TUBERCULOSIS.
Tuberculosis is a contagious disease produced by the action of Koch’s bacillus. It is common to man and all domesticated animals, but it specially affects animals of the bovine species. Its existence has long been recognised, although in oxen it was formerly confounded with the lesions of peripneumonia and echinococcosis.
It was not until the beginning of the nineteenth century that Laënnec (1811) described the tuberculous lesion from the anatomical and pathological standpoint. Gürlt pointed out for the first time in 1831 the similarity, the identity in fact, of tuberculous lesions in man and the ox.
In 1865 Villemin showed that tuberculosis could be conveyed from animal to animal, always producing similar lesions, and in 1868 Chauveau proved that, in the calf, infection might arise simply from the eating of tuberculous material.
At a somewhat later date doubts were entertained regarding the identity of human and bovine tuberculosis. Virchow denied the identity of the two diseases on the basis of a comparative study of the lesions. His opinion, however, has not prevailed, and the doctrine of the identity of tuberculosis in mammals still appears probable, in spite of the recent declarations of Koch (1901).
Causation. Tuberculosis is due solely to the activity of the tubercle bacillus. In 1884 Koch isolated and cultivated this bacillus in living animals, and always reproduced typical tuberculous lesions by injecting cultures. In 1887 Nocard and Roux described a rapid method of cultivating the bacillus, and in 1890 Koch announced the discovery of tuberculin.
The tubercle bacillus assumes the form of a little rod, five or six micromillimètres in length, and ·03 to ·05µ in thickness. It has a special staining reaction when treated with Ehrlich’s or Ziehl’s solution. It grows between 98° and 104° Fahr. (37° and 40° C.) in various artificial media containing glycerine.
Healthy subjects become infected by the accidental entrance of germs into their bodies, either by the respiratory and digestive tracts, or through solutions of continuity in the skin.
The material from tuberculous centres is virulent, whether consisting of sputum or discharge, saliva, fæces, urine, milk, etc., or tuberculous tissues derived from the different viscera.
The blood and muscular tissues are not always virulent, even in cases of generalised tuberculosis.
The virulent organisms usually enter the body through the lymphatic system; invasion proceeds from the point inoculated towards the nearest lymphatic glands and thence along the chain of lymphatic vessels, and the lesions extend, attacking the internal organs more or less rapidly. The body does not necessarily become fatally infected as a consequence of accidental or even experimental infection, for the bacillus may itself be destroyed by the phagocytes, or the lesion may remain purely local.
Although tuberculosis is the gravest and most widespread disease on the surface of the globe, its contagious character is relatively little marked, a fact which has unfortunately led to its receiving little attention in ordinary life.
Contagion is usually the result of cohabitation, although contact between diseased and healthy subjects for a period of some days or even weeks does not seem sufficient to produce the disease. Nocard has fixed a mean period of five to six months as necessary for the contraction of the disease by bovine animals, and Moussu has arrived at almost identical results by placing tuberculous and healthy cows together in a byre reserved for such researches. In this connection, however, very great differences of individual susceptibility exist, and these are difficult to appreciate in the present state of our knowledge. It thus happens that an animal of vigorous appearance and in good condition may easily contract tuberculosis, whilst a thinner and less vigorous one will resist it for a comparatively long time.
Speaking generally, it may be said that young animals contract tuberculosis by cohabitation in infected places more easily than adult or aged ones, and the fact that old animals contribute the larger
number of cases is to some extent due to their having in the course of their lives been more exposed to continued or successive infection.
Contagion does not occur in byres unless as the result of the presence of animals with open tuberculous lesions, such as caverns in the lungs, tuberculous bronchitis with ulceration of the mucous membrane, tuberculous metritis, enteritis, etc. The virulent germs are expelled in the saliva, nasal discharge, excrement, etc., and are distributed over the forage, manure, litter, and in the drinking water; after desiccation they may be spread by currents of air.
The mangers, racks, drinking pails, and various stable utensils become permanently contaminated, the air of the cowsheds contains virulent dust, and the animals there confined are continually exposed to infection either through the respiratory or digestive passages.
Contamination through the respiratory tract is by far the most frequent cause of the evil, and recent experiments at Pouilly-le-Fort (1900) have shown how easy it is to convey the disease experimentally by inhalation.
