This research paper provides a comprehensive analysis of the impact of architectural design in emergency psychiatric care, comparing traditional psychiatric wards in emergency departments with EmPATH (Emergency Psychiatric Assessment, Treatment and Healing) units. The study begins by addressing the urgent need for improved psychiatric crisis care, exploring historical and current challenges in behavioral health crisis management. It then delves into a multifaceted research approach, including interviews, literature reviews, and a critical space syntax analysis, comparing traditional emergency department psychiatric wards and EmPATH units. Case studies further illuminate the effectiveness of EmPATH units in fostering participatory, non-coercive, and healing caregiving environments. The findings underscore the importance of design in promoting patient dignity, safety, and autonomy, reducing stress, and enhancing communication. This research contributes to a broader understanding of psychiatric care design, advocating for participatory, non-coercive, supportive, and therapeutic environments in emergency psychiatric settings.
Keywords: EmPATH Unit, Behavioral Health Crises, Psychiatric Emergency Care, Therapeutic Environments, Mental Health Design, Participatory Caregiving, Space Syntax Analysis, PatientCentered Care, Non-Coercive Treatment, Healthcare Architecture.
As the behavioral health needs are increasing at an alarming rate, statistics indicate that 1 in 8 visits to U.S. emergency departments is related to mental health or substance abuse issues (Weiss, Barrett, Heslin, & Stocks, 2016). Unfortunately, the response to individuals experiencing behavioral and mental health crises at emergency departments often defaults to a “transfer-toinpatient-bed” status, contrasting with the swift assessment and follow-up care given to other medical emergencies. This has led to an overwhelming demand for psychiatric beds, resulting in untreated individuals enduring prolonged wait times, sometimes spanning several days.
Furthermore, the emergency department (ED) can prove to be a distressing and unsettling environment for individuals in a mental health crisis. Patients are often restrained or confined inside small cubicles under the supervision of attendants. The ED setting is surrounded by authorities and paramedics, harsh overhead lighting, loud noises, and chaotic activity, alongside the audible distress of others in pain nearby. It is well recognized that the conventional ED setting can worsen the symptoms of behavioral health patients in crises, yet there has been limited effort to address the growing demand and implement new care models in the ED (Garriga et al., 2016).
To tackle these challenges, Dr. Scott Zeller developed EmPATH Units (Emergency Psychiatric Assessment, Treatment, and Healing). These units provide a calm, supportive environment for behavioral health patients. Research shows that 75-80% of psychiatric emergencies can be stabilized within 24 hours in EmPATH units, reducing inpatient admissions and easing ED burdens (Zeller, Calma, & Stone, 2014). This research paper investigates how EmPATH units transform psychiatric crisis care through architectural design, serving as a valuable resource for architects and planners intending to design egalitarian, non-coercive, and participatory behavioral healthcare spaces for mental and behavioral health patients and staff.
Figure 1: For days, Melinda lived in a small, windowless room off the ER, awaiting an open spot in a psychiatric care unit. After a failed escape attempt, she was confined further—only allowed out to use the bathroom.
2.0 A Historical Perspective:
The Rise, Fall and Resurgence of Therapeutic Caregiving
Construction of the Kirkbride Asylums
(Kirkbride Buildings History, n.d.)
Architecture for treating mental health conditions has long struggled to achieve humane conditions. Before Dr. Thomas Story Kirkbride’s influence, mental health patients endured harsh, inhumane conditions, often confined in overcrowded, unsanitary facilities such as almshouses, jails, or makeshift asylums, where containment took precedence over treatment. Stigma surrounding mental illness led to severe neglect and abusive practices like restraint, isolation, and physical punishment. Kirkbride, a pioneering psychiatrist of the 1800s, played a key role in reforming mental healthcare in the United States with his patient-centered approach emphasizing compassion, dignity, and respect. He advocated for therapeutic environments designed to promote healing and recovery, with large buildings featuring extended wings arranged in staggered formations to maximize access to sunlight and fresh air, often located in peaceful, natural settings believed to encourage recovery. By combining compassionate care, supportive environments, and therapeutic activities, Kirkbride’s approach fostered trust and emotional well-being, shaping modern mental health care despite limited medical treatment options.
Influence of Pharmaceuticals
(Smith, 2016)
With the development of psychiatric towards prescribing and managing were effective in treating symptoms ‘modern’ approach to mental health medications was driven by the belief backed ability to correct mental health as biological or chemical imbalances However, this shift toward medication care resulted in decreased emphasis interactions and more standardized regimens, often at the expense emotional and social needs. While and treating a larger number of patients, personal, therapeutic relationships significantly altering the healthcare model and changing the treatment patients. As a result, patients often treatment that prioritized symptom
psychiatric medications, the focus shifted managing these drugs. These medications symptoms and were seen as a more care. The shift towards psychiatric belief in their precise, scientifically health conditions, increasingly viewed imbalances treatable with medication. medication management in mental health emphasis on one-on-one therapeutic standardized treatments focused on drug of holistic support for patient’s While beneficial for symptom control patients, this approach led to fewer relationships between caregivers and patients, healthcare delivery system toward a clinical treatment experience for behavioral health often felt depersonalized, receiving control over individualized care.
Going back to the Roots and Bringing Back Therapeutic Care giving (Smith, 2016)
By the late 20th century, nurses began re-evaluating therapeutic caregiving in response to the limitations of pharmaceutical interventions, especially in managing chronic mental illness. The widespread reliance on psychotropic drugs had overshadowed holistic, patient-centered care. However, nurses played a crucial role in facilitating recovery journeys guided by patients’ individual needs and long-term goals. Ethical challenges also influenced this significant shift. Nurses faced the difficult task of balancing patient-centered care with a healthcare system focused on managing risks. Ensuring the safety of both patients and staff while managing agitated behaviors added complexity to their evolving roles. Increasing criticism of excessive drug use, isolation, and physical restraints further fueled concerns about patients’ rights and ethical treatment. These historical challenges, combined with the recognized shortcomings of drug-based treatments, reinforced the importance of reintroducing therapeutic caregiving. This approach became central to mental and behavioral health (MBH) care, emphasizing compassion, respect, and personalized patient care in modern psychiatric treatment.
3.0 Challenges in ED Behavioral Health Care
Emergency departments nationwide are experiencing a critical crisis due to overcrowding caused by a well-documented phenomenon known as boarding. Boarding happens when patients are admitted to inpatient units but remain in the ED until an inpatient bed becomes available. Several factors contribute to this crisis, impacting both patients and healthcare provider and posing significant challenges to the providing behavioral health care:
(1) Deinstitutionalization of Psychiatric Services and Unreliability of Community Centers: Psychiatric care has shifted from hospital-based inpatient facilities to community-based crisis management solutions, resulting in significant deinstitutionalization. This change has reduced the number of available inpatient psychiatric beds to fewer than 50,000 nationwide. Consequently, psychiatric patients increasingly rely on outpatient services, medical management groups, and community centers, which are often ill-equipped to manage acute behavioral health crises, leaving emergency departments as the last resort.
(2) Increasing Number of Behavioral Health Patients: The prevalence of mental illnesses and substance use disorders has surged globally, affecting an es-timated 970 million people. In the United States, approximately 1 in 25 adults lives with a severe mental illness such as
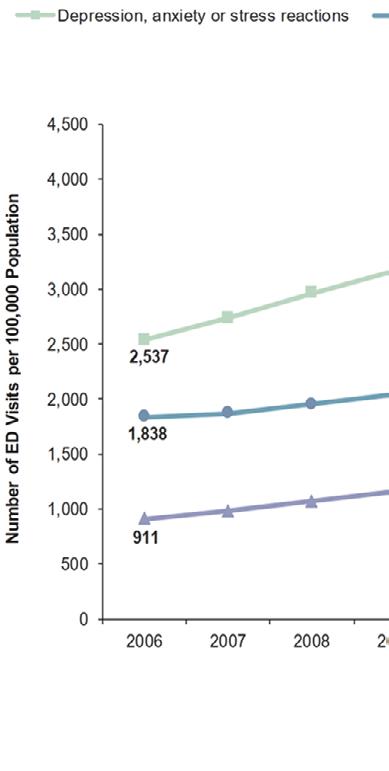
Figure 2: Population rates of ED visits disorders, 2006–2013. Weiss A., Barrett
visits involving mental & substance use
Barrett M., Heslin K., & Stocks C. (2016).
schizophrenia, depression, or substance use disorders, according to the National Alliance on Mental Illness. This growing mental health crisis has led to a significant rise in behavioral health emergencies in hospital EDs. Currently, behavioral health patients comprise 1 in every 8 ED visits, with average stays exceeding 30 hours (Weiss, Barrett, Heslin, & Stocks, 2016). Despite recognizing their responsibility to provide quality care, hospitals face challenges due to insufficient mental health planning and funding at state and local levels.
(3) Over-Reliance on Inpatient Admission in BH Emergencies: The standard response to behavioral health emergencies often involves securing inpatient beds rather than initiating immediate treatment in the emergency setting. This practice leads to unnecessary admissions into restrictive and costly care. For comparison, admitting all ED patients with chest pain would cause a shortage of hospital beds, even though only about 20% require hospitalization. Similarly, effective emergency behavioral health programs admit only about 20% of patients, with most emergencies managed within 24 hours. Since both cardiac and psychiatric emergencies require immediate evaluation, hospital EDs must adopt service models that provide prompt care without boarding patients (Zeller, Calma, & Stone, 2014).
