FIGURE 9.0 | Herd immunity protects a community from disease, much like a herd of animals protecting each other from danger.

CHAPTER 9
FIGURE 9.0 | Herd immunity protects a community from disease, much like a herd of animals protecting each other from danger.
CHAPTER 9
Here are a few essential terms introduced in the science and technology of vaccines and immunizations. By the end of this chapter, you should be able to apply these terms and understand how they relate to other critical concepts.
Adjuvants
Booster
Herd Immunity
Immunization
Inactivated Vaccines
Live Attenuated Vaccines
mRNA Vaccine
Subunit Vaccines
Vaccination
Vaccination Campaign
Vaccine Efficacy
Vaccine Hesitancy
Recombinant Vector Vaccine
Waning Immunity
Vaccination is a centuries-old technique that leverages the natural functions of our immune system to protect us against disease. The origins of vaccination began with the understanding that exposure to a pathogen, or a closely related pathogen, can lead to lasting immunity. Vaccines help to induce active immunity and immunological memory without exposing the individual to a full-blown infection—preparing the body to fight infections. It has been used to help prevent countless infectious diseases across human history.
Vaccines can be developed in different ways using various technologies. Vaccines can employ the whole pathogen, a portion of the pathogen, or a piece of its genome that encodes an antigen in order to build an immunological memory against it. Common types of vaccines include live attenuated, inactivated, subunit, and nucleic-acid based vaccines. Most vaccines are administered intramuscularly or subcutaneously but some are administered intradermally, nasally or orally.
Designing and developing a vaccine for human use is a process that takes many years, and emphasizes safety and efficacy from design to mass production and distribution. The process begins with researchers studying the pathogen and disease to identify vaccine targets. Once scientists choose their targets, vaccines can be designed; the best of these candidates enters pre-clinical and clinical research phases in which the efficacy and the safety of the vaccine in animals and humans are evaluated before its approval for public use. After their approval, mass production of the vaccine ramps up. These vaccines continue to be monitored for safety and efficacy long after their approval and distribution.
Herd immunity, elimination, and disease eradication can be achieved with effective vaccine distribution. Effective vaccine distribution requires collaboration across many groups and disciplines. On the logistical side, specific conditions are required to transport the vaccines, and keep them viable during transit. From a structural perspective, many organizations and countries typically need to work together in order to ensure equitable distribution and to protect the most vulnerable populations. On the community level, trust must be fostered between health professionals and those whose wellness they support.


After reading this chapter, you will know more about the history of vaccination and understand vaccine function, development, and distribution. You will also recognize the different types of vaccines, the technologies used to design them, routes of administration, and examples of vaccines currently in use. You will appreciate the process a vaccine follows from development at the research bench to the patient, as well as the factors that drive global vaccination efforts and the barriers to widespread adoption.
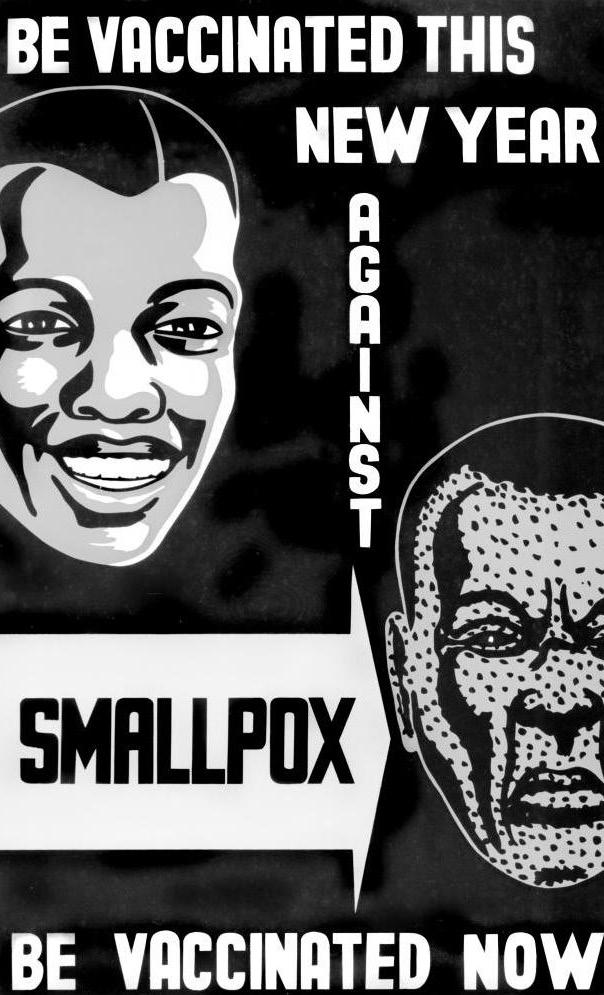
It’s 1706, and you’ve been taken against your will on the long, inhumane journey from West Africa to the British colonies to be sold into slavery. You are soon “purchased” by a Puritan church in Boston, Massachusetts, in the name of their minister, a man named Cotton Mather.
Mather often calls you useless and rebellious as you attempt to navigate the life that’s been thrust upon you. However, over the next few years, he’s forced to acknowledge your intelligence, and he grows increasingly intrigued by the life-saving medical practices you and your people have employed for generations. As the deadly disease known as smallpox makes its way through nearby communities, Mather asks if you’ve ever been infected, and you tell him about your ways of protecting people against this familiar disease back home. You explain to him how you were exposed to a small bit of pus from an infected person in order to gain future protection from
“I’m old enough to remember when the polio vaccine was still new. Also, it hadn’t been that long since most people who caught pneumonia died from it. These medical breakthroughs were practically miracles.”
—Pat Oren Kearny Cadigan, BritishAmerican science fiction author
the disease. You also inform him that although you still risked developing a full-blown, serious smallpox infection after this process, the chances of death were much lower than they would’ve been if you had contracted smallpox naturally. A few other enslaved people confirm your story, and Mather is convinced to spread the word.
Mather begins telling other community members, like physician Dr. Zabdiel Boylston, about your insight, and the two become major proponents for adopting the process in Massachusetts. However, you see that your message is met with immense resistance. Just as Mather was initially distrustful of your knowledge, the others with whom he shares your method immediately dismiss the experiences of a black slave and the knowledge you have brought. Eventually, anger over the idea and its African origins boils over, and Mather’s house is firebombed, with a note tied to the explosive saying, “Cotton Mather, You Dog, Dam You; I’ll inoculate you with this, with a Pox to you. [sic]”
In 1721, an intense smallpox outbreak hits Boston and convinces some residents of the importance of inoculation, this process you described in which a small amount of infectious material is introduced into a person’s body to stimulate protection. About half of the city’s population is stricken with the disease, with 1 out of every 7 infected individuals dying. Amid the devastation, and with the support for your approach that was gradually garnered over the past few years, Mather and Boylston were able to inoculate many individuals. They report their results, noting that amongst the inoculated, the mortality rate for those who later were infected with smallpox was 1 in 40. The numbers speak for themselves — a case fatality rate of 2.5%, compared to 14% for those not inoculated — and as a result, smallpox inoculation begins to gain popularity throughout the area.
Though you were barely regarded as human by those you helped to save, you’ve made a lasting impact on not only their lives, but also the lives of those who have continued to benefit from inoculation. Only centuries later have people
begun to appreciate your impact, and you are heralded in 2016 as one of the “Best Bostonians of All Time.” You are the man known as Onesimus – meaning “useful,” a name Mather assigned you as a reference to an enslaved man in the Bible – and you helped pave the way for modern vaccines.
Vaccines are one of the most significant determinants of global health. They have the power to prevent us from contracting or falling ill from some of the world’s most notorious diseases, or, at the very least, give our communities a fighting chance against them.
In the US, we rarely see people paralyzed from polio or scarred from smallpox, and most of us don’t have to worry about contracting lifethreatening tetanus from brushing against a rusty nail, or rabies from being bitten by a rabid dog. However, this wasn’t always the case, and is still a risk in many regions.
The history of vaccines is a long one. As you might remember from the story of Onesmius, in the early days, protection against many diseases was provided by inoculation (derived from the Latin term inoculationem, meaning “engrafting” or “budding”). For example, in 200 BCE China, powdered scabs of smallpox pustules were blown into the nostrils of healthy individuals, inducing lifelong immunity and dramatically decreasing case fatality rates. Inoculation against smallpox specifically is known as variolation, named after the scientific name for smallpox, Variola
Many years later, the ancient Greeks also noticed that previous exposures could prevent future infections. Thucydides, an Ancient Greek historian, described a plague that swept through Athens in 430 BCE. While there is still significant debate about the pathogen that caused this particular plague (perhaps smallpox, Ebola, typhoid, fungal contamination of crops — the list goes on), it was clearly incredibly deadly, and it killed about two thirds of the population. Thucydides observed that people who survived the infection could not
be reinfected, and thus described the basis of immunity.
The late 18th century brought immense activity, and a major breakthrough in our use of inoculations. It began with studies like that of Onesimus and Mather during the smallpox outbreak of 1721. However, the latter half of the century changed the enterprise altogether. At the time, there was a well-known adage, “as smooth as a milkmaid’s skin,” which referred to the fact that dairymaids never seemed to have the distinctive textured scars that resulted from a previous smallpox infection. The working theory was that they were protected by their exposure to cowpox – a similar disease that caused significant illness in cows, but less severe illness in people than smallpox did – an occupational hazard of working in the dairy industry.
Beginning in the 1760s, a number of scientists put the cowpox theory to the test, but it was an English physician named Edward Jenner who is credited with proving the theory. In 1796, Jenner hypothesized that exposure to cowpox protected against later smallpox infection. To prove this, he enlisted the help of Saran Nelmes, a milkmaid with cowpox, and used a knife to collect some fluid from her cowpox blister. He then used this contaminated knife to make a small incision in the arm of his gardener’s son, James, directly exposing the eight year old boy to the cowpox virus. Two months later, Jenner then intentionally exposed James to smallpox. Despite the clearly unethical nature of this experiment by modern standards, James’s clean bill of health showed the community the great potential benefit of the procedure: immunity against smallpox.
Jenner went on to repeat his experiment over 2 dozen times, including on his own 1-year-
old son, with continued success. He called the cowpox inoculation process vaccination, from the Latin vacca, which means cow. Vaccination differs from inoculation in a very important way: while inoculation introduces the pathogen itself into a person’s system in order to generate immunity (and therefore runs the risk of a full infection), vaccination instead introduces a substance that is highly unlikely to cause the disease (i.e., using cowpox without introducing live smallpox at all). From there, vaccination allows for immunization, which is the process of ultimately gaining protection against a disease. While not quite the formal definition, some people use the term immunizations as synonymous with vaccines. As you may recall from Chapter 1: Emerging Pathogens, a vaccine is now described more broadly as a lab-designed substance used to stimulate the production of antibodies and provide immunity against the disease without being previously infected.
At first, people were resistant to Jenner’s new procedure, i.e., the first ever vaccine, but with the support of esteemed doctors, the method
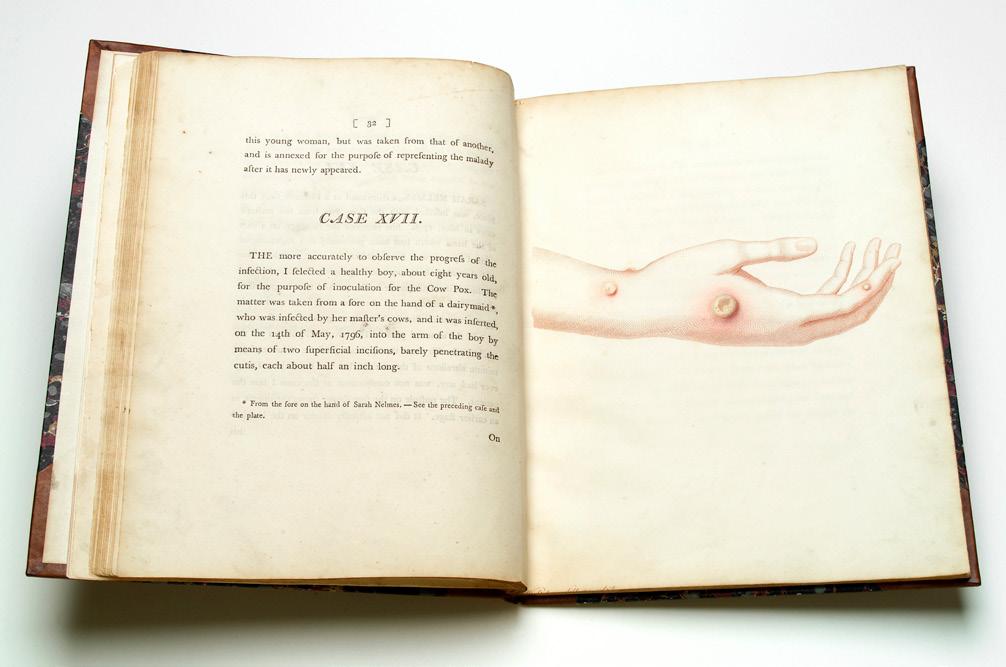
FIGURE 9.2 | Jenner’s reports of the first cowpox vaccination. The painting in the first edition of Jenner’s 1798 book, An Inquiry into the Causes and Effects of the Variolae Vaccine shows the hand of Sarah Nelmes, a milkmaid infected with cowpox and whose blister was used for Jenner’s first cowpox inoculation.
of vaccination spread widely. Eventually, President Thomas Jefferson and French Emperor Napoleon Bonaparte encouraged the use of smallpox vaccination within their countries. Throughout the rest of his life, Jenner would vaccinate anyone who asked and made no attempts to profit from his efforts.
Vaccination took another leap forward in the late 1800s, and, much like Alexander Fleming’s discovery of penicillin, it was due to another happy, vacation-related accident. In 1879, the “father of microbiology” Louis Pasteur was trying to figure out a way to prevent a type of chicken cholera that caused significant diarrhea and death within the chicken population. As part of this research, he asked a research assistant to inject the causative bacteria into chickens, which they knew would induce the disease in the recipient chickens. However, the assistant left for vacation without remembering to do the injections. Instead, he completed them when he came back about a month later, using the original (now month-old) bacteria. The chickens still became ill, but not nearly as ill as before.
With his attention now piqued, Pasteur decided to inject the same chickens again, this time with fresh bacteria. On this second round of injections, the chickens did not become ill. Pasteur and his assistant concluded that the original bacteria were still strong enough to induce an immune response, but had been weakened, or attenuated, by exposure to oxygen while they had been sitting around for a month. He named this process “atmospheric attenuation.” Attenuation is so valuable because it is a way to use a form of the pathogen itself to induce the immune system (rather than a close relative in the case of smallpox vaccination with cowpox), without nearly as much risk of severe illness as being directly exposed to a full-strength pathogen.
In 1880, another French scientist, Henry Toussaint, used a different strategy to produce an anthrax vaccine. He used heat to outright kill the bacteria that causes anthrax, then injected the killed material into the patient. In 1881, Pasteur himself used a similar approach to develop an additional anthrax vaccine. The subsequent decades brought a period of immense development of similar killed vaccines, including those against rabies, influenza, and pertussis. This began the development of what are known as inactivated vaccines (also known as killed whole organism vaccines): vaccines in which the pathogen is killed instead of attenuated.
Throughout the 20th century, as other vaccine strategies were developed and new vaccines were created, their impact skyrocketed. Pioneers like American microbiologist Dr. Maurice Hilleman, who is credited as one of the greatest vaccinologists of all time, and his gifted teammates developed 40 vaccines against serious diseases like chickenpox, and measles, mumps, and rubella (MMR vaccine). Hilleman’s discoveries increased our capacity to develop and broadly distribute vaccines, paving the way for extensive vaccination to combat infectious disease.
Take, for example, the impact of vaccines on containment of polio, a disease that has had many surges across human history, including in as early as 1570 BCE. Polio is a disease caused by the incredibly infectious poliovirus, and its effects can vary wildly. Around 75% of cases are asymptomatic, while others are so severe that they cause paralysis, potentially leading to either permanent disability or death. In the early 20th century, when this paralysis spread to the respiratory muscles, patients would have to be placed within breathing devices known as iron lungs (Figure 9.3).