Patients suffering from closed tuberculous lesions of the pleura, pericardium, spleen, peritoneum, etc., do not spread the bacilli. Healthy animals may remain in contact with them without danger, but it is well to remember that such cases are quite exceptional. As a rule the lesions are of a mixed character, and the general principle may be laid down that cohabitation of any duration with tuberculous subjects is dangerous.
Contagion spreads more easily, in proportion to the number of tuberculous subjects in a given byre, to the total number of animals in a herd, and to the neglect of cleanliness, good feeding, ventilation, etc.
Life in the open air and at grass greatly diminishes the chances of contagion. The virulent products are then disseminated in all directions and are soon destroyed by the general atmospheric conditions. Close confinement in ill-ventilated stables, on the contrary, strongly tends to the propagation and development of tuberculosis.
In calves infection may occur through the alimentary tract by means of tuberculous milk, whether such milk is obtained directly
from the udder or out of a pail. The same may be true of young pigs fed with skimmed milk.
Goats contract tuberculosis somewhat readily by confinement in byres with tuberculous cows, and Moussu declares that contagion afterwards spreads just as rapidly among goats as among cows. The vaunted great resistance of goats to tuberculosis, formerly so often spoken of, and by some wrongly considered as a condition of immunity, is deceptive, and if tuberculosis is less frequently seen in goats, this is solely because goats enjoy the greatest liberty at all seasons.
On the other hand, the disease is very rarely conveyed to sheep, even when they are kept for long periods with tuberculous cows. Moussu found that two years of close cohabitation were necessary for its development under these conditions.
Heredity is a factor of the highest importance in determining the causation of tuberculosis. At the present time a tendency exists to deny this, but such a view is erroneous.
Observation has clearly shown that tuberculosis is rarely conveyed from the mother to the fœtus, and that practically none of the calves borne by tuberculous mothers react to tuberculin (95 per cent.: Nocard and Bang); but even if this is absolutely correct, it only shows that great benefits might be derived if proper sanitary organisation and intelligent hygienic conditions in byres were found everywhere in the country. Unfortunately in practice this is far from being the case. These non-tuberculous calves are left in common contaminated byres, where they rapidly become infected and perpetuate the disease.
Physiologically these facts are easily explained. The placenta resists the passage of microbes, or at least only allows them to pass under quite exceptional conditions, and practically only when the blood-vessels are affected. As, on the other hand, tuberculosis of the ovaries, Fallopian tubes or uterus generally prevents pregnancy and causes sterility, there is nothing extraordinary in the fact that tuberculosis is not hereditary in the strict sense of the term. The influence of the sire has been invoked, but it has been proved that direct paternal infection is only possible where ulcerating tuberculous lesions of the testicle, prostate, or vesiculæ seminales
exist. Such conditions seldom or never occur in the sires of domestic animals.
As a general rule, therefore, it may be said that tuberculosis is not hereditary. New-born animals become infected during the months following birth, either directly through the alimentary tract when the mothers are suffering from mammary tuberculosis, or, perhaps more frequently, through the respiratory and digestive tracts.
But although microbic infection is not hereditary, it by no means follows that the offspring of tuberculous subjects are as well prepared for the struggle of life as the descendants of healthy subjects. What is transmitted is a greater tendency to contract the disease.
This aptitude or predisposition is of such importance that in Moussu’s opinion it should be regarded as one of the essential factors in the development of tuberculosis. The cause of tuberculosis is Koch’s bacillus. It does not always produce its full effects in animals born of healthy parents; but in one that suffers from a tuberculous hereditary taint tuberculosis appears.
Physiological and pathological researches cast considerable light on this question. In tuberculous mothers the organism not only suffers from the infection, but from a permanent intoxication which interferes with normal metabolism in the vital organs and the exchanges between mother and fœtus. If the microbes remain confined to the system of the mother, their poisons are conveyed by the blood and pass through the placental barrier. In a greater or less degree they saturate the tissues of the little creature in process of development, and communicate to it a peculiar hereditary taint. The effects of this taint are often noticeable from the moment of birth, for comparative physiological and pathological investigations have shown that the tissues of tuberculous animals assimilate given foods less perfectly and are the seat of greater losses of all kinds than those of healthy subjects.