3.1 The Boarding Problem: Bottle Neck & Inefficiency
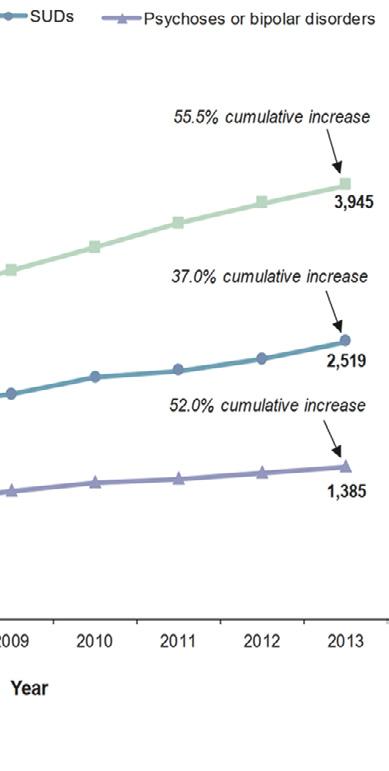
The combination of these factors leads to a classic bottleneck phenomenon, resulting in the prolonged stay, or boarding, of patients in the ED. This situation arises when a patient needs to be moved to an inpatient unit for further medical or psychiatric evaluation but cannot be admitted due to the lack of available beds. This shortage creates the bottleneck, with patients waiting in the ED until a bed becomes free (workweek, 2022).
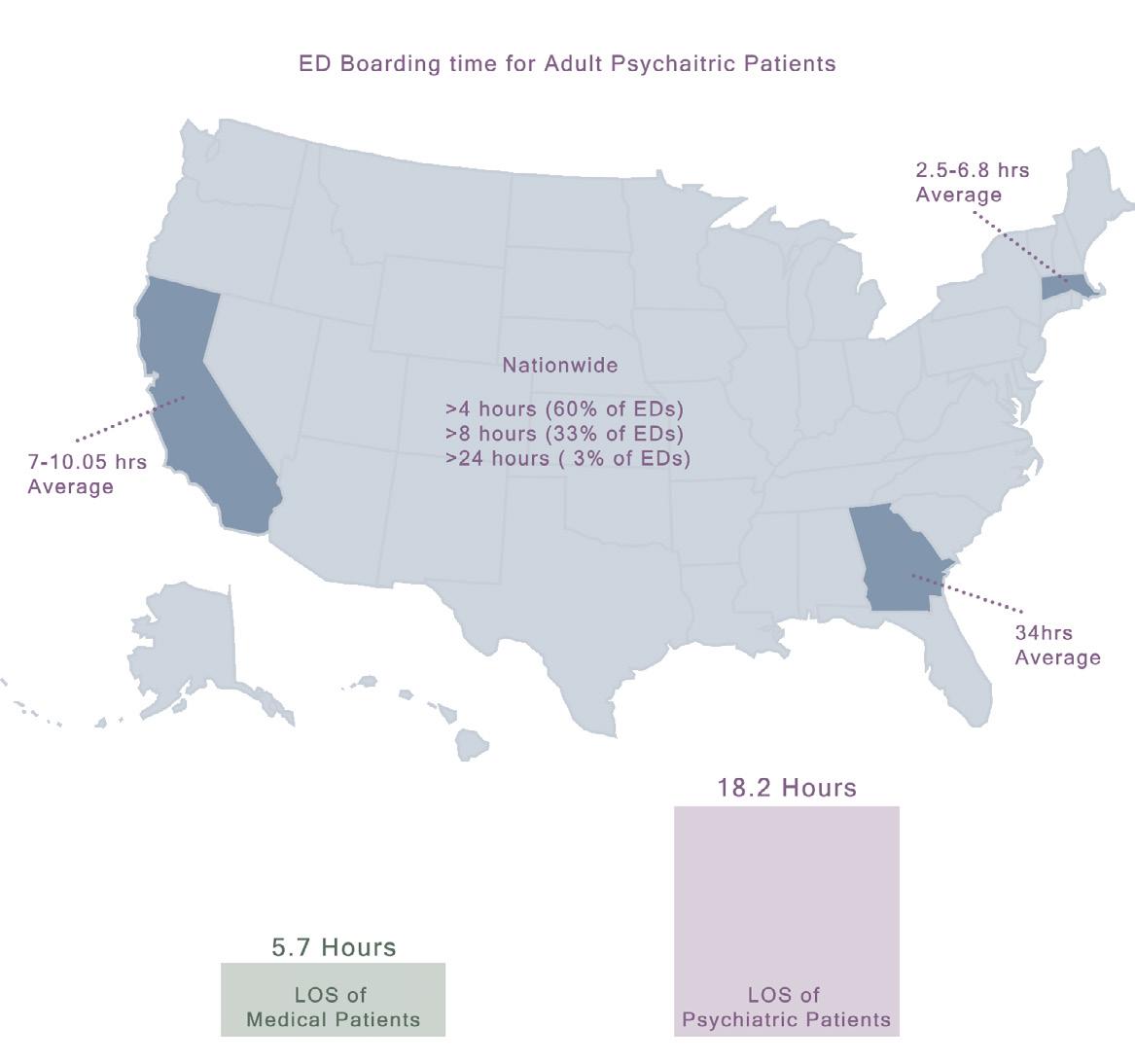
This boarding of patients directly impacts the Length of Stay (LOS) both in the ED and the inpatient unit. As more patients occupy beds for longer periods, the overall bed capacity of the hospital is strained. This, in turn, leads to longer wait times for beds, exacerbating the overcrowding in the ED (workweek, 2022). As a result of this, psychiatric patients spend 3x longer than other patients in Emergency Department (Zeller, n.d.).
Figure 3: The Vicious Boarding Cycle: Visualizing the interconnected challenges of boarding, length of stay, occupancy, and bed capacity in healthcare.
The Vicious Boarding Cycle
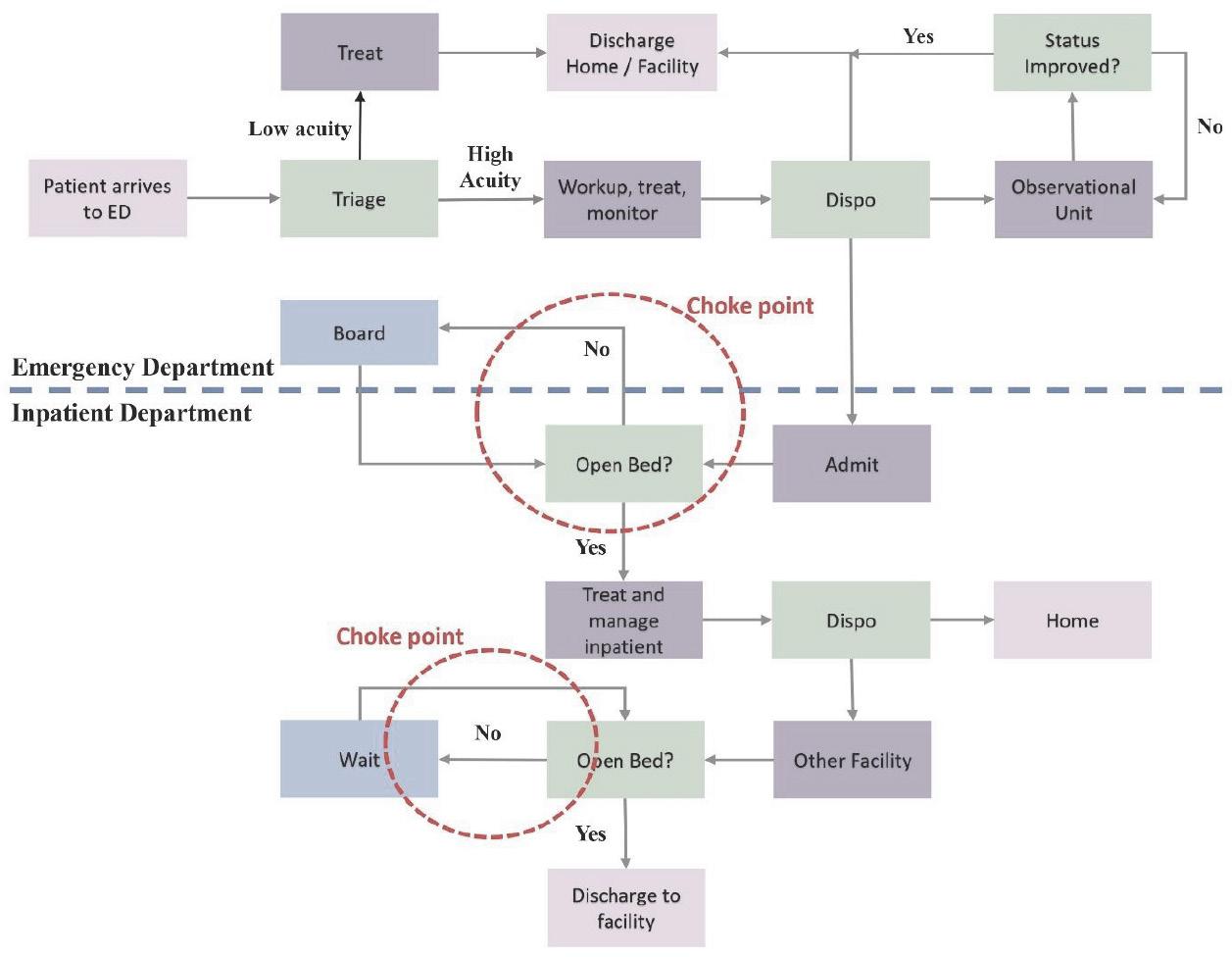
Figure 4 Patient flow through ED Highlighting choke points created due to Boarding. Graphical Adaptation from workweek. (2022, December 4).
3.2 Impact of Boarding
Boarding psychiatric patients in EDs disrupts care, strains staff, and burdens hospital resources:
(1) Chaotic Environment and Use of Cohesive Methods: Many EDs lack on-site psychiatrists, limiting access to specialized care. This gap forces ED staff, often untrained in psychiatric care, to manage patients in a stressful environment. The chaotic atmosphere can worsen psychiatric symptoms, leading to the increased use of physical or chemical restraints to maintain safety (Roy et al., 2019).
