Laser Hair Reduction in Aesthetic Dermatology: Mechanisms, Patient Factors and Aesthetic Outcomes
Hair Restoration in Androgenetic Alopecia
Exosomes in Aesthetic
Dermatology: Biological Basis, Clinical Evidence and Regulatory
Considerations Part- I
Botulinum Toxin Type A for Upper Facial Rejuvenation: Mechanisms, Injection Techniques and Aesthetic Outcomes
Management of Facial Melasma Using Red Orange Complex and a Topical Depigmenting Agent: A Case-Based Insight into Antioxidant-Driven Therapy
EXECUTIVE EDITOR & PUBLISHER
Dom Daniel CORPORATE OFFICE
22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.
EMAIL: theaestheticiansjournalindia@gmail.com
Website: www.theaestheticiansjournal.online
Printed, Published, Edited and Owned by Dom Daniel Printed at Swastik Printer, Gala No.9 & 10, Vishal Industrial Estate, Bhandup (West), Mumbai- 400078. Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“The Aestheticians Journal” takes no responsibility for unsolicited photographs or material
ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of February 2026
Aesthetic Dermatology: Principles, Progress and Promise
Aesthetic dermatology today stands at the intersection of science, technology, and refined clinical judgment. As patient expectations evolve— from mere correction to sustained skin and hair health—there is a growing emphasis on evidencebased, mechanism-driven, and outcome-oriented therapies. This issue is curated to reflect this paradigm shift, bringing together topics that highlight both established pillars and emerging frontiers in aesthetic practice.
Melasma remains a persistent therapeutic challenge due to its chronicity, relapsing course, and multifactorial pathogenesis. Management of Facial Melasma Using Red Orange Complex presents a case-based approach emphasizing antioxidantdriven therapy, highlighting the importance of oxidative stress modulation and photoprotection as integral components of comprehensive melasma management. Botulinum toxin type A continues to be a cornerstone of facial rejuvenation. The article on Upper Facial Rejuvenation revisits its mechanisms of action while underscoring the importance of anatomical precision, refined injection techniques, and individualized dosing to achieve natural, harmonious outcomes. Hair loss, particularly androgenetic alopecia, remains one of the most emotionally distressing concerns for patients. The section on Hair Restoration in Androgenetic Alopecia explores contemporary strategies focused on preserving follicular health and restoring confidence through scientifically grounded interventions. Laserbased technologies continue to redefine aesthetic dermatology. Laser Hair Reduction in Aesthetic Dermatology provides insights into laser–tissue interactions, patient-related variables, and treatment outcomes, enabling clinicians to optimize safety and efficacy. Finally, Exosomes in Dermatology reflects growing interest in regenerative, cell-free therapies, offering promise in skin rejuvenation, hair restoration, and inflammatory dermatoses while encouraging critical appraisal of evolving evidence.
Together, these contributions aim to bridge science with practice, offering clinically relevant insights to support thoughtful, evidence-driven aesthetic care.
Management of Facial Melasma Using Red Orange Complex and a Topical Depigmenting Agent: A Case-Based Insight into Antioxidant-Driven Therapy
Dr. Bhagyashri
Jaju
MD (Dermatology)
Dermatologist, Cosmetologist & Trichologist
Radiance Skin Clinic
Mumbai Introduction
Melasma is a common acquired pigmentary disorder characterized by chronic and recurrent hypermelanosis of sunexposed skin, predominantly affecting the face. It occurs most frequently in women of all racial backgrounds, with a higher prevalence in individuals with darker Fitzpatrick skin phototypes (III–IV), typically presenting during the third and fourth decades of life.
Clinically, melasma manifests as symmetrical, irregularly bordered, light- to darkbrown macules and patches, most commonly distributed in centrofacial, malar, and mandibular patterns. Owing to its conspicuous facial involvement, melasma represents one of the most distressing pigmentary conditions encountered in dermatological practice.1
The etiology of melasma is multifactorial and not yet fully elucidated, although a strong
genetic predisposition has been demonstrated. Nearly half of affected individuals report a positive family history, suggesting an inherited susceptibility. Environmental and hormonal factors play a crucial role in disease expression. Chronic sun exposure remains the most important precipitating and exacerbating factor, with ultraviolet radiation inducing melanocyte stimulation, endothelial activation, oxidative stress, and basement membrane disruption. In addition to ultraviolet light, visible light has been shown to contribute to melanogenesis through inflammatory pathways and enhanced melanocyte–keratinocyte interaction. At the molecular level, melasma is now recognized as a complex disorder involving multiple biochemical and cellular pathways rather than a simple increase in melanin production. Dysregulation of Wnt signalling pathways, characterized by
increased expression of Wntrelated genes and reduced levels of Wnt inhibitory factor-1, promotes melanocyte stem cell proliferation, melanogenesis, and enhanced melanosome transfer. Alterations in the PI3K/Akt pathway further modulate melanocyte activity, while structural damage to the basement membrane leads to loss of epidermal–dermal homeostasis and persistent low-grade inflammation. Histologically, melanocyte hyperactivity in melasma is primarily due to hypertrophy of existing melanocytes with increased melanosome density, rather than an increase in melanocyte number. Hormonal influences are well established in melasma pathogenesis, as evidenced by its frequent association with pregnancy, oral contraceptive use, and hormone replacement therapy. Estrogen and progesterone are known to upregulate melanogenic pathways, and a subset of women develop melasma following exposure to exogenous hormones. Notably, switching from combined oral contraceptives to hormonereleasing intrauterine devices has been associated with spontaneous improvement in some patients, further supporting the role of hormonal modulation.1
Melasma is commonly classified according to the depth of pigment deposition into epidermal, dermal, and mixed types, using tools such as Wood’s lamp examination and dermoscopy, which have important therapeutic and prognostic value. Although benign, melasma exerts a
significant psychosocial burden, often leading to reduced selfesteem, social avoidance, and impaired quality of life.1,2,3
Diagnosis is primarily clinical, based on symmetrical hyperpigmented macules and patches on sun-exposed facial areas. Wood’s lamp aids pigment depth assessment, particularly in lighter phototypes, while dermoscopy highlights pseudoridge pigmentation patterns. In select cases, biopsy or advanced imaging such as reflectance confocal microscopy may be used, and disease severity is commonly assessed using Melasma Area and Severity Index (MASI).1,4,5,6 Management remains challenging because of its chronic, relapsing nature and multifactorial pathogenesis, with frequent recurrence even after apparent clearance.
Here, we present a case of facial melasma successfully managed using a red orange complex-based formulation and a topical depigmenting agent, demonstrating notable clinical efficacy and an excellent patient response. The treatment protocol combined red orange complex-based formulation with a topical depigmenting regimen that included tranexamic acid cream, a broad-spectrum sunscreen and a gentle hydrating moisturizer. This multimodal approach targeted melanogenesis while supporting the skin barrier and minimizing irritation. Progressive lightening of pigmentation, improvement in skin tone uniformity, and enhanced overall radiance were observed, highlighting the potential role of red orange complex as an effective adjunct
in melasma management.
Case Report
A 32-year-old female presented to the dermatology clinic with a history of gradually progressive facial hyperpigmentation of several years’ duration. The pigmentation was bilateral and symmetrical, predominantly involving the malar regions, cheeks, and forehead. The condition was cosmetically distressing to the patient and was noted to exacerbate with sun exposure. Cutaneous examination revealed irregularly bordered light- to dark-brown macules and patches distributed over the centrofacial and malar regions, clinically consistent with melasma. The surrounding skin showed mild textural irregularity and features suggestive of dehydration, without evidence of active inflammation, erythema, or scaling. Based on the characteristic morphology and distribution of the lesions, a clinical diagnosis of facial melasma was established.
Treatment Protocol
The patient was initiated on a targeted depigmenting regimen combining an oral formulation containing 100 mg of red orange complex (ROC two times daily) and topical tranexamic acid cream 10% every night, both selected as active therapeutic agents for melasma management.
The red orange complex, rich in anthocyanins, flavanones, hydroxycinnamic acids, and vitamin C, provides potent antioxidant and photoprotective effects, helping to counter oxidative stress, inhibit melanogenesis, and modulate UV-induced inflammatory
pathways central to melasma pathogenesis.
Tranexamic acid was incorporated as a depigmenting agent due to its established role in suppressing melanocyte activation and reducing vascular and inflammatory mediators associated with pigmentation.
To support barrier repair and improve treatment tolerance, the following adjunctive measures were incorporated:
• Broad-spectrum sunscreen with high UVA and visible light protection prescribed for daily use to prevent pigment relapse and photodamage.
• Gentle hydrating moisturizer containing
humectants and barrier-restoring ingredients, applied twice daily to address epidermal dehydration, support epidermal barrier homeostasis and enhance skin resilience.
No aggressive depigmenting agents or procedures were used during the initial phase to minimize irritation and post-inflammatory hyperpigmentation risk.
Treatment Outcome and Follow-Up
Over the course of treatment, the patient showed progressive and noticeable lightening of facial pigmentation, with improved skin tone uniformity and enhanced radiance. A visible reduction in patch intensity over the malar and forehead regions was observed, along with improved skin hydration and texture. The treatment was well tolerated, with no reported adverse effects such as erythema, burning, or irritation. A meaningful reduction in disease severity from baseline was noted, correlating well with the clinical improvement, and these results were evident after 2 months of therapy.
As part of maintenance therapy, continuation of ROC as an oral antioxidant was advised for a few more months, followed by intermittent use during periods of increased sun exposure, such as the summer months or vacations.
Discussion
Melasma is a common, chronic, acquired hyperpigmentation
disorder that predominantly affects the facial skin. Its global prevalence may reach up to 41% in certain populations, and the conspicuous facial involvement significantly impairs patients’ quality
Before treatment
After 2 months treatment
Figure 1: Clinical improvement in facial melasma demonstrating enhanced skin tone uniformity and radiance following 2 months of treatment with the red orange complex
of life, with notable psychological and emotional consequences. Despite its high prevalence, the management of melasma remains challenging because of its recalcitrant nature, variable treatment response, and high rates of recurrence.7,8
The pathogenesis of melasma is complex and multifactorial. Traditionally, melasma has been attributed to increased melanin synthesis by hyperactive melanocytes and abnormal accumulation of melanosomes within the epidermis. However, contemporary evidence indicates that melasma is not solely a pigmentary disorder but involves multiple cellular and molecular pathways. Established triggering factors include ultraviolet (UV) radiation, genetic predisposition, and hormonal influences. More recent theories have highlighted the contributory roles of oxidative stress, inflammation, vascular and neural factors, impairment of the epidermal barrier, visible light exposure, and dysregulation of various molecular signalling pathways.8,9,10
Oxidative stress has emerged as a key pathogenic contributor in melasma. Elevated levels of circulating antioxidants in serum and increased expression of vascular endothelial growth factor (VEGF) within melasma lesions suggest an adaptive response to heightened oxidative injury and vascular involvement. Chronic UV exposure induces reactive oxygen species (ROS), which can stimulate melanogenesis directly and indirectly through inflammatory mediators, thereby perpetuating pigmentation and disease chronicity.
Red
Orange Complex (ROC): Antioxidant, Anti-inflammatory and Photoprotective Effects:
Red orange complex is a rich source of bioactive compounds with a robust antioxidant profile. The extract is highly concentrated in polyphenols and ascorbic acid, particularly anthocyanins, hydroxycinnamic acids, flavanones, and vitamin C, which collectively contribute to its potent free-radical scavenging capacity. The antioxidant activity of red orange extract has been extensively evaluated across diverse target populations, including athletes, individuals with diabetes, smokers, and subjects exposed to environmental air pollution.11,12
Beyond its systemic antioxidant effects, red orange extract has demonstrated significant skinprotective properties. Multiple experimental and clinical studies have investigated its role in protecting against ultraviolet (UV)-induced erythema and hyperpigmentation, particularly following sunlamp exposure. In a key experimental study, red orange complex H extract (ROC) was administered to evaluate its protective effects against UVA- and UVB-induced skin damage. ROC was shown to enhance endogenous scavenger activity, improve UVB protection, and exert antiinflammatory effects. These actions were mediated through modulation of inflammatory and stress-related signalling pathways, including activation of tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and nuclear factor-κB (NF-κB), along with downregulation of matrix
metalloproteinases (MMPs) in vitro, thereby limiting collagen degradation and photoagingrelated dermal damage.11,12
Clinical evidence further supports the photoprotective and anti-aging efficacy of ROC. Several studies have demonstrated that oral supplementation with red orange extract strengthens the skin’s physiological antioxidant defense mechanisms, reducing oxidative stress induced by UV radiation. In addition, ROC exhibits pronounced anti-inflammatory properties, primarily through suppression of IL-6 and TNF-α secretion and accumulation. Importantly, it has also been shown to downregulate melanogenesis, contributing to improved pigmentation and a more uniform skin tone.11,12 Collectively, these findings highlight red orange complex as a promising nutraceutical that protects against photo-induced damage, reduces inflammation and oxidative stress, and improves skin appearance and pigmentation.
