Lip Rejuvenation with Hyaluronic Acid: Anatomy, Techniques and the Light Lips Approach
Beyond Creams & Serums: The Power of CO₂ Fractional Laser for Eye Rejuvenation
Beyond Lesion
Clearance: Multimodal and Regenerative Strategies in the Management of Acne Vulgaris
A Gentle Glow: Managing Acne and Redness with Intense Pulsed Light (IPL) Therapy
HIFU for the Aging Face: Precision Skin Tightening with Minimal Downtime
EXECUTIVE EDITOR & PUBLISHER
Dom Daniel CORPORATE OFFICE
22, Shreeji Bhavan, 275-279, Samuel Street, Masjid Bunder (W), Mumbai-4000 03, INDIA.
EMAIL: theaestheticiansjournalindia@gmail.com
Website: theaestheticiansjournal.online
Printed, Published, Edited and Owned by Dom Daniel Printed at Swastik Printer, Gala No.9 & 10, Vishal Industrial Estate, Bhandup (West), Mumbai- 400078. Published at 22 Shreeji Bhavan, 275/279, Samuel Street, Masjid Bunder (West), Mumbai - 400003. India.
“The Aestheticians Journal” takes no responsibility for unsolicited photographs or material ALL PHOTOGRAPHS, UNLESS OTHERWISE INDICATED, ARE USED FOR ILLUSTRATIVE PURPOSE ONLY.
Views expressed in this Journal are those of the contributors and not of the publisher. Reproduction in whole or in parts of texts or photography is prohibited. Manuscripts, Photographs and art are selected at the discretion of the publisher free of charge (advertising excluded). Whether published or not, no material will be returned and remains the property of the publishing house, which may make use of it as seen fit. This may include the withdrawal of publication rights to other publishing houses.
All rights reserved. Reproducing in any manner without prior written permission prohibited.
Published for the period of December -2025
Winter Edition Highlights: Advancing Excellence in Aesthetic Dermatology
Welcome to the Winter edition of The Aestheticians Journal, December issue—an issue curated to inspire, educate, and empower every practitioner striving for excellence in aesthetic Dermatology. As the season brings its own set of skin and age-related challenges, we present a collection of evidence-based, technique-driven articles designed to elevate both clinical practice and patient outcomes.
This month, we explore Lip Rejuvenation with Hyaluronic Acid, focusing on detailed anatomy, advanced injection strategies, and the refined Light Lips approach for achieving natural, elegant enhancement. We then shift to periocular aesthetics with CO₂ Fractional Laser for Eye Rejuvenation, highlighting how energy-based devices now go far beyond creams and serums in addressing texture, laxity and fine lines.
Our feature on HIFU for the Aging Face offers a deep dive into precision lifting and tightening with minimal downtime—an increasingly essential modality for today’s busy patients seeking nonsurgical solutions. We then broaden the horizon with Multimodal and Regenerative Strategies for Acne Vulgaris, highlighting how contemporary acne care has evolved far beyond simple lesion clearance. Concluding this issue is A Gentle Glow: Managing Acne and Redness with Intense Pulsed Light (IPL) Therapy, which explores the benefits of IPL as a soothing yet effective tool in treating inflammatory skin concerns.
We hope this thoughtfully curated issue enriches your clinical perspective and supports your journey toward delivering confident, transformative care.
Hope you have a great read!
Thanks & Cheers
- Dom Daniel Executive Editor & Publisher
Dr. Vikramjeet Singh Dhingra,
Dr. Pramila Kanchan Aswani,
Dr. Damini Verma,
21st December'2025
Venue: Hotel Ginger, Near Domestic Airport, Vile Parle (East), Mumbai
Faculty for Bio Remodeller & Skin Booster
Dr. Pallavi Sule MBBS, DDV Dermatologist and Cosmetologist Dr. Pallavi Sule’s Clinic, Mumbai
Faculty for Threads
Dr. Dattatray Sonawane MD (Skin) Founder and Consultant Dermatologist La Peau Laser World, Thane
Registration Fees & Details
Registration
Registration
Aestheticconf Workshop
Faculty for Botulinum Toxin Type A
Dr. Abhay Talathi MD, DNB, FCPS, DVD Dermatologist and Cosmetologist SkinSpace Clinic, Mumbai
Dr. Pallavi Sule welocome message for
Editorial Board
Dr. Vikramjeet Singh Dhingra
M.Ch. Plastic Surgery
Consultant Plastic Surgeon
Bodysculpt, Mohali
Punjab
Dr. Pramila Kanchan Aswani
MBBS, DVD, FAGE
Consultant Dermatologist & Aesthetic
Physician
Mumbai
Dr. Damini Verma
MD, DNB (Dermatology, Venereology & Leprosy)
Associate Consultant Dermatologist
Apollomedics Super Speciality Hospital, Lucknow
Dr. Rashmi Soni
MD, DDV, DNB
Founder and Consultant Dermatologist
Cosmetologist and Dermatosurgeon
Skinsure Clinic, Pune
Consultant Dermatologist
KEM Hospital, Pune
Dr. Reeya Patel
MD (DVL)
Consultant Dermatologist
Surat
BRING BACK! Dry nails to life REGENAIL BD
5 In 1 Nourishing serum for perfect nails
Moisturises
Revitalises
Conditions
Restore Nails Grow Nails
Keratin Protein - Major component of natural nail
Solubilized keratin proteins bind to natural keratin proteins in nails, strengthen nail plate, fortify weak areas, bring back moisture lost to acetone and LED lights.
Jojoba Oil
Deeply penetrating natural oil acts as carrier, increases penetration of other ingredients moisturizes and conditions nails.
Sweet Almond Oil
Loaded with skin nourishing fatty acids ( oleic acid 55-86% & linolic acid 7-35%) treats dry brittle nails due to smoothening, softening and moisturizing properties.
Rowan Bioceuticals Pvt. Ltd.
(AN ISO 9001:2015 Certified Company)
Corporate Office: 324, Plot No-12, Vardhaman Big V Plaza, Road No-44, Community Centre, Pitampura, New Delhi -110034. Tel: +91-11-27018166, 47562736
Space-Inspire hub Western heights, J.P. Road, Opp., Gurudwara Four Bunglows, Village, Ambivali, Andheri West, Mumbai, Maharashtra- 400053. Tel.: +91-22-61984543, Email: rowancare@gmail.com, Web: www.rowanbio.in
Lip Rejuvenation with Hyaluronic Acid: Anatomy, Techniques and the Light Lips Approach
Dr. Vikramjeet Singh Dhingra
M.Ch. Plastic Surgery
Consultant Plastic Surgeon Bodysculpt, Mohali
Punjab
Introduction
The lip region represents a central focus in facial aesthetic enhancement, being, alongside the eyes, one of the most visually significant features of both male and female faces. Over time, intrinsic aging, photo-induced damage, hereditary factors, and lifestyle habits such as smoking contribute to progressive changes, including diminished lip volume, perioral rhytides and accentuation of mentolabial folds. Furthermore, genetically thin lips and lip asymmetries are frequent aesthetic concerns, often addressed through soft tissue augmentation with dermal fillers. Successful rejuvenation of the perioral region requires a nuanced approach, integrating advanced injection techniques with a judicious selection of technologies and materials. Among the various filler options explored, hyaluronic acid (HA) remains the gold standard due to its established safety profile, biocompatibility, and predictable outcomes, whereas polyacrylamide (PA)
has largely been abandoned due to granulomatous complications. HA fillers not only restore lip volume and contour but also play a pivotal role in comprehensive facial rejuvenation strategies aimed at restoring harmony and natural expression. Contemporary advancements, such as the Light Lips Technique, emphasize minimalistic yet effective interventions, employing microvolumes of small-particle HA strategically placed at anatomically defined points, including the GlogauKlein points of the cupid’s bow and corresponding areas of the lower lip. This technique achieves subtle lifting of the commissures and enhanced lip definition, delivering results that appear refined and natural. Nevertheless, despite remarkable progress in filler technology and technique, practitioners must remain vigilant regarding the potential for adverse effects, including late-onset complications, underscoring the importance of
expertise and patient selection in lip augmentation procedures.1,2,3
Anatomy, Aesthetic Concerns and Treatment Goals
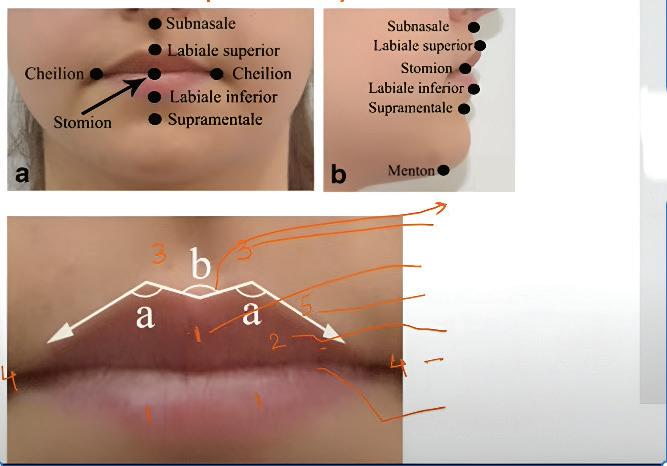
The upper lip extends from the base of the nose superiorly to the nasolabial folds laterally and to the free edge of the vermilion border inferiorly, while the lower lip extends from the superior vermilion edge to the oral commissures laterally and the mandible inferiorly. The vermilion–skin junction is accentuated by a fine pale line, creating a clear transition between lip and surrounding skin. Key landmarks include the Cupid’s bow, defined by two paramedian elevations along the vermilion border, and the philtrum, formed by paired vertical columns converging into a central midline depression. These anatomical features are critical to lip aesthetics and must be preserved or subtly enhanced during augmentation. Clinically, the most frequent concerns are vermillion deflation and drooping of the oral commissures, which contribute to a tired or “sad” appearance. Patients with adequate lip volume may benefit from contour refinement through vermilion border definition or targeted projection. For creating a pout, fillers can be placed in the submuscular plane. Treatment strategies should be individualized, depending on the defect and patient goals: genetically thin lips often require a staged approach with deep structural augmentation followed by superficial volume correction, whereas purely cosmetic enhancement is best achieved with superficially placed fillers emphasizing the white roll and vermilion expansion, ensuring natural balance between the upper and lower lips.1
Cupid’s Bow
Philtral Columns
Tubercles
White Roll
Vermilion Commissure
Red Roll
Patient Selection and Expected Outcomes
Optimal outcomes in lip augmentation depend on meticulous patient selection, a comprehensive medical history, and a detailed consultation that clearly communicates the potential benefits, limitations, and risks. Counselling must include discussion of transient post-procedure effects such as swelling and bruising, as many patients prefer discretion regarding cosmetic interventions. Emphasis should be placed on the expected downtime, typically
ranging from 2 days to 2 weeks, although the use of blunt cannulae instead of sharp needles has significantly reduced recovery time.1
Treatment Strategy
Lip augmentation involves reshaping and/or volumizing the vermilion, with additional refinement of the Cupid’s bow and the junction between the vermilion and the subnasal columella when indicated. A thorough evaluation should consider lip height in relation to incisor show, potential skeletal discrepancies such as maxillary hypoplasia or protrusion, and the patient’s occlusion status to ensure harmony and balance.1
Treatment Techniques
Local anesthesia is administered using a eutectic lidocaine–prilocaine preparation or regional nerve blocks (infraorbital for the upper lip, mental for the lower lip), with care taken to avoid anatomical distortion. Use of hyaluronic acid (HA) premixed with lidocaine minimizes injection-related discomfort. Post-procedural swelling or bruising may provoke patient anxiety and can be managed with ice application, nonsteroidal anti-inflammatory agents (avoided during the first 6 hours to prevent masking vascular compromise), or, if required, short courses of corticosteroids.1
Adverse events may arise from both filler characteristics and improper technique. Complications include postinjection nodularity, lumpiness, irregularities, or beading from overly superficial placement. More permanent fillers carry the added concern of long-
Figure 1: Lip anatomy
lasting undesirable results. Product-specific training is critical to minimize such risks, with overcorrection strongly discouraged. Simultaneous vermilion and vermilion border augmentation generally achieves a more balanced and complete aesthetic effect.1
Common HA injection techniques include serial puncture and linear threading (antegrade or retrograde). Technique selection should be guided by patient-specific anatomy and desired outcomes. The increasing use of cannulae has reduced downtime and improved patient satisfaction, though mastering this approach requires experience. A single access point at each oral commissure can provide safe and effective entry for augmentation of both upper and lower lips.1
Injection Technique4
• Product choice: HA is the preferred filler due to its safety and efficacy profile. In our practice, HA with cross-linking grade 3/6 and concentration of 25 mg/g was employed.
