





Dr. Bhaskar Pal President, FOGSI (2026)
Dear Colleagues and Future Torchbearers of FOGSI, Warm greetings from the Federation.
It gives me immense pride and optimism to address the Young Talent Promotion Committee — a vibrant platform that symbolizes the future strength, vision, and dynamism of FOGSI. The Young Talent Promotion Committee focuses on nurturing young obstetricians and gynaecologists through academic, social, and cultural engagement.
Our young members are not merely the doctors of tomorrow; they are the innovators, leaders, researchers, and compassionate caregivers of today. The Young Talent Promotion Committee stands as a testimony to FOGSI’s unwavering commitment to nurturing fresh ideas, encouraging academic excellence, and empowering emerging obstetricians and gynaecologists to rise with confidence and competence.
In a rapidly evolving era of medicine, where knowledge expands by the minute and technology reshapes clinical practice, it is the enthusiasm, curiosity, and adaptability of our young professionals that will keep FOGSI at the forefront of women’s healthcare. This committee provides the ideal ecosystem for learning, mentoring, sharing, and growing — a space where talent is recognized, skills are honed, and leadership is cultivated.
I encourage every young member to actively participate, question, innovate, and collaborate. Let this platform be your launchpad to explore research, develop academic brilliance, and contribute meaningfully to community health. Remember, leadership is not a position; it is a mindset nurtured through dedication, integrity, and service.
To the mentors and seniors guiding this initiative, I extend my heartfelt appreciation. Your guidance transforms potential into excellence and aspiration into achievement. Let us together build a generation of obstetricians and gynaecologists who are clinically sound, ethically strong, academically vibrant, and socially responsible.
The future of FOGSI is bright — because it rests in capable young hands.
With warm regards and best wishes,

EXECUTIVE EDITOR & PUBLISHER
Dom Daniel
CORPORATE OFFICE
22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.


EMAIL: paradigminfocomobgyn@gmail.com
Website: ytpfuturechronicles.com
Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“YTP FUTURE CHRONICLES” takes no responsibility for unsolicited photographs or material ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of February -2026





Dr. Suchitra Pandit
MD (Gynecology & Obstetrics)
Consultant - Gynecology & Obstetrics
Kokilaben Dhirubhai Ambani
Hospital, Mumbai Surya Hospitals, Santacruz, Mumbai
Dr. Parag Biniwale
MD, FICOG, FICMCH Diploma in Pelviscopy (Germany)
Consultant Ob - Gyn, Pune
Dr. Basab Mukherjee
MD FRCOG FICOG
Consultant Obstetrician & Gynecologist Kolkata
Dr. Charmila Ayyavoo
MD, DGO, DFP, FICOG, PGDCR Obstetrics & Gynaecology
Director, Aditi Hopsital and Aditi Pluro Fertility and IVF, Trichy
Dr. Neharika Malhotra
MD ObGyn (Gold Medallist) FICOG, DRM(Germany ) Infertility Specialist and high risk
Obstetrician Rainbow IVF Agra
Dr. Pratik Tambe
MD, FICOG, FICRM, FICMCH, FIAOG, Secretary, ICOG (2026-27)
Governing Council Member, ICOG (2020-25)
Governing Council Member, ICRM (2024-26)
Chairperson, FOGSI Endocrinology Committee (2017-19)
Chairperson, AMOGS Endocrinology Committee (2020-24)
Managing Council Member, MOGS, ISAR, MSR

Dr. Abha Rani Sinha Vice President FOGSI 2026
Dear Readers,
It gives me immense pleasure to congratulate Dr. Rohan Palshetkar Chair Young Talent Promotion Committee and his team for doing commendable work. It is nice to know that the Young Talent Promotion Committee chronicles as newsletter is published every month. This step taken by the Young Talent Promotion Committee will give FOGSIans a platform to explore their inner and hidden talents. My best wishes to all and wish you all a great year ahead.

FOGSI Young Talent Promotion Committee Chairperson
Dear Readers,
YTP FUTURE CHRONICLES sets the foundation for an academic dialogue responsive to emerging priorities in gynecological care. As women’s healthcare enters an era defined by precision medicine, metabolic awareness, and interdisciplinary collaboration, there is a growing need for platforms that not only disseminate knowledge but also stimulate critical clinical reflection. This edition has been conceptualized to bridge established clinical wisdom with emerging scientific evidence, offering gynecologists a forward-oriented perspective on care delivery.
The issue opens with The Glorious Legacy of the Young Talent Promotion Committee, FOGSI, highlighting institutional leadership and its enduring influence on professional excellence. This is complemented by an Interview with an eminent past Young Talent Promotion Committee Chairperson, offering thoughtful insights shaped by experience and vision. Contemporary challenges in obesity are addressed through The ‘Weight’ Is Over but the ‘Work’ Is Not, examining perceptions and longterm outcomes, alongside GLP-1–Based Therapies in Obesity, focusing on implications for women’s health and preconception Care in Current Practice, underscoring its growing relevance in modern obstetric care.
Together, these contributions aim to enrich clinical understanding, provoke thoughtful discourse, and reinforce a holistic, evidence-driven approach to women’s health. We trust this edition will serve as a meaningful academic companion in your ongoing professional journey.

Dr.Prerna Keshan
Consultant OBGYN, Infertility Specialist, Endoscopic Surgeon FICOG, FICMCH, FIAOG, MRCOG1
Masters in Cosmetic Gynecology National Coordinator, Young Talent Promotion Committee FOGSI

Dr. Gurkiran Kaur
MBBS, MS (Obstetrics and Gynaecology), Fellowship in Reproductive Medicine
Consultant Gynecologist and Infertlity specialist Kuldip Hospital and IVF Centre, Jalandhar
Dear Readers,
With immense pleasure, we are proud to present this edition of the YTP Future Chronicles. something which we had been working on to bring a new outlook for the next generation gynecologists across the nation.
Our esteemed organisation under the able leadership of revered president Dr. Bhaskar Pal sir is always keen on educating and enhancing new horizons in the upliftment of women’s health. This newsletter is aimed at focussing on the various issues revolving around women’s health beyond what routine textbook chapters enlighten us with. It’s a thorough attempt by our editorial contributors to bring into discussion the various societal factors that has an extra edge into the practice of the next generation gynecologists. Aimed at improving the understanding of our young fellow gynecologists this edition of the newsletter brings to you interesting insights by the stalwarts as well as real life inspirational values that can prove as major pathfinding routes for many.
We have the honour to have included extremely informative articles by few of the finest minds of the country inculcating the culture of constantly updating one’s academic treasure. The modern day advancements in women’s health management calls for frequent exercising of our futuristic approach to skill development and expertise amongst the Youth. The YTP FUTURE CHRONICLES aims to do that through the year ahead .
We extend our hearfelt gratitude to the chairperson FOGSI Young Talent Promotion Committee Dr. Rohan Palshetkar to have given us this opportunity to bring into life this edition of the newsletter. Wishing everyone a delightful and enriching reading experience.
Hello dear friends! This is Dr. Suchitra Pandit. I took over as the chairperson of Young Talent Promotion Committee in 2003. At that time, we had a five year tenure. I realized this is a wonderful platform for showcasing work done by our junior Fogsians. The various programs and workshops that we did, like caesarean skills, communication skills, safety first, writing skills, and so many more. We really had a great time.
I passed over the baton to Dr. Parag Biniwale. Then Dr. Bhaskar Pal took over and after that he handed over to Dr. Geeta Balsarkar, then Dr. Vinita Singh, followed by Dr. Neharika Malhotra and then the current chairperson Dr. Rohan Palshetkar.
And mind you, every chairperson has done some unique work that has left their stamp on the committee. I am sure when Dr. Prerna Keshan, who is an active member of the committee takes over as chairperson, she’ll also contribute something very different and unique of her own, to this committee.
I’d also like to say something else. I became FOGSI president in 2014. Dr. Parag Biniwale became Chairperson ICOG in 2025. And now Dr. Bhaskar Pal has taken over as President FOGSI in 2026. So this committee gives you all the practice, the luck and the skills to become something very big in FOGSI.
So my friends, long live the FOGSI Young Talent Promotion Committee!!

