Surgical & Cosmetic Dermatology is an official publication of the Brazilian Society of Dermatology (SBD) in partnership with the Brazilian Society of Dermatological Surgery. The technical and scientific content presented in this publication is co-owned by the Brazilian Society of Dermatology.
The advertisements published in this issue are the sole responsibility of the advertisers, just as the concepts expressed in signed articles are the sole responsibility of their authors, and do not necessarily reflect the opinion of the SBD.
All rights reserved and protected by law 9.610 of 02/19/98. No part of this publication may be reproduced without prior written authorization from the Brazilian Society of Dermatology, regardless of the means employed: electronic, mechanical, photographic, recording or any other. Material for distribution to the medical profession. The magazine is in the Legal Deposit, at the National Library, in accordance with Decree No. 1.825, of December 20, 1907.
Licença Creative Commons
Indexed
n Sumários. org (www.sumarios.org/)
n DOAJ (https://doaj.org/)
n Latindex (www.latindex.org)
n Lilacs (https://bases.bireme.br/)
n SCOPUS (http://www.scopus.com/home.url)
n Periódica (http://periodica.unam.mx)
n Redalyc (http://www.redalyc.org)
PUBLISHED QUARTERLY
Technical Team
Nazareno Nogueira de Souza
Librarian Vanessa Mafra
Subscription information on the website: www.surgicalcosmetic.org.br
SURGICAL & COSMETIC DERMATOLOGY / INSTRUCTIONS TO AUTHORS
GUIDE FOR AUTHORS
Surgical & Cosmetic Dermatology is an interdisciplinary open-access journal dedicated to publishing research on all aspects of Dermatologic Surgery. It also welcomes articles in Cutaneous Oncology, Cosmetic Surgery and Dermatology, Laser, and other Therapy Technologies.
Please see Editorial Policies to:
General information
Language
Open access
Authorship
Peer-review policy
Copyright and licensing
Ethical guidelines and research integrity
PREPRINT
We accept the submission of articles deposited in preprints repositories. Authors can share their preprint anywhere at any time.
If a preprint is accepted for publication, we encourage authors to link it to their formal publication through their Digital Object Identifier (DOI).
Authors can update their preprints on bioRxiv (https:// www.biorxiv.org/), medRxiv (https://www.medrxiv.org/) or others with their accepted manuscript.
DISCLAIMER
Statements and opinions expressed in the articles and communications published on Surgical & Cosmetic Dermatology are those of the author(s) and not necessarily those of the Editor(s), Publisher, or Society.
SUBMISSION GUIDELINES
Proper preparation of the manuscript makes the review and publication processes more efficient. Thus, we recommend some precautions that can significantly facilitate the preparation of papers.
Articles must be unpublished and written in the author’s original language (Portuguese or English): the editorial team will provide the necessary versions. The font must be Times New Roman or Arial, 12 points.
The study's title must be concise, informed in Portuguese and English, containing up to 150 characters without spaces, accompanied by a short title.
Abstracts in Portuguese and English must follow the appropriate format for the type of article.
4. Authors must inform full name, abbreviations, and their institutional affiliations, followed by city, state, and country. Links to institutions must be listed in hierarchical order (e.g., first the
Department, second the University). The inclusion of minicurriculums is not allowed.When an author is affiliated with more than one institution, each must be identified separately.When two or more authors are affiliated with the same institution, it should be identified only once. Authors belonging to Private Clinics must cite them as an institution. It is mandatory to mention the ORCID number used to identify researchers for the first and last authors. The author must assume at least one responsibility in the elaboration of the study and must inform the contribution of each one in the submission. One of the authors must be designated as the corresponding author, providing an email address. Authors must also mention the place where the work was conducted. Authors must clearly state any conflicts of interest and financial support.
The keywords must be cited in Portuguese and English, totaling 3 to 10 per language, and they must be included in all types of articles. We recommend that the keywords are obtained from DeCS (Health Science Descriptors) or MeSH (Medical Subject Headings), which can be accessed on the internet.
The limit number of words for texts must follow the type of article and calculated excluding references and abstracts in Portuguese and English.
Extensive and repetitive introductory information should be avoided, giving preference to the most recent, not yet published. Avoid repeating the same information in the abstract, introduction, and discussion.
Weights and measurements must be expressed in the decimal metric system and temperatures in degrees centigrade. Drugs must be mentioned by their generic names, followed by the dose and dosage used, avoiding commercial terms or brands. Descriptions of any equipment, instruments, tests, and reagents must contain the name of the manufacturer and the place of manufacture.
According to the ICMJE, only those who actively participated in the study can be designated as authors, thus assuming public responsibility for its content. Authorship credits must be based solely on substantial contributions to: discussion and planning of the topic and protocol, analysis or interpretation of data; writing of the article or its review; responsibility for final approval for publication.
Other minor contributions such as literature suggestions, data collection and analysis, funding obtaining, technical assistance in conducting routines, patients referral, routine test interpretation, and head of service or department that are not involved in the study do not constitute criteria for authorship. They can be recognized separately in the “Acknowledgments” session, according to the authors’ decision.
ARTICLE TYPES
A Surgical & Cosmetic Dermatology publishes the following article types:
REVIEW ARTICLES
Review articles deepen specific themes in the areas of interest of S&CD, algorithms, compilations, statistics, consensus, and guidelines.These papers have a free format; however, they must contain an unstructured abstract of up to 100 words and conclusions or final considerations. Limit: text up to 6000 words, 10 illustrations, and 60 references. Systematic review articles or meta-analyses must follow relevant guidelines (http://cochrane.org.br).
ORIGINAL ARTICLE
Original articles report original investigative research in Dermatological Surgery, Cutaneous Oncology, Imaging Diagnosis, Dermatology Technology, and Cosmetic Dermatology. Examples: experimental studies, clinical studies, comparisons and descriptions of techniques, or evaluation methods.The text should contain up to 4000 words, 10 illustrations, and 35 references and follow the IMRDC format (Introduction and objective, Methods, Results, Discussion, Conclusion).
Abstract: The abstract must contain up to 250 words and be structured, comprising: Introduction, Objective, Methods, Results, and Conclusions. It is not allowed to state that results or other data will be presented or discussed.
Introduction: State the reasons that motivated the study, describing the current state of knowledge on the subject. Use the last paragraph to specify the central question or objective of the research and the primary hypothesis tested, if any.
Methods: Explain how the study was conducted:
Study type: describe its design specifying the temporal direction (retrospective or prospective), the type of randomization, if any (pairing, drawing, sequencing, etc.), if the study was blind, comparative, placebo-controlled, etc.
Location: indicate where the study was conducted (private or public institution), mentioning the research’s approval by the Research Ethics Committee, the selection procedures, the inclusion and exclusion criteria, and the initial number of patients.
Procedures: describe the main characteristics of the interventions performed, detailing the technique and considering that the investigation study should be reproducible.
Methodology: Description of the methods used to evaluate the results.
Statistical analysis: Inclusion of descriptive and/or comparative statistical analysis describing the sample planning (representative of the universe to be studied), analysis and statistical tests, and presenting the adopted significance levels.We encourage using unusual statistical analyses, but a more detailed description should be made in this case.
Results: Report the main results that point estimates and measures of dispersion should accompany (e.g., mean and standard error) or interval estimates (e.g., confidence intervals), as well as the descriptive levels of the tests statistics used (e.g., “p-value”). Findings must also be interpreted from a clinical point of view.
Discussion: Emphasize the new and essential results found by the study, which will be part of the conclusion. Also, report observations from other relevant studies, mentioning the limitations of the findings and implications for future research.
Conclusions: Clearly and concisely answer the proposed objectives of the study. The same emphasis must be given to studies with positive or negative results.
DIAGNOSTIC IMAGING
Diagnostic Imaging addresses topics or clinical cases where imaging exams (dermoscopy, confocal microscopy, ultrasound, and other methods) are essential for diagnosis or treatment. It must contain unstructured abstract of up to 100 words, text up to 1200 words, 6 illustrations, and 5 references.
HOW I DO IT?
How do I do it? describes new techniques or details of procedures. It must contain unstructured abstract of up to 100 words, an introduction with a literature review, methods, results, discussion, and conclusion. Limit: 1200 words, 8 illustrations, and 30 references.
CASE REPORT
Case report is the description of cases or series of relevant cases in the areas of interest of S&CD, depicting treatments, complications, etc. It must contain unstructured abstract of up to 100 words, an introduction with a literature review, methods, results, discussion, and conclusion, whenever pertinent. Limit: text up to 1200 words, 8 illustrations and 30 references.
LETTERS TO THE EDITOR
Letters to the editor are objective, brief, and constructive comments on previously published studies or research. The text should be up to 600 words, with a maximum of 5 references.
ETHICS COMMITTEE
The authorization certificate by an Ethics Committee is only required for the Original Articles of prospective research.
REFERENCES
Bibliographic references must be listed on the last pages of the article and numbered according to the citation in the text (in sequential numerical order), following the Vancouver style, as indicated by the International Committee of Medical Journal Editors (ICMJE). References cited in table and figure legends must
keep the sequence with the citations in the text. If a document has six or more authors, provide the name of the first six authors followed by "et al".
Below are examples of the most common types of references taken from ICMJE:
Journal articles:
Hallal AH, Amortegui JD, Jeroukhimov IM, Casillas J, Schulman CI, Manning RJ, et al. Magnetic resonance cholangiopancreatography accurately detects common bile duct stones in resolving gallstone pancreatitis. J Am Coll Surg. 2005;200(6):869-75.
Book chapter:
Reppert SM. Circadian rhythms: basic aspects and pediatric implications. In: Styne DM, Brook CGD, editors. Current concepts in pediatric endocrinology. New York: Elsevier; 1987. p .91-125.
Website and online content:
With author: Fugh-Berman A. Pharmed OUT [Internet]. Washington: Georgetown University, Department of Physiology and Biophysics; c2006 [cited 2007 Mar 23]. Available from: http:// www.pharmedout.org/.
When the author is an organization: International Union of Biochemistry and Molecular Biology. Recommendations on Biochemical & Organic Nomenclature, Symbols & Terminology etc. [Internet]. London: University of London, Queen Mary, Department of Chemistry; [updated 2006 Jul 24; cited 2007 Feb 22]. Available from: http://www.chem.qmul.ac.uk/iubmb/
Previous presentation at events:
Bruhat M, Silva Carvalho JL, Campo R, Fradique A, Dequesne J, Setubal A, editors. Proceedings of the 10th Congress of the European Society for Gynaecological Endoscopy; 2001 Nov 22-24; Lisbon, Portugal. Bologna (Italy): Monduzzi Editore, International Proceedings Division; c2001. 474 p.
FIGURES
Figures, charts, and tables must be cited in sequential numerical order in the text in Arabic numerals (example: Figure 3, Chart 7), and the Editor is responsible for suppressing the redundant ones. Figure and charts legends and table titles and footnotes must accurately describe their content in short sentences, but sufficient for understanding, even if the article is not fully read. They must be uploaded in the system in the step corresponding to illustrations, avoiding using the field for the text, so the words within the figures are not counted.
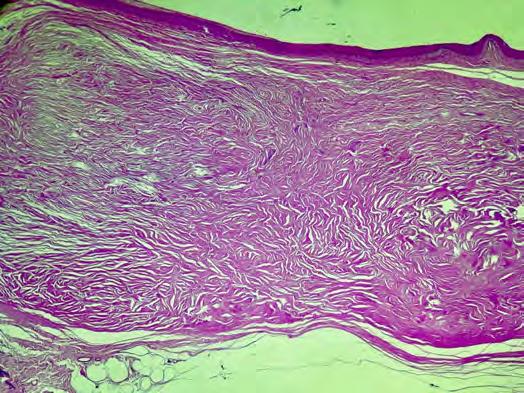
Figures must have a minimum resolution of 300 DPI, minimum width of 1,200 pixels with proportional height, and JPG or TIF formats. The photographs must be in focus, allowing the visualization of the details. Arrows or lines can be used to highlight areas of interest.The legends of histological images must specify staining and magnification. If a figure has been previously published, its source should be cited and included in the references.
The copyright holder's permission for its reproduction must be sent to the journal. The use of pictures that identify patients’ faces requires a written authorization (see the document Consent of Publishing Patient Photographs on the journal’s website).
Regarding videos, it is necessary to insert subtitles containing information such as the title of the manuscript, authorship, institution, and other relevant comments. When using patient images, their identity must be preserved; otherwise, written permission for disclosure must be attached.
Charts must be prepared in Microsoft Excel. Tables do not need to be described in the text because their objective is to supplement it and not augment it. The units used to express the results (m, g, g/100, mL, etc.) should appear at the top of each column. Patients must be identified by numbers or letters, and never by names, initials, or hospital registration numbers.
COVER LETTER
The cover letter must include the following information:
An explanation of why your manuscript is suitable for publishing in Surgical & Cosmetic Dermatology.
Confirmation that the manuscript's content is original and has not been published nor is being considered for publication elsewhere.
If the manuscript is being submitted for a particular special issue, its specific name must be mentioned in the cover letter. If the article reports the results of a health intervention in human participants, Surgical & Cosmetic Dermatology strongly recommends its record in an appropriate registry. The registration number and date must be indicated in this letter.
AUTHORS’ DECLARATIONS
The following final statements must be included in the final version of the manuscript. These declarations are expected to be submitted along with the cover letter since Surgical & Cosmetic Dermatology adopts a double-blind peer review.
‘Acknowledgments’ – list of people who contributed to the article (and does not meet the criteria for authorship), including contributors who provided professional writing services or materials.
‘Availability of data and materials’ – availability statements contain information on where data supporting the results reported in the article can be found, such as hyperlinks to publicly archived datasets. Example sentences are: ‘All data generated or analyzed during this study are included in this article’; ‘The datasets generated and/or analyzed during the current study are available in the [NAME] repository’, ‘The datasets generated during and/ or analyzed during the current study are available from the corresponding author on reasonable request’ or ‘Not applicable’ if no new data were created or analyzed in the study.
‘Financial support’ - all sources of funding of the study
should be disclosed; it is necessary to indicate grants that authors have received in support of the research.
‘Conflict of interest’ – all financial and non-financial competing interests must be declared in this section. If the authors do not have any competing interests, it is necessary to state ‘The authors declare that they have no conflict of interest’.
‘Authors’ contributions’ – Each author is expected to have made substantial contributions to the manuscript, which should be specified in this section. Please use initials to refer to each authors’ contribution. For example: ‘AB, CD, and EF conceived this research and designed experiments. GH participated in the design and interpretation of the data. IJ performed experiments and analysis. KL and MN wrote the paper and participated in the revisions of it. All authors read and approved the final manuscript’.
The maximum acceptable limit of authors is 5 (five); there will only be an exception for more complex works (ex. Original Article, Review) upon justification and approval by the editors.
‘Ethics approval/Ethics approval and consent to participate’: manuscripts reporting studies involving human participants or human data must include a statement on ethics approval and consent and include the name of the ethics committee that approved the study and the committee’s reference number. Studies involving animals must include a statement on ethics approval. If the manuscript does not report on or involve the use of any animal or human data, it is necessary to state ‘Not applicable’.
‘Consent for publication’if the manuscript contains any individual's personal data in any form, consent for publication must be obtained from that person, or in the case of children, their parent or legal guardian. All presentations of case reports must have consent for publication.
SUBMISSION
Manuscripts should be submitted through our online submission system (https://www.gnpapers.com.br/scd/default. asp?lang=en). The submitting author is responsible for the manuscript during the submission and peer-review process. They must ensure that all eligible co-authors have been included in the author list and have all read and approved the submitted manuscript. The following files are required to submit a manuscript:
The main manuscript file, which must not include the names of authors or co-authors (an anonymous file since the journal uses double-blind peer review). References and smaller tables should be included in this file.
A title page, which must contain the names of all authors and co-authors, their affiliations, emails, and all authors’ declarations.
A cover letter.
Figure files.
Any additional files as supplemental material to the manuscript.
All documents such as Copyright, Conflict of Interest, and Consent for Publishing Photographs are available on the journal’s website and in the online submission system. These documents must be signed by all participating authors and attached to the system when submitting the manuscript. Consent for Publishing Patient Photographs is only necessary when the patient’s face is fully identified. The editors will only request the Paper Participation document if necessary.
Table of contents
Official publication of the Brazilian Society of Dermatology
JULY - SEPTEMBER 2025 l Volume 17 l Number 3
ISSN:1984-5510
Online ISSN: 1984-8773
REVIEW ARTICLE
Synergistic Approaches in Facial Aesthetic Rejuvenation: Guidelines for Combining Hyaluronic Acid Fillers and
267 Laser/Energy-Based Technologies
Adriana Vilar inho, Alessandra Haddad, Cintia Cunha, Fernanda Nunes, Maria Paula Del Nero, Taciana Dal'Forno
Advances in evaluation and management of hyaluronic acid foreign body granulomas: a systematic review
274 Lina María Osorio Cock, Jaime Alberto Rengifo Palacios, María Paulina Uribe Posada, María Alejandra Sarabia de Capozzi, María Aida Angulo Morillo
ORIGINAL ARTICLE
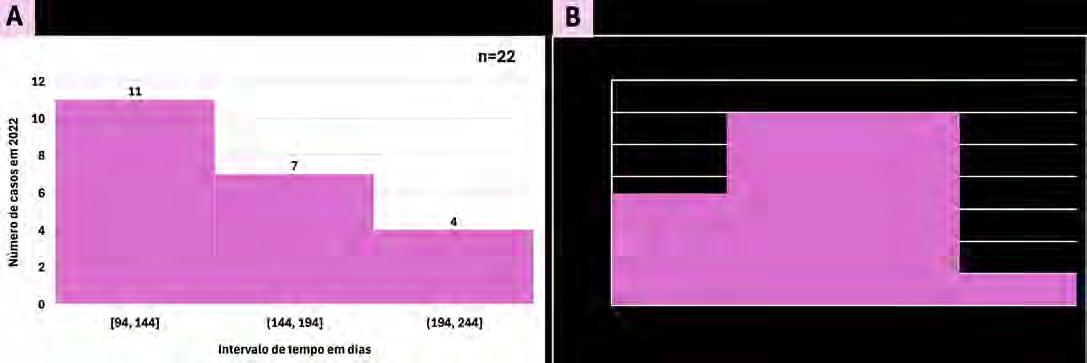
National Skin Cancer Prevention Campaign: Analysis of the Resolution Rate of Skin Tumors Diagnosed During
282 the 2022 and 2023 "Dezembro Laranja" Campaigns in Jundiaí
Isabella Melo Pompei, Célia Antônia Xavier de Moraes Alves, Annamaria Piovezan Lorenção, Bruna Mendes Almeida, Juliana Arêas de Souza Lima Beltrame Ferreira, Luciano Melo Pompei
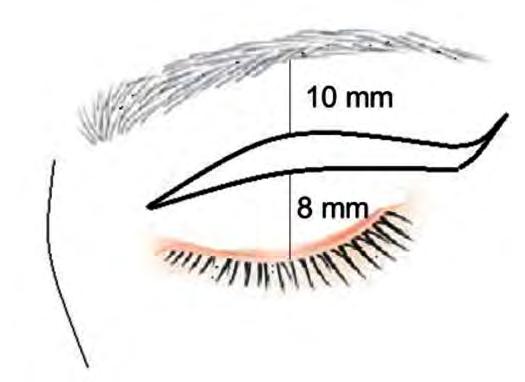
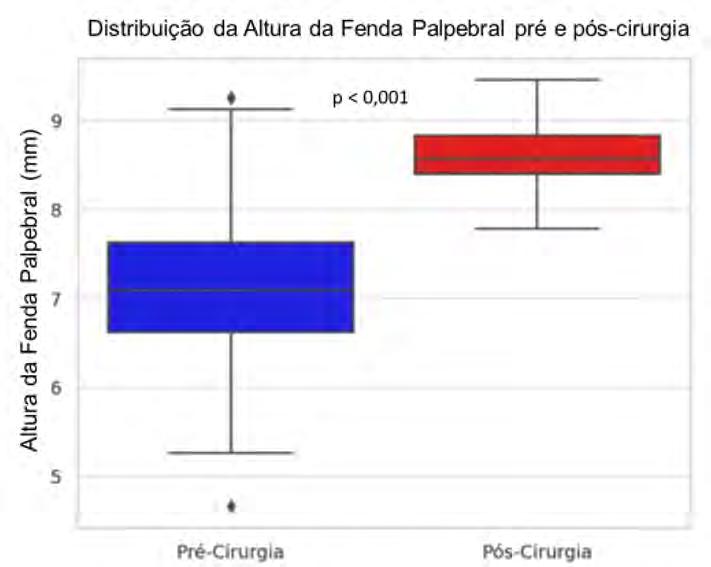
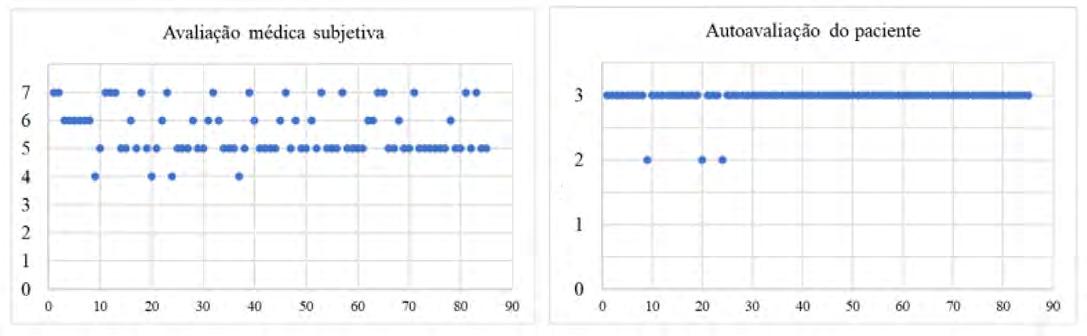
Quantitative and qualitative evaluation of upper blepharoplasty: a retrospective longitudinal study
Single-stage reconstruction of an upper third auricular defect with ipsilateral conchal cartilage graft and tunnelized preauricular flap
Roberto Klinger-Guerra, Jaime Zapata-Sepúlveda, Pablo Vargas-Mora, Pablo Muñoz-Alvear
Delayed closure of a scalp surgical wound using the Figueiredo technique: a case report
Rebecca Perez de Amorim, Hélio Amante Miot
Onychomatricoma - always a diagnostic challenge
Soraya Neves Marques Barbosa dos Santos, Sílvia Iovine Kobata, Isabela Boechat Morato, Natália de Paiva Sobreira
Bilateral lobuloplasty with inverted “snail”technique for correction of lobes deformed by prolonged use of gauges
Luiz Roberto Dal Bem Pires Júnior, Fernanda Nomoto Fujii, Rafaella Castilho,Waleska Ramos Alvim Lescowicz, Rodolfo Barros Leite, AnnaVictoria Valiente Engelhorn
Botulinum toxin in the treatment of pemphigus vegetans of the scalp
André Pozzobon Capeletti,Ana Paula Dornelles Manzoni, Rodrigo Pereira Duquia,VanessaVinderfeltes Padilha
A case of kidney transplant rejection secondary to cemiplimab for recurrent cutaneous squamous cell carcinoma
Nicole Russell, Siddharth Srikakolapu, Jane Scribner
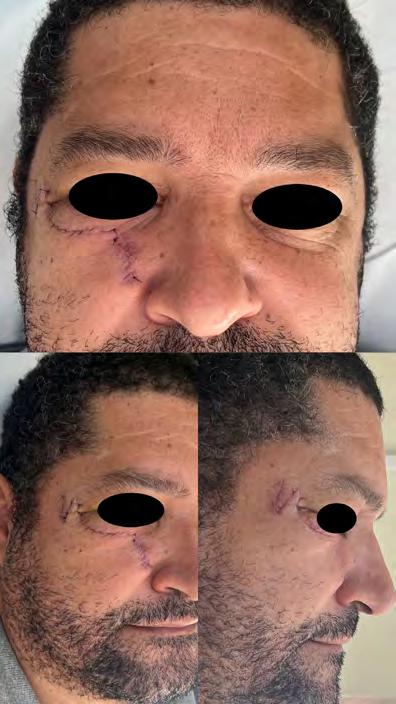
Reconstruction of the medial malar region and lower eyelid with a McGregor flap after resection of pigmented basal cell carcinoma
Luiz Roberto Dal Bem Pires Júnior, Carlos Augusto Silva Bastos, Rafaella Castilho, Waleska Ramos Alvim Lescowicz, Laurenlisiê Lourega Heitling Brittes
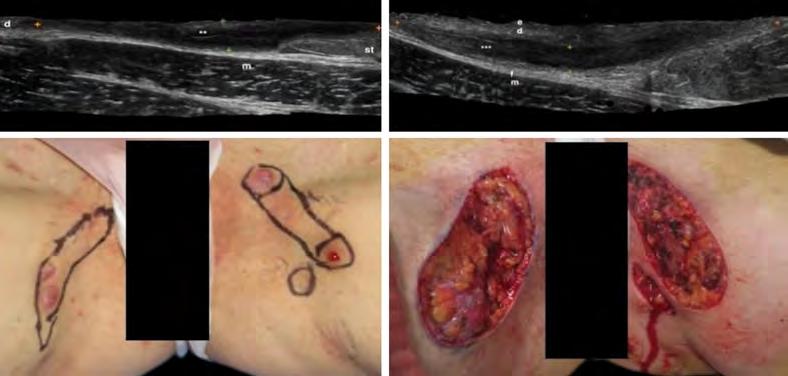
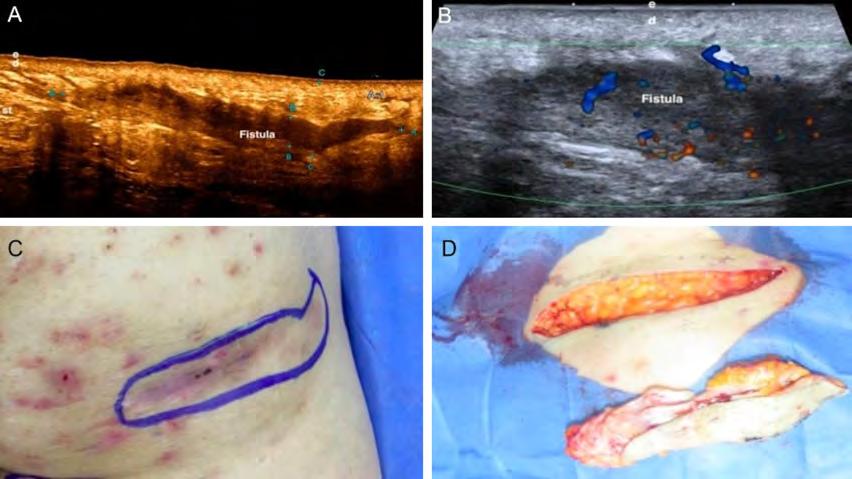
Ultrasound for a better surgical approach in hidradenitis suppurativa
Micaelly Samara Meneses Santos, José Roberto Pegas, Raissa Piagentini de Andrade, Leonardo Silva Grassi, Vanessa Cristina Coimbra, Bianca Sousa de Almeida Neves
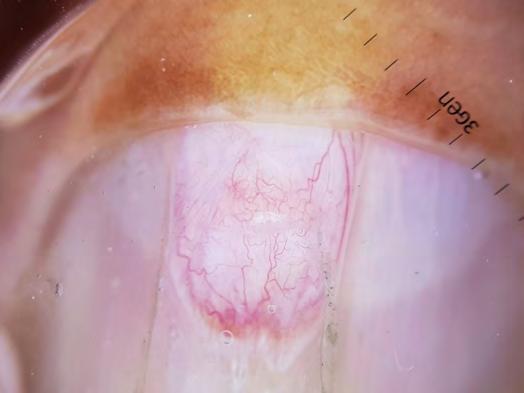
Atypical location of acquired digital fibrokeratoma
André Martins Ornelas, Clarissa Brito Farias, Isabelle Sousa Medeiros Torres Ferreira, Flauberto de Sousa Marinho
www.surgicalcosmetic.org.br/
Synergistic approaches in facial aesthetic rejuvenation: guidelines for combining hyaluronic acid fillers and laser/energy-based technologies
Abordagens sinérgicas no rejuvenescimento estético facial: diretrizes para utilização de ácido hialurônico combinado a tecnologias baseadas em laser e outras energias
This article presents practical guidelines for the synergistic use of HA and laser/energy-based technologies in facial rejuvenation.These recommendations originate from the collaborative interaction of a multidisciplinary group of physicians with experience in dermatology and plastic surgery, and can potentially be extended to treat other areas of the body, including neck and hands. The synergy between HA and lasers/intense pulsed light was recognized, emphasizing patient-tailored treatments and post-treatment care. These recommendations represent valuable guidelines, which can be adapted according to individual patient needs and to the continuous advancement of dermatological technologies.
1 Dermatologist, Private Practice, São Paulo (SP), Brazil
2 Plastic Surgeon, Universidade Federal de São Paulo - UNIFESP, Plastic Surgery Department, São Paulo (SP), Brazil
3 Plastic Surgeon, Hospital Israelita Albert Einstein, Plastic Surgery Department, São Paulo (SP), Brazil
4 Dermatologist, Private Practice, Uberlândia (MG), Brazil
5 Dermatologist, Private Practice, Porto Alegre (RS), Brazil
Correspondence:
Adriana Vilarinho
E-mail: adriana@adrianavilarinho.com.br
Funding: Galderma provided support for the board formation and manuscript writing.
RESUMO
Este artigo apresenta diretrizes práticas para o uso sinérgico de AH e tecnologias baseadas em laser/energia no rejuvenescimento facial. Essas recomendações se originam da interação colaborativa de um grupo multidisciplinar de médicos com experiência em dermatologia e cirurgia plástica e têm o potencial de serem estendidas para o tratamento de outras partes do corpo, incluindo pescoço e mãos. A sinergia entre AH e lasers/luz intensa pulsada foi reconhecida, enfatizando a personalização dos tratamentos e o cuidado pós-tratamento. Essas recomendações representam diretrizes valiosas, passíveis de adaptação conforme as necessidades individuais do paciente e o avanço contínuo das tecnologias dermatológicas.
Palavras-chave: Lasers; Luz; Rejuvenescimento; Ácido Hialurônico; Terapia a Laser; Terapia de Luz Intensa Pulsada.
Conflict of interest: Drs. Vilarinho, Cunha, Nunes, and Dal'Forno are affiliated with a speakers' bureau and hold positions as consultants for Galderma. Dr. Del Nero is a speaker, advisor, and consultant for Galderma. Dr. Haddad is a speaker, consultant, advisor, and investigator for Galderma. Dr. Nogueira is Medical Director at Galderma and Dr. Tomaz is Sr. Medical Manager at Galderma.
Submitted on: 03/07/2024
Final decision: 07/07/2025
How to cite this article: Vilarinho A, Haddad A, Cunha C, Nunes F, Del Nero MP, Dal’Forno T. Synergistic approaches in facial aesthetic rejuvenation: guidelines for combining hyaluronic acid fillers and laser/energy-based technologies. Surg Cosmet Dermatol. 2025;17:e20250385.
INTRODUCTION
The landscape of facial rejuvenation techniques has transformed substantially over the years, marked by the pursuit of a revitalized and youthful appearance. The realm of modern non-surgical cosmetic procedures now offers a wide range of solutions tailored to enhance the nuances of facial aesthetics while preserving the integrity of natural harmony and expressions.1-4 Hyaluronic acid (HA)-based dermal fillers have emerged as a cornerstone of this paradigm of minimally invasive aesthetic procedures.4,5 These fillers not only restore volume but also lift tissues to reduce the effects of fine lines, folds, hollowing, and wrinkles. Their strategic placement, including regions such as the forehead lines, temple, glabellar lines, lateral canthal lines, nasolabial folds, lips, jawline, marionette lines, chin, and tear troughs, leads to a contoured and rejuvenated aspect.3,5-7 In the context of HA for facial aesthetic rejuvenation, comprehensive characterization of the product holds pivotal clinical significance. Notably, NASHA® crosslinking technology provides HA with prolonged stability and bioavailability, enhancing its clinical utility. In addition, OBTTM technology8,9 finely regulates the physicochemical properties of HA, optimizing its integration within dermal tissues for superior outcomes.10,11 At the same time, lasers and energy-based treatments, exemplified by fractional laser resurfacing and radiofrequency devices, and intense pulsed light (IPL) therapy, have taken center stage. Their capacity to stimulate collagen production, tighten skin, and refine texture and tone has propelled them to the forefront of non-invasive modalities, amenable to individual or combined applications.7,12,13 As technological progress accelerates, the palette of non-surgical interventions for achieving facial rejuvenation is evolving with increasing diversity and efficacy. Yet, within this dynamic backdrop, the pursuit of facial rejuvenation is a nuanced process demanding comprehensive knowledge of individual patient demands, the complexities of aging physiology, facial anatomy, aesthetic principles, product characteristics, optimal technological choices, and the expertise of proficient practitioners3,6,12,14. Considering this multi-dimensional understanding, the aim of the present study is to create practical guidelines for HA treatment with laser/energy-based technologies while meeting evolving clinical needs for optimized outcomes, enhanced safety, and business viability within the particular context of minimally invasive aesthetic interventions of facial and non-facial areas.
METHODS
Participant Selection and Composition of Expert Group
A multidisciplinary group of nine medical experts with relevant knowledge and extensive clinical experience in HA treatment combined with laser/energy-based technologies convened in August 2023. The expert group included physicians specializing in dermatology and plastic surgery. The aim of this group was to provide insights and discuss best practices in facial treatments involving these modalities.
Questionnaire Development and Pre-Meeting Inquiry
Prior to the meeting, the members of the expert group were asked to answer a pre-meeting questionnaire consisting of 17 components relating to various aspects of the treatments:
1. Patient selection criteria
2. Clinical recommendations
3. Contraindications
4. Preoperative preparations
5. Varieties of hyaluronic acid products
6. Techniques of hyaluronic acid injection
7. Number of hyaluronic acid sessions
8. Interval between hyaluronic acid sessions
9. Laser/energy-based technologies used
10. Approaches in laser/energy-based techniques
11. Frequency of laser/energy-based sessions
12. Interval between laser/energy-based sessions
13. Sequencing of technology application
14. Guidelines for intraoperative care
15. Protocols for postoperative care
16. Potential adverse effects
17. Post-treatment follow-up strategies
Meeting Facilitation and Data Collection
During the meeting, organized by a neutral and trained medical facilitator (RT), discussions based on the responses to the questionnaire were captured on video. The facilitator steered the conversation, summarized key points, and facilitated clarifications to ensure equitable engagement and contribution from all participants. The discussions focused on comprehensive explanations of different treatment methods, the rationale underlying particular sequences, safety, and synergistic effects of combined treatments for facial aesthetic rejuvenation.
Formation of Guidelines
Open debates and dialogues were used to reach an agreement on potentially controversial topics. Participants drew from available evidence, their individual clinical experiences, and their concerns to identify high-relevance principles. These discussions, complemented by a review of current literature, formed the basis of a practical guideline encompassing facial aesthetic rejuvenation treatments.
Manuscript Development and Validation
Panel observations and suggestions from the discussions were assessed, resulting in the development of a manuscript. This manuscript was subsequently subjected to iterative revisions by all the authors, progressively refining its content. The culmination of this collaborative process led to unanimous agreement on the result. The final recommendations presented in this study represent the distilled expertise of the panel, grounded in clinical experience, and substantiated by previously published data
A, Haddad A, Cunha C, Nunes F, Del Nero MP, Dal’Forno T.
pertaining to the intersection of HA and laser/energy-based technologies in the field of facial aesthetic medicine focused on rejuvenation.
RESULTS AND RECOMMENDATIONS
Composition of Expert Group
The average age of the experts in the group was 48 years old, with an average of 25 years of medical practice, enhanced by advanced training acquired in residencies, master’s programs, and doctoral degrees within the specialized domains of general surgery, plastic surgery, dermatology, and internal medicine. After thorough discussions, the following recommendations were formulated based on a combination of scientific evidence and the collective clinical expertise of leading dermatologists, plastic surgeons, and researchers.
General Recommendations
The group emphasized the significance of patient selection and assessment, highlighting the importance of considering medical history. Pre-treatment evaluations should encompass detailed skin analysis to determine the most suitable HA formulation and laser/energy-based treatment for each patient. Sequential planning was recommended, with laser/IPL intervention typically preceding HA treatments, in the same session, to optimize skin response. A key aspect of the recommendations was determining the appropriate interval between laser/energy-based treatment and HA administration. The group recognized the potential for synergistic effects through the combination of HA and various laser modalities/IPL therapy within the same appointment to offer improvements in skin rejuvenation and overall aesthetic outcomes without requiring a minimum interval between procedures, unless the laser results in considerable swelling or heightened susceptibility to infection, in which case a 7-day interval between laser treatment and HA administration is advisable. The statements underscored the versatility of laser technologies that can be combined with HA, including fractional lasers, ablative technologies, nonablative lasers, and non-laser technologies, such as IPL therapy, tailored to each patient’s needs and manufacturer’s specifications. The optimal timing for laser/ IPL procedures before administering HA treatments was also debated, culminating in the conclusion that the time between the two interventions does not impact the aesthetic or safety outcomes of the procedure, as laser/IPL application can be immediately followed by the HA injection in the same session, though still accounting for exceptional circumstances related to technologies prone to significant edema or contamination, which can be seen in lasers with ablative potential, such as Er:YAG or CO2. In these cases, it may be necessary to delay HA application by 7 days. Customization emerged as a recurring theme in the recommendations, encouraging practitioners to tailor treatment plans based on individual patient characteristics and desired outcomes, while also accounting for specific laser/energy-based and HA formulations (considering the use of Restylane®
NASHA and/or OBT fillers for vertical projection and volume effect, alongside the incorporation of Restylane® Skinboosters™ for skin quality improvement, is advisable). Furthermore, the group emphasized post-treatment care as a pivotal element in minimizing downtime and adverse effects. The recommendations acknowledged that the combination of laser technologies, or IPL therapy, and HA is generally safe when administered by experienced practitioners. However, careful monitoring for potential adverse reactions and thorough patient education were considered essential. The expert group acknowledged the importance of maintaining comprehensive documentation and highlighted the need for further research to fully understand the long-term effects and potential advantages of combining laser/ energy-based treatments and HA.
Guideline Outcomes
The guidelines present the results for each of the 17 domains discussed by the expert group related to various aspects of the combination of treatments with laser/energy-based technologies and HA. It is important to note that these recommendations serve as guidelines and should be adapted to the specific needs of each patient and the evolving landscape of dermatological technologies. Clinicians are encouraged to keep up-to-date on the latest research and developments in the field to provide the highest standard of care when combining laser/energy-based technologies and HA for facial rejuvenation interventions. Table 1 presents recommendations for the optimal use of HA combined with laser/energy-based technologies for effective facial rejuvenation, table 2 provides guidelines on the effective use of laser/energy-based technologies combined with HA for enhanced facial rejuvenation outcomes, and table 3 provides comprehensive recommendations for an integrated approach to optimizing outcomes when combining laser/energy-based technologies and HA for facial rejuvenation.
DISCUSSION
The use of integrated therapeutic strategies for facial rejuvenation through protocols combining HA injection with laser/energy-based application is known to enhance patient satisfaction and achieve sustained efficacy.15 Nonetheless, the present article seems to represent a pioneering effort to establish practical guidelines for concurrent use of injectable HA treatments and laser/energy-based technologies. While attending to the growing worldwide interest in aesthetic medicine in the area of facial rejuvenation, it also emphasizes improved treatment results and the enhanced sustainability of clinical practice.7,12,16 Following prior findings,17 the expert group suggests that determining the most suitable approach depends on patient preferences, time constraints, anatomical factors, and financial considerations. Nevertheless, the core challenges of determining the extent of the intervention and the sequencing of its components remain a matter of dispute and are scarcely explored in clinical studies. Expert opinions have a key role in steering evidence-based prac-
Table 1: Recommendations for combining hyaluronic acid and laser/energy-based technologies in facial rejuvenation
HA Key recommendations
Patient selection criteria
Clinical recommendations
Contraindications
Preoperative preparations
Varieties of HA products
HA injection techniques
Number of HA injection sessions
Assess volume deficits, tissue projection, skin quality (wrinkles, furrows, dyschromia, pores, scars, dilated vessels), and appropriate laser/IPL choice for various phototypes and tanned skin. Consider tendency to post-inflammatory hyperchromia.
Enhance skin quality using laser/IPL and correct volumetric deficits with HA. Primary treatment areas: face, neck, and hands. Secondary sites include other body regions and intimate area.
Avoid use in case of local infection. There is increased risk of complications if a permanent filler, such as silicone or PMMA, is present in the same area.
Use local anesthetic and analgesic as needed. Prepare skin with suitable skincare regimen based on laser/IPL type, patient phototype, and clinical requirements.
Use Restylane® NASHA and/or OBT fillers, as well as Restylane® SkinboostersTM
Choose technique based on product and anatomical site: subdermal, subcutaneous, or supraperiosteal; cannula or needle. Amount of HA varies by site and individual assessment.
Tailor to individual patient assessment. For Restylane® SkinboostersTM: 2-4 sessions/ year, 1-3 syringes/area. Other Restylane® NASHA and/or OBT fillers for vertical projection and volume effect: 1 session/year/area.
Table 2: Recommendations for combining laser/energy-based technologies and hyaluronic acid in facial
rejuvenation
Laser/energy-based technologies
Laser/energy-based technologies used
Approaches to laser/energy-based techniques
Frequency of laser/energy-based sessions
Interval between laser/energy-based sessions
Key recommendations
Select laser type (or IPL therapy) based on individual patient clinical criteria. Examples include fractionated, ablative, and nonablative lasers. Note that IPL behaves similarly when combined with HA.
Choose technique according to technology and patient needs. Use appropriate energy levels to prevent burns, including suitable power and application time.
Tailor to individual patient assessment, generally ranging from 1 to 5 sessions.
Duration varies based on technology employed, typically ranging from 7 to 30 days.