• Volume restoration:
Injection into the vermilion via the vermilion border using a 30-gauge needle at an oblique angle of 30°, no deeper than 2.5 mm, prevents vascular injury. Small boluses (0.05–0.1 ml) are deposited retrograde in a linear threading manner, with a total of 1–1.5 ml per session for both lips.
• Shape refinement: Subtle enhancement of the vermilion border is achieved with 0.02–0.4 ml of HA per session, avoiding the white roll to prevent margin blunting. Careful retrograde
injections at a parallel angle preserve lip definition and natural contour.
• Correction of asymmetry: Additional micro-boluses (0.05–0.1 ml) are placed in targeted areas as needed.
4.3 Technique
The “4.3” technique is a hybrid lip augmentation method that merges the aesthetic precision of the vertical-lip technique with the efficiency of the retrograde linear approach. Designed to achieve naturallooking, harmonious, and well-defined lips, it utilizes hyaluronic acid (HA)-based fillers to enhance volume and contour with fewer entry points and minimal filler volume. This technique is useful to both male and female patients with standard anatomical lip features seeking subtle improvements in contour and fullness. Each procedure involved four injections in the upper lip and three in the lower lip, combining vertical and retrograde linear techniques. The filler, based on Tri-Hyal technology, contains a combination of free and crosslinked HA for enhanced cohesivity and durability, ensuring soft, hydrated, and natural results. The first injection was made at the apex of the right cupid’s bow, directed medially toward the upper labial tubercle (0.1 mL). Through the same entry point, a retrograde linear injection (0.05 mL) was performed along the vermilion border for contour enhancement, followed by another lateral injection (0.05 mL). The same steps were mirrored on the opposite side, resulting in four injections in the upper lip (0.4
mL total). For the lower lip, three injections were made: one at the midline vermilion border (0.1 mL) and two at the midpoint of each hemilip (0.05 mL each), totaling 0.3 mL. This combination of vertical and retrograde linear injections enhances the lips’ shape and projection while maintaining natural proportions. The remaining 0.3 mL was reserved for minor touch-ups according to patient needs. Proper depth of injection is essential to avoid superficial placement, which can cause visible irregularities, and to prevent deep injections that may increase the risk of vascular injury. The technique respects lip vascular anatomy—particularly the superior and inferior labial arteries, which course near the median line—minimizing the risk of complications. The “4.3” technique consistently achieved natural, symmetrical, and aesthetically pleasing outcomes in all patients. Improvements were observed in lip definition, volume, and surface smoothness, with reduced discomfort and a lower incidence of bruising or nodules due to fewer injection sites and limited filler volume. The TriHyal technology contributed to soft, hydrated, and long-lasting results. The “4.3” technique is a standardized, safe, and easily reproducible lip augmentation approach suitable for a wide range of patients. By combining vertical and retrograde linear injections at specific points, it delivers natural enhancement with minimal filler (0.7 mL) and fewer injection sites. This approach ensures predictable, refined, and harmonious results, making it an ideal method for
achieving subtle yet effective lip rejuvenation.5
Lip Categorization and Tailored Approach4
1. Normal-volume lips: Adequate baseline volume and definition with a desire for increased projection. Injection focuses on vermilion enhancement, not exceeding 1–1.5 ml per session. Reassessment occurs at 15 days, with incremental adjustments if necessary.
2. Thin lips: Characterized by hereditary or acquired atrophy, requiring staged augmentation to respect soft tissue expansion capacity. Typically, 0.5–1 ml of HA is injected into the thinner lip initially, followed by 0.5–1 ml in both lips at subsequent 30-day intervals until desired volume and proportion are achieved. Definition is then refined with conservative border injections.
3. Aged thin lips: Marked by volume loss, vermilion border effacement, elongation of the upper lip, and perioral rhytides. Initial sessions prioritize vermilion volume restoration (≤0.5 ml per session), followed by definition enhancement. Additional filler may be placed in perioral lines from the first session. Multiple staged sessions are essential for achieving natural rejuvenation.
Throughout the procedure, vigilance for intravascular injection is imperative. Warning signs such as blanching or severe pain necessitate immediate intervention with hyaluronidase, massage, warm compresses, and antiplatelet therapy until perfusion normalizes.
Aftercare4
• Gentle massage of the treated
area
• Cleansing with 0.9% saline
• Short-term application of ice packs to minimize edema and bruising
• Avoidance of strenuous activity, heat exposure, and hot beverages for 24 hours
• Follow-up assessments at 15 and 30 days to guide further treatment if needed
Advanced Considerations
Studies suggest HA augmentation can maintain aesthetic results for up to one year, with a very low incidence of allergic reactions. Prior to treatment, clinicians must assess for anticoagulant use, active or prior infections, herpes simplex history (requiring antiviral prophylaxis), or previous permanent filler placement.3
For improved patient comfort and safety, topical anesthesia (10% lidocaine and 3.5% prilocaine) is applied for 30 minutes before cleansing with 2% chlorhexidine. A 30-gauge needle facilitates precise dermal or subdermal delivery, reducing extrusion pressure and enhancing comfort. Six standardized injection points have been described, with cautious attention to depth to prevent Tyndall effect or subcutaneous overplacement.3
Blunt-tip microcannulae provide an alternative, associated with reduced bruising, ecchymosis, and post-procedure discomfort, while enabling more uniform filler distribution. Aspiration prior to injection is advised to avoid inadvertent intravascular delivery.6
Discussion
Lip augmentation with injectable fillers has become one of the
Result
Patient 1
Before treatment
After treatment
Patient 2
Lip Rejuvenation with Hyaluronic Acid: Anatomy,
most sought-after aesthetic procedures, largely due to its ability to deliver rapid results with minimal downtime. Hyaluronic acid (HA) fillers, in particular, dominate this field because of their favourable safety profile, ready availability, ease of application, and high levels of patient satisfaction. Successful augmentation depends on precisely targeting different anatomical regions of the lips to achieve individualized results. However, the choice of technique, filler quantity, and treatment strategy must always be tailored to each patient’s anatomy and expectations. Importantly, while treatment cost is a practical concern, it should not override clinical judgment; patients must be informed about the filler volume necessary to obtain natural, durable outcomes. Achieving consistently pleasing results requires more than technical skill—it demands a detailed understanding of lip anatomy, the dynamics of lip movement, and the structural changes that occur with aging. While cultural differences influence beauty ideals, certain features remain universally appealing: defined contours, a wellshaped Cupid’s bow, balanced vermilion height, gently elevated commissures, and harmonious proportions with surrounding facial structures. The lips inevitably undergo characteristic age-related changes, including elongation, volume depletion, flattening of the Cupid’s bow, drooping of the commissures, and the development of fine perioral rhytides. These alterations are driven by collagen and elastin loss, fat and muscle atrophy, and underlying skeletal
resorption. Patients therefore often seek lip treatments not only for beautification but also for restoration. Nevertheless, apprehension about unnatural, exaggerated outcomes remains common, highlighting the importance of adopting conservative, anatomyrespecting techniques. The “Light Lips” Technique was developed to address these concerns, offering subtle and harmonious enhancement using minimal filler volumes. By focusing on the lower segments of the philtral columns near the G and K points— while avoiding full-column augmentation—it restores central projection, delicate eversion, Cupid’s bow definition, and commissural support. This approach helps correct the age-related increase in the columella–vermilion distance while avoiding an overfilled appearance. The technique requires as little as 0.4 ml of HA across six points, making it cost-effective while also minimizing patient discomfort due to fewer injection sites. Its adaptability across age groups further underscores its clinical relevance. Younger patients typically desire sharper definition and minor enhancement, which this method delivers without excessive volume. Middleaged individuals benefit from a combination of contouring and commissural elevation to counteract early descent. In older patients, who often present with structural collapse and increased columella–vermilion distance, large filler volumes can appear heavy and unaesthetic; the “Light Lips” Technique instead provides subtle rejuvenation without exaggeration.1,3
Safety remains central to the procedure’s success. Anatomical studies reveal that most labial arteries lie within submucosal or intramuscular planes, with only a small minority in the subcutaneous layer. Superficial placement, as used in this technique, is therefore considered safe, and commissural injections remain distant from the facial artery. Still, vigilance is essential. A grayish hue may suggest overly superficial filler placement with risk of the Tyndall effect, while reduced resistance during injection may indicate deep subcutaneous placement. Aspiration and careful observation of tissue response are prudent safety practices.3
Clinically, the use of small filler volumes reduces the risks of vascular compromise, pain, and overtreatment while also lowering costs. The main drawback is a shorter duration of effect, as limited quantities of HA may resorb more quickly, necessitating earlier retreatments. Patients should be counselled about this trade-off so expectations remain realistic. Ultimately, lip aesthetics are a defining feature of facial beauty. Fuller lips with increased vermilion height and balanced upper-to-lower lip ratios (ideally 1:1.6 to 1:2) are widely associated with youthfulness and attractiveness. Conversely, disproportionate or excessive augmentation detracts from harmony. In this context, HA fillers remain the cornerstone of lip enhancement due to their safety, reversibility, and ability to deliver natural outcomes when applied with precision.
Lip Rejuvenation with Hyaluronic Acid: Anatomy, Techniques
The “Light Lips” Technique embodies these principles, offering an elegant solution that prioritizes subtlety, safety, and individualized care.6
Conclusion
Lip fillers, particularly hyaluronic acid–based injectables, remain a safe, effective, and customizable option for enhancing lip volume, definition, and symmetry. Success relies on a tailored approach— considering lip anatomy, patient expectations, and precise injection
References
1. Luthra, Amit. “Shaping Lips with Fillers.” Journal of cutaneous and aesthetic surgery vol. 8,3 (2015): 139-42. doi:10.4103/0974-2077.167269
2. Coppini M, Caponio VCA, Mauceri R, Pizzo G, Mauceri N, Lo Muzio L and Campisi G (2024) Aesthetic lip filler augmentation is not free of adverse reactions: lack of evidence-based practice from a systematic review. Front. Oral. Health 5:1495012. doi: 10.3389/ froh.2024.1495012
3. Cymrot N. Lip filler with hyaluronic acid - Light Lips Technique. Ann Dermatol Res. 2022; 6: 010-013.
4. Keramidas, Evangelos et al. “A Safe and Effective Lip Augmentation Method: The Step-by-Step Φ (Phi) Technique.” Plastic and reconstructive surgery. Global open vol. 9,2 e3332. 2 Feb. 2021, doi:10.1097/ GOX.0000000000003332
5. Castellaneta F, Lombardi M, D'Antonio S, Fabrizio T. The "4.3," A New Filler Lips Technique. J Cosmet Dermatol.
techniques—to achieve natural, harmonious results. With appropriate product selection and skilled administration, lip augmentation not only enhances aesthetics but also boosts patient confidence, while maintaining safety and reversibility as key advantages.
