
Shrewsbury and Telford Hospital NHS Trust Annual Report and Accounts 2022/23
Presented in accordance with the NHS Group Accounting Manual 2022/23 pursuant to the Companies Act 2006
2
Part 2: Accountability Report
Part 3: Annual Audited Accounts
3 Contents Page Foreword from the Chair and Chief Executive 4 Part
Performance Overview 9 Statement from the Chief Executive 9 Performance Analysis 21
1: Performance Report
Corporate Governance Report 50 Remuneration Report 71 Staff Report 81 Annual Governance Statement 101 Statement of Accountable Officer’s Responsibilities 127 Statement of Directors’ Responsibilities 128
129 External Auditor’s Opinion 2022/23 External Auditor's Completion Letter (Audit Certificate) Annual Audited Accounts 2022/23 134 136
Foreword from the Chair and Chief Executive
This year has undoubtedly been challenging for the Trust, and the NHS nationally, with a need to balance unprecedented demand for emergency and community care, alongside restoring elective services and continuing to deliver quality care during difficult flu and COVID-19 peaks. Despite its challenges, 2022/23 has brought real examples of innovation, collaboration and genuine progress against our journey of continuous improvement.
Against this backdrop, we have continued to focus on our local priorities including our response to the first and final Ockenden Reports published in December 2020 and March 2022, as well as making steady progress on our Getting to Good improvement programme. At the heart of this work is our commitment to providing safe care for our patients, and we are incredibly grateful for the dedication, resilience and compassion of our colleagues
Colleagues in maternity services have been working hard to deliver the 210 Ockenden actions set out in the Ockenden Reports.
Meaningful and sustainable change takes time, but we are pleased to report we are making good progress with 162 actions now delivered, putting us slightly ahead of our delivery plan. We are working at pace to progress the outstanding actions, supporting external parties where necessary change is outside our control. Alongside this, we are continuing with our wider improvement work and we are engaging with service users, and benefitting from their feedback to inform our approach, and working with stakeholders where necessary to take this forwards.
We owe it to those who experienced poor care, and to those in our communities who are pregnant or considering parenthood, to deliver safe, compassionate and personalised care. We want women to feel confident about giving birth at the Shrewsbury and Telford Hospital NHS Trust (SaTH) and to be assured that supporting and informing families to have the birthing experience they want is our absolute priority. We have further to go but we are determined to continue delivering real and effective change.
At the time of writing this report, we continue to face significant pressures on our services
Although this is a national challenge, we recognise that elements of our local environment, including system capacity and workforce pressures, have sometimes led to significantly longer waiting times in our emergency departments and for ambulance handovers. This is not the
4
standard of care that we would want to provide for the families and communities we serve, and we are doing everything we can to reduce waiting times and working with partners to improve flow through and out of our hospitals. We would like to thank patients and their families for their ongoing support as we have responded to these extreme pressures.
Throughout the year, we have seen examples of innovation as our teams trialled new ways of working to provide better care for patients. Throughout this report you will read examples of these new ways of working, including the launch of a dedicated Acute Floor at the Royal Shrewsbury Hospital in December 2022. Its aim is to ensure patients are being seen by the right clinician, at the right place, at the right time. However, almost 2,000 patients benefited from the new Acute Floor facility up to the year end, with the majority of those patients avoiding using the emergency departments altogether. Ultimately, this delivers better care and a better experience for our patients and enables greater flow within our hospitals.
Maintaining flow through our hospitals and the safe discharge of patients has been a consistent challenge, necessitating the continued use of surge plans and escalation beds throughout the year. Lack of flow through the hospital resulted in the loss of some of our elective activity, and the associated ongoing challenges associated with the restoration of activity which we are now working hard to recover.
Our partnership with Shropshire Community Health NHS Trust, and the wider system, has also led to an acceleration of the Virtual Ward programme. At the time of writing, over 100 patients are now using the Virtual Ward programme, which supports patients to receive the care they need in the community, enabled by digital technology. Our collective aspiration is to further grow this service, providing better health outcomes for our patients
Our clinical and operational teams have worked tirelessly throughout the year to reduce waiting times for patients, offering additional clinics, validating our waiting lists and seeking mutual aid from partners, where appropriate. We have eradicated 104 week waits and eradicated 78 week waits by end of April 2023. Whilst falling short of the national target, an incredible amount of work has taken place to reduce 78 week waits from 2,121 in November 2022 to 57 at the end of March 2023.
In March, we were able to restore orthopaedic services at The Princess Royal Hospital after a temporary pause due to the COVID-19 pandemic and ongoing pressures in emergency care.
5
This is a significant step forward in our restoration journey and will support patients with the most complex needs to receive treatment locally. We recognise there is much more to do, and our focus is now to reduce waiting times for people waiting 65 weeks by March 2024 and maintain this momentum and focus until we have restored our waiting times to pre-pandemic levels.
The considerable pressures, resulting in the opening of significant escalation capacity, the ongoing workforce challenges, increased cost of agency and bank costs, together with the care of increasing numbers of Covid patients, have led to a deficit of £47.206m. We are working closely with system partners to ensure we are working effectively together to deliver high quality and sustainable care for our communities.
We recognise the importance of working together across the Shropshire Telford and Wrekin Integrated Care System (ICS) with our partners and have supported the newly formed NHS Integrated Care Board (ICB) to support greater collaboration across the health and social care sector. We would like to recognise and thank our partners, across Shropshire, Telford and Wrekin, Mid-Wales and our neighbouring trusts, for their ongoing support.
We could not deliver our services without the support and dedication of over 300 committed volunteers who come from a wide range of backgrounds and we really value the different skills, outlooks and experiences that these individuals bring to the organisation. They make a real difference to the experience of our patients, families and colleagues. All of our volunteers play an important role within our hospitals, working alongside staff in a variety of departments and we would like to thank them for their continued support.
Looking forward, it is clear that we cannot tackle these significant challenges if we do not transform the way we deliver services. Our Hospitals Transformation Programme is a vital part of the Trust, and wider ICS’ strategy, to deliver better health outcomes and a vastly improved experience of care for our communities. In August 2022 we received national approval for the Strategic Outline Case for the reconfiguration of acute hospital services, subject to a number of conditions. This was a major milestone and moves us another step closer to securing the funding we need to transform our services. Throughout 2023/24 we will continue to involve clinicians, patients, partners and local communities as we progress through the final stages. If successful, this will secure the national investment that will deliver better care for everyone.
6
Investing in our digital infrastructure is another key priority and enabler to our ambitious transformation priorities. The introduction of our Electronic Patient Record will involve all teams and represents the biggest investment in IT infrastructure in many years. A comprehensive training and development programme is underway, which will support the necessary technical and cultural change across the Trust.
Alongside our digital investment, we will continue to use capital funding to improve our estate and equipment, providing modern facilities that will improve care and outcomes for the communities we serve. We made significant progress in 2022/23, including upgrading our endoscopy and ophthalmology services 2023/24 will see the launch of a £24million planned care hub at The Princess Royal Hospital, increasing the number of surgical theatres, providing improved environments for patients, and further supporting us to reduce waiting times for our patients. Alongside this, the development of the main entrance of the site is well under way. In all our work we are mindful of our carbon footprint and the role we play for communities now and in the future, through this document you can find out more about our Sustainability Report.
We could not deliver this, without the support of our amazing colleagues and we recognise that maintaining their health and wellbeing is of upmost importance. We are proud that in our 2022 staff survey results saw improvements across many elements of the NHS People Promise. However, we recognise that we are on a journey of continuous improvement with much more to do. As a Board we will continue to prioritise initiatives that support the psychological wellbeing of our staff, provide opportunities for them to develop and grow, and we will continue to build a culture that delivers our Trust’s values.
2023/24 is a significant year for the NHS as it celebrates its 75th birthday. Despite the current pressures, this year will be a year for reflection and optimism and it is timely that we have a significant innovation and transformation programme planned during this important year. We hope that our communities, patients, colleagues and partners will join us in celebrating this important milestone for the NHS. We remain incredibly grateful for everyone’s engagement and their feedback, and for their continued support in all that we aim to achieve.
Dr Catriona McMahon Mrs Louise Barnett Trust Chair Chief Executive Officer


7
Part one: Performance Report
8
Performance Overview
This section of our report provides detail as to what it is that we do here at SaTH, who we are, and our values and ambitions. It outlines the principal risks that the Trust faces in the delivery of our strategy and objectives and provides some details on how we performed over the financial year, 1 April 2022 – 31 March 2023.
Statement from the Chief Executive
We reported last year, that on 4 April 2022, the Trust had 169 inpatients with Covid-19 on our wards – this was the highest number in over two years of the pandemic. The numbers of Covid patients on our wards has thankfully reduced through 2022/23, however we still had over 70 patients that have tested positive for Covid-19 in our beds at the end of March 2023.

Maintaining flow through our hospitals and the safe discharge of patients has been an ongoing challenge, necessitating the continuation of surge plans and use of escalation beds throughout the year This continued to impact on our elective activity, which we are working hard to recover with the re-commencement of elective orthopaedic inpatient activity at Princess Royal Hospital in March 2023.
We have continued to ensure that our most clinically urgent patients have access to our services. We appreciate the distress and the pain that long waits for treatment can have for
9
our patients, and we continue to work towards reducing waiting times for our patients. We have a long way to go to recover elective waiting times to pre-Covid19 levels, but we have made considerable progress by year-end in reducing the number of patients waiting over 104 weeks and over 78 weeks for treatment. We have plans in place to meet ambitious national recovery standards for no patients waiting longer than 65 weeks by March 2024.
Pressures on our urgent and emergency care services remained high throughout the year with poor performance against national A&E standards, including ambulance hand over delays. Joint work with West Midlands Ambulance Service (WMAS) provided vital mitigation with the development of an Ambulance Receiving Area at Shrewsbury which has a joint workforce of WMAS paramedics and our Trust’s nursing and medical teams. An Ambulance Receiving Area pod has also been built at Princess Royal Hospital in Telford. This is staffed with the Trust’s nursing and medical teams, and it opened on 5th April 2023.
One of our principal objectives during the year continued to be the development of the Hospitals Transformation Programme (HTP) Outline Business Case, which, aligned to both internal and external plans will support, subject to approval, the modernisation of some of our facilities and infrastructure to enable the delivery of safe, effective and sustainable care for the population we serve.
The estate improvement work in Shrewsbury’s A&E was completed in September 2022 and now has a dedicated space for children and young people, and improved facilities in both ‘majors’ and resuscitation areas, as well as an improved waiting area. The ‘front-door’ teams continue to work closely together, optimising ‘streaming’ to the urgent treatment centres, using the same day emergency care pathways in medicine and surgery, as well as working with the new ‘single point of access’ routing for patients (building on the existing rapid response and 111 pathways).
A new Acute Floor has also been created at Shrewsbury which means that patients that are referred from the GP to see an acute physician can go direct to the Acute Medical Assessment Area rather than waiting in A&E. The acute floor consists of 26 short stay beds, 20 beds in the acute medical unit and 14 trollies, 3 assessment rooms and a seating area for up to 15 patients in the Acute Medical Assessment area. A further expansion is planned in 2023 to utilise 9 enhanced care beds once staff have been recruited and fully trained. Since opening in December 2022, we have seen 1778 patients up to 31st March 2023; 1244
Part 1: Performance Report 10
patients (70%) have arrived directly without going through A&E and 25% of patients have been discharged home directly from the acute floor.
The discharge lounges at both sites expanded in 2022/23. At Royal Shrewsbury Hospital the discharge lounge is now based on ward 31 and accommodates up to 16 patients and at Princess Royal Hospital an additional space has extended the footprint within the Paul Brown building to enable a further 8 patients to be accommodated.
We have worked closely with system partners to develop new models of care. The Virtual Ward model developed in partnership with Shropshire Community Health NHS Trust, commenced in October 2022 initially supporting five patients. At the end of March 2023, the Virtual Ward caseload had capacity to care for over 100 patients. Through 2023/24 we will be further increasing the capacity for step up (admission avoidance) patients and step down (discharge) patients.
The number of patient falls per 1000 bed days has reduced through 2022/23 due to the significant focus and quality work that has been undertaken around reducing deconditioning for patients who were admitted to our bed base. In March 2022, we had 5.45 falls per 1000 bed days; in March 2023 this had fallen to 4.05 falls per 1000 bed days. All falls continue to be reviewed daily by the quality matron with feedback provided to the nurse caring for the patient at the time to include examples of good practice and aspects of care requiring improvement.
We continue to focus improvement efforts on completing the actions identified within the first and final Ockenden Reports received by the Trust on 10 December 2020 and 20 March 2022 respectively There continues to be an Ockenden Review Assurance Committee, attended by a number of stakeholders and which is live streamed in public, provides oversight scrutiny andreviews progress against the action plan.
We have had two MRSA bacteraemia reported this year: one in December 2022 and one in February 2023. There has also been an increase in Clostridium difficile (C.Diff) cases in 2022/23 with 60 cases being reported against a target of 33. The Director of Infection, Prevention and Control is undertaking a systematic review of all 60 cases and the divisions have a focussed action plan in place that is monitored via the Infection Prevention and Control Operational Group.
Part 1: Performance Report 11
Collaboration and relationships with our partners continue to strengthen as the Shropshire, Telford and Wrekin Integrated Care System was put onto a statutory footing in July 2022. Daily tactical meetings are in place with our partners to review unscheduled care demand and capacity and to determine the level of discharge activity required to support a reduction in delays within the Emergency Department and ambulance handovers. Meetings are held across the system to agree actions that will support both planned care recovery and improvement in unscheduled care delays.
Through the latter part of 2022/23 we saw a number of strikes across the NHS and public sector. The Trust planned effectively to mitigate the risk to patients over that period whilst supporting colleagues who wished to take industrial action.
Moving into 2023/24, the Trust continues to work closely with its regulators to improve its provision of healthcare, and to work towards its vision to provide excellent care for the communities we serve. Our ‘Getting to Good’ framework has remained in place through 2022/23 with a weekly Operational Delivery Group which reviews the actions undertaken by the Trust to support progress. The Trust remains rated at level 4 against the NHS Oversight Framework and is provided with mandated support through the National Recovery Support Porgramme.
As we look forward to 2023/24, there are exciting developments for the Trust as we develop the plans to move forward with the Hospital Transformation Programme (HTP) and also replace the thirty year old Electronic Patient Record system across the organisation.
About the Trust
The Shrewsbury and Telford Hospitals NHS Trust was established in its present form on 1 October 2003 and brought together healthcare organisations in Shrewsbury, Telford and elsewhere in Shropshire. The Trust is spread across several locations, with the main sites of the Royal Shrewsbury Hospital and the Princess Royal Hospital in Telford, being positioned approximately fifteen miles apart. Outreach and outpatient clinics managed by the Trust are also provided at Whitchurch Community Hospital, Bridgnorth Community Hospital, Ludlow Community Hospital, and the Wrekin Community Clinic. The Trust serves a community of circa half a million service users across Shropshire, Telford and Wrekin, and mid-Wales.
Part 1: Performance Report 12
The Trust’s management structure comprises four clinical divisions led by clinician and management partnerships, and one corporate division (including departments such as finance, estates, facilities, human resources, governance and risk). These are: Medicine & Emergency Care Division, Surgery, Anaesthetics & Cancer Division, Women and Children’sServices Division, Clinical Support Services Division and Corporate Services.
The two main hospitals provide a wide range of acute hospital functions including Accident & Emergency, outpatients, diagnostics, critical care and inpatient medical care. The Trust has over seven hundred beds in total.
The Princess Royal Hospital became the specialist centre for inpatient head and neck surgery in 2013, following the establishment of enhanced outpatient facilities and a dedicated head and neck ward. It is also the main centre for inpatient women and children’s services following the opening of the Shropshire Women and Children’s Centre in 2014. The Royal Shrewsbury Hospital became the main specialist centre for acute surgery with a surgical assessment unit, surgical short stay unit and ambulatory care facilities. In 2022 cardiology services were also centralised at Princess Royal Hospital.
The expansion of the Shrewsbury A&E department was completed as planned and a new 32-bed modular ward in Shrewsbury became operational in May 2022, being used to support the critical care service as part of the surge plan pending essential ward moves until February 2022. Transformation of the Trust’s Endoscopy and Decontamination services has been completed to include a total of three additional procedure rooms and state-of-the-art decontamination facilities. Finally, plans to move renal dialysis services from our Telford site to a new, £4.5m purpose-designed facility for lower risk patients are underway. The new facility will allow the Trust to meet future demand, together with updating the previous facility into a new inpatient ward.
This programme of improvement continues with £24m NHSE funding being secured for the development of an Elective Hub, the first phase due to open in summer 2023 and the second phase proposed to complete in early 2024. This facility is aligned with our Hospital Transformation Programme and is an important pillar in our referral to treatment (RTT) and cancer recovery plan, providing improved and additional operating theatres and ringfenced beds for elective day case patients. Our first Shropshire, Telford & Wrekin (STW) Community Diagnostic Centre (CDC) is expected to open its doors to patients in September this year. The CDC will be hosted by SaTH but will accept referrals from all
Part 1: Performance Report 13
primary and secondary healthcare providers in STW. The CDC is located on Stafford Park, Telford and will provide a wide range of diagnostic services away from the main hospital sites, including phlebotomy, imaging and Cardio-respiratory testing.
The Trust has 7,181 whole time equivalent members of staff, of which 6,273 are employed in a substantive capacity. With on-going recruitment campaigns, the Trust has increased the substantive whole time equivalent workforce by 300 over the last 12 months. With 470 vacancies, the Trust remains below its targeted whole-time establishment and continues to rely on bank and expensive agency staff. An increased need to open escalation areas along with waves of Covid over the last 12 months have created further staffing pressures, therefore increasing reliance on agency staff. Expenditure for temporary staff, including agency, for the 2022/23 financial year stood at £46,529m (2021/22: £32,845m) – as can be seen from note 8 to the accounts.
Following the conclusion of the formal ‘Improvement Alliance’ with University Hospitals Birmingham NHS Foundation Trust and NHS Improvement in March 2022, the organisation continues to work collaboratively in achieving its performance priorities and progressing the delivery of the Trust’s Quality Improvement Plan (‘Getting to Good’).
‘Getting to Good’ is a three year improvement programme This critical programme is helping to drive and embed change throughout the organisation, ensuring that any improvements we make now and in the future are high quality and sustainable. The programme will be further progressed with regular monitoring and oversight of additional improvements to ensure that we continue to improve the quality of care which we provide for our patients
The Care Quality Commission
The Trust’s latest inspection report was published on 18 November 2021 following a series of inspections over July and August 2021. A copy of the inspection report can be found on the CQC’s website at https://www.cqc.org.uk/provider/RXW
Part 1: Performance Report 14
Our current CQC ratings:

Although this inspection demonstrated tangible improvements across both Medicine and Urgent & Emergency Care at both hospitals but particularly at the Princess Royal Hospital site where each domain improved by one rating, the Trust remained rated overall as Inadequate.
Prior to the inspection in 2021, the Trust had 60 Section 31 conditions in place for the Trust, with 30 in place for each site as well as the previously received 6 Section 29a warning Notices. Following the inspection, a full review of all the Section 31 conditions took place by the CQC which led to a majority of these conditions being removed. At 31 March 2023, the Trust has a remaining 5 Section 31 conditions remain in place for the Trust and we continue to work hard on embedding the improvements required so that all remaining conditions can be removed
The ongoing implementation and monitoring of improvements is co-ordinated and overseen by the Trust’s Getting to Good improvement plan which sets out the workstreams which the Trust is progressing in order to improve quality of care for patients. Further detail can be found within our 2022/23 Quality Account on our website.
The Trust’s strategic direction, vision and values
In response to the NHS Long Term Plan, we are currently working in conjunction with our partners across Shropshire, Telford and Wrekin Integrated Care System (ICS) to develop a five-year Integrated Care Strategy, which focusses on the health and wellbeing needs of the local population.
Part 1: Performance Report 15
In parallel to the Integrated Care Strategy the ICB and their partner Trusts/Providers have a duty to prepare a first Joint Forward Plan before the start of the financial year 2023. The Joint Forward Plan will describe how services are provided to meet our populations physical and mental health needs over the next five years aligned to the ICS four core purposes of:
• improving outcomes in population health and healthcare,
• tackling inequalities in outcomes, experience and access,
• enhancing productivity and value for money and
• helping the NHS to support broader social and economic development.
The main principles of the Joint Forward Plan are to ensure that it is:
• Aligned with the wider system partnerships ambitions
• Supporting and building on existing local strategies and plans
• Delivery focussed.
As an organisation we continue to strengthen our relationships and work collaboratively with all of our partners to develop and progress our Operational, System Improvement and Resource Plans for 2023/24 alongside reviewing opportunities for further collaborative working that enhances our local population health and wellbeing needs.
‘Core20PLUS5’ is a national NHS England approach to inform action to reduce healthcare inequalities at both national and system level. Our Trust Strategy includes a focus on enhancing the wider health and wellbeing of communities and system-wide implementation of the National approach to Core20PLUS5 to target a population cohort and 5 focus clinical areas requiring accelerated improvement.
Internally we have recently launched our revised overarching Trust Strategy which sets out the future direction of our organisation for the next five years – our Vision, our Values, our Strategic Goals and Key Strategic Themes with defined outcomes. To support the realisation of our Vision “excellent care for the communities we serve” a review of our longer-term sustainability strategies such as clinical, quality, workforce, estate and digital technologies is currently underway.
Part 1: Performance Report 16
Our Vision stems from the Trust’s ambition to continuously improve the services which we provide to our patients, their families and our communities.
With stakeholder input, our values were updated in summer 2020 to: Partnering Ambitious Caring Trusted

We believe that by always working with our values in mind, we can behave in a way which will provide the foundation for the provision of safe, approriate care for the people who are very important to us – our patients and their families.
The Trust’s improvement journey for 2022/23 was based upon our five strategic goals: Our Patients & Community:
We deliver safe and excellent care, first time, every time.
We work closely with our patients and communities to develop new models of care that will transform our services.
Part 1: Performance Report 17
Our People:
Our staff are highly skilled, motivated, engaged and ‘live our values’. SaTH is recognised as a great place to work
Our high performing and continuously improving teams constantly strive to improve the services that we deliver
Our Service Delivery:
Our services are extremely efficient, effective, sustainable and deliver value for money.
We deliver our services utilising safe, high-quality estate and up to date digital systems and infrastructure
Our Governance:
We are a learning organisation that sets ambitious goals and targets, operates in an open and transparent way and delivers what is planned.
Our Partners:
We have outstanding relationships with our partners, working together to deliver best practice integrated care for our communities
SaTH Improvement
The Trust has a dedicated Service Improvement team called the SaTH Improvement Hub. The aim of the SaTH Improvement Hub team is:
To empower colleagues at all levels to have the confidence, capability, passion and knowledge, to test changes and make improvements at SaTH and the communities we serve
The outcome measure we use for this is responses to the staff survey question ‘I am able to make improvements happen in my area of work’. As you can see from the following graph, this has improved in the period under review, but still remains under 50%.
18
Part 1: Performance Report
In order to support colleagues to test changes in their areas of work, the team have developed a structured improvement methodology, incorporating learnings from the work undertaken under the Virginia Mason methodology delivered in previous years, the NHS service improvement courses (Quality Service Improvement and Redesign and other improvement methodologies. The team offer consultancy support to colleagues, but also provide teaching against a locally designed syllabus. During 2022/23, the team have trained:

Part 1: Performance Report 19
Level Definition Duration Colleagues trained Introduction All colleagues provided with an introduction to our philosophy and key concepts, as part of a local induction 15 mins (video) Fundamentals All colleagues provided with improvement tools & concepts, which can be transferred back into the workplace 1 Day 152 Practitioner An
will
colleagues to run individual & team projects 6 Months 35 Lean for Leaders Top Up Builds on previous training package to enable colleagues quickly advance to Practitioner level 1 Day 35
advanced understanding of improvement tools & techniques, which
enable
Going Concern Disclosure
The accounts have been prepared on a going concern basis. The financial reporting framework applicable to NHS bodies, derived from the HM Treasury Financial Reporting Manual, defines that the anticipated continued provision of the entity’s services in the public sector is normally sufficient evidence of going concern. The directors have a reasonable expectation that this will continue to be the case.
The Board has carefully considered the principle of ‘Going Concern’ in the context of the Trust continuing to operate under the HM Treasury’s Financial Reporting Guidelines (FReM). For the year ending 31 March 2023, the Trust is reporting a deficit of £47.206m on an adjusted financial performance basis, against a planned deficit of £19.135m.
In 2022/23, the Trust’s income has been driven through an allocative process, consisting of block payments with specific adjustments for agreed growth and prices, ongoing Covid expenditure, and funding achieved through the Elective Recovery Fund (ERF) to incentivise restoration of elective services. There has also been a convergence adjustment applied to bring the Trust back towards a fair-share allocation. As the Shropshire, Telford & Wrekin Integrated Care System (ICS) is currently consuming more than its fair share (on a population basis), the convergence factor applied is higher.
Contracts were constructed on an Intelligent Fixed Payment (IFP) basis within the ICS. This is an approach based on collaboration, concentrating on the cost of providing healthcare across the system in order to bring the health system back to clinical, operational and financial balance. Other contracts were constructed on a typical cost and volume contract or an aligned incentive payment approach.
The Trust maintains a cash balance of £3.301m at the end of 2022/23 (March 2022: £15.889m).
Every ICS/STP received a 2022/23 capital spending envelope derived from the systemlevel allocation, with The Shrewsbury and Telford Hospital NHS Trust receiving a total system envelope of £19.822m in 2022/23. Historically the Trust has had low levels of internally generated capital funds underpinned by public dividend capital.
Part 1: Performance Report 20
In the financial landscape for 2023/24, nationally the NHS funding allocation moves to an aligned payment and incentive approach (API). This consists of a fixed element for nonelective care, and elective care is reimbursed on a variable basis based on actual activity delivered. Tariffs have been uplifted for inflation and adjusted for efficiency and convergence factor. Covid funding has also been included within baseline tariffs and therefore will no longer be funded separately. The Elective Recovery Fund (ERF) remains in place to support restoration of elective activity. Low-Volume Activity (LVA) contracts, worth under £0.5m, will be paid on a block basis.
The Board of Directors have concluded that whilst the financial position for 2023/24 is very challenging, based upon enquiries with NHS Improvement and the Department of Health and Social Care, they have a reasonable expectation that the Trust will have access to adequate resources (as in previous years) to continue in operational existence for at least 12 months from the date of approval of the financial statements and continue to provide services to its patients. Based on this expected continuation of services, the Trust continues to adopt the going concern basis in preparing the financial statements.
Performance Analysis
This section provides a detailed analysis of the Trust’s performance throughout 2022/23, and in doing so, brings together some of the principal performance measures that we use to determine the level of risk that we carry in the organisation.
The Board’s role in monitoring the performance of the organisation is supported by an accountability structure which enables visibility by the public, staff and external stakeholders through itsmonthlymeetings streamed in public. It remains the responsibility of the Board of Directors to design and then implement agreed priorities, objectives and the overall strategy of the Trust.
The Board considers performance against national priorities set out in the NHS Oversight Framework, which describes how NHS England works alongside trusts to support the delivery of high quality and sustainable services for patients.
The Board hasalsodeveloped a setof key performance indicators (KPIs), which are set out within a local performance management framework. These cover quality and safety
Part 1: Performance Report 21
measures as well as those performance, financial and workforce KPIs outlined in national framework.
An Integrated Performance Report is presented to each meeting of the Board of Directors, in the form of a scorecard accompanied by exception reporting, and explanatory narrative. This information is provided for the previous month, trends over time, and, where available or relevant,againsta benchmark.ThesearelinkedtotheTrust’sstrategicobjectives,national priority indicators, and local priorities.
The Board is supported by the work of the Quality Safety and Assurance Committee in monitoring performance against quality and workforce indicators, whilst the Finance and Performance Assurance Committee reviews operational and financial performance. The Board of Directors is also supported by the Audit and Risk Assurance Committee which provides assurance regarding the organisation’s risk and control framework.
The executive directors continually review the performance of the Trust monthly through a series of regular meetings, and monthly meetings with divisional colleagues at the operational Performance Review Meetings.
Part 1: Performance Report 22
Part 1: Performance Report
Our Key Performance Indicators 2022/23, by quarter:
The Trust has had an extremely busy year throughout 2022/23 since national Covid-19 restrictions were lifted and the focus intensified on recovery of elective and cancer services. Reduction in Covid-related admissions enabled us to re-establish green elective pathways, re-open elective theatres and re-commence surgery, prioritising patients by clinical urgency and, also the patients who had been waiting longest for their treatment.
23
Measurement (metric) end of Q1 end of Q2 end of Q3 end of Q4 Total 2022-23 Total elective activity undertaken (IP/DC) 15,511 16,251 17,023 17,571 66,356 Patients waiting more than 104 weeks to start consultant-led treatment (English/Welsh) 18 3 1 0Patients waiting more than 78 weeks to start consultant-led treatment (English/Welsh) 315 344 549 57Patients waiting more than 52 weeks to start consultant-led treatment (English/Welsh) 3,049 3,618 4,018 4,228Total patients waiting over 62 days to begin cancer treatment 554 781 685 476Proportion of cancer patients meeting 62 days standard - Target 85% 52.4% 50.6% 48.9% 42.2% 48.4% Proportion of urgent suspected cancer patients meeting faster cancer diagnosis standard - Target 75% 62.9% 61.1% 57.3% 60.5% 60.4% Total outpatient attendances 137,468 139,406 140,789 152,552 570,215 Urgent and Emergency Care performance measure (4-hour performance (excluding planned returns) 57.2% 52.5% 47.9% 54.2% 52.9% 30-minute ambulance breaches (ambulance handover 30–60 minutes) 2,356 2,357 2,212 2,233 9,158 25.2% 26.8% 27.0% 26.0% 26.2% 60-minute ambulance breaches (ambulance handover > than 60 minutes) 3162 3493 3495 2536 12,686 33.8% 39.7% 42.7% 29.6% 36.3% Number of patients spending more than 12 hours in an emergency department 4,047 5,245 7,260 5,871 22,423 10.31% 14.08% 18.67% 17.24% 15.01% Summary hospital-level mortality indicator 111.4 100.0 not yet available not yet available not yet available Overall CQC rating (provision of highquality care) Inadequate Methicillin-resistant Staphylococcus aureus (MRSA) bacteraemia infection rate 0 0 1 1 2 Clostridium difficile infection rate 11 17 11 21 60 E. coli bloodstream infections 5 7 13 14 52
Due to pressures on urgent and emergency services coupled with a consistently high number of patients with no criteria to reside in our hospitals, the Trust has struggled to recover from the considerable backlog of patients awaiting treatment. Plans were put in place to reduce the backlog as quickly as possible in order to minimise the risk of potential harm to patients, some of whom had been waiting for significant periods of time for treatment.
The ongoing provision of a Vanguard theatre throughout the year enabled us to maintain an increased level of elective day surgery throughout 2022/23 and the Surgical Same-Day Emergency Care Unit has supported ambulatory emergency care pathways. We have also invested in insourcing providers to undertake additional theatre sessions over seven days a week. Due to sustained pressure on urgent and emergency pathways, the recommencement of elective orthopaedic surgery in June 2022, could not be sustained, but after careful planning, elective orthopaedic inpatient surgery recommenced in March 2023 with the support of Shropshire, Telford and Wrekin system partners and NHS England. We continue to work with The Robert Jones & Agnes Hunt Orthopaedic Hospital (RJAH) to improve the availability of services for patients and have also benefitted from Mutual Aid available nationally.
To support elective and cancer recovery, a national tiering system was introduced to support trusts struggling to recover RTT and cancer standards. Our Trust originally received tier 2 support but moved to tier 1 in January when our performance deteriorated after the Christmas period in part due to increased incidence of Covid-19, consistent high levels of escalation in our hospitals and consistently high numbers of patients with no criteria to reside. Since then, we have made good progress against our revised improvement trajectories despite the impact of the junior doctors’ industrial action in February and ended the year with no 104-week breaches and 57 breaches at 78 weeks (against a planned trajectory of 211).
Our 62-day cancer backlog has improved from its highest level of 626 in January to 412 by year-end. Similarly, our 104-day backlog has improved from its highest level of 215 in September to end the year at 155. Our most challenged pathways are urology, colorectal and gynaecology. The main constraints were diagnostics, workforce and outpatient capacity to manage increased referrals in all of these specialties. A mobile CT and MRI scanner were brought in to support elective recovery and we also invested in ultrasound and endoscopy insourcing. In addition, at the end of quarter three we commissioned a further outsourced
Part 1: Performance Report 24
reporting provider and incentivised our reporting radiographers. By the end of the financial year, this had resulted in a significant improvement in the turnaround time of imaging reports, which made a significant contribution to the improvement in our recovery position.
A&E attendances have remained on average at 5000 attendances per month and we have seen bed occupancy over 92% through the winter months. Entering quarter three, our operational challenges intensified with a significant number of delays in discharges, resulting in delays to admission to our wards. This continued into quarter four, with patients waiting in emergency departments, in the main hospital corridors at both sites and within ambulances to access the emergency department. Our Board Assurance Framework (BAF) includes a risk – BAF risk 10: The Trust is unable to meet the required national urgent and emergency standards – this risk is scored at 20, as an extreme risk. We continued to work across the ICS to address the unscheduled care pressures across the system, which, together with ongoing workforce challenges continue to adversely impact on the recovery of our elective capacity.
In October, we worked with system partners to agree our activity plan for the remainder of the year. To offset the impact of internal constraints, we continued providing additional elective capacity through the independent sector, partnership with RJAH and other organisations outside Shropshire through mutual aid. By the end of quarter four, 130 patients had been treated via mutual aid arrangements.
There has been a continuation in the prevalence of Covid-19 in the community and patients admitted with Covid. This had a significant impact on our staff availability and that of partner organisations, particularly in quarter three and quarter four, resulting in the Trust experiencing further, very significant difficulties in maintaining flow and discharging patients in a timely fashion to create the necessary capacity for newly admitted patients. The flow out of the hospitals to safely discharge our patients was constrained, necessitating the Trust to extend our surge plans.
Our work on unscheduled care continued with a view to improve flow at our ‘front door’ by reducing the time from being medically fit for discharge, to being discharged. We developed a comprehensive Urgent and Emergency Care (UEC) improvement programme that is focused on internal systems and processes to ensure timely “simple discharges”. And we continued to work closely with local authority and community partners to focus on discharge ready patients requiring social and community support, on pathways 1, 2 and 3 and to create
Part 1: Performance Report 25
earlier discharge timesin the day so that we can release beds to our Emergency Department admissions and enable ambulance handover to improve. In January 2023, the Integrated Discharge Team leadership moved from us to Shropshire Community Health NHS Trust (SCHT) to support an increased response from our system partners to the discharge of patients who had no criteria to reside in our hospital beds and had been assessed as requiring pathway 1-3.
Moving forward into 2023/24, we maintain a focus on sustaining the improvements in ward processes that have been made in 2022/23 and developing criteria-led discharge along with programmes of work to improve the number of patients utilising the discharge lounges and being discharged earlier in the day.
Details regarding our quality of care performance details can be found in our Quality Account 2022/23. From 1 July 2023, this will become available on our website, although copies may be obtained by contacting our Communications Department at communications@sath.nhs.uk
Quality Priorities – Priorities for Improvement
A detailed narrative which describes our quality improvement priorities and their outcomes for the year can be found in our Quality Account 2022/23 which is published on our website
The quality improvement priorities for 2022/23 were based around the three domains of our Trust’s Quality Strategy 2021/2024 In summary, the eight overarching quality priorities for 2022/23 were:
Domain: QUALITY PRIORITIES:
Priority 1: Learning from Events and Developing a Safety Culture
SAFE
Priority 2: The Deteriorating Patient
Priority 3: Inpatient Falls
Priority 4: Best clinical outcomes
EFFECTIVE
Priority 5: Right care, right place, right time
Priority 6: Learning from experience
PATIENT EXPERIENCE
Priority 7: Vulnerable patients
Priority 8: End of life care
Part 1: Performance Report 26
The Board of Directors considered the quality improvement priorities for 2023/24 at its meeting in April 2023. These nine priorities are detailed within our Quality Account 2022/23.
Financial Performance 2022/23
The operational planning process for 2022/23 returned to provision of a full year plan following the 2021/22 planning process which had been split into two halves
Building on the planning process in 2021/22, the Trust worked with system partners to develop a triangulated plan across activity, workforce and finance for 2022/23 in response to the following priorities set out by NHS England:
• accelerate plans to grow the substantive workforce and work differently as we keep our focus on the health, wellbeing and safety of our staff
• use what we have learnt through the pandemic to rapidly and consistently adopt new models of care that exploit the full potential of digital technologies
• work in partnership as systems to make the most effective use of the resources available to us across acute, community, primary and social care settings, to get above pre-pandemic levels of productivity as the context allows
• use the additional funding government has made available to us to increase our capacity and invest in our buildings and equipment to support staff to deliver safe, effective and efficient care.
The NHS continued to operate within a temporary finance regime for 2022/23 due to the COVID-19 pandemic. The Trust’s plan for 2022/23 was to deliver a deficit of £19.135m inyear, with a recurrent deficit of £32.663m.
The Trust recorded a full year deficit of £47.206m, £28.071m adverse to the £19.135m full year deficit plan, but in line with the revised forecast formally reported and agreed with NHS England at the end of quarter three The planned underlying deficit for the Trust, i.e. (the financial position after the removal of one-off income and expenditure items) was a deficit of £32.6m and the actual underlying deficit at the end of the year was £34.4m which is a deterioration driven by inflation.
The main source of income for the Trust was via contracting with commissioners for health
27
Part 1: Performance Report
care services. In 2022/23, most of the Trust’s income from NHS commissioners was in the form of block contract arrangements. The Trust receives block funding from its commissioners, where funding envelopes are set at an Integrated Care System level.
In 2022/23, the Elective Recovery Fund enabled systems to earn income linked to the achievement of elective activity targets including funding any increased use of independent sector capacity. Income earned by the system was distributed by local agreement and the Trust received £13.3m of funding to support elective waiting list recovery.
Within Trust expenditure, the largest category is pay expenditure totalling £411.1m which is equivalent to 69% of total operating expenditure. Other significant components include £93m on drugs and clinical supplies (16%) and estates and premises costs of £30.2m (5%)
The Trust invested £57.333m of capital expenditure on medical equipment, digital infrastructure, improvements to existing buildings and expansion of our estate during the financial year. £19.798m of the capital programme was funded through the Trust’s internally generated funds and the remainder of the capital expenditure of £37.535m
funded through Public Dividend Capital.
This funding has enabled the Trust to continue to improve and expand the physical estate and continue improvements in the Trust’s equipment and digital infrastructure.
of
Part 1: Performance Report 28
was
Total
2022/23 £'000 Income from patient care activities 523,227 Other Operating Income 33,378 Operating Expenses (596,088) Operating deficit (39,483) Other gains and (losses) (479) Deficit before interest (39,962) Investment income 604 Finance costs (212) Public dividend capital dividends paid (7,876) Retained deficit (47,446) Adjusted for: Impairments (289) Adjustments in respect of Donations / Grants 574 Remove net impact of inventories received from DHSC group bodies for COVID response (45) Adjusted financial performance (47,206)
£36.863m has been invested in the physical estate including the first phase of creation of offsite Community Diagnostic Centre (£5.280m) and offsite Renal Unit (£4.894m) at Telford; first phase of creation and expansion of Elective Centre at PRH (£14.526m) and continuation of the Hospitals Transformation Programme; purchase of additional equipment (£5.060m) and improvements to digital services (£15.410m), including Year 1 of Frontline Digitalisation Project (£6.049m).
The Trust continues to build on progress made in planning for 2023/24 to enable the delivery of the projects to be completed earlier in the financial year to allow for the management of the programme over the financial years, as required.
The Trust has collaborated with all system partners in the ICS to develop a triangulated system plan for activity, workforce and finance that is supported by the detailed work ongoing at Trust level.
Culture and Staff Engagement
Our culture journey has continued over the past twelve months. The focus is on improving working life at the Shrewsbury and Telford Hospital NHS Trust. The aim of our culture work is to enable the Trust to be a psychologically safe place to work, and for it to become the employer of choice within the region, a place where colleagues feel a sense of belonging.
The below diagram illustrates the Trust’s People Plan Winning Principles - these are the key areas highlighted in the People Strategy for the organisation. They are in place to ensure that we have direction and focus from the people perspective of the organisation. Under each principle there are actions and measures to ensure that we are delivering the strategy.
Part 1: Performance Report 29
The Trust’s People Plan Winning Principles:
Present in the strategy and everything we do, ‘The Golden Thread’.
All objectives and outcomes need to deliver the People Plan and link to the Winning Principles.

