















An exploration into the ins and outs of endovascular arteriovenous fistulae (endoAVF) creation will be laid bare this morning during a session dedicated to innovative solutions for creation and maintenance of AV-access.
In conversation with LINC Today, Ounali Jaffer (Barts Health NHS Trust, London, United Kingdom) walked through his experience in using endoAVF, and touched on the past, present and future insights that may potentially drive this field.
EndoAVF is an exciting addition to vascular-access options for dialysis. How has the evidence supporting its use evolved in recent years, and what new clinical data are most compelling? As is the case with any new technology, the evidence base grows as the number of centres which take up the technology increases. Initial Industry sponsored trials showed very favourable outcomes in terms of technical success, maturation and cumulative patency rates for both devices.1,2 We are now seeing similar outcomes in a host of independent studies from various centres worldwide.
Within the last year, perhaps the most compelling publication was by Klein et al. in CVIR. The study was a retrospective analysis of 112 patients who had fistulae created using the 4F WavelinQ device (BD) across three centres in Canda, USA and the UK. Technical success was 97.3%, with a functional maturation rate of 87% and a cumulative two-year patency of 91.7 %.3 This compares favourably with previous studies using the Ellipsys device, such as that by Beathard et al.,4 which demonstrated a two-year cumulative patency rate of 92.7%. Taken together, the data suggests that endoAVF creation using either device is a durable technique, and
should merit consideration for patients with chronic renal disease.
How does the efficacy and safety profile of endoAVF compare to that of surgical AVF, particularly in terms of maturation rates, patency, and the need for reintervention?
Surgical fistulae have been shown to require approximately four months to mature, with a primary failure rate of 23%, a cumulative two-year patency of 63% and a reintervention rate of 1.9 per patient year. Therefore, on the face of it, endoAVF appears more favourable.5–8 In reality, the argument is more nuanced, as the site of access creation can have a bearing on results, as can the experience, infrastructure and volumes of procedures performed in individual centres. Although various publications have looked into this, to date there are no randomised controlled trials (RCTs) to facilitate true comparison.9–11
Having said this, in my view, endoAVF should be considered as an ancillary option for fistula creation as opposed to a direct competitor to surgical AVF.
What are the critical considerations for determining patient eligibility for endoAVF creation, and how do you navigate cases with borderline anatomy?
Before considering ensure that patients to attend all follow-up because, if reintervention must be done in a eligibility then largely patient’s anatomy. anatomical feasibility approximately 50–60% screened. Personally, venturing off instructions chances of success If anatomy appears perhaps consider
As you mentioned, the WavelinQ and Ellipsys systems are the two primary devices for creating endoAVF. What are the key differences between them, and how do you decide which device to use?
“There will always be continuing refinements of techniques and evolution of EndoAVF devices as time progresses. We have seen this already with the addition of adjunctive procedures at the index procedure to improve outcomes and evolution of the WavelinQ device.”
Ounali Jaffer
Editors
Whilst both devices endovascular fistula forearm, they are in different devices. WavelinQ creates the fistula the deep venous system, close to the perforator, between either the ulnar or radial artery and one of its paired
veins. The Ellipsys fistula is between the proximal radial artery and the perforator/deep communicating vein. Aside from this, the sites for access, the AVF creation method and the image guidance requirements are also completely different.
When it comes to device selection, a lot resides on the anatomical screening but if both options are available, I would usually start with WavelinQ device, as an Ellipsys fistula can still be subsequently formed if required, but the same is not true vice-versa. Procedure times are generally quicker for the Ellipsys compared to WavelinQ.
Current studies highlight promising short- and mid-term outcomes for endoAVF. What do we know about long-term durability, and what research gaps still need addressing? In reality, we know very little beyond the two-year mark. The Ellipsys pivotal study reported a very respectable fiveyear cumulative patency rate of 82%.1 WavelinQ data I am sure will follow, but we have to be mindful that the system was changed from a 6 F to a 4 F device, so there is an understandable lag compared to the Ellipsys system. Perhaps the one thing that is really missing is an RCT comparing the two devices.

