The Aesthticians Journal Digital August'2025 issue
Efficacy and Safety of Picosecond Laser in the Management of Uneven Skin Tone in Indian Skin Types Treatment of Nevus Spilus with Q-Switched Nd:YAG Laser (Finebeam)
Lip Aesthetics and Rejuvenation with Dermal Fillers Expert Opinion on IV Infusion Therapy Safety in Dermatology & Aesthetics
Restoration of the Forehead Lines with Botulinum Toxin Type A
EXECUTIVE EDITOR & PUBLISHER
Dom Daniel
CORPORATE OFFICE
22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.
EMAIL: theaestheticiansjournalindia@gmail.com
Website: theaestheticiansjournal.com
Printed, Published, Edited and Owned by Dom Daniel
Printed at Swastik Printer, Gala No.9 & 10, Vishal Industrial Estate, Bhandup (West), Mumbai- 400078. Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“The Aestheticians Journal” takes no responsibility for unsolicited photographs or material
ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of August -2025
Cover Model: Paayel Gosh
Photography: Niloy Mukherjee
Make up & Hair: Rajendra Pardesi, Jyoti Sikder
Stylist: Tasneem Karachiwala
Advancing Aesthetic Practice: Expert Insights and Clinical Pearls
We are delighted to present the latest edition of The Aestheticians Journal, where science meets aesthetics through expert insights, clinical precision, and innovative protocols.
This issue brings together a dynamic collection of articles addressing both foundational and advanced concepts in aesthetic dermatology. From enhancing lip aesthetics and perioral rejuvenation with dermal fillers, to the aesthetic restoration of forehead lines using Botulinum Toxin Type A, our contributors delve into techniques that blend anatomical understanding with artistic finesse.
In our continued effort to foster evidence-based practice, we present a critical expert opinion on the safety and scope of IV infusion therapy in dermatology and aesthetics—a topic of increasing interest and importance in current practice.
On the technological front, the issue explores the use of Q-switched Nd:YAG laser for the treatment of nevus spilus, highlighting practical experience in targeting pigmented lesions. Additionally, for our readers managing hair loss, we go beyond monotherapy to introduce a multimodal approach for hair regrowth in androgenetic alopecia, integrating multiple therapeutic strategies for enhanced clinical outcomes.
This issue also examines the efficacy and safety of picosecond lasers in addressing uneven skin tone in Indian skin types, offering practical guidance on delivering results in melanin-rich skin.
This curated content aims to keep you at the forefront of dermatological advancements, offering both practical guidance and thought-provoking insights.
Efficacy and Safety of Picosecond Laser in the Management of Uneven Skin Tone in Indian Skin Types
Dr. Monisha
Aravind
MD (Dermatology)
Senior Consultant and Aesthetic
Armoraa Skin Solutions
Chennai, Tamil Nadu
Introduction
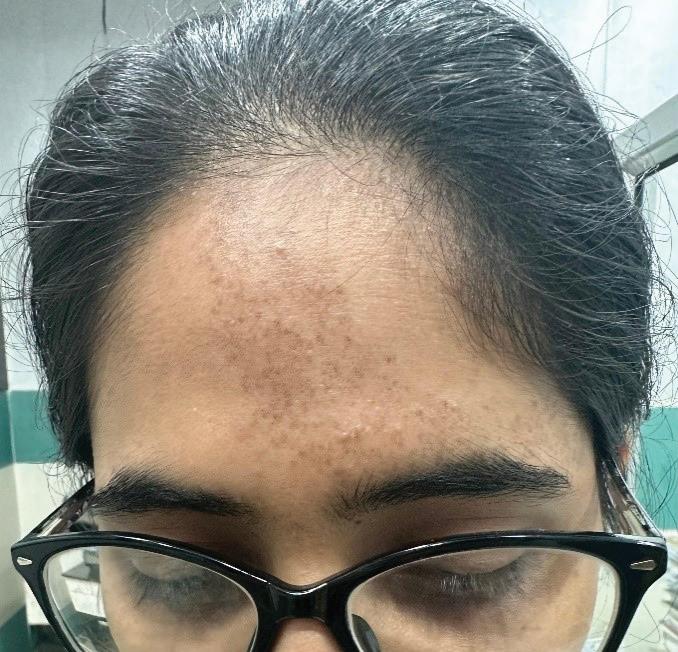
Uneven skin tone is a common dermatological concern among individuals with Indian skin types, particularly in the South Indian population, where increased melanin activity often results in more pronounced pigmentation over the forehead and perioral regions. This form of dyschromia, encompassing a spectrum of pigmentary disorders, necessitates treatment modalities that are both safe and efficacious for melanin-rich skin, with particular attention to minimizing the risk of post-inflammatory hyperpigmentation (PIH).
Cutaneous pigmentation is among the most visibly diverse human phenotypes, and disorders such as solar lentigines, PIH, melasma, and infraorbital hypermelanosis (dark circles) are frequently observed, especially in populations with darker phototypes. Individuals of Asian and Indian descent are particularly predisposed to these conditions due to intrinsic melanogenic tendencies and heightened responsiveness
Dermatologist
to environmental triggers. Ultraviolet (UV) radiation is a well-established exacerbating factor, known to stimulate melanocyte activity and worsen existing pigmentation. As a result, photoprotection remains a fundamental pillar in both the prevention and management of pigmentation disorders. Contemporary dermatologic approaches incorporate a range of interventions—including topical depigmenting agents, chemical peels, laser therapies, and systemic treatments— tailored to the unique needs of darker skin types. This review aims to consolidate current understanding of the pathophysiology, molecular mechanisms, and therapeutic strategies for pigmentary disorders, with a particular emphasis on their presentation and management within the Indian population.1
Technology Overview
The picosecond laser, a type of Q-switched laser, emits ultrashort pulses in the picosecond range—comparable in speed
Efficacy
to the trajectory of a bullet— allowing it to fragment pigment into minute, sand-like particles. Unlike traditional nanosecond lasers that rely heavily on photothermal effects, the picosecond laser primarily utilizes a photoacoustic mechanism of action. This minimizes thermal damage to surrounding tissues, making it particularly suitable for treating pigmentation disorders in Fitzpatrick skin types IV–VI.2,3
The picosecond laser exerts its clinical effects through two primary mechanisms of action: photo-thermo-mechanical ..... disruption (PTMD) and laserinduced optical breakdown (LIOB). In non-fractionated delivery, PTMD is the dominant mechanism, wherein ultrashort picosecond pulses induce rapid thermal expansion within targeted chromophores, generating intense acoustic shock waves. These shock waves create tensile stresses that surpass the mechanical rupture threshold of the chromophore, leading to precise photomechanical fragmentation with minimal collateral damage. This mechanism is particularly effective when the laser pulse duration is shorter than the tissue’s stress relaxation time, thereby maximizing mechanical disruption while minimizing thermal diffusion to surrounding tissues. In fractional mode, enhanced by delivery systems such as diffractive lens arrays (DLA), microlens arrays (MLA), and holographic beam splitters, the laser beam is subdivided into a matrix of high-fluence microspots interspersed with untreated skin. At these focal points, LIOB occurs in the
epidermis, where localized high energy induces plasma formation and vacuolization without breaching the skin barrier, while laser-induced cavitation (LIC) occurs in the superficial dermis, promoting controlled dermal injury. These subclinical microinjuries serve as a stimulus for collagen remodeling, elastin regeneration, and epidermal turnover, ultimately leading to clinical improvements in skin texture, pigmentation, scars, and other signs of photoaging.4,5
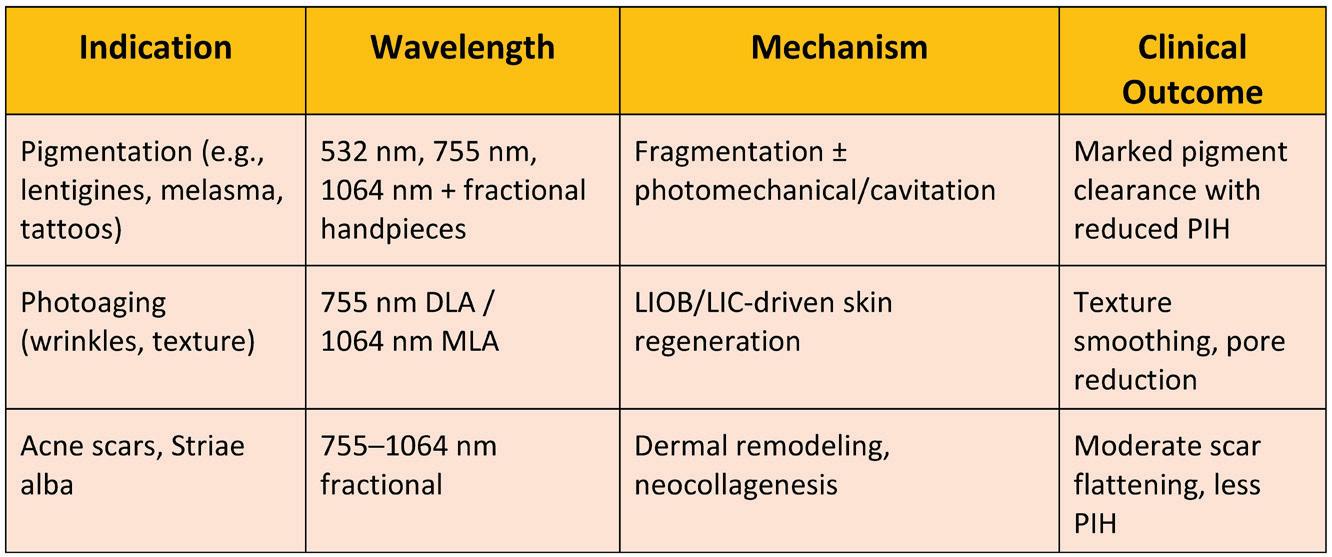
Clinical evidence confirms that fractional picosecond lasers effectively address multiple dermatologic concerns with minimal downtime and low incidence of post-inflammatory hyperpigmentation (PIH). Documented benefits include:4
• Pigmented lesions: Effective clearance of benign hyperpigmented lesions—such as solar lentigines, freckling, caféau-lait macules, melasma, postinflammatory hyperpigmentation, Nevus of Ota, and tattoo pigments—thanks to selective photomechanical fragmentation with reduced thermal side effects.4
• Photoaging manifestations: Significant improvements in skin texture, dyspigmentation, fine lines, wrinkles, and pore size following treatment with 755 nm or 1064 nm fractional systems. Patient-reported outcomes typically include noticeably smoother and more even-toned skin, with only transient erythema and a low incidence of postinflammatory hyperpigmentation (PIH).4
• Atrophic acne scars & striae: Multiple sessions have led to moderate to marked improvements in scar volume
and texture, with lower pain and PIH rates compared to ablative or non-fractional lasers.6
Mechanistically, LIOB in the epidermis creates controlled vacuolation leading to epidermal turnover, while LIC in the dermis generates microcavitation and stimulates collagen/elastin regeneration—a phenomenon supported by histopathology and reflectance confocal imaging Emerging in vitro data using melanocytecontaining 3D skin models highlight upregulation of tissue remodeling markers—such as matrix metalloproteinases, heatshock proteins, and collagen synthesis—following 1064 nm fractional picosecond irradiation; when combined with posttreatment dexpanthenol, dermal repair is accelerated.3
Comparative studies highlight distinctive advantages of picosecond technology.3
• More effective pigment clearance with fewer sessions and reduced risk of PIH versus ablative or nanosecond lasers.
