INDUSTRY LEADING AUTHORISING ENGINEERS & TECHNICAL ADVISORS.
“We are proud that Paul Crothers our Senior Authorising Engineer and Head of Training has led our training centre’s growth over the last two years. We offer regular Ventilation courses in our training centre to support our clients with certified CPD. We also have the flexibility to provide our training at a local site to support our clients. We have delivered training all over the British Isles and as far away as the Falklands.”
Graham P. Taylor, BSc, PGDip, C.Eng, FIHEEM, MIET, MSVHS, MWMSoc. Authorising & Consulting Engineer. Member Hospital Infection Society.
Compliance and regulatory standards must be met to keep buildings safe and operational. Risks, quality and compliance must be managed and maintained within healthcare Whether you are a hospital, a doctor’s surgery, or a dental practice, fmfirst® can support:
Asset management
Cleanliness audits
Document management
Efficacy audits
Incident reporting
Risk assessments
Task management - Helpdesk
£300 million for NHS tech
Ahead of the budget, the government confirmed that £300 million of new capital investment will go into technology for the
New digital tools will be rolled out to NHS staff to support their work and improve productivity, by automating administrative tasks and providing swifter access to patient information, as well as ensuring better staff communication and better coordinated care.
By upgrading technology, it is hoped that productivity will be improved so that nurses and doctors can focus on caring for patients and patients will be treated more quickly.
Health minister, Karin Smyth said: “Neighbourhood Health Centres fundamentally reimagine how the NHS works – bringing care closer to home and making sure the NHS is organised around patients’ needs, not the other way round.
“The Chancellor is rightly boosting investment in the NHS after we inherited a health service on its knees – with Lord Darzi’s investigation uncovering a £40 billion black hole. But funding will only get us so far. We need to use every measure available to us, which is why we’re leveraging in private investment to construct some of these centres, making the most of all expertise and every tool at our disposal.
“Our new NHS Rebuild approach will give the health service the investment it needs, repurposing and building a new generation of Neighbourhood Health Centres across the country. It will go hand in hand with reform and efficiency – ensuring proper value for money for taxpayers.”...
HEALTHCARE
Funding confirmed for new Neighbourhood Health Centres
The government has confirmed investment for hundreds of new Neighbourhood Health Centres.
250 new Neighbourhood Health Centres will house teams of GPs, nurses, dentists and pharmacists together under one roof to best meet the needs of the community.
These centres are part of a new Neighbourhood Health Service that will provide end-to-end care and tailored support.
As outpatient care is moved out of hospitals, the centres will house clinics in the community.
Neighbourhood health services will initially focus on improving access to general practice and supporting people with complex needs and long-term conditions, in the areas of highest deprivation.
Chancellor of the Exchequer Rachel Reeves said: “At the Budget I’ll set out how we’ll deliver on the country’s priorities to cut NHS waiting times, cut debt and cut the cost of living.
“We’re driving down waiting lists by bringing healthcare to patients’ doorsteps and turbocharging NHS productivity with cuttingedge technology.
“Our record investment, combined with ruthless efficiency and reform, will deliver the better care and better outcomes our NHS patients deserve.”
It has also been confirmed that £300 of new capital investment will go into technology for the NHS. New digital tools will be rolled out to to NHS staff to support their work and...
Enhancing Healthcare with BlueSky Messaging Serve
The state-of-the-art IOT messaging server focusing on critical alarm and alert messaging, ensuring that vital alerts reach the correct personnel swiftly, reducing response times and maximising efficiency.
The server’s modularity, scalability, and comprehensive support make it ideal for diverse healthcare settings.
+44
Billions from NHS reform to be redirected to patient care
The health secretary has announced that billions of pounds from NHS reform will be redirected back into patient care.
Reforms include ending duplication and reducing bureaucracy. 18,000 administrative posts will be removed, potentially saving more than £1 billion, which will be redirected in to patient care.
NHS leaders are also expected to cut 50 per cent of staff in ICBs.
The government has also confirmed it will deliver on the planned timetable of bringing NHS England back into the Department of Health and Social Care (DHSC) within two years.
Health secretary Wes Streeting said: “The government is protecting investment in the NHS at the Budget, worth an extra £29 billion to the health service. I want to reassure taxpayers that every penny they are being asked to pay will be spent wisely.
“We have already cut waiting lists for the first year in 15 years, recruited 2,500 more GPs, and cut ambulance waits for patients with conditions like heart attacks and strokes. Our investment to offer more services at evenings and weekends, arm staff with modern technology, and improve staff retention is working. At the same time, cuts to wasteful spending on things like recruitment agencies saw productivity grow by 2.4 per cent in the most recent figures – we are getting better bang for our buck...
Trusts given new powers to improve care
The best performing NHS trusts will be given more independence and power to improve care.
The highest performing hospitals and community health trusts will be given the status of “advanced foundation trust”.
Leaders of these trusts will be given greater freedom to make decisions locally, including how services are organised and how money is spent.
Eight of the highest performing trusts have been nominated to become the first advanced foundation trusts. Trusts that can prove they deliver good services and have sound finances will be able to spend any money they’ve saved since last year on new equipment, buildings and improving patient care. If the amount trusts want to invest is less than £100 million, the level of paperwork will be vastly reduced.
The trusts nominated for assessment are: Berkshire Healthcare NHS FT; Dorset Healthcare University NHS FT; Central London Community Healthcare NHS Trust; Northamptonshire Healthcare NHS FT; Northumbria Healthcare NHS FT; Alder Hey Children’s NHS FT; Norfolk Community Health and Care NHS Trust; and Cambridgeshire Community Services NHS Trust.
These trusts will be expected to deliver faster improvements in patient care, waiting times and productivity, work closely with staff and commissioners, and help drive positive change across the wider NHS...
£2 million to improve digital mental health tech
The Medicines and Healthcare products
Regulatory Agency (MHRA) and the National Institute for Health and Care Excellence (NICE) are to receive £2 million from Wellcome to improve the safety and effectiveness of digital mental health technologies.
The funding will allow the MHRA and NICE to continue developing clear, proportionate guidance for digital mental health technologies, supporting safer, more effective tools for people across the UK.
It is hoped, that as a result, people in the UK will have better access to high-quality, safe and effective digital mental health support.
The funding will run until Autumn 2028, and the support builds on activities already underway to help people across the UK access safe and effective digital mental health technologies.
Digital mental health technologies are being used more and more, including symptomtracking apps, AI-powered assessments and virtual reality therapy.
NHS research shows that they can provide real benefits by managing depression, anxiety and stress.
The next phase of work will establish a digital mental health technology AI airlock; explore international reliance and mutual recognition for the regulation of digital mental health technologies; drive increased quality and evidence for digital mental health technologies on the UK market; and consider challenges...
Men’s Health Strategy published: READ MORE
Prescription charges frozen: READ MORE
Chair appointed to Health Data Research Service: READ MORE
Record number of online GP requests in October: READ MORE
Most GPs now offer online access: READ MORE
Digital solutions saving time in social care: READ MORE
Plan to embed AI in Welsh health service
The Welsh Government has launched a new plan to embed the benefits of AI across public services, including the health service, and shape its influence to improve the lives of people across Wales.
The Plan will act as a long term roadmap and establish the building blocks for exploring the potential of AI in a responsible, ethical, and collaborative way.
Welsh public services are already using AI for example with personalised learning in schools, automation in local government, and faster diagnoses in the NHS.
A pilot in Cwm Taf Morgannwg University Health Board, in partnership with the Centre for Digital Public Services (CDPS), is exploring how AI scribing technology could reduce the administrative burden for clinical teams working in children’s neurodevelopmental services.
Feedback already suggests it could shorten assessments and reporting processes while maintaining quality and accuracy.
Kath Bowen, operational/AHP lead for the Paediatric Neurodiversity Assessment Service at Cwm Taf Morgannwg University Health Board said: “AI scribe technology has been a valuable addition to our service. It’s saving staff hours each week, allowing us to see more children and focus on meaningful conversations with ...
D J Hill Engineering Ltd.
Smarter workflows: how the right monitor transforms healthcare productivity
As clinical workflows grow more complex, technology, including monitors must evolve to meet these pressures with clarity, efficiency, and comfort
Healthcare professionals face unprecedented demands on their time and attention. Between managing electronic health records, reviewing diagnostic images, coordinating with colleagues and serving patients, a modern workflow requires seamless multitasking across multiple systems. The Philips 34B2U3600C business monitor offers a comprehensive solution that enhances both productivity and wellbeing.
One cable, endless possibilities
The standout feature of the 34B2U3600C is its USB-C docking capability with integrated RJ45 ethernet. This single-cable USB-C connection delivers video, data, network access and up to 90 W of power delivery to charge your laptop simultaneously. For healthcare settings where desk space is precious and security paramount, eliminating cable clutter whilst maintaining robust wired network connectivity is invaluable. IT departments will appreciate the simplified deployment, whilst clinicians benefit from instant connectivity when moving between workstations.
Work smarter with MultiView and SmartKVM
The 34-inch WQHD curved display with a 3440x1440 resolution provides exceptional screen real estate, but it’s the intelligent features that truly set this monitor apart. MultiView technology allows two devices to be displayed simultaneously in picture-bypicture or picture-in-picture mode, perfect for comparing patient records or monitoring multiple systems. The SmartKVM function enables effortless switching between connected devices, maintaining workflow momentum when juggling multiple computers or systems.
Protecting
your most valuable asset Healthcare professionals spend countless hours in front of screens, making eye comfort critical. The 34B2U3600C features TÜV Rheinland Eyesafe certification, with an always-on blue light filter that reduces eye strain without compromising colour accuracy. The FlickerFree technology further minimises fatigue during extended shifts. The curved VA panel delivers stunning image quality, ensuring diagnostic images and patient data are rendered with clarity and precision.
Peace of mind
In environments where every second counts and accuracy is paramount, the Philips 34B2U3600C delivers the connectivity, functionality and comfort that modern workflows demand. Knowing that it fulfils the strict environmental, social, and circular economy criteria to warrant TCO Certified, generation 10, a global sustainability certification for IT products, and comes with an extended 5-year warranty period further aligns with sustainability goals by promoting longer product lifecycles and reducing e-waste. M
The Government’s 10 Year Health Plan promises to reinvent the NHS through three radical shifts – hospital to community; analogue to digital; and sickness to prevention
Back in July, the Government set out the longawaited 10 Year Health Plan for England.
The 10 Year Health Plan is part of the government’s health mission to build a health service fit for the future. It sets out how the government will reinvent the NHS through three radical shifts: hospital to community; analogue to digital; and sickness to prevention.
The government will ensure that the NHS is ready to deliver these three shifts through a new operating model, by bringing in a new era of transparency, by creating a new workforce model, delivering a reshaped innovation strategy and by taking a new approach to NHS finances.
But what does this all mean in practice? Since July, the NHS and the government have published a few updates that answer some of our questions.
At the time of the plan’s launch, it was pointed out that patients were struggling to get appointments with their GP, waiting lists were long, staff demoralised and patient outcomes behind other countries. 250,000 ideas were submitted to the Change NHS website.