9.3 | Pediatric polio patient in an iron lung. Before widespread vaccination, polio infection was common, as was its most feared outcome: paralysis. When the paralysis spread to the respiratory muscles, patients needed to enter an “iron lung” that would force respiration. Image credit: © World Health Organization/Paul Palmer, 1956. Before the first poliovirus vaccine in 1955, children affected by polio depended on an iron lung for their survival.
The year 1952 saw an incredible polio outbreak in the US: 57,628 cases, resulting in more than 3,000 deaths, mostly in children. Fear gripped the country, schools closed, and parents kept their children away from other crowded areas like swimming pools and movie theaters. Their fears were finally abated in 1955 when the first polio vaccine, produced by Jonas Salk, came on the market. A second vaccine option, produced by Albert Sabin, became available in 1960, and together, these vaccines reduced the number of polio cases to near-zero by 1963 (Figure 9.4).
Since it became a common practice, vaccination has dramatically decreased worldwide mortality, improving public health worldwide. A 2019 WHO report found that
The polio vaccine clinical trials started in 1954.
The polio vaccine was introduced in 1955. There were 13,850 cases of paralytic polio that year.
FIGURE 9.4 | Polio cases in the US and vaccine introduction. This chart shows polio cases between 1937 and 2013, with a significant surge in 1952. Cases started to decline back to endemic levels in 1953, and large-scale polio vaccine trials began in 1954. After the introduction of the vaccine in 1955, the number of cases dropped significantly, reaching almost zero by 1963. Surges of this magnitude have not occurred in the US since then.
vaccines prevent 4-5 million deaths every year, and many diseases that have long plagued humanity have almost been completely eradicated. In some regions of the world, infectious disease is no longer the leading cause of death. Instead it has been replaced by noninfectious diseases like cancer and heart disease, which have lifestyle and genetic bases. In the context of human history, this is a completely new phenomenon, and it is in great part due to the efficacy of vaccine use and distribution (as well as to the success of antibiotics). That said, infectious diseases remain the leading cause of death in many regions, and they continue to pose a weighty, disproportionate burden on the developing world. With the permanent threat posed by emerging diseases (such as COVID-19), vaccines will always remain critical for maintaining and improving global health.
A timeline highlighting important events in vaccine development events is presented in Figure 9.5.
By now you know that vaccines protect us from being infected by or made ill by an infectious pathogen, but how do they do it? Vaccines prepare our bodies to respond to a pathogen in the future, by safely inducing an immune response; in essence giving us early practice defending against a potential threat. As you learned in Chapter 6: Immune System and Host Defenses, when the immune system is exposed to an antigen, it develops antibodies that protect against the specific antigen. Afterward, specialized B cells retain a memory of the invader after the infection is over. This process
430 BCE Thycydides describes immunity in survivors of the great plague in Athens
220 BCE Smallpox inoculation documented in China

1721 Smallpox outbreak in Boston curbed by Onesimus’ innoculation techniques
1796 Jenner demonstrates vaccination with cowpox protects against smallpox
1879 Pasteur discovers attenuation in chicken cholera

1880 Toussaint introduces inactivated vaccine for anthrax

1930s Egg-based vaccine production becomes the norm

1940s Cell-based vaccine production methods are developed

1955 Collier devises a freeze-dried vaccine for smallpox

1955 Salk’s polio vaccine becomes available

1960 Sabin’s polio vaccine becomes available

1969 First hepatitis B vaccine developed

1974 WHO Expanded Programme on Immunization is established
1980 Smallpox is eradicated worldwide

2020 mRNA vaccines become available, developed against COVID-19

FIGURE 9.5 | Timeline of vaccine milestones. Here, we summarize some of the most important breakthroughs for vaccine development.
is known as active immunity. Vaccines mimic the pathogen in some way to trigger the same response and protect against future exposure to the pathogen.
Vaccines trigger active immunity by introducing an antigen (or several antigens) of the pathogen to our bodies. This introduction sets off the immune response, thereby priming the body to fight off future infections without actually contracting the disease. (To note, there are other components in a vaccine that contribute to this response, and we will learn about these in the next section). When the vaccine recipient later encounters the pathogen in the wild, the memory B cells spring to action and activate
the adaptive immune system a second time. Since it’s now been primed and doesn’t have to start from scratch, the body is able to produce neutralizing antibodies much faster and more effectively than when first exposed (Figure 9.6).
Vaccines differ from other preventative measures that you saw in previous chapters. In Chapter 8: Therapeutics, you learned about the use of convalescent plasma to help recipients either fight off or prevent infection to achieve passive immunity. Unlike active immunity, passive immunity is temporary – it does not last as long as the protection from a vaccine – but gives immediate protection that can last for a few months.