Observation: Although not a form of laser technology, these recommendations also apply to intense pulsed light (IPL) therapy
Table 3. Comprehensive recommendations for combining hyaluronic acid and laser/energy-based technologies in facial rejuvenation
Clinical guidelines
Sequencing of technology application
Key recommendations
Opt for laser or IPL therapy before HA injection, potentially during a single appointment. Exception: if the ablative laser induces significant postoperative edema or risk of infection, allow for a 7-day interval between laser and HA.
Guidelines for intraoperative care Maintain asepsis and antisepsis.
Protocols for postoperative care
Potential adverse effects
Post-treatment follow-up strategies
IPL: intense pulsed light
Apply local cooling or soothing masks according to laser used. Use LED therapy and prescribe moisturizing, healing, soothing, or lightening creams based on diagnosis. Advise against sun exposure and recommend high-SPF sunscreen until skin recovery is complete.
Monitor for vascular occlusion and address hematoma, post-inflammatory hyperchromia, or hypochromia. Manage unsightly scars and guard against local infection and herpetic reactivation.
Engage in remote monitoring (telephone contact) within 24 hours post-procedure. Schedule photographic follow-up 3 to 6 months after the procedure.
tice and the advancement of aesthetic medicine, particularly within clinical contexts such as the current one which is marked by the limitations of the literature.18,19 In this scenario, practical guidelines developed by unanimous agreement and addressing core clinical topics such as those covered by the present recommendations (patient assessment, emerging technologies, personalized treatment, safety issues, and long-term results, among others) may serve as a valuable resource for both practitioners and patients seeking guidance to fully understand the field, its challenges, and the dynamic landscape of treatments.20,21 From a comprehensive standpoint, the present practical guidelines encompass patient preferences, volume deficits, and skin quality assessment, coupled with the selection of suitable lasers based on phototypes. The clinical emphasis lies in enhancing skin quality via lasers (or IPL therapy) and addressing volume deficits with HA. The integration of HA with lasers/energy-based interventions in the same session involves sequencing technologies before HA, with exceptions for a 7-day interval due to edema or infection risks. Preoperative measures involve skincare preparation and local anesthesia. The use of Restylane® NASHA and/or OBT fillers, alongside the incorporation of Restylane® Skinboosters™, follows techniques tailored to specific sites. The number of sessions depends on patient assessment, with intervals ranging from 7 to 30 days. Intraoperative care requires asepsis, while postoperative care involves soothing masks, LED therapy, and sun protection. Monitoring adverse effects including vascular occlusion, hematoma, pigmentation, scars, and infection is vital, and management strategies should be guided by the diagnosis. Follow-up requires remote monitoring within 24 hours and photographic documentation 3 to 6 months after the procedure. The recommendations also apply to IPL therapy, which, although not technically a form of laser technology, parallels the findings of Fodor et al. (2004), demonstrating its pivotal role in facial aesthetic rejuvenation. IPL effectively addresses various concerns raised by medical experts, including pigmentation irregularities, vascular anomalies, signs of aging, acne, and unwanted hair growth. This non-invasive modality boasts a favorable safety profile and minimal interruption, making it a versatile and effective solution for comprehensive facial enhancement and rejuvenation.22 Given the predilection of contemporary patients for achieving facial rejuvenation swiftly and cost-effectively, one should consider comprehensive treatments in a single session,17 following the recommendations outlined in the present practical guidelines, which start patients with medical-grade skincare to create more favorable responses to various interventions, including minimal filler augmentation. Following the protocol, laser/ IPL procedures before HA injection are endorsed because this sequence facilitates the modulation of skin texture with minimal edema, thereby enabling subsequent volumization with HA.17 The rationale behind this clinical sequencing is the physiological
response of the skin induced by laser/IPL treatment. This response encompasses augmented dermal thickness, decreased skin anisotropy, and discernible clinical enhancement characterized by improved texture, diminished pore size, improved wrinkles, and enhanced skin laxity, collectively extending the retention period of HA filler in the treated area.22-26 The proposed guidelines on the volume of HA to be administered and the periodicity of treatment in the context of laser/IPL-filler synergy are grounded on the evidence that diminished dermal thickness attributed to the reorganization of newly formed collagen fibers, a phenomenon known to develop over time, may lead to a discernible aesthetic compromise.15,27 However, it is important to highlight that the persistent impact of laser/IPL treatment, combined with the effects of HA, especially when based on NASHA28 and/or OBT technologies,29 remains effective over up to 12 months.30
Limitations
The practical guidelines in this article are rooted in the real-world experience of experts, though this approach has limitations due to subjectivity and lack of standardization. However, the elective nature of aesthetic procedures makes the design of comprehensive long-term studies challenging. Thus, the current understanding of emerging facial rejuvenation methods comes mainly from the collective experiences of individual practitioners.17 Therefore, these recommendations would benefit from future controlled clinical trials.19,21
CONCLUSIONS
Best practices for synergistic approaches in facial rejuvenation interventions involve the direct sequence of lasers/IPL before HA if administered in the same session. A 7-day interval due to edema or infection risks is advisable when using lasers with ablative potential. Application of Restylane® NASHA and/ or OBT fillers combined with technologies follows techniques tailored to specific sites and products while the number of sessions depends on patient assessment. Intraoperative care requires asepsis, while postoperative care involves soothing masks, LED therapy, sun protection, and customized topical treatment. Monitoring and management of adverse effects are key. Follow-up is based on remote monitoring within 24 hours and photographic documentation at 3 to 6 months post-procedure. Furthermore, strategically performing laser/energy-based interventions before HA treatments in the same session to optimize synergistic effects and consequently enhance treatment outcomes during a single session can also be consistent with contemporary patient preferences while enhancing business prospects in the field of facial aesthetics. Based on their expertise, the expert group emphasizes that the combination of Restylane® NASHA and/or OBT fillers with lasers or IPL is an effective and safe strategy for optimizing clinical outcomes in Aesthetic Medicine. l
A, Haddad A, Cunha C, Nunes F, Del Nero MP, Dal’Forno T.
REFERENCES:
1. Sadick NS, Manhas-Bhutani S, Krueger N. A novel approach to structural facial volume replacement. Aesthetic Plast Surg. 2013;37(2):266-76.
2. Hart DR, Fabi SG, White WM, Fitzgerald R, Goldman MP. Current concepts in the use of PLLA: clinical synergy noted with combined use of microfocused ultrasound and poly-l-lactic acid on the face, neck, and décolletage. Plast Reconstr Surg. 2015;136(5 Suppl):180S-7S.
3. Urdiales-Gálvez F, Martín-Sánchez S, Maíz-Jiménez M, Castellano-Miralla A, Lionetti- Leone L. Concomitant use of hyaluronic acid and laser in facial rejuvenation. Aesthetic Plast Surg. 2019;43(4):1061-70. Erratum in: Aesthetic Plast Surg. 2019 Sep 17.
4. Melo F, Carrijo A, Hong K, Trumbic B, Vercesi F, Waldorf HA, et al. Minimally invasive aesthetic treatment of the face and neck using combinations of a PCL-based collagen stimulator, plla/plga suspension sutures, and cross-linked hyaluronic acid. Clin Cosmet Investig Dermatol. 2020;13:333-44.
5. Bertossi D, Giampaoli G, Lucchese A, Manuelli M, Albanese M, Nocini R, et al. The skin rejuvenation associated treatment-fraxel laser, Microbotox, and low G prime hyaluronic acid: preliminary results. Lasers Med Sci. 2019;34(7):1449-55.
6. Langelier N, Beleznay K, Woodward J. Rejuvenation of the upper face and periocular region: combining neuromodulator, facial filler, laser, light, and energy-based therapies for optimal results. Dermatol Surg. 2016;42(Suppl 2):S77-82.
7. Goldman MP, Alster TS, Weiss R. A randomized trial to determine the influence of laser therapy, monopolar radiofrequency treatment, and intense pulsed light therapy administered immediately after hyaluronic acid gel implantation. Dermatol Surg. 2007;33(5):535-42.
8. Rzany B, Cartier H, Kestemont P, Trevidic P, Sattler G, Kerrouche N, et al. Full-face rejuvenation using a range of hyaluronic acid fillers: efficacy, safety, and patient satisfaction over 6 months. Dermatol Surg. 2012;38(7 Pt 2):1153-61.
9. Philipp-Dormston WG, Schuster B, Podda M. Perceived naturalness of facial expression after hyaluronic acid filler injection in nasolabial folds and lower face. J Cosmet Dermatol. 2020;19(7):1600-6.
10. Weiss RA, Moradi A, Bank D, Few J, Joseph J, Dover J, et al. Effectiveness and safety of large gel particle hyaluronic acid with lidocaine for correction of midface volume deficit or contour deficiency. Dermatol Surg. 2016;42(6):699-709. Erratum in: Dermatol Surg. 2016;42(10):1233.
11. Jones DH, Hessler J, Chapas A, Jonas B, Crider J, Chopra R. Microcannula injection of large gel particle hyaluronic acid for cheek augmentation and the correction of age- related midface contour deficiencies. Dermatol Surg. 2020;46(4):465-72.
12. Kim H, Park KY, Choi SY, Koh HJ, Park SY, Park WS, et al. The efficacy, longevity, and safety of combined radiofrequency treatment and hyaluronic acid filler for skin rejuvenation. Ann Dermatol. 2014;26(4):447-56.
13. Akerman L, Mimouni D, Nosrati A, Hilewitz D, Solomon-Cohen E. A Combination of non-ablative laser and hyaluronic acid injectable for postacne scars: a novel treatment protocol. J Clin Aesthet Dermatol. 2022;15(3):53-6.
14. Hsu SH, Chung HJ, Weiss RA. Histologic effects of fractional laser and radiofrequency devices on hyaluronic acid filler. Dermatol Surg. 2019;45(4):552-6.
15. Leheta T, El Garem Y, Hegazy R, Abdel Hay RM, Abdel Halim D. Non-ablative 1540 fractional laser: how far could it help injection lipolysis and dermal fillers in lower-face rejuvenation? A randomized controlled trial. J Cosmet Laser Ther. 2013;15(1):13-20.
16. Kim JE, Hong JY, Lee HJ, Lee SY, Kim HJ. Picosecond-domain fractional laser treatment over hyaluronic acid fillers: in vivo and clinical studies. Lasers Surg Med. 2020;52(10):928-34.
17. Kontis TC, Bunin L, Fitzgerald R. Injectable fillers: panel discussion, controversies, and techniques. Facial Plast Surg Clin North Am. 2018;26(2):225-36.
18. Carruthers J, Burgess C, Day D, Fabi SG, Goldie K, Kerscher M, et al. Consensus recommendations for combined aesthetic interventions in the face using botulinum toxin, fillers, and energy-based devices. Dermatol Surg. 2016;42(5):586-97.
19. Signorini M, Liew S, Sundaram H, De Boulle KL, Goodman GJ, Monheit G, et al. Global aesthetics consensus: avoidance and management of complications from hyaluronic acid fillers-evidence- and opinion-based review and consensus recommendations. Plast Reconstr Surg. 2016;137(6):961e-71e.
20. Philipp-Dormston WG, Bergfeld D, Sommer BM, Sattler G, Cotofana S, Snozzi P, et al. Consensus statement on prevention and management of adverse effects following rejuvenation procedures with hyaluronic acid-based fillers. J Eur Acad Dermatol Venereol. 2017;31(7):1088-95.
21. Urdiales-Gálvez F, Delgado NE, Figueiredo V, Lajo-Plaza JV, Mira M, Ortíz-Martí F, et al. Preventing the complications associated with the use of dermal fillers in facial aesthetic procedures: an expert group consensus report. Aesthetic Plast Surg. 2017;41(3):667-77.
22. Fodor L, Peled IJ, Rissin Y, Ramon Y, Shoshani O, Eldor L, et al. Using intense pulsed light for cosmetic purposes: our experience. Plast Reconstr Surg. 2004;113(6):1789-95.
23. Ross EV, Sajben FP, Hsia J, Barnette D, Miller CH, McKinlay JR. Nonablative skin remodeling: selective dermal heating with a mid-infrared laser and contact cooling combination. Lasers Surg Med. 2000;26(2):186-95.
24. Fournier N, Dahan S, Barneon G, Diridollou S, Lagarde JM, Gall Y, et al. Nonablative remodeling: clinical, histologic, ultrasound imaging, and profilometric evaluation of a 1540 nm Er:glass laser. Dermatol Surg. 2001;27(9):799-806.
25. Fournier N, Dahan S, Barneon G, Rouvrais C, Diridollou S, Lagarde JM, et al. Nonablative remodeling: a 14-month clinical ultrasound imaging and profilometric evaluation of a 1540 nm Er:glass laser. Dermatol Surg. 2002;28(10):926-31.
26. Lupton JR, Williams CM, Alster TS. Nonablative laser skin resurfacing using a 1540 nm erbium glass laser: a clinical and histologic analysis. Dermatol Surg. 2002;28(9):833-5.
27. Imayama S, Braverman IM. A hypothetical explanation for the aging of skin. Chronologic alteration of the three-dimensional arrangement of collagen and elastic fibers in connective tissue. Am J Pathol. 1989;134(5):1019-25.
28. Cartier H, Hedén P, Delmar H, Bergentz P, Skoglund C, Edwartz C, et al. Repeated full- face aesthetic combination treatment with abobotulinumtoxinA, hyaluronic acid filler, and skin-boosting hyaluronic acid after monotherapy with abobotulinumtoxinA or hyaluronic acid filler. Dermatol Surg. 2020;46(4):475-82.
29. Hedén P, Hexsel D, Cartier H, Bergentz P, Delmar H, Camozzato F, et al. Effective and safe repeated full-face treatments with abobotulinumtoxinA, hyaluronic acid filler, and skin boosting hyaluronic acid. J Drugs Dermatol. 2019;18(7):682-9.
30. Carruthers JDA, Glogau RG, Blitzer A; Facial Aesthetics Consensus Group Faculty. Advances in facial rejuvenation: botulinum toxin type A, hyaluronic acid dermal fillers, and combination therapies--consensus recommendations. Plast Reconstr Surg. 2008;121(5 Suppl):5S-30S.
AUTHOR’S CONTRIBUTION:
Adriana Vilarinho 0009-0006-7381-6299
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Alessandra Haddad 0000-0002-5552-7251
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Cintia Cunha 0009-0009-4919-4882
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Fernanda Nunes 0009-0002-2057-7344
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Maria Paula Del Nero 0000-0002-5369-3504
Author’s contribution: Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Taciana Dal'Forno 0000-0003-0848-9042
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
www.surgicalcosmetic.org.br/
Advances in evaluation and management of hyaluronic acid-induced foreign body granulomas: a systematic review
Avanços na avaliação e tratamento de granulomas de corpo estranho de ácido hialurônico: uma revisão sistemática
We conducted a systematic review following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) of cases of foreign body granuloma (FBG) induced by hyaluronic acid (HA).
A total of 27 patients with HA filler-induced FBG reported in literature were included. The estimated incidence of HA-induced FBG is 0.02%-0.6%. Several factors are involved, including cross-linking agents and impurities. The most frequent clinical presentation is asymptomatic nodules, although other lesions may occur. Histopathological examination is the gold standard for diagnosis, but ultrasound is a promising tool. Treatment options include expectant management, hyaluronidase, corticosteroids, 5-fluorouracil, and surgery.
Foi realizada uma revisão sistemática seguindo os critérios da declaração Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) de casos de granuloma de corpo estranho (GCE) causados por ácido hialurônico (AH). Foram incluídos 27 pacientes de GCE causado por preenchimento com AH encontrados na literatura. Estima-se que a incidência de GCE causado por AH seja de 0,02%-0,6%.Vários fatores estão envolvidos, incluindo agentes de reticulação e impurezas. Nódulos assintomáticos são a apresentação clínica mais frequente, mas outras lesões podem ser observadas. Embora o estudo histopatológico seja o padrão-ouro para diagnóstico, a ultrassonografia é uma ferramenta promissora. As opções de tratamento incluem conduta expectante, hialuronidase, corticoides, 5-fluorouracil e cirurgia.
Palavras-chave: Ácido Hialurônico; Preenchedores Dérmicos; Granuloma de Corpo Estranho.
Review Article
Authors:
Lina María Osorio Cock1
Jaime Alberto Rengifo Palacios1
María Paulina Uribe Posada1
María Alejandra Sarabia de Capozzi2
María Aida Angulo Morillo3
1 Universidad Pontificia Bolivariana, Department of Dermatology, Medellín, Antioquia, Colombia
2 Venezuelan Society of Dermatology, Venezuelan Society of Dermatology, Valencia, Carabobo, Venezuela
3 Oncology Hospital Dr. Miguel Pérez Carreño, Department of Pathology, Valencia, Carabobo, Venezuela
Submitted on: 03/27/2025. Final decision: 07/02/2025.
How to cite this article: Osorio Cock LM, Rengifo Palacios JA, Uribe Posada MP, Sarabia de Capozzi MA, Angulo Morillo MA. Advances in evaluation and management of hyaluronic acid-induced foreign body granulomas: a systematic review. Surg Cosmet Dermatol. 2025;17;e20250457.
INTRODUCTION
Hyaluronic acid (HA) injection is the second most common aesthetic nonsurgical procedure, with a 28.9% increase over the past 5 years.1 Although minimally invasive, it can lead to complications. Classically, complications are divided into 3 groups based on the time of onset: early (within 14 days), late (14 days to 1 year), and delayed (over 1 year).2 Among the late and delayed complications, foreign body granulomas (FBGs) are noteworthy. FBG is a histological inflammatory reaction to an antigen, characterized by the aggregation of macrophages and foreign body giant cells.3
Under normal circumstances, HA integrates into tissues without inflammatory infiltrates or epidermal or dermal alterations.4 With few reports and studies available, HA-induced FBG appears to be rare, with an estimated frequency of 0.02%-0.4% in retrospective reviews.5 However, biopsies required for histological confirmation are rarely performed because of concerns regarding the cosmetic outcomes of aesthetic procedure complications. Underdiagnosis is therefore suspected, and whether histological findings correlate with current clinical and imaging diagnoses remains uncertain.
As a result, few studies are available, and empirical treatment remains the norm, with variable outcomes. We aim to review case reports and case series in the literature to improve understanding, explore alternative diagnostic methods, and propose more accurate and effective treatment approaches.
METHOD OF LITERATURE SEARCH
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement in January 2025. A natural language search was performed to identify potentially relevant articles. The search terms used were “hyaluronic acid” and “granuloma,” combined with the Boolean operator “AND.” The Title/Abstract field tag was applied in PubMed, Embase, Scopus, and LILACS.
Inclusion criteria were primary studies, case reports, or case series describing HA filler-induced FBG. Exclusion criteria were failure to meet inclusion criteria (reason 1); absence of histopathological confirmation of FBG (reason 2); combination with other fillers (reason 2); genitourinary applications (reason 3); and animal studies (reason 4). No language or time restrictions were applied. After screening, 17 studies were included (Figure 1). Articles were manually reviewed, and data were extracted into Excel forms. The included studies are presented in the results.
RESULTS
We identified 17 case reports or case series of HA-induced FBG, comprising 32 patients. All patients were female, with the exception of 1 male. A histology-focused study reported 5 cases of HA filler-induced FBG among other dermal fillers; however, because clinical data were presented only as means and
modes that included other fillers, it was not included in the subsequent analysis. The cases are summarized in Table 1.
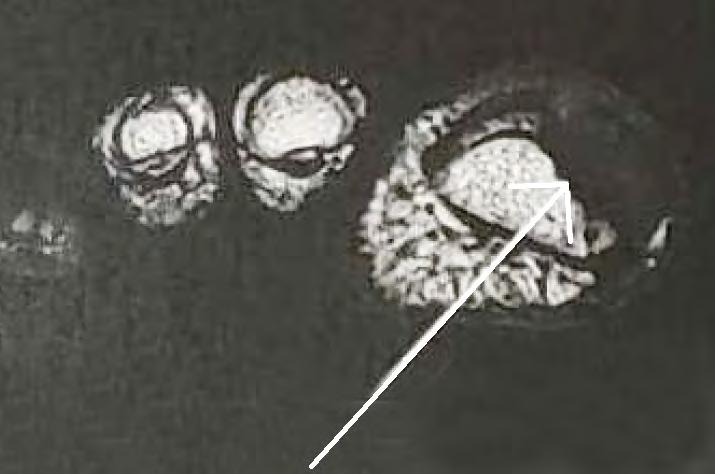
Table 1. Summary of reported cases. Magnetic resonance imaging (MRI), computed tomography (CT), and ultrasound (US). The mean age of patients was 44 years (range, 21–70), and the mean time to onset was 35 months (range, 0.5-120). Juvederm was the most frequently reported product; however, in most cases, the product used was unknown or not reported. A total of 4 cases described relevant background factors months before onset, including dental cleaning, blepharoplasty, COVID-19 vaccination, and breast cancer diagnosis and treatment. Nodules and masses, either inflammatory or noninflammatory, were the most common clinical presentations, but inflammatory plaques, papules, scar-like lesions, and blisters that progressed to ulcerative or fibrotic manifestations were also reported. The most frequently affected sites were perioral (n = 8), cheeks (n = 7), periocular (n = 5), and nose (n = 2), among others. Imaging modalities included MRI, CT, and US. Surgery was the most common treatment, generally with favorable outcomes, although corticosteroids, antibiotics, and hyaluronidase were also used.
DISCUSSION
Epidemiology
Approximately 15 years ago, the frequency of HA-induced FBG was estimated at 0.02%-0.4% in retrospective reviews.5 A more recent meta-analysis of 1,496 participants who underwent HA lip augmentation reported a frequency of 0.6%.23 In contrast, a retrospective analysis of 492 patients who underwent nonsurgical rhinoplasty with HA found no cases of FBG.24
This variability is likely related to multiple factors, as discussed later in pathogenesis and etiology. However, discrepancies in terminology (ie, delayed-onset nodules [DONs], inflammatory nodules, noninflammatory nodules, granulomas) and diagnostic methodology also contribute, as further discussed.
When considering DONs, the Manufacturer and User Facility Device Experience (MAUDE) database of the US Food and Drug Administration (FDA) showed that 71.8% of delayed-onset reactions were nodules (42.1% inflammatory and 29.7% noninflammatory), whereas 6.7% were granulomas, without a distinct classification.25 Another retrospective study found an overall incidence of DONs of 0.33% in 2,139 patients who underwent HA injections. Of these, 7 patients presented with DONs, but only 1 biopsy was performed, confirming FBG.6
These findings suggest that HA-induced FBG may be underdiagnosed, since biopsies are rarely performed owing to concerns about unfavorable cosmetic outcomes after aesthetic procedures.26
Pathogenesis
Although HA is generally thought to integrate into tis-
Identification of studies via databases and registers
Records identified from*:
PubMed n = 94
Embase n = 110
LILACS n = 3
Scopus n = 158
Databases (n = 365)
Records screened (n = 182)
Reports sought for retrieval (n = 182)
Reports assessed for eligibility (n = 180)
Records removed before screening:
Duplicate records removed (n = 183)
Records excluded** (n = 0 )
Reports excluded: Reason 1 (n = 91)
Reason 2 (n = 19)
Reason 2 (n = 16)
Reason 3 (n = 5)
Reason 4 (n = 33)
Reports not retrieved (n = 2 )
Studies included in review (n = 17)
sues without inflammation,4 some studies suggest the presence of a mild inflammatory reaction that goes unnoticed, characterized by a discrete population of macrophages with vacuolated cytoplasm and rare small giant cells, reflecting normal resorption.27 In contrast, FBGs, characterized by the aggregation of macrophages and foreign body giant cells, are formed through 4 phases3:
Recognition and inflammation: Implantation of the foreign material is followed by an innate immune response involving polymorphonuclear leukocytes — mainly neutrophils — along with complement activation and cytokine release.
Macrophage adhesion: The progression of inflammation directs monocytes, through cytokine signaling, to migrate into tissues and differentiate into macrophages.
Macrophage fusion: Aggregation and fusion of macrophages, mediated by interleukin-4 and interleukin-13, likely
occur in response to particle size, leading to the formation of foreign body giant cells.
Crosstalk between macrophages and foreign body giant cells: Both cell types secrete cytokines that recruit and activate fibroblasts, leading to the formation of a fibrous capsule around the foreign material.
HA-induced FBGs are considered an abnormal or exaggerated reaction to exogenous stimuli, often described as allergy or hypersensitivity. Although the central role of macrophages is well established, a type IVa hypersensitivity reaction has been inferred.28 However, this reaction is a T cell-mediated response, and the extent to which the adaptive immune system participates remains controversial. T cells have been identified in case reports of HA-induced FBG and are hypothesized to perpetuate ongoing macrophage activation around the granuloma.9,12,15,20,22,29 In contrast, a series of 18 biopsies from patients
Figure 1: Preferred Reporting Items for Systematic Reviews and Meta-Analyses flow diagram of the study selection process
with late-onset inflammatory adverse events to different fillers, including HA, showed no CD3-positive immune cells corresponding to T cell populations.30
Moreover, some authors have reported no adverse effects after HA re-exposure, leading to the hypothesis that HA-induced FBG may not represent a type IVa hypersensitivity reaction.5,6 Nonetheless, diagnostic tests for type IV hypersensitivity reactions have limited sensitivity and specificity.31 Patch testing is considered the gold standard for diagnosing type IV hypersensitivity,32 yet its sensitivity and specificity for delayed hypersensitivity drug eruptions are 32% and 92%, respectively,33 indicating a high rate of false-negative results. Another factor less frequently considered is the potential role of HA as an adjuvant in immune responses.
34
Etiology
HA is a glycosaminoglycan naturally present in the human body and, therefore, should not normally be recognized as foreign by the immune system. Nonetheless, HA functions as an extracellular matrix component and serves as an adhesive substrate for cellular migration, which may enhance immune responses.
34 Several mechanisms have been proposed as potential antigenic triggers of HA-induced FBG10,35,36:
Cross-linker: Agents such as 1,4-butanediol diglycidyl ether (BDDE), methacrylamide, hydrazide, carbodiimide, divinyl sulfone, and poly(ethylene glycol) diglycidyl ether are used to delay HA degradation by endogenous hyaluronidases. This effect is achieved through covalent bonding between HA molecules, reducing enzymatic exposure. BDDE is currently the most commonly used cross-linker due to its stability, biodegradability, and long safety record. Residual unreacted BDDE at levels < 2 ppm is considered safe; however, byproducts are not always adequately evaluated.
37
Impurities: During production, HA may come into contact with unintended molecules. Traces of stainless steel, aluminum, silicone, sodium hydroxide, and streptococcal endotoxins have been identified. Threshold limits for particulate matter in prefilled syringes are 6,000 and 600 per container for particles ≥ 10 µm and ≥ 25 µm, respectively.35,38
Infection: Delayed-onset reactions, including FBG, have been reported after infections, likely due to inoculation into previously implanted dermal fillers and subsequent inflammatory responses.39 Several authors have associated granuloma formation with biofilm development.13 Biofilms on HA surfaces may enable persistent infection with minimal host immune response.10
Immune system: FBG has frequently been reported following immune challenges such as vaccination, infections, and dental procedures. Cases of delayed hypersensitivity to HA after influenza-like illness have been described.31 In a study of 2,139 patients treated with HA, 7 developed DONs, 6 of whom had undergone dental procedures 1-168 days before nodule formation. A seasonal pattern was also noted, with most cases (71%) occurring between September and December.6 Another study
of 3,255 patients receiving 8,067 filler syringes reported higher granuloma rates in the post-COVID-19 period (0.3% vs 0.0%, P = .009).40 Both COVID-19 infection and vaccination have been implicated, as reexposure appears to trigger faster responses.41,42 The SARS-CoV-2 spike protein, which binds angiotensin-converting enzyme 2 (ACE2) receptors, favors a proinflammatory local Th1 cascade, promoting CD8+ T cell–mediated reactions to incipient granulomas.43 A heightened immune state may enable recognition of previously undetected antigens, thereby triggering granulomatous inflammation.35
HA molecular weight: Low-molecular weight HA (< 1,000 kDa) has been shown to be proinflammatory, whereas high-molecular weight HA is generally considered anti-inflammatory.44 Vycross technology has been associated with higher rates of DONs,6,25 although this remains controversial, as HA degradation would inherently release low-molecular weight fragments.35
Injection volume and technique: In a study of 4,500 patients, those who developed DONs had received a higher cumulative injection volume (5.0 mL) compared with those without nodules (0.5-1.5 mL lower cumulative volume), suggesting volume as a risk factor.45 Other studies, however, did not replicate this finding.6 Expert consensus nonetheless suggests that larger bolus volumes may increase the risk of FBG and other complications.46 Repeated injections using the droplet technique and incorrect injection depth have also been implicated,36 consistent with the heightened immune surveillance in dermal tissues compared with subcutaneous fat and deeper planes.
Clinical manifestations
Reports have documented HA-induced FBGs as early as a few weeks after injection and as late as 10 years post-procedure. This variability challenges the clinical value of categorizing HA-induced complications into early, late, or delayed presentations.2 Patient history is often unremarkable, and clinicians may be unaware of prior cosmetic procedures.47
HA-induced FBG appears more common in periorificial areas, similar to DONs. The most frequently affected sites are the lips (41.1%), followed by the nasolabial folds (23.6%), marionette lines (22.1%), perioral region (19.3%), and tear troughs (12.1%).25 Similar patterns have been observed with other dermal fillers.48 These regions may be more susceptible to complications due to repetitive movement and fixed points of origin and insertion, which facilitate filler deposition and increase the risk of FBG formation.
In a review of 11 cases of orofacial FBG following HA injection, the most common presentation was noninflammatory nodules,10 consistent with findings in the present report. However, atypical manifestations have also been described, including maculopapular lesions,7 papules, plaques,49 scar-like lesions,22 and blisters progressing to ulcerative-fibrotic changes,15 sometimes associated with inflammatory signs such as erythema and/ or edema.50 Consequently, categorizing FBG solely under broa-
der clinical groups such as “DONs,” “inflammatory nodules,” or “noninflammatory nodules”26 is imprecise and not diagnostic.
Pathology
In a retrospective review of 6 patients who underwent biopsy for facial nodules persisting > 3 months after HA injection, 4 cases were classified as “nongranulomatous” nodules containing only HA, while 2 were identified as granulomatous nodules.51 Normal resorption is characterized by discrete populations of macrophages with vacuolated cytoplasm and occasional small giant cells.27
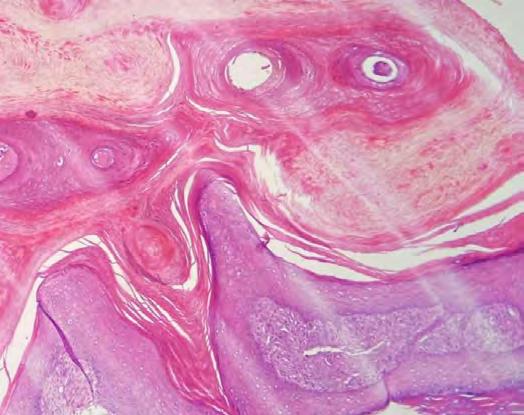
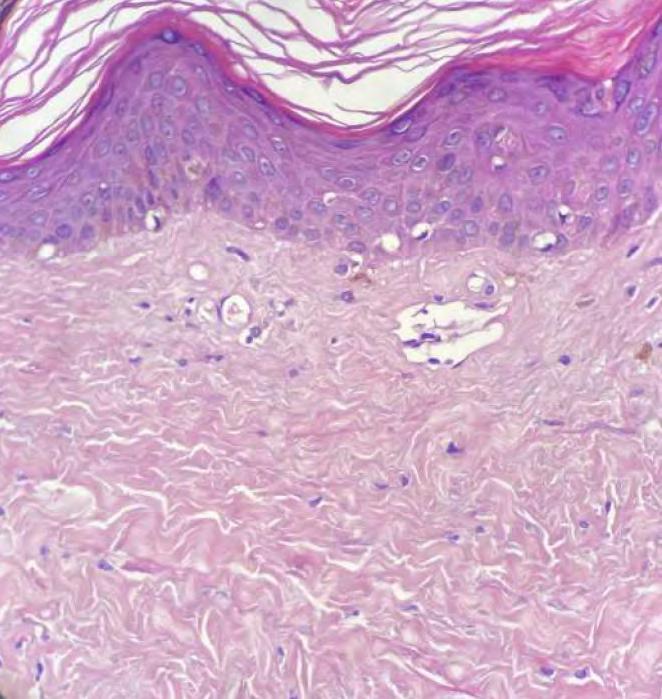
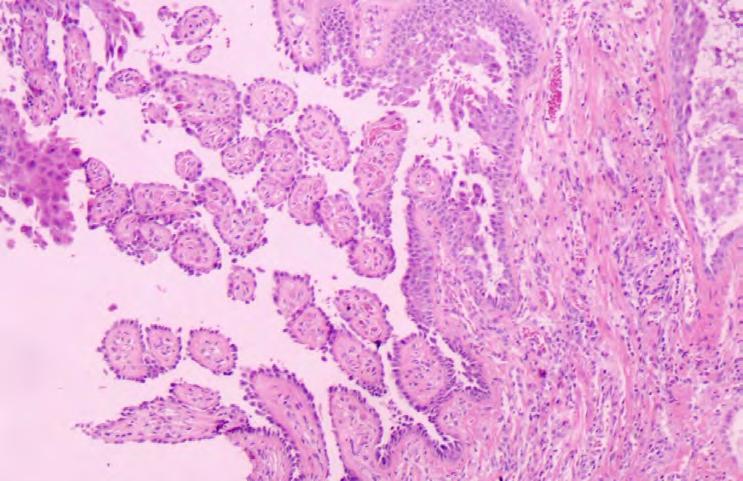
In a histopathologic review of 15 cases, foreign body granulomatous reactions to HA filler were predominantly characterized by vacuoles of basophilic material surrounded by palisading histiocytes, with variable numbers of eosinophils and foreign body giant cells.52 Multiple stains can be used to identify HA deposits. Hematoxylin-eosin reveals HA as gray to pale blue, while Alcian blue and colloidal iron stains demonstrate HA as bright blue to green-blue. Although the latter provide improved visualization, they are not mandatory.53 Morphologically, biphasic HA fillers typically appear granular, filamentous, or wispy, whereas monophasic HA is usually amorphous.10
Evaluation
Imaging studies can support the diagnostic work-up of HA-induced FBG. US findings typically include hypoechoic lesions with internal particulate echoes, peripheral hypoechogenicity, increased vascularity within and around the deposits, and increased echogenicity and thickness of the subcutaneous tissue.
54–56 Conversely, some deposits are described as anechoic areas with sharp, regular borders.57 Magnetic resonance imaging and computed tomography have also been used to evaluate nonvascular complications of HA, one of which is FBG.56 Nevertheless, FBG remains primarily a histological diagnosis, and no studies have established diagnostic accuracy. Despite this, imaging techniques are promising as complementary evaluation tools.
Treatment
Current guidelines are limited by reliance on clinical diagnosis, typically distinguishing between inflammatory and noninflammatory nodules. Granulomas are often grouped with the latter,58 even though, as noted, they may present with diverse clinical features distinct from noninflammatory nodules. The absence of a definitive diagnosis has led to a “scatter-gun” polypharmacy approach, which carries risks of adverse effects and suboptimal outcomes.26 The reluctance to perform biopsies in aesthetic complications, due to concerns about scarring, further limits histological confirmation. In this context, US emerges as a noninvasive tool that can aid more accurate evaluation.
Watchful waiting may be appropriate for noninflammatory nodules,46 as some granulomas resolve spontaneously within 2 years.59 Several therapeutic approaches have been described, including hyaluronidase, oral or intralesional corticosteroids,
antihistamines, anti-inflammatories, antibiotics, intralesional 5-fluorouracil, and surgery.36 Consistent with prior reviews, most HA-induced FBG have been successfully managed with surgical excision.60 However, this may reflect a bias toward excision in cases selected for histological analysis, which suggests underdiagnosis in nonoperated patients.
From a treatment rationale perspective, since FBGs are composed of HA deposits, inflammatory infiltrates, fibrosis, and/ or capsule formation, management with hyaluronidase, intralesional corticosteroids, and 5-fluorouracil is recommended, preferably under US guidance to ensure precise injection. Combining intralesional triamcinolone with 5-fluorouracil appears to reduce the risk of skin atrophy associated with higher triamcinolone doses.61 Oral corticosteroids may also be effective but are generally reserved due to systemic side effects.
The use of antibiotics should be limited to their anti-inflammatory properties, as alternative agents can achieve similar effects and concerns about global antibiotic resistance remain. Multiple sessions of hyaluronidase combined with triamcinolone and 5-fluorouracil may be required. US guidance not only improves injection accuracy but also helps determine whether hyaluronidase is indicated, given its activity against extracellular HA deposits but limited effect on inflammatory infiltrates, fibrosis, or capsule. Surgical excision should be considered the last resort.62
Limitations
As noted, HA-induced FBG is primarily a histological diagnosis, with limited correlation to clinical presentation and uncertain correlation between histological findings and imaging studies, although imaging remains promising. The overlap among clinical, imaging, and histopathological terminology related to HA-induced FBG obscures diagnosis and consequently hampers research. Some studies cited in the discussion were not included in the results due to the absence of histopathological confirmation. Furthermore, the number of available studies is scarce, and underreporting is likely. Additional research is therefore required.
CONCLUSION
Although the exact prevalence of HA-induced FBG remains uncertain, it is undoubtedly a potential complication. The current time-based classification of complications may warrant reevaluation. To date, HA-induced FBG continues to be a histological diagnosis, underscoring the need for biopsies to ensure accurate diagnosis and appropriate treatment. US is a valuable evaluation tool and a promising diagnostic method, but further studies are needed to establish correlations between imaging and histological findings. Tailoring treatment to the presence of HA deposits, inflammatory infiltrates, fibrosis, and/ or capsule formation may reduce adverse effects and optimize outcomes. More studies are also required to define effective therapeutic strategies. l
1. Triana L, Palacios Huatuco RM, Campilgio G, Liscano E. Trends in surgical and nonsurgical aesthetic procedures: a 14-year analysis of the International Society of Aesthetic Plastic Surgery —ISAPS. Aesthetic Plast Surg. 2024;48(20):4217–27.
2. Zaccaria G, Dotti A, Benanti E, Vigliarolo C, Vaienti L. A treatment algorithm for hyaluronic acid filler related complications of the face. J Plast Reconstr Aesthet Surg. 2024;91:207–17.
3. Lee JM, Kim YJ. Foreign body granulomas after the use of dermal fillers: pathophysiology, clinical appearance, histologic features, and treatment. Arch Plast Surg. 2015;42(2):232–9.
4. Tran C, Carraux P, Micheels P, Kaya G, Salomon D. In vivo bio-integration of three hyaluronic acid fillers in human skin: a histological study. Dermatology. 2014;228(1):47–54.
5. Lemperle G, Gauthier-Hazan N, Wolters M, Eisemann-Klein M, Zimmermann U, Duffy DM. Foreign body granulomas after all injectable dermal fillers: part 1. possible causes. Plast Reconstr Surg. 2009;123(6):1842–63.
6. Rivers JK. Incidence and treatment of delayed-onset nodules after VYC filler injections to 2139 patients at a single canadian clinic. J Cosmet Dermatol. 2022;21(6):2379–86.
7. Lai D, Liu H, Kong L, Cheng S. Delayed complication of botulinum toxin and hyaluronic acid filler injections: a case report. J Cosmet Dermatol. 2022;21(6):2374–8.
8. Denkova R, Georgieva I, Kantardjiev V. Immune system triggers as a factor for the formation of foreign body granuloma after hyaluronic acid fillers treatment: a case report and treatment protocol. J Appl Cosmetol. 2024;42(2).
9. Arici C, Tosuner Z. Infraorbital mass long after dermal filler injection: a report of two cases. J Cosmet Dermatol. 2023;22(4):1245–8.
10. Delayed foreign body granulomas in the orofacial region after hyaluronic acid injection. Chin J Dent Res. 2020;23(4):289–96.
11. Zhang FF, Xu ZX, Chen Y. Delayed foreign body granulomas in the orofacial region after hyaluronic acid injection. Chin J Dent Res. 2020;23(4):289–96.
12. Parulan MAA, Sundar G, Lum JH, Ramachandran U. A case report on dermal filler-related periorbital granuloma formation. Orbit. 2019;38(2):169–72.
13. Tamiolakis P, Piperi E, Christopoulos P, Sklavounou-Andrikopoulou A. Oral foreign body granuloma to soft tissue fillers. Report of two cases and review of the literature. J Clin Exp Dent. 2018;10(2):e177–84.
14. Kaczorowski M, Nelke K, Luczak K, Halon A. Filler migration and florid granulomatous reaction to hyaluronic acid mimicking a buccal tumor. J Craniofac Surg. 2020;31(1):e78–9.
15. Cecchi R, Spota A, Frati P, Muciaccia B. Migrating granulomatous chronic reaction from hyaluronic acid skin filler (restylane): review and histopathological study with histochemical stainings. Dermatology. 2014;228(1):14–7.
16. Tonin B, Colato C, Bruni M, Girolomoni G. Late granuloma formation secondary to hyaluronic acid injection. Dermatol Online J. 2020;26(7):13030.
17. Leupe P, Menger DJ. The injectable filler in rhinoplasty: not a complication-free alternative. B-ENT. 2016;12(2):137–42.
18. Dryden SC, Gabbard RD, Meador AG, Stoner AE, Klippenstein KA, Wesley RE. A case of orbital granuloma secondary to dermal filler injection. Cureus. 2021;13(12):e20606.
19. Nishimura M, Sakamoto S, Hoshino M, Miyazaki Y, Yamamoto J, Sakashita H, et al. Histological features of delayed foreign body granuloma with epithelioid histiocyte aggregation and eosinophilic reaction due to hyaluronic acid injection. Case Rep Dent. 2024;2024:5565324.
20. Kim JH, Choi JS, Yun JH, Kang HK, Baek JO, Roh JY, et al. Foreign body reaction to injectable hyaluronic acid: late granuloma formation. Ann Dermatol. 2015;27(2):224–5.
21. Alcântara CEP, Noronha MS, Cunha JF, Flores IL, Mesquita RA. Granulomatous reaction to hyaluronic acid filler material in oral and perioral region: a case report and review of literature. J Cosmet Dermatol. 2018;17(4):578–83.