Although the disease itself, therefore, is not hereditary, it is otherwise with the organic taint which plays so important a part in its development. This organic taint consists in a special condition of the tissues or cells of the parents, which show a diminished power of resistance to the action of the germs of tuberculosis; it is therefore
easy to understand how important a part these influences may play under certain conditions.
Without doubt, in the case of bovine animals, the predisposition could be neutralised in carefully managed studs by the immediate isolation of the new-born under conditions which shield them from tuberculous infection, and experiment has shown the benefits derived from such precautions; but it must not be forgotten that intelligently managed studs are the exception, and that for a long time to come we must in practice take cognisance of the actual conditions under which the disease develops.
The lesions of tuberculosis vary greatly in appearance, according to the organs affected, though the method of development is always identical.
The primary lesion corresponds to what has been termed tuberculous granulation, or anatomical tubercle properly so called; this, the macroscopical, pathological entity, assumes the form of a small prominent centre, semi-transparent, greyish, opaque or yellowish, according to its age.
These tubercles, produced by the presence of colonies of bacilli, are due to the defensive reaction of the invaded tissues, which gradually undergo change and are destroyed in a direction radiating from the centre towards the periphery. The tubercle in itself has no very specific character—only the bacillus.
The elementary lesion may remain isolated, but very frequently it is closely surrounded by other similar tubercles, and becomes enveloped in a common inflammatory area. A large portion of an organ may appear as if riddled with tubercles of different age and size, while the interstitial connective tissue reacts and forms fibrous separating partitions. The general appearance is that described under the term “diffuse tuberculous infiltration.”
At a still more advanced stage in the development of the disease conglomerations are produced, consisting of tuberculous masses the size of a hazel-nut, a walnut, an egg, a man’s fist, or even larger. These lesions, irrespective of size, undergo caseous degeneration from the centre towards the periphery.
In exceptional cases the tubercles remain fibrous. More frequently, particularly in animals of the bovine species, they become infiltrated
with lime salts. Caseous degeneration not only invades the centre of the tubercles but also the peripheral layers, and sometimes the whole of a conglomerated mass.
Steadily pursuing their course of pathological development, the tuberculous masses become softened and are transformed into tuberculous abscesses, which open towards any free passage, leaving behind sometimes ulcerations, sometimes caverns of varying sizes, or blind simple or bifurcated fistulæ.
Recent experiments by Nocard and Rossignol (1900) prove conclusively that a certain time (always more than a fortnight) elapses between the moment of entry of the contagion into the organism and that at which its effects become manifest by furnishing a reaction to tuberculin. Calcification or softening of the lesions, moreover, never occurs in less than fifty days.
According to the organs studied, these tuberculous lesions assume certain appearances, which in each locality seem almost always to be identical.
Thus, as regards the larynx, trachea, and bronchi, the tubercles develop in the depths of the mucous membrane, rapidly undergoing caseous transformation, softening and purulent degeneration, and producing numerous isolated or confluent ulcerations in the air passages.
According to the case and the kind of animal affected, the lung presents either disseminated tuberculous formation, tuberculous infiltration, tuberculous conglomeration, or cavern formation.
The lung may be affected to such a degree that it appears incredible that the blood can have been sufficiently aerated to support life.
The lungs may be transformed into yellowish, caseous, calcareous, or softened masses enveloped in thick, fibrous, resistant walls. The intervening pulmonary tissue may be healthy in appearance, or reddened, congested, and sometimes hepatised.
The pleural, pericardial, and peritoneal membranes may be covered with exuberant tuberculous lesions, like ripe mulberries, in consequence of fusion and massing of the tuberculous growths. The primary tubercles are surrounded with fibrous walls, which granulate when on the surface of a serous membrane, and impart to
the membrane a vegetative, sometimes villous appearance, and a colour varying from pink to light or dark red.
The collective lesions lining the cavities are described by butchers under the significant term of “grapes.” In the interior of these exuberant masses, which sometimes form layers an inch or more in thickness, the tuberculous lesions undergo the usual developmental changes, that is to say, they become caseated or infiltrated with lime salts, but they do not so readily undergo softening as those of the lung. The parietal and visceral serous membranes readily become adherent at numerous points, setting up union between the lung and the walls of the chest, or the intestine and the walls of the abdomen, etc.
