
APP2026 CPD Handbook
Proudly sponsored by:





Overview
The Pharmaceutical Society of Australia (PSA), through the Australasian College of Pharmacy (the College or ACP), is the official education partner of the APP2026 conference.
The activities at the APP2026 conference have been accredited for a total of up to 13 hours of Group 1 CPD (or 13 CPD credits) suitable for inclusion in an individual pharmacist's CPD plan which can be converted to up to 13 hours of Group 2 CPD (or 26 CPD credits) upon successful completion of relevant assessment activities (current as of 11 March 2026).
Although the College was acquired by the PSA on 19 December 2025, the process for completing APP2026 CPD assessments remains unchanged. To confirm, online APP2026 CPD assessments and certificates of completion are only available on the College CPD Library, not the PSA online learning platform.
Representatives of the PSA | ACP will be present at the APP2026 conference on trade stand #343.
How to record your CPD Credits
Group 1 CPD Credits
Eligibility: Attendance at an accredited APP2026 session.
Group 1 activities do not require completion of an assessment. You may self-record Group 1 credits on your preferred CPD platform or recording tool. This can be the College CPD Library, or another recording system, however, ensure that you do not record the same activity more than once across multiple platforms.
To self-record your Group 1 credits on your preferred CPD recording platform, refer to the essential CPD information included in this Handbook (e.g. accreditation codes and competency standards)
Group 2 CPD Credits
Eligibility: Attendance at an accredited APP2026 session and 100% pass rate of associated MCQs
Group 2 assessments are hosted in the College CPD Library. To access and complete assessments, you must login to your existing College account or create a new College account.
If you are not yet registered with the College, please visit acp.edu.au/APP2026 for information on how to create a free account in the College CPD Library.
Important information
• Enrolment into Group 2 assessments opens once the session has commenced (AEST – Queensland time). You may enrol and complete assessment questions during the session or after it concludes.
• A 100% pass rate on all assessments is required.
• You are provided with unlimited attempts per assessment.
Accessing Group 2 assessments
For those registered with the College, please use one of the following methods to access your Group 2 APP2026 assessments:
Method 1: Using direct links via this CPD Handbook
1. Locate the relevant session in this Handbook.
2. Click or type the Bitly link listed for that session.
3. If prompted, login to the College CPD Library using your existing account.
4. Click Enrol on the session page.
5. Open the session module and click the assessment link.
6. Complete the assessment and achieve a 100% pass rate.
7. Important: After successfully passing the assessment, download your certificate. This triggers the system to add the CPD credits to your transcript and mark the activity as 'Complete'.
Method 2: Self-enrolment into multiple APP2026 sessions
1. Login to the College CPD Library
2. Select the Conferences tab from the top menu, then APP2026.
3. Use the checkbox on each course tile to select one or more sessions.
4. Click Enrol all to enrol in your selected sessions.
5. Select the Your Learning tab from the top menu
6. Open the session module and click the assessment link.
7. Complete the assessment and achieve a 100% pass rate.
8. Important: After successfully passing the assessment, download your certificate. This triggers the system to add the CPD credits to your transcript and mark the activity as 'Complete'.
Bridging knowledge and practice in compounding: A clinical services perspective
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Marina Holt
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
OR
CPD accreditation code: PSAAPP2603
THURSDAY 12 MARCH 2026 11:00AM – 11:30AM
Competencies: 1.3, 1.5, 1.6, 3.1, 3.2, 3.3, 3.4, 3.5, 4.7
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2603.

• Identify the importance of adjusting calculations based on specific lot numbers, using the appropriate Certificate of Analysis, and the impact on patient outcomes
• Apply perioperative guidance for low-dose naltrexone by determining an appropriate cessation timeframe before elective surgery.
• Evaluate thromboembolism risk considerations in patients with Factor V Leiden mutation when considering use of estrogen hormone replacement.
• Identify areas where improvements to risk assessment forms may be appropriate to address patient safety
Multiple Choice Questions
1. A new lot of Naltrexone HCl (Dihydrate) has an assay of 100.0% and total solvents of 6.6%. How much API should be weighed for 100 capsules of 4.5mg strength?
A. 0.4500 g
B. 0.4818 g
C. 0.4200 g
D. 0.5000 g
2. How long before elective surgery should low-dose naltrexone (1-7mg) be ceased according to institutional guidelines?
A. 12 hours
B. 24 hours
C. 72 hours
D. 1 week
3. Which route of estrogen administration shows NO increased VTE risk in Factor V Leiden carriers when using transdermal treatment at 50 ug or less?
A. Oral estrogen tablets
B. Transdermal patches/gels
C. Sublingual troches
D. Intramuscular injections
4. Following concerns about melatonin safety, which question should be added to the risk assessment form for melatonin prescriptions?
A. What is your preferred flavour?
B. Have you previously purchased melatonin from the internet or iHerb?
C. Do you prefer tablets or capsules?
D. What time do you usually go to bed?
- Questions complete -
Pharmacy and the great GORD divide: Ins and outs of the scope of practice
Venue: GCCEC, Meeting Rooms 5 & 6
Speakers: Associate Professor Treasure McGuire and Anthony Vo
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
OR
CPD accreditation code: PSAAPP2604
THURSDAY 12 MARCH 2026 11:35AM – 12:05PM
Competencies: 1.5, 2.1, 2.3, 2.4, 3.1, 3.2, 3.3, 3.5, 3.6
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2604
• Summarise the key points of pharmacist led management of reflux and GORD.
• Outline the key steps and skills required to confidently and appropriately assess patients with symptoms of reflux.
• Identify common causes of reflux and the importance of personalising management.
Multiple Choice Questions
1. Which of the following statements are correct?
A. All pharmacists are able to initiate a trial of a standard dose PPI for up to 8 weeks
B. Pharmacists are able to recommend standard-dose and high-dose PPIs
C. All pharmacists are able to initiate a trial of a standard dose PPI for up to 14 days
D. Following failure of an initial trial of a PPI, pharmacists cannot initiate a second trial of a PPI
2. Pharmacists are recommended to personalise the management of reflux and GORD utilising which of the following:
A. Lifestyle measures
B. Antacid-alginate combination therapies
C. PPIs and H2RAs
D. All of the above
3. Which statement is correct about antacid-alginate products?
A. They have a lesser role in management for pharmacists with access to prescribing privileges
B. They play a complementary role in patients with frequent and/or severe reflux, with a different action to PPIs and providing symptom relief during the time it takes the PPI to take effect
C. There is no head-to-head evidence supporting the preference of an antacid-alginate as a first-line treatment option for patients with reflux
D. Patients on PPI experiencing breakthrough symptoms would not benefit from adding an antacid-alginate therapy to their regimen
4. In assessing a patient with symptoms of reflux, which of the following criteria can help determine the management approach.
A. Description of symptoms
B. Frequency of episodes
C. Severity of episodes
D. Trigger factors for symptoms
E. All of the above
5. Which of the following are instances where pharmacists may be able to assist patients with optimised reflux management based on guideline evidence?
A. First-time symptoms of reflux
B. Experiencing breakthrough symptoms when on a PPI
C. Experiencing symptoms when attempting to step down or off a PPI
D. All of the above - Questions complete -
When sunshine isn’t enough: Supporting maternal and neonatal bone health with vitamin D – evidence and optimal doses
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Associate Professor Treasure McGuire
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
OR
THURSDAY 12 MARCH 2026 12:10PM – 12:40PM
CPD accreditation code: PSAAPP2605 Competencies: 1.5, 1.6, 2.1, 2.3, 3.1, 3.2, 3.3, 3.5, 3.6
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2605.
• Explain the role and physiological actions of vitamin D in maternal and fetal skeletal development.