22. Hwang MJ, Lee YP, Jin YT, Chiang CP. Hyaluronic acid-induced foreign body granuloma in the upper lip. J Dent Sci. 2023;18(3):1429–30.
23. Czumbel LM, Farkasdi S, Gede N, Mikó A, Csupor D, Lukács A, et al. Hyaluronic acid is an effective dermal filler for lip augmentation: a meta-analysis. Front Surg. 2021;8:681028.
24. Jalali A. Nonsurgical rhinoplasty using the hyaluronic acid filler VYC-25L: safety and patient satisfaction in a retrospective analysis of 492 patients. J Cosmet Dermatol. 2024;23(2):426–33.
25. Cohen JL, Hicks J, Nogueira A, Lane V, Andriopoulos B. Postmarket safety surveillance of delayed complications for recent fda-approved hyaluronic acid dermal fillers. Dermatol Surg. 2022;48(2):220–4.
26. Convery C, Davies E, Murray G, Walker L. Delayed-onset nodules (dons) and considering their treatment following use of hyaluronic acid (ha) fillers. J Clin Aesthetic Dermatol. 2021;14(7):E59–67.
27. Plantier F. Lessons on reactions to aesthetic fillers. Ann Pathol. 2024;44(6):491– 7. [French]
28. Jutel M, Agache I, Zemelka-Wiacek M, Akdis M, Chivato T, Del Giacco S, et al. Nomenclature of allergic diseases and hypersensitivity reactions: adapted to modern needs: an eaaci position paper. Allergy. 2023;78(11):2851–74.
29. Alijotas-Reig J, Fernández-Figueras MT, Puig L. Inflammatory, immune-mediated adverse reactions related to soft tissue dermal fillers. Semin Arthritis Rheum. 2013;43(2):241–58.
30. Decates TS, Velthuis PJ, Jhingoerie R, Gibbs S, Bachour Y, Niessen FB. No association found between late-onset inflammatory adverse events after soft tissue filler injections and the adaptive immune system. J Cosmet Dermatol. 2023;22(2):458–63.
31. Turkmani MG, De Boulle K, Philipp-Dormston WG. Delayed hypersensitivity reaction to hyaluronic acid dermal filler following influenza-like illness. Clin Cosmet Investig Dermatol. 2019;12:277–83.
32. Muthupalaniappen L, Jamil A. Prick, patch or blood test? A simple guide to allergy testing. Malays Fam Physician. 2021;16(2):19–26.
33. Hassoun-Kheir N, Bergman R, Weltfriend S. The use of patch tests in the diagnosis of delayed hypersensitivity drug eruptions. Int J Dermatol. 2016;55(11):1219–24.
34. Alijotas-Reig J, Hindié M, Kandhaya-Pillai R, Miro-Mur F. Bioengineered hyaluronic acid elicited a nonantigenic T cell activation: implications from cosmetic medicine and surgery to nanomedicine. J Biomed Mater Res A. 2010;95A(1):180–90.
35. Lee W, Shah-Desai S, Rho NK, Cho J. Etiology of delayed inflammatory reaction induced by hyaluronic acid filler. Arch Plast Surg. 2024;51(1):20–6.
36. Singh K, Nooreyezdan S. Nonvascular complications of injectable fillers—prevention and management. Indian J Plast Surg. 2020;53(3):335–43.
37. Fidalgo López J, Deglesne PA, Arroyo R, Sepúlveda L, Ranneva E, Deprez P. Detection of a new reaction by-product in BDDE cross-linked autoclaved hyaluronic acid hydrogels by LC–MS analysis. Med Devices Evid Res. 2018;11:367–76.
38. Lee W, Rho NK, Yang EJ. Determination of hyaluronic acid dermal filler impurities using SEM/EDS Analysis. Polymers. 2023;15(7):1649.
39. Ibrahim O, Overman J, Arndt KA, Dover JS. Filler nodules: inflammatory or infectious? A review of biofilms and their implications on clinical practice. Dermatol Surg. 2018;44(1):53–60.
40. Michel JC, Perenack JD, Chapple AG, Christensen BJ. Are delayed dermal filler granulomas more common since COVID-19? J Oral Maxillofac Surg. 2023;81(1):42–8.
41. Witt J, Hooper D, Munavalli GG. Delayed inflammatory reaction to hyaluronic acid filler following shingrix and fluzone vaccines treated with lisinopril. JAAD Case Rep. 2022;23:133–5.
42. Alijotas-Reig J, García-GImenez V, Velthuis PJ, Niessen FB, Decates TS. Inflammatory immune-mediated adverse reactions induced by COVID -19 vaccines in previously injected patients with soft tissue fillers: a case series of 20 patients. J Cosmet Dermatol. 2022;21(8):3181–7.
43. Munavalli GG, Guthridge R, Knutsen-Larson S, Brodsky A, Matthew E, Landau M. COVID-19/SARS-CoV-2 virus spike protein-related delayed inflammatory reaction to hyaluronic acid dermal fillers: a challenging clinical conundrum in diagnosis and treatment. Arch Dermatol Res. 2022;314(1):1–15.
44. Rayahin JE, Buhrman JS, Zhang Y, Koh TJ, Gemeinhart RA. High and low molecular weight hyaluronic acid differentially influence macrophage activation. ACS Biomater Sci Eng. 2015;1(7):481–93.
45. Humphrey S, Jones DH, Carruthers JD, Carruthers A, Beleznay K, Wesley N, et al. Retrospective review of delayed adverse events secondary to treatment with a smooth, cohesive 20-mg/mL hyaluronic acid filler in 4500 patients. J Am Acad Dermatol. 2020;83(1):86–95.
46. Philipp-Dormston WG, Goodman GJ, De Boulle K, Swift A, Delorenzi C, Jones D, et al. Global approaches to the prevention and management of delayed-onset adverse reactions with hyaluronic acid-based fillers. Plast Reconstr Surg - Glob Open. 2020;8(4):e2730.
47. Cuylits N. Complications of hyaluronic acid injections in aesthetic medicine: an emerging pathology? Rev Med Brux. 2024;45(4):414–8.
48. Machado RA, Oliveira LQ, Martelli-Júnior H, Pires FR, Carvas JB, Rogerio VE, et al. Adverse reactions to the injection of face and neck aesthetic filling materials: a systematic review. Med Oral Patol Oral Cirugia Bucal. 2023;28(3):e278–84.
49. Bowles A, Ghalili S, Ojong OB, Vasile GF, Li YM, Aguilera SB. Novel management of granuloma formation secondary to dermal filler: a multi-modality approach. J Cosmet Dermatol. 2023;22(4):1233–7.
50. Rozas-Muñoz E, Gamé D, Piquero-Casals J, Mir-Bonafé JF, Ocampo-López C, Madariaga JA. Persistent nose swelling in a teenage girl: answer. Am J Dermatopathol. 2022;44(12):1003–4.
51. Modarressi A, Nizet C, Lombardi T. Granulomas and nongranulomatous nodules after filler injection: different complications require different treatments. J Plast Reconstr Aesthet Surg. 2020;73(11):2010–5.
52. Mu EW, Stokar E, Franks L, Meehan SA. Histopathologic reaction patterns to differentially cross-linked hyaluronic acid fillers: a retrospective case series. J Cutan Pathol. 2021;48(6):758–62.
53. Agosti V, Stefanini G. Granulomatous reaction to hyaluronic acid dermal filler: clinical and histological features. Aesthetic Med. 2024;10(1):e2024002.
54. Vandeputte J, Leemans G, Dhaene K, Forsyth R, Vanslembrouck J, Hatem F, et al. Spreading pattern and tissue response to hyaluronic acid gel injections in the subcutis: ultrasound videos, ultrasound measurements, and histology. Aesthet Surg J. 2021;41(2):224–41.
55. Gonzalez C, Duque-Clavijo V, Kroumpouzos G, Garcia Concha AM, Olmos Perez M. Ultrasonographic features of nonvascular complications of hyaluronic acid fillers: a retrospective study at a reference center for dermatologic ultrasonography. Clin Dermatol. 2024;42(5):538–46.
56. Mlosek RK, Migda B. The use of high-frequency ultrasonography for the diagnosis of palpable nodules after the administration of dermal fillers. J Ultrason. 2020;20(83):248–53.
57. Mlosek RK, Skrzypek E, Skrzypek DM, Malinowska S. High-frequency ultrasound-based differentiation between nodular dermal filler deposits and foreign body granulomas. Skin Res Technol. 2018;24(3):417–22.
58. Signorini M, Liew S, Sundaram H, De Boulle KL, Goodman GJ, Monheit G, et al. Global Aesthetics Consensus: avoidance and management of complications from hyaluronic acid fillers—evidence- and opinion-based review and consensus recommendations. Plast Reconstr Surg. 2016;137(6):961e–71e.
59. Zein M, Tie-Shue R, Pirakitikulr N, Lee WWL. Complications after cosmetic periocular filler: prevention and management. Plast Aesthetic Res. 2020;7:44.
60. Trinh LN, McGuigan KC, Gupta A. Delayed granulomas as a complication secondary to lip augmentation with dermal fillers: a systematic review. Surg J. 2022;8(1):e69–79.
61. Kroumpouzos G, Harris S, Bhargava S, Wortsman X. Complications of fillers in the lips and perioral area: Prevention, assessment, and management focusing on ultrasound guidance. J Plast Reconstr Aesthet Surg. 2023;84:656–69.
62. Kroumpouzos G, Treacy P. Hyaluronidase for dermal filler complications: review of applications and dosage recommendations. JMIR Dermatol. 2024;7:e50403.
AUTHOR’S CONTRIBUTION:
Lina María Osorio Cock
0000-0002-5591-7954
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Jaime Alberto Rengifo Palacios
0009-0009-1797-4534
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
María Paulina Uribe Posada
0009-0002-1956-8491
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
María Alejandra Sarabia de Capozzi
0009-0003-0155-2544
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
María Aida Angulo Morillo
0009-0000-3928-3392
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
www.surgicalcosmetic.org.br/
National Skin Cancer Prevention Campaign: analysis of the resolution rate of skin tumors diagnosed during the 2022 and 2023 Skin Cancer Awareness Month campaigns in Jundiaí, Brazil
Campanha Nacional de Prevenção ao Câncer de Pele: análise da taxa de resolutividade dos tumores cutâneos diagnosticados durante as campanhas do Dezembro Laranja de 2022 e 2023, realizadas em Jundiaí ABSTRACT
Introduction: Cutaneous malignant tumors are preventable and have a high cure rate when diagnosed early, resulting in reduced morbidity and mortality. Early-stage cancer detection allows for timely treatment, leading to a better prognosis.
Objective: To evaluate the effectiveness of the “Skin Cancer Awareness Month” campaign in identifying potential cases of skin cancer and its resolution rate based on the time required for lesion treatment.
Method: A retrospective analytical cross-sectional study with descriptive-quantitative characteristics.
Results: In 2022, the time between biopsy and curative surgery ranged from 94 to 218 days, with a median of 153 days. In 2023, the time between biopsy and curative surgery ranged from 12 to 249 days, with a median of 129 days. A statistically significant difference (p=0.04) was observed between the years 2022 and 2023 in the median time from biopsy to surgery.
Conclusion: Improved efficiency in performing biopsies and surgeries, as well as enhanced patient adherence to treatment, was necessary.
Keywords: Carcinoma; Carcinoma, Squamous Cell; Skin Neoplasms; Health Promotion; Time-to-Treatment.
1 Faculdade de Medicina de Jundiaí (FMJ), Dermatology, Jundiaí, São Paulo (SP), Brazil
2 Faculdade de Medicina do ABC, Gynecology, São Paulo (SP), Brazil
Research Ethics Committee approval protocol number: 68423723.1.0000.5412
Funding: None.
Conflict of interest: None.
Submitted on: 11/16/2024
Final decision: 06/05/2025
RESUMO
Introdução: Tumores malignos cutâneos são preveníveis e apresentam alta taxa de cura quando diagnosticados precocemente, resultando em redução da morbimortalidade. Assim, a identificação dos estágios iniciais do câncer permite tratar a doença de forma precoce, favorecendo um melhor prognóstico.
Objetivo: Definir a eficácia da campanha Dezembro Laranja na identificação de casos prováveis de câncer de pele e sua taxa de resolutividade, considerando o tempo hábil para a resolução das lesões.
Método: Estudo transversal analítico retrospectivo, com características descritivo-quantitativas.
Resultados: Em 2022, o tempo transcorrido entre a biópsia e a cirurgia curativa variou de 94 a 218 dias, com mediana de 153 dias. Em 2023, esse intervalo variou de 12 a 249 dias, com mediana de 129 dias. Foi observada diferença estatisticamente significativa (p = 0,04) entre os anos de 2022 e 2023 para a mediana do tempo entre a biópsia e a cirurgia.
Conclusão: Uma maior agilidade na realização de biópsias/cirurgias, além de uma melhor adesão dos pacientes ao tratamento, mostrou-se necessária.
Palavras-chave: Carcinoma de Células Escamosas; Carcinoma Basocelular; Neoplasias Cutâneas; Promoção da Saúde; Tempo para o Tratamento.
How to cite this article: Pompei IM, Alves CAXM, Lorenção AP, Almeida BM, Ferreira JASLB, Pompei LM. National Skin Cancer Prevention Campaign: analysis of the resolution rate of skin tumors diagnosed during the 2022 and 2023 Skin Cancer Awareness Month campaigns in Jundiaí, Brazil. Surg Cosmet Dermatol. 2025;17:e20250422.
INTRODUCTION
Malignant skin tumors, such as basal cell carcinomas (BCCs), squamous cell carcinomas (SCCs), and melanomas, account for a large share of all cancers in Brazil and worldwide. Among all malignant neoplasms, non-melanoma skin cancer is the most frequent type in both sexes.1 According to Brazil’s National Cancer Institute, approximately 30% of all malignant tumors are skin neoplasms, and diagnosis of new cases is expected to increase in coming years to about 180 thousand new cases/year.2,3 The increase in annual incidence rates highlights the trend of increased prevalence of the condition, not only due to global increases in life expectancy but primarily due to the combination of improved diagnostic capacity and longer exposure to risk factors, such as exposure to ultraviolet radiation. The significant increase in the number of skin tumors should come as a warning to health care systems, as well as encourage the deployment of new measures for early screening and diagnosis of skin neoplasms.4,5,6
Overall, skin tumors are caused by the abnormal and uncontrolled proliferation of skin cells. Depending on the skin layers affected, tumors can be divided into several types. The three most common types of skin cancer are, in decreasing order of incidence, BCCs, SCCs, and melanomas.7 BCCs, originating from the basal cells of the skin and skin appendages, primarily affect the H-zone of the face, with 70% of all cases found on the face and head, but may also affect the trunk and limbs. They are characterized by slow growth and low risk of metastases, which gives them high cure rates when detected early.8 SCCs originate from the squamous cells and may be found in any part of the body, and are more common on the lips, ears, scalp, areas of chronic inflammation, scars, and burns.8 Melanomas, in turn, are a more aggressive and fatal form of tumor, although fortunately rarer than the other two. While its diagnosis is a source of patient anxiety, when made early and assertively, the condition has cure rates of over 90%.9,10 The risk factors for developing this form of cancer are well known, facilitating primary prevention and health promotion by raising awareness about risk behaviors, warning signs, and periodicity of prevention.
Therefore, skin neoplasms are a preventable disease when exposure to carcinogenic agents is reduced or eliminated, and when individual susceptibility to those agents is likewise limited.11 In addition, malignant skin tumors, when diagnosed early, are known to have high cure rates—approximately 90%—resulting in lower morbidity and mortality.9,10 They are also a preventable type of cancer, with exposure to ultraviolet radiation without the use of photoprotection the primary risk factor. Therefore, early-stage detection of a neoplasm allows for timely treatment, leading to a better prognosis. Meanwhile, one should pursue means of implementing primary prevention measures, encourage the use of educational programs in schools and communities, increase early detection campaigns, improve therapeutic management of diagnosed cases, and reduce morbidity and costs to the health care system through early screening and effective treatment of lesions.4
With regard to early treatment of skin cancer, it should be stressed that health awareness campaigns represent an advancement in patient care, encompassing both primary and secondary prevention. Primary prevention is performed before the disease—in other words, it is based on unspecific protective measures against risk and damage through reduced exposure of individuals to disease risk factors in order to lower its incidence.12 Secondary prevention, in turn, occurs when the disease is subclinical or in its early stages. Despite our inability to change genetic predisposition, this stage enables us to lower the exposure to the factors causing tumors.13
Accordingly, the relevance of skin cancer prevention campaigns deserves more attention. The National Skin Cancer Prevention Campaign (NSCPC), established by the Brazilian Society of Dermatology in 2014, aims at preventing skin neoplasms through health promotion by warning, informing, and raising awareness among the population, focusing on primary prevention. The campaign also has a secondary prevention component based on screening efforts for early diagnosis of potential malignant skin lesions. Thus, it enables rapid treatment, lower mortality, and increased survival for patients.5
Currently, there are few Brazilian and/or Latin American studies on the resolution rates of primary and/or secondary prevention measures adopted to fight and treat skin cancer. The paucity of recent studies requires better assessment of dermatology practitioners, justifying the need to assess the effectiveness of measures adopted after a skin neoplasm has been diagnosed, since the number of patients with skin tumors only tends to increase, as do the impact and the consequences of the disease on their lives.
OBJECTIVES
To evaluate the effectiveness of NSCPC in identifying potential cases of skin cancer and its resolution rate based on the time required for lesion treatment. In addition, the study aimed at determining the epidemiological pattern found in the 2022 and 2023 NSCPCs.
METHODS
This is a retrospective analytical cross-sectional study with descriptive-quantitative characteristics. It was conducted based on records collected during NSCPC at the Faculdade de Medicina de Jundiaí (FMJ) outpatient dermatology service in Jundiaí, São Paulo, Brazil. The sample size corresponded to the maximum number of participants the researchers were able to approach during the 2022 and 2023 NSCPCs and who fit the inclusion criteria, totaling 158 individuals. The survey included all patients aged 18 years and older, as well as those with suspected diagnosis of skin cancer as assessed by FMJ dermatologists. Participants who did not agree to sign an informed consent form were excluded. This study was submitted to the FMJ Research Ethics Committee (REC). Analysis of the data collected from
NSCPC survey forms began once the REC gave its approval. The data were input in a Microsoft Excel® (Microsoft Corporation®, San Diego, USA) electronic spreadsheet. Statistical analysis was performed using the StatPlus® (AnalystSoft Inc.) plugin for Excel, with numerical data presented as mean (SD) or median (IQR). The Mann-Whitney U test was used to compare the years 2022 and 2023. The level of significance was set at 5%.
RESULTS
The total number of participants in the 2022 NSCPC who met the selection criteria for this study was 44, the majority of which consisted of 27 women (61.4%), compared to 17 men (38.6%). In 2023, 114 patients met the inclusion criteria and were referred for further investigation, with 71 women accounting for the majority of the sample (62.3%) and 43 men accounting for 37.7% of the total (Table 1).
In 2022, individuals aged 61-70 years had the highest rate of participation in the study, with 17 participants (38.6%), followed by those aged 71-80 years, with 10 participants (22.7%). Only two patients (4.5%) were older than 90 years, and the least represented age group consisted of individuals under 30 years of
age, with a single individual (2.3%). There were no participants aged 30-40 years. In 2023, incidence rates were similar, differing only in the switch between the two dominant age groups: the largest group of participants was 71-80 years of age, with 33 individuals (28.9%), followed by the 61-70 years age group, with 23 individuals (20.1%). In addition, there was an increase in the total number of participants over 90 years of age, totaling 17 individuals (14.9%) (Table 1).
The phototype most affected by skin tumors, in both 2022 and 2023, was phototype 2, accounting for 19 (43.1%) and 56 participants (49.1%), respectively, followed by phototype 3, with 13 (29.5%) and 27 (23.6%). However, a great number of records were found to lack this piece of information: six records (13.6%) in 2022 and 14 records (12.2%) in 2023, which may hinder proper data analysis (Table 1). Regarding personal history of skin cancer, a high number of records were found to lack this piece of information, totaling 10 records (22.7%). From the data available, 21 patients (47.7%) were found to have no personal history of the disease. The 2023 data on personal history of neoplasms were not analyzed in this study.
= National Skin Cancer Prevention Campaign.
Table 1: Data on participants selected during 2022 NSCPC (n = 44), 2023 NSCPC (n = 114), and total for both NSCPCs (n
In terms of the type of skin lesion found by dermatological examination, in 2022 most lesions consisted of BCC, with 25 cases (44.6%), followed by actinic keratosis (AK), with 10 cases (17.8%), and SCC, with seven cases (12.5%). Pigmented lesions, suggestive of melanoma, accounted for one case (1.7%). It should be noted that lesions outnumber participants because some patients had more than one lesion. In 2023, the largest share consisted of non-neoplastic lesions, totaling 41 cases (32.3%), followed by BCC, with 29 lesions (22.8%), and SCC, with 12 cases (9.4%). That same year, no pigmented lesion suggestive of melanoma was diagnosed (Table 2).
Regarding the site where the lesions were found, similar rates were observed in both 2022 and 2023. In the head and neck region, 28 cases (49.1%) were found in 2022 and 56 cases (45.1%) in 2023, totaling almost half of all lesions. In the trunk, 14 lesions (24.5%) were recorded in 2022 and 32 lesions (25.8%) in 2023. Percentages for lesions found on the limbs remained similar, with 12 lesions (21.1%) in 2022 and 29 lesions (23.3%) in 2023 (Table 3).
Cases assessed with possible outcomes of skin neoplasms were referred for biopsy in order to determine follow-up for each patient. In 2022, only one patient was directly referred for clinical follow-up with 5-fluorouracil (2.3%), while the remaining 43 (97.7%) were referred for biopsy. Out of these, six (14.0%) were lost to follow-up, 35 (81.3%) underwent punch
biopsy, and only two (4.7%) underwent resection. After biopsy results, four patients (9.3%) had no surgical indication, six (14.0%) were lost to follow-up, and 33 (76.7%) had indication for surgical procedures and their procedures were scheduled (Flowchart 1).
In 2023, out of 114 patients, only five (4.4%) failed to attend on the day of the biopsy. Among those who continued follow-up, 38 (34.9%) underwent resection and 71 (65.1%) underwent punch biopsy. After biopsy results, clinical follow-up was recommended for five patients (4.6%), there was no surgical indication for 45 patients (41.3%), and the remaining 59 (54.1%) were referred for surgical procedures (Flowchart 2).
The time between the 2022 NSCPC and the biopsy of the lesions assessed on the screening day ranged from 34 to 100 days, with a mean (SD) of 49.8 (13.1) days between the two events and a median of 47.0 days (IQR 40-53). Out of 37 patients referred for biopsy, 20 (54.1%) waited between 34 and 48 days to complete this step. An additional 11 patients (29.7%) required from 49 to 62 days, and only one (2.7%) waited over 90 days (Graph 1A). In 2023, the time between the NSCPC and the biopsy of the lesions assessed during the event ranged from 0 to 86 days, with a mean (SD) of 39.2 (26.2) days between the two events and a median of 47.0 days (IQR 12-58). Out of 109 patients who showed up on the day scheduled for their biopsies, 31 (28.4%) underwent the procedure in less than 20 days. The
= National Skin Cancer Prevention Campaign;
NSCPC = National Skin Cancer Prevention Campaign.
Table 2: Types of lesions diagnosed during 2022 NSCPC (n = 56), 2023
Table 3: Site of lesions diagnosed during 2022 NSCPC (n = 57), 2023 NSCPC (n = 124), and total for
(n = 181)
Flowchart 1: Representation of events and respective number of patients undergoing each intervention during 2022 NSCPC NSCPC = National Skin Cancer Prevention Campaign
majority, 41 (37.6%), waited between 39 and 57 days, and only 10 (9.2%) required 77 to 95 days to undergo biopsy (Graph 1B).
A major difference between the 2022 and 2023 NSCPCs was the performance of excisional biopsies and punch biopsies on the same date. In total, 27 patients (23.7%) underwent the procedure on the screening day, with 14 (48.3%) undergoing excisional biopsy and the other 15 (51.7%) undergoing punch biopsy. However, no statistically significant difference (p = 0.1) was observed between the years 2022 and 2023 in the median time from NSCPC to biopsy. The time between the biopsy of lesions identified during the 2022 NSCPC and the date of the surgical procedure for patients with formal indication for re-
section ranged from 94 to 218 days, with a mean (SD) of 152.8 (40.3) days and a median of 153.0 days (IQR 111.5-183.2). Out of 33 patients referred for surgical procedures, 11 (33.3%) were lost to follow-up and 22 (66.7%) underwent operations and were treated. Among surgical patients, 11 cases (50.0%) waited between 94 and 144 days to complete this stage, while four cases (18.9%) required over 194 days for resolution (Graph 2A). In 2023, however, the time ranged from 12 to 249 days, with a mean (SD) of 125.2 (57.9) days between the two events and a median of 129.0 days (IQR 91-172). A statistically significant difference (p = 0.04) was observed between 2022 and 2023 in the median time from biopsy to surgery. Out of 59 patients referred for sur-
Flowchart 2: Representation of events and respective number of patients undergoing each intervention during 2023 NSCPC NSCPC = National Skin Cancer Prevention Campaign
DISCUSSION
gical procedures, only 33 (55.9%) were operated on, while the remaining 26 (44.1%) were lost to follow-up. Among patients who underwent surgical procedures, seven (21.2%) were cured within 75 days, and for only two (6.1%) did resolution take more than 201 days (Graph 2B).
Data from the 2022 and 2023 NSCPCs were collected for this study to check whether there were any changes in resolution rate due to the application of different measures on each of the 2 years. Most malignant skin neoplasms are known to affect patients of advanced age, especially after the fifth decade of life.8,14 This 2023 NSCPC Biopsy
Graph 1: A - Distribution of cases versus time interval between 2022 NSCPC and biopsy, and B - Distribution of cases versus time interval between 2023 NSCPC and biopsy
NSCPC = National Skin Cancer Prevention Campaign
Graph 2: A - Distribution of cases versus time interval between biopsy and curative surgical procedures, 2022 NSCPC B) Distribution of cases versus time interval between biopsy and curative surgical procedures, 2023 NSCPC
corroborates the results from the present study, given that 88.6% of patients in the 2022 NSCPC and 92.1% in the 2023 NSCPC were older than 50 years. The largest age groups were 61-70 years (38.6%) in 2022 and 71-80 years (28.9%) in 2023.
Skin cancer is the result of accumulated mutations caused by photodamage, and so the number cellular changes increases for older age groups.15 This explains why the incidence of skin neoplasms is proportional to age.
Skin tumors have been described in the literature as more prevalent among men.6,8 However, more recent studies have shown an inversion of this prevalence, ie, more women are being diagnosed with BCC, SCC, or melanoma.3,14 In the present study, 61.4% of patients in 2022 and 62.3% in 2023 were women, in
line with the epidemiology found in other recent studies. One hypothesis for this inversion in prevalence is that tanned skin has come to be valued aesthetically in recent decades, making it a standard of beauty sought after by women. This attitude has led to the dissemination of outdoor activities and to the exposure of larger areas of the skin to UV radiation.16,17 An additional factor that might explain this change in incidence is the greater resistance among men to seek health care services. Moreover, women generally pay more critical attention and worry more about their own health.18,19
In terms of patient phototype, most (75.0% in 2022 and 81.6% in 2023) had low Fitzpatrick phototypes (1 to 3). In 2022 and 2023, only 11.4% and 6.1%, respectively, were classified as
Fitzpatrick 4 and 5. This finding is in line with expectations, given that the risk of developing skin carcinomas is 10 to 20 times higher for light skin compared to dark skin.20,21 This can be explained by the fact that a low phototype is a risk factor for developing skin cancer, given the lower amount of melanin (a pigment found in the epidermis), which in turn provides less protection against ultraviolet radiation, responsible for cancerous mutations.
In 2022, the most prevalent types of lesions among participants were skin neoplasms and their precursors. BCC accounted for 44.6% of lesions, followed by AK (17.8%) and SCC (12.5%). Melanoma accounted for less than 2.0% of cases. These findings are in line with epidemiological data from various regions of Brazil and other countries, in addition to reflecting the same profile observed in NSCPCs in other Brazilian cities.4,5,6,14
On the other hand, in 2023, most lesions (32.3%) diagnosed in pathological examination were non-neoplastic benign conditions. Meanwhile, several patients with suspected skin neoplasms had other benign conditions, leading to the discharge of 41.3% of patients who underwent biopsies. It should be noted that lesions outnumber participants because some patients had more than one lesion.
In 2023, the largest share of lesions consisted of non-neoplastic conditions, totaling 41 cases (32.2%), followed by BCC, with 29 lesions (22.8%), and SCC, with 12 cases (9.4%). That same year, no pigmented lesion suggestive of melanoma was diagnosed. In terms of lesion topography, the head region was the most affected (49.1% in 2022 and 45.2% in 2023), followed by the limbs (24.6% in 2022 and 25.8% in 2023), and finally the trunk (21.1% in 2022 and 23.4% in 2023). This may be explained by the fact that the face is less well-protected and more photoexposed, while the trunk often remains covered by clothing most of the time, blocking UV radiation.14,22
In terms of previous personal history of skin cancer, considering only the year 2022, 47.7% of participants denied any personal history of skin neoplasms. However, it should be noted that the field “personal history” was left blank in a significant number of records (22.7%), indicating the item is often ignored or forgotten by health care professionals. In other studies, the variable was also hard to analyze due to improperly filled survey forms.23 Given these facts, the correlation between personal history of skin cancer and outcomes could not be properly assessed. In the comparative analysis between the 2022 and 2023 NSCPCs, there was an increase in indications for continued investigation of suspected lesions (clinical follow-up or biopsy), with an added 70 patients (159.1%) referred for continued examinations.
In the 2024 study by Grana et al., the annual average linear increase in cases was higher than expected from the 2022 data, indicating an accelerated growth in incidence.6 It is worth questioning the cause for that increase. Possible causes include the population acquiring better information on the issue, leading to more individuals seeking care, or more comprehensive follow-up criteria to prevent any lesion, no matter how low the degree of suspicion, from going unnoticed.
Biopsy is known to be the only method capable of providing a definitive diagnosis of skin cancer.9,10,24 Therefore, cases of suspected neoplasms identified during NSCPC were referred for biopsy in order to confirm the diagnosis and establish the proper management for each case.25
In terms of procedures performed, most patients underwent punch biopsy (81.3% in 2022 and 65.1% in 2023). Excisional biopsy ensures the lesion is fully removed and, when margins are found to be free, patient treatment is considered complete. If melanoma is suspected, excisional biopsy should be performed whenever possible.26 On the other hand, because of their site or size, some lesions must be subjected primarily to punch biopsy, given their potential effects on staging and prognosis.26,27
In the present study, it was also possible to assess rates of patient adherence to outpatient follow-up. A large number of participants were lost to follow-up, either for failing to visit outpatient services or for not reporting to the services to which they had been referred. Biopsies from lesions examined during the 2022 NSCPC began to be performed in January 2023, and were given high priority compared to new referrals to the FMJ outpatient dermatology service. Even so, 14.0% of patients were lost to follow-up at the first stage of the investigation and failed to attend their scheduled biopsies.
During the 2023 NSCPC, new measures were implemented in an attempt to shorten the time between suspicion and resolution. Unlike what happened 1 year earlier, the choice was made to begin performing biopsies on the same day as the NSCPC, which likely contributed to the significant reduction in absences on the day of the biopsy, with that number falling to just 4.4% of patients. In addition, in order to shorten the interval between biopsy and curative surgery, other medical specialties (minor surgery, head and neck surgery, thoracic surgery, and plastic surgery) as well as the medical staff at FMJ helped perform the procedures, consequently contributing to the shorter time to cure.
Regarding time between NSCPC and lesion biopsy, in 2022, the mean interval between events was approximately 50 days, and in 2023 that average fell to approximately 40 days. However, the medians were the same, indicating there was no statistically significant difference between the 2 years. Out of all patients with formal indication for surgical procedures, 33.3% did not attend their scheduled procedure in 2022, as did 44.1% in 2023. As well as showing poor adherence to the treatment plan, these data reveal one of the difficulties faced in the present study.
The mean time between biopsy and curative surgery, in 2022, was approximately 153 days, falling to approximately 123 days in 2023, indicating an improvement over the previous year. Although the maximum time was higher in 2023 (249 days) than in 2022 (218 days), the 24-day reduction in median time between the two events was statistically significant, indicating the new method adopted for the 2023 NSCPC was more effective. The literature does not provide a set period between can-
JASLB, Pompei LM.
cer detection and performance of curative procedures. However, several studies highlight the importance of speedy resolution in order to halt disease progress, prevent metastases, avoid deformities, and lower treatment costs.5,9,10,28 The progression time of in situ BCC and SCC to their invasive form is, on average, 2 to 5 years. However, the tumor may present with a more rapid and aggressive growth,28,29 and it may also not be possible to determine exactly when the lesion first started. Therefore, it is indicated that curative therapy begin as soon as possible.
When assessing total loss to follow-up between the 2022 (38.6%) and 2023 NSCPCs (27.2%), we find that despite the rate remaining high, there was an 11.4% decrease, showing higher rates of patient adherence to treatment plans. Based on other studies, hypotheses that might justify absences include lack of transportation due to impaired mobility or poor financial conditions, forgotten appointments, and the long wait period to problem resolution. These situations deserve attention and the development of social services policies, given that absenteeism leads to delayed and postponed diagnosis and treatment.30
While surgery is the first-line therapy for definitive treatment of skin tumors because of its lower rate of recurrence, there are other therapeutic resources for surface BCC in low-risk areas.8-10,12,24,31 Ablative surgical methods and topical therapies (imiquimod or 5-fluorouracil) may be used, either combined or in sequence.32,33 However, between 25% and 75% of patients treated with these alternative methods require retreatment within 12 months due to field cancerization and the onset of new lesions. Therefore, surgical treatment should be adopted whenever possible.33 Given these facts, and to ensure the needs of each individual patient would be met, during the 2022 NSCPC, clinical follow-up with topical therapy (5-fluorouracil) was chosen for a single patient, given their advanced age, multiple comorbidities, and consequent short life expectancy. In 2023, the same treatment plan was adopted for five patients, again for these
REFERENCES:
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global Cancer Statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68(6):394-424.
2. Instituto Nacional de Câncer. Estimativa 2020: incidência de câncer no Brasil. Rio de Janeiro: Instituto Nacional de Câncer; 2019.
3. Instituto Nacional de Câncer. Estimativa 2023: incidência de câncer no Brasil. Rio de Janeiro: Instituto Nacional de Câncer; 2022.
4. Pessoa DL, Ferreira LP, Silva RS, Teixeira FFN, Abreu CB, Silva EHO, et al. Analysis of the epidemiological profile of non-melanoma skin cancer in the state of Roraima in the period from 2008 to 2014. Braz J Hea Rev. 2020;3(6):18577-90.
5. Sociedade Brasileira de Dermatologia. Data analysis of the Brazilian Society of Dermatology skin cancer prevention campaign, 1999 to 2005. An Bras Dermatol. 2006;81(6):533-9.
6. Grana AG, Gonçalves HS, Barcaui CB, Talhari C, Miot HA. Trends on detecting malignant skin neoplasms during the national campaigns of skin cancer prevention (2000-2023). An Bras Dermatol. 2024;99(6):946-50.
reasons.
This research is subject to at least two limitations. The first is that the study data do not include a sample representative of all Brazilian cities and states, comprising only participants from the city of Jundiaí during the 2022 and 2023 NSCPCs. This means the data cannot be generalized. However, the epidemiological data obtained during the events are in line with the studies found in the references. Second, despite attempts to contact patients lost to follow-up, it was not possible to determine precisely why treatment was abandoned, which might interfere with the accuracy of the outcome analysis. Although the exact reason for participant withdrawal remains unknown, it can be observed that with the changes implemented in the 2023 NSCPC, enabling faster biopsies and subsequent curative surgeries, the absenteeism rate was lowered efficiently.
CONCLUSIONS
Regardless of their limitations, the data from this study allow us to conclude that, although NSCPC is a valuable initiative for the identification of lesions suspected to be early-stage neoplastic lesions and skin neoplasms, its impact on reducing morbidity and mortality has yet to reach its full potential. For various reasons, time between diagnosis and case resolution is noticeably longer than the timelines recommended in the literature. Therefore, enhanced efficiency in performing biopsies and surgical procedures, alongside greater patient adherence to treatment, is needed. It should be noted that the improvements implemented in the 2023 NSCPC led to reduced time to cure and more rigorous and successful patient follow-up. Although the NSCPC methodology for combating skin cancer remains distant from an optimal standard, the pattern changes observed in this study and similar studies allow us to consider additional measures that may bring NSCPC closer to achieving excellence. l
7. Eufrásio LS, Lucena BCM, Almeida DKFH, Lima ESG, Souza KWDD, Silva APS, et al. Educação em saúde com campanhas nacionais de conscientização: porque toda informação importa! Julho a dezembro. Santa Cruz (RN): FACISA; 2022.
8. Rivitti EA. Dermatologia de Sampaio e Rivitti. 4th ed. São Paulo: Grupo a Educação; 2018. 1648 p.
9. National Comprehensive Cancer Network. Squamous cell skin cancer. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®); 2022.
10. National Comprehensive Cancer Network. Basal cell skin cancer. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®); 2022.
11. Cestari MEW, Zago MMF. Cancer prevention and health promotion: a challenge for the 21st century. Rev Bras Enferm. 2005;58(2):218-21.
12. Rojas KD, Perez ME, Marchetti MA, Nichols AJ, Penedo FJ, Jaimes N. Skin cancer: primary, secondary, and tertiary prevention. Part II. J Am Acad Dermatol. 2022;87(2):271-88.
13. Gill PS, Tattersall, MHN. Rastreamento e detecção precoce. In: Love RR, Editor. Manual de oncologia clínica. 6th ed. São Paulo: Fundação Oncocentro; 1999. p.117-38.
14. Oliveira TP, Andrade HD, Pegas JR, Bechara CS. Prevalence of pathological diagnoses and epidemiological profile of patients with non-melanoma skin cancer suspicious lesions. Surg Cosmet Dermatol. 2021;13:e20210031.
15. Wright CY, du Preez DJ, Millar DA, Norval M. The epidemiology of skin cancer and public health strategies for its prevention in southern Africa. Int J Environ Res Public Health. 2020;17(3):1017.
16. Keesling B, Friedman HS. Psychosocial factors in sunbathing and sunscreen use. Health Psychol. 1987;6(5):477-93.
17. Arthey S, Clarke VA. Suntanning and sun protection: a review of the psychological literature. Soc Sci Med. 1995;40(2):265-74.
18. Levorato CD, Mello LM, Silva AS, Nunes AA. Factors associated with the demand for health services from a gender-relational perspective. Cien Saude Colet. 2014;19(4):1263-74.
19. Instituto Brasileiro de Geografia e Estatística (IBGE). Pesquisa nacional de saúde: 2019: informações sobre domicílios, acesso e utilização dos serviços de saúde: Brasil, grandes regiões e unidades da federação / IBGE, Coordenação de Trabalho e Rendimento. Rio de Janeiro: IBGE; 2020. 85p.
20. Roewert-Huber J, Lange-Asschenfeldt B, Stockfleth E, Kerl H. Epidemiology and aetiology of basal cell carcinoma. Br J Dermatol. 2007;157(Suppl 2):47–51.
21. Lear W, Dahlke E, Murray CA. Basal cell carcinoma: review of epidemiology, pathogenesis, and associated risk factors. J Cutan Med Surg. 2007;11(1):19–30.
22. Souza CFD, Menegotto PF, Shibue JRT, Thomé EP, Schmitt JV, Tarlé RG. Topography of basal cell carcinoma and their correlations with gender, age and histologic pattern: a retrospective study of 1042 lesions. An Bras Dermatol. 2011;86(2):272-7.
23. Teixeira MA, McManus C, Pinheiro AMC, Abbud CBB, Fernandes AGO, Santos LRS, et al. Social epidemiological profile of patients with suspected skin cancer in the Federal District, Brazil. Rev Enferm Atual Derme. 2023;97: e023110.
24. Lim JL, Asgari M. Cutaneous squamous cell carcinoma (cSCC): clinical features and diagnosis. UptoDate; 2023.
26. Blakeman JM. The skin punch biopsy. Can Fam Physician. 1983;29:971-4.
27. Pickett H. Shave and Punch Biopsy for Skin Lesions. Am Fam Physician. 2011;84(9):995-1002.
28. John SM, Trakatelli M, Gehring R, Finlay K, Fionda C, Wittlich M, et al. Consensus report: recognizing non- melanoma skin cancer, including actinic keratosis, as an occupational disease - a call to action. J Eur Acad Dermatol Venereol. 2016;30(Suppl 3):38-45.
29. Rigel DS, Stein Gold LF. The importance of early diagnosis and treatment of actinic keratosis. J Am Acad Dermatol. 2013;68(1 Suppl 1):S20-7.
30. Bittar OJNV, Magalhães A, Martines CM, Felizola NBG, Falcão LHB. Absenteeism in outpatient care specialties in São Paulo. Boletim Epidemiológico Paulista. 2016;13(152):19-32.
31. Urun YG, Can N, Bagış M, Solak AA, Urun M. Adequacy of surgical margins, re-excision, and evaluation of factors associated with recurrence: a retrospective study of 769 basal cell carcinomas. An Bras Dermatol. 2023;98(4):449-59.
32. Work Group; Invited Reviewers; Kim JYS, Kozlow JH, Mittal B, Moyer J, et al. Guidelines of care for the management of basal cell carcinoma. J Am Acad Dermatol. 2018;78(3):540-59.
33. Smit JV, Sévaux RGL, Blokx WAM, Van De Kerkhof PCM, Hoitsma AJ, Jong EMGJ. Acitretin treatment in (pre) malignant skin disorders of renal transplant recipients: histologic and immunohistochemical effects. J Am Acad Dermatol. 2004;50(2):189-96.
