WHAT WOULD YOU DO? 3YR OLD THOROUGHBRED FILLY Rabecca McKenzie rabeccam@energyvets.co.nz
BACKGROUND Filly was normally boxed in a concrete brick and thick meshnetted stall. Injury occurred overnight and horse was travelled to the track and worked, despite lameness. Trainer mentioned she ‘worked out of it’. The primary phone call was from the trainer who wanted to administer antibiotics himself.
GENERAL PLAN AT REFERRAL HOSPITAL GREG QUINN
In keeping with principals for antimicrobial stewardship I asked some questions, including location of the wound and level of lameness. After not being satisfied to prescribe ‘over the counter’ a call was booked within the hour. On arrival the wound was obvious [Figure 1]. The horse had a normal physical examination. She was 4/5 lame at the walk. Figure 2: Showing debris in joint including hair (arrows).
Figure 1: Wound at first presentation
WHAT WOULD YOU DO? The wound was clipped and aseptically prepared. A sterile probe was placed which hit bone and on retraction of the probe there was a flush of serosanguineous fluid. A 20-gauge 25mm needle was placed, and a small amount of bloody synovial fluid was aspirated, after which 180mg of gentamicin was injected. Sterile swabs were then placed over the wound and two-layer bandage placed for transport. Photographs of the wound were sent immediately to the referring surgeon and transport arranged for the filly. Systemic medications were started with gentamicin (6.6mg/kg IV minus the 180mg in the joint), ceftiofur (5mg/kg IV), flunixin meglumine (1.1.mg/kg IV) and a 1500units TAT SC.
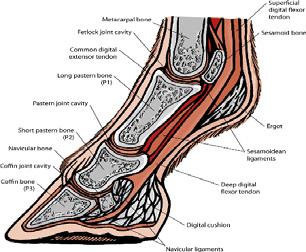
After initial assessment of vital parameters and comfort, the filly would be sedated for further evaluation. Following bandage removal, an initial survey set of four standard radiographic films would be the first task undertaken. The wound would then be prepped for ultrasound with protection of the wound from additional contamination prior to clipping. The adjacent soft tissue and bony structures would be assessed. It would be unusual for a horse that is 4/5 lame, not to have damaged something deeper and more vital. After placement of an abaxial nerve block, the respective synovial structures would be evaluated for their integrity. The ultrasound examination would help determine which structure to assess by following the trajectory of the wound penetration, if possible. With this location shown in Figure 1, there could be involvement of underlying bone and collateral ligament, distal interphalangeal (coffin) joint, or proximal interphalangeal (pastern) joint. Ideally, if there is insufficient fluid identified on ultrasound for synoviocentesis, the respective joints would be dissented with sterile isotonic fluids from the opposite side of the limb (palmar/plantar pastern) or abaxial to the midline (coffin) joint away from the wound. A small volume of antibiotic (gentamicin or amikacin), would be injected after sterile fluid distension. Any egress of fluid would indicate a breach of the synovial environment and the recommendation then would then be an arthroscopically guided surgical flush, with particular attention being paid to removing all fibrin and foreign material such as grit and hair [Figure 2]. If samples of joint fluid could be obtained, these should be cytologically evaluated and fluid sent for culture using a blood culture broth bottle.
Eq Vet Pract 2021 September; 46 (3) 49