MEASLES UPDATE: CLINICAL
MANAGEMENT AND FACILITY PREPAREDNESS
Regina Chinsio-Kwong, DO
Anissa Davis, MD, MPH
Christopher Zimmerman, MD, MPH Orange County Health Care Agency
February 20, 2026
Regina Chinsio-Kwong, DO
Anissa Davis, MD, MPH
Christopher Zimmerman, MD, MPH Orange County Health Care Agency
February 20, 2026
Clinical presentation and Infection Control
Epidemiology and Surveillance
The speakers for this Continuing Medical Education (CME) activity have no relevant financial relationships or disclosures with any commercial interests related to the content of this presentation.
• RNA Virus
• Only infects humans
• It is a paramyxovirus and so distantly related to Mumps and parainfluenza virus
• Measles Virus (MeV) is most closely related to rinderpest virus (RPV) which has been eradicated
• A recent study suggested that MeV and RPV diverged about that time that humans first started living in large cities roughly 3,000 years ago
• In the US measles became nationally notifiable disease in 1912
• In the first 10 years of reporting 6,000 deaths were reported per year
• In the decade before vaccine became available 1953-1963
• Nearly all children were infected by 15 years of age
• Each year:
• 3-4 million cases
• 400-500 measles deaths
• 48,000 measles hospitalizations
• 1,000 cases of encephalitis
• Prodromal illness of
• Malise
• Cough
• Coryza
• Conjunctivitis
• Sometimes Koplik spots
• Fever
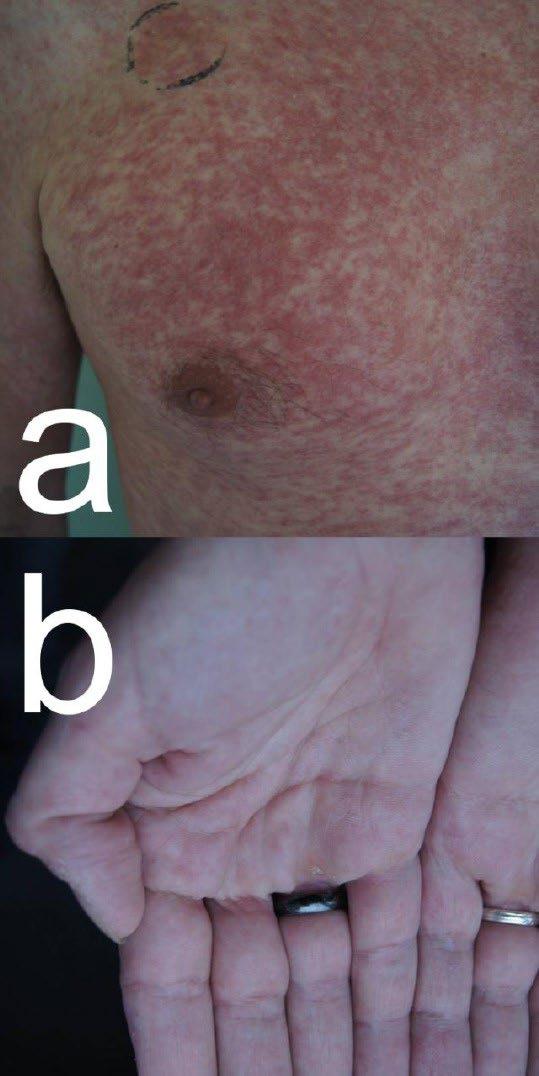
• Rash
• Maculopapular rash
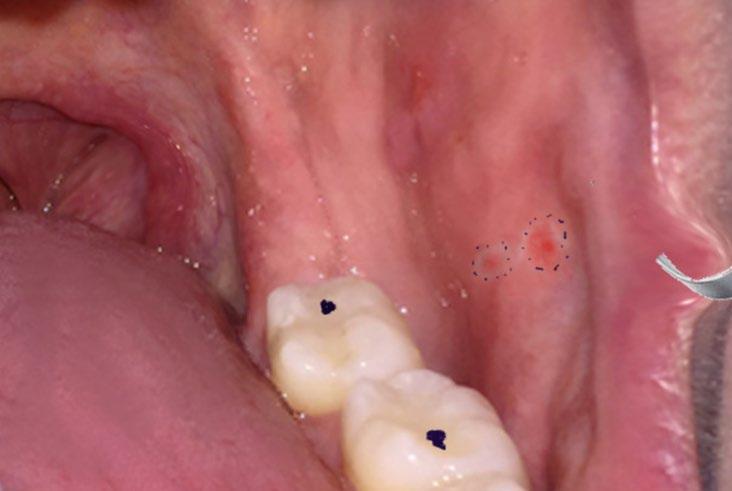
• Starting on the face spreading down the body and out to extremities

• Incubation period
• Typically, 14 days after exposure but can range from 7-21 days
• Infectious Period
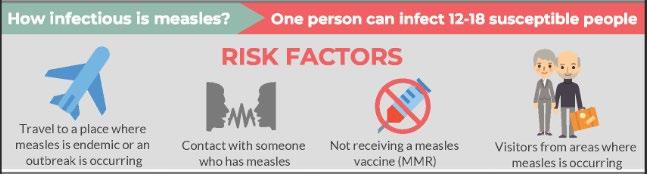
• Measles is the most contagious disease known
• Airborne transmission
• People with measles are infectious from 4 days before through 4 days after rash onset
• Fever and rash is a common presentation of many viral illness in children and adults
• Enteroviruses Measles
• Varicella Measles Vaccine
• HIV Human Herpes Virus 6 and 7
• Parvovirus B 19 Rubella
• Fever and rash can also be can also have bacterial causes
• Scalet fever Impetigo
• Pseudomonas folliculitis Neisseria (meningococcemia, gonococcemia)
• Non- infectious
• Allergic reactions/ drug reactions Erythema multiforme
• Public Health is looking for clinical suspicion of measles
• Measles is not a clinical diagnosis
• We want lab confirmation or rule out
• Degree of contagiousness
• Consequences of missing cases
• Viral testing allows us to do molecular epidemiology link cases to others to identify gaps in surveillance


714-834-8180 (24/7)
• What is the local epidemiology
• Make sure you are signed up for CD Health Alerts
• Known exposure to measles
• Travel International? Domestic?
• Visiting large venues (concerts, amusement parks)
• Measles Immunity status

• It happens!
• 23% of measles cases reported to CDC since January 2025 have been in those 20+ years of age