(2) Reverse Triaging in Psychiatric Care: With a limited number of psychiatric beds available, psychiatrists often have to use a method called reverse triaging. This means that as soon as psychiatric patients show even a slight improvement, they are sent back to their previous environment to free up beds for patients at higher risk. This approach can lead to a cycle where the same patients repeatedly enter and leave the ED and inpatient psychiatric care. (Kelen et al., 2017)
(3) Physician Burnout and Challenges: Overcrowded EDs increase emergency physician’s stress and risk of burnout. This issue is exacerbated by dealing with involuntary psychiatric holds, which carry a higher risk of violence. Physicians also experience moral distress, feeling responsible for patients but lacking the specialized training needed for effective psychiatric care (Kelen et al., 2017).
(4) Financial Strain on Hospitals: Boarding psychiatric patients causes significant financial losses for hospitals. A study found that each psychiatric patient held in the ED costs hospitals $2,400, leading to a 40% drop in physician reimbursement. Since psychiatric patients stay longer than other patients, each case reduces the capacity to treat two additional patients, further straining hospital finances (Zeller, n.d.).
Figure 5 Psychiatric patients bear the burden of systemic inefficiencies, enduring prolonged boarding times and extended ED stays—a stark reflection of unresolved challenges in healthcare delivery. Graphical Adaptation (Zeller S, Thomas S)
4.0
The EmPATH Unit
An EmPATH Unit (Emergency Psychiatric Assessment, Treatment and Healing Unit) is a standalone unit or section of the ED introduced as a response to resolve the issues generated as due to the ipact of bottleneck and inefficiencies of behavioral health patient Boarding in an emergency department. They streamline emergency department assessment of the health needs of mental health consumers and quickly transitions them out of emergency departments into These units that offer a calm, home-like, supportive milieu reminiscent of drop-in crisis programs. On top of that, because EmPATH Units are hospital-based and ED-affiliated, they are able to treat high-acuity, dangerous, intoxicated/in withdrawal, and/or medically comorbid individuals who normally would be excluded from community-based programs. (Zeller, n.d.)
The EmPATH units were designed and established by Dr. Scott Zeller, MD, Psychiatrist, on the basis of his Six Goals for Emergency Psychiatric Care which outlines a compassionate and effective approach to treating patients in crisis:
• Exclude medical causes and ensure stability: Rule out physical health causes for psychiatric symptoms.
• Rapidly stabilize the crisis: Quickly address the psychiatric emergency.
• Avoid coercion: Ensure treatment is consensual and respects patient autonomy.
• Treat in the least restrictive setting: Provide care in an open, supportive environment.
• Form a therapeutic alliance: Build trust and support with the patient.
• Plan aftercare: Develop a comprehensive post-care plan.
These units improve patient and staff satisfaction while reducing involuntary holds and intensive resource use. (Zeller, n.d.)
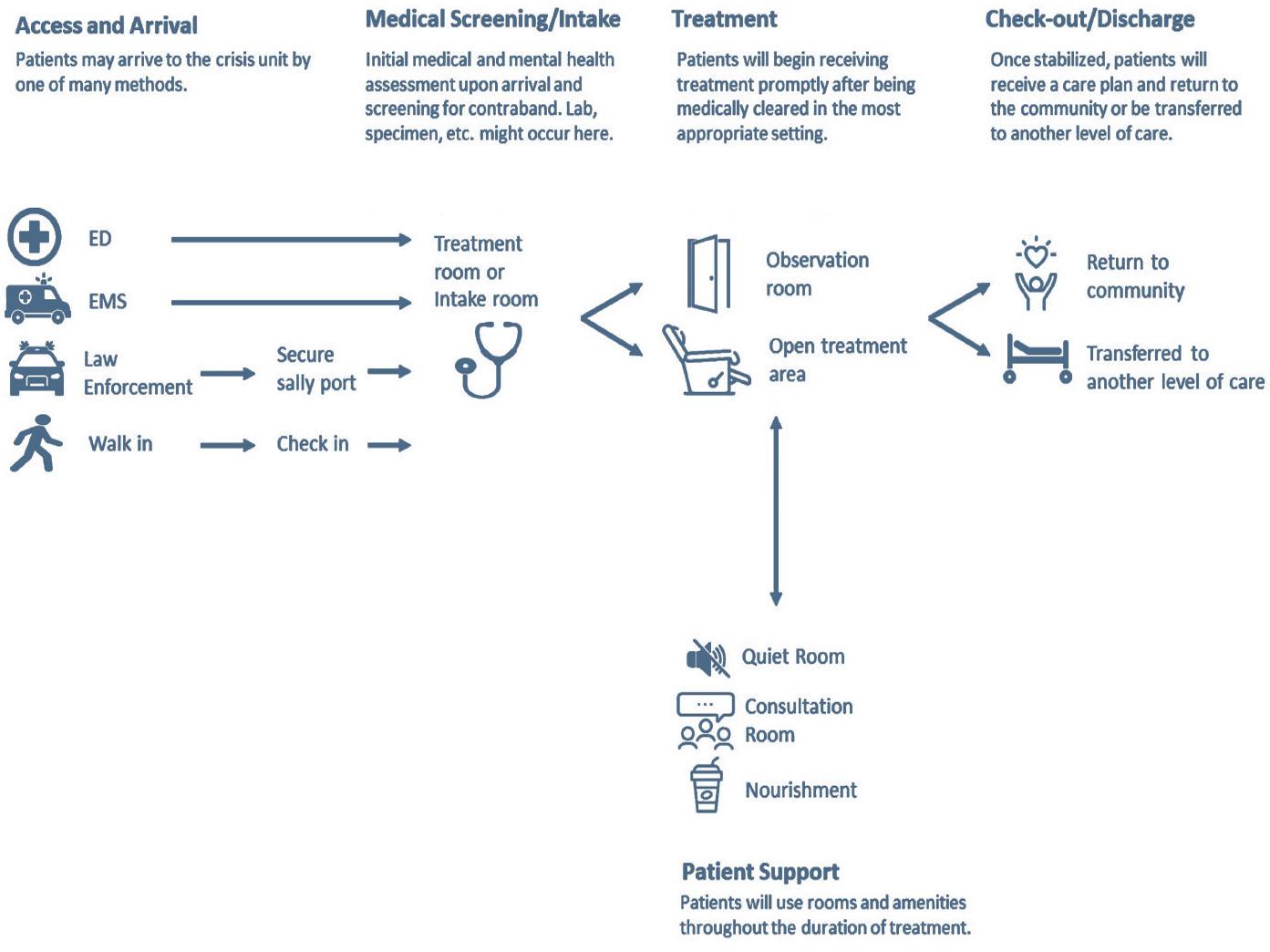
4.1 Journey through EmPATH Unit
The journey of a behavioral health patient from the emergency department (ED) to an EmPATH (Emergency Psychiatric Assessment, Treatment, and Healing) unit and beyond begins when the patient arrives at the ED experiencing a severe mental health crisis. This crisis may involve extreme psychosis, self-harm, or suicidal ideation, necessitating immediate medical attention.
Upon arrival, the patient undergoes triage and a preliminary assessment conducted by ED medical staff. This assessment evaluates the patient’s mental state, the severity of their condition, potential risks to themselves or others, and any urgent physical health concerns. The aim is to determine the most appropriate level of care. If the patient is experiencing an acute behavioral health crisis that requires specialized intervention, they are transferred to the EmPATH unit, designed specifically for mental health stabilization.The EmPATH unit provides an environment focused on intensive, personalized care. The patient receives a comprehensive psychiatric evaluation and individualized treatment plan. Crisis intervention strategies, including medication management, counseling, and therapy, are implemented to stabilize the patient’s mental health. The EmPATH team also addresses co-occurring conditions such as substance use disorders or underlying medical issues that could complicate the patient’s recovery process.
During their stay, patients benefit from a therapeutic setting aimed at reducing distress and fostering emotional stabilization. The multidisciplinary care team works collaboratively, offering supportive interventions tailored to the patient’s unique needs. Peer support specialists and case managers may also be involved, helping patients navigate their recovery journey with empathy and understanding.
