
UNICAMILLUS
Editor-in-Chief
Gianni Profita
Editor
Giorgia Martino
Graphic Design
Giulia Francini
Federico Calogero
Images and Contributions
Federica Alota
Giusy Condorelli
Damiano Giani
Ginevra Guidoni
Daniela Mariani
Claudia Romano
Translations
University Language Center
Ylenia Marcucci Faure
6 agEism and mEntal hEalth:
isolation, dEprEssion and stigma
Prof. Angelo Giovanni Icro Maremmani
10 thE agE of valuE: thE paradox of carE bEtwEEn rElationships and wElfarE
Prof. Donatella Padua
14 hormonEs, agEing and sExuality
Prof. Rosa Maria Paragliola
Prof. Salvatore Maria Corsello
18 agEism: bEtwEEn discrimination and a culturE of rEsignation
Prof. Alessandro Boccanelli
22 agEism in mEdicinE
Prof. Nicola Veronese
26 agEism and public hEalth an intErviEw with prof. gualano
Dr. Giorgia Martino


by Gianni Profita Rector
It seems that medicine, technology, and knowledge are advancing faster than our ability to understand them and make them accessible to everyone. Even in the most advanced societies, forms of inequality and exclusion persist, silently undermining public health. Ageism, or age-based discrimination, is one such form. In a culture of efficiency and productivity, age is sometimes seen as a limitation rather than an asset. We must remember that ageing is not a problem to be solved, but a process to be supported and appreciated. Combating ageism means promoting dignified medicine, where every person—young or old—is welcomed, listened to, and cared for with humanity and dignity. In this issue, our academic community addresses the topic from many perspectives, including mental health, ethics, communication, medical treatments, and sexuality in old age. This is a journey of knowledge and reflection that encourages us to look beyond prejudice in order to build a culture of health that is more equitable and respectful. However, the concept of inclusion is not limited to age. UniCamillus pursues its humanitarian mission with the same conviction: health is a universal right, not a geographical privilege. Our projects in Africa —in countries such as Benin, Somalia, Cameroon, Ethiopia, and Libya—demonstrate our commitment to developing local healthcare skills and providing assistance to areas affected by conflict, fragile healthcare systems, and limited resources. This issue will also address these topics. The experience of our tutors and students in the field brings UniCamillus’ humanitarian mission to life: for example, Massimo Gravante, a lecturer in Dermatology at UniCamillus and Vice-President of the non- profit organisation ‘Medici e Professionisti Senza Vacanze’, travels several times a year to the La Croix hospital in Zinvié, Benin, where he treats patients with leprosy, albinism, and congenital malformations. He also restores dignity and hope through dermatological surgery and local support programmes. Meanwhile, UniCamillus is developing structured training projects such as the CPD course in Traumatology in Libya and the ITESHS (Integrated Transcultural Educational Synergy in Health Sciences) project, which aims to strengthen orthopaedic, nursing, and psychological skills in Somalia, Cameroon, and Ethiopia. Thanks to state-ofthe-art laboratories, collaborations with local hospitals, and practical internship programmes for students, these initiatives build enduring capacity and create a real and measurable impact on the health and well-being of communities, rather than being limited to temporary interventions. UniCamillus is more than just an academic institution: it is a university that cares, teaches and learns simultaneously, bringing medicine where it is most needed and training professionals with a global and humanistic outlook. UniCamillus is also a place where research and innovation meet science and ethics. In this issue, we explore the new frontiers of diagnosis and treatment opened through Artificial Intelligence (AI), with the help of Professor Donatella Padua, UniCamillus’ Third Mission Delegate. At the same time, we are reminded of the need to keep human beings and their dignity at the centre of all progress. These themes are united by care: not only technical care, but also care as attention, listening and responsibility. Combating ageism, training medical professionals to be sensitive to diversity, building skills in the most fragile countries and questioning the ethical use of new technologies all respond to the same vision: uniting science and humanity to promote health and justice. UniCamillus was founded on this principle, and continues to grow with it and to nurture it.



agEism and mEntal
hEalth: isolation, dEprEssion and stigma
Professor Angelo giovAnni icro MAreMMAni
Angelo Giovanni Icro Maremmani is an Associate Professor of Psychiatry at UniCamillus. He completed his specialist training in Psychiatry at the University of Pisa and obtained a PhD in Biochemistry and Molecular Biology (BiBiM 2.0 “Pegaso Project”, Cycle XXXII) at the University of Siena.
He also completed a CPD secondlevel course in Pharmacological, Toxicological and Behavioral Addictions at the University of Pisa, as well as an advanced training course in ‘Systematic Reviews and MetaAnalyses for the Development of EvidenceBased Guidelines—Cochrane Methodology’ at the University of Milan.
In contemporary societies characterised by an increasing average life expectancy, the issue of ageing is becoming ever more significant. However, alongside this rise in population age, stereotypes and prejudices that reduce older individuals to a condition of inevitable frailty are increasingly common. Ageism, a term used to describe discrimination based on age, manifests not only in overt forms of social exclusion, but also in subtle, widespread attitudes. For example, it is commonly believed that a loss of energy, curiosity, or interest in life are ‘normal’ aspects of old age. In fact, many of these beliefs are not supported by scientific evidence. Although some physiological changes are a natural part of ageing, functional decline is not inevitable: psychological and relational wellbeing can remain high into advanced age, provided the dignity of the individual is preserved and implicit prejudices that associate ‘old age’ with ‘less value’ are challenged. In an ageing population, it is crucial to overcome stereotypes that risk turning a natural process into a form of exclusion.
Thinking that it is ‘normal’ to lose vitality or interest simply because one is elderly means accepting a reduced and limiting view of old age. Yet science and experience show that it is possible to maintain
balance, curiosity, and a desire for relationships until a very advanced age. Combating ageism means recognising that every stage of life deserves the same attention, care, and opportunities for participation.
loneliness And the trAnsforMAtion of fAMily bonds In Mediterranean cultures, the family has been a fundamental point of reference and a bond between generations for centuries. Older people were not only recipients of care, but also sources of support, memory, and guidance. Today, however, rapid demographic and social change is profoundly altering this balance. On the one hand, the progressive ageing of the population and the decline in the number of births are creating a growing disparity between young and old. On the other hand, job mobility— which is often necessary—means that many children live far from their parents, reducing the possibility of daily support and weakening the emotional and practical role that once guaranteed inclusion and intergenerational exchange. As the family network contracts, the risk of isolation increases. This, in turn, raises the likelihood of developing mood disorders, anxiety, or social withdrawal. If these issues are not recognised, they can evolve into conditions of psychological vulnerability. It is now well established that loneliness contributes to premature mortality. Furthermore, society is struggling to adapt to this new reality. Services dedicated to the elderly are often insufficient, and there is a lack of social spaces designed to foster a sense of belonging and purpose. Local communities, health institutions,
and cultural organisations should address this issue by creating opportunities for social interaction and participation that recognise and value the experience and expertise of older people. It is no coincidence that the retirement often marks a significant turning point for those entering old age, as they experience a profound and sudden change in their social role. Many specialist outpatient consultations begin precisely because individuals perceive this transition as a ‘loss of social role’. Combating ageism also means rethinking the role of the community and restoring older people to their rightful place at the heart of social relations and the transmission of values between generations.
debunking the dAngerous Myth of dePression And quAlity of life
One of the most insidious aspects of ageism in mental health is the tendency to consider depression or demotivation as ‘normal’ with advancing age. Depression is never a physiological consequence of ageing. It should not be confused with sadness or the understandable melancholy that may accompany certain losses. Depression is a genuine pathology that affects mood, concentration, motivation, and the ability to enjoy life. In older people, depression often manifests in atypical ways, such as reduced energy levels, loss of interest, cognitive impairment, sleep disturbances, appetite changes, and somatic symptoms. These symptoms are sometimes interpreted as ‘natural’ or attributed to cognitive decline, which can lead to late or missed diagnoses. The term ‘depressive pseudodementia’ is
used to describe cases in which symptoms mimic a reversible form of cognitive deterioration. Therefore, it is essential to make the correct diagnosis, as treating depression can improve not only mood, but also memory and cognitive efficiency, restoring individuals to their ‘physiological’ level of functioning for their age. Promoting quality of life means refusing a fatalistic view of old age and ensuring that mental health is assessed and treated with the same attention as in other stages of life. Prevention, early diagnosis, and integrated care are crucial for maintaining wellbeing in old age.