• Identify risk factors and consequences of vitamin D deficiency during pregnancy, including maternal and neonatal outcomes.
• Evaluate current evidence and guidelines on vitamin D supplementation in pregnancy, including recommended doses and controversies.
• Apply clinical trial findings (e.g., MAVIDOS) to counsel pregnant women on safe and effective vitamin D supplementation strategies.
Multiple Choice Questions
1. Which form of vitamin D is primarily synthesised in the skin following sunlight exposure?
A. Ergocalciferol
B. Colecalciferol
C. Calcitriol
D. Calcidiol
E. Cholecystokinin
2. What is the globally accepted threshold for vitamin D deficiency based on serum 25(OH)D levels?
A. <75 nmol/L
B. <50 nmol/L
C. <30 nmol/L
D. <20 nmol/L
E. <10 nmol/L
3. Which of the following is a recognised consequence of maternal vitamin D deficiency during pregnancy?\
A. Venous thromboembolism
B. Osteomalacia
C. Hypercalcemia
D. Increased maternal iron absorption
E. Large for gestational age
4. According to the MAVIDOS trial, what daily dose of vitamin D was used during pregnancy?
A. 200 IU
B. 400 IU
C. 600 IU
D. 1000 IU
E. 2000 IU
5. Which statement about vitamin D supplementation in pregnancy is TRUE?
A. WHO recommends universal vitamin D supplementation for all pregnant women
B. NICE recommends vitamin D 1000 IU daily for all pregnant women
C. No guidelines support supplementation during pregnancy
D. RANZCOG recommends vitamin D 200 IU daily for all pregnant women
E. International consensus suggests 600–1000 IU daily to reduce rickets risk
- Questions complete -
Heads up Australia: The untold cost of dandruff
Venue: GCCEC, Meeting Rooms 5 & 6
Speakers: Trent Playford, Dr Emily Shao and Catherine Bronger
CPD Credits
0.5 Group 1 CPD credits
Session attendance only. Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
• Explain the cause of dandruff.
CPD accreditation code: PSAAPP2609
Competencies: 3.1, 3.2, 3.5, 3.6
THURSDAY 12 MARCH 2026 2:00PM – 2:30PM
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2609.
• Describe the social and emotional burden of dandruff.
• Summarise the main reasons individuals may not seek assistance from pharmacists to manage dandruff
• Explain how to optimise the treatment of dandruff.
Multiple Choice Questions
1. Dandruff is caused by:
A. Headlice infestations
B. Allergic reactions
C. Malassezia overgrowth
D. An autoimmune disease
2. Which of the following statements is true?
A. Dandruff is a trivial condition, with only minor psychosocial consequences
B. Dandruff is a self-limiting condition that will resolve without treatment
C. Once dandruff has been effectively treated and cleared the person is cured of this condition
D. Dandruff typically requires ongoing treatment to prevent its recurrence
3. Which of the following statements is NOT true?
A. Dandruff can undermine a person’s self-esteem
B. Only the more severe seborrhoeic dermatitis, and not dandruff, can negatively impact a person’s mental health
C. Dandruff is associated with perceptions of poor hygiene
D. Dandruff can impact personal relationships and going out in public
4. Which of the following is NOT a contributing factor to people with dandruff not approaching pharmacists for assistance with their dandruff?
A. The belief that dandruff is too minor a condition to involve a pharmacist
B. The vast majority of people with dandruff can effectively self-manage their dandruff
C. Dandruff associated stigma and embarrassment
D. Many people are unaware that the pharmacist can assist with the management of dandruff
5. How do patients prevent the recurrence of dandruff?
A. No preventative measures are required as dandruff is a curable condition
B. After clearing their dandruff with an antifungal shampoo, regularly wash their hair with a non-medicated shampoo
C. After clearing their dandruff with an antifungal shampoo, use a keratolytic shampoo to keep the formation of dandruff under control
D. After clearing their dandruff with an antifungal shampoo, continue to use the use antifungal shampoo
- Questions complete -
Accelerating Adult Care in Pharmacy: Practical tips to support your community + grow your business
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Christopher Dunne
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
OR
CPD accreditation code: PSAAPP2665
THURSDAY 12 MARCH 2026 3:10PM – 3:40PM
Competencies: 1.6, 2.1, 2.3, 3.1, 3.2, 3.3, 3.6
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2665
• Recognise the prevalence of incontinence and identify common life-stage and health factors that place people at risk in their community.
• Match the appropriate continence product to an individual’s needs and know where to access further guidance or product information.
• Advise consumers on where to access additional support including continence services, health professionals, and available funding programs.
Multiple Choice Questions
1. A customer aged 52 asks whether bladder leakage is ‘normal’for someone their age. Based on prevalence data, how would you best respond?
A. Explain that bladder leakage affects over 2 in 3 women 25+ and almost 1 in 2 men 45+, and reassure them it is common and manageable
B. Advise them it affects 1 in 2 people, so they do not need further support
C. Tell them it is uncommon and may indicate a serious issue
D. Inform them it only affects 1 in 4 women and 1 in 6 men
2. A customer tells you they are experiencing heavy, unexpected leakage most days and are having to change their pad frequently. They are looking for something that will provide reliable all-day support. Based on leakage severity, which type of product would be most appropriate?
A. Liners
B. Pads
C. Garments
D. Reusable Underwear
3. A customer tells you they are having constant night-time leaks and have started doubling up products to cope. According to what you have learned today, when should a pharmacist refer this person for continence assessment?
A. Only if they have used the same products for more than six months
B. Only if the leakage occurs only during the day
C. Only if they can no longer afford products
D. When someone is using multiple products or still leaking despite correct use
4. Which two life-stage factors are commonly associated with an increased likelihood of experiencing bladder leakage?
A. Pregnancy / birth + menopause
B. Adolescence + marriage
C. Playing sport + new job
D. Mid-life + retirement
5. A customer newly diagnosed with bladder leakage mentions they also have diabetes and a history of prostate cancer treatment. Which combination of health conditions is commonly associated with incontinence?
A. Diabetes + Prostate Cancer
B. Heart disease + sensory impairment
C. Osteoporosis + asthma
D. High blood pressure + depression
- Questions complete -
Mobility matters: Reframing osteoarthritis care in pharmacy practice
Venue: GCCEC, Meeting Rooms 5 & 6
Speakers: Joyce McSwan, Professor David Hunter and Nicolete Ellis
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
OR
CPD accreditation code: PSAAPP2616
THURSDAY 12 MARCH 2026 4:00PM – 4:30PM
Competencies: 2.1, 2.2, 2.3, 3.1, 3.2, 3.3, 3.5, 3.6
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2616
• Explain the impact of osteoarthritis on mobility, functional independence and quality of life in ageing Australians, and recognise its growing burden on the healthcare system.
• Identify evidence-based guideline recommendations to the pharmacological management of osteoarthritis, together with non-pharmacological strategies including movement, exercise and self-management approaches to support effective, person-centred osteoarthritis care.
• Summarise practical pharmacy-based interventions to identify, counsel and refer patients with osteoarthritis, supporting multidisciplinary care and healthy ageing.
Multiple Choice Questions
1. Which of the following is a NOT a contributing factor of mobility limitations in adults?
A. Increased risk of falls
B. Age-related muscle weakening
C. Accumulation of chronic disease
D. Reduced cognitive function
2. Which set of changes is directly associated with OA and contributes to falls and loss of independence?
A. Increased strength, faster walking speed
B. Muscle fatigue, improved balance
C. Reduced flexibility, longer stride length
D. Gait changes, slower walking speed, reduced stability
3. Approximately how many people in Australia were living with osteoarthritis in 2022?
A. 1.7 million
B. 2.1 million
C. 8.3 million
D. 4.5 million
4. Which of the following statements is a common misconception related to OA?
A. Weight bearing damages joints
B. Graduated loading exercises benefits joints
C. Pain is common one year after joint surgery
D. Exercise-based interventions can improve pain and function
5. Which of the following statements is true, based on findings from the 2017 systematic review/meta-analysis by Liu et al.?