6 Flow Chart for a Behavioral Health Care Unit. Montgomery, M., Upton, S., State, W., & Zeller, S. (2022).
Figure
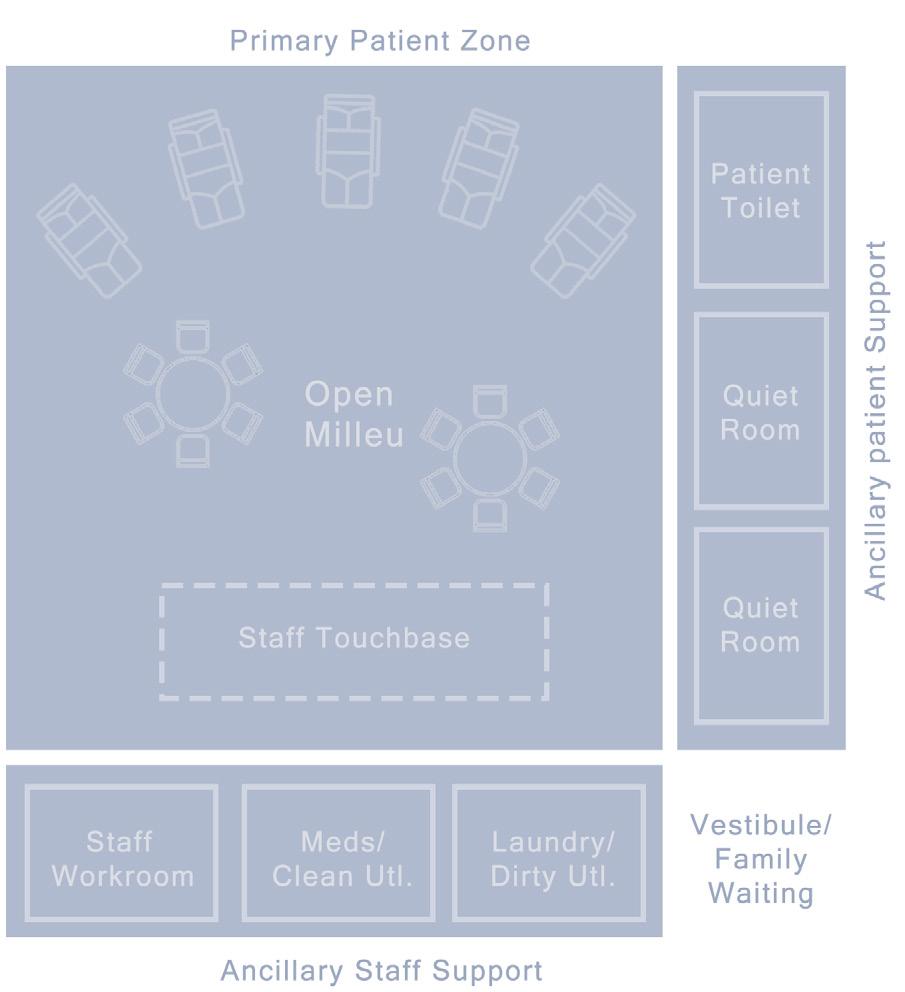
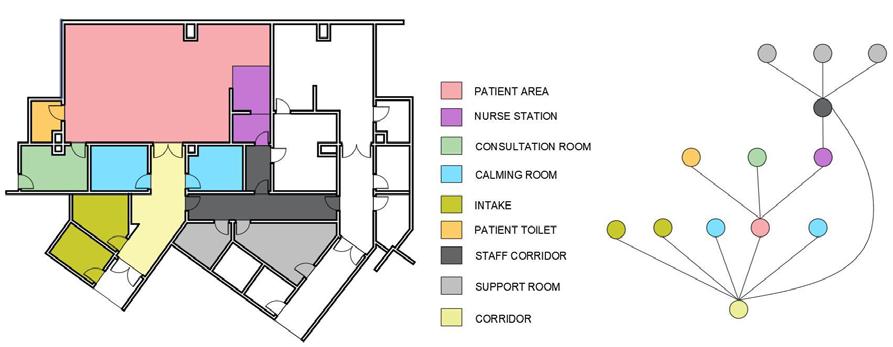
4.2 Space Planning Principles for EmPATH
The EmPATH unit is designed to support patients experiencing acute behavioral or mental health crises through a therapeutic caregiving environment. Its core feature is the central open area, the “milieu,” where patients and staff interact, fostering continuous observation and a sense of community.Key Design Features:
• Open milieu: A spacious, high-ceilinged area with calming decor, ambient lighting, and soothing textures.
• Patient spaces: Recliners with 40 sq. ft. of personal space promote comfort and reduce confinement. Tables encourage small-group interactions.
• Calming rooms: Voluntary quiet rooms provide a stress-free retreat, eliminating the need for locked seclusion.
• Safety and freedom: The unit layout ensures patient safety while supporting free movement and autonomy.
• Nourishment area: A self-serve snack area fosters independence and daily routine normalcy.
• Support apaces: Family waiting areas, patient toilets, and quiet rooms support holistic care.
• Healing Environment: Access to natural light, outdoor views, and secure outdoor areas enhances therapeutic recovery.
With a recommended 80 sq. ft. per patient, the EmPATH unit is purposefully designed to create a secure, compassionate, and healing space tailored to behavioral health needs.
Figure 7 Schematic Zoaning of EmPATH Unit Components.
4.3 Patient Benefits of Having an EmPATH
Behavioral health patients benefit significantly from the therapeutic caregiving environment of an EmPATH unit. As a trauma-informed unit, it offers a home-like setting distinct from the often chaotic emergency department, fostering a sense of calm and safety. Patients are encouraged to engage in relaxation, movement, and recreational activities, contributing to a more positive and active recovery process. The calm atmosphere of the EmPATH unit is designed to meet patients’ needs effectively. They have the autonomy to serve themselves snacks, beverages, and linens, which promotes independence and comfort. The multidisciplinary treatment team’s involvement from arrival to disposition ensures continuous and coordinated care.
Rapid evaluations by psychiatrists facilitate the integration of care with the development of comprehensive care plans tailored to each patient’s needs. This approach, along with constant observation and re-evaluation, significantly increases the likelihood of patients being diverted from hospitalization. Additionally, the EmPATH unit aims to eliminate restraints, typically reducing their use to far less than 1%, thereby minimizing trauma and promoting dignity and respect in patient care.
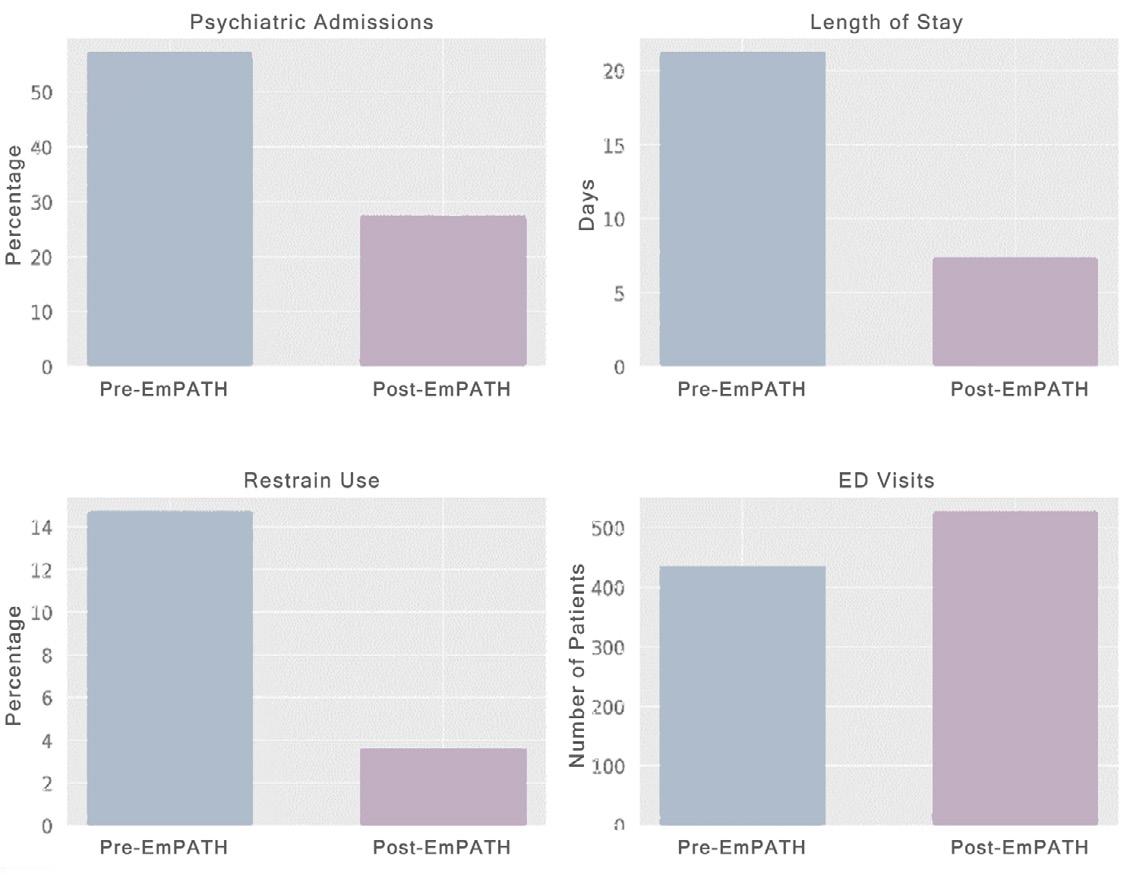
Figure 8, highlights the statistical data from the study at a 60,000-visit ED in Johnson County, Iowa, evaluating the EmPATH unit’s impact on 962 patients with suicidality. It compared 435 patient’s pre-implementations to 527 post-implementation without demographic differences. The study aimed to examine the unit’s effect on clinical outcomes in a rural setting. Results showed reduced IPD admissions, Average Length of Stay (LOS), use of restraint and ED boarding, plus improved 30-day follow-up rates after EmPATH’s introduction, confirming its effectiveness.
Figure 8 Impact of EmPATH Unit Implementation on ED Boarding Issues. ( By Author) Data From: Kim, A. K., Vakkalanka, J. P., Van Heukelom, P., Tate, J., & Lee, S. (2021).
5.0 Literature Review
Architectural Design of Psychiatric Care Spaces in Emergency Departments and Restraint Use
The architectural design of emergency departments (EDs) plays a crucial role in managing mental and behavioral health patients. The use of restraints in psychiatric care, recommended only as a last resort (Jenkins, 2006), is directly influenced by spatial layout and visibility. Jenkins (2006) stresses that restraint and seclusion should be applied only when there’s an immediate risk of harm, making ED design essential for safe patient management. Pati, Harvey, and Pati (2014) explored how ED design affects safety and operational efficiency, identifying 16 critical design elements such as entrances, waiting areas, and treatment spaces. Enhanced patient visibility in waiting areas supports early intervention, reducing the need for restraints. Additionally, centralized treatment layouts promote better staff coordination and timely care.
In conclusion, thoughtful ED design goes beyond aesthetics, directly impacting patient safety and care efficiency. Continued research is essential to explore how specific design features influence restraint use in psychiatric settings.
The Role of Participatory escalation in Psychiatric Crises
The literature on participatory caregiving emergency departments (EDs) highlights and improve patient care. Nordstrom psychiatric treatment during extended to high patient volumes. Wilson et medication, noting premature use can emphasizing the need for balanced (2012) argue that verbal de-escalation efficient than restraints, fostering sedation-related risks. Project BETA non-coercive strategies like verbal centered care and minimizing restraint
In all, the literature suggests that designing to promote participatory caregiving escalation techniques can effectively crises. This approach minimizes the injuries, and fosters a more therapeutic
Caregiving and Verbal DeCrises
caregiving and verbal de-escalation in highlights strategies to reduce violence
Nordstrom et al. (2019) stress active extended ED stays, often overlooked due et al. (2012) highlight the timing of can hinder psychiatric evaluations, balanced intervention. Holloman and Zeller de-escalation is more effective and resourcepatient cooperation and reducing BETA guidelines further advocate verbal de-escalation, promoting patientrestraint use.
designing emergency care processes caregiving and employing verbal deeffectively manage agitation in psychiatric the need for restraints, reduces staff therapeutic environment for patients.
