. This support makes a tangible impact on adult and pediatric cancer research at Vanderbilt-Ingram.
Pictured here:
1. StretchLab offers complimentary stretches to Clip In 4 the Cure attendees between spin sessions.
2. Ben Ho Park, MD, PhD, right, director of Vanderbilt-Ingram Cancer Center, and participant Brent Turner enjoy a Clip In spin session.
3. CycleHaus instructors Emmy Neisz, left, and Ali Ellis kick off the first spin session of the morning.
4. Participant Jeneth Aquino writes who she Clips In for; photos of participants and their “I Clip In for” signs were featured on TV screens during the event.
5. Laura Benjey passes out prizes to Clip In 4 the Cure attendees. Attendees compete to raise the most money, and the more money they raise, the more prizes they win.
6. Clip In is for anyone. Instructor Johna Germany leads the popular children’s spin session.
7. M&E Tour de Cure Team members Megan Pruce, Julia Dunagan, Dylan Palin and Sarah Lohrmann, left to right, pose for a photo after their ride. On average, each Clip In rider fundraised 92% more and received donations from 45% more donors compared to last year’s event.
Visit clipin4thecure.org to complete our interest form to be one of the first to know about registration for our 2025 event.
Olivia Leow
GLI MA WARRIORS
ALLIANCE TAKES ON BRAIN CANCER
On a sunny June day, Olivia Leow was driving her sons to a friend’s swimming pool when she briefly lost her peripheral vision. Later that afternoon, while watching them splash about in the water, her right hand temporarily went numb.
After some online research that evening with her husband, she figured she had experienced an aura, the warning signs of an approaching migraine, but the symptoms returned. Hospital evaluations determined she had a glioma, medical parlance for a brain tumor.
Her diagnosis occurred in the prime of her life as a mother with two young sons and a busy career as executive director of the Rotary Club of Nashville. Glioma is a cancer that afflicts people of all ages, including children. It is the deadliest pediatric cancer, and it’s also perplexing, evading the advances made in recent decades for other cancers.
STORY BY TOM WILEMON
PHOTOGRAPH BY ERIN O. SMITH
Janet and David Greene, of Knoxville, Tennessee, know the frustration of the slow pace of treatment advancements. It’s been 30 years since their son, Michael, died at age 16 from glioblastoma, the deadliest form of glioma. So does Leslie South. She lost her husband, Eric, in 2023 to the disease. They and Leow have formed an alliance to raise funds for Vanderbilt-Ingram Cancer Center to establish a preeminent Brain Tumor Center that will hasten discovery, expand clinical trials and train glioma specialists. The overarching goal is to develop better treatments and to make care more accessible.
“This is not a bricks and mortar project; it’s bringing together a group of like-minded people at the top of their fields and allowing them to collaborate to address this vexing problem of brain cancer,” said Reid Thompson, MD, the William F. Meacham Professor of Neurological Surgery and chair of Neurological Surgery.
There are different types of brain cancer, and the most common type is metastatic disease from another type of cancer that originates elsewhere in the body. Researchers have made progress in treating some of these tumors.
“A relentless focus on research has absolutely moved the dial and flipped the switch on certain types of brain tumors; I’m talking about melanoma,” Thompson said. “When I was a resident back in the 1990s, if a patient came in with metastatic melanoma to the brain, that was a death sentence. Survival was measured in mere months. A brilliant group of people made it their life’s work to understand and unravel the biology of melanoma. Through a lot of philanthropy and federal funding, this research led to a better understanding of melanoma, and specifically a recognition of the biology that drives melanoma. From that came drugs specifically targeted to melanoma.”
Vanderbilt was one of the leading cancer research centers conducting clinical trials for new melanoma treatments – treatments so effective that former President Jimmy Carter lived to be 100 after recovering from melanoma that had metastasized to his brain.
But gliomas, which originate in the brain, have not had a comparable research focus or treatment successes. One reason may be that glioma is a rare cancer, with an incidence rate of just 6 cases per 100,000 people.
“The vision is to create a center that will include imaging scientists, basic biologists and chemists to design drugs rapidly and screen them,” Thompson said. “This will include neuro-oncologists, who are clinical trial leaders, and researchers who can take discoveries from the lab and rapidly translate them to patients and do that at a pace that’s fast.”
This emphasis on glioma occurs during an inflection point for cancer, when new treatment modalities — such as immunotherapies, nanoparticle delivery and CRISPR technology — show promise for greatly improving survival rates and bringing about cures.
Olivia Leow’s story
It was Father’s Day, Sunday, June 20, 2021, when Leow had the symptoms that led to her diagnosis of astrocytoma, a glioma that develops in the astrocytes, which are star-shaped cells in the brain. That week when the symptoms returned, she called her doctor who advised her to go to an emergency room. She took her laptop along, not worrying too much and thinking she could get some work done while waiting to be seen.
The emergency room physician ordered an MRI of her brain, listed what the suspicious imaging might be, and then told her it was most probably a tumor.
Reid Thompson, MD, left, and Ryan Merrell, MD, coordinated on a treatment plan for Leow’s cancer.
“I want to be the mother of my children for as long as I can. That’s what I pray about — to be the mother of my children. I want to see them grow up and get married and have babies.” – Olivia Leow, above, with her husband and two sons
“It was like I’m in a movie,” Leow said. “I just kind of blacked out and didn’t hear anything. Then he read it again, and that’s when it settled in.”
She was hospitalized, underwent more testing and learned that she needed an awake craniotomy. The hospital recommended that she travel to California for the procedure, but with two young children, she immediately worried about the logistics of traveling so far for treatment. Friends and acquaintances who heard about her predicament kept recommending that she go to Vanderbilt and see Thompson.
“He was phenomenal,” she said. “I felt so sure after the first time that I met him that this was where I needed to be.”
She asked if she could wait for the surgery long enough to walk beside her 5-year-old son on his first day of kindergarten. Two weeks afterward, she was in the operating room. Thompson asked her what music she wanted to hear during the procedure. Leow told him he could decide. He turned up the Eagles. (She later organized a karaoke fundraising event for the brain cancer program at Vanderbilt, and Thompson sang “Take It Easy.”)
“It was pretty wild; I was awake for the majority of it,” Leow said. “I was talking. I was reading. I was telling stories. They wanted me to be continually talking and thinking and reading. I even called my husband in the middle of it.”
She spent one night in the ICU and went home the next day. Within a week, she was at her son’s T-ball game. Her treatment proceeded to 26 rounds of radiation followed by six months of taking an oral chemotherapy under the care of Ryan Merrell, MD, associate professor of Clinical Neurology and division chief of Neuro-Oncology.
