


AAMI eXchange25 in New Orleans was a great success, as anticipated, and the ACCE contributed to the conference program as we do every year. This year we showcased in our annual symposium the “Impact of AI – An Evolving Landscape.” The discussion looked at how this technical advance will make fundamental changes to the way medical devices are designed and maintained in the future. Along with the symposium, we sponsored an additional session on the “Hospital at Home” that examined how home monitoring has grown in recent years and transformed the approach to patient care in four other developed nations outside the U.S.
Michele Manzoli and I had the honor of presenting this year’s Advocacy Awards and the ACCE student paper competition and scholarships awards to the worthy recipients. We also added three new members to the Clinical Engineering Hall of Fame at our 35th annual members reception on Sunday June 22nd. This is one of the best opportunities we have to highlight the outstanding contributions of our hardworking and innovative colleagues to the broader CE/HTM community. I have felt personally privileged to carry out this duty the last few years. It amazes me how well the events we carry out at AAMI eXchange and other conferences, are completed without a hitch every time! Certainly, this is partially due to the great ACCE volunteers who are truly committed to our profession. However, I cannot overstate the role of Suly Chi in organizing these events. She tirelessly keeps all of us on time and on track. Many Thanks Suly!
As we look forward to the start of our new operating year, the leadership and committees of the ACCE are hard at work planning upcoming educational programs and conference symposiums, advocating for our profession, and updating parts of our Advocacy Awards program. I want to personally thank all our volunteer speakers for bringing these education sessions to us over the last year. For many of our colleagues, these webinars are important in keeping them up to date on new advances and challenging safety issues impacting healthcare and our profession.
This will be my last message as ACCE President as my term ends on August 15th. I want to thank all our membership for allowing me the opportunity to serve as your President over the last two years. It has truly been an honor and a privilege to hold this office. I am particularly proud that our Board of Directors has moved forward in a few areas in the last two years that will help advance our profession. We have made great progress improving our working relationship with HTCC and the two Boards of Examiners. A big shout-out to Katherine Navarro for her dedicated leadership of the CCE Audit Group Committee.
I hope all of you have time to enjoy the summer months with your family and friends. See you in the fall.
This column provides example questions and information regarding preparation for the CCE exam. The questions are based on topics from the ACCE Body of Knowledge survey and the CCE Study Guide, Version 13. Note that the instructors for the ACCE CCE Prep courses, and the writers for this column, do NOT have any affiliation with the CCE Board of Examiners and have no access to the actual exam questions. If you have specific topics you would like us to cover please contact editor@accenet.org
1) What should a Clinical Engineering Manager typically NOT include in their operating budget?
a. Leasing of the biomed shop
b. Continuous training of employees
c. Cost of spare parts and service contracts
d. Cost of personnel
2) What is meant by a payback period for a medical device?
a.The length of time it takes to pay for the acquisition cost to the seller of the device through a loan
b.The length of time to become profitable once an initial investment is made