A. Pycogenol and curcumin reported little to no effects of clinical importance on OA pain reduction
B. Fish oil demonstrated clinically important effects for OA pain at medium and long term
C. Widely used supplements like glucosamine & chondroitin are not clinically effective in reducing pain in patients with OA
D. Overall, all supplements reviewed were unsafe and should not be used
6. Which of the following best reflects the pharmacist’s role in supporting patients with OA?
A. Supply analgesics when requested and advise rest during pain flares
B. Screen for symptoms, counsel on medicines and self-management, provide non-pharmacological advice, and refer to appropriate health professionals when needed
C. Recommend supplements as first-line therapy before lifestyle modification
D. Refer all patients with joint pain directly to a specialist
- Questions complete -
Advancing cognitive health in pharmacy: Evidence informed omega 3 strategies
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Dr Liza Oates
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform. OR
Learning Outcomes
CPD accreditation code: PSAAPP2623
Competencies: 2.2, 2.3, 3.1, 3.2, 3.3, 3.5
FRIDAY 13 MARCH 2026 9:50AM – 10:20AM
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2623.
• Explain the increasing prevalence of dementia and need for evidence-informed prevention strategies.
• Describe the contribution of omega-3 fatty acids for brain health, and the clinical evidence to support cognition
• Outline patient groups most likely to benefit from evidence-informed interventions for cognitive health.
• Apply evidence-based dosing, dietary, and lifestyle strategies to promote cognition.
Multiple Choice Questions
1. Which statement best reflects the current evidence on dementia prevention?
A. Dementia is largely genetically determined and minimally influenced by lifestyle
B. Dementia prevention strategies are only effective once symptoms appear
C. Up to forty-five per cent of dementia cases are linked to modifiable risk factors
D. Supplements alone can prevent most cases of dementia
2. Which omega-3 fatty acid is the most structurally important for brain tissue and cognition?
A. Alpha-linolenic acid (ALA)
B. Eicosapentaenoic acid (EPA)
C. Docosahexaenoic acid (DHA)
D. Linoleic acid (LA)
3. In which population group is omega-3 supplementation most consistently associated with cognitive benefit?
A. Individuals with established moderate-to-severe dementia
B. Cognitively healthy adults and those with early or mild cognitive changes
C. Only individuals with vascular dementia
D. Only individuals taking cholinesterase inhibitors
4. Which dietary pattern has the strongest evidence for supporting long-term cognitive health?
A. High-protein, low-carbohydrate diet
B. Ketogenic diet
C. Mediterranean and MIND dietary patterns
D. Low-fat, low-omega-3 diet
5. Which statement best reflects appropriate counselling by pharmacists regarding omega-3 use for cognition?
A. Omega-3 supplements reverse dementia once diagnosed
B. Omega-3s should replace lifestyle interventions for brain health
C. Omega-3s are best positioned as part of a broader lifestyle-based cognitive health strategy
D. Omega-3 supplementation is unsafe in older adults
- Questions complete -
Understanding dry eye and its psychological impact: A patient centred approach
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Shaina Zheng
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
OR
CPD accreditation code: PSAAPP2625
FRIDAY 13 MARCH 2026 10:45AM – 11:15AM
Competencies: 1.4, 2.1, 2.2, 2.3, 3.1, 3.2, 3.3, 3.6
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2625.
• Outline what Dry Eye Disease is and the relationship between DED and mental health disorders.
• List the main cause of evaporative DED.
• Determine appropriate initial management for an individual presenting to the pharmacy with DED
• Summarise the pharmacist’s role in DED treatment and management
Multiple Choice Questions
1. According to TFOS DEWS III, Dry Eye Disease (DED) is primarily characterised by which of the following?
A. Reduced blink rate only
B. Tear film homeostasis loss with inflammation and neurosensory changes
C. Purely aqueous tear deficiency
D. Age-related degeneration only
2. Which statement best describes the relationship between Dry Eye Disease and mental health disorders?
A. Mental health disorders are rarely associated with DED
B. Only anxiety is linked to DED severity
C. Depression is associated with an increased risk and severity of DED
D. DED improves mental health outcomes
3. Approximately what proportion of Dry Eye Disease cases are evaporative in nature, most commonly linked to Meibomian Gland Dysfunction (MGD)?
A. 25%
B. 45%
C. 65%
D. 85%
4. A patient presents to the pharmacy with burning, gritty eyes that worsen with prolonged screen use. Which is the most appropriate initial management strategy?
A. Recommend an aqueous-only lubricating drop to use as needed
B. Recommend a lipid-based eye drop supporting lipid, aqueous, and mucin layers, used four times daily for 4 weeks
C. Advise immediate referral to an optometrist
D. Suggest reducing screen time only
5. What is the most appropriate pharmacist action if dry eye symptoms persist after 4–12 weeks of consistent treatment?
A. Increase dosing frequency indefinitely
B. Switch to an aqueous-only lubricant
C. Reassure the patient that symptoms are normal
D. Refer the patient to an optometrist for further assessment
- Questions complete -
TikTok trends vs therapeutic reality: What pharmacists need to know about magnesium evidence
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Jamil Karaki
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
OR
CPD accreditation code: PSAAPP2628
Competencies: 2.3, 3.1, 3.2, 3.3, 3.5
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2628.
FRIDAY 13 MARCH 2026 11:55AM – 12:25PM
• Explain how social media influences patient beliefs around magnesium and the impact of misinformation.
• Distinguish between various magnesium forms, including their bioavailability, pharmacokinetics, and clinical applications.
• Identify key contributors to magnesium depletion, including pharmaceutical agents and lifestyle factors.
• Describe pharmacists’ role in relation to delivering evidence-based advice to patients navigating digital health.
Multiple Choice Questions
1. Which feature of social media health content most commonly contributes to misinformation?
A. Use of cautious, qualified language
B. Discussion of contraindications and limitations
C. Reliance on anecdotal experiences and absolute claims
D. Citation of systematic reviews
2. A patient is enquiring about forms of magnesium for stress and sleep support. Which form is most suitable?
A. Magnesium oxide
B. Magnesium carbonate
C. Magnesium sulphate
D. Magnesium glycinate
3. Which patient scenario raises the greatest concern for potential magnesium depletion?
A. A healthy adult using magnesium occasionally after exercise
B. A patient on long term proton pump inhibitor therapy presenting with muscle cramps
C. A patient using ibuprofen daily for osteoarthritis
D. A patient taking magnesium gummies for general wellbeing
4. A patient tells you:“TikTok says magnesium is safe for everyone and has no interactions.” Which response best reflects the pharmacist’s evidence based advisory role?
A. “That’s incorrect, TikTok information shouldn’t be trusted”
B. “Magnesium is natural, so it’s safe to try”
C. “Let’s review your medications, health conditions, and goals to see if magnesium is appropriate for you”
D. “Everyone should supplement magnesium daily”
- Questions complete -
Dehydration in diabetes – safe use of oral rehydration salts (ORS)
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Deborah Hawthorne
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform. OR
Learning Outcomes
FRIDAY 13 MARCH 2026 12:30PM – 1:00PM
CPD accreditation code: PSAAPP2629
Competencies: 1.1, 1.6, 2.1, 2.2, 2.3, 3.1, 3.2, 3.3, 3.5, 3.6
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2629.
• Describe why people with diabetes are at increased risk of fluid loss and dehydration.