overcoMing stigMA in cAre
When stigma surrounding mental health is combined with stigma surrounding age, a double prejudice is created: ‘They are elderly’ and ‘They are depressed’, therefore ‘They cannot improve’. This attitude can discourage diagnosis and reduce the intensity of proposed treatments. However, scientific literature now confirms that even people over the age of 85 can benefit from targeted therapeutic interventions. Assessment must always be personalised, taking into account medical comorbidities and tolerability of prescribed treatments. There are, however, no age limits to the possibility of improvement. If chosen carefully and monitored prudently, antidepressants can resolve mild or moderate depression, restoring dignity, motivation, and serenity. Similarly, brief psychotherapeutic interventions and psychosocial support have been shown to significantly improve quality of life, even in older age groups. Overcoming stigma means
recognising that treatment is not only a therapeutic act, but also a gesture of respect towards the individual and their history. Age should not be a barrier, but rather a factor that requires sensitivity and professional expertise. Truly humane medicine must look beyond age and recognise the potential of every individual, even when their body or memory seems to limit their ability to express themselves.
A culturAl And educAtionAl chAnge is needed
Combating ageism requires social sensitivity and a transformation in the way health professionals are trained. Old age presents clinical peculiarities that deserve specific attention: symptoms can be subtle, comorbidities are common, and the family or care context can greatly affect the response to treatment. For this reason, it is essential that university programmes and CPD courses in the health sector include modules dedicated to the mental health of older adults. This would equip health professionals with the tools needed to recognise and treat these conditions appropriately. Training should also help to overcome stigma by promoting the idea that individuals of all ages have the capacity to change and respond to treatment. Viewing depression or cognitive decline as ‘natural’ outcomes of ageing would mean abandoning a fundamental principle of medicine: protecting quality of life and dignity. Ageing is not a decline; it is a phase of life that can be meaningful and offer opportunities if society and medicine can provide support, respect, and care. The most tangible way to build an inclusive
healthcare system that values every stage of life is to invest in training that recognises older people as individuals with both needs and skills.
conclusion
Ageism in mental health care is a silent yet pervasive phenomenon that denies many older people their right to be seen, understood, and treated with the same attention afforded to younger individuals. Recognising this is the first step towards creating a culture that values age not in terms of productivity, but in terms of experience, affection, and meaning. Investing in the mental health of older people is both an ethical duty and an act of civilisation, as it reflects the belief that psychological wellbeing has no age limits. It is also a collective investment, because a society that respects and values its older members becomes more cohesive, more empathetic, and better equipped to build the future.
Three common myths about mental ageing:
• ‘It is normal to be sad when you are elderly.’
False. Chronic sadness and loss of interest are symptoms of depression that can and must be treated; they are not part of physiological ageing.
• ‘Older people cannot respond to treatment.’
False. With appropriate therapies and careful monitoring, significant improvements in mood and quality of life can be achieved even in those over 80.
• ‘Memory loss is always dementia.’ False. In many cases, cognitive
decline is linked to mood disorders, medication use, or reversible medical conditions. Accurate assessment enables effective intervention.

thE agE of valuE:
thE paradox of carE bEtwEEn rElationships and wElfarE.
Professor donAtellA PAduA
Donatella Padua has been an Associate Professor of General Sociology at UniCamillus since 2022. She is Delegate for Third Mission and Social Impact, Chair of the Third Mission Committee, and Secretary General of the Advisory Board. She is also a member of the University Quality Committee and of the Equal Opportunities Committee.
Specialised in the Sociology of Health and Digital Sociology, she is the author of ‘Digital Cultural Transformation. Building Strategic Mindsets via Digital Sociology’ (Springer).
We tend to tackle our problems with statistics. According to United Nations projections, people over 65 will represent 16% of the world’s population by 2050, with peaks exceeding 25% in Europe and 34.6% in Italy. This is a structural as well as a systemic transformation, affecting not only demographics and health, but also institutions, families, care networks and intergenerational relationships, with implications for welfare and citizenship. ‘Ageing’—a term that often carries a certain linguistic distance in public discourse—is not simply a statistical fact. It is a transformation that runs through the social body like a silent crack, reshaping institutions and the relationships between people. Population ageing is not something that happens to society; it is society reshaping itself, moving toward a form that we have not yet learned to inhabit.
From this perspective, sociology has an important task: analysing how old age is constructed, experienced and interpreted in contemporary societies, capturing the plurality of experiences and the processes of inclusion and exclusion, in order to inform policy decisions. These social policies significantly impact health and welfare.
They relate to ‘care systems’— integrated networks of health, social and local services that sustain a delicate ‘welfare balance’. While older people are recipients of health and care services, they also play an important (and sometimes indispensable) role in providing care for families and communities. Consider the economic impact of grandparents in family life. This genuine form of ‘family welfare’ supports the household budget by providing practical assistance, replacing paid services, offering childcare and help with schoolwork, managing leisure time, providing financial and asset support, and making property available. Today, all of this is estimated to generate €40 billion in annual savings for families (Fortune Health Italia, 2023).
Sociology can measure, classify and predict. However, the oldest and most unsettling question remains unresolved: what does it mean to grow old in a culture that has made youth its dominant myth? A culture that celebrates speed, efficiency and productivity, and views older people not as a resource but as a burden; not as a repository of memory but as a trace. In summary, the fact that older people are both recipients and providers of care is a real paradox that characterises our times and is rarely acknowledged. The word care comes from the Latin cura and encompasses not only healthcare, but also attention, thought, concern and responsibility. Caring is not just about providing medical treatment; it is also about making space for another person in one’s life and assuming responsibility for their wellbeing. The quality of social policies is
measured by this interweaving of health, relationships and social responsibility.
The tradeoff between care understood as the cost of older people (i.e. healthcare, welfare and social security) and care understood as value creation (i.e. savings or reduced costs for families and communities) must also be analysed over time. While an ageing population and increased life expectancy are placing significant pressure on welfare systems—particularly healthcare—by increasing demand for pensions, care services and home care, longer life expectancy also opens up opportunities for active participation in family life, work, volunteering, politics and community life. This generation of value must be protected and promoted through preventive healthcare projects for older adults. One such initiative is the PREVASC2 study, which is currently underway at national level and is being scientifically coordinated by Dr Boccanelli. The study aims to investigate the prevalence of cardiovascular diseases in a population aged 65 and over in Italy. Promoted by UniCamillus in collaboration with Tor Vergata, the project offers free cardiovascular prevention to over65s, raising awareness and fostering a culture of prevention while simultaneously conducting epidemiological screening. PREVASC2 is a concrete example of the university’s Third Mission: through this project, the university plays an innovative role with significant social and health impact, activating local welfare systems and promoting healthy and active ageing—a genuine driver of social
value creation. However, there are social determinants that constitute sociocultural obstacles, the most significant of which is ageism, which we discuss below.
AgeisM: when Age becoMes fAte Age is not a neutral biological fact; it is a social category that determines roles, rights, expectations and marginalisation. People do not simply become ‘elderly’ by passing the years; rather, they become so within cultural contexts that define what it means to be old and how older people are expected to live. While the term ‘ageing’ refers to the natural process of growing older, with biological, cultural and relational dimensions, ‘ageism’ (Butler, 1969) describes the discrimination and stereotypes associated with later life, which devalue older people by attributing to them fragility, dependence and social irrelevance (Calasanti & Slevin, 2006; Phillipson, 2013). While ageing is universal, it is also differentiated by gender, class, ethnicity and historical context. Ageism, however, is a social construct that produces inequalities. Ageism is intertwined with other structural inequalities, such as low income, limited education, insecure employment, family responsibilities, gender and inadequate welfare provision, all of which amplify vulnerability and isolation in later life. The digital divide exacerbates this exclusion by limiting access to tools that could promote autonomy and participation. Media narratives also influence the collective imagination, portraying older people as either a burden or a resource and thus conditioning public policy and selfperception (Phillipson, 2013). These factors
all accelerate marginalisation, creating a divide between those who can still generate social value and those who are relegated to the role of care recipients, thereby highlighting the complex interplay between social, economic and health aspects. It is crucial to separate the concept of ageing from that of ageism for sociological analysis and public policy, as ageing does not only imply loss, but also entails gains in experience and perspective. Countering ageism means promoting active and inclusive ageing as well as recognising and valuing the abilities of older people.