Now, she sees Merrell every four months to make sure the glioma has not recurred. Glioma is a stubborn cancer with a very high recurrence rate. Survival rates vary according to the type of glioma, the tumor grade, the age of the patient and other factors.
“I talked to Dr. Merrell at one of my last visits about if the cancer comes back what do we do next. He mentioned that there’s a new drug after a successful clinical trial. It is for my specific tumor, down to the mutation type. It would be an incredible life-extending drug. That matters so much to me. Obviously, I want to live as long as I can. I want to be the mother of my children for as long as I can. That’s what I pray about — to be the mother of my children. I want to see them grow up and get married and have babies.”
In August 2024, the Food and Drug Administration approved vorasidenib for Grade 2 astrocytoma or oligodendroglioma with a susceptible IDH1 or IDH2 mutation. It was the first drug the FDA had approved for the disease in 20 years. However, there have been no new drug approvals for glioblastoma for an even longer time.
Michael Greene’s story
Michael Greene was a trumpet player, strikeout pitcher, exceptional student and only 14 years old when he was diagnosed with glioblastoma. More than 30 years later, David and Janet Greene remember the day vividly.
“When I drove into our driveway on May 20, 1993, and Janet told me that doctors said Michael had a brain tumor, I was really worried. I went upstairs and gave
him a hug and said, ‘We’re going to work through this together. We are going to be with you all the way.’ Then we went to the children’s hospital in our town that evening,” David Greene said.
He wasn’t prepared for the doctor’s words.
“Your son is going to die, and it’s going to be hard,” the doctor told him.
The couple determined that they were not going to give up on their son.
“I remember calling doctors all over the country to ask them,” he said. “I didn’t get a second opinion. I got a fifth and a sixth opinion. They all told me the same thing.”
“They said it in a kinder way,” Janet Greene said.
The couple decided to take Michael to Vanderbilt for treatment.
“I remember feeling like I was always carrying around a big rock in my stomach for the next year or so, ” David Greene said. “The only place that offered any hope at all was Vanderbilt, and even they were very clear that the chances were essentially nothing.”
Because of the blood-brain barrier — a natural defense system within the brain that restricts the passage of large molecules — delivering drugs to a tumor in the organ was problematic. To compensate, doctors increased the amount of chemotherapy, which multiplied the adverse side effects.
The glioblastoma spread despite their efforts. Michael wound up in a wheelchair and blind in one eye, but when Vanderbilt doctors told him and his parents about a clinical trial for a new drug called temozolomide being offered at Children’s National Hospital in Washington, D.C., the family decided he would participate. They got a glimmer of promise for what a new treatment could do. Michael stepped out of the wheelchair and even participated in the fun walk portion of a 10K race.
However, the positive response was temporary. Michael died in September 1994. Even after his passing, David and Janet Greene did not give up fighting on his behalf. They supported research at Vanderbilt to better understand brain tumor cells. They have given of their time as well, advocating for advances in cancer research and treatment. Janet Greene serves on the Board of Advisors for Vanderbilt-Ingram.
Thirty years after his death, they have pledged $1 million for the Brain Tumor Center in honor of Michael Greene.
“Collaboration is a really important word to everybody at Vanderbilt University Medical Center,” said Janet Greene. “They collaborate with each other within their department, with other departments, with other parts of Vanderbilt University and with other institutions. They are not ego people. They are ‘Let’s fix this’ people.’”
Eric South’s story
Eric South put up a fight after being diagnosed with glioblastoma at age 42 in February 2021. He sought out clinical trials and novel therapies, receiving treatment in Houston, Los Angeles and Nashville. A consultant in information technology and an executive in that field, he used his organizational skills along with his passion for golf to also fight for others. He cofounded Gladiator Project with his wife, Leslie South. The nonprofit raises money for glioblastoma research and patient support through annual golf tournaments in Franklin, Tennessee, each autumn, and at the Plainfield Country Club in Edison, New Jersey, each spring.
“It was entirely his idea to start Gladiator Project,” said Leslie South. “Not long after he awoke from his first surgery, he mentioned starting a nonprofit. I just brushed it off at the time. I was like, ‘That’s great,’
David and Janet Greene, parents of Michael Greene, left, have supported glioma research at Vanderbilt and have made a $1 million donation in their son’s honor for the Brain
Tumor Center.
SUSAN URMY
knowing he was on medication. But he was insistent that he wanted to start a charity.”
The couple met in Nashville in 2005 as government interns, got married in 2009, established a home in the Grassland Community of Williamson County and had two sons, who are now 10 and 12 years old.
Despite their hectic schedules of working, parenting and dealing with cancer treatments, they established the nonprofit in June 2021, within four months of his diagnosis.
After his initial treatment, he had a recurrence the following year, a scenario that is all too familiar for glioblastoma patients and their families. After completing his second clinical trial in Los Angeles, he decided to receive care at Vanderbilt-Ingram with Merrell, who had recently been recruited to Vanderbilt.
“He and Eric clicked instantly,” said Leslie South. “We learned about Dr. Merrell’s personal history with glioblastoma, and we saw his deep-seated desire and devotion to this specific cause.”
Merrell was in his third year of medical school when his father died from glioblastoma at age 63. That life experience led him to become a neuro-oncologist.
“Under Dr. Merrell’s care, Eric was able to access other treatments that the FDA has approved for different types of cancer, but not for glioblastoma and that weren’t in available clinical trials. That gave Eric a lot of hope and meaning. He had the attitude of ‘Hey, if this drug doesn’t work for me, we may learn something that helps it work for somebody else or that finally leads researchers and doctors onto the path to finding a real cure.’”
Eric South died on Aug. 31, 2023.
In Eric’s honor, Gladiator Project recently made a $500,000 commitment to establish the Gladiator Project Brain Tumor Research Fund to advance brain tumor clinical research at Vanderbilt-Ingram.
Path Forward
The funding raised for brain tumor research will help Vanderbilt leverage its strengths for research on gliomas. They include the Vanderbilt Brain Institute, BioVU, the Vanderbilt University Institute of Imaging Science, the Department of Neurological Surgery, the Division of Neuro-Oncology within the Department of Neurology, the Department of Cell and Developmental Biology, the Department of Radiation Oncology and the Department of Pharmacology.
The support will enable Vanderbilt to recruit top glioma researchers who will connect the dots between these resources and create collaborations with current investigators. It will also help establish a neuro-oncology fellowship, so that patients and their families will not have to travel across the country to receive care for glioma, which, because it’s rare, has few highly specialized programs.
Thompson is one of the nation’s top neurosurgeons, but he yearns for more knowledge at the cellular level about gliomas so better therapies can be developed for his patients after they leave the operating room.