FIGURE 9.6 | Vaccines induce a protective immune response. When a vaccine enters the human body, the immune system responds by targeting the foreign antigen and neutralizing it with antibodies, in line with our immune response to natural pathogens. In addition, as plasma B cells produce antibodies against the antigen, memory B cells “remember” the produced antibodies to be prepared in case of later infection with the actual pathogen.
A vaccine, on the other hand, is training your own body to defend against an invading pathogen, and aims to give your body the ability to produce antibodies to protect itself. Ideally, a vaccine should provide lifelong immunity, but now we know that’s not always the case; there is always the possibility that immunity may fade over time as our immunological memory “forgets” certain vaccines or pathogen exposures — an effect called waning immunity. The duration of conferred immunity depends on the type of disease and vaccine.
There are a number of reasons that some vaccines confer a shorter immunological memory than others. For example, inactivated vaccines typically don’t produce as strong an immune reaction as live vaccines. Also, vaccines against particular pathogens are known to be less effective than others, possibly due to the length of the pathogen’s incubation period; if a pathogen is particularly fast-acting, there may not be enough time for the immune system to build up a lifelong immunological memory, so it can’t “study” the pathogen long enough to build a robust memory.
This is why, even though some vaccines provide lifelong immunity with only one dose, others require a booster shot – an extra administration of a vaccine after an earlier dose. Some
vaccines need a booster in order to facilitate full immunity, which can be thought of as having multiple doses in a series, as you need for the human papillomavirus (HPV) vaccine and some COVID-19 vaccines. Booster shots can also be used to maintain immunity over time (Figure 9.7). Vaccines such as yellow fever, rubella, HPV, tetanus, and whooping cough all require a booster dose.
It is also important to note that an additional vaccine shot may be required as an “update” rather than a “reminder,” like your annual flu shot. As you’ve already read in previous chapters, including Chapter 8: Therapeutics, pathogens mutate and change over time. Importantly, certain pathogens mutate and change faster than others, which means that your body will need updated vaccines every so often to stay current on the pathogen’s information. You can think of this like taking a new mugshot photo that captures the pathogen’s current appearance every time it changes; with this process, your immune system’s enforcers can always recognize the potential threat.

Scan this QR code or click on this link to watch a video explaining measles and the benefits of vaccination.
antibodies decrease below threshold over time stronger response
First shot Second shot
TIME protective immune threshold
FIGURE 9.7 | Booster shots are needed for some vaccines to stimulate sufficient antibody production. Immunological memory induced by vaccination provides protection, and the generation of antibodies is increased after the administration of a second dose of the vaccine.
1. What is vaccination, and how does it relate to inoculation and immunization?
2. What does it mean to attenuate a pathogen, and how was this approach first applied to develop vaccines?
3. How does a vaccine trigger active immunity?
4. Why do some vaccines require a booster shot?
Now that we’ve discussed the core principles behind vaccines, we’ll go over the basics regarding some of the most common types of vaccines, how they are packaged for delivery to your immune cells, and how they are administered.
Let’s start by learning about the different types of vaccines. Much like you saw in Chapter 8: Therapeutics, there are a number of different ways to classify vaccines; the broadest distinction is between vaccines that use the whole pathogen and those that do not. We’ll begin with discussing whole pathogen vaccines, as you have already been introduced to a number of these vaccines earlier in this chapter.
As the name suggests, whole pathogen vaccines use the entirety of a pathogen, in varying forms, to induce an immune response. There are multiple subtypes of whole pathogen vaccines, which differ in how the pathogen material is prepared.
Live attenuated vaccines are prepared using a weakened version of the virus or bacteria of interest. There are a few ways to attenuate the pathogen, such as exposure to heat or various chemicals. In the 1930s an egg-based method for attenuation became the norm to attenuate viruses for vaccine production. In the 1940s, another way to attenuate organisms was introduced, repeated passages in mammalian cell culture, a procedure that uses cells that are grown in the laboratory. In this method, the pathogen is grown in successive generations of mammalian cells, growing weaker with each generation as it becomes increasingly adapted to the cells in the culture, and less effective
at infecting human cells. We will discuss eggbased and cell-culture methods further in the vaccine production section.
This weakened pathogen must replicate within the host to produce an immune response, but since it was weakened, it is incredibly unlikely to cause the full disease. Live attenuated vaccines resemble the natural pathogen so closely that the immune system has no means to differentiate between the two. This similarity allows live attenuated vaccines to confer long-lasting immunity and some of the best protection of all vaccine types, as these resemble the natural pathogen most closely.
That said, there are some risks to live attenuated vaccines, in that a full infection is possible if the pathogen replicates uncontrollably. This is typically only a concern in particular populations – those with weakened immune systems or pregnant people, and children under one year old – given that their immune systems are not quite at full strength, as well as immunocompromised people, including people with HIV. Other types of vaccines can be a better approach for such populations. Examples of live attenuated vaccines in use in the US include the measles-mump-rubella (MMR), varicella, rotavirus, and some influenza vaccines.
As we have discussed, inactivated vaccines, also known as killed whole organism vaccines, utilize a version of the pathogen that has been inactivated by heat, chemicals, or radiation rather than simply weakened. They, therefore, have the benefit of not being able to reproduce or induce an infection. However, these killed vaccines tend to provide shorter immunological memory than live attenuated vaccines and – as you might recall – may require booster
shots as a result. Examples of whole-pathogen inactivated vaccines are polio, hepatitis A, and rabies vaccines.
Some vaccines do not use the whole pathogen; rather, they use just a component or subunit. These subunit vaccines utilize a portion of the pathogen itself that is immunogenic – able to trigger an immune response. These subunits can be various antigens: pathogen proteins, the toxic compounds that the pathogens produce, or sugar molecules on the surface of pathogen. An antigen alone cannot cause infection; thus, subunit vaccines can elicit an immune response without the risk of contracting the disease. Subunit vaccines can include one antigen, multiple antigens, or the genetic material that encodes for the antigen(s).
This leads us to one of the limitations of subunit vaccines, which might not surprise you: they are typically not as effective as whole pathogen vaccines. Out of all the ways that your immune system could recognize a given pathogen, with its many antigens, subunit vaccines only expose it to one or a few of them. For instance, to return to our mugshot example, it is much easier to catch a perpetrator if you have a picture of their whole face rather than just their ear or nose.
There are many different types of subunit vaccines. They can be classified by which type of antigen(s) they use to trigger the immune system or by the way the antigens are packaged for delivery into cells.
Protein vaccines, as their name suggests, aim to deliver a protein antigen(s) from the target
pathogen. These can include surface proteins, which typically bind to receptors in order to enter cells, and other essential proteins from the pathogen that are capable of eliciting an immune response. They are the most common type of subunit vaccine, and examples include those for hepatitis B (HPV), HPV, pertussis, and COVID-19.
Toxoid vaccines, as the name implies, induce an immune response with toxoids, which are toxic substances produced by the pathogen. Since toxoids are produced by the pathogen, but not themselves infectious, they are a safer choice for immunocompromised individuals. Examples of toxoid vaccines include the combined tetanus and diphtheria vaccines, which are often administered together with the pertussis vaccine, as the DTaP or TDaP vaccines (depending on the patient’s age).
Polysaccharide vaccines induce an immune response by delivering polysaccharides (complex sugar molecules) found on the surface of some bacteria. Like protein antigens, polysaccharide antigens bind to immune cell receptors, stimulating an immune response and generating polysaccharide-specific antibodies. Polysaccharides are weaker antigens, and often produce less robust responses than protein and toxoid antigens, particularly in children. An example of a polysaccharide subunit vaccine is the pneumococcal vaccine, which protects against the bacterium Streptococcus pneumoniae, which can cause pneumonia and meningitis. This pneumococcal vaccine is generally recommended for those 65 and older, and does not work as well in young children.
One way to enhance the immune response to a particular vaccine is to include additional antigens in its components. These are known as conjugated vaccines, and it is a way
scientists were able to create a pneumococcal vaccine in children. Conjugate vaccines are made by attaching a weak antigen, typically a polysaccharide, to a stronger antigen, usually a protein. Interestingly, the proteins used in conjugate vaccines are usually from a source other than the targeted pathogen, and are typically from other bacteria or toxoids. For example, the Haemophilus influenzae B vaccine uses this approach by adding diphtheria, meningococcal, and tetanus components to boost the immune response to the H. influenzae B material.
While many types of vaccines use subunits, we describe subunit vaccines as those that rely on purified antigens that are delivered directly to the immune system. These breakdown further into two subgroups, traditional and recombinant subunit vaccines.
Traditional subunit vaccines are produced from the pathogens themselves. That is, these involve the chemical extraction and purification of the desired protein or other component directly from the cultivated pathogen. These subunits are produced in large quantities, which can be quite time- and labor-intensive to generate the level of pathogenic material necessary to mass-produce the vaccines. While most modern vaccines no longer use this traditional approach, one example still in use is the Pneumovax vaccine used to protect against infection by Streptococcus pneumoniae
In order to create a more efficient and safe production process, most subunit vaccines now utilize another host organism to produce only the antigen of interest. These recombinant subunit vaccines, referred to as recombinant vaccines, use recombinant DNA technology.
They are created by inserting the material for the gene that produces the desired immunogenic antigen into a benign host, typically yeast or bacterial cells. The geneticallyaltered hosts then churn out large volumes of the desired immunogenic proteins, which are purified and introduced to the vaccine recipient. The introduced material then triggers the recipient’s immune response. There are many examples of recombinant vaccines such as the HBV and HPV vaccines, and other vaccines described under the types of subunits above.
Recombinant vector vaccines, often denoted as vector vaccines, allow for not only the preparation but also the delivery of pathogenic genetic material by integrating it into another usually benign microbe as a carrier. These vectors can be a virus – like vesicular stomatitis virus (VSV) and adenovirus – or bacteria, like Mycobacterium bovis. These vectors can be killed and therefore non-replicating, or alive and able to replicate, therefore known as replicating Either way, they allow the vaccine to be produced and delivered to the immune system in one go, with no intermediaries. The genomes of the vector are modified to include the genetic material encoding for the desired antigen, which can then be replicated by the body’s cellular machinery without causing the disease.
The first Ebola vaccine approved in the US, rVSV-ZEBOV, uses VSV, to carry the Ebola glycoprotein, a surface antigen known to elicit a neutralizing immune response. A number of other recombinant vector vaccines have been developed that use viral and bacterial vectors. The Johnson & Johnson and Oxford/ AstraZeneca COVID-19 vaccines use human and chimpanzee adenoviruses as their vectors, respectively. The tuberculosis vaccine BCG,
uses as its vector a live attenuated version of the bacteria Mycobacterium bovis, a relative of Mycobacterium tuberculosis
These recombinant vector vaccines have a number of benefits. Given their microbial carrier, they have relative ease of delivery. By encoding the immunogenic genetic material in their carrier, these vaccines also induce a process that is very close to natural infection. Recombinant vector vaccines are, in a way, their own conjugate vaccine, as the vector pathogen also stimulates the immune system, along with the desired antigenic material. They are able to trigger both the innate and adaptive immune responses, and some can even include the immunogenic material for more than one antigen, strengthening the effects of the vaccine. They can thus often be delivered in a single dose. However, recombinant vector vaccines also have some important limitations. Pre-existing immunity to the viral vector could potentially reduce the effectiveness of the vaccine. Additionally, large-scale production of these vaccines can be challenging and timeconsuming.
The final subtype of subunit vaccines that we’ll discuss here are nucleic-acid vaccines, which can be either DNA vaccines or mRNA vaccines. These subunit vaccines also present a component of the pathogen to elicit an immune response, but rather than introduce the component itself, they introduce that component’s genetic material and let our own bodies act as factories to produce it.
In Chapter 2: Fundamentals of Genetics, we described how your cells convert DNA to RNA, and RNA to protein — the central dogma of biology. The development of nucleic acid-
based vaccines was inspired by the central dogma: when you receive a nucleic acid-based vaccine, your own cells convert the genetic material from the vaccine into pathogenspecific antigenic proteins. Your body then generates an immune response against these newly-built antigens and develops immunological memory to neutralize the actual pathogen if it’s ever encountered.
You may have heard a lot about mRNA vaccines lately, as two of the vaccines against COVID-19 are mRNA vaccines, showcasing the power of the technology. mRNA vaccines deliver a small portion of the pathogen’s genome in the form of mRNA that encodes for a specific pathogen protein. In the case of the COVID-19 mRNA vaccines, this mRNA carries the instructions to make the SARS-CoV-2 spike protein. After injection, the mRNA enters human host cells, which in turn manufacture the pathogenic protein fragments on their surface. In turn, these antigens trigger an immune response.
Nucleic-acid and, specifically, mRNA vaccines have incredible potential in the outbreak setting, as they are incredibly modular and therefore (comparatively) easy to update once the pathogen’s genome sequence is known. They also have the added benefit of not needing to wait for pathogenic material to be grown or manufactured over time.
While a relatively new technology, mRNA vaccines have proven safe, despite concerns raised about its mechanism of action. Specifically, it’s important to note that the mRNA from the vaccine does not stay in the body for long. It is broken down and eliminated shortly after it’s used to make the antigen. Moreover, the mRNA cannot be integrated into the person’s DNA because it does not enter the nucleus of the cell where the DNA is located.
FIGURE 9.8 | Types of vaccines. There are many different types and subtypes of vaccines. We have organized them in two main groups: whole pathogen vaccines (left) and subunit vaccines (right). Whole-pathogen vaccines can be produced by either attenuating or inactivating the pathogen. Subunit vaccines can be produced by the traditional method of culturing the subunit from the pathogen itself or by using a recombinant organism to produce the subunit more efficiently. Subunit vaccines can also be produced and delivered to the body in a recombinant vector containing the pathogen’s genetic material, which is then used by the human’s cellular machinery to produce the subunit. Nucleic acid vaccines deliver the genetic material of a pathogen subunit, and let the human cells act as factories to produce it.














































