






Instant Glow
Exfoliates dead skin cells, stimulates mild skin renewal, and brightens the complexion for an instant glow.
Blend of Arginine 20%, Lactic Acid 40%, Alantion 1%
For Active Acne/Acne with Pigmentation
Penetrates pores to remove excess oil, reduces acne and inflammation, and promotes gradual skin renewal.
Blend of Salicyclic acid 20% and Mandelic acid 30%
Epidermal Melasma/Hyperpigmentation
Targets excess melanin, gradually lightens dark spots, and promotes controlled, gentle exfoliation.
Blend of Glycolic Acid 22%, Lactic acid 10%, Pyruvic acid 3%, Kojic acid 7%




Dr. Bhaskar Pal President, FOGSI (2026)
Dear Colleagues and Future Torchbearers of FOGSI, Warm greetings from the Federation.
It gives me immense pride and optimism to address the Young Talent Promotion Committee — a vibrant platform that symbolizes the future strength, vision and dynamism of FOGSI. The Young Talent Promotion Committee focuses on nurturing young Obstetricians and Gynaecologists through academic, social and cultural engagement.
Our young members are not merely the doctors of tomorrow; they are the innovators, leaders, researchers and compassionate caregivers of today. The Young Talent Promotion Committee stands as a testimony to FOGSI’s unwavering commitment to nurturing fresh ideas, encouraging academic excellence, and empowering emerging Obstetricians and Gynaecologists to rise with confidence and competence.
In a rapidly evolving era of medicine, where knowledge expands by the minute and technology reshapes clinical practice, it is the enthusiasm, curiosity and adaptability of our young professionals that will keep FOGSI at the forefront of women’s healthcare. This committee provides the ideal ecosystem for learning, mentoring, sharing and growing — a space where talent is recognized, skills are honed, and leadership is cultivated.
I encourage every young member to actively participate, question, innovate and collaborate. Let this platform be your launchpad to explore research, develop academic brilliance and contribute meaningfully to community health. Remember, leadership is not a position; it is a mindset nurtured through dedication, integrity and service.
To the mentors and seniors guiding this initiative, I extend my heartfelt appreciation. Your guidance transforms potential into excellence and aspiration into achievement. Let us together build a generation of Obstetricians and Gynaecologists who are clinically sound, ethically strong, academically vibrant and socially responsible.
The future of FOGSI is bright — because it rests in capable young hands.
With warm regards and best wishes,
- Dr. Yuvraj Singh Jadeja
- Dr. Parul Saoji
BEYOND COPPER T: WHAT GYNECOLOGY SHOULD OFFER IN 2026 - Dr. Vaidehi Marathe
HEALTH
GYNAECOLOGIST: BURNOUT IS REAL - Dr. Sujata Dalvi, Dr. Palak Bansal
- Dr. Manish Machave

EXECUTIVE EDITOR & PUBLISHER
Dom Daniel
CORPORATE OFFICE
22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.


EMAIL: paradigminfocomobgyn@gmail.com
Website: ytpfuturechronicles.com
Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“YTP FUTURE CHRONICLES” takes no responsibility for unsolicited photographs or material
ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of April -2026






Dr. Geetha Balsarkar
Professor and Unit head
Nowrosjee Wadia Maternity Hospital
Seth G. S. Medical. College Parel, Mumbai
Dr. Yuvraj Singh Jadeja
M.D Obs and Gynaec, FRM, Dip RM, DIAGE, DCG.
Medical Director Nimaaya Center for Womens Health. Vadodara, Ahmedabad, Anand Delhi.
Dr. Parul Saoji
MS, DNB, MNAMS, FMAS, Dip. (CosGyn)
Cosmetic Gynaecologist, Laparoscopic Surgeon and Infertility Specialist Oracle Clinic, Nagpur
Dr. Vaidehi Marathe
Past President NOGS
Past Chair, PAC Committee AMOGS
Dr. Sujata Dalvi
Consultant Obstetrician & Gynaecologist, Mumbai
Affiliated with Gleneagles, Saifee, Bhatia & St. Elizabeth Hospitals
Honorary Clinical Associate, Nowrosjee Wadia Maternity Hospital
Dr. Palak Bansal
MBBS (Gold Medalist), MS OBG (Gold Medalist), MRCOG Part 1
Dr. Manish Machave
President POGS 2025-26
Ex-Chairman Ethics and Medicolegal Committee FOGSI

Dr. Abha Rani Sinha Vice President FOGSI 2026
Dear Readers,
It gives me immense pleasure to congratulate Dr. Rohan Palshetkar Chair Young Talent Promotion Committee and his team for doing commendable work. It is nice to know that the Young Talent Promotion Committee chronicles as newsletter is published every month. This step taken by the Young Talent Promotion Committee will give FOGSIans a platform to explore their inner and hidden talents. My best wishes to all and wish you all a great year ahead.

FOGSI Young Talent Promotion Committee Chairperson
Dear Readers,
In an era of rapidly advancing medical science and shifting clinical priorities, the need for platforms that encourage thoughtful exchange and practical learning in Gynaecology is more important than ever. YTP Future Chronicles, in association with FOGSI, is envisioned as one such initiative—bringing together emerging perspectives, evolving evidence, and real-world clinical experiences to support the next generation of Gynaecologists in navigating the complexities of modern women’s healthcare.
Aligned with the vision of fostering excellence in women’s health, this edition brings together a diverse range of topics that reflect both contemporary challenges and future directions in Gynaecology. From an engaging interview with Dr. Geeta Balsarkar to a thoughtprovoking discussion on Building a Personal Brand as a First-Generation Gynaecologist, the issue highlights the importance of professional identity and growth in modern practice.
Key clinical and public health themes in this edition include HPV Vaccination in Gynaecology Practice: Current Evidence and Implementation, highlighting the importance of preventive care. Contraception Beyond Copper T: What Gynecology Should Offer in 2026 reflects evolving patient-centered choices. Mental Health of Gynaecologists: Burnout is Real brings focus to physician well-being. Medical Negligence and the Bharatiya Nyaya Samhita, 2023 emphasizes the growing importance of medico-legal awareness in contemporary practice.
Through this collection of contributions, the edition aims to offer meaningful insights that enhance clinical understanding while encouraging reflective practice and professional growth. It serves as a valuable academic resource, supporting young Gynaecologists in their pursuit of excellence and commitment to delivering highquality, evidence-based care.

Dr. Prerna Keshan
Consultant OBGYN, Infertility Specialist, Endoscopic Surgeon FICOG, FICMCH, FIAOG, MRCOG1
Masters in Cosmetic Gynecology
National Coordinator, Young Talent Promotion Committee FOGSI

MS, DNB, MNAMS, FMAS, Dip. (CosGyn) Cosmetic Gynaecologist, Laparoscopic
Surgeon and Infertility Specialist Oracle Clinic, Nagpur

Dr. Palak Bansal
MBBS (Gold Medalist), MS OBG (Gold Medalist), MRCOG Part 1
Because the future of gynecology doesn’t just happen… it is created.
Dear Future Game-Changers,
Welcome to the Young Talent Promotion Committee (YTPC) Chronicles—not just another newsletter, but a space where ideas spark, conversations matter, and gynecologists find their voice (and sometimes their sanity ).
Let’s be honest—being a gynecologist today is equal parts passion and pressure. One moment you’re delivering life, the next moment you’re explaining to a patient why “Google diagnosis” isn’t the same as medical science. Somewhere between night duties, OPDs, and trying to remember if you’ve eaten your own meals, you’re also expected to stay updated, be empathetic, skilled, and… somehow still human.
And that’s exactly why this Chronicles exists.
In this edition, we have topics like
The Real Talk: Burnout is Real where we need to talk about the silent epidemic—burnout in gynecology.
The emotional load, long hours, medicolegal stress, expectations from patients, family, and society—it all adds up.HPV Vaccination – The Game Changer We Can’t Ignore, Let’s upgrade the conversation - NewAge Contraception – Beyond “Routine Advice”. And yes Learning from the Legends because Growth doesn’t happen in isolation.
YTPC – More Than a Committee. Let’s redefine what YTPC stands for. It’s not just about events or academic sessions—it’s about:
• Building confidence before competence (and then both!)
• Creating a safe space to ask “silly” questions (which are never silly)
• Encouraging leadership, innovation, and expression
Whether it’s presenting your first paper, conducting your first workshop, or simply finding your tribe—YTPC is where young gynecologists grow beyond textbooks.
A Little Note from Us to You
To every young gynecologist reading this:
You are doing better than you think.
Even on days when everything feels overwhelming. Even on days when outcomes don’t go your way.
Even on days when you question your choices.
Because this profession is not just about perfection—it is about presence, persistence, and purpose.
And Finally…
This Chronicles is not just ours—it’s yours. Your ideas, your struggles, your wins, your voice— This platform exists to amplify all of it.
So write, speak, share, question, challenge.
Because the future of gynecology is not going to be built in silence. It’s going to be built by young minds who dare to think differently. With energy, empathy, and a little bit of madness (the good kind ;), Let’s keep learning, evolving, and leading. Because the best version of gynecology… is still in the making.

Professor and Unit head
Nowrosjee Wadia Maternity Hospital
Seth G. S. Medical. College Parel, Mumbai
1) Can you describe your journey in FOGSI as a member and prominent leader? How did you start out? How has your experience been through all these years in this organisation?
Ans- I became a member of FOGSI in 1995 when I became a life member of The Mumbai Obstetric and Gynaecology society, which is its member body. When I joined The Nowrosjee Wadia Hospital and Seth G. S. Medical College, Mumbai in 1992 to do postgraduation, I was encouraged to present papers and posters in conferences. Slowly I graduated to becoming a master of ceremony in some programmes. Collecting biodata from Seniors in the organisation to introduce them at conferences helped me to get to know them and they also got to know me better. Both The Mumbai Obstetric society and FOGSI are vibrant organisations and I had a fantastic experience working for them. There is no other professional organisation as large as FOGSI and still united in its efforts to serve the society at large. My involvement in the organisation is living example that hard work, people’s skills and work ethics go a long way in your professional life. After all, work is worship.
2) How do manage to be so active in trainings and academics with your daily practice?
Ans- As a medical postgraduate teacher and fellowship of foetal medicine guide academics has been a way of life for me from the very beginning. I believe that if I use my knowledge to treat patients, I will be able to help a handful, but if I train more
people to think like me, thousands of patients will be benefitted. My students from all over the country who are senior consultants now are still in touch with me, many years after passing and still discuss their difficult cases with me. Trainings and academics are very important part of a doctor’s life abroad, unfortunately in India it has taken a backseat. But the scenario is rapidly changing for the better.
3) Who has been your mentor or guide who has inspired you all these years?
Someone whom you look up to and learn from every day?
Ans- Dr. Amarnath Bhide, Dr. Vandana Walvekar, Dr. Adi Dastur, Dr. C.N. Purandare, Dr. P.K. Shah, Dr. M.Y.Raval, Dr. M.N. Parikh and Dr. Vijaya Badhwar were all my mentors and guide because of whom I am able to negotiate this walk of life. Numerous registrars and lecturers with whom I have worked over these years have influenced me. My students have also taught me patience, courage, understanding and technology and contributed largely to my personality.
4) Can you describe some of your best moments or achievements in all these years in FOGSI?
Ans- Every time I deliver a lecture which is appreciated by audience I feel really blessed. Being an Editor for 15 years in the Journal of Obstetric and Gynaecology of India which culminated in being Editor in chief for three years gave me the ability to connect with each and every FOGSI member through my editorials. Being a chairperson of the Young talent promotion committee of FOGSI gave me the thrill of interacting and mentoring the junior members of FOGSI who are the future of this organisation.
5) What would be your message to the young generation of FOGSI who wants to follow in your footsteps?
Ans- There is no substitute to sincerity and hard work in any professional field. Mentors appear along the way of your progress if your intentions are good. There is enough work to be done in the society and getting a post in FOGSI does help you to achieve that better. Not having a post does not prevent you from working for the society. Where there is a will, there is a way!


