
Navigating Uterine Cancer Recurrence
Olivia W. Foley, MD Assistant Professor, Department of Obstetrics and Gynecology, Division of Gynecologic Oncology
February 25, 2026

Disclosures
No Disclosures
Thank you to Dr. Emily Hinchcliff for sharing graphics.

Roadmap
• Signs/symptoms of endometrial cancer recurrence
• Surveillance after endometrial cancer
• Treatment tools
• Categorizing endometrial cancer recurrence
- How does category affect treatment decision making?
- Role of molecular testing
• What’s new + clinical trials
• Living with recurrent endometrial cancer
Finding Recurrent Endometrial Cancer
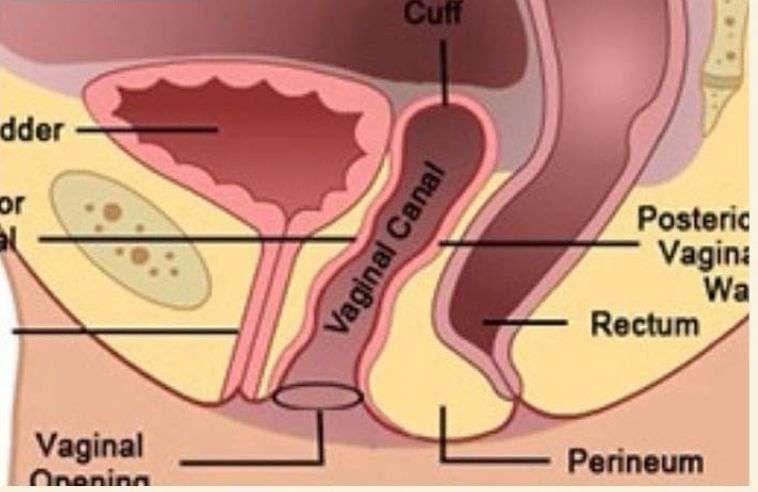
• Where does endometrial cancer come back?
- Top of the vagina*
- Pelvic/lower abdominal lymph nodes*
- Distant sites (lung, abdominal lining, other organs)
• When does endometrial cancer come back?
- Usually first 2 years (almost all in 5 years)
Finding Recurrent Endometrial Cancer Symptoms
•Vaginal bleeding
• Pelvic/abdominal pain
• Bloating
• Weight loss
• Nausea/vomiting
Surveillance After Endometrial Cancer
• Years 1-3 After Treatment
- Physical exam (including pelvic) every 3-6 months
• Years 4-5 After Treatment
- Physical exam (including pelvic) every 6-12 months
• OTHER TOOLS (CAN be used, not always indicated):
- CA-125 - Imaging *Regardless of surveillance plan, symptoms should be evaluated*
Treatment Tools
What are potential options?

Categorizing Endometrial Cancer Recurrence
Location
Symptoms and Performance Status
1) Local/Regional
2) Distant
DISTANT
How is recurrence and/or other medical issues affecting the patient?
Prior Treatment and Toxicities What has already been done, how has it worked, and what are side effects?
Histology/Grade
Molecular Features
How does the cancer look under the microscope? (Traditional classification)
The way of the future…
Categorizing Endometrial Cancer Recurrence
Location
1) Local/Regional – [surgery, radiation]
2) Distant – [systemic treatment]
DISTANT
Symptoms and Performance Status How is recurrence and/or other medical issues affecting the patient?
Prior Treatment and Toxicities What has already been done, how has it worked, and what are side effects?
Histology/Grade
Molecular Features
How does the cancer look under the microscope? (Traditional classification)
The way of the future…
Categorizing Endometrial Cancer Recurrence
Location
Symptoms and Performance Status
1) Local/Regional
2) Distant
DISTANT
How is recurrence and/or other medical issues affecting the patient?
Shared decision-making about options
Prior Treatment and Toxicities What has already been done, how has it worked, and what are side effects?
Shared decision-making about options
Histology/Grade
Molecular Features
How does the cancer look under the microscope? (Traditional classification)
The way of the future…
Categorizing Endometrial Cancer Recurrence
Location
1) Local/Regional
2) Distant
Symptoms and Performance Status
Prior Treatment and Toxicities
Histology/Grade
Molecular Features
DISTANT
How is recurrence and/or other medical issues affecting the patient?
What has already been done, how has it worked, and what are side effects?
How does the cancer look under the microscope? (Traditional classification)
The way of the future…
Traditional Categorization
Characteristic Type I Type II
Histology Endometrioid Non-endometrioid (serous, clear cell, carcinosarcoma)
Grade Usually low (less aggressive) Usually high (more aggressive)
Stage Often early Often advanced
Etiology Unopposed estrogen Sporadic
Treatment Considerations Generally more radiation Generally more systemic tx Can we do better?
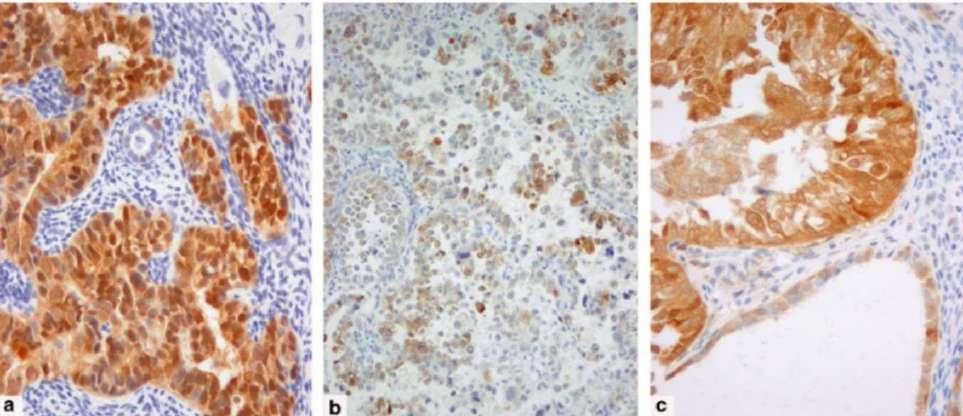
Molecular Features
We are far beyond traditional histology!