As you see, there are many different types of vaccines, all with their own unique characteristics, and therefore strengths and weaknesses. We have summarized the types of vaccines presented in this section in Figure 9.8.
Different vaccine technologies can be used to protect against the same pathogen. Recent examples of this are the COVID-19 vaccines. Currently in use in the US, there is a protein subunit COVID-19 vaccine, a (recombinant) viral vector COVID-19 vaccine and an mRNA COVID-19 vaccine. The diagram in Figure 9.9 shows how these three vaccines work. Interestingly, while they all are developed through different technologies, they all use as a subunit the viral spike protein, which mediates attachment and entry to the host cell, to induce immunity.
You now know a lot about the “active” components of vaccines, which are the components that induce the immune response in the recipient. Let’s spend some time learning about what else goes into vaccines.




F IGURE 9.9 | Different types of COVID-19 vaccines. Different technologies can be applied to develop vaccines for the same disease. To date, three different types of vaccines against COVID-19 have been approved by the FDA: protein subunit, viral vector, and mRNA. They all have the spike protein subunit as the vaccine target.
Scan this QR code or click on this link to watch an interview with Özlem Türeci and Uğur Şahin about how their work with mRNA revolutionized vaccine development, saving millions of lives.
In addition to the vaccine’s active ingredient, which are the pathogen antigens that will induce active immunity without causing the disease, there are many components in vaccines that help them to be maximally effective, and induce as large of a response as possible. This is a particular consideration for subunit vaccines because subunit vaccines are often less immunogenic than whole pathogen vaccines as they only carry a few components of the pathogen for the immune system to react to. We have previously discussed the use of conjugate vaccines, using multiple different components of a pathogen as subunits to elicit a stronger immune response.
Another way scientists can increase the strength of an immune response is by incorporating other substances, known as adjuvants, into the vaccine.
From the Latin “adiuvare” meaning “to help,” vaccine adjuvants include compounds, such as aluminum, that activate the innate immune system, thus priming the adaptive immune system to respond to the antigen(s) included in the subunit vaccine. Adjuvants increase immunological memory and strengthen the neutralizing response; in combination with the appropriate antigens in the subunit vaccine, they can help induce lifelong immunity. Aluminum was the primary adjuvant used for most of the 20th century, but today we have newer ones like MF59, an adjuvant used in the seasonal influenza vaccine that employs a naturally occurring oil called squalene to stimulate the immune response.
What else is in a vaccine? In addition to the active ingredients and adjuvants, vaccines contain trace components, stabilizers, antibiotics, and preservatives. Trace components are residues of the vaccine development process:








ACTIVE INGREDIENTS
Viral or bacterial antigens that directly stimulate the immune system but do not cause the disease.
ADJUVANTS
Help in boosting the immune response to the vaccine.
for example, small compounds that were used to kill the original pathogen in inactivated vaccines. Stabilizers are compounds that are able to protect the active ingredients while the vaccine is in storage or being transported; a common stabilizer is gelatin. Vaccines are also typically packed with at least a small amount of antibiotic molecules and preservatives to stop contaminating pathogenic material from growing within the vaccine vial. One preservative that has come under much scrutiny and controversy lately is thimerosal, which contains mercury. Even though extensive and rigorous studies have not found any harm from this preservative, due to public concern over mercury exposure, it has still been withdrawn from many vaccines, particularly childhood vaccines.
Keep the vaccine stable after manufacturing, and maintaining its e ectiveness during storage.
ANTIBIOTICS
Prevent contamination by bacteria during the vaccine manufacturing process.













COMPONENTS













Residual inactivating ingredients such as formaldehyde, and residual cell culture materials.


Protect the integrity of the active ingredients during manufacture, storage, and transportation.
As you can see, there are many components of vaccines. While they all serve different purposes, they all contribute to their safety and effectiveness (Figure 9.10). STABILIZERS PRESERVATIVES































9.10 | Vaccine ingredients. In addition to the active ingredients, vaccines contain other components that are needed to support and preserve the vaccine material. These usually include adjuvants, trace components, stabilizers, antibiotics, and preservatives.
Another distinction in the type of vaccine is whether or not it uses a delivery system. In the case of whole genome vaccines or recombinant vector vaccines, there is no need for a means to package and deliver them, as they are generally stable and easily administered. However, in other cases, we must make use of a delivery system, which can be thought of as a carrier that protects the somewhat delicate active material of the vaccine. These strategies are ways to pack and protect molecules that otherwise could be degraded before they can induce an immune response.
One delivery system utilizes nanoparticles, which are specialized carriers that can prevent vaccine material from degrading over time. A nanoparticle is a small particle, ranging between 1 to 100 nanometres in size, undetectable by the human eye. With nanoparticles carrying vaccines, the antigen or nucleic acid material is carried on the inside or embedded on the surface of the nanoparticle. Use of nanoparticles have recently risen to global attention as the technology behind the COVID-19 mRNA vaccines employ nanoparticles to enter cells.
Another type of delivery system is virosomes Virosomes are tiny lipid vesicles that are imbued with the membrane proteins found on viruses which allow viruses to invade and therefore infect the cell. However, virosomes do not contain the genetic material of the natural virus. This allows for delivery of the active material of the vaccine to the cell without infection.
Vaccine “production” in the times of Jenner was just procurement of the desired infectious
material, such as extracting pus from a milkmaid or another person infected with cowpox. As you might imagine, this was a somewhat unreliable and inefficient way to procure the needed material. In the next generation, Pasteur used rabbits to grow the immunogenic material used in his anthrax vaccine. This in vivo approach – meaning production within a living organism – was the norm until the 1930s.
In the 1930s, scientists started to cultivate viruses on the membranes of chick embryos. This laboratory technique is known as an egg-based – or in ovo (ovo meaning “egg”) – method, and led to the production of the influenza and yellow fever vaccines. This method uses fertilized chicken egg tissue. It’s a very interesting and effective technique: it starts with inoculating the virus into the egg cells. Then, as the virus grows in successive generations of egg cells, it becomes more and more adapted to infecting chicken tissue. This shift makes it less effective in infecting humans. So, over time, the virus becomes “weaker,” i.e., less capable of causing full disease in humans. When it’s weak enough, it can be extracted and used to create the vaccine. This approach was first used to develop a vaccine for influenza, and is still used to produce yellow fever, rabies, and most influenza vaccines.
In the 1940s, broader cell culture methods that allowed vaccines of all kinds – including varied whole pathogens and subunit vaccines – to be produced in mammalian cells in the laboratory emerged, kicking off a revolution within the world of vaccine production. The mammalian cells are kept alive in flasks with the nutrients they need. From there the selected pathogen or recombinant strain is grown within mammalian cells for a few days before harvesting. Benefits of this approach
include the fact that it is much faster than the egg-based method, and doesn’t rely on a large supply of eggs to be ready on demand, bothof which make it easier to produce vaccines rapidly in outbreak settings. It is also a much more cost-effective approach, and makes the vaccine safe for people with egg allergies, who previously couldn’t be vaccinated. Examples of vaccines that are produced through a cellbased method include the inactivated polio vaccine, as well as a major COVID-19 vaccine.
As you learned above, mRNA vaccines were critical for rapid response to COVID-19 partly due to the fact that their production is comparatively simple. Since mRNA vaccines simply utilize the desired genetic material of the pathogen, they do not require extended periods of growth in eggs nor cell culture, and therefore can be produced much more quickly and efficiently than other vaccine types.
There are many different routes of administration for vaccines, which differ depending on the type of vaccine and its target disease. As you might infer from reading in Chapter 8: Therapeutics, the route of administration is the path the vaccine takes into the body, and it is generally classified by the location at which the vaccine is administered. There are five primary ways to administer vaccinations, some of which will look familiar from the Therapeutics chapter as well: oral, intranasal, intramuscular, subcutaneous, and intradermal (Figure 9.11).
Convenient to distribute and receive, oral vaccines are typically administered in the form of coated capsules or sometimes ingested as drops.
In fact, Albert Sabin’s oral polio vaccine was administered by putting drops of the vaccine on sugar cubes, and then giving the sugar cubes to the children to eat. Given that oral vaccines require no needles and can be selfadministered, they are very useful in resourcelimited settings. The oral polio vaccine and rotavirus vaccine are among the most common oral vaccines used globally. Intranasal vaccination delivers the vaccine material by way of spraying into an individual’s nasal cavity (nostrils). Similar to oral vaccines, the intranasal route offers unique advantages compared to its counterparts, such as ease of self-administration. Intranasal vaccination has also been shown to ‘jumpstart’ an individual’s immune response by passing the vaccine material through the nasal mucus, which stimulates a pathway known as the mucosal immune response. The influenza vaccine is primarily administered intramuscularly, but influenza is also the only vaccine currently approved for intranasal administration in the US. More vaccines are being developed for intranasal delivery due to the benefits of this route.