• The same considerations should be made as when evaluating children
• Local epidemiology, exposures, travel, immunization status
• Providers include measles in the differential diagnosis when evaluating patients https://pmc.ncbi.nlm.nih.gov/articles/PMC6910791/
• Legal responsibility
• Suspected measles is immediately reportable per Title 17 Section 2500
• We can
• Help expedite testing
• Discuss specimen collection requirements
• Approve testing at the OC Public Health Laboratory
• Arrange specimen transport
• Provide Infection control recommendations
• Isolation measures
• Exposed Contacts
• Provide Postexposure prophylaxis recommendations
• MMR
• Immunoglobulin
• Viral Testing (PCR for Measles Virus)
• OC Public Health Lab (PHL) can turn around a result quickly usually within 24 hours of receipt
• Use synthetic swab (no cotton or wood)
• Place in viral transport media (VTM) or Universal transport media (UTM)
• Sources (two sources preferred)
• Oral pharyngeal (easiest and most preferred by the lab)
• Nasopharyngeal
• Urine (not required except in cases that rash was >4 days ago)
• You MUST call CDCD for a specimen to be accepted
• Measles IgM testing used to be the go-to test, but no longer
• Sensitivity and specificity of PCR is much better
• Can be helpful for late diagnosis
• IgG testing can confirm immunity in someone without vaccination records
• Commercial labs or OC PHL can do serological testing both IgG and IgM testing through CDCD
• Early compilations
• Dehydration
• Viral pneumonia
• Secondary bacterial pneumonias
• Encephalitis 1/1,000
• Death from respiratory or CNS complications
1-3/1,000
• Hearing loss
• Encephalitis
• Immune amnesia
• Loss of existing repertoire of memory B-cells and T-cells
• May last for 2-3 years
• Subacute sclerosing panencephalitis (SSPE)
• Occurrence 7-11/100,000
• Uniformly fatal progressive neurodegenerative process
• Risk is highest for those infected in infancy
• Documentation of 2 doses of MMR vaccine
• Birth prior to 1957
• Documentation of a positive measles IgG titer
• Infants < 1 year of age
• Immunocompromised without prior immunity
• Pregnant people
• Severely immunocompromised
• Primary immunodeficiencies
• Chemo
• HIV with CD4 counts < 200
• Immunosuppressive therapy
• Persons with documented immunity do not need PEP
• MMR
• Anyone without prior immunity without a contraindication should receive MMR vaccine within 72 hours of exposure
• Includes children 6-11 months of age
• Immunoglobulin (IG) PEP
• For those with contraindication to MMR vaccine
• Infants < 6 months, severely immunocompromised, non-immune pregnant people
• May be administered up through 6 days after initial exposure
• After 6 days IG PEP is not indicated as it is too late to interrupt illness
• Those who receive IG PEP must quarantine for 28 days from last exposure
• There is no specific treatment for Measles
• Vitamin A is recommended for children and adults diagnosed with measles
"Vitamin A does not prevent measles and is not a substitute for vaccination.