2025;24(1):e16601. doi:10.1111/ jocd.16601
6. de Queiroz Hernandez, P.M., Cotrin, P., Valarelli, F.P. et al. Evaluation of the attractiveness of lips with different volumes after filling with hyaluronic acid. Sci Rep 13, 4589 (2023). https://doi. org/10.1038/s41598-023-31332-1
Beyond Creams & Serums: The Power of CO₂ Fractional Laser for Eye Rejuvenation
Dr. Pramila Kanchan Aswani
MBBS, DVD, FAGE
Consultant Dermatologist & Aesthetic Physician
Mumbai Introduction
The periorbital region — the delicate skin encircling the eyes — is often the first to display visible signs of aging. Fine lines, crepey texture, skin laxity, and pigmentation changes gradually appear, reflecting both intrinsic aging and cumulative environmental insults. While topical creams and home remedies provide only mild support, meaningful rejuvenation requires interventions that act beneath the surface, stimulating regeneration and restoring dermal architecture. Periorbital aging is a multifactorial process involving structural changes at every layer of facial anatomy — from the underlying bone to the epidermis. Age-related resorption of the orbital rim, particularly along the superomedial and inferolateral margins, contributes to deepening tear troughs and accentuated hollowing. Since the eyes form the focal point of facial expression and recognition, even subtle alterations in this region
can influence perceived attractiveness, emotional expressivity, and self-esteem. Genetics largely determine the intrinsic pace of aging; however, extrinsic factors such as ultraviolet exposure, smoking, oxidative stress, and repetitive facial movements accelerate collagen and elastin degradation. The resulting loss of dermal support leads to thinning, reduced elasticity, and the formation of fine lines and folds. The periorbital skin, uniquely thin (approximately 0.2 mm) and poor in sebaceous and collagenous support, is especially vulnerable to these changes. Constant blinking and limited vascularity further predispose the area to wrinkling, pigmentation, and laxity, making it one of the most challenging regions for aesthetic correction. Periorbital rejuvenation aims to reverse these multifactorial changes through a combination of topical agents, chemical peels, lasers, neuromodulators, dermal fillers, and surgical approaches. Each modality
addresses specific components of aging: neuromodulators soften dynamic wrinkles by reducing muscle activity, while dermal fillers restore lost volume and improve tear trough deformities. However, filler treatments are temporary and carry the risk of irregularities if not precisely administered.1,2,3
In recent years, energy-based devices have emerged as cornerstone technologies in non-surgical periorbital rejuvenation. Among them, ablative fractional lasers (AFLs), particularly carbon dioxide (CO₂) and erbium: YAG lasers, have shown remarkable efficacy in improving wrinkles, pigmentation, and texture. The ultrapulsed fractional CO₂ laser, operating at 10,600 nm, delivers controlled microthermal zones of ablation and coagulation, triggering collagen remodeling and skin tightening. This process effectively enhances skin smoothness and elasticity while minimizing downtime compared with traditional resurfacing techniques. Fractional CO₂ laser therapy has demonstrated superior outcomes in improving photodamage, fine lines, and acne scars, with shorter recovery periods and minimal adverse effects such as erythema or post-inflammatory pigmentation. For many patients seeking subtle rejuvenation without the downtime or risks associated with surgery, laser-based alternatives offer an appealing balance between safety, efficacy, and cosmetic satisfaction. Continuouswave microspot CO₂ lasers, known for generating controlled nonscarring heat, provide an innovative approach to skin tightening and textural improvement. By inducing collagen denaturation and neocollagenesis, these lasers enhance skin firmness and resistance to gravitational descent. Furthermore, treatments can be performed safely in outpatient settings, reducing overall costs and making rejuvenation more accessible to a broader patient population. The quest for periorbital rejuvenation has evolved from purely surgical correction to sophisticated, energy-based modalities that offer safe, reproducible, and natural results. Continuous-wave and fractional CO₂ lasers, through their ability to tighten skin, remodel collagen, and enhance dermal structure, have established themselves as indispensable tools in modern aesthetic dermatology. Their precision, safety, and efficacy make them particularly suited for the delicate periorbital area — where even the smallest improvement can profoundly enhance facial harmony and patient confidence.1,2,3
Mechanism of Action: Fractional CO₂ Laser in Eye Rejuvenation
Fractional CO₂ laser resurfacing works by delivering controlled beams of fractionated light energy to the skin, creating microscopic zones of thermal injury known as microthermal treatment zones. These precisely spaced micro-spots, typically about 350 nm apart, target the dermis while leaving surrounding tissue intact. This fractional patterning limits thermal damage, promotes rapid healing, and enhances patient safety. The laser energy induces immediate collagen contraction through selective vaporization and residual dermal heating. This is followed by fibroblast activation, leading to neocollagenesis, elastin remodeling, and deposition of new extracellular matrix components over the following weeks. As a
result, the treated skin undergoes progressive tightening, improved elasticity, and refinement in texture. In the periorbital region, these effects translate to visible reduction in fine lines and superficial rhytides, correction of skin laxity, and widening of the eyelid aperture — collectively contributing to a more refreshed and youthful appearance. The procedure is noninvasive, welltolerated, and associated with minimal downtime (typically 2–3 days). By harnessing the skin’s intrinsic healing capacity, fractional CO₂ laser achieves both immediate and long-term rejuvenation. Its dual mechanism of precise tissue ablation and collagen remodeling makes it a highly effective modality for restoring periorbital firmness and smoothness while minimizing risks of scarring or distortion in this delicate anatomical zone.3,4
Figure 1: Fractional CO₂ Laser
Beyond Creams & Serums: The Power of CO₂ Fractional Laser for Eye Rejuvenation
Benefits of Fractional CO₂ Laser
Fractional CO₂ laser resurfacing provides a transformative, nonsurgical option for rejuvenating the delicate periorbital skin. It effectively addresses fine lines, crow’s feet, under-eye laxity, crepey texture, and early lowerlid sagging while improving pigmentation and dark circles caused by sun exposure or dryness. By generating controlled microthermal zones, the laser stimulates collagen remodeling and dermal tightening, resulting in smoother, firmer, and more luminous skin. Noticeable lifting and wrinkle reduction often occur after a single session, with progressive enhancement over the following weeks due to ongoing collagen regeneration. The treatment refines texture, minimizes pores, and softens superficial scars, producing a more uniform appearance.
Fractional CO₂ resurfacing also corrects subtle agerelated eyelid changes that may not require surgical blepharoplasty, inducing skin and muscle tightening without excision. Additionally, CO₂ laser technology has applications in functional eyelid procedures, including entropion, ectropion, and ptosis correction, offering impressive rejuvenation with minimal downtime and rapid recovery.5
Eye Protection during CO₂ Laser Procedures
The CO₂ laser emits energy that is highly absorbed by water and penetrates only the upper 200 µm of tissue. As the cornea is composed of more than 75% water and measures
approximately 500–600 µm in thickness, it is particularly susceptible to laser-induced injury. Accidental exposure can result in corneal burns or even globe perforation. Therefore, strict ocular safety measures are imperative for the patient, surgeon, and all operating room personnel. Everyone in the treatment area must wear protective eyewear with side shields rated for the CO₂ laser wavelength (10,600 nm), as ordinary glasses offer no protection. For patients, corneal shields are mandatory. Plastic shields are contraindicated because they can melt or ignite under repeated laser exposure. In contrast, metallic corneal shields—preferably stainless steel—remain structurally stable and reflective, ensuring optimal thermal protection and preventing ocular injury during CO₂ laser procedures.5
Pre-Laser Preparation
Local cutaneous anesthesia was achieved using a combination of lidocaine 23% and tetracaine 7%, applied as a thin film twice at 45-minute intervals before the procedure. To ensure patient comfort, oral oxycodone and ibuprofen were administered for analgesia, along with oral promethazine and alprazolam for anxiolytic and antiemetic effects. For ocular safety, protective eyewear carefully positioned to provide effective protection during the treatment.3
Laser technique
The patient was placed in a supine position, with the operator positioned behind the patient’s head for optimal
access and visibility. The treatment area included the facial and supraorbital regions, extending from the upper eyelid lash line to just below the brow. Using 300 μm and 180 μm handpieces, two laser passes were performed in each area, with power levels titrated to achieve visible skin retraction. The passes were applied at 45° angles to each other to ensure uniform energy distribution and optimal coverage. Laser parameters included a density of 20%, an index setting of six or eight depending on the patient’s skin type, and power levels ranging from 10 to 15 W, adjusted according to skin response and tolerance.3
Post-Procedure Care
• Moisturization: Postprocedure care involves applying a gentle petrolatumbased moisturizer regularly to support barrier repair.
• Sun Protection: Use a broad-spectrum sunscreen (SPF ≥30) and follow strict sunavoidance measures; advise the use of UV-protective glasses to shield the periocular region.
• Edema/Exudate/ ..........
Sloughing: Manage with cool compresses, head elevation, saline/water soaks, petrolatum ointment application, and consider mid-potency topical steroids when indicated.
• Severe Periocular Edema: A short 3–5-day course of low-dose oral steroids may be prescribed.
• Pruritus: Treat with topical steroids and oral antihistamines as required.
Discussion
In recent years, laser and light-based technologies have transformed aesthetic dermatology, particularly in periorbital rejuvenation. The delicate skin around the eyes, with its thin dermis, minimal sebaceous glands, and limited collagen and elastin, presents unique therapeutic challenges. Aging and photoexposure accelerate collagen degradation, leading to dermal thinning, laxity, rhytides, hyperpigmentation, and fat herniation. Traditionally, surgical blepharoplasty corrected these changes by addressing skin, muscle, and orbital fat, but potential complications—such as scarring, ectropion, prolonged downtime, and psychological distress—have prompted a shift toward minimally invasive alternatives. This global trend aligns with the growing demand for safe, effective treatments that require little recovery time. Laser and light-based modalities, including ablative and nonablative fractional resurfacing, intense pulsed light (IPL), fractional radiofrequency (RF), and laser-assisted lipolysis, now play a central role in managing periorbital laxity, wrinkles, and pigmentation, offering
precise, predictable, and natural-looking rejuvenation outcomes.6
A major milestone in this evolution was the introduction of fractional photothermolysis (FP) by Manstein et al. in 2003. This concept led to the development of fractional CO₂ lasers, which deliver controlled microthermal zones (MTZs) of injury surrounded by intact tissue, facilitating faster recovery and robust collagen remodeling. Hantash et al. demonstrated that fractional CO₂ laser treatment induces deep
Beyond Creams & Serums: The Power of CO₂ Fractional Laser for Eye Rejuvenation
Before Treatment
After Treatment
dermal coagulation, collagen contraction, and progressive neocollagenesis mediated by heat shock proteins (HSP72 and HSP47). This dual effect— immediate tightening and sustained dermal remodeling— makes fractional CO₂ lasers particularly effective for static periorbital wrinkles caused by dermal atrophy. Overall, advancements in laser and lightbased modalities have provided safe, precise, and efficient alternatives to surgery, achieving natural, long-lasting rejuvenation in the challenging periorbital region.6 Wu et al. reported that low-energy, high-density CO₂ ablative fractional laser (AFL) settings—specifically 10–12.5 mJ with 15% density—yielded optimal results for treating static periorbital wrinkles. These parameters effectively stimulated dermal collagen synthesis while minimizing adverse effects such as prolonged erythema and postinflammatory hyperpigmentation (PIH). The achieved penetration depth of 0.3–0.4 mm is ideal for the thin lower eyelid skin, which averages only 0.5 mm in thickness, ensuring adequate dermal stimulation without excessive tissue damage. Clinical improvements continued for up to six months post-treatment, reflecting the gradual and sustained process of collagen remodeling and maturation. These long-term outcomes are consistent with findings by Ross et al., who observed persistent collagen remodeling several months after CO₂ laser therapy. Histologic studies further confirm fibroblast proliferation, new collagen deposition, and restoration of dermal elasticity following
fractional CO₂ laser resurfacing, highlighting its dual advantage of immediate tissue contraction and progressive neocollagenesis-driven rejuvenation.2
Looking ahead, the integration of newer technologies—such as laser-assisted transdermal delivery systems, nanogelbased photodynamic therapy, and RF microneedling— may further refine periorbital rejuvenation. The ultimate goal remains achieving maximal aesthetic benefit with minimal invasiveness, reduced downtime, and superior safety.
