Specsavers has officially been named the 4th Best Workplace in Australia by Great Place To Work® – a testament to our vibrant, inclusive, and people-first culture.
This recognition reflects our ongoing commitment to delivering exceptional hearing care while creating a workplace where everyone feels valued, supported, and inspired to grow. Join a team that’s setting the standard – in hearing care and in culture. Explore careers at audiology-anz.com.au
AUDIOLOGIST SHORTAGE FOR AUSTRALIA BUT NO SCARCITY OF AUDIOMETRISTS, SAYS JSA
Australia has a shortage of audiologists nationwide, according to Jobs and Skills Australia’s latest data, but audiometry bodies dispute the notion that there is no shortage of audiometrists.
The Australian Government agency also said there were shortages of otolaryngologists in all states but sufficient ear, nose and throat (ENT) surgeons in Northern Territory and the Australian Capital Territory (Canberra).
Jobs and Skills Australia (JSA) is an independent government agency that provides the government with expert advice on the nation's current, emerging, and future workforce and skills needs. Its reports provide a ‘point-in-time’ assessment of occupations shortages in the Australian labour market.
Its latest data from 2024 and 2025 was updated on 28 July 2025. It was the first edition of a new job classification standard, the Occupation Standard Classification for Australia (OSCA) which replaces the former Australian and New Zealand Standard Classification of Occupations (ANZSCO).
JSA said that in 2024 and 2025 there were shortages of audiologists nationwide and in every Australian state and territory but no shortages of audiometrists nationwide or in any state or territory.
The Australian College of Audiology incorporating the Hearing Aid Audiology Society of Australia (ACAud inc. HAASA), disputed this point, stating there was an audiometrist shortage in rural areas.
ACAud inc. HAASA is the
only professional membership body representing audiologists and audiometrists in Australia, with most members being audiometrists.
“The latest Jobs and Skills shortage list suggests there is no shortage of audiometrists in Australia,” ACAud inc. HAASA told HPA . “That conclusion doesn’t reflect the lived reality in rural and regional practices.”
Mr Mark Paton, ACAud inc. HAASA board member with extensive experience in
ATO: AUDIOLOGISTS’ WAGES STAGNATE
The average taxable income for an audiologist in Australia was just under $97,000 in 2022-2023, according to the latest salary data released by the Australian Taxation Office (ATO). Audiologists earned slightly less in 2022-2023 than in 2021-2022 – overall $41 less or, for females, an average $93 less. Women again earned less than men in every job category in the sector. Female audiologists earned about $25,000 on average less than their male counterparts. And the average taxable income for female audiometrists was about $18,000 less than males. However, this figure needs to be interpreted cautiously as audiometrists were grouped in the broader medical technicians category in 2022-2023.
Ear, nose and throat (ENT) surgeons remained the nation’s fourth highest income earners, earning just over $595,000 on average, a rise of about $18,000 on the previous year.
The gender wage gap was far greater for ENT surgeons as otorhinolaryngologists who are women earned about $232,000 less than men.
The ATO released its taxation statistics for 2022-2023 on its website and updated the data on 13 November 2025.
For professions where a greater proportion work part-time, this can skew salaries down so when comparing between men and women, it may not necessarily be a like-for-like comparison.
Based on tax returns filed by 3,403 audiologists, the average taxable income of audiologists
in 2022-2023 was $96,892. In 2021-2022 it was $96,933.
For female audiologists, it was $90,979, based on 2,565 tax returns. This dropped $93 from the 2021-2022 figure of $91,072.
For their male counterparts, average taxable income was $114,988, based on information provided by 838 men. This amount fell $27 from $115,015 in 2021-2022.
The average taxable income for otorhinolaryngologists –combining male and female ENT surgeons – was $595,362, a rise of $18,680 from the previous year’s $576,925.
Male ENT surgeons earnt on average $641,204 compared with female ENTs on $408,600. This data was based on tax
continued page 8
rural and regional practice, added: “Most rural audiology businesses have essentially given up trying to attract clinicians. They would certainly employ anyone who was available but they tend to just work harder and do it themselves.”
ACAud inc. HAASA said that, in practice, smaller providers often invested heavily in training their own staff, only to face the risk that those newly skilled clinicians leave for metropolitan centres.
“Larger employers, meanwhile, continue to run international recruitment programs precisely because they cannot fill rural and provincial roles locally,” it said.
“This disconnect highlights a deeper issue: the data may not
continued page 8
Hearing loss in pregnancy
British ENT registrar Dr Sara Timms, currently undertaking a fellowship in Sydney, discusses a systematic review she jointly undertook to evaluate the effect of pregnancy and pregnancy syndromes on the function of the inner ear.
JSA says there’s not enough audiologists. Image: Prostock-studio/stock.adobe.com.
IN THIS ISSUE
16 Expression Audiology milestone
Guests at its 50th anniversary event celebrated a trip down memory lane.
22 Post Professional Doctor of Audiology
Hear from an ATSU manager, graduate and student of the program.
24
Sentio System launches in Australia
It's Oticon Medical's first active transcutaneous bone anchored hearing system.
OTITIS MEDIA: STRIVING TO CLOSE THE GAP
This edition, HPA takes an in depth look at otitis media through the eyes of three people at the coalface of what has been an ongoing issue in First Nations children.
Australia’s Indigenous children have some of the world’s highest rates of otitis media.
These painful middle ear infections can become chronic, leading to infection, burst eardrums and if untreated, hearing loss.
According to Perth audiologist Dr Lara Shur, in the field they say, ‘Can’t hear, can’t learn, can’t earn’ because, if not addressed early, the condition can cause lifelong effects.
Australia’s first Indigenous ENT surgeon, Professor Kelvin Kong, famously described hearing loss as a “developmental emergency”, saying that because it’s not life-threatening, it can be deemed less urgent. But as waiting lists for grommet surgery grow, children’s learning, linguistics and development can fall behind.
34 Specsavers Audiology Clinical Conference
The event was a big hit with Partners from Australia and New Zealand.
Addressing an audiometry nurses conference last year, audiometry nurse Ms Gisella Laughton said the OMOZ 2024 Conference heard the disturbing statistic that otitis media lasts for about three years in an Aboriginal child versus three months in other children.
All this information adds up to an alarming picture but those working in Australia’s hearing care and research sectors are coming at it from all fronts.
Our interview with Dr Shur, co-founder of Earbus Foundation, shows that with persistence and the right approach, positive outcomes are possible and there is hope. Dr Shur was recently nominated for an Australian of the Year Award for her team’s incredible work in helping to reduce the incidence of middle ear infections in Indigenous children.
ENT surgeon Professor Shyan Vijayasekaran from Perth Children’s Hospital also discusses two promising innovations he is helping to trial –Blitz-OM and Spritz-OM – developed by Western Australian researchers.
And Hearing Australia audiologist, Ms Sally-Anne Regan, says data from its HAPEE (Hearing Assessment Program Early Ears) could indicate a change in disease patterns from the more severe chronic suppurative otitis media to otitis media with effusion.
Turn to page 18 to read the full story.
HELEN CARTER Editor
Image: Heidi Modrovich.
Image: Oticon Medical.
Image: Specsavers.
Australia’s Leading Manufacturer of Hearing testing rooms
Our hearing testing rooms are designed in house, with expert knowledge, made from premium materials and individualised to your specific needs.
Product Offering
• Micro booth relocatable solution for testing in industrial and medical situations. Commonly used for work screenings and pre-employment scans.
• Modular Micro Booth Modular booths are demountable, making them easily adaptable to fit through smaller, unique spaces. These units are brilliant for testing
• Test Lab person booth with increased noise attenuation, creates an environment to give more data for an audiologist or an ENT specialist.
• Large Testing Room customisable rooms aimed to achieve the lowest possible ambient noise level to be used in paediatrics, bone conduction testing, or VROA.
Contact us to assist you in selecting the room that will suit your clients needs.
E. admin@adfi.com.au
P. 03 9775-0340
adfindustries.com.au
UPFRONT
Just as HPA went to print, the NATIONAL ACOUSTIC LABORATORIES received a HCF Research Foundation Translational Research Grant to develop and implement the Universal Language Independent AI Powered Speech Test (ULIPlus). Designed to work across more than 40 languages, the AI powered hearing care solution will improve diagnosis of hearing impairment for the one in five Australians who speak a language other than English
OFF THE BEATEN TRACK
Weird
Traffic noise is one pressure faced by rare southern Australia songbird, the threatened Southern Emu-wren, reports a Flinders University study.
“Anthropogenic (human) noise has the potential to negatively impact wildlife by disrupting communication and reducing overall fitness. This includes the effects of traffic noise and other loud noises on signalling behaviour of this rather sedentary and territorial songbird,” said PhD candidate Mr Julian Behrens. .
Wonderful
A cinema in Cornwall, England offers smart glasses to people with hearing problems so they can view subtitles while watching movies, the BBC reports. It said staff at White River Cinema in St Austell said the glasses were introduced to increase accessibility to film screenings. Subtitles appear through the glasses as captions with a handheld controller allowing the viewer to change the size, position, colour, focal-length and brightness of the text.
Wacky
at home. IN OTHER NEWS, the Bionics Institute will partner with Swinburne University of Technology in a first-of-its-kind collaboration to accelerate the development of life-changing medical devices. They will combine their cutting-edge facilities, scientific expertise and resources to progress medical device innovation into the clinic for the benefit of patients worldwide. The partnership builds on decades of experience across both organisations. The institute is a world-leading medical research institute with 40 years’ experience in taking medical devices from
concept to clinical reality, including the cochlear implant. FINALLY, Deaf Connect has launched a new Melbourne office alongside its community, partners, and stakeholders. It said the event marked a significant milestone in its commitment to the Deaf, Deafblind, and hard of hearing community in Victoria. “We envision the new office at 250 Victoria Parade to be more than just a workplace for our staff,” Deaf Connect said. “It's a purpose-built hub to enhance our service delivery, foster connection and provide a welcoming Deaf space for culture to thrive.”
Cover – Earbus cofounder, nurse audiometrist Dee Parker, checking a client’s ears. Image: Earbus.
Male and female mice develop sound preferences depending on their early auditory environment, a study shows. When exposed as pups to Beethoven’s Symphony No 9 or to silence, male mice showed strong, lasting behavioural changes. But neural activity in the brain's auditory cortex was correlated with music preference in female mice. This revealed sex-dependent differences in how early sound exposure shapes brain activity and emotional preferences later in life.
WHAT'S ON
Until 18 January
Audiology Australia Online Conference recordings are available offering up to eight CPD points. audiology.eventsair.com/ audaonline25
12-14 February
HBA’s 2026 Seminar will be in Brisbane, Australia. All HBA members, staff and non-members are welcome. hearbusiness.com.au
be asking the right people about gaps in the profession. On paper, the workforce looks sufficient. On the ground, however, the shortage is felt acutely in communities outside the cities, where access to hearing care is most needed.
"Ahpra’s new regulation of audiologists — which excludes audiometrists — is already having negative consequences in rural communities, worsening an already difficult situation.”
The Australasian College of Audiometry (AuCA), a Registered Training Organisation for audiometrists, also disputed there were enough audiometrists, suggesting JSA’s data could be skewed due to the new audiometrist classification scheme.
Mr Chedy Kalach, AuCA managing director, said JSA asked those advertising for positions to complete a survey to see if their ads were successful and asked about their employment history. “The hit rate for such surveys is very low, and I know large employers from other fields are never approached to complete the survey,” he said. “The survey is open for a short period of time and doesn’t have great reach, making the data unreliable. I haven’t found
the data behind this, but I suspect the data sample size is not valid.”
Kalach said that, more importantly, the ANZSCO code had changed to OSCA recently, debuting the newly created audiometrist standard through OSCA.
“Previously audiometrists were classified under medical technicians which included audiometrists, dialysis technicians, electroencephalographic technicians, mortuary technicians, ophthalmic technicians, respiratory technicians, orthotic and prosthetic technicians, perfusionists, and renal and sleep technicians,” he said.
“This was a vast range of professions and industries, with some having shortages and others not, hence the data wasn’t specific.”
Looking at the history of the new audiometrist OSCA standard, he believed JSA may have used the previous data for medical technicians.
“I’ll be waiting for mid 2026 data to be released as that will give us a better understanding,” Kalach said.
He said many audiometry roles were filled by upskilling current front of house staff to become audiometrists so there weren’t as many job adverts for audiometrists as jobs being filled compared to audiologists being hired.
Image: Chedy Kalach.
“MID
2026 DATA WILL GIVE US A BETTER UNDERSTANDING.”
CHEDY KALACH, AUCA.
Ms Heather Joseph, AuCA general manager, said it was difficult to read from parameters used by JSA. “I expect that audiologists are definitely advertised for much more than audiometrists,” she said. “Most of our students are already working in hearing clinics with audiometry used as an opportunity for people who are working in administration or reception to progress their career and become audiometrists.
“Not everyone is able to take two years full time to complete a Master’s degree in audiology so audiometry fills this gap to support the industry but often flies under the radar as it's not regularly advertised outside of the clinic.”
Joseph said that, with an aging population, the hearing industry would need more clinicians and if there was a job shortage in audiology, it made sense that there was also a shortage of audiometrists, albeit not recognised.
JSA obtains data from sources including surveys like the Recruitment Experiences and Outlook Survey where employers are surveyed about labour market conditions. It analyses online job ads and uses data from government agencies and other organisations including the Australian Bureau of Statistics.
MALES CONSISTENTLY EARNED MORE THAN FEMALES
continued from page 3
returns from 110 men and 27 women.
For the second year running, ophthalmology was the nation’s highest paid profession.
Ophthalmologists had an average taxable income of $643,389 in 2022-2023 followed by neurosurgeons on $611,754, plastic and reconstructive surgeons on $595,969 and otorhinolaryngologists on $595,362.
There was no specific category for audiometrists as in 2022-2023, they were classified under the broader category of medical technicians (other).
On average, yearly taxable income for medical technicians was $69,696. Men earned $18,812 more than females – $80,060 for males versus $61,248 for females.
The combined male/female figure was on parity with 2021-2022 when it was $69,694.
Other relevant salary details for the hearing health sector include health practice managers whose average taxable income was $83,534.
Again, males earned more on average ($105,059) than females ($80,695).
There was no category for audiometry nurses, but child and family health nurses had an average taxable income of $76,154.
Male nurses earnt about $25,000 more than females - approximately $95,000 versus $75,000.
The situation was similar for community health nurses who overall earned $75,830 or about $88,000 if they were male and $74,000 if they were female.
School teachers of the hearing impaired earned an average $78,782 – or about $96,000 for males and $77,000 for females while university lecturers took home $118,668 (about $128,000 for males versus $108,000 for females.)
Female audiologists earned an average $25,000 less than male audiologists. Image: Peakstock/ Shutterstock.com.
Interpreters, including Auslan interpreters, earned just under $50,000. The average taxable income was $49,623. For females it was $48,315 and males, $52,500.
The Australian Government’s Jobs and Skills Australia data defines interpreters as those who transfer spoken or signed languages into other spoken or signed languages, usually within a limited timeframe in the presence of the participants requiring the translation.
HEALTH MINISTER ASSURES AUDIOMETRISTS THEY WILL RECEIVE CONTINUED HSP RECOGNITION
Federal health minister Mr Mark Butler has assured audiometrists that they will continue to be recognised as qualified providers under the Hearing Services Program and other relevant Commonwealth-funded programs.
T he Australian College of Audiology incorporating HAASA (ACAud inc. HAASA) said the Hearing Health Sector Alliance (HHSA) had received a response from the minister about audiometrists’ roles. It confirmed they would remain eligible to deliver services under government programs despite upcoming registration of audiologists under the National Registration and Accreditation Scheme (NRAS).
“Recently, HHSA wrote to Minister Butler seeking assurance that audiometrists will continue to be recognised as qualified providers under the Australian Government Hearing Services Program (HSP) and other relevant Commonwealth-funded programs, due to the indispensable role audiometrists play in
strengthening Australia’s hearing health workforce,” ACAud inc.
HAASA said.
“As an executive member of the Hearing Health Sector Alliance (HHSA), we’re proud to stand alongside other leaders and organisations representing the full breadth of Australia’s hearing health community.
“Through this joint advocacy, we are now seeing tangible benefits for our members and meaningful progress across the sector.”
ACAud inc. HAASA said it had specifically sought the government’s assurance on two critical points:
• Audiometrists will remain eligible to deliver services under the Hearing Services Program and other relevant Commonwealth programs, irrespective of NRAS registration status; and
a response has been received from Minister Butler, stating that "funding for hearing services under the program is expected to remain largely unchanged" and that "the HMM (Health Ministers Meeting) decision (on audiologist registration) is not intended to reduce the scope of practice of audiometrists,” ACAud inc. HAASA said.
Mr Butler also said: “Audiology and audiometry are distinct yet complementary disciplines, each playing a vital and valued role in delivering high-quality hearing healthcare to Australians."
ACAud inc. HAASA said this was a positive step forward, reflecting recognition of the essential contributions that audiometrists make in delivering hearing health services to Australians.
• T hat the government is committed to supporting a diverse and sustainable hearing health workforce, inclusive of both audiometrists and audiologists.
“We are pleased to share that
“ACAud inc. HAASA and HHSA will continue to advocate for a strong, inclusive hearing health workforce, ensuring all professionals in this sector are valued and supported,” ACAud inc. HAASA said on 12 November 2025.
OPSM ADDS HEARING CARE TO ANZ SERVICES AND NUANCE AUDIO GLASSES GO ON SALE
OPSM has started delivering audiology services in Australia and New Zealand, and its Nuance Audio Glasses for people with mild to moderate hearing loss are also on sale, its parent company EssilorLuxottica has announced.
EssilorLuxottica said it had launched its first direct-to-consumer audiology service, with the goal of audiology being in at least nine practices across ANZ by the end of 2025, and additional locations to be consistently added over 2026.
“Vision and hearing loss affect similar demographics, particularly older adults, and integrating eye and hearing tests in the same location provides a more holistic and efficient approach for our patients by addressing multiple sensory issues at a single point of service,” Essilor Luxottica said.
“The introduction of audiology services marks a significant milestone in OPSM’s commitment to providing customers with accessible, integrated care for two of their most important senses.
Nuance Audio Glasses are over-the-counter hearing aids. Image: EssilorLuxottica.
director of audiology services at EssilorLuxottica, said: “By bringing professional audiology services into our OPSM network we are extending our promise of everyday excellence to hearing health, offering comprehensive, coordinated care for those facing sensory decline.
“Together, we can better support our communities’ well-being, accessibility, and connection to the world."
EssilorLuxottica said dual sensory impairment (loss of vision and hearing) affected up to 3% of adults aged 60-69 and nearly 22% of those aged 80 plus. Its rising prevalence underscored the importance of integrated sensory care for helping to preserve independence, communication, and quality of life.
Nuance is on sale in OPSM, Laubman & Pank, and EyeQ optometry stores, an EssilorLuxottica spokesperson said.
“Nuance is an over-the-counter hearing aid so optometrists and retail dispensers can sell them,” she said. “There is no requirement of a hearing test beforehand.”
The glasses will also be available at independent audiology and optometry stores in Australia, the spokesperson said. Meanwhile, Cearvol has introduced Aquarius Hearing Glasses overseas.
Health Minister Mark Butler. Image: Mark Butler.
IN BRIEF
TURNING EARBUDS INTO HEARING AIDS
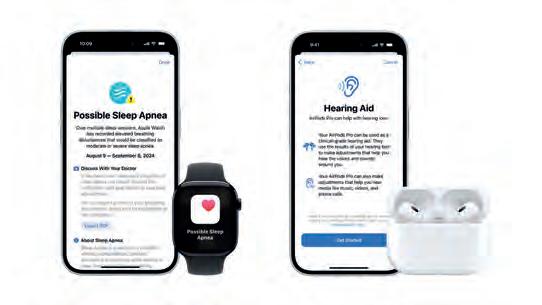
Israeli company Tuned has received Food and Drug Administration clearance for its software platform that transforms standard hearables such as earbuds and headphones into self-fitting hearing aids. Tuned said its hearing aid software brought medical-grade hearing accessibility to everyday hearables. It is the second company in the world, after Apple, to offer self-fitting hearing aid functionality in consumer-grade hearables. The FDA previously authorised Apple’s AirPods Pro 2 and Pro 3 to be used as the first over-the-counter hearing aid software device. “Tuned’s FDA-cleared solution offers a fully customisable self-fitting experience, allowing users to precisely adjust amplification to their personal hearing profile, without professional intervention,” Tuned said.
WORLD FIRST AUSLAN EMERGENCY APP
Expression Australia has launched its new Auslan Emergency Interpreting (AEI) App to provide three million Australians in the Deaf and Hard-of-hearing (DHoH) community with Auslan interpreting for the triple zero (000) emergency number. The app is a world-first emergency communications solution, providing the DHoH community with direct access to 000 for police, fire, or ambulance services, 24/7, 365 days a year, via real-time video calls with qualified Auslan interpreters. Current services only offer Auslan video call support during Australian Eastern Standard Time (AEST) business hours, but the new move extends this access to after hours. While Expression Australia self-funded the app’s launch, it is urging governments to consider funding long term sustainability.
DEMANT TO SELL OTICON MEDICAL
Hearing healthcare group Demant has signed an agreement to sell Oticon Medical, which provides bone anchored hearing solutions, to investment company Impilo. Impilo focuses on investments in Nordic healthcare companies and will develop Oticon Medical into a stand-alone business. Demant said it was selling the business “for a total contractual consideration of up to A$143 million (600 million Danish Kroner), thereby concluding the process of divesting its hearing implants business area”. “The agreement ensures the continuity of Oticon Medical’s business operations, its sustained strong position in the market, further growth as well as investments in future innovation for the benefit of customers and patients,” Demant said.
MANY OVER 50 WITH HL DON’T USE HEARING AIDS
An inaugural nationwide survey of hearing loss has revealed that about 40% of Australians aged 50 and over have some form of bilateral hearing impairment, but alarmingly, nearly one-third of people in this age group with significant hearing loss don’t use hearing aids.