In this context, Red Orange Complex (ROC) appears to be a promising adjunctive strategy in melasma management. ROC has been shown to significantly reduce UVB-induced erythema and hyperpigmentation, leading to a more uniform and homogeneous skin tone. These effects are particularly relevant in melasma, where UV-induced inflammation and oxidative stress are major aggravating factors. Both in vitro and clinical studies have demonstrated the potent antioxidant capacity of ROC, supporting cellular defense mechanisms under
conditions of oxidative imbalance.7,8,9,10,11,12
Tranexamic acid is a plasmin inhibitor with antifibrinolytic, antiinflammatory, anti-melanogenic, and anti-angiogenic properties. Owing to its proven efficacy and favorable safety profile, it is widely used and considered a effective therapy for melasma.13
Fatima et al. concluded that sunscreen improves melasma, with combination therapy being more effective. Regular photoprotection using broadspectrum UV and visible light sunscreen is essential
References
1. Gonzalez-Botello, Ana-Lorena. Oral Supplementation in the Treatment of Melasma: A Systematic Review. Journal of Dermatology and Dermatologic Surgery 29(1):p 10-16, Jan–Jun 2025. | DOI: 10.4103/jdds.jdds_31_24
2. Coricciati L, Gabellone M, Donne PD, Pennati BM, Zingoni T. The 675-nm wavelength for treating facial melasma. Skin Res Technol. 2023; 29:e13434. https://doi.org/10.1111/srt.13434
3. Sarkar R, Chugh S, Garg VK. Newer and upcoming therapies for melasma. Indian J Dermatol Venereol Leprol 2012;78:417428
4. Sanchez, Nestor P. et al. Melasma: A clinical, light microscopic, ultrastructural, and immunofluorescence study. Journal of the American Academy of Dermatology, Volume 4, Issue 6, 698 - 710
5. Gao, Tian-Wen1; Gu, Hua2; He, Li2,*; Lei, Tie-Chi3; Li, Ming4; Li, Tie-Nan5; Li, Chun-Ying1; Lin, Tong6; Mu, Kuan-Hou7; Tu, Cai-Xia8; Wen, Hai9; Wu, Ji-Yuan10; Xu, Ai-E11,*; Zhang, Jun-Ling12; Zhen, Zhi-Zhong13. Consensus on the Diagnosis and Treatment of Melasma in China (2021 Version)#. International Journal of Dermatology and Venereology 4(3):p 133139, September 2021. | DOI: 10.1097/ JD9.0000000000000164
6. Honigman A, Rodrigues M. Differential diagnosis of melasma
in melasma prevention and treatment.14 Moisturizing skincare products increase epidermal hydration, restore skin barrier function, reduce dryness and peeling, and improve skin smoothness.15
Conclusion
This case underscores the pivotal role of oxidative stress and photoinduced inflammation in melasma pathogenesis. Use of red orange complex (ROC) as a core therapeutic agent produced significant clinical improvement through its antioxidant, anti-inflammatory, and melanogenesis-modulating effects. Topical tranexamic acid cream enhanced efficacy by inhibiting melanocyte activation and vascular-inflammatory pathways. When combined with supportive skincare measures, including adequate moisturization and strict photoprotection, treatment outcomes were optimized and relapse minimized. ROC-based therapy emerges as a safe, well-tolerated, and effective demelanizing option, reinforcing the importance of a holistic, barrier-friendly approach in managing this chronic, relapsing disorder.
and hyperpigmentation. Dermatological Reviews. 2023; 4: 30-37. doi:10.1002/ der2.144
7. Khurana, Neelam; Mehdi, Mohammad M.; Sawhney, Mohinder P. S.1; Bansal, Sanjiv K.2. Assessment of Systemic Oxidative Stress Modulation in Melasma Following Treatment with Yellow Light Laser 577 nm and Topical 0.3% 4N Butyl Resorcinol: A Comparative Prospective Study. Indian Journal of Dermatology 70(2):p 57-62, Mar–Apr 2025. | DOI: 10.4103/ijd.ijd_11_24
8. Wang L-J, Pang Y-B, Li W-Q, He Q-Y, Zhang X-E, Liu E and Guo J (2024), Global research trends on melasma: a bibliometric and visualized study from 2014 to 2023. Front. Pharmacol. 15:1421499. doi: 10.3389/ fphar.2024.1421499
9. Aishwarya K, Bhagwat PV, John N. Current concepts in melasma - A review article. J Skin Sex Transm Dis 2020;2(1):13-7.
12. Puglia, C., Offerta, A., Saija, A., Trombetta, D. and Venera, C. (2014), Protective effect of red orange extract supplementation against UV-induced skin damages: photoaging and solar lentigines. J Cosmet Dermatol, 13: 151-157. https:// doi.org/10.1111/jocd.12083
13. Zehua Chen, Lvping Huang. Different administration routes of tranexamic acid in the treatment of melasma. Chinese Journal of Plastic and Reconstructive Surgery. Volume 6, Issue 3, 2024, Pages 154-158, ISSN 2096-6911, https://doi. org/10.1016/j.cjprs.2024.06.006.
14. Fatima, S., Braunberger, T., Mohammad, T. F., Kohli, I., & Hamzavi, I. H. (2020). The Role of Sunscreen in Melasma and Postinflammatory Hyperpigmentation. Indian journal of dermatology, 65(1), 5–10. https://doi. org/10.4103/ijd.IJD_295_18
15. Wang, Y., Zhao, J., Jiang, L., & Mu, Y. (2021). The Application of Skin Care Product in Melasma Treatment. Clinical, cosmetic and investigational dermatology, 14, 1165–1171. https:// doi.org/10.2147/CCID.S323748
11. Kim, Y. H., Lim, C. Y., Jung, J. I., Kim, T. Y., & Kim, E. J. (2023). Protective effects of red orange (Citrus sinensis [L.] Osbeck [Rutaceae]) extract against UVA-B radiation-induced photoaging in Skh:HR-2 mice. Nutrition research and practice, 17(4), 641–659. https://doi.org/10.4162/ nrp.2023.17.4.641
Management
AI at the Bedside: Transforming Vitiligo Management
Current developments in vitiligo management highlight the transformative role of artificial intelligence (AI) and deep learning algorithms in diagnosis, progression tracking, and treatment forecasting. Traditional assessment tools, such as the Vitiligo Area Scoring Index (VASI) and Vitiligo Disease Activity (VIDA) score, rely heavily on clinician judgment and are inherently semi-quantitative, limiting objective monitoring and treatment evaluation. AI-assisted imaging, including clinical photography, dermoscopy, and multisource fusion, combined with deep learning models such as CNNs and attention-based algorithms, achieves over 90% diagnostic accuracy, distinguishes vitiligo from mimickers, and enables precise lesion segmentation. These tools quantify depigmented areas, detect early disease, and track subtle activity changes more objectively than conventional scoring. Automated progression tracking with serial imaging and optical coherence tomography allows near-histological assessment of melanocyte loss and re-pigmentation, while mobile AI applications support remote monitoring and enhance patient engagement. Predictive AI models integrating clinical, imaging, and laboratory data can forecast individualized responses to therapies like narrowband UVB or JAK inhibitors, optimizing outcomes and reducing ineffective treatments. Challenges remain for AI in vitiligo, including small, heterogeneous datasets, underrepresentation of darker skin types, and need for large-scale validation. Priorities include standardizing imaging, improving model interpretability, and establishing regulatory frameworks. Addressing these could make AI a reliable bedside tool, enabling personalized, data-driven care and transforming vitiligo management.
Lasers and Energy-Based Devices: Modulating Cellular Senescence for Skin Rejuvenation
Emerging evidence suggests that lasers and energy-based devices may target cellular senescence, offering a potential avenue for fundamental skin rejuvenation at the molecular level. Cellular senescence, a key feature of skin aging, is characterized by cell cycle arrest, altered secretory profiles, and disrupted tissue homeostasis. A recent systematic review evaluated whether dermatologic technologies can modulate these senescent pathways, identifying studies examining lasers, light-based therapies, radiofrequency, ultrasound, photobiomodulation, photodynamic therapy, and intense pulsed light. Despite variability in study protocols and endpoints, most reports demonstrated reductions in markers of cellular senescence accompanied by improvements in age-related skin changes. Some studies further suggested a potential role in reducing neocarcinogenesis, indicating that modulating senescent signalling could influence longterm oncologic risk. Across modalities, treatment appeared to restore more youthful cellular signalling patterns, improving cell function and promoting clinical and microscopic signs of skin rejuvenation. These findings support the concept that controlled, low-level stress from lasers and energy-based devices may induce hormesis, enhancing tissue resilience and potentially improving skin structure and longevity by targeting cellular senescence. Clinically, these treatments could offer benefits beyond resurfacing or tightening, but current evidence is limited, with small, heterogeneous studies. Larger, standardized trials are needed to define optimal parameters, patient selection, and safety, while clinicians should interpret results in the context of individual patient goals and evolving scientific knowledge.
Botulinum Toxin Type A for Upper Facial
Rejuvenation: Mechanisms, Injection Techniques and Aesthetic Outcomes
Dr. Harkanwal Sekhon MD (Dermatology) Consultant Dermatologist
Ludhiana,
Punjab
Introduction
Botulinum toxin is a potent neurotoxic protein produced by Clostridium botulinum, a grampositive, anaerobic, sporeforming bacterium. Controlled therapeutic formulations have become integral to modern medical and aesthetic practice. Initially introduced in the late 1970s, its clinical applications have since expanded significantly, with notable use in dermatology and related therapeutic fields.1, 2
Botulinum toxin exists as seven immunologically distinct serotypes, labeled A through G, each produced by Clostridium botulinum but differing in molecular structure, potency, and clinical relevance. Among these, only serotypes A and B are widely used in clinical practice due to their established safety profiles, predictable pharmacodynamics, and effectiveness in neuromuscular modulation. Serotype A predominates
in aesthetic applications and is available in multiple commercial formulations, including onabotulinumtoxinA, abobotulinumtoxinA, and incobotulinumtoxinA, each with specific dosing guidelines, diffusion properties, and reconstitution requirements. Serotype B, available as rimabotulinumtoxinB, is primarily utilized in therapeutic rather than cosmetic indications, such as certain dystonias and spasticity. Serotypes C, D, E, F, and G exist and have been studied experimentally, but they are not routinely used in clinical or aesthetic practice due to limited efficacy, shorter duration of action, or higher immunogenicity. The proven ability of botulinum toxin to soften dynamic wrinkles has driven its widespread adoption in aesthetic medicine, where it is routinely used to address glabellar lines, forehead rhytides, lateral canthal lines, perioral rhytids, marionette lines, and platysmal bands. Its therapeutic
Botulinum
effect arises from precise, localized chemical denervation that relaxes overactive facial muscles, allowing for natural smoothing of dynamic lines and improved facial symmetry, establishing botulinum toxin as a cornerstone in modern facial rejuvenation.1, 3
Mechanism of action
botulinum toxin type A
The mechanism of botulinum toxin type A (BTX-A) involves a highly specific, multistep process resulting in reversible chemodenervation of targeted muscles, forming the basis of its use in aesthetic medicine. The heavy chain of BTX-A binds selectively to high-affinity receptors on the presynaptic membrane of cholinergic neurons at the neuromuscular junction, mainly polysialogangliosides and synaptic vesicle proteins, ensuring precise action on hyperactive muscle fibers while minimizing systemic exposure. After binding, the toxin undergoes receptormediated endocytosis into the neuron within an endocytic vesicle, and acidification of the vesicle triggers a conformational change that allows the light chain to translocate into the cytosol. The light chain, a zincdependent endopeptidase, specifically cleaves SNAP-25, a key component of the SNARE complex responsible for vesicle docking and acetylcholine release. Cleavage of SNAP-25 blocks acetylcholine release into the synaptic cleft, producing localized, reversible muscle relaxation. In aesthetic applications, this relaxation softens dynamic facial lines
such as glabellar frown lines, forehead rhytides, lateral canthal lines, and nasal bunny lines without affecting overall facial expression. Effects typically last three to six months, as nerve terminals regenerate and new SNARE proteins restore neurotransmission. Botulinum toxin has become an essential tool in modern medical and aesthetic practice, with its precise mechanism, established safety, and effectiveness in softening dynamic facial lines forming the foundation for its widespread use in facial rejuvenation and related therapeutic applications. As a precise and controllable neuromodulator, botulinum toxin represents a pivotal advancement in managing dynamic facial lines, highlighting its growing significance in aesthetic medicine and related therapeutic fields.2, 4
Diagnostic Considerations in Aesthetic Botulinum Toxin Therapy
A comprehensive pre-treatment assessment is fundamental to achieving safe, effective, and predictable outcomes in aesthetic botulinum toxin therapy. A detailed medical and medication history should screen for neuromuscular disorders, hypersensitivity to botulinum toxin or its excipients, drugs that interfere with neuromuscular transmission, prior exposure to botulinum toxin, and physiological states such as pregnancy or lactation.5
Equally important is the evaluation of psychological factors, including body image concerns and unrealistic
expectations, which may influence patient satisfaction and treatment success. Clinical examination should include a thorough physical and functional assessment of the skin and underlying musculature, noting skin quality, scars, atrophy, infection, and distinguishing dynamic from static muscle activity to guide accurate injection planning. Baseline motor function assessment and standardized pre-procedure photography aid in treatment mapping and objective outcome evaluation. Adjunctive diagnostic tools further enhance precision. Electromyography (EMG) helps identify subtle muscle hyperactivity, asymmetry, or compensatory recruitment, particularly in smal l or overlapping facial muscles, enabling precise targeting while minimizing diffusion-related complications. Ultrasound imaging allows realtime visualization of deep or anatomically variable muscles, improving accuracy and safety by avoiding neurovascular structures. Advanced tools such as 3D facial imaging, infrared thermography, patient-reported outcome measures, and muscle force testing collectively support individualized treatment planning and optimize aesthetic outcomes.5,6,7,8,9,10
These combined assessments and adjunctive imaging tools support individualized, precise, and safe aesthetic outcomes.