dialysis patients? Do you anticipate proximal
then move into the proximal forearm if this is not an option. I suspect that as techniques and devices evolve –and if the body of evidence expands and remains favourable – the scope and utilisation of endoAVF will widen. Currently, for us, the device can be potentially used first line if an RCF is not an option and/or it is the express wish of the patient. In these groups, cosmesis is often cited as a reason for choosing endoAVF over surgical AVF.
Can you share details about any upcoming trials focused on endoAVF, and what key questions these trials are aiming to answer?
Both WavelinQ and Ellipsys are currently recruiting for their post-market surveillance studies in the USA. These datasets should be useful additions to the growing evidence base. Perhaps the most interesting will be two RCTs comparing endoAVF with surgical AVF. One of these is being conducted by the group from University of California, Los Angeles in the USA. Patient recruitment has already begun, with a target recruitment of 90 patients and a projected study completion date of mid-to-late 2027. The primary outcome measure for this trial is physiological maturation rates at six months.
The endoAVF study due to commence in France has also generated a lot of interest. The primary outcome measure for this study is the cost–utility differential with endoAVF vs open surgery, which I think is a very pertinent issue that needs addressing within a RCT setting. The study also has a wide ranging and fairly comprehensive set of secondary outcome measures.
“AVFs are lifelines for patients with endstage kidney disease, and we know there are limited anatomical options for surgical AVF creation, so anything that allows us to expand the potential real estate available to create these lifelines seems like a good idea.”
Ounali Jaffer
considered, and whether drug-coated balloons have a role.
Perhaps most interesting is the so called endoAVF 2.0 devices such as Velocity. Early results from the Venos-1 feasibility study appear to be quite promising, with the US-based Venos-2 study due to start recruiting this month.
References
1. Hull JE, Jennings WC, Cooper RI, et al. Longterm results from the pivotal multicenter trial of ultrasound-guided percutaneous arteriovenous fistula creation for hemodialysis access. J Vasc Interv Radiol. 2022;33(10):1143–1150.
The successful delivery of endoAVF requires collaboration across specialties. What lessons can you share about building a multidisciplinary framework to support this service?
From my own personal point of view, an effective multidisciplinary team (MDT) approach is crucial to the success of an endoAVF programme. To achieve this, you first need to ensure all key stakeholders are engaged and consulted early on in the process to ensure all relevant views are heard and considered. Each stakeholder then must be made aware of their defined roles in delivering the service. This then allows for a robust framework to build an MDT for shared decision making.
The MDT within our institution includes nephrologists, vascular-access surgeons, interventional radiologists, interventional radiology clinical nurse specialists (IR CNS), vascular scientists, anaesthetists, and dialysis nurses. Together we are able to formulate the patient’s dialysis life plan, safeguard appropriate patient selection, list (and timely so) the patient for their
procedures, re-discuss cases of nonmaturation and dysfunction, and plan the next steps in the patient’s dialysis life plan in cases of endoAVF failure. In the event of patient complications or suspected fistula malfunction, early rediscussion in the MDT through efficient feedback loops is essential. This should ideally be achieved through a central coordinator, who at our institution are the IR CNS.13
Looking ahead, how do you see the field of endoAVF evolving? Are there any new technologies, techniques, or procedural advancements on the horizon that excite you?
As has been the case with previous technologies, there will always be continuing refinements of techniques and evolution of endoAVF devices as time progresses. We have seen this already with the addition of adjunctive procedures at the index procedure to improve outcomes and evolution of the WavelinQ device. Talk now revolves around issues such as whether new sites for fistula formation using these devices within the arm should be
2. Lok CE, Rajan DK, Clement J, et al. Endovascular proximal forearm arteriovenous fistula for hemodialysis access: results of the prospective, multicenter novel endovascular access trial (NEAT). Am J Kidney Dis. 2017;70(4):486–497.
3. Klein E, Repko B, Alvarez A, et al. Multi-center two-year patency outcomes of endovascular arteriovenous fistulas (endoAVF) created with a 4 French system. Cardiovasc Intervent Radiol. 2024;47(8):1045–1054.
4. Beathard GA, Litchfield T, Jennings WC. Two-year cumulative patency of endovascular arteriovenous fistula. J Vasc Access. 2020;21(3):350–356.
5. Lok CE, Huber TS, Orchanian-Cheff A, et al. Arteriovenous access for hemodialysis: a review. JAMA. 2024;331(15):1307–1317.
6. Al-Jaishi AA, Oliver MJ, Thomas SM, et al. Patency rates of the arteriovenous fistula for hemodialysis: a systematic review and meta-analysis. Am J Kidney Dis. 2014;63(3):464–478.
7. Bylsma LC, Gage SM, Reichert H, et al. Arteriovenous fistulae for haemodialysis: a systematic review and meta-analysis of efficacy and safety outcomes. Eur J Vasc Endovasc Surg. 2017;54(4):513–522.
8. Rajan DK, Ebner A, Desai SB, et al. Percutaneous creation of an arteriovenous fistula for hemodialysis access. J Vasc Interv Radiol. 2015;26(4):484–490.
9. Inston N, Khawaja A, Tullett K, et al. WavelinQ created arteriovenous fistulas versus surgical radiocephalic arteriovenous fistulas: a single-centre observational study. J Vasc Access. 2020;21(5):646–651.
10. Harika G, Mallios A, Allouache M, et al. Comparison of surgical versus percutaneously created arteriovenous hemodialysis fistulas. J Vasc Surg. 2021;74(1):209–216.
11. Shahverdyan R, Beathard G, Mushtaq N, et al. Comparison of Ellipsys percutaneous and proximal forearm Gracz-type surgical arteriovenous fistulas. Am J Kidney Dis. 2021;78(4):520–529.e1.
12. Shahverdyan R, Beathard G, Mushtaq N, et al. Comparison of outcomes of percutaneous arteriovenous fistulae creation by Ellipsys and WavelinQ devices. J Vasc Interv Radiol. 2020;31(9):1365–1372.
13. Lie G, Ahmed N, Shah N, et al. Adapting a dialysis service for delivery of percutaneous arteriovenous fistulas. Radiographics. 2022;42(6):1795–1811.
Recent advancements in drug-eluting stent (DES) technology are reshaping the treatment landscape for below-the-knee (BTK) lesions, delegates will hear this afternoon when Elena Herrero (Jaén University Hospital, Spain) highlights how emerging evidence supports a shift from DES as a bailout strategy to a primary treatment option in select cases.
Studies like DESTINY-I have demonstrated significantly better primary patency rates with DES compared to bare-metal stents (BMS) in BTK lesions, underscoring their growing role in primary interventions. “I believe that the primary use of stents should be indicated in calcified lesions, especially in diabetic patients or bifurcations,” Dr Herrero told LINC Today However, she emphasised that primary stenting should focus on DES, not BMS.
Clinical trials, such as ACHILLES, have shown that sirolimus-eluting stents outperform standard angioplasty in tibial artery disease. Dr Herrero pointed to these findings as pivotal for evolving treatment strategies: “In heavily calcified lesions at the origin of the tibial arteries, the use of DES has better outcomes than standard angioplasty. Perhaps in this type of lesion, we should consider the primary use of stents.”
While long-term data from studies like Giaquinta et al. report promising three-year patency and limb salvage rates with everolimus-eluting stents, Dr Herrero highlighted a critical focus: “When we talk about critical limb ischaemia, the most important thing is limb salvage, independent of the durability or patency of the procedure.”
In SPORTS, the authors revealed superior performance of the Eluvia DES (Boston Scientific) compared to both BMS and drug-coated balloons in complex femoropopliteal lesions. For Dr Herrero, she anticipates similar advantages in BTK interventions,