c.The length of time required to recoup the funds and break even from the initial investment
d.The length of time from the planning of a new device to its first patient use
3) You want to add a new Bone Density service to your hospital. You know the following:
• The Bone Densitometer will cost $40,000 and room renovations cost $100,000. It will cost $10,000 to train the users on the equipment and you’ll purchase a service agreement for $5,000/year for 10 years. You’ve estimated disposables and utilities will be $1,000 per year.
ACCE News
ACCE News is the official newsletter of the American College of Clinical Engineering (ACCE).
Managing Editor
Ted Cohen tedcohen@pacbell.net
Co-Editors
Sonja Markez
Jason Launders editor@accenet.org
Circulation & Address Corrections
Suly Chi, ACCE Secretariat secretariat@accenet.org
Advertising
Dave Smith advertising@accenet.org
• You would be able to eliminate fee-basing your patients to a neighboring hospital which costs you $20,000/year and you estimate you will earn $40,000/year from medical reimbursement. Based on the ROI, should you do this?
a. No, the ROI is below 100%
b. No, the ROI is negative
c. Yes, the ROI is positive and above 100%
4) What is generally considered the best way to determine the number of BMET FTEs needed for a Clinical Engineering Department?
a. Determine the number of beds in the hospital and apply a 2.5 FTE per bed standard.
b. Determine the number of medical devices in the hospital and obtain 1 FTE per 1,000 devices.
c. Evaluate the work order history hours for all medical devices in the hospital and determine the FTEs needed based on work hours.
d. Determine the total acquisition cost for all of the medical equipment in the hospital and assign 1 FTE per $1M worth of medical equipment.
5) What device would you NOT expect to find in an OR:
a. Intra-Aortic Balloon Pump
b. Smoke Evacuation System
c. Patient Warmer
d. Electrosurgical Unit
e. Insufflator
f. None of the Above
ACCE News is a benefit of ACCE membership; non-members may subscribe for $100 per year.
To subscribe e-mail: secretariat@accenet.org
Copyright © 2025 by ACCE
The ACCE CE Symposium task force (Juuso Leinonen, Mike Powers, Carolyn Mohoney, Ashley O’Mara, Priyanka Shah, Suly Chi, Dean Skillicorn, Peter Dziedzic) organized a highly successful and informative Clinical Engineering Symposium at the AAMI eXchange25 in New Orleans, LA. This year, the CE symposium focused on “Impact of AI on HTM: An Evolving Landscape.”
ACCE President Kim Greenwood addressed the participants, thanked the symposium sponsor Asimily, and introduced Ashley O’Mara, moderator for Part 1. The speakers for this part, Peter Dziedzic, Nathan Licht, and Dr. Thomas McCoy, covered topics about the AI Technologies that are rapidly expanding across a broad range of healthcare applications.
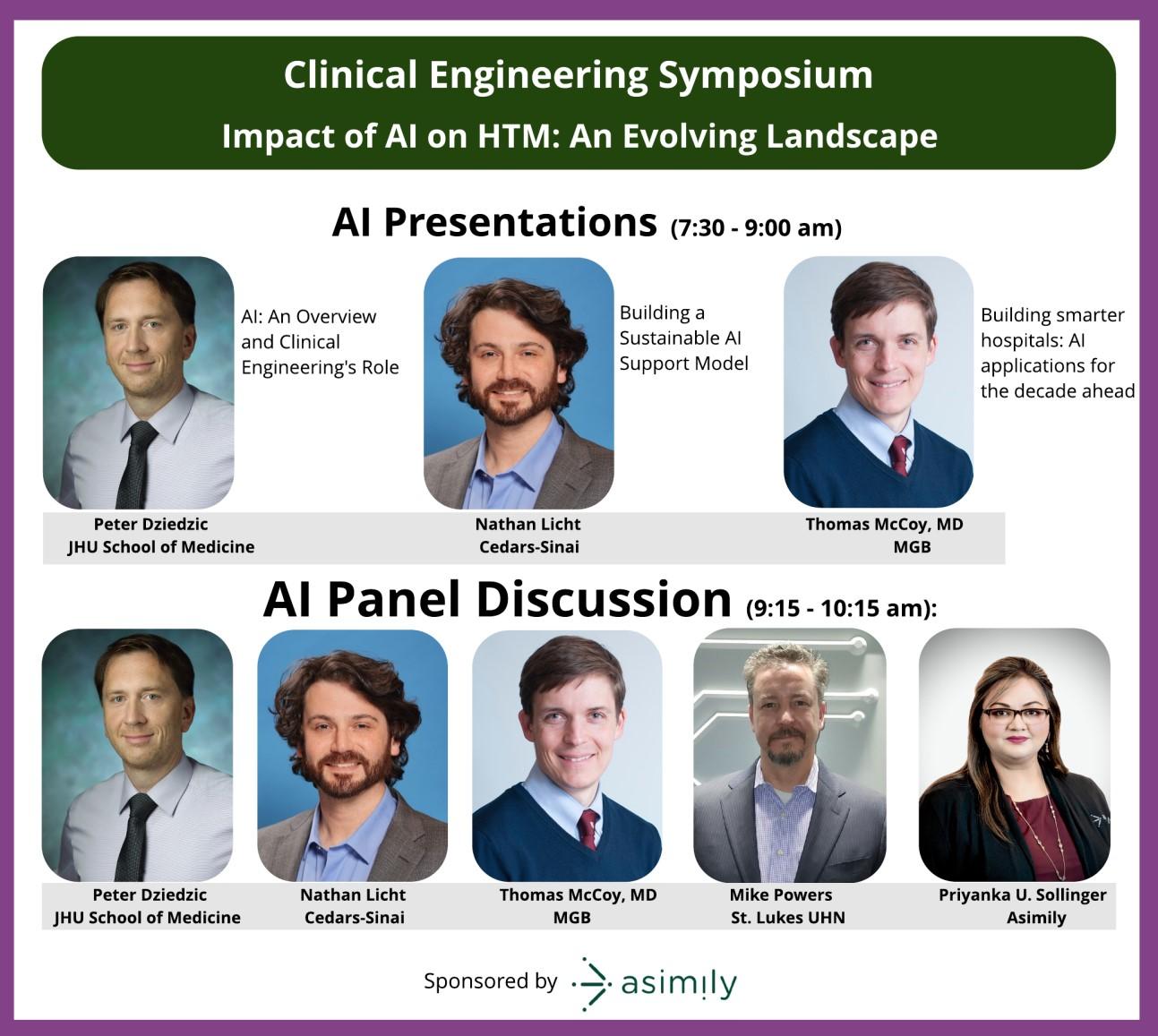
Peter H. Dziedzic of Johns Hopkins University opened the symposium with an overview of AI fundamentals and their direct relevance to clinical engineering. His talk, “Artificial Intelligence: An Overview and Clinical Engineering’s Role,” explored the layered concepts of machine learning, deep learning, and foundational models, framed through the essential triad of data, computing power, and models. Dziedzic highlighted how engineers play a critical role in transforming raw, heterogeneous clinical data into AI-ready systems by focusing on synchronization, infrastructure design, and system reliability. He shared real-world applications from the Johns Hopkins Neurosciences Critical Care Unit (NCCU), including a machine learning pipeline developed to analyze high-frequency intracranial pressure waveforms a task made possible only through thoughtful collaboration between data scientists and clinical engineers.


