

FUTURE CHRONICLES YTP

in
Coordinators:

Editor
Chief: Dr. Bhaskar Pal, Dr. Abha Rani Sinha, Dr. Rohan Palshetkar
Editorial
Dr. Prerna Keshan, Dr. Annesha Dutta


Dr. Bhaskar Pal President, FOGSI (2026)
Dear Colleagues and Future Torchbearers of FOGSI, Warm greetings from the Federation.
It gives me immense pride and optimism to address the Young Talent Promotion Committee — a vibrant platform that symbolizes the future strength, vision and dynamism of FOGSI. The Young Talent Promotion Committee focuses on nurturing young Obstetricians and Gynaecologists through academic, social and cultural engagement.
Our young members are not merely the doctors of tomorrow; they are the innovators, leaders, researchers and compassionate caregivers of today. The Young Talent Promotion Committee stands as a testimony to FOGSI’s unwavering commitment to nurturing fresh ideas, encouraging academic excellence, and empowering emerging Obstetricians and Gynaecologists to rise with confidence and competence.
In a rapidly evolving era of medicine, where knowledge expands by the minute and technology reshapes clinical practice, it is the enthusiasm, curiosity and adaptability of our young professionals that will keep FOGSI at the forefront of women’s healthcare. This committee provides the ideal ecosystem for learning, mentoring, sharing and growing — a space where talent is recognized, skills are honed, and leadership is cultivated.
I encourage every young member to actively participate, question, innovate and collaborate. Let this platform be your launchpad to explore research, develop academic brilliance and contribute meaningfully to community health. Remember, leadership is not a position; it is a mindset nurtured through dedication, integrity and service.
To the mentors and seniors guiding this initiative, I extend my heartfelt appreciation. Your guidance transforms potential into excellence and aspiration into achievement. Let us together build a generation of Obstetricians and Gynaecologists who are clinically sound, ethically strong, academically vibrant and socially responsible.
The future of FOGSI is bright — because it rests in capable young hands.
With warm regards and best wishes,
INTERVIEW WITH Dr. VINITA SINGH - Dr. Vinita Singh
ROLE OF A MENTOR IN SKILL
- Dr. Geetha Balsarkar
- Dr. Girish Mane
OF MATERNAL AND CHILD HEALTH: AN INDIAN PERSPECTIVE
- Dr. Poonam Goyal, Dr. Prerna Keshan
FRESH TAKE ON CLASSIC PROBLEM - OHSS REVISITED
- Dr. Annesha Dutta, Dr. Mohil Patel

EXECUTIVE EDITOR & PUBLISHER
Dom Daniel
CORPORATE OFFICE
22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.

FUTURE CHRONICLES YTP
Editorial Contributors

EMAIL: paradigminfocomobgyn@gmail.com
Website: ytpfuturechronicles.com
Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“YTP FUTURE CHRONICLES” takes no responsibility for unsolicited photographs or material
ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of March -2026






Dr. Vinita Singh
Professor OBGYN DEPT NMCH, Patna
Dr. Geetha Balsarkar
Professor and Unit head
Nowrosjee Wadia Maternity Hospital
Seth G. S. Medical. College Parel, Mumbai
Dr. Girish Mane
MBBS, DGO, MD, FICOG, MBA
State Coordinator, AMOGS (2024–2026)
Past Chairperson – Adolescent Health Committee, FOGSI (2019–2021)
Past Chairperson – Adolescent Gynaecology Committee, AMOGS (2018–2020 & 2022–2024)
Dr. Poonam Goyal
MD, FICOG, FICMCH, CIMP
HOD, IVF & Infertility Max Hospital Vaishali, Delhi NCR
Director and HOD, OBG, Panchsheel Hospital, Delhi Chairpersons Safe Motherhood Committee, FOGSI VP Delhi Medical Association
Dr. Prerna Keshan
Consultant OBGYN, Infertility Specialist, Endoscopic Surgeon FICOG, FICMCH, FIAOG, MRCOG1
Masters in Cosmetic Gynecology
National Coordinator, Young Talent Promotion Committee FOGSI
Dr. Annesha Dutta
MBBS, DNB, MNAMS, FIAOG, FRM, FMAS
Consultant, IVF Specialist, Ankur Fertility Clinic, Kolkata
Dr. Mohil Patel
Consultant Endoscopic Surgeon, Ahmedabad, Gujarat

Dr.
Abha Rani Sinha Vice President FOGSI 2026
Dear Readers,
It gives me immense pleasure to congratulate Dr. Rohan Palshetkar Chair Young Talent Promotion Committee and his team for doing commendable work. It is nice to know that the Young Talent Promotion Committee chronicles as newsletter is published every month. This step taken by the Young Talent Promotion Committee will give FOGSIans a platform to explore their inner and hidden talents. My best wishes to all and wish you all a great year ahead.

Dr. Rohan Palshetkar
FOGSI
Young Talent Promotion Committee Chairperson
Dear Readers,
YTP FUTURE CHRONICLES serves as a dynamic platform for academic dialogue, addressing the evolving priorities in Gynecological care. As women’s healthcare enters an era defined by precision medicine, metabolic awareness, and interdisciplinary collaboration, there is a growing need for forums that not only disseminate knowledge but also encourage critical clinical reflection. In line with its mission, and in alignment with FOGSI’s commitment to advancing women’s health, YTP FUTURE CHRONICLES continues to bridge academic rigor with practical insights, fostering dialogue and professional growth among young Gynecologists.
This edition brings together a diverse collection of contributions that reflect these goals. It begins with an exclusive Interview with Dr. Vinita Singh, offering valuable perspectives on leadership and innovation in healthcare. The article on the Role of Mentorship in Skill Development emphasizes how guidance and experience shape the next generation of professionals.
Contemporary social and clinical concerns are also addressed, including the Impact of Social Media on Adolescent Health and Sexuality and the Socioeconomic Determinants of Maternal Health in India, highlighting the interplay between societal factors and health outcomes. In addition, the article Informed Consent in Gynecology and a Revisitation of Ovarian Hyperstimulation Syndrome (OHSS) reinforces the importance of patient-centered, evidence-based clinical practice.
Together, these contributions aim to enrich understanding, provoke thoughtful discussion and provide a holistic view of women’s health challenges. This edition is intended to serve as a valuable academic companion, supporting continued professional growth and commitment to excellence in care.
Editorial Coordinators

Dr. Prerna Keshan
Consultant OBGYN, Infertility Specialist, Endoscopic Surgeon FICOG, FICMCH, FIAOG, MRCOG1
Masters in Cosmetic Gynecology
National Coordinator, Young Talent Promotion Committee FOGSI