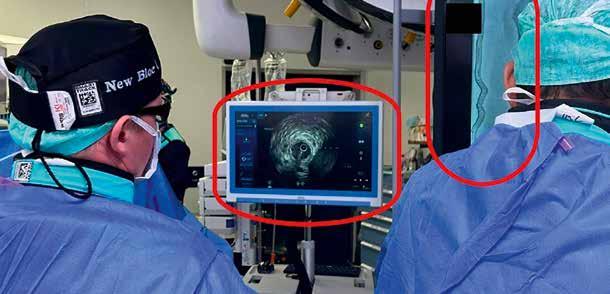
“The preparation of the vessel prior to stent implantation and the use of intravascular ultrasound for correct diameter and length measurement from healthy area to healthy area are very important for good results.”
Elena Herrero
especially in heavily calcified lesions. “We are increasingly using vessel preparation devices, such as atherectomy or intravascular lithotripsy, which will contribute to better outcomes in DES treatment,” she noted.
Indeed, she underscored the importance of procedural preparation in maximising DES success in BTK revascularisation. “The preparation of the vessel prior to stent implantation and the use of intravascular ultrasound for correct diameter and length measurement from healthy area to healthy area are very important for good results,” she explained.
As drug-eluting technology evolves, Dr Herrero also highlighted the increasing use of limus-eluting stents, which have shown superior benefits over paclitaxelcoated devices in studies and meta-analyses. “We will see if more studies confirm these results,” she added.
In the other hand, as DES platforms become more widely adopted for complex BTK disease, Dr Herrero remains cautious about overextending their use. “As long as the vessel preparation is correct and we cover the entire lesion, our results will improve. However, my view is that we should not extend the use of DES to very large lesions,” she advised.
Looking ahead, bioresorbable scaffolds may play a role in BTK interventions, especially at the belowthe-ankle level where metallic DES is not currently indicated, Dr Herrero remarked, adding a glimpse into the next frontier for BTK revascularisation.
Recent meta-analyses and trials, such as DESTINY II, continue to demonstrate improved outcomes with DES in longer BTK lesions. For now, Dr Herrero advocates for expanding their use beyond bailout scenarios. “We should consider the use of primary DES in certain circumstances, such as in calcified lesions, anterior tibial artery origins, or BTK bifurcations,” she said in closing.

