RandomizedtrialofthreeIVIgdosesfor treatingchronicinflammatory demyelinatingpolyneuropathy
DavidR.Cornblath,1 PieterA.vanDoorn,2 Hans-PeterHartung,3,4,5,6 IngemarS.J.Merkies,7,8 HansD.Katzberg,9 DorisHinterberger,10 ElisabethClodi10 andtheProCIDInvestigators
Intravenousimmunoglobulintreatmentforchronicinflammatorydemyelinatingpolyneuropathyusuallystarts witha2.0g/kginductiondosefollowedby1.0g/kgmaintenancedosesevery3weeks.Nodose-rangingstudieswith intravenousimmunoglobulinmaintenancetherapyhavebeenpublished.
TheProgressinChronicInflammatoryDemyelinatingpolyneuropathy(ProCID)studywasaprospective,doubleblind,randomized,parallel-group,multicentre,phaseIIIstudyinvestigatingtheefficacyandsafetyof10%liquid intravenousimmunoglobulin(PanzygaV R )inpatientswithactivechronicinflammatorydemyelinatingpolyneuropathy.Patientswererandomized1:2:1toreceivethestandardintravenousimmunoglobulininductiondoseand theneither0.5,1.0or2.0g/kgmaintenancedosesevery3weeks.Theprimaryendpointwastheresponseratein the1.0g/kggroup,definedasanimprovement 51pointinadjustedInflammatoryNeuropathyCauseand TreatmentscoreatWeek6versusbaselineandmaintainedatWeek24.Secondaryendpointsincludeddoseresponseandsafety.ThistrialwasregisteredwithEudraCT(Number2015–005443-14)andclinicaltrials.gov (NCT02638207).
BetweenAugust2017andSeptember2019,thestudyenrolled142patients.All142wereincludedinthesafety analyses.Asnopost-infusiondatawereavailableforthreepatients,139wereincludedintheefficacyanalyses,of whom121werepreviouslyoncorticosteroids.Theresponseratewas80%(55/69patients)[95%confidenceinterval (CI):69–88%]inthe1.0g/kggroup,65%(22/34;CI:48–79%)inthe0.5g/kggroup,and92%(33/36;CI:78–97%)inthe 2.0g/kggroup.Whiletheproportionofresponderswashigherwithhighermaintenancedoses,logisticregression analysisshowedthattheeffectonresponseratewasdrivenbyasignificantdifferencebetweenthe0.5and2.0g/ kggroups,whereastheresponseratesinthe0.5and2.0g/kggroupsdidnotdiffersignificantlyfromthe1.0g/kg group.Fifty-sixpercentofallpatientshadanadjustedInflammatoryNeuropathyCauseandTreatmentscoreimprovement3weeksaftertheinductiondosealone.Treatment-relatedadverseeventswerereportedin16(45.7%), 32(46.4%)and20(52.6%)patientsinthe0.5,1.0and2.0g/kgdosegroups,respectively.Themostcommonadverse reactionwasheadache.Therewerenotreatment-relateddeaths.
Intravenousimmunoglobulin(1.0g/kg)wasefficaciousandwelltoleratedasmaintenancetreatmentforpatients withchronicinflammatorydemyelinatingpolyneuropathy.Furtherstudiesofdifferentmaintenancedosesof intravenousimmunoglobulininchronicinflammatorydemyelinatingpolyneuropathyarewarranted.
1DepartmentofNeurology,JohnsHopkinsUniversity,Baltimore,MD21287,USA 2DepartmentofNeurology,ErasmusUniversityMedicalCenter,Rotterdam3015CE,TheNetherlands 3DepartmentofNeurology,HeinrichHeineUniversity,Du¨sseldorf40225,Germany 4BrainandMindCenter,UniversityofSydney,Sydney,NSW2050,Australia 5DepartmentofNeurology,MedicalUniversityofVienna,Vienna1090,Austria
ReceivedAugust16,2021.RevisedOctober15,2021.AcceptedNovember09,2021.AdvanceaccesspublicationJanuary17,2022 V C TheAuthor(s)(2022).PublishedbyOxfordUniversityPressonbehalfoftheGuarantorsofBrain. ThisisanOpenAccessarticledistributedunderthetermsoftheCreativeCommonsAttribution-NonCommercialLicense(https://creativecommons.org/licenses/ by-nc/4.0/),whichpermitsnon-commercialre-use,distribution,andreproductioninanymedium,providedtheoriginalworkisproperlycited.For commercial re-use,pleasecontactjournals.permissions@oup.com https://doi.org/10.1093/brain/awab422BRAIN2022:Page1of10
6DepartmentofNeurology,PalackyUniversity,Olomouc77147,CzechRepublic 7DepartmentofNeurology,MaastrichtUniversityMedicalCenter,Maastricht6229HX,TheNetherlands 8Curac¸aoMedicalCenter,Willemstad,Curac¸ao 9DepartmentofNeurology,UniversityofToronto,TorontoM5G2C4,Canada 10ClinicalR&D,OctapharmaPPG,Vienna1100,Austria
Correspondenceto:DavidR.Cornblath,MD DepartmentofNeurology,JohnsHopkinsUniversity,Meyer6-181a 600NorthWolfeSt.,Baltimore,MD21287,USA E-mail:dcornbl@jhmi.edu
Keywords: chronicinflammatorydemyelinatingpolyneuropathy;intravenousimmunoglobulin;ProCIDstudy; panzygaV R ;randomizedcontrolledtrial
Abbreviations: CIDP=chronicinflammatorydemyelinatingpolyneuropathy;I-RODS=InflammatoryRasch-built OverallDisabilityScale;INCAT=InflammatoryNeuropathyCauseandTreatment;IVIg=intravenousimmunoglobulin;MRC=MedicalResearchCouncil;ProCID=progressinchronicinflammatorydemyelinatingpolyneuropathy; TEAE=treatment-emergentadverseevents
Introduction
Chronicinflammatorydemyelinatingpolyneuropathy(CIDP)isa rare,auto-immunemediatedpolyneuropathyandcanbediagnosedusingguidelinesfromtheEuropeanFederationof NeurologicalSocieties/PeripheralNerveSociety(EFNS/PNS).1 2 However,thediagnosisofCIDPisnotstraightforward,3 andanumberofdisorderscanbemistakenforCIDP.4
ThreetreatmentshavebeenproveneffectiveforCIDP:intravenousimmunoglobulin(IVIg),corticosteroids,andplasmaexchange.5 Whereavailable,IVIgisthemostfrequentlyused first-linetreatmentduetoitssafetyandefficacy.Basedonseveral clinicalstudies,treatmentwithIVIginCIDPusuallystartswithan inductiondoseof2.0g/kgover2to5daysfollowedbymaintenance dosingof1.0g/kgevery3weeks.6–8
Theoptimalmaintenancedosemayvarybetweenpatients, andtheEFNS/PNSguidelinesrecommendthatthemaintenance dosemayneedtobeadjustedtosuitanindividualpatient’s needs.2 Whilsttailoreddosinghasbeenlongadvocatedandissupportedbyretrospectiveandreal-lifedata,9–12 therehavebeenno randomized,prospectivetrialsevaluatingdifferentIVIgmaintenancedoseregimensinpatientswithCIDP.Onlyonesmallopen, randomizedstudyhasevaluateddifferentinductiondosesofIVIg forCIDPandmultifocalmotorneuropathy,andtheresultsshowed apotentialdose-relatedeffect5weeksafterinductiontreatment.13
ThePATHstudyevaluatedtwodosesofsubcutaneousimmunoglobulin(SCIg),0.2and0.4g/kgeveryweek,inpatientswithCIDP andshowednosignificantdifferencesinoutcomesbetweenthose twoSCIgdosesduringastudyperiodof24weeks.14
TheProgressinChronicInflammatoryDemyelinatingpolyneuropathy(ProCID)studyinvestigatedtheefficacyandsafetyof IVIgaftera2.0g/kginductiondosefollowedbyastandardmaintenancedoseof1.0g/kggivenevery3weeks,andtwootherdoses, 0.5g/kgand2.0g/kg,onoutcomesinpatientswithCIDPduringa studyperiodof24weeks.