Dr. Annesha Dutta
MBBS, DNB, MNAMS, FIAOG, FRM, FMAS
Consultant, IVF Specialist, Ankur Fertility Clinic, Kolkata
Dear Readers,
With immense pleasure, we are proud to present this edition of the YTP Future Chronicles. Something which we had been working on to bring a new outlook for the next generation Gynecologists across the nation.
Our esteemed organisation under the able leadership of revered president Dr. Bhaskar Pal sir, is always keen on educating and enhancing new horizons in the upliftment of women’s health. This newsletter is aimed at focussing on the various issues revolving around women’s health beyond what routine textbook chapters enlighten us with. It’s a thorough attempt by our editorial contributors to bring into discussion the various societal factors that has an extra edge into the practice of the next generation Gynecologists. Aimed at improving the understanding of our young fellow Gynecologists this edition of the newsletter brings to you interesting insights by the stalwarts as well as real life inspirational values that can prove as major pathfinding routes for many.
We have the honour to have included extremely informative articles by few of the finest minds of the country inculcating the culture of constantly updating one’s academic treasure. The modern day advancements in women’s health management calls for frequent exercising of our futuristic approach to skill development and expertise amongst the youth. The YTP FUTURE CHRONICLES aims to do that through the year ahead.
We extend our heartfelt gratitude to the chairperson Young Talent Promotion Committee, FOGSI Dr. Rohan Palshetkar to have given us this opportunity to bring into life this edition of the newsletter.
Wishing everyone a delightful and enriching reading experience.
AN INTERVIEW WITH Dr. VINITA SINGH

1) Can you describe your early years in FOGSI? How did you start out and rise with this organization?
Ans- I started my FOGSI journey from the year 1995 after my post graduation. I was pretty nervous when I was first assigned to do a workshop in the rural area, which later I came to know was the dream project of Dr. Pankaj Desai (past president FOGSI). Still today he praises me for my first work done in Patna. Later I was the organizing secretary of BOGSCON, and from there onwards there was no looking back for me! In 2017, I became the Young Talent Promotion Committee chairperson for three years where I really enjoyed working with Dr. Rishma Pai, Dr. Nandita Palshetkar & Dr. Jaideep Malhotra. After that I became the ICOG Governing council member for two tenures and aspire to become the Vice President of FOGSI as well
2) What keeps you motivated and driven in your work?
Ans- Whenever you get appreciated for your work, I think that`s what keeps someone motivated and enthusiastic and keeps us driven for doing more and more for FOGSI.
3) Where do you see yourself in the next five years, at a personal and Professional level?
Ans- At present I am a Professor at an OBGY college where I had done my post graduation. Also this place is very nostalgic for me. When I see the younger students, I want to be known to them as a good teacher, yet an excellent clinician. If I get a chance to become the future Vice - President of FOGSI, I would like to focus and make our country aware on NCDs especially anaemia, diabetes and hypothyroidism, which can be prevented and treated at an earlier stages to help reduce the maternal mortality rate.
4) What is your message to the young aspiring members of FOGSI who are starting their journey in this organization?
Ans- FOGSI is an organization with more than 44,000 Gynaecologists as member. So my message to all aspiring Gynaecologists is to become members of FOGSI, because this is an organization, where we get to meet so many people at the pan India level with diversity and multiple qualities, making friends, learning from each other and updating ourselves.FOGSI makes us academically strong. My message to all the aspiring Gynaecologists is – Join FOGSI if you want to make a change in the society and try to give your best. I am really very much thankful to FOGSI and family for supporting me whole heartedly during my Young Talent Promotion tenure as a committee chairperson. Thanks a lot Dr. Prerna and Dr. Annesha, love you both!
Dr. Vinita Singh Professor OBGYN DEPT NMCH, Patna

ROLE OF A MENTOR IN SKILL DEVELOPMENT

FDr. Geetha Balsarkar Professor and Unit head
Nowrosjee Wadia Maternity Hospital
Seth G. S. Medical. College Parel, Mumbai
amous mentors such as Virgil in Dante's Inferno, Yoda in Star Wars and Gandalf in the Lord of the Rings Trilogy were guides for the challenging journey towards fulfilling their protégés’ potential.
Mentorship is a collaborative relationship between individuals or within groups who share responsibility for the achievement of individual development. Success in these relationships is often based on luck and personal compatibility and is measured by attainment of personal or professional goals. Such goals are often ill-
defined and evolve over time.
Mentorship can be distinguished from “coaching” which directs the learning or refining of specific skills needed for improved performance. Mentorship places greater emphasis on the process of individual development and survival skills. Both coaching and mentorship are essential to achieve potential. However, mentorship is about relationships constructed to help the mentee anticipate and navigate challenges specific to their developmental path and not a mechanism to achieve mastery of specific
knowledge or technical skills, although this may occur. The journey from medical college to an established ObstetricianGynaecologist is long, with lots of ups and downs in today’s fast-changing world of Obstetrics and Gynaecology. The best way to get through these tough times is through mentorship. Lack of guidance and professional support from senior colleagues, difficulty maintaining work-life balance, and uncertainties related to career paths and training are among the most common stressors leading to physician burnout. Residency training is associated with increased risk of burnout, with prevalence rates varying from 18 to 82%. Thus, organizational interventions are needed to address the curricular, training, and system factors that contribute to the high prevalence of distress and burnout among medical residents[1].
MENTORSHIP IN ACADEMIC MEDICINE
Mentorship is invaluable in medical colleges and fellowship programmes where experts are ambivalent, untrained, or unskilled in administrative leadership. Their increased responsibility for the productivity and performance of other professionals detracts from time for the specialties for which they were recruited. Mentorship helps bring balance in training in superspecialities, where we are limited by experience.
NEED FOR MENTORSHIP IN EARLY RESIDENCY
The transition from medical college to residency can be
overwhelming for any student. The OBS-GYN residencies are usually very demanding: long hours, high-stress situations, and steep learning curves. This is where mentorship becomes crucial.
Emotional Support: The mentor will provide the muchneeded emotional support during the challenging times of residency. They help the residents cope with stress and avoid burnout, one of the most prevalent factors in medical professions.
Guidance: Experienced mentors can provide the necessary advice on how to negotiate the entire maze of OBS-GYN residency programs and allow the residents to make appropriate decisions regarding career choices.
Skill Building: A good mentor is able to advance hands-on training with practical tips beyond that in a book, thus allowing the resident’s learning process to accelerate.
CHARACTERISTICS OF AN EFFECTIVE OBSGYN MENTORING SYSTEM
Effective mentorship in OBSGYN should be:
• Structured: A well-defined mentorship program with clear mentorship goals will enable both the mentor and mentee to stay focused and maximize their relationship.
• Tailored: Each resident carries with him different needs and aspirations. Mentorship must be offered based on individual strengths, weaknesses, and career goals.
• Continuous: Mentorship
is not a one-time event but rather a process that ought to continue throughout residency and thereafter.
• Reciprocal: While mentees gain knowledge and experience, fresh perspectives also mean a mentor obtains the satisfaction of nurturing the next generation of OBS-GYNs.
SEVEN KEY ROLES OF A MENTOR
1. Teacher/Knowledge Provider: Shares expertise, skills, and industry insights to help mentees understand tasks, navigate company culture, and access relevant resources, notes TriNet.
2. Role Model: Demonstrates integrity, professionalism, and ethical behaviour, setting a positive example for the mentee to emulate, as mentioned in ATS Journals and Excelsior University.
3. Coach/Challenger: Encourages mentees to explore new ideas, take calculated risks, and push their thinking by asking probing questions and offering challenges, according to ATS Journals and Education Week.
4. Advisor/Guide: Offers timely, practical advice and direction, helping mentees set realistic goals and providing the “steady hand” or “roadmap” for their career path.
5. Sponsor/Advocate: Actively supports the mentee's advancement by making introductions, promoting their work, and helping build their professional network, writes Indeed.com Canada.
6. Confidante/Supporter: Provides a safe, confidential space for mentees to share
concerns, stresses, and challenges, offering emotional support and reassurance, say ATS Journals and Elo Mentoring.
7. Resource Identifier: Points mentees toward useful tools, contacts, and opportunities, connecting them with information and people crucial for their development.
WHAT IS THE ROLE OF A MENTOR IN HEALTHCARE?
Mentoring facilitates the transfer of knowledge, expertise and experience from experienced doctors to their mentees. The mentees will gain valuable insights, learn
REFERENCES
new skills and enhance their professional capabilities, potentially leading to increased job satisfaction.
MENTORSHIP AND ORGANIZATIONAL PERFORMANCE
For the local and national organisation, competitive advantage is dependent on the development of committed leaders and innovators throughout the organization who are aligned with clearly articulated institutional values and goals. Depth in institutional leadership is a core asset. Mentorship enhances job satisfaction and retention of valuable health professionals –valuable interventions in the prevention of burnout. Over time, a supportive mentoring culture will help to increase institutional strength by endorsing the value of the individual while developing leadership throughout the organization to champion change and to support innovation. Mentorship takes on increased importance in academic medicine due to the challenges pose by rapid change in the healthcare environment and by career fatigue or burnout. The challenge of professional burnout and early identification of individuals struggling with personal and professional growth may be mitigated by such professional relationships.
1. Fishman A, Kenett R, Biron-Shental T. Implementing Personal Mentoring in an Obstetrics and Gynecology Residency Program-3Year Evaluation. Med Sci Educ. 2020 Jan 2;30(1):293-297. doi: 10.1007/s40670-019-00902-2. PMID: 34457670; PMCID: PMC8368510.
2. Jay A. Fishman, Mentorship in academic medicine: Competitive advantage while reducing burnout?, Health Sciences Review, Volume 1, 2021, 100004, ISSN 2772-6320, https://doi.org/10.1016/j.hsr.2021.100004. (https://www.sciencedirect.com/science/article/ pii/S2772632021000039)
ULTRASOUND-BASED RISK STRATIFICATION OUTPERFORMS RMI IN PREMENOPAUSAL OVARIAN CANCER TRIAGE
major prospective, multicenter diagnostic accuracy study published in The BMJ has demonstrated that

