ARCHIVES OF MEDICAL SCIENCE
Menopause and women’s cardiovascular health: is it really an obvious relationship?
Kamila Ryczkowska, Weronika Adach, Kamil Janikowski, Maciej Banach, Agata Bielecka-Dabrowa
EDITOR’S CHOICE:
1. Treatment goal attainment for secondary prevention in coronary patients with or without diabetes mellitus – Polish multicenter study POLASPIRE
2. Telomere-telomerase system status in patients with acute myocardial infarction with ST-segment elevation – relationship with oxidative stress
3. The prevalence of depression in children and adolescents under 18 years of age treated for mental disorders in Poland between 2005 and 2016
4. Clinical efficacy and safety of rituximab with membranous nephropathy: a meta-analysis
5. Menopause and women’s cardiovascular health: is it really an obvious relationship? www.archivesofmedicalscience.com
VOL. 19 | MARCH | ISSN 1734-1922 | EISSN 1896-9151 | BIMONTHLY 2/2023
NEW IF: 3.707

Termedia Publishing House
Editorial Board
George Bakris (Chicago, USa)
Jeroen J. Bax (Leiden, The Netherlands)
andrzej Bednarek (Lodz, Poland)
Hans G. Beger (Ulm, Germany)
ariela Benigni (Bergamo, italy)
Joseph J. Biederman (Boston, USa)
Natan Bornstein (Tel aviv, israel)
dirk L. Brutsaert (antwerp, Belgium)
Hugh Calkins (maryland, USa)
John Camm (London, UK)
andrew J.S. Coats (Sydney, australia)
antonio Colombo (milan, italy)
mark Crowther (Ontario, Canada)
Bjorn dahlof (New York, USa)
Undurti N. das (Shaker Heights, OH, USa)
Kenneth dickstein (Stavanger, Norway)
Steven m donn (ann arbor, mi, USa)

Joachim W. dudenhausen (Berlin, Germany)
adam dziki (Lodz, Poland)
moses elisaf (ioannina, Greece)
N. a mark estes iii (Boston, USa)
Gerasimos Filippatos (athens, Greece)
Guillermo Garcia-manero (Houston, USa)
mario Gaudino (rome, italy)
andrea r. Genazzani (Pisa, italy)
Bernard J. Gersh (rochester, USa)
m eric Gershwin (davis, USa)
Charles H. Hennekens (Washington, USa)
Gerd Heusch (essen, Germany)
Walter H. Hörl (Vienna, austria)
Stein Kaasa (Trondheim, Norway)
Vijay V. Kakkar (London, UK)
Norman m. Kaplan (dallas, USa)
Sverre e. Kjeldsen (Oslo, Norway)
marek L. Kowalski (Lodz, Poland)
Harlan m. Krumholz (New Haven, USa)
Piotr Kuna (Lodz, Poland)
Norbert Lameire (Ghent, Belgium)
Carlo La Vecchia (milan, italy)
Krista Lentine (St. Louis, mO, USa)
amir Lerman (rochester, USa)
Paweł Liberski (Lodz, Poland)
Gregory Y.H. Lip (Liverpool, UK)
Jolanta małyszko (Warsaw, Poland)
Joann e manson (Boston, USa)
maurie markman (Houston, USa)
Uwe mehlhorn (Cologne, Germany)
dimitri P. mikhailidis (London, UK)
Naoyuki miura (Hamamatsu, Japan)
Joanna Narbutt (Lodz, Poland)
Keiji Naruse (Okayama, Japan)
eva Negri (milan, italy)
Grzegorz Opolski (Warsaw, Poland)
Jose m. Ordovas (Boston, USa)
Jean-Paul Ortonne (Nice, France)
Kapil Parakh (Baltimore, USa)
Hendri H. Pas (Groningen, Netherlands)
Fausto J. Pinto (Lisbon, Portugal)
Herman m. van Praag (maastricht, Netherlands)
mahendra rao (Carlsbad, USa)
Kausik K. ray (London, UK)
Giuseppe remuzzi (Bergamo, italy)
robert roberts (Ottawa, Canada)
Bernardo rodriguez-iturbe (maracaibo, Venezuela)
denis roy (montreal, Canada)
Brian m. Salzberg (Pennsylvania, USa)
Ola didrik Saugstad (Oslo, Norway)
Jochen d. Schipke (duesseldorf, Germany)
Yehuda Y. Shoenfeld (Tel-aviv, israel)
alain Simon (Paris, France)
Helmut Sinzinger (Vienna, austria)
Vincent Soriano (madrid, Spain)
michał Stachowiak (Buffalo, USa)
Nicholas J. Talley (Jacksonville, USa)
Lip-Bun Tan (Leeds, UK)
eric J. Topol (La Jolla, USa)
anetta Undas (Cracow, Poland)
Tetsumei Urano (Hamamatsu, Japan)
Panos e. Vardas (Heraklion, Greece)
Jacob Vinten-Johansen (atlanta, USa)
Francesco Visioli (milan, italy)
david Vlahov (New York, USa)
avi a. Weinbroum (Tel aviv, israel)
Wojciech Zareba (New York, USa)
marian Zembala (Zabrze, Poland)
douglas P. Zipes (indianapolis, USa)
Carmine Zoccali (reggio Calabria, italy)
Joseph B. Zwischenberger (Galveston, USa)
Archives of Medical Science
Editor-in-Chief
Maciej Banach, MD, Prof. (Lodz, Poland)
Managing Editor
Marco Proietti, MD, Prof. (Rome, Italy)
Karel Allegaert (Rotterdam, Belgium)
Henedina Antunes (Portugal)
Majid Assadi (Bushehr, Iran)
Kengo Ayabe (Los Angeles, United States)
Dimitros Bogdanos (London, United Kingdom)
Claudia Regina Bonini-Domingos (São José do Rio Preto, Spain)
Alexandru Burlacu (Iasi, Romania)
Ali Cadili (Edmonton, Kanada)
Gunadi (Yogyakarta, Indonesia)
Ayse Cakir Gungor (Canakkale, Turkey)
Erwin Chiquete (Mexico City, Mexico)
Adrian Covic (Iasi, Romania)
Undurti Das (Federal Way, United States)
Anupam Dhasmana (McAllen, United States)
Jolanta Dorszewska (Poznan, Poland)
Sagar Dugani (United States)
Theodosios Filippatos (Greece)
Georgia Gerolouka-Kostopanagiotou (Athens, Greece)
Mojgan_Gharipour (Isfahan, Iran)
Souvik Ghosh (Sapporo, Japan)
Katja Goričar (Ljubljana, Slovenia)
Shinya Goto (Isehara, Japan)
Shafiul Haque (Jazan, Saudi Arabia)
Martin Horvath (Czech Republic)
Ahmed Idbaih (Paris, France)
Aleksandra Jezela-Stanek (Katowice, Poland)
Jacek Jóźwiak (Poland)
Mine Kanat-Pektas (Afyonkarahisar, Turkey)
Niki Katsiki (Thessaloniki, Greece)
Co-Editors
Wilbert S. Aronow, MD, Prof. (New York, United States)
Amirhossein Sahebkar, PharmD, PhD (Mashhad, Iran)
Statistics Editor
Małgorzata Misztal, PhD (Lodz, Poland)
Section Editors
Haseeb A. Khan (Riyadh, Saudi Arabia)
Veronika Kralj-Iglič (Ljubljana, Slovenia)
Martina Krüger (Dusseldorf, Germany)
Metka Lenassi (Slovenia)
Fenge Li (Texas, USA)
Ana Lleo (Rozzano, Italy)
Marios Lukas (St. George, Grenada)
Saurav Mallik (Boston, United States)
Giovanni Mariscalco (Varese, Italy)
Fleur Mason (Göttingen, Germany)
Michail Matalliotakis (Crete, Greece)
Colm McAlinden (United Kingdom)
Muhammad Miftahussurur (Surabaya, Indonesia)
Irina Milisav (Ljubljana, Slovenia)
Peter Müller (Munich, Germany)
Seyed Mohammad Nabavi (Teheran, Iran)
Thomas Niethammer (Germany)
Dragana Nikolic (Italy)
Ionut Nistor (Romania)
Demostenes Panagiotakos (Kalithea, Athens, Greece)
Nikolaos Papanas (Greece)
Narasimha Reddy Parine (Riyadh, Saudi Arabia)
Panagiotis Peitsidis (Southend, United Kingdom)
Leonard Peruski (Guatemala, Guatemala)
Antonio Picardi (Rome, Italy)
Gabriele Piffaretti (Varese, Italy)
Adam Reich (Rzeszów, Poland)
Kannan RR Rengasamy (Seoul, South Korea)
Language Editor
Richard Ashcroft (Oxford, UK)
Addresses
Lucie Riedlbauchova (Czech Republic)
Manfredi Rizzo (Palermo, Italy)
Lisa Qia Rong (New York, United States)
Paweł Rzymski (Poznan, Poland)
Piotr Rzymski (Poland)
Khaled Saad (Assiut, Egypt)
Pierre Sabouret (Paris, France)
Kamal Kant Sahu (Worcester, USA)
Motoaki Sano (Japan)
Alessandra Scaparrotta (Chieti, Italy)
Consolato Maria Sergi (Alberta and Ontario, Canada)
Eduard Shantsila (Birmingham, United Kingdom)
Bartosz Simonides (Warsaw, Poland)
Stanislaw Surma (Katowice, Poland)
Zheng Zachory Wei (Atlanta, USA)
Jelena Vekic (Serbia)
Josef Veselka (Prague, Czech Republic)
Jean-Louis Vincent (Brussels, Belgium)
Niels Voigt (Göttingen, Germany)
Stephan von Haehling (Göttingen, Germany)
Chengming Wang (Auburn, USA)
Jiexiong Xie (Merelbeke, Belgium)
İlhan Yaylim (Istanbul, Turkey)
Christos Zavos (Thessaloniki, Greece)
Hongliang Zhang (Beijing, China)
Lvyun Zhu (Hunan, China)
Natalya Zinkevich (Waukesha, United States)
Dorota Zozulińska-Ziółkiewicz (Poznan, Poland)
Editor-in-Chief
Prof. Maciej Banach, MD, PhD
Polish Mother’s Memorial Hospital Research Institute (PMMHRI)
Rzgowska 281/289, 93-338 Lodz, Poland
Fax: +48 42 271 11 24
ArchivesofMedicalScience
Managing Editor
Prof. Marco Proietti
Department of Clinical Sciences and Community Health
University of Milan
Via della Commenda
19,20122, Milan, Italy
E-mail: marco.proietti@unimi.it
AMS is indexed in ISI Master Journal List, ISI Science Citation Index Expanded/ISI Web of Science, PubMed Central/PubMed, EMBASE, Chemical Abstracts CAS, CAB Abstracts, Scopus, Index Copernicus (IC), National Library of Medicine (NML), Directory of Open Access Journals (DOAJ), Academic Journals Database, Global Health Databases, MNISW, J-Gate, OpenMED and Polish Medical Library (GBL). Impact Factor 2021: 3.707 , IC Valued: 176.07 pts, MEiN Value: 100 pts, Google Index H5: 37, CiteScore 2021: 5.3
President of the Management Board of the Termedia Publishing House
Marketing and Advertising Department
Anita Jóźwiak
Termedia Publishing House
Kleeberga 2, 61-615 Poznań, Poland
Phone/fax: +48 61 822 77 81
E-mail: termedia@termedia.pl
www.termedia.pl
www.ams.termedia.pl
Contact
E-mail: s.sekula@termedia.pl
Circulation of 1000 copies
Janusz Michalak
Production Editor
Marzena Demska
E-mail: m.demska@termedia.pl
Phone: +48 61 822 77 81 ext. 500
E-mail: a.jozwiak@termedia.pl
Distribution Subscription Department
Phone: +48 61 656 22 02
Archives of Medical Science was founded by Prof. Maciej Banach & Termedia Publishing House. Archives of Medical Science is supported and published by Termedia Publishing House.
Copyright: © 2023 Termedia & Banach. This is an Open Access journal, all articles are distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY-NC-SA 4.0) License (http://creativecommons.org/licenses/by-nc-sa/4.0/), allowing third parties to copy and redistribute the material in any medium or format and to remix, transform, and build upon the material, provided the original work is properly cited and states its license. The advertisers shall be liable for the contents of advertisement placed in Archives of Medical Science. Advertisements of prescription drugs are intended only for physicians licensed to prescribe them.
Clinical research
Cardiology/Editor’choice
305 Treatment goal attainment for secondary prevention in coronary patients with or without diabetes mellitus – Polish multicenter study POLASPIRE
M. Haberka, P. Jankowski, D.A. Kosior, M. Szpakowicz, K. Szóstak-Janiak, P. Kozieł, A. Krzykwa, M. Łapińska, M. Setny, K. Kamiński, A. Kubica, D. de Bacquer, G. de Backer, K. Kotseva, D. Wood, A. Pająk, D. Czarnecka, and Z. Gąsior (Poland, Belgium, Ireland)
313 Telomere-telomerase system status in patients with acute myocardial infarction with ST-segment elevation – relationship with oxidative stress
A. Vukašinović, B. Ostanek, A. Klisic, S. Kafedžić, M. Zdravković, I. Ilić, M. Sopić, S. Hinić, M. Stefanović, L. Memon, B. Gaković, N. Bogavac-Stanojević, V. Spasojević-Kalimanovska, J. Marc, A.N. Nešković, and J. Kotur-Stevuljević (Serbia, Slovenia, Montenegro)
Acute Coronary Syndrome
324 Twelve-month clinical results from the new cobalt-chromium sirolimus-eluting dedicated bifurcation stent BiOSS LIM C Registry
R.J. Gil, A. Kern, T. Pawłowski and J. Bil (Poland)
Thrombosis and Hemostasis
331 Percutaneous left atrial appendage closure for stroke prevention in patients with chronic renal disease
A. Lind, O. Azizy, J. Lortz, A. Janosi, T. Rassaf and C. Rammos (Germany)
Pulmonology
337 What is the right moment for noninvasive ventilation in amyotrophic lateral sclerosis?

J. Maskovic, A. Ilic, V. Zugic, Z. Stevic and M.I. Stjepanovic (Serbia)
Oncology
343 Prognostic value of XIAP and survivin expression in locally advanced breast cancer patients treated with anthracycline-based neoadjuvant chemotherapy
P. Pluta, D. Jesionek-Kupnicka, A. Pluta, K. Brzozowski, M. Braun, J. Kubicka-Wołkowska and J. Piekarski (Poland)
355 Prognostic value of midkine, syndecan-1, hyaluronan synthase-2, sestrin-1, laminin subunit alpha-4 and fibulin-3 for malignant pleural mesothelioma
H. Akgun, S. Metintas, G. Ak, S. Demirkol Canlı, M. Isbilen, A.O. Gure and M. Metintas (Turkey)
General Surgery
365 Can the POLARS tool accurately predict low anterior resection syndrome in rectal cancer patients undergoing laparoscopic resection?
P. Bogacki, J. Krzak, T. Gach, W. Szwed and M. Szura (Poland, Denmark) Paediatrics/Editor’choice
371 The prevalence of depression in children and adolescents under 18 years of age treated for mental disorders in Poland between 2005 and 2016
M. Lisiecka-Biełanowicz, D. Biechowska, E. Orłowska and B. Molenda (Poland)
381 How common is attention deficit hyperactivity disorder (ADHD) in a cohort of children with functional constipation, and does ADHD treatment improve functional constipation?
H. Bazmamoun, A. Momeni, L. Jahangard, F. Asnaashari and N. Pezeshki (Iran)
Radiology
385 How can we use positron emission tomography/computed tomography more accurately for characterization of asbestos-related pleural thickening?
F. Selcuk Simsek, M. Cakmak, D. Kuslu, T.A. Balci, E. In, I.H. Ozercan and Y. Narin (Turkey)
Arch Med Sci 2, 1st March / 2023 V
Contents
Diagnostics, laboratory
392 Platelet reactivity expressed as a novel platelet reactivity score is associated with higher inflammatory state after coronary artery bypass grafting
M. Wilczyński, M. Krejca, P. Stepinski, M. Rozalski and J. Golanski (Poland)
401 Integrated analysis of microbiota with bile acids for the phototherapy treatment of neonatal jaundice
K. Zhang, S. Fan, A. Lv, Y. Ma, X. Fang and J. Zhang (China)
Systematic review and meta-analysis
Nephrology
411 Clinical efficacy and safety of rituximab with membranous nephropathy: a meta-analysis
H. Zhong, H.Y. Li, T. Zhou and Z. Zhong (China)
Experimental research
Cardiology
420 Dichloroacetate ameliorates myocardial ischemia-reperfusion injury via regulating autophagy and glucose homeostasis
S. Li, B. Xie, W. Zhang and T. Li (China)
Obstetrics and Gynecology
430 Mechanisms underlying the improvement of preeclampsia through salvianolic acid B-regulated miRNA-155/CXCR4
C. Zhang, X. Han and X. Wang (China)
448 Evaluation of protective effects of GnRH agonist or antagonist on ovarian reserve with anti-Müllerian hormone and histological analysis in a rat model using cisplatin
M. Tas, G. Oner, P. Ulug, A. Yavuz and B. Ozcelik (Turkey)
Osteoporosis
452 Amarogentin promotes osteoblast differentiation in oestrogen-deficiency-induced osteoporosis rats by modulating the Nrf-2/MAPK/ERK signalling pathway
S. Li, X. Li, F. He, R. Jiao, S. Zhang and Z. Li (China)
State of the art paper
Women’s Cardiology/Editor’choice
458 Menopause and women’s cardiovascular health: is it really an obvious relationship?
K. Ryczkowska, W. Adach, K. Janikowski, M. Banach and A. Bielecka-Dabrowa (Poland)
Endocrinology and Metabolic Disorders
467 The role of selected adipokines in tumorigenesis and metabolic disorders in patients with adrenal tumors
A. Babinska, P. Kmieć and K. Sworczak (Poland)
Basic research
Oncology
478 Long non-coding RNA LINC00336 as an independent prognostic indicator and an oncogenic lncRNA in bladder cancer
X. Guo, N. Liu and M. Liu (China)
488 Induction of apoptosis in RL95-2 human endometrial cancer cells by combination treatment with docosahexaenoic acid and triacsin C
S.H. Chung, H.H. Lee, Y.S. Kim, K. Song and T.H. Kim (Republic of Korea)
VI Arch Med Sci 2, 1st March / 2023
Urology
499 Expression differences between proteins responsible for DNA damage repair according to the Gleason grade as a new heterogeneity marker in prostate cancer
D. Jaworski, A. Gzil, P. Antosik, I. Zarębska, J. Dominiak, I. Neska-Długosz, A. Kasperska, D. Grzanka, and Ł. Szylberg (Poland)
Research letters
Cardiology
507 The emerging role of ferroptosis in myocardial fibrosis of atrial fibrillation
H. Yue, Y. Zhan, Z. Zhang, W. Liang and Z. Wu (China)
Heart Failure
513 Eicosanoids in human heart failure: pilot study of plasma epoxyeicosatrienoic and dihydroxyeicosatrienoic acid levels
P. Kala, T. Hnat, K. Padrova, K. Kotaška and J. Veselka (Czech Republic)
Neurology
518 Impact of platelet endothelial aggregation receptor 1 genotypes and DNA methylation on platelet reactivity in patients with recurrent ischemic stroke treated with clopidogrel
J. Yang, Z. Bao, G. Hu, X. Luo and Z. Zhao (China)
Hematology
523 Determining the current prevalence of b-thalassemia variants in Jordan
D. Hasan, A. Al Tibi, G. Burghel and A. Abdelnour (Jordan, UK)
Letters to the Editor
Diabetology
528 Should SGLT2 inhibitors be prescribed in all diabetic type 2 patients?
M. Bernardi, L. Spadafora, M. Galli, G. Biondi-Zoccai and P. Sabouret (Italy, France)
Rheumatology
532 Involvement of anterior chest structures accompanied with chest pain in patients with gout
G. Wang, Y. Luo, B. Li, Z. Wen and J. Li (China)
536 Scleroderma renal crisis with posterior reversible encephalopathy syndrome
G. Wang, Y. Luo, J. Li, F. Yao and Z. Wen (China)
539 Seronegative rheumatoid arthritis as the first manifestation of multiple myelomaassociated amyloid arthropathy
G. Wang, N. Zhuo, M. Tang, L. Xue and Z. Liu (China)
542 Hypertrophic osteoarthropathy
G. Wang, M. Tang, L. Xue and Z. Liu (China)
544 Mesenteric vasculitis with inferior vena cava thrombosis associated with systemic lupus erythematosus
G. Wang, B. Li, Y. Luo, J. Li and Z. Wen (China)
Otolaryngology
546 Dystrophic calcification in the masseter muscle
A. Walulik, M. Rutkowska, P. Gajdzis and P. Czarnecka (Poland)
550 Effect of different surgical modalities on swallowing-related quality of life in patients with glottic laryngeal squamous cell carcinoma: how should we choose?
N. Shao, X. Wei, Y. Zhang, H. Luo, Y. Su, L. Liang, B. Chen, N. Li, X. Ren and H. Yang (China)
Arch Med Sci 2, 1st March / 2023 VII
Retraction notices
555 Retracted: Antiproliferative and apoptotic activity of glycyrrhizinic acid in MCF-7 human breast cancer cells and evaluation of its effect on cell cycle, cell migration and m-TOR/PI3K/Akt signalling pathway
556 Retracted: Antitumor and apoptotic effects of 5-methoxypsoralen in U87MG human glioma cells and its effect on cell cycle, autophagy and PI3K/Akt signaling pathway
557 Retracted: MicroRNA-1179 regulates proliferation and chemosensitivity of human ovarian cancer cells by targeting the PTEN-mediated PI3K/AKT signaling pathway
558 Retracted: Long non-coding RNA HOTAIR regulates proliferation, migration and invasion of human cervical cancer cells by modulating expression of MAPK1
Treatment goal attainment for secondary prevention in coronary patients with or without diabetes mellitus –Polish multicenter study POLASPIRE
Maciej Haberka1, Piotr Jankowski2, Dariusz A. Kosior3,4, Małgorzata Szpakowicz5, Karolina Szóstak-Janiak1, Paweł Kozieł2, Agnieszka Krzykwa4, Magda Łapińska5, Małgorzata Setny4, Karol Kamiński5, Aldona Kubica6, Dirk de Bacquer7, Guy de Backer7, Kornelia Kotseva8, David Wood8, Andrzej Pająk9, Danuta Czarnecka2, Zbigniew Gąsior1
1Department of Cardiology, School of Health Sciences, Medical University of Silesia, Katowice, Poland