Carotid revascularisation was placed under the spotlight on Tuesday afternoon, beginning with an exploration of carotid artery surgery in 2025 and beyond by Reza Ghotbi (Helios Klinikum München West, Munich, Germany).
Dr Ghotbi began by framing the landscape of carotid artery interventions in his practice, including transcarotid artery revascularisation (TCAR), carotid endarterectomy (CEA), and stenting (CAS). “Approximately 20% of all patients who undergo CEA, transfemoral CAS [TFCAS], or TCAR for carotid artery stenosis are at least 80 years old,” he said. “Among octogenarians, the adjusted hazard of TCAR relative to CEA is similar for both 30-day stroke and death. Regarding the high perioperative risk of these patients, I expect an increase in the absolute numbers.”
Recent data shows that TCAR represented 65% of high-risk carotid stenting cases (by 2021), so how does Dr Ghotbi expect this proportion to evolve by 2025? “The prevalence of carotid artery stenosis and its need for operative revascularisation will increase substantially in the next few decades,” he continued. “These patients have more comorbidities, decreased functional status, and greater anaesthesia risks relative to their younger counterparts, placing them at higher perioperative risks for adverse events.
“TCAR may serve as a promising less invasive treatment for carotid disease in older patients who have high anatomic, surgical or clinical risk for CEA.”
With studies indicating that TCAR is associated with decreased odds of stroke and death compared to TFCAS, Dr Ghotbi commented on how this might this impact patient selection and treatment algorithms in 2025. “Recently published data (meta-analysis) shows that TFCAS has higher rates of 30-day and 1-year stroke/death than TCAR. These associations remained particularly
“Carotid surgery for asymptomatic patients only makes sense in a setting that is able to identify asymptomatic patients with high risk for stroke.”
Reza Ghotbi

true for octogenarians, one of the most expanding group of patients. Therefore, I expect an increasing uptake of TCAR procedures.”
For Dr Ghotbi, even if there is to be increased adoption of TCAR, he reasoned that CEA is still the option with best clinical results and cost-effectiveness, thus CEA will likely remain the gold standard for most patients. However, results need to be improved to reflect the statistical decrease in stroke rate caused by carotid artery stenosis under strict application of best medical treatment, he added.
The ACST-2 trial found similar longterm protective effects against strokes for both stenting and surgery, so it begs the question of how outcomes such as this might this influence decision-making between the two approaches in 2025?
“For sure, the long-term protective effects against stroke is an important part of the puzzle,” said Dr Ghotbi.
“Periprocedural outcome is the first
step, and the healthcare system should be able to cover the considerable cost difference between the two procedures.”
The management of asymptomatic carotid stenosis in 2025 could be swayed when considering the ongoing debates about best medical therapy, which Dr Ghotbi noted as a ‘game-changer’: “We need high-volume centres with high-volume surgical expertise for carotid surgery. Carotid surgery for asymptomatic patients only makes sense in a setting that is able to identify asymptomatic patients with high risk for stroke.
“We should take in account that every patient with a symptomatic carotid artery stenosis had a primary asymptomatic stenosis. Best medical therapy is indicated for every patient even if it is not the only solution for them; we will for sure need to turn to experienced surgeons and interventionalists as well.”
As safety improvements continue in the field of carotid interventions, the
next frontier in optimising outcomes for patients with carotid artery disease in 2025 and beyond lies in “centres, centres, centres!”, according to Dr Ghotbi: “Specialised centres for carotid artery interventions (neurology, neuroradiology, vascular surgery, cardiology) are, in my opinion, the only way to collect experiences and resources from a multidisciplinary approach that truly reflects the nature of the disease.”
Indeed, it is this expert-driven, multidisciplinary decision-making – even in a growing landscape of revised clinical guidelines and reimbursement policies – that will be crucial in improving carotid interventions in 2025 and beyond.
“Clinical guidelines and reimbursement policies play a crucial role, but we should not forget that we have to make many individual decisions in our daily work, and we can hopefully continue to do so.
Individualised decisions must also have a place,” concluded Dr Ghotbi.