Combination Approach
CO₂ Laser with Platelet-Rich Plasma (PRP)
For patients seeking a more regenerative and synergistic approach to periorbital rejuvenation, the combination of fractional CO₂ laser and platelet-rich plasma (PRP) has shown remarkable promise. When performed in the same session, PRP significantly accelerates post-laser healing, minimizes downtime, and enhances the overall quality of results. Rich in growth factors, PRP nourishes the treated skin, stimulates collagen synthesis, and promotes faster tissue regeneration, making it especially beneficial for delicate, crepey under-eye skin. Clinical evidence supports the superior efficacy of this combination. Studies in cosmetic dermatology have demonstrated that autologous PRP, when used alongside fractional CO₂ laser, produces more pronounced improvement in acne scars and skin texture compared to laser monotherapy. PRP injections are
considered safe, well-tolerated, and effective, offering mild to moderate rejuvenation benefits in aging skin. Moreover, PRP has shown potential as an adjunct therapy for chronic wounds and pigmentary disorders such as vitiligo, owing to its regenerative properties and excellent safety profile. Recent investigations on low-energy ultrapulsed CO₂ fractional laser (LEUCO₂FL) combined with autologous PRP for periorbital rejuvenation have highlighted the enhanced outcomes achieved with this approach. The combination offers superior wrinkle reduction, improved skin elasticity, and higher patient satisfaction compared to CO₂ laser treatment alone, reinforcing its role as a safe and effective modality for achieving natural, regenerative skin rejuvenation.1
CO₂ Followed by Eye Boosters / Injectable Skin Hydrators
An effective companion to fractional CO₂ laser treatment is the use of injectable eye boosters, including polynucleotides, hyaluronic acid (HA) hydrators, and peptidebased bio-remodeling solutions. Following laser resurfacing, the creation of micro-channels in the skin enhances the penetration and efficacy of these boosters, resulting in superior smoothness, prolonged hydration, and improved elasticity. The combined effect restores a healthy glow, firmness, and luminosity to the periorbital skin.
Hydration plays a vital role in maintaining the skin’s radiance, texture, and biomechanical integrity. Hyaluronic acid, a key glycosaminoglycan within
Beyond Creams & Serums: The Power
the dermal extracellular matrix, is renowned for its exceptional ability to bind water up to 1,000 times its weight. This property makes HA-based injectables the gold standard for skin hydration and rejuvenation. Non–cross-linked HA fillers, commonly used in delicate regions such as the under-eye area, diffuse evenly with minimal surface irregularities, providing subtle hydration and elasticity without volumizing effects. In contrast, cross-linked HA formulations offer longer-lasting volume correction and are better suited for thicker skin regions. Injectable skin boosters aim not only to restore moisture but also to enhance overall skin quality, radiance, and firmness. The inclusion of biopolymers, amino acids, and synthetic polymers further supports dermal regeneration. When combined with laser therapy, these boosters amplify results through synergistic rejuvenation. However, the lack of robust clinical data underscores the need for well-designed studies to define optimal combinations, delivery methods, and treatment protocols for safe and effective periorbital rejuvenation.7,8,9
Conclusion
The eyes represent one of the most expressive and emotionally central areas of the face. When this region appears rested, hydrated, and supple, the entire face reflects vitality and youthfulness. Fractional CO₂ laser rejuvenation offers these benefits without surgery, maintaining a completely natural appearance—free from any “done” or frozen look. Laser and light-based modalities have revolutionized the management of periorbital aging. Among them, low-energy, high-density fractional CO₂ laser treatment stands out as an effective, reproducible, and safe option for addressing periorbital wrinkles, pigmentation, and skin laxity. Its ability to stimulate long-term collagen remodeling and deliver progressive improvements over several months highlights its significance in modern aesthetic dermatology. Continued research
References
1. Qi, Y., Sun, C., Zhou, Y., Luo, L., & Wang, C. (2025). Low Energy Ultrapulse CO2 Fractional Laser Combined with Autologous Platelet-Rich Plasma in Periorbital Rejuvenation Treatment. Journal of Investigative Surgery, 38(1). https://doi.org/10.1080/08941939.202 5.2484543
2. Wu, X., Cen, Q., Jin, J. et al. An Effective and Safe Laser Treatment Strategy of Fractional Carbon Dioxide Laser for Chinese Populations with Periorbital Wrinkles: A Randomized Split-Face Trial. Dermatol Ther (Heidelb) 15, 1307–1317 (2025). https://doi.org/10.1007/s13555025-01404-3
3. Toyos M. M. (2017). Continuous Wave Fractional CO2 Laser for the Treatment of Upper Eyelid Dermatochalasis and Periorbital Rejuvenation. Photomedicine and laser surgery, 35(5), 278–281.
https://doi.org/10.1089/pho.2016.4225
4. D. Ancona. Periorbital rejuvenation with fractional CO2 laser.September 2008 Journal of Plastic Dermatology 4(3):317-321
5. Mak ST. Carbon dioxide laser safety issues in blepharoplasty and eyelid surgery. Hong Kong J Ophthalmol. 2012 Dec 1; 16(1):6–10.
6. Liying Cheng, Lu Zhang, Xiaoming Sun, Xiyuan Mao, Liucheng Zhang, Yuguang Zhang, Ying Zhang. Progress of laser and light treatments for lower eyelid rejuvenation. Chinese Journal of Plastic and Reconstructive Surgery, Volume 3, Issue 4, 2021, Pages 218-223, ISSN 2096-6911, https://doi.org/10.1016/j. cjprs.2021.12.003.
7. Rho, N. K., Kim, H. S., Kim, S. Y., & Lee, W. (2024). Injectable "Skin Boosters" in Aging Skin Rejuvenation: A
aimed at refining parameters, assessing long-term outcomes, and integrating synergistic modalities will further enhance precision and efficacy in periorbital rejuvenation.
Final Takeaway
• Eye creams help maintain — but CO₂ fractional laser helps transform.
• One of the most effective non-surgical treatments for periorbital rejuvenation.
• Can be performed alone, or in combination with PRP or PRF (Platelet-rich fibrin) or regenerative eye boosters for enhanced results.
• Promotes collagen remodeling, skin tightening, and improved texture in the delicate eye area.
• Visible results: fresher, firmer, and more youthful eyes within 1–2 sessions.
• Minimal downtime: usually 3–5 days of mild redness or dryness, depending on treatment intensity.
Current Overview. Archives of plastic surgery, 51(6), 528–541. https://doi. org/10.1055/a-2366-3436
8. Rho, N. K., Kim, H. S., Kim, S. Y., & Lee, W. (2024). Injectable "Skin Boosters" in Aging Skin Rejuvenation: A Current Overview. Archives of plastic surgery, 51(6), 528–541. https://doi. org/10.1055/a-2366-3436
9. Yi, K. H., Winayanuwattikun, W., Kim, S. Y., Wan, J., Vachatimanont, V., Putri, A. I., Hidajat, I. J., Yogya, Y., & Pamela, R. (2024). Skin boosters: Definitions and varied classifications. Skin research and technology : official journal of International Society for Bioengineering and the Skin (ISBS) [and] International Society for Digital Imaging of Skin (ISDIS) [and] International Society for Skin Imaging (ISSI), 30(3), e13627. https:// doi.org/10.1111/srt.13627
Beyond Lesion Clearance: Multimodal and Regenerative Strategies in the Management of Acne Vulgaris
Dr. Damini Verma
MD, DNB (Dermatology, Venereology & Leprosy)
Associate Consultant Dermatologist
Apollomedics Super Speciality Hospital
Lucknow
Introduction
Acne vulgaris is a chronic inflammatory disorder of the pilosebaceous unit, commonly affecting areas with a high density of sebaceous glands, including the face, neck, chest, back, and shoulders. While it typically begins during adolescence due to androgen-induced activation of sebaceous glands, a significant number of women continue to experience acne beyond the age of 25, a condition referred to as adult female acne (AFA). Epidemiological data indicate that adult acne is more prevalent in females than in males, with its incidence decreasing with age, affecting approximately 7.5% of women aged 16–29 years, 5% of women aged 30–39 years, and less than 2% of women aged 40–49 years. Adult female acne is clinically classified into persistent acne, which originates during adolescence and persists into adulthood, and late-onset acne, which develops for the first
time after the age of 25. Studies also recognize a recurrent subtype characterized by intermittent flare-ups following periods of remission. Clinically, AFA differs from adolescent acne in its presentation, with most adult women exhibiting mild to moderate lesions, characterized by inflammatory papules, comedones, and fewer nodulocystic lesions, typically localized to the mandibular and perioral regions.1, 2
The pathophysiology of acne vulgaris is highly complex and multifactorial, involving a dynamic interplay of intrinsic and extrinsic factors that contribute to lesion development and persistence. At the core of its pathogenesis are increased sebum production by hyperactive sebaceous glands, abnormal follicular keratinization leading to comedone formation, colonization by Cutibacterium acnes, and dysregulated inflammatory
responses that perpetuate lesion progression. Epigenetic mechanisms, including DNA methylation and histone modifications, may further influence gene expression governing sebaceous gland activity, keratinocyte behaviour, and immune responses, thereby modulating individual susceptibility and disease severity. Genetic predisposition underlies variations in sebaceous gland size, hormone receptor sensitivity, and inflammatory threshold, which can explain differences in clinical presentation and response to treatment. Hormonal influences, particularly androgen excess, play a pivotal role in stimulating sebum production, while cyclical fluctuations associated with the menstrual cycle frequently exacerbate acne in adult women, underscoring the significance of hormonal regulation in pathophysiology. Additional factors, such as diet, stress, sleep disturbances, and suboptimal skincare practices, may further exacerbate inflammation and lesion formation by influencing sebum composition, skin barrier integrity, and microbial colonization. Collectively, these mechanisms demonstrate that acne vulgaris arises from a complex interplay of systemic, genetic, hormonal, and environmental factors, which together dictate both the clinical severity and chronicity of the condition.1, 2
Beyond the cutaneous manifestations, acne vulgaris substantially impacts quality
of life, often resulting in psychological distress, lowered self-esteem, anxiety, and social withdrawal. Patients may experience persistent concern over facial appearance, which can interfere with social interactions, professional activities, and overall mental well-being. Adult female acne, in particular, may carry additional emotional and psychosocial burdens due to its chronicity and potential for scarring.2 Given this multifaceted etiology and the profound psychosocial implications, a comprehensive, individualized approach to assessment and management is essential, incorporating both targeted therapeutic interventions and attention to lifestyle, hormonal, and psychological factors to optimize outcomes and improve overall quality of life.
Case Report
A 22-year-old female presented with concerns of persistent facial acne characterized by multiple comedones, including whiteheads, fleshcolored papules, keratin plugs, and closed comedones predominantly over both cheeks. The patient also reported uneven skin texture and dullness. Clinical examination revealed multiple non-inflammatory comedonal lesions with post-acne atrophic changes and mild textural irregularities involving the malar region bilaterally. There were no signs of active inflammation or nodulocystic lesions at presentation. The patient, with minimal response to prior
topical treatments, underwent a personalized protocol including topical retinoids for comedolysis and follicular normalization, followed by periodic comedone extraction and sequential chemical peels to enhance epidermal renewal, reduce pigmentation and improve overall skin texture. Subsequently, microneedling sessions were introduced to stimulate collagen remodeling and enhance dermal regeneration, targeting atrophic scarring and surface irregularities. Platelet-rich plasma (PRP) therapy was combined with microneedling to accelerate healing, promote neocollagenesis, and optimize rejuvenation outcomes. Over multiple sessions, the patient demonstrated progressive improvement with marked reduction in comedonal activity, smoother skin texture, and visible reduction in the appearance of atrophic scars. The overall facial complexion appeared brighter, healthier, and more uniform. The treatment was well tolerated without any adverse events. This case underscores the efficacy of a multimodal, individualized therapeutic strategy in addressing both active acne and post-acne sequelae. The integration of medical therapy, mechanical extraction, controlled exfoliation, and collagen-inducing procedures such as microneedling with PRP yielded superior aesthetic and structural results, highlighting the importance of comprehensive acne management beyond lesion clearance.
