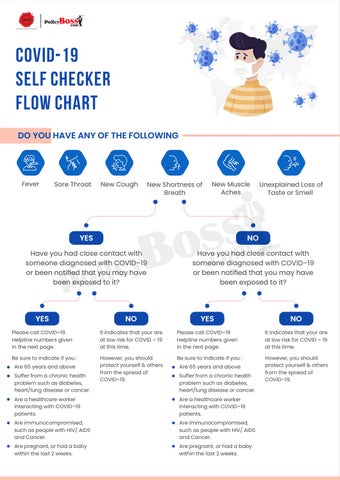
COVID-19 Self Checker Flow Chart DO YOU HAVE ANY OF THE FOLLOWING
Fever
Sore Throat
New Cough
New Shortness of Breath
New Muscle Aches
Unexplained Loss of Taste or Smell
YES
NO
Have you had close contact with someone diagnosed with COVID–19 or been notified that you may have been exposed to it?
Have you had close contact with someone diagnosed with COVID–19 or been notified that you may have been exposed to it?
YES
NO
YES
NO
Please call COVID–19 Helpline numbers given in the next page.
It indicates that your are at low risk for COVID – 19 at this time.
Please call COVID–19 Helpline numbers given in the next page.
It indicates that your are at low risk for COVID – 19 at this time.
Be sure to indicate if you :
However, you should protect yourself & others from the spread of COVID–19.
Be sure to indicate if you :
However, you should protect yourself & others from the spread of COVID–19.
Are 65 years and above Suffer from a chronic health problem such as diabetes, heart/lung disease or cancer.
Are 65 years and above Suffer from a chronic health problem such as diabetes, heart/lung disease or cancer.
Are a healthcare worker interacting with COVID–19 patients.
Are a healthcare worker interacting with COVID–19 patients.
Are immunocompromised, such as people with HIV/ AIDS and Cancer.
Are immunocompromised, such as people with HIV/ AIDS and Cancer.
Are pregnant, or had a baby within the last 2 weeks.
Are pregnant, or had a baby within the last 2 weeks.