AUTHOR’S CONTRIBUTION:
Isabella Melo Pompei 0000-0001-9438-1163
Statistical analysis; Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Critical review of the literature; Critical revision of the manuscript
Célia Antônia Xavier de Moraes Alves 0000-0002-8421-8837
Approval of the final version of the manuscript; Conception and design of the study; Effective participation in the conduct of the study; Critical review of the literature; Critical revision of the manuscript
Annamaria Piovezan Lorenção 0009-0001-6094-8595
Statistical analysis; Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Critical revision of the manuscript
Bruna Mendes Almeida 0000-0002-0804-5401
Approval of the final version of the manuscript; Conception and design of the study; Critical review of the literature; Critical revision of the manuscript
Juliana Arêas de Souza Lima Beltrame Ferreira 0000-0001-7338-3442
Approval of the final version of the manuscript; Conception and design of the study; Effective participation in the conduct of the study; Critical revision of the manuscript
Luciano Melo Pompei 0000-0001-7084-037X
Statistical analysis; Acquisition, analysis and interpretation of data; Critical revision of the manuscript
www.surgicalcosmetic.org.br/
Quantitative and qualitative evaluation of upper blepharoplasty: a
retrospective longitudinal study
Avaliação quantitativa e qualitativa da blefaroplastia superior: um estudo longitudinal retrospectivo
Introduction: The eyelids have specific functions, such as eye protection. Aging can lead to excess upper eyelid skin (upper dermatochalasis), causing functional and aesthetic impairment. Subjective assessments of improvement pre- and post-blepharoplasty may be underestimated, since even small increases in palpebral fissure height (PFH) can improve the visual field.
Objective: To measure PFH to check for improvements in dermatochalasis after upper blepharoplasty performed by dermatologists and compare the subjective assessments of independent dermatologists and patients.
Methods: Medical record review of patients who underwent upper blepharoplasty. Photographs taken before and two months after the procedure were compared. Independent dermatologists evaluated the photographs (subjective assessment). Patients’ subjective perception was also assessed. PFH before and after the procedure was calculated in millimeters (mm).
Results: A total of 170 eyelids were analyzed. There were significant differences in mean PFH values before and after the procedure (7.088 vs. 8.618 mm; p < 0.001) and in patient self-assessment (p = 0.001),but no differences between the subjective assessments by independent dermatologists (p = 0.665).
Conclusion: There was an improvement in mean PFH after blepharoplasty, which probably resulted in improved visual field. Dermatology is a specialty qualified to perform the procedure.
Introdução: As pálpebras desempenham funções específicas, como a proteção ocular. O envelhecimento pode levar ao excesso de pele palpebral superior (dermatocálase superior), causando prejuízos funcionais e estéticos. As avaliações subjetivas de melhora, pré e pós-blefaroplastia, podem ser subestimadas, já que mesmo um aumento mínimo na altura da fenda palpebral pode melhorar o campo visual.
Objetivo: Verificar, por meio da aferição da altura da fenda palpebral, se houve melhora da dermatocálase após a blefaroplastia superior realizada por dermatologistas, e comparar as avaliações subjetivas de dermatologistas independentes e dos pacientes.
Métodos: Estudo baseado na revisão de prontuários dos pacientes submetidos à blefaroplastia superior. Fotografias obtidas antes e 2 meses após a cirurgia foram comparadas. Dermatologistas independentes avaliaram as imagens (avaliação subjetiva), e a percepção subjetiva dos pacientes também foi verificada. A altura da fenda palpebral, em milímetros, foi calculada antes e após as cirurgias.
Resultados: Foram analisadas 170 pálpebras. Houve diferenças significativas nas médias da altura da fenda palpebral pré e pós-cirurgia (7,088 versus 8,618 mm; p < 0.001) e na autoavaliação dos pacientes (p = 0,001), mas não entre as avaliações subjetivas dos dermatologistas independentes (p = 0,665).
Conclusão: Houve aumento da média da altura da fenda palpebral após blefaroplastia, o que provavelmente resultou em melhora do campo visual. A dermatologia é uma especialidade apta a realizar o procedimento. Palavras-chave: Blefaroplastia; Pálpebras; Envelhecimento da Pele; Olho.
Original Article
Authors:
Gabriele Harumi Seko1
Jéssica Pagan Faria1
Eldislei Mioto1
Luan Yudi Prando Kasuga2
Melissa Caroline Godoi Prestes2
Rogerio Nabor Kondo1
1 Universidade Estadual de Londrina (UEL), Dermatology, Londrina (PR), Brazil
Correspondence: Gabriele Harumi Seko E-mail: gabrieleseko@gmail.com / kondo.dermato@gmail.com
Funding: None
Conflict of interest: None
Submitted on: 03/04/2025
Final decision: 04/14/2025
Acknowledgments
We would like to thank Ricardo Kazuhito Yamamoto, ophthalmologist and member of the Brazilian Society of Ophthalmology, for the guidance he provided to the study from the point of view of ophthalmology.
How to cite this article:
Seko GH, Faria JP, Mioto E, Kasuga LYP, Prestes MCG, Kondo RN. Quantitative and qualitative evaluation of upper blepharoplasty: a retrospective longitudinal study. Surg Cosmet Dermatol. 2025;17:e20250446.
INTRODUCTION
The eyelids are complex structures with specific functions, such as protecting the eyeball from trauma, shielding it from excessive light, and executing movements towards the tear drainage system, in addition to contributing to the eye’s beauty and expression.1,2 Some factors, primarily chronological skin aging, may lead to loss of elasticity and excess upper eyelid skin (upper dermatochalasis), causing visual impairment and impacting periocular aesthetics.3 Lower dermatochalasis has greater impact on cosmetic appearance.4 Laser and radiofrequency may be used to treat dermatochalasis,5 but a surgical procedure (blepharoplasty) is still the most widely used technique, given its low cost and low invasiveness.3 Traditionally, ophthalmology and plastic surgery are the two medical specialties that perform blepharoplasties.3,4,6 However, given the current public health care scenario, both specialties are in high demand, leading to extremely long waiting lists for blepharoplasty. Dermatology, as a medical-surgical specialty, can also perform the procedure, and having dermatologists perform blepharoplasties is an alternative to help reduce waiting times.7 In addition, it would be important to assess whether dermatology is able to achieve satisfactory postoperative outcomes. However, considering the subjective assessment of primary surgeons themselves alone would be suboptimal, and including the assessment of other physicians, combined with objective evaluation, would lower potential performance biases.3,6 A previous study proposed assessing the surgical outcomes of upper blepharoplasty performed by dermatologists objectively by comparing pre- and postoperative measures of palpebral fissure height (PFH).3 However, that study had a limited sample size (only nine patients) and suggested additional studies should be conducted.3 The aim of the present study was to determine if there was any improvement in dermatochalasis after upper blepharoplasty performed by a local dermatology service, thus investigating the qualification of that specialty to perform the procedure. The improvement was assessed both quantitatively, by comparing pre- and postoperative PFH measures, and qualitatively, based on the pre- and postoperative subjective assessments by independent dermatologists and the patients themselves.
METHODS Study design
A retrospective longitudinal study reviewed the medical records and photographs of patients who underwent upper blepharoplasty performed at the dermatology service of the university where the study was conducted.
Inclusion and exclusion criteria
The patient inclusion criteria for this study were having undergone upper blepharoplasty at the dermatology service between April 1, 2014, and March 31, 2023. The exclusion criteria, in turn, were absence of return after surgical procedure, lack of data that could not be obtained through invitations or by telephone, photographs taken by professionals other than the lead investigator, and use of cameras other than a Canon T3i.
Assessment methods
Photographs taken at a standardized distance of 50 cm with a Canon® T3i camera and 55 mm macro lens, before the procedure and 2 months after, were compared using the Scion Image 4.0 software. PFH, defined as the distance from the upper eyelid to the lower eyelid passing through the pupil, was calculated based on the stored photographs (Figure 1). The Pixel Converter software application was used to convert pixels into millimeters, using decimal thousandths to assign the PFH values in millimeters.
The photographs taken before and after the procedures were distributed to three independent dermatologists for assessment, without telling the specialists which had been taken before and which after the procedure (photograph A vs. photograph B). Next, the professionals assigned a numerical score comparing the evolution of photograph A to B and of photograph B to A, according to the following scale developed by the researchers: significant worsening (-3), moderate worsening (-2); mild worsening (-1), no change or no improvement (0), mild improvement (+1), moderate improvement (+2), and significant improvement (+3). Only the researchers knew that, for instance, a -3 score might actually indicate a +3 improvement. Patients’ subjective assessments were also scored based on functional (visual
Figure 1: Palpebral fissure height measurement
A - Pre-blepharoplasty.
B - Post-blepharoplasty
Seko GH, Faria JP, Mioto E, Kasuga LYP, Prestes MCG, Kondo RN.
field) and/or aesthetic improvement, using the following scale: improvement (+1), no improvement (0), and worsening (-1).
Statistical analysis
The data were provided via survey forms developed by the researchers themselves. The information collected was compiled into a Microsoft Excel spreadsheet for statistical analysis using the Stata® (version 13.0, StataCorp, Texas) and Jamovi software applications. Fisher’s exact test was used to compare categorical variables and the chi-square test for trends. Continuous variables were analyzed using the Wilcoxon-Mann-Whitney test. After checking the normality of quantitative variables using the Shapiro-Wilk test, nonparametric Mann-Whitney and Kruskal-Wallis tests were used to compare the results. Statistical significance was set at p < 0.05, with a 95% confidence interval. The minimum sample size calculation resulted in 170 eyelids (85 patients), considering a significant difference of at least 0.900 mm in PFH between pre- and post-blepharoplasty measurements, with a significance level of 5%, power of 80%, and a standard deviation of 0.300 mm.
Research Ethics Committee
The study was approved by the Human Research Ethics Committee of the hospital where the study was conducted, and received Certificate of Presentation for Ethical Evaluation number 69513623.0.0000.5231.
Detailed description of surgical technique
a) With the patient in horizontal supine position and eyes closed, a fusiform marking of the skin to be excised was made using a surgical marking pen or methylene blue. The lower limit was drawn at a distance greater than 8 mm from the
Figure 2: Marking of fusiform area. The inferior margin should be at least 8 mm from the ciliary edge, at the midpalpebral line. The upper edge should be 10 mm from the lower edge of the eyebrow
lash line, and the upper limit of the fusiform area was marked more than 10 mm from the lower edge of the eyebrow (measures adopted to avoid lagophthalmos).1 At the lateral ends, a slight arching was performed. (Figure 2)
B) Antisepsis with topical 10% polyvinyl-iodine solution;
C) Subcutaneous infiltration of upper eyelid with 2% lidocaine and vasoconstrictor;
D) Incision of the marked area with a 15 blade and excision of tissue to subcutaneous depth;
E) Hemostasis;
F) Sutures with 6-0 Mononylon, single stitches;
G) Cleaning and dressing with sterile Micropore tape.
RESULTS
Table 1 lists the main findings of the present study. The study analyzed 170 eyelids of 85 individuals, with mean age of 61.4 years, predominantly female (83.5%) and White (85.9%). There was a significant difference in mean pre- and post-blepharoplasty PFH (7.088 vs. 8.618 mm; p < 0.001). Graph 1 compares pre- and postoperative PFH measurements.
For dermatologists, a subjective assessment of mild improvement (52.9%) predominated over all other findings (47.2%) (p = 0.665). Comparing rates of improvement vs. non-improvement, the post-blepharoplasty outcome was significant (94.3 vs. 4.7%; p = 0.001). In patient self-assessments, however, a significant improvement was found (96.5 vs. 3.5%; p = 0.001). Graph 2 shows the assessments of dermatologists and patients. Regarding PFH correlations after blepharoplasty, there was an inverse correlation with patient age (r = -0.230; p = 0.032). Dermatologists’ assessments and patient self-assessments were not significantly correlated with post-blepharoplasty PFH (p > 0.05) (Table 2). However, comparing dermatologists’ assessments to patient self-assessments (disregarding PFH measurements), the result was statistically significant (r = 0.351; p < 0.001).
DISCUSSION
The sample was predominantly comprised of female patients, with mean age higher than 60 years, consistent with the literature.8,9 Mean preoperative PFH was 7.088 mm and mean postoperative PFH was 8.618 mm (p < 0.001), values close to those found by Schellini et al.3 Mean PFH without dermatochalasis, ie, in the young adult population, can vary by race, country, and sex. A Turkish study found an average of 10.4 mm for females and 10.3 mm for males.10 There are no consolidated data on mean post-blepharoplasty PFH. However, Schellini et al.3 report a postoperative mean PFH of 7.92 mm for nine patients, also smaller than the mean average observed in individuals without dermatochalasis, and similar to the results of the present study. Subjective assessments by dermatologists and patient self-assessments were not correlated with postoperative PFH (p > 0.05).
Table 1: Clinical and demographic profile
SD = standard deviation.
NA = not applicable.
# racial self-identification every patient provides when filling out their registration form at the hospital. & seamstress, sales clerk, manicurist, general services assistant, administrative assistant, radiology technician, shopkeeper, farmer, cleaning woman, construction worker, security technician, civil servant, unemployed.
*subjective assessment by three independent dermatologists without the aid of measurement devices. ¶ patient self-assessment.
r = Pearson’s correlation coefficient For
Table 2: Correlation coefficients between postoperative measurement of palpebral fissure height (mm) and selected characteristics (n = 170)
Distribution of pre- and postoperative palpebral fissure height
Palpebral fissure height (mm)
Preoperative
Subjective medical assessment
Graph 1. Distribution of pre- and postoperative PFH
PFH = palpebral fissure height.
Postoperative
Patient self-assessment
Graph 2: Comparative scatterplot of subjective assessments. The subjective medical assessment was ranked from 1 to 7 (1 = significant worsening; 2 = moderate worsening; 3 = mild worsening; 4 = no change or no improvement; 5 = mild improvement; 6 = moderate improvement; 7 = significant improvement). Self-assessments were ranked from 1 to 3 (1 = worsening; 2 = no change or no improvement; 3 = improvement)
The authors considered the hypothesis that pre- and post-blepharoplasty comparisons are barely perceptible to the naked eye, given that no assessment indicated a worsening (p < 0.05). That finding might suggest that even small improvements in PFH, measured in millimeters, would favor visual acuity. Visual field tests are the standard examination to assess the visual field before and after a blepharoplasty. However, that test depends on information provided by the patient and is also a subjective parame-
ter.8 This test was not performed in our study, as was also the case in the work of Schellini et al. Surgical indication was based on the patient’s complaint and the physical examination of excess upper eyelid skin. To date, there are no studies in the plastic surgery literature that employ PFH or some other objective measurement to assess upper blepharoplasty. Furthermore, no study has concomitantly applied three methods of assessing surgical outcomes (PFH, assessment by independent specialists, and patient
Seko GH, Faria JP, Mioto E, Kasuga LYP, Prestes MCG, Kondo RN.
self-assessment). Study limitations include the absence of visual field tests, which could have provided additional information, and the fact that it was conducted in a single referral center. In addition, 10 patients had to be excluded due to information bias, with 10 others from the consecutive listing included to maintain the sample size. Despite these limitations, the authors replicated a quantitative assessment (PFH)3 and compared it to qualitative parameters, finding superior postoperative outcomes in a more objective manner, evidence that dermatology may also be qualified to perform upper blepharoplasty.
CONCLUSION
By analyzing a quantitative parameter (PFH), the present study found a significant improvement in patients who underwent upper blepharoplasty performed at a dermatology service, indicating that the specialty may also be qualified to perform this type of procedure. l
REFERENCES:
1. Kondo RN, Singh BS, Ferreira VP, Araújo MCP. Upper eyelid transposition flap for reconstruction of a lower eyelid defect: a case report. Surg Cosmetic Dermatol. 2022;14:e20220156.
2. Zhou J, Ding J, Li D. Blepharochalasis: clinical and epidemiological characteristics, surgical strategy and prognosis -- a retrospective cohort study with 93 cases. BMC Ophthalmol. 2021;21(1):313.
3. Schellini SA, Preti RC, Yamamoto RK, Padovani CR, Padovan CR. Eyelid measures before and after upper blepharoplasty -- quantitative evaluation. Arq Bras Oftalmol. 2005;68(1):85-8.
4. Fagien S. Advanced rejuvenative upper blepharoplasty: enhancing aesthetics of the upper periorbita. Plast Reconstr Surg. 2002;110(1):278-91.
5. Biesman BS. Blepharoplasty: laser or cold steel? Skin Therapy Lett. 2003;8(7):5-7.
6. Lima CG, Siqueira GB, Cardoso IH, Sant'Anna AE, Osaki MH. Evaluation of dry eye in the preoperative and postoperative period of blepharoplasty. Arq Bras Oftalmol. 2006;69(3):377-82.
7. Scawn R, Gore S, Joshi N. Blepharoplasty basics for the dermatologist. J Cutan Aesthet Surg. 2016;9(2):80-4.
8. Pemberton JD, Salter M, Fay A, Thuro B, Spencer H, Dajani O. Investigation of goldmann perimetry in evaluation of patients for upper eyelid blepharoplasty. Orbit. 2018;37(1):48-52.
9. Homer NA, Zhou S, Watson AH, Durairaj VD, Nakra T. Wound dehiscence following upper blepharoplasty: a review of 2,376 cases. Ophthalmic Plast Reconstr Surg. 2021;37(3S):S66-9.
10. Bozkir MG, Karakaş P, Oĝuz O. Measurements of soft tissue orbits in Turkish young adults. Surg Radiol Anat. 2003;25(1):54-7.
AUTHOR’S CONTRIBUTION:
Gabriele Harumi Seko 0000-0001-6661-4070
Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Critical review of the literature; Critical revision of the manuscript.
Jéssica Pagan Faria 0000-0001-8727-2348
Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Critical review of the literature.
Eldislei Mioto 0000-0001-5376-9292
Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Critical review of the literature.
Luan Yudi Prando Kasuga
0009-0006-3724-0034
Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Critical review of the literature.
Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Critical review of the literature.
Rogerio Nabor Kondo 0000-0003-1848-3314
Statistical analysis; Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical review of the literature; Critical revision of the manuscript.
www.surgicalcosmetic.org.br/
Combination of chemical peels and oral isotretinoin in the treatment of acne scars
Combinação de peelings químicos e isotretinoína oral no tratamento de cicatrizes de acne
Introduction: Acne is a prevalent chronic disease that can cause physical, emotional, and social effects. Isotretinoin and chemical peels are available as treatment, but their combination has historically been avoided due to reports of abnormal healing. Recent studies suggest that the combination with superficial or medium-depth peels is safe, but there are no studies considering the specific characteristics of the Brazilian population.
Objective: To evaluate the safety and efficacy of combining isotretinoin and chemical peels in the treatment of acne scars.
Methods: A clinical trial was conducted with patients aged 15 to 25 years undergoing acne treatment with isotretinoin. The intervention group underwent three Jessner’s peels during isotretinoin use, while the control group underwent the same peels after treatment with isotretinoin was completed. Outcomes were assessed using the QGSGS and IGA scales by two blinded evaluators.
Results: Peels performed concomitantly with isotretinoin did not result in worse outcomes on the QGSGS and IGA scales compared to the control group.
Conclusion: The combination of isotretinoin and chemical peels proved to be safe, but further studies with larger samples are needed to establish recommendations.
Introdução: A acne é uma doença crônica prevalente que pode causar efeitos físicos, emocionais e sociais. A isotretinoína e os peelings químicos são tratamentos disponíveis, mas sua combinação foi historicamente evitada devido a relatos de cicatrização anormal. Estudos recentes sugerem que a combinação com peelings superficiais ou médios é segura, mas faltam estudos que levem em conta as características da população brasileira.
Objetivo: Avaliar a segurança e eficácia da combinação de isotretinoína e peelings químicos no tratamento de cicatrizes de acne.
Métodos: Ensaio clínico com pacientes de 15 a 25 anos em tratamento de acne com isotretinoína. O grupo de intervenção realizou três peelings de Jessner durante o uso de isotretinoína, e o grupo controle, após o término do tratamento com isotretinoína. A avaliação foi feita com as escalas EQGACA e IGA por dois avaliadores cegos.
Resultados: Os peelings concomitantes ao uso de isotretinoína não resultaram em piores desfechos nos escores EQGACA e IGA em comparação com o grupo controle.
Conclusão: A combinação de isotretinoína e peelings químicos foi segura, mas estudos com amostras maiores são necessários para estabelecer recomendações.
How to cite this article: Silverio MS, Andrade DS, Murari CM, Vasconcelos RCF, Rytenband F. Combination of chemical peels and oral isotretinoin in the treatment of acne scars. Surg Cosmet Dermatol. 2025;17:e20250427.
INTRODUCTION
Acne vulgaris is the eighth most common disease globally, affecting over 0.5 billion people,1 and it is estimated that 50% to 95% of adolescents have some degree of the disease. It is classified as a chronic inflammatory disorder of the pilosebaceous unit, and its pathogenic basis involves the following mechanisms: increased and abnormal sebum production under androgenic influence; altered keratinization leading to comedone formation; follicular colonization by Cutibacterium acnes (C. acnes); and the release of inflammatory mediators in the skin such as interleukin-1 alpha and TNF-alpha.2 In addition to acne vulgaris, there is also adult female acne, characterized by acne affecting women aged 25 years and older and which may persist from adolescence or begin in adulthood.
With regard to etiopathogenesis, this condition differs from acne vulgaris in its strong hormonal influence, involving alterations in androgen metabolism, worsening during the premenstrual period, and greater association with endocrinological disorders such as polycystic ovary syndrome, late-onset congenital adrenal hyperplasia, hyperinsulinism, and peripheral insulin resistance. In addition, it presents a tendency to relapse, requiring a different therapeutic approach compared to acne vulgaris as well as making maintenance treatment essential.3 The condition causes painful lesions and may lead to scarring in up to 95% of patients with the disease,4 leading to physical, emotional, and social impairment. It carries a high global disease burden and, among dermatological diagnoses, accounts for the second highest impact on DALYs (disability-adjusted life years, or the number of years of life lost due to premature death and disability), behind only eczema, and surpassing conditions such as urticaria, psoriasis, and a number of infections.5
To prevent unfavorable outcomes, it is important that effective treatments be initiated promptly. The main treatments for mild acne vulgaris include topical retinoids, benzoyl peroxide, topical antibiotics, salicylic acid, and azelaic acid. Isotretinoin, systemic antibiotics, and hormonal agents such as oral contraceptives and spironolactone may be used to treat moderate to severe acne. Even recent guidelines such as the American Academy of Dermatology’s “Guidelines of care for the management of acne vulgaris”6 describe the current evidence for other forms of treatment, such as chemical peels, photodynamic therapy, lasers, and mechanical extraction, as insufficient to warrant a recommendation.
Isotretinoin (13-cis-retinoic acid), a vitamin A derivative, approved for use in the United States in 1982 and in Brazil in 1990, stands out as one of the main forms of treatment. It has been widely used since then, and is currently indicated for nodulocystic acne, moderate papulopustulosa acne resistant to other treatments, acne with a tendency to scarring, and cases associated with social and emotional impairment. As monotherapy, it can induce remission in approximately 80% of patients.7 The mechanisms of action against acne include the involution of the pilosebaceous unit,8 normalization of infundibular hyper-
keratinization,7 immunomodulation with decreases in TNF-alpha, interleukin-4, interleukin-17, and interferon gamma levels,9 and decreases in populations of C. acnes.7 Isotretinoin is thus considered a first-line treatment, as it can treat acne effectively, prevent scarring, and promote rapid improvements in patient quality of life.
The most common adverse effects of isotretinoin are cheilitis, occurring in 94% to 100% of users, and xeroderma, or mucosal dryness, in 47% of cases. In general, neither requires the medication be discontinued, and both can be easily managed with topical moisturizers and ocular or nasal lubricants. Less frequent events include conjunctivitis, hair loss, brittle nails, pyogenic granulomas, headache, and myalgia.10 Laboratory abnormalities occurred in 2% of patients, primarily hypertriglyceridemia, elevated cholesterol, and elevated transaminases.11
However, all these adverse effects are dose-dependent and tend to normalize after treatment is discontinued. The most serious risk, which is dose-independent, is teratogenicity; pregnancies may result in miscarriage in up to 20% of cases and embryopathies in up to 28%.7 Therefore, the drug is contraindicated in pregnant women, and requires effective contraception and testing to rule out pregnancy in women of childbearing age. Another reported adverse effect is a potential increase in the risk of depression and suicide. However, a 2007 systematic review found no evidence to support this theory,12 and some studies have even observed a trend toward a reduction in depressive symptoms during treatment with isotretinoin.2 The literature also discusses the possibility of abnormal scarring after surgical or cosmetic procedures.
Currently, the isotretinoin label contraindicates aggressive dermabrasion, chemical peels, and laser skin treatments for 5 to 6 months after completing treatment. This recommendation is due to the risk of hypertrophic scarring in atypical areas, as well as hyper or hypopigmentation in treated areas.13 The change to the label was based on three small case series published in the 1980s, which reported keloid formation and delayed healing in a total of 11 patients following dermabrasion and argon laser treatment.14 The hypotheses suggested for this alteration in healing were that angiogenesis stimulation or the production of collagenase inhibitors would result in collagen accumulation.15 However, since then, several animal studies have shown similar wound healing rates between intervention and control groups.8
In support of the idea that wound healing occurs normally in patients undergoing isotretinoin treatment, a Brazilian retrospective observational study concluded that: (1) no significant differences in the prevalence of keloids or hypertrophic scars were observed between isotretinoin users and non-users; (2)there was no worsening of preexisting keloids in patients on the medication; and (3) a retrospective analysis of patients with keloids found a low prevalence of prior isotretinoin use.16 The contraindication against performing certain adjuvant procedures during isotretinoin treatment runs counter to excellence in care,
Silverio MS, Andrade DS, Murari CM, Vasconcelos RCF, Rytenband F.
since patients with acne severe enough to require isotretinoin are precisely those who could benefit most from cosmetic procedures.8
Given the current availability of minimally invasive procedures such as microdermabrasion, microneedling, fractional lasers, and superficial peels, it is necessary to revisit old recommendations. Among adjuvant therapies for acne, chemical peels stand out due to their advantages; they are relatively affordable compared to new technologies, can be performed at the physician’s office, and involve minimal downtime.17
Several formulations may be used as chemical peels, aiming to induce controlled therapeutic exfoliation of the skin.This results in partial or complete renewal of the epidermis, and may or may not reach the dermis, and is thus indicated for the treatment of pigmentation disorders and skin irregularities. In acne-prone skin, peels may be used both during the active phase of the disease, targeting comedones and inflammatory lesions, and during the healing phase, to reduce hyperchromias and scarring.
Because it works during both phases, Jessner’s peel, consisting of a solution of 14% salicylic acid, 14% resorcinol, and 14% lactic acid in 95% ethanol, is widely used. Salicylic acid has a sebosuppressive, keratolytic, and anti-inflammatory effect18; resorcinol is keratolytic; and lactic acid reduces hyperchromias, being safe even for darker skin.19 It can act as superficial to medium-depth peels depending on the number of applied layers, and the main adverse effects are the risk of contact dermatitis from resorcinol, with consequent post-inflammatory hyperpigmentation. Thus, its use requires caution in patients with higher Fitzpatrick skin phototypes.17
Some studies have analyzed the safety of chemical peels during oral isotretinoin therapy and found similar or even better aesthetic outcomes when both treatments were combined.8,18,20-22 This has led to the inclusion of superficial chemical peels among therapeutic options for isotretinoin users in major guidelines such as the 2017 Consensus of the American Society for Dermatologic Surgery (ASDS)8 and the 2019 Brazilian Consensus on isotretinoin use.7 However, there is still a lack of studies in the Brazilian population, which has unique skin characteristics. In addition, some recent guidelines, such as the “Guidelines of care for the management of acne vulgaris” from the American Academy of Dermatology,6 state that while there is no evidence in the literature to contraindicate chemical peels in patients with acne, there is also no evidence to recommend them. Therefore, further studies are needed on the subject.
In summary, acne is a chronic and disfiguring disease with a major impact on patients’ lives. It is therefore crucial to initiate effective treatments promptly and not postpone adjuvant procedures that can prevent scarring, which means chemical peels represent a valuable addition to the therapeutic arsenal alongside isotretinoin. However, due to previous recommendations against using both treatments concurrently, many physicians still postpone peels until after the disease has resolved. Given the paucity of literature on the subject, this study aims to gather evidence to
support the use of peels in combination with isotretinoin, taking into account the specific skin characteristics of the Brazilian population.
METHODS
This research project involving human subjects was submitted to the Research Ethics Committee of Universidade Santo Amaro and approved under protocol no. 7.004.647. It is a controlled, open-label clinical trial with blinded evaluators, to be conducted during 2024 at Complexo de Saúde Dr. Wladimir de Arruda, located at Rua Cássio de Campos Nogueira, 2031, in São Paulo (SP), Brazil. Participants were randomly assigned to two groups: one group underwent three Jessner’s peels concomitantly with isotretinoin use, at a frequency of one peel per month for three months (4th, 5th, and 6th months of treatment); the other group underwent three Jessner’s peels after completing isotretinoin treatment, on the 3rd, 4th, and 5th months following discontinuation of the medication. Throughout the isotretinoin and peeling treatment period, patients were instructed to use sunscreen (SPF 50 or higher) every day. If patients did not already have a preferred product, sunscreen was provided by the study. Peels were performed in the following steps:
Photographic documentation;
Skin degreasing with alcohol;
Application of three layers of Jessner’s solution using gauze, with a three-minute interval between each application;
Removal with water after three minutes.
Throughout the study, patients were able to contact the investigators in case of complications. All patients at the service were photographed before initiation of treatment; images were archived in electronic medical records and made available for research purposes with patient consent. At the end of treatment, additional photographs were taken using the following standard views: frontal face, full right profile, full left profile, right semi-profile, and left semi-profile. After the interventions, patients’ before and after photographs were scored by two blinded evaluators using the Quantitative Global Scarring Grading System for Post-acne Scarring (QGSGS) and Investigator Global Assessment (IGA) scales.23 Both evaluators were dermatologists with no access to patient identification data or to which group patients were assigned. Finally, scores were analyzed statistically to determine which group attained greater improvement in facial acne scars.
The product used in the procedures was: Jessner’s peel: 14% salicylic acid, 14% resorcinol, 14% lactic acid, 95% ethanol. Compounded formulation – Farmácia Drogaderma (CNPJ 43.342.542/0002-36); Application: 546095; Registration: 1656844. Pharmacist in charge: Dr. Marcio Nogueira Garcia (CRF-SP: 39016). Prescribing physician: Marina Soares Silvério (CRM-SP: 231.782).
INCLUSION CRITERIA
All patients aged 15 to 24 years seen at the Dermatology Service of Universidade Santo Amaro, diagnosed with grade 2 or 3 acne, and already receiving oral isotretinoin treatment independently of this study were invited to participate. In addition, participants were required to read and sign both the Informed Consent Form and the Image Use Authorization Form.
EXCLUSION CRITERIA
Pregnant patients or those planning to get pregnant during the study or within the subsequent 6 months, patients younger than 15 years or aged 25 years and older, and individuals who did not agree to sign the Informed Consent Form or the Image Use Authorization Form were excluded from the study. During the study, patients who failed to attend scheduled appointments or who did not adhere to isotretinoin treatment as prescribed were also excluded.
DATA ANALYSIS
The QGSGS and IGA scales were applied to photographs taken of each patient at the beginning of treatment and upon completion. Assessments were performed by blinded evaluators, two dermatologists who did not take part in the intervention stages and were not informed about to which group each patient had been assigned. Scores were then analyzed statistically to compare patients in the intervention and control groups. The Mann–Whitney test24 was used to compare variables between intervention and control groups, and the Wilcoxon signed-rank test24 to compare the periods before and after treatment.
RESULTS AND DISCUSSION
During the recruitment stage, a total of 46 patients agreed to take part in the study. Of these, 21 patients completed all study stages: 12 in the intervention group (4 male and 8 female; 9 aged 15–19 years and 3 aged 20–25 years) and 9 in the control group (7 male and 2 female; 6 aged 15–19 years and 3 aged 20–25 years). Discontinuing treatment due to severe adverse events related to either the peels or isotretinoin use was not necessary for any patient. The main reasons for patient exclusion were discontinuation of isotretinoin treatment (8 patients across both groups); missing scheduled appointments (9 patients across both groups); completion of isotretinoin treatment but unwillingness to undergo peels afterward (3 patients in the control group); undergoing other aesthetic facial procedures concurrent with the study (3 patients across both groups); and continued isotretinoin use at the time of study completion (2 patients in the control group). In addition to statistical analysis, representative patient photographs from each group were included, standardized before and after treatment, to illustrate the clinical progression observed (Figures 1 and 2).
The scores for before and after photographs for both groups as assessed using the IGA and QGSGS scales by the evaluators (Evaluator 1 and Evaluator 2) can be found in table 1 and table 2.
Silverio MS, Andrade DS, Murari CM, Vasconcelos RCF, Rytenband F.
Figure 1: Patients from the intervention group (A and B), with comparative photographs before (top row) and after (bottom row) treatment
Figure 2: Patients from the control group (A and B), with comparative photographs before (top row) and after (bottom row) treatment
Table 1: Scores attributed to photographs of patients in intervention group by evaluators
Treatment 1 (intervention group)
Evaluator 1
Table 2: Scores attributed to photographs of patients in control group by evaluators
Treatment 2 (control group)
Evaluator 1
Evaluator 2
Regarding the characteristics of the study groups, the difference in sample size (n) between groups stands out, as well as the heterogeneity of its composition in terms of sex: the intervention group included 4 male and 8 female patients, while the control group included 7 male and 2 female patients. This discrepancy between the two groups resulted from simple ran-
domization but also mainly from the need to exclude individuals who chose to withdraw from the study or who did not meet project requirements (missed appointments, failure to complete the tests required to maintain isotretinoin use, undergoing other treatments that could interfere with outcomes, among others). Therefore, the composition of the sample can be considered a
Table 3. Variation in scores of patients in intervention group
Patient Evaluator 1
Treatment 1 (intervention group)
Evaluator 2
Table 4: Variation in scores of patients in control group
Evaluator 1
Patient
Treatment 2 (control group)
Evaluator 2
(μ)
potential source of bias. Based on these scores, the variation in IGA and QGSGS scores before and after treatment was also calculated for each patient, resulting in ∆IGA and ∆QGSGS values, quantifying the degree of improvement or worsening of acne lesions and scars for each patient. From these data, the average of variations in scores (μ) was calculated using the scores from both evaluators, resulting in μ∆IGA and μ∆QGSGS, as shown in table 3 and table 4.
A preliminary analysis indicated that most scores had neutral or negative results. This means there was a decrease in the number of lesions (measured by IGA) and scars (measured by QGSGS) for both intervention and control group patients. Exceptionally, Patient E showed an increase in QGSGS assigned by Evaluator 1, and Patient B showed an increase in QGSGS assigned by Evaluator 2. A possible explanation for the increases in QGSGS for these two outliers is that active acne lesions may interfere with the initial assessment of preexisting scars, leading to an artificially low initial QGSGS score.The median and arithmetic mean of scores are shown in table 5 and table 6. Initially, the Wilcoxon signed-rank test was applied to compare the before and after treatment datasets, as shown in table 7 and table 8.
MS, Andrade DS, Murari CM, Vasconcelos RCF, Rytenband F.
Table 5: Median and arithmetic mean of intervention group scores
Treatment 1 (intervention group)
Evaluator 1
Table 6: Median and arithmetic mean of control group scores
Treatment 2 (control group)
Evaluator 1
Table 7: Wilcoxon signed-rank test - Intervention group
Wilcoxon signed-rank test (before vs. after)
Treatment 1 – (intervention group)
Evaluator 2
Evaluator 1
Evaluator 2
Evaluator 2
Table 8: Wilcoxon signed-rank test - Control group
Wilcoxon signed-rank test (before vs. after)
Treatment 2 – Control Group
Evaluator 1
Evaluator 2
The test showed that IGA and QGSGS values were higher before treatment than after for both groups and for both evaluators, with statistical significance, except for QGSGS in the control group according to Evaluator 1. The data confirm the expected hypothesis that both treatments promoted improvements in skin quality for patients, resulting in fewer acne lesions (measured by IGA) and fewer scars (measured by QGSGS). Al-
though this outcome was anticipated, it is worth emphasizing that the peels were not harmful to patients and may have had a neutral or beneficial effect. The Mann-Whitney test was also applied, resulting in the comparative analysis shown in table 9. The first piece of data shown in table 9 is that participants in both groups had similar ages. It can also be observed that when comparing the intervention and control group scores, the-
Table 9: Mann-Whitney test for scores attributed by each evaluator
Evaluator 1
Mann-Whitney test (compares the two study groups) Age
Evaluator 2
Legend:
NS = not significant
z = z score
p = probability of significance
Table 10: Mann-Whitney test for average of variations in scores
Mann-Whitney
Average of variation (μ) μ∆IGA
re were no statistically significant differences for the following parameters: IGA before (Evaluator 1), IGA after (Evaluator 1), QGSGS after (Evaluator 1), IGA before (Evaluator 2), QGSGS before (Evaluator 2), IGA after (Evaluator 2), and QGSGS after (Evaluator 2). This enables us to infer that performing Jessner’s peels during isotretinoin treatment likely did not significantly influence the variation in patient IGA and QGSGS scores. A single statistically significant difference was observed when comparing QGSGS before values according to Evaluator 1, with higher scores in the intervention group. This may indicate a selection bias, with patients randomized to the intervention group having more severe scarring before starting treatment. However, the scores assigned by Evaluator 2 did not corroborate these data. It is also worth noting that the number of participants in this study was small. With larger groups, results might have been statistically significant. When the Mann-Whitney test was applied to the average of variations in scores between before
and after photographs, no significant differences were found between groups either, as shown in table 10.
CONCLUSION
This study allows us to conclude that the use of Jessner’s chemical peel as an adjuvant to isotretinoin therapy for acne at different moments (during or after isotretinoin treatment) did not have harmful effects. Both the intervention and control groups showed statistically significant improvements in acne and scar reduction at the end of the study. The peels may have had neutral or beneficial effects. Therefore, there is no reason Jessner’s peels should be contraindicated during isotretinoin therapy. However, it was not possible to determine when peels should be performed, as no statistically significant differences were found between study groups. Further studies are required to establish a solid base to support recommending the use of Jessner’s peels as part of standard treatment. l
MS, Andrade DS, Murari CM, Vasconcelos RCF, Rytenband F.
REFERENCES:
1. Mavranezouli I, Daly CH, Welton NJ, Deshpande S, Laura B, Bromham N, et al. A systematic review and network meta-analysis of topical pharmacological, oral pharmacological, physical and combined treatments for acne vulgaris. Brit J Dermatol. 2022;187(5):639-49.
2. Simonart T. Newer approaches to the treatment of acne vulgaris. Am J Clin Dermatol. 2012;13(6):357-64.
3. Bagatin E, Freitas THP, Machado MCR, Ribeiro BM, Nunes S, Rocha MAD. Adult female acne: a guide to clinical practice. An Bras Dermatol. 2019;94(1):62-75.
4. Cachafeiro TH, Escobar GF, Maldonado G, Cestari TF. Translation into brazilian portuguese and validation of the "quantitative global scarring grading system for post-acne scarring". An Bras Dermatol. 2014;89(5):851-3.
5. Institute for Health Metrics and Evaluation (IHME). Global burden of disease 2021: findings from the GBD 2021 study. Seattle, WA: IHME; 2024.
6. Strauss JS, Krowchuk DP, Leyden JJ, Lucky AW, Shalita AR, Siegfried EC, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2007;56(4):651-63.
7. Bagatin E, Costa CS, Rocha MAD, Picosse FR, Kamamoto CSL, Pirmez R, et al. Brazilian Society of Dermatology consensus on the use of oral isotretinoin in dermatology. An Bras Dermatol. 2020;95(Suppl 1):19-38.
8. Waldman A, et al. ASDS Guidelines Task Force: consensus recommendations regarding the safety of lasers, dermabrasion, chemical peels, energy devices, and skin surgery during and after isotretinoin use. Dermatol Surg.2017;43(10):1249-62.
9. Karadag AS, Ertugrul DT, Bilgili SG, Takci Z, Akin KO, Calka O. Immunoregulatory effects of isotretinoin in patients with acne. Brit J Dermatol. 2012;167(2):433-5.
10. Brito MFM, Sant’Anna IP, Galindo JCS, Rosendo LHP, Santos JB. Evaluation of clinical adverse effects and laboratory alterations in patients with acne vulgaris treated with oral isotretinoin. An Bras Dermatol. 2010;85(3):331-7.
11. Costa CS, Bagatin E, Martimbianco ALC, Silva EMK, Lúcio MM, Magin P, et al. Oral isotretinoin for acne. Cochrane Database of Syst Rev. 2018;11(11): CD009435.
12. Marqueling AL, Zane LT. Depression and suicidal behavior in acne patients treated with isotretinoin: a systematic review. Semin Cutan Med Surg. 2007;26(4):210-20.
13. Roacutan (isotretinoína): produtos Roche Químicos e Farmacêuticos S.A: capsulas gelatinosas: 20 mg. [Bula para pacientes]. Eberbach, Alemanha: Roche; 2022.
14. Spring LK, Krakowski AC, Alam M, Bhatia A, Brauer J, Cohen J, et al. Isotretinoin and timing of procedural interventions. JAMA Dermatol. 2017;153(8):802-9.
15. Picosse FR, Yarak S, Cabral NC, Bagatin E. Early chemabrasion for acne scars after treatment with oral isotretinoin. Dermatol Surg. 2012;38(9):1521-6.
16. Guadanhim LRS, Gonçalves RG, Bagatin E. Observational retrospective study evaluating the effects of oral isotretinoin in keloids and hypertrophic scars. Int J Dermatol. 2016;55(11):1255-8.
17. Handog EB, Datuin MSL, Singzon IA. Chemical peels for acne and acne scars in asians: evidence based review. J Cutan Aesthet Surg. 2012;5(4):239-46.
18. Chandrashekar BS, Vadlamudi SR, Shenoy C. Safety of performing superficial chemical peels in patients on oral isotretinoin for acne and acne-induced pigmentation. J Clin Aesthetic Dermatol. 2021;14(11):41-3.
19. Yokomizo VMF, Benemond TMH, Chisaki C, Benemond PH. Chemical peels: review and practical applications. Surg Cosmet Dermatol. 2013;5(1):58-68.