Consistent with guidance from the American Academy of Pediatrics, vitamin A may be administered to infants and children in the United States with measles under the supervision of a healthcare provider as part of supportive management.
Children with severe measles, such as those who are hospitalized, should be managed with vitamin A.
Overuse of Vitamin A can lead to toxicity and cause damage to the liver, bones, central nervous system, and skin. Pregnant women should avoid taking high levels of vitamin A as it has been linked to severe birth defects."
HTTPS://WWW.CDC.GOV/MEASLES/HCP/CLINICALOVERVIEW/INDEX.HTML ACCESSED FEBRUARY 20, 2026 OC HEALTH CARE AGENCY | 21
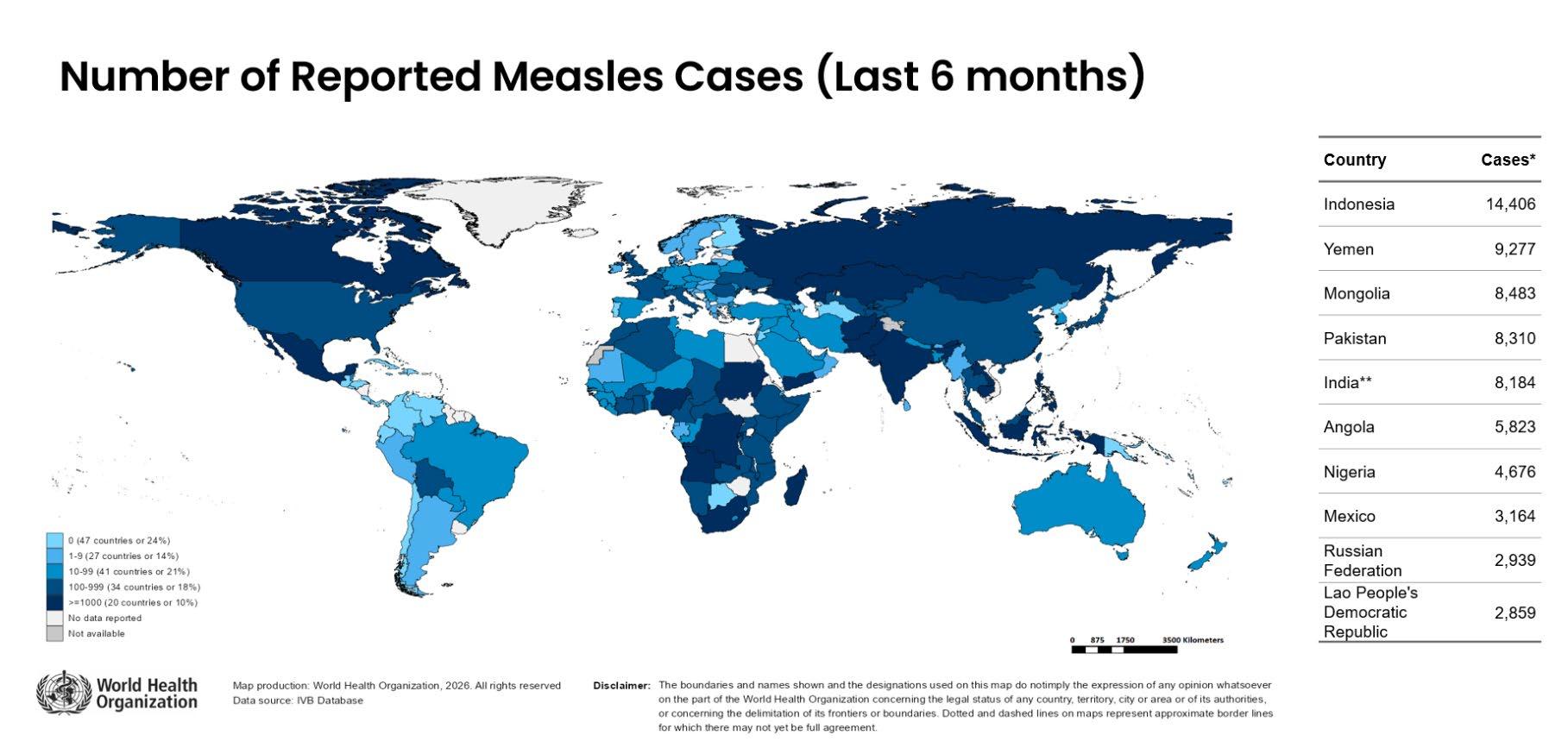
• 6 European Countries Recently Lost
Elimination Status:
• Armenia
• Austria
• Azerbaijan
• Spain
• United Kingdom
• Uzbekistan
• Other Countries with Endemic Measles
• France • Germany • Canada
India
Cambodia
Philippines
Vietnam
Italy • China?
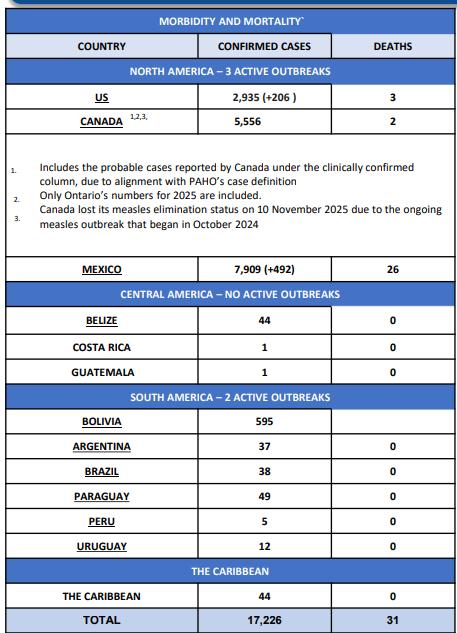
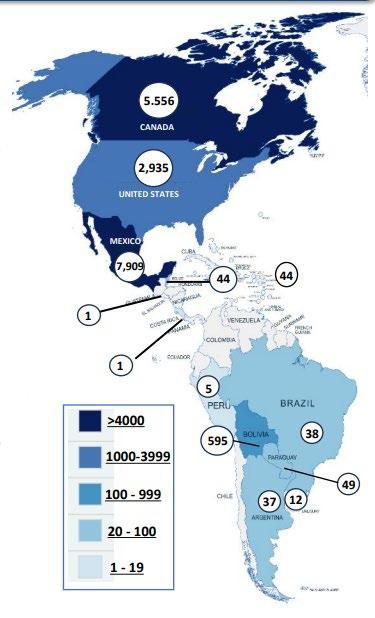
2025/26
• 17,226 cases
• 31 deaths
• 12 countries and the Caribbean
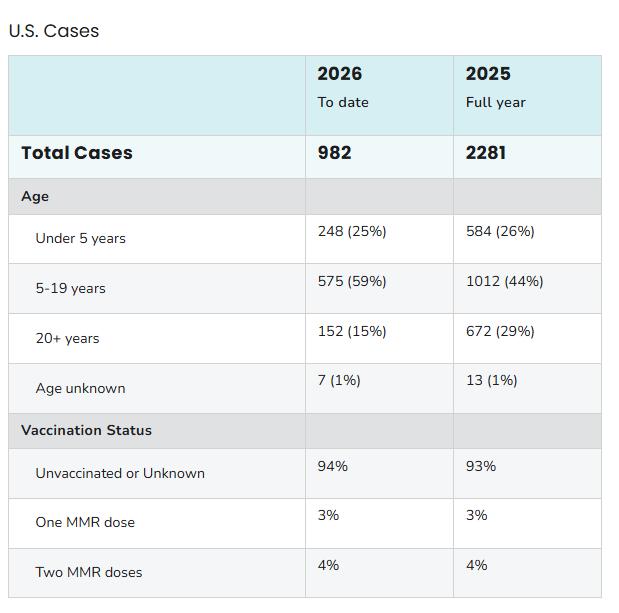
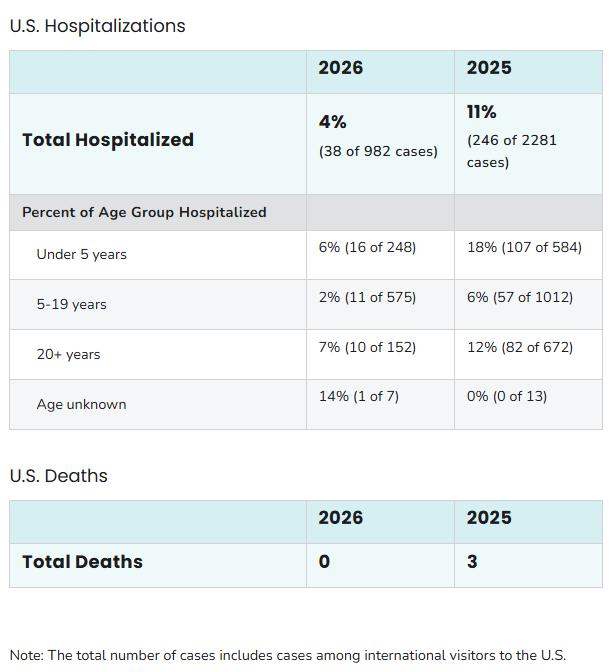
While majority of those hospitalized occurred in those < 5, they also occurred in adults
FROM HTTPS://WWW.CDC.GOV/MEASLES/DATARESEARCH/INDEX.HTML (LAST UPDATED FEBRUARY 20 , 2026) OC HEALTH CARE AGENCY | 27
• South Carolina
• Arizona
• Utah
• Florida
Many states have very few cases
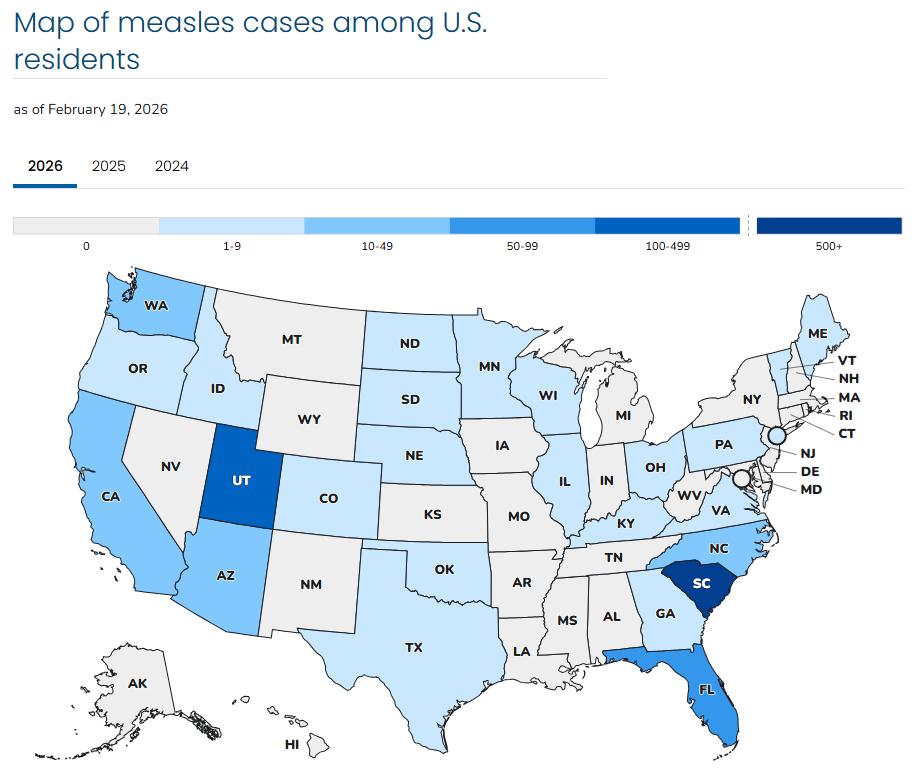
MEASLES CASES AND OUTBREAKS | MEASLES
Southwest Utah 2025-2026
Multiple churches/congregations
Hildale, Utah and Colorado City
Arizona 2025-2026
Fundamentalist LDS (FLDS)
Vaccine rates among Kindergarten children: 7-17%
El Paso, Texas