MD (Gynecology & Obstetrics) Consultant - Gynecology & Obstetrics
Kokilaben Dhirubhai Ambani Hospital, Mumbai Surya Hospitals, Santacruz, Mumbai


MD, FICOG, FICMCH Diploma in Pelviscopy (Germany)
Consultant Ob - Gyn, Pune
Q.1 Can you describe your early years in FOGSI? How did you start out and rise with this organization?
Ans- My first exposure to FOGSI was in the year 1996 when Pune Obs Gyn society had hosted the AICOG and as a young member of the society, I was roped in as the convenor of office administration committee of the organizing committee and I was supposed to look after the communication with all the delegates and faculties. So this was how I got to know FOGSI a bit closely and how it conducts all the activities and conferences. I was very lucky to be motivated by Late Dr. AV Umranikar and Late Dr. Subhash Nargolkar, past Vice Presidents of FOGSI, who have mentored and groomed me right from my post graduation days till today. My next close exposure was in the year 2002 when I, as a young secretary of the Pune ObsGyn society, on Dr. Nargolkar’s motivation, attended my first ever FOGSI managing committee meeting in Meerut and got to meet some of the stalwarts who were leading FOGSI in those times.
My big break came in the year 2003 when Dr. Suchitra Pandit became the chairperson of the Young Talent Promotion Committee and I, along with so many others like Dr. Bhaskar
Pal, Dr. Geetha Balsarkar and so many others, got the opportunity to work under her in this committee and participate in all the activities, youth melas she started and that helped in grooming us and being in the limelight.
I took over as the chairperson of Young Talent Promotion Committee in 2007 when Dr. Suchitra Pandit graciously promoted me for this post. Some of the activities and initiatives we took during my tenure were the communication skills workshops, awareness programs for adolescent boys, the best activity of Young Talent Promotion Committee yet, the assisted vaginal delivery workshops that we conducted all over India. So through all these activities we got to interact with obstetricians from all over India, learn the nuances of assisted vaginal birth with them, which was again a brainchild of Dr. Nargolkar.
My first exposure to ICOG was as an observer in the governing council meetings where I was given the role of taking down important points discussed in the meeting which had to be included in the minutes at a later date. My second break with ICOG came when I got its membership at one of its first convocations, and later became its governing council member in 2012-2014, 2015-2017. In 2017, I was elected unopposed as the honorary secretary of ICOG, and in 2018, as the last secretary with a three year tenure in the ICOG. As secretary ICOG, I got the opportunity to be examiner for MRCOG on two occasions, during covid in 2020, we started exploring virtual activities with Dr. Mandakini Megh as chairperson. Since then we have conducted these workshops regularly with various specialists whose knowledge and skill is valuable and should be shared in these activities.
Q.2 What keeps you motivated and driven in your work as ICOG Chairperson?
Ans- My keen interest in academics has always
drawn me towards ICOG, and during my tenure as chairperson, in 2025 we started a new program called odessy of teachers, wherein we have drafted modules for training teachers according to the new NMC guidelines. Another program we started was Harmony, in collaboration with Endocrinology Committee, covering the basics of gynaec hormones and endocrinology for post graduates and their clinical applications.
So I find fulfillment in teaching and learning, the only thing that has got me through ICOG, climbing it’s ladder right from a member, to secretary and now finishing my term as a chairperson.
On the clinical front as well, I started private practice in 1993, along with my role as a unit head in Kamla Nehru College which is again a teaching hospital.
Q.3 Where do you see yourself in the next five years? At a professional and personal level?
Ans- Five years down the line, I would still continue working as an obstetrician. Personally, I enjoy doing obstetrics and find happiness in every new birth, be it at one am or four am in the morning.
As far as the organization is concerned, working in ICOG was always my main thing, that I have now completed. I am now taking a cooling period, sort of a break and a year long hiatus. I hope to come back after this break a more refined person, ready to take on bigger organizational responsibilities and positions. So time will only tell what is on the cards!
Q.4 What is your message to the young aspiring members of FOGSI who are starting their journey in this organization?
Ans- My message to youngsters is that besides your clinical work and your patients, your family should be your priority. You must give them the time they deserve. But organizations also need enthusiastic workers, because we, through organizations are sharing our knowledge with people in lesser privileged areas, who do not have access to latest
information and guidelines, are benefitted with your knowledge and experience.
It is also important for seniors in various societies to motivate their juniors. Because unless someone pushes them, youngsters may not like to venture into something they’ve never tried. So organizational work can sometimes be thankless, but its definitely gratifying. I was lucky to have got involved in activities of POGS as a post graduate, and then after my PG, I was working without any role in the society, then slowly progressed to a managing committee member. I have always enjoyed working in the society as it gave me the opportunity to communicate with different members, and at a larger scale, FOGSI has given me friends from all over India, interacting with consultants all over India, understanding their thought processes, their clinical experiences and learning new things from them.
So I would definitely advise youngsters to keep working in various organizations. My personal choice was FOGSI. But I’ve also had the opportunity to work in the Indian Menopause Society and the ISOPARB. So whatever is your interest, you should definitely take that forward and give back to the society.
I take this opportunity to thank the current Chairperson of Young Talent Promotion Committee, Dr Rohan Palshetkar. And the National Coordinator of the Young Talent Promotion Committee, Dr Prerna Keshan, for giving me this opportunity to share my thoughts and experiences in FOGSI.

‘WORK’