• Better safety and comparable efficacy versus fractional CO₂, erbium, and 1550 nm lasers in treating pigmentation, scars, and striae—often with less downtime and discomfort.3
Safety profile is favorable, particularly in darker phototypes, with common side effects limited to mild erythema and edema. PIH is rare when conservative fluences and proper intervals are used.3
Clinical Application
In clinical dermatology, picosecond laser treatment has proven effective in targeting uneven pigmentation, leading to
a more uniform and radiant skin tone. Commonly treated areas such as the forehead and perioral regions exhibit progressive pigment clearance with minimal discomfort. The procedure is associated with negligible downtime and a very low risk of post-inflammatory hyperpigmentation (PIH), making it especially suitable for patients with darker skin types. Its favorable safety profile encourages patient compliance, as most individuals can return to their daily routines immediately following treatment, provided they adhere to adequate photoprotection measures. This balance of efficacy and safety has made picosecond lasers a preferred choice in pigment correction therapies.
Table 1: Clinical Highlights3
Treatment Protocol and Adjunctive Care
A standard clinical approach to picosecond laser therapy for pigmentation involves a structured, multi-phase regimen designed to maximize efficacy and ensure sustained results:
• Initial Phase: Patients undergo four treatment sessions spaced two weeks apart, targeting melanin-rich areas and initiating gradual pigment fragmentation.
• Consolidation Phase: Two further sessions at one-month intervals help reinforce pigment clearance and stabilize results.
• Maintenance Phase: To prevent recurrence and support longterm improvement, one session every three months for up to a year is recommended, especially in recurrent or dermal pigmentation like melasma.7
Comprehensive Skincare Integration
Laser outcomes are significantly enhanced when combined with a tailored skincare routine:6,7
• Photoprotection: Broad-spectrum sunscreens (SPF 50+, with PA+++) are essential to prevent UV-induced pigmentation rebound and reduce melanocyte stimulation post-treatment. Daily reapplication is advised.8
• Topical agents: Use of pigment-regulating and skin-repairing ingredients enhances clearance and reduces the risk of postinflammatory hyperpigmentation (PIH):
o Niacinamide (2–5%): Anti-inflammatory, reduces melanin transfer.
o Tranexamic acid (2–5%): Inhibits melanin synthesis and has
shown synergistic effects with laser therapy, especially in melasma.7,8,9
• Oral antioxidants: In selected patients, supplementation with agents like Polypodium leucotomos, vitamin C, glutathione, or proanthocyanidins can support skin defense against oxidative stress and UV-induced pigmentation, especially in photodamaged or high-risk individuals.7,8
A holistic protocol combining precision laser therapy with a scientifically grounded topical and systemic regimen offers superior, sustained pigment correction with a high safety profile.
Discussion
Picosecond lasers offer a refined and minimally invasive approach to dermatologic therapy, characterized by their ultra-short pulse durations and reliance on the mechanism of laser-induced optical breakdown (LIOB). This mechanism generates intraepidermal and intradermal vacuoles that initiate dermal remodeling, promoting neocollagenesis and elastin fiber regeneration. Compared to traditional Q-switched lasers, picosecond devices demonstrate improved clinical outcomes with reduced thermal diffusion, resulting in fewer adverse effects, lower treatment-associated discomfort, and shorter recovery times. Beyond their wellestablished role in managing pigmentary disorders, emerging evidence supports the utility of picosecond lasers in nonpigmentary applications, including acne scarring,
Efficacy and Safety of Picosecond Laser in the Management of Uneven Skin Tone in Indian Skin Types
photoaging, and general skin rejuvenation. Studies using wavelengths in the 700–1,064 nm range have shown that LIOB formation within the dermis can effectively stimulate structural remodeling, thereby improving skin texture and elasticity. These devices operate on the principle of selective photothermolysis but with enhanced precision due to the rapid delivery of energy, which confines the photomechanical effect to the target chromophores while
References
1. Nouveau, Stephanie et al. “Skin Hyperpigmentation in Indian Population: Insights and Best Practice.” Indian journal of dermatology vol. 61,5 (2016): 487-95. doi:10.4103/0019-5154.190103
2. Kim BJ, Kim SH, Cha HG, Park ES. Combination treatment for post-traumatic facial scars: 1,064-nm Nd:YAG picosecond laser with micro-lens array after fractional ablative CO<sub>2</sub> laser. Medical Lasers 2022;11:92-96. https://doi. org/10.25289/ML.2022.11.2.92
3. Zhou, Yanjun et al. “An update on fractional picosecond laser treatment: histology and clinical applications.” Lasers in medical science vol. 38,1 45. 20 Jan. 2023, doi:10.1007/s10103-02203704-y
4. Berkala Ilmz Kesehatan Kulit dan Kelamin – Periodical of Dermatology and Venereology Vol. 35 / No. 2 / April 2023
sparing adjacent tissues. As a result, picosecond lasers not only exhibit superior efficacy in pigment clearance but also deliver regenerative benefits with a high safety margin, making them an advanced tool in aesthetic and therapeutic dermatology.10,11
Conclusion
In conclusion, while picosecond laser therapy represents a highly effective tool for treating uneven skin tone in Indian and other melanin-rich skin types, its optimal results are achieved when integrated into a comprehensive, multimodal treatment strategy. This approach not only enhances pigment clearance but also improves skin texture, patient satisfaction, and longterm outcomes—firmly establishing the picosecond laser as a key component in the aesthetic management of pigmentary disorders in darker skin tones.
5. Kroma-Szal A, Pawlaczyk M, Urbańska M, Cieślawska J, Sobkowska D, Pordąb I, Gornowicz-Porowska J. Medical Applications of Picosecond Lasers for Removal of NonTattoo Skin Lesions—A Comprehensive Review. Applied Sciences. 2025; 15(9):4719. https://doi.org/10.3390/ app15094719
6. Li J, Duan F, Kuang J. Fractional picosecond laser for atrophic acne scars: A meta-analysis. J Cosmet Dermatol. 2023; 22: 2205-2217. doi:10.1111/jocd.15862
7. Jiryis B, Toledano O, Avitan-Hersh E, Khamaysi Z. Management of Melasma: Laser and Other Therapies—Review Study. Journal of Clinical Medicine. 2024; 13(5):1468. https://doi.org/10.3390/ jcm13051468
8. Cassiano, D.P., Espósito, A.C.C., da Silva, C.N. et al. Update on Melasma—Part II: Treatment. Dermatol Ther (Heidelb)
9. Park SJ, Park JW, Seo SJ, Park KY. Evaluating the tolerance and efficacy of laser-assisted delivery of tranexamic acid, niacinamide, and kojic acid for melasma: A single center, prospective, split-face trial. Dermatologic Therapy. 2022;35(3):e15287. doi:10.1111/ dth.15287
10. Nguyen, Lynhda et al. “Pikosekundenlaser in der Dermatologie” [Picosecond lasers in dermatology]. Dermatologie (Heidelberg, Germany) vol. 74,6 (2023): 440-447. doi:10.1007/ s00105-023-05144-3
11. Hong JK, Seok J, Choi SY, Li K, Kim BJ, Yoo KH. Review of picosecond lasers in nonpigmented disorders. Med Lasers 2022;11:125-133. https://doi. org/10.25289/ML.2022.11.3.125 Efficacy and
Treatment of Nevus Spilus with Q-Switched Nd:YAG Laser (Finebeam)
Dr. Megha Singh Pundir
MD (Dermatology)
Aesthetic Laser Specialist
Derm Elixir Clinic
Varanasi, Uttar Pradesh
Introduction
Nevus spilus, also known as speckled lentiginous nevus,
presents as a light brown (caféau-lait–like) patch with overlying darker macules or papules. While benign, these lesions can be cosmetically distressing, especially when located on visible areas such as the face, neck, or arms.
The Q-switched Nd:YAG laser, particularly with platforms like Finebeam, offers a highly effective and minimally invasive solution by targeting pigmentation with precision and minimal damage to surrounding skin.
Understanding Nevus Spilus Nevus spilus typically manifests in early life and consists of two pigmentary components:
• A tan or light brown background macule.
• Overlying darker speckled macules or small nevi.
Though medically harmless, its appearance can cause psychological or aesthetic concern in patients.
Why Q-Switched Nd:YAG (Finebeam)?
The Q-switched Nd:YAG laser (1064 nm) works by emitting ultra-short, high-intensity pulses that selectively target melanin in both the epidermis and dermis. The Finebeam platform enhances safety and efficacy— particularly in darker skin tones (Fitzpatrick types III–V)—by delivering energy precisely while minimizing thermal damage.
Key Benefits:
• High specificity for melanin
• Minimal epidermal disruption
• Safe for darker skin types
• Quick recovery and minimal downtime
Figure 1: Q-switched Nd:YAG laser
Procedure Protocol
Pre-treatment:
• Detailed clinical and dermoscopic evaluation.
• Informed consent and baseline photography.
Laser Parameters (customized per lesion depth and skin type):
• Wavelength: 1064 nm
• Spot size: 3–5 mm
• Fluence: 4.8–6 J/cm²
• Frequency: As per device setting
• Sessions: 5 sessions at 3-week intervals
Post-treatment Care:
• Use of broad-spectrum sunscreen (SPF 50+)
• Gentle cleansers and moisturizers.
• Avoidance of direct sun exposure and harsh skin treatments.
Clinical Outcome
Most patients observe the following improvements after a series of treatments:
• Gradual fading of the background pigmentation.
• Noticeable reduction in darker speckled macules.
• Enhanced skin texture and tone uniformity.
Typically, 70–80% clearance is achieved after 4–5 sessions, with minimal downtime and no scarring.
Before & After Summary
Visible improvement is typically seen by the fourth session with Q-switched Nd:YAG (Finebeam) laser.
There is significant reduction in pigmentation, leading to a more even skin tone and improved cosmetic appearance.
After 4 Sessions of Q-switched Nd:YAG (Finebeam) laser
After 4 Sessions of Q-switched Nd:YAG (Finebeam) laser
Conclusion
The Q-switched Nd:YAG (Finebeam) laser represents a safe, effective, and cosmetically rewarding modality for the treatment of nevus spilus. With proper patient selection, parameter settings, and post-care, excellent aesthetic results can be achieved with minimal risks.
Patient 1
Patient 2
Treatment of Nevus Spilus with Q-Switched Nd:YAG Laser (Finebeam)
Expert Opinion on IV Infusion Therapy Safety in Dermatology & Aesthetics
The recent IV therapy-related incident has indeed raised serious concerns around patient safety, clinical protocols, and the increasing commercialization of aesthetic procedures— particularly those involving IV drips.
As a practicing dermatologist with over 27 years of clinical and aesthetic experience and a network of 37+ clinics under the Sakhiya Skin Clinic brand, I am happy to share my views based on real-world practice and clinical responsibility.
1. What is your opinion of IV infusion therapies in dermatology?
IV infusion therapy can have a role in dermatology when used for specific clinical indications under strict medical supervision. However, its widespread use for "instant glow" or "energy boost" without medical necessity or evaluation is concerning.
2. What is your experience with IV infusion therapies, including safety and patient outcomes?
We have used IV glutathione, vitamin C, and nutritional drips in limited cases, mainly for pigmentary disorders or deficiency-related skin conditions. Outcomes are generally modest and vary by individual. Safety has been good in our setup because we follow stringent protocols and perform all infusions in a medical environment with crash cart readiness.
3. In your practice, do you recommend IV infusion therapy for any dermatological indications or just Aesthetics? If in clinical kindly specify which.
We recommend IV therapy only in:
• Refractory melasma
• Lichen planus pigmentosus (in specific settings)
• Nutritional deficiencies affecting skin and hair (e.g., B12, iron)
We do not recommend IV therapy just for aesthetic glow or social media trends
4. Based on your experience, which indications do you treat, and which IV formulations are most commonly requested?
Patients often request glutathione, vitamin C, B-complex, and amino acid infusions. Among these, glutathione for pigmentation is the most commonly asked. We strictly evaluate indication and fitness before considering it.