In the pericardium the vegetations are frequently of a fungoid character.
Tuberculosis of lymphatic glands sometimes assumes a disseminated, discrete form or that of a diffuse infiltration, or, again, in old-standing cases it constitutes a massive tuberculous conglomeration. In point of fact, the lymphatic glands as such no longer exist, their tissue having undergone total degeneration; they are represented only by an enlarged, thick, fibrous shell, forming the envelope which encloses caseated and calcareous masses of a more or less soft nature.
Tuberculous infiltration of the submaxillary and sub-parotideal lymphatic glands interferes with swallowing and breathing, compresses the pharynx, œsophagus and larynx, and deforms the head.
Compression of the arteries, veins, nerves, etc., at the entrance to the chest may cause various symptoms which are not difficult to interpret. The glands at the entrance to the chest and the whole of the anterior mediastinum may form a single mass. Lesions in the posterior mediastinum, however, are of even greater importance and explain certain symptoms, such as difficulty in swallowing, spasm of the œsophagus, mechanical contraction of the œsophagus, permanent tympanites, etc., for which the state of the lungs alone would not account.
Even when the lungs are unaffected it may happen that the lymphatic glands of the mediastinum (superior or inferior
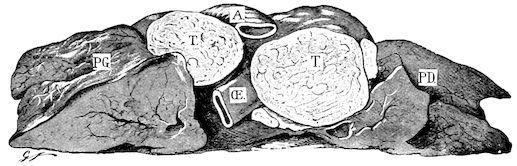
œsophageal lymphatic glands) and the bronchial lymphatic glands may be so diseased that the œsophagus is completely surrounded and compressed by them, and its function thus seriously impaired (Fig. 276).
In the abdomen the mesenteric glands are most exposed to disease, and when infected through the intestinal tract they assume the form of large flattened masses arranged along the mesentery.
In the digestive tract, as in the trachea and bronchi, tuberculosis has a marked tendency to assume the ulcerative form. Disseminated or aggregated tubercles develop in the thickness of the mucous membrane, and, after rapidly softening, become ulcerated. The nature of these lesions can only be determined by noting their character and examining the discharge.
F��. 276. Tuberculosis of lymphatics. PG, Left lung; PD, right lung; TT, tuberculous œsophageal lymph glands; A, aorta; Œ, œsophagus (the lung is divided transversely near its centre).
The ulcerations are localised in the mouth and pharynx, in the second half of the small intestine towards the ileum, and in Peyer’s patches.
Tuberculous lesions develop in the vaginal sheath of the male genital organs exactly in the same way as in an ordinary closed serous cavity; tubercles may also develop on the surface or in the substance of the testicle. They become aggregated, undergo softening, spread towards the interior, and may break down, thus forming abscesses. In the female genital passages the disease invades
the thickness of the walls, but shows a marked tendency to ulceration, as in the intestine or trachea.
In the udder tuberculosis is generally diffuse, shows a tendency to hypertrophy and the free formation of fibrous or sclerous tissue; only tubercles in the glandular layer of the acini become ulcerated. In time the whole of the secreting structure undergoes diffuse tuberculous suppuration, fibro-caseous masses form in the depths of the tissue and may soften, producing deep-seated tuberculous “cold abscesses.” The mammary lymphatic glands are affected in the same way as other lymphatic glands.
In the joints tubercles appear either on the synovial membrane or in the thickness of the bony epiphyses, very often at both points simultaneously. The synovial membrane is covered with vegetations and villous growths, the ends of the bones are attacked by a destructive ostitis, tubercles or tuberculous centres form in the thickness of the spongy tissue, the articular cartilages are destroyed, the ends of the bones become deformed, and in the last stages fungoid arthritis in various forms may be produced.
In bones the tubercles originate in the depths of the spongy tissue. They produce destructive hypertrophic ostitis, in which the bony tissue is replaced by tuberculous centres or masses divided by fibrous partitions. On section, these lesions exhibit the same yellowish caseated or calcified appearance as the lesions of other affected organs. The compact layer may sometimes be perforated at several points before being destroyed.