Before Treatment
After Treatment
Figure 1: Improved skin texture with reduced comedones on the cheeks following a multimodal treatment approach combining chemical peels, microneedling, and platelet-rich plasma (PRP) therapy
Diagnosis
Acne vulgaris is primarily diagnosed through clinical examination, based on lesion morphology, anatomical distribution, and severity. The disease is broadly graded into four categories: Grade 1, characterized by open and closed comedones; Grade 2, presenting with erythematous papules; Grade 3, featuring pustules; and Grade 4, comprising nodulocystic lesions.3 Clinical evaluation of lesion type and severity remains fundamental for accurate diagnosis and management planning. Standardized grading systems enhance diagnostic precision and treatment monitoring. Commonly used systems include the Global Acne Grading System (GAGS), Investigator Global Assessment (IGA), Pillsbury scale, Cook acne grading scale, and Leeds acne grading system. These scales provide objective classification of comedonal, papular, pustular, and nodulocystic lesions, supporting consistent evaluation and longitudinal follow-up of therapeutic outcomes. Dermoscopy serves as a valuable non-invasive diagnostic adjunct, offering enhanced visualization of pilosebaceous units and distinguishing between
open and closed comedones, inflammatory papules, pustules, and nodulocystic lesions. Similarly, digital imaging techniques facilitate accurate documentation of baseline lesion distribution and severity, enabling objective assessment of disease progression and response to treatment over time. In females with severe, recalcitrant, or atypical acne, hormonal evaluation is crucial to identify underlying endocrine disorders. This includes measuring serum androgens (testosterone, DHEA-S, androstenedione), LH/FSH ratio (for polycystic ovarian syndrome), 17-hydroxyprogesterone (for congenital adrenal hyperplasia), and prolactin (in cases of menstrual irregularities or galactorrhea).4,5,6,7
Accurate diagnosis of acne vulgaris is essential for determining lesion type and severity, thereby guiding the selection of appropriate and targeted therapeutic interventions.
Treatment
Medical management of acne vulgaris focuses on reducing lesions, inflammation, and scarring by targeting key pathogenic factors. Topical agents include retinoids, antibiotics, and combination formulations, while systemic options such as oral retinoids, antibiotics, and hormonal therapies are reserved for moderate to severe or hormonally influenced cases to achieve comprehensive control.7
Beyond
Comedone extraction is an adjunctive procedure in acne management, particularly during isotretinoin maintenance or premenstrual acne. It provides immediate improvement by removing open and closed comedones, though refilling can occur. The procedure should be performed under aseptic conditions with gentle steam, careful pressure, and pre- and post-treatment exfoliation and topical antimicrobial or anti-inflammatory therapy. Mechanistically, extraction relieves follicular obstruction, reduces Cutibacterium acnes colonization, and limits inflammation. Timing the procedure around ovulation may enhance efficacy in premenstrual acne by preventing sebum-induced blockage and subsequent inflammatory lesions.8
Chemical peels are an effective therapeutic option in acne management, tailored to skin type and clinical presentation. Salicylic acid 30% peel exerts keratolytic, comedolytic, and anti-inflammatory effects, reducing sebum, unclogging follicles, and improving pore appearance. Glycolic acid promotes epidermal exfoliation, reduces inflammation, and inhibits Cutibacterium acnes, decreasing lesion formation. Trichloroacetic acid peels stimulate collagen production and dermal remodeling, improving mild acne scars and skin texture. Peel depth, whether superficial, medium, or deep, is determined by skin type and acne severity. Mechanistically,
chemical peels enhance epidermal turnover, reduce follicular obstruction, modulate inflammation, and promote dermal regeneration, resulting in clearer, smoother, and healthier skin.9 Microneedling is a minimally invasive procedure for acne-prone skin that creates controlled microinjuries, stimulating collagen and elastin production, improving skin texture, and reducing acne scars. Devices such as dermarollers, pens, and stamps are chosen based on treatment area and severity. The procedure enhances penetration of topical agents, normalizes sebaceous gland activity, reduces sebum, decreases follicular obstruction, and limits Cutibacterium acnes proliferation, preventing new lesions. Proper aseptic technique is essential, and microneedling improves both the structure and function of acne-affected skin, promoting smoother, healthier skin.10 Platelet-rich plasma (PRP) therapy is an adjunctive treatment for acne and acne scars, using autologous plasma rich in growth factors such as PDGF, VEGF, and TGF-β to stimulate collagen and elastin synthesis, promote dermal regeneration, and accelerate wound healing. Mechanistically, PRP modulates local inflammation, enhances angiogenesis, supports remodelling of damaged tissue, and may reduce sebaceous gland activity, decreasing follicular inflammation and promoting resolution of lesions.
By improving both structural and functional integrity of acneaffected skin, PRP enhances skin texture and reduces scar formation.11
The combination of medical therapy, comedone extraction, chemical peels, microneedling, and PRP is beneficial in acne management, targeting inflammation, follicular obstruction, collagen regeneration, and scar improvement. Advanced non-invasive acne treatments include fractional CO₂, Er:YAG, and pulsed dye lasers for collagen remodeling and scar improvement. Photodynamic therapy, IPL, and blue light reduce bacterial load and inflammation. Fractional microneedle RF, LED therapy, HIFU, and LLLT further promote sebaceous regulation, dermal regeneration, and overall skin rejuvenation.
Appropriate management of acne requires a multimodal approach addressing inflammation, obstruction, and scarring to restore skin health and function.12,13
Discussion
Acne vulgaris is a multifactorial, chronic inflammatory disorder of the pilosebaceous unit with a global prevalence of approximately 9.38%, ranking as the eighth most common dermatological condition worldwide. It primarily affects adolescents, with prevalence approaching 100% in certain populations; however, an increasing incidence among
adults is now recognized. Shah et al. reported a prevalence of 0.74% for adult acne, likely reflecting greater health awareness and diagnostic recognition.14
Clinically, acne presents in several variants with distinct features. Acne conglobata is a severe nodulocystic form characterized by interconnecting abscesses and sinus tracts, often resulting in disfiguring scars without systemic symptoms. Acne fulminans, conversely, is an acute ulcerative and hemorrhagic variant that may be accompanied by systemic manifestations such as fever, arthralgia, and osteolytic lesions. Acne excoriée commonly affects young females and is associated with compulsive picking, leading to secondary excoriations and scarring. Infantile acne results from transient androgen excess from the adrenal glands or testes and typically resolves spontaneously as androgen levels normalize. Acne can also occur as part of systemic syndromes such as SAPHO (synovitis, acne, pustulosis, hyperostosis, and osteitis) and PAPA (pyogenic arthritis, pyoderma gangrenosum, and acne), reflecting underlying autoinflammatory mechanisms.
Comprehensive clinical evaluation is essential and
1. Telkkälä A, Sinikumpu SP, Huilaja L. Etiology of Adult Female AcneSystematic Review. Health Sci Rep. 2025; 8(5):e70697. Published 2025 Apr 30. References
should include assessment of disease onset, duration, medical and medication history, family predisposition, menstrual irregularities, features of virilization, systemic symptoms, and psychosocial burden. Physical examination must document lesion morphology and distribution—monomorphic eruptions suggest drug-induced acne or Malassezia folliculitis, whereas polymorphic lesions favor acne vulgaris. Evaluation for hyperandrogenism, postinflammatory hyperpigmentation, and scarring is vital for accurate grading and treatment planning. The differential diagnosis includes rosacea (absence of comedones, presence of telangiectasia), perioral dermatitis (papules sparing the vermilion border), and Demodex folliculitis (refractory to antibiotics). Other mimickers include facial angiofibromas, pseudofolliculitis barbae, nevus comedonicus, sebaceous hyperplasia, adnexal tumors, and Favre-Racouchot syndrome.1
Complications of acne extend beyond cutaneous involvement to include considerable psychosocial distress, anxiety, and depression, often resulting from persistent inflammation and scarring. Severe variants like acne fulminans may present with systemic symptoms and osteolytic bone lesions, while prolonged antibiotic use can lead to Gram-negative folliculitis. Morbihan’s disease, or solid facial edema, is another rare but challenging complication characterized by chronic erythema and swelling. Preventive strategies emphasize gentle, pH-balanced, non-comedogenic cleansing and dietary regulation, particularly reducing high-glycemic foods and excessive dairy intake.1 A multimodal treatment approach integrating medical therapy, comedone extraction, chemical peels, microneedling, and platelet-rich plasma (PRP) therapy effectively targets multiple pathogenic pathways—reducing inflammation, promoting collagen synthesis, and improving texture—thereby achieving sustained remission and superior aesthetic outcomes in acne management.
Conclusion
Acne vulgaris is a prevalent dermatological condition with considerable psychosocial impact, often affecting patient quality of life and self-esteem. A tailored, multimodal management strategy incorporating medical therapy, comedone extraction, chemical peels, microneedling, and PRP has demonstrated efficacy in improving skin texture, reducing lesions, and promoting overall cutaneous health, and future advancements in non-invasive and regenerative therapies hold promise for further enhancing outcomes and patient satisfaction.
doi:10.1002/hsr2.70697.
2. Vasam M, Korutla S, Bohara RA. Acne vulgaris: A review of the pathophysiology,
treatment, and recent nanotechnology based advances. Biochem Biophys Rep. 2023; 36:101578. Published 2023 Nov 23. doi:10.1016/j.bbrep.2023.101578.
3. Sutaria AH, Masood S, Saleh HM, Schlessinger J. Acne Vulgaris. In: StatPearls. Treasure Island (FL): StatPearls Publishing; August 17, 2023.
4. Bae IH, Kwak JH, Na CH, Kim MS, Shin BS, Choi H. A Comprehensive Review of the Acne Grading Scale in 2023. Ann Dermatol. 2024; 36(2):65-73. doi:10.5021/ad.23.094.
5. Alma A, Sticchi A, Chello C, et al. Dermoscopy, Reflectance Confocal Microscopy and Optical Coherence Tomography Features of Acne: A Systematic Review. J Clin Med. 2022; 11(7):1783. Published 2022 Mar 24. Doi: 10.3390/jcm11071783.
6. Bergman H, Tsai KY, Seo SJ, Kvedar JC, Watson AJ. Remote assessment of acne: the use of acne grading tools to evaluate digital skin images. Telemed J E Health. 2009; 15(5):426-430. doi:10.1089/ tmj.2008.0128.
7. Elsaie ML. Hormonal treatment of acne vulgaris: an update. Clin Cosmet Investig
Dermatol. 2016; 9:241-248. Published 2016 Sep 2. doi:10.2147/CCID.S114830.
8. Steventon K. Expert opinion and review article: The timing of comedone extraction in the treatment of premenstrual acne--a proposed therapeutic approach. Int J Cosmet Sci. 2011; 33(2):99-104. doi:10.1111/j.1468-2494.2010.00610.x.
9. Jaiswal S, Jawade S, Madke B, Gupta S. Recent Trends in the Management of Acne Vulgaris: A Review Focusing on Clinical Studies in the Last Decade. Cureus. 2024; 16(3):e56596. Published 2024 Mar 20. doi:10.7759/cureus.56596.
10. Măgerușan ȘE, Hancu G, Rusu A. Current Understanding of Microneedling Procedures for Acne Skin: A Narrative Review. Cosmetics. 2024; 11(6):193. https://doi. org/10.3390/cosmetics11060193
11. Ibrahim ZA, Gheida SF, El-Halaby AR, Hassan GFR, Mohammed DA. Platelet rich plasma injection versus topical erythromycin 2% in treatment of acne vulgaris. J Dermatolog Treat. 2022; 33(2):946-953. doi
:10.1080/09546634.2020.1793884.