Adult population- (2/3 cases)
School age (7%)
clustered in schools/clinics
Gaines County, Texas 2025
Old Colony Mennonite, Plautdietsch (low German speaking) community


Spartanburg County, SC 2026
Eastern European/Slavic Immigrant Communities- Eastern European immigrant and Slavicspeaking households
OC
Florida College
• Factors contributing to lower vaccination rates with certain groups
• religious beliefs that prioritize spiritual approaches to health
• concerns about vaccine safety
• historical experiences
• mistrust of government
• strong emphasis on personal and religious freedoms
January 21, 2026
• Child returning from South Carolina
January 28, 30, 31, 2026
• Young Adult - recently returned from international travel
• Toddler (no travel)
• LA case - traveled to Disneyland on January 28 (infectious period)
February 7, 2026
• Visitors from another county who visited Disney January 22
February 9, 2026
• Unvaccinated child without history of international or out of state travel
February 13, 2026
• Outbreak- 1 adult and 1 child
January 30 and 31, 2026
• Resident who recently travelled internationally
• International traveler February 2, 2026
• Resident who traveled internationally February 19, 2026
• Resident returning from international travel
January 31, 2026
• Minor- who returned from travel to San Francisco and Southern California February 10, 19, 2026- Outbreak- 8 cases
February 6, 2026
• Unvaccinated minor visiting from another state
San Mateo
January
• Unvaccinated Adult returned from international travel
• 1/28 Adult who recently traveled internationally
• Sites case visited during infectious period:
• gym
• Urgent care
• Hospital
• 159 total contacts
• 1/30 Toddler without travel