an ultrasound-based risk prediction model substantially outperforms the currently recommended NHS triage tool, the Risk of Malignancy Index (RMI), in detecting ovarian cancer among premenopausal women presenting with non-specific symptoms in primary and secondary care settings. The ROCkeTS (Refining Ovarian Cancer Test Accuracy Scores) trial recruited women across multiple hospitals over several years and conducted a rigorous head-to-head comparison of six diagnostic strategies, including RMI, ROMA, CA125 alone, and three ultrasound-based models developed by the International Ovarian Tumor Analysis group. At a defined risk threshold, the ultrasound-based model achieved a sensitivity of 89.1% with 75.1% specificity, identifying approximately nine out of ten malignancies, whereas RMI at the standard threshold demonstrated a markedly lower sensitivity of 42.6% despite high specificity of 96.5%, missing more than half of cancers, particularly in women who had not undergone menopause. Although the higher sensitivity was associated with modestly reduced specificity and the potential for increased additional testing, investigators highlighted that a two-step ultrasound strategy initially classifying clearly benign lesions before applying the risk model optimizes cost-effectiveness and clinical consequences within the NHS framework. Notably, most malignancies detected were early-stage (FIGO I/II), underscoring the potential survival benefit of improved triage accuracy. Ultrasound examinations were performed predominantly by NHS sonographers trained and quality-assured in the methodology, supporting scalability across the health service. The findings follow complementary results in postmenopausal cohorts published in The Lancet Oncology, further consolidating evidence that this ultrasound-based risk model represents the most sensitive validated approach for ovarian cancer risk stratification, with implications for earlier specialist referral, reduction of unnecessary oophorectomy in low-risk patients, and improved psychological and clinical outcomes.
GENETIC AND OBESITY-RELATED RISK IN ENDOMETRIAL CANCER
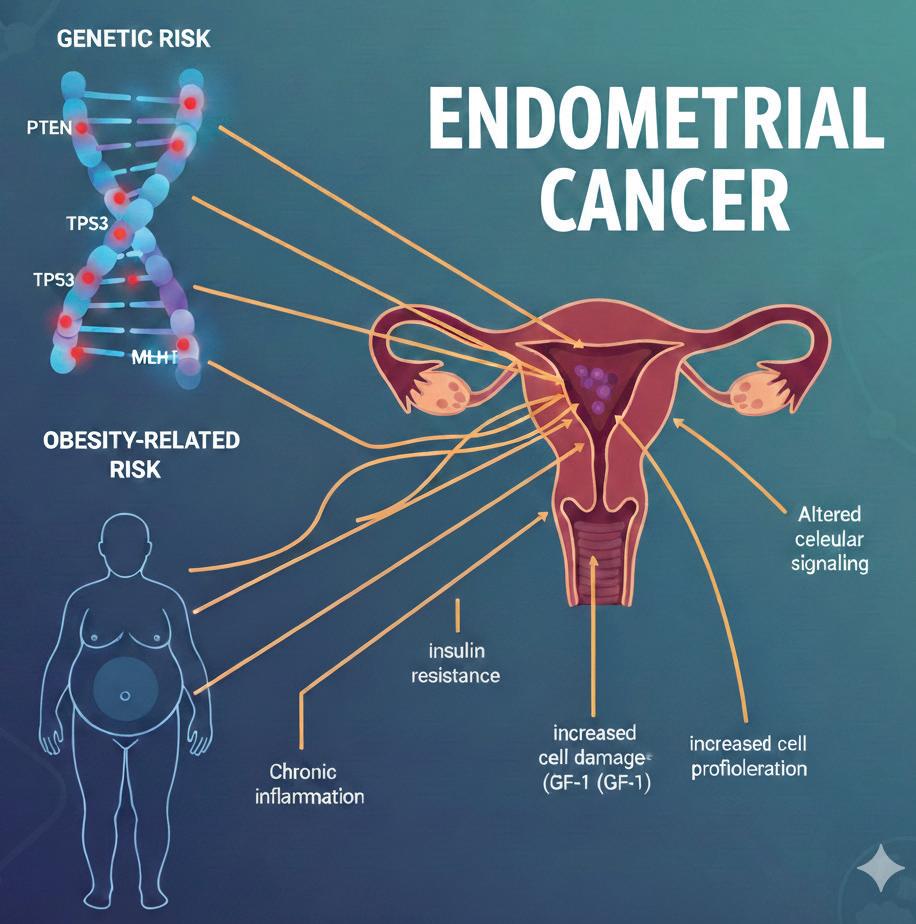
Amajor new study has reported that inherited genetic susceptibility may rival obesity as a key and independent driver
of endometrial cancer risk, challenging the long-standing paradigm that excess body weight is the predominant determinant of disease. Published in BMC Medicine, the large-scale analysis evaluated data from a substantial cohort of women and demonstrated that those in the highest category of a polygenic risk score (PRS) had a significantly increased risk of developing endometrial cancer, even when body mass index (BMI) was within the healthy range. Importantly, women with both elevated genetic risk and obesity experienced a markedly higher risk, underscoring the additive and independent contributions of genetic predisposition and adiposity rather than a single dominant pathway. These findings represent some of the first robust evidence that polygenic risk and BMI operate as separate yet synergistic determinants of disease development.
Endometrial cancer remains an under-recognized yet increasingly prevalent gynaecological malignancy, with incidence rates rising, particularly among younger women. Traditionally, clinical risk stratification has relied heavily on obesity as the principal modifiable risk factor, with genetic evaluation largely reserved for rare hereditary cancer syndromes. However, the current findings suggest that a substantial subgroup of women with normal BMI may still carry significant inherited risk that would not be detected through conventional screening approaches. Incorporating polygenic risk assessment alongside established clinical factors could enhance individualized risk prediction, enabling earlier surveillance, more targeted preventive strategies, and informed patient counselling. Furthermore, expanding understanding of the genetic architecture underlying endometrial carcinogenesis may facilitate the identification of novel molecular pathways and therapeutic targets, advancing precision medicine and improving long-term outcomes.