Treatment
The increasing demand for minimally invasive facial rejuvenation has established botulinum toxin injections as a
Botulinum Toxin Type A for Upper Facial Rejuvenation:
cornerstone of contemporary aesthetic medicine. These procedures are widely utilized for the management of dynamic facial rhytides and selected contouring indications, particularly in the upper face. Appropriate application requires comprehensive facial analysis, precise anatomical knowledge, and an individualized, patientcentred treatment approach to ensure optimal outcomes while minimizing complications. Aesthetic indications for botulinum toxin include treatment and prevention of dynamic wrinkles such as glabellar frown lines, forehead rhytides, and lateral canthal lines. It is also used for correcting brow asymmetry, brow descent, and achieving a chemical brow lift by weakening brow depressor muscles. Additionally, botulinum toxin prevents progression of dynamic to static wrinkles and serves as an adjunct to fillers, resurfacing procedures, and aesthetic surgery to enhance and prolong outcomes.
In patients with combined dynamic and static lines, muscle relaxation is performed first, followed by reassessment and targeted treatment of residual static wrinkles.11, 12
Pre-Procedure Assessment and Patient Selection
A comprehensive pre-treatment evaluation is essential, including a detailed medical history, review of prior aesthetic procedures and assessment of contraindications such as pregnancy, breastfeeding, neuromuscular disorders, hypersensitivity, local infection, or medications that potentiate
neuromuscular blockade. Facial analysis at rest and during animation should document muscle activity, symmetry, wrinkle patterns, and brow position, with standardized photography for baseline reference. Informed consent must be obtained, and correct dosing, dilution, and injection technique are critical to ensure safety and efficacy.11, 12
Procedural Setting and Preparation
Botulinum toxin injections are performed on an outpatient basis with the patient in an upright or semi-reclined position. The treatment area is cleansed thoroughly to remove cosmetics and debris, followed by antiseptic skin preparation. Target muscles are identified using palpation during voluntary contraction to accurately locate the muscle belly and zones of maximal activity. Injection sites may be marked to ensure symmetry and precision. Fine-gauge needles are used to minimize discomfort and tissue trauma. The procedure is generally well tolerated, although topical aesthetic is used for patient comfort.11, 12
Injection Technique and Upper Face Applications
Glabella
Treatment of the glabella represents the only FDAapproved cosmetic indication for BTX-A. Targeting this area alleviates the appearance of an angry crown or fatigued look, imparting a more relaxed and pleasant facial expression. Early intervention with BTX-A can prevent the development of static lines.13
Technique
Procerus and corrugators are treated with 3–5 low-volume, concentrated injections. The procerus is injected intramuscularly at the midpoint of an imaginary X between inner brows and contralateral inner canthi; elongated muscles may require two points (6–12 U). Corrugators are palpated during frowning/squinting and injected in the muscle belly with 6–8 U, needle directed upward and away from the globe ~1 cm above the orbital rim. Outcomes are better in thinner skin and finer wrinkles (positive glabellar spread test); thick sebaceous skin and deep furrows are harder to treat. Total doses range 10–40 U (higher in males). Effect duration depends on muscle size and dose—typically 4–6 months. BTX-A alone suits dynamic lines; if static lines persist, fillers may be added after 2 weeks. Repeat BTX-A at 4–6 months can further improve static lines with fewer side effects than fillers.13
Bunny Lines (Oblique Nasal Furrows)
Bunny lines are oblique wrinkles that appear bilaterally on the dorsum of the nose, oriented at approximately a 45° angle. These lines are primarily formed by the contraction of the levator labii superioris alaeque nasi muscle, with a secondary contribution from the medial fibers of the orbicularis oculi muscle. For cosmetic attenuation of these wrinkles, a total dose of 2 units of botulinum toxin should be administered into the upper portion of the levator labii superioris alaeque nasi muscle
Botulinum
on each side. The injection site is at the intersection of a horizontal line at the rhinion and a vertical line through the medial canthus, ensuring precise muscle relaxation while minimizing diffusion to adjacent muscles.14
Periorbital Area
Periorbital rhytides (crow’s feet) result primarily from hyperactivity of the orbital fibers of the orbicularis oculi muscle.13
Technique
Injections are delivered subcutaneously, 1 cm lateral to the orbital rim at three sites (2–4 U per site) targeting lateral orbicularis oculi fibers while avoiding the zygomaticus. Doses may be increased in males with hyperfunctional musculature. In cases of deeply resistant crow’s feet, additional temporal injection points may be beneficial. Total doses of 10–30 U have been reported, with effects lasting approximately 3–4 months.13
Forehead
The frontalis muscle elevates the forehead and eyebrows, producing transverse forehead wrinkles. In most individuals, two bellies of the frontalis are separated by a central tendinous aponeurosis, but some males and females have central muscle fibers detectable via palpation during active eyebrow movement.13
Technique
Pre-existing brow asymmetry should be documented, and patients counselled that treatment may diminish or accentuate asymmetry. Injection sites are marked and 1–2 U of BTX-A administered
subcutaneously or intramuscularly at 1.5–2 cm intervals along a “V” or horizontal pattern, starting 1 cm above the medial eyebrow and finishing at the hairline. When central muscle fibers are present, midline injections are performed; otherwise, they are avoided. Typically, 6–15 U is administered across 6–8 sites for the entire forehead, with results persisting 3–6 months.13
Chemical Brow Lift
The ideal female brow has a medial point on the alar base–medial canthus line, an arch ~1 cm above the supraorbital rim, and a lateral endpoint on the alar base–lateral canthus line; male brows are flatter. Brow elevation reflects frontalis activity opposed by medial (corrugators, procerus) and lateral (orbicularis oculi) depressors; selective paralysis of depressors permits unopposed frontalis lift. Injections target the glabella and lateral orbicularis oculi below the brow; lateral lift is enhanced with 2–4 U BTX-A at the lateral orbital orbicularis oculi just above the supraorbital ridge or along the superior temporal line. Absolute contraindications include neuromuscular disorders (e.g., myasthenia gravis, ALS), active infection, BTX-A hypersensitivity, pregnancy/lactation, drugs affecting neuromuscular transmission (aminoglycosides, curaretype blockers, quinidine, magnesium sulphate, succinylcholine), and psychiatric disorders.13
Post-Procedure Care
Patients are observed briefly following injection and provided with standardized post-procedure instructions. These include remaining upright for several hours, avoiding massage or manipulation of the treated areas, and limiting strenuous physical activity for the remainder of the day. Patients are advised that clinical effects typically begin within a few days, peak within one to two weeks, and gradually diminish over several months. Follow-up assessment may be scheduled to evaluate treatment response.13
Result
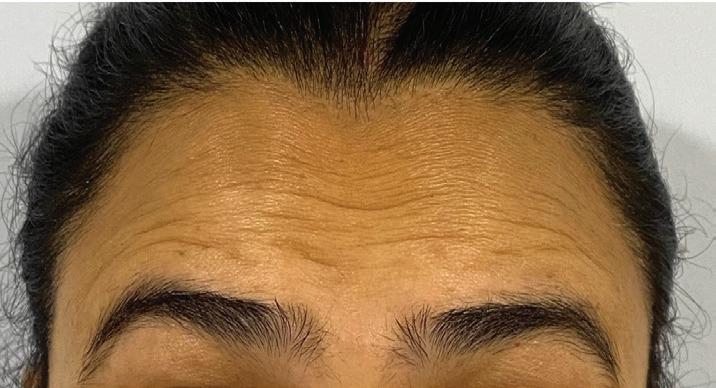
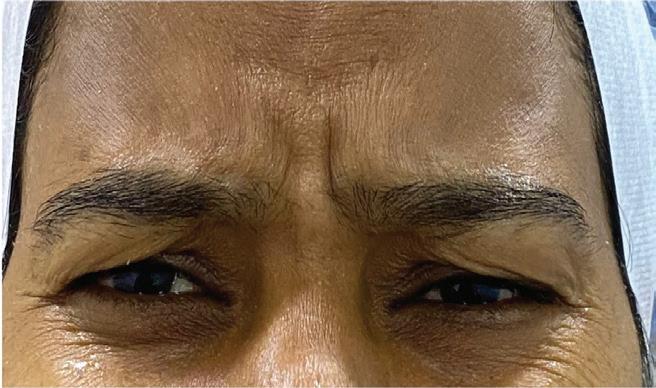
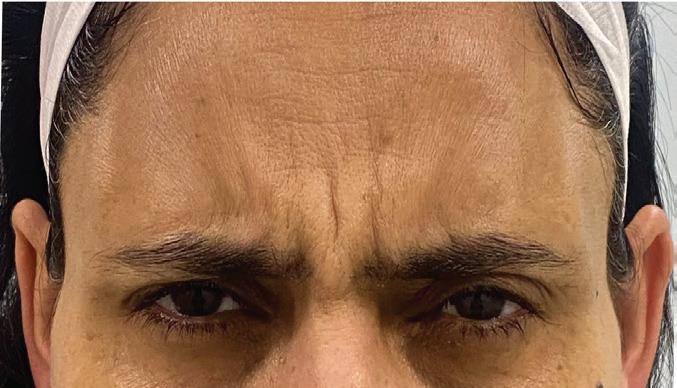
Patient 1 - Frown lines treated with Botulinum Toxin Type A
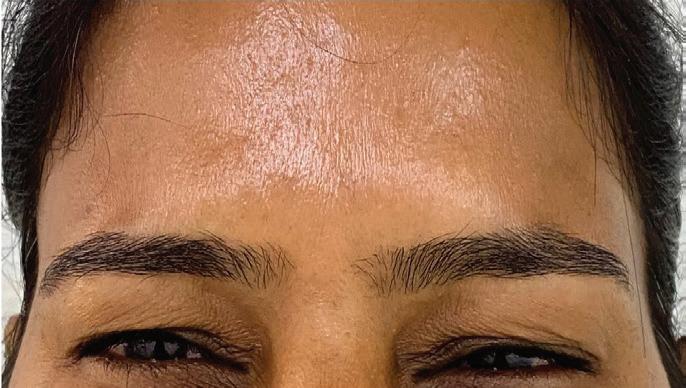
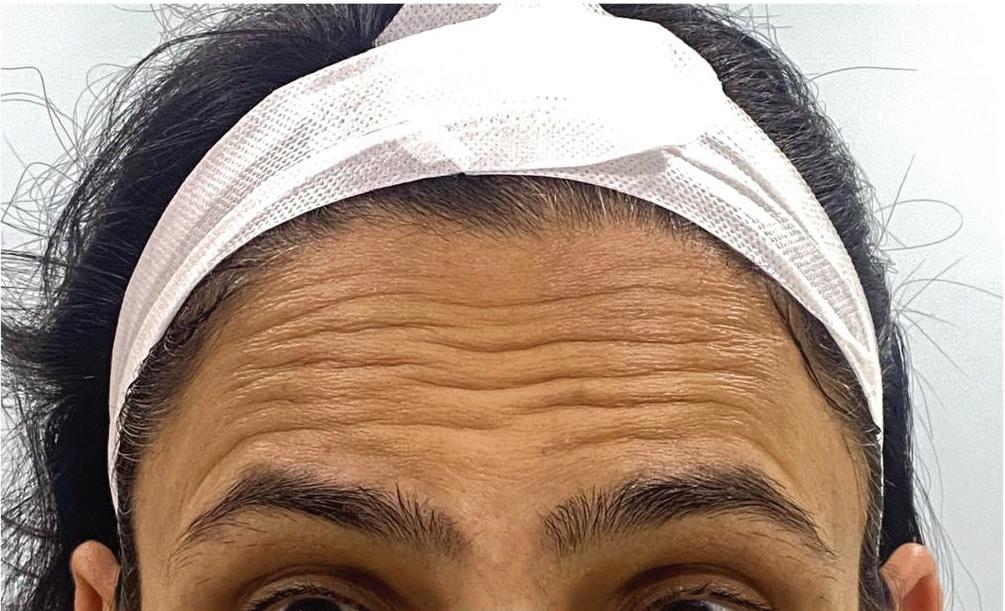
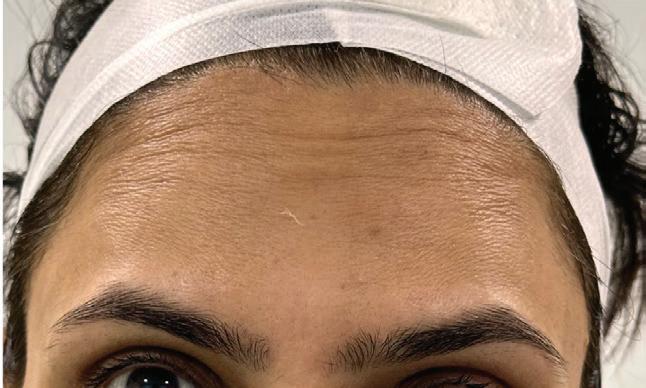
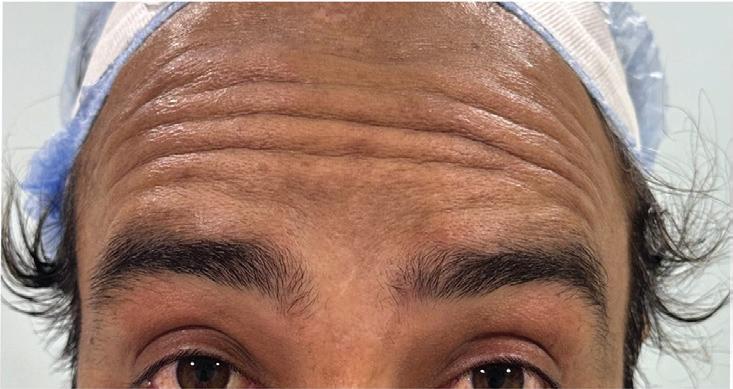
Patient 1 - Forehead lines treated with Botulinum Toxin Type A
Patient 2 - Forehead lines treated with Botulinum Toxin Type A
Patient 4 - Frown lines treated with Botulinum Toxin Type A
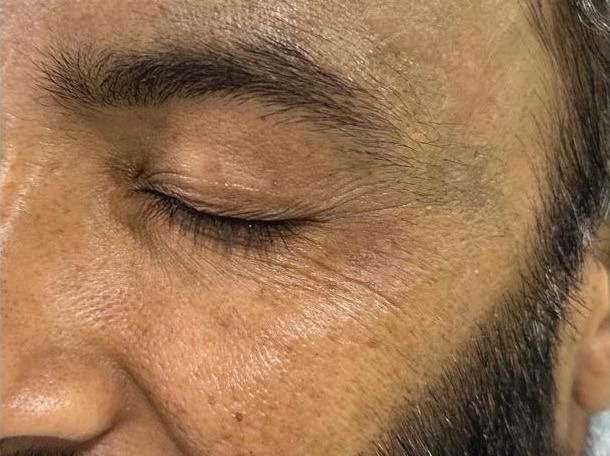
Patient 5 - Crow's Feet treated with Botulinum Toxin Type A
Patient 2 - Frown lines treated with Botulinum Toxin Type A
Patient 3 - Forehead lines treated with Botulinum Toxin Type A
Patient 2 - Crow's Feet treated with Botulinum Toxin Type A
Discussion
Botulinum toxin (BoNT) is an indispensable tool in aesthetic medicine, with botulinum toxin type A (BTX-A) being the most extensively studied and widely used formulation. Among available preparations, onabotulinumtoxinA is the most commonly utilized worldwide for both cosmetic and therapeutic indications, while abobotulinumtoxinA and incobotulinumtoxinA are also in clinical use. In the upper face, BTX-A injections represent a cornerstone of minimally invasive aesthetic practice, offering reliable improvement in facial appearance along with meaningful psychosocial benefits. Facial aging is an inevitable process resulting from cumulative structural and volumetric changes involving the skin, subcutaneous fat, ligaments, muscles, and underlying bone, collectively shaping the aging phenotype and influencing self-perception and social interactions. Increasingly, younger adults are seeking BTX-A for preventive use, a concept termed “prejuvenation,” aimed at preserving youthful facial dynamics and delaying wrinkle formation. By targeting frown muscles, BTX-A reduces dynamic lines and modulates emotional feedback, contributing to improved mood, self-confidence, and social engagement beyond purely cosmetic outcomes.15, 16, 17
Optimal outcomes with BTX-A depend on meticulous patient selection, a thorough understanding of facial anatomy and muscle dynamics, and
Patient 6 - Forehead lines treated with Botulinum Toxin Type A