Dr. Yuvraj Singh Jadeja
M.D Obs and Gynaec, FRM, Dip RM, DIAGE, DCG.
Medical Director Nimaaya Center for Womens Health. Vadodara, Ahmedabad, Anand Delhi.
There are two ways to become a doctor.
One is to inherit it. The other is to build it.
I belong to the second category.
I was not born into a family of stethoscopes and hospital corridors. I did not grow up overhearing dinner table discussions about surgical cases. I did not inherit a clinic board with my surname already etched in gold. I inherited something else instead —
aspiration, responsibility, and the quiet pressure of being the first.
And that changes everything. This is not just the story of building a fertility and women’s health centre. It is the story of building identity. Of creating trust from scratch. Of understanding that in modern medicine, clinical excellence alone is not enough — visibility, clarity, and authenticity matter just as much.
This is the story of how Nimaaya began in Vadodara… and how it grew to serve six cities.
Being a first-generation doctor is humbling. There is no safety net of legacy. No guaranteed referrals. No inherited goodwill.
You build every brick.
In the early years, I understood something deeply: I had to earn not just degrees, but credibility. Not just patients, but belief. Not just money but legacy.
When you are young in a conservative medical ecosystem, patients often look at you with silent questions:
“Is he experienced enough?”
“Has he handled complex cases?”
“Can we trust him with our child, our family, our hope?”
I learned early that trust is not demanded. It is demonstrated — repeatedly, patiently, ethically.
And that is where brand begins.
Doctoryuvi More than a clinic, more than a white coat, and every conversation had to be more than a consultation.
When we conceptualised Nimaaya - Women’s Health & Fertility Centre, it was never meant to be “just another IVF centre.”
It was meant to feel different.
Women’s health, especially fertility, is not transactional medicine. It is emotional medicine. It is vulnerability medicine. It is the medicine of waiting rooms filled with silent prayers.
From day one, we focused on three pillars:
1. Scientific Excellence
2. Emotional Safety
3. Ethical Transparency
4. Individual Branding that conveys clear crisp
We did not want a hospital that felt intimidating or I never wanted to be that doctor who was intimidating we wanted a space that felt warm. And a team that felt like friends. Where the lighting softened anxiety. Where consultations were conversations, not lectures.
In the beginning, we started small in Vadodara. One centre. Limited resources. Immense conviction.
Every success story was personal. Every negative cycle felt personal too.
I realised early that if I wanted to build a personal brand in today’s world, I could not remain confined to clinic walls.
Medicine has changed. Patients Google before they visit. They search, compare, question, verify.
So I chose not to resist that shift — I embraced it.
That is how “Doctoryuvi” was born on social media.
Not as a vanity project. But as a bridge.
On Instagram and digital platforms, I started with COVID. Since the need of the year was COVID awareness, though I was a Gynaecologist. I fell. The need of the yard was not women health. It was more about a credible doctor giving information in a pandemic that that was affecting millions of people. I kept my Gynaec work aside and started working for Covid awareness.
I feel since the intent was right destiny favoured me.
I became a go to Instagram page and a credible source for information by COVID and COVID vaccination was concerned.
This gave me credibility nationwide later, we started a COVID helpline number exclusively for pregnant women, as many of them were finding it extremely difficult to access emergency care and treatment during the pandemic.
This initiative was appreciated by the nation.
A lot of politicians, celebrities and Media started praising us for our work, which added on to my followers and credibility again on social media once COVID subsided, the credibility still remain, and then pivoted to my area of expertise, which was women health, infertility, surrogacy, etc.
For many young couples, the first introduction to me was not in the OPD. It was through a 60-second reel explaining AMH.
Personal branding in medicine
is often misunderstood. It is not about self-promotion. It is about self-positioning.
It is about ensuring that when someone types “fertility specialist near me,” they don’t just find a name — they find clarity.
The goal was never followers. The goal was familiarity.
When a patient walks in and says, “Doctor, I saw your video,” the consultation begins with trust already built.
Growth stories are often romanticised. They shouldn’t be.
There were days of self-doubt.
Days when cases failed.
Days when I questioned whether expanding too soon was risky.
There is also a unique challenge of being a young male Gynaecologist.
You must work twice as hard to create comfort. To ensure women feel heard, respected, understood.
In fertility medicine, outcomes are not entirely within your control. Biology is complex. And yet, accountability remains yours.
When you are building a brand, your mistakes feel heavier. Because now your name is not just on the prescription — it is online.
That pressure teaches discipline.
It forces you to remain updated. To audit your own
practice. To invest in training, embryology, lab standards, protocols.
Your brand becomes a daily responsibility.
Vadodara was our foundation.
But as word spread and cases became more complex, referrals began to come from neighbouring districts.
Soon, our practice expanded to:
• Anand
• Bharuch
• Ahmedabad
• Delhi
• And continuing presence in Vadodara
Each city came with its own demographic, culture, expectations.
In Anand and Bharuch, conversations often required reassurance and affordability sensitivity. In Ahmedabad, there was heightened awareness and comparison. Delhi brought scale, speed, and a different level of clinical scrutiny.
Expanding to six cities was not about ego. It was about accessibility.
When patients travel 200 kilometres for consultation, it tells you something — the system needs decentralisation of quality care.
But expansion demands systems:
• Standardised protocols
• Lab quality consistency
• Unified communication
• Training teams in shared philosophy
Scaling medicine without diluting ethics is one of the
hardest tasks.
Growth without compromise became our mantra.
BUILDS A MEDICAL BRAND? A personal brand in medicine is not built by advertising.
It is built by:
• Outcomes
• Communication
• Integrity
• Presence
• Education
The reason Doctoryuvi worked online is because it mirrored who I am offline.
If there is dissonance between digital personality and clinical behaviour, patients sense it immediately.
Authenticity scales. Pretence collapses.
Your brand must be sustainable at 8 pm after a long OT day.
Most doctors are trained clinically, not entrepreneurially.
No one teaches you:
• Financial modelling
• HR conflicts
• Marketing ethics
• Negotiating rents
• Managing digital reputation
• Handling medico-legal risks
And yet, if you run a centre, you must learn all of it.
There were months when operational expenses felt
overwhelming. Months when reinvesting in equipment meant personal sacrifice.
But I chose long-term equity over short-term gain.
Infertility is not a disease alone. It is social pressure. Family expectation. Silent comparison.
In India, a woman’s identity is still unfairly linked to motherhood.
As a Gynaecologist, you witness:
• Marriages under strain
• Women blaming themselves
• Men struggling with ego around sperm counts
• Families whispering I realised that branding in this field must carry sensitivity.
You cannot be flamboyant in fertility medicine. You must be dignified.
You cannot overpromise. You must understate and over deliver.
That balance built loyalty. REPUTATION IS COMPOUND INTEREST
In the beginning, progress feels slow. Then something shifts.
A patient you treated five years ago refers her sister.
An IVF baby grows up and comes back for a sibling cycle.
A complex endometriosis case travels from another city after reading your research insights online.
Being young in leadership brings another challenge: managing teams older than you.
Nurses, embryologists, administrative staff — many have years more life experience
Leadership cannot be authoritarian.
It must be collaborative.
We built a culture of:
• Weekly reviews
• Transparent discussions
• No blame for failed cycles
• Continuous training
When your internal team believes in your vision, patients feel it.
Brand is not what you say externally. It is what your staff says about you internally.
As your following grows online, so does scrutiny. Every statement must be evidence-based.
Every claim must be defendable.
In healthcare, misinformation spreads quickly. I consciously chose to remain educational rather than sensational.
No miracle language.
No exaggerated success rates. No celebrity-style hype.
Just clarity.
Because the long game in medicine is credibility.
1. Start Before You Feel Ready
If you wait for perfect
infrastructure, you will never begin.
2. Invest in Design
The aesthetic of Nimaaya matters. Healing environments influence perception.
3. Document, Don’t Perform
Share your journey honestly instead of curating artificial perfection.
4. Consistency Beats Virality
One viral post does not build a practice. Years of steady communication do.
5. Stay Clinically Obsessed
Branding without clinical excellence is hollow.
6. Protect Your Energy
Not every criticism deserves response. Not every comparison deserves attention.
I realised early on India does not lack doctors. It lacks accessible quality.
When we expanded to Anand and Bharuch, we reduced travel burden for couples.
When we entered Ahmedabad, we raised the bar of patient experience.
When we connected with Delhi, we stepped into nationallevel competitiveness.
Each expansion was strategic, not impulsive.
Growth must be thoughtful. Especially in healthcare.
Ambition in medicine is delicate.
If misdirected, it becomes commercialisation.
If guided correctly, it becomes service at scale. We were very sure we never wanted commercialisation.
My ambition has always been simple:
To make Doctoryuvi synonymous with trust in women’s health.
To make Doctoryuvi a reliable digital educator.
To ensure that being a firstgeneration doctor never feels like a limitation again — for me or for those who follow.
People see expansion. They see social media numbers.
They see city names. What they don’t see:
• Sleepless nights after failed cycles
• The emotional toll of patient grief
• The administrative chaos of multi-city operations
• The financial risk of growth
But that is the reality of building something meaningful.
And I would choose it again.
From one centre in Vadodara to six cities including Anand, Bharuch, Ahmedabad, and Delhi — the journey has been deeply personal.
I do not measure success by geography.
I measure it by:
• Babies born
• Women empowered
• Men educated
• Teams mentored
• Young doctors inspired
If one first-generation
medical student reads this and believes that legacy can be built — not inherited — then the brand has meaning.
Building a personal brand as a young Gynaecologist is not about visibility alone. It is about alignment.
Alignment between:
• Who you are
• What you practice
• What you communicate
• What you stand for
Nimaaya began as a dream in Vadodara. It became a movement across cities.
Doctoryuvi began as a digital voice. It became a trusted identity.
I am still learning. Still growing. Still refining.
Because in medicine, humility must grow alongside ambition.
And perhaps that is the most important brand principle of all.
Build with heart.
Scale with integrity. Serve with science.
re-eclampsia is a serious pregnancy complication characterized by elevated