At Sakhiya Skin Clinic, we use IV glutathione therapy very selectively—and only after detailed patient assessment. We do not recommend it as a routine glow or fairness treatment.
We consider it in patients who had naturally normal skin tone in childhood but later developed pigmentation due to specific conditions such as:
• Outdoor tanning caused by professional exposure like sports, swimming, or field jobs
Dr. Jagdish Sakhiya MD
Founder & Chief Dermatologist
Sakhiya Skin Clinic – India’s No.1 Skin Clinic Chain, Surat
• Exposed-skin darkness in contrast to normal covered skin tone
In some cases, we may consider short-term IV therapy for special personal occasions such as weddings, media appearances, or matrimonial events—but only when all safety parameters are met and expectations are realistic.
5. What baseline evaluations, including necessary laboratory tests, must be performed before initiating aesthetic IV therapy?
Before IV infusions, we check:
• LFT
• RFT
• CBC
• G6PD (especially with high-dose vitamin C or glutathione)
• Allergy history
• BP & vitals monitoring on the day of infusion
• Serum lipase and amylase
6. Do you utilize a standard informed consent document before administering IV drip therapy in your practice?
Yes, we have a standard, written informed consent specific to IV therapy which includes potential risks, benefits, off-label disclaimers (especially for glutathione), and emergency contact backup.
7. Are there specific contraindications or patient conditions for which you avoid doing IV infusion therapies even if the patient asks for it?
We do not offer IV therapy to patients with:
• G6PD deficiency
• Liver or kidney dysfunction
• Pregnancy/lactation
• History of drug allergy or anaphylaxis
• Immunocompromised or severely ill patients
8. What are the risks associated with IV drips given by unauthorized Non-medico providers without proper medical supervision?
This is the most dangerous trend. IV infusions by non-medical, salon, or home-based providers without any medical degree or emergency setup can lead to:
• Sepsis
• Allergic shock
• Air embolism
• Death in extreme cases
Unfortunately, such practices are increasing due to influencer culture.
9. Have you encountered patients who have had a negative IV treatment experience from unauthorized providers and later came to you?
Yes, we’ve had patients come with rashes, fever, or panic symptoms after unsafe infusions from unauthorized setups. Most of them were unaware of the ingredients injected into their body.
10. How do you counsel patients who express interest in self-injecting aesthetic or vitamin therapies?
We strongly discourage self-injections. I explain to patients that IV therapy, even if vitamin-based, is not risk-free. The route of administration (intravenous) is sensitive and must never be taken casually.
11. What patient education or counselling do you provide before administering any aesthetic IV drips?
We explain:
• What is being injected
• What benefits are scientifically proven
• What are the risks
• That this is not a fairness treatment, and
. results may vary
• That it’s not a permanent glow solution and requires lifestyle improvement
12. What is your opinion on "feel good" party/ after party IV drips?
We do not endorse or offer these at Sakhiya Skin Clinic. Any IV drip given casually without clinical need is unethical. “Hangover” drips promoted as a wellness fix is unsafe commercialization of medicine.
13. In your opinion, what should be the safety protocols for using IV drips in aesthetic practice—or should it be stopped due to potential risks as seen in the recent high-profile case? They should not be banned entirely, but their use must be restricted to qualified dermatologists or physicians, in a clinical setting, and only after proper screening, documentation, and monitoring. Self-
promotion and off-label use must be regulated.
14. To what extent is social media marketing influencing the use of IV drips for aesthetic purposes?
It has a huge impact. Celebrities and influencers promote “beauty drips” without understanding the medical risks. This creates unrealistic expectations among young audiences and bypasses medical logic.
15. In your opinion, who should take responsibility in the case of an adverse event—the injector or the product company?
The injector holds primary responsibility, especially in off-label or elective treatments. However, product companies too must take responsibility if formulations are promoted as “wellness solutions” without proper safety data or clear usage protocols.
In conclusion, I strongly believe that we, as responsible medical professionals, must draw a clear line between evidence-based care and trend-driven experiments. IV infusion therapy is a medical procedure, not a beauty add-on. We must uphold this distinction to protect our patients and our profession.
Whole-Body Cryotherapy in Atopic Dermatitis: A NonPharmacologic Adjunct
Whole-body cryotherapy (WBC) is emerging as a promising nonpharmacologic adjunctive treatment for atopic dermatitis (AD), a chronic inflammatory skin condition affecting up to 10% of the global population. Despite progress in conventional therapies, many patients continue to experience pruritus, erythema, and disrupted sleep. Unlike localized cryotherapy, WBC involves full-body exposure to ultra-cold temperatures (–100 °C to –180 °C) for 2–3 minutes in a cryochamber, with proposed mechanisms including reduced peripheral nerve conduction velocity, suppression of acetylcholine synthesis, and downregulation of Th2 cytokines such as IL-4 and IL-5. Cold exposure may also enhance antioxidative capacity and modulate systemic inflammation. Early clinical reports suggest improvements in pruritus, SCORAD scores, transepidermal water loss (TEWL), and sleep quality, with minimal adverse effects such as transient xerosis and rare acral frostbite. Safety protocols including real-time monitoring and emergency stop features are recommended. WBC may be particularly beneficial for patients with mild-to-moderate AD who show incomplete response to standard treatments, reflecting growing interest in nonpharmacologic strategies within multidisciplinary care for chronic inflammatory skin diseases.
Advances in Laser Therapy for Acne Vulgaris: Emerging Modalities and Clinical Integration
Laser therapies are emerging as effective adjuncts in acne vulgaris (AV) management, targeting both inflammatory and noninflammatory lesions. Visible light lasers, including 532-nm KTP and 585/595-nm pulsed dye lasers (PDL), act on C. acnes porphyrins, inducing bacterial lysis through photodynamic activity. PDL additionally modulates inflammatory pathways by downregulating IL8 and enhancing TGF-β expression, though its use is limited in darker skin types due to the risk of post-inflammatory hyperpigmentation (PIH). The 1064-nm Nd:YAG laser provides deeper dermal penetration, targeting sebaceous glands and attenuating proinflammatory cytokines (TNF-α, IL-1), with demonstrated safety in Fitzpatrick skin types III–VI. Sequential PDL–Nd:YAG application may yield enhanced therapeutic outcomes. Mid-infrared lasers (1320–1540 nm) and the 1726-nm diode laser offer selective sebocyte photothermolysis via water-based thermal injury, with favorable clinical responses and minimal adverse effects. Fractional ablative CO₂ lasers (FACL) address both active acne and associated scarring through dermal remodeling, modulating pathways such as TGF-β, FOXO1, and PPAR-γ.While heterogeneity exists in current study designs, accumulating clinical evidence supports the integration of laser therapies as early-intervention, non-antibiotic treatment options, particularly in patients with suboptimal response to conventional modalities.
Enhancing Lip Aesthetics and Rejuvenation with Dermal Fillers
Dr. Gayatri Bharadwaj MBBS, DVD
Consultant
Dermatologist
Dr Gayatri's Skin Clinic, Mumbai
Vida Clinics, Goa
Abstract
Lip enhancement with dermal fillers is a widely sought aesthetic procedure for improving volume, contour, and hydration of the lips. This case report highlights the successful use of hyaluronic acid-based filler for lip rejuvenation in a patient seeking a more youthful and defined appearance. A marked improvement in lip volume, symmetry, and color tone was noted post-treatment, contributing to an overall refreshed look.
Introduction
The lips are a vital element of facial aesthetics, contributing significantly to expressions, symmetry, and a youthful appearance. With advancing age and exposure to environmental factors such as sunlight and pollutants, the lips often lose their natural volume, definition, and moisture. This transformation may also be accelerated by habits like smoking or genetic predisposition. As a result, lip augmentation has gained widespread popularity as a cosmetic intervention aimed at restoring or enhancing lip
contours. Among various methods, the use of dermal fillers—particularly hyaluronic acid (HA)-based formulations— has become the preferred choice due to their favorable safety profile, reversibility, and natural-looking outcomes. The perioral area, including the lips, often undergoes changes such as the flattening of the Cupid’s bow, development of vertical lines, and accentuation of the mentolabial fold. In genetically thin lips or those with acquired asymmetry, soft tissue augmentation offers a minimally invasive solution that yields gratifying aesthetic improvements. Temporary and permanent fillers have been used for lip enhancement, although long-term complications like granulomas are more commonly associated with permanent agents. Clinical experience and published evidence continue to affirm the effectiveness and safety of HA fillers in aesthetic medicine. The ever-growing demand for non-surgical rejuvenation has positioned lip volumization and perioral enhancement among the most requested procedures
in cosmetic dermatology. However, achieving optimal results depends on selecting the appropriate HA filler tailored to individual patient needs and anatomical considerations. Key parameters influencing filler performance include hyaluronic acid concentration, particle size, crosslinking technology, extrusion force, elasticity (G'), viscosity (G"), and cohesiveness. These properties directly affect the filler’s behavior in tissue, its longevity, and the final aesthetic outcome. A comprehensive understanding of these variables enables clinicians to make informed decisions, ensuring both efficacy and patient satisfaction in lip and perioral rejuvenation treatments.1,2,3
In this case, we present a successful aesthetic outcome following the use of hyaluronic acid-based dermal fillers for lip enhancement and perioral rejuvenation. The patient underwent a minimally invasive procedure aimed at restoring lip volume, redefining contours and improving overall harmony of the lower facial region. The treatment resulted in excellent aesthetic improvement with enhanced lip fullness, hydration, and definition, contributing to a more youthful and balanced facial appearance. This case highlights the efficacy and safety of dermal fillers in achieving natural-looking lip rejuvenation with high patient satisfaction.
Case Presentation
A 28-year-old female patient presented with aesthetic concerns regarding her lips, specifically describing them as dull, dehydrated and asymmetrical. She expressed dissatisfaction with the overall
appearance of her lips, noting a gradual loss of volume and definition over time, especially in the upper lip. Upon clinical examination, the lips appeared thin and lacked contour, with diminished vermilion border definition and a flattened Cupid’s bow. The upper-tolower lip ratio was imbalanced, and the texture appeared dry, contributing to an overall aged and tired appearance. The patient’s primary goal was to achieve subtle, naturallooking enhancement, focusing on improved hydration, symmetry and contour, without the exaggerated fullness often associated with lip augmentation. She was particularly keen on maintaining facial harmony and avoiding an overfilled or artificial appearance. A hyaluronic acid-based dermal filler was chosen to restore volume, improve definition, and rejuvenate the perioral area while preserving a soft, natural outcome.
Treatment
Following a thorough clinical assessment and discussion of the patient’s expectations, a detailed treatment plan was formulated. After obtaining informed consent, a hyaluronic acid-based dermal filler, selected for its soft, pliable consistency and suitability for lip enhancement, was chosen to achieve natural-looking results.
The procedure was performed under topical anesthesia using a numbing cream to ensure patient comfort. A microbolus injection technique was employed, allowing for precise and controlled placement of the filler. This approach helped to achieve subtle volume enhancement
while maintaining lip mobility and natural expression. Particular attention was given to defining the vermilion border, enhancing the Cupid’s bow, and balancing the upper and lower lips to create symmetry and proportion. Small aliquots of filler were strategically placed to smooth out surface irregularities, improve hydration, and support the overall lip architecture. Gentle molding was performed post-injection to ensure even distribution and optimal contour. The entire procedure was completed in a single session with no immediate complications, and the patient tolerated the treatment well.
Results
Immediately after the procedure, the patient demonstrated a notable improvement in lip volume, contour, and overall aesthetic harmony. The lips appeared fuller yet natural, with enhanced definition of the vermilion border and a more pronounced, well-shaped Cupid’s bow. The subtle augmentation restored balance between the upper and lower lips, correcting the previously noted asymmetry.