Nathan Licht from Cedars-Sinai Medical Center shared a deeply practical session titled “Building a Sustainable AI Support Model.” Drawing from a decade of experience in analytics and visualization, Licht emphasized the importance of culture, communication, and governance in implementing AI across a large healthcare institution. He described Cedars-Sinai’s multi-pronged approach, which included education series, user engagement metrics, and the formation of an AI Committee and Intake Group to triage and support AI initiatives. Licht’s presentation offered valuable lessons for HTM professionals looking to scale AI responsibly, rooted not only in technology but in human behavior, organizational learning, and clear metrics for success.
(Continued on page 4)

Part 1 of the CE Symposium concluded with a compelling keynote Dr. Thomas H. McCoy of Mass General Brigham and Harvard Medical School. His talk, “Building Smarter Hospitals: Artificial Intelligence Applications for the Decade Ahead,” offered a syslevel vision for the future of AI in healthcare. McCoy introduced the concept of Smart and Autonomous Medical Systems driven solutions capable of sensing, thinking, and acting with minimal human input. He argued that the urgency to deploy AI is growing due to demographic pressures, workforce shortages, and the need to improve safety and reduce cost.
provoking comparisons and data-backed insights, McCoy made it clear that the hospitals of tomorrow must embrace agile architectures and continuous learning environments, fueled by data but grounded in ethical and operational rigor.
Peter Dziedzic Education Committee Member CE Symposium Task Force Member phd@jhu.edu
The symposium’s second part was a panel discussion on Artificial Intelligence in Healthcare. Erin Sparnon, from ICA, Inc., moderated the session and posed questions to the panelists, including some from the audience, to delve into key questions about the practical management of AI in clinical engineering. The expert panel of speakers included Peter Dziedzic from Johns Hopkins University School of Medicine, Nathan Licht from Cedars-Sinai Medical Center, Thomas McCoy from MGH, Mike Powers from St. Lukes UHN, and Priyanka Upendra Sollinger from Asimily.

Panelists shared some early wins with AI deployments in the aggregation and interpretation of multiple data streams. Powers is using AI on the back end of EHR data to help detect patients at risk for deterioration, leading to interventions an average of 4 hours earlier than at baseline. This is driving improved outcomes, as their rates of severe episodes of care are about half of state averages. Licht is using AI to query and aggregate multiple individual dashboards to get a single meaningful trend indicator of fetal heart rate to help detect alkalosis.
Discussion then switched to governance issues, as one noted, “How do we address lifecycle issues when equipment lasts 20 years and AI lasts 6?” Panelists agreed that no governance exists by default and you need to build it. Upendra suggested defining key outcomes for AI systems and regularly auditing their performance. To do this, facilities will need to provide a feedback loop that’s easy for clinicians to use. It’s critical that this feedback loop is non-punitive, as Dziedzic notes, “physicians are often remembered only for their mistakes, so no one wants their name associated with an error or incident.” One way to do this is to encourage clinicians to report patient harm related to AI recommendations in the same manner they use to report medical device incidents and use error. Without this continuous tracking of real-word performance, it’s impossible to truly assess local performance of AI systems.
Discussion then turned to the promise of data sharing and the practical challenges of navigating legal permissions, agreeing on what counts as proper anonymization, and reconciling inconsistent terms and practices in documenting service and repair. McCoy noted that other domains are further along this path, as data sharing is going well with ARPA for a federated network of HDOs to surface data for particular commercial uses. Attendees shared a lot of energy around the concept of standardized terminology and documentation, and are looking forward to more content from various AAMI committees and workgroups focused on standardizing CMMS workflows and repair vocabularies.
Discussion then turned to practical nonclinical uses of AI to support clinical engineering activities. As McCoy noted, reality is there are 200 staff maintaining 100 thousand de-
vices - maybe start with easy wins first to get some quick returns. Think of all the work involved reconciling Excel files with a few columns and a few thousand rows- use AI for a first pass at it.” Attendee Michael Brilling from DartmouthHitchcock agreed with the promise of using AI to reduce the technical burden of using tools like querying, but cautioned that this comes with a training responsibility, in that you need a way to talk to clinical people using data tools to help them understand what they’re seeing.
In closing, the panel also talked about situations where AI may not be the best tool for the job. An attendee, Sudhee Tumkur, recounted a situation in which he was called in to troubleshoot an anesthesia machine that wasn’t working, but quickly discovered that the issue at hand was a misseated endotracheal tube instead. He’d wondered if we could use AI to help clinicians troubleshoot problems to see if it’s really the device or a clinical problem, but the discussion quickly turned to using existing tools like safety incident reporting and additions to pre-op checklists to ensure the knowledge is captured and available for the next time an anesthesia machine isn’t working. Attendees also recommended documenting these types of situations in CMMS to establish a pattern for later training and ingestion by AI.
If you missed the CE Symposium, the presentation slides are available for download on the ACCE website. ACCE looks forward to continuing its coverage of the impact of AI on HTM through our upcoming educational webinars.