F IGURE 9.11 | Vaccine routes administration. Vaccines are administered in different ways. This diagram shows the ways vaccines are most commonly administered.
When we think of vaccine administration, we usually think of an injection in your arm or a child’s thigh. That is because you likely received an intramuscular injection at a doctor’s office the last time you got a vaccine, like the flu shot. A common practice in modern medicine, intramuscular vaccinations are administered at a 90-degree angle to the skin, and are used to deliver vaccine materials deep into the muscles. Examples of intramuscular injections include the tetanus and COVID-19 vaccines. Subcutaneous vaccination is administered into the fatty tissue just under the skin; the vaccine material injected in this manner is usually absorbed more slowly, sometimes over a period
of 24 hours. The MMR vaccine is administered subcutaneously. Intradermal vaccination is a shallow and technically precise injection of a vaccine into the middle layer of skin known as the dermis. These vaccines are used for molecules that absorb easily into the cell and often cause a swift, high immune response. Due to its difficult technique, intradermal injection is not often used, with the exception of the Bacille Calmette-Guérin (BCG) vaccine, which is a live attenuated vaccine that protects against tuberculosis.
1. Name three different types of vaccines.
2. What are adjuvants, and how do they promote immunity?
3. What are three routes of vaccine administration?
As you will see in this section, the ultimate goal of vaccine development is to maximize vaccine efficacy – a measure of a vaccine’s ability to prevent disease – as well as its safety. There is an incredibly rigorous process to ensure that both of these aims are met, with tons of oversight. Let’s learn about how efficacy and safety are ensured through the entire process.
From initial research to testing, manufacturing, and government oversight, vaccine development is quite a long process. You might recognize its similarities to the process of therapeutic development, which you learned about in Chapter 8: Therapeutics.
From research to approval, vaccine development follows six main steps (Figure 9.12):
1. Vaccine Research and Development
2. Preclinical Research
3. Clinical Research
• Phase I
• Phase II
• Phase III
4. Manufacturing
The vaccine approval process then follows these additional steps:
5. FDA Vaccine Review
6. Post-Market Clinical Research (Phase IV)
Vaccine development begins with research in a laboratory setting, most commonly at a university, biotechnology company, or government agency. During the research and discovery process, scientists begin with one main goal: understand how the pathogen of interest causes disease in humans. As they learn about the pathogen and how it interacts with the host’s immune system, they can start to set up experiments to design vaccines that mimic these specific pathogen-host interactions. During this investigation, scientists will analyze the pathogen of interest to identify a component that will be the best vaccine target – the specific antigen used to trigger an immune response. As you have learned, this could be a killed or weakened version of the whole pathogen itself, some of its subunits, or part of its genome.
There are many techniques that help researchers identify the best vaccine target. The first one we’ll talk about is called reverse vaccinology, and it is used to develop subunit vaccines. This process reviews a pathogen’s full genome and applies sequencing techniques to identify the genes that code for specific antigens. Once these antigens and their sequences are identified, researchers then study their characteristics at the nucleotide level to determine if any are particularly important to a host’s immune response and if they could be used to make a vaccine. With these techniques, scientists can more easily develop subunit vaccines by rapidly identifying immunogenic antigens, i.e., those that will have the highest capacity to confer immunity. Structural vaccinology is another novel approach to vaccine development, which applies chemical testing methods to build 3D models of the antigens that have been
determined via reverse vaccinology. These models can then be used to make more refined vaccine antigens.
Once a vaccine target is determined, researchers will tweak, test, and improve this vaccine candidate, as well as brainstorm the best ways to administer the vaccine and deliver it to the immune cells until they have developed a ‘rough draft’ of the vaccine. Altogether, this discovery period typically takes two to four years under standard, nonemergency conditions.
Once a vaccine candidate shows promise in the lab tests, it moves onto the one- to twoyear preclinical research step. During this period, the candidate is often tested on animal models such as mice and monkeys, aiming to demonstrate its efficacy and safety. As you might remember from Chapter 8: Therapeutics, although the use of animals in biomedical research remains controversial, it is widely accepted to be more ethical than immediately testing on human recipients. Furthermore, when researchers are working with animals, they are required to adhere to ethical and safety protocols and to comply with significant oversight initiatives.
Once successful preclinical trials are completed, the clinical research for vaccine development begins. The goal of this step is to evaluate the efficacy and safety of the vaccine in humans. Within the US, just like with therapeutics, the FDA is the institution responsible for authorizing vaccines. Before a new vaccine is approved to go on the market, the FDA rigorously evaluates and reviews its safety, efficacy, and possible side effects. The FDA
requires that vaccines undergo three phases of clinical testing. As the trials move into a new phase, both the number of participants and the length of time increase to ensure that the vaccine is being tested on a sufficiently large group of people and that any side effects are documented.
Phase I: evaluates the vaccine’s basic safety and ability to elicit an immune response in humans. Runs over the course of 1-2 years.
Phase II: investigates the safest and most efficacious dosage, immunization schedule, and route of administration in further detail. Runs over the course of 2-3 years.
Phase III: tests safety and efficacy in thousands of participants and analyzes the occurrences of rare side effects. Runs over the course of 2-4 years.
Historically, under non-emergency conditions, it takes roughly 15 years for a vaccine to reach the market after the start of development. However, this timeline has greatly accelerated through recent technological advances, as well as the urgency of the COVID-19 pandemic. As evidenced by the long and arduous research development process, creating a safe and potent vaccine that has the capacity to produce an immune response with long-lasting success can be a challenge, but the impact it can have on the world is well worth the effort.
The goal of this step is to find a consistent and reliable manufacturing method that efficiently can produce thousands of vaccine doses. Importantly, this step involves more than just packaging and processing. A key part of manufacturing is the determination of the lot release protocol, which is the set of tests that
each batch of vaccines will undergo before they are released for distribution. These tests help assess whether each batch has been properly produced, and it helps to catch potential errors before the vaccine is given to patients. Under standard conditions, manufacturing takes approximately one year to complete.
Once the clinical trials are over and a release protocol has been set, the vaccine manufacturer submits a Biologics License Application (BLA) to the FDA, which includes preclinical and clinical data about the vaccine and its commercial manufacturing process. The FDA team that reviews the BLA is composed of a diverse group of specialists from different disciplines, including physicians, chemists, statisticians, pharmacologists, manufacturing facility investigators, and labeling and communications experts. The review of the vaccine data, manufacturing process, and the marketing regulations is extremely comprehensive.
Once the FDA determines the vaccine is safe and effective, that the benefits are greater than the risks, and that the manufacturing process meets the requirements for quality control, the FDA approves the vaccine and provides a license. This review typically takes 1-2 years.
Even after a vaccine reaches the market and is distributed, the manufacturer will continue surveillance to monitor its safety and efficacy, and will respond to any adverse outcomes from the vaccine. This is the final step and the Phase IV of clinical trials.
Phase IV: studies the safety and efficacy of the vaccine in the general public. These trials
begin when the vaccine is approved by the FDA, and continue after it becomes available on the market. This is also called postmarketing surveillance. The FDA also continues to routinely inspect vaccine manufacturing facilities to carefully monitor the process for vaccine production and evaluate compliance with FDA’s requirements. This stage lasts at least a year, and typically far longer.
Refinement
4
Verification of safety and e cacy in hundreds of participants PHASE III
Verification of safety and e cacy in thousands of participants
MANUFACTURING
Identification
F IGURE 9.12 | Phases of Vaccine Development. This process is divided in six steps and can take more than 17 years under normal conditions, from the moment researchers begin to explore novel vaccine targets, to the moment a vaccine makes it into the market for human use. In the setting of urgent public health needs, this process can sometimes be accelerated.
Every vaccine developer’s goal is to maximize a vaccine’s efficacy without diminishing the vaccine’s safety and tolerability, which is the extent to which side effects can be tolerated by individuals. This has largely been achieved with vaccines being incredibly effective, while remaining safe for almost the entirety of the population. That said, it is important to note that vaccines do have some side effects. Most of these are short term, such as the typical soreness or muscle aches you might have felt at some point after getting a shot. In very rare circumstances, they can produce serious and adverse side effects in a small proportion of the population, such as disease-like symptoms in people with weakened immune systems, e.g., certain pregnant people, or people who have AIDS.
However, vaccines can have varying impacts on different individuals. Additionally, unintended side effects can also emerge due to aberrations in the vaccine manufacturing process, such as contaminants in the manufacturing, or, in
extremely rare cases, insufficient inactivation of the active ingredient. Other concerns include potential allergic reactions to other vaccine components such as stabilizers, antibiotics or preservatives necessary for growing and maintaining the vaccine material.
Fortunately, severe adverse events are exceedingly rare, and we have significant oversight systems that identify these events and respond appropriately. For example, in 2020 there was a nationwide pause of one of the COVID-19 vaccines in the US due to infrequent blood clots (four cases per one million doses administered were reported in 2021). Even extremely uncommon side effects can cause regulatory intervention, and they may cause a break in vaccine distribution. While some might interpret these temporary suspensions as evidence that the vaccine development and approval processes are not trustworthy, they are actually evidence of how carefully the vaccine roll-out process is monitored, as well as how responsive the regulatory authorities are to new information.
1. What is a vaccine target?
2. What is vaccine efficacy?
3. What’s the main goal of Phase I of the Clinical Research step in the vaccine development process?
As you likely already appreciate, there are many benefits of vaccines, at the individual, community, and population level.
At the individual level, the people who receive the vaccine themselves are protected against the pathogen. Some vaccines protect against all infection by a given pathogen, meaning that whoever receives the vaccine is incredibly unlikely to become infected with the pathogen. Others protect against severe disease, meaning that while the recipient can still become infected, they are unlikely to become severely ill or transmit the disease after.
Although vaccines are often incredibly effective against many serious diseases, no vaccine is 100% effective, and efficacy can vary widely between different vaccines. For example, the polio vaccine has a 99% efficacy rate, while the flu vaccine ranges between 20% and 60% efficacy for each of the past 10 years. This is due to a number of factors, namely that the exact strain of flu that circulates changes every year, so researchers have to do their best to forecast what the dominant strain will be with enough lead time to actually produce the vaccine, which may or may not be accurate. However, even with only a low efficacy, that’s still protection for millions of people.
Another component that affects vaccine efficacy is the recipient. Immunocompromised people might not be able to produce enough antibodies against the active material for the vaccine to be truly effective, and as you know, some vaccines might not be safe for immunocompromised people to receive at all, given the risk of re-activation of attenuated material. Other people might not be able
to get vaccinated if they’re allergic to some component of the vaccine, or a material involved in its production, like eggs. These people, therefore, cannot directly benefit from vaccines. So how will we protect them? We’ll detail some options in the next section.
Vaccines protect more than just the individual recipient; they also protect entire communities. This is due to the social nature of communicable diseases. As you know, infectious diseases follow chains of transmission, meaning that they are passed from an infected individual to a susceptible individual. Once a person gets an effective vaccine, they are much less susceptible to the disease, and therefore less likely to pass it on. As the number of vaccinated individuals in a population grows, the number of susceptible people decreases, and the potential chain of transmission is “shortened.” This powerful concept is known as herd immunity, a name derived from packs of animals gathering to surround and protect their more vulnerable members from predators. Herd immunity is achieved when a sufficiently high enough proportion of a population has been made immune to a disease to make an outbreak incredibly unlikely, indirectly protecting those who have not been or cannot be immunized. This phenomenon has saved countless lives.
To visualize how herd immunity can stop pathogen spread, you can think of an outbreak like falling dominoes, with each domino representing a person in the population. For an outbreak to spread, the proportion of susceptible individuals must be above a certain threshold, so that an infected individual
can encounter and pass the disease to a susceptible individual, who then spreads it to other susceptible individuals, and so on. There must be enough upright ‘dominoes’ in the population such that when one falls, it can knock over another and continue the chain. However, if enough intervening dominoes are laid flat, and therefore removed from the chain of susceptibility, the ones that remain will be so spaced out from each other that even if one were to fall, it would have very few, if any, nearby dominoes to take down with it, thus preventing a full-blown outbreak. By increasing the number of immune individuals through vaccination, we can decrease the proportion of susceptible individuals (dominoes) in the total population until it’s low enough to prevent pathogens with pandemic potential from infecting a significant number of hosts (Figure 9.13). This domino metaphor can also be applied to explain social distancing to reduce the spread of infectious disease. In this example, the dominoes would just be physically spaced far enough apart from each other that they can not knock down the next domino as they fall.
The proportion of the population that must be immune to a disease in order to achieve herd immunity varies depending on the
specific properties of the pathogen, disease, and population. These include how easily the pathogen spreads, how effective immunity to disease is, and how densely the population is structured. Nevertheless, one rule is true regardless of these details: the more immune individuals there are in a population, the fewer susceptible individuals there will be who may become infected. By increasing immunity with vaccines, we can decrease both the chances of outbreaks, as well as the probability that the few individuals in the population who can’t protect themselves from the disease will ever encounter it (Figure 9.14).
As an example, let’s examine the impact of vaccination and herd immunity on the spread of measles – an alarmingly transmissible infectious disease – in the US. Before the measles vaccine, the threat of serious complications from a measles infection was common, and out of the 3-4 million yearly infections in the US alone, over 500 people (many of them children) would die. This was before the development of a measles vaccine in 1963 (improved by Dr. Hillman in 1968), trials of which across the US and West Africa showed an incredible reduction in transmission rates. The CDC announced a goal to eliminate measles in the US by 1982, and by 1981, measles cases had decreased by 80% from the previous year.