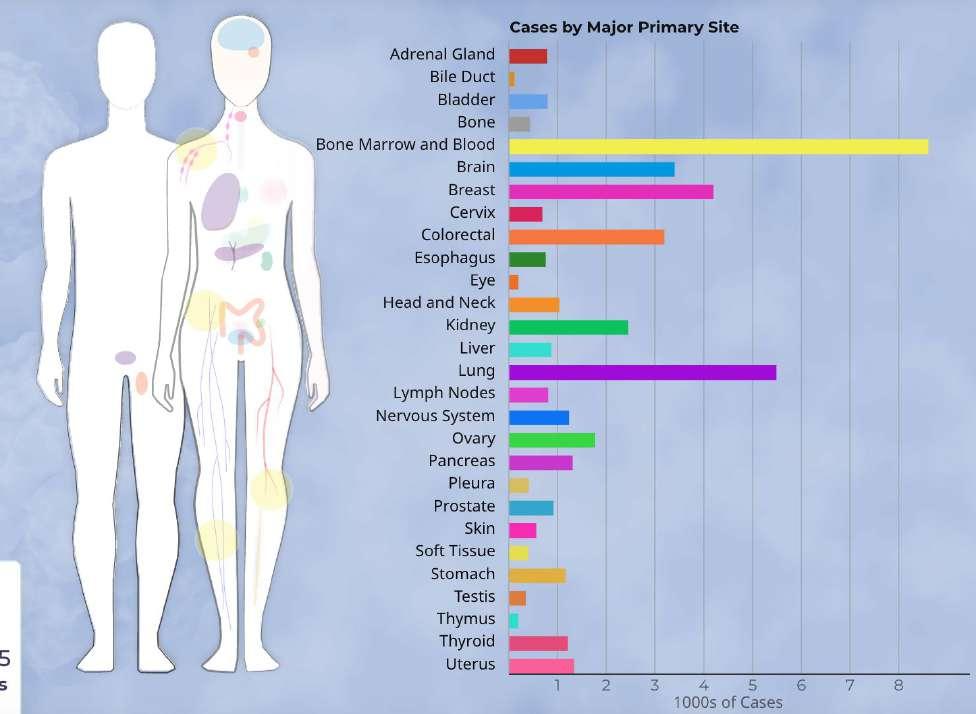
The Cancer Genome Atlas (TGCA)
• Landmark cancer genetics program
• Molecularly characterized multiple cancer types with matched normal samples
- 2664 cases of uterine cancer
Molecular Features
POLE Mutated Mismatch Repair Deficient No Specific Molecular Profile (NSMP)