The Outcome of Positive Distractions in Healthcare Environments
The literature on positive distractions in mental and behavioral health settings highlights their critical role in reducing patient stress and staff dependency. Positive distractions are environmental features that evoke positive emotions and hold attention without causing mental strain, helping block distressing thoughts. Dabrowska (2020) reviewed 40 studies on positive distractions in healthcare environments, focusing on elements like nature views, art, music, light, and audiovisual displays. Findings showed these interventions significantly reduced anxiety and perceived pain among patients, enhancing their well-being.Similarly, Jiang (2020) explored positive distractions in pediatric healthcare, identifying six key themes: art, spatial design, social interactions, play technologies, sensory features, and nature access. These elements improved emotional well-being, reduced stress, and facilitated smoother healthcare experiences.
In conclusion, incorporating positive distractions into healthcare design supports patient relaxation, reduces anxiety, and minimizes staff intervention, fostering a therapeutic and efficient care environment.
6.0 Space Syntax Analysis
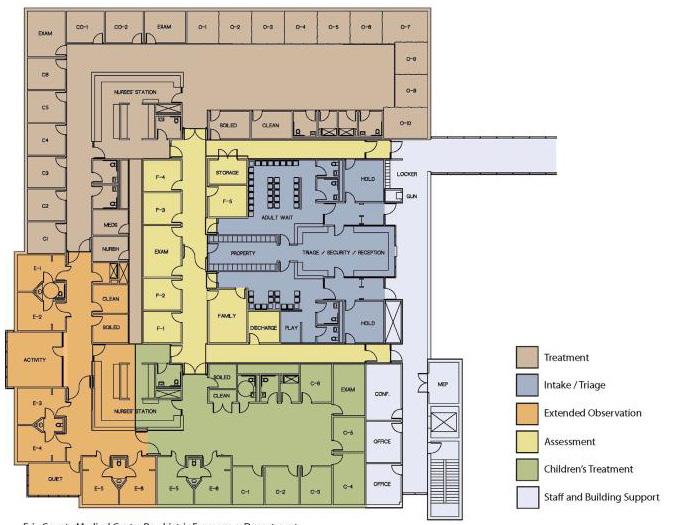
This section of the research paper delves into a comparative study between a traditional psychiatric ED ward and an EmPATH unit. The objective is to understand how the spatial layout impacts caregiving methods and patient behavior. For this study, we consider a portion of the Erie County Medical Center psychiatric emergency department to represent the traditional ED ward and the EmPATH unit at Central Care Hospital in Saint Cloud, Minnesota. The analysis focuses on examining design elements such as patient flow, visibility, privacy, and therapeutic environments within these settings. Insights gained from this comparison aim to inform architectural strategies that enhance patient outcomes and support effective caregiving practices in mental health facilities.
Boundary Mapping and Spatial Connectivity Analysis are Space Syntax tools used to study the relationships and interactions within spatial layouts. Boundary map analysis examines the physical barriers within a space, such as walls and doors, and their impact on movement and visibility. Spatial connectivity analysis, on the other hand, looks at how spaces are linked to each other, considering the directness and accessibility of these connections, and how they facilitate or hinder movement.
Traditional ED Psychiatric Ward
Spatial Adjacencies
• Traditional ED Psychiatric Ward : In the traditional ED ward, spatial programming follows a corridor-centric layout, requiring patients and staff to navigate the corridor to access rooms, leading to linear and segmented flow. This design can cause inefficient space utilization and bottlenecks, reflecting a compartmentalized approach that limits spatial connectivity.and accessibility.
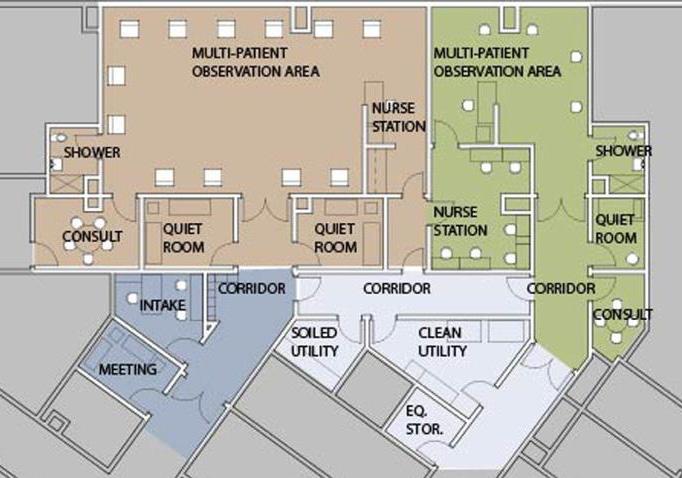
• EmPATH Unit: In contrast, the EmPATH unit features a spatial arrangement revolving around a central open patient area. This innovative design minimizes corridor dependency, using it mainly for the initial transfer of patients from outdoor to indoor settings post-assessment. The central open area encourages free movement, fostering an environment conducive to independence and interaction among users. This approach enhances spatial connectivity by creating a more integrated and accessible layout. The design underlines an egalitarian philosophy, improving not only the functionality of the space but also promoting a sense of community and openness in the care environment.
Flexibility and Adaptability
• Traditional ED Psychiatric Ward :The traditional ED ward lacks flexibility in its layout, relying on a narrow corridor structure that restricts movement to a linear path and facilitates transit between rooms. The rooms, separated by fixed partition walls, have designated uses, limiting adaptability and functional range. This rigid design constrains opportunities for innovative caregiving methods, as the environment does not support varied or adaptive uses.
EmPATH Unit
• EmPATH Unit: In stark contrast, the EmPATH unit features reconfigurable spaces with no fixed separations in the open patient area, allowing significant flexibility in use. This adaptability accommodates various activities and patient needs, fostering a dynamic care environment. Caregivers can conduct group therapy sessions or collective activities, promoting interaction and versatility.
Safety
• Traditional ED Psychiatric Ward :In the traditional ED ward, the layout of staff corridors raises safety concerns, featuring a dead-end corridor that connects only to two support rooms with limited access to other areas. This design poses risks during emergencies, such as fires, by restricting escape routes and hindering quick evacuations. The lack of multiple egress options compromises the effectiveness of emergency response and overall safety.
• EmPATH Unit: The unit prioritizes safety and accessibility with a staff-specific corridor restricted from patient access, ensuring a secure operational zone. The nurse station is strategically positioned for full visibility of the hall, including patient restroom doors, enabling constant monitoring and swift responses to emergencies. This design reflects a thorough integration of safety protocols, addressing security concerns more effectively.
Privacy and Openness
• Traditional ED Psychiatric Ward : The traditional ED ward features private, enclosed spaces that prioritize individual privacy. While ensuring personal space, this compartmentalized layout limits patient interaction, communal engagement, and the sense of openness essential for a healing environment.
• EmPATH Unit: The EmPATH unit eliminates partition walls, fostering visual connectivity and promoting community and interaction while respecting privacy. Calming rooms offer secluded spaces for patients needing rest, balancing communal openness with individual needs. This holistic design addresses both engagement and privacy, unlike the traditional ED ward.
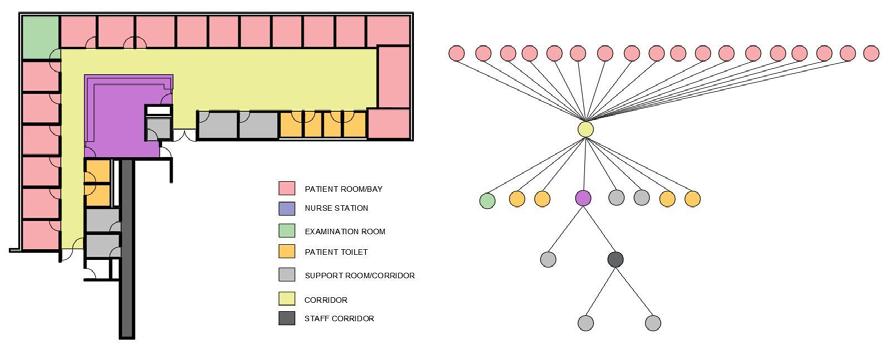
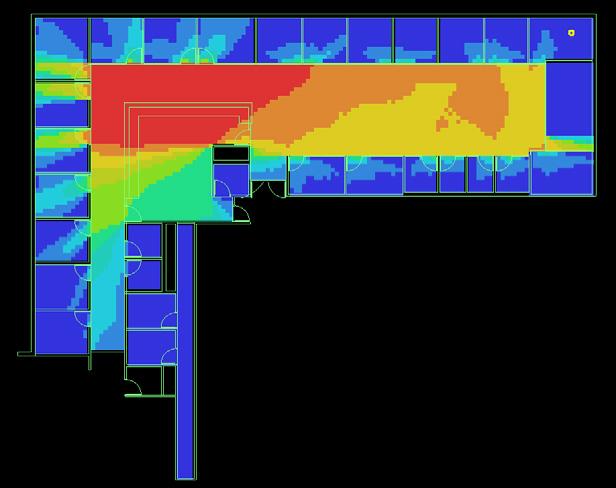
6.2 Visibility Graphic Analysis
Visibility Graphic Analysis is a spatial examination tool that quantifies the visible area from a specific point in a layout, offering insight into how space unfolds visually. This method delineates the direct line-of-sight regions and assesses how layout configurations affect visibility and, consequently, interactions within a given environment.