FDr. Basab Mukherjee MD, FRCOG, FICOG, Consultant Obstetrician & Gynecologist Kolkata
rom New Year resolutions to bucket lists to occupying our mental bandwith – the earnest desire ‘to lose weight’ reigns supreme. In a country where the national language is food, it is nearly impossible to avoid the temptation of the extra samosa or jalebi. Compounded is a patchy fitness culture, addictive internet habit and limited urban green spaces. All in all this makes us a fat and unfit population scoring high on BMIs and close to half fitting into the WHO defined obesity brackets.
In our clinical practice, we see only a small fraction of our overweight PCO and sub fertile
women who are able to adopt ‘lifestyle modification’ which we most liberally prescribe. This struggle has been an integral and frustrating aspect of our management in this group of patients. At the end of the discussion was the soft refrain ‘is there a medicine’. For decades, weight management has been framed as a willpower problem—an endless cycle of “eat less, move more,” followed by frustration, stigma, and relapse.
On this backdrop, in comes the magic bullet, GLP-1 agonists the ‘fat busters’ of the decade.
The news headlines hits us first – the brand of Tirzepatide from Eli Lilly propelled the company to be the first healthcare firm to achieve a $1 trillion market valuation in late 2025 thus joining the elite tech giants. In the social media, there has been a flood of weight loss drug-related posts – wegovy, ozempic, mounjaro et al. The question is where does this fit into our endorsements as health care providers?
Before we adopt a medicine, it is prudent to know what is it and how it acts. For the uninitiated, glucagon-like peptide-1 (GLP-1) receptor agonists mimic a natural gut hormone involved in appetite and glucose regulation. In simple terms, they help people feel full sooner reducing hunger and slowing down stomach emptying. Tirzepatide is a dual agonist (GIP/GLP-1), which may help explain its stronger weight-loss results in many studies and real-world use. Initially approved for diabetes now indications have extended to obesity with co-morbidities.
So what advantages do these new drugs bring to the table?
• Compared to the older antiobesity drugs, these have been associated with substantial greater average weight loss.
• The benefits go beyond the scale and the medicines are extremely valuable for Type 2 diabetes mellitus or candidates with high cardiometabolic risk.
• Visceral fat reduction is
pivotal for improving metabolic health, reducing cardiovascular risk and supporting sustained disease prevention.
• With every 5% of weight loss, proven benefits extend from MASH and OSA correction to remission of T2DM at more than 15% loss.
• There are lesser effective pills for those who fear the weekly injections.
• The medicine phase may help people to adopt healthy eating habits and instil a sense of confidence for those individuals who never lost weight in their life.
However all is not rosy and there is a dark side to these drugs.
• The gastrointestinal side effects in the form of nausea, indigestion, vomiting and diarrhoea are fairly common and limit users from reaching the highest doses for maximum efficacy.
• Another concern is the loss of lean muscle mass which should not exceed more than a quarter of the total weight loss.
• The drugs are contraindicated in pancreatitis, gall bladder disease, pregnancy, thyroid history, severe mental illness among other conditions and a careful medical history should precede their use.
The other question is ‘how long’? To answer this many argue much like hypertension and diabetes this should ideally go on lifelong as obesity is a
chronic disease. The real life scenario is that most users stop after a short period of time. This results in regaining a significant portion of the lost weight. A consistent use of these drugs month on month does not presently come cheap. However with the introduction of generic brands cost reduction in the future is inevitable.
The drugs at best are support tools and not short cuts. They cannot replace discipline, healthy eating and regular exercise. It is true that they cause meaningful medical weight loss, a rarity in the past and offer new hope for obesity related diseases. Theses medicines should be viewed as a part of a long term treatment plan which includes clinician-led screening, slow dose titration, side effect management, protein and resistance training for muscle protection and a realistic maintenance strategy.
GLP-1s may be life-changing but there is a great potential for misuse and abuse. The horizon looks exciting yet use without any medical supervision can be harmful. As prescriptions are expected to flood the market in the months and years to come, they should be associated with responsible recommendations, honest expectations and long term support.


Dr. Charmila Ayyavoo MD, DGO, DFP, FICOG, PGDCR Obstetrics & Gynaecology Director, Aditi Hopsital and Aditi Pluro Fertility and IVF, Trichy
The identification by mothers of decreased foetal movements
INTRODUCTION or foetal kick counts is an important clinical indicator of adverse perinatal outcomes. Stillbirths can be reduced with apt detection and appropriate management of women perceiving reduced foetal movements. Stillbirth is a serious issue with short
term and long-term adverse consequences for both families and communities. Lancet published the 2011 and 2016 stillbirth series and has made a strong statement for reduction of stillbirth.1 But scientific evidence is still lacking regarding the correct pathway of management of reduced foetal movements perceived by the mother.
The perception of fetal movements by the mother is perceived to be an indicator of well-being of the baby. The movements of the baby reflect the neurological development in-utero. It also reflects adequate foetal oxygenation. In acute or chronic placental deficiency, there is activation of the peripheral chemoreceptors. This will cause vascular redistribution to vital organs with a subsequent reduction in peripheral movements to conserve energy and reduce oxygen consumption.2
The perception of movements by the mother starts at 16-20 weeks of pregnancy. Mothers can describe the movements as flutter, movements like butterflies, or as bubbling movements.3 With increasing gestation, the pattern of movements may evolve. They are described as complex limb and body movements with increasing strength. The movements have a diurnal pattern in healthy pregnancies. The strong fetal movements are felt by most of the patients in the evening and at night time.
If movements are not felt well in the evening, it indicates a higher risk of stillbirth according to a study by Bradford.4 Another study called the STARS study pointed out that there if the fetus is active at bedtime, the chance of stillbirth is low. A change in the diurnal pattern where the baby is quiet in the evening should be given importance.5
There is a popular misconception that fetal movements tend to reduce in frequency and strength at later gestational ages because of less space in the uterus. The term healthy fetus appears to move less because it takes longer period of rest in between activities.13
If there is less perception of fetal movements at term at bedtime, the mothers should be advised to come for a checkup. The causes for reduced perception may also be due to size of the baby, the gestational age, the liquor volume, medicines taken by the mother, the sleep pattern of the baby, location of the placenta, weight of the mother, and maternal smoking habits.6
There will be periods of movements and rest. The typical kicking movement may change to rolling, tottering, shoving, and stretching movements. Healthy babies move well throughout the day and show strong movements even during the labor process.7
Small for gestational age babies
Reduced liquor volume
Preterm labor
Congenital anomalies
Chromosomal malformations
Fetal maternal hemorrhages
Perinatal neurological damage and abnormal neurodevelopment
Intrauterine infections
Perinatal hypoglycemia
Umbilical cord complications
Placental causes like insufficiency