Active Ageing: beyond the Myth of retireMent
Sociological theories have depicted old age in various ways. The disengagement theory (Cumming & Henry, 1961), for example, describes the progressive withdrawal from social roles, suggesting that ageing naturally involves isolation. In contrast, the continuity theory (Atchley, 1989) highlights the consistency between past and present identities, interpreting old age as a process of memory and selfreconciliation. Focusing on a different aspect, the activity theory (Havighurst & Albrecht, 1953) has inspired active ageing policies, suggesting that maintaining meaningful social roles is key to a good quality of life. The World Health Organization defines active ageing as “the process of optimising opportunities for health, participation and security in order to enhance quality of life as people age” (WHO, 2002). Promoting active ageing improves quality of life by enhancing social participation, dignity,
functional abilities and meaningful relationships. This requires robust disabilityprevention programmes, accessible and agefriendly services, and appropriate training for professionals and carers. This approach feeds into the ‘welfare balance’ previously described: if older people are not only recipients of care—and therefore a cost—but also a resource for promoting care within families and communities, then it is reasonable to suggest that active ageing policies generate a virtuous cycle of social and economic value. Healthy and wellsupported older people represent both human and social capital. Empirical research confirms that active social roles improve quality of life (Lakomý, 2023). Contexts that integrate intergenerational perspectives enjoy greater wellbeing and social sustainability (Walker & Zaidi, 2016). This demonstrates that a society that cares for its older population is more just, more cohesive and more forwardlooking.
the vAlue of relAtionshiPs: coMbAtting loneliness
Ageing is not just about policies and statistics; it is also about relationships and meaning. The quality of life of older people depends on social capital: family and friendship networks, as well as community participation, promote wellbeing, independence and a sense of usefulness. Conversely, isolation and loneliness can pose significant risks to mental and physical health. Multidisciplinary research, such as the aforementioned PREVASC2 Project, integrates clinical and social investigation, demonstrating the close link between
socioeconomic conditions and health vulnerability. This supports an approach that considers the individual’s life course, combining medical care with existential and relational dimensions. From this perspective, ageing should be studied as a relational process. Living conditions in old age depend on intergenerational connections—such as caring for grandchildren and supporting families—as well as on social inclusion, including social and civic participation and volunteering. The relationship with welfare institutions is also important. Sociology therefore highlights an important aspect of circularity: social connections act as a catalyst for healthy ageing, generating value, while simultaneously helping to preserve or even improve the health of older people. Policies that focus on life trajectories rather than chronological age are therefore essential for reducing the risk of exclusion and for promoting genuinely inclusive and equitable active ageing.
“Sociology can measure, classify and predict. However, the oldest and most unsettling question remains unresolved: what does it mean to grow old in a culture that has made youth its dominant myth?
A culture that celebrates speed, efficiency and productivity, and views older people not as a resource but as a burden; not as a repository of memory but as a trace.
hormonEs, agEing and sExuality
s
Salvatore Maria Corsello is a Full Professor of Medicine at UniCamillus, and a specialist in Endocrinology and Internal Medicine. Author of more than 140 scientific publications and numerous contributions to volumes on Endocrinology and Endocrine Surgery, he is a member of the leading national and internationa scientific societies in the field.
Rosa Maria Paragliola is an Associate Professor of Endocrinology at UniCamillus. She holds a PhD in Endocrine-Metabolic and Endocrine-Surgical Sciences, has authored more than 70 PubMed-indexed publications, and is a member of the major scientific societies in her discipline.
Ageing is an inevitable and complex biological process that affects all living organisms. It is characterised by a progressive decline in physiological functions linked to the accumulation of cellular damage, a reduced capacity to adapt to internal and external stressors, and an increased susceptibility to disease. Although not a disease in itself, ageing is a natural and unavoidable condition that manifests differently among individuals depending on genetic predisposition, environmental factors, and lifestyle. One of the most remarkable achievements—and at the same time one of the greatest challenges—of recent decades is the substantial increase in life expectancy, driven by advances in medicine, improved hygiene and social conditions, better nutrition, and the adoption of healthier lifestyles by a growing proportion of the population. In just a century, average life expectancy in Italy has risen by more than thirty years. The longevity of the population compels us to ensure that older adults not only live longer but also maintain good health and, whenever possible, remain free from chronic diseases. During a recent audience, Pope Leo XIV remarked: “The elderly are a gift and a blessing to be welcomed. Longer life expectancy is a positive development and one of the signs of hope in our time, in every part of the world.
Of course, it is also a challenge, because the growing number of elderly people is an unprecedented historical phenomenon that calls for new forms of discernment and understanding”. Ageing is accompanied by changes in hormone secretion, many of which represent normal adaptive responses aimed at gradually reducing reproductive and metabolic functions in order to prioritise energy conservation and survival. However, although ‘endocrine ageing’ is a physiological phenomenon, it can be particularly pronounced in some individuals, significantly contributing to vulnerability and reduced quality of life. The relationship between hormones and ageing is therefore one of the most compelling areas of modern medicine. The key challenge lies in distinguishing normal physiological changes from true hormonal deficiencies that may be treatable and capable of substantially improving patient wellbeing.
horMones And Ageing: A focus on sex steroids
Progressive changes in hormone secretion occur with advancing age. Thyroid secretion decreases slightly but progressively, resulting in lower circulating levels of thyroid hormones—particularly the most active form, FT3—accompanied by higher TSH levels and reduced tissue sensitivity to thyroid hormones. The somatotropic axis also shows a characteristic decline: pulsatile GH secretion diminishes, as do IGF1 levels, leading to reduced lean mass and increased visceral adiposity. At the adrenal level, DHEA secretion decreases markedly, while alterations in cortisol rhythm result in greater exposure to evening peaks. With regard to renal function, agerelated reductions in
neurohypophyseal sensitivity to antidiuretic hormone may impair urine concentration and increase the risk of dehydration. Among these changes, those affecting the hypothalamic–pituitary–gonadal axis play a central role in quality of life. Sex steroids—oestrogen and progesterone in women, and testosterone in men— profoundly influence wellbeing, including sexual health. Sexuality remains an integral component of wellbeing throughout life, although it inevitably evolves due to hormonal, psychological, and social changes associated with ageing. Beyond their reproductive and sexual functions, sex steroids contribute to numerous biological processes, including metabolism, body composition, bone health, cognitive function, and mood regulation. In women, menopause marks the progressive decline of ovarian function. Rather than a single event, it is best understood as a gradual transition occurring over several years (typically between ages 45 and 55), characterised by fluctuating hormone levels. This period— often referred to as the climacteric or perimenopause—may be accompanied by symptoms such as hot flushes, night sweats, sleep disturbances, vaginal dryness, and reduced libido. In the medium and long term, oestrogen deficiency accelerates bone loss and increases the risk of osteoporosis and fractures. It also alters lipid and carbohydrate metabolism, raising cardiovascular risk. Body composition shifts toward increased abdominal adiposity. Psychologically, hormonal fluctuations and oestrogen deficiency may contribute to irritability, impaired memory and attention, and a decline in perceived wellbeing. In men, the process is more
gradual and less pronounced. Testosterone levels begin to decline after the age of 40 due to reduced testicular production and increased levels of transport proteins, which lower the amount of free, biologically active testosterone. Clinical consequences may include reduced muscle mass and strength, increased visceral fat, decreased bone mineral density, and, in some cases, anaemia. From a sexual perspective, reduced libido and occasional erectile dysfunction may occur, although these often have concomitant vascular or metabolic causes. Low testosterone levels have also been associated with an increased risk of metabolic syndrome, type 2 diabetes mellitus, and cardiovascular disease, indicating that the role of sex hormones extends far beyond reproductive function. In both sexes, sexuality does not disappear in older age but evolves in response to hormonal changes, psychological and social factors, chronic diseases, and medications that may interfere with sexual function. Appropriate medical support can help individuals and couples maintain satisfying sexual activity as part of overall wellbeing.