Conducting an VGA analysis on a traditional ED ward and an EmPATH unit, I am able to compare and determine the extent to which each layout promotes visibility for monitoring by staff, the potential for patient interaction, and the overall spatial experience. Enhanced visual connectivity may correlate with improved patient outcomes, as it influences movement, interaction, and the perception of space. By comparing the results, I can discern which environment better facilitates a non-coercive, participatory approach to care, essential for fostering a supportive, healing atmosphere that encourages patient solidarity and staff engagement.
Traditional ED Psychiatric Ward EmPATH Unit
Visibility and Surveillance
• Traditional ED Psychiatric Ward : Positioned as central hubs within the ward, these stations facilitate a high level of oversight over the patient doors to supervise patient movement. None of the patient beds are in direct sight of the nurses, and only a small area of the room is exposed when doors are open due to enclosed cubicles. This highlights that here nurse stations are primarily designed for surveillance and medical caregiving, underscoring the role of nurses in constant monitoring and rapid response. While efficient for surveillance, this design can inadvertently create a sense of detachment between nurses and patients, focusing more on observation and less on participatory care.
• EmPATH Unit: The EmPATH unit reimagines the role and positioning of the nurse station, integrating it into the environment but not as the focal point and only partly visible from patient areas. This reflects a shift from constant surveillance to promoting independence and selfsufficiency among patients while ensuring necessary care and oversight. Nurses also have access to private areas, serving as breakspaces and workspaces, balancing professional responsibilities with personal well-being. This layout fosters participatory caregiving, enhancing patient care and supporting the mental and emotional health of nursing staff.
Staff and Patient Interaction
• Traditional ED Psychiatric Ward : In traditional ED wards, the enclosed nurse station, separated by glass partitions, emphasizes observation over participation in care. While offering a clear visual overview, this design limits direct interaction and spontaneous communication, creating a barrier that can impact the patient experience and care quality.
• EmPATH Unit: The EmPATH unit integrates staff and patient areas in an open-plan design, eliminating physical barriers. This fosters frequent, casual interactions, promoting collaboration, inclusivity, and a sense of community. The design enhances communication, understanding, and creates a therapeutic atmosphere, improving care outcomes.
Patient- Patient Interaction
• Traditional ED Psychiatric Ward : In traditional ED wards, patient areas are confined to individual rooms, limiting their space to assigned areas and potentially causing feelings of confinement. The design emphasizes privacy and separation, with minimal visual access to others, restricting social interaction and communal engagement, which are crucial for mental and emotional well-being.
• EmPATH Unit: Conversely, the EmPATH unit features an open layout where patients share a communal space, promoting visibility and interaction while maintaining personal privacy. This design fosters casual communication and a sense of community, supporting mental health through social engagement and enhancing the therapeutic environment.
Ease of Navigation
• Traditional ED Psychiatric Ward : Iraditional ED wards feature enclosed, complex corridor layouts that can cause confusion and disorientation for patients and staff. The lack of visual connectivity & intuitive pathways adds to stress, hindering movement efficiency & functionality.
• EmPATH Unit: The EmPATH unit features an open, intuitive layout with clear paths and extensive visibility, empowering patients to choose their activities and locations, enhancing autonomy and reducing stress. This design improves navigation, fosters solidarity, and creates a supportive environment for both patients and staff.
Access to Daylight and View
• Traditional ED Psychiatric Ward : with no natural light or views in central corridor and some of the rooms it tends to create a stressful, isolating environment and missing opportunities to support mental well-being.
• EmPATH Unit: through its cental layout, Provides natural light and views for all, promoting well-being, reducing stress, and fostering a healing environment.
7.1 Case Study: Crisis Stabilization Unit, Iowa University of Iowa Hospitals and Clinics
• Observations Following Empath Unit Inauguration:
• 58,000 Total ED visits/ year,
• 4,400 MBH ED visits/year
• 04 M/BH Care Staff on Site
• 25% decrease in admissions.
• Boarding Time Decreased from 28 hr to 6 hr
• 14hrs Average MBH LOS
• Use of physical restraints decreased.
• Patient Walkouts reduced from 7% to 1.2%.
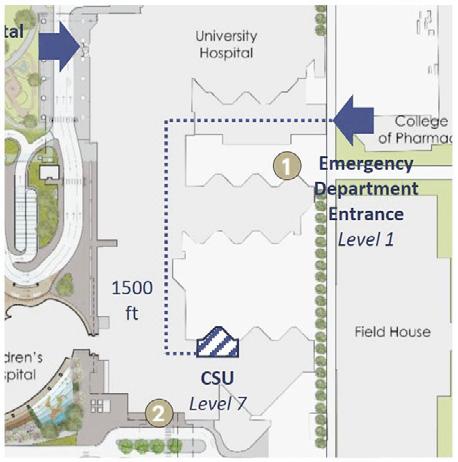
Figure 9 The CSU is strategically located
• Patient Demographics and Challenges: UIHC, with 73 psychiatric beds, faced increasing demand as patients sought emergency care, straining the 36-bed ED. Prolonged wait times and limited psychiatric care led to untreated cases and dissatisfaction.
• Development of the CSU: To address these issues, UIHC transformed a vacant pediatric ICU into the CSU at a cost of $1.1 million, completing the project in eight months. The unit is located on the seventh floor and spans 3,185 square feet
• Operational Workflow and Safety: The CSU, located away from the primary ED, minimizes noise, distractions, and public visibility, enhancing privacy and reducing stress. Its open layout ensures clear visibility between staff and patients, promoting safety and communication. An enclosed staff workroom provides a secure retreat during patient aggression.
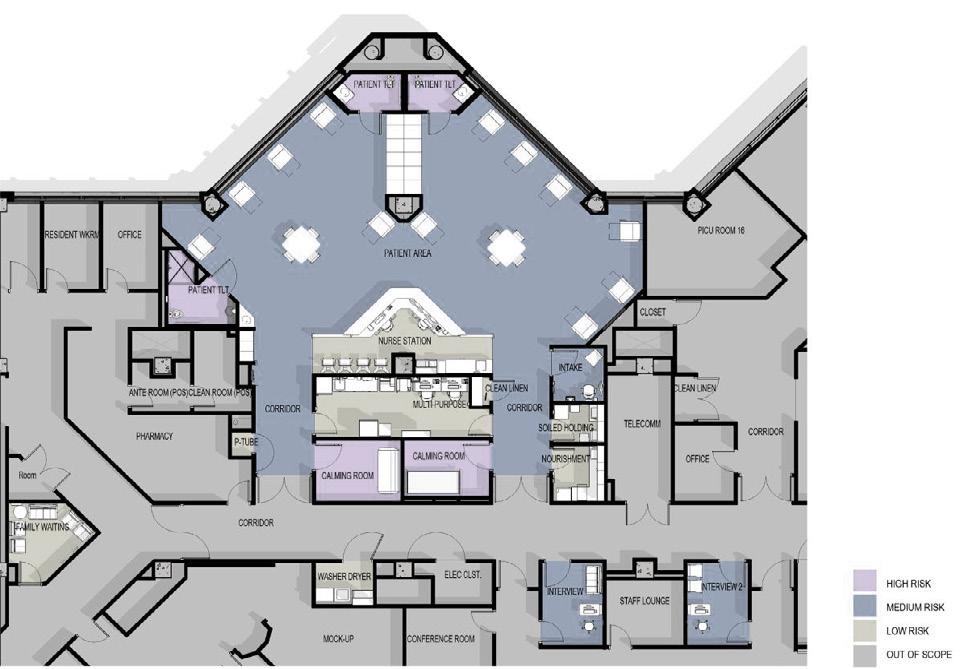
• Design Philosophy and Patient-Centered Features: The CSU is divided into three zones based on patient risk to ensure safety and tailored care:
• High-Risk Areas: Calming rooms and bathrooms with ligature-resistant fixtures and inaccessible ceilings to prevent self-harm.
• Medium-Risk Areas: Open treatment spaces and interview rooms with constant observation, weighted furniture, tamper-resistant fixtures, and accessible ceilings for a less restrictive environment.
• Low-Risk Areas: Staff-only zones with standard construction, not requiring ligatureresistant features.
Figure 10 Floor Plan of the UIHC CSU (Shultz, Hannah 2020)
• Patient Comfort and Dignity: The CSU provides shower facilities, clean clothes, and an onsite laundry room to foster normalcy and respect for patients.
• Security and Safety Measures: The CSU employs civilian-clothed security to reduce feelings of institutionalization and discreet measures like a distress button under the nurse’s desk and enclosed spaces to ensure staff safety during patient aggression.
• Nurse Station and Staff-Patient Interaction: The nurse station features an open design without glass barriers, using a lowered soffit and floor demarcation to define a soft boundary that encourages interaction. A private team workroom behind the station supports confidential discussions while maintaining unit observation.
Figure 11 The unit has calming graphics, controlled windows, and dimmable lighting for a soothing atmosphere.
• Open Layout and Social Environment: The main treatment area’s open layout, featuring recliners and ample space, encourages patient mobility and interaction. The design choice reduces feelings of confinement and promotes socialization which is crucial in mitigating feelings of isolation often associated with psychiatric conditions.
• Social Platform: Communal areas with games, television, and puzzles provide patients with choices and create an inclusive, engaging environment. An accessible water dispenser supports patient independence.
• Calming Rooms: Private spaces are available for patients to de-escalate or for staff interventions, ensuring a supportive and safe environment.
• Natural Light and Soothing Aesthetics: The unit’s location along an exterior wall allows for natural daylight and exterior views, contributing significantly to creating a calming atmosphere. Wall graphics, soft pastel colors, and thoughtful interior design further soothe patients, reducing anxiety and the sense of confinement.
• Safety Integration and Private Conversations: Safety Features: The unit includes features like pick-proof sealant, weighted furniture, secure TV enclosures, and acrylic shatterproof protection on exterior windows.