Reduced fetal movements can be associated with poor perinatal outcomes.
Reduced perception of fetal movements can be associated with fetal low Apgar scores, acidemia, increased chance of cesarean delivery, induction of labor, stillbirths, and perinatal deaths.
One of the commonest reasons for reduced fetal movements is fetal growth restriction (FGR). In an Australian study conducted on 18,000 births, 16% of women with FGR reported reduced fetal movements at term.8
In a systematic review, reduced foetal movements were perceived more by Caucasian women, women with smoking habit, anterior location of the placenta, reduced amniotic fluid and increase in amniotic fluid volume. There was no difference due to maternal age or parity of the mother. Certain conditions like previous caesarean, post term pregnancy, diabetes and hypertension were not predictive for reduced foetal movements.9
Many studies have shown that foetal movement counting does not help prevent adverse perinatal outcomes. The total stillbirths were not reduced in a Cochrane systematic review when mothers were asked to keep a count of daily foetal movements but the overall late stillbirth rate reduced. This was attributed to increased awareness and alertness.10
In another study, the maternal counting of foetal kicks helped in the identification of FGR.11
The AFFIRM trial which is the ‘Awareness of fetal movements and care package to reduce fetal mortality’ has been conducted to identify the utility of the maternal counting of fetal kicks. An eLearning module was provided to clinical staff and pregnant women were given a leaflet about the importance of checking daily fetal movements during pregnancy. Data was collected from 33 maternity hospitals and 40,000 deliveries. The trial revealed that there was no significant reduction in stillbirth with use of daily fetal movement counting by mothers. The intervention rate and neonatal morbidity was higher in this group. There was a reduction of SGA babies being born post term. There was a rise in induction of labor, reduction in spontaneous vaginal deliveries, increase in cesarean births, and increase in neonatal care admissions. The AFFIRM trial has identified the unintended effects of the mother keeping a count of the fetal movements. But the trial did not identify any direct harm due to the practice of maintaining fetal movement count charts.12 Further studies are being conducted to provide evidence that a change in practice is advisable.
MANAGEMENT ............ STRATEGIES:
The Australian Safer Baby Bundle (the Bundle) had been promoted to help in the reduction of stillbirths after 28 weeks of pregnancy by at least 20% by 2023.13 The
components of the bundle are as follows:
Reduction in smoking by the mother
Identification and management of fetal growth restriction (FGR)
Identification of decreased fetal movements
Sleeping position of the mother
Clinical decision for delivery of mothers with high risk for stillbirths.
1. The mothers are provided written information on the bundle approach. They are asked to report immediately if there are concerns with reduced fetal movements.
2. If the mother reports decreased fetal movements (RFM), the following questions should be asked:
• The duration of RFM?
• Is this the first episode?
• When did she perceive the fetal movement last?
3. She is screened for risk factors for stillbirth.
4. Appropriate investigations are done and she is subjected to a medical review.
5. The foetal heart is auscultated with a hand held doppler device or a Pinnard fetoscope to confirm viability. The growth trajectory of the baby is then reviewed using the previous ultrasound reports, symphysio-fundal height measurement charts.
6. Cardiotocography (CTG) is done to confirm the foetal heart.
If available, a computerized CTG is done.
7. A foetal ultrasound is then performed for growth, and amniotic fluid volume. Doppler studies of the umbilical artery are done if computerised CTG is not available or there is a suspicion of the foetus being small for gestational age (SGA) on clinical examination.
If the patient presents with recurrent episodes of RFM after 28 weeks of pregnancy, ultrasound for foetal growth, amniotic fluid volume, and umbilical artery doppler should be offered.
If ultrasound has been done in the past two weeks, a repeat ultrasound of the foetus is not needed.
If the patient presents with RFM after 38+6 weeks, there should be a discussion on induction of labour with her.
If the patient presents with recurrent episodes of RFM after 38+6 weeks, decision for delivery should be taken.
The mother and her attenders are informed about the reports. She is encouraged to review if she has more concerns regarding RFM.
The monitoring of fetal movements is considered as an important part of antenatal care but the definition of danger based on maternal perception of fetal movements is not defined yet. It is proved that inappropriate follow up and management can lead to stillbirths or iatrogenic preterm deliveries. More studies are needed to identify the correct
algorithm of management in cases of reduced fetal movements.
1. de Bernis L, Kinney MV, Stones W, ten Hoope-Bender P, Vivio D, Leisher SH, for the Lancet Ending Preventable Stillbirths series study group. Stillbirths: Ending preventable deaths by 2030. Lancet 2016; 387(10019): 703-16.
2. Levy M, Kovo M, Barda G, et al. Reduced fetal movements at term, low-risk pregnancies: is it associated with adverse pregnancy outcomes: ten years of experience from a single tertiary center. Arch Gynecol Obstet. 2020;301(4):987-993.
3. Raynes-Greenow CH, Gordon A, Li Q, Hyett JA. A cross-sectional study of maternal perception of fetal movements and antenatal advice in a general pregnant population, using a qualitative framework. BMC pregnancy and childbirth 2013; 13: 32.
4. Bradford BF, Cronin RS, McKinlay CJD, et al. A diurnal fetal movement pattern: findings from a cross-sectional study of maternally perceived fetal movements in the third trimester of pregnancy. PLoS One 2019; 14(6): e0217583
5. Warland J, O’Brien LM, Heazell AE, Mitchell EA. An international internet survey of the experiences of 1,714 mothers with a late stillbirth: the STARS cohort study. BMC Pregnancy & Childbirth 2015; 15(172): 1.
6. De Vries JI, Fong BF. Normal fetal motility: an overview. Ultrasound in Obstetrics and Gynecology 2006; 27(6): 701-11
7. Bradford B, Maude R. Maternal perception of fetal movements in the third trimester: a qualitative description. Women and Birth 2018; 31(5): e287-e93
8. Flenady V, Frøen F, MacPhail J, et al. Maternal perception of decreased fetal movements for the detection of the fetus at risk: the Australian experience of the international FEMINA collaboration. International Stillbirth Alliance (ISA) conference; 2008; Oslo, Norway; 2008.
9. Carroll L, Gallagher L, Smith V. Risk factors for reduced fetal movements in pregnancy: A systematic review and meta-analysis. Eur J Obstet Gynecol Reprod Biol. 2019 Dec;243:72-82. doi: 10.1016/j.ejogrb.2019.09.028. Epub 2019 Oct 18. PMID: 31677496.
10. Frøen JF, Heazell AE, Tveit JV, Saastad E, Fretts RC, Flenady V. Fetal movement assessment. Semin Perinatol 2008; 32(4): 243-6.
11. Saastad E, Winje BA, Stray Pedersen B, Froen JF. Fetal movement counting improved identification of fetal growth restriction and perinatal outcomes-a multi-centre, randomized, controlled trial. PLoS One 2011; 6(12): e28482.
12. Norman JE, Heazell AEP, Rodriguez A, et al. Awareness of fetal movements and care package to reduce fetal mortality (AFFIRM): a stepped wedge, cluster-randomised trial. The Lancet 2018; 392(10158): 1629-38.
13. Centre of Research Excellence Stillbirth. Safer baby bundle handbook and resource guide: working together to reduce stillbirth. Centre of Research Excellence Stillbirth; 2019. Accessed March 4, 2021. https://www.acn.edu.au/wp-content/uploads/sbbhandbook-v1.7-02092019.pdf
14. National Health Service England. Saving babies' lives version 2: a care bundle for reducing perinatal mortality. National Health Service England; 2019. Accessed March 4, 2021. https://www.england.nhs.uk/wp-content/uploads/2019/03/Saving-Babies-Lives-CareBundle-Version-Two-Updated-Final-Version.pdf