20. Mysore V, Mahadevappa OH, Barua S, Majid I, Viswanath V, Bhat RM, et al. Standard guidelines of care: performing procedures in patients on or recently administered with isotretinoin. J Cutan Aesthet Surg. 2017;10(4):186-94.
21. Mahadevappa OH, Mysore V, Viswanath V, Thurakkal S, Majid I, Talwar S, et al. Surgical outcome in patients taking concomitant or recent intake of oral isotretinoin: a multicentric study-iso-aims study. J Cutan Aesthet Surg. 2016;9(2):106-14.
22. Kar BR, Tripathy S, Panda M. Comparative study of oral isotretinoin versus oral isotretinoin + 20% salicylic acid peel in the treatment of active acne. J Cutan Aesthet Surg. 2013;6(4):204-8.
23. Bae IH, Kwak JH, Kim MS, Shin BS, Choi H.Comprehensive review of the acne grading scale in 2023. Ann Dermatol. 2024;36(2):65-73.
24. Siegel S, Castellan Jr NJ. Estatística não-paramétrica para ciências do comportamento. 2nd. ed. Porto Alegre: Artmed; 2006. 448 p.
AUTHOR’S CONTRIBUTION:
Marina Soares Silverio 0009-0005-0039-1667
Statistical analysis; Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical review of the literature; Critical revision of the manuscript.
Daniel Simão de Andrade 0009-0003-4002-5288
Approval of the final version of the manuscript; Acquisition, analysis and interpretation of data; Critical revision of the manuscript.
Carolina Malavassi Murari 0000-0001-6688-5145
Approval of the final version of the manuscript; Acquisition, analysis and interpretation of data; Critical revision of the manuscript.
Rossana Cantanhede Farias de Vasconcelos 0000-0002-6185-1840
Approval of the final version of the manuscript; Critical revision of the manuscript.
Fernanda Rytenband 0000-0002-2882-1658
Statistical analysis; Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical review of the literature; Critical revision of the manuscript.
www.surgicalcosmetic.org.br/
Assessing the impact of anti-nuclear antibodies on the severity and types of vitiligo: a retrospective clinical investigation
Avaliando o impacto dos anticorpos antinucleares na gravidade e nos tipos de vitiligo: estudo clínico investigativo retrospectivo
Introduction: Vitiligo is an autoimmune pigmentary disorder characterized by depigmented macules on the skin. It is associated with a range of autoimmune diseases. Antinuclear antibodies (ANA) are implicated in vitiligo, but their association with disease severity remains unclear.
Objective: This study aims to assess antinuclear antibody (ANA) serum levels and evaluate their relationship with the severity and types of vitiligo.
Methods and Patients: This is a retrospective study using preexisting patient records from the Pigmentary Disorders Unit of the Cairo Hospital of Dermatology and Venereology. The analysis included patients with complete medical records, including demographic data, clinical evaluation (VIDA and VASI scores), and laboratory results for ANA titer. Their correlation with disease severity and patient demographics was analyzed.
Results: The study found that 462 patients (33%) were positive for ANA, with a higher prevalence in females (350 patients; 75.8%). A significant correlation was observed between ANA positivity and family history of vitiligo and systemic autoimmune diseases such as type 1 diabetes mellitus and thyroid disease. Weak positive correlations were found between ANA, different types of vitiligo, and disease severity scores.
Conclusion: Vitiligo is strongly associated with systemic autoimmune conditions. Routine monitoring of autoimmune markers in patients with vitiligo is recommended.
Introdução: O vitiligo é uma doença pigmentar autoimune caracterizada por máculas despigmentadas na pele. Está associado a uma série de doenças autoimunes. Os anticorpos antinucleares (ANA) estão implicados no vitiligo, mas a sua associação com a gravidade da doença permanece obscura.
Objetivo: Este estudo tem como objetivo avaliar os níveis séricos de ANA e sua relação com a gravidade e os tipos de vitiligo.
Métodos e Pacientes: Este é um estudo retrospectivo usando registros de pacientes preexistentes da Unidade de Distúrbios Pigmentares do Hospital de Dermatologia e Venereologia do Cairo. A análise incluiu pacientes com registros médicos completos, incluindo dados demográficos, avaliação clínica (escores VIDA e VASI) e resultados laboratoriais dos títulos de ANA. Sua correlação com a gravidade da doença e a demografia dos pacientes foi analisada. Resultados: O estudo determinou que 462 pacientes (33%) eram positivos para ANA, com maior prevalência no sexo feminino (350 pacientes; 75,8%).
Conclusões: Foi observada uma correlação significativa entre positividade para ANA e histórico familiar de vitiligo e doenças autoimunes sistêmicas, como diabetes mellitus tipo 1 e doenças da tireoide. Correlações positivas fracas foram encontradas entre ANA e diferentes tipos de vitiligo e escores de gravidade da doença.
Conclusão: Há uma forte associação entre vitiligo e condições autoimunes sistêmicas. Recomenda-se o monitoramento de rotina de marcadores autoimunes em pacientes com vitiligo.
1 Cairo Hospital of Dermatology and Venereology (Al Haud Al Marsoud), Egyptian Ministry of Health and Population, Dermatology Department, Cairo, Egypt
Correspondence: Shaimaa Farouk
E-mail: dr.shaimaafarouk@gmail.com
Funding: None Conflict of interest: None
Submitted on: 12/18/2024 Final decision: 03/20/2025
How to cite this article: Aoun R, Hossam D, Sadek A, Farouk S. Assessing the impact of anti-nuclear antibodies on the severity and types of vitiligo: a retrospective clinical investigation. Surg Cosmet Dermatol. 2025;17:e20250432.
Aoun R, Hossam D, Sadek A, Farouk S.
INTRODUCTION
Vitiligo is a pigmentary disorder of autoimmune etiology characterized by depigmented macules or patches on the skin. Its worldwide prevalence is estimated at around 0.5%–2%.1 Though not a life- or organ-threatening condition, it has a significant impact on the psychological well-being and quality of life of patients.
Clinically, it can be classified into three main types: segmental, non-segmental, and mixed (segmental and non-segmental).2 The Vitiligo Area Scoring Index (VASI) and the Vitiligo Disease Activity Score (VIDA) are two key tools used to assess vitiligo in clinical practice. VASI calculates a score based on the percentage of affected skin in order to evaluate the extent and degree of depigmentation, making it useful for tracking treatment response over time.3 VIDA, on the other hand, measures disease activity based on patient-reported progression over the previous six months, offering insight into how active it is.4 Together, they provide a comprehensive view of both disease severity and progression.
Vitiligo is thought to have a complex pathogenesis and to be a multifactorial polygenic disorder.The exact cause of the loss of epidermal melanocytes in vitiligo is still unknown, despite a number of proposed theories, including autoimmune, autocytotoxic, biochemical, neural, and genetic mechanisms.5 Currently, the most likely explanation is the autoimmune theory.6 Autoantibodies known as antinuclear antibodies (ANA) target various cellular components.
Many different types of connective tissue diseases typically have positive ANA levels, and laboratory tests are often used to screen for systemic lupus erythematosus (SLE) and other connective tissue diseases due to their extremely high sensitivity but low specificity.7 There is debate over whether to check ANA levels in patients with vitiligo. According to a recent meta-analysis, the prevalence of ANA is higher among patients with vitiligo compared to the general population.8 As an autoimmune condition involving T lymphocytes, ANA positivity may be highly prevalent among patients with vitiligo. The objective of this study was to assess antinuclear antibody levels and their relationship with the severity of different types of vitiligo.
MATERIALS AND METHODS
This was a retrospective clinical investigation using preexisting patient records from the Pigmentary Disorders Unit of the Cairo Hospital of Dermatology and Venereology (Al-Haud Al-Marsoud). It included patients with a confirmed diagnosis of vitiligo based on clinical and Wood’s lamp examination and who had complete medical records, including demographic data, clinical evaluation (VIDA and VASI scores), and laboratory results for ANA titer. The study was conducted from September 2023 to October 2024. Patients with vitiligo were included regardless of sex and age. Records of pregnant or lactating women, as well as patients with a history of malignancies, were excluded.
Data Collection
Patient data were extracted from the medical records of the Pigmentary Disorders Unit at the Cairo Hospital of Dermatology and Venereology, including:
1. Demographic data (age, sex, and family history of vitiligo).
2. Clinical history (onset, course, duration of the lesion, history of medications, systemic diseases such as diabetes mellitus, systemic lupus erythematosus, and thyroid disease) and associated dermatological disorders (eg, alopecia areata and psoriasis).
3. Vitiligo Disease Activity Score (VIDA);
This includes a six-point scale to measure vitiligo activity (scoring from +4 to -1) as shown in the figure.4
3.1 Active disease:VIDA score +4 to +1
3.2 Stable disease:VIDA score 0 to -1
4. Vitiligo Area Scoring Index (VASI).21
The formula comprises involvement of all body areas (probable range, 0–100) as follows: VASI = ∑ All body sites (hand units) × (remaining depigmentation). One hand unit, consisting of the palm plus the volar surface of all fingers, represents approximately 1% of the total body surface area. The degree of remaining depigmentation is recorded as the closest percentage: 0%, 10%, 25%, 50%, 75%, 90%, or 100%. At 100% depigmentation, no pigment remains; at 90%, there are specks of pigment; at 75%, the depigmented area exceeds the pigmented area; at 50%, the depigmented and pigmented areas are identical; at 25%, the pigmented area exceeds the depigmented area; at 10%, there are only specks of depigmentation.
5. Laboratory test results:
Antinuclear antibodies (ANA) were detected by immunofluorescence staining on Hep-2 sections. ANA were classified as positive when detectable at 1:80, 1:160, and 1:320 dilution or higher.
According to the inclusion and exclusion criteria, 2390 patients were eligible for this study but only 1400 had complete medical records, including demographic data, clinical evaluation, VIDA and VASI scores, and laboratory results for ANA titer.
Statistical analysis:
All statistical analyses were performed using SPSS, version 28 (SPSS Inc., Chicago, IL). The data are presented as n and %. P-values of ≤0.05 and ≤0.01 were considered the cutoff point for statistically significant differences between variables. Categorical variables are presented as frequency and percentage, while continuous variables are presented as mean (SD). Categorical variables were compared using the chi-square (χ2) test,
and Pearson’s correlation coefficient when necessary. Statistical significance was set as p < 0.05. Two-way ANOVA was used to assess differences in mean changes in quantitative variables.
RESULTS
This study included 1400 patients diagnosed with vitiligo. The mean age of patients was 24.71 (13.432) years, ranging from 3 to 55 years. By age group, 37% of patients were 3–17 years old, 27% were 18–30 years old, and 36% were 31–55 years old. Most participants were female (77%), with males comprising 23% of the total. Mean disease duration was 2.45 (1.359) years, ranging from 1 to 10 years. Disease duration was distributed
as follows: 84% of patients had vitiligo for 1 to 3 years, 15% for 4 to 6 years, and only 1% for 7 to 10 years. Positive family history was reported by 24% of patients, whereas 76% had no family history. In terms of associated dermatological disorders, 7% of patients reported having alopecia areata (AA) and 4% had psoriasis. However, 89% of patients had no associated dermatological disorders. In addition, 6% had type 1 diabetes mellitus (DM), 10% had thyroid disease (TD), 6% had SLE, and 4% had rheumatoid arthritis (RA), while 74% had no associated systemic disorders. Finally, 33% were positive for ANA and 67% were negative (Table 1).
Table 1: Sociodemographic characteristics of the study patients
Aoun R, Hossam D, Sadek A, Farouk S.
A weak positive correlation was found between ANA and age group, sex, and disease duration (χ² = 1.85, p = 0.397χ² = 0.043, p = 0.512, and χ² = 2.307, p = 0.316, respectively). A highly significant positive correlation was found between family history of vitiligo and ANA positivity (χ² = 56.388, p < 0.0001). Among patients with a family history of vitiligo, 69.7% were positive for ANA, compared to 30.3% of patients with no family history of the disease. A weak positive correlation was found between ANA and associated dermatological disorders (χ² = 1.580, p = 0.110). A highly significant positive correlation was found between ANA and associated systemic disorders (χ² = 50.758, p < 0.0001) due to all patients (100%) with type 1 DM. TD was the most frequent among patients positive for ANA (30.3%), followed by type 1 DM and SLE (18.2%), and RA (12.1%) (Figure 1).
A weak positive correlation was observed between ANA values and different types of vitiligo. Negative ANA <1:40 was more frequent across all types of vitiligo except universalis (Table 2).
A weak positive correlation was found between ANA values and types of vitiligo (χ² = 14.573, p = 0.951). The acrofacial (NSV) and generalized (NSV) forms were the most frequent
types of vitiligo in relation to ANA levels (Table 3).
A weak positive correlation was observed between VASI scores,VIDA scores, and ANA values (Table 4).
DISCUSSION
Vitiligo is a dermatological disorder characterized by melanocytic abnormalities that result in depigmentation of the skin, mucous membranes, and hair. Although vitiligo can develop at any age and in any ethnic group, it usually manifests before the age of thirty. The onset of vitiligo has been linked to a number of etiological factors, including the immune, neurological, and endocrine mechanisms, environmental exposures, and genetics. Although vitiligo and autoimmune diseases can coexist, these associations do not always result in depigmentation.9
The present study included 1400 patients with vitiligo ranging in age from 3 to 55 years (mean, 24.7 years), consistent with other reports. In one study of 246 vitiligo cases, the average age was 25.9 years, while another reported a mean age of 34.5 years for 69 patients with vitiligo. Moreover, in a study of 74 patients with vitiligo, age ranged from 5 to 68 years (mean, 31.5 years), similar to the findings of the present study.10
Figure 1: Correlation between antinuclear antibodies (ANA) and demographic characteristics ofthe studypatients
Figure 1: Correlation between antinuclear antibodies (ANA) and demographic characteristics of the study patients
Correlation between ANA groups and types of vitiligo
ANA: antinuclear antibodies.
Table 3: Correlation between ANA values and types of vitiligo
In this study, 322 patients were male (23%), while 1078 (77%) were female. Morales-Sánchez et al. (2017) report that among 150 patients with vitiligo recruited for their study, 103 (68.7%) were women and 47 (31.3%) were men.11 In contrast, Dégboé et al. (2017) had more males (131; 53.3%) affected than females (115; 46.7%).12 The number of female patients with vitiligo may be higher because women notice changes in appearan-
ce and approach doctors sooner than men; in addition, because of social stigma, younger women tend to report the condition earlier due to matrimonial concerns.13
Duration of vitiligo in this study ranged from 1 to 10 years, most commonly 1 to 3 years (84%). Taneja et al. (2021) report durations of 2 to 4 years, very similar to the results of the present study; the small difference may be due to the larger number of patients (200 cases).14
Table 2:
ANA: antinuclear antibodies.
Table 4: Correlation between VASI and VIDA scores and ANA levels
Aoun R, Hossam D, Sadek A, Farouk S.
A positive family history of vitiligo was present in 24% of cases in the present study, while 76% of cases had no family history. Alenizi et al. (2014) report that 18% of patients had a positive family history of vitiligo; with the small difference possibly explained by the difference in sample size (the present study included 1400 patients, Alenizi et al. had 74).15
In terms of dermatological disorders associated with vitiligo, AA was found in 7% of patients and psoriasis in 4%, while 83% had none. Barbulescu et al. (2020) report that vitiligo and AA are common autoimmune conditions characterized by white spots on the skin and bald spots on the scalp.16 A retrospective study of 1098 patients with vitiligo found AA to be the most common autoimmune disease associated with vitiligo.17
Associated systemic disorders found in the present study included type 1 DM (6%), TD (10%), SLE (6%), and RA (4%). The large-scale cross-sectional study by Choi et al. (2017) found that 86,210 patients with vitiligo were at an increased risk of SLE.18 In a descriptive cross-sectional study, 7.79% of 154 patients with vitiligo also had psoriasis.19 In line with the results of the present study, Percivalle et al. (2009) report that among 712 patients with vitiligo, only 3% had associated psoriasis.20 In a 10-year retrospective study involving 3280 patients, Sheth et al. (2013) showed that comorbid autoimmune conditions occur in approximately 23% of patients with vitiligo, including TD, RA, inflammatory bowel disease (IBD), SLE, and type 1 DM.21
Several studies have suggested vitiligo is associated with various other autoimmune diseases, including thyroid conditions, AA, type 1 DM, pernicious anemia, and RA. Among these, thyroid disorders were frequent among patients with vitiligo.21,22
The prevalence of positivity for antinuclear antibodies (ANA) in the present study was 33%. The findings are consistent with those reported by Chaiyabutr et al. (2020) in their study of 85 Thai patients with vitiligo, where ANA prevalence was 35.3%. That study concluded that the positive speckled ANA pattern was the most common, while the homogenous pattern ANA was the most common in the present study.23 ANA positivity was higher in females (75.8%) than males (24.2%); in line with those reported by Chaiyabutr et al. (2020), who concluded that female gender was a factor associated with ANA positivity (90%).23
There was no statistically significant correlation between age group and ANA positivity; patients aged 3 to 17 years had the highest positivity for ANA (39.4%), followed by those aged 18 to 30 years (33.3%). These findings are in line with the report by Chaiyabutr et al. (2020), who concluded that “ANA-positive was not associated with age but associated with the female gender.”23
Kroon et al. (2013) found no correlation between presence of antibodies and recent disease activity or other clinical characteristics such as age, sex, extension, and duration of vitili-
go; likewise, the present study found no significant correlation between ANA positivity and disease duration.24 There was a significant correlation between ANA positivity and family history of vitiligo; the same finding was reported by Lin X et al. (2011).25 A positive correlation was found between ANA positivity and associated dermatological disorders such as AA and psoriasis, in line with the findings reported by Garg et al. (2015).26 There was a significant correlation between ANA positivity and associated systemic disorders for all patients with type 1 DM, TD, SLE, and RA, in line with the findings of Chivu et al. (2022).9 Kanani et al. (2023) concluded that there is a significant association between vitiligo and other autoimmune diseases.
The identification and characterization of antinuclear autoantibodies in patients with vitiligo are vital indicators that support the findings of previous research indicating vitiligo is an autoimmune disease and may help pave the way for determining the potential incidence of other autoimmune conditions.27 The present study found a weak positive correlation between ANA positivity and VASI scores, with 37.1% and 33.8% ANA-positive for VASI scores from 2 to 7 and for more than 7 to 13, respectively; similar to the findings of Chivu et al. (2022).9 There was a weak positive correlation between ANA positivity and different types of vitiligo, with 35% for the acrofacial (NSV) form and 33.8% for the generalized (NSV) form. This is in line with the findings of Ekhlas et al. (2023),27 but higher than the findings of Kasumagic-Halilovic et al. (2013),28 who detected ANA in 17% of patients with vitiligo; the difference may be due to the larger sample size in the present study.
CONCLUSION
The present study reported a significant prevalence of antinuclear antibodies in patients with vitiligo. Therefore, to enable early detection and timely interventions, screening for autoimmune diseases among patients with vitiligo is recommended. Vitiligo should be considered a systemic rather than a skin disease.
Recommendations
1. Dermatologists should routinely screen for anti-thyroid and antinuclear antibodies in patients with vitiligo, especially those with a family history of autoimmune disease.
2. For better outcomes, encourage a multidisciplinary approach, involving dermatologists, endocrinologists, and rheumatologists, to optimize care for patients with vitiligo with autoimmune markers.
3. Educate patients about the potential link between autoimmune markers and vitiligo, stressing the importance of regular monitoring and management of autoimmune conditions. l
2. Zhang Y, Cai Y, Shi M, Jiang S, Cui S, Wu Y, et al. The prevalence of vitiligo: a meta-analysis. PloS one. 2016;11(9):e0163806.
3. Al Hammadi A, Castro CCS, Parmar NV, Ubogui J, Hatatah N, Ahmed HM, Llamado L. Prevalence and burden of vitiligo in Africa, the Middle East and Latin America. Skin Health and Disease. 2024;4(1):e317.
4. Al-Shammari SA, Alotaibi HM, Assiri MA, Altokhais MI, Alotaibi MS, Alkhowailed MS. Quality of life in vitiligo patients in central Saudi Arabia. Saudi Med J. 2021;42(6):682-7.
5. Ezzedine K, Lim HW, Suzuki TA, Katayama I, Hamzavi I, Lan CC, et al. Revised classification/nomenclature of vitiligo and related issues: the Vitiligo Global Issues Consensus Conference. Pigment Cell Melanoma Res. 2012;25(3):E1-13.
7. Dwivedi M, Kemp EH, Laddha NC, Mansuri MS, Weetman AP, Begum R. Regulatory T cells in vitiligo: implications for pathogenesis and therapeutics. Autoimmunity Rev. 2015;14(1):49-56.
8. Alkhateeb A, Fain PR, Thody A, Bennett DC, Spritz RA. Epidemiology of vitiligo and associated autoimmune diseases in caucasian probands and their families. Pigment Cell Res. 2003;16(3):208-14.
9. Chivu AM, Bălășescu E, Pandia LD, Nedelcu RI, Brînzea A, Turcu G, et al. Vitiligo— thyroid disease association: when, in whom, and why should it be suspected? a systematic review. J Personal Med. 2022;12(12):2048.
10. Rashed L, Hay RA, Mahmoud R, Hasan N, Zahra A, Fayez S. Association of angiotensin-converting enzyme (ace) gene polymorphism with inflammation and cellular cytotoxicity in vitiligo patients. PloS one. 2015;10(7):e0132915.
11. Morales-Sánchez MA, Vargas-Salinas M, Peralta-Pedrero ML, Olguín-García MG, Jurado-Santa Cruz F. Impact of vitiligo on quality of life. Actas Dermosifiliogr. 2017;108(7):637-42.
12. Dégboé B, Atadokpèdé F, Saka B, Adégbidi H, Koudoukpo C, Yédomon H, do Ango‐ Padonou F. Vitiligo on black skin: epidemiological and clinical aspects in dermatology, Cotonou (Benin). Int J Dermatol. 2017;56(1):92-6.
13. Vora RV, Patel BB, Chaudhary AH, Mehta MJ, Pilani AP. A clinical study of vitiligo in a rural set up of Gujarat. Indian J Community Med. 2014;39(3):143-6.
14. Taneja N, Sreenivas V, Sahni K, Gupta V, Ramam M. Disease stability in segmental and non-segmental vitiligo. Indian Dermatol Online J. 2022;13(1):60-3.
15. Alenizi DA. Consanguinity pattern and heritability of vitiligo in Arar, Saudi Arabia. J Family Community Med. 2014;21(1):13-6.
16. Barbulescu CC, Goldstein NB, Roop DR, Norris DA, Birlea SA. Harnessing the power of regenerative therapy for vitiligo and alopecia areata. J Invest Dermatol. 2020;140(1):29-37.
17. Gill L, Zarbo A, Isedeh P, Jacobsen G, Lim HW, Hamzavi I. Comorbid autoimmune diseases in patients with vitiligo: a cross-sectional study. J Am Acad Dermatol. 2016;74(2):295-302.
18. Choi CW, Eun SH, Choi KH, Bae JM. Increased risk of comorbid rheumatic disorders in vitiligo patients: a nationwide population‐based study. J Dermatol. 2017;44(8):909-13.
19. Yazdanpanah MJ, Banihashemi M, Pezeshkpoor F, Moradifar M, Feli S, Esmaeili H.Evaluation between association of psoriasis and vitiligo. J Cutan Med Surg. 2015;19(2):140-3.
20. Percivalle S, Piccinno R, Caccialanza M. Concurrence of vitiligo and psoriasis: a simple coincidence? Clin Exp Dermatol. 2009;34(1):90-1.
21. Sheth VM, Guo Y, Qureshi AA. Comorbidities associated with vitiligo: a ten-year retrospective study. Dermatology. 2014;227(4):311-5.
22. McLeod DS, Cooper DS. The incidence and prevalence of thyroid autoimmunity. Endocrine. 2012;42(2):252-65.
23. Chaiyabutr C, Wongpraparut C, Charoenpipatsin N, Pruksaeakanan C, Silpa‐archa N. The necessity of antinuclear antibody investigation in pre‐phototherapy vitiligo patients: a retrospective study. Photodermatol Photoimmunol Photomed. 2020;36(5):373-7.
24. Kroon MW, Kemp EH, Wind BS, Krebbers G, Bos JD, Gawkrodger DJ, et al. Melanocyte antigen‐specific antibodies cannot be used as markers for recent disease activity in patients with vitiligo. J Eur Acad Dermatol Venereol. 2013;27(9):1172-5.
25. Lin X, Tian H, Xianmin M. Possible roles of B lymphocyte activating factor of the tumour necrosis factor family in vitiligo autoimmunity. Med Hypotheses. 2011;76(3):339-42.
26. Garg S, Mahajan VK, Mehta KS, Chauhan PS, Gupta M, Yadav RS, et al. Vitiligo and associated disorders including autoimmune diseases: a prospective study of 200 Indian patients. Pigment Internatinal. 2015;2(2):91-6.
27. Kanani E, Issa A, Al-Ahmadi K. Evaluation of autoimmune biomarkers in vitiligo patients’ serum. J Population Ther Clin Pharmacol. 2023;30(2):283-90.
28. Kasumagic-Halilovic E, Ovcina-Kurtovic N, Jukic T, Karamehic J, Begovic B, Samardzic S. Vitiligo and autoimmunity. Med Arch. 2013;67(2):91.
AUTHOR’S CONTRIBUTION:
Rasha Aoun 0009-0008-3863-4275
Approval of the final version of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study.
Dalia Hossam 0000-0001-9806-1714
Approval of the final version of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature.
Ahmed Sadek 0000-0002-1603-2790
Approval of the final version of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature.
Shaimaa Farouk 0000-0003-2415-2511
Statistical analysis, Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
www.surgicalcosmetic.org.br/
Diagnosis-to-treatment intervals for melanoma in Brazil: a matter of geography?
Intervalo de tempo entre o diagnóstico e o tratamento do melanoma no Brasil: uma questão de geografia?
Introduction: Melanoma is a type of skin cancer originating from melanocytes which may also affect mucous membranes, leptomeninges, and the uveal tract. Although less prevalent than other skin cancers, it has high lethality due to its aggressiveness, making it a significant public health problem in Brazil.
Objective: The primary objective of this study was to assess the time elapsed between diagnosis and treatment initiation for patients with melanoma in different regions of the country in 2024. In addition, it sought to identify possible regional disparities in this interval, as well as to correlate this information with existing data in the literature.
Methods: This cross-sectional study analyzed 4,405 cases of melanoma diagnosed in 2024, focusing on the diagnosis-to-treatment interval based on data from the Brazilian public health information systems (SISCAN, SIH, and SIA). The study assessed compliance with the 60-day legal maximum waiting time established by Law No. 12.732/2012 across the country's five macroregions.
Results: Regional disparities were observed: the South Region had the best indicators (34.25% of cases treated within 30 days), while the North Region had the worst performance (22.41%). A high percentage of cases had no recorded treatment initiation dates (60.86% nationwide; 68.10% in the North), revealing weaknesses in health information systems and possibly in treatment delivery. Persistent delays and regional inequalities highlight structural deficiencies in the provision of oncology care.
Conclusion: The findings underscore the need to strengthen the regionalization of care, improve recordkeeping, and implement effective mechanisms to enforce legal time limits.
Keywords: Melanoma; Diagnosis; Brazil.
RESUMO
Introdução: O melanoma é um tipo de câncer de pele originado dos melanócitos, podendo acometer também as mucosas, as leptomeninges e o trato uveal. Embora menos prevalente que outros cânceres cutâneos, apresenta alta letalidade devido à sua agressividade, configurando um importante problema de saúde pública no Brasil.
Objetivo: O presente estudo teve como objetivo principal avaliar o tempo decorrido entre o diagnóstico e o início do tratamento de pacientes com melanoma em diferentes regiões do país no ano de 2024. Além disso, buscou-se identificar possíveis disparidades regionais nesse intervalo, bem como correlacionar com dados já existentes na literatura.
Métodos: Este estudo transversal analisou 4.405 casos de melanoma diagnosticados em 2024, com foco no tempo entre odiagnóstico e o início do tratamento, conforme dados do Sistema de Informação do Câncer, do Sistema de Informações Hospitalares e do Sistema de Informações Ambulatoriais do Sistema Único de Saúde (SUS). Avaliou-se o cumprimento do prazo legal máximo de 60 dias, estabelecido pela Lei nº 12.732/2012, nas cinco macrorregiões do país.
Resultados: Observou-se uma importante variação regional: a região Sul apresentou os melhores indicadores (34,25% dos pacientes tratados em até 30 dias), enquanto a região Norte teve o pior desempenho (22,41%). Destaca-se o elevado percentual de casos sem registro da data de início do tratamento (60,86% no Brasil; 68,10% no Norte), o que evidencia falhas nos sistemas de informação e, possivelmente, na efetivação do próprio tratamento. Além disso, a persistência de atrasos e as desigualdades regionais revelam deficiências estruturais na oferta de cuidados oncológicos. Conclusões: Os resultados indicam a necessidade de fortalecer a regionalização da atenção, qualificar os registros e garantir o monitoramento dos prazos legais.
Palavras-chave: Melanoma; Diagnóstico; Brasil.
Original Article
Authors:
Isabela Karina Vilas Boas1
Maria Julia de Medeiros Pedroza1
Milena Dias da Silva1
Beatriz Bernaud Coelho1
Magda Blessmann Weber1
1 Universidade Federal de Ciências da Saúde de Porto Alegre (UFCSPA), Medicine, Porto Alegre (RS), Brazil
Correspondence: Isabela Karina Vilas Boas E-mail: isabelak.vilasboas@gmail.com
Funding: None. Conflict of interest: None.
Submitted on: 06/22/2025
Final decision: 08/07/2025
How to cite this article: Vilas Boas IS, Pedroza MJM, Silva MD, Coelho BB, Weber MB. Diagnosis-to-treatment intervals for melanoma in Brazil: a matter of geography? Surg Cosmet Dermatol. 2025;17:e20250483.
INTRODUCTION
Melanoma is a malignant skin neoplasm originating from melanocytes. The cutaneous form is the most common, but melanoma can also originate from mucous membranes, leptomeninges, and the uveal tract of the eye.¹ Although less frequent than nonmelanoma skin cancers (basal cell carcinoma and squamous cell carcinoma), which have the highest incidence rates according to the 2023 INCA estimate, melanoma has greater invasive and metastatic potential, as well as higher mortality rates. In Brazil, according to the same estimate, there were 1,923 deaths due to melanoma in 2020.² Therefore, early diagnosis and timely access to treatment are essential to halt its invasive potential and ensure better prognosis for patients and therapeutic success.
In recent years, more widespread dissemination of knowledge about melanoma risk factors that are well established in the scientific literature, such as unprotected sun exposure, white skin, and aging, along with the promotion of protective measures, such as photoprotection, routine skin exams, and public awareness campaigns, has contributed to an increase in treatment rates for malignant skin cancer.²,³ However, an analysis of historical trends shows an alarming scenario for melanoma with regard to incidence rates, mortality rate, and—most importantly—the diagnosis-to-treatment interval.³ Therefore, melanoma represents an important public health problem, particularly because many deaths are primarily linked to delays between diagnosis and treatment (diagnosis-to-treatment intervals longer than 30 days).
Given the impact of increased diagnostic intervals on prognosis and, consequently, on patient mortality, Brazilians are legally entitled, under Law No. 12.732/2012, to begin undergoing treatment in the Brazilian Unified Health System (SUS, Sistema Único de Saúde) within 60 days of reported diagnosis. This first treatment may involve surgery, radiation therapy, or chemotherapy, depending on the case.⁴ The main objective of this study was to assess the time elapsed between diagnosis and initiation of treatment for patients with melanoma across different regions of Brazil in 2024. In addition, the study sought to identify potential regional disparities in this interval as well as to correlate the findings with data already reported in the literature.¹
METHODS
An analytical cross-sectional study was conducted using data from the Outpatient Information System (SIA, Sistema de Informação Ambulatorial), the Hospital Information System (SIH, Sistema de Informação Hospitalar), and the Cancer Information System (SISCAN, Sistema de Informações de Câncer), available from the IT Department of the Brazilian Unified Health System (DATASUS).³ Case definition was based on matching data from the National Health Card to the International Classification of Diseases (ICD) code reported. Cases were selected using ICD code “C43: Malignant melanoma of skin.” The study included cases from January 2024 to December 2024,
taking into account Brazil’s five macroregions. The time in days between diagnostic examination and initiation of treatment was divided into up to 30 days, 31 to 60 days, more than 60 days, and no treatment information. Surgical procedures performed prior to diagnosis were included in the up to 30 days interval. The data extracted were tabulated in an Excel spreadsheet for detailed analysis.³ According to Brazilian National Health Council Resolution 510/2016, studies using public-domain data do not require review by a Research Ethics Committee.
RESULTS
In the North Region of Brazil, 116 cases of malignant skin melanoma were recorded in 2024 (Table 1). An analysis of the interval between diagnosis and initiation of treatment showed a concerning scenario regarding the effectiveness of oncological lines of care in the region. Of the 116 cases, only 26 (22.41%) initiated treatment within 30 days after diagnosis, below the national average of 32.10%.³ This is particularly relevant given that early treatment is directly associated with improved clinical outcomes in melanoma, a neoplasm known for its high metastatic potential.⁵ In addition, only 4 patients (3.45%) began treatment within 31 to 60 days, a period still compliant with Brazilian legislation (as established by Law No. 12.732/2012). In contrast, 7 patients (6.03%) began treatment more than 60 days after diagnosis, representing severe delays that potentially compromises patient prognosis. The most alarming finding, however, was the lack of information on treatment initiation for 79 cases (68.10%). This number represents more than two-thirds of all cases in the North and is well above the national average of 60.86%.¹,⁴ This gap may reflect both failures in recordkeeping and data monitoring and the absence of treatment delivery, suggesting a possible collapse in information and care systems in the region.⁶
In the Northeast Region, according to DATASUS databases, 572 malignant skin melanoma cases were recorded in 2024 (Table 2). Analysis of diagnosis-to-treatment intervals found more favorable indicators compared to the North but still highlighted significant challenges in access to and the effectiveness of oncology care. Of the total, 185 patients (32.34%) began
Source: Adapted from DATASUS, 2025
Vilas Boas IS, Pedroza MJM, Silva MD, Coelho BB, Weber MB.
Table 1: Diagnosis-to-treatment interval in the North Region
Table 2: Diagnosis-to-treatment
interval in the Northeast Region
Diagnosis-to-treatment interval Cases
Up to 30 days
31 to 60 days
185 (32.34%)
24 (4.20%)
More than 60 days 45 (7.87%)
No information
Source: Adapted from DATASUS, 2025
318 (55.59%)
treatment within 30 days of diagnosis. This percentage is consistent with the national average (32.10%), indicating that approximately one-third of patients in the Northeast received treatment within the time period considered optimal in the scientific literature, consistently associated with higher survival and lower progression rates in melanoma.⁷ ⁹ In addition, 24 patients (4.20%) began treatment within 31 to 60 days. Although initiation in these cases came after the optimal time period, they were still within the legal limit established by Law No. 12.732/2012, which sets a maximum of 60 days between diagnosis and initiation of treatment in SUS. However, 45 patients (7.87%) only began receiving treatment more than 60 days after diagnosis, the highest rate of severe delays among all regions analyzed so far. This is concerning, given that it suggests structural barriers directly affecting the health care system’s resolution rates and response times in treating melanoma.⁶ Another important point is the large number of cases with no data on treatment initiation. The study found 318 cases (55.59%) with no data on treatment delivery, compromising the analysis of this line of care and the assessment of public policies. Although lower than the Northern average, this figure still represents more than half of all cases in the Northeast, reflecting potential weaknesses in recordkeeping, tracking, and monitoring systems for melanoma patients.⁶,⁷
In the Central-West Region, 238 malignant skin melanoma cases were recorded in 2024, according to data from DATASUS information systems (Table 3). The case distribution by diagnosis-to-treatment intervals shows an intermediate scenario compared to other regions of Brazil, with records predominantly lacking information on treatment initiation. Of the total, 71 patients (29.83%) began treatment within 30 days of diagnosis, slightly below the national average (32.10%). Although not the worst-performing region, this percentage indicates that fewer than one-third of patients began receiving treatment within the ideal time period set by clinical best practices, which recommends initiating treatment as soon as possible in order to increase the likelihood of controlling the disease.⁷-⁹ An additional 6 cases (2.52%), a very small number, started treatment within 31 to 60 days, an interval still allowed by current legislation (Law No. 12.732/2012). These data highlight that most patients do not initiate treatment within 30 days of diagnosis nor within the legal limit, which may suggest longer-lasting barriers in the
Table 3: Diagnosis-to-treatment
interval in the Central-West Region
Diagnosis-to-treatment interval Cases
Up to 30 days
71 (29.83%)
31 to 60 days 6 (2.52%)
More than 60 days
No information
Source: Adapted from DATASUS, 2025
14 (5.88%)
147 (61.76%)
patient care flow.⁴ In addition, 14 patients (5.88%) began treatment more than 60 days after diagnosis, after the legal limit and representing a critical delay, with potential negative consequences for their clinical prognosis.10-13 This is a significant rate, and similar to those found in other regions with greater structural problems, such as the North and the Northeast. The most significant datum, however, was the number of cases with no information on treatment initiation, totaling 147 records (61.76%). This rate is higher than the national average (60.86%) and ranks as the third-highest among the five regions, behind only the North and the Southeast. The absence of this information severely compromises analyses of care effectiveness and hinders the process of monitoring public cancer policies in the region. The Southeast Region accounted for the highest absolute number of malignant melanoma cases in 2024, totaling 1,733 records (Table 4). This substantial figure represents a significant share of the national sample included in this study, reflecting both the population density of the region and the greater capillarity of its reporting systems. In terms of diagnosis-to-treatment intervals, 534 patients (30.81%) initiated treatment within 30 days. Although slightly below the national average (32.10%), this rate demonstrates relatively efficient responsiveness for cases that do undergo treatment. However, when one considers the total number of patients, this percentage means that fewer than one-third initiated treatment within the optimal time period, showing timeliness is not universal even where there is greater service availability. Only 37 cases (2.14%) began treatment within 31 to 60 days, a much lower percentage than observed in other regions.This rate suggests that, in practice, cases not treated
Table 4 - Diagnosis-to-treatment interval in the
Southeast Region
Diagnosis-to-treatment interval
Up to 30 days
31 to 60 days
More than 60 days
Cases
534 (30.81%)
37 (2.14%)
71 (4.10%)
No information 1,091 (62.95%)
Source: Adapted from DATASUS, 2025
quickly tend to exceed the legal time limit or may not even be recorded as treated. In addition, 71 patients (4.10%) started treatment more than 60 days after diagnosis, after the time limit established by Law No. 12.732/2012.While this number is comparable to other regions, the absolute number is significant due to the large volume of cases in the Southeast. The most concerning finding, however, was the 1,091 records (62.95%) with no information on treatment initiation data. That figure is equivalent to nearly two-thirds of all cases in the region and is higher than the national average (60.86%), evidence of serious issues in tracking patient care.¹⁴ The magnitude of that number in one of Brazil’s most structurally developed regions suggests that missing data may be associated with both failures in information systems and real gaps in access or continuity of care.¹⁴,¹⁵
In the South Region, 1,746 cases of malignant skin melanoma were recorded in 2024, making it the second-highest absolute number among Brazil’s five macroregions (Table 5). An analysis of diagnosis-to-treatment intervals shows slightly more efficient performance compared to the national average, especially regarding treatment initiation within the optimal period. Out of the total, 598 patients (34.25%) began treatment within 30 days of diagnosis. This is the highest rate among all regions, and above the national average (32.10%). This suggests that a higher proportion of patients in the South had timely access to treatment, possibly reflecting better organization of health care networks and greater capillarity of specialized services.¹⁶ Within the 31 to 60 days range, only 34 patients (1.95%) initiated treatment, the lowest percentage among all regions. Though still within the time limit established by Law No. 12.732/2012, the small number of cases in this interval may suggest a trend towards polarization: patients are either treated promptly or experience more severe delays.³,⁴ The share of patients initiating treatment more than 60 days after diagnosis was 3.89% (68 cases), similar to that found in other regions, such as the Southeast (4.10%). Although the two rates are similar, this indicator also shows a significant group of patients outside the legal time limit, which may directly compromise clinical outcomes in melanoma, a highly lethal neoplasm when treated late.⁴, ¹⁰ ,¹³ Finally, 1,046 cases (59.91%) had no information on treatment initiation, a figure close to the national average (60.86%). Though the lo-
west rate among all regions, it still represents a substantial gap that hinders a full assessment of the effectiveness of health care networks. Information may be missing both due to recording failures and to actual lack of treatment initiation.
DISCUSSION
Regional inequality in access to treatment
Diagnosis-to-treatment
to 30 days
to 60 days
than 60 days
Source: Adapted from DATASUS, 2025
The data highlight a striking pattern of regional inequality in access to treatment for patients diagnosed with malignant skin melanoma in Brazil. When analyzing the percentage of patients who initiated treatment within 30 days of diagnosis—considered the optimal interval for better clinical outcomes—significant variations were observed among the country’s macroregions.³ The South had the best performance, with 34.25% of cases treated within the ideal time period, followed by the Northeast (32.34%), Southeast (30.81%), Central-West (29.83%), and, finally, the North (22.41%), the most critical in this respect (Figure 1). These data reveal that while some regions can achieve rates close to or above the national average (32.10%), others, such as the North, face systemic challenges in ensuring timely treatment initiation, despite legislation guaranteeing this right (Law No. 12.732/2012). This asymmetry can be understood in light of historical and structural inequalities among Brazilian regions. The geographic distribution of specialized services, such as oncology and dermatology services, is clearly concentrated in the South and Southeast Regions, which have the highest number of high-complexity hospitals, specialized professionals, and logistical infrastructure. On the other hand, the North faces challenges related to a shortage of professionals, vast geographic distances, transportation limitations, and low density of specialized hospitals, directly compromising the diagnostic-therapeutic flow of oncology patients.⁴, ⁶ ,¹⁶ The literature supports this scenario. Oliveira et al., in a study conducted in 2020, demonstrated that regions with lower human development indices have higher rates of late-stage diagnoses, a result directly associated with the scarcity of specialized services and the low resolution rate of primary care. This finding is in line with those for the North Region, where only 22.41% of cases began receiving treatment within 30 days, and nearly 68% had no record of treatment initiation. The weakness of the oncology network in the region manifests itself not only as limited access but also as an inability to record, monitor, and ensure continuity of care. Complementarily, the thesis of Oliveira et al. broadens this perspective by showing that socioeconomic inequalities and poor territorial distribution of health care resources are reflected not only in cancer mortality indicators, but also in the conditions under which patients access the system—often in advanced stages of the disease and without a clear prospect of prompt therapeutic referral.⁶ This scenario is reinforced by our findings for the Northeast and Central-West regions, where the rates of delays greater than 60 days, although variable, coexist with high rates of incomplete or missing records, hindering any evidence-based planning action.³
Vilas Boas IS, Pedroza MJM, Silva MD, Coelho BB, Weber MB.