In tuberculosis of the brain the primary lesions develop at the expense of the serous layers of the arachnoid and on the pia mater, towards the base of the brain and the fissure of Sylvius, or at the expense of the small vessels which penetrate the depths of the nerve substance itself. Some tubercles remain isolated, become confluent or are collected in masses of different sizes, and provoke symptoms which vary with the locality attacked.
Symptoms. Tuberculosis is the most protean of all diseases, and at first sight it often seems impossible to assign to one group, clinical conditions presenting such essentially different appearances. All the tissues may be attacked, from the bones to the most delicate of the viscera, a fact which explains why all aspects of tuberculosis cannot be described. Certain forms, however, occur very frequently, and
may be regarded as classic; these will be considered in the order of their frequency.
TUBERCULOSIS OF THE RESPIRATORY APPARATUS.
Without doubt this form of tuberculosis is by far the most frequent. It assumes the form either of bronchitis, laryngobronchitis, or pulmonary tuberculosis.
Tuberculous Bronchitis.—The symptoms of tuberculous bronchitis do not essentially differ from those of ordinary bronchitis, though the disease develops more insidiously and slowly, and is seldom accompanied by fever. At first the cough is dry and suppressed; later it becomes paroxysmal, and at a still more advanced period liquid and rough. The least irritation brings on these attacks of coughing; changes from the warmth of the stable to the coldness of the outer air or vice versâ, the presence of dust or the action of liquids when drinking, etc., etc. During the first stage coughing is not followed by expectoration, but later yellowish-grey, glairy mucus may be discharged: more frequently it is coughed into the pharynx and swallowed.
These symptoms continue for weeks or months without showing any tendency to abate. If the larynx is attacked inspiration becomes rattling and difficult, while the neck and head are held extended, and the least pressure over the larynx produces coughing.
Tuberculosis of the larynx, trachea, and bronchi is usually accompanied by disease of the lung, but may occur by itself.
When there is a discharge it consists of thick, viscous, sticky mucus of a peculiar greyish-yellow colour. Microscopical examination shows it to contain tuberculous bacilli.
Pulmonary Tuberculosis usually assumes the chronic form, and is almost always preceded by specific bronchitis. The patients retain their appearance and condition for a longer or shorter time, and, without the experience resulting from continued observation, it would be difficult to believe them to be suffering from the slow development of a serious disease.
Frequent coughing without any apparent reason is the only symptom likely to arouse suspicion.
At a later stage these animals lose condition, feed less eagerly or exhibit capricious appetite, and sometimes well-marked and repeated digestive disturbance, such as slight tympanites with constipation or diarrhœa, moderate impaction of the rumen, relative atony and slackening of peristaltic movements. The wasting gradually becomes more marked or, in the case of pregnant or milch cows, makes intermittent progress, until the animals become anæmic and finally cachectic. The cough is more frequent and more severe, and is followed by discharge from the nose or by swallowing movements. From this time phthisis, properly so called, exists.
The course of the disease is not invariable. Certain animals may appear ill for years without clinically showing the least apparent aggravation; others on the contrary, though living under similar conditions, are rapidly attacked, and in six to twelve months exhibit all the signs of advanced phthisis. Pregnancy, suckling, and prolonged lactation favour the development of the disease by taxing the physical resources of the animal.
Animals suffering from phthisis exhibit a peculiar appearance. They are extremely thin, all their soft tissues are wasted, the limbs are dragged in moving, respiration is rapid and sometimes jerky, the mucous membranes are pale and discoloured, and the skin is tight and adherent to the subjacent tissues.
These general signs, however, would not warrant a diagnosis, for, apart from the cough, certain other diseases present all the external appearances of the last period of tuberculosis (chronic diarrhœa, chronic forms of poisoning—bacterial or otherwise—dyspepsia, etc.).
In cases of doubt it is essential to discover by percussion and auscultation that the external signs are really the result of lesions of the lung, and that the lung disease has developed gradually in accordance with the signs shown by simple external inspection.
The symptoms presented during the development of the pulmonary lesions may be divided into three phases.