blood pressure and placental dysfunction, posing significant risks to both the mother and fetus. Early diagnosis remains challenging because the condition is frequently recognized only after clinical manifestations become evident. Recent research published in Genome Biology has provided new insights into the molecular mechanisms underlying placental development and suggests potential pathways for earlier detection of the disorder. The study highlights the role of retroelement-derived regulatory sequences in controlling the expression of placental genes. Retroelements contribute to the structural and expression evolution of pregnancy-specific glycoprotein (PSG) genes, facilitating lineagespecific placental evolution. In particular, the LTR8B/PSG9 regulatory network appears to play a critical role in syncytiotrophoblast differentiation and normal placental function. Dysregulation of key transcriptional regulators, including DLX5 and GATA3, has been associated with increased expression of PSG9, suggesting disruption of this pathway in placental pathology. Because PSG9 is expressed during early pregnancy and its altered regulation may reflect early placental dysfunction, it demonstrates promising potential as a predictive biomarker for pre-eclampsia. Detection of such molecular alterations in maternal circulation may enable the development of non-invasive screening approaches for early risk assessment and improved monitoring of pregnancies susceptible to this life-threatening complication.

Arecent study published in Hypertension suggests that women
who experience adverse pregnancy outcomes may face an increased risk of long-term cardiovascular complications, particularly when exposed to persistent psychosocial stress. Pregnancy complications such as Preeclampsia, Preterm Birth, Stillbirth, and Small for Gestational Age were associated with higher blood pressure levels several years after delivery among women who also reported elevated stress during and after pregnancy. Researchers assessed stress levels during pregnancy and
followed participants for up to seven years postpartum, observing that women with pregnancy complications and sustained stress showed modest but clinically relevant increases in blood pressure compared with those with lower stress levels. According to the American Heart Association, even small increases in blood pressure at a young age may contribute to greater long-term cardiovascular risk. The findings emphasize the importance of monitoring blood pressure and addressing psychosocial stress in women with complicated pregnancies to reduce the risk of future cardiovascular disease. Researchers also noted that further studies are needed to better understand the biological mechanisms linking stress, adverse pregnancy outcomes, and long-term heart health.

Dr. Parul Saoji
MS, DNB, MNAMS, FMAS, Dip. (CosGyn)
Cosmetic Gynaecologist, Laparoscopic Surgeon and Infertility Specialist Oracle Clinic, Nagpur
Human papillomavirus (HPV) vaccination is one of the most
ABSTRACT effective cancer-prevention interventions available in Gynaecology. Robust evidence shows substantial protection against persistent infection with oncogenic HPV types, highgrade cervical intraepithelial neoplasia (CIN2/3), and downstream cervical cancer, with major population-level benefits when vaccination is
delivered before sexual debut. Global guidance has also evolved: the World Health Organization (WHO) now endorses simplified schedules (one- or two-dose strategies for adolescents and young adults, and multi-dose schedules for immunocompromised individuals), enabling programmatic scale-up. In India, professional bodies (e.g., FOGSI) and national policy signals support routine
vaccination of girls 9–14 years, alongside catch-up strategies and integration with screening. This article summarizes indications, age-based schedules, special situations relevant to Gynaecology practice (pregnancy, lactation, immunocompromised, prior HPV exposure, post-treatment CIN), and a clinic-ready implementation workflow. It also provides evidence-based counselling approaches for vaccine-hesitant patients and caregivers, emphasizing empathetic communication, myth correction, and shared decisionmaking (SCDM) for adults where benefits are individualized.
Keywords: HPV vaccine, cervical cancer prevention, Gynaecology practice, immunization schedule, vaccine hesitancy, counselling, CIN recurrence, implementation.

Cervical cancer prevention is increasingly a “two-pillar” strategy: primary prevention with HPV vaccination plus secondary prevention with HPV-based screening. WHO’s cervical cancer elimination strategy positions vaccination as foundational. Gynaecologists sit at the most influential touchpoints—adolescent counselling (via mothers), contraception visits, infertility workups, postpartum checks, preconception counselling, and colposcopy/ CIN clinics—making routine vaccination discussions feasible and impactful.
Even when vaccination occurs after sexual debut, it can still provide protection against HPV types not yet acquired; however, effectiveness is highest before exposure. CDC and ACOG continue to recommend routine vaccination through age 26 when not previously vaccinated, regardless of sexual activity history.
Efficacy against persistent infection and pre-cancer Randomized trials and long-term follow-up studies consistently
show strong protection against vaccine-type HPV infection and pre-cancer endpoints. ACOG notes “unequivocal” high efficacy, particularly when administered before HPV exposure.
Single-dose evidence and schedule simplification
Programmatic constraints (missed second/third doses, cost, school access, followup loss) led to major interest in single-dose schedules. WHO’s 2022 position update supports one- or two-dose schedules for girls 9–14 and for girls/women 15–20, while recommending at least two (and where possible three) doses for immunocompromised individuals.
High-quality clinical trial evidence supports strong protection after a single dose against persistent oncogenic HPV infection (e.g., KEN SHE). Long-term immunogenicity data from Costa Rica show sustained antibody responses years after a single dose of bivalent vaccine, supporting durability.
Practical takeaway: while global evidence and some guidance support simplified schedules, your clinic should follow the schedule approved/ endorsed by your national regulator and professional guidance for the product you are using, documenting clearly when any “reduced-dose” approach is off-label in your setting (FOGSI notes reduceddose schedules may await specific regulatory approval in India).
Adjuvant vaccination after CIN treatment: promising but
Observational data and metaanalyses suggest adjuvant HPV vaccination around the time of excisional treatment may reduce recurrent CIN2+ risk; ACOG (2023) cites a metaanalysis reporting meaningful risk reduction. However, newer randomized evidence has produced mixed results, so counselling should be balanced: potential benefit, low risk, but not guaranteed.
Primary prevention (routine + catch-up)
Core indication: prevention of HPV-related cancers (especially cervical) and other HPV-related disease, with maximal benefit when given prior to HPV exposure.
Secondary prevention adjunct (special situations)
HPV vaccines are prophylactic, not therapeutic: they do not treat existing infection or established lesions. Still, vaccination may reduce risk of future infection with other types and may have a role as adjuvant around CIN treatment in selected patients after shared counselling.
Boys and herd protection (relevant for counselling families)
Many immunization schedules include boys to reduce transmission and prevent HPV-related cancers in males. Indian paediatric guidance has recommended HPV vaccination for boys as well. Even if your Gyne practice vaccinates mostly girls/women, counselling mothers about
vaccinating sons can be valuable.
Global (WHO) schedule framework
WHO (Dec 2022) recommends:
• Girls 9–14 years: one or two doses.
• Girls/women 15–20 years: one or two doses.
• Women >21 years: two doses (6-month interval).
• Immunocompromised / HIV: at least two doses, ideally three where feasible.

CDC/ACIP (useful for evidence-based counselling and for patients abroad)
• Start 11–12 years (can start at 9).
• 2 doses if series begins before 15th birthday (0, then 6–12 months).
• 3 doses if starting at 15–26 years, and for immunocompromised persons (0, 1–2, 6 months, depending on product guidance).
• Adults 27–45 years: vaccination is shared clinical decisionmaking (SCDM), not routine.
India-facing practical schedule (FOGSI)
Professional guidance in India commonly operationalizes:
• 9–14 years: 2 doses (0, 6 months).
• 15–26 years: 3 doses (0, 2, 6 months).
• FOGSI’s cervical cancer guidance lists these schedules and discusses reduced-dose approaches with regulatory caveats.
Product-specific example (CERVAVAC® SmPC):
• 9–14 years: 2 doses (0, 6 months)
• 15–26 years: 3 doses (0, 2, 6 months)
Adolescents (9–14): the “best buy” group
Message: “This is a cancer-preventing vaccine, best before exposure.” WHO prioritizes this age group for maximum impact and program feasibility
Who decides: parents/caregivers—so your counselling is often directed at the mother during her own visit.
Late adolescents and young adults (15–26): catch-up
Benefits remain strong, especially if not previously vaccinated. ACOG recommends vaccination through 26 years regardless of sexual history, acknowledging that prior exposure does not eliminate potential benefit against unacquired types.
Adults 27–45: shared decisionmaking
This group needs individualized counselling because many will have already been exposed and average population benefit is smaller; still, some individuals (new partners, not in mutually monogamous relationships, etc.) may benefit. CDC explains the rationale for SCDM, including lower effectiveness with prior infection and lower exposure risk in monogamy.
Pregnancy and lactation
Most guidelines advise deferring vaccination during pregnancy (not because of proven harm, but because vaccination is not routinely recommended in pregnancy); if pregnancy occurs after starting the series, complete remaining doses postpartum. (Use your country/product guidance in clinic policy; document pregnancy status.)
Breastfeeding: generally considered acceptable to vaccinate postpartum; many programs include postpartum catch-up.
Immunocompromised ........ (including HIV, transplant, long-term steroids, autoimmune biologics)
WHO emphasizes immunocompromised ........ individuals should receive at least two doses, ideally three.
In practice: prefer 3-dose schedule and ensure documentation and follow-up.
Prior HPV infection, abnormal Pap/HPV positive, or genital warts
Key counselling: vaccine does not treat current infection
or lesions, but may protect against other vaccine types not yet acquired. Keep screening per guidelines.
Post-treatment CIN (LEEP/conization): adjuvant discussion
If you run a colposcopy/CIN service, consider a standard script:
• Evidence suggests reduced recurrence in some studies/metaanalyses
• But randomized evidence is mixed; benefit not guaranteed
• Safety profile is reassuring; cost and patient preference matter This is ideal for shared decision-making with clear informed consent.
Build an “HPV vaccine pathway” (simple and repeatable)
Step A: Identify eligible patients
• Every OPD intake form: include “HPV vaccine status: 0/1/2/3 doses; year received; product if known.”
• Ask mothers: “Any girl child 9–14 at home?”
Step B: Standardize counselling (2-minute version + 8-minute version)