The Australian Eye & Ear Health Survey provides the first nationwide data on the prevalence of hearing impairment in non-Indigenous and Indigenous Australians.
Report authors said the finding that only 69% of people with moderate or worse bilateral hearing impairment had used a hearing aid “highlights a major concern about unaddressed hearing loss in the older Australian population”.
Mr Mark Butler, Minister for Health and Ageing, Disability and the NDIS, launched the report of eye and ear health, vision and hearing impairment at Parliament House on World Sight Day, 9 October 2025.
It is the second National Eye Health Survey (NEHS) but this time ear health was added, providing the most comprehensive study of its kind, and a contemporary snapshot of the nation’s eye and ear health.
One of the report’s authors, Professor Bamini Gopinath, Cochlear Chair in Hearing and Health at Macquarie University Hearing, said: “The release of the report ensures we now have the data we need to plan hearing services, target prevention, and ensure equitable access to hearing care for all Australians.”
likely to reflect frequent hearing disability.
Hearing aid usage was similar among Indigenous and non-Indigenous Australians, but, concerningly, only about two-thirds of those with moderate or worse bilateral hearing impairment reported using hearing aids.
“Despite frequent hearing impairment, the uptake of hearing devices remains relatively low, including by many who were clinically eligible for them,” the report said.
“Only 69% of persons with moderate or worse bilateral hearing impairment had used a hearing aid. This suggests a potential gap between clinical need and device use, even among those who met the Australian criteria for subsidised hearing aid eligibility as outlined in the Australian Government Hearing Services Program (64% of all participants).
“This likely gap between need and use highlights a major concern about unaddressed hearing loss in the older Australian population.”
Hearing impairment appeared to occur at an earlier age and was more prevalent in the ‘younger’ group of Indigenous Australians aged 50 years or older compared to non-Indigenous Australians. Indigenous people were also more likely to report having hearing problems for longer and were less likely to consult a hearing professional.
Below: (L-R) Prof Bamini Gopinath and Prof Paul Mitchell at the launch. Image: Vision2020.
The report revealed that, after age standardisation, about 40% of Australians aged 50+ years have some form of bilateral hearing impairment but most of this is mild hearing impairment.
About one in seven (or 14%) aged 50+ have moderate or worse bilateral hearing impairment, a level
“These findings suggest there may be considerable unmet need in addressing hearing impairment in older Australians generally, and particularly among the ‘younger’ group of Indigenous Australians aged 50 years or older,” researchers said.
Hearing impairment was more frequent and severe in males than females in both groups. Prevalence of any bilateral hearing impairment was 58.5% for Indigenous males and 39.7% for females, compared with 55.9% for non-Indigenous males and 46.9% for females.
Over the past three years, 4,519 Australians aged 50 years and older, living at 30 randomly selected sites across six states and two territories, answered questions and had comprehensive eye and ear examinations. Ear examinations included video otoscopy, pure tone audiometry and tympanometry. More than 600 Aboriginal and Torres Strait Islanders participated.
REVIEW FINDS STRONG LINK BETWEEN TYPE 2 DIABETES AND HEARING LOSS
The risk of hearing loss is four times higher in people with type 2 diabetes than those without diabetes, a systematic review and meta-analysis show.
Researchers said the result was more pronounced than in other studies and findings indicated that comprehensive diabetes care should include hearing assessment. Additionally, hearing loss could be an early indicator of microvascular disease, potentially prompting earlier intervention to prevent further complications.
The authors analysed data from 17 studies encompassing 3,910 people with diabetes and 4,084 controls.
“The findings of this meta-analysis suggest that the prevalence of hearing loss among individuals with diabetes ranges from 40.6% to 71.9%,” they said in the November 2025 issue of Otolaryngology-Head and Neck Surgery. “The risk of hearing loss is 4.19 times higher in this group compared to the control group.”
This risk was predominantly observed at higher frequencies. Mean pure-tone audiometric thresholds of the diabetic group were 3.19 dB higher. They were higher for low frequencies and, more severely, for high frequencies. Additionally, HbA1c levels appeared to be correlated with severity of hearing loss. Patients with moderate or severe-to-profound hearing loss had higher mean HbA1c levels than controls, suggesting poorer glucose control was linked to more severe hearing impairment.
Authors said diabetes care should include hearing assessment. Image: Fizkes/stock.adobe.
Duration of diabetes also appeared to be a significant factor in the prevalence of hearing loss. Hearing loss prevalence was significantly higher among patients with a diagnosis of diabetes for more than 10 years, with these people facing a 2.07 times higher risk compared to those with shorter disease duration.
Authors suggested hearing loss in type 2 diabetes may result from microcirculatory alterations affecting the cochlea, leading to changes in the ultrastructure of the inner ear capillaries, including thickening of the basilar membrane and atrophy of the stria vascularis.
“Hearing loss in diabetes mellitus may be a consequence of subclinical microvascular disease,” they said. “This fact could potentially serve as an early warning sign, suggesting that closer monitoring is necessary, as well as the adaptation of treatment plans to minimise the occurrence or progression of hearing loss.”
GUIDELINES LAUNCHED TO TRANSFORM PATHWAY FOR ADULT COCHLEAR IMPLANTATION IN ANZ
The Australia and New Zealand Hearing Health Collaborative has launched the first ANZ Living Guidelines for Cochlear Implantation in Adults.
Guideline authors said the landmark initiative was designed to improve access, consistency, and outcomes in hearing healthcare for adults across the region.
Only one in 10 adults who could benefit from cochlear implants in Australia receive them, a figure that has not changed in 25 years.
The collaborative, comprising more than 70 clinicians, researchers, and individuals with a lived experience of hearing loss, adapted Global Living Guidelines to the Australian and New Zealand (ANZ) context through six national workshops in 2023 and 2024.
They adapted global evidence for cochlear implant (CI) referral, evaluation, candidacy and outcome evaluation.
The result is a set of practical, consensus-based recommendations tailored to the needs of adults in Australia and New Zealand.
Four co-chairs lead the ANZ HCC; audiologist Dr Jaime Leigh,
clinical lead of the Victorian Cochlear Implant Program at The Royal Victorian Eye and Ear Hospital; audiologist and Macquarie University Cochlear Chair in Hearing and Health, Professor Bamini Gopinath; Sydney ENT surgeon and Macquarie University Clinical Professor Payal Mukherjee; and Macquarie University professor of audiology, Professor Catherine McMahon.
Dr Leigh led a working group in developing the guidelines. “This is about more than clinical practice – it’s about restoring connection, participation, and wellbeing for thousands of adults,” she said.
“It marks a significant milestone in cochlear implant access and care across Australia and New Zealand.
“I am incredibility proud of what we have achieved, but most importantly, once implemented, how these guidelines will improve access, safety and quality of CI services in ANZ. The consumers of our services deserve to know what their options are and have access to CI technology irrespective of where they live and their financial status.”
People with lived experience who
Dr
helped co-design the guidelines included Mr John Ross, Ms Sue Walters, Ms Gillian Woodhouse, Mr Brendan Lonergan, Mr David Brady and Ms Hannah McPierzie. The working group that developed the guidelines were audiologists Dr Leigh, Associate Professor Holly Teagle, Professor Melanie Ferguson, Dr Cathy Sucher, Ms Emma Scanlan, Dr Colleen Psarros, Ms Nina Swiderski, Dr Katie Neal, Ms Jane Brew, Ms Eleanor McKendrick, Dr Dayse Távora-Vieira; and ENT surgeons Dr Claire Iseli, Dr Jafri Kuthubutheen, Professor Mukherjee and Dr Mike Bergin.
Above:
Jaime Leigh presenting at the September 2025 launch at Macquarie University. Image: Duncan Meldrum.
com.
EARBUS FOUNDATION CO-FOUNDER AN AUSTRALIAN OF THE YEAR AWARDS NOMINEE
A paediatric audiologist who 12 years ago co-founded Earbus Foundation to help save the hearing of Aboriginal and at-risk children was nominated in the 2026 Australian of the Year Awards.
Dr Lara Shur, who oversees a fleet of mobile ear clinics that deliver free care to thousands of children annually, was nominated in the Australia’s Local Hero for Western Australia award category.
She is CEO of Earbus Foundation, an organisation she created with Mr Paul Higginbotham, a teacher of the Deaf and former Earbus CEO, now executive director, and Ms Dee Parker, a nurse audiometrist.
The Earbus was the brainchild of ENT Professor Harvey Coates AO, now the foundation’s clinical patron, who launched the first Australian Earbus after seeing the concept in action in New Zealand.
Dr Shur served a decade as director of clinical services and outcomes and, after vast experience working in paediatric and regional settings, started in the role of Earbus CEO in April 2023.
A media release on 30 October 2025 which announced nominees
said Dr Shur was “making it possible for hearing-impaired Aboriginal and at-risk children in Western Australia to hear”.
“Ear infections are more prevalent among Aboriginal children than non-Indigenous children. If left untreated, they can cause hearing loss and serious, life-long limits on learning and development,” the release said.
“Lara co-founded Earbus Foundation around her kitchen table in 2013, where she and her co-founders worked for 12 months before they were able to pay themselves a salary.”
She has since mapped hearing services across WA, focusing on Indigenous communities.
“Under Lara’s leadership, a fleet of mobile ear clinics travel to schools, daycare centres and kindergartens at 200 locations in regional and remote communities,” it said. “Up to 5,200 Aboriginal and at-risk children are treated for free each year.”
Dr Shur, from Perth, has also facilitated ENT surgery clinics to treat children seen in Earbus programs across WA.
“It was a privilege to stand alongside fellow nominees whose work is shaping a more inclusive, compassionate WA. Congratulations to all the category winners –your impact is real, and your leadership matters.”
AUDIOLOGIST IS WESTERN AUSTRALIA’S EARLY CAREER ALLIED HEALTH PROFESSIONAL OF THE YEAR
A Perth audiologist who created two major innovations – paediatric and advanced scope registries – to help patients in her first year of practise is Western Australia’s Early Career Allied Health Professional of the Year for 2025.
Ms Caris Bogdanov has worked at Fiona Stanley Hospital, Perth for four years, initially as a research assistant and an intern audiologist then as an audiologist for the past two years.
She was among 11 allied health professionals and teams who were recognised for their “outstanding contributions to patient care” at the second annual WA Excellence in Allied Health Awards on 14 October at the University of Western Australia.
“I was completely surprised but also deeply moved – I truly didn’t expect to receive this recognition,” Bogdanov said.
The award, supported by North Metropolitan Health Service, was for nominees who had shown
exceptional potential during their first two years of practice. The program document said Bogdanov had demonstrated passion and commitment in providing quality, safe and compassionate care to patients, their families and caregivers.
“Caris is an early-career audiologist whose work blends clinical rigour with deep compassion,” the document stated.
She helped create the Paediatric Hearing Registry and the Advanced Scope Audiology Registry which are improving care across the South Metropolitan Health Service.
The paediatric registry supports tracking for more than 1,000 children, improving continuity of care and enabling earlier, more coordinated interventions.
The Advanced Scope Registry, implemented across South, East, and North Metropolitan Health Services, features a live dashboard that tracks referral sources, clinical outcomes, and waiting times. This
provides real-time data to inform service planning and improve patient flow.
“Both registries are the result of a collaborative effort closely tied to ongoing research and quality improvement projects,” Bogdanov said.
Bogdanov is a final-year PhD student under the supervision of audiologist, Associate Professor Dayse Távora–Vieira who was a finalist in the Allied Health Team of the Year Award. A/Prof Távora–Vieira was among 24 people in the South Metropolitan Health Service and Curtin Allied Health Research Unit nominated for the award.
Unit director, physiotherapist Associate Professor Vin Cavalheri, received the Allied Health Leader of the Year award for developing and implementing the unit’s demand-driven research strategy which has become a model locally, nationally and internationally for building allied health research capacity and culture.
Above: (Third from left) Dr Lara Shur with other nominees at the WA Government House ceremony on 13 November 2025.
Image: Australian of the Year Awards.
Caris Bogdanov with her award.
Image: Chief Allied Health Officer WA.
BLOODSPOT TEST DETECTS CMV
Testing for congenital cytomegalovirus (cCMV) at birth using the dried blood spot test is a reliable and effective method to identify newborns at risk for long-term developmental challenges, a study shows.
Congenital CMV is a virus passed to infants in the womb and occurs in about one in 200 infants. About 20% of babies with cCMV infection have birth defects or other long-term health problems including hearing loss.
Associate Professor Valerie Sung, paediatrician and principal research fellow at The Centre for Community Child Health, said cCMV was the leading infectious cause of childhood sensorineural hearing loss. She said Australia was lagging behind in cCMV screening despite robust evidence for targeted screening.
The centre is a department of The Royal Children’s Hospital and a research group of Murdoch Children’s Research Institute, Melbourne.
The new study, from the University of Minnesota Medical School, was published in JAMA Open Network.
Researchers said findings demonstrated the PCR-based test performed on dried blood spots was just as useful in identifying infants who needed follow-up for their congenital CMV infection as other tests that used urine or saliva.
The blood spot method detected more than 90% of symptomatic CMV cases, effectively identifying babies who were most in need of early interventions and ongoing developmental monitoring.
“Babies born with CMV infection, more often than not, do just fine,” said paediatrican Professor Mark Schleiss from the University of Minnesota Medical School. “However, enough infants experience complications – such as hearing loss and developmental delay – that there has long been debate about screening all newborns.”
A/Prof Sung said cCMV was not routinely screened for in Victoria and Australia. This meant it was less likely that infants with cCMV would be detected in time to offer potential antiviral treatment.
“Targeted CMV screening using saliva tests in babies who do not pass their newborn hearing check would allow for early and accurate cCMV diagnosis and could help prevent lifelong disabilities,” she said. “It should be rolled out nationwide through newborn hearing screening programs.”
Below: About 20% of babies with cCMV infection have birth defects or health problems including hearing loss.
Image: Antibydni/stock.adobe.com.
TODDLER BORN DEAF CAN HEAR AFTER GENE THERAPY
British toddler Opal Sandy, aged three, who was born profoundly deaf in both ears, can now hear normally on her own two years after receiving groundbreaking gene therapy, her parents have revealed.
She is one of 11 out of 12 children who experienced “clinically meaningful hearing improvements, including three who achieved normal hearing” after receiving the gene therapy, according to updated data. Eight with longer follow-up have showed stability or continued improvement in their hearing, researchers said.
Opal was 11 months old in September 2023 when she received gene therapy via an intra-cochlear infusion into her right ear. Good Morning America aired footage from BBC News of Opal and her parents Jo and James Sandy revealing her progress.
Opal was born deaf due to an inherited condition which led to mutations of the otoferlin (OTOF) gene. The infusion under general anaesthesia delivered a working copy of the OTOF gene into her right cochlea, and surgeons also placed a cochlear implant in her left ear.
Two years later, her parents said she can hear normally, even when the cochlear implant sound processor on her left ear is turned off. Her mother said the transformation was “mind blowing” and her father described it
as life changing. Three weeks after the surgery, Opal could hear her mother clapping behind her and turned around despite not having her cochlear implant sound processor turned on. “It was mind-blowing, even at that stage,” Jo said.
Six months post-surgery Opal could hear whispers and doctors described the level of hearing in her right ear as “near normal.” Opal is one of 11 patients who received the treatment to experience clinically meaningful hearing improvements, according to Regeneron Pharmaceuticals which developed the DB-OTO gene therapy. It reported latest data at the American Academy of Otolaryngology-Head and Neck Surgery 2025 annual meeting and published results in New England Journal of Medicine on 12 October.
AUDIOLOGISTS ADVISED TO GET HEALTHCARE IDENTIFIER
Above: Without the identifier, audiologists won’t be able to access My Health Record.
Image: Australian Digital Health Agency.
Audiology Australia (AudA) is recommending all audiologists apply for a Healthcare Provider Identifier –Individual (HPI-I) to enable access to digital health records.
The call follows Healthcare Identifier amendments passing the House of Representatives in September 2025, making self-regulating allied health professionals eligible for an HPI-I.
Ms Leanne Emerson, AudA CEO, said it strongly recommended all audiologists apply. “Without this identifier, audiologists won’t be able to access My Health Record and gain access to the digitalisation of the health care system,” she said. “This change ensures audiologists are recognised alongside other allied health professionals within Australia’s national digital health infrastructure.”
Audiologists should not wait until regulation, she said.
“Having a HPI-I now ensures audiologists can immediately access My Health Record and participate in national e-health programs. Waiting would mean missed opportunities for patient care and professional recognition.
AudA said it would provide guidance on application steps to members. Practitioners need proof of their profession (their AudA membership certificate from the AudA member hub), personal identification documents, and should link details if they work for an organisation with a Healthcare Provider Identifier-Organisation (HPI-O) number.
Healthcare Identifiers are 16-digit numbers assigned to patients, healthcare providers, and healthcare provider organisations to enable connections across healthcare settings.
Above: Opal Sandy pictured at a younger age with her parents Jo and James. Image: Cambridge University Hospitals NHS Foundation Trust.
MRFF FUNDS $4 MILLION HYDROGEN PEROXIDE OM TRIAL, USHER SYNDROME TREATMENTS
Innovative research, including a trial investigating hydrogen peroxide for otitis media, and a project to grow inner ear tissue from patient stem cells to test new treatments for Usher syndrome, has received federal government funding.
The research is among eight hearing related projects that received funds from the Medical Research Future Fund.
The Department of Health, Disability and Ageing updated a report on grant details on 24 September 2025.
The otitis media trial involves using hydrogen peroxide for persistent chronic suppurative otitis media (CSOM) in First Nations children. Funding of $4.2 million will allow researchers to compare topical hydrogen peroxide followed by the topical antibiotic ciprofloxacin, with ciprofloxacin treatment alone, to manage CSOM that has failed to resolve with standard treatment.
“It’s time to test a cheap,
frequently recommended, antiseptic treatment for the most severe form of middle ear disease CSOM,” said chief investigator, Dr Jemima Beissbarth from Menzies School of Health Research.
“CSOM is the most severe form of middle ear disease, characterised by a hole in the eardrum, through which discharge drains (for longer than two weeks). It disproportionally impacts children living in low socioeconomic conditions, including remote-living First Nations children.”
Other grants are for:
• Usher syndrome: A UWA and Lions Eye Institute project to grow inner ear tissue from patient stem cells to test new treatments for Usher syndrome.
• D ementia care at home: A University of Queensland home hearing and vision care project to improve quality of life for those with dementia and carers.
the trial.
• D ementia care in aged care: The University of Queensland SENSEcog aged care project focusing on hearing and vision support to improve quality of life for people with dementia in residential aged care.
• E arGenie for infants: A Bionics Institute innovation for earlier intervention for infants with auditory neuropathy, providing lifelong benefit.
• O lder Indigenous people: UWA research understanding hearing loss to address health needs of older Aboriginal and Torres Strait Islander people.
• O titis media pathways: A Macquarie University case-study approach to improving care pathways for otitis media in Aboriginal children aged up to 12.
• O vercoming racism: The Systematically and Together Overcoming Racism Model will co-design a framework aiming to reduce racism across the hearing health sector.
NOMINATIONS OPEN FOR 2026 ENDEAVOUR AWARDS INCLUDING NEW HEALTH AWARD
Nominations are open for the 2026 Endeavour Awards, Australia’s premier celebration of excellence and innovation in manufacturing and, for the first time, the healthcare sector is included.
Innovators in Australia’s healthcare and hearing care sectors are invited to nominate for the new Innovation in Healthcare Technology Award which recognises technologies that improve healthcare and medical manufacturing.
This category is for companies developing innovative health solutions, including medical devices, digital health platforms, biotechnologies, and pharmaceuticals.
Eligible technologies must have undergone advancements within two years before nominations close on 13 February 2026.
Products and technologies must be manufactured and/or commercially available in Australia. Nominees may also be eligible for the Manufacturer of the Year Award chosen from the winners of the other awards categories. This
organisations who are driving Australian manufacturing forward. They are presented annually by M anufacturers’ Monthly magazine and website published by Melbourne-based company
Prime Creative Media, a trade media and events company that also publishes Hearing Practitioner Australia.
Winners will be announced at a gala dinner on 13 May 2026 during Australian Manufacturing Week in
Brisbane. The event is recognised as the manufacturing industry’s night of nights, bringing together leaders, innovators, and rising stars to celebrate success, share stories, and connect with peers shaping the future of Australian manufacturing. Companies and individuals from across the hearing care sector are invited to submit their nominations and showcase the projects, technologies, and people making an impact on the industry’s growth and resilience. Visit endeavourawards. com.au to learn more and submit an entry.
Dr Jemima Beissbarth is leading
Image: Jemima Beissbarth.
The 2024 Endeavour Awards ceremony. Image: Prime Creative Media.
Fifty years of changing lives
Expression Audiology has celebrated its 50th anniversary with a commemorative event in Melbourne. Guests heard that the teachings of its predecessor, H.E.A.R Service, became foundational concepts in hearing rehabilitation and skills that audiologists are taught nationwide.
When the late Mrs Patricia Pengilley and Mrs Kathleen Herron, both teachers of the Deaf, co-founded the Hearing Education and Rehabilitation (H.E.A.R) Service in Melbourne in 1975, little did they know the impact it would have on the rehabilitation of generations of people with hearing loss.
The pioneers established the service for people with acquired hearing loss who had lost their hearing later in life. Few resources existed at that time for this growing segment of the population.
The story was revisited at Expression Audiology’s 50th anniversary celebrations on 15 October 2025, when former and current staff, family members, board members and others from the sector attended the golden jubilee event at the organisation’s new Collingwood headquarters.
The milestone represents the founding of Expression Audiology’s predecessor, the H.E.A.R Service in Melbourne which came under the umbrella of Expression Audiology in 2018.
Expression Audiology is part of Expression Australia which was established in 1884 as the Victorian Deaf Society (Vicdeaf). In 2018, Vicdeaf’s services rebranded to become Expression Australia although it still legally operates as the Victorian Deaf Society.