Patient 6 - Frown lines treated with Botulinum Toxin Type A
Patient 7 - Crow's Feet treated with Botulinum Toxin Type A
Patient 8 - Crow's Feet treated with Botulinum Toxin Type A
Botulinum
precise injection technique with individualized dosing. Younger patients often report higher satisfaction, as their wrinkles are predominantly dynamic and respond more predictably to treatment. Preservation of partial frontalis muscle activity— especially in the lateral fibers—is crucial to prevent an unnatural or “frozen” appearance. Dose customization is essential: men typically require higher doses due to greater muscle mass, while lower doses are advisable in patients with dermatochalasis or pre-existing eyebrow ptosis. Technical nuances include recognizing and managing the Mephisto sign, which results from unopposed lateral frontalis activity, and addressing arched supraciliary wrinkles using targeted, superficial injections. Improper lateral placement may lead to a “cockeyed” brow, correctable with small doses administered medial to the temporal fusion line. Brow ptosis can be minimized by maintaining injection points at
References
1. Nigam PK, Nigam A. Botulinum toxin. Indian J Dermatol. 2010; 55(1):8-14. doi:10.4103/0019-5154.60343
2. Satriyasa BK. Botulinum toxin (Botox) A for reducing the appearance of facial wrinkles: a literature review of clinical use and pharmacological aspect. Clin Cosmet Investig Dermatol. 2019; 12:223-228. Published 2019 Apr 10. doi:10.2147/ CCID.S202919
3. Kaji R, Endo A, Sugawara M, Ishii M. Efficacy of botulinum toxin type B (rimabotulinumtoxinB) in patients with cervical dystonia previously treated with botulinum toxin type A: A postmarketing observational study in Japan. eNeurologicalSci. 2021; 25:100374. Published 2021 Oct 27. doi:10.1016/j. ensci.2021.100374
4. Padda IS, Tadi P. Botulinum Toxin. In: StatPearls. Treasure Island (FL):
least 1.5–2 cm above the orbital rim. When appropriately performed, temporal hairline injections for supraciliary wrinkles are safe and effective, underscoring the versatility of BTX-A in tailored upper facial rejuvenation.15, 16, 17
Botulinum toxin is a safe and effective aesthetic treatment widely used to reduce dynamic facial lines, including frown lines, forehead wrinkles, and crow’s feet, thereby improving facial symmetry and overall appearance. High patient satisfaction reflects both visible aesthetic enhancement and psychosocial benefits such as improved self-confidence and mood. Adverse effects are typically mild and transient, including injection-site pain, edema, erythema, ecchymosis, headache, and temporary hypoesthesia. More significant complications, such as eyelid ptosis or facial asymmetry, are uncommon and can be minimized with appropriate dosing, precise injection technique, and sound anatomical knowledge. When combined with complementary modalities such as dermal fillers, chemical peels, or laser resurfacing, botulinum toxin effectively addresses both dynamic and static facial changes, delivering reliable and gratifying outcomes in upper facial rejuvenation.15, 16, 17
Conclusion
Botulinum toxin has gained widespread popularity as a safe and effective treatment for upper facial rejuvenation. It is commonly used to reduce dynamic wrinkles, such as glabellar frown lines, forehead lines, crow’s feet, and nasal bunny lines, while improving facial symmetry and boosting self-confidence. Its minimally invasive nature, reliable results, and rapid recovery contribute to its broad appeal among patients. The growing popularity of botulinum toxin highlights the need for ongoing research to better understand its long-term safety, effectiveness, and psychological as well as aesthetic benefits.
StatPearls Publishing; November 6, 2023.
5. Marinelli G, Inchingolo AD, Trilli I, Pezzolla C, Sardano R, Inchingolo F, Palermo A, Maspero CMN, Dipalma G, Inchingolo AM. Proactive Aesthetic Strategies: Evaluating the Preventive Role of Botulinum Toxin in Facial Aging. Muscles. 2025; 4(3):31. https://doi.org/10.3390/ muscles4030031
6. Gonzalez C, Rengifo J, Macias-Arias P, Duque-Clavijo V, Noreña-Rengifo BD. HighResolution Ultrasound for Complications of Botulinum Toxin Use: A Case Series and Literature Review. Cureus. 2024; 16(6):e63232. Published 2024 Jun 26. doi:10.7759/cureus.6323
7. Pradel R, Lerhe B, Kestemont P, Helmer C, Savoldelli C, Rios O. ThreeDimensional Photogrammetric Assessment of Facial Symmetry Improvement Following Botulinum Toxin Treatment in Patients with
Facial Palsy: An Observational Study. J Clin Med. 2025; 14(20):7298. Published 2025 Oct 16. doi:10.3390/jcm14207298
8. Kytko O, Vasil'ev Y, Emelyanova E, et al. Evaluation of the Effectiveness of Botulinum Therapy Based on the Anthropometric Characteristics of the Face Using Non-Invasive Thermal Imaging Data. Diagnostics (Basel). 2025; 15(19):2519. Published 2025 Oct 4. doi:10.3390/diagnostics15192519
9. Van Soest M, Remijn L, Tak I, van der Hoeve E, Koppendraaier L, de Ruiter M. Patient-Reported Outcome Measures After Botulinum Toxin for Temporomandibular-Related Myalgia: A Prospective Study. J Clin Med. 2025; 14(21):7494. Published 2025 Oct 23. doi:10.3390/jcm14217494.
Botulinum Toxin Type A for Upper Facial Rejuvenation: Mechanisms,
hand dynamometry: measuring outcomes following upper limb botulinum toxin-A injections in adults with acquired brain injury. J Rehabil Med. 2014; 46(4):314320. doi:10.2340/16501977-1781
11. Satriyasa BK. Botulinum toxin (Botox) A for reducing the appearance of facial wrinkles: a literature review of clinical use and pharmacological aspect. Clin Cosmet Investig Dermatol. 2019; 12:223-228. Published 2019 Apr 10. doi:10.2147/ CCID.S202919
12. Etrusco A, Geru M, Laganà AS, Chiantera V, Giannini A, Buzzaccarini G. Use of botulinum toxin in aesthetic medicine and gynaecology: current approaches, controversies, and future directions.
13. Nanda S, Bansal S. Upper face rejuvenation using botulinum toxin and hyaluronic acid fillers. Indian J Dermatol Venereol Leprol 2013; 79:32-40
14. Yi KH, Lee JH, Hu HW, Kim HJ. Novel Anatomical Guidelines on Botulinum Neurotoxin Injection for Wrinkles in the Nose Region. Toxins (Basel). 2022;14(5):342. Published 2022 May 15. doi:10.3390/ toxins14050342
15. Li K, Meng F, Li YR, et al. Application of Nonsurgical Modalities in Improving Facial Aging. Int J Dent. 2022; 2022:8332631. Published 2022 Feb 24.
doi:10.1155/2022/8332631
16. Vargas-Laguna E, Silvestre-Torner N, Magaletskyy-Kharachko K. [Translated article] Botulinum Toxin for Aesthetic Use in Facial and Cervical Regions: A Review of the Techniques Currently Used in Dermatology. Actas Dermosifiliogr. 2025; 116(3):T245-T253. doi:10.1016/j. ad.2024.12.007
17. Michon A. Botulinum toxin for cosmetic treatments in young adults: An evidence-based review and survey on current practice among aesthetic practitioners. J Cosmet Dermatol. 2023; 22(1):128-139. doi:10.1111/jocd.15513.
Androgenetic alopecia (AGA) is the most prevalent form of hair loss and is a genetically predisposed, androgendependent condition. It results from increased sensitivity of hair follicles to dihydrotestosterone (DHT), leading to progressive follicular miniaturization, shortening of the anagen (growth) phase, and gradual transformation of terminal hairs into fine, vellus-like hairs. Clinically, AGA presents as patterned hair loss with frontotemporal recession and vertex thinning in men, while women typically exhibit diffuse thinning over the crown with relative preservation of the frontal hairline. Affecting up to 50% of both males and females at some point after puberty, AGA follows a characteristic and predictable distribution pattern. Although often considered a cosmetic concern, AGA has a significant psychosocial impact, influencing self-esteem and quality of life. Emerging evidence also suggests associations with metabolic and cardiovascular comorbidities, highlighting its
importance as a condition with implications beyond hair loss alone.1,2,3
The pathophysiology of androgenetic alopecia (AGA) is multifactorial, involving genetic susceptibility, androgen signaling, follicular dynamics, and environmental influences. Normal hair growth follows a cyclical pattern comprising anagen (active growth, 2–7 years), catagen (involution, 1–2 weeks), and telogen (resting phase, approximately 2–3 months). In AGA, there is progressive shortening of the anagen phase with relative prolongation of telogen, leading to a reduced anagen-to-telogen ratio. This results in follicular miniaturization, progressive thinning of the hair shaft, and conversion of terminal hairs into vellus-like hairs, producing characteristic patterned hair loss. Androgen signaling plays a central role, particularly follicular sensitivity to dihydrotestosterone (DHT), generated from testosterone by type 1 and type 2 5α-reductase. Local modulation by enzymes such
as 17β- and 3β-hydroxysteroid dehydrogenases, steroid sulfatase, and aromatase further influences androgen activity. Paracrine mediators, including transforming growth factor-β1 (TGF-β1) and insulin-like growth factor-1 (IGF-1), contribute to follicular regression. Androgenmediated suppression of stem cell factor and detachment of the arrector pili muscle may explain the partial irreversibility of miniaturization. Genetically, AGA is polygenic, with key associations involving the androgen receptor gene on the X chromosome, loci on chromosomes 20 and 7, and epigenetic mechanisms such as DNA methylation. Mild perifollicular inflammation, oxidative stress, and microbial factors may further accelerate miniaturization without causing true scarring.1,2
Androgenetic alopecia causes significant psychosocial distress, particularly in women. Its predictable progression has led to surgical options, with FUE providing natural, durable results in stable AGA. Success depends on careful selection, meticulous technique, counseling, and longterm follow-up.
