
6 minute read
VITREORETINAL CASES

from OT April/May 2023
by TheAOP

Dr José Ares Gómez PhD, MSc, OD (EC), DipTp (IP), Prof Cert Glauc
IN BRIEF This feature presents a series of ultra-widefield retinal images. Readers are invited to review the cases and use additional resources where necessary to answer the questions.
Advertisement

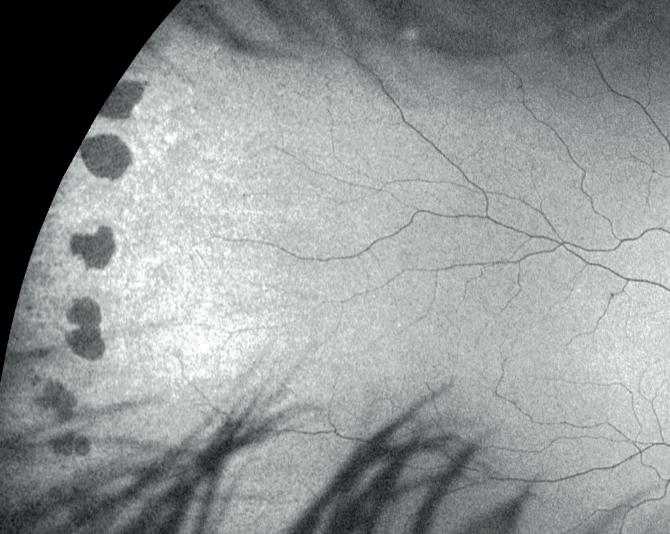
A 63-year-old asymptomatic male patient presents for routine examination a) Degenerative retinoschisis b) White without pressure c) Lattice degeneration with associated atrophic holes d) Retinal detachment with associated fluid a) Degeneration of the neural elements of the retina leading to atrophy of the tissues with lipid deposits in the internal retinal layers b) Due to an area of unusually strong attachment between the vitreous and retina c) Localised inner limiting membrane thinning, overlying vitreous liquefaction and marginal vitreoretinal adhesion d) Microcystoid degeneration of the neurosensory retina with splitting at the outer plexiform layer of the retina a) No treatment is required b) Laser photocoagulation to the area of degeneration c) Cryotherapy to the abnormal area of the retina d) Scleral buckling
01 What is the peripheral retinal degeneration shown in the image?
02 What is the aetiology of this condition?
03 What is the most likely type of treatment to be applied?
A 72-year-old asymptomatic female patient presents for routine examination a) Serous retinal detachment with associated subretinal fluid b) Degenerative retinoschisis c) White without pressure d) Horseshoe retinal break a) No treatment is required b) Localised laser photocoagulation to seal the break c) Cryopexy treatment d) Pneumatic retinopexy a) A fresh retinal break that requires emergency referral for vitrectomy and serous retinal detachment repair b) Migration of pigment from the retinal pigment epithelium c) Chronicity of this peripheral microcystoid degeneration of the neurosensory retina with splitting at the outer plexiform layer of the retina d) Previous laser treatment for an old retinal break a) Honeycomb degeneration associated with vitreous floaters b) Degenerative retinoschisis c) Retinal detachment with associated subretinal fluid d) Horseshoe retinal tear secondary to posterior vitreous detachment a) Rhegmatogenous as this retinal tear is associated with posterior vitreous detachment b) Tractional as this lesion has been caused by neovascularisation c) Exudative as this lesion has been caused by accumulation of subretinal fluid from a mass lesion d) Rhegmatogenous as this retinal lesion is associated with an intraocular foreign body a) Scleral buckling b) 360⁰ argon laser retinopexy to seal the tear c) No treatment has been undertaken d) None of these options a) Operculated retinal hole b) White without pressure c) Lattice degeneration with associated atrophic hole d) Paving stone retinal degeneration a) 14 to 35% of cases b) It is inevitable during a patient’s typical expected lifetime c) It is a benign degeneration and is not usually associated with complications such as retinal detachment d) 33% in males and 75% in females a) Usually located between the ora serrata and equator with a size of one to several disc diameters b) More commonly located in the infero-nasal and temporal quadrants c) The prevalence of this finding is approximately 4–28%, usually bilateral, no sexual predilection and increasingly common with age d) All of these options
04 What is the peripheral retinal anomaly shown in the image?
05 What is the most likely type of treatment for this case?
06 What does the pigment found in the far temporal retina indicate?
07 What is the posterior segment anomaly shown in the image?
08 What type of retinal detachment can this finding lead to?