Erin Sparnon Part 2 Moderator CE Symposium Task Force Member erin.sparnon@gmail.com
Hospital at Home: Worldwide Clinical Engineering Approaches to Mansession at AAMI Exchange 2025 was one of the highlights of my experience in New Orleans. Organized by ACCE, this session brought together a global panel of clinical engineering Umberto Nocco (Italy), Jean Ngoie (Canada/ who offered invaluable perspectives on how different healthcare sys-based care.
I was particularly inspired by how each speaker highlighted the expanding role of clinical engineers in shaping telehealth infrastructure, device integration, (Continued on page 6)
(Continued from page 5)
and even the architectural reimagining of patient homes. It was a powerful reminder that our profession is not only evolving but becoming even more critical to the future of patient-centered care.
What stood out to me most was the balance between visionary thinking and practical case studies - from Italy’s robust telemonitoring initiatives and Canada’s CHEO dialysis-at-home program to Germany’s structured approach to homecare devices and electronic health records. The international lens made it clear that while each country has unique challenges, we share common goals: safety, accessibility, and continuity of care beyond hospital walls. Many thanks to ACCE for organizing such a timely discussion.
Michele Manzoli ACCE Secretary and Session Moderator michele.manzoli@cshs.org


The 2025 members meeting/awards reception was held on Sunday, June 22, at Hilton New Orleans Riverside, Louisiana. ACCE thanks our co-sponsors, Intelas and Schiller Americas for their generous support. The 2025 Awardees received congratulations and plaques from Kim Greenwood, ACCE President.




ACCE 2025 Lifetime Achievement Award Winner: Carol Davis-Smith
2024 CE Hall of Fame Inductee: Mark Bruley

2025 CE Hall of Fame Inductee: Dr. James Philip
*Joseph F. Dyro and Anthony C. Easty also inducted into 2025 CE HOF but not present at Awards Ceremony
Undergraduate Division Winner: Ana Cristina
Master Division Winner:

Congratulations to all awards recipients who were at the 35th Members meeting & Awards reception as well as to those who were unable to travel to New Orleans to accept their awards in person.

Congratulations to 2025 Class Fellow Member: Axel Wirth, FACCE

Axel









L-R: Binseng Wang, Michele Manzoli, Umberto Nocco (A.H. International CE Award Winner), Suly Chi
L-R: Suly Chi, Shashi Avadhani, Erin Sparnon, Larry Hertzler, Danielle McGeary


As always, the ACCE booth has been a spot to learn about new activities and a networking point for our members new and old!
A big shout-out to our members/volunteers who helped us set-up/dismantle and monitor the ACCE Booth: Kim Greenwood, Ishtar Al-Tahir, Michele Manzoli, Peter Dziedzic, Gianna Vanchieri, Jenn Nichols, Ashley O’Mara, Alan Lipschultz, Dean Skillicorn and Binseng Wang. We couldn’t do it without your support.
Suly Chi ACCE Secretariat secretariat@accenet.org
At the 2025 AAMI eXchange, Dr. Binseng Wang of Sodexo and G. Wayne Moore of Acertera Acoustic Laboratories met for a rematch of their 2024 debate on medical device remanufacturing and servicing regulations.
The session was conducted in point-counterpoint format, with attendees voting on which questions the speakers debated. AAMI Board member and InterMed Group COO Larry Hertzler graciously moderated this discussion on what he called “regulating the unregulated.”
As a neutral convener, AAMI does not take a stance on contested policy areas like remanufacturing and right to repair. But the Association gladly provides an open forum for debate among members. If you missed this session, be sure to look out for future events like it – the debate over remanufacturing is unlikely to go away soon.
2Hertzler: If Original Equipment Manufacturers (OEMs) should provide the materials for service, then shouldn’t the servicers be registered just as the OEMs are?
Moore answered, “It depends on what type of servicing we’re actually talking about.” He sees a fundamental difference among repair, parts replacement, and making a modification that may not be appropriate to add to a finished, cleared medical device in the field. That said, Moore believes manufacturers should make the necessary information to conduct on-site repairs available to independent service organizations (ISOs), provided they act on behalf of a hospital.
But Moore made his position clear. If an ISO asks for information beyond the scope of what an OEM feels is appropriate or necessary to perform repairs in a hospital setting, then that activity has “crossed a line into potential remanufacturing.” If so, that ISO should be regulated in the same fashion as any OEM.
Wang responded by pointing out that FDA already has the legal authority to regulate ISOs in the same way as OEMs if the agency deems it necessary. “First of all, we are all regulated, like it or not.” He cited a 2018 FDA report that concluded there is no significant record of major issues related to ISO remanufacturing activities. To date, FDA has chosen not to regulate ISOs in this way. Based on this finding, Wang argued that there is no reason for FDA to invest its limited resources in regulating ISOs in the same way as OEMs. Further, he posited that the remanufacturing issues discovered by FDA were likely the result of a lack of access to OEM information.
Wang then drew an analogy to the U.S. Constitution, stating, “If I am required to abide by the Constitution but I’m not allowed to read the Constitution, how am I going to be able