12. Pei S, Inamadar AC, Adya KA, Tsoukas MM. Light-based therapies in acne treatment. Indian Dermatol Online J. 2015; 6(3):145-157. doi:10.4103/22295178.156379.
13. Hamadani F, Vranis NM. The Role of Fractional Radiofrequency in Longterm Acne Remission and Reduction of Acne Scar Load. Aesthet Surg J. 2025; 45(Supplement_1):S23-S31. doi:10.1093/asj/sjae150.
14. Dabash D, Salahat H, Awawdeh S, et al. Prevalence of acne and its impact on quality of life and practices regarding self-treatment among medical students. Sci Rep. 2024;14(1):4351. Published 2024 Feb 22. doi:10.1038/s41598-02455094-6.
HIFU for the Aging Face: Precision Skin Tightening with Minimal Downtime
Dr. Rashmi Soni MD, DDV, DNB
Founder and Consultant Dermatologist, Cosmetologist and Dermatosurgeon
Skinsure Clinic, Pune
Consultant Dermatologist, KEM Hospital, Pune
Introduction
In recent years, growing public interest in addressing facial wrinkles and age-related skin laxity has driven the development of multiple treatment modalities. Conventional approaches such as chemical peels, microdermabrasion, fractional lasers, and radiofrequency therapies have shown varying degrees of success in managing facial aging; however, a universally ideal treatment has yet to be established. More recently, ultrasound-based therapies have gained attention for both therapeutic and aesthetic purposes, with HighIntensity Focused Ultrasound (HIFU) emerging as a leading non-invasive option.1,2
"High-Intensity Focused Ultrasound was first applied in aesthetic dermatology by White and colleagues in 2008."HIFU received U.S. FDA approval in 2009 for brow lifting and has since been applied off-label
for a range of cosmetic goals, including facial rejuvenation, skin tightening, and body contouring. The mechanism of HIFU involves the delivery of focused ultrasound energy to targeted tissue layers, where it generates controlled thermal injury in the form of microcoagulation zones. This precise energy delivery stimulates collagen remodeling and tissue contraction without affecting the surrounding epidermis or adjacent structures. Clinical evidence indicates that HIFU is effective in tightening skin, particularly in areas such as the lower face, neck, and periorbital region, with reported improvements in skin laxity ranging from 18% to 30%. These findings underscore HIFU’s potential as a dependable, non-invasive solution for individuals seeking noticeable facial rejuvenation with minimal recovery time. In body contouring applications, reductions in circumference
of 2.5 to 4.5 cm have been observed in areas such as the abdomen and thighs. While not equivalent to surgical results, HIFU offers a compelling noninvasive alternative with a high safety profile. Technological advancements, including the introduction of parallel-beam ultrasound systems, have further enhanced the precision, comfort, and efficacy of HIFU treatments. Despite its growing popularity and positive clinical outcomes, standardization of treatment protocols remains an area for improvement. Key variables such as optimal energy levels, treatment depth, and appropriate patient selection need further clarification. Overall, HIFU represents a promising, low-risk alternative to surgical procedures, offering significant improvements in skin tone, texture, and body contours with minimal recovery time.1,2
Case Report
A 47-year-old female presented with aesthetic concerns of skin laxity, loss of definition in the nasolabial folds, and midface sagging, seeking a non-invasive option for facial rejuvenation. Clinical evaluation revealed moderate lower face laxity, prominent nasolabial folds, and uneven skin texture. A single session of high-intensity focused ultrasound (HIFU) was performed targeting the lower face and midface using standardized parameters for dermal tightening and facial lifting. The procedure was well tolerated without the need for anesthesia. Pre-treatment images demonstrated deepened
nasolabial folds and mild sagging. At the 8-week follow-up, there was visible softening of the nasolabial lines, improved skin texture, and enhanced dermal tightening with better facial contouring. The patient expressed high satisfaction with the outcome and experienced no adverse effects, supporting the efficacy of HIFU as a safe and effective non-invasive modality for facial rejuvenation in cases of moderate skin laxity.
Figure 1: Clinical outcome of HIFU therapy showcasing visible softening of the nasolabial lines, improved skin texture and enhanced dermal tightening with better facial contouring.
Treatment
High-Intensity Focused Ultrasound (HIFU) has emerged as a transformative, non-invasive technology in aesthetic dermatology, providing an effective and scientifically validated alternative to surgical facial rejuvenation. It is particularly beneficial in addressing facial laxity, deep wrinkles, and structural skin aging through precisely delivered thermal stimulation at targeted tissue depths. HIFU functions by focusing ultrasound energy into specific skin layers, notably the dermis and the superficial musculoaponeurotic system (SMAS), generating controlled thermal coagulation zones at temperatures between 65–75°C. This results in collagen contraction and stimulation of neocollagenesis, promoting dermal tightening and lifting without damaging the epidermis or surrounding structures.
Before treatment
After treatment
HIFU for the Aging Face: Precision Skin Tightening with Minimal Downtime
Unlike laser or radiofrequencybased treatments that primarily affect superficial layers, HIFU penetrates deeper, making it more effective for structural remodeling.3,4
The treatment protocol involves cleansing the skin, mapping target zones, and applying ultrasound coupling gel to facilitate energy conduction. Ultrasound is delivered in an anti-gravity direction to counteract tissue descent, with firm probe contact ensuring optimal energy delivery. Three depth-specific transducers are employed in sequence: the 4.5 mm cartridge targets the SMAS layer for foundational lifting, the 3.0 mm cartridge stimulates deep dermal collagen, and the 1.5 mm cartridge addresses superficial dermal remodeling and improves texture. Parameters such as pulse count and energy levels are customized based on skin thickness, degree of laxity, and aesthetic goals.3,4
HIFU triggers a structured three-phase healing response. The initial inflammatory phase (0–48 hours) is characterized by mild erythema, edema, and tenderness due to microthermal injury. This is followed by the proliferative phase (2–6 weeks), during which fibroblast activation and extracellular matrix (ECM) remodeling occur, progressively enhancing collagen production. Finally, the remodeling phase (3 weeks to 6 months) leads to the maturation and reorganization of collagen
and elastin fibers, resulting in visible skin tightening and improved elasticity. The majority of patients typically observe initial improvements within 2 to 3 months, with peak results becoming more apparent between 3 and 6 months posttreatment. In addition to its mechanical effects, HIFU also exerts significant molecular influences that enhance tissue regeneration. It downregulates caveolin-1 (Cav-1), a protein that suppresses fibroblast activity in aged skin, thereby restoring fibroblast function and stimulating the production of collagen types I and III, elastin, and epidermal growth factor (EGF). These changes contribute to dermal renewal, skin firming, and wound healing.3,4
HIFU’s applications extend beyond facial rejuvenation to include jawline contouring, submental tightening, brow lifting, and skin brightening. It is also used in body contouring (abdomen, thighs) and to treat dermatologic conditions such as seborrheic keratosis, sebaceous hyperplasia, vascular lesions, nevus sebaceous and hyperpigmentation.3,4
The procedure is considered safe overall, with less than 5% of individuals reporting temporary side effects. Nevertheless, careful patient selection is essential. Treatment should be avoided in cases of active skin infections, open wounds, metal implants (except dental work), implantable devices like pacemakers,
recent botulinum toxin use, pregnancy, permanent dermal fillers, bleeding disorders, or unrealistic treatment expectations. Extra caution is necessary when applying the 4.5 mm transducer to prevent nerve-related complications. Utilizing real-time imaging and precisely guided cartridges improves both the safety and effectiveness of the treatment.3,4
To maintain results, patients are encouraged to stay hydrated, apply broadspectrum sunscreen, and follow a customized skincare regimen. While a single session often produces satisfactory outcomes, some individuals may benefit from a repeat session after 3–6 months. For enhanced results, adjunctive treatments like botulinum toxin can be used in combination to refine dynamic wrinkle areas. Overall, HIFU offers a reliable, non-invasive approach to longlasting facial rejuvenation and contouring.3,4
Discussion
High-Intensity Focused Ultrasound (HIFU) has established itself as a cornerstone in aesthetic and regenerative dermatology, offering a non-invasive, energybased modality for facial rejuvenation, skin tightening, and overall dermal restoration. Its therapeutic efficacy lies in its ability to deliver precisely focused ultrasound energy to targeted tissue depths, specifically the dermis and the superficial musculoaponeurotic
system (SMAS), inducing controlled thermal coagulation. This process triggers collagen denaturation, followed by neocollagenesis and dermal remodeling, ultimately enhancing skin firmness, elasticity, and contour definition. In addition to these thermal effects, HIFU exerts non-thermal biomechanical mechanisms, such as acoustic cavitation, which contribute to localized tissue disruption and structural reorganization, further supporting its regenerative capabilities.5,6,7
The efficacy, precision, and safety of HIFU are governed by three primary technological components: the focused ultrasound transducer responsible for controlled energy delivery; real-time imaging modalities such as sonography or MRI that enable accurate visualization and targeting of anatomical planes; and a central control unit that modulates treatment parameters including energy intensity, frequency, and penetration depth. Frequency selection is critical in determining the treatment depth—lower-frequency ....... transducers allow for deeper tissue penetration, while higher-frequency transducers target more superficial layers— facilitating highly customized protocols based on anatomical and clinical considerations. By selectively treating various skin layers with precision, HIFU effectively addresses agerelated skin laxity and dermal
degradation with minimal recovery time and low complication rates.5,6,7
Healing outcomes following HIFU are generally favourable and vary depending on lesion depth, size, and histologic characteristics. Superficial lesions tend to exhibit rapid re-epithelialization with minimal fibrosis, while deeper or more structurally complex lesions undergo slower, yet controlled, collagen remodeling and dermal regeneration over several weeks. Transient hyperpigmentation may occur in certain individuals but typically resolves spontaneously. Dermoscopic monitoring throughout the healing phase provides valuable insights into vascular and pigmentary changes, aiding clinicians in adjusting follow-up care and recognizing early signs of complications.5,6,7
The application of High-Intensity Focused Ultrasound (HIFU) has been shown to significantly enhance dermal penetration and bioavailability of active agents through localized thermal and mechanical effects that transiently increase skin permeability. This mechanism not only stimulates dermal remodeling via collagen denaturation and neocollagenesis but also serves as an effective physical enhancer for transdermal drug delivery. Clinically, combining HIFU with topical treatments demonstrates excellent tolerability, with minimal risk of scarring, post-inflammatory hyperpigmentation, or textural changes, highlighting the safety of this integrated approach. A limitation of this study was its use of a parallel-group design, which introduces inter-individual variability and reduces comparative precision; employing split-face designs would better control patient-specific factors and improve internal validity. Overall, HIFU represents a versatile, non-invasive modality with proven regenerative and therapeutic benefits, extending beyond facial rejuvenation and tissue tightening to enhanced transdermal drug delivery. Continued technological advancements and protocol refinements are expected to further solidify HIFU’s role as a cornerstone treatment in dermatologic and aesthetic medicine, offering safe, effective and customizable care across diverse patient populations.5,6,7
Conclusion
High-Intensity Focused Ultrasound (HIFU) has transformed noninvasive facial rejuvenation by providing effective results with minimal downtime. It precisely targets deeper dermal layers, creating controlled thermal zones that trigger immediate collagen tightening and stimulate neocollagenesis—enhancing skin firmness and elasticity without affecting the epidermis. With optimized protocols and patient selection, HIFU has become a precision-driven modality offering sustained, individualized aesthetic outcomes. Its versatility, safety, and minimal recovery have established it as a key tool in modern aesthetic dermatology.