In the first phase percussion gives no information, though auscultation reveals rough respiration, inspiration and expiration being also unequal. Expiration, which, in the healthy subject, is
silent, becomes clearly perceptible, not over the whole lung, but usually over the anterior lobes, particularly the cardiac lobes. This sign is the result of tuberculous infiltration and of the neighbouring pulmonary tissue having lost its elasticity.
Inspiration is rough and rasping, and sometimes occurs in several stages, the act being interrupted or jerky; expiration lasts longer than inspiration, is rough and prolonged, but never blowing in character. These peculiarities are only found in one other condition of the lung, viz., emphysema.
The patients appear little affected in this, the first, stage of tuberculosis. But for the cough they may seem perfectly healthy.
In the second phase the tuberculous infiltration extends and ends in the massing, by fusion or centrifugal growth, of the tuberculous masses.
Percussion may now indicate localised dulness, but this is not invariable, because the diseased anterior and middle lobes of the lung are concealed beneath the muscles of the shoulder. When dulness is noted, it is usually over the lower part of the posterior lobes, very rarely at any higher point on the side of the chest. Frequently the dulness is only partial.
On auscultation the signs met with during the first stage become much more marked. Inspiration is always rough, rasping, painful and difficult at certain points, particularly in the anterior zones. In this region expiration is rough, prolonged and sometimes of a clearly marked blowing character. This is particularly the case in the subscapular zone and the auscultation zones 2 and 3 (Fig. 166). In the dorsal region and in zone No. 1, respiration may appear normal. Nevertheless, the sounds are propagated to a distance, the infiltrated lung steadily loses its elastic qualities, the vesicular murmur entirely disappears from the affected regions, and the sounds noted are of bronchial origin.
Like the first, the second phase may vary in intensity, extent, and in the diffusion or localisation of the tuberculous lesions. Blowing respiration may be noted over different areas, accompanied by sibilant, snoring and migratory mucous râles. The vesicular murmur is exaggerated in the healthy parts, coughing, accompanied by expectoration or followed by swallowing movements, is frequent, the
appetite becomes capricious, and the general condition suffers. In this second phase almost the whole of one lung may be diseased and exhibit the signs described.
The third phase corresponds to the softening of the tuberculous masses, and the formation of ulcers and caverns. The zones of dulness or partial dulness may be more extensive, though cavern formation is usually confined to the anterior or middle lobes. Percussion still affords no precise information.
As the tuberculous masses undergo softening and ulceration, their contents are gradually passed into the bronchi, and auscultation reveals signs indicative of the existence of caverns, which signs vary with the dimensions of the caverns themselves. On auscultation the respiration is always found to have at certain points a blowing character, and it may even develop into a true tubal souffle. In other areas, where the caverns are merely in course of formation, gurgling sounds are all that are heard, but where true caverns exist there is an incessant cavernous souffle.
The lesions peculiar to the third phase are seldom seen in practice; because the animals become anæmic, exhausted and cachectic, they are usually slaughtered early. Nevertheless, the third stage occasionally develops in an astonishingly short time, six to eight months at most.
Very frequently the patients, although cachectic and even phthisical, do not yield on auscultation the sounds described as peculiar to the third stage, because the tendency to softening is not very marked in bovine animals. The lungs exhibit massive infiltration, and, whilst pulmonary consumption is not uncommon, the development of caverns is comparatively rare.
The expectoration or discharge in this third form is puriform, glairy, viscous, and of a dirty-yellow or even greenish-yellow colour. Bacteriological examination reveals the presence of tubercle bacilli and adventitious organisms.
These conditions are always associated with various complications, and the second and third stages of chronic tuberculosis are frequently accompanied by lesions of the pleura, of the mediastinal lymphatic glands, of the liver, etc.