2I Department of Cardiology, Interventional Electrocardiology and Hypertension, Institute of Cardiology, Jagiellonian University Medical College, Krakow, Poland
3Mossakowski Medical Research Centre, Polish Academy of Sciences, Warsaw, Poland
4Department of Cardiology and Hypertension with the Electrophysiological Lab, Central Research Hospital the Ministry of the Interior and Administration, Warsaw, Poland
5Department of Population Medicine and Civilization Diseases Prevention, Medical University of Bialystok, Bialystok, Poland
6Department of Health Promotion, Collegium Medicum, Nicolaus Copernicus University, Bydgoszcz, Poland
7Department of Public Health and Primary Care, Ghent University, Belgium
8Cardiovascular Medicine, National Heart and Lung Institute, Imperial College London and National Institute of Preventive Cardiology, National University of Ireland-Galway, Galway, Ireland
9Department of Clinical Epidemiology and Population Studies, Institute of Public Health, Jagiellonian University Medical College, Krakow, Poland
Submitted: 25 July 2019; Accepted: 22 September 2019
Online publication: 23 January 2020
Arch Med Sci 2023; 19 (2): 305–312
DOI: https://doi.org/10.5114/aoms.2020.92558
Copyright © 2020 Termedia & Banach
Abstract
Introduction: Cardiovascular disease is still a leading cause of death in Poland and across Europe. The aim of this study was to assess the attainment of the main treatment goals for secondary cardiovascular prevention in coronary patients with or without diabetes mellitus (DM) in Poland.
Material and methods: The study group included 1026 patients (65.5 ±9 y.o.; males: 72%) included at least 6 months after the index hospitalisation for myocardial infarction, unstable angina, elective percutaneous coronary intervention or coronary artery bypass surgery. The target and treatment goals were defined according to the 2016 European Society of Cardiology guidelines on cardiovascular prevention.
Results: Patients with DM ( n = 332; 32%) were slightly older compared to non-diabetic ( n = 694) individuals (67.2 ±7 vs. 64.6 ±9 years old; p < 0.0001). The DM goal was achieved in 196 patients (60%). The rate of primary (LDL: 51% vs. 35%; p < 0.0001) and secondary (non-HDL: 56% vs. 48%; p < 0.02) goal attainment was higher in DM(+) compared to DM(–) patients. The rate of target blood pressure was lower in DM(+) than in normoglycemic patients (52% vs. 61% at < 140/90 mm Hg, p < 0.01. As expected, goal achievement of normal weight (9.5% vs. 19%; p < 0.0001) and waist circumference (7% vs. 15%; p < 0.001) was lower in diabetic patients and the rate of regular physical activity was similar (DM+ 12% vs. DM– 14%; p = ns). Finally, there was no difference in active smokers (DM+ 23% vs. DM– 22%; p = ns).
Corresponding author: Maciej Haberka MD PhD
Department of Cardiology
School of Health Sciences
Medical University of Silesia
45/47 Ziołowa St.
40-635 Katowice, Poland
E-mail: mhaberka@op.pl
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Clinical research Cardiology
Conclusions: Great majority of Polish patients in secondary prevention do not achieve treatment goals. Although lipid goals attainment is better in DM and the rate of smokers is similar, the management of all risk factors needs to be improved.
Key words: mischemic heart disease, coronary artery disease, diabetes, obesity, secondary prevention, goal attainment.
Introduction
Cardiovascular disease (CVD) is still a leading cause of death in Poland and across Europe [1]. Diabetes mellitus (DM) is a main risk factor for coronary artery disease (CAD) [2], which is associated with a more complex multivessel CAD [3] and worse clinical prognosis [4]. Therefore patients with CAD and DM require optimal medical therapy and high rates of treatment goal attainment [5]. Despite recent progress in methods of invasive treatment of CAD and its better availability [6], the 1-year mortality rate following myocardial infarction is still relatively high – 10% [7, 8]. Several studies and registries suggest that more efforts should be made to improve secondary CVD prevention to achieve better control of risk factors and lifestyle modifications [9–12].
The European Society of Cardiology (ESC) published guidelines on CVD prevention in clinical practice in 2016 [5] promoting clinical recommendations and providing target treatment goals. The available data on the recent efficacy of secondary prevention in Poland are scarce and limited to single measures. Therefore, the aim of our study was to provide a comprehensive assessment of the attainment of main treatment goals in secondary prevention in coronary patients with or without DM.
Material and methods
POLASPIRE was a multicenter, cross-sectional study performed among Polish patients from 4 geographical areas (Krakow, Katowice, Bialystok, Warszawa) and 14 departments of cardiology representing various reference levels, including departments within medical universities and secondary care hospitals. The study had two parts performed independently in all departments (2017–2018): retrospective identification of patients (eligibility criteria) from hospital discharge lists of 14 departments and a prospective visit of study patients performed in leading centers of 4 geographical regions. All consecutive patients, men and women (≥ 18 years and < 80 years of age at the time of their index event or procedure) hospitalized more than 6 months earlier in one of the 14 departments for acute myocardial infarction, unstable angina, elective percutaneous coronary intervention (PCI) or coronary artery bypass surgery (CABG) were identified and invited for a study visit. The aim was to obtain prospective survey data on at least
200 patients in each geographical area using similar standardized methods and instruments according to the manufacturer’s manual in all centers. All parts of the study were performed by centrally trained research staff. Retrospective data regarding demographic information, clinical diagnoses, CV diseases and risk factors or laboratory tests were obtained from medical records. The study visit provided updated data on CV risk factors, attainment of treatment goals, medications and lifestyle. The visit included an interview with a patient using a detailed questionnaires of the European Action on Secondary Prevention through Intervention to Reduce Events (EUROASPIRE V) registry translated and validated for Poland. Additional available medical records were used for information on CV risk factors and current treatment. Moreover, the following measurements were performed during the visit: office blood pressure (mean value from two measurements), height and weight, waist circumference. Fasting venous blood was drawn for serum glycated hemoglobin (HbA1c), total cholesterol (TCH), high-density lipoprotein (HDL-C), triglycerides (TG) and low-density lipoprotein (LDL-C) was calculated according to Friedewald’s formula [13]. Definitions of risk factors and target treatment goals were based on the 2016 European Society of Cardiology guidelines on CVD prevention [5].
The diagnosis of dyslipidaemia was defined as abnormal plasma lipid levels (TCH > 190 mg/dl, LDL cholesterol > 115 mg/dl, TG > 150 mg/dl, HDL cholesterol < 40 mg/dl in men and < 50 mg/dl in women) or prior diagnosis and/or treatment [14]. Overweight was defined as a body mass index (BMI) ≥ 25 < 30 kg/m2 and obesity as a BMI ≥ 30 kg/m². Waist circumference (WC) was measured using a tape applied at the point midway in the mid-axillary line between the lowest rim of the rib cage and the superior iliac crest of the patient standing. Abdominal overweight was defined as a WC of ≥ 80 cm for women and ≥ 94 cm for men. Arterial hypertension was defined as systolic blood pressure (SBP) ≥ 140 mm Hg and/or diastolic blood pressure (DBP) ≥ 90 mm Hg. Smoking was defined at the time of interview and physical activity was estimated in an interview-based questionnaire. Chronic kidney disease was included in the patient’s characteristics based on a prior diagnosis and/or treatment on the retrospective discharge list from the index hospitalization [15]. Total cholesterol, HDL-C and
306 Arch Med Sci 2, 1st March / 2023
M. Haberka, P. Jankowski, D.A. Kosior, M. Szpakowicz, K. Szóstak-Janiak, P. Kozieł, A. Krzykwa, M. Łapińska, M. Setny, K. Kamiński, A. Kubica, D. de Bacquer, G. de Backer, K. Kotseva, D. Wood, A. Pająk, D. Czarnecka, Z. Gąsior
TG were analyzed in serum, and HbA1c in whole blood. The main aim and the outcome measure of this analysis was the rate of patients with IHD and DM (known and treated since the index hospitalization) achieving the lifestyle, risk factors and therapeutic targets in comparison with individuals with IHD and not known DM. The study group was divided into two subgroups with (DM+) and without known DM (DM–) based on the retrospective medical records, including the discharge hospital documents (diagnosis and/or treatment).
The following goals were defined according to the 2016 guidelines [5]: controlled DM (HbA1c < 7.0%), lipid primary (LDL < 70 mg/dl) and secondary goal (non-HDL < 100 mg/dl), normal blood pressure (SBP < 140 and DBP < 90 mm Hg for all), normal BMI (20.0–25.0 kg/m), normal WC (women < 80 cm or men < 94 cm), smoking abstinence and regular physical activity with an equivalent of at least intensive activity for 20 min twice a week. The total number of attained goals was the sum of the above defined. An additional result for the attainment of BP target < 140/85 mm Hg was provided in the group with DM.
The coordinators of 4 geographical areas were responsible for obtaining Local Ethics Committees approvals and a written informed consent form was obtained from all the participants and stored in the patient’s file.
Statistical analysis
All results presented in the text, tables and figures are expressed as means ± standard deviation or number and percentage. Figure 1 is the exception and presents a box-and-whisker plot with medians, interquartile range and extreme values. The normality of distributions was analyzed using the Kolmogorov-Smirnov test. Baseline clinical parameters and the measures were compared between the subgroups using the t-tests for normally distributed continuous variables (Student’s t-test); in case of non-normal distribution, the Mann-Whitney U test was used. The Pearson χ2 test was applied to all categorical variables. A value p < 0.05 was considered statistically significant. Statistical analysis was undertaken using MedCalc software (version 19.0.5, Belgium).
Results
Clinical characteristics in patients with and without diabetes mellitus
The study group included 1026 patients (65.5 ±9 years old, male/female: 72%/28%), who accepted the invitation for the interview and the examination > 6 months after the index hospitalization for acute myocardial infarction (39%), unstable angina (22%), elective percutaneous coronary in-
tervention (35%) or coronary artery bypass surgery (4%). The study group represented a population of a very-high CV risk with several risk factors: dyslipidemia (100%), hypertension (81%), DM (32%), overweight (42.5%), obesity (43%) and active tobacco smoking (31%). Patients with known DM at the index hospitalization were included in the DM(+) group.
Patients DM(+) (n = 332; 32%) were slightly older compared to DM(–) individuals (67.2 ±7 vs. 64.6 ±9 years; p < 0.0001) with similar gender distribution (p = ns). Most patients with DM used oral antihyperglycemic medications (79%) with a minority treated with insulin (10%) or both (11%). The mean number of antihypertensive drugs was significantly increased in patients with DM (DM+ 2.93 ±0.66 vs. DM– 2.54 ±0.8; p < 0.0001). The clinical characteristics of the study group based on the retrospective hospital discharge list and medical records with the lipid-lowering treatment are presented in Table I.
There were 44 patients (6.3%) with undiagnosed DM (no DM or antihyperglycemic agents in medical records of the index event). Most of them (41) were diagnosed with DM in the outpatient clinics (oral glucose tolerance test or fasting plasma glucose) and were given oral antihyperglycemic drugs. Moreover, 246 patients (35%) in the DM(–) group had increased fasting plasma glucose at the prospective study visit suggestive of impaired fasting glucose.
Treatment goal attainment
The follow-up visit showed that patients with DM had significantly higher SBP, BMI, WC, TG and lower LDL-C and HDL-C compared to individuals without DM (Table II).
Figure 1. Total number of the main therapeutic goals attained. Box-and-whisker plot showing median, interquartile range (1st and 3rd quartiles) and extreme values. Therapeutic goals: low-density lipoproteins cholesterol < 70 mg/dl; non-high-density lipoprotein < 100 mg/dl, smoking abstinence, blood pressure < 140/90 mm Hg, regular physical activity = at least 20 min twice a week of intensive activity, normal body mass index = 20.0–25.0 kg/m², normal waist circumference – women < 80 cm or men < 94 cm
Treatment goal attainment for secondary prevention in coronary patients with or without diabetes mellitus – Polish multicenter study POLASPIRE Arch Med Sci 2, 1st March / 2023 307
8 7 6 5 4 3 2 1 0
Diabetes
Number
Diabetes (–)
(+)
Table
Data are presented as mean ± SD or No. (%).
The attainment of particular treatment goals is shown in Figure 2. In brief, the glycemic goal was achieved in 196 patients (60%) (Figure 3).
The rates of primary (LDL-C: 51% vs. 35%; p < 0.0001) and secondary (non-HDL-C: 56% vs. 48%; p < 0.02) lipid goal attainment were higher in DM(+) compared to DM(–) patients, but they had a smaller proportion of normal TG levels (65% vs. 76%; p < 0.001) (Figure 4). The rate of blood pressure < 140/90 mm Hg was lower in DM(+) than in normoglycemic patients (52% vs. 61%; p < 0.01). When the recommended target for patients with DM was used (< 140/85 mm Hg), the rate of target BP in the DM group was even lower (45%).
As expected, goal achievement of normal weight (9.5% vs. 19%; p < 0.0001) and waist circumference (7% vs. 15%; p < 0.001) were lower in diabetic patients. The rate of individuals with regular physical activity was similar and low (DM(+): 12%
vs. DM(–): 14%; p = ns). Finally, the proportions of active smokers were comparable but unacceptably high in both groups (DM(+): 23% vs. DM(–): 22%; p = ns) (Figure 2).
The total number of achieved goals was similar between both subgroups (DM(+): 2.56 ±1.3 vs. DM(–): 2.6 ±1.2; p = 0.6) (Figure 1). However, there was a small difference in total goal achievement among male patients (DM(+): 2.97 ±4.7 vs. DM(–): 2.77 ±1.4; p < 0.001) with no differences between female groups (DM(+) 2.55 ±3.2 vs. DM(–) 2.54 ±1.2; p = 0.9).
Figure 5 presents rates of patients of both groups reaching particular number of treatment goals.
Most patients with DM reported having a regular glucose check-up (88%) and a regular BP measure (DM+: 91% vs. DM–: 81%; p < 0.05). Only one-third of patients reported following a specific lipid-lowering diet (DM+: 33% vs. DM–: 28%;
308 Arch Med Sci 2, 1st March / 2023
M. Haberka, P. Jankowski, D.A. Kosior, M. Szpakowicz, K. Szóstak-Janiak, P. Kozieł, A. Krzykwa, M. Łapińska, M. Setny, K. Kamiński, A. Kubica, D. de Bacquer, G. de Backer, K. Kotseva, D. Wood, A. Pająk, D. Czarnecka, Z. Gąsior
Parameter Ischemic heart disease Diabetes (+) ( n = 332) Diabetes (–) ( n = 694) P -value Systolic blood pressure [mm Hg] 138 ±21 132 ±18 < 0.0001 Diastolic blood pressure [mm Hg] 80 ±12 80 ±10 1.0 Low-density lipoprotein cholesterol [mg/dl] 79 ±31 86 ±37 0.003 High-density lipoprotein cholesterol [mg/dl] 47.6 ±14.3 52 ±14.5 < 0.0001 Triglycerides [mg/dl] 143 ±77 125 ±90 0.002 Body mass index [kg/m²] 30.1 ±4.6 28.9 ±4.5 0.0001 Waist circumference [cm] 105.6 ±11.7 100.8 ±13 < 0.0001
Table II. Clinical assessment on follow-up visit in patients with and without diabetes mellitus
Parameter Ischemic heart disease Diabetes (+) ( n = 332) Diabetes (–) ( n = 694) P -value Clinical characteristics: Patients 332 (32%) 694 (68%) < 0.0001 Age [years] 67.2 ±7 64.6 ±9 < 0.0001 Males 233 (70%) 499 (72%) 0.6 Dyslipidemia 332 (100%) 694 (100%) 1.0 Hypertension 298 (89.8%) 637 (91.7%) 0.3 Overweight 101 (31%) 303 (43%) 0.0001 Obesity 194 (59%) 260 (37%) 0.0001 Chronic kidney disease 33 (9.6%) 32 (4.6%) 0.002 Lipid-lowering treatment: Statins 289 (89%) 623 (90%) 0.6 Atorvastatin 218 (65%) 441 (63%) 0.5 Rosuvastatin 64 (19%) 160 (23%) 0.14 Simvastatin 14 (4.2%) 19 (2.7%) 0.2 Fibrates 19 (5.8%) 17 (2.4%) 0.005 Ezetimibe 7 (2.1%) 20 (2.9%) 0.45
± SD or No. (%).
I. Clinical characteristics of study patients with and without diabetes mellitus
Data are presented as mean
p < 0.05). The particular lipid-lowering treatment is presented in Table I. The proportion of patients who were able to quit smoking just after the in-
dex event was higher in the DM(–) group (DM+: 28.5% vs. 36.6%; p < 0.05).
The proportion of patients who attempted to attain their weight was higher in DM patients (DM(+): 67.8% vs. DM(–): 60%; p = 0.01) and that of individuals who attempted to lose weight was
PhysicalactivityNosmokingWC<80cm(F) orWC<94cm(M)
of patients with and without diabetes mellitus reaching different target goals of low-density lipoprotein cholesterol (A) and non-high-density lipoprotein cholesterol (B)
goals
of therapeutic goals attained in patients with (A) and without (B) diabetes mellitus. Therapeutic goals: low-density lipoproteins cholesterol < 70 mg/dl; non-high-density lipoprotein < 100 mg/dl, smoking abstinence, blood pressure< 140/90 mm Hg, regular physical activity = at least 20 min twice a week of intensive activity, normal body mass index = 20.0–25.0 kg/m², normal waist circumference – women < 80 cm or men < 94 cm and HbA1c < 7.0% for patients with diabetes mellitus
Treatment goal attainment for secondary prevention in coronary patients with or without diabetes mellitus – Polish multicenter study POLASPIRE Arch Med Sci 2, 1st March / 2023 309
0 1 2 3 4 5 6 7 8 Total number of
attainment 0 1 2 3 4 5 6 7 8 Total number of goals attainment 30 25 20 15 10 5 0 Relative frequency (%) A B 30 25 20 15 10 5 0 Relative frequency (%)
Figure 5. Total number
100 90 80 70 60 50 40 30 20 10 0 (%) Diabetes (+) Diabetes (–) < 70 mg/dl < 70–99 mg/dl ≥ 100 mg/dl < 100 mg/dl < 100–129 mg/dl ≥ 130 mg/dl Diabetes (+) Diabetes (–) 100 90 80 70 60 50 40 30 20 10 0 (%) A B 100 90 80 70 60 50 40 30 20 10 0 (%)
Figure 4. Proportion
#p < 0.05 DM(+) DM(–) 12 12 78.5 76.6 15.1 7.1 62.5 40.5 19 9.5 61 45 76 65 48 56 35 51 61 0
Figure 2. Therapeutic goal achievements in patients with and without diabetes mellitus
BMI=20–30BMI=20–25 DM(+)BPDM(–)<140/90;<140/85mmHgTG<150mg%Non-HDL<100mg%LDL<70mg%HbA1c <7.0%
40 35 30 25 20 15 10 5 0 Relative frequency (%) 4 5 6 7 8 9 10 11 12 13 14 15 Diabetes control – HbA1c
Figure 3. Diabetes control: HbA1c in patients with diabetes mellitus with the relative frequency in the study group
similar in both groups (DM(+): 37.6% vs. DM(–): 33%; p = 0.15). The proportion of patients reporting engagement in physical activity aimed at weight loss was low and similar between both subgroups (DM(+): 21% vs. DM(–): 20.5%; p = 0.85).
Discussion
Our study of goal attainment in coronary patients with or without DM provided several important findings. First, despite a very high CV risk, the mean number of achieved goals was low in patients with and without DM. Second, diabetic or lipid goals revealed moderate rates of attainment in subjects with DM. Third, BMI, WC and physical activity revealed poor control, especially in DM patients. Fourth, about 6% (44 patients) of participants had previously undetected DM. Finally, drug therapies of dyslipidemia and DM are not optimal and need to be improved.
We present the most recent and comprehensive findings on the attainment of therapeutic goals in Polish patients since the ESC 2016 guidelines [5].
Our study sample was a relatively large group of patients with myocardial infarction or PCI as major index events. Patients with DM constituted one third of all individuals, with slightly higher mean age, similar gender distribution and significantly increased rates of obesity and CKD compared to non-DM patients. The great majority of patients with DM were treated with oral antihyperglycemic medication, but the target HbA1c was reached in only 60%. Twenty-nine percent of all participants in the recent EUROASPIRE-V registry (EAV) [9] had DM with a higher rate in insulin treatment (EAV: 32%) and slightly lower rate of patients with HbA1c target (54%).
There were 6.3% of patients with undetected DM during the index event hospitalization, which was mostly diagnosed in ambulatory outpatients. This screening failure was a cause of delay in diagnosis and more intensive treatment or lifestyle modifications. Moreover, one-third of patients in the DM(–) group had increased fasting plasma glucose at the prospective visit, suggesting a pre-diabetes state. This is even more interesting and important as those individuals would need intensive lifestyle modification to prevent or delay development of DM. Given that most patients in both groups had overweight or obesity and did not reach the recommended physical activity target, it is very probable that a considerable number of those patients will develop DM in the future. Undetected pre-diabetes or DM is quite common in patients with IHD [16] and it is associated with an unfavorable prognosis [17]. HbA1c is a test historically used for glycemic control, which helps to identify individuals with increased risk of microvascular complications [18].
The target BP was achieved in less than half of the patients with DM in spite of more intensive antihypertensive therapy. Additionally, the rates of CKD and obesity were significantly higher in patients with DM compared to non-DM patients. It suggests that hypertension is more advanced and difficult to control compared to normoglycemic patients [19, 20].
The rates of primary and secondary lipid goal attainment were significantly higher in patients with DM compared to non-DM subjects. Still, the LDL target was achieved only in one in two (DM+) or three (DM–) patients. There were no differences in statin use between the two groups. In spite of a very high CV risk of all patients, rosuvastatin was used only in one fifth of patients and atorvastatin was the most popular lipid-lowering drug. The prevalence of ezetimibe was very low in both subgroups and fibrates were used more frequently in DM. Finally, the rate of hypertriglyceridemia was higher in patients with DM. Only 1 in 3 patients used a specific lipidlowering diet with a slightly better rate among diabetic patients. Those findings are consistent with previous reports on the mechanisms of dyslipidemia in DM [21]. Obesity and DM are associated mainly with harmful changes in the quality (not the quantity) of LDL particles and higher levels of triglycerides [22]. This may explain better rates of LDL-C and non-HDL-C goal attainment in patients with DM, while scheduled lipid-lowering therapy was similar between both subgroups. Another potential explanation could be better real compliance of individuals with DM to medical recommendations. In the EAV study, the rates of LDL goal achievement in all participants (29%) and patients with DM (39%) were even worse compared to our study groups [9]. Moreover, the results of the EA-IV [23] focused on patients with a previously known DM showed a similar attainment of BP target < 140/ 90 mm Hg (53%), HbA1c goal (53%) but significantly lower rate of LDL-C goal achievement (28%).
As expected, the rates of lifestyle goal attainment were alarming in both groups, especially in subjects with DM. An unhealthy lifestyle is a major risk factor for the development of DM [24]. Most patients reported making an attempt to maintain their weight target, but only one third of both subgroups reported aiming at weight loss. The number of patients reporting engagement in physical activity in order to lose weight was very small and similar in both subgroups. The rates of overweight and obesity in our study group with DM were higher compared to the overall rates in EAV (overweight 44%, obesity 38%) [9]. Although patients with an early stage of obesity without vascular or metabolic complications may have similar prognosis to non-obese individuals [25], obesity is the most important factor leading to DM.
310 Arch Med Sci 2, 1st March / 2023
M. Haberka, P. Jankowski, D.A. Kosior, M. Szpakowicz, K. Szóstak-Janiak, P. Kozieł, A. Krzykwa, M. Łapińska, M. Setny, K. Kamiński, A. Kubica, D. de Bacquer, G. de Backer, K. Kotseva, D. Wood, A. Pająk, D. Czarnecka, Z. Gąsior
Our study provided the most recent results on a real-life therapeutic effects in secondary prevention among Polish patients. The main strength of our multicenter study is that it was performed in cardiac centers of various reference levels using standardized interviews rather than retrospective medical records only. The survey was extensive and comparable with results of a large crosssectional EAV study [9].
The final list of medical centers enrolling patients did not cover all the regions of Poland and therefore we cannot state that it was a nationwide epidemiologic study representative for Poland. All the participants were volunteers in a prospective visit and survey of their cardiovascular health. This is an obvious bias as the study group consisted of patients with an interest in CV prevention, suggesting that our results on therapeutic goal attainment in everyday practice might be even worse. Moreover, our invitation was limited only to patients hospitalized due to acute coronary syndrome or a revascularization procedure. Moreover, patients at higher risk who died within the first months after hospitalization might have presented even worse attainment of therapeutic goals. The retrospective data on study patients is based on medical records with all their imperfections, including the diagnosis of DM and the primary allocation to one of the subgroups. For the same reason we do not have patients’ HbA1c taken in the index hospitalization (not performed routinely), which would be used for a comparison with a prospective test. For logistic reasons, we did not perform OGTT at the prospective visit in all patients, which limits our knowledge on the current glucose state in the subgroup without DM.
In conclusion, this study provides the most recent and comprehensive results on secondary prevention among Polish coronary patients. A great majority of patients with DM in secondary prevention do not achieve treatment goals, particularly regarding lifestyles. Although lipid goal attainment is better in DM, the management of all risk factors needs to be improved. Routine screening for DM in coronary patients without known DM should become routine. Patients with DM need more intensive DM treatment as only 60% reached the diabetic goal. Smoking, obesity and low physical activity are the most important adverse lifestyles to be improved in both patients with and without DM.
Conflict of interest
The authors declare no conflict of interest.
2. Center for Disease Control and Prevention. National diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention; 2011. www.cdc.gov/diabetes/pubs/pdf/ndfs_ 2011.pdf (Accessed: May 2019)
3. Norhammar A, Malmberg K, Diderholm E, et al. Diabetes mellitus: the major risk factor in unstable coronary artery disease even after consideration of the extent of coronary artery disease and benefits of revascularization. J Am Coll Cardiol 2004; 43: 585-91.
4. De Bacquer D, De Smedt D, Kotseva K, et al. Incidence of cardiovascular events in patients with stabilized coronary heart disease: the EUROASPIRE IV follow-up study. Eur J Epidemiol 2019; 34: 247-58.
5. Piepoli MF, Hoes AW, Agewall S, et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J 2016; 37: 2315-81.
6. Kleczyński P, Siudak Z, Dziewierz A, et al. The network of invasive cardiology facilities in Poland in 2016 (data from the ORPKI Polish National Registry). Kardiol Pol 2018; 77: 805-7.
7. Gierlotka M, Zdrojewski T, Wojtyniak B, et al. Incidence, treatment, in-hospital mortality and one-year outcomes of acute myocardial infarction in Poland in 2009-2012 –nationwide AMI-PL database. Kardiol Pol 2015; 73: 14258.
8. Jankowski P, Gąsior M, Gierlotka M, et al. Coordinated care after myocardial infarction. The statement of the Polish Cardiac Society and the Agency for Health Technology Assessment and Tariff System. Kardiol Pol 2016; 74: 800-11.
9. Kotseva K, De Backer G, De Bacquer D, et al. Lifestyle and impact on cardiovascular risk factor control in coronary patients across 27 countries: results from the European Society of Cardiology ESC-EORP EUROASPIRE V registry. Eur J Prev Cardiol 2019; 26: 824-35.
10. Jankowski P, Czarnecka D, Badacz L, et al. Practice setting and secondary prevention of coronary artery disease. Arch Med Sci 2018; 14: 979-87.
11. Kotseva K, De Bacquer D, Jennings C, et al. Time trends in lifestyle, risk factor control, and use of evidence-based medications in patients with coronary heart disease in Europe: results from 3 EUROASPIRE Surveys, 1999–2013. Glob Heart 2017; 12: 315-22.
12. Jernberg T, Hasvold P, Henriksson M, et al. Cardiovascular risk in post-myocardial infarction patients: nationwide real world data demonstrate the importance of a longterm perspective. Eur Heart J 2015; 36: 1163-70.
13. Vujovic A, Kotur-Stevuljevic J, Spasic S, Bujisic N, Martinovic J, Vujovic M. Evaluation of different formulas for LDL-C calculation. Lipids Health Dis 2010; 9: 27-36.
References
1. Wilkins E, Wilson L, Wickramasinghe K, et al. European Cardiovascular Disease Statistics 2017. Brussels: European Heart Network; 2017.
14. Reiner Z, Catapano AL, De Backer G, et al. ESC/EAS Guidelines for the management of dyslipidaemias: the Task Force for the management of dyslipidaemias of the European Society of Cardiology (ESC) and the European Atherosclerosis Society (EAS). Eur Heart J 2011; 32: 1769-818.
15. Kidney Disease: Improving Global Outcomes (KDIGO) CKD Work Group. KDIGO clinical practice guideline for
Treatment goal attainment for secondary prevention in coronary patients with or without diabetes mellitus – Polish multicenter study POLASPIRE Arch Med Sci 2, 1st March / 2023 311
the evaluation and management of chronic kidney disease. Kidney Int Suppl 2013; 3: 1-150.
16. Norhammar A, Tenerz A, Nilsson G, et al. Glucose metabolism in patients with acute myocardial infarction and no previous diagnosis of diabetes mellitus: a prospective study. Lancet 2002; 359: 2140-4.
17. Tamita K, Katayama M, Takagi T, et al. Impact of newly diagnosed abnormal glucose tolerance on long-term prognosis in patients with acute myocardial infarction. Circ J 2007; 71: 834-41.
18. International Expert Committee report on the role of the A1C assay in the diagnosis of diabetes. Diabetes Care 2009; 32: 1327-34.
19. Haberka M, Stolarz-Skrzypek K, Biedroń M, et al. Obesity, visceral fat and hypertension-related complications. Metab Syndr Relat Disord 2018; 16: 521-9.
20. Hall JE, do Carmo JM, da Silva AA, Wang Z, Hall ME. Obesity, kidney dysfunction and hypertension: mechanistic links. Nat Rev Nephrol 2019; 15: 367-85.
21. Grundy SM. Small LDL, atherogenic dyslipidemia and the metabolic syndrome. Circulation 1997; 95: 1-4.
22. Haberka M, Okopień B, Gąsior Z. Obesity, ultrasound indexes of fat depots and lipid goal attainment in patients with high and very high cardiovascular risk: a novel approach towards better risk reduction. Nutr Metab Cardiovasc Dis 2016; 26: 123-33.
23. Gyberg V, De Bacquer D, De Backer G, et al. Patients with coronary artery disease and diabetes need improved management: a report from the EUROASPIRE IV survey: a registry from the EuroObservational Research Programme of the European Society of Cardiology. Cardiovasc Diabetol 2015; 14: 133.
24. Khavandi K, Amer H, Ibrahim B, Brownrigg J. Strategies for preventing type 2 diabetes: an update for clinicians. Ther Adv Chronic Dis 2013; 4: 242-61.
25. De Lorenzo A, Carazza M, Lima R. All-cause mortality of metabolically healthy or unhealthy obese: risk stratification using myocardial perfusion imaging. Arch Med Sci Atheroscler Dis 2018; 3: e90-5.
312 Arch Med Sci 2, 1st March / 2023
M. Haberka, P. Jankowski, D.A. Kosior, M. Szpakowicz, K. Szóstak-Janiak, P. Kozieł, A. Krzykwa, M. Łapińska, M. Setny, K. Kamiński, A. Kubica, D. de Bacquer, G. de Backer, K. Kotseva, D. Wood, A. Pająk, D. Czarnecka, Z. Gąsior
Telomere-telomerase system status in patients with acute myocardial infarction with ST-segment elevation – relationship with oxidative stress
Aleksandra Vukašinović1, Barbara Ostanek2, Aleksandra Klisic3, Srdjan Kafedžić4,5, Marija Zdravković5,6, Ivan Ilić4,5, Miron Sopić1, Saša Hinić6, Milica Stefanović4, Lidija Memon7, Branka Gaković4, Nataša Bogavac-Stanojević1, Vesna Spasojević-Kalimanovska1, Janja Marc2, Aleksandar N. Nešković4,5, Jelena Kotur-Stevuljević1
1Department of Medical Biochemistry, Faculty of Pharmacy, University of Belgrade, Belgrade, Serbia
2Department of Clinical Biochemistry, Faculty of Pharmacy, University of Ljubljana, Ljubljana, Slovenia
3Primary Health Care Center, University of Montenegro, Faculty of Medicine, Podgorica, Montenegro
4Department of Cardiology, Clinical Hospital Center Zemun, Belgrade, Serbia
5Faculty of Medicine, University of Belgrade, Belgrade, Serbia
6Department of Cardiology, Clinical Hospital Center Bezanijska kosa, Belgrade, Serbia
7Clinical Chemistry Laboratory, Clinical Hospital Center Bezanijska kosa, Belgrade, Serbia
Submitted: 26 November 2020; Accepted: 24 April 2021
Online publication: 30 April 2021
Arch Med Sci 2023; 19 (2): 313–323
DOI: https://doi.org/10.5114/aoms/136074
Copyright © 2021 Termedia & Banach
Abstract
Introduction: Telomeres are protective chromosomal ends. Short telomeres are a proven biomarker of biological aging. We aimed to find an association of telomere length and telomerase activity in circulating leukocytes and thromboaspirates of patients with acute myocardial infarction. Furthermore, association of the telomere-telomerase system with oxidative stress markers (as common risk factors for coronary artery disease (CAD)) was tested. Material and methods: Patients were selected from the patients admitted to the intensive care unit with acute myocardial infarction with ST-segment elevation (STEMI), with the following inclusion criteria – STEMI patients between 18 and 80 years old of both genders and candidates for primary percutaneous coronary intervention, with infarction pain present for a maximum of 12 h. In all the patients leukocyte telomere length, telomerase activity and scores related to oxidative-stress status (Protective, Damage and OXY) were evaluated.
Results: Patients were divided into different groups: with stable angina pectoris (AP) ( n = 22), acute myocardial infarction with: STEMI ( n = 93), non-obstructive coronary arteries (MINOCA) ( n = 7), blood vessel rupture ( n = 6) at three time points, and compared to the group of 84 healthy subjects. Telomerase activity was significantly higher in all CAD sub-groups compared to the control group (AP = 0.373 (0.355–0.386), STEMI = 0.375 (0.349–0.395), MINOCA = 0.391 (0.366–0.401), blood vessel rupture = 0.360 (0.352–0.385) vs. CG = 0.069 (0.061–0.081), p < 0.001), while telomeres were significantly shorter in STEMI, MINOCA and blood vessel rupture groups compared to the control group (STEMI = 1.179 (0.931–1.376), MINOCA = 1.026 (0.951–1.070), blood vessel rupture = 1.089 (0.842–1.173) vs. CG = 1.329 (1.096–1.624), p = 0.030]. Values of OXY score were significantly higher in STEMI and MINOCA patients compared to the control group and AP patients (5.83 (4.55–7.54) and 10.28 (9.19–10.72) vs. 4.94 (3.29–6.18) and 4.18 (2.58–4.86),
Corresponding author: Dr. Aleksandra Klisic
Primary Health Care Center
University of Montenegro
Faculty of Medicine
Podgorica, Montenegro
Phone: +382 20 481 999 aleksandranklisic@gmail.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Clinical research Cardiology
p < 0.001). Longer telomeres and higher telomerase activity were found in thromboaspirates, compared to the peripheral blood leukocytes in the same patients (1.25 (1.01–1.84) vs. 1.18 (0.909–1.516), p = 0.036; and 0.366 (0.367–0.379) vs. 0.366 (0.367–0.379), p < 0.001, respectively). In addition, telomere length and telomerase activity had good diagnostic ability to separate STEMI patients from healthy persons.
Conclusions: Leukocyte telomere length and telomerase activity can differentiate CAD patients from healthy persons, and relate CAD to oxidative stress.
Key words: cardiovascular disease, oxidative stress, telomere length, telomerase activity.
Introduction
Cardiovascular diseases (CVD) still account for 45% of all deaths worldwide [1, 2]. The underlying cause of many CVD is coronary atherosclerosis, a highly complex entity characterized by chronic, low-grade inflammation and occlusive plaque formation that leads to inadequate oxygen supply of the myocardium [3]. A common coronary artery disease (CAD) manifestation is acute coronary syndrome (ACS), which comprises unstable angina pectoris (AP), acute myocardial infarction (AMI) without ST-segment elevation (NSTEMI) and ST-segment elevation myocardial infarction (STEMI) [4]. According to the Vidal-Perez research group, between 5% and 25% of all myocardial infarctions are myocardial infarction with non-obstructive coronary arteries (MINOCA) [5].
Telomere deoxyribonucleic acid (DNA) is composed of repeating, non-coding, hexameric sequences d(TTAGGG) that protect chromosome endpoints from end-to-end fusion and degradation, prevent loss of genetic information and provide genome stability [6]. Telomere length and integrity are regulated through the activity of telomerase enzyme [6], a ribonucleic complex with enzymatic activity that adds short, repeating sequences d(TTAGGG) on the 3′-end of telomere DNA, thus prolonging telomeres and the lifespan of cells [7].
A close connection between oxidative stress and CVD has been established [8, 9]. Oxidative stress might cause oxidative damage of DNA, including telomeres, leading to their shortening, although the precise mechanism is not well understood [10, 11]. A number of sources of evidence suggest that telomere dysfunction might be a key molecular event in the pathogenesis of CVD, although most studies were performed on in vitro models, and there is still a lack results confirming this hypothesis on human samples [12]. Likewise, oxidative stress is thought to impact telomerase activity causing its deactivation, but the direct link with telomerase structure damage remains unclear. Still, there are conflicting conclusions on this topic, and there are limited results for a complex human medium like peripheral blood [13–15].
The aim of this study was to evaluate telomere length and telomerase activity in human samples, i.e. circulating leukocytes and thromboaspirates
of patients with AMI. Comparing the elements of the telomere-telomerase system in separate cardiovascular entities was performed in order to better understand the stages of CVD progression. The elements of the telomere-telomerase system were also analysed to associate them with oxidative stress markers and evaluate possible use of mentioned circulating parameters as diagnostic or prognostic markers in AMI patients.
Material and methods
Experimental design
The study was conducted from 2015 to 2016, and patients were followed for the next 4 years for the outcome (until December 2019). Patients with acute myocardial infarction were selected from the patients admitted to the intensive care units of Clinical Hospital Center Zemun and Clinical Hospital Center “Bezanijska kosa”. Inclusion criteria were: patients with acute myocardial infarction with STEMI from 18 to 80 years old of both genders, with infarction pain present for a maximum of 12 h and candidates for primary percutaneous coronary intervention. Patients were excluded from the study if they had STEMI caused by thrombosis of the previous stent, received thrombolytic therapy, had STEMI after previous coronary artery bypass graft surgery, cardiogenic shock, pregnant women and those who did not give their consent. Patients were enrolled in the study after they had received appropriate treatment. Since it was not possible to separate MINOCA patients from non-MINOCA patients during selection, we further divided them in three entities: STEMI, MINOCA or patients with AMI but without an implanted stent because of blood vessel rupture (hereinafter null-stent patients (NSP)). In order to better understand the relation of the telomere-telomerase system, oxidative stress and coronary artery disease, we selected AP patients as a group that presents all the cardiovascular risk factors but did not develop AMI. AP patients were recruited among the patients from the cardiology department of Clinical Hospital Center Zemun and Clinical Hospital Center “Bezanijska kosa” with programmed coronary angiography examination.
314 Arch Med Sci 2, 1st March / 2023
A. Vukašinović, B. Ostanek, A. Klisic, S. Kafedžić, M. Zdravković, I. Ilić, M. Sopić, S. Hinić, M. Stefanović, L. Memon, B. Gaković, N. Bogavac-Stanojević, V. Spasojević-Kalimanovska, J. Marc, A.N. Nešković, J. Kotur-Stevuljević
Telomere-telomerase system status in patients with acute myocardial infarction with ST-segment elevation – relationship with oxidative stress
Parallel with patients, the control group of 84 healthy persons, matched patients according to gender and age, was evaluated. The control group was selected for the study based on the following exclusion criteria: high blood pressure (systolic above 140 mm Hg; diastolic above 90 mm Hg), presence of cardiovascular disease, presence of renal, hepatic or malignant disease or previous infections, trauma and surgery interventions. Additionally, the absence of cardiovascular diseases in the control group was confirmed by electrocardiogram, echocardiogram and cardiac stress test performed by a cardiologist in Clinical Hospital Center Zemun and Clinical Hospital “Bezanijska kosa”.
All the participants were appropriately informed about the purpose and the aim of the study, and signed an informed consent form before they were included in the research. The Ethical Committees of Clinical Hospital Center Zemun (n. 325/1, from September 24th 2015), Clinical Hospital Center
“Bezanijska kosa” (n. 4705/4, from May 31st 2016 and General hospital “Medigroup” (n. 1080/15, from June 18th 2016) approved this study protocol.
Sample collection
Blood samples from the patients were obtained: i) upon admission to the Emergency centre, before the primary percutaneous coronary intervention (pPCI) procedure, for the first time point, ii) after the pPCI procedure was finished, for the second time point, and iii) 6 months after the acute event and after overnight fasting, for the third time point.
We collected peripheral venous blood (i.e. serum, plasma and whole blood samples (i.e. for telomerase enzyme and DNA isolation)) at indicated time points. In addition, aspirated occlusive lesions (thromboaspirates) were collected when indicated, during the pPCI procedure. The peripheral blood samples were obtained in the control group after overnight fasting.
Assays
Telomerase enzyme activity was measured using modified Real-Time Telomeric Repeat Amplification Protocol (RTq-TRAP) as described in our previous work [16]. Briefly, total leukocytes were collected from the whole blood, resuspended in ice cold CHAPS buffer, incubated for 30 min on ice and afterwards centrifuged for 20 min at 16,000 g. The supernatant was collected for further analysis. The telomerase activity was measured using primers TS: 5′-AATCCGTCGAGCAGAGTT-3′ and ACX: 5′-GCGCGGCTTACCCTTACCCTTACCCTAACC-3′ in 10 μL of the final mix containing qPCR Master Mix (5x HOT FIREPol EvaGreen qPCRSuperMix, Solis Biodyne, Tartu, Estonia), TS primer, ACX primer
and protein extract. PCR amplification followed the protocol: i) telomerase extension reaction for 30 min at 25ºC, ii) 95°C for 12 min, iii) 50 cycles of 95°C for 15 s, 60°C for 15 s, 72°C for 35 s, and iv) dissociation curve with settings 95°C for 1 s, 50°C for 1 s, 95°C continuously. The telomerase activity was calculated according to the formula by Elmore et al. [17].
Leukocyte telomere length (LTL) was determined with modified qPCR and calculated as T/S ratio [18]. LTL was determined with modified qPCR [19, 20]. In short, genomic DNA was extracted using a commercial DNA kit (Flexi GENE DNA kit, Qiagen). We opted for albumin as a single copy reference gene. The primers used in PCR reaction were:
Tel-forward (5′-ACACTAAGGTTTGGGTTTGGGTTTGGGTTTGGGTTAGTGT-3′), Tel reverse (5′-TGTTAGGTATCCCTATCCCTATCCCTATCCCTATCCCTAACA-3 ′), Alb forward (5′-CGGCGGCGGGCGGCGCGGGCTGGGCGGAAATGCTGCACAGAATCCT TG-3′) and Alb reverse (5′-GCCCGGCCCGCCGCGCCCGTCCCGCCGGAAAAGCATGGTCGCCTGTT-3′). The final reaction mixtures for the telomere length and the single copy reference gene (albumin) contained: qPCR Master Mix (5x HOT FIREPol EvaGreen qPCR SuperMix, Solis Biodyne, Tartu, Estonia), forward primer, reverse primer and DNA template. The thermal cycling profile for the telomere length included the following steps: i) 95 ºC for 12 min, ii) 4 cycles of 95°C for 15 s, 49°C for 20 s, iii) 40 cycles of 95°C for 15 s, 62°C for 10 s, 72°C for 15 s, and iv) dissociation curve with settings 95°C for 1 s, 50°C for 1 s, 95°C continuously. The PCR profile for albumin amplification contained the following steps: i) 95°C for 12 min, ii) 40 cycles of 95°C for 15 s, 62°C for 10 s, 87°C for 15 s, followed by iv) dissociation curve with settings 95°C for 1 s, 50°C for 1 s, 95°C continuously. PCR measurements for both the telomerase activity and telomere length were carried out on the LighCycler 480 II System (F. Hoffmann-La Roche Ltd, Basel, Switzerland). Until now, there is no evidence for clinical implementation of the mentioned biomarker, although they were strongly suggested [21–23].
The oxidative stress was evaluated through comprehensive scores: Protective, Damage and OXY score suggested by Veglia et al. [24]. In short, the Protective score was calculated as the average z-score of beneficial antioxidant parameters (total antioxidative status, content of sulfhydryl groups, paraoxonase activity, superoxide-dismutase activity), while the Damage score was the average z-score of pro-oxidant markers (pro-oxidative-antioxidative balance, total oxidative status, advanced oxidation protein products). The OXY score was calculated as the difference between average z-scores of Protective and Damage scores calculated as previously explained. The expected value of
Arch Med Sci 2, 1st March / 2023 315
the OXY score is near zero if levels of pro-oxidant markers are completely compensated by antioxidant defences [19]. All three scores are presented in arbitrary units.
Biochemical parameters (total cholesterol, triglycerides and creatine-kinase activity (CK)) were measured using routine enzymatic methods, while high-density lipoprotein cholesterol (HDL-C) was evaluated by the direct enzymatic method on the ILAB 600 analyser (Instrumentation Laboratory, Milan, Italy). To calculate the concentration of low-density lipoprotein cholesterol (LDL-C) the Friedewald formula was used. Levels of troponin I were determined using the commercial Access Immunoassay system (UniCelDxI 600 Access Immunoassay System, Beckman Coulter Inc, USA). All haematology parameters were measured using the ADVIA haematology system (Siemens Healthcare GmbH, Erlangen, Germany).
Statistical analysis
Normality distribution for all variables was checked by the Kolmogorov-Smirnov test or the Shapiro-Wilk test for groups with less than 50 patients. Data are presented as mean ± standard deviation for normally distributed variables, absolute frequencies for categorical variables or medians with 25th and 75th percentile value for variables with non-normal distribution. Parameters with normal distribution were analysed with ANOVA followed by Tukey’s post-hoc test for the differences in subgroups, while asymmetrically distributed variables were analysed by the Mann-Whitney and Kruskal-Wallis test and frequencies with the chisquare test. Data from different time points were evaluated using Friedman’s test for repeated measures. Parameters with a value of 0 were not included in the comparison. To evaluate the potential impact of certain parameters on each other, multiple regression analysis (forward selection) was used. Potential ability of parameters to distinguish patients from healthy persons was checked by receiver operating characteristic curve (ROC) analysis. All statistical analyses were done using PASW Statistic v.18 (Chicago, Illinois, USA) software. The p-value < 0.05 was set as statistically significant, while the groups with non-parametric distribution were corrected using Bonferroni adjustment and the significance level was p-value < 0.005. All the parameters in Figure 1 and Table I were taken into consideration before Bonferroni corrections. After Bonferroni corrections, parameters with a p-value < 0.005 were not statistically significant.
Data processing
Telomere length and telomerase activity might be influenced by various factors, such as gender, smoking habit, body mass index (BMI), comorbid-
ity with diabetes mellitus type 2, use of hypolipidemic drugs (e.g., statins) [24–29].
The data with non-normal distribution were first logarithmically transformed (data not shown) and included in the multiple linear regression (forward selection). We started from all the parameters that represent the risk factors for CVD, and the final best model consisted of telomerase activity, total cholesterol, HDL-C, and LDL-C.
A receiver operating characteristic (ROC) analysis of the selected parameters was conducted to test their discriminatory ability regarding healthy population and STEMI patients or STEMI patients and AP patients. After initial ROC analysis we constructed a model of parameters using logistic regression analysis generated predictive probabilities. A cut-off value was calculated using the Youden index (sensitivity + specificity – 1), where the highest calculated Youden index values indicated the corresponding cut-off.
Results
This study included 128 cardiovascular patients. The patient groups included 106 patients admitted with AMI, candidates for the primary percutaneous coronary intervention (pPCI) procedure (among them 93 patients with STEMI, 7 MINOCA patients and 6 patients with AMI without an implanted stent because of blood vessel rupture (further NSP)), and 22 patients with AP selected for angiography analysis. The control group of 84 healthy persons, matched to patients according to gender and age, was evaluated.
The overview of all the participants included in the study and basic patients’ clinical data are summarised in Table II. All groups were similar in age, BMI and diastolic blood pressure. Significantly higher values of systolic blood pressure were noted in the groups of STEMI patients and patients without an implanted stent compared to the control group. The basic biochemical and haematological parameters of the participants included in the study are summarised in Table III.
The telomere length, telomerase activity and oxidative-stress scores for the five main groups of patients and the control group in the study are presented in Figure 1. Significantly shorter telomeres were noted in all three groups compared to the control and AP groups. Among patient groups, the LTL were similar. Significantly higher values of telomerase activity were noted in all the subgroups of patients compared to the control group.
The MINOCA patients had the largest Damage score compared to other groups. The Protective score was the highest in the AP group compared to all the other groups. Values of OXY score was the highest in the MINOCA patients compared to the control group, AP and STEMI groups. In null-
316 Arch Med Sci 2, 1st March / 2023
A. Vukašinović, B. Ostanek, A. Klisic, S. Kafedžić, M. Zdravković, I. Ilić, M. Sopić, S. Hinić, M. Stefanović, L. Memon, B. Gaković, N. Bogavac-Stanojević, V. Spasojević-Kalimanovska, J. Marc, A.N. Nešković, J. Kotur-Stevuljević
Telomere-telomerase system status in patients with acute myocardial infarction with ST-segment elevation – relationship with oxidative stress
Control Angina STEMI MINOCA Null-stent subject pectoris
Arch Med Sci 2, 1st March / 2023 317
4 3 2 1 0 18 16 14 12 10 8 6 4 2 0 –2 20 18 16 14 12 10 8 6 4 2 0 –2 4 3 2 1 0 –1 –2 –3 –4 –5 –6 0.6 0.5 0.4 0.3 0.2 0.1 0 Telomere length, T/S ratio Damage score OXY score Protective score Telomerase activity, log activity A C E D B
Figure 1. Telomere length, telomerase activity and oxidative-stress scores for the four main groups of patients and the control group
Control Angina STEMI MINOCA Null-stent subject pectoris
Control Angina STEMI MINOCA Null-stent subject pectoris
p < 0.05 p < 0.05 p < 0.01 p < 0.01 p < 0.01 p < 0.01 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.05 p < 0.01 p < 0.05 p < 0.05 p < 0.01 p < 0.01 p < 0.01 p < 0.01 p < 0.01 p < 0.05
Control Angina STEMI MINOCA Null-stent subject pectoris Control Angina STEMI MINOCA Null-stent subject pectoris
a,b,c,d < 0.05 vs. control group, acute state, after pPCI intervention respectively; aa,bb,cc,ddp < 0.001 vs. control group, acute state, after pPCI intervention respectively. All results are variables with non-normal distribution and are presented as medians with 25th and 75th percentile value. Variables are analysed using Friedman’s test for repeated measures and the Wilcoxon test for paired values. STEMI – ST-segment elevation myocardial infarction, pPCI – primary percutaneous coronary intervention.
< 0.05 vs. control, AP, STEMI, MINOCA group (a vs. control subjects, b vs. AP, c vs. STEMI); aa,bbp < 0.001 vs. control, AP, STEMI, MINOCA group. Results are presented as frequencies or mean ± standard deviation for normally distributed variables (#). ANOVA followed by Tukey’s post-hoc test for differences in subgroups was used for normally distributed parameters. Frequencies were analysed with the c2 test. BMI – body mass index, BP – blood pressure, AP – angina pectoris, STEMI – ST-segment elevation myocardial infarction, MINOCA –myocardial infarction with non-obstructive coronary arteries, NSP – null-stent patients.
stent patients, Damage and OXY scores were significantly lower than in the MINOCA patients, while its Protective score was significantly lower as compared to the AP patients (Figure 1).
Table I summarises the results for STEMI patients obtained at different time points, and in different sample types (i.e. peripheral blood and thromboaspirates). LTL was, interestingly, significantly higher in the STEMI patients after the pPCI procedure compared to the same patients in the
acute state. Six months after the acute event, following the pPCI procedure and appropriate subsequent cardiovascular therapy, LTL remained significantly lower compared to the control subjects, similar as it was at the time of the acute event.
The telomerase activity showed significantly higher values in the acute state than in the control group. The telomerase activity values remained increased even at the follow-up 6 months after the acute event, compared to the controls and the
318 Arch Med Sci 2, 1st March / 2023
A. Vukašinović, B. Ostanek, A. Klisic, S. Kafedžić, M. Zdravković, I. Ilić, M. Sopić, S. Hinić, M. Stefanović, L. Memon, B. Gaković, N. Bogavac-Stanojević, V. Spasojević-Kalimanovska, J. Marc, A.N. Nešković, J. Kotur-Stevuljević
Parameter Control subjects ( n = 84) STEMI patients P -value Acute state ( n = 25) After pPCI intervention ( n = 25) 6-month follow-up ( n = 25) Thromboaspirate ( n = 17) Telomere length (T/S ratio) 1.39 (1.110–1.628) 1.18 (0.909–1.516)a 1.62 (1.18–2.05)aa,bb 1.15 (0.93–1.33)a 1.25 (1.01–1.84)c 0.036 Telomerase activity (log activity) 0.069 (0.061–0.081) 0.359 (0.345–0.394)aa 0.363 (0.354–0.395)aa 0.395 (0.367–0.421)aa, b 0.366 (0.367–0.379)aa < 0.001 Damage score 4.62 (3.62–5.49) 5.71 (4.09–7.87)a 4.47 (3.70–6.15)b 4.14 (3.08–5.38)b 4.81 (2.33–19.93)b 0.001 Protective score 0.357 (–0.205–0.885) 0.363 (0.071–1.189) –0.313 (–0.67–0.64)a,b –1.94 (–0.59––3.61)a,b 12.23 (0.376–28.33)aa, bb < 0.001 OXY score 4.79 (3.21–5.84) 4.99 (4.05–6.73) 4.69 (3.51–6.13)b 5.86 (4.71–7.52)a,b –3.04 (–22.81–46.47)aa,bb < 0.001
Table I. Telomere length, telomerase activity and oxidative-stress scores in STEMI patients through the different time points after the acute coronary event in blood and in thromboaspirate
Parameter Control subjects ( n = 84) AP patients ( n = 22) STEMI patients ( n = 93) MINOCA patients ( n = 7) NSP ( n = 6) P -value Age# [years] 56 ±5 60 ±10 61 ±11 59 ±13 60 ±10 0.923 BMI# [kg/m2] 26.2 ±3.9 28.4 ±4.2 25.8 ±4.5 25.9 ±2.9 26.6 ±7.7 0.195 Cigarette smoking, yes/no 16/68 6/16 67/93aa,bb 3/4 2/4 < 0.001 Systolic BP# [mm Hg] 127 ±18 131 ±11 136 ±24a 161 ±30 127 ±17a 0.004 Diastolic BP# [mm Hg] 82 ±10 79 ±7 85 ±14 96 ±26 82 ±11 0.093 Number of blood vessels with clinical significant stenosis – 1–3 1–5 0 1–3 –Number of implanted stents – 0 1–3 0 0 –Dyslipidaemia, % – 40.9a 45.2a 42.9a 33.3a < 0.001 Statins, % – 40.9a 17.2a 0 0 < 0.001 Diabetes mellitus, % – 0 9.7a 28.6a 0 < 0.001 Glucose intolerance, % – 36.4a 8.6a 57.1a 0 < 0.001 a,b,c
Table II. Demographic and clinical data of study participants
a,b,c,d < 0.05 vs. control, AP, STEMI, MINOCA groups (a vs. control subjects, b vs. AP, c vs. STEMI); aa,bb,cc,dd p < 0.001 vs. control, AP, STEMI, MINOCA groups respectively. Results are presented as medians with 25th and 75th percentile value or as mean ± standard deviation for normally distributed variables (#). ANOVA followed by Tukey’s post-hoc test for differences in subgroups was used for normally distributed parameters, Mann-Whitney and Kruskal-Wallis tests were used for parameters with non-normal distribution. AP – angina pectoris, STEMI – ST-segment elevation myocardial infarction, MINOCA – myocardial infarction with non-obstructive coronary arteries, NSP – null-stent patients.
same STEMI patients in the acute state. In fact, 6 months after the acute event STEMI patients’ telomerase activity was even more pronounced.
The Damage score was significantly higher in the STEMI patients’ acute state compared to the point after the pPCI intervention and 6 months after the acute event as well. On the other hand, the protective score was significantly lower after the pPCI intervention than in the acute state. The comprehensive OXY score was significantly lower after the pPCI procedure and at the 6-month follow-up compared to the STEMI patients in their acute state.
Regarding thromboaspirates, we noted longer telomeres in this patient sample than in peripheral blood leukocytes’ telomeres, but still shorter compared to LTL after the pPCI procedure. The telomerase activity in thromboaspirates was
higher than in peripheral blood leukocytes of the control group. The protective score showed significantly higher values in thromboaspirates compared to the peripheral blood samples of the same patients, while the OXY score calculated for thromboaspirates was significantly lower compared to its OXY scores in blood samples (Table I).
Logarithmic transformation of non-parametrically distributed variables allowed multiple regression analysis (forward selection) to predict leukocyte telomere length and telomerase activity in the STEMI patients. Table IV presents the best model of parameters predicting LTL, consisting of telomerase activity, total cholesterol, HDL-C and LDL-C, able to significantly predict leukocyte telomere length values in the STEMI patients. The adjusted R2 value (0.564) indicates that the selected model explained almost 60% of variability in LTL.
Table IV. Models predicting telomere length in STEMI patients according to multiple linear regression analysis
R2adj = 0.564 (N = 58, p < 0.001). SE – standard error for B, CI – confidence interval for B.
Arch Med Sci 2, 1st March / 2023 319
Telomere-telomerase system status in patients with acute myocardial infarction with ST-segment elevation – relationship with oxidative stress
Parameter Control subjects ( n = 84) AP patients ( n = 22) STEMI patients ( n = 93) MINOCA patients ( n = 6) NSP ( n = 7) P -value Total cholesterol# [mmol/l] 5.70 ±0.82 4.47 ±1.12 5.52 ±1.22 6.83 ±0.61 5.41 ±0.84 0.080 Triglycerides [mmol/l] 1.25 (0.87–1.72) 0.94 (0.74–1.70) 1.72 (1.19–2.44)aa,b 1.78 (0.64–2.11)aa 2.31 (1.72–4.74) < 0.001 HDL-C# [mmol/l] 1.50 ±0.37 1.30 ±0.212 1.14 ±0.395aa 1.65 ±0.334aa 0.88 ±0.198 < 0.001 LDL-C [mmol/l] 3.27 (2.77–3.78) 3.17 (2.77–3.78) 3.33 (2.64–4.47) 4.62 (3.71–5.08) 2.95 (2.52–4.13)a 0.009 Creatine kinase [IU/l] – 53 (47–150) 204 (100–487) 178 (78–611) 206 (90–319) 0.367 Troponin I [mg/l] – – 0.14 (0.002–3.00) 0.002 (0.002–2.5) 0.002 (0.001–6.0) 0.732 Red blood cells# [× 1012/l] 4.85 ±0.36 4.5 ±0.61 4.8 ±0.57 5.0 ±0.71 4.4 ±0.53 0.085 Haemoglobin# [g/l] 143 ±8.5 137 ±10.3 144 ±16.2b 149 ±17.3c 125 ±18.4 < 0.001 White blood cells# [× 109/l] 6.8 ±1.64 9.3 ±2.65 12.2 ±4.29aa,bb 9.4 ±2.30 15.6 ±9.25aa,b 0.001 Platelets [× 109/l] 271 (230–313) 213 (183–247) 246 (204–303) 222 (135–278) 408 (349–494)b,c,d < 0.001 CRP [mg/l] 0.50 (0.20–1.80) 3.09 (0.85–6.89)a 4.40 (2.05–9.68)aa,bb 58.45 (2.98–133.57)aa,bb 3.27 (1.20–5.83)a < 0.001
Table III. Basic biochemical and haematological parameters of study participants
Parameter B B (SE) 95th CI b P -value log Telomerase activity –0.444 0.441 –1.328 – 0.439 –0.117 < 0.001 Total cholesterol –0.153 0.034 –0.221 – (–0.084) –1.405 < 0.001 log LDL-C 1.163 0.279 0.603–1.724 1.260 < 0.001 HDL-C 0.168 0.048 0.071–0.264 0.500 < 0.001
Table V. Model for evaluation of telomere length clinical accuracy in STEMI patients
Table V shows the most important selected ROC parameters of the model. Comparison of ROC curves showed that separate curves have comparable discriminatory capability towards STEMI status. The construction of a model consisting of these two independent parameters (leukocyte telomere length and telomerase activity) using logistic regression analysis showed that the new ROC curve had a good discriminatory ability to separate the STEMI patients from healthy persons (AUC = 0.711, cut-off (95% CI) = 0.544 (0.632–0.790)). Other tested models were not significant enough to be able to predict different subgroups. Furthermore, the STEMI patients were followed additionally after the pPCI interventions for the next 4 years. Re-infarction and death occurrence were followed as the long-term outcomes. A total of two lethal outcomes and one re-infarction were recorded. In order to understand the role LTL in CAD progression, we divided STEMI telomere length in tertiles. Both patients with a lethal outcome had values in the lowest tertile (LTL 0.933 and 0.975), while the result of the patient with re-infarction was on the border between the lowest and the middle tertile (LTL 1.074).
Discussion
In the current study we found significantly shorter leukocyte’s telomere length in all four CVD subgroups (i.e. AP, STEMI, MINOCA and the patients who experienced blood vessel rupture during the emergency post-infarction treatment). To our best knowledge, this was the first time that telomere length and telomerase activity were measured in MINOCA patients and in thrombus obtained during the pPCI intervention in combination with oxidative stress markers. The lack of difference in telomere length between cardiovascular entities suggests that the presence of the common pathological processes leading to CVD development is the main cause of telomere integrity impairment, independently of the further specific cardiovascular sub-cause. Margaritis et al. [30] reported LTL as a potential predictive parameter for CAD patients’ outcomes, but also as a possible predictive marker of circulating oxidative stress. However, the study used peripheral blood cells of AMI patients for LTL measurement at just one point combined with ex vivo studies on peripheral blood mononuclear cells for oxidative stress analysis. Along with that, we evaluated the balance between pro-oxidants and antioxidants through the several calculated com-
prehensive redox status scores in our patients. In the STEMI patients, the oxidative stress condition was evidenced through the high Damage score and exhausted antioxidative protection (Table I). This result suggests a possible influence of circulating pro-oxidants on LTL shortening, which could be one of the CAD triggers acting through the genomic instability amplification [31, 32]. On the other hand, increased BMI, diabetes mellitus and glucose intolerance (Table II) that were present as comorbidities in the CAD groups could certainly contribute to further LTL shortening as well as smoking habit, stress and anxiety that are often present in CAD patients, but they were not further evaluated in this study [25, 26, 27].
We also noted increased telomerase activity (as a key telomere length maintenance enzyme) in all four cardiovascular subgroups compared to the healthy persons. The exact mechanism of telomerase activity increasing in cardiovascular patients is unknown, but it is considered to be mediated by telomerase catalytic subunit (TERT) stimulation via formation of 8-oxo-7,8-dihydro-2′-deoxyguanine (8-oxoG) in telomeric DNA [13]. Similarly to telomeres, we did not observe a difference in telomerase activity among four different patient subgroups, which suggests that the enzyme might have overall cardiovascular protection capability.
Recent studies have associated statin therapy, common therapy in CAD patients, with higher telomerase activity [28, 29]. The percentage of patients using statin in their therapy is reported in Table II. A significantly higher percentage of AP patients reported statins in their common therapy compared to the STEMI subgroup, while none of the MINOCA nor NSP patients had them in their therapy. By telomerase activity we compared the patients on statin therapy with those that did not use them, and we did not detect an increase of the telomerase enzyme activity in the patients who used hypolipidemic therapy.
Focusing on the STEMI patients, severe oxidative stress has been found in our results. We also observed that pPCI intervention worsened oxidative stress in the STEMI patients. It is well known that reperfusion could increase free radical generation and thus complicate the redox situation in already damaged endothelium [33]. Coluzzi et al. [34], working on primary human fibroblasts, explained that oxidative stress damages telomeres probably by making modified bases (8-oxoG) and causing single strand breaks in telomere DNA capable of triggering genome instability, whereas
320 Arch Med Sci 2, 1st March / 2023
A. Vukašinović, B. Ostanek, A. Klisic, S. Kafedžić, M. Zdravković, I. Ilić, M. Sopić, S. Hinić, M. Stefanović, L. Memon, B. Gaković, N. Bogavac-Stanojević, V. Spasojević-Kalimanovska, J. Marc, A.N. Nešković, J. Kotur-Stevuljević
AUC Standard error Asymptotic significance Cut-off (95% CI) 0.711 0.040 < 0.001 0.544 (0.632–0.790) CI – confidence interval
for B. Cut-off calculated using Youden index.
Tian and collaborators reported a close connection between peripheral leukocyte telomere shortening and premature CAD [10]. The appearance of shorter LTL in atherosclerotic patients might be attributed to the increased leukocyte consumption during inflammatory processes and accelerated telomere loss per replication in enhanced oxidative stress conditions [35]. The reperfusion procedure, contrary to our expectations, did not cause LTL shortening. We found significant LTL elongation after the recanalization of occluded arteries (Table I). The exact cause of the mechanism of this process has not been elucidated, but we suppose that massive pro-oxidant generation after the recanalization intervention triggers survival compensatory mechanisms mirrored here in LTL telomere elongation to enable longer life of these important immune system players. A rising number of studies have reported that telomere shortening upon oxidative stress is likely to be tissueand time-dependent. Dynamics of pro-oxidant change is probably faster than telomere length alteration [36], and this fact raises the question of the factors influencing our finding regarding telomere length change caused by pPCI. So, we hypothesized that forced blood flow, following recanalization of the occluded artery, brought unaffected leukocytes that could cause apparent leukocyte telomere lengthening, as seen in this study. Leukocytes are mobilized within hours of the AMI onset as part of a tissue injury healing response. On its way from bone marrow to the injured myocardium they must travel through the systemic circulation, and constitute part of the circulating blood cells [37, 38].
Our results showed increased telomerase activity in the STEMI patients at admission (Table I). The effects of oxidative stress on telomerase are still not well understood. While some studies [12, 13] suggested that reactive oxygen species promote telomerase activity, the Aeby research group [39] proposed repression of telomerase activity upon oxidative stress conditions. We confirmed that telomerase activity is upregulated with impairment of oxidative stress, which happened after occluded artery recanalization. Moreover, it remained highly active even 6 months after the acute event. This finding proves that still severe prooxidant levels promote telomerase activity most likely via destabilisation of G-quadruplex structures in the DNA due to formation of 8-oxoG in telomeric DNA, as suggested by Fouquerel et al. [14]. In concordance with still short telomeres and a high Damage score, these results confirm the direct relation between telomeres and STEMI pathology, as well as suggesting that a period longer than 6 months is needed for the whole recovery process after the AMI.
Silvain et al. reported a highly complex composition of the thrombus [40]. Our analysis of telomere length and telomerase activity directly in thrombus material showed results similar to the acute state, suggesting that once CAD has appeared it could impair the telomere structure, making it incapable of performing its physiological function and modifying telomerase by continuously accelerating its activity rate, most likely using the same mechanisms of telomerase stimulation by 8-oxoG formation as previously mentioned. Narducci et al. performed a similar experiment and also observed high telomerase activity in polymorphonuclear neutrophils of the coronary plaques obtained from angioplasty washing medium [41]. Redox status related scores in our study indicate the state of severe oxidative stress that is probably related to the telomere structure change and telomerase activity performance. To the best of our knowledge, this is the first time that a relation has been reported between the telomere-telomerase system and oxidative stress status of the whole atherosclerotic thrombus obtained during a pPCI intervention.
A moderate correlation was reported between leukocyte telomere length and triglyceride (negative) and HDL-C levels (positive) [42], and negative with hypercholesterolaemia in young individuals, as well [43]. We noted a different association in our research. Namely, we found that telomere length as a parameter could be strongly predicted by telomerase activity and total cholesterol, HDL-C and LDL-C (Table I). Short leukocyte telomeres might be connected to lipid status through various molecular mechanisms, such as increased inflammation and oxidative damage, conditions that have been already associated with the telomere attrition rate [44], but the precise mechanism still remains unclear. These results also suggest the potential role of LTL as a marker for CAD progression.
Our results are in accordance with the literature data by showing that LTL might be associated with CAD patients’ outcomes, as also suggested by other authors [25] who reported LTL as a predictor of post-AMI cardiovascular outcomes regardless of age. Indeed, the two deceased patients and the patient who experienced re-infarction in our study according to 4-year follow-up data had the LTL in the lowest tertile group. Still, further research is needed to understand this crosstalk better.
The results of the present study should be interpreted carefully. Our study included only Serbian subjects, and it should not be extended to other groups without additional confirmatory studies being conducted on other populations. The measurement of leukocyte telomere length, telomerase activity and oxidative stress parameters may not have clinical utility at the moment,
Arch Med Sci 2, 1st March / 2023 321
Telomere-telomerase system status in patients with acute myocardial infarction with ST-segment elevation – relationship with oxidative stress
but a great number of similar studies might emphasise the importance of finding novel, less complex analytical methods for those parameters that would qualify them as relevant and applicable for clinical use.
The findings of this study have to be considered in light of certain limitations. The first is the limited sample size. The restrictive inclusion criteria cause a small size of samples included in the study, especially in the MINOCA patient group, which has the prevalence of 5–6% [5] of all acute myocardial infarctions. The second limitation concerns the risk factors such as smoking habit, stress and anxiety that are often present in CAD patients. The stress and anxiety evaluations require specialised questionnaires, and they were not included in our study. Regarding the number of smokers, there is a discrepancy between the patients and the control group, with more smokers being in the patient group. To eliminate its effect, the control group should consist of only healthy smokers, which this study could not provide. Stress and anxiety could also cause imbalance in the obtained results. Their impact should be evaluated using more complex and specialised questionnaires that were unfortunately not included in this study.
In conclusion, our study suggests a close connection between the telomere-telomerase system and oxidative stress as one of the significant factors in CAD development. Leukocyte telomere length and telomerase activity have the ability to differentiate CAD patients from healthy persons.
The data obtained in this hypothesis-generating study suggest that shorter telomeres in these patients could be connected with poor patients’ outcome. However, due to the small sample size and confounding factors mentioned above, a more comprehensive study with an adequate number of patients would probably unveil this tight crosstalk between the telomere-telomerase system, oxidative stress and CAD.
Acknowledgments
This work was supported by the Ministry of Education, Science and Technological Development, Republic of Serbia (Grant no. 451-03-9/202114/200161) and Slovenian Research Agency (Grants P3-0298 and J3-5511). We would like to thank Professor Natasa Glisic, PhD, for her expert and excellent help in English language correction and critical revision of the manuscript.
Conflict of interest
The authors declare no conflict of interest.
References
1. Piepoli MF, Hoes AW, Agewall S, et al. ESC Scientific Document Group. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur Heart J 2016; 37: 2315-81.
2. Kappagoda CT, Amsterdam EA. Improving guidelines for the management of coronary heart disease risk factors. Arch Med Sci 2011; 7: 923-4.
3. Boudoulas KD, Triposciadis F, Geleris P, Boudoulas H. Coronary atherosclerosis: pathophysiologic basis for diagnosis and management. Prog Cardiovasc Dis 2016; 58: 676-92.
4. Makki N, Brennan TM, Girotra S. Acute coronary syndrome. J Intensive Care Med 2015; 30: 86-200.
5. Vidal-Perez R, Abou Jokh Casas C, Agra-Bermejo RM, et al. Myocardial infarction with non-obstructive coronary arteries: a comprehensive review and future research directions. World J Cardiol 2019; 11: 305-15.
6. Diotti R, Loayza D. Shelterin complex and associated factors at human telomeres. Nucleus 2011; 2: 119-35.
7. Zvereva IM, Scherbakova MD, Dontsova AO. Telomerase: structure, function and activity regulation. Biochemistry 2010; 75: 1569-83.
8. Kotur-Stevuljevic J, Memon L, Stefanovic A, et al. Correlation of oxidative stress parameters and inflammatory markers in coronary artery disease patients. Clin Biochem 2007; 40: 181-7.
9. Toualbi LA, Adnane M, Abderrezak K, et al. Oxidative stress accelerates the carotid atherosclerosis process in patients with chronic kidney disease. Arch Med Sci Atheroscler Dis 2020; 5: e245-54.
10. Tian R, Zhang LN, Zhang TT, et al. Association between oxidative stress and peripheral leukocyte telomere length in patients with premature coronary artery disease. Med Sci Monit 2017; 23: 4382-90.
11. Mazidi M, Kengne AP, Sahebkar A, Banach M. Telomere length is associated with cardiometabolic factors in US adults. Angiology 2018; 69: 164-9.
12. Uryga A, Gray K, Bennett M. DNA damage and repair in vascular disease. Annu Rev Physiol 2016; 78: 45-66.
13. Lee HT, Bose A, Lee CY, Opresko PL, Myong S. Molecular mechanisms by which oxidative DNA damage promotes telomerase activity. Nucleic Acids Res 2017; 45: 11752-65.
14. Fouquerel E, Lormand J, Bose A, et al. Oxidative guanine base damage regulates human telomerase activity. Nat Struct Mol Biol 2016; 23: 1092-100.
15. Mazidi M, Kengne AP, Cheskin LJ, Banach M. Serum lipophilic antioxidants levels are associated with leucocyte telomere length among US adults. Lipids Health Dis 2018; 17: 164.
16. Vukašinović AR, Kotur-Stevuljević JM, Mlakar V, et al. Telomerase stability and evaluation of real-time telomeric repeat amplification protocol. Scand J Clin Lab Invest 2019; 79: 188-93.
17. Elmore LW, Forsythe HL, Ferreira-Gonzalez A, Garrett CT, Clark GM, Holt SE. Real-time quantitative analysis of telomerase activity in breast tumor specimens using a highly specific and sensitive fluorescent-based assay. Diagn Mol Pathol 2002; 11: 177-85.
322 Arch Med Sci 2, 1st March / 2023
A. Vukašinović, B. Ostanek, A. Klisic, S. Kafedžić, M. Zdravković, I. Ilić, M. Sopić, S. Hinić, M. Stefanović, L. Memon, B. Gaković, N. Bogavac-Stanojević, V. Spasojević-Kalimanovska, J. Marc, A.N. Nešković, J. Kotur-Stevuljević
Telomere-telomerase system status in patients with acute myocardial infarction with ST-segment elevation – relationship with oxidative stress
18. Jodczyk S, Pearson JF, Aitchison A, Miller AL, Hampton MB, Kennedy MA. Telomere length measurement on the Roche LightCycler 480 Platform. Genet Test Mol Biomarkers 2015; 19: 63-8.
19. Klisic A, Kavaric N, Stanisic V, et al. Endocan and a novel score for dyslipidemia, oxidative stress and inflammation (DOI score) are independently correlated with glycated hemoglobin (HbA1c) in patients with prediabetes and type 2 diabetes. Arch Med Sci 2019; 16: 42-50.
20. Gardner M, Bann D, Wiley L, et al. Halcyon study team. Gender and telomere length: systematic review and meta-analysis. Exp Gerontol 2014; 51: 15-27.
21. Wisman GB, Hollema H, de Jong S, et al. Telomerase activity as a biomarker for (pre)neoplastic cervical disease in scrapings and frozen sections from patients with abnormal cervical smear. J Clin Oncol 1998; 16: 2238-45.
22. Zisuh AV, Han TQ, Zhan SD. Expression of telomerase & its significance in the diagnosis of pancreatic cancer. Indian J Med Res 2012; 135: 26-30.
23. Bhattacharyya J, Mihara K, Bhattacharjee D, Mukherjee M. Telomere length as a potential biomarker of coronary artery disease. Indian J Med Res 2017; 145: 730-7.
24. Veglia F, Werba JP, Tremoli E, et al. Assessment of oxidative stress in coronary artery bypass surgery: comparison between the global index OXY-SCORE and individual biomarkers. Biomarkers 2009; 14: 465-72.
25. Gielen M, Hageman GJ, Antoniou EE, et al.; TELOMAAS group. Body mass index is negatively associated with telomere length: a collaborative cross-sectional metaanalysis of 87 observational studies. Am J Clin Nutr 2018; 108: 453-75.
26. Piplani S, Alemao NN, Prabhu M, Ambar S, Chugh Y, Chugh SK. Correlation of the telomere length with type 2 diabetes mellitus in patients with ischemic heart disease. Indian Heart J 2018; Suppl 3: S173-6.
27. Andujar P, Courbon D, Bizard E, et al. Smoking, telomere length and lung function decline: a longitudinal population-based study. Thorax 2018; 73: 283-5.
28. Boccardi V, Barbieri M, Rizzo MR, et al. A new pleiotropic effect of statins in elderly: modulation of telomerase activity. FASEB J 2013; 27: 3879-85.
29. Strazhesko ID, Tkacheva ON, Akasheva DU, et al. Atorvastatin therapy modulates telomerase activity in patients free of atherosclerotic cardiovascular diseases. Front Pharmacol 2016; 7: 347.
30. Margaritis M, Sanna F, Lazaros G, et al. Predictive value of telomere length on outcome following acute myocardial infarction: evidence for contrasting effects of vascular vs. blood oxidative stress. Eur Heart J 2017; 38: 3094-104.
31. Aviv A. Genetics of leukocyte telomere length and its role in atherosclerosis. Mutat Res 2012; 730: 68-74.
32. Deng Y, Chang S. Role of telomeres and telomerase in genomic instability, senescence and cancer. Lab Invest 2007; 87: 1071-6.
33. Granger DN, Kvietys PR. Reperfusion injury and reactive oxygen species: the evolution of a concept. Redox Biol 2015; 6: 524-51.
34. Coluzzi E, Colamartino M, Cozzi R, et al. Oxidative stress induces persistent telomeric DNA damage responsible for nuclear morphology change in mammalian cells. PLoS One 2014; 9: e110963.
35. Yeh JK, Wang CY. Telomeres and telomerase in cardiovascular diseases. Genes 2016; 7: 58.
36. Spyridopoulos I, Hoffmann J, Aicher A, et al. Accelerated telomere shortening in leukocyte subpopulations of
patients with coronary heart disease: role of cytomegalovirus seropositivity. Circulation 2009; 120: 1364-72.
37. Tourki B, Halade G. Leukocyte diversity in resolving and nonresolving mechanisms of cardiac remodelling. FASEB J 2017; 31: 4226-39.
38. Mazidi M, Penson P, Banach M. Association between telomere length and complete blood count in US adults. Arch Med Sci 2017;13: 601-5.
39. Aeby E, Ahmed W, Redon S, Simanis V, Lingner J. Peroxiredoxin 1 protects telomeres from oxidative damage and preserves telomeric DNA for extension by telomerase. Cell Rep 2016; 17: 3107-14.
40. Silvain J, Collet JP, Nagaswami C, et al. Composition of coronary thrombus in acute myocardial infarction. J Am Coll Cardiol 2011; 57: 1359-67.
41. Narducci ML, Grasselli A, Biasucci LM, et al. High telomerase activity in neutrophils from unstable coronary plaques. J Am Coll Cardiol 2007; 50: 2369-74.
42. Rehkopf DH, Needham BL, Lin J, et al. Leukocyte telomere length in relation to 17 biomarkers of cardiovascular disease risk: a cross-sectional study of US adults. PLoS Med 2016; 13: e1002188.
43. Banach M, Penson PE. Cellular senescence, telomeres, and cardiovascular risk in familial hypercholesterolaemia. Eur J Prev Cardiol 2022: 29: 718-20.
44. Révész D, Milaneschi Y, Verhoeven JE, Penninx BW. Telomere length as a marker of cellular aging is associated with prevalence and progression of metabolic syndrome. J Clin Endocrinol Metab 2014; 99: 4607-15.
Arch Med Sci 2, 1st March / 2023 323
Twelve-month clinical results from the new cobalt-chromium sirolimus-eluting dedicated bifurcation stent BiOSS LIM C Registry
Robert J. Gil1, Adam Kern2, Tomasz Pawłowski1, Jacek Bil1
1Department of Invasive Cardiology, Centre of Postgraduate Medical Education, Central Clinical Hospital of the Ministry of Interior and Administration, Warsaw, Poland
2Department of Cardiology and Cardiosurgery, Faculty of Medical Sciences, University of Warmia and Mazury, Olsztyn, Poland
Submitted: 20 April 2019; Accepted: 6 August 2019
Online publication: 10 February 2020
Arch Med Sci 2023; 19 (2): 324–330
DOI: https://doi.org/10.5114/aoms.2020.92974
Copyright © 2020 Termedia & Banach
Abstract
Introduction: Percutaneous coronary interventions (PCI) in bifurcations are still challenging and are associated with higher risks of periprocedural complications as well as restenosis and stent thrombosis. The aim of this paper was to summarize 12 months of clinical results of the prospective, first-inman registry assessing the BiOSS LIM C stent (Balton, Poland)
Material and methods: In the prospective two-center registry we enrolled patients with non-ST-segment elevation acute coronary syndrome (NSTEACS) and stable coronary artery disease. Provisional T-stenting was the default treatment strategy. The primary endpoint was defined as the rate of cardiac death, myocardial infarction (MI) and clinically driven target lesion revascularization (TLR) in 12-month follow-up
Results: The study population consisted of 95 patients (mean age: 66.8 ± 9.8 years, 17.9% were females). A BiOSS LIM C stent was implanted in the left main (LM) in 53 (55.8%) cases. There were 25.2% of patients with NSTE-ACS, 33.7% with diabetes, 90.5% with hypertension, and 53.7% had previous MI. The device success rate was 100%. An additional regular drug-eluting stent was deployed in the side branch in 18.9% of cases. Proximal optimization technique and final kissing balloon (FKB) technique were used in 53.7% and 30.5% of cases, respectively. MI type 4a was registered in 4 (4.2%) cases. At 12 months the MACE rate was 9.5%, cardiac death 1.1%, MI 2.1% and clinically driven TLR 6.3%. All incidents, apart from one TLR, appeared in the LM subgroup.
Conclusions: Our registry might suggest that PCI using the BiOSS LIM C in coronary bifurcations is feasible and might be an option for percutaneous revascularization.
Key words: coronary bifurcation, left main, dedicated bifurcation stent, drug-eluting stent, sirolimus-eluting stent.
Introduction
Percutaneous coronary interventions (PCI) in bifurcations are still challenging and are associated with higher risks of periprocedural complications as well as in-stent restenosis and stent thrombosis [1, 2]. Dedicated bifurcation stents were proposed as one of the resolutions to these
Corresponding author: Jacek Bil MD PhD FESC
Department of Invasive Cardiology
Centre of Postgraduate Medical Education
Central Clinical Hospital of the Ministry of Interior and Administration
137 Woloska St
02-507 Warsaw, Poland
E-mail: biljacek@gmail.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/).
research
Clinical
Acute Coronary Syndrome
Twelve-month clinical results from the new cobalt-chromium sirolimus-eluting dedicated bifurcation stent BiOSS LIM C Registry
issues [3]. However, few of them have been tested in large randomized clinical trials [4, 5].
In response to this interest, the Polish dedicated bifurcation stent was designed. The BiOSS Clinical Program started in 2008. Initially, the BiOSS stent was the only stainless steel stent, but shortly after in 2010 a paclitaxel-eluting stainless steel stent, the BiOSS Expert stent, was developed. Moreover, going with the times, in 2012 the sirolimus-eluting stainless steel BiOSS LIM stent was released. We gathered a lot of data coming from both randomized clinical trials as well as from real world evidence (RWE) studies [6–14]. The data were acceptable and encouraging, but still a way for enhancement was sought. In consequence, a cobalt- chromium sirolimus-eluting version was created – the BiOSS LIM C stent. Research on an animal model met the expectations as to the safety profile and effectiveness, and thus the BiOSS LIM C stent started the phase of clinical trials [15].
Previously, we presented 3-month results of the interim analysis of the BiOSS LIM C Registry [16]. The aim of this research was to summarize 12 months’ complete clinical results of the prospective, first-in-man BiOSS LIM C registry.
Material and methods
Study population and device description
Between August 2016 and December 2017 we enrolled consecutive patients meeting exclusion and inclusion criteria with stable coronary artery disease or non-ST-elevation acute coronary syn-
drome (NSTE-ACS). Procedures were performed in two centers in Poland (Warsaw, Olsztyn). Prior to the procedure, written, informed consent was obtained. The Local Ethics Committee approved the registry protocol (No. 84/2016).
The BiOSS LIM C is a balloon-expandable sirolimus-eluting stent made of cobalt-chromium (strut thickness 70 μm). Sirolimus (1.4 μg/mm2) is released from the biodegradable coating built of a copolymer of lactic and glycolic acids (Figure 1). The BiOSS LIM C stent can be characterized as having two parts different in the diameter. The proximal part is joined with the distal part by only two struts. The details of patient population/ device description were presented in detail previously [16].
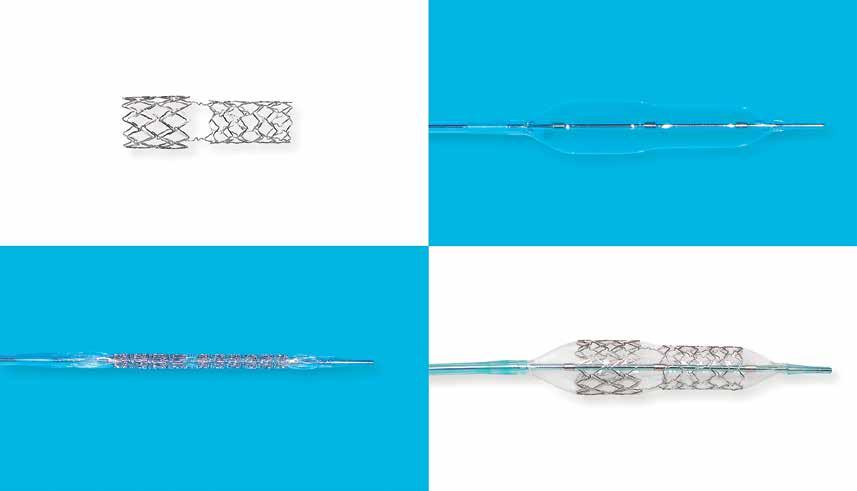
Interventional procedure and concomitant medications
Provisional T-stenting (PTS), i.e. single stent deployment in the main vessel-main branch across a side branch, was the default strategy in all patients. Medina classification was used to assess bifurcation lesions, where the value of 1 indicated stenosis greater than 50% (visual estimation) [17]. No restriction was applied in terms of lesion length. If necessary, an additional regular sirolimus-eluting stent was deployed. A drug-eluting stent was deployed in a side branch only if proximal residual stenosis was greater than 70% after balloon dilatation and/or significant blood flow disturbances after main vessel–main branch stenting and/or blood flow limiting dissection were observed.
Arch Med Sci 2, 1st March / 2023 325
A B C D
Figure 1. A – BiOSS LIM C stent alone, B – bottle balloon catheter, C – BiOSS LIM C crimped on the balloon, D – the fully deployed BiOSS LIM C
Table I. Baseline characteristics
the side branch. Final kissing balloon technique is mandatory when two stents are implanted, and is based on simultaneous inflation of two balloons – one located in the main vessel/main branch, and one located in the side branch.
In patients with NSTE-ACS a loading dose of P2Y12 inhibitor was given (clopidogrel 600 mg or ticagrelor 180 mg), and if necessary, also a loading dose of acetylsalicylic acid (ASA) was administered (300 mg). In planned cases 72 h before the procedure patients received ASA (75 mg/day) and clopidogrel (75 mg/day) or ticagrelor (90 mg b.i.d). All percutaneous coronary interventions (PCIs) were performed via radial or femoral access using 6 Fr or 7 Fr guiding catheters, and periprocedurally unfractionated heparin was administered (100 IU/kg). Dual antiplatelet therapy was recommended for 12 months.
All patients had TnI, CK and CK-MB levels determined before PCI, and 6 and 24 h after. Periprocedural myocardial infarction (MI) (type 4a) was defined according to the third universal definition [19].
Endpoints
The composite primary endpoint (major adverse cardiovascular events – MACE) was defined as the rate of cardiac death, MI and clinically driven target lesion revascularization (TLR) in 12-month follow-up. Secondary endpoints were as follows: death rate, MI rate, stent thrombosis (ST) rate as well as the device, angiographic and procedure success. Clinically driven TLR was defined as the reintervention within the target lesion because of a symptomatic ≥ 50% diameter stenosis within 12 months after the index procedure. Further details were presented previously [16].
The stent deployment protocol was based on the recent European Bifurcation Club guidelines and it was as follows [18]:
• wiring of both branches,
• main vessel predilatation and/or side branch predilatation according to the operator’s judgment,
• stent deployment (inflation for at least 20 s),
• proximal optimization technique (POT; highly recommended, but at operator’s judgment),
• side branch postdilatation/side branch stent deployment if required,
• final kissing balloon inflation after 2nd stent implantation or at operator’s judgment in other cases,
• re-POT after final kissing balloon technique. Proximal optimization technique is a technique in which a short balloon is expanded in the proximal part of the stent in the main vessel. This ensures full expansion and complete apposition of the stent as well as facilitating re-crossing into
Statistical analysis
Continuous variables are shown as mean ± standard deviation. Categorical data are shown as numbers (%). Continuous variables were compared using an unpaired two-sided Student t-test, and categorical data using the χ2 test or Fisher’s exact test, as appropriate. If the distribution was not normal in the Shapiro-Wilk test, the Wilcoxon signed-rank and Mann-Whitney U-tests were applied. P-values of < 0.05 were recognized as statistically significant. The time to event analysis was performed with the Kaplan-Meier estimator of survival curves. Statistical analyses were performed using R 3.0.2 software for OS (R Foundation, Vienna, Austria).
Results
The study population consisted of 95 patients. The mean age was 66.8 ±9.8 years and 17.9% (n = 17) were females. In the study population
326 Arch Med Sci 2, 1st March / 2023
Robert J. Gil, Adam Kern, Tomasz Pawłowski, Jacek Bil
Parameter BiOSS group, n = 95 (%) Age [years] 66.8 ±9.8 Women (%) 17 (17.9) Hypertension 86 (90.5) Hypercholesterolemia 77 (81.1) Diabetes type 2 32 (33.7) Prior MI 51 (53.7) Prior PCI 44 (46.3) CABG 14 (14.7) Peripheral artery disease 10 (10.5) Chronic kidney disease 13 (13.7) History of smoking 21 (22.1) Clinical indication for PCI: Planned PCI 70 (73.7) UA 14 (14.7) NSTEMI 10 (10.5) STEMI 0 Lesion location: LM 53 (55.8) LAD 26 (27.4) LCx 13 (13.7) RCA 3 (3.2) MI – myocardial infarction, PCI – percutaneous coronary intervention, CABG – coronary artery bypass graft, UA – unstable angina, NSTEMI – non-ST elevation myocardial infarction.
hypertension (90.5%) and dyslipidemia (81.1%) were the most common risk factors. The target lesion was located in the left main most commonly (55.8%, n = 53) (Table I). In Table II baseline clinical characteristics in subgroups LM vs. non-LM are presented. In the LM subgroup significantly more patients had diabetes (43.4% vs. 21.4%, p < 0.05) and dyslipidemia (84.9% vs. 52.4%, p < 0.05). Baseline angiographic characteristics are presented in Table III. It is noteworthy that true bifurcations were present in 52.6% (n = 50).
The procedure characteristics are shown in Table IV. The device and angiographic success rates were 100%. The procedure success rate was 95.8%. Main branch predilatation was performed in 80% of cases. The side branch required additional dilatation in over a third of lesions (38.9%),
and in 18 cases (18.9%) the classical DES was deployed, mostly in T and protrusion (TAP) technique (n = 15, 15.8%). The proximal optimization technique was performed in 53.7% of cases, and the final kissing balloon inflation was used in 29 (30.5%) patients.
Myocardial infarction type 4a was registered in 4 (4.2%) patients and was caused by temporary side branch occlusion. In the 12-month follow-up the MACE rate was 9.5% (n = 9), including 1 (1.1%) cardiac death due to heart failure exacerbation, 2 (2.1%) MI and 6 (6.3%) clinically driven TLR (Table V). Kaplan-Meier curves are presented in the Figure 2. All incidents, apart from one TLR, appeared in the LM subgroup (Table VI). In the case of TLR 2 cases were treated with plain old balloon angioplasty (POBA), 3 with another DES and 1 with CABG (Figure 3).
Twelve-month clinical results from the new cobalt-chromium sirolimus-eluting dedicated bifurcation stent BiOSS LIM C Registry Arch Med Sci 2, 1st March / 2023 327
Parameter LM subgroup, n = 53 (%) Non-LM subgroup, n = 42 (%) Age [years] 68.3 ±8.6 65.8 ±7.4 Women (%) 12 (22.6) 5 (11.9) Hypertension 47 (88.7) 39 (92.9) Hypercholesterolemia 45 (84.9) 22 (52.4)* Diabetes type 2 23 (43.4) 9 (21.4)* Prior MI 30 (56.6) 21 (50) Prior PCI 28 (52.8) 16 (38.1) CABG 11 (20.8) 3 (7.1) Peripheral artery disease 6 (11.3) 4 (9.5) Chronic kidney disease 6 (11.3) 7 (16.7) History of smoking 13 (24.5) 8 (19.1) MI – myocardial infarction, PCI – percutaneous coronary intervention, CABG – coronary artery bypass graft, *p < 0.05 between LM and non-LM groups.
Table II. Baseline characteristics in left main (LM) and non-LM subgroups
Parameter Whole population, n = 95 (%) LM subgroup, n = 53 (%) Non-LM subgroup, n = 42 (%) SYNTAX score 26.09 ±3.4 27.6 ±4.2 24.2 ±2.8 EuroSCORE II 0.86 ±0.21 0.94 ±0.32 0.76 ±0.29 Medina classification: 1.1.1 22 (23.2) 12 (22.6) 10 (23.8) 1.0.1 13 (13.7) 6 (11.3) 7 (16.7) 0.1.1 15 (15.8) 7 (13.2) 8 (19.1) 1.0.0 12 (12.6) 8 (15.1) 4 (9.5) 0.1.0 10 (10.5) 6 (11.3) 4 (9.5) 1.1.0 23 (24.2) 7 (13.2) 16 (38.1) LM – left main.
Table III. Baseline angiographic characteristics
Table IV. Procedural characteristics
– major adverse cardiovascular event, MI – myocardial infarction, TLR – target lesion revascularization. *Periprocedural MI type 4a. **Ruptured aortic aneurysm. #Mediastinitis.
A B
Free survival (%)
93.66% (95% CI: 86.43–97.10%) 90.50% (95% CI: 82.54–94.94%)
328 Arch Med Sci 2, 1st March / 2023
Robert J. Gil, Adam Kern, Tomasz Pawłowski, Jacek Bil
Parameter BiOSS group N (%) LM subgroup n = 53 (%) Non-LM subgroup n = 42 (%) Successful implantation 95 (100) 53 (100) 42 (100) Main vessel predilatation 76 (80.0) 45 (84.9) 31 (73.8) Side branch predilatation 25 (26.3) 20 (37.7) 5 (11.9)* Both branches’ predilatation 19 (20.0) 17 (32.1) 2 (4.8)* Nominal stent diameter in main vessel [mm] 3.89 ±0.45 4.17 ±0.36 3.78 ±0.35* Nominal stent diameter in main branch [mm] 3.18 ±0.42 3.42 ±0.35 3.01 ±0.23* Nominal stent length [mm] 19.51 ±3.29 19.94 ±3.16 18.78 ±3.43 Side branch postdilatation 37 (38.9) 23 (43.4) 14 (33.3) POT 51 (53.7) 37 (69.8) 14 (33.3)* FKB 29 (30.5) 22 (41.5) 7 (16.7)* Additional stent in SB 18 (18.9) 15 (28.3) 3 (7.1)* Dissection requiring an additional stent in main vessel 11 (11.6) 7 (13.2) 4 (9.5) Fluoroscopy time [min] 19.6 ±12.4 21.2 ±12.1 17.6 ±9.5 Contrast volume [ml] 197 ±66 211 ±75 180 ±43 Vascular access femoral/radial 6.3%/93.7% 5.7%/94.3% 7.1%/92.9% Guiding catheter 6F/7F 95.8%/5.3% 90.6%/9.4% 100%/0 LM – left main, POT
proximal optimization
balloon; *p < 0.05 between LM and non-LM groups.
Parameter 1 month n = 95 (%) 3 months n = 95 (%) 6 months n = 95 (%) 12 months n = 95 (%) MACE 0 1 (1.1) 3 (3.2) 9 (9.5) Death 0 0 1 (1.1)** 2 (2.1)# Cardiac death 0 0 0 1 (1.1) MI 4 (4.2)* 0 0 2 (2.1) TLR clinically driven 0 1 (1.1) 3 (3.2) 6 (6.3)
–
technique, FKB – final kissing
Table V. BiOSS LIM C clinical results
MACE
Free survival (%) 100 90 80 70 60 50 0 5 10 Time [months] 0 5 10 Time [months] 100 90 80 70 60 50
Figure 2. Kaplan-Meier curves showing event-free survival for major adverse cardiovascular events (A) and target lesion revascularization (B), respectively
Discussion
The 12-month results of BiOSS LIM C deployment are acceptable and encouraging. The stent was successfully deployed in 100% without major difficulties, even in direct stenting. The MACE rate was 9.5%, and the clinically driven TLR rate 6.3%.
When analyzing results, a high predilatation rate was observed (80%). It could have been associated with a significant portion of true bifurcations (52.6%). However, the relatively low proportion of POT cases might be surprising. Nevertheless, one must bear in mind the POT-like effect associated with the BiOSS LIM C structure. When sizing the BiOSS stent the operator might overestimate the main vessel diameter and therefore be convinced that he obtains a POT-like effect. However, we still believe that POT should be highly recommended.
BiOSS LIM C is the improved version of BiOSS stent differing in strut thickness (70 μm vs. 120 μm). This difference might translate into better clinical outcomes. The results observed in the porcine model with the BiOSS LIM C stent seemed to confirm our hope [20]. Interestingly, Table VII presents numerical comparisons of clinical results between BiOSS LIM C, BiOSS LIM and BiOSS Expert. The results suggest that BiOSS LIM C might be superior to BiOSS Expert, but the advantages of BiOSS LIM C over BiOSS LIM need further elucidation, especially when we analyze the LM population.
In the BiOSS LIM LM Registry the rate of MACE rate was 9.5% (n = 7), whereas the rate of clini-
cally driven TLR was 6.8% (n = 5) [7]. In the BiOSS LIM C Registry, these values were 15.1% (n = 8) and 9.4% (n = 5), respectively. These results are difficult to explain since the rate of true bifurcations, nominal stent parameters, and the rate of FKB were comparable or even higher in the case of the POT rate. Nevertheless, the factors negatively affecting the BiOSS LIM C results might be as follows: SYNTAX score (27.6 ±4.2 vs. 22.42 ±4.38) and the rate of additional stent implantation in the side branch (28.3% vs. 14.9%). Also, one should remember that the difference in radial force exerted by different stent platforms (cobalt-chromium vs. stainless steel) could play a significant role [21].
However, regarding the true value of the BiOSS LIM C stent, the two ongoing multicenter international studies will decide. The first one, POLBOS 3 (NCT03548272), will assess the stent in non-LM coronary bifurcations, and the second, POLBOS LM (NCT03508219), will evaluate the use of the BiOSS LIM C stent in the treatment of LM distal stenosis.
And finally, we should put our registry into the perspective of the European Society of Cardiology guidelines on myocardial revascularization from 2018 [22]. They recommend PCI in LM in patients with a low (class I) or intermediate (class IIa) SYNTAX score, and they recommend PCI in three-vessel CAD without diabetes only in patients with a low SYNTAX score (class I). In patients with three-vessel disease, diabetes and a low SYNTAX score PCI has class IIb recommendations. In our study population 33.7% of patients had diabetes and the mean SYNTAX score was 26.09 ±3.4. When choosing between PCI and CABG it is also worth remembering about
MACE – major adverse cardiovascular event, MI – myocardial infarction, TLR – target lesion revascularization.
Arch Med Sci 2, 1st March / 2023 329
Twelve-month
clinical results from the new cobalt-chromium sirolimus-eluting dedicated bifurcation stent BiOSS LIM C Registry
Parameter BiOSS LIM C, n = 95 (%) BiOSS LIM, n = 60 (%)
n = 63 MACE 9 (9.5) 3 (5) 9 (14.3) Death 2 (2.1) 1 (1.67) 2 (3.2) Cardiac death 1 (1.1) 1 (1.67) 2 (3.2) MI 2 (2.1) 1 (1.67) 0 TLR clinically driven 6 (6.3) 1 (1.67) 7 (11.1)
Table VII. 12-month follow-up from three BiOSS Registries
BiOSS Expert,
Figure 3. Restenosis location in BiOSS LIM C stent 1 6 2
5 3
4
Parameter 12 months n = 95 (%) LM n = 53 (%) Non-LM n = 42 (%) MACE 9 (9.5) 8 (15.1) 1 (2.4) Death 2 (2.1)# 2 (3.8) 0 Cardiac death 1 (1.1) 1 (1.9) 0 MI 2 (2.1) 2 (3.8) 0 TLR clinically driven 6 (6.3) 5 (9.4) 1 (2.4)
Table VI. Clinical results of BiOSS LIM C: LM vs. non-LM
MACE – major adverse cardiovascular event, MI – myocardial infarction, TLR – target lesion revascularization. #Mediastinitis.
the patient’s preferences, prior history of CABG, comorbidities (e.g. severe chronic obstructive pulmonary disease) and coronary artery anatomy (especially in patients with diabetes), in which sometimes there is no possibility to implant a well-functioning graft [23, 24].
The number of patients is relatively small. Patients with coronary bifurcation lesions a priori planned for a two-stent strategy were excluded. Also, no identical deployment techniques were used. However, PCIs were performed by operators experienced in BiOSS stent deployment. And finally, no control group was gathered to compare the use of this dedicated bifurcation stent and stenting with other devices and techniques.
In conclusion, our registry might suggest that PCI using the BiOSS LIM C in coronary bifurcations is feasible and might be the option for percutaneous revascularization.
Conflict of interest
The authors declare no conflict of interest.
References
1. Chatzizisis YS, Jonas M, Coskun AU, et al. Prediction of the localization of high-risk coronary atherosclerotic plaques on the basis of low endothelial shear stress: an intravascular ultrasound and histopathology natural history study. Circulation 2008; 117: 993-1002.
2. Jankowski P, Czarnecka D, Badacz L, et al. Practice setting and secondary prevention of coronary artery disease. Arch Med Sci 2018; 14: 979-87.
3. Mishra S. Dedicated bifurcation stents – mechanistic, hardware, and technical aspects. Indian Heart J 2016; 68: 841-50.
4. Pellegrini D, Cortese B. Focus on STENTYS((R)) Xposition S Self-Apposing((R)) stent: a review of available literature. Future Cardiol 2019; 15: 145-59.
5. Konigstein M, Srdanovic I, Gore AK, et al. Outcomes of the Tryton-dedicated bifurcation stent for the treatment of true coronary bifurcations: individual-patient-data pooled analysis. Catheter Cardiovasc Interv 2019; 93: 1255-61.
6. Gil RJ, Bil J, Grundeken MJ, et al. Regular drug-eluting stents versus the dedicated coronary bifurcation sirolimus-eluting BiOSS LIM(R) stent: the randomised, multicentre, open-label, controlled POLBOS II trial. EuroIntervention 2016; 12: e1404-12.
7. Gil RJ, Bil J, Grundeken MJ, et al. Long-term effectiveness and safety of the sirolimus-eluting BiOSS LIM(R) dedicated bifurcation stent in the treatment of distal left main stenosis: an international registry. EuroIntervention 2016; 12: 1246-54.
8. Gil RJ, Bil J, Dzavik V, et al. Regular drug-eluting stent vs dedicated coronary bifurcation bioss expert stent: multicenter open-label randomized controlled POLBOS I trial. Can J Cardiol 2015; 31: 671-78.
9. Gil RJ, Bil J, Vassiliev D, Inigo Garcia LA. First-in-man study of dedicated bifurcation sirolimus-eluting stent: 12-month results of BiOSS LIM(R) Registry. J Interv Cardiol 2015; 28: 51-60.
10. Bil J, Gil RJ, Vassilev D, Rzezak J, Kulawik T, Pawlowski T. Dedicated bifurcation paclitaxel-eluting stent BiOSS Ex-
pert(R) in the treatment of distal left main stem stenosis. J Interv Cardiol 2014; 27: 242-51.
11. Gil RJ, Vassilev D, Michalek A, et al. Dedicated paclitaxel-eluting bifurcation stent BiOSS(R) (bifurcation optimisation stent system): 12-month results from a prospective registry of consecutive all-comers population. EuroIntervention 2012; 8: 316-24.
12. Bil J, Grundeken MJ, Pawlowski T, Gil RJ. Self-positioning properties of dedicated bifurcation coronary stent BiOSS LIM(R) in the eye of 3D optical coherence tomography. Minerva Cardioangiol 2017; 65: 194-6.
13. Springler A, Hessenberger S, Reisinger N, et al. Deoxynivalenol and its metabolite deepoxy-deoxynivalenol: multi-parameter analysis for the evaluation of cytotoxicity and cellular effects. Mycotoxin Res 2017; 33: 25-37.
14. Salat K, Podkowa A, Malikowska N, et al. Novel, highly potent and in vivo active inhibitor of GABA transporter subtype 1 with anticonvulsant, anxiolytic, antidepressant and antinociceptive properties. Neuropharmacology 2017; 113: 331-42.
15. Bil J, Gil RJ, Pawlowski T, Milewski KP. Assessment of vascular response to BiOSS LIM C((R)) stents vs Orsiro((R)) stents in the porcine coronary artery model. Cardiovasc Ther 2017; 35. doi: 10.1111/1755-5922.12267.
16. Gil RJ, Bil J, Kern A, Pawlowski T. First-in-man study of dedicated bifurcation cobalt-chromium sirolimus-eluting stent BiOSS LIM C(R) – three-month results. Kardiol Pol 2018; 76: 464-70.
17. Medina A, Suarez de Lezo J, Pan M. A new classification of coronary bifurcation lesions. Rev Esp Cardiol 2006; 59: 183.
18. Lassen JF, Holm NR, Banning A, et al. Percutaneous coronary intervention for coronary bifurcation disease: 11th consensus document from the European Bifurcation Club. EuroIntervention 2016; 12: 38-46.
19. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Circulation 2012; 126: 2020-35.
20. Bil J, Gil RJ, Pawlowski T, Milewski KP. Assessment of vascular response to BiOSS LIM C((R)) stents vs Orsiro((R)) stents in the porcine coronary artery model. Cardiovasc Ther 2017; 35: e12267.
21. Chichareon P, Katagiri Y, Asano T, et al. Mechanical properties and performances of contemporary drug-eluting stent: focus on the metallic backbone. Expert Rev Med Devices 2019; 16: 211-28.
22. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/ EACTS Guidelines on myocardial revascularization. Eur Heart J 2019; 40: 87-165.
23. Jager B, Piackova E, Haller PM, et al. Increased platelet reactivity in dyslipidemic patients with coronary artery disease on dual anti-platelet therapy. Arch Med Sci 2019; 15: 65-71.
24. Dziedzic EA, Gasior JS, Pawlowski M, et al. Vitamin D level is associated with severity of coronary artery atherosclerosis and incidence of acute coronary syndromes in non-diabetic cardiac patients. Arch Med Sci 2019; 15: 359-68.
330 Arch Med Sci 2, 1st March / 2023
Robert J. Gil, Adam Kern, Tomasz Pawłowski, Jacek Bil
Percutaneous left atrial appendage closure for stroke prevention in patients with chronic renal disease
Alexander Lind, Obayda Azizy, Julia Lortz, Alexander Janosi, Tienush Rassaf, Christos Rammos
Department of Cardiology and Vascular Medicine, West German Heart and Vascular Center Essen, University of Duisburg-Essen, Essen, Germany
Submitted: 14 February 2019; Accepted: 24 August 2019
Online publication: 25 February 2020
Arch Med Sci 2023; 19 (2): 331–336
DOI: https://doi.org/10.5114/aoms.2020.92987
Copyright © 2020 Termedia & Banach
Abstract
Introduction: Atrial fibrillation (AF) is the most common cardiac arrhythmia in the general population. Atrial fibrillation is associated with an increased risk of thromboembolic events, particularly stroke. Chronic kidney disease (CKD) is associated with a higher prevalence of AF and is an independent risk factor of increased mortality and stroke in AF patients. Left atrial appendage closure (LAAC) for stroke prevention plays an important role in the treatment of patients with AF and increased bleeding risk. The impact of CKD on outcomes after LAAC has not been deeply investigated. We assessed whether percutaneous LAAC is safe and feasible in CKD patients.
Material and methods: Ninety-seven patients (mean age: 73.9 ±8.5 years) with AF and contraindications for oral anticoagulation (OAC) or complications under OAC underwent LAAC with the Amplatzer Cardiac Plug and the Amplatzer Amulet Occluder in an open-label observational single-center study. We classified patients as having normal to mild (KDOQI stage I–II) or moderate to severe (KDOQI stage III–V) CKD.
Results: Patients with moderate to severe CKD ( n = 49) had increased CHA 2DS 2-VASc and HAS-BLED scores and were at higher thromboembolic and bleeding risk (CHA 2DS 2-VASc: 4.08 ±0.79, HAS-BLED: 4.76 ±0.69) than patients with mild to moderate CKD ( n = 48, CHA 2DS 2-VASc: 3.69 ±1.1, HASBLED: 4.06 ±0.66; p < 0.001 for both). In both groups, procedural and occlusion success was similar (97.9% vs. 95.9%; p = 0.479). Follow-up of 6 months and from 12 to 36 months revealed effective stroke prevention and no bleeding complication in both groups.
Conclusions: In spite of a higher thromboembolic and bleeding risk in patients with severe CKD, LAAC is a safe and feasible option for stroke prevention.
Key words: complications, stroke, bleeding, chronic renal disease, left atrial appendage closure.
Introduction
Atrial fibrillation (AF) is the most common cardiac arrhythmia. Patients with AF are at increased risk of thromboembolism and stroke [1]. More than 95% of thrombi are found in the left atrial appendage (LAA) [2].
During AF, contractility in the LAA is low, which decreases flow velocities and raises the risk of thrombus formation and stroke. Oral anticoagulation (OAC) is the preferred therapy for stroke prevention for patients with a CHA2DS2-VASc score ≥ 2 [3]. Atrial fibrillation is common in patients with chronic kidney disease (CKD), and 1-year mortality after stroke in patients with CKD is approximately 30% [4]. Additionally,
Corresponding author: Christos Rammos
Department of Cardiology and Vascular Medicine
West German Heart and Vascular Center Essen
University of Duisburg-Essen
Essen, Germany
E-mail: christos.rammos@uk-essen.de
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
and Hemostasis
Clinical research Thrombosis
patients with CKD have a high risk of bleeding complications under OAC [5]. In patients with severe chronic kidney disease OACs are contraindicated [6]. Novel anticoagulants such as rivaroxaban, dabigatran and apixaban have recently been demonstrated to exhibit non-inferior or superior efficacy to warfarin in clinical trials [7–9] and are indicated for use in non-valvular atrial fibrillation based on recent American College of Cardiology (ACC) and European Society of Cardiology (ESC) guidelines [10, 11]. However, major bleeding risk of OACs remain high and higher costs of OACs lead to poorer cost effectiveness [12]. Recently, LAA closure (LAAC) has been shown not to be inferior to OAC for stroke prevention, according to the PROTECT-AF and PREVAIL clinical trials [13–15]. Left atrial appendage closure thus plays an important role as an alternative to OAC for stroke prevention in patients with AF, reducing the bleeding risk [16–18], and could be a potential alternative to OAC in patients with AF and CDK. However, patients with CKD are well known to be at high risk for procedural complications and to have a worse outcome after transcatheter interventions [19–23].
The aim of our study was to examine the procedural safety and efficacy of LAAC in patients with AF and CKD.
Material and methods
The objective of the study was to evaluate the safety and efficacy of the percutaneous LAAC procedure in patients with CKD. Ninety-seven patients with AF and an indication for LAAC were included in this observational single-center study in the Department of Cardiology and Vascular Medicine at the West-German Heart and Vascular Center Essen between 01/2011 and 01/2017. The study was performed in accordance with the Declaration of Helsinki. The institutional Ethics Committee of the University of Duisburg-Essen approved the study protocol (16-7080-BO). All subjects provided informed consent.
Patients with at least one of the following conditions were eligible: bleeding complications while using OACs, bleeding history leading to markedly elevated risk of recurrence with OAC use, HAS-BLED score ≥ 3, difficulty managing the dose of warfarin to maintain a stable INR level, or OAC refusal.
The procedure was performed by well-trained and experienced operators under fluoroscopy and transesophageal echocardiography (TOE) guidance using dedicated Amplatzer devices (first- and second-generation), as previously described in detail. Left atrial appendage closure was performed with the patient under conscious sedation [24]. Intravenous heparin was administered as a bolus dose to achieve an activated clotting time (ACT) of > 250 s in all patients. Transesophageal echo-
cardiography and an LAAC angiogram were used to determine the optimal device size. Based on instructions for use (IFU), all devices met the 5 signs of device stability (lobe compression, lobe perpendicular to LAA wall, disc of lobe with concave shape, disc separation from lobe, midpoint of lobe distal to left circumflex artery) prior to device release and were successfully implanted.
The post-implant drug regimen was discontinuation of OAC followed by dual-antiplatelet therapy with aspirin 100 mg and clopidogrel 75 mg daily for 3 to 6 months, following a loading dose of clopidogrel of 600 mg [15]. All patients were followed up with TOE after 6 months. Clinical follow-up to monitor major adverse events was done through outpatient or telephone assessments at 6 months. A long-term follow-up by telephone was carried out to monitor bleeding, stroke and mortality between 12 and 36 months after intervention.
Patient and procedural characteristics and follow-up results were collected in a dedicated database (Table I). In-hospital complications were reported for both groups including bleeding according to the ISTH definitions of bleeding in non-surgical patients [25], device embolization, need for surgery or cardiopulmonary resuscitation, pericardial effusion, and pericardial tamponade. Vessel complication was defined as access site vascular injury requiring surgical repair, access site-related bleeding requiring transfusion, or access site-related nerve injury that is permanent or requires surgery. Stroke was defined as an irreversible neurological deficit, as classified by the treating neurologist, on the basis of supporting information, including brain images and neurological evaluation.
Due to the number of patients included in this study we stratified patients according to CKD stage as normal to mild (KDOQI stage I–II) and moderate to severe (KDOQI stage III–V) CKD. The primary endpoint was safety of the procedure and complications within the 6-month post-procedure follow-up in patients with mild to moderate as compared to severe CKD. A 36-month long-term follow-up by telephone was carried out to control for bleeding complications, stroke and mortality.
Statistical analysis
The data were expressed with mean ± standard deviation (SD) and compared using the t-test or Mann-Whitney U test. Normal distribution was checked using the Kolmogorov-Smirnov test. Data analysis was performed with SPSS Statistics 22 (IBM for Windows). A p-value < 0.05 was considered statistically significant.
Results
Ninety-seven patients (mean age of 73.9 ±8.5 years) with AF and contraindications for OAC or
332 Arch Med Sci 2, 1st March / 2023
Alexander Lind, Obayda Azizy, Julia Lortz, Alexander Janosi, Tienush Rassaf, Christos Rammos
Percutaneous left atrial appendage closure for stroke prevention in patients with chronic renal disease
Table I. Baseline characteristics of patients undergoing left atrial appendage closure grouped according to the presence of chronic kidney disease
complications under OAC (i.e. gastrointestinal bleeding, intracranial bleed, poorly adjustable INR value) underwent LAAC with the Amplatzer Cardiac Plug and the Amplatzer Amulet Occluder. The baseline characteristics are listed in Table I. There was no significant difference in age (73.1 ±8.4 vs. 75.8 ±7.7 years), gender, body mass index (BMI) (27.6 ±4.7 vs. 28.6 ±5.4 kg/m2), coronary
artery disease (60.4 vs. 69.3%) or hypertension (100%). Patients with severe CKD (n = 49) had significantly higher CHA2DS2-VASc and HAS-BLED scores and were at higher thromboembolic and bleeding risk (CHA2DS2-VASc: 4.08 ±0.79, HASBLED: 4.76 ±0.69) due to minimally higher age and more PAD than patients with mild to moderate CKD (n = 48, CHA2DS2-VASc: 3.69 ±1.1, HAS-BLED:
Arch Med Sci 2, 1st March / 2023 333
Parameter KDOQI I or II ( n = 48) KDOQI III–V ( n = 49) P -value Age [years], mean ± SD 73.1 ±8.4 75.8 ±7.7 0.098 Male gender, n (%) 30 (62.5) 28 (57.1) 0.371 BMI [kg/m2], mean ± SD 27.6 ±4.7 28.6 ±5.4 0.387 CAD, n (%) 29 (60.4) 34 (69.3) 0.23 PAD 21 (43.7) 26 (53.1) 0.213 Hypertension, n (%) 48 (100) 49 (100) Atrial fibrillation, n (%): Paroxysmal 21 (43.8) 19 (38.7) 0.385 Permanent 26 (54.1) 25 (51.1) 0.457 Persistent 1 (2.1) 5 (10.2) 0.112 Hb [mg/dl] 12.6 ±3.1 11.9 ±2.9 0.319 EuroSCORE II (%), mean ± SD 5.1 ±3.1 5.3 ±2.4 0.082 CHA2DS2-VASc-Score, mean ± SD 3.69 ±1.1 4.08 ±0.79 < 0.01 STS-Score (%), mean ± SD 2.84 ±1.8 3.12 ±1.4 0.02 HAS-BLED-Score, mean ± SD 4.06 ±0.66 4.76 ±0.69 < 0.01 EGFR [ml/min], mean ± SD 69.4 ±9.7 43.6 ±10.9 0.03 EF (%), mean ± SD 50.7 ±7.7 50.4 ±8.3 0.172 Creatinine [mg/dl] mean ± SD 1.03 ±0.16 1.59 ±0.6 0.017 BMI – body mass index, CAD – coronary artery disease, eGFR – glomerular filtration rate, EF – ejection fraction, PAD – peripheral artery disease. 9 8 7 6 5 4 3 2 1 0 STS score Euro II score KDOQI I–IIº KDOQI III–Vº 6 5 4 3 2 1 0 HAS-BLED score CHA2DS2-VASc score KDOQI I–IIº KDOQI III–Vº
Figure 1. Periprocedural risk was elevated in patients with chronic kidney disease stage III–V. *p < 0.05
% %
Figure 2. Patients with chronic kidney disease stage III–V° were at higher thromboembolic and bleeding risk. *p < 0.05
4.06 ±0.66; p < 0.001 for both). Calculated STS score and EuroSCORE II predicted higher thromboembolic, bleeding, and periprocedural risk in patients with severe CKD (Figures 1 and 2).
The primary endpoints were safety and successful device implantation, including complications during follow-up. Successful device implantation into the LAA was achieved in 97% of cases.
The rate of successful device implantation was 98% in the CKD I–II group and 96% in the CKD III–V group. None of the patients needed surgery, but 1 patient in each group developed serious pericardial effusion. None of the patients
experienced periprocedural device embolization or vascular complications. During the 6-month and long-term follow-up between 12 months and 36 months after intervention, none of the patients in either group had bleeding complications or stroke (Tables II and III).
During the long-term follow-up 4 patients died in the KDOQI I–II group vs. 5 patients in the KDOQI III–V group (8.3% vs. 10.6%, p = 0.512) (Table III).
Secondary endpoints were the effects of contrast medium used (138.1 ±75.5 ml vs. 141.6 ±84.2 ml, p = 0.347) and subsequent changes in renal function. During the 6-month follow-up, renal function was unchanged in both groups (Figure 3).
334 Arch Med Sci 2, 1st March / 2023
Alexander Lind, Obayda Azizy, Julia Lortz, Alexander Janosi, Tienush Rassaf, Christos Rammos
Parameter KDOQI I or II ( n = 48) KDOQI III-V ( n = 49) P -value Successful occluder implantation, n (%) 48 (97.9) 48 (95.9) 0.479 Contrast amount used [ml], mean ± SD 138.1 ±75.5 141.6 ±84.2 0.347 Device embolization, n (%) 0 0 Major access-vessel complication, n (%) 0 0 Need for cardiovascular surgery, n (%) 0 0 Stroke, n (%) 0 0 Serious pericardial effusion, n (%) 1 (2.1) 1 (2.04) 0.631 Peripheral vascular complication, n (%) 0 0 Acute kidney injury stage III, n (%) 0 0 Death periprocedural (72 h), n (%) 0 0
Table II. Periprocedural results of patients undergoing left atrial appendage closure grouped according to chronic kidney disease
Adverse event KDOQI I–II ( n = 48) KDOQI III–V ( n = 47) P -value Stroke, n (%) 0 0 Peripheral vascular complication, n (%) 0 0 Bleeding complication, n (%) 0 0 Hb [mg/dl] 13.1 ±2.6 12.2 ±2.2 0.367 Leakage, n (%) 2 (4.2) 1 (2.1) 0.574 eGFR, mean ± SD 67.5 ±8.6 42.8 ±11.2 0.04 Residual interatrial shunt 1 (2.1) 3 (6.3) 0.422 Death 0 0
Table IV. Adverse events during follow-up
Variable KDOQI I–II ( n = 48) KDOQI III–V ( n = 47) P -value Stroke, n (%) 0 0 Bleeding complication, n (%) 0 0 36-month mortality, n (%) 4 (8.3) 5 (10.6) 0.512
Table III. Post-procedural follow-up between 12 months and 36 months after procedure
Percutaneous left atrial appendage closure for stroke prevention in patients with chronic renal disease
One patient in the KDOQI I–II group and 3 patients in the KDOQI III–V group had residual interatrial shunt after transseptal puncture (2.1% vs. 6.3%, p = 0.442), and 2 patients from the KDOQI I–II group and 1 patient from the KDOQI III–V group had leakage next to the device (4.2% vs. 2.1%, p = 574) (Tables II and IV).
Discussion
Left atrial appendage closure plays an important role as an alternative to OAC for stroke prevention in patients with AF who experienced complications under OAC. Patients with CKD have a high risk for cardiovascular morbidity and mortality and worsened outcomes after cardiovascular surgery and intervention.
Additionally, they are at high risk for complications such as bleeding, infections, and thromboembolism [26–28]. We investigated whether elevated periprocedural bleeding risk and stroke risk (STS score, EuroSCORE II, CHA2DS2-VASc score and HAS-BLED score) in patients with moderate to severe CKD (KDOQI stage III–V) results in equally successful intervention rates and low complication rates as compared to patients with normal or mild CKD (KDOQI stage I–II).
In our study population, the follow-up after 6 months and between 12 and 36 months after intervention showed similar results and a low general complication rate in both patient groups. Of the 95 patients who received LAAC no patient suffered from stroke or peripheral vascular complications. TOE showed similar intermediate results in terms of leakage (4.2 vs. 2.1%, p = 0.574) in patients with normal to mild (KDOQI stage I–II) CKD and moderate to severe (KDOQI stage III–V) CKD. It is known that patients with CKD undergoing invasive cardiology procedures have a higher risk of complications [22, 23].
In our study, patients with CKD had complex clinical conditions that may have led to bleeding, including pacemaker implantation, wounds, cancer and previous operations; however, compared to patients without CKD, the risk of major bleeding did not increase. Baseline hemoglobin was similar in both groups (12.6 ±3.1 vs. 11.9 ±2.9, p = 0.319) and did not change significantly in the follow-up. This may be because LAAC avoids long-term OAC therapy, which increases the bleeding risk.
The number of peri- and post-procedural complications during short-term and long-term follow-up in our study are surprisingly low. There was only one major complication, i.e. pericardial effusion or pericardial tamponade, in each group. No minor adverse events were reported. No patient needed cardiovascular surgery. Mortality during long-term follow-up was equal in both groups.
This is in accordance with other studies investigating the LAAC and chronic renal function. Kefer et al. [29] presented in their study the procedural safety and efficacy of LAAC with the ACP device. Stroke reduction was similarly high in patients with CKD and patients with normal renal function with no impact of the CKD stages on the periprocedural major adverse events. This is confirmed by Xue et al. [30], whose study using the Watchman Device documented no differences in complications in the CKD vs. the non-CKD group. Moreover, the observed bleeding rate reduction was significantly higher in the CKD group compared to the non-CKD group.
Left atrial appendage closure is not the first choice of therapy in patients with non-valvular AF, but studies have proven the non-inferiority of LAAC as compared to warfarin. Our study has shown that LAAC is safe, even in patients with advanced renal disease, despite increased procedural risk.
At present however, very few nephrologists are aware of and confident with LAA occlusion, a non-pharmacological alternative to oral anticoagulation, for their patients with CKD and AF. For this reason, these patients are rarely discussed with interventional cardiologists or with electrophysiologists for clinical evaluation. On the other hand, cardiologists are often not keen to perform invasive procedures in a fragile population such as renal disease patients, fearing major complications.
The present study has several limitations that should be acknowledged. This was a nonrandomized, retrospective, observational study, which included only 97 patients who underwent LAAC with the Amplatzer device. The follow-up with TOE and laboratory values was restricted to 6 months. Post-procedural long-term follow-up included a range from 12 months to 36 months. Long-term follow-up was restricted to bleeding complications and stroke. Only general mortality between 12 months and 36 months after the procedure could be determined.
Arch Med Sci 2, 1st March / 2023 335
100 80 60 40 20 0
GFR [ml/min]
Figure 3. Change in glomerular filtration rate (eGFR) in patients with mild to moderate and severe kidney disease
KDOQI I–IIº KDOQI III–IVº
GFR baseline Follow-up GFR baseline Follow-up
In conclusion, in spite of a higher thromboembolic and bleeding risk in patients with severe CKD, LAAC is an equally safe and a feasible option for stroke prevention in patients irrespective of kidney disease stage.
Acknowledgments
Alexander Lind and Azizy Obayda contributed equally to this work and should be considered cofirst authors.
Conflict of interest
The authors declare no conflict of interest.
References
1. Wolf PA, Abbott RD, Kannel WB. Atrial fibrillation as an independent risk factor for stroke: the Framingham Study. Stroke 1991; 22: 983-8.
2. Blackshear JL, Odell JA. Appendage obliteration to reduce stroke in cardiac surgical patients with atrial fibrillation. Ann Thorac Surg 1996; 61: 515.
3. Camm AJ, Lip GY, De Caterina R, et al.; ESC Committee for Practice Guidelines (CPG) 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. Developed with the special contribution of the European Heart Rhythm Association. Eur Heart J 2012; 33: 2719-47.
4. Reinecke H, Brand E, Mesters R, et al. Dilemmas in the management of atrial fibrillation in chronic kidney disease. J Am Soc Nephrol 2009; 20: 705-11.
5. Olesen JB, Lip GY, Kamper AL, et al. Stroke and bleeding in atrial fibrillation with chronic kidney disease. N Engl J Med 2012; 367: 625-35.
6. Schlieper G, Schwenger V, Remppis A, et al. Antikoagulation bei Patienten mit chronischer Niereninsuffizienz. Internist 2017; 58: 512-21.
7. Connolly SJ, Ezekowitz MD, Yusuf S, et al. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med 2009; 361: 1139-51.
8. Patel MR, Mahaffey KW, Garg J, et al. Rivaroxaban versus warfarin in nonvalvular atrial fibrillation. N Engl J Med 2011; 365: 883-91.
9. Granger CB, Alexander JH, McMurray JJ, et al. Apixaban versus warfarin in patients with atrial fibrillation. N Engl J Med 2011; 365: 981-92.
10. Kirchhof P, Benussi S, Kotecha D, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J 2016; 37: 2893-962.
11. January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/ HRS Focused Update of the 2014 Guideline for Management of Patients with Atrial Fibrillation. A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol 2019; 74: 104-32.
12. Reddy VY, Akehurst RL, Armstrong SO, Amorosi SL, Beard SM, Holmes DR. Time to cost-effectiveness following stroke reduction strategies in AF warfarin versus NOACs versus LAA closure. J Am Coll Cardiol 2015; 66: 2728-39.
13. Holmes DRJ, Fountain R. Stroke prevention in atrial fibrillation: WATCHMAN versus warfarin. Expert Rev Cardiovasc Ther 2009; 7: 727-9.
14. Holmes DRJ, Kar S, Price MJ, et al. Prospective randomized evaluation of the Watchman Left Atrial Appendage Closure device in patients with atrial fibrillation versus long-term warfarin therapy: the PREVAIL trial. J Am Coll Cardiol 2014; 64: 1-12.
15. Azizy O, Rammos C, Lehmann N, Rassaf T, Kälsch H. Percutaneous closure of the left atrial appendage in patients with diabetes mellitus. Diab Vasc Dis Res 2017; 14: 407-14.
16. Brass LM, Krumholz HM, Scinto JM, Radford M. Warfarin use among patients with atrial fibrillation. Stroke 1997; 28: 2382-9.
17. Urena M, Rodés-Cabau J, Freixa X, et al. Percutaneous left atrial appendage closure with the AMPLATZER cardiac plug device in patients with nonvalvular atrial fibrillation and contraindications to anticoagulation therapy. J Am Coll Cardiol 2013; 62: 96-102.
18. Tzikas A, Shakir S, Gafoor S, et al. Left atrial appendage occlusion for stroke prevention in atrial fibrillation: multicentre experience with the AMPLATZER Cardiac Plug. EuroIntervention 2016; 11: 1170-9.
19. Henry RM, Kostense PJ, Bos G, et al. Mild renal insufficiency is associated with increased cardiovascular mortality: the Hoorn Study. Kidney Int 2002; 62: 1402-7.
20. Muntner P, He J, Hamm L, Loria C, Whelton PK. Renal insufficiency and subsequent death resulting from cardiovascular disease in the United States. J Am Soc Nephrol 2002; 13: 745-53.
21. Garg AX, Clark WF, Haynes RB, House AA. Moderate renal insufficiency and the risk of cardiovascular mortality: results from the NHANES I. Kidney Int 2002; 61: 1486-94.
22. Yamamoto M, Hayashida K, Mouillet G, et al. Prognostic value of chronic kidney disease after transcatheter aortic valve implantation. J Am Coll Cardiol 2013; 62: 869-77.
23. Wanitschek M, Pfisterer M, Hvelplund A, et al. Longterm benefits and risks of drug-eluting compared to bare-metal stents in patients with versus without chronic kidney disease. Int J Cardiol 2013; 168: 2381-8.
24. Rassaf T, Balzer J, Zeus T, et al. Safety and efficacy of deep sedation as compared to general anaesthesia in percutaneous mitral valve repair using the MitraClip system. Catheter Cardiovasc Interv 2014; 84: E38-42.
25. Schulman S, Kearon C; Subcommittee on Control of Anticoagulation of the Scientific and Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J Thromb Haemost 2005; 3: 692-4.
26. Chan KE, Giugliano RP, Patel MR, et al. Nonvitamin K anticoagulant agents in patients with advanced chronic kidney disease or on dialysis with AF. J Am Coll Cardiol 2016; 67: 2888-99
27. Evans EP, Branch RA, Bloom AL. A clinical and experimental study of platelet function in chronic renal failure. J Clin Pathol 1972; 25: 745-53.
28. Chonchol M, Whittle J, Desbien A, Orner MB, Petersen LA, Kressin NR. Chronic kidney disease is associated with angiographic coronary artery disease. Am J Nephrol 2008; 28: 354-60.
29. Kefer J, Tzikas A, Freixa X, et al. Impact of chronic kidney disease on left atrial appendage occlusion for stroke prevention in patients with atrial fibrillation. Int J Cardiol 2016; 207: 335-40.
30. Xue X, Jiang L, Duenninger E, et al. Impact of chronic kidney disease on Watchman implantation: experience with 300 consecutive left atrial appendage closures at a single center. Heart Vessels 2018; 33: 1068-75.
336 Arch Med Sci 2, 1st March / 2023
Alexander Lind, Obayda Azizy, Julia Lortz, Alexander Janosi, Tienush Rassaf, Christos Rammos
What is the right moment for noninvasive ventilation in amyotrophic lateral sclerosis?
Jovana Maskovic1, Aleksandra Ilic1,2, Vladimir Zugic1,2, Zorica Stevic2,3, Mihailo I. Stjepanovic1,2
1Clinic of Pulmonology, Clinical Center of Serbia, Belgrade, Serbia
2Medical Faculty, University of Belgrade, Belgrade, Serbia
3Clinic of Neurology, Clinical Center of Serbia, Belgrade, Serbia
Submitted: 5 April 2019; Accepted: 8 September 2019
Online publication: 8 December 2019
Arch Med Sci 2023; 19 (2): 337–342
DOI: https://doi.org/10.5114/aoms.2019.90465
Copyright © 2019 Termedia & Banach
Abstract
Introduction: The most common cause of death in patients with amyotrophic lateral sclerosis (ALS) is respiratory failure, often in the period of 2–5 years, with a small percentage of patients surviving up to 10 years or more. The aim of the study was to evaluate the significance of pulmonary function tests in prediction of mortality and definition of indications for noninvasive mechanical ventilation (NIMV).
Material and methods: This retrospective-prospective study was performed at the Clinic of Pulmonology, Clinical Centre of Serbia in the period from January 2015 to December 2017. Patients with diagnosis of ALS established according to El Escorial criteria were included.
Results: The study included 76 patients with ALS, 50 (65.85%) with spinal and 26 (34.2%) with bulbar form of disease. Forced vital capacity (FVC) and forced expiratory volume in 1 s (FEV 1) were higher in spinal form of ALS, and the difference was statistically significant when compared to bulbar form. Form of disease, FVC < 70%, maximum inspiratory pressure (PI max) < 50 and maximum expiratory pressure (PE max) < 50 were significant factors for survival. The patients with bulbar form of disease had 2.174 (95.0% CI: 1.261–3.747) higher risk for death.
Conclusions: Our study points to the significance of timely application and early start of NIMV in patients with ALS as an important approach to defer functional impairment, which would mean that the criteria, in our country, for application of these devices must be changed, not only regarding the value of current functional diagnostic tests used in everyday practice in patients with ALS but also in regard to the introduction of new diagnostic tests, such as sniff nasal inspiratory pressure and/or polysomnographic testing.
Key words: pulmonary function, amyotrophic lateral sclerosis, noninvasive ventilation.
Introduction
Amyotrophic lateral sclerosis (ALS) is a progressive neuromuscular disease that causes skeletal muscle weakness, including muscles involved with respiration. Amyotrophic lateral sclerosis belongs to a group of neurological diseases, and affects the upper and lower motor neurons. It is one of the most common motor neuron diseases, and can occur indi-
Corresponding author: Mihailo I. Stjepanovic
Clinic of Pulmonology
Clinical Center of Serbia
Koste Todorovica 26 11000, Belegrade, Serbia
E-mail: mihailostjepanovic@gmail.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/).
Clinical research Pulmonology
vidually or as a hereditary family illness. The most common cause of death in these patients is respiratory failure, often in the period of 2–5 years, with a small percentage of patients surviving up to 10 years and more. Accordingly, monitoring respiratory status is critical to ALS management. Pulmonary function tests (PFTs) are used for evaluation of respiratory impairment and decision-making including the timing of noninvasive ventilation. Recognizing different respiratory tests in relation to disease progression and survival may help determine which tests are most suitable [1].
Poor prognosis and decreased survival time of patients with ALS correlate with their nutritional status. Various studies have evaluated weight, body mass index (BMI), survival time and ALS Functional Rating Scale-Revised (ALSFRS-R) in order to determine the best nutrition management methods for this patient population [2].
The aim of the study was to determine the significance of pulmonary function tests in prediction of mortality and define indications for noninvasive mechanical ventilation (NIMV).
Material and methods
This cross-sectional retrospective study was performed at the Clinic of Pulmonology, Clinical Centre of Serbia in the period from January 2015 to December 2017. Approval granted by the local ethics committee was not required. Patients with a diagnosis of ALS established according to El Escorial criteria were included [3]. The diagnosis of disease was made at the Clinic of Neurology, Clinical Centre of Serbia.
The following PFTs were performed in all patients: spirometry, impulse oscillometry, maximal inspiratory and expiratory mouth pressures, and arterial blood gases analysis. Spirometry was performed by means of a Lilly’s pneumotachometer (MasterScreen Pneumo, Viasys Healthcare, Germany), impulse oscillometry and maximal inspiratory and expiratory pressures (PImax and PEmax) at the mouth during occlusion were performed using commercial systems (MasterScreen IOS, Viasys Healthcare, Germany, and MasterScreen Body, Viasys Healthcare, Germany, respectively). The analysis of the arterial blood gasses was also performed on a commercial analyzer (ABL5, Radiometer, Denmark). All PFTs were performed according to European Respiratory Society/American Thoracic Society joint recommendations [4–8].
Informed consent was not obtained because all study procedures were routinely performed in all patients with ALS at our clinic.
The current criteria for assigning the noninvasive mechanical ventilation (NIMV) in our country are forced vital capacity (FVC) less than 50% of the predicted, and global respiratory failure or elevat-
ed bicarbonate levels (more than 27–28 mmol/l) in arterial blood gases analyses. The criteria were determined by the Republic Fund of Health Insurance, which has been providing non-invasive mechanical ventilation devices for home treatment to insured persons since 2007. Since that time, these criteria have been widely accepted as indications for home ventilation in our country.
Blood samples were collected from patients for laboratory analysis (urea (normal values 2.5–7.5 mmol/l), creatinine (normal values 45–84 μmol/l), creatine kinase (CK) (normal values 0–150 U/l), CK-MB (normal values < 25 U/l)); all tests were performed in an Accredited Medical Laboratory, ATC03-001, SRPS EN 150 15189-2014.
Primary outcome was the time from diagnosis to the establishment of indications for NIMV, as well as the secondary outcome – the time from diagnosis to death.
The outcome was determined by direct contact with patients or their families during regular clinical visits or by telephone contact or with family members when returning the NIMV device.
Statistical analysis
Descriptive statistics was calculated for the baseline demographic and clinical features. Normality of distribution was tested using graphical and mathematical methods. Continuous variables were presented as means with standard deviations or median with 25th–75th percentile, if required. Categorical variables were reported in numbers and percentages. Differences between groups were analyzed using Student’s t-test for normally distributed continuous variables or the Mann-Whitney test for non-normally distributed continuous variables and Pearson’s χ2 test for categorical variables.
Survival was computed by means of KaplanMeier survival analysis, and two groups were compared using the log-rank test. Cox-regression analysis was used to determine factors influencing survival. The level of significance was set at 0.05. Statistical analysis was performed using the IBM SPSS 21 (Chicago, IL, 2012) package.
Results
The clinical characteristics of patients are presented in Table I. The study included 76 patients with ALS, 50 (65.8%) with spinal and 26 (34.2%) with bulbar form of disease. There was no difference in age, gender or BMI between these two groups. Forced vital capacity and forced expiratory volume in 1 s (FEV1) were higher in spinal form of ALS, and the difference was statistically significant when compared to bulbar form. There was no difference in R5HZ, R20HZ, PImax or PE max be-
338 Arch Med Sci 2, 1st March / 2023
Jovana Maskovic, Aleksandra Ilic, Vladimir Zugic, Zorica Stevic, Mihailo I. Stjepanovic
Table I. Clinical characteristics of amyotrophic lateral sclerosis patients
*Data are presented as n (%). BMI – body mass index, FVC – forced vital capacity, FEV1 – forced expiratory volume in 1 s, PImax – maximum inspiratory pressure, PEmax – maximum expiratory pressure, CK –creatine kinase.
Table II. Factors influencing survival at the time of amyotrophic lateral sclerosis diagnosis
Figure 1. Survival from noninvasive mechanical ventilation (NIMV) between the spinal and bulbar form
tween the groups. Laboratory parameters – urea, creatinine and creatine kinase (CK) – did not differ between the groups. CK-MB was higher in spinal form, and the difference was statistically significant in comparison with bulbar form.
Mean follow-up time was 31.1 (minimum–maximum 2.0–81.0) months. Overall median survival was 32.0 (95% CI: 28.1–35.9) months from ALS diagnosis to outcome.
A non-invasive ventilation machine (NIVM) was introduced after a median of 23.0 (12.0–31.0) months in spinal and 13.5 (8.0–23.0) months in bulbar form of disease (p < 0.05).
Median survival from NIMV introduction to outcome was 12.0 (95% CI: 9.98–14.03) months.
Figure 2. Survival from amyotrophic lateral sclerosis (ALS) diagnosis between the spinal and
form
Median survival from NIMV introduction to final outcome (death) in patients with spinal form was 14.0 (95% CI: 11.36–16.64), and 10.0 (95% CI: 7.64–12.35) months in patients with bulbar form of disease (Figure 1). According to the log-rank test, this difference was statistically significant (p < 0.05).
Median survival from diagnosis to final outcome (death) in patients with spinal form was 37.0 (95% CI: 29.74–44.26) months, and 25.0 (95% CI: 20.20–29.80) months in patients with bulbar form of disease (Figure 2). According to
Arch Med Sci 2, 1st March / 2023 339
What is the right moment for noninvasive ventilation in amyotrophic lateral sclerosis?
Factor Spinal n = 50 Mean ± SD Bulbar n = 26 Mean ± SD P -value Age 54.3 ±8.3 53.9 ±10.2 0.870 Sex (male)* 26 (52.0%) 10 (38.5%) 0.262 BMI 25.7 ±6.6 27 ±8.5 0.484 FVC 93.8 ±31.2 78.7 ±26.7 0.039 FEV1 94.6 ±32.2 77.4 ±27.9 0.024 R5HZ 83.4 ±41.8 93.3 ±43 0.336 R20HZ 73.4 ±34.6 73.7 ±28.4 0.976 PI max 37.3 ±17.4 32.6 ±12.1 0.173 PE max 39.7 ±25.2 42 ±25.5 0.707 Urea 5.1 ±1.5 5 ±1.4 0.832 Creatinine 58.6 ±15.9 58.6 ±19.7 0.997 CK 153.5 ±60.4 131.8 ±55.8 0.131 CK-MB 4.6 ±1.3 4 ±1.3 0.047
Variable HR 95% CI for HR P -value Lower Upper Bulbar form 2.174 1.261 3.747 0.005 FVC < 70% 1.945 1.019 3.713 0.044 R20HZ < 120 0.739 0.315 1.736 0.488 R5HZ < 120 0.669 0.371 1.206 0.181 PI max < 50 1.957 1.014 3.775 0.045 PE max < 50 2.156 1.117 4.162 0.022 FVC – forced vital capacity, PImax – maximum inspiratory pressure, PE max – maximum expiratory pressure. 1.0 0.8 0.6 0.4 0.2 0 Time from NIMV to outcome Cumulative survival 0 5 10 15 20 Disease:
–
Bulbar – censored
Spinal Bulbar Spinal
censored
1.0 0.8 0.6 0.4 0.2 0 Time from ALS diagnosis to outcome Cumulative survival 0.00 20.00 40.00 60.00 80.00 100.00 Disease: Spinal Bulbar Spinal – censored Bulbar – censored
bulbar
the log-rank test, this difference was statistically significant (p < 0.05).
Cox-regression analysis was performed to determine the effect of pulmonary function parameter values recorded at the time of making the ALS diagnosis to survival, the results being presented in Table II.
Form of disease, FVC < 70%, PImax < 50 and PEmax < 50 were significant factors for survival. R20HZ < 120 and R5HZ < 120 were not significant factors for survival in patients with ALS. The patients with bulbar form of disease had 2.17 (95% CI: 1.26–3.75) higher risk for death. The patients with FVC < 70% of disease had 1.94 (95% CI: 1.02–3.71), PImax < 50 and PE max < 50 1.96 (95% CI: 1.01–3.77) higher risk.
Discussion
Our study showed that the patients with FVC less than 70% at the time of making their diagnosis as compared to the expected values carried two times higher risk of a lethal outcome. In addition, it was noted that the values of PImax and PE max lower than 80% in relation to the expected values represented a twice-higher risk of lethal outcome. On the other hand, impulse oscillometry parameters did not show any significant association with the length of survival of these patients.
A large number of former cross-section studies have pointed to FVC limitations in detecting an early respiratory dysfunction. It is questionable whether the employment of the FVC value is a relevant criterion as well as whether its value should be confined to the decision on timely application of NIMV [9–12]. In the study by Gordon et al., 50 patients having required tracheotomy underwent spirometry tests and their FVC values were recorded 30 days prior to the aforesaid event; FVC was 50% of the expected value or higher in 11 patients, 60% of the expected value or higher in 7 patients and 70% of the expected value or higher in 5 patients. All the aforementioned data indicate a possible disadvantage of FVC as a tool for evaluation of patient survival [13].
Longitudinal follow-up of ALS patients by Polkey et al. confirmed that the differences in FVC values showed low amplitudes either until death occurred or need for NIMV appeared, while the values of respiratory muscle tests manifested significant amplitudes; accordingly, it directly suggested that the measurement of respiratory muscle strength could be a more beneficial marker for assessing the most optimal timing of NIMV application [14].
Forced vital capacity values during the maneuver of spirometry testing with the patient assuming a recumbent position designated the preservation of diaphragmal musculature strength.
Lechtzin et al. recommended applying NIMV in all patients with FVC < 70% recorded during spirometry in a lying position [12]. Polkey et al. underlined the inferiority of the FVC value in ALS patients. This study pointed to worse prognosis in patients whose value of this parameter was even higher than 80% and in whom the NIMV was not started yet [14–16].
Measurement of the maximum static inspiratory pressure that a subject can generate at the mouth (PImax) or the maximum static expiratory pressure (PEmax) is a simple way to gauge inspiratory and expiratory muscle strength. The pressure measured during these maneuvers reflects the pressure developed by the respiratory muscles (Pmus), plus the passive elastic recoil pressure of the respiratory system including the lung and the chest wall (Prs) [17–21].
When respiratory muscle weakness occurs, PImax can be more sensitive than VC because the relationship between VC and PImax is curvilinear, so that decreases in respiratory muscle strength which develop before decreases in lung volume can be identified [22, 23].
Different studies have confirmed that the strength of respiratory muscles is one of the more significant prognostic markers in ALS patients; a recent study has underscored the need for adequate physical rehabilitation for musculature strengthening. The research studies suggest that this program of respiratory physical rehabilitation is well tolerated and leads to improvement of respiratory and bulbar functions [16].
During routine pulmonary function testing of ALS patients, it has been noted that some of them have elevated R20 and R5. Our study, however, did not find any correlation between the values of impulse oscillometry and time of survival of ALS patients (p = 0.488 for R20Hz and p = 0.181 for R5Hz), in spite of our high expectations that the patients with higher values of extrathoracic and intrathoracic airways resistance would have shorter time of survival. It is particularly true if we inspect the results suggesting that the time of survival in patients with bulbar disease is significantly shorter than in patients with the spinal form of the condition. Anyway, these results call for additional research in future as well as an analysis of the potential prognostic significance of airway resistance.
Presently recommended Medicare criteria (a federal government website managed and paid for by the U.S. Centers for Medicare & Medicaid Services) for NIMV application in ALS patients include any of the following: FVC < 50% of the expected, SAT O2 < 88% during at least 5 min, and PaCO2 44 mm Hg. Upon updating the American Academy of Neurology Database, two additional criteria
340 Arch Med Sci 2, 1st March / 2023
Jovana Maskovic, Aleksandra Ilic, Vladimir Zugic, Zorica Stevic, Mihailo I. Stjepanovic
were added, sniff nasal inspiratory pressure (SNIP) < 40 cm H2O and orthopnea, which may justify the introduction of noninvasive ventilation. In our country, the criteria of providing home care NIMV are FVC < 50% of the expected, and global respiratory insufficiency with HCO3 > 28 mmol/l obtained from arterial blood gas analysis. The study by Vitaca et al. revealed that the NIMV, in the Italian pulmonological units, was introduced in patients with neuromuscular conditions in case of diurnal hypercapnia, nocturnal desaturation and FVC < 50% of expected. Nevertheless, a large number of centers take the position that mere presence of symptoms such as dyspnea or orthopnea are adequate criteria for starting the ventilation [24].
The above result is immensely significant given that, in our country, the indication for NIMV application is FVC below 50%. But, our results demonstrate that FVC is a powerful predictive factor.
Our study has several limitations. First of all, measurement of maximal SNIP was not performed in our patients due to lack of equipment. SNIP has been shown to be strongly correlated with maximal sniff oesophageal pressure [25], is well established as a non-invasive method for assessing inspiratory muscle strength [26], and its values better correlate with onset of respiratory failure than FVC [27]. Next, SVC measurement was also not performed in our patients, despite the fact that change in SVC predicts respiratory failure or death in patients with ALS [28]. Similarly, nocturnal hypoventilation, known to be associated with poor prognosis, has not been studied in this analysis, in spite of the fact that an increasing number of experts nowadays believe that nocturnal hyperventilation is an indication of NIMV [18]. Finally, other prognostic factors in ALS, such as delay from symptom onset to diagnosis [29], progression rate of revised ALS Functional Rating Scale (ALSFRS-R) score [30], psychological distress [31], and frontotemporal lobar dementia [32], were not taken into account. All these factors, and several more, strongly affect quality of life and have an influence on survival of patients with ALS. A couple of prognostic scores based on mentioned and other parameters were developed for patients with ALS [33, 34]. Excluding these factors from our analysis could potentially have an influence on the results of this study, despite the fact that decline in lung function, measured primarily by FVC [35–37], is a strong independent prognostic factor in ALS.
The increasing number of clinicians and the authors of scientific and research papers agree on the fact that the sequential diagnostic procedures, especially if used in combination with sophisticated techniques as described by Carreiro et al., could offer an alternative predictive strategy [17].
In conclusion, our study points to the significance of timely application and early start of NIMV in patients with ALS as an important approach to defer functional impairment, which would mean that the criteria, in our country, for application of these devices must be changed, not only regarding the value of current functional diagnostic tests used in everyday practice in patients with ALS but also in regard to the introduction of new diagnostic tests, such as SNIP and/or polysomnographic testing.
Conflict of interest
The authors declare no conflict of interest.
References
1. Lechtzin N, Cudkowicz ME, de Carvalho M, Genge A, Hardiman O, Mitsumoto H. Respiratory measures in amyotrophic lateral sclerosis. Amyotroph Lateral Scler Frontotemporal Degener 2018; 19: 321-30.
2. Kellogg J, Bottman L, Arra EJ, Selkirk SM, Kozlowski F. Nutrition management methods effective in increasing weight, survival time and functional status in ALS patients: a systematic review. Amyotroph Lateral Scler Frontotemporal Degener 2018; 19: 7-11.
3. Brooks BR, Miller RG, Swash M, Munsat TL, World Federation of Neurology Research Group on Motor Neuron Diseases. El Escorial revised: world Federation of Neurology Criteria for the diagnosis of amyotrophic lateral sclerosis. Amiotroph Lateral Scler Other Motor Criteria for the diagnosis of amyotrophic lateral sclerosis. Amyotroph Lateral Scler Other Motor Neuron Disord 2000; 1: 293-9.
4. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J 2005; 26: 319-38.
5. Smith HJ, Reinhold P, Goldman MD. Forced oscillation technique and impulse oscillometry. Eur Respir Mon 2005; 31: 72-105.
6. Troosters T, Gosselink R, Decramer M. Respiratory muscle assessment. Eur Respir Mon 2005; 31: 57-71.
7. Roca J, Rabinovich R. Clinical exercise testing. Eur Respir Mon 2005; 31: 146-65.
8. Hughes JMB. Pulmonary gas exchange. Eur Respir Mon 2005; 31: 106-26.
9. Raaphorst J, Tuijp J, Verweij L, et al. Treatment of respiratory impairment in patients with motor neuron disease in the Netherlands: patient preference and timing of referral. Eur J Neurol 2013; 20: 1524-30.
10. Capozzo R, Quaranta VN, Pellegrini F, et al. Sniff nasal Inspiratory pressure as a prognostic factor of tracheostomy or death in amyotrophic lateral sclerosis. J Neurol 2015; 262: 593-603.
11. Morgan RK, McNally S, Alexander M, Conroy R, Hardiman O, Costello RW. Use of sniff nasal inspiratory force to predict survival in ALS. Am J Respir Crit Care Med 2005; 171: 269-74.
12. Lechtzin N, Wiener CM, Shade DM, Clawson L, Diette GB. Spirometry in the supine position improves the detection of diaphragmatic weakness in patients with amyotrophic lateral sclerosis. Chest 2002; 121: 436-42.
13. Gordon PH, Corcia P, Lacomblez L, et al. Defining survival as an outcome measure in amyotrophic lateral sclerosis. Arch Neurol 2009; 66: 758-61.
Arch Med Sci 2, 1st March / 2023 341
What is the right moment for noninvasive ventilation in amyotrophic lateral sclerosis?
14. Polkey M, Lyall R, Yang K, Johnson E, Leigh N, Moxham J. Respiratory muscle strength as a predictive biomarker for survival in amyotrophic lateral sclerosis. Am J Respir Crit Care Med 2017; 195: 86-95.
15. Wijesekera LC, Leigh PN. Amyotrophic lateral sclerosis. Orphanet J Rare Dis 2009; 4: 3.
16. Hamnegård CH, Wragg SD, Mills GH, et al. Clinical assessment of diaphragm strength by cervical magnetic stimulation of the phrenic nerves. Thorax 1996; 51: 1239-42.
17. Carreiro AV, Amaral PM, Pinto S, Tomás P, de Carvalho M, Madeira SC. Prognostic models based on patient snapshots and time windows: predicting disease progression to assisted ventilation in amyotrophic lateral sclerosis. J Biomed Inform 2015; 58: 133-44.
18. Vrijsen B, Buyse B, Belge C, et al. Noninvasive ventilation improves sleep in amyotrophic lateral sclerosis: a prospective polysomnographic study. J Clin Sleep Med 2015; 11: 559-66.
19. Calverley PMA. Control of breathing. In: Lung Function Testing: European Respiratory Monograph. Gosselink R, Stam H (eds.). European Respiratory Society 2005.
20. Troosters T, Gosselink R, Decramer M. Respiratory muscle assessment. Eur Respir Mon 2005; 31: 57-71.
21. Stanojevic S, Hall GL. Reference values for spirometry: the way forward for our patients. Respirology 2011; 16: 869.
22. Stanojevic S, Wade A, Stocks J. Reference values for lung function: past, present and future. Eur Respir J 2010; 36: 12-9.
23. Evans JA, Whitelaw WA. The assessment of maximal respiratory mouth pressures in adults. Respir Care 2009; 54: 1348-59.
24. Aboussouan LS, Mireles-Cabodevila E. Respiratory supportin patients with amiotrophic lateral sclerosis. Respir Care 2013; 58: 1555-8.
25. Heritier F, Rahm F, Pasche P, Fitting JW. Sniff nasal inspiratory pressure. A non-invasive assessment of inspiratory muscle strength. Am J Respir Crit Care Med 1994; 150: 1678-83.
26. Uldry C, Fitting JW. Maximal values of sniff nasal inspiratory pressure in healthy subjects. Thorax 1995; 50: 371-5.
27. Lyall RA, Donaldson N, Polkey MI, Leigh PN, Moxham J. Respiratory muscle strength and ventilatory failure in ALS. Brain 2001; 124: 200-13.
28. Andrews JA, Meng L, Kulke SF, et al. Association between decline in slow vital capacity and respiratory insufficiency, use of assisted ventilation, tracheostomy, or death in patients with amyotrophic lateral sclerosis. JAMA Neurol 2018; 75: 58-64.
29. Testa D, Lovati R, Ferrarini M, Salmoiraghi F, Filippini G. Survival of 793 patients with amyotrophic lateral sclerosis diagnosed over a 28-year period. Amyotroph Lateral Scler 2004; 5: 208-12.
30. Kimura F, Fujimura C, Ishida S, et al. Progression rate of ALSFRS-R at time of diagnosis predicts survival time in ALS. Neurology 2006; 66: 265-7.
31. McDonald E, Wiedenfeld SA, Hillel A, Carpenter CL, Walter RA. Survival in amyotrophic lateral sclerosis. The role of psychological factors. Arch Neurol 1994; 51: 17-23.
32. Armon C, Brandstater ME. Motor unit number estimate based rates of progression of ALS predict patient survival. Muscle Nerve 1999; 22: 1571-5.
33. Elamin M, Bede P, Montuschi A, Pender N, Chio A, Hardiman O. Predicting prognosis in amyotrophic lateral sclerosis: a simple algorithm. J Neurol 2015; 262: 1447-54.
34. Westeneng HJ, Debray TPA, Visser AE, et al. Prognosis for patients with amyotrophic lateral sclerosis: development and validation of a personalised prediction model. Lancet Neurol 2018; 17: 423-33.
35. Chiò A, Mora G, Leone M, et al. for the Piemonte and Valle d’Aosta Register for ALS. Early symptom progression rate is related to ALS outcome: a prospective population-based study. Neurology 2002; 59: 99-103.
36. Armon C, Moses D. Linear estimates of rates of disease progression as predictors of survival in patients with ALS entering clinical trials. J Neurol Sci 1998; 160 (Suppl 1): S37-41.
37. Magnus T, Beck M, Giess R, Naumann M, Toyka KV. Disease progression in amyotrophic lateral sclerosis: predictors of survival. Muscle Nerve 2002; 25: 709-14.
342 Arch Med Sci 2, 1st March / 2023
Jovana Maskovic, Aleksandra Ilic, Vladimir Zugic, Zorica Stevic, Mihailo I. Stjepanovic
Prognostic value of XIAP and survivin expression in locally advanced breast cancer patients treated with anthracycline-based neoadjuvant chemotherapy
11st Department of Surgical Oncology, Copernicus Memorial Hospital, Lodz, Poland
2Department of Cancer Pathology, Medical University of Lodz, Lodz, Poland
3Department of Hematology, Medical University of Lodz, Copernicus Memorial Hospital, Lodz, Poland
4General Oncology Counseling Center, Copernicus Memorial Hospital, Lodz, Poland
5Department of Surgical Oncology, Medical University of Lodz, Copernicus Memorial Hospital, Lodz, Poland
Submitted: 19 May 2019; Accepted: 19 August 2019
Online publication: 7 October 2019
Arch Med Sci 2023; 19 (2): 343–354
DOI: https://doi.org/10.5114/aoms.2019.88509
Copyright © 2019 Termedia & Banach
Abstract
Introduction: Neoadjuvant treatment in locally advanced breast cancer (LABC) is intended to decrease the cancer mass, increase the likelihood of radical resection and improve survival. Resistance to chemotherapy may depend on cellular expression of anti-apoptotic proteins. XIAP and survivin are the most potent inhibitors of apoptosis (IAP), but their role in drug-induced cancer cell apoptosis remains unclear. This study was designed to evaluate the impact of pre-treatment expression of XIAP and survivin on pathological complete response and survival in LABC patients.
Material and methods: The study included 60 LABC patients treated with anthracycline-based chemotherapy. XIAP and survivin expression was assessed immunohistochemically in pre-treatment core biopsy specimens.
Results: Pathological complete response was achieved in 33% of the LABC patients. Low/intermediate expression of both XIAP and survivin was significantly associated with pathological complete response ( p ≤ 0.04 and p < 0.001, respectively) and positively correlated with disease-free survival ( p = 0.017 and p < 0.001) and overall survival ( p = 0.052 and p < 0.001). The area under receiver operating characteristics curves (AUC) revealed predictive value of survivin expression for relapse and death in breast cancer patients (AUC = 0.63, p = 0.001 and AUC = 0.8, p < 0.001, respectively).
Conclusions: Our findings suggest that downregulation of XIAP and survivin in LABC patients might predict better treatment outcomes after anthracycline-based chemotherapy. This, in turn, may indicate XIAP and survivin proteins as potential targets for innovative anticancer therapies.
Key words: apoptosis, prognosis, breast neoplasm.
Introduction
Despite broad access to screening programmes, there has been little reduction in the number of advanced stage breast cancers at diagnosis [1–3]. Locally advanced breast cancer (LABC) is a non-metastatic and potentially curable disease, which presents a wide variety of clinical charac-
Corresponding author: Piotr Pluta MD, PhD
1st Department of Surgical Oncology Copernicus Memorial Hospital in Lodz 62 Pabianicka St 93-513 Lodz, Poland
Phone: +48 604 188 815 E-mail: drpiotrpluta@gmail.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Piotr Pluta1, Dorota Jesionek-Kupnicka2, Agnieszka Pluta3, Kamil Brzozowski3, Marcin Braun2, Joanna Kubicka-Wołkowska4, Janusz Piekarski5
Clinical research Oncology
teristics such as large invasive tumour, extension to the skin or chest wall, massive nodal involvement or inflammatory breast cancer [4]. In such patients, the neoadjuvant treatment is intended to decrease the cancer mass and increase the likelihood of radical resection. Additionally, the therapy response positively correlates with the survival [5, 6]. Despite introduction of novel hormonal agents and chemotherapeutic regimens, LABC patients’ treatment still remains challenging due to the high risk of disease recurrence [7, 8]. One prospective way to improve the long-time outcome in the disease is through a molecular tailored strategy based on exploration of cancer cell biology.
Apoptosis is a process by which aberrant, damaged or unwanted cells are eliminated from a multicellular body [9]. In the case of cancer cells, resistance to apoptosis is one of the principle mechanisms of their immortalization. The Inhibitors of Apoptosis Proteins (IAP) play a key role in this process and their upregulation is likely to be inherent to cancer cell development [10, 11]. The IAP family is a class of anti-apoptotic proteins defined by the presence of one or three Baculovirus IAP repeat (BIR) domains, which are hence also termed BIR-containing proteins (BIRCs). These domains are responsible for inhibiting apoptosis by binding the active sites of caspases, which are the crucial proteases in apoptotic pathways. However, inhibiting caspases is not the sole function of IAPs; they also contribute to cell cycle control, ubiquitination of proteins and receptor-mediated signalling [12]. Eight mammalian IAP proteins have been described including cellular IAP1 (cIAP1), cellular IAP2 (cIAP2), X chromosome-linked IAP (XIAP), survivin, BIR repeat-containing ubiquitin-conjugating enzyme system (BRUCE), neuronal apoptosis inhibitory protein (NAIP), melanoma IAP (MLIAP) and IAP-like protein 2 (ILP2) [10].
XIAP is considered the most potent caspasebinding protein and is known to inhibit both the intrinsic (mitochondrial directed) and extrinsic (death receptor directed) apoptosis pathways [13]. It contains three BIR domains and is the only IAP family member to inhibit caspases through a direct physical interaction [14]. High expression of XIAP has been found to be associated with resistance to chemotherapy in various malignancies and a few studies have presented its clinical role in breast cancer patients [13, 15–21].
Survivin contains a single BIR domain and with its molecular weight of 16.389 kDa it is the smallest member of the IAP family [22]. It is typically present during fetal development but is almost absent in normal adult tissues [23]. Survivin expression is markedly increased in most malignancies; however, its impact on chemoresistance and a poor prognosis in breast cancer patients is still uncertain [24–28]. The oncogenic role of survivin depends mainly
on its role in inhibiting both the intrinsic and extrinsic apoptosis pathways and enabling aberrant proliferation by mitotic control [10, 23].
A previous flow cytometry analysis in early breast cancer demonstrated XIAP and survivin to have higher median expression in more advanced tumours, and hence to possess the most significant prognostic importance among IAP family members [19]. Following these findings, the present study seeks to verify the role of XIAP and survivin in LABC and to assess their impact on the pathological response after chemotherapy and on long-term survival. To assess protein expression the present study uses immunohistochemistry rather than flow cytometry, as it is, in our opinion, a more affordable and practical technique.
Material and methods
Patient inclusion
The Research Ethics Committee of the Medical University of Lodz has approved the project protocol. The study group involved female patients with locally advanced breast cancer (LABC) who received neoadjuvant chemotherapy followed by surgery and adjuvant treatment between January 2006 to December 2011 in the Department of Chemotherapy and the Department of Surgical Oncology, Copernicus Memorial Hospital, Lodz, Poland. Inclusion criteria encompassed LABC patients with complete clinical data and available tissue samples. We excluded LABC male patients and those who received preoperative endocrine therapy. The pathological assessment of XIAP and survivin protein expression was conducted in pre-chemotherapy tumours. All the patients gave their written informed consent.
The retrospective clinical data of consecutive patients were retrieved from the medical record system. Of the 98 LABC patients whose data were available in our database, 60 of them met the eligibility criteria and were included in the study group. The median age of those patients was 53.5 years (range: 29–74 years).
The initial clinical stage of the disease was classified according to the 7th edition of the Union for International Cancer Control TNM Classification of Malignant Tumours [29]. The study group patients received the neoadjuvant chemotherapy with four to six cycles, performed every 3 weeks and consisting of doxorubicin (60 mg/m2) and cyclophosphamide (600 mg/m2), or doxorubicin (50 mg/m2) and docetaxel (75 mg/m2). Subsequently, all the patients underwent a modified mastectomy with axillary lymph node dissection and were irradiated postoperatively. Adjuvant hormone therapy and trastuzumab were administered depending on the receptor expression.
344 Arch Med Sci 2, 1st March / 2023
Piotr Pluta, Dorota Jesionek-Kupnicka, Agnieszka Pluta, Kamil Brzozowski, Marcin Braun, Joanna Kubicka-Wołkowska, Janusz Piekarski
Prognostic value of XIAP and survivin expression in locally advanced breast cancer patients treated with anthracycline-based neoadjuvant chemotherapy
Pathological assessment and immunohistochemistry
The diagnosis of invasive breast carcinoma was performed according to the standard pathological protocol, which encompassed tumour type and grading, the status of the oestrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor type 2 (HER-2). ER and PR receptor statuses were assessed using immunohistochemistry (IHC) and scored according to the Allred system [30]. Immunohistochemical expression of HER-2 receptor was evaluated using the standard protocol (0 and 1+ – negative, 2+ – equivocal, 3+ – positive). For IHC equivocal HER-2 (2+) status, fluorescent in situ hybridization (FISH) was performed so as to examine gene amplification.
The pathological complete response (pCR) to chemotherapy in the postoperative specimens was defined as the absence of invasive cancer in postoperative breast specimens, irrespective of ductal carcinoma in situ and axillary lymph node status (ypT0/is). A non-pathological complete response (non-pCR) was established in cases which did not fulfil the above criterion.
In order to examine the pre-treatment expression of XIAP and survivin, formalin-fixed, paraffin-embedded blocks (FFPE) of core biopsy were examined immunohistochemically as previously described [31]. Monoclonal IgG1 anti-hXIAP antibody, clone 117318 (RD Systems, Minneapolis, MN, USA) in dilution 1 : 40, pH 6.0 and IgG antihSurvivin antibody, clone AF886 (RD Systems, Minneapolis, MN, USA) in dilution 1 : 100, pH 6.0 were used for XIAP and survivin examination, respectively. Prostate specimens were used as positive controls according to the recommendation of the antibody manufacturer.
Two pathologists scored the results independently according to Perrone et al., with modifications [32]. The extent of expression was scored based on the percentage of immunopositivity cells as follows: 0 for < 1%; 1 for 1–20%; 2 for 21–50%; 3 for 51–80%; 4 for > 80%. The intensity of staining was classified as 0 for weak, 1 for moderate and 2 for strong. The immunopositivity and intensity scores were summed up to give a final score, interpreted as low expression for a score of 0, intermediate expression for 2–4 and high expression for 5–6. XIAP and survivin expression was assessed in the whole cells, collectively for cytosol and nuclear staining.
Statistical analysis
The dichotomic variables were compared using the c2 test with the corresponding corrections to the numbers of cases in the subgroups. The Tau-b Kendall rank correlation coefficient
(R tau-b) was calculated using the c2 test. The coefficient of correlation was assessed on the basis of ranges established by Cohen: a correlation coefficient greater than 0.6 indicated a strong correlation, 0.3–0.6 indicated a moderate correlation, and less than 0.3 indicated a poor correlation [33]. Disease-free survival (DFS) was calculated from the date of diagnosis until the documentation of relapse. Overall survival (OS) was calculated from the date of diagnosis until death or the date of the last contact with the patients. DFS and OS were assessed applying the Kaplan-Meier method. The logrank test was used to compare OS and DFS in the subgroups. The impact of clinicopathological factors on OS and DFS was calculated using the Cox proportional-hazards model univariate and multivariate analyses. Median follow-up was calculated using reverse Kaplan-Meier curves [34]. To calculate the best cut-off we used receiver operating characteristics (ROC) curves and Youden’s index. The area under ROC curves (AUC) was calculated to assess the predictive value of the tested factors [35]. P-values less than 0.05 were considered statistically significant. Statistica 13 software (Dell inc, Tulsa, OK, USA) was used for statistical calculation.
Results
XIAP and survivin expression in the pre-treatment biopsies
In the core biopsy, XIAP expression was assessed as low, intermediate and high in 17 (28%), 29 (48%) and 14 (23%) cases, respectively. Similarly, survivin expression was scored as low in 16 (27%) cases, intermediate in 24 (40%) cases and high in 20 (33%) cases. Figure 1 depicts examples of XIAP and survivin expression related to the scoring subdivision. In the dichotomic analysis, low/intermediate expression of XIAP and survivin comprised 46 (76%) cases and 40 (67%) cases, respectively vs. high expression of XIAP (14 cases; 23%) and survivin (20 cases; 33%). A positive correlation was observed between XIAP and survivin expression (p < 0.001; R tau-b = 0.42).
Relationship between XIAP and survivin expression and clinical/pathological parameters
Regarding the relationship between IAP protein expression and clinical and pathological parameters, expression of XIAP moderately correlated with disease stage, as lower XIAP expression prevailed in the more advanced disease (96% low/ intermediate vs. 71% high XIAP expression in stage III; p = 0.033). Neither XIAP nor survivin expression was correlated with other clinical and pathological factors. The detailed results are presented in Tables I and II.