Consider and include the key elements of the Equality, Diversity and Inclusion Strategy.
To ensure all colleagues live and breathe the Trust’s values and are valued for their unique difference.
To demonstrate equitable and fair processes so that all colleagues feel valued and able to challenge discrimination.
To support the mechanisms in place to create, maintain and sustain a diverse and talented workforce
To ensure all patients receive the best quality care regardless of their protected characteristics.
Culture Dashboard
The Culture Dashboard continues to be a key metric for the focus on cultural transformation within the Trust from the staff survey results. The six key themes have enabled there to be a focused approach to support, and cultural interventions to drive, the increase in scores. To further support the governance around the cultural work, a Culture Group was established in August 2022. With key stakeholders taking ownership and accountability for
Part 1: Performance Report 30
the six key themes, we have been able to leverage our resources to the departments and areas that need more cultural transformation support. Each stakeholder is responsible for providing a progress update at each meeting In 2022 we have seen an increase since the 2021 results, as can be seen within the following graph:
The implementation of a Trust wide Civility and Respect programme began in September 2022, with a Board Development Session facilitated by Dr Chris Tuner, Helen Turner, FTSU Lead and Lisa Baker-Murray, Head of Culture. The next steps have been to train a team of facilitators to enable the sessions to be rolled out across the Trust. The focus of the sessions is on raising awareness about behaviours that do not meet with the Trust Values, enabling and allowing all colleagues to consider what changes they can make when they interact with their fellow colleagues to make the experience more civil and respectful.
Staff Awards
In November 2022, our Trust held its first Annual Recognition week where we celebrated all the amazing work our colleagues do. A Long Service, special afternoon tea was held where over 60 colleagues attended to receive thanks for having served 25-40 years at the NHS.
Part 1: Performance Report 31
20% 30% 40% 50% 60% 70% 80% Compassion Teamwork Health & Wellbeing Vision & Values Goals & Performance Learning and Innovation SaTH 2020 SaTH 2021 SaTH 2022
Throughout the week a number of presentations were given, our colleagues who had achieved Learning and Development goals were presented with achievement awards. Our Volunteers were thanked at a celebratory lunch, and we finished the week with a very moving service of thanks for Remembrance Day.
The Recognition week led in our virtual Trust Annual Awards. More than 400 nominations were received, with over 30 awards presented. Colleagues were given their awards in person by the executive directors, whilst the presentations were filmed and edited into an hour long ‘Staff Awards’ video which was live streamed, which added the surprise element for viewers with over 3,000 friends and colleagues able to watch the awards from anywhere.
A list of all our fabulous award winners can be found below:
Partnering
Emma-Jane Beattie and the Emergency Planning Team
Ambitious
Rachel Bl Healthcare Assistant, Pre-op PRH
Caring
Emma Hicks and Ursula Owen, Macmillan Clinical Specialist Occupational Therapists
Trusted
Rebecca Bromley, Patient Journey Facilitator
Learning and Development
Sian Burley, Advanced Practitioner and Lucy Celieski, Advanced Clinical Practitioner in Breast Imaging at RSH
Clinical Rising Star
Samantha Petridis from the neonatal unit at PRH
Non-Clinical Rising Star
Phil Evans, Administrator, Therapy Centre RSH
Quality Improvement Award
Leeanne Morgan, Falls Specialist Nurse from Corporate Nursing at RSH
Quality Improvement Award
Kev Malton, Porter from Medical Devices at RSH
Innovation Award
Devaki Nayak, Consultant Ophthalmic Surgeon from Ophthalmology at RSH
Part 1: Performance Report 32
Volunteer of the Year Award
Ethan Holmes, A&E at RSH
Partner of the Year Award
Steve Lovell from Ezec Medical Transport
Clinical Leadership Award
Hayley Pearson, Deputy Chief Pharmacist from Pharmacy at RSH
Non-Clinical Leadership Award
John Skelton, Head of Leadership and Organisational Development from the People and OD Directorate
Shropshire Star Public Recognition Award
Lorna McQuaid, Bank Healthcare Assistant at PRH
We continue to celebrate with colleagues who have reached 25 or 40 years working for the NHS by presenting them with their Long Service Awards. We are looking forward to continuing to recognise our colleagues throughout the year along with our Recognition Week and Trust Awards in November 2023.
We are incredibly proud of all of our colleagues who were nominated, or received, Trust awards during 2022/23
In the Summer of 2021 Her Majesty the Queen announced that the NHS would be presented with a George Cross to acknowledge the outstanding dedication, care and courage shown by NHS staff during the Covid-19 pandemic.
The award, created in 1940, sits at the top of the UK honour’s system joint with the military Victoria Cross and is the highest civilian gallantry award. It is given for acts of the greatest heroism or of the most conspicuous courage in circumstances of extreme danger. Our Trust produced a replica George Cross badge and as part of Recognition week, each member received a George Cross badge, this included our Bank Staff and our Volunteers.
Equality, Diversity and Inclusion
The Trust’s Equality Diversity & Inclusion Strategy was reviewed and refreshed in April 2022 and aligns with the Trust’s People Plan and our values, which remain at the core of everything we do.
Part 1: Performance Report 33
Our Annual Equality, Diversity & Inclusion (EDI) report provides to our Board of Directors a progress update of our ambition to make SaTH a great place to work and receive excellent care regardless of our protected characteristics. We continue to work to achieve everything we set out in 2022; our commitment to improve the working lives of our people and provide excellent care for the communities we serve remains.
The Trust has governance and regulatory frameworks and mechanisms in place to ensure that assurances are provided in relation to the discharging of our equality duties. We have three EDI Staff networks for disability (Disability, Ability and Wellbeing Network), race (Race and Equality Network) and LGBTQIA+ (SaTH Pride Network). Each staff network has an executive sponsor from the leadership team. We continue to work towards building EDI champions from Board to ward level on the principle of inclusivity. Our governance structure includes: the EDI Group which is chaired by the Medical Director for Strategy and Partnership and reports into the Operational People Group; and a Patient Advocacy Group which engages with our community with representation from the Patient Experience Team and Public Participation team via the Community Engagement Facilitator.
For our people, the aim is to ensure we create a positive working environment and promote a culture of trust where our people work together and feel motivated and confident to challenge and be innovative. A key objective is to recruit and retain a workforce which is representative of the communities we serve, and to provide an environment that values the differences people bring with them, where they feel safe and supported throughout their career.
The Trust has fourteen individuals who have been supported to become Cultural Ambassadors via the Royal College of Nursing (RCN) development programme, with two main purposes of recruitment and employee relations. Workforce are leading on the employee relations and have introduced a process for involving cultural ambassadors which will include running a refresher cohort of training via the RCN with support from the People Governance and Projects Manager. The ambassadors will work with us to improve recruitment and the employment relation experience and decision-making processes.
Part 1: Performance Report 34
For our patients, the aim is to ensure that we are working with our key partners to provide the best possible service to our communities, ensuring everyone has fair access to all services and always treating everyone with respect. The group will engage across Shropshire, Telford and Wrekin to deliver a service which meets the needs of communities, especially those that are seldom heard, to reduce health inequalities.
As part of the Trust’s Safer Recruitment Workshops, we continue to support the Disability Confident Scheme and our commitment to guaranteeing an interview for applicants who meet the essential requirements of the advertised role. We became a level 2 Disability Confident Employer in 2022 and are continuing review of our job adverts and templates to ensure they are fully inclusive in this way. We also continue to work with local partners to ensure we reach all communities to encourage and support careers in the NHS.
In November 2022, we launched our six months Leadership Programme for ethnic minority colleagues called ‘Galvanise’. This programme was provided with collaboration between the Equality, Diversity and Inclusion team, Leadership and Organisation Development team and a Trust junior doctor who was instrumental in initiating the idea of the programme. It incorporated mentor allocation both internal and external, monthly senior leadership activity with Trust Mentor, two-monthly personal mentor meeting, twomonthly action learning group sessions, two-monthly public board meetings, Strengths Deployment Inventory (SDI) self-scoring motivation assessment, 360 feedback and personal coaching, and personal reflection. This culminated in final essay and a closing celebration on the 22nd of March 2023.
Leadership and Organisational Development Leadership Development Framework
Our Leadership Development Framework is underpinned by our Values and Behaviours; this has continued to be reviewed and updated over the last 12 months. Our Framework identifies leadership development at different levels from aspiring leaders through to senior leaders. We offer both internal and external development programmes and apprenticeship routes in level 3 supervisory management, through to degree level and masters level management and leadership apprenticeship routes with Chartered Management Institute registration.
Part 1: Performance Report 35
The Framework provides opportunities to attend leadership modules and briefings including values-based interviews, emotional intelligence, resilience, coaching skills for leaders and new on-line modules via our talent and career portal.
Our new Galvanise programme for colleagues from ethnic backgrounds started in November 2022 with a pilot programme.
Our Improvement methodology also features as part of the framework, including an introduction to improvement, improvement fundamentals and improvement practitioner courses.
Leadership Courses
Our Leadership Programmes continue to be delivered throughout the year. For the first time we are in a position where all of our current cohorts for SaTH 1, 2, 3 and 4 programmes are being delivered by our internally trained facilitators.
In the last 12 months, we have introduced a new senior leadership and coaching programme for two cohorts.
We have been working with the Shropshire, Telford & Wrekin Integrated Care Board (ICB) on the High Potential Scheme for aspiring Directors. We have supported with recruiting to the programme, providing interview and psychometric feedback and identifying stretch placements.
Our Values Based Interviewing course continues to be popular and well received, over the last 12 months we have delivered SDI workshops, team development, away days and 360 feedback sessions. During March 2023 we re-launched emotional intelligence and resilience workshops. This year we have also re-launched our coaching skills for leaders’ course, co-facilitated by our ILM qualified coaches.
In November 2022, we commenced a pilot ‘Galvanise’ programme, aimed at colleagues from ethnic backgrounds. We are working in conjunction with one of our junior doctors and EDI lead to design and deliver the programme.
Performance Report 36
Part 1:
The Programme includes a launch event, action learning, SDI assessment and feedback, access to Board meetings, internal mentors, career coaching and external mentoring, concluding with a celebration event (pictured) on 28th March 2023 with final essays, presentations and certificates. Following some great feedback and a review we plan to deliver a further cohort from 27th September 2023.
Strive Towards Excellence Programme (STEP)

New for this year has been the launch of a pilot Strive Towards Excellence Management Skills Programme. Running alongside our leadership development framework, providing our managers with technical skills development and signposting during the first 6 months of employment and transitioning into leadership behaviours.


Part 1: Performance Report 37
Our ision To provide excellent care for the communities we serve
Part 1: Performance Report
The Strive Towards Excellence Programme is underpinned by our Values and Behaviours and supported by our leadership and management competency framework, to support our managers on their continued journey.
The final celebration and closure event was held in December 2022. Following review and evaluation, the next cohort open to all managers is planned to start on 24th April 2023.
Leadership Masterclasses
Our Leadership Masterclasses continue to be delivered at least once per month; topics have included compassionate, inclusive and effective leadership, improvement reporting, empathic listening, courageous conversations and resilience. Masterclasses are well received due to their accessibility, delivered via MS Teams during the lunchtime period.
Cultural Reviews and behaviour frameworks
Our cultural reviews and development of team-based behaviour frameworks has continued this year. We continue to deliver culture, values, behaviour and wellbeing sessions as part of the corporate welcome and induction sessions.
Coaching
Regular supervision is provided for our internal pool of ILM qualified coaches, this will be opened up to other coaches and master coaches. Structured coaching continues to take place as part of our programmes and independently.
Talent Management
Our approach to talent management has involved reviewing and replacing the previous appraisal guidance with new talent conversation documentation and guidance, informed by staff feedback.
This has coincided with our involvement in the scope for growth pilot programme and subsequent launch of career conversation briefings for our managers. During March 2023, we launched our talent and career platform, providing our people with access to career planning tools, self-assessments, events updates, wellbeing information and learning modules. Out talent conversations briefings will be launched later in April 2023.
38
Schwartz Rounds
Over the last year we have transitioned our work on ‘team time’ into ‘schwartz rounds’. A steering group meet on a monthly basis, and we have a number of trained schwartz facilitators who co-deliver rounds covering topics such as ‘mission impossible’, ‘when I have been racially harassed at work’ and ‘here we go again’. The rounds continue to gain momentum with the next one planned for May 2023 titled ‘a day I felt proud’.
SaTH Education
The main aim of our education function is to ensure colleagues feel there are opportunities to develop their career, they feel supported to develop to their potential and they are able to access the right learning and development opportunities when they need to, as measured by the NHS Staff Survey. Within the year we have seen progress against these measures:
There have been a number of interventions undertaken by the team to achieve this progress. In last year’s annual report, our main aim for SaTH Education was to have a successful introduction of our new Learning Management System. This was launched in April 2022 with the aim that the system would ensure visibility of staff training and support improvements with mandatory training compliance, and, in turn, improve quality and safety. In April 2023, 90% of our colleagues are registered on the system and our mandatory training compliance has risen above our target of 90% for the first time, as can be seen within the below graph:

Part 1: Performance Report 39
The team have also seen other successes in year including:
• Improved Health Education England (HEE) rating for our library function
• Increase in our apprenticeship levy spend
• Improvement in the proportion of healthcare support workers who have successfully completed their care certificates
• Designed and launched a prospectus for SaTH Education
• Moved our libray materials to the Health Libraries West Midlands system
• Rebranded to ‘SaTH Education’
• Trained all colleagues within Education in SaTH improvement methodology.
In the next 12 months we plan to continue to test changes, using structured improvement methodology to attempt to continue to improve against our agreed outcome measures for each service, and for the relevant staff survey questions.

Nurse Education
The pre and post registration nursing teams have undergone change and development in the last twelve months, in order to strengthen the structure and have the right expertise to deliver the work within their remits. The pre-registration team continue to support preregistration learners, trainee nurse associates and nurse degree apprenticeship students within the clinical learning environments across the Trust; whilst the post registration team deliver nurse preceptorship, core clinical skills training, OSCE preparation and transition
Part 1: Performance Report 40
for internationally educated nurses and also support with the health care support worker academy at Telford College. The intention is to create the first non-medical education annual report later in 2023, in conjunction with the director and deputy directors of nursing.
Medical Education
Director of Medical Education (DME), Dr Gordon Wood, was appointed in February 2023. This role has a strategic medical education focus and now oversees both undergraduate and postgraduate education. Dr Adrian Marsh has been appointed Clinical Tutor to work with the DME leading postgraduate education. The Hospital Dean Professor Koottalai Srinivasan will continue to lead undergraduate education. The Medical Education Team now seamlessly supports postgraduate education, undergraduate education, locally employed doctors and Advanced Care Practitioners (ACP).
Our ACP programme has been extremely successful. Currently there are 60 ACPs in post and it is estimated that overall workforce numbers will increase to 75 by 2024. There are also between 15-20 ACPs in training at any one time. The strategic direction for this service now sits under the Director of Medical Education and investment has been agreed to strengthen the current staffing model with a more robust governance structure. The ACP programme will expand further via the workforce modelling for the Hospital Transformation Programme.
The Clinical Fellowship Programme continues with a current headcount of 93 junior clinical fellows/locally employed doctors and 34 senior clinical fellows. Each of the 127 doctors has an allocated named supervisor, access to study leave, medical portfolio and bespoke induction programme that mirror that of postgraduate doctors in training. The programme offers access to study leave for doctors on a 12-month contract and a fully funded postgraduate certificate in clinical medicine through Keele University for those clinical fellows who wish to enrol. 15 places per year are made available.
Freedom to Speak Up
The Freedom to Speak Up (FTSU) team is made up of a FTSU Lead and two FTSU Guardians, one of whom is on a fixed-term appointment. Supporting the team are approximately 35 ambassadors whose role is to promote FTSU and signpost colleagues whose experience ranges from a variety of clinical and non-clinical backgrounds and who represent the diversity of the workforce across our Trust. The ambassadors undertake these roles on a voluntary basis in addition to their substantive posts.
Part 1: Performance Report 41
The Freedom To Speak up Vision and Strategy 2022-25 was published in October 2022 following approval by the Board of Directors with nine priorities and a focus on four of those during 2022/23:
Priority 1 Ensure all groups who face barriers to speak up are supported with a focus on people of colour (BAME):
• We led the 30 Voice project to highlight the lived experience of BAME colleagues and improvements in tackling racism.
Priority 2 Ensure FTSU processes are fit for purpose in line with best practice:
• Internal audit of all processes with associated actions was undertaken.
Priority 3 Working with leaders to listen up and follow up:
• We developed the managers handbook and was one of the first trusts to mandate the FTSU online training, speak up, listen up and follow up.
Priority 4 Alongside our cultural team, lead the civility and respect social movement:
• Over 500 people within the Trust have taken the Civility and Respect workshops.
During 2022/23, 282 concerns were raised through the FTSU mechanism to the FTSU team, a decrease of 24% on the previous year.
FTSU concerns raised by quarter and year:
Part 1: Performance Report 42
Q1 Q2 Q3 Q4 Total number of concerns raised % Increase /decrease on previous year % National Average Increase/ decrease 2022/23 71 73 79 59 282 24% Not yet available 2021/22 100 113 90 66 369 22% 0% 2020/21 41 82 103 78 304 108% 33.7% 2019/20 22 17 57 49 145 120% 32% 2018/19 10 18 18 20 66 106% 73% 2017/18 4 7 12 9 32 N/A N/A
During 2022/23, 34% of the concerns brought to the attention of our FTSU teams were relating to behaviours/relationships, 22% of concerns raised were regarding worker safety and wellbeing, 21% related to concerns about patient safety, 12% of concerns were associated with systems and processes, and 11% to bullying and harassment. All the concerns raised were escalated.
Of those speaking up, 29% were nurses and midwifery registered; 19% administrative colleagues; 14% estates and ancillary; 12% allied health professionals; 11% medical and dental; 8% additional clinical services; 5% unknown or other; and 2% additional clinical services and healthcare scientists.
The senior FTSU team has continued to work closely during the year with colleagues, including the executive team, non-executive directors, the senior nursing team, unions, workforce department, organisational improvement team, the Guardian of Safe Working and numerous clinical colleagues including junior doctor forums.
Sustainability Report Climate Change
Our everyday activities are having a profound impact on the environment with irrevocable consequences - biodiversity loss and mass extinction, plastics in our food chain, acidification of our seas and climate change that will bring about frequent and often disastrous weather events. We must therefore maintain momentum in minimising our contribution to carbon in the atmosphere, products that persist in nature, and the destruction of other species due to loss of natural habitats. Extreme weather events and infectious diseases are now a very real and tangible part of our lives. Human activities have already set in motion these occurrences and therefore, we must adapt.
The NHS is responsible for circa 4% of the nation’s carbon emissions. In October 2020, NHS England published ‘Delivering a Net-Zero National Health Service’, a report that details the scale of the environmental problems faced by the NHS and the country. This report set ambitious targets requiring all NHS organisations to become net zero by 2040 for the NHS Carbon Footprint, and by 2045 for the NHS Carbon Footprint Plus.
Part 1: Performance Report 43
Green Plan
An organisational Green Plan has been approved by the Board of Directors. In addition, the Shropshire, Telford & Wrekin Integrated Care System Green Plan 2022-2025 has been developed and co-ordinated by the ICS Climate Change Group and was supported by the Board of Directors on 9 June 2022. The system plan brings together organisational green plans in the system. This document forms the basis for performance against the national climate change agenda and is the base for co-operation between system partners. The ICS Climate Change Group is also developing a system-wide Carbon Footprint assessment which will support the prioritisation of work going forward.
Measuring sustainability
One of the ways we have measured our impact is through the Green Plan. The trust has undertaken risk assessments and has a Trust Green Plan which takes account of UK Climate Projections 2018 (UKCP18).
NHS England is developing a new tool which the Trust is currently piloting and will be adopted when it is officially launched.
Carbon Management
The Trust has procured REGO-certified renewable energy over the past 4 years and will continue to do so into 2023/24. The Trust will continue to procure zero emissions from electricity imported from the national grid.
We have continued to invest in our Business Management System (BMS) utilising computerised control systems to reduce any unwarranted use of energy in the Trust’s hospitals. We are therefore able to identify trends in energy consumption enabling better prediction of energy need and therefore more effective utilisation of the Combined Heat and Power (CHP).
Energy Management
A Decarbonisation Strategy for Shrewsbury Hospital site has been developed and will inform future site infrastructure and backlog programmes. It also includes a proposal for a new zero carbon energy centre and heat network. We have also implemented electric vehicle charging points at our Royal Shrewsbury Hospital (RSH) site and developing the infrastructure at our other sites, and conversion of our fleet cars to become electrically powered, is also being explored.
Part 1: Performance Report 44
At our RSH sites we have installed photovoltaics on two areas – ward 37 and outpatients roof. There are plans for 2023/24 to expand this initiative further and across other sites.
Energy Usage
The general pattern of energy consumption for the Trust is included in the following table. Electricity usage overall has increased slightly compared to 2021/22 and could be attributed to the reintroduction of services following the COVID-19 pandemic, with more staff returning to work on site. Whilst the cost of energy has increased compared to 2021/22, we also expect a further inflation in energy prices as a result of international cost pressures