The NHS’s founding principles remain in place, universal care, free at the point of delivery, based on need and funded through general taxation, but the NHS will be reimagined so that patients can have choice and control over their care.
The NHS will be reinvented with science and technology at its centre and will be equipped to narrow health inequalities.
From hospital to community
The first shift is from hospital to community. The Neighbourhood Health Service offers an
The NHS will be reinvented with science and technology
at its centre
alternative to a hospital-centric, detached, fragmented system. This will bring care into the community and bring professionals into patient-centred teams. Access to general practice will be revitalised, enabling hospitals to focus on providing specialist care. Over time, the Neighbourhood Health Service will combine
with the genomics population health service to provide predictive and preventative care that anticipates need, rather than just reacting to it.
To put it simply, care should happen as locally as possible, digitally by default and in a patient’s home if possible. Care should be delivered in a neighbourhood health centre (NHC) when needed and in a hospital if necessary.
In order to achieve this, the pattern of health spending will be altered. The share of expenditure on hospital care will fall, with proportionally greater investment in out-ofhospital care.
A key goal is to end the 8am scramble by training thousands more GPs and building online advice into the NHS App. The government has said that anyone who needs a same-day appointment will be able to get one.
Two new contracts will be introduced to encourage GPs to work over larger geographies and lead new neighbourhood providers.
Patients will be supported to be active participants in their own care with a goal of ensuring 95 per cent of people will have an agreed care plan by 2027. The government will at least double the number of people offered a personal health budget (PHB) by 2028 to 2029, offer one million people a PHB by 2030, and ensure it is a universal offer for all who would benefit by 2035.
Patients will be able to use the NHS App to book appointments, communicate with professionals, receive advice, draft or view their care plan and self-refer to local tests and services.
An NHC will be established in every community, with priority going to areas with E
F the lowest life expectancy. These will be a one-stop shop for patient care and the place from which multidisciplinary teams operate. NHCs will be open at least 12 hours a day and six days a week.
Community pharmacy will have an increased role in the management of long-term conditions. They will also be linked to the single patient record.
There is a goal to improve access to NHS dentistry, improve children’s oral health and increase the number of NHS dentists working in the system by making the dental contract more attractive and introducing tie-ins for those trained in the NHS.
The government plans to deliver more urgent care in the community, in people’s homes or through NHCs, to end hospital outpatients as we know it by 2035.
The government has also committed to ending corridor care and restoring the NHS constitutional standard of 92 per cent of patients beginning elective treatment within 18 weeks.
Same-day emergency care services and co-located urgent treatment centres will be expanded and patients will be supported to book the most appropriate urgent care service.
Analogue to digital
In some aspects, the NHS has been lagging behind when it comes to technology. The plan is
to leverage the unique advantages of the NHS’s healthcare model, including world-leading data, its power in procurement and its means to deliver equal access to create the most digitally accessible health system in the world.
By harnessing digital, the government plans to ensure rapid access for those in generally good health, free up physical access for those with the most complex needs and help ensure financial sustainability.
For the first time, patients will be given control over a single, secure and authoritative account of their data, known as their single patient record, to enable more co-ordinated, personalised and predictive care.
The NHS App will be transformed into a worldleading tool for patient access, empowerment and care planning. It is hoped that by 2028, the app will be a full front door to the entire NHS.
Using the app, patients will be able to get instant advice for non-urgent care, and help finding the most appropriate service first time.
The NHS App will be transformed into a worldleading tool for patient access
Through the My Choices section, they will be able to choose their preferred provider looking at outcomes, feedback or distance from home.
Patients will be able to use the My Specialist section to book directly into tests where appropriate and hold consultations with My Consult.
Through My Medicines, they will be able to manage their medicines and through My Vaccines, they will be able to book vaccines.
My Care will enable patients to manage longterm conditions and My Companion will provide extra care support.
Patients will be able to upload health data through My Health and manage a loved one’s care through My Children or My Carer.
Elsewhere, patients will be able to leave feedback on the care they have received which will be compiled and passed back to providers.
There will be a single sign on for staff and technology like AI scribes will be scaled to free staff from bureaucracy and administration, so they have more time to focus on patients.
A ‘HealthStore’ will be built which will enable patients to access approved digital tools to manage or treat their conditions, enabling innovative businesses to work more collaboratively with the NHS and regulators.
The government has a plan to halve the gap in healthy life expectancy between the richest and poorest regions
Sickness to prevention
The government has a plan to halve the gap in healthy life expectancy between the richest and poorest regions, while at the same time, increasing it for everyone. The key to this is prevention.
The government plans to work with businesses, employers, investors, local authorities and mayors to create a healthier country.
The Tobacco and Vapes Bill means future generations of children will never be able to legally buy tobacco and restrictions have been placed on the advertisement and sale of vapes.
There are restrictions on junk food advertising targeted at children and a ban on the sale of high-caffeine energy drinks to children.
Healthy Start will be restored from the 2026 to 2027 financial year and free school meals expanded to all children with a parent in receipt of Universal Credit. E
There are plans to make the NHS the most AI-enabled health system in the World
F Other initiatives include weight loss medication, alcohol standards, expanded mental health support and increased uptakes of the HPV vaccine.
There are also plans to create a new genomics population health service by the end of the decade. Universal newborn genomic testing will be introduced, alongside populationbased polygenic risk scoring and other diagnostic tools, enabling early identification and intervention for individuals at high risk of developing common diseases.
New operating model
Perhaps one of the most well-known changes is the abolition of NHS England. NHS England will be combined with DHSC, reducing headcount by 50 per cent.
ICBs will be built up and commissioning support units closed so that ICBs become the strategic commissioners of local healthcare services.
New standards have been introduced for trusts and leaders, with pay tied to performance and good work rewarded.
Workforce
Central to plans to save costs are cuts to staff. In November, it was announced that 18,000 administrative posts will be cut across the NHS. The government plans for staff to be better treated and more motivated, with better training and development. Every member of staff will have their own personalised career coaching and development plan.
Innovation
A key part of the goal to transform the NHS is innovation. Five transformative technologies have been identified – data, AI, genomics, wearables and robotics – which will be harnessed to personalise care, improve
outcomes, increase productivity and boost economic growth.
A Health Data Research Service will be launched, backed by £600 million. This will transform the access to NHS data by providing a secure single access point to national-scale data sets, slashing red tape for researchers.
There are plans to make the NHS the most AI-enabled health system in the World, with AI integrated into clinical pathways.
Wearables will be standard in preventative, chronic and post-acute NHS treatment by 2035 and surgical robot adoption will be expanded.
Productivity
The NHS has a target to deliver a 2 per cent year-on-year productivity gain.
The practice of providing additional funding to cover deficits will end. The government has set a target for the NHS to move into surplus with the majority of providers achieving that by 2030.
Organisations will be asked to prepare robust five-year plans to break the cycle of short-term planning.
Organisations will be asked to prepare robust five-year plans
The 10-Year Health Plan sets out a comprehensive programme to reshape the NHS over the next decade. At its core are three major shifts: moving care from hospitals into communities, embedding digital tools across the system, and focusing on prevention to improve healthy life expectancy and reduce inequalities. To support these changes, the plan introduces a new operating model that streamlines leadership and governance, alongside workforce reforms designed to improve training, motivation and career development. It also places innovation at the centre of healthcare delivery, harnessing technologies such as data, AI, genomics, wearables and robotics to personalise care and boost productivity. Financial reforms aim to ensure long-term sustainability, with a focus on efficiency, transparency and surplus planning. Together, these measures are intended to modernise the NHS while preserving its founding principles of universal, free care, ensuring patients have greater choice, access and control over their health. L
Informed and empowered: the future of consent in healthcare
Informed consent is evolving as a central pillar of patient safety. As digital transformation reshapes clinical practice, new approaches are helping clinicians and patients engage in consent conversations
Informed consent has always been a cornerstone of ethical healthcare, but today it is more than a formality – it is a vital patient right, a safety mechanism, and a legal safeguard for clinicians and providers. With the acceleration of digital transformation, the landscape of consent is changing rapidly. At the forefront of this evolution is EIDO Healthcare, now part of Radar Healthcare, which is working to transform how clinicians and patients navigate the consent journey.
We spoke with Matthew Ravenscroft, Managing Director of EIDO Healthcare, about why informed consent matters more than ever, what risks poor practice can create, and how technology can strengthen the delicate balance between efficiency, safety, and patient empowerment.
Empowering patients, protecting clinicians
EIDO Healthcare was founded in 2000 by a clinician who recognised the gap between patients signing forms and patients truly understanding their treatment options.
“Informed consent isn’t just about a signature,” Matthew explains. “It’s about ensuring patients know what should go right, what could go
wrong, and what their options are, so they can make a truly considered decision.”
Today, EIDO is recognised as the gold standard in consent, offering PIF TICK certified resources for accuracy, clarity, and impartiality. For clinicians, this means trusted, ready-made materials that reduce administrative burden and potential legal challenges. For patients, it ensures they receive information that is accessible, balanced, and reliable.
Through its partnership with Radar Healthcare, EIDO has embedded consent into broader patient safety and quality monitoring systems.
“Consent done badly is both a patient safety risk and a medico-legal one,” says Matthew. “Through Radar Healthcare’s dashboards, organisations gain visibility into where consent is working well and where risks lie. It moves consent from a tick-box exercise to being part of continuous improvement.”
Trust begins with consent
The consequences of poor consent are significant. When patients are not fully informed, the impact is threefold: patient harm, professional liability, and reputational damage for providers.
Landmark cases such as Montgomery v Lanarkshire Health Board (2015) and high-profile reviews including the Cumberlege Review (2018) and Ockenden Review (2017-2022) have repeatedly placed consent in the spotlight. Each has underscored the principle that consent must not be rushed, minimised, or treated as a procedural hurdle.
“Informed consent is about patient rights and clinician protection,” Matthew notes. “Getting it wrong is not just about compliance – it’s about trust, safety, and the integrity of the whole care system.”
The post-pandemic shift
The COVID-19 pandemic reshaped the dynamics of healthcare delivery. With backlogs and stretched resources, hospitals needed to move patients through pathways more quickly.
Matthew states: “Consent is a complex medicolegal process. It takes time. The challenge has been how to make it more efficient without cutting corners.”
The solution has been digitisation and standardisation: providing patients with information in advance, enabling more meaningful face-to-face discussions, and reducing wasted time. This approach ensures efficiency without losing the human element.
“It’s about balancing speed with humanity –making sure patients still feel seen and heard.” Additionally, allowing patients time to process information beforehand means they can come prepared, making appointments more meaningful.
Communication as the core risk
More often than not, consent failures are not about medical errors but about communication gaps. Patients may not understand jargon, may not speak English fluently, or may feel rushed or pressured. These gaps can lead to misunderstandings, mistrust, and legal claims.
“Language is powerful,” says Matthew. “Every patient deserves information in a format they can understand and use.”