horMone rePlAceMent therAPy: indicAtions And liMitAtions Research into hormone replacement therapy has been driven by the consequences of the ageing process involving the hypothalamic–pituitary–gonadal axis. The aim is to counteract the clinical disorders associated with this process and to prevent the longterm complications of hormone deficiencies, especially in women. However, is it appropriate to intervene pharmacologically to ‘treat’ what is essentially a physiological event? There are
no absolute rules, and, as is often the case in medicine, clinical decisions must be made using sound, commonsense judgement, with management tailored to each individual patient. According to the guidelines issued by leading gynaecological societies, “menopause is not a disease and does not require treatment, but some women may be affected by the hormonal decline and therefore need replacement therapy” (SIG and SIGiTE, 2020). For menopausal women, hormone replacement therapy (HRT) with oestrogen alone (for hysterectomised patients) or in combination with progestogens (to prevent endometrial hyperplasia and cancer) represents the most effective treatment for vasomotor symptoms (hot flushes and night sweats), genitourinary syndrome (vaginal dryness, painful intercourse, recurrent infections), sleep disturbances and certain moodrelated symptoms. HRT is also useful for preventing accelerated bone loss after menopause and reducing the risk of fractures. However, HRT should not be offered as a standard option, but rather reserved for women experiencing symptoms and for whom there are no contraindications, such as breast or endometrial cancer, thrombosis or embolism, active cardiovascular disease or severe liver disease. Where considered, the therapeutic approach now aims to be highly personalised, offering maximum benefit with minimal risk. Several therapeutic options are available (e.g. estradiol, conjugated oestrogens, tibolone and tissueselective oestrogen complexes) with different routes of administration (oral, transdermal and vaginal) and various dosages and regimens (continuous or cyclical). Starting treatment at
the right time is very important: benefits are greater and risks lower if HRT is started in women who are still relatively young (ideally before the age of 60), symptomatic, in the perimenopausal period or within the first ten years after menopause. Although there are no strict limitations on the duration of HRT use, decisions about whether to continue, adjust or discontinue treatment should be guided by careful clinical judgement, taking into account individual conditions, personal and family risk factors, clinical goals and the woman’s preferences and motivations. Several studies have also shown that HRT can improve skin elasticity and hydration, a key aspect of the ageing process, although results may vary depending on environmental factors such as sun exposure, smoking and pollution. In men, testosterone therapy is indicated in cases of confirmed and symptomatic hypogonadism. As a general principle, treatment is appropriate for older symptomatic patients with total testosterone levels below 2.5 ng/ml. Replacement therapy improves body composition, bone density and sexual function, but requires careful monitoring (PSA and haematocrit) and should not be initiated in the presence of prostate or breast cancer.
horMones And AntiAgeing: Myth or reAlity?
Beyond HRT, there has been considerable interest in other hormonebased therapies with potential antiageing effects.
• Growth hormone (GH): the physiological decline in GH has been associated with sarcopenia and reduced quality of life. However, recombinant GH therapy in older adults has not demonstrated consistent
benefits and is associated with significant risks, including a potentially increased neoplastic risk.
• DHEA: oral supplementation has produced mixed results, with no robust evidence of a true antiageing effect.
• Melatonin: due to its action on circadian rhythm and sleep, it may have favourable effects on psychological wellbeing, but evidence remains inconclusive.
• Vitamin D: essential for bone and immune function, with antiinflammatory and antioxidant properties. Supplementation is recommended for older adults at risk of deficiency, but it cannot be considered an antiageing therapy on its own.
Therefore, none of these approaches can currently be regarded as a safe and effective antiageing strategy, and any therapy should be approached with balance and clinical prudence, within the broader framework of personalised medicine
conclusions
The relationship between hormones, ageing and sexuality is extremely complex. While hormonal decline is a natural part of ageing, it can contribute to frailty and reduced wellbeing in older adults. If indicated and well monitored, sex steroid replacement therapy is a useful tool for correcting specific disorders, whereas there is no solid evidence supporting ‘nonconventional’ therapies. The aim is not to ‘halt’ the physiological ageing process, but to improve its overall quality.

ag E ism : b E tw EE n discrimination and a cultur E of r E signation
Professor AlessAndro boccAnelli
Alessandro Boccanelli teaches Narrative Medicine within the Moral Philosophy course at UniCamillus. A physician and cardiologist, he previously served as Head of Cardiology and Director of the Department of Cardiovascular Diseases at San Giovanni Hospital in Rome. A former President of ANMCO, he is currently President of the Italian Society of Geriatric Cardiology and of the nonprofit association ‘Salute e Società’. He is the author of approximately 300 scientific publications in national and international journals.
Ageism refers to the discrimination, exclusion, stigmatisation or any other form of disadvantage experienced by older adults on the basis of chronological age. It is rooted in a cultural heritage that associates advancing age with an inevitable decline, to the point that corrective actions are considered futile and unjustifiable. This objective discrimination is mirrored by a subjective sense of resignation, as individuals view the progressive decline in organ and system function as inevitable and not something that can or should be addressed. This applies not only to physical decline, but also to the social roles individuals assume. As a result, individuals lose the opportunity to improve their quality of life, and society loses the chance to benefit from intellectual capacities that remain vibrant—and are often strengthened—by experience.
Over the past few decades, there has been a dramatic increase in life expectancy at birth and in remaining life expectancy across all age groups (see Table 1).
Over the past thirty years, there has been huge progress, but this has outstripped the pace of cultural adaptation to the new reality. Attitudes towards older people have remained unchanged, and the different ways of ageing
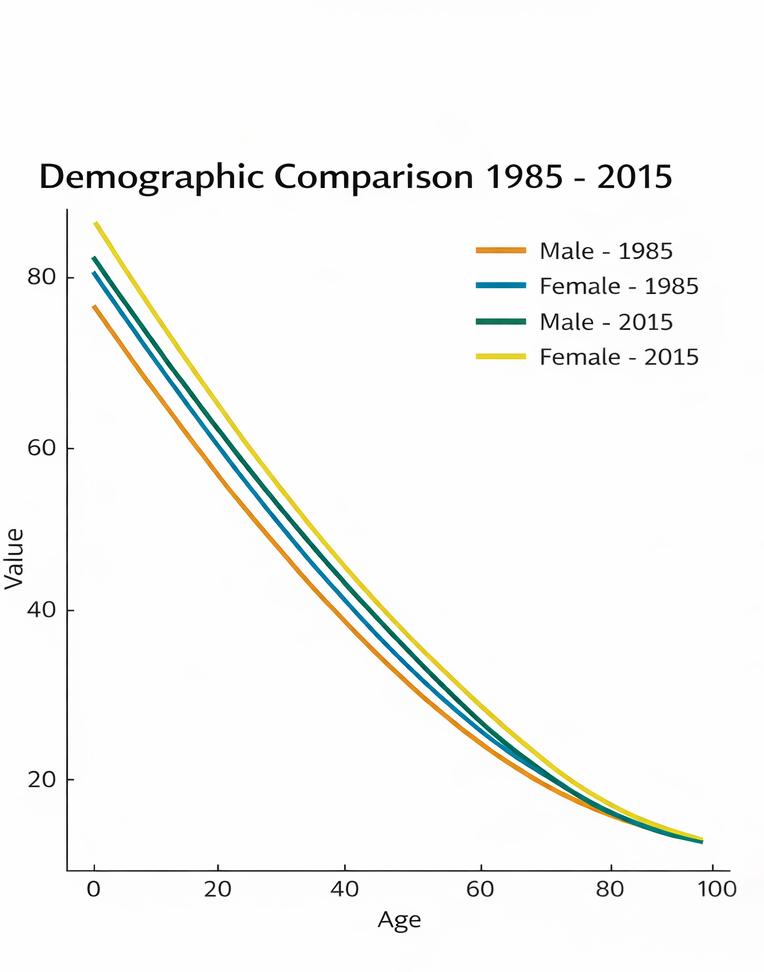
have not been taken into account. In 2024, life expectancy at birth is estimated at 81.4 years for men and 85.5 years for women. Alongside rising life expectancy at birth, it is essential to consider life expectancy in older age, an indicator that reflects the health and prospects of people who have already reached a certain age.
italy is among thE countriEs with thE highEst lifE ExpEctanciEs.