Arch Med Sci 2, 1st March / 2023 345
expression
XIAP (25% of cells positive (2 points); intensity: strong (2 point); total score): 4. B – High expression of XIAP (90% of cells positive (4 points); intensity: strong (2 points); total score: 6). C – High expression of survivin in cytosol and nuclei (100% of cells positive (4 points); intensity: strong (2 points); total score: 6). D – Case negative for expression (0% of cells positive)
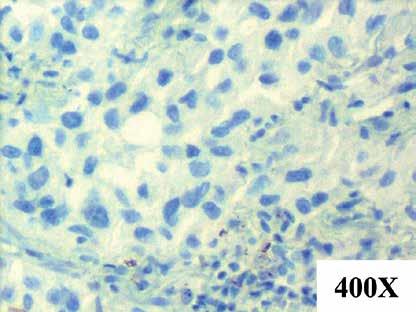
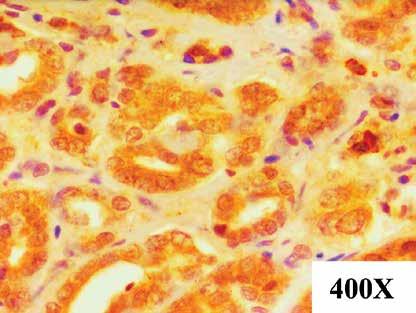
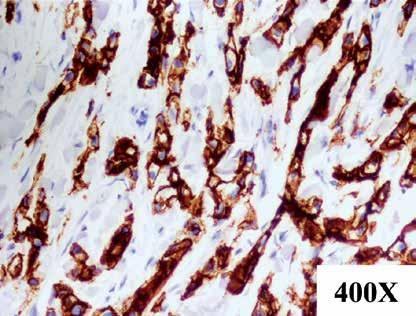
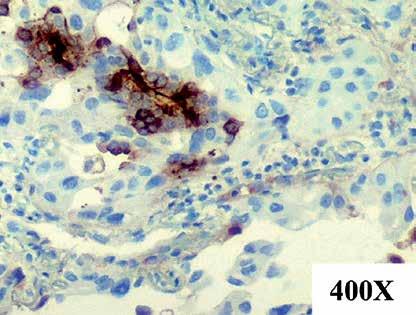
XIAP and survivin expression and pathological response to chemotherapy
Pathological complete response was achieved by 20 out of the 60 study participants (33%). Low/ intermediate XIAP expression was significantly associated with pCR (41% low/intermediate vs. 7% high XIAP expression in the pCR subgroup; p = 0.04). Similarly, low/intermediate expression of survivin in tumour correlated with post-chemotherapy achievement of pCR (50% low/intermediate vs. 0% high survivin expression in the pCR subgroup; p < 0.001). Among the clinical and pathological parameters, HER-2 positive receptor status inversely correlated with pCR (15% pCR in the HER-2 positive patients vs. 47% pCR in the HER-2 negative patients; p = 0.021). The association between clinicopathological variables and pCR rates is shown in Table III.
XIAP and survivin expression and survival
At a median follow-up of 96.5 months, 19 patients developed locoregional recurrence or distant metastases. Fifteen patients died during the follow-up.
The Kaplan-Meier analyses revealed that lower XIAP and survivin expression was associated with longer disease-free survival (DFS) (p = 0.017 and p < 0.001, respectively, Table IV, Figures 2 A, B). Better DFS was also observed in the patients with lack of a HER2 receptor and PCR achievement (p = 0.019 and p = 0.001, respectively).
Longer overall survival (OS) was observed in the patients with low/intermediate survivin expression in comparison to high expression (p < 0.001, Table IV, Figure 2 C). The patients with pCR had longer OS as compared to the non-PCR group (p = 0.001, Table IV).
In the multivariate Cox analysis survivin ex- pression was confirmed as the only independent risk factor for a longer DFS and OS (in both cases p < 0.001, Table V). Additionally, the area under ROC curves (AUC) analysis revealed a predictive value of survivin expression for relapse and death in breast cancer patients (AUC = 0.63, p = 0.001 and AUC = 0.8, p < 0.001 respectively; Table VI). Survivin had low sensitivity to non-PCR anticipation. Prediction of non-PCR, relapse and death was not confirmed in relation to XIAP expression.
346 Arch Med Sci 2, 1st March / 2023
Piotr Pluta, Dorota Jesionek-Kupnicka, Agnieszka Pluta, Kamil Brzozowski, Marcin Braun, Joanna Kubicka-Wołkowska, Janusz Piekarski
400× A C B D 400× 400× 400×
Figure 1. Examples of immunohistochemical staining of XIAP and survivin in pretreatment specimens of locally advanced breast cancer (LABC). A – Intermediate
of
Discussion
Overexpression of IAP family members has been repeatedly encountered in various cancers cells, yet their prognostic and predictive roles in various clinical scenarios remain uncertain [13]. The present report assesses expression of XIAP and survivin, two highly potent IAP proteins, in LABC patients undergoing an anthracycline-based chemotherapy with regard to pCR and survival.
In the study, high XIAP expression was detected in 33% of patients and was inversely associated with disease stage. In contrast, Xu et al. did not observe any significant correlation between high XIAP expression and breast cancer stage, as a high cytosolic fraction of this protein was detected in 18% of patients in stage II and in 12% of patients in stage III [20]. In a large cohort presented by Hussain et al. XIAP protein was overexpressed in 29.5% of 1009 breast cancer patients, irrespective of the tumour stage and lymph node involvement [18].
Preclinical studies have demonstrated that XIAP down-regulation increases sensitivity to
a cytotoxic therapy in inflammatory breast cancer cell lines, thus confirming the protective role of XIAP in drug-induced cancer cell apoptosis [36, 37]. Our results further support this hypothesis, as low/intermediate expression of XIAP was found to correlate with a higher rate of a pathological complete response to chemotherapy. To our knowledge, our report is the first to demonstrate that XIAP expression influences the pathological response to neoadjuvant chemotherapy. Nevertheless, Parton et al. failed to confirm that the pre-treatment expression of XIAP correlated with a clinical response in a previous study of 35 LABC patients [21]. On the contrary, in advanced head and neck squamous cell carcinoma, overexpression of XIAP was significantly associated with clinical resistance to the neoadjuvant cisplatin chemotherapy [17].
The survival analysis revealed a negative impact of high XIAP expression for DFS and OS in LABC patients. This is in concordance with a study conducted in a large group of breast cancer pa-
Arch Med Sci 2, 1st March / 2023 347
Prognostic value of XIAP and survivin expression in locally advanced breast cancer patients treated with anthracycline-based neoadjuvant chemotherapy
Parameter XIAP expression P -value Contingency coefficient Tau b Kendall Low/intermediate n (%) High n (%) Patients, n 60 46 (77) 14 (23) Age [years] < 50 16 (27) 5 (8) 0.949 0.008 –0.01 ≥ 50 30 (50) 9 (15) Tumour size T1/T2 23 (38) 7 (12) 1.000 0.00 0.00 T3/T4 23 (38) 7 (12) TNM stage IIB 2 (3) 4 (7) 0.033 0.32 –0.34 III 44 (73) 10 (17) Histological type NST 43 (72) 11(18) 0.104 0.21 0.21 LOB 3 (5) 3 (5) Histological grade G2 22 (37) 8 (13) 0.542 0.08 –0.08 G3 24 (40) 6 (10) ER status Negative 26 (43) 6 (10) 0.370 0.12 0.12 Positive 20 (33) 8 (13) PR status Negative 25 (42) 5 (8) 0.222 0.16 0.16 Positive 21 (35) 9 (15) HER-2 status Negative 28 (47) 6 (10) 0.234 0.15 0.15 Positive 18 (30) 8 (13) Triple negative No 30 (50) 11 (18) 0.347 0.12 –0.12 Yes 16 (27) 3 (5) NST – invasive carcinoma of no special type, LOB – invasive lobular carcinoma, ER – oestrogen receptor, PR – progesterone receptor, HER2 – human epidermal growth factor receptor type 2.
Table I. Relationship between XIAP expression and clinicopathological factors of the 60 locally advanced breast cancer patients
clinicopathological factors of the 60 locally advanced breast cancer patients
tients (n > 1000), which showed that overexpression of XIAP is an independent poor prognostic factor for survival [18]. In contrast, Xu et al. noted a lack of correlation between XIAP expression and survival, except for a subgroup of triple negative breast cancer, in which the presence of high XIAP levels in the tumour was associated with an increased risk of a relapse [20].
Unlike XIAP, the clinical role of survivin was thoroughly explored in breast cancer patients including those with LABC. Survivin overexpression has been found both in breast cancer cell lines and in tumour tissues [21, 38]. In our study expression of survivin was correlated with XIAP expression, which suggests a similar contribution of this protein to breast cancer development. We did not find any relationship between survivin expression and clinicopathological factors of LABC patients, but in a meta-analysis conducted by Li et al., high survivin expression was observed significantly more frequently in stage III/IV of the disease [25]. In the present study, survivin overexpression was
detected in 23% of the pre-treatment biopsies; these findings are similar to those of Zhao et al., who noted high staining of survivin in 33% of stage III breast cancer patients [39].
Our findings also indicate a correlation between survivin and pCR, since low/intermediate expression of this protein had a significant impact on pCR achievement. Zhao et al. also found that lack of survivin expression in IHC assessment was significantly associated with pCR [39]. However, another study found high survivin expression to be associated with a good response to chemotherapy [40, 41]. Lin et al. observed that in LABC patients the response rate to anthracycline/taxanes preoperative chemotherapy was higher in survivin positive breast tumours [40]. Sensitivity to preoperative chemotherapy in LABC patients may depend not only on the main “wild-type” survivin variant, but also on different transcript forms such as survivin-3B, survivin-ΔEx3 and survivin-2B [42]. Moreover, Faversani et al. demonstrated that overexpression of survivin-ΔEx3 preserves breast
348 Arch Med Sci 2, 1st March / 2023
Piotr Pluta, Dorota Jesionek-Kupnicka, Agnieszka Pluta, Kamil Brzozowski, Marcin Braun, Joanna Kubicka-Wołkowska, Janusz Piekarski
Parameter Survivin expression P -value Contingency coefficient Tau b Kendall Low/intermediate n (%) High n (%) Patients, n 60 40 (67) 20 (33) Age [years] < 50 15 (25) 6 (10) 0.774 0.07 –0.07 ≥ 50 25 (42) 14 (23) Tumour size T1/T2 21 (35) 9 (15) 0.584 0.07 –0.07 T3/T4 19 (32) 11 (18) TNM stage II B 3 (5) 3 (5) 0.361 0.12 0.12 III 37 (62) 17 (28) Histological type NST 36 (60) 18 (30) 1.000 0.00 0.00 LOB 4 (7) 2 (3) Histological grade G2 18 (30) 12 (20) 0.273 0.14 0.14 G3 22 (37) 8 (13) ER status Negative 22 (37) 8 (13) 0.273 0.14 –0.14 Positive 18 (30) 12 (20) PR status Negative 23 (38) 9 (15) 0.360 0.12 –0.12 Positive 17 (28) 11 (18) HER-2 status Negative 25 (42) 9 (15) 0.197 0.16 –0.17 Positive 15 (25) 11 (18) Triple negative No 25 (42) 16 (27) 0.170 0.17 0.18 Yes 15 (25) 4 (7) NST – invasive carcinoma of no special type, LOB – invasive lobular carcinoma, ER – oestrogen receptor, PR – progesterone receptor, HER-2 – human epidermal growth factor receptor type 2.
Table II. Relationship between survivin expression and
– invasive carcinoma of no special type, LOB – invasive lobular carcinoma, ER – oestrogen receptor, PR – progesterone receptor, HER-2 – human epidermal growth factor receptor type 2, pCR – pathological complete response, non-pCR – non-pathological complete response.
cancer cells from the first-line anthracycline-based chemotherapy [43]. They also found that the anti-survivin small molecule sepantronium bromide (YM155), which acts as a transcriptional suppressant of the survivin locus, incorporated into a doxorubicin regimen, induced apoptosis in tumour cells.
In the present study low pre-treatment survivin expression and survival correlated with better OS and DFS. In the multivariate analysis we also found that survivin expression is an independent risk factor for DFS and OS. We also demonstrated predictive value of survivin expression for relapse and death. These findings are similar to the study of Zhao et al., which also revealed that LABC patients with low survivin protein expression treated with anthracycline-based neoadjuvant chemotherapy
had a better prognosis [39]. A gene expression study confirmed that survivin overexpression can serve as a negative prognostic factor but only in a subgroup of breast cancer patients, who did not achieve pCR after the neoadjuvant chemotherapy [44]. In contrast, Span et al. reported that patients in a post-chemotherapy subgroup with high cytosolic survivin expression achieved significantly longer progression-free survival than those with a low level [28]. Two meta-analyses of breast cancer patients found high survivin expression to be a poor prognostic factor for overall survival, irrespective of the disease stage [25, 26].
There are some limitations of our study. In the study, 33% of the patients achieved pCR, which is higher than in many other previous studies [45, 46]. This difference may partly result from the
Arch Med Sci 2, 1st March / 2023 349
Prognostic value of XIAP and survivin expression in locally advanced breast cancer patients treated with anthracycline-based neoadjuvant chemotherapy
Parameter non-pCR n (%) pCR n (%) P -value Contingency coefficient Tau b Kendall Age [years] < 50 13 (22) 8 (13) 0.775 0.074 –0.074 ≥ 50 27 (45) 12 (20) Tumour size T1/T2 19 (32) 11 (18) 0.587 0.07 –0.07 T3/T4 21 (35) 9 (15) TNM stage IIB 4 (7) 2 (3) 0.648 0.00 0.00 III 36 (60) 18 (30) Histological type NST 36 (60) 18 (30) 0.648 0.00 0.00 LOB 4 (7) 2 (3) Histological grade G2 20 (33) 10 (17) 1.000 0.00 0.00 G3 20 (33) 10 (17) ER status Negative 19 (32) 11 (18) 0.587 0.07 –0.07 Positive 21 (35) 9 (15) PR status Negative 21 (35) 11 (18) 0.856 0.02 –0.02 Positive 19 (32) 9 (15) HER-2 status Negative 18 (30) 16 (27) 0.021 0.32 –0.33 Positive 22 (37) 4 (7) Triple negative No 29 (48) 12 (20) 0.331 0.13 0.13 Yes 11 (18) 8 (13) XIAP expression Low/ intermediate 27 (45) 19 (32) 0.040 0.29 –0.31 High 13 (22) 1 (2) Survivin expression Low/ intermediate 20 (33) 20 (33) < 0.001 0.45 0.50 High 20 (33) 0 NST
Table III. Clinicopathological parameters and expression of XIAP and survivin in relation to pathological complete response (pCR)
Table IV. Clinicopathological parameters and expression of XIAP and survivin in relation to disease-free survival and overall survival
DFS – disease-free survival, OS – overall survival, ND – not enough data, NST – invasive carcinoma of no special type, LOB – invasive lobular carcinoma, ER – oestrogen receptor, PR – progesterone receptor, HER-2 – human epidermal growth factor receptor type 2, pCR – pathological complete response, non-pCR – non-pathological complete response.
350 Arch Med Sci 2, 1st March / 2023
Piotr Pluta, Dorota Jesionek-Kupnicka, Agnieszka Pluta, Kamil Brzozowski, Marcin Braun, Joanna Kubicka-Wołkowska, Janusz Piekarski
Parameter DFS OS Probability of 10-year DFS HR 95% CI Log-rank p -value Probability of 10-year OS HR 95% CI Log-rank p -value Age [years]: 0.653 0.157 < 50 65.8% 0.802 0.304–2.113 80.8% 0.418 0.114–1.48 ≥ 50 62.6% 63.6% Tumour size: 0.608 0.799 T1/T2 62.3% 1.271 0.508–3.182 66.7% 0.877 0.317–2.427 T3/T4 65.1% 70.4% TNM stage: 0.958 0.187 IIB 66.7% 1.041 0.239–4.53 40.0% 2.297 0.645–8.182 III 63.3% 72.3% Histological type: 0.618 0.117 NST 67.3% 0.747 0.217–2.571 65.5% ND ND LOB 27.8% 100% Histological grade: 0.101 0.674 G2 53.3% 2.193 0.832–5.779 68.7% 0.805 0.291–2.225 G3 76.4% 67.5% ER status: 0.432 0.375 Negative 69.9% 0.696 0.279–1.735 74.2% 0.63 0.227–1.773 Positive 56.2% 61.7% PR status: 0.092 0.950 Negative 75.1% 0.46 0.181–1.168 67.5% 1.033 0.374–2.854 Positive 51.6% 70.3% HER-2 status: 0.019 0.379 Negative 73.6% 0.329 0.128–0.844 74.1% 0.637 0.231–1.76 Positive 51.2% 61.5% Triple negative: 0.408 0.601 No 59.5% 1.513 0.544–4.206 68.1% 1.349 0.429–4.24 Yes 70.6% 68.8% pCR 88.1% 0.124 0.028–0.554 0.001 100% ND ND 0.001 non-pCR 48.8% 51.2% XIAP expression: 0.017 0.052 Low/intermediate 75.1% 0.304 0.12–0.773 78.6% 0.332 0.114–0.97 High 0% 0% Survivin expression: < 0.001 < 0.001 Low/intermediate 82.8% 0.095 0.035–0.263 87.5% 0.087 0.025–0.311 High 0% 32.9%
Prognostic value of XIAP and survivin expression in locally advanced breast cancer patients treated with anthracycline-based neoadjuvant chemotherapy
broad definition of pCR used in the study, which in this case is based on the response of the tumour invasive component: the patients with residual ductal carcinoma observed in situ (ypT0/is) in the breast tissue specimen and with any axillary lymph node status were, therefore, also included in the pCR group. However, this approach did not diminish the prognostic role of pCR in our study, since the patients who attained pCR still demonstrated better OS and DFS.
There are several well-established clinicopathological factors for pCR achievement, e.g. younger age of patients, smaller tumour size or triple negative breast cancer [47, 48]. No such correlations were observed, which may result from the limited number of patients in our cohort or the sampling method. However, HER-2 positive receptor status
was found to have a significant impact on the chance of non-pCR and DFS. This may be associated with the lack of a targeted anti-HER-2 therapy in the preoperative regimen at that time: a combined chemotherapy with trastuzumab and/or pertuzumab is currently recommended in HER-2 positive LABC patients [49].
In contrast to XIAP, which is predominantly located in the cytosol compartment, survivin is expressed in both the cytoplasm and nucleus, which implicates different molecular mechanisms of action and has a potential prognostic value [15, 19, 25, 50]. In cancer cells, cytosol survivin has been related to inhibition of apoptosis, while nuclear survivin is more likely to be involved in aberrant proliferation. Collin et al., in a recently published case-control study encompassing a large patient
Arch Med Sci 2, 1st March / 2023 351 XIAP expression Survivin expression XIAP expression Survivin expression DFS DFS OS OS 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 0 24 48 72 96 120 144 168 Time [months] 0 24 48 72 96 120 144 168 Time [months] 0 24 48 72 96 120 144 168 Time [months] 0 24 48 72 96 120 144 168 Time [months] p = 0.01662 p = 0.00001 p = 0.05150 p = 0.00001 A C
D Low and intermediate expression High expression Figure 2.
for disease-free survival (DFS) (A, C) and overall survival (OS) (B, D) in 60 LABC patients LABC – locally advanced breast cancer.
B
Kaplan-Meier curves
Table V. Multivariate Cox regression analysis for disease-free survival (DFS) and overall survival (OS)
disease-free survival, OS – overall survival, ND – not enough data, NST – invasive carcinoma of no special type, LOB
invasive lobular carcinoma, ER – oestrogen receptor, PR – progesterone receptor, HER-2 – human epidermal growth factor receptor type 2, pCR – pathological complete response, non-pCR – non-pathological complete response.
Table VI. Predictive value of XIAP and survivin expression for non-PCR, relapse and death
AUC – area under the ROC curve, non-pCR – non-pathological complete response.
352 Arch Med Sci 2, 1st March / 2023
Piotr Pluta, Dorota Jesionek-Kupnicka, Agnieszka Pluta, Kamil Brzozowski, Marcin Braun, Joanna Kubicka-Wołkowska, Janusz Piekarski
Parameter DFS OS HR 95% CI P -value HR 95% CI P -value Age [years] <50 vs. ≥ 50 1.019 0.292–3.558 0.976 0.777 0.181–3.331 0.734 Tumour size: T1/T2 vs. T3/T4 3.668 0.997–13.493 0.06 1.912 0.586–6.238 0.282 TNM stage: IIB vs. III 1.587 0.234–10.785 0.636 1.258 0.222–7.139 0.795 Histological type: NST vs. LOB 0.306 0.036–2.592 0.277 ND ND ND Histological grade: G2 vs. G3 1.509 0.48–4.737 0.48 0.356 0.109–1.165 0.088 ER status: Negative vs. positive 5.302 0.692–40.598 0.108 0.749 0.111–5.051 0.767 PR status: Negative vs. positive 0.17 0.018–1.652 0.127 2.304 0.389–13.652 0.358 HER-2 status: Negative vs. positive 0.104 0.009–1.129 0.063 0.838 0.162–4.333 0.833 Triple negative: No vs. yes 0.094 0.006–1.556 0.099 0.872 0.082–9.235 0.909 pCR vs. non-pCR 0.329 0.047–2.316 0.264 ND ND ND XIAP expression: Low/intermediate vs. high 2.58 0.668–9.96 0.169 1.383 0.321–5.962 0.663 Survivin expression: Low/intermediate vs. high 0.05 0.011–0.266 < 0.001 0.04 0.007–0.218 < 0.001 DFS
–
–
Parameter Sensitivity Specificity AUC (95% CI) AUC p -value Prediction of non-PCR: XIAP low/medium vs. high (for cut-off: high) 0.325 0.950 0.638 (0.497; 0.778) 0.056 Survivin low/medium vs. high (for cut-off: high) 0.500 1.000 0.750 (0,630; 0.870) < 0.001 Prediction of relapse: XIAP low/medium vs. high (for cut-off: high) 0.421 0.842 0.632 (0.471; 0.792) 0.108 Survivin low/medium vs. high (for cut-off: high) 0,.632 0.868 0.750 (0.604; 0.896) 0.001 Prediction
XIAP low/medium vs. high (for cut-off: high) 0.400 0.822 0.611 (0.437; 0.785) 0.210 Survivin low/medium vs. high (for cut-off: high) 0.800 0.822 0.811 (0.676; 0.946) < 0.001
of death:
Prognostic value of XIAP and survivin expression in locally advanced breast cancer patients treated with anthracycline-based neoadjuvant chemotherapy
group (n = 541), did not confirm the association between cytoplasmic or nuclear survivin expression and breast cancer recurrence [51]. However, some previously conducted meta-analyses have revealed that cytoplasmic survivin overexpression is an unfavourable prognostic factor, while high expression of nuclear survivin has no impact on breast cancer prognosis [25, 26]. Nevertheless, in the present study we assessed the expression of both proteins throughout the cell with regard to their changes in cellular distribution during the cell lifetime and their uncertain prognostic impact.
In the era of novel cancer treatment IAP family proteins have become an attractive target for anticancer therapy. BIR domains of XIAP (as well as cIAP1/2) are the aim for the small molecules also known as SMAC mimetics, which play a role similar to that of the natural IAP antagonist SMAC/ DIABLO protein (Second Mitochondria-derived Activator of Caspases/Direct IAp Binding with Low pI) [52]. Preclinical and first clinical studies using SMAC mimetics in the treatment of solid tumour patients, such as breast and pancreatic cancer as well as lymphoma and leukaemia, are ongoing [52, 53]. Similarly, small molecules may block survivin through direct binding or more often by interacting with other cancer cell proteins [54, 55]. An alternative way of targeting survivin in cancer therapy is the use of survivin-based vaccines to generate a specific anti-survivin cytotoxic T-cell response. This type of immunotherapy has brought promising results in various cancers, including breast tumours [55, 56]. Further investigations of the novel IAP specific treatment complimenting the standard chemotherapy would be a prospect for improvement of the long-term prognosis of LABC patients.
In conclusion, low/intermediate expression of XIAP and survivin in the pre-treatment biopsies in LABC patients treated with anthracycline-based chemotherapy was significantly associated with pCR and positively correlated with disease-free survival and overall survival. However, to better understand the role of IAP proteins in the response of tumours to treatment, further studies with study groups including larger numbers of LABC patients are required. They should also be based around a complete IAP family panel that considers subcellular diversion and other treatment regimens, such as chemotherapy, biological and hormone therapy.
Acknowledgments
We thank Mr Edward Lowczowski from the Medical University of Lodz for language assistance.
This work was supported by the sources of the Medical University of Lodz (Grant No. 503/1-03401/503-06-100).
Conflict of interest
The authors declare no conflict of interest.
References
1. Harding C, Pompei F, Burmistrov D, Wilson R. Long-term relationships between screening rates, breast cancer characteristics, and overdiagnosis in US counties, 19752009. J Cancer 2019; 144: 476-88.
2. Augustynowicz A, Czerw AI, Deptała A. Health needs as a priority of local authorities in Poland based on the example of implementation of health policy cancer programs. Arch Med Sci 2018; 14: 1439-49.
3. Woźniacki P, Skokowski J, Bartoszek K, Kosowska A, Kalinowski L, Jaśkiewicz J. The impact of the Polish mass breast cancer screening program on prognosis in the Pomeranian Province. Arch Med Sci 2017; 132: 441-7.
4. Simos D, Clemons M, Ginsburg OM, Jacobs C. Definition and consequences of locally advanced breast cancer. Curr Opin Support Palliat Care 2014; 8: 33-8.
5. Adams S, Chakravarthy AB, Donach M, et al. Preoperative concurrent paclitaxel-radiation in locally advanced breast cancer: pathologic response correlates with five-year overall survival. Breast Cancer Res Treat 2010; 124: 723-32.
6. Rastogi P, Anderson SJ, Bear HD, et al. Preoperative chemotherapy: updates of National Surgical Adjuvant Breast and Bowel Project Protocols B-18 and B-27. J Clin Oncol 2008; 26: 778-85.
7. Dawood S, Ueno NT, Valero V, et al. Differences in survival among women with stage III inflammatory and noninflammatory locally advanced breast cancer appear early: a large population-based study. Cancer 2011; 117: 1819-26.
8. Brito RA, Valero V, Buzdar AU, et al. Long-term results of combined-modality therapy for locally advanced breast cancer with ipsilateral supraclavicular metastases: the University of Texas M.D. Anderson Cancer Center experience. J Clin Oncol 2001; 19: 628-33.
9. Hanahan D, Weinberg Ra. The hallmarks of cancer. Cell 2000; 100: 57-70.
10. Dubrez-Daloz L, Dupoux A, Cartier J. IAPs: more than just inhibitors of apoptosis proteins. Cell Cycle 2008; 15: 1036-46.
11. Crook NE, Clem RJ, Miller LK An apoptosis-inhibiting baculovirus gene with a zinc finger-like motif. J Virol 1993; 67: 2168-74.
12. Liston P, Fong WG, Korneluk RG. The inhibitors of apoptosis: there is more to life than Bcl2. Oncogene 2003; 22: 8568-80.
13. Mohamed MS, Bishr MK, Almutairi FM, Ali AG. Inhibitors of apoptosis: clinical implications in cancer. Apoptosis 2017; 22: 1487-509.
14. Deveraux QL, Takahashi R, Salvesen GS, Reed JC. X-linked IAP is a direct inhibitor of cell-death proteases. Nature 1997; 388: 300-4.
15. Gao X, Zhang L, Wei Y, et al. Prognostic value of XIAP level in patients with various cancers: a systematic review and meta-analysis. J Cancer 2019; 10: 1528-37.
16. Pluta A, Wierzbowska A, Cebula-Obrzut B, et al. Prognostic value of inhibitor of apoptosis protein family expression in patients with acute myeloid leukemia. Leuk Lymphoma 2015; 56: 2529-35.
17. Yang XH, Feng ZE, Yan M, et al. XIAP is a predictor of cisplatin-based chemotherapy response and prognosis for patients with advanced head and neck cancer. PLoS One 2012; 7: e31601.
Arch Med Sci 2, 1st March / 2023 353
18. Hussain AR, Siraj AK, Ahmed M, et al. XIAP over-expression is an independent poor prognostic marker in Middle Eastern breast cancer and can be targeted to induce efficient apoptosis. BMC Cancer 2017; 17: 640.
19. Pluta P, Jeziorski A, Cebula-Obrzut AP, et al. Expression of IAP family proteins and its clinical importance in breast cancer patients. Neoplasma 2015; 62: 666-73.
20. Xu YC, Liu Q, Dai JQ, et al. Tissue microarray analysis of X-linked inhibitor of apoptosis (XIAP) expression in breast cancer patients. Med Oncol 2014; 31: 764.
21. Parton M, Krajewski S, Smith I, et al. Coordinate expression of apoptosis-associated proteins in human breast cancer before and during chemotherapy. Clin Cancer Res 2002; 8: 2100-8.
22. Chen X, Duan N, Zhang C, Zhang W. Survivin and tumorigenesis: molecular mechanisms and therapeutic strategies. J Cancer 2016; 7: 314-23.
23. Ambrosini G, Adida C, Altieri DC. A novel anti-apoptosis gene, survivin, expressed in cancer and lymphoma. Nat Med 1997; 3: 917-21.
24. Wang W, Zhang B, Mani AM, et al. Survivin inhibitors mitigate chemotherapeutic resistance in breast cancer cells by suppressing genotoxic nuclear factor-kappaB activation. J Pharmacol Exp Ther 2018; 366: 184-93.
25. Li Y, Ma X, Wu X, Liu X, Liu L. Prognostic significance of survivin in breast cancer: meta-analysis. Breast J 2014; 20: 514-24.
26. Song J, Su H, Zhou YY, Guo LL. Prognostic value of survivin expression in breast cancer patients: a meta-analysis. Tumour Biol 2013; 34: 2053-62.
27. Kostadima L, Pentheroudakis G, Fountzilas G, et al. Survivin and glycodelin transcriptional activity in node-positive early breast cancer: mRNA expression of two key regulators of cell survival. Breast Cancer Res Treat 2006; 100: 161-7.
28. Span PN, Sweep FC, Wiegerinck ET, et al. Survivin is an independent prognostic marker for risk stratification of breast cancer patients. Clin Chem 2004; 50: 1986-93.
29. Sobin LH, Gospodarowicz MK, Wittekind C. TNM Classification of Malignant Tumours. 7th ed. Wiley-Blackwell, 2009.
30. Allred DC, Harvey JM, Berardo M, Clark GM. Prognostic and predictive factors in breast cancer by immunohistochemical analysis. Mod Pathol 1998; 11: 155-68.
31. Pluta P, Jesionek-Kupnicka D, Kubicka-Wołkowska J, et al. SMAC protein expression as a potent favorable prognostic factor in locally advanced breast cancer. Pol J Pathol 2018; 69: 33-41.
32. Perrone F, Suardi S, Pastore E, et al. Molecular and cytogenetic subgroups of oropharyngeal squamous cell carcinoma. Clin Cancer Res 2006; 12: 6643-51.
33. Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Lawrence Erlbaum, New Jersey 1988.
34. Schemper M, Smith TL. A note on quantifying follow-up in studies of failure time. Control Clin Trials 1996; 17: 343-6.
35. Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982; 143: 29-36.
36. Evans MK, Sauer SJ, Nath S, Robinson TJ, Morse MA, Devi GR. X-linked inhibitor of apoptosis protein mediates tumor cell resistance to antibody-dependent cellular cytotoxicity. Cell Death Dis 2016; 7: e2073.
37. Aird KM, Ghanayem RB, Peplinski S, Lyerly HK, Devi GR. X-linked inhibitor of apoptosis protein inhibits apoptosis in inflammatory breast cancer cells with acquired resistance to an ErbB1/2 tyrosine kinase inhibitor. Mol Cancer Ther 2010; 9: 1432-42.
38. Kennedy SM, O’Driscoll L, Purcell R, et al. Prognostic importance of survivin in breast cancer. Br J Cancer 2003; 88: 1077-83.
39. Zhao YC, Wang Y, Ni XJ, et al. Clinical significance of Smac and survivin expression in breast cancer patients treated with anthracycline-based neoadjuvant chemotherapy. Mol Med Rep 2014; 9: 614-20.
40. Lin Q, Liu Y, Chen H, et al. Survivin, Ki-67 and tumor grade as predictors of response to docetaxel-based neoadjuvant chemotherapy in locally advanced breast cancer. Mol Clin Oncol 2013; 1: 839-44.
41. Petrarca CR, Brunetto AT, Duval V, Brondani A, Carvalho GP, Garicochea B. Survivin as a predictive biomarker of complete pathologic response to neoadjuvant chemotherapy in patients with stage II and stage III breast cancer. Clin Breast Cancer 2011; 11: 129-34.
42. Boidot R, Vegran F, Lizard-Nacol S. Predictive value of survivin alternative transcript expression in locally advanced breast cancer patients treated with neoadjuvant chemotherapy. Int J Mol Med 2009; 23: 285-91.
43. Faversani A, Vaira V, Moro GP, et al. Survivin family proteins as novel molecular determinants of doxorubicin resistance in organotypic human breast tumors. Breast Cancer Res 2014; 16: R55.
44. Hamy AS, Bieche I, Lehmann-Che J, et al. BIRC5 (survivin): a pejorative prognostic marker in stage II/III breast cancer with no response to neoadjuvant chemotherapy. Breast Cancer Res Treat 2016; 159: 499-511.
45. Masood S. Neoadjuvant chemotherapy in breast cancers. Womens Health (Lond) 2016; 12: 480-91.
46. Cortazar P, Geyer CE Jr. Pathological complete response in neoadjuvant treatment of breast cancer. Ann Surg Oncol 2015; 22: 1441-6.
47. Untch M, Konecny GE, Paepke S, von Minckwitz G. Current and future role of neoadjuvant therapy for breast cancer. Breast 2014; 23: 526-37.
48. Kołacińska A, Chałubińska J, Błasińska-Morawiec M, et al. Pathological complete response in younger and older breast cancer patients. Arch Med Sci 2012; 8: 310-5.
49. https://www.nccn.org/professionals/physician_gls/pdf/ breast.pdf
50. Fortugno P, Wall NR, Giodini A, et al. Survivin exists in immunochemically distinct subcellular pools and is involved in spindle microtubule function. J Cell Sci 2002; 115: 575-85.
51. Collin LJ, Cronin-Fenton DP, Ahern TP, et al. Expression of survivin does not appear to influence breast cancer recurrence risk. Acta Oncol 2019; 58: 154-61.
52. Cossu F, Milani M, Mastrangelo E, Lecis D. Targeting the BIR domains of inhibitor of apoptosis (IAP) proteins in cancer treatment. Comput Struct Biotechnol J 2019; 25: 142-50.
53. Ali R, Singh S, Haq W. IAP proteins antagonist: an introduction and chemistry of Smac mimetics under clinical development. Curr Med Chem 2018; 25: 3768-95.
54. Xiao M, Xue Y, Wu Z, et al. Design, synthesis and biological evaluation of selective survivin inhibitors. J Biomed Res 2019; 22: 82-100.
55. Garg H, Suri P, Gupta JC, Talwar GP, Dubey S. Survivin: a unique target for tumor therapy. Cancer Cell Int 2016; 16: 49.
56. Onodi F, Maherzi-Mechalikh C, Mougel A, et al. High therapeutic efficacy of a new survivin LSP-cancer vaccine containing CD4+ and CD8+ T-Cell epitopes. Front Oncol 2018; 13: 517.
354 Arch Med Sci 2, 1st March / 2023
Piotr Pluta, Dorota Jesionek-Kupnicka, Agnieszka Pluta, Kamil Brzozowski, Marcin Braun, Joanna Kubicka-Wołkowska, Janusz Piekarski
Prognostic value of midkine, syndecan-1, hyaluronan synthase-2, sestrin-1, laminin subunit alpha-4 and fibulin-3 for malignant pleural mesothelioma
Hakan Akgun1,2, Selma Metintas1,3, Guntulu Ak1,2, Secil Demirkol Canlı4, Murat Isbilen4, Ali O. Gure4, Muzaffer Metintas1,2
1Eskisehir Osmangazi University Lung and Pleural Cancers Research and Clinical Center, Eskisehir, Turkey
2Department of Chest Diseases, Medical Faculty, Eskisehir Osmangazi University, Eskisehir, Turkey
3Department of Public Health, Medical Faculty, Eskisehir Osmangazi University, Eskisehir, Turkey
4Department of Molecular Biology and Genetics, İhsan Doğramacı Bilkent University, Ankara, Turkey
Submitted: 21 January 2019; Accepted: 22 September 2019
Online publication: 25 March 2021
Arch Med Sci 2023; 19 (2): 355–364
DOI: https://doi.org/10.5114/aoms/112525
Copyright © 2021 Termedia & Banach
Abstract
Introduction: The prognosis of malignant pleural mesothelioma (MPM) is poor, with a limited survival time. In this study, we aimed to examine expression levels of genes selected from relevant literature and to utilize in silico methods to determine genes whose expression could reflect the prognosis of patients with MPM by ex-vivo validation experiments.
Material and methods: The study group consisted of 54 MPM patients treated with chemotherapy. Expression of 6 genes – midkine (MDK), syndecan-1 (SDC1), hyaluronan synthase-2 (HAS2), sestrin-1 (SESN1), laminin subunit alpha-4 (LAMA4), and fibulin-3 (FBLN3) – was examined by qPCR in tumor tissues. Sestrin-1 and LAMA4 were identified using an in house R-based script: Unsupervised Survival Analysis Tool. Midkine, SDC1, HAS2, and FBLN3 were selected from current literature. We used two housekeeping genes, i.e. glucose-6-phosphate dehydrogenase and TATA-box binding protein, as controls.
Results: Of the patients, 43 (79.6%) had epithelioid mesothelioma. The median survival for all patients was 10 (±1.2 SE) months (95% CI: 7.7–12.3). In multivariate analyses, MDK ( p = 0.007), HAS2 ( p = 0.008) and SESN1 ( p = 0.014) expression levels were related to survival time in the whole group. In epithelioid type MPM patients, MDK ( p = 0.014), FBLN3 ( p = 0.029), HAS2 ( p = 0.014) and SESN1 ( p = 0.045) expression was related to survival time in multivariate analyses.
Conclusions: High HAS2 and SESN1 expressions and low MDK are potential biomarkers of good prognosis in MPM. High HAS2 and SESN1 expression and low MDK and FBLN3 can also be utilized as biomarkers of good prognosis for epithelioid MPM. Those results should be further investigated in sera, plasma, and pleural effusions.
Key words: prognosis, mesothelioma, midkine, sestrin-1, hyaluronan synthase-2, syndecan-1, fibulin-3, laminin subunit alpha-4.
Introduction
Malign pleural mesothelioma (MPM) is the primary malignant tumor of the pleura, which usually develops secondary to asbestos or erionite
Corresponding author: Muzaffer Metintas
Eskisehir Osmangazi University Lung and Pleural Cancers Research and Clinical Center
Eskisehir, Turkey
E-mail: muzaffermetintas@gmail.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/).
Clinical research Oncology
exposure [1, 2]. Overall, the prognosis is poor in patients with MPM, where the survival ranges from 6 to 17 months with a median of 12 months or less [3–5]. Though chemotherapy increases median survival slightly, the response to chemotherapeutic agents is reported to be around 50% [6]. Nevertheless, improved outcomes were reported with multimodal treatment in cases with early-stage, epithelioid-type tumors [7]. As almost all patients receive chemotherapy, identifying those patients with better prognosis via biomarkers is as important as early diagnosis. Moreover, determination of good prognostic factors is critical for the development of novel therapeutic regimens and identification of biologically distinct subgroups of the disease which will respond to the therapy.
Younger age, early-stage disease, epithelial type tumor, and good performance status are among well-accepted clinical factors indicative of better outcome. Positron emission tomography–computed tomography (PET-CT) and biomarkers also have potential value in this manner [8, 9]. Biomarkers draw great attention not only because of their ease of use in blood samples and being less expensive and repeatable, but also because the monitoring of their presences is relevant to the emergence and development of the tumor. However, no biomarker has been jointly agreed upon yet to determine the prognosis or to monitor the therapy in MPM.
In this study, we aimed to identify biological markers that could be used to determine the prognosis in MPM. To achieve this purpose, in tumor tissue, at diagnosis we examined midkine (MDK) [10], syndecan-1 (SDC1) [11], and hyaluronan synthase-2 (HAS2) [12], which we analyzed in our previous studies of MPM patients. We further studied sestrin-1 (SESN1) and laminin subunit alpha-4 (LAMA4), which was predicted to affect the prognosis by the Unsupervised Survival Analysis Tool (USAT) [13]. Fibulin-3 (FBLN3), which is widely studied as a potential diagnostic and prognostic marker [14, 15], was included in the study.
Material and methods
The study was performed between March 2015 and March 2017 in Eskisehir Osmangazi University Lung and Pleural Cancers Research and Clinical Center after being approved by the Ethics Committee for Clinical Research of Eskisehir Osmangazi University (Approval no: 80558721/69). Written informed consent was obtained from all patients.
Study population
A total of 54 patients who received chemotherapy and had an established diagnosis of MPM
were included in the study. At the planning stage of the study, the sample size was calculated as at least 54, assuming a medium effect size a error of 0.05 and b error (1-power) of 0.20. Age, sex, smoking status, asbestos exposure, clinical findings, and Karnofsky Performance Score (KPS) of the subjects were recorded. Their diagnostic, therapeutic, and prognostic follow-up data were documented with diagnosis data, histopathological type of the tumor, disease stage, chemotherapy regimens, treatment responses, and recurrence and mortality date. All of the patients included in the study have died. The stage was determined according to the 8th edition of TNM classification [16–18]. These parameters were further analyzed in the epithelioid MPM subgroup since such cases constitute the majority of all MPM patients and chemotherapy and other treatment modalities are more effective in these patients.
Biological analyses
We examined expression of MDK, SDC1, HAS2, SESN1, LAMA4 and FBLN3 in this study. We identified SESN1 and LAMA4 using an in house R-based script, Unsupervised Survival Analysis Tool (USAT), as defined elsewhere [13]. The GSE17118 dataset was analyzed using USAT to identify candidate genes that could be associated with prognosis of mesothelioma patients. USAT uses Cox proportional hazard regression, maximally selected rank statistics and log-rank tests with different types of expression data and stage stratification to determine stage-independent prognostic gene markers. Any gene is considered as significant when any of its probesets are significant in all those three statistical tests. We also chose to test FBLN3 as a potential prognostic marker [14, 15].
Pleural tissue specimens used in the study were histopathologically confirmed MPM samples that were obtained by diagnostic image-guided needle biopsy or medical thoracoscopy before the treatment. These tissue specimens were stored at –80°C until the laboratory studies were initiated.
RNA isolated from tissue samples (Norgen Animal Tissue RNA Isolation Kit [#25700] kit) were used for qPCR. cDNA was prepared from 200 ng of RNA (Genedirex GScript RTase kit). Glucose-6-phosphate dehydrogenase (G6PD) and TATA-box binding protein (TBP) were selected as housekeeping genes. Primers were designated to exon-span to avoid amplification of genomic DNA contamination. A Roche LightCycler 480 Real Time PCR (qPCR) device and ABM EvaGreen qPCR Mastermix-S kit were used to quantify expression of the determined genes in the tissue samples. qPCR results were pre-analyzed with Roche Relative Quantification. Crossing point (Cp) values of all samples were obtained after qPCR.
356 Arch Med Sci 2, 1st March / 2023
Hakan Akgun, Selma Metintas, Guntulu Ak, Secil Demirkol Canlı, Murat Isbilen, Ali O. Gure, Muzaffer Metintas
qPCR based expression of the 6 genes in the ex-vivo cohort was assessed and used for log-rank multiple cut-off analysis (LRMC) (Figure 1). The cut-off with the lowest p-value within the 10th and 90th percentiles was determined as threshold for each gene for further Kaplan-Meier analysis. The cut-off values
of MDK, SDC1, HAS2, SESN1, LAMA4, and FBLN3 genes were 2.04, 0.04, 0.55, 0.9, 0.9, 1.04 for good prognosis, respectively. The median survival times for low (< 0.9) and high expression (≥ 0.9) of LAMA4 were 9.0 (6.8–11.2) months and 10.1 (6.8–13.2) months, respectively (log-rank = 0.137; p = 0.711).
Arch Med Sci 2, 1st March / 2023 357
Prognostic value of midkine, syndecan-1, hyaluronan synthase-2, sestrin-1, laminin subunit alpha-4 and fibulin-3 for malignant pleural mesothelioma
2.5 2.0 1.5 1.0 0.5 0 A –log10( p ) B Expression threshold 1.5 1.0 0.5 0 –log10( p ) Expression threshold 1.5 1.0 0.5 0 C –log10( p ) D Expression threshold 2.5 2.0 1.5 1.0 0.5 0 –log10( p ) Expression threshold 3 2 1 0 E –log10( p ) F Expression threshold 1.5 1.0 0.5 0 –log10( p ) Expression threshold
Figure 1. Log rank multiple cut-off plots genrated for SESN1 (A), LAMA4 (B), MDK (C), FBLN3 (D), SDC1 (E), HAS2 (F) genes in ex-vivo cohort (n = 54). Horizontal line indicates log rank p value of 0.05. Vertical lines indicates 10th percentile, median and 90th percentile.
Table I. Patient characteristics
Cox regression analysis. Then, factors affecting the prognosis (genes, stage, histopathology and KPS) were determined by Cox regression analysis for all of the variables with p < 0.20. Statistical analyses were performed using IBM SPSS Version 15.0 Software (IBM Corp., Armonk, NY). Statistical power was calculated by G * Power (Version 3.1.9.2) statistical software. After the study, actual power in post-hoc power analysis was calculated as 0.8040880.
Results
In order to evaluate the prognostic value of the expression of MDK, SDC1, HAS2, SESN1, LAMA4, and FBLN3 genes, we used an ex-vivo MPM cohort. Demographic and clinical characteristics of the MPM patients in the study are presented at Table I.
Statistical analysis
Continuous variables were expressed as mean ± standard deviation (SD), median, and minimummaximum values whereas categorical variables were expressed as percentages. The ΔCp value was calculated by subtracting the reference gene’s Cp value from the test gene’s Cp value. The reference gene’s Cp value was the geometrical mean of the Cp value of housekeeping genes. The calculation of ΔΔCp involved subtraction by the ΔCp calibrator value. The fold changes for relative gene expression were determined by 2 Δ(ΔCp)
Log-rank multiple cut-off analysis was used to determine appropriate cut-off values for each gene as described previously [19]. Briefly, patients were divided into two groups based on all gene expression values, and log-rank p-values were calculated for the resulting strata. Graphs featuring –log10(p) values (y axis) and cut-off values (x axis) for each gene were then created. In all LRMC figures the first, second, and third vertical lines indicate the 10th percentile, median, and 90th percentile, respectively. The horizontal line indicates the negative logarithmic value (1.30) of p = 0.05, which was accepted as the margin of statistical value. Optimal cut-off values were determined by accepting the values above the horizontal line and between the 10th and 90th percentiles.
Overall survival was calculated from the date of diagnosis to death, or else censored at the last follow-up date. Survival analyses for each gene were performed with the Kaplan-Meier test based on the appropriate cut-off values. Adjustment was made according to stage and KPS to determine the effect of each gene on prognosis using
All patients had a history of asbestos exposure, 92.6% of which was environmental and the remaining 7.4% occupational. The percentage of MPM cases with smoking history was 37%. The chemotherapy regimen in the study was cisplatin plus pemetrexed.
The associations between patients’ median survival and studied gene expressions are shown in Figure 2.
The prognosis was significantly worse in patients with tumors overexpressing MDK (≥ 2.04) and FBLN3 (≥ 1.04) genes (Figures 2 A, E). On the other hand, the prognosis was significantly better in patients where SDC1 (≥ 0.04), HAS2 (≥ 0.55), and SESN1 (≥ 0.09) overexpression was detected (Figures 2 B, C, D). LAMA4 was not significantly associated with survival.
After adjustment for stage and KPS, Cox regression analysis showed that overexpression of MDK (p = 0.021), SDC1 (p = 0.009), HAS2 (p = 0.005), and SESN1 (p = 0.014) was associated with prognosis while FBLN3 (p = 0.657) and LAMA4 (p = 0.472) overexpression was not (Table II). In multivariate analysis, parameters of histopathology, stage, KPS and overexpression of MDK (p = 0.007), HAS2 (p = 0.008) and SESN1 (p = 0.014) genes were found to be independently and significantly associated with survival in MPM patients (Table II).
Epithelioid mesotheliomas constituted 79.6% of MPM cases in this study. After adjustment for stage and KPS, overexpression of HAS2 (p = 0.023) and SESN1 (p = 0.19) was associated with prognosis (Table III). Karnofsky Performance Score and overexpression of MDK (p = 0.014), FBLN3 (p = 0.029), HAS2 (p = 0.014) and SESN1 (p = 0.045) genes were found to be independently and significantly associated with survival in multivariable Cox regression analysis in epithelioid
358 Arch Med Sci 2, 1st March / 2023
Hakan Akgun, Selma Metintas, Guntulu Ak, Secil Demirkol Canlı, Murat Isbilen, Ali O. Gure, Muzaffer Metintas
III).
MPM patients (Table
Parameters Total Patients, n 54 Age [years], mean ± SD (min.–max.) 62.5 ±9.67 (36.0–82.0) Sex, n (%): Male 24 (44.4) Female 30 (55.6) Histopathology, n (%): Epithelioid 43 (79.6) Other (sarcomatoid, mixed) 11 (20.4) Stage, n (%): I–II 10 (18.5) III–IV 44 (81.5) KPS, median 80 (70–100) Survival [month], median (SE), (95% CI) 10.0 (1.2) (7.7–12.3) KPS – Karnofsky Performance Score, SD – standard deviation, SE – standard error, CI – confidence interval.
Prognostic value of midkine, syndecan-1, hyaluronan synthase-2, sestrin-1, laminin subunit alpha-4 and fibulin-3 for malignant pleural mesothelioma
Discussion
Determination of prognosis is very important in MPM both for life expectancy of the patient and selection and initiation of the best treatment options. There are some clinical factors associated with prognosis in MPM [20–22]. Nonetheless,
clinical factors are not useful for longitudinal follow-up of patients. With a focus on identifying prognostic biomarkers in MPM, this study evaluated the markers that we analyzed previously or were detected to be potentially effective by appropriate data software media yet there are no
Arch Med Sci 2, 1st March / 2023 359 Median survival (95% Cl) Log rank c2 = 6.36; p = 0.012 Low 11 (8.42–13.59) High 7 (5.64–8.36) 1.00 0.80 0.60 0.40 0.20 0 A Cumulative survival (%) B Survival [months] Cumulative survival (%) Survival [months] 0 10 20 30 40 50 0 10 20 30 40 50 1.00 0.80 0.60 0.40 0.20 0 1.0 0.8 0.6 0.4 0.2 0 C Cumulative survival (%) D Survival [months] Cumulative survival (%) Survival [months] 0 10 20 30 40 50 0 10 20 30 40 50 1.0 0.8 0.6 0.4 0.2 0 1.00 0.80 0.60 0.40 0.20 0 E Cumulative survival (%) Survival [months] 0 10 20 30 40 50 Midkine Median survival (95% Cl) Log rank c2 = 8.30; p = 0.004 Low 5 (3.20–6.80) High 10 (7.21–12.78) Syndecan-1 Median survival (95% Cl) Log rank c2 = 7.11; p = 0.008 Low 7 (4.85–9.14) High 11 (8.54–13.46) Sestrin-1 Median survival (95% Cl) Log rank c2 = 8.97; p = 0.003 Low 7 (5.32–8.67) High 11 (7.97–14.02) Hyaluronan synthase-2 Median survival (95% Cl) Log rank c2 = 6.98; p = 0.008 Low 10 (7.21–12.78) High 5 (0.19–9.80)
Fibulin-3
Figure 2. Kaplan-Meier survival curves of patients with mesothelioma classified by: A – midkine level in ex-vivo cohort (cutt-off: 2.04); B – syndecan-1 level in ex-vivo cohort (cutt-off: 0.04); C – hayluronan sybthase-2 level in ex-vivo cohort (cutt-off: 0.55); D – sestrin-1 level in ex-vivo cohort (cutt-off: 0.09); E – fibulin 3 level in ex-vivo cohort (cutt-off: 1.04)
known data in the literature. It might be thought that a prognostic biomarker could be elevated both in the blood and pleural fluid, facilitating the analysis of biomarkers in these body fluids. However, recent studies reported that investigation of prognostic biomarkers might be useful when initially analyzed in tumor tissues [23–25]. It may be more appropriate to examine tumor tissue since a limited number of samples will be studied in the first step of biomarker determination. If the presentation of a gene in the tumor tissue has been determined, then it can be analyzed in the body fluid samples of larger patient groups. Our study indicated that overexpression of MDK was associated with poor prognosis in tumor tissue of MPM patients whereas overexpression of HAS2 and SESN1 was associated with good prognosis, where a potential use of these biomarkers could be suggested.
Midkine encodes a heparin-binding growth factor that promotes survival, growth, and cellular mi-
multivariate analysis models
gration. Its genetic expression is especially present during embryogenesis [26], yet its level decreases until reaching a nadir in healthy adults [27]. Midkine is associated with a mitogenic effect, angiogenesis promoting effect, anti-apoptotic activity, and fibrinolytic activity in the development of malignancy. In the study where we investigated use of MDK and mesothelin in the diagnosis and prognosis of MPM, we detected that MDK was positively correlated with disease stage, and higher serum level of MDK was associated with poor prognosis after adjustment for disease stage, histological type, and treatment modalities [10]. In the current study, the prognosis was poorer in patients who had MDK overexpression, which was consistent with our previous findings.
Syndecan-1 encodes a cell surface proteoglycan, which regulates a variety of biological process including cellular division, differentiation, invasion, migration, and angiogenesis [28]. These functions imply a pathophysiological role for SDC1 in ma-
360 Arch Med Sci 2, 1st March / 2023
Hakan Akgun, Selma Metintas, Guntulu Ak, Secil Demirkol Canlı, Murat Isbilen, Ali O. Gure, Muzaffer Metintas
Parameter HR (95% CI)* P -value HR (95% CI)** P -value Histopathology: Epithelioid Ref 0.001 Ref 0.001 Others 3.70 (1.69–8.08) 4.51 (1.90–10.67) Stage: I–II Ref 0.020 Ref 0.027 III–IV 2.90 (1.18–7.10) 2.92 (1.13–7.59) KPS: ≥ 80 Ref 0.040 Ref 0.001 < 80 3.05 (1.05–8.83) 7.27 (2.22–23.79) MDK: Low Ref 0.021 Ref 0.007 High 2.91 (1.17–7.23) 3.89 (1.46–10.40) SDC1: High Ref 0.009 Ref 0.053 Low 3.47 (1.37-8.77) 2.77 (0.99-7.74) HAS2: High Ref 0.005 Ref 0.008 Low 2.72 (1.35–5.46) 2.77 (1.30–5.92) SESN1: High Ref 0.014 Ref 0.014 Low 3.67 (1.30-10.37) 4.0 (1.33-12.01) LAMA4: High Ref 0.472 Low 0.80 (0.44-1.46) FBLN3: Low Ref 0.657 High 0.78 (0.25–2.38)
and KPS-adjusted hazard ratios. **Multivariate hazard ratios.
Table II. Survival outcomes of malignant pleural mesothelioma patients in
*Stage-
Table III. Survival outcomes of epithelioid malignant pleural mesothelioma patients in multivariate analysis models
*Stage- and KPS-adjusted hazard ratios. **Multivariate hazard ratios.
lignant neoplasms [11]. The extracellular component of SDC1 undergoes proteolytic breakdown by the metalloproteinases, incorporating into the body fluids. Therefore, the level of SDC1 may alter in several pathological conditions such as during the course of the cancer, or development of metastasis, suggesting a potential target for association with prognosis. Kumar-Singh et al. in their study observed that the cases which had > 25% SDC1 immunoreactivity in their MPM tumor cells had better prognosis compared to those with < 25% SDC1 immunoreactivity. They further reported that disappearance of SDC1 genetic expression could play a key role in epithelial mesenchymal transformation [29]. In a study where our clinic was also included, when we accepted the estimation value of SDC1 in pleural fluid samples of MPM cases as 100.2 ng/ml, the prognosis was found to be poorer in patients who have SDC1 values above the estimation value compared with those below the estimation value (7.8 months vs. 17 months); however, no significant association was found between prognosis and serum SDC1 values [11]. This indicated that different findings were obtained when
SDC1 levels were measured in different biological products. In our study, the prognosis was better in patients in whom the SDC1 gene was overexpressed, which was also found after adjustment based on the stage and KPS but not confirmed in multivariate analysis. A study reported that SDC1 could have either a tumor suppressing or a tumor triggering function based on the type of the tumor [30]. It is obvious that SDC1 warrants further research in this respect.
Hyaluronan (HYA) is a high-molecular weight glycosaminoglycan found in nearly all tissues. It is produced by both tumor cells and stromal cells. Hyaluronan was shown to be the predominant glycosaminoglycan that forms the connective tissue within the tumor [31]. Its production is increased during wound healing and tissue repair. Recent experimental studies underlined the importance of HAS2 in HYA synthesis [32]. A study examined genetic expression profiles of HYA, HAS1, HAS2, and HAS3 in MPM cell lines and cell culture, where only HAS2 was found to be overexpressed in all cell lines and cell culture [33]. Naked mole rats have a relatively very long life-span
Arch Med Sci 2, 1st March / 2023 361
Prognostic value of midkine, syndecan-1, hyaluronan synthase-2, sestrin-1, laminin subunit alpha-4 and fibulin-3 for malignant pleural mesothelioma
Parameter HR (95% CI)* P -value HR (95% CI)** P -value Stage: I–II Ref 0.051 Ref 0.144 III–IV 2.93 (0.99–8.61) 2.30 (0.75–7.05) KPS: ≥ 80 Ref 0.362 Ref 0.043 < 80 1.98 (0.46–8.56) 5.17 (1.06–25.30) MDK: Low Ref 0.081 Ref 0.014 High 2.65 (0.89–7.96) 4.47 (1.35–14.78) SDC1: High Ref 0.058 Ref 0.074 Low 2.92 (0.97–8.83) 3.09 (0.90–10.63) HAS2: High Ref 0.023 Ref 0.014 Low 2.53 (1.14–5.64) 2.90 (1.24–6.80) FBLN3: Low Ref 0.133 Ref 0.029 High 3.12 (0.71–13.76) 5.93 (1.20–29.22) SESN1: High Ref 0.019 Ref 0.045 Low 4.11 (1.26–13.39) 3.74 (1.03–13.61) LAMA4: High Ref 0.214 Low 0.64 (0.32–1.27)
compared with equal-sized house mice (32 years vs. 4 years). A study reported that naked mole rats never developed cancer throughout their life-span [32]. The study by Tian et al. attributed this cancer refractoriness to excessive production of high-molecular weight HYA [34]. Reduced genetic expression of HAS2 that was involved in HYA synthesis was shown to cause tumor development in naked mole rats [32]. For this reason, HAS2 might be more useful than HYA for the prognosis of MPM. There has been no study yet to investigate the association of HAS2 and MPM prognosis.
In the study by Thylen et al., it was detected that elevation of serum HYA levels was positively correlated with tumor burden in MPM cases that featured high HYA levels in pleural fluid at the beginning, and it was further suggested that HYA could be used in clinical follow-up of these patients [35]. Another study by Creaney et al. reported poorer prognosis in MPM patients who had lower pleural levels of HYA compared to those having higher levels (12.6 months vs. 18 months) [23]. In our study, the prognosis was significantly better in patients with HAS2 gene overexpression. Similarly, the prognosis was also better in epithelioid MPM patients who had overexpression of the HAS2 gene. The association of HAS2 gene overexpression with survival was statistically significant in both overall MPM and epithelioid MPM.
Fibulin-3 is involved in formation of intercellular matrix, cellular replication, and migration, and mediates intercellular and cell-matrix connections [36]. Fibulin-3 is released from fibroblastic elastic tissues and vascular structures. Also, genetic overexpression of FBLN3 was observed in mesenchymal condensation and growth of bone and cartilaginous structures. A multicenter study by Pass et al. performed with MPM patients showed a significant decline of plasma FBLN3 levels after cytoreductive surgery and increased levels when progression occurred. It was further reported that FBLN3 level in pleural fluid was an independent prognostic indicator of survival in MPM patients who underwent cytoreductive surgery, where high pleural fluid FBLN3 level was associated with poor prognosis [37]. Creaney et al. reported that pleural fluid FBLN3 level was a significant independent prognostic factor in patients with MPM [14]. Consistently, Kirschner et al. reported an independent association of high pleural fluid FBLN3 level with poorer prognosis in MPM patients [15]. However, another study did not find any association between prognosis of MPM and plasma FBLN3 level [38]. Kaya et al. in their study where they accepted the threshold for serum FBLN3 level as 36.6 ng/ml reported the diagnostic sensitivity and specificity of this parameter to be above 90%, albeit insufficient to determine the prognosis [39].
In our study, the prognosis was poor in patients who had an overexpressed FBLN3 gene, but no effect on survival could be observed after it was adjusted according to the stage and KPS. However, our data showed the effect of FBLN3 on survival of epithelioid mesothelioma patients. Higher levels of FBLN3 in biphasic and sarcomatoid tumors and reduced FBLN3 genetic expression in epithelial tumors may explain the negative association of FBLN3 with the prognosis [14]. Moreover, inconsistent findings with previous studies could be attributed to the absence of a correlation between pleural fluid, plasma, and serum levels of FBLN3 [14, 37].
In order to identify novel independent biomarkers in MPM, SESN1 and LAMA4, the genes that were determined by USAT script were included in this study. Sestrin-1 encodes a member of the sestrin family which has regulatory functions in lipid deposition, and metabolic balance, muscle, and heart functions [40]. The protein encoded by SESN1 inhibits the protein target of rapamycin (TOR) by activating adenosine monophosphate activated protein kinase, and hence causing cessation of cellular growth [41]. Sestrin-1 was stressed to be a strong modulator of cellular growth and proliferation [42]. Sestrin-1 was suggested to be a potential therapeutic target in breast and colon cancers. However, no study has been undertaken so far in MPM. In our study, the prognosis was better in patients where the SESN1 gene was overexpressed both in the main MPM group and the epithelioid type subgroup. These findings might be explained by the strong modulatory role of SESN1 for cellular growth and proliferation. As there is no study in this respect, it appears very critical to test this unique finding in further research.
Laminin subunit alpha-4 encodes a member of the laminin family, which is a member of extracellular matrix glycoproteins and a major noncollagenous component of the basal membrane. They are involved in cellular adhesion, differentiation, migration, signaling, and axonal growth [43]. Genetic overexpression of LAMA4 in tumor cells was observed in tumor progression and epithelial-mesenchymal transition. Huang et al. reported overexpression of LAMA4 in tumor tissue, where they further associated this overexpression with tumor invasion and metastasis. The authors suggested that LAMA4 protein was located at the basal membrane of the tumor blood vessel, and could have a potential association with tumor angiogenesis [44]. In our study, LAMA4 expression was not associated with survival.
Mesothelin was not included in this study, because mesothelin is a well-studied biomarker for mesothelioma diagnosis and prognosis. In a re-
362 Arch Med Sci 2, 1st March / 2023
Hakan Akgun, Selma Metintas, Guntulu Ak, Secil Demirkol Canlı, Murat Isbilen, Ali O. Gure, Muzaffer Metintas
cent meta-analysis, high levels of mesothelin were associated with poor prognosis [45]. However, this is not always the case. It is known that mesothelin levels may vary depending on various factors. One of them is polymorphism in the mesothelin gene. It was reported that mesothelin levels were high in some healthy people due to polymorphism [46]. It should be taken into account by studies about mesothelin levels in mesothelioma.
The limitation of our study was the small size of the study population, which did not allow us to assess and discuss cellular subtypes other than MPM.
In conclusion, MDK, HAS2, and SESN1 were identified as potentially useful biomarkers in MPM patients, where overexpression of MDK was associated with poor prognosis and HAS2 and SESN1 overexpression was associated with better prognosis. Overexpression of the latter two genes was further found to be associated with good prognosis also in epithelioid MPM. However, overexpression of MDK and FBLN3 was associated with poor prognosis in epithelioid MPM patients. Our findings are unique assessments with respect to the biological markers. These results should be confirmed in a larger group of patients. Beyond this point, it will be possible to study these prognostic biomarkers in sera and pleural fluids of the mentioned patient groups.
Acknowledgments
This study was partly supported by the Research Fund of Eskişehir Osmangazi University.
Conflict of interest
The authors declare no conflict of interest.
References
1. Metintas M, Ozdemir N, Hillerdal G, et al. Environmental asbestos exposure and malignant pleural mesothelioma. Respir Med 1999; 93: 349-55.
2. Carbone M, Ly BH, Dodson RF, et al. Malignant mesothelioma: facts, myths, and hypotheses. J Cell Physiol 2012; 227: 44-58.
3. Rusch VW. A proposed new international TNM staging system for malignant pleural mesothelioma. From the International Mesothelioma Interest Group. Chest 1995; 108: 1122-8.
4. Metintas M, Metintas S, Ucgun I, et al. Prognostic factors in diffuse malignant pleural mesothelioma: effects of pretreatment clinical and laboratory characteristics. Respir Med 2001; 95: 829-35.
5. Ruffie PA. Pleural mesothelioma. Curr Opin Oncol 1991; 3: 328-34.
6. Vogelzang NJ, Rusthoven JJ, Symanowski J, et al. Phase III study of pemetrexed in combination with cisplatin versus cisplatin alone in patients with malignant pleural mesothelioma. J Clin Oncol 2003; 21: 2636-44.
7. Sugarbaker DJ, Flores RM, Jaklitsch MT, et al. Resection margins, extrapleural nodal status, and cell type deter-
mine postoperative long-term survival in trimodality therapy of malignant pleural mesothelioma: results in 183 patients. J Thorac Cardiovasc Surg 1999; 117: 54-63.
8. Basu S, Saboury B, Torigian DA, Alavi A. Current evidence base of FDG-PET/CT imaging in the clinical management of malignant pleural mesothelioma: emerging significance of image segmentation and global disease assessment. Mol Imaging Biol 2011; 13: 801-11.
9. Grigoriu BD, Scherpereel A, Devos P, et al. Utility of osteopontin and serum mesothelin in malignant pleural mesothelioma diagnosis and prognosis assessment. Clin Cancer Res 2007; 13: 2928-35.
10. Ak G, Tada Y, Shimada H, et al. Midkine is a potential novel marker for malignant mesothelioma with different prognostic and diagnostic values from mesothelin. BMC Cancer 2017; 17: 212.
11. Mundt F, Heidari-Hamedani G, Nilsonne G, et al. Diagnostic and prognostic value of soluble syndecan-1 in pleural malignancies. Biomed Res Int 2014; 419853.
12. Mundt F, Nilsonne G, Arslan S, et al. Hyaluronan and N-ERC/mesothelin as key biomarkers in a specific twostep model to predict pleural malignant mesothelioma. PLoS One 2013; 8: e72030.
13. İşbilen M. Identification of theranostic gene markers in cancers and prognostic validation in colorectal cancer. 2015. Repository: bilkent.edu.tr.
14. Creaney J, Dick IM, Meniawy TM, et al. Comparison of fibulin-3 and mesothelin as markers in malignant mesothelioma. Thorax 2014; 69: 895-902.
15. Kirschner MB, Pulford E, Hoda MA, et al. Fibulin-3 levels in malignant pleural mesothelioma are associated with prognosis but not diagnosis. Br J Cancer 2015; 113: 963-9.
16. Novak AK, Chansky K, Rice DC et al. The IASLC Mesothelioma Staging Project: proposals for revisions of the T descriptors in the forthcoming eighth edition of the TNM classification for mesothelioma. J Thorac Oncol 2016; 11: 2089-99.
17. Rice D, Chansky K, Nowak A, et al. The IASLC Mesothelioma Staging Project: Proposals for Revisions of the N Descriptors in the Forthcoming Eighth Edition of the TNM Classification for Pleural Mesothelioma. J Thorac Oncol 2016; 11: 2100-11.
18. Rusch VW, Chansky K, Kindler HL, et al. The IASLC Mesothelioma Staging Project: Proposals for the M Descriptors and for Revision of the TNM Stage Groupings in the Forthcoming (Eighth) Edition of the TNM Classification for Mesothelioma. J Thorac Oncol 2016; 11: 2112-9.
19. Demirkol S, Gomceli I, Isbilen M, et al. A combined ULBP2 and SEMA5A expression signature as a prognostic and predictive biomarker for colon cancer. J Cancer 2017; 8: 1113-22.
20. Curran D, Sahmoud T, Therasse P, et al. Prognostic factors in patients with pleural mesothelioma: the European Organization for Research and Treatment of Cancer experience. J Clin Oncol 1998; 16: 145-52.
21. Herndon JE, Green MR, Chahinian AP, et al. Factors predictive of survival among 337 patients with mesothelioma treated between 1984 and 1994 by the Cancer and Leukemia Group B. Chest 1998; 113: 723-31.
22. Francis RJ, Byrne MJ, Van Der Schaaf AA, et al. Early prediction of response to chemotherapy and survival in malignant pleural mesothelioma using a novel semiautomated 3-dimensional volume-based analysis of serial 18F-FDG PET scans. J Nucl Med 2007; 48: 1449-58.
23. Creaney J, Dick IM, Segal A, et al. Pleural effusion hyaluronic acid as a prognostic marker in pleural malignant mesothelioma. Lung Cancer 2013; 82: 491-8.
Arch Med Sci 2, 1st March / 2023 363
Prognostic value of midkine, syndecan-1, hyaluronan synthase-2, sestrin-1, laminin subunit alpha-4 and fibulin-3 for malignant pleural mesothelioma
24. Kang K, Huang YH, Li HP, Guo SM. Expression of UCA1 and MALAT1 long-chain non-coding RNAs in esophageal squamous cell carcinoma tissues is predictive of patient prognosis. Arch Med Sci 2018; 14: 752-9.
25. Solmaz ÖA. Prognostic significance of the tumor-stroma ratio in colon carcinoma: a retrospective study. Arch Med Sci Civil Dis 2018; 3: e190-e4.
26. Kadomatsu K, Muramatsu T. Midkine and pleiotrophin in neural development and cancer. Cancer Lett 2004; 204: 127-43.
27. Kadomatsu K, Tomomura M, Muramatsu T. cDNA cloning and sequencing of a new gene intensely expressed in early differentiation stages of embryonal carcinoma cells and in mid-gestation period of mouse embryogenesis. Biochem Biophys Res Commun 1988; 151: 1312-8.
28. http://www.ncbi.nlm.nih.gov/gene/6382.
29. Kumar-singh S, Jacobs W, Dhaene K, et al. Syndecan-1 expression in malignant mesothelioma: correlation with cell differentiation, WT1 expression, and clinical outcome. J Pathol 1998; 186: 300-5.
30. Garusi E, Rossi S, Perris R. Antithetic roles of proteoglycans in cancer. Cell Mol Life Sci 2012; 69: 553-79.
31. Ropponen K, Tammi M, Parkkinen J, et al. Tumor cellassociated hyaluronan as an unfavorable prognostic factor in colorectal cancer. Cancer Res 1998; 58: 342-7.
32. Gorbunova V, Seluanov A, Zhang Z, et al. Comparative genetics of longevity and cancer: insights from longlived rodents. Nat Rev Genet 2014; 15: 531-40.
33. Liu Z, Dobra K, Hauzenberger D, Klomınek J. Expression of hyaluronan synthases and hyaluronan in malignant mesothelioma cells. Anticancer Res 2004; 24: 599-604.
34. Tian X, Azpurua J, Hine C, et al. High-molecular-mass hyaluronan mediates the cancer resistance of the naked mole rat. Nature 2013; 499: 346-9.
35. Thylén A, Wallin J, Martensson G. Hyaluronan in serum as an indicator of progressive disease in hyaluronanproducing malignant mesothelioma. Cancer 1999; 86: 2000-5.
36. Segade F. Molecular evolution of the fibulins: implications on the functionality of the elastic fibulins. Gene 2010; 464: 17-31.
37. Pass HI, Levin SM, Harbut MR, et al. Fibulin-3 as a blood and effusion biomarker for pleural mesothelioma. N Engl J Med 2012; 367: 1417-27.
38. Pass HI, Goparaju C, Espin-Garcia O, et al. Plasma biomarker enrichment of clinical prognostic indices in malignant pleural mesothelioma. J Thorac Oncol 2016; 11: 900-9.
39. Kaya H, Demir M, Taylan M, et al. Fibulin-3 as a diagnostic biomarker in patients with malignant mesothelioma. Asian Pac J Cancer Prev 2014; 16: 1403-7.
40. http://www.ncbi.nlm.nih.gov/gene/27244.
41. Lee JH, Budanov AV, Park EJ, et al. Sestrin as a feedback inhibitor of TOR that prevents age-related pathologies. Science 2010; 327: 1223-8.
42. Sun G, Xue R, Yao F, et al. The critical role of Sestrin 1 in regulating the proliferation of cardiac fibroblasts. Arch Biochem Biophys 2014; 542: 1-6.
43. http://www.ncbi.nlm.nih.gov/gene/3910.
44. Huang X, Ji G, Wu Y, et al. LAMA4, highly expressed in human hepatocellular carcinoma from Chinese patients, is a novel marker of tumor invasion and metastasis. J Cancer Res Clin Oncol 2008; 134: 705-14.
45. Tian L, Zeng R, Wang X, et al. Prognostic significance of soluble mesothelin in malignant pleural mesothelioma: a meta-analysis. Oncotarget 2017; 8: 46425-35.
46. Garritano S, De Santi C, Silvestri R, et al. A common polymorphism within MSLN affects miR-611 binding site and soluble mesothelin levels in healthy people. J Thorac Oncol 2014; 9: 1662-8.
364 Arch Med Sci 2, 1st March / 2023
Hakan Akgun, Selma Metintas, Guntulu Ak, Secil Demirkol Canlı, Murat Isbilen, Ali O. Gure, Muzaffer Metintas
Can the POLARS tool accurately predict low anterior resection syndrome in rectal cancer patients undergoing laparoscopic resection?
Paweł Bogacki1, Jan Krzak2, Tomasz Gach1, Wojciech Szwed3, Mirosław Szura1
1Department of Experimental and Clinical Surgery, Jagiellonian University, Krakow, Poland
2Department of Surgery, South Jutland Hospital, Aabenraa, Denmark
3Department of General and Oncological Surgery, St John Grande Hospital, Krakow, Poland
Submitted: 27 February 2019; Accepted: 21 July 2019
Online publication: 9 September 2019
Arch Med Sci 2023; 19 (2): 365–370
DOI: https://doi.org/10.5114/aoms.2019.87760
Copyright © 2019 Termedia & Banach
Abstract
Introduction: Radical rectal cancer resection can lead to a long-term bowel function impairment known as low anterior resection syndrome (LARS). It remains unclear how to determine which patients are at a higher risk of developing LARS post-surgery. The POLARS tool was designed to predict the onset and severity of LARS in rectal cancer patients after surgery. The study aimed to assess the accuracy of POLARS in predicting the onset of LARS. Material and methods: A total of 66 rectal cancer patients treated laparoscopically between January 2016 and December 2017 were included in this retrospective study. Using POLARS, the predictive value for the occurrence of LARS was documented. During an average 17-month follow-up period, the bowel function of the patients was assessed using the dedicated LARS questionnaire. The predicted and actual scores were then compared. Results: Study participants included 36 women (54.5%) and 30 men (45.5%), with a mean age of 62.55 years (standard deviation: 10.2; range: 37–81). The mean predicted score according to POLARS was 24.5 (i.e. category “minor LARS”), and the mean actual score in the follow-up period was 16.42 (“no LARS” category). In only 39% of patients, the predicted LARS category was the same as the actual LARS category assessed by the questionnaire. Worse bowel function than reported at follow-up was predicted in 75% of all mispredictions.
Conclusions: POLARS did not prove to be accurate in predicting the risk and severity of LARS in these patients, although the average numbers appear promising. Further evaluation of the POLARS tool using a larger cohort is needed.
Key words: quality of life, rectal cancer, LARS, lower anterior resection, POLARS.
Introduction
Colorectal cancer is one of the most common human cancers, ranking third in terms of incidence and second in terms of mortality among all types of cancer. According to the 2018 GLOBOCAN report, the disease incidence is 19.7/100,000, and its associated mortality is 8.9/100,000 [1].
The standard of care in rectal cancer patients is surgical resection with
Corresponding author: Paweł Bogacki
Department of Experimental and Clinical Surgery
St. John Grande Hospital 11 Trynitarska St. 31-061 Krakow, Poland
E-mail: pawelbogacki1@gmail.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/).
Clinical research General Surgery
total mesorectal excision complemented by radiotherapy and/or chemotherapy, depending on disease severity [2, 3].
Improvements in surgical techniques and better adjuvant treatment has led to a decrease in the number of abdominoperineal resections (APR) performed in favour of less invasive operations with GI tract continuity restoration. Such treatment offers higher five-year survival rates and improves some aspects of patient quality of life [4–6]. However, an increase in low anterior resections of the rectum is associated with a higher incidence of postsurgical bowel dysfunction, known as lower anterior resection syndrome (LARS) [7]. According to numerous authors, LARS consists of over 30 different symptoms [8], thus making it difficult to clearly categorise and predict which patients are at considerable risk of developing LARS after undergoing lower anterior resection due to rectal cancer. In 2012, a Danish study was published in which the authors suggested five main aspects of LARS and created a dedicated questionnaire to objectively assess its onset and severity in individual patients [9]. Those five aspects were flatus control, liquid stool leakage, frequency of bowel emptying, need to empty bowels within 1 h of the last bowel emptying, and urgency. Each aspect is given a numerical score based on the patients’ response, and the sum of all scores place patients in either a no LARS, minor LARS, or major LARS group. The questionnaire made the preoperative conversation easier and allowed more unified comparison of patients; however, it still did not offer any benefit in terms of preoperative assessment of the risk of developing LARS post-surgery. In 2018, POLARS was developed. This internet tool is a clinical survey that considers several key factors in patients undergoing lower anterior resection due to rectal cancer to assess the risk of developing LARS post-surgery. To calculate the score, the following data are required: gender, age at surgery, total/partial mesorectal excision, tumour height, preoperative radiotherapy, and stoma. The tool calculates a numerical score of 0–42, which places patients in one of three categories: no risk of LARS (0–20 points), minor risk of LARS (21–29 points), or major risk of LARS (30–42 points). This tool potentially offers the opportunity to provide more patient-tailored treatment (altering postoperative care in high-risk patients) and acquire more adequate informed consent with better patient understanding of the potential for bowel dysfunction after surgery [10].
The aim of our study was to assess how accurately POLARS can predict the development of LARS in patients undergoing lower anterior resection due to rectal cancer. We also aimed to deter-
mine the actual severity and frequency of LARS in patients undergoing this procedure at our centre.
Material and methods
In this study, we analysed all consecutive patients undergoing lower anterior resection due to rectal cancer at our centre during a 2-year period between January 1st, 2016 and December 31st, 2017. For each patient, peri-operative data, including age at surgery, gender, total mesorectum excision (TME)/partial mesorectum excision (PME), tumour height, preoperative radiotherapy, and stoma, were gathered. Each patient was then assessed with POLARS retrospectively and categorised into one of three groups according to the risk of developing LARS based on their POLARS score (no risk of LARS, mild risk of LARS, major risk of LARS). The postop treatment was not altered in any way based on the results of the POLARS prediction score because the assessment occurred retrospectively long after surgery. After an average 17 months post-surgery, a check-up was performed via telephone interview, during which the LARS questionnaire was filled out with the patient. The LARS numerical score and LARS category were documented. The actual LARS score was then compared with the predicted POLARS score in each of the patients, and the level of agreement and its statistical significance were assessed. Further descriptive analysis of all mispredicted cases was performed in search of a pattern.
Statistical analysis
Descriptive statistics were used for quantitative analysis. Mean and standard deviation statistics were used where appropriate. Categorical variables were compared using the c2 test. The level of agreement between the POLARS and LARS scores and its statistical power was assessed using Cohen’s κ statistics. One-way ANOVA was used to compare characteristics between the three LARS groups.
Results
Between January 1st, 2016 and December 31st, 2017, 89 patients underwent laparoscopic lower anterior resection due to rectal cancer at our centre. Because of the need for conversion to an open procedure, 13 cases were excluded from the study. At the time of telephone check-up, 10 patients were lost to follow-up: 2 had died, and 8 could not be reached after numerous attempts. Thus, 66 patients were ultimately included in the study. The inclusion process is shown in Figure 1.
The mean age of the patients was 62.55 years (standard deviation (SD): 10.2 years; range: 37–81 years). The group consisted of 30 males (45.5%) and 36 females (54.5%). The mean POLARS score
366 Arch Med Sci 2, 1st March / 2023
Paweł Bogacki, Jan Krzak, Tomasz Gach, Wojciech Szwed, Mirosław Szura
was 24.5 points (SD 4.06 points, range: 19–35 points), and the median was 24 points, which would place the ‘average patient’ in the risk of minor LARS category. The no-LARS category included 10 patients, the mild-LARS category 48 patients, and the major-LARS category 8 patients. The group characteristics and detailed POLARS score data are presented in Table I.
The mean follow-up time was 17 months (SD 8.6, range: 11–29 months). On telephone check-up, the LARS score was calculated for each patient. The mean LARS score was 16.42 points (SD 13.62, range: 0–39 points) and the median score was 15 points, which put the ‘average patient’ in the no-LARS category, which did not correlate with the POLARS prediction.
Based on the LARS questionnaire, 36/66 patients (54.5%) were in the no-LARS category, 18/66 (27.3%) were in the minor-LARS category, and 12/66 (18.2%) were in the major-LARS category.
Interestingly, 10/10 (100%) patients who were predicted to be in the no-LARS category ended up in the same category after telephone check-up. Of 48 patients predicted to be in the mild-LARs category, only 14 (29.2%) ended up in this category, with 24 (50%) ending up in the no-LARS category and 10 (20.8%) ending up in the major-LARS category. Of 8 patients predicted to be in the major-LARS category, 2 (25%) stayed in the same category, 4 (50%) moved to the mild-LARS category, and 2 (25%) moved to the no-LARS category. A graphic representation of prediction vs. actual LARS score is depicted in Figure 2.
Overall, a correct prediction was noted in 26 (39.4%) cases, which was below expectations. Cohen’s κ statistic for the level of agreement was 0.130 (low level of agreement), p = 0.042. There were a total of 40 mispredicted cases (60.6%). Interestingly, upon analysis of the mispredicted cases, we found that 30/40 (75%) ended up in a lower LARS category than predicted, which means that on telephone check-up, patients expressed better bowel function than expected based on the POLARS tool assessment. Only 10/40 (25%) of mispredicted patients reported worse bowel function than
89 patients undergoing lower anterior resection for rectal cancer in 2016–2017
76 patients included in the study
13 patients excluded due to conversion to open surgery
10 patents lost to follow-up: – 2 died – 8 couldn’t be reached
66 patients completed the study
that predicted by the POLARS tool. Those patients ended up in a higher LARS category at follow-up.
Laparoscopic lower anterior resection is an increasingly common procedure to treat rectal
Arch Med Sci 2, 1st March / 2023 367
Can the POLARS tool accurately predict low anterior resection syndrome in rectal cancer patients undergoing laparoscopic resection?
Discussion
Figure 1. Schematic diagram of study design
Parameter All ( N = 66) No-LARS (n = 10) Mild-LARS (n = 48) Major-LARS ( n = 8) P -value Age, mean (SD; range) 62.5 (10.2; 37–81) 74.2 (4.1; 67–78) 61 (8.1; 48–81) 51.25(12.0;37–65) < 0.001 Gender: 0.332 Male 30 (45.5%) 6 (60%) 22 (45.8%) 2 (25%) Female 36 (54.5%) 4 (40%) 26 (54.2%) 6 (75%) Total mesorectum excision 66 (100%) 10 (100%) 48 (100%) 8 (100%) –Tumour height [cm], mean (SD) 12.4 (3.1) 14.4 (0.7) 12.8 (2.7) 7.25 (0.46) < 0.001 Stoma 0 (0%) 0 (0%) 0 (0%) 0 (0%) –Preoperative radiotherapy 22 (33.3%) 0 (0%) 16 (33.3%) 6 (75%) 0.004
Table I. Group characteristics according to POLARS prediction categories
POLARs predicted categories: Actual LARS categories: No-LARS n = 10 No-LARS n = 10 Mild-LARS n = 0 Major-LARS n = 0 No-LARS n = 24 Mild-LARS n = 48 Mild-LARS n = 14 Major-LARS n = 10 No-LARS n = 2 Major-LARS n = 8 Mild-LARS n = 4 Major-LARS n = 2 100% 0% 29.2% 50% 0% 20.8% 25% 50% 25%
Figure 2. Changes between POLARS prediction category and actual LARS category in each of the groups
cancer. Its obvious benefits include GI tract continuity restoration at the initial procedure, less invasiveness compared to APR, a better 5-year survival rate, and shorter recovery time after surgery [11]. However, lower anterior resection can lead to symptoms that negatively affect the quality of life. Those symptoms include urgency, faecal incontinence, frequent bowel movements, and difficulties in emptying the bowels [12]. This cluster of symptoms is referred to as LARS and is estimated to affect as many as 60–90% of all patients after lower anterior resection surgery [13].
The pathophysiology of this phenomenon is not fully understood. Surgical and radiotherapy-induced afferent visceral nerve damage could be the underlying cause [12]. A small study by Bregendahl et al. [14] showed that neoadjuvant radiotherapy in rectal cancer patients can cause neorectal hyposensitivity to both mechanical and thermal stimuli and can also lead to significantly lower anal resting pressure compared to patients who had not had radiotherapy before TME. The radiation-induced injury to the internal anal sphincter (which is more susceptible to ionising radiation than the external anal sphincter) may often lead to incontinence, because the internal anal sphincter is responsible for constant closure of the anal canal between bowel movements. In another study, Chen et al. [13] determined that major LARS was observed in 56% of patients who underwent TME with prior neoadjuvant radiotherapy compared to only 35% of those who did not have radiotherapy before TME surgery. The mean occurrence of major LARS in the study was 46% [13].
Another plausible hypothesis is a disturbance in colon and neorectal motility with enhanced postprandial response in patients after surgical rectal resection. Studies have shown a significant increase in neorectal pressure after a meal post-surgery in patients with major LARS compared to those with no LARS [15, 16]. The cause of this disturbance remains unidentified.
Neorectal reservoir dysfunction with reduced functional capacity may also play a role in LARS. Surgical denervation and a loss of stool-storing function of the rectum after resection are unavoidable. Reduced neorectal reservoir volume after end-to-end colorectal or coloanal anastomosis was believed to cause urgency and incontinence. A larger neorectal reservoir achieved with an altered surgical technique (colonic J pouch, coloplasty) showed benefits lasting only up to 12 months. Comparative studies analysing different techniques of anastomosis and creation of a larger reservoir volume of the neorectum have not shown any long-term benefits in terms of frequency and incontinence [17].
The treatment of LARS remains a challenge, and a multimodal approach should be implement-
ed. Therapy is empirical and symptom based. In minor-LARS patients, medical management is advised; however, few high-quality data are available regarding this matter. Loperamide treatment for diarrhoea, 5-HT3 receptor antagonists for postprandial urgency and incontinence, and simethicone for gas and bloating remain the treatments of choice in this group of patients [18–21]. Dietary restrictions, high fibre consumption, and probiotics are advised, although no data support the benefit of those agents. For major LARS patients, additional procedures such as pelvic floor rehabilitation (in the form of biofeedback, electrostimulation, pelvic floor muscle training, and volumetric training) and transanal irrigation are available and of some benefit [22–24].
With LARS being a significant problem greatly affecting the quality of life of patients undergoing low anterior resection surgery for rectal cancer, it is our duty to thoroughly inform patients of the possibility of developing life-altering symptoms post-surgery. Because LARS is multimodal and the pathophysiology is still not fully understood, it remains difficult to predict which patients will develop LARS and to what extent after surgery. The POLARS tool for predicting LARS scores in patients undergoing this procedure offered a promising opportunity to better inform the patient about possible bowel dysfunction after surgery. However, our study has shown a low level of agreement between predicted and actual LARS scores. Only 39% of patients ended up in the same category as predicted by POLARS, and Cohen’s κ agreement score was as low as 0.130. This finding was disappointing, although further analysis showed that the POLARS tool is rather conservative, and 75% of all mispredicted cases showed better bowel function on follow-up than predicted by POLARS. Furthermore, 100% of the patients who were grouped in the no-LARS category by the POLARS tool reported no LARS on follow-up. Thus, the predictive value in this group of patients is strong and may be useful during pre-operative counselling.
In our study, 30/66 (45%) patients reported some sort of bowel dysfunction on follow-up (mild or major LARS) showing how common this disorder is. Major LARS was noted in 12/66 (18%) of our patients. This group of patients showed the highest negative impact of surgery on quality of life. Of those 12 patients, only two were grouped in the “major LARS” category by the POLARS tool, whereas the remaining 10 were in the “mild LARS” category by POLARS prediction. This outcome should be remembered by physicians when dealing with patients categorised in the mild-LARS group upon perioperative assessment using POLARS.
Mild LARS was observed in 27% of patients, and no LARS in 55%. This is not consistent with Batersby’s findings published in 2018 with the
368 Arch Med Sci 2, 1st March / 2023
Paweł Bogacki, Jan Krzak, Tomasz Gach, Wojciech Szwed, Mirosław Szura
Can the POLARS tool accurately predict low anterior resection syndrome in rectal cancer patients undergoing laparoscopic resection?
introduction of the POLARS tool. He recorded the prevalence of major LARS at 43%, mild LARS at 23%, and no LARS at 34%. These differences may be due to a different patient cohort or a higher number of patients with a shorter distance between the tumour and the anal sphincter in Batersby’s study compared to ours. It has been shown that the higher the tumour, the smaller the risk of developing LARS post-surgery. van Heinsbergen et al. [25] showed a significant difference in the prevalence of major LARS between sigmoid resection patients (20%) and colon resection patients (90%).
It is important to remember that LARS is not the only tool developed for the classification of postsurgical bowel dysfunction. Keane et al. [8] conducted a meta-analysis of all topic-related studies published between 1986 and 2006; it was determined that researchers have used as many as 18 different tools to assess bowel function post-surgery and its effect on the quality of life. Most of the tools only assessed stool incontinence, and in 36% of the studies no established assessment tool was used, but only a combination of symptoms was recorded [8].
Perhaps the incidence of LARS may be related to the genetics of the disease, which are not captured in this study. Currently many rectal cancer studies are taking place that are trying to define the exact aetiology of the disease. One of such studies is focusing on the genetics of the disease and is attempting to determine certain gene variants that might be a specific early marker for the disease [26] – perhaps if we learn to catch the disease before it progresses to stages difficult to treat, we will no longer have to deal with LARs syndrome post-operatively. Not taking into account the complex background of the disease (including the genetic aspect) might be considered as a limitation of this study. Another suggested limitation of the study is not taking into account the post-operative radiotherapy in rectal cancer patients; this might be a confounding factor because the POLARS tool only takes into account the pre-operative radiotherapy in this group of patients. However, in our study, no patients underwent post-operative radiotherapy, so this could not have confounded the data.
In conclusion, POLARS is a promising tool in preoperative counselling and for tailoring postoperative care in patients undergoing low anterior resection. It was not as effective as we had hoped, but the low agreement level may stem from the fact that the number of patients included in the study was limited. It is important to highlight that this tool seems to be very effective in the no-LARS group, whereas in other groups the predictability of the LARS syndrome remains low. Further
research is needed to fully assess the value of POLARS and to give clinicians a better understanding of the information and consequences associated with POLARS scores.
Conflict of interest
The authors declare no conflict of interest.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68: 394-424.
2. Benson AB, Venook AP, Al-Hawary MM, et al. Rectal cancer, version 2. 2018, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw 2018; 16: 874-901.
3. Glynne-Jones R, Wyrwicz L, Tiret E, et al.; ESMO Guidelines Committee. Rectal cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2017; 28: iv22-iv40.
4. Brouwer NPM, Bos A, Lemmens V, et al. An overview of 25 years of incidence, treatment and outcome of colorectal cancer patients. Int J Cancer 2018; 143: 2758-66.
5. Allemani C, Matsuda T, Di Carlo V, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet 2018; 391: 1023-75.
6. Trenti L, Galvez A, Biondo S, et al. Quality of life and anterior resection syndrome after surgery for mid to low rectal cancer: a cross-sectional study. Eur J Surg Oncol 2018; 44: 1031-9.
7. Battersby NJ, Juul T, Christensen P, et al.; United Kingdom Low Anterior Resection Syndrome Study Group. Predicting the risk of bowel-related quality-of-life impairment after restorative resection for rectal cancer: a multicenter cross-sectional study. Dis Colon Rectum 2016; 59: 270-80.
8. Keane C, Wells C, O’Grady G, Bissett IP. Defining low anterior resection syndrome: a systematic review of the literature. Colorectal Dis 2017; 19: 713-22.
9. Emmertsen KJ, Laurberg S. Low anterior resection syndrome score: development and validation of a symptom-based scoring system for bowel dysfunction after low anterior resection for rectal cancer. Ann Surg 2012; 255: 922-8.
10. Battersby NJ, Bouliotis G, Emmertsen KJ, et al.; UK and Danish LARS Study Groups. Development and external validation of a nomogram and online tool to predict bowel dysfunction following restorative rectal cancer resection: the POLARS score. Gut 2018; 67: 688-96.
11. Steele RJ. Anterior resection with total mesorectal excision. J R Coll Surg Edinb 1999; 44: 40-5.
12. Bryant CL, Lunniss PJ, Knowles CH, Thaha MA, Chan CL. Anterior resection syndrome. Lancet Oncol 2012; 13: e403-8.
13. Chen TY, Wiltink LM, Nout RA, et al. Bowel function 14 years after preoperative short-course radiotherapy and total mesorectal excision for rectal cancer: report of a multicenter randomized trial. Clin Colorectal Cancer 2015; 14: 106-14.
14. Bregendahl S, Emmertsen KJ, Fassov J, et al. Neorectal hyposensitivity after neoadjuvant therapy for rectal cancer. Radiother Oncol 2013; 108: 331-6.
15. Mochiki E, Nakabayashi T, Suzuki H, et al. Barostat examination of proximal site of the anastomosis in pa-
Arch Med Sci 2, 1st March / 2023 369
tients with rectal cancer after low anterior resection. World J Surg 2001; 25: 1377-82.
16. Emmertsen KJ, Bregendahl S, Fassov J, Krogh K, Laurberg S. A hyperactive postprandial response in the neorectum –the clue to low anterior resection syndrome after total mesorectal excision surgery? Colorectal Dis 2013; 15: e599-e606.
17. Brown CJ, Fenech DS, McLeod RS. Reconstructive techniques after rectal resection for rectal cancer. Cochrane Database Syst Rev 2008; 2: CD006040.
18. Lazaraki G, Chatzimavroudis G, Katsinelos P. Recent advances in pharmacological treatment of irritable bowel syndrome. World J Gastroenterol 2014; 20: 8867-85.
19. Cohen LD, Levitt MD. A comparison of the effect of loperamide in oral or suppository form vs placebo in patients with ileo-anal pouches. Colorectal Dis 2001; 3: 95-9.
20. Hallgren T, Fasth S, Delbro DS, Nordgren S, Oresland T, Hultén L. Loperamide improves anal sphincter function and continence after restorative proctocolectomy. Dig Dis Sci 1994; 39: 2612-8.
21. Itagaki R, Koda K, Yamazaki M, et al. Serotonin (5-HT3) receptor antagonists for the reduction of symptoms of low anterior resection syndrome. Clin Exp Gastroenterol 2014; 7: 47-52.
22. Rosen H, Robert-Yap J, Tentschert G, Lechner M, Roche B. Transanal irrigation improves quality of life in patients with low anterior resection syndrome. Colorectal Dis 2011; 13: e335-8.
23. Pucciani F, Ringressi MN, Redditi S, Masi A, Giani I. Rehabilitation of fecal incontinence after sphincter-saving surgery for rectal cancer: encouraging results. Dis Colon Rectum 2008; 51: 1552-8.
24. Lin KY, Granger CL, Denehy L, Frawley HC. Pelvic floor muscle training for bowel dysfunction following colorectal cancer surgery: a systematic review. Neurourol Urodyn 2015; 34: 703-12.
25. van Heinsbergen M, Janssen-Heijnen ML, Leijtens JW, Slooter GD, Konsten JL. Bowel dysfunction after sigmoid resection underestimated: multicentre study on quality of life after surgery for carcinoma of the rectum and sigmoid. Eur J Surg Oncol 2018; 44: 1261-7.
26. Lamami Y, Mesediyeva R, Arikan S, et al. Preliminary report: one of the PD-1 gene variants may be a valuable marker for colorectal cancer. Arch Med Sci Civil Dis 2018; 3: e34-e40.
370 Arch Med Sci 2, 1st March / 2023
Paweł Bogacki, Jan Krzak, Tomasz Gach, Wojciech Szwed, Mirosław Szura
The prevalence of depression in children and adolescents under 18 years of age treated for mental disorders in Poland between 2005 and 2016
Mira Lisiecka-Biełanowicz1, Daria Biechowska2, Edyta Orłowska3, Bartłomiej Molenda2
1Department of the Prevention of Environmental Hazards and Allergology, Faculty of Health Sciences, Medical University of Warsaw, Warsaw, Poland
2Department of Public Health, Institute of Psychiatry and Neurology, Warsaw, Poland
3Institute of Psychology, University of Gdansk, Gdansk, Poland
Submitted: 7 March 2019; Accepted: 6 September 2019
Online publication: 18 April 2020
Arch Med Sci 2023; 19 (2): 371–380
DOI: https://doi.org/10.5114/aoms.2020.94530
Copyright © 2020 Termedia & Banach
Abstract
Introduction: The prevalence of depression in Polish children and adolescents under 18 years of age treated for mental disorders has increased in the last few years in Poland. The purpose of this study was to examine the prevalence of major depression in a population of Polish children and adolescents under 18 years of age treated for mental disorders, stratified by sex and place of residence, in the years 2005, 2009, 2014, and 2016.
Material and methods: We analysed the psychiatric treatment data of children and adolescents under the age of 18 years in Poland compiled by the Institute of Psychiatry and Neurology in Warsaw for these years.
Results: Major depression was moderately prevalent among children and adolescents treated in all evaluated types of mental health facilities, with a prevalence in this population ranging from 0.8% in 2005 to 4.3% in 2016. The rates of young patients with mood disorders increased from 3.1% in 2005 to 7.0% in 2016. Risk factors for developing major depression in our research group were: being female and living in an urban area.
Conclusions: Our findings suggest the need to increase the service capacity for children and adolescents as well as to intensify preventive measures to improve the mental health status of this age group.
Key words: depression, children and adolescents, psychiatric epidemiology.
Introduction
The World Health Organisation (WHO) predicts that, by the year 2020, major depression will be one of the most common mental disorders in the world [1]. Depression is a heterogeneous disease triggered by interaction between genetic, psychological, social, and lifestyle-related factors [2]. The incidence rates have been increasing systematically in adults, as well as in children and adolescents [3, 4]. As children and adolescents account for almost one-quarter of the global population, with 85% of them living in low- and middle-income countries, monitoring the prevalence of mental disorders in this age group is important [5, 6].
Empirical data show that mood disturbances during childhood are neither inevitable nor universal [7, 8]. Affective problems during these stages of physico-psychological development often involve major or mild
Corresponding author: Bartłomiej Molenda
Department of Public Health Institute of Psychiatry and Neurology
Sobieskiego St
02-957 Warsaw, Poland
Phone: +48 602 782 157
E-mail: bmolenda@ipin.edu.pl
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/).
Clinical research Paediatrics
Mira Lisiecka-Biełanowicz, Daria Biechowska, Edyta Orłowska, Bartłomiej Molenda
depression, which affect 20% of the underage population globally [9, 10]. The estimates differ depending on the country and diagnostic criteria. Studies are illustrating the growing rates of adolescent depression in developed countries, especially in individuals of young population between the ages of 13 and 18 years [11].
Research on the long-term physical health consequences of early-onset major depression has demonstrated that major depression is associated with considerable chronic physical health [12]. Over half of the individuals who recover from the first episode of depression will suffer at least one additional episode later in life, whereas approximately 80% of those with a history of two episodes will experience another recurrence [13].
As meta-analysis reports suggest, the proportion of the adult population experiencing any form of mood disorder represented by the available data in Eastern Europe is estimated at 0.47%, which is extremely low when compared with the corresponding proportion of 17–40% in Western European countries. These data refer to general mood disorders, particularly anxiety [6, 14]. However, this disproportion may be influenced by differences in reporting rates between countries representing various economic status. The data for the Polish population are limited because no national comorbidity surveys, which are routinely performed in other countries, have been performed in Poland. The first ever Polish population-based study on the epidemiology of psychiatric disorders (EZOP 2012) aimed at assessing the prevalence of selected mental disorders in the adult population [14].
Therefore, the purpose of this study was to determine the prevalence of major depression in the population of children and adolescents, stratified by sex and place of residence, in the years 2005, 2009, 2014, and 2016, in Poland, and to indicate an appropriate model of community-based treatment teams aimed at the specific needs of children and adolescents in Poland.
Material and methods
The assessment method adopted for this study included the analysis of data on the prevalence of depression among children and adolescents under 18 years of age treated for mental disorders in 2005–2016 in Poland, prepared by the Institute of Psychiatry and Neurology in Warsaw, Poland for the years 2005, 2009, 2014, and 2016. Our research was conducted mainly on the basis of the data collected from the following forms [15]:
(1) MZ-15, the operation of outpatient healthcare facilities for people with mental disorders; (2) MZ19, the activities of community mental-health teams; (3) MZ-30, the reported health care activity
of 24 h health care providers; and (4) MZ/Szp-11B, individual patient stays in 24 h mental health care settings.
The data for the purpose of our study were gathered from mental health hospitals, day-care centres, 24 h mental health facilities, and community mental health teams. More specific data, including patient sex and place of residence, were gathered mostly from the first two types of facilities mentioned above. Most medical units were located in urban areas. In Poland there is no regionalisation in the health care system, and as such the data should not be impacted by rural residence of the treated population.
Below we present the size and dynamics of the selected mental health problems in a population of children and adolescents under 18 years of age treated for mental disorders in 2005–2016 in Poland, based on existing routine information systems. For many years, information about Polish residents treated for mental disorders in mental health care centres (hospitals, care and treatment centres) was collected as part of the National Psychiatric Hospital Disease Examination implemented by the Institute of Psychiatry and Neurology in Warsaw.
Statistical analysis
The results are published in the statistical yearbook issued by the Institute. The presented coefficients are related to people, not cases, because, for the purposes of statistical analysis, multiple hospitalisations were combined in accordance with the identification key determined by the Institute.
Microsoft Excel (Microsoft, Redmond, Washington, USA) was used to analyse the statistical data provided in yearbooks and compiled by psychiatric and neurological care institutions in the years 2005, 2009, 2014, and 2016. Our analysis included the general mental health status of Polish children and adolescents and the proportions of this patient population treated for any mental conditions in general, those treated for mood disorders, and those treated for major depression in particular. Mental disorders were classified by psychiatrists according to the 10th revision of the International Classification of Diseases (ICD-10) [16] and reported on the basis of individual patient statistical cards.
Results
Over the analysed 12-year period, the number of children and adolescents under 18 years old who received treatment for any psychiatric conditions in mental-health hospitals and outpatient clinics for children and adolescents increased by
372 Arch Med Sci 2, 1st March / 2023
The prevalence of depression in children and adolescents under 18 years of age treated for mental disorders in Poland between 2005 and 2016
20,111. Over the same 12-year period, the number of underage psychiatric patients treated in day-care centres increased by 870, and the number of those treated by community mental-health teams increased by 1320 (993%). We noticed, however, a decrease (by 30%) in the number of patients treated in 24 h mental-health facilities. In 2009, a noticeable decrease occurred in the number of children and adolescents under 18 years old treated in mental-health outpatient clinics, daycare centres, and 24 h mental-health facilities. In comparison to the figures from 2005, the number of patients treated in all mental-health facilities increased by 17% by 2016. Specific numbers of children and adolescents receiving psychiatric treatment in different types of mental health facilities in Poland are presented in Table I.
Major depression (diagnosed according to the ICD-10 criteria) was moderately prevalent in the population of patients treated in mental health facilities, with the proportion of affected patients ranging from 0.8% to 4.3% over the evaluated 12year period. The specific figures for child and adolescent patients diagnosed with mood disorders in general and major depression in particular who were treated in mental hospitals and day-care centres are presented in Table II.
The data collected over the investigated time period indicated an increase in the prevalence of mood disorders among both day-care centres and mental hospital patients. The proportion of child and adolescent patients treated for mood disorders in day-care centres rose from 1.5% in 2005, to 2.0% in 2009, to 4.0% in 2014, and to 5.0% in 2016.
The rates of child and adolescent patients treated for mood disorders in mental hospitals were comparatively high, rising from 3.4% in 2005, to 4.9% in 2009, to 7.1% in 2014, and eventually to 7.5% in 2016. The rates in the combined population of child and adolescent patients treated in both of
these types of health care facilities increased from 3.1% to 7.0% between 2005 and 2016.
According to ICD-10, major depression is included in mood disorders (i.e. affective disorders); accordingly, these diagnoses were considered in our analysis. Our results showed a steady increase in the proportion of children and adolescents diagnosed specifically with depression out of all underage patients treated for mental problems. Between 2005 and 2016, this proportion increased from 0.8% to 3.4% among patients treated in daycare centres and from 2.0% to 4.3% among mental hospital patients. Of the combined population of children and adolescents treated in both these types of institutions, the rates of major depression were, respectively, 1.9% in 2005, 2.4% in 2009, 3.9% in 2014, and 4.1% in 2016.
Data from 2005, 2009, 2014, and 2016 indicate that, among children and adolescents undergoing treatment in day-care centres and mental hospitals, a certain group of individuals were most susceptible to developing major depression symptoms. The proportions of children and adolescents diagnosed with mood disorders in general and major depression in particular (stratified by sex and place of residence) and treated in day-care centres and mental hospitals in Poland are presented in Tables III and IV. These tables present the rates of treatment for the evaluated mental conditions per 100,000 residents. Our data indicate that depressive disorders were most common among female children and adolescents who were urban residents, in all the years studied. This finding is significant because more male than female patients in general received treatment in mental health facilities over the evaluated 12-year period. In 2005, similar rates of young male and female patients (33.3% and 66.7%, respectively) were treated in day-care centres for both mood disorders in general and depression in particular. Of the patients
Arch Med Sci 2, 1st March / 2023 373
Year Mental-health hospitals and out-patient clinics Day-care centres Community mental-health teams 24-hour mental-health facilities 2005 118,921 1771 133 9886 2009 114,121 2155 119 9494 2014 125,681 2545 1640 10,176 2016 139,032 2641 1453 9856 Difference between 2005 and 2016 +20,111 +870 +1,320 –30
Table I. Total numbers of children and adolescents treated for major depression in various types of mental health facilities
Source: Statistical reports from psychiatric and neurological health care facilities; the Polish statistical almanacs for the years 2005, 2009, 2014, and 2016 and the Institute of Psychiatry and Neurology, Warsaw.
II. Children and adolescents (Ch&A) diagnosed with mental health problems, including mood disorders in general and major depression in particular, treated in mental hospitals and daycare centres between 2005 and 2016
Source: Statistical reports from psychiatric and neurological health care facilities; Polish statistical almanacs for the years 2005, 2009, 2014, and 2016 and the Institute of Psychiatry and Neurology, Warsaw.
374 Arch Med Sci 2, 1st March / 2023
Numbers/ proportion 2005 2009 2014 2016 Ch&A
Ch&A
Ch&A treated
depres
sion Ch&A treated for
problem Ch&A treated for affective disorders Ch&A
sion Ch&A treated
Ch&A treated
disorders Ch&A treated specifically for depression Ch&A treated for
mental problem Ch&A treated for affective disorders Ch&A treated specifically for depression Ch&A treated in day-care centres: Absolute number 1771 27 15 2155 43 27 2545 101 70 2641 132 91 Proportion of those treated for mental problems 100 1.5 0.8 100 2.0 1.3 100 4.0 2.7 100 5.0 3.4 Ch&A treated in mental hospitals: Absolute number 9886 335 202 9494 466 252 10176 722 428 9856 744 424 Proportion of those treated for mental problems 100 3.4 2.0 100 4.9 2.7 100 7.1 4.2 100 7.5 4.3 Ch&A treated in both types of facilities: Absolute number 11657 362 217 11576 509 279 12721 823 498 12497 876 515 Proportion of those treated for mental problems 100 3.1 1.9 100 4.4 2.4 100 6.5 3.9 100 7.0 4.1
Mira Lisiecka-Biełanowicz, Daria Biechowska, Edyta Orłowska, Bartłomiej Molenda
Table
treated for any mental problem
treated for affective disorders
specifically for
-
any mental
treated specifically for depres
for any mental problem
for affective
any
The prevalence of depression in children and adolescents under 18 years of age treated for mental disorders in Poland between 2005 and 2016
Table III. Ch&A with mental health problems treated in day-care centres, stratified by sex and place of residence
Ch&A treated for affective disorders
Ch&A treated for any mental problem
Ch&A treated specifically for depression
Ch&A treated for affective disorders
Ch&A treated for any mental problem
Ch&A treated specifically for depression
Ch&A treated for affective disorders
Ch&A treated for any mental problem
Ch&A treated specifically for depression
Ch&A treated for affective disorders
Ch&A treated for any mental problem
Ch&A treated specifically for depression Percentage (stratified by sex and place of residence):
Source: Statistical reports from psychiatric and neurological health care facilities; Polish statistical almanacs for the years 2005, 2009, 2014, and 2016 and the Institute of Psychiatry and Neurology, Warsaw.
Ch&A treated specifically for major depression
Ch&A treated for mood disorders
Ch&A treated for any mental problem
Ch&A treated specifically for major depression
Ch&A treated for mood disorders
Table IV. Ch&A with mental health problems treated in mental hospitals, stratified by sex and place of residence
Ch&A treated for any mental problem
Ch&A treated specifically for major depression
Ch&A treated for mood disorders
Ch&A treated for any mental problem
Ch&A treated specifically for major depression
Ch&A treated for mood disorders
Ch&A treated for any mental problem
Percentage (stratified by sex and place of residence):
and the Institute of Psychiatry and Neurology, Warsaw.
and
Source: Statistical reports from psychiatric and neurological health care facilities; Polish statistical almanacs for the years
Arch Med Sci 2, 1st March / 2023 375
2005 2009 2014 2016
Demographic data
Male 53 29.3 21.3 59.7 41.2 38.9 55.5 32.7 28.3 52.3 32.4 29.4 Female 47 70.7 78.8 40.3 58.8 61.1 44.5 67.3 71.7 47.7 67.6 70.5 Urban 75 61.8 58.4 72.3 79.4 75.4 80.4 82.9 82.9 71.2 70.2 69.8 Rural 25 38.2 40.6 27.7 20.6 24.6 19.6 17.7 17.1 28.8 29.8 30.2 Rates of
Male 28.4 0.53 0.23 14.8 0.26 0.26 14.76 0.32 0.32 13.42 0.63 0.33 Female 23.58 1.2 0.81 10 0.72 0.41 11.83 1.27 0.80 12.23 1.31 0.78 Urban 31.66 0.88 0.51 17.93 0.97 0.5 21.38 1.55 0.93 18.27 1.36 0.77 Rural 16.77 0.87 0.56 6.87 0.25 0.16 5.22 0.33 0.19 7.38 0.58 0.33
treatment (per 100,000 residents):
2005, 2009,
2014,
2016
Demographic
2005 2009 2014 2016
data
Male 55.1 33.3 33.3 71.8 44.2 44.4 65.4 26.7 24.3 66.3 22.7 27.5 Female 44.9 66.7 66.7 28.2 55.8 55.6 34.6 73.3 75.7 33.7 77.3 72.5 Urban 80 81.5 80 91.3 86 81.5 91.4 93.1 97.1 84 84.8 85.7 Rural 20 18.5 20 8.7 14 18.5 8.6 6.9 2.9 16.0 15.2 14.3 Rates of treatment (per 100,000 residents): Male 5.3 0.05 0.03 4.07 0.03 0.03 4.35 0.04 0.04 4.56 0.08 0.07 Female 4 0.09 0.05 1.6 0.06 0.04 2.3 0.19 0.14 2.31 0.27 0.17 Urban 6 0.09 0.05 5.18 0.1 0.06 3.78 0.25 0.18 5.77 0.29 0.20 Rural 2.4 0.03 0.02 0.49 0.02 0.01 0.57 0.02 0.01 1.10 0.05 0.03
Mira Lisiecka-Biełanowicz, Daria Biechowska, Edyta Orłowska, Bartłomiej Molenda
diagnosed with mood disorders and treated in mental hospitals in 2005, 70.7% were female and 29.3% were male, whereas out of all patients diagnosed with major depression, 78.8% were female and 21.3% were male. This indicates that female children were twice or even three times more likely to develop mood disorders (particularly major depression) in 2005. High female-to-male patient ratios among mental hospital patients were also observed in the subsequent years. Among daycare centre patients treated in 2009, girls and boys constituted 55.8% and 44.2% of patients with mood disorders, respectively, and 55.6% and 44.4% of patients with major depression, respectively. Among mental-hospital patients treated in the same year, girls and boys constituted 58.8% and 41.2% of mood-disorder patients, respectively, and 61.1% and 38.9% of depression patients, respectively. In 2014, 73.3% of day-care centre patients diagnosed with mood disorders were female and 26.7% were male; of those diagnosed with major depression, 75.7% were female and 24.3% were male. In the same year, these proportions were similar in mental hospitals, where 67.3% of mood-disorder patients were female and 32.7% were male, and where 71.7% of major depression patients were female and 28.3% were male. The situation in 2016 was analogical, as 77.3% of patients receiving treatment in day-care centres due to mood disorders were female and 22.7% were male, and 72.5% of patients treated for depression were female and 27.5% were male. Among young mental-hospital patients, girls and boys constituted 67.6% and 32.4% of patients treated for mood disorders, respectively, and 70.5% and 29.5% of patients treated for depression, respectively.
An analysis of the collected data in terms of the place of residence revealed that, of all patients in this age group treated for mood disorders in daycare centres in 2005, urban residents constituted 81.5% in 2005, 86% in 2009, 93.1% in 2014, and 84.8% in 2016. The corresponding proportions of urban residents among young patients treated for major depression were 80% in 2005, 81.5% in 2009, 97.1% in 2014, and 85.7% in 2016.
The data for mental-hospital patients show that, of the patients in this age group treated for mood disorders, urban residents constituted 61.8% in 2005, 79.4% in 2009, 82.9% in 2014, and 70.2% in 2016. The corresponding proportions of urban residents among young patients treated for major depression were 58.4% in 2005, 75.4% in 2009, 82.9% in 2014, and 69.8% in 2016.
The rates of treatment per 100,000 population, stratified by sex and place of residence, were calculated based on the data published in Polish statistical yearbooks for the evaluated years and are presented in detail in Tables III and IV.
Discussion
Analysis of the data gathered for the evaluated years in the period from 2005 to 2016 demonstrated a 237% increase in the number of individuals under 18 years of age treated for major depression in our research group. The first ever Polish National Comorbidity Survey directed at the adult population showed the prevalence of depressive disorders among Polish adults to be very low, at 0.4% (95% confidence interval (CI): 0.3–0.5) [17], with adults of all ages and both sexes being affected evenly. This figure differed from those presented in earlier reports from other countries, where the prevalence of depressive disorders was estimated to be between 9.8% in Israel and 21.0% in France [18, 19]. The cited studies demonstrated higher prevalence rates in countries in which the survey response rate was higher than that in Poland. This discrepancy is not surprising because individuals refusing to participate in the study are often more severely affected by mental disorders than study participants [17]. Our analysis was based on the clinical data gathered by, and obtained from, daycare wards and psychiatric hospitals in the whole country. The research demonstrated a continually increasing number of children and adolescents treated for psychiatric disorders. This finding indicates an apparent worsening of the mental health status in this age group in Poland, because the actual prevalence of mental problems among children and adolescents in Poland is probably higher than what we observed. These findings raise concern because major depression is not a condition that can be completely cured. According to some studies, the risk of depressive episode recurrence in children and adolescents can be as high as 30–70% [20].
The increase in the rate of mental health issues recorded in Polish children and adolescents could be due to many factors within socio-economic changes after the dissolution of the Soviet Union. This was a great opportunity for rapid changes throughout the privatisation process in Poland but also introduced the risk of a negative impact on family life, especially for the young population. Rapid economic transformations could induce changes to the style of work, which also could affect the style of life and parents-children relations. Parents had less time to focus on their children and adolescents, which is one of the most important factors for their mental health.
The issue of the high prevalence rate of depression presented in our study cannot be explained with this basic data analysis, and more research is needed to explain this phenomenon. Evidently, because depression is a condition with complex aetiopathogenesis, many factors can contribute to this mental health problem being so common
376 Arch Med Sci 2, 1st March / 2023
[18, 20]. Literature provides a wide range of risk factors including biological, psychological, or social aspects of functioning [20]. Genetic susceptibility should not be responsible for disparity between the Polish population and young people living in other countries. Nevertheless, existing literature offers some evidence on risk factors connected with global changes in lifestyle of the younger population. Amongst them, spending more time on new media screen-based activities and less time on non-screen activities, obesity, the impact of social media, and peer-stress are strongly connected with increases in depression and suicide rates [21, 22]. Those factors are not entirely new but were more often observed in Poland between 1995 and 2011 [23].
What is more, early signs of depression in young individuals can easily be unnoticed or misinterpreted (i.e. interpreted as youth rebellion or as temporary problems) by their parents. Consequently, these youngsters are not provided with an accurate diagnosis and timely therapy and have more time to develop more severe clinical conditions [24–26].
As for other risk factors of developing depression, stressful life events are often mentioned in the literature. They include experiences of loss, marital discord or family conflicts, changes in family financial situation, interpersonal conflicts, emotional disappointments or losses, chronic diseases, or death of a loved one, and, often mentioned, experiencing abuse [27, 28]. There remains a need to conduct more studies, to include all those factors and explain their possible contribution to the high prevalence of depression amongst the young population.
The data we gathered from mental health institutions indicate an increase in the number of treated cases of both mood disorders and major depression among children and adolescents. The proportion of child and adolescent patients with major depression increased from 1.9% of all underage mental health patients in 2005 to 4.1% in 2016. Similarly, the proportion of child and adolescent patients with mood disorders rose from 3.1% of all underage mental patients in 2005 to 7.0% in 2016. This signifies the importance of intensifying the existing prevention programs, including those involving mental health screening among the general population of children and adolescents. Studies indicate that screening assessments among school youths lead to moderate (statistically significant) reductions in depression symptoms, and earlier intervention reduces the risk of depressive disorders in the future. Such preventive programs are especially effective in high-risk groups [29].
Mental health in Poland is deteriorating, which is indicated by the increased number of
children treated for mental health problems. We should consider better access to mental health in Poland, which could occur in the period under consideration, as well as the general increase in social acceptance of psychiatric care. For these reasons, the increase in the pace of mental health problems in Polish children and adolescents is unclear.
Among all child and adolescent mental health patients undergoing treatment, the proportion of patients diagnosed with depression was higher in mental hospitals than in day-care centres. However, both types of mental health facilities experienced an increase in the proportion of underage patients with depression over the investigated 12year period. This was also true for general mood disorders. Our study shows that, despite the availability of other diagnostic and treatment facilities for mood disorders (including major depression), most Polish children and adolescents seek help in mental hospital wards. This finding raises the concern given in earlier quality-of-care reports, which indicate a better quality of care in units that are smaller and in which not all patients have severe mental problems [30]. However, very few mental health facilities in low- and middle-income countries, including Poland, offer services targeted at children and adolescents, and the level of personnel training on child and adolescent mental health issues is insufficient [31].
The results of our study are consistent with global trends because both the prevalence and the rates of treatment for major depression are increasing worldwide [9, 32–34]. Moreover, there is no doubt that, according to the EZOP research, every fourth adult Pole has mental health problems [14, 17]. The use of specialty mental health providers is increasing, which leads to an increase in the use of prescribed medications and the rates of inpatient treatment [32, 33, 35–37].
Our analysis suggests that, in terms of sex, female children and adolescents are at a higher risk of developing depression, whereas, in terms of the place of residence, urban residents are at higher risk. Our results are consistent with those of other prevalence studies [17, 34, 38, 39] because women have been generally reported to be more likely than men to develop depression during their lifetime [40, 41].
Other findings also suggest that teenagers’ intention to seek help for mental disorders significantly depends on social factors as well as the individual’s sex (with girls being generally more likely to seek help than boys). The factor that inhibits help-seeking includes the gender norm regarding problem solving, with boys being more reluctant to seek help for depression than girls, and boys being expected to cope with problems on their own
Arch Med Sci 2, 1st March / 2023 377
The prevalence of depression in children and adolescents under 18 years of age treated for mental disorders in Poland between 2005 and 2016
Mira Lisiecka-Biełanowicz, Daria Biechowska, Edyta Orłowska, Bartłomiej Molenda
[42]. Relevant literature suggests that the female vulnerability to depression in the early years of life may be rooted in an intricate combination of genetic traits, normal female hormonal maturational processes, and gender socialisation [43].
The findings should be interpreted in the context of several limitations. Most notably, the study was not based on self-reports by children and adolescents but on clinical assessments reported by mental health institutions. Therefore, our survey (because we register treatment in the psychiatric care system) cannot be compared with traditional comorbidity surveys conducted in the general population of children and adolescents, because self-reports and parental reports are potentially more sensitive to capturing the initial symptoms of major depression [44, 45]. On the other hand, self-reporting has its own limitations and is prone to over interpretation. Therefore, a clinical assessment can be considered as this study’s advantage.
A second limitation is that our study addressed the population of patients already diagnosed with mood disorders and undergoing treatment. The current organisational solutions (regarding accessibility and the number of staff in health care facilities) within the Polish mental health care system better meet the needs of patients requiring comprehensive mental health care [46]. Changes in the way of thinking about mental health care for children and adolescents in Poland can also be seen to meet the objectives of the Polish National Mental Health Program, which stipulates the provision of child and adolescent mental health patients with any of the following: inpatient psychiatric care, outpatient mental health care, treatment at day wards, or care at home offered by a community-based team of health care professionals (Figure 1).
In conclusion, over the analysed period of 12 years, the number of children and adolescent patients undergoing anti-depression treatment increased for any psychiatric condition in mental-health outpatient clinics. Major depression
Hospital psychiatric treatment
Treatment at day wards
Mental Health Center
Treatment at home by community-based teams of HCPs
was moderately prevalent among children and adolescents treated in all evaluated types of mental health facilities, with its prevalence in this population ranging from 0.8% in 2005 to 4.3% in 2016. The rates of young patients with mood disorders increased from 3.1% in 2005 to 7.0% in 2016.
The increase in those treated for a mental disorder may be due to many reasons following the socio-economic changes which reshaped/redefined work and lifestyle, occurring over the last three decades in Poland. These kinds of changes could also be influenced by better access to psychiatric health care (with better quality of care in units that are smaller and in which not all patients have severe mental problems). Better access to health care could be improved by a socially higher – also in case of mental problems in children and adolescence – awareness about mental health through higher social acceptance of mental disorders. In the present study basic risk factors for developing major depression among young patients treated for mental disorders were being female and living in an urban area.
Our findings call for renewed efforts to expand the mental-health service capacity, intensify preventive measures, and better meet the mental health care needs of child and adolescent patients under the age of 18 years (especially for girls).
The National Mental Health Program is shifting the model of psychiatric treatment in Poland toward community-based care via Mental Health Centres in order to better meet the mental health care needs of children and adolescents, but we should continue to think about an appropriate model of community-based treatment teams aimed at the specific needs of this age group (children and adolescents) in Poland.
Conflict of interest
The authors declare no conflict of interest.
References
1. World Health Organization. Depression and Other Common Mental Disorders Global Health Estimates 2017.
2. Villas Boasad GR, Boerngen de Lacerdac R, Meirelles M, et al. Molecular aspects of depression: a review from neurobiology to treatment. Eur J Pharmacol 2019; 851: 99-121.
Outpatient mental healthcare
Figure 1. The model of mental health care currently being implemented in accordance with the National Mental Health Program includes the Centre for Mental Health, which incorporates hospital psychiatric treatment, outpatient mental health care, treatment at day wards, and treatment by community-based teams of healthcare professionals (HPCs) [46]
3. Bor W, Dean A, Najman J, Hayatbakhsh R. Are child and adolescent mental health problems increasing in the 21st century? A systematic review. Austral N Z J Psych 2014; 48: 606-16.
4. Flisher AJ, Dawes A, Kafaar Z, et al. Child and adolescent mental health in South Africa. J Child Adolescent Mental Health 2012; 24: 149-61.
5. United Nations. World Population Prospects – The 2017 Revision. United Nations: New York 2017.
6. Erskine HE, Baxter AJ, Patton G, et al. The global coverage of prevalence data for mental disorders in children and adolescents. Epidemiol Psych Sci 2017; 26: 395-402.
378 Arch Med Sci 2, 1st March / 2023
The prevalence of depression in children and adolescents under 18 years of age treated for mental disorders in Poland between 2005 and 2016
7. Ferdinand RF, Verhulst FC. Psychopathology in Dutch young adults: enduring or changeable? Soc Psychiatry Psychiatr Epidemiol 1995; 30: 60-4.
8. Patton GC, Coffey C, Romaniuk H, et al. The prognosis of common mental disorders in adolescents: a 14-year prospective cohort study. Lancet 1995; 383: 1404-11.
9. Kessler RC, Walters EE. Epidemiology of DSM-III-R major depression and minor depression among adolescents and young adults in the National Comorbidity Survey. Depress Anxiety 1998; 7: 3-14.
10. Cheung AH, Dewa CS. Canadian community health survey: major depressive disorder and suicidality in adolescents. Health Policy 2006; 2: 76-89.
11. Naicker K, Galambos NL, Zeng Y, et al. Social, demographic, and health outcomes in the 10 years following adolescent depression. J Adolesc Health 2013; 52: 533-8.
12. Thase ME. Managing medical comorbidities in patients with depression to improve prognosis. J Clin Psychiatry 2016; 77: 22-7.
13. Burcusa SL, Iacono WG. Risk for recurrence in depression. Clin Psychology Rev 2007; 27: 959-85.
14. Kiejna A, Adamowski T, Piotrowski P, et al. Epidemiology of mental disorders and access to mental health care. EZOP – Poland” – research methodology. Psychiatr Pol 2015; 49: 5-13.
15. Journal of Laws of 1995 No. 88 item 439 Act of June 29, 1995 on public statistics (the text available on: http:// isap.sejm.gov.pl/DetailsServlet?id=WDU19950880439), accessed on May 19, 2016.
16. World Health Organisation ICD-10 Classification of Mental and Behavioural Disorders: Clinical Descriptions and Diagnostic Guidelines. World Health Organisation, Geneva 1992.
17. Kiejna A, Piotrowski P, Adamowski T, et al. The prevalence of common mental disorders in the population of adult Poles by sex and age structure – an EZOP Poland study. Psychiatr Pol 2015; 49: 15-27.
18. Alonso J, Angermeyer MC, Bernert S, et al. ESEMeD/ MHEDEA 2000 Investigators, European Study of the Epidemiology of Mental Disorders (ESEMeD) Project. Prevalence of mental disorders in Europe: results from the European Study of the Epidemiology of Mental Disorders (ESEMeD) project. Acta Psychiatr Scand Suppl 2004; 420: 21-7.
19. Bromet EJ, Gluzman SF, Paniotto V, et al. Epidemiology of psychiatric and alcohol disorders in Ukraine: findings from the Ukraine World Mental Health survey. Soc Psychiatry Psychiatr Epidemiol 2005; 40: 681-90.
20. Birmaher B, Arbelaez C, Brent D. Course and outcome of child and adolescent major depressive disorder. Child Adolesc Psychiatr Clin N Am 2002; 11: 619-37.
21. Mojs E, Warchoł-Biedermann K, Głowacka M, Strzelecki W, Ziemska B, Samborski W. Are students prone to depression and suicidal thoughts? Arch Med Sci 2013; 11: 605-11.
22. Twenge JM, Joiner TE, Rogers ML, Martin GN. Increases in depressive symptoms, suicide-related outcomes, and suicide rates among U.S. adolescents after 2010 and links to increased new media screen time. Clin Psychol Sci 2018; 6: 3-17.
23. Dudek M, Kasznia-Kocot J, Giel K. Trends of selected health behaviors of Polish youth aged 13-15 the European and worldwide studies between 1995-2011. Environm Med 2015; 18: 74-80.
24. Fergusson DM, Woodward LJ. Mental health, educational, and social role outcomes of adolescents with depression. Arch Gen Psychiatry 2002; 59: 225-31.
25. Indic P, Murray G, Maggini C, et al. Multi-scale motility amplitude associated with suicidal thoughts in major depression. PLoS One 2012; 7: e38761.
26. Gladstone T, Beardslee WR, O’Connor E. The prevention of adolescent depression. Psychiatr Clin North Am 2011; 34: 35-52.
27. Shannon KE, Beauchaine TP, Brenner SL, Neuhaus E, Gatzke-Kopp L. Familial and temperamental predictors of resilience in children at risk for conduct disorder and depression. Dev Psychopathol 2007; 19: 701-27.
28. Mojs E, Bartkowska W, Kaczmarek ŁD, Ziarko M, Bujacz A, Warchoł-Biedermann K. Psychometric properties of the Polish version of the brief version of Kutcher Adolescent Depression Scale – assessment of depression among students. Psychiatr Pol 2015; 49: 135-44.
29. Stice E, Shaw H, Bohon C, Marti CN, Rohde P. A meta-analytic review of depression prevention programs for children and adolescents: factors that predict magnitude of intervention effects. J Consult Clin Psychol 2009; 77: 486-503.
30. Killaspy H, Cardoso G, White S, et al. Quality of care and its determinants in longer term mental health facilities across Europe: a cross-sectional analysis. BMC Psychiatry 2016; 16: 31.
31. Morris J, Belfer M, Daniels A, et al. Treated prevalence of and mental health services received by children and adolescents in 42 low-and-middle-income countries. J Child Psychol Psychiatry 2011; 52: 1239-46.
32. von Soest T, Wichstrøm L. Secular trends in depressive symptoms among Norwegian adolescents from 1992 to 2010. J Abnormal Child Psychol 2014; 42: 403-15.
33. Mojtabai R, Olfson M. National trends in the prevalence and treatment of depression in adolescents and young adults. Pediatrics 2016; 138: e20161878.
34. Twenge JM, Joiner TE, Rogers ML, Martin GN. Increases in depressive symptoms, suicide-related outcomes, and suicide rates among U.S. adolescents after 2010 and links to increased new media screen time. Clin Psychol Sci 2017; 6: 3-17.
35. Sigfusdottir ID, Asgeirsdottir BB, Sigurdsson JF, Gudjonsson GH. Trends in depressive symptoms, anxiety symptoms and visits to healthcare specialists: a national study among Icelandic adolescents. Scand J Public Health 2008; 36: 361-8.
36. Sweeting H, Young R, West P. GHQ increases among Scottish 15 year olds 1987–2006. Soc Psychiatry Psychiatr Epidemiol 2009; 44: 579-86.
37. Fleming TM, Clark T, Denny S, et al. Stability and change in the mental health of New Zealand secondary school students 2007-2012: results from the national adolescent health surveys. Austral N Z J Psychiatry 2014; 48: 472-80.
38. Avenevoli S, Swendsen J, He JP, et al. Major depression in the national comorbidity survey- adolescent supplement: prevalence, correlates, and treatment. J Am Acad Child Adolescent Psychiatry 2014; 54: 37-44.e2.
39. Skovlund CW, Kessing LV, Mørch LS, Lidegaard Ø. Increase in depression diagnoses and prescribed antidepressants among young girls. A national cohort study 2000–2013. Nordic J Psychiatry 2017; 71: 378-85.
40. Kuehner C. Why is depression more common among women than among men? Lancet Psychiatry 2017; 4: 146-58.
41. Polikandrioti M, Tzirogiannis K, Zyga S, et al. Effect of anxiety and depression on the fatigue of patients with a permanent pacemaker. Arch Med Sci Atheroscler Dis 2018; 3: 8-17.
Arch Med Sci 2, 1st March / 2023 379
42. Ando S, Nishida A, Usami S. et al. Help-seeking intention for depression in early adolescents: associated factors and sex differences. J Affective Disord 2018; 238: 359-65.
43. Born L, Shea A, Steiner M. The roots of depression in adolescent girls: is menarche the key? Curr Psychiatry Rep 2002; 4: 449-60.
44. Sourander A, Helstelä L, Helenius H. Parent-adolescent agreement on emotional and behavioral problems. Soc Psychiatry Psychiatr Epidemiol 1999; 34: 657-63.
45. Martin JL, Ford CB, Dyer-Friedman J, Tang J, Huffman LC. Patterns of agreement between parent and child ratings of emotional and behavioral problems in an outpatient clinical setting: when children endorse more problems. J Developm Behav Pediatr 2004; 25: 150-5.
46. Lisiecka-Biełanowicz M, Biechowska D, Cianciara D. Funkcjonowanie jednostek w różnych formach opieki psychiatrycznej w Polsce w latach 2010-2013. Analiza organizacyjna i ekonomiczno-finansowa. Psychiatr Pol 2018; 52: 143-56.
380 Arch Med Sci 2, 1st March / 2023
Mira Lisiecka-Biełanowicz, Daria Biechowska, Edyta Orłowska, Bartłomiej Molenda
Hassan Bazmamoun, Alireza Momeni, Leila Jahangard, Farzaneh Asnaashari, Nasrollah Pezeshki
Department of Pediatrics, Hamadan University of Medical Sciences, Hamadan, Iran
Submitted: 5 February 2019; Accepted: 19 August 2019
Online publication: 25 March 2021
Arch Med Sci 2023; 19 (2): 381–384
DOI: https://doi.org/10.5114/aoms/111841
Copyright © 2021 Termedia & Banach
Abstract
Introduction: Attention deficit hyperactivity disorder (ADHD) is one of the most common neurodevelopmental disorders in children. Functional constipation is common in children and has a significant impact on the quality of their life, affecting both physical and emotional well-being. The aim of this study was to evaluate the frequency of ADHD in functional constipation patients and its treatment effect on constipation.
Material and methods: In this clinical trial study, 80 children with simultaneous ADHD and functional constipation were allocated to two equal groups by the block randomization method. One group was treated only with ADHD drugs and the second group was treated for ADHD and functional constipation. Subsequently, the treatment outcome was evaluated in both groups.
Results: The frequency of ADHD in functional constipation patients was 13.87%. The frequency of functional constipation recovery in the first and second group was respectively 2 (5%) and 39 (97.5%) ( p < 0.001). ADHD treatment has no significant effect on the recovery of constipation. There was no statistically significant relationship between the response to treatment with age, sex and duration of having ADHD and constipation.
Conclusions: In patients with simultaneous ADHD and functional constipation, ADHD treatment did not influence the recovery of functional constipation and vice versa.
Key words: attention deficit hyperactivity disorder, constipation, children.
Introduction
Prevalence of constipation in the worldwide general population is very variable. It is estimated that between 0.7% and 29.6% of children suffer from constipation [1]. Functional constipation is constipation with no specific anatomical, medical or pharmaceutical causes, and is more common in children [2]. Functional constipation in children is multifactorial and two factors – inadequate dietary fiber intake and delayed bowel movements – often lead to progression of constipation [3]. Much effort has been made to standardize the terminology of children’s constipation and several international guidelines have been accepted for its definition, including NASPGHAN [4], PACCT [5], and ROME III [6], but none of them have been widely used in clinical practice or research work. Attention deficit hyperactivity disorder (ADHD) is one of the common behavioral problems
Corresponding author: Nasrollah Pezeshki
Department of Pediatrics
Hamadan University of Medical Sciences
Hamadan, Iran
E-mail: nasrpezeshk@yahoo.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
How common is attention deficit hyperactivity disorder (ADHD) in a cohort of children with functional constipation, and does ADHD treatment improve functional constipation?
Clinical research Paediatrics
Hassan Bazmamoun, Alireza Momeni, Leila Jahangard, Farzaneh Asnaashari, Nasrollah Pezeshki
in children [7, 8]. ADHD is defined as a sustained pattern of low attention or low attention with hyperactivity and impulsive behavior that is more than expected due to the age and level of development of the child [9]. The reported incidence of this disorder in school age children is between 3% and 8% [7, 10, 11]. It is more common in males than females (3 in 1 to 5 in 1) and the symptoms of the disease usually present by 3 years old [7]. Children with ADHD are at increased risk of other problems such as antisocial behavior, anxiety disorders, mood disorders, learning disorders, drug abuse and communication problems [12–14].
Experts have experimentally found that in children’s constipation, the importance of managing constipation-related behaviors is not less than that of a dietary or therapy regime [15].
Considering the higher prevalence of constipation and fecal incontinence among children with ADHD and the hypotheses explaining this relationship including behavioral problems, neurobiological disorders, defects in the relationship between the nervous system of the digestive system and the central nervous system, and the delay in maturation of the gastrointestinal tract [16], the aim of this study was to determine the frequency of ADHD in children with functional constipation and the effect of ADHD treatment on their constipation.
Material and methods
In this study, 2,090 children aged 4 to 12 years with constipation referred to the pediatric gastroenterology clinic of Besat Hospital in Hamadan City, Iran, during the years 2016 and 2017, after confirmation of the diagnosis of functional constipation by a pediatric gastroenterologist (based on the criteria of 2006 ROME III [6]), were evaluated to determine simultaneous existence of ADHD using the Conners Questionnaire.
If the patient had a total score of 34 points, he/ she was referred to a psychiatrist, and if ADHD was approved by a psychiatrist, he was entered into the study.
Patients with organic causes of constipation including Hirschsprung’s disease, hypothyroidism, spina bifida occulta, anorectal abnormalities, non-retentive fecal incontinency, chronic intestinal pseudo-obstruction, history of anorectal/colon surgery, and taking medications which could modify bowel habit, were excluded from the study.
This study was conducted with the approval of the Ethics Committee of Hamadan University of Medical Sciences (with the ethics code, Deputy of Research and Technology IR.UMSHA. REC.1395.535). All parents gave written informed consent and the parents took the oral assent of the children.
Eighty patients out of 290 patients with simultaneous ADHD and functional constipation were selected by simple randomization and then randomly divided by random blocks into two equal groups.
Non-treated group: They were only treated for ADHD by a standard method [17].
Treated group: At the same time, they were treated for ADHD and functional constipation including a dietary regimen and PEG without electrolyte at a maximum dose (0.7 g/kg/day, 13.8–40.0 g/daily), twice a day. For children with rectal impaction, disimpaction was initially performed with bisacodyl suppositories for 3–5 days (5 mg/daily > 4 years). No further treatment was allowed for constipation during the study.
Patients’ data were collected by a questionnaire including name, sex, age, duration of constipation, consistency/size/frequency of stool, number of painful defecations, fecal incontinence per week, and stool mass in the abdomen or rectum.
Parents were given dose regulation training to record the number and consistency of stools, frequency of stomach incontinence, abdominal pain, and pain relief.
Patients were examined and re-visited at 1, 3, 6 and 12 months after starting treatment, and drug dosage was adjusted.
To evaluate the response to treatment of ADHD, the Conners Questionnaire was used again, which would have been considered as improvement if the patient’s score was less than 34.
The definition of response to constipation treatment was ≥ 3 bowel movements weekly, ≤ 2 episodes of fecal incontinence per month and absence of abdominal pain.
Statistical analysis
In this study, quantitative variables were presented as mean and standard deviation, and qualitative variables were reported as percentages. The c2 test was used to evaluate the association between functional constipation improvement and sex/type of treatment. The Kolmogorov-Smirnov one sample test was used for normality detection. To compare disease duration between improved and non-improved patients, the Mann-Whitney U test was used, because distribution of disease duration was not normal. Data were analyzed using SPSS16 software. P-value < 0.05 was considered statistically significant.
Results
Eighty children with simultaneous ADHD and functional constipation were enrolled. Forty were in the non-treated group and forty in the treated group.
The percentage of male and female subjects in the non-treated group and treated group was respec-
382 Arch Med Sci 2, 1st March / 2023
How common is attention deficit hyperactivity disorder (ADHD) in a cohort of children with functional constipation, and does ADHD treatment improve functional constipation?
of having constipation [months], mean (SD)
Duration of having ADHD [months], mean (SD) *
test. **Student’s t-test. aPatients only treated for ADHD. bPatients treated for ADHD and constipation.
tively 55%, 45%, 57.5% and 42.5% (p = 0.822), with mean age 8.02 ±1.9 and 8.07 ±2.3 years (p = 0.458).
There were no significant differences regarding demographic data and duration of ADHD and constipation between the two groups (Table I).
The frequency of constipation recovery in the non-treated group was 5% (2) while it was 97.5% (39) in the treated group; the difference was statistically significant (p < 0.001).
There was no statistically significant relationship between functional constipation recovery in children with ADHD and age, sex, and duration of having functional constipation and ADHD (Table II).
The frequency of ADHD recovery in the nontreated group and treated group was 100%.
Discussion
In the present study, 13.87% of children with functional constipation had ADHD. The recovery of functional constipation in patients with ADHD who were simultaneously treated for constipation was higher than in patients who only received ADHD treatment. This means that treatment of ADHD has no effect on the treatment of constipation. There was no significant correlation between the recovery of functional constipation in children treated for ADHD and constipation with duration of having ADHD and functional constipation and patient’ age and sex.
Also the treatment of constipation did not significantly affect the frequency of ADHD recovery.
In a study by McKeown et al. in the United States between 2005 and 2007 in children aged 4 to 12 years old, the prevalence of ADHD was
4.4%, and the incidence of functional constipation in children with ADHD was 4.1%, while in children without ADHD it was 1.5%. Based on the findings of this study, although the risk of ADHD may increase the risk of functional constipation, ADHD treatment has no significant effect on the increase or decrease of constipation [18].
In the present study, similar to McKeown et al.’ findings, treatment of ADHD did not influence the functional constipation recovery.
In a study by Duel et al. in the United States whose results were published in 2003, in 28 patients with ADHD in comparison with 22 healthy persons with voiding dysfunction, measured by the Dysfunctional Voiding Symptom Survey (DVSS) questionnaire, the mean total score of the DVSS questionnaire in male subjects with ADHD and the control group was respectively 14.83 ±3.68 and 6.6 ±5.74, and in female subjects with ADHD and the control group it was respectively 19.0 ±5.3 and 5.83. The results of this study showed that in patients with ADHD, the mean score of the DVSS questionnaire (symptoms of fecal dysfunction) was significantly higher than in the control group in both males and females [19].
According to the results of the Benninga et al. study on children aged 5 to 17 years, due to problems with defecation of stool and abdominal and behavioral problems, it seems there is no relationship between colonic/anorectal function and behavioral profiles. However, children with gastrointestinal disorders had more behavioral problems than the control group [20].
The results of research by Becker et al. on the neural process of excitement and fecal inconti-
Arch Med Sci 2, 1st March / 2023 383
P -value Treated groupb Non-treated groupa Variable 0.822* 23 (57.5) 22 (55.0) Male sex, n (%) 0.458** 8.07 (2.3) 8.02 (1.9) Age [years], mean (SD) 0.594** 11.37 (2.78) 11.52 (2.89)
0.624** 13.14 (4.46) 13.47 (4.78)
χ
Table I. Comparison of demographic and clinical characteristic between treated and non-treated groups
Duration
2
P -value Not recovered Recovered Variable Gender, n (%): 0.485* 27 (67.5) 24 (60.0) Male 13 (32.5) 16 (40.0) Female 0.967** 8.06 (2.03) 8.04 (2.1) Age [years], mean (SD) 0.557** 13.61 (4.80) 13.00 (4.50) Duration of having ADHD [months], mean (SD) 0.531 11.61 (2.88) 11.21 (2.80) Duration
* χ2 test.
t-test.
Table II. Comparison of demographic and clinical characteristics between recovered and non-recovered groups
of having constipation [months], mean (SD)
**Student’s
nence in 14 children with fecal incontinence and constipation showed that in children with fecal incontinence, the response process to emotions and excitement was increased and could be considered as neurocognitive vulnerability due to the relation of the enteric nervous system with the central nervous system [16].
In a study by Niemczyk et al. in children aged 7 to 17 years with ADHD, delayed bowel control was significantly more prevalent than in children in the control group but treatment of ADHD, especially medication, can improve the treatment outcome of incontinence [21], which is different from the findings of the present study.
In our study, the treatment of constipation did not significantly affect the frequency of ADHD recovery. Unfortunately, no similar study was found for comparison.
Although functional constipation may be more prevalent in children with ADHD [18], or children with gastrointestinal disorders may have more behavioral disorders and neurobiological disorders, including deficiencies in the nervous and central nervous system, and delayed maturation of gastrointestinal motility may have a relation with functional constipation [16], according to our research, the treatment of ADHD or constipation has no significant effect on the recovery of the other condition. On the contrary, each disorder requires separate treatment.
In conclusion, in patients with functional constipation, ADHD is a common association and treatment of ADHD is not effective in the recovery of functional constipation. Also, treatment of constipation has no effect on the recovery of ADHD.
Acknowledgments
This article is a part of a pediatric medicine thesis supported by the Vice Chancellor for Research and Technology of Hamadan University of Medical Sciences (no. 9511267253). Thanks to the personnel of Besat Hospital and Hamadan Gastrointestinal Clinic who helped to collect the data.
Conflict of interest
The authors declare no conflict of interest.
References
1. Mugie SM, Benninga MA, Di Lorenzo C. Epidemiology of constipation in children and adults: a systematic review. Best Pract Res Clin Gastroenterol 2011; 25: 3-18.
2. Di Lorenzo C. Pediatric anorectal disorders. Gastroenterol Clin Notth Am 2001; 30: 269-87.
3. Rajindrajith S, Devanarayana NM. Constipation in children: novel insight into epidemiology, pathophysiology and management. J Neurogastroenterol Motil 2011; 17: 35-47.
4. Uc A, Hyman PE, Walker LS. Functional gastrointestinal disorders in African American children in primary care. J Pediatr Gastroenterol Nutr 2006; 42: 270-4.
5. Baker SS, Liptak GS, Colletti RB, et al. Constipation in infants and children: evaluation and treatment. A medical position statement of the North American Society for Pediatric Gastroenterology and Nutrition. J Pediatr Gastroenterol Nutr 1999; 29: 612-26.
6. Benninga M, Candy DC, Catto-Smith AG, et al. The Paris consensus on childhood constipation terminology (PACCT) group. J Pediatr Gastroenterol Nutr 2005; 40: 273-5.
7. Travis F, Grosswald S, Stixrud W. ADHD, brain functioning, and transcendental meditation practice. Mind Brain J Psychiatr 2011; 2: 73-81.
8. Wolraich M, Brown L, Brown RT, et al. ADHD: clinical practice guideline for the diagnosis, evaluation, and treatment of attention-deficit/hyperactivity disorder in children and adolescents. Pediatrics 2011; 128: 1007-22.
9. Sadock BJ, Sadock VA. Attention deficit disorder. In: Kaplan and Sadock’s Synopsis of Psychiatry: Behavioral Sciences/Clinical Psychiatry. 10th ed. Lippincott Williams & Wilkins; Philadelphia 2007. 1206-17.
10. Grizenko N, Shayan YR, Polotskaia A, Ter-Stepanian M, Joober R. Relation of maternal stress during pregnancy to symptom severity and response to treatment in children with ADHD. J Psychiatry Neurosci 2008; 33: 10-6.
11. Linnet KM, Dalsgaard S, Obel C, et al. Maternal lifestyle factors in pregnancy risk of attention deficit hyperactivity disorder and associated behaviors: review of the current evidence. Am J Psychiatry 2003; 160: 1028-40.
12. Amiri S, Fakhari A, Golmirzaei J, Mohammadpoorasl A, Abdi S. Tourette’s syndrome, chronic tics, and comorbid attention deficit/hyperactivity disorder in elementary students. Arch Iran Med 2012; 15: 76-8.
13. Faraone SV, Biederman J, Mennin D, Russell R, Tsuang MT. Familial subtypes of attention deficit hyperactivity disorder: a 4-year follow-up study of children from antisocial-ADHD families. J Child Psychol Psychiatry Allied Disciplines 1998; 39: 1045-53.
14. Dursun OB, Şengül F, Esin IS, Demirci T, Yücel N, Ömezli MM. Mind conduct disorders in children with poor oral hygiene habits and attention deficit hyperactivity disorder in children with excessive tooth decay. Arch Med Sci 2016; 12: 1279-85.
15. Di Lorenzo C. Childhood constipation: finally some hard data about hard stools! J Pediatr 2000; 136: 4-7.
16. Becker A, Rubly M, El Khatib D, Becker N, Von Gontard A. Central nervous system processing of emotions in children with faecal incontinence. Acta Paediatrica 2011; 100: e267-74.
17. Sadock BJ, Sadock VA, Ruiz P. Attention deficit/hyperactivity disorder. In: Kaplan and Sadock’s synopsis of psychiatry: Behavioral sciences/clinical psychiatry. 11st ed. Wolters Kluwer, Philadelphia 2015; 1169-80.
18. McKeown C, Hisle-Gorman E, Eide M, Gorman GH, Nylund CM. Association of constipation and fecal incontinence with attention-deficit/hyperactivity disorder. Pediatrics 2013; 132: e1210-5.
19. Duel BP, Steinberg-Epstein R, Hill M, et al. A survey of voiding dysfunction in children with attention deficithyperactivity disorder. J Urol 2003; 170: 1521-4.
20. Benninga MA, Voskuijl WP, Akkerhuis GW, Taminiau JA, Büller HA. Colonic transit times and behaviour profiles in children with defecation disorders. Arch Dis Child 2004; 89: 13-6.
21. Niemczyk J, Equit M, Hoffmann L, von Gontard A. Incontinence in children with treated attention-deficit/hyperactivity disorder. J Pediatr Urol 2015; 11: 141.e1-6.
384 Arch Med Sci 2, 1st March / 2023
Hassan Bazmamoun, Alireza Momeni, Leila Jahangard, Farzaneh Asnaashari, Nasrollah Pezeshki
1Department of Nuclear Medicine, Faculty of Medicine, Pamukkale University, Denizli, Turkey
2Department of Thoracic Surgery, Faculty of Medicine, Firat University, Elazig, Turkey
3Department of Nuclear Medicine, Antalya Education and Research Hospital, Antalya, Turkey
4Department of Pulmonology, Faculty of Medicine, Firat University, Elazig, Turkey
5Department of Pathology, Faculty of Medicine, Firat University, Elazig, Turkey
6Department of Nuclear Medicine, Elazig Medical Park Hospital, Elazig, Turkey
Submitted: 12 February 2019; Accepted: 6 August 2019
Online publication: 24 March 2021
Arch Med Sci 2023; 19 (2): 385–391
DOI: https://doi.org/10.5114/aoms/111529
Copyright © 2021 Termedia & Banach
Abstract
Introduction: There is no consensus about the standardized uptake value maximum (SUVmax) cut-off value to characterize pleural thickening worldwide. Sometimes, this causes unnecessary invasive diagnostic procedures. Our first aim is to determine a cut-off value for SUV max. Secondly, we try to answer the following question: If we use this cut-off value together with morphological parameters, can we differentiate benign thickening from malignant pleural mesothelioma (MPM) more accurately?
Material and methods: Thirty-seven patients who underwent 2-deoxy-2-fluoroD-glucose ([18F]FDG) positron emission tomography/computed tomography (PET/CT) before pleural biopsy were included the study. All of patients had histopathologically proven primary pleural disease. Their [18F]FDG-PET/CT imaging reports were re-assessed. If a patient’s SUVmax or size of the thickening was not mentioned in the report, we calculated it with their [18F]FDG-PET/CT.
Results: Age, pleural effusion, size, and SUVmax were found to have a relationship with MPM. We found the size > 14 mm, and SUVmax > 4.0 as cut-off values for MPM. The sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) for size > 14 mm were found to be 86.4%, 85.2%, 82.6%, 88.5%, respectively. For SUVmax > 4.0, sensitivity, specificity, PPV, NPV were 90.9%, 87.0%, 85.1%, 92.2%, respectively.
Conclusions: If a patient has SUVmax > 4.0 and/or size > 14 mm, the risk of MPM is high. These patients should undergo biopsy. If a patient’s SUVmax < 4.0, size < 14 mm and does not have pleural effusion, he/she has low risk for MPM. These patients can undergo the follow-up. If a patient’s SUVmax < 4, size < 14, and has pleural effusion the MPM risk is approximately 4%. These patients can undergo biopsy/cytology/follow-up. Novel studies are needed for these patients.
Key words: mesothelioma, cut-off value, pleural thickening, 18F-FDG-PET.
Introduction
Malignant pleural mesothelioma (MPM) and benign pleural thickenings (BPT) are rare diseases originating from mesothelial cells. Both of them are mostly associated with asbestos exposure. Malignant pleural
Corresponding author: Ass. Prof. F. Selcuk Simsek
Department of Nuclear Medicine
Faculty of Medicine Firat University
Elazig, Turkey
E-mail: fselcuksimsek@gmail.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
How can we use positron emission tomography/ computed tomography more accurately for characterization of asbestos-related pleural thickening?
F. Selcuk Simsek1, Muharrem Cakmak2, Duygu Kuslu3, Tansel A. Balci4, Erdal In4, Ibrahim H. Ozercan5, Yavuz Narin6
Clinical research Radiology
mesothelioma has aggressive behavior with very poor prognosis. Its median survival time is around 12 months. Recent studies reported that the incidence of the disease has increased [1–5]. Malignant pleural mesothelioma is generally detected in advanced stages after a long latency period. Early diagnosis is crucial for prolongation of survival [6–9] and can be achieved with imaging procedures. On the other hand, sometimes BPT and MPM cannot be differentiated properly with imaging methods. This causes unnecessary invasive approaches such as cytological examination or more invasive procedures [10].
Enhanced or unenhanced computed tomography (CT) is the most commonly used method to differentiate asbestos-related pleural pathologies. Nonetheless it does not have sufficient accuracy. Magnetic resonance imaging (MRI) is not commonly used for pleural lesion characterization due to its limited availability, costs and long time of the imaging. Moreover, if invasion does not exist in surrounding tissues, it is also not a reliable method [11]. Because we cannot achieve high accuracy with morphological techniques, 2-deoxy-2-[18F]fluoroD-glucose positron emission tomography/computed tomography ([18F]FDG-PET/CT) is used nowadays for this purpose. Although it has better results than morphological imaging modalities, [18F]FDG-PET/ CT also has insufficient accuracy. In addition, there is no consensus for a standardized uptake maximum (SUVmax) cut-off value to characterize pleural thickening [12, 13]. Because of all these difficulties, pleural thickening with suspected MPM is described as a ‘challenging disease to image by any modality’ by some scientists [7, 10]. At this point, radiologists/nuclear medicine specialists’ reports become very important for patient management. However, due to ambiguity of the imaging results in some patients, they undergo unnecessary cytological examination or biopsy [10].
Our first aim in this study is to determine a cut-off value for SUV max in patients with asbestos-related pleural thickening. Secondly, we try to answer this question: If we use this cut-off value together with morphological parameters, can we differentiate benign thickening from MPM more accurately? If we achieved a simple and practical diagnostic approach for these patients, it can help us to avoid unnecessary invasive diagnostic procedures. It can reduce costs of the Medicare system, save time for medical professionals and decrease complication rates caused by invasive methods.
Material and methods
Patient selection
The results of 98 patients who underwent [18F] FDG-PET/CT imaging for asbestos-related pleural
thickening between 1 January 2013 and 31 December 2017 were reviewed. Thirty-seven patients who did not have distant metastases in pre-biopsy [18F]FDG-PET/CT were included in the study. All of these patients had pathologically proven primary pleural disease. Thirty-one patients’ pleural lesions’ SUV max was > 2.5 and these patients directly underwent biopsy. Six patients’ SUVmax was < 2.5; however, three of them had pleural effusion and three of them had increasing size of the thickening in follow-up. These patients also underwent biopsy. Their anamnesis, demographic parameters, [18F]FDG-PET/CT and pathology results were found from our database. If size of the thickening, or lesions’ SUVmax value was not mentioned in a previous report, we calculated them from their re-examined [18F]FDG-PET/CT. Pathological results are accepted as gold standard.
Positron emission tomography/ computed tomography imaging
After at least 6 h of fasting, if a patient’s blood glucose level was appropriate for injection, approximately 6–8 millicuries of [18F]FDG were administered intravenously (IV). Patients rested in a warm and quiet room for about 60 min and then [18F]FDG-PET/CT (General Electric D600 16 slice, GE Healthcare, USA) was performed. Initially, morphologic imaging was performed with ‘care dose’ CT with 5 mm thickness from the vertex to the mid-thigh. Then, PET imaging was performed in 7–8 bed positions for approximately 3 min for each position. The patients underwent shallow breathing during the PET imaging. CT data were used for attenuation correction and anatomical localization. We did not use oral or IV contrast agents. Images were evaluated by us and SUVmax values of each suspicious lesion were measured.
Statistical analysis
Data were analyzed by Statistical Package for the MedCalc Statistical Software version 18.10.2 (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org; 2018). The numerical and categorical data were expressed as mean ± standard deviation and percentage, respectively. Kolmogorov-Smirnov and Shapiro-Wilk tests were used as tests of normality for continuous variables. Fisher’s exact test was used to determine the relationship between two groups and p < 0.05 was considered as statistically significant. Receiver operating characteristic (ROC) curve analysis was performed with Hanley and McNeil methodology. Sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were calculated.
386 Arch Med Sci 2, 1st March / 2023
F. Selcuk Simsek, Muharrem Cakmak, Duygu Kuslu, Tansel A. Balci, Erdal In, Ibrahim H. Ozercan, Yavuz Narin
Results
Fourteen (37.8%) patients were female. The total number of MPM diagnoses was 25 (67.6%). Approximately 61.0% of male and 78.0% of female patients were diagnosed with MPM. Although females had a higher rate of MPM, this was not statistically significant (p = 0.27). Patients’ mean age was 62.8 years (31–90; SD: 13.1). Mean age of the MPM and BPT patients was 65.6 and 62.6 years, respectively. Since 12 patients had BPT, we also calculated the geometric mean for them. This value was 56.0 years (41–75 and 95% CI was 43.7–65.9). Age had a statistically significant relationship with MPM (p = 0.049). The results are summarized in Table I.
Approximately 2 out of every 3 (66.7%) diffuse thickening patients had MPM. This rate was very similar for nodular thickening patterns (65.2%). The differences were not statistically significant. Approximately 44.4% of MPM patients had pleural calcification. This rate was 55.6% for patients with BPT. Although BPT patients had a higher pleural calcification rate, this also was not statistically significant. On the other hand, 83.3% of the patients with pleural effusion were diagnosed with MPM. The difference between MPM and BPT was statistically significant (p = 0.01). However, only 56.0% of MPM patients had pleural effusion. Mean size of the thickening and mean SUVmax values also had statistically significant differences between groups. The results are summarized in Table II.
We found size > 14 mm and SUV max > 4.0 as cutoff values for MPM. The sensitivity, specificity, PPV and NPV of size > 14 mm were calculated as 85.7%, 83.3%, 90.0% and 76.9%, respectively. Area under the ROC curve, standard error and confidence interval were 0.887, 0.05 and 95.0% (0.772–1.0), respectively. This cut-off value had 12.0% false negativity, and 8% of them were epithelioid, while 4% of them were non-epithelioid subtype MPM. For SUVmax > 4.0; sensitivity, specificity, PPV and NPV were 88.0%, 83.3%, 91.7%, 76.9%, respectively. Area under the ROC curve, standard error and confidence interval were 0.895, 0.05 and 95% (0.789–1.0), respectively. It also had 12.0% false negativity. All false patients in this group were epithelioid subtype. On the other hand, false positive results were associated with inflammation.
For example, 1 patient who was diagnosed with pleuritis had an SUVmax value of 5.8. ROC analysis is shown in Figure 1. 24 out of the 25 (96.0%) MPM patients had SUVmax > 4.0 or size > 14 mm. The remaining 1 patient with MPM had SUVmax < 4.0 and size < 14 mm. However, he had pleural effusion. When we examined BPT patients, 58.3% (7/12) of them had SUVmax < 4.0, size < 14 mm and had no pleural effusion. Figure 2 provides an example of this.
MPM – malignant pleural mesothelioma, BPT – benign pleural thickening.
Discussion
Malignant pleural mesothelioma is an aggressive tumor originating from mesothelial cells of the pleura. This malignancy is mostly related to asbestos exposure and the incidence of it has been increasing [1, 3, 14]. Early diagnosis is crucial for prolongation of survival and it can be achieved
Arch Med Sci 2, 1st March / 2023 387
How can we use positron emission tomography/computed tomography more accurately for characterization of asbestos-related pleural thickening?
P -value BPT ( n = 12; 32.4%) MPM ( n = 25; 67.6%) Factor 0.049 62.6 65.6 Mean age [years] 0.27 22% 78% Female 39% 61% Male
Table I. Relationship between age/sex and final diagnosis
P -value MPM, 95% CI BPT, 95% CI Factor 0.01 83.3 16.7 Pleural effusion > 0.1 44.4 55.6 Calcification > 0.1 66.7 33.3 Diffuse pattern > 0.1 65.2 34.8 Nodular pattern < 0.01 25.6 (SD ±12.5) 11.8 (SD ±3.2) Size of thickening [mm] < 0.01 10.6 (SD ±7.4) 2.96 (SD ±1.37) SUV max value MPM – malignant pleural mesothelioma, BPT – benign pleural thickening.
Table II. Relationship of some morphological/metabolic parameters and final diagnosis
100 80 60 40 20 0 0 100-Specificity 20 40 60 80 100 Size SUV max
Figure 1. ROC analysis of size and SUVmax
with imaging procedures. On the other hand, sometimes benign pleural thickening patients undergo unnecessary invasive procedures due to uncertainty of the imaging techniques’ reports. In such situations, cytological examination, which has low NPV, or more invasive procedures can be applied [10]. This increases costs of the Medicare system and is time consuming. Moreover, it can cause unnecessary morbidity, and increased complication rates in lots of patients.
Radiography is usually used as the first imaging method to evaluate the respiratory system [15]. If there are any suspicious findings, CT is the next step. Studies reported that CT imaging provides helpful information for pleural pathologies. However, CT parameters do not have sufficient accuracy for characterization of them. For example, Seely et al. reported that 43% of MPM patients had calcified pleural pathology, but 57% did not [16].
Leung et al. studied circumferential pleural thickening, nodular pleural thickening, parietal pleural thickening greater than 1.0 cm, and mediastinal pleural thickening patterns, and their relationship with MPM. They found that these parameters could be useful [17]. Hierholzer et al. reported that, if a patient had one or more of these four parameters, the sensitivity was 72% and specificity was 83% [18]. A study published in 2016 reported that circumferential thickening occurs in 31.1% of MPM patients. This rate was 59.2% for nodular thickening [19]. Kato et al. aimed to achieve more accurate results with irregularity. They found that low level pleural irregularity and BPT were associated. Scientists also reported that high level irregularity or mass formation and MPM were associated [20]. Finally, a recent study reported overall sensitivity, specificity, PPV and NPV of the CT imaging were 68.2%, 78.0%, 80.4% and 64.9%, respectively [21]. Due to the lack of highly reliable results with morphological CT imaging, some researchers studied contrast-enhanced CT parameters. Many studies have reported that venous phase contrast-
enhanced CT imaging provides more accurate results for pleural lesions’ evaluation [22, 23]. However, in a recent study, even if a venous phase was applied, and CT was reported by a thoracic radiologist, the sensitivity, specificity, PPV and NPV were 69%, 73%, 78% and 63%, respectively. If arterial phase imaging was applied, these values were 27%, 69%, 53% and 40%, respectively [24]. Moreover, Kato et al. reported that there were no significant differences between contrast enhanced and unenhanced CT imaging for characterized asbestos-related pleural thickening [20]. To overcome this difficulty, some other authors studied different MRI techniques. For example, Koc et al. aimed to obtain more reliable results with diffusion contrast enhanced MRI scanning. However, it could not provide high accuracy [25]. Tsim et al. used early contrast enhanced-MRI, which is a novel technique, to achieve high accuracy. With this method the authors reported sensitivity, specificity, PPV and NPV of 83%, 83%, 68% and 92%, respectively. Although it has higher accuracy compared to conventional ones, low PPV is noteworthy [26].
Our study had similar findings as those reported in the literature. 66.7% of the patients with diffuse thickening and 65.2% of the patients with nodular thickening were diagnosed with MPM. In addition, 44.4% of patients with pleural calcification had MPM, and 56.4% had BPT. These results were not statistically significant (p > 0.1). On the other hand, two CT parameters could differentiate BPT from MPM significantly. The first one was presence of effusion. In our patient population, 83.3% of the patients with pleural effusion were diagnosed MPM and only 16.7% of them had BPT. This was statistically significant (p = 0.01). A recent study also mentioned this relationship [27]. Ökten et al. reported that 83% of the pleural effusion patients had MPM. This value was very similar to our results [28]. Nonetheless, only 56.0% of the MPM patients had pleural effusion in our patient population. Chen et al. found that 60.0% of the MPM patients had pleural effusion [29]. According to findings, if a patient has pleural effusion and a history of asbestos exposure, he/she has high risk of MPM. However, if a patient does not have pleural effusion, this finding cannot exclude MPM. The second CT parameter related to MPM was size of the thickening. Moore et al. reported that if a lesion is > 10 mm, the likelihood of malignancy increases significantly [30]. In another study, if pleural thickening > 10 mm, sensitivity was found to be 56% and specificity was 88% [17]. We calculated size > 14 mm as an optimal cutoff value for pleural thickening characterization. With this cut-off value, the sensitivity, speci-