@ LINC 2025
Take a glimpse of upcoming lectures –and get a flavour of what you may have missed – with SNAPSHOTS @ LINC 2025.
Challenging cases: EVAR Speakers Corner Thursday 12:30
Fusion-guided in-situ laser fenestration to exclude descending thoracic penetrating aortic ulcer with no distal sealing zone




Background
Emergency endovascular exclusion of descending thoracic aortic pathologies near visceral branches often necessitate complex solutions such as surgeon-modified or in-situ fenestration with pre-stenting. Unfortunately, in cases of challenging narrow access vessels and small calibre visceral targets makes surgeonmodification techniques and prestenting a sub-optimal idea.
Case study
We present a case and the detailed process of fusion-guided in-situ laser fenestration to exclude a symptomatic penetrating aortic ulcer just above the coeliac artery with no appropriate distal sealing zone. Her narrow iliac vessels of 4–5 mm necessitated a low-profile endograft and small coeliac calibre.
Conclusion
In-situ laser fenestration using an
“In-situ laser fenestration using an off-the-shelf polyester endograft with fusion guidance (exclusively) is feasible.”
Jiaying Lau
off-the-shelf polyester endograft with fusion guidance (exclusively) is feasible. The key step is to perform fusion alignment in orthogonal planes with the undeployed device in-situ to limit displacement of target vessels.

When Shockwave Intravascular Lithotripsy (IVL), a technique that modifies both medial and intimal calcium while minimising trauma to the vessel wall, is best used in the iliac arteries was discussed by Ashish Patel, Clinical Senior Lecturer in Vascular Surgery and Consultant Vascular Surgeon at St Thomas’ Hospital (London, UK). With a special interest in peripheral arterial disease, the majority of Dr Patel’s patients have some chronic limb-threatening ischaemia. “In our unit we treat a large number of patients with aorto-iliac disease,” he told LINC Today ahead of his presentation, noting that iliac stenting is a large part of his work.
“We often use IVL as an adjunctive tool in calcified cases.”
Dr Patel was already familiar with Shockwave Medical’s IVL catheters. He has used the M5+ catheter for treatment of the superficial femoral and popliteal artery segments. “More recently, I’ve utilised the Shockwave L6 catheter, which is the bigger device,” he added. “So as a result, we now have the opportunity to treat calcified aortoiliac vessels either prior to, or in lieu of, stenting.”
Firstly, Dr Patel talked about how common aorta-iliac recanalisation is. “It’s one of those bread-and-butter operations that we should all be able to do really well,” he reasoned.
Then he addressed the benefits of IVL prior to stenting. “You can lower your stent zone,” said Dr Patel. “The main advantage is that, with the benefit of IVL, you may not need to encroach into the aorta.” That is important because these patients are ‘frequent flyers’, and the natural biology of their disease means that they have a significant likelihood of requiring further interventions in their lifetime. If you can avoid stenting across the aortic bifurcation, you are preserving options for subsequent
“If you see calcium in the aorto-iliac segment, and IVL might facilitate stent placement or reduce the risk of a complication such as a rupture, think about using Shockwave Intravascular Lithotripsy.”
Ashish Patel
re-interventions, Dr Patel noted. The implications of IVL when using bare-metal stents versus covered stents are quite interesting. Dr Patel’s group is currently participating in the ongoing Gore Medical FORWARD study comparing bare-metal with covered stents. And while his group have traditionally routinely used covered stents for aorto-iliac occlusive disease, he recognises that this might not be routine practice in other units. “These are highly effective stent grafts,” he commented. “But, due to cost implications, a lot of units have no choice but to use bare-metal stents as their go-to.”