HIFU for the Aging Face: Precision Skin Tightening with Minimal Downtime
References
1. Park, H., Kim, E., Kim, J., Ro, Y., & Ko, J. (2015). High-Intensity Focused Ultrasound for the Treatment of Wrinkles and Skin Laxity in Seven Different Facial Areas. Annals of dermatology, 27(6), 688–693. https://doi.org/10.5021/ ad.2015.27.6.688
2. Diala Haykal, Sonja Sattler, Ines Verner, Monisha Madhumita, Hugues Cartier, A Systematic Review of High-Intensity Focused Ultrasound in Skin Tightening and Body Contouring, Aesthetic Surgery Journal, Volume 45, Issue 7, July 2025, Pages 690–698, https://doi. org/10.1093/asj/sjaf053
3. Hong GW, Kim SB, Park SY, Wan J, Yi KH. Basic concepts in facial and neck thread lifting procedures. Skin Res Technol. 2024; 30(4):e13673. doi:10.1111/ srt.13673.
4. Kim, Jong Seo MD. Three-dimensional Analysis of Lifting Effects after Highintensity Focused Ultrasound (UltraformerMPT) across Seven Facial Aesthetic Units Considering SonoAnatomy. Plastic & Reconstructive Surgery-Global Open 12(10): p e6203, October 2024. | DOI: 10.1097/ GOX.0000000000006203.
5. Zargaran D, Zoller F, Zargaran A, Weyrich T, Mosahebi A. Facial skin ageing: Key concepts and overview of processes. Int J Cosmet Sci. 2022; 44(4):414-420. doi:10.1111/ics.12779.
6. Okuda I, Takeda M, Taira M, Kobayashi T, Inomata K, Yoshioka N. Objective analysis of the effectiveness of facial massage using breakthrough computed tomographic technology: A preliminary pilot study. Skin Res Technol. 2022; 28(3):472-479. doi:10.1111/srt.13152.
7. Biskanaki F, Tertipi N, Sfyri E, Kefala V, Rallis E. Complications and Risks of High-Intensity Focused Ultrasound (HIFU) in Esthetic Procedures: A Review. Applied Sciences. 2025; 15(9):4958. https://doi. org/10.3390/app15094958
Breakthrough IL-2 Pathway Agonist Shows Promising Advances in Treating Moderate to Severe Atopic Dermatitis
A novel IL-2 pathway agonist that selectively expands regulatory T cells offers a promising new approach for the treatment of moderate to severe atopic dermatitis by addressing the underlying immune dysregulation central to the disease's pathophysiology. Atopic dermatitis involves an imbalance in immune signaling, characterized by overactivation of Th2 cells and elevated levels of cytokines such as IL-4, IL-13, and IL-31, which contribute to skin barrier dysfunction, inflammation, and pruritus. This IL-2 agonist works by stimulating regulatory T cells, which play a critical role in maintaining immune tolerance and modulating excessive inflammation. Clinical benefits include marked reductions in skin lesions, itch intensity, and extent of affected skin, alongside improvements in sleep quality and pain control, which collectively enhance patients' quality of life. The treatment supports longterm disease control by restoring immune homeostasis rather than merely suppressing inflammatory pathways. It has demonstrated a favorable safety profile, with mostly mild and manageable adverse effects reported. This therapeutic strategy represents a significant advancement by targeting the root cause of immune dysregulation, providing hope for more durable and effective management of inflammatory skin conditions refractory to conventional therapies.
Obstructive Sleep Apnea and Skin Conditions: Emerging Associations and Clinical Considerations
Dermatological conditions such as atopic dermatitis and impaired wound healing have been increasingly linked to obstructive sleep apnea (OSA), a disorder defined by repetitive upper airway obstruction during sleep causing intermittent hypoxia and systemic inflammation. Studies indicate that patients with newly diagnosed OSA are at increased risk of developing atopic dermatitis, with this risk being more pronounced in male and younger populations, implicating age and sex as key factors in susceptibility. OSA impact on wound healing is also notable, with delayed recovery observed in both surgical and chronic wounds, attributed to oxidative stress, endothelial dysfunction, and persistent systemic inflammation. Additionally, the continuous positive airway pressure (CPAP) therapy frequently prescribed for OSA can lead to skin complications such as dermatitis due to friction, pressure, moisture, or material sensitivities, especially when masks are poorly fitted. While further research is needed to establish definitive causality, these findings emphasize the importance of recognizing skin manifestations in patients with OSA, advocating for integrated care approaches involving both dermatologists and sleep medicine specialists to address the complex interaction between respiratory and dermatologic health.
A Gentle Glow: Managing Acne and Redness with Intense Pulsed Light (IPL) Therapy
Dr. Reeya Patel MD (DVL)
Consultant
Dermatologist
Surat Introduction
Acne vulgaris is a chronic, multifactorial inflammatory dermatosis of the pilosebaceous unit and represents the most common dermatologic condition globally, affecting approximately 80% to 100% of individuals at some point in their lifetime. While predominantly a disease of adolescence, acne may persist into adulthood or present de novo. Clinically, acne vulgaris is characterized by the coexistence of noninflammatory lesions such as open and closed comedones, and inflammatory lesions such as papules, pustules, nodules, and cysts. Lesions typically localize to sebaceous glandrich regions including the face, chest, back, and proximal upper extremities. In adolescents, lesions commonly predominate in the T-zone, whereas in adults they may involve the lower face with variable distribution.1, 2
The pathogenesis of acne involves four fundamental processes: follicular hyperkeratinization, androgendriven sebum production,
colonization by Cutibacterium acnes, and chronic inflammation. Abnormal keratinocyte differentiation and infundibular obstruction initiate microcomedone formation. Androgens such as DHEAS, testosterone, and dihydrotestosterone activate androgen receptors in sebocytes and keratinocytes, stimulating the mTORC1–SREBP-1 pathway and promoting lipogenesis. Simultaneously, suppression of Wnt/β-catenin signaling via c-Myc enhances sebocyte differentiation, while PPARγ and PPARδ regulate sebocyte maturation and holocrine secretion. Increased sebum production—both quantitatively and qualitatively altered— favors C. acnes proliferation and biofilm formation. Insulinlike growth factor 1 (IGF-1) acts synergistically with androgens through the PI3K/Akt pathway, suppressing FoxO1 and AMPK, thereby augmenting lipid synthesis and androgen receptor activity. The absence of acne in Laron syndrome underscores IGF-1’s central
A
role. Inflammation begins with C. acnes-induced activation of Toll-like receptor 2 (TLR2) on keratinocytes and monocytes, leading to NLRP3 inflammasome activation and release of IL-1β, IL-6, IL-8, IL-12, TNF-α, and IFN-γ. These recruit neutrophils and matrix metalloproteinases (MMPs), causing matrix degradation and follicular rupture. Activation of AP-1 and NF-κB pathways further amplifies cytokine production, while the Th17 axis (IL-17, IL-23) sustains inflammation. Chronic lesions exhibit infiltrates of CD4⁺ T cells, B cells, plasma cells, and memory T cells, contributing to scarring. Exacerbating factors include corticosteroids, lithium, isoniazid, antiepileptics, mechanical irritation, comedogenic cosmetics, ultraviolet exposure, excessive cleansing, high-glycemic diets, dairy intake, stress, and genetic predisposition. Heritability estimates (81–90%) confirm acne’s strong genetic basis, linked to heightened innate immunity, lipid metabolism, and tissue remodeling genes.1,2
Clinically, acne vulgaris manifests across a broad spectrum, ranging from comedonal (Grade I) to nodulocystic (Grade IV) forms. Lesions may be accompanied by seborrhea and, in some cases, by notable atrophic (ice pick, boxcar, rolling) or hypertrophic/keloidal changes. Several distinct clinical variants exist: acne conglobata presents as a severe, chronic form with interconnecting nodules and draining sinuses; acne fulminans is an acute ulcerative type with systemic features requiring immunosuppression; and acne excoriée, commonly observed
in young women, is linked to compulsive picking and psychiatric comorbidities. Infantile acne, occurring between 3 and 6 months of age, is driven by transient adrenal androgen surges. Additionally, acne can be a cutaneous feature of systemic autoinflammatory syndromes such as SAPHO and PAPA, necessitating systemic immunomodulatory therapy. The emotional impact of acne can be profound, often exceeding the visible severity of the condition, with associations to low self-confidence, social isolation, anxiety, depression, and in severe cases, suicidal ideation.1, 2
These effects are especially prominent in adult populations and females, highlighting the importance of a comprehensive and patient-centered approach to care.
Case Report
A 28-year-old female presented with mild to moderate acne characterized by both inflammatory and non-inflammatory lesions distributed over the cheeks, nose, and forehead. Prominent erythema was noted over the forehead, accompanied by scattered papulopustular eruptions. Baseline evaluation revealed multiple erythematous papules and comedones with localized redness, contributing to uneven skin tone and textural irregularities. No evidence of nodulocystic or scarring lesions was observed. The patient underwent Intense Pulsed Light (IPL) therapy (Photofacial/Acne protocol), targeting the dual concern of active acne and associated erythema. The treatment aimed to reduce inflammation, control sebaceous activity, and improve overall skin clarity and texture. Following a series of IPL sessions, marked clinical improvement was observed. Post-treatment assessment demonstrated a significant reduction in inflammatory lesion count, resolution of erythema, and enhanced skin smoothness and tone. The patient reported high satisfaction with the aesthetic outcome, and no adverse effects were noted during or after the treatment course.
Figure 1: Clinical photograph of acneiform lesions on the
cheeks demonstrating visible improvement following a session of Intense Pulsed Light (IPL) therapy
Diagnosis
The diagnosis of acne vulgaris is primarily clinical, based on a detailed physical examination and comprehensive patient history to identify lesion morphology, distribution and potential aggravating factors such as medications, genetics, and lifestyle triggers. Hormonal evaluation is indicated in patients exhibiting features of hyperandrogenism. Recommended investigations include serum testosterone, DHEA/DHEAS, androstenedione, sex hormone-binding globulin (SHBG), LH/FSH ratio, 17-hydroxyprogesterone,........ prolactin, cortisol, insulin levels, ACTH stimulation, and dexamethasone suppression tests to identify androgen excess and related endocrine abnormalities.3 Microbiological swab culture may be performed to detect Cutibacterium acnes colonization or secondary bacterial infection, particularly in treatment-resistant or atypical cases.4 Sebum quantification using a Sebumeter provides an objective assessment of sebaceous gland activity; elevated readings correlate with disease severity and follicular obstruction.5 Several standardized grading systems are utilized for acne severity assessment, including the Pillsbury Scale, Cook’s Scale, Leeds System, Global Acne Grading System (GAGS), and Investigator’s Global Assessment (IGA).6 Lesion counting offers objective
quantification of comedones, papules, pustules, nodules, and cysts. Advanced imaging modalities—such as highresolution photography, polarized light, ultraviolet fluorescence, and threedimensional skin analysis— enhance visualization of surface and subsurface lesion characteristics.7 Comprehensive assessment facilitates accurate diagnosis, individualized therapy selection, and improved clinical outcomes.