• Recognise common settings and consequences associated with fluid loss and dehydration in diabetes.
• Review principles of sick day management to help manage hydration and prevent complications in people with diabetes, including safe use of oral rehydration solutions.
Multiple Choice Questions
1. Why are people with diabetes at an increased risk of fluid loss and dehydration?
A. Reduced thirst perception
B. Hyperglycaemia causing osmotic diuresis
C. Increased sweating
D. Reduced renal glucose filtration
2. Which situation commonly increases the risk of fluid loss and dehydration in people with diabetes?
A. Controlled fasting for weight management
B. Routine insulin titration
C. Use of continuous glucose monitoring
D. Intercurrent illness (sick days)
3. Significant fluid loss and dehydration in diabetes can lead to which of the following complications?
A. Improved insulin sensitivity
B. Reduced electrolyte loss
C. Diabetic ketoacidosis
D. Lower risk of acute kidney injury
4. Which action is an appropriate component of sick day management to help prevent dehydration-related complications in diabetes?
A. Reducing fluid intake to avoid nausea
B. Stopping all diabetes medications until recovery
C. Maintaining hydration and carbohydrate intake
D. Avoiding carbohydrate intake entirely
5. Which of the following statements best describes the role of glucose in oral rehydration solutions (ORS)?
A. Combines with potassium to activate SGLT1 pumps
B. Corrects acidosis caused by vomiting and diarrhoea
C. Replaces lost electrolytes during illness
D. Facilitates absorption of fluids and electrolytes
- Questions complete -
Empowering Pharmacists in Acne Management: Clear Skin, Full Scope
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Dr Leona Yip
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
OR
CPD accreditation code: PSAAPP2631
Competencies: 1.1, 3.1, 3.2, 3.5
FRIDAY 13 MARCH 2026 2:00PM – 2:30PM
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2631.
• Differentiate between types of acne including acne sequelae and referral points.
• Outline important considerations when prescribing acne treatments as part of pharmacists' expanded scope of practice.
• Describe the importance of holistic acne treatment and management strategies to improve patient outcomes.
Multiple Choice Questions
1. Which feature most strongly suggests a need for early referral to a dermatologist?
A. Mild comedonal acne with minimal inflammation
B. Acne resistant to several topical therapies and beginning to scar
C. Occasional papules limited to the T zone
D. Presence of post inflammatory erythema only
2. Which statement best describes the role of topical retinoids in acne management?
A. They primarily act as antibacterial agents
B. They should only be used for short term induction therapy
C. Their main benefit is rapid lesion clearance within 48 hours
D. They normalise desquamation, reduce inflammation and prevent microcomedone formation
3. What is the main purpose of moisturisation in the CTMP (Cleanse Treat Moisturise Protect) routine for acne patients?
A. Eliminate sebum production
B. Replace the need for retinoid therapy
C. Reduce dryness and irritation from topical treatments, improving adherence
D. Prevent all acne flare ups entirely
4. Which statement about acne scarring is correct?
A. Acne scarring occurs only in severe nodulocystic acne
B. Most acne scars are hypertrophic and occur on the chest
C. Atrophic scars result from collagen degradation during prolonged inflammation
D. Scars fully resolve once inflammation subsides
5. What key finding from the START study supports the use of trifarotene early in acne management?
A. It significantly reduces atrophic scar formation as early as Week 2
B. It clears acne lesions within 48 hours
C. It is less effective than vehicle for truncal acne
D. It cannot be used on the face
- Questions complete -
Optimising Type 2 Diabetes care: Practical use of diabetes specific nutritional formulas
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Anna Blackie
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform. OR
Learning Outcomes
FRIDAY 13 MARCH 2026 2:35PM – 3:05PM
CPD accreditation code: PSAAPP2632
Competencies: 1.6, 2.1, 2.3, 3.1, 3.2, 3.3, 3.6
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2632.
• Explain what Diabetes Specific Nutritional Formulas (DSNFs) are.
• Identify individuals who may benefit from the use of a DSNF based on nutritional needs and diabetes management goals.
• Apply the Clinical Practice Guide to make appropriate patient-centred DSNF recommendations.
Multiple Choice Questions
6. A Diabetes Specific Nutritional Formula is:
A. A weight-loss shake for people with type 2 diabetes
B. A replacement for a whole-food diet when diabetes management targets have not been achieved with multiple glucose-lowering medications
C. A specialised oral nutrition supplement for people with or at risk of diabetes that helps to manage malnutrition, dysglycaemia, and other cardiometabolic risk factors
D. A nutritional supplement containing high GI carbohydrates and low protein
7. Which of the following best describes who uses DSNFs?
A. People with or at risk of under-nutrition
B. People with or at risk of diabetes, irrespective of body weight
C. People with a BMI >30kg/m2 or BMI >27kg/m2 with diabetes
D. General population seeking weight loss
8. Which of the following people with type 2 diabetes would be least suitable for a DSNF?
A. Meeting dietary recommendations and HbA1c <7%
B. Using a GLP-1 receptor agonist and experiencing weight loss and GI adverse effects
C. Newly diagnosed with type 2 diabetes and feeling overwhelmed with dietary management advice
D. Using high doses of multiple glucose-lowering agents with fluctuating blood glucose levels
9. Greg is a 67-year-old man who has been living with type 2 diabetes for 7 years. He currently takes maximum doses of three oral glucose-lowering agents and his last HbA1c was 7.9%. His BMI is 28kg/m2, and he would like to lose weight. He lives alone and often has takeaway food as he finds cooking for one challenging. According to the DSNF Clinical Practice Guide, what is the most suitable plan for Greg?
A. 2 serves per day to replace meals or snacks
B. 1 serve per day to replace all or part of a meal
C. Total meal replacement with 3 serves per day
D. 2 serves per day in addition to main meals
10. Which of the following best describes a pharmacist’s role with DSNFs?
A. Diagnosing nutritional deficiencies and prescribing DSNFs as first-line therapy
B. Identifying appropriate patients, providing advice on DSNFs, and referring to other healthcare professionals when required
C. Replacing meals with DSNFs for all patients with type 2 diabetes and cardiovascular risk factors
D. Recommending DSNFs only when requested by a prescriber or dietitian
- Questions complete -
Breaking boundaries in MSK pain management: How pharmacists are redefining roles with expanded scope of practice
Venue: GCCEC, Arena 1A
Speakers: Grace Chong and Joyce McSwan
CPD Credits
0.75 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
OR
CPD accreditation code: PSAAPP2633
FRIDAY 13 MARCH 2026 2:45PM – 3:30PM
Competencies: 1.1, 1.3, 1.4, 1.5, 2.2, 2.3, 3.1, 3.2, 3.3, 3.5
1.5 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2633.
• Recall guideline recommendations for assessment and management of acute MSK pain.
• Describe the benefits of ibuprofen and ibuprofen/paracetamol combinations in the management of low back pain and other acute MSK conditions.
• Explain key counselling points to improve patient understanding of treatment goals and appropriate use of medicines for acute MSK pain
Multiple Choice Questions
1. Which of the following correctly describes the role of the Örebro Musculoskeletal Pain Questionnaire?
A. It is a diagnostic tool designed specifically for low back pain
B. It is a risk assessment tool that helps predict long-term disability and failure to return to work from four to 12 weeks following a soft tissue injury
C. It is a risk assessment tool that helps identify red flags for pharmacy-based management
D. It is a risk assessment tool used to predict likelihood of side effects of MSK pain treatment
2. Which of the following statements about the pharmacological management of MSK pain is FALSE?
A. NSAIDs are generally considered effective for MSK pain and inflammation and can be trialled in patients with no contraindications or precautions
B. Oral NSAIDs are recommended first-line for low back pain, neck pain, and osteoarthritis in low-risk patients
C. NSAIDs may be added to paracetamol to reduce risk of side effects and improve pain relief
D. NSAIDs are best trialled at maximum dose for a minimum duration of 5 days
3. Potential risk of adverse effects are important considerations for NSAID use in MSK pain. Which of the below statements accurately reflects the tolerability profile of ibuprofen?