• History of visitation to local public venue with many other international visitors during incubation period
• Patient isolated and fully vaccinated provider took sample at car
• No known exposures during infectious period
• 1/31 Los Angeles County Case
• International traveler who visited Disneyland while infectious 1/28/26
• 65 known exposures (restaurant staff)
• 2/6 Confirmed Case Visitor to OC
• Sites visited while infectious:
• Disneyland
• Dance studio
• Medical clinic
• 84 total contacts

Protocol to:
• Identify suspect measles cases ASAP
• Place them in an airborne infection isolation room (AIIR), if available or a private room with door closed ASAP
• Evaluate suspects outside if no AIIR
• Call Public Health immediately for any suspect case (714) 834-8180
• Call ahead if you refer patient out
• Train triage staff to rapidly recognize measles symptoms
• Determine which rooms most suitable (distance & high-risk people)
• Ensure all staff have documentation of immunity to measles
• Ensure you have PPE and providers are fit tested
• Identify measles strike team
• Logistics of testing and PEP administration
HTTPS://WWW.CDPH.CA.GOV/PROGRAMS/CID/DCDC/ CDPH%20DOCUMENT%20LIBRARY/IMMUNIZATION/M EASLES - HCFACILITYICRECS.PDF
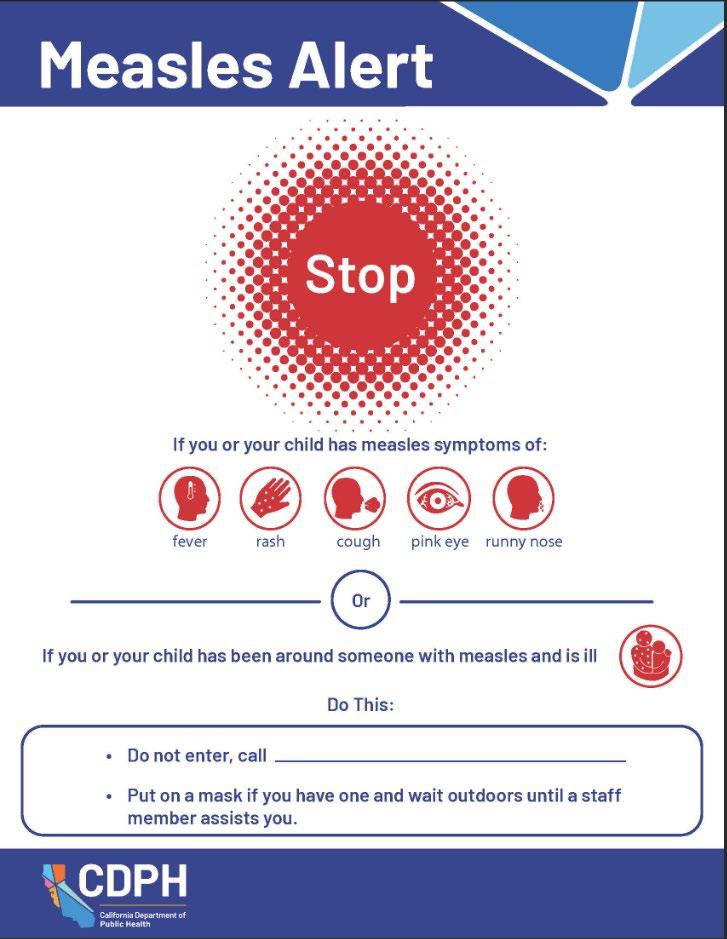
• Isolate and mask patient
• Ask about symptoms & epi risk factors:
• Epi risk factors in past 21 days
• Vaccination status of patient
• Symptoms: fever, rash (when and where), 3 C’s
• All healthcare workers entering the patient room regardless of immune status should use respiratory protection (N95)
• Limit staff & visitors entering isolation room
• Staff not known to be immune should not enter room
• Contact your infection control staff
• Keep exam room vacant for one hour before cleaning