09 What type of treatment is shown in the image?
10 What is the temporal retina finding shown in the image?
11 What is the likelihood of the finding in the image resulting in a retinal detachment?
12 Which of the following statements regarding the finding shown in the image is correct?
Dr José Ares Gómez was awarded a MSc in optometry in 2002. He returned to the University of Bradford the same year and was awarded a PhD in in 2007 which investigated retinal ganglion cell function in both normal and glaucomatous patients. He has held a position as a visiting research fellow in clinical optometry at the University of Bradford School of Optometry and Vision Science since September 2007 and has worked as a specialist optometrist at York Teaching Hospital NHS Foundation Trust since September 2008 with responsibilities in the glaucoma screening, cornea, specialist contact lens and medical retina treatment clinics.

“OPTICS LENDS ITSELF TO FLEXIBLE WORKING”
Frances Rus (pictured), managing director at Duncan and Todd, and Julie Mosgrove, retail director, on why flexibility is key at the Scottish independent optometry group

If someone wanted to work for Duncan and Todd, what is the first piece of advice you would offer?
Frances Rus (FR, pictured): We have fairly stable teams. Often people say that the first thing they notice is that the staff know all the patients by their names as soon as they walk through the door. It makes them feel that they have to up their game, to have that much knowledge about their patients. We give them time to get to know their patients. The biggest piece of advice is to take your time in the test, to understand your patients’ needs.
When shortlisting candidates, what is the first thing that you look for?
FR: Someone who wants to work in an independent practice, and understands that difference. Also, longevity: that they are looking to stay somewhere for a while.
How important is the cover letter?
Julie Mosgrove (JM): Cover letters give a bit of personality, rather than a CV, which is just a list of experience. It allows you to find out a bit more about the person.
What is the biggest mistake that someone can make in an interview for Duncan and Todd?
FR: Someone who is totally focused on the benefits. I would expect people to focus on the kind of environment they’ll be working in: testing times and the size of the team, for example. If I was interviewing somebody who didn’t show interest in the business, I think that would be a problem.
If you had a new employee preparing for their first week, what would you say to them?
FR: If they haven’t already, visit the practice, and meet the team and manager they will be working with.
JM: We have regular check-ins when someone is getting ready to start. Some people have a three-month notice period, so it can be a long time. We have touch points over that journey, so they feel engaged and ready to begin their role. We share information about what will happen on their induction day. We try to give as much information as possible, and advise on what to bring on their first day.
How do you approach flexible working?
FR: Duncan and Todd has always supported flexible working. The profession is predominantly female, so we are used to managing maternity
How important is employee wellbeing at Duncan
and Todd?
FR: Really important. I joined during my pre-reg year, as did Julie. Now that it is my business, I try really hard to hold onto what I loved about it. It is a caring profession.
As a management team, we all know each other really well. It’s a very approachable business. Whenever we have had external companies in, they tell me they have never had such honest and open feedback. We do exit interviews, and we’ll all sit down and discuss if there is anything there.
leave and people potentially wanting something different afterwards. Optics lends itself to flexible working. It just makes sense. If your people are happy, that’s a big part of work-life balance. Our percentage of part-timers must be 40%. It’s nearly half the workforce.
JM: We’ve always done certain things: for example, some lunches might be half an hour. Some colleagues work longer hours, but do fewer days. It is variable across practices. Some people do shifts: two weeks on, two weeks off. Everyone gets a weekend off.
Frances Rus
FR: We try to accommodate everybody. We have had people take a month or two off to go travelling. We even had a netball player who went to the Commonwealth Games.
0
It couldbe, if you're lookingfor a role that'sfocusedon clinicalcare and providinga high-quality serviceto NHS patients. Due to our recent expansion, we have vacancies in multiple locations, where you'll have the opportunity to work with some of the UK's leading ophthalmologists, nurses and HCTs. You'll benefit from fantastic training and professional development opportunities too.

Who Weare
We're patient-focused, providing clinical expertise and support for all our patients throughout every step of their patient journey.
We're busy-as the UK's largest provider of NHS cataract surgery, we have thousands of patients choosing our services and are proud to be able to support them in improving their sight and, ultimately, their quality of life.


Our patients really value the service we deliver-we've received 5-star reviews from more than 10,000 NHS patients across our 47 hospitals -you can read these on NHS UK.
CONTACTUS TODAY:

This is a great opportunity to join one of the UK's leading ophthalmology service providers. Please call or email us today if you're interested in joining our team.
WHAT WE'RE LOOKING FOR
You'll be GOC registered, with at least 12 months' post-registration experience -we provide full training so previous hospital experience isn't required.
You'll be someone that enjoys variety, is calm under pressure, great at problem solving and is willing to go the extra mile to provide the best service and advice for our patients.
Association of Optometrists
