to abide by it?” He also noted that the existing inspection and regulation regime for medical device manufacturers does not prevent all recalls or safety issues. Thus, he sees no reason why analogous regulations on ISOs would result in massively improved patient safety outcomes.
Moore offered a rejoinder, saying that “servicing can include component level change or a field replaceable unit modification,” but reiterated the point that there is no FDA definition for “bad servicing.” Instead, FDA differentiates servicing from remanufacturing, defining servicing as an “activity that returns a finished medical device to original equipment specifications, substantially...anything that doesn’t do that is classified as remanufacturing.” Moore indicated that he sees no issue with buying parts from the manufacturer, but it is vital to validate that those parts work as intended and align with the OEM’s intended purpose and function.
In Wang’s view, if ISOs do not have access to materials for software and software codes, “how can we be sure” if an intervention is correct and safe? He nevertheless clarified that he is not advocating for “anyone under the sun” to have access to OEM service material but rather the purchasers or owners of medical devices who could then share as needed with their contracted third parties.
Hertzler: Why don’t all HDOs require manufacturers to provide service documentation, service keys, etc., as a condition of purchase?
In Hertzler’s words, “Why isn’t this a requirement of purchase?” After all, there is an inherent pressure created by the fact that “hospitals are going to buy equipment no matter what.”
Wang stated that if OEMs included this demand with their purchases, it would benefit HTM professionals. Ideally, this would be a “standard demand” made by healthcare delivery organizations. He also said that the U.S. Secretary of Defense (DOD) recently issued a memo to secretaries of the various service branches demanding that equipment acquisitions by service branches include OEM information. However, “the issue is very simple. It’s called money.”
(Continued on page 16)
Healthcare organizations are increasingly looking to AI to streamline workflows, ease clinicians’ burdens, and cut costs. To meet the evolving needs of the healthcare landscape, ECRI is publishing a collection of AI resources and expanding its hands-on AI support services available to industry partners.
AI-enabled tools have benefits spanning the healthcare field, from identifying at-risk patients and enabling earlier interventions; to assisting clinical decision-making by surfacing relevant insights that might otherwise go unnoticed; to automating administrative tasks, leaving more time for direct patient care. Additionally, predictive AI is being tested and used in care delivery, with its scope set to expand into more applications.
However, AI also poses significant risks to patient safety if it is not properly assessed and managed. These systems depend on high-quality data, robust clinical validation, and a clear understanding of their intended use. Inadequate training data, poor integration, or lack of transparency can lead to inappropriate outputs and degraded care. Additionally, evolving regulatory requirements and clinician trust must be addressed.
The resources listed here and additional insights from ECRI address how to procure, integrate, and monitor AI solutions safely in healthcare.
ECRI’s AI Position Paper – This includes a seven-point plan with recommendations to use AI safely and mitigate risk, plus answers to the most pressing questions on regulatory clearance assurances and how to assess functionality.
White House AI Action Plan Recommendations – ECRI submitted practical recommendations to the Office of Science and Technology Policy (OSTP) to support their Artificial Intelligence Action Plan.
AI is the #1 Hazard in ECRI’s Top 10 Health Technology Hazards for 2025 Report – Download the report for recommendations on how to implement AI safely through a Total Systems Safety framework.
Webcast Recording: Managing Risks in AI-Enabled Health Tech – Seven percent of webinar attendees polled reported they were aware of instances at their facility in which AI could have contributed to an incident that did (or had potential to) cause harm in patient care.
Developing an Analytical Pipeline to Classify Patient Safety Event Reports Using Optimized Predictive Algorithms – This article shows how natural language processing and machine
learning techniques can rapidly categorize patient safety reports from multiple facilities.


The additional resources listed below are excerpts from ECRI’s member-only website that have been made accessible to non-members to meet an unmet need in the industry for insights into the safe, responsible use of AI applications in healthcare.
Managing the Risks of AI in Healthcare – This article addresses AI-enabled medical devices that use machine learning, including those that are “configuration locked” and those that are subject to ongoing updating.
Ethical Use of AI in Healthcare – This article provides guidelines for data management and privacy; bias and fairness; governance; monitoring and evaluation; and provider and patient education.
Understanding FDA’s Predetermined Change Control Plans (PCCPs) for AI-Enabled Medical Devices – Even with a PCCP, AI-enabled device performance may be unexpectedly altered, presenting new risks that require mitigation strategies.
Evidence Analysis: Application of AI in Histopathology and Cytology Practice – Evidence in this report indicates that AIenabled diagnostic reviews of high-resolution whole-slide images (WSI) demonstrate high sensitivity, specificity, and diagnostic accuracy relative to manual review across various malignancies including gastric, breast, and prostate cancer.
Evidence Analysis: AI Software for Improving Outpatient Scheduling and Patient Chart Management – This report focuses on the risks and benefits of using AI for administrative functions. AI applications may appear to predict patient behaviors and length of appointments and create efficiencies in appointment scheduling.
Keep in touch. We would love to hear about your thoughts and concerns about AI.
Ismael Cordero, Senior Project Engineer, Device Safety, ECRI icordero@ecri.org
In this issue, we highlight the journey of a legendary Clinical Engineer who has served in various capacities with ACCE and also volunteered with many task forces.