Dr. Neharika Malhotra
Obesity is a chronic, relapsing disease with unique
INTRODUCTION implications for women across the life course, influencing menstrual health, polycystic ovary syndrome (PCOS), fertility, pregnancy outcomes, menopause, cardiometabolic
risk, and quality of life. The emergence of glucagon-like peptide-1 (GLP-1)–based antiobesity medications (AOMs) has transformed obesity management from short-term weight loss to evidence-based long-term disease control.
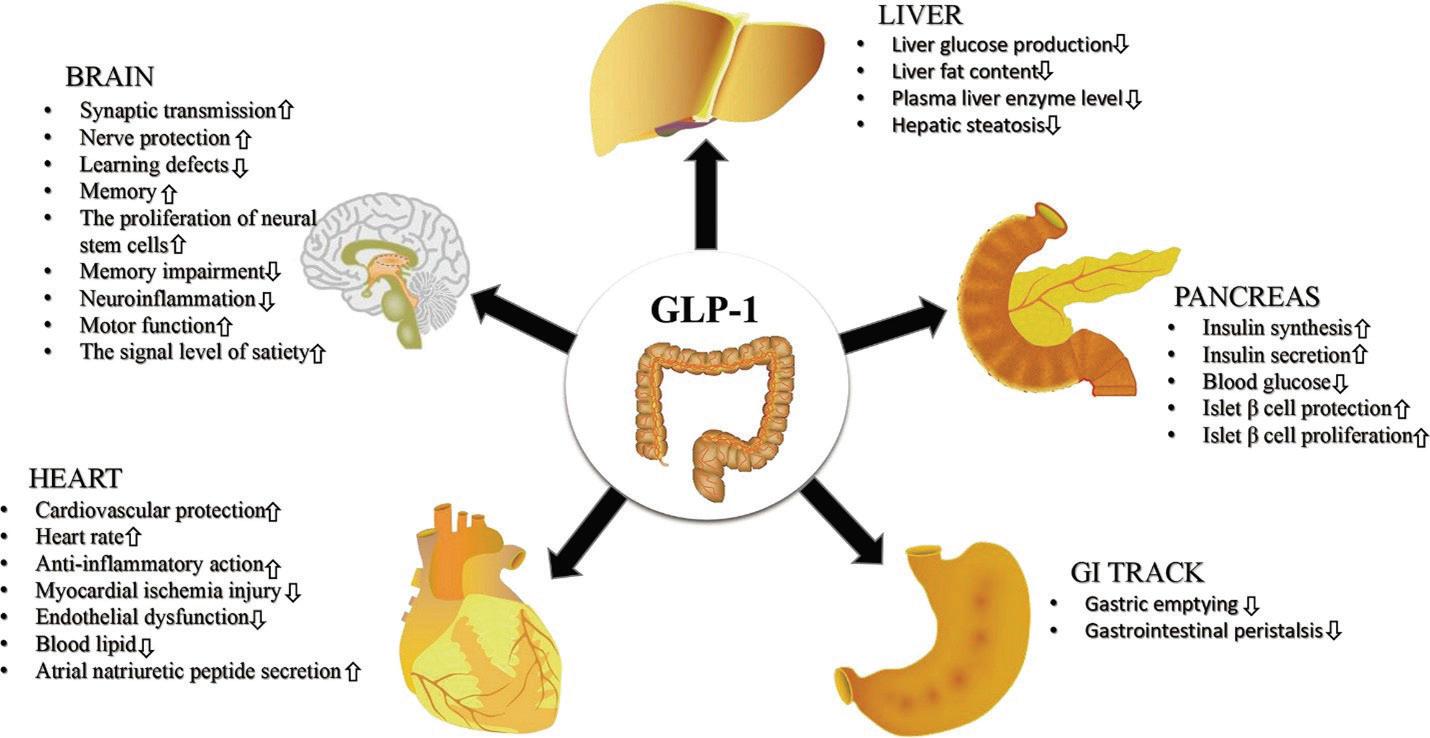
The figure shows: The effects of GLP-1RAs on multiple human organizations. GLP-1RAs exert a positive therapeutic effect on human brain, pancreas, heart, gastrointestinal tract (GI tract) and liver.
GLP-1 receptor agonists act centrally to reduce appetite and cravings, delay gastric emptying, and improve insulin sensitivity. Dual incretin agents such as tirzepatide also target glucosedependent insulinotropic polypeptide (GIP), leading to enhanced metabolic and weight-loss effects.
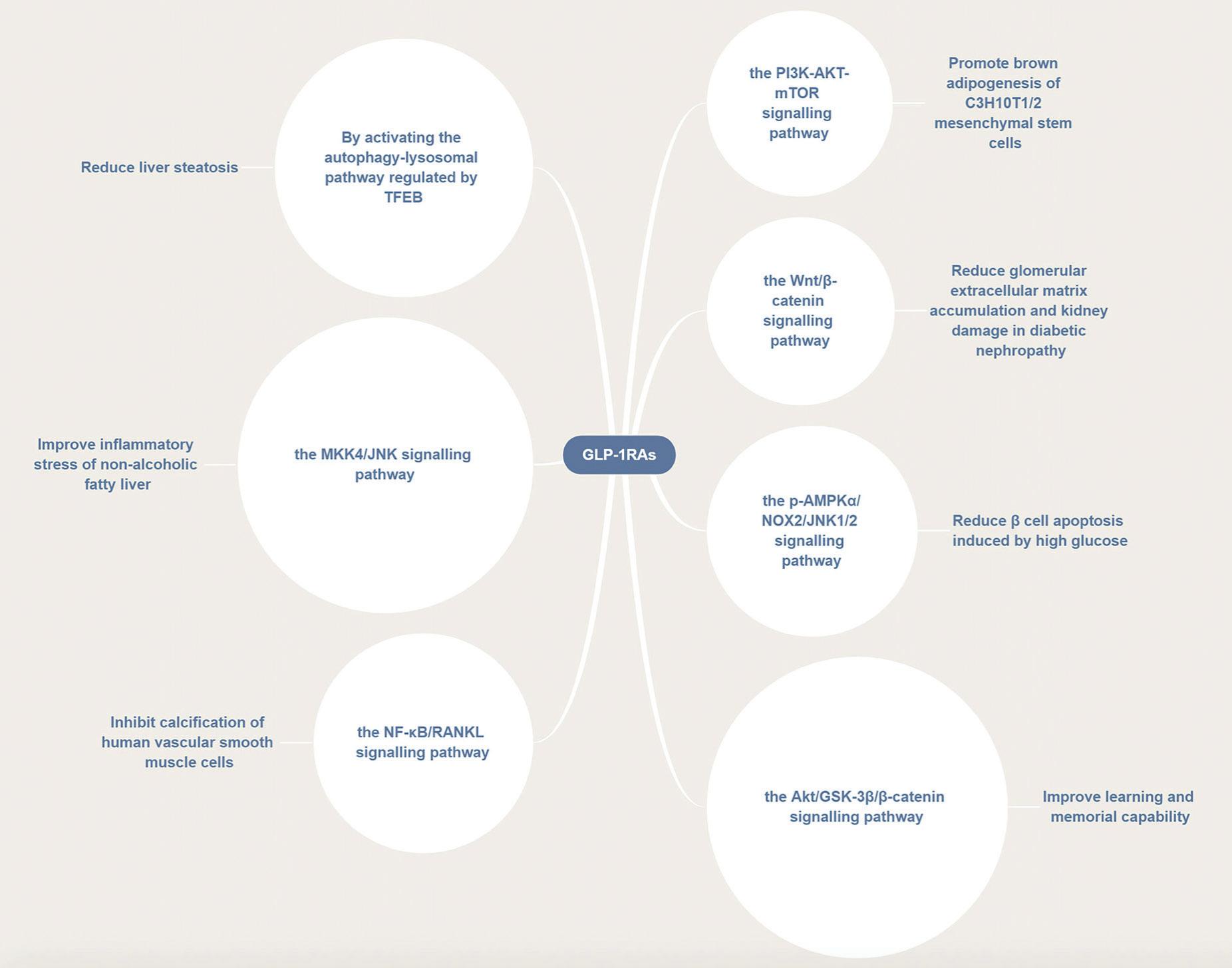
The figure shows: GLP-1RAs are involved in a variety of disease pathways. GLP-1RAs can activate several signaling pathways, such as the PI3K/AKT/mTOR, p-AMPKα/NOX2/JNK1/2, Wnt/β-catenin, Akt/GSK-3β/β-catenin, NF-κB/ RANKL, and MKK4/JNK pathways thus exerting a therapeutic effect in different diseases.
COMMONLY USED
GLP1 MEDICINES ARE:-
• Liraglutide 3.0 mg (daily SC)
• Semaglutide 2.4 mg (weekly SC)
• Tirzepatide (weekly SC; dual GIP/GLP-1)
• Oral semaglutide 50 mg (under obesity trials; oral peptide)
RELEVANCE IN WOMEN’S HEALTH
Women experience obesity differently due to hormonal fluctuations, reproductive events, and menopause-related metabolic shifts. GLP-1–based therapies have shown benefits in:
• PCOS: reduction in body weight, waist circumference, insulin resistance and androgen levels.
• Reproductive-age women: improved metabolic profile prior to conception (therapy must be discontinued before pregnancy).
• Perimenopause and menopause: reduction in visceral adiposity and cardiometabolic risk.
• Cardiovascular disease: semaglutide 2.4 mg has demonstrated cardiovascular risk reduction in obese patients without diabetes.
CLINICAL EVIDENCE
Semaglutide 2.4 mg and tirzepatide have demonstrated robust and sustained weight loss in large phase 3 trials. Cardiovascular outcome benefits have been shown with semaglutide in patients with obesity and established cardiovascular disease. Tirzepatide trials highlight the need for long-term continuation, as discontinuation leads to significant weight regain.
• Common adverse effects include nausea, vomiting, diarrhea, and constipation, particularly during dose escalation.
• GLP-1 therapies are contraindicated during pregnancy and breastfeeding.
• Tirzepatide may reduce the efficacy of oral contraceptives; nonoral contraception is advised during initiation and dose escalation.
• Counseling on long-term therapy, reproductive planning, and lifestyle integration is essential.
GLP-1–based anti-obesity therapies represent a paradigm shift in women’s health, offering meaningful weight reduction and metabolic benefits across reproductive stages. Their optimal use requires a chronic disease approach, individualized counseling, and integration with lifestyle and behavioral interventions.
1. World Health Organization. WHO guideline on the pharmacological treatment of obesity. Geneva: WHO; 2025.
2. Lincoff AM, et al. Semaglutide and cardiovascular outcomes in obesity without diabetes. N Engl J Med. 2023;389:2221–2232.
3. Jastreboff AM, et al. Tirzepatide once weekly for the treatment of obesity. N Engl J Med. 2022;387:205–216.
4. Aronne LJ, et al. Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity. JAMA. 2024.
5. De Hollanda BAA, et al. GLP-1 receptor agonists in women with polycystic ovary syndrome: a systematic review and meta-analysis. Clin Endocrinol (Oxf). 2024.
6. FDA. Wegovy (semaglutide) prescribing information. 2023.
7. FDA. Mounjaro (tirzepatide) prescribing information. 2022.
8. Kindel TL, et al. Multisociety clinical practice guidance for perioperative management of GLP-1 receptor agonists. 2024.
The kick start project of 2026 of YOUNG TALENT PROMOTION COMMITTEE FOGSI, the PRAYAS outreach programme on promoting responsive awareness of young adults through sexual education. The programme was conducted with students of classes 7 to 11 in association with the Rotary International Club District 3240. Around 150 students had a two hour interactive session with various queries answered on issues revolving around sensitive information on adolescent reproductive health and sexuality.
Earnest gratitude to revered Dr. Bhaskar Pal sir for approving this project, Dr. Abha Rani mam for her guidance and Dr. Rohan Palshetkar for the incessant support.