388 Arch Med Sci 2, 1st March / 2023
F. Selcuk Simsek, Muharrem Cakmak, Duygu Kuslu, Tansel A. Balci, Erdal In, Ibrahim H. Ozercan, Yavuz Narin
Figure 2. 58-year-old female patient. She had pleural thickening in the right lung. Lesion size was 13 mm, and SUV max value was 3.4. There was no sign of pleural effusion. After the histopathological examination the diagnosis was benign pleural thickening
How can we use positron emission tomography/computed tomography more accurately for characterization of asbestos-related pleural thickening?
ficity, PPV and NPV were found to be 85.7%, 83.3%, 90.0% and 76.9%. When we evaluated all unenhanced CT parameters, pleural thickening pattern (circumferential or nodular) or calcification could not differentiate benign lesions from MPM. On the other hand, presence of effusion, and size of the thickening were able to characterize it. However, if they are used alone, they are not reliable for differentiation of BPT from MPM.
At this point, [18F]FDG-PET/CT is a useful modality. Terada et al. reported that mean SUVmax was 5.3 for MPM and 1.2 for benign pleural disease [8].
Yeom et al. found that mean SUV max was 2.0 in benign tumors, while it was 3.6 in malignant cases [31]. We calculated that the mean SUVmax of BPT was 2.96 and the mean SUV max of MPM was 10.6. Our findings supported previous research. On the other hand, this is not the main problem in characterization of asbestos-related pleural thickening with [18F]FDG-PET/CT. The main problem is the lack of a consensus of the SUV max cut-off value.
Abe et al. accepted the SUVmax > 2.0 as a cutoff value, and 30/31 (96.7%) patients of MPM had positive uptake. The remaining 1 patient’s SUV max value was above 2.0 after the delayed image [13]. However, this value has insufficient NPV.
Elboga et al. reported that the sensitivity, specificity, PPV, NPV and accuracy of [18F]FDG-PET/CT were 91.8%, 61.5%, 87.1%, 72.7% and 84%, respectively [32]. In this study SUVmax > 2.5 was accepted as a cut-off value. Terada et al. accepted SUVmax > 3.5 as an optimal value. With this, they found 59.6% sensitivity, 93.1% specificity, 93.3% PPV and 58.7% NPV [8]. There are also some other studies performed to reach more satisfactory results with SUVmax. For example, Yamamoto et al. found that sensitivity, specificity, PPV and NPV were each 88% with qualitative analysis [33].
Yildirim et al. determined the SUV max > 2.2 as a cut-off value. Scientists reported that the sensitivity, specificity, PPV, and NPV were 94.1%, 100%, 100%, 93.3%, respectively [34]. The methodological differences between studies may have caused the differences. We found SUVmax > 4.0 as an optimal cut-off value by ROC analysis. The sensitivity, specificity, PPV and NPV were 88.0%, 83.3%, 91.7%, 76.9%, respectively. We think that although SUVmax > 4.0 has high PPV, and moderately high NPV, if used alone, it is not a reliable parameter for pleural lesion characterization.
On the other hand, when we used either SUVmax > 4.0 or size > 14 mm, 24 out of 25 (96.0%) MPM patients had one of them. The remaining 1 patient had pleural effusion. When we used SUVmax < 4.0, size < 14 mm, and lack of pleural effusion altogether, all of these patients had BPT. We think these results are within an acceptable range.
Asbestosis-related pleural thickening
When this criterion was applied to our patient population, 58.3% of BPT cases were correctly diagnosed without biopsy. This approach could also allow us to avoid one out of every five (7/37) invasive diagnostic methods.
Our study has some limitations. First of all, it has a retrospective nature and inherently has limitations due to this kind of design. Secondly, although our patient population was exposed to asbestos for a long period of their life, due to features of the region, the number of biopsies with proven BPT were still low. We think our biopsy selection criteria caused this. Thirdly, we did not include the MRI or contrast-enhanced CT results in the study. However, [18F]FDG-PET/CT examination is mostly performed without IV contrast and the current study design did not include these techniques. In addition, as mentioned in the text, enhanced CT or MRI techniques also lacked sufficient accuracy for characterization.
In conclusion, before deciding the invasive diagnostic approaches for asbestos related pleural thickening patients, according to unenhanced CT and [18F]FDG-PET/CT findings, we should check firstly the SUVmax value and size of the thickening. If a patient has SUVmax > 4.0, or size > 14 mm these patients must undergo the biopsy. If a patient’s SUVmax < 4.0, size < 14 mm and he/she has no pleural effusion, the likelihood of MPM is low. These patients can undergo the follow-up.
If a patient’s SUVmax < 4.0, size < 14 mm but the patient has pleural effusion, this patient has BPT with high likelihood. However, we cannot exclude MPM with this result. Due to the risk of misdiagnosing them, biopsy or cytology may be appropriate for them. This is another subject of research. Figure 3 summarizes this approach. Finally, we think multicentric and high-volume prospective studies may clarify the recommended approach’s usefulness.
Arch Med Sci 2, 1st March / 2023 389
Figure 3. Suggested diagnostic approach for asbestos-related pleural thickening
SUV max > 4.0 or size > 14 mm SUV max < 4.0 or size < 14 mm Biopsy Pleural effusion (–) Pleural effusion (+) Follow-up Follow-up/ cytology/biopsy
Acknowledgments
We wish to thank Professor Muzaffar Metintas for his advice and contribution.
Conflict of interest
The authors declare no conflict of interest.
References
1. Kang SR, Bok JS, Lee GD, Choi SH, Kim HR, Kim DW. Surgical options for malignant mesothelioma: a singlecenter experience. Korean J Thorac Cardiovasc Surg 2018; 51: 195-201.
2. Taioli E, Wolf AS, Camacho-Rivera M, et al. Determinants of survival in malignant pleural mesothelioma: a Surveillance, Epidemiology, and End Results (SEER) study of 14,228 patients. PLoS One 2015; 10: e0145039.
3. Lineeguida. Mesoteliomapleurico. AIOM 2016. Available from: http://www.aiom.it/ professionisti/documenti%2Dscientifici/linee%2dguida/mesotelioma%2dpleurico/ 1,2811 [Accessed: 20.06.2018].
4. Gatto MP, Tanna D. Distribution and trends in mesothelioma mortality in Italy from 1974 to 2006. Int Arch Occup Environ Health 2013; 86: 489-96.
5. Falaschi F, Romei C, Fiorini S, Lucchi M. Imaging of malignant pleural mesothelioma: it is possible a screening or early diagnosis program? A systematic review about the use of screening programs in a population of asbestos exposed workers. J Thorac Dis 2018; 10 (Suppl 2): 262-268.
6. Roca E, Laroumagne S, Vandemoortelea T, et al. 18F-fluoro-2-deoxy-d-glucose positron emission tomography/ computed tomography fused imaging in malignant mesothelioma patients looking from outside is not enough. Lung Cancer 2013; 79: 187-90.
7. Nowak AK, Armato SG, Ceresoli GL, Yildirim H, Francis RJ. Imaging in pleural mesothelioma: a review of imaging research presented at the 9th International Meeting of the International Mesothelioma Interest Group. Lung Cancer 2010; 70: 1-6.
8. Terada T, Tabata C, Tabata R, et al. Clinical utility of 18-fluorodeoxyglucose positron emission tomography/ computed tomography in malignant pleural mesothelioma. Exp Ther Med 2012; 4: 197-200.
9. Nickell LT Jr, Lichtenberger JP 3rd, Khorashadi L, Abbott GF, Carter BW. Multimodality imaging for characterization, classification, and staging of malignant pleural mesothelioma. Radiographics 2014; 34: 1692-706.
10. Franceschini MC, Ferro P, Canessa PA, et al. Mesothelin in serum and pleural effusion in the diagnosis of malignant pleural mesothelioma with non-positive cytology. Anticancer Res 2014; 34: 7425-9.
11. Yamamuro M, Gerbaudo VH, Gill RR, et al. Morphologic and functional imaging of malignant pleural mesothelioma. Eur J Radiol 2007; 64: 356-66.
12. Treglia G, Sadeghi R, Annunziata S, et al. Diagnostic accuracy of 18F-FDG-PET and PET/CT in the differential diagnosis between malignant and benign pleural lesions: a systematic review and meta-analysis. Acad Radiol 2014; 21: 11-20.
13. Abe Y, Tamura K, Sakata I, et al. Clinical implications of 18F-fluorodeoxyglucose positron emission tomography/computed tomography at delayed phase for diagnosis and prognosis of malignant pleural mesothelioma. Oncol Rep 2012; 27: 333-38.
14. Klabatsa A, Chicklore S, Barrington SF, Goh V, LangLazdunski L, Cook GJR. The association of 18F-FDG PET/CT parameters with survival in malignant pleural mesothelioma. Eur J Nucl Med Mol Imaging 2014; 41: 276-82.
15. Gill RR, Gerbaudo VH, Sugarbaker DJ, Hatabu H. Current trends in radiologic management of malignant pleural mesothelioma. Semin Thorac Cardiovasc Surg 2009; 21: 111-20.
16. Seely JM, Nguyen ET, Churg AM, Müller NL. Malignant pleural mesothelioma: computed tomography and correlation with histology. Eur J Radiol 2009; 70: 485-91.
17. Leung AN, Müller NL, Miller RR. CT in differential diagnosis of diffuse pleural disease. Am J Roentgenol 1990; 154: 487-92.
18. Hierholzer J, Luo L, Bittner RC, et al. MRI and CT in the differential diagnosis of pleural disease. Chest 2000; 118: 604-9.
19. Kim YK, Kim JS, Lee KW, Yi CA, Koo JM, Jung SH. Multidetector CT findings and differential diagnoses of malignant pleural mesothelioma and metastatic pleural diseases in Korea. Korean J Radiol 2016; 17: 545-53.
20. Kato K, Gemba K, Fujimoto N, et al. Pleural irregularities and mediastinal pleural involvement in early stages of malignant pleural mesothelioma and benign asbestos. Eur J Radiol 2016; 85: 1594-600.
21. Hallifax RJ, Haris M, Corcoran JP, et al. Role of CT in assessing pleural malignancy prior to thoracoscopy. Thorax 2015; 70: 192-3.
22. Arenas-Jiménez JJ, García-Garrigós E, Escudero-Fresneda C, et al. Early and delayed phases of contrast-enhanced CT for evaluating patients with malignant pleural effusion. Results of pairwise comparison by multiple observers. Br J Radiol 2018; 91: 20180254.
23. Helm EJ. Matin TM, Gleeson FV. Imaging of the pleura. J Magn Reson Imaging 2010; 32: 1275-86.
24. Tsim S, Stobo DB, Alexander L, Kelly C, Blyth KG. The diagnostic performance of routinely acquired and reported computed tomography imaging in patients presenting with suspected pleural malignancy. Lung Cancer 2017; 103: 38-43.
25. Koç M, Poyraz AK. The role of diffusion-weighted MR imaging in detecting malignant and benign pleural thickening in asbestos-related pleural diseases. Erciyes Med J 2017; 39: 44-7.
26. Tsim S, Humphreys CA, CowellGW, et al. Early contrast enhancement: a novel magnetic resonance imaging biomarker of pleural malignancy. Lung Cancer 2018; 118: 48-56.
27. Düzköprü Y, Oruç Z, Kaplan MA et al. The importance of serum and pleural fluid level of vascular ndothelial growth factor (VEGF) and VEGF fluid/serum ratio in the differential diagnosis of malignant mesothelioma-related pleural effusion. Contemp Oncol 2017; 21: 213-7.
28. Ökten F, Köksal D, Onal M, Özcan A, Simsek C, Ertürk H. Computed tomography findings in 66 patients with malignant pleural mesothelioma due to environmental exposure to asbestos. Clin Imaging 2006; 30: 177-80.
29. Chen D, Li X, Zhao H, et al. The efficacy of pemetrexed and bevacizumab intrapleural injection for malignant pleural mesothelioma-mediated malignant pleural effusion. Indian J Cancer 2014; 51 Suppl 3: S82-5.
30. Moore AJ, Parker RJ, Wiggins J. Malignant mesothelioma. Orphanet J Rare Dis 2008; 3: 34.
31. Yeom YK, Kim MY, Lee HJ, Kim SS. Solitary fibrous tumors of the pleura of the thorax: CT and FDG PET characte-
390 Arch Med Sci 2, 1st March / 2023
F. Selcuk Simsek, Muharrem Cakmak, Duygu Kuslu, Tansel A. Balci, Erdal In, Ibrahim H. Ozercan, Yavuz Narin
How can we use positron emission tomography/computed tomography more accurately for characterization of asbestos-related pleural thickening?
ristics in a tertiary referral center. Medicine 2015; 94: e1548.
32. Elboga U, Yılmaz M, Uyar M, Zeki Çelen Y, Bakır K, Dikensoy O. The role of FDG PET-CT in differential diagnosis of pleural pathologies. Rev Esp Med Nucl Imagen Mol 2012; 31: 187-91.
33. Yamamoto Y, Kameyama R, Togami T, et al. Dual time point FDG PET for evaluation of malignant pleural mesothelioma. Nucl Med Commun 2009; 30: 25-9.
34. Yildirim H, Metintas M, Entok E, et al. Clinical value of fluorodeoxyglucose-positron emission tomography/ computed tomography in differentiation of malignant mesothelioma from asbestos-related benign pleural disease: an observational pilot study. J Thorac Oncol 2009; 4: 1480-4.
Arch Med Sci 2, 1st March / 2023 391
1Department of Cardiac Surgery, Chair of Cardiology and Cardiac Surgery, Medical University of Lodz, Lodz, Poland
2Department of Haemostasis and Haemostatic Disorders, Medical University of Lodz, Lodz, Poland
Submitted: 28 May 2019; Accepted: 19 August 2019
Online publication: 12 December 2019
Arch Med Sci 2023; 19 (2): 392–400
DOI: https://doi.org/10.5114/aoms.2019.90470
Copyright © 2019 Termedia & Banach
Abstract
Introduction: Despite therapy, patients operated using a cardiopulmonary bypass demonstrate increased platelet aggregation, which rebounds to above preoperative levels. The aim of the study was to test the interaction between platelet reactivity/activation and selected inflammatory markers in the post-operative period.
Material and methods: In total, 103 patients with non-ST elevation acute coronary syndrome (NSTE-ACS) who were not eligible for percutaneous coronary interventions (PCI), and required urgent revascularization, were included. Platelet reactivity was measured using the PFA-100 platelet analyser, multiple electrode aggregometry, and was expressed as a novel platelet reactivity score (PRS). Patients were divided using their PRS scores into high platelet relativity or low platelet reactivity subgroups (HPR or LPR). Platelet basal activation was measured using immunoassays for soluble P-selectin and soluble CD40L. We measured high-sensitivity C-reactive protein (CRP), and used immunoassays for tumour necrosis factor α (TNF- α ) and interleukin 6 (IL-6) as inflammation markers.
Results: Significant differences between HPR and LPR groups were found for CRP (mg/l): 81.5 vs. 44.6, p < 0.02; and TNF- α (pg/l): 3.51 vs. 2.37, p < 0.02. A significant association was found between CRP, TNF- α , IL-6 and platelet reactivity (platelet reactivity score). Cohen’s κ showed: CRP = 0.49, p < 0.0001, TNF- α = 0.37, p < 0.002. Perioperative myocardial infarction and rhythm disturbances occurred more frequently in the high platelet reactivity group: 7 (16.3%) vs. 2 (3.3%), p < 0.04, and 9 (20.9%) vs. 4 (6.7%), p < 0.04, respectively.
Conclusions: Inflammatory parameters CRP and TNF- α are strongly associated with platelet reactivity (expressed as PRS) in cardiopulmonary bypass graft patients. Platelet hyperreactivity in the early post-operative period combined with a systemic inflammatory state correlates with a higher risk of post-operative rhythm disturbances and myocardial infarction.
Key words: platelet reactivity, platelet activation, inflammation, coronary artery bypass grafting, cardiopulmonary bypass.
Introduction
Antiplatelet treatment has proved to be effective in preventing bypass occlusion after coronary artery bypass grafting (CABG). Despite therapy, patients operated using a cardiopulmonary bypass showed
Corresponding author: Dr. Jacek Golański
Department of Haemostasis and Haemostatic Disorders
Chair of Biomedical Sciences
Medical University of Lodz
6/8 Mazowiecka St
92-215 Lodz, Poland
Phone: +48 42 272 57 20
E-mail: jacek.golanski@umed. lodz.pl
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Platelet reactivity expressed as a novel platelet reactivity score is associated with higher inflammatory state after coronary artery bypass grafting
Mirosław Wilczyński1, Michał Krejca1, Piotr Stepinski1, Marcin Rozalski2, Jacek Golanski2
laboratory
Clinical research Diagnostics,
Platelet reactivity expressed as a novel platelet reactivity score is associated with higher inflammatory state after coronary artery bypass grafting
increased platelet aggregation that rebounded to above preoperative levels [1, 2]. Considering the mechanism of early graft failure, it seems logical that potent platelet inhibition may improve graft patency [3–5]. By contrast, it is known that an impaired response to antiplatelet therapy underlies the increased risk of post-operative occlusions and can even result in death after CABG surgery [6]. Several potential explanations have been proposed for the nature of high on-treatment platelet reactivity, including modifiable factors: too low doses of anti- platelet drugs, high platelet turnover, oxidative stress, dyslipidaemia and inflammation [7–12]. Coronary artery bypass grafting surgery itself is associated with excessive activation of platelets, which results in stimulation of the production and release of young platelets [2, 13, 14].
It is noteworthy that platelet reactivity is strongly dependent on modifiable factors, especially on the inflammatory state [12, 15, 16]. The inflammation process, which is associated with CABG as a result of cardiopulmonary bypass, is affected by many factors, including surgical trauma, blood contact with the cardiopulmonary bypass (CPB) device’s artificial surfaces, as well as ischaemia and reperfusion injury. The pro-inflammatory cytokines interleukin (IL)-6 and IL-8, tumour necrosis factor-α (TNF-α), anti-inflammatory IL-10, and C-reactive protein (CRP) were found at increased levels following CABG [17].
Coronary artery bypass grafting surgery is associated with a systemic inflammatory response, endothelial damage and platelet activation, regardless of whether a CPB has been performed [18–20]. A number of publications indicate that this augmentation of platelet reactivity largely depends on a set of environmental factors, including the inflammatory state [15, 21]. The association between preoperative inflammatory parameters and early graft occlusion, as well as cardiovascular events following coronary artery bypass grafting, has not, however, been fully elucidated [22]. C-reactive protein is a powerful independent predictor of cardiovascular events in patients with coronary artery disease. Recent clinical trials targeting CRP have shown a reduction in major adverse cardiovascular events (MACE) after an acute coronary syndrome (ACS). Inflammation could be linked to high platelet reactivity (HPR), which is an independent predictor of MACE in patients with ACS [15]. A relation has been observed between CRP concentration and in-hospital outcome, following coronary artery bypass grafting [23]. It seems that a rise in the CRP level, as an inflammation marker, may be associated with transient platelet hyperactivity after CABG.
Therefore, the aim of this study was to evaluate the effect of an inflammatory state (measured by
CRP, IL-6 and TNF-α levels) on platelet reactivity in a short postoperative period (6th day) using two different platelet assays and to analyse the results comprehensively.
Material and methods
Patients
In total, 140 patients with NSTE-ACS, who were not eligible for PCI and required urgent revascularization, were enrolled in the study (source population). All CABG procedures were performed at the First Department of Cardiac Surgery, Medical University of Silesia in Katowice (Poland). Patients meeting inclusion criteria were enrolled consecutively. Patients presenting at least two of the following criteria were included in the study: 1) symptoms of chest pain lasting for at least 20 min within a period of 24 h preceding the coronary angiography; 2) elevated troponin levels; 3) ST-segment depression of at least 0.1 mV or a negative T wave of at least 0.2 mV in two or more contiguous leads. All the patients enrolled in the study presented with complex coronary lesions including left main disease, multiple-vessel disease or a coronary anatomy not amenable to PCI, which was reflected by a SYNTAX score > 22 points (intermediate and high risk).
The predefined exclusion criteria were: chest pain longer than 48 h, ST segment elevation, oral pre-treatment with clopidogrel, age over 80 years, percutaneous revascularization procedure within the previous 30 days, CABG within the previous 6 months, NYHA class IV heart failure preceding hospitalization, gastrointestinal or genitourinary bleeding within the previous 30 days, history of intracranial disorders (including stroke, primary and metastatic brain tumours and history of head trauma); major surgery or high level trauma within the previous 6 weeks; history of bleeding diathesis, thrombocytopenia defined as less than 100,000 PLT/mm3, anticoagulation with INR ≥ 1.8, impairment of liver function, renal impairment with creatinine level > 1.5 mg%, uncontrolled blood pressure exceeding 200/110 mm Hg, and hypersensitivity to any drug.
The characteristics of the overall (source) population of the study (n = 140) were: female sex: 40 (28.6%) patients; age: 63.0 ±9.4 years; body mass index (BMI) 28.2 ±3.9 kg/m2; hypertension: 109 (77.9%); dyslipidaemia: 132 (94.3%); peripheral artery disease: 9 (6.4%); diabetes mellitus: 35 (25.0%); EuroSCORE: 5.6 ±2.0 points. All the patients were on aspirin until the day of the operation. A complete set of all clinical and laboratory data was gathered for the target group (n = 103). The characteristics of this group are presented in detail in Table I.
Arch Med Sci 2, 1st March / 2023 393
Table
score) 6 days after the operation
Continuous data are presented as mean ±SD or as median (interquartile range: LQ-UQ). Categorical data are presented as absolute numbers and %. Significance of differences was analyzed using Mann-Whitney U test (continuous data) or Fisher’s exact test (categorical data). *Statistical significance of differences regards a comparison of the two subgroups. BMI – body mass index, CPB – cardiopulmonary bypass, PRBCs – packed red blood cells, FFP – fresh frozen plasma, PRP – platelet rich plazma, MI – myocardial infarction, Tnl – troponin I, Hb – hemoglobin, IL-6 – interleukin-6, CRP – C-reactive protein, TNF-a – tumour necrosis factor-a
Operative (surgery) techniques
Anaesthesia was induced and maintained using standard procedures. A median sternotomy was performed and patients were placed on CPB, under mild hypothermia at 34°C and cold cardioplegia at a 4 : 1 ratio to protect against myocardial ischaemia. Unfractionated heparin was delivered intravenously at a dose of 300 U/kg and then again every 60 min of CPB to maintain an acti-
vated clotting time of at least 480 s. Immediately after CPB was ceased, heparin was reversed with protamine sulphate at a dose of 3 mg/kg. Acetylsalicylic acid (aspirin) at a daily dose of 300 mg was reinitiated after the procedure, subsequently reduced to a daily dose of 150 mg on day 6 and maintained for the duration of the study. Clopidogrel at a daily dose of 75 mg was administered to each patient 6 days after the procedure.
394 Arch Med Sci 2, 1st March / 2023
Mirosław Wilczyński, Michał Krejca, Piotr Stepinski, Marcin Rozalski, Jacek Golanski
Variable Whole group n = 103 High platelet reactivity n = 43 Low platelet reactivity n = 60 P -value* Female sex (%) 35 (34.0) 15 (34.5%) 20 (33.3%) ns Age [years] 62.7 ±9.9 61.0 ±10.9 63.1 ±9.4 ns BMI [kg/m2] 27.7 ±3.3 28.7 ±3.5 27.6 ±3.2 ns Hypertension (%) 85 (82.5) 37 (86.0%) 48 (80.0%) ns Dyslipidaemia (%) 98 (95.1) 41 (95.3%) 57 (95.0%) ns Peripheral artery disease (%) 8 (7.6) 2 (4.7%) 6 (10.0%) ns Diabetes mellitus (%) 23 (22.3) 12 (27.9%) 11 (18.3%) ns EuroSCORE [points] 5.8 ±2.0 6.0 ±2.2 5.7 ±1.9 ns Duration of CPB [min] 87.4 ±21.6 85.4 ±26.2 88.3 ±23.3 ns Aorta clamping time [min] 48.2 ±19.0 47.3 ±19.0 48.7 ±13.9 ns Postoperative blood drainage [ml] 826 ±448 814 ±491 848 ±491 ns Need for PRBCs transfusion 1.61 ±1.39 1.60 ±1.29 1.62 ±1.47 ns Need for FFP transfusion 2.28 ±0.74 2.28 ±0.70 2.28 ±0.76 ns Need for PRP transfusion 0.90 ±0.58 1.16 ±0.69 0.57 ±0.69 ns CK-MB [UI] 24.00 (17.50–42.49) 24.00 (16.50–52.50) 24.00 (18.00–32.25) ns TnI [ng/ml] 0.92 (0.38–2.01) 0.99 (0.43–2.45) 0.86 (0.37–1.95) ns Perioperative MI 9 (8.7%) 7 (16.3%) 2 (3.3%) < 0.04 Postoperative rhythm disturbances 13 (12.6%) 9 (20.9%) 4 (6.7%) < 0.04 Hb [g/dl] 11.78 ±1.19 11.82 ±1.20 11.68 ±1.18 ns Leukocyte count [× 109/l] 9.75 ±1.37 9.66 ±1.42 9.87 ±1.26 ns Platelet count [× 109/l] 227.8 ±80.9 217.8 ±75.9 236.7 ±84.7 ns Mean platelet volume [fl] 10.38 ±1.49 10.39 ±1.57 10.35 ±1.47 ns IL-6 [pg/l] 22.8 (14.4–31.4) 24.4 (14.8–37.5) 21.4 (13.2–30.0) ns CRP [mg/l] 54.1 (36.7–82.0) 81.5 (44.7–104.8) 44.6 (36.5–62.7) < 0.02 TNF- α [pg/l] 2.59 (2.16–4.15) 3.51 (2.38–5.25) 2.37 (1.77–3.10) < 0.02
I. Characteristics of total group of coronary artery bypass grafting subjects and patients allocated to subgroups with high and low platelet reactivity (estimated using the platelet reactivity
Platelet reactivity expressed as a novel platelet reactivity score is associated with higher inflammatory state after coronary artery bypass grafting
Blood collection
Blood was collected by peripheral venipuncture into two plastic tubes (S-Monovette; Sarstedt, Nümbrecht, Germany). The first tube contained buffered 3.2% sodium citrate (Becton Dickinson, Plymouth, United Kingdom) with a final citrate to blood ratio of 1 : 9 vol/vol, while the second contained 250 μg/ml hirudin (Refludan, Schering AG, Germany), yielding a final concentration of 25 μg/ml in the blood sample. Whole blood was kept at room temperature. Blood samples for complete blood cell counts were collected in K2EDTA anticoagulated sample tubes. The samples were processed within 4 h.
Platelet reactivity
Determination of PFA-100 closure time
The closure time (CT expressed in seconds, maximal recorded value of 300 s) was measured using a PFA-100 flow analyser (Siemens Healthcare Diagnostics, Inc, Norwood, MA, USA). All blood samples were tested for closure times with collagen/epinephrine (CTCEPI) and collagen/ADP (CTCADP) cartridges in accordance with the manufacturer’s instructions, at least 30 min but not more than 1 h after the blood was withdrawn. PFA-100 measurements were performed in duplicate, and mean CT values were calculated.
Multiple electrode aggregometry
Whole blood aggregation was measured using a 5-channel, semi-automatic, dual measurement aggregometer (Multiplate Analyzer; Roche Diagnostics GmbH, Mannheim, Germany). The ADP Test (ADP; final concentration, 6.4 μmol) or AspiTest (arachidonic acid, final concentration, 0.5 mmol/l) was added as a platelet agonist, and an increase in electrical impedance caused by the growing platelet attachment to the electrodes was recorded continuously for 10 min. Platelet reactivity was expressed as the maximal aggregation (arbitrary units – AU).
Platelet reactivity score
In this paper, we suggest introducing a novel comprehensive score for assessing platelet reactivity: the platelet reactivity score (PRS). The rule for calculating PRS is shown below (medians are calculated on the basis of all the results of the given parameter (CTCEPI, CTCADP, ASPItest, ADPtest) in the studied group.
CTCEPI < median: 1; CTCEPI ≥ median: 0
CTCADP < median: 1; CTCADP ≥ median: 0
ASPItest > median: 1; ASPItest ≤ median: 0
ADPtest > median: 1; ADPtest ≤ median: 0
The PRS score range is from 0 to 4, with a cut-
off platelet reactivity score of > 2. Patients were allocated to the high platelet reactivity (HPR) group or the low platelet reactivity (LPR) group (PRS ≤ 2).
Platelet activation
Immunoassays for soluble P-selectin (soluble CD62) and soluble CD40L
To obtain plasma for immunoassays, EDTA blood was prepared following standard procedures and the samples were stored at –50°C until analysis. Levels of sP-selectin and sCD40L in patients’ plasma were measured using commercially available ELISA tests (respectively, Human P-Selectin/CD62P DuoSet ELISA Quantikine and Human CD40 Ligand/TNFSF5 Quantikine ELISA Kit; R&D Systems, Minneapolis, Minnesota, USA). The intra-assay variability for the lower assay range was less than 10%. The measurement ranges were 0–50 ng/ml for sCD62 and 62–4000 pg/ml for sCD40L.
Inflammatory markers and other laboratory parameters
CK-MB, high-sensitive troponin I (hTnI) and high-sensitivity C-reactive protein (hs-CRP) serum levels were measured using an ELISA test. To assess qualitative and quantitative changes in platelets the following parameters were analysed: mean platelet count (MPC), mean platelet volume (MPV) and large platelet concentration ratio (L-PCR). Cell blood counts were carried out using the Sysmex XE-2100 (Sysmex Corporation, Kobe, Kansai, Japan).
Immunoassays for tumour necrosis factor-α and interleukin-6
To obtain serum for immunoassays, non-anticoagulated blood was prepared following standard procedures and samples were stored at –50°C until analysis. Levels of TNF-α and IL-6 in patients’ serum were measured using commercially available ELISA tests (respectively, Human TNF-alpha Quantikine ELISA Kit and Human IL-6 Quantikine ELISA Kit, R&D Systems, Minneapolis, Minnesota, USA). The intra-assay variability for the lower assay range was less than 10%. The measurement ranges for TNF-α were 0.5–32 pg/ml and 3.1–300 pg/ml for IL-6.
Measurement points
Two time points were used to test all parameters: (T1) before CABG, (T2) 6 days after the surgery procedure.
Statistical analysis
Mean ± SD are given for normally distributed variables. Medians and interquartile ranges (Me,
Arch Med Sci 2, 1st March / 2023 395
IQ) are given for other parameters showing departures from normality (according to the ShapiroWilk W test). Simple paired comparisons were performed using unpaired Student t test, while non-normally distributed variables were analysed using the Mann-Whitney U test. Pearson’s χ2 test with Yates correction (if necessary) was used for categorical data. Cohen’s κ coefficient was calculated as a measure of agreement. A κ statistic value of < 0.4 represents poor-to-fair agreement, a value of 0.41–0.60 reflects moderate agreement, a value of 0.61–0.80 is considered good agreement, and a κ value of 0.81–1.0 is considered very good agreement. The odds ratio (OR) and 95% confidence interval (CI) were assessed to establish the correlation between PRS and inflammatory markers using logistic regression.
The statistical analysis was performed using Statistica 13.1 (StatSoft Inc., Tulsa, Oklahoma).
Results
Patients and procedural characteristics
Thirty-seven patients were excluded from the study due to incomplete laboratory parameters. In total, 103 NSTE-ACS patients, requiring urgent coronary artery bypass graft surgery, were included in the study. The characteristics of selected parameters in CABG patients before and 6 days after the operation are presented in Table II.
Platelet reactivity and activation on the 6th day after the operation
Platelet reactivity significantly increased in the postoperative period, as reflected by CTCEPI and CTCADP In the case of arachidonic acid (ASPItest) and ADP-
induced aggregation (ADPtest), there were no differences between the pre-operative period and on the 6th day after CABG (Figure 1).
Platelet activation significantly increased in the post-operative period, as reflected by the elevated levels of soluble P-selectin and soluble CD40L (Figure 2).
High platelet reactivity and low platelet reactivity groups
There was no association between individual parameters (analysed alone) of platelet reactivity dependent on aspirin (CTCEPI, ASPItest) and a very low association between parameters of platelet reactivity dependent on P2Y12 inhibitors (CTCADP, ADPtest) and inflammatory markers. However, in the next approach, we used a complex, comprehensive score (the novel PRS) and divided the whole group into high platelet reactivity (PRS > 2; HPR; n = 43) and low platelet reactivity (PRS ≤ 2; LPR; n = 60) subgroups. Using this approach, the elevation of two parameters, CRP and TNF-α, was found in the HPR subgroup in comparison with the LPR group of CABG patients (Table I).
Perioperative outcomes
Perioperative myocardial infarction and rhythm disturbances occurred more frequently in the high platelet reactivity group (differences close to statistical significance). Post-operative chest bleeding, prolonged ventilator use, renal failure and stroke were similar in both groups. Levels of cardiac markers, EuroSCORE and other clinical parameters were comparable in both tested groups (Table I).
Continuous data are presented as mean ±SD or as median (interquartile range: LQ–UQ). Categorical data are presented as absolute numbers (n) and %. Significance of differences was analyzed using Mann-Whitney U test (continuous data) or Fisher’s exact test (categorical data). Hb – hemoglobin, Tnl – troponin I, CRP – C-reactive protein, TNF- a – tumour necrosis factor- a, IL-6 – interleukin-6.
396 Arch Med Sci 2, 1st March / 2023
Mirosław Wilczyński, Michał Krejca, Piotr Stepinski, Marcin Rozalski, Jacek Golanski
Variable Before operation 6 days after operation P- value Hb [g/dl] 13.77 ±1.01 11.64 ±1.21 < 0.0001 Leukocyte count [× 109/l] 8.29 ±1.48 10.12 ±1.67 < 0.0001 Platelet count [× 109/l] 187.0 ±50.1 229.2 ±81.3 < 0.0001 Mean platelet volume [fl] 9.71 ±1.84 10.36 ±1.57 < 0.003 TnI [ng/ml] 0.22 (0.10–1.36) 0.89 (0.32–2.80) < 0.0001 CK-MB [UI/l] 18.00 (13.75–28.00) 25.00 (18.00–43.00) < 0.0001 CRP [mg/l] 16.05 (7.57–35.50) 54.05 (36.98–) < 0.0001 TNF- α [pg/l] 1.83 (1.07–2.38) 2.63 (2.19–4.10) < 0.0001 IL-6 [pg/l] 8.85 (4.90–17.5) 21.87 (14.28–34.41) < 0.0001
Table II. Characteristics of selected parameters of coronary artery bypass grafting patients (n = 103) before and 6 days after operation
Platelet reactivity expressed as a novel platelet reactivity score is associated with higher inflammatory state after coronary artery bypass grafting
Before surgery 6 days after surgery CEPI p < 0.02 CADP p < 0.005 PFA-100 – occlusion time [s] 150 125 100 75 50 25 25 50 75 100 125 150 Multiplate – whole blood platelet aggregation [AU]
Agreement and regression analysis of selected inflammatory markers with platelet reactivity or activation on the 6th day after CABG
AA (0.5 mmol/l) AA (6.4 µmol/l)
A logistic regression analysis showed that CRP and TNF-α were associated with platelet reactivity (Table IV).
Discussion
A significant association was found between CRP, TNF-α, IL-6 and platelet reactivity (platelet reactivity score) but not with platelet activation (sCD40L, sP-selectin). The agreement between the results was assessed using Cohen’s κ test and is presented in Table III. Concordance between platelet reactivity and inflammatory markers was in the poor to fair range but reached a level of statistical significance.
The inflammatory milieu that occurs after CABG as a result of cardiopulmonary bypass has been extensively studied and is the consequence of multiple factors, including surgical trauma, and blood contact with the foreign surfaces of the CPB [5, 17]. On the other hand, the relationship between inflammatory state, CABG and high platelet reactivity has rarely been discussed [20, 24]. There-
Arch Med Sci 2, 1st March / 2023 397
Figure 1. Platelet reactivity monitored in coronary artery bypass grafting (CABG) patients using PFA-100 and Multiplate (MEA – multiple electrode aggregometry) on the day before surgery and 6th day after surgery. Data shown as median (interquartile range, minimum and maximum values). Significance of differences was analysed using the Mann-Whitney U test
A B C D 300 250 200 150 100 50 50 100 150 200 250 300
Table IV. Logistic regression analysis to assess the correlation between PRS and inflammatory markers with platelet reactivity on 6th day after coronary artery bypass grafting
fore, the aim of this study was to analyse the association between platelet reactivity or platelet activation after CABG with selected markers of the inflammatory state. In our work, the simultaneous use of Multiplate and PFA-100 analysers and the PRS proved to be useful tools for detecting a connection between platelet reactivity and an inflammatory state.
Literature reports that high platelet reactivity after CABG has an incidence range of 10–90% [21, 25]. This is a transient phenomenon, more frequently observed during the first month after surgery, and some authors suggest that it may explain the elevated risk of graft thrombosis and death
after CABG [2, 21]. The response of platelets to CPB is complex, with a reduction in platelet count from a baseline during the first days, and then increasing to a higher count than before surgery [1, 13, 26, 27]. Cardiopulmonary bypass also causes a systemic inflammatory response and platelet activation [26]. Plasma levels of IL-6 significantly correlate with a systemic inflammatory response and reflect the severity of acute inflammation [24].
In this study, we found that the increased platelet reactivity was significantly associated with high levels of CRP, TNF and IL-6, but only when platelet reactivity was expressed as a complex PRS. We observed a significant increase in CRP level during the first week after CABG, peaking at the same time as the lowest anti-platelet therapy effectiveness was recorded. This phenomenon might account for the increased risk of occlusion of bypass
predicting risks of cardiovascular events.
We found that perioperative myocardial infarction and rhythm disturbances occurred more fre-
398 Arch Med Sci 2, 1st March / 2023
Mirosław Wilczyński, Michał Krejca, Piotr Stepinski, Marcin Rozalski, Jacek Golanski
grafts at this moment during the post-operative period [28, 29]. Measurements of residual platelet reactivity by PFA-100 [28] and whole blood platelet aggregometry [30] are considered adequate for
Figure 2. Platelet activation monitored in coronary artery bypass grafting (CABG) patients using immunoassays for soluble P-selectin and soluble CD40L on the day before surgery and 6th day after surgery. Data shown as median (interquartile range, minimum and maximum values). Significance of differences was analysed using the Mann-Whitney U test
Markers Observed agreement [%] Cohen’s κ Confidence interval (95% CI) P -value CRP 74.5 0.49 0.246–0.738 < 0.0001 TNF- α 68.3 0.37 0.019–0.612 < 0.002 IL-6 61.9 0.24 –0.011–0.432 < 0.03 CRP – C-reactive protein, TNF- a – tumour necrosis factor- a, IL-6 – interleukin-6.
Table III. Agreement of selected inflammatory markers with platelet reactivity on 6th day after coronary artery bypass grafting
Markers Odds ratio (OR) Confidence interval (95% CI) P -value CRP 1.1049 1.046–1.158 < 0.003 TNF- α 1.225 1.119–1.312 < 0.03 CRP – C-reactive protein, TNF- a – tumour necrosis factor- a
B Before surgery 6th day after surgery sP-selectin sCD40L 175 150 125 100 75 50 25 0 500 1000 1500 2000 2500 3000 5000 p < 0.0001 p < 0.003 Platelet activation [pg/ml]
A
Platelet reactivity expressed as a novel platelet reactivity score is associated with higher inflammatory state after coronary artery bypass grafting
quently in the high platelet reactivity group. By contrast, basal platelet activation was not associated with inflammatory markers in this study. In the literature, perioperative myocardial infarction and rhythm disturbances were observed but they have rarely been correlated with the inflammatory state and platelet reactivity [31–33]. Interestingly, Plicner et al. showed that clinical outcomes in the early postoperative period are associated with inflammation and platelet activation markers [20].
In our study, all patients displayed a rise in platelet reactivity, despite continuing the same antiplatelet treatment after surgery. The reduced antiplatelet effect of aspirin is associated with low-grade inflammation in patients with coronary artery disease [34]. In our study, we observed a similar tendency in CABG patients. Recent literature has confirmed that CRP promotes platelet activation [35]. Additionally, CRP was found in platelet aggregates and stimulated further platelet deposition at the arterial wall [36]. Moreover, an association was also observed between increased IL6 levels and increased platelet count.
In this study, we demonstrated the platelet hyperreactivity as measured by PFA-100 CTCADP (cartridges with ADP and collagen) and by aggregometry (multiplate with ADP as agonist). Interestingly, Gluckman et al. suggested platelet hyperreactivity measured by PFA-100 CTCADP to be a novel independent risk factor for early thrombosis after CABG surgery [28].
In our opinion, application of the PRS with a cutoff at PRS > 2 indicating platelet hyperactivity allows one to investigate complex dependencies between platelet reactivity and inflammatory state after CABG despite a small number of patients. We believe that the association between inflammatory state and platelet hyperreactivity as well as perioperative outcomes, demonstrated in this study, suggests a need of a combined analysis of both platelet reactivity and inflammatory markers (in particular CRP) in order to assess perioperative outcomes.
In conclusion, our study demonstrated that increased platelet reactivity, expressed as a novel PRS after CABG, is associated with a higher concentration of inflammation markers. Furthermore, following a cardiac operation with extra-corporeal circulation, platelet hyperreactivity in the early post-operative period, combined with a systemic inflammatory state, correlates with a higher risk of post-operative rhythm disturbances.
Conflict of interest
The authors declare no conflict of interest.
References
1. Gielen CLI, Brand A, van Heerde WL, Stijnen T, Klautz RJM, Eikenboom J. Hemostatic alterations during coronary artery bypass grafting. Thromb Res 2016; 140: 140-6.
2. Wilczynski M, Wybraniec MT, Milewski K, et al. Eptifibatide infusion versus placebo in high risk patients with non-ST segment elevation acute coronary syndromes managed with urgent coronary artery bypass graft surgery. A prospective multicenter randomized placebo-controlled clinical trial. J Cardiovasc Surg 2016; 57: 100-10.
3. Bomb R, Oliphant CS, Khouzam RN. Dual antiplatelet therapy after coronary artery bypass grafting in the setting of acute coronary syndrome. Am J Cardiol 2015; 116: 148-54.
4. Yang D, Peng C, Liao Z, Wang X, Guo W, Li J. The effect of the CYP2C19*2 allele on cardiovascular outcomes in patients with coronary artery stenting: a prospective study. Arch Med Sci 2018; 15: 837-44.
5. Januszek R, Siudak Z, Dziewierz A, Rakowski T, Dudek D, Bartuś S. Long-term outcomes of percutaneous coronary interventions within coronary artery bypass grafts. Arch Med Sci 2021; 17: 628-37.
6. Agarwal N, Mahmoud AN, Patel NK, et al. Meta-analysis of aspirin versus dual antiplatelet therapy following coronary artery bypass grafting. Am J Cardiol 2018; 121: 32-40.
7. Łabuz-Roszak B, Pierzchała K, Niewiadomska E, Skrzypek M, Machowska-Majchrzak A. Searching for factors associated with resistance to acetylsalicylic acid used for secondary prevention of stroke. Arch Med Sci 2015; 11: 106-14.
8. Jäger B, Piackova E, Haller PM, et al. Increased platelet reactivity in dyslipidemic patients with coronary artery disease on dual anti-platelet therapy. Arch Med Sci 2018; 15: 65-71.
9. Kuliczkowski W, Golanski R, Bijak M, et al. Relationship between high on aspirin platelet reactivity and oxidative stress in coronary artery by-pass grafted patients. Blood Coagul Fibrinolysis 2016; 27: 151-5.
10. Guirgis M, Thompson P, Jansen S. Review of aspirin and clopidogrel resistance in peripheral arterial disease. J Vasc Surg 2017; 66: 1576-86.
11. Jager B, Piackova E, Haller PM, et al. Increased platelet reactivity in dyslipidemic patients with coronary artery disease on dual anti-platelet therapy. Arch Med Sci 2019; 15: 65-71.
12. Sibbing D, Aradi D, Alexopoulos D, et al. Updated expert consensus statement on platelet function and genetic testing for guiding P2Y12 receptor inhibitor treatment in percutaneous coronary intervention. JACC Cardiovasc Interv 2019; 12: 1521-37.
13. Xu K, Chan NC, Hirsh J, et al. Quantifying immature platelets as markers of increased platelet production after coronary artery bypass grafting surgery. Eur J Haematol 2018; 101: 362-7.
14. Schneider DJ, Chava S. Factors influencing platelet reactivity in patients undergoing coronary artery bypass surgery. Coron Artery Dis 2016; 27: 185-90.
15. Cornara S, Crimi G, Somaschini A, et al. Systemic inflammatory status is associated with increased platelet reactivity in the early period after acute coronary syndromes. Platelets 2018; 29: 528-30.
16. Patti G, Mangiacapra F, Ricottini E, et al. Correlation of platelet reactivity and C-reactive protein levels to occurrence of peri-procedural myocardial infarction in patients undergoing percutaneous coronary intervention (from the ARMYDA-CRP study). Am J Cardiol 2013; 111: 1739-44.
Arch Med Sci 2, 1st March / 2023 399
17. Leyvi G, Vivek K, Sehgal S, et al. A comparison of inflammatory responses between robotically enhanced coronary artery bypass grafting and conventional coronary artery bypass grafting: implications for hybrid revascularization. J Cardiothorac Vasc Anesth 2018; 32: 251-8.
18. Weymann A, Popov AF, Sabashnikov A, et al. Baseline and postoperative levels of C-reactive protein and interleukins as inflammatory predictors of atrial fibrillation following cardiac surgery: a systematic review and meta-analysis. Kardiol Pol 2018; 76: 440-51.
19. Evora PR, Bottura C, Arcencio L, Albuquerque AA, Évora PM, Rodrigues AJ. Key points for curbing cardiopulmonary bypass inflammation. Acta Cir Bras 2016; 31 Suppl 1: 45-52.
20. Plicner D, Stolinski J, Wasowicz M, et al. Preoperative values of inflammatory markers predict clinical outcomes in patients after CABG, regardless of the use of cardiopulmonary bypass. Indian Heart J 2016; 68 Suppl 3: S10-5.
21. Golanski J, Chlopicki S, Golanski R, Gresner P, Iwaszkiewicz A, Watala C. Resistance to aspirin in patients after coronary artery bypass grafting is transient – Impact on the monitoring of aspirin antiplatelet therapy. Ther Drug Monit 2005; 27: 484-90.
22. Hedman A, Larsson PT, Alam M, Wallen NH, Nordlander R, Samad BA. CRP, IL-6 and endothelin-1 levels in patients undergoing coronary artery bypass grafting. Do preoperative inflammatory parameters predict early graft occlusion and late cardiovascular events? Int J Cardiol 2007; 120: 108-14.
23. Balciunas M, Bagdonaite L, Samalavicius R, Griskevicius L, Vuylsteke A. Pre-operative high sensitive C-reactive protein predicts cardiovascular events after coronary artery bypass grafting surgery: a prospective observational study. Ann Card Anaesth 2009; 12: 127-32.
24. Arazi HC, Doiny DG, Torcivia RS, et al. Impaired anti-platelet effect of aspirin, inflammation and platelet turnover in cardiac surgery. Interact Cardiovasc Thorac Surg 2010; 10: 863-7.
25. Wand S, Adam EH, Wetz AJ, et al. The prevalence and clinical relevance of ASA nonresponse after cardiac surgery: a prospective bicentric study. Clin Appl Thromb Hemost 2018; 24: 179-85.
26. Olechowski B, Khanna V, Mariathas M, et al. Changes in platelet function with inflammation in patients undergoing vascular surgery. Platelets 2019; 30: 190-8.
27. Ivert T, Dalen M, Ander C, Stålesen R, Lordkipanidzé M, Hjemdahl P. Increased platelet reactivity and platelet-leukocyte aggregation after elective coronary bypass surgery. Platelets 2019; 30: 975-81.
28. Gluckman TJ, McLean RC, Schulman SP, et al. Effects of aspirin responsiveness and platelet reactivity on early vein graft thrombosis after coronary artery bypass graft surgery. J Am Coll Cardiol 2011; 57: 1069-77.
29. Chakos A, Jbara D, Singh K, Yan TD, Tian DH. Network meta-analysis of antiplatelet therapy following coronary artery bypass grafting (CABG): none versus one versus two antiplatelet agents. Ann Cardiothorac Surg 2018; 7: 577-85.
30. Rafiq S, Johansson PI, Kofoed KF, et al. Thrombelastographic hypercoagulability and antiplatelet therapy after coronary artery bypass surgery (TEG-CABG trial): a randomized controlled trial. Platelets 2017; 28: 78693.
31. Wang A, Wu A, Wojdyla D, et al. Dual antiplatelet therapy for perioperative myocardial infarction following CABG surgery. Am Heart J 2018; 199: 150-55.
32. Haghjoo M. Postoperative rhythm disorders after adult cardiac surgery. Postoperative Critical Care for Adult Cardiac Surgical Patients. Springer 2018; 405-17.
33. Zakkar M, Ascione R, James AF, Angelini GD, Suleiman MS. Inflammation, oxidative stress and postoperative atrial fibrillation in cardiac surgery. Pharmacol Ther 2015; 154: 13-20.
34. Larsen SB, Grove EL, Kristensen SD, Hvas AM. Reduced antiplatelet effect of aspirin is associated with lowgrade inflammation in patients with coronary artery disease. Thromb Haemost 2013; 109: 920-9.
35. Boncler M, Rywaniak J, Szymanski J, Potempa LA, Rychlik B, Watała C. Modified C-reactive protein interacts with platelet glycoprotein Ibalpha. Pharmacol Rep 2011; 63: 464-75.
36. Badimon L, Pena E, Arderiu G, et al. C-reactive protein in atherothrombosis and angiogenesis. Front Immunol 2018; 9: 430.
400 Arch Med Sci 2, 1st March / 2023
Mirosław Wilczyński, Michał Krejca, Piotr Stepinski, Marcin Rozalski, Jacek Golanski
Integrated analysis of microbiota with bile acids for the phototherapy treatment of neonatal jaundice
Kun Zhang, Sainan Fan, Anping Lv, Yanan Ma, Xiaohui Fang, Jinping Zhang
Department of Pediatrics, Shanghai Jiao Tong University Affiliated Sixth People’s Hospital, Shanghai, China
Submitted: 19 February 2021; Accepted: 6 March 2021
Online publication: 18 March 2021
Arch Med Sci 2023; 19 (2): 401–410
DOI: https://doi.org/10.5114/aoms/134023
Copyright © 2021 Termedia & Banach
Abstract
Introduction: Infant jaundice is a common condition which results from a high concentration of serum bilirubin. Phototherapy is a widely used treatment for bilirubin clearance. We analyzed the effect of phototherapy on intestinal flora and metabolism of newborns. The aim was to assess the benefit of treatment for hyperbilirubinemia with phototherapy.
Material and methods: Fifty-three jaundiced infants hospitalized at our neonatal intensive care unit were treated with phototherapy. Of them, 29 were prescribed antibiotics during the hospitalization. Fecal samples were collected before and 24 h and 48 h after phototherapy. The bacterial species and relative abundance were identified with Macrogene sequencing. The bile acids in feces were identified using liquid chromatography-mass spectroscopy (LC-MS).
Results: Differential microbial species/genera and secondary bile acids were found after phototherapy. There are significant differences in the changes of the microbial species/genera between infants who did not receive antibiotic treatment and those who were given antibiotic treatment. Secondary bile acids were also significantly altered. At the same time, the differential microbial species/genera and the differential secondary bile acids interacted with each other.
Conclusions: This study identified several differential intestinal microbial species and secondary bile acids in fecal samples from infants with jaundice before and after phototherapy. Phototherapy can change the flora and its metabolism and its long-term impact needs further observation.
Key words: phototherapy, neonatal jaundice, intestinal flora, bile acids.
Introduction
Neonatal jaundice is a common condition worldwide, which may be physiological or pathological. Physiological jaundice results from hyperbilirubinemia, which presents as a high bilirubin concentration in the serum. Total serum bilirubin (TSB) is currently used as a diagnostic index for jaundice [1]. Most bilirubin comes from red blood cells (RBCs), which undergo hemolysis and release their hemoglobin content, with unconjugated bilirubin being the end-product of hemoglobin metabolism. After binding to serum albumin, unconjugated bilirubin is transported to the liver, where it will detach from the albumin and conjugate with glucuronic acid [2]. Conjugated bilirubin is water soluble and excreted into the small intestine with bile acids and then is further catabolized by colonic
Corresponding author: Jinping Zhang
Department of Pediatrics
Shanghai Jiao Tong
University Affiliated Sixth People’s Hospital 222 Huanhuxisan Road
Pudong New Area 201306
Shanghai, China
Phone: +17621710577
E-mail: zhang-jin-ping@163. com
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
Clinical research Diagnostics, laboratory
flora to urobilinogen, which is excreted from the body [3].
However, newborns have an increased bilirubin production because of the shorter lifespan of their RBCs and higher concentration of hemoglobin. On the other hand, newborns have a poorer capacity for the clearance of bilirubin. At birth, infants also have significantly lower levels of plasma albumin compared to adults [4]. The non-albumin-bound unconjugated bilirubin will pass through the blood-brain barrier and result in neuronal injury [5]. In the small intestine, the flora converts bilirubin monoglucuronides to urobilinogen, which is excreted from the body. In addition, the metabolites produced by intestinal microbiota contribute to the motility of the gastrointestinal tract (GIT). Nevertheless, newborns lack intestinal flora, and thus have a decreased intestinal motility [6]. Thus, a proportion of the bilirubin is deconjugated by b-glucuronidase and reabsorbed into the blood from the intestine [7].
Phototherapy is a treatment widely used to reduce serum bilirubin in jaundiced newborns, due to the safety and convenience of its use. As a yellow pigment, bilirubin strongly absorbs blue light in the 460 nm wavelength and then converts it irreversibly to lumirubin, a water-soluble and less toxic compound, which can be excreted with bile acids and urine [2].
The human GIT microbiota contributes to host metabolism. GIT microbiota produces short-chain fatty acids (SCFAs) and secondary bile acids, which play essential roles in host energy metabolism [8]. Primary bile acids, including cholic acid (CA) and chenodeoxycholic acid (CDCA), are synthesized in the liver and then converted to secondary bile acids by microbiota in the GIT [9–11]. Bile acids not only play roles in several metabolism processes, but also regulate the composition of the GIT microbiota [12]. In short, microbial richness is considered to be an indicator of a host’s heath status. Alterations to the microbiota may lead to functional amelioration of the GIT microbiota’s capacity to produce metabolites.
In the present study, the aim was to assess the benefit of treatment for hyperbilirubinemia with phototherapy. In this context, we characterized the 16S rRNA microbiome of jaundiced infants before and after phototherapy, with or without antibiotic treatment. We also quantified the concentrations of secondary bile acids and determined the relationship between the differential microbiota species and differential secondary bile acids. We observed several species/ genera and secondary bile acids which may well participate in the clearance of bilirubin in jaundiced infants after they had been treated with phototherapy.
Material and methods
Study cohort and patient characteristics
Fifty-three term neonates with jaundice were treated in the neonatal intensive care unit of the Pediatrics Department, Hospital between June 2017 and June 2018. The whole cohort comprised infants with birth weight ≥ 2,500 g and gestational age over 37 weeks. This study was approved by the ethics committee of our hospital. Written consent was obtained from the legal guardians of these neonates before they were included in the study. All neonates with jaundice were diagnosed according to the criteria defined in practical neonatology. Briefly, neonates with the following symptoms were diagnosed with jaundice. (1) jaundice appears within 24 h after birth; (2) a serum bilirubin concentration > 221 μmol/l (12.9 mg/dl), which was mainly indirect bilirubin, or the daily increase exceeded 85 μmol/l (5 mg/dl); (3) jaundice appears again after receding; (4) jaundice lasted for > 2 weeks and the serum conjugated bilirubin concentration was > 34 μmol/l (2 mg/dl). Exclusion criteria were: congenital malformation; surgical disease; chromosomal abnormalities; congenital metabolic abnormalities; neonatal asphyxia; sepsis or suspected sepsis; RH hemolysis requiring blood exchange; glucose-6-phosphate dehydrogenase (G6PD) deficiency; hemoglobin disease or congenital infection.
Treatment
The blue LED light of the jaundice treatment apparatus with a double-sided light source (peak wavelength 425–475nm) was used. The blue light source was about 40 cm away from the neonates. During phototherapy for 24 h or 48 h the whole body, except for the genitals and eyes, was fully exposed to the light. Breathing and heart rate were closely monitored during the phototherapy treatment.
Determination of serum bilirubin concentration
The routine biochemistry panel, including serum concentrations of bilirubin, was carried out. The fifth-generation Total Bile Acids Randox RX Series assay (Randox Laboratories, Crumlin, UK) was used to measure the total concentrations of bile acids in sera.
Fecal sample collection and storage
In this pilot study, only a subset of 8 samples at baseline, 9 samples after 24 h phototherapy and 12 samples after phototherapy for 48 h were selected for analysis. Samples were selected randomly. Sterile containers were used to collect the fecal
402 Arch Med Sci 2, 1st March / 2023
Kun Zhang, Sainan Fan, Anping Lv, Yanan Ma, Xiaohui Fang, Jinping Zhang
Integrated analysis of microbiota with bile acids for the phototherapy treatment of neonatal jaundice
samples. Samples were collected on the day of hospital admission, and 48 h and 72 h after phototherapy. Samples were immediately frozen at –20°C and stored until required for subsequent analysis.
Extraction of fecal genomic DNA
Fecal samples were collected in sterile containers and stored at –20°C until required for further analysis. Genomic DNA was purified using a QIAamp PowerFecal DNA Kit according to the instructions of the manufacturer. The libraries were constructed using a standard protocol and the sequencing was produced on the Illumina Hiseq system. Sequence reads were assembled with SOAP de novo. The relative abundance of the microbial species was analyzed using MetaPhlAn.
Quantification of fecal bile acids
The major bile acids (BAs) were identified using gas chromatography. For protein precipitation, each ~100 mg fecal sample was mixed with 0.3 ml of methanol, followed by vortex mixing for 1 min. After 10 min centrifugation (12,000g) at 4°C, the supernatant was transferred and diluted 10 times in methanol, followed by another 1 min of vortex. After a further additional 10 min centrifugation (12,000g) at 4°C, the supernatant (5 μl) was injected into the UPLC (Waters ACQUITY UPLC, US) for analysis.
Chromatographic separation was accomplished in a Thermo Ultimate 3000 system equipped with an ACQUITY UPLC BEH C18 (100 × 2.1 mm, 1.7 μm) Waters column maintained at 40°C. Gradient elution of analytes was carried out with 0.01% formic acid in water (A) and acetonitrile (B). An increasing linear gradient of solvent B (v/v) was used as follows: 0–4 min, 25 % B; 4–9 min, 25–30% B; 9–14 min, 30–36% B; 14–18 min, 36–38% B; 18–24 min, 38–50% B; 24–32 min, 50–75% B; 32–35 min, 75–100% B; 35–38 min, 100–25% B. The capillary temperature was 500°C. The Orbitrap analyzer scanned over a mass range of m/z 81–1000 for a full scan at a mass resolution of 70,000.
Data dependent acquisition (DDA) MS/MS experiments were performed with an HCD scan. The normalized collision energy was 30 eV. Dynamic exclusion was implemented to remove some unnecessary information in the MS/MS spectra.
Ethics approval
The study was approved by the Ethics Committee of Shanghai Sixth People’s Hospital East Campus. Approval No: 2017-009.
Statistical analysis
SPSS 23 was used to analyze the data, which are presented as the mean ± SE. The Wilcoxon
rank sum test was employed for comparisons between groups with a non-normal distribution. Correlations between variables were evaluated using the Spearman coefficient. A p-value < 0.05 was considered to be a statistically significant finding.
Results
Clinical characteristics of infants with jaundice
Of the 53 jaundiced infants enrolled in the study, all had been admitted to the NICU of the Sixth People’s Hospital Affiliated to Jiaotong University, Shanghai, between June 2017 and June 2018. The average gestational age was 271.2 ±8.77 days and birth weight 3.2 ±0.36 kg. The onset of jaundice occurred 2.17 ±1.43 days after birth. The mean total serum bilirubin (TSA) was 19.7 ±3.7 mg/dl, and transcutaneous bilirubin (TCB) concentration was 21.49 ±4.36 mg/dl. Twenty-nine of the babies were treated with antibiotics, and the others were not (Table I).
Phototherapy effects on total serum bilirubin
The concentration of total serum bilirubin was measured at baseline and after treatment. At the time of hospitalization, the mean serum bilirubin of all the patients combined was 19.7 ±3.7 mg/dl. It was 19.2 ±2.8 mg/dl and 20.1 ±4.3 mg/dl in the non-antibiotic-treated group and antibioticstreated group, respectively. As shown in Table II, the phototherapy cleared the bilirubin significantly. In the group of non-antibiotic-treated patients, the mean serum bilirubin level decreased to 13.7 ±2.7 mg/dl and 0.8 ±0.2 mg/dl 24 h and 48 h after phototherapy treatment, respectively. In the group of antibiotic-treated infants, it decreased to 13.2 ±3.2 mg/dl and 0.7 ±0.2 mg/dl 24 h and 48 h after
Table I. Baseline and clinical characteristics (n = 40)
Arch Med Sci 2, 1st March / 2023 403
Parameter Value Birth characteristics, mean ± SD: Gestational age [days] 271.20 ±8.77 Birth weight [kg] 3.2 ±0.36 Onset of jaundice [days] 2.18 ±1.40 Age [days] 7.10 ±5.24 Phototherapy duration [h] 88.51 ±41.92 TCB [mg/dl] 21.49 ±4.36 TSA [mg/dl] 19.7 ±3.7 Feeding type, n (%): Breastfeeding 36 (67.92) Mixture 17 (32.08) Antibiotics usage, n (%): Yes 29 (54.72) No 24 (45.28)
Table II. Effects of phototherapy on total serum bilirubin concentrations before and after phototherapy
s_Alistipesputrediniss_Cellvibriounclassifieds_Clostridiumbolteaes_Enterobactercloacaes-Enterococcusfaeciums_Eubacteriumsiraeums_Finegoldiamagnas_Veillonellaatypica
g_Alistipesg_Bacillusg-Cellvibriog_Enterobacterg_Finegoldiag-Lactococcus
S_bacteroidescaccaes_Doreaunclassifieds_Eubacteriumrectals_Faecalibacteriumprausnitzii
s_Pantoeaunclassifieds_Roseburiaunclassifieds_Veillonellaparvula
s_Veillonellaunclassified
g_Clostridiumg_Eubacteriumg_Faecalibacteriumg_Pantoeag-Prevotellag_Roseburiag_Veillonella
Figure 1. Differential gut microbial species and genera before and after phototherapy, as characterized by 16S rRNA sequencing. A – Samples are from infants without antibiotic treatment. B – Samples are from infants with antibiotic treatment
Kun
404 Arch Med Sci 2, 1st March / 2023
Zhang, Sainan Fan, Anping Lv, Yanan Ma, Xiaohui Fang, Jinping Zhang
Antibiotics usage Baseline [mg/dl] Phototherapy 24 h [mg/dl] Phototherapy 48 h [mg/dl] No (24 cases) 19.2 ±2.8 (24 cases) 13.7 ±2.7 (24 cases) 0.8 ±0.2 (21 cases) Yes (29 cases) 20.1 ±4.3 (29 cases) 13.2 ±3.2 (29 cases) 0.7 ±0.2 (20 cases)
40 30 20 10 40 30 20 10 1.5 1.0 0.5 0.10 0.08 0.06 0.04 0.02 0.0008 0.0006 0.0004 0.0002 0 0.00008 0.00006 0.00004 0.00002 0 Percentage Percentage A B
Baseline 24 h 48 h
Integrated analysis of microbiota with bile acids for the phototherapy treatment of neonatal jaundice
phototherapy, respectively. Furthermore, there was no significant difference between the two groups.
Phototherapy effects on abundance of microbiota in the GIT
To evaluate the alteration of GIT microbiota before and after phototherapy, Macrogene sequencing analysis was employed. Among the infants who did not receive antibiotic treatment (Figure 1 A), many species detected were significantly altered. Alistipes putredinis and Cellvibrio unclassified were found to be decreased after phototherapy, while Clostridium bolteae, Enterobacter cloacae, Enterococcus faecium, Eubacterium siraeum, Finegoldia magna and Veillonella atypica were found to be increased significantly. Genera including Alistipes, Bacillus, Cellvibrio, Enterobacter, Finegoldia and Lactococcus were altered significantly after phototherapy. On the other hand, among the infants who were given antibiotic treatment (Figure 1 B), species were also found to have been altered significantly after phototherapy. Many species increased including Bacteroides caccae, Dorea unclassified, Eubacterium rectale, Faecalibacterium prausnitzii, Roseburia unclassified, Veillonella parvula, and Veillonella unclassified. Only Pantoea unclassified was found to be decreased after phototherapy. The genera included Clostridium, Eubacterium, Faecalibacterium, Pantoea, Prevotella, Roseburia and Veillonella. These results indicated that phototherapy could modulate the relative abundance of some species and genera. It is noteworthy that the differential species or genera were quite different in infants who were treated with antibiotics and those who were not.
Phototherapy effects on relative abundance of BAs
The microbiota metabolizes the primary bile acids to secondary BAs. LC/MS was used to evaluate the fecal BA profiles in the infants enrolled in the study. Figure 2 demonstrates that phototherapy could induce alterations in some types of secondary bile acids, as indicated by analysis of the fecal samples. In the group of non-antibiotic-treated infants (Figure 2), the concentrations of 11 secondary bile acids were significantly altered after phototherapy, including LCA, 12-ketol LCA, b-UDCA, DCA, NorCA, GLCA, GUDCA, GDCA, TLCA, THDCA and TUDCA. All differential secondary bile acids were elevated 24 h after phototherapy and then reduced to a lower level 48 h after phototherapy, as compared with baseline. On the other hand, in the group of antibiotic-treated infants (Figure 3), levels of 8 secondary bile acids were altered after phototherapy, i.e. LCA, isoLCA, NorCA, GLCA, GUDCA, GDCA, LCA-3S and TLCA. In detail, levels
of LCA and LCA-3S were reduced 24 h or 48 h after phototherapy compared to baseline. isoLCA, NorCA, GLCA, GUDCA, GDCA and TLCA were elevated 24 h after phototherapy and then were reduced to lower concentrations 48 h after phototherapy compared to baseline values. These results strongly suggested that phototherapy could affect the production of bile acids.
Impact of differential species or genera on differential bile acids
To explore further the association between the differential species/genera and the differential secondary bile acids, multivariate logistic regression analyses were conducted. First, we assessed the effect of differential species or genera on bile acids’ alteration when adjusting for the use of probiotics or breastfeeding. Notably, among the infants who did not receive antibiotic treatment (Figure 4 A), the alteration of the genus Bacillus was associated with b-UDCA (OR: 1.2115 × 1017, 95% CI: 1.5561 × 109 –9.4322 × 1024). Among the infants given antibiotics (Figure 4 B), the alteration of LCA was associated with Bacteroides caccae (OR = 0.0033, 95% CI: 0.0003–0.0342), Veillonella parvula (OR = 66122791.02, 95% CI: 134159.7–32589693406), Veillonella unclassified (OR = 2.4282 × 10–8, 95% CI: 5.3115 × 10–11–1.1100 × 10–5) and the genus Veillonella (OR = 0, 95% CI: 0–6.3239 × 10–271). The alteration of LCA-3S was associated with Bacteroides caccae (OR = 1.6320 × 10–5, 95% CI: 2.9602 × 10–6–8.9978 × 10–5), Roseburia unclassified (OR = 0, 95% CI: 0–0), Veillonella parvula (OR = 145,925.7967, 95% CI: 1,569.550155–13,567,160.04), Veillonella unclassified (OR = 0.000547188, 95% CI: 6.2182 × 10–6–0.04815). The alteration of GDCA was associated with Pantoea unclassified (OR = 1.3752, 95% CI: 1.2344–1.5320).
Impact of differential bile acids on differential species or genera
Next, we assessed the effect of differential bile acids on differential species or genera after adjusting the data for the use of probiotics or breast-feeding. Notably, among the infants who were not treated with antibiotics (Figure 5 A), the alteration of the species Eubacterium siraeum was associated with 12-ketoLCA (OR = 1.0233, 95% CI: 1.0017–1.0453), DCA (OR = 1.0074, 95% CI: 1.0012–1.0136) and GLCA (OR = 0.7460, 95% CI: 0.5785–0.9619, p < 0.05). The alteration of the genus Bacillus was associated with b-UDCA (OR = 1.0088, 95% CI: 1.0030–1.0146), DCA (OR = 1.0043, 95% CI: 1.0015–1.0071) and GDCA (OR = 0.917, 95% CI: 0.8680–0.9692). On the other hand, alteration of the genus Lactococcus was
Arch Med Sci 2, 1st March / 2023 405
associated with GLCA alteration (OR = 0.1440 95% CI: 0.0318–0.6512). In contrast, among the infants given antibiotics (Figure 5 B), the species Bacteroides caccae was associated with isoLCA (OR = 3.2794 × 1016, 95% CI: 5.4541 × 1013–1.9718 × 1019) and GLCA (OR = 2.6089 × 10-64, 95% CI: 2.6234 × 10109–2.5944 × 10-19). Also, the species Eubacterium rectale (OR = 1.6634, 95% CI: 1.2759–2.1685) and Faecalibacterium prausnitzii (OR = 1.5533, 95% CI: 1.2476–1.9340) and the genera Eubacterium (OR = 1.6642, 95% CI: 1.2755–2.1712), Faecalibacterium (OR = 1.5533, 95% CI: 1.2476–1.9340), and Prevotella (OR = 1.6330, 95% CI: 1.2486–2.1357) were associated with alterations in TLCA.
Discussion
The neonatal intestinal microbiota was influenced by several factors including diet, the maternal microbiome and local culture, which may
*p < 0.05, **p < 0.01, ***p < 0.001.
have produced geographical differences in the microbiota composition in the cohort of infants [13]. However, neonatal jaundice is a common clinical sign in newborn infants worldwide, for which phototherapy is the simplest treatment. Hence, it will be necessary to determine the GIT microbiota composition in jaundiced infants before and after phototherapy in different regional-based cohorts. Antibiotics are widely used in neonatal medication, but they perturb a developing infant’s intestinal microbiota. In the present study, infants treated with antibiotics or not had quite a different differential species/genera before and after phototherapy, which supports the disruption effect of antibiotic therapy. More importantly, various factors, including antibiotic-resistant genes, should be taken into consideration when trying to understand the responses of infants to antibiotics.
Phototherapy could transform the unconjugated bilirubin into conjugated forms, which could
406 Arch Med Sci 2, 1st March / 2023
Kun Zhang, Sainan Fan, Anping Lv, Yanan Ma, Xiaohui Fang, Jinping Zhang
0.4 0.3 0.2 0.1 0 1.0 0.8 0.6 0.4 0.2 0 0.05 0.04 0.03 0.02 0.01 0 0.05 0.04 0.03 0.02 0.01 0 0.5 0.4 0.3 0.2 0.1 0 0.6 0.4 0.2 0 Percentage Percentage Percentage Percentage Percentage Percentage 12-ketoLCA DCA GDCA GLCA NorCA THDCA + TUDCA Baseline 24 h 48 h Baseline 24 h 48 h Baseline 24 h 48 h Baseline 24 h 48 h Baseline 24 h 48 h Baseline 24 h 48 h n = 18 n = 18 n = 18 n = 18 n = 18 n = 18 n = 17 n = 17 n = 17 n = 17 n = 17 n = 17 n = 19 n = 19 n = 19 n = 19 0.05 0.04 0.03 0.02 0.01 0 0.20 0.15 0.10 0.05 0 Percentage Percentage GUDCA LCA Baseline 24 h 48 h Baseline 24 h 48 h n = 18 n = 18 n = 17 n = 17 n = 19 n = 19 0.04 0.03 0.02 0.01 0 0.15 0.10 0.05 0 Percentage Percentage TLCA b-UDCA Baseline 24 h 48 h Baseline 24 h 48 h n = 18 n = 18 n = 17 n = 17 n = 19 n = 19 n = 19 n = 19
Figure 2. Comparison of the relative abundance of secondary bile acids in the fecal samples from infants without antibiotic treatment before and after phototherapy
*p < 0.05, **p < 0.01, ***p < 0.001. then be metabolized to urobilinoids by the GIT microbiota. In our study, the TSB of the jaundiced infants dropped drastically in the first 24 h after phototherapy, and then returned to normal values 48 h after phototherapy. By contrast, the relative abundance of fecal secondary bile acids rose rapidly in the first 24 h after phototherapy, but decreased to the level of baseline in the second 24 h. Accordingly, the correlated microbiota species also exhibited a higher relative abundance 24 h after phototherapy compared to baseline and then a reduction 48 h after phototherapy. This finding suggested that TSB reduction in the first 24 h is sufficient to induce the alteration of differential species/genera and secondary bile acids. The underlying mechanisms of this response remain to be investigated.
Reduction of enterohepatic circulation by accelerated bilirubin fecal excretion can reduce infant jaundice. It is well known that exposure to phototherapy provokes an increased rate of intestinal transit and thus diarrhea in jaundiced infants [14, 15]. It is worth thinking about how phototherapy can induce an alteration in the GIT microbiota species. Previous studies have indicated a significantly greater colon motility index for patients with diarrhea, as excess bile acid concentrations in the colon stimulate enteroendocrine cells and accelerate colonic transit. In our study, we observed elevation of fecal secondary bile acids after photo-
therapy, which leads to speculation that bilirubin metabolism after phototherapy might modulate colonic microbiota species and thus produce more fecal secondary bile acids accordingly. There is limited information on the mechanisms involved in the colon motility response to secondary bile acids. However, the bile acid-GIT microbiome axis has emerged as an important regulator of health and findings have indicated that species interacted with each other. Indeed, we find relationships between differential secondary bile acids and differential species/genera. TLCA (taurolithocholic acid) and DCA are activators of Gas-protein-coupled receptor G protein-coupled bile acid receptor1 (TGR5), whose activation protects the intestinal barrier function and reduces inflammation [16]. We found that changes in TLCA composition had an impact on several differential species alterations after phototherapy. Among them, Eubacterium rectale, Faecalibacterium prausnitzii, and the genus Prevotella, which are SCFA-producing bacteria [17, 18], were affected by TLCA. Several studies have reported that fecal DCA could be increased by a western diet and participate in intestinal carcinogenesis [19]. Nevertheless, carcinogenesis is a long-term process with stepwise accumulation of mutations. Therefore, transient elevation of DCA after phototherapy might be a stress reaction, and how it modulates GIT homeostasis after phototherapy remains to be explored.
Integrated analysis of microbiota with bile acids for the phototherapy treatment of neonatal jaundice Arch Med Sci 2, 1st March / 2023 407 0.25 0.20 0.15 0.10 0.05 0 6 4 2 0 0.20 0.15 0.10 0.05 0 8 6 4 2 0 0.25 0.20 0.15 0.10 0.05 0 0.4 0.3 0.2 0.1 0 0.8 0.6 0.4 0.2 0 0.25 0.20 0.15 0.10 0.05 0 Percentage Percentage Percentage Percentage Percentage Percentage Percentage Percentage GDCA LCA GLCA LCA-3S GUDCA NorCA isoLCA TLCA Baseline 24 h 48 h Baseline 24 h 48 h Baseline 24 h 48 h Baseline 24 h 48 h Baseline 24 h 48 h Baseline 24 h 48 h Baseline 24 h 48 h Baseline 24 h 48 h n = 12 n = 12 n = 12 n = 12 n = 12 n = 12 n = 12 n = 12 n = 8 n = 8 n = 8 n = 8 n = 8 n = 8 n = 8 n = 8 n = 9 n = 9 n = 9 n = 9 n = 9 n = 9 n = 9 n = 9
Figure 3. Comparison of the relative abundance of secondary bile acids in the fecal samples from infants with antibiotic treatment before and after phototherapy
s_Alistipes putredinis
s_Cellvibrio unclassified
s_Clostridium bolteae
s_Enterobacter cloacae
s-Enterococcus faecium
s_Eubacterium siraeum
s_Finegoldia magna
s_Veillonella atypica
g_Alistipes
g_Bacillus
g_Enterobacter
g-Lactococcus
s_bacteroides caccae
s_Dorea unclassified
s_Eubacterium rectale
s_Faecalibacterium prausnitzii
s_Pantoea unclassified
s_Roseburia unclassified
s_Veillonella parvula
s_Veillonella unclassified
g_Clostridium
g_Eubacterium
g-Prevotella
g_Roseburia
g_Veillonella
*p < 0.05, **p < 0.01, ***p < 0.001.
In conclusion, the present study revealed fluxes in bile acids and their association with differential species/genera before and after phototherapy treatment. We believe that a large-cohort study needs to be conducted to confirm the physiological roles of these differential species and BAs.
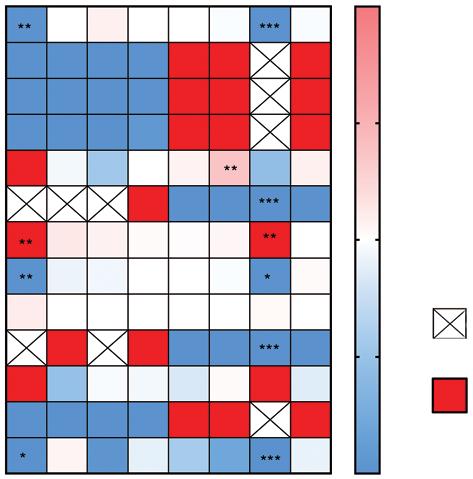
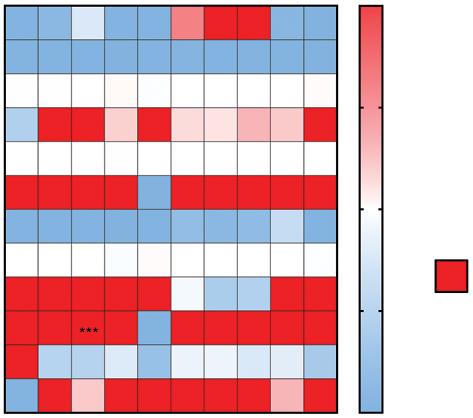
Acknowledgments
Kun Zhang and Sainan Fan contributed equally to this work.
This study was supported by the people’s livelihood research special funding of Shanghai Science and technology development (PKJ2017-Y09). This study was supported by Clinical Research
408 Arch Med Sci 2, 1st March / 2023
Kun Zhang, Sainan Fan, Anping Lv, Yanan Ma, Xiaohui Fang, Jinping Zhang
Figure 4. Differential gut microbial species/genera impact on secondary bile acids. A – Heatmap of odds ratio between differential gut microbial and differential secondary bile acids in infants without antibiotic treatment. B – Heatmap of odds ratio between differential gut microbial and differential secondary bile acids in infants with antibiotic treatment. Rows represent differential microbial species/genera and columns represent differential secondary bile acids
isoLCA12-ketoLCAb-UDCA DCANorCA GLCAGUDCA GDCA TLCA THDCA+TUDCA
> 2 > 2
LCA isoLCA NorCA GLCA GUDCA GDCA LCA-3S TLCA
A B 2.0 1.5 1.0 0.5 0 2.0 1.5 1.0 0.5 0 Infinite
s_Alistipes putredinis
s_Cellvibrio unclassified
s_Clostridium bolteae
s_Enterobacter cloacae
s-Enterococcus faecium
s_Eubacterium siraeum
s_Finegoldia magna
s_Veillonella atypica
g_Alistipes
g_Bacillus
g_Celivibrio
g_Enterobacter
g_Finegoldia
g-Lactococcus
s_bacteroides caccae
s_Dorea unclassified
s_Eubacterium rectale
s_Faecalibacterium prausnitzii
s_Pantoea unclassified
s_Roseburia unclassified
s_Veillonella parvula s_Veillonella unclassified
*p < 0.05, **p < 0.01, ***p < 0.001.
Plan of SHDC (SHDC2020CR3055B). This study was supported by Shanghai Pudong Health and Family Planning Commission Joint Public Relations Project (PW2017D-7). The funding organization played no role in the implementation of this study.
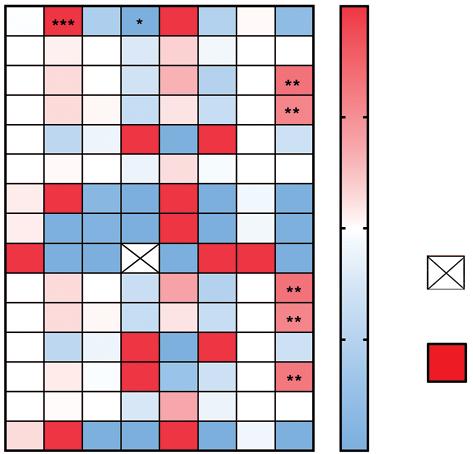
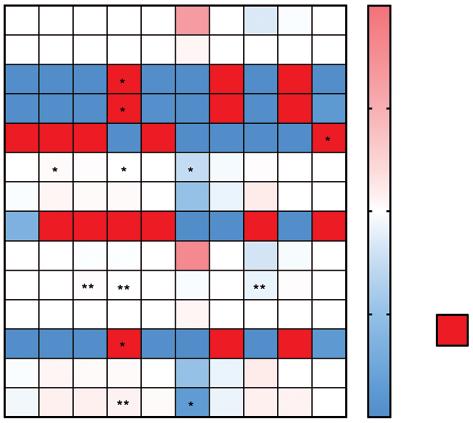
Conflict of interest
The authors declare no conflict of interest.
References
1. Watson RL. Hyperbilirubinemia. Crit Care Nurs Clin North Am 2009; 21: 97-120.
Integrated analysis of microbiota with
acids for the phototherapy treatment of neonatal
Arch Med Sci 2, 1st March / 2023 409
bile
jaundice
Figure 5. Differential secondary bile acids’ impact on gut microbial species/genera. A – Heatmap of odds ratio between differential gut microbial and differential secondary bile acids in infants without antibiotic treatment. B – Heatmap of odds ratio between differential gut microbial and differential secondary bile acids in infants with antibiotic treatment. Rows represent differential microbial species/genera and columns represent differential secondary bile acids
isoLCA12-ketoLCA
b-UDCA DCANorCA GLCAGUDCA GDCA TLCA
THDCA+TUDCA
> 2 > 2
LCA isoLCA NorCA GLCA GUDCA GDCA LCA-3S TLCA
g_Clostridium g_Eubacterium g_Faecalibacterium g_Pantoea g_Prevotella g_Roseburia g_Veillonella A B 2.0 1.5 1.0 0.5 0 2.0 1.5 1.0 0.5 0 Infinite
Kun Zhang, Sainan Fan, Anping Lv, Yanan Ma, Xiaohui Fang, Jinping Zhang
2. Dennery PA, Seidman DS, Stevenson DK. Neonatal hyperbilirubinemia. N Engl J Med 2001; 344: 581-90.
3. Takimoto M, Matsuda I. g-Glucruonidase activity in the stool of the newborn infant. Biol Neonate 1971; 18: 66-70.
4. Notarianni LJ. Plasma protein binding of drugs in pregnancy and in neonates. Clin Pharmacokinet 1990; 18: 20-36.
5. Sinclair CJ. A difference in mortality rate and incidence of kernicterus among premature infants allotted to two prophylactic antibacterial regimens, by William A. Silverman, et al, Pediatrics, 1956; 18: 614-624. Pediatrics 1998; 102: 225-7.
6. Koppen IJN, Benninga MA, Singendonk MMJ. Motility disorders in infants. Early Hum Dev 2017; 114: 1-6.
7. Mitra S, Rennie J. Neonatal jaundice: aetiology, diagnosis and treatment. Br J Hosp Med 2017; 78: 699-704.
8. Kapourchali FR, Cresci GAM. Early-life gut microbiome – the importance of maternal and infant factors in its establishment. Nutr Clin Pract 2020; 35: 386-405.
9. Lefebvre P, Cariou B, Lien F, Kuipers F, Staels B. Role of bile acids and bile acid receptors in metabolic regulation. Physiol Rev 2009; 89: 147-91.
10. Staels B, Fonseca VA. Bile acids and metabolic regulation: mechanisms and clinical responses to bile acid sequestration. Diabetes Care 2009; 32 Suppl 2: S237-45.
11. Kuver R. The expanding universe of bile acid physiology: delving into the mysteries of dark (green) matter. J Surg Res 2013; 182: 207-9.
12. Ridlon JM, Kang DG, Hylemon PB, Bajaj JS. Bile acids and the gut microbiome. Curr Opin Gastroenterol 2014; 30: 332-8.
13. Echarri PP, Graciá CM, Berruezo GR, et al. Assessment of intestinal microbiota of full-term breast-fed infants from two different geographical locations. Early Hum Dev 2011; 87: 511-3.
14. Sivan Y, Dinari G, Goodman C, Merlob P, Nitzan M. Small intestine transit time and lactose absorption during phototherapy. Biol Neonate 1985; 48: 10-4.
15. Rubaltelli F, Largajolli G. Effect of light exposure on gut transit time in jaundiced newborns. Acta Paediatr Scand 1973; 62: 146-8.
16. Brighton CA, Rievaj J, Kuhre RE, et al. Bile acids trigger GLP-1 release predominantly by accessing basolaterally located g protein-coupled bile acid receptors. Endocrinology 2015; 156: 3961-70.
17. Ferreira-Halder V, Faria AVS, Andrade SS. Action and function of Faecalibacterium prausnitzii in health and disease. Best Pract Res Clin Gastroenterol 2017; 31: 643-8.
18. Louis P, Flint HJ. Diversity, metabolism and microbial ecology of butyrate-producing bacteria from the human large intestine. FEMS Microbiol Lett 2009; 294: 1-8.
19. Jenkins GJ, Cronin J, Alhamdani A, et al. The bile acid deoxycholic acid has a non-linear dose response for DNA damage and possibly NF-kappaB activation in oesophageal cells, with a mechanism of action involving ROS. Mutagenesis 2008; 23: 399-405.
410 Arch Med Sci 2, 1st March / 2023
Clinical efficacy and safety of rituximab with membranous nephropathy: a meta-analysis
Hongzhen Zhong1, Hong-Yan Li2, Tianbiao Zhou1, Zhiqing Zhong1
1Department of Nephrology, the Second Affiliated Hospital of Shantou University Medical College, Shantou, China
2Department of Nephrology, Huadu District People’s Hospital of Guangzhou, Southern Medical University, Guangzhou, China
Submitted: 22 January 2019; Accepted: 2 August 2019
Online publication: 14 October 2020
Arch Med Sci 2023; 19 (2): 411–419
DOI: https://doi.org/10.5114/aoms.2020.99899
Copyright © 2020 Termedia & Banach
Abstract
Introduction: Membranous nephropathy (MN) is an organ-specific autoimmune disease, and its prevalence is increasing. B lymphocytes activated by T cells produce antibodies. CD19+/CD20+ plasma cells may contribute to autoantibody and alloantibody production. Rituximab has been effective in treating MN in many clinical trials. Thus, we conducted a meta-analysis to explore the clinical efficacy and safety of rituximab with MN. Material and methods: We searched Embase, PubMed, Cochrane Library and ClinicalTrials.gov without language or publication date limitations. Studies were classified in high-risk, medium-risk and low-risk groups based on baseline proteinuria. Follow-up periods and different administrations of rituximab were also compared. Complete remission (CR) and partial remission (PR) were assessed to measure the efficacy of rituximab, and adverse effects were also extracted. Dichotomous data were expressed by the odds ratio (OR), and the 95% confidence intervals (95% CI) were used for the recruited studies. Results: Fourteen articles, including 17 studies, were included in this metaanalysis. The pooled OR of overall PR and CR remission rate was 0.58 (95% CI: 0.53–0.63; p = 0.003). No studies belonged to the low-risk group. The overall PR and CR remission rate in the medium-risk group was 0.56 (95% CI: 0.36–0.73; p = 0.57). The pooled OR of overall PR and CR remission rate in the high-risk group was 0.59 (95% CI: 0.53–0.65; p = 0.03). At the 12-month follow-up, the pooled OR of overall PR and CR remission rate was 0.51 (95% CI: 0.43–0.59; p = 0.72). At the 24-month follow-up, the pooled OR of overall PR and CR remission rate was 0.71 (95% CI: 0.48–0.86; p = 0.07). The pooled OR of efficacy of rituximab at 375 mg/m2 × 4 was 0.63 (95% CI: 0.55–0.70; p = 0.001). Rituximab was tolerated in MN, and most adverse effects were mild. The pooled OR of infusion reaction rate of rituximab was 0.25 (95% CI: 0.13–0.44; p = 0.01) in MN. The pooled OR of cardiovascular-related event rate of rituximab in MN was 0.04 (95% CI: 0.02–0.11). The pooled OR of infection rate of rituximab in MN was 0.06 (95% CI: 0.03–0.12; p < 0.00001).
Conclusions: Rituximab is safe and effective in MN and a promising alternative treatment. More randomized control trials and studies on the role of MN are expected.
Key words: membranous nephropathy, rituximab, complete remission, partial remission, meta-analysis.
Introduction
In recent years, membranous nephropathy (MN) has increased in prevalence, and is a common glomerulonephritis [1, 2]. Studies have also
Corresponding author: Tianbiao Zhou
Department of Nephrology
The Second Affiliated Hospital of Shantou University Medical College
Shantou, China
E-mail: zhoutb@aliyun.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Nephrology
Systematic review and meta-analysis
Hongzhen Zhong, Hong-Yan Li, Tianbiao Zhou, Zhiqing Zhong
shown that membranous nephropathy is the most common glomerulonephritis in the elderly [3–6]. Membranous nephropathy is considered as an organ-specific autoimmune disease, and is histologically defined by subepithelial immune deposits. The major membranous nephropathy target antigen is podocyte phospholipase A2 receptor (PLA2R) [7]. It has been reported that approximately 70% and 80% of total idiopathic membranous nephropathy patients are found with elevated serum anti-PLA2R antibodies levels and enhanced glomerular PLA2R deposits, respectively [8].
B lymphocytes activated by T cells produce antibodies, which play an essential role in glomerular immunoglobulin deposits and complement activation [9, 10], and B cells have been suggested as antigen-presenting cells involved in the pathogenesis of MN [11]. CD20 is a pan-B cells marker due to its expression in the pre-B stage of B cells and absence after differentiating to plasma cells [11]. CD19+/CD20+ plasma cells may contribute to autoantibody and alloantibody production [12, 13].
Rituximab is a monoclonal antibody that specifically binds to the CD20 antigen. In recurrent MN [14–16], anti-CD20 antibody with classical immunosuppressant treatment may block the proliferation of B cells and the production of pathogenic antibodies in patients. Rituximab is also effective in treating other conditions associated with autoantibody production, such as systemic lupus erythematosus [17] and rheumatoid arthritis [18]. Although the effects of rituximab on MN have not been characterized in animal studies, clinical trials and case reports have reported that rituximab is associated with good remission rates and is safe in patients with MN. So far, only Zou et al. [19] have conducted studies prior to 2016 with 12-month follow-up to analyze the efficacy and safety of rituximab in idiopathic membranous nephropathy. However, Cravedi [20] suggests that nephrologists should note the limitations of this study and warn against an oversimplified interpretation of the data. Based on this literature, we analyzed the role of rituximab in membranous nephropathy in different stages of membranous nephropathy, different follow-up periods, and administered doses and adverse effects. This meta-analysis will provide evidence for the application of rituximab in MN.
Material and methods
Search strategy
The keywords “rituximab”, “CD20 antibody”, “glomerulonephritis, membranous”, “membranous nephropathy”, “idiopathic membranous nephropathy” and “membranous glomerulonephritis”. “(rituximab OR CD20 antibody) AND (glomerulonephritis membranous OR membranous nephro-
pathy OR idiopathic membranous nephropathy OR membranous glomerulonephritis)” was entered into PubMed, Embase, Cochrane Library and ClinicalTrials.gov for search without language or publication date limitations.
Inclusion and exclusion criteria
We included and excluded relevant studies according to the following criteria. Primary membranous nephropathy was eligible, and secondary membranous nephropathy was excluded. Rituximab as the first line in membranous nephropathy was included, and combined therapy or second line therapy was excluded. Patients were over 18 years old; pediatric trials were not considered. Reviews, case reports and editorials were excluded, and only randomized controlled trials, prospective studies, and retrospective studies were included in this meta-analysis.
Outcome measures and data collection
The numbers of complete remissions (CR) and partial remissions (PR) were extracted to measure the efficacy of rituximab in membranous nephropathy at 12 months and at 24 months. Basic information was collected from each study, including author, publish year, rituximab dose, study design, total subjects in completed trials and period of follow-up. Baseline values of proteinuria, serum albumin, serum creatinine and estimated glomerular rate (eGFR) of patients were also recorded. Finally, adverse effects were included. The most common adverse effects of rituximab in MN are infusion reactions, infections, cardiovascular events, bullous dermatitis and small patches of hair loss and thinning, and tumors. Infusion reactions included symptoms of skin rash, flu-like symptoms, and a metallic taste.
Statistical analysis
The primary aim of treatment is to reduce chronic proteinuria. The 2012 KIDGO guideline of idiopathic membranous nephropathy proposes a relationship between 24 h proteinuria and disease progression. We divided patients into low-risk (proteinuria was < 4 g/day), medium-risk (proteinuria was 4–8 g/day) and high-risk groups (proteinuria was > 8 g/day) according to their baseline level of proteinuria. The role of rituximab in membranous nephropathy was analyzed at different stages of disease progression and follow-up periods (12 months and 24 months). CR and PR values were extracted from the included studies, and pooled using the method of the inverse of the variance with logit transformed proportions [21]. Review Manager Version 5.3 software was used for further
412 Arch Med Sci 2, 1st March / 2023
Clinical efficacy and safety of rituximab with membranous nephropathy: a meta-analysis
analyses. The results were converted according to the formulae below [22], and the values were considered to denote the efficacy of rituximab. Dichotomous data were expressed by the odds ratio (OR), and the 95% confidence intervals (95% CI) were used for the recruited studies. A p-value less than 0.05 was considered as statistically significant. The heterogeneity was assessed withIsquare (I2). When I2 was less than 50% [23], a fixed-effects model was used; otherwise, a random-effects model was used [24, 25].
(1) The conversion formula for the effect indicator is: Pf = OR/(1 + OR).
(2) The conversion formula for 95% confidence interval upper limits is: LL = LLOR/(1 + LLOR).
(3) The conversion formula for 95% confidence interval lower limits is: UL = ULOR/(1 + ULOR).
Results
Search results
Results of every database are displayed in Figure 1. There were 150, 221, 22 and 12 articles in PubMed, Embase, Cochrane library and ClinicalTrials.gov, respectively. Removing article types based on the inclusion criteria and duplicates, 14 articles including 17 studies were included in this meta-analysis.
Study characteristics
Table I displays the basic characteristics of the included reports. There were 2 retrospective reports [26, 27] and 12 prospective reports
[28–39]. There are many administration protocols for rituximab, including four weekly doses of 375 mg/m2 (the most common), 15 days part of 1 g and titrated to circulating B cells. The total number of completed studies was 364. The follow-up period varied; eight studies [27, 30, 32, 33, 35, 37, 39] contained data to 12 months, four studies [28, 29, 36, 38] included data to 24 months. Patient characteristics of 17 studies are shown in Table II. Based on baseline proteinuria, no studies were classified as low-risk, three studies [26, 27, 31] were included in the mediumrisk group, and twelve studies [28–30, 32–39] were classified as high-risk. Seven studies [27–29, 32, 34–36] reported that rituximab was administered in four weekly rituximab doses of 375 mg/m2. Two studies [30, 31] reported that rituximab (375 mg/m2) was administered once or twice. Two reports [37, 38] contained a 1 g dose of rituximab twice, but the number of PR and CR could not be extracted.
Efficacy of rituximab in membranous nephropathy
Fifteen studies [26–39] were included to assess the efficacy of rituximab in MN. The I2 = 37%, fixed model was applied, which suggested that the heterogeneity between included documents was minimal. The pooled OR of initial results was 1.38 (95% CI: 1.12–1.71; p = 0.003; Figure 2 A), and after conversion, the pooled OR of overall PR and CR remission rate was 0.58 (95% CI: 0.53–0.63; p = 0.003), which was statistically significant.
Arch Med Sci 2, 1st March / 2023 413
PubMed 150 Article type type: (1) Case reports 44 (2) Review 45 (3) Editorial 5 (4) Comment 9 Embase 221 Cochrane library 22 Clinical trials 12 Publication type type: (1) Conference abstract 116 (2) Review 38 (3) Letter 7 (4) Note 3 (5) Editorial 2 (6) Erratum 1 54 47 135 Duplicates 12 Case report 7 Letter 1 Not nephrotic syndrome 15 Not rituximab 13 Without nephrotic syndrome and rituximab 12 Without related results 24 Without detailed data 12 Not published in English 2 < 18 years old 23 14
Figure 1. Flow chart of screening articles Note: + mean sum up; – mean subtraction
The baseline proteinuria of three studies [26, 27, 31] met criteria of the medium-risk group. The I2 = 63%, a random model, indicated heterogeneity of 1.25 (95% CI: 0.58–2.72; p = 0.57; Figure 2 B) between the included studies. After conversion, the pooled OR of overall PR and CR remission rate in the medium-risk group was 0.56 (95% CI: 0.36–0.73), not statistically significant.
According to baseline proteinuria, twelve studies [28–30, 32–39] were included in the high-risk group. The I2 = 33%, a fixed model was used, indicating a minimal heterogeneity between the included studies of 1.43 (95% CI: 1.13–1.82; p = 0.003; Figure 2 C). After conversion, the pooled OR of overall PR and CR remission rate in the high-risk group was 0.59 (95% CI: 0.53–0.65), which was statistically significant.
Eight studies [27, 30, 32, 33, 35, 37, 39] were assessed to analyze the efficacy of rituximab at the 12-month follow-up. The heterogeneity was low, with an I2 of 25%. The pooled OR of overall PR and CR was 1.06 (95% CI: 0.77–1.45; p = 0.72). After transformation, the pooled OR of overall PR and CR remission rate in 12-month follow-up was 0.51 (95% CI: 0.43–0.59), not statistically significant.
Four studies [28, 29, 36, 38] were assessed to analyze 24-month efficacy of rituximab. Since the I2 was 69%, a random model was executed, indicating heterogeneity between studies. The pooled OR of initial PR and CR rate was 2.40 (95% CI: 0.92–6.26; p = 0.07). After transformation, the pooled OR of overall PR and CR remission rate at the 24-month follow-up was 0.71 (95% CI: 0.48–0.86), not statistically significant.
The efficacy of rituximab administered at 375 mg/m2 × 4 was then assessed. The I2 was 44%; a fixed model indicated heterogeneity between the reports, with the pooled OR of initial PR and CR of 1.7 (95% CI: 1.24–2.35; p = 0.001). After conversion, the pooled OR of overall PR and CR was 0.63 (95% CI: 0.55–0.70), statistically significant. Studies of rituximab administered at 375 mg/m2 once or twice were not included.
Safety of rituximab in membranous nephropathy
The most common adverse effects of rituximab in MN are infusion reactions, infections, cardiovascular events, bullous dermatitis and small
414 Arch Med Sci 2, 1st March / 2023
Hongzhen Zhong, Hong-Yan Li, Tianbiao Zhou, Zhiqing Zhong
Author, year PMID Intervention Study design Total subjects Follow-up [months] Cravedi, 2011 21508634 Four weekly rituximab
(375 mg/m2
Prospective, matchedcohort study 11 24 Irazabal, 2013 22987142 RTX (375 mg/m2 × 4) Prospective study 20 24 Moroni, 2017 27387472 RTX (375 mg/m2) once or twice Prospective study 34 12 Bagchi, 2018 29942496 RTX (375 mg/m2) once or twice Prospective study 21 13.1 (10–23.9) Souqiyyeh, 2015 25579715 375 mg/m2 RTX every week for 2 to 4 weeks Multicenter, retrospective study 25 6–21 Ruggenenti, 2006 17699281 RTX (375 mg/m2 × 4) Prospective cohort study 9 12 Wang, 2018 29149305 RTX (375 mg/m2) according to circulating B cells Prospective cohort study 36 12 (9.0–19.3) Aleš Rigler, 2017 28664837 375 mg/m2 RTX in 4 weekly doses → RTX in a single dose of 375 mg/m2 Retrospective study 29 12 Ruggenenti, 2012 22822077 RTX (375 mg/m2 × 4) Prospective studies 68 29 (6–121) Ruggenenti, 2003 12819245 RTX (375 mg/m2 × 4) Prospective, observational study 8 12 Fervenza, 2010 20705965 RTX (375 mg/m2 × 4) Prospective cohort study 18 24 Fervenza, 2008 17943078 RTX 1 g × 2 Prospective cohort study 14 12 Beck, 2011 21784898 Group 1: RTX 1 g × 2; Group 2: RTX (375 mg/m2 × 4) Cohort studies 35 24 Cravedi, 2007 17702725 Group 1: four weekly doses of 375 mg/m2; group 2 titrated to circulating B cells Controlled clinical trial matched-cohort study 36 12
Table I. Studies included in this meta-analysis
doses
each)
patches of hair loss and thinning, and tumors. Infusion reactions included symptoms of skin rash, flu-like symptoms, and a metallic taste. The majority of these were acute and disappeared after treatment infusions were stopped or methylprednisolone infusion. Some resolved without any treatment. Cardiovascular-related events were atrial fibrillation, myocardial infarction and hypotension. These symptoms typically appeared several months following rituximab infusion.
No treatments were prescribed in the included studies. Infectious included soft tissue infections of lower extremities, herpes zoster, respiratory tract infection and pneumonia. These symptoms developed over 1–5 months after rituximab infusion. Oral antibiotics or anti-viral drugs were successfully used to treat these conditions. Bullous dermatitis often appeared 1 day after RTX. Hair loss and tumors were rare.
Six studies [28, 34–37, 39] were included to analyze the infusion reaction rate of rituximab in MN. The I2 was 74%, so a random model was ap-
plied. Heterogeneity was present in the included studies. The pooled OR of initial result was 0.33 (95% CI: 0.14–0.80; p = 0.01; Figure 3 A). After transformation, the pooled OR of infusion reaction rate of rituximab was 0.25 (95% CI: 0.13–0.44), which was statistically significant.
Three studies [30, 34, 36] were assessed to analyze the cardiovascular-related event rate of rituximab in MN. Due to an I2 of 0, there was no heterogeneity between the studies. The pooled OR of initial result was 0.04 (95% CI: 0.02–0.12; p < 0.00001; Figure 3 B). After conversion, the pooled OR of rate was 0.04 (95% CI: 0.02–0.11), which was statistically significant.
Five studies [30, 31, 33, 36, 37] reported infection with rituximab treatment of MN. The pooled I2 = 0%, a fixed model was conducted, with no heterogeneity between the reports. The pooled OR of initial result was 0.06 (95% CI: 0.03–0.14; p < 0.00001; Figure 3 C), and after transformation, the pooled OR of rate was 0.06 (95% CI: 0.03–0.12), statistically significant.
Clinical efficacy
Arch Med Sci 2, 1st March / 2023 415
and safety of rituximab with membranous nephropathy: a meta-analysis
Author, year PMID Age [years] Gender Proteinuria [g/day] Serum albumin Serum creatinine [mg/dl] eGFR [ml/min/ 1.73 m2] Cravedi, 2011 21508634 50.1 ±12.3 1 female, 10 male 10.3 (5.8–13.8) 2.1 ±0.6 g/dl 1.1 ±0.4 > 20 Irazabal, 2013 22987142 49.0 ±13.0 3 female, 17 male 11.9 ±4.9 2.7 ±0.6 g/dl 1.5 ±0.5 72.4 ±33.2 Moroni, 2017 27387472 52.8 ±15.2 11 female, 23 male 11.9 ±8.2 2.4 ±0.6 g/dl 1.3 ±0.6 67.2 ±30.8 Bagchi, 2018 29942496 33.3 ±12.3 33.3% were females 6.2 ±2.2 2.5 ±0.5 g/dl 0.9 ±0.3 95.8 ±26.9 Souqiyyeh, 2015 25579715 37.4 ±9.5 Total 25 6.2 ±4.7 34.1 ±6.2 g/dl – 96.1 ±46.1 Ruggenenti, 2006 17699281 51.2 ±13.2 5 female, 4 male 8.9 ±5.3 2.2 ±0.6 mg/dl 1.0 ±0.3 95.6 ±20.3 Wang, 2018 29149305 47.3 ±17.6 6 female, 30 male 12.3 ±5.9 21.9 ±5.8 g/l 2.1 ±1.4 55.7 ±33.9 Aleš Rigler, 2017 28664837 51.2 ±11.8 7 female, 19 male 7.9 ±4.4 – 1.5 ±0.7 80.4 ±43.8 Ruggenenti, 2012 22822077 51.5 ±5.9 28 female, 72 male 9.1 (5.8–12.8) 2.2 ±0.6 g/dl 1.2 (0.97–1.7) 60.0 ±4.0 Ruggenenti, 2003 12819245 52.8 ±19.6 5 female, 3 male 8.6 ±3.9 2.7 ±0.5 mg/dl 1.5 ±0.8 –Fervenza, 2010 20705965 48.6 ±12.9 17 male 3 female 11.9 ±4.9 2.7 ±0.6 g/100 ml 1.5 ±0.5 72.4 ±33.2 Fervenza, 2008 17943078 47.0 ±8.0 5 female, 3 male 13.0 ±5.7 2.3 ±0.6 g/100 ml 1.4 ±0.5 85.2 ±13.6 Beck, 2011 21784898 48.2 ±10.9 5 female, 28 male 12.4 ±5.1 – 1.5 ±0.5 77.9 ±31.3 Cravedi, 2007 17702725 57.0 ±13.0 67% male 10.3 ±8.9 2.3 ±0.8 g/dl 1.4 ±0.5 > 20 Cravedi*, 2007 17702725 55.0 ±15.0 67% male 9.1 ±3.8 2.4 ±0.6 g/dl 1.5 ±0.7 > 20 *Group 2 (rituximab was titrated to circulating B cells).
Table II. Baseline characteristics of included studies
Aleš Rigler A, 2017
Bagchi S, 2018
Beck LH Jr, 2011
Cravedi P, 2011
Cravedi P*, 2007
Cravedi P, 2007
Fervenza FC, 2008
Fervenza FC, 2010
Irazabal MV, 2013
Moroni G, 2017
Ruggenenti P, 2003
Ruggenenti P, 2006
Ruggenenti P, 2012
Souqiyyeh MZ, 2015 Wang X,
Discussion
membranous
Proteinuria is a marker of membranous nephropathy. With 4–120 months of observation, approximately 30–40% of patients can achieve spontaneous complete remission [40, 41]. With optimal supportive care combined with classical immunosuppressive therapy, less than 30% of cases progress to severe renal insufficiency [42–44]. Clinical studies indicate that severe proteinuria is a risk factor for progression of idiopathic membranous nephropathy to end-stage renal disease [45]. Thus, urine protein data are valuable to inform treatment-related decisions [46, 47].
(MN).
overall remission rate of rituximab in MN. B – The remission rate of rituximab in medium-risk group. C – The remission rate of rituximab in high-risk group
Proteinuria is also an indirect indicator of autoimmune activity and disease severity [48]. In this meta-analysis, the included studies were divided into high-risk, medium-risk and low-risk groups according to baseline proteinuria levels. The overall remission rate was 58% (p = 0.003), and the remission rate of the medium-risk and high-risk groups were 56% (p = 0.57) and 59% (p = 0.003), respectively, lower than some prospective studies included [26, 28, 31, 32, 34, 39]. The effective ratio of rituximab in some reports approached 80% [29, 35, 36]. In the randomized controlled trial from Dahan et al. [49], the rate
416 Arch Med Sci 2, 1st March / 2023
Hongzhen Zhong, Hong-Yan Li, Tianbiao Zhou, Zhiqing Zhong
0.01 0.1 1 10 100 Favours [experimental] Favours
[control]
2018 Total (95% CI) –0.49247648 0.48550782 –0.05715841 0.55961579 0.69314718 0.69314718 0.28768207 1.38629436 0.47000363 –0.23638878 0.69314718 0.69314718 0.80562516 0.7537718 –0.33647224 100.0% 0.382707 0.44935852 0.33819977 0.62678317 0.61237244 0.4330127 0.54006172 0.55901699 0.40311289 0.34539578 0.70710678 0.70710678 0.2624798 0.42874646 0.3380617 100.0% 8.0% 5.8% 10.3% 3.0% 3.1% 6.3% 4.0% 3.8% 7.2% 9.9% 2.4% 2.4% 17.1% 6.4% 10.3% 100.0% 0.61 [0.29, 1.29] 1.63 [0.67, 3.92] 0.94 [0.49, 1.83] 1.75 [0.51, 5.98] 2.00 [0.60, 6.64] 2.00 [0.86, 4.67] 1.33 [0.46, 3.84] 4.00 [1.34, 11.96] 1.60 [0.73, 3.53] 0.79 [0.40, 1.55] 2.00 [0.50, 8.00] 2.00 [0.50, 8.00] 2.24 [1.34, 3.74] 2.12 [0.92, 4.92] 0.71 [0.37, 1.39] 1.38 [1.12, 171] Heterogeneity: χ2 = 22.30, df = 14 (p = 0.07), I2 = 37% Test for overall effect: Z = 2.98 (p = 0.003) Study or subgroup Iog [odds ratio] SE Weight Odds ratio IV, fixed, 95% CI Odds ratio IV, fixed, 95% CI Study or subgroup Iog [odds ratio] SE Weight Odds ratio IV, random, 95% CI Odds ratio IV, random, 95% CI Odds ratio IV, fixed, 95% CI Aleš Rigler A, 2017 Bagchi S, 2018 Souqiyyeh MZ, 2015 Total (95% CI) –0.49247648 0.48550782 0.7537718 100.0% 0.382707 0.44935852 0.42874646 100.0% 35.6% 31.6% 32.8% 100.0% 0.61 [0.29, 1.29] 1.63 [0.67, 3.92] 2.12 [0.92, 4.92] 1.25 [0.58, 2.72] 0.01 0.1 1 10 100 Favours [experimental] Favours [control] Heterogeneity: Tau2= 0.29; χ2 = 5.34, df = 2 (p = 0.07); I2 = 63% Test for overall effect: Z = 0.57 (p = 0.57)
Beck LH
Cravedi
Cravedi
Cravedi
Fervenza
Fervenza FC, 2010 Irazabal MV, 2013 Moroni G, 2017 Ruggenenti P, 2003 Ruggenenti P, 2006 Ruggenenti P, 2012 Wang X, 2018 Total (95% CI) –0.05715841 0.55961579 0.69314718 0.69314718 0.28768207 1.38629436 0.47000363 –0.23638878 0.69314718 0.69314718 0.80562516 –0.33647224 100.0% 0.33819977 0.62678317 0.61237244 0.4330127 0.54006172 0.55901699 0.40311289 0.34539578 0.70710678 0.70710678 0.2624798 0.3380617 100.0% 12.9% 3.8% 3.9% 7.9% 5.1% 4.7% 9.1% 12.4% 3.0% 3.0% 21.4% 12.9% 100.0% 0.94 [0.49, 1.83] 1.75 [0.51, 5.98] 2.00 [0.60, 6.64] 2.00 [0.86, 4.67] 1.33 [0.46, 3.84] 4.00 [1.34, 11.96] 1.60 [0.73, 3.53] 0.79 [0.40, 1.55] 2.00 [0.50, 8.00] 2.00 [0.50, 8.00] 2.24 [1.34, 3.74] 0.71 [0.37, 1.39] 1.43 [1.13, 1.82] Heterogeneity: χ2 = 16.53, df = 11 (p = 0.12), I2 = 33% Test for overall effect: Z = 2.96 (p = 0.003) Study or subgroup Iog [odds ratio] SE Weight Odds ratio IV, fixed, 95% CI 0.01 0.1 1 10 100 Favours [experimental] Favours [control] A B C
Figure 2. The efficacy of rituximab in
nephropathy
A – The
Jr, 2011
P, 2011
P*, 2007
P, 2007
FC, 2008
The safety of rituximab in membranous nephropathy (MN). A – The infusion reaction rate of rituximab in MN. B – The cardiovascular related event rate of rituximab in MN. C – The infection rate of rituximab in MN
of CR or PR was 35% in the primary 6-month endpoint, but after an extended median follow-up of 17 months, 64.9% of rituximab-treated patients were in remission. In the prospective study from Aleš Rigler et al. [27], the remission rate was 37.9% following rituximab treatment. They attributed the results to a short follow-up period and low dose of rituximab. Based on this, we conducted another subgroup analysis. The remission rates were 51% (p = 0.72) and 71% (p = 0.07) in 12-month follow-up and 24-month follow-up, respectively. To some extent, the remission rate of rituximab was related to the observation time. Considering the dose administered, the pooled remission rate with rituximab (375 mg/m2 × 4) was 63%, similar to previous reports.
Rituximab is well tolerated in most patients [33]. In our meta-analysis, the most common adverse effects were infusion reaction (25%, p = 0.01); others were infection (6%, p < 0.00001) and cardiovascular events (4%, p < 0.000001). It has also been safer over the past 10 years compared to other immunosuppressive agent treatments for this disease [50, 51]. Rituximab ameliorated proteinuria and had minimal adverse effects on quality of life [52], where patients receiving cyclophosphamide had high-
er rates of hospitalization, liver toxicity, infection, and cardiovascular and thrombotic events [53]. In addition, rituximab can act in a B-cell-independent manner to prevent the disruption of the actin cytoskeleton and podocyte apoptosis [54].
Overall, rituximab is safe and effective alternative treatment. We speculate that the underlying mechanism is that rituximab is a monoclonal antibody that specifically binds to CD20 antigen, blocking the proliferation of B cells and the production of pathogenic antibodies in MN patients. The role of B cells in MN is unknown. B cells play an important role in the immune pathogenesis of glomerulonephritis, but their biological actions still need to be understood in order to determine the time, duration and conditions of the optimal therapeutic response to B cell targeting methods [55]. Furthermore, severe MN may involve spontaneous remission without treatment, and its progression was difficult to predict, which explains the treatment uncertainty that still exists today [44, 56, 57]. Rituximab treatment for the depletion of B cells to reduce urinary protein and promote clearance of autoantibodies [58–61] is still debated based on recent trials and metanalyses. A lack
Clinical
Arch Med Sci 2, 1st March / 2023 417
efficacy and safety of rituximab with membranous nephropathy: a meta-analysis
Study or subgroup Iog [odds ratio] SE Weight Odds ratio IV, random, 95% CI Odds ratio IV, random, 95% CI Cravedi P, 2011 Cravedi P, 2007 Fervenza FC, 2008 Fervenza FC, 2010 Ruggenenti P, 2003 Ruggenenti P, 2012 Total (95% CI) –2.30258509 –1.60943791 0 0.22314355 –1.94591015 –1.75785792 100.0% 1.04880885 0.4472136 0.53452248 0.47434165 1.06904497 0.34240528 100.0% 10.4% 19.9% 18.3% 19.4% 10.2% 21.7% 100.0% 0.10 [0.01, 0.78] 0.20 [0.08, 0.48] 1.00 [0.35, 2.85] 1.25 [0.49, 3.17] 0.14 [0.02, 1.16] 0.17 [0.09, 0.34] 0.33 [0.14, 0.80] 0.01 0.1 1 10 100 Favours [experimental] Favours [control] Heterogeneity: t2 = 0.29; χ2 = 18.94, df = 5 (p = 0.002); I2 = 74% Test for overall effect: Z = 2.47 (p = 0.01) Study or subgroup Iog [odds ratio] SE Weight Odds ratio IV, fixed, 95% CI Odds ratio IV, fixed, 95% CI Fervenza FC, 2010 Moroni G, 2017 Ruggenenti P, 2012 Total (95% CI) –2.77258872 –4.20469262 –2.83321334 100.0% 0.72886899 1.00743505 1.02899151 100.0% 49.4% 25.8% 24.8% 100.0% 0.06 [0.01, 0.26] 0.01 [0.00, 0.11] 0.06 [0.01, 0.44] 0.04 [0.02, 0.12] Heterogeneity: χ2 = 1.46, df = 2 (p = 0.48); I2 = 0% Test for overall effect: Z = 6.17 (p < 0.00001) Study or subgroup Iog [odds ratio] SE Weight Odds ratio IV, fixed, 95% CI Odds ratio IV, fixed, 95% CI Bagchi S, 2018 Fervenza FC, 2008 Fervenza FC, 2010 Moroni G, 2017 Wang X, 2018 Total (95% CI) –3.55534806 –1.79175947 –2.83321334 –2.77258872 –3.55534806 100.0% 1.01418511 0.76376262 1.02899151 0.72886899 1.01418511 100.0% 15.0% 26.4% 14.6% 29.0% 15.0% 100.0% 0.03 [0.00, 0.21] 0.17 [0.04, 0.74] 0.06 [0.01, 0.44] 0.06 [0.01, 0.26] 0.03 [0.00, 0.21] 0.33 [0.14, 0.80] Heterogeneity: χ2 = 2.84, df = 4 (p = 0.58); I2 = 0% Test for overall effect: Z = 7.02 (p < 0.00001) 0.01 0.1 1 10 100 Favours [experimental] Favours [control] 0.01 0.1 1 10 100 Favours [experimental] Favours [control]
A B C
Figure 3.
of response to rituximab treatment may be due to a lack of CD20 molecules in the plasma cell produced antibodies [62]. Therefore, B cell depletion may not be sufficient to maintain sustained remission [27, 30]. Multiple doses and protocols of rituximab have been used in different studies [20]. Some researchers have observed that the half-life of rituximab in MN patients is shorter than with other diseases, and attribute this to the molecular weight of rituximab (145 kDa), which may not be cleared in the urine [63, 64]. Some patients with rheumatoid arthritis [65] and idiopathic membranous nephropathy [49] are resistant to CD20 monoclonal anti-B cells, and this may increase the instability of rituximab in patients with MN.
There were some limitations in the present meta-analysis. Not all included studies were randomized controlled trials, making it more difficult to assess overall efficacy. Second, the number of patients included in our meta-analysis was small. The ideal method to classify membranous nephropathy is based on pathological manifestation, not proteinuria. However, few studies included pathological results, and classifying the severity of MN based on proteinuria is appropriate for clinical applications.
In conclusion, rituximab is a promising, safe and effective alternative treatment for MN. Additional randomized controlled trials of rituximab for MN are needed as well as additional studies on the role of B cells in MN.
Acknowledgments
Hongzhen Zhong and Hong-Yan Li contributed equally to this work and should be regarded as joint first authors.
This study was supported by the Natural Science Foundation of the Guangdong Province (no. 2015A030310386), Guangdong Medical Science and Technology Research Fund Project (no. A2018336), and Guangzhou Medical Key Discipline Construction Project.
Conflict of interest
The authors declare no conflict of interest.
References
1. Shin HS, Cho DH, Kang SK, et al. Patterns of renal disease in South Korea: a 20-year review of a single-center renal biopsy database. Renal Fail 2017, 39: 540-6.
2. Zhou Q, Yang X, Wang M, et al. Changes in the diagnosis of glomerular diseases in east China: a 15-year renal biopsy study. Renal Fail 2018; 40: 657-64.
3. Perkowska-Ptasinska A, Bartczak A, Wagrowska-Danilewicz M, et al. Clinicopathologic correlations of renal pathology in the adult population of Poland. Nephrol Dial Transplant 2017; 32: ii209-18.
4. Maixnerova D, Jancova E, Skibova J, et al. Nationwide biopsy survey of renal diseases in the Czech Republic during the years 1994-2011. J Nephrol 2015; 28: 39-49.
5. Perkowska-Ptasinska A, Deborska-Materkowska D, Bartczak A, et al. Kidney disease in the elderly: biopsy based data from 14 renal centers in Poland. BMC Nephrol 2016; 17: 194.
6. Nationwide and long-term survey of primary glomerulonephritis in Japan as observed in 1,850 biopsied cases. Research Group on Progressive Chronic Renal Disease. Nephron 1999; 82: 205-13.
7. Beck LH Jr, Salant DJ. Membranous nephropathy: from models to man. J Clin Invest 2014; 124: 2307-14.
8. Beck LH Jr, Bonegio RG, Lambeau G, et al. M-type phospholipase A2 receptor as target antigen in idiopathic membranous nephropathy. N Engl J Med 2009; 361: 11-21.
9. Biancone L, Andres G, Ahn H, DeMartino C, Stamenkovic I. Inhibition of the CD40-CD40ligand pathway prevents murine membranous glomerulonephritis. Kidney Int 1995; 48: 458-68.
10. Penny MJ, Boyd RA, Hall BM. Mycophenolate mofetil prevents the induction of active Heymann nephritis: association with Th2 cytokine inhibition. J Am Soc Nephrol 1998; 9: 2272-82.
11. Cohen CD, Calvaresi N, Armelloni S, et al. CD20-positive infiltrates in human membranous glomerulonephritis. J Nephrol 2005; 18: 328-33.
12. Cui Z, Zhao MH. Advances in human antiglomerular basement membrane disease. Nat Rev Nephrol 2011; 7: 697-705.
13. Jennette JC, Falk RJ. Pathogenesis of antineutrophil cytoplasmic autoantibody-mediated disease. Nat Rev Rheumatol 2014; 10: 463-73.
14. Grupper A, Cornell LD, Fervenza FC, Beck LH Jr, Lorenz E, Cosio FG. Recurrent membranous nephropathy after kidney transplantation: treatment and long-term implications. Transplantation 2016; 100: 2710-6.
15. Stahl R, Hoxha E, Fechner K. PLA2R autoantibodies and recurrent membranous nephropathy after transplantation. N Engl J Med 2010; 363: 496-8.
16. Cravedi P, Remuzzi G, Ruggenenti P. Rituximab in primary membranous nephropathy: first-line therapy, why not? Nephron Clin Pract 2014; 128: 261-9.
17. Smith KG, Jones RB, Burns SM, Jayne DR. Long-term comparison of rituximab treatment for refractory systemic lupus erythematosus and vasculitis: remission, relapse, and re-treatment. Arthritis Rheumat 2006; 54: 2970-82.
18. Edwards JC, Szczepanski L, Szechinski J, et al. Efficacy of B-cell-targeted therapy with rituximab in patients with rheumatoid arthritis. N Engl J Med 2004; 350: 2572-81.
19. Zou PM, Li H, Cai JF, Chen ZJ, Li C, Li XW. Therapy of rituximab in idiopathic membranous nephropathy with nephrotic syndrome: a systematic review and meta-analysis. Chinese Med Sci J 2018; 33: 9-19.
20. Cravedi P. Rituximab in membranous nephropathy: not all studies are created equal. Nephron 2017; 135: 46-50.
21. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986; 7: 177-88.
22. Chen YH, Du L, Geng XY, Liu GJ. Implement meta-analysis with non-comparative binary data in RevMan software. Chin J Evid Based Med 2014; 14: 889-96.
23. Sokouti M, Sadeghi R, Pashazadeh S, et al. A systematic review and meta-analysis on the treatment of liver hydatid cyst using meta-MUMS tool: comparing PAIR and laparoscopic procedures. Arch Med Sci 2019; 15: 284-308.
24. Hao JQ, Zhang QK, Zhou YX, Chen LH, Wu PF. Association between circulating leptin concentration and G-2548A gene polymorphism in patients with breast cancer: a meta-analysis. Arch Med Sci 2019; 15: 275-83.
25. Mazidi M, Rezaie P, Banach M on behalf of Lipid and Blood Pressure Meta-analysis Collaboration (LBPMC)
418 Arch Med Sci 2, 1st March / 2023
Hongzhen Zhong, Hong-Yan Li, Tianbiao Zhou, Zhiqing Zhong
Clinical efficacy and safety of rituximab with membranous nephropathy: a meta-analysis
Group. Effect of magnesium supplements on serum C-reactive protein: a systematic review and meta-analysis. Arch Med Sci 2018; 14: 707-16.
26. Souqiyyeh MZ, Shaheen FA, Alsuwaida A, et al. Rituximab as a rescue therapy in patients with glomerulonephritis. Saudi J Kidney Dis Transpl 2015; 26: 47-55.
27. Aleš Rigler A, Jerman A, Orsag A, et al. Rituximab for the treatment of membranous nephropathy: a singlecenter experience. Clin Nephrol 2017; 88: 27-31.
28. Cravedi P, Sghirlanzoni MC, Marasa M, Salerno A, Remuzzi G, Ruggenenti P. Efficacy and safety of rituximab second-line therapy for membranous nephropathy: a prospective, matched-cohort study. Am J Nephrol 2011; 33: 461-8.
29. Irazabal MV, Eirin A, Lieske J, et al. Low- and high-molecular-weight urinary proteins as predictors of response to rituximab in patients with membranous nephropathy: a prospective study. Nephrol Dial Transplant 2013; 28: 137-46.
30. Moroni G, Depetri F, Del Vecchio L, et al. Low-dose rituximab is poorly effective in patients with primary membranous nephropathy. Nephrol Dial Transplant 2017; 32: 1691-6.
31. Bagchi S, Subbiah AK, Bhowmik D, et al. Low-dose rituximab therapy in resistant idiopathic membranous nephropathy: single-center experience. Clin Kidney J 2018; 11: 337-41.
32. Ruggenenti P, Chiurchiu C, Abbate M, et al. Rituximab for idiopathic membranous nephropathy: who can benefit? Clin J Am Soc Nephrol 2006; 1: 738-48.
33. Wang X, Cui Z, Zhang YM, et al. Rituximab for non-responsive idiopathic membranous nephropathy in a Chinese cohort. Nephrol Dial Transplant 2018; 33: 1558-63.
34. Ruggenenti P, Cravedi P, Chianca A, et al. Rituximab in idiopathic membranous nephropathy. J Am Soc Nephrol 2012; 23: 1416-25.
35. Ruggenenti P, Chiurchiu C, Brusegan V, et al. Rituximab in idiopathic membranous nephropathy: a one-year prospective study. J Am Soc Nephrol 2003; 14: 1851-7.
36. Fervenza FC, Abraham RS, Erickson SB, et al. Rituximab therapy in idiopathic membranous nephropathy: a 2-year study. Clin J Am Soc Nephrol 2010; 5: 2188-98.
37. Fervenza FC, Cosio FG, Erickson SB, et al. Rituximab treatment of idiopathic membranous nephropathy. Kidney Int 2008; 73: 117-25.
38. Beck LH Jr, Fervenza FC, Beck DM, et al. Rituximab-induced depletion of anti-PLA2R autoantibodies predicts response in membranous nephropathy. J Am Soc Nephrol 2011; 22: 1543-50.
39. Cravedi P, Ruggenenti P, Sghirlanzoni MC, Remuzzi G. Titrating rituximab to circulating B cells to optimize lymphocytolytic therapy in idiopathic membranous nephropathy. Clin J Am Soc Nephrol 2007; 2: 932-7.
40. Tran TH, Hughes GJ, Greenfeld C, Pham JT. Overview of current and alternative therapies for idiopathic membranous nephropathy. Pharmacotherapy 2015; 35: 396-411.
41. Huh H, Lee H, Lee JP, et al. Factors affecting the longterm outcomes of idiopathic membranous nephropathy. BMC Nephrol 2017; 18: 104.
42. Glassock RJ. Pathogenesis of membranous nephropathy: a new paradigm in evolution. Contrib Nephrol 2013; 181: 131-42.
43. Ronco P, Debiec H. Advances in membranous nephropathy: success stories of a long journey. Clin Exp Pharmacol Physiol 2011; 38: 460-6.
44. Ponticelli C, Glassock RJ. Glomerular diseases: membranous nephropathy – a modern view. Clin J Am Soc Nephrol 2014; 9: 609-16.
45. Shiiki H, Saito T, Nishitani Y, et al. Prognosis and risk factors for idiopathic membranous nephropathy with nephrotic syndrome in Japan. Kidney Int 2004; 65: 1400-7.
46. du Buf-Vereijken PW, Branten AJ, Wetzels JF. Idiopathic membranous nephropathy: outline and rationale of a treatment strategy. Am J Kidney Dis 2005; 46: 1012-29.
47. Cattran D. Management of membranous nephropathy: when and what for treatment. J Am Soc Nephrol 2005; 16: 1188-94.
48. Honkanen E, Tornroth T, Gronhagen-Riska C. Natural history, clinical course and morphological evolution of membranous nephropathy. Nephrol Dial Transpl 1992; 7 Suppl 1: 35-41.
49. Dahan K, Debiec H, Plaisier E, et al. Rituximab for severe membranous nephropathy: a 6-month trial with extended follow-up. J Am Soc Nephrol 2017; 28: 348-58.
50. Gea-Banacloche JC. Rituximab-associated infections. Sem Hematol 2010; 47: 187-98.
51. Tan CS, Koralnik IJ. Progressive multifocal leukoencephalopathy and other disorders caused by JC virus: clinical features and pathogenesis. Lancet Neurol 2010; 9: 425-37.
52. Marasa M, Cravedi P, Ruggiero B, Ruggenenti P. Refractory focal segmental glomerulosclerosis in the adult: complete and sustained remissions of two episodes of nephrotic syndrome after a single dose of rituximab. BMJ Case Rep 2014; 2014: bcr2014205507.
53. van den Brand JA, van Dijk PR, Hofstra JM, Wetzels JF. Long-term outcomes in idiopathic membranous nephropathy using a restrictive treatment strategy. J Am Soc Nephrol 2014; 25: 150-8.
54. Fornoni A, Sageshima J, Wei C, et al. Rituximab targets podocytes in recurrent focal segmental glomerulosclerosis. Sci Transl Med 2011; 3: 85ra46.
55. Hoffman W, Lakkis FG, Chalasani G. B cells, antibodies, and more. Clin J Am Soc Nephrol 2016; 11: 137-54.
56. Godel M, Huber TB. Immunosuppression for membranous nephropathy. Lancet 2013; 381: 2161.
57. Hofstra JM, Fervenza FC, Wetzels JF. Treatment of idiopathic membranous nephropathy. Nat Rev Nephrol 2013; 9: 443-58.
58. Fiorentino M, Tondolo F, Bruno F, et al. Treatment with rituximab in idiopathic membranous nephropathy. Clin Kidney J 2016; 9: 788-93.
59. Cortazar FB, Leaf DE, Owens CT, Laliberte K, Pendergraft WF 3rd, Niles JL. Combination therapy with rituximab, low-dose cyclophosphamide, and prednisone for idiopathic membranous nephropathy: a case series. BMC Nephrol 2017; 18: 44.
60. van den Brand J, Ruggenenti P, Chianca A, et al. Safety of rituximab compared with steroids and cyclophosphamide for idiopathic membranous nephropathy. J Am Soc Nephrol 2017; 28: 2729-37.
61. Katsuno T, Ozaki T, Kim H, et al. Single-dose rituximab therapy for refractory idiopathic membranous nephropathy: a single-center experience. Int Med 2017; 56: 1679-86.
62. Bomback AS, Fervenza FC. Membranous nephropathy: approaches to treatment. Am J Nephrol 2018; 47 Suppl 1: 30-42.
63. Magnasco A, Ravani P, Edefonti A, et al. Rituximab in children with resistant idiopathic nephrotic syndrome. J Am Soc Nephrol 2012; 23: 1117-24.
64. Fogueri U, Cheungapasitporn W, Bourne D, Fervenza FC, Joy MS. Rituximab exhibits altered pharmacokinetics in patients with membranous nephropathy. Ann Pharmacother 2018; 2018: 1060028018803587.
65. Mei HE, Wirries I, Frolich D, et al. A unique population of IgG-expressing plasma cells lacking CD19 is enriched in human bone marrow. Blood 2015; 125: 1739-48
Arch Med Sci 2, 1st March / 2023 419
Dichloroacetate ameliorates myocardial ischemiareperfusion injury via regulating autophagy and glucose homeostasis
Shuo Li1,2, Boqia Xie3, Wenqian Zhang1, Tong Li1
1Department of Thoracic Surgery, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, China
2Department of Thoracic Surgery, The Affiliated Hospital of QingDao University, Qingdao, China
3Department of Cardiology, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, China
Submitted: 13 January 2019; Accepted: 21 July 2019
Online publication: 27 August 2019
Arch Med Sci 2023; 19 (2): 420–429
DOI: https://doi.org/10.5114/aoms.2019.87503
Copyright © 2019 Termedia & Banach
Abstract
Introduction: Autophagy occurs in response to myocardial ischemia-reperfusion (I/R) injury and plays both a protective and detrimental role in this pathological process. Dichloroacetate (DCA) has a protective role during myocardial I/R injury, but its effects on autophagy induction are less well understood. We established a rat myocardial I/R injury model and investigated the effects of DCA on autophagy induction.
Material and methods: Healthy Sprague-Dawley (SD) rats were used to establish a myocardial I/R model. The effect of DCA on cardiac infarct size, cardiac function, and serum levels of serum creatine kinase (CK), lactic dehydrogenase (LDH) and cardiac troponin I (cTnI) during I/R injury were assessed. Using cultured rat cardiac myocytes, we investigated the functional implications of DCA and explored the relevant mechanism(s) of DCA protection during I/R injury.
Results: DCA significantly decreases infarct size and arrhythmia scores, increases heart rate (HR), left ventricular developed pressure (LVDP), the maximal rate of pressure rise (+dp/dtmax) and coronary flow (CF), and reduces the levels of CK, LDH and cTnI after I/R. DCA treatment enhanced myocardial cell viability and alleviated apoptosis assessed through TUNEL assays and Bcl-2/Bax expression. Notably, the levels of the autophagy biomarkers Beclin-1, LC3II and reactive oxygen species (ROS) significantly decreased following DCA treatment. When Bcl-2 was silenced, Beclin-1 expression significantly decreased following DCA treatment, suggesting that DCA confers a protective role during I/R injury through autophagy regulation. Moreover, DCA was found to regulate glucose homeostasis through increasing the expression of Glut-1 and Glut-4.
Conclusions: DCA contributes to I/R injury protection through the regulation of autophagy and glucose homeostasis.
Key words: ischemia-reperfusion injury, dichloroacetate, autophagy, glucose metabolism.
Introduction
Ischemic heart disease is characterized by high morbidity and mortality and is a major cause of death worldwide [1]. Although rapid reperfusion is considered the most effective therapy for myocardial infarction
Corresponding author: Dr. Bo-qia Xie
Department of Cardiology
Beijing Chao-Yang Hospital
Capital University of Medical Science
8 Gongtinan Road
Beijing 100020, China
Phone: +86 10-85231000
Fax: +86 10-85231000
E-mail: dr.boqiaxie@hotmail.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/). Experimental research
Cardiology
Dichloroacetate ameliorates myocardial ischemia-reperfusion injury via regulating autophagy and glucose homeostasis
[2], it can induce injury during the early stages, termed myocardial ischemia/reperfusion (I/R) injury. It was reported that I/R injury disturbs ionic homeostasis, increases the production of reactive oxygen species (ROS) and inflammatory responses, induces mitochondrial disorders, and causes calcium overload [3].
Autophagy is a crucial house-keeping process that controls the degradation of long-lived proteins and damaged organelles, playing a vital role in I/R in the myocardium [4]. Autophagy is induced in response to stress conditions in the heart, including cardiac muscle hypertrophy and heart failure, and is regarded as a prominent feature of cardiovascular dysfunction [5–11]. It has been shown that autophagy exerts a dual function during I/R injury in the myocardium. On one hand, autophagy compensates for mitochondrial injury, providing support to proteostasis and the survival of damaged cardiomyocytes following I/R injury [12–14]. However, sustained autophagy during reperfusion can induce cell death through the digestion of essential proteins and organelles. Matsui et al. indicated that autophagy plays a protective role during ischemia, but can detrimentally affect the heart during reperfusion [15]. Regarding the early reperfusion of ischemic myocardium, a modest increase in autophagy protects against necrocytosis due to the degradation of damaged organelles and the provision of free fatty acids (FFA) and amino acids, but sustained up-regulation of autophagy drives cardiac cell apoptosis and/or injury, leading to cell death. In addition, autophagy is an important regulator of glucose homeostasis. He et al. revealed that autophagy controlled by exercise-induced Bcl-2 is essential for muscle glucose homeostasis, and that Bcl-2-knockout mice fail to increase GLUT4 localization at the plasma membrane, reducing glucose uptake [16]. Roy et al. revealed that TBC1D5 shuttling is dependent on autophagy as it controls the plasma membrane translocation of GLUT1 [17].
It has been reported that dichloroacetate (DCA) activates pyruvate dehydrogenase and stimulates glucose aerobic metabolism in perfused hearts [18, 19]. DCA also reduces oxygen consumption and lactate production [20]. These data demonstrate that DCA ameliorates cardiac dysfunction by depleting lactic acidosis [21]. Stacpoole et al. [22] reported that DCA elevates systolic pressure and cardiac output for those suffering from hypotension and lactic acidosis. Moreover, Burns et al. [23] suggested that DCA stimulates pyruvate dehydrogenase and restores myocardial ATP levels to augment myocardial protection in rat hearts. However, the role of DCA in I/R through its ability to regulate autophagy has not been reported.
In this study, we hypothesized that DCA may alleviate I/R injury through the inhibition of autophagy.
We further investigated the potential mechanism(s) involved in the regulation of autophagy by DCA.
Material and methods
Myocardial ischemia-reperfusion model in vivo
Healthy Sprague-Dawley (SD) rats weighing 250–300 g were purchased from the Institute of Laboratory Animal Sciences, Peking Union Medical College (Beijing, China). Rats were raised individually in plastic cages under conditions of a 12 h light/ dark cycle (temperature at 23 ±1°C; 12 h light/dark cycle, light on at 7 a.m.). Thirty SD rats were randomly divided into three groups: the control group (normal saline), the I/R group (normal saline and I/R) and the I/R + DCA (3 mM) group. Each group consisted of 12 rats. The study group was anesthetized with 3% sodium pentobarbital (i.p.) (60 mg/kg) and treated with heparin (i.p.) (150 U/kg). The rats in the control group underwent a sham operation. Myocardial I/R was produced in rats of the I/R group according to previous studies [24]. Briefly, the BIOPAC multi-guide biometric device was used to test the ECG with needle electrodes installed under the skin. A catheter was inserted into the carotid artery to take blood samples upon completion of the experiment. Following intubation, rats were ventilated mechanically using a rodent ventilator (SAR830, USA). The chest was opened, the pericardium was incised, and the heart was visible. Subsequently, the left anterior descending coronary artery was ligated to perform coronary artery occlusion, which was confirmed by ST segment elevation, an increase in R-wave amplitude and epicardial cyanosis. At 30 min post-occlusion, a snare was used to release the coronary artery occlusion, and the heart was reperfused for 120 min. Additionally, reperfusion was confirmed by the recovery from cyanosis and the inversion of ECG changes [25]. After reperfusion, hearts were separated and stained with 1% (w/v) triphenyl tetrazolium chloride (TTC) to assess infarct size. All procedures were strictly conducted in accordance with the national (D.L.n.26, March 4, 2014) and international regulations and policies (directive 2010/63/EU). This protocol was permitted by the Animal Experimental Ethics Committee, Beijing Chao-Yang Hospital, Capital University of Medical Science.
Evaluation of cardiac function
Arrhythmia was defined and determined based on the criteria of the Lambeth Conventions [26]. ECG recordings were analyzed during the first 30 min of reperfusion for ventricular arrhythmias. Arrhythmias were categorized into 6 groups and their severity scored [27]: 0 = no arrhythmia; 1 = less than 10 s of ventricular tachycardia or oth-
Arch Med Sci 2, 1st March / 2023 421
er arrhythmias, with no ventricular fibrillation (VF); 2 = 11 s to 30 s of ventricular tachycardia or other arrhythmias, with no VF; 3 = 31 s to 90 s of ventricular tachycardia or other arrhythmias, with no VF; 4 = 91 s to 180 s of ventricular tachycardia or other arrhythmias, and/or less than 10 s of reversible VF; 5 = greater than 180 s of ventricular tachycardia or other arrhythmias, and/or greater than 10 s of reversible VF; 6 = irreversible VF. In addition, the heart rate (HR), the left ventricular developed pressure (LVDP), and the maximal rate of pressure rise (+dp/dtmax) were recorded, and the coronary flow (CF) was measured to evaluate cardiac function.
Serum determination
After 120 min of reperfusion, 3 ml of blood was collected through the common carotid artery to detect the levels of serum creatine kinase (CK) (Abcam), lactic dehydrogenase (LDH) (Abcam) and cardiac troponin I (cTnI) (Abcam) by enzyme-linked immunosorbent assay (ELISA). Assays were performed according to the manufacturer’s instructions.
Cardiac myocyte culture
Cardiac myocytes in neonatal rats were isolated and maintained as previously described [28]. Briefly, isolated cells were cultured in serum-free, glucose-free Dulbecco’s modified Eagle’s medium (DMEM) (Thermo Fisher Scientific, Shanghai, China) in the anoxia chamber (95% N2, 5% CO2) at 37°C for 24 h. Reperfusion was then initiated through the replacement of normal culture media containing 10% fetal bovine serum (FBS) (Gibco) in 5% CO2 and 95% O2 for 2 h. At the beginning of the reperfusion, different concentrations of DCA were used to treat cells and were maintained for 12 h. Cells were then harvested for specific assays.
Myocardial cell viability and apoptosis
To gain insight into the role of DCA in cardiac myocytes, cell viability and apoptosis assays were performed. Treated myocardial cells were seeded into 96-well plates at a density of 10,000 cells per hole and viability was assessed via MTT assay. For the assessment of apoptosis, TUNEL staining was performed according to the manufacturer’s instructions. Apoptotic cells were counted in five random visual fields. The percentage of cells undergoing apoptosis was calculated using the following equation: Apoptosis % = number of apoptotic cells/total number of apoptotic cells × 100%.
Reverse transcription-quantitative polymerase chain reaction (RT-qPCR)
RNA isolation from myocardial cells was performed to analyze the expression of Bcl-2 and Bax
at the mRNA level using TaqMan assays (Life Technologies, CA, US). Tests were performed as previously described [29].
Immunofluorescence
For immunofluorescence, cardiac myocytes were first fixed with 4% paraformaldehyde (PFA) for 10 min. Cardiac myocytes were then permeabilized with 0.1% Triton X-100 for 10 min, blocked for 1 h with 1% bovine serum albumin (BSA), and incubated with anti-LC3 antibody (Abcam, dilution 1 : 100) and anti-Beclin-1 antibody (Abcam, dilution 1 : 100) for 12 h at 4°C. After incubation of primary antibodies, cardiac myocytes were incubated with anti-mouse IgG labeled with Alexa Fluor-488 for 1 h at 37°C and then stained with DAPI for 5 min. The immunofluorescence results were assessed under Laser confocal microscopy (Carl ZEISS, Oberkochen, Germany).
Intracellular ROS detection
The myocardium of the left ventricle was sectioned and fixed in 10% formalin, and frozen in liquid nitrogen prior to use. Assays were performed as previously described [30]. ROS positive cells were detected by DCFH-DA (Beyotime, China). Using fluorescence microscopy, cell images were obtained and ROS fluorescence intensity was quantified using Image J software (NIH, Bethesda, Maryland, USA).
siRNA treatment
Hairpin siRNA was used to silence Bcl-2 expression in myocardial cells. siRNA was synthesized by Thermo Fisher. Bcl-2 siRNA: 5′-GGGAGAACAGGGTACGATA-3′, scrambled control siRNA: 5′-GGGAAACGGTGCAGAGATA-3′. Following the transient transfection of myocardial cells with siRNA, cells were incubated under normal conditions. Samples were then prepared for further assays.
Western blot
Total proteins from cultured cells and the left ventricle were extracted according to our protocols. Western blot assays were conducted as previously described. Obtained proteins were incubated with anti-Beclin-1 (1 : 1000, Cell Signaling Technology), anti-Bcl-2 (1 : 1000, Cell Signaling Technology), anti-LC3 (1 : 1000, Cell Signaling Technology), anti-Glut1 (1 : 1000, Abcam) and anti-Glut4 primary antibodies (1 : 100, Abcam).
Statistical analysis
All data analysis was performed using SAS 9.3 software (SAS Institute, USA) and a p-value less than 0.05 was considered statistically significant.
422 Arch Med Sci 2, 1st March / 2023
Shuo Li, Boqia Xie, Wenqian Zhang, Tong Li
Dichloroacetate ameliorates myocardial ischemia-reperfusion injury via regulating autophagy and glucose homeostasis
Normally distributed data with homogeneous variance were expressed as the mean ± standard deviation (SD). A one-way analysis of variance was performed for multiple group comparisons, followed by post-hoc analysis for group-wise comparisons.
Results
Effects of DCA on the myocardial I/R model in vivo