Materialsandmethods
Studydrug
IVIg(PanzygaV R ,Octapharma)isaglycine-stabilized10%liquid humanIVIg15,16 withprovenefficacyandsafetyasreplacement
therapyinprimaryimmunodeficiency17 andforimmunomodulationinpatientswithimmunethrombocytopenicpurpura.18 This IVIgproductislicensedfordifferentindications(includingCIDP)in theUSA,19 Canada20 andtheEU.21
Studydesignandparticipants
TheProCIDstudy(EudraCTNumber2015–005443-14andclinical trials.gov identifierNCT02638207)wasdesignedin2016/2017and initiatedin2017.22 Thetrialprotocolandstatisticalanalysisplan werepublishedpreviously.22
Patientswereeligibleiftheywereatleast18yearsoldandhad beendiagnosedwithdefiniteorprobableCIDPaccordingtopublishedcriteria1 andiftheyweredependentontreatmentwith immunoglobulinsorcorticosteroids.Themainexclusioncriteria includedpreviousfailureofimmunoglobulintreatment,treatment withotherimmunomodulatory/suppressiveagentsintheprior 6months,treatmentwithimmuno-chemotherapeuticregimens, andclinicalevidenceofperipheralneuropathyfromanother cause.Fullinclusionandexclusioncriteriawerepublishedpreviously.22 Allpatientsgavewritteninformedconsentpriortoany study-relatedprocedures.Theethicscommitteesofallparticipatingcentresapprovedthestudyprotocol.
Procedures
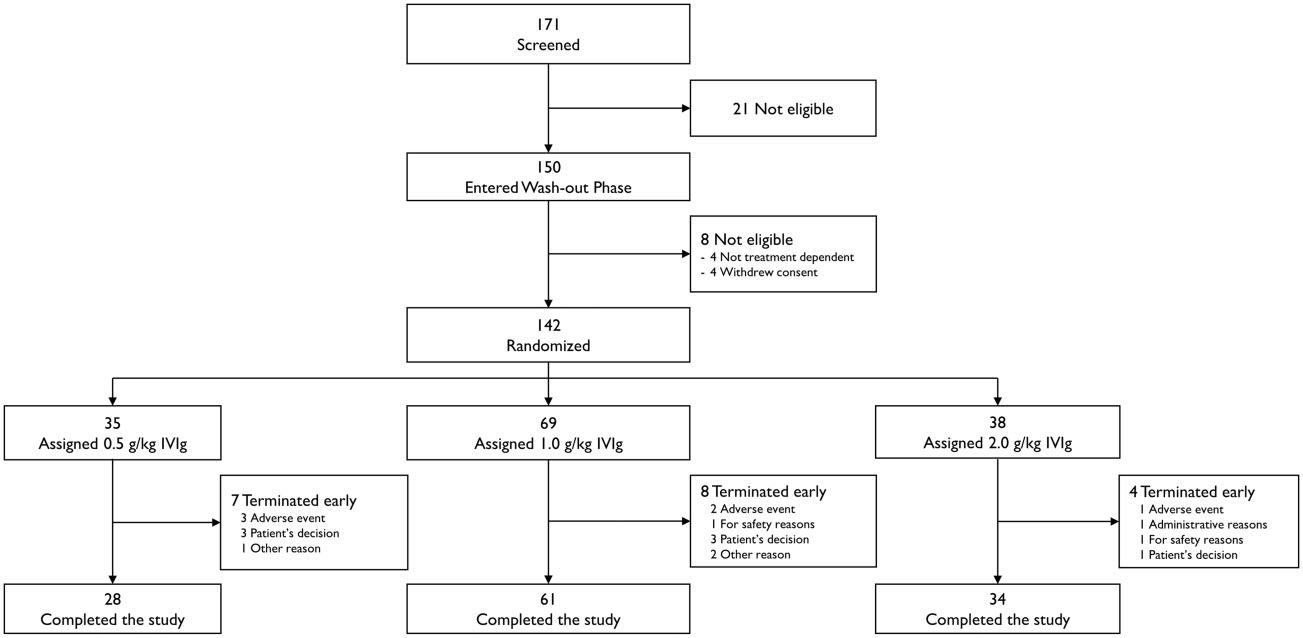
Thestudyconsistedofscreening,wash-out,anddose-evaluation phases(Fig.1).Patientswerescreened,and,ifeligible,enteredthe wash-outphase,duringwhichtheircurrentmedicationwas reducedinapredefinedstandardmanner,todeterminewhether theyhadactiveCIDP.ForthosepreviouslyonIVIg,thedosewas reducedby25%ateachsequentialinfusionuntildeterioration.For thosepreviouslyoncorticosteroids,thedosewasreducedatthe discretionoftheinvestigatorataratetoexpectstudyentrywithin 6–12weeksandtoadoseofprednisolone 420mg/dayorequivalentwhendeteriorationoccurred.Lowdosesofcorticosteroidsat deteriorationcouldbecontinuedduringthestudy.Thewash-out phasehadamaximumof12weeks,andonlypatientswhodeterioratedinthistimeframewereenrolledandrandomizedintothe dose-evaluationphase.Patientswhodidnotdeteriorateinthe wash-outphasewereconsiderednottohaveactiveCIDPandwere excludedfromthestudy.Deteriorationwasdeterminedby

worseningoftheiroverallstatusaccordingtothePatients’Global ImpressionofChangeScaleandeitheranincreaseinadjusted InflammatoryNeuropathyCauseandTreatment(INCAT)scoreby 51point,oradecreaseof 58kPaongripstrengthinonehand, orreachedtheInflammatoryRasch-builtOverallDisabilityScale (I-RODS)minimumclinicallyimportantdifferencerelatedtothe varyingstandarderrorscut-offof–1.96orless.23
Allpatientswhodeterioratedwererandomlyassigned1:2:1to maintenancedosesof0.5,1.0or2.0g/kgIVIginthe24-weekdoseevaluationphase.TheythenreceivedaninductiondoseofIVIg 2.0g/kg,followedbysevenmaintenanceIVIgdosesof0.5,1.0or 2.0g/kgevery3weeks(± 4days).Themaskedassignmentofthe correctdoseandtreatmentforeachstudyvisitwasmanagedusing aninteractivewebresponsesystem.Thetreatmentgroupassignmentwasonlyreportedtothehospitalpharmacistordesigneeby adedicatedemailtowhichnootherstudypersonnelhadaccess. Thepatientwasmaskedtothemedicationbytheuseofanopaque (non-transparent)infusionlineandoverpouches.Theevaluating investigatorwasnotinvolvedwithadministeringmedicationto thepatient.Dosingwasbasedonactualbodyweightandadministeredovertwoconsecutivedayswithoutpre-medication. Corticosteroids(prednisoloneorequivalent) 420mg/dayasconcomitantCIDPmedicationwerepermittedduringthedose-evaluationphaseforpatientswithpriorcorticosteroidtherapy.Forall patientsinthe0.5and1.0g/kgdosegroupswhowerestable(unimproved)atWeek6ordeterioratedbetweenWeeks3and18,there wastheoptiontoadministerrescuetreatmentwithtwoconsecutiveinfusionsofIVIg2.0g/kgat3-weekintervals(± 4days). FollowingthetwoIVIgrescuetreatments,patientsattendedan endofstudyvisit.PatientsdeterioratingafterWeek18or21 droppedoutandhadtheirendofstudyvisitatWeek21or24,respectively.Patientsinthe2.0g/kgarmwerediscontinuedfromthe studyiftheywerestable(unimproved)atWeek6ordeteriorated afterWeek3andbeforeWeek21.