In addition to volumization, the lips showed a healthier, more vibrant pink hue, indicative of improved hydration and circulation. The texture appeared smoother and softer, contributing to a refreshed and youthful perioral appearance. Mild post-injection swelling was observed, which is expected and self-limiting. Over the subsequent 3–5 days, as the swelling resolved, the final result became more refined and aesthetically pleasing. The filler integrated well into the tissue without any nodularity or
irregularities.
At the follow-up visit, the patient expressed a high level of satisfaction, highlighting the natural feel and look of the enhancement. She particularly appreciated that the results met her desire for subtle rejuvenation without an overfilled or artificial appearance. No adverse events or complications were noted during the recovery period.
Discussion2,4,5
This case exemplifies the effectiveness of hyaluronic acid (HA)based dermal fillers in addressing aesthetic concerns related to lip volume, shape, symmetry and definition. The results achieved were not only visually rejuvenating but also contributed significantly to the patient’s self-confidence and satisfaction. The success of the treatment lay in the combination of patient-specific planning, a conservative yet strategic injection technique, and a nuanced understanding of lip anatomy. Lip augmentation today is more than just volume enhancement—it is a precise art that involves restoring youthful features, improving proportional harmony, and maintaining natural expression.
Dermal fillers have become a foundational component of aesthetic facial treatments. Their applications have evolved from merely reversing signs of aging to reshaping facial contours, enhancing individual features, and even altering emotional expressions projected
by the face. As techniques have advanced, so has the understanding of how to optimize filler choice and placement for natural results while minimizing risks. The development of newer crosslinked HA fillers with varying rheological properties, along with improved delivery systems like cannulas, has contributed to more predictable outcomes and reduced complication rates.
Lip augmentation using HA fillers offers several advantages, immediate results, minimal downtime, and high patient satisfaction. HA remains the filler of choice for lip and perioral rejuvenation due to its biocompatibility, reversibility and hydrophilic nature, which enhances lip hydration. The versatility of HA fillers allows for precise sculpting of various anatomical components of the lips, including the vermilion border, Cupid’s bow, philtral columns, and oral commissures. Treatment can be customized to the patient's age, lip structure and aesthetic goals, whether the aim is subtle enhancement or restoration following age-related volume loss.
A thorough understanding of lip anatomy and its dynamic behavior is essential. The lips are highly vascular and innervated structures, making them both delicate and expressive. Successful outcomes depend on individualized treatment plans, anatomical precision, and proper technique. Prior to treatment, dynamic assessment should be performed to detect asymmetries, perioral muscle activity, and any underlying structural imbalances that may
Before Treatment
Figure 1: Dermal filler for lip rejuvenation
After Treatment
affect results. Additionally, agespecific considerations are crucial—while younger patients often seek volume and shape enhancement, older individuals may require comprehensive perioral rejuvenation, addressing rhytides, volume loss, and structural definition.
Patient selection and counseling play a pivotal role in achieving successful outcomes. A detailed medical history, discussion of treatment expectations, and explanation of possible side effects such as swelling, bruising, or herpetic flare-ups are essential. Patients should be informed about postprocedure downtime, which may range from a few days to two weeks, and reassured about the transient nature of most side effects. The growing use of blunttip cannulas has significantly reduced downtime, bruising and discomfort, allowing for greater patient satisfaction and quicker recovery. However, for those new to aesthetic practice, starting with needles can provide better control and familiarity with lip anatomy, before gradually transitioning to cannula-based techniques.
Several injection techniques— such as serial puncture, linear threading (both antegrade and
References
1. B.J. Mahmood Faris, The Use of Facial Fillers in Clinical Practice: The Level of Patient Satisfaction and an Overview of Common Clinical Complications, Actas Dermo-Sifiliográficas, Volume 115, Issue 5, 2024, Pages 458-465, ISSN 0001-7310, https://doi.org/10.1016/j. ad.2023.10.008.
2. Luthra A. (2015). Shaping Lips with Fillers. Journal of cutaneous and aesthetic surgery, 8(3), 139–142. https://doi.
retrograde), and depot or microbolus placements—are employed depending on the desired effect. Each technique offers specific advantages and must be tailored to the patient’s needs. Use of topical anesthetics, or nerve blocks in sensitive patients, helps ensure comfort, while HA fillers pre-mixed with lidocaine reduce procedural discomfort. Ice compresses and short courses of NSAIDs or corticosteroids can be used post-treatment to reduce swelling, though NSAIDs should be avoided in the immediate postinjection period to prevent masking signs of vascular compromise.
Though rare, complications can occur. These include the formation of nodules or lumps, which usually resolve with massage or hyaluronidase, and more serious events like vascular occlusion, presenting with blanching and pain. Prompt recognition and management—including warm compresses, topical nitroglycerin, or immediate use of hyaluronidase—are critical in such cases. Prophylactic antivirals should be considered in patients with a history of herpes simplex to avoid reactivation.
Ultimately, achieving natural, harmonious results in lip augmentation requires more than technical skill—it demands a refined aesthetic sense, comprehensive knowledge of anatomy, and an empathetic approach to patient care. Continuous education, practice refinement, and staying updated with evolving filler technologies and techniques are crucial for dermatologists and aesthetic practitioners to deliver consistently excellent outcomes.
Conclusion
Lip augmentation using dermal fillers offers a reliable, minimally invasive solution for restoring lip volume, enhancing contour and achieving youthful, natural-looking results. When performed with a thorough understanding of facial anatomy, careful patient evaluation and tailored technique selection, the procedure ensures both safety and high patient satisfaction. Long-term success hinges on an individualized approach that respects the unique lip proportions, dynamic movement and aesthetic goals of each patient. As techniques and filler technologies continue to advance, lip augmentation remains a key component of comprehensive facial rejuvenation strategies, blending art with science for refined and harmonious outcomes.
org/10.4103/0974-2077.167269
3. Díaz-Aguayo I, Urdiales-Gálvez F, Benítez PA, et al. Aesthetic management of lips and perioral region with Hylacross® and Vycross® hyaluronic-acid based fillers: A document of recommendations. J Cosmet Dermatol. 2024; 23: 2843-2856. doi:10.1111/jocd.16358
4. Taylor, Susan C et al. “Lip and Perioral Enhancement With Hyaluronic Acid Dermal
Fillers in Individuals With Skin of Color.” Dermatologic surgery : official publication for American Society for Dermatologic Surgery [et al.] vol. 45,7 (2019): 959-967. doi:10.1097/DSS.0000000000001842
5. Arora G. Fillers for aesthetics on the face – Newer perspectives. Cosmoderma 2021;1:6.
Paayel Ghosh – A talented actress, dedicated to holistic wellness and social impact, following a disciplined skin and hair care routine developed and maintained under the guidance of her Dermatologist.
In this exclusive interview, Paayel Ghosh outlines her approach to achieving optimal skin and hair health, underscoring the role of discipline and mindfulness in shaping her philosophy. Her holistic wellness routine focuses on nurturing internal health through a balanced diet, regular exercise, adequate hydration, and the inclusion of antioxidantrich green tea. Paayel believes that true beauty emerges from a foundation of balance, simplicity, and attentive self-care, along with expert guidance from her Dermatologist.
1.What does your daily skincare and hair care routine involve, and how do you maintain such healthy skin and hair?
Well, I would, first of all, acknowledge the fact that I am genetically blessed with good skin and hair. However, it is important not to take it for granted and to continue taking good care. Every morning, my day starts with washing my face using a face wash, and after that, I apply sunscreen with SPF 50. Once my day is done, and before I go to sleep at night, I make sure to wash my face again thoroughly with the same face wash. After that, I apply a Vitamin C serum followed by a moisturizer. As far as hair is concerned, I wash it daily, though not necessarily always with shampoo, but with good quality normal water. Once a week, I use hair oil and leave it on for an hour before shampooing. Usually, I limit my use of sunscreen and conditioner to three times a week. Also, I must say that at least once every week, I apply a hair mask, which I keep on for
around 30 minutes before applying shampoo and conditioner.
2.How do you adapt your hair care routine when travelling or working in different climatic conditions?
When I am traveling, I usually opt for hair botox. However, even with hair botox, I ensure that my hair receives proper care. I make it a point to apply a hair mask at least twice a week while traveling, and only after that do I proceed with shampoo and conditioner. I avoid using hair oil during travel. Under normal circumstances, I get a proper hair massage and leave the oil on for about an hour. Since that is not feasible when I am traveling, I make sure to apply a hair mask before shampooing to maintain nourishment and hydration.
3. What is one common hair care myth that you believe people should stop believing?
One common hair care myth that I believe people should stop believing is that using shampoo every day causes hair fall. In my opinion, that is a significant misconception.
4. How do you balance using natural remedies versus commercial skincare products in your routine, and what
has worked best for you?
I find that a combination of natural remedies and commercial products works best for me. Boiling neem and methi in oil and applying it once a week has been particularly effective. In addition to that, I use sulphate-free shampoo and conditioner, which suits my hair well.
5. How much does diet and hydration influence your skin health, and do you follow any particular practices in this regard?
Diet and hydration are very important for skin health. Eating a properly nourished diet helps significantly in keeping the skin young and vibrant. Adequate water intake is essential, as is consuming vegetable juice. At least 3-4 liters of water should be consumed daily to help flush out toxins from the body effectively.
6. How do you care for your skin during long shooting hours, especially under heavy makeup and lighting?
We cannot avoid heavy makeup or makeup during shooting. So, what I do is, immediately after pack-up, I remove all the makeup, wash my face with my regular face wash, and then apply a moisturizer. Only after this is done do I step out of my vanity van. I also make it a point to eat fruits and drink coconut water during the shoot to keep my skin hydrated from within.
7. What skin challenges, such as acne or pigmentation, have you encountered, and how have you successfully managed or overcome them?
Well, I have been blessed in a way that I have never had issues related to pigmentation.
8. What specific advice or treatments has your Dermatologist recommended to support your skin and hair health?
My Dermatologist has always advised me to drink a good amount of water daily and to exercise regularly, so that the toxins beneath the skin can be flushed out through the pores, which open up as you begin to sweat. Apart from this, I have been recommended to drink one cup of green tea daily, and I follow that dedicatedly.
9. What is the most valuable skincare advice you have received from a Dermatologist, and how has it influenced your routine?
Well, like I said, working out is important to ensure that toxins are flushed out through your skin pores. Additionally, staying hydrated and consuming the required amount of water daily is crucial. And yes, I started incorporating green tea into my routine after my Dermatologist suggested it, and it has helped me immensely. It is now a mandatory part of my daily life, no matter what.
10. What advice would you give to someone aiming to develop a comprehensive and effective skincare routine from the beginning?
Wash your face with water at least twice a day. Splash water on the face, use a sunscreen with SPF above 30, and also apply Vitamin C serum. These are essential steps. Additionally, applying moisturizer and lip balm before going to bed is paramount.