Digestive disturbances often occur; the appetite is capricious or in abeyance, there is atony of the rumen and chronic dyspeptic tympanites. These disturbances are easily understood where there are lesions of the liver, intestine, and mesenteric lymphatic glands, but not when the lung alone appears the seat of the disease. In this condition the patients probably suffer from permanent complex intoxication, due to toxins elaborated by the tubercle bacillus and other microbes which multiply on or in the lesions, and this chronic intoxication reacts on the vital functions (innervation, secretion, digestion and nutrition). Nor are the effects limited to these appearances; the heart’s action is also accelerated, and the temperature rises. During the first and part of the second phase there is comparatively little fever, but afterwards this is continuous or of a peculiar intermittent character. In the morning the patient’s temperature may be normal; in the evening it has risen from 1·5 to as much as 9° Fahr. (1·1 to 5·2° C.) above normal, and this recurs day by day. These attacks coincide with softening of the lesions, and when suppurating caverns exist they are more marked and more nearly continuous, assuming the characters of the hectic fever shown in consumption.
Often during the febrile periods the urine is albuminous.
In chronic tuberculosis of bovine animals bleeding from the lung is rare even when caverns exist, and Moussu, in spite of extensive experience, has seen only two cases. This is in striking contrast with the condition in human sufferers from pulmonary tuberculosis, twothirds of whom bleed at the lungs.
TUBERCULOSIS OF SEROUS MEMBRANES.
After pulmonary tuberculosis, tuberculosis of the pleural and peritoneal serous membranes is the most frequent clinical form of this disease. Sometimes both forms exist, and although the pleural and peritoneal lesions predominate or alone attract attention, there are also lesions in the lung or mediastinal lymphatic glands.
It is difficult to explain how the pleural and peritoneal serous membranes can be seriously invaded without the lung becoming
affected, though in point of fact such a state of things frequently exists.
Tuberculosis of the pleura without pulmonary lesions is suggested by very obscure symptoms. The general signs consist in diminution of appetite, loss of condition, tachycardia, elevation of temperature, and progressive organic wasting. These are always present, though in themselves they have no specific significance.
The local symptoms are still more vague. Percussion causes pain, and the practitioner might at first suspect peripneumonia. The patient edges away, and tries to avoid the application of the pleximeter hammer. Firm pressure over the intercostal spaces sometimes causes struggling, and produces indications of abnormal sensitiveness. There is generally extensive partial dulness, sometimes complete dulness towards the lower regions of the chest.
On auscultation the lung may reveal the different indications of chronic pulmonary tuberculosis, or simply diminution of the respiratory murmur at points, accompanied by crepitant, sibilant râles, and moist, crackling sounds. As the anterior portions of the pleural sacs are most commonly invaded, the anterior vena cava is compressed, causing some difficulty in the return circulation, and producing venous pulse, which may extend as high as the parotid gland; there is, however, no swelling of the dewlap.
Respiration is frequent and difficult in consequence of adhesions between the pleura and lungs, which are connected by bands of fibrous tissue of varying extent. Coughing is rarely absent, and if the lung is diseased may be followed by discharge containing numerous bacilli. Otherwise the cough exhibits the pleuritic character, that is, it remains slight, dry, paroxysmal, and painful. The pericardium may be affected as well as the pleura; if the conditions occur simultaneously the venous pulse in the jugulars will be particularly apparent.
The symptoms of tuberculous pericarditis are similar to those of ordinary pericarditis, except that the exudation is less abundant; in a word, the symptoms are those of rather trifling exudative pericarditis.
Tuberculosis of the peritoneum is frequently accompanied by that of the pleura or the abdominal viscera. The lesions are localised on
the parietal peritoneum and epiploon, producing in time adhesions between the viscera and walls of the peritoneal cavity, which affect the action of the digestive organs, gradually causing interference with the peristaltic movement both of the rumen and the intestines. The stagnation of alimentary matter favours fermentation, so that the rumen becomes permanently distended. The right flank also is swollen, and the abdomen exhibits a change in shape similar to that in peritonism, which is a constant symptom of tuberculous peritonitis.
As in the thorax, the tuberculous lesions seldom produce extensive liquid exudation, so that ascites does not occur, but on palpation the abdominal walls appear to have entirely lost their pliability and to be unyielding and greatly thickened, a point which is the more remarkable as the animals are thinner.
The wall of the abdomen is stiff, incapable of being depressed as in ordinary subjects, and gives to the fingers the sensation of a thick hard covering, through which the subjacent organs and their contents, that is, the rumen, intestine and alimentary material, can no longer be felt. This rigidity is always most marked in the lower abdominal region. The digestive peristaltic movement can no longer be detected, and on auscultation the normal sounds are manifestly much slower than usual.