• In Conclusion, the architectural and interior design of the CSU at UIHC is a testament to the thoughtful integration of safety, comfort, and therapeutic elements in a psychiatric care environment. By prioritizing patient dignity, encouraging open interactions, and ensuring safety and comfort, the CSU stands as a model of innovative design in mental health care facilities. Its environment is not only conducive to stabilization and recovery but also respects the individual needs and dignity of each patient, showcasing the future of compassionate and effective psychiatric care.
8.1 Results: Spatial Layout Observations
The result of this study has been divided into two parts. The first of the results discusses the outcomes of space syntax analysis better comparative study between a traditional psychiatric emergency department Ward and an empath unit to understand the impact of special layout on caregiving methods and patient Behavior. The second part of results gives a comprehensive list of design features that were used to design an empath unit in the case studies.
DESIGN
CONSIDERATION
Spatial Adjacencies
TRADITIONAL ED EmPATH UNIT INTERPRETATION
Corridor-centric layout imposes constraints on movement, leading to inefficiency and potential bottlenecks.
Central open area encourages free movement and interaction, enhancing spatial connectivity and community.
Flexibility and Adaptability
Safety
Lack of flexibility due to narrow corridor structure and fixed room designations restricts innovative caregiving.
Reconfigurable spaces in the open patient area allow for flexibility in use and a dynamic care environment.
Prioritizes safety with strategic nurse station placement for monitoring and quick response to emergencies.
EmPATH’s layout enhances spatial connectivity and egalitarian principles better than the traditional ED.
EmPATH’s adaptable design supports diverse caregiving approaches, offering a more dynamic environment.
EmPATH demonstrates a more comprehensive consideration of security and safety than the traditional ED.
DESIGN CONSIDERATION
TRADITIONAL ED EmPATH UNIT INTERPRETATION
Privacy and Openness
Visibility and Surveillance
Private, enclosed spaces limit opportunities for patient interaction and communal engagement.
Central nurse stations designed for surveillance, creating detachment and focusing less on participatory care.
Design eliminates partition walls, fostering open patient areas and communal spaces while respecting privacy.
Nurse stations promote independence with necessary oversight, balancing professional responsibilities and wellbeing.
EmPATH’s balance of privacy and openness provides a more holistic environment for patient care.
EmPATH’s approach to nurse station placement fosters a supportive care environment, enhancing patient well-being.
Staff-Patient Interaction
Patient-Patient Interaction
Enclosed nurse stations with glass partitions limit direct interaction and spontaneous communication. Integrates staff and patient areas, eliminating barriers and fostering casual, frequent interactions.
Individual room layout restricts patient interaction, leading to potential confinement and lack of communal engagement.
Open layout enhances visual connectivity and community among patients, beneficial for mental health.
EmPATH’s layout promotes egalitarian staff-patient interactions, contributing to a therapeutic atmosphere.
EmPATH’s open design promotes patient solidarity and interaction, supporting mental and emotional health.
Ease of Navigation
Complex, enclosed corridors are challenging to navigate, leading to stress and disorientation.
Intuitive and straightforward layout with clear paths simplifies navigation, reducing stress and promoting autonomy.
EmPATH’s design reduces stress and enhances patient and staff experience by simplifying navigation.
8.2 Results: Design Observations
SPACE INTENDED USES FEATURES &CHARACTERISTICS RATIONALE
Intake Room or Area initial assessment prior to beginning treatment
Nurse Station (Commonly
Referred to As A Care Team Station)
often considered home base for the care team. the care team will use this space to conduct clinical tasks and documentation; observe patient care areas, directly or via surveillance cameras; and meet with other staff.
located near entrance two means of retreat for staff safety typically designed as a high-risk space patient behavior is an unknown risk.
no glass partition separation between the nurse station and patient area.
provides good visibility to patient care areas promotes staff interaction with patients surveillance camera monitors (if present) shielded from patient view) an enclosed staff workroom allows staff to retreat while additional staff
The care team often requires a safe, designated staff space that allows for patient observation. where the nurse station is open to a multiple-patient observation area, provision of a directly accessible, lockable staff work area should be considered.
Medication
Safety Zone storage for medication to be administered on the unit. medication may be administered from this zone.
located out of circulation path separated with locked door from other spaces work counter handwashing facilities acoustic design to minimize sound transmission visible to the nurse station
most jurisdictions require medication to be stored in a secure location. separation with a locked door is a best practice.
SPACE INTENDED USES FEATURES & CHARACTERISTICS RATIONALE
Exam/ Treatment Room medical assessment and minor medical treatment for patients on the unit. this space might be used to medically clear a patient prior to admission to the EmPATH.
handwashing facilities often designed as a medium-risk space secure storage proper lighting as per clinical requirements
exam/treatment rooms located in the EmPATH will reduce the need for patients to leave the unit for medical examination or treatment.
Open Milleu provision of a therapeutic and comfortable setting in which patients can stabilize and receive therapy and treatment
The open-plan area, visible from the nurse station and supported by concealed camera surveillance, features soft warm lighting, movable recliners, small activity tables, and visible bays or nooks for privacy while maintaining visibility. It incorporates daylight access, non-institutional decor with a residential feel, and biophilic patterns on walls or ceilings for therapeutic benefits. If present, security guards wear civilian clothing to maintain a welcoming atmosphere.
a therapeutic stabilization and treatment space has proved to reduce average length of stay for many patients. an open area provides space for a variety of patient activities and direct visibility of patients by staff.
SPACE INTENDED USES FEATURES & CHARACTERISTICS RATIONALE
Patient Toilet Room when nature calls..
Shower Room patient hygiene
Laundry Room patients to have their clothes washed while stay
durable, tamper-resistant, and ligature-resistant fixtures, finishes, and hardware throughout anti-barricade door options designed as a high-risk space staff need to be able to monitor and access the room without compromising patient dignity and privacy.
durable, tamper-resistant, and ligature-resistant fixtures, finishes, and hardware throughout designed as a wet location designed as a high-risk space
Supervised access only, with durable, tamper-resistant, ligature-resistant fixtures and finishes, designed as a high-risk wet location.
Access to a shower ensures a hygienic shared environment, allowing staff to monitor and access the space while maintaining patient dignity and privacy.
quiet room a quiet space for patients to go when they are agitated
calming, color-changing lights visual access to outdoors with bed facing the window. minimal stimulation from other patients or the environment acoustic privacy from common areas often designed as a high-risk space
quiet rooms and similar spaces increase patient choice and can help calm a patient, reducing the need for involuntary medication or physical restraint.
SPACE INTENDED USES FEATURES & CHARACTERISTICS RATIONALE
secure holding room temporary holding space to provide patients a secure environment until they are ready for treatment or transfer to another facility
separated with locked door designed for one patient at a time observable from a constantly attended nurse station small window in the door or the wall adjacent to the door camera surveillance may be added design as a high-risk space
consultation room a private setting in which patients can meet with a provider considerations: barricaderesistant hardware vision panel for door or wall duress alarm options for staff retreat patientfacing design
this is a dedicated, patientsafe environment for shortterm use during a crisis for which other spaces on the unit may not be appropriate.
consultations with a psychiatrist, social worker, therapist, or other professional should occur in a private setting.
nourishment area storage for snacks and beverages for patient use
extent of patient access determined by the facility risk assessment and functional program work counter with easily accessed snacks and beverage dispenser so patients can serve themselves ice machine handwashing facilities patient food refrigerator storage for non-refrigerated food
designated space for patient nourishment increases choice and a sense of normalcy.
9.0 Conclusion
The potential of EmPATH units lies in their ability to redefine mental health emergency care by prioritizing patient dignity, healing, and operational efficiency. These units bridge the gap between crisis intervention and comprehensive treatment, offering a transformative model that benefits patients, providers, and healthcare systems alike. By integrating mental health specialists, rapid assessment protocols, and flexible spatial designs, EmPATH units optimize resource utilization while addressing critical gaps in psychiatric care.
Their growing presence across the U.S. signals a shift toward proactive mental health solutions, enabling healthcare systems to better respond to rising mental health challenges. States like South Carolina, with initiatives to expand EmPATH facilities, exemplify how strategic investments can
amplify impact on a broader scale. The success of EmPATH units offers inspiration for future innovations in healthcare design, fostering environments that blend medical efficiency with emotional well-being. By fostering collaboration between spatial planning, clinical practice, and policy, EmPATH units hold the potential to transform mental health crisis care—moving toward a system that ensures timely, compassionate, and effective support for all.
This research journey explored how the architectural design of psychiatric care spaces can transform the experience of mental health crises. Through comprehensive analyses, including interviews, literature reviews, space syntax methodologies, and case studies, significant insights emerged. The findings unequivocally demonstrate that well-designed EmPATH units create
participatory, non-coercive, and healing environments. These units are more than treatment spaces—they are sanctuaries that uphold patient dignity, respect privacy, and support autonomy.
The architectural design of EmPATH units fosters safety, reduces agitation, and lowers instances of violence and aggression, benefiting both patients and staff. By enhancing communication and ensuring a secure care environment, these units contribute to a holistic sense of well-being. Furthermore, the study highlights the interconnectedness of design strategies, emphasizing that calming design elements should be applied cohesively rather than in isolation, as they work together to create a therapeutic environment.
The broader implications of this research are profound. It challenges architects and designers to think creatively, considering patient needs, operational processes, and social contexts. The goal is to move beyond a checklist-based design approach and engage deeply with stakeholders to create spaces that are genuinely healing and supportive.
In conclusion, this research not only advances the understanding of psychiatric care design but also calls architects and healthcare designers to action. It urges them to design spaces that go beyond functionality—spaces that are humane, empathetic, and conducive to recovery. EmPATH units set a new benchmark in psychiatric emergency care, marking a pivotal shift toward a more compassionate and effective approach to mental health crisis management. Their success underscores the critical role of architectural innovation in shaping patient outcomes. As mental health challenges continue to rise, the need for thoughtful, researchinformed design has never been more urgent.