To assess whether DCA can alleviate myocardial I/R injury, we compared the cardiac infarct size,

Figure 1. Evaluation of arrhythmia and myocardial damage indicators in vivo A – TTC staining results of hearts in control, ischemia/reperfusion (I/R) and I/R+ dichloroacetate (DCA) groups (n = 4); B – infarct size of hearts in the three groups (n = 4); C – arrhythmia score changes in the three groups (n = 4); D – heart rate (HF) changes in the three groups (n = 4); E – left ventricular developed pressure (LVDP) changes in the three groups (n = 4); F – the maximal rate of pressure rise (+dp/dtmax) changes in the three groups (n = 4); G – coronary flow (CF) changes in the three groups (n = 4); H – I/R groups display higher creatine kinase (CK) levels compared to the control group (n = 4); I – serum lactic dehydrogenase (LDH) (n = 4); J – serum cardiac troponin I (cTnl) (n = 4). I/R represents ischemia/reperfusion group. Rats in the I/R + DCA group had ischemia/reperfusion and were treated with DCA
**P < 0.01 compared to the control group. ## P < 0.01 compared to the I/R group.

Arch Med Sci 2, 1st March / 2023 423
Control I/R I/R + DCA A B E H I J C F D G Infarct size (%) LVDP [mm Hg] Serum CK [U/l] Serum LDH [U/l] Serum cTnI [pg/ml] Arrhythmia scores +dp/dtmax [mm Hg/s] HR [bpm] CF [ml/min] 60 40 20 0 150 100 50 0 600 400 200 0 400 300 200 100 0 10 8 6 4 2 0 5 4 3 2 1 0 ** ** 2500 2000 1500 1000 500 0 400 300 200 100 0 15 10 5 0 Control I/R I/R + DCA Control I/R I/R + DCA Control I/R I/R + DCA Control I/R I/R + DCA Control I/R I/R + DCA Control I/R I/R + DCA Control I/R I/R + DCA Control I/R I/R + DCA Control I/R I/R + DCA ** ** * ** ** **
cardiac arrhythmia scores, HR, LVDP, +dp/dtmax, CF and serum myocardial injury markers during reperfusion in the three experimental groups. The infarct size in the I/R group was significantly higher than the control group, while DCA significantly reduced the infarct size compared to the I/R group (Figures 1 A, B). Notably, arrhythmia scores in the I/R groups were dramatically higher in comparison to the control group, but treatment with DCA strongly reduced the arrhythmia score, suggesting that it reverses the effects of IR (Figure 1 C). The HR, LVDP, +dp/dtmax, and CF were significantly lower in the I/R group compared to the control group, while they were significantly higher after treatment with DCA compared to the I/R group (Figures 1 D–G). In addition, we also observed an apparent increase in the serum levels of CK, LDH and cTnI in the I/R group, which was reversed by DCA treatment (Figures 1 H–J). Collectively, these results confirmed that DCA exerts a protective role in myocardial I/R models in vivo
the I/R group was lower than the control group (p < 0.01) (Figure 2 A). Notably this effect was reversed by DCA treatment. When the concentration of DCA was 30 μM, cell viability improved (Figure 2 A). When myocardial cell apoptosis was determined by TUNEL assay, the percentage of apoptotic cells in the I/R group was strongly elevated compared to the control group. It was noteworthy that DCA treatment reversed these effects and 30 μM DCA significantly alleviated cell apoptosis (Figure 2 B). In addition, when the expression of Bcl-2 and Bax was assessed at the mRNA level, qRT-PCR assays indicated that the Bcl-2/Bax ratio in the I/R group was strongly down-regulated, whilst DCA recovered the Bcl-2/Bax ratio (Figure 2 C). Taken together, these observations demonstrate that DCA promotes cell viability and inhibits apoptosis following I/R.
DCA attenuates I/R injury by suppressing reperfusion-induced autophagy
In vitro effects of DCA on myocardial cell viability and apoptosis
We next determined the viability of myocardial cells in vitro through MTT assays. Treated cells were divided into control, I/R, and I/R + DCA groups. The results showed that cell viability in
To explore the role of DCA in the regulation of autophagy, we analyzed its effects on Beclin-1 and LC3-II expression, considered reliable autophagy biomarkers. Western blot analysis indicated that Beclin-1 level (p < 0.05, Figures 3 A, B) and the ratio of LC3-II/LC3-I (p < 0.05, Figures 3 A, C) were significantly higher in the I/R group in comparison to A
B
Figure 2. Effects of dichloroacetate (DCA) on myocardial cell viability and apoptosis in vitro A – Cell viability was determined by MTT assays in the six groups (n = 4); B – effects of DCA on cell apoptosis induced by ischemia/reperfusion (I/R) assessed through TUNEL staining (n = 4); C – expression of Bcl/Bax in each group (n = 4).
**P < 0.01 compared to control group; ##p < 0.01 compared to the I/R group.
424 Arch Med Sci 2, 1st March / 2023
Shuo Li, Boqia Xie, Wenqian Zhang, Tong Li
C
MTT reduction (OD/mg wet wt) Cell apoptosis (%) Ratio of Bcl-2/Bax 0.8 0.6 0.4 0.2 0 25 20 15 10 5 0 1.5 1.0 0.5 0 Control I/R IR + IR + IR + IR + 10 µM 30 µM 50 µM 100 µM DCA DCA DCA DCA Control I/R IR + IR + IR + IR + 10 µM 30 µM 50 µM 100 µM DCA DCA DCA DCA Control I/R IR + IR + IR + IR + 10 µM 30 µM 50 µM 100 µM DCA DCA DCA DCA
Dichloroacetate ameliorates myocardial ischemia-reperfusion injury via regulating autophagy and glucose homeostasis
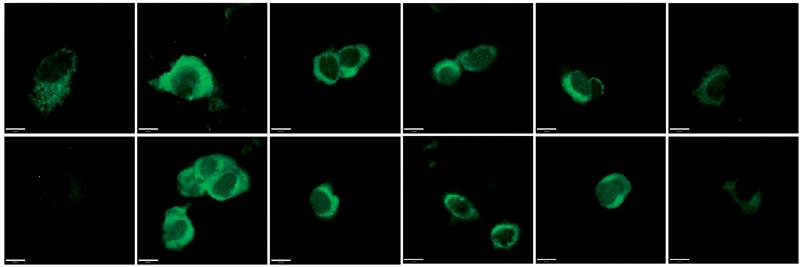
Figure 3. Dichloroacetate (DCA) attenuates ischemia/reperfusion (I/R) injury by suppressing reperfusion-induced autophagy. A – Western blot analysis of LC3-II/LC3-I and Beclin-1 following DCA treatment (n = 4); B – relative expression of LC3-II/LC3-I (n = 4); C – Beclin-1 expression was determined by western blot (n = 4); D – LC3, E – Beclin-1 mRNA levels in the six groups (n = 4); F – immunofluorescence results of LC3 and Beclin-1 in the six groups (n = 4) *P < 0.05 compared to control group. #P < 0.05 compared to I/R group. ##P < 0.01 compared to I/R group.
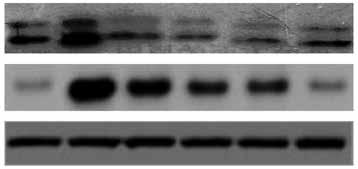
Arch Med Sci 2, 1st March / 2023 425
Control I/R IR + IR + IR + IR + 10 µM 30 µM 50 µM 100 µM DCA DCA DCA DCA LC3-I LC3-II Beclin-1 b-actin B C E F D A Protein expression of LC3-II/LC-I Protein expression of Beclin-1 mRNA expression of Beclin-1 mRNA expression of LC3 4 3 2 1 0 2.5 2.0 1.5 1.0 0.5 0 4 3 2 1 0 2.5 2.0 1.5 1.0 0.5 0 Control I/R IR + IR + IR + IR + 10 µM 30 µM 50 µM 100 µM DCA DCA DCA DCA Control I/R IR + IR + IR + IR + 10 µM 30 µM 50 µM 100 µM DCA DCA DCA DCA Control I/R IR + IR + IR + IR + 10 µM 30 µM 50 µM 100 µM DCA DCA DCA DCA Control I/R IR + 10 µM DCA IR + 30 µM DCA IR + 50 µM DCA IR + 100 µM DCA Control I/R IR + IR + IR + IR + 10 µM 30 µM 50 µM 100 µM DCA DCA DCA DCA LC3 Beclin-1
the control group. Conversely, this effect was significantly inhibited in a concentration-dependent manner by DCA treatment (Figures 3 A–C). These findings were confirmed at the mRNA level through qRT-PCR (Figures 3 D, E). In addition, the immunofluorescence results also showed that the expression of LC3 and Beclin-1 increased in the I/R group and decreased in the DCA treated group (Figure 3 F). Collectively, these results revealed that DCA inhibits reperfusion-induced autophagy through the down-regulation of potential indicators.
Effects of DCA on autophagy through ROS and Bcl-2
It has been reported that ROS accumulation drives the oxidative destruction of DNA, proteins and lipids, triggering cell damage and apoptosis [24]. ROS accumulation is also essential for autophagy induction under conditions of starvation or stress [25]. To assess the effects of ROS in the DCA-mediated inhibition of autophagy, we assessed the levels of ROS in myocardial cells using DCFH-DA. The results showed that ROS production increased after I/R, which was significantly reduced by DCA (Figure 4 A). These effects were
lost following treatment with N-acetyl-l-cysteine (NAC), a classical ROS inhibitor.
Hairpin siRNA was used to silence Bcl-2 and western blot analysis revealed that Beclin-1 expression decreased following DCA treatment. A significant difference in the LC3-II/LC3-I levels following Bcl-2 knock-down was not observed (Figures 4 B, C). These observations suggest that ROS and Bcl-2 contribute to DCA-mediated autophagy inhibition.
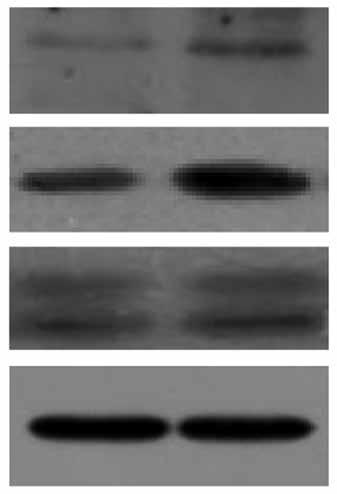
Effects of DCA on myocardial glucose homeostasis in vivo
We finally assessed the effects of DCA on myocardial glucose homeostasis after reperfusion in vivo. Data from both western blot and qRT-PCR assays revealed upregulation of Glut-1 and Glut-4 at both the protein and mRNA level in left ventricular tissue following DCA treatment Figures 5 A–E. This suggested that DCA promotes glucose uptake.
Discussion
Ischemic heart disease involving myocardial infarction leads to serious health issues. Rapid reper-
Figure 4. Effects of dichloroacetate (DCA) on autophagy through reactive oxygen species (ROS) and Bcl-2. A – ROS generation was detected by DCFH-DA in myocardial cells (n = 4); B – expression levels of Bcl-2, LC3-II/LC3-I and Beclin-1 after Bcl-2 siRNA silencing in ischemia/reperfusion (I/R) + DCA groups (n = 4); C – band intensities from western blots were calculated and normalized to GAPDH levels (n = 4). Protein expression is expressed as the fold change relative to experimental controls *P < 0.1, **p < 0.01.
426 Arch Med Sci 2, 1st March / 2023
Shuo Li, Boqia Xie, Wenqian Zhang, Tong Li
A
C Mean fluorescence intensity Relative protein expression to GAPDH 250 200 150 100 50 0 0.8 0.6 0.4 0.2 0
B
Control I/R IR + IR + IR + IR + IR + 10 µM 30 µM 50 µM 100 µM DCA + DCA DCA DCA DCA NAC Bcl-2
LC3-II/LC3-I siRNA-Bcl-2 Control I/R + DCA + + siRNA-Bcl-2 + –Bcl-2 Beclin LC3-I LC3-II GAPDH
Beclin
Dichloroacetate ameliorates myocardial ischemia-reperfusion injury via regulating autophagy and glucose homeostasis
fusion of the ischemic myocardium remains the fundamental therapy for myocardial infarction [2]. Importantly, an additional injury, termed myocardial I/R, occurs during the initial period. DCA can activate pyruvate dehydrogenase and improves cardiac function [31]. In this study, we explored the functional implications of DCA after I/R injury in vitro and in vivo and identified a protective role of DCA against reperfusion injury through the modulation of autophagy and glucose homeostasis.
Autophagy is an intracellular bulk degradation process that has the capacity to degrade and recycle cytosolic and long-lived proteins and organelles [4, 32, 33]. Autophagy occurs at low levels and is enhanced by stressors such as nutrient depletion [34]. Recent studies have shown that autophagy has both beneficial and adaptive roles depending
on the context and its magnitude of induction [35]. Autophagy is also implicated in I/R injury. At low levels, autophagy can prevent cell injury following I/R. In high concentrations or through sustained up-regulation, autophagy can promote cardiac cell apoptosis or cell injury through Beclin-1 [36]. This study indicated that DCA improves cardiac function, increases cell viability and inhibits apoptosis. Furthermore, the first evidence that DCA can inhibit Beclin-1 expression and influence the LC3-II/ LC3-I ratio is provided, suggesting that DCA reduces autophagy induction during the reperfusion period.
Growing evidence demonstrates that ROS-activated autophagy occurs during myocardial reperfusion [37, 38]. ROS functions as an essential signaling molecule that modulates a series of biological processes, including gene expression,
*P < 0.05 compared to the control group. **P < 0.01 compared to the control group.
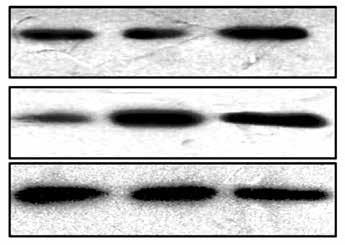
Arch Med Sci 2, 1st March / 2023 427
Protein expression of Glut-1 Protein expression of Glut-4 mRNA expression of Glut-1 mRNA expression of Glut-4 0.6 0.4 0.2 0 4 3 2 1 0 0.8 0.6 0.4 0.2 0 3 2 1 0 Control I/R i/R + DCA Control I/R i/R + DCA Control I/R i/R + DCA Control I/R i/R + DCA Control I/R I/R + DCA Glut-1 Glut-4 b-actin A B D C E
Figure 5. Effects of dichloroacetate (DCA) on myocardial glucose homeostasis in vivo. Glut-1 (A, B) and Glut-4 (A, C) expression levels were detected by western blot analysis in the three groups. Glut-1 (D) and Glut-4 (E) mRNA levels were also determined by RT-PCR (n = 4)
cell metabolism, growth and survival. However, excessive ROS is detrimental to cellular homeostasis, leading to cell damage and apoptosis [24, 39]. It has been reported that autophagy is upregulated through ROS accumulation during myocardial reperfusion. In this study, we found that DCA treatment strongly inhibited ROS production during myocardial reperfusion, but NAC (an ROS inhibitor) had the capacity to abolish this effect. Combined with the aforementioned data, these results indicate that ROS contributes to DCA-mediated autophagy inhibition, promoting myocardial cell protection during the reperfusion period.
It has been demonstrated that Bcl-2 is involved in apoptotic signaling. Interestingly, Bcl-2 family members regulate a variety of biological effects, including morphogenesis, glucose homeostasis, and autophagy [16, 40, 41]. Moreover, previous studies have shown that Bcl-2 decreases the levels of starvation-induced autophagy in vitro and in vivo, indicating its key role in autophagy regulation [42, 43]. In this in-vitro study, DCA significantly alleviated apoptosis by up-regulation of the Bcl-2/Bax ratio. Following Bcl-2 silencing, Beclin-1 was inhibited by DCA treatment, suggesting that it contributes to the ability of DCA to regulate autophagy. We also found that Bcl-2 silencing does not influence the LC3-II/LC3-I ratio, a finding that warrants further investigation.
It was recently reported that myocardial efficiency is reduced when the levels of FFA are elevated [44, 45]. We therefore predict that myocardial glucose abundance decreases oxygen consumption to improve myocardial efficiency. In addition, autophagy regulates glucose homeostasis [16]. We found that DCA dramatically enhanced Glut-1 and Glut-4 expression, raising the possibility that DCA represses autophagy to improve myocardial energy metabolism.
In conclusion, DCA regulates autophagy and glucose homeostasis to improve I/R injury. Importantly, we revealed the utility of DCA as a therapeutic strategy for I/R injury.
Acknowledgments
Shuo Li and Boqia Xie contributed equally to this article.
This study was supported by the National Natural Science Foundation of China (grant number 81400268).
Conflict of interest
The authors declare no conflict of interest.
in mice with myocardial ischemia/reperfusion injury through AMPK activation-mediated mitochondrial fission. Sci Rep 2016; 6: 37114.
2. Guo J, Wang SB, Yuan TY, et al. Coptisine protects rat heart against myocardial ischemia/reperfusion injury by suppressing myocardial apoptosis and inflammation. Atherosclerosis 2013; 231: 384-91.
3. Bystrom P, Foley N, Toledo-Pereyra L, et al. Ischemic preconditioning modulates ROS to confer protection in liver ischemia and reperfusion. EXCLI J 2017; 16: 483.
4. Thapalia BA, Zhou Z, Lin X. Autophagy, a process within reperfusion injury: an update. Int J Clin Exp Pathol 2014; 7: 8322-41.
5. Jensen BC, Bultman SJ, Holley D, et al. Upregulation of autophagy genes and the unfolded protein response in human heart failure. Int J Clin Exp Med 2017; 10: 1051-8.
6. Ren J, Sowers J R, Zhang Y. Metabolic stress, autophagy, and cardiovascular aging: from pathophysiology to therapeutics. Trends Endocrinol Metab 2018; 29: 699-711.
7. Miyata S, Takemura G, Kawase Y, et al. Autophagic cardiomyocyte death in cardiomyopathic hamsters and its prevention by granulocyte colony-stimulating factor. Am J Pathol 2006; 168: 386-97.
8. Li Z, Wang J, Yang X. Functions of autophagy in pathological cardiac hypertrophy. Int J Biol Sci 2015; 11: 672-8.
9. Shimomura H, Terasaki F, Hayashi T, Kitaura Y, Isomura T, Suma H. Autophagic degeneration as a possible mechanism of myocardial cell death in dilated cardiomyopathy. Jpn Circ J 2001; 65: 965-8.
10. Zhu H, Tannous P, Johnstone JL, et al. Cardiac autophagy is a maladaptive response to hemodynamic stress. J Clin Invest 2007; 117: 1782-93.
11. Ma S, Wang Y, Chen Y, Cao F. The role of the autophagy in myocardial ischemia/reperfusion injury. Biochim Biophys Acta 2015; 1852: 271-6.
12. Tannous P, Zhu H, Nemchenko A, et al. Intracellular protein aggregation is a proximal trigger of cardiomyocyte autophagy. Circulation 2008; 117: 3070-8.
13. Quinsay MN, Thomas RL, Lee Y, Gustafsson AB. Bnip3mediated mitochondrial autophagy is independent of the mitochondrial permeability transition pore. Autophagy 2010; 6: 855-62.
14. Ma X, Liu H, Foyil SR, Godar RJ, Weinheimer CJ, Diwan A. Autophagy is impaired in cardiac ischemia-reperfusion injury. Autophagy 2012; 8: 1394-6.
15. Matsui Y, Takagi H, Qu X, et al. Distinct roles of autophagy in the heart during ischemia and reperfusion roles of AMP-activated protein kinase and beclin 1 in mediating autophagy. Circ Res 2007; 100: 914-22.
16. He C, Bassik MC, Moresi V, et al. Exercise-induced BCL2regulated autophagy is required for muscle glucose homeostasis. Nature 2012; 481: 511-5.
17. Roy S, Leidal AM, Ye J, Ronen SM, Debnath J. Autophagy-dependent shuttling of TBC1D5 controls plasma membrane translocation of GLUT1 and glucose uptake. Mol Cell 2017; 67: 84-95.e5.
18. Jaimes R, Kuzmiak-Glancy S, Brooks DM, et al. Functional response of the isolated, perfused normoxic heart to pyruvate dehydrogenase activation by dichloroacetate and pyruvate. Pflügers Archiv 2016; 468: 131-42.
19. Kato T, Niizuma S, Inuzuka Y, et al. Analysis of metabolic remodeling in compensated left ventricular hypertrophy and heart failure. Circ Heart Fail 2010; 3: 420-30.
References
1. Fang L, Fan X, Yu Z, et al. Cardioprotection by combination of three compounds from ShengMai preparations
20. Niewisch MR, Kuçi Z, Wolburg H, et al. Influence of dichloroacetate (DCA) on lactate production and oxygen consumption in neuroblastoma cells: is DCA a suitable
428 Arch Med Sci 2, 1st March / 2023
Shuo Li, Boqia Xie, Wenqian Zhang, Tong Li
Dichloroacetate ameliorates myocardial ischemia-reperfusion injury via regulating autophagy and glucose homeostasis
drug for neuroblastoma therapy?. Cell Physiol Biochem 2012; 29: 373-80.
21. Barbee RW, Kline JA, Watts JA. Depletion of lactate by dichloroacetate reduces cardiac efficiency after hemorrhagic shock. Shock 2000; 14: 208-14.
22. Stacpoole PW, Barnes CL, Hurbanis MD, Cannon SL, Kerr DS. Treatment of congenital lactic acidosis with dichloroacetate. Arch Dis Child 1997; 77: 535-41.
23. Burns AH, Giaimo ME, Summer WR. Dichloroacetic acid improves in vitro myocardial function following in vivo endotoxin administration. J Crit Care 1986; 1: 11-7.
24. Ran X, Diao JX, Sun XG, et al. Huangzhi oral liquid prevents arrhythmias by upregulating caspase-3 and apoptosis network proteins in myocardial ischemia-reperfusion injury in rats. Evid Based Complement Alternat Med 2015; 2015: 518926.
25. Himori N, Matsuura A. A simple technique for occlusion and reperfusion of coronary artery in conscious rats. Am J Physiol 1989; 256: 1719-25.
26. Walker MJA, Curtis MJ, Hearse DJ, et al. The Lambeth conventions: guidelines for the study of arrhythmias in ischaemia, infarction, and reperfusion. Cardiovasc Res 1988; 22: 447-55.
27. Cai HB, Sun XG, Liu ZF, et al. Effects of dahuangzhechong pills on cytokines and mitogen activated protein kinase activation in rats with hepatic fibrosis. J Ethnopharmacol 2010; 132: 157-64.
28. Kang JX, Xiao YF, Leaf A. Free, long-chain, polyunsaturated fatty acids reduce membrane electrical excitability in neonatal rat cardiac myocytes. Proc Natl Acad Sci USA 1995; 92: 3997-4001.
29. Stather PW, Sylvius N, Wild JB, Choke E, Sayers RD, Bown MJ. Differential microRNA expression profiles in peripheral arterial disease. Cir Cardiovasc Genet 2013; 6: 490-7.
30. Tao R, Kim SH, Honbo N, Karliner JS, Alano CC. Minocycline protects cardiac myocytes against simulated ischemia-reperfusion injury by inhibiting poly(ADP-ribose) polymerase-1. J Cardiovasc Pharmacol 2010; 56: 659-68.
31. Piao L, Fang YH, Kubler MM, et al. Enhanced pyruvate dehydrogenase activity improves cardiac outcomes in a murine model of cardiac arrest. PLoS One 2017; 12: e0185046.
32. Bai Y, Chen Y, Chen X, et al. Trichostatin A activates FOXO1 and induces autophagy in osteosarcoma. Arch Med Sci 2019; 15: 204-13.
33. Pandurangan AK, Ismail S, Esa NM, et al. Inositol-6 phosphate inhibits the mTOR pathway and induces autophagy-mediated death in HT-29 colon cancer cells. Arch Med Sci 2018; 14: 1281-8.
34. Lum JJ, Deberardinis RJ, Thompson CB. Autophagy in metazoans: cell survival in the land of plenty. Nat Rev Mol Cell Biol 2005; 6: 439-48.
35. Schiattarella GG, Hill JA. Therapeutic targeting of autophagy in cardiovascular disease. J Mol Cell Cardiol 2015; 95: 86-93.
36. Munasinghe PE, Riu F, Dixit P, et al. Type-2 diabetes increases autophagy in the human heart through promotion of Beclin-1 mediated pathway. Int J Cardiol 2016; 202: 13-20.
37. Xu A, Szczepanek K, Maceyka MW, et al. Transient complex I inhibition at the onset of reperfusion by extracellular acidification decreases cardiac injury. Am J Physiol Cell Physiol 2014; 306: 1142-53.
38. Godar RJ, Ma X, Liu H, et al. Repetitive stimulation of autophagy-lysosome machinery by intermittent fasting
preconditions the myocardium to ischemia-reperfusion injury. Autophagy 2015; 11: 1537-60.
39. Dunn JD, Alvarez LA, Zhang X, Soldati T. Reactive oxygen species and mitochondria: a nexus of cellular homeostasis. Redox Biol 2015; 6: 472-85.
40. Danial NN, Korsmeyer SJ. Cell death: critical control points. Cell 2004; 116: 205-19.
41. Cleland MM, Norris KL, Karbowski M, et al. Bcl-2 family interaction with the mitochondrial morphogenesis machinery. Cell Death Differ 2011; 18: 235-47.
42. Levine B, Yuan J. Autophagy in cell death: an innocent convict? J Clin Invest 2005; 115: 2679-88.
43. Pattingre S, Tassa A, Qu X, et al. Bcl-2 antiapoptotic proteins inhibit beclin 1-dependent autophagy. Cell 2005; 122: 927-39.
44. Ma P, Han L, Lv Z, et al. In-hospital free fatty acids levels predict the severity of myocardial ischemia of acute coronary syndrome. BMC Cardiovasc Disord 2016; 16: 29.
45. Wang Y, Zhang HW, Guo YL, et al. Free fatty acids as a marker for predicting periprocedural myocardial injury after coronary intervention. Postgrad Med J 2019; 95: 18-22.
Arch Med Sci 2, 1st March / 2023 429
Experimental research
Obstetrics and Gynecology
Mechanisms underlying the improvement of preeclampsia through salvianolic acid B-regulated miRNA-155/CXCR4
Chuanlian Zhang1, Xue Han2, Xiaoxue Wang2
1Department of Obstetric Nursing, Linyi Central Hospital, Linyi Shandong, China
2Department of Ultrasonics, Linyi Central Hospital, Linyi Shandong, China
Submitted: 12 May 2019; Accepted: 21 July 2019
Online publication: 12 February 2020
Arch Med Sci 2023; 19 (2): 430–447
DOI: https://doi.org/10.5114/aoms.2020.92938
Copyright © 2020 Termedia & Banach
Abstract
Introduction: The aim of this study was to evaluate the effects and mechanisms of salvianolic acid B (Sal B) in preeclampsia treatment by in vivo and in vitro study.
Material and methods: Rats were randomly divided into 5 groups. In order to establish the model of preeclampsia, endotoxin was administered to the rats in the Sal B intervention and model groups. The systolic blood pressure (SBP) of the tail artery and urine protein concentration were observed at different points, the miRNA-155 and CXCR4 gene expression levels by RTPCR and the CXCR4 and p-AKT protein expression by WB assay. Using HTR8/ SVneo to explain the mechanisms; evaluating the miRNA-155 and CXCR4 mRNA expression by RT-PCR assay, measuring the cell invasion and migration by transwell and wound healing assay in different groups; evaluating the CXCR4 and p-AKT protein expression by WB assay and p-AKT nucleation volume by cellular immunofluorescence were evaluated.
Results: Compared with the normal group, the systolic blood pressure and urine protein were significantly increased in the model group ( p < 0.05), serum NO concentration was significantly down-regulated (all p < 0.05), CXCR4 and miRNA-155 mRNA expression was significantly different and CXCR4 and p-AKT protein expression was significantly suppressed (all p < 0.05). With Sal B supplement, the SBP, urine protein and NO concentration were significantly improved with dose-dependent (all p < 0.05). In the cell experiment, the cell invasion and migration ability were significantly improved with Sal B supplement (both p < 0.05). However, with miRNA-155 transfection, the cell invasion and migration ability were suppressed with Sal B treatment (both p < 0.05).
Conclusions: Sal B improved preeclampsia via regulation of miRNA-155/ CXCR4 in the in vitro and vivo study.
Key words: Sal B, preeclampsia, HTR8/SVneo cell, miRNA-155, CXCR4, p-AKT, Salvia miltiorrhiza.
Introduction
Preeclampsia (PE) is a type of hypertension specific to human pregnancy, with an incidence of 2% to 7%. PE is primarily clinically manifested as an increase in urinary protein and blood pressure after 20 weeks of gestation [1], and represents one of the main etiologies for maternal and perinatal morbidity and mortality. The high-risk factors for
Corresponding author: Xiaoxue Wang
Department of Ultrasonics Linyi Central Hospital
Linyi Shandong
276400, China
E-mail: wangxiaoxue190318@163. com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Mechanisms underlying the improvement of preeclampsia through salvianolic acid B-regulated miRNA-155/CXCR4
PE include primiparity age over 40 years, obesity, diabetes mellitus, assisted reproductive conception, a family history of PE, multiple pregnancies, a previous pregnancy of PE and chronic hypertension [2]. To date, the mechanisms of pathogenesis underlying PE remain unclear. MicroRNAs (miRNAs) are a group of single-stranded non-coding small RNA molecules that are 18–23 nucleotides in length. Accumulating studies in recent years have shown that some miRNAs are abnormally expressed when PE occurs; one of them is miR-155 [3–5]. Abnormal expression levels of miRNA-155 may be closely associated with the development of such dysfunctions as trophoblast invasion and migration [6], whereas the specific molecular mechanisms still warrant more explorations and studies. As a G protein-coupled receptor, CXCR4 is expressed in the villus tissue throughout pregnancy. After binding to its ligand, CXCR4 can activate the downstream PI3K/AKT signaling pathway to affect the expression levels of genes within cells, thereby regulating the invasion and migration of the trophoblasts within the human villus tissues in early pregnancy [7, 8].
Salvianolic acid B (Sal B) is an aqueous bioactive component in Salvia miltiorrhiza, and a polyphenolic compound highly abundant within this plant. Sal B has the molecular formula of C36H30O16, an important water-soluble active ingredient in Salvia miltiorrhiza, and possesses most of the biological activity of Salvia miltiorrhiza [9]. Studies have shown that Sal B has been extensively used in various diseases, such as angina pectoris, pulmonary fibrosis and malignancies [10–12]. Sal B is most commonly used for treatment of cardiovascular disease, such as myocardial infarction and heart failure [9, 13, 14]; however, the roles of Sal B in improving PE and related mechanisms underlying it remain elusive.
Herein, we for the first time explored the efficacy of Sal B in PE through in vivo experiments, and initially investigated the roles of miRNA-155/ CXCR4 in it; then, we validated the relevant mechanisms of action through cell experiments. By doing so, we investigated the mechanisms of action of Sal B in improving PE, and provided a solid experimental basis for the clinical treatment of PE.
Material and methods Materials
Sal B was purchased from MCE (MedChemExpress, USA), and endotoxin from Sigma, USA, with a purity of 99.9%; the NO kit was a product from Shanghai Yanjing Biotechnology Co., Ltd., early pregnancy human extravillous trophoblast HTR8/ SVneo from the Cell bank, Chinese Academy of Science, and fetal bovine serum and RPMI1640 me-
dium from Gibco, USA. miR-155 mimics, negative control (NC), miRNA-155 inhibitor and miRNA-155 inhibitor negative control (miRNA-155 inhibitor NC) were designed and synthesized by Shanghai Gene Pharma Co., Ltd., China. The sequences of miRNA-155 mimics (5′ to 3′) were: sense: UUAUGCUAAUCGUGAUAGGGGU; antisense: CCCUAUCACGAUUAGCAUUAAUU; the sequence of miRNA-155 inhibitor (5′ to 3′) was ACCCCUAUCACGAUUAGCAUUAA; the sequences of NC (5′ to 3′) were: sense: UUCUCCGAACGUGUCACGUTT; antisense: ACGUGACACGUUCGGAGAATT; and the sequence of miRNA-155 inhibitor NC (5′ to 3′) was CAGUACUUUUGUGUAGUACAA. The following materials were used: RPMI1640 medium (Hyclone), OptiMEM medium (Gibco), fetal bovine serum (FBS, Hangzhou Evergreen), trypsin (Geneview), transfection reagent Lipofectamine 2000 and Trizol (Invitrogen), RNA reverse transcription kit, SYBR green fluorescence Dye (Toyobo), Real-time PCR System, Transwell Chamber (BD Biosciences), protein concentration assay kit (Beijing CW Century Co., Ltd.), protein marker molecular marker (Geneview), rabbit anti-human CXCR4 monoclonal antibody, rabbit anti-human p-AKT monoclonal antibody, and rat anti-human b-actin monoclonal antibody (Abcam).
Experimental methods
Establishment and grouping of PE models
SD rats of clean grade with a body weight of 200–250 g were fed in a standard clean environment. The experiment was conducted in strict accordance with the National Institutes of Health (NIH) guidelines for feeding and use of laboratory animals. The male and female rats were housed in separate cages at a ratio of 2 : 1, with the finding of a vaginal plug as the 1st day of pregnancy. A total of 60 female rats were randomized to 5 groups, with 12 rats in each group. In addition to the normal group, the rats in the drug groups (low-, medium-, and high-dose groups) and the model control group were intravenously instilled with endotoxin 1.0 μg/(kg·d) at 2 ml/h at the 14th day of pregnancy for 4 days, and the rats in the blank control group were given normal saline of an equal dose. The conditions for H/R were hypoxia at 37°C with 2% O2 and 5% CO2 for 2 h, and reoxygenation at 37°C with 20% O2 and 5% CO2 for 6 h [15].
Methods of administration
From the 14th to the 21st day of pregnancy, the rats in the low-, medium- and high-dose drug groups were intraperitoneally injected with different concentrations of Sal B injection (20.0, 40.0, and 80.0 mg/kg), and the rats in the blank control and model control groups were administered nor-
Arch Med Sci 2, 1st March / 2023 431
Chuanlian Zhang, Xue Han, Xiaoxue Wang
mal saline of an equal dose until the 21st day of pregnancy.
Indicators for detection
The blood pressure of the tail artery, the content of 24 h urine protein and the concentration of plasma NO were monitored on the 19th and 21st days of pregnancy, respectively. 1) Test of blood pressure of the tail artery: the blood pressure of the rats’ tail artery was measured by means of the multi-channel non-invasive pressure measurement system. The rat was fixed in an incubator at 30°C for about 10 min, and the probe was fixed. The blood flow was blocked by the pressure increased by the tail compression sleeve until the blood flow of the tail artery had been blocked and the pulse wave had disappeared. After 3 to 5 s, the software was turned on and the external pressure was gradually decreased until the arterial pulsation appeared, at which time the blood pressure was recorded as systolic blood pressure of the experimental animal. Each rat was measured repeatedly 6 times at an interval of 2 min, with the mean value used. 2) Content of 24 h urine protein: the 24 h urine of the rat was collected, and the concentration of urine protein was determined through colorimetry. 3) Concentration of the plasma NO: 5 ml of blood from the abdominal aorta was collected and centrifuged, with the supernatant taken for use. The absorbance value of the supernatant was measured using the nitrate reductase method and converted to the concentration of NO.
HE staining
The placental tissues were removed, partially fixed in 4% paraformaldehyde for 24 h, embedded in paraffin, and sectioned (4 μm). The placental tissues underwent HE staining for pathological examination.
Total RNA extraction, reverse transcription and amplification
The placental tissues or cells were taken out from the rats and subjected to extraction of total RNA using the Trizol method, and the concentrations and purity of RNA in all groups were determined. 2 μg of RNA was reverse transcribed into cDNA, with the volume of the reverse transcription system being 20 μl. Amplification was performed after reverse transcription, with 3 replicate wells set in each group. Primers were synthesized by Shanghai Sangon Biotechnology Co., Ltd., and the primer sequences were as follows:
CXCR-4 F: 5′-ACTACACCGAGGAAATGGGCT-3′; R:
5′-CCCACAATGCCAGTTAAGAAGA-3′ ; b-actin F: 5′-GGGAAATCGTGCGTGACATTAAGG-3′; R: 5′-CAG-
GAAGGAAGGCTGGAAGAGTG-3′. miRNA-155 F: 5′-TTAATGCTAATCGTGACT-3′; R: 5′-ACCTGAGAGTAGACCAGA-3′. U6 F: 5′-CTCGCTTCGGCAGCACA-3′; R: 5′-AACGCTTCACGAATTTGCGT- 3′. The amplification procedure was pre-denaturation at 95°C for 10 min; 95°C for 15 s; 60°C for 1 min (40 cycles in total); prolongation at 72°C for 10 min. The relative expression levels of target genes were used as the criterion, and the relative expression levels of CXCR4 and miRNA-155 mRNA were calculated using 2–ΔΔCt
Cell culture, grouping and treatment
The RPMI1640 cell culture medium containing 10% fetal bovine serum was added to the HTR8/ SVneo cells and cultured in a constant-temperature incubator at 37°C with 5% CO2 and 95% saturated humidity. The cells were divided into the NC, H/R, BL, miRNA-155 mimics, miRNA-NC, inhibitor NC, miRNA-155 inhibitor, Sal B and Sal B + miRNA-155 groups.
Western blot
The fresh placenta tissues or cells from each group were placed, washed with pre-cooled PBS 3 times and then 50 μl of protein lysate (containing protease inhibitor and phosphatase inhibitor at 1 : 100) added to make the protein solution, whose concentration was determined using the BCA method. Protein loading was 80 μg, and 12% sodium dodecyl sulfate-polyacrylamide gel (SDSPAGE) was prepared by means of electrophoresis for separation of proteins, followed by membrane transfer. CXCR4 was blocked with 5% skim milk powder, and p-AKT with 5% BSA at room temperature for 2 h, after which the blocking solution was discarded. Primary antibody CXCR4 (diluted at 1 : 500), p-AKT (diluted at 1 : 5 000) and internal reference b-actin (diluted at 15,000) antibody were added, incubated at 4°C overnight, secondary antibody (diluted at 1 : 1 : 1000) was added, and it was incubated at room temperature for 2 h, protected from light. The ODYSSEY Clx detection and imaging system was used for scanning and photographing.
Transwell cell invasion test
Prior to seeding of cells, it was necessary to equilibrate the transwell chamber and the 24-well plate: 100 μl of serum-free medium and 600 μl of FBS were added to the upper and lower chamber, respectively, and placed at 37°C with 5% CO2 overnight. The cells in all the groups transfected and starved for 24 h were collected, counted, inoculated into the upper chamber at 2 × 104 cells/well, and cultured at 37°C with 5% CO2 for 36 h. Then, the cells in the upper chamber were erased, and
432 Arch Med Sci 2, 1st March / 2023
Mechanisms underlying the improvement of preeclampsia through salvianolic acid B-regulated miRNA-155/CXCR4
those in the lower chamber were fixed in methanol, and photographed after Giemsa staining. A total of 5 fields of view were used under high power microscope for counting, with the mean value used. The procedure for each group was repeated in triplicate.
Wound healing experiment
The cells underwent the scratch test at 24 h after transfection. After the medium in the six-well plate had been replaced with serum-free medium for 12 h starvation of cells, a “hyphen”-shaped scratch was created with a 200 μl pipette tip along the plate to form a central blank area. The tip was washed with PBS once, and the scratch area was photographed (0 h) under a microscope. Another 24 h culture was performed, and observation and photography (24 h) were done. The relative migration distance of cells was analyzed using Image J software. The experiment was repeated in triplicate, with the mean value used.
Cellular immunofluorescence
After the cells in each group were treated for 48 h, the medium was discarded. The cells were washed with pre-cooled PBS, fixed in 2 ml of 4% paraformaldehyde for 20 min, permeabilized and blocked with 1% polyethylene glycol octylphenyl ether, to which rabbit anti-human p-AKT monoclonal antibody (1 : 100) was added, and incubated in a wet box at 4°C overnight. To the cells were then added FITC-labeled goat anti-rabbit fluorescent secondary antibody (diluted at 1 : 50, American Arthox, USA) dropwise, and incubated at 37°C for 1 h. The nuclei were stained with propidium iodide (PI) and the sections were sealed with glycerin. The colored locations and the intensity of fluorescence were observed under a laser confocal microscope.
Statistical analysis
Statistical analysis was performed with the SPSS 20.0 statistical software. The experimental data in this study were represented by mean ± SD. One-way analysis of variance was adopted for inter-group comparisons, and the SNK-q test for multiple inter-group comparisons. The test level was a = 0.05.
Results
Histopathological effects of Sal B on placenta
nucleus vacuolarization of the syncytiotrophoblast cells was seen in the placental tissue in the model group, together with a large number of syncytial nodules, fibrinoid necrosis, and a decreased number of microvessels in the villi. After the administration of Sal B, occasional spiral arteries and some syncytial nodules were seen in the Sal B group, and constantly improved with the increase in the concentration of Sal B. See Figure 1 for details.
Effects of Sal B on systolic blood pressure and urine protein concentration in PE rats
After induction with endotoxin drugs (D19), the systolic blood pressure and urine protein of rats in the model group and other drug groups were significantly higher than in the blank control group (p < 0.05), suggestive of the successful establishment of the model. Model establishment between the low-, medium- and high-dose drug groups and the model group was comparable. At 4 days after the intervention of the various drug groups with the different concentrations of Sal B, the systolic blood pressure in each drug group was significantly lower than in the model group (p < 0.05), and with the increase in the drug dose, the decrease in the systolic blood pressure was more obvious and the systolic blood pressure in the high-dose group was significantly lower than in the low-dose group (p < 0.05). The concentration of urine protein in various drug groups was lower than in the model group, with the difference being statistically significant (p < 0.05). The content of urine protein also showed a dose-dependent manner in different drug groups. After drug intervention, the concentrations of plasma NO in rats in various drug groups were generally higher than those prior to drug intervention, and significantly higher than in the model group (p < 0.05, Table I).
Effects of Sal B on placental weight, body weight and body length of newborn rats
The placental weight, body weight and body length of the newborn rats in the model group were significantly lower than in the blank control group (p < 0.05). The placental weight, body weight and body length of the newborn rats in the medium- and high-dose groups were significantly higher than in the model group (p < 0.05). The placental weight, body weight and body length of the newborn rats in the low-dose group were higher than in the model control group, but the difference was not statistically significant (Table II).
Effects of Sal B on miRNA-155, CXCR4 and p-AKT in the placenta of PE rats
Marked
Trophoblastic nodules and fibrinoid necrosis were rare in the placenta in the NC group, capillaries were abundant in number, and vascular syncytium cell membranes were well formed.
RT-PCR quantitative analysis showed that compared with the normal group, the expression of
Arch Med Sci 2, 1st March / 2023 433
Sal (40.0 mg/ kg) based on PE model; Sal H-H – the rats were treated by high-dose Sal (80.0 mg/kg) based on PE model
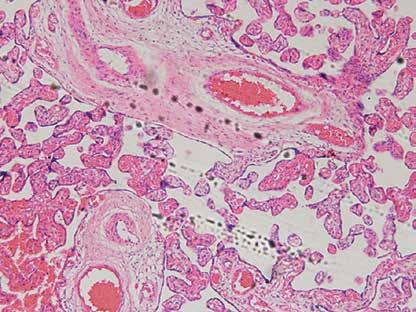
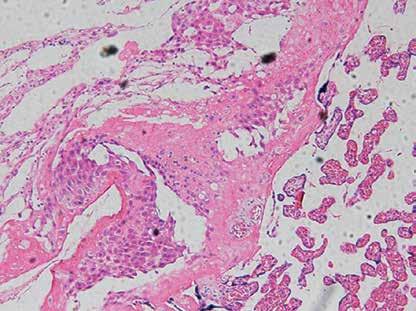
*P < 0.05, compared with normal group; Δp < 0.05, compared with model group; #p < 0.05, compared with Sal B-H group.
434 Arch Med Sci 2, 1st March / 2023
Chuanlian Zhang, Xue Han, Xiaoxue Wang
Normal
Model
Figure 1. Pathology of different groups by HE staining (×100). Normal – the rats were treated by normal treatment; Model – the rats were treated by PE model; Sal B-L – the rats were treated by low-dose Sal (20.0 mg/kg) based on PE model; Sal B-M – the rats were treated by medium-dose
Sal B-L Sal B-H
Sal B-M
Group N SBP [mm Hg] 24 h proteinuria [mg/l] NO [mmol/l] D19 D21 D19 D21 D19 D21 Normal 12 113.7 ±4.2 115.8 ±3.5 142.8 ±22.6 140.5 ±22.5 154.8 ±28.8 153.4 ±33.5 Model 12 139.6 ±3.8* 138.5 ±4.2* 351.6 ±42.9* 360.5 ±50.9* 52.8 ±9.4* 54.6 ±8.8* Sal B-L (20.0 mg/kg) 12 140.2 ±4.1* 128.1 ±3.8*Δ# 361.5 ±52.9* 208.5 ±35.9* 62.8 ±9.8* 72.8 ±10.8* Δ# Sal B-M (40.0 mg/kg) 12 139.7 ±4.0* 125.2 ±4.0 Δ 355.8 ±48.5* 175.4 ±9.5* 58.4 ±8.9* 97.6 ±15.7* Δ# Sal B-H (80.0 mg/kg) 12 139.5 ±4.8* 116.4 ±4.5 Δ 359.8 ±55.4* 153.7 ±10.5* 57.5 ±8.7* 130.5 ±20.6* Δ#
Table I. Comparison of systolic blood pressure and urine protein concentration in preeclampsia rats of different points
Mechanisms underlying the improvement of preeclampsia through salvianolic acid B-regulated miRNA-155/CXCR4
Table II. Placental weight, neonatal rats’ weight and neonatal rats’ body length in different groups
*P < 0.05, compared with normal group; Δp < 0.05, compared with model group; #p < 0.05, compared with Sal B-H group.
Figure 2. miRNA-155 and CXCR4 mRNA by RT-PCR and CXCR4 and p-AKT protein expression by WB assay. Normal – the rats were treated by normal treatment; Model – the rats were treated by PE model; Sal B-L – the rats were treated by low-dose Sal (20.0 mg/kg) based on PE model; Sal B-M – the rats were treated by medium-dose Sal (40.0 mg/kg) based on PE model; Sal H-H – the rats were treated by high-dose Sal (80.0 mg/kg) based on PE model. A – miRNA-155 and CXCR4 mRNA expression by RT-PCR assay. B – CXCR4 and p-AKT protein expression by WB assay
***P < 0.001, compared with normal group; #p < 0.05, ##p < 0.01, ###p < 0.001, compared with model group; Δp < 0.05, ΔΔp < 0.01, compared with Sal B-L group, $p < 0.05, compared with Sal B-M group.
Arch Med Sci 2, 1st March / 2023 435
Group N Placental weight [g] Neonatal rats’ weight [g] Neonatal rats’ body length [cm] Normal 12 0.73 ±0.13 5.24 ±0.55 3.89 ±0.35 Model 12 0.48 ±0.12 4.36 ±0.41* 3.12 ±0.35 Sal B-L (20.0 mg/kg) 12 0.51 ±0.14*# 4.56 ±0.49*# 3.24 ±0.40*# Sal B-M (40.0 mg/kg) 12 0.61 ±0.13* Δ 4.78 ±0.60* Δ 3.30 ±0.41 Δ Sal B-H (80.0 mg/kg) 12 0.66 ±0.15 Δ 5.00 ±0.54* Δ 3.62 ±0.35 Δ
miRNA-155 mRNA expression in difference groups (fold) CXCR4 mRNA expression in difference groups (fold) CXCR4/GAPDH (fold) p-AKT/GAPDH (fold) 4 3 2 1 0 1.5 1.0 0.5 0 1.5 1.0 0.5 0 1.0 0.8 0.6 0.4 0.2 0 Normal Model Sal B-L Sal B-M Sal B-H Normal Model Sal B-L Sal B-M Sal B-H Normal Model Sal B-L Sal B-M Sal B-H Normal Model Sal B-L Sal B-M Sal B-H Normal Model Sal B-L Sal B-M Sal B-H A B *** *** *** *** # # # # ##, Δ ##, Δ ##, Δ ##, Δ ###, ΔΔ, $ ###, ΔΔ $ ###, ΔΔ, $ ###, ΔΔ $ CXCR4 p-AKT GAPDH
the miRNA-155 gene was significantly increased while that of the CXCR4 gene was significantly decreased (p < 0.01, Figure 2 A) in the model group. Compared with the model group, the expression of the miRNA-155 gene was significantly inhibited while that of the CXCR4 gene was significantly elevated (p < 0.01, Figure 2 A) in the drug groups, with significant differences seen between the drug groups (p < 0.05, Figure 2 A). Semi-quantitative WB assay showed that compared with the normal group, the expression levels of the CXCR4 and p-AKT proteins in the model group were significantly lower (p < 0.01, Figure 2 B); compared with the model group, the expression levels of the CXCR4 and p-AKT proteins in the drug groups were significantly higher (p < 0.01, Figure 2 B), with significant differences seen between the drug groups (p < 0.05, Figure 2 B).
Expression of miRNA-155 and CXCR4 genes in cells in various groups
Compared with the NC group, the expression of the miRNA-155 gene in H/R, BL, miRNA-155 mimics, miRNA-NC and inhibitor NC groups was significantly higher while the expression of the CXCR4 gene was significantly lower (p < 0.001, Figure 3). However, compared with the H/R group, the expression of the miRNA-155 gene in the miRNAinhibitor group was significantly lower while the expression of the CXCR4 gene was significantly higher (p < 0.001, Figure 3).
Effects of miRNA-155 on invasion and migration of cells
The transwell cell invasion and wound healing experiments showed that compared with the NC group, the number of transmembrane cells and the rate of wound healing were significantly lower in the H/R, BL, miRNA-155 mimics, miRNA-NC and inhibitor NC groups (p < 0.001, Figure 4), and that compared with the H/R group, the number of
transmembrane cells and the rate of wound healing were significantly higher in the miRNA-inhibitor group (p < 0.001, Figure 4).
Effects of
miRNA-155
on related proteins and entry of p-AKT into the nucleus
Compared with the NC group, the expression of the CXCR4 and p-AKT proteins and the amount of p-AKT protein entering the nucleus in the H/R, BL, miRNA-155 mimics, miRNA-NC and inhibitor NC groups were significantly lower (p < 0.001, Figure 5). However, compared with the H/R group, the expression of the CXCR4 and p-AKT proteins and the amount of p-AKT protein entering the nucleus were significantly higher in the miRNA-inhibitor group (p < 0.001, Figure 5).
Effects of Sal B on expression levels of miRNA-155 and CXCR4 genes in cells in various groups
Compared with the NC group, the expression of the miRNA-155 gene was significantly higher in the H/R group and Sal B + miRNA-155 group, while the expression of the CXCR4 gene was significantly lower (p < 0.001, Figure 6). However, compared with the H/R group, the expression of the miRNA-155 gene was significantly lower in the Sal group, while the expression of the CXCR4 gene was significantly higher (p < 0.001, Figure 6).
Effects of Sal B on invasion and migration of cells
The transwell cell invasion and wound healing experiments showed that compared with the NC group, the number of transmembrane cells and the rate of wound healing were significantly lower in the H/R group and the Sal B + miRNA-155 group (p < 0.001, Figure 7); compared with the H/R group, the number of transmembrane cells and the rate of wound healing in the Sal B group were markedly higher (p < 0.001, Figure 7).
436 Arch Med Sci 2, 1st March / 2023
Chuanlian Zhang, Xue Han, Xiaoxue Wang
miRNA-155 mRNA expression in difference groups (fold) CXCR4 mRNA expression in difference groups (fold) 5 4 3 2 1 0 1.5 1.0 0.5 0 NC H/R BL miRNA- miRNA- Inhibitor miRNANC 155 NC 155 mimics inhibitor NC H/R BL miRNA- miRNa- Inhibitor miRNANC 155 NC 155 mimics inhibitor *** *** *** *** *** *** *** *** *** *** ### ###
Figure 3. miRNA-155 and CXCR4 gene expression in difference cell groups by RT-PCR ***P < 0.001, compared with NC group; ###p < 0.001, compared with H/R group.
Mechanisms underlying the improvement of preeclampsia through salvianolic acid B-regulated miRNA-155/CXCR4
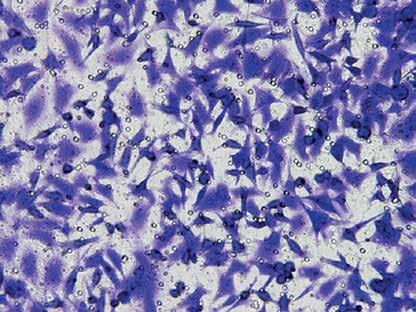
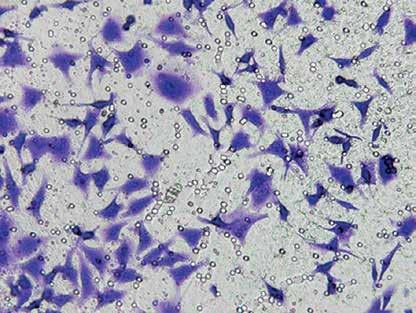
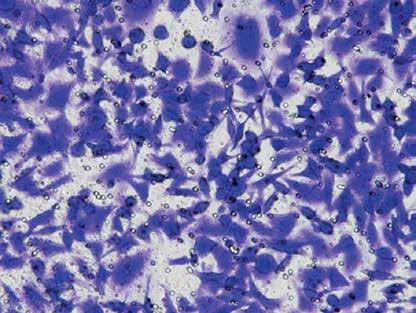
Arch Med Sci 2, 1st March / 2023 437
Figure 4. miRNA-155 effect on cell invasion and migration. A – miRNA-155 effect on cell invasion by transwell assay ***P < 0.001, compared with NC group; ###p < 0.001, compared with H/R group.
NC
miRNA-155 inhibitor
H/R BL
miRNA-NC
miRNa-155 mimics
The invasion cell number of difference groups 150 100 50 0 NC H/R BL
*** *** *** *** *** ### A
Inhibitor NC
miRNA- miRNa- Inhibitor miRNANC 155 NC 155 mimics inhibitor

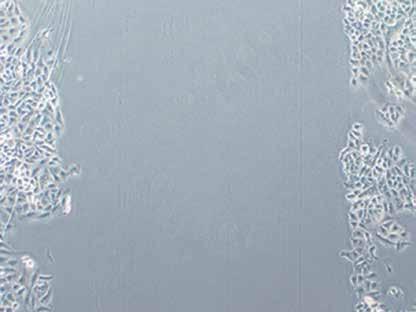

438 Arch Med Sci 2, 1st March / 2023
Chuanlian Zhang, Xue Han, Xiaoxue Wang
0 h B 24 h NC H/R BL miRNA-NC
Figure 4. Cont. B – miRNA-155 effect on cell migration by wound healing assay ***P < 0.001, compared with NC group; ###p < 0.001, compared with H/R group.
Mechanisms underlying the improvement of preeclampsia through salvianolic acid B-regulated miRNA-155/CXCR4
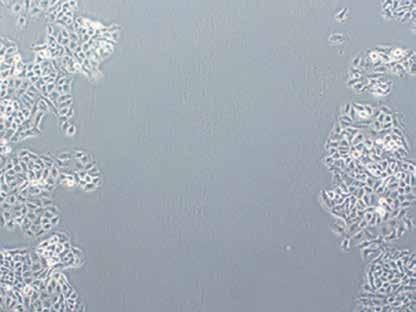
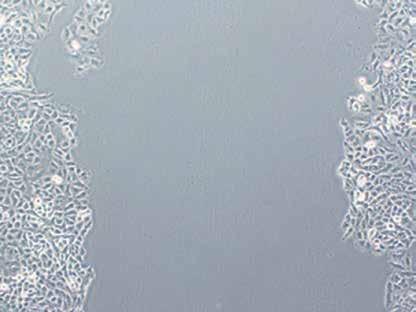
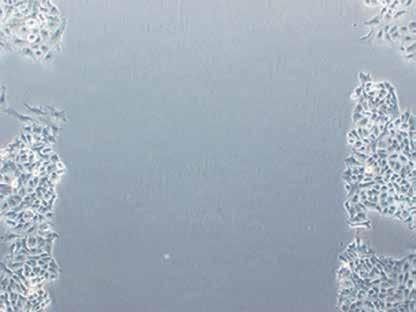
Arch Med Sci 2, 1st March / 2023 439
0 h 24 h miRNa-155 mimics Inhibitor NC miRNA-155 inhibitor Wound healing rate of difference groups (%) 100 80 60 40 20 0 NC H/R BL miRNA- miRNA- Inhibitor miRNANC 155 NC 155 mimics inhibitor *** *** *** *** *** ###
Figure 4. Cont. B – miRNA-155 effect on cell migration by wound healing assay ***P < 0.001, compared with NC group; ###p < 0.001, compared with H/R group.
Effects of Sal B on related proteins and entry of p-AKT into the nucleus
Compared with the NC group, the expression of CXCR4 and p-AKT proteins and the amount of p-AKT protein entering the nucleus in the H/R group and the Sal B + miRNA-155 group were significantly lower (p < 0.001, Figure 8); however, compared with the H/R group, the expression of CXCR4 and p-AKT proteins and the amount of p-AKT protein entering the nucleus in the Sal group were significantly higher (p < 0.001, Figure 8).
Discussion
PE represents an idiopathic hypertensive syndrome presenting with hypertension and proteinuria, etc. after 20 weeks of gestation in women with normal blood pressure. It can lead to serious maternal complications and is one of the main causes of maternal and perinatal death [16]. The incidence of PE in Europe and the United States at present is low (approximately 2–5%), while it is more common in developing countries, with an incidence of about 10%. PE accounts for 9% of maternal mortality in Asia and Africa [17]. Among 10 million pregnant women worldwide every year, gestational hypertension, especially PE,
leads to the death of 76,000 pregnant women and 500,000 fetuses or neonates [18]. The American College of Cardiology has also included PE among the risk factors for cardiovascular disease, and recommended that patients with a history of PE be understood and their lifestyles be improved [19, 20]. However, the mechanisms of pathogenesis underlying PE remain unclear, and there is still a lack of effective treatment options in clinical practice. Pregnancy has to be terminated early in many cases, causing pregnancy failure, and many epidemiological studies have also confirmed that the development of PE may have long-term adverse consequences in the offspring [21, 22]. The mechanisms of pathogenesis underlying PE may involve many factors, such as placental ischemia and hypoxia, inflammatory responses, changes in the PE-associated signaling pathways, trophoblastic infiltration abnormalities, abnormal maternal-fetal interface immunity, local coagulation of placenta and imbalanced anticoagulant mechanisms, and the abnormal expression profiles of miRNAs [23, 24].
Since the discovery of the first miRNA in Caenorhabditis elegans by Lee et al. in 1993 [25], more than 2,000 miRNAs have been discovered, and bioinformatics has predicted that miRNA may
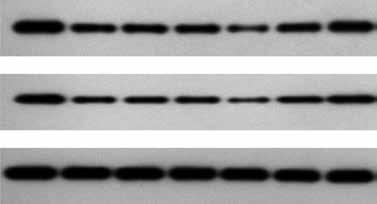
440 Arch Med Sci 2, 1st March / 2023 NC
CXCR4 p-AKT GAPDH CXCR4/GAPDH (fold) p-AKT/GAPDH (fold) 1.0 0.8 0.6 0.4 0.2 0 1.0 0.8 0.6 0.4 0.2 0 NC H/R BL
inhibitor NC
*** *** *** *** *** *** *** *** *** *** ### ###
Chuanlian Zhang, Xue Han, Xiaoxue Wang
H/R BL miRNA- miRNA- Inhibitor miRNANC 155 NC 155 mimics inhibitor
miRNA- miRNA- Inhibitor miRNANC 155 NC 155 mimics
H/R BL miRNA- miRNA- Inhibitor miRNANC 155 NC 155 mimics inhibitor
A
Figure 5. CXCR4 and p-AKT protein expression by WB assay and p-AKT nucleation volume. A – CXCR4 and p-AKT proteins expression by WB assay ***P < 0.001, compared with NC group; ###p < 0.001, compared with H/R group.
regulate 60% of genes encoding proteins within the human genome [26]. Great strides have been made in research on miRNAs in inflammation and tumors, while research on eclampsia-associated miRNAs has just started. miRNAs can regulate the post-translational expression of genes by undergoing complementary pairing with the 3′ non-coding region (3′UTR) of mRNA completely or incompletely, and plays an important role in the differentiation, development, proliferation, invasion, apoptosis and other biological processes of cells [27]. Encoded by the BIC gene, the miRNA-155 gene is located on human chromosome 21q21. 3, and is a miRNA closely associated with inflammation, tumors and immune regulation [28]. Recent studies have shown that miRNA-155 can target
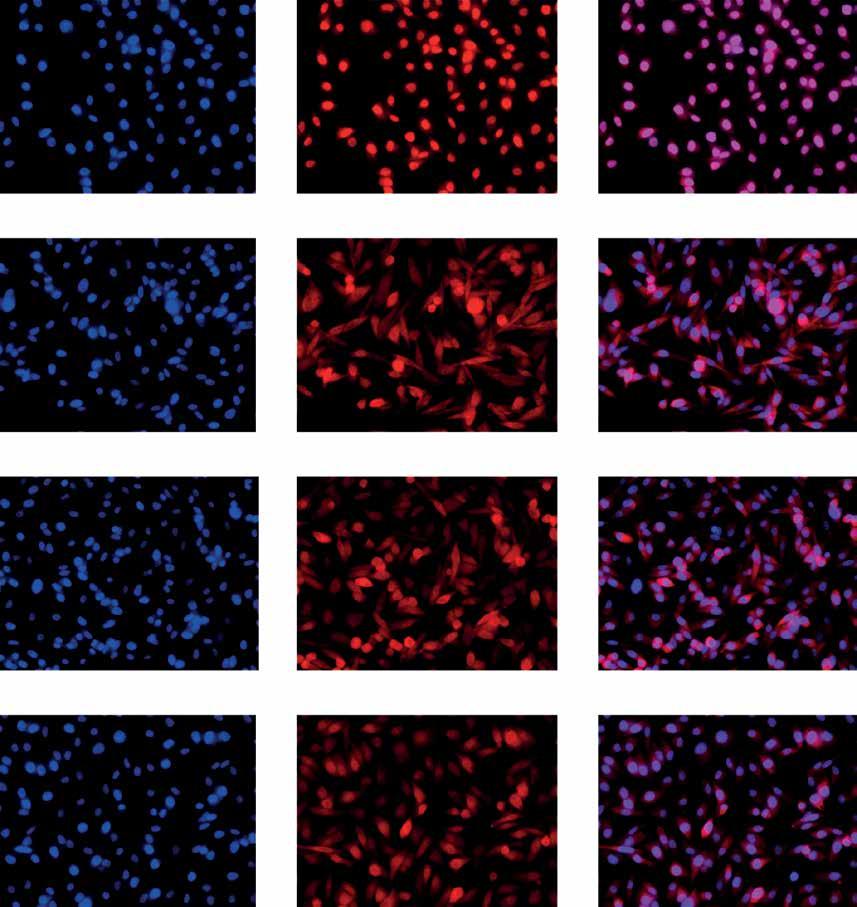
the regulation of expression of CXCR4, affect the proliferation and angiogenesis of cancer cells and increase the invasiveness of tumor cells in such diseases as gastric cancer and breast cancer [29, 30]. CXCR4, which is also known as chemokine receptor 4, is located on the human chromosome 2q21, and consists of 352 amino acids. It can be expressed on the membranes of various cells, including trophoblast cells, and is expressed in the villus tissues throughout pregnancy [31].
Sal B is an active ingredient from the traditional Chinese medicine Salvia miltiorrhiza. Pharmacological studies have shown that Sal B can regulate the vascular tone by blocking the b-receptors, reducing the calcium influx, antagonizing endothelin, and increasing the generation of NO in the
Arch Med Sci 2, 1st March / 2023 441
Mechanisms underlying the improvement of preeclampsia through salvianolic acid B-regulated miRNA-155/CXCR4
B DAPI p-AKT Merge NC
BL
Figure 5. Cont. B – p-AKT nucleation volume of different groups by cell immunofluorescence ***P < 0.001, compared with NC group; ###p < 0.001, compared with H/R group.
H/R
miRNA-NC
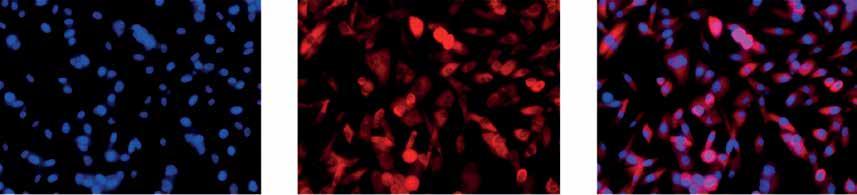
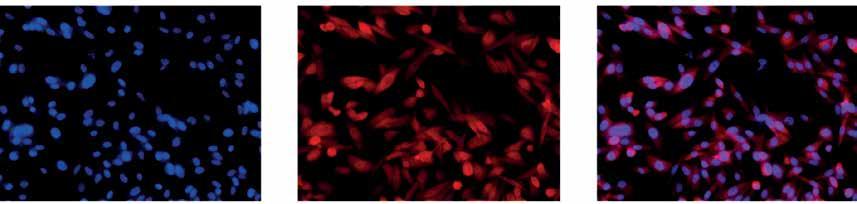
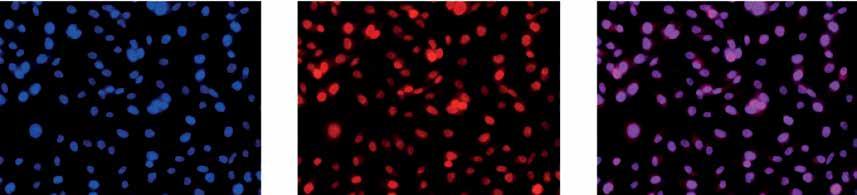
442 Arch Med Sci 2, 1st March / 2023
Chuanlian Zhang, Xue Han, Xiaoxue Wang
<
DAPI p-AKT Merge miRNA-155 mimics Inhibitor NC miRNA-155 inhibitor The nucleation volume of difference groups 15 10 5 0 NC H/R BL miRNA- miRNA- Inhibitor miRNANC 155 NC 155 mimics inhibitor *** *** *** *** *** ### miRNA-155 mRNA expression in difference groups (fold) CXCR4 mRNA expression in difference groups (fold) 6 4 2 0 1.5 1.0 0.5 0 NC H/R Sal B Sal B + miRNA-155 NC H/R Sal B Sal B + miRNA-155 *** *** *** *** ### ###
Figure 5. Cont. B – p-AKT nucleation volume of different groups by cell immunofluorescence
***P
0.001, compared with NC group; ###p < 0.001, compared with H/R group.
Figure 6. miRNA-155 and CXCR4 mRNA expression in different groups by RT-PCR assay ***P < 0.001, compared with NC group; ###p < 0.001, compared with H/R group.
platelets, etc., thus increasing the blood flow [32, 33]. These show that Sal B exhibits good effects in combating platelet aggregation, dilating small arteries, and improving microcirculation and hemorheology, and that it can improve the invasion and migration of chorionic trophoblast cells.
This study demonstrated that Sal B exhibited marked effects on improving the blood pressure and urine protein and promoting the development and maturation of young rats, suggestive of the good effects of Sal B in improving the vascular
tension of the placenta and improving hypoxia and ischemia of cells. In the meantime, it was found that Sal B could lead to an increased concentration of NO in the plasma and enhanced invasion and migration of trophoblast cells. The cell experiments showed that Sal B could restore the injury of invasion and migration of the chorionic trophoblast cells as a result of simulation of the hypoxia model of PE. The mechanisms underlying this may be associated with promoted CXCR4 expression levels and p-AKT protein activity and an
Arch Med Sci 2, 1st March / 2023 443 NC A
H/R
Mechanisms underlying the improvement of preeclampsia through salvianolic acid B-regulated miRNA-155/CXCR4
Sal B
The invasion cell number of difference groups 150 100 50 0
*** *** ###
Sal B + miRNA-155
NC H/R Sal B Sal B + miRNA-155
Figure 7. Cell invasion and migration in different groups by transwell and migration. A – Cell invasion of different groups by transwell assay ***P < 0.001, compared with NC group; ###p < 0.001, compared with H/R group.



444 Arch Med Sci 2, 1st March / 2023 0 h B 24 h NC H/R Sal B Sal B + miRNA-155 Wound healing rate of difference groups (%) 80 60 40 20 0 NC H/R Sal B Sal B + miRNA-155 *** *** ###
Chuanlian
Zhang, Xue Han, Xiaoxue Wang
Figure 7. Cont. B – Cell wound healing rate of different groups by wound healing assay ***P < 0.001, compared with NC group; ###p < 0.001, compared with H/R group.
increased nuclear load through inhibition of miRNA-155.
In conclusion, this study, through in vivo and in vitro experiments, demonstrated that Sal B could improve the pathological changes in PE by inhibiting miRNA-155, and its mechanisms may include activation of the CXCR4 /PI3K/AKT signaling pathway to affect such biological functions of trophoblasts as invasion and migration.
Conflict of interest
The authors declare no conflict of interest.
Arch Med Sci 2, 1st March / 2023 445 NC
CXCR4 p-AKT GAPDH A CXCR4/GAPDH (fold) p-AKT/GAPDH (fold) 1.0 0.8 0.6 0.4 0.2 0 1.0 0.8 0.6 0.4 0.2 0 NC H/R Sal B Sal B + miRNA-155 NC H/R Sal B Sal B + miRNA-155 *** *** *** *** ### ###
Mechanisms underlying the improvement of preeclampsia through salvianolic acid B-regulated miRNA-155/CXCR4
H/R Sal B Sal B + miRNA-155
Figure 8. CXCR4 and p-AKT protein expression by WB assay and p-AKT nucleation volume. A – CXCR4 and p-AKT protein expression by WB assay ***P < 0.001, compared with NC group; ###p < 0.001, compared with H/R group.
446 Arch Med Sci 2, 1st March / 2023 The nucleation volume of difference groups 15 10 5 0 NC H/R Sal
B +
*** *** ### DAPI p-AKT Merge B NC H/R Sal B Sal B + miRNA-155
Chuanlian Zhang, Xue Han, Xiaoxue Wang
B Sal
miRNA-155
Figure 8. Cont. B – p-AKT nucleation volume of different groups by cell immunofluorescence ***P < 0.001, compared with NC group; ###p < 0.001, compared with H/R group.
Mechanisms underlying the improvement of preeclampsia through salvianolic acid B-regulated miRNA-155/CXCR4
References
1. Lain KY, Roberts JM. Contemporary concepts of the pathogenesis and management of preeclampsia. J Am Med Assoc 2002; 287: 3183-6.
2. Saito S, Shiozaki A, Nakashima A, Sakai M, Sasaki Y. The role of the immune system in preeclampsia. Mol Aspects Med 2007; 28: 192-209.
3. Murphy MS, Casselman RC, Tayade C, Smith GN. Differential expression of plasma microRNA in preeclamptic patients at delivery and 1 year postpartum. Am J Obstet Gynecol 2015; 213: 367e1-9.
4. Lazar L, Rigo J. The role of microRNA in pathogenesis of preeclampsia-miRNA network analysis. Pregnancy Hypertens 2013; 3: 99.
5. Li XL, Li CF, Dong X, Gou W. MicroRNA-155 inhibits migration of trophoblast cells and comtributes to the pathogenesis of severe preeclampsia by regulating endothelial nitric oxide synthase. Mol Med Reports 2014; 10: 550-4.
6. Dai Y, Qiu Z, Diao Z, et al. MicroRNA-155 inhibits proliferation and migration of human extravillous trophoblast derived HTR-8/SVneo cells via down-regulating cyclin D1. Placenta 2012; 33: 824-9.
7. Wang L, Li X, Zhao Y, et al. Insights into the mechanism of CXCL12-mediated signaling in trophoblast functions and placental angiogenesis. Acta Biochim Biophys Sin (Shanghai) 2015; 47: 663-72.
8. Warner JA, Zwezdaryk KJ, Day B, Sullivan DE, Pridjian G, Morris CA. Human cytomegalovirus infection inhibits CXCL12-mediated migration and invasion of human extravillous cytotrophoblasts. Virol J 2012; 9: 255.
9. Ho JH, Hong CY. Salvianolic acids: small compounds with multiple mechanisms for cardiovascular protection. J Biomed Sci 2011; 18: 30.
10. Yu LJ, Zhang KJ, Zhu JZ, et al. Salvianolic acid exerts cardioprotection through promoting angiogenesis in animal models of acute myocardial infarction: preclinical evidence. Oxid Med Cell Longev 2017; 2017: 8192383.
11. Liu M, Xu H, Zhang L, et al. Salvianolic acid B inhibits myofibroblast transdifferentiation in experimental pulmonary fibrosis via the up-regulation of Nrf2. Biochem Biophys Res Commun 2018; 495: 325-31.
12. Sha W, Zhou Y, Ling ZQ, et al. Antitumor properties of Salvianolic acid B against triple-negative and hormone receptor-positive breast cancer cells via ceramide-mediated apoptosis. Oncotarget 2018; 9: 36331-43.
13. Li Y, Wang L, Dong Z, et al. Cardioprotection of salvianolic acid B and ginsenoside Rg1 combination on subacute myocardial infarction and the underlying mechanism. Phytomedicine 2019; 57: 255-61.
14. Yu J, Chen R, Tan Y, et al. Salvianolic acid B alleviates heart failure by inactivating ERK1/2/GATA4 signaling pathway after pressure overload in mice. PLoS One 2016; 11: e0166560.
15. Leach RE, Kilburn BA, Petkova A, Romero R, Armant DR. Diminished survival of human cytotrophoblast cells exposed to hypoxia/reoxygenation injury and associated reduction of heparin-binding EGF-like growth factor. Am J Obstet Gynecol 2008; 198: 471.e1-7.
16. Ghulmiyyah L, Sibai B. Maternal mortality from preeclampsia /eclampsia. Semin Perinatol 2012; 36: 56-9.
17. Duley L. The global impact of pre-eclampsia and eclampsia. Semin Perinatol 2009; 33: 130-7.
18. Khowaja AR, Mitton C, Bryan S, Magee LA, Bhutta ZA, von Dadelszen P. Economic evaluation of community level interventions for pre-eclampsia (CLIP) in south
Asian and African countries: a study protocol. Implement Sci 2015; 10: 76.
19. Mosca L, Benjamin EJ, Berra K, et al.; American Heart Association. Effectiveness-based guidelines for the prevention of cardiovascular disease in women-2011 update: a guideline from the American Heart Association. J Am Coll Cardiol 2011; 57: 1404-23.
20. Seely EW, Rich-Edwards J, Lui J, et al. Risk of future cardiovascular disease in women with prior preeclampsia: a focus group study. BMC Pregnancy Childbirth 2013; 13: 240.
21. Davis EF, Lazdam M, Lewandowski AJ, et al. Cardiovascular risk factors in children and young adults born to preeclamptic pregnancies: a systematic review. Pediatrics 2012; 129: E1552-61.
22. Lawlor DA, Macdonald-Wallis C, Fraser A, et al. Cardiovascular biomarkers and vascular function during childhood in the offspring of mothers with hypertensive disorders of pregnancy: findings from the Avon Longitudinal Study of Parents and Children. Eur Heart J 2012; 33: 335-45.
23. Chaiworapongsa T, Chaemsaithong P, Yeo L, Romero R. Pre-eclampsia part 1: current understanding of its pathophysiology. Nat Rev Nephrol 2014; 10: 466-80.
24. Chen DB, Wang W. Human placental microRNAs and preeclampsia. Biol Reprod 2013; 88: 130.
25. Lee RC, Feinbaum RL, Ambros V. The c. elegans heterochronic gene lin-4 encodes small RNAs with antisense complementarity to lin-14. Cell 1993; 75: 843-54.
26. Friedman RC, Farh KK, Burge CB, Bartel DP. Most mammalian mRNAs are conserved targets of microRNAs. Genome Res 2009; 19: 92-105.
27. Bushati N, Cohen SM. microRNA functions. Annu Rev Cell Dev Biol 2007; 23: 175-205.
28. Garo LP, Murugaiyan G. Contribution of MicroRNAs to autoimmune diseases. Cell Mol Life Sci 2016; 73: 2041-51.
29. Ma Z, Ma Y, Xia Q, et al. MicroRNA-155 expression inversely correlates with pathologic stage of gastric cancer and it inhibits gastric cancer cell growth by targeting cyclin D1. J Cancer Res Clin Oncol 2016; 142: 1201-12.
30. Liang Z, Wu H, Reddy S, et al. Blockade of invasion and metastasis of breast cancer cells via targeting CXCR4 with an artificial microRNA. Biochem Biophys Res Commun 2007; 363: 542-6.
31. Zhao HB, Tang CL, Hou YL, et al. CXCL12 /CXCR4 axis triggers the activation of EGF receptor and ERK signaling pathway in CsA-induced proliferation of human trophoblast cells. PLoS One 2012; 7: e38375.
32. Yang K, Luo Y, Lu S, et al. Salvianolic acid B and ginsenoside re synergistically protect against Ox-LDL-induced endothelial apoptosis through the antioxidative and antiinflammatory mechanisms. Front Pharmacol 2018; 9: 662.
33. Liu CS, Chen NH, Zhang JT. Protection of PC12 cells from hydrogen peroxide-induced cytotoxicity by salvianolic acid B, a new compound isolated from Radix Salviae miltiorrhizae. Phytomedicine 2007; 14: 492-7.
Arch Med Sci 2, 1st March / 2023 447
Evaluation of protective effects of GnRH agonist or antagonist on ovarian reserve with anti-Müllerian hormone and histological analysis in a rat model using cisplatin
1Department of Obstetrics and Gynecology, Acıbadem Mehmet Ali Aydınlar University, Acıbadem Kayseri Hospital, Kayseri, Turkey
2Department of Obstetrics and Gynecology, Magnet Hospital, Kayseri, Turkey
3Department of Obstetrics and Gynecology, Ömer Halisdemir University, Niğde, Turkey
4Department of Obstetrics and Gynecology, Erzincan University, Erzincan, Turkey
5Department of Obstetrics and Gynecology, Erciyes University, Kayseri, Turkey
Submitted: 19 February 2019; Accepted: 1 August 2019
Online publication: 27 August 2019
Arch Med Sci 2023; 19 (2): 448–451
DOI: https://doi.org/10.5114/aoms.2019.87540
Copyright © 2019 Termedia & Banach
Abstract
Introduction: The aim of this prospective trial was to evaluate the ovarian reserve with anti-Müllerian hormone (AMH), which is the best predictor of ovarian reserve, and perform histological analysis after exposure to cisplatin with a GnRH agonist or antagonist.
Material and methods: Twenty-four Wistar albino rats were randomly divided into three groups, each consisting of eight rats. In the GnRH agonist group (group 1), rats received a single dose of 50 mg/m 2 cisplatin with 1 mg/kg triptorelin. In the GnRH antagonist group (group 2), rats received a single dose of 50 mg/m 2 cisplatin with 1 mg/kg cetrorelix. In the control group (group 3), rats received 50 mg/m 2 cisplatin. Ovarian reserve was assessed by AMH and histology.
Results: Primary follicle counts were higher in group 2 (4.50 ±1.47 vs. 3.50 ±1.70 vs. 3.00 ±3.54) and secondary follicle counts were higher in group 1 (2.96 ±1.11 vs. 1.74 ±1.03 vs. 1.37 ±3.11). Numbers of tertiary follicles were higher both in groups 1 and 2 than the control group (1.36 ±0.83 vs. 0.84 ±0.99 vs. 0.50 ±0.75). The total follicle count of the study groups were significantly higher compared with the control group (14.32 ±5.96 vs. 12.48 ±4.12 vs. 10.63 ±6.80). AMH was significantly higher in groups 1 and 2 compared with the control group (18.56 ±25.33 vs. 16.48 ±24.66 vs. 9.37 ±26.54).
Conclusions: This is the first prospective randomized controlled study showing the protective effects of GnRH agonist and antagonist on ovarian reserve after cisplatin exposure in an animal model.
Key words: ovarian reserve, cisplatin, anti-Müllerian hormone.
Introduction
Chemotherapy is a pivotal part of cancer treatment and chemotherapy usage has been gradually increased in the world for this reason. It is known that chemotherapeutic agents damage ovaries and may cause ovarian failure and infertility [1]. Due to these damaging effects of chemotherapy on ovarian reserve, many prophylactic agents have been used to try to protect against destructive effects of chemotherapies on ovarian reserve [2].
Corresponding author: Mustafa Tas
Department of Obstetrics and Gynecology
Acibadem University
Turkey
E-mail: drmustafatas@yahoo. com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/).
Mustafa Tas1, Gokalp Oner2, Pasa Ulug3, Adem Yavuz4, Bulent Ozcelik5
Experimental research Obstetrics and Gynecology
Evaluation of protective effects of GnRH agonist or antagonist on ovarian reserve with anti-Müllerian hormone and histological analysis in a rat model using cisplatin
Cisplatin was the most commonly used alkylating agent in gynecological cancers. Most of the studies revealed that GnRH agonist or antagonist usage with chemotherapeutic agents may protect ovarian reserve [3, 4]. Alkylating agents may affect ovaries with cortical fibrosis, blood vessel damage, and severe reduction in primordial follicles and ovarian cell proliferation. Also arrest and apoptosis may start in granulosa cells.
The fertility of women may be determined by the ovarian reserve tests including counting the number of ovarian follicles and measuring the level of anti-Mullerian hormone (AMH). The tests are the most widely used parameters in infertility clinics [5].
To date, there has been no study clearly investigating ovarian reserve with anti-Müllerian hormone (AMH) and histological analysis after cisplatin exposure with a GnRH agonist or antagonist in an animal model. In this prospective randomized controlled trial, we evaluated the effects of a GnRH agonist or antagonist on ovarian reserve of rats exposed to cisplatin, which was the most commonly used chemotherapeutic agent in gynecological cancers.
Material and methods
Twenty-four five- to six-month-old female Wistar-Albino rats weighing 180–210 g were used in this study. All procedures were approved by Ethics Committee of Kobay Experimental Animal Laboratory. All procedures were carried out at Kobay Experimental Animal Laboratory. All rats were housed under controlled temperatures (22 ±2°C) and 12/12 h light/dark cycle with food and water ad libitum.
Twenty-four Wistar albino rats were randomly divided into three groups, each consisting of eight rats. In the GnRH agonist group (group 1), rats received a single dose of 50 mg/m2 cisplatin with 1 mg/kg Triptorelin. In the GnRH antagonist group (group 2), rats were received single dose 50 mg/m2 cisplatin with 1 mg/kg Cetrorelix. In the control group (group 3), rats received 50 mg/m2 cisplatin.
Blood samples (2 ml) were collected from the heart of the rats before laparotomy. The serum of the blood was separated from cells by centrifugation, and samples were frozen at –20°C until assayed. AMH levels (ng/ml) were determined by using ELISA (Cusabio Rat AMH kit; Biotek Synergy HT Microplate Reader, US) in Duzen Laboratory by a researcher blinded to the groups. All samples were tested in the same assay. The coefficients of intra- and inter- assay variations were 4.8% and 7.5%, respectively.
Ovarian samples were randomly prepared in 5-μm slices to assess follicles [6]. Hematoxylin-eosin was used for staining of the samples. The same
pathologist blindly examined the ovarian follicles and noted the counts of the follicles. Primordial, primary, secondary and tertiary follicles were defined according to the usual standard textbooks of microscopic anatomy [6].
Statistical analysis
The Statistical Package for the Social Sciences version 15.0 was used for the statistical analyses (SPSS Inc., Chicago, IL, USA) and groups were compared with the t test. P < 0.05 was considered statistically significant. Values were expressed as mean ± standard deviation.
Results
Ovarian reserve was assessed by AMH and histology. There was no difference in the primordial follicle count between the groups. Primary follicle counts were higher in group 2 (4.50 ±1.47 vs. 3.50 ±1.70 vs. 3.00 ±3.54) and secondary follicle counts were higher in group 1 (2.96 ±1.11 vs. 1.74 ±1.03 vs. 1.37 ±3.11). Tertiary follicle counts were higher both in group 2 and 3 compared to the control group (1.36 ±0.83 vs. 0.84 ±0.99 vs. 0.50 ±0.75). The total follicle count of the study groups was significantly higher compared with the control group (14.32 ±5.96 vs. 12.48 ±4.12 vs. 10.63 ±6.80). AMH was found to be significantly higher in groups 1 and 2 compared with the control group (18.56 ±25.33 vs. 16.48 ±24.66 vs. 9.37 ±26.54). Histological examination of the groups is demonstrated in Figure 1. There is no difference between the protective effect of GnRH agonist and GnRH antagonist (Table I).
Discussion
Fertility and premature menopause are major concerns for young women who are undergoing treatment for cancer. Premature ovarian failure caused by chemotherapy depends on type and dosage of the agents. Alkylating agents such as cisplatin are widely used chemotherapeutic agents and cause ovarian damage. Cisplatin has a heavy metal combination and antineoplastic effects on rapidly divided cells [7]. In this prospective randomized study, we evaluated how to decrease the detrimental effect of cisplatin on ovaries.
There are lots of experimental and clinical studies on protective agents such as gonadotropin-releasing hormone (GnRH) agonists and GnRH antagonists [8–10]. Our previous study showed that a GnRH agonist with cisplatin may protect ovarian reserve compared to solely cisplatin [11]. Controversially after this study meta-analyses showed that GnRH agonists had no effect to protect ovarian reserve against chemotherapy [12]. Then a committee opinion suggested that the data on
Arch Med Sci 2, 1st March / 2023 449
There is no statistically significant difference between groups sharing the same letter. All data sets of power of performed test with a = 0.050 (power of the study): 0.976–1.000.
the use of GnRH analogs for ovarian suppression have been conflicting in terms of the efficacy, so other fertility preservation options should be offered in addition to GnRH analog treatment [13]. But the studies and meta-analyses evaluated different types and dosages of chemotherapeutic agents. Additionally application of GnRH analogs was different. In our study we added a GnRH analog on the same day as cisplatin.
The protective mechanism of the GnRH agonists on the ovaries after exposure to cytotoxic effects on ovaries involves the GnRH receptors at the gonadal and pituitary levels. A GnRH agonist may downregulate the receptors of gonads and suppress primordial follicle development [14]. Additionally, the hypoestrogenic state decreases
ovarian perfusion and delivery of chemotherapy to the ovaries and a direct effect of the GnRH agonist on the ovary occurs independently of the gonadotropin level may be discussed for the protection of ovarian germ cells [15, 16]. Our study showed that GnRH agonist administration has a protective effect on ovarian reserve compared with the control group.
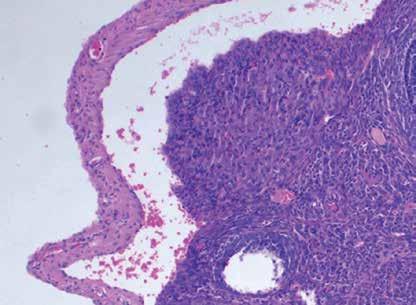
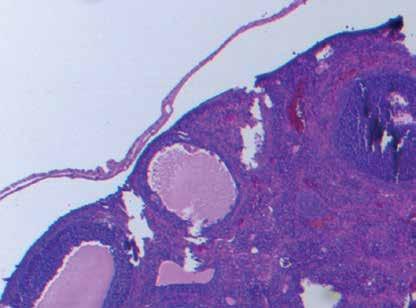
Recently, GnRH antagonists have been used to decrease the effects of chemotherapy on ovaries [17, 18]. A GnRH antagonist shows higher competitive blockade of the receptors than a GnRH agonist. Additionally a GnRH antagonist inhibits apoptosis triggered by chemotherapy [17]. To our knowledge, there has been no study comparing the protective effects of a GnRH agonist and antagonist on ova-
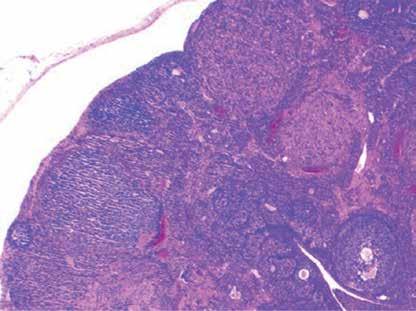
450 Arch Med Sci 2, 1st March / 2023
Mustafa Tas, Gokalp Oner, Pasa Ulug, Adem Yavuz, Bulent Ozcelik
A B C
Figures 1. Histological demonstration of the groups is shown. A – Follicles of control group. B – Follicles of group 1. C – Follicles of group 2
Parameter Control group 3 Group 1 (GnRH agonist) Group 2 (GnRH antagonist) Primordial follicles 5.76 ±6.97a 6.50 ±3.32a 5.50 ±4.33a Primary follicles 3.00 ±3.54a 3.50 ±1.70a,b 4.50 ±1.47b Secondary follicles 1.37 ±3.11a 2.96 ±1.11b 1.74 ±1.03a,b Tertiary follicles 0.50 ±0.75a 1.36 ±0.83b 0.84 ±0.99b Total follicles 10.63 ±6.80a 14.32 ±5.96b 12.48 ±4.12a,b AMH [ng/ml] 9.37 ±26.54a 18.56 ±25.33b 16.48 ±24.66b
Table I. Results of ovarian follicle tests and endometrium thickness of the groups
Evaluation of protective effects of GnRH agonist or antagonist on ovarian reserve with anti-Müllerian hormone and histological analysis in a rat model using cisplatin
ries exposed to chemotherapy. Our study was the first to show the effects of a GnRH agonist and antagonist on ovaries after application of cisplatin, which was the most commonly used chemotherapeutic agent in gynecological malignancies.
Various ovarian reserve tests have been used to predict the ovarian response and pregnancy outcomes in couples. Two of most widely used tests are AMH levels and AFC [19, 20]. AMH is an increasingly used reliable marker of present ovarian reserve and the number of follicles remaining in ovaries [21]. In this study, ovarian reserve tests such as AMH and histological follicles count were used.
This study clearly demonstrated that cisplatin had a cytotoxic effect on the ovaries and combination with a GnRH agonist and antagonist had statistically significant protective effects on the total follicle count but not the primordial follicles. Although primordial follicles did not significantly change, primary, secondary and tertiary follicles might be protected with a GnRH agonist and antagonist. Additionally, AMH levels supported this situation and increased with the GnRH agonist and antagonist.
In conclusion, ovarian reserve was first evaluated after exposure to cisplatin with a GnRH agonist and antagonist in an animal randomized prospective study using most common ovarian reserve tests including AMH and histological examination of ovarian follicles. These data represent an important benefit for understanding the effect of GnRH agonists and antagonists on ovarian reserve. Also, both GnRH agonists and antagonists have limited protective effects on ovarian reserve.
Conflict of interest
The authors declare no conflict of interest.
References
1. Gadducci A, Cosio S, Genazzani AR. Ovarian function and childbearing issues in breast cancer survivors. Gynecol Endocrinol 2007; 23: 625-31.
2. Yeh J, Kim BS, Liang YJ, Peresie J. Gonadotropin stimulation as a challenge to calibrate cisplatin induced ovarian damage in the female rat. Reprod Toxicol 2009; 28: 556-62.
3. Ozcelik B, Turkyilmaz C, Ozgun MT, et al. Prevention of paclitaxel and cisplatin induced ovarian damage in rats by a gonadotropin-releasing hormone agonist. Fertil Steril 2010; 93: 1609-14.
4. Bedaiwy MA, Abou-Setta AM, Desai N, et al. Gonadotropin-releasing hormone analog cotreatment for preservation of ovarian function during gonadotoxic chemotherapy: a systematic review and meta-analysis. Fertil Steril 2011; 95: 906-14.
5. Yeh J, Kim B, Peresie J, Liang YJ, Arroyo A. Serum and ovarian Müllerian inhibiting substance, and their decline in reproductive aging. Fertil Steril 2007; 87: 1227-30.
6. Ulug P, Oner G. Evaluation of the effects of single or multiple döşe methotrexate administration, salpingec-
tomy on ovarian reserve of rat with the measurement of anti-Müllerian hormone (AMH) levels and histological analysis. Eur J Obstet Gynecol Reprod Biol 2014; 181: 205-9.
7. Kalil NG, McGuire WP. Chemotherapy for advanced epithelial ovarian carcinoma. Best Pract Res Clin Obstet Gynaecol 2002; 16: 553-71.
8. Blumenfeld Z. Endocrine prevention of chemotherapy-induced ovarian failure. Future Oncol 2016; 12: 1671-4.
9. Blumenfeld Z. How to preserve fertility in young women exposed to chemotherapy? The role of GnRH agonist cotreatment in addition to cryopreservation of embrya, oocytes, or ovaries. Oncologist 2007; 12: 1044-54.
10. Lemos CN, Reis FM, Pena GN, Silveira LC, Camargos AF. Assessment of fertility protection and ovarian reserve with GnRH antagonist in rats undergoing chemotherapy with cyclophosphamide. Reprod Biol Endocrinol 2010; 8: 51.
11. Ataya KM, McKanna JA, Weintraub AM, Clark MR, LeMaire WJ. A luteinizing hormone-releasing hormone agonist for the prevention of chemotherapy-induced ovarian follicular loss in rats. Cancer Res 1985; 45: 3651-6.
12. Elgindy E, Sibai H, Abdelghani A, Mostafa M. Protecting ovaries during chemotherapy through gonad suppression: a systematic review and meta-analysis. Obstet Gynecol 2015; 126: 187-95.
13. Ethics Committee of the American Society for Reproductive Medicine. Fertility preservation and reproduction in cancer patients. Fertil Steril 2005; 83: 1622-8.
14. Blumenfeld Z, Avivi I, Eckman A, Epelbaum R, Rowe JM, Dann EJ. Gonadotropin-releasing hormone agonist decreases chemotherapy-induced gonadotoxicity and premature ovarian failure in young female patients with Hodgkin lymphoma. Fertil Steril 2008; 89: 166-73.
15. Sutcliffe SB. Cytotoxic chemotherapy and gonadal function in patients with Hodgkin’s disease. JAMA 1979; 242: 1898-901.
16. Shenns RJ. Gonadal dysfunction. In: Cancer – Principles & Practice of Oncology. DeVita VT Jr, Hellman S, Rosenberg SA (eds.). J.B. Lippincott Co., Philadelphia 1993; 2395-406.
17. Zhao XJ, Huang YH, Yu YC, Xin XY. GnRH antagonist cetrorelix inhibits mitochondria-dependent apoptosis triggered by chemotherapy in granulosa cells of rats. Gynecol Oncol 2010; 118: 69-75.
18. Meirow D, Assad G, Dor J, Rabinovici J. The GnRH antagonist cetrorelix reduces cyclophosphamide-induced ovarian follicular destruction in mice. Hum Reprod 2004; 19: 1294-9.
19. Cook CL, Siow Y, Taylor S, Fallat ME. Serum müllerian-inhibiting substance levels during normal menstrual cycles Fertil Steril 2000; 73: 859-61.
20. Maheshwari A, Fowler P, Bhattacharya S. Assessment of ovarian reserve – should we perform tests of ovarian reserve routinely? Hum Reprod 2006; 21: 2729-35.
21. Rajpert-De Meyts E, Jorgensen N, Graem N, Müller J, Cate RL, Skakkebaek NE. Expression of anti-Müllerian hormone during normal and pathological gonadal development: association with differentiation of Sertoli and granulosa cells. J Clin Endocrinol Metabol 1999; 84: 3836-44.
Arch Med Sci 2, 1st March / 2023 451
Experimental research
Osteoporosis
Amarogentin promotes osteoblast differentiation in oestrogen-deficiency-induced osteoporosis rats by modulating the Nrf-2/MAPK/ERK signalling pathway
Sirui Li1, Xianlong Li1, Feng He1, Rui Jiao2, Song Zhang1, Zhihua Li3
1The Second Clinical Medical College of Dalian Medical University, Dalian, China
2Clinical Medical College of Yangzhou University, Yangzhou, China
3Department of Orthopaedics, Xiaogan Central Hospital, Xiaogan, China
Submitted: 26 May 2019; Accepted: 24 July 2019
Online publication: 11 November 2019
Arch Med Sci 2023; 19 (2): 452–457
DOI: https://doi.org/10.5114/aoms.2019.89652
Copyright © 2019 Termedia & Banach
Abstract
Introduction: The beneficial effect of amarogentin in the management of osteoporosis was determined using in vivo and in vitro methods.
Material and methods: Experimental osteoporosis was induced in rats via bilateral ovariectomy. Rats were then treated for 5 weeks with amarogentin (50 and 100 mg/kg, p.o.). The levels of several biochemical markers of bone resorption and formation as well as bone mineral density (BMD) were measured in the rat serum. Isolated rat bone tissues were analysed using western blot assays In the in vitro study, MG63 human osteoblasts were treated with amarogentin (0–100 μ g/ml), after which alkaline phosphatase activity and osteoblast proliferation were evaluated. Osteoblasts treated with amarogentin and inhibitors of extracellular signal-regulated kinase (ERK) were further examined via western blotting.
Results: In the rat model of oestrogen-deficiency-induced osteoporosis, BMD was significantly enhanced ( p < 0.01) and levels of inflammatory cytokines were reduced in amarogentin-treated animals vs. the controls. Amarogentin treatment also attenuated the altered levels of osteocalcin , C-telopeptide of type 1 collagen, procollagen type I N-terminal propeptide, and bone-specific alkaline phosphatase, and the altered expression of Akt, Nrf-2, ERK, and nuclear factor- κ B p65 in the serum of rats with osteoporosis. In the in vitro study, amarogentin treatment enhanced alkaline phosphatase activity and osteoblast proliferation compared to the non-treated control. Amarogentin treatment alone enhanced the expression of p-ERK compared to treatment with an amarogentin + ERK inhibitor.
Conclusions: Both the in vivo and the in vitro studies demonstrated the protective effect of amarogentin against oestrogen-deficiency-induced osteoporosis in rats. The mechanism seems to involve the amarogentin-mediated enhancement of osteoblast differentiation via the Nrf-2/MAPK/ERK signalling pathway.
Key words: amarogentin, osteoporosis, oestrogen, ovary, osteoblast, inflammation.
Introduction
Osteoporosis is a bone disorder characterised by bone loss and destruction of the bone microarchitecture. This imbalance between bone resorption and formation results in fragile bones and increased suscepti-
Corresponding author: Zhihua Li
Department of Orthopaedics
Xiaogan Central Hospital
6 Square St
Xiaogan 432000, Hubei Province, China
Phone/fax: +86 0712-2335126
E-mail: zoeperez248@ hotmail.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Amarogentin promotes osteoblast differentiation in oestrogen-deficiency-induced osteoporosis rats by modulating the Nrf-2/MAPK/ERK signalling pathway
bility to fracture [1, 2]. Osteoporosis occurs worldwide – mostly in postmenopausal women due to the cessation of oestrogen production by the ovaries [3] and therefore the loss of the positive effect of oestrogen on bone formation [4]. Among the cellular pathways involved in the differentiation and growth of osteoblasts are those of mitogen-activated protein kinase (MAPK) and extracellular signal-regulated kinase (ERK) [5]. Osteoclast differentiation and thus bone resorption are controlled by nuclear factor-κB (NF-κB) [6]. Anabolics are used for the management of osteoporosis because they enhance osteoblast function and therefore bone formation. However, conventional treatments for the management of osteoporosis have several limitations. Thus, in the last few decades, interest has grown in the management of osteoporosis by alternative medicine approaches.
Amarogentin is a secoiridoid glycoside that has been isolated from Swertia and Gentiana roots [7]. Swertia mileensis (Gentianaceae) and S. chirayita (Roxb. ex Fleming) are used traditionally in the management of hepatitis, liver injury, and diabetes in China [8]. Amarogentin is reported to have anticancer, hepatoprotective, antioxidant, anti-infective, immunomodulatory, anti-inflammatory, and anti-diabetic properties [9–11]. The vasculo-metabolic effects of amarogentin were shown to be mediated by tumour necrosis factor-a (TNF-a) and MAPK [12].
Thus, in this study we used a rat model of oestrogen-deficiency-induced osteoporosis and a human osteoblast cell line to explore whether amarogentin has beneficial effects on osteoporosis.
Material and methods
Animal model
Female Sprague Dawley rats (weight: 200–250 g; age: 3 months) were procured from the Beijing Laboratory Animal Research Center, China, and housed under standard conditions (humidity: 60 ±5%; temperature: 24 ±3°C) with a 12 : 12-h light/dark cycle. All animals were acclimatised to the laboratory conditions and had free access to normal standard chow and tap water. The study protocols were approved by the Institutional Animal Care and Use Committee of Xiaogan Central Hospital, China (IACUC/XCH/2019/14).
Chemicals
Amarogentin was purchased from Sigma-Aldrich Ltd. (St. Louis, MO, USA) and the enzyme-linked immunosorbent assay (ELISA) kits from Thermo Fisher Scientific (Waltham, MA, USA). The primary antibodies used in the western blot assays were purchased from Santa Cruz Biotechnology (Santa Cruz, CA, USA) and Thermo Fisher Scientific.
Experimental procedures
Bilateral ovariectomy was performed in anaesthetised rats as described previously [13]. A 2-cm incision was made along the abdomen of the rats, and the ovaries were exposed using arterial forceps. After bilateral removal of the ovaries, the abdominal fat pad was repositioned, and the wound was closed by suturing. These rats were assigned to the ovariectomised (OVR) or amarogentin-treated (50 and 100 mg/kg, p.o., for 5 weeks) groups. Rats in the control (sham) group underwent the same surgery but their ovaries were not removed.
Determination of bone mineral density (BMD)
Dual energy X-ray absorptiometry was used to measure the BMD of the rats. Prior to scans of the total femur, lumbar vertebrae, and whole body, the rats were anaesthetised with a mixture of Zoletil-Rompun.
Determination of biochemical parameters
Blood was withdrawn from the retro-orbital plexuses of the anaesthetised rats and centrifuged at 2,000 rpm for 10 min to separate the serum. ELISA kits were used according to the manufacturer’s instructions to measure the serum levels of osteocalcin (OC), C-telopeptide of type 1 collagen (CTX), procollagen type I N-terminal propeptide (PINP), bone-specific alkaline phosphatase (BSAP), interleukin-1b (IL-1b), TNF-a, and IL-17. Bone resorption was estimated based on the concentration of tartrate-resistant acid phosphatase 5b (TRACP 5b).
Western blot assay
Protein was extracted from the right tibia via incubation of the bone in lysis buffer. The lysate was centrifuged at 12,000 rpm for 10 min and the supernatant was collected. The protein concentration was determined using a bicinchoninic acid quantification assay. Sodium dodecyl sulphate-polyacrylamide gel electrophoresis (SDSPAGE) using a 10% polyacrylamide gel was performed to separate the proteins, which were then transferred to a polyvinylidene difluoride (PVDF) membrane. The membrane was incubated with the following primary antibodies in a western blot assay: Akt (1 : 1,000; Santa Cruz Biotechnology), NF-κB p65 (1 : 100; Thermo Fisher Scientific), Nrf-2 (1 : 500; Santa Cruz Biotechnology), MAPK (1 : 100; Thermo Fisher Scientific), ERK (1 : 200; Thermo Fisher Scientific), and b-actin (1 : 2,000; Santa Cruz Biotechnology). Chemiluminescent signals were detected on the washed membrane using laboratory imaging software.
Arch Med Sci 2, 1st March / 2023 453
Data are presented as mean ± standard error of the mean (SEM; n = 8). **p < 0.01, vs. sham control group; #p < 0.05, ##p < 0.01, vs. ovariectomised (OVR) group.
In vitro study
Determination of alkaline phosphatase activity and osteoblast proliferation
The human osteoblast line MG63 was procured from the American Type Culture Collection, and an immunoassay kit based on the incorporation of bromodeoxyuridine into newly synthesised DNA was used to determine the effect of amarogentin. Alkaline phosphatase activity in pre-osteoblastic MC3T3-E1 cells was estimated using an ALP B-test kit according to the manufacturer’s instructions.
Western blot assay
MG63 cells were treated for 2 h with 100 μg/ml amarogentin with and without ERK inhibitor, after which cell proteins were extracted using PROPREP protein extraction solution and subjected to SDS-PAGE on a 10% polyacrylamide gel. The separated proteins were transferred to a PVDF membrane and incubated first with anti-p-ERK (1 : 200; Thermo Fisher Scientific) and anti-ERK (1 : 200; Thermo Fisher Scientific) and then with a horseradish-peroxidase-conjugated secondary antibody. BIO1D software (Scientific Software Group, Salt Lake City, UT, USA) was used for data analy-
sis and a chemiluminescent imaging system was used to visualise the signals on the immunoblots.
Statistical analysis
All data are expressed as the means ± standard error of the mean (n = 8). Results were compared among groups using one-way analysis of variance. A post-hoc comparison of means was carried out using Dunnett’s post-hoc test in Prism software (ver. 6.1; GraphPad Software Inc., San Diego, CA, USA). The level of statistical significance was set at a = 0.05.
Results
Effect of amarogentin on BMD
Figure 1 shows the effect of amarogentin on the BMD of the whole body, lumbar spine, and femur of rats with oestrogen-deficiency-induced osteoporosis. The mean BMD of OVR rats was lower than that of sham-operated rats. However, compared to OVR rats, amarogentin-treated rats exhibited enhanced whole-body and lumbar-spine BMD.
Amarogentin attenuates serum biochemical parameters
The levels of the markers of bone formation in the serum of rats with oestrogen-deficiency-induced osteoporosis that were treated or not treated with amarogentin are shown in Table I. Lower serum OC levels and higher serum CTX, PINP, and BSAP levels were measured in the OVR group than in the sham-operated group. However, amarogentin treatment improved the levels of all four markers in rats with osteoporosis
Amarogentin reduces the levels of inflammatory cytokines
The effect of amarogentin on inflammatory cytokine levels in the serum in the rat model is shown in Figure 2. The levels of IL-1b, IL-17, and TNF-a were higher in the OVR group than in the sham-operated group. In the amarogentin-treated group, the levels of all three cytokines were lower than in the OVR group.
454 Arch Med Sci 2, 1st March / 2023
Sirui Li, Xianlong Li, Feng He, Rui Jiao, Song Zhang, Zhihua Li
Figure 1. Effect of amarogentin on bone mineral density of the whole body, lumbar spine, and femur of rats with oestrogen-deficiency-induced osteoporosis
Whole body Lumbar Femur Sham OVR Amarogentin 50 mg/kg Amarogentin 100 mg/kg BMD [g/cm 2 ] 0.30 0.25 0.20 0.15 0.10 0.05 0 ** ** ** ## ## ## #
No. Group OC [pg/ml] CTX [ng/ml] PINP [ng/ml] BSAP [U/l]) 1 Sham 8.64 ±0.84 39.72 ±2.8 6.28 ±0.47 9.35 ±0.63 2 OVR 3.49 ±0.27** 126 ±7.43** 21.83 ±0.81** 12.71 ±0.86* 3 Amarogentin 50 mg/kg 5.12 ±0.31# 79.68 ±3.28## 14.62 ±0.49## 11.29 ±0.57 4 Amarogentin 100 mg/kg 6.81 ±0.79## 48.2 ±3.79## 9.37 ±0.62## 10.37 ±0.61# Mean ± SEM (n = 8); **p < 0.01 vs. sham group; #p < 0.05, ##p < 0.01 vs. OVR group.
Table I. Effect of amarogentin on biochemical markers in the serum of oestrogen-deficiency-induced osteoporosis rat model
Amarogentin promotes osteoblast differentiation in oestrogen-deficiency-induced osteoporosis rats by modulating the Nrf-2/MAPK/ERK signalling pathway
Amarogentin attenuates the expression of Akt, NF-κB p65, Nrf-2, MAPK, and ERK proteins
Figure 3 shows the levels of Akt, NF-κB p65, Nrf-2, and ERK protein expression in the bone tissues of rats with oestrogen-deficiency-induced osteoporosis that were treated with amarogentin. The expression of Akt, Nrf-2, and ERK decreased, whereas that of NF-κB p65 increased in the bone tissues of the OVR rats compared to the sham-operated rats. By contrast, the expression of Akt, Nrf-2, and ERK proteins was significantly enhanced and that of NF-κB p65 reduced in the bone tissues of the amarogentin-treated rats compared to that of the OVR rats.
Effect of amarogentin on alkaline phosphatase activity and osteoblast proliferation
Alkaline phosphatase activity and osteoblast proliferation were determined in MG63 cells that were treated or not treated with amarogentin (Figure 4). Amarogentin treatment (50 and 100 μg/ml) significantly enhanced MG63 osteoblast proliferation (p < 0.05 and p < 0.01, respectively) relative to the control group. Alkaline phosphatase activity
Data are presented as mean ± SEM (n = 8). **p < 0.01, vs. sham control group; ##p < 0.01, vs. OVR group.
was also significantly higher (p < 0.01) in amarogentin-treated (10–100 μg/ml) MG63 cells than in the untreated control cells
Effect of amarogentin on ERK/MAPK pathway
Figure 5 shows the effect of amarogentin (100 μg/ml) on the ERK/MAPK pathway of MG63 cells
Data are presented as mean ± SEM (n = 8). **p < 0.01, vs. sham control group; ##p < 0.01, vs. OVR group.
Data are presented as mean ± SEM (n = 8). *p < 0.05, **p < 0.01, vs. cells not treated with amarogentin (0 µg/ml).
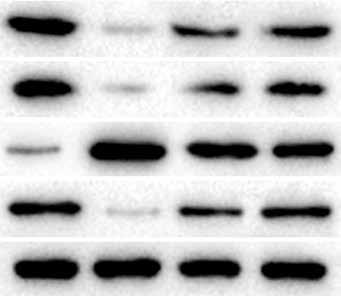
Arch Med Sci 2, 1st March / 2023 455
Figure 2. Effect of amarogentin on levels of inflammatory cytokines in the serum of rats with oestrogen-deficiency-induced osteoporosis
IL-1b IL-17 TNF-a Sham OVR Amarogentin 50 mg/kg Amarogentin 100 mg/kg Inflammatory cytokines [pg/ml] 100 90 80 70 60 50 40 30 20 10 0 ** ** ** ## ## ## ## ## ## Akt NF-κB p65 Nrf-2
Sham OVR Amarogentin
Amarogentin
mg/kg Relative expression 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0 ** ** ** ** ## ## ## ## ## ## ## ##
p-ERK
50 mg/kg
100
Figure 3. Effect of amarogentin on expression of Akt, NF-κB p65, Nrf-2, and ERK proteins in rats with oestrogen-deficiency-induced osteoporosis
Sham OVR Amarogentin Amarogentin
mg/kg 100 mg/kg Akt Nrf-2 NF-κB p65 p-ERK b-actin
50
Figure 4. In vitro effect of amarogentin on alkaline phosphatase activity and proliferation of MG63 cells (human osteoblasts)
0 10 25 50 100 Amarogentin [µg/ml] 0 10 25 50 100 Amarogentin [µg/ml] Osteoblast proliferation (%) Alkaline phosphatase activity (%) 160 140 120 100 80 60 40 20 0 200 180 160 140 120 100 80 60 40 20 0 ** ** * ** ** **
in the presence and absence of ERK inhibitor. The ratio of p-ERK/ERK protein expression was significantly higher in the amarogentin-treated group than in the sham-operated group, whereas p-ERK protein expression was significantly reduced in the group treated with amarogentin and an ERK inhibitor.
Discussion
Postmenopausal osteoporosis is the most common bone disorder in females, but current treatments have several limitations [14]. In this study, we evaluated the protective effect of amarogentin both in vivo – against oestrogen-deficiency-induced osteoporosis in rats – and in vitro – in a human osteoblast line. In the rats, serum levels of several biochemical markers of bone formation were evaluated, BMD was measured, and western blot assays of inflammatory cytokines and cellular pathways were conducted. In cultured MG63 cells, the effects of amarogentin on alkaline phosphatase activity and osteoblast proliferation were determined. In addition, the cells were assayed for ERK expression in the presence or absence of an ERK inhibitor.
CTX, OC, BSAP, and PINP are often used as markers of bone formation and resorption [15], and measurements of their levels are used to evaluate drugs designed for the management of osteoporosis [16]. Our study showed that amarogentin treatment attenuates the alterations in CTX, OC, BSAP, and PINP levels in the serum of OVR rats. Inflammatory cytokines play an important role in the regulation of bone resorption, but a deficiency of oestrogen results in their overexpression [17–20]. Our study revealed that amarogentin-treated rats exhibited a significant reduction in the levels of inflammatory cytokines (p < 0.01) compared to OVR rats.
The ERK/MAPK signalling pathway regulates osteoblast apoptosis and differentiation, and ERK participates in osteogenesis and bone metabolism [21]. Physiological inhibition of the ERK gene contributes to the development of osteoporosis by
inhibiting osteoblast differentiation and proliferation [22]. Many of the drugs with proven efficacy in the management of osteoporosis modulate the ERK/MAPK signalling pathway [18, 23]. Our study showed that amarogentin treatment enhances osteoblast differentiation in vitro and that ERK expression is reduced in osteoblasts treated with amarogentin and an ERK inhibitor. In addition, the expression of Akt, Nrf-2, and ERK proteins was shown to be significantly enhanced in the bone tissue of OVR rats. Akt and Nrf-2 proteins participate in the development of osteoporosis by altering osteoblast function, as reported previously.
In conclusion, our investigation demonstrated that amarogentin has a protective effect against oestrogen-deficiency-induced osteoporosis in a rat model. Amarogentin was shown to enhance osteoblast differentiation by regulating the Nrf-2/ MAPK/ERK signalling pathway.
Acknowledgments
The authors thank Xiaogan Central Hospital, China for providing the necessary facilities to conduct this study.
Conflict of interest
The authors declare no conflict of interest.
References
1. Sözen T, Özışık L, Başaran NÇ. An overview and management of osteoporosis. Eur J Rheumatol 2016; 4: 46-56.
2. Feng X, McDonald JM. Disorders of bone remodeling. Annu Rev Pathol 2011; 6: 121-45.
3. Clarke BL, Khosla S. Physiology of bone loss. Radiol Clin North Am 2010; 48: 483-95.