Consultant OBGYN, Infertility Specialist, Endoscopic Surgeon FICOG, FICMCH, FIAOG, MRCOG1 Masters in Cosmetic Gynecology
National coordinator, Young Talent Promotion Committee FOGSI

MUMBAI-21st December 2025
Hands-on Workshop on Facial Injectables
Standardizing Excellence in Advanced Facial Injectable Techniques
AESTHETICCON Mumbai, held on December 21st, 2025, the One-Day Hands-on Workshop on Facial Injectables offered participants DASIL certification. This workshop comprehensively covered key aesthetic modalities, including Bio-Remodeller, Skin Booster, Botulinum Toxin Type A and Threads





Each of faculties Dr. Pallavi Sule, Dr. Abhay Talathi, Dr. Dattatray Sonawane through Live demonstration showcased their expertise as their patiently guided the participants during the Hands-On session. The event concluded with the distribution of DASIL Certificate of Attendance to the participants.

MD, FICOG, FICRM, FICMCH, FIAOG, Secretary, ICOG (2026-27)
Governing Council Member, ICOG (2020-25)
Governing Council Member, ICRM (2024-26)
Chairperson, FOGSI Endocrinology Committee (2017-19)
Chairperson, AMOGS Endocrinology Committee (2020-24)
Managing Council Member, MOGS, ISAR, MSR
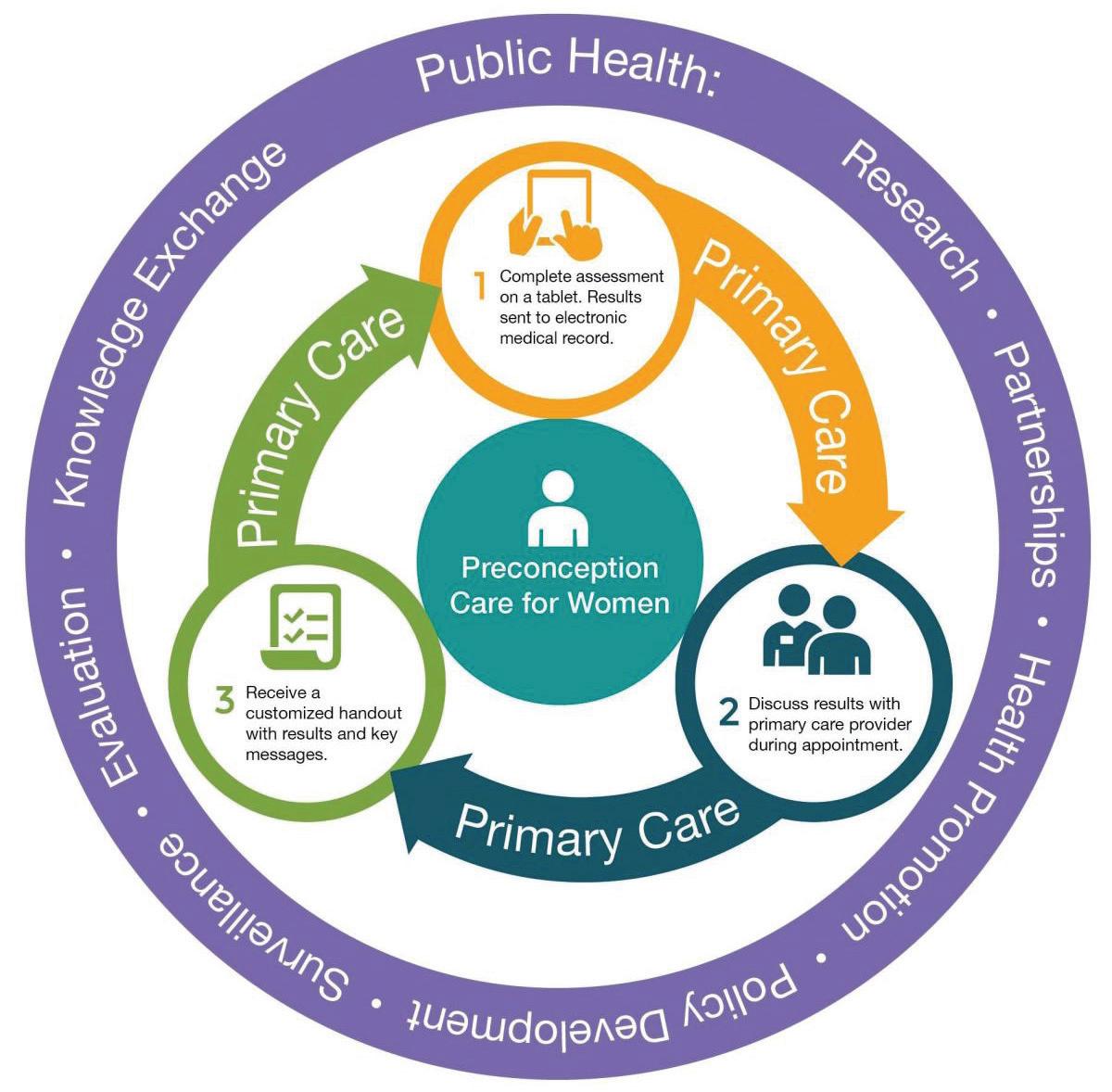
Preconception care is an essential aspect of maternal and reproductive health that focuses on providing care to women and couples planning for pregnancy. It encompasses a variety of interventions designed to optimise the health of couples intending to conceive, thereby improving pregnancy outcomes and the health of the offspring.
With the increasing awareness of the importance of maternal and paternal health before conception, healthcare providers are increasingly focusing on integrating comprehensive preconception care into standard practice. This article covers significant elements of preconception
care including its importance, components, implementation strategies, challenges and future directions while maintaining a focus on current clinical practices.
Preconception care is vital for several reasons which may not be immediately apparent. However, when you consider that most couples are getting married later today when compared to 2-3 decades ago and are putting off pregnancies until much later in life, these decisions carry a host of risks which are not immediately recognised.
With an increasing number of couples resorting to assisted reproductive techniques as a
shortcut to completing their family owing to a multitude of issues including late marriage, financial shortcomings, social pressure and family expectations, it is particularly relevant to give importance to preconception care in this high risk population.
Initiating the conversation with prospective parents is of paramount importance as this is not a subject traditionally taught in the medical curriculum in detail. Often these issues don’t enter the mind space of both clinicians and patients until much later during pregnancy. Fig 1 lists out the important components of preconception care.
Many health conditions can affect pregnancy outcomes. Medical disorders and silent undiscovered metabolic complications like diabetes, hypertension and obesity can lead to complications such as gestational diabetes, hypertensive disorders of pregnancy, preeclampsia or congenital anomalies. Recognising, screening, evaluating and addressing these risks preconceptionally helps pave the way forward for healthier pregnancies.
For couples with a family history of genetic disorders, preconception care allows for genetic counselling. This can include carrier screening for inherited conditions, which can inform reproductive choices and the management of potential risks.
Preconception care encourages healthy lifestyle modifications, including nutritional advice, avoiding alcohol consumption,
smoking cessation and refraining from recreational drug abuse which can lead to a shorter time to pregnancy, healthier pregnancies, avoid congenital anomalies and ensure better fetal development.
A thorough medical history and physical examination are crucial in assessing pre-existing conditions and risk factors. Clinicians should typically go through a checklist and review:
- Personal and family medical history
- Previous pregnancy outcomes
- Current medications and supplements
- Lifestyle choices (e.g., smoking, alcohol, drugs, diet)
Nutrition plays a foundational role in preconception health and optimising both partners’ bodies prior to conception and pregnancy is being now recognised as having a substantial bearing on pregnancy outcomes. Common nutrition recommendations include:
Folic acid supplementation
- widely recommended for women planning to conceive to take 400-800 micrograms of folic acid daily to reduce the risk of neural tube defects.
Balanced diet - emphasizing a diet rich in fruits, vegetables, whole grains and lean proteins helps achieve a healthy weight and reduces risks associated with obesity or malnutrition.
Weight management strategies - Addressing
underweight or obesity through behaviour modification, journalling and food diaries can help improve reproductive health and lower the risk of complications.
Reviewing and updating immunizations is critical. Vaccines against diseases like rubella, varicella, and hepatitis B should be administered preconceptionally to protect both the mother and the baby.
Screening for sexually transmitted infections (STIs), including HIV, syphilis and hepatitis is critical. Early detection can facilitate treatment and minimise risks of transmission to the fetus.
Mental health plays a significant role in overall health and these issues are being diagnosed with increasing frequency in modern times. Preconception care should include evaluations for anxiety, depression and other psychiatric conditions to ensure that potential parents are psychologically ready for pregnancy.
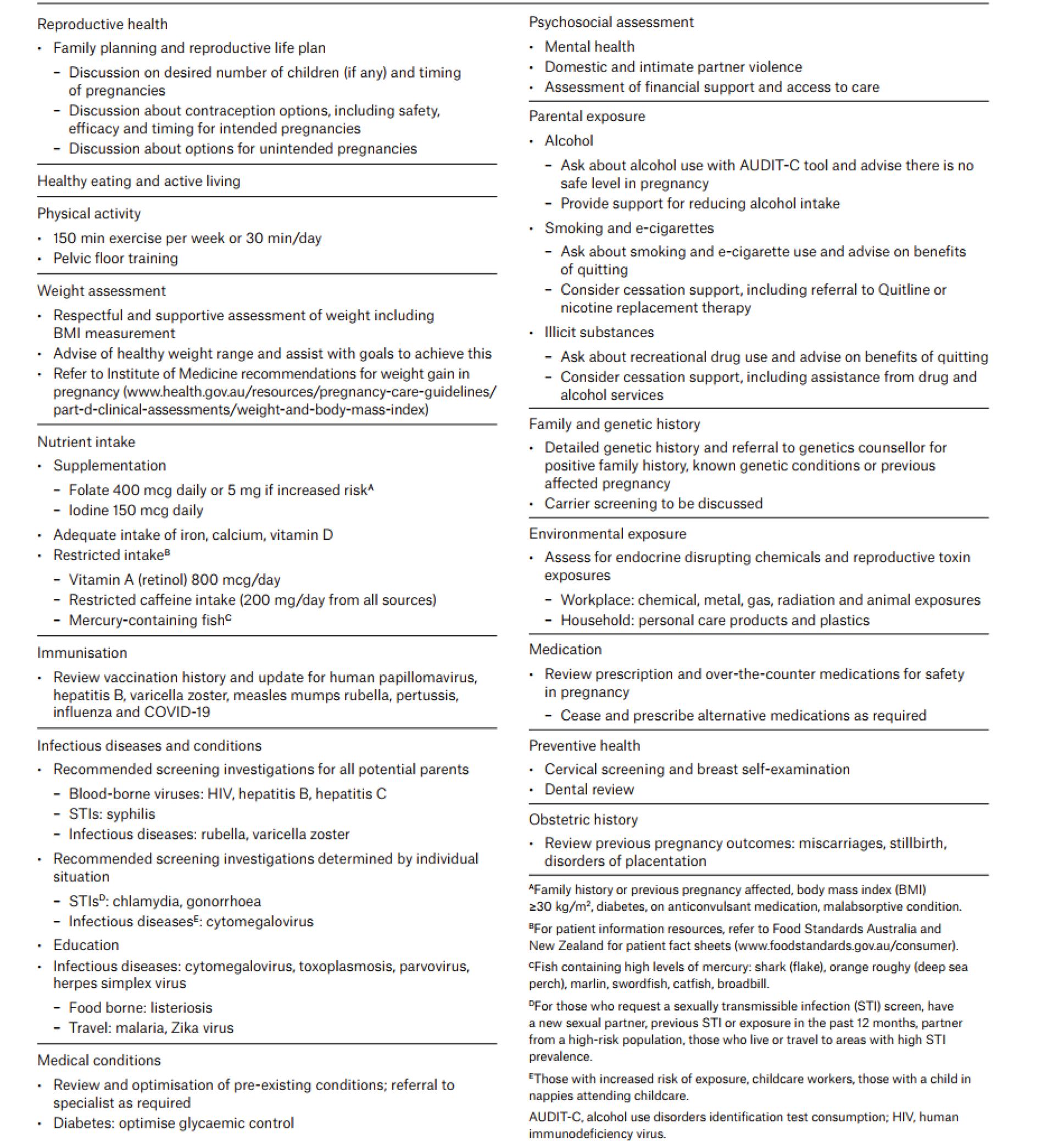
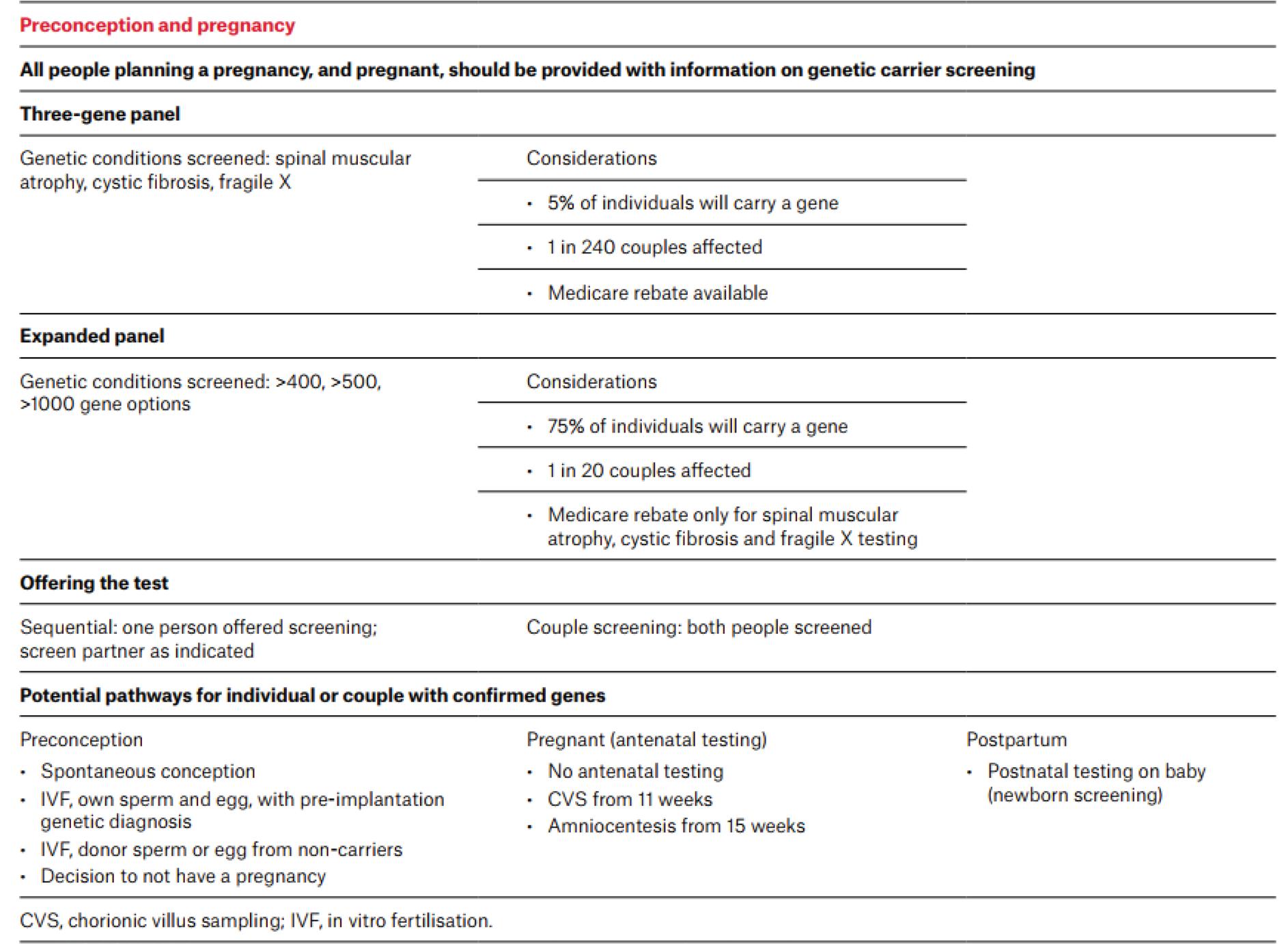
Table 1 presents a comprehensive preconception care checklist which has been implemented in Australia, while Table 2 presents the most important concepts in genetic counselling.
Table 1. Preconception care checklist
While the importance of preconception care is clear, the implementation in clinical practice varies widely. Several strategies can facilitate its integration into routine practice:
Education and trainingHealthcare providers should receive adequate training and education on preconception care to ensure they can effectively counsel patients. Incorporating preconception
care into obstetric training programs highlights its importance from an early stage.
Patient-centric policies - Implementing such an approach ensures that care is tailored to the individual’s needs and circumstances. Use of tools such as risk assessment questionnaires can help identify specific concerns for each couple.
Multidisciplinary team approach - Preconception care is multifaceted and often requires input from various healthcare professionals, including dietitians, mental health professionals and genetic counsellors. Collaborative care models can enhance comprehensive assessment and management.
Community outreach and access - involving NGOs and community health initiatives can raise awareness and provide resources for preconception care, especially in underserved populations. Programs that target at-risk groups can improve access and education around preconception health.
Despite its importance, several barriers hinder the effective implementation of preconception care: Lack of awareness among clinicians and lay personsmany patients and healthcare
providers remain unaware of the significance of preconception care, which can lead to missed opportunities for health optimisation before conception.
Access to care – political, geographical, financial and systemic barriers can impact access to preconception care services. Lowincome individuals or those living in rural areas may have limited access to healthcare resources.
Time constraints – obstetricians often operate under significant time constraints during appointments, making it challenging
to address comprehensive preconception care adequately.