• Standard cleaning procedures
• Patient instructions:
• stay home until measles is ruled out or until 4 days after rash onset
• public health will be calling
• Call ahead or inform healthcare providers if they need to seek additional medical care
In the past 21 days:
• Known contact with measles case or an ill person with fever and rash
• Contact with an international visitor who arrived in US in the past 21 days
• Travel outside the US
• Domestic travel through an airport
• Visited a US venue popular with international visitors, such as theme parks, tourist attractions
• Lives in or visited a US community where there are measles cases
•AIIR vs. room w door closed
•Closed room mitigates but may not eliminate risk of exposures due to shared air space
•Exposed persons are those who shared air space with patient, even if patient was masked
•Healthcare staff who wore appropriate PPE are still considered exposed
•There’s no guidance on length of time in shared airspace considered an exposure
•We will want proof of immunity in health workers

• 72 hour to 6-day window to provide prophylaxis (MMR or IG)
• Need to document when and where patient was in facility
• Line list of exposed staff and their immunity documentation
Those with no documented immunity by day 5 after exposure they will be excluded from work for up to 21 days
• Employer's responsibility
• Line list of exposed patients and visitors
• Particularly concerned for infants, pregnant people, severely immunocompromised
• We may need assistance reaching patients
• Plan for logistics of serologic testing, IVIG and IMIG and MMR

• Identify
• Exposed Visitors/Clients/Patients and High- Risk Individuals