“I’m in my 60s now, and I feel like I’m still asking some of the same questions I was asking about these cancers of the brain when I was in my 20s,” he said. “I don’t want to retire and find out that I am still asking the same questions.”
The recruitment of translational scientists to mine Vanderbilt’s resources with a laser-like focus on brain tumors, identify new paths of investigation and then bridge their findings into clinical relevancy is the path forward, Merrell said.
“I think of the patients we have had who died too young where we felt a sense of futility because of not being able to offer them other treatments,” Merrell said. “We want to change that.” n
Leslie South established a nonprofit, Gladiator Project, with her husband, Eric South, who died of gliobastoma.
DONN JONES
CHEMO ALLERGY
Researchers seek biomarkers to identify patients with chemotherapy allergies
Atrue allergy to a medication is not that common, and when it happens, there’s often a work-around, like substituting a drug in another class.
But what if you’re a patient with cancer and the drug you’re allergic to is a chemotherapy agent that offers the best, and sometimes only, chance of saving your life?
Physicians in the Drug Allergy Clinic at Vanderbilt University Medical Center are studying why that happens and how to best help patients tolerate the allergy-inducing chemotherapy.
STORY BY NANCY HUMPHREY • ILLUSTRATION BY AMANDA BAILEY
When your immune system mistakenly identifies a drug as a harmful substance, like it does for a virus or bacteria, it may develop an allergy antibody specific to that drug.
The next time you take the drug, the antibodies direct the immune system to release an attack on the substance, and an allergic reaction occurs. While the reaction may only result in itching or hives, sometimes it’s a more severe reaction that can lead to anaphylaxis, a life-threatening allergic reaction that can lead to low blood pressure, unconsciousness or even death.
Sam Manning, a 77-year-old retired real estate broker from Nashville, was diagnosed in April 2021 with Stage 4 peritoneal carcinoma, a gynecological cancer that arose from the lining of her abdomen.
But one day, after several treatments, the chemotherapy agent she was prescribed, carboplatin, resulted in anaphylaxis.
“There are certain drugs we give patients when we are treating their cancer that have a higher chance of the patient eventually becoming allergic to that drug. It’s particularly problematic for women getting treated with platinum drugs for ovarian cancer or other gynecological malignancies,” said Cosby Stone Jr., MD, MPH, assistant professor of Medicine in the Division of Allergy, Pulmonary and Critical Care Medicine. “Losing access to a drug that is working for your cancer can be a disaster. You can end up having a bad outcome.”
Stone said that chemotherapy drugs are the fifth most common category of drugs that result in patients having anaphylaxis.
“Chemotherapy reactions are also more likely to be fatal if we don’t get them under control, and that’s because the patients are sicker to begin with,” he said.
Manning’s oncologist, Marta Crispens, MD, professor of Obstetrics and Gynecology, director of the Division of Gynecologic Oncology and director of the Gynecologic Oncology Fellowship, said platinum drugs, specifically carboplatin and cisplatin, are the most active chemotherapy agents for cancers such as epithelial, ovarian and cervical cancers and are critical to the treatment of many other gynecological cancers such as endometrial cancer.
“Allergic reactions can limit our ability to use these critical drugs,” she said. “Being able to use these drugs in patients in whom anaphylactic reactions might have previously prevented their use allows us to offer patients their best chance of response and cure.”
A Wicked Strong Allergy
In 2021 Manning began having severe abdominal pains that became progressively worse. Her daughter, Tasha, took her to an urgent care clinic near her home, and they sent her to Stonecrest Hospital’s emergency
room in Smyrna where 24 hours later they determined that she had a large tumor in her abdomen.
After some insurance issues were resolved, she was sent to Vanderbilt-Ingram Cancer Center where she had more scans and met with her medical team. The 9 ½ pound tumor was removed by Marcus Tan, MD, associate professor of Surgery.
She was told she had one to two years to live and began chemotherapy after recovering from the surgery. But, after previously tolerating carboplatin for a while, one day she experienced a reaction to it. She broke out in hives over her entire body, wound up having a severe anaphylactic reaction to carboplatin, and had to be admitted to the hospital.
“The more doses of carboplatin a patient receives, the more likely they are to be allergic,” Stone said. “If you’ve had zero doses of carboplatin, your chance of being allergic is less than 1%. If you’ve had seven doses, it goes up to 27%; 10 doses, about 50%.”
“Sam had a wicked strong allergy, even stronger than the average allergy,” Stone remembers. “We started working through the process of desensitizing her so that she could still get carboplatin for her cancer. However, even with the first desensitization, she still had some very strong symptoms that first time.”
Stone, who called the hospital to check on Manning and was told she wasn’t doing well, spent the night in the cancer unit with her and eventually came up with a desensitization protocol to allow her to still receive carboplatin despite her allergy.
“She still had some breakthrough symptoms despite desensitization that were pretty bad. We treated the symptoms; I kept her company until she felt better; and
Stone Jr., MD, MPH, developed a desensitization protocol to allow Sam Manning to receive carboplatin despite her allergy.
Cosby
that’s how we got her through that first full treatment after becoming allergic,” he said. “After that, we kept working on it together. Each treatment got slowly better as we worked on controlling her allergy symptoms with an improved, personalized protocol.”
Diluting the chemo
The Drug Allergy Clinic began treating patients with chemotherapy allergies shortly after the COVID19 pandemic restrictions eased.
“We trained our nurses and pharmacists, working with our gynecologic oncologists and built this program from scratch. We were able to take advantage of the opportunity to implement some of the most up-todate protocols available in the drug allergy research space,” Stone said.
When a patient is allergic to a chemotherapy drug, the VUMC drug allergy and pharmacy teams take the drug that the patient is allergic to, at the concentration they need, and use a protocol that dilutes it by a factor of 10, then a factor of 100. Then, this very diluted drug is slowly administered to the patient.
“I was a mess. Dr. Crispens told me that carboplatin was the only chemo medicine that would do me any good with my cancer. They were able to keep using it, but only because Dr. Stone kept tweaking it and improving how they administered my allergy treatments with it. Every time, it got better.” – Sam Manning, pictured below.
“Over the course of three hours, we slowly double the concentration of the drug the patient is getting, starting with the really diluted drug, and slowly bumping it up every 15 minutes until they are at the concentration they need to actually get the full treatment,” Stone explained.
To do this, a patient must be admitted to the hospital and have a nurse dedicated solely to their care at the bedside.
“Depending on how well the patient tolerates it, we keep doing desensitization in the hospital, but some patients are able to tolerate it well enough to go back to the outpatient infusion center for the same protocol,” Stone said.
The Whys and Hows
The team is still searching for answers as to why patients become allergic to the platinum drugs.
“Either the interaction of the drug with the body creates a new allergen your body recognizes, or the repeated exposure makes it possible for it be recognized as an allergen. Those are questions we’re trying to answer,” Stone said.