A key indicator is life expectancy at age 65, which measures the average number of years a 65yearold can expect to live based on observed mortality rates in the reference year. In 1952, life expectancy at age 65 was 12.8 years for men and 14.1 years for women. In 2023, in the European Union (EU27), life expectancy at age 65 reached 21.8 years for women and 18.3 years for men. In Italy, the corresponding figures were 22.6 and 19.7 years, respectively. In light of this change,
the traditional age of 65 used to define the start of old age seems increasingly outdated: the age at which people become elderly has shifted further forward. Using remaining life expectancy at age 65 as a reference point, men would become ‘elderly’ from around age 74 in 2023, and women from age 75. Applying these dynamic thresholds would significantly reduce—almost halve—the share of people considered elderly in the total population compared with the static threshold of 65 years and over. This substantial reduction offers a different perspective on the impact of demographic ageing, taking into account the changing characteristics of the generations entering old age.
Up to at least age 75, a growing proportion of older adults are healthier, more active and more productive than in the past. However, the increase in healthy life expectancy has not kept pace with the overall rise in life expectancy. This gap between living longer and living longer in good health represents a major challenge for an ageing society (see Fig. 1).
Ageism is therefore an attitude that, due to a misguided sense of resignation—both objective and subjective—prevents individuals from taking the necessary steps to improve not only the quantity but also the quality of their lives. Healthy life expectancy is a key indicator for understanding the challenges posed by population ageing. Living longer is not enough: the additional years must be lived with autonomy, well-being, and the opportunity to participate actively in society.
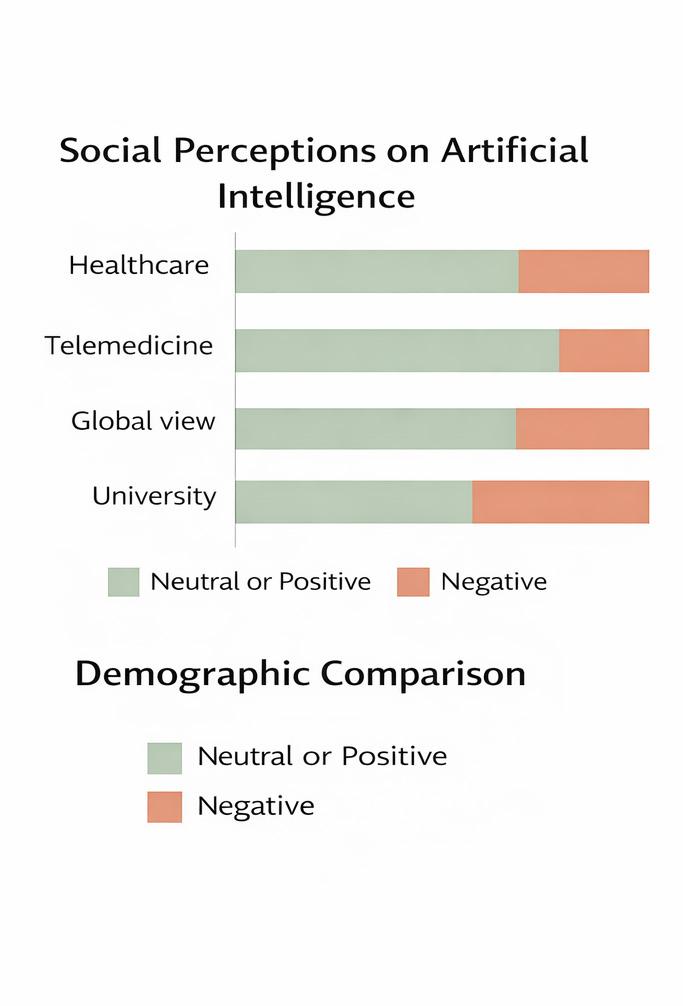
fig. 1: agEing modEls b = birth; d = dEath thE grEEn sEction of thE bar indicatEs yEars spEnt in good hEalth, whilE thE rEd sEction rEprEsEnts yEars affEctEd by chronic disEasEs that compromisE quality of lifE. if lifE ExpEctancy incrEasEs but thE agE at which disEasEs appEar rEmains unchangEd (Model B), The nuMBer of yeArS SpenT SufferIng also incrEasEs idEally, thE onsEt of illnEss-rElatEd limitations should bE postponEd as much as possiblE, confining thEm to thE pEriod immEdiatEly precedIng deATh (Model d).
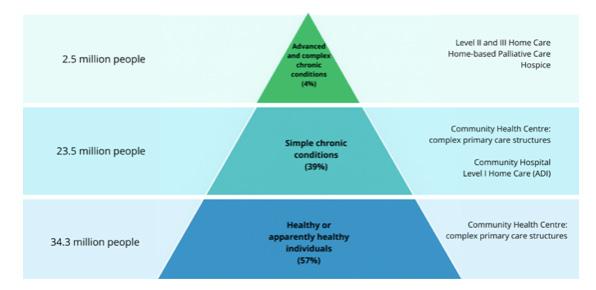
Over 14 million people in Italy suffer from chronic diseases. Of these, 8.4 million are aged over 65. More than half of those aged 65 to 75 live with one or more chronic conditions. Many diseases affecting people over 65 are either undiagnosed or diagnosed too late, with significant consequences in terms of acute health risks, reduced treatment effectiveness, and increased costs for the national health system.
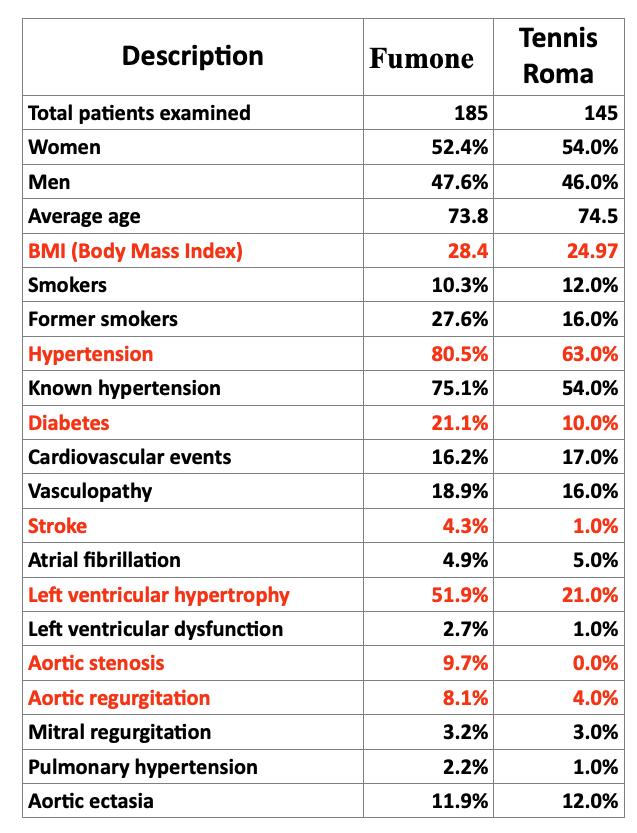
The social context in which people live is extremely important. For example, consider our screening experience involving individuals over the age of 65, carried out in a rural setting and in a sports club. Clear differences emerged in body mass index, arterial hypertension, diabetes and heart disease (Table 2).