F IGURE 9.13 | The domino effect of an outbreak. The fall of the chain is disrupted as individuals gain immunity and are removed from the susceptible population. In this way, vaccinations are especially helpful to prevent potential outbreaks, and protect large portions of the community.
Since the risk of measles transmission in any given interaction is so incredibly high, measles’ threshold for herd immunity is also incredibly high, requiring 95% immunity within the population. In a population of 330 million, in order to maintain this 95% herd immunity threshold, roughly 310 million people needed to remain immune to measles in order to prevent transmission—a difficult but attainable goal to maintain. This impressive coverage was eventually achieved.
F IGURE 9.14 | Herd immunity is achieved when the majority of the population is immune to the disease. Immunity can be achieved by vaccination or infection. Both decrease the number of hosts that a disease can spread to and infect. This diagram represents the spread of a disease when different percentages of the population have been vaccinated; here, herd immunity in this example, is achieved when ~75% of the population is vaccinated.
Once herd immunity is achieved, the next step is elimination, which is having no new cases of a disease in a defined geographic area. After years of focused efforts on measles vaccination, the CDC declared that the deadly disease had officially been eliminated from the US in 2000.
Another successful example of elimination is that of polio in the US. While it is still present in other parts of the world – for example, it is endemic in Afghanistan and Pakistan – there have been no cases of natural polio infection in the US since 1979, while there have been some polio cases reported within the US since ‘79, these have all been due to reactivation of vaccine materials, not transmission between infected people. (You might be glad to hear that the US now exclusively uses inactivated polio vaccines to avoid this issue.) Other viruses in the US that have been successfully eliminated in the US through vaccination campaigns, but that still exist elsewhere include rubella and measles. Since these diseases are still present in the world, there is always the risk that they will be brought back
into the US by travelers from endemic regions. For this reason, it’s crucial to still maintain high levels of vaccination and coordinate surveillance efforts against pathogens that have been considered eliminated.
After elimination has been achieved, hopefully, things can progress towards eradication , which is when there are no new cases of the specific disease anywhere in the world. While this is an incredibly challenging goal to achieve, it has been achieved, most notably with the eradication of smallpox in 1980 (Figure 9.15).
A key contributor to the success of smallpox eradication efforts is Leslie Harold Collier. In 1955, Collier, a professor of virology at the University of London, devised a smallpox vaccine that was stable at room temperature, making distribution much more feasible. Collier’s vaccine was freeze-dried, meaning that the vaccine was first frozen and then dried, so that it could stay preserved in the dried state at room temperature. This process decreased
the need for long-term refrigeration, making more extensive initiatives in limited resource areas (e.g., where the electricity needed for refrigeration is not readily available) possible. This allowed for unprecedented global vaccination efforts.
Smallpox was a particularly good candidate for eradication due to specific aspects of the virus’ genome and biology.
1. Low diversity: the virus responsible for smallpox has a DNA genome with a relatively low mutation rate, which means that its genome changes slowly, and there is less danger of new strains quickly emerging that would resist the vaccine.
2. Symptomatic transmission: since transmission only occurs after the individual has developed symptoms, it is comparatively easy to trace smallpox transmission because it can only be spread by infected individuals (i.e., it’s clear which interactions were risky).
3. No reservoir: since humans are the only animals that can be infected by smallpox, there is no animal or environmental reservoir. Thus, eradication within the human population would mean complete eradication.
We have not yet been successful in eradicating any other pathogens in the human population, because, unlike smallpox, most pathogens have some combination of a non-human reservoir, high mutation rate, or transmission before symptoms appear. All of these increase the risk of vaccine escape, or reintroduction into the human population, making eradication very difficult. However, as you already know, administration of even one vaccine has exponential protective benefits, and so we continue to vaccinate.
So what needs to be done in order to achieve herd immunity, or even elimination/eradication?
This level of vaccination is frequently achieved via vaccination campaigns, which are initiatives that aim to deliver large numbers of vaccines in a relatively short period of time.
Mass vaccination campaigns are an incredible undertaking. They require coordination between international organizations to help procure a sufficient number of vaccines of the
desired formulation. Organizations like the WHO, Gavi, The Vaccine Alliance® (GAVI®); the Bill and Melinda Gates Foundation® (BMGF); the Coalition for Epidemic Preparedness Innovations (CEPI®); and the United Nations International Children’s Emergency Fund (UNICEF®) have helped coordinate these procurement efforts. Their efforts typically aim to support equitable access for those who cannot afford vaccines and/or live in disease-endemic areas. It is important to note, however, that these organizations are not directly embedded in a nation’s healthcare system and often operate externally. Long-term reliance on these groups may not be in the best interest of the countries receiving assistance since their support may diminish as the threat of an outbreak declines. It is essential that local governments invest in local healthcare infrastructure to sustain their work.
The next step to a successful vaccination campaign is identifying local individuals who will be able to help administer the vaccines, or potentially bringing in healthcare workers from other regions to help. In addition to those who will actually physically administer the vaccines, many other employees and/or volunteers will be needed to coordinate the logistics of ensuring that there are sufficient supplies at each vaccination location, and ensuring that there is a way to log who has already received the vaccine(s) in order to avoid unnecessary duplication. Sometimes this is achieved by marking the patient’s finger with a long-lasting dye after they have received the vaccine (Figure 9.16).
Finally, local community members are recruited to help spread the word about vaccines, when and where to receive them, their benefits, and any other questions. Engaging community
| Post-vaccination finger dye. Some regions may not have the infrastructure to reliably keep track of who has received what vaccines using paper or electronic records. This long-lasting dye can be applied to the fingers of children who have already been vaccinated to avoid duplication.
leaders in this way ensures that efforts are culturally appropriate, and will work to build rapport with the surrounding communities.
One example of a comparatively recent mass vaccination initiative took place in Yemen in 2019. Measles is endemic in Yemen, but the country saw an incredible outbreak in 2018. In comparison to the 433 cases of measles reported in 2017, there were 10,640 in 2018; an estimated two thirds of these cases were seen in children. A particular driver of this outbreak was likely ongoing political conflict in the region disrupting healthcare delivery and driving mass migration and close-quarter living in refugee camps.
Aid organizations mobilized in early 2019, and 40,000 healthcare workers joined UNICEF and the WHO, as well as Yemeni health authorities, to help vaccination efforts. Their efforts focused on vaccine delivery to those aged 6 months15 years, and they were incredibly successful in their mission. All told, they vaccinated