EIDO addresses this by offering resources in multiple languages, plain English, audio, large print, and easy-read versions for people with learning disabilities. The goal is to remove barriers to understanding and ensure every patient is genuinely informed.
The double-edged sword of digital
In today’s digital-first world, patients often consult Google or AI tools before seeing a clinician. While this can increase awareness, it also introduces risks. “We’ve seen real-world cases where patients followed AI-generated advice with harmful consequences,” Matthew warns.
To combat this, EIDO ensures that all its patient materials are not only expertly written but also independently certified for quality. While
AI can play a role in generating drafts, the final word always comes from EIDO’s expert linguists and clinicians. This ensures patients can trust the information they receive.
The future: empowerment and interoperability
Looking forward, Matthew envisions a future where consent is both digital and deeply personal. Trusted information should be accessible directly through tools such as the NHS app, tailored to patients’ needs and available in multiple formats.
But he cautions that digital progress must not create new divides. “Not every patient or department is digitally ready at the same time. We must balance innovation with inclusivity, ensuring no one is left behind.”
The next frontier lies in data. Patient-reported outcomes and experiences will increasingly shape how consent processes evolve.
Clinicians, supported by technology, will have greater insight into patient values, needs, and expectations. This shift will support clinicians taking consent in new ways, whilst ensuring it remains a shared decision-making process rather than a tick box transaction.
“To be informed and empowered means recognising that consent is a two-way street. Patients must learn about their procedure, but clinicians must also learn about their patients. Technology can standardise the basics, freeing clinicians to focus on what really matters: the unique individual in front of them.”
Consent as the foundation of safer healthcare
As healthcare systems continue to transform, informed consent will remain a defining measure of safety, ethics, and trust. With the combined expertise of EIDO Healthcare and Radar Healthcare, providers are better placed to make consent not just a formality, but a genuine dialogue - one that empowers patients, supports clinicians, and strengthens organisational resilience.
Ultimately, informed consent isn’t just about avoiding litigation. It’s about building safer, more transparent, and compassionate healthcare journeys. When patients and clinicians are both informed and empowered, everyone benefits. M
Asckey’s continued partnership with GHC NHS Foundation Trust
Asckey’s Cleaning Monitoring System replaced the Trust’s outdated software, delivering reliable data, strong reporting, and responsive support
In 2012, Phil Wright, who was Asckey’s sales executive at the time and is now our commercial director, began conversations with Gloucestershire Health and Care Trust around their auditing needs. The Trust were using a legacy system that was basic and dated, with limited reporting options.
In 2018, the Trust put their requirements out to tender, and Asckey were successful in their bid to provide a Cleaning Monitoring System. Asckey worked closely with the Trust and were able to have the software up and running within four months of the contracts being signed.
We spoke to the performance and compliance manager at the Trust about how they’ve benefited from the system and working with Asckey.
What benefits have you seen since using the system?
“Over the time of the contract, the interface has developed to meet the needs of the auditors, and continues to be modern, stable, and easy to use. The system has good options for reporting; the 13-week report is easy to use and works well for our requirements.
The system has helped us to present highquality, credible data across the Trust. The system is stable, has no downtime, and ensures we are always adhering to the latest standards. For the price we pay, it is excellent value for money.”
How have you found working with Asckey?
“The response time to any of our queries is very quick and is either solved immediately or pushed through to the next system update. All our interactions over the last eight years have been excellent. I’ve been able to work closely with Phil, Michael, and other members of the team during the update to the 2021 standards. The rollout of these standards on the system is brilliant.”
Speaking of the partnership, Phil Wright, Asckey commercial director, said: “Since launching our application in the Trust, I’ve worked closely with them to help them get the most out of the product, whether it be training/ product enhancements or demonstrations of other modules available. Working closely and collaboratively with our clients is one of the ways we can maintain such strong long-term relationships with them.” M
FURTHER INFORMATION
If you would like to discover more about Asckey’s cleaning audit software or any other fmfirst® applications, then visit: www.asckey.com
What is the NHS Staff Survey?
The NHS Staff Survey (NSS) is one of the largest workforce surveys in the world. It has been carried out each autumn since 2003
The results of the survey are used by NHS organisations to understand staff experience on a local and national level. These insights can then be used to improve working conditions and then ultimately patient care.
Because it is carried out annually, researchers, leaders and interested parties can compare views over time. They can also compare the experiences of those working similar organisations.
The NHS Staff Survey is designed to capture a clear picture of working life through carefully tested and validated questions. Its development follows a gold standard process, drawing on proven questions from other surveys, engaging widely with experts and stakeholders, and trialling with staff across diverse roles and backgrounds to ensure reliability and relevance.
All NHS Trusts are required to participate in the NHS Staff Survey. Commissioning support units, social enterprises, ICBs and other NHS
organisations are invited to take part on a voluntary basis. Staff working at an organisation on 1 September will be included in that year’s survey.
Participation is not compulsory for staff, but it strongly encouraged, so that staff can have their voices heard. It is important that as many people as possible take part so the results are wide and representative.
The survey is carried out in the autumn with the results published the following spring.
From 2023, NHS Trusts with at least 200 eligible in-house bank only workers were required to extend the survey to those workers.
The data from the survey is anonymised and publicly available.
The Staff Survey is owned by NHS England and the Survey Coordination Centre at Picker Institute Europe and the independent Staff Survey Advisory Group support them with the implementation. E
The NSS reports on the seven elements of the People Promise
F The People Promise
The NSS is aligned to the People Promise, which is to work together to improve the experience of working in the NHS for everyone. The People Promise describes, through the voices of NHS staff, the changes that would most enhance their working lives. It highlights priorities such as access to health and wellbeing support, greater flexibility in how work is arranged, and fostering a sense of belonging for everyone, regardless of role or background.
The NSS reports on the seven elements of the People Promise: we are compassionate and inclusive; we are recognised and rewarded; we each have a voice that counts; we are safe and healthy; we are always learning; we work flexibly; and we are a team. It also reports on two longstanding themes: staff engagement and morale.
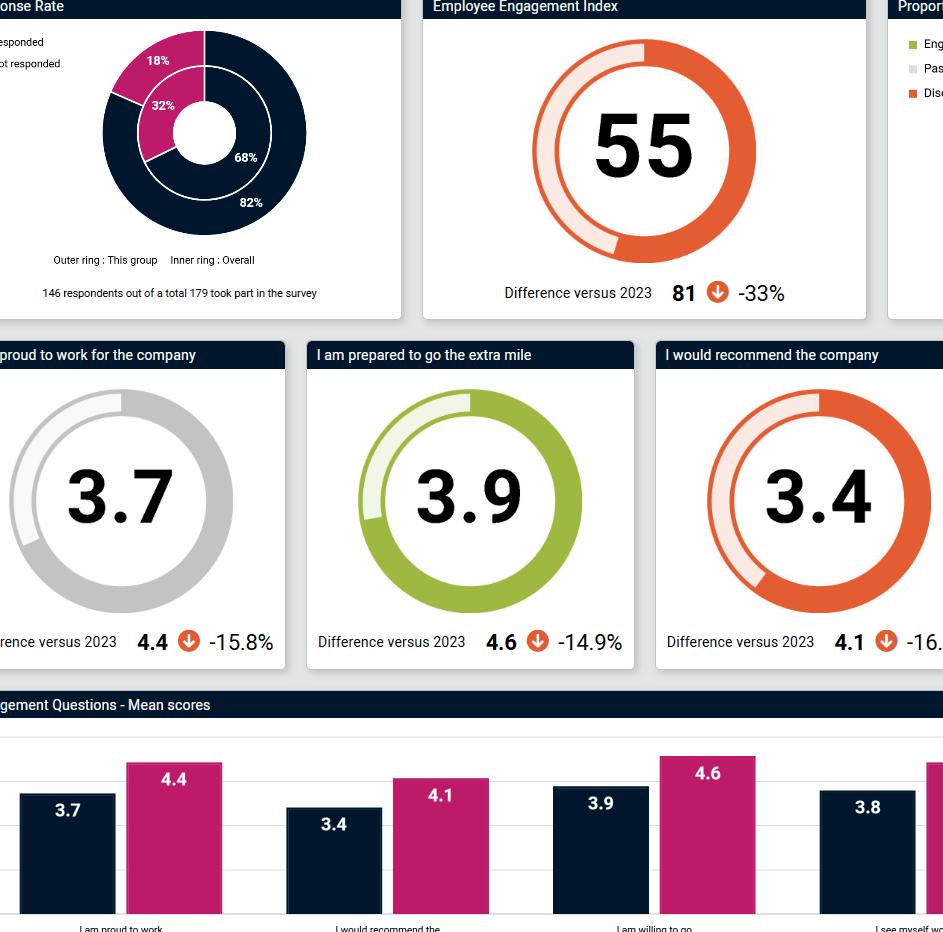
The results
On the whole, results from the 2024 survey have remained steady and generate similar results across all categories. Of the nine criteria, two of these have unchanged scores from 2023, which are rated out of ten: ‘We are recognised and rewarded’ (5.99), ‘We are a team’ (6.80). Four of these saw marginal gains: ‘We are safe and healthy’ (6.14 up from 6.13), ‘We are always learning’ (5.67 up from 5.64), ‘We work flexibly’ (6.31 up from 6.28), and morale (5.96 up from 5.94), and three of these saw slight decreases: ‘We are compassionate and inclusive’ (7.28 down from 7.30), ‘We each have a voice that counts’ (6.69 down from 6.72), and staff engagement (6.85 down from 6.89). Although most statements were met with similar responses to 2023, some are still considerably lower than 2020 outcomes, such as morale (6.08), staff engagement (7.05), although these have steadily increased since the COVID-19 pandemic.
Under the ‘We are safe and healthy bracket,’ staff gave ‘negative experiences’ a sub-score of 7.82 out of ten, a slight decrease from 7.83 in 2023. Although this may seem like a positive score, and few negative experiences among survey respondents, one in seven staff (14.38 per cent) have experienced at least one incident of violence by patients, service users, their relatives, or other members of the public,
making this the highest proportion since 2021. 0.78 per cent of staff experienced at least one incident of physical violence from managers, again up from 2023 (0.72 per cent), and 1.89 per cent from other colleagues, the highest proportion in a while.
Harassment, bullying and abuse, while incrementally decreasing, was still high: more than one quarter (25.08 per cent) of staff have experienced at least one incident of this within the past year from patients, service users, their relatives or other members of the public. Almost one in ten (9.46 per cent) and more than one sixth of survey respondents experienced this from managers and colleagues: both statistics are part of a wider decline, but these figures are still alarmingly high.
Since 2023, staff have been asked if they have received unwanted behaviour of a sexual nature, including jokes, touching, and assault, within the last year. 8.82 per cent of staff reported at least one incident from patients, service users, their relatives or other members of the public, an increase from last year (8.79
per cent). From staff and colleagues, this figure has seen a slight decrease, from 3.85 per cent in 2023 to 3.66 per cent in 2024. These figures starkly differ across sectors: around one in ten nurses and midwives said they have been the target of unwanted sexual behaviour at work, with ambulance staff most likely to experience this: incidents here were more than one in four (28.79 per cent).