Waste
The Trust continues to ensure compliance with disposal of its waste. All our domestic waste is sent to an energy recovery facility to generate electricity. The Trust is piloting a recycling scheme for dry mixed recycling and continues to segregate recyclable material, such as metal and cardboard, where possible.
Part 1: Performance Report 45
The waste figures for 2022-2023 at our acute sites are:
Following the introduction of the Clinical Waste Strategy in March 2023, the Trust is recruiting a Waste and Energy Manager to reduce our clinical waste in line with the current Health Technical Memorandum requirements.
The Trust also takes an environmentally friendly approach towards the disposal of ‘sharps’ waste, by employing a greener approach with the use of re-used sharps containers. Through this method, the Trust saved 44 tonnes of single use plastic bins from being burnt, leading to saving 252 tonnes of carbon dioxide by using this process.
A furniture reuse system is in place across our sites to enable staff to internally exchange furniture between departments. Fourteen percent of staff are now active members of this reuse, reduce furniture and office stationery scheme. We are proud of the fact that use of this scheme saved the Trust £40,000 and 16 tonnes of carbon dioxide.
Transport
The daily commute of our staff has a huge impact on the local environment in terms of vehicle numbers, noise, air quality and the demand for parking. We have a car-share web portal to encourage staff to share their commute and we also actively encourage staff to use public transport and the local cycle routes as means to get to work.
Approximately 27% of staff choose not to bring their car to work, and instead use buses, cycles, shared lifts, orwalking. The recent staff travel survey showed an increase in numbers not bringing their cars to works and an increase in staff walking from 6.8% to 7.5%.
46
Part 1: Performance Report
Waste bag type Royal Shrewsbury Hospital The Princess Royal Hospital Yellow bags 104,951.79 kg 65,381.50 kg Orange bags 566,759.22 kg 557,587.65 kg Tiger bags 6,187.45 kg 5,998.88 kg TOTAL: 677,898.46 kg 628,968.03 kg
Like most sectors, the Trust has also seen a significant increase in staff who can work from home, being able to do so, for at least part of their working week. The Trust’s 2021 Staff Travel survey indicated that pre-pandemic 4.7% of staff worked from home, although this rose to 17% of colleagues now working one or more days from home.
To help all visitors to find their way around the Trust, including our staff, a successful mapping project was carried out on Google Maps. So far, the mapping edits to the Trust sites have generated over 2 million views. For example, the newly created Captain Tom’s Garden has received 5,526 views and the RSH A&E has received 215,839 views.
47 Mode Share Travel Table Response Mode Share % Travel Mode 2011 2015 2018 2019 2021 2022 Walk 4.7% 7.8% 7.8% 8.0% 6.8% 7.5% Cycle 1.3% 5.5% 3.8% 5.9% 6.5% 3.9% Cycle Train not recorded 0.6% 0.3% 0.0% 0.0% 0.0% Electric Bike not recorded not recorded not recorded 0.2% 1.1% no data Bus 1.6% 2.8% 3.1% 3.1% 4.1% 4.4% Train 1.2% 1.2% 0.4% 0.5% 0.5% 0.3% Motorcycle 0.1% 0.3% 0.4% 0.7% 0.9% 0.5% Lift in car that than goes elsewhere not recorded not recorded 0.6% 1.7% 2.9% 1.8% Taxi not recorded not recorded 0.5% 0.7% 0.9% 1.8% Car Share 4.6% 3.3% 3.9% 4.0% 2.0% 5.0% SOV-Single Occupancy Vehicle 86.5% 73.1% 77.8% 75.2% 74.4% 73.0%
Part 1: Performance Report
Biodiversity
To enhance our Biodiversity across the Trust we have a Biodiversity and Green Space Strategy which links to our Trust and System-wide Green Plans.
Our planting includes more pollinators to attract butterflies, bees and insects.
Louise Barnett, Chief Executive Officer
15 June 2023
Part 1: Performance Report 48
Part two: Accountability Report
49
Corporate Governance Report
The Directors Report
The Board of Directors present their report and audited financial statements for the financial year ended 31 March 2023.
In accordance with its Establishment Order, the Board of Directors comprises seven nonexecutive directors and five executive directors, one of whom is the Chief Executive. All Directors are required to comply with Trust policies, including the need to declare any actual or potential conflict of interest, and must comply with the Fit and Proper Persons Test requirements.
Whilst non-executive directors are not employees of the Trust and are appointed to provide independent challenge to the Board of Directors, each board member brings a variety of individuals skills and experience to the Board.
Directors serving during the year were:
Non-executive directors (voting Board members)
Dr Catriona McMahon
Dr McMahon is Chair of the Trust, and chairs the Board of Directors, the Trust’s Remuneration Committee, and, jointly with Maxine Mawhinney the Trust’s Ockenden Report Assurance Committee.
Dr McMahon is passionate about the NHS, patient access to innovation and excellence in patient care. Her professional background includes anaesthetics / critical care and, from 1998, pharmaceutical medicine. She is currently the Lead Industry Member on the Scottish Medicines Consortium (SMC), where she works with both SMC and the pharmaceutical industry on health technology assessment and continuous process improvement. She is a former member of the Institute of Health and Care Excellence (NICE) Appeals Panel and NICE Neuroscience Guidelines Review Panel.
Before leaving the pharmaceutical industry to set up her own consultancy, she worked closely with the NHS to advance commercial clinical research in our healthcare system, including acting
Part 2: Accountability Report 50
as co-chair of the Ministerial and Industry Strategy Group (MISG) Clinical Research Working Group (2012 - 2014).
She is also a Non-Executive Director for University Hospitals Birmingham NHS Foundation Trust and owner of, and executive coach within, her own coaching business, specialising in supporting the development and delivery of senior leaders in the healthcare and life science sectors.
Dr McMahon attended Edinburgh Medical School and, prior to joining the pharmaceutical industry, she practised anaesthetics and critical care medicine in the north-east of England for nine years. She is a Fellow of the Faculty of pharmaceutical Medicine and holds a Master of Public Health (Healthcare Management; Liverpool University) and a Masters in Science (Executive Coaching; Ashridge Business School).
Teresa Boughey
Mrs Boughey is the Chair of our Charitable Funds Assurance Committee, and member of our Finance and Performance Assurance Committee, Quality and Safety Assurance Committee, and Remuneration Committee.
She is the founder and CEO of Jungle HR, a national, award-winning strategic HR consultancy, and has more than 25 years’ of HR experience at senior manager and director level after working across a variety of sectors. Mrs Boughey is a Business Board member of the All-Parliamentary Group for Women and Enterprise, chairing the Environmental, Social and Governance (ESG) Workstream, and is also a Board Advisor at Royal Holloway University, School of Business & Management. She has authored the Amazon number 1 bestselling book, ‘Closing the Gap – 5 Steps to Creating an Inclusive Culture’.
Mrs Boughey is a Chartered Fellow of CIPD, a member of the Institute of Directors and holds an MA in Human Resource Management. The Board appointed Mrs Boughey to the role of Senior Independent Director and Non-Executive Director lead for Doctor Case Management on 8 December 2022.
Part 2: Accountability Report 51
David Brown
Mr Brown is a member of our Audit and Risk Assurance Committee, Finance and Performance Assurance Committee, Quality and Safety Assurance Committee, and Remuneration Committee.
Since retiring from military service in 2000 as a Colonel, Mr Brown has gained senior executive experience as an MD and CEO in the engineering, and oil and gas sectors. Since 2014, he has run his own consultancy, specialising in business turn-around, management of change, strategic assessment and improving staff motivation.
Mr Brown graduated from the University of London with a BSc Hons in Geology, and has an MSc in Guided Weapons Technology, and and MSc in Business Management, as well as a PGDip in The Management of Change. He is a Fellow of the CMI and a Chartered Manager, as well as being a member of the Institute of Directors.
Mr Brown is also Chair of the Trust’s Organ Donation Group, and from January 2022, the recently established Public Assurance Forum .
Raj Dhaliwal (from 1 May 2022)
Raj has almost 20 years of banking experience, having covered roles across multiple disciplines and geographies.
Recently he led lending operations for business banking and mortgages, being responsible for ensuring over £36bn of lending approvals were safely disbursed within a controlled manner.
Currently he is Head of Group Change Risk owning the global Policy and Standard specifically for Technology Change.
Outside Raj spends time between volunteering as a special constable for West Midlands Police.
Part 2: Accountability Report 52
Rosi Edwards (From 1 June 2022 as associate non-executive director and substantial non-executive director from 1 February 2023)
Ms Edwards joined the Trust in June 2022. She has chaired the Trust’s Quality and Safety Assurance Committee from February 2023 and is a member of the Audit and Risk Assurance Committee, the Remuneration Committee and Charitable Funds Committee. At system level, she attends the Shropshire, Telford and Wrekin Integrated Care System Quality and Performance Committee.
She was previously a Non-Executive Director at the Royal Wolverhampton NHS Trust, from 2013 to 2021, where she chaired the Quality Governance Assurance Committee and was a member of the Audit Committee, Remuneration Committee and was NED lead for learning from Deaths, End of Life Care and Freedom to Speak Up.
During a career of over 30 years as a regulator in occupational health and safety and health, starting as HM Inspector of Factories and eventually as Regional Director for Wales, Midlands and the Southwest in the Health and Safety Executive, she developed practical expertise in risk management and the assessment of organisations’ ability to manage risk.
She speaks French and Italian and was appointed chair of a tripartite committee of international experts for the International Labour Organisation, producing within a tight schedule an agreed Code of Practice on Safety in the Use of Machinery, has worked as an Occupational safety and Health consultant for the Organisation for Economic Co-operation and Development on a project to streamline the regulatory system in Italy, and has been an Executive Reviewer for the Care Quality Committee.
She is Honorary President of Birmingham Health Safety and Environment Group, a wellregarded occupational health and safety group covering organisations in West Midlands.
Professor Trevor Purt
Professor Purt is the Chair of the Audit and Risk Assurance Committee, member of the Trust’s Ockenden Report Assurance Committee, and the Remuneration Committee.
He is both a Chartered Engineer and Chartered Surveyor after having initially trained in architecture. Professor Purt has been a CEO or equivalent both in the public and private
Part 2: Accountability Report 53
sectors for over 25 years, and as a senior NHS leader he has led some of the largest NHS organisations in the UK with experience from both the provider and commissioning sectors, as well as working at both regional and national levels, including ICS development.
Professor Purt’s last role was in the private sector where he was Vice President for IBM Watson’s Healthcare Consultancy business for Europe, the Middle East and Asia, with a specific remit around population health and wider health and social care system integration and service reconfiguration.
In addition, Professor Purt was a Secretary of State appointee to the NMC, has served as a trustee and board member of the NHS Confederation, and The Prince’s Trust.
Associate non-executive director (non-voting)
Dr Tim Lyttle (from 1 March 2022)
Joining the Trust on 1 March 2023, Dr Tim Lyttle is an Associate Non-Executive Director and Non-Executive Maternity and Neonatal Safety Champion. He has 25 years of clinical experience as a GP and has also served in several Board level medical leadership roles, including Wrexham Local Health Board and Shropshire Clinical Commissioning Group. Between 2017 and 2021, Dr Lyttle provided strategic leadership in the mergers of three small “at risk” GP practices in Whitchurch with Ellesmere Medical Practice to create a more sustainable practice, namely Churchmere Medical Group.
Dr Lyttle continues as Clinical Director of North Shropshire Primary Care Network, supporting the development of 7 GP practices. He is also developing a role with the Integrated Care System supporting senior GP retention, and additional specialist skills in leadership creativity and holistic well-being.
In addition to being a graduate of Queen’s University Belfast, Dr Lyttle is a member of the Royal College of GPs and has completed an Ashridge diploma in leadership for quality improvement, a post graduate degree in psychology and a diploma in psychotherapy.
Non-executive directors who left during the year:
Tony Bristlin, non-executive director - was the Deputy Chair of the Trust until 30 April 2022 when he stepped down from his role to take up a new opportunity closer to his own community.
Part 2: Accountability Report 54
Mr Bristlin was a member of the Audit and Risk Assurance Committee, the Quality and Safety Assurance Committee, the Remuneration Committee, the Quality Improvement Committee in Common, and the Trust’s Ockenden Report Assurance Committee. He was also the Trust’s non-executive Maternity Champion
Dr David Lee, non-executive director - was the Senior Independent Director, Chair of the Quality and Safety Assurance Committee, and member of the Audit and Risk Assurance Committee, the former Quality Improvement Committee in Common (to April 2022), and the Remuneration Committee. David left on 2 December 2022
Professor Clive Deadman, non-executive director - was Chair of the Finance and Performance Assurance Committee, and a member of Quality and Safety Assurance Committee, and Remuneration Committee. He left the Board 31 December 2022.
Professor Julie Green, associate non-executive director (non-voting) - was Associate Non-Executive Director and Maternity and Neonatal Safety Champion from 1 May 2022 to 28 February 2023.
Executive directors (voting Board members)
Louise Barnett – Chief Executive Officer
Mrs Barnett joined the Board of Directors as Chief Executive Officer (CEO) in February 2020, bringing with her extensive experience as both a CEO and board level director, having worked in both public and private sector organisations. She is also the Accounting Officer of the Trust and is accountable to Parliament.
Mrs Barnett is committed to addressing health inequalities and to working in partnership with stakeholders across Shropshire Telford and Wrekin Integrated Care System (ICS), and further afield, to improve health outcomes for the communities served by the Trust.
She is passionate about supporting teams and creating a positive and inclusive environment for all, where colleagues feel truly valued, and where patients receive excellent care.
Part 2: Accountability Report 55
Supporting a number of national and regional leadership programmes, Mrs Barnett is committed to developing leaders of the future to support the effective provision of sustainable high quality integrated services for our communities.
Hayley Flavell – Director of Nursing
A Registered General Nurse with over 30 years’ experience of working in the NHS, Mrs Flavell has broad experience of working as a senior nurse leader in a variety of acute hospital trusts and joined us from the University Hospitals Birmingham NHS Foundation Trust.
Originating from the West Midlands, Mrs Flavell is passionate about providing our patients and their families with high quality, safe and responsive care. She believes that this can be achieved only by listening to our patients, communities and growing and developing a workforce that is fit for purpose now, and in the future, and by leading others to be able to deliver to the best of their ability at all times. She can often be found on wards and in clinical areas whenever she has a spare moment, to listen to staff and patients about their experiences of being at the Trust.
Sara Biffen – Chief Operating Officer
Ms Biffen joined the NHS in 1986, the last 16 years of which have been at senior manager level at the Trust. She has worked operationally with clinical teams across several specialties/areas and was the Assistant Chief Operating Officer for Planned Care for 5 years.
Ms Biffen was appointed to the Deputy Chief Operating role in February 2016, where she led on 18-week RTT and cancer improvement and worked with the Divisions to improve emergency planning and business continuity. She took up her current role of Acting Chief Operating Officer in March 2022 before which, she covered the Divisional Director of Operations for Medicine and Emergency Care and was the senior responsible officer (SRO) for urgent and emergency care.
Helen Troalen – Director of Finance
Ms Troalen joined the NHS in 2003 as a graduate trainee and qualified as a management accountant in 2007. Her career has spanned nearly twenty years in the NHS with roles in both the provider and commissioner sectors. She has also worked in a regional role at NHS London. Prior to joining the Trust, Ms Troalen was Deputy Chief Financial Officer at The Royal Wolverhampton NHS Trust for four years. Prior to that she was the Deputy Chief Finance Officer
Part 2: Accountability Report 56
at a large collaborative of clinical commissioning groups in north-west London, also for four years.
Ms Troalen has a particular focus on improving services for patients and the role that robust financial stewardship can play in effective organisations. Being involved in the redesign of stroke and major trauma services in London remains a particular career highlight.
Dr John Jones – Medical Director
Dr Jones has lived in Shropshire and worked at the Trust for almost 20 years, primarily as a consultant physician and gastroenterologist.
Dr Jones was an undergraduate at Christ's College Cambridge University and then a clinical student at Oxford University. He has worked in hospitals in Gloucester, Oxford, Stoke-onTrent and the East Midlands before moving to Shropshire after completion of his PhD.
He has strong interest in medical education and regulation and carries out a number of roles for the GMC including as an educational visitor for new medical schools. He led the introduction of the first Keele University curriculum to our hospitals. He has previously worked for the Parliamentary and Health Service Ombudsman in Manchester.
Although the majority of Dr Jones’ time is now spent in the executive role, he continues in clinical practice with a particular focus on specialist endoscopy for patients with suspected cancer.
Executive directors (non-voting)
Rhia Boyode – Director of People & Organisational Development
Rhia has spent most of her career in Organisational Development in the private sector supporting Global FTSE companies.
She went on to pursue a career in Human Resources which progressed to her leading the full range of HR and OD services for many years as a Head of HR Globally within Transportation, Automotive and Aerospace before joining the NHS as a Deputy Director going on to become a Board level Executive Director.
Part 2: Accountability Report 57
She has a Master of Science degree in Human Resource Management from Salford University of Manchester (Business School) and is a Fellow of the Chartered Institute of Personnel and Development (CIPD).
In addition to her role at The Shrewsbury and Telford NHS Trust, Rhia is Co-Chair of the West Midlands NHS Providers HRD Network.
Nigel Lee – Chief Operating Officer – Interim Director of Strategy & Partnerships
Beginning his career as a helicopter pilot in the RAF both in Search and Rescue and as part of Special Forces, Mr Lee served in Northern Ireland, the Falkland Islands and Iraq. He completed tours in the Defence Procurement Agency and Ministry of Defence on major programmes and strategic planning, before starting his healthcare career in 2006 as a hospital director for a BUPA hospital in the Wirral. From there, he became divisional director at Alder Hey Children’s Hospital and Aintree University Hospital.
Mr Lee has had senior operational roles with the Cheshire and Merseyside Major Trauma Network as well as a range of service configuration developments in the Merseyside area. Before joining the Trust in March 2018 as the Chief Operating Officer, Mr Lee was working in his role as Director of Secondary Care for the North Wales Health Board, where he was responsible for four hospital sites, women’s services and the specialist cancer centre. He led elective and diagnostics improvement projects and played a lead role in the whole-system urgent and emergency care development programme.
On 13 March 2022, Mr Lee moved from his executive COO role and took up an interim role as Director of Strategy & Partnerships, to concentrate on progressing the Trust’s strategic work and development of integration with the Integrated Care system.
Anna Milanec – Director of Governance & Communications
During her career, Ms Milanec has gained both public and private sector experience in highly regulated environments, working both at home and abroad.
Beginning her working life in the global financial services sector, Ms Milanec worked as part of specialised compliance and governance teams, within portfolios encompassing multi-national organisations that required adherence to international law and regulatory requirements.
Part 2: Accountability Report 58
(Membership of the Chartered Institute for Securities and Investment was allowed to lapse upon leaving the finance industry, relocating to England, and joining the NHS in 2010.)
Since that time, Ms Milanec has supported Boards of Directors to improve their governance, risk and compliance frameworks. She has successfully led two NHS organisations to eliminate existing governance conditions on their Provider Licences. In November 2020, Ms Milanec joined the Trust to support it with its own improvement journey.
Ms Milanec is a Fellow of the International Compliance Association, a Chartered Governance Professional and Fellow of the Institute of Governance Professionals. She also holds a MSc in Corporate Governance and Administration.
Inese Robotham – Assistant Chief Executive (from 13 March 2023)
Ms Robotham joined the Trust in March 2023 from Swansea University Health Board where she was in the role of Chief Operating Officer, and she has held similar roles in Dorset County Hospital NHS Foundation Trust and Worcestershire Acute Hospitals NHS Trust.
Ms Robotham started her NHS career in 2001 as an Information Analyst and then progressed through a number of operational management and leadership posts. With over twenty years NHS experience in both high performing and challenged organisations, Ms Robotham brings a wealth of knowledge and expertise across a number of areas including partnership working, operational delivery and large-scale transformational change.
Ms Robotham holds a MSc in Leadership for Healthcare Improvement from the University of Birmingham and is passionate about creating the conditions for continuous improvement and enabling staff to deliver the best possible care to the local communities.
Executives who left during the year:
Dr Richard Steyn was Co-Medical Director (non-voting) until 31 March 2023.
Part 2: Accountability Report 59
The Board of Directors and Meetings
The Trust is governed by the Board of Directors. The overarching governance arrangements are described in detail within the organisation’s Standing Orders, Standing Financial Instructions and the Scheme of Delegation
The Chair proactively encourages Board members to constructively challenge and explore proposals made to the Board and assist in developing proposals on strategy, priorities, risk mitigations and standards.
Standing items on the Board meeting agenda relate to strategy, governance, patient feedback, quality of care, people issues, integrated performance and summary reports of meetings of the Board’s assurance committees. The Board Assurance Framework is also reported on a quarterlybasis as a standing agenda item and outlines the risks to achievement of the organisation’s goals/objectives Detailed reports have been received by theBoardon a broad range of other strategic issues during the year.
The importance of the triangulation of understanding, challenge and assurance between Committees is recognised and reflected through cross-membership and reporting between the groups and through the receipt of summary reports to the Board of Directors. Like other NHS organisations, meetings of the Board of Directors are usually held in public, but due to pandemic regulations, they were live streamed to members of the public throughout the financial year. The Board returned to meeting face-to-face in December 2022 and continues to live stream the meetings with the public. Members of the public can send in questions for the Board, the answers to which are then reported on the Trust website. Board papers are also published monthly on the Trust website before the meetings and can be found by following this link: https://www.sath.nhs.uk/about-us/trust-information/board-papers/
Part 2: Accountability Report 60
The Board of Directors formally met twelve times during the year:
The Board received reports from four committees chaired / co-chaired by the Non-Executive Directors:
Audit and Risk Assurance Committee
Quality and Safety Assurance Committee
Finance and Performance Assurance Committee
Ockenden Report Assurance Committee
In addition, the Trust has:
• a Remuneration Committee, its membership being made up of all the non-executive directors and chaired by the Trust Chair, with delegated authority to make decisions on behalf of the Board.
• a People Committee, made up of the members of the Board. This will change to a People & Organisation Development Assurance Committee during 2023/24.
• a Charitable Funds Assurance Committee, which reports to the Board when the Board meets as the Corporate Trustee of charitable funds.
61
Part 2: Accountability Report
Meeting Dates 14 Apr 2022 12 May 2022 9 Jun 2022 15 Jun 2022 14 July 2022 11 Aug 2022 7 Oct 2022 10 Nov 2022 8 Dec 2022 12 Jan 2023 9 Feb 2023 9 Mar 2023 Voting Board Members: Catriona McMahon √ √ √ √ √ √ √ √ √ √ √ √ Louise Barnett √ √ √ √ √ √ √ √ √ √ √ √ Sara Biffen x √ √ x √ √ √ √ √ √ √ √ Teresa Boughey √ √ x x √ x √ √ √ √ √ √ Tony Bristlin √ David Brown √ √ √ √ √ √ √ √ √ √ √ √ Clive Deadman √ √ √ x √ √ √ √ x Hayley Flavell √ √ √ √ √ x √ √ √ √ √ √ Dr John Jones √ √ √ √ √ √ √ x √ √ √ √ Dr David Lee √ √ √ √ √ √ √ √ Helen Troalen √ √ √ √ √ x √ √ x √ √ √ Trevor Purt √ √ √ √ √ √ √ √ √ √ √ x Raj Dhaliwal √ √ x √ √ √ √ √ √ √ √ Rosi Edwards √ √
Audit and Risk Assurance Committee
The Committee’s principal function is to assure the Board on the adequacy and effectiveness of the Trust’s system of internal control and its arrangements for risk management, integrated governance processes, financial reporting and ensuring that the organisation operates effectively.
The Committee met regularly throughout the year. Chaired by Non-Executive Director Professor Trevor Purt, the Committee comprises three Non-Executive Directors (including the committee chair). The other committee members during the year and their attendance are shown below:
* Full member of the committee from February 2023.
The priorities for the Committee are to monitor the integrity of the Trust’s financial statements and to review the Trust’s financial and non-financial controls and management systems.
TheCommitteereceives regularreportsfromthe Trust’s internal and external auditor and from the local counter fraud service. Executive directors and subject matter experts normally attend the meetings as well as the external auditor, KPMG LLP, and internal auditors, Merseyside Internal Audit (MIAA)
The Committee reviewed and updated its terms of reference during the year, which were approved by the Board in October 2022. It also reviewed the Trust’s Standing Financial Instructions, Standing Orders and Scheme of Reservation and Delegation, which were
Part 2: Accountability Report 62
2022/23 Meeting Dates 6 Apr 2022 4 May 2022 15 June 2022 8 Aug 2022 5 Oct 2022 30 Nov 2022 1 Feb 2023 Committee Members: Professor Trevor Purt (Chair) √ √ √ √ √ √ √ David Brown √ √ √ √ √ √ √ Dr David Lee x x √ √ √ √ N/A Rosi Edwards* N/A N/A √ √ √ √ √ Regular attendees: Helen Troalen √ √ √ √ √ √ √ Anna Milanec √ √ √ √ √ √ √
approved by Board in December 2022.
The Committee receives and monitors the policies and procedures associated with counter fraud and corruption An independent local counter fraud service provided by MIAA produces an anti-fraud progress report giving updates on both reactive and proactive work undertaken in the Trust. The Anti-Fraud Work Plan was subject to approval by the Audit and Risk Assurance Committee.
The purpose of internal audit is to provide the Trust, via the Audit and Risk Assurance Committee and the Chief Executive, with an independent and objective opinion on risk management, control and governance and their effectiveness in achieving the Trust’s agreed objectives. To provide this opinion, the internal auditor reviews the risk management and governance processes annually within the Trust and usually on a three-year cyclical basis the operation of internal control systems within the Trust. Further detail regarding the work of the internal auditors is included within the Annual Governance Statement.
External Auditors’ Remuneration
Fees payable to the external auditors (net of VAT) during the year for statutory audit services amounted to £116,000 (2021/22: £109,000). No additional work was undertaken by the external auditors for the Trust.
Public Sector Payment Policy – Better Payment Practice Code
In accordance with the Better Payments Practice Code and government accounting rules, the Trust’s payment policy is to pay creditors by the due date, or within 30 days of receipt of a valid invoice, (whichever is the later) unless other terms have been agreed.
In 2022/23, the Trust paid 66.4% (2021/22: 86.7%) of non-NHS trade invoices within target, and 61.4% (2021/22: 89.7%) of NHS trade invoices within target. More details can be found in note 48 to the accounts.
Fraud, Bribery and Corruption
The Trust’s Anti-Fraud, Bribery and Corruption Policy & Response Plan was updated in September 2021 and sets out the arrangements that the Trust maintains to deter, prevent, detect and investigate instances of fraud, corruption and bribery carried out against the Trust, and the
Part 2: Accountability Report 63
wider NHS. The policy was approved by the Board in January 2022 on a 3-year review and has been reviewed to confirm no further update is required during the year 2022/23.
The Trust has a qualified Local Counter Fraud Specialist (contracted from MIAA) that supports the Trust in reducing the risk of fraud through annual fraud risk assessment, which informs an annual Anti-Fraud Work Plan. The Anti-Fraud Work Plan is subject to approval by the Audit and Risk Assurance Committee, with Anti Fraud Progress Reports and an Annual Report presented to Audit and Risk Assurance Committee throughout the year.
Modern Slavery
Under Section 54 of the Modern Slavery Act, we are committed to ensuring that employees of the Trust are not exploited, that they are safe, that they have the right to work and remain in the country, and that their employment standards and human rights are adhered to. The Trust expects the same from its suppliers and is committed to working with them to ensure any issues are identified and proactively managed. Some controls in place include:
Employment checks of individuals and of agencies which supply temporary staff
Use of NHS General Terms and Conditions of Contract for Goods and Services which cover all suppliers to the Trust including medicines
Due diligence within our procurement and tendering processes to test that selected suppliers and third parties are complaint with the legislation.
Declaration from Directors as to audit information
The Directors are responsible for preparing the Annual Report and Accounts and consider the report to be a fair, balanced and understandable account of the performance for the year ended 2022/23
Each director knows of no information which would be relevant to the auditors for the purpose of their audit report and of which, the auditors are not aware and, that they have taken all the steps that he or she should have taken to make him or herself aware of any such information and to establish that the auditors are aware of it
Register of Interests
Directors are asked to declare any interests that are relevant or material on appointment and as soon as possible should a conflict arise during their term. The agendas of the Board and
Part 2: Accountability Report 64
meetings of its committees contain an item allowing directors to declare any interests which may conflict with the scheduled meeting business. The Board of Directors receives the Board member interests at itsmeeting held in public on a twice annual basis. The Register of Interests and Register of Gifts and Hospitality has been updated and maintained during the year, presented to the Audit & Risk Assurance Committee and placed on the Trust’s website. The registers can be found via the following link:
https://www.sath.nhs.uk/about-us/trust-information/registers-of-interests/


The Shrewsbury and Telford Hospital NHS Trust Charity (number 1107883)
Full details about the charity, including latest annual report and accounts, can be found on the Charity Commission website here:


https://register-ofcharities.charitycommission.gov.uk/charity -search/-/charity-details/4013618


Engagement with our Communities
The Shrewsbury and Telford Hospital NHS Trust is committed to ensuring that the patient-public voice is at the centre of shaping our health services, both now and in the future. As an organisation we are committed to ensuring that our patients and local community have the opportunity to get involved in a timely and meaningful way. In October 2021 our Board of Directors approved our 5-year Public Participation Plan, which outlines how we will engage with our local communities. We want to build greater public confidence, trust and understanding by listening and being responsive to the needs of our local communities.
Part 2: Accountability Report 65
To support increased engagement and transparency, in January 2022 the Trust formed a Public Assurance Forum, chaired by a NonExecutive Director. The Forum membership consists of Trust repesentatives from the Divisions and representatives from a wide range of health and community groups. The aim of the Public Assurance Forum is to bring a public and community perspective, and scrutiny of processes, decision making and wider work, which takes place at the Shrewsbury and Telford Hospital NHS Trust. It is an advisory group whose role is to ensure that decisions about services and the delivery of care are developed in partnership with our local communities.
To support our communities to get involved, we offer a free community membership scheme (for individuals and organisations). Our members receive a monthly email update which has information about what is happening in the Trust, opportunities to get involved/upcoming events and information from our system/community partners.
Our target for the year 2022/23 was to increase our community membership by 10% across both individual and organisational members, which we have exceeded. Currently we have over 3600 individual members and 350 organisations.
This year we have reached out to all Town and Parish Councils in our areas to ask them to sign up as a community member. The response was overwhelming and by the end of summer 2022, we were delighted to report that all 170 Town and Parish Councils in the areas covered by the Trust across Shropshire, Telford & Wrekin and Powys, had signed up. We also contacted all County and Borough councillors to offer them membership as a way of keeping up to date with their local hospitals – over 99% of elected councillors have signed up as members.

Part 2: Accountability Report 66
Community membership scheme type 01/04/2022 Target (10% ) 31/03/2023 Actual Individuals 2541 2795 3692 45% Organisations 98 108 351 258%
Alongside these projects, we have continued to grow our organisational membership across the voluntary and community sector. Key to this is regular attendance at network meetings, many of which returned to face-to-face over the past year.
Hospitals Transformation Programme Engagement
The Public Participation Team has been supporting the Trust to engage with local communities around the Hospitals Transformation Programme (HTP). The team has organised a number of events including:
Quarterly focus groups - which are aligned to the four clinical workstreams. Workstream focus groups have been planned over the next two years which will inform the plans as they develop towards implementation. We are also planning focus groups to help shape the retail offer in the new front entrance at PRH and to look at transport issues. The first focus groups were held in February and March 2023 and were well-attended with the next groups in May and June. We have also attended local health groups to update.
Quarterly About Health events - the first event this year in January 2023 was successful with over 100 individuals attending this online event. Future sessions are being arranged on a quarterly basis and we will publish these in our monthly newsletter update.
We have supported the Divisions to develop their Equality and Health Inequality Impact Assessments as part of the Trust’s Outline Business Case.
Over the next few years of the Hospitals Transformation Programme, the Trust is committed to ensuring that local communities are involved with the implementation of this programme.
Service Changes and Developments
When the Trust is considering service changes or developments, we work with our staff, local communities, and statutory bodies to ensure that we engage with our communities in a timely and meaningful way. The Trust has a legal duty under Section 242 of the of the NHS Act 2006 to involve the public and patients in decision making around service changes and developments.
In 2022/23 we have engaged with our local communities around the following service changes:
Part 2: Accountability Report 67
• Renal Dialysis, Princess Royal Hospital
• Audiology and ENT, Royal Shrewsbury Hospital (temporary service change)
• Breast Screening Mobile Unit, Market Drayton and Bridgnorth (temporary service change)
• Outpatient Echocardiography (temporary service change)
To ensure that our public can be kept informed and engaged on any proposed or approved service change, we place all information relating to the service change on our website. This includes:
• The presentation to our stakeholders and communities
• Equality Impact assessment
• Engagement Plan and Report
• Questions and Answers
The detail of all service change proposals and engagement can be found at: https://www.sath.nhs.uk/about-us/get-involved/public-participation-2/get-involved-with-us2/services-changes-and-development/
Social Inclusion
During the pandemic, the Public Participation Team applied for funding through NHS Charities Together to address some of the gaps in engagement with Black and Minority Ethnic (BAME) and other seldom heard communities.
A grant of £50,000 was received and this supported funding a Social Inclusion Facilitator role for 12 months. The aim of this role was to establish links and build relationships with seldom heard community groups and organisations and individuals across Shropshire, Telford & Wrekin, and Powys. In 2022/23 the area of focus of the project included: Young People, BAME, Faith Groups, Substance Abuse, and Armed Forces Veterans
The NHS Charities Together funded Social Inclusion project came to an end in October 2022, and we have been able to secure a substantive post within the Public Participation to continue this element of community engagement.
Part 2: Accountability Report 68
Following completion of the project, a 2022/23 Social Inclusion Report has been produced.
Volunteers
Our patients, their friends and families and our workforce are supported by an amazing group of people who give up their time to help – our volunteers.
At the Trust, volunteers are able to provide support from the age of 16 and we have no upper age limit. Currently we have 353 active volunteers providing over 2,000 hours of support every month. Most individuals volunteer for at least four hours a week, many giving far more hours to our hospitals each week.
Over the past year, our volunteers have supported the Trust during times of high demand and pressure, particulary in our A&E departments which have been immensely busy.

Feedback from our volunteers
“One dad who is absolutely tired and couldn't comfort his small child was so grateful that I spent time with him and little girl”
“I'm happy doing my bit ...”
Sophie, one of A&E volunteers
“It has been a great experience where I had to interact with all sort of different people and learnt a lot from it and am grateful for the opportunity”
Respondent to a volunteer survey
“I really enjoyed learning about the different pathways and the NHS attributes and values”
A young Peoples Academy delegate.
Part 2: Accountability Report 69
01/04/2022 Target (10% increase) 31/03/2023 Actual increase Number of volunteers 281 309 353 25.6%
Photo: Ethan - our Volunteer of the Year 2022
Following a sucessful bid grant from NHS Charities Together, over the past 15 months we have developed our Young Volunteer Programme. The Trust is one of only 16 Trusts across the country to be awarded funding to enhance our young volunteer scheme through a project to target young people, aged 16-18, in the area who may experience barriers to volunteering. To date over 250 young people have accessed the scheme since the project has began and we have seen a significant difference in the number of young people volunteering at the Trust (with over 40% being under the age of 25 years old). Many of our young volunteers are considering a career within health and social care, and the young volunteer scheme has supported a number of young people to gain the experience they need.
Our young volunteers are recognised as a potential future workforce. It is important that we engage and offer opportunities to our young people, and as a result we have developed a Young People’s Academy. The Academy is held over 1 day and participants are involved in practical sessions (such as sighted guiding training) as well as information sessions on the NHS, careers, volunteering and getting involved
Building on this success, the Trust’s volunteer team have launched a “ olunteer to Career” project, following funding from Health Education England. The project aims to give hands on experience to people contemplating a career in the NHS, through volunteering, developing their skills and knowledge and mentoring. The programme started in December 2022 and is focusing on careers within maternity. The aim of the programme is to support a mimimum of 25 volunteers into a NHS career.
A very BIG thank you to all our Volunteers, past and present.
Part 2: Accountability Report 70
Remuneration Report
This Remuneration Report considers the senior managers of the organisation. ‘Senior Managers’ are defined as those persons in senior positions having the authority or responsibility for directing or controlling the major activities of the Trust. The means, those persons who influence the decisions of the organsiation as a whole, rather than those who take decisions at divisional or departmental level. For the purposes of this report, this covers the Trust’s nonexecutive directors and executive directors (voting and non-voting)
Remuneration Policy
The Trust’s approach to Remuneration Policy for Directors is in line with guidance issued by NHSI/E in order that directors’ pay remains both competitive and provides value for money. The Trust has a Remuneration Committee that agrees the remuneration packages for executive directors and other senior managers on locally agreed pay. The Remuneration Committee has met regularly during the year and recently reviewed its terms of reference.
Remuneration figures in the following tables represent actual remuneration rather than full year effect, and the band of the highest paid directors’ remuneration excludes pension related benefits and is based on annualised, full time equivalent remuneration.
The expense payments for the Chair and non-executive directors are ‘home to base’ mileage, taxed at source.
The tables on the following pages are subject to audit.
Part 2: Accountability Report 71
Part 2: Accountability Report
Salary and Pensions entitlements of senior managers 2022/23
Remuneration of senior managers 2022/23 - subject to audit 2022/23
72
Name and Title Salary £000 Other Remuneration £000 Expense payments (taxable) £0 Performance pay and bonuses £000 Long term performance pay and bonuses £000 All pensionrelated benefits £000 TOTAL £000 Executive Directors: Louise Barnett Chief Executive 210-215 - - - - 95-100 305-315 Sara Biffen Acting Chief Operating Officer 145-150 - - - - 330-335 475-485 Hayley Flavell Director of Nursing 145-150 2 - - - 150-155 300-310 Dr John Jones Medical Director 200-205 18 - - - 55-60 275-285 Nigel Lee Interim Director of Strategy & Partnerships 145-150 - - -Opted out of NHS pension scheme 145-150 Helen Troalen Director of Finance 150-155 - - - - 90-95 240-250 Inese Robotham Assistant Chief Executive 5-10 - - - - 90-95 95-105 Rhia Boyode Director of People & Organisation Development 150-155 - - -Opted out of NHS pension scheme 150-155 Anna Milanec Director of Governance & Communications 115-120 - - - - 40-45 155-165 Richard Steyn Co-Medical Director 180-185 320-325 505-510 Non-Executive Directors (NED): Dr Catriona McMahon Chair 55-60 - 3,200 - - - 55-60 Teresa Boughey, NED 10-15 - - - - - 10-15 Anthony Bristlin, NED³ 1-5 - 400 - - - 1-5
Part 2: Accountability Report
73 David Brown, NED 10-15 - 300 - - - 10-15 Clive Deadman, NED¹ 5-10 - - - - - 5-10 Dr David Lee, NED² 5-10 - - - - - 5-10 Trevor Purt, NED 10-15 - 400 - - - 10-15 Rajinder Dhaliwal, NED* 10-15 - - - - - 10-15 Rosi Edwards, NED** 10-15 - - - - - 10-15 Timothy Little, Associate NED*** 1-5 - - - - - 1-5 Julie Green, Associate NED**** 10-15 - 200 - - - 10-15 Note: ¹ Left 31.12.22 ² Left 2.12.22 ³ Left 30.4.22 * Commenced 1.5.22 ** Commenced 1.6.22 *** Commenced 1.3.23 **** Commenced 1.5.22, left 28.2.23
Remuneration of senior managers reported in 2021/22
Part 2: Accountability Report 74
Name and Title Salary £000 Other Remuneration £000 Expense payments (taxable) £0 Performance pay and bonuses £000 Long term performance pay and bonuses £000 All pensionrelated benefits £000 TOTAL £000 Executive Directors: Louise Barnett Chief Executive 205-210 0-5 - - - 50-55 260-265 Sara Biffen Acting Chief Operating Officer 5-10 - - - - 50-55 55-60 Hayley Flavell Director of Nursing 125-130 - - - - 180-185 310-315 Dr John Jones Medical Director 55-60 50-55 - - - 145-150 250-255 Nigel Lee Chief Operating Officer 135-140 0-5 - -Opted out of NHS pension scheme 135-140 Dr Arne Rose Medical Director 110-115 25-30 Not in NHS pension scheme 135-140 Helen Troalen Director of Finance 130-135 0-5 - - - 115-120 250-255 Non-Executive Directors: Dr Catriona McMahon Chair 40-45 - 3,000 - - - 45-50 Teresa Boughey, NED 10-15 - - - - - 10-15 Anthony Bristlin, NED 10-15 - 700 - - - 15-20 David Brown, NED 10-15 - - - - - 10-15 Clive Deadman, NED 10-15 - 100 - - - 10-15 Dr David Lee, NED 10-15 - - - - - 10-15 Trevor Purt, NED 10-15 - 100 - - - 10-15
2021/22
All Pension Related Benefits
The value of pension benefits accrued during the year is calculated as the real increase in pension multiplied by 20, less the contributions made by the individual. The real increase excludes increases due to inflation or any increase or decrease due to a transfer of pension rights. This value does not represent an amount that will be received by the individual. Rather, is a calculation that is intended to convey an estimation of the benefit that being a member of the pension scheme could provide. The table below provides further information on the pension benefits accruing to the individual.
Salary and pension entitlements are provided for the ‘executive directors’ as non-executive directors do not receive pensionable remuneration
All Pension Related Benefits 2022/23 – subject to audit
2022/23
Part 2: Accountability Report 75
Name and Title Real increase in pension at pension age (bands of £2,500) Real increase in pension lump sum at pension age (bands of £2,500) Total accrued pension at pension age at 31 March 202 3 (bands of £5,000) Lump sum at pension age related to accrued pension at 31 March 202 3 (bands of £5,000) Cash Equivalent Transfer Value at 1 April 2022 Real increase in Cash Equivalent Transfer Value Cash Equivalent Transfer Value at 31 March 202 3 Employer's contribution to stakeholder pension £000 £000 £000 £000 £000 £000 £000 £000 Louise Barnett Chief Executive 2.5-5 0-2.5 60-65 95-100 973 48 1,080 0 Hayley Flavell Director of Nursing 5-7.5 10-12.5 55-60 120-125 831 109 986 0 Helen Troalen Director of Finance 2.5-5 2.5-5 35-40 60-65 469 48 552 0 Dr John Jones Medical Director (from 1/10/2021) 0-2.5 0 70-75 155-160 1,317 25 1,407 0 Sara Biffen Acting Chief Operating Officer (from 14/3/2022) 12.5-15 32.5-35 65-70 155-160 1,052 301 1,405 0
Part 2: Accountability Report
Cash equivalent transfer value (CETV) figures are calculated using the guidance on discount rates for calculating unfunded public service contribution rates that was extant on 31 March 2023. HM Treasury published updated guidance on 27 April 2023; this guidance will be used in the calculation of 2023/24 CETV figures.
Fair Pay Disclosure – subject to audit
Reporting bodies are required to disclose the relationship between the remuneration of the highest-paid director in their organisation and the median remuneration of the organisation’s workforce.
The banded remuneration of the highest paid director at the Shrewsbury and Telford Hospital NHS Trust in the financial year 2022-23 was in the salary banding of £215,000 to £220,000 (2021-22: £215,000 to £220,000). This was 6 82 times (2021-22: 7 35 times) the median remuneration of the workforce, which was £31,912 (2021-22, £28,915).
Total remuneration includes salary, non-consolidated performance-related pay, benefits-in-kind, but not severance payments. It does not include employer pension contributions and the cash equivalent transfer value of pensions.
The median remuneration ratio of the workforce decreased by 7.26%.
76 Inese Robotham Assistant Chief Executive (from 13/03/2023) 2.5-5 0-2.5 40-45 70-75 652 2 730 0 Anna Milanec Director of Governance & Communications 0-2.5 - 25-30 - 340 26 393 0 Richard Steyn Co-Medical Director 12.5-15 30-32.5 90-95 260-265 0 25 54 0
Part 2: Accountability Report
Exit Packages agreed in 2022/23
This section provides an analysis of exit packages agreed with staff during the year (along with a 2021-22 comparison) and is subject to audit. Redundancy and other departure costs have been paid in accordance with the provisions of the NHS Scheme.
Exit Packages 2022/23– subject to audit
77 The yearly percentage change in the highest paid director’s remuneration 1.82% The yearly percentage change in the total average employee remuneration 10.18% The ratio between the highest paid director's remuneration and the pay and benefits of the employee on the 25th percentile of pay and benefits of the Trust's employees for the financial year 8.96 The ratio between the highest paid director's remuneration and the pay and benefits of the employee on the 75th percentile of pay and benefits of the Trust's employees for the financial year 4 74
Exit packages 2022/23 Exit package cost band (incl. any special payment element.) Number of compulsory redundancies Number of other departures agreed Total number of exit packages <£10,000 20 20 £10,000 - £25,000 2 2 £25,001 - £50,000 £50,001 - £100,000 £100,001 - £150,000 £150,001 - £200,000 >£200,000 Total number of exit packages by type 0 22 22 Total cost (£) - £117,000 £117,000
Part 2: Accountability Report
Exit Packages 2021/22 (comparison) – subject to audit
Exit packages 2021/22
Exit package cost band (incl. any special payment element.)
Other non-compulsory departure payments – subject to audit
Of which, non-contractual payments requiring HMT approval made to individuals where the payment value was more than 12 months’ of their annual salary
78
Number of compulsory redundancies Number of other departures agreed Total number of exit packages <£10,000 2 10 12 £10,000 - £25,000 £25,001 - £50,000 1 1 £50,001 - £100,000 1 1 £100,001 - £150,000 £150,001 - £200,000 >£200,000 Total number of exit packages by type 3 11 14 Total cost (£) £41,000 £101,000 £142,000
Other non-compulsory departure payments 2022/23 2021/22 Type Number of payments agreed Total value of agreements £000 Number of payments agreed Total value of agreements £000 Voluntary redundancies including early retirement contractual costs - - -Mutually agreed resignations (MARS) contractual costs - - 1 76 Early retirements in the efficiency of the service contractual costs - - -Contractual payments in lieu of notice 22 117 10 25 Exit payments
Employment Tribunals or court orders - - -Non-contractual payments requiring HMT approval - - -Total 22 117 11 101
following
- - - -
Reporting related to the Review of Tax Arrangements of Public Sector Appointees
Following the Review of the tax arrangements of public sector appointees published by the Chief Secretary to the Treasury on 23 May 2012, departments and their arm’s length bodies must publish information on their highly paid and/or senior off-payroll engagements.
The Trust is required to disclose:
All off-payroll engagements as of 31 March 2023, greater than £245 per day and that last longer than six months.
All new off-payroll engagements, or those that reached six months in duration, between 1 April 2022 and 31 March 2023, greater than £245 per day and that last for longer than six months.
Any off-payroll engagements of board members, and/or, senior officials with significant financial responsibility, between 1 April 2022 and 31 March 2023
These disclosures are provided within the following three tables: For all off-payroll
Part 2: Accountability Report 79
Number 2021/22 Number 2022/23 Number of existing engagements as of 31 March 2023 10 17 Of which, the number that have existed: -for less than one year at the time of reporting 1 7 for between one and two years at the time of reporting 4 7 for between 2 and 3 years at the time of reporting 5 3 for between 3 and 4 years at the time of reporting -for 4 or more years at the time of reporting - -
engagements as of 31 March 2023, for more than £245 per day and that last longer than six months:
Part 2: Accountability Report
For all new off-payroll engagements, or those that reached six months in duration, between 1 April 2022 and 31 March 2023, for more than £245 per day and that last for longer than six months
Number of new engagements, or those that reached six months in duration, between 1 April 2022 and 31 March 2023
2021/22
2022/23
Of which: - -
Number assessed as caught by IR35 - -
Number assessed as not caught by IR35 10 17
Number engaged directly (via PSC contracted to department) and are on the departmental payroll - -
Number of engagements reassessed for consistency/assurance purposes during the year - -
Number of engagements that saw a change to IR35 status following the consistency review - -
For any off-payroll engagements of board members, and/or, senior officials with significant financial responsibility, between 1 April 2022 and 31 March 2023
Number of off-payroll engagements of board members, and/or senior officers with significant financial responsibility, during the financial year
Total number of individuals on payroll and off-payroll that have been deemed “board members, and/or, senior officials with significant financial responsibility”, during the financial year. This figure includes both on payroll and off-payroll engagements.
80
Number
Number
10
17
Number
Number
2021/22
2022/23
0 0
14 22
Staff Report
Shrewsbury and Telford Hospital NHS Trust’s Recruitment and Retention Strategy supports the Trust’s ambitions to be a well-led Trust, providing excellent care for the communities we serve. However, like most organisations, the national shortage of certain NHS roles means that workforce remains a challenge for the Trust. With its rural location, competition from organisations in nearby metropolitan areas, and reputational issues, the Trust is working hard to recruit and retain a competent, and agile workforce; this is a key priority for the Trust.
Average number of employees (WTE basis) – subject to audit
Recognising the importance of supporting new employees who join the Trust, we have provided an ‘onboarding service’ to include sending welcome cards, a revised welcome pack detailing key information, and contacting staff during the first six months of employment to support them to settle in.
Part 2: Accountability Report 81
2022/23 2021/22 Type Permanent number (WTE) Other number (WTE) Total number (WTE) Total number (WTE) Medical and dental 715 153 868 787 Ambulance staff 8 - 8 4 Administration and estates 1,283 87 1,370 1,206 Healthcare assistants and other support staff 1,217 284 1,501 1,431 Nursing, midwifery and health visiting staff 1,980 334 2,314 2,167 Nursing, midwifery and health visiting learners 24 - 24 9 Scientific, therapeutic and technical staff 703 50 753 713 Healthcare science staff 343 - 343 332 Social care staff - - -Other - - - 116 Total average numbers 6,273 908 7,181 6,765
of employees (WTE) engaged on capital projects 30 4 34 30
Of which, Number
Staff Costs – subject to audit
The Trust has now developed a monthly recruitment dashboard to provide key metrics on both medical and non-medical recruitment activity.
We have introduced a range of new programmes such as a Nursing Associate Top Up programme allowing development of Nursing Associates to become registered nurses.
Recruitment and Selection workshops have been implemented to support appointing managers during the hiring process. We have also re-introduced Trac (recruitment system) training sessions, which are delivered virtually.
In January 2022, the Trust launched an Academy to train Health Care Support Workers, alongside partner organisations within the county’s health and care system, and Telford College.
Our international nursing recruitment campaign was successfully completed in February 2022,
Part 2: Accountability Report 82
2022/23 2021/22 Type Permanent £000 Other £000 Total £000 Total £000 Salaries and wages 288,661 1,613 290,274 266,199 Social Security Costs 28,864 - 28,864 26,118 Apprenticeship levy 1,393 - 1,393 1,273 Employer’s contributions to NHS pension scheme 46,112 - 46,112 42,723 Pension cost - other - -Other post employment benefits - - -Other employment benefits - - -Termination benefits - - -Temporary Staff - 46,529 46,529 32,845 Total gross staff costs 365,030 48,142 413,172 369,158 Recoveries in respect of seconded staff - - -Total Staff Costs 365,030 48,142 413,172 369,158 of whichCosts capitalised as part of the assets 1,747 491 2,238 1,723
with 190 WTE nurses joining the Trust. The programme included robust objective structured clinical examination (OSCE) support, and development, and enhanced onboarding assistance to include support with travel, accommodation and overcoming the many challenges of the pandemic e.g., quarantine and delays with travel. In addition to the successful recruitment inyear, the Trust’s available workforce at year-end also included 1782 staff on the internal bank, in addition to staff working within the Trust via external agencies.
The Trust successfully introduced an internal Structured English Language Reference (SELR) programme achieving a 100% success rate for all assessments submitted.
Expenditure on Consultancy
The Trust spent £595,000 on consultancy during 2022/23 (£859,000 in 2021/22).
Analysis of staff numbers
The figures in the following tables are calculated based on headcount in the organisation at 31 March 2023, unless otherwise indicated.
The Trust had 314 new starters in medical and dental roles over the last 12 months (up to March 2023) inclusive of 185 Deanery doctors. During the same period, the organisation had 294 leavers, of which 188 were Deanery doctors. This represents an overall headcount increase of 7% across all medical and dental staff.
83
Part 2: Accountability Report
Medical & Dental Starters & Leavers (Headcount) Job Role New Starters Leavers Clinical Assistant (closed to new entrants) 0 1 Consultant 32 26 Specialist 1 0 Specialty Doctor 14 22 Deanery Postgraduate Doctor - Foundation Level 57 50 Deanery Postgraduate Doctor (ST1-8) 128 138 Locally Employed Doctor - Foundation Level 6 1 Locally Employed Doctor - Specialty Registrar (ST1-8) 76 56 Total: 314 294
Recruitment - disability
The Trust continues to demonstrate its commitment to supporting individuals with long-term health conditions and disabilities and has now progressed to level 2 of the Disability Confident Scheme. The Trust continues to raise awareness of the scheme by developing a supporting document for appointing managers on our commitments and also by delivering Safer Recruitment workshops to staff involved in the recruitment process.
The Trust has recently introduced a new supportive process for individuals going through the recruitment process and once newly employed, where a long-term health condition/disability has been identified and reasonable adjustments are required. This provides the Trust with a mechanism to monitor and identify any potential challenges at an early stage, to ensure that our new recruits have any adjustments in place in order to undertake their role.
During the financial year 2022/23, the Trust received a total of 1053 applications for jobs from candidates with disabilities. Of these, 483 (2021/22: 445) candidates were shortlisted and invited to interview, 302 candidates attended interview and 152 (2021/22: 118) applicants were appointed.
Part 2: Accountability Report 84
Staff with recorded disabilities Headcount Percentage No 6,537 87 24% Not Declared 644 8 59% Prefer not to Answer 28 0.37% Not Known 1 0 01% Yes 283 3.78% Grand Total 7493
Turnover
Turnover for the year 2022/23 reduced to 13.06% compared to 15.20% in 2021/22.
Sickness absence
The Trust’s staff sickness absence data for 2022/23 is provided below:
Staff gender distribution
A breakdown of the number of persons who were directors of the Trust, senior managers, and other employees is shown below.
Part 2: Accountability Report 85
Turnover by Staff Group
Doctors & Students) 2022/23 % Trust whole-time equivalent turnover % 13.06% Allied Health Professionals 16.54% Additional Professional Scientific and Technical 14.94% Administrative and Clerical 14.21% Additional Clinical Services 14.04% Estates and Ancillary 13.59% Healthcare Scientists 12.94% Medical and Dental 11.49% Nursing and Midwifery Registered 10.89%
(Excluding Junior
Gender Breakdown (headcount) 2022/23 Male Female Total Percentage of total Board level directors 2 7 9 0.12% Non-Executive Directors / Chair 4 3 7 0.09% Senior Managers 14 42 56 0.75% All other employees 1555 5866 7421 99.04% Grand Total 21.02% 78.98% 7493 Staff Sickness Absence 2022/23 2022/23 (Number) 2021/22 (Number) Total days lost 85,688 74,504 Total staff years 6,164 5,937 Average working days lost (per WTE) 14 13
Staff age distribution
Breaking down our workforce into age bandings as shown here, illustrates that most of our workforce are under the age of 50 years old. However, with 32% of our workforce being over the age of 50, it may pose a risk to the Trust in the future if many colleagues take retirement at a similar time. Recruitment mitigates some of this risk, and more integrated workforce planning across the system will become increasing required.
Staff ethnicity and religious belief
During the 2022/23 financial year, 21% of our workforce has an ethnicity from ethnic minority group which is an increase of 2% from the previous financial year. There has been an increase in Asian and Asian British ethnicity from 10.7% to 11.8% whilst numbers of Black or Black British have increased from 3.5% to 4.5%; there has been a decrease in White from 80% to 78%. This is shown in the following tables, together with the details of religious beliefs:
Part 2: Accountability Report 86
Age Band Headcount Percentage <=20 Years 55 0.73% 21-25 494 6.59% 26-30 987 13.17% 31-35 1054 14.07% 36-40 889 11.86% 41-45 819 10.93% 46-50 810 10.81% 51-55 926 12.36% 56-60 840 11.21% 61-65 491 6.55% 66-70 100 1.33% >=71 Years 28 0.37% Grand Total 7493
Control measures are in place to provide assurance that all obligations under equality, diversity and human rights legislation are complied with. Monitoring provides data which informs plans and strategies to achieve an inclusive workplace and make improvements to the working environment for all staff. The outcomes are reported to the Board annually, and the Equality and Diversity Action Plan is updated as appropriate.
During the financial year, we have continued to strengthen our partnership working across the Integrated Care System and with our partners As a system, we have committed to 10 overarching pledges which includes tackling the problems of ill health, health inequalities and access to health care, improving our leadership and governance and making our system a great place to work
Part 2: Accountability Report 87
Ethnicity Headcount Percentage Asian or Asian British 886 11.82% Black or Black British 336 4.48% Mixed 104 1.39% Not Stated 64 0.85% Other Ethnic Groups 244 3.26% White 5859 78.19% Grand Total 7493 Religious Belief Headcount Percentage Atheism 1130 15.08% Buddhism 50 0.67% Christianity 3938 52.56% Hinduism 256 3.42% I do not wish to disclose my religion/belief 1377 18.38% Islam 225 3.00% Jainism 3 0.04% Judaism 3 0.04% Other 457 6.10% Sikhism 54 0.72% Grand Total 7493
Trade union facility time disclosures
Entities within the scope of the Trade Union (Facility Time Publication Requirements) Regulations 2017, are required to publish details in their Annual Report. The Trust’s disclosures for the year 2022/2023 are shown in the following tables:
Paid trade union activities
Time spent on paid trade union activities as a percentage of total paid facility time hours calculated as:
hours spent on paid trade union activities by relevant union officials during the relevant period divided by total paid facility time hours, multiplied by 100.
88
Trade unions and numbers of representatives Number Total number of employees who were relevant union officials during the relevant period 27 Full-time equivalent number 23.54 Percentage (%) of time spend on facility time % 0% 12 0 – 50% 13 51 – 99% 0 100% 2 Percentage (%) of pay bill spent on facility time % / £ Total cost of facility time £94,767 Total pay bill £410,934,000 Percentage of the total pay bill spent on facility time 0.023% .
11%
Total
Staff Survey
Between September and November 2022, the National NHS Staff Survey was undertaken The overall aim of the survey is to gather views and thoughts from our staff so that we can listen to what our people think about working for the Trust.
The information from the staff survey, together with information from ‘Making a Difference Together’ the online conversation platform and the People Pulse, is used to inform action plans and help us to improve the working lives of our staff, and so provide better care for patients. The NHS People Pulse also supports identification of any incremental changes and trajectories allowing early intervention, should that be required. This was not available for the 2022 survey but will aid the 2023.