There is a consensus among the reviewed guidelines that a detailed personal and family history and risk factor assessment and counselling against smoking, alcohol and substance abuse are the main areas to focus when providing preconception care. In addition, assessment of immunisation status and screening for intimate partner violence and sexual coercion, as well as screening for human papillomavirus and cervical cancer, are unanimously recommended.
All medical societies also agree that counselling on diet, body mass index and physical activity should be routinely offered along with a review of supplements and advice on folic acid supplementation. The need of medication review for potential teratogenic effects and the importance of assessing for environmental and occupational exposure to teratogens are underlined by all guidelines.
Moreover, the American College of Obstetricians and Gynaecologists (ACOG) and Public Health Agency of Canada
(PHAC) recommend a discussion regarding contraception, support an optimal interpregnancy interval of at least 18 months and underline that screening for sexually transmitted infections should be offered only in cases with existing risk factors. ACOG and RANZCOG also suggest that patients should be offered guidance on proper food handling and traveling restrictions to prevent certain infectious diseases. Finally, ACOG and PHAC provide guidance on the preconception management of chronic medical conditions.
To enhance preconception care within clinical practice, several future directions can be pursued including policy development, public health campaigns, technology integration and well designed clinical trials. Advocating for policies that recognise and support preconception care as part of standard medical practice can improve access and funding for educational programs. Initiating public health campaigns focusing on the importance of preconception care can raise awareness among potential parents and encourage them to seek care.
Further research is needed to assess the long term beneficial impact of preconception care on maternal and infant health outcomes. This knowledge could guide improvements in care strategies and policy development. Utilising tele-health and digital health tools can help bridge gaps in access, allowing for virtual consultations and educational resources that facilitate preconception care, particularly in remote areas.
Preconception care represents a critical opportunity to enhance reproductive health, minimise risks, and promote healthy pregnancies. As the healthcare landscape continues to evolve, integrating comprehensive preconception care into routine practice will require concerted efforts from healthcare providers, policymakers and communities.
By addressing gaps in awareness, access and education, the potential for healthier families and communities will significantly improve. Promoting a culture that values preconception health can ultimately lead to better maternal and child health outcomes, reflecting the ongoing commitment to holistic health care.
1. Giouleka S, Papagera V, Siargkas A, Michos G, Liberis A, Kalogiannidis I, Mamopoulos A, Tsakiridis I, Dagklis T. Preconception Care: A Comparative Review of Major Guidelines. Obstet Gynecol Surv. 2025 Aug;80(8):491-505. doi: 10.1097/OGX.0000000000001425. PMID: 40758390.
2. Hemsing N, Greaves L, Poole N. Preconception health care interventions: A scoping review. Sex Reprod Healthc. 2017 Dec;14:24-32. doi: 10.1016/j.srhc.2017.08.004. Epub 2017 Aug 19. PMID: 29195631.
3. Dorney E, Black K. Preconception care. Aust J Gen Pract. 2024 Nov;53(11):805-812. doi: 10.31128/AJGP-08-23-6927. PMID: 39499834.


3-Days Program Highlights*

3 Half-days
Observership in Aesthetic Procedures
3 Half-days Lectures by DHA Certified Faculty with UAE DHA@CME Credits CME Credits# with
Package to be announced shortly
Inclusions:
* 3-Nights 4-Days Stay, in a 4-STAR Hotel with breakfast and dinner, Lunch at Academy/Aesthetic Centre, To and fro - Hotel to Academy/Aesthetic Centre SIC◊
Exclusions:
Air fare to Dubai and back , airport transfer, Sight seeing etc.
@ DHA- Dubai Health Authority
# Proposed s/t confirmation
◊ SIC- Seat in Coach
Interested Drs kindly call for further details: +91