Diagnosis
Androgenetic alopecia is primarily diagnosed on clinical grounds, based on a characteristic history of gradual hair thinning beginning after puberty, with or without a positive family history of patterned hair loss. In most cases, scalp biopsy is not required and is reserved for situations where the diagnosis is uncertain. Dermoscopic examination is a valuable adjunct, typically revealing
hair shaft diameter variability, follicular miniaturization, and brown peripilar casts. Dermoscopy also helps differentiate AGA from diffuse alopecia areata, which may mimic male pattern hair loss but characteristically shows tapered or fractured hairs, such as exclamation-point hairs. A thorough clinical evaluation should include a detailed review of systems, medical history, and current medications to exclude alternative causes of hair loss and identify potential contributing or triggering factors. Laboratory investigations may be considered in selected cases and can include thyroid function tests, complete blood count, and evaluation for iron deficiency using serum iron, total iron-binding capacity, and serum ferritin levels. When clinically indicated, screening for syphilis may also be performed. Additionally, a brief psychiatric assessment is advisable, as hair loss can be associated with significant psychological distress, including depressive symptoms.3
Accurate diagnosis of alopecia depends on the integration of these clinical findings to guide appropriate classification and management.
Treatment
Hair transplantation is a minimally invasive surgical procedure for treating hair loss from pattern baldness, scarring alopecia, trauma, burns, or gender-affirming surgery. Healthy follicles are harvested from donor sites, typically the occipital or lateral scalp, and implanted into thinning or bald areas to restore natural hairline, density, and growth while
minimizing scarring.4, 5
Indications: Hair transplantation is indicated for androgenetic alopecia, traction alopecia, inactive scarring alopecia, scars, and cosmetic or gender-affirming reconstruction, but should be deferred in active inflammation or unstable, progressive hair loss.4,5
Contraindications: Hair transplantation is contraindicated in active scalp inflammation, infections, trichotillomania, body dysmorphic disorders, allergy to anesthetics, bleeding disorders, or significant medical comorbidities.4, 5
Planning and Patient Evaluation
Hair transplantation can be performed in individuals aged 18 to 70 years, following thorough investigation, with preference given to those who have a stabilized pattern of hair loss. Family history helps predict progression and plan a sustainable hairline. Donor hair characteristics—color, quality, density, and hair–skin contrast—affect outcomes, with lower contrast and curly, wavy, or frizzy hair providing better visual density. Hairline planning is critical, guided by facial thirds: the midline hairline is ≥8 cm from the glabella, lateral hairlines 9.5–11.5 cm above the lateral canthus, with temporal angles sharper in men and rounded in women. Hairline shape is individualized to facial morphology and patient expectations.4, 5
Graft Selection and Hairline Design
Hairline reconstruction typically uses 250–300 single-hair
Hair Restoration in Androgenetic Alopecia
micrografts placed irregularly to mimic natural macro- and micro-irregularity. Two-hair follicular unit grafts are placed just behind the hairline, followed by three- or four-hair grafts posteriorly for density. Smaller grafts are favoured in poor hair–skin contrast, while 1–1.5 mm punch grafts are reserved for total baldness and avoided in areas with existing hair.4, 5
Donor Area Anaesthesia
The donor area procedure is performed under local anaesthesia using a solution of 30 mL of an anaesthetic agent diluted in 100 mL of normal saline, with 1 mL of a vasoconstrictor (1:1000) added to enhance haemostasis and prolong the anaesthetic effect. The donor hair is trimmed to 2–4 mm for optimal visualization. Tumescence with normal saline is performed to improve tissue firmness, minimize bleeding, and enhance patient comfort, followed by a 10–20 minute waiting period to ensure adequate anaesthesia and haemostasis before proceeding with the procedure.4, 5
Pre-Procedure Patient
Preparation Guidelines
Do’s
1. Medical History and Allergies:
Obtain a detailed history regarding drug allergies (e.g., penicillin, local anesthetic agents), other known allergies, existing medical conditions, prior surgeries, and all current medications.
2. Anticoagulant Use:
Assess whether the patient is taking blood-thinning
medications, as these may represent a contraindication to surgery. Common agents include clopidogrel, warfarin (Coumadin), and heparin.
3. Chronic Medications:
Medications for conditions such as hypertension, diabetes, and epilepsy may be continued. The usual morning dose on the day of the procedure is permitted.
4. Dietary Instructions:
Patients may consume light food before arriving at the hospital. The procedure should not be performed on an empty stomach.
5. Hair and Scalp Preparation:
Shampooing the hair prior to the procedure is mandatory. The use of hair sprays, gels, or other styling products is not permitted. Patients using hair systems should discontinue their use at least 7 days before the procedure, perform daily shampooing, and avoid wearing the system on the day of surgery.
6. Hair Dyeing:
In patients with white hair, dyeing the donor area light brown or darker may be done approximately three days prior to the procedure. The recipient area should not be dyed.
7. Body Hair Harvesting:
If body hair harvesting is planned, chest or back hair should be shaved approximately one week before surgery.
8. Pre-operative Medication and Scalp Care:
Patients should begin prescribed pre-operative medications one day before surgery. The scalp should be washed with Betadine
Cleansing Scrub 7.5% twice daily on the day before and on the day of the procedure.
Don’ts and Lifestyle Adjustments before Hair Transplant Surgery
Certain lifestyle habits and medications can significantly influence the safety and outcome of a hair transplant procedure. Proper preoperative preparation helps minimize complications such as excessive bleeding, poor graft survival, and delayed healing. Patients should strictly follow the instructions outlined below.
Pre-Procedure Lifestyle and Medication Restrictions
1. Driving:
Patients should not drive on the day of the procedure. A mild sedative may be administered, which can impair alertness and reaction time.
2. Blood-Thinning ............. Medications:
Avoid aspirin, Disprin, anticoagulants, and other blood-thinning drugs at least 7 days before surgery. Even a single dose of aspirin can affect blood clotting for up to two weeks. Over-the-counter medications and topical agents like minoxidil should also be discontinued one week prior to surgery.
3. Alcohol Consumption:
Alcohol must be strictly avoided for 48 hours before the procedure, and preferably up to 7 days prior, as it can thin the blood and interfere with anesthesia and wound healing.
4. Smoking:
Smoking negatively impacts blood circulation and graft survival. Patients should stop
or significantly reduce smoking at least one week before and continue abstinence for three weeks after surgery. Ideally, cessation one month prior to surgery is recommended.
5. Hair Cutting:
Patients should not cut their hair short before surgery. Hair trimming, if required (especially for FUE), will be done at the clinic under sterile conditions.
6. Clothing:
On the day of surgery, patients should avoid tight clothing such as T-shirts or pullovers. A button-down shirt is recommended to prevent graft displacement or bandage disruption.
7. Vitamins and Herbal Supplements:
All vitamin supplements and herbal products should be stopped 7 days before surgery, particularly Vitamin E and B-complex, as they may mildly increase bleeding risk.
Pre-Treatment Laboratory Investigations
The following investigations are required before the procedure:
1. Complete Blood Count (CBC)
2. Random Blood Sugar (RBS) and HbA1c
3. HIV
4. HBsAg (Hepatitis B)
5. Anti-HCV
6. PT and APTT
7. Bleeding Time and Clotting Time
8. ECG (for patients above 35 years or with cardiac history)
9. Serum TSH, Liver Function Test (LFT), Renal Function Test (RFT)
Additional investigations or
a fitness certificate may be requested based on the patient’s pre-existing medical conditions.
Physical Activity and Hair Preparation
Patients should avoid strenuous exercise, heavy lifting, or highintensity workouts for one week prior to surgery, as these activities may increase blood circulation and the risk of bleeding. Light activities such as walking are permitted.
Patients are advised to wash their hair thoroughly starting two days before surgery, including the morning of the procedure, using a mild shampoo. The scalp should be clean and free from oil or residue. Hair styling products such as gel, mousse, or hairspray must be avoided for at least seven days before surgery to ensure optimal scalp hygiene.
Hair on the back and sides of the scalp should not be cut prior to surgery. Maintaining a hair length of approximately 2–3 inches helps conceal the donor area and any suture line postprocedure.
Dietary Considerations before Surgery
Patients should consume a light, non-spicy meal the night before and on the morning of surgery to prevent nausea, acidity, or dizziness during the procedure. Caffeinated beverages should be avoided on the day of surgery, as caffeine may interfere with sedatives and increase restlessness.
Day of Surgery Guidelines
Wear loose, comfortable clothing, preferably a button-
down shirt and relaxed-fit trousers. Avoid T-shirts or pullovers. Patients must arrange transportation in advance, as driving is not permitted after the procedure due to sedation.
Donor Hair Harvesting
Follicular
Unit
Extraction (FUE) is a technique of donor hair harvesting in which individual follicular units are directly extracted from the donor area using manual or motorized steel punches measuring 0.7–1.2 mm in diameter. Both the donor and recipient sites are infiltrated with local anaesthetic to provide adequate tissue turgor and achieve haemostasis. Following extraction, the harvested grafts are preserved in chilled normal saline and implanted promptly to minimize out-of-body time and thereby optimize graft survival.4, 5
Graft Preparation
Harvested donor strips are placed in chilled saline on ice, divided into slivers, and excess fat trimmed to ~2 mm below the hair bulb. Follicular unit grafts (1–4 hairs) are prepared under 2X–3X magnification and stored in saline in Petri dishes or moist stockinette in groups of 25 until implantation.4, 5
Recipient Site Anesthesia and Preparation
Recipient area anaesthesia is achieved with supratrochlear and supraorbital nerve blocks along with a frontal ring block. The area is tumesced with normal saline, avoiding vasoconstrictors to reduce postoperative telogen effluvium while minimizing bleeding and pain. Recipient sites are created following the natural hair direction, maintaining a ragged
Hair
hairline, using 18–23 gauge needles in an organized yet irregular pattern. Approximately 250–300 micrografts are strategically implanted along the hairline, while recipient sites in the posterior region are created using needles appropriately sized to correspond with the graft dimensions. Increased bleeding in secondary or tertiary procedures, or after preoperative topical therapy, is controlled with adequate tumescence and a 10–15 minute interval before implantation.4, 5
Graft Insertion
Grafts are inserted atraumatically using fine angled forceps, grasping about 2 mm of subcutaneous tissue beneath the bulb to prevent trauma. They are positioned flush with the skin to avoid pitting or cobblestoning. Each session typically lasts 5–6 hours, with 2000–3000 follicular unit grafts transplanted, often with multiple operators working simultaneously to optimize efficiency and outcomes.4, 5
Postoperative Care
Sometimes, the patient can experience postoperative edema, which can be effectively managed with medications. Gentle hair washing with a mild shampoo is initiated on postoperative day 5 of procedure. Mechanical trauma to the scalp, use of hair oils or strong shampoos, and wearing helmets or tight or overhead garments should be avoided for approximately three weeks. Topical therapy is initiated after the first wash and continued for 2–6 months to Promote early graft growth.4, 5
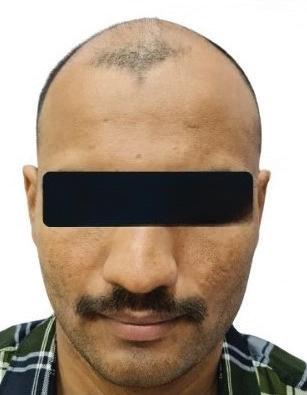
Result Patient 1
After 5 months of treatment
Before treatment
Patient 2
After treatment
Before treatment
3
Discussion
Hair loss is a highly prevalent condition affecting both men and women, with diverse clinical presentations and underlying pathogenetic mechanisms. The primary differential diagnosis of androgenetic alopecia (AGA), particularly in cases involving the frontal hairline, is frontal fibrosing alopecia, a scarring alopecia characterized by irreversible follicular destruction.6 In men, male androgenetic alopecia (MAA) affects up to 80% by the age of 70 and typically presents as gradual frontotemporal hairline recession and progressive vertex thinning, which may eventually coalesce into diffuse balding over the crown. The severity and progression of MAA are systematically assessed using the Hamilton–Norwood scale, a seven-stage classification that provides a standardized framework for clinical evaluation. Type I represents minimal or no recession of the anterior hairline, while Type II shows triangular or frontal temporal recession. Type III is characterized by deeper frontotemporal recession, often considered the earliest stage of clinically significant balding. The intermediate stages, Types IV
and V, demonstrate further vertex involvement and bridging of balding areas, whereas Type VI shows extensive hair loss with only scattered temporal and occipital hair remaining. Type VII represents the most advanced stage, with a narrow band of hair preserved along the sides and back of the scalp. This classification not only standardizes assessment but also assists in prognostication, treatment planning, and monitoring of disease progression over time.1, 7 Female pattern hair loss affects up to 40% of women, causing diffuse mid-frontal and vertex thinning with preserved hairline; graded by Ludwig scale and often psychologically distressing.1
Management of androgenetic alopecia (AGA) requires a targeted, pathophysiologybased approach aimed at preserving follicular integrity, preventing progressive miniaturization, and improving hair density. Early diagnosis enables timely intervention to slow disease progression. Core medical therapies include topical minoxidil to stimulate follicular activity and oral 5α-reductase inhibitors in men to reduce dihydrotestosteronemediated follicular damage. Supportive strategies such as lifestyle modification, optimal scalp care, and nutritional adequacy further support hair health. Emerging modalities— including low-level laser therapy, platelet-rich plasma, microneedling, prostaglandin analogues, and regenerative therapies—address oxidative stress, inflammation, impaired microcirculation, and follicular signaling to prolong anagen and
Hair Restoration in Androgenetic Alopecia
enhance hair regeneration.1,2
For patients with stable AGA, hair transplantation offers a permanent solution by relocating androgen-resistant follicles to areas of hair loss, restoring natural density and hairline architecture with minimal scarring. Follicular unit extraction (FUE) enables precise, customized graft placement, while transplanted follicles are
References
1. Kaliyadan F, Nambiar A, Vijayaraghavan S. Androgenetic alopecia: An update. Indian J Dermatol Venereol Leprol 2013; 79:613-625
2. Ntshingila S, Oputu O, Arowolo AT, Khumalo NP. Androgenetic alopecia: An update. JAAD Int. 2023; 13:150-158. Published 2023 Jul 22. doi:10.1016/j. jdin.2023.07.005
3. Ho CH, Sood T, Zito PM. Androgenetic Alopecia. [Updated 2024 Jan 7]. In: StatPearls [Internet]. Treasure Island (FL):
typically resistant to further androgen-mediated miniaturization, eliminating the need for ongoing therapy.