During the session, Dr Patel showed an example of a bare-metal stent being post-dilated following deployment into a heavily calcified vessel. He explained that they can sometimes not expand their intended diameter due to the calcium. “You try and the vessel ruptures much calcium,” he situations, you may wish ensure that the stent less calcified vessel stent is planned, such calcified common iliac benefit. “In this situation, plan is a primary covered stent within the iliac artery, without the need for ‘kissing’ stents, you may not necessarily need to use IVL. However, if you’re worried that the covered stent may not open adequately, or improve vessel compliance might facilitate more accurate deployment, then
you might want to consider IVL.”
Finally, Dr Patel addressed the patient cohort where IVL without stenting is possible for iliac lesions. Claudicants, who are failing best medical therapy, he said, are a cohort for whom IVL is a compelling application; however there is a paucity of data. “In stenosed, (not occluded) iliacs, greater luminal flow without stenting may be adequate for symptom control and an improvement in quality of life. This can often apply to those patients, particularly women, who have small, stenosed iliac vessels. “Improving vessel compliance, followed by controlled angioplasty, make senses in a claudicant, as you’re achieving luminal gain and improving inflow,” he added.
“Therefore, I think there’s a role for IVL in patients where you’d rather avoid stenting small vessels. They’re claudicating, and you are aiming to improve their quality of life by increasing their walking distance by a few hundred yards.”
For those clinicians thinking of using Shockwave’s L6 for any of these procedures, there is not much of a learning curve, said Dr Patel, especially if they have already used the M5+ and the S4 catheters. “It’s another device for bigger vessels and another territory,” he underlined. “The learning curve, for those who have never used IVL, is mainly about preparing the device and identifying appropriate lesions. Understanding that it’s not an angioplasty balloon, it’s a vessel preparation device prior to angioplasty or stenting is important.”
In conclusion, Dr Patel advocates for IVL, but only in certain circumstances. “If you see calcium in the aorto-iliac segment, and IVL might facilitate stent placement or reduce the risk of a complication such as a rupture, think about using Shockwave IVL,” he explained.
Registration hours
Tuesday, 28 January 07:00 – 18:00
Wednesday, 29 January 07:30 – 18:00
Thursday, 30 January 07:30 – 18:00
Your name badge
Your name badge must be worn at all times for admittance to all LINC sessions, including the exhibit area. No new badge will be printed in case of loss. No exceptions will be made.
Internet access
Internet is available for free in the exhibit area during the entire duration of the congress.
Network: Leipziger Messe, Username: linc2025, Password: leipzig
Exhibit hours/Program hours
Tuesday, 28 January 08:00 – 18:00
Wednesday, 29 January 08:00 – 18:00
Thursday, 30 January 08:00 – 18:00
Your certificate
Your certificate will be available for download in your personal registration account about one week after the congress.
Congress bags/Welcome bags
The bags can be collected in front of Multi purpose area 3 on level 0 in the CCL. 1 bag per participant.
Media restrictions
LINC strictly prohibits recording or streaming any of the scientific sessions and live cases in the plenary rooms.
The qr-code on your badge contains your encoded contact details. Only exhibitors who have the lead retrieval qr-code reader will be able to obtain them from you. By letting exhibitors scan your badge, you give your consent to share your data.
We will be taking photography throughout the event for use in future marketing and communication activities. If you DO NOT wish your photo to be included, please pick up a RED lanyard from the registration desks so that you can be identified by our photographer.
For your convenience we have arranged an information desk in hall 2 and CCL level 0. You will be able to obtain information/make reservations regarding local restaurants, hotels, ticket sales, etc.
Meeting rooms
All meeting rooms are located in the CCL. Please follow the signs from hall 2 to the CCL. A concierge at the information meeting rooms counter will show you the location of your meeting room.
At LINC you have the opportunity to visit the Self-Service Restaurant Snack Point, located at level 0, between hall 2 and the CCL.
Opening hours from Tuesday to Thursday: 08:00–17:00
Innovation forum Speakers Corner Thursday 11:15

Background
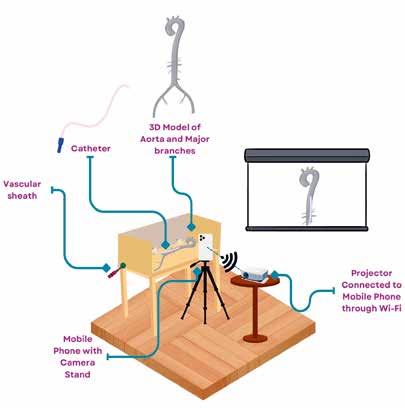
My presentation provides a step-by-step guide to constructing a cost-effective angio-simulator tailored for both at-home and in-hospital use. Crafted primarily from acrylic glass (polymethyl methacrylate), this simulator offers endovascular professionals and students the ability to experience hands-on training without the need for software. With an approximate cost of $200, this angio-simulator serves as an economical alternative to pricier commercial versions that often pose financial challenges for many educational institutions. The acrylic construction facilitates modifications,
Figure 1. This illustration highlights the main components of the angio-simulator, including the main body, which consists of the skeleton (3D model of the aorta) and DSA box, a mobile phone with a camera stand, and a Wi-Fi-enabled projector. The setup also incorporates a vascular sheath.
LEIPZIG INTERVENTIONAL COURSE 28–30 January 2025, Leipzig, Germany

