26
SF | CPD: ENDOCRINOLOGY
October 2021 | Vol. 21 No. 10 www.medicalacademic.co.za
This article was independently sourced by Specialist Forum.
Superior HbA1c REDUCTION REDUCTION with iGlarLixi
Please note that our CPD activities are only for practitioners registered with the HPCSA. Any other health professional should apply to their own Council for CPD purposes.
Type 2 diabetes (T2DM) is a progressive disease, associated with microvascular complication such as retinopathy, nephropathy, and neuropathy, as well as macrovascular complications including myocardial infarction. To prevent these complications, prompt treatment intensification is recommended.2,4,5
D
espite the high risk, studies show that it can take up to seven years before treatment intensification is initiated, further increasing the risk of diabetes-related complications. See box 1 for treatment intensification recommendations. 2
Treatment intensification options Guidelines recommend progressive addition of rapid-acting insulin to patients’ existing basal insulin regimen, multiple doses of premix insulin, addition of a glucagon-like peptide-1 receptor agonists (GLP-1 RA) or switching to a once-daily fixed-ratio combination (FRC) of basal insulin and a GLP-1 RA as intensification options, said Dr Adri de Kok, one of South Africa’s leading experts in diabetes care.1,3 Dr de Kok was the keynote speaker at the South African launch of of iGlarLixi (see box 2). The combination offers a once-weekly, singleinjection option for treatment intensification. 3 Dr de Kok discussed the findings of the Advancing therapy in suboptimally controlled basal insulin-treated type 2 diabetes: Clinical outcomes with iGlarLixi versus premix BIAsp 30 in the SoliMix randomized controlled trial, published in the June edition of Diabetes Care.3 SoliMix is the first head-to-head clinical trial comparing the safety and efficacy of iGlarLixi versus premix insulin (BIAsp30 [30% insulin aspart + 70% insulin aspart protamine]), plus one or two oral antidiabetic agents (OADs), in adult patients with insufficiently controlled T2DM.1
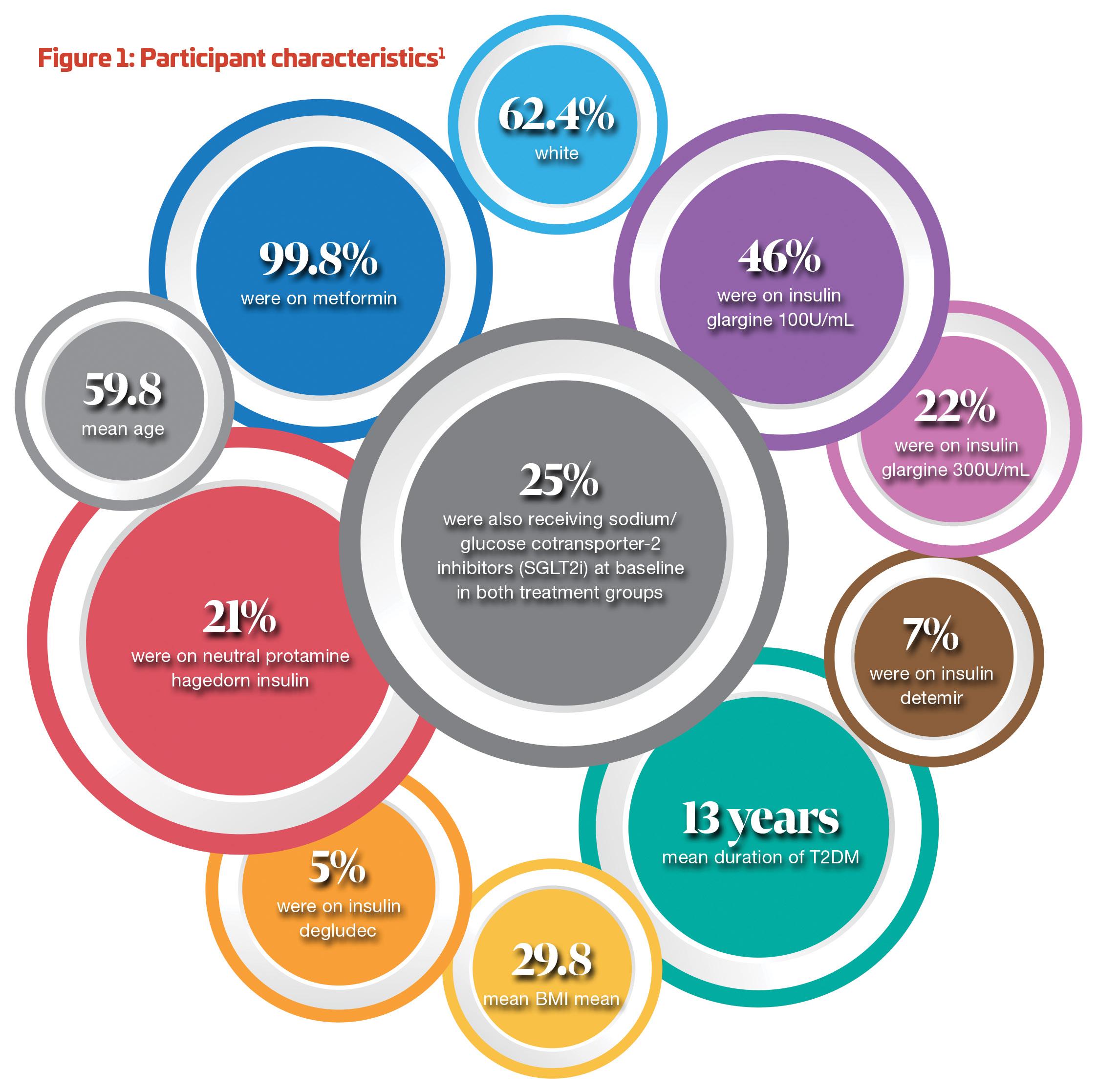
Solimix study design SoliMix was a 26-week, open-label study involving 89 centres in 17 countries. Participants (n=887) with T2DM, suboptimally controlled (HbA1c ≥7.5% and ≤10%) on basal
insulin were randomised to once-daily iGlarLixi (n=443) or twice-daily BIAsp 30 (n=444).1
Primary efficacy endpoints Primary efficacy endpoints were non-inferiority in HbA1c reduction (margin 0.3%) or superiority in bodyweight change for iGlarLixi versus BIAsp 30. The two primary objectives of this study were to demonstrate that, compared with BIAsp 30, iGlarLixi was non-inferior in terms of HbA1c reduction or superior in terms of bodyweight change from baseline to week 26.1