• Anyone in a shared airspace of the suspected case from an hour before until an hour after the person was put in isolation, consider waiting rooms, restrooms, hallways, offices where the person may have visited
• Are there expose who are high risk for severe disease (<12 months of age, severely immunocompromised, Non-immune pregnant women)
• Exposed staff
• Including healthcare, administrative, security, facilities, environmental staff, or any EMS workers present
• If you have Employee Health (EH), OC Public Health would expect EH to assess immunity of exposed staff
• Create a line list (be ready to share with Public Health)
• Include
• Name
• DOB
• Contact information, language
• measles immunity status if known

• What is the story
• Public Health will ask: How old, when did rash start, where on the body did the rash start, did they have a known exposure, travel
• Specimen coordination
• Public Health can discuss how to collect specimens, we can arrange specimen transport, testing and results
• PLEASE DO NOT SEND PATIENTS TO PUBLIC HEALTH FOR TESTING
• Please call us (714) 834-8180 while patient is at your office
• Contacts
• Ask for line list of exposed
• Provide recommendations on exposed individuals
• Who needs Post-exposure prophylaxis (PEP), what type of PEP
• Who needs to quarantine
• Monitoring
• Non-immune exposed individuals will be monitored, by phone, for the length of quarantine
• Document staff immune status NOW
• This will help avoid work exclusions
• Give people time to find their documentation or to get titers drawn
• Prepare for potential increased staffing needs to respond
• A single case linked to your facility can require significant effort and coordination with local officials for rapid notification and to ensure safety and health of staff and visitors.