Aesthetic Restoration of the Forehead Lines with Botulinum Toxin Type A
Dr. Madhuri Zanwar MBBS, DDV
Clinical and Aesthetic Dermatologist
Mumbai Introduction
The practice of aesthetic medicine continues to evolve, with botulinum toxin type A emerging as one of the most widely used and effective non-surgical treatments for facial aging. Among the various facial concerns addressed in clinical practice, forehead lines are particularly common and often among the earliest signs of aging that prompt individuals to seek cosmetic consultation. These lines, formed due to repeated muscle movements and gradual loss of skin elasticity, can create an impression of fatigue, stress, or age. Forehead wrinkles primarily result from the dynamic action of the frontalis muscle, which plays a critical role in facial expression—especially in raising the eyebrows. This muscle extends from the eyebrows up to the hairline, and repeated contractions over time contribute to the formation of horizontal forehead lines. However, these lines vary greatly in appearance, influenced by individual anatomy, genetic factors, facial habits, and lifestyle choices. This variation underscores the importance of personalized assessment in aesthetic treatments.1,2,3
Botulinum toxin injections have become the cornerstone of minimally invasive facial rejuvenation procedures worldwide. Clinically, botulinum toxin type A works by inhibiting the release of acetylcholine at the neuromuscular junction, temporarily reducing muscle activity and thereby softening dynamic lines. When administered precisely into overactive areas of the frontalis, it results in muscle relaxation and visible smoothening of forehead lines. The effects typically begin to appear within a few days, reaching their peak by two weeks, and persist for approximately three to four months. While botulinum toxin type A is FDA-approved for cosmetic indications such as glabellar frown lines and lateral canthal lines (crow’s feet), its use has expanded to include treatment of horizontal forehead lines. Additionally, it is approved for a range of medical conditions, including chronic migraines, cervical dystonia, upper limb spasticity, blepharospasm, severe axillary hyperhidrosis, and others. It is important to note that botulinum toxin is most
effective for dynamic rhytids— wrinkles that appear with movement—rather than static or deep lines caused by advanced photoaging. Despite this, its role in achieving a rejuvenated and relaxed forehead appearance remains unmatched, owing to its predictability, safety profile, and high patient satisfaction.1,2,3
Case Presentation
A 34-year-old female visited our dermatology clinic with concerns about prominent horizontal forehead lines that were particularly noticeable during facial expressions. These dynamic wrinkles, which had gradually deepened over time, contributed to a fatigued and prematurely aged appearance. The patient was specifically looking for a non-surgical, safe, and effective solution to achieve a smoother, more youthful, and refreshed look without downtime.
Following a detailed consultation that included assessment of her aesthetic goals, evaluation of medical history, and screening for any contraindications, the decision was made to proceed with botulinum toxin type A injections. This FDA-approved treatment was chosen for its proven efficacy in relaxing overactive facial muscles and softening expression lines. A customized injection protocol was designed, targeting the frontalis muscle—the primary contributor to forehead wrinkles. Botulinum toxin were strategically administered in a symmetric fashion across the forehead to ensure balanced results, natural expression retention, and optimal wrinkle reduction.
Procedure
• Technique: Intramuscular injections were performed using finegauge needles.
• Duration: The entire procedure was completed within 10–15 minutes.
• Pain Management: Minimal discomfort was reported; topical numbing was optional and not required in this case.
• Post-care Instructions: The patient was advised to avoid lying down, vigorous exercise, and massaging the area for 4–6 hours post-injection.
Results
Follow-up was done after two weeks to assess the results. The patient showed excellent clinical improvement, as evidenced by the provided before-and-after photographs.
• Before: Visible deep forehead lines, especially during expression.
• After: Remarkable smoothing of the forehead, with complete relaxation of dynamic lines and a refreshed, youthful, and friendly facial appearance.
Before treatment
After treatment
Figure 1: After botulinum toxin type A injection, remarkable smoothing of the forehead, with complete relaxation of dynamic lines and a refreshed, youthful and friendly facial appearance
Duration of Effect
The effect of the botulinum toxin is expected to last between 3 to 6 months, after which re-treatment may be considered.
Additional Benefits Discussed
The patient was educated about additional therapeutic and aesthetic uses of botulinum toxin, including treatment for:
• Glabellar lines (frown lines)
• Crow’s feet (periorbital wrinkles)
• Excessive axillary sweating (hyperhidrosis)
• Jawline reshaping (masseter hypertrophy)
• Chronic migraine management
Mechanism of Action
The development of facial wrinkles is primarily attributed to two factors: thinning of the dermis over time and the repetitive
contractions of underlying facial muscles. These dynamic muscle movements, particularly in areas like the forehead and around the eyes, contribute significantly to the formation of fine lines and folds. Botulinum toxin type A, a neurotoxic protein derived from the bacterium Clostridium botulinum, offers an effective therapeutic approach by temporarily relaxing targeted muscles involved in these expressions. At the molecular level, botulinum toxin acts at the neuromuscular junction, where it inhibits the release of acetylcholine—a neurotransmitter responsible for muscle contraction. It functions by targeting and disrupting a vital membrane protein known as synaptosomal-associated protein of 25 kilodaltons (SNAP-25), which is essential for nerve signal transmission. This disruption prevents the fusion of synaptic vesicles with the neuronal membrane, thereby halting acetylcholine release and inducing temporary chemodenervation. The result is localized muscle paralysis, which smooths the overlying skin and softens the appearance of dynamic wrinkles. With time, neuromuscular activity slowly returns as the body regenerates SNAP-25, leading to the restoration of muscle movement.3
Injection Technique
Before beginning the procedure, clinicians should assess and document any pre-existing brow asymmetry and inform the patient that treatment may either enhance or reduce this asymmetry. Injection points should be carefully marked, maintaining 1.5 to 2 cm spacing
between sites along either side of a deep wrinkle in a horizontal or V-shaped configuration. The injections generally begin about 1 cm above and medial to the eyebrow and proceed superiorly toward the hairline.4,5
When functional muscle fibers are present in the midline, central forehead injections may be included; otherwise, they should be avoided to prevent unintended effects. Typically, three to four injection points are placed on each side of the midline, totaling six to eight injection sites across the forehead. A critical safety zone— approximately one fingerbreadth above the orbital ridge and lateral to the mid-pupillary line— should be avoided to reduce the risk of brow or eyelid ptosis.4,5
To prevent the appearance of an excessively arched or "Spock-like" brow, an optional subcutaneous injection of 4–6 units of botulinum toxin A may be placed 1 to 1.5 cm above the supraorbital prominence at the mid-pupillary line. Overall, a total of 10 to 20 units of botulinum toxin is typically administered, with clinical results lasting between three to six months.4,5 Dose is adjusted according to muscle strength, desired outcome and previous use.
Indications and Contraindications
Botulinum toxin type A, originally developed for therapeutic applications, has demonstrated broad utility across both medical and aesthetic disciplines. Over the past two decades, it has been effectively used to treat a variety of neuromuscular and autonomic disorders, including blepharospasm, strabismus,
cervical dystonia, chronic migraine, muscle spasticity, and axillary hyperhidrosis. Its transition into aesthetic medicine was marked by a significant milestone in 2002, when the U.S. Food and Drug Administration (FDA) approved its use for the treatment of glabellar lines. This was followed by an additional approval in 2013 for lateral canthal lines, commonly known as crow’s feet.3,6
Although only a limited number of cosmetic applications are FDA-approved, the off-label use of botulinum toxin has expanded considerably. It is now widely regarded as the treatment of choice for dynamic wrinkles, particularly those in the upper third of the face—including forehead lines, glabellar lines, and periorbital wrinkles. The use of botulinum toxin in the lower face and neck is also gaining popularity; however, these areas require more advanced technique due to the complexity and interdependence of the involved muscle groups.3,6
Beyond the commonly treated regions, botulinum toxin is indicated for a wide array of wrinkles caused by persistent muscle activity. These include bunny lines on the nose, perioral lines around the mouth, and platysmal bands on the neck. It is most effective on dynamic wrinkles—those that appear during facial expressions—while static or fixed wrinkles may require adjunctive therapies such as dermal fillers, chemical peels, fractional lasers, or thread lifts to achieve optimal aesthetic outcomes. Non-cosmetic uses of botulinum toxin continue to evolve, with applications including palmar, plantar,
Aesthetic
and gustatory hyperhidrosis, treatment of migraines, facilitation of wound healing, and management of conditions like anal fissures.3,6
Although it offers wideranging benefits, it is important to be aware of specific contraindications to ensure it is used safely. Botulinum toxin should be avoided in patients with neuromuscular junction disorders or peripheral motor neuropathies, as it may exacerbate muscle weakness. It should also not be administered concurrently with aminoglycoside antibiotics or other drugs that may interfere with neuromuscular transmission. Treatment should be postponed in patients who have ongoing inflammatory skin issues at the proposed injection site. Moreover, its use is contraindicated during pregnancy and lactation due to the lack of conclusive safety data in these populations.3,6
Discussion
In recent years, the demand for botulinum toxin type
A injections for forehead rejuvenation has increased significantly, driven by the desire for a more refreshed and natural appearance. Achieving optimal and safe outcomes with this treatment requires a thorough understanding of the underlying forehead anatomy and recognition of individual anatomical variations to tailor the approach for each patient.4,5
The frontalis muscle, which lies directly beneath the forehead skin, is primarily responsible for elevating the eyebrows and producing horizontal forehead wrinkles. This muscle originates
from the galea aponeurotica and inserts into the skin near the eyebrows. Notably, it is the sole elevator of the brow, working in dynamic balance with the surrounding depressor muscles to maintain eyebrow position and shape. Anatomical studies have identified four morphological variations of the frontalis—full, V-shaped, central, and lateral forms—each contributing to distinct wrinkle patterns due to their differing fiber distribution and cutaneous insertions.4,5
Recent findings highlight that the forehead skin moves in two directions during muscle activity, offering improved insight into the mechanisms behind wrinkle development. The lower fibers of the frontalis pull the skin upward, elevating the brow, while the upper fibers exert a downward force, leading to hairline descent. These opposing movements converge at a horizontal line known as the line of convergence or C-line, typically located just below the hairline. This C-line represents a static anatomical point where both muscular actions neutralize each other, and it frequently corresponds to the second visible horizontal line on the forehead.4,5
Given the central role of the frontalis in generating forehead lines, botulinum toxin injection in this region has become the third FDA-approved indication for cosmetic use in facial wrinkles. Although the procedure is generally considered safe, potential complications can occur—ranging from mild, transient effects to more significant issues that may impair aesthetic outcomes. Many of
these complications can be reduced by targeting injections to the upper portion of the frontalis, thereby preserving the natural movement and position of the brows.4,5
Anatomically, the frontalis lacks a bony origin and is instead anchored by soft tissue structures. The previously mentioned bidirectional motion supports the hypothesis that the C-line could functionally act as a common point of origin for both the upper and lower muscle fibers. By targeting this zone for botulinum toxin injection, practitioners may achieve better control over both sets of muscle actions and effectively reduce wrinkles located above and below this line. Moreover, injecting along the C-line may offer a dual benefit—providing effective wrinkle reduction while minimizing the risk of adverse effects such as brow ptosis or asymmetry.4,5
The frontalis muscle generally has two sections, or bellies, divided by a central tendinous aponeurosis that usually contains few or no muscle fibers. However, in some individuals—particularly men and a subset of women— functional muscle fibers may be present in the central region. These fibers can be identified through gentle palpation as the patient actively raises and lowers the eyebrows.4,5
Conclusion
This case highlights the transformative potential of botulinum toxin type A in aesthetic dermatology. Through a simple and minimally invasive procedure, the patient experienced
Aesthetic Restoration of the Forehead Lines with Botulinum Toxin Type A
significant improvement in forehead lines, resulting in a smoother, more youthful, and refreshed facial appearance. Beyond the physical enhancement, the treatment contributed to increased self-esteem and patient satisfaction. Botulinum toxin type A remains a cornerstone
References
1. Biello A, Zhu B. Botulinum Toxin Treatment of the Upper Face. [Updated 2023 Sep 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/ NBK574523/
2. Alhallak K. (2024). Optimizing Botulinum Toxin A Administration for Forehead Wrinkles: Introducing the Lines and Dots (LADs) Technique and a Predictive Dosage
in cosmetic dermatology due to its established efficacy and favorable safety profile when administered by qualified professionals. Clinical improvements in dynamic wrinkles—particularly those between the eyebrows—are typically evident within four weeks of treatment. However,
practitioners should be mindful of potential adverse effects, such as transient eyelid ptosis, which may occur in some cases. With appropriate technique and individualized planning, botulinum toxin injections continue to offer reliable, reproducible, and high-impact aesthetic results.