And why diluting the chemotherapy then slowly bumping it back up works has not fully been determined.
“We can do more than we can understand,” Stone said. “We can make a patient not react to chemo, even when they’ve had anaphylaxis, or if they do react despite a desensitization, it’s not so bad that we can’t control it. But we don’t know exactly why it works. Honestly, the clinical care is a little further than the science, but we are trying to fix that,” he said.
“We think that desensitization gets below the patient’s reaction threshold, such that giving them the drug is more like a controlled burn rather than an explosion, and they have a reaction that’s lower than their level of ability to detect or experience. We control the reaction, so it doesn’t come on all at once, so all we have to do, if they have symptoms, is give them some antihistamines and hold off on the drug for a little bit, then restart it.”
Not all patients who are allergic to their
JOHN RUSSELL
Marta Crispens, MD, director of Gynecologic Oncology, worked closely with Stone to develop a treatment plan for Manning.
chemotherapy drugs have as strong of a reaction as Manning’s, Stone said.
“I was a mess,” Manning remembers. “Dr. Crispy (her nickname for Crispens) told me that carboplatin was the only chemo medicine that would do me any good with my cancer. They were able to keep using it, but only because Dr. Stone kept tweaking it and improving how they administered my allergy treatments with it. Every time, it got better.”
Stone said the team got Manning to the point of only minor symptoms with each chemotherapy treatment. “It allowed her to get another 10-20 treatments with this key drug for her cancer, despite being very allergic to it.”
Her case has provided the drug allergy team with valuable information on how to better treat patients who are allergic to their chemotherapy.
“Mrs. Manning’s allergy was so strong that we had to pull out all our tricks, and then we were able to apply them to other patients, with great benefit — in particular which additional medicines (extra antihistamines, montelukast, etc.) patients need to take for several days beforehand so they can get through their desensitization more smoothly,” Stone said.
Tolerable and Safe
About 95% of patients treated for chemotherapy allergies at VUMC have been patients with ovarian and endometrial cancers, but the team has also helped patients with gastrointestinal and head and neck cancers.
“This a patient-centered approach that allows the patient to keep getting the drug that’s working for their cancer. The whole program is built around trying to achieve two goals: making it as tolerable for the patient as possible and making it as safe for the patient as possible, despite the fact that they are allergic to this drug that they have to take,” Stone said.
Stone, Scott Smith, MD, PhD, associate professor of Medicine, and Elizabeth Phillips, MD, the John A.
“Sam had a wicked strong allergy, even stronger than the average allergy. We started working through the process of desensitizing her so that she could still get carboplatin for her cancer.”
– Cosby Stone, MD, MPH
Oates Professor of Clinical Research and professor of Medicine, Dermatology, Pharmacology and Pathology, Microbiology and Immunology, have a pilot grant funded by Chic Awearness to study chemotherapy allergy at VUMC.
Stone said he’s hopeful research can pinpoint the markers of these reactions and find the allergy antibodies patients are making against these drugs, so that a blood test can be developed, or a treatment can be identified that blocks the reaction.
“The first rule is: Take care of the patient. Do the best you can for the patient. Second: Use science to figure out how to do better next time,” he said.
Since most of the chemotherapy drugs that cause allergies are drugs that have been around for some time, the ultimate work-around on the drug allergy problem
may be developing new drugs that don’t result in allergic reactions.
“I don’t mind if the cancer doctors make me obsolete by coming up with better drugs for these cancers, but we’ll take care of all the patients who need us until they do,” Stone said.
Manning, who credits Stone and Crispens with saving her life, recently began immunotherapy at Vanderbilt-Ingram and is hopeful that will give her more time.
“I’ll never be cured. I’ve lost all my hair. I don’t have the energy I used to have, and I can’t do the things I used to do,” she said. “I used to be a big boater. I had a houseboat on the lake, and I can’t do any of that anymore. Cancer has dragged me down. But I’m here. I’m still here.” n
More women are at risk for chemotherapy allergy
Women are more likely than men to experience chemotherapy reactions and allergies.
70%
Up to 70% of female patients may develop an allergy to carboplatin with prolonged treatment.
70%
Up to 70% of female patients may experience a reaction to paclitaxel during chemotherapy treatment.
95%
Among women patients at Vanderbilt with chemotherapy allergies, 95% have ovarian or endometrial cancer.
Lily Hensiek
A Grateful Goal
A clinical trial saved Lily Hensiek’s life when she relapsed with childhood leukemia. Now, she’s helping other cancer patients.
Lily Hensiek doesn’t remember much about the first time she was diagnosed with pre-B cell acute lymphoblastic leukemia (ALL) when she was 7 years old.
“The big thing was the back pain that radiated down my legs. I could barely walk,” she said. “I mainly remember being shocked and confused. It was a big learning curve of what leukemia was and what I was about to go through.”
She didn’t know then that her cancer journey would last through her teenage years or that she would play an important role in improving treatment for other children with ALL. At first, she and her family had to deal with the frustration, shock and denial of a cancer diagnosis.
STORY BY DANNY BONVISSUTO • PHOTOGRAPH BY DONN JONES
Hensiek was learning how to do a back handspring in gymnastics when she complained of lower back pain,
so her mother, Larisa Featherstone, first thought it was a sprain. When Hensiek spiked a fever of 103, she then thought it was a virus or urinary tract infection. After two trips to the emergency room with no answers, Featherstone took Hensiek to her pediatrician who ordered blood work and discovered she had leukemia.
“I remember thinking, this can’t be happening. It’s not possible,” Featherstone said. “There were so many words that were foreign to me — not that cancer is a foreign word — but I kept thinking, surely this can’t be my kid they’re talking about. I kept waiting for the doctors to tell me they’d gotten her blood mixed up with someone else’s. When Lily first felt sick and we went to the ER, the doctors told me they ruled out ‘everything bad.’ I think back on the conditions they ruled out, and they were all better than cancer.”
She did her best to hold it together while trying to explain cancer to her child.
“Lily kept asking when she’d be able to go home. She was scheduled to have her ears pierced a few days after her diagnosis and wanted to know if it would be canceled,” Featherstone said. “Lily couldn’t conceive of it lasting more than a couple days because all she’d known was strep throat and ear infections.”
Hensiek enrolled in a clinical trial through the National Cancer Institute’s sponsored cooperative group for pediatric cancer, Children’s Oncology Group, and her leukemia went into remission within the first month of treatment. She continued in remission through two years of chemotherapy. She recalls a lot of nausea and a chemotherapy drug nicknamed the “Red Devil” for its color and ability to turn her urine red.