Conclusion
Hair transplantation is an effective procedure for restoring hair in appropriately selected patients with androgenetic alopecia (AGA), providing durable and natural results. Optimal outcomes depend on thorough patient evaluation, meticulous planning, precise surgical technique, careful graft handling, and diligent postoperative care. Advances in follicular unit extraction (FUE) have improved graft survival and minimized scarring, while ongoing innovations in follicular preservation and surgical precision continue to enhance long-term outcomes in hair restoration.
StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/ books/NBK430924/
4. Zhang X, Caulloo S, Zhao Y, Zhang B, Cai Z, Yang J. Female pattern hair loss: clinico-laboratory findings and trichoscopy depending on disease severity. Int J Trichology. 2012; 4(1):23-28. doi:10.4103/0974-7753.96082.
5. Razmi TM, Subburaj K. Hair transplantation: A brief review. Clin Dermatol Rev 2022; 6:80-7
6. Syed HA, Idoudi S. Frontal Fibrosing Alopecia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; June 7, 2024.
7. Asfour L, Cranwell W, Sinclair R. Male Androgenetic Alopecia. In: Feingold KR, Ahmed SF, Anawalt B, et al., eds. Endotext. South Dartmouth (MA): MDText. com, Inc.; January 25, 2023.
Intradermal Botulinum Toxin A Shows Promise for Post-Acne Erythema Management
Intradermal botulinum toxin A may offer a rapid and effective approach for managing post-acne erythema. A single-center, split-face study enrolled adults with persistent facial redness following inflammatory acne. Each participant received intradermal botulinum toxin A on one cheek and three sessions of broadband light therapy on the contralateral side at one-month intervals. Over three months, intradermal botulinum toxin A demonstrated faster and more pronounced reductions in Clinician Erythema Assessment scores, erythema index, colorimetric values, and sebum secretion compared with broadband light, with sustained sebum reduction at two and three months. Both modalities improved skin hydration and reduced transepidermal water loss, erythema scores, and colorimetric parameters relative to baseline. Pain scores were higher with intradermal injections, but patient satisfaction and safety profiles were comparable between treatments, with no significant adverse events reported. These findings indicate that intradermal botulinum toxin A may provide meaningful erythema and sebum reduction in a single session, offering a potential therapeutic option for patients with persistent post-acne redness. However, the study’s small sample size, single-center design, and limited follow-up underscore the need for larger, long-term trials before routine clinical adoption.
New Review Identifies Alternative Treatments to Hydroquinone for Melasma
A systematic review of topical therapies for melasma has identified effective alternatives to hydroquinone (HQ), emphasizing improved safety profiles while maintaining efficacy. The analysis included chemical agents such as thiamidol, tranexamic acid (TXA), topical metformin, tretinoin, flutamide, and methimazole, as well as natural compounds including niacinamide, kojic acid, azelaic acid, and ascorbic acid. HQ remains the most potent tyrosinase inhibitor, achieving high MASI score reduction, but its use is limited by adverse effects such as erythema, irritation, and dermatitis. Thiamidol demonstrated comparable or superior pigment reduction with minimal side effects, while TXA and topical metformin achieved similar MASI improvements with better tolerability. Tretinoin, flutamide, and methimazole showed variable efficacy with generally favourable safety profiles. Natural agents offer meaningful pigment reduction with high safety, making them suitable for maintenance or sensitive skin. Niacinamide showed efficacy comparable to HQ, kojic acid and azelaic acid provided clinically relevant improvements, and ascorbic acid offered delayed but significant pigment reduction. The review underscores that thiamidol, TXA, and topical metformin are promising HQ alternatives, while natural agents support safer long-term management, and future research should prioritize large-scale, rigorous trials to define optimal dosing, combination strategies, and long-term safety for these emerging therapies in melasma treatment.
Exosomes in Aesthetic Dermatology: Biological Basis, Clinical Evidence and Regulatory Considerations Part- I
Dr. Sama Rais
MBBS, DNB (Dermatology)
Clinical and Aesthetic Dermatologist
Medical Head & Founder Derma Hub
Mumbai Abstract
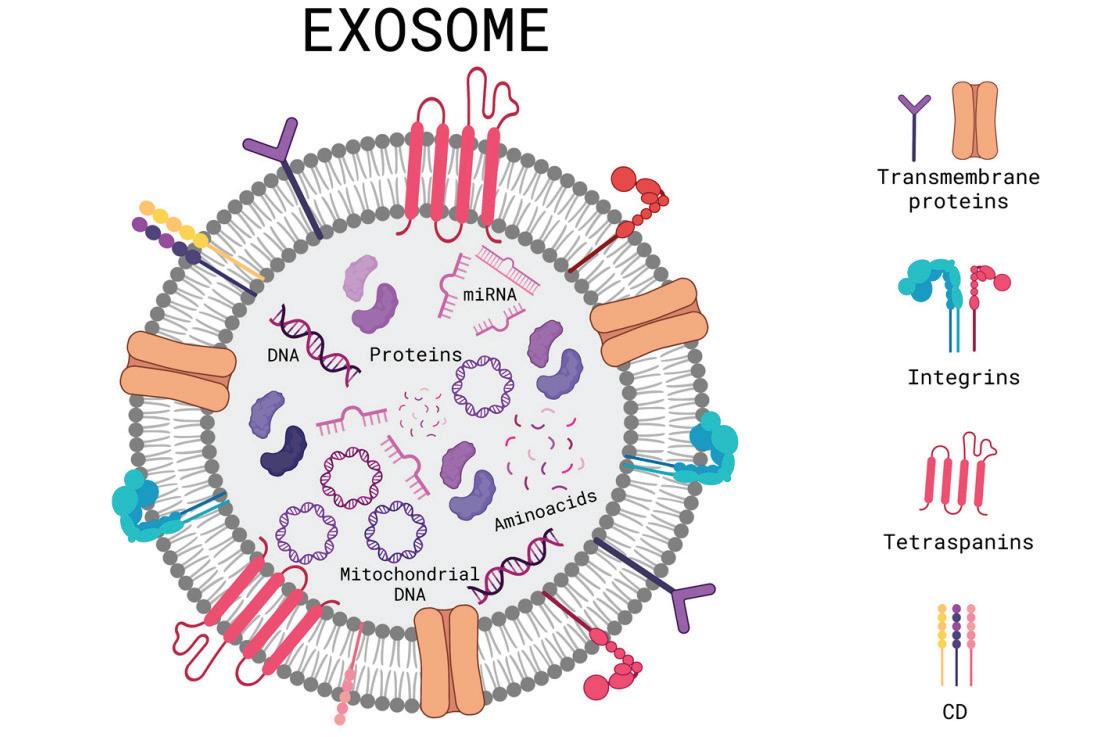
Exosomes are nanoscale extracellular vesicles that mediate intercellular communication through the transfer of proteins, lipids, and nucleic acids. Interest in their relevance to aesthetic dermatology has increased, particularly in exploratory research settings related to skin appearance optimization and post-procedure tissue responses. This review examines the biological basis of exosome activity in cutaneous systems, including keratinocyte–fibroblast signalling, extracellular matrix dynamics, and inflammatory pathway involvement as characterized primarily in experimental and translational studies. Available human clinical evidence—largely limited to small, non-randomized studies and case reports—is critically reviewed with attention to source material, route of administration, and outcome reporting. Clear distinctions are made between autologous, allogeneic, and commercially derived exosome preparations due to their differing safety,
manufacturing, and regulatory considerations. Current evidence does not establish standardized production methods, dosing parameters, or long-term safety for aesthetic indications. From a regulatory standpoint, exosomebased products intended for cosmetic or therapeutic application outside approved investigational frameworks raise significant classification and compliance challenges, particularly when claims exceed basic research or homologous use. Overall, while exosomes represent a biologically relevant research modality, their application in aesthetic practice should be regarded as investigational and limited to ethically approved research or strictly educational contexts.
Introduction
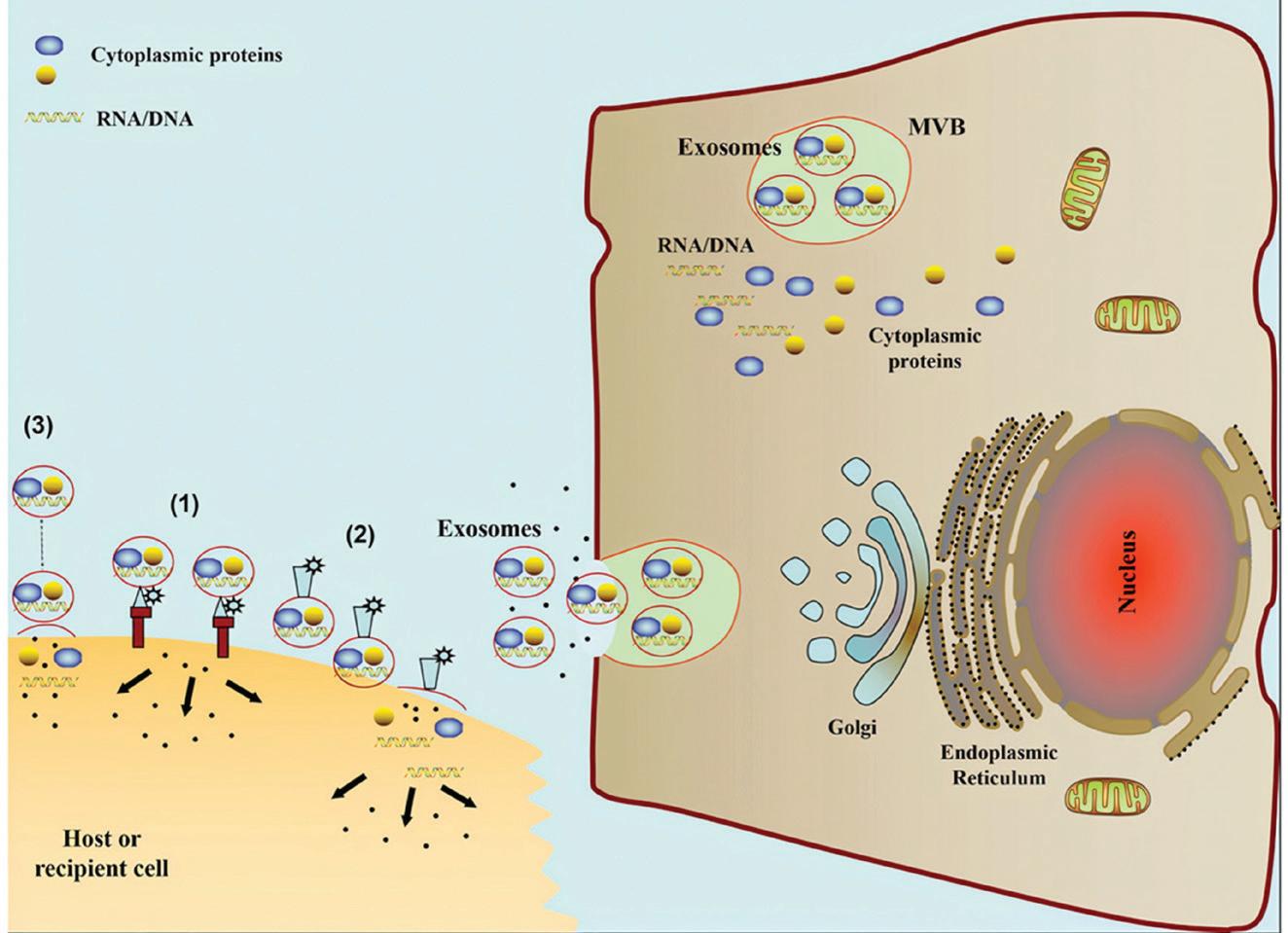
Exosomes are nano sized extracellular vesicular structures released by different cell types, with diameter ranging from 40–160 nm.1 They are important for intercellular communication and influence
neighbouring and distant cells through transfer of bioactive cargo which contain proteins, lipids and nucleic acid which help control both physiological and pathological processes in experimental and biological systems.