4. Ji MX, Yu Q. Primary osteoporosis in postmenopausal women. Chronic Dis Transl Med 2015; 1: 9-13.
5. Munshi A, Ramesh R. Mitogen-activated protein kinases and their role in radiation response. Genes Cancer 2013; 4: 401-8.
6. Song J, Jing Z, Hu W, Yu J, Cui X. Alpha-linolenic acid inhibits receptor activator of NF-kappaB ligand induced (RANKL-Induced) osteoclastogenesis and prevents inflammatory bone loss via downregulation of nuclear
456 Arch Med Sci 2, 1st March / 2023
Sirui Li, Xianlong Li, Feng He, Rui Jiao, Song Zhang, Zhihua Li
Ratio of p-ERK/ERK 2.5 2.0 1.5 1.0 0.5 0 ** ##
Control Amarogentin Amarogentin + PD98059
Figure 5. In vitro effect of amarogentin on the ERK/MAPK pathway in MG63 cells treated with an ERK inhibitor Data are presented as mean ± SEM (n = 8). **p < 0.01, vs. control cells; ##p < 0.01, vs. amarogentin-treated cells.
p-ERK ERK
Control Amarogentin Amarogentin + PD98059
Amarogentin promotes osteoblast differentiation in oestrogen-deficiency-induced osteoporosis rats by modulating the Nrf-2/MAPK/ERK signalling pathway
factor-kappa B-inducible nitric oxide synthases (NF-kappaB-iNOS) signalling pathways. Med Sci Monit 2017; 23: 5056-69.
7. Keil M, Härtle B, Guillaume A, Psiorz M. Production of amarogentin in root cultures of Swertia chirata. Planta Med 2000; 66: 452-7.
8. Kumar V, Van Staden J. A review of Swertia chirayita (Gentianaceae) as a traditional medicinal plant. Front Pharmacol 2016; 6: 308.
9. Zhang Y, Zhao H, Li H, et al. Protective effects of amarogentin against carbon tetrachloride-induced liver fibrosis in mice. Molecules 2017; 22: E754.
10. Patel K, Kumar V, Verma A, Rahman M, Patel DK. Amarogentin as topical anticancer and anti-infective potential: scope of lipid based vesicular in its effective delivery. Recent Pat Antiinfect Drug Discov 2019; 14: 7-15.
11. Wölfle U, Haarhaus B, Schempp CM. Amarogentin displays immunomodulatory effects in human mast cells and keratinocytes. Mediators Inflamm 2015; 2015: 630128.
12. Potunuru UR, Vishnu Priya V, Sai varsha MKN, et al. Amarogentin, a secoiridoid glycoside, activates AMP-activated protein kinase (AMPK) to exert beneficial vasculo-metabolic effects. Biochim Biophys Acta Gen Subj 2019: 1863: 1270-82.
13. Wang YG, Jiang LB, Gou B. Protective effect of vanillic acid on ovariectomy-induced osteoporosis in rats. Afr J Tradit Complement Altern Med 2017; 14: 31-8.
14. Lems WF, Raterman HG. Critical issues and current challenges in osteoporosis and fracture prevention. An overview of unmet needs. Ther Adv Musculoskelet Dis 2017; 9: 299-316.
15. Wheater G, Elshahaly M, Tuck SP, Datta HK, van Laar JM. The clinical utility of bone marker measurements in osteoporosis. J Transl Med 2013; 11: 201.
16. Lewiecki EM. Bisphosphonates for the treatment of osteoporosis: insights for clinicians. Ther Adv Chronic Dis 2010; 1: 115-28.
17. Zupan J, Jeras M, Marc J. Osteoimmunology and the influence of pro-inflammatory cytokines on osteoclasts. Biochem Med (Zagreb) 2013; 23: 43-63.
18. Moreno-Eutimio MA, Espinosa-Monroy L, Orozco-Amaro T, et al. Enhanced healing and anti-inflammatory effects of a carbohydrate polymer with zinc oxide in patients with chronic venous leg ulcers: preliminary results. Arch Med Sci 2018; 14: 336-44.
19. Yelumalai S, Giribabu N, Karim K, Omar SZ, Salleh NB. In vivo administration of quercetin ameliorates sperm oxidative stress, inflammation, preserves sperm morphology and functions in streptozotocin-nicotinamide induced adult male diabetic rats. Arch Med Sci 2019; 15: 240-9.
20. Eken KM, Ersoy GS, Kaygusuz EI, et al. Etanercept protects ovarian reserve against ischemia/reperfusion injury in a rat model. Arch Med Sci 2019; 15: 1104-12.
21. Matsushita T, Chan YY, Kawanami A, Balmes G, Landreth GE, Murakami S. Extracellular signal-regulated kinase 1 (ERK1) and ERK2 play essential roles in osteoblast differentiation and in supporting osteoclastogenesis. Mol Cell Biol 2009; 29: 5843-57.
22. Feng X, McDonald JM. Disorders of bone remodeling. Annu Rev Pathol 2011; 6: 121-45.
23. Kim HK, Kim MG, Leem KH. Osteogenic activity of collagen peptide via ERK/MAPK pathway mediated boosting of collagen synthesis and its therapeutic efficacy in osteoporotic bone by back-scattered electron imaging and microarchitecture analysis. Molecules 2013; 18: 15474-89.
Arch Med Sci 2, 1st March / 2023 457
Menopause and women’s cardiovascular health: is it really an obvious relationship?
Kamila Ryczkowska1, Weronika Adach1, Kamil Janikowski1,2, Maciej Banach1,2, Agata Bielecka-Dabrowa1,2
1Department of Preventive Cardiology and Lipidology, Medical University of Lodz, Lodz, Poland
2Department of Cardiology and Congenital Diseases of Adults, Polish Mother’s Memorial Hospital Research Institute (PMMHRI), Lodz, Poland
Submitted: 21 November 2022; Accepted: 9 December 2022
Online publication: 10 December 2022
Arch Med Sci 2023; 19 (2): 458–466
DOI: https://doi.org/10.5114/aoms/157308
Copyright © 2022 Termedia & Banach
Abstract
Cardiovascular diseases are common for men and women but there are differences between the sexes in terms of clinical symptoms, pathophysiology and response to the treatment. Cardiovascular diseases (CVD) in women is commonly underdiagnosed and often women tend to have a lower perception of the risk. That can lead to delayed diagnosis and failed recognition of symptoms. Women develop heart diseases later than men because of the protection in the reproductive phase of their life. Once they enter menopause the risk increases. Estrogen provides a protective effect against heart disease in women. Therefore, the risk of CVD increases after menopause in most cases. The presented work emphasizes the importance of the menopausal period as the time of increasing CVD risk. It also emphasizes the importance of monitoring the health of women in their middle age, a critical time in which early intervention strategies should be implemented to reduce the risk of CVD.
Key words: cardiovascular diseases, hypertension, hormone therapy, lipid disorders, estrogens.
Introduction
Cardiovascular disorders are the first cause of death in the world, the second is cancer. About 17.9 million people die from cardiovascular diseases (CVDs), an estimated 31% of deaths globally according to data presented by World Health Organization (WHO) in 2017.
CVDs include disorders like coronary heart disease, cerebrovascular disease, rheumatic heart disease, arterial disease, peripheral arterial disease, congenital heart disease, deep vein thrombosis and pulmonary embolism. CVD is the main cause of morbidity and mortality in both men and women in developed countries. Studies have shown that low estrogen levels correlate with coronary artery disease in men [1]. CVD occurs more frequently in men than in women before menopause [2].
As the increased risk of CVD coincides with menopause, studies have shown that female hormones, especially estrogens, are cardioprotective and play significant roles in both reproductive and non-reproductive systems [2]. Menopause is associated with a significant increase of blood
Corresponding author: Weronika Adach
Department of Preventive Cardiology and Lipidology
Chair of Nephrology and Hypertension Medical University of Lodz
4 Kościuszki St
90-419 Lodz, Poland
Phone: +48 42 271 15 99
E-mail: weronika.adach@ umed.lodz.pl
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/). State of the art paper
Women’s Cardiology
Menopause and women’s cardiovascular health: is it really an obvious relationship?
pressure, body mass index (BMI), obesity, and body fat distribution [3]. Moreover, they can be synthesized in non-reproductive tissues such as the bone, brain, liver, heart, and muscles [4].
Female sex hormones
Estradiol, which is also known as 17-beta-estradiol or estrogen (E2), is the most common form of circulating estrogens and is also considered to be the primary female sex hormone. Two other forms which are less abundant are estrone (E1) and estriol (E3). The third one (E3) is formed from E1 through 16a-hydroxylation. Their roles become more prominent during pregnancy when they are produced by the placenta in large quantities [5].
Estrogens like other sex hormones are delivered from cholesterol during estrogen biosynthesis [6]. E2 is considered as the major product of this process which plays an important role before menopause, while the significance of E1 grows after menopause [7]. E2 is principally synthesized by ovaries, corpus luteum and placenta but it is also produced by other tissues such as the brain, adipose tissue, bone, vascular endothelium, and aortic smooth muscle cells [5]. E2 synthesized in gonads works to a large extent as a hormonal factor influencing distal tissues, while nongonadal compartments act mainly locally in the tissue in which it is synthesized. Extragonadal production of E2 is crucial because it remains the only source of endogenous E2 in men and postmenopausal women [5].
Dyslipidemia and cholesterol accumulation are more common during menopause, which may be associated with an estrogen deficiency [8]. However, new reports have emerged that show that independent serum estrogen, follicle stimulating hormone (FSH) can increase the production of cholesterol in the liver. A recent study of 278 women found that in perimenopausal women, serum FSH, total cholesterol (TC), and low density lipoprotein cholesterol (LDL-C) levels were higher compared to premenopausal women, despite similar results in serum estrogen levels [9]. Another study involving 588 postmenopausal women confirmed that higher levels of FSH were associated with higher levels in both TC and LDL-C [10]. In a group of 400 postmenopausal women who showed similar values of FSH, TC and LDL-C in the serum, a significant improvement in the level of lipids was noticed only in women after hormone therapy whose FSH concentration decreased by about 30% [11].
Sex steroids have a great effect on the risk of coronary heart disease. Loss of ovarian hormones leads to an increase in LDL-C, triglycerides, and a decrease in high density lipoprotein cholesterol (HDL-C) [12]. These data suggest that blocking FSH signaling lowers serum cholesterol levels by inhibiting hepatic cholesterol biosynthesis [9].
Hormone therapy
The research group comprised women aged 53 to 73 years and not using hormone therapy (HT). Nevertheless, the results of postmenopausal hormone therapy on CVD risk remain controversial [13].
According to the data, oral or transdermal HT does not increase the risk of heart disease. On the contrary, observational studies showed the beneficial cardioprotective effect that can be obtained even with the use of low doses of oral HT (effect of 0.3 mg/day of oral conjugated equine estrogen was similar compared to a standard dose of 0.625 mg/day). The use of HT may delay the progression of the thickness of the intima-media layer of the carotid arteries, which in turn leads to atherosclerosis and coronary calcification [14, 15].
However, the clinical trials confirming the cardioprotective benefits of HT in primary prevention have not been acknowledged yet. In addition, recent data suggest that oral and transdermal HT, in a dose-dependent manner and independent of the HT formulation, may increase the risk of thromboembolism and stroke [13].
For these diseases, transdermal estrogen at a dose < 50 μg/day in combination with micronized progesterone seems to be an innocuous choice. Data suggest that low-dose transdermal and oral HT appears to be safe in relation to CVD risk in menopausal women and during the first years (e.g., 10 years) after menopause. Literature data suggest that TH can alleviate the majority of CVD risk factors to varying degrees, including visceral obesity, dyslipidemia, and glucose hemostasis. Depending on the type of estrogen, dose, route of administration and the type of progestogen, TC, LDL-C, Lp(a) can be lowered and the concentration of HDL-C may be increased [16–18].
When oral estrogen is used, an increase in triglyceride (TG) levels may be observed, however, when administered trans-dermally, TG levels may decrease or remain the same [16, 17]. Furthermore, transdermal estrogen has no effect on the coagulation system and is not associated with an increased risk of venous thromboembolism (VTE) [19].
Non-hormonal drugs are recommended as the first-line therapy for women with an increased baseline thromboembolic risk. If the first-line drugs do not bring the expected result, transdermal estradiol alone or with micronized progesterone application is considered. When HT is initiated > 10 years after the menopause (> 60 years old), because of the risks of coronary heart disease, venous thromboembolism and stroke, HT is recommended to be used for the shortest time conceivable and in the lowest possible dose. Transdermal administration is highly recommended. Nevertheless, individualized pharmacotherapy should be
Arch Med Sci 2, 1st March / 2023 459
Transdermal
Unmetabolized
applied when prescribing HT, which includes baseline CVD risk assessment [13].
Most international scientific societies agree that the early initiation of HT in patients with premature or surgical menopause is associated with cardiovascular benefits [20] (Table I).
The role of estrogens and estrogen receptors in the cardiovascular system
Growing proof highlights that the synthesis and signaling of estrogens can be both cell- and tissue-specific. It proves that estrogens are not only purely female sex hormones for gonadal organ growth and functioning [7].
Estrogens perform important functions in extragonadal tissues such as the liver, muscles, and the brain. Estrogen treatment is evaluated in clinical trials for dealing with age-related diseases. However, due to large discrepancies in research results, the question arises whether estrogen therapy is beneficial or harmful [7].
Therefore, it is important to understand the exact mechanism of estrogen’s impact on individual tissues in the body. Understanding of cell-specific, tissue estrogen and ERs is essential for studying physiological and pathological changes during aging, as well as being important for the development of new therapeutic agents for the prevention and treatment of heart diseases and other age-related diseases such as Parkinson’s disease (PD), and Alzheimer’s disease (AD) and osteoporosis. Estrogens play an important role in the early development of primary and secondary sexual characteristics. In addition, they are important for the embryonic and fetal development of brain networks. Estrogens have two types of receptors: classical nuclear receptors (ERa and ERb) and novel cell surface membrane receptors (GPR30 and ER-X) [7].
These two types of estrogen receptors are expressed with tissue- and cell-specific deliveries. Recent trials suggest that brain estrogens are neuroprotective thanks to cell surface membrane receptors and nuclear receptors. Ovarian estrogens play a key role in the management of the reproductive system such as puberty, fertility, and estrous cycle mostly via interaction with nuclear estrogen receptors [7].
During the reproductive period, estrogens secreted by the ovaries have a protective effect on lipid metabolism and the functions of the vascular endothelium. Postmenopausal lower estrogen levels contribute to increased vascular tone through endocrine and autonomic mechanisms that link impaired nitric oxide-dependent vasodilation [21, 22].
The cell- and tissue-specific operation of estrogens as well as their receptors provide healthy aging as well as conflicting outcomes from estrogen therapy in diseases that are related to aging [7].
There is now much evidence of the protective properties of endogenous estrogen against cardiovascular disease (CVD). First, it is known for its positive effect on plasma lipid profiles, as well as antiplatelet and antioxidant properties [23].
Protective role of estrogens
In premenopausal women, estrogens are synthesized mainly in the ovaries, corpus luteum and the placenta. Estrogens are also produced by organs such as the brain, skin, liver, and heart [4]. Three main forms of estrogens are estrone (E1), estradiol (E2, or 17b-estradiol), and estriol (E3) [24].
The risk of cardiovascular disease drastically increases after menopause when the level of estrogens is dropping down [25]. The protective role against cardiovascular disease in women during childbearing age is believed to be at least partially related to E2 as endogenous E2 levels and ER expression vary widely between the sexes. E2 is involved in its cardioprotective action by increasing angiogenesis and vasodilation, and by reducing ROS, oxidative stress, and fibrosis [5].
These mechanisms lead E2 to limit heart remodeling and reduce heart hypertrophy. Even if the usage of E2 as a therapeutic agent for human use is controversial, targeting specific ERs in the cardiovascular system could open new and perhaps safer therapeutic options for using E2 to protect the cardiovascular system [5] (Figure 1).
The protective role of estrogen in cardiovascular diseases is associated with a decrease in fibrosis, stimulation of angiogenesis and vasodilation, enhancement of mitochondrial function and reduction in oxidative stress [5].
Studies show that women who experienced premature menopause had a significantly in-
460 Arch Med Sci 2, 1st March / 2023
Kamila Ryczkowska, Weronika Adach, Kamil Janikowski, Maciej Banach, Agata Bielecka-Dabrowa
Table I. Comparison of transdermal E2 and oral CE delivery. Modified [17]
E2
CE delivery
delivery Oral
E2,
First pass liver metabolism
or ↔ TG ↑ TG
LDL/HDL ↓↓ LDL/HDL
Clotting factors ↑ Clotting factors
Inflammatory factors ↑ Inflammatory factors ↑ E2 delivery to non-hepatic tissues ↓ CE delivery to non-hepatic tissues
at lower doses, directly to the blood stream
↓
↓
↔
↔
Fibrosis
Decrease fibrosis migration and proliferation
Decrease collagen Deposition (MMP, AngII)
Mitochondria
Pro-survival/anti-apoptotic
Increase FAO, decrease infarct size
Decrease ROS production
Menopause and women’s cardiovascular health: is it really an obvious relationship?
Vasculature
Increase angiogenesis (VEGF)
Increase vasodilation (eNOS)
Protective role of estrogen (E2)
creased risk of a non-fatal cardiovascular event before the age of 60, but not after the age of 70 in comparison to women who reach menopause at the age of 50–51 years. Early menopausal women require close monitoring in clinical practice. Moreover, the age at which a woman reaches menopause may be considered as an important factor in assessing the risk of cardiovascular disease in women. Women who reach menopause at the age under 40 years were categorized as premature menopause, 40–44 years as early menopause, 45–49 years as relatively early, 50–51 years as the reference category, 52–54 years as relatively late and 55 years or older as late menopause. 301 438 women were included in this analysis which was done across five countries and regions (Australia, Scandinavia, the USA, Japan, and the UK) [26].
The menopausal transition is characterized by active changes in follicle-stimulating and estradiol hormone levels. Research done by the Study of Women’s Health Across the Nation (SWAN) and the Melbourne Women’s Midlife Health Project reported a decrease in estradiol level 2 years before the final menstrual period (FMP) and an increase in follicle-stimulating hormone 6 years before [27].
Cardiovascular disease
Women suffer from coronary heart diseases (CHD) a few years later than men. Women are more common to have stable plaques and a better occurrence of microvascular lesions compared to men [28]. Nevertheless, studies have shown that gender is not affecting the outcome of the hypertension treatment [3].
Men get sick more often and are diagnosed with CVD earlier than premenopausal women. After the menopause, the incidence of CVD in women increases significantly [2]. Epidemiological studies have reported that women get sick and die more often from CVD compared to men. There are an increasing number of studies that highlight the gender differences in pharmacokinetics (PK) of drugs for CVD. Differences in drug absorption may come from higher gastric pH in women and
Oxidative stress
Anti-oxidant properties
Increase cell survival
the longer gastrointestinal transit time. Differences were also noted in gastrointestinal glutathione S-transferase and cytochrome P450 enzymes. Women have a higher percentage of body fat but weigh less than men, which can have different drug distribution in the body. However, on the topic of pharmacotherapy, there is still a lack of consistent gender findings [29, 30].
The risk increases significantly in the middle age, which interferes with menopause. This observation suggests that the menopause transition (MT) contributes to an increased risk of heart disease [20, 31].
Long-standing studies of menopausal women have provided a better understanding of the relationship between MT and CVD. Research conducted for over 20 years has recognized different patterns of change in endogenous sex hormones and unfavorable changes in body fat distribution, lipids, and lipoproteins, likewise in structural and functional measures of blood vessel health during the MT period [32].
The results highlight the MT period as a colliding time with the CVD risk, which underlines the importance of health monitoring and potential intervention in midlife [20].
Epidemiological evidence has shown that the most common risk factors for CVD in menopausal women are central obesity, atherogenic dyslipidemia, glucose intolerance and hypertension [33] (Figure 2).
Increased sensitivity to sodium during menopause, which leads to fluid retention in the body causing swelling of the arms and legs, may also contribute to the cardiovascular risk [34].
Hypertension
Hypertension is one of the risk factors for cardiovascular disease [35]. Hypertension affects an increasing proportion of the world population and is one of the leading causes of morbidity and mortality worldwide [36].
Aortic stiffness is considered to lead to death due to cardiovascular events. Degradation of elas-
Arch Med Sci 2, 1st March / 2023 461
Figure 1. Protective role of estrogen (E2)
The main cardiovascular risk factors in the menopause
tin fiber, collagen accumulation, cellular element restructuring and calcium accumulation in the vascular wall, as well as arterial stiffness leads to mechanical adaptation of the arterial wall triggered by hypertensive heart disease [36].
The changes in hormone levels in the vascular system and metabolic changes that occur with age may be directly influenced by the increase in blood pressure, which is more common in postmenopausal women [22]. However, it is not clear whether this is a consequence of the aging process, which reduces vascular flexibility, or menopause [16]. However, several additional factors should be taken into account, i.e., smoking, low physical activity or obesity [37].
Adipose tissue in addition to being an energy storage is also an endocrine organ that produces adipokines such as leptin, resistin, adiponectin, and interleukin 6 [38]. Leptin is one of the biomarkers that may be used as an inflammation factor that may be considered to be responsible for interacting with the arterial wall [36]. Leptin receptors are found in the aorta and blood vessels, and their level is related to the amount of adipose tissue. Studies have shown that that higher levels of leptin in plasma lead to obesity, hypertension, and other heart diseases [36].
Currently available guidelines for the treatment of hypertension should be followed. Nevertheless, the rate of women with high blood pressure is generally under-diagnosed and under-treated [25]. In developed countries, it is estimated that 30% of adult women suffer from hypertension. Younger women have a lower absolute cardiovascular risk compared
to older ones. Nonetheless, effective treatment of hypertension should take place at any age. Hypertension occurs twice as often in postmenopausal women as in premenopausal women. Moderate or borderline hypertension (< 140/90 mm Hg) in women affects greater endothelial dysfunction and cardiovascular difficulties compared to men [25].
A recent meta-analysis confirmed that women with early menopause (EM < 45 years) had a higher risk of arterial hypertension (AH) compared to women with menopause > 45 years [39]. This is probably due to a decrease in estrogen levels, which in turn causes the production of vasoconstrictor factors, i.e. endothelin and angiotensinogen, as well as a lower estrogen to androgen ratio during the menopause [40].
Lipid disorders
Women have a higher level of total cholesterol concentration > 6.5 mmol/l compared to 50-yearold males or older in the UK. Raised cholesterol levels are one of the risk factors for heart diseases [25].
The main findings regarding the differences in the lipid profile in women before and after menopause indicate that unfavorable changes in the lipid profile in postmenopausal women expose them to a greater risk of cardiovascular diseases [41].
In the perimenopausal period, changes in the cardiovascular risk usually occur. The occurrence of metabolic syndrome in postmenopausal women is 2–3 times more likely than in premenopausal women [42]. Changes in the lipid profile show a decrease in HDL levels and an increase in
462 Arch Med Sci 2, 1st March / 2023
Kamila Ryczkowska, Weronika Adach, Kamil Janikowski, Maciej Banach, Agata Bielecka-Dabrowa
Figure 2. Menopause and cardiovascular disease
Reconstruction of the arteries
Type 2 diabetes Lipid disorders Obesity Hypertension Smoking Inactive lifestyle ↑ Activity of the sympathetic nervous system ↑ Oxidative stress ↑ Plasma renin activity ↑ Endothelin concentration Vascular tension Inflammation
the value of triglycerides and LDL cholesterol by about 10–15% in postmenopausal women [43]. An increase in BMI and abdominal obesity in postmenopausal women show about 5 times higher risk of central obesity compared to premenopausal women [44].
Postmenopausal women have increased levels of LDL-C, TC, and TG. Nevertheless, studies indicate that there is no significant difference in HDL-C levels in pre- and postmenopausal women. Future prospective studies are crucial for understanding properly HDL-C levels and functions in a larger group of women with different menopausal status [45].
An independent risk factor for cardiovascular diseases that should be mentioned is Lipoprotein (a) (Lp(a)). Its structure is similar to that of the LDL particle. The differences in structure of these molecules regarding size and electrophoretic mobility are related to the high molecular weight of apo (a). Lp(a) is involved in pro-thrombotic and atherogenic processes. It has the ability to freely penetrate the endothelial barrier and adhere to the arterial wall, which can lead to the development of atherosclerotic cardiovascular disease [46, 47]. Many studies have shown that Lp(a) levels may increase slightly in the perimenopausal period. Although studies are still inconsistent, it cannot be excluded that an elevated Lp(a) concentration may increase the incidence of coronary artery disease in postmenopausal women [48].
An increased incidence of dyslipidemia and cholesterol accumulation can be observed during menopause, traditionally it is associated with estrogen deficit [49]. Due to lack of evidence, the current guidelines for the prevention of heart disease do not contain specific recommendations for men and women separately. Therefore, the latest lipid-lowering guidelines recommend statins
as the first-line treatment to reduce the risk of CVD, regardless of gender and menopausal status [47, 50–52].
However, it should be remembered that there are studies suggesting that statin use, especially in high doses, in post-menopausal women may increase the risk of diabates, therefore, the recent recommendations prompt on how to optimally treat lipid disorders in women with metabolic disturbances without incrasing the risk of new onset diabates [53–55]. To reduce the risk of metabolic syndrome, osteoporosis, vascular events and dyslipidemia, lifestyle assessment and counseling for menopausal women should be an integral part of health care. Eating habits and proper care for a healthy lifestyle in the menopausal period are very important because they apply to all women and can be easily modified (Table II).
Postmenopausal women show an increase in blood pressure as well as subclinical vascular disease. This is because of the increased carotid and femoral artery intima media thickness, coronary artery calcium score and arterial stiffness, and impaired flow-mediated dilation. Women with early menopause before the age of 40 have a higher risk of developing diabetes than women with menopause at the age of 50–54 years. Menopause before the age of 40 increases this risk due to more prolonged E2 deficiency. The risk of obesity in women during menopause increases due to a decrease in metabolism and a lack of exercise. These factors can lead to the development of insulin resistance, type 2 diabetes, and many cardiovascular and lipid disorders [17, 20, 56] (Figure 2).
Obesity and diabetes
Diabetes mellitus, despite the advances in early diagnosis, still remains an independent factor showing a very high or high risk of cardiovascu-
Arch Med Sci 2, 1st March / 2023 463
Menopause and women’s cardiovascular health: is it really an obvious relationship?
Parameter Women with surgical menopause at age < 40 y Women with natural menopause at age < 40 y Women with menopause at age ≥ 40 y Menopausal hormone therapy (MHT) Hypertension ↑↑↑ [32, 52] ↑↑ [16, 21, 32] ↑ or ~ [32, 52] ↓ [32] Coronary heart disease ↑↑ [32, 52] ↑ [32, 52] ↑ [52] ↓ [32] Heart failure ↑↑ [52] ↑ [21, 52] ~ [32] ↓ [32] Lipid disorders ↑↑ [52] ↑ [21] ↑ [52] ↓ or ~ [32] Type 2 diabetes ↑↑ [17] ↑ [17, 52] ↑ or ~ [17, 52] ↓ [17] Obesity ↑ [52] ↑ [21] ↑ [17] ↓ [17] ↑↑↑ – high risk, ↑↑ – medium risk, ↑ – low risk, ~ – neutral, ↓ – reduced risk.
Table II. Assessment of risk factors for cardiovascular diseases and cardiovascular risk factors at different times of the menopause
lar events. This risk is closely correlated with the occurrence of organ damage, e.g. kidney disease. Diabetes is most often diagnosed along with other risk factors for cardiovascular diseases, including dyslipidemia, arterial hypertension or obesity [47]. An increasing number of studies report that the use of menopausal hormonal therapy (MHT) may have a beneficial effect on glucose homeostasis in perimenopausal women with and without type 2 diabetes. A summary of over 100 studies found that MHT reduced abdominal fat in nondiabetic women. In women with diabetes, the use of MHT lowers the level of fasting blood glucose by an average of about 30%, while improving the values of lipids and blood pressure. The beneficial effect of MHT on glucose metabolism is due to the increase in lipid oxidation and energy expenditure. As a consequence, fat storage in the abdominal area is reduced and the risk of central obesity is reduced [57].
In highly developed countries, the problem of obesity and the health burdens it entails are countless. This applies not only to cardiovascular diseases, but also to metabolic and cancerous diseases. Until now, increases in body fat and weight gain have usually been attributed to chronological aging. Current results suggest however that menopause may have an effect on weight and fat gain. During the menopause, there is a decrease in E2 and an increase in FSH. Both of these hormones are responsible for the energy balance, additionally E2 influences the regulation of lipid storage and metabolism in adipose tissue. Therefore, a decrease in E2 during the menopause may contribute to a slower metabolic rate, a decrease in physical activity and the consumption of more kcal. Still, the results of the effects of menopause on obesity are not consistent [58].
Menopause and genetics
Age when natural menopause occurs has a great impact on women’s fertility and health. It is said that the timing of menopause is mostly influenced by genetic factors. Menopausal age ranges usually between 40 and 60 years [59].
Genetic factors play a major role in determining this discrepancy in an age when menopause occurs as has been shown in more than a few mother-daughter studies, twins, and a pair of siblings. Estimated heritability timing of menopause ranges from 31% to 87% and it is a complex genetic trait [59].
In association studies, genes that could be associated with the disease (the so-called candidate genes) are analyzed. This method is based on comparing the frequency of specific alleles and genotype polymorphisms of a given gene in a group of unrelated sick and healthy patients. A given allele may be associated with a disease if it is more com-
mon in sick people. Association studies are particularly useful when analyzing multi-gene diseases. Genome-wide association studies show common genetic loci influencing several potential candidate genes in many molecular pathways. A candidate gene’s location is associated with a particular disease. Considering its location, the gene is suspected of causing the disease. These molecular pathways include immune function, ovarian function, neuroendocrine function and DNA repair [20].
Research suggests that genetic predisposition to age at natural menopause (ANM) increases the risk of heart disease in women. Negative genetic correlations between ANM and coronary artery disease and risk factors for cardiovascular disease in women indicate genetic pleiotropy. A few genetic variants related to earlier ANM are linked to increased coronary artery disease and cardiovascular risk factors like hip circumference, and BMI. There were no results that support claims that ANM declining variants have an influence on risk factors for coronary artery disease in men. This demonstrates the usefulness of genetic and gender-specific analyses for a better understanding of the relationship between the cardiovascular risk and ANM [60].
Conclusions
Prevention of cardiovascular diseases should begin early for both men and women. For women, consultations during the perimenopausal and menopausal periods are an ideal opportunity to assess the cardiovascular risk. Early menopause is generally referred to the superior risk of CVD and this factor should be a strong warning sign during a medical consultation [61, 62]. As perimenopause is a time of significant deleterious cardiovascular changes, new research may focus on estimating when a woman will pass the FMP. Anti-Müllerian hormone (AMH) is a new emerging biomarker of reproductive aging which can help to estimate when a woman will undergo her FMP, and, in general, does it better than FSH. Therefore, results of using this new biomarker should complement data gained from other perhaps more traditional hormone measurements [63].
Acknowledgments
Kamila Ryczkowska and Weronika Adach contributed equally to this work.
Conflict of interest
The authors declare no conflict of interest.
464 Arch Med Sci 2, 1st March / 2023
Kamila Ryczkowska, Weronika Adach, Kamil Janikowski, Maciej Banach, Agata Bielecka-Dabrowa
References 1. Bajelan M, Etehad Roodi N, Hasanzadeh Daloee M, Farhangnia M, Samadi Kuchaksaraei A. The effect of low testosterone and estrogen levels on progressive coro-
Menopause and women’s cardiovascular health: is it really an obvious relationship?
nary artery disease in men. Rep Biochem Mol Biol 2019; 8: 168-71.
2. Stanhewicz AE, Wenner MM, Stachenfeld NS. Sex differences in endothelial function important to vascular health and overall cardiovascular disease risk across the lifespan. Am J Physiol Hear Circ Physiol 2018; 315: H1569-88.
3. Paduszyńska A, Banach M, Maciejewski M, Dąbrowa M, Bielecka-Dąbrowa A. The outcomes of hypertension treatment depending on gender in patients over 40 years of age. Prz Menopauz 2021; 19: 174-8.
4. Zhao H, Zhou L, Shangguan AJ, Bulun SE. Aromatase expression and regulation in breast and endometrial cancer. J Mol Endocrinol 2016; 57: R19-33.
5. Iorga A, Cunningham CM, Moazeni S, Ruffenach G, Umar S, Eghbali M. The protective role of estrogen and estrogen receptors in cardiovascular disease and the controversial use of estrogen therapy. Biol Sex Differ 2017; 8: 33.
6. Hu J, Zhang Z, Shen WJ, Azhar S. Cellular cholesterol delivery, intracellular processing and utilization for biosynthesis of steroid hormones. Nutr Metab 2010; 7: 47.
7. Cui J, Shen Y, Li R. Estrogen synthesis and signaling pathways during aging: from periphery to brain. Trends Mol Med 2013; 19: 197-209.
8. Rossouw JE, Anderson GL, Prentice RL, et al.; Writing Group for the Women’s Health Initiative Investigators. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women’s Health Initiative randomized controlled trial. JAMA 2002; 288: 321-33.
9. Guo Y, Zhao M, Bo T, et al. Blocking FSH inhibits hepatic cholesterol biosynthesis and reduces serum cholesterol. Cell Res Feb 2019; 29: 151-66.
10. Serviente C, Tuomainen TP, Virtanen J, Witkowski S, Niskanen L, Bertone-Johnson E. Follicle-stimulating hormone is associated with lipids in postmenopausal women. Menopause 2019; 26: 540-5.
11. Song Y, Wang ES, Xing LL, et al. Follicle-stimulating hormone induces postmenopausal dyslipidemia through inhibiting hepatic cholesterol metabolism. J Clin Endocrinol Metab 2016; 101: 254-63.
12. Stevenson JC, Tsiligiannis S, Panay N. Cardiovascular risk in perimenopausal women. Curr Vasc Pharmacol 2018; 17: 591-4.
13. Oliver-Williams C, Glisic M, Shahzad S, et al. The route of administration, timing, duration and dose of postmenopausal hormone therapy and cardiovascular outcomes in women: a systematic review. Hum Reprod Update 2019; 25: 257-71.
14. Manson JE, Allison MA, Rossouw JE, et al.; WHI and WHI-CACS Investigators. Estrogen therapy and coronary-artery calcification. N Engl J Med 2007; 356: 2591-602.
15. Oppermann K, Colpani V, Spritzer PM. Risk factors associated with coronary artery calcification in midlife women: a population-based study. Gynecol Endocrinol 2019; 35: 904-8.
16. Anagnostis P, Paschou SA, Katsiki N, Krikidis D, Lambrinoudaki I, Goulis DG. Menopausal hormone therapy and cardiovascular risk: where are we now? Curr Vasc Pharmacol 2019; 17: 564-72.
17. Mauvais-Jarvis F, Manson JE, Stevenson JC, Fonseca VA. Menopausal hormone therapy and type 2 diabetes prevention: evidence, mechanisms, and clinical implications. Endocr Rev 2017; 38: 173-88.
18. Anagnostis P, Galanis P, Chatzistergiou V, et al. The effect of hormone replacement therapy and tibolone on lipo-
protein (a) concentrations in postmenopausal women: a systematic review and meta-analysis. Maturitas 2017; 99: 27-36.
19. Stuenkel CA, Davis SR, Gompel A, et al. Treatment of symptoms of the menopause: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metabol 2015; 100: 3975-4011.
20. El Khoudary SR, Aggarwal B, Beckie TM, et al. Menopause transition and cardiovascular disease risk: implications for timing of early prevention: a scientific statement from the American Heart Association. Circulation 2020; 142: 506-32.
21. Davis SR, Lambrinoudaki I, Lumsden M, et al. Menopause. Nat Rev Dis Primers 2015; 23: 15004.
22. Maas A, Rosano G, Cifkova R, et al. Cardiovascular health after menopause transition, pregnancy disorders, and other gynaecologic conditions: a consensus document from European cardiologists, gynaecologists, and endocrinologists. Eur Heart J 2021; 42: 967-84.
23. Miller VM, Lahr BD, Bailey KR, Heit JA, Harman SM, Jayachandran M. Longitudinal effects of menopausal hormone treatments on platelet characteristics and cell-derived microvesicles. Platelets 2016; 27: 32-42.
24. Thomas MP, Potter BVL. The structural biology of oestrogen metabolism. J Steroid Biochem Mol Biol 2013; 137: 27-49.
25. Newson L. Menopause and cardiovascular disease. Post Reprod Heal 2018; 24: 44-9.
26. Zhu D, Chung HF, Dobson AJ, et al. Age at natural menopause and risk of incident cardiovascular disease: a pooled analysis of individual patient data. Lancet Public Heal 2019; 4: 553-64.
27. El Khoudary SR, Thurston RC. Cardiovascular implications of the menopause transition: endogenous sex hormones and vasomotor symptoms. Obstet Gynecol Clin North Am 2018; 45: 641-61.
28. Harvey RE, Coffman KE, Miller VM. Women-specific factors to consider in risk, diagnosis and treatment of cardiovascular disease. Women’s Heal 2015; 11: 239-57.
29. Kalibala J, Pechère-Bertschi A, Desmeules J. Gender differences in cardiovascular pharmacotherapy-the example of hypertension: a mini review. Front Pharmacol 2020; 11: 564.
30. Jóźwiak JJ, Studziński K, Tomasik T, et al.; LIPIDOGRAM2015 Investigators. The prevalence of cardiovascular risk factors and cardiovascular disease among primary care patients in Poland: results from the LIPIDOGRAM2015 study. Atheroscler Suppl 2020; 42: 15-24.
31. Kannel WB, Hjortland MC, McNamara P, Gordon T. Menopause and risk of cardiovascular disease. The Framingham study. Ann Intern Med 1976; 85: 447-52.
32. El Khoudary SR. Gaps, limitations and new insights on endogenous estrogen and follicle stimulating hormone as related to risk of cardiovascular disease in women traversing the menopause: a narrative review. Maturitas 2017; 104: 44-53.
33. Anagnostis P, Goulis DG, Menopause and its cardiometabolic consequences: current perspectives. Curr Vasc Pharmacol 2019; 17: 543-5.
34. Ji H, Kim A, Ebinger JE, et al. Sex differences in blood pressure trajectories over the life course. JAMA Cardiol 2020; 5: 19-26.
35. Lewek J, Bielecka-Dąbrowa A, Maciejewski M, Banach M. Pharmacological management of malignant hypertension. Expert Opin Pharmacother 2020; 21: 1189-92.
36. Bielecka-Dabrowa A, Bartlomiejczyk MA, Sakowicz A, Maciejewski M, Banach M. The role of adipokines in the
Arch Med Sci 2, 1st March / 2023 465
development of arterial stiffness and hypertension. Angiology 2020; 71: 754-61.
37. Reckelhoff JF, Fortepiani LA. Novel mechanisms responsible for postmenopausal hypertension. Hypertension 2004; 43: 918-23.
38. Paduszyńska A, Sakowicz A, Banach M, Maciejewski M, Dąbrowa M, Bielecka-Dąbrowa A. Cardioprotective properties of leptin in patients with excessive body mass. Ir J Med Sci 2020; 189: 1259-65.
39. Anagnostis P, Theocharis P, Lallas K, et al. Early menopause is associated with increased risk of arterial hypertension: a systematic review and meta-analysis. Maturitas 2020; 135: 74-9.
40. Salpeter SR, Walsh JM, Ormiston TM, Greyber E, Buckley NS, Salpeter EE. Meta-analysis: effect of hormone-replacement therapy on components of the metabolic syndrome in postmenopausal women. Diab Obes Metabol 2006; 8: 538-54.
41. Ambikairajah A, Walsh E, Cherbuin N. Lipid profile differences during menopause: a review with meta-analysis. Menopause 2019; 26: 1327-33.
42. Hallajzadeh J, Khoramdad M, Izadi N, et al. Metabolic syndrome and its components in premenopausal and postmenopausal women: a comprehensive systematic review and meta-analysis on observational studies. Menopause 2018; 25: 1155-64.
43. Choi Y, Chang Y, Kim BK, et al. Menopausal stages and serum lipid and lipoprotein abnormalities in middle-aged women. Maturitas 2015; 80: 399-405.
44. Franz R, Maturana MA, Magalhães JA, Moraes RS, Spritzer PM. Central adiposity and decreased heart rate variability in postmenopause: a cross-sectional study. Climacteric J Int Menopause Soc 2013; 16: 576-83.
45. Li H, Sun R, Chen Q, et al. Association between HDL-C levels and menopause: a meta-analysis. Hormones 2021; 20: 49-59.
46. Kotani K, Sahebkar A, Serban C, et al. Tibolone decreases lipoprotein(a) levels in postmenopausal women: a systematic review and meta-analysis of 12 studies with 1009 patients. Atherosclerosis 2015; 242: 87-96.
47. Banach M, Burchardt P, Chlebus K, et al. PoLA/CFPiP/ PCS/PSLD/PSD/PSH guidelines on diagnosis and therapy of lipid disorders in Poland 2021. Arch Med Sci 2021; 17: 1447-547.
48. Yan XN, Jin JL, Hong LF, et al. Lipoprotein(a) is associated with the presence and severity of new-onset coronary artery disease in postmenopausal women. J Womens Health 2020; 4: 503-10.
49. Taneja C, Gera S, Kim SM, Iqbal J, Yuen T, Zaidi M. FSH-metabolic circuitry and menopause. J Mol Endocrinol 2019; 63: R73-80.
50. El Khoudary SR, Aggarwal B, Beckie TM, et al. Menopause transition and cardiovascular disease risk: implications for timing of early prevention: a scientific statement from the American Heart Association. Circulation 2020; 142: e506-32.
51. Nikolic D, Banach M, Mikhailidis DP, Rizzo M. Can the effects of gender, menopause and ageing on lipid levels be differentiated? Clin Endocrinol 2016; 85: 694-5.
52. Dobrowolski P, Prejbisz A, Kuryłowicz A, et al. Metabolic syndrome – a new definition and management guidelines: a joint position paper by the Polish Society of Hypertension, Polish Society for the Treatment of Obesity, Polish Lipid Association, Polish Association for Study of Liver, Polish Society of Family Medicine, Polish Society of Lifestyle Medicine, Division of Prevention and
Epidemiology Polish Cardiac Society, “Club 30” Polish Cardiac Society, and Division of Metabolic and Bariatric Surgery Society of Polish Surgeons. Arch Med Sci 2022; 18: 1133-56.
53. Banach M, Surma S, Reiner Z, et al. Personalized management of dyslipidemias in patients with diabetes-it is time for a new approach (2022). Cardiovasc Diabetol 2022; 21: 263.
54. Culver AL, Ockene IS, Balasubramanian R, et al. Statin use and risk of diabetes mellitus in postmenopausal women in the Women’s Health Initiative. Arch Intern Med 2012; 172: 144-52.
55. Katsiki N, Banach M. Statins and the risk of diabetes: the debate. Arch Intern Med 2012; 172: 895-6; author reply 896-7.
56. Honigberg MC, Zekavat SM, Aragam K, et al. Association of premature natural and surgical menopause with incident cardiovascular disease. JAMA 2019; 322: 2411-21.
57. Paschou SA, Marina LV, Spartalis E, et al. Therapeutic strategies for type 2 diabetes mellitus in women after menopause. Maturitas 2019; 126: 69-72.
58. Greendale GA, Sternfeld B, Huang M, et al. Changes in body composition and weight during the menopause transition. JCI Insight 2019; 4: e124865.
59. Voorhuis M, Onland-Moret NC, van der Schouw YT, Fauser BCJM, Broekmans FJ. Human studies on genetics of the age at natural menopause: a systematic review. Hum Reprod Update 2010; 16: 364-77.
60. Sarnowski C, Kavousi M, Isaacs S, et al. Genetic variants associated with earlier age at menopause increase the risk of cardiovascular events in women. Menopause 2018; 25: 451-7.
61. Bojar I, Mlak R, Homa-Mlak I, Prendecka M, Owoc A, Małecka-Massalska T. Association between myostatin serum concentration and body fat level in peri- and postmenopausal women. Arch Med Sci 2022; 18: 36575.
62. Bojar I, Raczkiewicz D, Gujski M, et al. Oestrogen receptor a gene polymorphisms, insomnia, and cognitive functions in perimenopausal and postmenopausal women in non-manual employment. Arch Med Sci 2022; 18: 1318-28.
63. Finkelstei JS, Lee H, Karlamangla A, et al. Antimullerian hormone and impending menopause in late reproductive age: the study of women’s health across the nation. J Clin Endocrinol Metab 2020; 105: E1862-71.
466 Arch Med Sci 2, 1st March / 2023
Kamila Ryczkowska, Weronika Adach, Kamil Janikowski, Maciej Banach, Agata Bielecka-Dabrowa
The role of selected adipokines in tumorigenesis and metabolic disorders in patients with adrenal tumors
Anna Babinska, Piotr Kmieć, Krzysztof Sworczak
Department of Endocrinology and Internal Medicine, Medical University of Gdansk, Gdansk, Poland
Submitted: 30 April 2019; Accepted: 12 August 2019
Online publication: 4 March 2020
Arch Med Sci 2023; 19 (2): 467–477
DOI: https://doi.org/10.5114/aoms.2020.93486
Copyright © 2020 Termedia & Banach
A bstract
Recently, more and more attention has been directed to the role of adipose tissue and adipocytokines in the pathogenesis of metabolic and inflammatory disorders in humans. Excess fat tissue has also been associated with a higher risk of malignancies. Advances in the research on the role of adipokines in adrenal tumors may elucidate the relationship between various types of adipose tissue (visceral, subcutaneous, and periadrenal) and metabolic disorders observed in hormonally active adrenal tumors, as well as associations with adrenal cortex cancer. In patients with active or cured Cushing syndrome, increased leptin and resistin concentrations as well as release of pro-inflammatory cytokines can be associated with cardiovascular risk. Also, the renin-angiotensin-aldosterone system in patients with primary hyperaldosteronism may affect the metabolic activity of the adipose tissue. Elevated resistin concentrations in this group of patients are associated with morphological changes of the myocardium independently of the effects of the metabolic syndrome. Further, it has been suggested that hypoadiponectinemia comprises an additional factor in the pathogenesis of carbohydrate metabolism disorders and the risk of cardiovascular complications in pheochromocytoma patients. Understanding the mechanisms of action of adipokines may be important in developing prophylactic and therapeutic strategies in hormonally active and malignant tumors of the adrenal glands.
Key words: adipokines, adipokine receptors, subclinical Cushing syndrome, Cushing syndrome, pheochromocytoma, primary hyperaldosteronism, adrenocortical carcinoma.
Introduction
Obesity is a major social problem. The number of obese people in the United States in 2010 was 78 million [1]. Obesity increases the risk of hypertension (HT), dyslipidemia, type 2 diabetes (DM2), coronary artery disease (CAD), stroke, gallbladder disease, osteoarthritis, and sleep apnea. Also, the relationship between obesity and many human cancers has been proven: in all malignancies, obesity was associated with an increased mortality rate – by 52% in men and 88% in women [1–3].
Apart from its role in the storage of lipids, the adipose tissue (AT) is considered the largest endocrine gland in humans. It regulates energy homeostasis, metabolism, inflammatory processes, immunity, hormonal equilibrium, and bone turnover [4–7]. Concerning metabolic homeo-
Corresponding author:
Anna Babinska MD
Department of Endocrinology and Internal Medicine
Medical University of Gdansk
7 Dębinki St
80-288 Gdansk, Poland
Phone: +48 58 349 28 40
Fax: +48 58 349 28 41
E-mail: a.mail@wp.pl
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
State
the
paper Endocrinology
of
art
and Metabolic Disorders
Anna Babinska, Piotr Kmieć, Krzysztof Sworczak
stasis, physiologically, hormones secreted by the AT (adipokines) signal functional status to other organs. In this respect, the crucial peptides are leptin and adiponectin. What is more, substances produced by the fat tissue are also involved in immunity and inflammation. Obesity and adipocyte dysfunction induce production of inflammatory cytokines (commonly, and also here, referred to as adipocytokines together with adipokines), the secretory profile of the AT becomes pathologic. Adipocytokines likely contribute to metabolic diseases and inflammation [8, 9].
Adipose tissue is considered to be involved in the pathology of rheumatoid arthritis (RA), systemic lupus erythematosus, and Behçet’s disease [10]. In active arthritis peri-articular fat and synovial tissue were shown to release leptin, resistin and adiponectin, and the secretion of proinflammatory adipokines was increased [10]. Excessive expression of adipokines was also demonstrated in the intestinal mesenteric fat tissue in patients with Crohn’s disease. Research on the effect of adipokines on acute pancreatitis is ongoing: it seems that serum concentrations of resistin and leptin are elevated in this disease and may constitute its marker [11]. Kumar et al. [12] described increased adipogenesis and increased expression of adiponectin and leptin in the orbital tissue of patients with active thyroid orbitopathy.
Chronic inflammation that takes place in the adipose tissue may affect the development of metabolic disorders related to obesity. In many studies, a relationship has been demonstrated between adipocytokine secretion observed in obesity and the development of insulin resistance, DM2, hypertension (HT), non-alcoholic steatohepatitis, and adverse lipid profile [8, 9].
Furthermore, a relationship has been investigated between various adipocytokines and human neoplasms, including benign and malignant tumors of the endocrine system. The main mechanisms underlying the association between obesity and the risk of malignancy include:
– insulin resistance and the insulin-like growth factor 1 (IGF1) system (insulin inhibits apoptosis and stimulates IGF1 synthesis, which is a growth factor and promotes cancer; in obesity IGF1-binding protein synthesis in the liver is reduced, as a result, IGF-1 bioavailability increases),
– impact of adiposity on the biosynthesis and bioavailability of endogenous sex hormones,
– obesity-induced low-grade chronic systemic inflammation,
– alterations in the levels of adipocyte-derived factors [3, 5, 13, 14].
In many human cancers (mainly those related to obesity) the role of leptin, which promotes carcinogenesis, as well as adiponectin, has been
investigated. In humans, leptin has been shown to increase the growth of tumor cells associated with obesity, but it has also been proven to affect cancers not associated with obesity, for example, central nervous system tumors – gliomas and meningiomas [15].
Adiponectin, on the other hand, has a protective effect and anti-proliferative properties. Decreased adiponectin concentration has been demonstrated in cancers of the stomach, prostate, endometrium and breast [5].
There are a few reports concerning the role of adipose tissue in endocrine diseases. In this review the role of adipokines in oncogenesis and metabolic disorders in the course of human adrenal gland tumors is discussed.
Methods
This review was based on an electronic search of literature using the PubMed database. Associations between adipokine and cytokine levels and the risk of cancers and metabolic disorders in adrenal tumors were investigated.
Characterization of selected adipokines Adiponectin
The best known adipokine is adiponectin [4, 5]. Adiponectin is believed to be a mediator of obesity-related cancers and exerts direct anticancer effects via its receptors [5, 16]. Adiponectin is mainly synthesized in the white adipose tissue; secretion in the brown adipose tissue is low [7, 17]. Researchers also noted the presence of adiponectin in other animal tissues: skeletal muscles [18], liver [19], colon [20], cardiac tissue [21], salivary glands [22], bone marrow [23], fetal tissue and placenta [24], as well as cerebrospinal fluid [25], and breast milk [26]. Its expression in various tissues may indicate its para- and autocrine action [4, 5]. Adiponectin is a 247-amino acid monomer protein that circulates in the form of trimers, low molecular weight hexamers (LMW), or multimeric form with high molecular weight (HMW). Various spatial forms have different physiological properties, and the HMW and trimeric forms have the highest biological activity [4, 5]. It seems that the key factor in exerted biological effects of adiponectin is not its total concentration but the ratio of the HMW fraction to total adiponectin [4, 5].
The effects of adiponectin are mediated via its receptors, which are present in various organs and tissues. Yamauchi was first to isolate adiponectin receptors in human and mouse tissues in 2003 [27]. To date, three adiponectin receptors have been identified: two main, i.e. AdipoR1 and AdipoR2, and one receptor similar to that in the cadherin family [5, 28]. Receptor expression cor-
468 Arch Med Sci 2, 1st March / 2023
The role of selected adipokines in tumorigenesis and metabolic disorders in patients with adrenal tumors
relates with insulin concentration, and decreases in diabetic mice [29]. Obesity seems to reduce the expression of AdipoR1/AdipoR2, thus reducing the sensitivity to adiponectin, which in turn leads to a vicious cycle of insulin resistance [30]. Aging and long-term consumption of high-fat foods were reported to reduce the concentration of adiponectin and increase the expression of its receptors [31].
Adiponectin, through its receptors, activates several intracellular signaling pathways, mainly AMPK, but also mammalian target of rapamycin (mToR), nuclear factor κB (NF-κB), c-Jun N-terminal kinase (JNK), and signal transducer and activator of transcription proteins, STATs [32, 33].
The negative correlations between circulating adiponectin and obesity (especially central), insulin resistance and DM2 are well known [34]. A meta-analysis of prospective studies involving a total of 14,598 participants and 2,623 DM2 cases showed that higher adiponectin concentration was associated with a lower risk of DM2 [34]. Higher adiponectin levels were also associated with a moderate reduction of coronary artery disease risk in men with DM [35]. In addition, hypoadiponectinemia was associated with an adverse atherosclerotic lipid profile [36]; the risk of cardiovascular complications was inversely proportional to adiponectin concentrations [37].
Adiponectin has insulin-sensitizing action and reports by some authors indicate that hypoadiponectinemia is associated not only with insulin resistance, DM, and CAD [38–40], but also with malignant tumors [6]. The anti-inflammatory effect of adiponectin is primarily conveyed by inhibition of T-cell activation and proliferation, and blocking of tumor necrosis factor a (TNF-a) release. Adiponectin also inhibits the synthesis of interferon γ (IFN-γ), a molecule that stimulates cytotoxicity of natural killer (NK) cells. Adiponectin induces the synthesis of interleukin (IL)-10, an anti-inflammatory molecule, and receptor antagonist for IL-1. It also increases monocyte apoptosis and phagocytosis by macrophages, and inhibits the expression of TNF-a-induced adhesion molecules [25].
The protective effect of adiponectin in cancer is based on its anti-proliferative properties. It inhibits angiogenesis and intracellular signaling associated with carcinogenesis [41]. Adiponectin reduces the proliferation of tumor and endothelial cells in the breast and prostate by binding mitogenic growth factors [41]. Several cancer cell lines express receptors for adiponectin, suggesting its possible direct effects on these cells. Expression of adiponectin receptors has been demonstrated in breast, prostate, liver, stomach, colorectal, pancreatic, and lung carcinoma [5, 16, 42–45].
Chou et al. analyzed the relationship between AdipoR1 and AdipoR2 expression in various human neoplasms and cancer progression assessed as presence of local lymphatic and distant metastases. A statistically significant relationship was found between AdipoR1 expression and kidney cancer with and without metastasis. In the course of kidney cancer, a neoplasm strongly associated with obesity, lower serum adiponectin levels and significantly higher expression of AdipoR1 receptors in tumor tissue are found than in non-obesity-associated neoplasms [16]. In breast cancer, high expression of AdipoR1 was associated with vascular invasion. In contrast, in gastric cancer, high AdipoR1 expression was associated with longer survival [16].
Leptin
Leptin is the second well-known human adipokine. It is mainly produced by differentiated adipocytes, and its effects are contrary to those of adiponectin [46]. Leptin suppresses appetite and induces energy expenditure, although in the obese elevated leptin levels are present presumably due to resistance to the hormone [8].
Leptin is a pro-inflammatory adipokine. It enhances the formation of free oxygen radicals and induces proliferation of endothelial cells and expression of metalloproteinases within the extracellular matrix. It also activates neutrophils, monocytes and cytotoxic NK cells, stimulates production of proinflammatory cytokines by monocytes and lymphocytes, increases proliferation of T-lymphocytes and monocytes, and promotes angiogenesis. Leptin acts via its receptor, Ob-R (located on the surface of endothelial cells and leukocytes) [4], regulates many intracellular pathways: JAK (Janus kinase), STAT (signal transducer and activator of transcription) protein, PI3K (phosphatidylinositol 3-kinases), AKT (protein kinase B), and MAPK (mitogen-activated protein kinase). In addition, leptin increases proliferation via a variety of growth factors such as vascular endothelial growth factor (VEGF), fibroblast growth factor 21 (FGF21), and IGF-1 [47, 48].
A positive relationship between leptin concentration and coronary artery calcification was demonstrated in 860 healthy adults, who had neither diabetes nor established cardiovascular risk factors [49]. Leptin induced C-reactive protein (CRP) secretion, which is a well-known marker of cardiovascular risk [49].
Leptin is one of the most potent adipokines in metabolic regulation. It regulates body weight by signaling the state of nutrition to other organs –in particular to the hypothalamus, which produces neuropeptides and neurotransmitters that affect energy delivery and expenditure. Leptin also plays
Arch Med Sci 2, 1st March / 2023 469
Anna Babinska, Piotr Kmieć, Krzysztof Sworczak
an important role in the regulation of homeostasis. It improves insulin sensitivity in the liver and skeletal muscles and regulates the function of pancreatic b cells. Interactions between leptin and inflammation are bi-directional: proinflammatory cytokines increase the synthesis and release of leptin, which in turn contributes to chronic inflammation in obesity [8].
Leptin was shown to increase the growth of breast, esophageal, stomach, pancreatic, prostate, ovarian, and lung cancer cells [50–52]. A relationship between leptin concentration and colon cancer cell proliferation was also suggested [53]. Further, it was indicated that leptin promotes the proliferation of some breast tumors in vitro as well as tumor invasiveness and angiogenesis in some animal models [53, 54]. The oncogenic effects of leptin have not been elucidated yet. It is believed this protein activates intracellular signal transduction pathways [55]. In addition to receptor effects of leptin, e.g. in gastric cancer, its direct paracrine and autocrine action not mediated by its receptor was proposed [51]. It seems that oncogenic effects of leptin are exhibited more prominently in obesity-related cancers (esophageal, breast, stomach, colon and pancreatic) compared to those in which obesity plays a smaller role [56]. In epidemiological studies, an association between serum leptin concentrations and tumor progression was suggested. The strongest relationship was demonstrated for colon, prostate and breast cancers [57–59].
The effect of leptin on endocrine tumors is very poorly understood. Ob-R presence was demonstrated in the human adrenal glands [60]. Associations between leptin levels and adrenocortical and adrenal medullary neoplasms have not been investigated yet.
Resistin
Resistin was first discovered as an obesity hormone in animal studies. In obesity, an increase in serum resistin concentration was observed [61]. In experimental studies, resistin was demonstrated to act antagonistically to insulin [62, 63]. It seems that in humans resistin acts on insulin signaling pathway, causing dephosphorylation of 3-phosphorylated phosphoinositide [64]. Recent research in humans also indicates its role in the pathogenesis of atherosclerosis. Its concentration was demonstrated to be independently associated with an increased risk of myocardial infarction and ischemic stroke in a large cohort of middle-aged subjects and in the Women’s Health Initiative Observation Study [65]. Also, high resistin concentration was associated with morphological changes in the heart independently of the presence of metabolic syndrome [66].
Recent reports indicate that high serum resistin levels are an important risk factor for heart failure in the elderly, independently of CRP, insulin resistance or obesity [67, 68].
Resistin is mainly produced by monocytes and macrophages (which is stimulated by TNFa and IL-6), and its synthesis is induced during adipogenesis [69–71]. In turn, resistin activates the NF-κB pathway and, as a result, induces TNF-a, IL-6, and IL-12 production. Resistin stimulates expression of adhesion molecules: vascular cell adhesion molecule 1 (VCAM-1) and intercellular adhesion molecule 1 (ICAM-1) in endothelial cells, and induces endothelin 1, a strong spasmogen.
Epidemiological studies in humans showed a relationship between elevated resistin concentration and higher risk of DM2, myocardial infarction, and atherosclerosis. It seems that resistin concentration may serve as a marker of metabolic diseases in humans [8].
Other proinflammatory cytokines secreted by the adipose tissue
Associations between a pathologic adipocytokine profile (reduced adiponectin and increased leptin as well as resistin levels) and the development of insulin resistance, DM, and the risk of cardiovascular diseases have been reported by many researchers [4, 72, 73]. In studies of the pathologies of cardiovascular and metabolic diseases as well as malignancies cytokines secreted by the AT other than the three adipokines above have also been investigated.
Pro-inflammatory cytokines, including IL-6, TNF-a, and monocyte chemoattractant protein 1 (MCP-1), are involved in many pathological processes including inflammation, endothelial damage, atherosclerosis, insulin resistance, HT, and bone remodeling [4, 74].
Interleukin 6 is a cytokine that plays an important role in the development of insulin resistance in obesity. Adipose tissue contributes to 10–35% of circulating IL-6 in humans. Hyperglycemia causes an increase in IL-6 concentration. Expression of IL-6 in the adipose tissue correlates positively with insulin resistance both in vivo and in vitro [8]. In a cohort of 1293 healthy elderly subjects followed prospectively for a mean of 11.6 years, elevated IL-6 levels were associated with a doubling of cardiovascular risk and all-cause mortality [36]. Also, elevated IL-6 concentrations were shown to constitute a risk factor of DM2 and myocardial infarction [34, 37].
Tumor necrosis factor a is part of the inflammatory system, capable of initiating a cytokine cascade including synergistic and inhibitory reactions that control the synthesis and expression of other proinflammatory cytokines [8].
470 Arch Med Sci 2, 1st March / 2023
The role of selected adipokines in tumorigenesis and metabolic disorders in patients with adrenal tumors
TNF-a promotes the expression of adhesive molecules in endothelial cells and synthesis of endothelin 1 and angiotensinogen, which contributes to HT. Pro-inflammatory effects aside, TNF-a and IL-6 lower adiponectin secretion [23, 27, 39].
Adipocytokines in benign human adrenal cortex tumors
Wide use of thoracic and abdominal imaging studies results in an increased prevalence of adrenal tumors, which amounts to 10% among the elderly [75]. Most of the discovered tumors are hormonally inactive; rarely they have subclinical or overt hormonal activity [75]. All hormonally active tumors may lead to many metabolic disorders and an increased risk of cardiovascular diseases [76–80]. There are also reports indicating increased risk of these diseases in non-functional adrenal incidentaloma patients (NFAI) [81].
Adipokines were shown to be secreted by the periadrenal fat tissue surrounding adrenal tumors and their receptors to be present in tumor tissues [16, 82, 83]. Researchers’ interest has been directed at a potential effect of adipokines on hormonal activity and metabolic disorders in hormonally active adrenal tumors.
Adrenal Cushing’s and subclinical Cushing’s syndrome
Endogenous Cushing’s syndrome (CS) is a consequence of chronically increased serum glucocorticoid concentrations. Authors of many studies have shown that glucocorticoid overproduction in both overt and subclinical Cushing’s syndrome (CS and SCS) increases the risk of metabolic diseases and cardiovascular events [72, 74, 81, 84–87]. In patients with CS, the mortality rate due to complications of metabolic diseases increases fourfold compared with the healthy population [72, 88].
In a number of studies a relationship has been shown between concentrations of cortisol and adipocytokines [72]. Wagenmakers et al. showed that an adverse adipokine profile (i.e. low adiponectin and high leptin and resistin levels) persisted even after CS patients had been cured [89]. Persisting central distribution of the AT negatively affects the adipocytokine profile and likely contributes to sustained increased cardiovascular risk, independently of active hypercortisolemia [89]. The authors of the current review observed higher TNF-a and IL-6 concentrations as well as lower adiponectin levels in 20 SCS patients compared to healthy volunteers [90].
Dogruk Unal et al. demonstrated that low adiponectin concentration is a valuable determinant of SCS in patients with accidentally discovered adrenal tumors [87]. Barahona et al. recorded lower concentrations of adiponectin in clinically active
CS female patients as well as those treated for CS (over the preceding 11 ±6 years) compared to healthy volunteers, although this difference was not significant when age was taken into account [91].
Concerning another adipokine, resistin, in a study by Krsek et al. [92], its concentration was higher in 10 female CS patients compared to healthy volunteers. Resistin levels positively correlated with body mass index (BMI). Resistin level reduction did not reach statistical significance 9 months after surgical treatment, although the amount of visceral fat decreased among enrolled patients.
Although hyperleptinemia has been repeatedly confirmed in CS patients, a relationship between cortisol and leptin levels is unclear [72, 93]. Gavrila et al. showed that cortisol and leptin circadian profiles are strongly related: their peak concentrations occur during morning hours. Peak leptin concentration followed that of cortisol with a 2-hour time difference, which suggests a relationship between these hormones [94]. Also, in human studies, administration of dexamethasone resulted in an increase in leptin in obese subjects, which was independent of sex, age, and insulin sensitivity [94]. Further, Widjaja et al. recorded a significant reduction in leptin concentration 2.5 years after transsphenoidal surgery for ACTH-dependent Cushing’s syndrome. In their small group of patients (n = 9), insulin, cortisol concentrations, and BMI returned to reference values for sex and age [95].
In contrast, Weise and co-authors found that diurnal leptin profile was normal in 18 patients with CS, and observed no correlation between leptin and cortisol levels. This lack of association between both hormones in CS was also underlined by the fact that corticotropin-releasing hormone (CRH) administration before and 10 days after surgical treatment of hypercortisolemia in 12 CS patients did not affect leptin concentration (despite significant differences in cortisol levels, i.e. basally and in response to CRH both before and after surgery) [96].
A possible explanation for these findings is the fact that so far no studies have investigated the relative amount of specific body fat stores (namely visceral and subcutaneous fat) and leptin concentration in CS patients. This distinction in tissue type is crucial because subcutaneous fat produces two to three times more leptin than visceral fat [97].
Although the pathogenesis of hypoleptinemia in CS patients is unclear, it is thought to be a compensatory mechanism for excess glucocorticoids, due to which food intake is inhibited (via suppression of neuropeptide Y and stimulation of proopiomelanocortin (POMC), which has anorectic effects) [72, 98].
Central obesity, a typical feature of CS, is associated with altered secretion of adipocytokines,
Arch Med Sci 2, 1st March / 2023 471
Anna Babinska, Piotr Kmieć, Krzysztof Sworczak
which contributes to metabolic and cardiovascular complications [5, 85, 88]. In CS patients, serum concentrations of leptin and resistin, as well as proinflammatory cytokines such as TNF-a and IL-6, are increased [72]. It is possible that a pathological adipocytokine profile constitutes an additional risk factor of metabolic and cardiovascular diseases in CS patients. The situation is not so clear in patients with SCS, in whom obesity and overweight are less frequent and less severe than in patients with overt CS [72, 86]. Probably, even small but chronic exposure to excess glucocorticoids in both CS and SCS can lead to central accumulation of adipose tissue, which results in a persistent, unfavorable profile of adipokines and cytokines. Despite reports on the influence of adipocytokines on the risk of metabolic diseases in CS and SCS patients, literature data are often contradictory [81, 99, 100]; therefore, future studies including larger patient populations are required.
Primary hyperaldosteronism
In primary hyperaldosteronism (PA) patients compared to primary hypertensives the risk of cardiovascular diseases and the frequency of metabolic syndrome are increased [101–104]. Resection of an aldosterone-producing adenoma leads to regression of these disorders. The role of adipocytokines in primary aldosteronism has been poorly studied.
A relationship between hyperaldosteronism and fat tissue function is indicated by reports on the presence of the mineralocorticoid receptor (MR) in the AT, which mediates actions of both aldosterone and glucocorticoids in adipocyte differentiation, adipocytokine secretion, and lipid accumulation [105]. The RAAS may be involved in the modulation of adipocytokines in individuals with excessive serum aldosterone [106, 107].
Letizia et al. showed that mineralocorticoids, such as aldosterone, play an important role in adipose tissue function, regulating differentiation of preadipocytes to mature adipocytes, and inducing inflammatory adipocytokines [108]. In their study, higher secretion of leptin and lower secretion of adiponectin in adrenal fat tissue surrounding aldosterone-producing tumors were observed [108].
Rossi et al. analyzed AdipoR1 and AdipoR2 receptor expression in normal adrenal glands (which were removed during renal cell carcinoma surgery) and aldosterone-secreting adenomas [109]. Significantly higher expression of adiponectin receptors in aldosteronomas compared to normal adrenal cortex was revealed. The authors speculated that adiponectin modulates aldosterone secretion by affecting adiponectin receptor subtypes in the adrenal cortex [109].
In another report, Iacobellis et al. compared adipocytokine levels in PA and essential hypertension patients. Higher concentrations of resistin were found in the former group, while leptin levels were higher and adiponectin lower after accounting for the presence of metabolic syndrome in both patient groups [66]. It is possible that high resistin concentrations in PA may be the result of abnormal adipocyte function due to exposure to prolonged high concentrations of aldosterone [66]. However, a direct effect of aldosterone on resistin concentration has not been demonstrated yet [66].
Similarly, lower adiponectin levels in PA patients compared to low renin essential hypertensives were also found by Fallo et al. [110]. Low adiponectin levels may contribute to endothelial dysfunction [66].
On the other hand, Haluzík et al. found that leptin concentrations were not different between PA and matched healthy controls at baseline; however, a significant increase in leptin levels was observed in PA patients after treatment (both surgical and pharmacological) [111]. The same observation concerning pre- and post-surgery leptin levels for PA was made by Torpy et al., who suggested that improved insulin secretion due to correction of hypokalemia may be the underlying reason for increase in leptinemia [112].
The few studies, in which only selected adipokines in PA patients were investigated, and in light of the presence of adipocyte receptors in the tissue of adenomas secreting aldosterone, indicate the need for further studies on larger groups of patients to explain the influence of the fat tissue on metabolic disorders observed in this group of patients.
Adrenocortical carcinoma
Research on the relationship between the adipose tissue and human neoplasms is largely observational, and there are limited data on rare malignancies, including those of the adrenal glands.
Chou et al. investigated expression of adiponectin receptors in various, including non-obesity-associated human neoplasms, and were the first to show their presence in adrenocortical cancer (ACC) [16]. The authors showed that AdipoR1 expression was much higher in obesity-associated neoplasms compared to those in which the influence of obesity as an etiological factor was not proven [16].
The authors of the current review evaluated differences in the expression of adiponectin receptors in benign and malignant adrenal tumors by immunohistochemistry. In an analysis of 128 resected adrenal tumors both AdipoR1 and AdipoR2 expression levels were significantly higher in ACC compared to benign adrenal hyperplasia and adrenocortical adenomas [82]. It seems that
472 Arch Med Sci 2, 1st March / 2023
The role of selected adipokines in tumorigenesis and metabolic disorders in patients with adrenal tumors
higher adipokine receptor expression in malignant adrenal tumors can be explained by down-regulation, which is present in epithelial breast cancer as well as Barrett’s adenocarcinoma [113, 114]. It can be assumed that low serum adiponectin levels are associated with tumorigenic effects, resulting in increased expression of AdipoR1 and R2 receptors in adrenal tumor tissue [82, 83].
An attempt to evaluate the proliferative effect of leptin in adrenal tumors was undertaken by Glasow et al. in 1999 [60]. The researchers examined normal and neoplastic adrenocortical tissue and found that leptin does not regulate the proliferation of adrenocortical tumors despite the presence of its receptor in the tumors [60].
In the above-mentioned study conducted by the authors of this review (resected adrenal tumors from 128 patients), it was demonstrated that leptin receptor expression was absent or minimal in half of examined benign tumors (nodular hyperplasia and adrenocortical adenomas), while being much higher in ACCs [82, 83]. We also sought for a relationship between the expression of adipokine and leptin receptors in ACC tissue and the progression of this rare human tumor [83], but none was demonstrated. Effective radical surgical treatment remains the established prognostic factor [115].
Considering the role of adipokines in neoplasia and the presence of adipokine receptors in adrenal tumors, it can be hypothesized that adipokines play a role also in human adrenocortical cancers, which are non-obesity-associated neoplasms.
Pheochromocytoma
Pheochromocytoma (PHEO) is a neoplasm that arises from chromaffin cells of the neural tube of the sympathetic and parasympathetic nervous system. It comprises approximately 1–8.7% of incidentally discovered adrenal tumors according to various reports [116–118]. PHEOs produce one or more catecholamine (epinephrine, norepinephrine, dopamine, which are metabolized to metanephrines, normetanephrines, and 3-methoxytramine, respectively), as well as other active substances, all of which lead to various clinical symptoms [116–118].
Obesity is rare in patients with PHEO due to the catabolic effect of excessive catecholamine secretion, which stimulates lipolysis [75, 119, 120]. However, adrenal glands are embedded in fat tissue, which has been shown to secrete adipokines that can affect PHEO [108]. There are reports assessing the influence of the adipose tissue on PHEO tumor metabolism that suggest its effect on metabolic disorders in this group of patients [119, 120].
Glucose metabolism disorders including DM are a relatively common feature in patients with
PHEO. According to the literature, impaired glucose tolerance was observed in 25% to 75% of patients with PHEO and about 33% developed DM [116, 119, 120]. Supraphysiological catecholamine concentrations reduce insulin secretion and are the main cause of DM in PHEO patients. Wiesner et al. reported that glucose intolerance in PHEOs is caused by increased insulin resistance [121]. Possibly, insulin resistance is another factor in the development of DM in pheochromocytoma patients.
In some studies, lower adiponectin concentrations compared to controls were observed in PHEO patients [119, 122]. Elenkova et al. suggested that hypoadiponectinemia was the missing link in the pathogenesis of carbohydrate metabolism disorders in these patients, and that it may be an additional risk factor for cardiovascular and metabolic complications [119].
Epinephrine up-regulates the expression of adiponectin receptors. It seems that high catecholamine concentrations present in PHEO, i.e. the cause of glucose intolerance and DM, induce compensatory expression of adiponectin receptors, particularly AdipoR1, in PHEO tumor tissue, probably due to decreased serum adiponectin concentration [122].
In the available literature, Isobe et al. speculated that, contrary to epinephrine, high levels of norepinephrine induce adiponectin secretion. It was suggested that this mechanism is protective against occurrence of DM in PHEO patients with excess norepinephrine secretion [122].
The authors of the current review investigated adipokine and leptin receptor expression in tumor tissues of 40 adrenal PHEO patients. AdipoR1 and R2 receptor expression was significantly higher in PHEO compared to both benign and malignant adrenocortical tumors [82]. Also, leptin receptor expression in PHEO tumors was higher than in adrenocortical tumors [82].
In studies by other authors, serum leptin concentrations in patients with PHEO tumors were evaluated [122]. It was shown that chronic overproduction of catecholamines that occurs in PHEO did not suppress leptin secretion in these patients. This may be related to the development of tolerance to a chronic excess of catecholamines in the adipose tissue [123].
The interplay between fat tissue surrounding PHEO and possible stimulation of leptin secretion by catecholamines may be associated with higher expression of Ob-R in this type of tumor. In fact, in our previous studies, expression of leptin receptor was significantly higher in PHEO compared to ACC. Higher expression of adiponectin and leptin receptors in PHEO may result from a significantly stronger effect of catecholamines on adipokine secretion by the AT in comparison to the effect of adrenocortical hormones [82].
Arch Med Sci 2, 1st March / 2023 473
Anna Babinska, Piotr Kmieć, Krzysztof Sworczak
Presence of adipokine receptors in PHEO tumors in humans as well as the relationship between low adiponectin concentration and increased risk of DM and insulin resistance in PHEO patients indicates the role of adipose tissue in metabolic disorders in this pathology.
Conclusions
The role of adipocytokines in hormonally active adrenal tumors and their possible effect on metabolic disorders and cardiovascular risk has been investigated scarcely. Elucidating the interplay between excess hormone levels and adipocytokines remains a challenge for future studies.
Presence of adipokine receptors in adrenal cortex and medulla tumors, and, particularly, their high expression in malignant tumors, suggest the possible effect of adipokines on neoplasia in these non-obesity-related neoplasms. Understanding the mechanisms linking adiponectin and leptin with proliferation may be important in the development of anticancer prophylaxis and therapy not only in obesity-associated malignancies. The pathophysiological significance of adipokine receptors and their potential prognostic value in assessment of the risk of cancer incidence, recurrence and treatment results in obesity-related cancers warrant the necessity of future studies. It is possible that treatment with adiponectin receptor analogues or clinical use of adiponectin may have direct beneficial effects in many human cancers. However, currently, lifestyle modifications remain the most important factor in the prevention of cancer and metabolic disorders related to obesity.
Conflict of interest
The authors declare no conflict of interest.
References
1. Executive summary: Guidelines (2013) for the management of overweight and obesity in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society published by the Obesity Society and American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Based on a systematic review from the The Obesity Expert Panel, 2013. Obesity (Silver Spring) 2014; 22 Suppl 2: S5-39.
2. Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med 2003; 348: 1625-38.
3. Park J, Euhus DM, Scherer PE. Paracrine and endocrine effects of adipose tissue on cancer development and progression. Endocr Rev 2011; 32: 550-70.
4. Siemińska L. Adipose tissue. Pathophysiology, distribution, sex differences and the role in inflammation and cancerogenesis. Endocrinol Pol 2007; 58: 330-42.
5. Dalamaga M, Diakopoulos KN, Mantzoros CS. The role of adiponectin in cancer: a review of current evidence. Endocr Rev 2012; 33: 547-94.
6. Kelesidis I, Kelesidis T, Mantzoros CS. Adiponectin and cancer: a systematic review. Br J Cancer 2006; 94: 1221-5.
7. Ziemke F, Mantzoros CS. Adiponectin in insulin resistance: lessons from translational research. Am J Clin Nutr 2010; 91: 258S-61S.
8. Jung UJ, Choi MS. Obesity and its metabolic complications: the role of adipokines and the relationship between obesity, inflammation, insulin resistance, dyslipidemia and nonalcoholic fatty liver disease. Int J Mol Sci 2014; 15: 6184-223.
9. Cao H. Adipocytokines in obesity and metabolic disease. J Endocrinol 2014; 220: T47-59.
10. Schäffler A, Müller-Ladner U, Schölmerich J, Büchler C. Role of adipose tissue as an inflammatory organ in human diseases. Endocr Rev 2006; 27: 449-67.
11. Schäffler A, Landfried K, Völk M, et al. Potential of adipocytokines in predicting peripancreatic necrosis and severity in acute pancreatitis: pilot study. J Gastroenterol Hepatol 2007; 22: 326-34.
12. Kumar S, Coenen MJ, Scherer PE, Bahn RS. Evidence for enhanced adipogenesis in the orbits of patients with Graves’ ophthalmopathy. J Clin Endocrinol Metab 2004; 89: 930-5.
13. van Kruijsdijk RC, van der Wall E, Visseren FL. Obesity and cancer: the role of dysfunctional adipose tissue. Cancer Epidemiol Biomarkers Prev 2009; 18: 2569-78.
14. Gallagher EJ, LeRoith D. Minireview: IGF, insulin, and cancer. Endocrinology 2011; 152: 2546-51.
15. Sergentanis TN, Tsivgoulis G, Perlepe C, et al. Obesity and risk for brain/CNS tumors, gliomas and meningiomas: a meta-analysis. PLoS One 2015; 10: e0136974.
16. Chou SH, Tseleni-Balafouta S, Moon HS, et al. Adiponectin receptor expression in human malignant tissues. Horm Canc 2010; 1: 136-45.
17. Maeda K, Okubo K, Shimomura I, et al. cDNA cloning and expression of a novel adipose specific collagen-like factor, apM1 (AdiPose Most abundant Gene transcript 1). Biochem Biophys Res Commun 1996; 221: 286-9.
18. Delaigle AM, Jonas JC, Bauche IB, Cornu O, Brichard SM. Induction of adiponectin in skeletal muscle by inflammatory cytokines: in vivo and in vitro studies. Endocrinology 2004; 145: 5589-97.
19. Kaser S, Moschen A, Cayon A, et al. Adiponectin and its receptors in non-alcoholic steatohepatitis. Gut 2005; 54: 117-21.
20. Fayad R, Pini M, Sennello JA, et al. Adiponectin deficiency protects mice from chemically induced colonic inflammation. Gastroenterology 2007; 132: 601-14.
21. Piñeiro R, Iglesias MJ, Gallego R, et al. Adiponectin is synthesized and secreted by human and murine cardiomyocytes. FEBS Lett 2005; 579: 5163-9.
22. Katsiougiannis S, Kapsogeorgou EK, Manoussakis MN, Skopouli FN. Salivary gland epithelial cells: a new source of the immunoregulatory hormone adiponectin. Arthritis Rheum 2006; 54: 2295-9.
23. Brochu-Gaudreau K, Rehfeldt C, Blouin R, et al. Adiponectin action from head to toe. Endocrine 2010; 37: 11-32.
24. Chen J, Tan B, Karteris E, et al. Secretion of adiponectin by human placenta: differential modulation of adiponectin and its receptors by cytokines. Diabetologia 2006; 49: 1292-302.
25. Schäffler A, Müller-Ladner U, Schölmerich J, Büchler C. Role of adipose tissue as an inflammatory organ in human diseases. Endocr Rev 2006; 27: 449-67.
474 Arch Med Sci 2, 1st March / 2023
The role of selected adipokines in tumorigenesis and metabolic disorders in patients with adrenal tumors
26. Bronsky J, Karpísek M, Bronská E, et al. Adiponectin, adipocyte fatty acid binding protein, and epidermal fatty acid binding protein: proteins newly identified in human breast milk. Clin Chem 2006; 52: 1763-70.
27. Yamauchi T, Kamon J, Ito Y, et al. Cloning of adiponectin receptors that mediate antidiabetic metabolic effects. Nature 2003; 423: 762-9.
28. Kadowaki T, Yamauchi T. Adiponectin and adiponectin receptors. Endocr Rev 2005; 26: 439-51.
29. Tsuchida A, Yamauchi T, Ito Y, et al. Insulin/Foxo1 pathway regulates expression levels of adiponectin receptors and adiponectin sensitivity. J Biol Chem 2004; 279: 30817-22.
30. Ouchi N, Kihara S, Arita Y, et al. Adiponectin, an adipocyte-derived plasma protein, inhibits endothelial NF-kappaB signaling through a cAMP-dependent pathway. Circulation 2000; 102: 1296-301.
31. Bullen JW Jr, Bluher S, Kelesidis T, Mantzoros CS. Regulation of adiponectin and its receptors in response to development of diet-induced obesity in mice. Am J Physiol Endocrinol Metab 2007; 292: E1079-86.
32. Miyazaki T, Bub JD, Uzuki M, Iwamoto Y. Adiponectin activates c-Jun NH2-terminal kinase and inhibits signal transducer and activator of transcription 3. Biochem Biophys Res Commun 2005; 333: 79-87.
33. Bråkenhielm E, Veitonmäki N, Cao R, et al. Adiponectin-induced antiangiogenesis and antitumor activity involve caspase-mediated endothelial cell apoptosis. Proc Natl Acad Sci USA 2004; 101: 2476-81.
34. Li S, Shin HJ, Ding EL, van Dam RM. Adiponectin levels and risk of type 2 diabetes: a systematic review and meta-analysis. JAMA 2009; 302: 179-88.
35. Schulze MB, Shai I, Rimm EB, Li T, Rifai N, Hu FB. Adiponectin and future coronary heart disease events among men with type 2 diabetes. Diabetes 2005; 54: 534-9.
36. Okada T, Saito E, Kuromori Y, et al. Relationship between serum adiponectin level and lipid composition in each lipoprotein fraction in adolescent children. Atherosclerosis 2006; 188: 179-83.
37. Pischon T, Girman CJ, Hotamisligil GS, et al. Plasma adiponectin levels and risk of myocardial infarction in men. JAMA 2004; 291: 1730-7.
38. Hivert MF, Sullivan LM, Fox CS, et al. Associations of adiponectin, resistin, and tumor necrosis factor-alpha with insulin resistance. J Clin Endocrinol Metab 2008; 93: 3165-72.
39. Weyer C, Funahashi T, Tanaka S, et al. Hypoadiponectinemia in obesity and type 2 diabetes: close association with insulin resistance and hyperinsulinemia. J Clin Endocrinol Metab 2001; 86: 1930-5.
40. Hotta K, Funahashi T, Arita Y, et al. Plasma concentrations of a novel, adipose-specific protein, adiponectin, in type 2 diabetic patients. Arterioscler Thromb Vasc Biol 2000; 20: 1595-9.
41. Bub JD, Miyazaki T, Iwamoto Y. Adiponectin as a growth inhibitor in prostate cancer cells. Biochem Biophys Res Commun 2006; 340: 1158-66.
42. Barb D, Williams CJ, Neuwirth AK, Mantzoros CS. Adiponectin in relation to malignancies: a review of existing basic research and clinical evidence. Am J Clin Nutr 2007; 86: s858-66.
43. Mistry T, Digby JE, Chen J, Desai KM, Randeva HS. The regulation of adiponectin receptors in human prostate cancer cell lines. Biochem Biophys Res Commun 2006; 348: 832-8.
44. Petridou ET, Mitsiades N, Gialamas S, et al. Circulating adiponectin levels and expression of adiponectin
receptors in relation to lung cancer: two case-control studies. Oncology 2007; 73: 261-9.
45. Dalamaga M, Migdalis I, Fargnoli JL, et al. Pancreatic cancer expresses adiponectin receptors and is associated with hypoleptinemia and hyperadiponectinemia: a case-control study. Cancer Causes Control 2009; 20: 625-33.
46. Cohen B, Novick D, Rubinstein M. Modulation of insulin activities by leptin. Science 1996; 274: 1185-8.
47. Nieman KM, Romero IL, Van Houten B, Lengyel E. Support tumorigenesis and metastasis. Biochim Biophys Acta 2013; 1831: 1533-41.
48. Ray A, Cleary MP. The potential role of leptin in tumor invasion and metastasis. Cytocine Growth Factor Rev 2017; 38: 80-97.
49. Qasim A, Mehta NN, Tadesse MG, et al. Adipokines, insulin resistance, and coronary artery calcification. J Am Coll Cardiol 2008; 52: 231-6.
50. Tilg H, Moschen AR. Adipocytokines: mediators linking adipose tissue, inflammation and immunity. Nat Rev Immunol 2006; 6: 772-83.
51. Wiwanitkit V. Interaction between leptin and leptin receptor in gastric carcinoma: gene ontology analysis. Rev Esp Enferm Di 2007; 99: 201-5.
52. Horiguchi A, Sumitomo M, Asakuma J, et al. Increased serum leptin levels and over expression of leptin receptors are associated with the invasion and progression of renal cell carcinoma. J Urol 2006; 176: 1631-5.
53. Husting SD, Berger NA. Energy balance, host-related factors, and cancer progression. J Clin Oncol 2010; 28: 4058-65.
54. Nkhata KJ, Ray A, Schuster TF, Grossmann ME, Cleary MP. Effects of adiponectin and leptin co-treatment on human breast cancer cell growth. Oncol Rep 2009; 21: 1611-9.
55. Pai R, Lin C, Tran T, Tarnawski A. Leptin activates STAT and ERK2 pathways and induces gastric cancer cell proliferation. Biochem Biophys Res Commun 2005; 331: 984-92.
56. Beales IL, Garcia-Morales C, Ogunwobi OO, Mutungi G. Adiponectin inhibits leptin-induced oncogenic signaling in oesophageal cancer cell by activation of PTP1B. Mol Cell Endocrinol 2014; 382: 150-8.
57. Stattin P, Lukanova A, Biessy C, et al. Obesity and colon cancer: does leptin provide a link? Int J Cancer 2004; 109: 149-52.
58. Chang S, Hursting SD, Contois JH, et al. Leptin and prostate cancer. Prostate 2001; 46: 62-7.
59. Wu MH, Chou YC, Chou WY, et al. Circulating levels of leptin, adiposity and breast cancer risk. Br J Cancer 2009; 100: 578-82.
60. Glasow A, Bornstein SR, Chrousos GP, Brown JW, Scherbaum WA. Detection of Ob-receptor in human adrenal neoplasms and effect of leptin on adrenal cell proliferation. Horm Metab Res 1999; 31: 247-51.
61. Janowska J, Zahorska-Markiewicz B, Olszanecka-Glinianowicz M. Relationship between serum resistin concentration and proinflammatory cytokines in obese women with impaired and normal glucose tolerance. Metabolism 2006; 55: 1495-9.
62. Steppan CM, Bailey ST, Bhat S, et al. The hormone resistin links obesity to diabetes. Nature 2001; 409: 307-12.
63. Steppan CM, Lazar MA. Resistin and obesity-associated insulin resistance. Trends Endocrinol Metab 2002; 13: 18-23.
Arch Med Sci 2, 1st March / 2023 475
Anna Babinska, Piotr Kmieć, Krzysztof Sworczak
64. Barnes KM, Miner JL. Role of resistin in insulin sensitivity in rodents and humans. Curr Protein Pept Sci 2009; 10: 96-107.
65. Rajpathak SN, Kaplan RC, Wassertheil-Smoller S, et al. Resistin, but not adiponectin and leptin, is associated with the risk of ischemic stroke among postmenopausal women: results from the Women’s Health Initiative. Stroke 2011; 42: 1813-20.
66. Iacobellis G, Petramala L, Cotesta D, et al. Adipokines and cardiometabolic profile in primary hyperaldosteronism. J Clin Endocrinol Metab 2010; 95: 2391-8.
67. Butler J, Kalogeropoulos A, Georgiopoulou V, et al. Serum resistin concentrations and risk of new onset heart failure in older persons: the health, aging, and body composition (Health ABC) study. Arterioscler Thromb Vasc Biol 2009; 29: 1144-9.
68. Frankel DS, Vasan RS, D’Agostino RB Sr, et al. Resistin, adiponectin, and risk of heart failure the Framingham offspring study. J Am Coll Cardiol 2009; 53: 754-62.
69. McTernan CL, McTernan PG, Harte AL, Levick PL, Barnett AH, Kumar S. Resistin, central obesity, and type 2 diabetes. Lancet 2002; 359: 46-7.
70. Patel L, Buckels AC, Kinghorn IJ, et al. Resistin is expressed in human macrophages and directly regulated by PPAR gamma activators. Biochem Biophys Res Commun 2003; 300: 472-6.
71. Lehrke M, Reilly MP, Millington SC, Iqbal N, Rader DJ, Lazar MA. An inflammatory cascade leading to hyperresistinemia in humans. PLoS Med 2004; 1: e45.
72. Valassi E, Biller BM, Klibanski A, Misra M. Adipokines and cardiovascular risk in Cushing’s syndrome. Neuroendocrinology 2012; 95: 187-206.
73. Iacobellis G, Petramala L, Cotesta D, et al. Adipokines and cardiometabolic profile in primary hyperaldosteronism. J Clin Endocrinol Metab 2010; 95: 2391-8.
74. Debono M, Bradburn M, Bull M, Harrison B, Ross RJ, Newell-Price J. Cortisol as a marker for increased mortality in patients with incidental adrenocortical adenomas. J Clin Endocrinol Metab 2014; 99: 4462-70.
75. Bednarczuk T, Bolanowski M, Sworczak K, et al. Adrenal incidentaloma in adults – management recommendations by the Polish Society of Endocrinology. Endokrynol Pol 2016; 67: 234-58.
76. Tauchmanova L, Rossi R, Biondi B, et al. Patients with subclinical Cushing’s syndrome due to adrenal adenoma have increased cardiovascular risk. J Clin Endocrinol Metab 2002; 87: 4872-8.
77. Swiatkowska-Stodulska R, Sworczak K. Disorders of hemostasis in overt and subclinical hypercortisolism. Exp Clin Endocrinol Diabetes 2013; 121: 588-94.
78. Terzolo M, Pia A, Ali A, et al. Adrenal incidentaloma: a new cause of the metabolic syndrome? J Clin Endocrinol Metab 2002; 87: 998-1003.
79. Tuna MM, Imga NN, Doğan BA, et al. Non-functioning adrenal incidentalomas are associated with higher hypertension prevalence and higher risk of atherosclerosis. J Endocrinol Invest 2014; 37: 765-68.
80. Di Dalmazi G, Vicennati V, Garelli S, et al. Cardiovascular events and mortality in patients with adrenal incidentalomas that are either non-secreting or associated with intermediate phenotype or subclinical Cushing’s syndrome: a 15-year retrospective study. Lancet Diabetes Endocrinol 2014; 2: 396-405.
81. Ermetici F, Malavazos AE, Corbetta S, et al. Adipokine levels and cardiovascular risk in patients with adrenal incidentaloma. Metabolism 2007; 56: 686-92.
82. Babińska A, Pęksa R, Wiśniewski P, Sworczak K. Expression of adiponectin receptors 1 and 2 and leptin
receptor in human adrenal tumors. Arch Med Sci 2019; 15: 1254-60.
83. Babińska A, Pęksa R, Wiśniewski P, Świątkowska-Stodulska R, Sworczak K. Diagnostic and prognostic role of SF1, IGF2, Ki67, p53, adiponectin, and leptin receptors in human adrenal cortical tumors. J Surg Oncol 2017; 116: 427-33.
84. Androulakis II, Kaltsas GA, Kollias GE, et al. Patients with apparently nonfunctioning adrenal incidentalomas may be at increased cardiovascular risk due to excessive cortisol secretion, J Clin Endocrinol Metab 2014; 99: 2754-62.
85. Fassnacht M, Arlt W, Bancos I, et al. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol 2016; 175: G1-G34.
86. Babinska A, Siekierska-Hellmann M, Błaut K, et al. Hormonal activity in clinically silent adrenal incidentalomas. Arch Med Sci 2012; 8: 97-103.
87. Dogruk Unal A, Ayturk S, Aldemir D, Bascil Tutuncu N. Serum adiponectin level as a predictor of subclinical Cushing’s syndrome in patients with adrenal incidentaloma. Int J Endocrinol 2016; 2016: 8519362.
88. Etxabe J, Vazquez JA. Morbidity and mortality in Cushing’s disease: an epidemiological approach. Clin Endocrinol (Oxf) 1994; 40: 479-84.
89. Wagenmakers M, Roerink S, Gil L, et al. Persistent centripetal fat distribution and metabolic abnormalities in patients in long-term remission of Cushing’s syndrome. Clin Endocrinol 2015; 82: 180-187.
90. Babinska A, Kaszubowski M, Kmieć P, Sworczak K. Adipokine and cytokine levels in patients with adrenocortical cancer, subclinical Cushing’s syndrome and healthy controls. Steroids 2018; 140: 39-44.
91. Barahona MJ, Sucunza N, Resmini E, et al. Persistent body fat mass and inflammatory marker increases after long-term cure of Cushing’s syndrome. J Clin Endocrinol Metab 2009; 94: 3365-71.
92. Krsek M, Silha JV, Jezková J, et al. Adipokine levels in Cushing’s syndrome; elevated resistin levels in female patients with Cushing’s syndrome. Clin Endocrinol 2004; 60: 350-7.
93. Masuzaki H, Ogawa Y, Hosoda K, et al. Glucocorticoid regulation of leptin synthesis and secretion in humans: elevated plasma leptin levels in Cushing’s syndrome. J Clin Endocrinol Metab 1997; 82: 2542-7.
94. Gavrila A, Peng CK, Chan JL, Mietus JE, Goldberger AL, Mantzoros CS. Diurnal and ultradian dynamics of serum adiponectin in healthy men: comparison with leptin, circulating soluble leptin receptor, and cortisol patterns. J Clin Endocrinol Metab 2003; 88: 2838-43.
95. Widjaja A, Schürmeyer TH, Von zur Mühlen A, Brabant G. Determinants of serum leptin levels in Cushing’s syndrome. J Clin Endocrinol Metab 1998; 83: 600-3.
96. Weise M, Abad V, Considine RV, Nieman L, Rother KI. Leptin secretion in Cushing’s syndrome: preservation of diurnal rhythm and absent response to corticotropin-releasing hormone. J Clin Endocrinol Metab 1999; 84: 2075-9.
97. Van Harmelen V, Reynisdottir S, Eriksson P, et al. Leptin secretion from subcutaneous and visceral adipose tissue in women. Diabetes 1998; 47: 913-7.
98. Schwartz MW, Baskin DG, Bukowski TR, et al. Specificity of leptin action on elevated blood glucose levels and hypothalamic neuropeptide Y gene expression in ob/ ob mice. Diabetes 1996; 45: 531-5.
476 Arch Med Sci 2, 1st March / 2023
The role of selected adipokines in tumorigenesis and metabolic disorders in patients with adrenal tumors
99. Harman E, Karadeniz M, Biray C, et al. The relation of adiponectin and tumor necrosis factor alpha levels between endothelial nitric oxide synthase, angiotensin-converting enzyme, transforming growth factor beta, and tumor necrosis factor alpha gene polymorphism in adrenal incidentalomas. J Endocrinol Invest 2009; 32: 881-88.
100. Lazúrová I, Spišáková D, Wagnerová H, et al. Clinically silent adrenal adenomas – their relation to the metabolic syndrome and to GNB3 C825T gene polymorphism. Wien Klin Wochenschr 2011; 123: 618-22.
101. Rossi GP, Bernini G, Caliumi C, et al. PAPY Study Investigators. A prospective study of the prevalence of primary aldosteronism in 1,125 hypertensive patients. J Am Coll Cardiol 2006; 48: 2293-300.
102. Born-Frontsberg E, Reincke M, Rump LC, et al. Participants of the German Conn’s Registry. Cardiovascular and cerebrovascular comorbidities of hypokalemic and normokalemic primary aldosteronism: results of the German Conn’s Registry. J Clin Endocrinol Metab 2009; 94: 1125-30.
103. Fallo F, Veglio F, Bertello C, et al. Prevalence and characteristics of the metabolic syndrome in primary aldosteronism. J Clin Endocrinol Metab 2006; 91: 454-9.
104. Giacchetti G, Ronconi V, Turchi F, et al. Aldosterone as a key mediator of the cardiometabolic syndrome in primary aldosteronism: an observational study. J Hypertens 2007; 25: 177-86.
105. Marzolla V, Armani A, Zennaro MC, et al. The role of the mineralocorticoid receptor in adipocyte biology and fat metabolism. Mol Cell Endocrinol 2012; 350: 281-8.
106. Oda N, Takeda Y, Zhu A, et al. Pathophysiological roles of the adrenal renin-angiotensin system in patients with primary aldosteronism. Hypertens Res 2006; 29: 9-14.
107. Sowers JR, Whaley-Connell A, Epstein M. Narrative review: the emerging clinical implications of the role of aldosterone in the metabolic syndrome and resistant hypertension. Ann Intern Med 2009; 150: 776-83.
108. Letizia C, Petramala L, Tiziana di Gioia CR, et al. Leptin and adiponectin mRNA expression from the adipose tissue surrounding the adrenal neoplasia. J Clin Endocrinol Metab 2015; 100: E101-4.
109. Rossi GP, Sticchi D, Giuliani L, et al. Adiponectin receptor expression in the human adrenal cortex and aldosterone-producing adenomas. Int J Mol Med 2006; 17: 975-80.
110. Fallo F, Della Mea P, Sonino N, et al. Adiponectin and insulin sensitivity in primary aldosteronism. Am J Hypertens 2007; 20: 855-61.
111. Haluzík M, Sindelka G, Widimský J Jr, Prázný M, Zelinka T, Skrha J. Serum leptin levels in patients with primary hyperaldosteronism before and after treatment: relationships to insulin sensitivity. J Hum Hypertens 2002; 16: 41-5.
112. Torpy DJ, Bornstein SR, Taylor W, Tauchnitz R, Gordon RD. Leptin levels are suppressed in primary aldosteronism. Horm Metab Res 1999; 31: 533-6.
113. Ogunwobi OO, Beales IL. Globular adiponectin, activing via adiponectin receptor-1, inhibits leptin-stimulated oesophageal adenocarcinoma cell proliferation. Mol Cell Endocrinol 2008; 285: 43-50.
114. Nakayama S, Miyoshi Y, Ishihara H, Noguchi S. Growthinhibitory effect of adiponectin via adiponectin receptor 1 on human breast cancer cell through inhibition of S-phase entry without inducing apoptosis. Breast Cancer Res Treat 2008; 112: 405-10.
115. Fassnacht M, Dekkers OM, Else T, et al. European Society of Endocrinology Clinical Practice Guidelines on the management of adrenocortical carcinoma in adults, in collaboration with the European Network for the Study of Adrenal Tumors. Eur J Endocrinol 2018; 179: G1-46.
116. Mansmann G, Lau J, Balk E, Rothberg M, Miyachi Y, Bornstein SR. The clinically inapparent adrenal mass: update in diagnosis and management. Endocr Rev 2004; 25: 309-40.
117. Grumbach MM, Biller BM, Braunstein GD, et al. Management of the clinically inapparent adrenal mass (“incidentaloma”). Ann Intern Med 2003; 138: 424-9.
118. Kloos RT, Gross MD, Francis IR, Korobkin M, Shapiro B. Incidentally discovered adrenal masses. Endocr Rev 1995; 16: 460-84.
119. Elenkova A, Matrozova J, Zacharieva S, Kirilov G, Kalinov K. Adiponectin – a possible factor in the pathogenesis of carbohydrate metabolism disturbances in patients with pheochromocytoma. Cytokine 2010; 50: 306-10.
120. Bosanska L, Petrak O, Zelinka T, Mraz M, Widimsky J Jr, Haluzik M. The effect of pheochromocytoma treatment on subclinical inflammation and endocrine function of adipose tissue. Physiol Res 2009; 58: 319-25.
121. Wiesner TD, Blüher M, Windgassen M, Paschke R. Improvement of insulin sensitivity after adrenalectomy in patients with pheochromocytoma. J Clin Endocrinol Metab 2003; 88: 3632-6.
122. Isobe K, Fu L, Tatsuno I, et al. Adiponectin and adiponectin receptors in human pheochromocytoma. J Atheroscler Thromb 2009; 16: 442-7.
123. Böttner A, Eisenhofer G, Torpy DJ, et al. Lack of leptin suppression in response to hypersecretion of catecholamines in pheochromocytoma patients. Metabolism 1999; 48: 543-5.
Arch Med Sci 2, 1st March / 2023 477
Long non-coding RNA LINC00336 as an independent prognostic indicator and an oncogenic lncRNA in bladder cancer
Xi Guo1,2, Naijiang Liu3, Mingkai Liu4
1Department of Urology, Xiangya Hospital, Central South University, Changsha, Hunan Province, China
2Department of Urology, Hunan Provincial People’s Hospital, Changsha, Hunan Province, China
3Department of Surgery, the Eighth People’s Hospital of Jinan City, Jinan, Shandong Province, China
4Department of Urology, the Affiliated Hospital of Hebei University, Baoding, Hebei Province, China
Submitted: 27 May 2019; Accepted: 11 August 2019
Online publication: 11 November 2019
Arch Med Sci 2023; 19 (2): 478–487
DOI: https://doi.org/10.5114/aoms.2019.89661
Copyright © 2019 Termedia & Bnach
Abstract
Introduction: Long non-coding RNAs (lncRNAs) have been implicated in the initiation and progression of malignant tumor. The aim of the present study was to investigate whether LINC00336 contributes to the tumorigenesis of bladder cancer (BCa).
Material and methods: LncRNA expression profiling in BCa tissues was analyzed using lncRNA microarray. Cell viability, invasion and apoptosis were detected using CCK8, Transwell and Annexin V-fluorescein isothiocyanate/ propidium iodide (Annexin V-FITC) double staining, respectively. Results: LncRNA microarray and RT-qPCR revealed that LINC00336 was significantly up-regulated in BCa tissues and cell lines compared with the corresponding control group. Kaplan-Meier and multivariate regression analysis demonstrated that LINC00336 could serve as an independent risk factor for predicting the prognosis of BCa patients. In vitro experimental measurements showed that knockdown of LINC00336 had the ability to block cell proliferation and invasion, as well as to induce cell cycle arrest and apoptosis. Conclusions: These findings indicated that LINC00336 might serve as an oncogene in the initiation and progression of BCa, and LINC00336 may be a valuable and promising therapeutic target for the treatment of BCa.
Key words: bladder cancer, LINC00336, long non-coding RNA, prognosis, apoptosis.
Introduction
Bladder cancer (BCa) is the ninth most common malignant tumor, accounting for 90–95% of all urothelial carcinomas, and the majority of BCa occurs in men [1, 2]. Global cancer statistics reveal that there were approximately 429,800 new cases of BCa and 165,100 deaths in 2012 worldwide [1]. Cancer statistics in China indicate that 80,500 cases were newly diagnosed and 32,900 deaths occurred in 2015 [3]. In fact, approximately 70% of BCa patients are diagnosed with a non-muscle invasive BCa (NMIBC), while 30% of BCa patients present with a muscle-invasive
Corresponding author: Dr. Mingkai Liu
Department of Urology
the Affiliated Hospital of Hebei University
718 East Dongfeng Road
Baoding 071000
Hebei Province, China
Phone/fax: +86 0312
5981792
E-mail: liu_mingkai123@ sina.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/). Basic research
Oncology
BCa (MIBC) or a metastatic disease [2]. Currently, transurethral resection of bladder tumor or radical cystectomy is recommended as first-line treatment for the primary therapy of NMIBC or MIBC respectively [4]. Generally, most patients with NMIBC have a good prognosis, but a small fraction of patients develop MIBC or a metastatic disease resulting in aggressive features and poor prognosis, with a 5-year survival rate less than 50% [5]. Therefore, it is extremely urgent to identify new prognostic biomarkers, which may be helpful for the treatment and management of BCa.
Long non-coding RNAs (lncRNAs) are originally transcribed from non-coding sequences, consisting of more than 90% of the human genome, and are longer than 200 nucleotides with lack of protein coding capability [6]. LncRNAs have been implicated in many biological processes, including carcinogenesis, and perform a dual role in tumor initiation, progression and metastasis by modulating oncogenic and tumor-suppressing genes [7–9]. Recently, lncRNAs have been reported as a class of biomarkers to predict the prognosis of patients with malignant neoplasms, such as gastric cancer [10], prostate cancer [11], esophageal squamous cell carcinoma [12] and hepatocellular carcinoma [13]. Several lncRNAs, including OIP5-AS1, DGCR5 and SNHG16, are identified as prognostic indicators and may be vital for the pathogenesis of BCa [14–16]. However, the roles of lncRNAs in BCa have not been completely clarified.
In the present study, we performed lncRNA microarray assays to explore lncRNA expression profiling in three pairs of BCa tissues and adjacent non-tumorous tissues. Microarray analysis revealed that lncRNA LINC00336 expression levels were significantly up-regulated in BCa tissues. Subsequently, we validated the expression of LINC00336 in ninety-eight pairs of BCa tissues and adjacent non-tumorous tissues using RT-qPCR analysis, and the association between LINC00336 and overall survival (OA) or disease-free survival (DFS) was investigated in BCa patients. Furthermore, in vitro experiments were performed to detect the roles of LINC00336 in BCa cell proliferation and apoptosis.
Material and methods
Patients and specimens
Sixty-two BCa patients were recruited from the Xiangya Hospital of Central South University (Changsha China), the Eighth People’s Hospital of Jinan City (Jinan China) and the Affiliated Hospital of Hebei University (Baoding China) from January 2010 to June 2013. Sixty-two pairs of BCa and adjacent non-tumorous tissues were obtained from BCa patients who had undergone surgery. All samples were immediately stored in an ultra-low
temperature refrigerator. Signed informed consent forms were obtained from all BCa patients. The Ethics Committee of the Xiangya Hospital of Central South University (Changsha China), the Eighth People’s Hospital of Jinan City (Jinan China) and the Affiliated Hospital of Hebei University (Baoding China) approved our study.
Cell culture
Human normal bladder epithelial cell line (SVHUC-1) and bladder cancer cell lines (5637, T24 and SW780) were purchased from the Cell Bank of Type Culture Collection of Chinese Academy of Sciences (Shanghai, China). Cells were cultured in Dulbecco’s modified Eagle’s medium (DMEM; Invitrogen, Carlsbad, CA, USA) with 5% fetal bovine serum (Thermo Scientific HyClone, Beijing, China), 5% CO2, 95% air atmosphere in a humidified incubator (Thermo, USA).
LncRNAs microarray
Differentially expressed lncRNAs in three pairs of BCa tissues and adjacent non-tumorous tissues were analyzed using the Agilent human lncRNA array V.2.0 platform (Agilent Technologies, Santa Clara, CA, USA).
Cell transfection
Short hairpin RNA (shRNA) was designed to specifically target LINC00336 using shRNA design tools (http://rnaidesigner.thermofisher.com/rnaiexpress/). Using BLAST (http://blast.ncbi.nlm.nih.gov/ Blast.cgi), we verified that the designed shRNA targeted only the LINC00336. Sh-LINC00336 and sh-NC were synthesized by GenePharma (Shanghai, China).
CCK-8
5637, T24 and SW780 cell viability was measured using the CCK-8 Cell Proliferation/Viability Assay Kit (Dojindo, Japan) as described previously [17]. Absorbance was calculated at 450 nm using an Elx800 Reader (Bio-Tek Instruments Inc., Winooski, VT, USA).
Transwell assay
Invasion of bladder cancer cells was determined using a transwell insert (8 μm, Corning) as described previously [18]. Absorbance was determined at a wavelength of 570 nm using an Elx800 Reader (Bio-Tek Instruments Inc., Winooski, VT, USA).
Cell cycle analysis
5637, T24 and SW780 cell cycle distribution was measured using the CycleTESTTM PLUS DNA Reagent Kit (BD Biosciences, San Jose, CA, USA) as described previously [19].
Long
Arch Med Sci 2, 1st March / 2023 479
non-coding RNA LINC00336 as an independent prognostic indicator and an oncogenic lncRNA in bladder cancer
Apoptosis
5637, T24 and SW780 cell apoptosis was analyzed using an Annexin V-FITC/PI double staining kit (Invitrogen, Carlsbad, Calif, USA) with flow cytometry (FACScan, BD Biosciences, San Jose, CA, USA) as described previously [20]. Apoptotic cell proportion was calculated using CELL Quest 3.0 software (BD Biosciences).
RT-qPCR
Total RNA was isolated using RNAiso (Takara, Dalian, China). The RT Kit (Toyobo Co. Ltd, Osaka, Japan) and KAPA SYBR Green FAST qPCR Kit (KAPA, Wilmington, MA, US) were used to measure the expression levels of LINC00336 using the Applied Biosystems 7300 Real-Time PCR System (Thermo Fisher Scientific, Inc.) and normalized to the inter-
nal control U6. LncRNAs expression levels were calculated using the 2–ΔΔCq method [21].
Ethics approval
Written informed consent was obtained from all of the participants prior to collection of samples. The Ethics Committee of the Xiangya Hospital of Central South University (Changsha China), the Eighth People’s Hospital of Jinan City (Jinan China) and the Affiliated Hospital of Hebei University (Baoding China) approved our study according to the Helsinki Declaration.
Statistical analysis
Data were presented as the mean ± standard error of the mean. Statistical analysis was performed using SPSS software version 19.0 (IBM Corp., Ar-
Figure 1. LncRNAs expression profiling in BCa tissues. A – Microarray and hierarchical cluster analysis were performed using the multiple experiment viewer 4.7.1 software, and 29 differentially expressed lncRNAs in three pairs of BCa tissues and adjacent non-tumorous tissues were selected out according to Log2|FC| ≥ 2.0, p < 0.001 and FDR < 0.001. B – Top 6 differentially expressed lncRNAs, i.e. OIP5-AS1, H19, LINC00336, POU3F3, NEF and SNHG15, were chosen for RT-qPCR assays in sixty-two pairs of BCa tissues and adjacent non-tumor tissues
*P < 0.05.
480 Arch Med Sci 2, 1st March / 2023
Xi Guo, Naijiang Liu, Mingkai Liu
N1 N2 N3 T1 T2 T3 Log2 FC ELF3-AS1 2.48 OXCT1-AS1 2.20 SNHG7 2.17 GAS6-AS2 2.19 UCA1 2.87 PVT1 2.72 CALML3-AS1 2.57 HOTAIR 2.31 OIP5-AS1 3.49 H19 3.13 LINC00336 3.41 POU3F3 3.33 LINC00261 –2.27 ADAMTS9-AS2 –2.09 LINC00052 –2.16 TFAP2A-AS1 –2.39 PICART1 –2.54 ZEB2-AS1 –2.42 RUNX1-IT1 –2.60 LINC02023 –2.06 MIR503HG –2.22 HERC2P2 –2.42 MT1JP –2.04 DGCR5 –2.84 CASC2 –2.70 NEF –3.48 SNHG15 –3.16 PINT –2.33 ARAP1-AS1 –2.95 –2 0 2 Relative lncRNA expression 15 10 5 0 N T OIP5-AS1 Relative lncRNA expression 10 8 6 4 2 0 N T H19 Relative lncRNA expression 15 10 5 0 N T LINC00336 Relative lncRNA expression 10 8 6 4 2 0 N T POU3F3 Relative lncRNA expression 4 3 2 1 0 N T NEF Relative lncRNA expression 4 3 2 1 0 N T SNHG15 A B
Long non-coding RNA LINC00336 as an independent prognostic indicator and an oncogenic lncRNA in bladder cancer
monk, NY, USA). Student’s t-test or Kruskal-Wallis test was used to analyze two-group differences. Differences between multiple groups were analyzed by one-way analysis of variance, followed by a post-hoc Tukey test. Pearson’s c2 test was used to evaluate differences between the clinical characteristics and LINC00336 expression levels in BCa patients. OS and DFS were calculated using the Kaplan-Meier method with the log-rank test applied for comparison. Univariate and multivariate regression analysis were performed to evaluate the correlation between clinical characteristics, LINC00336 expression and OS using a Cox proportional hazard model. P < 0.05 was considered to indicate a statistically significant difference.
Results
LncRNAs expression profiling in BCa tissues
As shown in Figure 1 A, microarray probes were used to detect differentially expressed lncRNAs in three pairs of BCa tissues and adjacent non-tumor tissues. Based on the Log2|FC| ≥ 2.0, p < 0.001 and FDR < 0.001, a total of 29 lncRNAs were significantly differentially expressed in three BCa tissues compared with adjacent non-tumor tissues. Among them, 12 and 17 lncRNAs were up-regulated and down-regulated, respectively. To further validate the results of microarray, the top 6 differentially expressed lncRNAs, i.e. OIP5AS1, H19, LINC00336, POU3F3, NEF and SNHG15, were chosen for RT-qPCR assays in sixty-two pairs of BCa tissues and adjacent non-tumor tissues. OIP5-AS1, H19, LINC00336 and POU3F3 were increased, while NEF and SNHG15 were decreased in sixty-two BCa tissues as compared to adjacent non-tumor tissues (Figure 1 B). These results were consistent with the microarray assay. The fold change (FC) of LINC00336 was 3.86 in BCa tissues compared with adjacent non-tumor tissues, which was higher than other lncRNAs. Therefore, we focused on LINC00336 in our study.
LINC00336 was an independent prognostic indicator in BCa patients
As shown in Table I, the up-regulation of LINC00336 expression level was significantly correlated with tumor stage T (p = 0.002), histological grade (p = 0.001) and vascular invasion (p = 0.043), while the expression level of LINC00336 were not associated with age, gender, tumor size or lymph node metastasis in BCa patients (Table I). We also found that age, gender, tumor size and lymph node metastasis had no obvious effect on OS in BCa patients (Figures 2 A–C, F). However, high tumor stage T (p= 0.014), histological grade (p = 0.004) and vascular invasion (p = 0.026) were significantly associated with poor prognosis of BCa
patients (Figures 2 D, E, G). Kaplan-Meier analysis and log-rank tests revealed that high LINC00336 expression level showed worse OS and DFS than those of BCa patients with low LINC00336 expression (Figures 2 H, I). COX univariate and multivariate analyses revealed that LINC00336, vascular invasion and histological grade were independent risk factors for predicting the prognosis of BCa patients (Table II).
Knockdown of LINC00336 repressed proliferation and invasion in BCa cells
We further determined the functions of LINC00336 in BCa cells in vitro. First, we found significant up-regulation of LINC00336 expression level in BCa cells compared with human normal SV-HUC-1 cells (Figure 3 A). Next, the LINC00336 specific shRNA was designed to target inhibition of LINC00336 expression level in BCa cells, and the results demonstrated that the expression level
Arch Med Sci 2, 1st March / 2023 481
Variables N LINC00336 expression P -value Low ( n = 25) High ( n = 37) Age [years]: 0.272 ≤ 55 37 17 20 > 55 25 8 17 Gender: 0.284 Male 42 15 27 Female 20 10 10 Tumor size [cm]: 0.233 ≤ 3 34 16 18 > 3 28 9 19 Tumor stage T: 0.002 Ta-T1 30 18 12 T2-T4 32 7 25 Histological grade: 0.001 L 27 17 10 H 35 8 27 Lymph node metastasis: 0.541 No 40 15 25 Yes 22 10 12 Vascular invasion: 0.043 No 30
Yes 32
Table I. Correlation between LINC00336 expression and clinicopathological variables of BCa patients
16 14
9 23
Figure 2. LINC00336 was an independent prognostic indicator in BCa patients. Kaplan-Meier analysis and logrank test indicated that age (A), gender (B), tumor size (C) and lymph node metastasis (F) have no relevance for survival prognosis in BCa patients. Tumor stage T (D), Histological grade (E) and vascular invasion (G) are correlated with OS in BCa patients
482 Arch Med Sci 2, 1st March / 2023
Xi Guo, Naijiang Liu, Mingkai Liu
OS (%) OS (%) OS (%) OS (%) OS (%) OS (%) OS (%) 100 80 60 40 20 0 100 80 60 40 20 0 100 80 60 40 20 0 100 80 60 40 20 0 100 80 60 40 20 0 100 80 60 40 20 0 100 80 60 40 20 0 0 20 40 60 80 100 Time [months] ≤ 55 > 55 0 20 40 60 80 100 Time [months] ≤ 3 > 3 0 20 40 60 80 100 Time [months] L H 0 20 40 60 80 100 Time [months] No Yes 0 20 40 60 80 100 Time [months] M F 0 20 40 60 80 100 Time [months] Ta-T1 T2-T4 0 20 40 60 80 100 Time [months] No Yes Age [years] Tumor size Histological grade Vascular invasion Gender Tumor stage T Lymph node metastasis A C E G B D F p = 0.248 p = 0.329 p = 0.004 p = 0.026 p = 0.723 p = 0.014 p = 0.385
Long non-coding RNA LINC00336 as an independent prognostic indicator and an oncogenic lncRNA in bladder cancer
of LINC00336 was significantly decreased in T24, 5637 and SW780 cells after transfection with shLINC00336 (Figure 3 B). After transfection with shLINC00336 into T24, 5637 and SW780 cells, the cell proliferation was markedly inhibited when the incubation time was more than 48 h (Figure 3 C). Transwell assay revealed that inhibition of cell invasion was observed in T24, 5637 and SW780 cells induced by silencing LINC00336 (Figure 3 D). These results indicated that LINC00336 had the ability to promote BCa cell proliferation and invasion.
Knockdown of LINC00336 induced cell cycle arrest and apoptosis in BCa cells
Flow cytometry was used to analyze whether LINC00336 regulated cell cycle and apoptosis of BCa cells. The results showed that the percentage of S-phase cells was significantly increased in T24, 5637 and SW780 cells induced by silencing LINC00336 (Figures 4 A, B). We also found that the apoptotic cell proportion was significantly elevated in T24, 5637 and SW780 cells after transfected with sh-LINC00336 (Figures 4 C, D). These findings suggested that knockdown of
LINC00336 induced S-phase cell cycle arrest and apoptosis in BCa cells.
Discussion
BCa usually exhibits an excellent prognosis, which critically depends on early diagnosis and treatment, after surgical resection combined with chemotherapy regimens [5]. However, the 5-year OS rate remains unsatisfactory for BCa patients with recurrence or metastasis [5]. Therefore, exploration of novel prognostic markers may be important for the treatment of BCa. At present, non-coding RNAs (ncRNAs), including microRNAs, lncRNAs and circular RNAs, as a novel class of molecular biomarkers, have been identified as prognostic biomarkers of several cancer types, including BCa [22, 23]. LncRNAs belong to the ncRNA family and play a crucial role in the progression of carcinogenesis [24]. With the rapid development of cancer genomics and high-throughput sequencing, thousands of lncRNAs are deregulated or mutated in various cancers [25]. In BCa, numerous lncRNAs, such as UCA1, HOXD-AS1, TUG1, MALAT1, MEG3 and H19, are associated with cell proliferation, mi-
Arch Med Sci 2, 1st March / 2023 483
OS (%) OS (%) 100 80 60 40 20 0 100 80 60 40 20 0 0 20 40 60 80 100 Time [months] Low High 0 20 40 60 80 100 Time [months] Low High LINC00336 LINC00336 H I p < 0.001 p = 0.002
Figure 2. Cont. High LINC00336 expression was correlated with poor OS (H) and DFS (I) in BCa patients
Variables Univariate Multivariate HR (95% CI) P -value HR (95% CI) P -value Age (> 55 vs. ≤ 55) 0.91 (0.43–1.90) 0.675 Gender (M vs. F) 1.21 (0.61–2.66) 0.341 Tumor size (> 3 vs. ≤ 3) 1.27 (0.72–2.79) 0.247 Lymph node metastasis (Yes vs. No) 1.72 (0.894–3.93) 0.091 Tumor stage T (T2-T4 vs. Ta-T1) 2.66 (1.13–4.87) 0.025 1.45 (0.812–3.77) 0.145 Histological grade (H vs. L) 5.63 (2.03–10.67) < 0.001 3.01 (1.67–7.59) 0.009 Vascular invasion (Yes vs. No) 2.78 (1.19–5.71) 0.012 2.49 (1.02–4.79) 0.037 LINC00336 (high vs. low) 3.15 (1.64–6.51) 0.004 2.82 (1.26–7.53) 0.019
Table II. Univariate and multivariate regression analysis of BCa patients for overall survival
Figure 3. Knockdown of LINC00336 repressed proliferation and invasion in BCa cells. A – Expression of LINC00336 in human normal bladder epithelial cell line (SV-HUC-1) and bladder cancer cell lines (5637, T24 and SW780) was measured using RT-qPCR. B – After transfection with sh-NC or shLINC00336 into 5637, T24 and SW780 cells, the expression of LINC00336 was measured using RTqPCR. C – Cell proliferation changes of 5637, T24 and SW780 cells were determined using CCK-8 assay. D – Invasive abilities of bladder cancer cells were determined using transwell assay
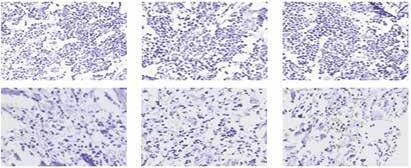
*P < 0.05, **p < 0.01, ***p < 0.001 compared with control group.
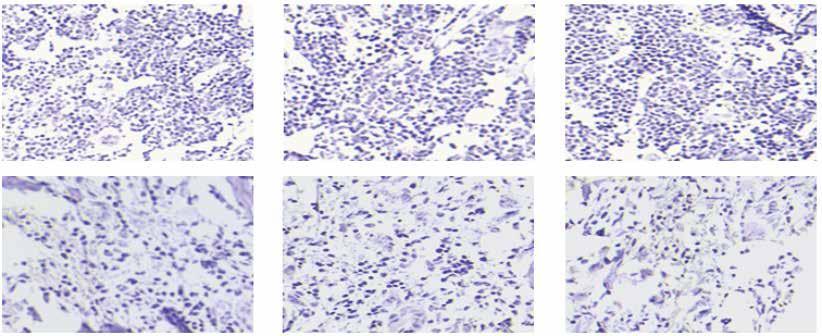
484 Arch Med Sci 2, 1st March / 2023 Relative expression of LINC00336 Relative expression of LINC00336 A C D B 4 3 2 1 0 1.5 1.0 0.5 0 SV-HUC-1 T24 5637 SW780 0 24 48 72 Time [h] sh-NC sh-LINC00336 0 24 48 72 Time [h] sh-NC sh-LINC00336 0 24 48 72 Time [h] sh-NC sh-LINC00336 T24 5637 SW780 sh-NC sh-LINC00336 Cell viability (OD 450) Cell viability (OD 450) Cell viability (OD 450) 1.5 1.0 0.5 0 1.0 0.8 0.6 0.4 0.2 0 1.5 1.0 0.5 0 T24 5637 SW780 sh-LINC00336 sh-NC T24 5637 SW780 OD (570 nm) 0.8 0.6 0.4 0.2 0 T24 5637 SW780 sh-NC sh-LINC00336
Xi Guo, Naijiang Liu, Mingkai Liu
Long non-coding RNA LINC00336 as an independent prognostic indicator and an oncogenic lncRNA in bladder cancer
sh-NCsh-LINC00336 sh-NCsh-LINC00336 sh-NCsh-LINC00336
Figure 4. Knockdown of LINC00336 induced cell cycle arrest and apoptosis in BCa cells. Flow cytometry assays were performed to analyze cell cycle progression (A, B) and apoptosis (C, D) of 5637, T24 and SW780 cells after transfection with sh-NC or sh-LINC00336
*P < 0.05.
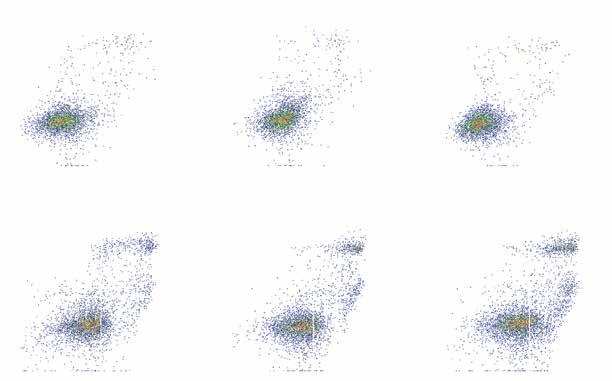
Arch Med Sci 2, 1st March / 2023 485
T24 5637 SW780 1000 800 600 400 200 0 600 400 200 0 60 40 20 0 50 40 30 20 10 0 0 20 40 60 80 100 120 0 30 60 90 120 0 20 40 60 80 100 120 0 30 60 90 120 0 20 40 60 80 100 120 0 20 40 60 80 100 120 1000 800 600 400 200 0 600 400 200 0 600 500 400 300 200 100 0 600 400 200 0 Number Cell cycle stage Apoptotic cell proportion (%) Channels (FL2-A) A B
D
T24 5637 SW780 T24 5637 SW780 G0/G1 s G2/M T24 5637 SW780 sh-NC sh-LINC00336 sh-LINC00336 sh-NC sh-LINC00336 sh-NC PI Annexin V-FITC Q1 104 103 102 101 100 104 103 102 101 100 104 103 102 101 100 104 103 102 101 100 104 103 102 101 100 104 103 102 101 100 100 101 102 103 104 100 101 102 103 104 100 101 102 103 104 100 101 102 103 104 100 101 102 103 104 100 101 102 103 104 Q1 Q1 Q1 Q1 Q1 Q2 2.51% 1.18% 12.1% 14.5% 2.75% 1.20% 15.3% 15.8% 1.86% 0.53% 16.7% 19.8% Q2 Q2 Q2 Q2 Q2 Q3 Q3 Q3 Q3 Q3 Q3 Q4 Q4 Q4 Q4 Q4 Q4
C
gration, invasion, drug resistance and prognosis [25, 26]. Although lncRNAs are implicated in BCa, understanding the roles of tremendously large numbers of lncRNAs in the initiation and progression of BCa is a challenging task.
In our study, lncRNA microarray and RT-qPCR revealed that LINC00336 expression levels were significantly increased in BCa tissues and cell lines compared with the corresponding control group. Kaplan-Meier, COX univariate and multivariate analyses confirmed that LINC00336 could serve as an independent risk factor for predicting the prognosis of BCa patients. In vitro experimental measurements demonstrated that knockdown of LINC00336 showed the ability to inhibit cell proliferation and invasion and induce cell cycle arrest and apoptosis. These findings suggest than LINC00336 may act as an oncogene in the initiation and progression of BCa, and LINC00336 may be a valuable and promising therapeutic target for the treatment of BCa. Recently, He et al. reported that LINC00336 is up-regulated in chromophobe renal cell carcinoma tissues and was identified to be significantly correlated with OS [27]. Wang et al. also demonstrated that LINC00336 is upregulated and performs an important role in pulmonic tumorigenesis, and overexpression of LINC00336 promotes cell growth, colony formation and tumor formation [28]. Moreover, high LINC00336 expression level is associated with poor prognosis in nonsmall cell lung cancer [28]. These results confirm that LINC00336 functions as an oncogene to facilitate tumor cell growth.
Previous studies corroborate that lymph node metastases constitute a strong prognostic factor in BCa [29, 30]. Mechanistic investigations highlight that lymphovascular invasion may be an important predictor for lymph node metastasis in multiple cancer types [31–33]. The present study reveals a significant increase in LINC00336 expression level in BCa patients with vascular invasion. However, there is no obvious association between LINC00336 expression level and lymph node metastasis, which may be attributed to the small sample size in our study.
To determine possible mechanisms of LINC00336 loss-of-function induced BCa cell growth inhibition, we hypothesized that knockdown of LINC00336 might affect cell cycle and apoptosis of BCa cells. We silenced the expression of LINC00336 by transfection with specific shRNA into three BCa cell lines, i.e. T24, 5637 and SW780 cells, and the inhibition rate of LINC00336 expression level reached up to 50% in in vitro experiments. Subsequently, we observed that S-phase cell cycle arrest and an increase in apoptotic cell proportion occurred in T24, 5637 and SW780 cells after transfection with sh-LINC00336. Our results
demonstrated that inhibition of cell growth rate might be associated with S-phase cell cycle arrest and elevation of apoptotic cell proportion in BCa cells after transfection with sh-LINC00336.
We need to make clear the limitations in our study. First, the roles of LINC00336 in cell growth have not been investigated in human BCa xenografts in nude mice. In addition, functions of LINC00336 with gene-gene interactions are not involved in the present study.
In conclusion, LINC00336 as an independent risk factor for predicting the prognosis of BCa was observed in our study, and knockdown of LINC00336 had the ability to suppress cell proliferation and invasion and induce cell cycle arrest and apoptosis in BCa cells. LINC00336 displayed aberrant expression of BCa tissues and showed strong potential for development of a novel therapeutic target for the treatment of BCa.
Conflict of interest
The authors declare no conflict of interest.
References
1. Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin 2015; 65: 87-108.
2. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 2015; 136: E359-86.
3. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin 2016; 66: 115-32.
4. Wu SQ, Xu R, Li XF, Zhao XK, Qian BZ. Prognostic roles of tumor associated macrophages in bladder cancer: a system review and meta-analysis. Oncotarget 2018; 9: 25294-303.
5. Yafi FA, Aprikian AG, Chin JL, et al. Contemporary outcomes of 2287 patients with bladder cancer who were treated with radical cystectomy: a Canadian multicentre experience. BJU Int 2011; 108: 539-45.
6. Hon CC, Ramilowski JA, Harshbarger J, et al. An atlas of human long non-coding RNAs with accurate 5’ ends. Nature 2017; 543: 199-204.
7. Mitra R, Chen X, Greenawalt EJ, Maulik U, Jiang W, Zhao Z. Decoding critical long non-coding RNA in ovarian cancer epithelial-to-mesenchymal transition. Nature Commun 2017; 8: 1604.
8. Russell MR, Penikis A, Oldridge DA, et al. CASC15-S is a tumor suppressor lncRNA at the 6p22 neuroblastoma susceptibility locus. Cancer Res 2015; 75: 3155-66.
9. Han X, Xu Z, Tian G, et al. Suppression of the long non-coding RNA MALAT-1 impairs the growth and migration of human tongue squamous cell carcinoma SCC4 cells. Arch Med Sci 2018; 15: 992-1000.
10. Li Y, Wen X, Wang L, et al. LncRNA ZEB1-AS1 predicts unfavorable prognosis in gastric cancer. Surg Oncol 2017; 26: 527-34.
11. Huang W, Su X, Yan W, et al. Overexpression of AR-regulated lncRNA TMPO-AS1 correlates with tumor progression and poor prognosis in prostate cancer. Prostate 2018; 78: 1248-61.
486 Arch Med Sci 2, 1st March / 2023
Xi Guo, Naijiang Liu, Mingkai Liu
Long non-coding RNA LINC00336 as an independent prognostic indicator and an oncogenic lncRNA in bladder cancer
12. Kang K, Huang YH, Li HP, Guo SM. Expression of UCA1 and MALAT1 long-chain non-coding RNAs in esophageal squamous cell carcinoma tissues is predictive of patient prognosis. Arch Med Sci 2018; 14: 752-9.
13. Jin L, He Y, Tang S, Huang S. LncRNA GHET1 predicts poor prognosis in hepatocellular carcinoma and promotes cell proliferation by silencing KLF2. J Cell Physiol 2018; 233: 4726-34.
14. Wang Y, Shi F, Xia Y, Zhao H. LncRNA OIP5-AS1 predicts poor prognosis and regulates cell proliferation and apoptosis in bladder cancer. J Cell Biochem 2019; 120: 7499-505.
15. Fang C, He W, Xu T, Dai J, Xu L, Sun F. Upregulation of lncRNA DGCR5 correlates with better prognosis and inhibits bladder cancer progression via transcriptionally facilitating P21 expression. J Cell Physiol 2019; 234: 6254-62.
16. Cao X, Xu J, Yue D. LncRNA-SNHG16 predicts poor prognosis and promotes tumor proliferation through epigenetically silencing p21 in bladder cancer. Cancer Gene Ther 2018; 25: 10-17.
17. Wang F, Ying HQ, He BS, et al. Upregulated lncRNA-UCA1 contributes to progression of hepatocellular carcinoma through inhibition of miR-216b and activation of FGFR1/ ERK signaling pathway. Oncotarget 2015; 6: 7899-917.
18. Zhan Y, Chen Z, Li Y, et al. Long non-coding RNA DANCR promotes malignant phenotypes of bladder cancer cells by modulating the miR-149/MSI2 axis as a ceRNA. J Exp Clin Cancer Res 2018; 37: 273.
19. Wang X, Wang L, Gong Y, et al. Long noncoding RNA LINC01296 promotes cancer-cell proliferation and metastasis in urothelial carcinoma of the bladder. Onco Targets Ther 2019; 12: 75-85.
20. Wang L, Wei Y, Yan Y, et al. CircDOCK1 suppresses cell apoptosis via inhibition of miR196a5p by targeting BIRC3 in OSCC. Oncol Rep 2017; 39: 951-66.
21. Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative PCR and the 2(-Delta Delta C(T)) method. Methods 2001; 25: 402-8.
22. Wieczorek E, Reszka E. mRNA, microRNA and lncRNA as novel bladder tumor markers. Clin Chim Acta 2018; 477: 141-53.
23. Yang C, Yuan W, Yang X, et al. Circular RNA circ-ITCH inhibits bladder cancer progression by sponging miR17/miR-224 and regulating p21, PTEN expression. Mol Cancer 2018; 17: 19.
24. Xie H, Ma B, Gao Q, et al. Long non-coding RNA CRNDE in cancer prognosis: review and meta-analysis. Clin Chim Acta 2018; 485: 262-71.
25. Bhan A, Soleimani M, Mandal SS. Long noncoding RNA and cancer: a new paradigm. Cancer Res 2017; 77: 3965-81.
26. Pan J, Li X, Wu W, et al. Long non-coding RNA UCA1 promotes cisplatin/gemcitabine resistance through CREB modulating miR-196a-5p in bladder cancer cells. Cancer Lett 2016; 382: 64-76.
27. He HT, Xu M, Kuang Y, Han XY, Wang MQ, Yang Q. Biomarker and competing endogenous RNA potential of tumor-specific long noncoding RNA in chromophobe renal cell carcinoma. Onco Targets Ther 2016; 9: 6399-406.
28. Wang M, Mao C, Ouyang L, et al. Long noncoding RNA LINC00336 inhibits ferroptosis in lung cancer by functioning as a competing endogenous RNA. Cell Death Differ 2019; 26: 2329-43.
29. Cha EK, Sfakianos JP, Sukhu R, Yee AM, Sjoberg DD, Bochner BH. Poor prognosis of bladder cancer patients
with occult lymph node metastases treated with neoadjuvant chemotherapy. BJU Int 2018; 122: 627-32.
30. Hugen CM, Daneshmand S. Lymph node dissection in bladder cancer: were do we stand? World J Urol 2017; 35: 527-33.
31. Werntz RP, Smith ZL, Packiam VT, Smith N, Steinberg GD. The impact of lymphovascular invasion on risk of upstaging and lymph node metastasis at the time of radical cystectomy. Eur Urol Focus 2018; pii: S24054569(18)30292-X.
32. Qian Y, Pollom EL, Nwachukwu C, et al. Extent of lymphovascular space invasion may predict lymph node metastasis in uterine serous carcinoma. Gynecol Oncol 2017; 147: 24-9.
33. Schiefer AI, Schoppmann SF, Birner P. Lymphovascular invasion of tumor cells in lymph node metastases has a negative impact on survival in esophageal cancer. Surgery 2016; 160: 331-40.
Arch Med Sci 2, 1st March / 2023 487
Induction of apoptosis in RL95-2 human endometrial cancer cells by combination treatment with docosahexaenoic acid and triacsin C
1Department of Obstetrics and Gynaecology, Soonchunhyang University College of Medicine, Bucheon, Republic of Korea
2Department of Interdisciplinary Program in Biomedical Science, Soonchunhyang University Graduate School, Asan, Republic of Korea
Submitted: 26 November 2018; Accepted: 26 August 2019
Online publication: 3 March 2021
Arch Med Sci 2023; 19 (2): 488–498
DOI: https://doi.org/10.5114/aoms/111947
Copyright © 2021 Termedia & Banach
Abstract
Introduction: Docosahexaenoic acid (DHA) supplementation has been reported to negatively correlate with cancer cell proliferation and tumour development in many cancer types. Although cumulative evidence has demonstrated the apoptotic effect and cytotoxicity of DHA against tumour development in many cell types, the precise cellular and biochemical mechanisms of DHA-induced apoptosis in human endometrial cancer cells have not been investigated.
Material and methods: MTT assay was performed to confirm the degree of apoptosis by combining treatment with DHA and triacsin C in endometrial cancer cell line. The synergistic effects of triacsin C and DHA were identified by performing flowcytometry and immunoblotting analysis.
Results: Combined treatment with DHA and triacsin C significantly induced apoptosis in RL95-2 endometrial carcinoma cells. Combined treatment with 125 μM DHA and 5 μM triacsin C significantly increased the sub-G1 population and apoptotic fragments in endometrial carcinoma cells. It was also demonstrated that DHA and triacsin C induced apoptosis through mitochondrial pathways via caspases-9, -3, and -7 as well as through the extrinsic pathway by activation of caspase-8/BID.
Conclusions: Further elucidation of the apoptotic mechanisms involving DHA treatment with ACS ablation could shed light on possible new treatment strategies for endometrial cancer. In addition, further research into the mechanisms of DHA and triacsin C-induced apoptotic mechanisms may lead to the development of therapeutic strategies for endometrial cancer.
Key words: docosahexaenoic acid, triacsin C, endometrial cancer, caspases, apoptosis.
Introduction
Endometrial carcinoma is the most common gynaecological malignancy, currently representing 13% of all female cancers [1, 2]. The American Cancer Society estimates that there were 43,470 new cases and 7950 deaths from endometrial cancer in 2010 [3]. Current therapies for advanced and recurrent endometrial cancer remain ineffective.
Dietary n-3 polyunsaturated fatty acids (PUFAs) inhibit the growth of endometrial cancers, which have been identified as the most com-
Corresponding author: Tae-Hee Kim MD, PhD
Department of Obstetrics and Gynaecology
Soonchunhyang University
Bucheon Hospital
170 Jomaru-ro, Wonmi-gu, Bucheon
14584, Republic of Korea
Phone: +82-32-621-5380
Fax: +82-2-6008-6874
E-mail: heeobgy@naver.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Soo-Ho Chung1, Hae-Hyeog Lee1, Yeon-Suk Kim2, Kisung Song2, Tae-Hee Kim1
Basic research Oncology
mon hormone-responsive tumours both in vitro and in vivo [4, 5]. Epidemiological data suggest an inverse relationship between endometrial cancer risk and consumption of a diet rich in PUFAs, including docosahexaenoic acid (DHA, 22:6n-3) and eicosapentaenoic acid (EPA, 20:5n-3) [6, 7]. DHA supplementation is negatively correlated with cancer cell proliferation and tumour development in many cancer types. Importantly, while DHA selectively inhibits such proliferation, it is significantly less toxic towards normal cells [8–10]. It has been suggested that DHA induces apoptosis by regulating mitochondrial-related mechanisms at the membrane [11]. Studies have demonstrated that the incorporation of DHA into mitochondrial membranes increases susceptibility to reactive oxygen species (ROS) damage generated in colonocytes [12] and the HT-29 human colon tumour cell line [13]. Specifically, the association between DHA and cardiolipin, a mitochondrial inner membrane phospholipid, contributes to a mitochondrial-dependent apoptotic pathway that initiates the release of cytochrome c from the mitochondrial intermembrane space, which is associated with the induction of oxidative stress, loss of mitochondrial membrane potential, and apoptotic signalling [14–16]. Two major apoptotic pathways have been proposed in normal human cells. The extrinsic apoptotic pathway involves the stimulation of death receptors including Fas and tumour necrosis factor receptor-1 and involves the adapter protein Fas-associated death domain, as well as the initiator caspase-8. In parallel, the intrinsic pathway of apoptosis results from changes in mitochondrial status, activation of the apoptosome, and release of mitochondrial cytochrome c into the cytosol, which initiates a caspase activation cascade [17, 18]. Activated caspase-8 in these systems directly activates the executioner caspase (caspase-3) or cleaves BID (a BH3-only member of the Bcl-2 family of proteins), which triggers its translocation to the mitochondria followed by the release of cytochrome c, Smac/DIABLO, and apoptosis inducing factor [19, 20]. Other studies have reported that pro-caspase-8 is translocated to the mitochondria, where it binds to cardiolipin, oligomerises, and is activated, leading to cleavage of truncated p15 BID (tBID) and the generation of proteolytically active p43 and p10 fragments [21]. An immunofluorescence analysis revealed that active caspase-8 and tBID are primarily located in the mitochondria, although a distinct portion of pro-caspase-8 also co-localised with tBID at the mitochondria following exposure to DHA and triacsin C. Therefore, it seems plausible that DHA and triacsin C induce translocation of caspase-8 to the mitochondria, where it binds BID, leading to activation of tBID in the mitochondria. In ad-
dition, a sub-G1 analysis revealed that DHA and triacsin C-induced apoptosis are completely suppressed by inhibition of caspase-8, indicating that apoptosis requires activation of caspase-8 and BID. Although these results show that apoptosis induced by DHA and triacsin C is involved in both the extrinsic and intrinsic apoptotic pathways, activation of caspase-8/Bid appears to play the most critical role in the induction of apoptosis in RL95-2 cells. Cumulative evidence has demonstrated the apoptotic effect and cytotoxicity of DHA against tumour development in many cell types [22, 23], but the precise cellular and biochemical mechanisms of DHA-induced apoptosis in human endometrial cancer cells have not been investigated.
Long-chain unsaturated fatty acids are normally processed by acyl-coA synthetases (ACSs). Acyl-coA synthetases catalyse the initial step of mammalian fatty acid metabolism by converting long-chain fatty acids to acyl-CoA, which function mainly as activated lipid intermediates for fatty acid b-oxidation, modulating cellular signal transduction [24, 25]. Studies with triacsin C have shown that inhibiting ACS leads to apoptosis in human T lymphoblastoma [26], glioma [27, 28], and hepatocellular carcinoma cells [29] through pathways mediated by mitochondria. Another study showed that treatment with simvastatin, a lipid-lowering drug, decreases proliferation of human acute monocytic leukaemia (THP-1) macrophage cells [30]. Based on these findings, it has been hypothesised that the inhibition of ACS by triacsin C would impair DHA metabolism, which contributes to cytotoxicity-induced apoptosis by DHA in RL95-2 endometrial carcinoma. Therefore, combining DHA with triacsin C might maximise the effect of apoptosis in endometrial cancer cell line.
In the present study, we evaluated whether triacsin C cooperatively induces apoptosis with DHA in RL95-2 cells. Then, we investigated whether the synergistic effects of triacsin C and DHA on apoptotic induction were mediated by changes in mitochondria accompanied by activation of caspase-8, -9, -7, and -3.
Material and methods
Cell culture
RL95-2 cells (human endometrial adenocarcinoma cell line; American Type Culture Collection, Manassas, VA, USA) were cultured in Dulbecco’s modified Eagle’s medium nutrient mixture with HAMS F-12 (Sigma, St. Louis, MO, USA) containing 10% foetal bovine serum (Invitrogen, Carlsbad, CA, USA) and 1.2 g/l sodium bicarbonate supplemented with 10 μg/ml penicillin-streptomycin (Invitrogen). The cells were incubated in a humidified incubator at 37°C with 5% CO2 and exposed to DHA or triacsin C when confluency reached 20%.
Arch Med Sci 2, 1st March / 2023 489
Induction of apoptosis in RL95-2 human endometrial cancer cells by combination treatment with docosahexaenoic acid and triacsin C
MTT cell viability assay
Cells were seeded in 12-well plates at a density of 5 × 105 cells per well. After an appropriate treatment time (24 or 48 h) with DHA and triacsin C, the culture medium was removed and replaced with a medium containing 0.5 mg 3-[4,5-dimethylthiazol-2-yl]-2.5-diphenyltetrazolium bromide; thiazolyl blue (MTT; Sigma) dissolved in phosphate-buffered saline (PBS, pH 7.2). After 4 h, the crystals were dissolved with 200 μl DMSO (Sigma). The intensity of the colour in each well was measured at a wavelength of 490 nm using a microplate reader (EL-312e; Biotek, Winooski, VT, USA).
Flowcytometric cell death assay
The cells were harvested, fixed in 95% ethanol for 24 h, incubated with 0.05 mg/ml propidium iodide (PI) and 1 μg/ml RNase A (Sigma) at 37°C for 30 min, and analysed by flow cytometry using Epics XL and analytic software (EXPO32 TM; Beckman Coulter, Brea, CA, USA). The cells belonging to the sub-G1 population were considered apoptotic cells; the percentage of each phase of the cell cycle was determined.
Hoechst 33258 staining
The cells were stained with Hoechst 33258 (4 μg/ml) for 30 min at 37°C, fixed for 10 min in 4% paraformaldehyde (PFA; Sigma), and observed under an Axiophot microscope (Carl Zeiss, Zena, Germany).
Annexin V cell death assay
The cells were stained using an Annexin V-FITC Apoptosis Detection kit (BD Biosciences, Parsippany, NJ, USA) according to the manufacturer’s instructions. The stained cells were analysed by flow cytometry.
Western blot analysis
Whole-cell lysates were prepared by incubating the cell pellets in lysis buffer (30 mM NaCl, 0.5% Triton X-100, 50 mM Tris-HCl (pH 7.4), 1 mM Na3VO4, 25 mM NaF, and 10 mM Na4P2O7) for 30 min on ice. After the insoluble fractions were removed by centrifugation at 14,000 rpm at 4°C for 30 min, the supernatants were collected, and protein concentration was determined with a BCA protein assay kit (Pierce Biotechnology, Woburn, MA, USA). The same amount of protein (~30 μg) was subjected to sodium dodecyl sulphate-polyacrylamide gel electrophoresis (SDS-PAGE) and transferred to a nitrocellulose membrane. The membranes were incubated for 1 h at room temperature (RT) with a primary antibody in Tris-buff-
ered saline containing 0.05% Tween-20 (TBS-T (pH 7.4)) in the presence of 5% nonfat dry milk. After the membranes were washed in TBS-T, secondary antibody reactions were performed with an appropriate antibody source conjugated with horseradish peroxidase. The signals were detected with an enhanced chemiluminescence detection kit (Amersham Pharmacia Biotech, Piscataway, NJ, USA) in an LAS-3000 detector (Fujifilm, Tokyo, Japan). Immunoblotting for b-actin was performed in every experiment as an internal control. All antibodies and reagents are summarised in Table I.
Immunocytochemistry
Harvested cells were attached on slide glasses by Cytospin centrifugation. The cells were fixed in 4% PFA, washed with PBS, and incubated with 0.2% Triton X-100. The cells were incubated with anti-cleaved caspase-3 and caspase-7 (Cell Signaling Technology, Beverly, MA, USA) primary antibodies in 1% bovine serum albumin at RT. The cells were incubated with FITC-conjugated anti-rabbit IgG and anti-mouse IgG, Texas Red-conjugated anti-rabbit IgG, and anti-mouse IgG (Vector Laboratories, Burlingame, CA, USA), and Alexa-conjugated anti-rabbit IgG (Invitrogen) secondary antibodies at RT. The cells were incubated with PI (50 μg/ml) at RT to counterstain the nucleus, if required. Finally, the cells were mounted and observed under a confocal microscope (LSM510; Carl Zeiss).
Statistical analysis
Data are expressed as the mean ± standard deviation of 3 or 4 separate experiments. Data were subjected to analysis of variance followed by Duncan’s post-hoc test. Means were considered significantly different at p < 0.05.
Results
DHA or triacsin C alone does not induce cell death in RL95-2 endometrial carcinoma cells
To evaluate the cytotoxic effects of DHA and triacsin C, RL95-2 cells were exposed to various concentrations of DHA (0–150 μM) or triacsin C (0–10 μM), respectively. Cell survival was estimated after 24 h of exposure to increasing drug concentrations using MTT and sub-G1 assays (PI staining). Cell viability was slightly reduced after increasing the concentrations of DHA or triacsin C (Figures 1 A, B). However, cell death as determined by sub-G1 analysis revealed that treatment with DHA or triacsin C alone did not induce significant cell death after 24 h at any of the concentrations tested (Figures 2 A, B).
490 Arch Med Sci 2, 1st March / 2023
Soo-Ho Chung, Hae-Hyeog Lee, Yeon-Suk Kim, Kisung Song, Tae-Hee Kim
Induction of apoptosis in RL95-2 human endometrial cancer cells by combination treatment with docosahexaenoic acid and triacsin C
Table I. Reagents and antibodies Variable Cooperation
Reagents:
Docosahexaenoic acid (DHA) Sigma (St. Louis, MO, USA)
Triacsin C (Tc) Sigma (St. Louis, MO, USA)
Hoechst 33258 Sigma (St. Louis, MO, USA)
Phenylmethyl-sulphonyl fluoride (PMSF) Sigma (St. Louis, MO, USA)
Antibodies:
Procaspase-8 Santa Cruz Biotech (Santa Cruz, CA, USA)
Procaspase-9 Santa Cruz Biotech (Santa Cruz, CA, USA)
ProBID Santa Cruz Biotech (Santa Cruz, CA, USA)
tBID Santa Cruz Biotech (Santa Cruz, CA, USA)
Cleaved caspase-8 Cell Signaling Tech (Beverly, MA, USA)
Cleaved caspase-9 Cell Signaling Tech (Beverly, MA, USA)
Cleaved caspase-3 Cell Signaling Tech (Beverly, MA, USA)
Cleaved d caspase-7 Cell Signaling Tech (Beverly, MA, USA)
Actin Sigma (St. Louis, MO, USA)
PARP Calbiochem (San Diego, CA, USA)
z-VAD Calbiochem (San Diego, CA, USA)
DEVD-CHO Calbiochem (San Diego, CA, USA)
IETD Calbiochem (San Diego, CA, USA)
LEHD Calbiochem (San Diego, CA, USA)
XIAP BD Pharmingen (San Diego, CA, USA)
Combination treatment with DHA and triacsin C significantly induces apoptosis in RL95-2 endometrial carcinoma cells
Figures 2 A, B shows that treatment with DHA or triacsin C alone was insufficient to induce cell death in RL95-2 cells. Based on these results, the
optimal concentrations to induce cytotoxicity with combined treatment were determined in a series of combination experiments (data not shown): DHA concentration of 125 μM and triacsin C at 5 μM. Figure 2 C shows that after RL95-2 cells were exposed to combined treatment with 5 μM triacsin C and 125 μM DHA for 24 h, cell death
Figure 1. Effect of docosahexaenoic acid (A) or triacsin c (B) on cell viability in RL95-2 endometrial cancer cells. Cell viability shown in cells treated with various concentrations of docosahexaenoic acid (0–150 μM) or triacsin c (0~10 μM) for 24 h and determined by 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide (MTT) assay.
DHA and Tc indicate docosahexaenoic acid and triacsin c, respectively
At least 3 independent experiments were performed, and data shown are the mean ± SD. *, p < 0.05 compared to 0 µM control.
Arch Med Sci 2, 1st March / 2023 491
120 100 80 60 40 20 0 120 100 80 60 40 20 0 0 50 100 125 150 DHA [µM] 0 0.5 1 5 10 Tc [µM] A B % Viability % Viability
increased significantly to 65.9 ±12.6% (p < 0.001). Hoechst staining of the cells exposed to combined treatment revealed nuclear fragmentation (Figures 3 A–D), while Annexin V staining revealed migration of the viable cell population (region i) toward late apoptosis (region iv) during treatment (Figures 3 B). These results suggest that the combined treatment of DHA and triacsin C synergised to induce cell death, which did not occur with treatment of DHA or triacsin C alone.
DHA and triacsin C-induced apoptosis initiates through caspase-8/tBID and subsequently activates caspase-9, -3, and -7
To clarify whether DHA and triacsin C-induced apoptosis involves caspase activity, activation of the initiator (-8 and -9) and effector (-3 and -7) caspases was analysed by western blot and immunocytochemistry. Anti-procaspase-8, procaspase-9, proBID, and tBID were obtained from Santa Cruz Biotechnology (Santa Cruz, CA, USA). Anti-cleaved caspase-8, -9, -3, and -7 were purchased from Cell Signaling Technology (Beverly, MA, USA). Anti-poly ADP ribose polymerase (PARP) was purchased
from Calbiochem (San Diego, CA, USA). Anti-XIAP was obtained from BD Pharmingen (San Diego, CA, USA). Anti-rabbit and mouse Ig-conjugated with horseradish peroxidase were purchased from Amersham Pharmacia Biotech. As shown in Figures 4 and 5, combined treatment with DHA and triacsin C invoked activation of caspases-3 and -7 as well as cleavage of PARP and XIAP (Figure 4). In addition, consistent with the western blot results, increased levels of caspase-3 and -7 were observed in DHA and triacsin C-treated RL95-2 cells (Figure 5).
Next, to explore the mechanisms by which DHA and triacsin C induce the extrinsic and intrinsic apoptosis pathways, activation of caspase-8 and -9 and BID was examined. Western blot analysis showed that the levels of cleaved caspase-8 (43/41 and 18 kDa) and -9 (37/35 kDa), and tBID (17 kDa), increased significantly with the combined treatment compared to DHA or triacsin C alone (Figure 6).
Activated caspase-8 directly activates caspase-3 or cleaves a BH3-only member of the Bcl-2 family of proteins, triggering its translocation to the mitochondria, where it causes release of cytochrome c To explore the contribution of caspase-8/tBID to mitochondrial function, the subcellular localisa-
Figure 2. Effect of DHA or triacsin C on cell death in RL95-2 endometrial cancer cells. A – Cell death of cells treated with various concentrations of DHA (0–150 μM) for 24 h and assessed by flow cytometry is shown. Effect of triacsin C on cell death in RL95-2 endometrial cancer cells. B – Cell death of cells treated with various concentrations of triacsin C (0–10 μM) for 24 h and assessed by flow cytometry is shown. C – Effect of combination treatment with DHA and triacsin C on cell death in RL95-2 endometrial cancer cells. Cells were treated with 125 μM DHA, 5 μM triacsin C, or a combination of 125 μM DHA and 5 μM triacsin C for 24 h. DHA and Tc indicate docosahexaenoic acid and triacsin C, respectively. The percentage of cells with a sub-G1 DNA content was taken as a measure of cell death
At least 3 independent experiments were performed, and data shown are the mean ± standard deviation. *p < 0.05 compared to 0 µM control. #p < 0.001 compared with control, DHA-treated, or triacsin C-treated group.
492 Arch Med Sci 2, 1st March / 2023
Soo-Ho Chung, Hae-Hyeog Lee, Yeon-Suk Kim, Kisung Song, Tae-Hee Kim
100 80 60 40 20 0 100 80 60 40 20 0 100 80 60 40 20 0 0 50 100 125 150 DHA [µM] 0 0.5 1 5 10 Tc [µM] DHA – + – + Tc – – + + A
C % Cell death % Cell death % Cell death
B
to fragmented nuclei. Original magnification: ×800. The proportion or type of cell death was identified by the Annexin V cell death assay. i, ii, iii, and iv denote viable (live), necrotic, early apoptotic, and late apoptotic regions, respectively (B)
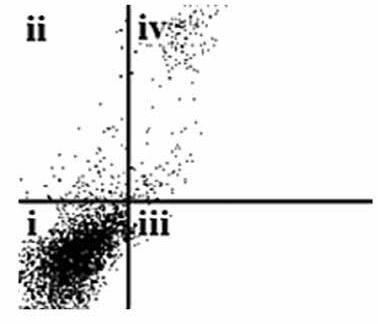
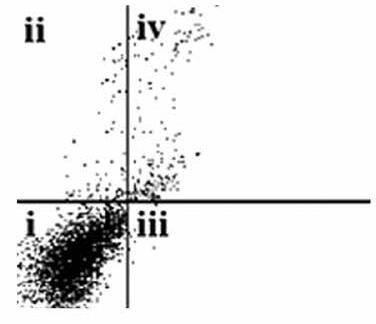
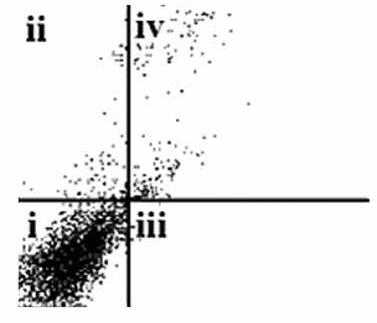

tion of active caspase-8 and tBID was confirmed by double immunostaining with active caspase-8 and tBID using mt-hsp60 as a mitochondrial marker protein. As shown in Figures 7 A and B, immunoreactivity of active caspase-8 and tBID can be mostly seen at the mitochondria following exposure to DHA and triacsin C. To examine whether caspase-8 co-localises with tBID at the mitochondria, double immunostaining was conducted
with confocal analysis. The fluorescence signal of the active portion of caspase-8 and tBID produced a yellow image when superimposed (Figure 7 C), suggesting that the 2 molecules were co-localised in the mitochondria. Our results suggest that combined treatment with DHA and triacsin C induces caspase-8 translocation to the mitochondria, where it binds BID, leading to activation of tBID in the mitochondria.
Arch Med Sci 2, 1st March / 2023 493 A a a c b d b c d
Induction of apoptosis in RL95-2 human endometrial cancer cells by combination treatment with docosahexaenoic acid and triacsin C
CON CON Tc DHA DHA + Tc DHA Tc DHA + Tc 103 102 101 100 103 102 101 100 103 102 101 100 103 102 101 100 100 101 102 103 Annexin-V 100 101 102 103 Annexin-V 100 101 102 103 Annexin-V 100 101 102 103 Annexin-V PI PI PI PI B
Figure 3. Nuclear fragmentation in RL95-2 endometrial cancer cells following exposure to combined treatment with DHA and triacsin C (A). Cells were treated with 125 μM DHA, 5 μM triacsin C, or a combined treatment of 125 μM DHA and 5 μM triacsin C for 24 h. Nuclear morphology was detected by Hoechst 33258 staining. Arrows point
treatment
DHA and
C. Cells were treated with 125 μM DHA, 5 μM triacsin C, or a combination of 125 μM DHA and 5 μM triacsin C for 24 h. A – Activation of caspase-3 and -7 following exposure to DHA and triacsin C, as shown by western blot analyses for caspase-3 and -7, and PARP cleavage. Equal amounts of protein (30 μg) were separated by sodium dodecyl sulphate-polyacrylamide gel electrophoresis and immunoblotted using cleaved caspase-3, cleaved caspase-7, PARP, and XIAP antibodies, respectively. Actin was used as an internal (loading) control