At the event, Kathleen Herron told guests: “It’s really special to see so many people here today including people we’ve known over the years and worked with, and to see how the organisation has moved with the times; I’m so glad I was able to be a part of it. It’s a special place today, a
wonderful plan and architecture.”
Earlier in a video reflection, she recalled that her father was a teacher at the NSW School for Deaf Children when she was a child. She would often go with him and was looked after by the older children. She also met Patricia Pengilley who was a teacher at the school.
“I loved all the contact I had with the deaf community; I saw what my father did and how happy he was, so I became a teacher of the deaf too,” Herron recalled.
Twenty years later, when at home with her two young daughters, a car pulled up and out stepped Pengilley, armed with a proposition.
“Pat said, ‘I’m starting a service for people who were born hearing but lost their hearing later in life. There’s really nothing here for them – they’re being told to buy a hearing aid and they’ll be right,” she recalled. “We chatted for ages, and it sounded really exciting.”
Pengilley had been running courses solo but after her visit, the couple approached the Victorian Deaf Society (Vicdeaf) and started running community education courses onsite. They began outreach into the community where people with hearing loss were, educating about assistance aids. They spoke to ENT specialists and people selling hearing aids, advising there was more to communication than hearing aids.
The pair knew there were good programs overseas and Pengilley received a Churchill Fellowship to go to Sweden to study some. A Hospitals and Charities Commission grant in 1972 helped establish their own service with a receptionist, teachers and nurses.
ASSISTED LISTENING DEVICES
These community educators went into the community and gave talks on devices such as amplified telephones, loop systems, systems to hear the television better, baby cry alarms, smoke alarms and special doorbells for those with hearing loss.
In 1975, a $3 million government grant enabled them to establish H.E.A.R Service to run courses and provide education soon after The University of Melbourne audiology course started.
“Patricia had a lot of input into that, and we had students come to us,” Herron said. “We employed the first audiologist to graduate from Melbourne Uni which was amazing. The grant money enabled us to build a sound treated room and a devices room where people could see assisted listening devices.
“I loved my time at H.E.A.R Service. Patricia was an amazing woman; she had the vision – I could work with her to help get that vision into operation – but I didn’t have that vision she had; she was determined.”
Patricia Pengilley’s daughters, Ms Penelope Pengilley, Ms Sara Timms and granddaughter Ms Florence Stewart, attended the recent celebration. Penelope’s video reflection revealed her mother was born in India, where she trained as a teacher and taught at a school for deaf children before returning to Australia to teach lipreading for the Australian Association of Better Hearing.
Later, on her husband Cecil’s sabbatical in Bangalore, a nun asked her to set up a school for deaf children which she did.
“During this time in 1968, she wrote the
Guests clapping in Auslan at the golden jubilee event.
book, By Word of Mouth coordinated approach to aural rehabilitation, which pulled together ideas she had about communication, working with people with acquired hearing loss and their family and colleagues,” her daughter said.
It suggested how to come to terms with hearing loss and explained tinnitus and potential treatment.
After she co-founded H.E.A.R Service, it was recognised as Community Educator of the Year due to its extensive outreach into communities and helping teach people how to deal with hearing loss, Penelope said.
“Everything had to be just right; the level of commitment she had for her clients was remarkable, the awareness she helped create, and encouragement of good communication skills in the community,” she added.
KEY MILESTONE
Lawyer, Ms Rebecca Adam, the first Deaf CEO to lead Expression Australia, said the anniversary was a key milestone, representing half a century of people connecting with sound and developing their confidence to connect to community.
“It’s also half a century of care, compassion, guidance and support for thousands of individuals to access the pleasure of being able to hear,” Adam said. “The 1970s was a bold and visionary time and that drive continues today.
“Access to community from a small clinic has grown to a trusted audiology service in Victoria and Tasmania, and in future it will become a national service.”
She paid tribute to its “exceptional audiologists”, innovations and “remarkable founders and pioneers of the service”, Patricia Pengilley and Kathleen Herron.
“The stories we hear and the smiles on our clients’ faces are testament to that legacy,” Adam said. “The work all Expression Audiology staff do, and their expertise, empathy and dedication have transformed lives. Thanks also to clients and families for trusting us; you’re the reason we do what we do.”
While audiology was a key component of what Expression Audiology provided, it also offered advocacy, information, interpreting, awareness programs and community support. “I hope the next 50 years continues to be innovative, enhancing communication for all, regardless of their level of hearing loss,” Adam said.
“Expression Audiology is led by Jenna Turner, head of audiology, senior audiologists Gloria Lee and Matt Grounds, and audiologist Evita Elango, who have done an extraordinary job of providing warmth and professionalism in everything they do.”
Turner reviewed its successes at the event and thanked clients whose support and loyalty had kept it going. “I’m so proud to work in an organisation which truly champions diversity,” she said. “It’s not just 50 years of Expression Audiology,
audiology practice rooted in the principles of empowerment, partnership and communication.”
FOUNDATIONAL CONCEPTS
A unique audiology service, it sat alongside the deaf and hard of hearing community, and was a visionary organisation with accessibility at its heart, she added.
“Pat and Kathleen’s work employing the first Melbourne Uni audiologist, educating the public on acquired hearing loss, running courses and information sessions on how to communicate and general communication skills were foundational concepts in hearing rehabilitation,” Turner said,
“They are now skills that audiologists are taught at university, and they championed these concepts. Patricia had the concept and the courage while Kathleen the connections and the knowledge of how to put these in place. One would not have existed without the other.”
Turner said Expression Audiology had a valued partnership with Word of Mouth Technology whose founders, Mr Bob Willis and his wife Betty, had pioneered assistive listening devices (ALDs) such as baby cry alarms and doorbell alarms. This legacy lived on through its Victorian and
“ They put ALDs in the space of audiologists and made them think about holistic care and the whole person, not just their ears and hearing,” she said.
In the 1990s and 2000s, the legacy of classes, public education, hearing screening and reduced price hearing aids continued, Turner said. In the 2010s, former CEO Ms Gina Birch expanded the audiology clinic to Oakleigh while East Melbourne and Box Hill clinics were refreshed. All clinics featured ALD displays and in 2008 a booth at Highpoint Shopping Centre offered free hearing screening. In 2011 Mr Matthew Grounds took the audiology leadership role. “He brought about great change and innovation and without it we wouldn’t be here today,” Turner said. “This encompassed the Hearing Services Program, the NDIS, opening a Geelong office, and expanding home assisted tech sessions." Turner said it was a legacy to learn from and be proud of.
“Our clients have also had a big role in this legacy; it’s a shared milestone,” she said. Fittingly, Pengilley and Herron have clinical rooms named after them at Expression Audiology. While their names and legacy will live on regardless, it’s a nice nod to two pioneers who helped change the face of hearing rehabilitation.
(From left) Expression Australia CEO Rebecca Adam, H.E.A.R. Service co-founder Kathleen Herron, Expression Audiology head of audiology Jenna Turner.
(From left) Patricia Pengilley and Kathleen Herron when they founded H.E.A.R Service.
Otitis media: breaking down the barriers
For otitis media in Australia, there’s an abundance of research and prevention activities, education, and management and treatment options. While there’s a long way to go in the fight against this pervasive condition, progress is being made. HPA examines some wins and innovations.
By the time an Australian child turns two, they’ve usually mastered a bunch of quintessential toddler milestones: wobbling into confident steps, perfecting the art of the tantrum and discovering the magic of playground slides. They’ve tasted their first choccy milk, learned to say “no” with gusto, and left a trail of half-eaten snacks throughout the house.
But there’s another milestone – far less charming – yet almost as universal. Most children will experience at least one middle ear infection, or otitis media (OM) episode, before blowing out their second birthday candles, according to the Australian Institute of Health and Welfare. And while it’s common, its impact on hearing, learning and quality of life can be anything but trivial.
One in four suffer repeat infections – recurrent or persistent OM – and for Aboriginal children, the figure increases to nearly one in two. This often results in hearing loss, requiring antibiotics and grommet surgery to insert tiny ventilation tubes and drain fluid from the eardrum. ENT surgeons perform about 35,000 grommet procedures a year in Australia to reduce risks of eardrum perforation, infection and improve hearing.
Indigenous Australian children have some of the highest rates of OM in the world, with prevalence in some remote communities reaching up to 90%. As a result, about 40% of Indigenous children aged 7–14 in remote areas have hearing loss, compared with 31% in regional areas and 23% in cities.
Overall, about 43% of First Nations people aged seven and over have hearing loss. Tragically, for some whose OM remains untreated for long periods, the damage
is lifelong with permanent hearing loss requiring hearing aids, hearing implants or cochlear implants.
One organisation that’s had phenomenal success in reducing incidence and harm from OM is Earbus Foundation of Western Australia. Its model has listened to community and is based on multidisciplinary teamwork.
In 12 years, Earbus has delivered more than 100,000 occasions of care in some of the remotest communities in WA. Its staff see about 10,000 children a year.
The difference the program has made is immense. “Our stats are unbelievable,” says co-founder, audiologist Dr Lara Shur, recently nominated for an Australian of the Year Local Hero Award for her tireless work.
“Once our program starts in a community, it takes between nine and 18 months, and rates of otitis media will drop.
“Some communities have been as high as 60%, 70%, 80% but rates of chronic suppurative otitis media (CSOM) have dropped after our visits to below the World Health Organization benchmark of 4% - a rate the WHO determines is a public health emergency.”
REDUCED CSOM RATES
CSOM is a persistent infection of the middle ear characterised by a perforated eardrum and continuous or recurring ear discharge (otorrhoea.)
“Earbus has helped to reduce rates of otitis media in 200 communities in remote WA,” Dr Shur says. “This is evidence that our program works.”
South African-born Dr Shur previously worked at the world’s third largest hospital, Chris Hani Baragwanath Academic Hospital in Soweto where she saw many OM cases.
After migrating to Australia, she worked in several audiology clinics in Perth before joining not-for-profit children’s charity, Telethon Speech and Hearing (now TSH), where she enjoyed working with First Nations people.
There she met Mr Paul Higginbotham, former Telethon Speech and Hearing CEO and a teacher of the Deaf. The pair and nurse audiometrist Ms Dee Parker founded the not-for-profit Earbus Foundation.
Earbus staff travel in mini-buses and four-wheel drives to remote communities to check and wash ears, perform hearing tests, diagnose and treat otitis media, and educate
“Studies have also found 90% to 94% of incarcerated adults in the Northern Territory have some form of ear disease.”
Dr Lara Shur Earbus Foundation
Image: Lara Shur.
An Earbus client having his hearing tested.
Image: Earbus.
communities and people unlike anything I've ever seen before. The three of us sat around my kitchen table one afternoon. We’d been talking about this outreach idea and that day, we decided to do it.”
NO WAGE FOR A YEAR
None of the founders received a wage for at least the first year of the organisation.
“Our (life) partners supported us financially and were all involved in the formation of the foundation as they could see we were passionate about making a difference to children’s lives,” Dr Shur says.
“It was 2013 and there were very few services going to community.”
Higginbotham was a pioneer of the model of taking services to communities, she says, and between the three of them, they “found a solution to this problem that had persisted in Aboriginal Australia, which is how to get kids’ ears clean and get them hearing”.
“We went into some communities, and almost every child had discharge full of pus pouring from their ears,” Dr Shur recalls. “Our team had to upskill to wash ears because there was so much discharge.
in Australia, a rich country with infrastructure
Solutions back then were mainly tertiary driven – seeing an ENT after damage to ears and hearing, she adds.
In their first year, the trio did 22 trips to areas such as Kalgoorlie and Port Hedland. They were on the road for more than five months in one car with equipment.
For four gruelling years they were on this conveyor belt of intensive work – flying in, being on the road all week, flying home, doing a week’s worth of paperwork and applying for funding (as the entire service was free for patients) ,then flying out again.
They changed things as they went along – if they saw improvements could be made, they did them. But none of it would have happened without the financial support of donors, Dr Shur says, and other incredible partners including audiologists who loaned them equipment as they had nothing when they started.
“I’d get on a plane and think, ‘I don't know how I'm going to do it this week, I'm so tired’,” Dr Shur recalls. “But come Monday, the first child who walked into the room, we were on it – that was it; we loved seeing those kids.
“We’d regularly take a GP or nurse
Chronic suppurative otitis media with tympanic membrane perforation.
“The kids got to know us, and we could really see the change in children and communities. In one community where we washed ears out constantly for four months, we returned a year later and were lucky if we washed out one ear.”
One GP wrote 28 scripts at a site but when she returned the next year, only wrote two.
“It’s a no brainer. If you take a doctor to a site once a month for a year, kids get better. It’s primary health care, it's not waiting for tertiary treatment,” Dr Shur says. “The children referred to ENT are complex cases or needing surgery.”
CAN’T HEAR, LEARN, EARN
Dr Shur believes otitis media is pervasive because of the social determinants of health; environmental factors in many of these communities keep the pathology high.
“If we can abolish social determinants of health that we know affect children and are parts of the pathology such as poverty, lack of access to housing, water and healthcare, that is a huge part of the answer,” she says.
“We say, ‘can't hear, can't learn, can’t earn’. If you arrive at school and you've got otitis media you don't hear the teacher, your speech and language is delayed, your literacy and numeracy isn't what it should be.
“You don't come out of school with a full education, so you don't get a great job and are more likely to engage with juvenile justice. These are children, not adults, incarcerated with ear disease, and juvenile justice doesn’t allow people to come in and screen hearing.”
One study found many women screened at one of WA’s women's prisons had ear disease or long-term ear pathology, Dr Shur says.
“Studies have also found 90% to 94% of incarcerated adults in the Northern Territory have some form of ear disease,” she says.
Primary prevention through programs such as EarBus aims to help halt these harrowing outcomes.
Earbus undertakes about 80 outreach trips a year and offers services in rural areas and Perth. It also treats adults with
Image: Mikhail V. Komarov/Shutterstock.com.
Earbus co-founder, audiologist Dr Lara Shur, testing a child’s hearing.
(From left) Earbus co-founders Paul Higginbotham, Dee Parker and Dr Lara Shur.
Ears to you! The Goldfields Earbus with co-founder Paul Higginbotham.
Image: Earbus.
Image: Earbus.
Image: Earbus.
“We found Haemophilus influenzae was the culprit associated with the worst otitis media, and people who had it cultured from their nose or middle ear were far more likely to need a second set of grommets.”
an 87-year-old being its oldest patient. “We don’t turn away anyone with ear troubles,” Dr Shur says.
Its permanent staff of six audiologists, five nurses, and a nurse practitioner are complemented by GP and nurse practitioner consultants who do several outreach trips annually. Local ENTs are also accessed wherever possible.
“But we’re only in WA and can’t get to some communities and towns because we don’t have enough funding,” Dr Shur says. “I don't think a month goes by that someone doesn't approach us and say, “I've seen your bus, I've seen your program, please come to us’.”
She believes other states would benefit from similar programs that are locally driven and have community buy-in. “You want local people to take the model and utilise it,” she says. “It is doable when we co-design with communities. They told us they wanted a regular, monthly visit, not every six months, the same people, rather than different ones every time, and they wanted all services to join up.
“They didn’t want to see one professional and wait for weeks to see another. This was across the board, whether in Esperance, the Pilbara or the Goldfields. They said, ‘make it easy for us, make us want to engage and we’ll come’.
“Families love their children; they will do the right thing if we just help them a bit.”
Prof Shyan Vijayasekaran Perth ENT surgeon
The deputy principal of one of the Earbus partnership schools sent Dr Shur an email stating Earbus had made a life-changing difference to the community. “She sees it on a day-to-day basis,” Dr Shur says. “It’s not just the kids who can now hear but the program’s also improved parent engagement at their school.”
VACCINE AND EARFLO
Earbus has also partnered with Griffiths University to partly fund researcher, PhD fellow Ms Ayesha Zayed, who is investigating an otitis media vaccine.
“Surveillance, identification and treatment are great but if we can stop people from getting otitis media, we absolutely should,” Dr Shur says.
Earbus awarded Zayed its Professor Harvey Coates Scholarship named after its clinical patron, “an inspiring man who changed audiology and outcomes across Australia by bringing newborn hearing screening to Australia and WA”.
“Prof Coates was instrumental in bringing the idea behind the Earbus program to Australia from New Zealand,” Dr Shur says.
She predicts the Australian-made innovation, Earflo, will have a big impact on OM. “Those involved with developing it have done an amazing job,” she says “I think it’s going to change otitis media for the world. Ideally, every family would have an Earflo
sippy cup; they’d start with this, and if it didn’t help, progress to a doctor and treatment.
“The cup pressurises through the nose. About 78% of kids who used it in a small Earbus trial improved from type B (OM with effusion) or C (developing infection or fluid buildup) to type A, which is normal.”
Earflo says ENT specialists and biomedical engineers developed the medical device, which is pending US Food and Drug Administration (FDA) approval. As a child drinks from the cup, its soft mask seals under the nose. Earflow senses the swallow and pushes air into their nose. This helps open the eustachian tube, and trapped fluid can flow out of the ear, relieving pressure and helping prevent hearing loss, Earflo says.
SPRITZ-OM
Two other Australian-developed OM innovations are Spritz-OM and Blitz-OM.
ENT surgeon Professor Shyan Vijayasekaran, who has worked at Perth Children's Hospital for 20 years and been involved in OM research for 25 years, is involved in trialling both.
The Curtin University and University of Western Australia Clinical Professor says that, on one hand, much has changed in those two decades, but on the other, little has changed.
“Influenza vaccination in the early 2000s put a bit of a dent in rates of otitis media but only marginally because a lot of bacteria the vaccines covered were replaced by non-vaccine serotypes,” he says.
“Bacteria are smart, they’ve evolved and, like humans, they want to survive. You take one step in their direction, and they move in another. You get a vaccine which kills certain serotypes and another pops up.”
Research he has collaborated on includes studying which bacteria in the middle ear, nasopharynx and adenoids were associated with otitis media.
“We found Haemophilus influenzae was the culprit associated with the worst otitis media, and people who had it cultured from their nose or middle ear were far more likely to need a second set of grommets,” he says.
Further research showed Haemophilus hemolyticus placed on adenoid tissue in the lab displaced Haemophilus influenzae In mice with Haemophilus influenzae -related middle ear infections, this replacement bacteria added to the nasopharynx stopped mice developing OM.
Research microbiologist Associate Professor Lea-Ann Kirkham and paediatric immunologist Professor Peter Richmond from The Kids Research Institute Australia in Perth turned this discovery into the nasal vaccine – Spritz-OM – to prevent ear infections.
It targets the major pathogen responsible for more than 50% of the 700 million annual ear infections worldwide.
“We're now heading into Spritz-OM’s phase one clinical trials in humans,” Prof Vijayasekaran says.
Image Shyan Vijayasekaran.
On the road again with the Earbus.
Image: Earbus.
BLITZ-OM
Other research he’s participating in involves trialling the medicine Blitz-OM given during grommet surgery to help clear the infection and prevent the need for repeat surgery. Blitz-OM was developed by clinical research scientist Dr Ruth Thornton and her team at Wesfarmers Centre of Vaccines and Infectious Diseases at The Kids Research Institute of Australia.
One third of children require repeat ventilation tube insertion (grommets) for OM. Disease recurrence is associated with persistent middle ear bacterial biofilms – slime that protects bacteria, Prof Vijayasekaran says.
The drug dornase alfa (DNase) is used in cystic fibrosis to dissolve biofilm in the lungs and reduce thickness of secretions. In Blitz-OM, DNase is a liquid given during grommet surgery to try to disrupt biofilm in the middle ear. It breaks down biofilm, allowing antibiotics to penetrate and kill bacteria in the ear and the human immune system to attack and dissolve the bacteria.
“The liquid turns into a slow-release gel,” Prof Vijayasekaran says. “Our study using a single dose found the grommet extrusion rate and blockage rate was reduced in the ear of patients who had one dose (versus their other ear, the control ear).” A second study gave DNase for five days but results are not yet in. Further trials are approaching. Other advances on the horizon include grommet guns to enable insertion under local, instead of general anaesthetic.
Perth has extensive waiting lists for grommet surgery which Prof Vijayasekaran says is due to insufficient theatre time as every speciality is competing for operating theatres. While category one surgery is always within a month and category two within three months, category three surgery waits have blown out to 12 months, he adds. Prof Vijayasekaran says risk factors for OM include not being fully vaccinated, genetics, and daycare attendance. The ideal is smaller daycares, better ventilation, hand hygiene, and enforcing non-attendance for sick kids, but he agrees these are hard to achieve. However, he says progress is being made.
Dr Shur adds: “There is so much hope for children, that's the exciting part. The ideal is
Otitis media guidelines update
Work is underway on an update to otitis media guidelines which will include new treatments, says audiologist, Ms Sally-Anne Regan, Hearing Australia’s head of community services.
The Otitis Media Guidelines for Aboriginal and Torres Strait Islander Children 2020 were developed by experts in the field of ear and hearing health.
Regan says other good news includes more audiologists now have access to the portable Visually Reinforced Orientation Audiometry (VROA) hearing test that Hearing Australia and its research division, the National Acoustic Laboratories (NAL) pioneered.
Since 2019, Hearing Australia has run HAPEE (Hearing Assessment Program Early Ears) providing free services nationwide to First Nations children aged six and under.
Regan says HAPEE, which is an initiative of Hearing Australia and funded by the Australian Government, is vital, with more than 10,000 children in over 300 metropolitan, rural and remote locations accessing hearing services through the program each year. Recent analysis of its data found more than 26% of children it assessed have undiagnosed ear disease and one-in-five have undiagnosed hearing loss.
Additionally, 8% have persistent ear trouble and these are the ones who are most at risk. She says Hearing Australia works with surgeons, community controlled, and state and territory health services to develop and implement treatment pathways to minimise the time these children experience ear disease and hearing loss.