• 2-minute: cancer prevention + best age + safety reassurance
• 8-minute: types, schedule, side effects, myths, screening link, cost, reminders
Step C: Consent + documentation
• Provide a one-page consent in local language: benefits, schedule, expected minor AEFIs, emergency advice.
• Record: brand, batch, expiry, site, date, next dose due, vaccinator name.
Step D: Cold chain & administration
• Follow vaccine label for storage and handling; train one nurse as “vaccine champion.”
• Observe 15 minutes post-shot (syncope precautions for adolescents).
Step E: Reminder system
• WhatsApp + SMS: schedule next dose at checkout.
• A weekly list: “due in next 2 weeks” phone call.
Step F: Integrate with screening Vaccination does not replace screening. FOGSI emphasizes continued screening as per guidelines. Your script: “Vaccine prevents most cancers, screening catches the rest early.”
Quality indicators to track monthly
• % eligible girls counselled
• Vaccine initiation rate
• Series completion rate (if multi-dose)
• AEFI log (minor/major; referral if needed)
• Missed-opportunity count (eligible patient not counselled)
Practice positioning and community linkage (India)
India’s policy environment has increasingly emphasized HPV vaccination for girls 9–14. Gyne clinics can complement public programs by:
• offering vaccination to those outside school programs,
• supporting awareness sessions (schools, corporates), coordinating with nearby paediatricians and family physicians for family-based vaccination.
COUNSELLING ........... VACCINE-HESITANT PATIENTS: ................ EVIDENCE-BASED COMMUNICATION THAT WORKS
Start with a “presumptive, confident recommendation”
A strong clinician recommendation is one of the most consistent predictors of vaccine uptake. Use:
“Today, she is due for the HPV vaccine—this prevents cervical cancer. We can give Dose 1 now.”
Then pause. If resistance appears, shift to empathy and questions.
Use motivational interviewing (MI) in 4 moves 1. Ask permission: “Can I share
what we know scientifically?”
2. Explore values: “What worries you most—safety, necessity, or fertility concerns?”
3. Reflect + affirm: “You’re trying to make the safest choice for your daughter.”
4. Offer a clear plan: “Let’s do Dose 1 today; I’ll message you the next due date.”
Address the 6 most common myths (with quick scientific counters)
Myth 1: “It will affect fertility.”
Response: HPV vaccines are designed to prevent infection and cancer risk; major professional bodies continue to recommend them broadly, including for adolescents, and do not list infertility as an expected outcome.
Myth 2: “It encourages early sexual activity.”
Response: The vaccine is a health intervention timed for immune response and preexposure prevention; it does not alter values or behaviour. Reframe: “We give seatbelts before accidents, not after.”
Myth 3: “My child is not at risk.”
Response: HPV is common and often acquired soon after sexual debut; vaccination is most effective before exposure.
Myth 4: “One dose/two dose confusion—so better wait.”
Response: WHO supports simplified schedules to improve coverage, but we follow the locally recommended/productapproved schedule in our clinic; delaying often leads to missed protection.
Myth 5: “It’s too new / not enough data.”
Response: HPV vaccines have extensive global use, and ongoing studies continue to refine optimal dosing; current evidence includes strong efficacy and long-term immunogenicity data.
Myth 6: “If screening exists, vaccine is unnecessary.”
Response: Screening detects disease early; vaccination prevents the infection that causes most disease. Best protection is both.
For adults 27–45: a clean shared decision-making script
Use CDC’s SCDM rationale as your base.
3 questions to personalize benefit:
1. “Are you likely to have a new sexual partner in the future?”
2. “Are you currently in a mutually monogamous relationship?”
3. “Have you been vaccinated earlier?”
If risk of future exposure is meaningful and vaccination status is incomplete → vaccination may be reasonable. Handling misinformation without confrontation
• Avoid debating social media claims directly.
• Use “truth sandwich” technique: truth → myth → truth.
• Offer credible handouts (WHO/FOGSI summary) and invite follow-up.
• Most reactions are mild and self-limited (injection-site pain, fever, fatigue).
• Syncope can occur in adolescents; a brief observation period is practical.
• True contraindication is severe allergy to a component or a prior dose. For pregnancy, defer remaining doses until postpartum if discovered after initiating the series (per clinic policy and product guidance).
HPV vaccination is a cornerstone of cervical cancer elimination and a high-yield intervention in Gynaecology practice. Current evidence supports strong protection, with increasing global endorsement of simplified schedules and sustained effectiveness data. A practical clinic pathway—systematic eligibility checks, standardized counselling, robust reminders, and documentation— can significantly improve uptake and completion. For vaccinehesitant families, empathetic, evidence-based counselling and confident recommendations outperform myth-versus-myth debates. Finally, vaccination should be integrated with continued screening to maximize lifetime protection against cervical cancer.
HPV Vaccination in Gynaecology Practice: Current Evidence and Implementation
1. World Health Organization. Human papillomavirus vaccines: WHO position paper. Wkly Epidemiol Rec. 2022;97(50):645–672.
2. World Health Organization. WHO updates recommendations on HPV vaccination schedule (news release). 20 Dec 2022.
3. World Health Organization. Human papillomavirus and HPV vaccines (WHO guidance page). Updated Dec 2022.
4. Centers for Disease Control and Prevention (CDC). HPV Vaccination Recommendations (ACIP/CDC).
5. CDC. ACIP Shared Clinical Decision-Making Recommendations. Updated 7 Jan 2025.
6. American College of Obstetricians and Gynaecologists (ACOG). Human Papillomavirus Vaccination. Committee Opinion No. 809. Obstet Gynecol. 2020; 136(2).
7. ACOG. Adjuvant Human Papillomavirus Vaccination for Patients Undergoing Treatment for CIN2+. Practice Advisory. 2023.
8. Barnabas RV, et al. Efficacy of Single-Dose Human Papillomavirus Vaccination among Young African Women. NEJM Evidence. 2022.
9. National Cancer Institute. One HPV Vaccine Dose Prevents Cancer-Causing Infections (KEN SHE trial summary). 2022.
10. Porras C, et al. HPV16/18 antibodies 11–16 years after single dose of bivalent HPV vaccine. JNCI Monographs. 2024.
11. Burdier FR, et al. An update on one-dose HPV vaccine studies and trials (meeting report). 2023.
12. Petráš M, et al. Timing of HPV vaccination as adjuvant treatment of CIN2+ recurrence: meta-analysis/meta-regression. 2023.
13. van de Laar RLO, et al. Adjuvant prophylactic HPV vaccination after excisional treatment: randomized evidence (abstract). 2025.
14. Federation of Obstetric and Gynaecological Societies of India (FOGSI). Preventing Cervical Cancer through HPV Vaccination in India. 2024.
15. FOGSI. GCPR: Prevention and Management of Cervical Cancer. June 2024.
16. Indian Academy of Pediatrics. Recommended Immunization Schedule / updates including HPV for boys and 2-dose 9vHPV for 9–14 years. Indian Pediatr. 2024.
17. Government of India, Press Information Bureau. Union Finance Minister announces vaccination programme for girls 9–14 years. 1 Feb 2024.
18. CDSCO (India). CERVAVAC® SmPC (qHPV) – dosage schedules 9–14 (2-dose) and 15–26 (3-dose). 2022.
19. Serum Institute of India. CERVAVAC® product indication (9–26 years; prevention of HPV-related cancers/warts).