P53 Mutated
Molecular classification has significant implications for response to treatment!
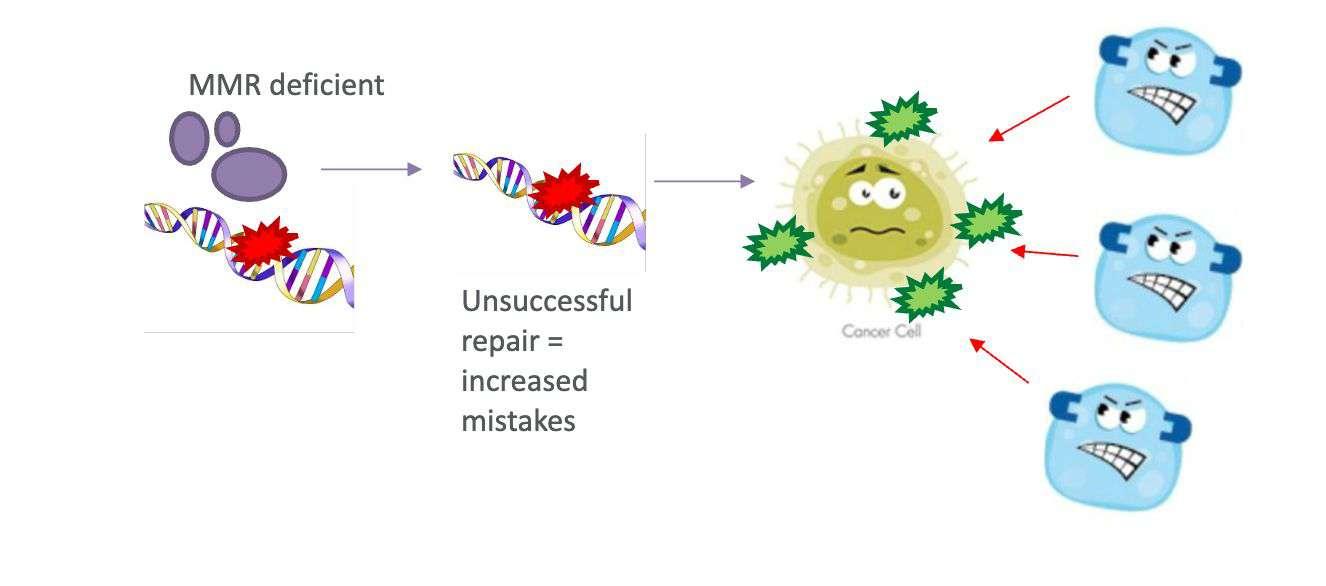
Mismatch Repair Deficiency
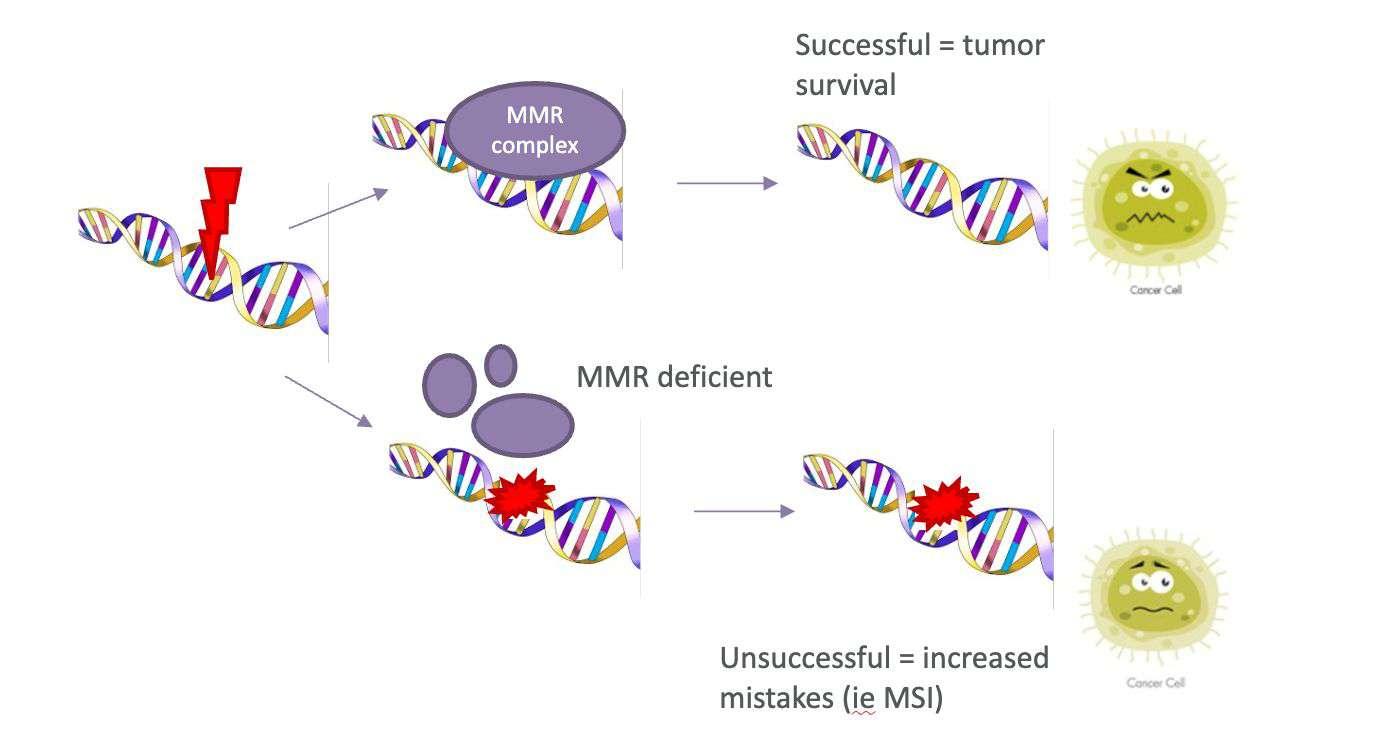
Mismatch Repair Deficiency: Immunogenic
Immunotherapy and Previously Treated Recurrent Endometrial Cancer