Outcomes
Theprimaryoutcomewastheproportionofrespondersinthe 1.0g/kgarmatWeek24.8,24 Aresponderwasdefinedasasubject
whoshowedanimprovement(decrease) 5 1pointinadjusted INCATscoreatWeek6comparedwithbaseline(firstvisitofthe dose-evaluationphase),completedthe24-weekstudy,andmaintainedtheresponseatWeek24.Anon-responderwasdefinedasa subjectwhodidnotachieveanimprovementof 51pointin adjustedINCATscorebyWeek6,orwhodeterioratedbetween Week3andWeek21,orwhodiscontinuedbeforeWeek24,irrespectiveofadjustedINCATscoreattermination.
Themainsecondaryoutcomesweretheproportionofrespondersinthe0.5g/kgand2.0g/kgarmsatWeek24relativetobaseline comparedwiththe1.0g/kgarmbasedontheadjustedINCAT score,gripstrength,I-RODSscore,andMedicalResearchCouncil (MRC)score,andtimetofirstconfirmedworseningontheadjusted INCATscoreby 51pointfromthevalueatbaseline.OthersecondaryoutcomeswerethePainIntensityNumericRatingScaleand thesumofthedistalevokedamplitudeofeightmotornerves.To assesssafetyandtolerability,treatment-emergentadverseevents (TEAEs)perinfusionandthenumberofpatientswithTEAEswere recorded.AnadverseeventwasdefinedasaTEAEiffirstonsetor worseningoccurredafterthestartofthefirstIVIgadministration inthestudy.Thefulllistofoutcomesvariableshaspreviously beenpublished.22
Statisticalanalysis
Thesamplesizecalculationwasbasedontheexpectedproportion ofrespondersbasedontheadjustedINCATscoreinthe1.0g/kg dosegroup.Atthetimethisstudywasdesigned,experienceswith thisdosingregimenwereavailablefromtheICE6 andPRIMA7 studies.InthePRIMAstudy,7 thelowerlimitofthe95%Wilson-Score confidenceinterval(CI)fortheproportionofresponders(R)was 42%,andthus42%wasselectedasthethresholdforevaluationof theprimaryendpoint:nullhypothesis(H0)R 5 0.42;alternative hypothesis(H1)R 5 0.42.Thiswastestedbycomparingthelower limitofthe95%Wilson-ScoreCIfortheobservedproportionofresponderswithapre-definedthresholdof0.42.Weestimatedthe truepercentageofrespondersinCIDPpatientstreatedwithIVIgas 60%.Incomparison,60.7%ofpatientswererespondersinthe PRIMAstudyand54.2%intheICEstudy.6,7 Weappliedthese
Figure1Trialdesign.
parameterstoacomputersimulationusingSASV R statisticalanalysissoftwareandcalculatedthataminimumof62evaluable patientsinthe1.0g/kgdosegroupwasneededtoachievea powerofatleast80%.Toaccountforpossibledropouts,itwas plannedtoenrol70patientsintothisgroup.Toallowforthe comparisonbetweendosegroups,itwasplannedtoenrolhalf thenumberofevaluablepatientsintothe0.5and2.0g/kg groups,resultinginatotalof124evaluablepatientsandanenrolmenttargetof140patients.Theprimaryevaluationofefficacyendpointswasbasedonthefullanalysissetinan intention-to-treatanalysis.
Theresponseratesinthealternativedosegroupswerecompareddescriptivelyandbyanoddsratioanalysis.Allotherend pointswereanalysedbymeansofdescriptivestatistics.Safetywas analysedinallpatientswhoreceivedanyamountofIVIginthe study.
Inaddition,anexploratorylogisticregressionanalysiswasperformedthatincludedthepretreatmentaswellasthedosegroup aspredictorvariablesforresponsebasedonadjustedINCATscore. Thesamemodelwasappliedtotreatmentresponsesbasedongrip strength,I-RODSscoresandMRCsumscore.
Dataavailability
Individualparticipantdatacollectedduringthetrialwillnotbe shared.Thestudyprotocolandmainresultsareavailableat https://clinicaltrials.gov/ct2/show/study/NCT02638207 (Accessed 24February2022).
Results
Patientdisposition
Patientswereenrolledfrom25centresworldwidebetween9 August2017and5September2019.Atotalof171patientswere screened,and150enteredthewash-outphase.Eightpatients werenoteligibleforinclusionintothedose-evaluationphase duetotheirdiseasenotbeingtreatmentdependent(n =4)or withdrawalofconsent(n =4).Atotalof142patientsexperienced deteriorationduringthewash-outphaseandwererandomized:
35(24.6%)toIVIg0.5g/kg,69(48.6%)toIVIg1.0g/kg,and38 (26.8%)toIVIg2.0g/kg.All142randomizedpatientsreceivedat leastoneinfusionofIVIgandwereincludedinthesafetyanalysisset.Theintention-to-treatpopulationconsistedof139 patientsbecausenopost-infusiondatawerecollectedinthree patients.Theper-protocolsetcomprised129patients:five patientswereexcludedduetodosingerrors,fourpatientswithdrewfromstudy,andonepatientwaslosttofollow-up.Intotal, 123patients(86.6%)completedthestudy(Fig.2).Ofthe19 patients(13.4%)whoterminatedearlyandwerethuscountedas non-responders,themostcommonreasonswerepatient’sdecision(n =7,4.9%)andTEAEs(n =6,4.2%).Thehighestincidence ofearlyterminationswasseeninthe0.5g/kggroup(20.0%),comparedwith11.6%inthe1.0g/kggroupand10.5%inthe2.0g/kg group.
Demographicandbaselinecharacteristics
Demographiccharacteristicsintheintention-to-treatpopulation (Table1)weresimilaracrossrandomizationstrataandinthe safetyanalysisset.Intotal,91.4%ofpatientshadahistoryoftypicalCIDP.Twelve(8.6%)patientshadatypicalCIDP:ninedistal acquireddemyelinatingsymmetricneuropathyandthreemultifocalacquireddemyelinatingsensoryandmotorneuropathy.One hundredandtwenty-onepatients(87.1%)hadbeentreatedpreviouslywithcorticosteroidsfortheirCIDP,and18patients(12.9%) withimmunoglobulins.Thepercentageofpatientspreviously treatedforCIDPwithimmunoglobulinsorwithcorticosteroids wasdistributedequallyacrossthethreedosegroups.Afterdeteriorationandatthestartofthedose-evaluationphase,44/121 patients(36%)previouslyoncorticosteroidsenteringthisphase werestilloncorticosteroids,andthiswasbalancedevenlyacross dosegroups(Table1).Thecorticosteroiddosewasreducedto 420mg/dayinallexcepttwoofthese44patients,oneinthe0.5g/ kggroupandoneinthe1.0g/kggroup,whowereonadoseof 25mg/dayprednisoloneequivalentduetoamiscalculationinthe conversionofmethylprednisolonetoprednisolone.Neitherof thesepatientswereexcludedfromtheanalyses.Twelveofthe18 patients(67%)previouslyonIVIgwerestillonIVIgatthestartof thedose-evaluationphase.