The requirement of caspase activation for DHA and triacsin C-induced apoptosis was examined using the following caspase-specific inhibitors: zVAD-FMK (pan-caspase inhibitor), DEVE-CHO (caspase-3/-7 inhibitor), IETD-CHO (caspase-8
inhibitor), and LEHD-CHO (caspase-9 inhibitor). RL95-2 cells were pretreated for 2 h with the inhibitors prior to treatment for 14 h with DHA and triacsin C. As shown in Figure 8, the pancaspase inhibitor (zVAD-FMK), caspase-8 inhibitor (IETD-CHO), and a combination of caspase-8/-9 inhibitors (IETD-CHO/LEHD-CHO) completely attenuated DHA and triacsin C-induced cleavage of caspase-8, -9, and -7, and PARP. However, the caspase-3/7 (DEVD-CHO) and caspase-9 inhibitor (LEHD-CHO) partially blocked cleavage of caspase-3, -9, and -7, and PARP, but not caspase-8. The p17 fragment of caspase-3 was only weakly detected following pre-incubation with the pancaspase inhibitor and caspase-8 and -8/9 inhibitors during combined treatment. Sub-G1 analysis showed that DHA and triacsin C-induced apoptosis was partially suppressed by the caspase-9 and -3/7 inhibitors, whereas it was completely blocked by the pan-caspase, caspase-8, and caspase-8/9 inhibitors (Figure 9). These results indicate that DHA and triacsin C-induced apoptosis is triggered through activation of caspase-8 and subsequent activation of caspases-9, -3, and -7.
Discussion
In recent decades, DHA has emerged as a promising anticancer agent. Although it exerts a selective cytotoxic effect on malignant tumour cells at physiological concentrations [9, 10], DHA alone was insufficient in the present study to induce apoptosis in the RL95-2 endometrial carcinoma line. ACS family enzymes, which activate and convert long-chain fatty acids, play a dominant role in
bined treatment with DHA and triacsin C. Cells were treated with 125 μM DHA, 5 μM triacsin C, or combined treatment with 125 μM DHA and 5 μM triacsin C for 24 h, cytospun, fixed, and immunostained with a cleaved caspase-3 or -7 antibody, respectively. Propidium iodide (PI, red) was employed for differential nuclear staining Microphotographs were taken using confocal microscopy. Original magnification: 800×.
494 Arch Med Sci 2, 1st March / 2023 DHA – + – + Tc – – + + Cleaved caspase-3 Cleaved caspase-7 PARP XIAP Actin ← 19 kDa ← 17 kDa ← 20 kDa ← 116 kDa ← 85 kDa ← 55 kDa ← 35 kDa ← 42 kDa
Soo-Ho Chung, Hae-Hyeog Lee, Yeon-Suk Kim, Kisung Song, Tae-Hee Kim
CON DHA Tc D + Tc
Figure 4. Activation of caspase-3 and -7, PARP cleavage, and XIAP in RL95-2 endometrial cancer cells by combined
with
triacsin
Figure 5. Immunocytochemical localisation of active caspase-3 and -7 in RL95-2 cells following exposure to com-
Active caspase-7
Active caspase-3
Induction of apoptosis in RL95-2 human endometrial cancer cells by combination treatment with docosahexaenoic acid and triacsin C
phospholipid biosynthesis, b-oxidation, and lipid metabolism [24, 25]. Therefore, we hypothesised that inhibiting ACS function would disrupt DHA metabolism, leading to the accumulation of exogenous DHA in the mitochondria and contributing to the induction of apoptosis in RL95-2 endometrial cancer cells. This study showed that 125 μM DHA or 5 μM triacsin C alone did not induce apparent cytotoxic effects. However, combined treatment with 125 μM DHA and 5 μM triacsin C increased the sub-G1 population and apoptotic fragments. Western blotting also demonstrated that DHA and triacsin C induced apoptosis through the mitochondrial pathways via caspase-9, -3, and -7, as well as through the extrinsic pathway by activating caspase-8/BID.
Mitochondria are particularly susceptible to oxidative stress; several studies have demonstrated that the accumulation and association of DHA with cardiolipin may lead to the generation of ROS and changes in cardiolipin and apoptosis signalling [31–33]. In addition, inhibiting ACS with triacsin C leads to the accumulation of exogenous free fatty acids [34, 35], which might affect mitochondrial status in cells undergoing apoptosis. Cardiolipin is generally believed to be localised at the inner membranes of mitochondria, but is also present at the contact sites formed between mitochondrial inner and outer membranes [36, 37]. Cardiolipin has also been shown to act as an activation platform for bringing together both caspase-8 and tBID. During apoptosis, the translocation of caspase-8/tBID at contact sites between the inner and outer mitochondrial membranes leads to a loss of cardiolipin content and dissociation of cytochrome c from the mitochondrial inner membrane [36, 38–40].
Therefore, it has been postulated that inhibition of ACSs by triacsin C would induce activation of caspase-8/tBID in RL95-2 cells by dissociating cytochrome c at the mitochondria membrane. The activation of caspase-8/tBID and subsequent translocation to the mitochondrial membrane (dependent on cardiolipin) is critical for inducing apoptosis and may affect mitochondrial membrane function and integrity, sequentially leading to ROS production in the electron transport chain [41]. In addition, inhibiting ACSs with triacsin C modifies the structure and content of cardiolipin [42], suggesting that ACSs are essential for the maintenance of cardiolipin content as well as cell survival.
Some limitations in our study should be mentioned. We did not observe the effect of apoptosis in heterogeneous endometrial cells treated with triacsin C and DHA. Therefore, it will be necessary to evaluate the combined effect on endometrial
exposure to combined treatment with DHA and triacsin C, as shown by western blotting analyses for procaspase-8, cleaved caspase-8, proBID, truncated BID (tBID), procaspase-9, and cleaved caspase-9. Cells were treated with 125 μM DHA, 5 μM triacsin C, or combined treatment with 125 μM DHA and 5 μM triacsin C for 24 h. Equal amounts of protein (30 μg) were separated by sodium dodecyl sulphate-polyacrylamide gel electrophoresis and immunoblotted using procaspase-8, cleaved caspase-8, proBID, tBID, procaspase-9, and cleaved caspase-9 antibodies, respectively. Actin was used as an internal (loading) control

cancer samples, such as heterogeneous tissue, in a further study. However, this is the first study to verify the apoptotic effect of the combination on endometrial cancer cells. The mechanisms of DHA and triacsin C-induced apoptosis may provide the basis for developing therapeutic strategies for endometrial cancer.
In conclusion, the synergistic effect between DHA and triacsin C has not been investigated in most clinical and preclinical studies. Nevertheless, further elucidation of the apoptotic mechanisms involving DHA and ACS inhibition could shed light on possible new treatment strategies for endometrial cancer.
Acknowledgments
This study was supported by the Soonchunhyang University Research Fund.
Conflict of interest
The authors declare no conflict of interest.
Arch Med Sci 2, 1st March / 2023 495 DHA – + – + Tc – – + + Pro caspase-8 Cleaved caspase-8 Pro BID tBID Pro caspase-9 Cleaved caspase-9 Actin ← 55 kDa ← 43 kDa ← 41 kDa ← 22 kDa ← 17 kDa ← 47 kDa ← 37 kDa ← 35 kDa ← 42 kDa
Figure 6. Activation of caspase-8, BID, and caspase-9 in RL95-2 endometrial cancer cells following
following exposure to combined treatment with DHA and triacsin C.
were treated with 125 μM DHA, 5 μM triacsin C, or combined treatment with 125 μM DHA and 5 μM triacsin C for 24 h, cytospun, fixed, and immunostained with cleaved caspase-8 (A), tBID (B), cleaved caspase-8, tBID (C), and Hsp60 (as a specific mitochondrial protein marker) antibodies, respectively. Hoechst 33258 (blue) dye was employed for differential nuclear staining. Co-localisation of active caspase-8 (green) and Hsp60 (red) on mitochondria following exposure to combined treatment with 125 μM DHA and 5 μM triacsin C for 24 h
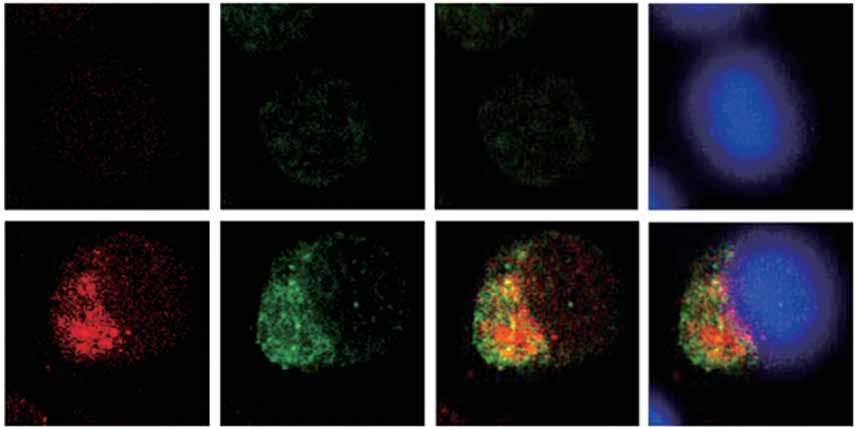
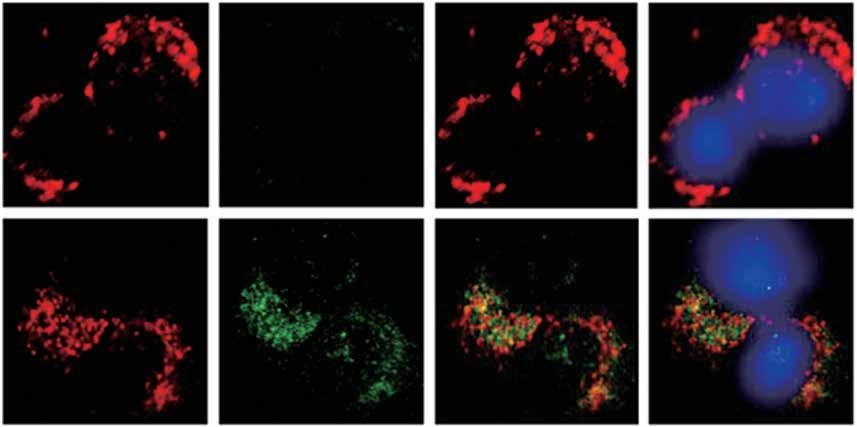
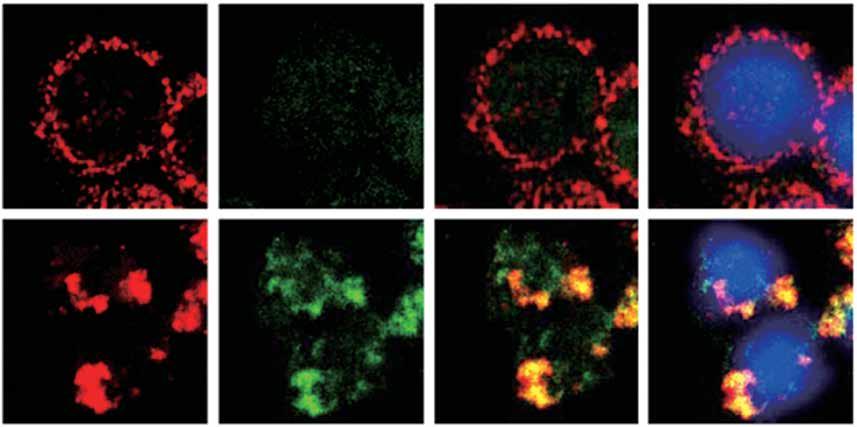
496 Arch Med Sci 2, 1st March / 2023 Hsp60
Hsp60
A B
Cas-8
C
Cas-8
tBID
tBID
Hsp60/Cas-8
Hsp60/tBID
Cas-8/tBID
Hsp60/Cas-8/Hoechst
Hsp60/tBID/Hoechst
DHA + Tc CON DHA + Tc CON DHA + Tc CON
Cas-8/tBID/Hoechst
Figure 7. Immunocytochemical localisation of active caspase-8 in RL95-2 cells
Cells
Induction of apoptosis in RL95-2 human endometrial cancer cells by combination treatment with docosahexaenoic acid and triacsin C
CON z-VAD DEVD-CHOIETD LEHD IETD/LEHD
Figure 8. Suppressed activation of caspase-8, -9, -3, and -7 by caspase inhibitors in RL95-2 endometrial cancer cells following combined treatment with DHA and triacsin C. Cells were exposed to 125 μM DHA and 5 μM triacsin C for 14 h in the absence or presence of zVAD-FMK (pan caspase inhibitor), DEVE-CHO (caspase-3/-7 inhibitor), IETD-CHO (caspase-8 inhibitor), LEHD-CHO (caspase-9 inhibitor), or IETD plus LEHD, respectively. Changes in caspases by caspase inhibitors in RL95-2 cells following exposure to DHA and triacsin C are shown by western blot analyses for caspase-8, -9, -3, and -7, and PARP cleavage. Equal amounts of protein (30 μg) were separated by sodium dodecyl sulphate-polyacrylamide gel electrophoresis and immunoblotted using a cleaved form-specific antibody for caspase-8, -9 -3, and -7, and PARP antibody. Actin expression was examined as a loading control
“-” – DHA and triacsin C without treatment, “+” – 125 µM DHA and 5 µM triacsin C treatment for 14 h.
References
1. Moxley KM, McMeekin DS. Endometrial carcinoma: a review of chemotherapy, drug resistance, and the search for new agents. Oncologist 2010; 15: 1026-33.
2. Moore SC, Gierach GL, Schatzkin A, Matthews CE. Physical activity, sedentary behaviours, and the prevention of endometrial cancer. Br J Cancer 2010; 103: 933-8.
3. Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin 2010; 60: 277-300.
4. Kim HJ, Vosseler CA, Weber PC, Erl W. Docosahexaenoic acid induces apoptosis in proliferating human endothelial cells. J Cell Physiol 2005; 204: 881-8.
5. Pandurangaan AK, Ismail S, Esa NM, Munusamy MA. Inositol-6 phosphate inhibits the mTOR pathway and induces autophagy-mediated death in HT-29 colon cancer cells. Arch Med Sci 2018; 14: 1281-8.
6. Bandera EV, Kushi LH, Moore DF, Gifkins DM, McCullough ML. Dietary lipids and endometrial cancer: the current epidemiologic evidence. Cancer Causes Control 2007; 18: 687-703.
7. Terry P, Wolk A, Vainio H, Weiderpass E. Fatty fish consumption lowers the risk of endometrial cancer: a na-
z-VADDEVD-CHO IETD LEHDIETD/LEHD
Figure 9. Suppression of apoptosis induced by combined treatment with DHA and triacsin C in the presence of caspase inhibitors in RL95-2 endometrial cancer cells. Cells were exposed to 125 μM DHA and 5 μM triacsin C for 14 h in the absence or presence of zVAD-FMK (pan caspase inhibitor), DEVE-CHO (caspase-3/-7 inhibitor), IETD-CHO (caspase-8 inhibitor), LEHD-CHO (caspase-9 inhibitor), or IETD plus LEHD, respectively. Cell death was assessed by flow cytometry. The percentage of cells with a sub-G1 DNA content was taken as a measure of cell death
At least 3 independent experiments were performed, and data shown are mean ± standard deviation.
*,#p < 0.05 and p < 0.001 compared with the DHA and triacsin C-treated group, respectively. “-” – DHA and triacsin C without treatment, “+” – 125 µM DHA and 5 µM triacsin C treatment for 14 h.
tionwide case-control study in Sweden. Cancer Epidemiol Biomarkers Prev 2002; 11: 143-5.
8. Zhang G Zha J, Liu J, Di J. Minocycline impedes mitochondrial-dependent cell death and stabilizes expression of hypoxia inducible factor-1a in spinal cord injury. Arch Med Sci 2018; 15: 475-83.
9. Begin ME, Ells G, Das UN, Horrobin DF. Differential killing of human carcinoma cells supplemented with n-3 and n-6 polyunsaturated fatty acids. J Natl Cancer Inst 1986; 77: 1053-62.
10. Begin ME, Das UN, Ells G, Horrobin DF. Selective killing of human cancer cells by polyunsaturated fatty acids. Prostaglandins Leukot Med 1985; 19: 177-86.
11. Serini S, Piccioni E, Merendino N, Calviello G. Dietary polyunsaturated fatty acids as inducers of apoptosis: implications for cancer. Apoptosis 2009; 14: 135-52.
12. Chapkin RS, Hong MY, Fan YY, et al. Dietary n-3 PUFA alter colonocyte mitochondrial membrane composition and function. Lipids 2002; 37: 193-9.
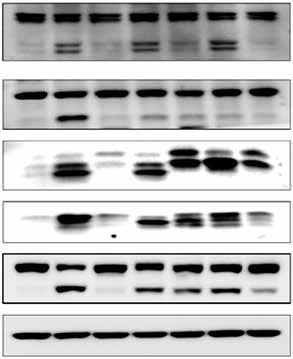
13. Watkins SM, Carter LC, German JB. Docosahexaenoic acid accumulates in cardiolipin and enhances HT-29 cell oxidant production. J Lipid Res 1998; 39: 1583-8.
14. Kolar SS, Barhoumi R, Callaway ES, et al. Synergy between docosahexaenoic acid and butyrate elicits p53-independent apoptosis via mitochondrial Ca(2+) accumulation in colonocytes. Am J Physiol Gastrointest Liver Physiol 2007; 293: G935-43.
15. Yang M, Zhang L, Wang X, Zhou Y, Wu S. Down-regulation of miR-203a by lncRNA PVT1 in multiple myeloma promotes cell proliferation. Arch Med Sci 2018; 14: 1333-9.
Arch Med Sci 2, 1st March / 2023 497 DHA + Tc – + + + + + + Cleaved caspase-8 Cleaved caspase-9 Cleaved caspase-3 Cleaved caspase-7 PARP Actin ← 55 kDa ← 43 kDa ← 41 kDa ← 47 kDa ← 35/37 kDa ← 21 kDa ← 19 kDa ← 17 kDa ← 20 kDa ← 116 kDa ← 86 kDa ← 42 kDa
CON
DHA + Tc – + + + + + + % Cell death 25 20 15 10 5 0
16. Mohamed EA, Kassem HH. Protective effect of nebivolol on doxorubicin-induced cardiotoxicity in rats. Arch Med Sci 2018; 14: 1450-8.
17. Hengartner MO. The biochemistry of apoptosis. Nature 2000; 407: 770-6.
18. Green DR, Reed JC. Mitochondria and apoptosis. Science 1998; 281: 1309-12.
19. Korsmeyer SJ, Wei MC, Saito M, Weiler S, Oh KJ, Schlesinger PH. Pro-apoptotic cascade activates BID, which oligomerizes BAK or BAX into pores that result in the release of cytochrome c. Cell Death Differ 2000; 7: 1166-73.
20. Li H, Zhu H, Xu CJ, Yuan J. Cleavage of BID by caspase 8 mediates the mitochondrial damage in the Fas pathway of apoptosis. Cell 1998; 94: 491-501.
21. Gonzalvez F, Schug ZT, Houtkooper RH, et al. Cardiolipin provides an essential activating platform for caspase-8 on mitochondria. J Cell Biol 2008; 183: 681-96.
22. Sun H, Berquin IM, Owens RT, O’Flaherty JT, Edwards IJ. Peroxisome proliferator-activated receptor γ–mediated up-regulation of syndecan-1 by n-3 fatty acids promotes apoptosis of human breast cancer cells. Cancer research 2008; 68: 2912-9.
23. Engelbrecht AM, du Toit-Kohn J-L, Ellis B, Thomas M, Nell T, Smith R. Differential induction of apoptosis and inhibition of the PI3-kinase pathway by saturated, monounsaturated and polyunsaturated fatty acids in a colon cancer cell model. Apoptosis 2008; 13: 1368-77.
24. Ellis JM, Frahm JL, Li LO, Coleman RA. Acyl-coenzyme A synthetases in metabolic control. Curr Opin Lipidol 2010; 21: 212-7.
25. Watkins PA. Very-long-chain acyl-CoA synthetases. J Biol Chem 2008; 283: 1773-7.
26. Iorio E, di Vito M, Spadaro F, et al. Triacsin C inhibits the formation of 1H NMR-visible mobile lipids and lipid bodies in HuT 78 apoptotic cells. Biochim Biophys Acta 2003; 1634: 1-14.
27. Mashima, T, Sato S, Okabe S, et al. Acyl-CoA synthetase as a cancer survival factor: its inhibition enhances the efficacy of etoposide. Cancer Sci 2009; 100: 1556-62.
28. Luo Z, Pan J, Ding Y, Zhang YS, Zeng Y. The function and clinical relevance of lncRNA UBE2CP3-001 in human gliomas. Arch Med Sci 2018; 14: 1308-20.
29. Sung YK, Park MK, Hong SH, et al. Regulation of cell growth by fatty acid-CoA ligase 4 in human hepatocellular carcinoma cells. Exp Mol Med 2007; 39: 477-82.
30. Çoban N, Güleç Ç, Selçuk BÖ, Erginel-Ünaltuna N. Role of simvastatin and RORa activity in the macrophage apoptotic pathway. Anatol J Cardiol 2017; 17: 362-6.
31. Ng Y, Barhoumi R, Tjalkens RB, et al. The role of docosahexaenoic acid in mediating mitochondrial membrane lipid oxidation and apoptosis in colonocytes. Carcinogenesis 2005; 26: 1914-21.
32. Hong MY, Chapkin RS, Barhoumi R, et al. Fish oil increases mitochondrial phospholipid unsaturation, upregulating reactive oxygen species and apoptosis in rat colonocytes. Carcinogenesis 2002; 23: 1919-25.
33. Shi X, Guan Y, Jiang S, Li T, Sun B, Cheng H. Renin-angiotensin system inhibitor attenuates oxidative stress induced human coronary artery endothelial cell dysfunction via the PI3K/AKT/mTOR pathway. Arch Med Sci 2019; 15: 152-64.
34. Perez R, Matabosch X, Llebaria A, Balboa MA, Balsinde J. Blockade of arachidonic acid incorporation into phospholipids induces apoptosis in U937 promonocytic cells. J Lipid Res 2006; 47: 484-91.
35. Arai T, Kawakami Y, Matsushima T, Okuda Y, Yamashita K. Intracellular fatty acid downregulates ob gene expres-
sion in 3T3-L1 adipocytes. Biochem Biophys Res Commun 2002; 297: 1291-6.
36. Kim TH, Zhao Y, Ding WX, et al. Bid-cardiolipin interaction at mitochondrial contact site contributes to mitochondrial cristae reorganization and cytochrome c release. Mol Biol Cell 2004; 15: 3061-72.
37. Stankova B, Tvrzicka E, Bayerova H, Bryhn AC, Bryhn M. Herring oil intake results in increased levels of omega-3 fatty acids in erythrocytes in an urban population in the Czech Republic. Arch Med Sci Civil Dis 2018; 3: 3-9.
38. Sorice M, Manganelli V, Matarrese P, et al. Cardiolipin-enriched raft-like microdomains are essential activating platforms for apoptotic signals on mitochondria. FEBS Lett 2009; 583: 2447-50.
39. Schug ZT, Gottlieb E. Cardiolipin acts as a mitochondrial signalling platform to launch apoptosis. Biochim Biophys Acta 2009; 1788: 2022-31.
40. Scorrano L. Caspase-8 goes cardiolipin: a new platform to provide mitochondria with microdomains of apoptotic signals? J Cell Biol 2008; 183: 579-81.
41. Ott M, Zhivotovsky B, Orrenius S. Role of cardiolipin in cytochrome c release from mitochondria. Cell Death Differ 2007; 14: 1243-7.
42. Mashima T, Oh-hara T, Sato S, et al. p53-defective tumors with a functional apoptosome-mediated pathway: a new therapeutic target. J Natl Cancer Inst 2005; 97: 765-77.
498 Arch Med Sci 2, 1st March / 2023
Soo-Ho Chung, Hae-Hyeog Lee, Yeon-Suk Kim, Kisung Song, Tae-Hee Kim
Damian
1Department of Clinical Pathomorphology, Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University in Torun, Poland
2Department of Pathomorphology, Military Clinical Hospital, Bydgoszcz, Poland
Submitted: 12 March 2019; Accepted: 4 August 2019
Online publication: 18 November 2019
Arch Med Sci 2023; 19 (2): 499–506
DOI: https://doi.org/10.5114/aoms.2019.89773
Copyright © 2019 Termedia & Banach
Abstract
Introduction: The purpose of this research was to explore the correlation between Gleason score and pattern and the expression of the MLH1, MSH2, MDC1, TP53BP1 proteins in prostate cancer (PC). Prostate cancer development is related to errors in DNA, among others double-strand breaks (DSB) and changes in the base sequence of the DNA. These errors should be repaired through mismatch (MMR) or DSB repair proteins such as MSH2, MLH1, MDC1 and TP53BP1.
Material and methods: A total of 500 prostate cancer specimens were recruited in this study. From among all gathered specimens the 52 most suitable cases were selected. The expression of examined proteins was detected by immunohistochemistry, and its correlation with the Gleason score and pattern were further analyzed through standard statistical algorithms.
Results: The results show a significant correlation between Gleason pattern and the nuclear expression of the MSH2 protein and the cytoplasmic expression of the MLH1 protein. Gleason score significantly correlates with the nuclear and the cytoplasmic expression of the MSH2 protein and the cytoplasmic expression of the MDC1 protein. There is no correlation between the nuclear or cytoplasmic expression of the TP53BP1 protein and Gleason pattern or score.
Conclusions: Our study suggests that the aberration in the MMR repair mechanism may be significantly more important regarding the grading among PC cells in comparison to the impact of alterations in the DSB repair mechanism. The lack of correlation between expression of the TP53BP1 protein and Gleason pattern and Gleason score suggests that the radiation resistance of PC is independent of alterations connected with TP53BP1.
Key words: radiotherapy, mismatch repair genes, double-strand breaks.
Introduction
Prostate adenocarcinoma (PC) is the most common cancer among men, with the cancer mortality approximately 16% per year [1]. The mortality risk after radical prostatectomy could be predicted using a grading system based on histopathological examination of postoperative material [2]. The histologic grading of PC is still based on the standard Gleason score (GS) [3] and the prognosis is closely negatively correlated
Corresponding author: Damian Jaworski
Department of Clinical Pathomorphology
Collegium Medicum
Nicolaus Copernicus University
9 Sklodowskiej-Curie St
85-094 Bydgoszcz, Poland
Phone: +48 52 585 42 00
Fax: +48 52 585 40 49
E-mail: jaworskiresearch@gmail.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Expression differences between proteins responsible for DNA damage repair according to the Gleason grade as a new heterogeneity marker in prostate cancer
Jaworski1, Arkadiusz Gzil1, Paulina Antosik1, Izabela Zarębska1, Joanna Dominiak1, Izabela Neska-Długosz1, Anna Kasperska1, Dariusz Grzanka1, Łukasz Szylberg1,2
Basic research Urology
with this grading. In the 2014 International Society of Urological Pathology proposed a modification of the aforementioned scale, reorganizing the previous GS into a 5-grade system [4]. However, the proper grading may be difficult, because of the multifocal growth of PC.
Prostate adenocarcinoma development is related to various errors in DNA. One of the major DNA error types arises because of single or double-strand breaks (DSBs). These errors are repaired by specific molecular pathways in which DSB repair proteins such as MDC1 and TP53 are involved. In this process, the TP53BP1 is involved by the MDC1 protein, which causes activation of downstream effector molecules and the initiation of repair [5].
BRCA1 and BRCA2 proteins are also involved in DSB repair. Studies show that loss of their specific functions in this pathway causes genomic instability and is connected with higher risk of breast, ovarian and pancreas cancers and PCs [6–9].
Another type of DNA errors stems from changes in the base sequence of the DNA and is recognized by the DNA mismatch repair (MMR) pathway. It results from the incorrect DNA replication made by DNA polymerase, wrong linked bases or the impact of drugs [10, 11]. Mistakes in DNA are detected by the MutSa complex. This complex is a homodimer and consists of MSH2 and MSH6 proteins [10].
The assembly of the MutSa complex with the hMutLa complex, which consists of MLH1 and PMS2 proteins, creates the hMutLa-hMutSa-heteroduplex complex. A formed complex initiates repair of the mismatch defects [11].
Conventionally, the loss of MMR proteins is associated with the development of adenocarcinomas, mostly colorectal cancers and also squamous cell carcinomas [11, 12]. The germline mutation in one of the MMR genes, such as MLH1, MSH2, MSH6 or PMS2, leads to hereditary nonpolyposis colon carcinoma (Lynch syndrome) [13–15].
The accumulation of DNA mutations could be caused by dysfunction of DNA repair pathways. An interesting question is whether there is a correlation between MMR protein alterations and histological grade of cancer. The grading of PC is specific and well defined, due to the fact that the authors of the current study wanted to investigate the association between MLH1, MSH2, MDC1 and TP53BP1 and Gleason pattern (GP) and GS.
Moreover, the results of this study could indicate the relevance of this protein expression assessment as valuable information in deciding on follow-up or adjuvant treatment, e.g. adjuvant radiotherapy. On the basis of this study we supposed that alterations in TP53BP1 might have significant value for selection of the treatment after prostatectomy, e.g. between immediate adjuvant radiotherapy and hormone therapy.
Material and methods
Patients and tissue samples
The study included 500 prostates with lymph nodes from patients who underwent radical prostatectomy for prostate carcinoma. The patients were aged between 52 and 78. All the material was fixed in 10% buffered formalin and processed according to the standard protocol. Finally, paraffin blocks were prepared. The inclusion criteria for material used in this study were the clear-cut diagnosis of PC that fits the Gleason classification criteria, and the presence of sufficient material for further work. Moreover, we specified the group and selected 26 patients in whom lymphadenectomy was performed during prostatectomy, N status was available and there were metastases to lymph nodes. Afterwards we selected a group of 26 patients with N status described as N0. Finally we created a group of the 52 most suitable cases. Subsequently, two independent pathologists verified specimens of those cases. We divided chosen specimens into 3 groups. The current study was focused on alterations of protein expression between different GS and GP, whereas for the further part of this study we needed a group with metastases to lymph nodes.
The first group included 29 specimens of GS 7, the second group 29 specimens of GS 8, and the third group 18 specimens of GS 9. Furthermore, we evaluated separately areas with the highest protein expression (hot spots) for GP 3, 4 and 5. For expression of the MDC1 protein, we evaluated 72 hot spots for GP3, 149 hot spots for GP4, and 13 hot spots for GP5. For expression of the TP53BP1 protein, we evaluated 62 hot spots for GP3, 116 hot spots for GP4, and 14 hot spots for GP5. For expression of the MLH1 protein, we evaluated 69 hot spots for GP3, 155 hot spots for GP4, and 10 hot spots for GP5. For expression of the MSH2 protein, we evaluated 77 hot spots for GP3, 133 hot spots for GP4, and 18 hot spots for GP5.
Selected places of specimens were evaluated by Remmele-Stegner immunoreactive score [16]. The expression of each examined protein among specimens was evaluated in reference to GS and GP.
Methods
The formalin-fixed, paraffin-embedded (FFPE) tissue specimens were cut into 3 μm paraffin sections, using a rotary microtome (Accu-Cut SRM 200; Sakura, Torrance, CA, USA). The sections were mounted on microscopic slides providing superior adhesion (SuperFrost Plus; Menzel-Glaser, Braunschweig, Germany). For deparaffinization, rehydration, and antigen retrieval, paraffin sec-
500 Arch Med Sci 2, 1st March / 2023
D. Jaworski, A. Gzil, P. Antosik, I. Zarębska, J. Dominiak, I. Neska-Długosz, A. Kasperska, D. Grzanka, Ł. Szylberg
Expression differences between proteins responsible for DNA damage repair according to the Gleason grade as a new heterogeneity marker in prostate cancer
tions were pre-treated with a high-pH buffer (Epitope Retrieval Solution) in an automated PT-link system (Dako; Agilent Technologies, Inc., Santa Clara, CA, USA). Thereafter, immunohistochemical staining was performed using rabbit polyclonal anti-MDC1 (1 : 200, Sigma-Aldrich; HPA006915), rabbit polyclonal anti-53BP1 (1 : 300, Novus Biologicals; NB100-304), rabbit monoclonal anti-MLH1 (1 : 100, Abcam; ab92312), mouse monoclonal anti-MSH2 (1 : 200, BD Pharmingen; G219-1129) and using the visualization system EnVision FLEX + HRP (Dako; Agilent Technologies, Inc. Inc., Santa Clara, CA, USA) on an Autostainer Link 48 platform according to well-known protocols [17, 18]. Finally, the slides were counterstained with hematoxylin, dehydrated in an alcohol gradient, cleared in xylene, and mounted (Dako; Agilent Technologies, Inc.).
Antigen expression for each studied antibody was evaluated by the Remmele-Stegner immunoreactive score [16].
The expression of each examined protein among specimens was evaluated in reference to the GS and GP. Three sections for every case were chosen, after which 3 different fields of view were evaluated and the average of those results was calculated. Positive controls were performed by immunohistochemical staining on every specimen on its own tissue without cancer involvement. The power of magnification was ×20.
Statistical analysis
All statistical analyses were performed using Statistica version 13 (StatSoft) and Microsoft Ex-
cel 2007. The comparative studies were analyzed statistically using the nonparametric KruskalWallis test. The p-value < 0.05 was considered statistically significant. The expression values of analyzed proteins were presented as the median and 25th and 75th percentiles.
Results
Association of MSH2 expression with Gleason score and Gleason pattern
In 97% of cases nuclear expression and in 68% of cases cytoplasmic expression of the MSH2 was revealed. Statistical analysis demonstrated a significant correlation between GP and nuclear expression of MSH2 (p = 0.004) (Figure 1 A).
Statistical analysis did not show any significant correlation between cytoplasmic MSH2 level and GP (Table I).
Statistical analysis showed a significant correlation between nuclear and cytoplasmic expression of MSH2 and GS (p = 0.044, p = 0.045 respectively) (Figures 2 A and 2 B respectively).
Association of MLH1 expression with Gleason score and Gleason pattern
In 93% of cases nuclear expression and in 74% of cases cytoplasmic expression of MLH1 was revealed. Statistical analysis demonstrated no significant correlation between the level of MLH1 in nuclei with reference to GP.
Statistical analysis demonstrated a significant correlation between cytoplasmic expression of MLH1 and GP (p = 0.0255) (Figure 1 B).
Arch Med Sci 2, 1st March / 2023 501
A B 14 12 10 8 6 4 2 0 –2 14 12 10 8 6 4 2 0 –2 p = 0.004 p = 0.0255 3 4 5 3 4 5 MSH – Gleason pattern MSH2 –nucleus MLH1 –cytoplasm Median 25–75% Min.-max. MLH1
Figure 1. Box plot of data with correlation between Gleason pattern and protein expression. A – Correlation between Gleason pattern and nuclear expression of MSH2 protein. B – Correlation between Gleason pattern and cytoplasmic expression of MLH1 protein
– Gleason pattern
Statistical analysis demonstrated no significant correlation between the level of MLH1 in nuclei and cytoplasm with reference to GS (Table II).
Association of TP53BP1 expression with Gleason score and Gleason pattern
In 95% of cases nuclear expression and in 96% of cases cytoplasmic expression of TP53BP1 was revealed. Statistical analysis demonstrated no correlation between cytoplasmic or nuclear expression of the TP53BP1 and GS and GP (Tables II and I respectively).
Association of MDC1 expression with Gleason score and Gleason pattern
In 71% of cases nuclear expression and in 69% of cases cytoplasmic expression of MDC1 was re-
vealed. Statistical analysis demonstrated no significant correlation between the level of MDC1 in nuclei and cytoplasm with reference to GP (Table I).
Statistical analysis showed a significant correlation between cytoplasmic expression of MDC1 and GS (p = 0.0108) (Figure 2 C).
Statistical analysis showed no significant correlation between the level of MDC1 in nuclei and with reference to GS (Table II).
Discussion
In the normal cell, the MMR system promotes repair during and after DNA replication mainly through the excision-repair reaction. This MMR mechanism engages numerous proteins, including MSH2 and MLH1, which were a part of this study [19–21]. MSH2 gene inactivation and the loss of MSH2 protein cause insufficient DNA repair
502 Arch Med Sci 2, 1st March / 2023
D. Jaworski, A. Gzil, P. Antosik, I. Zarębska, J. Dominiak, I. Neska-Długosz, A. Kasperska, D. Grzanka, Ł. Szylberg
A B C 14 12 10 8 6 4 2 0 –2 14 12 10 8 6 4 2 0 –2 14 12 10 8 6 4 2 0 –2 p = 0.044 p = 0.045 p = 0.0108 7 8 9 7 8 9 7 8 9 Gleason score Gleason score Gleason score MSH2 –nucleus MSH2 –cytoplasm MDC1 –cytoplasm
Median 25–75% Min.-max. Median 25–75% Min.-max. Median 25–75% Min.-max.
Figure 2. Box plot of data with the correlation between Gleason score and protein expression. A – Correlation between Gleason score and nuclear expression of MSH2 protein. B – Correlation between Gleason score and cytoplasmic expression of MSH2 protein. C – Correlation between Gleason score and cytoplasmic expression of MDC1 protein
Table II. Summarized medians and statistical significance of our results in reference to Gleason score
and the development of tumors with high levels of microsatellite instability [22–27]. Furthermore, a recent study showed that loss-of-function mutations of MSH2 were most common in PCa compared to another MMR protein, i.e. MLH1 [28–30].
Dominguez-Valentin et al. followed a similar approach in their study which was focused on patients with Lynch syndrome and PC. Their results showed that defect of MSH2 was associated with high GS (GS of ≥ 8) and more aggressive biological behavior of the prostatic carcinomas [31]. Another study that addressed a similar subject was that of Guedes et al., which revealed that the highest rates of MSH2 gene inactivation and loss MSH2 protein occurred among the most aggressive high-grade prostatic adenocarcinomas, especially among tumors with GP5 [32]. However, in our study the nuclear and cytoplasmic level of MSH2 according to GS did not support this concept. This fact may suggest other significant alterations in MSH2 expression among PCs in patients with and without Lynch syndrome.
Based on our results, we can suspect that in cases with GS of ≥ 7 there were significantly more incorrectly paired nucleotides, which caused increased nuclear expression of MSH2 to conduct sufficient DNA repair [33, 34]. The corresponding cytoplasmic and protein expression of the MSH2 in specimens with GS ≥ 7 could be a result of increased expression of the MSH2 gene caused by intensified DNA repair because of an increased level of mutations. Moreover, our study showed a decreased overall level of nuclear MSH2 according to GP. It revealed that MSH2 loss was more common among high grade prostatic cancer. In the group with GP4 the level of nuclear MSH2 was increased compared to samples with GP3. The greater number of incorrectly paired nucleotides might have been connected with higher demand of the MSH2. However, a decreased level of the nuclear MSH2 in GP5 might have resulted from a higher amount of mutations in the MSH2 gene, which prevented adequate DNA repair. The high GS in cancers with MSH2 deficien-
Arch Med Sci 2, 1st March / 2023 503
Expression differences between proteins responsible for DNA damage repair according to the Gleason grade as a new heterogeneity marker in prostate cancer
Protein Gleason pattern 3 Gleason pattern 4 Gleason pattern 5 P -value Median Percentile Median Percentile Median Percentile 25% 75% 25% 75% 25% 75% TP53BP1 – n 8.00 4.00 12.00 8.00 8.00 12.00 10.00 3.00 12.00 ns TP53BP1 – c 8.00 4.00 8.00 8.00 4.00 8.00 8.00 3.00 12.00 ns MDC1 – n 3.00 0.00 6.00 3.00 0.00 7.00 6.00 4.50 8.00 0.0591 MDC1 – c 2.50 0.00 7.50 3.00 0.00 6.00 8.00 2.50 8.00 ns MSH2 – n 8.00 4.00 12.00 8.00 8.00 12.00 3.00 0.25 8.75 0.004 MSH2 – c 3.00 0.00 4.00 3.00 0.50 4.00 0.00 0.00 2.50 ns MLH1 – n 8.00 4.000 12.00 8.00 3.00 12.00 12.00 8.75 12.00 ns MLH1 – c 4.00 0.00 7.00 8.00 4.00 12.00 8.00 6.25 12.00 0.0255 n – nuclear staining, c – cytoplasmic staining.
Table I. Summarized medians and statistical significance of our results in reference to Gleason pattern
Protein Gleason score 7 Gleason score 8 Gleason score 9 P -value Median Percentile Median Percentile Median Percentile 25% 75% 25% 75% 25% 75% TP53BP1 – n 8.00 6.00 12.00 8.00 6.00 12.00 8.00 6.00 12.00 ns TP53BP1 – c 8.00 4.00 8.00 8.00 4.00 8.00 8.00 4.00 12.00 ns MDC1 – n 4.00 1.00 6.00 2.00 0.00 6.00 5.00 0.00 8.00 0.046 MDC1 – c 4.00 2.00 8.00 2.00 0.00 4.00 4.00 0.00 8.00 0.0108 MSH2 – n 8.00 6.00 12.00 8.00 3.00 12.00 8.00 8.00 12.00 0.044 MSH2 – c 4.00 0.00 4.00 2.00 0.00 4.00 3.50 1.00 4.00 0.045 MLH1 – n 8.00 4.00 12.00 8.00 4.00 12.00 8.00 2.00 12.00 ns MLH1 – c 4.00 2.00 8.00 4.00 0.00 8.00 4.00 0.00 8.00 ns n – nuclear staining, c – cytoplasmic staining.
cy suggested more aggressive behavior compared to prostatic tumors without MSH2 defects. It might have been connected with a subset of prostatic carcinoma called “hypermutated” [35]. The Pritchard et al. study revealed that all hypermutated prostatic cancers had mutations in MMR genes and MSI. Complex structural rearrangements in the MSH2 gene (for example MSH2-KCNK12 inversion) were an important mechanism determining hypermutation in advanced PC. Thus, hypermutated prostatic cancers showed complete loss of MSH2 protein, as we observed in our study. According to Pritchard et al. prostatic cancers without hypermutation were microsatellite stable and had valid MSH2 protein [28]. In our study we observed the increase of MSH2 in cancers with higher GS and its decrease in cases with higher GP. This observation may result from intratumor heterogeneity in PC.
Another investigated protein of the MMR mechanism was MLH1. Studies suggested that MLH1 abnormalities could increase prostate tumor aggressiveness and indicated that expression of MLH1 among PC cells was significantly downregulated in comparison to normal prostate or benign hyperplasia [19, 36–39]. Numerous studies revealed the impact of alteration within the MLH1 gene on PC stage, but the results of those studies were diverse. Studies showed that simultaneously with growth of the GS, MLH1 gene expression declined [39, 40]. However, other studies showed the rising trend of the MLH1 gene expression among PC with the higher GS [41, 42]. The findings in our study could help to clarify the reason for these inconsis-
tencies among studies. Our study showed a relevant dependency for the cytoplasmic MLH1 expression among PCs with a higher GP, but no significant correlation among PCs regarding the GS.
We assumed that it could have resulted from the PC heterogeneity and the intratumoral heterogeneity of MLH1 gene expression, which could be the reason for these discrepancies between the results for the GS and GP.
The other investigated proteins engaged in DNA repair were TP53BP1 and MDC1. These proteins are involved in specific molecular pathways to detect DSB, which protects cells against DNA alterations and the initiation of carcinogenesis [43, 44]. Jäämaa et al. observed the accumulation of TP53BP1 and MDC1 at places of DNA damage induced by cytotoxic drugs and ionizing radiation in nonmalignant human prostate tissue, which implied a protective function of the DSB repair pathway against malignant transformation [45].
The current research is the first to center on TP53BP1 level according to histopathological grade. However, our results demonstrated no significant correlation between this protein level in all evaluated localizations and GP and GS.
As a consequence, we supposed that the TP53BP1 function does not undergo disorders during a process of PC dedifferentiation.
Different studies revealed only that TP53BP1 decreased during cancer clinical progression [46–48]. These observations suggested the independence of disease risk factors related to clinical progression and the factors leading to cancer progression.