DIGITAL THRESHOLDS: THE IMPACT OF
SOCIAL MEDIA ON ADOLESCENT HEALTH AND SEXUALITY IN INDIA

Dr. Girish Mane
MBBS, DGO, MD, FICOG, MBA
State Coordinator, AMOGS (2024–2026)
Past Chairperson – Adolescent Health Committee, FOGSI (2019–2021)
Past Chairperson – Adolescent Gynaecology Committee, AMOGS (2018–2020 & 2022–2024)
In the last decade, India has witnessed a digital revolution characterized
INTRODUCTION by the cheapest mobile data in the world and a flurishing population of "digital natives." For the nearly 253 million adolescents in India, social media is no longer a peripheral activity but a primary environment for identity formation, socialization, and health-seeking behavior. However, this digital immersion is a double-edged sword. While it offers unprecedented access to many good things with positive sexual health information and community
support, it simultaneously exposes vulnerable youth to unrealistic beauty standards, cyberbullying, and unregulated sexual content. This chapter explores the multi-dimensional impact of social media on adolescent health and sexuality in India, analyzing the intersection of traditional socio-cultural norms with globalized digital narratives.
1. INTRODUCTION: THE DIGITAL LANDSCAPE OF YOUNG INDIA
India’s adolescent population (aged 10–19) is the largest in the world. As of 2024–2025,
the proliferation of platforms like Instagram, YouTube, and WhatsApp has fundamentally altered the transition from childhood to adulthood. Unlike previous generations, today’s Indian adolescents navigate a "phygital" reality where their online personas are as significant as their physical presence.
The 2024–2025 Economic Survey of India recently flagged "digital addiction" as a major public health concern. With adolescents spending an average of 3–5 hours daily on screens, the impact on their physical health (sedentary lifestyles), mental health (anxiety and body dysmorphia), and sexual development (exposure to pornography and digital dating) has reached a critical juncture.
2. IMPACT ON PHYSICAL AND MENTAL HEALTH
2.1 The Sedentary Crisis and Sleep Debt
The most immediate impact of excessive social media use is the disruption of biological rhythms. Indian studies indicate a rising "sleep debt" among urban and semi-urban youth who engage in "revenge bedtime procrastination"—staying up late to scroll through reels.
• Physical Health: Reduced physical activity contributes to rising rates of adolescent obesity and PCOD (Polycystic Ovarian Disease) among young girls in India.
• The "Blue Light" Effect: Chronic exposure to screens interferes with melatonin production, leading to irritability, poor academic focus, and long-term metabolic issues.
2.2 Mental Health: The Validation Trap
Social media platforms are designed around "variable reward" systems (likes, comments, shares) that trigger dopamine releases similar to gambling.
• The Comparison Culture: Indian adolescents are increasingly prone to "Upward Social Comparison." Viewing the curated, "perfect" lives of influencers leads to feelings of inadequacy, referred to as the "Fear of Missing Out" (FOMO).
• Depression and Anxiety: National Mental Health Survey (NMHS) data suggests a correlation between high social media usage and the prevalence of depressive symptoms. In India, where mental health is still stigmatized, many adolescents turn to social media for "self-diagnosis," which can lead to misinformation and delayed professional help.
2.3 Body Image and the "Beauty Standard"
India has a complex relationship with beauty, historically rooted in "fairness" and now pivoting toward "Westernized" thinness and muscularity.
• Filters and Dysmorphia: The ubiquitous use of "beautifying" filters on Instagram and Snapchat has led to "Snapchat Dysmorphia," where adolescents desire surgical or cosmetic changes to match their filtered images.
• Gendered Pressures: Research in Indian metros shows that while girls face pressure to be thin and fair, boys are increasingly obsessed with "gym-culture" and muscle
dysmorphia, often fueled by fitness influencers promoting unregulated supplements.
3. SOCIAL MEDIA AND ADOLESCENT SEXUALITY IN INDIA
In a country where Comprehensive Sexuality Education (CSE) is often absent from school curricula and "sex" remains a taboo dinner-table topic, social media has filled the vacuum.
3.1 The Informal Sex Education
For many Indian teens, Instead of the teachers and parents, YouTube and Instagram are their primary sources of information regarding:
• Puberty and menstruation.
• Contraception and safe sex.
• LGBTQ+ identities and rights.
The Benefit: Digital platforms provide a "discreet" space. An adolescent in a conservative town can learn about consent or gender identity without the fear of immediate social judgment.
The Risk: The lack of a "gatekeeper" means that misinformation—such as myths about masturbation causing weakness or home remedies for STIs—spreads as quickly as factual data.
3.2 Digital Dating and the Change in Relationship Dynamics
Traditional Indian dating, often characterized by "secret" meetings, has shifted to DMs (Direct Messages).
• Online Grooming: The anonymity of the internet allows predators to pose as peers. Indian law enforcement
has seen a spike in cases under the POCSO (Protection of Children from Sexual Offences) Act originating from social media interactions.
• Sexting and Nudes: The "normalization" of sharing explicit images as a form of intimacy is a growing trend. However, in the Indian context, the fallout of such "leaks" is devastating due to the high stakes of "family honor" (izzat), often leading to extreme measures like self-harm or suicide.
3.3 Pornography and the Scripting of Desire
With easy access to highspeed internet, exposure to pornography is occurring at younger ages (often between 10–13).
• Unrealistic Expectations: Pornography often portrays aggressive, non-consensual, and physically unrealistic sexual acts. In the absence of formal education, Indian adolescents may internalize these scripts as the "norm."
• Impact on Consent: There is a growing concern that digital consumption of sexual violence is desensitizing young men to the importance of enthusiastic consent in realworld relationships.
4. EMERGING RISKS: CYBERBULLYING AND DIGITAL VIOLENCE
4.1 Cyberbullying in the Indian Context
Cyberbullying in India often takes the form of "slutshaming," casteist slurs, or religious trolling. Unlike physical bullying, cyberbullying
is persistent; the victim cannot "go home" to escape it.
• Gendered Violence: Girls are disproportionately targeted with "morphing" (using AI to put their faces on explicit bodies) and "doxing" (releasing private information).
• The "Bystander" Effect: The viral nature of Indian social media means that a single derogatory post can be shared across thousands of WhatsApp groups within minutes, magnifying the trauma.
4.2 AI and Deepfakes
As we enter 2025, the rise of "Deepfake" technology is the new frontier of digital violence. Adolescents now face the risk of their images being used to create non-consensual deepfake pornography, a tool often used for extortion or "revenge."
5. SOCIO-CULTURAL NUANCES: THE INDIAN FAMILY VS. THE ALGORITHM
The impact of social media in India cannot be understood without the context of the "Joint Family" and "Collectivist" culture.
• The Digital Divide: There is a significant gap between "Digital Parents" (who monitor usage) and "Analog Parents" (who may provide the device but have no understanding of its contents).
• Privacy vs. Surveillance: In many Indian households, privacy is a luxury. Adolescents often use "ghost apps" or multiple accounts to hide their digital lives from parents, leading to a "dual life" that increases psychological stress.
6. THE "DIGITAL DIVIDEND": POSITIVE IMPACTS AND OPPORTUNITIES
It is crucial not to view social media solely through a lens of pathology.
• Community Building: For marginalized youth, such as the LGBTQ+ community in India, social media is a lifeline. It provides access to "found families" and support groups that are unavailable in their physical vicinity.
• Health Campaigns: The Government of India’s "Rashtriya Kishor Swasthya Karyakram" (RKSK) has begun utilizing social media to reach adolescents with messages on nutrition, iron deficiency, and mental health.
• Creative Expression: Platforms like Instagram and YouTube have allowed Indian youth to bypass traditional gatekeepers in arts, music, and activism, fostering a sense of agency and self-worth.
7. RECOMMENDATIONS FOR STAKEHOLDERS
7.1 For Parents: Beyond "Screen Time"
• Media Literacy: Instead of just limiting hours, parents should engage in "active mediation"—discussing what the child is seeing and helping them deconstruct the "unreality" of influencers.
• Building Trust: Creating a "no-judgment" zone so that if an adolescent is harassed online, they feel safe coming to their parents rather than hiding it for fear of having their device confiscated.
7.2 For Educators: Integrating Digital Hygiene
• Digital Citizenship: Schools must move beyond "IT classes" and teach "Digital Citizenship," covering topics like cyber-laws (IT Act 2000), consent, and the ethics of sharing content.
• Peer Support Systems: Training "digital mentors" within schools who can provide first-line support for victims of cyberbullying.
7.3 For Policy Makers: Regulation and Accountability
REFERENCES
• Platform Responsibility: Strict enforcement of age-verification and "duty of care" for platforms operating in India.
• Legal Literacy: Simplifying the process for reporting cybercrimes and ensuring that police personnel are sensitized to adolescent victims.
8. CONCLUSION
The impact of social media on adolescent health and sexuality in India is a defining challenge of the 21st century. The algorithm is currently faster than our cultural adaptation. As India continues to digitize, the goal should not be to "disconnect" our youth, but to equip them with the "digital resilience" needed to navigate this threshold. By bridging the gap between traditional values and digital realities through empathy, education, and robust policy, we can ensure that the digital world becomes a space of empowerment rather than a source of harm.
1. NFHS-5 (2019-21): National Family Health Survey reports on adolescent nutrition and sexual health indicators.
2. Economic Survey of India (2024-25): Chapter on "Human Development and Health" regarding digital addiction.
3. NMHS 2016/updated 2023: National Mental Health Survey data on adolescent depression.
4. UNICEF India: Reports on "The State of the World's Children: Children in a Digital World."
5. Ministry of Health and Family Welfare (MoHFW): RKSK (Rashtriya Kishor Swasthya Karyakram) strategy documents.
6. IIPS Mumbai: Various studies on "Social Media and Body Image Dissatisfaction among Indian Youth."
SOCIAL DETERMINANTS OF MATERNAL AND CHILD HEALTH:

Dr. Poonam Goyal
MD, FICOG, FICMCH, CIMP
HOD, IVF & Infertility Max Hospital Vaishali, Delhi NCR
Director and HOD, OBG Panchsheel Hospital, Delhi
Chairpersons Safe Motherhood Committee, FOGSI VP Delhi Medical Association
AN INDIAN PERSPECTIVE

MDr. Prerna Keshan
Consultant OBGYN, Infertility Specialist, Endoscopic Surgeon FICOG, FICMCH, FIAOG, MRCOG1
Masters in Cosmetic Gynecology
National Coordinator, Young Talent Promotion Committee FOGSI
INTRODUCTION by medical care alone. While advances in obstetrics, neonatology, and public health programs have significantly improved outcomes, the social environment in which a woman is born, grows, lives, and works continues to exert a profound influence on her health and that of her child. These non-medical factors—collectively known as the social determinants of health—are particularly relevant in the Indian context, where stark social, economic, and genderbased disparities persist
aternal and Child Health (MCH) is not determined
NATCON ORATION -SOCIAL DETERMIN…
UNDERSTANDING
SOCIAL DETERMINANTS OF HEALTH
Social determinants of health encompass conditions such as education, income, nutrition,
housing, sanitation, gender equity, cultural practices, and access to healthcare services. These factors shape health behaviours, influence exposure to risks, and determine the ability to seek and receive timely care. In maternal and child health, their impact begins even before conception and extends across the life course of both mother and child.
MATERNAL AND CHILD HEALTH IN THE INDIAN SETTING
India remains a predominantly rural country, with nearly two-thirds of its population and approximately 70% of its workforce residing in rural areas. Despite increasing urbanization, projections suggest that more than half of India’s population will continue to live in rural settings even by 2050. The rural economy contributes nearly 46% of national income, yet health indicators in these regions often lag behind urban counterparts.
Women in rural India frequently face limited access to quality healthcare, compounded by poor transportation, inadequate health infrastructure, and shortage of skilled health professionals. Equally concerning is the lack of awareness regarding optimal health practices, including nutrition, antenatal care, institutional deliveries, and postnatal follow-up. These gaps directly translate into preventable maternal morbidity, mortality, and adverse neonatal outcomes.
GENDER BIAS AND ITS IMPACT ON WOMEN’S HEALTH
One of the most irrefutable and persistent social determinants affecting maternal health in India is gender bias. From early childhood, girls often receive less nutrition, fewer
educational opportunities, and delayed healthcare compared to boys. Early marriage, repeated pregnancies, limited decisionmaking autonomy, and financial dependence further compromise women’s health.
In many households, women seek healthcare only when complications become severe. Preventive services—such as antenatal check-ups, iron and folic acid supplementation, or contraception—are often neglected. This systemic undervaluation of women’s health perpetuates intergenerational cycles of poor maternal and child outcomes.
ACCESS TO BASIC SERVICES
Access to basic services such as safe drinking water, sanitation, electricity and clean cooking fuel plays a critical role in MCH outcomes. Poor sanitation and unsafe water increase the burden of infectious diseases, particularly diarrhea and parasitic infestations, which contribute to malnutrition and anemia in women and children.
Indoor air pollution from biomass fuel disproportionately affects pregnant women, increasing the risk of low birth weight, respiratory illnesses, and adverse pregnancy outcomes. Thus, infrastructure development and social welfare policies are as crucial to maternal health as medical interventions.
KEY DETERMINANTS OF CHILD HEALTH
Child health is intricately linked to maternal health and the surrounding social environment. Maternal education emerges as one of the strongest predictors of child survival and well-being. Educated mothers are more likely to seek antenatal care, ensure immunization, adopt appropriate
feeding practices, and recognize danger signs early.
Nutrition, particularly in the first 1000 days of life, is heavily influenced by household food security, cultural feeding practices, and maternal awareness. Poverty, coupled with inadequate healthcare access, results in undernutrition, stunting, and increased vulnerability to infections— factors that impair physical and cognitive development.
WHY DISCUSS SOCIAL DETERMINANTS OF MCH TODAY?
Despite multiple national programs and policy initiatives, medical solutions alone cannot bridge the gap in maternal and child health outcomes. Addressing social determinants is essential for achieving equitable, sustainable, and long-term improvements in MCH indicators.
A holistic approach— integrating healthcare delivery with education, women’s empowerment, poverty alleviation, and infrastructure development—is the need of the hour. Strengthening community awareness, promoting gender equity, and ensuring last-mile access to services can transform maternal and child health across India.
CONCLUSION
Maternal and child health is a mirror reflecting the social conscience of a society. In India, improving MCH outcomes requires looking beyond hospitals and clinics to the social realities shaping women’s lives. By acknowledging and actively addressing social determinants, we can move closer to the goal of safe motherhood, healthy childhood, and a stronger future generation.
ovarian hyperstimulation syndrome
FRESH TAKE ON CLASSIC PROBLEM - OHSS REVISITED
ABSTRACT
Ovarian