A. Coadministration with food has a significant influence on ibuprofen’s adverse effect profile
B. Ibuprofen has been found to have a similar cardiovascular risk profile to diclofenac
C. OTC doses of ibuprofen have comparable GI tolerability to paracetamol when taken as directed in patients without contraindications or precautions
D. OTC doses of ibuprofen are suitable for use in patients with gastric ulcer or bleeding
4. What is the benefit of combining ibuprofen and paracetamol for acute low back pain relief?
A. Provides synergistic analgesia
B. Found to reduce pain and disability in low back pain in a 2024 meta-analysis
C. Both A and B
D. None of the above
5. Which of the following is NOT an appropriate discussion point when counselling a patient on a management plan for mild, acute MSK pain?
A. Potential causes of the pain
B. Positive prognosis
C. Correct dosing and dosing intervals
D. The need for bed rest until the pain has completely gone
- Questions complete -
From QCPP to Quality and Safety: The next chapter
Venue: GCCEC, Meeting Rooms 5 & 6
Speakers: Natalie Willis and Erica Vowles
CPD Credits
0.75 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
FRIDAY 13 MARCH 2026 4:00PM – 5:30PM
CPD accreditation code: PSAAPP2640
Competencies: 1.5, 1.6, 2.1, 2.3, 4.1, 4.2, 4.3, 4.5, 4.6, 4.7
1.5 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2640
• Recognise why the transition from QCPP to QSPP is necessary, and how evolving expectations of safety, quality, and assurance have shaped the new program.
• Identify what is changing and what is not as pharmacies move from QCPP to QSPP, including accreditation cycles, assessment focus, and operational responsibilities.
• Outline how QSPP strengthens clinical governance expectations compared to QCPP, shifting focus from compliance evidence to governance in practice.
Multiple Choice Questions
1. Which factor most strongly explains why QCPP is transitioning to QSPP?
A. The need to reduce the administrative burden of accreditation
B. The expansion of pharmacy services requiring stronger safety and quality assurance
C. Changes to funding arrangements for community pharmacy
D. The introduction of digital assessment platforms
2. Which shift in expectations has most influenced the design of QSPP?
A. A move towards shorter accreditation cycles
B. Increased focus on financial governance and business performance
C. Greater system wide expectations for assurance of safe, quality care
D. Increased reliance on self assessment by pharmacies
3. How does the assessment focus under QSPP differ most from QCPP?
A. Assessments occur less frequently
B. Greater emphasis on documented policies and procedures
C. Increased focus on how governance systems operate in practice
D. Assessments apply only to pharmacies offering advanced services
4. Under QSPP, how are clinical governance expectations strengthened compared to QCPP?
A. Clinical governance is assessed only during initial accreditation
B. Responsibility for governance shifts primarily to individual pharmacists
C. Governance is embedded across systems, culture, and leadership
D. Governance requirements are limited to clinical services only
5. How does QSPP most significantly change expectations for patient and consumer engagement compared to QCPP?
A. Patient engagement is limited to collecting satisfaction surveys
B. Engagement is optional unless the pharmacy provides advanced clinical services
C. Patients and consumers are partners in safety, quality, and service improvement
D. Engagement is addressed only through complaints management processes
- Questions complete -
The role of VLED (Very Low Energy Diets) alongside GLP-1 medications
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Dr Terri-Lynne South
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
OR
CPD accreditation code: PSAAPP2645
Competencies: 2.2, 2.3, 3.1 3.2, 3.3, 3.5
SATURDAY 14 MARCH 2026 9:55AM – 10:25AM
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2645
• Explain how GLP-RAs function and the definition, purpose and application of VLED products
• Identify common nutritional challenges faced by patients using GLP-1 therapies and management strategies.
• Identify when a patient using GLP-1 medications are suitable for VLED products.
Multiple Choice Questions
1. What is the primary physiological rationale for combining a modified Very Low Energy Diet (mVLED) with GLP-1 receptor agonist therapy?
A. To offset the delayed gastric emptying caused by GLP-1 receptor agonists
B. To enhance thermogenesis through concurrent macronutrient restriction
C. To align rapid hepatic fat reduction with sustained appetite suppression and improved adherence
D. To prevent reactive hypoglycaemia by reducing insulin secretion
2. During concurrent GLP-1 and VLED therapy, which nutritional focus best mitigates the risk of sarcopenia and malnutrition?
A. Increasing total caloric intake by adding complex carbohydrates
B. Ensuring daily protein intake of ≥ 1.0–1.2 g/kg, adequate micronutrients, with monitoring
C. Prioritising high-fat, low-fibre foods to slow gastric emptying
D. Using collagen powders or “DIY shakes” to maintain lean mass
3. In which of the following scenarios is combination GLP-1 + VLED therapy most clinically justified?
A. A patient with mild overweight and no metabolic comorbidities
B. An individual with severe obesity and metabolic risk factors (e.g., NAFLD, OSA, or high insulin resistance)
C. A patient with recent myocardial infarction seeking gradual recovery
D. An adolescent with early-stage disordered eating patterns
4. According to Dr South’s implementation framework, what constitutes a critical sequencing error when initiating GLP-1 and VLED together?
A. Starting with a modified VLED before assessing tolerance to GLP-1s
B. Initiating both VLED and GLP-1 dose escalation simultaneously, increasing risk of intolerance and dehydration
C. Delaying VLED introduction until after 12 weeks of stable GLP-1 use
D. Maintaining GLP-1 dose stability during VLED transition phase
5. Which statement best reflects evidence-aligned patient messaging about GLP-1 + mVLED therapy?
A. “You’ll can remain on the VLED indefinitely .”
B. “Once appetite is suppressed, nutritional intake can safely decline.”
C. “This is a structured, time-limited metabolic intervention designed to preserve muscle and sustain results through chronic GLP-1 use.”
D. “GLP-1 therapy replaces the need for dietary modification.”
- Questions complete -
Unravelling key aspects of infant nutrition and common feeding conditions: Confusion to confidence
Venue: GCCEC, Meeting Rooms 5 & 6
Speakers: Dr Brett MacFarlane, Dr Janet Green and Kathy Beck
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
OR
SATURDAY 14 MARCH 2026 10:45AM – 11:15AM
CPD accreditation code: PSAAPP2648
Competencies: 2.1, 2.3, 3.1, 3.2, 3.6
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2648
• Outline why parents and carers may choose to use infant formula.
• Answer questions parents and carers have about nutritional strategies to manage cows’ milk allergy and reflux.
• Advise parents and carers on choosing specialist infant formulas for cows’ milk allergy and reflux and switching between formulas.
Multiple Choice Questions
1. Which of the following is a reason parents/carers may choose to use infant formula?
A. To eliminate the need for complementary foods until 12 months
B. Perceived or actual insufficient milk supply
C. Because all infant formulas are unregulated products
D. Because reflux always requires stopping breastfeeding
2. What do guidelines recommend as the core nutritional strategy for managing cows’milk allergy (CMA)?
A. Switching to lactose-free formula as first-line management
B. Using goat’s milk formula because it is less allergenic
C. Complete exclusion of the causal proteins
D. Using HA (hypoallergenic) formula for confirmed CMA
3. Which of the following statements about the management of cows’ milk protein allergy (CMPA) is INCORRECT?
A. Hydrolysed rice protein-based formula has been shown to significantly lower CMPA symptoms
B. Hydrolysed rice protein-based formulas contain other key nutrients and essential fatty acids
C. According to ASCIA, alternative animal formulas like goat or sheep are suitable for CPMA
D. Most young children become tolerant of cows’ milk as they age
4. For a formula-fed infant with uncomplicated gastro-oesophageal reflux (GOR), what nutritional approach is recommended in clinical guidelines?