Table 5 - Diagnosis-to-treatment interval in the South Region
The central critique that emerges from these data and from theoretical analyses is the fragility of the principle of equity, one of the pillars of SUS. Although SUS was conceived as a universal and egalitarian system, in practice it operates in a highly unequal way, penalizing populations in peripheral and more vulnerable territories. The combination of physical, logistical, and institutional barriers generates a cumulative effect that delays diagnosis, hinders access to care, and ultimately compromises the survival of patients with melanoma and other types of cancer.¹¹,¹⁷ Therefore, the results of this study reaffirm the existence of a deeply rooted pattern of regional inequality, which compromises equity in access to oncology care.⁶ ⁷ ¹⁷ Although melanoma is less prevalent than other types of skin cancer, its potential for invasiveness and mortality makes attention to the regional barriers that delay treatment even more urgent.⁷,¹⁰ Confronting these disparities must take into account the effective regionalization of oncology, the strengthening of infrastructure in remote areas, and the improvement of territorial planning for SUS, with the goal of guaranteeing timely and comprehensive access to health care for all Brazilians.
High rate of missing information on treatment
One of the most concerning findings of this study is the
high number of melanoma cases recorded without any information on treatment initiation.³ The national average, with 60.86% of records lacking data regarding therapeutic initiation, is alarming and compromises not only individual clinical care but also the formulation, evaluation, and oversight of oncology policy in Brazil. This lack of information affects all regions, especially the North, where 68.10% of cases have no record of treatment initiation, and the Southeast, where the highest absolute number of cases is concentrated and where this rate reaches 62.95%. Even the South Region, which had the best performance in terms of promptness of treatment initiation, had 59.91% incomplete records. These percentages show that the problem transcends regional inequalities and points to a systemic weakness in the processes of recording, reporting, and monitoring therapeutic actions.18
It is necessary, therefore, to reflect on whether this lack of information stems from a merely administrative failure—such as not filling mandatory fields in the SISCAN, SIH, or SIA systems—or whether it reveals an even more serious reality: the actual non-initiation of treatment for a significant portion of patients.⁶ ¹⁶ ¹⁸ Both hypotheses are cause for concern. In the first case, the failure compromises the reliability of the national health surveillance systems and prevents the correct assessment
Figure 1: Regional comparison of diagnosis-to-treatment intervals
of the effectiveness of Law No. 12.732/2012, which mandates that cancer treatment initiate within 60 days after diagnosis.⁴ In the second case, it implies the very right to health care is being denied, constituting a large-scale legal and ethical violation. The invisibility of these data is even more impactful in contexts of greater social and geographic vulnerability. Patients living in regions distant from urban centers, with low educational levels and less access to information and to justice, tend to be the most affected by this neglect toward recordkeeping and health care. As discussed by Oliveira et al. in 2020, this statistical invisibility is not neutral: it acts as an instrument of exclusion by erasing realities that would require urgent state action.⁶
The absence of data produces a false sense of control and effectiveness, masking inequalities and perpetuating institutional inaction. Furthermore, the lack of recorded data on treatment directly affects planning capacity and the evaluation of public managers. Without accurate data, measuring the effectiveness of the national cancer control policy, identifying logistical bottlenecks, prioritizing investments, and articulating health care networks that guarantee comprehensiveness and continuity of care become unfeasible.¹⁸ Therefore, addressing this gap should not be understood merely as a technical issue of improving information systems, but as an essential strategy of equity and health care justice. The qualification of records, systems integration, continuing training and education of professionals responsible for notifications, and the use of technology to automate and cross-check data are possible paths to make SUS more transparent, responsive, and committed to the lives of its users.¹⁴, ¹⁷
Delays beyond the legal limit
Law No. 12.732/2012, enacted with the aim of ensuring that patients diagnosed with cancer begin treatment within a maximum of 60 days, represents an important regulatory landmark in the struggle for equitable access to oncology care in Brazil.⁴ However, the data from this study show that, despite the existence of this legislation, there is still a significant share of patients whose rights are not enforced.3,6 In 2024, between 4.10% (Southeast) and 7.87% (Northeast) of recorded cases initiated treatment more than 60 days after diagnosis, exceeding the legal limit. While these percentages may seem modest at first, they are highly significant for patients with malignant melanoma, an aggressive subtype of skin cancer characterized by high metastatic potential and rapid progression.1,11 In such cases, delayed treatment initiation may mean the difference between a favorable prognosis and fatal progression.7,10,13 The persistence of these delays raises serious questions about the actual effectiveness of Law No. 12.732/2012.4
The absence of systematic oversight mechanisms, institutional accountability, and real-time monitoring means that, in practice, the law depends on the organizational capacity of health care services rather than its binding legal authority.17,18 This weakness enables the standards to be generally ignored, with no formal consequences for the health care managers and
institutions involved. In addition, the fragmentation of oncology networks, health care gaps in certain regions, and poor integration between primary, specialized, and hospital care make compliance with legal time limits difficult, especially in areas where centralized services force patients into long travel and waiting times. The Northeast, with the highest share of delays exceeding the legal limit (7.87%), exemplifies how a combination of structural, socioeconomic, and geographic factors negatively impacts the enforcement of current legislation.16,17
It should be emphasized that the biological nature of melanoma requires an immediate therapeutic response. Studies show that delays of eight weeks or more in treatment initiation are associated with increase mortality and onset of metastasis, particularly in thick or ulcerated melanomas.11,14 Thus, cases exceeding 60 days often represent irreversible losses of therapeutic opportunity. Therefore, a critical analysis of the data indicates that legislation by itself has been insufficient to ensure timely access to care. Without a strong surveillance system, institutional accountability, and active care flow management, the law runs the risk of becoming dead letter.18 It is crucial that the state take a more proactive role in expanding this right, investing in expanding oncology capacity, particularly in vulnerable regions, and promoting integrated systems that enable real-time tracking of diagnostic-treatment intervals.
Implications for clinical practice and public health
This study has important implications for clinical practice, health care planning, and policymaking, particularly for SUS. The analysis of diagnosis-to-treatment intervals for melanoma found not only marked regional disparities but also systemic weaknesses in mechanisms involving regulation, monitoring, and access to oncology care in Brazil.6,16,17 The high rate of patients without treatment information—over 60% across all regions—must be understood as a warning sign of institutional inefficiency. This statistical invisibility not only distorts the reality of actual health care practices but also hinders evidence-based decision-making.
The absence of reliable data compromises territorial planning for the oncology network, resource allocation, policy effectiveness evaluation, and prioritization of investments in vulnerable regions.18 The data indicate the urgent need for targeted interventions, prioritizing regions such as the North and Central-West, where rates of compliance with legal time limits for treatment initiation are lowest and incomplete records highest. These regions should be the focus of public policy that combine expanding installed capacity, training and retaining specialists, strengthening primary care, and improving health information systems such as SISCAN.16,17 In addition, the results underline the importance of regionalizing oncology care equitably, promoting access to specialized services outside major urban centers. Strategies such as teledermatology, mobile early-diagnosis centers, and integrated lines of care may be effective alternatives to reduce delays, especially in remote areas. Clinical practice
Vilas Boas IS, Pedroza MJM, Silva MD, Coelho BB, Weber MB.
should also be reassessed in light of these findings. Primary and specialized care professionals must be trained not only for early melanoma diagnosis but also to ensure immediate referral and proper recording of treatment.
Strengthening integration across primary, medium, and high-complexity care is essential to ensure continuity and comprehensiveness, core principles of SUS.17 Finally, these findings highlight the need to revise the implementation strategies of Law No. 12.732/2012, especially in terms of establishing active monitoring and institutional accountability systems. Enforcing legal time limits should be a high-priority task for health care managers, not a secondary one.4 This study contributes to the consideration of melanoma as a marker of the Brazilian health care system’s responsiveness and reinforces the urgency of more robust, region-sensitive, and data-driven public policy, aiming at more equitable access to effective therapies.
Study limitations
This study has some important limitations, especially regarding the source and nature of the data. The analysis was based on secondary data from SUS’s public information systems (SISCAN, SIH, SIA), which, though widely used in health research, are susceptible to inconsistencies, underreporting, and delayed input. This is reflected, for instance, in the high rate of cases without information on treatment initiation, which makes it difficult to accurately assess public policy effectiveness. Another relevant limitation is the absence of data on tumor staging at diagnosis, which prevents an analysis of diagnosis-to-treatment intervals as a function of clinical severity. This is particularly important for melanoma, where aggressiveness varies by lesion depth and extension. The absence of this information hinders the capacity of this study to correlate therapeutic delays to objective clinical outcomes. In addition, part of the data input into information systems may be self-reported or inconsistently entered across health care units, compromising uniformity and comparability between regions. This calls for caution in interpreting results and highlights the need to improve health records.6,16,18
Suggestions for future studies
Based on the limitations and findings above, future studies could further explore the effects of treatment delays on melanoma, especially in terms of the impact of diagnosis and delayed initiation of therapy on survival and disease progression. Longitudinal studies tracking patients over time would be particularly useful in identifying high-risk profiles and in assessing the effectiveness of interventions.17 In addition, qualitative
analyses of the experiences of patients and health care professionals involved in oncology care are recommended. Considering the lived experience, perceived barriers, and coping strategies could reveal subjective and contextual dimensions not captured by quantitative data, further enriching our understanding of these phenomena.6 Finally, further studies could explore predictive models based on territorial and socioeconomic data in order to identify priority areas for interventions as well as to assess the impact of local programs and public policies aimed at improving melanoma care in Brazil.16,18
CONCLUSION
The results of this study reaffirm the existence of significant regional inequalities and structural weaknesses in access to oncology care in Brazil, particularly regarding treatment for malignant skin melanoma. Analyzing the interval between diagnosis and initiation of treatment revealed not only frequent delays and noncompliance with current legislation but also alarming information gaps in national databases, undermining the effectiveness of public policies and of health governance itself. Inequality of access, marked by geographic, socioeconomic, and structural disparities, systematically disadvantages the populations of vulnerable regions, such as the North and Central-West, perpetuating a state of health inequity. In addition to representing an administrative failure, the high percentage of cases without information on treatment also serves as an indicator of invisibility to care, especially in historically neglected territories.
Persistent delays beyond the legal limit established by Law No. 12.732/2012 underline the need to revise mechanisms of implementation, monitoring, and accountability, since the existence of legislation has not, by itself, ensured an effective right to timely treatment. Given this situation, it is crucial that SUS improve its information system, regionalize oncology services equitably, and integrate various care levels more efficiently. Strategies such as strengthening primary care, expanding diagnostic and treatment centers in remote areas, and using technologies such as telemedicine may contribute to overcoming these barriers.
Finally, this study highlights the importance of high-quality data, attuned to the regional and social specificities of Brazil, in driving public policy. The aggressiveness and rapid progression of melanoma make it a relevant indicator of responsiveness in the Brazilian health care system, and addressing the inequalities discussed in this study is essential to ensuring the universal right to health care and guaranteeing comprehensive oncology care in Brazil. l
Vilas Boas IS, Pedroza MJM, Silva MD, Coelho BB, Weber MB.
REFERENCES:
1. Garbe C; Becker JC. Melanoma. In: Bolognia JL; Jorizzo JL; Schaffer JV. (Ed.). Dermatologia. Tradução de Adriana de Carvalho Corrêa et al.; coordenação da edição brasileira Célia Luiza Petersen Vitello Kalil. 3. ed. Rio de Janeiro: Elsevier; 2015. p.1883–910.
2. Instituto Nacional de Câncer José Alencar Gomes da Silva (INCA). Estimativa 2023: incidência de câncer no Brasil [recurso eletrônico]. Rio de Janeiro: INCA; 2022. Disponível em: https://www.inca.gov.br/publicacoes/livros/estimativa-2023-incidencia-de-cancer-no-brasil. Acesso em: 1 maio 2025.
3. Brasil. Ministério da Saúde. DATASUS. Tabnet. Brasília, DF: Ministério da Saúde; 2022. Disponível em: https://datasus.saude.gov.br/informacoes-de-saude-tabnet/. Acesso em: 3 ago. 2022.
4. Brasil. Lei nº 12.732, de 22 de novembro de 2012. Dispõe sobre o primeiro tratamento de paciente com neoplasia maligna comprovada e estabelece prazo para seu início. Diário Oficial da União: seção 1, Brasília, DF, 23 nov. 2012. Disponível em: https://www.planalto.gov.br/ccivil_03/_ato2011-2014/2012/lei/l12732.htm. Acesso em: 1 maio 2025.
5. Santos CAD; Souza DLB. Melanoma mortality in Brazil: trends and projections (1998-2032). Ciência & Saúde Coletiva. 2019;24(4):1551–61.
6. Oliveira MM; Andrade SSCA; Oliveira PP; Silva GA; Malta DC. Desigualdades sociais no diagnóstico do câncer do colo do útero no Brasil: um estudo de base hospitalar. Ciência & Saúde Coletiva. 2020;25(3):1003–14.
7. Conic RZ, Cabrera CI, Khorana AA, Gastman BR. Determination of the impact of melanoma surgical timing on survival using the National Cancer Database. J Am Acad Dermatol. 2018;78(1):40-6.
8. Davis LE, Shalin SC, Tackett AJ. Current state of melanoma diagnosis and treatment. Cancer Biol Ther. 2019;20(11):1366–79.
9. Dixon AJ, Sladden M, Zouboulis CC, et al. Primary cutaneous melanoma – management in 2024. J Clin Med. 2024;13(6):1607.
10. Xiong DD, Barriera-silvestrini P, Knackstedt TJ. Delays in the surgical treatment of melanoma are associated with worsened overall and melanoma- specific mortality: a population-based analysis. J Am Acad Dermatol. 2022;87(4):807-14.
11. Zhang MZ, Hines AS, Demer AM, Brewer JD. The impact of surgical delay in primary cutaneous melanoma: a systematic review. Dermatol Surg. 2024;50(6):501-6.
12. Stålhammar G. Delays between uveal melanoma diagnosis and treatment increase the risk of metastatic death. Ophthalmology. 2024;131(9):1094-104.
13. Conic RZ, Cabrera CI, Khorana AA, Gastman BR. Determination of the impact of melanoma surgical timing on survival using the National Cancer Database. J Am Acad Dermatol. 2018;78(1):40-6.
14. Pereira Shimada GD, Mota AA, Souza MC, Bernardes SS. Time-to-treatment initiation for cutaneous melanoma reflects disparities in healthcare access in Brazil: a retrospective study. Public Health. 2022;210:1-7.
15. Johansson M, Brodersen J, Gøtzsche PC, Jørgensen KJ. Screening for reducing morbidity and mortality in malignant melanoma. Cochrane Database Syst Rev. 2019;6(6):CD012352.
16. Puntel L. Acesso universal à saúde: um comparativo entre as cinco grandes regiões brasileiras. 2019. 56 f. Trabalho de Conclusão de Curso (Graduação em Ciências Econômicas) – Universidade Federal do Rio Grande do Sul, Porto Alegre, 2019. Disponível em: https://lume.ufrgs.br/handle/10183/201826. Acesso em: 2 maio 2025.
17. Campos, GWS. Reflexões temáticas sobre eqüidade e saúde: o caso do SUS. Saúde e Sociedade. 2006;15(2):23-33.
18. Teixeira SV, Pimentel TRO, Costa NR. Sistema de vigilância em saúde no brasil: avanços e desafios. Saúde em Debate. 2015;39(104):255-67.
AUTHOR’S CONTRIBUTION:
Isabela Karina Vilas Boas 0009-0007-9895-4687
Preparation and writing of the manuscript; acquisition, analysis and interpretation of data; intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; critical review of the literature.
Maria Julia de Medeiros Pedroza 0009-0009-6410-3870
Preparation and writing of the manuscript; acquisition, analysis and interpretation of data; intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied.
Milena Dias da Silva 0009-0006-4147-1644
Acquisition, analysis and interpretation of data.
Beatriz Bernaud Coelho 0009-0004-2604-7672
Preparation and writing of the manuscript.
Magda Blessmann Weber 0000-0001-5885-5851
Effective participation in the conduct of the study.
www.surgicalcosmetic.org.br/
Adapalene (0.3%)/benzoyl peroxide gel (2.5%) for adult female acne: a real-world case series
from Latin America
Gel de adapaleno (0,3%)/peróxido de benzoíla (2,5%) para acne da mulher adulta: uma série de casos reais da América Latina
Palavras-chave: Peróxido de Benzoíla; Adapaleno; Acne Vulgar
To the Editor:
Adult female acne (AFA) is a common condition affecting women aged 25 years and older, with a chronic and relapsing course.1 This multifactorial disorder is associated with hormonal imbalance (eg, polycystic ovary syndrome), psychological stress, genetics, and lifestyle factors, which collectively contribute to its complexity and challenging management.1,2 The Latin American population has diverse characteristics, influenced by demographics, race/ethnicity, and exposome.3 In Brazil, the population prevalence of AFA has been estimated at 41%.4
Controlled trials of AFA treatment are scarce, but the primary therapeutic options typically include topical retinoids, antimicrobial agents, combined oral contraceptive pills, and spironolactone.5-9
Letter to the Editor
Authors:
Marco Alexandre Rocha1
Leonel Fierro-Arias2
Patricia Troielli3
Anália Viana4
Hélio Amante Miot5
1 Universidade Federal de São Paulo (UNIFESP), Dermatology, São Paulo (SP), Brazil
2 Hospital General de Mexico, Dermatology, Ciudad del Mexico, Mexico
3 Universidad de Buenos Aires, School of Medicine, Buenos Aires (BA), Argentina
4 Galderma, Medical Affairs, São Paulo (SP), Brazil
5 Universidade Federal de São Paulo (UNIFESP), Dermatology, Botucatu (SP), Brazil
Correspondence:
Marco Alexandre Rocha E-mail: marcoderm@hotmail.com / heliomiot@gmail.com
Funding: Galderma Brasil Ltda funded medical writing assistance and the Article Publishing Charge.
Acknowledgments: To the patients who allowed us to publish their anonymized photos.
Conflict of interest: MAR received fees for classes and/or participation in advisory boards from Pierre-Fabre, FQM, Galderma, L'Oréal, Naos Group, Kenvue / J&J, Hypera, and Dove-Unilever. HAM received fees for classes and participation in advisory boards from Merz, Abbvie, Galderma, Kenvue, Pierre-Fabre, Pfizer, Eucerin / Beiersdorf, and L'Oréal. PT received fees for classes and/or participation in advisory boards from Galderma; L'Oréal, La Roche-Posay, and Eucerin / Beiersdorf. LF received fees for classes and/or participation in advisory boards from Galderma, Pierre-Fabre, Eucerin / Beiersdorf, NAOS / Bioderma, and ISDIN. AV is an employee of the Galderma Brazil Medical Affairs Department.
Submitted on: 03/25/2025
Final decision: 08/05/2025
How cite this article: Rocha MA, Fierro-Arias L, Troielli P, Viana A, Miot HA. Adapalene (0.3%)/benzoyl peroxide gel (2.5%) for adult female acne: a real-world case series from Latin America. Surg Cosmet Dermatol. 2025;17:e20250456.
Rocha MA, Fierro-Arias L, Troielli P, Viana A, Miot HA
Early recognition and proper treatment of AFA are crucial to minimize complications such as scarring and hyperpigmentation as well as to reduce its impact on quality of life. Currently, the management of AFA must be tailored to individual characteristics, mitigating triggers and addressing key pathophysiologic mechanisms, including inflammation, comedogenesis, sebogenesis, and skin microbiome abnormalities.2,9,10
In this retrospective case series, we present six cases of AFA from 3 Latin American countries (Brazil, Colombia, and Argentina) treated with a combination of adapalene 0.3%/benzoyl peroxide 2.5% gel (A0.3/BPO2.5) and other therapies. The primary reason for choosing these cases was to reflect the diversity in disease severity and the different treatment combinations applicable in real-world practice. These were consecutive cases treated in the authors’ practice between August and September 2023, and all patients provided written informed consent for the publication of their photographs and clinical data.The study was approved by the institutional ethics committee (approval number 7.082.589).
Patient characteristics, treatments, and outcomes are presented in table 1 and figure 1.
In the first case, pronounced inflammation marked by pustules and nodules required a regimen of oral antibiotics associated with spironolactone and topical A0.3/BPO2.5. After four months of treatment, only minor erythema and residual acne scars were observed.
The second case presented primarily with papules and comedones. The patient was treated with A0.3/BPO2.5 for three months, resulting in a substantial decrease in lesions, though some scarring remained.
In the third case, papules, pustules, and skin pigmentation were evident. Following three months of treatment with oral spironolactone and A0.3/BPO2.5, there was an almost complete elimination of lesions, total resolution of pigmentation, and an improvement in overall skin quality.
After six months of treatment with a cyproterone acetate combined oral contraceptive and A0.3/BPO2.5, the fourth case experienced complete clearance of acne lesions and a substantial improvement in overall skin quality.
In the fifth case, inflammatory papules, comedones, and nodules showed total reduction following six months of treatment with oral spironolactone and A0.3/BPO2.5.
In the last case, mild papular AFA was successfully treated with a combination of oral spironolactone and A0.3/BPO2.5, resulting in a complete clearance within three months.
The multifactorial nature of AFA requires an approach encompassing an assessment of hormonal imbalance alongside management of inflammation, sebogenesis, and comedogenesis. Beyond cleansers, moisturizers, and photoprotection, the association of oral and topical therapies is a common practice, depending on the clinical presentation of the lesions and individual patient characteristics.2,5
1 34 III
Lymecycline 300 mg/d for 60 days, spironolactone 100 mg/d, adapalene 0.3% / benzoyl peroxide gel 2.5%
2 25 II Adapalene 0.3% / benzoyl peroxide gel 2.5%
3 29 III
4 32 IV
5 22 III
6 31 I
Spironolactone 50 mg/d, adapalene 0.3% / benzoyl peroxide gel 2.5%
Figure 1: Clinical evolution of five cases of adult female acne.
Case 1: pretreatment
A - and after 4 months B. Case 2: pretreatment C - and after 3 months D. Case 3: pretreatment E - and after 3 months F. Case 4: pretreatment
G - and after 6 months H. Case 5: pretreatment
I and after 6 months J. Case 6: pretreatment
K - and after 3 months L
Topical combination of A0.3/BPO2.5 offers a synergistic strategy for treating acne. The comedolytic effect of adapalene, coupled with the antimicrobial, anti-inflammatory, and sebum-control properties of benzoyl peroxide, leads to superior performance compared to the use of either agent in isolation. In addition, adapalene reduces inflammation, making this combination appropriate for addressing various factors involved in the pathogenesis of different types of acne and skin phototypes.9,11 A0.3/BPO2.5 is a well-tolerated topical treatment; nevertheless, its use every other day and/or in combination with the prior application of non-comedogenic moisturizers are alternatives for sensitive skin.
Antiandrogens (eg, spironolactone) are usually prescribed for AFA, even in cases where hormonal workups are normal, leading to a reduction in sebogenesis and consequent improvement in acne lesions. Contraceptive pills containing progestins with antiandrogenic properties (eg, cyproterone) are both effective in treating acne and in preventing relapse following remission.2 Spironolactone can be used alone or together with combined oral contraceptive pills or intrauterine devices to achieve a synergistic effect, or in situations where counterbalancing the effects of levonorgestrel present in hormonal intrauterine devices is required.9,12,13
Oral antibiotics, particularly tetracyclines, are recommended for moderate-to-severe inflammatory acne, typically for up to three months. Combining oral antibiotics with topical benzoyl peroxide minimizes the risk of inducing antimicrobial resistance.14 Oral isotretinoin is reserved for refractory AFA; nevertheless, prescribing with caution and providing reassurance is essential for women of reproductive age.15
The present cases emphasize the need to customize treatment plans and consider factors such as patient preferences, lifestyle, side effects, and contraindications (such as pregnancy or hyperkalemia).
In conclusion, this case series highlights the efficacy and tolerability of a combination approach in the treatment of adult female acne in real-world settings. The tailored use of A0.3/ BPO2.5 alongside antiandrogens, combined oral contraceptive pills, and short courses of antibiotics highlights the need for individualized strategies to match disease severity and patient characteristics. l
Rocha MA, Fierro-Arias L, Troielli P, Viana A, Miot HA
REFERENCES:
1. Addor FASA, Schalka S. Acne da mulher adulta: aspectos epidemiológicos, diagnósticos e terapêuticos. An Bras Dermatol. 2010;85(6):789-95.
2. Dias da Rocha MA, Saint Aroman M, Mengeaud V, Carballido F, Doat G, Coutinho A, Bagatin E. Unveiling the nuances of adult female acne: a comprehensive exploration of epidemiology, treatment modalities, dermocosmetics, and the menopausal influence. Int J Womens Health. 2024;16:663-78.
3. Rocha M, Barnes F, Calderon J, Fierro-Arias L, Gomez CEM, Munoz C, Jannell O, et al. Acne treatment challenges - Recommendations of Latin American expert consensus. An Bras Dermatol. 2024;99(3):414-24.
4. Lange EP HG, Sampaio RP, Estella PC, Benedito BA, Schimitt JV. Adult female acne: prevalence and risk factors in a sample of the brazilian population. Surg Cosmet Dermatol. 2025;17:e20250363.
5. Medeiros Ribeiro B, Follador I, Costa A, Francesconi F, Neves JR, Almeida LMC. Acne da mulher adulta: revisão para o uso na prática clínica diária. Surg Cosmet Dermatol. 2015;7:10-9.
6. Bagatin E, Rocha M, Freitas THP, Costa CS. Treatment challenges in adult female acne and future directions. Expert Rev Clin Pharmacol. 2021;14(6):687-701.
7. Chilicka K, Rogowska AM, Szygula R, Dziendziora-Urbinska I, Taradaj J. A comparison of the effectiveness of azelaic and pyruvic acid peels in the treatment of female adult acne: a randomized controlled trial. Sci Rep. 2020;10(1):12612.
8. Thielitz A, Lux A, Wiede A, Kropf S, Papakonstantinou E, Gollnick H. A randomized investigator-blind parallel-group study to assess efficacy and safety of azelaic acid 15% gel vs. adapalene 0.1% gel in the treatment and maintenance treatment of female adult acne. J Eur Acad Dermatol Venereol. 2015;29(4):789-96.
9. Amuzescu A, Tampa M, Matei C, Georgescu SR. Adult female acne: recent advances in pathophysiology and therapeutic approaches. Cosmetics. 2024;11(3):74.
10. Dreno B, Nguyen JM, Hainaut E, Machet L, Leccia MT, Beneton N, Claudel JP, Celerier P, Le Moigne M, Le Naour S, et al. Efficacy of spironolactone compared with doxycycline in moderate acne in adult females: results of the multicentre, controlled, randomized, double-blind prospective and parallel female acne spironolactone vs doxyCycline Efficacy (FASCE) Study. Acta Derm Venereol. 2024;104:adv26002.
11. Dreno B, Bissonnette R, Gagne-Henley A, Barankin B, Lynde C, Kerrouche N, Tan J. Prevention and Reduction of Atrophic Acne Scars with Adapalene 0.3%/Benzoyl Peroxide 2.5% Gel in Subjects with Moderate or Severe Facial Acne: Results of a 6Month Randomized, Vehicle-Controlled Trial Using Intra-Individual Comparison. Am J Clin Dermatol. 2018;19(2):275-86.
12. Aguilar Medina DA, Cazarin J, Magana M. Spironolactone in dermatology. Dermatol Ther. 2022;35(5):e15321.
13. Searle TN, Al-Niaimi F, Ali FR. Spironolactone in dermatology: uses in acne and beyond. Clin Exp Dermatol. 2020;45(8):986-93.
14. Bagatin E, Florez-White M, Arias-Gomez MI, Kaminsky A. Algorithm for acne treatment: Ibero-Latin American consensus. An Bras Dermatol. 2017;92(5):689-93.
15. Bagatin E, Costa CS, Rocha M, Picosse FR, Kamamoto CSL, Pirmez R, Ianhez M, Miot HA. Consensus on the use of oral isotretinoin in dermatology - Brazilian Society of Dermatology. An Bras Dermatol. 2020;95(Suppl 1):19-38.
AUTHOR’S CONTRIBUTION:
Marco Alexandre Rocha 0000-0003-1090-177X
Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical review of the literature; Critical revision of the manuscript.
Leonel Fierro-Arias 0000-0001-6264-7342
Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical review of the literature; Critical revision of the manuscript.
Patricia Troielli 0000-0002-3070-3917
Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical review of the literature; Critical revision of the manuscript.
Anália Viana
0000-0002-1978-1367
Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical revision of the manuscript.
Hélio Amante Miot 0000-0002-2596-9294
Approval of the final version of the manuscript; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical review of the literature; Critical revision of the manuscript.
www.surgicalcosmetic.org.br/
Single-stage reconstruction of an upper third auricular defect with ipsilateral conchal cartilage graft and tunnelized preauricular flap
Reconstrução em estágio único de um defeito no terço superior da orelha com enxerto de cartilagem conchal ipsilateral e retalho préauricular tunelizado
Large upper-third auricular defects present complex reconstructive challenges, requiring restoration of both form and function. We describe a single-stage technique combining an ipsilateral conchal cartilage graft for structural support with a tunnelized preauricular transposition flap for soft tissue coverage. This approach provides rigid support to enable the use of glasses and hearing aids, along with good color and texture match. In a 79-year-old patient with a 30 × 28 mm post-Mohs surgical defect, the method yielded a satisfactory outcome with preserved ear contour and function. Only minor issues, such as slight forward auricular displacement, were noted at 8-month follow-up.
Grandes defeitos no terço superior da orelha representam desafios reconstrutivos, exigindo a restauração da forma e função. Descrevemos uma técnica em estágio único que combina um enxerto de cartilagem conchal ipsilateral para suporte estrutural com um retalho pré-auricular tunelizado para cobertura de tecidos moles. Essa abordagem garante suporte rígido, permitindo o uso de óculos e aparelhos auditivos, com boa compatibilidade de cor e textura. Em um paciente de 79 anos com um defeito pós-Mohs de 30 × 28 mm, a técnica preservou o contorno e a função auricular. Apenas questões menores, como um leve deslocamento anterior da orelha, foram observadas no seguimento de 8 meses.
How to cite this article: Klinger-Guerra R, Zapata-Sepúlveda J, Vargas-Mora P, Muñoz-Alvear P.
Single-stage reconstruction of an upper third auricular defect with ipsilateral conchal cartilage graft and tunnelized preauricular flap. Surg Cormet Dermatol. 2025;17:e20250468.
R, Zapata-Sepúlveda J, Vargas-Mora P, Muñoz-Alvear P
INTRODUCTION
The reconstruction of upper-third auricular defects presents a unique challenge due to the ear’s intricate anatomy and dual role in aesthetics and function.The loss of cartilage and skin, often following oncologic excision, necessitates techniques that preserve contour and rigidity.¹,2 This is particularly relevant for elderly patients who rely on the auricle’s structure for wearing glasses or hearing aids.3,4
Single-stage approaches offer a practical solution, minimizing surgical interventions and reducing complications associated with comorbidities such as diabetes or hypertension.3,4
The use of cartilage grafts and well-vascularized flaps has been shown to effectively restore structural integrity and improve functional outcomes.5,6
METHODS
A single-stage repair combining an ipsilateral conchal cartilage graft with a tunnelized preauricular flap was selected. Initially, cartilage from the ipsilateral concha was harvested through an incision in the conchal skin. The cartilage graft was placed over the defect and secured to the remaining cartilaginous framework with 4-0 Vicryl absorbable sutures. The donor site was closed with 5-0 Prolene sutures.
Next, a superiorly based ipsilateral preauricular transposition flap was planned, following natural skin lines. The flap dissection started distally and progressed upward to the level of the helical crus. An incision was made along the roof of the helix, creating a tunnel beneath it. The tunnel was carefully sized to match the flap’s width and thickness. The portion of the flap passing through the tunnel was deepithelialized. Next, the preauricular flap was advanced through the tunnel, placed over the defect on the cartilage graft, and secured with 4-0 Prolene sutures. The secondary defect in the preauricular area was closed using 4-0 Vicryl and 5-0 Prolene sutures.
RESULTS
Reconstruction was completed successfully in a single operative session. The immediate postoperative appearance of the ear showed restored contour of the upper third and a well-positioned skin flap with good color match to the surrounding auricular skin. The cartilage graft provided noticeable structural support, maintaining the projection and shape of the ear rim. The preauricular flap showed robust perfusion, and there were no signs of venous congestion or flap compromise in the postoperative period. In addition, minor complications were noted. The patient presented slight forward displacement of the upper
Figure 1: Post-MMS defects. MMS, Mohs micrographic surgery
Figure 2: Proposed flap design
third of the ear and the presence of hair-bearing skin in an area typically devoid of hair. However, these issues did not impact the overall functional outcome.
DISCUSSION
Cartilage grafts provide essential support in auricular reconstruction, maintaining contour and preventing long-term deformities.¹,2 Conchal cartilage, due to its similar curvature, is a favorable donor site for autologous grafts that avoids the morbidity associated with distant grafts.4 Preauricular flaps enhance vascularization, reducing the risk of necrosis and ensuring a stable soft tissue cover.³,7,8 Despite these advantages, minor complications were observed, including forward auricular displacement and the presence of hair-bearing skin in a typically hairless area. These issues, although not functionally limiting, highlight the importance of optimizing flap tension and graft fixation.3,5 Future refinements, such as precise flap positioning and controlled graft sizing, may further improve outcomes. In cases of hair-bearing skin transposition, laser hair removal or minor revisions could enhance cosmetic results.6,7
Previous studies confirm the effectiveness of combining cartilage grafts with preauricular flaps, demonstrating high structural stability and low complication rates.1,2,4,8 Our findings reinforce the need for meticulous surgical planning to balance aesthetic and functional demands.
Figure 3: Preauricular flap elevation and defect exposure
Figure 4: Immediate postoperative view
Figure 5: Postoperative month 8
CONCLUSION
The single-stage technique for upper-third auricular defect reconstruction, using an ipsilateral conchal cartilage graft and a tunnelized preauricular transposition flap, is a reliable and effective approach. This method successfully restores both the
REFERENCES:
1. Brent B. Technical advances in ear reconstruction with autogenous rib cartilage grafts: personal experience with 1200 cases. Plast Reconstr Surg. 1999;104(2):319-34.
2. Ebrahimi A. Reconstructive surgery of auricular defects: an overview. Plast Aesthet Res. 2015;2(5):219-26.
4. Helal HA. Reconstruction of post-traumatic full-thickness defects of the upper auricle using autologous conchal cartilage graft and temporoparietal fascia. World J Plast Surg. 2014;3(2):95-101.
form and function of the auricle, providing sufficient rigidity to support devices such as glasses and hearing aids. In addition, it avoids the need for multi-stage procedures, which is particularly advantageous for elderly patients or those with comorbidities that increase the risk of postoperative complications. l
5. Moreno-Vazquez S, Antoñanzas J, Oteiza-Rius I, Escudero-Nafs FJ, Espinoza-Mellado MD, Idoate MÁ, et al. Reconstructive procedures of the auricular concha after cutaneous oncologic surgery: a systematic review. J Clin Med. 2023;12(20):6521.
6. Hallak B, Bouayed S, Teiga PS. Two-stage reconstruction of a full-thickness defect of the upper third of the auricle, using an autologous ipsilateral conchal cartilage graft; surgical technique. Otolaryngol Case Rep. 2020;17:100231.
7. Schmidt M, Zaussinger M, Duscher D, Wenny R, Huemer GM. Preauricular pull-through flap for reconstruction of the auricle. J Plast Reconstr Aesthet Surg. 2021;74(1):130-4.
8. Pereira N, Tolkachjov SN, Weenig RH, Martires KJ. Tunnelized preauricular transposition flap for reconstruction of auricular defect. J Dermatol Treat. 2014;25(5):441-3.
AUTHOR’S CONTRIBUTION:
Roberto Klinger-Guerra
0009-0001-9504-2849
Statistical analysis; Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical review of the literature; Critical revision of the manuscript.
Jaime Zapata-Sepúlveda
0009-0000-1990-3275
Statistical analysis; Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical revision of the manuscript.
Pablo Vargas-Mora 0000-0002-9388-2940
Statistical analysis; Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical review of the literature; Critical revision of the manuscript.
Pablo Muñoz-Alvear 0000-0001-8214-649X
Statistical analysis; Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical review of the literature; Critical revision of the manuscript.
Klinger-Guerra R, Zapata-Sepúlveda J, Vargas-Mora P, Muñoz-Alvear P
www.surgicalcosmetic.org.br/
Delayed closure of a scalp surgical wound using the Figueiredo technique: a case report
Fechamento tardio de ferida cirúrgica do couro cabeludo pela técnica de
Not all surgical wounds are amenable to primary healing, particularly on the scalp where tissue inelasticity and lesion extent, such as in skin cancers, complicate the procedure. Grafts and flaps increase complexity, recovery time, and surgical costs.The Figueiredo technique reduces costs, protects the wound during its critical phase, maintains wound moisture, and promotes the effective development of granulation tissue. This previously unpublished report demonstrates the use of the technique on the scalp of an elderly patient with systemic scleroderma and a suspected squamous cell carcinoma lesion, showing good progress and satisfactory aesthetic results.
Authors: Rebecca Perez de Amorim1 Hélio Amante Miot1
1 Universidade Estadual Paulista (UNESP), Dermatology and Radiotherapy, Botucatu (SP), Brazil
RESUMO
Nem todas as feridas operatórias são passíveis de fechamento primário, especialmente no couro cabeludo, onde a inelasticidade do tecido e a extensão da lesão, como em neoplasias cutâneas, complicam o procedimento. Enxertos e retalhos aumentam a complexidade, o tempo de recuperação e o custo cirúrgico. A técnica de Figueiredo reduz custos, protege a ferida no período crítico, mantém sua umidade e promove o desenvolvimento do tecido de granulação. Este relato inédito apresenta a aplicação da técnica em couro cabeludo de um paciente idoso com esclerodermia sistêmica e lesão suspeita de carcinoma espinocelular, demonstrando boa evolução e resultado estético satisfatório. Palavras-chave: Oncologia Cirúrgica; Neoplasias cutâneas; Técnicas de Fechamento de Ferimentos; Couro Cabeludo.
Correspondence: Rebecca Perez de Amorim E-mail: rebeccapamorim@outlook.com / helio.a.miot@unesp.br
Funding: None. Conflict of interest: None.
Submitted on: 09/16/2024
Final decision: 01/28/2025
How to cite this article: Amorim RP, Miot HA. Delayed closure of a scalp surgical wound using the Figueiredo technique: a case report. Surg Cosmet Dermatol. 2025;17:e20250407.
INTRODUCTION
The Figueiredo surgical technique, published in 2017, demonstrated the use of a polypropylene prosthesis, obtained from a sterile saline solution bag, to cover traumatic fingertip injuries.1-3 The technique is based on the prior repair of the nail bed and placement of the prosthesis, shaped precisely to the surgical wound area, beneath the nail bed, fixed in place with simple or “U” stitches using nylon thread. The material temporarily replaces the nail, secured to the wound edges without exerting pressure on the nail bed as it heals.1,3 In this way, the wound heals by secondary intention while the prosthesis ensures protection of the treated area, reduces infection from local contamination, accelerates the formation of granulation tissue, and prevents dressings from adhering to the site.1,3 The first report on the use of this technique in dermatology was published in 2023. That article describes its application for lesions located in distal limb extremities, where graft take is more difficult, whether due to the extent of the surgical wound, the presence of shear forces, venous insufficiency, or peripheral edema.2 To date, there have been no reports of the use of the Figueiredo technique on the scalp. The technique may prove highly valuable in dermatological clinical practice, given limited local tissue redundancy and the frequent need for aggressive surgical approaches, depending on the extent of the tumor.
METHODS AND RESULTS
The patient, a 73-year old male with limited systemic scleroderma, reported a painful injury on his scalp for the previous six months. Upon physical examination, the lesion presented as a hyperkeratotic, infiltrated nodule with an erythematous base (Figure 1), 1.5 cm wide in the major axis, located on the left parietal region.The nodule was compatible with suspected squamous cell carcinoma (SCC). An excision with oncologic margins and secondary intention closure using the Figueiredo technique was chosen for the therapeutic surgical approach, given the medium-complexity outpatient setting. Site antisepsis was performed using alcoholic chlorhexidine, and local infiltrative anesthesia was administered with 2% lidocaine and vasoconstrictor. Lesion exeresis included a 4 mm lateral margin reaching the galea at the lower limit (Figure 2). The sterile saline bag was cut and the polypropylene prosthesis placed, maintaining dimensions similar to the surgical defect (Figure 3). To avoid tissue ischemia, the prosthesis was fixed with well-spaced simple stitches using 3-0 nylon. A compressive dressing was applied with gauze, bandage, and Micropore tape. The patient was instructed to remove the secondary dressings 48 hours after the procedure and return in 21 days for prosthesis removal. After 21 days, the patient returned for removal of the prosthesis. The area presented an erythematous, viable granulation tissue, level with the surrounding skin. No debridement was necessary (Figure 4). The patient progressed well, with no complaints, and returned after 45 days with the surgical defect completely healed, reportedly since the 30th day. The histopathological examination repor-
Figure 1: Preoperative period: Hyperkeratotic, infiltrated plaque with an erythematous base measuring approximately 1.5 cm located on the left parietal region
Figure 2: Intraoperative wound, lesion exeresis with 4-mm lateral margin reaching the galea at the deep margin
ted well-differentiated SCC and exeresis with free margins. The satisfactory aesthetic outcome can be seen in figure 5, 6 months after the procedure.