Dr. Annesha Dutta
MBBS, DNB, MNAMS, FIAOG, FRM, FMAS
Consultant, IVF Specialist, Ankur Fertility Clinic, Kolkata

Dr. Mohil Patel
Consultant Endoscopic Surgeon, Ahmedabad, Gujarat
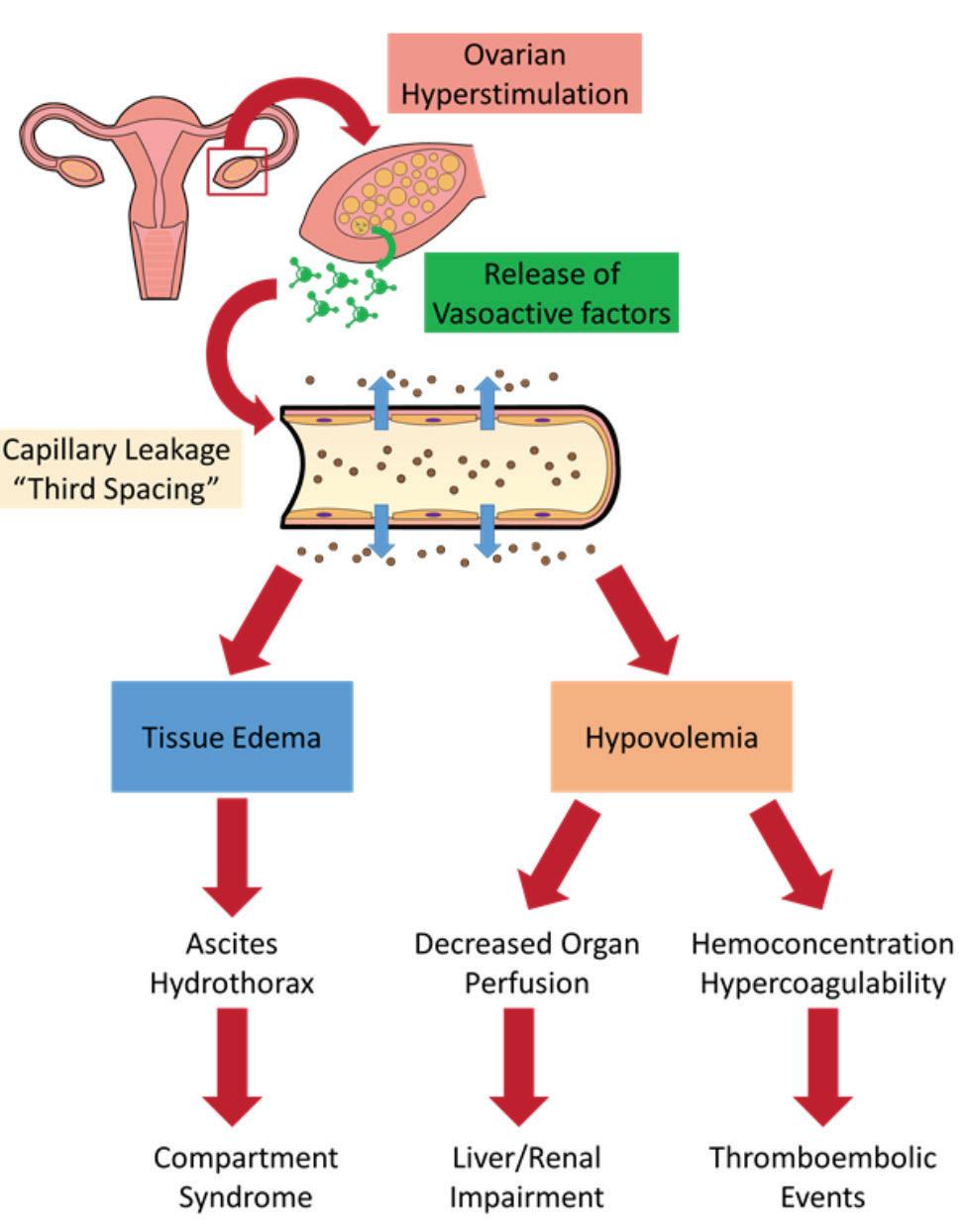
Hyperstimulation..... Syndrome (OHSS) is a serious complication of ovulation induction that usually occurs after gonadotropin stimulation, followed by human chorionic gonadotropin administration, for infertility treatment. In this manuscript, the existing knowledge of the pathophysiology, risk factors, primary, secondary methods of prevention alongwith clinical manifestations and characteristics of mild, moderate, severe and critical forms are reviewed. Methods of handling of outpatient cases as well as in-hospital management methods with indications of hospitalization are summarized in this review. Various
drugs,medical treatment strategies including indications for aspiration of the ascitic fluid and pleural effusion, and rare indications for surgery are briefly explained in this article. Severe OHSS, which was considered life threatening some decades ago, can now be easily and effectively prevented, besides the establishment of an OHSS-free clinic.
KEYWORDS:
Ovarian hyperstimulation syndrome, pathophysiology, risk factors, prevention, classification, management
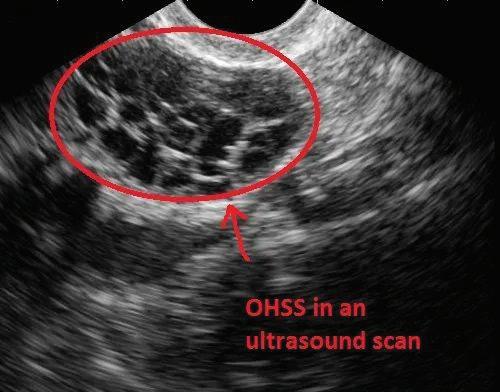
DEFINITION:
Exaggerated response to ovarian stimulation characterized by ovarian enlargement and increased capillary permeability. Incidence of about 3-8% in moderate to severe form and 20 to 30% milder forms in COS(1)
ETIOPATHOGENESIS:
The syndrome is known to be dependent on HCG. OHSS does not occur if hcg is withheld. Ongoing hcg stimulation by early pregnancy is a risk factor for persistent and severe OHSS hcg mediated VEGF seems to have critical role. Many of the angiogenic factors implicated in the development of the syndrome, act directly or indirectly through VEGF. Renin – angiotensin –
aldosterone system, prostagandins endothein-1 TNF apha and various inflammatory mediators have a been implicated in the etiopathogenesis.
RISK FACTORS:
Young age (< 33years predicts OHSS)
High AMH >3.4 ng/ml
High AFC > 24
Previous OHSS
High or rapidly rising E2 levels (>3500 pg/ml)
Development of >= 25 follicles >= 24 oocytes retrieved PCOS
BMI (lower BMI predicts OHSS: <18.44 kg/m2)
Race (black race predicts OHSS)
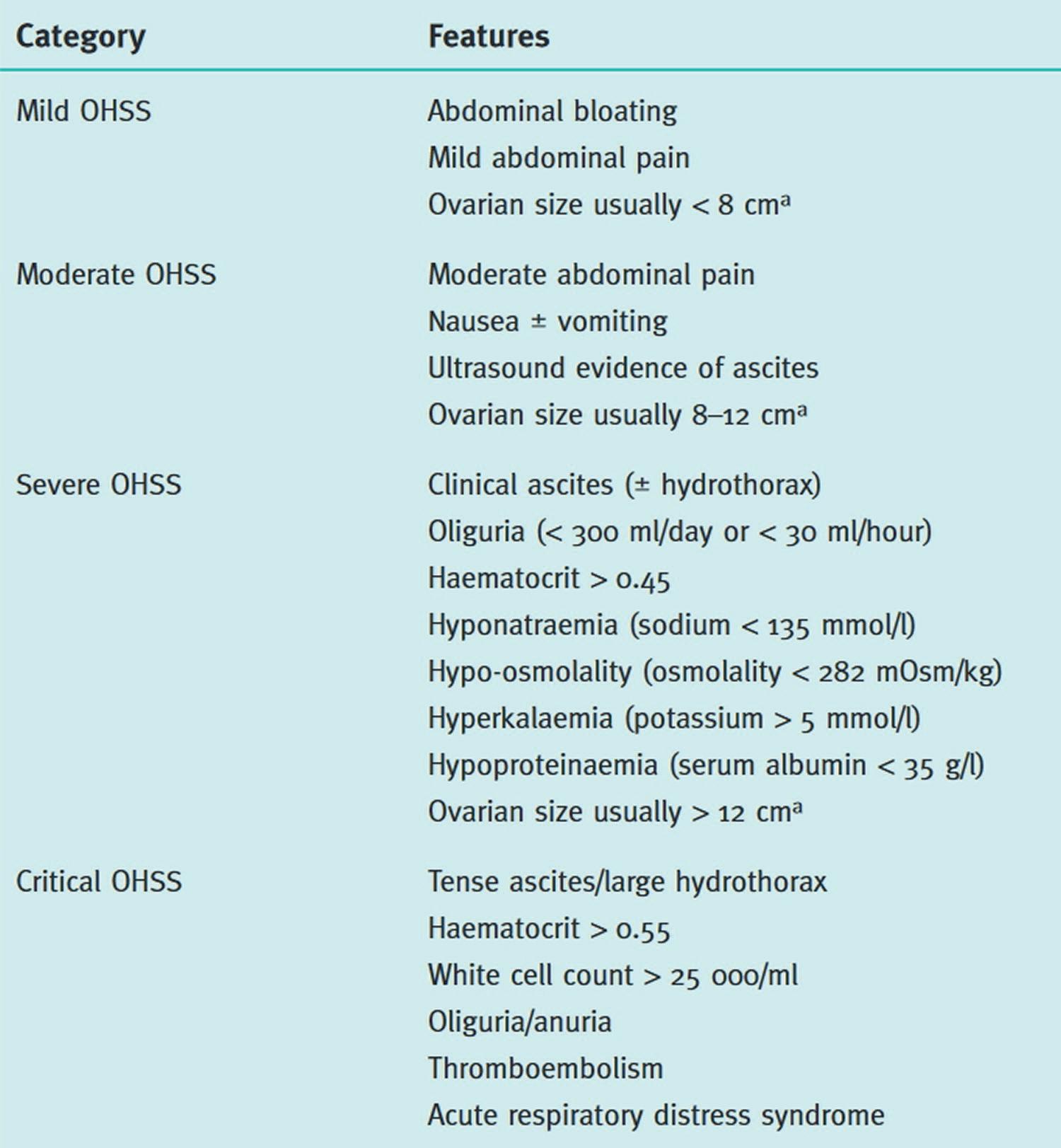
CLASSIFICATIONS:
1) Mild, moderate, severe, critical
2) Early, late
BASED ON THE DISEASE SEVERITY
EARLY OR LATE
Early OHSS
hCG
Exogenous
Late OHSS
Endogenous
Time of onset < 9 days after hCG trigger >=9 days after hCG trigger
Occurrence Occurs in a stimulated cycle Occurs in a setting of pregnancy
Associated with Higher peak Estradiol levels, greater gonadotropin levels
PRIMARY PREVENTION:
Singleton or Multiple pregnancy
1. Reducing gonadotrophin dose and duration: Using low dose of gonadotropins for stimulation in high risk patients reduces reduces the risk of OHSS
2. Avoiding adjunct GnRH agonist: GnRHa prevent the luteal phase of FSH rise causing recruitment of large number of follicles and preventing follicles from becoming atretic.
3. GnRH antagonist protocol: More physiological follicular selection, recruitment of smaller no. of follicles. Lesser doses of gonadotropins required.
4. Avoidance of hcg for luteal phase support: GnRHa can be used instead of hCG for trigger resulting in a lower incidence of OHSS.
5. Insulin sensitizing agents (Metformin): By improving intraovarian hyperandrogenism, metformin reduces the no. of nonperiovulatory follicles and thereby reduce estradiol secretion and preventing OHSS
6. Letrozole: Letrozole in a dose of 7.5 mg OD from the day of hCG trigger for 5 days reduces moderate and severe early onset OHSS. Further evidences are needed.
7. Glucocorticoids:...................
Prednisolone 10 mg thrice daily x 5days alongwith letrozole from the day of hCG trigger in the luteal phase reduces the risk of OHSS. More evidences are needed.
8. Aspirin: Decreases the level of histamine, serotonin, PDGF, thereby preventing the cascade of OHSS
9. Clomiphene Citrate: Insufficient evidence
SECONDARY
..............
PREVENTION:
1) Alternative agents for triggering ovulation (GnRHa): GnRHa has a shorter and moderated gonadotropin surge and hence completely eliminates the risk of OHSS
2) Cryopreservation of all embryos: A part of the segmentation approach for an OHSS free clinic.
3) Cycle cancellation: Prevents early OHSS but still not recommended due to financial
and psychological burden it causes to the patient
4) Coasting: Coasting involves withholding gonadotropins and delaying hCG administration until E2 levels platues or significantly decreases. It decreases VEGF level by causing atresia of the small follicles but it should not be more than 3 days as it is detrimental for oocyte quality.
5) Dopamine agonists: A daily administration of 0.5mg of cabergoline or 2.5mg BD bromocriptine for 8 days starting from the day of hCG trigger, prevents the phosphorylation of VEGF receptor and reduces the release of vasoactive angiogenic agents.