Uptake Mechanisms:
Exosomes mediate intercellular communication via a number of characterized uptake mechanisms, including soluble and juxtacrine signalling, fusion, phagocytosis, receptor- and raft-mediated endocytosis, and pinocytosis.
Exosome Mechanisms in Skin and Hair Biology:
I. Skin: Mechanisms of Action:
• Intercellular ..................
Communication
Exosomes are extracellular vesicles that facilitate intercellular communication by transporting protected bioactive cargo across the extracellular environment1 as demonstrated in experimental models. They are generated through the endosomal pathway, where intraluminal vesicles form within multivesicular bodies and are subsequently released following membrane fusion.1
Their molecular cargo includes membrane proteins (CD9, CD63, CD81), lipids, and regulatory nucleic acids capable of influencing recipient cell signalling pathways1 in vitro and in vivo. Cellular uptake occurs via receptor-mediated interactions, membrane fusion, or endocytic processes, enabling downstream modulation of gene expression1 under experimental conditions.
• Epidermal Homeostasis and Barrier Function
Exosome signalling has been
shown to influence keratinocyte proliferation and differentiation, processes essential for epidermal renewal and barrier integrity2 in preclinical studies. Experimental data suggest that stem cell–derived exosomes may support lipid synthesis pathways associated with epidermal barrier repair2 in laboratory models.
• Immune Regulation and Inflammatory Microenvironment
Exosomes participate in immune signalling networks and have demonstrated immunomodulatory effects in experimental models by influencing cytokine balance.3 Specifically, reductions in pro-inflammatory mediators such as IL-6 and TNF-α alongside enhancement of antiinflammatory signalling have been reported3 in non-clinical systems. In inflammatory skin disease models, exosomemediated communication between keratinocytes and immune cells has been shown to modulate inflammatory cascades without implying clinical therapeutic use.4
Mesenchymal stem cell–derived exosomes have demonstrated inhibition of complement activation and attenuation of IL-17–associated signalling in psoriasis-like models limited to experimental disease models.4
• Tissue Repair and Regenerative Pathways
Exosomes have been associated with angiogenic signalling through delivery of vascular endothelial growth factor, supporting neovascularization in wound-healing models5 in preclinical contexts.5 They also influence fibroblast activity, promoting extracellular matrix remodelling through regulation
of collagen and elastin synthesis in experimental systems.3 Enhanced migration and proliferation of keratinocytes and fibroblasts have been observed in experimental systems, supporting re-epithelialization processes without establishing clinical efficacy.6
• Cellular Aging and Oxidative Stress
Cellular senescence is a recognized contributor to skin aging and tissue dysfunction.7 Exosome-mediated signalling has been investigated for its role in modulating senescenceassociated inflammatory pathways in experimental research settings. Additionally, exosomes have been studied for their capacity to enhance antioxidant defences, mitigating oxidative stress–related cellular damage in vitro and animal studies.8
• Pigmentation Biology
Keratinocyte-derived exosomes have been shown to influence melanocyte behaviour through transfer of regulatory microRNAs in experimental pigmentation models.3 This mechanism contributes to modulation of melanogenesis within experimental pigmentation models and has not been validated clinically.3
II. Hair: Mechanisms of Action
• Hair Follicle Cycle Regulation
Hair follicles undergo cyclic transitions between anagen, catagen, and telogen phases, regulated largely by dermal papilla cell signalling. Disruption of dermal–epidermal interactions has been associated with hair follicle dysfunction and hair loss disorders in biological and clinical observational contexts.9
• Growth Factor–Associated Signalling
Mesenchymal stem cell–derived exosomes have been observed to contain growth factors such as VEGF, IGF-1, and TGF-β, which are relevant to follicular biology based on experimental analyses.5
These signalling molecules are associated with vascular support, cellular survival, and matrix interactions within the follicular microenvironment in non-clinical models.5
• Dermal Papilla Cell Activation
Exosome signalling has been shown to influence dermal papilla cell proliferation and functional activity in experimental models. This interaction is relevant to maintenance of hair follicle cycling and follicular microenvironment stability in laboratory systems.6
• Oxidative Stress and Cytoprotection
Oxidative stress has been implicated in follicular aging and inflammatory hair disorders.8 Exosomes have been studied for their antioxidant-associated cargo, which may contribute to cellular protection in follicular systems in preclinical research only.5,8
Schematic diagram 1: General structure of an exosome. Created with BioRender.com10
Schematic diagram 2: Depicting cell to cell communication
pathways; (1) Exosomes signal recipient cells via direct surfacebound ligands. (2) Exosomes transfer activated receptors to recipient cells. (3) Exosomes may epigenetically reprogram recipient cells via delivery of functional proteins, lipids, and RNAs11
Dermatologic Indications
Investigated for ExosomeBased Interventions
1. Skin aging / rejuvenation
Mechanism: MSC-derived exosomes modulate fibroblast activity, collagen synthesis, angiogenesis, and extracellular matrix remodelling via paracrine signalling rather than cellular replacement12 as proposed in experimental and early clinical studies.
Small human trials and reviews report modest wrinkle reduction and elasticity improvement; results are variable and shortterm12,13 and do not establish durable clinical efficacy.
2. Hair loss (androgenetic alopecia, telogen effluvium)
Mechanism: Exosomes influence dermal papilla signalling and hair-cycle regulators, promoting anagen entry and follicular survival¹³ in exploratory human and experimental studies.
Clinical studies show increases in hair density and thickness, with adipose- and placentaderived sources showing the most consistent signals13,14 with heterogeneity and limited follow-up.
Immunomodulatory effects include cytokine down-regulation (TNF-α, IL-17, IL-23) and normalization of keratinocyte
proliferation15 demonstrated primarily in preclinical disease models.
Strong preclinical and animal data demonstrate lesion and epidermal thickness reduction; human evidence remains indirect15,16 and noninterventional.
4. Wound healing / postprocedure recovery
Mechanism: Exosomes enhance angiogenesis, keratinocyte migration, and macrophage polarization toward reparative phenotypes12 in translational research settings.
Translational and limited clinical studies suggest accelerated epithelialization and improved healing quality12 without regulatory approval.
References
1. Wei H, Chen Q, Lin L, et al. Regulation of exosome production and cargo sorting. Int J Biol Sci. 2021;17(1):163–177.
2. Senoo M, Pinto F, Crum CP, McKeon F. p63 is essential for the proliferative potential of stem cells in stratified epithelia. Cell. 2007;129:523–536.
3. Xiong M, Zhang Q, Hu W, et al. The novel mechanisms and applications of exosomes in dermatology and cutaneous medical aesthetics. Pharmacol Res. 2021;166:105490.
4. Zhang B, et al. Topical application of mesenchymal stem cell exosomes alleviates imiquimod-induced psoriasislike inflammation. Int J Mol Sci. 2021;22(2).
5. Kim WS, Park BS, Sung JH. The woundhealing and antioxidant effects of adiposederived stem cells. Expert Opin Biol Ther. 2009;9(7):879–887.
6. Shabbir A, Cox A, Rodriguez-Menocal L, Salgado M, Van Badiavas E. Mesenchymal stem cell exosomes induce proliferation and migration of normal and chronic wound fibroblasts, and enhance angiogenesis in vitro. Stem Cells Dev. 2015;24(14):1635–1647. doi:10.1089/ scd.2014.0316. PMID: 25782006.
7. Chin T, Lee XE, Ng PY, et al. The role
5. Acne and acne scarring
Mechanism: Anti-inflammatory signalling and regulation of fibroblast collagen deposition may reduce post-inflammatory damage.12
Evidence is limited to exploratory studies; controlled human data are sparse (weak support).12
Mechanism: Proposed regulation of melanocyte signalling and oxidative stress pathways.12 Evidence is largely experimental; human clinical validation is lacking (very low support).12
8. Radiation- or laser-induced skin injury
Mechanism: Cytoprotective and anti-inflammatory effects reduce tissue damage and promote regeneration.12 Supported mainly by preclinical and early translational data (low certainty).12
Note: Stay tuned for Part II, Coming in the March 2026 issue!
of cellular senescence in skin aging and age-related skin pathologies. Front Physiol. 2023;14:1297637.
8. Rinnerthaler M, Bischof J, Streubel MK, et al. Oxidative stress in aging human skin. Biomolecules. 2015;5(2):545–589.
9. R H Mahmoud, E Peterson, E V. Badiavas, M Kaminer, Al E. Eber.Exosome: A Comprehensive Review for the Practicing Dermatologist. J Clin Aesthet Dermatol. 2025;18(4):33–40.
10. Tienda-Vázquez MA, Hanel JM, Márquez-Arteaga EM, Salgado-Álvarez AP, Scheckhuber CQ, Alanis-Gómez JR, Espinoza-Silva JI, Ramos-Kuri M, Hernández-Rosas F, Melchor-Martínez EM, Parra-Saldívar R. Exosomes: A Promising Strategy for Repair, Regeneration and Treatment of Skin Disorders. Cells. 2023 Jun 14;12(12):1625. doi: 10.3390/ cells12121625. PMID: 37371095; PMCID: PMC10296902.
11. Zhang Y, Liu Y, Liu H, Tang WH. Exosomes: biogenesis, biologic function and clinical potential. Cell Biosci. 2019 Feb 15;9:19. doi: 10.1186/s13578-019-02822. PMID: 30815248; PMCID: PMC6377728.
12. Dal’Forno-Dini T, Birck MS, Rocha M, Bagatin E. Exploring the reality of exosomes in dermatology. An Bras Dermatol. 2025;100(1):121–130. doi:10.1016/j.
13. Al Ameer MA, Alnajim AT, Al Ameer A, et al. Exosomes and hair regeneration: a systematic review of clinical evidence across alopecia types and exosome sources. Clin Cosmet Investig Dermatol. 2025;18:2215–2227. doi:10.2147/CCID. S543451. PMID: 409XXXXX.
14. Siriphanit R, Thanasarnaksorn W, Boonpethkaew S, et al. Comparative study of adipose- and umbilical cord-derived MSC exosomes in dermatologic models. Exp Dermatol. 2025;34(11):e70176. doi:10.1111/exd.70176. PMID: 41217063.
15. Huang YC, Chang CY, Huang CJ. Effectiveness of exosomes from different mesenchymal stem cells in psoriasis: murine study and meta-analysis. Biomedicines. 2025;13(9):2093. doi:10.3390/biomedicines13092093. PMID: 41007656; PMCID: PMC12467663.
16. Dal’Forno-Dini T, Bagatin E. Immunomodulatory and regenerative implications of exosomes in inflammatory skin disease. An Bras Dermatol. 2025. PMID: 39562240.