In addition to the time she spent in the hospital, she spent a lot of time in the clinic after her diagnosis. When she finished two years of treatment, she followed up monthly for the first year; every two months for the second year; every three months for the third year; every four months for the fourth year and annually after five years. After five years she was considered cured because the chances of relapse after five years of remission are less than a few percent.
The Relapse
One day in September 2016, when Hensiek was 15, and 5½ years out of treatment, she told her mother, “My back’s hurting, and I’m running a fever, but I don’t feel bad.”
“One thing about being a cancer mom is that you tend to overreact, so in an effort to not overreact I said, ‘Let’s see how you feel in the morning.’ She woke up fine,” Featherstone said. “A week and a half later, she was playing the last game of her volleyball season, and I thought she looked pale and tired, but because of the chemo she went through, she tires more quickly than most kids her age.”
That night Hensiek ran another fever and experienced more back pain. They went to her doctor’s office in the morning, which offered a blood test to put everyone’s mind at ease. The call Featherstone received with the results was that her daughter’s leukemia had returned.
“I was with Larisa a week before Lily came in with her relapse — at a fundraising event for Monroe Carell,” said Debra Friedman, MD, director of Pediatric Hematology and Oncology at Monroe Carell Jr. Children’s Hospital at Vanderbilt, and Lily’s treating physician for what they call her second round. “Larisa spoke at the event and said how well Lily was doing and that she’d finally gotten to the point where she woke up and didn’t worry about leukemia. And literally a week later, Lily was in my clinic complaining of back pain that didn’t make sense. I got a blood count, and she had relapsed.”
When Hensiek was originally diagnosed in December 2008, the standard of care for her type of leukemia was chemotherapy. Eight years later, when she relapsed, another clinical trial was available at Vanderbilt through the Children’s Oncology Group, designed specifically for patients without early relapses.
Debra Friedman, MD, cared for Hensiek during her second clinical trial.
9,620
About 9,620 children in the United States under the age of 15 will be diagnosed with cancer in 2024. Cancer incidence rates in children overall have stabilized since 2015, after increasing since at least 1975.
Source: American Cancer Society
85%
Because of major treatment advances in recent decades, about 85% of children with cancer now live five years or more after being diagnosed with cancer. Overall, this is a huge increase since the mid-1970s, when the five-year survival rate was about 58%.
1,040
After accidents, cancer is the second leading cause of death in children ages 1 to 14. About 1,040 children under the age of 15 are expected to die from cancer in 2024. The cancer death rate has declined by more than half from 1970 to 2021 in both children and adolescents, largely due to improvements in treatment and high participation in clinical trials.
“Lily relapsed very late — way out of normal late,” said Friedman, holder of the E. Bronson Ingram Chair in Pediatric Oncology. “The standard of care at the time for someone who relapsed as late as she did was reinduction chemotherapy and cycles of rotating intensive and nonintensive chemotherapy, which is what she did the first time but more intensive. The open clinical trial, a Phase 3 randomized trial, was comparing the standard of care with chemotherapy backbone to that with a new agent incorporated called blinatumomab. In the Phase 3 trials, the standard arm is always the standard of care, and the alternative arm is, ‘Hey, can we do better?’ It’s almost like a no-lose situation.”
According to Friedman, blinatumomab, which Hensiek and her family call blina, is a bi-specific T cellengaging immunotherapy that has a receptor for CD19, which is on leukemia cells, and a receptor for CD3 on immune system T cells, so it brings the T cells to the leukemia cells to destroy them. In other words, it trains the body to fight off the cancer cells.
“If you’ve heard of CAR-T cell therapy, this is a similar concept, but it’s actually a pharmaceutical agent, so to say,” Friedman said. “Some people call it a poor man’s CAR-T, but it’s neither cheap nor poor. It’s on the top 10 list of most expensive drugs in oncology.”
New Treatment Path
Hensiek and her family had a difficult time deciding whether to participate in the study.
“It was a hard decision. We struggled with it a lot, talked with doctors and did a lot of research,” Featherstone said. “We decided to participate and put whether or not Lily would receive the chemo side only or the
chemo-plus-blina side in God’s hands and knew it was a blessing in disguise, because this was an option she didn’t have the first time.”
Hensiek was placed in the experimental arm of the study to receive both chemotherapy and blinatumomab, and she was the third Vanderbilt University Medical Center patient to get blinatumomab on the clinical trial.
She said her doctors gave her a weekend to “be normal and hang out with friends” before she went inpatient for a month as the first step in another two years of treatment, which altered the course of her teenage years.
“I had all the support in the beginning, but everyone has so much going on at that age, and it was hard to keep friendships. I had one good friend throughout my entire treatment who was there and would visit me in the hospital consistently,” Hensiek said. “I missed out on football games and having a normal high school experience. I tried to go to classes when I could, but I had to have an immune system, feel OK and have enough stamina to last the entire school day. It was difficult to keep up with my schoolwork, but my big goal was to graduate with my friends and classmates, even though it was recommended that I take a year off to focus on treatment.”
When Hensiek was on the blinatumomab portion of treatment, it was infused intravenously 24/7 for a month.
“I had a little backpack that I’d carry around with me. I was very forgetful of the backpack and would walk away and get yanked backward,” she said. “I felt almost 100% when I was on that drug, which is crazy compared to the chemotherapy, on which I’d always feel exhausted and nauseated. On the blinatumomab, I always felt like a normal human and never nauseated. I felt like I could go hang out with people and wasn’t as tired. I was also able to go to classes.”
The whole family felt better when she felt better.
“Drugs are hard. Most people don’t realize how brutal cancer treatment is unless they’ve walked it themselves or with a family member,” Featherstone said. “When Lily was on the blinatumomab, she felt good and was able to be a more normal kid, which is what she really wanted.”
According to Friedman, Hensiek did very well in the clinical trial, went into remission quickly after the first month of therapy, tolerated the blinatumomab well, and finished therapy in 2018. She has remained in continued clinical remission ever since.
The study she participated in was closed and analyzed, and the arm that incorporated blinatumomab had better event-free survival. It is now the standard of care for patients with late leukemia relapses.
“It was such a positive result, we all said, ‘Well, can
we integrate this into up-front therapy?’ Or is it only effective in relapse therapy?” Friedman said.
In recent years, another Phase 3 randomized clinical trial opened up within the Children’s Oncology Group for patients with standard risk pre-B cell acute lymphoblastic leukemia, and patients were randomized to standard of care chemotherapy or chemotherapy with the addition of blinatumomab in a few cycles. At an analysis at three years, the blinatumomab arm was statistically and clinically superior to the chemotherapy-only arm — so much so that the study closed early, and most patients are getting blinatumomab added to their chemotherapy-only protocol.