The questions from the staff survey are also aligned to the People Promise. This is in keeping with the wider NHS vision of making the NHS a great place to work.
Sadly, the Trust did not score well against the indicators versus our benchmark trusts which has been the trajectory for the last two years, as can be seen within the following table. However, all people promises and themes have seen an increase year on year. Seeing the lowest increase at 0.02 to the highest increase at 0.20 within the “We work flexibly promise”, a key flagship programme from the 2021 staff survey results.
89
A total of 7029 members of staff were eligible to respond to the survey, and 49% of staff completed the survey in line with the target in the People Strategy, which equated to a total of 3392 respondents. This was the highest number of responses received since the survey has been taking place in the Trust, and an increase of 4% on the previous year. The following table shows that we have seen an increase in the last few years in our staff participation in the staff survey.
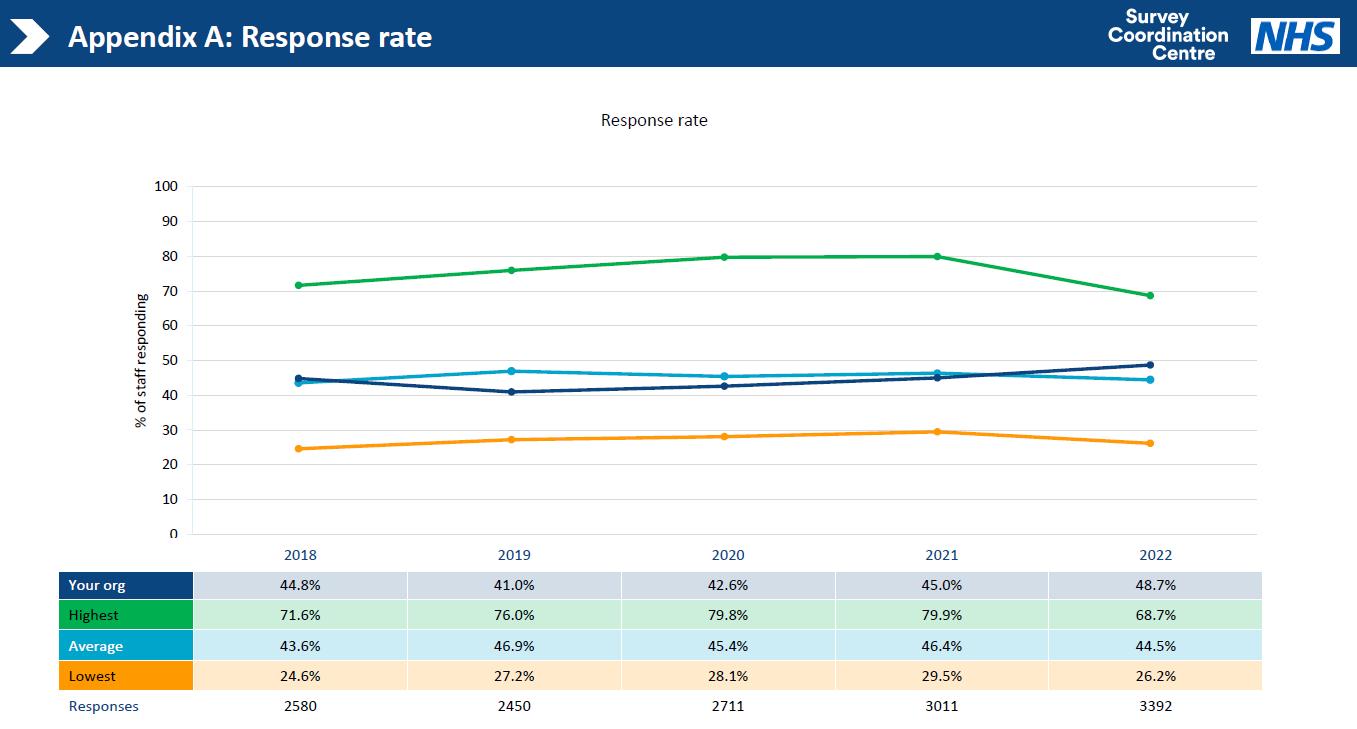

90
The staff engagement score has seen a steady decline over the last six years, from 6.6 in 2018 to 6.55 in 2020 and then to 6.29 in 2021. 2022 saw it rise to 6.32, as can be seen in the following table. This is not deemed a significant increase but a shoot of growth, nonetheless. We remain 0.5% behind our average benchmark trusts.

This indicates that we have more work to do in the staff engagement area. The research in the Messenger review, the government Engaging for Success: enhancing performance through employee engagement report, and in a 2020 report for NHSE, West and Dawson cite that, “Engagement has been shown to have many significant associations with patient satisfaction, mortality rates, infection rates, employee absenteeism and turnover”. Engagement is a key focus in this year’s work in the Trust.
The questions where we have seen significant declines year on year are pertinent to the level of pay, feeling secure to raise concerns around clinical practice and the standard of care provided by the organisation.
Where we have significantly better scores than our benchmark Trusts are all pertinent to the ‘We are compassionate and inclusive’ people promise.
91
We are concerned to see that the number of colleagues experiencing violence had increased and we are currently looking into this in detail.
We also undertook a bank staff survey as part of the Trust’s commitment to making the Trust an inclusive and great place to work, with over 200 colleagues taking part. This equated to 20% of the bank only staff that support our organisation. This is 5% higher than our comparable Trusts.
We are awaiting our comparative data versus the national picture. However, reviewing their engagement-led questions these show encouraging numbers such as
1. I look forward to going to work 67% (Motivation)
2. I am enthusiastic about my job 74% (Motivation)
3. I would recommend my organisation as a place to work 53.2% (Advocacy)

Involvement is an opportunity for us to focus on, to improve this score in 2023.
The National Staff Survey is an important method of data collection as it allows us to evaluate how we are doing and to show that we are listening by acting on the issues that our staff anonymously say are important to them. The Trust shared its internal results for 2022 with all key stakeholders prior to the embargo lift this year. A yearly timeline was produced to ensure that each month there was communication and action taking place. We felt that this was important to provide more time for actions to come to life before the fieldwork begins again in October. We have also launched a new dashboard available on Mangers Resources so midlevel managers can see, own, and act on their data with their teams to drive real change. To accompany this, we created an online offer on our Learning Management System (LMS) for managers and team leaders. The purpose of this is to support in the interpretation of their results
92
and where to go within the People and OD Directorate, FTSU and Patient Safety teams to gain support. There are a variety of tools and downloads to support their work and to gain knowledge within this platform.
Data from the National Staff Survey feeds into the Trust’s Culture Dashboard and our performance in relation to vision and values, goals and performance, learning and innovation, compassion, teamwork and health and wellbeing.
The National Staff Survey measures are aligned to key targets in our People Strategy, which in turn, are set as individual performance targets for our senior leaders:
The outcome of the National Staff Survey tells us that we made progress against all measures. But some real challenges include our overall people promise, staff engagement and staff morale scores which are below average for our sector.
Evidence shows engagement is a key driver to staff survey results and positive staff engagement has been linked to reduced staff turnover, lower sickness absence, reduced presenteeism and improved patient experience. Therefore, engagement is a top priority this year, along with, motivation, involvement, and advocacy (sub-components of employee engagement) and have a direct correlation to patient care.
93
2020/21 baseline 2022/23 target 2021/22 actual 2022/23 actual Number of people experiencing discrimination at work in the staff survey 7.5% 5.6% 9.6% 8.9% People reporting effective leadership in the staff survey 57.9% 74.5% 56% 60.2% Staff survey engagement score (score not %) 6.6 6.9-7.0 6.29 6.32 % of staff recommending the Trust as a place to work or receive treatment 49% 55-58% 44% 39% (care) 41% (work) NHS staff survey response rate 41% 45% 45-48% 49%
Health and Wellbeing
The wellbeing of our colleagues is of upmost importance to us. The wellbeing team continue to regularly walk around the hospital sites to speak to staff, offer support and promote health and wellbeing. The wellbeing team wear distinct purple wellbeing t-shirts and give out wellbeing support packs which include all the health and wellbeing offer available to staff such as psychological, physical, emotional, financial, and healthy lifestyles support.
Alongside the existing sources of psychological support available to staff including the Employee Assistance Programme, Phoenix Psychology, Mental Health First Aider’s and ICS Wellbeing Hub, the Trust commissioned its own Staff Psychology Service consisting of a Consultant Psychologist, two Principal Psychologists, two Senior Applied Psychologists and a Lead Counsellor, alongside the Trust Lead Consultant Psychologist.
The service takes a stepped-care approach, providing interventions at individual, team and service levels including critical incident debriefing, and in addition supports the organisation to embed psychological thinking across all that it does. The service went ‘live’ on 1 March 2023, and prior to this the Trust Lead Psychologist began identifying key priorities, for example focusing on the Critical Care and Emergency Department.
Bereavement support has been a priority, with a new ‘Bereavement Guide for Managers and Staff’ developed to encourage and support line managers to be compassionate leaders who consider the different ways in which our colleagues may experience a bereavement. Monthly bereavement cafés have also been introduced and facilitated by the End-of-Life Care Lead.
Whilst the Menopause offer continues to grow and be promoted around the Trust, to ensure the wellbeing offer is diverse and inclusive to all, there has been a focus on men’s health. A men’s health speaker and advocate has facilitated sessions to our male staff to provide a safe space to speak out and end the stigma around men’s mental health. These sessions have also been delivered to the female workforce to help them spot signs that their male colleagues may be struggling and how to approach those sensitive conversations.
The wellbeing team have worked closely with the ICS Wellbeing Group to create a wellbeing offer for staff across the system. This includes menopause and men’s health bi-monthly meet ups and burnout support sessions, along with the newest addition of the sleep school
94
programme to provide staff with the tools and advice to help improve their sleep quality and manage daytime stress, mentally detach from work and optimise energy through diet and exercise.

Cost of Living Crisis – Support for our people
In addition to the above, we recognised that the cost-of-living crisis would be affecting all of our workforce in some way, therefore we developed a Financial Wellbeing package for our staff who found themselves struggling. Our aim is to support staff to manage their finances, as well as ensuring they are able to eat, drink, and support their family during school and winter months; further work is being launched for Spring and Summer. At the time during 2022-23 the package included:


95
COVID Pandemic – Support to our People
In addition to the above, there have been several key achievements in our response to the pandemic that has contributed to supporting and engaging our people including:
91% of staff received two doses of the COVID 19 vaccine
Redeployment/mutualaid of staff in response to staff needing to shield or supporting gaps due to high levels of absence. This included both corporate teams being redeployed (over 30 staff) on to ward and clinical areas and military aid to support teams across the Trust.
We established a ‘listening ear’ service where our peer-to-peer listeners and coaches providing listening support. A counselling service was provided by ‘Care First’, we have mental health first aiders and have over 25 trained Trauma and Resilience Management (TRiM) Practitioners to support our staff who have experienced a traumatic incident. 51 individuals have used this service. This service will now be available through our psychological hub.
We work with Shropshire Mental Health Services, the ICS TRiM Hub and the Shropshire, Telford & Wrekin Staff Psychological Wellbeing Hub to provide additional psychological support for our people.
Our partnerships with Midlands Partnership University NHS Foundation Trust and Phoenix Psychology ensured that we had access to specialist clinical psychologists for supporting staff through traumatic incidents and post-traumatic stress, prior to our own hub being launched.
A centralised absence line for all staff was used for part of the year (up to September 2022) to help staff report sickness absence during the COVID-19 pandemic. This has helped staff record absence, seek advice and submit a referral for testing. It also provided an accurate real-time picture of staffing gaps across the Trust.
We have organised additional support for those suffering with long-term health conditions linked to COVID-19. This has included extensions to sick pay and adjustments to job roles, duties, etc., where required.
Gender pay gap reporting and actions
Gender pay reporting legislation requires employers with 250 or more employees to publish statutory calculations every year showing how large the pay gap is between their male and female employees.
Average gender pay gap as a mean average: 25.24% (This 2022 data shows that there is a difference of 25.24% between the mean hourly rate of pay for male
96
employees and mean hourly rate of pay for female employees, with men earning £5.61 per hour more on average.
Average gender pay gap as a median average: 9.24% (This data shows that there is difference of 9.24% between the median rate of pay for male employees compared with that of female employees, with men earning on average £1.49 more an hour).
Average bonus gender pay gap as a mean average: 35.56% (There is a 35.56% difference in favour of male employees in the level of mean bonus payments made to male employees when compared with female employees).
Average bonus gender pay gap as a median average: 33.33% (There is a 33.33% difference again in favour of male employees when comparing the median bonus level for male employees with that of female employees).
Proportion of males receiving a bonus payment: 5.09% and proportion of females receiving a bonus payment: 0.53%.
Proportion of males and females when divided into four groups ordered from lowest to highest pay:
Male and female employees in each quartile - including medical staff:
Note: 1st Quartile = lowest. 4th Quartile = highest.
Note: In considering the gender profile across these quartiles pay bands it is evident that as of 31st March 2022, according to their average hourly earnings, men are less well represented in the Upper quartile.
The Trust’s 2022 gender pay gap information is published on the Trust’s website, and can be accessed via the link below:
https://www.sath.nhs.uk/wp-content/uploads/2023/03/GenderPayGap_Report2022.pdf
97
Quartile Female (number) Male (number) Female % Male % 2020 2021 2022 2020 2021 2022 2020 2021 2022 2020 2021 2022 1 1327 1450 1395 325 339 311 80.33% 81.05% 81.77% 19.67% 18.95% 18.23% 2 1369 1477 1707 287 311 332 82.67% 82.61% 83.72% 17.33% 17.39% 16.28% 3 1435 1538 1472 213 251 211 87.08% 85.97% 87.46% 12.92% 14.04% 12.54% 4 1160 1254 1203 502 536 527 69.80% 70.06% 69.54% 30.2% 29.94% 30.46%
A trend of positive improvements can be seen in relation to the average gender pay gap for all staff over the last three years. The average difference per hourly rate between men and women continues to narrow from £5.94 (2020) to £5.76 (2021) and £5.61 (2022).
This narrowing gender pay gap trend is also reflected in the average hourly bonus pay and the median hourly rate of pay for all staff, with the median bonus pay gap maintaining the same percentage of 33.33% over the last three years. However, the Trust continues to see a gap between the earnings of men and women with a higher percentage of the male workforce receiving bonus pay than the female workforce. When medical staff are excluded from the data, there is a difference in favour of female employees of 5.24%. This has increased by 2.21% since the data was last reported in 2021, with women on average earning more per hour at £0.46 in 2021 and £0.82 in 2022, giving an increase of £0.36 since 2021, thereby resulting in an increase in pay gap.
This data will be reviewed and used to inform the SaTH Equality, Diversity and Inclusion Group, and to update our EDI strategy, objectives and action plans for improvement, with a commitment to addressing any areas of inequality which may be identified.
Medical Leadership
The Medical Leadership Programme (supported by the Faculty of Medical Leadership and Management - FMLM) has been completed by 75 Medical Leaders. This focussed on the contextual, personal and relational leadership development. A final celebration day was held in November 2022, in person, which was well attended and received excellent feedback. A consistent theme from the feedback was the importance of networking and peer support that had been provided by the programme.
Further continued professional development programme for all those who attended and those who have since taken up Medical Leadership roles will be proposed in the coming year, along with a programme for Aspiring Medical Leaders.
Consultant Welcome event
Following the success of the new Consultant Welcome which took place in March 2022, there was a further event held in October 2022. The programme was led by Medical Director and
98
Deputy Medical Director providing comprehensive insights into the Integrated Care System, Public Health, patient safety and much more. The success of this programme has led to a collaborative, system-wide approach with the Integrated Care Board for the next event in May 2023 which will include new colleagues from primary care, Shropshire Community Health NHS Trust, Robert Jones and Agnes Hunt Orthopaedic Hospital and Midlands Partnership University NHS Foundation Trust. The objective is to create stronger bonds and peer support for our system network.
The feedback from the October event was very positive with 54% rating it as excellent and 38% rating it as good.
Medical Director’s Internal Continued Professional Development (CPD)
This year, the Medical Director’s Internal CPD events for all senior medical staff has been launched. The events are held twice per year with wide ranging and relevant subjects important to all specialities. It is also an opportunity for the senior medical staff to have time for discussion directly with the Medical Director with several in person and virtual events for each programme enabling participation. Feedback has been good, with most evaluation scores in the range of ‘good’ to ‘excellent’.
GP and Consultant Exchange Programme
2022 saw the launch of the Shropshire, Telford and Wrekin GP and Consultant Exchange Programme. This was led by Dr Mary Eardley and supported by Alison Jones, GP Liaison Manager. The national scheme identified the importance of collaborative working across primary and secondary care which influenced patient care through improved communication and better understanding of each area’s challenges.
There were 27 pairings of Consultants and GPs with reciprocal visits taking place over a fourmonth period. A celebration event was held in November 2022 where learning and feedback was shared with all those who took part as well as the Medical Director and Deputy Medical Director for the Trust, and the Chief Medical Office for the Integrated Care Board. It has generated a renewed understanding of the challenges of each area and an enthusiasm for this to be repeated.
99
There has been agreement that the GP and Consultant Exchange Programme will continue as an annual event.
Specialty Doctors and Specialist Grade Doctors (SAS) Development Day
In February 2023, there was the first development day specifically for our Specialty Doctors and Specialist Grade doctors (SAS). The Trust’s SAS Advocate and Deputy Medical Director organised the day to focus on personal development and an opportunity for peer networking. This event is the first of a programme of events demonstrating the Trust’s commitment to the SAS Charter and investment in this valuable workforce. SAS Doctors who attended the day provided 100% feedback on the event which was rated largely excellent. A programme of continual professional development is being developed with a view to holding two events per year.
Medical Leadership Recruitment
There has been successful recruitment to the substantive Executive Medical Director role, with Dr John Jones being appointed in December 2022 following an interim period within the role.
There have been some changes in the Medical Leadership roles within the Divisions with Mr Martyn Underwood, Divisional Medical Director for Women’s and Children’s stepping down from Women’s and Children’s and Mr Andrew Sizer being successfully appointed. Also, Dr Steve McKew being successfully recruited into the substantive position of Divisional Medical Director role for Surgery, Anaesthetics and Cancer.
During September 2022, the Trust became the first trust in the region to appoint a SAS Advocate, Dr Katie Shellis, to support the SAS charter and be champion for the SAS doctors in a medical leadership capacity.
Louise Barnett, Chief Executive Officer
15 June 2023
100
Annual Governance Statement – 2022/23
1 Scope of Responsibility
As Accountable Officer, I have responsibility for maintaining a sound system of internal control that supports the achievement of The Shrewsbury and Telford Hospital NHS Trust’s policies, aims and objectives, whilst safeguarding the public funds and departmental assets for which I am personally responsible, in accordance with the responsibilities assigned to me. I am also responsible for ensuring that the NHS trust is administered prudently and economically and that resources are applied efficiently and effectively. I also acknowledge my responsibilities as set out in the NHS Trust Accountable Officer Memorandum.
2 The purpose of the system of internal control
The system of internal control is designed to manage risk to a reasonable level rather than to eliminate all risk of failure to achieve policies, aims and objectives; it can therefore only provide reasonable and not absolute assurance of effectiveness. The system of internal control is based on an ongoing process designed to identify and prioritise the risks to the achievement of the policies, aims and objectives of the Shrewsbury and Telford Hospital NHS Trust, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically. The system of internal control has been in place in the Shrewsbury and Telford Hospital NHS Trust (the Trust) for the year ended 31 March 2023 and up to the date of approval of the annual report and accounts.
3 Capacity to handle risk
I have the overall responsibility as Chief Executive and Accountable Officer, for the management of risk in the organisation.
101
Shrewsbury
The
and Telford Hospital NHS Trust Organisation Code: RXW
Each member of the executive team has an area of responsibility for risk management in accordance with their portfolios and as reflected in their role descriptions, which supports me in my role as Accountable Officer.
I am also supported in my role through the assurance committees of the Board of Directors, each under the chairmanship of a Non-Executive Director, with appropriate membership or input from members of the Executive Team. These committees comprise the Audit and Risk Assurance Committee, Quality and Safety Assurance Committee, Finance and Performance Assurance Committee, People and Organisational Development Assurance Committee and the Ockenden Report Assurance Committee (a time limited committee which was established and held its first meeting in March 2021).
The Audit & Risk Assurance Committee comprising of independent Non-Executive Directors, oversees the system of internal control and the overall assurance processes associated with managing risk.
A framework of operational committees sits below the board assurance committees, which provide the process through which risks are monitored throughout the organisation and up to the Board (ward to board). In addition, the Senior Leadership Committee (Operational and Transformation), the monthly communications cascade, and divisional and operational meetings, all provide forums at which risks to the organisation are considered.
The role of the Board of Directors is to effectively govern the organisation, and in doing so, to deliver high quality care for the population it serves. The Board of Directors receives the Chairs’ highlight reports and assurances from the Quality & Safety Assurance Committee relating to the management of all serious incidents, including Never Events, as well as receiving the monthly integrated performance report which includes performance on all quality and performance matters
The Trust continues on its journey of improvement with conditions remaining on its Provider Licence, imposed by both principal healthcare regulators. There have been improvements and innovation in some services, as highlighted through a number of external visits and independent reports. However, the Trust recognises that there are still areas that need more focus. However, the foundations that have been built over the last
102
two to three years have provided recognisable healthcare performance frameworks that existing, and newly recruited, colleagues now recognise and can work with as part of our improvement journey.
There has also been a change in several Non-Executive and Executive director posts in recent years, leading to a restructure of executive portfolios and bringing in more experience and skills to the Board. In-year changes to the voting directors can be found within the accountability report section of the annual report.
Following the peak of the Covid-19 pandemic, and with the national vaccination programme having remained in place during 2022-23, the more usual cycle of Trust business continued to strengthen during the financial year, with some meetings being held in public, albeit live streamed. The first face to face meeting of the Board of Directors for over two years was held in November 2022, with observing members of the public continuing to join via the live stream. The Board is working towards public observers joining future meetings in person, subject to infection, prevention and control, and practical considerations.
There are governance arrangements throughout the divisional triumvirate structures where divisional performance is overseen and monitored by the executive team, and key risks to delivery of services are identified via Performance Review Meetings, the focus of which has been strengthened in-year. The divisional triumvirates also played a more confident role in improvement across the organisation this financial year, with a greater knowledge and understanding of their own leadership roles and their part in the Trust’s continual improvement journey.
4. The risk and control framework
The Trust seeks to manage and mitigate risk as far as possible. However, it is understood that delivering healthcare carries inherent risks that cannot be completely eradicated but can be reduced through effective identification and mitigation where possible. The process begins with the systematic identification of risks via structured risk assessments and incorporated within risk registers. All risks are assessed and scored using an approved scoring matrix which considers the potential likelihood, consequence, and overall severity of each risk. This results in each risk being awarded
103
a score of between 1 (low) to 25 (extreme). The effectiveness of the existing control measures is assessed, and associated gaps and action plans agreed and monitored to ensure management of the risk.
The Board Assurance Framework provides the Trust with a system to identify and monitor risks which may affect achieving the strategic objectives/goals. Each risk is mapped to corresponding controls and assurances, both internal and external.
Work has continued during 2022-23 to improve the Trust’s risk management framework and functions following a review of this area and work which began in 2020-21. Further to a review of the IT system used to monitor and record risk (4Risk), the Trust introduced the Datix system to monitor and record risk in June 2022, with a transfer of risk registers from 4Risk to Datix. This provides a more integrated approach to management of risk, enabling the triangulation of incidents and complaints.
A Risk Management Strategy is in place (approved June 2021) and the Risk Management Policy was refreshed and approved in March 2022. An improved quarterly Board Assurance Framework (BAF) document was introduced from quarter 1 in 2022-23 and has continued to develop throughout the year and be actively considered by the Board, following prior consideration at its committees. Three new risks were added to the BAF in quarter 1, 2022-23. It was further identified that training should be rolled out across the organisation to support the development of a robust risk management framework and the Trust’s capability to consistently manage and mitigate risk and which was progressed in 2022/23.
A whole suite of risk management guidance, toolkits, education and training materials was incorporated into a ‘SATH Risk Management’ Teams channel during the financial year, with a digitised learning programme due to go live during 2023/24.
It remains the case that whilst a working BAF is in place, there is still further work to be carried out to ensure that it properly aligns with an overall medium to long-term Trust strategy which includes the long-term clinical strategy.
104
The risk appetite is set by the Board, forms part of the Risk Management Policy, and was last reviewed in March 2023.
We have a Senior Independent Director in place who is available to any colleague should they have concerns that they feel they are unable to raise via normal communication channels with the Chair, Chief Executive or any of the Board members.
5. Major risks to the organisation
The Annual Governance Statement for 2021/22 identified a number of risks that would also be carried forward into 2022/23 and which continue to remain current. A commentary for each of these risks is provided below.
a) Quality of care, including standards of performance and licence conditions
This relates to the failure to deliver high quality patient care, leading to poor patient experience, avoidable harm and poor clinical outcomes.
The Trust continues to focus on a number of areas of improvement including VTE, number of falls with harm, healthcare acquired infections and the timely response to patient concerns and complaints. The need for the Trust to maintain its continuous improvement journey is paramount.
The published report (dated 18th November 2021) following the last CQC inspection confirmed the overall CQC ratings remained as follows:
Safe – Inadequate
Effective – Requires Improvement
Caring – Requires Improvement
Responsive – Inadequate
Well-led – Requires Improvement
Use of Resources – Requires Improvement
Whilst improvements were noted by the inspection team, the Trust remained rated ‘Inadequate’ overall.
105
Prior to the CQC inspection in 2021, the Trust had 60 Section 31 conditions in place across the Trust, with thirty conditions for each site, as well as the previously received 6 Section 29a warning Notices. Following the inspection, a full review of all the Section 31 conditions took place by the CQC which led to most of these conditions being removed. The Trust now has a remaining 5 Section 31 conditions in place and continues to work hard on embedding the improvements required so that the remaining conditions can be removed once the organisation meets all the requirements set by the regulator.
Work continues to ensure that actions to improve the ratings, are embedded and consistently applied. Monthly reports in relation to the actions in place or planned, relating to our remaining Section 31 conditions are provided to the CQC. The Trust also has quarterly engagement meetings with the CQC to discuss and showcase improvements made in core services provided by the Trust.
The ongoing implementation and monitoring of improvements is coordinated and monitored by the Trust’s “Getting to Good” improvement plan which sets out the workstreams which the Trust is progressing in order to improve quality of care for patients. This includes a focus on clinical and corporate governance, as well as culture to support the required improvements.
There are also regular updates on progress to the Board with “Getting to Good” programme updates and external reporting to the monthly System Oversight and Assurance Group, which is attended by representatives from the ICS, national regulators, and key regional stakeholders.
Ongoing improvements during 2022/23 to the Integrated Performance Report, provided to every meeting of the Board of Directors, has extended the breadth and range of indicators provided and has continued to ensure the Board has clear sight, on performance delivery and issues which may affect the quality of care.
The Trust continues to implement and strengthen its Quality Governance Framework. All potential serious incidents and near misses continue to be discussed at the weekly Review Action and Learning from Incidents Group (RALIG) chaired by the Medical Director. The Nursing Incident Quality Assurance Meeting (NIQAM) ensures oversight of
106
the serious incident investigation process relating to falls, pressure ulcers and hospital acquired infections. These two meetings ensure the timely review of incidents and learning by the organisation.
b) Access and waiting time performance
Urgent and emergency care demand remained high throughout the year, and A&E performance, including ambulance handover delays, were a challenge. The Trust ended the year at 52.9% achievement of the 4-hour A&E wait standard, with 36.3% of ambulance waits of 60 minutes or more.
Maintaining flow through our hospitals and the safe discharge of patients has also been a consistent challenge, necessitating the continued use of significant surge plans and escalation beds throughout the year.
Lack of flow through the hospital resulted in the loss of some of our elective activity, and the associated ongoing challenges associated with the restoration of activity which we are now working hard to recover.
Several Trust and systemwide initiatives were implemented throughout the year to progress improvement in this area, such as the programme of Multi Agency Discharge Events (MADE) which are regularly undertaken across the Trust.
However, we have a long way to go to recover elective wait times to pre-Covid-19 levels, although we made some progress by year-end in reducing the number of patients waiting over 104 weeks and over 78 weeks for treatment.
Our programme of improvement has continued during the year with £24m NHS England (NHSE) funding being secured for the development of an Elective Hub, the first phase due to open in summer 2023 and the second phase due to complete by early 2024. This facility is aligned with our Hospital Transformation Programme and is an important pillar in our referral to treatment (RTT) and cancer recovery plan during 2023/24, providing improved and additional operating theatres and ringfenced beds for elective day case patients.
107
Detail on our performance during the year can be found in more detail within the Performance Report section of the annual report.
c) Implementing recommendations of the independent review of maternity services
The first Ockenden report1 which reviewed the provision of maternity services at the Trust, was published in December 2020, and was followed by the final report2 which was published in March 2022. These reports highlighted significant failings in maternity care at the Trust.
The Review, chaired by Mrs Donna Ockenden, examined cases mainly arising between 2000 and 2019, involving 1,486 families and the review of 1,592 clinical incidents.
The Review found repeated failures in the quality of care and governance at the Trust, as well as failures from external bodies to effectively monitor the care provided. These failures arose from there not being enough qualified staff, a lack of ongoing training, a lack of investigation and governance at the Trust and a culture of not listening to the families involved.
By the time of the publication of the final Report, the Trust had delivered all the ‘immediate and essential actions’ from the first Report which the Trust had independently led on.
An unreserved public apology from the Trust was provided on the day of publication of the Final Report. A public commitment was given by the Chief Executive to implement all the actions arising from the Review, a commitment which was later reiterated by the Board of Directors on 15 April 2022.
The combined reports include 210 actions, 93 ‘Local Actions for Learning’ to be implemented solely by the Trust and 117 ‘Immediate and Essential Actions’ for implementation of all providers of maternity care in England.
1 Ockenden Review (December 2020), Emerging Findings and Recommendations from the Independent Review of Maternity Services at Shrewsbury and Telford NHS Trust.
2 Ockenden Review (March 2022), findings Conclusions and Essential Actions from the Independent Review of Maternity Services at Shrewsbury and Telford NHS Trust; Our Final Report
108
Based on a rigorous assurance validation process, at the time of writing, March 2023, and a year since the publication of the final Report, the latest formally reported position to the Board was as at 14 February 2023. At that time, 162 of the 210 total actions (i.e., 77%) have been implemented, comprising 130 (62%) actions that have been ‘evidenced and assured’, and 32 (15%) ‘delivered and not yet evidenced’. Of the 48 (23%) of actions ‘not yet delivered’, over two-thirds are in progress. Ten of the ‘not yet delivered’ actions have been ‘de-scoped’ as falling out of the Trust’s control to deliver and they are dependent upon actions of third parties, such as NHS England or the Care Quality Commission. The Trust remains absolutely committed to implementing all the required actions in full at a pace, which is consistent with ensuring that they are fully embedded and sustainable for the future, in keeping with the Trust’s assurance approach.
We owe it to those families we failed, and to those we care for today and in the future, to continue to make improvements, so that we are delivering the best possible care for the communities that we serve.
The Ockenden Report Assurance Committee was established and held its first monthly meeting in March 2021. Its purpose was to consider progress against the recommendations and actions from both reports in more detail. The Committee is cochaired by an external Chair, alongside the Trust’s Chair. Members include Trust colleagues (both Executive and Non-Executive Directors), together with representatives from the Shropshire Telford & Wrekin Integrated Care Board, Maternity Voices Partnership, Healthwatch, and NHS England. Each of the meetings of the Committee has been livestreamed in public and, to date, it has met on seventeen occasions.
Progress from the Committee is reported monthly to the Board of Directors which is in addition to regular reporting of progress against each of the Ockenden Reports’ actions. This work is also underpinned by the work of the Maternity Transformation Assurance Committee, which is responsible for reviewing progress and delivery for each of the Ockenden actions. We are beginning to see positive assurance from reports and observations from several external organisations, that service improvements at the Trust are being made and are being embedded.
109
The Clinical Negligence Scheme for Trusts (CNST) handles all clinical negligence claims against member NHS bodies. The Maternity Safety Strategy set out the Department of Health and Social Care’s ambition to reward those who have taken action to improve maternity safety, and these actions are being embedded within the Maternity Transformation Project’s work. At the end of May 2023, the Trust achieved ten out of ten of the year four safety actions within the CNST Maternity Incentive Scheme. This was following a period of specific focus in this area and provision of the required evidence. The achievement of these year four safety actions will assist the Trust to mitigate the maternity risks highlighted within this AnnualGovernance Statement and Annual Report.
Finally, after the initial announcement of their intentions in June 2020, West Mercia Police continue to investigate allegations of poor maternity care at the Trust. The independent police investigation will explore whether there is evidence to support a criminal case against the Trust or any individuals involved. The Trust continues to co-operate fully with the investigation.
d) Improving financial performance
The key objective for 2022/23 was to secure better budget holder engagement and education and to redesign the business case framework, which is the process that budget holders follow to secure investment in services. The Trust also focused on capital processes to develop a five-year capital programme and on the processes to secure workforce both on a temporary and permanent basis.
There was also a focus on training and engagement of finance staff with vacant posts recruited to and a small restructure to better align the resources of the team with the needs of the Trust.
By strengthening all of the above processes it is expected that there will be more informed and effective financial decision making and controls
The Trust planned to have an in-year deficit of £19.1m with an underlying exiting deficit position of £33.5m. (The underlying exiting deficit position denotes what the net income and expenditure position is after adjusting for non-recurrent or one-off items that arose in-year.)
110
The Trust recorded a deficit of £47.206m in-year which is £28.071m adverse to the inyear plan. The planned underlying deficit for the Trust, i.e. (the financial position after the removal of one-off income and expenditure items) was a deficit of £32.6m and the actual underlying deficit at the end of the year was £34.4m
The main driver of the deficit was the use of additional escalation capacity to help prevent overcrowding in the emergency departments and to cope with the pressures on services.
The cause of the potential overcrowding was the lack of available ward beds into which, patients from the emergency departments, could be admitted. This in turn was because of the failure to discharge sufficient numbers of patients with no criteria to reside. This was due to several factors, relating to hospital flow processes, and to insufficient out of hospital provision to meet their needs.
At times up to 26% of the core bed base of the hospital was being occupied by patients who no longer needed to be in hospital. The cost of this capacity over the year was £22m and as such is the largest driver of the deterioration in the Trust’s financial position.
Whilst the Trust took a risk-based approach to planning for 2022/23, the extent to which the risk materialised was significant and mitigation insufficient.
Increasing covid pressures in the earlier half of the financial year affected capacity more than planned, added to which additional funding for the Hospital Discharge Programme ceased in March 2022.
Due to the physical constraints within the wards and emergency departments, the additional capacity required for 2022/23, and failure to improve elective care sufficiently, was more costly than planned even taking account of a continuing pandemic and ongoing workforce challenges.
In planning for the new financial year, the Trust has agreed to a very stretching financial plan.
There are several significant risks to the delivery of the plan. In particular, the potential
111
ongoing reliance on escalation capacity, and the associated dependency on workforce costs, including the continued use of agency staff.
The ongoing challenge to discharge patients with no criteria to reside will continue to be a significant area of focus. Our emergency care transformation programme will play a pivotal role in supporting the delivery of our plans.
The Trust is committed to strengthen partnership working across health and care, and a number of the critical actions are dependent upon these collaborative arrangements.
The Trust is committed to a series of actions to mitigate these risks, to ensure that services are delivered in the most cost-efficient way and has a very stretching cost improvement plan in place.
NHS England has supported the Trust with the provision of a Finance Improvement Director who is working closely with the Trust regarding our planned delivery of our plan, and the mitigation of risks associated with that delivery.
During the year, an exercise was commissioned across all NHS organisation in England to complete a self-assessment “improving financial health” checklist that was developed by the Healthcare Finance Managers Association. This was to assess the robustness of a number of financial functions within the Trust including budgeting, forecasting, financial planning, governance arrangements and the culture, training and development. The Trust achieved good scores (largely, four or five out of five for each domain) which were validated by internal audit. An area of focus will continue to be culture, training and development. This reflects the stage we are at in our financial improvement journey, and the output of this work will support our planning to further develop the function and organisational capability and capacity next year.
Finally, it was reported in last year’s statement that the Trust would be working towards Future Finance Focused level two accreditation This was achieved during the year, and the Trust is committed to achieving level three.
112
d) Regulatory Fire Issues
The Trust received a Prohibition Notice (served under Article 31 of the Regulatory Reform (Fire Safety) Order 2005) from Shropshire & Wrekin Fire Authority, dated 15 November 2022, with regard to Block 42, Ward 22 (staff area and handover room), Royal Shrewsbury Hospital. This notice was subsequently lifted following the Trust having successfully complied with the requirements. A ward block fire safety improvement plan was put in place by the Trust in response to the requirements raised, together with enhanced fire safety officer, advisor, and management resource.
The Trust was also issued with two Fire Enforcement Notices on 28 November 2022, following which, the required actions were then incorporated into the ward block fire safety improvement plan. Actions to address these Enforcement Notices remain ongoing and include staff training, evacuation procedures, staff awareness of fire risk, fire stopping, housekeeping, managing building work and alterations, maintenance and contractors working on site. The Trust continues to work closely with Shropshire Wrekin Fire Authority regarding our improvement action plan The first notice, in the main, relates to staff training with a plan for compliance by 30th June 2023. The second notice relates mainly to the building with a view to achieving full by 30th April 2025.
6. Provider Licence
The NHS Provider Licence is the main tool for regulating providers of NHS services. While NHS Trusts were exempt from the requirement to apply for and hold the licence during 2022-23, directions from the Secretary of State require NHSE to ensure that NHS Trusts comply with conditions equivalent to the licence as it deems appropriate. Several additional undertakings applied during 2021-22 to the Trust by NHSI/E, increased the number of requirements with which to comply.
Oversight of all NHS trusts, NHS foundation trusts and Integrated Care Boards is undertaken by NHSE using the NHS Oversight Framework. Following the publication of the new Code of Governance for NHS Providers which applies to all NHS Trusts from 1 April 2023, the Trust plans to adhere to the Code on a ‘comply or explain’ basis.
With reference to the requirements of the Trust’s Standing Orders and Standing Financial Instructions, no gaps in legal compliance have been identified during the year.
113
7. Fit and Proper Person Independent Investigation Report (Scolding Report) and Board Governance Review
Following receipt of a letter by the Chief Executive from two complainants in July 2020 concerning Mr Ben Reid (the former Chair of the Trust), Ms Fiona Scolding KC was commissioned by the Trust to carry out an independent investigation with regard to whether or not the issues raised in that letter gave rise to matters which engage the Fit and Proper Persons Regulations (FPPR), such that Mr Reid’s actions meant that he should no longer be considered to be a fit and proper person in accordance with the FPPR.
Ms Scolding was asked to examine the actions and conduct of Mr Ben Reid, who was the Chair of the Trust between February 2018 and August 2020. Further, in commissioning the independent investigation, the Trust was conscious that the matters raised by the complainants in relation to Mr Reid in his role as Chair may also necessarily involve the Trust Board’s actions and those of its Board Directors during the period in question.
In her report, Ms Scolding concluded that the complaints against Mr Reid did not amount to matters which would be considered to meet the test of “unfitness” as set out in the FPPR.
She concluded that whilst mistakes were made and that, although the actions of Mr Reid were not always correct, they did not meet the threshold of “serious” mismanagement by way of deliberate activity or standards which fall significantly below the level of the competent Chair.
Given the importance of Ms Scolding’s report and findings as they related to Board Governance, a proposal for a Board Governance Review was received and approved at the July 2022 meeting of the Board of Directors held in private, whilst awaiting Ms Scolding’s final report.
Ms Scolding’s final report was received by the Trust and complainants in August 2022 and shared with the Board of Directors, in public, on 13 October 2022, including the
114
Trust’s response to the final report and the thematic summary of the findings of the report. The Board fully accepted the findings of Ms Scolding’s report.
The Board Governance Review has progressed during the year and the Board received findings from the feedback received from an internal self-assessment of the functioning of the Board at its development session in December 2022. A further development session held in January 2023 covered Board effectiveness, committee effectiveness, and the themes from the Scolding review. The Board has also undertaken a review of its Standing Orders, Scheme of Reservation and Delegation and Standing Financial Instructions during the year, along with reviewing the terms of reference of its committees.
The Board intends to undertake an external independent Well Led review during 2023.
8. Committees of the Board
The principal board assurance committee structure which discharges overall responsibilities for risk management is summarised below:
The Board of Directorsis responsible for establishing principal strategic and corporate objectives and for driving the organisation forward to achieve these. It is also responsible for ensuring that effective systems are in place to identify and manage the risks associated with the achievement of these objectives through the Board Assurance Framework and the Corporate Risk Register.
The Audit and Risk Assurance Committee, on behalf of the Board, reviews the establishment and maintenance of an effective system of internal control and risk management across the whole of the Trust’s activities (both clinical and non-clinical) that supports the achievement of the Trust’s objectives and also ensures effective internal and external audit.
The Quality and Safety Assurance Committee (QSAC) is set up to provide assurance to the Board and the Audit and Risk Assurance Committee that there are adequate controls in place to monitor the care given to patients using the services provided by the Trust, and to ensure that their experience of our services and outcomes are as expected.
115
The Finance and Performance Assurance Committee (FPAC) is responsible for scrutinising aspects of financial performance, as well as conducting scrutiny of major business cases and proposed investment decisions.
The Ockenden Report Assurance Committee (a time limited committee) is established to provide assurance to the Board on progress against the Report’s recommendations and, in response, the Trust’s actions. Board members met as a People Committee during the year to consider elements such as workforce risks, inclusion and culture. The Board has formally established a People & Organisation Development Assurance Committee to receive assurances that staffing processes are safe, sustainable and effective and that the NHS People Promises are being delivered. The terms of reference for this committee were considered by the Board in April 2023.
Risk assessment is a key feature of all ‘business-as-usual’ management processes. All areas of the Trust have an ongoing programme of risk assessment which inform local risk registers. Operational risks are identified and evaluated using a five-by-five risk matrix, which feeds into the risk appraisal process. The risk registers are reviewed regularly through governance structures at both operational and corporate level, dependent on the severity of each risk. Each risk and related action have an identified owner who is responsible for risk monitoring, reporting and for implementing actions to mitigate the risk within a specified period. The Senior Leadership Committee reviews the highest rated risks on a monthly basis.
The Board of Directors is responsible for the approval of the Trust’s Risk Management Strategy. The strategy describes an integrated approach to ensure that all risks to the achievement of the Trust’s objectives are identified, evaluated, monitored and managed appropriately. It defines how risks are linked to one or more of the Trust’s strategic or operational objectives, and clearly defines the risk management structures, accountabilities, and responsibilities throughout the Trust.
The Board Assurance Framework (BAF) is the mechanism which is used to identify and monitor the Trust’s strategic objectives/goals and manage the associated risks that may compromise their achievement. The BAF is reviewed on a quarterly basis by the Executive
116
Directors and is formally reviewed quarterly by board assurance committees and the Board of Directors.
Operational and other corporate risks categorised as ‘extreme’ risks, are also reviewed by the Audit and Risk Assurance Committee as part of its regular monitoring of risk management.
There continues to be gaps in workforce that impacts on service delivery. However, we have a number of mechanisms in place which allow us to monitor staffing levels to provide safe and effective care. Information about staffing levels is published monthly on our Trust external website, and we publish links to the Nursing & Midwifery Staffing papers discussed in public at our Board meetings. The Trust also undertakes a nursing and midwifery establishment review every six months, which is reported to the Board of Directors. The Guardian of Safe Working regularly reports Junior Doctor compliance to safe working hours and formally notifies the Board of Directors of any exception reports.
A gap analysis has been completed in relation to the ‘Developing Workforce Safeguards’ published by NHS Improvement in October 2018. Additional actions in relation to workforce safeguards have been developed. The Trust is ensuring compliance with these recommendations with its use of evidence-based workforce planning, implementation of People Strategy and Recruitment and Retention Strategy. We will continue to explore and develop new roles, including widening our offer of Apprenticeships across the organisation, which will support care delivery. We currently have several new roles and programmes in place including Nursing Associates, Operating Department Practitioners, Nurse Apprentices, Physician Associated and Advanced Clinical Practitioners. We have also undertaken several system collaboration projects including the introduction of a Health Care Support Worker academy, and international recruitment for both nursing and Allied Health Professional’s.
The Board receives monthly workforce data via the Integrated Performance Report reported to the Board. In addition, the Board receives six-monthly updates specifically on nurse staffing. In accordance with the recommendations of ‘Developing Workforce Safeguards’ the Trust uses a triangulated approach to maintaining assurance around workforce strategies and safe staffing systems.
117
The Shrewsbury and Telford Hospital NHS Trust is required to register with the Care Quality Commission (CQC). The Trust is not fully compliant with the registration requirements of the CQC and the current conditions which have been imposed are described earlier in this statement within its major risks.
The Trust appeared in court on 18 May 2022 to answer three charges brought against it by the Care Quality Commission in relation to failures of care in October 2019 and May 2020. The Trust accepted responsibility, entered a plea of guilty to the charges and was ordered to pay a total of £1,375,712.
A series of immediate actions were implemented following the incidents, and internal investigations and external reviews were undertaken to ensure that improvements were made to address the failings. All involved have worked extremely hard to improve the quality of care in these areas and strong progress continues to be made against the actions.
In accordance with the requirements of ‘Managing Conflicts of Interests in the NHS’ guidance (June 2017), the Trust has published on its website an up-to-date register of interests, including gifts and hospitality, for decision-making staff (as defined by the Trust with reference to the guidance) within the past twelve months. An internal audit review in 2020/21 found that a low number of declarations had been made and a number of requirements as required by the ‘Managing Conflicts of Interest in the NHS’ guidance had not been met. As a result, a number of internal audit recommendations were made, accepted by management, and an action plan put in place to address the shortcomings.
Delivery of this action plan has progressed during 2022-23, with regular progress updates provided to Audit & Risk Assurance Committee. The number of declarations of interest made has significantly increased during 2022-23. The associated policy and processes have also been reviewed. The Trust intends to make the process of making declarations of interest easier for staff from May 2023 via use of the Electronic Staff Record. Once introduced, compliance with declarations made by those classed as decision makers will have enhanced reporting and monitoring, ensuring that the Trust can further improve on its position.
118
As an employer with staff entitled to membership of the NHS Pension Scheme, control measures are in place to ensure all employer obligations contained within the Scheme regulations are complied with. This includes ensuring that deductions from salary, employer’s contributions, and payments into the Scheme are in accordance with the Scheme rules, and that member Pension Scheme records are accurately updated in accordance with the timescales detailed in the Regulations.
Control measures are in place to provide assurance that all obligations under equality, diversity and human rights legislation are complied with. Monitoring provides data which informs plans and strategies to achieve an inclusive workplace and make improvements to the working environment for all staff. The outcomes are reported to the Board annually, and the Equality and Diversity Action Plan is updated as appropriate. The Gender Pay report is also published annual showing the difference between the average earnings of men and women. It can also help us to assess the levels of equality in the workplace, female and male participation, and how effectively talent is being managed and maximised.
The Equality Duty requires public bodies to have due regard to the need to eliminate discrimination, advance equality of opportunity, and foster good relations in the course of developing policies and delivering services. Equality analysis is completed on all policies, procedures, strategies and service developments. The Equality Delivery System is designed to specifically support service delivery that is fair, providing equality of access to employment and delivery that meets the needs of a diverse population.
The Trust has an Equality, Diversity and Inclusion (EDI) Group which includes representation from the community, meets bi-monthly and reports to the Operational People Group. During November 2022, the Patient Advocacy EDI group meeting was reinstated. Dedicated Equality, Diversity & Inclusion Leads are in post at the Trust in recognition of increasing BAME representation within our workforce and communities.
The Trust is fully committed to the significant improvement required to create a fully inclusive, supportive environment free from discrimination for staff and for patients.
119
The Trust has undertaken risk assessments and has plans in place which take account of the ‘Delivering a Net Zero Health Service’ report under the Greener NHS programme. The trust ensures that its obligations under the Climate Change Act and the Adaptation Reporting requirements are complied with.
9. Review of economy, efficiency, and effectiveness of the use of resources
The Board of Directors and its assurance committees have a key role in review of the effective use of resources. The Board of Directors retains oversight of the overall business planning process, budgets and use of staffing resources and establishment. The Finance and Performance Assurance Committee meets monthly and has a key role in review of operational and relevant workforce matters, investment decisions, and monthly financial performance, providing assurance to the Board of Directors.
In 2022/23, the Audit and Risk Assurance Committee focused on the effectiveness of controls in relation to: quality spot checks; the Assurance Framework; HfMA financial sustainability; quality of patient records; key financial systems – general ledger; key financial systems – accounts receivable; key financial systems – accounts payable; key financial systems – treasury management; Ockenden report 1 – follow up actions; end of life pathways – CQC action plan; Data Security and Protection Toolkit 21-22; ESR/payroll & sickness; and risk management divisional governance.
The Quality and Safety Assurance Committee has provided assurance to the Board of Directors on efficient and effective quality of patient care. The Committee monitored progress against the Trust’s quality improvement plan and key safety metrics.
Internal and external auditors provide assurance in respect of the internal control environment and the use of the organisation’s resources. Audit findings and recommendations are monitored and progressed by operational committees and the Audit and Risk Assurance Committee has an overarching overview for assurance purposes through the internal audit progress reports.
Any report which offers Limited assurance results in the development of a management action plan with an agreed timescale for improvement, and progress is monitored by the
120
Audit and Risk Assurance Committee. Serious issues are escalated to the Board of Directors.
The governance structure at Executive level and below provide opportunities for specific divisions, service lines and departments to be challenged on their efficient, effective and economic use of resources within the respective services which they provide. All budget holders are provided with monthly financial information to help them ensure resources are used economically, efficiently and effectively.
10. Information Governance
The Trust has an established process for managing the Information Governance agenda, led by the Director of Governance and Communication (Trust Senior Information Risk Owner), the Medical Director as Caldicott Guardian, and supported by a Data Protection Officer, who is also the Head of Information Governance.
The Trust uses NHS Digital’s Data Security and Protection Toolkit (DSPT) to measure performance, and improvements over the previous year have been noted for 2021/22, although the Trust continues to work through its agreed improvement plan with NHS Digital. The Trust aims to submit its 2022/23 submission by the end of June 2023.
The Information Governance Committee’s purpose is to support and drive the broader information governance agenda and to provide the Board of Directors with the assurance that effective information governance best practice mechanisms are in place within the organisation. It is responsible for monitoring and controlling risks relating to data security and to sign off the Data Security and Protection Toolkit (DSPT) submissions.
The Trust reported three incidents to the Information Commissioners Office between 1st April 2022 to 31st March 2023 relating to information governance including data losses or confidentiality breaches. At the time of writing, the ICO has not acted against the Trust for any of the reportable incidents to date.
The Trust manages threats to cyber security on an ongoing basis. Frequent reports of progress in implementing recommendations regarding nationally circulated cyber security
121
threat information is issued to a number of senior leaders in the organisation, with a role to oversee the oversight of cyber threats and management risks to the organisation.
11. Data Quality and governance
Data quality remains a key focus for the Trust. A Patient Data Quality Group (PDQG) has recently been put in place to provide the strategic direction for data quality and oversee and gain assurance on the quality of the data within the Trust’s Patient Administration System used at the Trust and any other system which directly affects key standards (e.g., A&E, Maternity, SUS), patient safety or financial sustainability.
Ensuring the quality and accuracy of our elective waiting list data has been an essential aspect of our recovery agenda at the Trust and this will be further facilitated by the PDQG in 2023/24 as our key focus area. A data quality dashboard is also in development which will primarily focus on waiting list metrics and this will be used as the driver in ensuring that processes are appropriately implemented to ensure key patient data is fit for purpose, quality-assured and valid.
The integrated performance report was redesigned in 2022/23 and shared with the Board monthly. The document continues to be developed in response to the requirements of the organisation. The Board of Directors remain assured that there are effective processes and controls in place to ensure the accuracy of data at the end of the reporting year ending 31 March 2023.
12. Review of effectiveness
As Accountable Officer, I have responsibility for reviewing the effectiveness of the system of internal control. My review of the effectiveness of the system of internal control is informed by the work of the internal auditors, clinical audit and the executive managers and clinical leads within The Shrewsbury and Telford Hospital NHS Trust who have responsibility for the development and maintenance of the internal control framework. I have drawn on the information provided in this annual report and other performance information available to me. My review is also informed by comments made by the external auditors in their management letter and other reports. I have been advised on the implications of the result of my review of the effectiveness of the system of internal
122
control by the board, the Audit and Risk Assurance Committee and a plan to address weaknesses and ensure continuous improvement of the system is in place.
The Board of Directors and its committees have met regularly and kept arrangements for internal control under review through discussion and approval of policies and practice and monitoring of outcomes agreed as indicators of effective controls. The Board and its committees review the Integrated Performance Report monthly, which covers the key national priority and regulatory indicators and locally derived key performance indicators. The report provides more detailed briefings on any areas of adverse performance. This report is supplemented by several more granular reports reviewed by board committees, and regular performance review meetings with the Divisions. The selection of appropriate metrics is subject to regular review, with changes in definitions or strategic priorities reflected in the selection.
Internal and external auditors provide assurance in respect of the internal control environment and the use of the organisation’s resources. Audit findings and recommendations are monitored and progressed by the committees of the Board and the Audit and Risk Assurance Committee has an overarching overview for assurance purposes through the internal audit progress reports.
The purpose of the Head of Internal Audit Opinion is to contribute to the assurances available to the Accountable Officer and the Board which underpin the Board’s own assessment of the effectiveness of the organisation’s system of internal control. The opinion has assisted in the preparation of this Annual Governance Statement.
The Head of Internal Audit provides me with an opinion on the overall arrangements for gaining assurance through the Board Assurance Framework and on the controls reviewed as part of the internal audit work. The Head of Internal Audit opinion for 202223 gave an overall Substantial Assurance opinion on the system of internal control in place during the year:
“The overall opinion for the period 1st April 2022 to 31st March 2023 provides Substantial Assurance that there is a good system of internal control designed to meet the organisation’s objectives, and that controls are generally being applied consistently.”
123
This opinion has greatly improved since the limited assurance opinion received for 2021/22.
Issues relating to the formulation of the opinion included work conducted through the risk based internal audit plan for 2022/23, as can be seen in the following table:
Title
2 high assurance opinions: Key Financial Systems – General Ledger.
Key Financial Systems – Accounts Receivable.
6 substantial assurance opinions: Key Financial Systems – Accounts Payable.
Key Financial Systems – Treasury.
Management Ockenden 1 - Follow up Actions.
End of Life Pathways – CQC Action Plan.
ESR/Payroll & Sickness.
Data Protection and Security Toolkit 21-22
1 moderate assurance opinion: Quality Spot Checks
1 limited assurance opinion: Risk Management Divisional Governance
Zero no assurance opinions
3 reviews without an assurance rating
N/A
HfMA Financial Sustainability Checklist. Assurance Framework.
Quality of Patient Records – Advisory Review.
A report was produced at the conclusion of each audit assignment and, where scope for improvement is found, recommendations are made, and appropriate action plans agreed with management. 28 recommendations were raised during the year relating to the riskbased audits, all of which were accepted by management. None of the recommendations were critical, but three were high risk recommendations in relation to the Divisional Risk Management and Quality Spot Checks reviews.
124
Opinion provided
risk-based
of core and
review
My review as Accountable Officer is also informed by:
Opinion and reports from our external auditors
Financial accounts and systems of internal control
Matters brought before the Board of Directors, and Board Assurance Committees
Trust risk registers
In-year submissions against performance to NHSI/E
Department of Health performance requirements/indicators
Compliance with the Care Quality Commission essential standards for quality and safety for all regulated activities
Progress against the Information governance assurance framework including the Data Security and Protection Toolkit
Investigation reports and action plans following serious incidents (RALIG, NIQAM)
The work of the Trust’s Anti-Fraud Specialist who carries out a detailed work plan and specialist investigations.
13.Conclusion
As the Accountable Officer, I am reporting that there are no significant internal control issues that have been identified for 2022/23 year.
However, as highlighted above, there are several significant risks which may affect delivery of the Trust’s objectives, which are reflective of the CQC’s ‘inadequate’ rating for the Trust, and the provision of NHS England’s oversight through their Recovery Support Programme.
Formal action plans have been agreed to address the risks in all areas where these have been identified. Implementation of the recommendations are being tracked and reported to the Board of Directors, and regulators, on a continuing basis.
125
The system of internal control has been in place at the Trust for the year ended 31 March 2023 and up to the date of approval of the Annual Report and Accounts.
Accountable Officer: Louise Barnett
Organisation: The Shrewsbury and Telford Hospital NHS Trust
Louise Barnett, Chief Executive Officer 15
June 2023
126
Statement of chief executive’s responsibilities as the accountable officer of the Trust
The Chief Executive of NHS England has designated that the Chief Executive should be the Accountable Officer of the trust. The relevant responsibilities of Accountable Officers are set out in the NHS Trust Accountable Officer Memorandum. These include ensuring that: there are effective management systems in place to safeguard public funds and assets and assist in the implementation of corporate governance value for money is achieved from the resources available to the trust the expenditure and income of the trust has been applied to the purposes intended by Parliament and conform to the authorities which govern them effective and sound financial management systems are in place and annual statutory accounts are prepared in a format directed by the Secretary of State to give a true and fair view of the state of affairs as at the end of the financial year and the income and expenditure, other items of comprehensive income and cash flows for the year.
As far as I am aware, there is no relevant audit information of which the trust’s auditors are unaware, and I have taken all the steps that I ought to have taken to make myself aware of any relevant audit information and to establish that the entity’s auditors are aware of that information.
To the best of my knowledge and belief, I have properly discharged the responsibilities set out in my letter of appointment as an Accountable Officer.
Louise Barnett, Chief Executive Officer
15 June 2023
127
Statement of directors’ responsibilities in respect of the accounts
The directors are required under the National Health Service Act 2006 to prepare accounts for each financial year. The Secretary of State, with the approval of HM Treasury, directs that these accounts give a true and fair view of the state of affairs of the Trust and of the income and expenditure, other items of comprehensive income and cash flows for the year. In preparing those accounts, the directors are required to: apply on a consistent basis accounting policies laid down by the Secretary of State with the approval of the Treasury make judgements and estimates which are reasonable and prudent state whether applicable accounting standards have been followed, subject to any material departures disclosed and explained in the accounts. Prepare the financial statement on a going concern basis and disclose any material uncertainties over going concern.
The directors are responsible for keeping proper accounting records which disclose with reasonable accuracy at any time the financial position of the Trust and to enable them to ensure that the accounts comply with requirements outlined in the above-mentioned direction of the Secretary of State. They are also responsible for safeguarding the assets of the Trust and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities.
The directors confirm to the best of their knowledge and belief they have complied with the above requirements in preparing the accounts.
The directors confirm that the annual report and accounts, taken as a whole, is fair, balanced and understandable and provides the information necessary for patients, regulators and stakeholders to assess the NHS Trust’s performance, business model and strategy.
By order of the Board:
15 June 2023. Louise Barnett, Chief Executive Officer
 15 June 2023 Helen Troalen, Director of Finance
15 June 2023 Helen Troalen, Director of Finance
128
INDEPENDENT AUDITOR’S REPORT TO THE BOARD OF DIRECTORS OF THE SHREWSBURY AND TELFORD HOSPITAL NHS TRUST
REPORT ON THE AUDIT OF THE FINANCIAL STATEMENTS Opinion
We have audited the financial statements of The Shrewsbury and Telford Hospital NHS Trust (“the Trust”) for the year ended 31 March 2023 which comprise the Statement of Comprehensive Income, the Statement of Financial Position, the Statement of Changes in Taxpayers Equity and the Statement of Cash Flows, and the related notes, including the accounting policies in note 1
In our opinion the financial statements:
• give a true and fair view of the state of the Trust’s affairs as at 31 March 2023 and of its income and expenditure for the financial year then ended;
• have been properly prepared in accordance with the accounting policies directed by the Secretary of State for Health and Social Care with the consent of HM Treasury on 23 June 2022 as being relevant to NHS Trusts in England and included in the Department of Health and Social Care Group Accounting Manual 2022/23; and
• have been prepared in accordance with the requirements of the National Health Service Act 2006 (as amended).
Basis for opinion
We conducted our audit in accordance with International Standards on Auditing (UK) (“ISAs (UK)”) and applicable law Our responsibilities are described below We have fulfilled our ethical responsibilities under, and are independent of the Trust in accordance with, UK ethical requirements including the FRC Ethical Standard We believe that the audit evidence we have obtained is a sufficient and appropriate basis for our opinion
Going concern
The Directors have prepared the financial statements on the going concern basis as they have not been informed by the relevant national body of the intention to either cease the Trust’s services or dissolve the Trust without the transfer of its services to another public sector entity They have also concluded that there are no material uncertainties that could have cast significant doubt over their ability to continue as a going concern for at least a year from the date of approval of the financial statements (“the going concern period”).
In our evaluation of the Directors’ conclusions, we considered the inherent risks associated with the continuity of services provided by the Trust over the going concern period. Our conclusions based on this work:
• we consider that the Directors’ use of the going concern basis of accounting in the preparation of the financial statements is appropriate; and
• we have not identified, and concur with the Directors’ assessment that there is not, a material uncertainty related to events or conditions that, individually or collectively, may cast significant doubt on the Trust’s ability to continue as a going concern for the going concern period.
However, as we cannot predict all future events or conditions and as subsequent events may result in outcomes that are inconsistent with judgements that were reasonable at the time they were made, the above conclusions are not a guarantee that the Trust will continue in operation.
kpmg 129
Fraud and breaches of laws and regulations – ability to detect Identifying and responding to risks of material misstatement due to fraud
To identify risks of material misstatement due to fraud (“fraud risks”) we assessed events or conditions that could indicate an incentive or pressure to commit fraud or provide an opportunity to commit fraud. Our risk assessment procedures included:
• Enquiring of management, the Audit and Risk Assurance Committee and internal audit and inspection of policy documentation as to the Trust’s high-level policies and procedures to prevent and detect fraud including the internal audit function, and the Trust’s channel for “whistleblowing”, as well as whether they have knowledge of any actual, suspected or alleged fraud.
• Assessing the incentives for management to manipulate reported financial performance as a result of the need to achieve financial performance targets delegated to the Trust by NHS England.
• Reading Board and Audit and Risk Assurance Committee minutes.
• Using analytical procedures to identify any unusual or unexpected relationships.
We communicated identified fraud risks throughout the audit team and remained alert to any indications of fraud throughout the audit.
As required by auditing standards, and taking into account possible pressures to meet delegated targets, we performed procedures to address the risk of management override of controls in particular the risk that Trust management may be in a position to make inappropriate accounting entries. On this audit we did not identify a fraud risk related to revenue recognition due to the block nature of the funding provided to the Trust during the year, and the simple recognition criteria and low individual value of other income streams. We therefore assessed that there was limited opportunity for the Trust to manipulate the income that was reported.
In line with the guidance set out in Practice Note 10 Audit of Financial Statements of Public Sector Bodies in the United Kingdom we also recognised a fraud risk related to nondepreciation expenditure recognition, particularly in relation to completeness of year-end accruals This fraud risk is in response to pressure to manipulate expenditure in order to report that the planned financial position has been met.
We performed procedures including:
• Identifying journal entries and other adjustments to test based on risk criteria and comparing the identified entries to supporting documentation. These included unexpected account combinations with revenue, expenditure, borrowings and cash
• Assessing whether the judgements made in making accounting estimates are indicative of a potential bias.
• Inspecting cash payments and expenditure transactions in the period following 31 March 2023 to verify expenditure had been recognised in the correct accounting period.
Identifying and responding to risks of material misstatement related to compliance with laws and regulations
We identified areas of laws and regulations that could reasonably be expected to have a material effect on the financial statements from our general sector experience and through discussion with the directors and other management (as required by auditing standards), and from inspection of the Trust’s regulatory and legal correspondence and discussed with the directors and other management the policies and procedures regarding compliance with laws and regulations.
kpmg 130
We communicated identified laws and regulations throughout our team and remained alert to any indications of non-compliance throughout the audit.
The potential effect of these laws and regulations on the financial statements varies considerably.
The Trust is subject to laws and regulations that directly affect the financial statements including the financial reporting aspects of NHS legislation We assessed the extent of compliance with these laws and regulations as part of our procedures on the related financial statement items.
We are also required to make a referral to the Secretary of State under section 30 of the Local Audit and Accountability Act 2014 if we have reason to believe that the Trust, or an officer of the Trust, is about to make, or has made, a decision which involves or would involve the body incurring unlawful expenditure, or is about to take, or has begun to take a course of action which, if followed to its conclusion, would be unlawful and likely to cause a loss or deficiency.
As outlined in the section of this report dealing with other legal and regulatory matters, we made a Section 30 referral to the Secretary of State on 16 May 2023, relating to the Trust’s failure to comply with its “breakeven duty” set out in paragraph 2(1) of Schedule 5 to the National Health Service Act 2006.
Whilst the Trust is subject to many other laws and regulations, we did not identify any others where the consequences of non-compliance alone could have a material effect on amounts or disclosures in the financial statements.
Context of the ability of the audit to detect fraud or breaches of law or regulation
Owing to the inherent limitations of an audit, there is an unavoidable risk that we may not have detected some material misstatements in the financial statements, even though we have properly planned and performed our audit in accordance with auditing standards. For example, the further removed non-compliance with laws and regulations is from the events and transactions reflected in the financial statements, the less likely the inherently limited procedures required by auditing standards would identify it.
In addition, as with any audit, there remained a higher risk of non-detection of fraud, as these may involve collusion, forgery, intentional omissions, misrepresentations, or the override of internal controls. Our audit procedures are designed to detect material misstatement. We are not responsible for preventing non-compliance or fraud and cannot be expected to detect noncompliance with all laws and regulations.
Other information in the Annual Report
The Directors are responsible for the other information, which comprises the information included in the Annual Report, other than the financial statements and our auditor’s report thereon. Our opinion on the financial statements does not cover the other information and, accordingly, we do not express an audit opinion or, except as explicitly stated below, any form of assurance conclusion thereon.
Our responsibility is to read the other information and, in doing so, consider whether, based on our financial statements audit work, the information therein is materially misstated or inconsistent with the financial statements or our audit knowledge Based solely on that work:
• we have not identified material misstatements in the other information; and
• in our opinion the other information included in the Annual Report for the financial year is consistent with the financial statements
Annual Governance Statement
We are required by the Code of Audit Practice published by the National Audit Office in April 2020 on behalf of the Comptroller and Auditor General (the “Code of Audit Practice”) to report
kpmg 131
to you if the Annual Governance Statement has not been prepared in accordance with the requirements of the Department of Health and Social Care Group Accounting Manual 2022/23 We have nothing to report in this respect.
Remuneration and Staff Reports
In our opinion the parts of the Remuneration and Staff Reports subject to audit have been properly prepared in all material respects, in accordance with the Department of Health and Social Care Group Accounting Manual 2022/23.
Directors’ and Accountable Officer’s responsibilities
As explained more fully in the statement set out on page 128, the directors are responsible for the preparation of financial statements that give a true and fair view. They are also responsible for: such internal control as they determine is necessary to enable the preparation of financial statements that are free from material misstatement, whether due to fraud or error; assessing the Trust’s ability to continue as a going concern, disclosing, as applicable, matters related to going concern; and using the going concern basis of accounting unless they have been informed by the relevant national body of the intention to either cease the services provided by the Trust or dissolve the Trust without the transfer of its services to another public sector entity
As explained more fully in the statement of the Chief Executive's responsibilities, as the Accountable Officer of the Trust, on page 127 the Accountable Officer is responsible for ensuring that annual statutory accounts are prepared in a format directed by the Secretary of State
Auditor’s responsibilities
Our objectives are to obtain reasonable assurance about whether the financial statements as a whole are free from material misstatement, whether due to fraud or error, and to issue our opinion in an auditor’s report Reasonable assurance is a high level of assurance, but does not guarantee that an audit conducted in accordance with ISAs (UK) will always detect a material misstatement when it exists Misstatements can arise from fraud or error and are considered material if, individually or in aggregate, they could reasonably be expected to influence the economic decisions of users taken on the basis of the financial statements.
A fuller description of our responsibilities is provided on the FRC’s website at www.frc.org.uk/auditorsresponsibilities
REPORT ON OTHER LEGAL AND REGULATORY MATTERS
Report on the Trust’s arrangements for securing economy, efficiency and effectiveness in its use of resources
Under the Code of Audit Practice, we are required to report if we identify any significant weaknesses in the arrangements that have been made by the Trust to secure economy, efficiency and effectiveness in its use of resources.
We have nothing to report in this respect.
Respective responsibilities in respect of our review of arrangements for securing economy, efficiency and effectiveness in the use of resources
As explained in the statement set out on page 127, the Chief Executive, as the Accountable Officer, is responsible for ensuring that value for money is achieved from the resources available to the Trust. We are required under section 21(2A) of the Local Audit and Accountability Act 2014 to be satisfied that the Trust has made proper arrangements for securing economy, efficiency and effectiveness in its use of resources.
We are not required to consider, nor have we considered, whether all aspects of the Trust’s arrangements for securing economy, efficiency and effectiveness in its use of resources are operating effectively
kpmg 132
We have planned our work and undertaken our review in accordance with the Code of Audit Practice and related statutory guidance having regard to whether the Trust had proper arrangements in place to ensure financial sustainability, proper governance and to use information about costs and performance to improve the way it manages and delivers its services. Based on our risk assessment, we undertook such work as we considered necessary
Statutory reporting matters
We are required by Schedule 2 to the Code of Audit Practice issued by the Comptroller and Auditor General (‘the Code of Audit Practice’) to report to you if we refer a matter to the Secretary of State under section 30 of the Local Audit and Accountability Act 2014 because we have reason to believe that the Trust, or an officer of the Trust, is about to make, or has made, a decision which involves or would involve the body incurring unlawful expenditure, or is about to take, or has begun to take a course of action which, if followed to its conclusion, would be unlawful and likely to cause a loss or deficiency.
On 16 May 2023 we made a section 30 referral to the Secretary of State in respect of the Trust’s breach of its “breakeven duty” set out in paragraph 2(1) of Schedule 5 to the National Health Service Act 2006. The Trust had previously breached its five-year breakeven duty and reported an in-year deficit of £47.206 million in 2022/23, resulting in a cumulative deficit of £178.063 million at 31 March 2023.