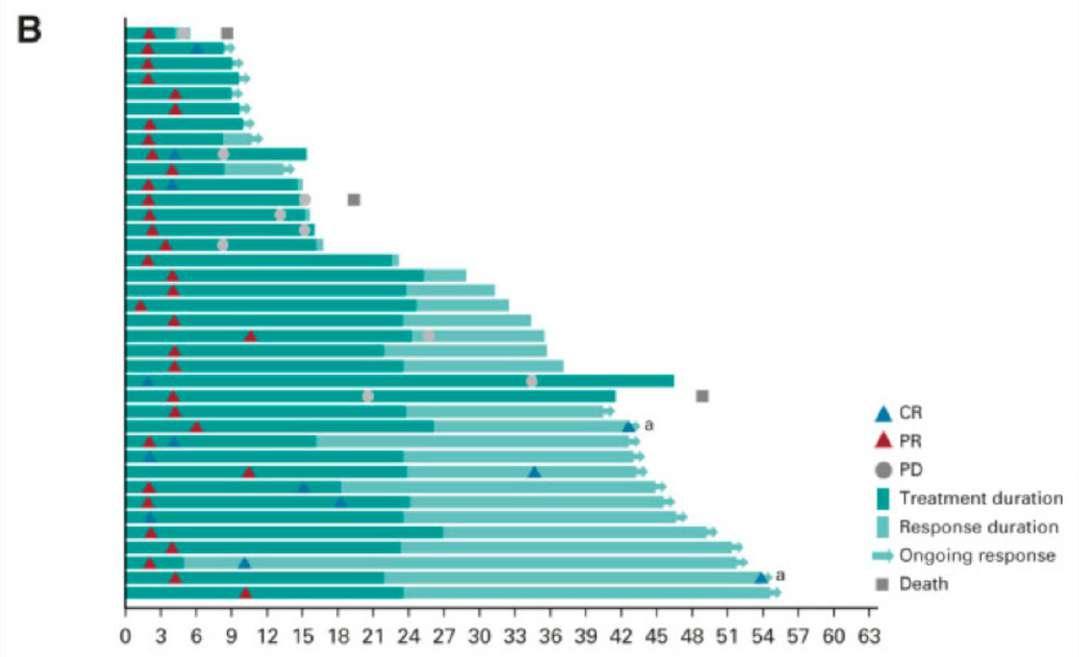
Keynote – 158 // PEMBROLIZUMAB
• 79 patients (previously treated)
• Mismatch repair deficient
• 48% response rate
• 2/3 patients with a response >3yrs
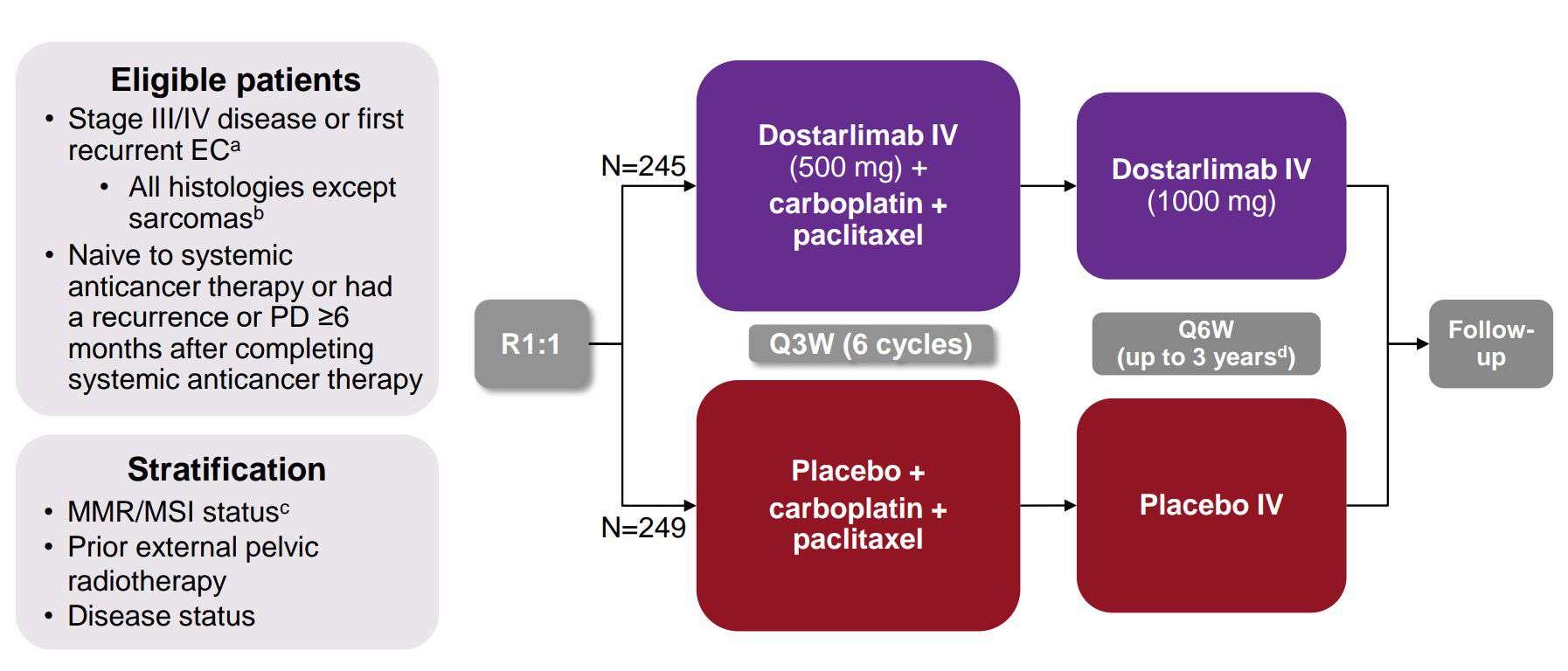
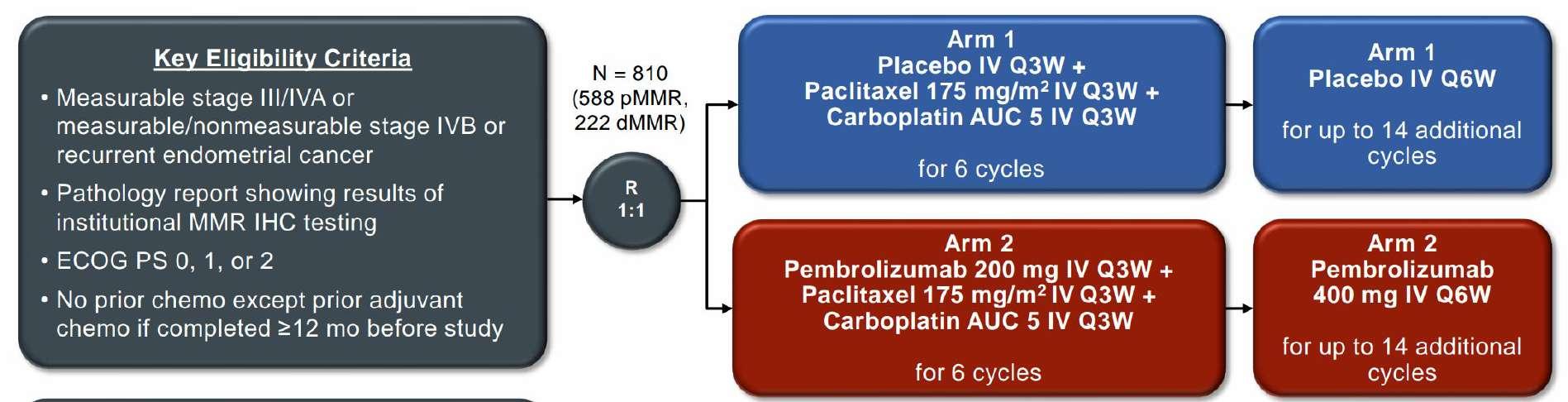
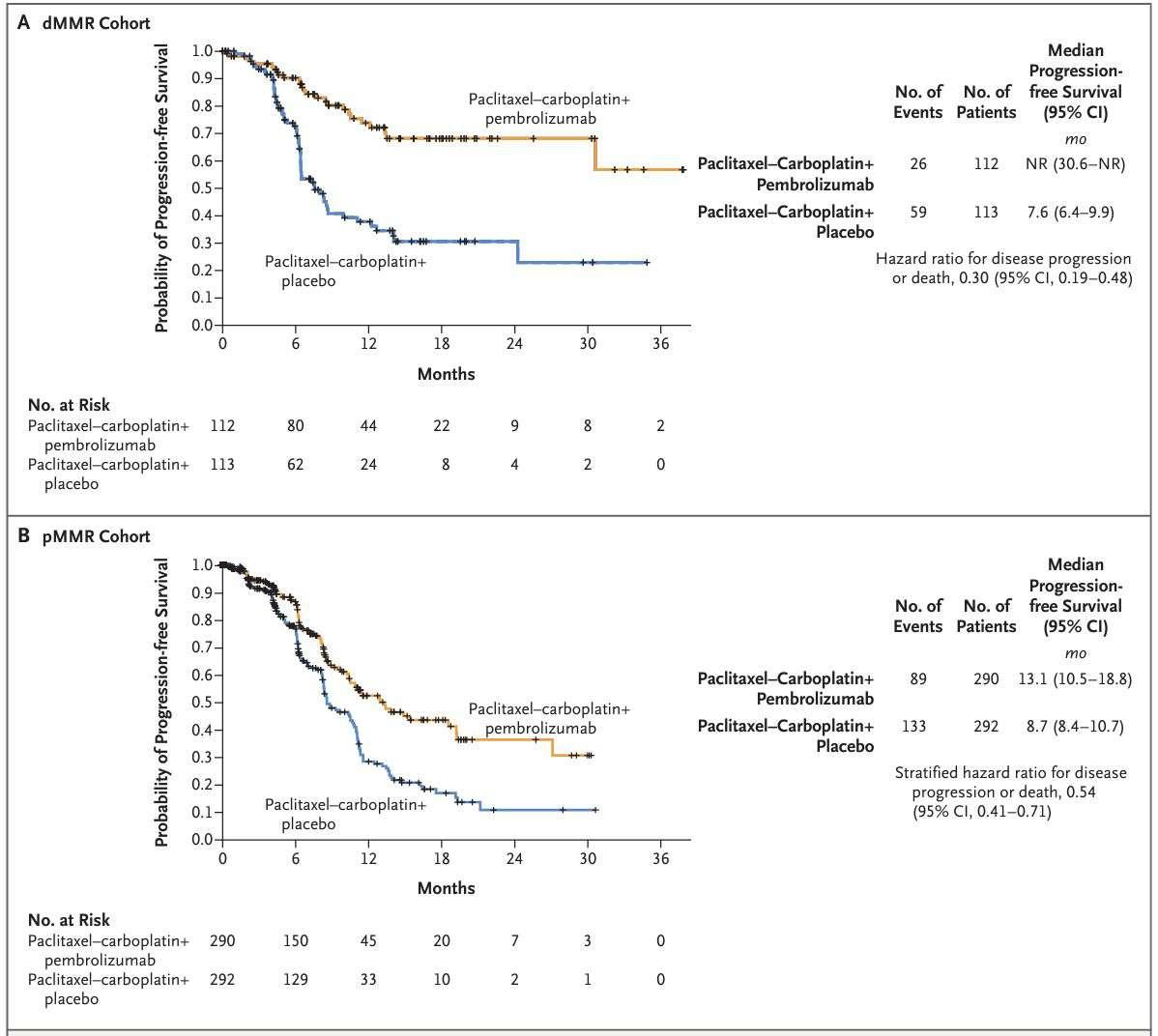