“Now our standard of care for all pediatric patients with B-ALL, whether they’re in the standard or highrisk category, whether they’re little or older, is to give them a regimen that incorporates chemotherapy and blinatumomab,” Friedman said. “It really has changed the face of how we’re treating ALL because we’re incorporating immunotherapy for all patients. Virtually every program in the country has incorporated this as the standard of care.”
Friedman said the next step may be to substitute some chemotherapy with blinatumomab.
“We’ve added blinatumomab to the chemo regimen, but we haven’t substituted,” Friedman said. “I think that may come in future studies, as well as the introduction of other new agents. Though it occasionally has very bad side effects, which is why we start it inpatient and monitor patients for several days, blinatumomab is much better tolerated than chemotherapy, generally
speaking, although more burdensome because it is a continuous, 24/7, 28-day infusion. The results of the trials testing the addition of blinatumomab for relapsed and newly diagnosed B-ALL show the power of clinical trials.”
Lily’s Garden
Although she was just a child when she received her first diagnosis, Hensiek wanted to do something to take some type of action against cancer.
“It was such an unfair thing we were going through, not just for us but for everyone, and we wanted to make it less unfair in the future,” Hensiek said. “My family and I wanted to support the Medical Center in treating kids with cancer and hopefully finding better ways to treat them.”
She started with a goal of $100 and increased it to $1 million when her mother challenged her to reach higher. Featherstone never thought they’d raise that much money, but, through community fundraisers, gifts from family and friends, donations from local foundations and businesses, and support from Johnston & Associates, a workplace safety consulting firm founded by Hensiek’s grandfather, Ron Johnston, she surpassed her goal and created the Lily’s Garden Endowed Lecture in Childhood Cancer and the Lily’s Garden Research Fund. These funds have supported visiting professors, research at Monroe Carell and Vanderbilt-Ingram Cancer Center and the leaders of the future — oncology fellows and junior faculty.
The garden theme was born of the way Hensiek’s doctor originally explained treatment to her: that cancer
Lily Hensiek, a leukemia survivor, and her family created multiple funds to support pediatric cancer research and training at Monroe Carell Jr. Children’s Hospital at Vanderbilt through community fundraisers and individual donors.
“My family and I wanted to support the Medical Center in treating kids with cancer and hopefully finding better ways to treat them.” – Lily Hensiek, right, with her mother, Larisa Featherstone
was the weeds that had overtaken her garden of cells, and chemotherapy would remove those weeds and allow her garden to grow again.
“Once we surpassed the goal, Lily said, ‘There’s still cancer,’” said Featherstone, who is CEO of Johnston & Associates and chair of the Monroe Carell Advisory Board. “A lot of people asked her to set a new goal, and she said it was for there to be no cancer. Unfortunately, it’s not about a dollar amount — it’s about finding a cure and getting better treatment in place, and that work is not done yet.
“When Lily was first diagnosed, I decided I was going to do all this crazy research, which was ridiculous but my way of dealing with it,” Featherstone said. “I researched every single thing about all these drugs and didn’t understand 99% of it because I’m not a doctor, but what I found fascinating was that sometimes there are wild ideas or out-of-the-box thinking, and that’s what drives innovation. And so, encouraging these doctors and providing them with funds so they can do what they do so children can have more successful outcomes — that’s really the goal.”
Hensiek’s family, Larisa and Phillip Featherstone and Carol and Ron Johnston, continued their philanthropic support with the establishment of the Lily’s Garden Fellowship in 2018 to support pediatric oncology fellows. In 2022, the family made a new commitment to endow the Lily’s Garden Discovery Researcher Fund to support researchers in pediatric cancer.
Featherstone said she had just started feeling like
their lives were back to normal when her daughter relapsed in 2016.
“She finally got caught up in school. She was playing volleyball,” Featherstone said. “The doctors give you these road maps when your kids have treatment, and I’m very methodical. I checked off literally every medication and visit. We felt like we’d done everything we were supposed to do, and it was smooth sailing. My younger daughter, Sophie, said it best: The first time was horrible, but starting Lily’s Garden gave our lives purpose. The second time was like, do we really need to go through this again? I realize that’s not how it works, but that’s how it felt.”
Because she relapsed so late, the thought that it could happen again lives in the back of their minds.
“I always tell people, she’s out of treatment longer this time than she was the first time, but the chance she could relapse late is still there,” she said. “I fear relapse, but I continue to see more advancements are being made. If something were to happen again, which would be horrendous, there are even more options, which gives her more chances.”
The Future
Hensiek, now 23, accomplished her goal of graduating with her high school class in 2019 and graduated from the University of South Carolina in 2023. While working as a clinical research assistant at the UT Southwestern Medical Center in Dallas, she set a new goal: to be a physician assistant. She started the PA program at Kansas State University in January.
“For as long as I can remember I’ve wanted to be in the medical field. I loved my nurses during my first diagnosis — I even had a few who’d gone through cancer treatment. There were times when I didn’t want to take my medicine, and they were the only ones who could convince me to take it,” Hensiek said. “I want to be that person for future patients. I hope to bring a perspective of understanding that’s different from other medical professionals.”
Friedman, who has had many conversations with Hensiek over the years about her interest in the medical field, said she will make a wonderful physician assistant.
“She always asks good questions. She was always eager to learn. If something was going on, she always wanted to know why it was going on and what we could be doing differently,” Friedman said. “She has an inquisitive mind and is truly a lovely human being who cares about other people. She also understands the reality of pediatric cancer and the medical field. She’s not going in with blinders on thinking she’s going to cure the world. Over the years, she saw people around her not survive their malignancy. She’s lived it. She’s going in with her eyes wide open, and I know that she will make an impact for so many in the future, as she has already done.” n
SOUND POWER
New technology sends ultrasound waves to destroy tumors
In October 2023 the Food and Drug Administration approved a groundbreaking treatment for patients with liver cancer or liver metastases that uses focused ultrasound waves to destroy tumors. With philanthropic assistance, Vanderbilt University Medical Center will begin to offer this innovative therapy, known as histotripsy, in early 2025.
Unlike surgery and other localized but invasive ablation treatments that rely on heat, cold or chemicals, histotripsy employs precisely targeted ultrasound waves to break down cancer cells through mechanical forces alone. The procedure typically takes half an hour and allows most patients to return home the same day.
“A lot of patients with liver cancer or liver metastases are unfortunately not surgical candidates, and they run out of options. We can offer this treatment to selected patients, and what excites me is that it’s completely noninvasive,” said Kamran Idrees, MD, MSCI, MMHC, professor of Surgery and Ingram Associate Professor of Cancer Research, who is helping to lead the introduction of histotripsy at VUMC. He serves as chief of the Division of Surgical Oncology and Endocrine Surgery and director of Pancreatic and Gastrointestinal Surgical Oncology.
these small micro bubbles that oscillate and cause tissue disruption,” Idrees said. “It liquefies the tumor cells completely.” The destroyed tissue is naturally eliminated by the body within weeks to months.