A further 35% have fluctuating ear disease where otitis media changes over time and need ongoing monitoring as they may progress to chronic disease.
“According to our data, these percentages have not shifted significantly over the past six years,” Regan says. But Hearing Australia isn’t seeing a high rate of perforations, she says, and believes this reflects a change in disease patterns from the more severe chronic suppurative otitis media – associated with perforations – to otitis media with effusion or glue ear.
“Both problems require specialist attention,” she says. “OME can be treated successfully at an early age whereas repair of perforations is not usually undertaken until the child is at school. Assuming
children have access to the required ENT treatment, early identification can reduce the amount of time spent with hearing loss and its effects on development.”
Hearing Australia works with communities to design services to meet local needs. Through HAPEE, Hearing Australia’s team has supported the upskilling of more than 1,000 health workers in hearing health.
Additionally, the PLUM (parent-evaluated listening and understanding measure) tool, developed by NAL, is available to everyone. The questionnaire helps early childhood educators and health workers ask parents about their child's listening behaviours to help identifying kids likely to have long term ear and hearing trouble. Hearing Australia can train health practitioners who wish to use the tool.
“Hearing Australia is striving to halve the rate of hearing loss in Aboriginal and Torres Strait Islander children by 2029,” Regan says. “This is an ambitious goal and one that we cannot achieve on our own. Through HAPEE, we’ve taken important first steps towards this by raising awareness of the need for early identification and treatment and by working with our many partners to streamline and strengthen referral pathways.”
The HAPEE program also integrates with Hearing Australia’s rehabilitation services, ensuring timely provision of amplification devices whenever required, Regan says.
“Reduction in the rate of chronic disorders is going to take time, but we believe that by 2029 there should be significant improvements," she says. "We’ll continue to work closely with our many amazing partners to improve the ear and hearing health outcomes of First Nations children.”
Image: Hearing Australia.
Ayesha Zayed is investigating an otitis media vaccine.
A Hearing Australia team member performing a hearing check.
Image: Hearing Australia.
Image: Griffiths University.
Becoming a Doctor of Audiology
The Post-Professional Doctor of Audiology Program from America’s A.T. Still University is gaining momentum with audiologists from Australia and around the world seeking to elevate their expertise and develop new skills.
Confidence is one of the biggest benefits Tasmanian audiologist Dr Heidi Modrovich gained from studying for her doctorate of audiology online at A.T. Still University (ATSU). That, along with gaining new skills and knowledge in clinical practice, have helped transform her career.
“It's given me a new lease on life as an audiologist and a professional confidence that I didn't feel before,” she says.
Dr Modrovich put her newfound knowledge into practise while studying the program and has found it immensely helpful since graduating. “As I was learning, I was updating protocols in the clinic,” she says.
“For example, I had more structure to talk to clients about the latest tinnitus treatments and ideas on what treatments were good.
“Beyond knowledge gained, the doctorate helped me step into my confidence as a clinician. It gave me the foundation to handle different cases, know my scope, discuss
theories with patients, and find the research I need. I’m backing myself now – the program gave me the vehicle to get there.”
Previously based in Melbourne, Dr Modrovich moved to Tasmania with her audiologist husband Nick in 2007 to take ownership of AudioClinic Hobart due to its owner’s retirement. She completed her MBA and had two children while expanding to seven clinics statewide. After 10 years, the clinic was sold to Oticon Australia and in 2017, the Modrovichs established Ability Hearing and Balance in Hobart, which now includes a Launceston clinic and outreach services. “I’d always wanted to do the audiology doctorate,” she says. “I was impressed with the ATSU website and course subjects.
“The second time around setting up our clinic, we didn't want to just focus on hearing aid rehab, we wanted to work to our full scope. Nick was passionate about vestibular
Left: ATSU Australian alumni, current students and staff at an Independent Audiologists Australia conference in Queensland, (L-R) Dr Heidi Modrovich, Dr Signe Steers, Melanie Gibson (ATSU), Rachel Gibson, Nicole Eglinton and Colleen Campbell.
testing, and with my psychotherapy background and being a tinnitus sufferer, that was a major interest for me, along with auditory processing testing and auditory training.”
WORLD CLASS EXPERTS
Dr Modrovich didn’t feel she had a solid grasp of those areas from her university training of 25 years ago. “For my ATSU electives I chose auditory processing disorders, tinnitus and implantable devices,” she says. “The subjects were great because I received in-depth knowledge into the latest evidence-based practice such as new tinnitus protocols and I can now confidently create a tinnitus protocol for my clinic. The program’s world class and we’re taught by experts in each field.”
She mostly studied on weekends and says having a supportive husband and independent teenage children helped.
The program is designed so students can study around working and family life. “It’s doable and interesting because it's directly related to what you see in the clinic,” she says. “While I was studying neuroimaging, patients were showing me their MRI or CT, and I knew how to look at them which keeps you motivated.
“Lectures are recorded and it’s well-structured because you watch them in your own time. There are class discussions (on noticeboards) where you write your opinion and research. Your peers respond in a time that suits them to facilitate class discussions.”
Assignments are short or long papers, and there are multiple choice open book quizzes. Organisation is critical when balancing many commitments, so when going on holidays, Dr Modrovich ensured she was on top of things in her course beforehand.
She found it interesting learning about audiology in other countries from classmates and another highlight was going to the ATSU health sciences campus in Arizona to graduate. Her husband is now undertaking the program, as is Brisbane audiologist Ms Rachel Gibson who started in July 2025.
BOOST FOR COMPLEX CASES
Rachel, founder of All Ears in Hearing, was inspired by friends and colleagues who achieved the audiology doctorate. “They all said how much benefit they got out of it, that it improved their knowledge, and gave them that extra confidence in managing complex cases,” she says. “I see many complex cases and thought it’d level up my knowledge as it’s been 25 years since I was at uni.”
Rachel, president of Independent Audiologists Australia (IAA), has many
Image: IAA.
performs a lot of auditory processing tests. “I want to ensure I give those patients, and all my clients, the best service I can,” she says.
She studies nightly and at weekends to reach the recommended 12 hours weekly.
“Having lectures recorded is really good as you can pause it if you didn't quite understand something, rewind it and listen again,” Rachel says. “You’ve got time to write notes, and can adjust the timing to speed it up or slow it down.”
She also likes the variety – lectures with course lecturers, readings, quizzes and discussion boards which foster connection and a sense of belonging. “You’re given a topic to write about, post it on a discussion board, colleagues respond and it’s interesting because on some topics, such as ethics, students raise issues you might not have thought about,” she says.
ETHICS MANUAL
Rachel is already putting into practise what she’s learning; an ethics manual she compiled for the core ethics subject is being used by her staff. She’s found it’s enhanced her critical thinking; for example, studying the core neuroscience subject is making her think more critically about her tinnitus and auditory processing patients.
“I think about things in a different way and at the end I’ll have increased confidence to handle more complex cases,” she says. “There were many interesting electives to choose from; I chose tinnitus, cochlear implants, vestibular management, and auditory processing.”
A fully online course was a key reason for choosing the program, so she could study around running her business, practising and family life. “Because you can do it in your own time it’s easier than driving somewhere or attending a lecture at a set time,” she says. “I was nervous at first because two years is a big commitment but I'm glad I’m doing it now. The staff understand most of us are working, have families and are busy. The biggest thing is to communicate if you’re struggling, or something’s come up and you need more help or time.”
If people want to test the waters before committing to the full program, there’s an
unsure about committing, trying one subject can help. IAA members receive a 20% discount on non-degree seeking courses.
For more than two decades, the Post-Professional Doctor of Audiology Program has helped audiologists worldwide advance clinical and leadership skills. Program manager and instructional designer Ms Melanie Gibson, who has been part of the program since its early years, says alumni also qualify for this tuition discount.
Having received her own Master of Arts (teaching) degree online while balancing work and raising young children, she understands firsthand the importance of flexibility and support. Melanie serves as the first point of contact for students, guiding them through initial weeks and remaining a consistent source of assistance until graduation. She can meet via Zoom if there are questions or students feel overloaded.
“The biggest thing is communication with instructors or the department because we'll work with you,” she says. “My goal is to ensure all courses are top level and offer enough variety to meet students’ diverse needs”.
She regularly reviews student feedback to ensure the program stays current and valuable. There are 26 subjects and each student’s academic degree plan includes 12 to 18 courses (subjects) with course materials frequently updated to reflect emerging trends and technologies. Lectures are pre-recorded, and there are transcripts and PowerPoints for easy access. “We’re constantly exploring new topics such as artificial intelligence, how to use AI ethically in your practice and how it’s being integrated into hearing aids,” Melanie adds.
COMPREHENSIVE CURRICULUM
The program features four core subjects; ethics (professional roles and responsibilities), neuroscience and neuroimaging (foundational skills), global
health care and audiology (learning about audiology in other countries), and culminating case experience. “The case experience enables students to synthesise what they've learnt by presenting or writing up a complex patient case, based on a course they’ve taken. They demonstrate how they'd diagnose, treat and counsel within real-world clinical contexts,” Melanie says. “There are clinical and business electives including how to open a practice and marketing. Another unique subject, pharmacology, studies the relationship between medication and the auditory-vestibular system. A pharmacologist teaches initial weeks and an audiologist covers ototoxicity. One valuable aspect is peer learning. “Students realise others face similar challenges and share how they handle them,” she explains. “Our exit interviews consistently show how much students value connecting with audiologists from around the world and learning new approaches and perspectives they hadn’t considered before.”
Many instructors are alumni, sustaining a strong global community dedicated to advancing the field. Australia has seen significant growth due to word of mouth and the program's reputation, with 21 students and 18 graduates. “Our graduates love the program and share their experiences," Melanie says. "We love our Australian students; they bring enthusiasm and positivity and have been a wonderful addition to our global classroom.”
For more information, visit atsu.edu
Above: Dr Heidi Modrovich (second from left) at her graduation in Arizona with ATSU colleagues.
Above: Rachel Gibson studying online.
Image: Rachel Gibson.
(From left) At the IAA gala dinner are Dr Signe Steers, Dr Heidi Modrovich, Nicole Eglinton, Melanie Gibson from ATSU, and Rachel Gibson.
Image: IAA.
Image: Heidi Modrovich.
SENTIO: The smallest transcutaneous hearing implant
Oticon Medical’s first active transcutaneous bone anchored hearing system – the Sentio System – launched in Australia in August 2025. Audiologist KATHRYN DARK and business unit manager TRACEY KING reveal the benefits of the new hearing implant and outline funding options.
More audiologists could present the option of a bone anchored hearing system (BAHS) to patients especially as wider candidacy and sophisticated systems nowadays mean additional patients can benefit.
This is the view of Ms Kathryn Dark and the leading hearing implant manufacturer she works for, Oticon Medical.
“The onus is on audiologists to give people the best options, and not just offer hearing aids or cochlear implants,” says Dark, Oticon Medical’s clinical sales specialist for Queensland and South Australia. “Bone conduction implants can be life changing for these patients.”
Despite the benefits, increased patient awareness and education are needed among Australian hearing practitioners and the public, she says.
Ms Tracey King, Oticon Medical’s business unit manager ANZ, believes offering comprehensive solutions can attract more patients to audiology clinics. Apart from financial benefits of increased patronage are positive recommendations about a practitioner who goes the extra mile to offer everything.
“If you want a practice that makes a point of difference, it’s all about providing good service and all options,” she says. “Every audiologist should know about these solutions, the difference they make to people's lives and be offering them to the right candidates because they can be a game-changer.”
TRY BEFORE DECIDE
One great advantage of BAHS is that potential clients get to try before they decide. Wearing a soft headband with a sound processor indicates beforehand what their hearing would be like if they had implant surgery.
It’s quick and easy for audiologists to set up using a demonstration device that Oticon Medical provides for the pre-operative trial, says Dark.
“While giving patients a good indication of what their hearing would be like with an implant, it also forms part of the candidacy assessment,” she says. "Candidates who go on to have surgery experience greater improvements in sound compared to the softband trial because the system transmits vibrations directly to the bone.”
Oticon Medical has always made this option available to patients considering implants, and to those people who prefer utilising the softband only. Now the company is providing even more choice through its revolutionary new Sentio System.
The Sentio is a transcutaneous active bone conduction implant system with the implant fully implanted below the skin. The only external part is the sound processor.
“Sentio delivers the proven benefits of our Ponto System, but in a transcutaneous option,” explains Dark.
“The Ponto is a percutaneous implant system that uses a small implant and connecting abutment for leading or transmitting vibration to the bone.”
While the sound processor clips onto the Ponto’s external abutment, the Sentio sound processor is magnetically attached behind the ear. Both vibrate the temporal bone, which stimulates movement of fluid in the cochlea, facilitating hearing.
INDUSTRY LEADING FEATURES
Key features of the Sentio System include the Sentio Ti implant which is placed under the skin. Oticon Medical says it is the smallest transcutaneous implant available, being 28% smaller than alternatives.
It combines with the Sentio 1 Mini – the slimmest, smallest and lightest transcutaneous sound processor which the company says is 26% lighter and 12% smaller than alternative devices available on the market today.
The Sentio has the same very wide frequency bandwidth as the Ponto, from 200 Hz up to 9,500 Hz, making it the widest bandwidth for any transcutaneous implant,
Dark adds. It also has a 360-degree sound experience.
“Wider bandwidth means better sound quality, especially for music appreciation and speech discrimination in noise,” Dark says.
The sound processor is held over the implant by a magnet, and its light weight means the processor is more likely to stay in place even in active situations. There’s also less pressure against underlying skin.
The processor has a 60-hour average battery life, can connect through Bluetooth to mobile phones and is compatible with a range of wireless devices, Oticon Medical says.
The Sentio 1 Mini provides as close to natural hearing as possible including high frequency sounds, the company adds. It uses innovative noise reduction technology – OpenSound Navigator – to deliver “remarkable sound quality and speech understanding”, adapting to the environment. Additionally, the OpenSound Optimizer stops audible feedback before it occurs, Oticon Medical says.
Dark says feedback has been positive from audiologists and ENT surgeons who attended roadshow launches across Australia.
“Everybody was rather excited by it as soon as they saw it. The big point of difference is the size of the implant – it’s much smaller and thinner,” she says.
“This gives surgeons greater flexibility in placement so they’re more likely to place the implant in the ideal position. This means the external sound processor is also in the
Above: The Sentio Ti implant is 28% smaller than alternatives, says Oticon Medical.
ideal position behind the ear. ” Additionally, microphones are in the ideal position, producing the best sound quality, she adds.
The size and weight of the sound processor is not only aesthetically pleasing, Dark says, but aids comfort.
CANDIDACY HAS BROADENED
She believes the Sentio will revolutionise hearing implants. “One system does not replace the other, but certain people might be better candidates for Ponto while others are better candidates for Sentio,” she says.
BAHS is suitable for patients with conductive or mixed hearing loss, single-sided deafness, or sensorineural hearing loss. It’s also an option for those with medical contraindications to air conduction hearing aids such as those with allergies to device materials, skin issues including psoriasis or eczema in the ear, ear canal stenosis or ear infections.
In particular, Sentio is suitable for candidates with thinner bones, poorer osseointegration or thinner skin. Ponto has the largest fitting range of any bone anchored hearing system.
Dark says more awareness and education are needed for Australian hearing practitioners and the public about this option.
Ponto surgery can be done under local anaesthetic if people cannot tolerate general anaesthesia in as little as 15 minutes, and Sentio surgery is typically done in under an hour, she says.
AUDIOLOGIST ROLES
“We have a way to go in Australia, with awareness around bone conduction devices and implants, and how easy it is to work with bone conduction devices,” she adds. “If an audiologist can fit a hearing aid, they can fit a bone conduction device.
“They’ve come a long way in the past 15 years, thanks to innovation from Oticon Medical. They have sophisticated sound
Audiologists play a key part in candidacy assessment by presenting options and helping patients choose an implant. This is based on communication and lifestyle goals and clinical suitability in discussion with the ENT surgeon.
Fitting the sound processor post-surgery is less intense than for a cochlear implant, Dark adds, and more akin to fitting an air conduction hearing aid. Patients require yearly checkups for follow-up and adjustment.
“To use a bone conduction implant system the inner ear hearing must be quite good, so speech testing is needed to confirm this,” Dark says. “Speech testing by an audiologist indicates whether a patient would be a bone conduction implant candidate.”
Audiologists can contact their local implant clinic or Oticon Medical to help explore if their patient is a good candidate.
FUNDING OPTIONS
King says the team is working to get Sentio on the prescribed list for private health funding in 2026. Private health insurance covers the cost of the system if it's on the prescribed list although other hospital fees may be out of pocket, she says. Health insurance can also cover sound processor upgrades – important for new technology.
In the interim, patients with the right level of health insurance can access the system through ex gratia applications. The Oticon Medical team can provide support in this application process, King says.
Oticon Medical has also been working with Hearing Australia to achieve support for Sentio sound processors for public patients who are eligible. “The Ponto is on the prescribed list and is supported by Hearing Australia which fits Pontos largely on a soft
and other public hospitals may fund both, she adds.
For public patients, it depends on each state and its support and funding in public hospitals for bone anchored hearing systems, King says.
“Some states have no dedicated public funding for bone anchored hearing systems,” she says. “It just depends on the state, the hospital, surgeons and audiologists who work in public hospitals to be able to motivate for why they need it.”
Public hospitals may require paperwork and applications, Dark adds, and while the NDIS provides funding towards sound processors, the process is complex.
HELP WITH PAPERWORK
The business unit and the Oticon Medical clinical team, which has good success with private hospitals and health funds, help audiologists with the trial process and paperwork. The unit also supports ENT surgeons, operating room teams, hospital central sterilising departments and teachers.
“We can provide the product to trial, be there for the trial, train audiologists on the software which is simple to use, and support them getting comfortable with bone anchored hearing if they haven't worked in that sphere,” King says.
Sentio launched in New Zealand, the US and Europe last year where it has had very good traction, Dark says.
“For patients who are candidates, bone anchored solutions make a world of difference,” King adds. “You just have to hear some of the patients’ stories – they truly change people's lives.”
For more information, visit oticonmedical.com/au
A patient during a Sentio sound processor fitting. A safety line from the processor to clothing reduces risk of loss or damage.
Images: Oticon Medical.
Outstanding response to Edge AI
Starkey Australia has received overwhelmingly positive feedback about its Edge AI hearing aids from both patients and audiologists across Australia and New Zealand. This enthusiastic response is largely driven by the device’s top five standout benefits, which continue to set it apart in the market.
“
It’s the first time I have heard well in 20 years,” said the patient, crying. “I’ve never had a pair of hearing aids that work like this.”
This was the emotional comment from an elated Australian client recently fitted with Edge AI hearing aids which were released to the national market ten months ago.
Her audiologist told Starkey: “I had a patient come in for her follow up appointment after her Edge AI mRIC (micro receiver-in-canal) fitting last week. She cried guys! She loves them. Zero complaints!”
Another audiologist asked a patient if she would like to demo the devices. “The patient agreed, I fit them on her and was interrupted mid-sentence,” the audiologist said. “The patient said, ‘Am I supposed to hear this?’, and I said, ‘What do you mean?’ They replied, ‘These are so pure, why haven’t I had these before?
“She took them, and her husband will probably buy a set too.”
These are just two of many positive testimonials Starkey Australia has received after asking audiologists for feedback on what it says is a groundbreaking new platform built to help every degree of hearing loss.
Audiologist Ms Dawn Rollings, managing director of Starkey Hearing Technologies ANZ, says that since launching Edge AI in February 2025, the company has been excited by the outstanding response from its partners
across Australia and New Zealand.
“Our customers consistently report that Edge AI’s natural sound processing and seamless adaptation set it apart from anything else on the market,” she says. “Clients frequently praise the remarkable improvement in speech clarity and how Edge AI makes listening effortless, even in challenging environments.
“With record-breaking adoption rates and exceptional customer satisfaction, Edge AI is quickly becoming the new standard in hearing technology.”
THE TOP FIVE ADVANTAGES
1. The AI
Not all artificial intelligence is created equal, Rollings says, and that’s particularly true of Edge AI’s seventh generation AI technology.
“Like the human brain’s auditory cortex, Edge AI’s G2 Neuro Processor features the industry’s only fully integrated neural processing unit (NPU) dedicated to DNN processing to deliver unparalleled speech
Above (L-R): Clients praise the improvement in speech clarity and effortless listening; Edge AI maintains an industry-leading battery life of up to 51 hours for its RIC RT.
enhancement and noise reduction,” she says.
“We’re the only ones who have the deep neural network (DNN) chip integrated into one neural processing unit which means we can increase features.
“By using this powerhouse, we can mimic the brain and classify speech and speech babble – what we want to hear versus what we don’t want to hear.”
Its sophisticated always-on DNN architecture utilises a speech probability predictor to classify speech 30% more accurately in noisy environments compared to previous technology, Rollings adds.
2. All day wear
Starkey says Edge AI maintains an industry-leading battery life of up to 51
“Our customers consistently report that Edge AI’s natural sound processing and seamless adaptation set it apart from anything else on the market.”
Dawn Rollings
Starkey Hearing Technologies ANZ
hours for its RIC RT (receiver–in–canal rechargeable telecoil) while performing 100 times more DNN processing than its predecessor.
“We're making technology that after five years use will outperform many brand-new hearing aids’ battery life,” Starkey says.
3. Edge Mode+
Wearers can use on demand Edge Mode+ for increased comfort and clarity through the MyStarkey App.
The company says Edge Mode+ is an industry first on-demand DNN-powered noise management and comfort feature. It uses the integrated NPU for fast and efficient processing of the environment, classifying complex soundscapes and using AI to select the best setting based on each sound scene.
4. Future forward connectivity
Edge AI’s superior connectivity features a Bluetooth Low Energy (LE) Audio streaming protocol, which consumes less power and delivers the next-generation connectivity standard.
“Edge AI devices pair more easily, connect more quickly, stream more robustly and are Auracast ready,” Rollings adds.
5. Beyond hearing
Other industry-leading benefits beyond better hearing include activity and social engagement tracking, and a world first balance assessment tool.