Figure2Trialprofile.
Table1Baselinecharacteristics
Characteristic Treatmentgroup(intention-to-treat)
0.5g/kg(n =34)1.0g/kg(n =69)2.0g/kg(n =36)
Female, n (%)
Age,years
13(38)31(45)13(36)
57(40–64)59(51–67)61(49–66)
Bodyweight,kg83(72–97)80(71–93)77(66–89)
Bodymassindex,kg/m2 27(25–31)27(24–30)25(23–29)
EFNS/PNScriteria, n (%)
DefiniteCIDP
34(100)68(99)36(100)
ProbableCIDP 01(1)0
TypeofCIDP, n (%)
Typical 33(97)62(90)32(89)
Atypical 1(3)7(10)4(11)
Priortreatment, n (%)
Corticosteroids 29(85)60(87)32(89)
Immunoglobulins5(15)9(13)4(11)
Patientsstilloncorticosteroidsatstartofdose-evaluationphase, n (%)11(38)20(33)13(41)
Prednisoloneequivalent/day(mg)
Median(range)20(2.5–25)18(2.5–25)20(2.5–20)
PatientsstillonIVIgatstartofdose-evaluationphase, n (%)2(40)6(67)4(100)
IVIg(g/kg)
Median(range)0.9(0.3–1.4)0.4(0.3–0.8)0.4(0.2–0.7)
Efficacyscoresatscreening
AdjustedINCATscore(range0–10)4(4–5)4(4–5)4(4–5) I-RODS(range0–48)27(20–32)25(21–31)29(21–32)
Maximumgripstrength(kPa;range0–160)
Dominanthand51(32–68)53(39–78)52(41–64)
Non-dominanthand52(28–70)54(38–76)54(38–67)
MRCsumscore(totalrange0–80)46(42–50)46(42–52)47(43–53)
Allvaluesarethemedian(interquartilerange)unlessotherwisestated(intention-to-treat).
Efficacy
Fortheprimaryendpoint,theresponserateinthe1.0g/kggroup was80%(55/69patients;95%CI:69–88%)(Table2).ThelowerCI limitof69%exceededthepredefinedthresholdof42%,thusthe primaryendpointwasmet.
TheadjustedINCATscoreresponseratesinthe0.5and2.0g/kg maintenancedosegroupswere65%(22/34patients;95%CI: 48–79%)and92%(33/36patients;95%CI:78–97%)atWeek24,respectively.Inpatientspreviouslyoncorticosteroids,theresponse rateacrossallthreedosegroupswas82%(99/121patients;95%CI: 74–88%)and66%,83%and94%inthe0.5,1.0and2.0g/kggroups, respectively.Inpatientspreviouslyonimmunoglobulintherapy, theresponserateacrossallthreedosegroupswas61%(11/18 patients;95%CI:39–80%)and60%,56%and75%inthe0.5,1.0and 2.0g/kggroups,respectively.
Responderratesinthe1.0g/kgdosegroupforgripstrength, I-RODSandMRCsumscorewere65%,55%and72%,respectively (Table2).Responserateswere56%,38%and59%forthe0.5g/kg cohortand83%,72%and86%forthe2.0g/kgcohort,respectively (Table2).
Usinglogisticregressionanalysis,thedosegrouphadaneffect onthetreatmentoutcomesofadjustedINCATscore(P =0.040), gripstrength(P =0.047),andI-RODS(P =0.038),butnotMRCsum score(P =0.066).Oddsratioanalysescomparingthe0.5and2.0g/ kggroupstothe1.0g/kggroupshowedoverlappingCIs(Table3). Furtheranalysesshowedthatthestatisticaldifferenceswerenot driveninastepwisefashionbydose,butduetothedifferencesbetweenthe0.5g/kgand2.0g/kgdosegroups(Table3),withanodds ratioof5.8(95%CI:1.4–23.6)foradjustedINCATscore.
Animprovementinleastsquaremeanschangefrombaseline toendofstudywasachievedinalldosegroupsforadjustedINCAT score,gripstrength,I-RODS,andMRCsumscore(datanotshown).
Ofthe29non-respondersacrossthedosegroups,22wereon corticosteroidspriortostudyenrolmentand11werestilloncorticosteroidsduringthestudy.Ofthe29non-responders,13received rescuetreatment;sixinthe0.5g/kggroupandseveninthe1.0g/kg group(SupplementaryTable1).Thethreeremainingnon-responderswereinthe2.0g/kggroupandthereforenoteligibleforrescue treatment.Threeoutofsix(50%)patientsinthe0.5g/kggroupand 4of7(57%)patientsinthe1.0g/kggrouphadanimproved adjustedINCATscorefollowingrescuetreatment(Supplementary Table1).Inthe0.5g/kggroup,oneofthesepatientsreceivedrescue treatmentdespitetheadjustedINCATscorenotreturningtobaseline.Inthe1.0g/kggroup,anotherpatientreceivedrescuetherapy inerror.Theother16non-respondersdroppedoutofthestudyfor variousreasonsandwereconsideredstudynon-responders,irrespectiveofwhethertheiradjustedINCATscorehadimprovedat thetimetheydroppedout:sixinthe0.5g/kggroup,seveninthe 1.0g/kggroup,andthreeinthe2.0g/kggroup.Atthetimeofearly termination,animprovementof 51pointinadjustedINCATscore hadbeenachievedbyallsixpatientsinthe0.5g/kggroup,fiveof thesevenpatientsinthe1.0g/kggroup,andnoneofthethree patientsinthe2.0g/kggroup.
Oneresponderineachdosegroupdidnotreceiverescuemedication(0.5g/kgand1.0g/kggroup)orwasnotdiscontinued(2.0g/ kggroup)accordingtoprotocoldespitebeingstableatWeek6and subsequentlyhadaresponseatWeek9(0.5and1.0g/kgpatients) orWeek12(2.0g/kgpatient)thatwasmaintainedatWeek24.In theperprotocolset,whichexcluded10intention-to-treatpatients
Table2Proportionofrespondersattheendofstudy
ParameterTreatmentgroup(intention-to-treat)Overall P-value
0.5g/kg(n =34)1.0g/kg(n =69)2.0g/kg(n =36)
AdjustedINCATscore65(48–79)
80(69–88)
92(78–97)0.040
Gripstrength56(40–71)65(53–75)83(68–92)0.047
I-RODS38(24–55)55(43–66)72(56–84)0.038
MRCsumscore59(42–74)72(61–82)86(71–94)0.066
Allvaluesare%ofpatients(95%Cl).Theprimaryendpoint(adjustedINCATscoreresponseinpatientstreatedwith1.0g/kgIVIg)isindicatedinitalics.Theoverall P-valueis calculatedusingatype3logisticregressionanalysisofeffectsmodellingresponsefromtreatment,randomizationstratum,CIDPvariant,andbaselinescorewithout interactions.