A28-year-old woman with heavy periods and poor pill
INTRODUCTION compliance comes to the OPD asking for something more reliable than a Copper T or daily tablets. Situations like this are now common in practice. Contraceptive care has moved far beyond the traditional trio of Copper T, daily pills, and condoms. Women today want methods that are reliable, low maintenance, reversible, private, and aligned with their medical profile and lifestyle. Many discontinue conventional methods due to bleeding problems, daily adherence burden, or side
effects. Missed opportunities in postpartum and postabortal periods continue to contribute to unintended pregnancies. Current global and national guidance emphasizes expanding the contraceptive basket and prioritizing long acting reversible contraception and user controlled options.[1, 2]
This chapter provides a practical, clinic-ready framework covering mechanisms, eligibility, initiation, efficacy, side effects, contraindications, counseling, follow up, and special situations based on major international and Indian
recommendations.[1–6]
NEED FOR......................
OPTIONS BEYOND........
CONVENTIONAL ........... METHODS
Copper IUDs are highly effective but are associated with increased menstrual bleeding and pain in a significant proportion of users, contributing to discontinuation.[1,3] Combined oral pills are highly effective with perfect use but show higher failure with typical use due to missed doses. Typical use failure rates for pills, patch, and ring are about 7 percent per year.[1,2] Condoms are user dependent and require consistent partner co-operation.
Newer methods reduce user error, improve continuation, and allow better matching with comorbidities such as anemia, heavy menstrual bleeding, migraine, or estrogen contraindication. Long acting reversible contraception shows efficacy comparable to sterilization with reversibility.[2,3]
METHOD ELIGIBILITY FRAMEWORK
Method choice should follow Medical Eligibility Criteria categories. Conditions are classified from category 1 with no restriction to category 4 with unacceptable risk. This framework should be routinely applied for hypertension, migraine with aura, thromboembolic disease, breast cancer, liver disease, obesity, and postpartum status before prescribing or inserting a method.[1]
MODERN
a) Levonorgestrel intrauterine system
Examples: Mirena, Kyleena, Levosert, Benilexa
b) Subdermal etonogestrel implant
Example: Nexplanon (Implanon NXT)
c) Reusable combined hormonal vaginal ring
Example: Annovera
Also monthly vaginal ring: NuvaRing
d)..Self-administered DMPA subcutaneous injection
Example: Sayana Press (DMPASC)
e)..Newer progestin only pills
Examples: Drospirenone-only pill formulations such as Slynd
f)..Combined hormonal patch and ring systems
Examples: Transdermal patch — Xulane, Twirla
vaginal ring — NuvaRing
g)..On demand non hormonal vaginal gel
Example: Phexx
h)..Immediate postpartum and postabortal LARC use
Methods include Copper IUDs, LNG IUS (for example Mirena type), and etonogestrel implant (Nexplanon)[1-5]
Hormonal contraceptives act mainly by ovulation suppression, cervical mucus thickening, and endometrial thinning. Progestin dominant methods primarily suppress ovulation and alter cervical
mucus. Levonorgestrel intrauterine systems act mainly locally on the endometrium and cervical mucus with low systemic levels. Vaginal pH modulators reduce sperm motility by maintaining an acidic environment.[1,2]
• Levonorgestrel Intrauterine System
Mechanism: Local levonorgestrel release produces endometrial suppression and thick cervical mucus. Ovulation is often preserved.[1, 3]
Insertion: Same as copper IUD technique. Insert anytime if pregnancy is reasonably excluded. Immediate postpartum and postabortal insertion is acceptable with proper screening and training.[1, 2]
Efficacy: Less than 1 percent failure per year.[2, 3]
Additional benefits: Reduces heavy menstrual bleeding and dysmenorrhea. Useful in heavy menstrual bleeding and for endometrial protection with estrogen therapy.[3, 4]
Side effects: Initial irregular spotting, later lighter periods or amenorrhea.
Contraindications: Pregnancy, active pelvic infection, distorted uterine cavity, unexplained vaginal bleeding, current breast cancer.[1]
Follow up: Review at 4 to 6 weeks, then yearly.[2]
• Subdermal Etonogestrel Implant
Mechanism: Continuous progestin release suppresses ovulation and thickens cervical
mucus. [1, 2]
Insertion: Minor office procedure under local anesthesia. Insert within first 5 days of cycle for immediate protection, otherwise add 7 day backup. Approved duration is 3 years. Evidence for extended use exists but may be off label.[2, 3]
Efficacy: About 0.1 percent failure per year.[2]
Side effects: Irregular bleeding, possible amenorrhea, acne, mild weight change.
Contraindications: Current breast cancer, severe liver disease, unexplained vaginal bleeding. Past VTE is not an absolute contraindication under MEC.[1]
• Reusable Combined Hormonal Vaginal Ring
Mechanism: Estrogen plus progestin suppress ovulation.[2]
Use: Self inserted for 21 days, removed for 7 days. Some products allow reuse for up to one year. Availability varies by region.[2, 5]
Efficacy: Typical use failure about 7 percent.[2]
Contraindications: All estrogen contraindications apply, including migraine with aura, VTE, uncontrolled hypertension, smoking above 35 years, severe liver disease, and current breast cancer.[1]
• Self-Administered DMPA
Subcutaneous
Mechanism: Depot progestin suppresses ovulation for 3 months.[1, 2]
Use: Subcutaneous injection every 12 to 13 weeks. Suitable for self-administration after training.[2, 6]
Efficacy: Typical use failure
about 4 percent.[2]
Side effects: Irregular bleeding, amenorrhea, weight gain in some users, delayed fertility return, reversible bone density reduction.[1, 2]
Contraindications: Current breast cancer, unexplained vaginal bleeding, severe liver disease.[1]
• Newer Progestin Only Pills
Mechanism: Ovulation suppression and cervical mucus effect.[2]
Use: Daily pill. Newer formulations allow a longer missed pill window than older progestin only pills.[2]
Role: Useful where estrogen is contraindicated.[1]
• On Demand Non-Hormonal Vaginal Gel
Mechanism: Maintains acidic vaginal pH and reduces sperm motility.[2]
Use: Applied before each act of intercourse as directed.
Efficacy: Lower than LARC and hormonal methods. Suitable for on demand use. Combine with condoms for higher protection.[2]
• Initiation and Switching
Quick start is acceptable for most hormonal methods if pregnancy is reasonably excluded. If started beyond day 5 of cycle, use 7 day backup. LARC can be inserted anytime with backup advice. Switching methods should include overlap or backup protection to avoid gaps.[2]
• Postpartum and Postabortal Contraception
Immediate postpartum and postabortal insertion of IUD, IUS, and implant
is recommended to reduce missed opportunities. Estrogen methods should be delayed in early postpartum, especially in breastfeeding women. Progestin only methods are generally safe early postpartum.[1, 2, 4]
• Drug Interactions
Enzyme inducing drugs such as certain antiepileptics and rifampicin reduce efficacy of pills, patch, and ring. LARC methods are preferred in these users.[1, 2]
• Side Effect Management
Irregular bleeding with progestin methods can be managed with NSAIDs or short hormonal courses in eligible women. Amenorrhea is not harmful once pregnancy is excluded. Good pre counseling improves continuation.[2, 3]
• Warning Signs
Estrogen methods: Severe headache, visual symptoms, chest pain, breathlessness, leg swelling.[1]
IUD or IUS: Severe pelvic pain, fever, foul discharge, missing strings.[2]
• Failure with Method in Situ
If pregnancy occurs with implant, remove implant and evaluate. If pregnancy occurs with IUD or IUS, rule out ectopic pregnancy and remove the device if strings are visible.[1, 2]
• Dual Protection
Condoms should be advised with any primary method where STI risk exists. Other contraceptive methods do not protect against STI.[1]
• Follow Up
LARC methods: One early review at 4 to 6 weeks if needed,
then yearly.[2]
Short acting methods: Review at 3 months, then yearly with blood pressure check for estrogen users.[2]
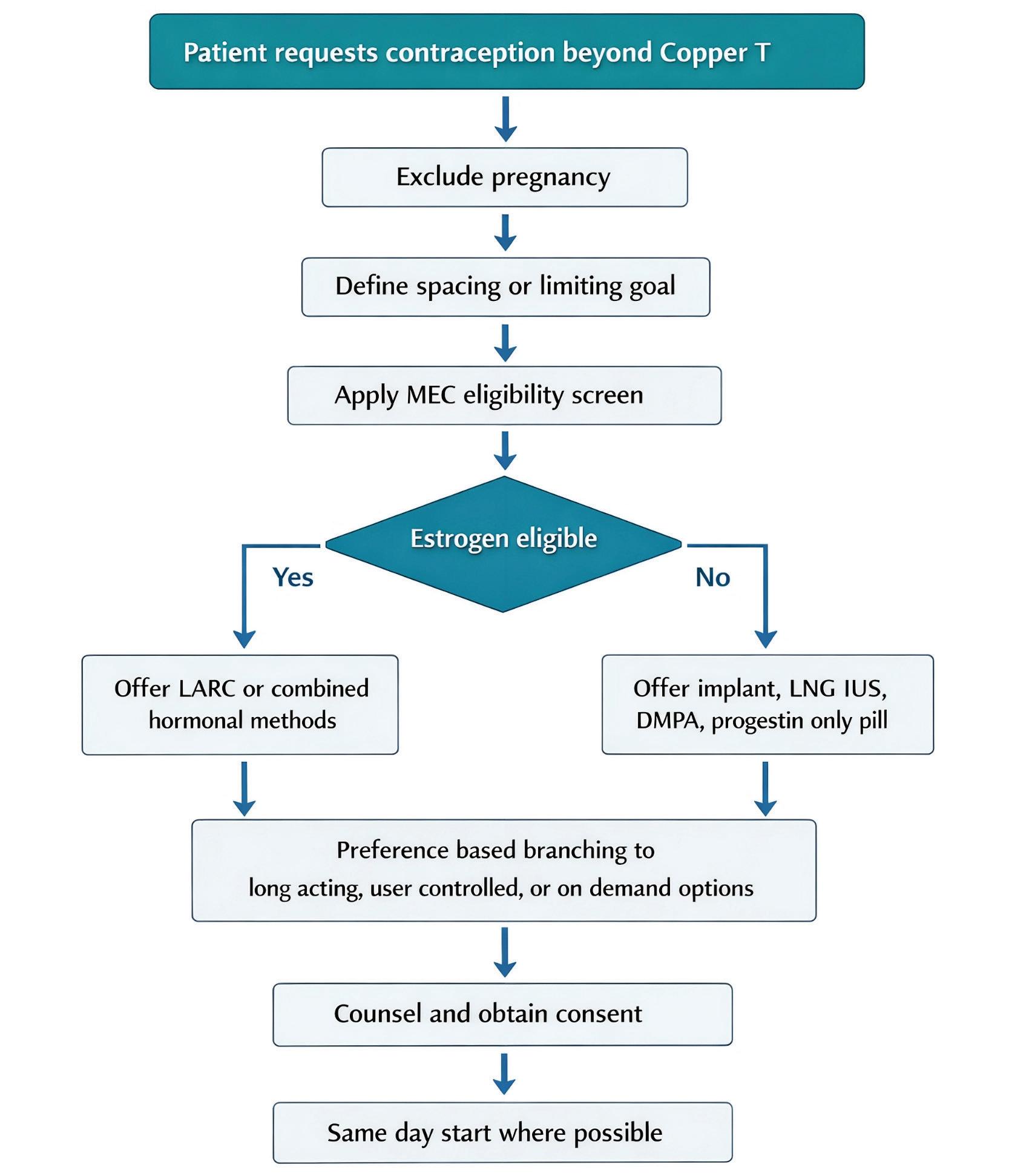
Step 1- Confirm pregnancy exclusion and define spacing or limiting goal.
Step 2- Apply MEC screening for estrogen risk, breast cancer, liver disease, VTE risk, and postpartum status.[1]
Step 3- If eligible and wants highest efficacy with low maintenance, offer LARC first, LNG IUS or implant.[2, 3]
Step 4- If user prefers a self -controlled method, consider ring, progestin only pill, or DM PA SC depending on eligibility.[2]
Step 5- If user wants a non-hormonal on demand method, discuss vaginal gel and co ndoms with efficacy counseling.[2]
Figure 1. Decision Flow for Method Selection
Shared decision making is recommended by major guidelines. Discuss effectiveness, expected bleeding changes, side effects, risks, benefits, and alternatives in clear language. Respect patient preference when medically eligible. Document counseling, selected method, key risks discussed, and procedural consent for insertions and injections. This improves continuation and supports medicolegal safety.[2, 3]
AVAILABILITY AND COST CONSIDERATIONS IN INDIA
In India, copper IUDs, selected LNG IUS devices, DMPA, and pills are available through national programs, while implants, newer rings, and vaginal gels may have limited availability and higher out of pocket cost. Method choice should consider access and affordability along with medical eligibility.[6]
LNG IUS 3 to 8 years Less than 1 percent 2,3] Heavy bleeding plus contraception Early spotting
Implant 3 years About 0.1 percent [2] Highest reversible efficacy Irregular bleeding
DMPA SC 3 months About 4 percent [2]
Estrogen contraindication Weight gain and delayed fertility return
Vaginal ring Monthly use about 7 percent [2] No daily pill Estrogen contraindications
New progestin only pill Daily Higher failure than LARC [2]
Estrogen free Adherence
Vaginal gel Per act Higher failure than hormonal [2] On demand non hormonal Lower efficacy
Offering only pills and Copper T without discussing LARC options. [2,3]
Skipping MEC screening before prescribing estrogen methods. [1]
Under-counseling about irregular bleeding with implants and progestin methods.
Delaying postpartum contraception counseling until discharge. [2,4]
Ignoring drug interaction history. [1]
Not documenting counseling and consent.
[1–4]
• Offer multiple options beyond Copper T.
• Prefer LARC where suitable.
• Apply MEC criteria routinely.
• Use quick start and same day provision when possible.
• Set bleeding expectations clearly.
• Encourage dual protection when needed.
• Document counseling and consent.
1. World Health Organization. Medical Eligibility Criteria for Contraceptive Use. Latest edition.
2. World Health Organization. Selected Practice Recommendations for Contraceptive Use. Latest edition.
3. American College of Obstetricians and Gynecologists. Practice Bulletins on Long Acting Reversible Contraception and Hormonal Contraception.
4. Faculty of Sexual and Reproductive Healthcare. Clinical Guidelines on Contraceptive Methods.
5. Royal College of Obstetricians and Gynaecologists. Guidance on Contraception.
6. Government of India. National Family Planning and Contraceptive Guidelines.
recent study published in The Lancet Digital Health describes the development of an required before