CCE
DTS Director, Clinical Engineering
I have always prided myself in being a “Jill of all trades” in the sense that I have many different interests but no real mastery in anything. My wide range of afterschool activities (Student Council, newspaper, Speech Team) may have seemed like I was preparing for a life in politics, but I was also drawn to healthcare. Being an avid softball player, I considered careers in athletic training and physical therapy, but never felt quite settled with those choices. It wasn’t until, as a Junior in High School when someone mentioned they thought I’d be a great engineer, that I started to see a path forward. My friend’s mom was actually on a college tour for her older son, and while learning about biomedical engineering, she thought of me. My friend’s mom called me personally to tell me she thought it’d be a great fit for me. I think that’s so important for the folks out there helping to shape the next generation: that sometimes all we need to hear is that someone believes we can be successful. The rest is really history; I went to Milwaukee School of Engineering to pur-
sue a Bachelor’s degree in Biomedical Engineering and I dived right into a multitude of extracurricular activities (softball, BMES, becoming the president of my sorority, working full-time in the Student Accounts office). While I loved biomedical engineering, I knew I did not want to be stuck behind a desk for the rest of my life, limiting myself to working on one thing. It was then again that someone else in my life saw something in me and believed I would be a good Clinical Engineer. I consider myself incredibly lucky to have had Dr. Larry Fennigkoh as my college advisor. He encouraged me to pursue the University of Connecticut’s Clinical Engineering Master’s program. In preparation for that, I volunteered at the Milwaukee VA Hospital and shadowed clinical professionals in various hospitals. I was selected as the ABM Healthcare Support Services intern and worked at Women & Infants Hospital in Providence, RI for two (2) years while I completed my Master’s degree. After graduation, I worked there for another two (2) years before accepting a job at Yale New Haven Health on their device integration team. I worked on that team for four (4) years (through Covid) and had the incredible opportunity to work on several large projects including implementing a secondary alarm notification system in the neonatal intensive care unit, standing up anesthesia integration at one of our community hospitals, and bringing ventilator waveform data to our Tele-ICU at the height of the Covid-19 pandemic. I was promoted to Senior Manager in 2021, and recently accepted the Director of Clinical Engineering. I am incredibly humbled and honored to continue to lead Yale New Haven Health on its proud journey of in-house Clinical Engineering systemization.
I have been a member of ACCE for over ten (10) years. I took my membership to the next level by first working with the Education Committee and helping to develop the annual HIMSS symposium and other educational activities. I eventually became the Treasurer (20192021) and Member-At-Large (2021-2022), which was a challenging position but helped me learn about budgets and accounting. I am extremely grateful for this experience as it helps me tremendously in my current role. Currently, I am on the US Board of Examiners for Certification in Clinical Engineering Program.
(Continued on page 15)
The International Federation of Medical and Biological Engineering (IFMBE) recently reported a turnover in its Officers during recent elections for the period 2025–2028. With 114 out of 164 delegates voting from 66 countries and 5 international societies, this was the highest participation since electronic voting was introduced. The following appointments were officially confirmed by the Election Committee:

• Professor Virginia Laura Ballarin (Argentina), elected as Vice-President (2025–2028) with 69% of the vote, brings a distinguished academic and leadership profile. Virginia is Full Professor of Biomedical Engineering at Universidad Nacional de Mar del Plata, where she directs the Image Processing Lab and its Bioengineering PhD program. She has held key roles in IFMBE, IEEE-EMBS and regional bioengineering societies.

• Professor Leandro Pecchia (Italy), re-elected unopposed as Secretary General with 99% support. Leandro is Full Professor at the University Campus Bio-Medico of Rome and leads the Intelligent Health Technology for Health and Wellbeing lab. He also served the WHO as Innovation Manager for COVID-19 from 2020 to 2023, has authored over 200 peer-reviewed publications, and has a long track record of leading positions in Scientific Societies: President of EAMBES (2021-23), IUPESM (2018-22), and has served the IFMBE as IFMBE Clinical Engineering Division Treasurer (2018-25) and IFMBE Healthcare Technology Assessment Division Chair (2015-18) and Treasurer (2012-15).

(Continued from page 14)
What do you think of being female in engineering?
At times it can be difficult to be taken seriously, and I have often felt the need to work twice as hard as my male peers to prove I deserve to be here. It is also incredibly rewarding. Regardless of gender, everyone brings their own unique perspectives and talents to each situation and it’s great to collaborate on a solution with folks from different backgrounds. That’s one of the reasons I love healthcare so much - there’s always something new happening and new problems to solve with new people.
Who was your greatest influencer/advocate for choosing clinical engineering?
My friend’s mom and Dr. Larry Fennigkoh (story above). What surprises you in clinical engineering?
I was surprised to find that in the real-world clinical engineering setting we often act as the liaisons or the quarterback between different teams. We understand the technical side, so we can speak to the IT teams, but we also are fully entrenched in the clinical world and can communicate with nursing and other clinical providers. In my experience, those
on page 17)
groups often struggle to communicate with each other. Clinical Engineering is uniquely situated to act as project manager for multidisciplinary initiatives and as mediator when resolving complex technical issues. CEs also have a mathoriented mind, so it’s been interesting as a manager and director to be involved and even lead organizational financial conversations. Having a well-rounded background, like so many engineers do, has enabled me to have a seat at many tables and this elevates the Clinical Engineering department from basement-dwellers to technical solutions experts.
What would you tell other female when considering engineering?
Do it! It is incredibly rewarding and challenging. Clinical Engineering especially, is a great crossroad of technical aptitude and interpersonal skills that makes each day different from the last.
We welcome our newest members, approved by the Membership Committee, and supported by the Board of Directors:
Name Class
Waqas Mehmood Individual
Corey Lord Corporate/Associate
Joshua Varnes Corporate/Associate
Sarah Basenese Corporate/Associate
Ratish Kumar Associate
Olu Famewo Individual
Ansar Chishty Individual
Farhan Ahmed Individual
Alberto Vasquez, CCE Individual Faculty
Biomedical Engineer
Projects & Service
Khanum Memorial Cancer Hospital Pakistan
Sisters Mission Outreach IL/USA
Medical System Pakistan
Engineer Danaher UAE
University of Texas at San Antonio TX/USA
(Continued from page 12)
Amy Klemm, MS, CCE Membership Committee Chair Amy.s.klemm@gmail.com
Healthcare delivery organizations like hospitals do not have the same resources as the U.S. DOD. Further, Wang noted that some OEMs offer financing packages to HDOs that stipulate service contracts with the OEM. How many hospitals can say, “No, I don’t want the equipment”?
Moore countered, stating that while DOD has great deal of taxpayer resources, they are “not infinite.” During his career, he has observed some HDOs successfully make demands of OEMs. “It can be done.”
Wang also expressed concern with OEMs discontinuing devices deemed legacy devices and then indicating that it is unsafe to allow third parties or in-house staff to work on their cyber capabilities or software. Without concrete action by Congress or FDA, he believes this trend could become “more and more aggressive.”
Moore responded by pointing out that “the FDA does not know everything.” While he acknowledged the agency’s efforts and expertise, FDA simply does not have subject matter experts for every issue that may arise in HTM. Given the pace of technological change, this can create a challenging environment.
Hertzler: Instead of each state creating its own right-to-repair law, shouldn’t the federal government establish a single, uniform law for the country?
“Yes. Thank you.” But Moore elaborated, saying that he is skeptical that the U.S. Congress has the ability or willingness to act. If Congress does not settle the question of right-to-repair, a state-by-state approach may be a viable alternative.
Wang also favors a national right-to-repair law. Even if it is difficult to get Congress to act, “we still can come to some type of understanding even if we don’t have a nationwide law or regulation.” Given patients’ needs, ISOs “need a tool to provide prompt care.” His priority is ensuring that HTM professionals promote good patient outcomes by servicing medical devices.
AAMI Staff
Dan Visnovsky
Media Relations Manager dvisnovsky@aami.org
(Continued from page 15)