Secondary endpoints Key secondary efficacy endpoints were assessed at week 26, including HbA1c <7% without weight gain at week 26, HbA1c <7% without weight gain at week 26 and without hypoglycaemia (plasma glucose <3.9mmol/L) during the treatment period, and the superiority of iGlarLixi versus BIAsp 30 in terms of HbA1c reduction from baseline to week 26.1 Other secondary exploratory glycaemic endpoints included the proportion of patients reaching HbA1c target <7% at week 26, HbA1c target <7% without American Diabetes Association (ADA) level 2 hypoglycaemia (<3mmol/L), HbA1c <7 % without weight gain of >1kg, and HbA1c <6.5 %. Other secondary endpoints included change in total insulin dose and change in fasting plasma glucose (FPG), from baseline to week 26.1
Safety endpoints Safety endpoints were hypoglycaemia, adverse events (AEs), serious AEs (SAEs), AEs leading to treatment discontinuation and AEs leading to death. Hypoglycaemia was defined as: level 1 (<3.9 mmol/L and ≥3mmol/L]), level 2 or level 3 (severe hypoglycaemia), according to the ADA
Box 1: When should treatment be intensified? The majority of guidelines recommend a glycaemic target of <7% for non-pregnant adult patients. Suboptimal glycaemic control is defined as HbA1c >7%. 2 The 2021 ADA guideline recommends that treatment intensification for patients not meeting treatment goals should not be delayed. The early introduction of insulin (a GLP-1RA is preferred to insulin when possible) should be considered if there is evidence of ongoing catabolism (weight loss), if symptoms of hyperglycaemia are present, or when HbA1C levels are >10% or blood glucose levels are >16.7mmol/L. 5 If basal insulin has been titrated to an acceptable fasting blood glucose level (or if the dose is >0.5 units/kg/day with indications of need for other therapy) and HbA1c remains above target, consider an FRC.5 A patient-centred approach should be used to guide the choice of pharmacologic agents. Considerations include effect on cardiovascular (CV) and renal comorbidities, efficacy, hypoglycaemia risk, impact on weight, cost, risk for side effects, and patient preferences. 5 Among patients with T2DM who have established atherosclerotic CVD disease or indicators of high risk, established kidney disease, or heart failure, a SGLT2i or GLP1-RA with demonstrated CVD benefit is recommended as part of the glucoselowering regimen independent of HbA1C and in consideration of patient-specific factors. 5 The treatment programme should be reevaluated at regular intervals (every three to six months) and adjusted as needed to incorporate specific factors that impact choice of treatment. 5 classification. Nocturnal hypoglycaemia was also assessed post-hoc using two definitions: between bedtime and waking, and between 00h00-06h00.1
Study method iGlarLixi was injected before a meal using a prefilled disposable pen injector. BIAsp 30