8 minute read
CPD: Allergic rhinitis + asthma = united airways disease

Please note that our CPD activities are only for practitioners registered with the HPCSA. Any other health professional should apply to their own Council for CPD purposes.
Allergic rhinitis + asthma = united airways disease
Advertisement
Childhood allergic rhinitis (AR), an immunoglobulin (IgE) mediated condition, usually caused by sensitisation to inhaled allergens, is often missed, mistreated and misunderstood. AR is associated with significant comorbidities, can progress to asthma, or even worsen control of existing asthma, increasing the need for hospitalisation and doctor visits, as well as medicine costs.1
Kaplan et al2 found that 59%-78% of children with asthma also have rhinitis and Giavina-Bianchi et al5p2 showed that between 10%-40% of patients with rhinitis have asthma. Rhinitis is most commonly associated with early-onset allergic asthma.2
A survey by the International Study of Asthma and Allergies in Childhood (ISAAC) survey showed that asthma, rhinitis, and eczema symptoms have increased substantially over the past 15 years. The survey showed that the prevalence of AR increases from 85% in children aged six- to seven- years to 14.6% in those aged 13-14 years.1
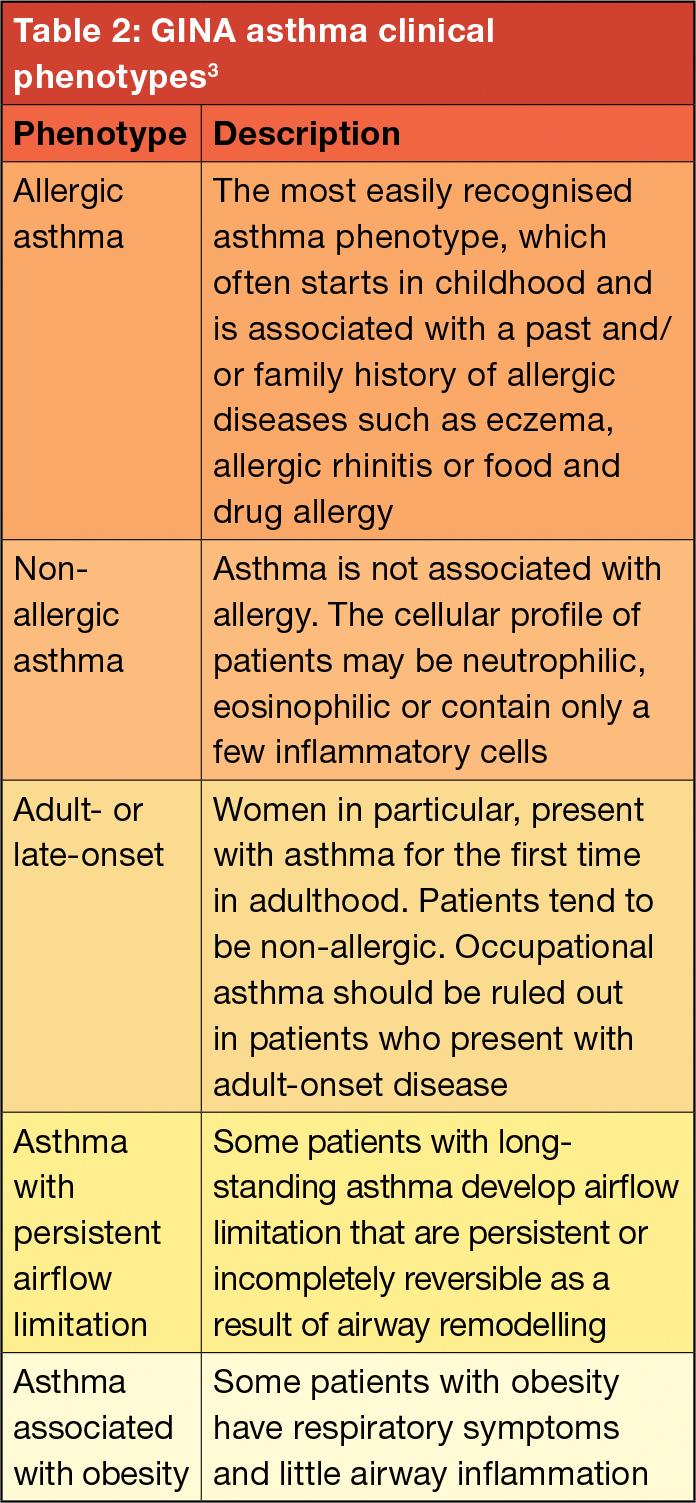
According to the Global Initiative for Asthma (GINA) an estimated 300 million people worldwide have asthma. The prevalence of asthma has increased in many developing countries, negatively affecting productivity and family dynamics.3
ISAAC also showed that environmental, rather than genetic factors are the likely causes of the increased prevalence in children. For example, children who eat fruit, vegetables and fish appear to be less affected than those who eat fast food.1
Asthma shows a similar trend. According to Cevhertas et al, the prevalence and incidence of asthma are increasing – especially in young adults aged 16-25-years. Environmental factors such as air pollution, genetic polymorphisms, and epigenetic factors all contribute to the development of asthma. Environmental interventions and exposure control can improve asthma control and exacerbations.4
Impact of AR and asthma on QoL
According to Scadding et al, AR is often trivialised, while in fact it represents a global health problem causing worldwide morbidity.1 The frequency of common colds in childhood means that AR may be misdiagnosed or ignored.1
An American study showed that 53% of children with asthma and comorbid rhinitis remained undiagnosed. Similar rates of underdiagnosis (32%-45%) have also been reported in adults and could be due to under reporting by patients or caregivers and poor recognition of rhinitis symptoms by doctors.2
AR and asthma severely impact patients’ quality of life (QoL). In children, AR can affect the sinuses, ears and chest and cause sleep problems, leading to reduced school performance, family difficulties and decreased involvement in outdoor activities.1
McDonald et al stress that QoL burden for patients with severe asthma is frequently underappreciated. Current public health messages erroneously promote that individuals with asthma can live normal lives unaffected by asthma symptoms and attacks. While this might be true for those with mild-to-moderate asthma, it causes additional difficulty for individuals with severe disease, for whom poor symptom control, exacerbations, and impacts on social life, physical activity, work, and school are often unavoidable.9
Symptoms of asthma and AR