Table3Oddsratioanalysisoftheeffectoftreatmentgrouponresponse
ParameterOddsratio(95% CI)(intention-to-treat)
0.5g/kgversus1.0g/kg2.0g/kgversus0.5g/kg2.0g/kgversus1.0g/kg
AdjustedINCATscore0.5(0.2–1.2)5.8(1.4–23.6)2.7(0.7–10.2) Gripstrength0.6(0.3–1.4)4.2(1.4–13.3)2.5(0.9–7.0)
I-RODS0.5(0.2–1.3)3.9(1.4–10.8)2.1(0.8–5.0) MRCsumscore0.6(0.2–1.4)4.1(1.2–13.2)2.3(0.8–6.7)
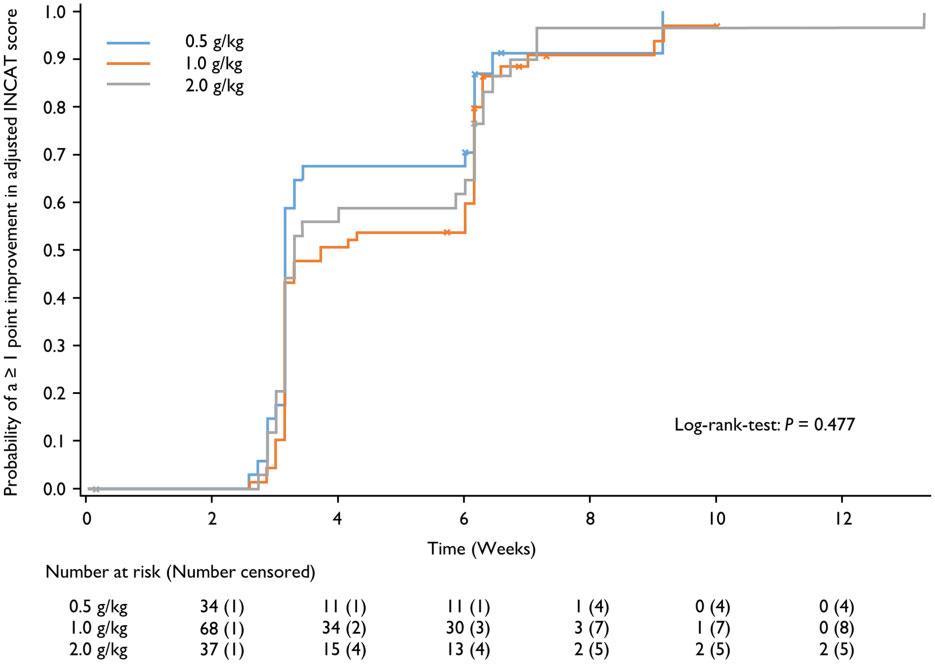
Figure3Timetoimprovementof 51pointinadjustedINCATscore. Databymaintenancedosegroupinpatientswhoachievedsuchanimprovementatanytimeduringthestudy(safetyanalysisset).
includingthosethreeresponders,theresponseratewas72%(21/ 29patients;95%CI:54–85%)inthe0.5g/kggroup,83%(54/65 patients;95%CI:72–90%)in1.0g/kggroup,and91%(32/35patients; 95%CI:78–97%)inthe2.0g/kggroup(SupplementaryTable2).
Morethanhalfofallpatients(n =78;56.1%)showedanimprovementof 51adjustedINCATscorepointaftertheinduction doseof2.0g/kg:23of34(67.6%)inthe0.5g/kggroup,35of69 (50.7%)inthe1.0g/kggroupand20of36(55.6%)inthe2.0g/kg group.ByWeek6,121of139(87.0%)patientshadanimprovement of 51adjustedINCATscorepoint:30of34(88.2%)inthe0.5g/kg group,59of69(85.5%)inthe1.0g/kggroupand32of36(88.9%)in the2.0g/kggroup.
Mediantimetoanimprovementof 51adjustedINCAT scorepointfrombaselinewas22,26and23daysinthe0.5,1.0and
2.0g/kggroups,respectively(Fig.3).Overall,91.2%ofpatientsin the0.5g/kggroup,88.4%ofpatientsinthe1.0g/kggroupand91.7% ofpatientsinthe2.0g/kggrouphadanimprovementof 51 adjustedINCATscorepointatsomepointinthestudy.Thesevaluesarehigherthanintheprimaryanalysisbecausepatientscould showanimprovementinthescoreduringthestudy,butsubsequentlydeclinedordroppedoutandwerethenconsiderednonresponders.MediantimetoresponseinI-RODSwas63,64,and 43.5daysinthe0.5,1.0,and2.0g/kggroups,respectively.
ThetimetofirstconfirmedworseninginadjustedINCATscore byatleast1pointfromthevalueatbaseline(Week0)revealed thatonlyasinglepatientinthe1.0g/kgdosegroupmetthiscriterion,andthereforethisanalysiswasnotpossible.Thiswasalsothe caseforthetimetofirstconfirmedworseninginI-RODSscoresas
Table4SummaryofrelatedTEAEsobservedin 55% ofpatients
TEAE
Treatmentgroup(safetyanalysisset)
0.5g/kg(n =35)1.0g/kg(n =69)2.0g/kg(n =38)
Patients,(% of patients)
Events,(% of infusions)
Patients,(% of patients)
Events,(% of infusions)
Patients,(% of patients)
Events,(% of infusions)
AnyrelatedTEAE16(45.7)37(16.1)32(46.4)80(16.6)20(52.6)56(20.8)
Headache1(2.9)1(0.4)10(14.5)12(2.5)9(23.7)14(5.2)
Somnolence2(5.7)3(1.3)001(2.6)1(0.4)
Allergicdermatitis4(11.4)4(1.7)5(7.2)10(2.1)4(10.5)5(1.9)
Urticaria3(8.6)4(1.7)0000
Pruritus00002(5.3)3(1.1)
Pyrexia3(8.6)4(1.7)6(8.7)6(1.2)2(5.3)3(1.1)
Chills3(8.6)4(1.7)2(2.9)2(0.4)1(2.6)1(0.4)
Bloodpressureincreased2(5.7)3(1.3)5(7.2)6(1.2)00
Bodytemperatureincreased2(5.7)2(0.9)2(2.9)5(1.0)3(7.9)3(1.1)
Bloodlactatedehydrogenaseincreased005(7.2)5(1.0)00
Nausea1(2.9)1(0.4)1(1.4)2(0.4)3(7.9)5(1.9)
thisoccurredinonlythreepatients:oneinthe0.5g/kggroupand twointhe1.0g/kggroup.
Theproportionofpatientsdeterioratingduringthedose-evaluationphaseofthestudywaslow,oneeachinthe0.5g/kgand 1.0g/kggroups,aswasthenumberofpatientswhowerestableat Week6:13(9.4%)patientsintotal,withfiveinthe0.5g/kggroup, sixinthe1.0g/kggroup,andtwointhe2.0g/kggroup (SupplementaryTable1).
MeanpainintensityaccordingtoPainIntensityNumericRating Scalescoreincreasedduringthewash-outphase,thentendedto decreasethroughWeek24.Mean ± standarddeviation(SD) changesfrombaselinewere–2.3 ± 3.0,–2.2 ± 2.9and–2.2 ± 3.3inthe 0.5,1.0and2.0g/kggroups,respectively.