• Professor Maria Fernanda Cabrera (Spain), reelected unopposed as Treasurer with 98% votes, is Associate Professor at Universidad Politécnica de Madrid, directs the Life Supporting Technologies Group, and has coordinated more than 20 EU-funded ICT projects. She has authored 100+ scientific articles and serves on editorial boards including IEEE Open Journal of Engineering in Medicine and Biology.
Looking forward, the biomedical engineering and medical physics communities will converge at the IUPESM World Congress 2025, scheduled 29 September – 4 October 2025 at the Adelaide Convention Centre, Australia. Themed
“Bridging the Gap: Science, Technology, and Clinical Practice for a Sustainable World”, the congress will showcase advances in AI, immersive technologies, particle therapy, 3D printing, and more. It will feature plenaries, parallel tracks, practical workshops, a major industry exhibition,
and special sessions on digital health and sustainability. Professor Pecchia will give an invited speech on Biomedical Engineering and Global Health.
The call for late-breaking abstracts remains open until 7 August 2025, and standard registration closes on 26 August 2025, offering a final opportunity to present cuttingedge work.
In summary, IFMBE celebrates both its newly elected leadership, boasting world-class expertise, and the forthcoming Adelaide congress, which promises to be a key interdisciplinary forum for the medical physics and biomedical engineering community.
Leandro Pecchia, PhD IFMBE Secretary Leandro.Pecchia@unicampus.it
The ACCE Secretariat is a critical position that serves as the backbone of the organization’s daily operations. You will wear many hats, providing comprehensive administrative and logistical support across various departments. This role offers a dynamic and fast-paced environment where you can contribute significantly to the success of ACCE.
Responsibilities
• Membership Management
• Support Board and Committees
• Coordinate Educational Webinars and ACCE News
• Manage collaborations & Social Media
• Support webmaster with website content, ensuring accuracy and functionality
Qualifications:
• Bachelor’s degree in relevant field (e.g., Business Administration, Communications) or equivalent experience preferred
• Proficiency in MS Office Suite, Intuit, Acrobat, Zoom
• Working knowledge of accounting software (QuickBooks preferred)

• Ability to work independently with minimal supervision, demonstrating initiative and problem-solving skills
• If you are interested, or know someone that would be willing to help the ACCE, please contact Bhaskar Iduri at: contact@accenet.org
Thank you for participating in the 2025 ACCE Officer and Board Election and casting your important vote. The election for ACCE’s new Board for the year 2025 has been finalized and the Board has approved the results.
The election ballot was emailed to 314 eligible members, including Individual, Fellow and Emeritus members in good standing. Institutional/Corporate Fellow and Individual members also participate in elections. Of the 314 members, 90 votes were received between July 7 and July 22, 2025.
The new Board of Directors will take office as the governance body for ACCE on August 15, 2025. We are pleased to announce the 2025-2026 team and, as always, we look forward to serving you and your needs.
The following Board members will be continuing their second 2-year term:
Member-at-Large Jim Panella
Member-at-Large Kevin Kreitzman
Member-at-Large Erin Sparnon
Member-at-Large Ashley O’Mara
The following Board member will remain as Immediate Past President when the new President takes office:
Michele Manzoli ACCE Secretary michele.manzoli@cshs.org