widespread implementation in routine healthcare practice artificial intelligence (AI)–based risk assessment tool capable of predicting the likelihood of breast cancer development within several years following routine screening. The algorithm, originally designed to detect malignancies on mammographic images, has been adapted into a predictive model known as the BRAIx risk score, which analyzes imaging data to estimate an individual’s future risk of breast cancer. The model was developed using mammographic data from a large cohort of women and subsequently validated in an additional population, with further confirmation in an independent group. The findings demonstrated that the BRAIx risk score outperformed traditional risk indicators commonly used in clinical practice, including breast density, family history, and demographic factors, in identifying individuals at increased risk. Among women categorized within the highest risk group according to the AI score, a notable proportion developed breast cancer within the following years despite having initially received negative screening results. These findings highlight the potential of AI-driven risk stratification to enhance the personalization of breast cancer screening programs, moving beyond the conventional uniform screening approach toward a model that tailors surveillance intensity according to individual risk profiles. Such tools may enable earlier detection through targeted monitoring of high-risk individuals while potentially reducing unnecessary screening and associated false positives among those at lower risk. Although the results underscore the promise of integrating AI-based predictive analytics into screening strategies, further prospective studies and clinical validation are can be considered.

Astudy published in the Journal of Applied Physiology indicates that hormonal fluctuations
across the menstrual cycle may influence women’s perception of exercise difficulty without significantly altering their physiological capacity for sustained high-intensity exercise. Female sex hormones, particularly estrogen and progesterone, vary throughout the menstrual cycle and play key roles in metabolic regulation and energy balance. However, their impact on exercise performance has remained unclear due to the limited representation of women in exercise physiology research. In this study, participants underwent repeated exercise testing to determine their maximal metabolic
steady state, the highest intensity of exercise that can be sustained primarily through aerobic metabolism. The findings showed that this threshold remained stable across different hormonal phases, suggesting that menstrual cycle–related hormonal changes do not significantly affect a woman’s ability to maintain intense aerobic exercise. Nevertheless, subjective assessments revealed that perceived exertion varied, with workouts reported as more difficult during phases associated with higher progesterone levels. Despite these perceptual differences, objective physiological markers, including heart rate and oxygen consumption, remained consistent. These findings highlight that while hormonal fluctuations may influence how strenuous exercise feels, they do not appear to compromise actual physical performance, emphasizing the importance of individualized training approaches that consider both physiological capacity and perceived effort.

Consultant Obstetrician & Gynaecologist, Mumbai
Affiliated with Gleneagles, Saifee, Bhatia & St. Elizabeth Hospitals
Honorary Clinical Associate, Nowrosjee Wadia Maternity Hospital