Therewerenocleartrendsovertimeinthenerveconduction studies.
Safety
MediandosesofIVIgadministeredperpatientperinfusion,includingtheinductiondose,were70g(0.7g/kg)inthe0.5g/kggroup, 101g(1.1g/kg)inthe1.0g/kggroup,and155g(2.0g/kg)inthe2.0g/ kggroup.Dosingwasbasedonactualbodyweight,andtherewas nomaximumdailydose.
Inthe0.5g/kggroup,16(45.7%)patientsexperienced37related TEAEsover230infusions(Table4).Inthe1.0g/kggroup,32(46.4%) patientsexperienced80relatedTEAEsover482infusions,andin the2.0g/kggroup20(52.6%)patientsexperienced56relatedTEAEs over270infusions.Overall,themostcommonlyreportedrelated TEAEswereheadachein20patients(14.1%),allergicdermatitisin 13patients(9.2%),pyrexiain11patients(7.7%),increasedblood pressureinsevenpatients(4.9%),andincreasedbodytemperature insevenpatients(4.9%).Headachewasthemostprevalentrelated TEAEinthe1.0and2.0g/kggroups(14.5%and23.7%,respectively), whilethemostcommonrelatedTEAEinthe0.5g/kggroupwasallergicdermatitis(11.4%ofpatients).Generally,theincidenceof relatedTEAEswassimilaracrossthetreatmentgroups.Theonly TEAEwhereadoseeffectwasapparentwasheadache,withanincidenceof2.9%inthe0.5g/kggroup,14.5%inthe1.0g/kggroup, and23.7%inthe2.0g/kggroup.
Fivepatients(3.5%)experiencedTEAEsthatledtodiscontinuationofthestudydrug,oneofwhich,allergicdermatitisinapatientreceiving1.0g/kgIVIg,wasconsideredrelated.
ElevenseriousTEAEswerereportedinsixpatients(4.2%).Two ofthese(headacheandvomiting)werereportedinonepatientin
the1.0g/kggroupandconsideredrelatedtoIVIgtreatment,butdid notleadtostudydiscontinuation.
Twopatients(1.4%)hadTEAEsleadingtodeath,butneither eventwasconsideredrelatedtothestudydrug.Onepatient aspiratedleadingtorespiratoryarrest,andonedeveloped meningoencephalitis.
Duringthestudy,nohaemolysisorthromboembolicevents werereported.Laboratoryanalysesofhaematology,clinicalchemistry,urinalysisandviralmarkersdidnotindicateanysafetyconcerns.Therewerenofindingsofnoteonphysicalexaminationor inthevitalsignsdata.
Discussion
TheProCIDstudyisthelargestrandomizedstudytoshowthat IVIgiseffectiveasmaintenancetherapyinpatientswithCIDPand thefirsttoexaminesystematicallyalowerandhigherIVIgmaintenancedose.Theprimaryobjectivewastoassesstheefficacyof IVIgadministeredasa2.0g/kginductiondosefollowedbyseven maintenancedosesof1.0g/kgevery3weeks.Theresponserateon thisregimenwas80%,andthelower95%CIlimitof69%exceeded thepredefinedthresholdof42%,indicatingthattheprimaryend pointhadbeenmet.Thisthresholdwasalsoexceededinthe0.5 and2.0g/kgmaintenancegroups.Similarresponseswereseenin otheroutcomemeasures.
Publishedguidelinesrecommendthatthemaintenancedoseof IVIgmayneedtobeadjustedindividually.2 TheProCIDstudywas thefirsttoexaminesystematicallyalower(0.5g/kg)andahigher (2.0g/kg)maintenancedoseofIVIginCIDPandcompareefficacy withstandarddosingof1.0g/kg.TheadjustedINCATscore responserateswere65,80and92%inthe0.5,1.0and2.0g/kg maintenancedosegroups,respectively.Similarincremental improvementsinresponserateswereobservedforsecondaryefficacyvariables.Despitethestudynotbeingpoweredtoshowastatisticallysignificantdoseresponse,astatisticallysignificanteffect ofdoseonresponsewasobservedacrossalldosegroupsusinglogisticregressionanalysis.However,statisticallysignificantdifferencesbetweenanytwooftheindividualdosegroupswereonly seenbetweenthe0.5and2.0g/kgmaintenancegroups.Ourdata thereforesuggestthatalowermaintenancedoseof0.5g/kgissufficienttoachieveandmaintainaresponsein65%ofpatientsbut thatahigherdosemaybebeneficialtoimprovethosenotrespondingtoloworstandarddosing.
ThePATHstudyexaminedtwodifferentdosesofSCIgmaintenancetherapy,0.2and0.4g/kgeveryweek,theequivalentof0.6 and1.2g/kgIVIgevery3weeks,inpatientswithCIDP.14 Thestudy evaluateda2-folddosedifferenceandfoundnodifferencesineithersafetyorefficacybetweenthesetwodoseswithastudyperiod of24weeks.14 InthePATHextensionstudy,theoverallrelapse rateswere10%inthe0.4g/kg/weekand48%inthe0.2g/kg/week group.24 Afterdosereductionfrom0.4to0.2g/kg/week,51%(27/53) ofpatientsrelapsed,ofwhom92%(24of26)improvedafterre-initiationofthe0.4g/kg/weekdose.24 Inourstudy,a2-folddosedifference,lowversusstandard,orstandardversushighdosing,also didnotresultinasignificantdifferenceinresponserate.Onlythe 4-folddosedifferencebetweenlow(0.5g/kg)andhigh(2.0g/kg) maintenancedosingdid,withanoddsratioof5.8(95%CI:1.4–23.6) foradjustedINCATscore.Thus,wepostulatethata2-folddosedifferencemightbetoosmalltodetectsignificantdifferencesinresponserate.Therefore,alargerstudy,statisticallypoweredto comparedifferentdoseratios,e.g.2-foldversus3-foldversus 4-fold,wouldbeneededtoconfirmacleardoserelationshipandto identifypotentialpatientcharacteristicsthatmighthelptopredict therequiredmaintenancedoseforanindividualpatient.