A. Start a proton pump inhibitor (PPI) immediately
B. Stop feeds and use cooled boiled water only
C. Change to a lactose-free formula
D. Use a thickened formula (commercially thickened preferred)
5. When transitioning between specialised formulas, what approach is recommended?
A. Switch to the new formula immediately (100% from the first feed)
B. Alternate feeds (one feed old formula, one feed new formula) for 2 days only
C. Gradually transition over ~5–7 days by mixing increasing proportions of the new formula
D. Dilute the new formula so the taste is weaker for the first week
- Questions complete -
New best practice guidelines: The role of the community pharmacists in acute wound care
Venue: GCCEC, Arena 1A
Speaker: Associate Professor John Smithson
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform. OR
Learning Outcomes
CPD accreditation code: PSAAPP2647
SATURDAY 14 MARCH 2026 11:00AM – 11:30AM
Competencies: 2.1, 2.3, 3.1, 3.2, 3.3, 3.5, 3.6
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2647
• Outline key points from the newly launched Best Practice Statement and its implications for pharmacy practice.
• Describe the pharmacist’s evolving role in wound care and why it matters for patient outcomes.
• Identify and classify common acute wounds using correct clinical terminology.
• Apply the T.I.M.E. framework for structured wound assessment.
• Select appropriate dressings based on wound characteristics and patient needs.
• Explain antimicrobial stewardship and recognise referral triggers.
Multiple Choice Questions
1. Which of the following most accurately reflects the newly adapted ‘Best Practice Statement: The role of the Australian Community Pharmacist in Wound care’ implications for day to day pharmacy practice?
A. Pharmacists should select dressings based only on cost and product familiarity
B. Pharmacists may independently diagnose chronic wounds without referral
C. Pharmacists should undertake structured wound assessment, provide evidence based dressing selection, and recognise clear referral thresholds
D. The Statement primarily promotes the exclusive use of advanced silver dressings in acute wounds
2. A deep traumatic wound is producing heavy exudate with frequent strike-through. Which dressing is most appropriate?
A. Film dressing
B. Hydrogel dressing
C. Alginate dressing
D. Hydrocolloid dressing
3. A patient presents with a clean, shallow abrasion producing minimal exudate. The wound is clean and shows no signs of infection. What is the most appropriate initial dressing?
A. Foam dressing
B. Alginate dressing
C. Film dressing
D. Hydrogel dressing
4. Which scenario best demonstrates the expanded, contemporary role of the community pharmacist in wound care?
A. Handing the patient a retail pamphlet and recommending they visit a GP for all wound related issues
B. Performing structured assessment, selecting an appropriate dressing, providing follow up advice, and escalating when red flags appear
C. Suturing all new lacerations that present to the pharmacy
D. Selling dressings but leaving assessment and triage entirely to the patient
5. A patient presents with a wound showing increased slough coverage, malodour, and stalled healing over the last two weeks. Which T.I.M.E. component is MOST clearly failing and requires priority attention?
A. T – Tissue: Non viable slough requires debridement
B. I – Inflammation/Infection: No infection indicators are present
C. M – Moisture: The wound is excessively dry
D. E – Edge: Robust epithelial migration is progressing well
6. A patient with diabetes presents with increasing wound pain, malodour, delayed healing, and spreading erythema beyond the wound margin. What is the most appropriate action?
A. Supply topical antimicrobial dressing only
B. Start oral antibiotics immediately
C. Optimise wound care and review in 48 hours
D. Urgently refer for medical assessment
- Questions complete -
The proactive pharmacist’s guide to UV’s impact on skin conditions
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Dr Melissa Manahan
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
CPD accreditation code: PSAAPP2650
SATURDAY 14 MARCH 2026 11:20AM – 11:50AM
Competencies: 1.1, 1.2, 1.3, 1.4, 2.1, 2.2, 2.3, 3.1, 3.2, 3.3, 3.5, 3.6
1.0 Group 2 CPD credits
OR
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2650.
• Explain the importance of UV protection and the risk of UV related skin damage in Australia.
• Discuss the impact of UV light on both acne and eczema-prone skin.
• Outline the important role of UV protection / sunscreen formulations in Australia
• Apply a personalized approach to UV protection and sunscreen recommendations for customers
Multiple Choice Questions
1. Reasons that acne patients should use sunscreen include:
A. Sunscreens by their very nature cannot clog pores
B. Reduction in risk of post inflammatory hyperpigmentation
C. Many acne treatments are photosensitising
D. B and C
2. Why does acne sometimes appear to improve immediately after sun exposure?
A. UV permanently reduces sebum
B. UV temporarily reduces inflammation
C. UV kills acne bacteria long term
D. UV strengthens the skin barrier
3. Photoaggravation occurs in what percentage of atopic dermatitis patients?
A. 0%
B. 1%
C. 10%
D. 30%
4. A 25-year-old customer visits your pharmacy in Sydney, concerned about worsening acne after increased sun exposure. She also mentions that her mother has eczema and struggles to find a sunscreen that doesn’t irritate her skin. Which of the following recommendations best demonstrates an understanding of UV protection, skin health, and personalized sunscreen advice in the Australian context?
A. Recommend any high SPF sunscreen, as all sunscreens offer equal protection and are suitable for all skin types
B. Advise the customer to reduce sunscreen use, as UV light often helps clear acne and eczema symptoms
C. Explain the high UV risk in Australia and recommend broad-spectrum SPF 50+ sunscreens with non-comedogenic or sensitiveskin formulations based on individual needs
D. Suggest relying solely on hats and clothing for UV protection, as sunscreen is unnecessary in mild weather
5. A 28-year-old woman living in Brisbane works as a dog walker and spends several hours outdoors daily. She reports new freckles on her cheeks, occasional sunburn, and worsening acne flare ups after long days in the sun. She also has a history of mild eczema that becomes itchy after beach days. She currently uses a moisturiser with SPF50 in the morning and rarely reapplies sunscreen because she dislikes ‘heavy’ textures. Which recommendation best addresses her UV related risks while considering her acne and eczema prone skin?
A. Switch to a rich, occlusive SPF50+ cream to strengthen the skin barrier and prevent UV induced dryness
B. Use a lightweight, non comedogenic SPF50+ broad spectrum sunscreen with high UVA protection, reapply every 2 hours outdoors, and pair with a gentle barrier supporting moisturiser
C. Continue using the SPF50 moisturiser daily but add a hat
D. Avoid sunscreen on acne prone areas and rely on tanning to reduce inflammation and improve breakouts
- Questions complete -
From handshake deals to legal headaches: The must know clauses to protect your pharmacy partnership SATURDAY 14 MARCH 2026 11:35AM – 12:05PM
Venue: GCCEC, Arena 1A
Speaker: Sarah Stoddart
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
CPD accreditation code: PSAAPP2649
Competencies: 1.3, 2.2, 2.4, 4.1, 4.2, 4., 4.4, 4.5, 4.6, 4.7
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2649.
• Articulate the risks associated with informal partnership arrangements in pharmacy business and how those risks can contribute to partnership disputes.
• Illustrate key partnership agreement provisions.
• Implement risk management principles to partnership planning and review.