The survey revealed a diversity and equality sub-score of 8.08, which although higher than its ‘We are compassionate and inclusive’ rating (7.28), is the lowest diversity score in five years (8.1 in 2021). In a similar vein, less than six in ten (55.93 per cent) of staff in 2024 felt that the NHS acts fairly towards career progression or promotion, regardless of protected characteristics like gender, religion or ethnic background. Discrimination among staff has also increased to its highest level in five years, with almost one in ten staff reporting discrimination within the last twelve months from patients, service users, their relatives, or other members of the public (9.25 per cent)
Around one in ten nurses and midwives said they have been the target of unwanted sexual behaviour at work
and from managers, team leaders or colleagues (9.22 per cent). The latter has seen a steady climb over the years, from 8.37 per cent in 2020, with 66 per cent citing discrimination on the grounds of their ethnicity.
Again, ambulance staff have reported the most incidents of workplace discrimination, (18.60 per cent), although nursing and healthcare assistants have been the biggest jump, from 14.38 percent reporting discrimination in 2023, to a concerning 16.44 per cent reporting discrimination in 2024. M
www.nhsstaffsurveys.com
Industry Insight: NHS staff experiences
Surveys reveal persistent anxiety and workload pressures across the NHS, while perceptions of staffing have improved slightly since 2020, burnout and discontent remain high
What trends are you seeing in NHS staff sentiment around anxiety and workload pressure and what effect does this have?
The NHSSS survey shows under half of NHS staff agree they are able to meet the demands on their time at work, just over half say that they have adequate materials and equipment and about a third say that they have enough staff within their organisation.
Agreement that staffing levels are adequate has improved over the last two to three years, but is still lower than the ‘high’ of 38 per cent reported in the 2020 survey. Is that really ‘high’?
The Royal College of Nursing survey highlights that two thirds of nurses are working when they should be on sick leave, and that stress is the most significant cause of illness, cited by nearly two-thirds of respondents, up from 50 per cent in 2017.
And these issues are not new, as noted already these issues were already at high levels in 2017, before the pandemic. In 2021, 35 per cent of NHS staff reported feeling burnt out because of work – in 2024, the levels are still high at 30 per cent – an improvement but still gravely concerning.
HR buzzwords like “quiet quitting” and “career cushioning” are everywhere. Do you think these buzzwords help us understand staff behaviour, or do they risk oversimplifying complex issues?
Staff that are worn out, feel neglected or undervalued, or just unheard – will often react with behaviours that are negative including “quiet quitting” (doing the minimum possible, no willingness to give discretionary effort), or “career cushioning” (focussing on learning new skills and perhaps focussing more on maintaining relationships with recruiters and/or
potential future employers in case they need to move jobs – not a bad thing of itself provided that it isn’t a distraction from doing their current job).
But those terms describe behaviours and avoid looking more closely at why these behaviours are occurring. Using these terms can also lead to ‘lazy’ solutions that do not address the root causes and create lack of engagement among staff.
The NHS is a unique organisation, but many of the challenges faced are similar to those faced by other organisations with concerns about job security, workload, confidence in leadership are concerns for those in commercial, charitable, not-for-profit and other public sector organisations too.
How can NHS organisations establish the root cause of staff discontent effectively?
While there may be signposts to more obvious challenges such as lack of staff or resources, high workload demands, balancing pay and reward with cost-of-living rises, keep looking. There may be other, less obvious reasons for discontent that are just as important and potentially easier to address.
It’s perhaps too easy to look at pay and benefits – prior to 2020 we were seeing a continued and consistent decline in perceptions of pay being fair – not just in healthcare, but across sectors and sizes of organisations. More recently there has been improvement in this measure, but pay and benefits on their own are not the sole factor to address.
Those thinking about leaving the NHS organisation they work at is high at 29 per cent, albeit having improved slightly from two years ago, so there are still strong challenging issues that need to be addressed regarding workload and effective communications throughout individual organisations that make up the NHS.
Once insight has been gathered, how can NHS organisations effectively address these issues, without falling into generic solutions?
Put in place initiatives and solutions that can be tracked, and ‘course-corrected’ or replaced if they are not having impact. Resources and budgets are obviously tight, but communicate what the initiative is trying to achieve and listen to the feedback from the target staff groups.
Avoid additional workload that initiatives may have – more paperwork or data generation to monitor targets won’t be welcome.
Match good intentions with senior management support – communications, presence and listening – to help action plans succeed.
Each team, trusts or type of service will have a specific element of culture which will layer together – aligning these elements so that they work together requires effort, but leads to more effective teams.
People feel connected to those they work closely with and in the NHS colleagues are seen to respect and support each other. This is a strong building block, add effective line management, good leadership and positive shared objectives to create success. M
Colin is a Market Research specialist with 30 years’ experience as a client and within agencies. A MRS Certified member, he has worked on a range of research projects, including brand, advertising, reputation, customer satisfaction, employee engagement and satisfaction, internal communications, and change management.
Colin Wheeler, managing director, Survey Solutions
Winter preparations
The NHS is bracing yet again for another tough winter, with early flu outbreaks, rising demand in A&E, and ongoing industrial action
Every year, colder months bring a surge in seasonal illnesses and hospital admissions, but this winter is expected to be particularly challenging. Health leaders have already warned of a “long, hard winter” ahead, as flu cases are arriving earlier than usual and are predicted to be the worst in a decade.
At the same time, the NHS is working to reduce waiting lists (now 230,000 lower than July last year), while managing record levels of ambulance callouts and emergency attendances
To prepare, NHS England has stress-tested winter plans across regions, ensuring hospitals and Integrated Care Boards have strategies in place for different demand scenarios.
These include expanding urgent care services, strengthening infection control measures, and accelerating vaccination programmes for flu and COVID-19.
Supply chains are also being reinforced to guarantee essential equipment and medicines remain available during peak demand.
Meanwhile, public campaigns are encouraging people to make informed choices about where to seek care, from self-care at home to NHS 111, in order to ease pressure on frontline staff.
Stress tests
In September, the Health Service started preparing by running stress test exercises. Local NHS leaders tested the robustness of their winter plans by participating in scenario exercises such as staff shortages, rapid increase in demand, and multiple virus outbreaks.
Teams also identified patients who would be the most vulnerable to winter viruses and hospital admission, so they could be provided with targeted care.
This year will see a different approach, with more power for NHS leaders on-the-ground to deliver bespoke plans for their local population.
The health service is also working closely with local authority and social care colleagues, so that discharge capacity can surge at times of peak demand.
Sir Jim Mackey, NHS chief executive, said:
“Despite record demand this year NHS teams have worked hard to improve waiting times, with last month’s Category 2 ambulance response times the fastest for four years – but we know the coming colder months will be much more challenging.
The health service is also working closely with local authority and social care colleagues
“The NHS has done more preparation to be ready for the winter months than ever before, because we know the last few winters have been particularly tough for patients and staff, and we are determined for this year to be better”.
Health and social care secretary Wes Streeting said: “Winter is always tough for the NHS, but this year we’re ramping up preparations and doing more to protect the country. From ‘war game’ exercises to extra checks for the most vulnerable, we’re making sure the health service is ready for whatever comes its way.
“But the public has a crucial role too. The single best way you can protect yourself, your family, and the NHS is by getting vaccinated. It takes pressure off hardworking staff and helps ensure care is there for patients when they need it most.
“By preparing together – government, NHS staff and the public – we can give the health service the best chance to weather the winter ahead”.
Healthy lifestyles
In November, the government launched a new campaign supported by Sport England that aims to help parents discover simple ways to build movement into daily life during the winter months.
According to research, almost three in five (57 per cent) parents say their children’s physical activity levels are likely to suffer a seasonal dip during autumn and winter, with cold or wet weather (60 per cent) and darker evenings (41 per cent) highlighted as the key barriers.
NHS guidance recommends that children get at least 60 minutes of physical activity each day – including 30 minutes outside of school hours. Yet the new survey reveals that 81 per cent of parents underestimate how much physical activity children need. Already, more than half of children in England aren’t getting the recommended amount of movement and, worryingly, the research shows this will increase during the colder months.
Supported by Joe Wicks, the ‘Let’s Move!’ campaign makes staying active easy and affordable, offering ideas from kitchen discos E
Regional teams made it as easy as possible for people to receive their vaccines
F to local activities and playground fun. It encourages families to move together – 80 per cent of parents believe their habits influence their child’s activity levels – and highlights how everyday routines can support healthy, active lifestyles. Regular movement boosts mood, focus, and family connections, with 78 per cent of parents agreeing that their child is happier after being active, has more energy (71 per cent) and has better concentration (68 per cent).
While just over half (52 per cent) of parents say their children really enjoy traditional forms of sport, others face barriers such as low confidence (31 per cent) or a dislike of competitiveness (30 per cent). However, 94 per cent of parents say their children enjoy physical play as a form of movement – with top activities including visiting the playground (56 per cent), riding a bike (46 per cent), dancing (44 per cent) and playing tag or chase (43 per cent).
‘Let’s Move!’ aims to support different ways for children to enjoy being active – from sport to play and everyday movement. The campaign features real families from local areas having fun getting active together in ways which suit them, such as dancing or playing in the playground.
Winter vaccinations began in October. Regional teams made it as easy as possible for people to receive their vaccines, for example, by hosting mobile vaccination buses to deliver vaccines closer to home, running family drop-in sessions in the community, and for the first time ever delivering flu vaccines to two- and three-yearolds in some community pharmacies.
Dr Amanda Doyle, national director for primary care and community services at NHS England, said: “It’s concerning to hear flu and COVID-19 cases are already creeping up ahead of winter – but vaccinations remain our best defence against these viruses and can be lifesaving. I urge everyone eligible to come forward for their jabs as soon as they can, with easy to book appointments or drop-in sessions now available closer to home.
“Teams across the country are working hard to make it as easy as possible to get vaccinated at your local GP, pharmacy, school or other community clinic, and for the first time ever parents will be able to get flu vaccines for their two- and three-year-olds at their high-street pharmacy to help busy families protect their children in a way that works for them.
“Get vaccinated today to protect yourself and others around you, it might keep you out of hospital this winter”.
Capacity
In Scotland, health secretary Neil Gray has confirmed £20 million to boost social care capacity.
Speaking to parliament, he shared updates on winter preparations for the NHS and urged people to get the flu vaccine.
The money will be targeted at initiatives by health boards to increase social care capacity and provide extra support at the front door of A&Es. This will reduce admissions and help to relieve pressure on acute services.
Gray also warned of an expected early and difficult flu season and urged everyone eligible to get their vaccination, particularly children and young people who can transmit the virus to vulnerable family members and friends.
To further help with winter pressures, the Scottish Ambulance Service (SAS) will recruit more than 290 new frontline A&E staff this year, including newly qualified paramedics and ambulance care assistants.