6) Calcium infusions: 10ml of 10% calcium gluconate in 200
ml saline on the day of oocyte retrieval and day 1-3 after oocyte retrieval helps in preventing severe OHSS and drecreases OHSS occurrence rates
7) Aspirin
8) Glucocorticoids
9) Colloid infusion (Albumin and HES)
10) Luteal GnRH antagonist administration
MANAGEMENT:
Depends on the relevant history from woman suspected to be suffering from OHSS
History
Time of onset of symptoms relative to trigger
Medication used for trigger (hCG or GnRH agonist)
Number of follicles on final monitoring scan
Number of eggs collected
Were embryos replaced and how many?
Polycystic ovary syndrome diagnosis?
Symptoms
Abdominal bloating
Abdominal discomfort/pain, need for analgesia
Nausea and vomiting
Breathlessness, inability to lie flat or talk in full sente
Reduced urine output
Leg swelling
Vulval swelling
Associated comorbidities such as thrombosis
EXAMINATION AND INVESTIGATIONS
Examination
General: assess for dehydration, oedema (pedal, vulval and sacral); record heart rate, respiratory rate, blood pressure, body weight
Abdominal: assess for ascites, palpable mass, peritonism; measure girth
Respiratory: assess for pleural effusion, pneumonia , pulmonary oedema
Investigations
Full blood count
Haematocrit (haemoconcentration)
C-reactive protein (severity)
Urea and electrolytes (hyponatraemia and hyperkalaemia)
Serum osmolality (hypo-osmolality)
Liver function tests (elevated enzymes and reduced albumin)
Coagulation profile (elevated fibrinogen and reduced antithrombin) hCG (to determine outcome of treatment cycle) if appropriate
Ultrasound scan: ovarian size, pelvic and abdominal free fluid. Consider ovarian Doppler if torsion suspected
Other tests that may be indicated
Arterial blood gases
D-dimers
Electrocardiogram (ECG)/echocardiogram
Chest X-ray
Computerised tomography pulmonary angiogram (CTPA) or ventilation/perfusion (V/Q) scan
DIFFERENTIAL DIAGNOSIS:
Pelvic abscess, pelvic infection, appendicitis, ectopic pregnancy, ovarian torsion or ruptured cyst, bowel perforation
• Outpatient management for mild and moderate OHSS:
1) Counselling regarding worsening of symptoms
2) Fluid intake guided by thirst
3) Avoid intense exercise, sexual intercourse
4) Weight and abdominal girth measurement
5) Input out chart
6) Analgesics: Paracetamol or opioids to be given, avoid NSAIDS as it increases renal impairment
7) Provide with a 24hr emergency contact number
8) Monitor every 2 to 3 days till symptoms resolve or menses occur
9) Baseline lab investigations should be repeated if the severity of OHSS is worsening
• Inpatient management for severe/critical OHSS,worsening signs of OHSS in case of outpatient management, inadequate fluid intake due to nausea,uncontrolled pain, non-compliant patient:
1) Daily assessment of full blood count, hematocrit, electrolytes, creatinine and liver function tests. Other imaging alongwith ABG,
ECG, C-XRAY may be needed depending on the clinical features.
2) Haematocrit guides about the degree of intravascular volume depletion
3) Analgesics and antiemetics
4) Oral fluid is the most physiological approach
5) IV crystalloids only if oral intake is inadequate
6) IV colloids in cases of persistent haemoconcentration and/or oliguria. Human albumin soln. 25% may be used as a plasma volume expander in doses of 50 to 100 g infused over 4hrs and repeated 4 to 12hrly. Strict fluid balance should be followed for these patients.
• Paracentesis: Indications
1) In case of raised serum creatinine
2) Tense ascites
3) Oliguria despite volume replacement
4) Non responsive haemoconcentration
5) Shortness of breath and respiratory compromise due to increased intraabdominal pressure
Method:
Drainage of around 2L ascitic fluid under usg guidance produces significant reductions in intraabdominal pressure and renal vascular resistance.If accidentally large volumes are removed, IV colloid therapy can be considered in them.
• Anticoagulation: Incidence of thrombosis in OHSS is between 0.7 to 10%, mainly affecting the upper body sites and frequently involves the arterial system.Vigilance about unusual symptoms like
dizziness, loss of vision and neck pain or unusual neurological symptoms.
• Surgical Management: Adnexal torsion, ovarian rupture, ectopic pregnancy, Haemorrhage
REFERENCES
• Termination Of Pregnancy: When the critical stage of OHSS is complicated by renal failure, thromboembolism, ARDS and multiorgan failure, potentially live saving TOP is the best choice.
• Awareness: Clinicians should be highly aware about pregnancies complicated by OHSS may end up in gestational diabetes, placental abruption, preeclampsia, preterm delivery and low birth weight.
1.Practice Committee of the American Society for Reproductive Medicine. Ovarian hyperstimulation syndrome.
2.Royal College of Obstetricians and Gynaecologists (RCOG). The management of Ovarian Hyperstimulation Syndrome.Green Top Guideline No 5.
A Young Talent Promotion Committee Event