Histotripsy works by delivering microsecond pulses of high-pressure sound waves that create rapid pressure changes in tumor tissue. These changes cause microscopic bubbles to rapidly form, expand and collapse, generating intense and highly localized mechanical forces strong enough to break apart cancer cells. Beyond treatment for liver tumors, potential additional applications for histotripsy remain under study.
“The ultrasound waves go into the liver and create
A key advantage of histotripsy is its ability to preserve important anatomical structures while destroying cancer cells. “The best part about it is tissue selectivity,” Idrees said. “It affects the tumor cells, but it doesn’t affect the key structures within the liver such as blood vessels and the bile ducts.”
This selective destruction represents a significant advancement over current treatments for liver cancer, which include surgical removal, thermal ablation, chemoembolization and radiation therapy. While these traditional methods can be effective, they come with significant limitations. Surgery is invasive and suitable for only 10% to 20% of patients. Other treatments risk complications such as bleeding or injury to normal
Histotripsy
structures such as bile ducts. These traditional techniques will continue to have a role in treatment of liver tumors and liver metastases, Idrees said, with histotripsy figuring as a new addition to the armamentarium.
The procedure itself is remarkably straightforward. It’s performed under general anesthesia to control breathing, as the liver sits close to the diaphragm. Using ultrasound imaging guidance, physicians identify the tumor’s location and program these coordinates into a robotic system that delivers the treatment with precision. With a specialized membrane placed over part of the patient’s abdomen, a water bath between the membrane and the machine helps transmit the ultrasound waves effectively.
While the procedure can take as little as five minutes for smaller tumors, average treatment time per tumor is about 34 minutes.
The treatment can be monitored by doctors in real time using ultrasound imaging like what’s used for seeing babies in the womb.
“The patient comes in under general anesthesia; we identify the lesions under ultrasound; and we can ablate from a single lesion up to three lesions,” Idrees said. “After destruction of a lesion or lesions, we wake the patient up. If the patient is doing well, they go home the same day or after 23 hours observation. We cannot do that with any surgery or any other technology as of now.”
Another significant advantage is its repeatability for patients who develop new tumors over time. “It’s not one and done,” Idrees said. “If they have more lesions or other lesions pop up, we can repeat the procedure as needed.”
Unlike chemotherapy or radiation therapy, histotripsy doesn’t create heat or ions that could damage healthy DNA. The destroyed cancer tissue simply turns
into a harmless liquid that gets naturally absorbed and eliminated by the body’s drainage systems.
One particularly notable advantage of histotripsy is that patients can continue their chemotherapy during treatment. As Idrees points out, “For any surgery and other procedures that we do, we stop chemotherapy for at least four to six weeks. Then they’re going to get the procedure, and if there’s no complication, they can restart the chemotherapy. But if they have a complication, there may be a delay in restarting the chemotherapy. With histotripsy, we don’t have to worry about any of that.”
And since the risk of bleeding with histotripsy is negligible, patients can continue blood thinners.
The treatment has shown promising results in clinical trials. In the HOPE4LIVER trial, which led to FDA approval, the technical success rate was 95%, with 42 out of 44 tumors successfully treated. The procedurerelated major complication rate was 7%, which is comparable to existing treatments. The trial included patients with both primary liver cancer and liver metastases from other cancers, including colorectal, breast and pancreatic cancers.
The treatment can also be combined with other approaches. For patients with tumors on both sides of the liver, doctors can use histotripsy to treat one side while surgically removing tumors on the other side. Additionally, histotripsy has been approved for “downstaging” liver tumors — reducing their size to make patients eligible for liver transplantation.
Idrees notes that, regarding the liver, histotripsy does have some current limitations; notably, the liver lesion must be visualized by ultrasound and the maximum treatment depth is 14 to 16 centimeters, making tumors near the top of the liver and certain right-sided liver lesions difficult to access and treat.
While currently approved only for liver tumors, research is ongoing to explore histotripsy’s potential use in treating other types of cancer. The technology’s ability to preserve healthy tissue while effectively destroying tumors makes it a promising addition to the cancer treatment arsenal. n
“A lot of patients with liver cancer or liver metastases are unfortunately not surgical candidates, and they run out of options. We can offer this treatment to selected patients, and what excites me is that it’s completely noninvasive.”
– Kamran Idrees, MD, MSCI, MMHC (seen left)
DONN
JONES
Sid Sadler
My Story
FIRST-PERSON ESSAY
It’s OK To Not Be OK
Men need to talk about cancer diagnoses
STORY BY SID SADLER PHOTOGRAPHS BY DONN JONES
At one point or another as a little boy you are told, “Get over it.” These three words you wouldn’t think could do much damage, but deep inside they deteriorate a man’s ability to trust his feelings. Feelings are one thing, but trusting your health is a whole other bag of worms. What do you do when you can’t trust your health or feelings? This is a deck of cards presented to many men when they are diagnosed with cancer.
By the time I got my cancer diagnosis at 32 years of age, I had been seeing a therapist monthly for almost four years. The loss of my mom, coupled with the pandemic and having a spouse who was on the front lines being an ICU nurse did a lot to both of us. I decided to start seeing someone. I wasn’t sure what I would “get” out of it, or better, I wasn’t sure if the person on the other side of the room would truly care about any of my problems. What came in the coming years was a better understanding of myself and the ability to admit, it’s OK to not be OK.
“What does all of this have to do with a cancer diagnosis?” you might ask. Well, with a cancer diagnosis you give up the ability to ignore the “what if,” because the “what if” is happening to you. I struggle the most with something called “catastrophizing.” This is a fancy way of saying, “I always expect the worst to happen, no matter what is in front of me. I throw logic out of the window for my good friend, anxiety.” Couple that with a cancer diagnosis, and BOOM, you have a recipe for disaster.
See, cancer, we can all agree, sucks for a variety of health reasons, but I’m here to tell you, the mental aspect of it can be just as bad, if not worse. You lose your ability to trust your body. The one body you were given for some reason or another has “betrayed” you.
Now what?
A lot of people will take refuge in groups, me included. Misery enjoys company, after all, doesn’t it? I noticed something in most of the
groups I joined. There were people from all walks of life telling their stories, asking questions, venting and much more. You know, the type of thing you expect from a support group. There was one thing lacking though, men ... This isn’t to say there were NO men. In fact, there were some men really getting to the core of their feelings. However, it takes just one glance at most support groups, both online and in person, to see that the tide shifts heavily toward women. Why is that? I have some thoughts, and I’m sure some of you reading this do too.