NHS 24 has also implemented a new call centre system backed by £5 million of investment. Over 90 per cent of callers triaged by NHS 24 as needing an ambulance response now have their call information transferred and referred digitally, removing repetitive stages of the call process and speeding up the process.
Health boards have been directed to undertake a new approach, working together to plan digital care and business systems, and make best use of available capacity for orthopaedic elective services.
Gray said: “We know pressure on the system exacerbates over winter and I am determined to ensure that pressure is relieved as much as possible. We have been preparing plans for this winter season throughout the past year with NHS boards and local authorities.
“Our investment of £20 million will be crucial in our efforts to bolster social care capacity, reduce unnecessary hospital admissions and
NHS 24 has also implemented a new call centre system backed by £5 million of investment Reduce
ensure people receive the right care in the most appropriate setting.
“A key part of our winter response is prevention and our national flu vaccination programme is well underway. Vaccination is one of the best ways to protect our own health and those around us – with flu cases rising and initial evidence suggesting this may be an early and potentially difficult flu season, I urge all those who are eligible to get vaccinated.”
“We have significantly increased Scottish Ambulance Service staffing and we are investing in capacity in our NHS 24 call centres so that people are getting the right support quickly and when they need it.
“Our dedicated health and social care staff are the cornerstone of our winter response every year – they will continue to work tirelessly in the coming months to provide excellent care, and I thank them for their outstanding efforts.” L
NHS warns of bad flu season
This year is expected to be a bad flu season. Here’s what you can do to help reduce the spread
Back in October, NHS leaders warned that this year’s flu season could be bad, with flu cases hitting the NHS a month earlier than usual and cases three times higher than the same time last year.
In a sign of things to come, Japan declared a flu epidemic with many schools shut. At the time, NHS leaders warned of a long and drawnout flu season.
By the end of October, more than 12 million flu jabs had been delivered. This included more than 6.7 delivered to the over 65s, 1.8 million to school-aged children and 366,000 to two and three-year-olds.
At the time, Duncan Burton, chief nursing officer for England, said: “This early rise of flu in children is particularly concerning – especially given that flu circulation in children normally precedes that in adults – so it’s vitally important those eligible come forward for their vaccine as soon as possible to avoid a long and drawn-out flu season.
“The flu virus changes every year, so it’s important to get a vaccination each year to ensure yours and your families protection and to help reduce the spread to others.
“Vaccines are one of the safest and most effective ways to help shield against the virus and prepare for what we expect to be a very challenging winter, so I would urge everyone eligible to come forward for their jabs as soon as they can, with easy to book appointments or drop-in sessions now available closer to home.
Dr Alex Allen, consultant epidemiologist at UKHSA, said: “We’re seeing an unusually early start to the flu season this year, with the latest data showing a sharp increase among children but also increases in other age groups, with the virus now starting to spread more widely in the community.
“If you’re eligible for a vaccine it is because you are at greater risk of severe illness – every year we see many thousands end up in hospital and far too many deaths from flu. It’s crucial that everyone eligible books their appointment as soon as possible. The vaccine is our best defence. “Parents should return school consent forms or arrange GP appointments for 2- to 3-year-olds. The nasal spray vaccine can help stop your child from getting very unwell and reduce the risk of passing flu to vulnerable family members.
“Anyone with flu or COVID-19 symptoms –including high temperature, cough, and E
Vaccines are one of the safest and most effective ways to help shield against the virus
F feeling tired or achy – should minimise contact with others, especially those who are vulnerable. If you need to go out with symptoms, consider wearing a face covering, wash hands regularly and ensure indoor spaces are well ventilated.”
Flu jab SOS
The following week the NHS issued a flu jab SOS, with England’s top nurse warning people to get protected as soon as possible. The NHS made available 2.4 million vaccination slots in the next week, enough to vaccinate the whole of Greater Manchester.
Eligible adults were urged to get their jab as soon as possible, after Australia had its biggest flu season in history.
By 6 November, more than 13 million jabs had been delivered included three in five of all care home residents. However, only a third of eligible toddlers had been vaccinated.
Duncan Burton, chief nursing officer for England, said: “With just weeks left to ensure best protection against the worst of the flu season, we are issuing an urgent SOS to the eligible people who have yet to get jabbed this year.
The flu vaccine is estimated to have prevented around 100,000 people from being hospitalised in England last winter
“It is vital that the public use the over 2.4 million available appointments we have running next week to stamp out this early wave of flu cases and help shield themselves ahead of winter, when viruses tend to circulate and the NHS faces increased pressure on its services.
“The vaccine is proven to be safe and help prevent those at risk from getting seriously ill and even hospitalised from flu – so please check your local pharmacy, book an appointment online or by calling 119, or speak to your GP practice today about your winter flu vaccine”.
Public health minister Ashley Dalton said: “Vaccination is the best form of defence against flu – particularly for the most vulnerable. “With flu cases already triple what they were this time last year, I urge everyone eligible to
take up one of the 2.4 million appointments available next week.
“Getting vaccinated now means you’ll have the best possible protection in place for yourself and your loved ones, and will also be protecting our NHS as we approach the challenging winter months.”
The UK Health Security Agency (UKHSA) found that the flu vaccine is estimated to have prevented around 100,000 people from being hospitalised in England last winter.
In healthcare environments
Healthcare environments are particularly vulnerable to flu outbreaks because of the close contact between patients, staff, and visitors. Preventing transmission is essential to protect vulnerable individuals and reduce pressure on services. One of the most effective measures is vaccination of healthcare workers. Staff immunisation reduces the likelihood of contracting flu and passing it on to patients, making it a cornerstone of infection control. Strict hand hygiene is another critical defence. Regular handwashing with soap and water, or using alcohol-based hand sanitiser, helps limit
Healthcare environments are particularly vulnerable to flu outbreaks
the spread of flu viruses from surfaces and equipment. Alongside this, the appropriate use of personal protective equipment (PPE) such as masks, gloves, and gowns is vital, particularly when caring for patients with suspected or confirmed flu.
Isolation and cohorting of patients can also play a major role. Those with flu symptoms should be separated where possible, or grouped together, to prevent cross-infection with nonflu patients. Enhanced cleaning protocols are equally important, with frequently touched surfaces such as bed rails, door handles, and medical equipment disinfected regularly to reduce viral contamination.
Visitor management is another key consideration. Limiting visits during peak flu season, and encouraging symptomatic visitors to stay away, helps protect patients and staff. Good ventilation in wards and waiting areas further reduces the concentration of airborne flu particles, lowering the risk of transmission. By combining vaccination with robust infection control practices, healthcare settings can significantly reduce the risk of flu outbreaks. These measures not only protect patients but also safeguard staff and maintain the resilience of the NHS during the winter months. L
What are benefits and the risks of AI in healthcare?
Professor Christina Pagel, director of UCL’s Clinical Operational Research Unit, and a member of The Operational Research Society explores how AI can boost efficiency, accuracy and patient care, while warning of risks around bias, over-diagnosis and ethics
Artificial intelligence (AI) is transforming industries worldwide. According to PwC’s 2025 AI Predictions report , top-performing organisations are shifting their focus from simply experimenting with AI use cases to embedding AI at the core of their business strategy. Healthcare is one example of where AI adoption is accelerating.
A survey of UK healthcare organisations by SOTI showed that in just one year the number of UK healthcare organisations using AI jumped from 47 per cent in 2024 to 94 per cent in 2025. Once limited to administrative functions, over half now use AI to help diagnose conditions or personalise treatment, though the most common use remains processing or analysing medical data.
AI in action
By 2027, the roll out of validated AI diagnostic tools and administrative aids, including AI scribes, across GP practices is set to save time, up the equivalent of more than 2,000 full-time GP positions . Meanwhile, NHS England is investing £6 million in an AI research screening platform to help hospitals trial tools that analyse images and detect abnormalities . This is a taster of how AI could reshape future diagnosis and treatment.
The UK government is fully invested in AI use across the NHS. Supporting its 10-Year Health Plan for England, a National Commission has just been established to make the NHS “the most AI-enabled care system in the world,” accelerating safe access to AI and shaping a regulatory framework.
Yet with any innovative technology, there are risks as well as benefits, and implementation will need to be planned carefully to ensure it’s successful and lives up to the expectations.
The benefits of AI
Understanding what is meant by AI matters. A few years ago, the term mainly referred to machine learning (ML) and neural networks, systems trained to recognise patterns, particularly in images. Today, AI usually refers to
large language models (LLMs) such as ChatGPT. The distinction matters. ML excels in pattern recognition, classification, and prediction tasks, while LLMs manage language, synthesis, and reasoning.
In my view, medical imaging offers the clearest success case so far. ML systems can analyse scans and flag anomalies with remarkable accuracy, making radiology and pathology ideal areas for AI support. These tools assist rather than replace human experts. However large language models (LLMs) are now emerging as practical tools to support clinicians in real-world decision-making. These can review, summarise, and synthesise patient data, identify subtle patterns that might be missed (particularly from text data), and offer alternative explanations, essentially acting as another pair of eyes. Rather than replacing clinical judgment, they complement it by reducing common sources of error, such as cognitive bias or communication gaps within teams. By providing input without regard to E
Understanding what is meant by AI matters
AI is only as good as the data it relies on
F hierarchy or status, LLMs have the potential to quietly strengthen the way care decisions are made. The key is that LLMs should not be used to replace clinical judgement and expertise, but to enhance it.
AI also promises to relieve administrative burdens. Tools that transcribe consultations, or draft letters, can save clinicians or support staff hours every week. In an overstretched NHS, time is precious, but efficiency must not compromise empathy, the human connection that data alone cannot capture.
Navigating the risks of AI
One of the biggest risks for ML systems analysing imaging data is that they can also
detect harmless irregularities, which can contribute to over-diagnosis. Given overdiagnosis is already a concern for some conditions such as thyroid or prostate cancers, the use-case for ML must be considered on a disease-by-disease basis.
Detecting more does not always mean treating better, and as diagnostic AI expands, the NHS must avoid over-testing and overtreatment. The seductive trap will be that the more healthy people are treated when they do not need to be, the better outcomes from your programme will look (because you are diluting the statistics with people who were always going to be fine).
AI is only as good as the data it relies on; incomplete or biased datasets risk perpetuating inequities. Historic underrepresentation of women, ethnic minorities, or older adults can skew outcomes, though AI does hold potential to correct these gaps too, for example, improving recognition of skin conditions on
darker skin or ensuring women’s symptoms are accurately assessed.
There is the question of ethics and consent. For example, a small pilot research study is currently being conducted at University College London Hospital (UCLH). Researchers led by an ICU doctor are using camera-based AI to monitor sedated patients (with their prior consent) for signs of pain or delirium. Early results suggest it can improve comfort and shorten hospital stays, but it raises concerns around surveillance and how consent is sought routinely if rolled out more broadly. Finally, data alone cannot capture (and will never capture) the full complexity of healthcare. Lifestyle factors, patient-reported symptoms, and in-person observations are often unrecorded but vital to effective care. AI can process information faster than any clinician, but human expertise remains essential to interpret results and apply context.