Individuals’ perception of their own health status is also influenced by a fatalistic acceptance of progressive physical deterioration, a phenomenon that could be described as ‘selfageing’. An example of this is our recently published study on a sample of individuals over the age of 65 (The PREVASC study: Prospective REgistry of Valve disease in Asymptomatic Italian elderly SubjeCts, Boccanelli et al., Aging Clinical and Experimental Research, 2025, 37:98). Although 20% of the assessed subjects were in a functional class higher than II
(moderate exertional dyspnoea), more than 70% reported a satisfactory quality of life. This occurs because a reduction in functional capacity is often accepted as an inevitable aspect of ageing.
whAt initiAtives cAn be tAken to coMbAt AgeisM?
The first challenge to be addressed is cultural, and the second is organisational. How can we help individuals become more aware of their health status and potential? An example comes from the communitybased prevention initiatives carried out by UniCamillus University in collaboration with the Department of Nursing Sciences at Tor Vergata (PREVASC2). This longitudinal study is being conducted on a population of individuals over the age of 65 who belong to community settings such as senior centres and local churches. Its primary objective is to define the current epidemiology of cardiovascular risk exposure and the prevalence of heart disease, with particular reference to: 1) define the distribution of cardiovascular risk factors in older adults, particularly the prevalence of atherogenic dyslipidaemia, and its correlation with social and economic status.
2) define the prevalence of atrial fibrillation in older adults.
3) define the prevalence of asymptomatic and symptomatic left ventricular dysfunction in older adults.
4) define the current epidemiology of heart valve
disease in older adults:
a. identify the different clinical characteristics of valve disease in older adults.
b. develop an observational study on the characteristics of mitral regurgitation in older adults, including current epidemiology and new treatment options.
c. conduct an observational study on atypical presentations and different natural histories of aortic stenosis in older adults.
d. define the current epidemiology of tricuspid regurgitation in older adults, and its relationship with chronic pulmonary embolism, pulmonary hypertension, and the presence and severity of tricuspid regurgitation.
This model leverages the Third Mission of Universities and can be replicated nationwide.
From an organisational perspective, intermediate care and the facilities that provide it—which are predominantly nurseled—must be strengthened by establishing multidisciplinary teams comprising general practitioners, internal outpatient specialists (including those working within complex organisational structures such as UCCPs), community nurses, and other healthcare professionals such as speech and language therapists, physiotherapists, dieticians, rehabilitation technicians and social workers.
The effects of the proposed measures on the quality of care and on the local community are summarised in Fig. 3:
• Improved communitybased care, unlike systems centred on specialist services, ensures a more equitable distribution of health across the population.
• A continuous point of reference for the population enables better care and more effective support for the local community.
• Greater social and healthcare integration, thanks to the ability to respond to the needs of individuals and families in a personalised way.
• The stronger the local care system, the lower the overall costs for the health service.
agEism in mEdicinE:
diffErEntiatEd diagnosEs and trEatmEnts
Professor nicolA veronese
Nicola Veronese is an Associate Professor at UniCamillus University and a boardcertified geriatrician. His research is primarily epidemiological and focuses on the most common diseases affecting older adults.
He is the author of more than 700 scientific articles published in national and international journals, as well as numerous abstracts accepted at major conferences. Since 2024, he has served as EditorinChief of ‘Aging Clinical and Experimental Research’.
Ageism, a term referring to discrimination based on age, is one of the most underestimated challenges in contemporary medical practice. While sexism and racism have received more attention in clinical and social settings, ageism often operates more quietly, influencing decisions about diagnosis, therapy and communication, and even the allocation of healthcare resources.
Understanding how age can generate stereotypes and prejudices is essential not only to improving the quality of care but also to ensuring fair treatment for all patients. This essay aims to explore the influence of ageism on diagnosis and treatment by analysing its mechanisms, consequences, and potential countermeasures.
definition And origins of AgeisM
The term ageism was first coined by psychiatrist Robert Butler in 1969 to describe discriminatory attitudes towards older people. Today, the term is applied to all age groups, but in medicine it primarily concerns the elderly population.
The origins of ageism are complex and multifaceted:
• cultural, linked to the glorification of youth and productivity;
• social, involving the marginalisation of older people in decisionmaking processes;
• healthrelated, shaped by the perception that old age is synonymous with illness, frailty and dependence.
These prejudices can result in unfair clinical practices in which patients are not assessed as individuals, but as ‘elderly’ individuals with a predetermined fate. The concept of ageism is often discussed alongside that of frailty, a widespread condition among older adults characterised by increased vulnerability to acute events. In clinical practice, frail individuals are frequently discriminated against—or rather, their frailty is not adequately taken into account—which ultimately contributes to ageist attitudes.
AgeisM in MedicAl diAgnosis
Underdiagnosis and late diagnosis
One common issue is the tendency to underestimate symptoms in older people. Conditions such as fatigue, joint pain and cognitive impairment are often dismissed as ‘normal for one’s age’ without further investigation. This can result in delayed diagnosis of conditions such as depression, neurodegenerative diseases or cancer. It is important to remember that some of these conditions can be reversed with appropriate treatment, so failing to diagnose them can result in a significant reduction in quality of life.
Overdiagnosis and medicalisation
On the opposite end of the spectrum, some older people undergo excessive diagnostic testing, including invasive procedures, based on the idea that an ageing body is ‘naturally sick’. This entails high costs and
additional risks, often without any real benefit.
Cognitive biases of the physician
Unconscious stereotypes can influence clinical reasoning. Some classic examples are:
• Not all chest pain in older people is attributable to coronary causes.
• Not all memory disorders imply dementia.
• Not all mobility declines are irreversible.
We must replace the mental shortcut of ‘it’s just old age’ with critical thinking and an evidencebased clinical approach.
AgeisM in therAPeutic treAtMents
Exclusion from clinical trials
Historically, medical research has excluded patients over the age of 65 from many clinical trials. This results in the elderly population being poorly represented in drug efficacy and safety data, creating gaps in therapeutic guidelines. It is important to remember that the Italian population is ageing rapidly, yet the available medicines have been tested on adults with pathologies and characteristics that differ substantially from those of older people.
Denial or reduction of therapies
It is not uncommon for older people to be denied aggressive treatments such as chemotherapy or cardiac device implantation on the basis of age alone, rather than due to individual clinical contraindications. This approach contrasts with the principles of personalised medicine. Rather than focusing on chronological age, it is important to assess individual frailty, which underlies
many of the failures of current therapies in older adults.
Overtreatment and polypharmacy
Conversely, in some contexts, numerous drugs are prescribed without careful evaluation of interactions and side effects. Polypharmacy is common among people over 80 and exposes patients to the risk of adverse events and not taking medications as prescribed.
Unequal access to innovative treatments
New technologies, such as immunotherapies, robotic surgery and advanced rehabilitation, are often offered primarily to younger patients. Older people are at risk of receiving ‘traditional’ therapies even when innovative options would be more appropriate.
AgeisM in the doctor–PAtient relAtionshiP
Ageism manifests itself not only in diagnosis and therapy, but also in communication.
• Some doctors adopt a paternalistic tone, infantilising elderly patients.
• Others tend to talk to family members rather than to the patients themselves.
• The qualityoflife aspect is sometimes overlooked in favour of standardised clinical parameters.
A truly patientcentred relationship requires consideration of a person’s preferences, expectations and values, regardless of age.
the consequences of AgeisM in Medicine
Ageism has concrete and measurable effects:
• Reduced life expectancy:
delayed diagnoses and inadequate treatment worsen prognosis.
• Reduced quality of life: exclusion from rehabilitation or preventive therapies can lead to greater disability.
• Increased healthcare costs: complications arising from inappropriate care or adverse drug events generate additional costs.
• Mistrust in the healthcare system: some older people avoid checkups and treatment due to perceived discrimination.
strAtegies to recognise And Address AgeisM
Specialised training in geriatrics Healthcare students must receive solid training on the physiology of ageing, distinct from pathology, so as not to confuse normal agerelated changes with disease.