Asthma and rhinitis share common risk factors and present common susceptibility to different agents, such as allergens (atopy) and infections.5
According to Cevhertas et al asthma and AR often co-exist because of ‘united airways’. Patients with AR show seasonal or perennial asthma-like symptoms, negative skin prick test, and/or specific IgE, but display positive bronchial and/or nasal allergen provocation test responses triggered by house dust mites.4
Giavina-Bianchi et al explain that the upper and lower respiratory tracts form a continuum, allowing the passage of air into and out of the lungs and sharing many anatomical and histological properties. They share common structures, including the ciliary epithelium, basement membrane, lamina propria, glands, and goblet cells, forming the so-called united airway.5
There are also some differences between the upper and lower airways. Nasal mucosa, which is attached to bone, is enriched with vessels, whereas bronchial mucosa, which is attached to cartilage, is enriched with smooth-muscle cells. Therefore, the major cause of airway obstruction, especially in the early phase of the allergic response is different – upper airway obstruction is caused by vasodilation and oedema, whereas lower airway obstruction arises from smooth-muscle constriction.5

How to treat asthma and AR
As rhinitis and asthma tend to coexist, the Allergic Rhinitis and its Impact on Asthma (ARIA) guideline highlights the importance of integrated care pathways centred around the patient with rhinitis and asthma.6 Similarly, GINA recommends an evaluation for comorbid AR in patients with asthma.3
According to the Joint Task Force guidelines set forth by the American Academy of Allergy, Asthma and Immunology, American College of Allergy, Asthma and Immunology and the Joint Council on Allergy, Asthma and Immunology, AR can be classified as seasonal (SAR), perennial (PAR) or episodic.7
PAR is typically caused by sensitisation to indoor allergens such as dust mites, mould, and animal dander, while SAR is most often due to sensitisation to pollen allergens. Episodic AR refers to sporadic exposures to aeroallergens that are not typically encountered, such as visiting a farm or home with animal allergens that an individual would not typically encounter.7
The ARIA guideline suggests categorising AR as intermittent or persistent. Intermittent refers to symptoms occurring less than four days a week or for less than four consecutive weeks, while persistent refers to symptoms present more than four days per week and for more than four consecutive weeks.7
The ARIA working group additionally classifies severity of AR as mild and moderate/ severe. Patients have mild AR if they do not have any of the following characteristics: sleep disturbance, impairment of daily activities, impairment of school/work and symptoms. Patients with one or more of the above characteristics are considered to have moderate/severe AR.7
The ARIA guideline recommends the following treatment for patients with AR:6
» In patients with SAR: A combination of intranasal corticosteroid (INCS) and an oral antihistamine (OAH) or INCS alone, but the choice of treatment depends on patient preferences. At initiation of treatment (first two weeks), a combination of an INCS and an inhaled AH (INAH) might act faster than an INCS alone and might therefore be preferred by some patients. In settings in which the additional cost of combination therapy is not large, a combination therapy might be a reasonable choice
» In patients with PAR: A combination of an INCS and an INAH or an INCS alone.