TUBERCULOSIS OF LYMPHATIC GLANDS.
It might perhaps have seemed more logical to place tuberculosis of the lymphatic glands at the commencement of these clinical divisions of tuberculosis, as when tuberculous lesions, of whatever kind, occur in the lung, pleura, abdomen, etc., the lymphatic glands in the neighbourhood are invariably invaded. In such cases, however, the lesions in question are not the dominant features.
Under this heading must be classed tuberculous lesions which, on the contrary, affect the lymphatic glands in so marked a manner that lesions in other organs may be regarded as secondary. This occurs somewhat frequently, because at the present day there is a tendency to believe that inoculation takes place mainly through the mucous membrane of the pharynx, and thence extends towards the
neighbouring lymphatic glands. At any rate, it is unquestionable that tuberculosis of the lymphatic glands may exist quite apart from any other lesion visible to the naked eye.
Two forms are very common, tuberculosis of the retro-pharyngeal region and of the neck, and tuberculosis of the mediastinal lymphatic glands.
Tuberculosis of the Retro-pharyngeal Glands.—In addition to the retro-pharyngeal glands the cervical chain of lymphatic glands, the subglossal, subatloid, preparotid, and even the prescapular lymphatic glands and those at the entrance to the chest, may also be invaded more or less.
This form of tuberculosis may remain latent for a long time, attention being attracted to it only when deglutition is impeded and local deformity becomes apparent.
Swelling of lymphatic glands resulting from tuberculous infection is slow and progressive, differing entirely from that which accompanies suppurative adenitis. The neighbouring connective tissue is certainly somewhat thickened or infiltrated, but the glands themselves can always be detected. The region of the gullet is enlarged, the depression marginating the lower jaw is filled up, the subatloid space disappears, the subglossal glands occupy the space beneath the tongue, and in cases where the lesions are very pronounced the œsophagus and larynx may even be pushed downwards.
Swallowing is difficult, in consequence of compression of the upper part of the œsophagus, and, as the laryngeal nerves may be included in the swelling, dyspnœa or roaring not uncommonly results.
By palpation with one or both hands it is easy to identify the glands and detect enlargement, hardness and sensitiveness. In exceptional instances the caseous masses they contain undergo softening and conversion into purulent material.
When the cervical lymphatic glands are attacked the jugular furrows disappear, and the whole of the pretracheal and lateral regions of the neck exhibit doughy swellings.
These swellings are rarely symmetrical, a fact which admits of this condition being distinguished from lesions due to lymphadenitis,
without examining the blood.
The prescapular glands are rarely attacked, but those at the entrance to the chest, which may be found on either side of the trachea by passing the fingers between the two first ribs, are frequently enlarged to the size of a fowl’s egg.
Tuberculosis
of the Mediastinum. Whenever the lungs are much involved, the bronchial glands are also invaded, though the glands of the anterior and posterior mediastina may escape. On the other hand, the mediastinal glands are sometimes much involved, whilst the lung remains intact.
The lymphatic glands, particularly those of the mediastinum, may be enormously enlarged, and the various accidents which result are due as much to mechanical interference with the functions of adjacent organs as to the lesions themselves.
When the glands of the anterior mediastinum are affected, they cause compression of the anterior vena cava, with stasis of blood in the jugular vein and venous pulse, then compression of the œsophagus and trachea, and of the nerves at the entrance to the chest, producing difficulty in swallowing, respiration and circulation.
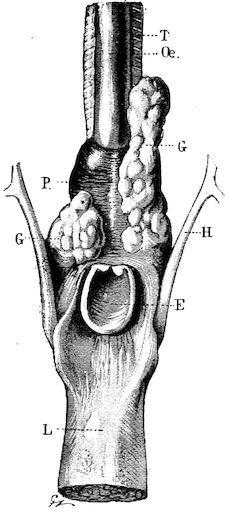
F��. 277.—Lesions in retro-pharyngeal tuberculosis. T, Trachea; Œ, œsophagus; P, pharynx; H, hyoid bone; E, epiglottis; L, tongue; G, tuberculous retro-pharyngeal glands.