Most clinicians cannot use advanced LLMs due to legal, ethical, and infrastructure limitations
Building an AI-ready future
While AI is proving effective in areas such as imaging, hospitals are far from fully AI-enabled. Most clinicians cannot use advanced LLMs due to legal, ethical, and infrastructure limitations. Real progress will require secure, ring-fenced models within hospitals, trained on local datasets under strict governance and with upgraded hardware and software. Just as much of an issue is that most UK healthcare settings are understaffed and clinical teams simply struggle to find the time or energy to learn new systems.
AI offers immense promise though to improve efficiency, accuracy, and patient care. It can streamline administrative work, enhance diagnosis, reduce bias, and support clinical decision-making. Yet its success depends on the people who design, deploy, and interpret it. AI will not replace health professionals, but when implemented responsibly, it can help them work smarter, placing patients at the centre of healthcare. L
Professor Christina Pagel, director of UCL’s Clinical Operational Research Unit, and a member of The Operational Research Society
Why bringing data together across the NHS is so crucial
Unlocking the true value of NHS data means moving beyond fragmented systems to a unified, cloud-based solution, delivering better patient care, efficiency, and national-level insight
Across the NHS there has been a push on collecting data for a variety of reasons.
Improve patient care
Unified data allows healthcare providers to access comprehensive patient information, leading to better diagnoses, treatment decisions, and overall care coordination, improving the patient pathway.
Efficiency
Centralising data streamlines administrative tasks, reduces duplication of efforts, and enhances resource allocation, ultimately leading to more efficient healthcare delivery.
Population health management
Integrated data enables health authorities to monitor population health trends, identify high-risk groups, and implement targeted interventions to improve public health outcomes.
Cost savings
By eliminating redundant systems and optimising healthcare processes, centralised data management can lead to cost savings for both healthcare providers and patients. Overall, bringing data together across the NHS will not only improve individual patient outcomes but also enhances the effectiveness, efficiency, and sustainability of the healthcare system as a whole.
The challenge
There are numerous software solutions required to enable the NHS to run it’s services. Within the Supply Chain environment alone we see various systems including, sourcing, contracting, cataloguing, requisitioning, procurement, top-up, inventory management, point-of-care scanning, and finance platforms.
Many NHS Trusts find that they have different solution providers for many or all of these solutions which in itself has led to huge data complexity with systems being built in different ways, data stored in different ways, and data being built and presented differently. Product item data, and a lack of any single point of truth is a huge reason that connecting this data has become so difficult, with a single item appearing under different coding from not only one organisation to another but in many cases this is present within a single organisation. This issue is further magnified when you expand out from a Trust to an ICS, ICB, and National level.
The NHS is left with a situation whereby the same item can appear in Trust/ICS data multiple times under different part coding and descriptions, with this in mind there is no easy solution to analyse product item data meaning that buying power and supply chain efficiencies are impacted negatively.
The age-old conundrum, how can the NHS mobilise the true value in its data?
So how can the NHS mobilise the true value in its data? To date we have all witnessed a growth in third party organisations springing up providing consultancy services to help consolidate data and make it usable for both trusts and ICSs alike.
The biggest area has been in trying to decipher item coding, so that a better procurement picture can be created and volumes realised to chase savings on item cost and review clinical variation. Whilst this is great, this is very much a short term and costly solution.
Would it not be more beneficial and even more powerful to resolve the route cause by looking for a unified Source to Pay solution
that can be deployed across multiple organisations (NHS and or public sector) no matter what the finance platform they have.
A unified solution provided by a single provider where data is cleansed and connected to a single point of truth (manufacturer data), is free flowing across modules, available and reportable at Trust, ICS, ICB, and national level without the need for an external entity to decipher it?
The solution is already here!
Since 2002, the Scottish Government has deployed Elcom’s cloud-based Purchase-toPay (P2P) solution named as PECOS, PECOS, as a shared service across 118+ public sector organisations, including central and local government, NHS Scotland, universities, and colleges. Processing £8-9 billion in annual spend, PECOS automates the full procurement lifecycle — from requisition and purchase order creation to receipting, invoice matching, and electronic payments. Delivered as a scalable Software-as-a-Service (SaaS) platform, it standardises processes across diverse entities while preserving operational autonomy.
Central to this transformation is the aggregation of PECOS’s clean, standardised transactional data into Scotland’s national Management Information (MI) platform,
provided by Elcom and operated by the Scottish Procurement and Property Directorate. Every purchase order, invoice, and receipt processed through PECOS feeds directly into this centralised MI system via secure, automated data pipelines, creating a single, trusted source of truth for national spend intelligence. This eliminates the historical burden of manual data collation, reconciliation errors, and inconsistent reporting formats that once plagued cross-entity analysis.
The benefits of this national MI integration are profound: Comprehensive Spend Visibility; Strategic Policy Alignment; Enhanced Accountability and Governance; CrossSector Benchmarking and Collaboration; and Predictive and Prescriptive Analytics.
In summary, Elcom’s solutions have redefined public sector procurement in Scotland. By delivering a single, cloud-based P2P solution that enforces data quality, integrates with diverse finance systems, and feeds a national MI platform, it has unlocked unprecedented visibility, accountability, and strategic capability — delivering tangible economic, operational, and societal benefits to taxpayers and public services alike. M
How do we make UK’s health and care sector digital ready?
As the UK’s health and care sector rapidly evolves to meet digital transformation targets, there’s a question mark over whether the workforce feels supported and equipped with the skills needed for such a significant transformation to succeed
Last year, Integrated Care Systems (ICSs) leaders flagged concerns that the sector would struggle to meet its digital ambitions without first ensuring the workforce is effectively supported. With these concerns in mind, Steven Hurst, Director of Corporate Learning at Arden University explores how health and care organisations can upskill their workforce effectively to keep pace with digital transformation. He also discusses how degree apprenticeships and learning pathways can help bridge the skills gap, ensuring healthcare professionals are equipped and motivated to use these tools effectively.
New systems, familiar challenges
The UK health and care sector is undergoing a significant digital transformation, with ICSs playing a pivotal role in meeting national digitisation targets. From implementing electronic patient records (EPRs) to building interoperable systems, technological advances promise to revolutionise patient care by enabling faster, more accurate decision-making and improving efficiency across the board. However, as the tools and systems evolve, a critical question looms over the workforce tasked with implementing and using these technologies: can the workforce keep pace? And
crucially, are healthcare leaders doing enough to ensure teams feel supported throughout this immense period of change?
The NHS’s Frontline Digitisation Programme launched in 2021, marking a significant step forward in modernising health and care services. By moving from paper-based records to digital patient databases, the health and care sector aims to make patient information accessible across care pathways, improving collaboration and efficiency. Despite the progress, workforce and training issues remain
The path to successful digital adoption is as much about people as it is about technology
significant barriers to meeting these goals, as highlighted in the NHS’s Confederation report. It also stated that leaders also recognised “the need to invest in people and the workforce alongside the investment in technology”, stressing that if the right balance isn’t achieved and the workforce isn’t effectively supported, “digital transformation ambitions won’t be realised”.
The challenge is twofold. First, equipping the workforce with new skills to use advanced technologies effectively. Second, addressing the cultural and psychological impact of such widespread transformation. Without regular, targeted engagement efforts, staff risk feeling overwhelmed and under-supported, which could derail even the most ambitious plans.
The path to successful digital adoption is as much about people as it is about technology.
What upskilling to a digital future looks like
Managing a digitalised workforce requires a distinct set of leadership qualities and management skills, as the dynamics of the workplace evolve with technological advancements. Leaders must not only E
Prioritising workforce education can lead directly to operational efficiency and better care delivery
F understand cutting-edge digital tools and systems but also foster a culture of adaptability and innovation to keep pace with rapid changes. Effective communication, data-driven decision-making, and the ability to guide teams through digital transformation are crucial competencies. This makes upskilling vital – not just for employees but also for the leadership teams themselves as it will ensure they can support, inspire, and maximise the potential of a tech-savvy workforce in a digitally driven environment.
Traditional leadership often emphasised hierarchy, authority, and stability, relying on established processes and long-term strategies to guide organisations. While these qualities remain valuable, the digital era demands a more dynamic and agile approach. Unlike conventional leadership, which may focus on maintaining the status quo, modern digital leadership prioritises adaptability, rapid problem-solving, and continuous innovation to thrive in a fast-changing landscape. Additionally, where traditional leadership might have been top-down, digital-first leadership encourages collaboration, cross-functional teams, and empowering individuals at all levels to contribute towards transformation.
This shift reflects the need to balance structure with flexibility, ensuring organisations remain competitive and resilient in an increasingly digital world.
The role degree apprenticeships play Degree apprenticeships offer healthcare organisations the unique tools to address this particular workforce readiness. These programmes combine practical on-the-job learning with academic study, enabling professionals to upskill while remaining in their roles. Covering topics such as strategy, leading teams and organisations, financial management and managing digital transformation, these courses allow NHS employees to develop a strong skillset and mindset that reflects the sector’s current and future needs.
This model benefits both employees and employers. For workers, it provides an opportunity to enhance their career prospects while staying financially secure. For employers, it addresses specific skill shortages within their organisation. To illustrate the impact degree apprenticeships can have on healthcare digitisation, consider the following example.
A medium-sized NHS trust in the Southeast initiated a bespoke training programme for clinical staff to improve data interpretation and patient record management. They partnered with a local university to offer apprenticeships tailored specifically to their needs. Within 18 months, the trust reported a 32 per cent reduction in time spent on administrative tasks and noted improved patient outcomes
thanks to better decision-making supported by accurate data.
This shows how prioritising workforce education can lead directly to operational efficiency and better care delivery. While 40 per cent of staff may have the basic digital skills needed for everyday tasks, a significant proportion may struggle with these fundamentals. From digital coordinators to clinical informatics specialists, degree apprenticeships can fill crucial roles in the delivery and maintenance of cutting-edge health technology.
Practical steps for supporting the workforce
Here’s how leaders can ensure their teams feel supported and capable during this digital transformation. First, conduct skill audits: before introducing new systems, map out the digital capabilities across your organisation. Identify gaps and prioritise roles that require immediate training. Second, invest in tailored training. Generic training sessions won’t cut it. Digital literacy training should be role-specific, with a practical focus on how employees can use digital systems to improve their daily workflows. Third, communicate a clear vision. Staff need to understand why digitisation matters and how it will improve their ability to deliver care. Regular engagement through town halls, workshops, and one-on-one discussions can foster stronger buy-in from teams. Fourth, foster collaborative learning. Encourage knowledge sharing between teams. Those with
Upskilling the workforce isn’t an optional add-on
advanced digital skills can mentor colleagues, reducing learning curves and increasing workplace camaraderie. Fifth, leverage external expertise. Partner with universities, private training providers, and digital consultancies to outsource specialist training, particularly for roles requiring advanced technical expertise. Finally, use learning platforms. Explore modern e-learning platforms that offer flexible, accredited courses in key areas such as senior leadership management, health and care management, and EPR functionality.