Immunotherapy in Treatment Naïve Endometrial Cancer
RUBY // DOSTARLIMAB
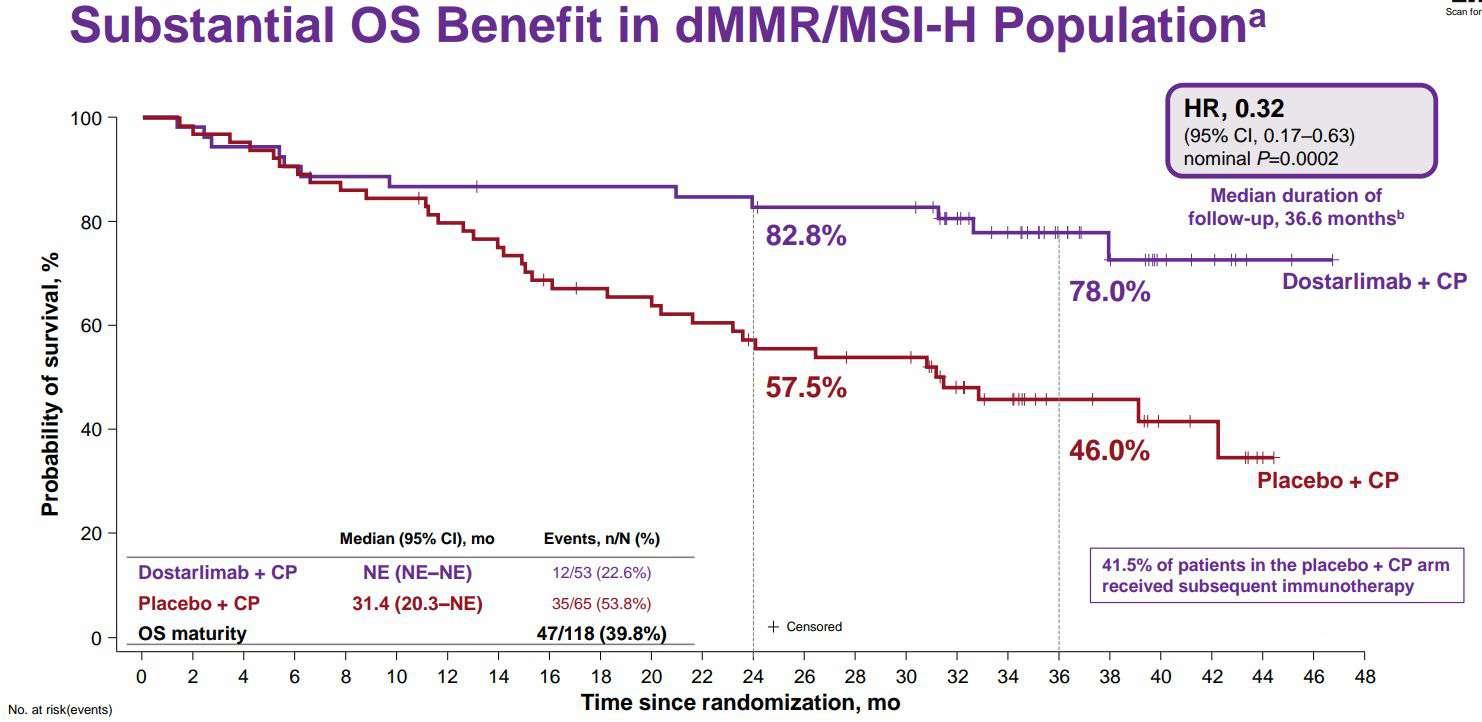
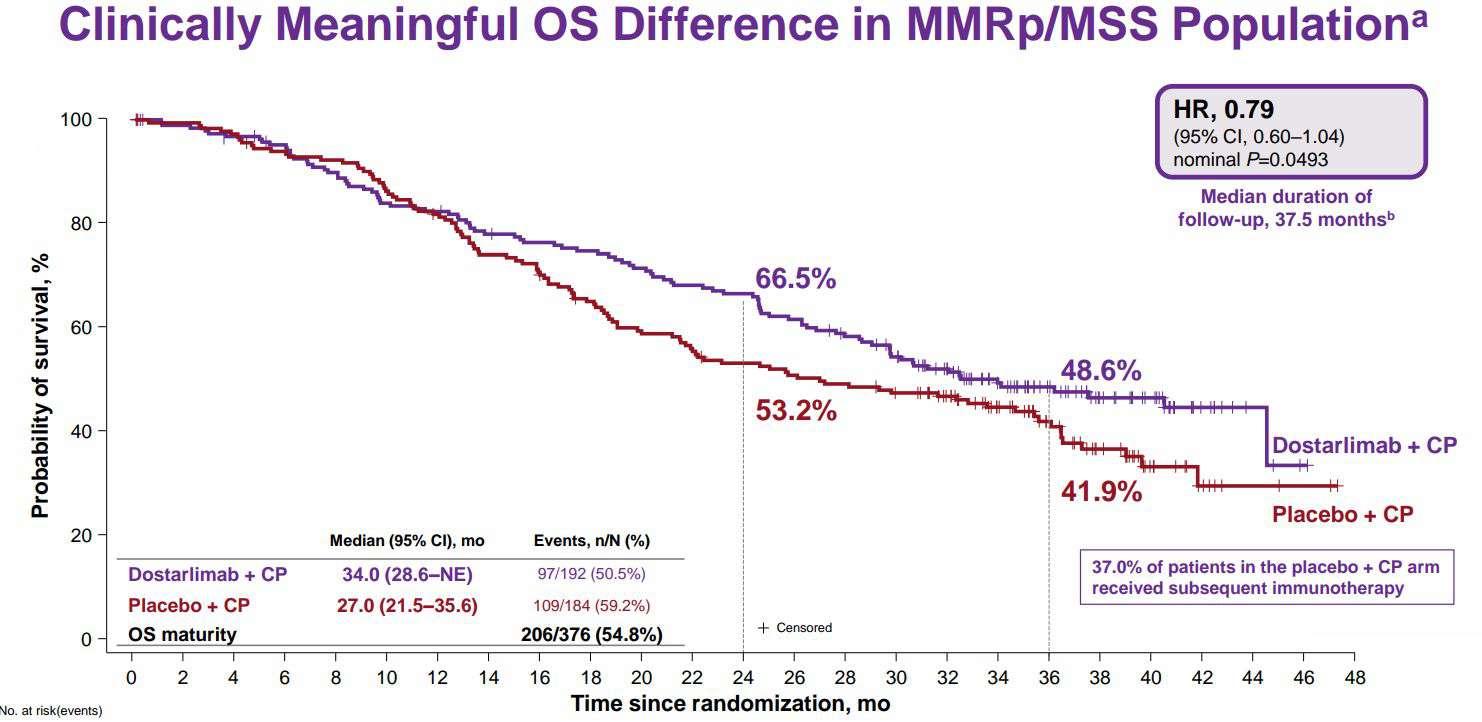
Immunotherapy in Treatment Naïve Endometrial Cancer
GY0-18 // PEMBROLIZUMAB
[Still
a Role for
Immunotherapy in Previously Treated Endometrial Cancer Without MMR Deficiency!]