Edge AI also continues Starkey's Fall Alert feature, the world's first and only fall detection system onboard a hearing aid.
Edge AI hearing aids are modern, discreet, comfortable and can be used in all listening situations and for people with all levels of hearing loss, Starkey says.
As Starkey’s leader in ANZ, Rollings is proud that local hearing practitioners can now give patients the edge they deserve to hear better and live better.
“Give your patients the competitive edge they deserve; with Edge AI, you’re delivering the very best,” she says.
Clarity, connection, confidence
Other encouraging comments and feedback that hearing practitioners from Australia and New Zealand have relayed to Starkey this year include:
• " My patients are often hesitant about new tech, but Edge AI hearing aids have been a game-changer. The setup is intuitive, and most users feel confident using them after just one appointment. It’s empowering to see them take control of their hearing without needing constant support."
• " The clarity is outstanding. Patients often tell me they’re hearing sounds they haven’t noticed in years – birds, conversations in cafés, even their own footsteps. Edge AI’s adaptive sound processing makes noisy environments manageable without overwhelming the user."
• " Edge Mode+ is a standout feature. I’ve had patients use it in unpredictable environments – windy parks, busy restaurants – and they’re amazed at how quickly the hearing aids adapt. Plus, the Bluetooth connectivity is seamless. Calls, music, even TV streaming, it just works."
• One of the first things my patients ask is, 'Will it last all day?' With Edge AI hearing aids, the answer is always yes. The battery performance is outstanding, reliable, long-lasting, and perfect for busy lifestyles. Whether it's a full day at work or a weekend outing, they don’t have to worry about charging. It’s peace of mind in a tiny device."
One hearing impaired audiologist from Australia, who has worn hearing aids for more than 40 years, said Edge AI was “by far the best hearing aids” she’d ever worn.
“I’d been wearing Genesis AI and was quite impressed with them then I went to the Edge AI launch and tried those,” she said. “I thought, ‘Wow, these are even better’. The performance in noise and superb clarity is what sets Edge AI apart from other hearing aids.
“I don't know how else to describe it, but they’ve got the ‘oomph’. That might not be for everybody but for me, it’s fantastic. It’s a clear, crisp sound; they’ve got guts and presence.
“ The AI and DNN automatically adjust everything; I hardly ever have to use the (My Starkey) app on my phone to make adjustments.”
The audiologist said she fits many Starkey hearing aids, not only because of their quality, but because “the local support is so good”. She hopes to wear her top of the range Edge AI devices for many years.
“My advice to anyone considering buying a hearing aid is to get Edge AI as they will be transformational,” she adds.
Images: Starkey.
Above: The G2 Neuro Processor features the industry’s only fully integrated neural processing unit dedicated to DNN processing, Starkey says.
Right: Edge Mode+ gives increased comfort and clarity through the MyStarkey App.
A hidden gem
Signia has launched the world's first rechargeable custom CIC (completely in the canal) hearing aid with directionality. It’s an innovative addition to its Integrated Xperience platform.
Aworld-first innovation from Signia means people with mild to moderate hearing loss can now enjoy exceptional sound quality and speech clarity – without sacrificing the discreet, invisible design many want in a hearing aid.
For years, people wanting a hearing aid that was invisible had to make a trade-off: subtlety for sound. Now, Signia’s new Insio Charge&Go IX CIC shatters that compromise, bringing crystal-clear speech and superior sound to those with mild to moderate hearing loss – without giving up the discreet, in-ear design they love.
“Patients no longer have to choose between aesthetics and performance,” says audiologist Mr Peter McKinnon, head of commercial acceleration for Signia’s parent company, WSA. “They can finally have both in one product.”
Unveiled across Australia and New Zealand in roadshows in November 2025, the world’s first rechargeable custom CIC with directionality redefines what’s possible in a device so small it virtually disappears.
Previously, this group of patients who ranked the aesthetics and unobtrusiveness of a custom CIC (completely in the canal) as a top priority were said to face
inferior outcomes because of the device’s small size that limited the number of microphones on the hearing aid to one.
Now they can have the best of both worlds – discreet design and superior performance thanks to an innovation in multi-microphone directionality, says Mckinnon.
NO COMPROMISE
“What’s exciting about this hearing aid is that we haven't had to compromise,” Mckinnon says. “It's rechargeable, which gives reliability, ease of use and convenience, but importantly, we’re the first ones to launch a rechargeable CIC with a directional microphone.”
Mckinnon says Signia is focused on ensuring people with hearing loss perform at their best, reflected by its tagline, ‘Be brilliant’.
“ We want our hearing aid wearers to hear well and be confident to contribute in a way that realises their true potential,” he says. “This is only possible if they are comfortable wearing hearing aids.
“Unfortunately, hearing aid stigma is a
major barrier that is impacting people taking the step to receive hearing aids and benefit from them.”
In fact, it’s estimated only 10% of people with mild hearing loss use hearing aids, and research shows a major reason is the perception of hearing aids and the stigma surrounding them, he adds.
“At Signia we’re focused on addressing this stigma through design and throughout our whole portfolio,” Mckinnon says.
“We have products where we've tried to reimagine what a hearing aid looks like and design them to be modern and look like high tech consumer electronics.”
DIRECTIONAL MICROPHONES
Design influences almost half of hearing aid buyers, according to a WSA study from 2024 that found 47% of the market indicated this was their primary consideration when choosing a hearing aid.
The challenge with hidden CIC devices historically was that as these products were so small, there had to be a compromise on performance, Mckinnon says.
“They basically missed out on technology and in many ways, were prioritising small design over performance,” he adds.
“Directional microphones enable wearers to hear better in challenging situations with background noise and are the number one technology to improve speech clarity. But this requires two microphones.”
With standard CIC designs, there was only enough space for one microphone.
“A normal CIC with one microphone will pick up sound all around and give the same level of emphasis or focus,” Mckinnon says.
“Directional microphones will focus on the speaker.”
Directional microphones are a technology for enhancing speech and reducing background noise, especially in noisy environments, by focusing on
Right: The portable rechargeable charger has 35 hours of run time on a single charge.
Signia says its Insio Charge&Go IX CIC is discreet and virtually invisible.
aesthetics but in the past, we've had to compromise on sound quality.”
Even though there is only one microphone for both the left and right hearing aid of an Insio pair, Signia uses an innovative high-speed binaural link between the devices called Binaural OneMic Directionality 2.0, Mckinnon says.
“The hearing aids act as one system using both microphones, creating directionality which provides performance that gives five times the speech enhancement in noise of competitor CIC hearing aids,” he says.
PORTABLE CHARGER
Being rechargeable is also highly beneficial for usability and convenience.
A CIC normally takes the smallest type of battery – disposable 10A batteries measuring 5.8mm x 3.6mm. These can be fiddly to change and especially difficult for older people who may have arthritis and dexterity problems.
“The Insio Charge&Go IX CIC is rechargeable, so clients never have to change a battery,” Mckinnon says. “It has 35 hours of run time on a single charge, so if the wearer charges it overnight, it’s ready to go for a whole day and a half.”
The charger is portable and pocket sized so it can be kept in a handbag or pocket and has its own inbuilt power bank that provides three extra charging cycles.
“If you’re gardening, on a weekend away or camping and you don’t have access to mains power, you’ll have four days of use before you have to charge your power bank.”
An additional quick charge feature of 30 minutes charging provides nine hours and is handy for an emergency charge. A full charge takes four hours and provides 35 hours of run time.
Another benefit of rechargeability is there is no requirement for a battery door; the hearing aid housing is sealed.
This provides a positive effect on reliability by limiting the impact when exposed to moisture and dust. In fact, the Insio Charge&Go IX CIC has a high Ingress Protection (IP) rating of IP 68, meaning it is both dust and water resistant.
CUSTOM COMFORT
Being custom made for each individual ear canal also means an ultra-comfortable fit, Mckinnon adds.
Many people with milder hearing losses are still active in the workforce and socially but it's in those challenging situations where they have the most difficulty.
“When things are quiet, they can manage but in social situations, it’s more difficult,” Mckinnon says. “This is a big innovation for them.”
And it’s also suitable for people with moderate hearing loss, he adds.
It’s virtually invisible as it sits deep in the ear, is tiny, and comes in three colours –dark brown, black and mocha.
CONVERSATION ENHANCEMENT
The electronics are positioned in the shell to deliver the smallest possible hearing aid and the shell is then printed. Turnaround time from impression to delivery is generally five to 10 days, he adds.
The Insio is part of Signia’s Integrated Xperience (IX) platform. The platform is
“It's rechargeable, which gives reliability, ease of use and convenience, but importantly, we’re the first ones to launch a rechargeable CIC with a directional microphone.”
Peter Mckinnon WSA
said to deliver world-class performance in noisy environments via its flagship technology, RealTime Conversation Enhancement (RTCE) available in Signia Behind-the-Ear (BTE), Receiver-in-Canal (RIC) and In-The-Ear (ITE) Styles.
Signia says RTCE is a breakthrough multi-stream architecture enabling wearers to focus on and hear more than one person talking in a noisy situation.
The feature automatically follows and boosts multiple voices, even in noisy places, it adds.
A recent study showed 86% of people performed better in noisy group conversation wearing hearing aids from the IX platform than a top competitor’s hearing aid.
Insio launched in the US in October 2025 to excellent feedback, Mckinnon says.
“People have been wanting this design for a long time, and we’ve noticed how much it’s helped them in terms of performance,” Mckinnon says.
“They want something invisible and aren’t going to accept anything else. Existing wearers of CICs are noticing the vast benefits and improvement w ith Insio.”
Above: The tiny hearing aids come in three colours – black, dark brown and mocha.
Being custom made means an ultracomfortable fit.
Images: Signia.
A monumental achievement
ADF Industries was the mastermind behind 22 new soundproof rooms at Sydney’s MARCS Institute for Brain, Behaviour and Development. Here’s how it executed the project – thought to be the largest installation of audiology rooms at a single location in the southern hemisphere.
When an institute that’s considered a global leader in auditory research relocated to a new building on Western Sydney University campus, one of the biggest challenges it faced was that it was next to NSW’s largest, busiest hospital.
The MARCS Institute for Brain, Behaviour and Development needed a quiet environment to test the brain. But moving to the new Westmead Innovation Quarter premises next to Westmead Hospital meant much of that important work was going to be carried out with a helipad, railways, and traffic nearby.
This environment was not conducive to silent testing and an optimal solution was needed.
Enter Melbourne-based All Duct Fabrications (ADF) Industries – experts in sound booth design, manufacture and installation. The company and Western Sydney University had previously worked together for more than a decade at MARCS’ original site.
Dr Leidy Castro-Meneses, technical team leader for the institute, says there were 10 booths on the initial site, some from ADF Industries.
“We liked the design and also ADF’s flexibility with booth design,” she says. “The managing director Jono Davies was able to custom size the booths for us.”
This was why the NSW-based MARCS chose the Victorian business over local providers to design, manufacture and install the 22 audiology rooms in the benchmark project. The institute occupies floors four
to seven of the Westmead Innovation Quarter, a research, health, education and business hub.
“We had conversations and back and forth changes and iterations. Jono always had a workable solution to any request,” Dr Castro-Meneses says.
“We now have four types of booths, based on acoustic rating and electromagnetic rating, ranging in size from 6 sqm to 17 sqm. Jono worked with the building design as the building structure had to plan for the weight of the booths – the smallest weighing three tonnes.”
SOMETHING SPECIAL
Davies recalls the university proposing the idea for the project about four years ago. “We went back and forth on concepts and designs,” he says. “Working with the researchers and scientists to develop what was required, it became clear this wasn’t just a pipe dream, but something very special.”
Dr Castro-Meneses, with a degree in psychology and a PhD in human cognition
and brain sciences, says she loves research, in particular, understanding how the brain and mind process information and make inference. This is the field that MARCS researchers work in.
MARCS was formed as a research centre –Music and Auditory Research Centre – and initial research was in auditory perception including music.
“After 20 years, the institute expanded its scope but it remains a global leader in auditory research,” she says. “We look at how babies learn language, how being bilingual postpones some aspects of ageing and how music can elevate our mood.”
It’s also leading the way in understanding how the human brain develops across the lifespan. This includes research on how the brain responds and can be enhanced to visual, auditory, sensory and technological stimulus.
MARCS also paves the way in developing systems that can leverage evolutionary strategies to process information, Dr Castro-Meneses adds.
“For example, some researchers at our BabyLab investigate how babies from three months old perceive and categorise the world before they produce language, how cognition and language interact and influence each other,” she says.
“We also have the AgedLab where researchers investigate how the elderly brain ages and optimises wellbeing.”
Other researchers at the institute investigate how creativity and improvisation shape the human brain and benefits associated with this.
“We have researchers in biomedical sciences, trying to develop better technologies to improve medical sciences, for example, enhancing perception in people with perception deficiencies such as peripheral neuropathy which often leads to amputations,” she adds.
“The MARCS Institute also has the International Centre for Neuromorphic System, which is a team of dedicated engineers implementing technologies that mimic human processing.”
“I recommend ADF because it’s flexible, serious about making required changes and punctual on delivery. Prices are also affordable.”
Dr Leidy Castro-Meneses MARCS Institute
One of ADF's soundproof rooms at MARCS.
Image: Leidy Castro-Meneses
Images: MARCS.
CONTROLLED ENVIRONMENT
But to carry out much of this important work, Dr Castro-Meneses says conducting research with human participants requires a controlled environment.
That’s where it’s collaboration with ADF comes in.
“For example, if you are testing how the brain perceives a talker in a noisy environment such as a party, you also need to test the brain in a quiet environment, so you can make comparisons,” she says.
“We often measure the brain’s electrical signals, for example, and these require isolation of other sources of electrical noise.
“Our rationale was that at Westmead, we could potentially have more sources of noise acoustically, electromagnetically and through vibration, such as flying helicopters passing the next door hospital, a light rail and heavy rail next door, people walking and talking in corridors next to labs and even air conditioning ramping up suddenly when the cooling system detects temperature changes in the whole floor.”
The open office plan with access to window views meant labs were designed to be inside, at the core of each floor, but this also translated to more people nearby, making potential noise – not ideal for lab testing, she adds.
AUSTRALIAN-MADE MATERIALS
As a leading Australian manufacturer of quality audiometric rooms and soundproof booths, ADF’s custom-made products feature in audiology clinics, hospitals, institutes, mining sites and mobile hearing testing vehicles worldwide.
The family-owned and operated business has existed for more than 50 years and has specialised in design and manufacture of hearing test rooms and sound booths for 30 years. It uses the latest technology, does everything inhouse and only uses Australian-made materials.
Davies, a mechanical engineer, says ADF has designed, constructed and installed
hundreds of audiometric rooms and soundproof booths across Australia and overseas including New Zealand, Samoa and Singapore.
Most jobs are one to two booths and can be delivered within a few months but for bigger projects such as hospitals or institutes, the paperwork can take two months, and that’s when an assignment can go for a year.
“The MARCS Institute job was amazing,” he recalls. “It was in the middle of the COVID pandemic so that provided another layer of complexity because we weren't allowed to cross the border for planning.
“All planning was done remotely over Zoom, with the main challenge not being able to see the site and environment.
“We couldn’t fly up to measure; other trades onsite had to provide information so we could be confident that the rooms would fit.”
ADF’s skilled team designed and manufactured the rooms in its Melbourne facility in Seaford and a fleet of 10 semi-trailers transported them to Sydney where they were stored before installation.
“It was our biggest job and the most booths installed in the southern hemisphere,” Davies says. All rooms were for different purposes from studies on equipment to testing patients.
RF ATTENUATION
All rooms installed for the MARCS project were required to meet various standards. These included Australian Standards AS/ NZS1269.4-2014 Occupational Noise Management Auditory Assessment, Australian Standards ISO-8253-2-2009, Acoustic Audiometric Test Methods 2014, and International Standards ISO8253.2-2009.
“In an exciting first for us, the rooms incorporated radiofrequency (RF) and electromagnetic frequency attenuation technology,” Davies says.
The business set out to achieve and beat the standard, he adds, going the extra mile and putting in a lot of background work to surpass the client’s expectations. This included engaging extra parties to ensure everything was spot on.
Planning started in 2020 and the job was completed in February 2022 with a team of installers fitting the rooms over eight weeks.
Davies says there were stressful times and late nights because of the scale of the project and its timing due to COVID.
“But everyone – my family, my staff and the installation crew – came together to deliver an exceptional outcome. That’s what makes me proud,” he says.
“The result was 100% successful, and we were able to double the attenuation required in the RF (radiofrequency) rooms.”
Dr Castro-Meneses agrees. “The end result is that our researchers feel more stable knowing that vibration, acoustics and electromagnetic interference can be successfully managed during lab testing," she says. "They're very happy with the rooms’ efficiency.
“I recommend ADF because it’s flexible, serious about making required changes and punctual on delivery. Prices are also affordable.”
For more information see adfindustries.com.au.
MARCS Institute occupies four floors of the Westmead Innovation Quarter.
Images: MARCS.
Above: A smaller audiometric room ADF designed at MARCS.
All 22 rooms were different sizes and shapes.
Image: Arthur Vay.
Images: MARCS.
Translating research into practice
Dr BEC BENNETT, principal research audiologist at the National Acoustic Laboratories, details her experience with converting research into practice at Hearing Australia’s Innovation Centre.
In the ever-evolving world of audiology, bridging the gap between research and clinical practice can often be a slow and complex process. As a researcher at the National Acoustic Laboratories (NAL), I’ve long been focused on developing practical, evidence-based tools that can be applied immediately within clinical settings to support adults with hearing loss. That’s why my recent experience working with the Innovation Centre – a unique collaboration between Hearing Australia and NAL – has been so transformative.
WHAT IS THE INNOVATION CENTRE?
The Innovation Centre is an operational audiology clinic embedded within Hearing Australia, functioning like any other client-facing centre, with a front-of-house
as a testbed for innovation.
It’s here that researchers like myself can work side-by-side with clinicians to trial new ideas, co-develop tools, and understand how innovations function in the real world, with real clients, and in real time. It's a space where research is not confined to labs or publications but brought to life in the environments where it matters most.
access to the Innovation Centre is an incredible opportunity.
Backed by Hearing Australia, the nation’s largest provider of government-funded hearing services, and supported by NAL’s research leadership, the Innovation Centre bridges the gap between discovery and delivery.
A RESEARCHER’S DREAM: WHY THE CENTRE MATTERS
Rather than developing a tool in isolation and hoping it will be used, I can embed intervention(s) directly into a working clinic, observe its use in context, gather feedback, and refine the intervention(s) iteratively. This process allows for fast, agile learning that not only improves the product but also enhances our understanding of what implementation might look like at scale. I’ve been fortunate to work alongside two exceptional colleagues throughout this journey; Ms Raisse Tjoa, a Hearing Australia innovation audiologist based at the Innovation Centre in Rouse Hill, Sydney, and audiologist Ms Kate Rutledge, Innovation Centre project manager, based at NAL. Their expertise, dedication, and collaborative spirit have been integral to the success of our recent project.
HearWB HEARING WELLBEING APP
The project we’ve been trialling in the Innovation Centre is focused on a new digital health tool: HearWB (short for Hearing Wellbeing). This mobile app is designed to support adults with hearing difficulties by offering evidence-based educational content, skill-building exercises, and wellbeing tracking tools. HearWB provides:
• Lessons: Interactive modules to increase knowledge about hearing loss, identify unhelpful behaviours, and empower users to manage the communication, social, and emotional aspects of hearing loss.
• Skills: Practical exercises that put those lessons into action, encouraging new, positive behaviours.
• Tracking: Tools for monitoring wellbeing over time, reinforcing self-efficacy.
• Progress reporting: Visual feedback that links behaviour changes to improvements in wellbeing and quality of life.
We’re currently in the usability testing phase, but as part of our research, we wanted to understand how the app might fit into clinical workflows. What would clinicians need to feel confident
Dr Bec Bennett, NAL principal research audiologist.
(From left) Hearing Australia innovation audiologist Raisse Tjoa and Innovation Centre manager Julie Till.
Image: Bec Bennett.
Image: Hearing Australia.
Under Rutledge’s guidance, we designed a four-week implementation sprint at the Rouse Hill Innovation Centre, with Tjoa acting as our clinician partner. We trained Tjoa on the app, equipped her with a prototype brochure and simple clinical tools, and supported her in integrating HearWB into her appointments.
Each week, we had stand-up/mini sprint meetings to review what Tjoa had learned, gather her feedback, and iterate based on real-world experience.
In week one, we quickly hit our first challenge: brochure confusion. Clients received a flyer for HearWB and another for their hearing aid management app but it wasn’t clear they were for different apps. Some clients assumed they were different versions of the same tool. Tjoa flagged this with us immediately.
Thanks to the agile nature of the Innovation Centre, we were able to redesign the HearWB brochure within 24 hours, aligning it visually with the style of the other app’s materials. This small change helped clients clearly differentiate the apps and make informed decisions about downloading them.
Over the four weeks, Tjoa continuously refined her language when introducing the app, testing different ways of framing its value. She documented her evolving script and shared insights about what worked and what didn’t when engaging clients. This helped us refine not only the app materials, but also our clinician guidance and implementation plan.
WHY THIS WORK MATTERS
Our research often hinges on the question: How will this be used in the real world? With the Innovation Centre, that question isn’t an afterthought – it’s front and centre.
We’re not just designing a good app; we’re designing a good app that clinicians want to recommend and clients want to use. And we’re doing it in collaboration with the very people who will use it and recommend it.
Through this process, we’ve been able to:
• Identify and resolve real-time implementation barriers
• Co-create clinician tools with direct user feedback
• Observe authentic client reactions and refine our approach.
This is the kind of translational research that makes a difference.
ACKNOWLEDGING COLLABORATORS
None of this would have been possible without the incredible team at the Innovation Centre.