3. Small R. (2014). Botulinum toxin injection for facial wrinkles. American family physician, 90(3), 168–175.
4. El-Garem YF, Eid AA, Leheta TM. Locking the line of convergence by botulinum toxin type A for the treatment of dynamic forehead wrinkles. J Cosmet Dermatol. 2023; 22: 186-192. doi: 10.1111/jocd.15468
5. Nanda S, Bansal S. Upper face rejuvenation using botulinum toxin and hyaluronic acid fillers. Indian J Dermatol Venereol Leprol 2013;79:32-40
6. Shetty M K. Guidelines on the use of botulinum toxin Type A. Indian J Dermatol Venereol Leprol 2008;74:13-22
Polynucleotide-Based Injectables (PDRN): A Regenerative Breakthrough in Aesthetic Dermatology
Polynucleotide-based injectables, primarily composed of polydeoxyribonucleotide (PDRN) derived from salmon sperm DNA, are emerging as effective biostimulatory agents in aesthetic dermatology. These injectables promote cutaneous regeneration by activating dermal fibroblasts and stimulating collagen and extracellular matrix synthesis, key to improving skin firmness, elasticity, and structural integrity. Clinically indicated for fine rhytides, periorbital aging, dermal laxity, and impaired epidermal barrier function, PDRN exhibits notable regenerative, anti-inflammatory, and wound-healing effects. Delivery methods include mesotherapy, microneedling, and direct intradermal injections, depending on target depth and skin condition. Unlike hyaluronic acid-based boosters, polynucleotides enhance dermal remodeling through fibroblast proliferation and neoangiogenesis while improving hydration due to their hygroscopic properties. With a low immunogenic profile, they are well tolerated across all Fitzpatrick skin types and have shown additional benefits in post-laser healing and scar modulation. A standard treatment protocol involves 3–4 sessions, offering minimal downtime and a strong safety profile, making them a compelling option in regenerative aesthetic practice.
Advances in Hyaluronic Acid-Based
Nonsurgical Rhinoplasty for Asian Nasal
Nonsurgical Rhinoplasty (NSR) using hyaluronic acid (HA) fillers is rapidly becoming a preferred option for nasal contouring, particularly among Asian patients, due to its minimally invasive approach and quick recovery. HA fillers enhance nasal structure by retaining water through glycosaminoglycans, allowing softtissue remodelling and volumization. Given the anatomical features of the Asian nose typically a flatter dorsum, wider alar base, and thicker skin biphasic HA fillers with high elasticity (G′) and larger particle size are favoured for improved projection, stability, and reduced risk of migration or edema. Key target areas include the radix, dorsum, glabella, tip, columella, and nasolabial angle, with filler delivered supraperiosteally or sub-SMAS via microbolus or linear threading techniques. In addition to volumizing effects, HA stimulates neocollagenesis and extracellular matrix remodelling, contributing to long-term tissue support. However, detailed knowledge of nasal vascular anatomy remains critical to avoid serious complications like vascular occlusion. Proper filler selection, precise technique, and readiness to administer hyaluronidase are essential for safe outcomes. Ongoing innovations aim to refine filler formulations and injection strategies tailored to ethnic nasal anatomy, enhancing both the safety and aesthetic results of NSR procedures.
Beyond Monotherapy: A Multimodal Protocol for Hair Regrowth in Androgenetic Alopecia
Dr. Saloni Vora-Gala
MBBS, DDV
Medical Head and Consultant Dermatologist
Dr. Sheth’s Skin and Hair Clinics
Mumbai Introduction
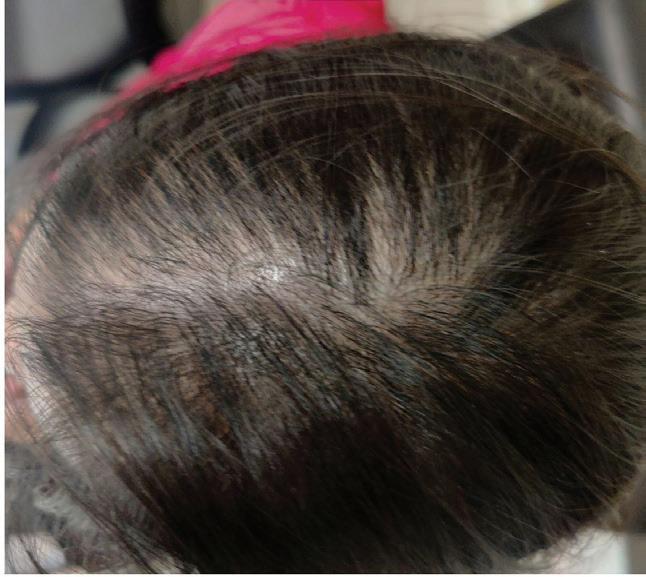
Androgenetic alopecia (AGA), often referred to as pattern baldness, remains the leading contributor to hair loss worldwide, affecting both men and women. It has a strong genetic component and is largely driven by androgenic hormones, particularly dihydrotestosterone (DHT). However, new insights reveal that AGA is a multifactorial condition influenced by hormonal, nutritional, inflammatory, and environmental factors.[1,2]
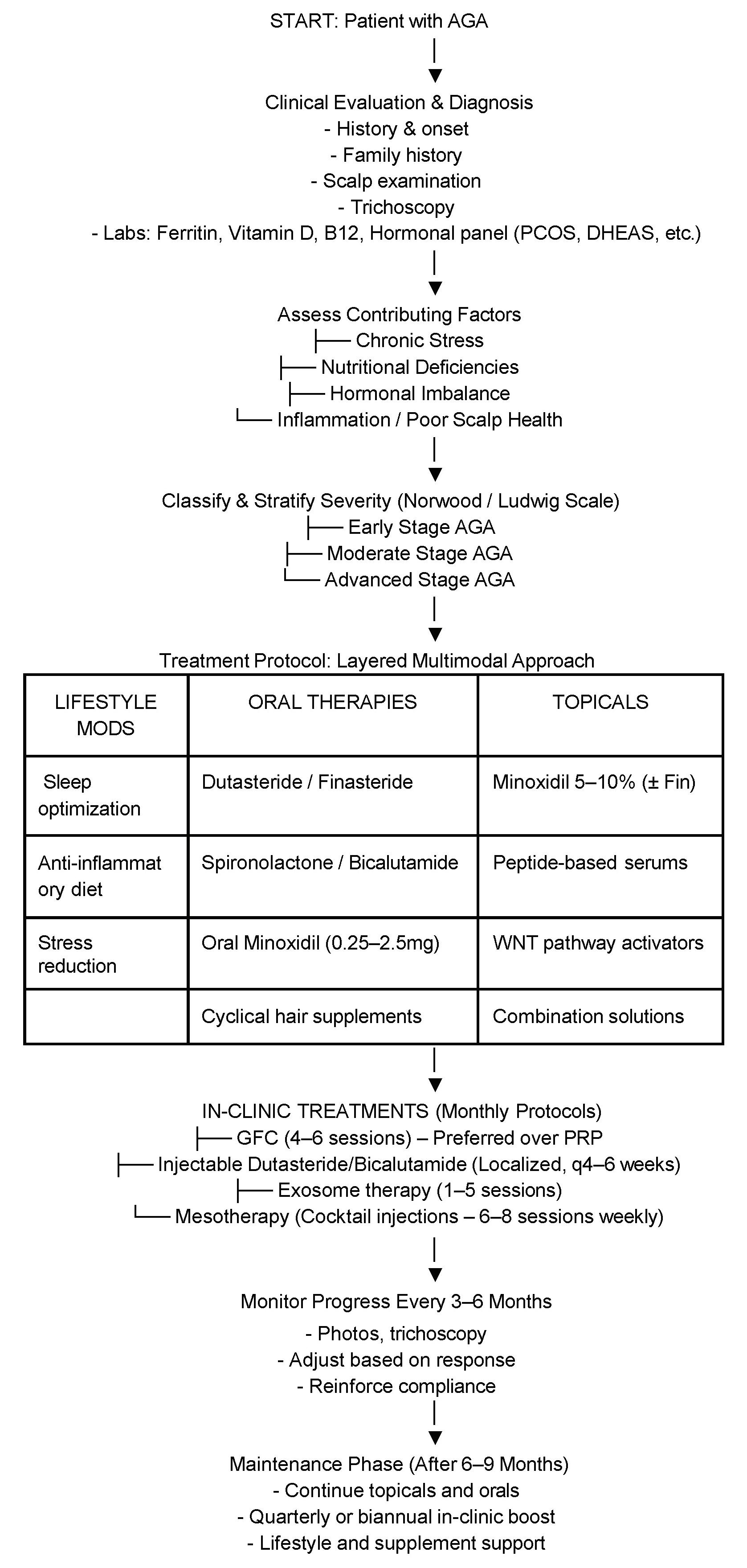
Traditionally, treatments for AGA have been limited to monotherapies such as topical minoxidil and oral finasteride. While effective for some, these therapies often fall short in producing satisfactory regrowth, especially in moderate to advanced stages. The last few years have seen a paradigm shift in how dermatologists approach AGA. By integrating lifestyle changes, targeted oral and topical therapies, and in-clinic regenerative treatments, we can achieve significantly improved hair regrowth outcomes.[3,4]
Understanding the Pathophysiology of AGA AGA occurs due to the progressive miniaturization of hair follicles over successive growth cycles. This process is primarily driven by DHT (dihydrotestosterone), a more potent derivative of testosterone that binds to androgen receptors in genetically susceptible hair follicles. Once bound, DHT triggers a cascade of molecular events that shrink the hair follicle, shorten the anagen (growth) phase, prolong the telogen (resting) phase, and over time convert thick terminal hairs into thin, short, non-pigmented vellus hairs.[1,2] [5,6]
AGA is a polygenic condition, with variations in genes related to androgen receptor expression, WNT signaling, and prostaglandin metabolism contributing to follicular sensitivity to DHT rather than just its concentration.[7] [8]
Histopathological studies reveal that AGA is not a purely non-inflammatory condition. Subclinical inflammation
surrounding hair follicles may alter the scalp microenvironment, potentially leading to scarring and irreversible follicle loss.[2] [9]
Vascular factors also play a critical role. Hair follicle health depends on adequate blood flow to the dermal papilla, and compromised circulation may hinder its function. This underlies the therapeutic action of vasodilators like minoxidil.[5]
Nutritional deficiencies such as iron, zinc, vitamin D, B12, and amino acids like L-lysine are commonly associated with impaired hair cycling and are especially prevalent in women with AGA.[6,7]
Stress-induced activation of the HPA axis can result in elevated cortisol, disrupting hair cycling and compounding AGA. Chronic stress is increasingly recognized as both a trigger and an aggravator of hair loss conditions.[9]
Recent molecular insights also reveal that elevated PGD2 levels in balding areas are believed to suppress hair growth, contributing to the progression of AGA, while prostaglandin E2 (PGE2) levels, which support hair growth, are reduced. In addition, fibroblast growth factor 5 (FGF5), known to promote catagen transition, is increasingly studied as a therapeutic target.[10,11]
Why Combination Therapy Works
Most monotherapies address only a single factor in the multifaceted biology of AGA. For instance, finasteride and dutasteride effectively reduce systemic and scalp DHT levels, thereby addressing the hormonal axis of AGA. However,
they have no impact on vascular insufficiency, oxidative stress, nutritional deficiencies, or follicular stimulation. Similarly, topical minoxidil, though FDAapproved and widely used, promotes blood flow to the scalp but does not directly address hormonal imbalances or inflammation contributing to AGA.[12]
Combination therapy is rooted in the understanding that AGA is a multifactorial disorder.[4] [13]
A multimodal, layered treatment strategy allows dermatologists to simultaneously address:
• Hormonal factors through oral 5-alpha-reductase inhibitors or anti-androgens.[1]
• Circulatory deficiencies with minoxidil or low-level laser therapy.[14]
• Inflammation and oxidative stress with topical corticosteroids, ketoconazole, or antioxidants.[9]
• Nutritional imbalances via dietary correction and supplementation.[11]
• Regenerative signaling through platelet-derived treatments (PRP, GFC), peptides, or exosomes.[15,16]
Clinical studies have shown that combination regimens provide superior outcomes in both male and female AGA. For example, the combination of oral finasteride and topical minoxidil has been proven to result in higher hair density and thickness compared to either agent alone. [13,17] In women, combining low-dose oral minoxidil with spironolactone or bicalutamide yields both hormonal regulation and follicular stimulation.[4] [13]
In my clinical experience, layering therapies also improves
patient satisfaction and compliance. As patients begin to notice improvements in density, reduced shedding, and improved hair texture within the first 3–6 months, they are more likely to remain adherent to the regimen. Additionally, combination therapy allows for customization and tapering, reducing the need for longterm dependence on any single modality.[13,18]
Emerging regenerative tools like exosomes and GFC further support this synergistic approach, delivering signaling molecules and growth factors that activate dormant follicles and enhance angiogenesis.[5,6] [15,16]
Therefore, a strategic and personalized combination of therapies is not just more effective—it is increasingly becoming the standard of care in trichological practice.