504 Arch Med Sci 2, 1st March / 2023
D. Jaworski, A. Gzil, P. Antosik, I. Zarębska, J. Dominiak, I. Neska-Długosz, A. Kasperska, D. Grzanka, Ł. Szylberg
A
C D
Figure 3. Collage of representative area photographs with protein expression. A – Photograph of area with MSH2 protein expression. B – Photograph of area with MLH1 protein expression. C – Photograph of area with MDC1 protein expression. D – Photograph of area with TP53BP1 protein expression
B
Expression differences between proteins responsible for DNA damage repair according to the Gleason grade as a new heterogeneity marker in prostate cancer
An interesting fact is that other studies showed that alterations in TP53BP1 function resulted in insensitivity to radiotherapy [49–52].
However, an earlier clinical study has demonstrated that the radiotherapy relapse rate increases in the case of prostatic cancer with an increasing GS value [53]. Our results suggest nevertheless that the mechanism of this radiation resistance might not arise from alterations of TP53BP1. Moreover, there is a lack of studies about another clinical context and further research is needed in this field.
MDC1 was another investigated component of the DNA damage response that participates in the DNA damage checkpoint and protects the integrity of the genome [54]. The latest study showed that there was overexpression of MDC1 in cells of several cancer types in comparison to normal cells [55, 56]. Zou et al. found that MDC1 was a positive co-activator of the estrogen receptor a (ERa) in breast cancer [55]. They detected that down-regulation of MDC1 decreased the expression of the endogenous estrogen responsive genes and, therefore, the growth of the tumor [55]. Similar correlations have been described by Wang et al. for PC. They proved that MDC1 was an androgen receptor co-activator involved in PC suppression. Moreover, they showed that MDC1 participated in suppression of PCa cell growth and migration [56]. However, our results showed no significant correlation between the level of MDC1 in nuclei and cytoplasm with reference to GP. On the other hand, we demonstrated a significant decrease of the cytoplasmic expression of MDC1 in cases with GS 8. This process may be caused by PC heterogeneity and the results may differ according to the PC group, which is examined [57].
In conclusion, our study suggested that the aberration in the MMR repair mechanism may be significantly more crucial regarding grading among PC cells in comparison to the impact of alterations in the DSB repair mechanism. Moreover, the present study indicated divergences among expression of the respective proteins in GP and GS. There was a significant positive correlation between GS and nuclear expression of MSH2, but a negative correlation between GP and MSH2 nuclear expression. According to this, there was no relevant correlation between MLH1 cytoplasmic expression and GS, whereas there was a significant positive correlation between cytoplasmic expression of MLH1 and GP. This may indicate significant heterogeneity among PC. Furthermore, we concluded due to the lack of a correlation between expression of the TP53BP1 protein and GP and GS that the radiation resistance of prostate cancer seems to be independent of alterations connected with TP53BP1 (Figure 3).
Conflict of interest
The authors declare no conflict of interest.
References
1. Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017. CA Cancer J Clin 2017; 67: 7-30.
2. Ham WS, Chalfin HJ, Feng Z, et al. New prostate cancer grading system predicts long-term survival following surgery for Gleason score 8-10 prostate cancer. Eur Urol 2017; 71: 907-12.
3. Humphrey PA, Moch H, Cubilla AL, Ulbright TM, Reuter VE. The 2016 WHO classification of tumours of the urinary system and male genital organs – part B: prostate and bladder tumours. Eur Urol 2016; 70: 106-19.
4. Epstein J, Egevad L, Amin MB, Delahunt B, Srigley JR, Humphrey PA; Grading Committee. The 2014 International Society of Urological Pathology (ISUP) Consensus Conference on Gleason Grading of Prostatic Carcinoma: definition of grading patterns and proposal for a new grading system. Am J Surg Pathol 2016; 40: 244-52.
5. Oberle C, Blattner C. Regulation of the DNA damage response to DSBs by post-translational modifications. Curr Genomics 2010; 11: 184-98.
6. Breast Cancer Linkage Consortium. Cancer risks in BRCA2 mutation carriers. J Natl Cancer Inst 1999; 91: 1310-6.
7. O’Donovan PJ, Livingston DM. BRCA1 and BRCA2: breast/ ovarian cancer susceptibility gene products and participants in DNA double-strand break repair. Carcinogenesis 2010; 31: 961-7.
8. Tirkkonen M, Johannsson O, Agnarsson BA, et al. Distinct somatic genetic changes associated with tumor progression in carriers of BRCA1 and BRCA2 germ-line mutations. Cancer Res 1997; 57: 1222-7.
9. Thompson D, Easton DF; Breast Cancer Linkage Consortium. Cancer Incidence in BRCA1 mutation carriers. J Natl Cancer Inst 2002; 94: 1358-65.
10. Reyes GX, Schmidt TT, Kolodner RD, Hombauer H, Diego S, Jolla L. New insights into the mechanism of DNA mismatch repair. Chromosoma 2015; 124: 443-62.
11. Poulogiannis G, Frayling IM, Arends MJ. DNA mismatch repair deficiency in sporadic colorectal cancer and Lynch syndrome. Histopathology 2010; 56: 167-79.
12. Chui MH, Ryan P, Radigan J, et al. The histomorphology of Lynch syndrome-associated associated ovarian carcinomas: toward a subtype-specific screening strategy. Am J Surg Pathol 2014; 38: 1173-81.
13. Montenegro YM, Ramírez AT MC. Hereditary colo-rectal cancer. Rev Colomb Cir 2002; 17: 31-6.
14. Hashmi AA, Ali R, Hussain ZF, et al. Mismatch repair deficiency screening in colorectal carcinoma by a fourantibody immunohistochemical panel in Pakistani population and its correlation with histopathological parameters. World J Surg Oncol 2017; 15: 4-11.
15. Yoshioka Y, Togashi Y, Chikugo T, et al. Clinicopathological and genetic differences between low-grade and highgrade colorectal mucinous adenocarcinomas. Cancer 2015; 121: 4359-68.
16. Remmele W, Stegner HE. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987; 8: 138-40.
17. Kowalewski A, Szylberg Ł, Tyloch J, et al. Caspase 3 as a novel marker to distinguish chromophobe renal cell carcinoma from oncocytoma. Pathol Oncol Res 2019; 25: 1519-24.
Arch Med Sci 2, 1st March / 2023 505
18. Sadlecki P, Jóźwicki J, Antosik P, Grabiec M. Expression of selected epithelial-mesenchymal transition transcription factors in serous borderline ovarian tumors and type I ovarian cancers. Tumour Biol 2018; 40: 1010428318784807.
19. Reyes GX, Schmidt TT, Kolodner RD, Hombauer H. New insights into the mechanism of DNA mismatch repair. Chromosoma 2015; 124: 443-62.
20. Fishel R. Mismatch repair. J Biol Chem 2015; 290: 26395-403.
21. Fukuhara S, Chang I, Mitsui Y, et al. DNA mismatch repair gene MLH1 induces apoptosis in prostate cancer cells. Oncotarget 2014; 5: 11297-307.
22. Peltomaki P, Lothe RA, Aaltonen LA, et al. Microsatellite instability is associated with tumors that characterize the hereditary non-polyposis colorectal carcinoma syndrome. Cancer Res 1993; 53: 5853-5.
23. Aaltonen L, Peltomäki P, Leach F, et al. Clues to the pathogenesis of familial colorectal cancer. Science 1993; 260: 812-6.
24. Papadopoulos N, Lindblom A. Molecular basis of HNPCC: mutations of MMR genes. Hum Mutat 1997; 10: 89-99.
25. Peltomäki P, Vasen HF. Mutations predisposing to hereditary nonpolyposis colorectal cancer: database and results of a collaborative study. The International Collaborative Group on Hereditary Nonpolyposis Colorectal Cancer. Gastroenterology 1997; 113: 1146-58.
26. Lynch HT, de la Chapelle A. Hereditary colorectal cancer. N Engl J Med 2003; 348: 919-32.
27. Nagasaka T, Rhees J, Kloor M, et al. Somatic hypermethylation of MSH2 is a frequent event in Lynch syndrome colorectal cancers. Cancer Res 2010; 70: 3098-108.
28. Pritchard CC, Morrissey C, Kumar A, et al. Complex MSH2 and MSH6 mutations in hypermutated microsatellite unstable advanced prostate cancer. Nat Commun 2014; 5: 4988.
29. Abeshouse A, Ahn J, Akbani R, et al. The molecular taxonomy of primary prostate cancer. Cell 2015; 163: 1011-25.
30. Robinson D, Van Allen EM, Wu YM, et al. Integrative clinical genomics of advanced prostate cancer. Cell 2015; 161: 1215-28.
31. Dominguez-Valentin M, Joost P, Therkildsen C, Jonsson M, Rambech E, Nilbert M. Frequent mismatch-repair defects link prostate cancer to Lynch syndrome. BMC Urol 2016; 16: 15.
32. Guedes LB, Antonarakis ES, Schweizer MT, et al. MSH2 loss in primary prostate cancer. Clin Cancer Res 2017; 23: 6863-74.
33. Geng H, Sakato M, DeRocco V, et al. Biochemical analysis of the human mismatch repair proteins hMutSa MSH2(G674A)-MSH6 and MSH2-MSH6(T1219D). J Biol Chem 2012; 287: 9777-91.
34. Heinen CD, Cyr JL, Cook C, et al. Human MSH2 (hMSH2) protein controls ATP processing by hMSH2-hMSH6. J Biol Chem 2011; 286: 40287-95.
35. Kumar A, White TA, MacKenzie AP, et al. Exome sequencing identifies a spectrum of mutation frequencies in advanced and lethal prostate cancers. Proc Natl Acad Sci 2011; 108: 17087-92.
36. Supek F, Lehner B. Differential DNA mismatch repair underlies mutation rate variation across the human genome. Nature 2015; 521: 81-4.
37. Soni A, Bansal A, Singh LC, et al. Gene expression profile and mutational analysis of DNA mismatch repair genes in carcinoma prostate in Indian population. Omi A J Integr Biol 2011; 15: 319-24.
38. Chen Y, Wang J, Fraig MM, et al. Alterations in PMS2, MSH2 and MLH1 expression in human prostate cancer. Int J Oncol 2003; 22: 1033-43.
39. Chen Y, Wang J, Fraig MM, et al. Defects of DNA mismatch repair in human prostate cancer. Cancer Res 2001; 61: 4112-21.
40. Burger M, Denzinger S, Hammerschmied CG, et al. Elevated microsatellite alterations at selected tetranucleotides (EMAST) and mismatch repair gene expression in prostate cancer. J Mol Med 2006; 84: 833-41.
41. Wilczak W, Rashed S, Hube-Magg C, et al. Up-regulation of mismatch repair genes MSH6, PMS2 and MLH1 parallels development of genetic instability and is linked to tumor aggressiveness and early PSA recurrence in prostate cancer. Carcinogenesis 2017; 38: 19-27.
42. Norris AM, Gentry M, Peehl DM, D’Agostino R, Scarpinato KD. The elevated expression of a mismatch repair protein is a predictor for biochemical recurrence after radical prostatectomy. Cancer Epidemiol Biomarkers Prev 2009; 18: 57-64.
43. Shibata A. Regulation of repair pathway choice at twoended DNA double-strand breaks. Mutat Res 2017; 803805: 51-5.
44. Lukas J, Lukas C, Bartek J. More than just a focus: the chromatin response to DNA damage and its role in genome integrity maintenance. Nat Cell Biol 2011; 13: 1161-9.
45. Jäämaa S, Af Hällström TM, Sankila A, et al. DNA damage recognition via activated ATM and p53 pathway in nonproliferating human prostate tissue. Cancer Res 2010; 70: 8630-41.
46. Kurfurstova D, Bartkova J, Vrtel R, et al. DNA damage signalling barrier, oxidative stress and treatment-relevant DNA repair factor alterations during progression of human prostate cancer. Mol Oncol 2016; 10: 879-94.
47. Du R, Zheng L, Huang W, Zhang H, Jiang Z. Correlation of 53BP1 gene mutation with prostatic adenocarcinoma. Zhonghua Bing Li Xue Za Zhi 2011; 40: 449-53.
48. Lewinska A, Jarosz P, Czech J, et al. Capsaicin-induced genotoxic stress does not promote apoptosis in A549 human lung and DU145 prostate cancer cells. Mutat Res 2015; 779: 23-34.
49. Xiao Y, Zheng X, Huang A, Liu T, Zhang T, Ma H. Deficiency of 53BP1 inhibits the radiosensitivity of colorectal cancer. Int J Oncol 2016; 49: 1600-8.
50. Gou Q, Xie Y, Liu L, et al. Downregulation of MDC1 and 53BP1 by short hairpin RNA enhances radiosensitivity in laryngeal carcinoma cells. Oncol Rep 2015; 34: 251-7.
51. Squatrito M, Vanoli F, Schultz N, Jasin M, Holland EC. 53BP1 is a haploinsufficient tumor suppressor and protects cells from radiation response in glioma. Cancer Res 2012; 72: 5250-60.
52. Wang W, Song Z, Zhang Y. Efficacy of brain radiotherapy plus EGFR-TKI for EGFR-mutated NSCLC patients who develop brain metastasis. Arch Med Sci 2018; 14: 1298-307.
53. Brawer MK. Radiation therapy failure in prostate cancer patients: risk factors and methods of detection. Rev Urol 2002; 4 Suppl 2: S2-11.
54. Stewart GS, Wang B, Bignell CR, Taylor AMR, Elledge SJ. MDC1 is a mediator of the mammalian DNA damage checkpoint. Nature 2003; 421: 961-6.
55. Zou R, Zhong X, Wang C, et al. MDC1 enhances estrogen receptor-mediated transactivation and contributes to breast cancer suppression. Int J Biol Sci 2015; 11: 992-1005.
56. Wang C, Sun H, Zou R, et al. MDC1 functionally identified as an androgen receptor co-activator participates in suppression of prostate cancer. Nucleic Acids Res 2015; 43: 4893-908.
57. Tolkach Y, Kristiansen G. The heterogeneity of prostate cancer: a practical approach. Pathobiology 2018; 85: 108-16.
506 Arch Med Sci 2, 1st March / 2023
D. Jaworski, A. Gzil, P. Antosik, I. Zarębska, J. Dominiak, I. Neska-Długosz, A. Kasperska, D. Grzanka, Ł. Szylberg
The emerging role of ferroptosis in myocardial fibrosis of atrial fibrillation
Honghua Yue, Yujia Zhan, Zheng Zhang, Weitao Liang, Zhong Wu
Department of Cardiovascular Surgery, West China Hospital, Sichuan University, Chengdu, China
Submitted: 18 November 2022; Accepted: 5 February 2023
Online publication: 24 February 2023
Arch Med Sci 2023; 19 (2): 507–512
DOI: https://doi.org/10.5114/aoms/160941
Copyright © 2023 Termedia & Banach
Abstract
Introduction: The aim of this study was to investigate the relationship between ferroptosis and myocardial fibrosis in atrial fibrillation (AF).
Methods: The patient’s left atrial appendage tissue was obtained in cardiac surgery. Sirius red staining, Prussian blue and Western blot were used to detect staining to assess histological fibrosis and ferroptosis changes.
Results: There is a certain correlation between the degree of tissue fibrosis and ferroptosis in AF ( r = 0.7763, p = 0.0004). The key proteins related to the regulation of ferroptosis were significantly abnormal in the AF group.
Conclusions: Ferroptosis is involved in myocardial fibrosis of AF and is a potential target for the diagnosis, prevention and treatment of AF.
Key words: ferroptosis, myocardial fibrosis, atrial fibrillation.
Atrial fibrillation (AF) is one of the most common cardiac arrhythmias, with studies reporting that it affects more than 33 million people worldwide, and its prevalence is expected to more than double over the next 40 years. AF is associated with important major adverse cardiovascular events, such as heart failure, major stroke, and myocardial infarction, and is also a significant burden on healthcare expenditures [1–4]. Many studies have found that atrial structural remodeling plays an important role in the management of AF. Myocardial fibrosis is the main marker of atrial structural remodeling, which can interrupt the continuity of muscle bundles, interfere with the formation of tight junctions containing connexins, and interfere with cardiac electrical conduction, resulting in slow conduction and conduction block [5]. In addition, coupling between cardiomyocytes and fibroblasts/myofibroblasts can alter cardiomyocyte electrical activity, promote ectopic firing, and promote AF development [6]. Therefore, it is of great clinical significance to clarify the pathogenesis of myocardial fibrosis in AF for the treatment of AF.
Ferroptosis is a kind of cell death mediated by iron-dependent lipid peroxidation. Recent studies have found that ferroptosis can promote liver fibrosis, pulmonary fibrosis and renal fibrosis, and targeted inhibition of ferroptosis can help improve tissue fibrosis [7–9]. However, the role of ferroptosis in myocardial fibrosis in AF has not yet been studied, so this study aimed to explore the relationship between ferroptosis and myocardial fibrosis in AF.
Corresponding author: Zhong Wu
Department of Cardiovascular Surgery
West China Hospital
Sichuan University
Chengdu, China
Phone: +86-028-85422897
E-mail: wuzhong71@scu.edu.cn
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/). Research letter Cardiology
Honghua Yue, Yujia Zhan, Zheng Zhang, Weitao Liang, Zhong Wu
Methods. The subjects of this study were patients with valvular disease who underwent heart valve surgery (Table I). Patients with persistent AF were used as the experimental group (AF group), and patients with sinus rhythm were used as the control group (SR group). The study was conducted in accordance with the Declaration of Helsinki, and the research protocol was approved by the Ethics Committee of West China Hospital of Sichuan University (approval No: [2021] No. 143). During the surgery, the left atrial appendage tissue was removed, and one portion was immediately fixed in a 4% paraformaldehyde solution for histological examination. The other part was stored in a freezer at –80°C for western blotting (Wb) analysis (Antibody, Abcam plc, Shanghai, China). The PVDF membrane was incubated with primary antibodies specific for FTH1, GSH, GPX4 and xCT (1 : 2000), GSDMD, cleaved GSDMD, pro-caspase-1, caspase-1, cleaved caspase-1, pro-IL-1b (1 : 1000), and GAPDH (1 : 5000). The results for each protein are representative of three independent repeated measurements. Sirius red staining and Prussian blue staining were used to assess histological fibrosis and ferroptosis changes in the left atrial appendage. Wb detects ferroptosis-related protein expression in the left atrial appendage. The statistical analysis was performed with the software Prism 8 (GraphPad, San Diego, CA, USA). Categorical variables are presented as the number and percentage of patients, and continuous data are shown as mean ± standard deviation. P-values < 0.05 were considered statistically significant. Correlations were calculated using the Pearson or Spearman correlation. Results. Here, we found that compared with patients in sinus rhythm, patients with AF had significantly increased myocardial fibrosis (SR group 13.35 ±1.81% vs. AF group 25.8 ±2.72%, p = 0.0018) in the left atrial appendage (Figure
1 A). Prussian blue staining found that iron particles in the left atrial appendage tissue of patients with AF increased significantly (SR group 0.012 ±0.003% vs. AF group 0.045 ±0.011%, p = 0.016), indicating that iron metabolism in the myocardium of patients with AF was abnormal (Figure 1 B). There is a certain correlation between the degree of tissue fibrosis and ferroptosis in AF (r = 0.7763, p = 0.0004, Figure 1 C). Wb detection of left atrial appendage tissue confirmed that key proteins related to the regulation of ferroptosis were significantly abnormal in the AF group (Figure 1 D).
Discussion. Ferroptosis is a newly discovered nonapoptotic regulatory cell death mode that is characterized by iron-dependent lipid peroxidation-mediated cell death. Increasing evidence indicates that ferroptosis mediated by iron metabolism imbalance, abnormal lipid peroxidation, decreased glutathione peroxidase 4 activity and inhibition of the cystine/glutamate transport system are closely related to the occurrence and development of tissue fibrosis [10, 11]. FTH1 (ferritin heavy chain 1) plays an important role in iron absorption and transportation and participates in the formation of stored iron. When the expression of FTH1 decreases, the production of stored iron decreases, which leads to the accumulation of intracellular Fe2+ and induces ferroptosis [12]. When ferroptosis occurs, the intracellular antioxidant glutathione (GSH) is continuously consumed, the activity of glutathione peroxidase 4 (GPX4) decreases, and the oxidation-antioxidant balance is broken. The continuous accumulation of ROS (reactive oxygen species) leads to the loss of cell integrity and cell death after lipid peroxidation occurs in the cell membrane [10]. xCT (SLC7A11) promotes GSH synthesis by mediating cystine uptake and glutamate release, protecting cells from oxidative stress, maintaining cellular redox bal-
508 Arch Med Sci 2, 1st March / 2023
Parameter AF ( n = 8) SR ( n = 8) P -value Age [years] mean ± SD 58.19 ±7.57 54.29 ±8.73 0.35 Male, n (%) 4 (50) 5 (62.5) 0.5 NYHAII/III, n (%) 3 (37.5) 2 (25) 0.6 Diabetes, n (%) 2 (25.0) 1 (12.5) 0.5 Smoking, n (%) 3 (37.5) 0 (0.0) 0.05 ACEI or ARB, n (%) 2 (25) 1 (12.5) 0.5 RAD [mm] mean ± SD 42.31 ±7.22 37.86 ±6.62 0.22 LAD [mm] mean ± SD 55.75 ±6.95 49.43 ±5.97 0.07 LVD [mm] mean ± SD 51.12 ±6.70 49.43 ±5.74 0.59 RVD [mm] mean ± SD 23.31 ±3.09 21.29 ±1.60 0.13 EF (%) mean ± SD 53.62 ±8.48 61.29 ±9.20 0.1 AF – atrial fibrillation, SR – sinus rhythm, ACEI – angiotensin converting enzyme inhibitor, ARB – angiotensin receptor inhibitor, RAD – right atrial diameter, LAD – left atrial diameter, LVD – left ventricle diameter, RVD – right ventricle diameter, EF – ejection fraction.
Table I. Clinical characteristics of study group
The emerging role of ferroptosis in myocardial fibrosis of atrial fibrillation
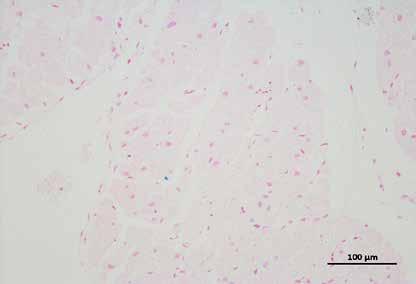
r = 0.7763 p = 0.0004
Figure 1. A
Sirius red staining of the left
appendage: the collagen ratio was significantly increased in the AF group, indicating that the myocardial fibrosis in the AF group was severe (SR group 13.35 ±1.81% vs. AF group 25.8 ±2.72%, n = 8, p = 0.0018). B – Prussian blue staining showed that iron particles in the left atrial appendage tissue of patients with AF increased significantly, indicating that iron metabolism in the myocardium of patients with AF was abnormal (SR group 0.012 ±0.003% vs. AF group 0.045 ±0.011%, n = 8, p = 0.016). C – There is a certain correlation between the degree of tissue fibrosis and ferroptosis in AF (r = 0.7763, p = 0.0004)
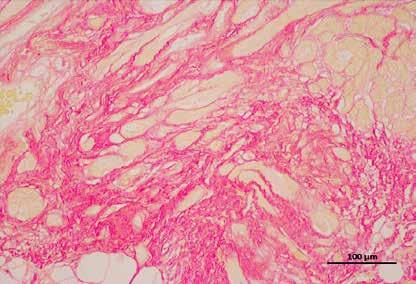
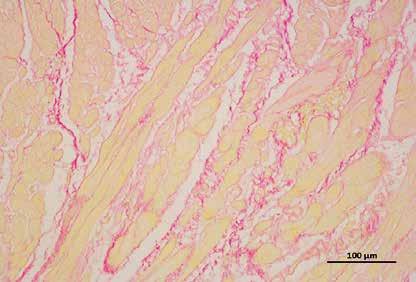
Arch Med Sci 2, 1st March / 2023 509
Sirius red Prussian-blue A B SR 200× AF 200× SR 200× AF 200× 40 30 20 10 0 0.10 0.08 0.06 0.04 0.02 0 Collagen volume fraction (%) Ferrum particles fraction (%) SR AF SR AF 50 40 30 20 10 0 Collagen volume fraction (%) 0 0.05 0.10 0.15 Ferrum particles fraction (%) C
–
atrial
Figure 1. Cont. D – Expression levels of key regulatory proteins of ferroptosis: FTH1, GPX4, and xCT were significantly downregulated in the AF group, suggesting an important relationship between ferroptosis and AF. The apoptosis-related cytokines (caspase-1, GSDMD, and pro-IL-1b) were significantly elevated in the AF group, suggesting that apoptosis also has an important link with AF
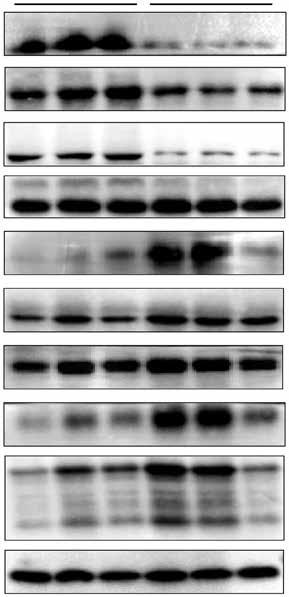
510 Arch Med Sci 2, 1st March / 2023
Honghua Yue, Yujia Zhan, Zheng Zhang, Weitao Liang, Zhong Wu
D FTH1 GPX4 xCT GSDMD Cleaved-GSDMD pro-Caspase1 Caspase1 Cleaved-Caspase1 pro-IL-1b Cleaved-IL-1b GAPDH SR AF 1.5 1.0 0.5 0 1.5 1.0 0.5 0 1.5 1.0 0.5 0 2.5 2.0 1.5 1.0 0.5 0 1.5 1.0 0.5 0 1.5 1.0 0.5 0 FTH1/GAPDH GPX4/GAPDH xCT/GAPDH Cleaved-GSDMD/GAPDH GSDMD/GAPDH pro-Caspase1/GAPDH FTH1 GPX4 xCT Cleaved-GSDMD GSDMD pro-Caspase1
ance, and preventing lipid peroxidation-induced cell death [13]. These three key regulatory proteins responding to ferroptosis were significantly downregulated in the AF group, suggesting an important relationship between ferroptosis and AF. Meanwhile, we know that caspase-1 cleaves GSDMD (gasdermin D) and cytokines and that the pro-IL-1b precursor is activated by proteolysis to produce its proinflammatory form IL-1b Visualization of these important cytokines can be achieved by using specific antibodies. Importantly, caspase-1 also cleaves the amino terminal fragment of the key protein GSDMD, causing it to oligomerize and form holes in the cell membrane, leading to cytokine secretion, water intake and eventual cell rupture [14]. These typical apoptosis-related cytokines were significantly elevated in the AF group, suggesting that apoptosis also has an important link with AF.
In conclusion, ferroptosis is a new type of cell death that is neither apoptosis nor necrosis, and has characteristics different from other forms of regulated cell death. However, as a form of death regulated by a variety of substances, it is still unclear which are the most key executive molecules in the process of ferroptosis. At present, there are few studies on the relationship between ferropto-
sis and cardiovascular disease, and they mainly focus on the mechanism of ischemia-reperfusion injury. However, regarding the pathological mechanism of myocardial fibrosis, there is little research on ferroptosis, especially the mechanism by which ferroptosis regulates myocardial fibrosis in AF. We have preliminarily confirmed that ferroptosis is related to myocardial fibrosis in AF, which will provide theoretical support for targeting the inhibition of myocardial fibrosis and the treatment of AF.
Acknowledgments
This study was funded by the National Natural Science Foundation of China (grant number: 82172060), Post-Doctor Research Project, West China Hospital, Sichuan University (grant number: 2020HXBH106), and funded by the Department of Science and Technology of Sichuan Province (grant number: 2022YFS0362, 2022YFS0363).
Honghua Yue and Yujia Zhan contributed equally to this article.
Conflict of interest
The authors declare no conflict of interest.
Arch Med Sci 2, 1st March / 2023 511
The emerging role of ferroptosis in myocardial fibrosis of atrial fibrillation
2.0 1.5 1.0 0.5 0 2.0 1.5 1.0 0.5 0 2.0 1.5 1.0 0.5 0 2.0 1.5 1.0 0.5 0 Caspase1 pro-IL-1 b
Figure 1. Cont. D – Expression levels of key regulatory proteins of ferroptosis: FTH1, GPX4, and xCT were significantly downregulated in the AF group, suggesting an important relationship between ferroptosis and AF. The apoptosis-related cytokines (caspase-1, GSDMD, and pro-IL-1b) were significantly elevated in the AF group, suggesting that apoptosis also has an important link with AF
/GAPDH
b
Cleaved-Caspase1/GAPDH Cleaved-IL-1
GAPDH/GAPDH Caspase1 pro-IL-1
b
Cleaved-Caspase1 Cleaved-IL-1b
Honghua Yue, Yujia Zhan, Zheng Zhang, Weitao Liang, Zhong Wu
References
1. Wijesurendra RS, Casadei B. Mechanisms of atrial fibrillation. Heart 2019; 105: 1860-7.
2. Chung MK, Refaat M, Shen WK, et al. Atrial fibrillation: JACC council perspectives. J Am Coll Cardiol 2020; 75: 1689-713.
3. Wańkowicz P, Nowacki P, Gołąb-Janowska M. Risk factors for ischemic stroke in patients with non-valvular atrial fibrillation and therapeutic international normalized ratio range. Arch Med Sci 2019; 15: 1217-22.
4. Wańkowicz P, Nowacki P, Gołąb-Janowska M. Atrial fibrillation risk factors in patients with ischemic stroke. Arch Med Sci 2021; 17: 19-24.
5. Begg GA, Holden AV, Lip GY, Plein S, Tayebjee MH. Assessment of atrial fibrosis for the rhythm control of atrial fibrillation. Int J Cardiol 2016; 220: 155-61.
6. Nattel S. How does fibrosis promote atrial fibrillation persistence: in silico findings, clinical observations, and experimental data. Cardiovasc Res 2016; 110: 295-7.
7. Yu J, Wang JQ. Research mechanisms of and pharmaceutical treatments for ferroptosis in liver diseases. Biochimie 2021; 180: 149-57.
8. Xu W, Deng H, Hu S, et al. Role of ferroptosis in lung diseases. J Inflamm Res 2021; 14: 2079-90.
9. Yang L, Guo J, Yu N, et al. Tocilizumab mimotope alleviates kidney injury and fibrosis by inhibiting IL-6 signaling and ferroptosis in UUO model. Life Sci 2020; 261: 118487.
10. Li J, Cao F, Yin HL, et al. Ferroptosis: past, present and future. Cell Death Dis 2020; 11: 88.
11. Shojaie L, Iorga A, Dara L. Cell death in liver diseases: a review. Int J Mol Sci 2020; 21: 9682.
12. Doll S, Freitas FP, Shah R, et al. FSP1 is a glutathione-independent ferroptosis suppressor. Nature 2019; 575: 693-8.
13. Sönmez Aydın F, Hukkamlı B, Budak H. Coaction of hepatic thioredoxin and glutathione systems in iron overload-induced oxidative stress. J Biochem Mol Toxicol 2021; 35: e22704.
14. Wang J, Deng B, Liu Q, et al. Pyroptosis and ferroptosis induced by mixed lineage kinase 3 (MLK3) signaling in cardiomyocytes are essential for myocardial fibrosis in response to pressure overload. Cell Death Dis 2020; 11: 574.
512 Arch Med Sci 2, 1st March / 2023
Eicosanoids in human heart failure: pilot study of plasma epoxyeicosatrienoic and dihydroxyeicosatrienoic acid levels
Petr Kala1,2, Tomas Hnat1, Karolina Padrova3, Karel Kotaška3, Josef Veselka1
1Department of Cardiology, University Hospital Motol and 2nd Faculty of Medicine, Charles University, Prague, Czech Republic
2Center of Experimental Medicine, Institute of Clinical and Experimental Medicine, Prague, Czech Republic
3Department of Medical Chemistry and Biochemistry, University Hospital Motol and 2nd Faculty of Medicine, Charles University, Prague, Czech Republic
Submitted: 18 October 2022; Accepted: 14 January 2023
Online publication: 6 February 2023
Arch Med Sci 2023; 19 (2): 513–517
DOI: https://doi.org/10.5114/aoms/159313
Copyright © 2023 Termedia & Banach
Abstract
Introduction: The role of eicosanoids, metabolites of arachidonic acid with cardio-renal activity, remains unclear in human heart failure (HF).
Methods: We enrolled 50 patients with HF to measure plasma 14,15-EET and 14,15-DHET levels using commercial ELISA kits and compared them with 25 age- and sex-matched controls.
Results: Both of the measured eicosanoids were significantly higher in the HF group: 14,15-EET (91.3 ±25.7 ng/ml vs. 64.95 ±35.4 ng/ml) and 14,15DHET (10.58 ±2.06 ng/ml vs. 9.07 ±1.60 ng/ml), p for both < 0.001.
Conclusions: We found that peripheral plasma eicosanoid (14,15-EET, 14,15-DHET) levels are raised in patients with HF compared to age- and sex-matched controls.
Key words: heart failure, eicosanoids, epoxyeicosatrienoic acid, dihydroxyeicosatrienoic acid.
Heart failure (HF) is the leading cause of cardiovascular morbidity and mortality, and with its increasing prevalence, the healthcare systems worldwide face an HF pandemic [1–3]. Despite modern pharmacotherapy, including angiotensin receptor-neprilysin inhibitor (ARNI) and sodium-glucose cotransporter-2 inhibitors (SGLT2i), the prognosis of patients, especially those with advanced HF, remains poor [4].
Eicosanoids have been studied previously in basic cardiovascular and renal research. These metabolites of the cytochrome P-450 (CYP)-dependent epoxygenase pathway of arachidonic acid (AA), especially epoxyeicosatrienoic acids (EETs), importantly contribute to the regulation of cardiovascular and renal systems through their vasodilatory and natriuretic effect. Furthermore, in preclinical studies, they exert organ-protective actions [5–7]. Under physiological conditions, EETs are produced dominantly by endothelial cells (as endothelium-derived hyperpolarization factor – EDHF) and exhibit autocrine and paracrine action. EETs are rapidly transformed by soluble epoxide hydrolase (sEH) to biologically less active dihydroxyeicosatrienoic acids (DHETs) [5, 8] and excreted mainly
Corresponding author: Petr Kala MD, PhD
Department of Cardiology
University Hospital Motol and 2nd Faculty of Medicine
Charles University
Center of Experimental Medicine
Institute of Clinical and Experimental Medicine
Prague, Czech Republic
E-mail: petrkala@gmail.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/).
Research letter Heart Failure
by the kidney. The role of eicosanoids in human HF, however, remains unclear.
Our translational project (Eicosanoids in Human Heart Failure) aims to evaluate the role of eicosanoids in human HF. Here we present pilot data of the peripheral plasma levels of eicosanoids (14,15-EET and 14,15-DHET) measured by enzyme-linked immunosorbent assay (ELISA) in patients with HF in comparison to healthy controls.
Methods. A total of 50 consecutive adult patients with de novo or acute decompensated HF with reduced left ventricular ejection fraction (LVEF, HFrEF) admitted between July and September 2021 to our tertiary cardiovascular center were enrolled in this study; the only exclusion criterion was advanced renal failure before or during renal replacement therapy or a transplant program. The median age of the whole cohort was 70 years; 33% were women. As controls, we used blood samples of age- and sex-matched patients from our central hospital laboratory, where we excluded subjects with a diagnosis of HF in the medical records or with higher N-terminal pro B-type natriuretic peptide (NT-proBNP) in any of the blood tests available.
The blood samples were collected before breakfast in the morning the day after admission into
tubes coated with microscopic silica particles as a clot activator. After centrifugation (10 min, 4000 rpm, 8°C), the serum was separated, aliquoted, directly analyzed (eicosanoid analysis) and the rest was stored at –80°C. The concentration of eicosanoids (14,15-EET and 14,15-DHET) was assessed using commercially available sandwich ELISA assays (MyBiosource, USA). Analyses were performed according to the manufacturer’s instructions. The sensitivity of 14,15 EET kit is 1 ng/ml, and the detection range is 3.12–100 ng/ml. Reproducibility – intra-assay CV (%) and inter-assay CV (%) are less than 15% [CV(%) = SD/mean ×100]. The sensitivity of 14,15 DHET was 0,1 ng/ml.
We compared HF patients’ plasma EET and DHET levels with controls and analyzed the potential correlations with age, sex, New York Heart Association (NYHA) class, NT-proBNP, estimated glomerular filtration rate by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) equation (eGFR), and LVEF.
Clinical variables were summarized by a median or mean for continuous variables and by N (percentage) for categorical variables. Comparisons between two groups were performed using the two-tailed Student’s t-test or the Mann-Whitney U test as appropriate according to the Shapiro-Wilk normality test. The linear bivariate correlations
514 Arch Med Sci 2, 1st March / 2023
Petr Kala, Tomas Hnat, Karolina Padrova, Karel Kotaška, Josef Veselka
200 180 160 140 120 100 80 60 40 20 0 * * 20 15 10 5 0 20 15 10 5 0 A B C 14,15-EET [ng/ml] 14,15-DHET [ng/ml] EET/DHET Controls HF Controls HF Controls HF NS
Figure 1. Peripheral plasma levels of 14,15-EET (A) and 14,15-DHET (B) in HF and control groups. The 14,15-EET to 14,15-DHET ratio (C)
Eicosanoids in human heart failure: pilot study of plasma epoxyeicosatrienoic and dihydroxyeicosatrienoic acid levels
were measured by the Pearson correlation coefficient (Pearson’s r). Plasma levels are presented by mean ± SD; p < 0.05 indicates a statistically significant difference (* in the figure). Statistical analysis was performed using SPSS Statistics 28 (IBM, Armonk, NY, USA), Prism 9 (GraphPad, San Diego, CA, USA) and Med.Calc 13 (MedCalc Software, Ostende, Belgium).
All participants provided written informed consent. The study protocol following the principles of the Declaration of Helsinki was approved by the University Hospital Motol ethics committee. ClinicalTrials.gov Identifier: NCT05305170 (Eicosanoids in Human Heart Failure).
Results. Both of the measured eicosanoids were significantly higher in patients with HF: 14,15-EET (91.3 ±25.7 ng/ml vs. 64.95 ±35.4 ng/ml, p < 0.001) (Figure 1 A) and 14,15-DHET (10.58 ±2.06 ng/ml vs. 9.07 ±1.60 ng/ml, p < 0.001) (Figure 1 B). The combination of peripheral levels of EET and DHET (i.e., total EET production) was also significantly higher in patients with HF (101.92 ±25.64 ng/ml vs. 74.02 ±35.92 ng/ml, p < 0.001), but the EET/DHET ratio, a parameter of EET degradation and decreased peripheral bioavailability of EETs (i.e., sEH activity), was not statistically different between the HF group and controls (8.75 ±3.0 vs. 7.24 ±4.06, p = 0.07) (Figure 1 C).
In patients with HF, the mean NT-proBNP was 8840 ng/l, NYHA class III, eGFR 52.2 ml/ min/1.73 m2, LVEF 38%, high-sensitivity C-reactive
protein (hsCRP) 14.58 mg/l (Table I). The 14,15EET levels did not correlate with age, NYHA class, NT-proBNP, eGFR, or LVEF, but there was a significant correlation with sex (r = –0.285, p = 0.013), with higher levels in men (89.26 ±31.39 ng/ml vs. 70.76 ±29.86 ng/ml, p = 0.013). Therefore, we compared men and women separately in HF and control groups with a significant intergroup difference (HF vs. controls) for men (93.88 ±27.99 ng/ ml vs. 76.19 ±37.82 ng/ml, p = 0.016) and women (85.57 ±19.06 ng/ml vs. 55.96 ±31.84 ng/ml, p = 0.004). The 14,15-DHET levels did not correlate with age, sex, NT-proBNP, NYHA class, eGFR, or LVEF.
Discussion. In this proof-of-method part of our academic translational study, we found that peripheral plasma levels of both eicosanoids, active 14,15-EET and its inactive metabolite 14,15-DHET, were higher in patients with de novo or acute decompensated HFrEF compared to controls. The production of EETs was increased, but not their degradation to DHETs (EET/DHET ratio). The levels of 14,15-EET correlated with sex and were higher in men, both in the HF group and the control group.
One possible explanation could be higher production in the failing heart or peripheral tissue as a compensatory mechanism for tissue deficiency or decreased degradation either in the heart or in peripheral compartments. That needs to be elucidated by collecting blood samples from more body
Arch Med Sci 2, 1st March / 2023 515
Parameter HF SD Controls SD Diff. ( t -test) N 50 25 Age (mean) 70 13 69 14 0.80838 Female (%) 32 36 0.77406 LVEF (%) 38 16 60 5 < 0.00001 NTproBNP [ng/l] 8840 9145 202 144 < 0.00001 Hypertension (%) 78 54 0.02161 Type 2 diabetes mellitus (%) 48 19 0.00909 Coronary artery disease (%) 76 27 < 0.00001 COPD (%) 24 0 0.00013 Chronic kidney disease (%) (eGFR < 60 ml/min/1.73 m2) 58 7 < 0.00001 eGFR [ml/min/1.73 m2] 52.21 25.23 79.84 19.29 < 0.00001 hsCRP [mg/l] 14.58 17.53 4.75 4.38 0.00054 LDL [mmol/l] 2.36 1.00 2.70 0.66 0.05671 Total cholesterol [mmol/l] 3.95 1.23 4.58 0.74 0.00759 Statin (%) 56 58 0.44494 BMI [kg/m2] 29.27 2.28 29.16 5.29 0.47296 Weight [kg] 86.24 18.21 81.26 15.93 0.12288 LVEF – left ventricle ejection fraction, NT-proBNP – N-terminal pro B-type natriuretic peptide, COPD – chronic obstructive pulmonary disease, eGFR – estimated glomerular filtration rate, hsCRP – high-sensitivity C-reactive peptide, LDL – low-density lipoprotein, BMI – body mass index.
Table I. Patients’ characteristics
compartments (i.e. peripheral venous, peripheral arterial, central venous, central arterial and coronary sinus). So far, we can only extrapolate from our previous preclinical animal studies.
According to preclinical studies, the therapeutic potential of eicosanoids (due to their vasodilatory and natriuretic effect) seems promising in HF [5, 7]. Since EETs are rapidly transformed by sEH to biologically inactive DHETs, sEH inhibition was employed in most previous studies in which anti-hypertensive, cardio-, and renoprotective effects were reported [8]. However, this strategy might prove less successful whenever endogenous EET biosynthesis is compromised; thus, EET-agonistic analogs designed to resist degradation represent an alternative approach [9, 10]. In our recent animal study, we found that in a rodent volume-overload HF model induced by aortocaval fistula, the tissue EET deficiency in the left ventricle and kidney contributes to the poor prognosis and that pharmacological strategies that include EET analogs improve survival of this model by reducing bilateral cardiac eccentric hypertrophy and decreasing lung congestion [11].
The EET/DHET ratio is commonly used to assess the bioavailability of active metabolites [5, 6, 12], as validated in our preclinical study, where this ratio was reduced by around 65% in the kidney and left ventricle (LV) in an animal HF model when compared to controls. There were no significant differences in the kidney and LV protein expression of the enzymes responsible for EET production. However, the expression of sEH protein, an enzyme responsible for converting EETs to DHETs, was significantly increased in the animal HF model in LV tissue [11]. In this pilot human study, we did not measure the direct tissue concentrations of eicosanoids in the heart or kidney, where we expect the deficiency of active EETs according to our previous preclinical data [11].
It was proposed that intrarenal EETs may also act as an endogenous compensatory system opposing increased renin-angiotensin system (RAS) activity [12, 13]. Therefore, the increased peripheral concentration of eicosanoids might compensate for decreased availability in heart and renal tissue and countervail the activated RAS. Several body compartments contribute to the eicosanoid peripheral plasma levels because various cell types produce eicosanoids as paracrine and autocrine agents [5].
Any inflammatory diseases or steroid intake may influence the results of plasma eicosanoid levels, although this possible interaction has not been studied yet, especially in human HF. In our cohort, there was no patient or control on steroidal medication during blood collection, index hospitalization, or chronically. Although we found high-
er plasma hsCRP levels in the HF cohort than in controls (some of the HF decompensations were due to acute inflammatory diseases), there was no correlation between hsCRP and eicosanoid levels, suggesting no full explanation of our findings.
Since this was a pilot study to prove the feasibility of measuring the peripheral plasma levels of eicosanoids in HF patients by the ELISA method, the number of patients and controls is relatively low, limiting further analyses. We only enrolled de novo or acute decompensated HFrEF patients; thus, plasma eicosanoid levels of stable HFrEF patients and patients with only mildly reduced (HFmrEF) or preserved LVEF (HFpEF) remain to be elucidated in the next part of our project.
In conclusion, we found that levels of peripheral plasma eicosanoids (14,15-EET, 14,15-DHET) measured by ELISA are raised in patients with de novo or acute decompensated HFrEF compared to age- and sex-matched controls. These findings support further research into eicosanoids in HF.
Acknowledgments
This work was supported by Charles University Grant Agency (GAUK 68121). The work was supported by the Project development of research organization Czech Republic.
Supported by Ministry of Health, Czech Republic – conceptual development of research organization, Motol University Hospital, Prague Czech Republic 00064203.
Conflict of interest
The authors declare no conflict of interest.
References
1. Conrad N, Judge A, Tran J, et al. Temporal trends and patterns in heart failure incidence: a population-based study of 4 million individuals. Lancet 2018; 391: 572-80.
2. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2021; 42: 3599-726.
3. Arundel C, Lam PH, Faselis C, et al. Length of stay and readmission in older adults hospitalized for heart failure. Arch Med Sci 2021; 17: 891-9.
4. Vaduganathan M, Claggett BL, Jhund PS, et al. Estimating lifetime benefits of comprehensive disease-modifying pharmacological therapies in patients with heart failure with reduced ejection fraction: a comparative analysis of three randomised controlled trials. Lancet 2020; 396: 121-8.
5. Imig JD, Cervenka L, Neckar J. Epoxylipids and soluble epoxide hydrolase in heart diseases. Biochem Pharmacol 2022; 195: 114866.
6. Fan F, Roman RJ. Effect of cytochrome P450 metabolites of arachidonic acid in nephrology. J Am Soc Nephrol 2017; 28: 2845-55.
7. Lai J, Chen C. The role of epoxyeicosatrienoic acids in cardiac remodeling. Front Physiol 2021; 12: 642470.
516 Arch Med Sci 2, 1st March / 2023
Petr Kala, Tomas Hnat, Karolina Padrova, Karel Kotaška, Josef Veselka
Eicosanoids in human heart failure: pilot study of plasma epoxyeicosatrienoic and dihydroxyeicosatrienoic acid levels
8. Fleming I. The pharmacology of the cytochrome P450 epoxygenase/soluble epoxide hydrolase axis in the vasculature and cardiovascular disease. Pharmacol Rev 2014; 66: 1106-40.
9. Imig JD, Elmarakby A, Nithipatikom K, et al. Development of epoxyeicosatrienoic acid analogs with in vivo anti-hypertensive actions. Front Physiol 2010; 1: 157.
10. Gawrys O, Husková Z, Baranowska I, et al. Combined treatment with epoxyeicosatrienoic acid analog and 20-hydroxyeicosatetraenoic acid antagonist provides substantial hypotensive effect in spontaneously hypertensive rats. J Hypertens 2020; 38: 1802-10.
11. Kala P, Miklovič M, Jíchová Š, et al. Effects of epoxyeicosatrienoic acid-enhancing therapy on the course of congestive heart failure in angiotensin ii-dependent rat hypertension: from mRNA analysis towards functional in vivo evaluation. Biomedicines 2021; 9: 1053.
12. Elmarakby AA. Reno-protective mechanisms of epoxyeicosatrienoic acids in cardiovascular disease. Am J Physiol Regul Integr Comp Physiol 2012; 302: R321-30.
13. Sporková A, Redd RN, Falck JR, et al. Interlobular arteries from 2-kidney, 1-clip goldblatt hypertensive rats’ exhibit-impaired vasodilator response to epoxyeicosatrienoic acids. Am J Med Sci 2016; 351: 513-9.
Arch Med Sci 2, 1st March / 2023 517
Impact of platelet endothelial aggregation receptor 1 genotypes and DNA methylation on platelet reactivity in patients with recurrent ischemic stroke treated
with clopidogrel
1Department of Neurology, Zhuzhou Hospital Afliated to Xiangya Medical College, Central South University, Zhuzhou, Hunan, China
2Department of Hematology, Zhuzhou Hospital Affiliated to Xiangya Medical College, Central South University, Zhuzhou, Hunan, China
Submitted: 4 October 2022, Accepted: 10 January 2023
Online publication: 16 February 2023
Arch Med Sci 2023; 19 (2): 518–522
DOI: https://doi.org/10.5114/aoms/159180
Copyright © 2023 Termedia & Banach
Abstract
Introduction: The aim of this study is to investigate the role of genetic variation and DNA methylation of PEAR1 rs12041331 in high on-treatment platelet reactivity (HPR) and recurrent ischemic stroke (RIS).
Methods: Genotype, methylation, and mRNA of PEAR1 rs12041331 were detected in patients with cerebral ischemia, for the analysis of the effect of PEAR1 rs12041331 on HPR and RIS.
Results: The major G allele of PEAR1 rs12041331 was associated with hypermethylation, which was associated with HPR. This link was not observed for RIS.
Conclusions: The PEAR1 rs12041331 genetic polymorphism and DNA methylation may be among the genetic factors affecting HPR. The correlation between PEAR1 and RIS needs to be studied further.
Key words: DNA methylation, ischemic stroke, platelet aggregation, platelet endothelial aggregation receptor 1.
The 5-year recurrence rate of ischemic stroke (IS) patients is more than 30% in China [1]. Recurrent ischemic stroke (RIS) is associated with a higher risk of mortality and disability. Clopidogrel, an antiplatelet agent that prevents adenosine diphosphate (ADP)-induced platelet aggregation by irreversibly binding to the ADP receptor P2Y12 on the platelet membrane, has always been an important secondary prevention strategy for IS. However, many regular clopidogrel users have the same platelet reactivity as non-treated individuals and they cannot avoid blood clots because the platelet aggregation was not inhibited. This phenomenon is called “high on-treatment platelet reactivity (HPR)” [2], which is an independent risk factor for RIS [3].
Platelet endothelial aggregation receptor 1 (PEAR1) is a membrane protein encoded by the PEAR1 gene and is expressed on the surface of platelets and endothelial cells; PEAR1 rs12041331 is one of the most strongly expressed PEAR1 variants at many reported loci. Polymorphism
Corresponding author: Zhen Zhao
Department of Neurology
Zhuzhou Hospital
Affiliated to Xiangya Medical College
Central South University
China
E-mail: hijenny@126.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/).
Jiahui Yang1, Zhengjun Bao1, Guoyu Hu2, Xiaopeng Luo1, Zhen Zhao1
Research letter Neurology
Impact of platelet endothelial aggregation receptor 1 genotypes and DNA methylation on platelet reactivity in patients with recurrent ischemic stroke treated with clopidogrel
of PEAR1 rs12041331 is believed to contribute to HPR in patients with ischemic stroke; however, this is controversial [4, 5]. One potential reason for this divergence may be that only about 12% of HPR occurrences are associated with gene polymorphism [6]. PEAR1 rs12041331 is the first functional CpG-SNP related to platelet function whose regulatory mechanism depends on DNA methylation [7]. The major G allele forming the CpG pair is associated with higher gene expression in platelets in comparison to the minor A allele [7]. We speculate that PEAR1 rs12041331 polymorphisms and DNA methylation are associated with the risk of HPR and recurrent stroke. As far as we know, there is no research focusing on the potential association between PEAR1 DNA methylation and clopidogrel HPR in ischemic stroke patients.
Our study is the first to investigate the relationship between PEAR1 rs12041331, locus-specific DNA methylation, and gene expression alterations in RIS patients, and its possible correlation with clopidogrel HPR.
Methods. A total of 90 patients diagnosed with acute minor ischemic stroke were recruited and sorted into two groups: 46 cases of primary ischemic stroke (PIS group) and 44 cases of RIS. The RIS group consisted of patients either with a history of IS and relapsing or with newly diagnosed IS after onset of the first infarction [8]. Patients did not have hematologic disorders and were not taking any other antiplatelet or anticoagulant drug. All patients were placed on clopidogrel 75 mg once daily for at least 8 days and atorvastatin calcium 20 mg daily after admission.
Evaluation of ADP-triggered platelet aggregation inhibition rate was performed through thromboelastography on the eighth day after admission. The HPR and normal on-treatment platelet reactivity (NPR) were defined using the 5 μmol/l ADP-induced platelet inhibition rate as the criterion (< 50% and ≥ 50%, respectively).
On the eighth day after admission whole blood samples were taken and DNA was extracted from them using a TIANamp Genomic DNA Kit (Tiangen, DP304-03, Beijing) according to the manufacturer’s instructions. The genotype of the PEAR1 rs12041331 polymorphism was confirmed by polymerase chain reaction (PCR) amplification and Sanger sequencing according to the manufacturer’s instructions. Primer 5.0 was used to design primers: PEAR1-F (5′ GAGGAGTGGGACTGAGAAT 3′) and PEAR1-R (5′ GACAGGCAGGGTGTTGAG 3′).
CpG sites were analyzed by pyrosequencing. Bisulfite conversion reaction was performed using an EpiTect Bisulfite Kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. Converted DNA was amplified by PCR using the PyroMark PCR Kit (Qiagen). PCR primers were as
follows: forward: 5′ GTGGGGGGGATTAGAGTT 3′ ; reverse: 5′ AACCCCTAAAAAAATCCCTTCTACTATCTC 3′. The cycling conditions were recommended by the manufacturer. 20 μl of PCR product was pyrosequenced using the PyroMark Gold Q96 Kit and a pyrosequencer (QIAGEN).
Ribonucleic acid (RNA) was extracted from serum samples using miRNeasy Serum/Plasma Kits (QIAGEN, Hilden, Germany, catalog number 217184) according to the manufacturer’s instructions. Quantitative PCR (qPCR) was conducted using the PerfectStart Green qPCR SuperMix in a Light Cycler 480 Gene Scanning system (Roche, Swiss). Primers used were as follows: forward: 5′ CCAGGATGGGAGCTGTAT 3′, and reverse: 5′GGAGCAGTTAGCACCAAAT 3′. Glyceraldehyde-phosphate dehydrogenase (GAPDH) was used as an internal reference (forward: 5′CCTCACAGTTGCCATGTAGA3′, and reverse: 5′TGGTACATGACAAGGTGCG 3′). Real-time PCR reactions were prepared, and the qPCR conditions were according to the manufacturer’s recommendations. Fluorescence intensity was then detected with a melting curve from 60°C to 97°C.
Ethics statement. The studies involving human participants were reviewed and approved by the Ethics Committee of ZhuZhou Central Hospital Affiliated to Central South University Xiangya School of Medicine. The study participants provided their written informed consent to be included in this study.
Statistical analysis. The PEAR1 rs12041331 genotypic distribution was in Hardy-Weinberg equilibrium. Differences in the distributions of demographic characteristics, frequencies of genotypes and levels of DNA methylation mRNA between two independent groups were evaluated using the independent t-test or Mann-Whitney U test (for continuous variables) and the c2 test or Fisher’s exact test (for categorical variables). Statistical analysis was performed using IBM SPSS software (SPSS 23.0 for Windows; IBM, Chicago, IL, USA), and p ≤ 0.05 was considered statistically significant.
Results. Age (p = 0.019) and the proportion of HPR (p = 0.029) were higher in the RIS group. There were no differences between the PIS and RIS groups in other traditional risk factors for AIS, including gender, body mass index (BMI), hypertension, diabetes mellitus, smoking history, high-density lipoprotein cholesterol (HDL-c), and low-density lipoprotein cholesterol (LDL-c) (p > 0.05) (Table I). A significant fraction of HPR (47.8%, p = 0.014) patients were homozygous for the major G allele (GG) of PEAR1 rs12041331; this allele has been related to HPR (p = 0.007) (Table I, Figure 1 A). The PEAR1 DNA methylation level (33.53 ±14.28% vs. 26.11 ±14.53%, p = 0.044) and mRNA
Arch Med Sci 2, 1st March / 2023 519
Table
Values are presented as mean ± SD or number of patients (percentage) as appropriate. P-values represent the statistical difference of each variable by PIS group and RIS group or HPR group and NPR group. SNP – single nucleotide polymorphism, BMI – body mass index, HDL-C – high-density lipoprotein cholesterol, LDL-C – low-density lipoprotein cholesterol, ADP – adenosine diphosphate, HbA1c – glycated hemoglobin, PIS – primary ischemic stroke group, RIS – recurrent ischemic stroke, HPR – high on-treatment platelet reactivity, NPR – normal on-treatment platelet reactivity.
expression (6.28 ±1.11 vs. 5.75 ±1.36, p = 0.046) were significantly higher in the HPR group compared to the NPR group (Figure 1 B). The PEAR1 DNA methylation level was the highest for GG homozygotes, who had significantly higher methylation levels than GA and AA individuals (Figure 1 C).
The PEAR1 mRNA expression was independent of PEAR1 rs12041331 genotype (Figure 1 D) and DNA methylation (r = 0.157, p = 0.139). There was no significant difference when comparing the PEAR1 rs12041331 genotypes, methylation and mRNA levels between the PIS and RIS groups (data not shown). Multivariate logistic regression analysis showed that carriage of the G allele, higher mRNA expression, and RIS are independently associated with a higher risk of HPR (Figure 1 E).
Discussion. In this study we were the first to analyze the PEAR1 rs12041331 genetic polymorphism, DNA methylation, and mRNA expression level and its correlation with HPR in patients with RIS. Our data indicate that the G allele is associated with a higher prevalence of HPR. Li et al. [5] also observed an association between the GG genotype and HPR in patients with IS treated with aspirin. It is worth noting that patients with coronary artery disease carrying the A allele as-
sociated with lower platelet reactivity are at high risk for cardiovascular events [5]. This high risk was also reported in a retrospective study showing that the A allele was more frequent than the G allele in RIS patients [9]. This result contradicts the idea that HPR is linked to a poorer clinical outcome including ischemic stroke. One possible explanation is that the A allele could positively affect the migration of endothelial cells and promote thrombosis [10]. In our study, we did not observe an association between the PEAR1 rs12041331 polymorphism and RIS, although we did find that the G allele is related to HPR linked with RIS. As suggested in two other studies published by Yue et al., PEAR1 rs12041331 AA carriers with stroke are highly sensitive to aspirin therapy [5]. Another study proposed that genetic variations in PEAR1 rs12041331 do not contribute to atherothrombotic risk in stroke patients [11]. Unlike our study, the latter did not involve measurements of platelet reactivity; none of these studies considered DNA methylation and mRNA levels. Nevertheless, scant research has been devoted to the role of PEAR1 on the risk of RIS. Contrary to our study, Du et al. found that the polymorphism at PEAR1 was independently associated with RIS in Chinese patients.
520 Arch Med Sci 2, 1st March / 2023
Jiahui Yang, Zhengjun Bao, Guoyu Hu, Xiaopeng Luo, Zhen Zhao
Characteristics PIS group ( n = 46) RIS group ( n = 44) P - value HPR group ( n = 53) NPR group ( n = 37) P - value Age [years] 61.8 ±11.4 67.2 ±10.0 0.019 64.8 ±10.3 63.9 ±12.0 0.846 Male sex, n (%) 32 (69.6) 32 (72.7) 0.741 32 (69.6) 32 (72.7) 0.741 BMI [kg/m2] 24.6 ±3.0 24.3 ±3.0 0.606 24.6 ±3.1 24.4 ±2.9 0.765 Previous or current Smoker, n (%) 23 (50.0) 15 (34.1) 0.127 16 (34.8) 22 (50.0) 0.144 Diabetes mellitus, n (%) 18 (39.1) 20 (45.5) 0.544 18 (39.1) 20 (45.5) 0.544 Hypertension, n (%) 35 (76.1) 34 (77.3) 0.894 34 (73.9) 35 (79.5) 0.528 HbA1c [g/l] 6.1 (5.6, 7.2) 6.0 (5.5, 7.9) 0.997 6.0 (5.6, 7.7) 6.1 (5.5, 7.7) 0.707 LDL-C [mmol/l] 2.81 (2.17, 3.38) 2.51 (2.04, 3.15) 0.199 2.81 (2.11, 3.22) 2.49 (2.05, 3.25) 0.483 HDL-C [mmol/l] 1.03 (0.85, 1.22) 0.98 (0.84, 1.20) 0.809 0.98 (0.86, 1.21) 1.05 (0.83, 1.22) 0.774 HPR, n (%) 22 (47.8) 31 (70.5) 0.029 ADP-induced platelet inhibition rate (%) 45.5 (28.9, 63.1) 34.0 (16.6, 56.5) 0.071 22.7 (16.5, 41.2) 61.4 (37.5, 81.2) < 0.001 PEAR1 rs12041331 genotypes, n (%): GG 15 (32.6%) 14 (31.8%) 0.247 22 (41.5%) 7 (18.9%) 0.014 GA 20 (43.5%) 25 (56.8%) 26 (49.1%) 19 (51.4%) AA 11 (23.9%) 5 (11.4%) 5 (9.4%) 11 (29.7%) Allele, n (%): G 50 (54.3) 53 (60.2) 0.425 44 (66.0) 38 (44.6) 0.007 A 42 (45.7) 35 (39.8) 27 (44.0) 50 (55.4)
I. Baseline characteristics of patients within the different groups
Impact of platelet endothelial aggregation receptor 1 genotypes and DNA methylation on platelet reactivity in patients with recurrent ischemic stroke treated with clopidogrel
Figure 1. A – A higher proportion of HPR patients were homozygous for the major G allele (GG) of PEAR1 rs12041331 (p = 0.014). The difference in genotype between the RIS and PIS groups was not statistically significant (p = 0.247).
B – The PEAR1 DNA methylation level (p = 0.044) and mRNA expression (p = 0.046) were higher in the HPR group compared to the NPR group. C – The PEAR1 DNA methylation level is highest for GG homozygotes, who had significantly higher methylation levels than GA and AA individuals (p < 0.001). D – The mRNA expression was independent of PEAR1 rs12041331 genotype. E – Forest plot of associations between HPR and common conditions
Arch Med Sci 2, 1st March / 2023 521 OR (95% CI) P-value Hypertension 1.355 (0.415–4.431) 0.615 (References: No) Diabetes 0.383 (0.136–1.074) 0.068 (References: No) Recurrence of IS 3.876 (1.352–11.109) 0.012 (RIs vs. PIS) PEAR1 genotypes 8.140 (1.840–26.013) 0.006 (CG + GA vs. AA) PEAR1 mRNA 2.010 (1.212–3.335) 0.007 expression 100 80 60 40 20 0 80 60 40 20 0 10 8 6 4 2 0 60 40 20 0 8 6 4 2 0 % The methylation level of PEAR1rs12041331 (%) The mRNA level of PEAR1rs12041331 The methylation level of PEAR1rs12041331 (%) The mRNA level of PEAR1rs12041331 A C E D B PIS group RIS group HPR group NPR group AA GA GG GG (n = 29) GA (n = 45) AA (n = 16) GG (n = 29) GA (n = 45) AA (n = 16) NPR group (n = 37) HPR group (n = 53)
ns ns 0 2 4 6 8 10 12 14 16 18 20 22 24 26 Odds ratio (OR)
Therefore, we speculate that the antiplatelet effect is influenced not only by the mutation of PEAR1, but also by DNA methylation [12].
Consistent with our findings, a study showed that a low methylation level was significantly associated with the minor A allele [7]. However, inconsistent with an vitro experiment showing greater platelet expression of the PEAR1 protein in relation to the G allele of the PEAR1 rs12041331 [13], no direct correlation was found between the G allele, hypermethylation and mRNA levels in our study. One likely reason for this inconsistency is the complex genetic regulation of gene expression by other loci or epigenetic regulatory mechanisms. Despite this, we speculate that there is a correlation between methylation and mRNA levels of PEAR1 because the hypermethylation and high mRNA levels are both associated with HPR in our results. However, this hypothesis differs from the generally accepted theory that gene expression is negatively associated with DNA methylation. To explain this phenomenon, Izzi et al. proposed that the methylation level of PEAR1 is positively correlated with its expression during the early stages of cell differentiation [14]. Regrettably, no association between RIS, genotype and methylation of PEAR1 was observed in our study, possibly because RIS is often caused by multiple factors, and a single genetic factor may not be sufficient to detect the risk associated with RIS.
Our study has some limitations such as an insufficient sample size and the fact that we studied only one locus (PEAR1 rs12041331). Further studies should focus on protein levels as well. In conclusion, carriers of the G allele of PEAR1 rs12041331 and promoter hypermethylation may also have increased HPR risk. However, the association between PEAR 1 rs12041331 and RIS has not been proved.
Acknowledgments
This work was supported by the Hunan Provincial Natural Science Joint Fund Project (2017JJ4066) and a research grant from the Hunan Provincial Health Commission (No. B2017158).
The authors thank AiMi Academic Services (www.aimieditor.com) for English language editing and review services.
Conflict of interest
The authors declare no confict of interest.
References
1. Wang Y, Xu J, Zhao X, et al. Association of hypertension with stroke recurrence depends on ischemic stroke subtype. Stroke 2013; 44: 1232-7.
2. Zhao X, Ma S, Kang Y, et al. Antiplatelet effect, safety, and pharmacokinetics of vicagrel in patients with coronary artery disease undergoing percutaneous coronary intervention. Eur Heart J Cardiovasc Pharmacother 2022; 8: 806-14.
3. Rao Z, Zheng H, Wang F, et al. The association between high on-treatment platelet reactivity and early recurrence of ischemic events after minor stroke or TIA. Neurol Res 2017; 39: 719-26.
4. Peng LL, Zhao YQ, Zhou ZY, et al. Associations of MDR1, TBXA2R, PLA2G7, and PEAR1 genetic polymorphisms with the platelet activity in Chinese ischemic stroke patients receiving aspirin therapy. Acta Pharmacol Sin 2016; 37: 1442-8.
5. Li Z, Jiang H, Ding Y, et al. Platelet endothelial aggregation receptor 1 polymorphism is associated with functional outcome in small-artery occlusion stroke patients treated with aspirin. Front Cardiovasc Med 2021; 8: 664012.
6. Shuldiner AR, O’Connell JR, Bliden KP, et al. Association of cytochrome P450 2C19 genotype with the antiplatelet effect and clinical efficacy of clopidogrel therapy. JAMA 2009; 302: 849-57.
7. Izzi B, Pistoni M, Cludts K, et al. Allele-specific DNA methylation reinforces PEAR1 enhancer activity. Blood 2016; 128: 1003-12.
8. Samsa GP, Bian J, Lipscomb J, et al. Epidemiology of recurrent cerebral infarction: a medicare claims-based comparison of first and recurrent strokes on 2-year survival and cost. Stroke 1999; 30: 338-49.
9. Zhao J, Chen F, Lu L, et al. Effect of 106PEAR1 and 168PTGS1 genetic polymorphisms on recurrent ischemic stroke in Chinese patient. Medicine 2019; 98: e16457.
10. Fisch AS, Yerges-Armstrong LM, Backman JD, et al. Genetic variation in the platelet endothelial aggregation receptor 1 gene results in endothelial dysfunction. PLoS One 2015; 10: e138795.
11. Zhang XG, Gu JY, Fu QQ, et al. Impact of platelet endothelial aggregation receptor-1 genotypes on long-term cerebrovascular outcomes in patients with minor stroke or transient ischemic attack. Front Neurol 2021; 12: 649056.
12. Izzi B, Noro F, Cludts K, et al. Cell-specific PEAR1 methylation studies reveal a locus that coordinates expression of multiple genes. Int J Mol Sci 2018; 19: 1069.
13. Faraday N, Yanek LR, Yang XP, et al. Identification of a specific intronic PEAR1 gene variant associated with greater platelet aggregability and protein expression. Blood 2011; 118: 3367-75.
14. Izzi B, Gianfagna F, Yang WY, et al. Variation of PEAR1 DNA methylation influences platelet and leukocyte function. Clin Epigenetics 2019; 11: 151.
522 Arch Med Sci 2, 1st March / 2023
Jiahui Yang, Zhengjun Bao, Guoyu Hu, Xiaopeng Luo, Zhen Zhao
Determining the current prevalence of b-thalassemia variants in Jordan
Diya Hasan1, Ahmad Al Tibi2, George Burghel3, Amid Abdelnour2
1Al Balqa Applied University, Allied Medical Sciences, Jordan
2Biolab Diagnostic Laboratories, Amman, Jordan
3Manchester University NHS Foundation Trust, Manchester Centre for Genomics Medicine, Manchester, UK
Submitted: 12 January 2023; Accepted: 10 February 2023
Online publication: 10 March 2023
Arch Med Sci 2023; 19 (2): 523–527
DOI: https://doi.org/10.5114/aoms/161096
Copyright © 2023 Termedia & Banach
Abstract
Introduction: This study aimed to define and update the prevalence of b -pathogenic thalassemia variants in Jordan.
Methods: A total of 158 patients with suspected b -thalassemia minor were examined using CBC and Hb-electrophoresis, and polymerase chain reaction with hybridization to identify the type of pathogenic variants.
Results: Five common and seven rare b -thalassemia pathogenic variants were identified in this study, in addition to three variants that had not been previously reported: -101 [C>T], IVS 1.130 [G>C], and codon 44 [-C].
Conclusions: The results provide a new update on the existing Jordanian b -thalassemia variant database that will aid the enhancement of diagnostic and treatment protocols for patients.
Key words: hemoglobinopathies, b -thalassemia, pathogenic variants, hemoglobin.
b-thalassemia is a common hereditary disorder, especially in the Middle East [1], and is the most common hemoglobinopathy in Jordan with a carrier rate of approximately 2–4% [2]. Clinical classifications often focus on disease severity, and cases fall into one of three broad categories: b-thalassemia minor, b-thalassemia intermedia, and b-thalassemia major [3].
More than 300 different pathogenic variants affecting diverse levels of b-globin gene expression and b-thalassemia have been discovered [4]. However, these variants are not spread uniformly; they have geographical and racial origins, as each is distinguished by a few common variants and a varying number of unusual variants [5].
The carrier prevalence rate of thalassemia in Jordan is currently reported as around 2–4%. The number of registered cases treated by the Ministry of Health (MOH) is 656 patients (550 with b-thalassemia major and 106 with b-thalassemia intermedia). The number of patients in the four thalassemia treatment centers overseen by the MOH was 1228 according to the national registry in 2017, representing 86% of the total of 1450 thalassemia patients in the Hashemite Kingdom of Jordan [2]. Therefore, we aimed to investigate and update the prevalence of b-thalassemia variants in Jordan and compare it with other studies in Jordan and neighboring countries.
Corresponding author: Diya Hasan PhD Al Balqa Applied University Allied Medical Sciences
Jordan
E-mail: diyahasan@bau. edu.jo
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Research letter Hematology
Diya Hasan, Ahmad Al Tibi, George Burghel, Amid Abdelnour
Methods. Patient cohort. The study population consisted of 158 individuals, 82 females aged 1 to 74 years with mean age of 22.39 ±16.46 and 76 males aged 1 to 80 years with mean age of 20.55 ±18.27. Amman had the highest share of b-thalassemia patients with 65.8%, followed by Irbid at 14.5%, Zarqa at 8.9%, and Ma’an at 2.5%, while Mafraq and Tafilah had 1.9% each; Aqaba, Jarash, and Madaba had 1.3% each; and Balqa had 0.6%.
The current study received ethical approval from the ethical committee and institutional review board (IRB) of Al-Balqa Applied University in Amman, Jordan (IRB number: 26/3/2/274). Informed consent was obtained in all cases.
Methods. Patients underwent hematological testing, including CBC, Hb electrophoresis, and genetic testing, to screen for b-thalassemia. Vacutainer blood samples (4 ml) containing ethylenediaminetetraacetic acid K3 (EDTA) anticoagulant (Becton Dickinson, Franklin Lakes, NJ, USA) were drawn from the patients for routine hematological investigations, including complete blood count (CBC) using Sysmex XN-1000 (Sysmex Corporation, Kobe, Japan) and Hb electrophoresis using MINICAP (Sebia, Lisses, France). DNA was subsequently extracted from the blood samples using an automated nucleic acid extraction instrument, EZ1 (Qiagen, Hilden, Germany). A dsDNA high-sensitivity assay kit was used to measure the DNA concentration in ng/μl using the QuBit 4 fluorometer, following the manufacturer’s instructions (Thermo Fisher Scientific, USA).
The isolated DNA was amplified by multiplex PCR (Veriti Thermal 96-Well Thermal Cycler Applied Biosystems, USA) using commercial b-globin strip assay, allowing the multiplication of 22 targets of b-globin and detection using reverse hybridization (Vienna Lab Labor diagnostika GmbH, Austria). The extrapolation of the results from the membrane strip was performed using StripAssay Online Calculator v2.17. Samples were processed at the hematology and genetics departments of Biolab Diagnostic Laboratories, Amman, Jordan.
Statistical analysis. Complete data analyses were performed using Microsoft Excel (Redmond, WA, US, 365) and GraphPad Prism 9 (San Diego, USA, version 9.0.0) software.
Results. The study population was screened for 16 b-thalassemia variants, all of which were found to be b-thalassemia carriers (heterozygous mutants). No homozygous or compound heterozygous variants were identified in this study. The distribution of variants is classified by common and rare variants [6]. Sixteen different b-thalassemia variants have been reported. Five of them were represented in about 65.82% of the total Jordanian thalassemic variants and were classified
as common variants: IVS 1.6 [T>C] (17.72%), IVS 1.110 [G>A] (13.29%), IVS 2.1 [G>A] (13.29%), IVS 1.1 [G>A] (11.39%), and IVS 2.745 [C>G] (10.13%). Another eleven variants were classified as rare variants and represented about 25.93% of the total Jordanian thalassemic variants and include codon 8 [-AA] (5.06%), codon 5 [-CT] (4.43%), codon 39 [C>T] (4.43%), IVS 1.5 [G>C] (3.16%), -30 [T>A] (2.53%), -87 [C>G] (1.9%) and equal frequencies for these variants: codon 6 [-A], IVS 1.130 [G>C], codon 44 [-C], IVS 2.848 [C>A] with 0.63%, -101 [C>T] with -87 [C>G] 1.9% for both. In addition, these three variants have not been previously reported in Jordan: -101 [C>T], IVS 1.130 [G>C], and codon 44 [-C]. The different thalassemia mutations observed in Jordan are listed in Table I.
The percentage of b-thalassemia variants in our study differed from those provided in previously published studies in the Jordanian population and neighboring countries. Table II shows the distribution of the variants in previous studies compared with that in the current study and indicates that the common and rare variants are still in the same category but at different percentages, which means that the prevalence of b-thalassemia variants should be updated regularly to reflect the dominant variant in the current population in order to understand the community distribution for these variants. In addition, it shows the comparison of this study with other studies conducted in neighboring countries and indicates that these common variants are rare in other countries and vice versa, which means that every population has a unique distribution of variants depending on their proximity or distance from each other and the social relations between them.
Discussion. Few studies have been conducted on the prevalence and distribution of b-thalassemia in Jordan. Three common variants were observed during the molecular characterization of b-thalassemia in northern Jordan: IVS 1.110 [G>A], IVS 2.1 [G>A], and IVS 2.745 [C>G], in 54% of total samples. This study demonstrated the diversity of b-thalassemia alleles in North Jordan and is in line with the outcomes of the current study, in which three variants were classified as common at different percentages [7]. The common frequent alleles in Jordan are generally similar to those found in other studies in Jordan [8, 9]. If supported by future research, these findings can provide updated data on the spectrum of b-thalassemia variants in Jordan, making the study valuable and reference-worthy [10].
The types and frequencies of the common b-thalassemia variants in Jordan are generally similar to those reported in surrounding countries and have more differences from those reported in the Arabian Peninsula. Additionally, there is a dif-
524 Arch Med Sci 2, 1st March / 2023
Determining the current prevalence of b-thalassemia variants in Jordan
Table I. Distribution of b-thalassemia variants (common and rare)
The analysis is presented as the mean percentage of the total number of patients. *ªNever been reported or published in a Jordanian population. HGVS – Human Genome Variation Society [1, 26]. Available at HbVar database: http://globin.bx.psu.edu/hbvar.
ference between variants’ distribution; the IVS 1.5 [G>C] mutation, which is rare in Jordan, Syria, Lebanon, Palestine, Tunisia, Algeria, and Turkey [11], has a much higher frequency in Oman, the United Arab Emirates, Kuwait, and Saudi Arabia and constitutes the most common mutation in Oman as well as in UAE [12]. This difference could be the result of continuous links between the Jordanian population and northeastern Mediterranean countries, as compared to the geographic isolation between the Jordanian population and other Arab countries.
The IVS 1.6 [T>C] variant was found to be the most recurrent in Palestine, accounting for 28.7%,
and 40% in Egypt; IVS 1.1 [G>A] ranked third among the most recurrent b-thalassemia variants in Palestine and Egypt, with 9% and 24%, respectively, which is most likely due to the close relationship between these populations in Jordan [13]. These variants are a rarity in Saudi Arabia, Bahrain, Oman, and Tunisia [12]. In the present study, the most recurrent variant was IVS 1.6 [T>C], and IVS 1.1 [G>A] ranked third among the most recurrent variants of b-thalassemia, consistently with previous findings.
IVS 1.110 [G>A] (13.29%) is ranked as the second most common variant in Jordan, but is the variant most distributed in the countries sur-
Arch Med Sci 2, 1st March / 2023 525
Common variants HGVS Type of variants Phenotype Distribution N % IVS 1.6 [T>C] HBB:c.92+6T>C RNA processing/ Consensus splice sites b ++ Mediterranean 28 17.72 IVS 1.110 [G>A] HBB:c.93-21G>A RNA processing/ Cryptic splice sites b + Mediterranean 21 13.29 IVS 2.1 [G>A] HBB:c.315+1G>A RNA processing/ Splice junction bθ Mediterranean, U.S. Blacks 21 13.29 IVS 1.1 [G>A] HBB:c.92+1G>A RNA processing/ Splice junction bθ Mediterranean 18 11.39 IVS 2.745 [C>G] HBB:c.316-106C>G RNA processing/ Cryptic splice sites b + Mediterranean 16 10.13 Rare variants Codon 8 [-AA] HBB:c.25_26delAA RNA translation/ Frameshift bθ Mediterranean 8 5.06 Codon 5 [-CT] HBB:c.17_18delCT RNA translation/ Frameshift bθ Mediterranean 7 4.43 Codon 39 [C>T] HBB:c.118C>T RNA translation/ Nonsense codons bθ Mediterranean 7 4.43 IVS 1.5 [G>C] HBB:c.92+5G>C RNA processing/ Consensus splice sites b + Asian Indian, SE Asian 5 3.16 -30 [T>A] HBB:c.-80T>A Transcriptional variants/Promoter regulatory elements b + Mediterranean, Bulgarian 4 2.53 -87 [C>G] HBB:c.-137C>G Transcriptional variants/Promoter regulatory elements b ++ Mediterranean 3 1.90 -101 [C>T]*ª HBB:c.-151C>T Transcriptional variants/Promoter regulatory elements b ++ (Silent) Mediterranean 3 1.90 Codon 6 [-A] HBB:c.20delA RNA translation/ Frameshift bθ Mediterranean, U.S. Blacks 1 0.63 IVS 1.130 [G>C]*ª HBB:c.93-1G>C RNA processing/ Splice junction bθ Italian, Japanese, UAE 1 0.63 Codon 44 [-C]*ª HBB:c.135delC RNA translation/ Frameshift bθ Kurdish 1 0.63 IVS 2.848 [C>A] HBB:c.316-3C>A RNA processing/ Consensus splice sites b + UB Blacks, Egyptian, Iranian 1 0.63
Table
Oman
II. Frequency of b -thalassemia alleles in the previous studies in Jordan and 12 Arab populations with Turkey compared with the current study. Saudi Arabia (SA), Turkey (TU), Lebanon (L), United Arab Emirates (UAE), Syria (S), Egypt (E), Palestine (P), Kuwait (K), Bahrein
526 Arch Med Sci 2, 1st March / 2023
Diya Hasan, Ahmad Al Tibi, George Burghel, Amid Abdelnour
(O),
(T), Algeria (A), Iraq (I) Variant Phenotype This study Study 1 [12] Study 2 [13] Study 3 [14] Study 4 [15] S [12] I [24] S. A [22] P [20] L [25] E [21] K [18] UAE [19] B [18] O [18] T [23] A [23] TU [26] IVS 1.6 [T>C] b + 17.72 6.6 8.3 9.9 NP** 5 3.90 1 28.7 15.0 40 7.3 1.5 ––6 3.3 6.6 IVS 1.110 [G>A] b + 13.29 22 25 23 22 21 30.10 13.5 17.6 33.0 48 –1.0 1.5 0.5 12.3 24.7 41.7 IVS 2.1 [G>A] b θ 13.29 19.8 15 6.1 20 9 18.40 17.5 2.9 10.0 7 29 2.8 6.1 3.1 ––7.2 IVS 1.1 [G>A] b θ 11.39 6.6 10 16.9 12 11 7.80 4 9.0 16.0 24 7.3 –3 1 0.9 11.7 8.9 IVS 2.745 [C>G] b + 10.13 12 14.2 7 NP** 3 ––0.3 1.0 8 –––––0.9 8.6 Codon 8 [-AA] b θ 5.06 NP** 0.8 2.6 NP** 8 0.97 ––2.5 1 3 2.2 ––––7.7 Codon 5 [-CT] b θ 4.43 3.3 3.8 5.5 NP** 4 3.90 1 2.5 4.0 1 –2.1 –0.5 1.8 –1.9 Codon 39 [C>T] b θ 4.43 2 4.6 6.7 NP** 17 1.90 7.7 4.6 0.5 4 7.3 2.2 24.2 1 27 27.6 4.6 IVS 1.5 [G>C] b + 3.16 5.5 1.3 2.6 NP** 4 9.70 19.2 1.1 0.5 10 18.8 44.5 –62.4 –0.4 2.2 -30 [T>A] b + 2.53 NP** NP** 2.3 NP** 2 ––2.1 0.5 –––––2.6 0.4 1.0 -87 [C>G] b + 1.90 2 1.3 NP** NP** 1 –0.34 –1.5 3 ––––––1.0 -101 [C>T] *ª b ++ (Silent) 1.90 NP** NP** NP** NP** 2 ––––––0.2 ––––1.1 Codon 6 [-A] b θ 0.63 1 1.3 1.7 NP** –––0.3 –1 ––––10.5 17 –IVS 1.130 [G>C] *ª b θ 0.63 NP** NP** NP** NP** 1 0.97 0.67 ––––––––––Codon 44 [-C] *ª b θ 0.63 NP** NP** NP** NP** 2 4.90 2 –1.0 –1 0.4 4.5 11.1 4.4 –1.3 IVS 2.848 [C>A] b + 0.63 2 1.3 0.6 NP** 1 2.90 –2.5 –9 –0.4 ––0.9 0.4 –*ªIt has never been reported or published in a Jordanian population. **NP –not performed.
(B),
Tunisia
rounding Jordan including Syria, Iraq, Lebanon, Egypt, and Turkey [8, 14]. Its neighboring countries are in agreement with the possible ancient Greek origin of this mutation [11]. Furthermore, the frequency distribution of the IVS 1.110 [G>A] variant is less than 2% in UAE, Bahrain, and Oman [12, 15].
The IVS 2.1 [G>A] variant, which is co-ranked with the IVS 1.110 [G>A] variant (13.29%) as the second most common variant in Jordan, is also the second ranked variant in Iraq, Saudi Arabia, and Bahrain. It is the most common variant in Kuwait with 29% [12]. The lowest frequency was reported in Palestine, the UAE, and Oman [12, 13, 15].
The current study reported three variants that had not been previously reported in Jordan. The first one is -101 [C>T]; this variant was reported in Syria, UAE, and Turkey. IVS 1.130 [G>C] is the second variant and has been reported in Syria, Iraq, and Saudi Arabia. The third variant is codon 44 [-C]; this variant has been reported in Syria, Iraq, Saudi Arabia, Lebanon, Kuwait, UAE, Bahrain, Oman, Tunisia, and Turkey [8, 12, 15].
In conclusion, this study compared the spectrum and distribution of various variants with other studies to determine the current prevalence of b-thalassemia variants in Jordan. The b-thalassemia variants -101 [C>T], IVS 1.130 [G>C], and codon 44 [-C] have never been reported in a Jordanian population.
Acknowledgments
We would like to acknowledge the biomedical scientists at Biolab diagnostic laboratories for supporting this work and the financial support obtained through the Deanship of Scientific Research at Al-Balqa Applied University, Salt, Jordan (grant 44229).
Conflict of interest
The authors declare no conflict of interest.
References
1. Elmezayen AD, Kotb SM, Sadek NA, Abdalla EM. Beta-globin mutations in Egyptian patients with beta-thalassemia. Lab Med 2015; 46: 8-13.
2. Ministry of Health – Jordan. Health & economic burden of b-thalassemia in Jordan for 2019.
3. Vucak J, Turudic D, Milosevic D, et al. Genotype-phenotype correlation of beta-thalassemia in Croatian patients: a specific HBB gene mutations. J Pediatr Hematol Oncol 2018; 40: e77-82.
4. Taher AT, Musallam KM, Cappellini MD. Beta-thalassemias. N Engl J Med 2021; 384: 727-43.
5. Asadov C, Abdulalimov E, Mammadova T, Gafarova S, Guliyeva Y, Aliyeva G. Genotype-phenotype correlations of beta-thalassemia mutations in an Azerbaijani population. Turk J Haematol 2017; 34: 258-63.
6. Khan AM, Al-Sulaiti AM, Younes S, Yassin M, Zayed H. The spectrum of beta-thalassemia mutations in the 22
Determining the current prevalence of b-thalassemia variants in Jordan
Arab countries: a systematic review. Expert Rev Hematol 2021; 14: 109-22.
7. Sadiq MF, Huisman TH. Molecular characterization of beta-thalassemia in north Jordan. Hemoglobin 1994; 18: 325-32.
8. Jarjour RA, Murad H, Moasses F, Al-Achkar W. Molecular update of beta-thalassemia mutations in the Syrian population: identification of rare beta-thalassemia mutations. Hemoglobin 2014; 38: 272-6.
9. Faraon R, Daraghmah M, Samarah F, Srour MA. Molecular characterization of beta-thalassemia intermedia in the West Bank, Palestine. BMC Hematol 2019; 19: 4.
10. Alshorman A, Maghayreh M, Al Shorman A, Lafi M. The impact of mean corpuscular volume in identifying thalassemia trait through the premarital screening program in Northern Jordan. Jordan Med J 2010; 44: 476-80.
11. Sadiq MF, Eigel A, Horst J. Spectrum of beta-thalassemia in Jordan: identification of two novel mutations. Am J Hematol 2001; 68: 16-22.
12. Daar S, Gravell D. Diagnosis of Beta-thalassaemia carriers in the sultanate of oman. Sultan Qaboos Univ Med J 2006; 6: 27-31.
13. Darwish HM, El-Khatib FF, Ayesh S. Spectrum of beta-globin gene mutations among thalassemia patients in the West Bank region of Palestine. Hemoglobin 2005; 29: 119-32.
14. El-Shanshory M, Hagag AA, Shebl SS, et al. Spectrum of beta globin gene mutations in Egyptian children with beta-thalassemia. Mediterr J Hematol Infect Dis 2014; 6: e2014071.
15. Baysal E. Molecular basis of beta-thalassemia in the United Arab Emirates. Hemoglobin 2011; 35: 581-8.
Arch Med Sci 2, 1st March / 2023 527
Should SGLT2 inhibitors be prescribed in all diabetic type 2 patients?
Marco Bernardi1, Luigi Spadafora1, Mattia Galli2, Giuseppe Biondi-Zoccai3,4, Pierre Sabouret5,6
1Department of Clinical, Internal Medicine, Anesthesiology and Cardiovascular Sciences, Sapienza University of Rome, Rome, Italy
2Catholic University of the Sacred Heart, Rome, Italy
3Department of Medical-Surgical Sciences and Biotechnologies, Sapienza University of Rome, Rome, Italy
4Mediterranea Cardiocentro, Naples, Italy
5Heart Institute, 47-83 Boulevard de l’Hôpital, ACTION Study Group-CHU PitiéSalpétrière Paris, France
6Collège National des Cardiologues Français (CNCF), Paris, France
Submitted: 13 November 2022; Accepted: 28 January 2023
Online publication: 3 February 2023
Arch Med Sci 2023; 19 (2): 528–531
DOI: https://doi.org/10.5114/aoms/160006
Copyright © 2023 Termedia & Banach
The sodium-glucose cotransporter 2 inhibitors (SGLT2i) or gliflozins are considered as a major class in the therapeutic strategy of type 2 diabetes mellitus (T2DM) due to their proven efficacy in reducing blood sugar levels and, more importantly, in decreasing major cardiovascular events (MACE) [1].
This new class of drugs has sparked tremendous enthusiasm among the medical community, due to its impressive and unexpected reduction of MACE in heart failure (HF) patients and chronic kidney disease (CKD) patients, diabetic as well as non-diabetic [2, 3]. Thus, SGLT2i have been compared to paradigm-shifting drugs such as Aspirin and penicillin for their major clinical benefits, leading to the question recently posed: “Could flozins be the statins for risk-based primary prevention of heart failure?” [4, 5]. Hence, the question arises spontaneously: should a SGLT2i be prescribed in all T2DM patients?
SGLT2i act on the proximal tubule of kidney and inhibit renal glucose’s reabsorption, increasing glucose and sodium excretion, with an excellent safety profile [6].
In 2015, the first cornerstone randomized controlled trial (RCT) was published: the Empagliflozin, Cardiovascular Outcomes and Mortality in Type 2 Diabetes (EMPA-REG) Trial [2]. In this placebo-controlled trial, 7,020 patients with type 2 diabetes and established cardiovascular disease were randomized to receive either empagliflozin or placebo. Compared to the placebo arm, the SGLT2i arm surprisingly had a lower risk of death from cardiovascular causes (HR = 0.62; 95% CI: 0.49 to 0.77; p < 0.001), hospitalization for heart failure (HHF) (HR = 0.65; 95% CI: 0.50 to 0.85; p = 0.002), and death from any cause (HR = 0.68; 95% CI: 0.57 to 0.82, p < 0.001).
The next randomized study evaluated the impact of dapagliflozin in the Dapagliflozin Effect on Cardiovascular Events–Thrombolysis in Myocardial Infarction (DECLARE-TIMI 58) trial [7]. In this RCT, T2DM patients at risk for atherosclerotic cardiovascular disease or in secondary prevention were randomly assigned to dapagliflozin or placebo. A lower rate of cardiovascular death (HR = 0.83; 95% CI: 0.73 to 0.95; p = 0.005) or HHF
Corresponding author: Pierre Sabouret MD
Cardiology Department
Heart Institute
47-83 Bld de l’hôpital
Pitié-Salpétrière Hospital
Sorbonne University
F-75013 Paris, France
Phone: + 33 4 96 20 62 70 (assistant Missis Bezah)
E-mail: cardiology.sabouret@ gmail.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/). Diabetology Letter to the Editor
(HR = 0.73; 95% CI: 0.61 to 0.88) was reported in the dapagliflozin group, confirming its cardiovascular benefits.
Further positive results with SGLT2i were reported in the CANVAS Program, a combination of two RCTs in which 10,142 participants with T2DM and high cardiovascular risk were randomized to receive canagliflozin or placebo [8]. Canagliflozin was found to reduce the risk of cardiovascular events compared to placebo (HR = 0.86; 95% CI: 0.75 to 0.97; p < 0.001 for noninferiority; p = 0.02 for superiority). Notably, the treated arm revealed a greater risk of amputation, not observed in other trials. Another major RCT evaluating canagliflozin versus placebo was the Canagliflozin and Renal Events in Diabetes with Established Nephropathy Clinical Evaluation (CREDENCE) trial [9]. In this study, canagliflozin reduced the risk of kidney failure and cardiovascular events compared to placebo (HR = 0.70; 95% CI: 0.59 to 0.82; p = 0.00001).
In the same therapeutic class, ertugliflozin was evaluated in the eValuation of ERTugliflozin effIcacy and Safety CardioVascular outcomes trial (VERTIS-CV), which randomized 8,246 patients with type 2 diabetes and atherosclerotic cardiovascular disease to ertugliflozin or placebo [10]. Ertugliflozin was non-inferior to placebo concerning MACE (a composite of death from cardiovascular causes, nonfatal myocardial infarction, or nonfatal stroke) (HR = 0.97; 95.6% CI: 0.85 to 1.11; p < 0.001), but failed to reduce events.
The high level of proofs of clinical benefits of SGLT2i was reinforced by a meta-analysis (MA) of 6 RCTs in patients with T2DM [11]. In this MA, SGLT2i reduced the risk of MACE (HR = 0.90; 95% CI: 0.85-0.95; Q statistic, p = 0.27), mainly driven by a reduction of HHF and cardiovascular mortality. Nevertheless, apparent heterogeneity was observed: empagliflozin was associated with a lower risk of cardiovascular death, canagliflozin with a lower risk for MACE and incidence of kidney disease, whereas dapagliflozin was associated with a reduced risk for HHF, to be interpreted cautiously due to methodological limitations of this MA.
The spectrum of the clinical benefits of gliflozins has become wider since they are equally effective in diabetic and non-diabetic patients, as reported in heart failure patients and in individuals with a chronic kidney disease (CKD) [12–14]. More recently, the EMPEROR Preserved trial and DELIVER trial reported clinical benefits on hard endpoints in patients with heart failure with preserved ejection fraction (HFpEF), leading to the current perspective of the wide use of SGLT2i among the heart failure population, independently of ejection fraction (EF) [15]. Notably, a recent RCT evaluating dapagliflozin and empagliflozin in HF or CKD versus optimal medical therapy (OMT)
Should SGLT2 inhibitors be prescribed in all diabetic type 2 patients?
reported similar efficacy and safety for both drugs, suggesting a class effect [16].
The underlying mechanisms explaining the cardiovascular and renal benefits of SGLT2i remain not entirely elucidated. Hypotheses include a reduction of preload promoted by osmotic diuresis, a decrease of afterload mediated by improved endothelial function and potential inhibition of cardiac fibrosis [17, 18]. Weight loss resulting from glycosuria, improved endothelial function, modulation of inflammation markers and growth factors may also contribute to the cardiovascular benefits [19]. Due to these cumulative benefits, SGLT2i are indicated in T2DM patients with comorbidities, target organ damage and/or in secondary prevention, often in combination with metformin, which still plays a key role in glycaemic control [20]. Notably, particular concern should be given to patients with latent autoimmune diabetes in adults (LADA), where the assumption of SGLT2i is linked with a higher risk of ketoacidosis [21].
Despite these impressive results, there are also preferred indications for the class of the glucagon-like peptide 1 receptor agonists (GLP1-RA), which reduce MACE in T2DM patients with a more pronounced heterogeneity (Figure 1). Indeed, GLP1-RA provide a more potent decrease of glycated haemoglobin and weight loss in indirect comparison with a good safety profile [22, 23]. In this context, a recent meta-analysis tried to enlighten differences among GLP1-RA and SGLT2i in T2DM patients and assessed their efficacy and safety in this population. The effectiveness of both therapeutic classes was similar when compared with OMT, by reducing MACE with comparable effects on myocardial infarction (MI), cardiovascular mortality, and all-cause mortality [24]. Even though SGLT2i provide better nephroprotection and prevention of HHF than GLP1-RA, some uncertainties remain about their indication in all T2DM patients. Firstly, no RCT of SGLT2i versus OMT reported a reduction in acute coronary syndromes (ACS), whereas the LEADER trial demonstrated the efficacy of liraglutide in this field [25]. Furthermore, GLP1-RA reduced ischemic strokes in the REWIND and SUSTAIN-6 studies, whereas only sotagliflozin in the SOLOIST-WHF trial showed a stroke reduction [26–28].
Interestingly, two ongoing trials, DAPA-MI and EMPACT-MI, recruiting 6,400 and 6,500 patients respectively (in the early phase after an acute MI), are providing additional information on the widespread usage of gliflozins. These RCTs are evaluating the ability of dapagliflozin or empagliflozin to decrease the risk of HHF and cardiovascular death compared with placebo in post-myocardial infarction patients with low left ventricular ejection fraction (LVEF) compared to OMT [29, 30].
Arch Med Sci 2, 1st March / 2023 529
Due to the inclusion criteria of these RCTs, questions about the efficacy of gliflozins to reduce ischemic events will remain and require dedicated studies in coronary patients with normal LVEF.
Additionally, evidence suggests that combination therapy with GLP1RA and SGLT2i may improve glycaemic control, weight loss, systolic blood pressure, NAFLD, and renal function. There is therefore a need for further research to refine the combined effects on cardiovascular and renal disease [31, 32].
In conclusion, SGLT2i are a unique story of serendipity [33]. Their wide effects, accidentally discovered, are still changing medical practice and may lower the burden of MACE. Indeed, gliflozins are effective in the following ways: reducing blood sugar, improving outcomes in patients with HFrEF and HFpEF irrespective of T2DM, slowing the development of end-stage kidney disease in patients with chronic kidney disease.
Even though SGLT2i treatment reduces cardiovascular events, its long-term effectiveness is still unknown, particularly in atherosclerosis. In contrast, some GLP1-RA already have proven efficacy in this field, in combination with a more potent decrease in weight and glycated haemoglobin. In this context, the choice of antidiabetic agents in T2DM patients should be tailored to each patient according to all the clinical characteristics in order to apply the most effective strategy. In conclusion, it is crucial to improve the awareness among general practitioners and diabetologists of the high incidence of HF in diabetic patients in order to start SGLT2i therapy earlier.
Conflict of interest
Giuseppe Biondi-Zoccai has consulted for Balmed, Cardionovum, Crannmedical, Eukon, In-
novheart, Guidotti, Meditrial, Microport, Opsens Medical, Replycare, Teleflex, and Terumo. Pierre Sabouret reports consulting fees from Astra Zeneca, BI, BMS, Lilly, Les laboratoires Servier, Novartis, Recordati, Sanofi, Vifor outside the submitted work.
References
1. Zelniker TA, Braunwald E. Mechanisms of cardiorenal effects of sodium-glucose cotransporter 2 inhibitors: JACC state-of-the-art review. J Am Coll Cardiol 2020; 75: 422-34.
2. Zinman B, Wanner C, Lachin JM, et al.; EMPA-REG OUTCOME Investigators. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med 2015; 373: 2117-28.
3. Braunwald E. Gliflozins in the management of cardiovascular disease. N Engl J Med 2022; 386: 2024-34.
4. Braunwald E. SGLT2 inhibitors: the statins of the 21st century. Eur Heart J 2022; 43: 1029-30.
5. Freaney PM, Lloyd-Jones DM, Khan SS. Could flozins be the statins for risk-based primary prevention of heart failure? JAMA Cardiol 2021; 6: 741-2.
6. Clar C, Gill JA, Court R, Waugh N. Systematic review of SGLT2 receptor inhibitors in dual or triple therapy in type 2 diabetes. BMJ Open 2012; 2: e001007.
7. Wiviott SD, Raz I, Bonaca MP, et al.; DECLARE–TIMI 58 Investigators. Dapagliflozin and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2019; 380: 347-57.
8. Neal B, Perkovic V, Mahaffey KW, et al.; CANVAS Program Collaborative Group. Canagliflozin and cardiovascular and renal events in type 2 diabetes. N Engl J Med 2017; 377: 644-57.
9. Perkovic V, Jardine MJ, Neal B, et al.; CREDENCE Trial Investigators. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med 2019; 380: 2295-306.
10. Cannon CP, Pratley R, Dagogo-Jack S, et al.; VERTIS CV Investigators. Cardiovascular outcomes with ertugliflozin in type 2 diabetes. N Engl J Med 2020; 383: 1425-35.
530 Arch Med Sci 2, 1st March / 2023
Marco Bernardi, Luigi Spadafora, Mattia Galli, Giuseppe Biondi-Zoccai, Pierre Sabouret
Weight goal BMI Heart failure Atherothrombotic risk or status Risk of hypoglycemia Renal function Efficacy on HbA1c Patient’s preferences Optimal therapeutic strategy
Figure 1. Criteria which influence a tailored strategy in T2DM patients
11. McGuire DK, Shih WJ, Cosentino F, et al. Association of SGLT2 inhibitors with cardiovascular and kidney outcomes in patients with type 2 diabetes: a meta-analysis. JAMA Cardiol 2021; 6: 148-58.
12. McMurray JJV, Solomon SD, Inzucchi SE, et al.; DAPA-HF Trial Committees and Investigators. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med 2019; 381: 1995-2008.
13. Packer M, Anker SD, Butler J, et al.; EMPEROR-Reduced Trial Investigators. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med 2020; 383: 1413-24.
14. McDonagh TA, Metra M, Adamo M, et al.; ESC Scientific Document Group. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J 2021; 42: 3599-726.
15. Anker SD, Butler J, Filippatos G, et al.; EMPEROR-Preserved Trial Investigators. Empagliflozin in heart failure with a preserved ejection fraction. N Engl J Med 2021; 385: 1451-61.
16. Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al.; DAPA-CKD Trial Committees and Investigators. Dapagliflozin in patients with chronic kidney disease. N Engl J Med 2020; 383: 1436-46.
17. Kalra S. Sodium-glucose cotransporter 2 (SGLT2) inhibitors and cardiovascular disease: a systematic review. Cardiol Ther 2016; 5: 161-8.
18. Lee TM, Chang NC, Lin SZ. Dapagliflozin, a selective SGLT2 Inhibitor, attenuated cardiac fibrosis by regulating the macrophage polarization via STAT3 signaling in infarcted rat hearts. Free Radic Biol Med 2017; 104: 298-310.
19. van Bommel EJ, Muskiet MH, Tonneijck L, Kramer MH, Nieuwdorp M, van Raalte DH. SGLT2 inhibition in the diabetic kidney-from mechanisms to clinical outcome. Clin J Am Soc Nephrol 2017; 12: 700-10.
20. Cosentino F, Grant PJ, Aboyans V, et al.; ESC Scientific Document Group. 2019 ESC Guidelines on diabetes, pre-diabetes, and cardiovascular diseases developed in collaboration with the EASD. Eur Heart J 2020; 41: 255-323.
21. Clark A, Mohammed AS, Raut A, Moore S, Houlden R, Awad S. Prevalence and clinical characteristics of adults presenting with sodium-glucose cotransporter-2 inhibitor-associated diabetic ketoacidosis at a Canadian Academic Tertiary Care Hospital. Can J Diabetes 2021; 45: 214-9.
22. Marso SP, Bain SC, Consoli A, et al.; SUSTAIN-6 Investigators. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016; 375: 1834-44.
23. Marso SP, Daniels GH, Brown-Frandsen K, et al.; LEADER Steering Committee; LEADER Trial Investigators. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016; 375: 311-22.
24. Sabouret P, Bocchino PP, Angelini F, et al. Comparing benefits from sodium-glucose cotransporter-2 inhibitors and glucagon-like peptide-1 receptor agonists in randomized clinical trials: a network meta-analysis. Minerva Cardiol Angiol 2022 Feb 23. doi: 10.23736/ S2724-5683.22.05900-2.
25. Marso SP, Daniels GH, Brown-Frandsen K, et al.; LEADER Steering Committee; LEADER Trial Investigators. Liraglutide and cardiovascular outcomes in type 2 diabetes. N Engl J Med 2016; 375: 311-22.
26. Gerstein HC, Colhoun HM, Dagenais GR, et al.; REWIND Investigators. Dulaglutide and cardiovascular out-
Should SGLT2 inhibitors be prescribed in all diabetic type 2 patients?
comes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet 2019; 394: 121-30.
27. Marso SP, Bain SC, Consoli A, et al.; SUSTAIN-6 Investigators. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med 2016; 375: 1834-44.
28. Bhatt DL, Szarek M, Steg PG, et al.; SOLOIST-WHF Trial Investigators. Sotagliflozin in patients with diabetes and recent worsening heart failure. N Engl J Med 2021; 384: 117-28.
29. DAPA-MI: ClinicalTrials.gov Identifier: NCT04564742.
30. EMPACT-MI: ClinicalTrials.gov Identifier: NCT04509674.
31. Brown E, Heerspink HJL, Cuthbertson DJ, Wilding JPH. SGLT2 inhibitors and GLP-1 receptor agonists: established and emerging indications. Lancet 2021; 398: 262-76.
32. Frías JP, Guja C, Hardy E, et al. Exenatide once weekly plus dapagliflozin once daily versus exenatide or dapagliflozin alone in patients with type 2 diabetes inadequately controlled with metformin monotherapy (DURATION-8): a 28 week, multicentre, double-blind, phase 3, randomised controlled trial. Lancet Diabetes Endocrinol 2016; 4: 1004-16.
33. Rosano G, Iacoviello M, Filardi PP. Serendipity of sodium-glucose co-transporter 2 inhibitors: a new paradigm in the management of heart failure with reduced ejection fraction. G Ital Cardiol 2021; 22: 277-83.
Arch Med Sci 2, 1st March / 2023 531
Involvement of anterior chest structures accompanied with chest pain in patients with gout
Gang Wang1, Ying Luo2, Bihui Li2, Zhenhua Wen1, Jie Li2
1Department of Rheumatology and Immunology, Zhuzhou Hospital Affiliated to Xiangya Medical College, Central South University, Zhuzhou, Hunan, China
2Department of Nephrology, Zhuzhou Hospital Affiliated to Xiangya Medical College, Central South University, Zhuzhou, Hunan, China
Submitted: 17 December 2022; Accepted: 28 January 2023
Online publication: 22 February 2023
Arch Med Sci 2023; 19 (2): 532–535
DOI: https://doi.org/10.5114/aoms/160005
Copyright © 2023 Termedia & Banach
Gout is a rheumatic disease caused by the deposition of monosodium urate crystals. Studies have shown that monosodium urate crystals are more likely to be deposited in areas with relatively low temperatures and pH, so gout nodules are mostly found in the olecranon bursa, peroneal tendon, Achilles tendon, the helix of the ear, peripheral joints, especially the first metatarsophalangeal joint, and some rare sites of gout such as the spine, nose, eyes, and heart have also been reported [1]. Anterior chest pain is common in the population and its causes usually include heart disease, muscle strain, rib fracture, pneumothorax, costochondritis, intercostal neuralgia, lobar pneumonia, aortic dissection, malignancy of the lungs, reflux esophagitis, and autoimmune diseases. However, anterior chest pain caused by gout has rarely been reported and is very easily overlooked. There is no summary in this regard. The purpose of this article is to analyze the clinical features of gout presenting as anterior chest pain, a rare entity, using a database of published literature and to suggest a comprehensive clinical and diagnostic evaluation of patients with joint pain and swelling.
We conducted a systematic literature review in PubMed up to and including October 1, 2022. We used a combination of the following terms: “sternoclavicular joint”, “sternum-clavicle joint”, “manubriosternal joint”, “sternocostal joint, “rib”, “costal cartilage”, “costochondral”, “sternum”, “sternal”, “manubrium”, “clavicle”, “xiphoid process”, “gout”, and “gouty arthritis” and excluded articles for which the full text was not available and the lesion was not located in the anterior chest wall region. Articles involving the acromioclavicular joint that does not present as anterior chest pain and subcutaneous gout are also excluded. The literature search yielded 26 articles after eliminating duplicates. After screening the titles and abstracts and the references of the included papers, eight articles were found to be relevant. The eligible articles included 8 case reports [2–9]. A total of 8 patients were identified, with a male/female ratio of 7/1 and a mean age of 52 years (range: 44–61), with a median age of 52 years (Table I). Seven patients had peripheral joint gout or risk factors for monosodium urate crystal deposits such as hyperuricemia, poorly controlled type 2 diabetes, obesity, alcohol intake, overweight, renal insufficiency, and cardiovascular disease before being diagnosed with gout presenting with anterior chest pain. Only 1 patient had no risk factors or family history and later presented with a painful, increasing bony mass in the sternal notch that resembled a malig-
Corresponding author: Jie Li
Department of Nephrology
Zhuzhou Hospital
Affiliated to Xiangya Medical College
Central South University
Zhuzhou, Hunan
412007, China
E-mail: lijiecsu2021@163.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/).
Rheumatology Letter to the Editor
Table I. General clinical characteristics of 8 patients with gout presenting with anterior chest pain
Febuxostat; colchicine; diclofenac
Heart disease
10.1 (reference range 2.6–7.0) mg/dl
Dual-energy CT
Involvement of anterior chest structures accompanied with chest pain in patients with gout
joints
Anterior chest pain
Gout; hyperuricemia
No
Costal cartilage
M/44
Mass excision
Malignancy
/
Mass excision biopsy
A painful and increasing bony mass in the sternal notch
No
/
Sternoclavicular joint
F/52
NSAIDs; febuxostat; corticosteroids; anakinra
Neoplasia
Recovered 3 [4]
Normal limit (263 mmol/l)
Dual-energy CT
Widespread pain, especially at the chest level; fever; night sweats
Chronic gouty arthritis; type 2 diabetes; lumbosacral radicular syndrome; obesity
Yes
M/50 Sternoclavicular joint
Antibiotic therapy; colchicine
/
8 mg/dl
Joint fluid aspiration analysis reveals monosodium urate crystals
Arthralgia; fever
Recovered 4
Gouty arthritis; alcoholism
Yes
M/54 Sternoclavicular joint
Prednisone; colchicine; allopurinol
Infection
8.6 mg/dl
CT-guided core biopsy
Pleuritic chest pain; fever
Gout; viral cardiomyopathy; heart transplantation
Yes
Recovered 5 [6]
First costochondral junction
M/49
Prednisone; NSAIDs; allopurinol
/
9.1 mg/dl
Joint fluid aspiration analysis reveals monosodium urate crystals
Intense, acute, anterior thoracic pain located on the sternum
Gout; alcohol intake
Recovered 6 [7]
Yes
M/52 Manubriosternal joint
Recovered
/
Osteomyelitis; malignancy
Slightly elevated
Tissue biopsy
A progressive tumor over the left sternoclavicular joint.
Carcinoma of the tongue
Recovered 7 [8]
Colchicine
Ischemic heart disease
9.6 mg/dl
Arthrocentesis and polarizing microscopy
Tenderness and mild swelling over the upper sternum
Type 2 diabetes; hypertension; renal insufficiency
Yes
No
M/61 Sternoclavicular joint
Recovered 8 [9]
M/54 Manubriosternal joint
F –female, M –male, NSAIDs –non-steroidal anti-inflammatory drugs.
Arch Med Sci 2, 1st March / 2023 533
No. Sex/
Medical
Clinical manifestations Confirmation
Uric acid level Differential diagnosis Treatment Prognosis 1 [2]
age Site Gout in peripheral
history/ risk factors
examinations
Recovered 2 [3]
[5]
Gang Wang, Ying Luo, Bihui Li, Zhenhua Wen, Jie Li
nant tumor [3]. Of all the sites of gout attacks, the sternoclavicular joint was the most common (n = 4), the others being the costal cartilage (n = 2) and manubriosternal joint (n = 2). Almost all patients presented with anterior chest pain accompanied by localized joint swelling, and in some patients with pain that mimicked myocardial infarction and pleurisy [2, 6]. In addition, some patients presented with night sweats, fever, and other symptoms similar to sternal tuberculosis and infection [4–6]. The main tools for confirming the diagnosis include joint aspiration for polarizing microscopy, mass excision biopsy, and dual-energy CT (DECT). The vast majority of patients had abnormal serum uric acid levels. The differential diagnosis of this disease mainly includes malignant tumors, acute chest pain, costochondral chest wall syndrome, and pyogenic arthritis. Pharmacological treatment included NSAIDs, steroid hormones, allopurinol, febuxostat, colchicine, antibiotics, and the IL-1 receptor antagonist anakinra. In the articles that mentioned treatment outcomes, all patients had a good prognosis.
Our study indicates that the mean age of onset of gout mimicking anterior chest pain is older (52 years) and that this disease does not occur in younger populations, which increases the differential range of this disease such as acute myocardial infarction, aortic dissection, etc. In addition, the gender ratio of 7 : 1 in this disease is much higher than the 2 : 1 to 4 : 1 gender ratio in epidemiological studies on gout in European and North American population-based studies, indicating that males are the most prevalent group of this rare entity [10]. In terms of laboratory tests, most patients have abnormal serum uric acid levels, but normal uric acid levels do not exclude gout. Anterior chest pain is the most common clinical characteristic of this rare entity in this article. Gout involving the anterior chest (especially at the joints) can mimic painful disorders of the anterior chest region such as acute myocardial infarction, pulmonary embolism, costochondritis, septic arthritis, neoplastic lesions, and rheumatic diseases (e.g., SAPHO syndrome, rheumatoid arthritis, osteoarthritis, relapsing polychondritis, axial spondyloarthritis, fibromyalgia). Notably, there is a strong link between hyperuricemia, gout and cardiovascular risk. Studies have shown that hyperuricemia and gout negatively impact vascular function by exerting pro-oxidant effects and reducing nitric oxide bioavailability, thereby inducing inflammation and endothelial dysfunction, which may contribute to hypertension, metabolic syndrome and cardiovascular disease [11]. Gout itself is a factor in the acceleration of atherosclerosis and subsequent cardiovascular events, including chest pain [11]. In addition, there may be an overlap between
the articular-skeletal gout manifestation and the “cardiovascular disease presentation: chest pain”, and there are some suggestions for differential diagnosis, including that patients can be investigated for these episodes of chest pain by blood tests (including troponin), electrocardiogram, echocardiography, and chest CT. In the sample summarized in this article, some patients have completely normal tests mentioned above and even no abnormalities were seen at the chest wall and peripheral joints. Synovial fluid of joints showing monosodium urate crystals under polarized light microscopy is the gold standard for the diagnosis of gout [10]. For some atypical sites such as the spine, heart, lungs, and other organs, the biopsy is difficult, but for sites such as sternoclavicular joints, sternocostal joints, etc., tissue biopsy can accurately diagnose gout [12]. Given the high specificity of dual-energy CT for the detection of urate crystals and its advantages of non-invasiveness, reproducibility, and accurate assessment of atypical sites, it is considered a promising clinical screening tool for gout [13]. Treatment is based on drugs that relieve symptoms and lower blood uric acid, including glucocorticoids, colchicine, NSAIDs, and interleukin-1 receptor antagonists if necessary [1]. All patients have a positive prognosis after treatment. This article explores the general basic features of gout mimicking anterior chest pain using a database of published literature and suggests that chest pain can be a rare manifestation of gout and should be considered as one of the “clinical masks” of the disease; however, the cardiovascular causes of the pain should always be considered and may be a co-existing phenomenon. However, the limitation of this article is that 8 cases are not sufficient to elucidate the clinical features of the disease, and publication bias needs to be considered, so there may be more cases in reality. Further research is needed regarding the more detailed clinical characteristics of the rare entity described in this article.
Acknowledgments
We would like to thank the members and staff of the Department of Rheumatology and Immunology of the Zhuzhou Central Hospital who contributed to this manuscript.
Conflict of interest
The authors declare no conflict of interest.
References
1. Dalbeth N, Merriman TR, Stamp LK. Gout. Lancet 2016; 388: 2039-52.
2. Yoshida Y, Harada Y, Shimizu T. Costochondral gout. CMAJ 2022; 194: E845.
534 Arch Med Sci 2, 1st March / 2023
Involvement of anterior chest structures accompanied with chest pain in patients with gout
3. Sahdev N, Smelt J, Avila Z, et al. Tophaceous gout in the sternoclavicular joint. J Surg Case Rep 2020; 2020: rjaa398.
4. Fedeli MM, Vecchi M, Rodoni Cassis P. A Patient with complex gout with an autoinflammatory syndrome and a sternoclavicular joint arthritis as presenting symptoms. Case Rep Rheumatol 2020; 2020: 5026490.
5. Serra S, Monteiro P, Vaz A, et al. Septic arthritis and gout: a case report. Acta Reumatol Port 2012; 37: 70-4.
6. Chang PC, Seeger LL, Motamedi K, et al. Tophaceous gout of the first costochondral junction in a heart transplant patient. Skeletal Radiol 2006; 35: 684-6.
7. Perez-Ruiz F, Calabozo M, Alonso-Ruiz A. Gouty arthritis in the manubriosternal joint. Ann Rheum Dis 1997; 56: 571.
8. Kern A, Schunk K, Thelen M. Gout in the area of the cervical vertebrae and the sternoclavicular joint. RoFo 1999; 170: 515-7.
9. Kernodle GW Jr, Allen NB. Acute gout presenting in the manubriosternal joint. Arthritis Rheum 1986; 29: 570-2.
10. Dalbeth N, Gosling AL, Gaffo A, Abhishek A. Gout. Lancet 2021; 397: 1843-55.
11. Perez-Ruiz F, Becker MA. Inflammation: a possible mechanism for a causative role of hyperuricemia/gout in cardiovascular disease. Curr Med Res Opin 2015; 31 Suppl 2: 9-14.
12. Wang G, Zhuo N, Tian F, et al. Spinal gout with erector spinae muscle entrapment. Rheumatology 2022; 61: e129.
13. Choi HK, Al-Arfaj AM, Eftekhari A, et al. Dual energy computed tomography in tophaceous gout. Ann Rheum Dis 2009; 68: 1609-12.
Arch Med Sci 2, 1st March / 2023 535
Scleroderma renal crisis with posterior reversible encephalopathy syndrome
Gang Wang1, Ying Luo2, Jie Li2, Fangling Yao1, Zhenhua Wen1
1Department of Rheumatology and Immunology, Zhuzhou Hospital Affiliated to Xiangya Medical College, Central South University, Zhuzhou, Hunan, China
2Department of Nephrology, Zhuzhou Hospital Affiliated to Xiangya Medical College, Central South University, Zhuzhou, Hunan, China
Submitted: 13 October 2022; Accepted: 31 October 2022
Online publication: 17 February 2023
Arch Med Sci 2023; 19 (2): 536–538
DOI: https://doi.org/10.5114/aoms/156169
Copyright © 2023 Termedia & Banach
The patient was a 58-year-old female with a thin build who was admitted to the hospital with swollen and hardened skin for 2 years and convulsions with impaired consciousness for 5 h. She had a 2-year history of diffuse cutaneous systemic sclerosis (SSc) with regular hospital review and maintenance treatment with methylprednisolone 8 mg QD. She had no history of hypertension with a baseline blood pressure of 100/75 mm Hg, a baseline creatinine value of 49 μmmol/l, and a body mass index (BMI) of 18.2 kg/m2 before admission. On examination, she presented with transient extremity twitches, normal post-episode extremity muscle strength and tone, and negative bilateral pathological signs; thickened skin on the face and the back of both hands and wrists – sclerodactyly. Laboratory tests showed elevated lactate dehydrogenase (486 IU/l), anemia (HB: 107 g/l), and perfect urine routine suggesting positive urine protein (++) and urine occult blood (+). Blood pressure accelerated to 157/100 mm Hg (new-onset hypertension) over a short period, while serum creatinine rose to 85 μmmo/l (more than a 50%/two-fold increase from baseline). The cranial magnetic resonance imaging (MRI) showed patchy abnormal signal foci in the right frontal lobe, right occipital lobe, and bilateral parietal lobes, and the diagnosis requires consideration of posterior reversible encephalopathy syndrome (Figures 1 A-C). The head computed tomography (CT) revealed no hemorrhage or occupancy, and no other evidence of neurological damage was found, including intracranial infection, cerebrovascular disease, electrolyte balance disorders, craniocerebral trauma, exogenous poisoning, metabolic disease, and hypoglycemia. The initial diagnosis was considered early scleroderma renal crisis with secondary posterior reversible encephalopathy syndrome [1, 2]. The treatment was initiated with an angiotensin-converting enzyme inhibitor (ACEI) against hypertension and methylprednisolone 6 mg QD for the primary condition, supplemented by treatment of seizures to make significant improvements in convulsion symptoms. Serum creatinine decreased to 48 μmol/l on recheck and blood pressure gradually decreased to normal. Repeat cranial MRI showed that the original intracranial patchy abnormal signal foci were absorbed than before (Figures 1 D-F).
Posterior reversible encephalopathy syndrome, a group of rare neuroimaging syndromes with acute or subacute onset, mainly manifested as headache, dizziness, nausea, vomiting, seizure, visual abnormality, consciousness impairment and disturbance of mental behavior [3]. The typical imaging findings of posterior reversible encephalopathy syndrome
Corresponding author: Zhenhua Wen
Department of Rheumatology and Immunology
Zhuzhou Hospital
Affiliated to Xiangya Medical College
Central South University
Zhuzhou Hunan, China
E-mail: zhenhuawen2021@126.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/).
Rheumatology Letter to the Editor
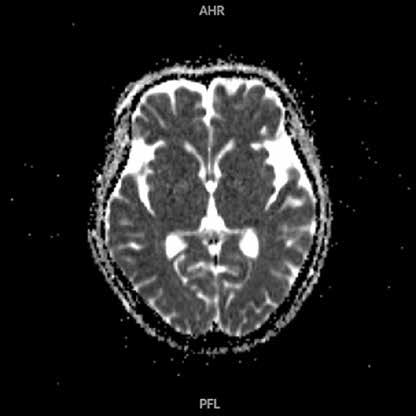
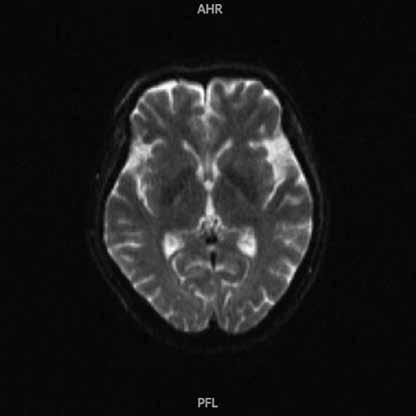
Arch Med Sci 2, 1st March / 2023 537
Scleroderma renal crisis with posterior reversible encephalopathy syndrome
A
Figure 1. A–C – The cranial magnetic resonance imaging showed patchy abnormal signal foci in the right frontal lobe, right occipital lobe, and bilateral parietal lobes. D–F – Repeat cranial magnetic resonance imaging showed that the original intracranial patchy abnormal signal foci were absorbed than before
C E B D F
are reversible and symmetric lesions in white matter of the posterior brain areas. There are no specific diagnostic criteria for posterior reversible encephalopathy syndrome, and in certain clinical situations (especially hypertension, renal disease, immunosuppressive therapy), patients presenting with acute onset neurological symptoms such as headache, visual abnormalities, impaired consciousness and seizures, and with characteristic imaging changes on MRI of the head, should be highly suspicious of posterior reversible encephalopathy syndrome when other possible diseases are excluded [3]. Scleroderma renal crisis is a rare and serious complication of SSc characterized by sudden onset of hypertension and acute kidney injury, manifested by elevated blood pressure, elevated plasma renin levels and progressive rise in serum creatinine, which may be accompanied by headache, malaise, encephalopathy and pulmonary edema, microvascular hemolytic anemia, and thrombocytopenia [4]. The patient had an underlying history of diffuse cutaneous SSc and was on long-term hormone therapy, with a short-term increase in blood pressure from baseline normal to hypertension grade I, accompanied by a more than 50%/two-fold increase in serum creatinine values from baseline, with urinary protein (++) and urinary occult blood (+), and an improvement in blood pressure and serum creatinine from before after treatment with ACEI. Although no renal puncture biopsy was performed, scleroderma renal crisis was a comprehensive diagnosis based on clinical and laboratory findings. Fa’ak reported a 73-year-old female patient with scleroderma who developed posterior reversible encephalopathy syndrome induced by scleroderma renal crisis [5]. Chen described a 36-year-old man with diffuse cutaneous SSc who developed scleroderma renal crisis and acute chronic renal failure, ultimately requiring maintenance hemodialysis [6]. However, the coexistence of these two diseases has rarely been described.
The core mechanism of posterior reversible encephalopathy syndrome due to scleroderma renal crisis may be that the sudden rise in blood pressure breaks the cerebrovascular autoregulation and causes vascular endothelial cell damage, resulting in blood-cerebrospinal fluid barrier disruption, increased vascular permeability and vasogenic edema [7]. Studies have shown that scleroderma renal crisis can occur in 10–15% of patients with SSc, and predisposing factors include diffuse cutaneous SSc with extensive progressive cutaneous involvement and positive anti-RNA polymerase I and III autoantibodies, and long-term hormone use [8]. Hormones can trigger or exacerbate SRC, and it is important to weigh the pros and cons of this strategy. In this case, the patient reduced the
dosage after the onset of the disease. Although SSc involving the peripheral nervous system is common, regardless of creatinine levels, a diagnosis of scleroderma renal crisis should be considered when a patient presents with sudden onset of central nervous system symptoms in the setting of abnormal renal function and rapidly developing hypertension over a short period of time and may be diagnosed with a combination of secondary posterior reversible encephalopathy syndrome in conjunction with characteristic imaging findings.
Acknowledgments
We would like to thank the members and staff of the Department of Rheumatology and Immunology of the Zhuzhou Central Hospital who contributed to this manuscript.
Conflict of interest
The authors declare no conflict of interest.
References
1. Rhew EY, Barr WG. Scleroderma renal crisis: new insights and developments. Curr Rheumatol Rep 2004; 6: 129-36.
2. Chen X, Zhao JG, Gao B, et al. Posterior reversible encephalopathy syndrome with a special focus on seizures. J Clin Neurosci 2022; 95: 38-43.
3. Shankar J, Banfield J. Posterior reversible encephalopathy syndrome: a review. Canad Assoc Radiol J 2017; 68: 147-53.
4. Bose N, Chiesa-Vottero A, Chatterjee S. Scleroderma renal crisis. Semin Arthritis Rheum 2015; 44: 687-94.
5. Fa’ak F, Al-Bahadili H, Shah N, et al. Posterior reversible encephalopathy syndrome induced by scleroderma renal crisis in a patient with undiagnosed scleroderma. J Clin Rheumatol 2021; 27: S825-6.
6. Chen CY, Hung SY, Lee YJ, et al. Delayed onset of posterior reversible encephalopathy syndrome in a case of scleroderma renal crisis with maintenance hemodialysis: case report and literature review. Medicine 2016; 95: e5725.
7. Bartynski WS. Posterior reversible encephalopathy syndrome, part 2: controversies surrounding pathophysiology of vasogenic edema. AJNR Am J Neuroradiol 2008; 29: 1043-9.
8. Mouthon L, Bérezné A, Bussone G, et al. Scleroderma renal crisis: a rare but severe complication of systemic sclerosis. Clin Rev Allergy Immunol 2011; 40: 84-91.
538 Arch Med Sci 2, 1st March / 2023
Gang Wang, Ying Luo, Jie Li, Fangling Yao, Zhenhua Wen
Seronegative rheumatoid arthritis as the first manifestation of multiple myeloma-associated amyloid arthropathy
1Department of Rheumatology and Immunology, The Second Affiliated Hospital of Soochow University, Suzhou, China
2Department of Nephrology, The Second Xiangya Hospital of Central South University, Changsha, Hunan, China
Submitted: 24 January 2023; Accepted: 15 February 2023
Online publication: 24 February 2023
Arch Med Sci 2023; 19 (2): 539–541
DOI: https://doi.org/10.5114/aoms/161285
Copyright © 2023 Termedia & Banach
A 74-year-old man with a history of hypertension presented to the rheumatology department with polyarticular swelling and tenderness, followed by progressive pain in the hip. Physical examination revealed stiffness of the joints of both hands in a fixed position with limited joint motion. Ultrasound of the hand joints showed symmetric synovitis with bone erosion involving the proximal interphalangeal joints, metacarpophalangeal joints, and wrist joints. Subsequent magnetic resonance imaging of the hip revealed a swollen mass of soft tissue around the right hip joint, measuring approximately 16 × 16 × 10 cm, along with severe synovial hyperplasia in both hips (Figure 1 A). Histopathological examination showed massive amyloid deposition and calcification (Figure 1 B, Congo red staining), along with massive synovial cell proliferation and inflammatory cell infiltration (Figure 1 C, Crystal violet staining), and immunohistochemistry showed positivity for λ chains (Figure 1 D). Laboratory tests were negative for rheumatoid factor, anti-citrullinated protein antibody, antinuclear antibodies, ANCA, HLA-B27; hemoglobin was 80 g/l, blood calcium 3.11 mmol/l, serum creatinine 322 μmol/l, serum b2-microglobulin 13943.7 ng/ml, urine protein was 5.85 g/day. Inflammatory indicators showed that erythrocyte sedimentation rate of 60 mm/h and C-reactive protein of 43.2 mg/l.
Serum immunofixation electrophoresis showed that IgG-λ M-type protein accounted for 14.9%, and urine λ light chain concentration of 585 mg/l (κ light chain 23.8 mg/l), and peripheral blood λ free light chain concentration > 1470 mg/l (κ free light chain 182 mg/l). Bone marrow aspiration revealed plasma cells comprising 51% of the cells, and immunophenotyping indicated that these cells were clonal plasma cells. A diagnosis of multiple myeloma (IgG-λ type D-S stage IIIB)-associated amyloid arthropathy (MAA) was made with seronegative rheumatoid arthritis at the first presentation. At the 6-month follow-up, the patient received chemotherapy in the hematology department and experienced a reduction in symptoms.
Approximately 20% of multiple myeloma cases can be associated with immunoglobulin light chain amyloidosis. Of these, 3.7–9.2% of patients have immunoglobulin light chain amyloidosis involving the joints, leading to multiple myeloma-associated amyloid arthropathy [1–4], a rare complication of multiple myeloma with mechanisms relat-
Corresponding author: Zhichun Liu MD
Department of Rheumatology and Immunology
The Second Affiliated Hospital of Soochow University
Suzhou, China
E-mail: zcliurheu@suda.edu.cn
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
Gang Wang1, Ning Zhuo2, Mei Tang1, Leixi Xue1, Zhichun Liu1
Rheumatology Letter to the Editor
ed to light chain amyloid deposition. A systematic review revealed that of 101 patients with amyloid arthropathy associated with multiple myeloma, 63 presented with arthritis prior to the diagnosis of multiple myeloma, 33 of which were initially misdiagnosed as RA [5]. There were 72 cases of polyarthritis, 17 of oligoarthritis, and 3 of monoarthritis. The shoulder joint was most frequently involved, followed by the knees and small hand joints [5]. Multiple myeloma-associated amyloid arthropathy mainly presents as symmetrical rheumatoid factor-negative nonerosive symmetric polyarthritis and is easily confused with rheumatoid arthritis [6]. Studies have shown that multiple myeloma-associated amyloid arthropathy usually has a relatively bland synovitis, with a few presenting with massive synovial inflammation. It is helpful to distinguish RA from multiple myeloma-associated amyloid arthropathy in synovial
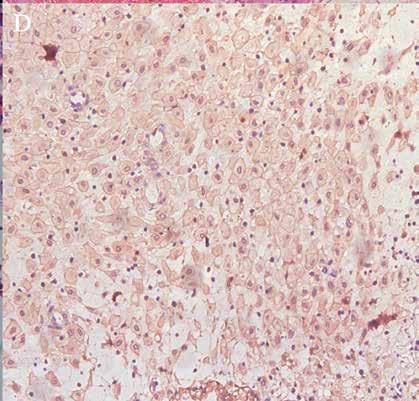
biopsies, for example, by finding synovial plasma cells, which are a common feature of RA. The absence of plasma cells in synovial biopsies should raise a suspicion of multiple myeloma-associated amyloid arthropathy [5]. Previous studies have shown that multiple myeloma and amyloid bone lesions can be complicated in patients with seropositive rheumatoid arthritis [7]. This case was seronegative rheumatoid arthritis and met the diagnostic criteria for rheumatoid arthritis [8]. More importantly, this case brings to light the fact that rheumatoid arthritis can be the first presentation in patients with multiple myeloma-associated amyloid arthropathy, which has not been previously described in the literature, and highlights the diagnostic value of magnetic resonance imaging, histopathology, and immunofixation electrophoresis in the field of rheumatology. Future studies are necessary to investigate the variability of clinical
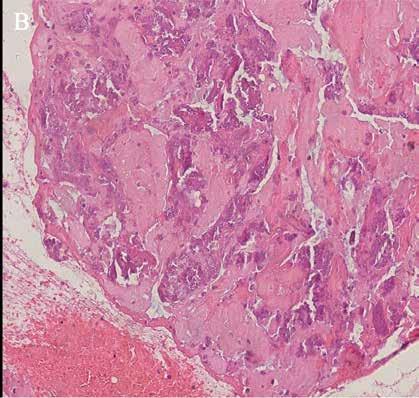
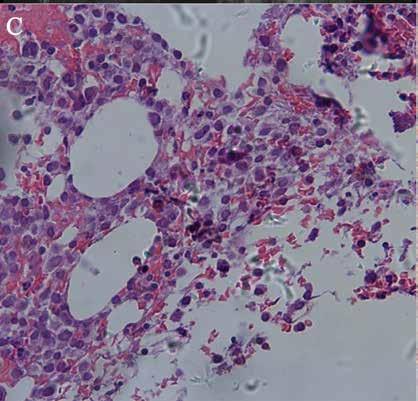
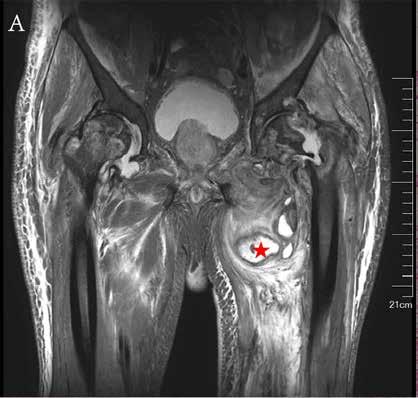
540 Arch Med Sci 2, 1st March / 2023
Gang Wang, Ning Zhuo, Mei Tang, Leixi Xue, Zhichun Liu
A
B D
Figure 1. A – Magnetic resonance imaging of the hip revealed a swollen mass of soft tissue around the right hip joint, measuring approximately 16 × 16 × 10 cm, along with severe synovial hyperplasia in both hips. Histopathological examination showed massive amyloid deposition and calcification (B, Congo red staining), along with massive synovial cell proliferation and inflammatory cell infiltration (C, Crystal violet staining), and immunohistochemistry showed positivity for λ chains (D)
C
Seronegative rheumatoid arthritis as the first manifestation of multiple myeloma-associated amyloid arthropathy
features between multiple myeloma-associated amyloid arthropathy with seronegative or seropositive rheumatoid arthritis and multiple myeloma-associated amyloid arthropathy with or without combined rheumatoid arthritis.
Acknowledgments
We would like to thank the members and staff of the Department of Rheumatology and Immunology of the Second Affiliated Hospital of Soochow University who contributed to this manuscript. This manuscript was supported by the Jiangsu Provincial Health Key Research and Development Project (ZD2022032).
Conflict of interest
The authors declare no conflict of interest.
References
1. Goldberg A, Brodsky I, Mccarty D. Multiple myeloma with paramyloidosis presenting as rheumatoid disease. Am J Med 1964; 37: 653-8.
2. Gordon DA, Pruzanski W, Ogryzlo MA, et al. Amyloid arthritis simulating rheumatoid disease in five patients with multiple myeloma. Am J Med 1973; 55: 142-54.
3. Alpay N, Artim-Esen B, Kamali S, et al. Amyloid arthropathy mimicking seronegative rheumatoid arthritis in multiple myeloma: case reports and review of the literature. Amyloid 2009; 16: 226-31.
4. He C, Ge XP, Zhang XH, et al. Multiple myeloma presenting with amyloid arthropathy as the first manifestation: two case reports. World J Clin Cases 2022; 10: 13028-37.
5. Elsaman AM, Radwan AR, Akmatov MK, et al. Amyloid arthropathy associated with multiple myeloma: a systematic analysis of 101 reported cases. Semin Arthritis Rheum 2013; 43: 405-12.
6. Fujishima M, Komatsuda A, Imai H, et al. Amyloid arthropathy resembling seronegative rheumatoid arthritis in a patient with IgD-kappa multiple myeloma. Intern Med 2003; 42: 121-4.
7. Fam AG, Lewis AJ, Cowan DH. Multiple myeloma and amyloid bone lesions complicating rheumatoid arthritis. J Rheum 1981; 8: 845-50.
8. Arnett FC, Edworthy SM, Bloch DA, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 1988; 31: 315-24.
Arch Med Sci 2, 1st March / 2023 541
Hypertrophic osteoarthropathy
Gang Wang, Mei Tang, Leixi Xue, Zhichun Liu
Department of Rheumatology and Immunology, The Second Affiliated Hospital of Soochow University, Suzhou, China
Submitted: 8 December 2022; Accepted: 26 December 2022
Online publication: 17 February 2023
Arch Med Sci 2023; 19 (2): 542–543
DOI: https://doi.org/10.5114/aoms/158560
Copyright © 2023 Termedia & Banach
A 51-year-old man presented to the rheumatology department with 30 years of progressive bilateral enlargement of the palms, forearms, and ankles and 10 years of limited knee motion. He had a previous history of diabetes mellitus and no family history of similar symptoms. On examination, finger and toe clubbing were observed (Figure 1 A). Restricted knee motion was observed on palpation, and enlargement of the forearms and lower legs was also observed. There was no hyperhidrosis or skin thickening. Radiographs of the forearm, knee and lower leg showed increased periosteal bone formation (Figures 1 B, C). Serum laboratory tests including thyroid function tests and echocardiogram were normal. Whole-body positron emission tomography-computed tomography showed osteophytes at multiple sites throughout the body showing increased FDG uptake changes (Figure 1 D). 99mTc-MDP bone scintigraphy was performed, which showed diffusely symmetrical increased tracer uptake in the large joint areas of the extremities, suggesting hypertrophic osteoarthropathy (Figure 1 E) [1]. The patient was diagnosed with hypertrophic osteoarthropathy, characterized by periosteal bone proliferation, clubbing, hyperhidrosis and facial skin thickening, in the absence of systemic disease. The patient was initially treated with nonsteroidal anti-inflammatory drugs for 1 week and an intra-articular injection of sodium hyaluronate into the knee. Subsequent follow-up was followed for symptom resolution.
Hypertrophic osteoarthropathy is a syndrome clinically characterized by abnormal skin and periosteal proliferation of the distal extremities [2]. Most cases of this disease are associated with neoplastic disease, most commonly lung cancer, while primary hypertrophic osteoarthropathy is a rare autosomal recessive inherited multisystemic disease [2]. The pathogenesis of the disease involves increased circulation to distal peripheries and the release of growth factors, leading to an increase in osteoblast activity and fibroblasts, which leads to a clinical triad of digital clubbing, usually distal and symmetrically distributed osteochondritis and arthritis [3, 4]. Treatment options for this disease include NSAIDs, bisphosphonates, and octreotide, which can be effective in treating bone pain [5]. In addition, trunk vagotomy has shown relief in refractory patients [6], and in some cases, aspiration of knee fluid and intra-articular injections for pain have been found to be effective.
Acknowledgments
This manuscript was supported by the Jiangsu Provincial Health Key Research and Development Project (ZD2022032).
Corresponding author: Zhichun Liu
Department of Rheumatology and Immunology
Second Affiliated Hospital of Soochow University
Suzhou, China
E-mail: zcliurheu@suda.edu.cn
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Letter to the Editor
Rheumatology
We would like to thank the members and staff of the Department of Rheumatology and Immunology of the Second Affiliated Hospital of Soochow University who contributed to this manuscript.
Conflict of interest
The authors declare no conflict of interest.
References
1. Martínez-Lavín M. Hypertrophic osteoarthropathy. Best Pract Res Clin Rheumatol 2020; 34: 101507.
2. Pineda C, Martínez-Lavín M. Hypertrophic osteoarthropathy: what a rheumatologist should know about this uncommon condition. Rheum Dis Clin N Am 2013; 39: 383-400.




3. Yao Q, Altman RD, Brahn E. Periostitis and hypertrophic pulmonary osteoarthropathy: report of 2 cases and
review of the literature. Semin Arthritis Rheumatism 2009; 38: 458-66.
4. Treasure T. Hypertrophic pulmonary osteoarthropathy and the vagus nerve: an historical note. J Royal Soc Med 2006; 99: 388-90.

5. Nguyen S, Hojjati M. Review of current therapies for secondary hypertrophic pulmonary osteoarthropathy. Clin Rheumatol 2011; 30: 7-13.
6. Ooi A, Saad RA, Moorjani N, et al. Effective symptomatic relief of hypertrophic pulmonary osteoarthropathy by video-assisted thoracic surgery truncal vagotomy. Ann Thorac Surg 2007; 83: 684-5.
Arch Med Sci 2, 1st March / 2023 543
Hypertrophic osteoarthropathy
A C D B E
Figure 1. A – Finger clubbing. B, C – Radiographs of the forearm, knee and lower leg showed increased periosteal bone formation. D – Whole-body positron emission tomography-computed tomography showed increased FDG uptake changes. E – 99mTc-MDP bone scintigraphy showed diffusely symmetrical increased tracer uptake in the large joint areas of the extremities
Mesenteric vasculitis with inferior vena cava thrombosis associated with systemic lupus erythematosus
Gang Wang1, Bihui Li2, Ying Luo2, Jie Li2, Zhenhua Wen1
1Department of Rheumatology and Immunology, Zhuzhou Hospital Affiliated to Xiangya Medical College, Central South University, Zhuzhou, Hunan, China
2Department of Nephrology, Zhuzhou Hospital Affiliated to Xiangya Medical College, Central South University, Zhuzhou, Hunan, China
Submitted: 24 September; Accepted: 24 December 2022
Online publication: 17 February 2023
Arch Med Sci 2023; 19 (2): 544–545
DOI: https://doi.org/10.5114/aoms/158532
Copyright © 2023 Termedia & Banach
A 14-year-old girl presented to our hospital with acute abdominal pain and vomiting for 2 days. A diagnosis of systemic lupus erythematosus (SLE) as well as secondary Evans syndrome, due to a combination of autoimmune haemolytic anaemia and immune thrombocytopaenia, was made at our hospital 6 months ago – a diagnosis predicated on the simultaneous exclusion of sepsis, paroxysmal nocturnal haemoglobinuria, thrombotic thrombocytopaenic purpura, and Kasabach-Merritt syndrome. Her condition improved after treatment with prednisone (60 mg/day) and mycophenolate mofetil (0.75 g/day). No significant family history was present. Physical examination revealed jaundice and periumbilical tenderness with no rebound pain. Laboratory data showed a white blood cell of 9.78 × 109/l (normal range: 4–10), haemoglobin of 132 g/l (normal range: 110–155), platelets of 131 × 109/l (normal range: 100–300), erythrocyte sedimentation rate of 37 mm/h (normal range: 0–15), C-reactive protein of 4.8 mg/l (normal range: 0–10), PCT of 0.17 μg/ml (normal range: 0–0.5), C3 of 0.78 g/l (normal range: 0.9–1.8), and C4 of 0.03 g/l (normal range: 0.1–0.4). The stool culture was negative. Positive for antinuclear antibodies (ANA), direct and indirect Coombs test. There were elevated titres of anti-cardiolipin and anti-b2-glycoprotein-I (b2-GPI) antibodies of IgM and IgG isotypes, along with the presence of lupus anticoagulants. The systemic lupus erythematosus disease activity index (SLEDAI) score was greater than 10. Enhanced abdominal computed tomography showed diffuse intestinal wall thickening, engorgement of mesenteric vessels (Figures 1 A, B), and inferior vena cava thrombosis (Figure 1 C), with no evidence of intestinal infection or tumour. The final diagnosis of lupus mesenteric vasculitis, secondary antiphospholipid syndrome (APS), and inferior vena cava thrombosis was made. Initially, she was given 1 mg/kg of methylprednisolone as the first choice of treatment, but her symptoms did not resolve. Subsequently, methylprednisolone 500 mg/day was given for 3 days and then gradually reduced to 0.5 mg/kg for maintenance, combined with cyclophosphamide 0.6 g to enhance immunosuppression and enoxaparin 4000 U/day for anticoagulation, along with fasting, anti-infection, parenteral nutrition, and other symptomatic supportive treatment. She recovered well and was discharged 2 weeks later with regular follow-up.
Corresponding author: Zhenhua Wen
Department of Rheumatology and Immunology
Zhuzhou Hospital
Affiliated to Xiangya Medical College
Central South University
Zhuzhou Hunan, China
E-mail: zhenhuawen2021@126.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/).
Rheumatology Letter to the Editor
The serological examination of gastrointestinal tract involvement in SLE lacks specific markers, and its clinical manifestations are not specific, especially requiring differentiation from gastrointestinal tract infection, inflammatory bowel disease, pseudo-intestinal obstruction, adverse drug reactions, and other diseases [1]. Abdominal contrast-enhanced CT is helpful for early diagnosis, and the common imaging findings are target sign (thickening and oedema of the intestinal wall) and engorgement of mesenteric vessels. Buck et al. found that the incidence of mesenteric vasculitis was significantly higher in patients with SLEDAI scores above 8 than in those with scores below 8. Therefore, computed tomography is recommended as a routine for the diagnosis of vasculitis in patients with SLEDAI scores above 8 and subacute abdominal pain [2]. The inflammatory mechanism represented by intestinal vasculitis and the intestinal vascular thrombotic mechanisms induced by antiphospholipid antibodies may activate each other and participate in the development of gastrointestinal involvement and inferior vena cava thrombosis in this case of SLE [3]. Studies have shown that b2-GPI inhibits ADP-induced platelet aggregation and activation of coagulation factors and is thought to control thrombus formation [4]. Vein thrombosis in APS occurs mostly in the veins of the extremities and pulmonary system, while obstruction in the portal, mesenteric, and inferior vena cava is rare. The present case is an uncommon example of combined mesenteric vasculitis and inferior vena cava thrombosis associated with APS. Treatment usually requires long-term anticoagulant therapy. In conclusion, lupus mesenteric vasculitis is the most common cause of acute abdominal pain in childhood-onset SLE, and it usually occurs during the active phase of the disease, with the possibility of combined inferior vena cava thrombosis requiring vigilance.

Acknowledgments
We would like to thank the members and staff of the Department of Rheumatology and Immu-
nology of the Zhuzhou Central Hospital who contributed to this manuscript.
Conflict of interest
The authors declare no conflict of interest.
References
1. Trapani S, Rubino C, Simonini G, et al. Gastrointestinal and hepatic involvement in paediatric systemic lupus erythematosus. Clin Exp Rheumatol 2021; 39: 899-906.
2. Buck AC, Serebro LH, Quinet RJ. Subacute abdominal pain requiring hospitalization in a systemic lupus erythematosus patient: a retrospective analysis and review of the literature. Lupus 2001; 10: 491-5.
3. Brewer BN, Kamen DL. Gastrointestinal and hepatic disease in systemic lupus erythematosus. Rheum Dis Clin N Am 2018; 44: 165-75.
4. Ruiz-Irastorza G, Crowther M, Branch W, et al. Antiphospholipid syndrome. Lancet 2010; 376: 1498-509.
Arch Med Sci 2, 1st March / 2023 545
Mesenteric vasculitis with inferior vena cava thrombosis associated with systemic lupus erythematosus
A B C
Figure 1. A, B – Enhanced abdominal computed tomography showed diffuse intestinal wall thickening and engorgement of mesenteric vessels C – Enhanced abdominal computed tomography showed a large thrombus in the inferior vena cava
Dystrophic calcification in the masseter muscle
Agata Walulik1, Monika Rutkowska2, Paweł Gajdzis3, Paulina Czarnecka2
1Student Scientific Circle of Head and Neck Surgery; Otolaryngology, Head and Neck Surgery Clinic, 4th Military Clinical Hospital, Wroclaw, Poland
2Department of Maxillofacial Surgery, Otolaryngology, Head and Neck Surgery Clinic, 4th Military Clinical Hospital, Wroclaw, Poland
3Department of Pathomorphology and Oncological Cytology, Faculty of Medicine, Wroclaw Medical University, Wroclaw, Poland
Submitted: 17 November 2022; Accepted: 14 February 2023
Online publication: 24 February 2023
Arch Med Sci 2023; 19 (2): 546–549
DOI: https://doi.org/10.5114/aoms/161229
Copyright © 2023 Termedia & Banach
Ectopic calcification is a pathological condition resulting from abnormal deposition of salt ions in the soft tissues of the body. There are several types of ectopic calcifications, including calciphylaxis, metastatic calcifications, nodular calcifications, idiopathic calcifications and dystrophic calcifications, the latter type being the subject of this paper [1]. This particular type of biomineral disorder is most often associated with a history of trauma, infection or infestation of the affected area, and it progresses without visible abnormalities in blood calcium levels [2]. In some cases, calcifying lesions may represent a local, non-specific response of unknown origin [3]. Dystrophic calcification can occur in any soft tissue, with the most prevalent location being the vascular and cardiac tissue, particularly often occupying a myocardial or valvular mass [4]. The lesions in head and neck tissues are extremely rare. They are asymptomatic, and the disease is diagnosed incidentally [5]. Based on the literature analysis, the case presented below represents the 6th described dystrophic masseter muscle calcification in the world.
A 12-year-old female patient was admitted to the Clinical Department of Maxillofacial Surgery at the 4th Military Clinical Hospital in Wroclaw for biopsy of the left mandibular angle due to an interstitial lesion of the left masseter muscle, which had been discovered several months earlier. On palpation, lesions were perceptible from external and internal access in the form of two associated nodules, superficially and deeply located in relation to each other. The lesion was non-painful, hard, movable relative to the unchanged skin. Activity and function of nerves V and VII and Stensen’s ducts were bilaterally normal. The ultrasound image revealed two well-demarcated hyperechoic lesions measuring approx. 8 × 6 mm and 4 × 4 mm with an acoustic shadow visible below. The lesion was located within the masseter muscle, slightly forward of the anterior margin of the parotid gland. The image suggested calcification/stone (Figure 1). Orthopanthomogram (OPG) and cone beam computed tomography (CBCT) scan revealed two highly saturated foci within the masseter muscle (Figures 2 and 3). In laboratory tests, no abnormalities in ionic and endocrine metabolism were observed, total calcium was at 2.65 mmol/l. It was decided to have an open biopsy of the nodules. The lesion was removed bluntly after dissection of the masseter muscle with access through the oral vestibule. The removed material was sent for histopathological examination, which described two lesions with diameters of 0.8 cm and 0.6 cm. Cross-sections showed fibrous tissue with
Corresponding author: Paulina Czarnecka MD, PhD
Department of Maxillofacial Surgery
Otolaryngology, Head and Neck Surgery Clinic
4th Military Clinical Hospital
Wroclaw, Poland
Phone: +48 261 660 216
E-mail: paulina.j.czarnecka@ gmail.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
Otolaryngology Letter to the Editor
foci of calcification and central necrosis (Figure 4). After excluding calcium disorders, a diagnosis indicating calcifications of the dystrophic type of the masseter muscle was made.
Based on the available English literature, the case presented here is the first report of dystrophic calcification in the masseter muscle in Central Europe and the second such condition reported in a female patient.
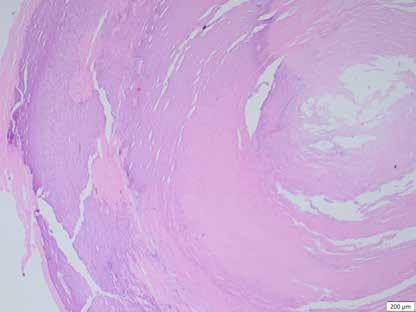
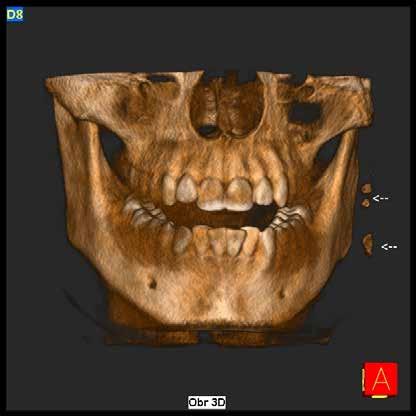

The pathomechanism of dystrophic calcification is characterized by the occurrence of soft tissue damage leading, through a series of phenomena, to the deposition of calcium salts within the tissue, including hydroxyapatite and amorphous calcium phosphate. This process takes place without any noticeable variation in the concentrations of the above elements
blood.
Arch Med Sci 2, 1st March / 2023 547
Dystrophic calcification in the masseter muscle
in the
The dying cells
Figure 1. Ultrasound image of a well-demarcated hyperechoic lesion measuring 4x4 mm within the left masseter muscle (white arrow), MM – masseter muscle, M – mandible
Figure 2. OPG image showing two highly saturated lesions in the left masseter muscle (white arrows)
Figure 3. CBCT image showing two highly saturated lesions located near the left mandibular angle (white arrows)
Figure 4. Cross-section showing fibrous tissue with foci of calcification (left side) around central necrosis (right side)
Agata Walulik, Monika Rutkowska, Paweł Gajdzis, Paulina Czarnecka
within the lesion release phosphorus-binding proteins. High concentrations of calcium and phosphate are released in the mitochondria of cells, thus leading to crystal formation and cell necrosis. This process is further exacerbated by tumor necrosis factor (TNF), interleukin (IL) 6 (IL-6) and IL-1. This condition may be accompanied by chronic inflammation and vascular hypoxia [6].
The medical history of the 12-year-old patient we describe, admitted to the Clinical Department of Maxillofacial Surgery at the 4th Military Clinical Hospital in Wroclaw, did not indicate a history of infection or trauma to the affected area. Analyzing the case we present and the cases published in the literature collected in the table below, it is possible to notice a tendency for dystrophic calcification to appear in an area of soft tissue not covered by previous pathology. Thus, it can be concluded that the dystrophic changes described so far, differ in their nature from textbook features and only Kim et al. when describing the case of a 26-yearold woman, indicated a previous injury to the muscle in the patient’s 4th year of life [3]. However, it should be borne in mind that in many cases, the lack of information about past medical conditions may not reflect the facts of the patient’s history, particularly with regard to early childhood injuries.
In the light of the described case, special attention should be paid to the importance of appropriately selected diagnostics. A number of calcifying lesions can be located within the facial region, such as calcifying lymph nodes, dystrophic calcifications, venous malformations and neoplastic lesions [1]. The first step towards an accurate diagnosis should be to narrow down the range of possible diseases on the basis of imaging studies, supplemented by laboratory tests. The imaging study of choice in pediatric patients should be ultrasound. Due to the lower adipose tissue content in the head and neck region compared to the adult population, there is better tissue penetration by ultrasound in children, allowing for better resolution images to be obtained. The use of Doppler ultrasound also allows the vascularization of the lesion to be assessed. Ultrasound-based diagnostics allows an initial assessment of palpably detected pathology without exposing the patient to high doses of X-rays and without the need for sedation, often required for computed tomography (CT) or magnetic resonance imaging (MRI) scans in children [7]. Pediatric patients show particular sensitivity to the radiation used in CT scans, so it should be performed as an adjunct to ultrasound after assessing the need for expanded diagnostic imaging. It is important to remember the recommended reduction in radiation doses for children [8].
Presented to stomatology in 1998, CBCT has become an extremely helpful imaging test in the
diagnosis of diseases located in the head and neck region [9]. This innovative maxillofacial imaging technique produces accurate, high-resolution images using doses much lower than those used in CT scans [10]. The examination results in a three-dimensional image of the dental structures and bones in the craniofacial region in a single scan, which enables more precise treatment planning. It is important to remember that the correct imaging modality, regardless of the age of the patient, is one that provides as much information as possible about the lesion in the safest way for the individual and as quickly as possible to perform.
Pediatric patients are significantly less likely to develop a malignant neoplastic lesion in the head and neck than the adult patient population [11]. However, this does not preclude the need for a biopsy to accurately assess the palpable soft tissue lesion. Cytological examination of a palpable lesion should be considered the gold standard and be the final step towards an accurate diagnosis. Fine needle aspiration (FNA) biopsy has a number of advantages, including being a quick and inexpensive procedure that does not require hospitalization, with a low risk of complications. For pediatric patients, however, sedation is often required during FNA so an open surgical biopsy may be a much better option here, not only providing material for histopathological examination but also forming a part of the treatment based on removal of the entire lesion.
As a consequence of the particular rarity of dystrophic calcification in head and neck tissues, there is no clear protocol for the treatment of the above condition. Reports of drug treatment include lesions of other regions, including the bladder and skin. In the above cases, it has been reported that smaller lesions respond to warfarin, ceftriaxone while larger lesions show sensitivity to diltiazem, bisphosphonates, probenecid and aluminum hydroxide [6, 12, 13]. Regardless of the size of the lesion, surgical removal of the calcification should also be considered, with factors such as size, location, age and general condition of the patient guiding the final decision. The surgical access to the lesion should be as small and subtle as possible in order to avoid additional potentially lesion causing trauma.
Analyzing the entirety of the presented case, we can undoubtedly state that dystrophic calcification is a discrete condition whose diagnosis relies on the vigilance of the patient or a skillful examining doctor, and in the area we have described – especially the dentist. Although calcification of the masseter muscle is not a serious pathology, it is important that, if a similar lesion is observed, a diagnosis is made as soon as possible to exclude other, more serious lesions. Due to
548 Arch Med Sci 2, 1st March / 2023
the rarity of the condition, there are no long-term observation reports of cases without any surgical or pharmacological interventions. Therefore, it is difficult to determine further development without treatment.
In conclusion, dystrophic calcification of the masseter muscle is a rare lesion of head and neck tissues. Diagnostic success and correct treatment are based on imaging, laboratory blood tests and histopathological examination of the affected tissue.
Conflict of interest
The authors declare no conflict of interest.
References
1. Chislett SP, Liming BJ, Rogers DJ. Dystrophic calcification: a rare pediatric parotid mass. Int J Pediatr Otorhinolaryngol 2016; 81: 38-40.
2. Kim HY, Park JH, Lee JB, Kim SJ. A case of dystrophic calcification in the masseter muscle. Maxillofac Plast Reconstr Surg 2017; 39: 31.
3. Nagaraja A, Kumar NG, Kumar BJ, Naik RM, Sangineedi YJ. A solitary phlebolith in the buccal mucosa: report of a rare entity and clinicopathologic correlation. J Contemp Dent Pract 2016; 17: 706-10.
4. Ananthakrishna R, Moorthy N. Dystrophic myocardial calcification. Indian Heart J 2016; 68 (Suppl 2): S180-1.
5. Gozgec E, Ogul H. Intense soft tissue calcification of the head and neck following tracheostomy. J Craniofac Surg 2021; 32: e145-7.
6. Le C, Bedocs PM. Calcinosis cutis. 2022 Jul 12. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan. PMID: 28846311.
7. Friedman ER, John SD. Imaging of pediatric neck masses. Radiol Clin North Am 2011; 49: 617-32.
8. Levin TL. Pediatric imaging: radiation exposure and how we image. Pediatr Rev 2018; 39: 50-2.
9. Kapila SD, Nervina JM. CBCT in orthodontics: assessment of treatment outcomes and indications for its use. Dentomaxillofac Radiol 2015; 44: 20140282.
10. Li G. Patient radiation dose and protection from conebeam computed tomography. Imaging Sci Dent 2013; 43: 63-9.
11. Liu ES, Bernstein JM, Sculerati N, Wu HC. Fine needle aspiration biopsy of pediatric head and neck masses. Int J Pediatr Otorhinolaryngol 2001; 60: 135-40.
12. Róbert L, Kiss N, Medvecz M, Kuroli E, Sárdy M, Hidvégi B. Epidemiology and treatment of calcinosis cutis: 13 years of experience. Indian J Dermatol 2020; 65: 105-11.
13. Jeon SW, Park YK, Chang SG. Dystrophic calcification and stone formation on the entire bladder neck after potassium-titanyl phosphate laser vaporization for the prostate: a case report. J Korean Med Sci 2009; 24: 741-3.
Dystrophic calcification in the masseter muscle
Arch Med Sci 2, 1st March / 2023 549
Effect of different surgical
1The Second Affiliated Hospital of Xi’an Jiaotong University, Department of Otolaryngology Head and Neck Surgery, Xi’an, China
2The Second Clinical Medical College of Lanzhou University, Lanzhou, China
3The Second Affiliated Hospital of Xi’an Jiaotong University, Nursing Department, Xi’an, China
4The Second Clinical Medical College of Xi’an Jiaotong University, Xi’an, China
Submitted: 30 December 2022; Accepted: 14 February 2023
Online publication: 9 March 2023
Arch Med Sci 2023; 19 (2): 550–554
DOI: https://doi.org/10.5114/aoms/161230
Copyright © 2023 Termedia & Banach
Laryngeal cancer is a more common type of disease in the clinical otolaryngology department, and it is generally treated with surgical resection [1, 2]. Laryngeal cancer is the most common malignant tumors of head and neck in our country. The incidence is about 1.12/100 000 and the standardized death rate is 0.61/100 000 [3, 4]. Surgery for laryngeal cancer requires as much laryngeal function as possible while undergoing removal of the lesion [5]. There are different surgical methods for different stages of laryngeal cancer. The choice of surgical procedure is based on tumor size, location, possible post-operative dysfunction, surgical or radiation physician’s treatment level and experience, occurrence function, quality of life, and treatment outcome [6–8]. For T1-2N0 laryngeal cancer patients, oral laser resection of laryngeal cancer and oral robotic surgery are the most common options. Both of them have the characteristics of little trauma, no incision on the body surface, short hospital stay, low cost, and good functional recovery after surgery [9, 10]. For laryngeal cancer patients with T1-2N1-3/T3N0-3, surgery with or without radiotherapy or radiotherapy with cisplatin is recommended first if the patient can tolerate both surgery and cisplatin. Surgery is preferred for patients who can tolerate surgery but are intolerant to cisplatin. For patients who cannot tolerate surgery and can tolerate cisplatin, radiotherapy with cisplatin chemotherapy is preferred. For patients who cannot tolerate both surgery and cisplatin, radiotherapy alone is preferred [11]. For laryngeal cancer with a locally advanced stage or distant metastasis, an appropriate radiotherapy program can be selected according to lymph node involvement, major vessel involvement, incisal margin status, etc. [12].
In traditional surgical treatment, total larynx resection postoperative patients lose laryngeal function, are prone to swallowing disorders, and poor quality of life [13]. With the continuous development of surgical techniques, the emergence of partial laryngectomy makes it possible to preserve laryngeal function in patients with laryngeal cancer [14]. Partial laryngectomy currently includes horizontal partial laryngectomy and vertical partial laryngectomy. Both surgical methods are ideal in treating laryngeal cancer, and there is no unified clinical standard for which surgi-
Corresponding authors: Hui Yang
Xiaoyong Ren
Department of Otolaryngology Head and Neck Surgery
The Second Affiliated Hospital of Xi’an
Jiaotong University
157, Xiwu Road
710004 Xi’an City
Shanxi Province, China
E-mail: yanghui1866@163.com
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License
(http://creativecommons.org/licenses/by-nc-sa/4.0/).
modalities on swallowingrelated quality of life in patients with glottic laryngeal squamous cell carcinoma: how should we choose?
Na Shao1, Xinyuan Wei2, Yue Zhang3, Huanan Luo1, Yonglong Su4, Lixia Liang1, Boyan Chen1, Na Li1, Xiaoyong Ren1, Hui Yang1
Otolaryngology Letter to the Editor
Effect of different surgical modalities on swallowing-related quality of life in patients with glottic laryngeal squamous cell carcinoma: how should we choose?
cal treatment is taken, and the difference between the two surgical procedures is rarely reported [15]. To further determine the impact of the two surgeries on laryngeal cancer patients, this paper retrospectively analyzes the data of patients treated by the two surgeries in our hospital, analyzes the impact of the two surgeries on the quality of life and swallowing function. It is hoped that this study provides a theoretical basis for the clinical treatment of laryngeal cancer.
General data of 68 patients with glottic laryngeal squamous cell carcinoma admitted to our hospital between January 2020 and December 2021 were also retrospectively included. General information of the selected objects is shown in Table I.
Inclusion criteria: (1) patients with first onset and first surgical treatment; (2) patients with preoperative pathological biopsy suggesting glottic laryngeal squamous cell carcinoma; (3) all patients underwent preoperative imaging examination to determine the primary lesion and the scope of invasion, without distant metastases; and (4) patients with complete clinical data. Exclusion criteria: (1) patients treated with chemoradiotherapy before surgery; (2) patients complicated with other malignancies; (3) patients with congenital laryngeal malformations; (4) patients with a history of laryngeal surgery; and (5) patients participating in other researchers. The prevalence of all subjects is shown in Table I.
According to the patient surgical procedure, only patients with simple vertical partial laryngeal resection or simple partial vertical laryngectomy were included, and 5 partial horizontal vertical laryngectomies and patients with metastases were excluded, and 63 patients were finally included as the study subjects.
The patient was intubated with a low endotracheal tube after local anesthesia. The curved transverse incision was centered on the ring methyl membrane, and the skin and the flap were separated layer by layer, and the white neck line was cut to fully expose the larynx. The annular cartilage cut the ring nail membrane to the vocal cord process and examined the glottis. The split carformate cartilage was detected in the median deviation, and the larynx was explored. After splitting the formoid cartilage, the affected formoid cartilage endoperiosteum should be peeled off, and the upper edge of the ventricular zone should be cut horizontally along the upper edge of the formoid cartilage toward the arytenoid epiglottitis. The upper and lower incision is combined, if necessary, and the arytenoid cartilage can be excised. The glottic defect was repaired in the pyriform fossa mucosa. The anterior residual edge of the lateral ventricular band and the vocal cord and
Table I. General information of the patients
Arch Med Sci 2, 1st March / 2023 551
Variable X±s/ N (%) Sex: Man 64 (94.1) Woman 4 (5.9) Age 61.9 ±9.3 Nation: The Han nationality 65 (95.6) Other 3 (4.4) Degree of education: An illiterate person 11 (16.2) Primary school or junior high school 33 (48.5) High school or technical secondary school 16 (23.5) College or above 8 (11.8) Marital status: Married 62 (91.2) Divorced/widowed 6 (8.8) Occupation: Be on the job/active worker/being employed 6 (8.8) Retired 34 (50.0) Other 28 (41.2) Smoking: Deny 19 (27.9) Yes 40 (58.8) Has quit smoking 9 (13.2) Drinking: Deny 38 (55.9) Yes 23 (33.8) Has quit the wine/drinking 7 (10.3) Tumor stage: Issues/stage 1 and issues/stage 2 58 (85.3) Stage 3 and 4 10 (14.7) T-stage: T1 44 (64.7) T2 14 (20.6) T3/T4 10 (14.7) M: M0 65 (95.6) M1 3 (4.4) N-stage: N0 54 (79.4) N1/ N2 14 (20.6) Type of surgery: Vertical partial laryngectomy 45 (66.2) Horizontal partial laryngectomy 18 (26.5) Horizontal vertical partial laryngectomy 5 (7.4) Pathology type: Malignant (squamous cell carcinoma) 68 (100)
the medial edge of the lateral ribbon muscle with the fascia band, bypassing the anterior counter-suture edge of the formoid cartilage plate, and stretching the anterior and posterior diameter of the throat. A notch at the upper end and the lower end of the thyroid cartilage plate was fixed, the anterior cervical ribbon muscle was strengthened, the drainage skin piece was placed, and the subcutaneous tissue was stitched in the opposite position.
After tracheotomy under local anesthesia, intubation, and general anesthesia, with a horizontal arc incision in the neck, the median lowest point was located in the middle of the parathyroid cartilage, at both ends of the leading edge of the sternocleidomastoid muscle. The latissimus neck flap was isolated and the hyoid and formoid cartilage were exposed. The superior hyoid muscle group on the upper side of the hyoid was cut close to the lesion, and cut in the middle of the hyoid or biased to the healthy side of the hypus on the affected side, which fully exposed the formoid cartilage. The hydromandrium was cut along the upper margin of the thyroid cartilage and dissected down, and the subpharyngeal constrictor attached to the lateral margin of the thyroid cartilage was severed, fully exposing the working thyroid cartilage. The inner periosteum was dissected, the upper half and upper angle of the affected parathyroid cartilage were removed, and the incision was slightly tilted up to avoid injuring the anterior combination. When cutting to the contralateral side, it was gradually tilted from the midline to retain the upper thyroid cartilage angle at the contralateral side. Cut the piriform nest on the affected side, the scissors toward the direction of the tongue will be wrinkled, cut to between the epiglottis and the root of the tongue for the whole layer cut, cut to the countermeasure tongue will be wrinkled. Observe the tumor range and wrinkle into the laryngeal vestibule in the contralateral laryngeal element, cut horizontally along the laryngeal chamber, separate the detection chamber and the vocal cord to the anterior combination, cut horizontally from the anterior to the posterior chamber in the
affected laryngeal chamber, and remove the compartment above the vocal cord process to remove the specimen. When both sides of the arytenoid wrinkle into the laryngeal chamber, damage to the arytenoid cartilage should be avoided. Closing the arytenoid will wrinkle the mucosa and repair the residual medial mucosa and vocal cord margin of the piriform socket. The affected lateral hyoid was removed, the hyoid and formoid cartilage margin were closed with line 4, the hypopharyngeal mucosa was layered with suture, and the ribbon muscle was strengthened. The skin patch was drained, and the skin was sutured.
Total quality and dimension score levels of 2, 4, 12, 24, and 48 weeks, including distress, feeding process, swallowing symptom frequency, food choice, verbal communication, swallowing fear, panic, mental health, social life, fatigue and sleep frequency, and food texture, were observed. The correlation of the total quality of life (QoL) score with each dimension score was analyzed. The swallowing function classification was observed at different time points, and the correlation between swallowing function grade and quality of life was analyzed.
Using SPSS 23.0 statistical software, measurement data were represented as ± s, t-test, count data as percentage, using c2 test, the contrast between multiple groups was detected by repeated measure variance, and p < 0.05 was considered statistically significant.
The swallowing QOL scores varied at different time points (p < 0.001); no significant difference between time and group interaction (p > 0.05) was observed; and the total swallowing QOL score between different groups is significant difference (p < 0.05) (Table II).
Statistical differences occurred at different time points (p < 0.001); no significant difference between time and group interaction was observed (p > 0.05); and distress scores between different groups are significant difference (p < 0.01) (Table III).
In recent years, with the change of people’s lifestyle and eating habits and the aggravation of environmental pollution, the incidence of throat can-
552 Arch Med Sci 2, 1st March / 2023
Na Shao, Xinyuan Wei, Yue Zhang, Huanan Luo, Yonglong Su, Lixia Liang, Boyan Chen, Na Li, Xiaoyong Ren, Hui Yang
Variable Vertical half throat Horizontal half throat Two weeks after surgery 2083.33 ±1096.05 1536.11 ±690.44 Four weeks after surgery 2586.11 ±979.09 1948.61 ±585.39 Twelve weeks after surgery 3290.00 ±702.66 2851.67 ±781.90 Twenty-four weeks after surgery 3843.89 ±481.21 3280.59 ±1059.13 Forty-eight weeks after surgery 3833.50 ±1398.72 3457.00 ±1462.58 FTime dye time, p 50.689, < 0.001 FBetween groups of endometrium, p 5.832, 0.019 FIntergroup of time electrode, p 0.324, 0.861
Table II. Comparison of the two surgical swallowing-related total scores of QoL
Effect of different surgical modalities on swallowing-related quality of life in patients with glottic laryngeal squamous cell carcinoma: how should we choose?
cer has increased year by year. Clinical treatment of laryngeal cancer is mainly to improve the local control rate, preoperative evaluation of tumor scope, intraoperative protection of the cricoarytenoid joint, and postoperative swallowing function [6, 7]. At present, clinical partial laryngectomy is used to treat laryngeal cancer patients and good results are achieved [8, 9]. With the early detection of laryngeal cancer, the strengthening of the comprehensive treatment concept and the progress of repair and reconstruction means, laryngeal cancer surgery emphasizes the preservation of the laryngeal function as much as possible to improve the quality of life of patients [10, 11]. Therefore, how to choose surgical methods to improve the postoperative quality of life of patients has become the focus of clinical attention [12].
This paper retrospectively analyzes the clinical data of patients with glottic laryngeal squamous cell carcinoma in our hospital, compares the postoperative quality of life of patients with partial and horizontal laryngectomy, the results of two kinds of patients are better/different at different time points than patients at different time points, suggesting that the postoperative quality of life of patients treated by vertical partial resection is better. The comparison of the scores of the other dimensions of the quality of life also showed that the vertical hemithroat patients were significantly better than those of the other dimensions. The swallowing function of both surgical patients was also graded later, and the results showed that the swallowing function grade was also significantly different between the two groups. This was because the partial horizontal laryngectomy was performed above the level of the vocal cord, the complete removal of the supraglottic structure, the normal movement of the lateral arytenoid cartilage, and the vocal cord was retained intact [1]. However, with the loss of laryngeal vestibular structure, the protective function of the larynx was completely compensated by the glottis closure, and the chance of vocal cord mucosal impact was increased, resulting in mucosal thickening and affecting the swallowing function and quality of life
[3]. However, vertical laryngeal partial resection can retain the normal swallowing and occurrence of the function to the greatest extent, due to the more preserved tissue, the postoperative swallowing function and quality of life of patients are not affected [13]. When observing the relationship between swallowing function grade and QOL, it was found that the two groups of surgical patients were mostly negatively correlated with the total score of quality of life, indicating that the higher the QOL score, the lower the swallowing function grade, and the better the swallowing function. This paper compares the quality of life and swallowing function in the patients of the two different surgical methods, and thus provides a basis for the clinical treatment of laryngeal cancer. This will provide more reference for the selection of laryngeal cancer surgery.
However, this paper still has some limitations:
(1) Small sample size. Only 63 patients were included in this study; (2) The comparison between primary outcome indicators and secondary outcome indicators is not clear so it is difficult to draw an accurate and complete clinical conclusion; (3) The evaluation system is relatively simple, and more authoritative and comprehensive scales can be further adopted to evaluate it in the follow-up process. The next step will be a multicenter large-sample control study to further verify the accuracy of the results.
In conclusion, vertical partial laryngectomy for patients with glottic laryngeal squamous cell carcinoma is helpful to improve the postoperative quality of life and significantly improve the swallowing function, which is worthy of clinical application and promotion.
Acknowledgments
I would like to thank my hospital and department for its support and help.
Conflict of interest
The authors declare no conflict of interest.
Arch Med Sci 2, 1st March / 2023 553
Variable Vertical half throat Horizontal half throat Two weeks after surgery 71.13 ±66.84 32.81 ±33.81 Four weeks after surgery 84.38 ±62.45 54.69 ±49.34 Twelve weeks after surgery 129.38 ±45.95 89.06 ±30.23 Twenty-four weeks after surgery 163.12 ±42.74 140.63 ±34.00 Forty-eight weeks after surgery 188.75 ±19.57 168.75 ±42.33 FTime dye time, p 53.354, < 0.001 FBetween groups of endometrium, p 8.313, 0.006 FIntergroup of time electrode, p 1.244, 0.304
Table III. Comparison of the two types of postoperative distress-related QoL scores
References
1. Steuer CE, El-Deiry M, Parks JR, Higgins KA, Saba NF. An update on larynx cancer. CA Cancer J Clin 2017; 67: 31-50.
2. Hou Y, Yang X, Miao S, Qu G, Meng H. Interactive regulation of laryngeal cancer and neuroscience. Biochim Biophys Acta Rev Cancer 2021; 1876: 188580.
3. Obid R, Redlich M, Tomeh C. The treatment of laryngeal cancer. Oral Maxillofac Surg Clin North Am 2019; 31: 1-11.
4. Hajmohammadi E, Molaei T, Mowlaei SH, et al. Sonodynamic therapy and common head and neck cancers: in vitro and in vivo studies. Eur Rev Med Pharmacol Sci 2021; 25: 5113-21.
5. Zenga J, Goldsmith T, Bunting G, Deschler DG. Rehabilitation of speech and swallowing after total laryngectomy. Oral Oncol 2018; 86: 38-47.
6. Cox SR, Daniel CL. Racial and ethnic disparities in laryngeal cancer care. J Racial Ethn Health Disparities 2022; 9: 800-11.
7. Kolator M, Kolator P, Zatoński T. Assessment of quality of life in patients with laryngeal cancer: a review of articles. Adv Clin Exp Med 2018; 27: 711-5.
8. Hrelec C. Management of laryngeal dysplasia and early invasive cancer. Curr Treat Options Oncol 2021; 22: 90.
9. Topaloğlu İ, Bal M, Salturk Z, Berkiten G, Atar Y. Analysis of vocal and swallowing functions after horizontal glottectomy. Ear Nose Throat J 2016; 95: E8-13.
10. Ferlito A, Silver CE, Howard DJ, Laccourreye O, Rinaldo A, Owen R. The role of partial laryngeal resection in current management of laryngeal cancer: a collective review. Acta Otolaryngol 2000; 120: 456-65.
11. Ellington TD, Henley SJ, Senkomago V, et al. Trends in incidence of cancers of the oral cavity and pharynxUnited States 2007-2016. MMWR Morb Mortal Wkly Rep 2020; 69: 433-8.
12. Machiels JP, René Leemans C, Golusinski W, Grau C, Licitra L, Gregoire V. Squamous cell carcinoma of the oral cavity, larynx, oropharynx and hypopharynx: EHNS-ESMO-ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol 2020; 31: 1462-75.
13. Luo C, Lv K, Liu Q, et al. Comparison of laser microsurgery and open partial laryngectomy for T1-2 laryngeal cancer treatment. Ann Transl Med 2021; 9: 464.
14. Mosaddad SA, Beigi K, Doroodizadeh T, et al. Therapeutic applications of herbal/synthetic/bio-drug in oral cancer: an update. Eur J Pharmacol 2021; 890: 173657.
15. Werner J, Scaglioni MF, Ko SS, Rajan GP. Preservation of laryngeal function through reconstruction of the supraglottis and thyrohyoid membrane with a chimeric anterolateral thigh flap after supraglottic laryngectomy: a case report and literature review. Microsurgery 2021; 41: 462-7.
554 Arch Med Sci 2, 1st March / 2023
Na Shao, Xinyuan Wei, Yue Zhang, Huanan Luo, Yonglong Su, Lixia Liang, Boyan Chen, Na Li, Xiaoyong Ren, Hui Yang
Arch Med Sci 2023; 19 (2): 555
DOI: https://doi.org/10.5114/aoms/162278
Retracted: Antiproliferative and apoptotic activity of glycyrrhizinic acid in MCF-7 human breast cancer cells and evaluation of its effect on cell cycle, cell migration and m-TOR/PI3K/Akt signalling pathway
Zhen Zhang, Yun Feng, Zhen-Yu Li, Xiao-Zhong Cao
Departments of General Surgery, Luoyang Central Hospital Affiliated to Zhengzhou University, Luoyang, Henan, China
Arch Med Sci 2019; 15, 1: 174–182
DOI: https://doi.org/10.5114/aoms.2018.79429
Online publication: 8 November 2018
PMCID: PMC6348358, PMID: 30697268
This article has been withdraw because of scientific misconduct regarding used in articles images.
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/). Retraction notice
Arch Med Sci 2023; 19 (2): 556
DOI: https://doi.org/10.5114/aoms/162281
Retracted:
and PI3K/Akt signaling pathway
Department of Pediatrics, Nanfang Hospital, Southern Medical University, Guangzhou, Guangdong, China
Arch Med Sci 2019; 15 (6): 1530–1538
DOI: https://doi.org/10.5114/aoms.2019.81729
Online publication: 30 January 2019
PMCID: PMC6855158, PMID: 31749882
This article has been withdraw because of scientific misconduct regarding used in articles images.
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/).
Antitumor and apoptotic effects of 5-methoxypsoralen in U87MG human glioma cells and its effect on cell cycle, autophagy
Retraction notice
Haixia Guo, Yuelin He, Chaoke Bu, Zhiyong Peng
Arch Med Sci 2023; 19 (2): 557
DOI: https://doi.org/10.5114/aoms/162282
Retracted: MicroRNA-1179 regulates proliferation and chemosensitivity of human ovarian cancer cells by targeting the PTEN-mediated PI3K/AKT signaling pathway
1Department of Oncology, Gong’an County People’s Hospital, Gong’an County, Hubei Province, China
2Department of Radiology, Gong’an County People’s Hospital, Gong’an County, Hubei Province, China
Arch Med Sci 2020; 16 (4): 907–914
DOI: https://doi.org/10.5114/aoms.2019.86798
Online publication: 22 July 2019
PMCID: PMC7286340, PMID: 32542094
This article has been withdraw because of scientific misconduct regarding used in articles images.
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/).
Retraction notice
Zhang Zhihong1, Chen Rubin2, Lu Liping2, Mao Anpeng1, Guo Hui1, Wu Yanting1, Shan Zhenxiu1
Arch Med Sci 2023; 19 (2): 558
DOI: https://doi.org/10.5114/aoms/162283
1Department of Oncology, Affiliated Hospital of Jining Medical University, Jining, Shandong Province, China
2Communicable Disease Control Division in Qingdao Chengyang District Center for Disease Control and Prevention, Qingdao, Shandong Province, China
3Department of Breast Surgery, Affiliated Hospital of Jining Medical University, Jining, Shandong Province, China
Arch Med Sci 2020; 16 (5): 1158–1165
DOI: https://doi.org/10.5114/aoms.2019.83512
Online publication: 11 March 2019
PMCID: PMC7444711, PMID: 32864005
This article has been withdraw because of scientific misconduct regarding used in articles images.
Creative Commons licenses: This is an Open Access article distributed under the terms of the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International (CC BY -NC -SA 4.0). License (http://creativecommons.org/licenses/by-nc-sa/4.0/).
Retracted: Long non-coding RNA HOTAIR regulates proliferation, migration and invasion of human cervical cancer cells by modulating expression of MAPK1
Retraction notice
Haiying Liu1, Jing Liu2, Guangzhang Zhao3
Instructions for authors
Aims and scope
Archives of Medical Science (AMS) publishes high quality original articles and reviews of recognized scientists that deal with all scientific medicine. Original papers from young scientists are especially welcomed.

AMS opens the possibilities for young, capable scientists. AMS would like to give them a chance to have a publication following matter-of-fact, professional review by outstanding, famous medical scientists. Thanks to that they will have an opportunity to present their study results and/or receive useful advice about the mistakes they have made so far.
The second equally important aim is a presentation of review manuscripts of recognized scientists about the educational capacity, in order that young scientists, often at the beginning of their scientific carrier, could constantly deepen their medical knowledge and be up-to-date with current guidelines and trends in world-wide medicine. The fact that our educational articles are written by world-famous scientists determines their innovation and the highest quality.
Full length articles should not exceed 8 printed pages (4400 words including tables and references – about 20 typewritten double-spaced 8˝” 11’’ sheets). Each article should contain structured abstract (200-250 words), divided such as the text of the manuscript. Subject matter should be organized under suitable headings and subheadings such as: Structured Abstract, Introduction, Materials and Methods, Results, Discussion, Conclusions, Acknowledgments and References. Footnotes should be avoided and their contents incorporated into the text. Manuscripts should be in their final form when submitted.
Reserach Letters and Letters to the Editor should be no more than 1000 words – 3-4 manuscript pages, excluding structured abstract (100 words – only for the Research Letters) references, name(s) and address(es) of the signers. The authors are strongly recommended to prepare the letters with no more than 10-15 references, no more than 2 tables or 1 figure, and no more than 5 authors, all of whom should sign the copyright release form. Keywords and name and mailing address of all authors should be included.
Review articles should follow the format for a regular article, but should be submitted only after consultation with the Editors. Each article should contain unstructured abstract (100-150 words) and up to 5 key words.
Ethical consideration
Papers describing animal experiments can be accepted for publication only if the experiment conforms to the legal requirements in Poland as well as with the European Communities Council Directive of November 24, 1986 or the National Institute of Health Guide (National Institute of Health Publications No. 80-23, Revised 1978) for the care and use of Laboratory Animals for experimental procedure. Authors must provide a full description of their anesthetics and surgical procedures. Papers describing experiments on human subjects must include a statement that experiments were performed with the understanding and consent of each subject, with the approval of the appropriate local ethics committee.
Submission of manuscripts
All manuscripts written in English should be submitted to Editorial Office by electronic Editorial System of Archives of Medical Science at the following URL: http://panel.termedia.pl/?ams (the link to Editorial System is also given on the main web page of the journal).
Tables and figures should be submitted separately; linked files such as images or charts should also be provided. Authors are requested not to submit the manuscripts by post or e-mail.
In of Legal aspects
In sending the manuscript the author(s) confirm(s) that (s)he has (they have) not previously submitted it to another journal (except for abstracts of no more than 250 words) or published it elsewhere. The author(s) also agree(s), if and when the manuscript is accepted for publication, to automatic and free transfer of copyright to the Publisher allowing for the publication and distribution of the material submitted in all available forms and fields of exploitation (Copyright © Termedia & Banach). The author(s) accept(s) that the manuscript will not be published elsewhere in any language without the written consent of the copyright holder, i.e. the Publisher.
All manuscripts submitted should be accompanied by a covering letter including signed confirmation of the above and confirming that this publication has been approved by all co-authors (if any), as well as by the responsible authorities at the institution where the work has been carried out. Generally no more than six authors should be listed (except multicenter studies). All authors must sign the covering letter (available online) and send to Editors with the manuscript. Materials previously published should be accompanied by written consent for reprinting from the relevant Publishers. In the case of photographs of identifiable persons, their written consent should also be provided. Any potential conflict of interest will be dealt with by the local court specific to the Publisher. Legal relations between the Publisher and the author(s) are in accordance with Polish law and with international conventions binding on Poland.
Instructions for authors
Anonymous review
All manuscripts will be subject to a process of anonymous editorial review (the name of authors and their affiliations will be disclosed to the referees only when the review process is complete). In order to achieve this, the first page and the acknowledgements page will be removed from the manuscripts sent to referees. Manuscripts will be sent to independent reviewers, and the information about acceptance should be limited to 4 weeks.
Archives of Medical Science may also consider high quality papers under the Fast Track Review scheme. This scheme relies on a dedicated group of top class reviewers to deliver a final decision on reviewed manuscripts within fourteen days and the possibility of online publishing in next 2 weeks after acceptance. The authors need to indicate that they want to have their paper proceed as a fast-track review during the submission process and additionally inform the Editor about this (m.banach@termedia.pl).
The scheme requires an additional fee to the standard one from authors (all together 1600 Euro).
Preparation of manuscripts
Articles must be written in English, with either British or American spelling used consistently throughout. Authors not entirely familiar with English usage are advised to seek the assistance of an English speaker; correct style is the responsibility of the authors.
• The length of original article should not exceed 20 printed pages including text, illustrations, tables, and references. Short research notes should not exceed 4 printed pages.
• Manuscripts should be typed, double-spaced, and fully corrected. Allow a margin at least 3 cm at the top, bottom and left side of the page. Text should not be justified, but flush left.
• The first page of each paper should indicate: the author’s name, title of the paper, the institute where the work was conducted, complete name and address for correspondence with telephone and fax numbers, and e-mail address if available; running head not exceed 40 characters including space.
• The second page contains the abstract which should be written in an informative style. Avoid generalizations and give essential details of research findings. For indexing purposes, a list of 3–5 key words (according to Index Medicus) in English and not included in the title should be typed below the abstract.
• The textual material of the article should be organized in a standard form with separate: Introduction, Material and Methods, Results, Discussion, Conclusion and References. Review articles should be divided into sections and subsections as appropriate without numbering.
• Do not underline in the text. Avoid footnotes. When essential, they are numbered consecutively and typed at the foot of the appropriate page.
• All dimensions and measurements must be specified in the metric system.
• The source of any drug and special reagent should be identified. Indicate doses and use the international names
• Particular attention needs to be paid to the selection of appropriate analysis of data and the results of statistical test should be incorporated in the results section. The Statistics Editor will check the statistical analysis of each submitted manuscript. The Editors reserve the right to check raw data.
• The nomenclature used should conform to the current edition of the Nomina Anatomica, Nomina Anatomica Veterinaria or to the Nomina Anatomica. Avium, Eponyms (e.g., Fallopian tube, Eustachian tube) should not be used.
• Legends of figures should be typed on separate sheet.
• Tables (numbered in Roman numerals) and illustrations (numbered in Arabic numerals) should be prepared on separate sheets.
• Abbreviations should be explained in full when first used in the text, table or figure.
• The editor reserves the right to make corrections.
Tables
• Tables require a brief but descriptive heading.
• The major divisions of the table should be indicated by horizontal rules.
• Explanatory matter should be included in footnotes, indicated in the body of the table in order of their appearance.
• Tables must not duplicate material in the text or in illustration.
Illustrations
• The desired position of the figures and tables in the text should be indicated in the left margin. When possible, group several illustrations on one block for reproduction; figures and photographs should be attached as separate printouts (in the electronic version, as separate files); figures should be saved in one of the following formats: .cdr, .tif, .jpg, .ai, .bmp or .eps. Photographs sent in the electronic form should be of the resolution of 300 dpi and in .tif or .jpg format. Do not place figures and photographs in MS Office files. Like all other figures, block should be prepared within a�rectangular frame to fit within a�single or double column width of 84 and 174 mm, respectively, and a�maximum page height of 226 mm.
• Each figure should include scale magnification bar; do not use magnification factors in the figure legends.
• All figures, whether photographs, graphs or diagrams, should be numbered consecutively throughout. Do not give explanations on a�back of illustrations.
Instructions for authors
• Only good drawings and original photographs can be accepted; negatives, photocopies or xerocopies cannot be used.
• On the back of each illustration indicate its number and top.
• Color illustrations can be included, but the expense must be borne by the authors. The cost of color print for every successive 8 pages is 200 Euro (VAT exclusive) irrespective of the number of color pages, i.e., the price remains the same whether there is one or eight pages. The Publisher makes out the bill to the Author.
References
The list of references (written on a separate sheet) should include only those publications that are cited in the text. Number references consecutively in the order in which they first appear in the text. Numbers in square brackets should give citation of literature references in the text at the appropriate places. All authors cited and only these must be included in the reference list. List all authors when there are six or fewer; when there are seven or more, list the first three, then “et al.”. References should be written as follows:
Journal papers: initials and names of all authors, full title of paper, journal abbreviation (according to Index Medicus), year of publication, volume (in Arabic numerals), first and last page (example below):
Banach M, Kosmider A, Zwolinski R, Walczak A, Okonski P, Zaslonka J. Mechanical aortic valve replacement in patients with stenosis or aortic valve regurgitation. The influence on improvement of haemodynamic parameters of heart. Eur J Heart Failure 2004; 3: 98-102.
If a cited work has been published in a language other than English, its title should be stated in English, and the original language should be included in square brackets (example below):
Stefaniak B, Jaszewski R, Kosmider A, Zwolinski R, Knopik J, Walczak A, et al. Early and subsequent results of operation of trivalvular diseases [Polish]. Wiad Lek 2003; 56: 348-52.
Book and monographs: initials and names of all authors, full title, edition, publisher, place, year (examples below): Ringsven MK, Bond D. Gerontology and leadership skills for nurses. 2nd ed. Albany (NY): Delmar Publishers; 1996.
Chapter in a book: Phillips SJ, Whisnant JP. Hypertension and stroke. In: Laragh JH, Brenner BM, editors. Hypertension: pathophysiology, diagnosis, and management. 2nd ed. New York: Raven Press; 1995. p. 465-78.
Conference proceedings:
Kimura J, Shibasaki H, editors. Recent advances in clinical neurophysiology. Proceedings of the 10th International Congress of EMG and Clinical Neurophysiology; 1995 Oct 15-19; Kyoto, Japan. Amsterdam: Elsevier; 1996.
Reference to articles that are accepted for publication may be cited as “in press”, whereas manuscripts that are still in preparation or submitted for publication should be referred to as “unpublished data”.
This journal should be cited in lists as Arch Med Sci.
Proofs
Authors should keep a copy of their article, as proofs will be sent to them without the manuscript. Corrections to the proofs should be restricted to printer’s errors only; other alterations will be charged to the authors. In order to maintain rapid publication, proofs should be returned within 48 h after receipt, preferably by fax, courier mail or e-mail. If the Publisher receives no response from the authors after 5 days, it will be assumed that there are no errors to correct and the article will be published.
The Instruction for Authors and covering letter are also available online on page www.ams.termedia.pl
Publication charge
Please note that there is an obligatory charge (= 800 Euro) for each manuscript which is accepted for publication in Archives of Medical Science journal. We send invoices for payment after articles are accepted for publication.
Subscription information
The journal is published in one volume per year consisting of six numbers. The annual subscription price for 2020 is 250 Polish zloty for subscribers from Poland and 300 Polish zloty for foreign subscribers.
Payment should be made to:
Termedia sp. z o.o., ul. Kleeberga 8, 61-615 Poznań
BZ WBK III O/Poznań PL 61 1090 1359 0000 0000 3505 2645
SWIFT: WBKPPLPP
The publisher must be notified of a cancellation of a subscription not later than two months before the end of the calendar year. After that date the subscription is automatically prolonged for another year.
Publishing, Subscription and Advertising Office: TERMEDIA Publishing House
ul. Kleeberga 2
61-615 Poznań, Poland
phone/fax +48 61 822 77 81
e-mail: termedia@termedia.pl http://www.ams.termedia.pl
WWW.TERMEDIA.PL 9 771734 19232 3