I am immensely grateful to Kate Rutledge, whose deep knowledge of innovation processes and agile methodology has guided this project every step of the way. Her ability to create space for fast learning while maintaining clinical rigour is what makes the Innovation Centre so special.
And to Raisse Tjoa – thank you for your thoughtful, skilful, and generous contribution.
Balancing full-time clinical work with research innovation is no small task, and your engagement has truly elevated this work. Your insights, feedback, and genuine care for your clients have ensured this project is grounded in the reality of clinical practice.
LOOKING AHEAD
HearWB is still in development, but thanks to the Innovation Centre, we now have rich, practical insights to guide the next phase of implementation planning.
We’re confident that when the app is ready for broader rollout, it will have the clinical tools and strategies needed to succeed in the real world – because it’s been built in the real world.
The Innovation Centre represents what’s possible when clinical excellence and research innovation come together. It has been a privilege to be part of this collaboration, and I look forward to sharing more learnings as we continue this work.
(From left) Raisse Tjoa, and Kate Rutledge, in the Innovation Centre.
=Image:
Monika Wisniewska/stock.adobe.com.
The app is designed to support adults with hearing difficulties through educational content, skill-building exercises and wellbeing tracking tools.
Image: Hearing Australia.
Elevating clinical practice and trust
More than 150 Specsavers Audiology Partners from around Australia and New Zealand converged on Melbourne for the second annual Specsavers Audiology Clinical Conference. The event centred on elevating clinical expertise and left attendees feeling inspired, connected and ready for professional growth.
The Specsavers Audiology Clinical Conference 2025 opened with a clear message: clinical excellence and patient connection are at the heart of Specsavers’ mission. Chief audiologist Mr Nick Taylor set the tone in his opening address, urging delegates to reflect on their practice and embrace continuous improvement.
“Our mission is to change lives through better hearing,” he said. “A part of this is keeping up with the latest technology and making it accessible to people who need it, but at the core of our purpose is that human connection – listening, building trust and understanding every customer so we can meet them where they are and improve their life in a way that's meaningful to them.
“We’re here to challenge ourselves, learn from each other and the many experts who lead in their field who have joined us today.
“We’re here to celebrate the individuals who have been helped by the people in this room – the grandparents who can now have a close relationship with their grandchildren, those working who can remain in employment, those who don’t feel isolated anymore and have the confidence to go out and be social again. We’re here to celebrate them and to celebrate audiology, to learn, improve and develop our skills, to network and enjoy each other’s company.”
Specsavers professional development managers Ms Natalie Braude and Ms Annette Newland-Nell, who organised the conference, ensured content was aligned with Specsavers’ visions and values.
“We're in a profession that is continuously evolving and changing to meet the needs of today’s customers. Our clinicians can’t rest on their laurels or qualifications; they need to have opportunities available to challenge the status quo and grow their expertise,” Braude said.
NAVIGATING AI IN AUDIOLOGY
Keynote speaker, audiologist Dr Dianne Rafter from New Zealand, brought deep clinical insight and knowledge gained from a Masters in Technological Futures to help clinicians navigate AI’s role in audiology and communicate its value in clinical practice.
“The future belongs to people who are curious and courageous. As audiologists, we’re wonderfully placed because we can use this technology to make a true difference for customers,” she said. She simplified concepts of mechanical AI, DNN AI, generative AI and agentic AI and provided clinical case studies to highlight how practitioners can adapt their language about AI to suit customers’ health and technology literacy.
Machine learning and deep neural networks (DNNs) are now integral to hearing aids, classifying sound scenes and adjusting to environments, Dr Rafter said. “Speech in noise is the most exciting part of AI in hearing aids,” she added. “Small DNNs separate speech from noise. They extract speech and enhance it which is true ‘de-noising’ and a very exciting development for hearing aids. “It’s
fundamentally changing the processing of sound,” she said.
It was important for clinicians to explain to their customers that DNNs were trained on millions of sound samples of voices, noises, and languages but do not record or listen to clients, she said. In future, users may be able to train hearing aids to prioritise preferred voices.
CLINICAL EDUCATION
In a clinical education session, Dr Rafter challenged clinicians to think about tools, skills and mindsets to be ready for the future patient. Discussion on future healthcare trends concluded clinicians needed to continuously learn and keep updated to provide the best care.
“With awareness of the technology available and a solid understanding of the impact it can have on customers, you can enhance your expertise and provide solutions that change lives,” Dr Rafter said.
One delegate said the sessions on AI were incredible. “Best presenter I have ever seen. Learnt so much!” the delegate said.
Dr Tim McLean and Dr Justin Zakis also delivered clinical education. Dr McLean, an ENT surgeon, discussed vestibular schwannoma and otologic conditions. He said vestibular schwannoma affected one in 100,000 people, often causing dizziness and sudden sensorineural hearing loss. Tumour size dictated symptoms.
Partners found networking a valuable part of the event.
Specsavers Audiology Partners enjoying Dr Dianne Rafter’s AI presentation.
“Utility of the auditory brainstem response (ABR) is pretty low as it lacks sensitivity for small tumours,” he said. “The ABR will miss 30% of tumours less than 1.5cm so an MRI is recommended if there are any concerning features on an audiogram.
“Often patients are panicked when they get a referral. When people hear ’tumour’, they think cancer so say we’re looking for benign things, not cancer, and that destresses the situation. Vestibular schwannoma is slow growing – 1mm a year – 40% don’t grow and 10% shrink.”
Most cases undergo active surveillance with periodic MRI, and hearing preservation is best achieved without radiation or surgery. Observation generally provides a better quality of life than surgery or radiation, Dr McLean said. “About a third of patients eventually need treatment, mainly for tumour growth,” he said.
He described superior semicircular canal dehiscence, where patients hear internal body noises such as eye or joint movements. This can cause imbalance and low-frequency conductive hearing loss. Most are managed conservatively; canal-plugging surgery helps severe cases.
He said otosclerosis could present with conductive hearing loss and be confirmed by CT imaging showing bony overgrowth around the stapes.
IMPORTANCE OF REMS IN FITTING
Dr Zakis, principal researcher at National Acoustic Laboratories (NAL), delivered a research-backed presentation on the importance of verifying hearing aid fittings with real ear measures (REMs) rather than relying solely on manufacturer first-fit prescriptions.
He provided compelling evidence that fitting and fine-tuning devices without verification often leads to settings being around 7-10dB below target. In contrast, when verified with REMs, devices are within 1.5-2.5dB of target levels – a significant improvement. “Speech understanding in noise is improved by about 10% when the fitting targets are verified with REMs,” Dr Zakis said. He said performing REMs accounts for individual real ear unaided
Doug Perkins Award recipients
Winners of the inaugural Specsavers Audiology Doug Perkins Medal for Clinical Excellence were announced at the conference.
Named in honour of Specsavers co-founder, optometrist Mr Doug Perkins CBE, the award celebrates one store in Australia and one in New Zealand exemplifying the highest standards of clinical care, customer outcomes, and a strong culture of excellence.
The winners were Ms Nil Koca, Specsavers Audiology Dandenong (Victoria, Australia), and Ms Iris Shin, Specsavers Audiology Albany (Auckland, New Zealand).
Mr Nick Taylor presented the awards which he said were a cornerstone of clinical recognition within the Specsavers network.
“These stores have set the benchmark for clinical excellence,” he said. “To determine the winner, we analyse nationwide clinical data, customer feedback, and health outcomes to identify finalists – and these two stores stood out for their unwavering commitment to quality care, accessible hearing health, and fostering a thriving store culture.”
Taylor said the six ANZ finalists represented the top 3% of stores in each country, selected for their consistent excellence across all areas of audiology practice. “Their achievements set a high bar for future winners,” he said.
“We were looking for practices that lead in delivering exceptional customer outcomes, provide consistently outstanding patient experiences, and continuously improve store processes to ensure high-quality hearing care.
“These stores demonstrate a deep commitment to accessible hearing health and contribute positively to their workplace culture.”
gain, ensuring each customer receives a truly personalised fitting. The improved outcomes of device fittings provide not only a professional advantage for clinicians but improve customer loyalty, with less chance of hearing aids ending up “in-the-drawer”.
Dr Zakis discussed NAL’s next generation hearing aid fitting system, NAL-NL3. He detailed why the evolution of the new fitting prescription was necessary and highlighted how it incorporates specialised targets for specific populations, including comfort in noise and minimal hearing loss. These changes and improvements are designed to address different unmet customer needs, helping clinicians build expertise and strengthen the trust customers place in their hearing care professional.
Specsavers’ invited special guest Dr Emma West, senior emergency physician and director of education at Royal Melbourne Hospital Emergency and Trauma Centre, shared lessons learnt from the frontline of emergency healthcare. She said connection is more than performing tasks – it’s about words, tone, body language, and agility in building trust with each patient. Her personal stories resonated with attendees, reinforcing the conference’s central theme.
An interactive workshop complemented her talk, highlighting the importance of trust language and communication. Delegates reflected on their own communication styles and considered how small changes could have a big impact on outcomes.
ADVANCE 73 LAUNCH
Audiologist Ms Sylvia Soong from Sonova Australia presented the new Advance 73 hearing aid platform, now available at Specsavers. She highlighted its AI-powered sound scene classification which adapts to each environment, improved speech enhancement, and universal connectivity. The technology, available across all five levels, was demonstrated live, including submerging hearing aids in water to showcase durability.
Soong said Advance 73 features the most advanced chipset in the Specsavers Advance range, offering stability and power in a compact design. Improvements in Bluetooth connectivity, battery life, and water resistance made it a standout choice for clinicians and customers, she said.
Specsavers Audiology said its clinical conference was fast becoming a feature CPD event on the Specsavers calendar, with delegates praising its thoughtful content, engaging speakers, and networking opportunities. “Everything was great. I hope we keep having these. So great to see what different partners are doing,” one attendee said. Taylor echoed these sentiments: “Engaging learning and development is one of our priorities. As we continue to expand and evolve our CPD offering, we hope that in time our employees, team members and the wider audiology community will have the chance to attend this wonderful conference our team creates. Our goal is to make it the highlight of the professional development calendar for audiologists."
Audiology Unchained 2025 report
Independent Audiologists Australia’s flagship event, Audiology Unchained 2025 on Queensland’s Sunshine Coast, brought together 116 delegates from across Australia, New Zealand, and as far as the USA and UK.
By Julie Watts, IAA executive officer
It was a privilege to host Independent Audiologists Australia (IAA)’s Audiology Unchained 2025 conference, with the event exceeding all expectations for professional development and collegial exchange.
The conference theme, Full scope: Real impact, captured the essence of independent audiology practice –embracing the full breadth of clinical expertise while making tangible contributions to patient outcomes and community wellbeing.
Attendees enjoyed an immersive two-day program at Mantra Mooloolaba Beach on 17 to 18 October 2025 which balanced rigorous clinical content with networking, mentorship, and celebration of professional achievement.
International guest Mr Neel Raithatha from the UK – known to many as ‘The wax whisperer’ thanks to his online presence and advocacy in cerumenology – attended to showcase his “revolutionary WaxScope system”, and host pre and post-event training sessions. The WaxScope system is TGA-approved and distributed by event sponsor The ENT Store.
Instructional designer and program manager for A.T. Still University’s Post Professional Doctor of Audiology Program, Ms Melanie Gibson, from Arizona also attended and took the opportunity to connect with several ATSU alumni and current AuD students in attendance.
DEPTH AND DIVERSITY
Friday’s lecture program opened with a powerful keynote from Ms Rachael Robertson, Australia’s first female Antarctic expedition leader and author of the book, Leading on the Edge. She delivered a standout address on leadership, teamwork, and resilience.
Drawing from her year leading 18 people through the Antarctic winter, Robertson’s message – “Respect trumps harmony” – resonated deeply with audiologists navigating professional and organisational challenges.
Her humour and honesty about isolation, leadership under pressure, and accountability earned enthusiastic accolades from delegates.
“Absolutely first class! Rachael is a wonderful presenter with a highly motivational message,” one delegate said.
“Sensational speaker! What a treat to be able to listen to such an inspirational story and woman,” another said.
A full day of presentations followed, spanning clinical innovation, research translation, and the human side of practice.
Key topics included hyperacusis and sound sensitivities, genetic testing in Ménière’s disease, the use of otoacoustic emissions in routine audiological practice, auditory processing, patient-centred care, and the role of artificial intelligence in audiology.
Saturday offered a full day of workshops, with delegates participating in practical, small-group sessions across two curated
streams. Topics included bedside vestibular testing, clinical APD testing, single-sided deafness pathways, hands-on WaxScope demonstrations, hearing protection, and infection control.
A members-only masterclass on billing and reimbursement rounded out the day, before the annual general meeting and networking drinks.
HANDS-ON LEARNING AND COLLABORATION
The interactive workshop structure on day two proved to be one of the event’s greatest successes. Each session was designed to maximise practical learning, peer discussion, and equipment handling.
Delegates chose between Stream One, Full Scope Whole-Person Rehabilitation, or Stream Two, Full Scope Diagnostic and Implantable Pathways, completing a curated series of themed workshops and masterclasses.
Stand-out sessions included the Stream Two ENT panel where Dr Kristy Fraser-Kirk, Dr Brendan Perry and Dr Andrew Chang shared practical insights on audiologist-ENT collaboration.
Perth audiologist Dr Dayse Távora-Vieira’s playbook for decision-making in single-sided deafness was also a highlight, along with Dr Tegan Keogh’s clinical masterclass on auditory processing from testing to interpretation.
Psychologist Dr Jacqui Truter’s thoughtful Stream One discussion on mental health in the audiology clinic, covering everything from managing distressed patients to tackling clinician burnout, was also well received.
The gala dinner at The Wharf Mooloolaba was one of many highlights.
(From left) Cristy Newall, Jonathan Galt, Prof Philip Newall and Dr Yazdaneh Galt.
EXPO AND INDUSTRY ENGAGEMENT
An energetic trade exhibition ran alongside both conference days, featuring displays from hearing aid manufacturers, service providers, and clinical support partners.
Platinum sponsor Cochlear showcased its Nucleus Nexa System. Gold sponsors were WSA, Phonak and MED-EL; silver sponsors included Starkey, A.T. Still University, The ENT Store, Pacific Ears, and Pengwen Bookkeeping.
Cochlear, Phonak, and WSA also contributed insights on new technologies and practice differentiation during day one's presentation sessions.
A ‘creatives’ corner’ in the trade hall was a new addition, where IAA members showcased their non-audiology passion projects. Books by Melbourne audiologists Mr Keith Chittleborough and Ms Khatija Halabi and Tasmanian audiologist Dr Heidi Modrovich were on sale while Brisbane audiologist Ms Erin Seamer shared custom earrings.
With the trade hall open during all catering
Recognising excellence
The event also saw the launch of IAA’s inaugural Indy Awards. The awards were a defining moment for IAA, celebrating members who embody the association’s values of quality, integrity, and independence.
Award recipients were:
ommunity champion: Ms Seray Lim and Mrs Laura Drexler (joint winners)
lying start award: Ms Kathryn Penno
entor of the year: Ms Philippa Carter
ractice innovation: Ms Sara Patterson
AA values award: Ms Nicole Eglinton
ervice awards: 2024–2025 executive committee – Ms Rachel Gibson, Dr Heidi Modrovich, Mr Mo Helou, Dr Tegan Keogh, Dr Greg Butcher, Mr Grant Collins and Dr Signe Steers.
ecade of service award: Mr Grant Collins
istinguished service award: Dr Louise Collingridge. Nobody has worked harder to achieve audiologist registration than my highly respected predecessor, IAA’s former CEO Dr Collingridge. It was an honour to present her with this award.
The ‘unchained dinner experience’ included an interactive lucky door prize with each table working together to unlock a set of keys. The winning key held by Queensland audiologist Mrs Penelope Woods unlocked a prize cage containing premium wine and a coveted golden ticket of free registration to a year’s worth of IAA events including Audiology Unchained in Canberra in October 2026.
Signature cocktails on arrival cheekily named the Ahpra-ol Spritz celebrated IAA’s long-fought win on national registration for audiologists. After dinner, guests admired
the unchained ice sculpture, hit the dance floor, and posed in the 360° photo booth.
CONNECTION BEYOND THE LECTERN
More than just a professional conference, Audiology Unchained 2025 fostered genuine connection across the independent audiology community. Delegates described the event as rejuvenating and reinvigorating, offering space for reflection, exchange, and renewed pride in their professional identity.
Their comments included:
“Literally one of the best conferences I’ve been to in the last 10 years.”
“The line-up of speakers and topics were spot on.”
“Terrific speakers, with interesting and clinically relevant topics.”
“I was very impressed with the IAA conference experience. All your speakers were brilliant, and the organisation was very impressive.”
“Loved the content, speakers and overall vibe!”
With Audiology Unchained 2026 confirmed for Canberra on 23–24 October, IAA is already planning how to build on this year’s success. If 2025 was about unlocking ideas and breaking boundaries, 2026 promises to take that energy to a national stage.
Post-event registrations are available, with a curated package of recordings from the conference and workshops.
For membership or event information, visit independentaudiologists.net.au.
Above: (Top L-R then clockwise) IAA's inaugural Indy Award winners, Nicole Eglinton, Seray Lim, Laura Drexler, Kat Penno, Phillippa Carter and Sara Patterson. Above (right): Distinguished service award recipient, Dr Louise Collingridge.
Images: IAA.
Keith Chittleborough introduces puppet Kevin Sanders Kettletown to Penelope Woods.
(From left) The IAA executive committee, Grant Collins, Dr Signe Steers, Dr Greg Butcher, Dr Tegan Keogh, executive officer Julie Watts, Dr Heidi Modrovich and Rachel Gibson.
Audiometry nurses upskill
The Audiometry Nurses of Australia Association has celebrated its annual conference in Penrith, NSW, mastering new skills in ear health including performing otoacoustic emissions.
Audiometry nurses are a vital but often overlooked part of the hearing-health ecosystem.
As an early point of contact, they help identify hearing issues, conduct accurate screening, and ensure patients are referred appropriately, supporting earlier intervention and better long-term outcomes.
In many regional and remote areas, audiometry nurses enable access to hearing care, reducing delays and supporting families who rely on regular testing. They also boost health literacy by educating patients on ear health, hearing protection, and the need for follow-up.
They nurses work anywhere across Australia, including in private organisations, audiology clinics, community health services and school programs, enhancing reach, efficiency and quality of hearing care. They also perform hearing tests in mobile vans at field days and other events.
These practitioners are registered or enrolled nurses who have completed a post graduate qualification in audiometry through the Australian College of Nursing. In NSW, they work mainly in community health centres. A large part of their work in community health settings is working with children and childhood hearing assessments.
As most work as sole practitioners, events such as the Audiometry Nurses of Australia Association’s annual conference are important get togethers not just for networking but for keeping up with the latest advances in the field.
Audiometry nurses from across NSW recently gathered for their 2025 conference from 15 to 17 October 2025 at the Log Cabin Hotel, Penrith, an historic hotel on beautiful Dharug land with spectacular views over the Nepean River.
About 40 delegates attended, mostly from NSW. Apart from presentations, there were trade displays from Natus, Interacoustics – Diatec, TAFE Eartrain, Myo Munchee, Sonic and Baxter.
Association president, Ms Kate Norton, said an otoacoustic emissions workshop by audiologist Ms Jean Tsembis from TAFE NSW was particularly interesting as many audiometry nursing services have started performing otoacoustic emissions (OAEs) as part of the battery of testing.
“Ongoing education is vital in this area,” said Norton, a clinical nurse consultant
in audiometry from Grafton.
OAEs are an objective and non-invasive test that measures the health of the inner ear by recording soft sounds produced by the cochlea. It is used for hearing screening, especially in newborns and young children who cannot respond to traditional tests, and to help diagnose hearing conditions by assessing the function of the outer hair cells.
The first day provided a great array of speakers, Norton said.
Ms Elissa Haddrick, ENT clinical nurse consultant from The Children’s Hospital at Westmead, discussed statewide ENT referral criteria. This criteria is aimed at improving the quality and appropriateness of referrals, outlines tests required before ENT appointments, streamlines patient experiences and streamlines the service.
Another ENT clinical nurse consultant, Ms Jess Muscatt, discussed grommet management. Norton said this was also a great topic to review as most clients of audiometry nurses have conductive hearing loss.
NEWBORN HEARING SCREENING
On the second day, chiropractor Dr Mary Bourke, CEO of Myo Munchee, showed her product which is designed to help with the management of eustachian tube dysfunction. Her dentist father Dr Kevin Bourke invented the TGA and FDA certified device.
Ms Judy Noonan from Nepean Blue Mountain Local Health District and Ms Judy McClosky from Western Sydney Local Health District discussed the NSW newborn hearing screening program.
She explained why children have eustachian tube dysfunction, including not actively chewing, and how her product can help. She said the Myo Munchee helps with chewing and swallowing exercises that strengthen the muscles around the ear.
Above: Delegates at the conference dinner dressed to the dinner’s theme of a day at the races.
(From left) All committee members were re-elected, Gisella Laughton, Helen Gee, Belinda Wilson, Kirsten Biddle, Kate Norton, Sarah Austin and Lee Lewis.
issues including adenotonsillectomies and grommets.
His colleague, adult and paediatric ENT surgeon Dr Vanaja Siva, also from the ENT Institute, Penrith, discussed otitis media, complications and treatment.
“As audiometry nurses mainly see children with otitis media with effusion, we found these talks most informative,” Norton said.
MASKING AND ACOUSTIC REFLEXES
Ms Jan Pollard, chief audiologist at Sonic, presented on masking and acoustic reflexes. “These are difficult concepts to grasp and are part of the battery of testing for audiometry nurses,” Norton said.
Tracy Hawes as life member
“Learning more about these components of audiometry is vital.”
Norton presented on hearing conservation audiometry.
Day three kicked off with itinerant support teacher Ms Nina Scott discussing the criteria for hearing support in the public education system. Audiometry nurses work closely with itinerant support teachers for hearing to ensure children maximise their learning potential at school.