The bigger picture
Amid widespread discussions about funding constraints and operational inefficiencies, it’s tempting to focus primarily on technical infrastructure during the digital transformation process. However, without addressing the human element, even the most sophisticated systems risk being underused. Upskilling the workforce isn’t an optional add-on; it’s a core component of digital transformation.
A long-term commitment to professional development, supported by innovative learning models like degree apprenticeships, is critical. Not only does it empower individuals, but it enables organisations to harness the full potential of modern technology. L
How NHS Supply Chain led a national response to a hand hygiene crisis
When a large supplier of hand hygiene products collapsed overnight, NHS Supply Chain led a national response to protect patient safety
The silent guardian of patient safety
Imagine delivering care without washing your hands. For most of us, that sounds unthinkable. Yet, on 30 April 2024, this scenario became a looming reality. When GOJO UK – the largest supplier of hand hygiene products on our framework and into the NHS – unexpectedly went into administration, the foundations of safe care were at risk.
With 90 per cent market share and proprietary wall-fixed dispensers installed across hundreds of trusts and bespoke cartridges limiting interchangeability, the challenge was immense. Around 300 customers relied on these products, with each trust typically having 50,000 dispensers installed. With fitters able to replace only 50 dispensers per day on average, a full national transition was projected to take six to nine months but at the point of disruption, only eight weeks of stock remained.
Without urgent action, hospitals, clinics, and community services faced serious disruption, and patient safety incidents were a real possibility.
Responding under pressure
The disruption came without warning. “It felt like being in a pressure cooker with expectations, urgency, and complexity compounding as new issues surfaced,” said Tom Brailsford, head of resilience, NHS Supply Chain.
NHS Supply Chain immediately mobilised its Resilience, Patient Safety and Category Teams and convened a national response. Working closely with NHS England and the Department of Health and Social Care (DHSC) for strategic oversight, Integrated Care System (ICS) Advisory Groups for regional coordination, and suppliers and trusts for operational execution, the aim was clear: maintain patient safety and continuity of care.
“This response was truly collaborative across the whole of the NHS. Without the support of trust colleagues to ensure the right products were switched out at the right time to enable an orderly transition, the recovery would have been significantly more problematic,” said Tom Brailsford.
Internally, a cross-functional Working Group was established to manage risks, align expertise and accelerate decision making. Daily meetings supported rapid progress, while communication with customers was prioritised. Over 25 weekly webinars, each attended by 150-200 participants, provided updates and enabled two-way dialogue throughout the process.
A clinician from Central and North West London NHS Foundation Trust reflected: “We couldn’t have done it without you. NHS Supply Chain’s influence and leverage were invaluable,
A detailed data dashboard ensured decisions were based on evidence, not assumptions
helping mediate a resolution that was a win-win for everyone involved.”
Practical steps to maintain supply
There was no option to pause. NHS Supply Chain worked to secure remaining stock from GOJO entities in the US and Europe while navigating regulatory requirements to import emergency supplies. Clinical risk stratification guidance was developed with NHS England and the DHSC, to ensure products were prioritised based on clinical need – particularly for mental health trusts where switching to freestanding products posed higher risks.
Behind the scenes, supply chain intelligence tools validated alternative suppliers, warehouse capacity was expanded, and logistics were coordinated to support the transition. Manual tracking of product usage and switching intentions, labour-intensive but essential, helped maintain visibility. A detailed data dashboard ensured decisions were based on evidence, not assumptions.
“Our supply partners stepped up to massively increase production capacity in a very short amount of time, supporting the needs of the NHS and putting patients first,” said Tom Brailsford.
The outcome
The objectives were clear: avoid uncontrolled disruption, maintain supply and protect patient safety. Despite the complexity, no critical incidents were reported. Continuous supply was maintained across all settings. By the end of 2024, 85 per cent of customers had transitioned to new products, with the remainder on track for April 2025.
Customer feedback reinforced the success: 69 per cent felt disruption management was effective; 61 per cent expressed confidence in handling future disruptions; and 79 per cent found communications effective, though only 41 per cent felt well supported in switching suppliers, highlighting areas for improvement.
As Simon Marriott, assistant director of supply chain at Nottingham University Hospitals NHS Trust, summed up: “The country could have fallen down, but it didn’t, which is a testament to how this was managed by NHS Supply Chain.”
Lessons learned
This disruption highlighted the importance of collaboration and resilience. Daily working group meetings accelerated progress, while clear, proactive communication proved essential. It also underscored the risks of heavy reliance on a single supplier with proprietary products.
Although processes were tested and stretched, they improved over time. Most importantly, GOJO stock was maintained throughout the transition – an achievement that reflects the collective effort behind the scenes.
Looking ahead
Building on these lessons, the hand hygiene crisis of 2024 was more than a supply chain challenge – it was a shared test of adaptability and commitment to patient safety. To strengthen resilience and reduce further risk of disruption, NHS Supply Chain is implementing the following initiatives: a Supply Disruption Incident Management Process with clear roles and governance; a Resilience Capability Programme to upskill teams; enhanced supplier financial monitoring standards; and exploration of universal dispenser options to reduce dependency on proprietary systems.
Because resilience isn’t just about reacting to disruption, it’s about being ready for what comes next. M
FURTHER INFORMATION
www.supplychain.nhs.uk
Legionella Risk Assessments –is yours suitable and sufficient?
It is a legal requirement to assess the risk posed by Legionella bacteria in all commercial properties, which should inspire confidence that compliance is essential for safety and peace of mind. The Risk Assessment must be “suitable” and “sufficient”. As the complexity of water systems increases, along with the number of outlets and components, the need for expert external help tends to increase
There is clear guidance on what a good LRA should contain, provided by the British Standard (BS8580-1) and the Legionella Control Association (LCA). These documents make it clear that your risk assessment needs to identify any risks present – both Inherent and Residual – and determine what is low as reasonably practicable (ALARP). HC Legionella’s assessments thoroughly identify these risks, emphasising our expertise in delivering comprehensive evaluations for your water systems.
The legal responsibility for commissioning an LRA lies with the Duty Holder; this is usually the business holder or head of the organisation, although often delegated to the Responsible Person (RP), who takes responsibility for specific day-to-day Legionella control tasks on behalf of the DH.
One of the outcomes of a good LRA is the identification of the tasks required to manage the risk posed by Legionella moving forward; this ensures that every task is considered. Both HSG 274 Part 2 Table 2.1 and HTM0401 Table 1 list the main tasks that need to be allocated to a Hot & Cold-water system in domestic and Healthcare environments, respectively.
An Executive Summary should provide a brief overview of the report, highlight key risks identified, and outline the mitigation measures to reduce them. The Executive Summary is the part of the document that gives the assessor free rein to comment on your specific system, risks and challenges, and to state their thoughts and concerns clearly, suggesting remediation.
If a significant issue has been identified, the Risk Assessor should debrief the site and ensure they understand the risk and its implications before leaving on the day of assessment and not leave this until the final written report is issued.
HC Legionella has the knowledge, skills and competence to undertake a bespoke Legionella Risk Assessment for your site. We work in line with the LCA Service Standards, BS 8580-1 and BS 8680 guidance, ensuring your assessment aligns with trusted standards and giving you confidence in the process and results.
For clients working within the Healthcare sector, our experience goes even further, as HC Legionella is a Company Affiliate Member of the Institute of Healthcare Engineering and Estate Management (IHEEM). We have a wealth of experience and knowledge, meaning no system is beyond our combined expertise. M
www.hclegionella.co.uk
Keep calm and carry on flushing
Charlie Brain, senior consultant, at the Water Hygiene Centre explains how to manage less used water outlets
Above all, three factors determine the likelihood of Legionella bacteria colonising a water system: water temperature; cleanliness, i.e. availability of nutrients and shelter; and water age; i.e. the rate of water movement & turnover within a system.
Much like a game of rock-paper-scissors, no single one of these factors can trump the others in importance.
Legionella control
Water temperature control is made more difficult in a dirty system where the temperature cannot penetrate the sediment or where the movement of water is restricted so that hot water cools and cold water warms up. A clean system is all very well, but if the water temperature is not controlled or if water is allowed to stagnate then bacteria will find a place to grow and biofilms will form.
Finally, even where water turnover is high, bacteria will find a place of shelter amongst sediment and sludge or hide out in pockets of
the system that struggle to achieve the required temperature and adequate flow rates.
In most cases, the control of Legionella bacteria can be achieved by considering these three concerns and addressing any shortfalls in the design, installation, maintenance or operational performance of the water system. In this blog, we look at ways in which regular movement of water can be achieved.
Right first time
“Right first time” has become a bit of a catchphrase here at the Water Hygiene Centre. Successful water safety begins with the correct design and installation of water systems. Failures at the first hurdle increase the inherent risk of a water system, and is, therefore, more troublesome, throughout its life cycle. HSG274 Part 2 states that: “storage tanks, water heaters, pipework and components and associated equipment containing water” should be “designed to avoid water stagnation by ensuring flow through all parts of the system”. E
F Well-designed water systems that are properly installed and commissioned can minimise the potential for stagnation, which can be caused by a vast range of design and engineering defects, some examples of which include: versized storage vessels, in particular where there is more than 24-hour storage capacity; uneven flow through parallel storage vessels; oversized pipes or excessively long pipe runs; pipework constrictions; unauthorised isolation of services; unbalanced hot water circulation; standby equipment; low draw-off outlets positioned at the end of the line e.g. water coolers or ice-making machines; and over-provision of services resulting in reduced frequency of use.
Whilst operational estate managers may have the necessary authority and resources to correct physical defects, often, designers and project managers can address these defects either on the drawing board or at least before water systems enter service.
This leaves operational managers to devise and implement a programme of inspection and testing that will determine the operational temperature performance and hygienic condition of a water system; however, when it comes to identifying those outlets that are simply underused by the building occupants things start to become a little more difficult.
Infrequently used outlets
In the workplace, there may be outlets that are required for operational, welfare or safety purposes that do not receive regular and frequent use and/or areas that are temporarily out of use. Estates managers require the assistance of building occupants to identify them and whilst in some cases estates teams will have the resources to implement a Legionella flushing regime, in others this duty will fall to the building occupants themselves. Any outlet that is subject to infrequent or intermittent use is classed as an infrequently used outlet . The definition of “infrequent use” may vary between applications and will depend not only on frequency and duration of use but also on other risk factors, such as water temperature and the vulnerability of the population which may potentially be exposed.
The Health & Safety Executive’s HSG274 Legionnaires’ Disease: Technical Guidance Part 2 states: “Any outlet not used for a period equal to or greater than seven days” should be classed as an infrequently used outlet and that “for
It should first be established if the outlets are surplus to requirements
high-risk populations, e.g. healthcare and care homes, more frequent flushing may be required as indicated by the Legionella risk assessment”.
For healthcare premises, the Department of Health’s HTM04-01 Part B: Operational Management states: “water draw-off should form part of the daily cleaning process. The procedure for such practice should be fully documented and covered by written instructions”.