As a medical professional it can be difficult to keep track of the broad landscape of related first-class vascular events. With PEO you will have a simple tool to overview all upcoming educational live events such as webinars, conferences and workshops. Furthermore PEO offers the possibility to easily find interesting on-demand content and podcasts.
· Tag an event that you don’t want to miss
· Add it to your personal calendar
· Get your reminding notification
· Share it with your colleagues
You will find many helpful features to keep informed about all professional updates of your special field.
The PEO congress app is available in the app store for free


“Commercially available angiosimulators, essential tools for training in endovascular procedures, frequently remain inaccessible for most hospitals due to their prohibitive costs.”
Khaled Elhendawy
allowing for the simulation of specific pathologies, anatomical variations, and testing of new endovascular devices in a safe, in vitro environment.
The angio-simulator I developed consists of three primary components: the main body, a cell phone camera, and a projector. The main body includes a skeleton (3D model of the aorta) constructed from acrylic glass and a DSA box. During my presentation, I will demonstrate stepby-step how to build the simulator, starting with the skeleton. The cell phone camera is then set up to capture high-quality video, complemented by proper lighting to ensure clarity and precision. The final component is a WiFi-enabled projector, which allows for easy real-time integration.
Innovation in medicine does not necessarily require high costs; impactful advancements can often be achieved frugally and resourcefully. Commercially available angiosimulators, essential tools for training in endovascular procedures, frequently remain inaccessible for most hospitals due to their prohibitive costs, with access often limited to conferences and expensive training courses.


Introduction
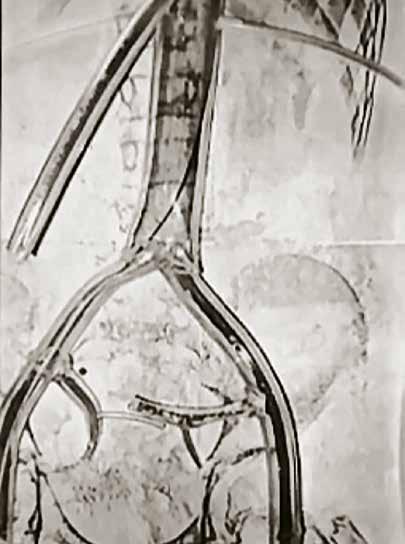
We report our method to perform the covered endovascular reconstruction of aortic bifurcation (CERAB) technique without contrast medium

(such as iodinated agents or CO 2). Some patients have chronic kidney disease or iodine allergies, thereby precluding the use of iodinated contrast medium. Furthermore, CO 2 angiography is not always available, as is the case in our centre.
Procedural detail
Our contrast-free CERAB technique, conducted under fluoroscopy and assisted by intravascular ultrasound




“Our contrastfree CERAB technique, conducted under fluoroscopy and assisted by intravascular ultrasound, is easy.”
Arnaud Kerzmann
(IVUS), is easy. IVUS is used to identify the occlusive lesions, the level of the aortic bifurcation and the iliac bifurcations. Those levels are sketched on the fluoroscopy screen. The covered stents are then deployed under fluoroscopy at the level drawn on the screen. IVUS is once again used to check stent positioning and opening; IVUS can detect technical defects not seen with angiography in 25% of cases, and intraoperative correction is possible.
Closing remarks
The use of IVUS with fluoroscopy to perform percutaneous CERAB without contrast medium is
feasible. It facilitates identification of potential technical defects not viewable with angiography.
One caveat is the cost of IVUS, especially in countries where there is no reimbursement.
LEIPZIG INTERVENTIONAL COURSE 28–30 January 2025, Leipzig, Germany





At the unique Moritzbastei. Thursday, January 30 from 19:00.
Within walking distance from the inner city hotels.
Get your ticket for 79,00 Euro at the registration desk. Available from Tuesday.
Challenging cases: EVAR Speakers Corner Thursday 12:30
Innovative approach: Common channel inner branch for bilateral renal arteries and superior mesenteric artery fenestration in physician-modified endograft for symptomatic Type 1a endoleak treatment post-chimney endovascular aneurysm repair