Hearing Australia audiologists, Ms Arveen Kaur and Ms Sally Wood, discussed services for children and when to refer. They also shared valuable tips when testing children.
journey. “Personal stories always touch the heart,” Norton said. “They show how our part, no matter how big or small can help in the big picture.”
The Shepherd Centre also gave a general overview of the services it provides.
LIONS ASSISTANCE DOGS
Raffles which ran over the three days raise money each year to go to hearing health charities. This year, delegates raised $750 for Lions Assistance Dogs, previously known as Australian Lions Hearing Dogs.
“It takes $40,000 to train an assistance dog,” Norton said. “This is all raised by generous donations. The dog is then placed with a person at no cost.
“Lions Assistance Dogs advocate and recipient Ms Faye Yarroll and her dog Sydney gave us a demonstration of how a hearing dog works before accepting our donation. We were all in awe of what little Sydney could do for Faye.”
The association’s annual general meeting was during the conference, and the committee was re-elected to the same positions. They are: president Ms Kate Norton, vice-president Ms Belinda Wilson, secretary Ms Kirsten Biddle, treasurer Ms Sarah Austin, editor Ms Lee Lewis and committee members, Ms Helen Lee and Ms Gisella Laughton – who was also the conference organiser.
The Audiometry Nurses of Australia Association (ANAA) inducted Ms Tracy Hawes as a life member, and she graciously accepted the nomination although she was unable to attend the conference.
The audiometry nurse from Western Sydney Local Health District previously served over the years as ANAA president.
“Tracy built strong connections between our association and other groups involved in hearing health,” ANAA president Ms Kate Norton said. “She raised our profile and showed everyone that we’re here, doing amazing work.
“One of her standout moments was on 6 April 2017 when she represented ANAA at the Inquiry into Hearing Health and Wellbeing in Australia at Parliament House.
“How brave she was to stand there in parliament giving evidence and recommendations for the betterment of hearing health of our nation. She attended many meetings before and after the inquiry, continuing to advocate for those hard of hearing.”
Norton said Hawes also organised and assisted the running of several ANAA conferences, going well beyond what was expected of her at work – all for the benefit of audiometry nursing. “Tracy served on many committees, often giving her own time or using lunch breaks to represent our organisation,” she said.
(From left) Conference organiser, audiometry nurse Gisella Laughton with Penrith surgeon Dr Vanaja Siva.
Lions Assistance Dogs advocate and recipient Faye Yarroll and her dog Sydney.
HBA seminar: BUILDING RESILIENT AND PROFITABLE BUSINESSES
The 2.5-day Hearing Business Alliance 2026 Seminar will be in February in Brisbane.
Hearing Business Alliance (HBA), which supports the business aspects of audiology practice in Australia, will host its major event for the year at the Sofitel Brisbane Central in February.
Organisers are expecting independent audiologists and audiometrists from around the nation to attend the seminar, from 12 to 14 February 2026. It will feature expert presentations, workshops, a trade exhibition, and gala dinner.
Workshops on Thursday afternoon will be followed by welcome drinks on Thursday night, presentations on Friday and Saturday, and a gala dinner on Friday night.
Building resilient and profitable businesses will be a major theme and a new topic to be introduced will be the ethical application of AI in audiology healthcare.
Mr Stephen Logan, HBA’s business manager, says this year’s program has been carefully curated to reflect the incredible
pace of change shaping both the audiology profession and the small business landscape.
“From AI and branding to leadership and financial strategy, our speakers bring diverse expertise and real-world insight,” he says. “We’re excited about the focus on ethical AI, showing how innovation can drive both patient care and business growth, and exploring how technology can be leveraged responsibly to improve patient care and business efficiency.
“These sessions set the tone for a seminar that’s not just about keeping up but leading the way in modern hearing healthcare.”
Mrs Jane MacDonald, HBA’s CEO, says the 2026 seminar is all about future-proofing the small to medium-sized audiology businesses working within the hearing health sector.
“We’re combining sessions on technology and leadership with hands-on workshops
and presentations on finance, HR, compliance and more – everything clinics need to thrive,” she says.
“Our speakers, from Brad Seymour to Natasha Hawker, bring expertise that goes straight to the heart of running a sustainable practice. I’m also looking forward to sharing the latest HBA priorities and hearing how members are adapting in this exciting period of change.”
HBA recommends people planning to attend book their accommodation and flights now as the Edinburgh Military Tattoo, from 12 to 15 February, coincides with the seminar.
“If you look at the various hotel booking sites, reasonably priced options at nearby hotels and Airbnbs are still available.
Southbank is only a 10-minute taxi/uber drive to the Sofitel Brisbane Central,” MacDonald says.
Register at hearbusiness.com.au
PRESENTATIONS
OPENING ADDRESS AND SEMINAR OVERVIEW
Mr Stephen Logan, Hearing Business Alliance business manager.
THE ADVANTAGES OF NALTECH FOR YOUR BUSINESS
Bringing COSI 2.0. Virtual Personas, and NAL-NL3 to Practice
Dr Brent Edwards, National Acoustic Laboratories director.
STRATEGIC LEADERSHIP
Scaling authentic resilience and building local success and resilience
Mr Brad Seymour, management consultant and co-founder of Yellow Brick Road and Wizard Home Loans.
THE HEARING SERVICES PROGRAM Program update
Ms Gabriela Luksza, director, Hearing Policy and Compliance, Hearing Services Branch, Department of Health, Disability and Ageing, and Mr Rob Aked, director Hearing Voucher Operations, Hearing Services Branch, Department of Health, Disability and Ageing.
NAVIGATING EMPLOYMENT LAWS
Key Australian legislation compliance essentials (Fair Work Act, NES, WHS) and avoiding legal pitfalls
Ms Belinda McLean, HR Focus general manager.
HBA KEY ACTIVITIES
Strategic insights and small business update
Ms Jane MacDonald, Hearing Business Alliance CEO.
AI IN AURAL REHAB
Driving compliance, outcomes, and practice growth
Mr Rick Carlson, Neurotone CEO.
BECOMING THE GO-TO AUDIOLOGY CLINIC
How to build a brand that attracts patients; Branding inside the office; From first visit to lifelong advocate; Strengthening patient loyalty through in-office branding and automation
Dr Adam Locker, AuD, founder, Audiology AI and Delray Hearing Center, Florida, USA.
WORKSHOPS
ETHICAL AI IMPLEMENTATION FOR HEARING CLINICS
FINANCIAL MANAGEMENT STRATEGIES FOR SMALL BUSINESSES
Mrs Katie Bryan, Propeller Advisory founder and CEO.
Time-saving tools you can use tomorrow
Mrs Lizette Fourie, business mentor, Hearpreneur Solutions.
INTRODUCING AUDZONE
The first Australian AI platform for audiology clinics
Audiometrist Mr Daniel Fechner, director, AudZone.
BRAND IN ACTION
MASTER CLASSES FROM PAIN POINT TO POWERHOUSE
The three pillars of recruitment, culture and contract confidence
Ms Natasha Hawker, Employee Matters founder and managing director.
CERUMEN MANAGEMENT
VorOtek
Mr Charles Vorrath, director, VorOtek.
The Australian-developed VorOtek O Scope is an in-practice tool for wax removal and deep canal procedures.
CERUMEN MANAGEMENT
Clear Ears Learning
Registered nurse, co-founder and director of Clear Ears Learning, Ms Meg Bumpstead.
A hands-on workshop to bring your personal and practice branding to life
Audiologist Dr Adam Locker, founder Audiology AI marketing agency which helps hearing businesses grow through automation, and Delray Hearing Center, Florida, USA will lead this workshop. Dr Locker bought a failing audiology practice for $21,000 in 2007, expanded it to four offices and five years later sold it for $4.6 million.
Year in review
2025
Confirmation of Ahpra registration for audiologists, a new hearing aid fitting formula and gene therapy breakthroughs were among the big stories of the year for the hearing care sector. Here’s a snapshot of news across the industry.
Australia’s audiologists will remember 2025 as the year the profession achieved a long-awaited regulation breakthrough, the NAL-NL3 hearing aid fitting formula gained worldwide acclaim and Auracast arrived in Australia.
Clinically, AI advances continued to transform the industry, enabling new hearing aids to deliver better sound and
January
clarity, and a 'smart' cochlear implant debuted. The audiology landscape kept changing with technology developments including Apple’s Air Pods Pro 2 hearing aid feature receiving Therapeutic Goods Administration (TGA) approval, EssilorLuxottica moving into the audiology space – offering its Nuance audio glasses for sale in Australian audiology and optometry stores – and George & Matilda
The Therapeutic Goods Administration approved Apple’s AirPods Pro 2 for use as hearing aids in adults with mild to moderate hearing loss in Australia. But its Hearing Aid Feature was not yet available until Apple updated software. The software also contained a hearing test feature.
Audiometrists received their own job classification recognised by the Australian Government and no longer had to be categorised under medical technicians for taxation and other purposes. They received their own code under a new classification scheme, the Occupation Standard Classification for Australia.
A story on hearing practitioner wages was a popular read. Income data released by the Australian Taxation Office revealed the average taxable income for an audiologist in Australia in 2021-2022 – the latest information available – was $96,933. For ENT (ear, nose and throat) surgeons it was $576,925, making them Australia’s fourth most highly paid profession.
Right: Apple’s Air Pods Pro 2 received TGA approval for use in Australia as hearing aids.
Eyecare selling Audeara ear buds. Many in the sector again received government, health and association awards and nominations for their dedication to the hearing needs of the Australian public.
Australian-first cochlear implant guidelines for adults also launched, and research discoveries from Australia and overseas continued in hearing loss, dementia, Menière’s disease, and tinnitus.
February
Scientists from the Kolling Institute and the University of Sydney discovered a new gene mutation for Ménière’s disease which they said meant the inherited or genetic form of the disease may be more common than first realised.
The American pioneers of Tinnitus Retraining Therapy, neuroscientists Drs Pawel and Margaret Jastreboff, delivered face-to-face training in Melbourne for audiologists from around the world. Melbourne tinnitus expert, Ms Mini Gupta, organised the course during tinnitus awareness week.
Starkey launched its Edge AI hearing aids in Australia and New Zealand. ANZ managing director, Ms Dawn Rollings, said the deep neural network was 100 times more powerful than its predecessor, Genesis AI, enhancing sound clarity and streaming range. Other features were 30% better speech identification than existing devices, improved signal to noise ratio, and a two-fold increase in streaming range.
The State Insurance Regulatory Authority, which manages NSW workers’ compensation, proposed cost cutting for hearing aid fitting and rehabilitation for people who sustained workplace-related hearing loss.
March
The Hearing Business Alliance Seminar in Melbourne achieved record attendance – 184 delegates from 121 independent businesses – reflecting continued growth of the organisation in membership, strength and as an influential industry voice.
The Australian Society of Otolaryngology Head & Neck Surgery celebrated its 75th annual scientific meeting in Sydney, attracting more than 600 ENT surgeons from around Australia and overseas.
Sydney Opera House became the first major cultural institution globally to introduce Auracast broadcast technology, setting a benchmark for accessibility in the arts and removing barriers for people with hearing loss. GN, Hearing Australia and National Acoustic Laboratories also collaborated on the world first.
Hearing Australia launched the landmark Profit for Purpose program to provide free hearing assessments, hearing aids and support to at risk people ineligible for Australian Government funded hearing services.
And University of Melbourne research suggested cochlear implants may improve cognitive function and slow dementia symptoms in older adults.
April
The National Acoustic Laboratories revealed its NAL-NL3 hearing aid fitting formula at the American Academy of Audiology conference. It was the first time in 15 years there had been an update to the formula which is used by most audiologists worldwide. It features a suite of prescriptions and will help practitioners solve one of the biggest problems – how to fit hearing aids to people with audiometrically normal hearing tests.
More than 1,000 delegates – one in four audiologists in Australia – attended the nation’s premier hearing health event of the year, the Audiology Australia 2025 conference in Adelaide. Many were honoured with awards including Professor Louise Hickson who was made an AudA life member.
A new $82 million clinical teaching building was announced for La Trobe University, Melbourne. It will house a new audiology clinical service, training and research. It will also offer audiology services to the public, and help relieve Australia’s allied health workforce shortage.
May
Sydney ENT surgeon Clinical Professor Catherine Birman OAM achieved an incredible milestone, performing her 2,000th cochlear implant operation, the second most in Australia, and a rare feat worldwide. The operation at Macquarie University Hospital was on Mr Leslie Harris, 72.
A La Trobe University study found high rates of bullying of audiology interns and students on placement across Australia. Nearly a third of those who answered questions about bullying said they had experienced this. Healthscope, Australia’s second largest private hospital operator entered administration. It said the group’s 37 hospitals nationwide, which employ 19,000 staff including 108 ENT surgeons, would remain open while a buyer was sought.
Dr Angela Alexander, an audiologist who specialises in and trains practitioners to diagnose and treat auditory processing disorder (APD), launched a global directory of practitioners who test and treat APD remotely: The Auditory Processing Services on Zoom Directory.
June
Cochlear launched a world-first platform in Australia and New Zealand, featuring its new NEXOS chipset embedded in a novel “smart”, upgradable cochlear implant capable of evolving with future innovations. The Nucleus Nexa System is the first and only hearing implant featuring internal memory and upgradeable firmware. Conventional implants access future innovation by upgrading their external sound processor but in the new system, wearers can access future technology via updates to firmware in the smart implant and the sound processor.
NSW audiologist, Emeritus Professor Philip Newall, and Canberra ENT and cochlear implant surgeon Dr Edward Peter Chapman were recognised in the 2025 King’s Birthday Honours List for decades of giving generously of their skills and time. Prof Newall was awarded an AM in the General Division “for significant service to audiology education and research, and to the community”. Dr Chapman received an OAM in the General Division “for service to medicine in otorhinolaryngology”.
Right: Delegates at the Audiology Australia 2025 Conference in Adelaide.
Right: Celeste Strings playing at the Auracast launch at Sydney Opera House.
Right: TRT creator Prof Pawel Jastreboff, left, delivered a TRT course in Melbourne; Starkey’s Edge AI hearing aids.
Right: Professor Catherine Birman OAM performed 2,000 cochlear implant surgeries.
Right: (From left) Dr John Newall, his father Prof Philip Newall and Prof Newall's wife Cristy Newall. Images:
July
Melbourne audiologist Ms Mini Gupta’s case report for the inaugural World Misophonia Day was widely read. She successfully treated a young boy, Hunter, who has misophonia and autism and previously wore earmuffs almost 95% of the time.
The Hearing Professional Conduct and Complaints Body warned against live streaming and/or audiovisual recording of patient appointments for training purposes. It said it was a potential breach of the Code of Conduct for audiologists and audiometrists, and was “unethical, and illegal in most cases” to record or view a client appointment without the client’s informed consent.
Early signs of hearing improvement were seen in an Australian toddler who received gene therapy for congenital deafness, confirmed Sensorion, the company developing the treatment. An Australian surgeon involved in the trial, Prof Catherine Birman OAM, reported “encouraging onset of early auditory responses” in all five patients treated plus a good safety profile for the treatment and procedure.
August
Cochlear implant pioneer, Professor Graeme Clark AC, celebrated his 90th birthday at a tribute event at The Royal Victorian Eye and Ear Hospital. Former colleagues – including those instrumental in helping develop the implant – patients, staff, industry, friends and family gathered in the hospital auditorium to honour the ENT surgeon. Another milestone celebrated was the hospital’s 5,000th cochlear implant with recipient, Mrs Margaret Pearce, who was 95 when she received her implant, attending.
Charles Darwin University announced enrolments in its Master of Clinical Audiology had increased by more than 500% since 2022 when the program launched as the only one of its kind nationally to offer online study paired with intensive, hands-on clinical training.
Meanwhile, Specsavers continued its upward trajectory as a major Australian employer ranking fourth in the large business category of the 2025 Best Workplaces list.
September
In one of the biggest developments in the history of audiology in Australia, the Health Ministers Meeting in Perth on 12 September confirmed audiologists would be regulated under the National Registration and Accreditation Scheme (NRAS). Audiologists will join the Australian Health Practitioner Regulation Agency (Ahpra) which administers the NRAS scheme.
The Australian College of Audiology incorporating HAASA (ACAud inc. HAASA) said it was concerning that audiometrists would be excluded from regulation. But in November, ACAud inc. HAASA said health minister Mr Mark Butler had reassured it that audiometrists would continue to be recognised as qualified providers under the Hearing Services Program and other relevant Commonwealth-funded programs.
Meanwhile, the Therapeutic Goods Administration approved Neuromod Devices’ Lenire tongue stimulation device for use by adults with tinnitus in Australia, with audiologists and ENT surgeons likely to have major roles in its prescription and management.
October
The Australia and New Zealand Hearing Health Collaborative launched the first ANZ guidelines for cochlear implantation in adults to improve access, consistency, and outcomes.
Eyecare provider OPSM started delivering audiology services in Australia and New Zealand, and its Nuance Audio Glasses for people with mild to moderate hearing loss went on sale in EssilorLuxottica Group’s optometry stores.
ACAud inc. HAASA lodged a submission to the MBS Review Advisory Committee advocating for audiometrists to be eligible providers under seven audiology and allied health Medicare items.
British toddler Opal Sandy, born profoundly deaf, can now hear normally on her own two years after receiving groundbreaking gene therapy, her parents revealed.
Fiona Stanley Hospital audiologist Ms Caris Bogdanov, who created paediatric and advanced scope registries, was crowned Western Australia’s Early Career Allied Health Professional of the Year.
And more than 150 Specsavers Audiology Partners from around Australia and New Zealand converged on Melbourne for the second annual Specsavers Audiology Clinical Conference.
November
A paediatric audiologist who 12 years ago co-founded Earbus Foundation to help save the hearing of Aboriginal and at-risk children, Dr Lara Shur, was nominated in the 2026 Australian of the Year Awards, Local Hero for Western Australia section. Earbus has delivered more than 100,000 occasions of care.
Israeli company Tuned received Food and Drug Administration clearance for its software platform that transforms standard hearables such as earbuds and headphones into self-fitting hearing aids. It’s the second company, after Apple, to offer self-fitting hearing aid functionality in consumer-grade hearables.
Independent Audiologists Australia presented its inaugural Indy Awards, which celebrate excellence in independent audiology, at its Audiology Unchained 2025 conference in Queensland.
Meanwhile a systematic review and meta-analysis found the risk of hearing loss was four times higher in people with type 2 diabetes than those without diabetes. Findings indicated diabetes care should include hearing assessment, researchers said.
Right: Dr Lara Shur was nominated for an Australian of the Year Award; Tuned software turns earbuds into hearing aids.
Right: Toddler Sandy Opal can hear after receiving gene therapy.
Right: Neuromod’s Lenire tinnitus device received TGA approval.
Right: Prof Graeme Clark AC (third from right) at his 90th birthday tribute, and 5,000th cochlear implant recipient Margaret Pearce (far right).
Right: Hunter, 10, received successful treatment for his misophonia.
WHAT HAPPENS TO THE INNER EAR DURING PREGNANCY?
ENT registrar Dr SARA TIMMS and otolaryngologist Dr EMMA STAPLETON undertook a systematic review to evaluate the effect of pregnancy and pregnancy syndromes on the function of the inner ear. DR TIMMS explains.
IN PREGNANCY SYNDROMES SUCH AS PRE-ECLAMPSIA THESE CHANGES MAY BE PERMANENT DUE TO MICROVASCULAR ISCHAEMIA.
DR SARA TIMMS
The inner ear is a complex organ responsible for the conversion of mechanical sound, head position and movement stimuli into electrical signals. It depends on a fine balance of electrolyte and fluid content in the endolymph and perilymph, as well as correctly functioning sensory hair cells.
Research has established that hearing thresholds fluctuate during the menstrual cycle, a pattern which suggests that circulating oestrogen is protective for the inner ear. Vestibular function similarly shows subtle hormonal cycle variability.
In pregnancy, persistent high circulating levels of oestrogen and progesterone lead to much greater physiological changes than those of the menstrual cycle. Cardiac output and circulating volume increase, haemodilution occurs, a thrombotic state develops, and the immune system adapts to become ‘tolerant’ of the developing foetus.
Sensorineural hearing loss and vestibular loss of function caused by trauma, ototoxicity and ageing are understood to be irreversible, whereas other inner ear conditions demonstrate a degree of reversibility.
Pregnancy, with its physiological changes that are reversed post-partum, offers insight into the reversibility of vestibulocochlear dysfunction.
contained original research, 29 of which were prospective studies of an observational nature and eight were retrospective reviews. There were no interventional randomised controlled trials, but many observational studies included matched controls. The remaining 32 articles included case series, case studies and reviews.
We reviewed the published work in two categories: those that assessed the effects of normal pregnancy on the inner ear, and those that considered the effect of pregnancy syndromes such as gestational diabetes and preeclampsia.
NORMAL PREGNANCY –HEARING
Three studies reported a statistically significant but subtle hearing loss in pregnancy, particularly in the lower frequencies and in the third trimester of pregnancy. These studies all suggested that this subclinical hearing loss is reversible after delivery.
A small study with 100 participants tested the normal otoacoustic emissions produced by a healthy cochlea. It found them to be absent in 4% of non-pregnant individuals, but in 26% of pregnant women. Another study found a higher incidence of tinnitus in low-risk pregnancy than in non-pregnant controls.
studies raises the possibility that women with significant nausea and vomiting in pregnancy, including hyperemesis gravidarum, may have underlying undiagnosed vestibular pathology.
Supporting this hypothesis, it was found that a history of motion sickness or migraine is more common in those who experience nausea in pregnancy.
PREGNANCY SYNDROMES
Three studies found a statistically significant worsening in hearing thresholds in women with pre-eclampsia compared with pregnant women without pre-eclampsia. One of these studies repeated the assessment after delivery and found the changes to persist, which may be due to the permanent microangiopathy (damage to small blood vessels) caused by the condition.
Similarly, patients with gestational diabetes had significantly worse pure tone thresholds in the higher frequencies (8 kHz to 14 kHz) when compared with pregnant controls, a finding that did not normalise postpartum.