The Pillars of Holistic Hair Regrowth Therapy
A. Lifestyle Modifications Lifestyle choices directly influence hair health by modulating inflammation, circulation, and hormonal balance. Chronic stress increases cortisol, leading to telogen effluvium and aggravating AGA. Incorporating stress-relieving practices such as yoga, meditation, or mindfulness-based therapy is critical. Inadequate sleep has also been linked to impaired hair growth due to hormonal disruption. Regular cardiovascular exercise enhances blood flow to the scalp, supporting follicular oxygenation and nutrient delivery.[19,20]
Dietary habits are equally important. A protein-rich diet with adequate iron, omega-3 fatty acids, vitamin D, and antioxidants can support healthy hair cycling. Smoking cessation and limiting alcohol intake are strongly recommended, as these habits can impair vascular health and nutrient absorption. [19,20]
B. Oral Interventions
• Dutasteride (0.1–0.5 mg/ day or 0.5 mg weekly): A dual 5-alpha-reductase inhibitor (Type I and II), offering more potent and sustained DHT suppression than finasteride. It is highly effective in treating male AGA and increasingly used off-label in women under monitoring.[21]
• Finasteride (1 mg/day): Selectively inhibits Type II 5-alpha-reductase. Approved for male AGA, with studies confirming its efficacy in slowing hair loss and promoting regrowth.[22]
• Spironolactone (50–200 mg/day): A potassium-sparing diuretic with anti-androgenic effects, widely used in women with female pattern hair loss, especially those with signs of hyperandrogenism. Spironolactone reduces androgen effects by inhibiting receptor binding and dampening adrenal hormone output. [23]
• Bicalutamide (25–50 mg/ day): A non-steroidal antiandrogen used off-label in women with AGA, particularly effective in PCOS. It is better tolerated than spironolactone in some patients.[23]
• Oral Minoxidil (0.25–2.5 mg/day): An emerging lowdose option that acts as a
potassium channel opener to prolong the anagen phase. Particularly useful in patients who cannot tolerate topical minoxidil. Common side effects include hypertrichosis and postural hypotension.[18,24]
• Hair Supplements and Nutraceuticals: Supplements play a supportive role by correcting deficiencies and promoting an environment conducive to hair growth. Key ingredients include [11,19, 25]:
◽ Zinc and Iron: Critical in hair matrix production
◽ Vitamin D and B12: Essential for follicular cycling
◽ Plant-Based DHT Blockers: Such as beta-sitosterol, saw palmetto, pygeum, pumpkin seed oil—used for their 5-alpha-reductase inhibition properties [25,26]
◽ Amino acids (L-cysteine, methionine): Precursors for keratin synthesis
• The cyclical therapy model for hair supplements involves rotating different supplements on alternate days or weekly cycles to prevent overdose and improve compliance. For example, iron + vitamin C on one day, followed by amino acid-based supplements on another, and plant-based DHT blockers on the third day. This method is gaining popularity for long-term maintenance.[6,19]
C. Topical Therapies [17, 27]
• Minoxidil (5% to 10%): A vasodilator that prolongs the anagen phase and increases hair shaft thickness. The 10% strength may offer superior benefits in refractory cases but is associated with higher irritation potential. Foam and solution forms are available. It may be used once or twice
daily, with titration based on tolerance. Combination topical formulations that include minoxidil with finasteride, minoxidil with peptides, and even WNT pathway activators have shown synergistic results, especially in early to moderate AGA. These combination solutions are increasingly popular for patients who prefer a comprehensive regimen in a single application.[7]
• Peptide-based Serums: These serums contain biomimetic peptides, copper peptides (GHK-Cu), and growth factors that stimulate dermal papilla cells and support extracellular matrix remodeling. They are particularly useful in patients with intolerance to minoxidil or as adjuncts postprocedure.[9] [17]
D. In-Clinic Regenerative Therapies
• GFC (Growth Factor Concentrate): GFC is derived from autologous blood and enriched with concentrated growth factors after platelet activation and separation. Compared to PRP, GFC has the advantage of being free from platelet debris and inflammatory cytokines, thereby offering a more consistent and refined outcome. Typically, 4–6 sessions spaced 4 weeks apart are recommended. Most patients begin to observe tangible results after the third treatment session.[10] [15]
• Exosome Therapy: Derived from mesenchymal stem cells, exosomes are nanoscale vesicles that carry growth signals—including RNA, proteins, and peptides—to revive inactive hair follicles. Though still experimental, they
offer potential for follicular rejuvenation. Dosage protocols vary, but 1–5 sessions spaced monthly are common.[16, 28]
• Injectable Dutasteride/ Bicalutamide: Used for localized hormonal blockade, injectable dutasteride (0.05–0.1 mL of 0.5 mg/mL solution) or bicalutamide (0.25–0.5 mL at 5 mg/mL) is administered intradermally every 4–6 weeks in affected scalp areas. This approach minimizes systemic side effects while enhancing local efficacy.[21] [23] [28]
• Mesotherapy: A technique involving microinjections of a cocktail of vitamins, peptides, and medications directly into the dermis. Often used as an adjunct to stimulate local circulation and nutrient delivery. Protocols typically involve 6–8 sessions spaced fortnightly.[12] [29]
Case Series Disclaimer:
The following case studies and treatment protocols are derived from the author’s clinical experience at Dr. Sheth’s Skin and Hair Clinics. All patient data has been anonymized and shared with informed consent for educational purposes.
Case 1: Male, 29 years old, AGA
• Complaints: Receding hairline, vertex thinning
• Protocol: LDOM 1.25 mg/ day, nutraceuticals, topical 5% minoxidil with finasteride and peptides, GFC x 2 sessions, exosomes x 2 sessions
• Result: 50% increase in hair density at 5 months; reduced shedding and improved hair quality
Case 2: Female, 33 years old, Diffuse AGA with PCOS, 13 months post-partum
• Complaints: Thinning along mid-part and crown, receding hairline
• Protocol: Iron, vitamin B12 and vitamin D supplementation, 5% minoxidil + peptide serum, Wnt pathway activator serum, GFC x 2 sessions, exosomes x 2 sessions
• Result: Noticeable improvement in volume, density and texture over 5 months
Case 3: Female, 41 years old, Diffuse AGA
• Complaints: Thinning along mid-part and crown, receding hairline
• Protocol: LDOM 1.25 mg/day, Oral Finasteride 5%, nutraceuticals, Vitamin D supplementation, topical 5% minoxidil with finasteride and peptides, GFC x 8 sessions
• Result: Noticeable improvement in volume, density and texture over 8 months
Case 4: Female, 65 years old, Diffuse AGA, NRI
• Complaints: Thinning along mid-part and crown
• Protocol: LDOM 1.25 mg/day, dutasteride 0.5 mg, nutraceuticals cyclical therapy, topical 5% minoxidil and peptides, GFC x 2 sessions, Injectable dutasteride and bicalutamide x 2 sessions, Exosomes x 1 session
• Result: Noticeable improvement in volume, density and texture over 10 months
Case 5: Male, 42 years old, AGA
• Complaints: Receding hairline, temple and vertex thinning
• Protocol: LDOM 1.25 mg/day, Oral Finasteride 1 mg, nutraceuticals cyclical therapy, topical 5% minoxidil with finasteride and peptides, GFC x 4 sessions, Injectable dutasteride x 2 sessions, Exosomes x 2 sessions
• Result: Increase in hair density at 8 months; improved hair quality, good coverage
Case 6: Female, 24 years old, Diffuse AGA with PCOS
• Complaints: Thinning along mid-part and crown, receding hairline
Androgenetic alopecia (AGA) is not a one-size-fits-all condition. Variability in patient demographics, severity, hormonal profiles, and treatment tolerability necessitate a personalized protocol for optimal outcomes. The treatment plan must be dynamic—adapting over time to evolving needs, preferences, and responses. [3]
• Early-Stage AGA: In patients with minimal recession or thinning (Norwood I–II or Ludwig I), the goal is to preserve density and prevent progression. Primary interventions include:
◽ Topical minoxidil 5%, potentially in combination with finasteride or peptides
◽ Lifestyle optimization and early use of nutraceuticals [1]
• Female AGA: Requires careful hormonal assessment. Polycystic ovarian syndrome (PCOS) and insulin resistance must be ruled out.[3] Management focuses on:
◽ Spironolactone or bicalutamide for hormonal control
◽ Correcting iron deficiency (target ferritin >70 ng/mL)
◽ Topical therapies (minoxidil 5–7%, peptides)
◽ Adjunctive exosome therapy or mesotherapy in diffuse thinning [16, 29]
• Advanced-Stage AGA (Norwood IV–VI): In these cases, hair follicles have significantly miniaturized or been replaced by fibrotic tissue. Aggressive and regenerative approaches are warranted:
◽ Oral dutasteride (0.5 mg
Beyond Monotherapy: A Multimodal Protocol for Hair Regrowth in Androgenetic Alopecia
daily or weekly) [13, 21]
◽ GFC therapy (4–6 sessions) [15]
◽ Injectable dutasteride or bicalutamide (q4–6 weeks) [21, 23]
◽ Microneedling, exosomes, or PRP as combinatory boosters [4,5]
• Maintenance Phase (Post 6–9 Months): Once visible results plateau, treatment can be simplified to reduce burden and cost. A typical maintenance strategy includes:
◽ Nutraceuticals (e.g., cyclical therapy with plant-based DHT blockers) [19]
◽ Quarterly in-clinic boosters (e.g., GFC or mesotherapy)
Counseling, Compliance & Expectations
Patient education is key to achieving long-term success in AGA management. Unrealistic expectations often lead to early discontinuation. Effective counseling should include:
• Initial Shedding Phase: Patients may experience increased hair fall during the first 2–4 weeks of minoxidil or regenerative therapy— this is a sign of dormant follicles re-entering the anagen phase.[6]
• Timeline for Results:
◽ Early signs of improvement (reduced shedding, new hair) appear in 3–4 months
◽ Peak cosmetic outcomes typically occur at 9–12 months
• Continued Maintenance: Since AGA tends to worsen over time, maintaining hair growth through long-term therapy is crucial to preserve results.[7]
Additional techniques to enhance compliance include:
◽ Realistic before-after images from similar cases
2. Whiting DA. Diagnostic and predictive value of horizontal scalp biopsy sections in male pattern androgenetic alopecia. Journal of the American Academy of Dermatology. 1993 May;28(5 Pt 1):755–763. doi:10.1016/0190-9622(93)701064
3. Blume-Peytavi U, Blumeyer A, Tosti A, et al. Evidence-based (S3) guideline for the treatment of androgenetic alopecia in women and in men. Journal der Deutschen Dermatologischen Gesellschaft. 2011 Oct;9 Suppl 6:S1–S57. doi:10.1111/ j.1610-0379.2011.07802.x
4. Rossi A, Antiga E, Ganzetti G, et al.
Comparative effectiveness of finasteride vs dutasteride in androgenetic alopecia: a meta-analysis. Journal of Dermatological Treatment. 2012 Dec;23(6):392–395. doi:1 0.3109/09546634.2011.649113
5. Sawaya ME, Price VH. Different levels of 5α-reductase type I and II, aromatase, and androgen receptor in hair follicles of women and men with androgenetic alopecia. Journal of Investigative Dermatology. 1997 Mar;109(3):296–300.