THE PURPOSE OF OUR AUDIT WORK AND TO WHOM WE OWE OUR RESPONSIBILITIES
This report is made solely to the Board of Directors of The Shrewsbury and Telford Hospital NHS Trust, as a body, in accordance with Part 5 of the Local Audit and Accountability Act 2014 Our audit work has been undertaken so that we might state to the Board of the Trust, as a body, those matters we are required to state to them in an auditor’s report and for no other purpose To the fullest extent permitted by law, we do not accept or assume responsibility to anyone other than the Board of the Trust, as a body, for our audit work, for this report or for the opinions we have formed.
kpmg 133
Andrew Cardoza for and
Chartered Accountants One Snowhill Snow Hill Queensway Birmingham B4 6GH 30 June 2023
on behalf of KPMG LLP
Helen Troalen Director of Finance
The Shrewsbury and Telford Hospital NHS Trust
Royal Shrewsbury Hospital
Mytton Oak Road
Shrewsbury
Shropshire
SY3 8XQ
2 August 2023
Dear Helen
Independent Auditor’s Report to the Board of Directors of The Shrewsbury and Telford Hospital NHS Trust
Issue of audit opinion on the financial statements

In our audit report for the year ended 31 March 2023 issued on 30 June 2023 we reported:
In our opinion, the financial statements:
• give a true and fair view of the state of the Trust’s affairs as at 31 March 2023 and of its income and expenditure for the year then ended;
• have been properly prepared in accordance with the accounting policies directed by NHS England with the consent of the Secretary of State in March 2023 as being relevant to NHS Foundation Trusts and included in the Department of Health and Social Care Group Accounting Manual 2022/23; and
• have been prepared in accordance with the requirements of the National Health Service Act 2006 (as amended).
Issue of value for money conclusion
In our audit report for the year ended 31 March 2023 issued on 30 June 2023 we reported the following in respect of the Trust’s arrangements for securing economy, efficiency and effectiveness in its use of resources:
KPMG LLP Tel +44 (0) 121 232 3147 One Snowhill Fax +44 (0) 121 232 3500 Snow Hill Queensway Birmingham B4 6GH United Kingdom KPMG LLP, a UK limited liability partnership and a member firm of the KPMG global organisation of independent member firms affiliated with KPMG International Limited, a private English company limited by guarantee. Registered in England No OC301540 Registered office: 15 Canada Square, London, E14 5GL For full details of our professional regulation please refer to ‘Regulatory information’ under ‘About’ at www.kpmg.com/uk Document Classification - KPMG Confidential Private & confidential
Your ref Our ref Contact Tony Felthouse 0121 232
3247
Under the Code of Audit Practice, we are required to report if we identify any significant weaknesses in the arrangements that have been made by the Trust to secure economy, efficiency and effectiveness in its use of resources.
We have nothing to report in this respect.
Certificate of completion of the audit
In our Year End Report 2022/23 issued on 30 June 2023, we explained that we could not certify the audit as complete as we had not yet issued our Auditor’s Annual Report We have now issued that report and there are no further matters to bring to your attention.
We certify that we have completed the audit of the accounts of The Shrewsbury and Telford Hospital NHS Trust for the year ended 31 March 2023 in accordance with the requirements of the Local Audit and Accountability Act 2014 and the Code of Audit Practice.
Yours sincerely,
 Andrew Cardoza Director, KPMG LLP
Andrew Cardoza Director, KPMG LLP
KPMG LLP 2 August 2023 2 Document Classification - KPMG Confidential
Annual Accounts for the year ending 31
March 2023
134
Statement of Comprehensive Income
2022/23 2021/22 Note £000 £000 Operating income from patient care activities 3 523,227 493,237 Other operating income 4 33,378 41,905 Operating expenses 7, 9 (596,088) (545,023) Operating surplus/(deficit) from continuing operations (39,483) (9,881) Finance income 11 604 16 Finance expenses 12 (212) 4 PDC dividends payable (7,876) (6,694) Net finance costs (7,484) (6,674) Other gains / (losses) 13 (479) (99) Surplus / (deficit) for the year from continuing operations (47,446) (16,654) Surplus / (deficit) on discontinued operations and the gain / (loss) on disposal of discontinued operations 15 -Surplus / (deficit) for the year (47,446) (16,654) Other comprehensive income Will not be reclassified to income and expenditure: Impairments 8 (1,204) (1,337) Revaluations 18 8,731 4,419 May be reclassified to
Fair value gains/(losses) on financial assets mandated at fair value through OCI 22 -Recycling gains/(losses) on disposal of financial assets mandated at fair value through OCI 13 -Foreign exchange gains / (losses) recognised directly in OCI -Total comprehensive income / (expense) for the period (39,918) (13,572) Adjusted financial performance (control total basis): Surplus / (deficit) for the period (47,446) (16,654) Remove net impairments not scoring to the Departmental expenditure limit (289) 5,514 Remove I&E impact of capital grants and donations 574 (178) Remove net impact of inventories received from DHSC group bodies for COVID response (45) 428 Adjusted financial performance surplus / (deficit) (47,206) (10,890) 136
income and expenditure when certain conditions are met:
Statement of Financial Position
The notes on pages 141 to 191 form part of these accounts.
Name Louise Barnett Position Chief Executive
Date 15 June 2023