HTM04-01 also states “during the temporary closure of wards or departments, a flushing regime should be instigated to maintain system hygiene. Flushing should be continued until stable temperatures are achieved. Advice and guidance is also provided in BSI’s PD855468”.
According to PD855468, ‘hygiene flushing’ (i.e. drawing off water for the avoidance of stagnation) should be carried out weekly or “twice weekly in healthcare premises”.
The hierarchy of control
Where infrequently used outlets are identified, it should first be established if the outlets are surplus to requirements. If no longer required, outlets should be removed – ensuring that all associated supply pipework is taken out and that no live dead-end pipework remains in situ. Where this cannot be achieved a regular Legionella flushing regime will be required.
Periodically flushing outlets can be an effective means of achieving a regular changeover of the water
Reasons for a Legionella flushing regime
Periodically flushing outlets can be an effective means of achieving a regular changeover of the water contained in the infrequently used outlet and its associated supply pipework, this ensures: introduction of fresh cold water containing residual disinfectant, either from the mains supply or from a supplementary water treatment system, if fitted; regular exposure of hot water pipework to temperatures at which Legionella and other bacteria are discouraged; and disturbance of biofilms through the sheering action of running water.
Process for flushing
A Legionella flushing regime should be devised as part of the organisation’s “written scheme of control” or “ water safety plan ” and will need to take account of: the responsibility structure for management & execution of the programme including arrangements for holiday cover and E
All staff training should be recorded
F absenteeism; the technical specification for the task; the task risk assessment & safe method of work, i.e. how to flush outlets safely; the process for identifying infrequently used outlets and keeping the list of outlets under review; Legionella training requirements for personnel carrying out flushing activities and those supervising them; training and supervision of operatives carrying out flushing activities; and water safety record keeping requirements.
The HSG274 Part 2 and HTM04-01 Part B guidance both advise that outlets should be flushed “until the temperature at the outlet stabilises and is comparable to supply water”. The time that this takes in practice will depend on a range of variables including: length of the supply pipework; ambient temperature; frequency of use; localised heat sources; quality of pipework insulation; and flow rate.
The list could go on… let’s just say the duration for flushing will vary between installations!
HTM04-01 adds that regular flushing applies to all infrequently used outlets and that monitoring water temperature when flushing to confirm that the temperature is comparable
to the parent supply which indicates that any standing water has been replaced with fresh water from the system.
Flushing frequency
The guidance recommends that flushing is carried out at least weekly but also suggests that Legionella risk assessments should be used to determine if flushing is required more frequently. For example, it is not uncommon in healthcare premises to find that the routine flushing of infrequently used outlets is carried out twice weekly or even daily where a particular risk has been identified (daily flushing is required in Augmented Care areas of a hospital).
Exposure to aerosols
Water emitted from the outlet during flushing should be purged to drain safely. To reduce the risk of exposure to Legionella bacteria, the British Standards Institutes published document PD855468 suggests: “flushing should be carried out in a safe manner which minimises aerosol production e.g. removing showerheads prior to flushing”.
Water hygiene record keeping
HSG274 highlights concerns that lapsed flushing programmes “can result in a critical increase in Legionella at the outlet”. Either hard-copy
or electronic records are acceptable as long as they include details of: a list of the individual outlets to be flushed; the date, time and duration of flushing; the initials of the person carrying out the work; the water temperature achieved; biocide concentration, if applicable;
Good design practices are essential
any faults and other observations; further actions required; and sign-off by an authorised person . In addition to the flushing task records, all staff training should be recorded.
When can we stop flushing?
For occupied areas, checks should be made with local staff to ensure that the list of littleused outlets reflect current practices and usage levels. Outlets should be added and removed from the list as necessary. As such a regular review of the scheme and the list of outlets is required to ensure they remain up to date. Management reporting procedures should be in place to ensure that flushing teams are kept abreast of changes in building and/or department occupancy.
Summary
The prevention of stagnation within water systems starts on the drawing board. Good design practices are essential to minimise resource-intensive control measures and remedial works later.
It might not sound difficult to flush water from a tap, and perhaps this leads to complacency amongst duty holders, but developing and implementing a dynamic and effective system for identifying infrequently used outlets can be difficult.
It requires ongoing leadership, communication and cooperation throughout organisations to nail it down. In our experience, there is no “one-size fits all” solution but organisations could start by identifying the key players and bringing them into the discussion. This includes: those who can provide information on whether outlets are used or not; those responsible for administering & managing the flushing programmes; those responsible for operational maintenance of the water systems; and designers and installers.
Some or all of these stakeholders may already be members of an organisation’s Water Safety Group, which is the ideal forum for such discussions. M
FURTHER INFORMATION
What are the definitions for ‘little use’ of an outlet?
The essential role of passive fire protection in building safety
This article from the FIA explores the critical role of Passive Fire Protection, its integration with active systems, and the regulatory standards that shape its implementation to contain fire and smoke from the moment ignition occurs. Understanding how PFP functions and why it must operate alongside active systems is key to safeguarding lives, property, and business continuity.
Fire safety in modern buildings depends on a balance between active and passive fire protection systems. While active systems such as sprinklers, alarms, and extinguishers respond once a fire starts, passive fire protection (PFP) is built into the structure itself, working silently
What is passive fire protection?
Passive fire protection refers to the permanent fire-resistant features integrated into a building’s design. These systems require no activation or human input; instead, they are designed to delay fire spread, limit smoke movement, and protect escape routes. A central principle of PFP is compartmentation dividing a building into fire-resistant zones. By containing fire within one area, compartmentation slows its progress, protects occupants, and makes firefighting safer and more effective. Limiting smoke movement is equally vital, as smoke inhalation remains one of the leading causes of fire-related fatalities.
Examples of passive fire protection system
Fire and smoke doors
Fire doors are engineered to resist flames, smoke, and heat for a defined period typically
30, 60, or 120 minutes. When closed, they act as fire barriers; when open, they provide evacuation routes or access for emergency crews.
These doors differ from standard ones in weight, thickness, and construction, often incorporating fire-rated hinges, self-closing mechanisms, and smoke seals. The seals, usually brush, or intumescent types prevent toxic gases from leaking through gaps. Proper fitting is crucial to ensure they do not obstruct door closure.
Fire curtains
Used in open-plan areas such as theatres, shopping centres, and offices, fire curtains are deployable barriers designed to contain fire and smoke. They can operate automatically or manually, providing additional time for evacuation and firefighting. Although they move, their role in containment aligns them closely with passive protection principles.
Fire walls
Fire walls are structural barriers, often constructed from reinforced concrete or masonry, that extend from foundation to roof. E
Fire curtains are deployable barriers designed to contain fire and smoke
Establishing a robust PFP strategy begins with a comprehensive fire risk assessment
F Their non-combustible composition allows them to resist fire for several hours, stopping flames and heat from spreading between sections of a building or adjacent properties.
Intumescent coatings
These specialised coatings protect loadbearing steel structures. When exposed to high temperatures, they expand to form an insulating layer that slows heat transfer, helping to preserve the building’s structural integrity and delay collapse.
How passive differs from active protection
The main difference between passive and active fire protection lies in their mode of operation. Passive systems are preventive built into the structure and continuously providing protection without activation.
Active systems are reactive triggered by heat, smoke, or manual action to detect, alert, or extinguish fires.
Both are vital. Passive systems buy time by containing the fire, while active systems use that time to suppress it. Increasingly, new technologies blur the line between the two, but
their interdependence remains clear: neither can function as a complete solution alone.
Implementing an effective PFP strategy
Establishing a robust PFP strategy begins with a comprehensive fire risk assessment. This identifies hazards, evaluates how a building is used, and highlights where passive systems are most needed.
A typical plan should: divide the building into fire-resistant compartments; use approved fire-resistant materials; protect the structural framework; install barriers to restrict fire and smoke spread
Attention to detail is essential. Even small gaps around pipes, ducts, cables, and electrical outlets can allow fire and smoke to pass through walls or floors. Specialist sealing materials should be used to maintain compartment integrity.
Good ventilation also plays a role, helping to clear dangerous gases and maintain safe escape routes. All PFP installations should be carried out by qualified professionals, with detailed records maintained for audits and compliance. Regular inspection and maintenance are not optional, they are legal and practical necessities to ensure systems perform as designed.
Common challenges and how to overcome them
Retrofitting in older buildings
Integrating PFP systems into existing structures can be complex and expensive. Many older buildings were constructed before modern fire safety standards, requiring structural modifications to accommodate fire-resistant materials or compartmentation barriers.
Ongoing maintenance and testing
PFP elements can degrade over time due to wear, building movement, or accidental damage. Without routine inspections, a system may fail when most needed. Installation of other services may cause damage to the fire resisting elements of the building. Controlling and monitoring of such works is important to ensure that the PFP systems has not been compromised. Establishing a planned maintenance schedule ensures early detection of issues and compliance with regulations.
Evolving regulations
Fire safety legislation is constantly evolving. The Building Safety Act 2022 and updates to the
PFP elements can degrade over time due to wear
Building Regulations 2010 have reinforced the importance of competence, record-keeping, and product certification. Staying compliant E
Neither active nor passive fire protection can function effectively in isolation
F requires ongoing attention and investment, particularly for complex or high-rise buildings.
Cost and resource constraints
High-quality fire-resistant materials and professional installation can be costly. However, the financial and reputational impact of inadequate fire protection is far greater. Cutting corners compromises safety and may expose building owners to legal liability.
Regulatory standards and compliance
In the UK, passive fire protection systems must comply with the Building Regulations 2010, particularly Approved Document B (Fire Safety), which governs compartmentation, escape routes, and fire resistance.
Materials and systems should meet British Standards such as: BS 476: Part 20–24:1987 –Fire resistance tests for building elements; BS EN 13501 – Fire classification of construction products and building elements; BS EN 13631:2020 – Fire resistance testing for construction products; and BS EN 1634-1:2014 – Testing for fire doors and shutters.
Ensuring compliance not only protects occupants but also supports insurance coverage
and legal defensibility. Documentation such as fire stopping certificates, installation records, and inspection logs forms part of the Golden Thread of information required under the Building Safety Act.
Why integration matters
Neither active nor passive fire protection can function effectively in isolation. Passive systems
Passive fire protection forms the structural backbone of building fire safety
contain the fire, while active systems detect and suppress it. Together, they provide a layered defence strategy that protects life safety, preserves property, and enables business continuity after an incident.
For designers, facilities managers, and responsible persons, the goal should always be integration, ensuring that both systems complement one another through coordinated design, installation, and maintenance.
Conclusion
Passive fire protection forms the structural backbone of building fire safety. Through fire-resistant walls, doors, coatings, and compartmentation, it restricts fire and smoke spread, maintains structural stability, and preserves vital escape routes.
When combined with active systems such as alarms and sprinklers, PFP enables a comprehensive approach that not only meets regulatory requirements but also saves lives and limits damage.
In the words of many fire safety professionals: active systems fight fire, passive systems buy time. Both are indispensable, and together they define the resilience of the built environment. M