Multiple Choice Questions
1. Which of the following is not a risk of an informal partnership arrangement?
A. No record of how decisions are to be made
B. Cannot prove ownership of the pharmacy business
C. Potential for costly and lengthy disputes
D. Inadequate provision for annual and personal leave periods
2. Which of the following are key clauses in a partnership agreement?
A. Dispute resolution
B. Retirement
C. Distributions
D. All of the above
3. When is the best time to enter into a partnership agreement?
A. After the partnership buys its first pharmacy
B. When the partnership is formed
C. When a dispute arises
D. When the partnership objectives have been achieved
4. The best process for resolving partnership disputes is …?
A. For the majority partner to make the decision
B. To do what the partnership legislation says
C. To have a dispute resolution process to follow
D. Do nothing and let it resolve naturally
5. Which of the following life events is least likely to impact on a partnership arrangement?
A. Buying a house
B. Divorce
C. Parental leave
D. Permanent disablement
- Questions complete -
Vaping cessation in practice
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Jarrod McMaugh
CPD Credits
0.5 Group 1 CPD credits
Session attendance only. Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
OR
CPD accreditation code: PSAAPP2652
SATURDAY 14 MARCH 2026 11:55AM – 12:25PM
Competencies: 1.5, 2.1, 2.3, 3.1, 3.2, 3.3, 3.5, 3.6
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2652
• Identify key clinical and psychological differences in vaping and smoking.
• Reiterate the evidence-based strategies for vaping cessation.
• Recognise when nicotine replacement therapy is appropriate for supporting cessation of vaping in simulated scenario.
Multiple Choice Questions
1. All of the following factors have been identified as increasing difficulty ceasing vaping when compared to smoking EXCEPT:
A. Increased access to nicotine products
B. Higher frequency of use
C. Greater situational triggers
D. Lower patient insight into nicotine consumption levels
2. Which of the following is TRUE regarding current evidence-based strategies for vaping cessation?
A. Current evidence suggests that vaping cessation relies on behavioural counselling with limited therapeutic options
B. Vaping specific strategies have been extensively researched, and distinct frameworks have been identified for vaping cessation
C. Smoking cessation evidence can be directly extrapolated to vaping cessation as there are no distinct behavioural or clinical differences between the two
D. Much of the evidence is currently mostly extrapolated from smoking cessation frameworks with new evidence emerging regarding specific behavioural influences
3. Patrick is a 41-year-old man who attends the pharmacy seeking advice to seek vaping. He smoked for 10 years before swapping to vaping 5 years ago. Following further discussion, you determine that Patrick knows his triggers and has a plan in place for delaying cravings, but he would like to avoid withdrawal symptoms. Which of the following is the most appropriate course of action based on what you have learned in this presentation?
A. Refer to a medical practitioner for pharmacotherapy
B. Initiate NRT in the form of a patch alongside referral for further support
C. Initiate NRT in the form of a mouth spray alongside support for specific psychosocial challenges
D. Refer for further support as there are no approved products for vaping cessation
- Questions complete -
Fluorides 101 and the pharmacist role in caries prevention
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Jasmine Bell
CPD Credits
0.5 Group 1 CPD credits
Session attendance only. Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
SATURDAY 14 MARCH 2026 2:00PM – 2:30PM
CPD accreditation code: PSAAPP2658
Competencies: 1.1, 1.4, 1.5, 1.6, 2.1, 2.3, 2.4
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2658.
• Discuss the continuing importance of fluoride in caries prevention, and the evidence base supporting the use of fluorides
• Outline the key information from the current Australian Guidelines for the use of fluorides and how these can be applied to a pharmacy practice.
• Compare the different fluoridated toothpastes available and how to make appropriate product recommendations for patients and consumers.
Multiple Choice Questions
1. Which TWO of the following describe how fluoride works for caries prevention?
A. Fluoride inhibits demineralisation by lowering the critical pH for enamel
B. Fluoride increases the risk of critical mineral loss from the enamel structure
C. Calcium Fluoride globules form on tooth surface and in plaque – and acts as a fluoride reservoir
D. The lower the concentration of fluoride, the more effective caries reduction
2. True or False. The Australian Fluoride Guidelines recommend, no fluoride toothpaste for children under 18 months, however, can be used if there is elevated caries risk.
A. True
B. False
3. A high concentrated fluoride toothpaste containing 5000ppm can be recommended for patients (Select 4 correct answers):
A. With active caries or a high caries risk, and those over the age of 10 years
B. Wearing orthodontic appliances
C. Who don’t like the flavour of regular supermarket toothpaste
D. Consuming a high sugar diet
E. Taking long term medication that causes dry mouth
F. Under the age of 10 years for caries prevention
4. Which of the following statements is incorrect?
A. Fluoride mouthrinses can form an important part of a caries management plan for patients (over 6 years old) who are at moderate to high risk of caries
B. A fluoride mouthrinse should ideally be used separate from morning and evening brushing events
C. Fluoride mouthrinses are suitable at any age
D. A Fluoride mouthrinse increases frequency of fluoride exposure
5. Which of the following is not correct for a regular concentration toothpaste?
A. They contain between 1000-1500 parts per million fluoride
B. They are generally recommended for children over the age of 6 years
C. They available in supermarkets, pharmacies and dental surgeries
D. They are only found behind the counter
- Questions complete -
The business of sleep: Building a high-performing sleep study and CPAP Clinic in pharmacy
Venue: GCCEC, Meeting Rooms 7 & 8
Speaker: Justin Chan
CPD Credits
0.5 Group 1 CPD credits
Session attendance only. Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
SATURDAY 14 MARCH 2026 2:00PM – 2:30PM
OR
CPD accreditation code: A2609PC11 Competencies: 2.2, 2.3, 4.5, 4.6, 4.7
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/2609PC11.

• Describe the incidence and health impacts of sleep disorders including Obstructive Sleep Apnoea (OSA).
• List the key components of a sleep service.
• Describe important considerations when choosing a sleep provider
Multiple Choice Questions
1. What percent of Australians suffer from a sleep disorder at some time in their lives?
A. 30%
B. 50%
C. 70%
D. 90%
2. Which of the following are key components of a sleep service?
A. Bulk billed home sleep studies
B. Respiratory & Sleep physician telehealth
C. CPAP services
D. All of the above
3. Which of the following are benefits of the HST device?
A. Fast hookup of 5 minutes
B. Whole pharmacy team can be trained to use it
C. Disposable electrodes, reducing staff time cleaning and better signal quality
D. All of the above
4. What is a requirement to claim a bulk-billed at-home sleep study (MBS 12250)?
A. Age: 16+
B. Epworth Sleepiness Scale ≥ 8
C. Has not claimed a home sleep study under Medicare in the last 24 months
D. STOP-BANG score ≥ 5
5. What would be the best option for a patient that fails the Epworth Sleepiness Scale or STOPBANG questionnaire?
A. Don’t get a sleep test
B. Recommend lifestyle modifications
C. Repeat the questionnaire in 1 month
D. Have a Respiratory & Sleep Physician consultation to determine whether a sleep study is clinically justified
- Questions complete -
The clinical and public health impact of FluMist (Influenza virus vaccine nasal spray) availability in 2026
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Professor Paul Van Buynder
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform.
Learning Outcomes
OR
CPD accreditation code: PSAAPP2660
SATURDAY 14 MARCH 2026 2:35PM – 3:05PM
Competencies: 1.1, 1.3, 1.4, 2.1, 2.2, 2.3, 3.1, 3.2, 3.5, 3.6
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2660.
• Identify key features of influenza disease severity in children, including the risk of hospitalisation and death in young age groups.
• State the minimum age for use of the live attenuated influenza vaccine (LAIV) and explain why it is not recommended for children under 24 months.
• Describe which paediatric age groups are eligible for publicly funded LAIV in Australian states.
• Describe key practical characteristics of LAIV relevant to pharmacy practice, including route of administration, cold chain needs, and differences from inactivated influenza vaccines.