31 March 2023 31 March 2022 Note £000 £000 Non-current assets Intangible assets 15 21,067 15,809 Property, plant and equipment 16 302,140 259,490 Right of use assets 19 21,262 Receivables 25 2,002 1,723 Total non-current assets 346,471 277,022 Current assets Inventories 24 9,774 9,039 Receivables 25 23,507 10,190 Cash and cash equivalents 29 3,301 15,889 Total current assets 36,582 35,118 Current liabilities Trade and other payables 30 (86,267) (66,175) Borrowings 32 (3,651)Provisions 34 (347) (321) Other liabilities 31 (297) (1,554) Total current liabilities (90,562) (68,050) Total assets less current liabilities 292,492 244,090 Non-current liabilities Borrowings 32 (17,969)Provisions 34 (828) (932) Total non-current liabilities (18,797) (932) Total assets employed 273,694 243,158 Financed by Public dividend capital 415,207 344,753 Revaluation reserve 81,423 73,896 (222,936) (175,491) 273,694 243,158 Income and expenditure reserve Total taxpayers' equity
137
Statement of Changes in Equity for the year ended 31 March 2023
Statement of Changes in Equity for the year ended 31 March 2022
Public dividend capital Revaluation reserve Income and expenditure reserve Total £000 £000 £000 £000 Taxpayers' and others' equity at 1 April 2022 - brought forward 344,753 73,896 (175,491) 243,158 Implementation of IFRS 16 on 1 April 2022 - - -Surplus/(deficit) for the year - - (47,445) (47,445) Impairments - (1,204) - (1,204) Revaluations - 8,731 - 8,731 Public dividend capital received 70,454 - - 70,454 Taxpayers' and others' equity at 31 March 2023 415,207 81,423 (222,936) 273,694
Public dividend capital Revaluation reserve Income and expenditure reserve Total £000 £000 £000 £000 Taxpayers' and others' equity at 1 April 2021 - brought forward 322,816 70,814 (158,837) 234,793 Surplus/(deficit) for the year - - (16,654) (16,654) Impairments - (1,337) - (1,337) Revaluations - 4,419 - 4,419 Public dividend capital received 21,937 - - 21,937 Taxpayers' and others' equity at 31 March 2022 344,753 73,896 (175,491) 243,158 138
Information on reserves
Public dividend capital
Public dividend capital (PDC) is a type of public sector equity finance based on the excess of assets over liabilities at the time of establishment of the predecessor NHS organisation. Additional PDC may also be issued to trusts by the Department of Health and Social Care. A charge, reflecting the cost of capital utilised by the trust, is payable to the Department of Health as the public dividend capital dividend.
Revaluation reserve
Increases in asset values arising from revaluations are recognised in the revaluation reserve, except where, and to the extent that, they reverse impairments previously recognised in operating expenses, in which case they are recognised in operating income. Subsequent downward movements in asset valuations are charged to the revaluation reserve to the extent that a previous gain was recognised unless the downward movement represents a clear consumption of economic benefit or a reduction in service potential.
Financial assets reserve
This reserve comprises changes in the fair value of financial assets measured at fair value through other comprehensive income. When these instruments are derecognised, cumulative gains or losses previously recognised as other comprehensive income or expenditure are recycled to income or expenditure, unless the assets are equity instruments measured at fair value through other comprehensive income as a result of irrevocable election at recognition.
Merger reserve
This legacy reserve reflects balances formed on previous mergers of NHS bodies.
Income and expenditure reserve
The balance of this reserve is the accumulated surpluses and deficits of the Trust.
139
Statement of Cash Flows
2022/23 2021/22 Note £000 £000 Cash flows from operating activities Operating surplus / (deficit) (39,482) (9,881) Non-cash income and expense: Depreciation and amortisation 7.1 21,294 14,744 Net impairments 8 (289) 5,514 Income recognised in respect of capital donations 4 (403) (1,140) (Increase) / decrease in receivables and other assets (13,923) 13,020 (Increase) / decrease in inventories (735) 271 Increase / (decrease) in payables and other liabilities 6,164 3,554 Increase / (decrease) in provisions (97) (383) Net cash flows from / (used in) operating activities (27,471) 25,699 Cash flows from investing activities Interest received 604 16 Purchase of intangible assets (4,165) (5,964) Purchase of PPE and investment property (42,304) (36,352) Sales of PPE and investment property 925 1,961 Receipt of cash donations to purchase assets 403 1,140 Net cash flows from / (used in) investing activities (44,537) (39,199) Cash flows from financing activities Public dividend capital received 70,454 21,937 Capital element of lease liability repayments (3,067)Other interest (1)Interest element of lease liability repayments (192)PDC dividend (paid) / refunded (7,774) (7,953) Net cash flows from / (used in) financing activities 59,420 13,984 Increase / (decrease) in cash and cash equivalents (12,588) 484 Cash and cash equivalents at 1 April - brought forward 15,889 15,405 Cash and cash equivalents at 31 March 28.1 3,301 15,889 140
Note 1 Accounting policies and other information
Note 1.1 Basis of preparation
The Department of Health and Social Care has directed that the financial statements of the Trust shall meet the accounting requirements of the Department of Health and Social Care Group Accounting Manual (GAM), which shall be agreed with HM Treasury. Consequently, the following financial statements have been prepared in accordance with the GAM 2022/23 issued by the Department of Health and Social Care. The accounting policies contained in the GAM follow International Financial Reporting Standards to the extent that they are meaningful and appropriate to the NHS, as determined by HM Treasury, which is advised by the Financial Reporting Advisory Board. Where the GAM permits a choice of accounting policy, the accounting policy that is judged to be most appropriate to the particular circumstances of the Trust for the purpose of giving a true and fair view has been selected. The particular policies adopted are described below. These have been applied consistently in dealing with items considered material in relation to the accounts.
Accounting convention
These accounts have been prepared under the historical cost convention modified to account for the revaluation of property, plant and equipment, intangible assets, inventories and certain financial assets and financial liabilities.
Note 1.2 Going concern
These accounts have been prepared on a going concern basis. The financial reporting framework applicable to NHS bodies, derived from the HM Treasury Financial Reporting Manual, defines that the anticipated continued provision of the entity’s services in the public sector is normally sufficient evidence of going concern. The directors have a reasonable expectation that this will continue to be the case.
The Board has carefully considered the principle of ‘Going Concern’ in the context of the Trust continuing to operate under the HM Treasury’s Financial Reporting Guidelines (FReM). For the year ending 31 March 2023, the Trust is reporting a deficit of £47.206m on an adjusted financial performance basis, against a planned deficit of £19.135m.
In 2022/23, the Trust’s income has been driven through an allocative process, consisting of block payments with specific adjustments for agreed growth and prices, ongoing Covid expenditure, and funding achieved through the Elective Recovery Fund (ERF) to incentivise restoration of elective services. There has also been a convergence adjustment applied to bring the Trust back towards a fair-share allocation. As the Shropshire, Telford & Wrekin Integrated Care System (ICS) is currently consuming more than its fair share (on a population basis), the convergence factor applied is higher.
Contracts were constructed on an Intelligent Fixed Payment (IFP) basis within the ICS. This is an approach based on collaboration, concentrating on the cost of providing healthcare across the system in order to bring the health system back to clinical, operational and financial balance. Other contracts were constructed on a typical cost and volume contract or an aligned incentive payment approach.
The Trust maintains a cash balance of £3.301m at the end of 2022/23 (March 2022: £15.889m).
Every ICS/STP received a 2022/23 capital spending envelope derived from the system-level allocation, with The Shrewsbury and Telford Hospital NHS Trust receiving a total system envelope of £19.822m in 2022/23. Historically the Trust has had low levels of internally generated capital funds underpinned by public dividend capital.
In the financial landscape for 2023/24, nationally the NHS funding allocation moves to an aligned payment and incentive approach (API). This consists of a fixed element for non-elective care, and elective care is reimbursed on a variable basis based on actual activity delivered. Tariffs have been uplifted for inflation and adjusted for efficiency and convergence factor. Covid funding has also been included within baseline tariffs and therefore will no longer be funded separately. The Elective Recovery Fund (ERF) remains in place to support restoration of elective activity. Low-Volume Activity (LVA) contracts, worth under £0.5m, will be paid on a block basis.
Notes to the
Accounts
141
The Board of Directors have concluded that whilst the financial position for 2023/24 is very challenging, based upon enquiries with NHS Improvement and the Department of Health and Social Care, they have a reasonable expectation that the Trust will have access to adequate resources (as in previous years) to continue in operational existence for at least 12 months from the date of approval of the financial statements and continue to provide services to its patients. Based on this expected continuation of services, the Trust continues to adopt the going concern basis in preparing the financial statements.
Note 1.3 Interests in other entities NHS Charitable Fund
The Trust is the Corporate Trustee to the Shrewsbury and Telford Hospital NHS Trust Charity. The Trust has assessed its relationship to the charitable fund and determined it not to be a subsidiary because the Trust is not exposed to, or has rights to, variable returns and other benefits for itself, patients and staff from its involvement with the charitable fund and has the ability to affect those returns and other benefits through its power over the fund.
The charitable fund’s statutory accounts are prepared to 31 March in accordance with the UK Charities Statement of Recommended Practice (SORP) which is based on UK Financial Reporting Standard (FRS) 102.
Note 1.4 Revenue from contracts with customers
Where income is derived from contracts with customers, it is accounted for under IFRS 15. The GAM expands the definition of a contract to include legislation and regulations which enables an entity to receive cash or another financial asset that is not classified as a tax by the Office of National Statistics (ONS).
Revenue in respect of goods/services provided is recognised when (or as) performance obligations are satisfied by transferring promised goods/services to the customer and is measured at the amount of the transaction price allocated to those performance obligations. At the year end, the Trust accrues income relating to performance obligations satisfied in that year. Where the Trust’s entitlement to consideration for those goods or services is unconditional a contract receivable will be recognised. Where entitlement to consideration is conditional on a further factor other than the passage of time, a contract asset will be recognised. Where consideration received or receivable relates to a performance obligation that is to be satisfied in a future period, the income is deferred and recognised as a contract liability.
Revenue from NHS contracts
The main source of income for the Trust is contracts with commissioners for health care services. Funding envelopes are set at an Integrated Care System (ICS) level. The majority of the Trust’s income is earned from NHS commissioners in the form of fixed payments to fund an agreed level of activity.
In 2022/23 fixed payments are set at a level assuming the achievement of elective activity targets. These payments are accompanied by a variable-element to adjust income for actual activity delivered on elective services and advice and guidance services. Where actual elective activity delivered differs from the agreed level set in the fixed payments, the variable element either increases or reduces the income earned by the Trust at a rate of 75% of the tariff price. Elective recovery funding provides additional funding for the delivery of elective services. In 2022/23 elective recovery funding was included within the aligned payment and incentive contracts. In 2021/22 income earned by the system based on achievement of elective recovery targets was distributed between individual entities by local agreement and income earned from the fund was accounted for as variable consideration.
The Trust also receives income from commissioners under Commissioning for Quality Innovation (CQUIN) and Best Practice Tariff (BPT) schemes. Delivery under these schemes is part of how care is provided to patients. As such CQUIN and BPT payments are not considered distinct performance obligations in their own right; instead, they form part of the transaction price for performance obligations under the overall contract with the commissioner. In 2022/23 payment under these schemes is included in fixed payments from commissioners based on assumed achievement of criteria. Adjustments for actual performance are made through the variable element of the contract payments.
142
Revenue from research contracts
Where research contracts fall under IFRS 15, revenue is recognised as and when performance obligations are satisfied. For some contracts, it is assessed that the revenue project constitutes one performance obligation over the course of the multi-year contract. In these cases, it is assessed that the Trust’s interim performance does not create an asset with alternative use for the Trust, and the Trust has an enforceable right to payment for the performance completed to date. It is therefore considered that the performance obligation is satisfied over time, and the Trust recognises revenue each year over the course of the contract. Some research income alternatively falls within the provisions of IAS 20 for government grants.
NHS injury cost recovery scheme
The Trust receives income under the NHS injury cost recovery scheme, designed to reclaim the cost of treating injured individuals to whom personal injury compensation has subsequently been paid, for instance by an insurer. The Trust recognises the income when performance obligations are satisfied. In practical terms this means that treatment has been given, it receives notification from the Department of Work and Pension's Compensation Recovery Unit, has completed the NHS2 form and confirmed there are no discrepancies with the treatment. The income is measured at the agreed tariff for the treatments provided to the injured individual, less an allowance for unsuccessful compensation claims and doubtful debts in line with IFRS 9 requirements of measuring expected credit losses over the lifetime of the asset.
Note 1.5 Other forms of income
Grants and donations
Government grants are grants from government bodies other than income from commissioners or trusts for the provision of services. Where a grant is used to fund revenue expenditure it is taken to the Statement of Comprehensive Income to match that expenditure. Where the grant is used to fund capital expenditure, it is credited to the consolidated statement of comprehensive income once conditions attached to the grant have been met. Donations are treated in the same way as government grants.
Apprenticeship service income
The value of the benefit received when accessing funds from the Government's apprenticeship service is recognised as income at the point of receipt of the training service. Where these funds are paid directly to an accredited training provider from the Trust's Digital Apprenticeship Service (DAS) account held by the Department for Education, the corresponding notional expense is also recognised at the point of recognition for the benefit.
Note 1.6 Expenditure on employee benefits
Short-term employee benefits
Salaries, wages and employment-related payments such as social security costs and the apprenticeship levy are recognised in the period in which the service is received from employees. The cost of annual leave entitlement earned but not taken by employees at the end of the period is recognised in the financial statements to the extent that employees are permitted to carry-forward leave into the following period.
Pension costs
NHS Pension Scheme
Past and present employees are covered by the provisions of the two NHS Pension Schemes. Both schemes are unfunded, defined benefit schemes that cover NHS employers, general practices and other bodies, allowed under the direction of Secretary of State for Health and Social Care in England and Wales. The scheme is not designed in a way that would enable employers to identify their share of the underlying scheme assets and liabilities. Therefore, the scheme is accounted for as though it is a defined contribution scheme: the cost to the trust is taken as equal to the employer's pension contributions payable to the scheme for the accounting period. The contributions are charged to operating expenses as and when they become due.
Additional pension liabilities arising from early retirements are not funded by the scheme except where the retirement is due to ill-health. The full amount of the liability for the additional costs is charged to the operating expenses at the time the Trust commits itself to the retirement, regardless of the method of payment.
143
Note 1.7 Expenditure on other goods and services
Expenditure on goods and services is recognised when, and to the extent that they have been received, and is measured at the fair value of those goods and services. Expenditure is recognised in operating expenses except where it results in the creation of a non-current asset such as property, plant and equipment.
Note 1.8 Discontinued operations
Discontinued operations occur where activities either cease without transfer to another entity, or transfer to an entity outside of the boundary of Whole of Government Accounts, such as private or voluntary sectors. Such activities are accounted for in accordance with IFRS 5. Activities that are transferred to other bodies within the boundary of Whole of Government Accounts are ‘machinery of government changes’ and treated as continuing operations.
Note 1.9 Property, plant and equipment
Recognition
Property, plant and equipment is capitalised where:
•it is held for use in delivering services or for administrative purposes
•it is probable that future economic benefits will flow to, or service potential be provided to, the Trust
•it is expected to be used for more than one financial year
•the cost of the item can be measured reliably
•the item has cost of at least £5,000, or
•collectively, a number of items have a cost of at least £5,000 and individually have cost of more than £250, where the assets are functionally interdependent, had broadly simultaneous purchase dates, are anticipated to have similar disposal dates and are under single managerial control.
Where a large asset, for example a building, includes a number of components with significantly different asset lives, eg, plant and equipment, then these components are treated as separate assets and depreciated over their own useful lives.
Subsequent expenditure
Subsequent expenditure relating to an item of property, plant and equipment is recognised as an increase in the carrying amount of the asset when it is probable that additional future economic benefits or service potential deriving from the cost incurred to replace a component of such item will flow to the enterprise and the cost of the item can be determined reliably. Where a component of an asset is replaced, the cost of the replacement is capitalised if it meets the criteria for recognition above. The carrying amount of the part replaced is de-recognised. Other expenditure that does not generate additional future economic benefits or service potential, such as repairs and maintenance, is charged to the Statement of Comprehensive Income in the period in which it is incurred.
Measurement
Valuation
All property, plant and equipment assets are measured initially at cost, representing the costs directly attributable to acquiring or constructing the asset and bringing it to the location and condition necessary for it to be capable of operating in the manner intended by management.
Assets are measured subsequently at valuation. Assets which are held for their service potential and are in use (ie operational assets used to deliver either front line services or back office functions) are measured at their current value in existing use. Assets that were most recently held for their service potential but are surplus with no plan to bring them back into use are measured at fair value where there are no restrictions on sale at the reporting date and where they do not meet the definitions of investment properties or assets held for sale.
Revaluations of property, plant and equipment are performed with sufficient regularity to ensure that carrying values are not materially different from those that would be determined at the end of the reporting period. Current values in existing use are determined as follows:
• Land and non-specialised buildings – market value for existing use
• Specialised buildings – depreciated replacement cost on a modern equivalent asset basis.
144
For specialised assets, current value in existing use is interpreted as the present value of the asset's remaining service potential, which is assumed to be at least equal to the cost of replacing that service potential. Specialised assets are therefore valued at their depreciated replacement cost (DRC) on a modern equivalent asset (MEA) basis. An MEA basis assumes that the asset will be replaced with a modern asset of equivalent capacity and meeting the location requirements of the services being provided. Assets held at depreciated replacement cost have been valued on an alternative site basis where this would meet the location requirements.
Properties in the course of construction for service or administration purposes are carried at cost, less any impairment loss. Cost includes professional fees and, where capitalised in accordance with IAS 23, borrowing costs. Assets are revalued and depreciation commences when the assets are brought into use.
IT equipment, transport equipment, furniture and fittings, and plant and machinery that are held for operational use are valued at depreciated historic cost where these assets have short useful lives or low values or both, as this is not considered to be materially different from current value in existing use.
Depreciation
Items of property, plant and equipment are depreciated over their remaining useful lives in a manner consistent with the consumption of economic or service delivery benefits. Freehold land is considered to have an infinite life and is not depreciated.
Property, plant and equipment which has been reclassified as ‘held for sale’ cease to be depreciated upon the reclassification. Assets in the course of construction and residual interests in off-Statement of Financial Position PFI contract assets are not depreciated until the asset is brought into use or reverts to the Trust, respectively.
Revaluation gains and losses
Revaluation gains are recognised in the revaluation reserve, except where, and to the extent that, they reverse a revaluation decrease that has previously been recognised in operating expenses, in which case they are recognised in operating expenditure.
Revaluation losses are charged to the revaluation reserve to the extent that there is an available balance for the asset concerned, and thereafter are charged to operating expenses.
Gains and losses recognised in the revaluation reserve are reported in the Statement of Comprehensive Income as an item of ‘other comprehensive income’.
Impairments
In accordance with the GAM, impairments that arise from a clear consumption of economic benefits or of service potential in the asset are charged to operating expenses. A compensating transfer is made from the revaluation reserve to the income and expenditure reserve of an amount equal to the lower of (i) the impairment charged to operating expenses; and (ii) the balance in the revaluation reserve attributable to that asset before the impairment.
An impairment that arises from a clear consumption of economic benefit or of service potential is reversed when, and to the extent that, the circumstances that gave rise to the loss is reversed. Reversals are recognised in operating expenditure to the extent that the asset is restored to the carrying amount it would have had if the impairment had never been recognised. Any remaining reversal is recognised in the revaluation reserve. Where, at the time of the original impairment, a transfer was made from the revaluation reserve to the income and expenditure reserve, an amount is transferred back to the revaluation reserve when the impairment reversal is recognised.
Other impairments are treated as revaluation losses. Reversals of ‘other impairments’ are treated as revaluation gains.
De-recognition
Assets intended for disposal are reclassified as ‘held for sale’ once the criteria in IFRS 5 are met. The sale must be highly probable and the asset available for immediate sale in its present condition. Following reclassification, the assets are measured at the lower of their existing carrying amount and their ‘fair value less costs to sell’. Depreciation ceases to be charged and the assets are not revalued, except where the 'fair value less costs to sell' falls below the carrying amount. Assets are de-recognised when all material sale contract conditions have been met.
Property, plant and equipment which is to be scrapped or demolished does not qualify for recognition as ‘held for sale’ and instead is retained as an operational asset and the asset’s useful life is adjusted. The asset is de-recognised when scrapping or demolition occurs.
145
Donated and grant funded assets
Donated and grant funded property, plant and equipment assets are capitalised at their fair value on receipt. The donation/grant is credited to income at the same time, unless the donor has imposed a condition that the future economic benefits embodied in the grant are to be consumed in a manner specified by the donor, in which case, the donation/grant is deferred within liabilities and is carried forward to future financial years to the extent that the condition has not yet been met.
The donated and grant funded assets are subsequently accounted for in the same manner as other items of property, plant and equipment.
146
Useful lives reflect the total life of an asset and not the remaining life of an asset. The range of useful lives are shown in
Note 1.10 Intangible assets
Recognition
Intangible assets are non-monetary assets without physical substance which are capable of being sold separately from the rest of the Trust’s business or which arise from contractual or other legal rights. They are recognised only where it is probable that future economic benefits will flow to, or service potential be provided to, the Trust and where the cost of the asset can be measured reliably.
Internally generated intangible assets
Internally generated goodwill, brands, mastheads, publishing titles, customer lists and similar items are not capitalised as intangible assets.
Expenditure on research is not capitalised. Expenditure on development is capitalised where it meets the requirements set out in IAS 38.
Software
Software which is integral to the operation of hardware, eg an operating system, is capitalised as part of the relevant item of property, plant and equipment. Software which is not integral to the operation of hardware, eg application software, is capitalised as an intangible asset.
Measurement
Intangible assets are recognised initially at cost, comprising all directly attributable costs needed to create, produce and prepare the asset to the point that it is capable of operating in the manner intended by management.
Subsequently intangible assets are measured at current value in existing use. Where no active market exists, intangible assets are valued at the lower of depreciated replacement cost and the value in use where the asset is income generating. Revaluations gains and losses and impairments are treated in the same manner as for property, plant and equipment. An intangible asset which is surplus with no plan to bring it back into use is valued at fair value where there are no restrictions on sale at the reporting date and where they do not meet the definitions of investment properties or assets held for sale.
Intangible assets held for sale are measured at the lower of their carrying amount or fair value less costs to sell.
Amortisation
Intangible assets are amortised over their expected useful lives in a manner consistent with the consumption of economic or service delivery benefits.
Useful lives of property, plant and equipment Min life Max life Years Years Land -Buildings, excluding dwellings 7 71 Dwellings 14 46 Plant & machinery 2 27 Transport equipment 10 10 Information technology 3 10 Furniture & fittings 5 23
147
Useful lives of intangible assets Min life Max life Years Years Information technology 5 12 Development expenditure -Websites -Software licences 5 10 Licences & trademarks -Patents -Other (purchased) -Goodwill -148
Note 1.11 Inventories
Inventories are valued at the lower of cost and net realisable value using the replacement cost formula. This is considered to be a reasonable approximation to fair value due to the high turnover of stocks.
The Trust received inventories including personal protective equipment from the Department of Health and Social Care at nil cost. In line with the GAM and applying the principles of the IFRS Conceptual Framework, the Trust has accounted for the receipt of these inventories at a deemed cost, reflecting the best available approximation of an imputed market value for the transaction based on the cost of acquisition by the Department.
Note 1.12 Investment properties
Investment properties are measured at fair value. Changes in fair value are recognised as gains or losses in income/expenditure.
Only those assets which are held solely to generate a commercial return are considered to be investment properties. Where an asset is held, in part, for support service delivery objectives, then it is considered to be an item of property, plant and equipment. Properties occupied by employees, whether or not they pay rent at market rates, are not classified as investment properties.
Note 1.13 Cash and cash equivalents
Cash is cash in hand and deposits with any financial institution repayable without penalty on notice of not more than 24 hours. Cash equivalents are investments that mature in 3 months or less from the date of acquisition and that are readily convertible to known amounts of cash with insignificant risk of change in value.
In the Statement of Cash Flows, cash and cash equivalents are shown net of bank overdrafts that are repayable on demand and that form an integral part of the Trust’s cash management. Cash, bank and overdraft balances are recorded at current values.
Note 1.14 Financial assets and financial liabilities
Recognition
Financial assets and financial liabilities arise where the Trust is party to the contractual provisions of a financial instrument, and as a result has a legal right to receive or a legal obligation to pay cash or another financial instrument. The GAM expands the definition of a contract to include legislation and regulations which give rise to arrangements that in all other respects would be a financial instrument and do not give rise to transactions classified as a tax by ONS.
This includes the purchase or sale of non-financial items (such as goods or services), which are entered into in accordance with the Trust’s normal purchase, sale or usage requirements and are recognised when, and to the extent which, performance occurs, ie, when receipt or delivery of the goods or services is made.
Classification and measurement
Financial assets and financial liabilities are initially measured at fair value plus or minus directly attributable transaction costs except where the asset or liability is not measured at fair value through income and expenditure. Fair value is taken as the transaction price, or otherwise determined by reference to quoted market prices or valuation techniques.
Financial assets or financial liabilities in respect of assets acquired or disposed of through leasing arrangements are recognised and measured in accordance with the accounting policy for leases described below.
Financial assets are classified as subsequently measured at fair value through income and expenditure.
Financial liabilities classified as subsequently measured at fair value through income and expenditure.
Financial assets and financial liabilities at amortised cost
149
Financial assets and financial liabilities at amortised cost are those held with the objective of collecting contractual cash flows and where cash flows are solely payments of principal and interest. This includes cash equivalents, contract and other receivables, trade and other payables, rights and obligations under lease arrangements and loans receivable and payable.
After initial recognition, these financial assets and financial liabilities are measured at amortised cost using the effective interest method less any impairment (for financial assets). The effective interest rate is the rate that exactly discounts estimated future cash payments or receipts through the expected life of the financial asset or financial liability to the gross carrying amount of a financial asset or to the amortised cost of a financial liability.
Interest revenue or expense is calculated by applying the effective interest rate to the gross carrying amount of a financial asset or amortised cost of a financial liability and recognised in the Statement of Comprehensive Income and a financing income or expense. In the case of loans held from the Department of Health and Social Care, the effective interest rate is the nominal rate of interest charged on the loan.
Financial assets measured at fair value through other comprehensive income
A financial asset is measured at fair value through other comprehensive income where business model objectives are met by both collecting contractual cash flows and selling financial assets and where the cash flows are solely payments of principal and interest. Movements in the fair value of financial assets in this category are recognised as gains or losses in other comprehensive income except for impairment losses. On derecognition, cumulative gains and losses previously recognised in other comprehensive income are reclassified from equity to income and expenditure, except where the Trust elected to measure an equity instrument in this category on initial recognition.
Financial assets and financial liabilities at fair value through income and expenditure
Financial assets measured at fair value through profit or loss are those that are not otherwise measured at amortised cost or at fair value through other comprehensive income. This category also includes financial assets and liabilities acquired principally for the purpose of selling in the short term (held for trading) and derivatives. Derivatives which are embedded in other contracts, but which are separable from the host contract are measured within this category. Movements in the fair value of financial assets and liabilities in this category are recognised as gains or losses in the Statement of Comprehensive income.
Impairment of financial assets
For all financial assets measured at amortised cost including lease receivables, contract receivables and contract assets or assets measured at fair value through other comprehensive income, the Trust recognises an allowance for expected credit losses.
The Trust adopts the simplified approach to impairment for contract and other receivables, contract assets and lease receivables. All debts more than three months old are set up as potential credit losses except those that could be offset against any salary payments. All overseas accounts are set up as potential credit losses on a monthly basis. The Trust does not normally recognise expected credit losses in relation to other NHS bodies.
The Trust does not have any other financial assets that require impairment.
Expected losses are charged to operating expenditure within the Statement of Comprehensive Income and reduce the net carrying value of the financial asset in the Statement of Financial Position.
Derecognition
Financial assets are de-recognised when the contractual rights to receive cash flows from the assets have expired or the Trust has transferred substantially all the risks and rewards of ownership.
Financial liabilities are de-recognised when the obligation is discharged, cancelled or expires.
150
Note 1.15 Leases
A lease is a contract or part of a contract that conveys the right to use an asset for a period of time in exchange for consideration. An adaptation of the relevant accounting standard by HM Treasury for the public sector means that for NHS bodies, this includes lease-like arrangements with other public sector entities that do not take the legal form of a contract. It also includes peppercorn leases where consideration paid is nil or nominal (significantly below market value) but in all other respects meet the definition of a lease. The trust does not apply lease accounting to new contracts for the use of intangible assets.
The Trust determines the term of the lease term with reference to the non-cancellable period and any options to extend or terminate the lease which the Trust is reasonably certain to exercise.
The Trust as a lessee Recognition and initial measurement
At the commencement date of the lease, being when the asset is made available for use, the Trust recognises a right of use asset and a lease liability.
The right of use asset is recognised at cost comprising the lease liability, any lease payments made before or at commencement, any direct costs incurred by the lessee, less any cash lease incentives received. It also includes any estimate of costs to be incurred restoring the site or underlying asset on completion of the lease term.
The lease liability is initially measured at the present value of future lease payments discounted at the interest rate implicit in the lease. Lease payments includes fixed lease payments, variable lease payments dependent on an index or rate and amounts payable under residual value guarantees. It also includes amounts payable for purchase options and termination penalties where these options are reasonably certain to be exercised.
Where an implicit rate cannot be readily determined, the Trust’s incremental borrowing rate is applied. This rate is determined by HM Treasury annually for each calendar year. A nominal rate of 0.95% applied to new leases commencing in 2022 and 3.51% to new leases commencing in 2023.
The Trust does not apply the above recognition requirements to leases with a term of 12 months or less or to leases where the value of the underlying asset is below £5,000, excluding any irrecoverable VAT. Lease payments associated with these leases are expensed on a straight-line basis over the lease term. Irrecoverable VAT on lease payments is expensed as it falls due.
Subsequent measurement
As required by a HM Treasury interpretation of the accounting standard for the public sector, the Trust employs a revaluation model for subsequent measurement of right of use assets, unless the cost model is considered to be an appropriate proxy for current value in existing use or fair value, in line with the accounting policy for owned assets. Where consideration exchanged is identified as significantly below market value, the cost model is not considered to be an appropriate proxy for the value of the right of use asset.
The Trust subsequently measures the lease liability by increasing the carrying amount for interest arising which is also charged to expenditure as a finance cost and reducing the carrying amount for lease payments made. The liability is also remeasured for changes in assessments impacting the lease term, lease modifications or to reflect actual changes in lease payments. Such remeasurements are also reflected in the cost of the right of use asset. Where there is a change in the lease term or option to purchase the underlying asset, an updated discount rate is applied to the remaining lease payments.
The Trust as a lessor
The Trust assesses each of its leases and classifies them as either a finance lease or an operating lease. Leases are classified as finance leases when substantially all the risks and rewards of ownership are transferred to the lessee. All other leases are classified as operating leases.
Where the Trust is an intermediate lessor, classification of the sublease is determined with reference to the right of use asset arising from the headlease.
Finance leases
Amounts due from lessees under finance leases are recorded as receivables at the amount of the Trust’s net investment in the leases. Finance lease income is allocated to accounting periods to reflect a constant periodic rate of return on the Trust’s net investment outstanding in respect of the leases.
Operating leases
151
Income from operating leases is recognised on a straight-line basis or another systematic basis over the term of the lease. Initial direct costs incurred in negotiating and arranging an operating lease are added to the carrying amount of the leased asset and recognised as an expense on a straight-line basis over the lease term.
Initial application of IFRS 16
IFRS 16 Leases as adapted and interpreted for the public sector by HM Treasury has been applied to these financial statements with an initial application date of 1 April 2022. IFRS 16 replaces IAS 17 Leases, IFRIC 4 Determining whether an arrangement contains a lease and other interpretations.
The standard has been applied using a modified retrospective approach with the cumulative impact recognised in the income and expenditure reserve on 1 April 2022. Upon initial application, the provisions of IFRS 16 have only been applied to existing contracts where they were previously deemed to be a lease or contain a lease under IAS 17 and IFRIC 4. Where existing contracts were previously assessed not to be or contain a lease, these assessments have not been revisited.
The Trust as lessee
For continuing leases previously classified as operating leases, a lease liability was established on 1 April 2022 equal to the present value of future lease payments discounted at the Trust’s incremental borrowing rate of 0.95%. A right of use asset was created equal to the lease liability and adjusted for prepaid lease payments. Hindsight has been used in determining the lease term where lease arrangements contain options for extension or earlier termination.
No adjustments have been made on initial application in respect of leases with a remaining term of 12 months or less from 1 April 2022 or for leases where the underlying assets has a value below £5,000. No adjustments have been made in respect of leases previously classified as finance leases.
The Trust as lessor
Leases of owned assets where the Trust is lessor were unaffected by initial application of IFRS 16.
2021/22 comparatives
Comparatives for leasing transactions in these accounts have not been restated on an IFRS 16 basis. Under IAS 17 the classification of leases as operating or finance leases still applicable to lessors under IFRS 16 also applied to lessees. In 2021/22 lease payments made by the Trust in respect of leases previously classified as operating leases were charged to expenditure on a straight line basis.
152
The Trust recognises a provision where it has a present legal or constructive obligation of uncertain timing or amount; for which it is probable that there will be a future outflow of cash or other resources; and a reliable estimate can be made of the amount. The amount recognised in the Statement of Financial Position is the best estimate of the resources required to settle the obligation. Where the effect of the time value of money is significant, the estimated riskadjusted cash flows are discounted using HM Treasury's discount rates effective from 31 March 2023:
HM Treasury provides discount rates for general provisions on a nominal rate basis. Expected future cash flows are therefore adjusted for the impact of inflation before discounting using nominal rates. The following inflation rates are set by HM Treasury, effective from 31 March 2023:
Early retirement provisions and injury benefit provisions both use the HM Treasury's pension discount rate of 1.70% in real terms (prior year: minus 1.30%).
Clinical negligence costs
NHS Resolution operates a risk pooling scheme under which the trust pays an annual contribution to NHS Resolution, which, in return, settles all clinical negligence claims. Although NHS Resolution is administratively responsible for all clinical negligence cases, the legal liability remains with the Trust. The total value of clinical negligence provisions carried by NHS Resolution on behalf of the trust is disclosed at note 34.2 but is not recognised in the Trust’s accounts.
Non-clinical risk pooling
The Trust participates in the Property Expenses Scheme and the Liabilities to Third Parties Scheme. Both are risk pooling schemes under which the Trust pays an annual contribution to NHS Resolution and in return receives assistance with the costs of claims arising. The annual membership contributions, and any excesses payable in respect of particular claims are charged to operating expenses when the liability arises.
Note 1.17 Contingencies
Contingent assets (that is, assets arising from past events whose existence will only be confirmed by one or more future events not wholly within the entity’s control) are not recognised as assets, but are disclosed in note 34 where an inflow of economic benefits is probable.
Contingent liabilities are not recognised, but are disclosed in note 34, unless the probability of a transfer of economic benefits is remote.
Contingent liabilities are defined as:
•possible obligations arising from past events whose existence will be confirmed only by the occurrence of one or more uncertain future events not wholly within the entity’s control; or
•present obligations arising from past events but for which it is not probable that a transfer of economic benefits will arise or for which the amount of the obligation cannot be measured with sufficient reliability.
Note 1.16 Provisions Nominal rate Prior year rate Short-term Up to 5 years 3.27% 0.47% Medium-term After 5 years up to 10 years 3.20% 0.70% Long-term After 10 years up to 40 years 3.51% 0.95% Very long-term Exceeding 40 years 3.00% 0.66% Inflation rate Prior year rate Year 1 7.40% 4.00% Year 2 0.60% 2.60% Into perpetuity 2.00% 2.00%
153
Note 1.18 Public dividend capital
Public dividend capital (PDC) is a type of public sector equity finance based on the excess of assets over liabilities at the time of establishment of the predecessor NHS organisation. HM Treasury has determined that PDC is not a financial instrument within the meaning of IAS 32.
The Secretary of State can issue new PDC to, and require repayments of PDC from, the trust. PDC is recorded at the value received.
A charge, reflecting the cost of capital utilised by the trust, is payable as public dividend capital dividend. The charge is calculated at the rate set by HM Treasury (currently 3.5%) on the average relevant net assets of the Trust during the financial year. Relevant net assets are calculated as the value of all assets less the value of all liabilities, with certain additions and deductions as defined by the Department of Health and Social Care.
This policy is available at https://www.gov.uk/government/publications/guidance-on-financing-available-to-nhs-trustsand-foundation-trusts.
In accordance with the requirements laid down by the Department of Health and Social Care (as the issuer of PDC), the dividend for the year is calculated on the actual average relevant net assets as set out in the “pre-audit” version of the annual accounts. The dividend calculated is not revised should any adjustment to net assets occur as a result of the audit of the annual accounts.
Note 1.19 Value added tax
Most of the activities of the trust are outside the scope of VAT and, in general, output tax does not apply and input tax on purchases is not recoverable. Irrecoverable VAT is charged to the relevant expenditure category or included in the capitalised purchase cost of fixed assets. Where output tax is charged or input VAT is recoverable, the amounts are stated net of VAT.
Note 1.20 Corporation tax
The Trust is not required to pay corporation tax as it is an NHS trust and has no trading company.
Note 1.21 Climate change levy
Expenditure on the climate change levy is recognised in the Statement of Comprehensive Income as incurred, based on the prevailing chargeable rates for energy consumption.
Note 1.22 Foreign exchange
The functional and presentational currency of the trust is sterling.
A transaction which is denominated in a foreign currency is translated into the functional currency at the spot exchange rate on the date of the transaction.
Where the trust has assets or liabilities denominated in a foreign currency at the Statement of Financial Position date:
•monetary items are translated at the spot exchange rate on 31 March
•non-monetary assets and liabilities measured at historical cost are translated using the spot exchange rate at the date of the transaction and
•non-monetary assets and liabilities measured at fair value are translated using the spot exchange rate at the date the fair value was determined.
Exchange gains or losses on monetary items (arising on settlement of the transaction or on re-translation at the Statement of Financial Position date) are recognised in income or expense in the period in which they arise.
Exchange gains or losses on non-monetary assets and liabilities are recognised in the same manner as other gains and losses on these items.
Note 1.23 Third party assets
Assets belonging to third parties in which the Trust has no beneficial interest (such as money held on behalf of patients) are not recognised in the accounts. However, they are disclosed in a separate note to the accounts in accordance with the requirements of HM Treasury’s FReM
154
Note 1.24 Losses and special payments
Losses and special payments are items that Parliament would not have contemplated when it agreed funds for the health service or passed legislation. By their nature they are items that ideally should not arise. They are therefore subject to special control procedures compared with the generality of payments. They are divided into different categories, which govern the way that individual cases are handled. Losses and special payments are charged to the relevant functional headings in expenditure on an accruals basis.
The losses and special payments note is compiled directly from the losses and compensations register which reports on an accrual basis with the exception of provisions for future losses.
Note 1.25 Gifts
Gifts are items that are voluntarily donated, with no preconditions and without the expectation of any return. Gifts include all transactions economically equivalent to free and unremunerated transfers, such as the loan of an asset for its expected useful life, and the sale or lease of assets at below market value.
Note 1.26 Transfers of functions to/from other NHS bodies/local government bodies
There have been no functions that have been transferred to/from the Trust from/to other NHS/local government bodies.
155
Note 1.27 Early adoption of standards, amendments and interpretations
No new accounting standards or revisions to existing standards have been early adopted in 2022/23.
Note 1.28 Standards, amendments and interpretations in issue but not yet effective or adopted
IFRS17 Insurance Contracts - the effective date for IFRS17 is now 2023/24 but work has not yet started on understanding its impact on the NHS.
Note 1.29 Critical judgements in applying accounting policies
The following are the judgements, apart from those involving estimations (see below) that management has made in the process of applying the Trust's accounting policies and that have the most significant effect on the amounts recognised in the financial statements:
Charitable Funds: Following Treasury’s agreement to apply IAS 27 (Consolidation and Separate Financial Statements) to NHS Charities from 1 April 2013, The Shrewsbury and Telford Hospital NHS Trust has established that as the Trust is the Corporate Trustee of the linked NHS Charity, it effectively has the power to exercise control so as to obtain economic benefits so therefore may have needed to consolidate its NHS Charity Accounts into its NHS Trust Accounts. The Trust has considered the income, expenditure, assets and liabilities of the NHS Charity to be immaterial in the context of the accounts of the NHS Trust and have not consolidated these into the Trust’s accounts.
Note 1.30 Sources of estimation uncertainty
The following are assumptions about the future and other major sources of estimation uncertainty that have a significant risk of resulting in a material adjustment to the carrying amounts of assets and liabilities within the next financial year:
In the application of the NHS Trust’s accounting policies, management is required to make judgements, estimates and assumptions about the carrying amounts of assets and liabilities that are not readily apparent from other sources. The estimates and associated assumptions are based on historical experience and other factors that are considered to be relevant. Actual results may differ from those estimates and the estimates and underlying assumptions are continually reviewed. Revisions to accounting estimates are recognised in the period in which the estimate is revised if the revision affects only that period or in the period of the revision and future periods if the revision affects both current and future periods.
Accruals: The Trust uses, wherever possible, advice from specialist providers or information from counterparty organisations to support estimated values within the accounts. If these are not available, the Trust uses own data and experience to calculate estimated amounts to reduce material errors from the estimated values included in the accounts.
Provisions: Provisions are made from probable legal and constructive obligations of uncertain timings and amount as at the reporting date. These are based on estimates using relevant and reliable information as is available at the time the financial statements are prepared. These provisions are estimates of the actual costs of future cash flows and are dependent on future events. Any difference between expectations and the actual future liability will be accounted for in the period when such determination is made.
Revaluation: The Trust commissioned Cushman and Wakefield (‘C&W’) to undertake a desktop update valuation of the Trust’s estate as at 31 March 2023. Specialised buildings are valued at Depreciated Replacement Cost defined as Modern Equivalent Asset.
Land and building assets are valued on the basis explained in Notes 1.9 and 16. A professional firm of valuers has provides the Trust with a valuation based on estimated fair value and remaining useful life. As the Trust’s land and buildings are infrastructural in nature, and thus do not have a conventional market value in use; the valuations are based on estimates provided by suitably qualified professionals in accordance with HM Treasury guidance. Future revaluations of property may result in further changes to the carrying values of the non-current assets. The Trust’s management determines the estimated useful lives and depreciation charges for all property, plant and equipment assets (with the exception of land). These estimates are based on past experience and practice across the health sector, as well as drawing on the technical expertise within the Trust. Management will increase the depreciation charges where useful lives are less than previously estimated, or it will write off or write down assets that are obsolete, abandoned or sold. Useful lives for land, buildings and dwellings are determined by independent valuers and management reviews these for reasonableness.
156
Market Conditions