DISCUSSION
The Figueiredo technique is a viable option to manage the healing process in sterile scalp lesions. Considered easy to perform, it does not require a dermatologic surgeon with advanced surgical expertise or a surgical support center at a tertiary hospital. In addition, the technique relies on low-cost, widely available materials, which reduces the burden on the health care system.2-6 Oncologically, it allows for early detection of recurrences and facilitates reintervention, unlike rotation flaps.6-8 It is highly applicable in elderly patients, who have reduced vascular supply, which hinders graft take, as in the case of systemic sclerosis. It also avoids the need to operate on a second surgical site (donor area) in graft procedures, reducing patient discomfort, the likelihood of complications, postoperative recovery time, and the morbidity associated with the procedure. In cases involving flaps, there is also the need to enlarge the surgical area to allow for rotation, increasing both operative time and the amount of anesthesia required. Moreover, many patients have equally photodamaged areas adjacent to the skin tumor to be excised, making them unsuitable for
Figure 3: Immediate postoperative period: polypropylene prosthesis fixed with well-spaced simple stitches using 3-0 nylon
Figure 4: Postoperative day 21: removal of polypropylene prosthesis, presence of granulation tissue, level with lateral margins
Figure 5: Late postoperative period at 180 days, fully healed injury
coverage.2,4,5,6 During the healing process, the exudate is replaced by yellowish fibrin. Gradually, this tissue gives way to granulation tissue, which ultimately leads to complete epithelialization of the surgical wound. Because the polypropylene prosthesis is transparent, it allows for reassessment, important in cases involving extensive lesions that require the prosthesis to remain in place for longer than reported in the present case. Healing time depends on wound-related factors, such as infection, and patient-related factors, such as age and skin quality (thickness, vascularization, photodamage degree, etc.).3,4 Some publications have described secondary intention healing in scalp and forehead wounds following Mohs micrographic surgery.6,7 Secondary intention healing relies on two main stages: wound contraction and re-epithelialization. In this case, wound contraction in the area is minimal due to poor tissue elasticity, meaning that healing occurs predominantly through re-epithelialization.7,8 The reepithelialization process begins at the wound edges. Granulation tissue (GT) has to “fill in” the wound before epithelial migration can occur, and GT formation depends on maintaining moisture in the surgical wound (SW). The literature describes cleaning the SW with hydrogen peroxide, using topical antibiotics, daily cleaning, daily application of petrolatum, and four-layer dressings (Vaseline, gauze, cotton, and tape) to prevent secondary infection and allow scar tissue formation. Some authors also suggest using purse-string
REFERENCES:
1. Figueiredo LA, Ribeiro RS, Melo ALB, Lima AL, Terra BB, Ventim FC. Polypropylene prosthesis for the treatment of fingertip injuries. Description of surgical technique and results. Rev Bras Ortop. 2017;52(6):685-92.
2. Carrai LHM, Rodrigues EF, Lima TFM, Sasseron MGM, Gomes Neto A. Delayed surgical closure (secondary intention) using the Figueiredo Technique: a case series study. Surg Cosmet Dermatol. 2023;15:e20230212.
3. Muniz AAS, Muniz MT, Figueiredo LA, Figueiredo PH, Oliveira BG. Use of the Figueiredo Technique for the treatment of ring avulsion injury: a case report. BioRes Scientia. 2024;2(2):1-4.
4. Figueiredo LA, Ribeiro RS, Figueiredo PH, Lima ALM, Oliveira FM, Oliveira Júnior DS. Comparison between Atasoy-Kleinert V-Y Advancement Flap and Figueiredo Techniques for the treatment of transverse and dorsal oblique fingertip injuries. Rev Bras Ortop. 2022;59(5): e712–e718.
AUTHOR’S CONTRIBUTION:
Rebecca Perez de Amorim 0000-0002-1170-5685
sutures at the wound edges in order to enhance tissue contraction.7,8 In the circumstances described in this case report, the use of a polypropylene prosthesis offers several advantages. It is durable, remains in place for the period required, protects the operative bed, maintains a moist environment, does not exert compression, and stimulates granulation tissue formation. After the first 48 hours, secondary dressings and ointments can be discontinued while the prosthesis remains in place, and contact with water is permitted. Furthermore, suturing the wound edges enhances the tissue contraction component described above.2,3,4,7,8 Prospective, randomized, controlled trials comparing this method to conventional dressings are needed to assess the potential advantages of the Figueiredo technique in repairing scalp surgical defects undergoing secondary intention healing.
CONCLUSION
Primary closure is the most common method of skin restoration and should be considered as long as it generates satisfactory aesthetic results and no anatomical distortion. However, there are circumstances when that is not possible. Allowing healing by secondary intention is an alternative to grafts and flaps.6 The Figueiredo technique has been shown to be safe and effective in this case report, there was no local infection associated with prosthesis use, and the patient obtained a satisfactory aesthetic outcome. l
5. Carvalho RSS, Leitão Júnior PSL, Dias Neto VS, Souza IGL, Rosal LCF, Gomes ACS. Use of polypropylene prosthesis using the Figueiredo Technique for treating thumb degloving in the interior of Minas Gerais – case report. Braz J Health Rev. 2024;7(3):1-11.
6. Sin-Soler M, Yébenes M, Gamissans M, Riera-Martí N, Lara A, Sàbat M. The use of bone wax versus dermal regeneration matrix for the reconstruction of scalp defects. Int J Dermatol. 2024;63(9):1236-41.
7. Becker GD, Adams LA, Levin BC. Secondary intention healing of exposed scalp and forehead bone after Mohs surgery. Otolaryngol Head Neck Surg. 1999;121(6):751-4.
8. Wong N, Zloty D. Secondary intention healing over exposed bone on the scalp, forehead, and temple following Mohs micrographic surgery. J Cutan Med Surg. 2022;26(3):274-9.
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Hélio Amante Miot 0000-0002-2596-9294
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Onychomatricomas are rare and benign tumors of the nail apparatus. Clinical findings, dermoscopic features and possibly imaging and histopathology exams confirm the diagnosis. We report the case of a 15-year-old male patient who had undergone multiple previous treatments for other diagnoses with no response. The transverse hypercurvature and digitiform projections on the nail plate, complemented by histopathological analysis, confirmed the hypothesis of onychomatricoma. The relevance of proper diagnosis and therapeutic management in these cases spares the patient and optimizes the use of public resources that would otherwise be spent on countless consultations and the long period until diagnosis. Keywords: Neoplasms, Adnexal and Skin Appendage; Nails; Onychomycosis; Nails, Malformed.
Case report
Authors:
Soraya Neves Marques Barbosa dos Santos1
Sílvia Iovine Kobata1
Isabela Boechat Morato1 Natália de Paiva Sobreira1
1 Universidade Federal de Minas Gerais (UFMG), Dermatology, Belo Horizonte (MG), Brazil
RESUMO
O onicomatricoma é um tumor raro e benigno do aparelho ungueal. Achados clínicos, dermatoscópicos e eventualmente exames de imagem e histopatologia confirmam o diagnóstico. Relatamos o caso de um paciente masculino de 15 anos submetido a múltiplos tratamentos prévios para outros diagnósticos sem resposta. A hipercurvatura transversa e as projeções digitiformes na lâmina ungueal, complementadas pela análise histopatológica, confirmaram a hipótese de onicomatricoma. A relevância do diagnóstico correto e da devida condução terapêutica nesses casos poupa sofrimento para o paciente e otimiza recursos públicos que seriam gastos em inúmeras consultas e longo período até o diagnóstico. Palavras-chave: Unhas Malformadas; Onicomicose; Unhas; Neoplasias de Anexos e de Apêndices Cutâneos.
Correspondence:
Soraya Neves Marques Barbosa dos Santo
E-mail: snmbsantosdermato@hotmail. com / snmbsantosdermato@gmail.com
Funding: None. Conflict of interest: None.
Submitted on: 09/18/2024
Final decision: 02/27/2025
How to cite this article: Santos SNMB, Kobata SI, Morato IB, Sobreira NP. Onychomatricoma: always a diagnostic challenge. Surg Cosmet Dermatol. 2025;17:e20250408.
INTRODUCTION
An onychomatricoma (OM) is a rare and benign tumor of the nail apparatus, of unknown origin, found primarily in the nail matrix of the fingers. The classical clinical presentation includes a thick yellow band on the nail plate, tending toward transverse hypercurvature, often accompanied by findings of splinter hemorrhage and cavitations in the distal portion of the nail plate.1-3 Generally asymptomatic and rarely associated with chronic paronychia, OMs may cause severe pain and impair quality of life.2 In the literature, we find several reports of patients with long care pathways before proper diagnosis and treatment.4,5 This article reports on a clinical case referred to the dermatology department, treated for years as onychomycosis but with a clinical and histopathological diagnosis matching OM. Clinical and complementary criteria for an earlier and more assertive diagnosis are discussed below.
CASE REPORT
A patient, Caucasian, male, 48 years old, employed as an information technology assistant, visited the dermatology department complaining of an alteration in the thickness and coloring of the nail on the right hallux. The alteration began approximately 15 years earlier, and had been accompanied by intense pain for 1 year, with progressive worsening and impaired walking. The patient had undergone several earlier treatments for onychomycosis, such as oral terbinafine and topical antifungal medications, without improvement. He reported episodes of acute pain with drainage of purulent periungual secretion requiring systemic antibiotic therapy on several occasional, as well as frequent use of nonsteroidal anti-inflammatory drugs for pain relief. Upon dermatological examination, the right hallux was found to have a thickened and yellowish nail plate, with a well-defined band of hyperkeratosis and transverse hypercurvature containing digitiform projections and areas of splinter hemorrhage, more clearly seen in dermoscopy. There was also edema and warmth of the proximal nail fold (Figures 1 and 2). Direct mycological examination of the nail bed was negative, but a culture found growth of Trichophyton mentagrophytes. In an X-ray of the right hallux (Figure 3), there was doubt regarding the presence of a punched-out lesion of the distal phalanx in the area underlying the nail injury. Magnetic resonance imaging of the right hallux was requested (Figures 4 and 5), showing an oval injury to the nail matrix, hypointense on T1 and with heterogeneous signal on T2, with poorly-defined limits and no soft tissue infiltration, but also found remodeling of the bone contour. A surgical approach with excisional biopsy of the lesion to confirm the diagnosis was chosen. The procedure consisted of a distal anesthetic block, detachment of the nail plate, and exeresis of an exophytic lesion measuring 1.5 cm by 0.5 cm in the nail matrix. The presence of digitiform projections of the nail plate toward the nail matrix lesion was observed during the procedure (Figure 6). Histopathological analysis using hematoxylin and eosin staining found nail plate cavitations filled with
1: Thickened and yellowish nail plate, with a well-defined band of hyperkeratosis and transverse hypercurvature containing digitiform projections and areas of splinter hemorrhage
Figure 2: Thickened and yellowish nail plate, with a well-defined band of hyperkeratosis and transverse hypercurvature containing digitiform projections and areas of splinter hemorrhage
SNMB, Kobata SI, Morato IB, Sobreira NP.
Figure
plasma and fibroepithelial tumor with digitiform projections of the matrix epithelium and interspersed mastocytes, compatible with the diagnosis of OM (Figures 7 A,B).
DISCUSSION
OMs are rare and benign fibroepithelial tumors of the nail matrix and still represent a diagnostic challenge. Originally described by Baran and Kint in 1992,6 OM shows peculiar CD34 expression in the connective tissue portion.2,7 The incidence is higher in Caucasians, with more reports among women, though some authors claim they are not more frequent in either sex. It occurs mainly around the fifth decade of life, but there are case reports in children.7,8 The fingernail matrix is affected more often (63%), with the index finger accounting for two-thirds of cases; toes are affected in 36% of cases. Multiple fingers and toes may be affected simultaneously, but that is unusual.2
Clinical features consist of a well-demarcated portion of the nail plate with evident thickening, presence of splinter hemorrhage, transverse hypercurvature, and xanthonychia, the latter the most frequent sign, found in a little over 50% of all cases.2 Other characteristics include: erythema and edema of the proximal nail fold, prominent longitudinal groove, onychodystrophy, and dorsal pterygium.2,9 Pain may or may not be associated with the condition. Digitiform projections after surgical avulsion of the nail plate are highly suggestive.5 The primary differential diagnoses are fibrokeratoma and periungual fibroma, but also include squamous cell carcinoma, Bowen’s disease, subungual verruca vulgaris, keratoacanthoma, osteochondroma, and fungal and bacterial infections. It may also present with associated lon-
Figure 3: Radiograph of the hallux
Figure 4 and 5: Magnetic resonance imaging
Figure 6: The presence of digitiform projections of the nail plate toward the nail matrix lesion was observed during the procedure
BAgitudinal melanonychia, with the differential diagnosis including disorders of proliferation and activation of nail matrix melanocytes.2 OM and onychomycosis frequently coexist, since cavitations make the nail plate more susceptible to secondary fungal infections. OM cases are frequently treated as onychomycosis, leading to delayed diagnosis and unnecessary use of ineffective medications.10,11 Therefore, the finding of septate hyaline hyphae
upon direct mycological examination and fungal growth in culture media do not rule out OM, and the absence of response to standard therapy should suggest the hypothesis of other differential diagnoses.4 Dermoscopy evidences thickening of the nail plate with multiple honeycombed cavitations (70%), hemorrhagic striae (72%), and white longitudinal grooves corresponding to nail plate channels (71%). Honeycombed cavitations may be filled by yellowish or red-black pigmentation material. While the patterns of plaque thickening and splinter hemorrhage do not have high specificity and may be present in isolated cases of onychomycosis, the presence of parallel longitudinal white grooves associated with lateral demarcation of the lesion and honeycombed cavitations have high specificity.2,4,5,7,12 Complementary tests may be requested to rule out skeletal involvement and explore the presence of OM, but they are not required for diagnostic confirmation. Ultrasonography has higher predictive value when performed by an experienced professional and may find hypoechoic areas on the nail matrix with adjacent hyperechoic linear areas corresponding to digitiform projections.5,11 Radiography of the affected finger or toe is easily available and may rule out skeletal involvement, but it does not show typical signs for a conclusive diagnosis. Magnetic resonance imaging, although not routinely necessary, shows low signal uptake in the lesion and in the nail matrix and high uptake of adjacent signal corresponding to tumor projections.3,5 In this case report, the radiograph showed an equivocal image of the distal phalanx of the right hallux, which might correspond to skeletal involvement (punched-out lesion), so a second imaging examination was requested before the surgical procedure to enable better planning. In terms of histology, OM are fibroepithelial tumors comprising two distinct parts. The proximal zone is characterized by having deep epithelial invaginations occupied by overlapping nail protrusions. The distal zone corresponds to epithelial digitations originating from the matrix epithelium, which proliferate and cause perforations in the nail plate.2,13,14 Immunohistochemistry is of great diagnostic aid, with OM positive for CD34, whereas CD99 markers, S-100 protein, epithelial membrane antigen, actin, and desmin are negative.1 Clinical suspicion combined with complementary examinations, such as radiography, ultrasonography, magnetic resonance imaging, and dermoscopy, are valuable, but diagnosis can only be confirmed by histopathological analysis.5,7 Treatment consists of full surgical excision of the tumor, including the normal nail matrix proximal to the lesion to prevent local relapse.Though a benign tumor, long-term follow-up is recommended due to the risk of relapse. Permanent nail dystrophy is not an infrequent complication.2,15 Despite classical clinical and intraoperative characteristics, the lack of knowledge about the condition and its tendency to be asymptomatic contribute to late diagnosis. Given what appears to be a case of intractable onychomycosis associated with transverse hypercurvature, nail thickening, and splinter hemorrhages, underlying OM should be suspected. l
Figure 7: A and B - Slide and nail matrix (hematoxylin-eosin, 10x)
REFERENCES:
1. Figueiredo LA, Ribeiro RS, Melo ALB, Lima AL, Terra BB, Ventim FC. Polypropylene prosthesis for the treatment of fingertip injuries. Description of surgical technique and results. Rev Bras Ortop. 2017;52(6):685-92.
2. Carrai LHM, Rodrigues EF, Lima TFM, Sasseron MGM, Gomes Neto A. Delayed surgical closure (secondary intention) using the Figueiredo Technique: a case series study. Surg Cosmet Dermatol. 2023;15:e20230212.
3. Muniz AAS, Muniz MT, Figueiredo LA, Figueiredo PH, Oliveira BG. Use of the Figueiredo Technique for the treatment of ring avulsion injury: a case report. BioRes Scientia. 2024;2(2):1-4.
4. Figueiredo LA, Ribeiro RS, Figueiredo PH, Lima ALM, Oliveira FM, Oliveira Júnior DS. Comparison between Atasoy-Kleinert V-Y Advancement Flap and Figueiredo Techniques for the treatment of transverse and dorsal oblique fingertip injuries. Rev Bras Ortop. 2022;59(5): e712–e718.
5. Carvalho RSS, Leitão Júnior PSL, Dias Neto VS, Souza IGL, Rosal LCF, Gomes ACS. Use of polypropylene prosthesis using the Figueiredo Technique for treating thumb degloving in the interior of Minas Gerais – case report. Braz J Health Rev. 2024;7(3):1-11.
6. Sin-Soler M, Yébenes M, Gamissans M, Riera-Martí N, Lara A, Sàbat M. The use of bone wax versus dermal regeneration matrix for the reconstruction of scalp defects. Int J Dermatol. 2024;63(9):1236-41.
7. Becker GD, Adams LA, Levin BC. Secondary intention healing of exposed scalp and forehead bone after Mohs surgery. Otolaryngol Head Neck Surg. 1999;121(6):751-4.
8. Wong N, Zloty D. Secondary intention healing over exposed bone on the scalp, forehead, and temple following Mohs micrographic surgery. J Cutan Med Surg. 2022;26(3):274-9.
AUTHOR’S CONTRIBUTION:
Soraya Neves Marques Barbosa dos Santos
0000-0001-5138-8584
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Sílvia Iovine Kobata 0000-0002-9079-6940
Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript.
Isabela Boechat Morato
0000-0002-2542-4454
Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied.
Natália de Paiva Sobreira 0000-0002-8460-1289
Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied.
www.surgicalcosmetic.org.br/
Bilateral lobuloplasty with inverted “snail” technique for correction of lobes deformed by prolonged use of gauges
Lobuloplastia bilateral com técnica “snail” invertida para correção de lóbulos deformados por uso prolongado de alargadores
Case report
Authors:
Luiz Roberto Dal Bem Pires Júnior1
Fernanda Nomoto Fujii1
Rafaella Castilho1
Waleska Ramos Alvim Lescowicz1
Rodolfo Barros Leite1
Anna Victoria Valiente Engelhorn2
1 Hospital de Clínicas, Universidade Federal do Paraná (UFPR), Dermatology, Curitiba (PR), Brazil
Earlobe stretching dates back to various ancient cultures, symbolizing social status, cultural identity, and spirituality. Since the 1970s, it has gained popularity in the West as a form of self-expression. However, the use of gauges can lead to deformities requiring surgical correction. Numerous techniques have been developed over the past century to address this issue. This case report describes the use of the inverted “snail” technique, which employs two flaps, folding the medial flap into a spiral, and allows for a harmonious and symmetrical adjustment. It can be a viable alternative for correcting extensive deformities and asymmetries.
Keywords: Body modification, non-therapeutic; Ear deformities, acquired; Esthetics; Plastic surgery procedures.
2 Hospital de Clínicas, Universidade Federal do Paraná (UFPR), Clinical Medicine, Curitiba (PR), Brazil
RESUMO
O alargamento dos lóbulos das orelhas remonta a diversas culturas ancestrais, nas quais simbolizava status social, identidade cultural e espiritualidade. A partir da década de 1970, popularizou-se no Ocidente como forma de autoexpressão. No entanto, o uso de alargadores pode resultar em deformidades que necessitam de correção cirúrgica. Diversas técnicas foram desenvolvidas ao longo do último século para esse fim. Este relato descreve o uso da técnica “snail” invertida, que utiliza dois retalhos, dobrando o retalho medial em espiral e possibilitando um ajuste harmonioso e simétrico, uma alternativa viável para correção de deformidades extensas e assimetrias. Palavras-chave: Modificação Corporal não Terapêutica; Deformidades Adquiridas da Orelha; Estética; Procedimentos de Cirurgia Plástica.
Correspondence:
Luiz Roberto Dal Bem Pires Júnior E-mail: lrdalbem@gmail.com / ldalbem@ymail.com
Funding: None.
Conflict of interest: None.
Submitted on: 11/04/2024
Final decision: 02/13/2025
How to cite this article:
Pires Júnior LRDB, Fujii FN, Castilho R, Lescowicz WRA, Leite RB, Engelhorn AVV. Bilateral lobuloplasty with inverted “snail” technique for correction of lobes deformed by prolonged use of gauges. Surg Cosmet Dermatol. 2025;17:e20250418.
INTRODUCTION
Earlobe stretching dates back to various ancient cultures. In Ancient Egypt, for instance, Pharaoh Tutankhamun wore ear gauges, a common practice among elites symbolizing status and power.1 In Africa, tribes such as the Maasai in Kenya and the Mursi in Ethiopia practice earlobe stretching to this day, with gauge size associated with age, wisdom, and how respected an individual is in their community. Earlobe stretching also has spiritual significance among some tribes in South America and indigenous peoples of Asia, who believe the practice opens “gateways” or “connections” with the spirit world.2 In the modern Western world, gauges rose in popularity in the 1970s and 1980s as part of counterculture movements, and became consolidated as a form of self-expression associated with alternative groups and subcultures during the 1990s and 2000s. Earlobe stretching came to be seen as a form of body modification connected to individuality and self-expression, untethered from tradition and part of the modern urban context.3 Although gauges have historically been used in many cultures to symbolize social status, cultural identity, and spirituality, prolonged use can cause earlobe deformities, which may in turn require surgical correction. The search for approaches that ensure aesthetic and functional results while preserving natural earlobe anatomy and promoting discreet scars has encouraged the development of new repair techniques. In this case report, we describe the use of the inverted “snail” technique for the reconstruction of bilateral earlobes deformed by prolonged use of gauges. It differs from the technique as previously described in terms of the transection site of the enlarged branch of the lobe.4
CASE REPORT
The patient, a 29-year old male with no comorbidities, sought specialized care in order to correct deformities in both earlobes caused by prolonged use of gauges, with gradual increase in size since adolescence. Clinical presentation included earlobes with large-diameter orifices and irregular margins, as well as bilateral asymmetry, making repair an aesthetic challenge (Figure 1). After careful assessment, bilateral lobuloplasty using the innovative inverted “snail” technique was indicated. The technique was chosen due to its capacity to recreate the natural contour of the earlobe, minimizing visible scars and restoring symmetry. In an outpatient setting, the procedure began with marking the skin around the circumference of the stretched branch of the earlobe (Figure 2A), with specific points on the medial and lateral regions. After asepsis and antisepsis, local infiltration using a modified Klein solution was performed, providing adequate anesthesia and vasoconstriction. Next, the stretched branch was sectioned at its lateral portion (Figure 2B), resulting in a longer medial flap and a shorter lateral flap (Figure 2C). To ensure harmonization of the new earlobes, scarification was carried out on the inner surface of the whole lateral flap and on the outer surface of the medial flap, preserving part of the outer surface of the lateral flap to form the lower border of the new lobe. The medial flap was then folded over its own
Figure 1: Preoperative period
Figure 2: Stages of the “snail” technique Image A - Stretched earlobe Image B - Transection Image C - Flaps Image D - Rotation and suture
axis, taking on a spiral shape—the “snail”—and joined to the raw areas of both flaps. Stabilization was achieved with simple stitches using 4-0 Vicryl sutures between the scarified areas, followed by a continuous 5-0 nylon suture along the entire length for skin closure (Figure 2D). In the postoperative period, the patient progressed favorably, with no complications, pain, or signs of infection (Figure 3). Proper healing was observed, along with a satisfactory aesthetic outcome, featuring symmetrical earlobes and a harmonious contour, in contrast to the asymmetries and deformities observed previously (Figure 4).
DISCUSSION
Earlobe deformity caused by prolonged ear gauge use has driven the search for surgical techniques that enable effective aesthetic and functional repair, given that individuals with earlobe defects caused by piercings are more likely to suffer negative image effects.5 Repairing these deformities demands special care due to the anatomic complexity and aesthetic requirements involved, including preserving the natural contour of the earlobe and minimizing visible scarring. Given existing surgical options, the technique chosen is generally that which makes the lobe more similar to the original, with a rounded shape and no notches or level differences.6,7 Throughout history, several techniques have been developed, from Miller’s simple wedge excision in 1925 to more complex techniques, such as Hamilton and
La Rossa’s Z-plasty in 1975. The evolution in lobuloplasty techniques reflects the ongoing effort to improve both aesthetic and functional outcomes for patients.6,8 Techniques such as Pardue’s, which aims to preserve the lobe orifice, may lead to level differences in the lower border,8 while methods such as Kalimuthu’s “V”-shaped flap and Fatah and Fearon’s “L”-shaped flap do not preserve the lobe orifice.9-11 Despite these variations, the satisfaction rate for lobuloplasty outcomes is approximately 92% to 100%,12,13 and the rate of postoperative complications is low, ranging from 0% to 33.3%. Reported complications include hypertrophic, depressed, or wide scars, recurrence of clefts, and surgical wound infections.14,15 In the present case, the “snail” technique proved effective by folding the medial flap into a spiral to form the new earlobe margin, enabling the lobe to regain a harmonious and symmetrical contour. The creation of flaps of different sizes, with selective scarification, contributes to a more precise fit between the medial and lateral flaps. The procedure enables the correction of asymmetries, preserves vascularization, ensures a smooth contour, and promotes healing without excessive tension, minimizing the formation of unsightly scars. This makes the technique an alternative for patients with significant deformities caused by prolonged use of large-diameter gauges. This case report contributes to the literature by introducing a technique that provides an aesthetically adequate outcome, widening treatment options to correct extensive deformities with high aesthetic demand. l
12. Miller TR, Eisbach KJ. Repair of enlarged pierced-ear openings. Ear Nose Throat J. 2005;84(5):276-7.
13. Reiter D, Alford EL. Torn earlobe: a new approach to management with a review of 68 cases. Ann Otol Rhinol Laryngol. 1994;103(11):879-84.
14. Ribeiro AA, Lourenço L, Matsuda TMHB, Ferrari NM. Split earlobe repair: literature review and new technique proposal. Surg Cosmet Dermatol. 2009;1(3):141-4.
15. Sharma R, Krishna S, Kumar S, Verma M. Rotation flap lobuloplasty: technique and experience with 24 partially torn earlobes. Int J Oral Maxillofac Surg. 2014;43(10):1206-10.
AUTHOR’S CONTRIBUTION:
Luiz Roberto Dal Bem Pires Júnior 0009-0001-6728-420X
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Fernanda Nomoto Fujii 0000-0001-5421-5865
Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied
Rafaella Castilho 0009-0003-1437-2024
Critical revision of the manuscript
Waleska Ramos Alvim Lescowicz 0000-0002-0106-1097
Critical revision of the manuscript
Rodolfo Barros Leite 0009-0008-0854-3030
Critical revision of the manuscript
Anna Victoria Valiente Engelhorn 0000-0002-9427-6459
Critical review of the literature, Critical revision of the manuscript
www.surgicalcosmetic.org.br/
Botulinum toxin in the treatment of pemphigus vegetans of the scalp
Toxina botulínica no tratamento de pênfigo vegetante de couro cabeludo
Case Report
Authors:
André Pozzobon Capeletti1
Ana Paula Dornelles Manzoni1
Rodrigo Pereira Duquia1
Vanessa Vinderfeltes Padilha1
1 Santa Casa de Misericórdia de Porto Alegre, Dermatology, Porto Alegre (RS), Brazil
Pemphigus vegetans is a rare clinical form of pemphigus vulgaris, and scalp involvement is even rarer. Treatment can be challenging, often requiring systemic immunosuppression. Botulinum toxin can be an effective and low-risk alternative for the treatment of pemphigus vegetans unresponsive to conventional treatments. We report an unprecedented case in the literature of successful treatment of scalp lesions through the application of botulinum toxin type A.
Keywords: Pemphigus; Scalp; Botulinum Toxins, Type A
RESUMO
O pênfigo vegetante é uma forma clínica rara de pênfigo vulgar, sendo o acometimento do couro cabeludo ainda mais incomum. O tratamento pode ser desafiador, com frequente necessidade de imunossupressão sistêmica. A toxina botulínica pode ser uma alternativa efetiva e de baixo risco para o tratamento do pênfigo vegetante não responsivo aos tratamentos convencionais. Relatamos um caso inédito na literatura, com sucesso terapêutico das lesões em couro cabeludo através da aplicação de toxina botulínica tipo A. Palavras-chave: Pênfigo; Couro Cabeludo; Toxinas Botulínicas Tipo A
Correspondence: André Pozzobon Capeletti E-mail: pozzobon.capeletti@hotmail. com
Funding: None.
Conflict of interest: None.
Submitted on: 09/01/2024
Final decision: 02/17/2025
How to cite this article: Capeletti AP, Manzoni APD, Duquia RP, Padilha VV. Botulinum toxin in the treatment of pemphigus vegetans of the scalp. Surg Cosmet Dermatol. 2025;17;e20250399.
INTRODUCTION
Pemphigus encompasses a group of autoimmune bullous diseases of the skin and mucous membranes, with variable geographic distribution worldwide, and pemphigus vulgaris is its most frequent subtype.1,2,3 Pemphigus vegetans is a rare clinical form,6,8 and scalp involvement is even rarer.3,6,7,8 Treatment can be challenging, often requiring systemic immunosuppression.2,3,4,5,6
The present study aims at presenting an unprecedented case in the literature of pemphigus vegetans on the scalp, refractory to conventional treatment, achieving good clinical response to botulinum toxin type A.
CASE REPORT
A 50-year-old male patient, White, previously diagnosed with pemphigus vulgaris, had bullous lesions on his nose, scalp, oral mucosa, trunk, abdomen, arms, and legs. A laboratory assessment found no relevant alterations. The initial therapeutic options were prednisone, azathioprine, and mycophenolate, but they had to be discontinued due to their side effects. Except for the lesions on the patient’s scalp, which progressed to a vegetative appearance, all other lesions were controlled by using rituximab (Figure 1A and 1B). Pathologic examination of the scalp
Alesion found suprabasal acantholysis, hyperkeratosis, acanthosis, and moderate lymphocytic inflammatory infiltrates (Figure 2). Direct immunofluorescence found IgG positivity, with intercellular pattern in the epidermis. Clinical-histological correlation corroborated the diagnosis of pemphigus vegetans. The choice was made to administer botulinum toxin as an experimental treatment for the scalp lesions. After topical application of 4% lidocaine cream (Dermomax®) on the scalp plaques for 30 minutes and antisepsis with 0.2% aqueous chlorhexidine, botulinum toxin type A (Botox®), 2 UI/cm², was injected intradermally (Table 1). After 6 weeks, lesion verrucosity had improved by over 50%. At reassessment, a new dose of botulinum toxin was administered, following the same procedure, achieving progressive improvement (Figure 3A and 3B).
DISCUSSION AND CONCLUSION
Currently, there is no literature on the use of botulinum toxin to treat pemphigus vegetans. Nevertheless, it has shown promise as a low-risk therapeutic alternative for this dermatosis.9, 12,13,14 The mechanisms of action of botulinum toxin are not yet fully understood. One hypothesis suggests that the inhibi-
Capeletti AP, Manzoni APD, Duquia RP, Padilha VV.
Figure 1: A - Vegetative plaque on the left occipital region before treatment with botulinum toxin; B - Vegetative plaque on the right occipital region before treatment with botulinum toxin
Table 1: Application of botulinum toxin to pemphigus vegetans lesions on the scalp
Description of application technique
1 Topical application of 4% lidocaine cream (Dermomax®) on lesions 30 minutes before the procedure
2 Antisepsis with 0.2% aqueous chlorhexidine, with full removal of topical anesthetic from application sites
3 Intradermal injection of botulinum toxin type A (Botox®), 2 UI/cm², into lesions
Figure 3: A - Left occipital region 6 months after the first application of botulinum toxin; B - Right occipital region 6 months after the first application of botulinum toxin
tion of acetylcholine binding to the neuromotor receptors of sweat glands may reduce both sweating and neural activity of the eccrine glands.12,13,15,16 In addition, it has been proposed that botulinum toxin blocks the release of neuropeptides and other substances involved in the local inflammatory process.11,14 In the present case, a marked improvement in the lesions was observed, with a reduction of more than 50% in verrucosity in only 6 weeks, and progressive disappearance over a 6-month period. The leading hypothesis is that the anhidrotic and anti-inflammatory effects of botulinum toxin decrease the risk of
REFERENCES:
1. Porro AM, Seque CA, Ferreira MCC, Enokihara MMSS. "Penphigus vulgaris." An Bras Dermatol. 2019;94(3):264-78.
2. Messersmith L, Krauland K. Pemphigus Vegetans. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022.
3. Zaraa I, Sellami A, Bouguerra C, Sellami MK, Chelly I, Zitouna M, et al. Pemphigus vegetans: a clinical, histological, immunopathological and prognostic study. J Eur Acad Dermatol Venereol 2011;25(10):1160-7.
4. Danopoulou I, Stavropoulos P, Stratigos A, Chatziolou E, Chiou A, Georgala S, et al. Pemphigus vegetans confined to the scalp. Int J Dermatol. 2006;45(8):1008-9.
5. Mori M, Mariotti G, Grandi V, Gunnella S, Maio V. "Pemphigus vegetans of the scalp". J Eur Acad Dermatol Venereol. 2016;30(2):368-70.
6. Noama D, Ouafaa H, Nadia A, Said A, Anass F, Hanane R, et al. Pemphigus végétant: une forme rare de pemphigus. La Presse Médicale. 2014;43(5):e119-e134.
7. Lakhmiri M, Maouni S, Znati K, Meziane M, Ismaïli N, Benzekri L, et al. Pemphigus végétant [Pemphigus vegetans]. Ann Dermatol Venereol. 2020;147(1):78-9.
8. Huei LT, Yee EYW. Scalp involvement in pemphigus vegetans. J Cutan Med Surg. 2021;25(3):329.
local infections, both micro and macro, which could otherwise exacerbate the proinflammatory process and worsen the clinical condition. Based on reports of the use of botulinum toxin to treat other dermatoses, we believe that periodic reapplications (every 6 months, for example) may be necessary to optimize outcomes. Botulinum toxin may represent an effective and low-risk alternative for the treatment of pemphigus vegetans unresponsive to conventional treatments. However, clinical trials are still required to clarify the best use and the mechanism of action of this therapy. l
9. Zhang H, Tang K, Wang Y, Fang R, Sun Q. Botulinum toxin in treating Hailey-Hailey disease: asystematic review. J Cosmet Dermatol. 2021;20(5):1396-402.
10. Messikh R, Atallah L, Aubin F, Humbert P. La toxine botulique dans les maladies dermatologiques invalidantes. Ann Dermatol Vénéréol. 2009;136(4):S129-S136.
11. Bansal C, Omlin KJ, Hayes CM, Rohrer TE. Novel cutaneous uses for botulinum toxin type A. J Cosmet Dermatol. 2006;5(3):268-72.
12. Martina E, Diotallevi F, Radi G, Campanati A, Offidani A. Therapeutic use of botulinum neurotoxins in Dermatol: systematic review. Toxins. 2021;13(2):120.
13. Lewandowski M, Świerczewska Z, Barańska-Rybak W. Off-Label use of botulinum toxin in dermatology-current state of the art molecules. 2022;27(10):3143.
14. Alster TS, Harrison IS. Alternative clinical indications of botulinum toxin. Am J Clin Dermatol 2020;21(6):855-80.
15. Kim YS, Hong ES, Kim HS. "Botulinum toxin in the field of dermatology: novel indications." Toxins. 2017,9(12):403.
16. Campanati A, Martina E, Giuliodori K, Consales V, Bobyr I, Offidani A, et al. Botulinum toxin off-label use in dermatology: a review. Skin appendage disord. 2017;3(1):39-56.
AUTHOR’S CONTRIBUTION:
André Pozzobon Capeletti
0000-0002-7226-0042
Approval of the final version of the manuscript; Conception and design of the study; Preparation and writing of the manuscript; Acquisition, analysis and interpretation of data; Effective participation in the conduct of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; Critical review of the literature; Critical revision of the manuscript
Ana Paula Dornelles Manzoni 0000-0001-6184-4440
Approval of the final version of the manuscript; Conception and design of the study; Effective participation in the conduct of the study; Critical revision of the manuscript
Rodrigo Pereira Duquia 0000-0001-6308-3585
Author’s contribution: Approval of the final version of the manuscript; Conception and design of the study; Effective participation in the conduct of the study; Critical revision of the manuscript
Vanessa Vinderfeltes Padilha 0000-0001-6794-985X
Author’s contribution: Approval of the final version of the manuscript; Conception and design of the study; Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied
Capeletti AP, Manzoni APD, Duquia RP, Padilha VV.
www.surgicalcosmetic.org.br/
A case of kidney transplant rejection secondary to cemiplimab for recurrent cutaneous squamous cell carcinoma
Um caso de rejeição de transplante renal secundária a cemiplimabe para carcinoma espinocelular cutâneo recorrente
Case report
Authors: Nicole Russell1
Siddharth Srikakolapu2 Jane Scribner2
1 University of South Carolina School of Medicine Greenville, School of Medicine, Greenville (SC), United States
We report a case involving a 71-year-old male with a history of kidney transplant on immunosuppressive therapy and non-melanoma skin cancers who developed persistent lesions on the cheek and forehead after multiple skin cancer treatments. Biopsies identified poorly differentiated cutaneous squamous cell carcinoma. The patient underwent excisional salvage therapy with flap reconstruction, complicated by infection requiring debridement. He subsequently presented with in-transit dermal metastases and began treatment with cemiplimab. Unfortunately, after two cycles, he faced graft rejection and transitioned to hemodialysis. A recent PET-CT revealed no evaluable disease, and there were no clinical signs of recurrence at his last follow-up.
2 Medical University of South Carolina, Department of Dermatology and Dermatologic Surgery, Charleston (SC), United States
RESUMO
Relatamos o caso de um paciente do sexo masculino, 71 anos, com histórico de transplante renal em uso de terapia imunossupressora e cânceres de pele não melanoma, que desenvolveu lesões persistentes na bochecha e testa após múltiplos tratamentos para câncer de pele. As biópsias evidenciaram carcinoma espinocelular cutâneo pouco diferenciado. O paciente foi submetido a terapia de salvamento excisional com reconstrução por retalho, que evoluiu com infecção necessitando de desbridamento. Posteriormente, apresentou metástases dérmicas em trânsito e iniciou tratamento com cemiplimabe. Infelizmente, após dois ciclos, evoluiu com rejeição ao enxerto e necessidade de hemodiálise. Uma PET-CT recente não revelou doença passível de avaliação e não havia sinais clínicos de recidiva em seu último seguimento. Palavras-chave: Receptor de Morte Celular Programada 1; Carcinoma Espinocelular; Rejeição ao Enxerto; Doenças Renais.
Correspondence: Nicole Russell E-mail: nrussell@email.sc.edu
Funding: None. Conflict of interest: None.
Submitted on: 09/22/2024 Final decision: 01/30/2025
How to cite this article: Russel N, Srikakolapu S, Scribner J. A case of kidney transplant rejection secondary to cemiplimab for recurrent cutaneous squamous cell carcinoma. Surg Cosmet Dermatol. 2025;17:e20250409.
Russel N, Srikakolapu S, Scribner J.
CASE REPORT
A 71-year-old male with a history of kidney transplant secondary to IgA nephropathy on tacrolimus and prednisone and multiple non-melanoma skin cancers, treated with photodynamic therapy, 5-fluorouracil, and Mohs surgery, presented to dermatology clinic with non-healing lesions of the left cheek and central forehead adjacent to previous Mohs scars. Examination revealed a scaly papule with an erythematous base on the left cheek and left forehead, a reddish-purple papule adjacent to a scar on the central forehead, and an ulcerated violaceous papule adjacent to a scar on the left anterior cheek/temple region. Previous biopsies from the sites of concern found moderately well-differentiated squamous cell carcinoma. Biopsies obtained during the current visit revealed dermal deposition of poorly differentiated cutaneous squamous cell carcinoma extending to deep and peripheral margins. Special stains were positive for P63 and CD10 and negative for desmin and SOX-10 (Figure 1A and 1B).
In addition, the central forehead lesion had special stains positive for CK903, P40/CK 5/6, GATA-3, and PAX-8. The patient was diagnosed with recurrent locally aggressive cutaneous squamous cell carcinoma (T1N0M0) induced by post-transplant immunosuppressive therapy. He subsequently underwent excisional salvage therapy and local flap reconstruction. The postoperative course was complicated by skin graft wound healing and deterioration. Bacterial cultures grew Serratia marcescens resistant to augmentin, and the patient completed a course of Bactrim with concurrent wound debridement. The patient was found to have progressive gross residual in-transit dermal metastases at the graft site, for which cemiplimab was initiated (Figure 2). Initiation of cemiplimab required discontinuation of tacrolimus and initiation of sirolimus. The patient received two cycles of cemiplimab. Unfortunately, the patient presented to the emergency department with graft rejection secondary to cemiplimab. The patient was placed on hemodialysis and cemiplimab was discontinued. A recent PET-CT scan revealed no obviously evaluable disease. The patient had no clinical signs of recurrence at his most recent follow-up visit (Figure 3).
B AFigure 1: A - Initial clinical presentation and histology of central forehead biopsy showing a dermal deposit of poorly differentiated carcinoma. B - Initial clinical presentation and histology of central forehead biopsy showing a dermal deposit of poorly differentiated carcinoma.