TheadjustedINCATscoreoverallresponserateof80%witha 1.0g/kgmaintenancedoseinourstudywashigherthanreported inotherIVIgstudies:ICE54%,PRIMA61%andPRISM76%.6–8 Itisof interesttocomparegroupsofpatientsinthedifferentstudiesthat havebeentreatedpreviouslywithcorticosteroidsorIVIg.Selection ofpatientswhohadpreviouslyrespondedtoIVIgmayimpactthe IVIgresponserateinatrial.14 OurstudyisthefirstIVIgstudytoincludeahighpercentageofpatientswhowerepreviouslytreated withcorticosteroidsandnotwithIVIg.Thehigherproportionof patientshavingbeentreatedwithcorticosteroidsmightbedueto loweravailabilityofIVIginsomeofthecountries.ThePATHstudy preselectedpatientsbasedonIVIgresponse.14 Corticosteroidsare afirst-linetreatmentoptionforCIDP.2 Corticosteroidsarewidely availableandinexpensive,butlong-termusehaspotentiallyserioussideeffects.5,25,26 UnliketheProCIDstudy,patientspreviously oncorticosteroids(410mg/dayprednisoloneorequivalent)were excludedfromtheICEstudy,6 patientspreviouslyon‘high-dose’ corticosteroidswereexcludedfromthePRISMstudy8 and,althoughcorticosteroidusewasnotspecificallyexcluded,noinformationonpriorcorticosteroidusewasprovidedinthePRIMA study.7 Furthermore,thepercentageofpatientsclassifiedasIVIgnaı¨ve,butpotentiallyonpriorcorticosteroids,was23%,6 54%7 and 55%8 intheICE,PRIMAandPRISMstudies,respectively,compared with87%whowereIVIg-naı¨veandonpriorcorticosteroidsinour study.Thesedifferencesinpriortreatment,alongwithotherdifferencesinpatientandstudycharacteristics,mighthaveinfluencedresponseratesacrossstudiesandmakecomparisons betweenthestudiesdifficult.Nevertheless,sincetheProCIDstudy clearlydifferentiatedbetweenpatientspreviouslysuccessfully treatedwithIVIgandthosepreviouslytreatedwithcorticosteroids, withmostsubjectsbeinginthelatterstratum,thestudyprovided auniqueopportunitytoassesstheeffectsofswitchingfromcorticosteroidstoIVIg.Thehighresponseratesinthecorticosteroids stratum,66%,83%and94%inthe0.5g/kg,1.0g/kgand2.0g/kg arms,respectively,clearlyshowthatsubjectspreviouslyoncorticosteroidscansuccessfullyandsafelybetransitionedtoIVIg.
Theincidenceoftreatment-relatedTEAEs,exceptforheadache, wassimilaracrossthedosegroups.Treatmentwaswelltolerated eveninIgG-naı¨vepatientsandinthoseregularlytreatedwithhigh doseIVIg.ThesedatashowthatpatientscanswitchfromcorticosteroidstoIVIgwithconfidencetopotentiallyavoidtheside effectsassociatedwithcorticosteroiduse.
Inthisstudy,56%ofallpatientsand62%ofrespondersshowed animprovementof 51adjustedINCATscorepointafterthe
inductiondosealone,i.e.byWeek3.Incomparison,thepercentageofresponderswhohadanimprovedadjustedINCATscore aftertheinductiondosewas44%intheICEstudy,27 50%inthe PRIMAstudy7 and22%inthePRISMstudy.8 Thishasimportant implicationsforclinicalpractice.OurstudyandtheICEtrial27 showthatnearlyallpatientswhowillrespondtoIVIgdosowithin 6–8weeks,thatis,asingleinductiondoseandtwomaintenance doses.Giventheissuesabovewithactualpatientinclusion,the translationofthistothetreatment-naı¨vepatientislessclear. WhentodecidethatapatientisnotrespondingtoIVIgremainsa clinicaldecision,butthesedatasuggestthattreatinglongerthan 3monthswhilewaitingforasignificantresponseisnotuseful.2
Alimitationofthestudyasdetailedabove,incommonwith otherstudiesevaluatingIVIginpatientswithCIDP,isthatitevaluatesrescuetreatmentmainlyofpreviouslysuccessfullytreated CIDPpatientswhoseconditionhasbeenallowedtodeteriorate priortotreatment,andnotnewlydiagnosedanduntreatedCIDP patients.Giventhatthestudyperiodwas24weeks,thelongertermefficacy,safetyandrelapseratewiththedifferentmaintenancedoseswerenotassessedinthisstudy.However,thestudy demonstratedalowrateofdeterioration(1.4%)afterWeek6across alldosegroups.Otherlimitationsofthestudywerethatitwasnot placebocontrolledandwasnotstatisticallypoweredtodetecta doseresponsebetweenthethreedosingregimens.
Insummary,theProCIDstudydemonstratedthat1.0g/kgIVIg isefficaciousandwelltoleratedasmaintenancetreatmentfollowinga2.0g/kginductiondoseinpatientswithactiveCIDP,evenin thosepatientshavingbeensuccessfullytreatedwithcorticosteroidspreviously.Alowerorhighermaintenancedosemaybe beneficialinsomepatients,althoughfurtherstudiesareneededto confirmthisfinding.
Acknowledgements
ThisstudywassponsoredbyOctapharmaPharmazeutika Produktionsges.m.b.H.(Vienna,Austria)whothankinvestigators, trialpersonnelandpatientsfortheirparticipation.Medicalwriting assistancewasprovidedbynspmltd,Meggen,Switzerland,and fundedbyOctapharma.
Funding
ThisstudywasfundedbyOctapharmaPharmazeutika Produktionsges.m.b.H.(Vienna,Austria).
Competinginterests
D.R.C.reportsconsultingforAmgen,AnnexonBiosciences,argenx SE,BiotestPharmaceuticals,CignaHealthManagement,CSL Behring,Grifols,Johnson&Johnson,MomentaPharma,New EnterpriseAssociates,Octapharma,Pfizer,Pharnext,Polyneuron Pharmaceuticals,SeattleGenetics,andUCB.D.R.C.isontheData SafetyMonitoringBoardforthefollowing:Alnylam Pharmaceuticals,Anavex,PledPharma,HansaMedical,and MitsubishiTanabePharmaCorporation.D.R.C.wasinvolvedwith technologylicensingforAstraZenecaPharmaceuticals,LP Pharmaceuticals(Xiamen),Genentech,Levicept,SeattleGenetics, MerrimackPharmaceuticals,andDisarmTherapeutics,outsidethe submittedwork.P.A.v.D.reportsgrantsfromSanquinBlood SupplyandPrinsesBeatrixSpierfonds,duringtheconductofthe study;andgrantsfromGrifols,Takeda,Annexion,Argenx, CommonwealthSerumLaboratories,Octapharma,andHansa,outsidethesubmittedwork.H.P.H.reportsconsultingCSLBehring, SanofiGenzyme,andUCB.H.P.H.receivedpaymentsorhonoraria fromCSLBehringandOctapharma.H.D.K.isonSteering
CommitteesforOctapharmaandSanofiGenzyme.I.S.J.M.reports grantsfromTalecrisTalentsprogram,GBS/CIDPFoundation InternationalandFP7EUprogram,outsidethesubmittedwork; Furthermore,aresearchfoundationattheUniversityofMaastricht receivedhonorariaonbehalfofhimforparticipationinsteering committeesoftheTalecrisImmuneGlobulinIntravenousFor ChronicInflammatoryDemyelinatingPolyneuropathyStudy, CommonwealthSerumLaboratories,Behring,Octapharma,LFB, Novartis,UnionChimiqueBelge,outsidethesubmittedwork. H.D.K.reportstravelsupportandconsultingfeesfrom Octapharmainrelationtoastudydesignadvisoryboard.H.D.K. reportsconsultingforUCB,Terumo,Akcea,Alnylam,andCSL Behring.H.D.K.isonDataSafetyMonitoringBoardsorAdvisory BoardsforUCBandOctapharma.H.D.K.receivedagrantfrom Takedaforinvestigator-initiatedresearch.D.H.andE.C.are employeesofOctapharmaPPG,Vienna,Austria.
Supplementarymaterial
Supplementarymaterial isavailableat Brain online.
AppendixI
ProCIDstudyinvestigators
Fulldetailsareprovidedinthe Supplementarymaterial
S.Kastrev,V.Rizova,R.Massie,R.Talab,M.Bednar,P.Ridzon,J. Schmidt,J.Zschu¨ntzsch,C.Ro´zsa,L.Vecsei,K.Rejdak,M. Koszewicz,S.Budrewicz,A.Dulamea,M.Marian,A.Kadar,L. Zecheru-Lapusneanu,V.Mikhailov,D.Zakharov,N.Suponeva,M. Piradov,N.Smolko,DSmolko.