10.0 Limitations and Future Scope
This study was limited by the inability to conduct in-person evaluations of traditional psychiatric wards and EmPATH units. Without direct observation, the research relied on secondary data and prior studies, restricting a nuanced understanding of spatial layouts, operational challenges, and the real-life experiences of patients, families, and caregivers. The absence of firsthand engagement with stakeholders further limited the incorporation of valuable insights into how these environments function in practice and their impact on mental health outcomes.
Future research must prioritize a human-centered and evidence-based approach by integrating field studies with stakeholder engagement. Direct visits to both traditional wards and EmPATH units can uncover how spatial design impacts recovery, caregiving efficiency, and family involvement. Observing these spaces and documenting real-world interactions will yield richer insights into participatory and non-coercive caregiving practices, as well as the practical challenges faced by users. Additionally, this hands-on approach can help identify potential design gaps that may not be evident through secondary data alone.
As EmPATH units are still in their formative stages, this presents a unique opportunity to analyze their impact and refine their design beyond foundational layouts. Research should explore how spatial interventions can further enhance patient autonomy, caregiver workflows, and family inclusion. By mapping patient journeys, conducting focus groups, and gathering feedback, future studies can establish innovative design strategies that transform these spaces into truly restorative environments, setting new benchmarks for mental health care while fostering a sense of dignity, comfort, and holistic healing.
11.0 Bibliography
• Zeller, S., Calma, N., & Stone, A. (2014). Effect of a Regional Dedicated Psychiatric Emergency Service on Boarding and Hospitalization of Psychiatric Patients in Area Emergency Departments. Western Journal of Emergency Medicine, 15(1), 1–6. https://doi.org/10.5811/ westjem.2013.6.17848
• Zeller, S., and S. Thomas. “The Myriad Components of Creating a Comprehensive Patient Safety System.” The Joint Commission Journal on Quality and Patient Safety 47, no. 1 (January 2021):3-4. https://doi.org/10.1016/j.jcjq.2020.10.002.
• Zeller, S. (n.d.). Update on EmPATH: Expanding an Effective ED Boarding Solution Update on EmPATH The Missing Link in Crisis/Emergency Behavioral Healthcare. Retrieved from https://calhospital.org/wp-content/uploads/2022/12/Update-on-EmPATH_Zeller_Orrock_2up.pdf
• workweek. (2022, December 4). Part II: Why is the Emergency Department So Crowded? -. Retrieved from workweek.com website: https://workweek.com/2022/12/03/part-ii-why-is-the-emergency-department-so-crowded/
• Wirz-Justice, A. (2009). How does light therapy work? Omega, 60(3), 227-237.
• Weiss, A., Barrett, M., Heslin, K., & Stocks, C. (2016). Trends in Emergency Department Visits Involving Mental and Substance Use Disorders, 2006-2013. Retrieved from https://hcup-us.ahrq.gov/reports/statbriefs/sb216-Mental-Substance-Use-Disorder-ED-VisitTrends.pdf
• Ulrich, R. S. (1984). View through a window may influence recovery from surgery. Science, 224(4647), 420-421.
• This Simple Strategy Prevents 70 Percent of Psych Admissions. (n.d.). Retrieved December 20, 2023, from www.vituity.com website: https://www.vituity.com/healthcare-insights/this-simple-strategy-prevents-70-percent-of-psych-admissions/
• Smith, K. (2016). Recovery and Reflection: The Role of History in Nursing Education. Retrieved from https://www.jhrehab.org/wp-content/ uploads/2016/10/JHR_Fall_2016_Smith.pdf
• Scott Zeller, “emPATH Units as a Solution to ED Psychiatric Patient Boarding,” Psychiatry Advisor website, September 7, 2017, https:// www.psychiatryadvisor.com/home/practice-management/ empath-units-as-a-solution-for-ed-psychiatric-patient-boarding.
• Roy, A., Lachner, C., Dumitrascu, A., Dawson, N. L., Vadeboncoeur, T. F., Maniaci, M. J., … Burton, M. C. (2019). Patients on Involuntary Hold Status in the Emergency Department. Southern Medical Journal, 112(5), 265–270. https://doi.org/10.14423/smj.0000000000000968
• Roadmap to the Ideal Crisis System. (n.d.). Retrieved December 20, 2023, from National Council for Mental Wellbeing website: https:// www.thenationalcouncil.org/resources/roadmap-to-the-ideal-crisis-system/
• Quigley, P. A. (2013). Reducing the risk of falls and fall-related injuries in hospitals. In Falls and Fall Risk: Clinical Assessment and Management (Vol. 9, pp. 1-17).
• Psychiatric Care Unit Opens in Minnesota - Renovations. (n.d.). Retrieved December 20, 2023, from Healthcare Facilities Today website: https://www.healthcarefacilitiestoday.com/posts/Psychiatric-Care-Unit-Opens-in-Minnesota--26569
• Pati, D., Harvey, T. E., Jr., & Redden, P. (2008). Nurse’s station design: More than meets the eye. HERD: Health Environments Research & Design Journal, 1(2), 75-89.
• Pati, D., Harvey, T. E., and Pati, S. (2014). Physical design correlates of e#iciency and safety in emergency departments: A qualitative examination. Critical Care Nursing Quarterly, 37(3), 299–316. https://doi.org/10.1097/ CNQ.0000000000000032
• Nordstrom, K., Berlin, J., Nash, S., Shah, S., Schmelzer, N., & Worley, L. (2019). Boarding of Mentally Ill Patients in Emergency Departments: American Psychiatric Association Resource Document. Western Journal of Emergency Medicine, Volume 20, Issue 5, 20(5), 690–695. https://doi.org/10.5811/westjem.2019.6.42422
• Montgomery, M., Upton, S., State, W., & Zeller, S. (2022). Design of Behavioral Health Crisis Units. Retrieved from https://fgiguidelines. org/wp-content/uploads/2022/06/FGI-Design-of-BHCUs_2022-06.pdf
• M. P. Wilson and S. L. Zeller, “Introduction: Reconsidering psychiatry in the emergency department,” Journal of Emergency Medicine 43, no. 5 (November 2012):771-72, https://doi.org/10.1016/j.annemergmed.2017.01.036
• Kirkbride Buildings History. (n.d.). Retrieved December 20, 2023, from www.kirkbridebuildings.com website: https://www. kirkbridebuildings.com/about/history.html
• Kim, A. K., Vakkalanka, J. P., Van Heukelom, P., Tate, J., & Lee, S. (2021). Emergency psychiatric assessment, treatment, and healing (EmPATH) unit decreases hospital admission for patients presenting with suicidal ideation in rural America. Academic Emergency Medicine. https://doi.org/10.1111/acem.14374
• Kelen, G. D., Troncoso, R., Trebach, J., Levin, S., Cole, G., Delaney, C. M., … Sauer, L. (2017). Effect of Reverse Triage on Creation of Surge Capacity in a Pediatric Hospital. JAMA Pediatrics, 171(4), e164829. https://doi.org/10.1001/jamapediatrics.2016.4829
• Kaplan, S. (1990). The restorative benefits of nature: Toward an integrative framework. Journal of Environmental Psychology, 15(3), 169182.
• Kaplan, R., & Kaplan, S. (1989). The experience of nature: A psychological perspective. Cambridge University Press.
• Joseph, A. (2006). The impact of light on outcomes in healthcare settings. The Center for Health Design.
• Jiang, S. (2020). Positive Distractions and Play in the Public Spaces of Pediatric Healthcare Environments: A Literature Review. HERD: Health Environments Research & Design Journal, 13(3), 193758672090170. https://doi.org/10.1177/1937586720901707
• Jenkins, P. (2006). Emergency Department Treatment of the Psychiatric Patient: Policy Issues and Legal Requirements. Retrieved from https://ebookcentral.proquest.com
• International Interior Design Association (IIDA). (2010). Design Matters: Methodologies in Healthcare IIDA Best Practices Case Study.
• Holloman, G., & Zeller, S. (2012). Overview of Project BETA: Best Practices in Evaluation and Treatment of Agitation. Western Journal of Emergency Medicine, 13(1), 1–2. https://doi.org/10.5811/westjem.2011.9.6865
• Gonzalez, M. T. (2014). Therapeutic landscapes and mental health. In The Routledge Handbook of Health Geography.
• Gifford, R. (2007). Environmental psychology: Principles and practice. Optimal books.
• Garriga, M., Pacchiarotti, I., Kasper, S., Zeller, S. L., Allen, M. H., Vázquez, G., … Hidalgo-Mazzei, D. (2016). Assessment and management of agitation in psychiatry: Expert consensus. The World Journal of Biological Psychiatry, 17(2), 86–128. https://doi.org/10.3109/156229 75.2015.1132007
• Designing for Empathy and Resilience in Mental and Behavioral Health. (n.d.). Retrieved from HKS Architects website: https://www. hksinc.com/our-news/articles/designing-for-empathy-and-resilience-in-mental-and-behavioral-health/
• Decompression Space In Behavioral Health Design - HCD Magazine. (2020, June 5). Retrieved December 20, 2023, from HCD Magazine - Architecture & Interior Design Trends for Healthcare Facilities website: https://healthcaredesignmagazine.com/trends/operationsfacility-management/decompression-space-in-behavioral-health-design/
• Dabrowska, M. A. (2020). The Role of Positive Distraction in the Patient’s Experience in Healthcare Setting: A Literature Review of the Impacts of Representation of Nature, Sound, Visual Art, and Light. Repository.gatech.edu. Retrieved from https://repository.gatech.edu/ entities/publication/97388436-0a5f-4a05-9a87-0d8cd2fb9115
• Boyce, P., Hunter, C., & Howlett, O. (2003). The Benefits of Daylight through Windows. Rensselaer Polytechnic Institute.
• Bluyssen, P. M., Aries, M., & van Dommelen, P. (2011). Comfort of workers in office buildings: The European HOPE project. Building and Environment, 46(1), 280-288.
• Augustin, S., & Coleman, C. (2015). Color psychology and color therapy: A factual study of the influence of color on human life.
A study driven by the belief that spaces can inspire hope, foster recovery, and strengthen connections.