F IGURE 9.17 | A health care worker in Aden, Yemen vaccinating children against measles and rubella in 2019. UNICEF-backed the measles-rubella vaccination campaign in Yemen, during which millions of children received the vaccine across several nations. Image credit: © UNICEF/UN0284455/Fadhel.
an estimated 13 million kids, and covered approximately 92% of their target population (Figure 9.17).
Even though we may theoretically have the technology and resources to build herd immunity against, eliminate, or even eradicate many of the world’s preventable diseases, there are several challenges we still face with the access and distribution of vaccines, particularly in low-resource regions. Reducing this burden requires not only the development of efficacious and safe vaccines for diseases that affect the most vulnerable, but also broad vaccine manufacturing rights, convenient vaccine transportation strategies, affordable vaccine prices, readily available emergency doses, and coordinated efforts to administer and distribute the vaccine in every region that needs it, among many other elements. While there are many factors that influence vaccine availability and uptake, two
key ones are vaccine distribution channels and social factors.
Even the best-designed vaccine is useless if you can’t deliver it to the people who need it. The ways that vaccines are physically distributed to patients are known as vaccine distribution channels (VDCs). VDCs can typically be broken down into four general stages (Figure 9.18). Smooth transition within and between these stages typically requires involvement from stakeholders at the national, regional, and district levels, as well as at recipient healthcare facilities. From the production line to the recipients, the four stages are: 1. Sourcing 2. Storage 3. Transportation 4. Administration
Sourcing goes beyond just identifying the company that’s producing the desired vaccine, and buying up as much as you can afford. It’s actually a very complex process. Sourcing is typically taken up at the national level by the government, and for LMICs, is often mediated by a humanitarian group like UNICEF or GAVI in order to attempt equitable distribution at (somewhat) reasonable prices.
These stakeholders must determine what vaccines they need to buy in what formulations (including the size of the vials), and where would be the best place to buy from. For example, perhaps there’s a vaccine production plant in a neighboring country, but for whatever reason, the government has reason to have higher confidence in a vaccine that is produced on a different continent, but with higher shipping costs; which one should they choose? In these scenarios, government officials might have to weigh trade-offs between perceived efficacy, and purchasing more doses of the potentially-less effective vaccine for the same price.
The vast majority of vaccines need to be kept at cold temperatures at all times, at the risk of inactivating the vaccine if it gets too warm. Therefore, proper equipment and logistics are needed to maintain a completely uninterrupted production, storage and distribution cycle at the desired low-temperature range – known as a cold chain. Cold chain limitations were recently emphasized during the development of the COVID-19 vaccine; one of the highlyanticipated mRNA vaccines had to be kept at between -112 °F (-80 °C) and -76 °F (-60 °C), an ultra-cold temperature that the majority
of health facilities around the world did not have the equipment to maintain. While the other mRNA vaccine could be stored at a more manageable temperature of -4 °F (-20 °C), many more rural areas still lack the infrastructure to maintain the necessary cold chain requirements.
There are a few ways to try to work around these cold chain concerns. One approach is to use solar powered cold boxes, or other storage devices that use ice and isolation to keep the vaccines cool enough. However, these will eventually require some access to a power source. Additionally, there are ongoing efforts to develop more thermostable vaccines, but as of yet, these are not the norm. You might be surprised to learn that in many LMICs, vaccines are stored in the country for 4-18 months before they’re administered, and so the need is large.
Vaccine manufacturing plants are not evenly distributed around the globe, and are instead concentrated in higher income countries. As a result, vaccines must be transported to lowerincome destinations via plane or boat. From there, they are distributed on cold shipping trucks – either belonging to the country’s government, or to private third party shipping companies – to national, regional, or district storage centers. From there, they are dispersed to individual clinics or providers. This final stage is known as last mile distribution.
This last mile varies widely depending on where the vaccine is in the world. For example, for healthcare clinics in cities, the last mile will likely be covered in a truck or car. But the same is not true for remote regions. Sometimes vials of vaccines are carried on bikes or by hand across regions without roads or otherwise
variable terrain, and their final destination isn’t always a clinic. In some particularly remote cases, healthcare workers trek straight to individual people who need the vaccine, and administer the vaccines on site.
Once the vaccines have arrived at their destination, the final step is administration.
Even though the end is in sight, administration is still a long complicated process involving many steps (Figure 9.18). After all, it involves getting health care workers, interested patients, active vaccines, and the right administration supplies (including everything from syringes to alcohol wipes) all in the same place at the same time. Some methods to reduce the barriers to vaccine administration include using oral formulations that can be