For the most part, men for a long time were taught to simply “suck it up.” Stop the whining and complaining, “or else.” As time has passed, we have seen this sentiment lessen, in my opinion, for the better. However, we are now seeing the disaster this has produced in millions of men that aren’t sure how to deal with their feelings. We can see this take root in various aspects of everyday life, in relationships, and friendships as well. When a “problem” arises in a man’s life, you will see one of three routes taken usually:
• The do-nothing approach — which we all likely know too well. This leads to distress, anger, depression, anxiety and much more. You get the drift.
• The do-something approach — this is when a problem arises when the man does have some form of healthy learned behaviors, and choses to “do something.” This could be talking it out with friends, a therapist, spouse, etc.
• The in-between — this is as it sounds, is a mixture of the two, but can still present unhealthy habits for men to cope with their feelings. (I believe more men are here than we think.)
Prior to seeing my therapist, I would say I was a mixture of one and three. This led to unhealthy habits in the form of drinking, keeping feelings in and various other “outlets.” This isn’t to frown on a nice cold alcoholic beverage either, but for many men, there is a disconnect with enjoying one and depending on 10.
Fast forward to early December 2023. I found myself waiting to speak to my doctor about a CT he ordered due to concerning symptoms I was having. He said, “Sid, you have an approximately 11 centimeter mass on your left kidney. It’s likely something called clear cell
“I have found the men that do open up about their feelings are nothing short of exceptional, and I have met some outstanding men that have truly shaped the way I view the way I share my own cancer experience.”
renal carcinoma.” Better known as kidney cancer. A flood of “what ifs” pop into my head, and to make matters worse, Rachel, my amazing wife, who is a nurse practitioner, wasn’t there in person but on FaceTime due to her having to work. I felt alone, cold, sad, depressed, and a sudden rush of emotions flooded my thoughts. I called one of my good buddies right after who isn’t local, but we speak daily. He was basically with me during this whole ordeal from my onset of symptoms to finding out I likely had kidney cancer. I turned to a friend to release some of these emotions. I turned to my wife as well, who is nothing short of amazing. While stressful for both of us, she soon allowed me space to speak about my fears. With her background she knew exactly how to navigate a lot of the medical nuances I wasn’t sure about. I turned to many groups online and found refuge with patients, caregivers and advocates alike. I knew more than anything that I wanted to learn what I could as fast as I could about this stupid mass in me.
While scouring social media and the internet, I found some awesome people who I will forever be grateful for. They allowed me space to talk about my feelings and at no time made me feel uncomfortable sharing. Men must feel comfortable sharing, or they won’t share. Allowing this open space is vital to men across the board. I don’t think the issue is there’s “no space” for men to share. I think the issue is men just aren’t comfortable with sharing. I have found the men that do open up about their feelings are nothing short of exceptional, and I have met some outstanding men that have truly shaped the way I view the way I share my own cancer experience.
See, this isn’t just a man issue, but a society
“My hope is that even if ONE person reads this story and decides to open up or allows their friend to open up, it makes a difference.”
My Story
FIRST-PERSON ESSAY
issue. We must allow men to open up about their feelings. If you are reading this and don’t believe that we are lacking men speaking out in the cancer community, I encourage you to check out any of the hundreds of cancer support groups online or in person. You will find most people posting (patients/caregivers) are women. As I said earlier, this isn’t to complain about that fact. This essay isn’t stating that NO men talk about their feelings. However, there is a lack, and we must address this.
How do we do this?
Allow room for men to speak without judgment about how “manly” they are. This is the biggest issue in the way. Men don’t want to be seen as “weak” or “bothering” someone, especially strangers they don’t know online. Secondly, we need to continue to see more men encourage this open space! If I hadn’t seen the select few men I saw when I was first diagnosed, I’m not sure if I would’ve felt as compelled to share my story within groups. As simple as it sounds, men want to see other men share; it’s a domino effect. It’s such a freeing feeling that you have when you genuinely believe you can share your feelings and share without the fear of repercussion or judgment.
The “ask” to allow men to be open about their feelings, isn’t a big ask in my opinion. Sure, that’s half the battle. The other half is men coming forward to speak about their feelings/fears. If, however, men see there’s an open and willing space, my belief is eventually they will take to that idea. I know I did, and I’m sure many will.
If you have made it this far into this essay, I’m assuming you have been touched by cancer, or have someone in your life you care about who’s a man, or both. Although I might’ve made it seem like it’s a simple thing to do, it’s not. Many men will continue to not speak about their feelings and feel helpless. We
can change that narrative though. Changing a narrative doesn’t happen overnight, but over countless days, months and years. It’s the snowball effect in action. My hope is that even if ONE person reads this story and decides to open up or allows their friend to open up, it makes a difference. I believe we owe this to ourselves as a society. Opening an avenue for men to openly speak about their feelings won’t just benefit them, but their possible treatment. It will also benefit countless families and quite possibility could build back broken relationships. I still don’t have all the answers on how to navigate a cancer diagnosis, but I do know one thing.
It’s OK to not be OK. n
Psycho-Oncology Program Counseling Services
Psychiatric medication consultation and psychotherapy (counseling) services are available to Vanderbilt-Ingram Cancer Center patients throughout treatment and up to two years posttreatment. If you would like more information about these services or to discuss a referral, please contact your oncologist or social worker.
Sid Sadler said his wife, Rachel, provided emotional support during his cancer diagnosis and treatment.
VICC Ambassador Breakfast
Tuesday, April 8, at 7 a.m.
Westin Nashville
VICC Ambassadors
The Vanderbilt-Ingram Cancer Center Ambassadors invite you to the annual breakfast showcasing their support of innovative, groundbreaking research at Vanderbilt-Ingram. The program will feature presentations from promising VICC researchers, and the audience will help select a discovery grant recipient for 2025.
will
For more information, contact Casey Holden, Director of Community Development, at casey.n.holden@vumc.org JOIN US AS WE CELEBRATE 15 YEARS OF THE
Nathan Dudney and Hannah Dudney, MD, founding members of the VICC Ambassadors, will receive this year's EB and Todd Jackson Ambassador Award.
VANDERBILT UNIVERSITY MEDICAL CENTER
VANDERBILT-INGRAM CANCER CENTER
Office of News and Communications
T-5200 Medical Center North Nashville, TN 37232-2390
You can help conquer cancer At Vanderbilt-Ingram Cancer Center, philanthropy drives innovative research into cancer’s most vexing questions, helps fund clinical trials in search of new and better treatments, supports training for the next generation of cancer experts, and has the power to help save lives. Join us with a charitable gift to make expert, compassionate cancer care possible. Help us create a world without cancer. Give today.