The UK and other countries continue to experience heightened uncertainty due to a number of factors. Inflationary pressures continue to weigh on the economy and whilst having peaked still remain at high levels having a very material effect on higher cost of living expenses. Base rates have increased rapidly to combat the inflationary conditions and the expectation is for further rises still to come. The cost of debt has risen, and its availability reduced which together with the outward movement in gilt yields from historically low levels has weighed on investor sentiment and had an adverse impact on property values. Confidence in the banking sector is fragile as seen in the recent actions around a handful of banks but most particularly Credit Suisse and this is likely to result in the further tightening of debt available to investors. Whilst the UK is now expected to escape a recession, despite this having been widely predicted, it is clear that economic conditions remain challenging in the short to medium term. In recognition of the potential for market conditions to move rapidly in response to wider political and economic changes, we highlight the importance of the Valuation Date as it is important to understand the market context under which the valuation opinion was prepared. At this point we anticipate longer marketing periods being required to elicit bids.
Building Safety – Market Uncertainty
The aftermath of the Grenfell Fire on 14 June 2017 resulted in a wholesale review of the regime relating to building safety. A public inquiry commenced in 2018 with a report on the findings of the first phase of the inquiry published in October 2019. The second phase of the inquiry commenced in January 2020 and is still ongoing.
An Independent Review of Building Regulations and Fire Safety led by Dame Judith Hackitt was published in May 2018. This included recommendations for a new Building Regulations regime for residential buildings of 10 storeys (30m) or higher. The Government subsequently announced that Building Regulations would be amended from 21 December 2018 to ban the use of combustible materials on the external walls of new buildings over 18m containing flats, as well as, inter alia, buildings such as new hospitals, residential care homes and student accommodation. Due to the changes to the building regulations the ban will affect existing buildings undergoing major works or a change of use. On 20 January 2020 MHCLG published “Building safety advice for building owners, including fire doors” which consolidated the previously published advice notes including Advice Note 22. The advice note specifically deals with aluminium composite material panels, high pressure laminate panels, spandrel panels, balconies and external wall insulation systems as well as smoke control system and fire doors. The advice note does not cover all types of wall systems for buildings below 18 metres, but consideration is to be given to the spread of fire externally through the fire risk assessment taken into consideration the buildings occupancy and other factors which may result in remedial actions being required.
The Fire Safety Act 2021 came into force in May and aims to improve fire safety in multi-occupancy domestic premises. The Act requires responsible persons to assess, manage and reduce the fire risks posed by the structure and external walls of the buildings for which they are responsible (including cladding, balconies and windows). It applies to all multioccupied residential buildings and is not dependent on the height of the building. The Act allows the Fire & Rescue Service to enforce against non-compliance in relation to the external walls and the individual doors opening onto the common parts of the premises, but the Act does not address remediation costs in relation to cladding or its replacement.
Market participants continue to be affected by details of construction, health and safety, and particularly fire prevention, mitigation and means of escape from buildings where people sleep. The Government’s proposed legislation is far reaching and will provide a new regime for building regulations compliance. In the light of these circumstances, valuations are undertaken in the context of a changing regulatory environment and we would therefore recommend that it is kept under regular review.
Pensions: The NHS Pensions Scheme provides cover for past and present employees, and is subject to a full valuation every five years (see note 10). The Trust carries provisions in certain instances relating to early retirement, based on latest actuarial information provided by the NHS Pensions Agency. This is therefore subject to change which is recognised in the period to which it arises.
Insurance: The Trust maintains insurance against potential legal claims, which are managed by the NHS Resolution. The Trust makes provisions for the estimated excess liabilities due under this policy, in line with information provided by the NHS Resolution. Uncertainty in estimation may relate to the timing of potential settlements, although the liability to the Trust will be limited to the level of excess.
157
Note 2 Operating Segments
The Trust operates in one material segment which is the provision of healthcare services with the Trust Board as its chief operating decision maker deciding how to allocate resources and assessing performance.
Note 3 Operating income from patient care activities
All income from patient care activities relates to contract income recognised in line with accounting policy 1.4.
Note 3.1 Income from patient care activities (by nature)
*Aligned payment and incentive contracts are the main form of contracting between NHS providers and their commissioners. More information can be found in the 2022/23 National Tariff payments system documents. https://www.england.nhs.uk/publication/past-national-tariffs-documents-and-policies/
**The employer contribution rate for NHS pensions increased from 14.3% to 20.6% (excluding administration charge) from 1 April 2019. Since 2019/20, NHS providers have continued to pay over contributions at the former rate with the additional amount being paid over by NHS England on providers' behalf. The full cost and related funding have been recognised in these accounts.
*** In March 2023 the government announced an additional pay offer for 2022/23, in addition to the pay award earlier in the year. Additional funding was made available by NHS England for implementing this pay offer for 2022/23 and the income and expenditure has been included in these accounts as guided by the Department of Health and Social Care and NHS England. In May 2023 the government confirmed this offer will be implemented as a further pay award in respect of 2022/23 based on individuals in employment at 31 March 2023.
2022/23 2021/22 £000 £000 Acute services Income from commissioners under API contracts* 444,876 435,500 High cost drugs income from commissioners (excluding pass-through costs) 2,473 4,954 Other NHS clinical income 1,489 1,301 All services Private patient income 1,273 1,257 Elective recovery fund 13,381 2,487 Agenda for change pay award central funding*** 12,168Additional pension contribution central funding** 13,982 12,950 Other clinical income 33,585 34,788 Total income from activities 523,227 493,237
158
Note 3.2 Income from patient care activities (by source)
Note 3.3 Overseas visitors (relating to patients charged directly by the provider)
2022/23 2021/22 Income from patient care activities received from: £000 £000 NHS England 98,794 80,386 Clinical commissioning groups 92,228 375,505 Integrated care boards 294,740Other NHS providers 819 1,301 Non-NHS: private patients 1,273 1,257 Non-NHS: overseas patients (chargeable to patient) 230 87 Injury cost recovery scheme 1,259 904 Non NHS: other 33,884 33,797 Total income from activities 523,227 493,237 Of which: Related to continuing operations 523,227 493,237 Related to discontinued operations - -
2022/23 2021/22 £000 £000 Income recognised this year 230 87 Cash payments received in-year 34 50 Amounts added to provision for impairment of receivables 203 51 Amounts written off in-year 33 43 159
Note 4 Other operating income
* This includes donated equipment from group bodies for COVID response.
** This includes inventories and equipment below capitalisation threshold for COVID response.
*** The majority of 'Other income' is for Car-Parking, Pathology, Therapies, Radiology, Midwifery, and Intensive Support funding.
Note 5.1 Additional information on contract revenue (IFRS 15) recognised in the period
Revenue recognised in the reporting period that was included in within contract liabilities at the previous period end
Revenue recognised from performance obligations satisfied (or partially satisfied) in previous periods
Note 5.2 Fees and charges
The Trust undertakes income generation schemes with an aim of achieving profit, which is then used in patient care. The Trust has no income generation activities whose full cost exceeded £1m.
Note 6 Operating leases - The Shrewsbury And Telford Hospital NHS Trust as lessor
The Trust has no operating lease agreements where it is acting as the lessor.
Contract income Non-contract income Total Contract income Non-contract income Total £000 £000 £000 £000 £000 £000 Research and development 766 - 766 575 - 575 Education and training 17,310 - 17,310 14,498 - 14,498 Non-patient care services to other bodies 1,353 1,353 1,932 1,932 Reimbursement and top up funding 1,722 1,722 8,826 8,826 Receipt of capital grants and donations and peppercorn leases* 403 403 1,140 1,140 Charitable and other contributions to expenditure** 1,483 1,483 1,786 1,786 Other income*** 10,341 - 10,341 13,148 - 13,148 Total other operating income 31,492 1,886 33,378 38,979 2,926 41,905 Of which: Related to continuing operations 33,378 41,905 Related to discontinued operations - -
2022/23 2021/22 £000 £000 1,554 1,512 -
2022/23 2021/22
160
Note 7.1 Operating expenses
2022/23 2021/22 £000 £000 Purchase of healthcare from non-NHS and non-DHSC bodies 115 265 Staff and executive directors costs 410,934 367,435 Remuneration of non-executive directors 160 133 Supplies and services - clinical (excluding drugs costs) 41,960 40,180 Supplies and services - general 6,496 6,296 Drug costs (drugs inventory consumed and purchase of non-inventory drugs) 51,234 47,931 Inventories written down 286 165 Consultancy costs 595 859 Establishment 7,548 6,217 Premises 30,150 22,814 Transport (including patient travel) 737 651 Depreciation on property, plant and equipment and right of use assets 18,815 12,901 Amortisation on intangible assets 2,479 1,843 Net impairments (289) 5,514 Movement in credit loss allowance: contract receivables / contract assets 484 400 Increase/(decrease) in other provisions 162 143 Change in provisions discount rate(s) (10) (4) Fees payable to the external auditor* audit services- statutory audit 140 131 Internal audit costs 114 114 Clinical negligence 14,541 15,470 Legal fees 290 193 Insurance 88 90 Education and training 2,189 2,454 Expenditure on short term leases (current year only) 61Variable lease payments not included in the liability (current year only) 5,315Operating lease expenditure (comparative only) - 10,495 Car parking & security 868 720 Losses, ex gratia & special payments 16 12 Other 610 1,601 Total 596,088 545,023 Of which: Related to continuing operations 596,087 545,023 Related to discontinued operations -* audit services - statutory audit of £116,280 plus £23,256 of VAT 161
Note 7.2 Other auditor remuneration
No other auditor remuneration was paid to the external auditor.
Note 7.3 Limitation on auditor's liability
The limitation on auditor's liability for external audit work is £5 million (2021/22: £5 million).
Note 8 Impairment of assets
The Trust commissioned Cushman and Wakefield to undertake a desktop update valuation of the Trust's Estate as at 31 March 2023. The valuation has resulted in the following:
- impairments to the value of £936k have been charged to Statement of Comprehensive Income and previous impairments of £1,225k have been reversed, giving a net reversal of impairments of £289k to Statement of Comprehensive Income;
- impairments of £1,663k have been charged to the Revaluation Reserve and previous impairments of £459k have been reversed, giving a net impairment of £1,204k to the Revaluation Reserve.
Note 9 Employee benefits
Note 9.1 Retirements due to ill-health
During 2022/23 there were 8 early retirements from the trust agreed on the grounds of ill-health (6 in the year ended 31 March 2022). The estimated additional pension liabilities of these ill-health retirements is £545k (£554k in 2021/22).
These estimated costs are calculated on an average basis and will be borne by the NHS Pension Scheme.
2022/23 2021/22 £000 £000 Net impairments charged to operating surplus / deficit resulting from: Changes in market price (289) 5,514 Total net impairments charged to operating surplus / deficit (289) 5,514 Impairments charged to the revaluation reserve 1,204 1,337 Total net impairments 915 6,851
2022/23 2021/22 Total Total £000 £000 Salaries and wages 290,274 266,199 Social security costs 28,864 26,118 Apprenticeship levy 1,393 1,273 Employer's contributions to NHS pensions 46,112 42,723 Temporary staff (including agency) 46,529 32,845 Total gross staff costs 413,172 369,158 Recoveries in respect of seconded staff -Total staff costs 413,172 369,158 Of which Costs capitalised as part of assets 2,238 1,723
162
Past and present employees are covered by the provisions of the two NHS Pension Schemes. Details of the benefits payable and rules of the Schemes can be found on the NHS Pensions website at www.nhsbsa.nhs.uk/pensions. Both are unfunded defined benefit schemes that cover NHS employers, GP practices and other bodies, allowed under the direction of the Secretary of State for Health and Social Care in England and Wales. They are not designed to be run in a way that would enable NHS bodies to identify their share of the underlying scheme assets and liabilities. Therefore, each scheme is accounted for as if it were a defined contribution scheme: the cost to the NHS body of participating in each scheme is taken as equal to the contributions payable to that scheme for the accounting period.
In order that the defined benefit obligations recognised in the financial statements do not differ materially from those that would be determined at the reporting date by a formal actuarial valuation, the FReM requires that “the period between formal valuations shall be four years, with approximate assessments in intervening years”. An outline of these follows:
a) Accounting valuation
A valuation of scheme liability is carried out annually by the scheme actuary (currently the Government Actuary’s Department) as at the end of the reporting period. This utilises an actuarial assessment for the previous accounting period in conjunction with updated membership and financial data for the current reporting period, and is accepted as providing suitably robust figures for financial reporting purposes. The valuation of the scheme liability as at 31 March 2023, is based on valuation data as at 31 March 2022, updated to 31 March 2023 with summary global member and accounting data. In undertaking this actuarial assessment, the methodology prescribed in IAS 19, relevant FReM interpretations, and the discount rate prescribed by HM Treasury have also been used.
The latest assessment of the liabilities of the scheme is contained in the report of the scheme actuary, which forms part of the annual NHS Pension Scheme Accounts. These accounts can be viewed on the NHS Pensions website and are published annually. Copies can also be obtained from The Stationery Office.
b) Full actuarial (funding) valuation
The purpose of this valuation is to assess the level of liability in respect of the benefits due under the schemes (taking into account recent demographic experience), and to recommend contribution rates payable by employees and employers.
The latest actuarial valuation undertaken for the NHS Pension Scheme was completed as at 31 March 2016. The results of this valuation set the employer contribution rate payable from April 2019 at 20.6% of pensionable pay.
The actuarial valuation as at 31 March 2020 is currently underway and will set the new employer contribution rate due to be implemented from April 2024.
Note 10 Pension costs
163
Note 11 Finance income
Finance income represents interest received on assets and investments in the period.
Note 12.1 Finance expenditure
Finance expenditure represents interest and other charges involved in the borrowing of money or asset financing.
Note 12.2 The late payment of commercial debts (interest) Act 1998 / Public Contract Regulations 2015
Note 13 Other gains / (losses)
Note 14 Discontinued operations
There are no discontinued operations.
2022/23 2021/22 £000 £000 Interest on bank accounts 604 16 Total finance income 604 16
2022/23 2021/22 £000 £000 Interest expense: Interest on lease obligations 192Interest on late payment of commercial debt 1Total interest expense 193Unwinding of discount on provisions 19 (4) Total finance costs 212 (4)
2022/23 2021/22 £000 £000
legislation 1 -
Amounts included within interest payable arising from claims made under this
2022/23 2021/22 £000 £000 Losses on disposal of assets (479) (99) Total gains / (losses) on disposal of assets (479) (99) Total other gains / (losses) (479) (99)
164
Note 15.1 Intangible assets - 2022/23
Software licences Internally generated information technology Intangible assets under construction Total £000 £000 £000 £000 Valuation / gross cost at 1 April 2022 - brought forward 4,797 11,455 5,423 21,675 IFRS 16 implementation - reclassification of
assets - - -Additions 133 2,518 5,076 7,727 Reclassifications - 1,760 (1,750) 10 Disposals / derecognition - (16) - (16) Valuation / gross cost at 31 March 2023 4,930 15,717 8,749 29,396 Amortisation at 1 April 2022 - brought forward 771 5,095 - 5,866 IFRS 16 implementation - reclassification of
of
assets - - -Provided during the year 634 1,845 - 2,479 Disposals / derecognition - (16) - (16) Amortisation at 31 March 2023 1,405 6,924 - 8,329 Net book value at 31 March 2023 3,525 8,793 8,749 21,067 Net book value at 1 April 2022 4,026 6,360 5,423 15,809 165
existing finance leased assets to right of use
existing finance leased assets to right
use
Note 15.2 Intangible assets - 2021/22
Software licences Internally generated information technology Intangible assets under construction Total £000 £000 £000 £000 Valuation / gross cost at 1 April 2021 - as previously stated 4,370 7,803 4,389 16,562 Additions 389 2,419 2,274 5,082 Reclassifications 38 1,233 (1,240) 31 Disposals / derecognition - - -Valuation / gross cost at 31 March 2022 4,797 11,455 5,423 21,675 Amortisation at 1 April 2021 - as previously stated 210 3,813 - 4,023 Provided during the year 561 1,282 - 1,843 Disposals / derecognition - - -Amortisation at 31 March 2022 771 5,095 - 5,866 Net book value at 31 March 2022 4,026 6,360 5,423 15,809 Net book value at 1 April 2021 4,160 3,990 4,389 12,539 166
Note 16.1 Property, plant and equipment - 2022/23
Land Buildings excluding dwellings Dwellings Assets under construction Plant & machinery Transport equipment Information technology Furniture & fittings Total £000 £000 £000 £000 £000 £000 £000 £000 £000 Valuation/gross cost at 1 April 2022 - brought forward 13,500 178,311 1,450 25,963 53,740 388 23,455 2,369 299,176 IFRS 16 implementation - reclassification of existing finance leased assets to right of use assets - - - - - - - -Additions - 6,649 - 37,249 6,738 6 643 127 51,412 Impairments - (3,955) - - - - - - (3,955) Reversals of impairments - 547 3 - - - - - 550 Revaluations - 4,833 49 - - - - - 4,882 Reclassifications - 10,921 1 (16,711) 5,325 19 157 278 (10) Disposals / derecognition - - - (925) (2,599) - - - (3,524) Valuation/gross cost at 31 March 2023 13,500 197,306 1,503 45,576 63,204 413 24,255 2,774 348,531 Accumulated depreciation at 1 April 2022 - brought forward - 397 - - 28,936 354 8,883 1,116 39,686 IFRS 16 implementation - reclassification of existing finance leased assets to
of use assets - - - - - - - -Provided during the year - 6,364 37 - 4,760 14 3,761 229 15,165 Impairments - (1,356) - - - - - - (1,356) Reversals of impairments - (1,131) (3) - - - - - (1,134) Revaluations - (3,815) (34) - - - - - (3,849) Reclassifications - - - - 26 - - (26)Disposals / derecognition - - - - (2,121) - - - (2,121) Accumulated depreciation at 31 March 2023 - 459 - - 31,601 368 12,644 1,319 46,391 Net book value at 31 March 2023 13,500 196,847 1,503 45,576 31,603 45 11,611 1,455 302,140 Net book value at 1 April 2022 13,500 177,914 1,450 25,963 24,804 34 14,572 1,253 259,490 167
right
Note 16.2 Property, plant and equipment - 2021/22
Land Buildings excluding dwellings Dwellings Assets under construction Plant & machinery Transport equipment Information technology Furniture & fittings Total £000 £000 £000 £000 £000 £000 £000 £000 £000 Valuation / gross cost at 1 April 2021 - as previously stated 13,500 170,651 1,447 14,976 54,114 388 16,267 2,141 273,484 Additions - 10,627 38 19,568 2,352 - 6,954 199 39,738 Impairments - (9,679) (37) - - - - - (9,716) Reversals of impairments - 136 2 - - - - - 138 Revaluations - 1,298 - - - - - - 1,298 Reclassifications - 5,278 - (8,581) 3,009 - 234 29 (31) Disposals / derecognition - - - - (5,735) - - - (5,735) Valuation/gross cost at 31 March 2022 13,500 178,311 1,450 25,963 53,740 388 23,455 2,369 299,176 Accumulated depreciation at 1 April 2021 - as previously stated - 338 - - 28,469 337 6,241 923 36,308 Provided during the year - 5,870 37 - 4,142 17 2,642 193 12,901 Impairments - (1,811) (4) - - - - - (1,815) Reversals of impairments - (879) (33) - - - - - (912) Revaluations - (3,121) - - - - - - (3,121) Reclassifications - - - - - - - -Disposals / derecognition - - - - (3,675) - - - (3,675) Accumulated depreciation at 31 March 2022 - 397 - - 28,936 354 8,883 1,116 39,686 Net book value at 31 March 2022 13,500 177,914 1,450 25,963 24,804 34 14,572 1,253 259,490 Net book value at 1 April 2021 13,500 170,313 1,447 14,976 25,645 51 10,026 1,218 237,176 168
Valuation Assumptions
There are a variety of factors which drive the valuation both in terms of base data such as floor areas, in-year capital expenditure and change in building usage but also several judgemental assumptions applied by the Valuer e.g. build cost indices, remaining useful lives, Modern Equivalent Asset, obsolescence adjustments and judgements around land values. Some of these are outlined below:
On the commencement of the contract in March 2021, the Valuer undertook an initial full valuation of the Trust's owned property assets at Royal Shrewsbury Hospital and Princess Royal Hospital, Telford.
The building assets were first assessed to ascertain whether they should be valued on a sales comparison basis or by the depreciated replacement cost method. The Trust's land and buildings were strictly categorised into property assets and their major components, in accordance with the RICS Valuation - Global Standards, (in that the whole of a site is designated as the property asset, with the land, the separate buildings upon it and the external works being the major components of the asset).
Obsolescence
The major components of the property asset were then surveyed for the purpose of categorising for use and quality and a detailed survey of each was undertaken in order to assess the condition/physical obsolescence.
To assess the physical obsolescence of a building/major component, the Valuer breaks it down into 26 elements, such as the foundations, walls and roof etc and the remaining useful life of each of these elements is then assessed against the lifespan, through inspection. The proportion of build costs for each element is calculated based on comparable build cost information published by the RICS Building Cost Information Service (BCIS), enabling the cost weighted physical obsolescence of the building/major component to be assessed. For the areas of the buildings, the departments within them and the land, the Valuer relies on information provided by the Trust, they do not undertake any on-site measurement, but do review a sample of buildings against plans provided by the Trust to confirm accuracy.
From their detailed site inspection they assessed the level of functional obsolescence to the hospital and also to each building/component. This is stated as a percentage reduction applied to the rebuild cost. The valuation is therefore based on the existing buildings and their gross internal areas rather than the area of the modern equivalent replacement, enabling the Trust to effectively measure the change in value to a block associated with future alterations or a change in usage etc. The valuer, then met with the Trust's Estates and Finance Teams to review their assessment of the level of obsolescence and obtain the Trust's opinion based on its detailed knowledge to the estate and its function.
Functional obsolescence is where the design or specification of the building no longer fulfils the function for which it was designed efficiently compared with the modern equivalent. Examples of functional obsolescence are poor energy performance and disabled accessibility of the existing buildings. In addition the modern equivalent reprovision of the existing service could be from a smaller area than the existing.
The same process was undertaken to assess the level of economic obsolescence for each of the buildings. A common example of economic obsolescence is where there is over capacity against the demand and therefore this should be reflected in the value of the asset regardless of how modern or efficient it may be.
Through meetings with the Trust and the Valuer's site inspections, any assets under construction (AUC) as at the valuation date, being 31 March 2021, were identified and the valuation adjusted appropriately. Additionally, proposed future works, with business case approval, which would impact the valuation of the existing property were identified through consultation with the Trust and taken into account in the valuation.
The current cost of replacement was assessed, based on comparable build cost information and the Regional Location Factor published by the RICS Building Cost Information Service. The current cost of replacement was then reviewed to take account of physical obsolescence, functional obsolescence, economic obsolescence, AUC and future works to arrive at a depreciated replacement cost valuation as at 31 March 2021 in accordance with RICS Guidance Note - Global Standards. A 5 year average BCIS Location factor was utilised to iron out fluctuations.
169
Land (Alternative Site)
In assessing the value of the land the Valuer considered if the actual site was clearly one a hypothetical buyer would no longer consider appropriate because it would be commercially wasteful or would be an inappropriate use of resources. The fundamental principle is that the hypothetical buyer for a modern equivalent asset would purchase the least expensive site which would be suitable and appropriate for the existing operations. therefore the modern equivalent site may be smaller or in a different location of the existing is considered unnecessarily expensive.
Remaining Useful life Assessment
In order to calculate the depreciation for the major components of the Trust's property assets an assessment of their remaining useful lives was required as at 31 March 2021, which in accordance with RICS Guidance NoteDepreciated Replacement Cost Method of Valuation for Financial Reporting, reflects the varying remaining useful lives of the in-situ constituent parts.
Desktop and Interim Revaluations
Following the initial full valuation as at 31 March 2021, the Valuer has provided desktop updates as at 31 March 2022, 2023 and will also do so for 2025). The desktop update applies an index based uplift to the previous valuation (reviewing new acquisitions, disposals, AUC, alterations and levels of obsolescence). For 31 March 2024, an interim revaluation will be carried out. The service is the same as for the desktop update revaluation, except that rather than applying an index based uplift, the build cost for all specialist property assets will be reassessed based on comparable build cost information published by the RICS Build Cost Information Service. The reason for an Interim revaluation at the mid-point in the cycle is to address any variance which may arise between the BCIS "All-in" Tender Price Index and comparable build cost information specific to the healthcare sector.
170
* Note 16.3 Property, plant
- 31 March 2023
Land Buildings excluding dwellings Dwellings Assets under construction Plant & machinery Transport equipment Information technology Furniture & fittings Total £000 £000 £000 £000 £000 £000 £000 £000 £000 Owned - purchased 13,500 188,603 1,167 45,563 27,993 45 11,571 1,371 289,813 Owned - donated/granted - 8,244 336 13 3,610 - 40 84 12,327 Total net book value at 31 March 2023 13,500 196,847 1,503 45,576 31,603 45 11,611 1,455 302,140
and equipment financing
Land Buildings excluding dwellings Dwellings Assets under construction Plant & machinery Transport equipment Information technology Furniture & fittings Total £000 £000 £000 £000 £000 £000 £000 £000 £000 Owned - purchased 13,500 170,061 1,122 25,468 21,207 34 14,525 1,138 247,055 Owned - donated/granted - 7,853 328 495 3,597 - 47 115 12,435 Total net book value at 31 March 2022 13,500 177,914 1,450 25,963 24,804 34 14,572 1,253 259,490
Note 16.4 Property, plant and equipment financing - 31 March 2022
Land Buildings excluding dwellings Dwellings Assets under construction Plant & machinery Transport equipment Information technology Furniture & fittings Total £000 £000 £000 £000 £000 £000 £000 £000 £000 Subject to an operating lease - - - - - - - -Not subject to an operating lease 13,500 196,847 1,503 45,576 31,603 45 11,611 1,455 302,140 Total net book value at 31 March 2023 13,500 196,847 1,503 45,576 31,603 45 11,611 1,455 302,140 171
Note 16.5 Property plant and equipment assets subject to an operating lease (Trust as a lessor) - 31 March 2023
Note 17 Donations of property, plant and equipment
During 2022/23 donations have been received from Royal Shrewsbury Hospital League of Friends; The Shrewsbury and Telford Hospital NHS Trust Charitable Funds; Lingen Davies Cancer Fund and MacMillan Cancer Services for the purchase of medical equipment and building works.
Note 18 Revaluations of property, plant and equipment
The Trust commissioned Cushman and Wakefield to undertake a desktop update valuation of the Trust's Estate as at 31 March 2023. The properties were inspected internally and externally by Craig Chatwin BSc (Hons) MRICS, Adam Griffiths BSc (Hons) MRICS and Steven Gandley BSc (Hons) MRICS on 15 and 16 February 2021. David Wilson MRICS has been signatory of Valuation Reports provided to Shrewsbury and Telford Hospitals NHS Trust for a continuous period since 31 March 2021. Jonathan Stickells is a signatory of this report but has had no previous involvement. The valuation has been prepared in accordance with the RICS Valuation – Global Standards, which incorporate the International Valuation Standards (“IVS”) and the RICS UK National Supplement (the “RICS Red Book”), edition current at the Valuation Date. It follows that the valuation is compliant with IVS.
As a result of these revaluations the Net Book Value of the Estate was valued upwards by £7,816k as follows: Revaluation Reserve – total £7,527k increase, representing a revaluation upwards of £8,731k and net decrease of £1,204k relating to reversals £459k and £1,663k impairments charged. The Impairment Charge to SoCI is a positive £289k - representing an impairment charge to the value of £936k and reversal of previous impairments of £1,226k.
Note 19 Leases - The Shrewsbury And Telford Hospital NHS Trust as a lessee
The Trust is a lessee in a number of leases relating to property and equipment. These include property leases for a number of the Trust's services including Fertility Service and Maternity Services. In addition, the Trust has several leases for equipment including MRI and CT Scanners; X-Ray equipment and Endoscopy and Pathology Services equipment.
The Trust has applied IFRS 16 to account for lease arrangements from 1 April 2022 without restatement of comparatives. Comparative disclosures in this note are presented on an IAS 17 basis.
172
Note 19.1 Right of use assets - 2022/23
IFRS 16 implementation - reclassification of existing finance leased assets from PPE or intangible assets
- adjustments for existing operating leases
IFRS 16 implementation - reclassification of existing finance leased assets from PPE or intangible assets
- adjustments for existing subleases
Property (land and buildings) Plant & machinery Transport equipment Total Of which: leased from DHSC group bodies £000 £000 £000 £000 £000
- - - -IFRS
implementation
/ subleases 12,071 9,047 341 21,459 4,732 Transfers by absorption - - - -Additions 3,888 81 - 3,969 349 Remeasurements of the lease liability (509) - - (509) (730) Movements in provisions for restoration / removal costs - - - -Impairments - - - -Reversal of impairments - - - -Revaluations - - - -Reclassifications - - - -Disposals / derecognition - - (7) (7)Valuation/gross cost at 31 March 2023 15,450 9,128 334 24,912 4,351
16
- - - -IFRS
implementation
- - - -Transfers by absorption - - - -Provided during the year 1,514 2,029 107 3,650 562 Impairments - - - -Reversal of impairments - - - -Revaluations - - - -Reclassifications - - - -Disposals / derecognition - - - -Accumulated depreciation at 31 March 2023 1,514 2,029 107 3,650 562 Net book value at 31 March 2023 13,936 7,099 227 21,262 3,789 Net book value of right of use assets leased from other NHS providers 1,941 Net book value of right of use assets leased from other DHSC group bodies 1,848 173
16
Note 19.2 Revaluations of right of use assets
No Right of use assets have been revalued in 22/23.
Note 19.3 Reconciliation of the carrying value of lease liabilities
Lease liabilities are included within borrowings in the statement of financial position. A breakdown of borrowings is disclosed in note 32.1.
Lease payments for short term leases, leases of low value underlying assets and variable lease payments not dependent on an index or rate are recognised in operating expenditure. These payments are disclosed in Note 7.1. Cash outflows in respect of leases recognised on-SoFP are disclosed in the reconciliation above.
Income generated from subleasing right of use assets in £0k and is included within revenue from operating leases in note 4.
Note 19.4 Maturity analysis of future lease payments at 31 March 2023
Undiscounted future lease payments payable in:
2022/23 £000 Carrying value at 31 March 2022IFRS 16 implementation - adjustments for existing operating leases 21,234 Lease additions 3,969 Lease liability remeasurements (509) Interest charge arising in year 192 Early terminations (7) Lease payments (cash outflows) (3,259) Carrying value at 31 March 2023 21,620
Total Of which leased from DHSC group bodies: 31 March 2023 31 March 2023 £000 £000
-not later than one year; 3,651 570 -later than one year and not later than five years; 12,066 1,823 -later than five years. 5,903 1,422 Total gross future lease payments 21,620 3,815 Finance charges allocated to future periods -Net lease liabilities at 31 March 2023 21,620 3,815 Of which: Leased from other NHS providers 1,945 Leased from other DHSC group bodies 1,870
174
Note 19.5 Maturity analysis of finance lease liabilities at 31
March 2022 (IAS 17 basis)
The Trust had no leases determined to be finance leases under IAS17.
Note 19.6 Commitments in respect of operating leases at 31 March 2022 (IAS 17 basis)
This note discloses costs incurred in 2021/22 and commitments as at 31 March 2022 for leases the trust previously determined to be operating leases under IAS 17.
2021/22 £000 Operating lease expense Minimum lease payments 10,495 Total 10,495 31 March 2022 £000 Future minimum lease payments due: -not later than one year; 8,920 -later than one year and not later than five years; 23,568 -later than five years. 14,425 Total 46,913 Future minimum sublease payments to be received 544
175
IFRS 16 as adapted and interpreted for the public sector by HM Treasury has been applied to leases in these financial statements with an initial application date of 1 April 2022.
The standard has been applied using a modified retrospective approach without the restatement of comparatives. Practical expedients applied by the Trust on initial application are detailed in the leases accounting policy in note 15.
Lease liabilities created for existing operating leases on 1 April 2022 were discounted using the weighted average incremental borrowing rate determined by HM Treasury as 0.95%.
Reconciliation of operating lease commitments as at 31 March 2022 to lease liabilities under IFRS 16 as at 1 April 2022
Note 20 Investment Property
The Trust has no investment property that require disclosure within this note.
Note 21 Investments in associates and joint ventures
The Trust has no investments in associates or joint ventures.
Note 22 Other investments/financial assets
The Trust has no other investments/financial assets.
Initial
IFRS
1
1 April 2022 £000 Operating lease commitments under IAS 17 at 31 March 2022 46,913 Impact of discounting at the incremental borrowing rate IAS 17 operating lease commitment discounted at incremental borrowing rate 46,432 Less: Commitments for short term leases (214) Commitments for leases of low value assets (25) Irrecoverable VAT previously included in IAS 17 commitment (1,984) Services included in IAS 17 commitment not included in the IFRS 16 liability (23,950) Other adjustments: Differences in the assessment of the lease term 2 Rent increases/(decreases) reflected in the lease liability, not previously reflected in the IAS 17 commitment 973 Total lease liabilities under IFRS 16 as at 1 April 2022 21,234
Note 19.7
application of
16 on
April 2022
176
Inventories recognised in expenses for the year were £98,869k (2021/22: £93,102k). Write-down of inventories recognised as expenses for the year were £286k (2021/22: £165k).
In response to the COVID 19 pandemic, the Department of Health and Social Care centrally procured personal protective equipment and passed these to NHS providers free of charge. During 2022/23 the Trust received £1,483k of items purchased by DHSC (2021/22: £1,786k).
The deemed cost of these inventories was charged directly to expenditure on receipt with the corresponding benefit recognised in income.
Of which receivable from NHS and DHSC group bodies:
*Contract receivables in 22/23 includes £12.2m pay award funding from NHS England.
24 Inventories 31 March 2023 31 March 2022 £000 £000 Drugs 3,206 2,830 Consumables 6,141 5,941 Energy 427 268 Total inventories 9,774 9,039 of which: Held at fair value less costs to sell -Note 25.1 Receivables 31 March 2023 31 March 2022 £000 £000 Current Contract receivables* 20,249 6,216 Allowance for impaired contract receivables / assets (1,130) (839) Prepayments (non-PFI) 2,568 2,535 PDC dividend receivable 257 359 VAT receivable 1,315 1,767 Other receivables 248 152 Total current receivables 23,507 10,190 Non-current Contract receivables 1,259 904 Other receivables 743 819 Total non-current receivables 2,002 1,723
Current 17,339 3,480 Non-current 743 819
Note
177
Note 25.2 Allowances for credit losses
Note 25.3 Exposure to credit risk
The majority of the Trust's revenue comes from contracts with other public sector bodies therefore the Trust has low exposure to credit risk. The maximum exposures as at 31 March 2023 are in receivables from customers, as disclosed
in the trade and other receivables note.
Contract receivables and contract assets All other receivables Contract receivables and contract assets All other receivables £000 £000 £000 £000 Allowances as at 1 April - brought forward 839 - 844New allowances arising 553 - 439Reversals of allowances (69) - (38)Utilisation of allowances (write offs) (193) - (405)Allowances as at 31 Mar 2023 1,130 - 840 -
2021/22 2022/23 178
Note 29.1 Cash and cash equivalents movements
Cash and cash equivalents comprise cash at bank, in hand and cash equivalents. Cash equivalents are readily convertible investments of known value which are subject to an insignificant risk of change in value.
Note 29.2 Third party assets held by the trust
The Shrewsbury And Telford Hospital NHS Trust held cash and cash equivalents which relate to monies held by the Trust on behalf of patients or other parties and in which the trust has no beneficial interest. This has been excluded from the cash and cash equivalents figure reported in the accounts.
2022/23 2021/22 £000 £000 At 1 April 15,889 15,405 Net change in year (12,588) 484 At 31 March 3,301 15,889 Broken down into: Cash at commercial banks and in hand 16 16 Cash with the Government Banking Service 3,285 15,873 Total cash and cash equivalents as in SoFP 3,301 15,889 Bank overdrafts (GBS and commercial banks) -Drawdown in committed facility -Total cash and cash equivalents as in SoCF 3,301 15,889
31 March 2023 31 March 2022 £000 £000 Bank balances 3 1 Total third party assets 3 1
179
Note 30.1 Trade and other payables
Of which payables from NHS and DHSC group bodies:
Note 30.2 Early retirements in NHS payables above
The payables note above includes amounts in relation to early retirements as set out below:
- to buy out the liability for early retirements over 5 years -
- number of cases involved
31 March 2023 31 March 2022 £000 £000 Current Trade payables 14,709 10,482 Capital payables 29,402 16,731 Accruals 41,158 38,218 Receipts in advance and payments on account 35 40 Social security costs 283 216 Other taxes payable 471 406 Pension contributions payable 119 28 Other payables 90 54 Total current trade and other payables 86,267 66,175 Non-current Trade payables -Capital payables -Accruals -Receipts in
and payments
-PFI lifecycle replacement
-VAT payables -Other taxes payable -Other payables -Total non-current trade and other payables - -
advance
on account
received in advance
Current 1,962 2,647 Non-current - -
31 March 2023 31 March 2023 31 March 2022 31 March 2022 £000 Number £000 Number
-
-180
In 22/23 deferred income was released to offset non-recurrent expenditure.
*The Trust has applied IFRS 16 to lease arrangements within these accounts from 1 April 2022 without restatement of comparatives. More information about leases and the impact of this change in accounting policy can be found in note 19.
Note 31 Other liabilities 31 March 2023 31 March 2022 £000 £000 Current Deferred income: contract liabilities 297 1,554 Total other current liabilities 297 1,554 Non-current -Total other non-current liabilities - -
Note 32.1 Borrowings 31 March 2023 31 March 2022 £000 £000 Current Lease liabilities* 3,651Total current borrowings 3,651Non-current Lease liabilities* 17,969Total non-current borrowings 17,969 -
181
Note 32.2 Reconciliation of liabilities arising from financing activities - 2022/23
2022
Note 32.3 Reconciliation of liabilities arising from financing activities - 2021/22
Carrying
at 1 April 2021
Note 33 Other financial liabilities
The Trust has no other financial liabilities.
Lease Liability Total £000 £000
-Cash movements: Financing cash flows - payments and receipts of principal (3,067) (3,067) Financing cash flows - payments of interest (192) (192) Non-cash movements: Impact of implementing IFRS 16 on 1 April 2022 21,234 21,234 Additions 3,969 3,969 Lease liability remeasurements (509) (509) Application of effective interest rate 192 192 Early terminations (7) (7) Carrying value at 31 March 2023 21,620 21,620
Carrying value at 1 April
Lease Liability Total £000 £000
-Cash movements: Financing cash flows -
and
-Financing cash flows - payments of interest -Non-cash movements: Additions -Application of effective interest rate -Early terminations -Carrying value at
March
- -
value
payments
receipts of principal
31
2022
182
Note 34.1 Provisions for liabilities and charges analysis
IFRS 16 implementation - adjustments for onerous
Early departure costs and injury benefits relate to a provision for future payments payable to NHS Pensions Agency in respect of former employees.
Legal claims relate to NHS Resolution non clinical cases with employees and members of the general public.
Clinicians who are members of the NHS Pension Scheme and who as a result of work undertaken face a tax charge in respect of the growth of their NHS pension benefits above their pension savings annual allowance threshold will be able to have this charge paid by the NHS pension scheme. A contra entry has been set up in Receivables (see Note 25.1).
Pensions: early departure costs Pensions: injury benefits Legal claims Clinicians Pension Provision Total £000 £000 £000 £000 £000 At 1 April 2022 43 185 197 828 1,253
provisions - - - -Change in the discount rate (1) (9) - (671) (681) Arising during the year 41 33 106 600 780 Utilised during the year (42) (70) (71) (10) (193) Reversed unused - - (18) - (18) Unwinding of discount 2 17 - 15 34 At 31 March 2023 43 156 214 762 1,175 Expected timing of cash flows: - not later than one year; 43 71 214 19 347 - later than one year and not later than five years; - 85 - 49 134 - later than five years. - - - 694 694 Total 43 156 214 762 1,175
lease
183
Note 34.2 Clinical negligence liabilities
At 31 March 2023, £372,224k was included in provisions of NHS Resolution in respect of clinical negligence liabilities of The Shrewsbury And Telford Hospital NHS Trust (31 March 2022: £561,600k).
Note 35 Contingent assets
The contingent liabilities represent the difference between the expected values of provisions for legal claims carried at note 34.1 and the maximum potential liability that could arise from these claims.
Note 36 Contractual capital commitments
Note 37 Other financial commitments
The Trust has no other financial commitments.
Note 38 Defined benefit pension schemes
The Trust has no other defined benefit pensions schemes.
Note 39 On-SoFP PFI, LIFT or other service concession arrangements
The Trust has no on-SOFP PFI, LIFT or other service concession arrangements.
Note 40 Off-SoFP PFI, LIFT and other service concession arrangements
The Trust has no off-SOFP PFI, LIFT or other service concession arrangements.
liabilities 31 March 2023 31 March 2022 £000 £000 Value of contingent liabilities NHS Resolution legal claims (32) (76) Gross value of contingent liabilities (32) (76) Amounts recoverable against liabilities -Net value of contingent liabilities (32) (76) Net value of contingent assets - -
and
31 March 2023 31 March 2022 £000 £000 Property, plant and equipment 7,604 2,632 Intangible assets 455 78 Total 8,059 2,710
184
Note 41 Financial instruments
Note 41.1 Financial risk management
Financial reporting standard IFRS 7 requires disclosure of the role that financial instruments have had during the period in creating or changing the risks a body faces in undertaking its activities. Because of the continuing service provider relationship that the NHS Trust has with commissioners and the way those commissioners are financed, the Trust is not exposed to the degree of financial risk faced by business entities. Also financial instruments play a much more limited role in creating or changing risk that would be typical of listed companies, to which the financial reporting standards mainly apply. The Trust has limited powers to borrow or invest surplus funds and financial assets and liabilities are generated by day-to-day operational activities rather than being held to change the risks facing the Trust in undertaking its activities.
The Trust's treasury management operations are carried out by the finance department, within parameters defined formally within the Trust's standing financial instructions and policies agreed by the Board of Directors. The Trust's treasury activity is subject to review by the Trust's internal auditors.
Currency risk
The Trust is principally a domestic organisation with the great majority of transactions, assets and liabilities being in the UK and sterling based. The Trust has no overseas operations. The Trust therefore has low exposure to currency rate fluctuations.
Interest rate risk
The borrowings are for 1-25 years, in line with the life of the associated assets, and interest is charged at the National Loans Fund rate fixed for the life of the loan. The Trust therefore has low exposure to interest rate fluctuations.
The Trust may also borrow from government for revenue financing subject to approval by NHS England & NHS Improvement. Interest rates are confirmed by the Department of Health and Social Care (the lender) at the point borrowing is undertaken. The Trust has no revenue or capital loans in place as at 31 March 2023.
The Trust therefore has low exposure to interest rate fluctuations.
Credit risk
Because the majority if the Trust's revenue comes from contracts with other public sector bodies, the Trust has low exposure to credit risk. The maximum exposure as at 31 March 2023 are in receivables from customers as disclosed in the trade and other receivables note.
Liquidity risk
The Trust's operating costs are incurred under contracts with Clinical Commissioning Groups, which are financed from resources voted annually by Parliament. The Trust funds its capital expenditure from funds obtained within its prudential borrowing limit. The Trust is not, therefore, exposed to significant liquidity risks subject to the availability of temporary revenue support funding and the demonstration of cash requirement.
185
Note 41.2 Carrying values of financial assets
Note 41.3 Carrying values of financial liabilities
Carrying values of financial assets as at 31 March 2023 Held at amortised cost Total book value £000 £000 Trade and other receivables excluding non financial assets 21,369 21,369 Cash and cash equivalents 3,301 3,301 Total at 31 March 2023 24,670 24,670 Carrying values of financial assets as at 31 March 2022 Held at amortised cost Total book value £000 £000 Trade and other receivables excluding non financial assets 7,251 7,251 Cash and cash equivalents 15,889 15,889 Total at 31 March 2022 23,140 23,140
Carrying values of financial liabilities as at 31 March 2023 Held at amortised cost £000 Obligations under leases 21,620 Trade and other payables excluding non financial liabilities 85,478 Provisions under contract 1,175 108,273 Carrying values of financial liabilities as at 31 March 2022 Held at amortised cost £000 Trade and other payables excluding non financial liabilities 65,513 Provisions under contract 197 65,710 Total at 31 March 2022 Total at 31 March 2023 186
Note 41.4 Maturity of financial liabilities
The following maturity profile of financial liabilities is based on the contractual undiscounted cash flows. This differs to the amounts recognised in the statement of financial position which are discounted to present value.
Note 41.5 Fair values of financial assets and liabilities
The book value (carrying value) is a reasonable approximation of fair value for the Trust's financial assets and liabilities.
31 March 2023 31 March 2022 £000 £000 In one year or less 90,304 65,710 In more than one year but not more than five years 12,066In more than five years 5,903Total 108,273 65,710
187
Note 42 Losses and special payments
£71k of the ex-gratia payments in 2022/23 (£92k in 2021/22) are included in legal claims in Note 34.1 Provisions for liabilities and charges analysis rather than Note 7.1 Operating expenses.
The Trust has set aside £1.3m in relation to a fine, charged by Shropshire Magistrates Court, for two negligence cases which occurred between October 2019 and May 2020. (This is not included in the table above as it has not yet been paid, it is due to be paid by 18 May 2024.)
Note 43 Gifts
Gifts made
Total number of cases Total value of cases Total number of cases Total value of cases Number £000 Number £000 Losses Cash losses - - 1 0 Bad debts and claims abandoned 365 250 406 406 Stores losses and damage to property 42 287 38 165 Total losses 407 537 445 571 Special payments Ex-gratia payments 57 204 61 1,033 Total special payments 57 204 61 1,033 Total losses and special payments 464 741 506 1,604 Compensation payments received
Total number of cases Total value of cases Total number of cases Total value of cases Number £000 Number £000
- - - -
2022/23 2021/22 2022/23 2021/22
A corrective payment of £788k was included in 2021/22 relating to the Flowers legal case and the treatment of overtime payments, in particular payments for voluntary overtime in the calculation of holiday pay and the interpretation of the Working Time Directive. 188
Note 44 Related parties
The Department of Health and Social Care is regarded as the parent department. The main entities within the public sector that the trust has had dealings with during the year are listed below. These are entities where income and/or expenditure has been in excess of £250,000.
NHS Shropshire, Telford and Wrekin CCG
NHS South East Staffs and Seisdon Peninsular CCG
NHS Stafford and Surrounds CCG
NHS Herefordshire and Worcestershire CCG
NHS Shropshire, Telford and Wrekin ICB
NHS Black Country ICB
NHS Cheshire and Merseyside ICB
NHS Staffordshire and Stoke-on-Trent ICB
NHS Herefordshire and Worcestershire ICB
NHS England
Health Education England
NHS Property Services
NHS Resolution
Mid Cheshire Hospitals NHS Foundation Trust
Shropshire Community Health NHS Trust
St Helens and Knowsley Teaching Hospitals NHS Trust
The Robert Jones and Agnes Hunt Orthopaedic Hospital NHS Foundation Trust
The Royal Wolverhampton NHS Trust
University Hospitals Birmingham NHS Foundation Trust
University Hospitals of North Midlands NHS Trust
Powys Local Health Board
Betsi Caclwaladr University Local Health Board
Cwm Taf Local Health Board
NHS Pension Scheme
NHS Blood and Transplant
HM Revenue and Customs
The Trust is linked to the Shrewsbury and Telford Hospital NHS Trust Charity. The Annual Report and Accounts for the Shrewsbury and Telford Hospital NHS Charity are submitted separately to the Charity Commission and are not consolidated into the Trust's Accounts.
The Trust is also linked to Royal Shrewsbury Hospital League of Friends, Friends of Princess Royal Hospital and Lingen Davies Cancer Fund, who donate various pieces of medical equipment to the Trust. The Trust hires facilities from Shropshire Education and Conference Centre.
Note 45 Transfers by absorption
There were no transfers by absorption in the year where the Trust has been either the receiving or divesting party.
Note 46 Prior period adjustments
The Trust has made no prior period adjustments where comparative information has been restated due to either a change in accounting policy or material prior period error.
Note 47 Events after the reporting date
There are no events after the reporting date that need to be included in this note.
189
Note 48 Better Payment Practice code
The Better Payment Practice code requires the NHS body to aim to pay all valid invoices by the due date or within 30 days of receipt of valid invoice, whichever is later.
Note 49 External financing limit
The trust is given an external financing limit against which it is permitted to underspend
Note 50
Note 51 Breakeven duty financial performance
2022/23 2022/23 2021/22 2021/22 Non-NHS Payables Number £000 Number £000 Total non-NHS trade invoices paid in the year 154,683 239,467 137,133 209,477 Total non-NHS trade invoices paid within target 102,687 157,849 118,912 186,763 Percentage of non-NHS trade invoices paid within target 66.4% 65.9% 86.7% 89.2% NHS Payables Total NHS trade invoices paid in the year 2,025 12,847 1,921 13,854 Total NHS trade invoices paid within target 1,244 8,285 1,724 12,437 Percentage of NHS trade invoices paid within target 61.4% 64.5% 89.7% 89.8%
2022/23 2021/22 £000 £000 Cash flow financing 79,975 21,452 External financing requirement 79,975 21,452 External financing limit (EFL) 80,779 31,212 Under / (over) spend against EFL 804 9,760
2022/23 2021/22 £000 £000 Gross capital expenditure 62,599 44,820 Less: Disposals (1,410) (2,060) Less: Donated and granted capital additions (403) (1,140) Charge against Capital Resource Limit 60,786 41,620 Capital Resource Limit 61,590 45,207 Under / (over) spend against CRL 804 3,587
Capital Resource Limit
2022/23 2021/22 £000 £000 Adjusted financial performance surplus / (deficit) (control total basis) (47,206) (10,890) Breakeven duty financial performance surplus / (deficit) (47,206) (10,890)
190
Note 52 Breakeven duty rolling assessment
1997/98 to 2008/09 2009/10 2010/11 2011/12 2012/13 2013/14 2014/15 2015/16 £000 £000 £000 £000 £000 £000 £000 £000 Breakeven duty in-year financial performance 712 26 59 81 65 (12,130) (14,649) Breakeven duty cumulative position (22,891) (22,179) (22,153) (22,094) (22,013) (21,948) (34,078) (48,727) Operating income 262,882 277,980 299,850 309,362 314,106 316,794 326,477 Cumulative breakeven position as a percentage of operating income (8.4%) (8.0%) (7.4%) (7.1%) (7.0%) (10.8%) (14.9%) 2016/17 2017/18 2018/19 2019/20 2020/21 2021/22 2022/23 £000 £000 £000 £000 £000 £000 £000 Breakeven duty in-year financial performance (5,631) (17,400) (18,743) (25,715) (3,752) (10,890) (47,206) Breakeven duty cumulative position (54,358) (71,758) (90,501) (116,216) (119,968) (130,858) (178,063) Operating income 350,244 359,041 369,186 421,853 511,443 535,142 556,605 Cumulative breakeven position as a percentage of operating income (15.5%) (20.0%) (24.5%) (27.5%) (23.5%) (24.5%) (32.0%) 191
This document is also available on request in other formats, including large print and translation into other languages for people in Shropshire, Telford & Wrekin and mid-Wales. Please contact us at communications@sath.nhs.uk to request other formats.
192