Laser Hair Reduction in Aesthetic
Dermatology: Mechanisms, Patient Factors and Aesthetic Outcomes
Dr. Ayushi Bothra
MD (Dermatology)
Consultant Dermatologist
Dr. Ayushi Bothra’s Skin and Hair Clinic
Mumbai Introduction
Unwanted hair growth is a common aesthetic and, at times, medical concern that can significantly impact quality of life. Conventional hair- reduction methods— including shaving, threading, waxing, plucking, and chemical depilatories—provide only shortterm results and necessitate frequent repetition to maintain hair-free skin. With increasing patient expectations for safe, effective, and long-lasting outcomes, laser and light-based technologies have emerged as the preferred modalities for long-term hair reduction in modern dermatological practice. Laser hair reduction has gained widespread acceptance over the past decade owing to its efficacy, precision, and relatively favorable safety profile. Among the various available options—including electrolysis, topical eflornithine, and intense pulsed light (IPL) systems— laser devices remain the most effective for achieving sustained hair reduction. These systems operate on the principle of
selective photothermolysis, wherein specific wavelengths of light (600–1200 nm) are selectively absorbed by melanin within the hair shaft and follicular structures, leading to thermal damage of the hair bulb, bulge, and dermal papilla while sparing the surrounding skin. Although laser hair reduction does not result in complete and permanent eradication of hair, it produces significant and prolonged reduction in terminal hair density. A single session can reduce hair growth by approximately 10–40%, while repeated treatments may achieve up to 90% reduction, with results persisting for several months to years. Posttreatment regrowth is typically finer and lighter, often converting terminal hairs into vellus hairs. The effectiveness of treatment is greatest in individuals with light skin and dark hair, though advances in technology have expanded its applicability across a wider range of skin phototypes. Multiple laser systems—including
ruby, alexandrite, diode, and Nd:YAG lasers, as well as IPL devices—are currently used for hair reduction, each differing in wavelength, depth of penetration, and suitability for various skin types. Emerging techniques such as low-fluence, high-repetition “in-motion” laser systems further enhance safety and efficacy by achieving gradual follicular heating while protecting the epidermis. Despite these advances, laser hair reduction is not devoid of risks, and outcomes may vary depending on patient-related and device-related factors. Therefore, appropriate patient selection, adequate training, and a thorough understanding of laser physics and hair biology are essential to optimize results and minimize adverse effects.1,2,3,4
Case Report
A 31 year old female patient with a known diagnosis of polycystic ovary syndrome (PCOS) presented with complaints of unwanted terminal hair growth over the chin, associated with significant cosmetic concern and frequent reliance on mechanical hair reduction methods. On baseline clinical examination, the chin area demonstrated increased hair density with coarse, thick, pigmented terminal hairs, consistent with hormonally mediated facial hirsutism commonly observed in PCOS. The underlying skin showed mild perifollicular pigmentation without evidence of active inflammation, folliculitis, or scarring. The patient underwent a single session of laser hair reduction (LHR) using an appropriate wavelength and treatment parameters
individualized according to her skin phototype and hair characteristics. Standard pre-procedural precautions were adhered to, and the procedure was well tolerated, with no immediate or delayed adverse effects. Post-treatment evaluation at follow-up revealed a notable early therapeutic response. There was a visible reduction in hair density, with fewer terminal hairs across the treated region. The residual hairs appeared thinner, lighter, and less coarse, indicating effective follicular targeting and early miniaturization. Hair regrowth was slower and more sparse, and overall skin texture appeared smoother with improved cosmetic uniformity. Importantly, no post-procedural complications such as hyperpigmentation, scarring, or folliculitis were observed. This case highlights the effectiveness of laser hair reduction even after a single session in achieving early reduction in hair thickness, coarseness, and density. The patient reported high satisfaction owing to reduced hair visibility and decreased dependence on mechanical hair reduction, reinforcing the role of LHR as a safe and effective adjunctive treatment for hirsutism in PCOS, with progressive improvement expected over subsequent sessions.
Before treatment
After treatment
Figure 1: Marked early clinical improvement following a single laser hair reduction session, demonstrating significant reduction in hair thickness, coarseness, and overall hair density
Technique and Treatment Protocol
Laser hair reduction begins with thorough cleansing of the treatment area to remove oils and debris, followed by comfortable patient positioning and mandatory eye protection for both patient and operator. Laser parameters are individualized based on skin type, hair characteristics, and the device used. The handpiece is held perpendicular to the skin and applied with gentle pressure to approximate follicles to the surface and reduce local blood flow. Transient perifollicular erythema and edema are expected and should be explained prior to treatment.1
Mechanism of Action: Selective Photothermolysis
Laser hair reduction is based on the principle of selective photothermolysis, which refers to the precise, site-specific thermal destruction of target tissues through selective absorption of light energy by specific chromophores, while sparing the surrounding
structures. In laser hair reduction, melanin acts as the primary chromophore. It selectively absorbs electromagnetic radiation within the wavelength range of approximately 300–1200 nm. When laser energy of an appropriate wavelength, pulse duration, and fluence is delivered, melanin within the hair shaft, hair matrix, and follicular epithelium absorbs the energy and converts it into heat. This localized rise in temperature causes thermal injury to critical follicular structures responsible for hair growth, without significant damage to adjacent epidermal and dermal tissues. In clinical practice, absorption of laser energy within the target is not always uniform. The extended theory of selective photothermolysis explains that in such situations, thermal damage can still be achieved through heat conduction from areas of high chromophore concentration to adjacent structures with lower absorption. In hair follicles, melanin concentration is greatest within the hair shaft and matrix cells, whereas the surrounding follicular epithelium and bulge stem cell region contain relatively less melanin. Upon laser irradiation, the melanin-rich hair shaft and matrix act as heat reservoirs, capturing laser energy and transferring thermal energy to the surrounding follicular structures. This secondary heat diffusion results in damage to the hair matrix and bulge stem cells, leading to delayed regrowth and long-term reduction of terminal hair.1
Patient-Related Factors
The ideal candidate for
conventional laser hair reduction is an individual with thick, dark terminal hairs, light skin, and a normal hormonal profile, as these factors strongly influence treatment efficacy and safety. Skin type is a critical determinant, particularly in darker phototypes (IV–VI), where increased epidermal melanin acts as a competing chromophore, reducing follicular selectivity and increasing the risk of adverse effects such as burns and post-inflammatory pigmentary changes. To minimize complications, lower fluences are often used in dark skin, which may compromise clinical efficacy. The longpulsed Nd:YAG laser is therefore preferred in dark or tanned skin because its longer wavelength penetrates deeper and is less absorbed by epidermal melanin, although its reduced melanin affinity may limit effectiveness. Tanned skin further increases the risk of epidermal injury, especially with shorter wavelengths, often necessitating suboptimal parameters. Hair characteristics are equally important: thick, pigmented terminal hairs respond best due to higher melanin content, whereas fine or vellus hairs (<30 µm diameter), such as those on the upper lip, respond poorly. Hair color also affects outcomes, with black and brown hair showing the most sustained reduction, while light blonde, white, or gray hairs—lacking melanin—respond minimally. Attempts to enhance response in non-pigmented hair using exogenous chromophores have shown only temporary benefit and do not reliably destroy follicular stem cells, limiting longterm efficacy.4
Post-Procedure Care
Post-treatment cooling with ice packs or cooling devices helps reduce pain and swelling. Topical antibiotics may be used if epidermal injury occurs, while short courses of topical corticosteroids can minimize erythema. Strict photoprotection and regular sunscreen use are essential. Because hair follicles are most responsive during the anagen phase, multiple sessions are required. Typically, 4–6 sessions at 4–6 week intervals are needed initially, with maintenance treatments every 6–12 months.1
Factors Affecting Outcome and Complications
Treatment response depends on hair site, skin and hair color, hair growth phase, laser type, hormonal status, and treatment planning. Common adverse effects include erythema, pain, and burning, while less frequent complications include blistering, dyspigmentation, scarring, ocular injury, and rarely paradoxical hypertrichosis, especially with IPL systems.1
Discussion
Laser hair reduction (LHR) is one of the most commonly performed cosmetic procedures worldwide. LHR offers superior outcomes in terms of precision, speed, patient comfort, and durability of results. However, like any medical or aesthetic procedure, it is not entirely free of complications. Adverse effects may occur immediately or develop over time, depending on patient-related factors, device parameters, and operator expertise. Importantly, most complications are preventable with appropriate
patient selection, correct laser settings, and adherence to pre- and post-procedure care, while others can be effectively managed with minimal intervention. Post-treatment management plays a critical role in optimizing outcomes and minimizing complications. Commonly used measures include topical corticosteroids to reduce inflammation, emollients and moisturizers to restore the skin barrier, topical analgesics for discomfort, and selective antiviral or antibiotic agents when indicated. Strict photoprotection and patient education further contribute to safe recovery. Ongoing technological advancements in laser systems, including improved cooling mechanisms and refined pulse parameters, continue to enhance safety and efficacy, reducing the incidence of adverse events. The efficacy of LHR is based on the principle
References
1. Vaidya T, Hohman MH, Kumar D D. Laser Hair Removal. [Updated 2023 Jul 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm. nih.gov/books/NBK507861/
2. Thomas, M. M., & Houreld, N. N. (2019). The “in’s and outs” of laser hair removal: a mini review. Journal of Cosmetic and Laser Therapy, 21(6), 316–322. https://
of selective photothermolysis, wherein laser energy selectively targets melanin within the hair shaft and follicle, converting light energy into heat that damages follicular germ cells. This process is most effective during the anagen phase of the hair growth cycle, explaining the need for multiple sessions followed by maintenance treatments. Optimal results are traditionally achieved in individuals with light skin and dark hair due to greater contrast between hair and skin pigmentation, although newer technologies have expanded treatment options across diverse skin types. Despite its limitations in lighter hair colors, LHR remains a cornerstone of modern aesthetic dermatology for long-term hair reduction.5
Conclusion
Laser hair reduction is a widely practiced and effective method for the management of unwanted hair, based on the principle of selective photothermolysis. The use of integrated cooling systems and appropriate laser parameters enhances safety by minimizing thermal injury to the skin. Treatment outcomes and complication rates are influenced by multiple factors. Importantly, the majority of adverse effects can be prevented through careful patient selection, proper technique, adequate training, and strict adherence to pre- and post-procedure protocols. Patient education regarding preventive measures and realistic expectations is essential. With continued advancements in technology and a strong emphasis on safety-oriented practices, laser hair reduction can achieve optimal outcomes with minimal risk, reinforcing its role as a cornerstone procedure in aesthetic dermatology.
doi.org/10.1080/14764172.2019.16054 49
3. Bhat, Y. J., Bashir, S., Nabi, N., & Hassan, I. (2020). Laser Treatment in Hirsutism: An Update. Dermatology practical & conceptual, 10(2), e2020048. https://doi. org/10.5826/dpc.1002a48
4. Arsiwala SZ, Majid IM. Methods to overcome poor responses and challenges
of laser hair removal in dark skin. Indian J Dermatol Venereol Leprol 2019;85:3-9
5. Naik PP. Laser hair removal: Mechanisms and complications. Journal of Clinical Practice. 2021;18(1):1570–1577.
Radiofrequency Microneedling Shows Promising Results for Rosacea Management
A new systematic review and network metaanalysis evaluated multiple randomized controlled trials comparing laser and energy-based devices (EBDs) for rosacea, including pulsed dye laser (PDL), intense pulsed light (IPL), potassium titanyl phosphate laser (KTP), neodymium-doped yttrium aluminum garnet laser (Nd:YAG), radiofrequency microneedling (RFMN), and combination regimens with oxymetazoline or niacinamide. Primary outcomes were patient satisfaction, erythema and telangiectasia improvement, and long-term adverse events, while secondary outcomes included shortterm effects such as erythema, swelling, and crusting. Radiofrequency microneedling (RFMN) ranked highest for patient satisfaction and erythema improvement, while oxymetazoline plus pulsed dye laser (PDL) was most effective for telangiectasia, followed by potassium titanyl phosphate laser (KTP). Shortterm adverse events were mild and resolved quickly, and long-term effects such as post-inflammatory hyperpigmentation and atrophic scarring were rare. Limitations of the evidence include small sample sizes, heterogeneous outcomes, unclear risk of bias, and insufficient long-term follow-up, and limited representation of darker skin types. Clinically, lasers and energy-based devices (EBDs) are effective for erythema and telangiectasia but require multiple sessions and careful counseling on risks, healing, and limitations in darker skin. Future research should optimize device parameters, treatment intervals, patient-specific factors, and combination therapies to improve personalized and durable outcomes.
Enhanced Outcomes with Combination Therapies for Keloids and Hypertrophic Scars
Keloids and hypertrophic scars remain a persistent challenge in dermatology and surgical practice, especially in patients with skin of colour, due to high recurrence rates and the risk of pigmentary changes. A recent systematic analysis assessed the effectiveness of multiple treatment modalities and highlighted that monotherapies, including surgical excision, intralesional cryotherapy, corticosteroids, radiation, and bleomycin, provide moderate success but are frequently associated with recurrence or adverse pigmentary outcomes. Radiation-based approaches and intralesional therapies were effective in scar reduction but carried risks of pigment alteration, dermatitis, and tissue atrophy. Combination therapies, particularly surgical excision paired with radiation or with corticosteroids, verapamil, or cryotherapy, achieved markedly higher rates of scar resolution, and tension offloading devices showed promising outcomes in areas prone to high mechanical stress. The analysis emphasizes the critical importance of balancing therapeutic efficacy with pigment preservation and tailoring strategies to individual patients. Limitations of the current evidence include heterogeneous reporting, inconsistent outcome definitions, and reliance on retrospective studies, underscoring the urgent need for high-quality, controlled research to develop personalized, evidence-based protocols for scar management in patients with skin of colour.
Rowan Bioceuticals Pvt. Ltd.
(AN ISO 9001:2015 Certified Company)
Corporate Office: 324, Plot No-12, Vardhaman Big V Plaza, Road No-44, Community Centre, Pitampura, New Delhi -110034. Tel: +91-11-27018166, 47562736
Space-Inspire hub Western heights, J.P Road, Opp., Gurudwara Four Bunglows, Village, Ambivali, Andheri West, Mumbai, Maharashtra- 400053. Tel.: +91-22-61984543, Email: rowancare@gmail.com, Web: www.rowanbio.in
Pincode:
OBSERVERSHIP IN AESTHETICS
3-Nights, 4-Days
Program Highlights* 2 Half-days
Lectures by DHA Certified Faculty 2 Half-days
Observership in Aesthetic Procedures with upto 6 DHA@CME Credits# CME Credits# with
Package to be announced shortly
Inclusions:
* 3-Nights 4-Days Stay, in a 4-STAR Hotel with breakfast and dinner, Lunch at Academy/Aesthetic Centre, To and fro - Hotel to Academy/Aesthetic Centre SIC◊
Exclusions:
Air fare to Dubai and back , airport transfer, Sight seeing etc.
@ DHA- Dubai Health Authority
# Proposed s/t confirmation
◊ SIC- Seat in Coach
Interested Drs kindly call for further details: +91