Use of multidimensional assessment
The Comprehensive Geriatric Assessment (CGA) integrates clinical, functional, cognitive and social aspects to provide a more realistic picture of the patient’s condition. The CGA can determine whether a person is frail, offering clear and reproducible guidance that, more effectively than chronological age alone, helps physicians choose the most appropriate treatment.
An inclusive, evidencebased approach
It is essential that clinical research systematically includes older people so that guidelines and protocols are valid for all age groups.
Personcentred communication
The doctor–patient relationship should value autonomy and individual preferences while avoiding infantilising or stereotypical language.
Ethics and distributive justice
In contexts where resources are limited, clinical decisions cannot be based solely on chronological age. Instead, they must take into account individual prognoses, expected quality of life and patient wishes.
tAngible exAMPles of clinicAl AgeisM
The following examples illustrate the significant issue of clinical ageism.
Case 1: Acute myocardial infarction
An 82yearold patient is admitted to the emergency room with chest pain. In some hospitals, advanced age may discourage the immediate use of primary angioplasty, despite scientific evidence demonstrating its effectiveness in selected elderly patients.
Case 2: Diagnosis of depression
A 75yearold woman experiences loss of interest and insomnia. These symptoms are often dismissed as ‘normal for her age’ without a psychiatric evaluation or consideration of early dementia. Failure to diagnose depression compromises quality of life and increases the risk of suicide.
Case 3: Cancer treatment
A 79yearold man with colon cancer was offered palliative care instead of curative surgery solely because of his age. A more thorough evaluation could have supported surgery with a chance of recovery.
the future: intergenerAtionAl Medicine
Twentyfirstcentury medicine must prepare for a world in which the elderly population is growing both in number and in societal relevance. The goal is not only to add years to life, but life to years.
Combating ageism means:
• Promoting inclusive clinical research.
• Offering proportionate and personalised treatments.
• Educating future doctors to see the patient as an individual, not an age group.
conclusion
Ageism in medicine is not a marginal issue; it affects diagnosis, treatment, communication and the overall quality of care. For medical students, recognising and combating ageism is a fundamental step towards achieving ethical, fair and truly patientcentred clinical practice. Selecting treatments based on individual clinical conditions rather than chronological age is an act of justice and professionalism. In an ageing society, overcoming generational bias will be one of the most important skills for the doctors of tomorrow.


An interview with Professor Maria Rosaria Gualano, a lecturer in General and Applied Hygiene at UniCamillus
by Giorgia Martino
Discrimination is not always easy to spot. Sometimes it is subtle, manifesting in everyday attitudes, common phrases, or deep-rooted stereotypes that shape the way we perceive age. This is the case with ageism—a form of prejudice based on age that can result in social exclusion, reduced attention to healthcare, or simple indifference to the needs of older people. This is by no means a minor issue.
According to the World Health Organization (WHO), ageism poses a real threat to global public health. It affects people’s physical and mental well-being, and contributes to widening inequalities in access to care.
When age-related prejudices influence diagnosis, doctorpatient communication or health policies, the entire public health system is affected. Therefore, combating ageism means promoting equity, prevention, and quality care for all age groups. We discussed this issue with Professor Maria Rosaria Gualano, a lecturer in General and Applied Hygiene at UniCamillus University, who has been working for years in the fields of health promotion, prevention, and health communication.
Together, we have explored how ageism affects physical and mental health, access to services, and social perceptions of ageing, and what we, as citizens and communities, can do to combat it.
whAt Are the MAin consequences of AgeisM for the PhysicAl And MentAl heAlth of older PeoPle?
“Scientific literature has demonstrated that ageism has several unpleasant consequences for older people. First and foremost, it has a negative effect on mental health, essentially leading to an increase in depression, anxiety and social isolation, all of which stem from a collapse in self-esteem linked to feeling ‘useless’ and ‘no longer productive’. Additionally, those experiencing ageism often neglect their personal care and reduce their physical activity, which can lead to early cognitive and motor deterioration. This can also lead to an increased incidence of chronic diseases, an increased risk of hospitalisation, and slower recovery after accidents. Overall, both life expectancy and quality of life tend to deteriorate”.
cAn discriMinAtion AgAinst older PeoPle Affect the quAlity of cAre or Access to heAlth services?
“Unfortunately, yes. Symptoms are often underestimated, partly because some older people tend to communicate less and ]neglect to report certain symptoms to healthcare professionals or caregivers. This can result in minimising symptoms or leading to inadequate diagnoses, with serious consequences for health. Sometimes, older people may receive less accurate and personalised treatment because they are considered a lower priority than younger patients. Furthermore, we must consider the barrier of the so- called ‘digital divide’, which in this case means not having easy access to online health services. The risk is that this group will be excluded, if there is no caregiver who can provide digital support”. a g E ism and public h E alth : why ag E discrimination harms E v E ryon E – including young p E opl E
cAn AgeisM Also Affect other Age grouPs?
“It can affect society as a whole, especially because it limits older people’s active participation in the community, depriving it of valuable resources in terms of knowledge and experience. Moreover, the perception of ageing can influence younger people, creating a negative view of old age and leading them to imagine a bleak future for themselves. When ageism is internalised in this way, the idea that ‘ageing is only getting worse’ can accompany people throughout their lives, creating negative moods that can seriously affect their mental health. The negative stereotype of old age can therefore fuel a cycle that places little value on human life. Instead, we need to create a culture that values the positive aspects of every age group and recognises their unique characteristics and potential. For example, consider that, as an older adult, you may now have the time and financial resources to embark on trips and experiences that were not possible for you earlier in life. A culture that fails to value the skills and experience of older people certainly reduces the transmission of intergenerational knowledge and weakens the social fabric. A more cohesive society is healthier, with positive effects on both physical and mental well-being”.
Are there Any effective ProgrAMMes or cAMPAigns thAt Address AgeisM in heAlthcAre?
“In 2021, the WHO published the Global Report on Ageism, which primarily aimed to raise global awareness of this cultural issue and provide scientific evidence to support the development of concrete courses of action. These include promoting accurate and non-misleading messages about ageing as a normal, rich and productive stage of life through the media, schools, institutions and healthcare. The campaign emphasises that combating ageism is an important form of investment in the future, and that the way we view ageing today will determine how we experience old age tomorrow. In this regard, the WHO has also developed an online toolkit with infographics that can be downloaded. Such campaigns should also be implemented and disseminated at a grassroots level. Therefore, there is still a long way to go in raising institutional awareness of these issues, also through scientific societies and citizens’/patients’ associations”.
so, let’s tAlk About whAt we As ordinAry citizens cAn do. whAt everydAy behAviours cAn we AdoPt to coMbAt AgeisM?
“A few years ago, I collected and published scientific evidence on the promotion of so-called ‘intergenerational programmes’, which I believe are a fundamental resource for our societies. These strategies are now recognised internationally and institutionally as effective in combating ageism because they bring young and old people together to promote the mutual exchange of experiences and learning between generations, with each person contributing their emotional, ethical and knowledge-based background. In addition to these more structured practices, it’s clear that the message to convey is to promote a culture that respects people of all ages. Each of us makes daily choices about how to behave. We can choose to respect others, avoid making offensive remarks about older people, listen to and value the stories of those who are older and have meaningful experiences to share, and support older people without making them feel ‘useless’. Certainly, each of us can do our part to combat stereotypes and discrimination every day, in order to build a more integrated and inclusive society that benefits everyone’s well-being”.
c ould lariocidin b E a n E w hop E in th E fight against antimicrobial r E sistanc E ?
Antimicrobial resistance (AMR) is an increasingly serious global problem, causing more than 1 million deaths worldwide every year. The ability of bacteria, viruses, fungi, and parasites to develop resistance to antibiotics poses one of the most serious challenges to modern medicine.
A study published in The Lancet in September 2024 predicts that over 39 million people could die from antibiotic-resistant infections by 2050. Conducted by the Global Research on Antimicrobial Resistance (GRAM) Project, the research analysed the evolution of AMR between 1990 and 2021, providing worrying predictions for the coming decades. The study examined 204 countries, revealing a growing trend that could escalate into a global health crisis if urgent action is not taken.