Protection begins with awareness.


Proud to be part of a meaningful vaccination awareness initiative in collaboration with IMA Maharashtra State Sexual Committee, FOGSI Young Talent Promotion Committee, and FOGSI SEXUAL HEALTH COMMITTEE and Sudarshan School, Nagpur. FOR 48 girls. These are the girls whose mothers reside in red light areas and have prostitution as their profession . Unfortunately at young age of 13 -14 years these girls drop out from school to enter in the line!
When we educate children, we empower families.
When we vaccinate, we prevent.
When we act together, we build a healthier future.
OBSERVERSHIP IN AESTHETICS


3-Nights, 4-Days
Program Highlights* 2 Half-days
Lectures by DHA Certified Faculty 2 Half-days
Observership in Aesthetic Procedures with upto 6 DHA@CME Credits# CME Credits# with

Package to be announced shortly
Inclusions:
* 3-Nights 4-Days Stay, in a 4-STAR Hotel with breakfast and dinner, Lunch at Academy/Aesthetic Centre, To and fro - Hotel to Academy/Aesthetic Centre SIC◊
Exclusions:
Air fare to Dubai and back , airport transfer, Sight seeing etc.
@ DHA- Dubai Health Authority
# Proposed s/t confirmation
◊ SIC- Seat in Coach
Interested Drs kindly call for further details: +91