• Adjust clinical workflows and patient triage to minimize potential measles exposures
• Consider prescreening protocols
• For patients with cough, conjunctivitis, fever or rash, recent visit to areas with outbreaks
• Measles vaccination status
• Consider:
• Waiting outside
• Isolation protocols
• PPE protection REVIEW CDPH QUICKSHEET AT HTTPS://WWW.CDPH.CA.GOV/PROGRAMS/CID/DCDC/CDPH%20DOCUMENT%20LIBR
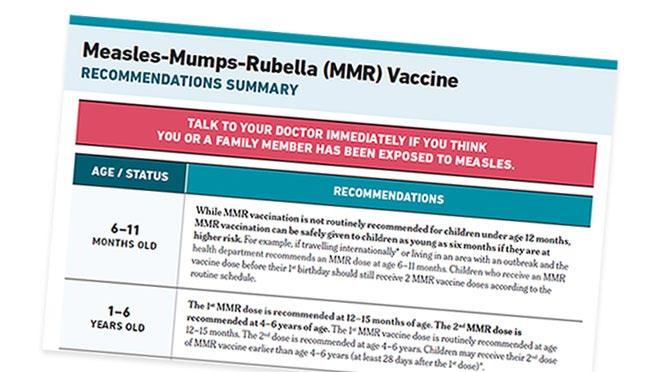
MMR vaccines are our best defense against the disease and its complications.
Two doses of MMR (measles, mumps, rubella) vaccine for optimal protection
• Children: one dose at 12 months of age and another at 4–6 years
• Older children, adolescents and non-pregnant adults without documented doses of MMR vaccine:
• Two doses of MMR separated by at least 28 days
• Talk to your health care provider or visit MyTurn.ca.gov to make a vaccine appointment.
• Unsure if you’re vaccinated against measles?
• Check your CA Digital Vaccine Record (DVR) or ask your healthcare provider.
• If no records exist, get vaccinated.

Whether you’re visiting family or exploring the world (or settings with potential of interaction with many travelers), ensure you are up to date with the MMR vaccine.
• Aim for getting vaccinated two weeks before departure or arrival of visitors. Before international travel or travel to regions with ongoing outbreaks consider following immunization for international travel:
• Babies 6–11 months of age should receive one dose of MMR vaccine *this is an additional dose and is not considered part of the 2-dose MMR vaccination for routine vaccines.
• Ensure everyone 12 months and older are up to date with two doses of MMR vaccine.
• If they’re not up to date, they should get two doses at least 28 days apart.




Utilize resources from our website and Subscribe to our advisory list and monthly newsletter!
Orange County Health Care Agency Website
• www.ochealthinfo.com/
• https://www.ochealthinfo.com/services-programs/disease-prevention/diseasesconditions/measles
Health Corner Webpage
• www.ochealthinfo.com/healthcorner
• Communicable Disease Surveillance
https://ochealthinfo.com/cdcd/data
• Respiratory Virus Surveillance
https://www.ochealthinfo.com/respiratoryvirus
Provider Advisory List
Clinicians, receive immediate notification of communicable disease related alerts.
Sign up at this link: Provider Advisory Email Advisory.
Subscribe to receive the County Health Officer newsletter by scanning the QR Code (right) or by entering your email here: Health Officer Newsletter Subscription


www.ochealthinfo.com/healthcorner

For Communicable Disease Control contact #'s in other counties or cities across California, go to LHD Communicable Disease Contact List.