However, recent research published in Nature could mark a significant turning point in tackling this threat to health. Lariocidin, a potent new antibiotic derived from soil bacteria, may offer a solution for treating strains that are resistant to commonly used antibiotics.
An old resource, A new discovery
Lariocidin was discovered in soil samples collected from a lab technician’s garden. Researchers from McMaster University (Canada) and the University of Illinois (Chicago) analysed soil bacteria over a long period of time and, after a year of study, identified a micro-organism belonging to the genus Paenibacillus, capable of naturally producing a new antibiotic, lariocidin, which has the ability to inhibit protein synthesis in bacteria.
Lariocidin acts by binding directly to the ribosome, the cellular ‘factory’ that produces proteins. By interfering with this fundamental process, the molecule prevents bacteria from correctly synthesising their proteins, hindering their growth and replication.
resistAnt to resistAnce
One of the most promising features of lariocidin is its ability to avoid the common antibiotic resistance mechanisms developed by bacteria. Moreover, this antibiotic is not toxic to human cells, a crucial aspect for its potential therapeutic use.
Experiments have shown lariocidin to be surprisingly effective in treating serious infections, confirming its potential as a new weapon in the fight against difficult-to-treat bacterial infections.
So, have we found a solution to AMR? Not quite. We spoke to Gianpiero D’Offizi, lecturer in Gastroenterology at UniCamillus University who is also an expert in allergology and infectious diseases.
to re A d the full A rticle A nd find out M ore A bout the to P ics covered , sc A n the qr code A nd visit the unic AM illus website .
l E gal and E thical p E rsp E ctiv E s on b alancing i nnovation and h E alth r ights
This chapter delves into the legal and ethical perspectives surrounding the complex relationship between pharmaceutical innovation, intellectual property (IP) rights, and the global right to health. While patents and other forms of IP protection are critical for fostering innovation in the pharmaceutical industry, they often create barriers to accessing life-saving medicines, particularly in LMICs. Striking a balance between the need to incentivize innovation and ensuring global access to essential medicines is one of the most pressing challenges in contemporary global health policy. This chapter will explore the ethical responsibilities of pharmaceutical companies, the role of governments and international organizations, and alternative IP models aimed at balancing these competing interests.
the ethicAl resPonsibility of PhArMAceuticAl coMPAnies
Pharmaceutical companies play a pivotal role in the global health ecosystem. They are responsible for developing new treatments and cures that save millions of lives each year. However, these companies are also profit-driven entities, and their primary obligation is often seen as maximizing shareholder value. This tension between corporate profit motives and broader public health needs raises important ethical questions about the role of pharmaceutical companies in society. [...]
Questo capitolo approfondisce le prospettive legali ed etiche che circondano la complessa relazione tra innovazione farmaceutica, diritti di proprietà intellettuale (IP) e diritto globale alla salute. Mentre i brevetti e altre forme di protezione della proprietà intellettuale sono fondamentali per promuovere l’innovazione nell’industria farmaceutica, spesso creano ostacoli all’accesso ai farmaci salvavita, in particolare nei LMIC. Trovare un equilibrio tra la necessità di incentivare l’innovazione e garantire l’accesso globale ai farmaci essenziali è una delle sfide più urgenti nella politica sanitaria globale contemporanea. Questo capitolo esplorerà le responsabilità etiche delle aziende farmaceutiche, il ruolo dei governi e delle organizzazioni internazionali e i modelli di PI alternativi volti a bilanciare questi interessi concorrenti.
lA resPonsAbilità eticA delle Aziende fArMAceutiche
Le aziende farmaceutiche svolgono un ruolo fondamentale nell’ecosistema sanitario globale. Sono responsabili dello sviluppo di nuovi trattamenti e cure che salvano milioni di vite ogni anno. Tuttavia, queste società sono anche entità orientate al profitto e il loro obbligo principale è spesso visto come la massimizzazione del valore per gli azionisti. Questa tensione tra le motivazioni del profitto aziendale e le più ampie esigenze di salute pubblica solleva importanti questioni etiche sul ruolo delle aziende farmaceutiche nella società. [...]
TO READ THE FULL ARTICLE AND FIND OUT MORE ABOUT THE TOPICS COVERED, SCAN THE QR CODE AND DOWNLOAD THE LATEST ISSUE OF UNICAMILLUS GLOBAL HEALTH JOURNAL
RESEARCH / A bstr A ct
A selection of the M ost recent A nd interesting rese A rch conducted by u ni c AM illus rese A rchers .
Abstracts of the work are available. To view the full text, scan the relevant QR code. Access to the research is subject to specific subscriptions or affiliations to the platforms containing the extended work.
2025 National Guidelines on the Mediterranean Diet: Executive Summary of a Joint Report by Italian Scientific Societies and the National Institute of Health Task Force on Clinical Practice Guidelines
Nicola Veronese , Vincenza Gianfredi , Massimo Volpe , Michela Zanetti , Graziano Onder , Marco Silano , Daniele Nucci, MSc , Luigi Fontana , Alessandro Laviano , Cornel Sieber , Stefania Maggi , Italian Mediterranean Guideline Group
The paradox of sleep where sleep is no longer possible: a neurophysiological perspective and a human rights imperative
Di Gennaro, G., Romigi, A. The paradox of sleep where sleep is no longer possible: a neurophysiological perspective and a human rights imperative. Neurol Sci 47, 30 (2026). https:// doi.org/10.1007/s10072-025-08722-6
Preclinical evidence and therapeutic perspectives on carnosine for the treatment of neurodegenerative disorders
Saviana Antonella Barbati 1,2 , Giuseppe Carota 3 , Konstantinos Partsinevelos 3 , Lucia Di Pietro 3 , Anna Privitera 4 , Vincenzo Cardaci 5 , Andrea Graziani 1 , Renata Mangione 1,2, Giuseppe Lazzarino 6 , Barbara Tavazzi 1,2 , Valentina Di Pietro 7 , Emiliano Maiani 1,2, Francesco Bellia 3 , Angela Maria Amorini 3 , Giacomo Lazzarino 1,2 , Shahid Pervez Baba 8,9, Giuseppe Caruso 1,2
Hypoprolactinemia: Biology, Clinical Relevance, and Diagnostic Challenges
Rosa Maria Paragliola, Andrea Corsello, Gianluca Cera, Pietro Locantore, Manolo Piccirilli, Roberto Salvatori
A blood-based DNA damage signature in patients with Parkinson’s disease is associated with disease progression
Sproviero, D., Payán-Gómez, C., Milanese, C. et al. A blood-based DNA damage signature in patients with Parkinson’s disease is associated with disease progression. Nat Aging 5, 1844–1861 (2025). https://doi.org/10.1038/s43587-025-00926-x
Protecting the future of vaccine development amidst US funding withdrawal for mRNA vaccine research
Eskild Petersena ∙ Giuseppe Ippolitob ∙ Markus Maeurerc ∙ Francine Ntoumid,e ∙ Jean B Nachegaf,g ∙ David S Huih ∙ Alimuddin Zumlai,j
Duchenne Muscular Dystrophy: Integrating Current Clinical Practice with Future Therapeutic and Diagnostic Horizons
Costanza Montagna1 Emiliano Maiani1,2, Luisa Pieroni1,2 and Silvia Consalvi1,2,*
Real- world data and patient- reported outcomes in diabetes in Emilia–Romagna (REWINDER): protocol of a federated cohort study for the regional evaluation of quality of care during and after COVID- 19
Fabrizio Carinci,1 Rossella Messina,2,3 Massimo Michelini,4 Amelia Bici,4 Arianna Berardo,2 Alessandra Dei Cas,5,6 Elisa Iezzi,6 Concetta Tania Di Iorio,7 Stefano Gualdi,8 Raffaella Aldigeri,5 Maria Pia Fantini , 3 Riccardo C Bonadonna,5,9,10 Massimo Massi Benedetti,11 Paolo Di Bartolo 2,3