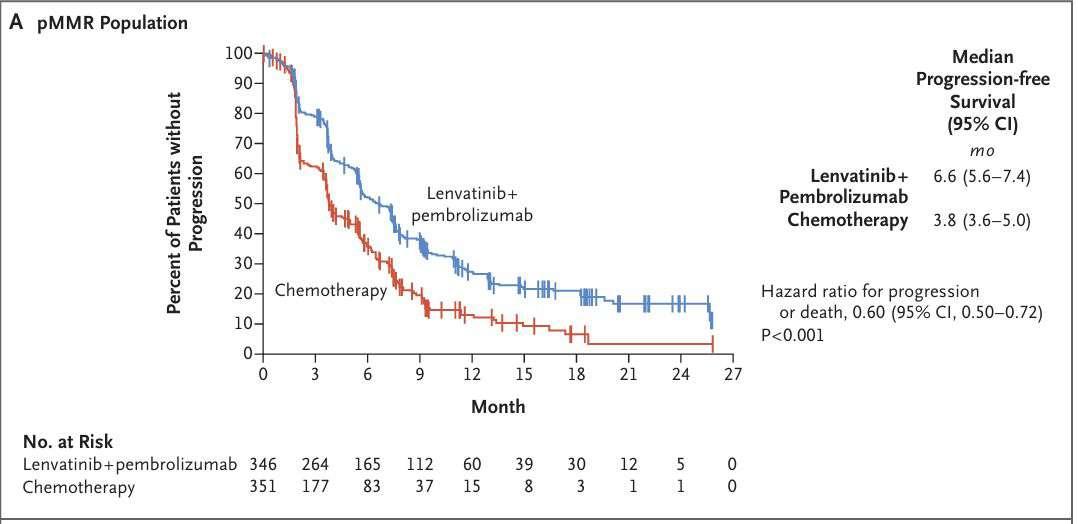
KEYNOTE – 775 // PEMBROLIZUMAB/LENVIMA
Molecular Features
POLE Mutated Mismatch Repair Deficient No Specific Molecular Profile (NSMP) P53 Mutated
Excellent prognosis –de-escalate treatment??
Consider hormone receptors, other molecular testing
More likely to spread distantly – think chemotherapy
Now incorporates molecular profile!
The Way of the Future
What Next?
Antibody-Drug Conjugates
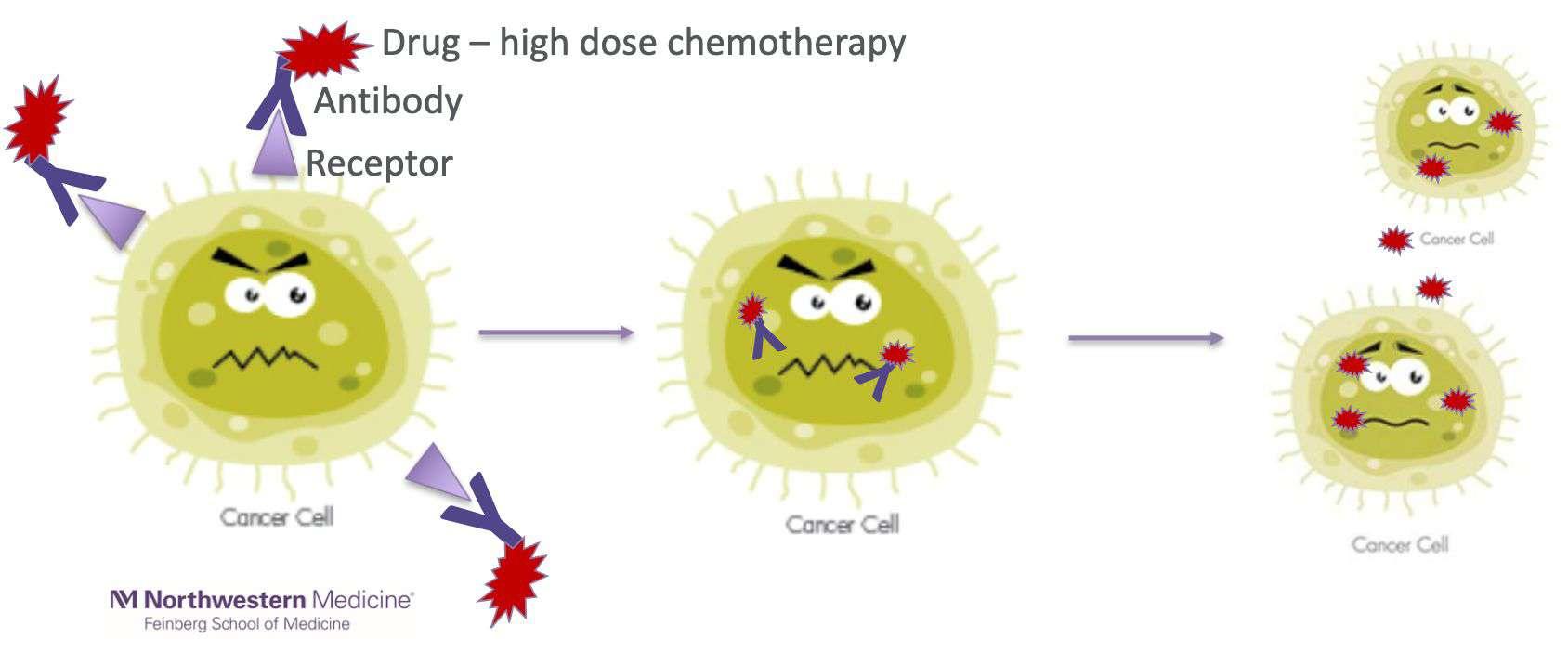
Antibody Drug Conjugates