References
1. vandenBerghPYK,HaddenRDM,BoucheP,etal.;Peripheral NerveSociety.EuropeanFederationofNeurologicalSocieties/ PeripheralNerveSocietyguidelineonmanagementofchronic inflammatorydemyelinatingpolyradiculoneuropathy:Report ofajointtaskforceoftheEuropeanFederationofNeurological SocietiesandthePeripheralNerveSociety-firstrevision. EurJ Neurol.2010;17(3):356–363.
2. vandenBerghPYK,vanDoornPA,HaddenRDM,etal.European AcademyofNeurology/PeripheralNerveSocietyGuidelineon diagnosisandtreatmentofchronicinflammatorydemyelinatingpolyradiculoneuropathy:ReportofajointTaskForce-secondrevision. JPeripherNervSyst.2021;26(3):242–268.
3. AllenJA,LewisRA.CIDPdiagnosticpitfallsandperceptionof treatmentbenefit. Neurology.2015;85(6):498–504.
4. NeliganA,ReillyMM,LunnMP.CIDP:Mimicsandchameleons. PractNeurol.2014;14(6):399–408.
5. OaklanderAL,LunnMP,HughesRA,vanSchaikIN,FrostC, ChalkCH.Treatmentsforchronicinflammatorydemyelinating polyradiculoneuropathy(CIDP):Anoverviewofsystematic reviews. CochraneDatabaseSystRev.2017;1:CD010369.
6. HughesRAC,DonofrioP,BrilV,etal.;ICEStudyGroup. Intravenousimmuneglobulin(10%caprylate-chromatography purified)forthetreatmentofchronicinflammatorydemyelinatingpolyradiculoneuropathy(ICEstudy):Arandomisedplacebo-controlledtrial. LancetNeurol.2008;7(2):136–144.
7. LegerJ-M,BleeckerJL,deSommerC,etal.;PRIMAstudyinvestigators.EfficacyandsafetyofPrivigenV R inpatientswithchronic inflammatorydemyelinatingpolyneuropathy:Resultsofaprospective,single-arm,open-labelPhaseIIIstudy(thePRIMA study). JPeripherNervSyst.2013;18(2):130–140.
8. Nobile-OrazioE,PujolS,KasiborskiF,etal.Aninternational multicenterefficacyandsafetystudyofIqYmuneininitialand maintenancetreatmentofpatientswithchronicinflammatory demyelinatingpolyradiculoneuropathy:PRISMstudy. JPeripher NervSyst.2020;25(4):356–365.
9. RajaballyYA,SeowH,WilsonP.Doseofintravenousimmunoglobulinsinchronicinflammatorydemyelinatingpolyneuropathy. JPeripherNervSyst.2006;11(4):325–329.
10.RajaballyYA,AfzalS.Clinicalandeconomiccomparisonofan individualisedimmunoglobulinprotocolvs.standarddosing forchronicinflammatorydemyelinatingpolyneuropathy. J Neurol.2019;266(2):461–467.
11.KuitwaardK,FokkinkW-JR,BrusseE,etal.MaintenanceIVimmunoglobulintreatmentinchronicinflammatorydemyelinatingpolyradiculoneuropathy. JPeripherNervSyst.2017;22(4): 425–432.
12.LunnMP,EllisL,HaddenRD,RajaballyYA,WinerJB,ReillyMM. Aproposeddosingalgorithmfortheindividualizeddosingof humanimmunoglobulininchronicinflammatoryneuropathies. JPeripherNervSyst.2016;21(1):33–37.
13.KuboriT,MezakiT,KajiR,etal.Theclinicalusefulnessofhighdoseintravenousimmunoglobulintherapyforchronicinflammatorydemyelinatingpolyneuropathyandmultifocalmotor neuropathy. NotoShinkei.1999;51(2):127–135.
14.vanSchaikIN,BrilV,vanGelovenN,etal.;PATHstudygroup. Subcutaneousimmunoglobulinformaintenancetreatmentin chronicinflammatorydemyelinatingpolyneuropathy(PATH): Arandomised,double-blind,placebo-controlled,phase3trial. LancetNeurol.2018;17(1):35–46.
15.MersichC,AhrerK,BuchacherA,etal.Biochemicalcharacterizationandstabilityofimmuneglobulinintravenous10%liquid (PanzygaV R ). Biologicals.2017;45:33–38.
16.RadomskiKU,LattnerG,SchmidtT,Ro¨mischJ.Pathogensafety ofanewintravenousimmuneglobulin10%liquid. BioDrugs 2017;31(2):125–134.
17.BorteM,MelamedIR,PulkaG,etal.Efficacyandsafetyof humanintravenousimmunoglobulin10%(PanzygaV R )in patientswithprimaryimmunodeficiencydiseases:Atwostage,multicenter,prospective,open-labelstudy. JClin Immunol.2017;37(6):603–612.
18.ArbachO,TaumbergerAB,WietekS,CervinekL,SalamaA. Efficacyandsafetyofanewintravenousimmunoglobulin (PanzygaV R )inchronicimmunethrombocytopenia. Transfus Med.2019;29(1):48–54.
17.panzygaV R USPI.2021.https://www.fda.gov/media/115397/down load.Accessed16July2021.
20.panzygaV R CanadianProductMonograph.2017.https://pdf.hres. ca/dpd_pm/00041520.PDF.Accessed16July2021.
21.panzygaV R SmPC.2019.https://www.medicines.org.uk/emc/prod uct/7317/smpc#gref.Accessed16July2021.
22.CornblathDR,HartungH-P,KatzbergHD,MerkiesISJ,van DoornPA.Arandomised,multi-centrephaseIIIstudyof3differentdosesofintravenousimmunoglobulin10%inpatients withchronicinflammatorydemyelinatingpolyradiculoneuropathy(ProCIDtrial):Studydesignandprotocol. JPeripherNerv Syst.2018;23(2):108–114.
23.DraakTHP,VanhoutteEK,vanNesSI,etal.;PeriNomSStudy Group.Changingoutcomeininflammatoryneuropathies: Rasch-comparativeresponsiveness. Neurology.2014;83(23): 2124–2132.
24.vanSchaikIN,MielkeO,BrilV,etal.;PATHstudygroup.Longtermsafetyandefficacyofsubcutaneousimmunoglobulin IgPro20inCIDP:PATHextensionstudy. NeurolNeuroimmunol Neuroinflamm.2019;6(5):e590.
25.BunschotenC,JacobsBC,vandenBerghPYK,CornblathDR,van DoornPA.Progressindiagnosisandtreatmentofchronic inflammatorydemyelinatingpolyradiculoneuropathy. Lancet Neurol.2019;18(8):784–794.
26.HughesRA,MehndirattaMM,RajaballyYA.Corticosteroidsfor chronicinflammatorydemyelinatingpolyradiculoneuropathy. CochraneDatabaseSystRev.2017;11:CD002062.
27.LatovN,DengC,DalakasMC,etal.;IGIV-CCIDPEfficacy(ICE) StudyGroup.Timingandcourseofclinicalresponseto intravenousimmunoglobulininchronicinflammatorydemyelinatingpolyradiculoneuropathy. ArchNeurol.2010;67(7): 802–807.