1
TThe field of Obstetrics & Gynaecology is recognized as demanding and challenging in healthcare profession. They often encounter extended and irregular working hours, unforeseen delivery outcome, complications during childbirth and occasional maternal death. These circumstances contribute physical and mental fatigue. There is predominance of female practitioners in some parts of India in this field. They face high levels of mental stress like burnout, anxiety, depression. This is
driven by long and erratic working hours, high stakes, unpredictable outcome of patients and heavy patient workload. Most professionals attribute traumatic stress to adverse medical outcome. The word ‘stresses’ originated from Latin word ‘stringere’ meaning starvation, pain, sting and physical hardship.1 High levels of stress can impair performance and result in negative behavioural / attitudinal environment. Obstetricians and Gynaecologists are no exception to this and may have post-traumatic stress disorder (PTSD). Residency training program leads to severe burnout with postgraduates encountering multitude of stressors.
1) Environment with Stakes: High Pressure of Handling both Maternal and fetal lives, fertility patients for success often leads to severe stress. Pregnancy and childbirth being joyful, at times can cause complications like still birth / maternal death. Such events have very high emotional impact on treating Obstetricians & Gynaecologist. The rate of suicide is 16 % among Indian Medical Fraternity in this branch.2 Knowledge of lethal suicide methods, easy access to potentially lethal drugs, apathy and fearlessness towards death are also additional contributing factors.
2) Burnout / Fatigue: Long unpredictable working hours leads to tremendous physical and mental exhaustion. Enormous patient workload, huge expectations from medical
personnel, limited resources, inadequately skilled support staff, non-supportive peer group causes more stress / burnout and their concern take a backseat. Major event gets noticed but day to day issues that jeopardize safety / quality of service by Obstetricians & Gynaecologists are least addressed. Additional issue of keeping oneself calm under all circumstances while still maintaining interaction with patient’s relatives is challenging. External issues of family, finances and high goals also have effect on stress.
3) Covid 19 impact: Pandemic exacerbated mental health issues causing anxiety, depression and insomnia over trivial matters.
4) Gender specific challenges: Certain working environmental areas face social pressure as most working faculties are females. High rates of anxiety have been faced and observed as compared to male colleagues.
5) Barriers to Care: Fear of professional judgement, stigma and lack of Institutional support system prevents medical personnel from seeking support.
• Commonly reported symptoms are Anxiety (81%), Guilt (62%) and Sleep disturbance (58%).
• Complication of birth / death of patient and uncertainty about the future.
• Burnout can contribute to increase in medical errors and decrease in quality care Ob
Gyn residency has highest rate of Burn Out as compared to other departments.³
• There is always stress at work due to too much paperwork, prolonged working hours, less time for family - friends - hobbies, unhealthy food, new learning of a subject, expectation to perform well in clinical situations, experiencing any of patients.
• Some may feel colloquial depression (feeling of sadness / despondency).
• Few may have clinical depression (prolonged / severe state of despondency unrelated to typical grief related experience).
• Some cannot pursue hobbies because they did not have enough time or interest.
• Burnout can lead to absenteeism, intent to leave, substance abuse and mood disorder.
• Long term sequel of stressful environment could be depersonalization and reduced personal accomplishment.
• In extreme cases, stress can lead to suicide.
• Those who are private sector in smaller nursing homes or hospitals of their own, do face this burn out especially at the time of adverse outcome for the lack of support, reputation at stake, fear of decrease in patient turnout after the episode, episode of violence, possibility of damage to the clinic - hospital and facing medico legal consequences.
Table 1: Stress Related Symptoms2
• Engaging in stress free / diverted activities:
➢ Talking with friends, family and partner, listen to music, going for movie if time permits, social media, exercise - gym, eating junk food, sleep - relax, shopping offline - online.
➢ Occasionally writing research paper and indulging in religious activities can help.
However, all these may not prevent patient aggression / violence and work conflict.
• Start day with good nutrition, proper planning, positive attitude and bit of physical activity.
➢ Organize oneself to be free from clutter and more efficient at work.
➢ Avoid multitasking especially, while handling emergency.
• Adapt relaxation strategies like meditation, deep breathing exercises and mindfulness.
➢ This is the state of actively observing present experiences / thoughts without judging them.
➢ Focus mind on simple activities like breathing, walking, enjoying meal which will grow stronger over a period of time so that it can be applied to different aspects of life.
• Relaxation response is Calming Focus and Let go relax.
➢ This could be small prayer, positive.
➢ Brief word - sound - phrase, yoga, meditation.
➢ Doing this for 10 - 20 minutes a day can bring about physiological slowdown of
heart rate / breathing, decreases lactate levels and hence anxiety attacks.
• COPE (Brief Coping Orientation Problems Experienced) is a measure to cope up with Health care professionals.
➢ Handling of difficult situations are divided into adaptive or maladaptive.
➢ Adaptive strategies like acceptance, humour or planning help improve functioning.
➢ Maladaptive strategies like venting out, denial, and substance abuse may maintain or increase level of stress or distress.
➢ Most doctors usually prefer maladaptive measures.
Unsure of reaching OPD / OT on time
Overworked / Burned out
Systemic Reforms: Implementation of systemic, manageable working hours with better work life balance need to be done. Suggestions to have 8 hours duty have been made in public sector hospitals, as there are enough qualified staff available to look after the work.4
However, in private sector, though workload is less, such limited hours duty may not be feasible. Private sector faculty at times work with limited staff whereas in public sector environment there are many helping hands especially in case of emergency. It is advisable for Private sector medical fraternity with smaller nursing homes / hospitals to have core group of few colleagues who can be of immediate help in case of emergence. This may include peer group of other relevant medical branches.
Changing Mind set of public and authorities managing healthcare system is of utmost importance. They need to consider medical personnel as Human Beings and not supernatural power.
Confidential Support: Access to confidential counselling and mental health services to combat stigma is of immense importance.
Training / awareness: Regular workshops and stress management
training is necessary to reduce mental burnout.
Futuristic Way:
The current generation of Postgraduates who have taken up Ob Gyn branch, desires to do Fellowship in Assisted Reproductive Technology (ART), Fetal Medicine or minimally access surgery (MAS + Robotic) after Masters’ degree. This not only gives an opportunity to become expert in super speciality but also provides an advantage of scheduled work, no erratic hours of work, no emergencies and no sleep disturbance. This gives an opportunity of proper planning of family time, social activities and persuasion of co-curricular interest.
We stand where first cries split the night, Where fragile breaths begin their fight. Where joy and grief in one room stay, And strength must not give way.
We stitch the torn, we guard the womb, We speak of hope in shadowed rooms. But who will see the silent cost— The healer bent, the spirit lost?
Behind each calm and measured tone Is weariness the charts don’t own. For even those who bring forth life May carry unseen, quiet strife.
Burnout in Obstetrics and Gynaecology is increasingly recognized as a serious professional and public health concern. Characterized by emotional exhaustion, depersonalization, and a reduced sense of personal accomplishment, burnout reflects the cumulative psychological strain of sustained occupational stress. Within Obstetrics and Gynaecology, the risk is amplified by unpredictable emergencies, surgical intensity, medico-legal vulnerability, and profound emotional labour.
Burnout does not emerge in a single moment; it evolves across the professional lifespan. Its character shifts from acute exhaustion during residency to transitional stress in early independent practice and later into a more chronic, morally complex fatigue five to ten years beyond training. Understanding this progression is critical for prevention, intervention, and sustainability in the specialty.
Residency in Obstetrics and Gynaecology is one of the most demanding phases in medical training. Long duty hours, night calls, emergency obstetrics, and surgical learning curves create a relentless environment. Sleep deprivation becomes routine, and emotional exposure to maternal and neonatal morbidity is frequent.
Research consistently demonstrates high burnout rates among OB-GYN residents, with emotional exhaustion being particularly prominent. The training environment often prioritizes endurance and performance over psychological processing. Residents witness maternal deaths, obstetric catastrophes, and reproductive loss, frequently without structured debriefing. These experiences accumulate quietly.
Depersonalization may develop as a coping mechanism. Emotional distancing can protect against immediate distress but may also erode empathy over time. Reduced personal accomplishment can emerge when residents feel they are functioning merely to survive shifts rather than growing as clinicians.
The residency stage resembles sustained physiological stress activation. Disrupted sleep patterns and persistent cognitive vigilance alter emotional regulation. The identity of the young physician is shaped in this furnace. Idealism may persist, but it is tempered by fatigue and responsibility.
Burnout during residency is not merely a reaction to workload; it reflects the psychological cost of formation under pressure.
Completion of residency brings professional autonomy, but it also introduces new stressors. The early years of independent practice are marked by full accountability for clinical decisions. Litigation
fears become tangible realities. Financial pressures and productivity expectations increase. Administrative tasks multiply.
The landmark study by Rath and colleagues examining members of the Society of Gynaecologic Oncology reported that approximately 32 percent met criteria for burnout. Emotional exhaustion was the most common component. Importantly, 33 percent screened positive for depression and 13 percent reported a history of suicidal ideation. These findings underscore the intersection between burnout and broader mental health vulnerabilities.
The early consultant stage can feel isolating. During residency, peers share the burden; in independent practice, stress is often experienced alone. Young gynaecologists may feel compelled to demonstrate competence continuously. Despite these pressures, many still report a high sense of professional accomplishment, illustrating the complex coexistence of pride and distress.
Burnout at this stage often manifests as anxiety intertwined with responsibility. It is less about survival and more about sustaining performance without a safety net.
By five to ten years beyond residency, many gynaecologists have established reputations, leadership roles, and stable clinical practices. Technical confidence increases, but
cumulative stress may deepen.
The surgical dimension of the specialty contributes significantly. A systematic review by Galaiya and colleagues identified long working hours, medico-legal concerns, and work-life imbalance as major contributors to burnout in surgeons. These findings align closely with the realities of obstetrics and Gynaecology, where emergency procedures and high-risk surgeries are routine.
At this stage, burnout often transforms into moral distress. Physicians may feel constrained by systemic limitations that prevent ideal patient care. Resource shortages, staffing challenges, and administrative demands generate ethical tension.
The work of Afulani and colleagues studying maternity providers in rural Kenya demonstrated that both psychological and physiological stress indicators were associated with burnout. High patient load, poor working conditions, and limited institutional support were significant situational predictors. Although conducted in a resource-limited context, the broader message is universal: burnout is shaped not only by individual resilience but by systemic structures.
Mid-career burnout is frequently quieter than in residency. It may present as chronic fatigue, cynicism, emotional withdrawal, or diminished enthusiasm. It is less dramatic but more persistent.
The distinction between burnout and depression is clinically important but practically intertwined. Rath and colleagues demonstrated strong correlations between burnout and depressive symptoms among gynaecologic oncologists. Prolonged occupational exhaustion may increase vulnerability to major depressive episodes.
Burnout is occupationally triggered, but when left unaddressed, it can extend beyond professional boundaries. Sleep disturbances, irritability, and emotional blunting affect personal relationships and overall wellbeing.
Recognizing early signs is essential. Burnout is not weakness. It is a predictable response to sustained imbalance between demands and resources.
Burnout persists because it is embedded within healthcare systems. Obstetrics and Gynaecology operate under constant urgency. The expectation of availability is culturally ingrained. Stigma around seeking mental health support remains a barrier.
Evidence suggests that institutional structures significantly influence burnout risk.
Environments that encourage mentorship, allow reflective practice, and promote balanced scheduling tend to demonstrate lower distress levels. Conversely, systems characterized by excessive workload, limited
autonomy, and inadequate support foster higher burnout rates.
The data from Afulani and colleagues reinforce the role of situational predictors. Structural conditions matter. Burnout cannot be addressed solely through individual coping strategies; organizational accountability is critical.
The Human Cost and Professional Imperative
Burnout affects not only physicians but also patient safety and healthcare systems. Emotional exhaustion impairs concentration and communication. Depersonalization diminishes therapeutic connection. Reduced personal accomplishment erodes motivation.
In Obstetrics and Gynaecology, where clinical decisions can carry life-altering consequences, provider well-being is directly linked to maternal and neonatal outcomes. Protecting the mental health of Gynaecologists is therefore not a luxury but a professional imperative.
Across residency, early practice, and mid-career stages, burnout evolves but remains recognizable. It begins as fire, transitions into tension, and may settle into chronic heaviness if unattended.
Burnout in Obstetrics and Gynaecology is real, measurable, and deeply human. It is shaped by long hours, emotional intensity, systemic pressures, and the profound responsibility of bringing life safely into the world. Yet awareness offers hope. When the profession acknowledges the silent cracks beneath the white coat, it creates space for repair. Sustainable care for women begins with sustainable care for those who provide it.
“Strength in medicine is not measured by silent endurance, but by the courage to recognize when healing must begin within.”
Stress is a major contributor to chronic illness and significantly
affects Obstetricians and Gynaecologists due to prolonged and erratic working hours, administrative workload, and high-risk clinical responsibilities. Across residency, early practice, and mid-career stages, sustained occupational stress may lead to burnout characterized by emotional exhaustion, anxiety, depression, depersonalization, and reduced professional accomplishment, potentially impacting physician well-being and patient care. Effective management requires individual coping strategies along with institutional support, including mental health awareness, confidential counselling services, peer support, and structured assistance following adverse clinical outcomes. Incorporating resilience and coping training in the medical curriculum and promoting systemic reforms that support balanced work schedules are essential to reduce stigma, enhance physician well-being, and ensure safe, high-quality patient care.
1. Kaur B: Workplace Stress in Obstetricians - Gynaecologist in India: Open Access Journal of Gynaecology; 2019, 4 (3), DOI: 10.23880 / oaig 16000181
2. Nishant Das et al: Suicide among Healthcare Professionals - An Indian Perspective; Healthcare; 2022 Feb 11; 10(2):354. doi: 10.3390/ healthcare10020354
3. Shikha Madan et al: What are Primary Stressors faced by Ob Gyn Residents; Indian Journal of Obstetrics & Gynaecology Research;2024, 11 (3), 558 - 562
4. Dushad Ram et al: Mental Health Challenges among Doctors in India: a Scoping Review of Existing Research; Indian Journal of Psychological Medicine; July 2025, https://doi.org/10.1177/02537176251349766
5. Rath KS, Huffman LB, Phillips GS, Carpenter KM, Fowler JM. Burnout and associated factors among members of the Society of Gynecologic Oncology. American Journal of Obstetrics and Gynecology. 2015;213(6):824.e1–824.e9.
6. Afulani PA, Ongeri L, Kinyua J, Temmerman M, Mendes WB, Weiss SJ. Psychological and physiological stress and burnout among maternity providers in a rural county in Kenya: individual and situational predictors. BMC Public Health. 2021;21:453.
7. Galaiya R, Kinross J, Arulampalam T. Factors associated with burnout syndrome in surgeons: a systematic review. Annals of the Royal College of Surgeons of England. 2020;102(6):401–407.