6. Olsen EA, Hordinsky M, Whiting D, et al. The importance of dual 5α-reductase inhibition in male pattern hair loss: a randomized controlled study of dutasteride vs finasteride. Journal of the American Academy of Dermatology. 2006 Dec;55(6):1014–1023. doi:10.1016/j. jaad.2006.08.006
7. Heilmann-Heimbach S, Hochfeld LM,
◽ Visual documentation using trichoscopy or scalp photography every 3 months
◽ Patient diaries to track subjective improvement
◽ Simplified regimens and once-daily products to reduce treatment fatigue
Conclusion
Androgenetic alopecia management has evolved from singular, symptomatic treatments to personalized, root-cause-based protocols. By layering lifestyle support, hormonal balance, topicals, regenerative therapies, and patient education, dermatologists can now offer results that are more predictable, visible, and sustainable.
This integrative approach not only addresses the follicle but also the patient’s overall health, well-being, and self-confidence—making it a cornerstone of modern dermatological care.
Paus R, et al. Hunting the genes in malepattern baldness: insights from targeting regulatory loci and WNT signaling. Scientific Reports. 2017 Mar;7(1):45419. doi:10.1038/srep45419
8. Higgins CA, Chen JC, Cerise JE, et al. Fibroblast Growth Factor 5 is a key regulator of hair growth. Experimental Dermatology. 2014 Aug;23(8):543–6. doi:10.1111/exd.12418
9. Kanti V, Hillmann K, Kottner J, Blume-Peytavi U. Perifollicular inflammation in male pattern baldness: a clinicopathological investigation. European Journal of Dermatology. 2018 Dec;28(6):799–806. doi:10.1684/ ejd.2018.3364
10. Garza LA, Liu Y, Yang Z, et al. Prostaglandin D2 inhibits hair growth and is elevated in bald scalp of
men with androgenetic alopecia. Science Translational Medicine. 2012 Jul;4(126):126ra34. doi:10.1126/ scitranslmed.3003122
11. Trost LB, Bergfeld WF, Calogeras E. Diagnosis and treatment of iron deficiency and its relationship to hair loss. Journal of the American Academy of Dermatology. 2006 May;54(5):824–844. doi:10.1016/j. jaad.2005.12.008
12. Messenger AG, Rundegren J. Minoxidil: mechanisms of action on hair growth. British Journal of Dermatology. 2004 Feb;150(2):186–194. doi:10.1111/ j.1365-2133.2004.05785.x
13. Suchonwanit P, McMichael AJ, Leerunyakul K. Therapeutic potential of combination therapy in androgenetic alopecia. Dermatology Practical & Conceptual. 2021 Jan;11(1):e2021031. doi:10.5826/dpc.1101a31
14. Ablon G. A study of a peptide complex for hair growth improvement. Journal of Drugs in Dermatology. 2016 Mar;15(3):311–315.
15. Moreno Arrones OM, Saceda Corralo D, Vano Galvan S, et al. Injectable treatments in androgenetic alopecia: safety and efficacy. Dermatologic Therapy. 2021 Jan;34(1):e14537. doi:10.1111/ dth.14537
16. D’Agostini F, Cinque B, Bregoli M, et al. Efficacy of mesotherapy in AGA: a prospective cohort study. Journal of Cosmetic Dermatology. 2022 Apr;21(3):1234–1240. doi:10.1111/ jocd.14422
17. Faghihi G, Khezri S, Firooz A, et al. Efficacy of peptide-based topical therapy in male pattern hair loss: a randomized controlled trial. Dermatologic Therapy. 2021 Feb;34(1):e14537. doi:10.1111/ dth.14537
18. Ramos PM, Miot HA. Efficacy and safety of low-dose oral minoxidil for hair loss: A systematic review. Journal of the American Academy of Dermatology. 2020 May;82(2):443–455. doi:10.1016/j. jaad.2019.08.065
19. Dhurat R, Sukesh M, Avhad G, et al. A randomized comparative study of platelet-rich plasma versus growth factor concentrate for androgenetic alopecia. International Journal of Trichology. 2015 Jul–Sep;7(3):128–132. doi:10.4103/09747753.162909
20. Kaufman KD, Olsen EA, Whiting D, et al. Finasteride in the treatment of men with androgenetic alopecia. Journal of the American Academy of Dermatology. 1998 Apr;39(4 Pt 1):578–589. doi:10.1016/ S0190-9622(98)70206-0
21. Sinclair R, Wewerinke M, Jolley D. Treatment of female pattern hair loss with oral antiandrogens. British Journal of Dermatology. 2005 Mar;152(3):466–473. doi:10.1111/j.1365-2133.2005.06218.x
22. Yazdabadi A, Sinclair R. Treatment of female-pattern hair loss with the androgen receptor antagonist flutamide: a case report. Australasian Journal of Dermatology. 2011 May;52(2):132–134. doi:10.1111/ j.1440-0960.2010.00735.x
23. Haeck IM, van der Steen PH, van der
Ziel HM, et al. An overview of herbal alternatives in androgenetic alopecia treatment. Phytotherapy Research. 2007 Mar;21(3):237–245. doi:10.1002/ ptr.2042
24. Rushton DH. Nutritional factors and hair loss. Clinical and Experimental Dermatology. 2002 Jul;27(5):396–404. doi:10.1046/j.1365-2230.2002.01076.x
25. Caserini M, Preda L, Previtali S, et al. Topical finasteride: efficacy and systemic exposure in a randomised, double-blind, placebo-controlled study. Skin Appendage Disorders. 2016 Apr;2(3–4):117–123. doi:10.1159/000450601
26. Rossi A, Cantoresi F, Elena A, et al. Minoxidil side effects and efficacy in male pattern hair loss: a meta-analysis. Journal of Dermatological Treatment. 2012 Oct;23(5):368–371. doi:10.3109/09546 634.2011.652549
27. Saeed L, Kaboodkhani R, Amiri S, et al. Exosome therapy for androgenetic alopecia: A systematic review. Stem Cell Reviews and Reports. 2021 Dec;17(6):2041–2052. doi:10.1007/ s12015-021-10244-1
29. Tosti A, et al. Mesotherapy protocols with dutasteride in AGA: a pilot clinical study. Dermatologic Therapy. 2019;32(6):e13059. doi:10.1111/ dth.13059
Emerging Research Highlights 2-Deoxy-D-Ribose as a Potential Pro-Angiogenic Agent for Male Pattern Baldness Therapy
A naturally occurring sugar, 2-deoxy-D-ribose (2dDR), is showing strong potential as a new approach to treating hair loss. This pentose sugar, known for its role in biological processes, has been found to stimulate angiogenesis the formation of new blood vessels around hair follicles. Increased vascularization boosts the supply of oxygen and nutrients essential for hair follicle regeneration and growth. In a testosterone-induced mouse model simulating male pattern baldness, topical application of 2dDR significantly promoted hair regrowth, with results comparable to Minoxidil, the only FDA-approved topical treatment for androgenic alopecia. The key mechanism behind 2dDR’s effectiveness lies in its pro-angiogenic activity, which improves microvascular blood flow to the follicular environment. This enhances follicle health and supports the growth of new hair. Unlike synthetic drugs, 2dDR is naturally derived, stable, cost effective, and poses fewer risks. Its compatibility with various delivery systems such as gels, creams, and dressings adds practical benefits for patients. Given that androgenic alopecia affects up to 50% of men globally and current treatments are limited, 2dDR could offer a novel, accessible alternative. This discovery paves the way for further research into natural compounds that promote hair regrowth by improving blood supply potentially offering new hope to millions affected by hair loss.
New Dual Therapy Shows Promise in Advancing Vitiligo Treatment
A new analysis signals a breakthrough in vitiligo care, highlighting the effectiveness of combining platelet-rich plasma (PRP) therapy with fractional laser treatment. The findings show that patients receiving both therapies experienced significantly improved skin repigmentation and greater satisfaction compared to those treated with either approach alone. The science behind the success lies in the synergy of both modalities. Fractional lasers commonly CO₂ and erbium: YAG creates controlled micro-injuries that activate the skin healing process and improve melanocytes activity. These microchannels also allow for deeper penetration of PRP, which is rich in growth factors like VEGF and PDGF. Together, they enhance skin regeneration, stimulate pigment-producing cells, and promote vascular remodeling.Unlike many existing options; this combination therapy reduced the number of non-responders without increasing side effects. Reported reactions were mild and temporary, such as slight redness or discomfort. Importantly, PRP may also reduce inflammation following laser treatment, improving comfort and adherence. While results are encouraging, experts caution that more research is needed. The reviewed studies were geographically limited and showed variability in treatment protocols. Nevertheless, this combined approach offers new hope for patients with stubborn, stable vitiligo, marking a potential shift toward more personalized, regenerative skin therapies.
A recent systematic review has confirmed that topical omega-3 polyunsaturated fatty acids (PUFAs) deliver significant benefits for skin conditions such as atopic dermatitis, wounds, contact dermatitis, and melanoma. These findings underscore the expanding therapeutic potential of omega3s beyond their traditional oral use.The review examined key fatty acids including alpha-linolenic acid (ALA), linoleic acid (LA), eicosapentaenoic acid (EPA), and docosahexaenoic acid (DHA) known for their anti-inflammatory and skin-repairing effects. The analysis showed that topical application improves skin hydration, reduces inflammation and irritation, accelerates wound healing, and alleviates symptoms in inflammatory skin disorders. Mechanistically, omega-3 PUFAs inhibit NF-κB and COX-2 inflammatory pathways and decrease proinflammatory cytokines such as IL-1β, IL-6, and TNF-α. They also promote skin barrier repair by enhancing keratinocyte function, maintaining lipid balance, and protecting against UV-induced oxidative damage.EPA and DHA formulations demonstrated strong efficacy and were well tolerated, with no significant adverse events reported. The review positions topical omega-3 PUFAs as a promising and scientifically supported adjunct in the management of inflammatory and barrier-compromised skin diseases.
New Review Uncovers Critical Diagnostic Gaps in Hair and Scalp Disorders for Skin of Color Patients
A new review has shed light on critical diagnostic challenges in identifying hair and scalp disorders in patients with skin of color (SoC), exposing major gaps in dermatology education and clinical practice. Misdiagnosis is common and can delay treatment, with serious conditions like leukemia and T-cell lymphoma sometimes mistaken for benign skin issues. Black women with vertex hair loss are frequently misdiagnosed with central centrifugal cicatricial alopecia (CCCA), though further testing often reveals conditions like alopecia areata or lichen planopilaris. Scalp biopsies corrected half of misdiagnoses and resolved all complex cases, while trichoscopy provided moderate support. The review stresses the need for mechanism-based diagnosis rather than relying on visual cues, which may be misleading in SoC patients. It also highlights systemic flaws in medical education, including limited SoC representation in training materials and insufficient instruction on SoC-specific conditions. These gaps contribute to clinician bias and reduced diagnostic confidence. Experts urge updates to dermatology curricula, increased use of diagnostic tools, and targeted training to improve care for patients with skin of color.