Two treatment tracks:
» Track 1 (preferred approach): As-needed low dose inhaled corticosteroids (ICS)/ formoterol as reliever therapy. Reduces the risk of severe exacerbation compared to regimens with short-acting β-agonists (SABAs) as reliever therapy
» Track 2 (alternative approach): As-needed SABA as reliever if track 1 is not possible or is not preferred by a patient who do not experience with exacerbations on their current therapy.
According to Kaplan et al there is conflicting evidence on the benefits of adequately treating rhinitis in terms of its impact on asthma outcomes. One meta-analysis reported no significant improvement in asthma symptoms or lung function by treating rhinitis with INCS, even though a trend in improvement was noted.2
Other studies have shown that treatment does improve disease control and quality of life in asthma patients. For example, in adults, the use of INCS was associated with a significantly reduced risk of asthma-related emergency room treatments and hospitalisations.2
Tiotiu et al pointed out that numerous studies provide evidence that appropriate treatment of AR results in the improvement of asthma. Although the use of AHs (first-line treatment in AR), is not recommended ARIA guidelines for treating asthma, evidence suggests that this treatment appears to delay asthma development in highrisk atopic infants and has beneficial effects on asthma outcomes when it is used to treat AR.8
Guideline recommended dosages of AH is associated with a significant improvement in AR and asthma symptoms and QoL without a significant impact on the lung function probably related to the fact that more elevated doses are needed to obtain a bronchodilator effect.8
INCS therapy in patients with both AR and asthma significantly decreased asthma symptom scores, disease severity and rescue medication use, could prevent the increase in bronchial hyperresponsiveness associated with seasonal pollen exposure and exercise-induced asthma, and improved lung function.8
The benefit of allergen immunotherapy has been proven in AR (improvement of symptom score and QoL with decrease in medication use) and asthma (increase in time to first asthma exacerbation following weaning of inhaled corticosteroids).8
Kaplan et al add that consideration should be given to optimal management of sleep disturbances including sleep apnoea (a common comorbid condition in asthma) as a consequence of upper airway obstruction in patients with persistent asthma and comorbid rhinitis. Sleep disturbances can lead to tiredness, irritability, memory deficit, daytime sleepiness and depression, thereby reducing QoL.2

References
1. Scadding GK, Smith PK, Blaiss M, et al. Allergic Rhinitis in Childhood and the New EUFOREA Algorithm. Frontiers in Allergy, 2021.
2. Kaplan A, Szefler SJ and Halpin DMG. Impact of comorbid conditions on asthmatic adults and children. Primary Care Respiratory Medicine, 2020.
3. GINA. 2020 Pocket Guide for Asthma Management and Prevention (for adults and children older than 5 years). https://ginasthma.org/wp-content/uploads/2020/04/ Main-pocket-guide_2020_04_03-final-wms.pdf
4. Cevhertas L, Ogulur I, Maurer DJ, et al. Advances and recent developments in asthma in 2020. Allergy, 2020.
5. Giavina-Bianchi P, Aun MV, Takejima P, Kalil J and Agondi RC. United airway disease: current perspectives. Journal of Asthma and Allergy, 2016.
6. Bousquet J, Schunemann HJ, Togias A, et al. Nextgeneration Allergic Rhinitis and Its Impact on Asthma (ARIA) guidelines for allergic rhinitis based on Grading of Recommendations Assessment, Development and Evaluation (GRADE) and real-world evidence. J Aller Clin Immunol, 2019.
7. Egan M and Bunyavanich S. Allergic rhinitis: the “Ghost Diagnosis” in patients with asthma. Asthma Research and Practice, 2015.
8. Tiotiu A, Plavec D, Novakova S, et al. Current opinions for the management of asthma associated with ear, nose and throat comorbidities. Eur Respir Rev, 2018. SF
To complete the quiz, go to www.medicalacademic.co.za and click on the CPD tab