Answers
Question 1
Correct answer: A
Explanation: Space for biomed shops are typically covered under a separate budget.
Question 2
Correct answer: C
Explanation:
Don’t be confused by B. Once you start making a profit, you’ve gone past the payback period. If we, for example, pay $1M for a CT scanner and we start seeing patients and charge an average of $1,000 per test and do 10 tests a day:
$1,000 x 10 = $10,000 per day
$1,000,000/$10,000 = 100 days to break even
This is very simplified; you’d have to take into account a lot more than just the initial purchase price (like installation costs, training, consumables, utilities, etc.)
Question 3
Correct answer: C
Explanation:
Cost of Investment
= $40,000 equipment + $100,000 renovation + $10,000 training + ($5,000x10) + ($1,000x10) = $210,000
Gain from Investment:
= ($20,000 x 10 Fee base) + ($40,000 x 10 Reimbursement) = $200,000 + $400,000 = $600,000
Return on Investment (ROI)
= (Gain from Investment Cost of Investment) Cost of Investment = (600,000-210,000)/210,000 = 1.86 or 186%
Question 4
Correct answer: C
Question 5
Correct answer: F
Explanation:
• IABPs are typically placed during cardiac surgery, using x-ray imaging to guide the balloon and catheter up to the patient’s aorta
• Smoke Evacuation Systems are used to capture and filter surgical smoke to remove odors and particulates during electrosurgical procedures
• Patient warmers (sometimes called Bair Huggers) are used to maintain a patient’s body temperature
• Electrosurgical Units are used to make incisions
• Insufflators blow CO2 into a patient cavity, allowing more room for surgical procedures
Questions written by the ACCE CCE Written Exam Study Group Instructors.
Jenn Nichols, MSE, CCE, CHTM BOK Committee Chair jennie_nichols@yahoo.com
On June 12th, 2025, ACCE held its final session of the 2024-2025 term, titled “What does ‘Clinical’ mean to you in Clinical Engineering?” We were honored to welcome esteemed guests Izabella Gieras from Cedars Sinai and Jennifer McFarlane from Huntington Hospital. The latter offered a unique perspective having transitioned from Biomedical Technician to Nursing early in her career. The session emphasized the critical role Clinical Engineering/HTM plays in enhancing hospital workflows. As one of the key stakeholders, CE/HTM must work very closely with clinical and medical staff, IT, Supply Chain, and Infection Control. The session highlighted the importance of partnering with nursing education departments to boost customer satisfaction and improve patient safety. The discussions included case studies of large-scale projects showcasing successful collaborations between Clinical Engineering and end-users. The session also stressed the significance of involving Clinical Engineering early in projects to foster effective partnerships with clinical stakeholders and ensure successful implementations.


(Continued from page 20)
The Education Committee would like to thank our speakers/panelists from the 2024-2025 Educational Webinar series. They made it possible to have a very successful Webinar Series. We had a lot of distinguished speakers from all over the country, representing manufacturers and hospital staff. We had clinical engineers, IT representatives, managers, directors, administrators, etc. We would like to thank all of them for taking time out of their busy schedules to share with us their knowledge, help us advance the Clinical Engineering profession, and support ACCE through the Webinar Series.
From all of us in the Education Committee – THANK YOU!
Currently the Education Committee is working to finalize the line-up of topics for the 2025-2026 Webinar series.
The new series will kick off on Thursday, September 11, 2025 with Nick Everson, MHM, covering the topic “Patient Monitoring System Integration.”
Click here to register.
Sponsorship opportunities:
The ACCE Board and the Education Committee continue working to maintain the goal of providing the Educational Webinar Series FREE to all members thanks to our generous supporters. If you are interested in supporting this upcoming series, please contact us at secretariat@accenet.org.
Join these generous organizations to support our 2025-2026 educational webinar series!



If you are interested in volunteering within the ACCE Education Committee or its task force (symposiums), please complete this volunteer form.
Juuso Leinonen & Mike Powers, Education Committee co-chairs Suly Chi, Webinar Coordinator secretariat@accenet.org
The Journal of Clinical Engineering is a compilation of articles, papers, and extensive manuscripts relevant to clinical/biomedical engineering or biomedical technology. Subject matter directly relates to the engineering or technology involved in patient care and treatment or technology in the broad field of health care delivery.
ACCE members receive a discounted subscription to the Journal of Clinical Engineering for only $99! (Originally $378). You must login to the ACCE website to view the code. Then visit LWW.com to enter code.

editor@accenet.org
29 Sept 202504 Oct 2025 2025 IUPESM World Congress on Medical Physics and Biomedical Engineering 2025
Location: Adelaide Convention Centre, Australia
Click here for more information.
30 Sept 2025 5:00 pm Last day to renew your 2025 CCE (with late fee) After this date, certification is lost. Click here for details and to renew.
15 Oct 202516 Oct 2025 2025 NESCE - Northeastern Healthcare Technology Symposium
Registration is now open!
Location: Doubletree by Hilton, Manchester, NH 03101
Click here to learn more.
21 Oct 2025 2025 Global Clinical Engineering Day
06 Mar 202608 Mar 2026
09 Mar 202612 Mar 2026
29 May 202601 June 2026
CMIA Connect 26
Location: San Ramon Marriott, San Ramon, California
Click here for more information and to register.
HIMSS26 Global Health Conference & Exhibition
Location: Las Vegas, NV
Click here for more information and to register.
2026 AAMI eXchange
Location: Denver, CO
Stay tuned for more information.