Rapidly Expanding Option
• >190 ADCs in development
• Vary by TARGET (cell receptor) and PAYLOAD (chemo drug attached)
ADCs in Endometrial Cancer
DESTINY-PanTumor02 // Trastuzumab Deruxtecan (Enhertu)
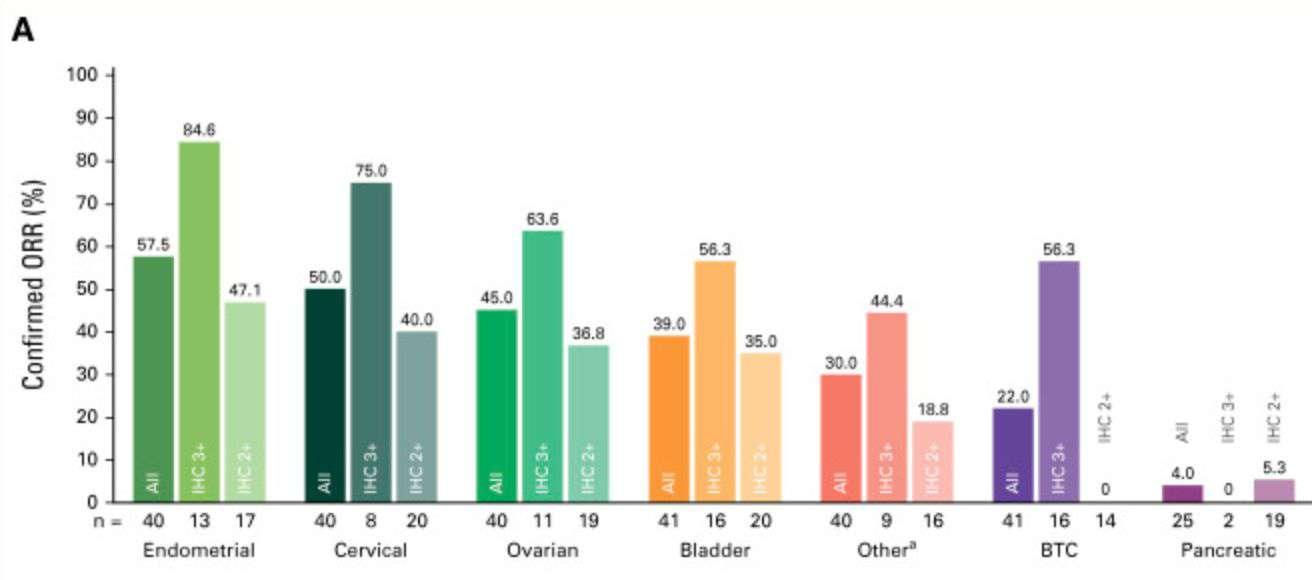
Target: HER2 receptor
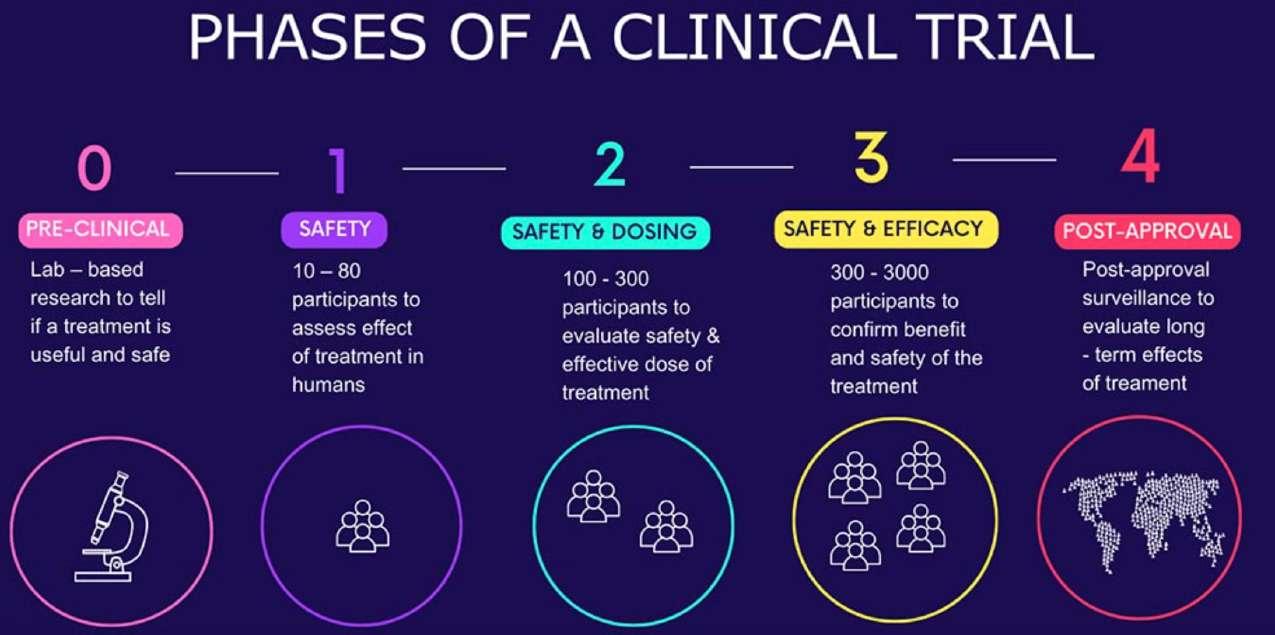
Clinical Trials

Living with Recurrent Endometrial Cancer
• Toxicities of hormones, immunotherapy, and targeted therapy are different than chemotherapy (many easier to manage!)