2: Progressive gross residual in-transit dermal metastases at the graft site 2 months after surgery
Figure 3: 5 months after surgery and 2 cycles of cemiplimab with no evidence of recurrence
DISCUSSION
Solid organ transplant recipients receiving chronic immunosuppression therapy have a markedly increased risk of developing cutaneous squamous cell carcinoma, accounting for 40% of all malignancies in organ transplant recipients. Cemiplimab is a monoclonal antibody directed at PD-1 which has shown significant responses in patients with locally advanced or metastatic cutaneous squamous cell carcinoma and has become a mainstay of treatment. Hanna et al. report that no kidney
allograft rejection events were observed during a phase I study of cemiplimab for kidney transplant recipients with advanced cutaneous squamous cell carcinoma when used in combination with pulsed-dose corticosteroids and mTOR inhibitors. Cui et al. report that solid organ transplant rejection rates may be as high as 40% with anti PD-L1 agent monotherapy and suggest PD-L1 positive expression in graft biopsy may be an effective marker for predicting transplant rejection. l
Figure
Russel N, Srikakolapu S, Scribner J.
REFERENCES:
1. Hanna GJ, Dharanesswaran H, Giobbie-Hurder A, Harran JJ, Liao Z, Pai L, et al. Cemiplimab for kidney transplant recipients with advanced cutaneous squamous cell carcinoma. J Clin Oncol. 2024;42(9):1021-30.
2. Cui X, Yan C, Xu Y, Li D, Guo M, Sun L, et al. Allograft rejection following immune checkpoint inhibitors in solid organ transplant recipients: a safety analysis from a literature review and a pharmacovigilance system. Cancer Med. 2023;12(5):5181-94.
AUTHOR’S CONTRIBUTION:
Nicole Russell 0009-0009-3745-6902
Conception and design of the study, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature
Siddharth Srikakolapu 0000-0002-2606-1042
Approval of the final version of the manuscript, Preparation and writing of the manuscript
Jane Scribner
Author’s contribution: Approval of the final version of the manuscript
www.surgicalcosmetic.org.br/
Reconstruction
of the medial malar region and lower eyelid with a McGregor
flap after resection of pigmented basal cell carcinoma
Reconstrução de região malar medial e pálpebra inferior com retalho de McGregor após exérese de carcinoma basocelular pigmentado
Basal cell carcinoma is the most common skin cancer, most often found in the head and neck region. We present the case of a 47-year-old male patient with pigmented basal cell carcinoma in the right medial malar region. After confirmatory biopsy, the lesion was excised with a 5 mm safety margin, extending to the lower eyelid. Reconstruction was performed using the McGregor flap, a technique that enables effective tissue advancement with minimal tension, minimizing the risk of complications. The patient had an uncomplicated recovery with satisfactory oncologic, aesthetic, and functional outcomes, demonstrating the technique’s efficacy in complex periocular reconstructions.
O carcinoma basocelular é o câncer de pele mais comum, ocorrendo com maior frequência na região de cabeça e pescoço. Apresentamos o caso de um paciente do sexo masculino, 47 anos, com carcinoma basocelular pigmentado na região malar medial direita. Após biópsia confirmatória, a lesão foi excisada com margem de segurança de 5 mm, abrangendo a pálpebra inferior. Optou-se pela reconstrução com retalho de McGregor, técnica que possibilita bom avanço dos tecidos sem tensão, minimizando o risco de complicações. O paciente evoluiu sem complicações, com resultados oncológicos, estéticos e funcionais satisfatórios, demonstrando ser uma abordagem eficaz para reconstruções complexas na região periocular.
Luiz Roberto Dal Bem Pires Júnior E-mail: lrdalbem@gmail.com / ldalbem@ymail.com
Funding: None. Conflict of interest: None.
Submitted on: 11/05/2024
Final decision: 01/28/2025
How to cite this article: Pires Júnior LRDB, Bastos CAS, Castilho R, Lescowicz WRA, Predolin KFB, Brittes LLH. Reconstruction of the medial malar region and lower eyelid with a McGregor flap after resection of pigmented basal cell carcinoma. Surg Cosmet Dermatol. 2025;17:e20250420.
INTRODUCTION
Basal cell carcinoma (BCC) is the most common malignant neoplasm in the world, accounting for most cases of skin cancer.1 Nodular BCC has the highest prevalence, and is often found in the head and neck region.2 In addition, the incidence of BCC is increasing annually—in Brazil, according to estimates from the National Cancer Institute, for the 2023-2025 period, 101,920 new cases in males and 118,520 new cases females are expected.3 Although BCC has low metastasis potential (0.03%), it is locally invasive,3 which can compromise structures around the lesion.The pigmented form accounts for only approximately 6% of BCC cases,4 making differential diagnosis with other pigmented lesions, such as intradermal nevus, sebaceous hyperplasia, trichoepithelioma, and melanoma, even more important.5
The malar region is considered one of the most important for facial aesthetics, and is also one of the most affected by BCC. It can be divided into four anatomical subunits: medial, lateral, zygomatic, and buccal. Skin characteristics vary gradually among these subunits.6 The medial portion is limited by the lower eyelid, medial epicanthus, nasofacial sulcus, perialar area, and upper part of the nasogenian sulcus. Its proximity to areas at high risk of complications, such as the lower eyelid, makes surgical planning challenging, requiring techniques that ensure minimal tension, lead to discreet scars that respect the natural lines of the skin, and hide incisions efficiently in such a delicate and heterogeneous region.7
CASE REPORT
A 47-year-old male patient, with no comorbidities and no personal or family history of skin neoplasms, was referred from primary care due to a reportedly fast-growing pigmented papule measuring approximately 1 cm in the right upper medial malar region (Figure 1). Lesion dermoscopy revealed arborizing vessels, rainbow pattern, gray-blue ovoid nests, and blue globules, consistent with pigmented BCC (Figure 2), as confirmed by incisional biopsy.
Surgical treatment was planned based on these findings. After lesion resection with a 5 mm safety margin, the surgical wound included the lower eyelid, leading to the choice of performing a McGregor flap reconstruction (Figure 3). The technique consists of a lateral incision following the curvature of the eyelid, which may extend to the area anterior to the preauricular hairline depending on the width of the defect to be covered. In the case of the patient in this report, extending the main incision was not necessary. The curvature of the incision is essential to provide adequate vertical length for the flap.
A Z-plasty was performed at the lateral end of the incision, with defect width corresponding to the central limb of the “‘Z.” The descending and ascending limbs were of equal length to the central limb and formed a 60-degree angle with it, facilitating flap mobilization. Dissection was performed in the subcutaneous plane, allowing advancement of the flap and its subsequent transposition in the Z-plasty, culminating in closure
of the defect after compensation with a Burow’s triangle perpendicular to the main incision line. The suture was performed with 5-0 Vicryl and 6-0 Nylon (Figure 4).
The patient had an uncomplicated recovery with satisfactory functional, oncologic, and aesthetic outcomes (Figures 5 and 6).
DISCUSSION
In high-risk BCC cases, a category which includes the present case due to its location, the primary treatment options are surgical, with radiation therapy reserved for patients unable to undergo surgical procedures. Standard resection, with surgical
Figure 1: Macroscopy of pigmented basal cell carcinoma in right malar region
margins evaluated by histopathological examination, is a common practice in Brazil. In these procedures, 4 to 6 mm margins, but which can be as wide as 8 mm, are drawn around the visible tumor, with pathologic examination performed subsequently.8
The surgical procedure should follow the principles of oncology, with complete removal of the tumor as its primary goal. However, when planning periocular interventions, considering the preservation of function in order to optimize oncologic, functional, and aesthetic outcomes is key.9
In lower eyelid reconstruction, rotation flaps are traditionally effective given their horizontal vector, which minimizes the risk of postoperative ectropion and canthal distortion.10 Since the lateral rotation skin flap technique for the malar region proposed by Mustardé in 1966, several others have been developed based on medially advancing lateral skin to correct lower eyelid defects. In general, there is skin laxity in the lateral facial region, and this advancement is limited; without measures to reduce flap tension, it tends to return to its original position in the postoperative period.11
Figure 2: Dermoscopy of pigmented basal cell carcinoma
Figure 4: Immediate postoperative period –McGregor flap technique
In 1973, McGregor introduced a technique to correct lower eyelid defects involving lateral periorbital Z-plasty, enabling medial advancement of the tissues and relieving tension on the advancement flap. This approach represents an excellent alternative within the reconstructive arsenal for complex lower eyelid defects. It was originally indicated for the reconstruction of V-shaped defects involving up to two-thirds of the eyelid width
and is applicable to both the lower and upper eyelids. After 15 years applying this technique, McGregor reported favorable surgical outcomes, with high-quality scars and preservation of the natural appearance of the lateral canthus.12 In the present case, this technique was successfully used in the reconstruction of the lower eyelid and medial malar region, resulting in a satisfactory outcome and establishing itself as a valuable option within the surgical arsenal. l
1. Kim JYS, Kozlow JH, Mittal B, Moyer J, Olencki T, Rodgers P. Guideline of care for the management of basal cell carcinoma. J Am Acad Dermatol. 2018;78(3):540-59.
2. Basset-Seguin N, Herms F. Update in the management of basal cell carcinoma. Acta Derm Venereol. 2020;100(11):adv00140.
3. Instituto Nacional de Câncer (INCA). Estimativa de câncer no Brasil 2023-2025 [Internet]. Disponível em: https://www.gov.br/inca/pt-br/ assuntos/cancer/numeros/estimativa/estado- capital/brasil.
4. Cameron MC, Lee E, Hibler BP, Barker CA, Mori S, Cordova M, et al. Basal cell carcinoma: epidemiology; pathophysiology; clinical and histological subtypes; and disease associations. J Am Acad Dermatol. 2019;80(2):303-17.
5. Kim DP, Kus KJB, Ruiz E. Basal cell carcinoma review. Hematol Oncol Clin North Am. 2019;33(1):13–24.
6. Sanchez FLE. Manejo dos tumores perioculares com cirurgia micrográfica de Mohs. Surg Cosmet Dermatol. 2014;6(4):226-32.
8. National Comprehensive Cancer Network® (NCCN®). Guidelines Version 2.2022; 24 de março de 2022.
9. Cerci FB, Fantini BC. Retalhos e enxertos em cirurgia micrográfica de Mohs. São Paulo: Editora Atheneu; 2022.
10. Harris J, Perez N. Anchored flaps in post-Mohs reconstruction of the lower eyelid, cheek, and lateral canthus: avoiding eyelid distortion. Ophthalmic Plast Reconstr Surg. 2003;19(1):5 - 13.
11. Mustardé JC. The use of flaps in the orbital region. Plast Reconstr Surg. 1970;45(2):146-50.
12. McGregor IA. Eyelid reconstruction following subtotal resection of upper or lower lid. Br J Plast Surg. 1973;26(4):346-54.
AUTHOR’S CONTRIBUTION:
Luiz Roberto Dal Bem Pires Júnior
0009-0001-6728-420X
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Carlos Augusto Silva Bastos
Conception and design of the study
Rafaella Castilho
0000-0003-0255-2696
0009-0003-1437-2024
Critical review of the literature; Critical revision of the manuscript
Waleska Ramos Alvim Lescowicz
Critical review of the literature
Karina Fernanda Bortoloto Predolin
Critical revision of the manuscript
Laurenlisiê Lourega Heitling Brittes
Critical review of the literature
0000-0002-0106-1097
0009-0003-2745-7481
0009-0004-9918-087X
www.surgicalcosmetic.org.br/
Ultrasound for a better surgical approach in hidradenitis suppurativa
Ultrassom para uma melhor abordagem cirúrgica na hidradenite supurativa
Case report
Authors:
Fernando Bulla-Alcala1
Claudia González2
Sara Cataño3
Juan Felipe Ochoa-Bermudez4
1 Univesidad el Bosque, Dermatology, Bogotá, Colombia
2 Access Medical Center, Radiology, Bogotá, Colombia
3 Pontificia Universidad Javeriana, Dermatology, Bogotá, Colombia
Hidradenitis suppurativa (HS) is a chronic inflammatory disease affecting intertriginous areas of the body, characterized by painful nodules, abscesses, sinusoidal tracts, and fistulas. Surgery is crucial for treatment, being potentially curative and achieving high satisfaction levels. Pre-surgical evaluations are often limited by the difficulty of detecting fistulous tracts and deep nodules. Ultrasound has emerged as a staging, follow-up, treatment response evaluation, and preoperative management method for HS. It enables accurate localization of subclinical lesions and optimizes surgical results. This report presents two representative cases of pre-surgical ultrasound evaluation in HS.
A hidradenite supurativa (HS) é uma doença inflamatória crônica que afeta áreas intertriginosas, caracterizada por nódulos dolorosos, abscessos, trajetos sinuosos e fístulas. A cirurgia é fundamental no tratamento, sendo potencialmente curativa e alcançando alta satisfação. Porém, avaliações pré-cirúrgicas enfrentam limitações para identificar trajetos fistulosos e nódulos profundos. O ultrassom surgiu como ferramenta para estadiamento, monitoramento, avaliação de resposta ao tratamento e planejamento pré-operatório, permitindo localizar lesões subclínicas e otimizar resultados cirúrgicos. Este estudo apresenta dois casos ilustrativos que demonstram a utilidade da ultrassonografia na avaliação pré-cirúrgica em pacientes com HS.
Juan Felipe Ochoa-Bermudez E-mail: juanfelipeochoab@gmail.com
Funding: None
Conflict of interest: None
Submitted on: 12/28/2024
Final decision: 01/30/2025
How to cite this article:
Bulla-Alcala F, González C, Cataño S, Ochoa-Bermudez JF. Ultrasound for a better surgical approach in hidradenitis suppurativa. Surg Cosmet Dermatol. 2025;17:e20250433.
INTRODUCTION
Hidradenitis suppurativa (HS) is a chronic inflammatory disease characterized by painful nodules, abscesses, sinusoidal tracts, and fistulas, primarily affecting intertriginous regions such as the axillae and groin.1,2 Treatment is comprehensive, encompassing antibiotics, retinoids, biological therapies, and surgical interventions.3 Surgery remains crucial, as it is the only potentially curative option, achieving high satisfaction levels regardless of disease severity.4
Several classifications are used to assess HS severity. The most widely recognized is the Hurley system, which stages the disease into three levels.2 However, traditional classifications have limitations, including inaccurate assessment of inflammation.5,6 To address these, new scales have been developed. The Modified Hurley scale evaluates body surface area involvement, inflammation, and migratory lesions,7 while the IHS4 (International Hidradenitis Suppurativa Severity Score System) dynamically assesses nodules, abscesses, and fistulous tracts over time.5,6
Physical examination of HS patients has limitations, as fistulous tracts and deep nodules are often undetectable by palpation alone.7 This limitation may lead to inadequate medical and surgical treatment.7-11 Imaging addresses these challenges by clarifying lesion morphology and severity, tracking disease progression, and assisting in pre-surgical mapping.12 Imaging modalities include ultrasound and MRI.13-15 High-resolution ultrasound with Doppler analysis is particularly effective, providing safe, accurate detection of subclinical lesions and active inflammation. It is now considered the standard of care for diagnosis, staging, and preoperative localization of target lesions in HS.7,16-23
METHOD
We present two cases of patients treated at a Dermatologic Surgery Center in Bogotá, Colombia. Both patients, diagnosed with HS and referred for surgical intervention, underwent high-frequency ultrasound for lesion localization and marking. Informed consent was obtained.
CLINICAL CASES
Case 1
A 25-year-old woman with severe HS (Hurley stage III; IHS4: 19 points) was treated with combined medical management (oral antibiotics) and surgery. Preoperative ultrasound identified isolated dermal edema, follicular dilation, cystic nodules, and fistulas in the bilateral inguinal regions. A complex type II fistula extended from the distal right inguinal region to the proximal thigh, while a type III fistula was observed in the left inguinal region. Ultrasound-guided marking of target lesions facilitated surgical resection (Figure 1). Six months postoperatively, the patient showed adequate healing without recurrence.
Case 2
A 58-year-old woman with HS in the inguinal, intergluteal, and gluteal regions had a history of biological treatment and multiple surgical resections. Preoperative ultrasound identified a type III fistula with significant fibrosis in the proximal right buttock and a type II fistula with mild fibrosis and edema in the infragluteal fold. The marking of lesions ensured precise surgical resection (Figure 2). Postoperative outcomes were successful, with no complications or recurrence at one-year follow-up.
RESULTS
Satisfactory postoperative outcomes were achieved in both patients, showing the efficacy of ultrasound-guided surgical resection in improving surgical precision and reducing recurrence.
DISCUSSION
Pre-surgical planning based solely on clinical parameters often underestimates the extent and severity of HS lesions.22 Visual examination and palpation fail to identify deep or subclinical lesions, resulting in incomplete surgical margins and increased risk of recurrence.7,23 Imaging, particularly ultrasound, addresses these limitations by providing detailed information about lesion boundaries, subclinical activity, and severity.7,18 High-resolution ultrasound with Doppler analysis is especially useful for staging disease, monitoring treatment response, and guiding preoperative planning.7,18,24-26
The modified Sonographic Scoring of Hidradenitis Suppurativa (mSOS-HS) is a validated tool for staging HS based on ultrasound findings27:
Stage I includes one fluid collection and changes in the dermis, such as pseudocysts or follicular dilations.
Stage II involves two to four fluid collections or a fistulous tract with dermal changes affecting up to two body segments.
Stage IIIA includes five or more fluid collections or multiple fistulous tracts, while Stage IIIB involves extensive, bilateral, or interconnected fistulas.
Ultrasound also categorizes fistulas based on fibrosis and edema into three types25:
1. Type I: Minimal fibrosis and low edema.
2. Type II: Moderate fibrosis and low edema.
3. Type III: Severe fibrosis and significant edema.
Detecting fibrosis is particularly important, as fibrotic lesions are less likely to respond to medical therapy.25,28 These cases often require combined medical and surgical management.18 By delineating subclinical lesions and determining fistula depth, ultrasound significantly improves surgical precision.7,17,18,24-27
Certain patient factors increase the likelihood of inadequate surgical margins, including obesity, male gender,
A C
B D
Figure 1: A - High-resolution ultrasound with 18-24 MHz linear golf club transducer of the inner third of the right thigh showing a tubular, elongated structure with well-defined borders corresponding to a Type II fistula with fibrosis in the wall. Asterisks (**) indicate a retained monofilament hair tract in the fistula. Green calipers (+) delineate the fistula thickness, which extends to the muscle fascia (m), and orange calipers indicate the fistula length. B - High-resolution ultrasound with 18-24 MHz linear golf club transducer of the inner third of the left thigh showing a tubular, elongated structure with well-defined borders corresponding to a Type III fistula with fibrosis in the wall and edema in the periphery. Asterisks (**) indicate a retained monofilament hair tract in the fistula. Green calipers (+) delineate the fistula thickness, which extends to the fascia (f) of the muscle (m), and orange calipers indicate the fistula length. C - Fistula and nodule marking. D - Surgical resection guided by prior ultrasound marking.
Figure 2: A - High-resolution ultrasound with an 18-24 MHz linear golf club transducer of the external aspect of the left buttock showing a tubular, elongated structure with well-defined borders corresponding to a Type III fistula with fibrosis in the wall and edema in the periphery, located in the deep dermis-hypodermis. Calipers B + delineate the fistula thickness, and Calipers A + indicate its actual length. Calipers C + measure the depth of the fistula from the epidermis (e) to the deepest plane of the subcutaneous tissue. Dermis (d). B - Magnified Color Doppler image of part of the fistula described in A showing an important vascularized component within the fistula, consistent with an active inflammatory process of the disease. C - Ultrasound-marked lesions in the right gluteal region. D - Surgical resection guided by prior ultrasound marking.
Hurley stage II disease, and elevated IHS4 scores. 23 These patients benefit most from preoperative ultrasound examination, as it improves lesion localization, reduces recurrence rates, and optimizes surgical outcomes. 7,18,24-26 Studies have shown that ultrasound-guided surgical procedures improve margin delineation and decrease recurrence within 24 weeks postoperatively. 23
In the cases presented, wide local resections guided by ultrasound ensured complete lesion removal and successful postoperative healing. Ultrasound provided detailed preoperative insights, detecting subclinical lesions and guiding precise resection, ultimately minimizing recurrence and enhancing outcomes.
REFERENCES:
1. Lyons A, Zubair R, Kohli I, Hamzavi I. Preoperative ultrasound for evaluation of hidradenitis suppurativa. Dermatol Surg. 2019;45(2):294–6.
2. Goldburg SR, Strober BE, Payette MJ. Hidradenitis suppurativa: epidemiology, clinical presentation, and pathogenesis. J Am Acad Dermatol. 2020;82(5):1045–58.
3. Martorell A, García FJ, Jiménez-Gallo D, Pascual JC, Pereyra-Rodríguez J, Salgado L, et al. Update on hidradenitis suppurative (Part II): treatment. Actas Dermosifiliogr. 2015;106(9):716–24.
4. Fertitta L, Hotz C, Wolkenstein P, Méningaud JP, Sawan D, Hersant B, et al. Efficacy and satisfaction of surgical treatment for hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2020;34(4):839–45.
5. Zouboulis CC, Tzellos T, Kyrgidis A, Jemec GBE, Bechara FG, Giamarellos- Bourboulis EJ, et al. Development and validation of the International Hidradenitis Suppurativa Severity Score System (IHS4), a novel dynamic scoring system to assess HS severity. Br J Dermatol 2017;177(5):1401–9.
6. Horváth B, Janse IC, Blok JL, Driessen RJB, Boer J, Mekkes JR, et al. Hurley staging refined: a proposal by the Dutch hidradenitis suppurativa expert group. Acta Derm Venereol 2017;97(3):412–3.
7. Martorell A, Alfageme Roldán F, Vilarrasa Rull E, Ruiz-Villaverde R, Romaní De Gabriel J, García Martínez F, et al. Ultrasound as a diagnostic and management tool in hidradenitis suppurativa patients: a multicentre study. J Eur Acad Dermatol Venereol. 2019;33(11):2137–42.
8. Wortsman X, Castro A, Figueroa A. Color Doppler ultrasound assessment of morphology and types of fistulous tracts in hidradenitis suppurativa (HS). J Am Acad Dermatol 2016;75(4):760–7.
9. Napolitano M, Calzavara-Pinton PG, Zanca A, Bianchi L, Caposiena Caro RD, Offidani AM, et al. Comparison of clinical and ultrasound scores in patients with hidradenitis suppurativa: results from an Italian ultrasound working group. J Eur Acad Dermatol Venereol. 2019;33(2):e84–7.
10. Gutfilen-Schlesinger G, Lopes De Souza SA, Gutfilen B. Should we scan hidradenitis suppurativa patients? A systematic review of radiologic findings. Adv Skin Wound Care. 2021;34(7):1–10.
11. Lyons AB, Narla S, Kohli I, Zubair R, Nahhas AF, Braunberger TL, et al. Assessment of inter-rater reliability of clinical hidradenitis suppurativa outcome measures using ultrasonography. Clin Exp Dermatol. 2022;47(2):319–24.
12. Mendes-Bastos P, Martorell A, Bettoli V, Matos AP, Muscianisi E, Wortsman X. The use of ultrasound and magnetic resonance imaging in the management of hidradenitis suppurativa: a narrative review. Br J Dermatol 2023;188(5):591–600.
13. Lopes AA, Moraes GN, De Lima Dias BMM, De Souza GD, De Souza LQ. Preoperative imaging assessment of hidradenitis suppurativa. Rev Bras Cir Plast. 2019;34(2):264–7.
14. Wortsman X, Jemec GBE. A 3D ultrasound study of sinus tract formation in hidradenitis suppurativa. Dermatol Online J. 2013;19(6):18564.
CONCLUSION
HS is a chronic disease with significant demands on the treating physician due to its complex management. Surgery is critical, being the only potentially curative intervention. High-frequency ultrasound plays an invaluable role in preoperative planning, enabling the detection of subclinical lesions, precise lesion mapping, and improved surgical outcomes. Incorporating ultrasound into the standard management of HS enhances treatment efficacy, reduces recurrence, and ensures better patient care. l
15. Elkin K, Daveluy S, Avanaki K. Hidradenitis suppurativa: current understanding, diagnostic and surgical challenges, and developments in ultrasound application. Skin Res Technol 2020;26(1):11–9.
16. Marasca C, Marasca D, Megna M, Annunziata M, Fabbrocini G. Ultrasound: an indispensable tool to evaluate the outcome of surgical approaches in patients affected by hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2020;34(8):413–4.
17. Martorell A, Wortsman X, Alfageme F, Roustan G, Arias-Santiago S, Catalano O, et al. Ultrasound evaluation as a complementary test in Hidradenitis Suppurativa: proposal of a standarized report. Dermatol Surg. 2017;43(8):1065–73.
18. Wortsman X. Color Doppler ultrasound: a standard of care in hidradenitis suppurativa. J Eur Acad Dermatol Venereol 2020;34(10):e616–7.
19. Lacarrubba F, Dini V, Napolitano M, Venturini M, Caposiena Caro DR, Molinelli E, et al. Ultrasonography in the pathway to an optimal standard of care of hidradenitis suppurativa: the Italian Ultrasound Working Group experience. J Eur Acad Dermatol Venereol. 2019;33(Suppl 6):10–4.
20. Wortsman X, Moreno C, Soto R, Arellano J, Pezo C, Wortsman J. Ultrasound in-depth characterization and staging of hidradenitis suppurativa. Dermatol Surg. 2013;39(12):1835–42.
22. Wortsman X. Imaging of Hidradenitis Suppurativa. Dermatol Clin. 2016;34(1):59–68.
23. Cuenca-Barrales C, Salvador-Rodríguez L, Arias-Santiago S, Molina-Leyva A. Preoperative ultrasound planning in the surgical management of patients with hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2020;34(10):2362–7.
24. Wortsman X, Calderon P, Castro A. Seventy-MHz Ultrasound detection of early signs linked to the severity, patterns of keratin fragmentation, and mechanisms of generation of collections and tunnels in Hidradenitis Suppurativa. J Ultrasound Med. 2020;39(5):845–57.
25. Reyes-Baraona F, Isabel Herane M, Wortsman X, Figueroa A, García-huidobro I, Giesen L, et al. Guía clínica chilena para el estudio y tratamiento de hidradenitis supurativa. Rev Med Chile. 2021;149(artículo especial):1620-35.
26. Wortsman X. Strong validation of ultrasound as an imaging biomarker in hidradenitis suppurativa. Br J Dermatol. 2021;184(4):591–2.
27. Wortsman X. Update on ultrasound diagnostic criteria and new ultrasound severity and activity scorings of Hidradenitis Suppurativa. J Ultrasound Med. 2024;43(1):207–13.
Author’s contribution: Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Claudia González 0000-0003-2618-308X
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Sara Cataño 0000-0001-5183-6973
Approval of the final version of the manuscript, Conception and design of the study, Preparation and writing of the manuscript, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
Juan Felipe Ochoa-Bermudez 0000-0003-0038-4692
Approval of the final version of the manuscript, Preparation and writing of the manuscript, Acquisition, analysis and interpretation of data, Effective participation in the conduct of the study, Intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied, Critical review of the literature, Critical revision of the manuscript
www.surgicalcosmetic.org.br/
Atypical location of acquired digital fibrokeratoma
Fibroqueratoma digital adquirido de localização atípica
Case report
Authors:
André Martins Ornelas1,2
Clarissa Brito Farias2
Isabelle Sousa Medeiros Torres Ferreira3 Flauberto de Sousa Marinho2
1 Hospital das Clínicas - UFPE, Department of Dermatology, Recife (PE), Brazil
2 Faculdade de Medicina Nova Esperança, Department of Dermatology, João Pessoa (PB), Brazil
Acquired digital fibrokeratoma is a rare, benign, fibroepithelial tumor, which commonly presents as a finger-shaped normochromic nodule, typically located at the extremities. When affecting the nails, it usually emanates from the proximal nail fold, rarely arising from the matrix or nail bed. In this report, we describe an unusual case of acquired digital fibrokeratoma located under the nail plate of the right thumb. We describe the clinical, dermoscopic, and histopathological aspects of the lesion, as well as the surgical treatment used, and present a brief literature review on the subject.
Keywords: Nail Diseases; Fibroma; Nails; Skin Neoplasms
RESUMO
O fibroqueratoma digital adquirido é um tumor raro, benigno, de natureza fibroepitelial, que se apresenta como pápula normocrômica em forma de dedo, localizado tipicamente nas extremidades. Quando acomete as unhas, costuma emanar da prega proximal, raramente surgindo a partir da matriz ou do leito ungueal. Neste relato, descrevemos um caso incomum de fibroqueratoma digital adquirido localizado sob a placa ungueal de polegar direito. Descrevemos os aspectos clínicos, dermatoscópicos e histopatológicos da lesão, bem como o tratamento cirúrgico empregado, e apresentamos uma breve revisão bibliográfica sobre o assunto. Palavras-chave: Fibroma; Doenças da unha; Unhas; Neoplasias cutâneas
Correspondence:
André Martins Ornelas E-mail: andre-ornelas@hotmail.com
Funding: None
Conflicts of interest: None
Submitted on: 01/17/2025
Accepted on: 06/05/2025
How to cite this article: How to cite this article: Ornelas AM, Farias CB, Ferreira ISMT, Marinho FS. Atypical location of acquired digital fibrokeratoma. Surg Cosmet Dermatol. 2025;17:e20250435.
INTRODUCTION
Acquired digital fibrokeratoma (ADFK) is an uncommon benign tumor, typically observed on the fingernails or toenails. Its etiology is not fully understood, with trauma considered a possible triggering factor. Clinically, it tends to present as a solitary, asymptomatic, finger-like or dome-shaped nodule, which may cause nail deformities and aesthetic impairment. The diagnosis is based on characteristic histopathological features, including acanthosis, hyperkeratosis, and abundant fibrous tissue. Since the tumor does not regress spontaneously, surgical treatment is usually indicated.
The objective of this report was to describe a case of ADFK originating from the nail matrix of the right thumb, an uncommon site compared to its usual occurrence at the proximal nail fold or nail bed. We present a detailed analysis of the clinical, dermoscopic, and histopathological aspects of the lesion, along with a description of the surgical treatment performed. We conclude with a brief literature review aimed at deepening the understanding of this condition. For this review, we selected articles indexed in the PubMed, SciELO, and Periódicos Capes databases, published between 2009 and 2025. The descriptors used were: “acquired digital fibrokeratoma,” “digital fibrokeratoma,” and “nail tumor,” applying the Boolean operator “and” in the following combinations: “acquired digital fibrokeratoma and histopathology,” “acquired digital fibrokeratoma and dermoscopy,” and “acquired digital fibrokeratoma and surgery.”
CASE REPORT
A 59-year-old man with a prior history of systemic hypertension and basal cell carcinoma on the face presented to the dermatology service with a complaint of a nail lesion on the right first finger, persisting for 10 years. The patient denied associated symptoms or previous treatments. There was no history of local trauma preceding the onset of the lesion.
Physical examination revealed a nail plate with canaliform dystrophy and a subungual lesion located at the lunula (Figure 1). On onychoscopy, a homogeneous white area and arborizing vessels were observed (Figure 2). The diagnostic hypotheses considered were fibrokeratoma and superficial acral fibromyxoma.
After proximal digital block, the nail plate was distally elevated to expose the nail bed and matrix. A longitudinal incision was then made in the distal nail matrix, followed by separation and excision of the lesion. The surgical defect in the nail matrix was repaired using 4.0 polyglycolic acid sutures, and the nail plate was repositioned onto the nail bed.
Histological analysis, performed with hematoxylin–eosin staining, demonstrated proliferation of fibroblastic cells and numerous thick, closely packed collagen bundles, regularly distributed within the dermis (Figure 3).These findings are consistent with the diagnosis of ADFK.
DISCUSSION
ADFK is a rare benign fibroepithelial tumor, first described by Bart in 1968.1 It is most commonly found on the fingers and toes, although cases have been reported in nondigital areas such as the hands, feet, knees, elbows, and forearms, among others. ADFK specifically located in the nail apparatus was designated by Cahn in 1977 as acquired ungual fibrokeratoma, classified into two variants: periungual fibrokeratoma and subungual fibrokeratoma, depending on the location of the tumor.2
ADFK occurs across all races, being more common in men between 12 and 70 years of age, with peak incidence in middle age.3 Its etiopathogenesis is not fully understood, although traumatic events have been suggested as potential contributors. However, a history of trauma is not always reported by patients.4 Local infections by Staphylococcus aureus may also act as triggering factors. Studies have demonstrated increased migration of fibroblasts incubated with S. aureus enterotoxin B.5,6 In addition, some researchers have observed an increased presence of factor XIIIa-positive dermal dendrocytes in ADFK, suggesting they may play a role in collagen synthesis and tumor formation.6 Qiao et al.7 reported the case of a transplant patient who developed concomitant gingival hyperplasia and ADFK while undergoing treatment with cyclosporine. The lesions regressed after discontinuation of the medication, suggesting that the drug may have triggered tumor development. However, no other cases associated with cyclosporine use were found in the literature,
Figure 1: Canaliform dystrophy and subungual lesion located at the lunula
indicating that this association warrants further investigation. The diagnosis of ADFK is based on characteristic clinical and histological features. Nevertheless, it often represents a true diagnostic challenge, given its rarity and wide range of clinical presentations.2 ADFK generally presents as a solitary, normochromic tumor with a slightly hyperkeratotic tip,5 typically measuring less than 1 cm in diameter and asymptomatic, although there are reports of lesions larger than 1 cm and associated with pain.1 Morphologically, it may present as rod-shaped, dome-shaped, flat, or branching.2 In our literature review, we found that
the rod-shaped (47.7%) and dome-shaped (37.3%) types are the most prevalent (Table 1).
ADFK usually arises from the proximal nail fold or, less commonly, from the nail matrix or bed. In a study involving 20 participants, subungual lesions were observed in only 1 patient.4 Another study, with 21 Chinese patients, identified subungual lesions in only 2 cases.1 When compiling three case series, we observed that 56% of patients presented with lesions on the fingers and 44% on the toes (Table 1).
The lesion may exert pressure on the nail matrix, resulting in nail plate deformities such as longitudinal depression8 (as observed in the patient in the present case), thinning of the nail plate, abnormal growth, trachyonychia, onycholysis, subungual hyperkeratosis, and hemorrhagic crust.5 The presence of a collarette at the lesion base is an important clinical finding for differentiating ADFK from other nail tumors.9
Studies investigating in detail the dermoscopic features of ADFK are scarce. In general, onychoscopy demonstrates a central homogeneous light-yellow area surrounded by a hyperkeratotic scaly collarette, reflecting the acanthosis and hyperkeratosis frequently associated with this tumor. Some patients have light white cracks on the nail surface, which may present as punctate blood vessels.1,10 Homogeneous red lacunae have also been described, divided by white meshwork-like keratotic septi, which may correspond to the histologically retracted hyperkeratotic epidermis. This wide variability of dermoscopic findings may be related to the varying degree of vascular formations and collagen fiber accumulation observed in the tumor.6,10 None of these findings, however, provide diagnostic accuracy. In the present case, arborizing vessels were observed – which had not been previously described in the reviewed literature.
In the presence of a fibrous tumor located in the nail apparatus, particularly when elongated in shape, the diagnosis of ADFK should be strongly considered. Differential diagnoses include supernumerary digit, verruca vulgaris, cutaneous horn, Koenen’s tumor, eccrine poroma, and superficial acral fibromyxoma.2,9 In a retrospective study, Wang et al.11 reported five cases of ADFK that had been misdiagnosed as eccrine poroma, verruca vulgaris, rudimentary polydactyly, pyogenic granuloma, and acral fibroma. Vance and Hohnadel12 documented the youngest patient with ADFK described to date: a 6-year-old child with a persistent 6-mm nodule on the right first digit, initially misdiagnosed as verruca vulgaris. The high rates of diagnostic error suggest that physicians may not be sufficiently familiar with ADFK.11
The histology of ADFK shows acanthotic epidermis, hyperkeratosis, and focal thickening of the granular layer. In the dermis, thick collagen bundles are observed, arranged irregularly or parallel to the tumor axis. Elastic fibers are generally thin and sparse, and the dermis is usually highly vascularized.1,9 Surgical treatment is recommended, particularly in the presence of pain or cosmetic impairment, since the tumor does not tend to regress spontaneously.4,5 Complete surgical excision
Figure 2: Onychoscopy showing a homogeneous white area and arborizing vessels
Figure 3: Thick collagen bundles arranged parallel to the tumor axis
Author No. of cases
Liu et al., 20231
Hwang et al., 20174
Palaniappan et al., 202210
Wang et al., 202411
*One case was observed on the palm.
1: Literature review of ADFK
Periungual: 16/21
Intraungual: 3/21
Subungual: 2/21
Periungual: 15/20
Intraungual: 4/20
Subungual: 1/20
Dome-shaped: 9/21
Rod-shaped: 11/21
Branching: 1/21
Flat: 0/21
Dome-shaped: 8/20
Rod-shaped: 3/20
Branching: 5/20
Flat: 4/20
Dome-shaped: 8/26
Rod-shaped: 8/26
Dome-shaped: 2/5
Rod-shaped: 3/5
Periungual: 31/41 (75.6%)
Intraungual: 7/41 (17%)
Subungual: 3/41 (7.3%)
Dome-shaped: 27/72 (37.5%)
Rod-shaped: 35/72 (48.6%)
Branching: 6/72 (8.3%)
Flat: 4/72 (5.5%)
Table
Figure 4: A - Postoperative outcome after 2 years. B - Onychoscopy of the nail plate 2 years after surgery
is the treatment of choice, as partial removal is frequently associated with local recurrence.2,5 The lesion should be dissected back to its most proximal origin in the nail unit and excised at that site to prevent recurrence.8 To avoid further damage to the nail matrix and ensure complete tumor removal, Jahan et al.3 recommend careful elevation of the lesion and retraction of the proximal nail fold, which allows better visualization of the structures during surgery. Lesions located above the nail plate may also be removed by shaving followed by phenolization or CO2 laser vaporization 3,4 Electrosurgery and cryosurgery have also been reported as alternative treatment options by some authors.10,11
Figures 4A and B show the postoperative outcome 2 years after surgery. To date, no signs of tumor recurrence have been observed.
CONCLUSION
ADFK is a benign fibroepithelial tumor that usually presents as a solitary, painless nodule measuring less than 1 cm, and only rarely arises beneath the nail plate. The true incidence of ADFK may be underestimated, as it resembles several benign lesions that generally do not require routine histopathological examination. Early recognition and adequate treatment are essential to prevent nail deformities. The recommended therapeutic approach is surgical excision, which must be performed with caution to avoid damage to the nail matrix.
The diagnosis of nail tumors represents a true challenge in dermatologic practice, particularly when lesions occur beneath the nail plate. Biopsy is often required for diagnostic clarification, which entails high cost and the risk of permanent nail dystrophy. Therefore, in the presence of a fibrous nodule located at the nail fold, bed, or matrix –especially when dome-shaped or finger-like – ADFK should be considered as a differential diagnosis. l
REFERENCES:
1. Liu Y, Zhu Y, Chen G, Xu H, Rao Y, Liu K. A retrospective study on the clinical features of skin lesions in Chinese acquired digital fibrokeratoma patients. J Cosmet Dermatol. 2023;23(1):172–8.
2. Sung KY, Lee S, Lee SY. An unusual presentation of acquired periungual fibrokeratoma: a mixed form of dome‐shaped and branching type. Clin Case Reports. 2020;8(11):2129–31.
3. Jahan N, Padubidri Kombettu Ashwini, S. Chethana, Jayadev Betkerur, Shastry
4. V. Horn on the nail: acquired ungual fibrokeratoma. J Cutan Aesth Surg. 2021;14(1):121–4.
5. Hwang S, Kim M, Baik Kee Cho, Hyun Jeong Park. Clinical characteristics of acquired ungual fibrokeratoma. Indian J Dermatol Venereol Leprol. 2017;83(3):337–7.
6. Ballan A, Zeinaty P, Tomb R, Kechichian E, El Hachem L, Nasr M, et al. Acquired ungual fibrokeratoma: a systematic review of the literature. Int Dermatol. 2020;60(5):533–9.
7. Shih S, Khachemoune A. Acquired digital fibrokeratoma: review of its clinical and dermoscopic features and differential diagnosis. Int Dermatol. 2018;58(2):151–8.
8. Qiao J, Liu YH, Fang K. Acquired digital fibrokeratoma associated with ciclosporin treatment. Clin Exp Dermatol. 2009;34(2):257–9.
9. Hare AQ, Rich P. Nail tumors. Dermatol Clin. 2021;39(2):281–92.
10. Pegas JR, Cade KV, Kiyomura MY, Soares A, Mayer L, Tebcherani AJ. Fibroqueratoma digital adquirido: a propósito de um caso clínico. Surg Cosmet Dermatol. 2012;4(4):357–9.
11. Palaniappan V, Sadhasivamohan A, Sankarapandian J, Karthikeyan K. Acquired fibrokeratoma: a retrospective study in a tertiary centre in South India. Indian J Dermatol. 2022;67(3):312.
12. Wang X, Zhang D, Lin Q, Niu C, Fan H, Zhang M, et al. Acquired digital fibrokeratoma: a report of five cases and review of the literature. Clin Cosmet Invest Dermatol. 2024;17:247–52.
13. Vance P, Hohnadel M. Acquired digital fibrokeratoma in a 6‐Year‐Old patient: the youngest reported case. Pediatr Dermatol. 2025;42(4):892-3.
AUTHOR’S CONTRIBUTION:
André Martins Ornelas 0009-0002-0393-7205
Study conception and design; manuscript drafting and writing; data collection, analysis, and interpretation; intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; critical review of the literature.
Clarissa Brito Farias 0009-0009-5395-045X
Manuscript drafting and writing; data collection, analysis, and interpretation; critical review of the manuscript.
Isabelle Sousa Medeiros Torres Ferreira
Data collection, analysis, and interpretation.
Flauberto de Sousa Marinho
0000-0002-9597-3272
0000-0002-9337-9931
Final approval of the manuscript; study conception and design; data collection, analysis, and interpretation; intellectual participation in the propaedeutic and/or therapeutic approach to the cases studied; critical review of the manuscript.