Treatment
Intense Pulsed Light (IPL) therapy is a non-invasive modality used in the management of moderate to severe inflammatory acne, post-acne erythema, and hyperpigmentation. It offers an effective alternative for patients who cannot tolerate or prefer to avoid systemic medications. Contraindications include photosensitivity disorders, use of photosensitizing drugs, recent tanning, pregnancy, active infections, keloid tendency, and darker skin phototypes, where the risk of post-inflammatory hyperpigmentation (PIH) can be minimized through careful parameter adjustment.8
IPL emits high-intensity, noncoherent, polychromatic light within the wavelength range of 400–1200 nm, produced by flashlamps with bandpass filters. The emitted light targets chromophores such as porphyrins produced by Cutibacterium acnes, inducing selective photothermal destruction of bacteria. Additionally, IPL reduces sebaceous gland activity by photothermolysis of its vascular supply and
modulates inflammation through downregulation of TNF-α and upregulation of TGF-β1/ Smad3 signaling. Treatment parameters—including fluence, pulse duration, and pulse mode (single or burst)—are individualized according to skin type and acne severity. Sessions are typically conducted every 2–4 weeks for a total of 4–6 treatments. Each session involves systematic coverage of affected areas, avoiding pulse overlap. Post-procedure, transient erythema, edema, or pigmentary changes may occur. IPL’s combined photothermal, photochemical, and immunomodulatory effects reduce bacterial load, sebum secretion, and inflammation, leading to improved acne control and minimized scarring.9,10
Intense Pulsed Light (IPL) therapy exhibits significant therapeutic efficacy in the management of inflammatory acne vulgaris through a constellation of synergistic mechanisms. The principal mode of action is selective photothermolysis, wherein endogenous porphyrins produced by Cutibacterium acnes absorb light energy, leading to photodynamic bacterial destruction. In addition to its antimicrobial properties, IPL demonstrates antiangiogenic effects by thermally coagulating the microvasculature that supplies sebaceous glands, thereby reducing sebaceous gland volume and sebum secretion. IPL further modulates cutaneous inflammation by downregulating pro-inflammatory mediators such as tumor necrosis factor-α
(TNF-α) and upregulating transforming growth factor-β1 (TGF-β1)/Smad3 signaling pathways. This promotes dermal remodeling, enhances extracellular matrix synthesis, and supports collagen and elastin regeneration—processes that improve post-acne skin texture and minimize scarring. Acne vulgaris comprises both non-inflammatory (open and closed comedones; Grades 1–2) and inflammatory lesions, the latter being more susceptible to scarring. IPL is particularly effective against inflammatory acne through combined photothermal, photochemical, and photoimmunological effects. The use of continuous or doublepulse modes ensures uniform energy delivery, augmenting antibacterial and antiinflammatory outcomes while preventing lesion recurrence. Customization of pulse duration below the thermal relaxation time (TRT) of target tissues enhances safety and efficacy, especially in darker phototypes, minimizing the risk of postinflammatory hyperpigmentation and promoting uniform lesion resolution.10, 11, 12
Advantages of Intense Pulsed Light (IPL) therapy include its noninvasive nature, minimal patient discomfort, and lack of systemic side effects, allowing simultaneous targeting of multiple pathogenic factors involved in acne. IPL effectively improves inflammatory lesions as well as residual erythema and offers additional benefits of skin rejuvenation through collagen induction. The ability to customize treatment parameters and pulse modes enhances therapeutic safety and
efficacy, particularly in patients with darker skin phototypes, by reducing the risk of hyperpigmentation and scarring. Furthermore, IPL therapy involves minimal downtime, making it an attractive option for patients seeking efficient acne management with rapid recovery and improved cosmetic outcomes.10, 11, 12
Discussion
Acne vulgaris is a common inflammatory disorder of the pilosebaceous units, most prevalent during puberty but often persisting into adulthood. Several dermatoses can mimic its clinical presentation and must be differentiated. Rosacea presents with telangiectasia and lacks comedones, while perioral dermatitis manifests as grouped erythematous papules around the mouth, sparing the vermilion border. Demodex folliculitis causes papules and pustules resistant to conventional acne therapy. Facial angiofibromas in tuberous sclerosis appear as pink or red papules on the cheeks and nose in children. Pseudofolliculitis barbae affects the beard area, particularly in individuals with tightly curled hair, leading to papules, pustules, and scarring. Nevus comedonicus presents as grouped congenital comedones, whereas sebaceous hyperplasia produces small, umbilicated yellow papules on the forehead and cheeks. Adnexal tumors such as trichoepithelioma, trichodiscoma, and fibrofolliculoma appear as flesh-colored facial papules. Favre-Racouchot syndrome, associated with chronic photodamage, presents with open and closed comedones
on the upper lateral cheeks of older adults. Acne vulgaris may result in significant complications, both physical and psychological. Emotional distress, including depression, anxiety, and diminished selfesteem, often arises from active lesions and post-acne scarring. Acne fulminans represents a severe, ulcerative variant presenting with sudden onset of painful nodules, ulceration, and hemorrhagic crusting— typically in adolescent males— and may be spontaneous or isotretinoin-induced, with systemic symptoms such as fever and arthralgia. Solid facial edema (Morbihan’s disease) manifests as chronic erythema and swelling requiring isotretinoin, corticosteroids, or clofazimine. Gram-negative folliculitis develops in patients on long-term antibiotics, producing pustules and nodules resistant to standard therapy due to organisms like Enterobacter or Klebsiella.1
Management of acne vulgaris begins with patient education about its chronic course, realistic expectations, and the need for sustained therapy, as visible improvement often requires 2–3 months. Counseling helps prevent premature discontinuation and supports long-term maintenance, typically with topical retinoids. Patients should use gentle cleansers, avoid harsh scrubs and lesion manipulation, and select non-comedogenic products. Although high-glycemic diets and milk intake may exacerbate acne, dietary advice should be individualized due to limited evidence.1,2
Mild acne is treated with topical
A Gentle Glow: Managing Acne and Redness with Intense Pulsed Light (IPL) Therapy
retinoids, benzoyl peroxide, topical antibiotics, azelaic acid, or salicylic acid. Moderate to severe cases may require oral isotretinoin, systemic antibiotics, or hormonal therapy. Post-inflammatory hyperpigmentation is managed with photoprotection, depigmenting agents, and chemical peels, while residual erythema responds to pulsed dye laser, microneedling radiofrequency, LED therapy, or topical tranexamic acid. Acne scars are treated according to type using CROSS technique, punch elevation, subcision, laser resurfacing, fillers, excision, intralesional therapy, cryotherapy, or CO₂ laser vaporization. Though many
References
1. Sutaria AH, Masood S, Saleh HM, Schlessinger J. Acne Vulgaris. In: StatPearls. Treasure Island (FL): StatPearls Publishing; August 17, 2023.
2. Chilicka K, Gold MH, Nowicka D. Acne vulgaris and the most popular and new cosmetological treatments. J Cosmet Dermatol. 2023; 22(7):1946-1950. doi:10.1111/jocd.15757.
3. Elsaie ML. Hormonal treatment of acne vulgaris: an update. Clin Cosmet Investig Dermatol. 2016; 9:241-248. Published 2016 Sep 2. doi:10.2147/CCID.S114830.
4. Yadav AK, Bhooshan S, Johnson A, Asati DP, Nema S, Biswas D. Association of Antimicrobial Susceptibility and Treatment Outcome in Acne Vulgaris Patients: A Pilot Study. J Lab Physicians. 2020; 12(4):233-238. Doi: 10.1055/s0040-1720943
5. Jaalouk D, Pulumati A, Algarin YA, Humeda J, Goldberg DJ. The impact of
options exist, Intense Pulsed Light (IPL) therapy is a versatile and effective treatment that simultaneously targets bacterial colonization, sebaceous gland activity, inflammation, and vascular abnormalities. IPL is non-invasive, minimizing systemic risks and irritation, with minimal downtime to enhance adherence. Its customizable pulses improve safety, especially in darker skin types, by reducing postinflammatory hyperpigmentation risk. Additionally, IPL promotes dermal remodeling and scar prevention by stimulating collagen and elastin synthesis, making it a well-tolerated, comprehensive option for active acne and residual lesions.10, 12
Conclusion
Acne vulgaris is a chronic cutaneous disorder involving complex pathogenic pathways that commonly affects visible areas and can impact patient well-being. Intense Pulsed Light therapy has emerged as a clinically effective, non-invasive treatment option for managing both active lesions and post-inflammatory erythema, offering minimal adverse effects and reduced downtime compared to conventional systemic therapies. By improving clinical outcomes and treatment satisfaction, IPL contributes to better patient care. Nevertheless, further controlled studies are necessary to standardize treatment protocols and evaluate long-term efficacy.
energy-based devices on sebum in acne vulgaris: A systematic review. J Cosmet Dermatol. 2024; 23(10):3066-3077. doi:10.1111/jocd.16466
6. Bae IH, Kwak JH, Na CH, Kim MS, Shin BS, Choi H. A Comprehensive Review of the Acne Grading Scale in 2023. Ann Dermatol. 2024; 36(2):65-73. doi:10.5021/ad.23.094.
7. Agnew T, Furber G, Leach M, Segal L. A Comprehensive Critique and Review of Published Measures of Acne Severity. J Clin Aesthet Dermatol. 2016; 9(7):40-52.
8. Kumaresan M, Srinivas CR. Efficacy of ipl in treatment of acne vulgaris: comparison of single- and burst-pulse mode in ipl. Indian J Dermatol. 2010; 55(4):370-372. doi:10.4103/0019-5154.74550
9. Pei S, Inamadar AC, Adya KA, Tsoukas MM. Light-based therapies in acne treatment. Indian Dermatol Online J. 2015; 6(3):145-157. doi:10.4103/22295178.156379.
10. Deshpande AJ. Efficacy and Safety Evaluation of High-density Intense Pulsed Light in the Treatment of Grades II and IV Acne Vulgaris as Monotherapy in Darkskinned Women of Child Bearing Age. J Clin Aesthet Dermatol. 2018; 11(4):4348.
11. Mathew ML, Karthik R, Mallikarjun M, Bhute S, Varghese A. Intense Pulsed Light Therapy for Acne-induced Post-inflammatory Erythema. Indian Dermatol Online J. 2018; 9(3):159-164. doi:10.4103/idoj.IDOJ_306_17
12. Jean-Pierre P, Tordjman L, Ghodasara A, Nwosu C, Nouri K. Emerging lasers and light-based therapies in the management of acne: a review. Lasers Med Sci. 2024; 39(1):245. Published 2024 Sep 28. Doi: 10.1007/s10103-024-04196-8.
Extended-Release Oral Minoxidil: A Promising Advancement in Androgenetic Alopecia Management
Extended-release oral minoxidil is emerging as a promising advancement in the treatment of androgenetic alopecia (AGA), a common Dermatologic condition with significant psychosocial impact. While topical minoxidil remains a standard treatment, it is often limited by poor adherence due to scalp irritation, cosmetic concerns, and delayed efficacy. Immediate-release oral minoxidil, though increasingly used off-label, poses cardiovascular risks related to rapid plasma peaks and short systemic exposure, limiting its safety and effectiveness. The extended-release formulation is designed to maintain steady plasma concentrations within the therapeutic window necessary for follicular stimulation, while avoiding supratherapeutic levels that may affect cardiovascular function. In a blinded retrospective comparison with immediate-release oral and 5% topical minoxidil, patients receiving the extendedrelease formulation showed significantly greater clinical improvement, with earlier and more visible hair regrowth noted within four months. These findings suggest a more favourable efficacy and tolerability profile, potentially improving adherence and patient satisfaction. However, given the retrospective design and cross-trial comparisons, prospective randomized studies are needed to confirm long-term safety and sustained efficacy. If validated, extended-release minoxidil could represent a clinically meaningful improvement in AGA management.
Seboselective 1726-nm Laser Demonstrates Long-Term Efficacy and Safety in Treating Moderate-to-Severe Acne across Diverse Skin Types
A long-term follow-up study has demonstrated that the seboselective 1726-nm laser offers a safe and effective treatment option for moderate-to-severe acne across a wide range of skin types, including darker skin tones. The treatment produced significant and sustained reductions in both inflammatory and non-inflammatory lesion counts, with a steady increase in clinical response rates over time. The proportion of patients achieving an Investigator Global Assessment score of clear or almost clear improved markedly throughout the study period. Improvements were consistent across demographic subgroups including age, gender, and skin type, suggesting broad applicability. Safety data confirmed a favorable profile, with adverse events being mild, transient, and self-limiting, and no reported pigmentary changes, scarring, or vesiculation. The study also reported high levels of patient satisfaction and improved self-confidence, particularly among adolescents and young adults, a group especially vulnerable to the psychosocial burden of acne. While the open-label design and absence of a control group are limitations, standardized photographic assessments provided valuable comparative insights. These findings highlight the potential of the 1726-nm laser to deliver durable acne clearance while minimizing treatment burden and side effects. Further randomized controlled trials are needed to validate these promising outcomes and support wider adoption in diverse patient populations.