• Treatment toxicity should always be part of the treatment conversation
• Supportive care/symptom management is critical
- Medications
- Physical/occupational therapy + physical activity
- Nutrition
- Psychological health
Education for Patients and Families


Know your tumor’s molecular profile!

Support
Take Home Points
1) Not all recurrent endometrial cancer is the same – treatment should be individualized to the patient and the tumor.
2) There is still an important role for traditional treatments like chemotherapy and radiation – but many new options.
3) Living well with recurrent endometrial cancer is critical - in this for the long haul.
References
Uterine neoplasms. NCCN Clinical Practice Guidelines in Oncology. Version 2.2026. https://www.nccn.org/professionals/physician_gls/pdf/uterine.pdf.
Morton M, Yao M, Chalif J, et al. Association of clinical trial participation with improved overall survival for recurrent, platinum-resistant ovarian cancer. Obstet Gynecol 2023;142(3):459-466.
Meric-Bernstam F, Makker V, Oaknin A, et al. Efficacy and safety of trastuzumab deruxtecan in patents with HER2-expressing solid tumors: Primary results from the DESTINY-PanTumor02 phase II trial. J Clin Oncol 2024;42(1):47-58.
Makker V, Colombo N, Casado Herraez A, et al. Lenvatinib plus pembrolizumab for advanced endometrial cancer. NEJM 2022;386:437-448.
Clinical trials explained. Rare Disease Clinical Trial Network. https://rarediseaseresearch.ie/clinical-trials-explained/
Reid-Nicholson M, Iyengar P, Hummer AJ, et al. Immunophenotypic diversity of endometrial adenocarcinomas: implications for differential diagnosis. Modern Path 2006;19:1091-1100.
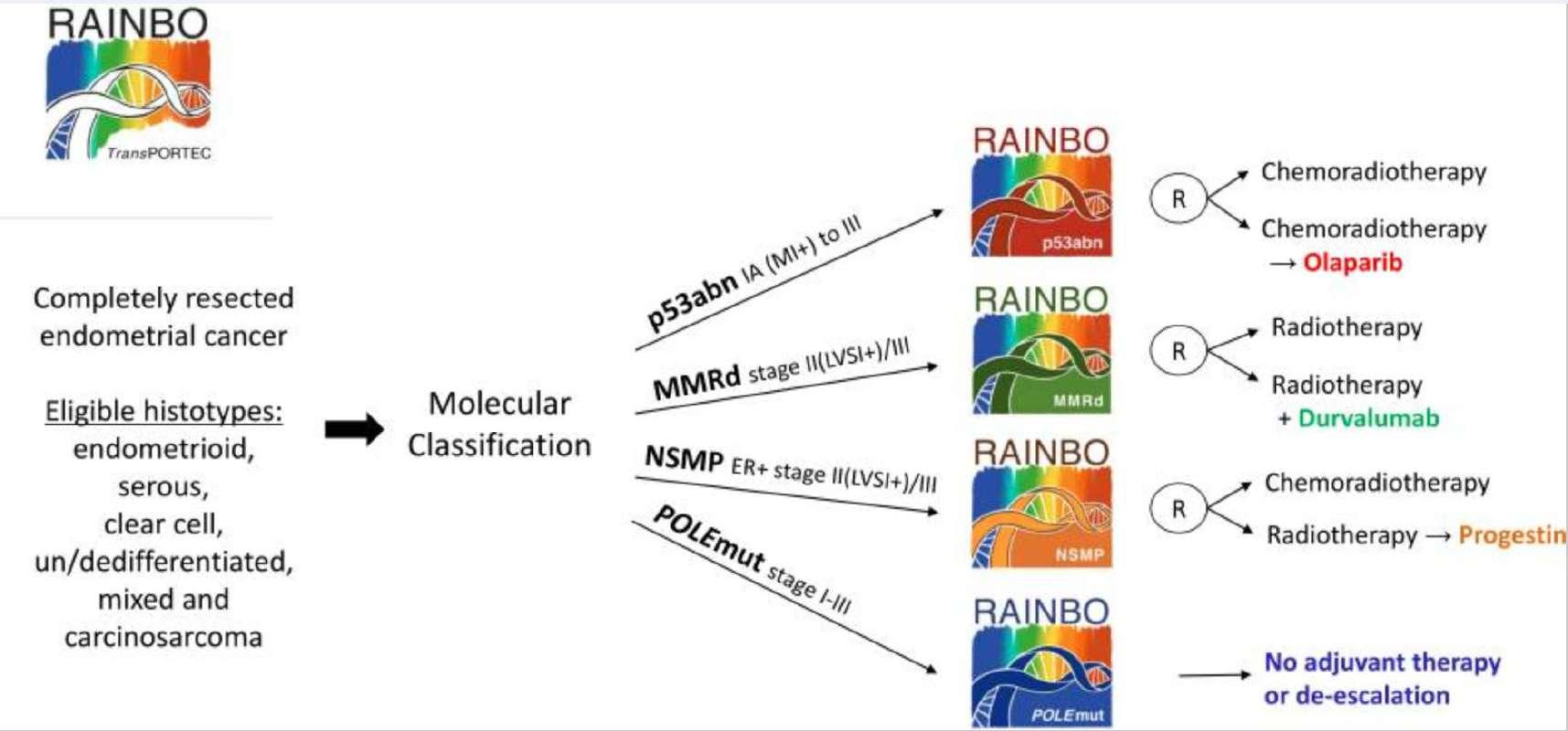
RAINBO Research Consortium. Refining adjuvant treatment in endometrial cancer based on molecular features: the RAINBO clinical trial program. Int J Gynecol Cancer 2022;33(1):109-117.
Berek JS, Matias-Guiu X, Creutzberg C, et al. FIGO staging of endometrial cancer: 2023. Int J Gynaecol Obstet 2023;162(2):383-394.
Eskander RN, Sill MW, Beffa L, et al. Pembrolizumab plus chemotherapy in advanced endometrial cancer. NEJM 2023;388:2159-2170.
O’Malley D, Bariani GM, Cassier PA, et al. Pembrolizumab in patients with microsatellite instability – high advanced endometrial cancer: Results from the KEYNOTE-158 study. J Clin Oncol 2022;40:752-761.
Mirza MR, Chase DM, Slomovitz BM. Dostarlimab for primary advanced or recurrent endometrial cancer. NEJM 2023;388:2145-2158.