CONCLUSION
Below: Those with nausea and vomiting may have vestibular pathology.
We performed a systematic review, published in the Journal of Laryngology and Otology online on 1 October 2025, to evaluate the effect of pregnancy and pregnancy syndromes on the function of the inner ear. The initial searches identified 341 articles, of which 69 were included in the final analysis.
Of the 69 articles reviewed, 37
Many studies investigated sudden sensorineural hearing loss (SSNHL) in pregnancy, largely from the perspective of establishing safe treatment guidelines, for example the use of intratympanic steroids. In large whole-population analyses from Taiwan and South Korea, it was found that SSNHL occurs less commonly in pregnancy than in the general population.
NORMAL PREGNANCY –BALANCE
Vestibular migraine was a common cause of dizziness in pregnancy in one study, a symptom that might wrongly be attributed to ‘normal’ pregnancy nausea. This group of Image: Prostock-studio/stock.adobe.com
Several observational studies found changes in vestibular function test results in pregnancy, such as reduced gain on the video head impulse test (VHIT) and abnormalities in the vestibular evoked myogenic potentials (VEMPs), particularly in the first trimester.
Despite the heterogeneity of the literature, the hearing practitioner can draw several valuable conclusions from this review. The inner ear is sensitive to physiological changes that occur in pregnancy which can affect hearing and balance.
Reasons for this may include altered electrolyte balance in endolymph and perilymph, hypercoagulability affecting small inner ear vessels, or direct effects of pregnancy hormones. In pregnancy syndromes such as pre-eclampsia these changes may be permanent due to microvascular ischaemia. It is important to take a thorough history, including motion sickness, and consider vestibular diagnoses in a patient presenting with balance symptoms in pregnancy.
ABOUT THE AUTHOR: Dr Sara Timms is an ENT registrar training in Manchester, UK who has an interest in otology and hearing implants. She is currently undertaking the Graham Fraser Otology Fellowship in Sydney working with Professor Catherine Birman OAM in the University of Sydney and department members of the Royal Prince Alfred Hospital, Children’s Hospital at Westmead and Nextsense Cochlear Implant Program.
Image: Sara Timms.
11–13 May 2026
Accor Stadium, Sydney
Experience audiology in action.
Step into The Sound Exchange ’26 – Australia’s #1 hands-on, immersive audiology event. Join leading audiologists, researchers, and innovators to explore the future of hearing care.
Attend the main event
Select one of four interactive Masterclass streams on 12–13 May, and gain a deep dive into specialised areas of audiology through practical sessions, live demonstrations and real-world learning.
Looking to extend your learning?
Enhance your experience with optional pre-conference workshops on 11 May – broadening your learning before diving into your chosen stream.
Registrations open now!
For more information, visit audiology.eventsair.com/sound-exchange-2026
HEARING LOSS HIGHER IN RURAL AREAS
Prevalence of hearing loss is higher in Australia’s rural than urban areas says LIAN GIJO, which is all the more reason for hearing care practitioners to practise in country regions.
HEALTHCARE PROFESSIONALS STAND AT THE FRONTLINE OF A QUIET REVOLUTION, ONE WHERE MORE PEOPLE CAN HEAR.
Hearing loss remains one of the most overlooked public health issues and a silent epidemic. The World Health Organization (WHO) reports that 430 million people in the world's population require hearing rehabilitation. This is expected to grow to more than 700 million by 2050.
In this context, in underserved regions ranging from the remote villages of Africa to the Pacific island communities, access to hearing healthcare remains out of reach. By comparison, Australia has an upper hand with its strong public system that makes hearing care widely accessible. About one in 10 adults over the age of 65 years and one in 20 between 45-59 years experience some degree of hearing loss. Studies have found that prevalence of hearing loss is higher in rural Australia compared to urban areas, especially in parts of Western Australia and the Northern Territory.
A study that evaluated the key enablers and barriers in Australian hearing healthcare included the lack of knowledge about hearing and hearing health among primary health care providers, accessibility factors such as location of services and available educational resources, psychosocial support and reduced awareness of tele-audiology services. The insufficient number of hearing health specialists is often one other important barrier to meeting the demands in remote and rural communities. In this lens, the value of audiometrists and their global outreach work becomes clearer.
The shortage of audiological professionals in rural Australia has been established by several studies, with approximately 600 professionals serving a population of seven million. The trend of audiologists to move from regional areas to the cities as their career progresses is also widely seen.
Another aggravator was the limited access to audiological training for rural students or the unwillingness to travel to study in metropolitan areas; or if they did, reluctance to return to rural areas upon graduation. This gap has been resolved with the introduction of remote study options for Cert IV in Audiometry and the Diploma in Audiometry, training audiometrists to tackle challenges in the hearing healthcare sector and meet the increased demand of hearing healthcare professionals in rural Australia.
Audiometrists are essential to provide hearing healthcare services through mobile hearing units, outreach teams and community clinics, conducting hearing assessments, dispensing of hearing aids and referral of complex cases to audiologist and ENTs. As the trend in hearing loss prevalence is changing, they play a critical role in the early intervention of children through play audiometry and hearing rehabilitation among adult populations.
The situation is even more pressing when it comes to the Indigenous communities. Hearing loss among Indigenous communities of Australia such as Aboriginal and Torres Strait Islander children and young adults is high in prevalence and characterised by early onset, persistence, and greater severity.
When left untreated, it can lead to chronic hearing loss and affect long-term wellbeing. This also focuses on the need for more Indigenous workers trained through courses such as Cert IV in Audiometry for Aboriginals and Torres Strait Islanders provided at the Australasian College of Audiometry. Here, professionals are uniquely positioned to help, focusing on practical care and community engagement, which
aligns with the needs of culturally diverse populations, helping build trust and provide more culturally appropriate care.
BRINGING GLOBAL SKILLS TO RURAL AUSTRALIA
Some skills that translate powerfully in rural Australian settings, eliminating some of the common barriers are:
• The ability to work with limited resources and creative solutions
• Being able to communicate across cultural differences
• The skills to navigate community dynamic with respect and humanity
• A focus on education and empowerment, not just treatment.
PATHWAYS AND POSSIBILITIES: GETTING INVOLVED
For audiometrists keen to make a difference in their communities, there are several meaningful ways to become involved, including:
• Volunteering with NGOs which focus on global hearing health
• Initiating and/or joining outreach programs in remote and regional Australia
• Supporting Indigenous-led organisations as clinicians and advocates.
A PROFESSION WITH GLOBAL AND LOCAL PURPOSE
The global trend of hearing loss affects millions worldwide and disproportionately affects vulnerable communities. Hearing healthcare professionals stand at the frontline of a quiet revolution, one where more people can hear, connect, learn, and thrive. Their hands-on skills, growing global experience and human-centered approach make them invaluable not only overseas, but in Australia where hearing healthcare equity has a long way to go. Whether you are early in your career or an experienced audiologist or audiometrist, there has never been a more important time to broaden your horizons. The world and Australia need you.
*References will be included in the online version.
LIAN GIJO
ABOUT THE AUTHOR: Ms Lian Gijo is a clinical audiologist and educator with the Australasian College of Audiometry.
Below: Rural towns such as Stanley, Tasmania have a lot to offer including lifestyle.
Image: Lian Gijo.
PROTECTING PRIVACY: PREPARING FOR CHANGE
GEORGIE HAYSOM looks at what recent changes to Australian privacy laws mean for healthcare providers.
THIS CHANGE MARKS A SIGNIFICANT SHIFT IN AUSTRALIAN PRIVACY LAW AS INDIVIDUALS CAN NOW BRING A PERSONAL CLAIM FOR COMPENSATION OR DAMAGES FOR THE FIRST TIME.
GEORGIE HAYSOM
The new tort of serious invasion of privacy is the most significant of a suite of legal reforms for Australian privacy laws. These changes reflect growing community concern about how organisations collect, use and protect personal information, particularly sensitive health information.
The new tort will apply where someone intentionally or recklessly intrudes on another’s seclusion – for example by “watching”, ”listening to,” or “recording”– or misuses private information, including unauthorised collection, use or disclosure of personal information. As the name indicates, the privacy breach must be serious.
This change marks a significant shift in Australian privacy law as individuals can now bring a personal claim for compensation or damages for the first time. This change compliments the increased powers the government has bestowed on the Office of the Australian Information Commissioner (OAIC) to issue infringement and compliance notices from 10 June 2025, which impose financial penalties for lower level breaches of privacy.
Above: Responsibility may not stop with rogue employees, with the potential for employers to be held vicariously liable if they cannot demonstrate they took reasonable steps to protect patient privacy.
patients’ personal information and establishing policies to respond to requests for access to information.
LOOKING AHEAD: AUTOMATED DECISION-MAKING
The government has made it clear the tort is not intended to capture appropriate healthcare or research activities. Even so, it will have implications for healthcare settings.
ENSURE ROBUST POLICIES AND PROCEDURES
Australian courts have yet to test the extent of the new provisions. Some situations that have occurred in health contexts might now be covered by the tort, including, for example, covertly filming or sharing images of unconscious patients, publishing patient contact or health information, or stalking patients.
As with other civil causes of action such as negligence, employers could face vicarious liability for an employee’s actions if they cannot demonstrate they took reasonable steps to protect patient privacy. Healthcare providers and practices must now ensure their privacy systems are robust. This includes implementing privacy policies and procedures, updating existing privacy policies, restricting access to information only to those who need it, and ensuring staff are trained on their responsibilities when handling
Healthcare professionals working in hospitals can also expect increasing vigilance around privacy and records management policies as hospitals will also need to demonstrate they have reasonable safeguards in place. In a hospital context, it is even more important to be sure you understand and follow hospital policies to avoid an inadvertent breach, which may also impact your employment obligations.
ARE YOUR PRIVACY POLICIES UP TO DATE?
Under current privacy law, all healthcare providers must have a clearly expressed and up-to-date privacy policy that explains how the practice manages personal information. This is a legal obligation, not a ‘nice to have’.
We too often see avoidable medico-legal issues tracing back to outdated, unclear, or incomplete policies. The OAIC now has expanded powers to issue infringement notices and civil penalties for lower-level privacy breaches, including if healthcare providers fail to ensure their privacy policy is compliant or fail to appropriately respond to their privacy obligations (such as providing access to records).
Practitioners and practices may face financial penalties via an infringement notice if they do not ensure they comply with their privacy obligations. If your practice lacks a privacy policy that contains the required content, you should update it immediately.
From December 2026, privacy legislation will also require practices to disclose in their privacy policies whether they use any automated decision-making tools including software that assists in diagnosing or interpreting conditions, or supporting surgical planning based on biometric data.
Even if your practice does not currently use such tools, you will need to keep patients informed as technology advances. You must be transparent about the use of these tools, if and when you use them, to meet future obligations and maintain patient trust.
The changes to privacy law present a timely opportunity, and increased incentives, to strengthen your practice’s approach to privacy. Patients trust you not only with their hearing but also their personal information. You can best protect both your patients and your practice against financial penalty by demonstrating that you take that responsibility seriously, through sound policies, secure systems, and informed staff.
Note: For more guidance, Avant members can access its privacy collection page via avant.org.au/ cyber-collection and view its webinar on the changes at www.youtube.com/ watch?v=5xUj4p6PWpM&t=1251s
Image: XiXinXing/Shutterstock.com.
ABOUT THE AUTHOR: Georgie Haysom, BSc, LLB (Hons) LLM (Bioethics), GAICD, is the general manager of advocacy, education and research at Avant.
Image: Georgie Haysom
SOAPBOX
BREAKING THROUGH NDIS BARRIERS
Parents of Deaf Children has created free workbooks to break through barriers and make the NDIS more accessible for families with Deaf/deaf children.
In 2025 Parents of Deaf Children (PODC) rolled out its Breaking Through Barriers Advocacy
Series – a collection of practical, plain-language and free workbooks designed to make Australia’s National Disability Insurance Scheme (NDIS) more accessible for families raising Deaf/deaf children. We know how overwhelming the NDIS can feel. Policies and processes change constantly, and families are often left trying to interpret complex information while juggling therapy, schooling, and day-to-day life. Our goal in creating these resources was simple – to take the pressure off families by turning that complexity into clear, functional tools that make sense in the real world.
There’s no shortage of NDIS information online, but much of it is hard to understand. We wanted to bridge that gap – to create something that reflects lived experience, language access, and the practical realities of raising Deaf/deaf children. Each workbook is grounded in what we hear every day from parents, what we see as advocates, and what we’ve experienced navigating the system alongside families ourselves.
THE FOUR CORE WORKBOOKS
1. NDIS 101 – What Every Parent of a Deaf
Child Needs
This first workbook lays the foundation. It breaks down how the NDIS works for children with hearing loss, explains eligibility and evidence requirements, and walks families through setting clear, achievable goals. It also covers plan management options and funding categories in plain English, helping parents feel prepared and confident from their first planning meeting.
2. The NDIS Game Plan –Planning, Prep and Pathways
Once families understand the basics, Game Plan helps them take charge of implementation. It includes templates, mapping tools, and examples of what quality evidence looks like. Families learn how to build stronger reports, work with providers, and link supports directly to their child’s goals. This resource also unpacks the latest reforms under the new PACE central computer system, helping families stay ahead in a constantly changing environment.
3. Fixing Broken Plans – NDIS Reviews, Variations and Knowing Your Rights
Sometimes, plans fall short or decisions feel unfair. Fixing Broken Plans gives families step-by-step guidance through reviews and appeals, including plan variations under Section 48 and internal reviews under Section 100 of the NDIS Act. It includes practical scripts, templates, and timelines so parents can advocate confidently. Importantly, it reminds families they have rights to safety, respect, privacy, and fair treatment throughout every stage of the process.
This workbook recognises the emotional toll of constant advocacy. It helps families find balance and avoid burnout, using tools like the advocacy weather check-in and push grid to work out when to act, when to rest, and when to seek support. It’s about sustainability – reminding parents that their wellbeing matters as much as their child’s progress.
CREATING FUNCTIONAL RESOURCES THAT WORK
Each workbook was designed to be more than information – it’s a functional tool families can use. We didn’t want these to be tokenistic or overly technical. We wanted them to create real-world change – to be the kind of resource a parent could print out, take to a meeting, and use to advocate effectively.
Feedback has been incredible. Families are telling us the workbooks make the NDIS finally feel understandable. Many have shared
them with their child’s therapists, support coordinators, planners, and Teachers of the Deaf. We’ve also seen them used by other community and disability groups because so much of the information applies across different support needs.
That was our hope from the start –that these workbooks wouldn’t just inform one parent, but would ripple outward. When a parent learns how to advocate, they share that knowledge with others – families just starting the journey and those yet to come. That’s the power of parent voices.
This series also led to the creation of a fifth resource – Language Access Lens: High School. Built on ideas first introduced in Push, Pause, Pivot, it focuses on how language access continues through education. While it’s a new addition, families have begun using it to start meaningful conversations in schools about communication, inclusion, and access.
With the completion of these workbooks, PODC’s NDIS advocacy series is now finalised. In 2026, we’ll turn our focus to supporting families as they navigate the education system – creating resources that equip parents with the knowledge and confidence to ensure their children have genuine access to language and learning throughout their schooling years.
This work was made possible through funding from the NSW Government’s Disability Advocacy Futures Program, and we are deeply grateful. Its support allows PODC to continue creating practical, rights-based resources that make a real difference for families.
Breaking Through Barriers is more than a name; it’s our purpose. Each workbook represents the strength, resilience, and lived experience of the families we serve. Together, they're helping parents turn uncertainty into action, and advocacy into lasting change.
People can access the free resources at podc.org.au.
Name: Suzanne Robertson
Affiliation: President of Parents of Deaf Children, a non-profit organisation supporting families with babies, children and teenagers with hearing loss in NSW and the ACT.
Location: Sydney Australia.
“THERE'S NO SHORTAGE OF NDIS INFORMATION ONLINE BUT MUCH OF IT IS HARD TO UNDERSTAND.”
Suzanne Robertson Image: Suzanne Robertson.
People on the move
NEW ROLE FOR ANDREA ROMAS
Ms Andrea Romas has been promoted to audiology clinical project lead at Specsavers. Having worked in professional services for the brand for six years, and before that for Phonak and Hearing Australia, Romas has a strong background in audiology partner support and transformation. Specsavers said her experience in designing workflows, training strategies, and change management initiatives will ensure it continues to change lives through better hearing. Her career spans leadership roles where she championed digital enablement, optimised customer journeys and training. Passionate about empowering Partners for success, she combines strategic insight with clinical expertise to deliver impactful solutions that elevate service standards and efficiency.
GN PROMOTES PAUL JONES
GN Hearing has promoted Mr Paul Jones to general manager for Australia and New Zealand. GN said Jones brought 27 years of extensive management experience, including seven with GN. During this time, he led the ANZ sales team, drove sales excellence for the APAC region, and most recently served as country director for Australia. Jones shared his vision to deepen relationships with partners and the hearing health community through his new role. “My focus will be on building even stronger, more collaborative relationships with our partners and the broader hearing health community,” he said. “GN has always been at the forefront of innovation, but equally important is how we listen, understand, and respond to the needs of those we serve.”
DWM AUDIOLOGY HANDOVER
Ms Myriam Westcott (right) has retired from clinical practice after 25 years of being an owner/director of DWM Audiology. She leaves the clinic in the safe hands of co-director and close friend Ms Kate Moore, (left) now sole owner/director. “Kate and I have enjoyed many years of harmonious and collaborative partnership, and I'm thankful for her support of my gently paced exit. I will continue to be active in the field of tinnitus and sound intolerance, coordinating research and providing training, lectures, presentations and webinars,” Westcott says. “We’ve had a wonderful partnership; Kate will do a great job steering DWM into the future.” Westcott is proud of its international reputation for tinnitus, hyperacusis therapy programs and personalised and ethical care.
WIDEX WELCOMES YVY NGUYEN
Ms Yvy Nguyen is Widex’s new account and product manager for Victoria and Tasmania. Nguyen has extensive experience in the retail audiology sector and a deep commitment to advancing natural hearing through innovation, collaboration, and exceptional client outcomes. She has a Master of Clinical Audiology and a Bachelor of Applied Science from La Trobe University where she was awarded the Vice Chancellor’s Scholarship for Academic Excellence. She's also an Audiology Australia member. Her experience across clinical and retail environments has given her a deep understanding of what clients value. Widex sales director ANZ, Ms Geraldine Todd, says Yvy’s clinical expertise makes her an invaluable asset to Widex and the professionals it supports.
APAC POSITION FOR ANDERHOV
Mr Andreas Anderhov is GN Hearing’s new Asia Pacific (APAC) regional president. He was promoted from his previous role as cluster managing director for Australia, New Zealand, India and South Korea. Anderhov said trust in local leadership was central to his plan for the region. “I have strong confidence in our local leadership, whose deep understanding of regional markets, cultural nuances, and customer needs allows them to navigate complexities effectively while aligning with GN’s global objectives,” he said. “I believe that fostering a culture of trust and transparency reflects the value we have over our local leaders and allows them to drive performance and innovation within their teams.”
MARIANA REIS JOINS FLINDERS UNI
Dr Mariana Reis joined the audiology team at Flinders University College of Nursing and Health Sciences, Adelaide in August 2025 as a lecturer in the Master of Audiology program. Her role includes contributing to the design and delivery of the program curriculum as well as supporting audiology students at the Flinders University Health2Go interprofessional clinic. Trained as an audiologist in Brazil, Dr Reis completed her PhD in aural rehabilitation at Macquarie University in 2019. Her career spans clinical, research, and education roles across the not-for-profit, public, and private sectors. She is passionate about driving impact through education, and empowering future audiologists to deliver evidence-based, person-centred hearing healthcare.
Image: Mariana Reis.
EVENTS CALENDAR 2026
To list an event in our calendar please email helen.carter@primecreative.com.au
JANUARY 2026
AUDIOLOGY AUSTRALIA ONLINE CONFERENCE 2025 RECORDINGS Online Until 18 January portal.audiology.asn.au/all-events
FEBRUARY 2026
TINNITUS AWARENESS WEEK 2026 Nationwide and worldwide 2-8 February soundfair.org.au/tinnitus-awareness
HEARING BUSINESS ALLIANCE 2026 SEMINAR Brisbane, Australia 12-14 February hearbusiness.com.au
MARCH 2026
WORLD HEARING DAY Worldwide 6 March who.int/campaigns
76TH ASOHNS ASM Hobart, Australia 20-22 March asm.asohns.org.au
APRIL 2026
ACAUD INC.HAASA NATIONAL CONGRESS 2026 Gold Coast, Australia 22-24 April acaud.com.au
AMERICAN ACADEMY OF
MAY 2026
AUDIOLOGY AUSTRALIA'S SOUND EXCHANGE '26 Sydney, Australia 11-13 May soundexchange.com.au
IAA MEANS BUSINESS: BOOKKEEPING LIKE A BOSS Online recording 19 May independentaudiologists.net.au
WCA 2026 WORLD CONGRESS OF AUDIOLOGY Seoul, Korea 24-27 May wca2026seoul.com
JULY 2026
The Sound Exchange ’26, an Audiology Australia event, will be in Sydney in May.
WCA 26, The World Congress of Audiology, will be in Seoul, Korea in May, towards the end of the cherry blossom season.
The 2026 Australian Deaf Games will be on the Sunshine Coast in July.
Image: Aerial Film Studio.
Not all AI is created equal
Like the human brain’s auditory cortex, Edge AI’s all NEW G2 Neuro Processor features the industry’s only fully integrated neural processing unit (NPU) dedicated to DNN processing to deliver unparalleled speech enhancement and noise reduction. Edge AI’s sophisticated DNN architecture is doing 100x more DNN processing and utilizes our Speech Probability Predictor to classify speech 30% more accurately in noisy environments (compared to previous technology).
To find out more or order call 1800 024 985 or speak to your local product specialist. Visit us at starkeypro.com.au