F IGURE 9.18 | The long road to vaccination. This flowchart visualizes the chain of events that take a vaccine from the factory to the clinic to the recipient. Along this long road, most vaccines require being stored at cool temperatures to remain effective. Maintaining this cold chain is critical during vaccine delivery.
administered by individuals with less training, require fewer supplies, and do not need safe needle storage/disposal.
Additional barriers to administration include getting the word out about when and where vaccines are available. In some communities, vaccines can be offered at standard doctor or pharmacy appointments. In others, where there is limited ability to store the vaccines long-term, or insufficient health professionals to administer the vaccine each day, or just a need to move very quickly, there can be popup vaccine clinics, where people can come get vaccinated at a particular place and time. However, spreading the word about these clinics can be tricky, especially in areas where people live far apart, and/or have limited access to communications and media.
Further, many vaccines require multiple doses, scheduled weeks, months, or even years apart, in order to be fully effective and maintain efficacy over time. As the number of required visits increases, the rate of individuals completing the series decreases, as it can be hard to come back to a clinic repeatedly. This poses particular challenges to rural and remote populations who have to travel long distances to receive their vaccines. This can sometimes result in under-protection against infectious disease in these communities, which already face unique health risks and vulnerabilities.
Many different factors influence vaccine uptake, which is the proportion of people in a population who receive a vaccine. These both include issues of accessibility to vaccination services as well as attitudes towards vaccination.
One of the most pressing factors affecting vaccine access is cost; many people can simply not afford to be vaccinated, particularly if a long journey to receive them means spending lots of gas money, or taking time off work. This means reduced protection for people of low socioeconomic status, a group that already faces disproportionate vulnerability to infectious disease. On a global scale, the current methods of vaccine distribution and access give richer nations access to vaccines at staggeringly disproportionate rates in comparison to other nations, as these markets promise higher profit returns. Beyond being unjust, this is an especially inefficient strategy in an outbreak setting, as it allows greater opportunity for pathogen mutation, and then re-introduction to populations that were previously immune.
In a different vein, it’s important to appreciate that different cultures and communities also perceive vaccinations and their safety differently. As the example of Oneismus and Cotton Mather shows, distrust of immunizations has been around as long as the immunizations themselves. In the context of vaccinations, this distrust and concern, despite their documented safety and efficacy is known as vaccine hesitancy. This likely started with a very legitimate fear of the unknown – of course it was alarming to be exposed to known pathogenic materials back in the days when vaccination meant facing Jenner’s puss-covered knife. In modern times, there have been a number of incidents, such as the Trovan trial conducted in Nigeria that we told you about in Chapter 8: Therapeutics, that triggered distrust of therapeutics and vaccines within the harmed communities, and also more broadly. Since then, there has been a learning process to reach optimal efficiency and safety
levels vaccines now have. There are also some legitimate social factors that drive vaccine hesitancy. These include previous medical mistreatment of the community, or their administration by people who are not part of the local community, i.e. western aid agencies.
These social factors, as well as incredibly rare adverse vaccine reactions, might make vaccines seem like they’re not worth the perceived risks — at least in the modern US, when the diseases that the vaccines protect against are basically unheard of. For example, do you know anybody who has had diphtheria? Would you be able to describe what would happen during a diphtheria infection? For most people in the US, the answer is no, yet we ask people to get 6 vaccines against it before they’re 13 years old. (If you’re curious, diphtheria causes a fever and sore throat, then creates a large white plaque on the back of the throat that can be large enough to fatally block the airway in 5-10% of cases). Just as any costbenefit analysis is skewed when the costs are immediate and the benefits are abstract, when people are not accustomed to seeing people suffer from these diseases, they often overlook the advantages of a vaccine.
But not all vaccination concerns are grounded in evidence. While vaccine hesitancy may have originally been due to concern about a new technology, and lack of evidence for its safety to that point, it has since been propagated by broader fears, myths, theological ideologies and reactions to political mandates. In the 19th century, in the UK and in the US, the anti-vaccination leagues emerged. These were mainly a response to mandatory child vaccination campaigns. The anti-vaccination leagues claimed that the smallpox vaccine did not work, made you sick, contained poisonous chemicals and suggested that
vaccine mandates were the manifestation of a cruel, overbearing government. These claims were preserved in the groups of people against vaccination in the 20th century and anti-vaccine movements, and later became popularized by celebrities and high-profile political figures.
The early popular claim about vaccination is the repeatedly debunked assertion that vaccines cause autism. Despite the fact that the original study suggesting this link was retracted due to fraud and insufficient evidence and numerous other scientific studies performed since have found no association between the two, this claim continues to circulate.
As a result of both founded and unfounded claims about vaccines, there are particular groups who choose not to vaccinate themselves or their children, even when they are able to do so. This trend to opt out of vaccinations is demonstrated by groups of people who oppose vaccination completely and may even promote misinformation about vaccine safety. These groups are described as anti-vaccination, and are sometimes called antivaxxers. However, this term is commonly avoided by medical and public health professionals, due to concerns about alienating groups who would greatly benefit from building increased trust with healthcare professionals.
When vaccine hesitancy becomes popular, it can disrupt vaccination campaigns and affect global public health by prolonging disease spread in a community. That is, many unvaccinated individuals benefit from herd immunity, so do not face the consequences of susceptibility to disease. However, as the numbers of unvaccinated people goes up, communities are at risk. This leads to preventable diseases and sometimes avoidable deaths.
An example of a resurgence of a disease that was previously controlled with vaccines is the 2018 measles outbreak in the US. This outbreak mainly occurred within Orthodox Jewish communities in New York; this is thought to be at least partially due to low rates of vaccination throughout the close-knit community. A number of factors are believed to contribute to this insufficient vaccine coverage, including larger average family size (it can be hard to round up multiple kids to get to the doctor), as well as misinformation campaigns targeting community members who are less likely to use the internet or otherwise have access to fact-check vaccine-related claims. The outbreak started when one unvaccinated child came home from a visit to Israel with measles. 649 cases followed, at least 557 of whom were unvaccinated. Fortunately, there were no deaths as a result of this outbreak, but 37 children had to be hospitalized. In addition to the toll on the sick individuals and their families, the New York City Department of Health and Mental Hygiene spent an estimated $8.4 million responding to this outbreak.
The 2018 measles outbreak demonstrates the importance of culturally sensitive and
appropriate information, and outbreak response initiatives. Messaging around the demographics of those affected by the outbreak seemed to refresh a false, antisemitic narrative that Jewish people spread disease, as was claimed in the 14th century with the spread of the Black Death plague, and more recently by Nazi doctors in the run-up to World War II. These feelings were exacerbated by a perceived lack of engagement of the Orthodox community by public health responders when designing containment initiatives. Therefore, the response to this outbreak imposed additional harm on an already vulnerable community.
Cases like these more broadly highlight how diseases can quickly and dangerously reemerge without vaccination to keep them at bay, and remind us that pathogens remain a threat, even in times of relative quiet. While these measles cases were mostly contained to unvaccinated people, reduced community vaccination can lead to disease spread even among those who themselves received vaccines via pathogen mutation and vaccine escape, with life-threatening consequences. In this way, vaccination is not a purely individual choice and can impact the global population.
1. An existing strain of influenza has erupted into a global outbreak, and you are assigned to organize the vaccination campaign. Name four practical factors you need to consider for a successful vaccination campaign.
2. What are three specific pathogen-related factors that make a pathogen a good candidate for eradication?
3. Why is herd immunity important and how does it protect susceptible individuals in a population?
1. Vaccination is the act of introducing a killed or weakened version or piece of a pathogen to a host organism in order to induce immunity if it were to encounter the pathogen again. Inoculation is a precursor to vaccination that introduces the direct, pathogenic agent to the host in order to induce immunity. Immunization is the broad process by which a person becomes protected from – or immune to – a pathogen. This is typically through vaccination but can also occur through natural infection.
2. Attenuation is the process of making a pathogen weak enough that it can be safely introduced into the host via a vaccine without risking full-blown infection. This approach was first applied by Pasteur when he exposed pathogens to the oxygen in the air for extended periods of time until they became less immunogenic.
3. Vaccines trigger active immunity by introducing components of a pathogen to the body. This prompts a response by B cells to produce antibodies against the pathogen’s antigen and subsequent memory of the pathogen by memory B cells. This memory allows the immune system to advance a faster and more efficient immune response when the pathogen is encountered in the future. Vaccines might also trigger strong T cell responses to enhance overall immunity.
4. Some vaccines require a booster shot, likely due to a number of reasons. including waning immunity, pathogen incubation period, and changes to the pathogen over time.
1. Any combination of 3 below (definitions in the text and glossary):
b. Live attenuated vaccines
c. Inactivated vaccines
d. Subunit vaccines
i. Protein vaccines
ii. Polysaccharide vaccines
iii. Conjugated vaccines
iv. Toxoid vaccines
v. Nucleic-acid vaccines
d. Recombinant vector vaccines
e. DNA vaccines
f. mRNA vaccines
2. Adjuvants are substances added to vaccines. They boost immune response, increase immunological memory and can help induce lifelong immunity.
3. There are five primary routes of vaccine administration: oral, intranasal, intramuscular, subcutaneous, and intradermal. They are chosen based on the specific vaccine being given and the disease being targeted.
1. A vaccine target is the selected antigen(s) that will trigger the desired immune response.
2. Vaccine efficacy is a measure to evaluate how good a vaccine is at preventing a disease in a safe manner. Specifically, it is the percentage reduction of disease in a vaccinated group compared to an unvaccinated group under optimal conditions.
3. The main goal of Phase 1 of the Clinical Research stage (Stage 3) is to evaluate the vaccine’s basic safety and ability to elicit an immune response in humans.
1. Answers may vary, but will likely include some of the following: (1) affordable vaccine prices, (2) broad vaccine manufacturing rights, (3) readily available emergency doses, (4) coordinated efforts to administer and distribute the vaccine in every region that needs it, (5) eliminating infrastructural disparities across the healthcare systems of different nations, (6) equalizing healthcare systems of all countries due to limited resources
regarding their manufacturing capacities, (7) personnel for vaccine administration, (8) cold chain and refrigeration capacity, (9) perceived vaccination safety to eliminate vaccine hesitancy.
2. Answers may vary, but should include the some of the following components: (1) The virus responsible for the disease has a relatively low gene sequence diversity; thus, there will be less danger of new strains quickly emerging that would resist the vaccine, (2) transmission only occurs after the disease’s symptoms manifest, making it easier to detect potential spread of the disease through infected individuals, (3) if humans are the only disease reservoir, you could eradicate the disease fully by stopping human-to-human transmission and by thus removing the human reservoir altogether.
3. Herd immunity is important because immune individuals can buffer those who cannot be vaccinated effectively or at all, breaking up chains of transmission before many people become infected.
Adjuvants: Substances added to vaccines in order to increase the magnitude or strength of an immune response.
Attenuated: When a pathogen is weakened so it can induce immunity without risk of harmful infection.
Booster: Extra administration of a vaccine after a previous dose.
Cell Culture: The growth of microorganisms such as bacteria and yeast (microbiological culture), human and mammalian cells (cell culture), and plants (plant tissue culture) in the laboratory. Cultures are used in the diagnosis of infections, testing of new drugs, and in general in research.
Cold Chain: A temperature-controlled supply chain that includes all vaccine-related procedures, beginning with the cold storage unit at the manufacturing plant, extending to the transport and delivery of the vaccine and proper storage at the provider facility, and ending with administration of the vaccine to the patient.
Conjugated Vaccines: Vaccines that pair weaker antigens with stronger antigens from the target pathogen or other microbes in order to elicit a more robust and longer-lasting immune response.
DNA Vaccines: Vaccines composed of a small portion of the pathogen’s DNA, to instruct cells in the recipient’s body to produce a subunit of the target pathogen, triggering an immune response for protection.
Elimination: When the number of new cases of a disease is reduced to zero in a defined geographic area.
Eradication: When the number of new cases of a disease is reduced to zero across the entire global population.
Herd Immunity: A certain threshold of immune individuals within a population that greatly restricts the pathogen’s ability to spread through the population, indirectly protecting the population as a whole.
Immunization: The process of receiving protection from a disease through vaccination.
Immunogenic: The ability or extent to which a substance is able to stimulate an immune response or confer immunity.
Inactivated Vaccines: Vaccines that use the killed version of the pathogen to induce an immune response. They are also known as killed vaccines.
Inoculation: The act of introducing a pathogen or its antigen(s) into a living organism to stimulate the production of an immune response.
Intradermal Vaccination: Vaccine administration through a shallow or superficial injection into the dermis, which is located underneath the epidermis (skin).
Live Attenuated Vaccines: A vaccine that contains the weakened (attenuated) but still live version of a pathogen.
mRNA Vaccines: Vaccines composed of a small portion of the pathogen’s mRNA to instruct cells in the recipient’s body to produce a subunit of the target pathogen, triggering an immune response for protection.
Nanoparticles: Small particles that can carry vaccines and help with their efficacy by incorporating adjuvants, protecting the vaccine, and improving their stability.
Polysaccharide Vaccines: Vaccines composed of polysaccharides (complex sugar molecules) found on the surface of some bacteria. Like protein antigens, polysaccharide antigens bind to immune cell receptors, stimulating an immune response and generating polysaccharide-specific antibodies.
Protein Vaccines: Vaccines composed of protein antigen(s) from the target pathogen. These can include surface proteins, which typically bind to receptors in order to enter cells, and other essential proteins from the pathogen that are capable of eliciting an immune response.
Recombinant Vector Vaccines (aka Vector Vaccines): Vaccines that utilize a genetically modified version of a non-disease-causing microbe – bacteria or virus – as a vector to transport antigens from the target pathogen to your cells.
Subunit Vaccines: Vaccines that use specific antigens (e.g. proteins, toxoids, polysaccharides) rather than all components of the pathogen to stimulate the immune system.
Tolerability: The extent to which side effects can be tolerated by individuals.
Toxoid Vaccines: Vaccines that use a toxin (harmful product) made by the pathogen to stimulate the immune system.
Vaccination: The act of introducing a vaccine – a harmless version of part of a pathogen –into the body in order to produce an immune response, resulting in protection from a specific disease.
Vaccination Campaigns: Intense efforts that work to vaccinate many people in diseaseendemic areas in a short period of time; these efforts can have a positive, lasting effect on the health systems of a country and are commonly used by the WHO and other international organizations. When the efforts aim to target whole populations they are described as mass vaccination campaigns.
Vaccine Efficacy: A measure used to describe how good a vaccine is at preventing disease.
Vaccine Hesitancy: Delay in acceptance or refusal of vaccination despite availability of vaccination services, influenced by factors such as fear or distrust of the safety and necessity of vaccines, religious beliefs, and beliefs in personal freedoms.
Vaccine Target: the chosen antigen(s) of a pathogen that will induce the desired immune response, on which a vaccine is based.
Variolation: The process of inoculation –introducing a pathogen or antigen into a living organism to stimulate the production of antibodies – specific to smallpox, and named after the scientific name for smallpox, Variola.
Virosomes: Vaccine delivery system; uses lipid vesicles that contain viral membrane proteins to deliver active vaccine ingredients to the cell.
Waning Immunity: The loss of protective immune response to a pathogen over time after vaccination or natural infection.