Supong Worathanmanon Prince of Songkla University, Songkhla, Thailand
Introduction
The management of symptomatic Type 1a endoleaks (T1aELs) poses considerable challenges, particularly in cases characterised by complex anatomy and prior endovascular interventions. These scenarios are often complicated by intricate vascular configurations, the alignment of previously deployed devices, and the urgency of the clinical condition, all of which demand innovative and adaptable strategies. Physician-modified endografts (PMEGs) have emerged as a promising solution to address these complexities, offering a customisable approach to endovascular repair. However, the need for precise tailoring to accommodate individual anatomical variations underscores the demanding nature of this intervention.
Report
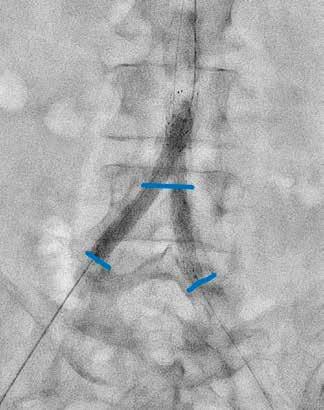
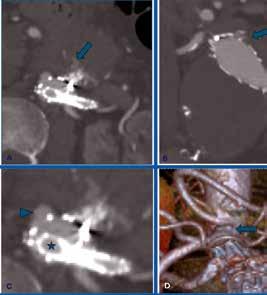
We report the management of a 79-year-old male with compromised functional status who presented with a symptomatic T1aE following a previous chimney endovascular aneurysm repair (ChEVAR) for an infrarenal abdominal aortic aneurysm. The endoleak was identified at the greater curvature of
1. A–B)
tomography angiography showed


“This report underscores the feasibility and efficacy of employing a physician-modified endograft featuring a commonchannel inner branch for the management of Type 1 endoleak following chimney endovascular aneurysm repair.”
Supong Worathanmanon
the aneurysm neck and was further complicated by challenging anatomical features, including the proximity of the chimney graft to the right renal artery and the close alignment of the celiac and superior mesenteric arteries (SMAs). To address these complexities, a PMEG was developed, incorporating a common-channel inner branch for bilateral renal arteries and fenestration for the SMA, accompanied by celiac artery embolisation.
The procedure was conducted under general anaesthesia using a fully percutaneous approach. Sequential cannulation facilitated the deployment of stents for the SMA and renal arteries, employing a kissing stent technique followed by balloon moulding to ensure precise alignment and optimal outcomes. Post-operative imaging confirmed the accurate positioning of the stents and the successful resolution of the endoleak. The patient experienced an uneventful recovery, requiring only a one-day stay in the intensive care unit, and was discharged on the fifth postoperative day. At eight-month follow-up, the patient remained asymptomatic, with imaging confirming stable stent positioning and no recurrence of the endoleak.
This report underscores the feasibility and efficacy of employing a PMEG featuring a commonchannel inner branch for the management of
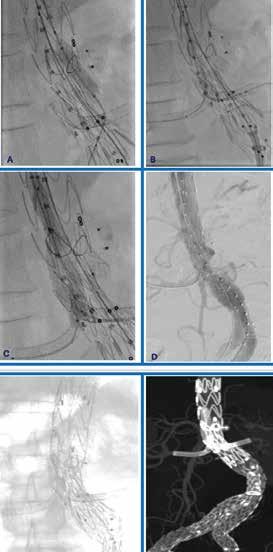
3. A) Superior mesenteric artery stent deployment; B) cannulation of both renal arteries; C) kissing stenting of both renal arteries; D) final aortogram showed no endoleak; E–F) single-shot and reconstruction images of the physicianmodified endograft.
T1aEL following ChEVAR. It highlights the potential of physician-modified techniques in addressing complex anatomical and procedural challenges, thereby enhancing patient outcomes in advanced endovascular interventions. Continued investigation through further studies and case reports is essential to validate these findings and evaluate the long-term effectiveness of such innovative approaches across diverse patient populations.
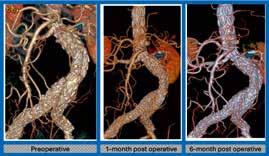
Figure 4: Preoperative computed tomography angiography (CTA) reconstruction revealed the presence of Type 1a endoleak (<). Notably, follow-up CTA assessments were conducted at 1 and 6 months.


Elevate your vascular surgery skills and knowledge

Customized online training program for early career physicians in vascular surgery
▪ Specialized focus on pathologies and treatment options
▪ Targeted educational support designed to address the educational needs of physicians in early stages of their career
▪ Comprehensive learning experience with real-life case studies and discussions
▪ Access to a European community and networking opportunities
▪ Personalized learning path with live and on-demand sessions (more than 40 videos with clinical cases available)
Learn more — visit www.gorevascularmastery.com/eCampus