Multiple Choice Questions
1. Influenza disease:
A. Is only very serious and a problem for old people and those living in aged care
B. Is very serious in young children and can lead to hospitalisation and death
C. Is mild in very young children and children of school age
D. Is only serious for children with immune suppression
2. What is the approved age range for the intranasal live attenuated influenza vaccine (LAIV) according to the product information presented in this activity?
A. From 6 months to <5 years
B. From 6 months to <18 year
C. From 24 months to <18 years
D. From 12 months to <5 years
3. LAIV is funded for:
A. All children from 2 years to 18 years
B. All children from 2 years to 5 years
C. Children from 2 years to 5 years in some states
D. Children from 2 years to 18 years in some states
4. Which statement about the storage requirements for the intranasal live attenuated influenza vaccine (LAIV) is correct?
A. LAIV can be stored safely at room temperature for the entire season
B. LAIV must be stored frozen and thawed before use
C. LAIV requires cold chain storage at 2–8 °C, with one permitted temperature excursion to 25 °C
D. LAIV must be stored between 0–2 °C to maintain stability
- Questions complete -
Breathe freely, sleep deeply: The pharmacist’s role in airway wellness
Venue: GCCEC, Meeting Rooms 5 & 6
Speaker: Professor Brendon Yee
CPD Credits
0.5 Group 1 CPD credits
Session attendance only.
Please self-record Group 1 credits using your preferred CPD recording platform. OR
Learning Outcomes
SATURDAY
14 MARCH 2026 3:10PM – 3:40PM
CPD accreditation code: PSAAPP2662
Competencies: 2.2, 2.3, 3.1, 3.2, 3.3, 3.5
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2662.
• Outline the importance of sleep and the impact of sleep disturbance, including common sleep disorders and their symptoms, and the importance of the nose for good sleep.
• Answer questions customers may have about the management of nasal obstruction and congestion, in particular as it relates to OSA and CPAP use.
• Advise customers on choosing treatment options for managing nasal symptoms and improving CPAP use.
Multiple Choice Questions
1. Which of the following is often forgotten as a cause of sleep disturbances?
A. Nasal symptoms of obstruction and congestion
B. Emotional regulation
C. Immunity
D. Substance abuse
2. What do guidelines recommend as a management strategy for nasal obstruction and congestion which can impact sleep?
A. Antibiotics to prevent infection
B. Sedating antihistamines to help get to sleep
C. Intranasal saline or high-volume irrigation to clear nasal and sinus passages
D. Cold and flu medications to dry up a runny nose
3. A customer with diagnosed obstructive sleep apnoea is experiencing a nasal symptom of dryness and congestion with their use of CPAP, what can be recommended according to evidence?
A. Increasing the pressure of the CPAP machine for push more air through the nasal passages
B. Cleaning the CPAP mask
C. Stop using the CPAP machine immediately
D. Introducing a high-volume nasal irrigation to restore mucociliary clearance
- Questions complete -
Insuring innovation: Risk management for expanding pharmacist roles
Venue: GCCEC, Meeting Rooms 7 & 8
Speaker: Claire Bekema
CPD Credits
0.5 Group 1 CPD credits
Session attendance only. Please self-record Group 1 credits using your preferred CPD recording platform. OR
Learning Outcomes
SATURDAY 14 MARCH 2026 3:10PM – 3:40PM
CPD accreditation code: PSAAPP2661
Competencies: 1.6, 2.1, 2.3, 3.1, 3.2, 3.3, 3.6
1.0 Group 2 CPD credits
Session attendance and 100% pass rate of associated MCQs. To record your MCQ answers, visit bit.ly/APP2661.
• Identify key practical benefits that can be gained from being proactive about risk management.
• List the five predominant categories of risk that can present in pharmacy practice.
• Explain why it is important to define the risk question for a new service or role.
Multiple Choice Questions
1. Which of the following is NOT a possible benefit of being proactive in risk management when implementing new pharmacy services?
A. Improved patient safety and health outcomes by implementing documented processes that prevent near misses and incidents
B. Minimised operational losses (e.g time, resources) by having clear policies and procedures
C. Reduced workflow efficiency due to more policies and procedures
D. Increased protection from reputational or professional consequences
2. According to PDL, what are the five predominant types of risk encountered in pharmacy practice?
A. Regulatory and Compliance Risk, Business Risk, Clinical Risk, Professional Risk, Operational Risk
B. Regulatory and Strategic Risk, Clinical Risk, Professional Risk, Ethical Risk, Operational Risk
C. Regulatory and Compliance Risk, Clinical Risk, Uncertainty-based Risk, Professional Risk, Operation Risk
D. Regulatory and Compliance Risk, Clinical Risk, Professional Risk, Ethical Risk, Operational Risk
3. Complete the following sentence with the most correct answer. It important to define the risk question for a new service or role…
A. …to give staff the opportunity to express their objection
B. …to prompt reflection on the variety of risk that might be present and drive action to minimise these
C. …to allow reflection and discussion of the benefits of implementation
D. …to drive the change management process
- Questions complete -
Frequently asked questions and troubleshooting steps
Question Answer
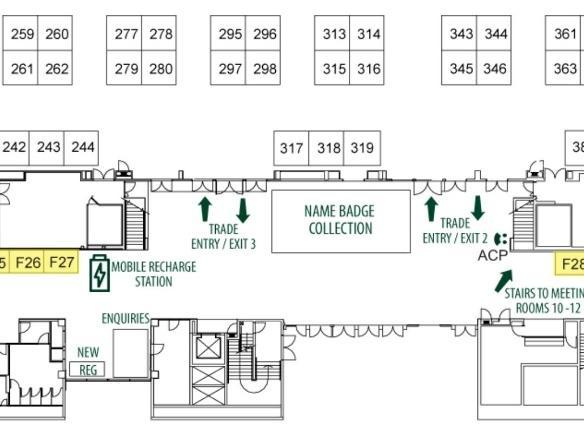
Where can I find the PSA | ACP Team at the conference?
From 8:30am - 5:30pm on Thursday 12 March 2026, the PSA | ACP Team will be available at a kiosk beside the APP2026 name badge collection station.
From Thursday, 5:30pm (the APP2026 Welcome Reception), the PSA | ACP trade stand will move into the main exhibition hall for the remainder of the conference. We are located at stand #343.
I cannot login to the College CPD Library.
Check that you are using the correct URL to access to the College CPD Library here: https://guilded.guild.org.au/login.
Please also ensure you are entering the same email address that you have registered with the College as your username to login and/or reset your password.
If you are unsure of your College CPD Library username, or you are unable to reset your password, please contact the PSA | ACP Team.
I can login to the CPD Library, but I cannot see the 'Conferences' tab or APP2026 activities.
I can see the APP2026 activities, but I cannot enrol into them.
You do not yet have the correct permissions assigned to your account. This may be because:
• You did not indicate that you intended to collect CPD points on your APP2026 registration.
• The email you used to register for the conference is different to the address attached to your College CPD Library account.
• Your permissions have not yet been assigned e.g. if you registered onsite at the conference.
Please contact the PSA | ACP Team who will update the relevant permissions on your account.
Enrolment into Group 2 assessments opens once the session has commenced or passed (AEST – Queensland time).
Please refer to the enrolment start date within the course description and enrol once the session time has commenced or passed.
If you are still unable to enrol, please contact the PSA | ACP Team who can check your account permissions.
How to contact the PSA | ACP Team
If you have any questions regarding your APP2026 CPD activities, logging in to the College CPD Library, or general enquiries relating to the College or PSA, please:
• Visit the PSA | ACP trade stand. We are located at stand #343.
• Email the PSA | ACP at info@acp.edu.au
• Phone the PSA | ACP on 07 3144 3680.