Dr. Manish Machave
President POGS 2025-26
Ex-Chairman Ethics and Medicolegal Committee FOGSI
TINTRODUCTION Sanhita, Bharatiya Nyay Sanhita, and Bharatiya Sakshya Adhiniyam—were passed with a few revisions and modifications in 2023, were published on December 25, 2023, in the Official Gazette. It has been enforced on July 1, 2024. There have been claims of a rise in unresolved cases, low conviction rates, and inadequate use of technology.
he three criminal laws—Bharatiya Nagarik Suraksha
As the Indian criminal justice system has struggled to keep up with technological advancements, according to lawmakers, it is important to modernise the criminal system. These three pieces of legislation purport to “decolonize” British criminal laws.
The Oxford Dictionary defines negligence as a lack of proper care or inadequate attention. Legally, medical negligence is defined as a duty
of care, breach of such duty and consequential harm. The patient may suffer financial losses, health consequences, worsening of their condition, trauma, irreversible impairment that lasts for the rest of their life, etc.
In general terms, it is either an act of commission or omission.
1. Duty of Care: The healthcare provider owes a legal duty to care for the patient.
2. Breach of Duty: The healthcare provider fails to meet the required standard of care, disregarding the patient’s needs.
3. Injury: The patient suffers injury or harm due to the breach of duty.
4. Causation: A clear link must exist between the breach of duty and the injury sustained by the patient…..causa causans.
To establish medical negligence all these essentials have to be proven in a court of law by the complainant.
• In the Landmark case Jacob Mathew v. State of Punjab and Another, The Supreme Court of India defined negligence as: “Negligence is defined as when a defendant fails to use ordinary care or skill towards a person to whom he/she owes a duty, resulting in the plaintiff suffering damage to his person or property”. The Court also distinguished between medical negligence and criminal negligence, noting that not all unfavourable outcomes constitute criminal negligence.
• In the case of Bolam v. Friern Hospital Management
Committee, The court held that negligence occurs when a competent professional fails to meet the standard expected of them. However, if a mistake could be made by a reasonable person exercising ordinary caution, it may not constitute negligence.
• The SC of India, in the case of Kusum Sharma v. Batra Hospital and Medical Research, held that being negligent means either failing to do something that a reasonable man would do or doing something that a prudent & reasonable man would not do, guided by those considerations that commonly direct the conduct of human affairs.
1. Indian Penal Code, 1860 (IPC)
Section 304A: Causing death by negligence
Whoever causes the death of any person by doing any rash or negligent act not amounting to culpable homicide, shall be punished with imprisonment which may extend to 2 years, or with a fine, or both.
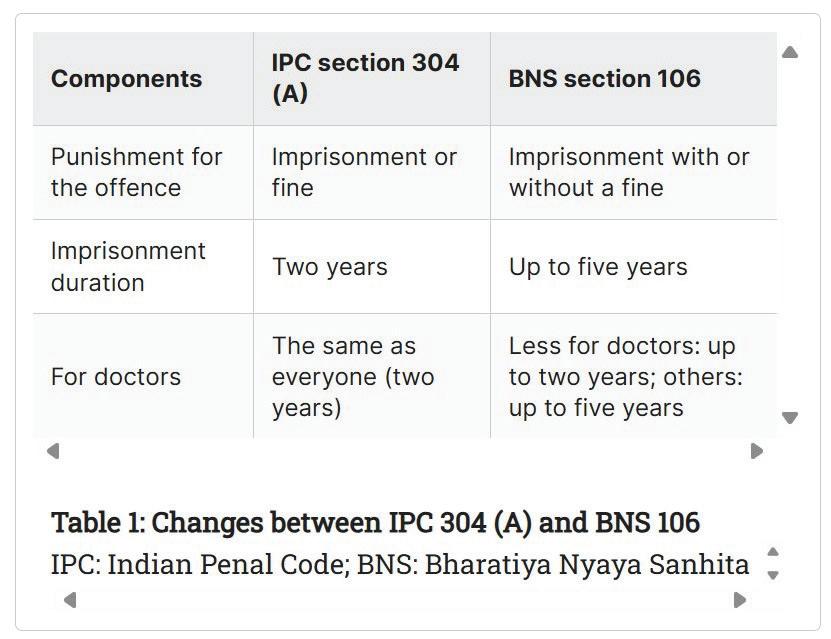
Under tort law, patients can claim compensation for harm caused by negligence. This encompasses civil wrongs. Civil negligence is a form of negligence in which a patient brings an action for damages in a Civil Court against a medical attendant, who owed a duty of care if the patient had suffered injury in consequence of negligence or unskilled treatment.
3. Consumer Protection Act, 1986
Medical services fall under the Consumer Protection Act, enabling patients to seek redress for deficiencies in service OR unfair trade practices through the District/State/National Consumer Disputes Redressal Commission (CDRC).
4. Code of Medical Ethics, 2002: The Indian Medical Council (IMC) Regulations, 2002,
Samhita, 2023
originated in accordance with the IMC Act, 1956, regulate disciplinary action taken against medical practitioners. Healthcare professionals who engage in improper conduct (professional misconduct) may face disciplinary action from the IMC and State Medical Councils
Section 106(1) CAUSING
BY NEGLIGENCE
Whoever causes death of any person by doing any rash or negligent act not amounting to culpable homicide, shall be punished with imprisonment of either description for a term which may extend to five years, and shall also be liable to fine; and if such act is done by a registered medical practitioner while performing medical procedure, he shall be punished with imprisonment of either description for a term which may extend to two years, and shall also be liable to fine.
For the purposes of this subsection, “registered medical practitioner” means a medical practitioner who possesses any medical qualification recognised under the National Medical Commission Act, 2019 and whose name has been entered in the National Medical Register or a State Medical Register under that Act.
COMPARISON of The Indian Penal Code, 1860(IPC) and The Bharatiya Nyaya Samhita, 2023 Under Section 304A of IPC, if reckless or careless behaviour results in
another person’s death, but the act does not amount to culpable homicide, the person responsible can be imprisoned for up to two years, fined, or both.
However, under Section 106 of the BNS, the general punishment is up to five years of imprisonment and a fine. But if the negligent act is committed by a “registered medical practitioner” while performing a medical procedure, the punishment is comparatively less, with imprisonment of up to two years and shall also be liable to a fine.
Thus, under BNS, if found guilty, imprisonment could be mandatory.
The implementation of BNS is expected to significantly impact medical practice in India. These new laws aim to reduce incidents of negligence. They promise better patient protection and trust in the healthcare system.
However, balancing regulations with practical realities remains a challenge. Continuous debates between healthcare providers, regulators, and patients are crucial to refine these laws and ensure they achieve the intended outcomes without hampering medical practice.
Both patients & healthcare providers face distinct challenges within the legal framework:
Patients: often bear the burden of proof in legal cases and a lack of awareness about their legal rights can discourage them from pursuing compensation.
Doctors: The risk of litigation leads to a defensive approach to practice, which can affect their decisions.
The Bharatiya Nyaya Sanhita (BNS) changes medical negligence laws in significant ways that improve patient safety and responsibility. These improvements provide difficulties for healthcare professionals. Clear guidelines and continuous education are necessary to enable the unexpected finding of a balance between regulation and practical realities in order to ensure effective implementation. To create a fair and efficient system that serves patients and medical professionals the same, it will be essential to address issues and improve the laws.
The Bharatiya Nyaya Sanhita (BNS) introduces significant changes to medical negligence laws aimed at improving patient safety and accountability. While these changes present challenges for healthcare professionals, clear guidelines, continuous education, and ongoing dialogue are necessary to strike a balance between regulation and practical realities. Addressing these concerns will be essential to creating a fair and effective system that serves both patients and healthcare providers. Medical Negligence and The
1. Oxford University Press. (n.d.). Negligence. In Oxford Learner’s Dictionaries. https://www.oxfordlearnersdictionaries.com/ definition/american_english/negligence
2. (2005) 6 SCC 1, Appeal (crl.) 144-145 of 2004
3. [1957] 1 WLR 582
4. (2010) 3 SCC 480
5. Section 26 of BNS: Act not intended to cause death, done by consent in good faith for person’s benefit.
6. The New Indian Express. (2024, July 2). Doctor up in arms as laws dealing with negligence suggest jail term, fine. The New Indian Express. Medical

We the team Young Talent Promotion Committee FOGSI take the proud privilege to congratulate our esteemed Chairperson Dr. Rohan Palshetkar for having been installed as the Youngest secretary of the Association of Maharashtra ObGyn Societies at the 39th Annual Conference of AMOGS held at Mumbai.
The dedication, resilience and the willingness to serve that so well describes Dr. Rohan Palshetkar is a living example for all the youngsters to follow.
With devotion beyond compare and talent galore, we wish our beloved chairperson a legendary tenure and hoping that such superstars of the NextGen be pathfinders of many across the globe.
Team Fogsi Young Talent Promotion Committee
Alarge longitudinal study, published in JAMA Cardiology, has demonstrated
that women experiencing premature menopause before the age of 40 have an increased lifetime risk of developing coronary heart disease (CHD) compared to those with later onset menopause. The analysis included postmenopausal women from longterm cohort studies, followed over several decades, during which numerous CHD events were recorded. Even after adjusting for traditional cardiovascular risk factors including smoking, obesity, hypertension, and diabetes, premature menopause remained independently associated with increased CHD risk; notably, it was also more prevalent among Black women. The underlying mechanisms are thought to be related to early estrogen deficiency, which contributes to adverse metabolic and vascular changes such as dyslipidemia, elevated blood pressure, central fat redistribution, and impaired glucose metabolism, and increased arterial stiffness, thereby accelerating atherosclerotic processes. These findings highlight the importance of incorporating menopausal history into cardiovascular risk assessment, recognizing premature menopause as an early clinical marker of increased long-term risk, and implementing timely preventive strategies. The study further underscores the need for a multidisciplinary approach, as menopause has systemic implications beyond Gynaecological health, particularly in influencing cardiovascular outcomes.
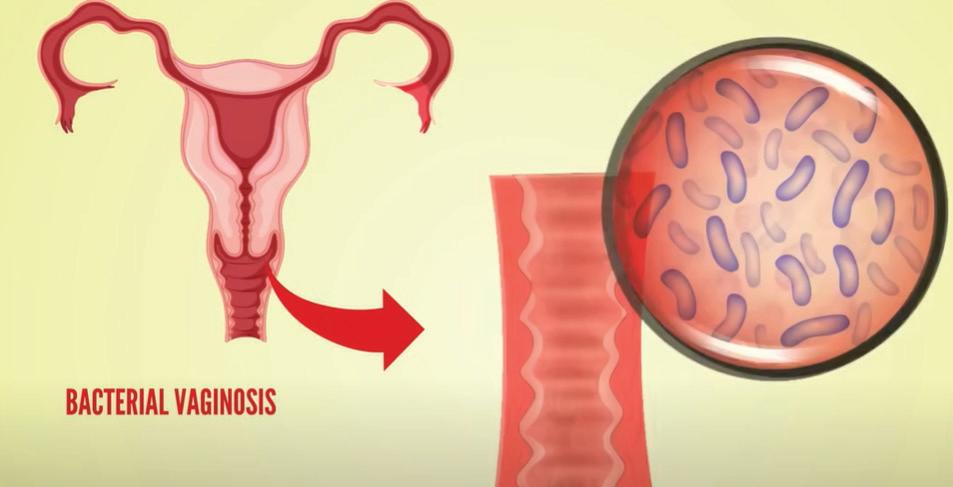
Arecent randomized clinical trial has demonstrated that multi-strain
probiotic therapy may offer a promising strategy for reducing recurrence of bacterial vaginosis (BV), a common condition affecting a significant proportion of women globally. The study, published in Cell Host & Microbe, evaluated a live biotherapeutic product containing multiple strains of Lactobacillus crispatus, aimed at restoring the vaginal microbiome following standard antibiotic treatment. BV is characterized by
disruption of the normal vaginal flora and is associated with symptoms such as discharge, odor, and irritation, as well as increased risk of adverse reproductive outcomes including preterm birth and susceptibility to infections such as HIV. While conventional antibiotic therapy provides short-term symptom relief, recurrence rates remain high due to inadequate restoration of protective lactobacilli. In this trial, participants received antibiotics followed by varying regimens of placebo or multi-strain probiotic therapy over a short duration, and microbiome assessment was conducted using genetic sequencing techniques. The findings demonstrated successful colonization of protective L. crispatus in a substantial proportion of participants within the initial weeks, with persistence observed in a subset during extended follow-up. Importantly, the presence of these beneficial bacteria was associated with a reduced likelihood of BV recurrence during the study period. These results highlight the potential of microbiome-directed therapies in addressing the limitations of conventional treatment by promoting sustained restoration of vaginal microbial balance. Further studies are underway to optimize dosing strategies and evaluate long-term clinical efficacy, with the aim of advancing this approach toward larger-scale trials and potential regulatory approval.



Credits# with
3-Nights, 4-Days Program Highlights* 2 Half-days
Lectures by DHA Certified Faculty 2 Half-days
Observership in Aesthetic Procedures with upto 6 DHA@CME Credits#
Package to be announced shortly
Inclusions:
* 3-Nights 4-Days Stay, in a 4-STAR Hotel with breakfast and dinner, Lunch at Academy/Aesthetic Centre, To and fro - Hotel to Academy/Aesthetic Centre SIC◊
Exclusions:
Air fare to Dubai and back , airport transfer, Sight seeing etc.
@ DHA- Dubai Health Authority
# Proposed s/t confirmation
◊ SIC- Seat in Coach
Interested Drs kindly call for further details: +91